User login
Lapatinib, paclitaxel combo didn’t score for HER2-positive gastric cancers
Lapatinib in combination with paclitaxel conferred no overall survival benefit over paclitaxel alone for patients with advanced HER2-positive gastric cancer.
However, the combined treatment did show some benefit for those whose cancers were highly expressed, Dr. Taroh Satoh and his colleagues wrote online May 27 in the Journal of Clinical Oncology (J. Clin. Oncol. 2014 May 27 [doi: 10.1200/JCO.2013.53.6136]).
The Asian study also found that Chinese patients responded better to the combination treatment than did Japanese patients, said Dr. Satoh of Osaka University, Japan, and his coauthors.
The year-long TyTAN (Tykerb with Taxol in Asian HER2-Positive Gastric Cancer) study randomized 261 patients (mean age, 60 years) to two treatment arms: oral lapatinib (Tykerb) 1,500 mg once per day plus paclitaxel (Taxol) 80 mg/m2 infusions on days 1, 8, and 15 of a 4-week cycle; or paclitaxel 80 mg/m2 alone.
The study included patients from Japan, mainland China, South Korea, and Taiwan. All cancers were HER2-positive by fluorescence in situ hybridization.
There was no difference in median overall survival between the combination and monotherapy groups (11 vs. 9 months, respectively; P = .104). The median progression-free survival time and time to progression were similar in the combination and monotherapy groups (5.5 vs. 4.4 months, respectively).
Response duration was numerically longer with the combination treatment (7.4 vs. 5 months), but that difference was not statistically significant. However, significantly more patients taking the combination did respond to treatment (27% vs. 9%; odds ratio, 3.85).
Subgroup analyses revealed some significant differences in treatment effect. Patients who had not undergone a gastrectomy did better when they took the combination therapy, with an overall 37% decrease in the risk of disease progression or death compared with paclitaxel alone. Patients with highly expressed HER2 cancers did better on the combination as well, with a 41% reduced risk of death, a longer period of progression-free survival (5.6 vs. 4.2 months), and a 46% reduction in the risk or death. Patients with poorly or moderately expressed HER2 didn’t experience any significantly improved benefits with the combination over paclitaxel alone.
The subgroup analysis also found that Chinese patients responded better to the combination treatment than to monotherapy, with significantly better overall survival (9.7 vs. 7.6 months) and progression-free survival (7.2 vs. 4.7 months). Japanese patients did not experience significant benefits in either of these outcomes.
The most common adverse events were diarrhea, alopecia, and neutropenia. Combination therapy was associated with more adverse events leading to discontinuation than paclitaxel alone (16% vs. 9%). The most frequent of these were diarrhea (3 patients) and decreased appetite (3) in the combination group, and peripheral sensory neuropathy (3) in the monotherapy group.
There was a high incidence of neutropenia (65% in the combination group; 50% in the monotherapy group), with nine patients in the combination group and two in the monotherapy group developing febrile neutropenia.
There were more nonfatal serious adverse events in the lapatinib plus paclitaxel group than in the paclitaxel-alone group (26% vs. 15%). These included febrile neutropenia, reduced appetite, neutropenia, pneumonia, abdominal pain, nausea, device-related infection, diarrhea, and vomiting. Diarrhea, alopecia, neutropenia, and leucopenia were more common in Japanese than Chinese patients.
Nine patients experienced a total of 10 fatal adverse events. Six of these were in the combination group, with four considered to be treatment related (diarrhea, acute myocardial infarction, acute left ventricular failure, and cardiac arrest).
Three patients in the monotherapy group experienced a total of four fatal adverse events (subileus, gastrointestinal perforation, and gastrointestinal hemorrhage), but they were not considered treatment related. Three of the fatal events were cardiac and considered to be paclitaxel related. All occurred in Chinese patients.
The study was sponsored by GlaxoSmithKline. Dr. Satoh has received honoraria from GlaxoSmithKline and Bristol-Myers Squibb. Many of the coauthors also disclosed relationships with GlaxoSmithKline and other companies.
Lapatinib in combination with paclitaxel conferred no overall survival benefit over paclitaxel alone for patients with advanced HER2-positive gastric cancer.
However, the combined treatment did show some benefit for those whose cancers were highly expressed, Dr. Taroh Satoh and his colleagues wrote online May 27 in the Journal of Clinical Oncology (J. Clin. Oncol. 2014 May 27 [doi: 10.1200/JCO.2013.53.6136]).
The Asian study also found that Chinese patients responded better to the combination treatment than did Japanese patients, said Dr. Satoh of Osaka University, Japan, and his coauthors.
The year-long TyTAN (Tykerb with Taxol in Asian HER2-Positive Gastric Cancer) study randomized 261 patients (mean age, 60 years) to two treatment arms: oral lapatinib (Tykerb) 1,500 mg once per day plus paclitaxel (Taxol) 80 mg/m2 infusions on days 1, 8, and 15 of a 4-week cycle; or paclitaxel 80 mg/m2 alone.
