User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
2023 GOLD update: Changes in COPD nomenclature and initial therapy
Airways Disorders Network
Asthma & COPD Section
The 2023 GOLD committee proposed changes in nomenclature and therapy for various subgroups of patients with COPD.
The mainstay of initial treatment for symptomatic COPD should include combination LABA/LAMA bronchodilators in a single inhaler. For patients with features of concomitant asthma or eosinophils greater than or equal to 300 cells/microliter, an ICS/LABA/LAMA combination inhaler is recommended.
People with “young COPD” develop respiratory symptoms and meet spirometric criteria for COPD between the ages of 25 and 50 years old. Other terminology changes center around those with functional and/or structural changes suggesting COPD, but who do not meet the postbronchodilator spirometric criteria to confirm the COPD diagnosis.
Those with “pre-COPD” have normal spirometry, including the FEV1 and FEV1/FVC ratio, but have functional and/or structural changes concerning for COPD. Functional changes include air trapping and/or hyperinflation on PFTs, low diffusion capacity, and/or decline in FEV1 of > 40 mL per year.
Structural changes include emphysematous changes and/or bronchial wall changes on CT scans. “PRISm” stands for preserved ratio with impaired spirometry, where the postbronchodilator FEV1/FVC is greater than or equal to 0.70, but FEV1 is < 80% predicted with similar functional and/or structural changes to those with “pre-COPD.” People with PRISm have increased all-cause mortality. Not all people with pre-COPD or PRISm progress clinically and spirometrically to COPD; however, they should be treated because they have symptoms as well as functional and/or structural abnormalities. Despite increasing data regarding pre-COPD and PRISm, many gaps remain regarding optimal management.
Maria Ashar, MD, MBBS
Airways Disorders Network
Asthma & COPD Section
The 2023 GOLD committee proposed changes in nomenclature and therapy for various subgroups of patients with COPD.
The mainstay of initial treatment for symptomatic COPD should include combination LABA/LAMA bronchodilators in a single inhaler. For patients with features of concomitant asthma or eosinophils greater than or equal to 300 cells/microliter, an ICS/LABA/LAMA combination inhaler is recommended.
People with “young COPD” develop respiratory symptoms and meet spirometric criteria for COPD between the ages of 25 and 50 years old. Other terminology changes center around those with functional and/or structural changes suggesting COPD, but who do not meet the postbronchodilator spirometric criteria to confirm the COPD diagnosis.
Those with “pre-COPD” have normal spirometry, including the FEV1 and FEV1/FVC ratio, but have functional and/or structural changes concerning for COPD. Functional changes include air trapping and/or hyperinflation on PFTs, low diffusion capacity, and/or decline in FEV1 of > 40 mL per year.
Structural changes include emphysematous changes and/or bronchial wall changes on CT scans. “PRISm” stands for preserved ratio with impaired spirometry, where the postbronchodilator FEV1/FVC is greater than or equal to 0.70, but FEV1 is < 80% predicted with similar functional and/or structural changes to those with “pre-COPD.” People with PRISm have increased all-cause mortality. Not all people with pre-COPD or PRISm progress clinically and spirometrically to COPD; however, they should be treated because they have symptoms as well as functional and/or structural abnormalities. Despite increasing data regarding pre-COPD and PRISm, many gaps remain regarding optimal management.
Maria Ashar, MD, MBBS
Airways Disorders Network
Asthma & COPD Section
The 2023 GOLD committee proposed changes in nomenclature and therapy for various subgroups of patients with COPD.
The mainstay of initial treatment for symptomatic COPD should include combination LABA/LAMA bronchodilators in a single inhaler. For patients with features of concomitant asthma or eosinophils greater than or equal to 300 cells/microliter, an ICS/LABA/LAMA combination inhaler is recommended.
People with “young COPD” develop respiratory symptoms and meet spirometric criteria for COPD between the ages of 25 and 50 years old. Other terminology changes center around those with functional and/or structural changes suggesting COPD, but who do not meet the postbronchodilator spirometric criteria to confirm the COPD diagnosis.
Those with “pre-COPD” have normal spirometry, including the FEV1 and FEV1/FVC ratio, but have functional and/or structural changes concerning for COPD. Functional changes include air trapping and/or hyperinflation on PFTs, low diffusion capacity, and/or decline in FEV1 of > 40 mL per year.
Structural changes include emphysematous changes and/or bronchial wall changes on CT scans. “PRISm” stands for preserved ratio with impaired spirometry, where the postbronchodilator FEV1/FVC is greater than or equal to 0.70, but FEV1 is < 80% predicted with similar functional and/or structural changes to those with “pre-COPD.” People with PRISm have increased all-cause mortality. Not all people with pre-COPD or PRISm progress clinically and spirometrically to COPD; however, they should be treated because they have symptoms as well as functional and/or structural abnormalities. Despite increasing data regarding pre-COPD and PRISm, many gaps remain regarding optimal management.
Maria Ashar, MD, MBBS
In metastatic NSCLC, better QoL outcomes tied to better outcomes
The authors, including Fabio Salomone of the University of Naples Federico II, department of clinical medicine and surgery, also observed trends toward an association between QoL improvement and PFS among patients treated with chemotherapy and immunotherapy.
The new research was presented during a poster session at European Lung Cancer Congress 2023.
“The findings of the study support the thesis that QoL and survival in patients with NSCLC are linked. Although this is documented in the literature, this study sums up the evidence of a large number of RCTs, and provides detail in the QoL/survival relationship by treatment type. The subgroup analysis by treatment type is a key strength of the study showing that the QoL/survival link is stronger and more reliable in target(ed) therapies,” George Kypriotakis, PhD, who was not involved with the study, said in an interview.
Combining efficacy and quality of life improvement is an important consideration in clinical practice. “It is important that clinicians provide therapies that are also palliative and improve QoL,” said Dr. Kypriotakis, assistant professor of behavioral sciences at University of Texas MD Anderson Cancer Center, Houston. He noted that the finding of a PFS benefit is a good indicator of overall benefit, which is important since OS outcomes require a larger number of patients and longer follow-up to determine.
“PFS can still be a valid surrogate for OS, especially when it is positively associated with QoL,” noted Dr. Kypriotakis.
The study included 81 trials. Sixteen of the studies investigated immunotherapy, 50 investigated targeted therapy, and 17 investigated chemotherapy regimens. Thirty-seven percent of the trials found an improvement in QoL in the treatment arm compared with the control arm, 59.3% found no difference between arms, and 3.7% found a worse QoL in the treatment arm. There was no statistically significant association between an improvement in OS and QoL among the trials (P = .368).
Improved QoL tied to improved PFS
The researchers found an association between improved QoL and improved PFS. Among 60 trials that showed improved PFS, 43.3% found a superior QoL in the treatment arm, 53.3% showed no difference, and 3.3% showed reduced QoL. Among 20 trials that found no improvement in PFS, 20% demonstrated an improved QoL, 75% found no change, and 5% showed worse QoL (P = .0473).
A subanalysis of 48 targeted therapy trials found a correlation between PFS and QoL improvement (P = .0196). Among 25 trials involving patients receiving epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) inhibitors showing an improved PFS, 60% showed improved QoL, 36% showed no difference, and 4% showed worsening (P = .0077). Seven of these trials showed no PFS benefit and no change in QoL.
Industry sponsorship may affect QOL results
The researchers found potential evidence that industry sponsorship may lead to a spin on QoL outcomes. Among 51 trials that showed no QoL benefit associated with treatment, the description of the QoL outcome in 37 industry-sponsored was judged to be neutral and coherent with the study findings in 26 cases, but unjustifiably favorable in 11 cases. Among 14 with nonprofit support, descriptions of QoL results were found to be neutral in all cases (P = .0232).
“Obviously, industry may be motivated to overemphasize treatment benefits, especially in measures that also have a qualitative/subjective dimension such as QoL. Assuming that the authors used a reliable criterion to evaluate “inappropriateness,” industry may be more likely to emphasize QoL improvements as a surrogate for OS, especially when seeking drug approval,” Dr. Kypriotakis said.
The study is retrospective and cannot prove causation.
Dr. Salomone and Dr. Kypriotakis have no relevant financial disclosures.
The authors, including Fabio Salomone of the University of Naples Federico II, department of clinical medicine and surgery, also observed trends toward an association between QoL improvement and PFS among patients treated with chemotherapy and immunotherapy.
The new research was presented during a poster session at European Lung Cancer Congress 2023.
“The findings of the study support the thesis that QoL and survival in patients with NSCLC are linked. Although this is documented in the literature, this study sums up the evidence of a large number of RCTs, and provides detail in the QoL/survival relationship by treatment type. The subgroup analysis by treatment type is a key strength of the study showing that the QoL/survival link is stronger and more reliable in target(ed) therapies,” George Kypriotakis, PhD, who was not involved with the study, said in an interview.
Combining efficacy and quality of life improvement is an important consideration in clinical practice. “It is important that clinicians provide therapies that are also palliative and improve QoL,” said Dr. Kypriotakis, assistant professor of behavioral sciences at University of Texas MD Anderson Cancer Center, Houston. He noted that the finding of a PFS benefit is a good indicator of overall benefit, which is important since OS outcomes require a larger number of patients and longer follow-up to determine.
“PFS can still be a valid surrogate for OS, especially when it is positively associated with QoL,” noted Dr. Kypriotakis.
The study included 81 trials. Sixteen of the studies investigated immunotherapy, 50 investigated targeted therapy, and 17 investigated chemotherapy regimens. Thirty-seven percent of the trials found an improvement in QoL in the treatment arm compared with the control arm, 59.3% found no difference between arms, and 3.7% found a worse QoL in the treatment arm. There was no statistically significant association between an improvement in OS and QoL among the trials (P = .368).
Improved QoL tied to improved PFS
The researchers found an association between improved QoL and improved PFS. Among 60 trials that showed improved PFS, 43.3% found a superior QoL in the treatment arm, 53.3% showed no difference, and 3.3% showed reduced QoL. Among 20 trials that found no improvement in PFS, 20% demonstrated an improved QoL, 75% found no change, and 5% showed worse QoL (P = .0473).
A subanalysis of 48 targeted therapy trials found a correlation between PFS and QoL improvement (P = .0196). Among 25 trials involving patients receiving epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) inhibitors showing an improved PFS, 60% showed improved QoL, 36% showed no difference, and 4% showed worsening (P = .0077). Seven of these trials showed no PFS benefit and no change in QoL.
Industry sponsorship may affect QOL results
The researchers found potential evidence that industry sponsorship may lead to a spin on QoL outcomes. Among 51 trials that showed no QoL benefit associated with treatment, the description of the QoL outcome in 37 industry-sponsored was judged to be neutral and coherent with the study findings in 26 cases, but unjustifiably favorable in 11 cases. Among 14 with nonprofit support, descriptions of QoL results were found to be neutral in all cases (P = .0232).
“Obviously, industry may be motivated to overemphasize treatment benefits, especially in measures that also have a qualitative/subjective dimension such as QoL. Assuming that the authors used a reliable criterion to evaluate “inappropriateness,” industry may be more likely to emphasize QoL improvements as a surrogate for OS, especially when seeking drug approval,” Dr. Kypriotakis said.
The study is retrospective and cannot prove causation.
Dr. Salomone and Dr. Kypriotakis have no relevant financial disclosures.
The authors, including Fabio Salomone of the University of Naples Federico II, department of clinical medicine and surgery, also observed trends toward an association between QoL improvement and PFS among patients treated with chemotherapy and immunotherapy.
The new research was presented during a poster session at European Lung Cancer Congress 2023.
“The findings of the study support the thesis that QoL and survival in patients with NSCLC are linked. Although this is documented in the literature, this study sums up the evidence of a large number of RCTs, and provides detail in the QoL/survival relationship by treatment type. The subgroup analysis by treatment type is a key strength of the study showing that the QoL/survival link is stronger and more reliable in target(ed) therapies,” George Kypriotakis, PhD, who was not involved with the study, said in an interview.
Combining efficacy and quality of life improvement is an important consideration in clinical practice. “It is important that clinicians provide therapies that are also palliative and improve QoL,” said Dr. Kypriotakis, assistant professor of behavioral sciences at University of Texas MD Anderson Cancer Center, Houston. He noted that the finding of a PFS benefit is a good indicator of overall benefit, which is important since OS outcomes require a larger number of patients and longer follow-up to determine.
“PFS can still be a valid surrogate for OS, especially when it is positively associated with QoL,” noted Dr. Kypriotakis.
The study included 81 trials. Sixteen of the studies investigated immunotherapy, 50 investigated targeted therapy, and 17 investigated chemotherapy regimens. Thirty-seven percent of the trials found an improvement in QoL in the treatment arm compared with the control arm, 59.3% found no difference between arms, and 3.7% found a worse QoL in the treatment arm. There was no statistically significant association between an improvement in OS and QoL among the trials (P = .368).
Improved QoL tied to improved PFS
The researchers found an association between improved QoL and improved PFS. Among 60 trials that showed improved PFS, 43.3% found a superior QoL in the treatment arm, 53.3% showed no difference, and 3.3% showed reduced QoL. Among 20 trials that found no improvement in PFS, 20% demonstrated an improved QoL, 75% found no change, and 5% showed worse QoL (P = .0473).
A subanalysis of 48 targeted therapy trials found a correlation between PFS and QoL improvement (P = .0196). Among 25 trials involving patients receiving epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase (ALK) inhibitors showing an improved PFS, 60% showed improved QoL, 36% showed no difference, and 4% showed worsening (P = .0077). Seven of these trials showed no PFS benefit and no change in QoL.
Industry sponsorship may affect QOL results
The researchers found potential evidence that industry sponsorship may lead to a spin on QoL outcomes. Among 51 trials that showed no QoL benefit associated with treatment, the description of the QoL outcome in 37 industry-sponsored was judged to be neutral and coherent with the study findings in 26 cases, but unjustifiably favorable in 11 cases. Among 14 with nonprofit support, descriptions of QoL results were found to be neutral in all cases (P = .0232).
“Obviously, industry may be motivated to overemphasize treatment benefits, especially in measures that also have a qualitative/subjective dimension such as QoL. Assuming that the authors used a reliable criterion to evaluate “inappropriateness,” industry may be more likely to emphasize QoL improvements as a surrogate for OS, especially when seeking drug approval,” Dr. Kypriotakis said.
The study is retrospective and cannot prove causation.
Dr. Salomone and Dr. Kypriotakis have no relevant financial disclosures.
FROM ELCC 2023
Malpractice risks for docs who oversee NPs or PAs
Even in states that have abolished requirements that NPs be physician-supervised, physicians may still be liable by virtue of employing the NP, according to William P. Sullivan, DO, an attorney and emergency physician in Frankfort, Ill.
Indeed, the vast majority of lawsuits against NPs and PAs name the supervising physician. According to a study of claims against NPs from 2011 to 2016, 82% of the cases also named the supervising physician.
Employed or contracted physicians assigned to supervise NPs or PAs are also affected, Dr. Sullivan said. “The employed physicians’ contract with a hospital or staffing company may require them to assist in the selection, supervision, and/or training of NPs or PAs,” he said. He added that supervisory duties may also be assigned through hospital bylaws.
“The physician is usually not paid anything extra for this work and may not be given extra time to perform it,” Dr. Sullivan said. But still, he said, that physician could be named in a lawsuit and wind up bearing some responsibility for an NP’s or PA’s mistake.
In addition to facing medical malpractice suits, Dr. Sullivan said, doctors are often sanctioned by state licensure boards for improperly supervising NPs and PAs. Licensure boards often require extensive protocols for supervision of NPs and PAs.
Yet more states are removing supervision requirements
With the addition of Kansas and New York in 2022 and California in 2023, 27 states no longer require supervision for all or most NPs. Sixteen of those states, including New York and California, have instituted progressive practice authority that requires temporary supervision of new NPs but then removes supervision after a period of 6 months to 4 years, depending on the state, for the rest of their career.
“When it comes to NP independence, the horse is already out of the barn,” Dr. Sullivan said. “It’s unlikely that states will repeal laws granting NPs independence, and in fact, more states are likely to pass them.”
*PAs, in contrast, are well behind NPs in achieving independence, but the American Academy of Physician Associates (AAPA) is calling to eliminate a mandated relationship with a specific physician. So far, Utah, North Dakota and Wyoming have ended physician supervision of PAs, while California and Hawaii have eliminated mandated chart review. Other states are considering eliminating physician supervision of PAs, according to the AAPA.
In states that have abolished oversight requirements for NPs, “liability can then shift to the NP when the NP is fully independent,” Cathy Klein, an advanced practice registered nurse who helped found the NP profession 50 years ago, told this news organization. “More NPs are starting their own practices, and in many cases, patients actually prefer to see an NP.”
As more NPs became more autonomous, the average payment that NPs incurred in professional liability lawsuits rose by 10.5% from 2017 to 2022, to $332,187, according to the Nurses Service Organization (NSO), a nursing malpractice insurer.
The number of malpractice judgments against autonomous NPs alone has also been rising. From 2012 to 2017, autonomous NPs’ share of all NP cases rose from 7% to 16.4%, the NSO reported.
The good news for physicians is that states’ removal of restrictions on NPs has reduced physicians’ liability to some extent. A 2017 study found that enacting less restrictive scope-of-practice laws for NPs decreased the number of payments made by physicians in NP cases by as much as 31%.