The study included patients from Japan, mainland China, South Korea, and Taiwan. All cancers were HER2-positive by fluorescence in situ hybridization.
There was no difference in median overall survival between the combination and monotherapy groups (11 vs. 9 months, respectively; P = .104). The median progression-free survival time and time to progression were similar in the combination and monotherapy groups (5.5 vs. 4.4 months, respectively).
Response duration was numerically longer with the combination treatment (7.4 vs. 5 months), but that difference was not statistically significant. However, significantly more patients taking the combination did respond to treatment (27% vs. 9%; odds ratio, 3.85).
Subgroup analyses revealed some significant differences in treatment effect. Patients who had not undergone a gastrectomy did better when they took the combination therapy, with an overall 37% decrease in the risk of disease progression or death compared with paclitaxel alone. Patients with highly expressed HER2 cancers did better on the combination as well, with a 41% reduced risk of death, a longer period of progression-free survival (5.6 vs. 4.2 months), and a 46% reduction in the risk or death. Patients with poorly or moderately expressed HER2 didn’t experience any significantly improved benefits with the combination over paclitaxel alone.
The subgroup analysis also found that Chinese patients responded better to the combination treatment than to monotherapy, with significantly better overall survival (9.7 vs. 7.6 months) and progression-free survival (7.2 vs. 4.7 months). Japanese patients did not experience significant benefits in either of these outcomes.
The most common adverse events were diarrhea, alopecia, and neutropenia. Combination therapy was associated with more adverse events leading to discontinuation than paclitaxel alone (16% vs. 9%). The most frequent of these were diarrhea (3 patients) and decreased appetite (3) in the combination group, and peripheral sensory neuropathy (3) in the monotherapy group.
There was a high incidence of neutropenia (65% in the combination group; 50% in the monotherapy group), with nine patients in the combination group and two in the monotherapy group developing febrile neutropenia.
There were more nonfatal serious adverse events in the lapatinib plus paclitaxel group than in the paclitaxel-alone group (26% vs. 15%). These included febrile neutropenia, reduced appetite, neutropenia, pneumonia, abdominal pain, nausea, device-related infection, diarrhea, and vomiting. Diarrhea, alopecia, neutropenia, and leucopenia were more common in Japanese than Chinese patients.
Nine patients experienced a total of 10 fatal adverse events. Six of these were in the combination group, with four considered to be treatment related (diarrhea, acute myocardial infarction, acute left ventricular failure, and cardiac arrest).
Three patients in the monotherapy group experienced a total of four fatal adverse events (subileus, gastrointestinal perforation, and gastrointestinal hemorrhage), but they were not considered treatment related. Three of the fatal events were cardiac and considered to be paclitaxel related. All occurred in Chinese patients.
The study was sponsored by GlaxoSmithKline. Dr. Satoh has received honoraria from GlaxoSmithKline and Bristol-Myers Squibb. Many of the coauthors also disclosed relationships with GlaxoSmithKline and other companies.
Lapatinib in combination with paclitaxel conferred no overall survival benefit over paclitaxel alone for patients with advanced HER2-positive gastric cancer.
However, the combined treatment did show some benefit for those whose cancers were highly expressed, Dr. Taroh Satoh and his colleagues wrote online May 27 in the Journal of Clinical Oncology (J. Clin. Oncol. 2014 May 27 [doi: 10.1200/JCO.2013.53.6136]).
The Asian study also found that Chinese patients responded better to the combination treatment than did Japanese patients, said Dr. Satoh of Osaka University, Japan, and his coauthors.
The year-long TyTAN (Tykerb with Taxol in Asian HER2-Positive Gastric Cancer) study randomized 261 patients (mean age, 60 years) to two treatment arms: oral lapatinib (Tykerb) 1,500 mg once per day plus paclitaxel (Taxol) 80 mg/m2 infusions on days 1, 8, and 15 of a 4-week cycle; or paclitaxel 80 mg/m2 alone.
The study included patients from Japan, mainland China, South Korea, and Taiwan. All cancers were HER2-positive by fluorescence in situ hybridization.
There was no difference in median overall survival between the combination and monotherapy groups (11 vs. 9 months, respectively; P = .104). The median progression-free survival time and time to progression were similar in the combination and monotherapy groups (5.5 vs. 4.4 months, respectively).
Response duration was numerically longer with the combination treatment (7.4 vs. 5 months), but that difference was not statistically significant. However, significantly more patients taking the combination did respond to treatment (27% vs. 9%; odds ratio, 3.85).
Subgroup analyses revealed some significant differences in treatment effect. Patients who had not undergone a gastrectomy did better when they took the combination therapy, with an overall 37% decrease in the risk of disease progression or death compared with paclitaxel alone. Patients with highly expressed HER2 cancers did better on the combination as well, with a 41% reduced risk of death, a longer period of progression-free survival (5.6 vs. 4.2 months), and a 46% reduction in the risk or death. Patients with poorly or moderately expressed HER2 didn’t experience any significantly improved benefits with the combination over paclitaxel alone.