However, the top location for NP payouts remains the physician’s office, not the autonomous NP’s practice, according to the latter NSO report. Plaintiffs sue NPs’ and PAs’ supervising physicians on the basis of legal concepts, such as vicarious liability and respondeat superior. Even if the physician-employer never saw the patient, he or she can be held liable.
Court cases in which supervising physician was found liable
There are plenty of judgments against supervising or collaborating physicians when the NP or PA made the error. Typically, the doctor was faulted for paying little attention to the NP or PA he or she was supposed to supervise.
Dr. Sullivan points to a 2016 case in which a New York jury held a physician 40% liable for a $7 million judgment in a malpractice case involving a PA’s care of a patient in the emergency department. The case is Shajan v. South Nassau Community Hospital in New York.
“The patient presented with nontraumatic leg pain to his lower leg, was diagnosed by the PA with a muscle strain, and discharged without a physician evaluation,” Dr. Sullivan said. The next day, the patient visited an orthopedist who immediately diagnosed compartment syndrome, an emergent condition in which pressure builds up in an affected extremity, damaging the muscles and nerves. “The patient developed irreversible nerve damage and chronic regional pain syndrome,” he said.
A malpractice lawsuit named the PA and the emergency physician he was supposed to be reporting to. Even though the physician had never seen the patient, he had signed off on the PA’s note from a patient’s ED visit. “Testimony during the trial focused on hospital protocols that the supervising physician was supposed to take,” Dr. Sullivan said.
When doctors share fault, they frequently failed to follow the collaborative agreement with the NP or PA. In Collip v. Ratts, a 2015 Indiana case in which the patient died from a drug interaction, the doctor’s certified public accountant stated that the doctor was required to review at least 5% of the NP’s charts every week to evaluate her prescriptive practices.
The doctor admitted that he never reviewed the NP’s charts on a weekly basis. He did conduct some cursory reviews of some of the NP’s notes, and in them he noted concerns for her prescribing practices and suggested she attend a narcotics-prescribing seminar, but he did not follow up to make sure she had done this.
Sometimes the NP or PA who made the mistake may actually be dropped from the lawsuit, leaving the supervising physician fully liable. In these cases, courts reason that a fully engaged supervisor could have prevented the error. In the 2006 case of Husak v. Siegal, the Florida Supreme Court dropped the NP from the case, ruling that the NP had provided the supervising doctor all the information he needed in order to tell her what to do for the patient.
The court noted the physician had failed to look at the chart, even though he was required to do so under his supervisory agreement with the NP. The doctor “could have made the correct diagnosis or referral had he been attentive,” the court said. Therefore, there was “no evidence of independent negligence” by the NP, even though she was the one who had made the incorrect diagnosis that harmed the patient.
When states require an autonomous NP to have a supervisory relationship with a doctor, the supervisor may be unavailable and may fail to designate a substitute. In Texas in January 2019, a 7-year-old girl died of pneumonia after being treated by an NP in an urgent care clinic. The NP had told the parents that the child could safely go home and only needed ibuprofen. The parents brought the girl back home, and she died 15 hours later. The Wattenbargers sued the NP, and the doctor’s supervision was a topic in the trial.
The supervising physician for the NP was out of the country at the time. He said that he had found a substitute, but the substitute doctor testified she had no idea she was designated to be the substitute, according to Niran Al-Agba, MD, a family physician in Silverdale, Wash., who has written on the Texas case. Dr. Al-Agba told this news organization the case appears to have been settled confidentially.
Different standards for expert witnesses
In many states, courts do not allow physicians to testify as expert witnesses in malpractice cases against NPs, arguing that nurses have a different set of standards than doctors have, Dr. Sullivan reported.
These states include Arkansas, Illinois, North Carolina, and New York, according to a report by SEAK Inc., an expert witness training program. The report said most other states allow physician experts in these cases, but they may still require that they have experience with the nursing standard of care.
Dr. Sullivan said some courts are whittling away at the ban on physician experts, and the ban may eventually disappear. He reported that in Oklahoma, which normally upholds the ban, a judge recently allowed a physician-expert to testify in a case involving the death of a 19-year-old woman, Alexus Ochoa, in an ED staffed by an NP. The judge reasoned that Ms. Ochoa’s parents assumed the ED was staffed by physicians and would adhere to medical standards.
Supervision pointers from a physician
Physicians who supervise NPs or PAs say it is important to keep track of their skills and help them sharpen their expertise. Their scope of practice and physicians’ supervisory responsibilities are included in the collaborative agreement.
Arthur Apolinario, MD, a family physician in Clinton, N.C., says his 10-physician practice, which employs six NPs and one PA, works under a collaborative agreement. “The agreement defines each person’s scope of practice. They can’t do certain procedures, such as surgery, and they need extra training before doing certain tasks alone, such as joint injection.
“You have to always figure that if there is a lawsuit against one of them, you as the supervising physician would be named,” said Dr. Apolinario, who is also president of the North Carolina Medical Society. “We try to avert mistakes by meeting regularly with our NPs and PAs and making sure they keep up to date.”
Collaborating with autonomous NPs
Even when NPs operate independently in states that have abolished supervision, physicians may still have some liability if they give NPs advice, Dr. Al-Agba said.
At her Washington state practice, Dr. Al-Agba shares an office with an autonomous NP. “We share overhead and a front desk, but we have separate patients,” Dr. Al-Agba said. “This arrangement works very well for both of us.”
The NP sometimes asks her for advice. When this occurs, Dr. Al-Agba said she always makes sure to see the patient first. “If you don’t actually see the patient, there could be a misunderstanding that could lead to an error,” she said.
Conclusion
Even though NPs now have autonomy in most states, supervising physicians may still be liable for NP malpractice by virtue of being their employers, and physicians in the remaining states are liable for NPs through state law and for PAs in virtually all the states. To determine the supervising physician’s fault, courts often study whether the physician has met the terms of the collaborative agreement.
Physicians can reduce collaborating NPs’ and PAs’ liability by properly training them, by verifying their scope of practice, by making themselves easily available for consultation, and by occasionally seeing their patients. If their NPs and PAs do commit malpractice, supervising physicians may be able to protect themselves from liability by adhering to all requirements of the collaborative agreement.
*Correction, 4/19/2023: An earlier version of this story misstated the name of the AAPA and the states that have ended physician supervision of PAs.
A version of this article first appeared on Medscape.com.
Even in states that have abolished requirements that NPs be physician-supervised, physicians may still be liable by virtue of employing the NP, according to William P. Sullivan, DO, an attorney and emergency physician in Frankfort, Ill.
Indeed, the vast majority of lawsuits against NPs and PAs name the supervising physician. According to a study of claims against NPs from 2011 to 2016, 82% of the cases also named the supervising physician.
Employed or contracted physicians assigned to supervise NPs or PAs are also affected, Dr. Sullivan said. “The employed physicians’ contract with a hospital or staffing company may require them to assist in the selection, supervision, and/or training of NPs or PAs,” he said. He added that supervisory duties may also be assigned through hospital bylaws.
“The physician is usually not paid anything extra for this work and may not be given extra time to perform it,” Dr. Sullivan said. But still, he said, that physician could be named in a lawsuit and wind up bearing some responsibility for an NP’s or PA’s mistake.
In addition to facing medical malpractice suits, Dr. Sullivan said, doctors are often sanctioned by state licensure boards for improperly supervising NPs and PAs. Licensure boards often require extensive protocols for supervision of NPs and PAs.
Yet more states are removing supervision requirements
With the addition of Kansas and New York in 2022 and California in 2023, 27 states no longer require supervision for all or most NPs. Sixteen of those states, including New York and California, have instituted progressive practice authority that requires temporary supervision of new NPs but then removes supervision after a period of 6 months to 4 years, depending on the state, for the rest of their career.
“When it comes to NP independence, the horse is already out of the barn,” Dr. Sullivan said. “It’s unlikely that states will repeal laws granting NPs independence, and in fact, more states are likely to pass them.”
*PAs, in contrast, are well behind NPs in achieving independence, but the American Academy of Physician Associates (AAPA) is calling to eliminate a mandated relationship with a specific physician. So far, Utah, North Dakota and Wyoming have ended physician supervision of PAs, while California and Hawaii have eliminated mandated chart review. Other states are considering eliminating physician supervision of PAs, according to the AAPA.
In states that have abolished oversight requirements for NPs, “liability can then shift to the NP when the NP is fully independent,” Cathy Klein, an advanced practice registered nurse who helped found the NP profession 50 years ago, told this news organization. “More NPs are starting their own practices, and in many cases, patients actually prefer to see an NP.”
As more NPs became more autonomous, the average payment that NPs incurred in professional liability lawsuits rose by 10.5% from 2017 to 2022, to $332,187, according to the Nurses Service Organization (NSO), a nursing malpractice insurer.
The number of malpractice judgments against autonomous NPs alone has also been rising. From 2012 to 2017, autonomous NPs’ share of all NP cases rose from 7% to 16.4%, the NSO reported.
The good news for physicians is that states’ removal of restrictions on NPs has reduced physicians’ liability to some extent. A 2017 study found that enacting less restrictive scope-of-practice laws for NPs decreased the number of payments made by physicians in NP cases by as much as 31%.
However, the top location for NP payouts remains the physician’s office, not the autonomous NP’s practice, according to the latter NSO report. Plaintiffs sue NPs’ and PAs’ supervising physicians on the basis of legal concepts, such as vicarious liability and respondeat superior. Even if the physician-employer never saw the patient, he or she can be held liable.
Court cases in which supervising physician was found liable
There are plenty of judgments against supervising or collaborating physicians when the NP or PA made the error. Typically, the doctor was faulted for paying little attention to the NP or PA he or she was supposed to supervise.
Dr. Sullivan points to a 2016 case in which a New York jury held a physician 40% liable for a $7 million judgment in a malpractice case involving a PA’s care of a patient in the emergency department. The case is Shajan v. South Nassau Community Hospital in New York.
“The patient presented with nontraumatic leg pain to his lower leg, was diagnosed by the PA with a muscle strain, and discharged without a physician evaluation,” Dr. Sullivan said. The next day, the patient visited an orthopedist who immediately diagnosed compartment syndrome, an emergent condition in which pressure builds up in an affected extremity, damaging the muscles and nerves. “The patient developed irreversible nerve damage and chronic regional pain syndrome,” he said.
A malpractice lawsuit named the PA and the emergency physician he was supposed to be reporting to. Even though the physician had never seen the patient, he had signed off on the PA’s note from a patient’s ED visit. “Testimony during the trial focused on hospital protocols that the supervising physician was supposed to take,” Dr. Sullivan said.
When doctors share fault, they frequently failed to follow the collaborative agreement with the NP or PA. In Collip v. Ratts, a 2015 Indiana case in which the patient died from a drug interaction, the doctor’s certified public accountant stated that the doctor was required to review at least 5% of the NP’s charts every week to evaluate her prescriptive practices.
The doctor admitted that he never reviewed the NP’s charts on a weekly basis. He did conduct some cursory reviews of some of the NP’s notes, and in them he noted concerns for her prescribing practices and suggested she attend a narcotics-prescribing seminar, but he did not follow up to make sure she had done this.
Sometimes the NP or PA who made the mistake may actually be dropped from the lawsuit, leaving the supervising physician fully liable. In these cases, courts reason that a fully engaged supervisor could have prevented the error. In the 2006 case of Husak v. Siegal, the Florida Supreme Court dropped the NP from the case, ruling that the NP had provided the supervising doctor all the information he needed in order to tell her what to do for the patient.
The court noted the physician had failed to look at the chart, even though he was required to do so under his supervisory agreement with the NP. The doctor “could have made the correct diagnosis or referral had he been attentive,” the court said. Therefore, there was “no evidence of independent negligence” by the NP, even though she was the one who had made the incorrect diagnosis that harmed the patient.
When states require an autonomous NP to have a supervisory relationship with a doctor, the supervisor may be unavailable and may fail to designate a substitute. In Texas in January 2019, a 7-year-old girl died of pneumonia after being treated by an NP in an urgent care clinic. The NP had told the parents that the child could safely go home and only needed ibuprofen. The parents brought the girl back home, and she died 15 hours later. The Wattenbargers sued the NP, and the doctor’s supervision was a topic in the trial.
The supervising physician for the NP was out of the country at the time. He said that he had found a substitute, but the substitute doctor testified she had no idea she was designated to be the substitute, according to Niran Al-Agba, MD, a family physician in Silverdale, Wash., who has written on the Texas case. Dr. Al-Agba told this news organization the case appears to have been settled confidentially.
Different standards for expert witnesses
In many states, courts do not allow physicians to testify as expert witnesses in malpractice cases against NPs, arguing that nurses have a different set of standards than doctors have, Dr. Sullivan reported.
These states include Arkansas, Illinois, North Carolina, and New York, according to a report by SEAK Inc., an expert witness training program. The report said most other states allow physician experts in these cases, but they may still require that they have experience with the nursing standard of care.
Dr. Sullivan said some courts are whittling away at the ban on physician experts, and the ban may eventually disappear. He reported that in Oklahoma, which normally upholds the ban, a judge recently allowed a physician-expert to testify in a case involving the death of a 19-year-old woman, Alexus Ochoa, in an ED staffed by an NP. The judge reasoned that Ms. Ochoa’s parents assumed the ED was staffed by physicians and would adhere to medical standards.
Supervision pointers from a physician
Physicians who supervise NPs or PAs say it is important to keep track of their skills and help them sharpen their expertise. Their scope of practice and physicians’ supervisory responsibilities are included in the collaborative agreement.
Arthur Apolinario, MD, a family physician in Clinton, N.C., says his 10-physician practice, which employs six NPs and one PA, works under a collaborative agreement. “The agreement defines each person’s scope of practice. They can’t do certain procedures, such as surgery, and they need extra training before doing certain tasks alone, such as joint injection.
“You have to always figure that if there is a lawsuit against one of them, you as the supervising physician would be named,” said Dr. Apolinario, who is also president of the North Carolina Medical Society. “We try to avert mistakes by meeting regularly with our NPs and PAs and making sure they keep up to date.”
Collaborating with autonomous NPs
Even when NPs operate independently in states that have abolished supervision, physicians may still have some liability if they give NPs advice, Dr. Al-Agba said.
At her Washington state practice, Dr. Al-Agba shares an office with an autonomous NP. “We share overhead and a front desk, but we have separate patients,” Dr. Al-Agba said. “This arrangement works very well for both of us.”
The NP sometimes asks her for advice. When this occurs, Dr. Al-Agba said she always makes sure to see the patient first. “If you don’t actually see the patient, there could be a misunderstanding that could lead to an error,” she said.
Conclusion
Even though NPs now have autonomy in most states, supervising physicians may still be liable for NP malpractice by virtue of being their employers, and physicians in the remaining states are liable for NPs through state law and for PAs in virtually all the states. To determine the supervising physician’s fault, courts often study whether the physician has met the terms of the collaborative agreement.
Physicians can reduce collaborating NPs’ and PAs’ liability by properly training them, by verifying their scope of practice, by making themselves easily available for consultation, and by occasionally seeing their patients. If their NPs and PAs do commit malpractice, supervising physicians may be able to protect themselves from liability by adhering to all requirements of the collaborative agreement.
*Correction, 4/19/2023: An earlier version of this story misstated the name of the AAPA and the states that have ended physician supervision of PAs.
A version of this article first appeared on Medscape.com.
Even in states that have abolished requirements that NPs be physician-supervised, physicians may still be liable by virtue of employing the NP, according to William P. Sullivan, DO, an attorney and emergency physician in Frankfort, Ill.
Indeed, the vast majority of lawsuits against NPs and PAs name the supervising physician. According to a study of claims against NPs from 2011 to 2016, 82% of the cases also named the supervising physician.
Employed or contracted physicians assigned to supervise NPs or PAs are also affected, Dr. Sullivan said. “The employed physicians’ contract with a hospital or staffing company may require them to assist in the selection, supervision, and/or training of NPs or PAs,” he said. He added that supervisory duties may also be assigned through hospital bylaws.
“The physician is usually not paid anything extra for this work and may not be given extra time to perform it,” Dr. Sullivan said. But still, he said, that physician could be named in a lawsuit and wind up bearing some responsibility for an NP’s or PA’s mistake.
In addition to facing medical malpractice suits, Dr. Sullivan said, doctors are often sanctioned by state licensure boards for improperly supervising NPs and PAs. Licensure boards often require extensive protocols for supervision of NPs and PAs.
Yet more states are removing supervision requirements
With the addition of Kansas and New York in 2022 and California in 2023, 27 states no longer require supervision for all or most NPs. Sixteen of those states, including New York and California, have instituted progressive practice authority that requires temporary supervision of new NPs but then removes supervision after a period of 6 months to 4 years, depending on the state, for the rest of their career.
“When it comes to NP independence, the horse is already out of the barn,” Dr. Sullivan said. “It’s unlikely that states will repeal laws granting NPs independence, and in fact, more states are likely to pass them.”
*PAs, in contrast, are well behind NPs in achieving independence, but the American Academy of Physician Associates (AAPA) is calling to eliminate a mandated relationship with a specific physician. So far, Utah, North Dakota and Wyoming have ended physician supervision of PAs, while California and Hawaii have eliminated mandated chart review. Other states are considering eliminating physician supervision of PAs, according to the AAPA.