The subgroup analysis also found that Chinese patients responded better to the combination treatment than to monotherapy, with significantly better overall survival (9.7 vs. 7.6 months) and progression-free survival (7.2 vs. 4.7 months). Japanese patients did not experience significant benefits in either of these outcomes.
The most common adverse events were diarrhea, alopecia, and neutropenia. Combination therapy was associated with more adverse events leading to discontinuation than paclitaxel alone (16% vs. 9%). The most frequent of these were diarrhea (3 patients) and decreased appetite (3) in the combination group, and peripheral sensory neuropathy (3) in the monotherapy group.
There was a high incidence of neutropenia (65% in the combination group; 50% in the monotherapy group), with nine patients in the combination group and two in the monotherapy group developing febrile neutropenia.
There were more nonfatal serious adverse events in the lapatinib plus paclitaxel group than in the paclitaxel-alone group (26% vs. 15%). These included febrile neutropenia, reduced appetite, neutropenia, pneumonia, abdominal pain, nausea, device-related infection, diarrhea, and vomiting. Diarrhea, alopecia, neutropenia, and leucopenia were more common in Japanese than Chinese patients.
Nine patients experienced a total of 10 fatal adverse events. Six of these were in the combination group, with four considered to be treatment related (diarrhea, acute myocardial infarction, acute left ventricular failure, and cardiac arrest).
Three patients in the monotherapy group experienced a total of four fatal adverse events (subileus, gastrointestinal perforation, and gastrointestinal hemorrhage), but they were not considered treatment related. Three of the fatal events were cardiac and considered to be paclitaxel related. All occurred in Chinese patients.
The study was sponsored by GlaxoSmithKline. Dr. Satoh has received honoraria from GlaxoSmithKline and Bristol-Myers Squibb. Many of the coauthors also disclosed relationships with GlaxoSmithKline and other companies.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Lapatinib plus paclitaxel conferred no overall survival benefit in advanced, HER-positive gastric cancer.
Major finding: There was no difference in median overall survival between the combination and monotherapy groups (11 vs. 9 months; P = .104).
Data source: The TyTAN study randomized 261 patients to oral lapatinib 1,500 mg once daily plus paclitaxel 80 mg/m2 infusions on days 1, 8, and 15 of a 4-week cycle; or paclitaxel 80 mg/m2 alone.
Disclosures: The study was sponsored by GlaxoSmithKline. Dr. Satoh has received honoraria from GlaxoSmithKline and Bristol-Myers Squibb. Many of the coauthors also disclosed relationships with GlaxoSmithKline and other companies.
Type 2 diabetes remits in some bariatric surgery patients
In a group of moderately obese patients with type 2 diabetes, Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding resulted in complete disease remission in 17% and 23%, respectively.
Partial remission was significantly more common among the Roux-en-Y patients, with 50% achieving it, compared with 27% of the gastric banding patients, Dr. Anita Courcoulas and her colleagues reported in the June 4 online issue of JAMA Surgery (JAMA Surg. 2014 [doi:10.1001/jamasurg.2014.467]). There were no partial or complete remissions in the study’s third arm – a year-long intensive lifestyle-management program.

The results are encouraging, but because the study had only 69 patients with just 1 year of follow-up, "no definitive conclusions can be drawn," about the durability of disease remission, Dr. Courcoulas, a bariatric surgeon at the University of Pittsburgh Medical Center, and her associates wrote.
"Nevertheless, the [lifestyle management arm] had no remission, so these results suggest that the gastric banding procedure – low risk and potentially reversible – may have a place as a treatment option for patients with low body mass index and type 2 diabetes. Further studies will be needed to confirm these results," the investigators wrote.
The patients were an average of 47 years old, with a mean body mass index (BMI) of 35 kg/m2. The mean duration of type 2 diabetes was 6 years. The average HbA1c was 8%. Almost all were taking some kind of antidiabetic medication; 40 were on oral drugs, and 26 were taking insulin.
By 1 year, there were no cases of partial or complete remission in the lifestyle intervention group. In the Roux-en-Y group, 50% experienced a partial remission and 17% a complete remission. In the gastric banding group, 27% experienced a partial remission and 23% a complete remission.
Patients in the Roux-en-Y group lost significantly more weight than those in the banding or lifestyle groups (27% vs. 17% and 10% respectively). HbA1c improved significantly more in the Roux-en-Y group than in the banding or lifestyle groups as well. Significantly more surgical patients than lifestyle patients were able to be off all antidiabetic medications (58% vs. 36% and 4%, respectively).
Surgical safety was good, with six patients needing one additional hospital night for nausea or glucose management. One banding patient needed a port replacement, and three others had minor clinical problems. There were three serious adverse events, including an anastomotic ulcer in one Roux-en-Y patient and dehydration requiring a hospital stay in two gastric banding patients.
The study also highlighted some of the problems with accruing and retaining patients in weight loss trials, the investigators noted. Of 667 screened patients, 69 (10%) were randomized. Of these, seven refused their assigned treatment, and one was excluded from treatment on the procedure day. Six had incomplete follow-up and five – all in the lifestyle intervention arm – withdrew by 6 months.
Because the planned 12-month follow-up was too short to allow any conclusions about the stability of diabetes remission in treated patients, longer follow-up is crucial and will require considerable financial investments.
"These important feasibility issues – the need for targeted screening, the thorough assessment of clinical equipoise to reduce the likelihood of postrandomization dropout, the challenging retention in the [lifestyle] arm, and funding – raise a number of concerns for the scalability of this type of study to a larger multicenter trial. For this reason, pursuing alternative methods to obtain high-order evidence regarding outcomes of surgical vs. nonsurgical treatment may be more reasonable for people with a relatively low BMI," they said.
The study was funded by the National Institutes of Health. Dr. Courcoulas disclosed financial relationships with Covidien, EndoGastric Solutions, Nutrisystem, and Ethicon J&J Healthcare. Some of the other authors disclosed financial relationships with a variety of pharmaceutical companies.
In a group of moderately obese patients with type 2 diabetes, Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding resulted in complete disease remission in 17% and 23%, respectively.
Partial remission was significantly more common among the Roux-en-Y patients, with 50% achieving it, compared with 27% of the gastric banding patients, Dr. Anita Courcoulas and her colleagues reported in the June 4 online issue of JAMA Surgery (JAMA Surg. 2014 [doi:10.1001/jamasurg.2014.467]). There were no partial or complete remissions in the study’s third arm – a year-long intensive lifestyle-management program.
The results are encouraging, but because the study had only 69 patients with just 1 year of follow-up, "no definitive conclusions can be drawn," about the durability of disease remission, Dr. Courcoulas, a bariatric surgeon at the University of Pittsburgh Medical Center, and her associates wrote.
"Nevertheless, the [lifestyle management arm] had no remission, so these results suggest that the gastric banding procedure – low risk and potentially reversible – may have a place as a treatment option for patients with low body mass index and type 2 diabetes. Further studies will be needed to confirm these results," the investigators wrote.
The patients were an average of 47 years old, with a mean body mass index (BMI) of 35 kg/m2. The mean duration of type 2 diabetes was 6 years. The average HbA1c was 8%. Almost all were taking some kind of antidiabetic medication; 40 were on oral drugs, and 26 were taking insulin.
By 1 year, there were no cases of partial or complete remission in the lifestyle intervention group. In the Roux-en-Y group, 50% experienced a partial remission and 17% a complete remission. In the gastric banding group, 27% experienced a partial remission and 23% a complete remission.
Patients in the Roux-en-Y group lost significantly more weight than those in the banding or lifestyle groups (27% vs. 17% and 10% respectively). HbA1c improved significantly more in the Roux-en-Y group than in the banding or lifestyle groups as well. Significantly more surgical patients than lifestyle patients were able to be off all antidiabetic medications (58% vs. 36% and 4%, respectively).
Surgical safety was good, with six patients needing one additional hospital night for nausea or glucose management. One banding patient needed a port replacement, and three others had minor clinical problems. There were three serious adverse events, including an anastomotic ulcer in one Roux-en-Y patient and dehydration requiring a hospital stay in two gastric banding patients.
The study also highlighted some of the problems with accruing and retaining patients in weight loss trials, the investigators noted. Of 667 screened patients, 69 (10%) were randomized. Of these, seven refused their assigned treatment, and one was excluded from treatment on the procedure day. Six had incomplete follow-up and five – all in the lifestyle intervention arm – withdrew by 6 months.
Because the planned 12-month follow-up was too short to allow any conclusions about the stability of diabetes remission in treated patients, longer follow-up is crucial and will require considerable financial investments.
"These important feasibility issues – the need for targeted screening, the thorough assessment of clinical equipoise to reduce the likelihood of postrandomization dropout, the challenging retention in the [lifestyle] arm, and funding – raise a number of concerns for the scalability of this type of study to a larger multicenter trial. For this reason, pursuing alternative methods to obtain high-order evidence regarding outcomes of surgical vs. nonsurgical treatment may be more reasonable for people with a relatively low BMI," they said.
The study was funded by the National Institutes of Health. Dr. Courcoulas disclosed financial relationships with Covidien, EndoGastric Solutions, Nutrisystem, and Ethicon J&J Healthcare. Some of the other authors disclosed financial relationships with a variety of pharmaceutical companies.
In a group of moderately obese patients with type 2 diabetes, Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding resulted in complete disease remission in 17% and 23%, respectively.
Partial remission was significantly more common among the Roux-en-Y patients, with 50% achieving it, compared with 27% of the gastric banding patients, Dr. Anita Courcoulas and her colleagues reported in the June 4 online issue of JAMA Surgery (JAMA Surg. 2014 [doi:10.1001/jamasurg.2014.467]). There were no partial or complete remissions in the study’s third arm – a year-long intensive lifestyle-management program.