In states that have abolished oversight requirements for NPs, “liability can then shift to the NP when the NP is fully independent,” Cathy Klein, an advanced practice registered nurse who helped found the NP profession 50 years ago, told this news organization. “More NPs are starting their own practices, and in many cases, patients actually prefer to see an NP.”
As more NPs became more autonomous, the average payment that NPs incurred in professional liability lawsuits rose by 10.5% from 2017 to 2022, to $332,187, according to the Nurses Service Organization (NSO), a nursing malpractice insurer.
The number of malpractice judgments against autonomous NPs alone has also been rising. From 2012 to 2017, autonomous NPs’ share of all NP cases rose from 7% to 16.4%, the NSO reported.
The good news for physicians is that states’ removal of restrictions on NPs has reduced physicians’ liability to some extent. A 2017 study found that enacting less restrictive scope-of-practice laws for NPs decreased the number of payments made by physicians in NP cases by as much as 31%.
However, the top location for NP payouts remains the physician’s office, not the autonomous NP’s practice, according to the latter NSO report. Plaintiffs sue NPs’ and PAs’ supervising physicians on the basis of legal concepts, such as vicarious liability and respondeat superior. Even if the physician-employer never saw the patient, he or she can be held liable.
Court cases in which supervising physician was found liable
There are plenty of judgments against supervising or collaborating physicians when the NP or PA made the error. Typically, the doctor was faulted for paying little attention to the NP or PA he or she was supposed to supervise.
Dr. Sullivan points to a 2016 case in which a New York jury held a physician 40% liable for a $7 million judgment in a malpractice case involving a PA’s care of a patient in the emergency department. The case is Shajan v. South Nassau Community Hospital in New York.
“The patient presented with nontraumatic leg pain to his lower leg, was diagnosed by the PA with a muscle strain, and discharged without a physician evaluation,” Dr. Sullivan said. The next day, the patient visited an orthopedist who immediately diagnosed compartment syndrome, an emergent condition in which pressure builds up in an affected extremity, damaging the muscles and nerves. “The patient developed irreversible nerve damage and chronic regional pain syndrome,” he said.
A malpractice lawsuit named the PA and the emergency physician he was supposed to be reporting to. Even though the physician had never seen the patient, he had signed off on the PA’s note from a patient’s ED visit. “Testimony during the trial focused on hospital protocols that the supervising physician was supposed to take,” Dr. Sullivan said.
When doctors share fault, they frequently failed to follow the collaborative agreement with the NP or PA. In Collip v. Ratts, a 2015 Indiana case in which the patient died from a drug interaction, the doctor’s certified public accountant stated that the doctor was required to review at least 5% of the NP’s charts every week to evaluate her prescriptive practices.
The doctor admitted that he never reviewed the NP’s charts on a weekly basis. He did conduct some cursory reviews of some of the NP’s notes, and in them he noted concerns for her prescribing practices and suggested she attend a narcotics-prescribing seminar, but he did not follow up to make sure she had done this.
Sometimes the NP or PA who made the mistake may actually be dropped from the lawsuit, leaving the supervising physician fully liable. In these cases, courts reason that a fully engaged supervisor could have prevented the error. In the 2006 case of Husak v. Siegal, the Florida Supreme Court dropped the NP from the case, ruling that the NP had provided the supervising doctor all the information he needed in order to tell her what to do for the patient.
The court noted the physician had failed to look at the chart, even though he was required to do so under his supervisory agreement with the NP. The doctor “could have made the correct diagnosis or referral had he been attentive,” the court said. Therefore, there was “no evidence of independent negligence” by the NP, even though she was the one who had made the incorrect diagnosis that harmed the patient.
When states require an autonomous NP to have a supervisory relationship with a doctor, the supervisor may be unavailable and may fail to designate a substitute. In Texas in January 2019, a 7-year-old girl died of pneumonia after being treated by an NP in an urgent care clinic. The NP had told the parents that the child could safely go home and only needed ibuprofen. The parents brought the girl back home, and she died 15 hours later. The Wattenbargers sued the NP, and the doctor’s supervision was a topic in the trial.
The supervising physician for the NP was out of the country at the time. He said that he had found a substitute, but the substitute doctor testified she had no idea she was designated to be the substitute, according to Niran Al-Agba, MD, a family physician in Silverdale, Wash., who has written on the Texas case. Dr. Al-Agba told this news organization the case appears to have been settled confidentially.
Different standards for expert witnesses
In many states, courts do not allow physicians to testify as expert witnesses in malpractice cases against NPs, arguing that nurses have a different set of standards than doctors have, Dr. Sullivan reported.
These states include Arkansas, Illinois, North Carolina, and New York, according to a report by SEAK Inc., an expert witness training program. The report said most other states allow physician experts in these cases, but they may still require that they have experience with the nursing standard of care.
Dr. Sullivan said some courts are whittling away at the ban on physician experts, and the ban may eventually disappear. He reported that in Oklahoma, which normally upholds the ban, a judge recently allowed a physician-expert to testify in a case involving the death of a 19-year-old woman, Alexus Ochoa, in an ED staffed by an NP. The judge reasoned that Ms. Ochoa’s parents assumed the ED was staffed by physicians and would adhere to medical standards.
Supervision pointers from a physician
Physicians who supervise NPs or PAs say it is important to keep track of their skills and help them sharpen their expertise. Their scope of practice and physicians’ supervisory responsibilities are included in the collaborative agreement.
Arthur Apolinario, MD, a family physician in Clinton, N.C., says his 10-physician practice, which employs six NPs and one PA, works under a collaborative agreement. “The agreement defines each person’s scope of practice. They can’t do certain procedures, such as surgery, and they need extra training before doing certain tasks alone, such as joint injection.
“You have to always figure that if there is a lawsuit against one of them, you as the supervising physician would be named,” said Dr. Apolinario, who is also president of the North Carolina Medical Society. “We try to avert mistakes by meeting regularly with our NPs and PAs and making sure they keep up to date.”
Collaborating with autonomous NPs
Even when NPs operate independently in states that have abolished supervision, physicians may still have some liability if they give NPs advice, Dr. Al-Agba said.
At her Washington state practice, Dr. Al-Agba shares an office with an autonomous NP. “We share overhead and a front desk, but we have separate patients,” Dr. Al-Agba said. “This arrangement works very well for both of us.”
The NP sometimes asks her for advice. When this occurs, Dr. Al-Agba said she always makes sure to see the patient first. “If you don’t actually see the patient, there could be a misunderstanding that could lead to an error,” she said.
Conclusion
Even though NPs now have autonomy in most states, supervising physicians may still be liable for NP malpractice by virtue of being their employers, and physicians in the remaining states are liable for NPs through state law and for PAs in virtually all the states. To determine the supervising physician’s fault, courts often study whether the physician has met the terms of the collaborative agreement.
Physicians can reduce collaborating NPs’ and PAs’ liability by properly training them, by verifying their scope of practice, by making themselves easily available for consultation, and by occasionally seeing their patients. If their NPs and PAs do commit malpractice, supervising physicians may be able to protect themselves from liability by adhering to all requirements of the collaborative agreement.
*Correction, 4/19/2023: An earlier version of this story misstated the name of the AAPA and the states that have ended physician supervision of PAs.
A version of this article first appeared on Medscape.com.
Lack of food for thought: Starve a bacterium, feed an infection
A whole new, tiny level of hangry
Ever been so hungry that everything just got on your nerves? Maybe you feel a little snappy right now? Like you’ll just lash out unless you get something to eat? Been there. And so have bacteria.
New research shows that some bacteria go into a full-on Hulk smash if they’re not getting the nutrients they need by releasing toxins into the body. Sounds like a bacterial temper tantrum.
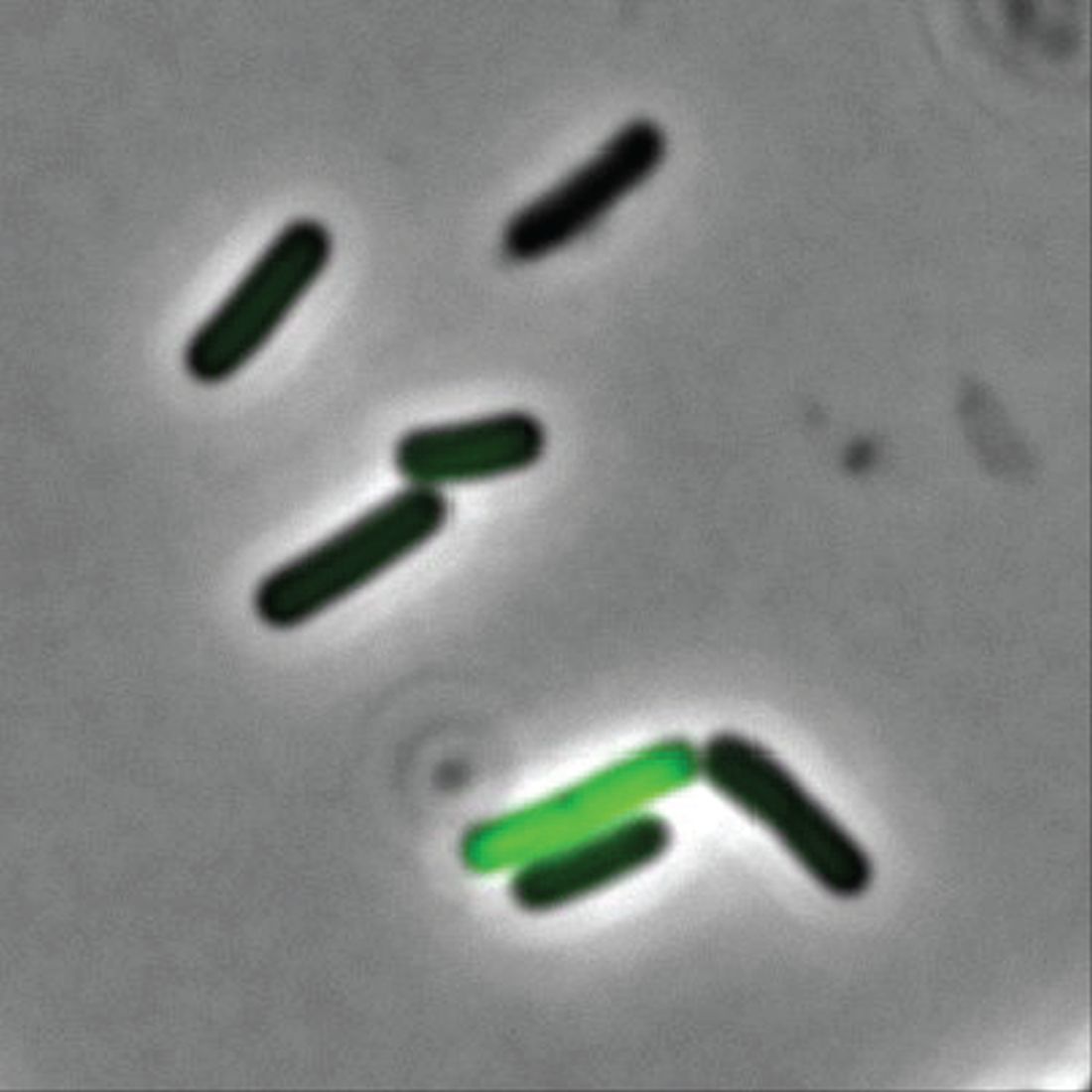
Even though two cells may be genetically identical, they don’t always behave the same in a bacterial community. Some do their job and stay in line, but some evil twins rage out and make people sick by releasing toxins into the environment, Adam Rosenthal, PhD, of the University of North Carolina and his colleagues discovered.
To figure out why some cells were all business as usual while others were not, the investigators looked at Clostridium perfringens, a bacterium found in the intestines of humans and other vertebrates. When the C. perfringens cells were fed a little acetate to munch on, the hangry cells calmed down faster than a kid with a bag of fruit snacks, reducing toxin levels. Some cells even disappeared, falling in line with their model-citizen counterparts.
So what does this really mean? More research, duh. Now that we know nutrients play a role in toxicity, it may open the door to finding a way to fight against antibiotic resistance in humans and reduce antibiotic use in the food industry.
So think to yourself. Are you bothered for no reason? Getting a little testy with your friends and coworkers? Maybe you just haven’t eaten in a while. You’re literally not alone. Even a single-cell organism can behave based on its hunger levels.
Now go have a snack. Your bacteria are getting restless.
The very hangry iguana?
Imagine yourself on a warm, sunny tropical beach. You are enjoying a piece of cake as you take in the slow beat of the waves lapping against the shore. Life is as good as it could be.
Then you feel a presence nearby. Hostility. Hunger. A set of feral, covetous eyes in the nearby jungle. A reptilian beast stalks you, and its all-encompassing sweet tooth desires your cake.
Wait, hold on, what?
As an unfortunate 3-year-old on vacation in Costa Rica found out, there’s at least one iguana in the world out there with a taste for sugar (better than a taste for blood, we suppose).

While out on the beach, the lizard darted out of nowhere, bit the girl on the back of the hand, and stole her cake. Still not the worst party guest ever. The child was taken to a local clinic, where the wound was cleaned and a 5-day antibiotic treatment (lizards carry salmonella) was provided. Things seemed fine, and the girl returned home without incident.
But of course, that’s not the end of the story. Five months later, the girl’s parents noticed a red bump at the wound site. Over the next 3 months, the surrounding skin grew red and painful. A trip to the hospital in California revealed that she had a ganglion cyst and a discharge of pus. Turns out our cake-obsessed lizard friend did give the little girl a gift: the first known human case of Mycobacterium marinum infection following an iguana bite on record.
M. marinum, which causes a disease similar to tuberculosis, typically infects fish but can infect humans if skin wounds are exposed to contaminated water. It’s also resistant to most antibiotics, which is why the first round didn’t clear up the infection. A second round of more-potent antibiotics seems to be working well.
So, to sum up, this poor child got bitten by a lizard, had her cake stolen, and contracted a rare illness in exchange. For a 3-year-old, that’s gotta be in the top-10 worst days ever. Unless, of course, we’re actually living in the Marvel universe (sorry, multiverse at this point). Then we’re totally going to see the emergence of the new superhero Iguana Girl in 15 years or so. Keep your eyes open.
No allergies? Let them give up cake
Allergy season is already here – starting earlier every year, it seems – and many people are not happy about it. So unhappy, actually, that there’s a list of things they would be willing to give up for a year to get rid of their of allergies, according to a survey conducted by OnePoll on behalf of Flonase.

Nearly 40% of 2,000 respondents with allergies would go a year without eating cake or chocolate or playing video games in exchange for allergy-free status, the survey results show. Almost as many would forgo coffee (38%) or pizza (37%) for a year, while 36% would stay off social media and 31% would take a pay cut or give up their smartphones, the Independent reported.
More than half of the allergic Americans – 54%, to be exact – who were polled this past winter – Feb. 24 to March 1, to be exact – consider allergy symptoms to be the most frustrating part of the spring. Annoying things that were less frustrating to the group included mosquitoes (41%), filing tax returns (38%), and daylight savings time (37%).
The Trump arraignment circus, of course, occurred too late to make the list, as did the big “We’re going back to the office! No wait, we’re closing the office forever!” email extravaganza and emotional roller coaster. That second one, however, did not get nearly as much media coverage.
A whole new, tiny level of hangry
Ever been so hungry that everything just got on your nerves? Maybe you feel a little snappy right now? Like you’ll just lash out unless you get something to eat? Been there. And so have bacteria.
New research shows that some bacteria go into a full-on Hulk smash if they’re not getting the nutrients they need by releasing toxins into the body. Sounds like a bacterial temper tantrum.
Even though two cells may be genetically identical, they don’t always behave the same in a bacterial community. Some do their job and stay in line, but some evil twins rage out and make people sick by releasing toxins into the environment, Adam Rosenthal, PhD, of the University of North Carolina and his colleagues discovered.
To figure out why some cells were all business as usual while others were not, the investigators looked at Clostridium perfringens, a bacterium found in the intestines of humans and other vertebrates. When the C. perfringens cells were fed a little acetate to munch on, the hangry cells calmed down faster than a kid with a bag of fruit snacks, reducing toxin levels. Some cells even disappeared, falling in line with their model-citizen counterparts.
So what does this really mean? More research, duh. Now that we know nutrients play a role in toxicity, it may open the door to finding a way to fight against antibiotic resistance in humans and reduce antibiotic use in the food industry.
So think to yourself. Are you bothered for no reason? Getting a little testy with your friends and coworkers? Maybe you just haven’t eaten in a while. You’re literally not alone. Even a single-cell organism can behave based on its hunger levels.
Now go have a snack. Your bacteria are getting restless.
The very hangry iguana?
Imagine yourself on a warm, sunny tropical beach. You are enjoying a piece of cake as you take in the slow beat of the waves lapping against the shore. Life is as good as it could be.
Then you feel a presence nearby. Hostility. Hunger. A set of feral, covetous eyes in the nearby jungle. A reptilian beast stalks you, and its all-encompassing sweet tooth desires your cake.
Wait, hold on, what?
As an unfortunate 3-year-old on vacation in Costa Rica found out, there’s at least one iguana in the world out there with a taste for sugar (better than a taste for blood, we suppose).
While out on the beach, the lizard darted out of nowhere, bit the girl on the back of the hand, and stole her cake. Still not the worst party guest ever. The child was taken to a local clinic, where the wound was cleaned and a 5-day antibiotic treatment (lizards carry salmonella) was provided. Things seemed fine, and the girl returned home without incident.