The results are encouraging, but because the study had only 69 patients with just 1 year of follow-up, "no definitive conclusions can be drawn," about the durability of disease remission, Dr. Courcoulas, a bariatric surgeon at the University of Pittsburgh Medical Center, and her associates wrote.
"Nevertheless, the [lifestyle management arm] had no remission, so these results suggest that the gastric banding procedure – low risk and potentially reversible – may have a place as a treatment option for patients with low body mass index and type 2 diabetes. Further studies will be needed to confirm these results," the investigators wrote.
The patients were an average of 47 years old, with a mean body mass index (BMI) of 35 kg/m2. The mean duration of type 2 diabetes was 6 years. The average HbA1c was 8%. Almost all were taking some kind of antidiabetic medication; 40 were on oral drugs, and 26 were taking insulin.
By 1 year, there were no cases of partial or complete remission in the lifestyle intervention group. In the Roux-en-Y group, 50% experienced a partial remission and 17% a complete remission. In the gastric banding group, 27% experienced a partial remission and 23% a complete remission.
Patients in the Roux-en-Y group lost significantly more weight than those in the banding or lifestyle groups (27% vs. 17% and 10% respectively). HbA1c improved significantly more in the Roux-en-Y group than in the banding or lifestyle groups as well. Significantly more surgical patients than lifestyle patients were able to be off all antidiabetic medications (58% vs. 36% and 4%, respectively).
Surgical safety was good, with six patients needing one additional hospital night for nausea or glucose management. One banding patient needed a port replacement, and three others had minor clinical problems. There were three serious adverse events, including an anastomotic ulcer in one Roux-en-Y patient and dehydration requiring a hospital stay in two gastric banding patients.
The study also highlighted some of the problems with accruing and retaining patients in weight loss trials, the investigators noted. Of 667 screened patients, 69 (10%) were randomized. Of these, seven refused their assigned treatment, and one was excluded from treatment on the procedure day. Six had incomplete follow-up and five – all in the lifestyle intervention arm – withdrew by 6 months.
Because the planned 12-month follow-up was too short to allow any conclusions about the stability of diabetes remission in treated patients, longer follow-up is crucial and will require considerable financial investments.
"These important feasibility issues – the need for targeted screening, the thorough assessment of clinical equipoise to reduce the likelihood of postrandomization dropout, the challenging retention in the [lifestyle] arm, and funding – raise a number of concerns for the scalability of this type of study to a larger multicenter trial. For this reason, pursuing alternative methods to obtain high-order evidence regarding outcomes of surgical vs. nonsurgical treatment may be more reasonable for people with a relatively low BMI," they said.
The study was funded by the National Institutes of Health. Dr. Courcoulas disclosed financial relationships with Covidien, EndoGastric Solutions, Nutrisystem, and Ethicon J&J Healthcare. Some of the other authors disclosed financial relationships with a variety of pharmaceutical companies.
FROM JAMA SURGERY
Key clinical point: Bariatric surgery was linked to type 2 diabetes remission in some moderately obese patients.
Major finding: Complete remission occurred in 17% of Roux-en-Y bypass patients and 23% of gastric banding patients, but in none of those assigned to a lifestyle intervention.
Data source: The three-way randomized trial of 69 patients.
Disclosures: The study was funded by the National Institutes of Health. Dr. Courcoulas disclosed financial relationships with Covidien, EndoGastric Solutions, Nutrisystem, and Ethicon J&J Healthcare. Some of the other authors disclosed financial relationships with a variety of pharmaceutical companies.

Chronic migraine affects education, employment, and income
PHILADELPHIA – People with chronic migraine have higher levels of headache-related disability and unemployment and under-employment, which correspond to lower personal and household income.
Demographic findings of the CaMEO (Chronic Migraine Epidemiology and Outcomes) study confirm that chronic migraine exerts serious, long-lasting effects on personal and family well-being, Dr. Richard Lipton said at the annual meeting of the American Academy of Neurology.

CaMEO was a 13-month, Web-based survey that garnered input from almost 81,000 people who reported headache within the past year, said Dr. Lipton, director of the Montefiore Headache Center, Bronx, New York.
They completed a validated questionnaire that used diagnostic questions from the International Classification of Headache Disorders system to identify episodic migraine (less than 15 headache days/month) and chronic migraine (more than 15 headache days/month). After the initial assessment, they completed additional assessments every 3 months for the duration of the study.
Of the entire study population, 16,789 (21%) were found to have migraine. Of those, 1,476 (8.8%) had chronic migraine (CM). The rest had episodic migraine (EM).
Mean ages were similar in both groups (41 years). Those with CM were significantly more likely to be female (81% vs. 74%), obese (42% vs. 35%), and white (88% vs. 83%). The mean score on the MIDAS (Migraine Disability Assessment) test, a measure of headache-related disability, was significantly higher (worse) for those with CM (61 vs. 13).
Chronic migraine was associated with a significantly lower educational level, with 35% having at least a bachelor’s degree, compared with 46% of those with EM (odds ratio, 0.63). Full- or part-time employment was less common among those with CM (56% vs. 66%; OR, 0.66).
There were also significant differences in annual income. At every income level, those with CM had significantly higher odds of making less than did those with EM (OR, 0.65). People with CM also were significantly more likely to have low household income (OR, 0.63).
"The CM group was more likely to have individual incomes of less than $50,000/year (79% vs. 69%) and household incomes of less than $50,000 year (50% vs. 39%)," Dr. Lipton said.
"We have previously shown that people from low-income households and low educational backgrounds have a higher incidence of migraine onset," Dr. Lipton said. "This suggests there are some factors associated with low income, stressful life events, or even family history – you might come from a low-income family because your parents had migraine that was disabling to them."
In addition to baseline characteristics, the study is looking at barriers to care; migraine phenotypes and comorbidities; and family burden on both spouses and children.
Allergan Inc. sponsored the study. Dr. Lipton has received honoraria from the company.
On Twitter @alz_gal
PHILADELPHIA – People with chronic migraine have higher levels of headache-related disability and unemployment and under-employment, which correspond to lower personal and household income.
Demographic findings of the CaMEO (Chronic Migraine Epidemiology and Outcomes) study confirm that chronic migraine exerts serious, long-lasting effects on personal and family well-being, Dr. Richard Lipton said at the annual meeting of the American Academy of Neurology.
CaMEO was a 13-month, Web-based survey that garnered input from almost 81,000 people who reported headache within the past year, said Dr. Lipton, director of the Montefiore Headache Center, Bronx, New York.
They completed a validated questionnaire that used diagnostic questions from the International Classification of Headache Disorders system to identify episodic migraine (less than 15 headache days/month) and chronic migraine (more than 15 headache days/month). After the initial assessment, they completed additional assessments every 3 months for the duration of the study.
Of the entire study population, 16,789 (21%) were found to have migraine. Of those, 1,476 (8.8%) had chronic migraine (CM). The rest had episodic migraine (EM).
Mean ages were similar in both groups (41 years). Those with CM were significantly more likely to be female (81% vs. 74%), obese (42% vs. 35%), and white (88% vs. 83%). The mean score on the MIDAS (Migraine Disability Assessment) test, a measure of headache-related disability, was significantly higher (worse) for those with CM (61 vs. 13).
Chronic migraine was associated with a significantly lower educational level, with 35% having at least a bachelor’s degree, compared with 46% of those with EM (odds ratio, 0.63). Full- or part-time employment was less common among those with CM (56% vs. 66%; OR, 0.66).
There were also significant differences in annual income. At every income level, those with CM had significantly higher odds of making less than did those with EM (OR, 0.65). People with CM also were significantly more likely to have low household income (OR, 0.63).
"The CM group was more likely to have individual incomes of less than $50,000/year (79% vs. 69%) and household incomes of less than $50,000 year (50% vs. 39%)," Dr. Lipton said.
"We have previously shown that people from low-income households and low educational backgrounds have a higher incidence of migraine onset," Dr. Lipton said. "This suggests there are some factors associated with low income, stressful life events, or even family history – you might come from a low-income family because your parents had migraine that was disabling to them."
In addition to baseline characteristics, the study is looking at barriers to care; migraine phenotypes and comorbidities; and family burden on both spouses and children.
Allergan Inc. sponsored the study. Dr. Lipton has received honoraria from the company.
On Twitter @alz_gal
PHILADELPHIA – People with chronic migraine have higher levels of headache-related disability and unemployment and under-employment, which correspond to lower personal and household income.
Demographic findings of the CaMEO (Chronic Migraine Epidemiology and Outcomes) study confirm that chronic migraine exerts serious, long-lasting effects on personal and family well-being, Dr. Richard Lipton said at the annual meeting of the American Academy of Neurology.
CaMEO was a 13-month, Web-based survey that garnered input from almost 81,000 people who reported headache within the past year, said Dr. Lipton, director of the Montefiore Headache Center, Bronx, New York.
They completed a validated questionnaire that used diagnostic questions from the International Classification of Headache Disorders system to identify episodic migraine (less than 15 headache days/month) and chronic migraine (more than 15 headache days/month). After the initial assessment, they completed additional assessments every 3 months for the duration of the study.
Of the entire study population, 16,789 (21%) were found to have migraine. Of those, 1,476 (8.8%) had chronic migraine (CM). The rest had episodic migraine (EM).
Mean ages were similar in both groups (41 years). Those with CM were significantly more likely to be female (81% vs. 74%), obese (42% vs. 35%), and white (88% vs. 83%). The mean score on the MIDAS (Migraine Disability Assessment) test, a measure of headache-related disability, was significantly higher (worse) for those with CM (61 vs. 13).
Chronic migraine was associated with a significantly lower educational level, with 35% having at least a bachelor’s degree, compared with 46% of those with EM (odds ratio, 0.63). Full- or part-time employment was less common among those with CM (56% vs. 66%; OR, 0.66).