But of course, that’s not the end of the story. Five months later, the girl’s parents noticed a red bump at the wound site. Over the next 3 months, the surrounding skin grew red and painful. A trip to the hospital in California revealed that she had a ganglion cyst and a discharge of pus. Turns out our cake-obsessed lizard friend did give the little girl a gift: the first known human case of Mycobacterium marinum infection following an iguana bite on record.
M. marinum, which causes a disease similar to tuberculosis, typically infects fish but can infect humans if skin wounds are exposed to contaminated water. It’s also resistant to most antibiotics, which is why the first round didn’t clear up the infection. A second round of more-potent antibiotics seems to be working well.
So, to sum up, this poor child got bitten by a lizard, had her cake stolen, and contracted a rare illness in exchange. For a 3-year-old, that’s gotta be in the top-10 worst days ever. Unless, of course, we’re actually living in the Marvel universe (sorry, multiverse at this point). Then we’re totally going to see the emergence of the new superhero Iguana Girl in 15 years or so. Keep your eyes open.
No allergies? Let them give up cake
Allergy season is already here – starting earlier every year, it seems – and many people are not happy about it. So unhappy, actually, that there’s a list of things they would be willing to give up for a year to get rid of their of allergies, according to a survey conducted by OnePoll on behalf of Flonase.
Nearly 40% of 2,000 respondents with allergies would go a year without eating cake or chocolate or playing video games in exchange for allergy-free status, the survey results show. Almost as many would forgo coffee (38%) or pizza (37%) for a year, while 36% would stay off social media and 31% would take a pay cut or give up their smartphones, the Independent reported.
More than half of the allergic Americans – 54%, to be exact – who were polled this past winter – Feb. 24 to March 1, to be exact – consider allergy symptoms to be the most frustrating part of the spring. Annoying things that were less frustrating to the group included mosquitoes (41%), filing tax returns (38%), and daylight savings time (37%).
The Trump arraignment circus, of course, occurred too late to make the list, as did the big “We’re going back to the office! No wait, we’re closing the office forever!” email extravaganza and emotional roller coaster. That second one, however, did not get nearly as much media coverage.
A whole new, tiny level of hangry
Ever been so hungry that everything just got on your nerves? Maybe you feel a little snappy right now? Like you’ll just lash out unless you get something to eat? Been there. And so have bacteria.
New research shows that some bacteria go into a full-on Hulk smash if they’re not getting the nutrients they need by releasing toxins into the body. Sounds like a bacterial temper tantrum.
Even though two cells may be genetically identical, they don’t always behave the same in a bacterial community. Some do their job and stay in line, but some evil twins rage out and make people sick by releasing toxins into the environment, Adam Rosenthal, PhD, of the University of North Carolina and his colleagues discovered.
To figure out why some cells were all business as usual while others were not, the investigators looked at Clostridium perfringens, a bacterium found in the intestines of humans and other vertebrates. When the C. perfringens cells were fed a little acetate to munch on, the hangry cells calmed down faster than a kid with a bag of fruit snacks, reducing toxin levels. Some cells even disappeared, falling in line with their model-citizen counterparts.
So what does this really mean? More research, duh. Now that we know nutrients play a role in toxicity, it may open the door to finding a way to fight against antibiotic resistance in humans and reduce antibiotic use in the food industry.
So think to yourself. Are you bothered for no reason? Getting a little testy with your friends and coworkers? Maybe you just haven’t eaten in a while. You’re literally not alone. Even a single-cell organism can behave based on its hunger levels.
Now go have a snack. Your bacteria are getting restless.
The very hangry iguana?
Imagine yourself on a warm, sunny tropical beach. You are enjoying a piece of cake as you take in the slow beat of the waves lapping against the shore. Life is as good as it could be.
Then you feel a presence nearby. Hostility. Hunger. A set of feral, covetous eyes in the nearby jungle. A reptilian beast stalks you, and its all-encompassing sweet tooth desires your cake.
Wait, hold on, what?
As an unfortunate 3-year-old on vacation in Costa Rica found out, there’s at least one iguana in the world out there with a taste for sugar (better than a taste for blood, we suppose).
While out on the beach, the lizard darted out of nowhere, bit the girl on the back of the hand, and stole her cake. Still not the worst party guest ever. The child was taken to a local clinic, where the wound was cleaned and a 5-day antibiotic treatment (lizards carry salmonella) was provided. Things seemed fine, and the girl returned home without incident.
But of course, that’s not the end of the story. Five months later, the girl’s parents noticed a red bump at the wound site. Over the next 3 months, the surrounding skin grew red and painful. A trip to the hospital in California revealed that she had a ganglion cyst and a discharge of pus. Turns out our cake-obsessed lizard friend did give the little girl a gift: the first known human case of Mycobacterium marinum infection following an iguana bite on record.
M. marinum, which causes a disease similar to tuberculosis, typically infects fish but can infect humans if skin wounds are exposed to contaminated water. It’s also resistant to most antibiotics, which is why the first round didn’t clear up the infection. A second round of more-potent antibiotics seems to be working well.
So, to sum up, this poor child got bitten by a lizard, had her cake stolen, and contracted a rare illness in exchange. For a 3-year-old, that’s gotta be in the top-10 worst days ever. Unless, of course, we’re actually living in the Marvel universe (sorry, multiverse at this point). Then we’re totally going to see the emergence of the new superhero Iguana Girl in 15 years or so. Keep your eyes open.
No allergies? Let them give up cake
Allergy season is already here – starting earlier every year, it seems – and many people are not happy about it. So unhappy, actually, that there’s a list of things they would be willing to give up for a year to get rid of their of allergies, according to a survey conducted by OnePoll on behalf of Flonase.
Nearly 40% of 2,000 respondents with allergies would go a year without eating cake or chocolate or playing video games in exchange for allergy-free status, the survey results show. Almost as many would forgo coffee (38%) or pizza (37%) for a year, while 36% would stay off social media and 31% would take a pay cut or give up their smartphones, the Independent reported.
More than half of the allergic Americans – 54%, to be exact – who were polled this past winter – Feb. 24 to March 1, to be exact – consider allergy symptoms to be the most frustrating part of the spring. Annoying things that were less frustrating to the group included mosquitoes (41%), filing tax returns (38%), and daylight savings time (37%).
The Trump arraignment circus, of course, occurred too late to make the list, as did the big “We’re going back to the office! No wait, we’re closing the office forever!” email extravaganza and emotional roller coaster. That second one, however, did not get nearly as much media coverage.
Genetic analysis shows causal link of GERD, other comorbidities to IPF
Relationships between 22 unique comorbidities and idiopathic pulmonary fibrosis (IPF) were assessed by a bidirectional Mendelian randomization (MR) approach in a retrospective study. Three of the comorbidities that were examined appeared causally associated with an increased risk of IPF.
Researchers used summary statistics of large-scale genomewide association studies (GWAS) obtained from the IPF Genetics Consortium. For replication, they used data from the Global Biobank Meta-Analysis Initiative.
Pulmonary or extrapulmonary illnesses are regularly observed to be comorbidities associated with IPF. Although randomized control trials can provide strong deductive evidence of causal relationships between diseases, they are also often subject to inherent practical and ethical limitations. MR is an alternative approach that exploits genetic variants of genes with known function as a means to infer a causal effect of a modifiable exposure on disease and minimizes possible confounding issues from unrelated environmental factors and reverse causation. Bidirectional MR extends the exposure-outcome association analysis of MR to both directions, producing a higher level of evidence for causality, Jiahao Zhu, of the Department of Epidemiology and Health Statistics, Hangzhou, China, and colleagues wrote.
Study details
In a study published in the journal Chest, the researchers reported on direction and causal associations between IPF and comorbidities, as determined by bidirectional MR analysis of GWAS summary statistics from five studies included in the IPF Genetics Consortium (4,125 patients and 20,464 control participants). For replication, they extracted IPF GWAS summary statistics from the nine biobanks from the GBMI (6,257 patients and 947,616 control participants). All individuals were of European ancestry.
The 22 comorbidities examined for a relationship to IPF were identified through a combination of a PubMed database literature search limited to English-language articles concerning IPF as either an exposure or an outcome and having an available full GWAS summary statistic. The number of patients in these studies ranged from a minimum of 3,203 for osteoporosis to a maximum of 246,363 for major depressive disorder.
To estimate causal relationships, single-nucleotide polymorphism selection for IPF and each comorbidity genetic instrument were based on a genomewide significance value (P < 5x10–8) and were clumped by linkage disequilibrium (r2 < 0.001 within a 10,000 kB clumping distance). Evidence from analysis associating each comorbidity with IPF was categorized as either convincing, suggestive, or weak. Follow-up studies examined the causal effects of measured lung and thyroid variables on IPF and IPF effects on blood pressure variables.
Convincing evidence
The bidirectional MR and follow-up analysis revealed “convincing evidence” of causal relationships between IPF and 2 of the evaluated 22 comorbidities. A higher risk of IPF was associated with gastroesophageal reflux disease (GERD). Importantly, a multivariable MR analysis conditioning for smoking continued to show the causal linkage between GERD and a higher risk of IPF. In contrast, the genetic liability of COPD appeared to confer a protective role, as indicated by an associated decrease in risk for IPF. The researchers suggest that this negative relationship may be caused by their distinct genetic architecture.
Suggestive evidence
“Suggestive evidence” of underlying relationships between IPF and lung cancer or blood pressure phenotype comorbidities was also found with this study. The MR results give support to existing evidence that IPF has a causal effect for a higher lung cancer risk. In contrast, IPF appeared to have a protective effect on hypertension and BP phenotypes. This contrasted with VTE: Evidence suggestive that genetic liability to hypothyroidism could lead to IPF was also found (International IPF Genetics Consortium, P < .040; MR PRESSO method; and GBMI, P < .002; IVW method).
Limitations
The primary strengths of the study was the ability of MR design to enhance causal inference, particularly when large cohorts for perspective investigations would be inherently difficult to obtain. Several noted limitations include the fact that causal estimates may not be well matched to observational or interventional studies and there was a low number of single-nucleotide polymorphisms available as genetic instruments for some diseases. In addition, there was a potential bias because of some sample overlap among the utilized databases, and it is unknown whether the results are applicable to ethnicities other than those of European ancestry.
Conclusion
Overall, this study showed that a bidirectional MR analysis approach could leverage genetic information from large databases to reveal causative associations between IPF and several different comorbidities. This included an apparent causal relationship of GERD, venous thromboembolism, and hypothyroidism with IPF, according to the researchers. These provide the basis to obtain “a deeper understanding of the pathways underlying these diverse associations” that may have valuable “implications for enhanced prevention and treatment strategies for comorbidities.”
The authors disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Relationships between 22 unique comorbidities and idiopathic pulmonary fibrosis (IPF) were assessed by a bidirectional Mendelian randomization (MR) approach in a retrospective study. Three of the comorbidities that were examined appeared causally associated with an increased risk of IPF.
Researchers used summary statistics of large-scale genomewide association studies (GWAS) obtained from the IPF Genetics Consortium. For replication, they used data from the Global Biobank Meta-Analysis Initiative.
Pulmonary or extrapulmonary illnesses are regularly observed to be comorbidities associated with IPF. Although randomized control trials can provide strong deductive evidence of causal relationships between diseases, they are also often subject to inherent practical and ethical limitations. MR is an alternative approach that exploits genetic variants of genes with known function as a means to infer a causal effect of a modifiable exposure on disease and minimizes possible confounding issues from unrelated environmental factors and reverse causation. Bidirectional MR extends the exposure-outcome association analysis of MR to both directions, producing a higher level of evidence for causality, Jiahao Zhu, of the Department of Epidemiology and Health Statistics, Hangzhou, China, and colleagues wrote.
Study details
In a study published in the journal Chest, the researchers reported on direction and causal associations between IPF and comorbidities, as determined by bidirectional MR analysis of GWAS summary statistics from five studies included in the IPF Genetics Consortium (4,125 patients and 20,464 control participants). For replication, they extracted IPF GWAS summary statistics from the nine biobanks from the GBMI (6,257 patients and 947,616 control participants). All individuals were of European ancestry.
The 22 comorbidities examined for a relationship to IPF were identified through a combination of a PubMed database literature search limited to English-language articles concerning IPF as either an exposure or an outcome and having an available full GWAS summary statistic. The number of patients in these studies ranged from a minimum of 3,203 for osteoporosis to a maximum of 246,363 for major depressive disorder.
To estimate causal relationships, single-nucleotide polymorphism selection for IPF and each comorbidity genetic instrument were based on a genomewide significance value (P < 5x10–8) and were clumped by linkage disequilibrium (r2 < 0.001 within a 10,000 kB clumping distance). Evidence from analysis associating each comorbidity with IPF was categorized as either convincing, suggestive, or weak. Follow-up studies examined the causal effects of measured lung and thyroid variables on IPF and IPF effects on blood pressure variables.
Convincing evidence
The bidirectional MR and follow-up analysis revealed “convincing evidence” of causal relationships between IPF and 2 of the evaluated 22 comorbidities. A higher risk of IPF was associated with gastroesophageal reflux disease (GERD). Importantly, a multivariable MR analysis conditioning for smoking continued to show the causal linkage between GERD and a higher risk of IPF. In contrast, the genetic liability of COPD appeared to confer a protective role, as indicated by an associated decrease in risk for IPF. The researchers suggest that this negative relationship may be caused by their distinct genetic architecture.
Suggestive evidence
“Suggestive evidence” of underlying relationships between IPF and lung cancer or blood pressure phenotype comorbidities was also found with this study. The MR results give support to existing evidence that IPF has a causal effect for a higher lung cancer risk. In contrast, IPF appeared to have a protective effect on hypertension and BP phenotypes. This contrasted with VTE: Evidence suggestive that genetic liability to hypothyroidism could lead to IPF was also found (International IPF Genetics Consortium, P < .040; MR PRESSO method; and GBMI, P < .002; IVW method).
Limitations
The primary strengths of the study was the ability of MR design to enhance causal inference, particularly when large cohorts for perspective investigations would be inherently difficult to obtain. Several noted limitations include the fact that causal estimates may not be well matched to observational or interventional studies and there was a low number of single-nucleotide polymorphisms available as genetic instruments for some diseases. In addition, there was a potential bias because of some sample overlap among the utilized databases, and it is unknown whether the results are applicable to ethnicities other than those of European ancestry.
Conclusion
Overall, this study showed that a bidirectional MR analysis approach could leverage genetic information from large databases to reveal causative associations between IPF and several different comorbidities. This included an apparent causal relationship of GERD, venous thromboembolism, and hypothyroidism with IPF, according to the researchers. These provide the basis to obtain “a deeper understanding of the pathways underlying these diverse associations” that may have valuable “implications for enhanced prevention and treatment strategies for comorbidities.”
The authors disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Relationships between 22 unique comorbidities and idiopathic pulmonary fibrosis (IPF) were assessed by a bidirectional Mendelian randomization (MR) approach in a retrospective study. Three of the comorbidities that were examined appeared causally associated with an increased risk of IPF.
Researchers used summary statistics of large-scale genomewide association studies (GWAS) obtained from the IPF Genetics Consortium. For replication, they used data from the Global Biobank Meta-Analysis Initiative.
Pulmonary or extrapulmonary illnesses are regularly observed to be comorbidities associated with IPF. Although randomized control trials can provide strong deductive evidence of causal relationships between diseases, they are also often subject to inherent practical and ethical limitations. MR is an alternative approach that exploits genetic variants of genes with known function as a means to infer a causal effect of a modifiable exposure on disease and minimizes possible confounding issues from unrelated environmental factors and reverse causation. Bidirectional MR extends the exposure-outcome association analysis of MR to both directions, producing a higher level of evidence for causality, Jiahao Zhu, of the Department of Epidemiology and Health Statistics, Hangzhou, China, and colleagues wrote.
Study details
In a study published in the journal Chest, the researchers reported on direction and causal associations between IPF and comorbidities, as determined by bidirectional MR analysis of GWAS summary statistics from five studies included in the IPF Genetics Consortium (4,125 patients and 20,464 control participants). For replication, they extracted IPF GWAS summary statistics from the nine biobanks from the GBMI (6,257 patients and 947,616 control participants). All individuals were of European ancestry.
The 22 comorbidities examined for a relationship to IPF were identified through a combination of a PubMed database literature search limited to English-language articles concerning IPF as either an exposure or an outcome and having an available full GWAS summary statistic. The number of patients in these studies ranged from a minimum of 3,203 for osteoporosis to a maximum of 246,363 for major depressive disorder.
To estimate causal relationships, single-nucleotide polymorphism selection for IPF and each comorbidity genetic instrument were based on a genomewide significance value (P < 5x10–8) and were clumped by linkage disequilibrium (r2 < 0.001 within a 10,000 kB clumping distance). Evidence from analysis associating each comorbidity with IPF was categorized as either convincing, suggestive, or weak. Follow-up studies examined the causal effects of measured lung and thyroid variables on IPF and IPF effects on blood pressure variables.
Convincing evidence
The bidirectional MR and follow-up analysis revealed “convincing evidence” of causal relationships between IPF and 2 of the evaluated 22 comorbidities. A higher risk of IPF was associated with gastroesophageal reflux disease (GERD). Importantly, a multivariable MR analysis conditioning for smoking continued to show the causal linkage between GERD and a higher risk of IPF. In contrast, the genetic liability of COPD appeared to confer a protective role, as indicated by an associated decrease in risk for IPF. The researchers suggest that this negative relationship may be caused by their distinct genetic architecture.