There were also significant differences in annual income. At every income level, those with CM had significantly higher odds of making less than did those with EM (OR, 0.65). People with CM also were significantly more likely to have low household income (OR, 0.63).
"The CM group was more likely to have individual incomes of less than $50,000/year (79% vs. 69%) and household incomes of less than $50,000 year (50% vs. 39%)," Dr. Lipton said.
"We have previously shown that people from low-income households and low educational backgrounds have a higher incidence of migraine onset," Dr. Lipton said. "This suggests there are some factors associated with low income, stressful life events, or even family history – you might come from a low-income family because your parents had migraine that was disabling to them."
In addition to baseline characteristics, the study is looking at barriers to care; migraine phenotypes and comorbidities; and family burden on both spouses and children.
Allergan Inc. sponsored the study. Dr. Lipton has received honoraria from the company.
On Twitter @alz_gal
AT THE 2014 AAN ANNUAL MEETING
Key clinical point: Survey findings show that chronic migraine has serious negative effects on income, disability, and educational attainment.
Major finding: Compared with those with episodic migraine, people with chronic migraine were up to 38% less likely to be employed, have advanced degrees, and make more than $50,000/year.
Data source: CaMEO is a Web-based study of almost 17,000 migraineurs.
Disclosures: Allergan Inc. sponsored the study. Dr. Lipton has received honoraria from the company.

Etrolizumab leads to clinical remission in some patients with refractory ulcerative colitis
The investigational monoclonal antibody etrolizumab effected clinical remission in significantly more patients with refractory ulcerative colitis than did placebo, an industry-sponsored trial showed.
Two tested doses of the drug achieved significant benefit over placebo, although the larger – 300 mg biweekly with a 420-mg loading dose – was slightly less effective, Dr. Séverine Vermeire and colleagues wrote in the May 9 issue of the Lancet (2014 [dx.doi.org/10.1016/S0140-6736(14)60661-9]).
The drug also significantly improved the incidence of endoscopic remission, which the authors said was a more stringent test of effect than was the clinical score.
"In our study, a relatively high proportion of patients in the placebo group achieved a clinical response – probably because ... this endpoint is less rigorous," wrote Dr. Vermeire of the University of Leuven (Belgium) and coauthors. "By contrast, endoscopic remission is an extremely rigorous endpoint, especially for the treatment-refractory patients included in this study, and thus was achieved in a small proportion of actively treated patients compared with no patients in the placebo group."
The 10-week phase II study comprised 124 patients with ulcerative colitis who had been unresponsive to conventional therapy. They were randomized to placebo injections or to etrolizumab: either 100 mg at weeks 0, 4, and 8, with placebo at week 2, or a 420-mg loading dose at week 0 followed by 300 mg at weeks 2, 4, and 8.
By 10 weeks, clinical remission had occurred in 21% of the 100-mg group, 10% of the 300-mg group, and none of the placebo group. Clinical response had occurred in 33% of the 10-mg group, 31% of the 300-mg group, and 29% of the placebo group – not significantly different.
By week 8, endoscopic and rectal bleeding subscores of 0 (endoscopic remission) had occurred in one patient in the placebo group, three in the 100-mg group, and one in the 300-mg group – also not significantly different.
By week 10, however, this endpoint did reach statistical significance, with no patients in the placebo group achieving the 0 score, compared with four in the 100-mg group and three in the 300-mg group.
Adverse events occurred in 61% of the 100-mg group, 48% of the 300-mg group, and 72% of the placebo group. These included rash (7%, 3%, and 2%, respectively), influenzalike illness (7%, 0%, and 2%), and arthralgia (15%, 5%, and 9%).
There were 12 serious adverse events: 5 (12%) in the 100-mg group, 2 (5%) in the 300-mg group, and 5 (12%) in the placebo group. These were related to the disease, the investigators said. There were no serious opportunistic infections. Four patients in the 300-mg group and two in the placebo group experienced mild injection site reactions.
Etrolizumab works by inhibiting the interaction of alpha-4 beta-7 integrin with mucosal addressin cell adhesion molecule-1. This action inhibits the movement of immune cells into the intestine while avoiding the broad immunosuppressive effects of other antibodies.
Genentech sponsored the study. Dr. Vermeire had no financial ties with the company, although she disclosed relationships with other pharmaceutical companies. The coauthors also had multiple relationships with drug manufacturers, including Genentech.
On Twitter @Alz_Gal
The investigational monoclonal antibody etrolizumab effected clinical remission in significantly more patients with refractory ulcerative colitis than did placebo, an industry-sponsored trial showed.
Two tested doses of the drug achieved significant benefit over placebo, although the larger – 300 mg biweekly with a 420-mg loading dose – was slightly less effective, Dr. Séverine Vermeire and colleagues wrote in the May 9 issue of the Lancet (2014 [dx.doi.org/10.1016/S0140-6736(14)60661-9]).