Suggestive evidence
“Suggestive evidence” of underlying relationships between IPF and lung cancer or blood pressure phenotype comorbidities was also found with this study. The MR results give support to existing evidence that IPF has a causal effect for a higher lung cancer risk. In contrast, IPF appeared to have a protective effect on hypertension and BP phenotypes. This contrasted with VTE: Evidence suggestive that genetic liability to hypothyroidism could lead to IPF was also found (International IPF Genetics Consortium, P < .040; MR PRESSO method; and GBMI, P < .002; IVW method).
Limitations
The primary strengths of the study was the ability of MR design to enhance causal inference, particularly when large cohorts for perspective investigations would be inherently difficult to obtain. Several noted limitations include the fact that causal estimates may not be well matched to observational or interventional studies and there was a low number of single-nucleotide polymorphisms available as genetic instruments for some diseases. In addition, there was a potential bias because of some sample overlap among the utilized databases, and it is unknown whether the results are applicable to ethnicities other than those of European ancestry.
Conclusion
Overall, this study showed that a bidirectional MR analysis approach could leverage genetic information from large databases to reveal causative associations between IPF and several different comorbidities. This included an apparent causal relationship of GERD, venous thromboembolism, and hypothyroidism with IPF, according to the researchers. These provide the basis to obtain “a deeper understanding of the pathways underlying these diverse associations” that may have valuable “implications for enhanced prevention and treatment strategies for comorbidities.”
The authors disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM CHEST
SBRT: Alternative to surgery in early stage lung cancer?
, according to population-based data from a German cancer registry.
“From a public health perspective, SBRT is a good therapeutic option in terms of survival, especially for elderly and inoperable patients,” noted the study authors, led by Jörg Andreas Müller, MD, department of radiation oncology, University Hospital of Halle, Germany.
The analysis was published online in the journal Strahlentherapie Und Onkologie.
Surgery remains the standard of care for early stage NSCLC. However, many patients are not eligible for surgery because of the tumor’s location, age, frailty, or comorbidities.
Before the introduction of SBRT, conventional radiation therapy was the only reasonable option for inoperable patients, with study data showing only a small survival improvement in treated vs. untreated patients.
High-precision, image-guided SBRT offers better tumor control with limited toxicity. And while many radiation oncology centers in Germany adopted SBRT as an alternative treatment for surgery after 2000, few population-based studies evaluating SBRT’s impact on overall survival exist.
Using the German clinical cancer registry of Berlin-Brandenburg, Dr. Müller and colleagues assessed SBRT as an alternative to surgery in 558 patients with stage I and II NSCLC, diagnosed between 2000 and 2015.
More patients received surgery than SBRT (74% vs. 26%). Those who received SBRT were younger than those in the surgery group and had better Karnofsky performance status.
Among patients in the SBRT group, median survival was 19 months overall and 27 months in patients over age 75. In the surgery group, median survival was 22 months overall and 24 months in those over 75.
In a univariate survival model of a propensity-matched sample of 292 patients – half of whom received SBRT – survival rates were similar among those who underwent SBRT versus surgery (hazard ratio [HR], 1.2; P = .2).
Survival was also similar in the two treatment groups in a T1 subanalysis (HR, 1.12; P = .7) as well as in patients over age 75 (HR, 0.86; P = .5).
Better performance status scores were associated with improved survival, and higher histological grades and TNM stages were linked to higher mortality risk. The availability of histological data did not have a significant impact on survival outcomes.
Overall, the findings suggest that SBRT and surgery offer comparable survival outcomes in early stage NSCLC and “the availability of histological data might not be decisive for treatment planning,” Dr. Müller and colleagues said.
Drew Moghanaki, MD, chief of the thoracic oncology service at UCLA Health Jonsson Comprehensive Cancer Center, Los Angeles, highlighted the findings on Twitter.
A thoracic surgeon from Germany responded with several concerns about the study, including the use of statistics with univariate modeling and undiagnosed lymph node (N) status.
Dr. Moghanaki replied that these “concerns summarize how we USED to think. It increasingly seems they aren’t as important as our teachers once thought they were. As we move into the future we need to reassess the data that supported these recommendations as they seem more academic than patient centered.”
The study authors reported no specific funding, and no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to population-based data from a German cancer registry.
“From a public health perspective, SBRT is a good therapeutic option in terms of survival, especially for elderly and inoperable patients,” noted the study authors, led by Jörg Andreas Müller, MD, department of radiation oncology, University Hospital of Halle, Germany.
The analysis was published online in the journal Strahlentherapie Und Onkologie.
Surgery remains the standard of care for early stage NSCLC. However, many patients are not eligible for surgery because of the tumor’s location, age, frailty, or comorbidities.
Before the introduction of SBRT, conventional radiation therapy was the only reasonable option for inoperable patients, with study data showing only a small survival improvement in treated vs. untreated patients.
High-precision, image-guided SBRT offers better tumor control with limited toxicity. And while many radiation oncology centers in Germany adopted SBRT as an alternative treatment for surgery after 2000, few population-based studies evaluating SBRT’s impact on overall survival exist.
Using the German clinical cancer registry of Berlin-Brandenburg, Dr. Müller and colleagues assessed SBRT as an alternative to surgery in 558 patients with stage I and II NSCLC, diagnosed between 2000 and 2015.
More patients received surgery than SBRT (74% vs. 26%). Those who received SBRT were younger than those in the surgery group and had better Karnofsky performance status.
Among patients in the SBRT group, median survival was 19 months overall and 27 months in patients over age 75. In the surgery group, median survival was 22 months overall and 24 months in those over 75.
In a univariate survival model of a propensity-matched sample of 292 patients – half of whom received SBRT – survival rates were similar among those who underwent SBRT versus surgery (hazard ratio [HR], 1.2; P = .2).
Survival was also similar in the two treatment groups in a T1 subanalysis (HR, 1.12; P = .7) as well as in patients over age 75 (HR, 0.86; P = .5).
Better performance status scores were associated with improved survival, and higher histological grades and TNM stages were linked to higher mortality risk. The availability of histological data did not have a significant impact on survival outcomes.
Overall, the findings suggest that SBRT and surgery offer comparable survival outcomes in early stage NSCLC and “the availability of histological data might not be decisive for treatment planning,” Dr. Müller and colleagues said.
Drew Moghanaki, MD, chief of the thoracic oncology service at UCLA Health Jonsson Comprehensive Cancer Center, Los Angeles, highlighted the findings on Twitter.
A thoracic surgeon from Germany responded with several concerns about the study, including the use of statistics with univariate modeling and undiagnosed lymph node (N) status.
Dr. Moghanaki replied that these “concerns summarize how we USED to think. It increasingly seems they aren’t as important as our teachers once thought they were. As we move into the future we need to reassess the data that supported these recommendations as they seem more academic than patient centered.”
The study authors reported no specific funding, and no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to population-based data from a German cancer registry.
“From a public health perspective, SBRT is a good therapeutic option in terms of survival, especially for elderly and inoperable patients,” noted the study authors, led by Jörg Andreas Müller, MD, department of radiation oncology, University Hospital of Halle, Germany.
The analysis was published online in the journal Strahlentherapie Und Onkologie.
Surgery remains the standard of care for early stage NSCLC. However, many patients are not eligible for surgery because of the tumor’s location, age, frailty, or comorbidities.
Before the introduction of SBRT, conventional radiation therapy was the only reasonable option for inoperable patients, with study data showing only a small survival improvement in treated vs. untreated patients.
High-precision, image-guided SBRT offers better tumor control with limited toxicity. And while many radiation oncology centers in Germany adopted SBRT as an alternative treatment for surgery after 2000, few population-based studies evaluating SBRT’s impact on overall survival exist.
Using the German clinical cancer registry of Berlin-Brandenburg, Dr. Müller and colleagues assessed SBRT as an alternative to surgery in 558 patients with stage I and II NSCLC, diagnosed between 2000 and 2015.
More patients received surgery than SBRT (74% vs. 26%). Those who received SBRT were younger than those in the surgery group and had better Karnofsky performance status.
Among patients in the SBRT group, median survival was 19 months overall and 27 months in patients over age 75. In the surgery group, median survival was 22 months overall and 24 months in those over 75.
In a univariate survival model of a propensity-matched sample of 292 patients – half of whom received SBRT – survival rates were similar among those who underwent SBRT versus surgery (hazard ratio [HR], 1.2; P = .2).
Survival was also similar in the two treatment groups in a T1 subanalysis (HR, 1.12; P = .7) as well as in patients over age 75 (HR, 0.86; P = .5).
Better performance status scores were associated with improved survival, and higher histological grades and TNM stages were linked to higher mortality risk. The availability of histological data did not have a significant impact on survival outcomes.
Overall, the findings suggest that SBRT and surgery offer comparable survival outcomes in early stage NSCLC and “the availability of histological data might not be decisive for treatment planning,” Dr. Müller and colleagues said.
Drew Moghanaki, MD, chief of the thoracic oncology service at UCLA Health Jonsson Comprehensive Cancer Center, Los Angeles, highlighted the findings on Twitter.
A thoracic surgeon from Germany responded with several concerns about the study, including the use of statistics with univariate modeling and undiagnosed lymph node (N) status.
Dr. Moghanaki replied that these “concerns summarize how we USED to think. It increasingly seems they aren’t as important as our teachers once thought they were. As we move into the future we need to reassess the data that supported these recommendations as they seem more academic than patient centered.”
The study authors reported no specific funding, and no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM STRAHLENTHERAPIE UND ONKOLOGIE
Nasal COVID treatment shows early promise against multiple variants
if used within 4 hours after infection inside the nose, new research reveals.
Known as TriSb92 (brand name Covidin, from drugmaker Pandemblock Oy in Finland), the viral inhibitor also appears effective against all coronavirus variants of concern, neutralizing even the Omicron variants BA.5, XBB, and BQ.1.1 in laboratory and mice studies.
Unlike a COVID vaccine that boosts a person’s immune system as protection, the antiviral nasal spray works more directly by blocking the virus, acting as a “biological mask in the nasal cavity,” according to the biotechnology company set up to develop the treatment.
The product targets a stable site on the spike protein of the virus that is not known to mutate. This same site is shared among many variants of the COVID virus, so it could be effective against future variants as well, researchers note.
“In animal models, by directly inactivating the virus, TriSb92 offers immediate and robust protection” against coronavirus infection and severe COVID, said Anna R. Mäkelä, PhD, lead author of the study and a senior scientist in the department of virology at the University of Helsinki.
The study was published online in Nature Communications.
A potential first line of defense
Even in cases where the antiviral does not prevent coronavirus infection, the treatment could slow infection. This could happen by limiting how much virus could replicate early in the skin inside the nose and nasopharynx (the upper part of the throat), said Dr. Mäkelä, who is also CEO of Pandemblock Oy, the company set up to develop the product.
“TriSb92 could effectively tip the balance in favor of the [the person] and thereby help to reduce the risk of severe COVID-19 disease,” she said.
The antiviral also could offer an alternative to people who cannot or do not respond to a vaccine.
“Many elderly people as well as individuals who are immunodeficient for various reasons do not respond to vaccines and are in the need of other protective measures,” said Kalle Saksela, MD, PhD, senior author of the study and a virologist at the University of Helsinki.
Multiple doses needed?
TriSb92 is “one of multiple nasal spray approaches but unlikely to be as durable as effective nasal vaccines,” said Eric Topol, MD, a professor of molecular medicine and executive vice president of Scripps Research in La Jolla, Calif. Dr. Topol is also editor-in-chief of Medscape, WebMD’s sister site for medical professionals.
“The sprays generally require multiple doses per day, whereas a single dose of a nasal vaccine may protect for months,” he said.
“Both have the allure of being variant-proof,” Dr. Topol added.
Thinking small
Many laboratories are shifting from treatments using monoclonal antibodies to treatments using smaller antibody fragments called “nanobodies” because they are more cost-effective and are able to last longer in storage, Dr. Mäkelä and colleagues noted.
Several of these nanobodies have shown promise against viruses in cell culture or animal models, including as an intranasal preventive treatment for SARS-CoV-2.
One of these smaller antibodies is being developed from llamas for example; another comes from experiments with yeast to develop synthetic nanobodies; and in a third case, researchers isolated nanobodies from llamas and from mice and showed they could neutralize the SARS-CoV-2 virus.
These nanobodies and TriSb92 target a specific part of the coronavirus spike protein called the receptor-binding domain (RBD). The RBD is where the coronavirus attaches to cells in the body. These agents essentially trick the virus by changing the structure of the outside of cells, so they look like a virus has already fused to them. This way, the virus moves on.
Key findings
The researchers compared mice treated with TriSb92 before and after exposure to SARS-CoV-2. When given in advance, none of the treated mice had SARS-CoV-2 RNA in their lungs, while untreated mice in the comparison group had “abundant” levels.
Other evidence of viral infection showed similar differences between treated and untreated mice in the protective lining of cells called the epithelium inside the nose, nasal mucosa, and airways.
Similarly, when given 2 or 4 hours after SARS-CoV-2 had already infected the epithelium, TriSb92 was linked to a complete lack of the virus’s RNA in the lungs.
It was more effective against the virus, though, when given before infection rather than after, “perhaps due to the initial establishment of the infection,” the researchers note.
The company led by Dr. Mäkelä is now working to secure funding for clinical trials of TriSb92 in humans.
A version of this article first appeared on WebMD.com.
if used within 4 hours after infection inside the nose, new research reveals.
Known as TriSb92 (brand name Covidin, from drugmaker Pandemblock Oy in Finland), the viral inhibitor also appears effective against all coronavirus variants of concern, neutralizing even the Omicron variants BA.5, XBB, and BQ.1.1 in laboratory and mice studies.
Unlike a COVID vaccine that boosts a person’s immune system as protection, the antiviral nasal spray works more directly by blocking the virus, acting as a “biological mask in the nasal cavity,” according to the biotechnology company set up to develop the treatment.
The product targets a stable site on the spike protein of the virus that is not known to mutate. This same site is shared among many variants of the COVID virus, so it could be effective against future variants as well, researchers note.
“In animal models, by directly inactivating the virus, TriSb92 offers immediate and robust protection” against coronavirus infection and severe COVID, said Anna R. Mäkelä, PhD, lead author of the study and a senior scientist in the department of virology at the University of Helsinki.
The study was published online in Nature Communications.
A potential first line of defense
Even in cases where the antiviral does not prevent coronavirus infection, the treatment could slow infection. This could happen by limiting how much virus could replicate early in the skin inside the nose and nasopharynx (the upper part of the throat), said Dr. Mäkelä, who is also CEO of Pandemblock Oy, the company set up to develop the product.
“TriSb92 could effectively tip the balance in favor of the [the person] and thereby help to reduce the risk of severe COVID-19 disease,” she said.
The antiviral also could offer an alternative to people who cannot or do not respond to a vaccine.
“Many elderly people as well as individuals who are immunodeficient for various reasons do not respond to vaccines and are in the need of other protective measures,” said Kalle Saksela, MD, PhD, senior author of the study and a virologist at the University of Helsinki.
Multiple doses needed?
TriSb92 is “one of multiple nasal spray approaches but unlikely to be as durable as effective nasal vaccines,” said Eric Topol, MD, a professor of molecular medicine and executive vice president of Scripps Research in La Jolla, Calif. Dr. Topol is also editor-in-chief of Medscape, WebMD’s sister site for medical professionals.
“The sprays generally require multiple doses per day, whereas a single dose of a nasal vaccine may protect for months,” he said.
“Both have the allure of being variant-proof,” Dr. Topol added.
Thinking small
Many laboratories are shifting from treatments using monoclonal antibodies to treatments using smaller antibody fragments called “nanobodies” because they are more cost-effective and are able to last longer in storage, Dr. Mäkelä and colleagues noted.
Several of these nanobodies have shown promise against viruses in cell culture or animal models, including as an intranasal preventive treatment for SARS-CoV-2.
One of these smaller antibodies is being developed from llamas for example; another comes from experiments with yeast to develop synthetic nanobodies; and in a third case, researchers isolated nanobodies from llamas and from mice and showed they could neutralize the SARS-CoV-2 virus.
These nanobodies and TriSb92 target a specific part of the coronavirus spike protein called the receptor-binding domain (RBD). The RBD is where the coronavirus attaches to cells in the body. These agents essentially trick the virus by changing the structure of the outside of cells, so they look like a virus has already fused to them. This way, the virus moves on.
Key findings
The researchers compared mice treated with TriSb92 before and after exposure to SARS-CoV-2. When given in advance, none of the treated mice had SARS-CoV-2 RNA in their lungs, while untreated mice in the comparison group had “abundant” levels.
Other evidence of viral infection showed similar differences between treated and untreated mice in the protective lining of cells called the epithelium inside the nose, nasal mucosa, and airways.
Similarly, when given 2 or 4 hours after SARS-CoV-2 had already infected the epithelium, TriSb92 was linked to a complete lack of the virus’s RNA in the lungs.
It was more effective against the virus, though, when given before infection rather than after, “perhaps due to the initial establishment of the infection,” the researchers note.
The company led by Dr. Mäkelä is now working to secure funding for clinical trials of TriSb92 in humans.
A version of this article first appeared on WebMD.com.
if used within 4 hours after infection inside the nose, new research reveals.
Known as TriSb92 (brand name Covidin, from drugmaker Pandemblock Oy in Finland), the viral inhibitor also appears effective against all coronavirus variants of concern, neutralizing even the Omicron variants BA.5, XBB, and BQ.1.1 in laboratory and mice studies.
Unlike a COVID vaccine that boosts a person’s immune system as protection, the antiviral nasal spray works more directly by blocking the virus, acting as a “biological mask in the nasal cavity,” according to the biotechnology company set up to develop the treatment.
The product targets a stable site on the spike protein of the virus that is not known to mutate. This same site is shared among many variants of the COVID virus, so it could be effective against future variants as well, researchers note.
“In animal models, by directly inactivating the virus, TriSb92 offers immediate and robust protection” against coronavirus infection and severe COVID, said Anna R. Mäkelä, PhD, lead author of the study and a senior scientist in the department of virology at the University of Helsinki.
The study was published online in Nature Communications.
A potential first line of defense
Even in cases where the antiviral does not prevent coronavirus infection, the treatment could slow infection. This could happen by limiting how much virus could replicate early in the skin inside the nose and nasopharynx (the upper part of the throat), said Dr. Mäkelä, who is also CEO of Pandemblock Oy, the company set up to develop the product.
“TriSb92 could effectively tip the balance in favor of the [the person] and thereby help to reduce the risk of severe COVID-19 disease,” she said.
The antiviral also could offer an alternative to people who cannot or do not respond to a vaccine.
“Many elderly people as well as individuals who are immunodeficient for various reasons do not respond to vaccines and are in the need of other protective measures,” said Kalle Saksela, MD, PhD, senior author of the study and a virologist at the University of Helsinki.
Multiple doses needed?
TriSb92 is “one of multiple nasal spray approaches but unlikely to be as durable as effective nasal vaccines,” said Eric Topol, MD, a professor of molecular medicine and executive vice president of Scripps Research in La Jolla, Calif. Dr. Topol is also editor-in-chief of Medscape, WebMD’s sister site for medical professionals.
“The sprays generally require multiple doses per day, whereas a single dose of a nasal vaccine may protect for months,” he said.
“Both have the allure of being variant-proof,” Dr. Topol added.
Thinking small
Many laboratories are shifting from treatments using monoclonal antibodies to treatments using smaller antibody fragments called “nanobodies” because they are more cost-effective and are able to last longer in storage, Dr. Mäkelä and colleagues noted.
Several of these nanobodies have shown promise against viruses in cell culture or animal models, including as an intranasal preventive treatment for SARS-CoV-2.
One of these smaller antibodies is being developed from llamas for example; another comes from experiments with yeast to develop synthetic nanobodies; and in a third case, researchers isolated nanobodies from llamas and from mice and showed they could neutralize the SARS-CoV-2 virus.
These nanobodies and TriSb92 target a specific part of the coronavirus spike protein called the receptor-binding domain (RBD). The RBD is where the coronavirus attaches to cells in the body. These agents essentially trick the virus by changing the structure of the outside of cells, so they look like a virus has already fused to them. This way, the virus moves on.
Key findings
The researchers compared mice treated with TriSb92 before and after exposure to SARS-CoV-2. When given in advance, none of the treated mice had SARS-CoV-2 RNA in their lungs, while untreated mice in the comparison group had “abundant” levels.
Other evidence of viral infection showed similar differences between treated and untreated mice in the protective lining of cells called the epithelium inside the nose, nasal mucosa, and airways.
Similarly, when given 2 or 4 hours after SARS-CoV-2 had already infected the epithelium, TriSb92 was linked to a complete lack of the virus’s RNA in the lungs.
It was more effective against the virus, though, when given before infection rather than after, “perhaps due to the initial establishment of the infection,” the researchers note.
The company led by Dr. Mäkelä is now working to secure funding for clinical trials of TriSb92 in humans.
A version of this article first appeared on WebMD.com.
FROM NATURE COMMUNICATIONS
High-dose prophylactic anticoagulation benefits patients with COVID-19 pneumonia
High-dose prophylactic anticoagulation or therapeutic anticoagulation reduced de novo thrombosis in patients with hypoxemic COVID-19 pneumonia, based on data from 334 adults.
Patients with hypoxemic COVID-19 pneumonia are at increased risk of thrombosis and anticoagulation-related bleeding, therefore data to identify the lowest effective anticoagulant dose are needed, wrote Vincent Labbé, MD, of Sorbonne University, Paris, and colleagues.
Previous studies of different anticoagulation strategies for noncritically ill and critically ill patients with COVID-19 pneumonia have shown contrasting results, but some institutions recommend a high-dose regimen in the wake of data showing macrovascular thrombosis in patients with COVID-19 who were treated with standard anticoagulation, the authors wrote.
However, no previously published studies have compared the effectiveness of the three anticoagulation strategies: high-dose prophylactic anticoagulation (HD-PA), standard dose prophylactic anticoagulation (SD-PA), and therapeutic anticoagulation (TA), they said.
In the open-label Anticoagulation COVID-19 (ANTICOVID) trial, published in JAMA Internal Medicine, the researchers identified consecutively hospitalized adults aged 18 years and older being treated for hypoxemic COVID-19 pneumonia in 23 centers in France between April 2021 and December 2021.
The patients were randomly assigned to SD-PA (116 patients), HD-PA (111 patients), and TA (112 patients) using low-molecular-weight heparin for 14 days, or until either hospital discharge or weaning from supplemental oxygen for 48 consecutive hours, whichever outcome occurred first. The HD-PA patients received two times the SD-PA dose. The mean age of the patients was 58.3 years, and approximately two-thirds were men; race and ethnicity data were not collected. Participants had no macrovascular thrombosis at the start of the study.
The primary outcomes were all-cause mortality and time to clinical improvement (defined as the time from randomization to a 2-point improvement on a 7-category respiratory function scale).
The secondary outcome was a combination of safety and efficacy at day 28 that included a composite of thrombosis (ischemic stroke, noncerebrovascular arterial thrombosis, deep venous thrombosis, pulmonary artery thrombosis, and central venous catheter–related deep venous thrombosis), major bleeding, or all-cause death.
For the primary outcome, results were similar among the groups; HD-PA had no significant benefit over SD-PA or TA. All-cause death rates for SD-PA, HD-PA, and TA patients were 14%, 12%, and 13%, respectively. The time to clinical improvement for the three groups was approximately 8 days, 9 days, and 8 days, respectively. Results for the primary outcome were consistent across all prespecified subgroups.
However, HD-PA was associated with a significant fourfold reduced risk of de novo thrombosis compared with SD-PA (5.5% vs. 20.2%) with no observed increase in major bleeding. TA was not associated with any significant improvement in primary or secondary outcomes compared with HD-PA or SD-PA.
The current study findings of no improvement in survival or disease resolution in patients with a higher anticoagulant dose reflects data from previous studies, the researchers wrote in their discussion. “Our study results together with those of previous RCTs support the premise that the role of microvascular thrombosis in worsening organ dysfunction may be narrower than estimated,” they said.
The findings were limited by several factors including the open-label design and the relatively small sample size, the lack of data on microvascular (vs. macrovascular) thrombosis at baseline, and the predominance of the Delta variant of COVID-19 among the study participants, which may have contributed to a lower mortality rate, the researchers noted.
However, given the significant reduction in de novo thrombosis, the results support the routine use of HD-PA in patients with severe hypoxemic COVID-19 pneumonia, they concluded.
Results inform current clinical practice
Over the course of the COVID-19 pandemic, “Patients hospitalized with COVID-19 manifested the highest risk for thromboembolic complications, especially patients in the intensive care setting,” and early reports suggested that standard prophylactic doses of anticoagulant therapy might be insufficient to prevent thrombotic events, Richard C. Becker, MD, of the University of Cincinnati, and Thomas L. Ortel, MD, of Duke University, Durham, N.C., wrote in an accompanying editorial.
“Although there have been several studies that have investigated the role of anticoagulant therapy in hospitalized patients with COVID-19, this is the first study that specifically compared a standard, prophylactic dose of low-molecular-weight heparin to a ‘high-dose’ prophylactic regimen and to a full therapeutic dose regimen,” Dr. Ortel said in an interview.
“Given the concerns about an increased thrombotic risk with prophylactic dose anticoagulation, and the potential bleeding risk associated with a full therapeutic dose of anticoagulation, this approach enabled the investigators to explore the efficacy and safety of an intermediate dose between these two extremes,” he said.
In the current study, , a finding that was not observed in other studies investigating anticoagulant therapy in hospitalized patients with severe COVID-19,” Dr. Ortel told this news organization. “Much initial concern about progression of disease in patients hospitalized with severe COVID-19 focused on the role of microvascular thrombosis, which appears to be less important in this process, or, alternatively, less responsive to anticoagulant therapy.”
The clinical takeaway from the study, Dr. Ortel said, is the decreased risk for venous thromboembolism with a high-dose prophylactic anticoagulation strategy compared with a standard-dose prophylactic regimen for patients hospitalized with hypoxemic COVID-19 pneumonia, “leading to an improved net clinical outcome.”
Looking ahead, “Additional research is needed to determine whether a higher dose of prophylactic anticoagulation would be beneficial for patients hospitalized with COVID-19 pneumonia who are not in an intensive care unit setting,” Dr. Ortel said. Studies are needed to determine whether therapeutic interventions are equally beneficial in patients with different coronavirus variants, since most patients in the current study were infected with the Delta variant, he added.
The study was supported by LEO Pharma. Dr. Labbé disclosed grants from LEO Pharma during the study and fees from AOP Health unrelated to the current study.
Dr. Becker disclosed personal fees from Novartis Data Safety Monitoring Board, Ionis Data Safety Monitoring Board, and Basking Biosciences Scientific Advisory Board unrelated to the current study. Dr. Ortel disclosed grants from the National Institutes of Health, Instrumentation Laboratory, Stago, and Siemens; contract fees from the Centers for Disease Control and Prevention; and honoraria from UpToDate unrelated to the current study.
A version of this article originally appeared on Medscape.com.
High-dose prophylactic anticoagulation or therapeutic anticoagulation reduced de novo thrombosis in patients with hypoxemic COVID-19 pneumonia, based on data from 334 adults.
Patients with hypoxemic COVID-19 pneumonia are at increased risk of thrombosis and anticoagulation-related bleeding, therefore data to identify the lowest effective anticoagulant dose are needed, wrote Vincent Labbé, MD, of Sorbonne University, Paris, and colleagues.
Previous studies of different anticoagulation strategies for noncritically ill and critically ill patients with COVID-19 pneumonia have shown contrasting results, but some institutions recommend a high-dose regimen in the wake of data showing macrovascular thrombosis in patients with COVID-19 who were treated with standard anticoagulation, the authors wrote.
However, no previously published studies have compared the effectiveness of the three anticoagulation strategies: high-dose prophylactic anticoagulation (HD-PA), standard dose prophylactic anticoagulation (SD-PA), and therapeutic anticoagulation (TA), they said.
In the open-label Anticoagulation COVID-19 (ANTICOVID) trial, published in JAMA Internal Medicine, the researchers identified consecutively hospitalized adults aged 18 years and older being treated for hypoxemic COVID-19 pneumonia in 23 centers in France between April 2021 and December 2021.
The patients were randomly assigned to SD-PA (116 patients), HD-PA (111 patients), and TA (112 patients) using low-molecular-weight heparin for 14 days, or until either hospital discharge or weaning from supplemental oxygen for 48 consecutive hours, whichever outcome occurred first. The HD-PA patients received two times the SD-PA dose. The mean age of the patients was 58.3 years, and approximately two-thirds were men; race and ethnicity data were not collected. Participants had no macrovascular thrombosis at the start of the study.
The primary outcomes were all-cause mortality and time to clinical improvement (defined as the time from randomization to a 2-point improvement on a 7-category respiratory function scale).
The secondary outcome was a combination of safety and efficacy at day 28 that included a composite of thrombosis (ischemic stroke, noncerebrovascular arterial thrombosis, deep venous thrombosis, pulmonary artery thrombosis, and central venous catheter–related deep venous thrombosis), major bleeding, or all-cause death.
For the primary outcome, results were similar among the groups; HD-PA had no significant benefit over SD-PA or TA. All-cause death rates for SD-PA, HD-PA, and TA patients were 14%, 12%, and 13%, respectively. The time to clinical improvement for the three groups was approximately 8 days, 9 days, and 8 days, respectively. Results for the primary outcome were consistent across all prespecified subgroups.
However, HD-PA was associated with a significant fourfold reduced risk of de novo thrombosis compared with SD-PA (5.5% vs. 20.2%) with no observed increase in major bleeding. TA was not associated with any significant improvement in primary or secondary outcomes compared with HD-PA or SD-PA.
The current study findings of no improvement in survival or disease resolution in patients with a higher anticoagulant dose reflects data from previous studies, the researchers wrote in their discussion. “Our study results together with those of previous RCTs support the premise that the role of microvascular thrombosis in worsening organ dysfunction may be narrower than estimated,” they said.
The findings were limited by several factors including the open-label design and the relatively small sample size, the lack of data on microvascular (vs. macrovascular) thrombosis at baseline, and the predominance of the Delta variant of COVID-19 among the study participants, which may have contributed to a lower mortality rate, the researchers noted.
However, given the significant reduction in de novo thrombosis, the results support the routine use of HD-PA in patients with severe hypoxemic COVID-19 pneumonia, they concluded.
Results inform current clinical practice
Over the course of the COVID-19 pandemic, “Patients hospitalized with COVID-19 manifested the highest risk for thromboembolic complications, especially patients in the intensive care setting,” and early reports suggested that standard prophylactic doses of anticoagulant therapy might be insufficient to prevent thrombotic events, Richard C. Becker, MD, of the University of Cincinnati, and Thomas L. Ortel, MD, of Duke University, Durham, N.C., wrote in an accompanying editorial.
“Although there have been several studies that have investigated the role of anticoagulant therapy in hospitalized patients with COVID-19, this is the first study that specifically compared a standard, prophylactic dose of low-molecular-weight heparin to a ‘high-dose’ prophylactic regimen and to a full therapeutic dose regimen,” Dr. Ortel said in an interview.
“Given the concerns about an increased thrombotic risk with prophylactic dose anticoagulation, and the potential bleeding risk associated with a full therapeutic dose of anticoagulation, this approach enabled the investigators to explore the efficacy and safety of an intermediate dose between these two extremes,” he said.
In the current study, , a finding that was not observed in other studies investigating anticoagulant therapy in hospitalized patients with severe COVID-19,” Dr. Ortel told this news organization. “Much initial concern about progression of disease in patients hospitalized with severe COVID-19 focused on the role of microvascular thrombosis, which appears to be less important in this process, or, alternatively, less responsive to anticoagulant therapy.”
The clinical takeaway from the study, Dr. Ortel said, is the decreased risk for venous thromboembolism with a high-dose prophylactic anticoagulation strategy compared with a standard-dose prophylactic regimen for patients hospitalized with hypoxemic COVID-19 pneumonia, “leading to an improved net clinical outcome.”
Looking ahead, “Additional research is needed to determine whether a higher dose of prophylactic anticoagulation would be beneficial for patients hospitalized with COVID-19 pneumonia who are not in an intensive care unit setting,” Dr. Ortel said. Studies are needed to determine whether therapeutic interventions are equally beneficial in patients with different coronavirus variants, since most patients in the current study were infected with the Delta variant, he added.
The study was supported by LEO Pharma. Dr. Labbé disclosed grants from LEO Pharma during the study and fees from AOP Health unrelated to the current study.
Dr. Becker disclosed personal fees from Novartis Data Safety Monitoring Board, Ionis Data Safety Monitoring Board, and Basking Biosciences Scientific Advisory Board unrelated to the current study. Dr. Ortel disclosed grants from the National Institutes of Health, Instrumentation Laboratory, Stago, and Siemens; contract fees from the Centers for Disease Control and Prevention; and honoraria from UpToDate unrelated to the current study.
A version of this article originally appeared on Medscape.com.
High-dose prophylactic anticoagulation or therapeutic anticoagulation reduced de novo thrombosis in patients with hypoxemic COVID-19 pneumonia, based on data from 334 adults.
Patients with hypoxemic COVID-19 pneumonia are at increased risk of thrombosis and anticoagulation-related bleeding, therefore data to identify the lowest effective anticoagulant dose are needed, wrote Vincent Labbé, MD, of Sorbonne University, Paris, and colleagues.
Previous studies of different anticoagulation strategies for noncritically ill and critically ill patients with COVID-19 pneumonia have shown contrasting results, but some institutions recommend a high-dose regimen in the wake of data showing macrovascular thrombosis in patients with COVID-19 who were treated with standard anticoagulation, the authors wrote.
However, no previously published studies have compared the effectiveness of the three anticoagulation strategies: high-dose prophylactic anticoagulation (HD-PA), standard dose prophylactic anticoagulation (SD-PA), and therapeutic anticoagulation (TA), they said.
In the open-label Anticoagulation COVID-19 (ANTICOVID) trial, published in JAMA Internal Medicine, the researchers identified consecutively hospitalized adults aged 18 years and older being treated for hypoxemic COVID-19 pneumonia in 23 centers in France between April 2021 and December 2021.
The patients were randomly assigned to SD-PA (116 patients), HD-PA (111 patients), and TA (112 patients) using low-molecular-weight heparin for 14 days, or until either hospital discharge or weaning from supplemental oxygen for 48 consecutive hours, whichever outcome occurred first. The HD-PA patients received two times the SD-PA dose. The mean age of the patients was 58.3 years, and approximately two-thirds were men; race and ethnicity data were not collected. Participants had no macrovascular thrombosis at the start of the study.
The primary outcomes were all-cause mortality and time to clinical improvement (defined as the time from randomization to a 2-point improvement on a 7-category respiratory function scale).
The secondary outcome was a combination of safety and efficacy at day 28 that included a composite of thrombosis (ischemic stroke, noncerebrovascular arterial thrombosis, deep venous thrombosis, pulmonary artery thrombosis, and central venous catheter–related deep venous thrombosis), major bleeding, or all-cause death.
For the primary outcome, results were similar among the groups; HD-PA had no significant benefit over SD-PA or TA. All-cause death rates for SD-PA, HD-PA, and TA patients were 14%, 12%, and 13%, respectively. The time to clinical improvement for the three groups was approximately 8 days, 9 days, and 8 days, respectively. Results for the primary outcome were consistent across all prespecified subgroups.
However, HD-PA was associated with a significant fourfold reduced risk of de novo thrombosis compared with SD-PA (5.5% vs. 20.2%) with no observed increase in major bleeding. TA was not associated with any significant improvement in primary or secondary outcomes compared with HD-PA or SD-PA.
The current study findings of no improvement in survival or disease resolution in patients with a higher anticoagulant dose reflects data from previous studies, the researchers wrote in their discussion. “Our study results together with those of previous RCTs support the premise that the role of microvascular thrombosis in worsening organ dysfunction may be narrower than estimated,” they said.
The findings were limited by several factors including the open-label design and the relatively small sample size, the lack of data on microvascular (vs. macrovascular) thrombosis at baseline, and the predominance of the Delta variant of COVID-19 among the study participants, which may have contributed to a lower mortality rate, the researchers noted.
However, given the significant reduction in de novo thrombosis, the results support the routine use of HD-PA in patients with severe hypoxemic COVID-19 pneumonia, they concluded.
Results inform current clinical practice
Over the course of the COVID-19 pandemic, “Patients hospitalized with COVID-19 manifested the highest risk for thromboembolic complications, especially patients in the intensive care setting,” and early reports suggested that standard prophylactic doses of anticoagulant therapy might be insufficient to prevent thrombotic events, Richard C. Becker, MD, of the University of Cincinnati, and Thomas L. Ortel, MD, of Duke University, Durham, N.C., wrote in an accompanying editorial.
“Although there have been several studies that have investigated the role of anticoagulant therapy in hospitalized patients with COVID-19, this is the first study that specifically compared a standard, prophylactic dose of low-molecular-weight heparin to a ‘high-dose’ prophylactic regimen and to a full therapeutic dose regimen,” Dr. Ortel said in an interview.
“Given the concerns about an increased thrombotic risk with prophylactic dose anticoagulation, and the potential bleeding risk associated with a full therapeutic dose of anticoagulation, this approach enabled the investigators to explore the efficacy and safety of an intermediate dose between these two extremes,” he said.
In the current study, , a finding that was not observed in other studies investigating anticoagulant therapy in hospitalized patients with severe COVID-19,” Dr. Ortel told this news organization. “Much initial concern about progression of disease in patients hospitalized with severe COVID-19 focused on the role of microvascular thrombosis, which appears to be less important in this process, or, alternatively, less responsive to anticoagulant therapy.”
The clinical takeaway from the study, Dr. Ortel said, is the decreased risk for venous thromboembolism with a high-dose prophylactic anticoagulation strategy compared with a standard-dose prophylactic regimen for patients hospitalized with hypoxemic COVID-19 pneumonia, “leading to an improved net clinical outcome.”
Looking ahead, “Additional research is needed to determine whether a higher dose of prophylactic anticoagulation would be beneficial for patients hospitalized with COVID-19 pneumonia who are not in an intensive care unit setting,” Dr. Ortel said. Studies are needed to determine whether therapeutic interventions are equally beneficial in patients with different coronavirus variants, since most patients in the current study were infected with the Delta variant, he added.
The study was supported by LEO Pharma. Dr. Labbé disclosed grants from LEO Pharma during the study and fees from AOP Health unrelated to the current study.
Dr. Becker disclosed personal fees from Novartis Data Safety Monitoring Board, Ionis Data Safety Monitoring Board, and Basking Biosciences Scientific Advisory Board unrelated to the current study. Dr. Ortel disclosed grants from the National Institutes of Health, Instrumentation Laboratory, Stago, and Siemens; contract fees from the Centers for Disease Control and Prevention; and honoraria from UpToDate unrelated to the current study.
A version of this article originally appeared on Medscape.com.
Sleep duration of Black infants increased by intervention
An intervention tailored for Black first-time mothers helped increase their infants’ sleep time, researchers have found, a notable result as many studies have shown Black infants get less sleep on average than White infants.
Less sleep has historically put Black children at higher risk for negative outcomes including obesity and poorer social-emotional functioning and cognitive development. These disparities persist into adulthood, the researchers note, as previous studies have shown.
Justin A. Lavner, PhD, with the department of psychology at the University of Georgia in Athens, led this post hoc secondary analysis of the Sleep SAAF (Strong African American Families) study, a randomized clinical trial of 234 participants comparing a responsive parenting (RP) intervention with a safety control group over the first 16 weeks post partum. The original analysis studied the effects of the intervention on rapid weight gain.
In the original analysis, the authors write that “From birth to 2, the prevalence of high weight for length (above the 95th percentile) is 25% higher among African American children compared to White children. From age 2 to 19, the rate of obesity is more than 50% higher among African American children compared to White children. Similar disparities persist into adulthood: rates of obesity are approximately 25% higher among African American adults compared to White adults.”
The differences in early rapid weight gain may be driving the disparities, the authors write.
Elements of the intervention
The intervention in the current analysis included materials delivered at the 3- and 8-week home visits focused on soothing and crying, feeding, and interactive play in the babies’ first months. Families were recruited from Augusta University Medical Center in Augusta, Ga., and had home visits at 1, 3, 8, and 16 weeks post partum.
Mothers got a packet of handouts and facilitators walked through the information with them. The measures involved hands-on activities, discussion, and videos, all tailored for Black families, the authors state.
Mothers were taught about responding appropriately at night when their baby cries, including giving the baby a couple of minutes to fall back to sleep independently and by using calming messages, such as shushing or white noise, before picking the baby up.
Babies learn to fall asleep on their own
They also learned to put infants to bed early (ideally by 8 p.m.) so the babies would be calm but awake and could learn to fall asleep on their own.
The control group’s guidance was matched for intensity and session length but focused on sleep and home safety, such as reducing the risk of sudden infant death syndrome (SIDS), keeping the baby’s sleep area close to, but away from, the mother’s bed, and preventing shaken baby syndrome.
In both groups, the 3-week visit session lasted about 90-120 minutes and the 8-week visit lasted about 45-60 minutes.
Longer sleep with the intervention
A total of 212 Black mothers, average age 22.7, were randomized – 108 to the RP group and 104 to the control group. Answers on questionnaires were analyzed and at 16 weeks post partum, infants in the RP group (relative to controls) had:
- Longer reported nighttime sleep (mean difference, 40 minutes [95% confidence interval, 3-77]).
- Longer total sleep duration (mean difference, 73 minutes [95% CI, 14-131]).
- Fewer nighttime wakings (mean difference, −0.4 wakings [95% CI, −0.6 to −0.1]).
- Greater likelihood of meeting guidelines of at least 12 hours of sleep per day (risk ratio, 1.4 [95% CI, 1.1 to 1.8]) than controls.
Findings were published in JAMA Network Open.
Additionally, mothers in the RP group more frequently reported they engaged in practices such as letting babies have a few minutes to fall back to sleep on their own (RR, 1.6 [95% CI, 1.0-2.6]) and being less likely to feed their infant just before the baby’s bedtime (RR, 0.5 [95% CI, 0.3-0.8]).
In an accompanying invited commentary, Sarah M. Honaker, PhD, department of pediatrics, Indiana University, Indianapolis, and Alicia Chung, EdD, Center for Early Childhood Health and Development at New York University, write that though the added average sleep duration is one of the most significant findings, there is a possibility of desirability bias because it was reported by the mothers after specific guidance by the facilitators.
“Nonetheless,” the editorialists write, “even if the true effect were half as small, this additional sleep duration could yield notable benefits in infant development if the effect persisted over time. The difference in night wakings between the intervention and control groups (1.8 vs 1.5 per night) at 16 weeks postpartum was statistically significant, though it is unclear whether this difference is clinically meaningful to families.”
They note that it is unclear from the study how the intervention was culturally adapted and how the adaptation might have affected outcomes.
Sleep intervention trials have focused on White families
The editorialists write that much is known about the benefits of behavioral sleep intervention in controlled trials and general population settings, and no adverse effects on infant attachment or cortisol levels have been linked to the interventions.
However, they add, “Unfortunately, this substantial progress in our understanding of infant BSI [behavioral sleep intervention] comes with a caveat, in that most previous studies have been performed with White families from mid-to-high socioeconomic backgrounds.”
Dr. Honaker and Dr. Chung write, “[I]t is important to note that much work remains to examine the acceptability, feasibility, and efficacy of infant BSI in other groups that have been historically marginalized.”
Dr. Lavner and colleagues point out that before their study, there had been little emphasis on interventions to encourage better sleep in general for Black infants, “as most early sleep interventions for this population have focused on SIDS prevention.”
“To our knowledge, Sleep SAAF is the first study to show any benefits of [an] RP intervention on sleep and sleep practices among Black infants and their families,” they write.
The researchers note that a limitation of the study is that the study sample was limited to Black first-time mothers recruited from a single medical center in Georgia.
The study by Dr. Lavner et al. was funded by the National Institutes of Health, a Harrington Faculty Fellowship from the University of Texas, and an award from the Penn State Clinical and Translational Sciences Institute supported by the National Center for Advancing Translational Sciences. Editorialist Dr. Honaker reported receiving grants from Nationwide Children’s Hospital (parent grant, Centers for Disease Control and Prevention) to evaluate the acceptability of infant behavioral sleep intervention in Black families.
An intervention tailored for Black first-time mothers helped increase their infants’ sleep time, researchers have found, a notable result as many studies have shown Black infants get less sleep on average than White infants.
Less sleep has historically put Black children at higher risk for negative outcomes including obesity and poorer social-emotional functioning and cognitive development. These disparities persist into adulthood, the researchers note, as previous studies have shown.
Justin A. Lavner, PhD, with the department of psychology at the University of Georgia in Athens, led this post hoc secondary analysis of the Sleep SAAF (Strong African American Families) study, a randomized clinical trial of 234 participants comparing a responsive parenting (RP) intervention with a safety control group over the first 16 weeks post partum. The original analysis studied the effects of the intervention on rapid weight gain.
In the original analysis, the authors write that “From birth to 2, the prevalence of high weight for length (above the 95th percentile) is 25% higher among African American children compared to White children. From age 2 to 19, the rate of obesity is more than 50% higher among African American children compared to White children. Similar disparities persist into adulthood: rates of obesity are approximately 25% higher among African American adults compared to White adults.”
The differences in early rapid weight gain may be driving the disparities, the authors write.
Elements of the intervention
The intervention in the current analysis included materials delivered at the 3- and 8-week home visits focused on soothing and crying, feeding, and interactive play in the babies’ first months. Families were recruited from Augusta University Medical Center in Augusta, Ga., and had home visits at 1, 3, 8, and 16 weeks post partum.
Mothers got a packet of handouts and facilitators walked through the information with them. The measures involved hands-on activities, discussion, and videos, all tailored for Black families, the authors state.
Mothers were taught about responding appropriately at night when their baby cries, including giving the baby a couple of minutes to fall back to sleep independently and by using calming messages, such as shushing or white noise, before picking the baby up.
Babies learn to fall asleep on their own
They also learned to put infants to bed early (ideally by 8 p.m.) so the babies would be calm but awake and could learn to fall asleep on their own.
The control group’s guidance was matched for intensity and session length but focused on sleep and home safety, such as reducing the risk of sudden infant death syndrome (SIDS), keeping the baby’s sleep area close to, but away from, the mother’s bed, and preventing shaken baby syndrome.
In both groups, the 3-week visit session lasted about 90-120 minutes and the 8-week visit lasted about 45-60 minutes.
Longer sleep with the intervention
A total of 212 Black mothers, average age 22.7, were randomized – 108 to the RP group and 104 to the control group. Answers on questionnaires were analyzed and at 16 weeks post partum, infants in the RP group (relative to controls) had:
- Longer reported nighttime sleep (mean difference, 40 minutes [95% confidence interval, 3-77]).
- Longer total sleep duration (mean difference, 73 minutes [95% CI, 14-131]).
- Fewer nighttime wakings (mean difference, −0.4 wakings [95% CI, −0.6 to −0.1]).
- Greater likelihood of meeting guidelines of at least 12 hours of sleep per day (risk ratio, 1.4 [95% CI, 1.1 to 1.8]) than controls.
Findings were published in JAMA Network Open.
Additionally, mothers in the RP group more frequently reported they engaged in practices such as letting babies have a few minutes to fall back to sleep on their own (RR, 1.6 [95% CI, 1.0-2.6]) and being less likely to feed their infant just before the baby’s bedtime (RR, 0.5 [95% CI, 0.3-0.8]).
In an accompanying invited commentary, Sarah M. Honaker, PhD, department of pediatrics, Indiana University, Indianapolis, and Alicia Chung, EdD, Center for Early Childhood Health and Development at New York University, write that though the added average sleep duration is one of the most significant findings, there is a possibility of desirability bias because it was reported by the mothers after specific guidance by the facilitators.
“Nonetheless,” the editorialists write, “even if the true effect were half as small, this additional sleep duration could yield notable benefits in infant development if the effect persisted over time. The difference in night wakings between the intervention and control groups (1.8 vs 1.5 per night) at 16 weeks postpartum was statistically significant, though it is unclear whether this difference is clinically meaningful to families.”
They note that it is unclear from the study how the intervention was culturally adapted and how the adaptation might have affected outcomes.
Sleep intervention trials have focused on White families
The editorialists write that much is known about the benefits of behavioral sleep intervention in controlled trials and general population settings, and no adverse effects on infant attachment or cortisol levels have been linked to the interventions.
However, they add, “Unfortunately, this substantial progress in our understanding of infant BSI [behavioral sleep intervention] comes with a caveat, in that most previous studies have been performed with White families from mid-to-high socioeconomic backgrounds.”
Dr. Honaker and Dr. Chung write, “[I]t is important to note that much work remains to examine the acceptability, feasibility, and efficacy of infant BSI in other groups that have been historically marginalized.”
Dr. Lavner and colleagues point out that before their study, there had been little emphasis on interventions to encourage better sleep in general for Black infants, “as most early sleep interventions for this population have focused on SIDS prevention.”
“To our knowledge, Sleep SAAF is the first study to show any benefits of [an] RP intervention on sleep and sleep practices among Black infants and their families,” they write.
The researchers note that a limitation of the study is that the study sample was limited to Black first-time mothers recruited from a single medical center in Georgia.
The study by Dr. Lavner et al. was funded by the National Institutes of Health, a Harrington Faculty Fellowship from the University of Texas, and an award from the Penn State Clinical and Translational Sciences Institute supported by the National Center for Advancing Translational Sciences. Editorialist Dr. Honaker reported receiving grants from Nationwide Children’s Hospital (parent grant, Centers for Disease Control and Prevention) to evaluate the acceptability of infant behavioral sleep intervention in Black families.
An intervention tailored for Black first-time mothers helped increase their infants’ sleep time, researchers have found, a notable result as many studies have shown Black infants get less sleep on average than White infants.
Less sleep has historically put Black children at higher risk for negative outcomes including obesity and poorer social-emotional functioning and cognitive development. These disparities persist into adulthood, the researchers note, as previous studies have shown.
Justin A. Lavner, PhD, with the department of psychology at the University of Georgia in Athens, led this post hoc secondary analysis of the Sleep SAAF (Strong African American Families) study, a randomized clinical trial of 234 participants comparing a responsive parenting (RP) intervention with a safety control group over the first 16 weeks post partum. The original analysis studied the effects of the intervention on rapid weight gain.
In the original analysis, the authors write that “From birth to 2, the prevalence of high weight for length (above the 95th percentile) is 25% higher among African American children compared to White children. From age 2 to 19, the rate of obesity is more than 50% higher among African American children compared to White children. Similar disparities persist into adulthood: rates of obesity are approximately 25% higher among African American adults compared to White adults.”
The differences in early rapid weight gain may be driving the disparities, the authors write.
Elements of the intervention
The intervention in the current analysis included materials delivered at the 3- and 8-week home visits focused on soothing and crying, feeding, and interactive play in the babies’ first months. Families were recruited from Augusta University Medical Center in Augusta, Ga., and had home visits at 1, 3, 8, and 16 weeks post partum.
Mothers got a packet of handouts and facilitators walked through the information with them. The measures involved hands-on activities, discussion, and videos, all tailored for Black families, the authors state.
Mothers were taught about responding appropriately at night when their baby cries, including giving the baby a couple of minutes to fall back to sleep independently and by using calming messages, such as shushing or white noise, before picking the baby up.
Babies learn to fall asleep on their own
They also learned to put infants to bed early (ideally by 8 p.m.) so the babies would be calm but awake and could learn to fall asleep on their own.
The control group’s guidance was matched for intensity and session length but focused on sleep and home safety, such as reducing the risk of sudden infant death syndrome (SIDS), keeping the baby’s sleep area close to, but away from, the mother’s bed, and preventing shaken baby syndrome.
In both groups, the 3-week visit session lasted about 90-120 minutes and the 8-week visit lasted about 45-60 minutes.
Longer sleep with the intervention
A total of 212 Black mothers, average age 22.7, were randomized – 108 to the RP group and 104 to the control group. Answers on questionnaires were analyzed and at 16 weeks post partum, infants in the RP group (relative to controls) had:
- Longer reported nighttime sleep (mean difference, 40 minutes [95% confidence interval, 3-77]).
- Longer total sleep duration (mean difference, 73 minutes [95% CI, 14-131]).
- Fewer nighttime wakings (mean difference, −0.4 wakings [95% CI, −0.6 to −0.1]).
- Greater likelihood of meeting guidelines of at least 12 hours of sleep per day (risk ratio, 1.4 [95% CI, 1.1 to 1.8]) than controls.
Findings were published in JAMA Network Open.
Additionally, mothers in the RP group more frequently reported they engaged in practices such as letting babies have a few minutes to fall back to sleep on their own (RR, 1.6 [95% CI, 1.0-2.6]) and being less likely to feed their infant just before the baby’s bedtime (RR, 0.5 [95% CI, 0.3-0.8]).
In an accompanying invited commentary, Sarah M. Honaker, PhD, department of pediatrics, Indiana University, Indianapolis, and Alicia Chung, EdD, Center for Early Childhood Health and Development at New York University, write that though the added average sleep duration is one of the most significant findings, there is a possibility of desirability bias because it was reported by the mothers after specific guidance by the facilitators.
“Nonetheless,” the editorialists write, “even if the true effect were half as small, this additional sleep duration could yield notable benefits in infant development if the effect persisted over time. The difference in night wakings between the intervention and control groups (1.8 vs 1.5 per night) at 16 weeks postpartum was statistically significant, though it is unclear whether this difference is clinically meaningful to families.”
They note that it is unclear from the study how the intervention was culturally adapted and how the adaptation might have affected outcomes.
Sleep intervention trials have focused on White families
The editorialists write that much is known about the benefits of behavioral sleep intervention in controlled trials and general population settings, and no adverse effects on infant attachment or cortisol levels have been linked to the interventions.
However, they add, “Unfortunately, this substantial progress in our understanding of infant BSI [behavioral sleep intervention] comes with a caveat, in that most previous studies have been performed with White families from mid-to-high socioeconomic backgrounds.”
Dr. Honaker and Dr. Chung write, “[I]t is important to note that much work remains to examine the acceptability, feasibility, and efficacy of infant BSI in other groups that have been historically marginalized.”
Dr. Lavner and colleagues point out that before their study, there had been little emphasis on interventions to encourage better sleep in general for Black infants, “as most early sleep interventions for this population have focused on SIDS prevention.”
“To our knowledge, Sleep SAAF is the first study to show any benefits of [an] RP intervention on sleep and sleep practices among Black infants and their families,” they write.
The researchers note that a limitation of the study is that the study sample was limited to Black first-time mothers recruited from a single medical center in Georgia.
The study by Dr. Lavner et al. was funded by the National Institutes of Health, a Harrington Faculty Fellowship from the University of Texas, and an award from the Penn State Clinical and Translational Sciences Institute supported by the National Center for Advancing Translational Sciences. Editorialist Dr. Honaker reported receiving grants from Nationwide Children’s Hospital (parent grant, Centers for Disease Control and Prevention) to evaluate the acceptability of infant behavioral sleep intervention in Black families.
FROM JAMA NETWORK OPEN
‘Excess’ deaths surging, but why?
This transcript has been edited for clarity.
“Excess deaths.” You’ve heard the phrase countless times by now. It is one of the myriad of previously esoteric epidemiology terms that the pandemic brought squarely into the zeitgeist.
As a sort of standard candle of the performance of a state or a region or a country in terms of health care, it has a lot of utility – if for nothing more than Monday-morning quarterbacking. But this week, I want to dig in on the concept a bit because, according to a new study, the excess death gap between the United States and Western Europe has never been higher.
You might imagine that the best way to figure this out is for some group of intelligent people to review each death and decide, somehow, whether it was expected or not. But aside from being impractical, this would end up being somewhat subjective. That older person who died from pneumonia – was that an expected death? Could it have been avoided?
Rather, the calculation of excess mortality relies on large numbers and statistical inference to compare an expected number of deaths with those that are observed.
The difference is excess mortality, even if you can never be sure whether any particular death was expected or not.
As always, however, the devil is in the details. What data do you use to define the expected number of deaths?
There are options here. Probably the most straightforward analysis uses past data from the country of interest. You look at annual deaths over some historical period of time and compare those numbers with the rates today. Two issues need to be accounted for here: population growth – a larger population will have more deaths, so you need to adjust the historical population with current levels, and demographic shifts – an older or more male population will have more deaths, so you need to adjust for that as well.
But provided you take care of those factors, you can estimate fairly well how many deaths you can expect to see in any given period of time.
Still, you should see right away that excess mortality is a relative concept. If you think that, just perhaps, the United States has some systematic failure to deliver care that has been stable and persistent over time, you wouldn’t capture that failing in an excess mortality calculation that uses U.S. historical data as the baseline.
The best way to get around that is to use data from other countries, and that’s just what this article – a rare single-author piece by Patrick Heuveline – does, calculating excess deaths in the United States by standardizing our mortality rates to the five largest Western European countries: the United Kingdom, France, Germany, Italy, and Spain.
Controlling for the differences in the demographics of that European population, here is the expected number of deaths in the United States over the past 5 years.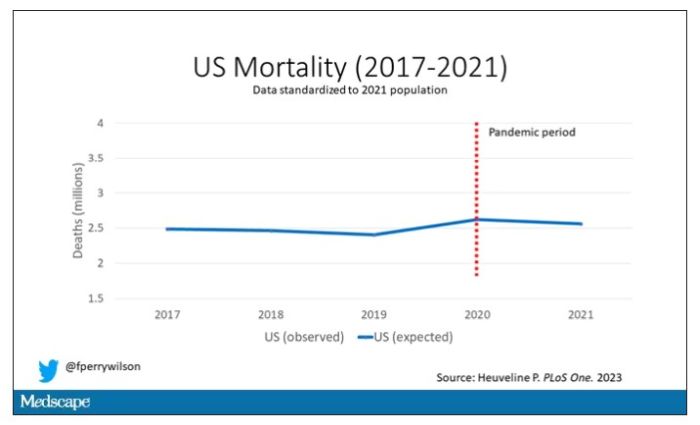
Note that there is a small uptick in expected deaths in 2020, reflecting the pandemic, which returns to baseline levels by 2021. This is because that’s what happened in Europe; by 2021, the excess mortality due to COVID-19 was quite low.
Here are the actual deaths in the US during that time.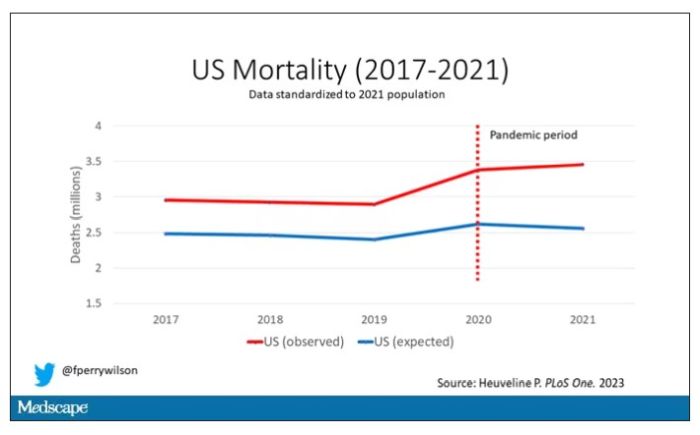
Highlighted here in green, then, is the excess mortality over time in the United States.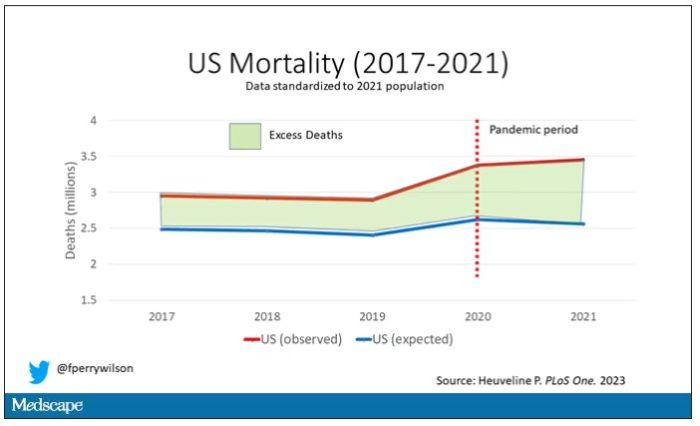
There are some fascinating and concerning findings here.
First of all, you can see that even before the pandemic, the United States has an excess mortality problem. This is not entirely a surprise; we’ve known that so-called “deaths of despair,” those due to alcohol abuse, drug overdoses, and suicide, are at an all-time high and tend to affect a “prime of life” population that would not otherwise be expected to die. In fact, fully 50% of the excess deaths in the United States occur in those between ages 15 and 64.
Excess deaths are also a concerning percentage of total deaths. In 2017, 17% of total deaths in the United States could be considered “excess.” In 2021, that number had doubled to 35%. Nearly 900,000 individuals in the United States died in 2021 who perhaps didn’t need to.
The obvious culprit to blame here is COVID, but COVID-associated excess deaths only explain about 50% of the excess we see in 2021. The rest reflect something even more concerning: a worsening of the failures of the past, perhaps exacerbated by the pandemic but not due to the virus itself.
Of course, we started this discussion acknowledging that the calculation of excess mortality is exquisitely dependent on how you model the expected number of deaths, and I’m sure some will take issue with the use of European numbers when applied to Americans. After all, Europe has, by and large, a robust public health service, socialized medicine, and healthcare that does not run the risk of bankrupting its citizens. How can we compare our outcomes to a place like that?
How indeed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven,Conn. He reported no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
“Excess deaths.” You’ve heard the phrase countless times by now. It is one of the myriad of previously esoteric epidemiology terms that the pandemic brought squarely into the zeitgeist.
As a sort of standard candle of the performance of a state or a region or a country in terms of health care, it has a lot of utility – if for nothing more than Monday-morning quarterbacking. But this week, I want to dig in on the concept a bit because, according to a new study, the excess death gap between the United States and Western Europe has never been higher.
You might imagine that the best way to figure this out is for some group of intelligent people to review each death and decide, somehow, whether it was expected or not. But aside from being impractical, this would end up being somewhat subjective. That older person who died from pneumonia – was that an expected death? Could it have been avoided?
Rather, the calculation of excess mortality relies on large numbers and statistical inference to compare an expected number of deaths with those that are observed.
The difference is excess mortality, even if you can never be sure whether any particular death was expected or not.
As always, however, the devil is in the details. What data do you use to define the expected number of deaths?
There are options here. Probably the most straightforward analysis uses past data from the country of interest. You look at annual deaths over some historical period of time and compare those numbers with the rates today. Two issues need to be accounted for here: population growth – a larger population will have more deaths, so you need to adjust the historical population with current levels, and demographic shifts – an older or more male population will have more deaths, so you need to adjust for that as well.
But provided you take care of those factors, you can estimate fairly well how many deaths you can expect to see in any given period of time.
Still, you should see right away that excess mortality is a relative concept. If you think that, just perhaps, the United States has some systematic failure to deliver care that has been stable and persistent over time, you wouldn’t capture that failing in an excess mortality calculation that uses U.S. historical data as the baseline.
The best way to get around that is to use data from other countries, and that’s just what this article – a rare single-author piece by Patrick Heuveline – does, calculating excess deaths in the United States by standardizing our mortality rates to the five largest Western European countries: the United Kingdom, France, Germany, Italy, and Spain.
Controlling for the differences in the demographics of that European population, here is the expected number of deaths in the United States over the past 5 years.
Note that there is a small uptick in expected deaths in 2020, reflecting the pandemic, which returns to baseline levels by 2021. This is because that’s what happened in Europe; by 2021, the excess mortality due to COVID-19 was quite low.
Here are the actual deaths in the US during that time.
Highlighted here in green, then, is the excess mortality over time in the United States.
There are some fascinating and concerning findings here.
First of all, you can see that even before the pandemic, the United States has an excess mortality problem. This is not entirely a surprise; we’ve known that so-called “deaths of despair,” those due to alcohol abuse, drug overdoses, and suicide, are at an all-time high and tend to affect a “prime of life” population that would not otherwise be expected to die. In fact, fully 50% of the excess deaths in the United States occur in those between ages 15 and 64.
Excess deaths are also a concerning percentage of total deaths. In 2017, 17% of total deaths in the United States could be considered “excess.” In 2021, that number had doubled to 35%. Nearly 900,000 individuals in the United States died in 2021 who perhaps didn’t need to.
The obvious culprit to blame here is COVID, but COVID-associated excess deaths only explain about 50% of the excess we see in 2021. The rest reflect something even more concerning: a worsening of the failures of the past, perhaps exacerbated by the pandemic but not due to the virus itself.
Of course, we started this discussion acknowledging that the calculation of excess mortality is exquisitely dependent on how you model the expected number of deaths, and I’m sure some will take issue with the use of European numbers when applied to Americans. After all, Europe has, by and large, a robust public health service, socialized medicine, and healthcare that does not run the risk of bankrupting its citizens. How can we compare our outcomes to a place like that?
How indeed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven,Conn. He reported no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
“Excess deaths.” You’ve heard the phrase countless times by now. It is one of the myriad of previously esoteric epidemiology terms that the pandemic brought squarely into the zeitgeist.
As a sort of standard candle of the performance of a state or a region or a country in terms of health care, it has a lot of utility – if for nothing more than Monday-morning quarterbacking. But this week, I want to dig in on the concept a bit because, according to a new study, the excess death gap between the United States and Western Europe has never been higher.
You might imagine that the best way to figure this out is for some group of intelligent people to review each death and decide, somehow, whether it was expected or not. But aside from being impractical, this would end up being somewhat subjective. That older person who died from pneumonia – was that an expected death? Could it have been avoided?
Rather, the calculation of excess mortality relies on large numbers and statistical inference to compare an expected number of deaths with those that are observed.
The difference is excess mortality, even if you can never be sure whether any particular death was expected or not.
As always, however, the devil is in the details. What data do you use to define the expected number of deaths?
There are options here. Probably the most straightforward analysis uses past data from the country of interest. You look at annual deaths over some historical period of time and compare those numbers with the rates today. Two issues need to be accounted for here: population growth – a larger population will have more deaths, so you need to adjust the historical population with current levels, and demographic shifts – an older or more male population will have more deaths, so you need to adjust for that as well.
But provided you take care of those factors, you can estimate fairly well how many deaths you can expect to see in any given period of time.
Still, you should see right away that excess mortality is a relative concept. If you think that, just perhaps, the United States has some systematic failure to deliver care that has been stable and persistent over time, you wouldn’t capture that failing in an excess mortality calculation that uses U.S. historical data as the baseline.
The best way to get around that is to use data from other countries, and that’s just what this article – a rare single-author piece by Patrick Heuveline – does, calculating excess deaths in the United States by standardizing our mortality rates to the five largest Western European countries: the United Kingdom, France, Germany, Italy, and Spain.
Controlling for the differences in the demographics of that European population, here is the expected number of deaths in the United States over the past 5 years.
Note that there is a small uptick in expected deaths in 2020, reflecting the pandemic, which returns to baseline levels by 2021. This is because that’s what happened in Europe; by 2021, the excess mortality due to COVID-19 was quite low.
Here are the actual deaths in the US during that time.
Highlighted here in green, then, is the excess mortality over time in the United States.
There are some fascinating and concerning findings here.
First of all, you can see that even before the pandemic, the United States has an excess mortality problem. This is not entirely a surprise; we’ve known that so-called “deaths of despair,” those due to alcohol abuse, drug overdoses, and suicide, are at an all-time high and tend to affect a “prime of life” population that would not otherwise be expected to die. In fact, fully 50% of the excess deaths in the United States occur in those between ages 15 and 64.
Excess deaths are also a concerning percentage of total deaths. In 2017, 17% of total deaths in the United States could be considered “excess.” In 2021, that number had doubled to 35%. Nearly 900,000 individuals in the United States died in 2021 who perhaps didn’t need to.
The obvious culprit to blame here is COVID, but COVID-associated excess deaths only explain about 50% of the excess we see in 2021. The rest reflect something even more concerning: a worsening of the failures of the past, perhaps exacerbated by the pandemic but not due to the virus itself.
Of course, we started this discussion acknowledging that the calculation of excess mortality is exquisitely dependent on how you model the expected number of deaths, and I’m sure some will take issue with the use of European numbers when applied to Americans. After all, Europe has, by and large, a robust public health service, socialized medicine, and healthcare that does not run the risk of bankrupting its citizens. How can we compare our outcomes to a place like that?
How indeed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven,Conn. He reported no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.