The drug also significantly improved the incidence of endoscopic remission, which the authors said was a more stringent test of effect than was the clinical score.
"In our study, a relatively high proportion of patients in the placebo group achieved a clinical response – probably because ... this endpoint is less rigorous," wrote Dr. Vermeire of the University of Leuven (Belgium) and coauthors. "By contrast, endoscopic remission is an extremely rigorous endpoint, especially for the treatment-refractory patients included in this study, and thus was achieved in a small proportion of actively treated patients compared with no patients in the placebo group."
The 10-week phase II study comprised 124 patients with ulcerative colitis who had been unresponsive to conventional therapy. They were randomized to placebo injections or to etrolizumab: either 100 mg at weeks 0, 4, and 8, with placebo at week 2, or a 420-mg loading dose at week 0 followed by 300 mg at weeks 2, 4, and 8.
By 10 weeks, clinical remission had occurred in 21% of the 100-mg group, 10% of the 300-mg group, and none of the placebo group. Clinical response had occurred in 33% of the 10-mg group, 31% of the 300-mg group, and 29% of the placebo group – not significantly different.
By week 8, endoscopic and rectal bleeding subscores of 0 (endoscopic remission) had occurred in one patient in the placebo group, three in the 100-mg group, and one in the 300-mg group – also not significantly different.
By week 10, however, this endpoint did reach statistical significance, with no patients in the placebo group achieving the 0 score, compared with four in the 100-mg group and three in the 300-mg group.
Adverse events occurred in 61% of the 100-mg group, 48% of the 300-mg group, and 72% of the placebo group. These included rash (7%, 3%, and 2%, respectively), influenzalike illness (7%, 0%, and 2%), and arthralgia (15%, 5%, and 9%).
There were 12 serious adverse events: 5 (12%) in the 100-mg group, 2 (5%) in the 300-mg group, and 5 (12%) in the placebo group. These were related to the disease, the investigators said. There were no serious opportunistic infections. Four patients in the 300-mg group and two in the placebo group experienced mild injection site reactions.
Etrolizumab works by inhibiting the interaction of alpha-4 beta-7 integrin with mucosal addressin cell adhesion molecule-1. This action inhibits the movement of immune cells into the intestine while avoiding the broad immunosuppressive effects of other antibodies.
Genentech sponsored the study. Dr. Vermeire had no financial ties with the company, although she disclosed relationships with other pharmaceutical companies. The coauthors also had multiple relationships with drug manufacturers, including Genentech.
On Twitter @Alz_Gal
The investigational monoclonal antibody etrolizumab effected clinical remission in significantly more patients with refractory ulcerative colitis than did placebo, an industry-sponsored trial showed.
Two tested doses of the drug achieved significant benefit over placebo, although the larger – 300 mg biweekly with a 420-mg loading dose – was slightly less effective, Dr. Séverine Vermeire and colleagues wrote in the May 9 issue of the Lancet (2014 [dx.doi.org/10.1016/S0140-6736(14)60661-9]).
The drug also significantly improved the incidence of endoscopic remission, which the authors said was a more stringent test of effect than was the clinical score.
"In our study, a relatively high proportion of patients in the placebo group achieved a clinical response – probably because ... this endpoint is less rigorous," wrote Dr. Vermeire of the University of Leuven (Belgium) and coauthors. "By contrast, endoscopic remission is an extremely rigorous endpoint, especially for the treatment-refractory patients included in this study, and thus was achieved in a small proportion of actively treated patients compared with no patients in the placebo group."
The 10-week phase II study comprised 124 patients with ulcerative colitis who had been unresponsive to conventional therapy. They were randomized to placebo injections or to etrolizumab: either 100 mg at weeks 0, 4, and 8, with placebo at week 2, or a 420-mg loading dose at week 0 followed by 300 mg at weeks 2, 4, and 8.
By 10 weeks, clinical remission had occurred in 21% of the 100-mg group, 10% of the 300-mg group, and none of the placebo group. Clinical response had occurred in 33% of the 10-mg group, 31% of the 300-mg group, and 29% of the placebo group – not significantly different.
By week 8, endoscopic and rectal bleeding subscores of 0 (endoscopic remission) had occurred in one patient in the placebo group, three in the 100-mg group, and one in the 300-mg group – also not significantly different.
By week 10, however, this endpoint did reach statistical significance, with no patients in the placebo group achieving the 0 score, compared with four in the 100-mg group and three in the 300-mg group.
Adverse events occurred in 61% of the 100-mg group, 48% of the 300-mg group, and 72% of the placebo group. These included rash (7%, 3%, and 2%, respectively), influenzalike illness (7%, 0%, and 2%), and arthralgia (15%, 5%, and 9%).
There were 12 serious adverse events: 5 (12%) in the 100-mg group, 2 (5%) in the 300-mg group, and 5 (12%) in the placebo group. These were related to the disease, the investigators said. There were no serious opportunistic infections. Four patients in the 300-mg group and two in the placebo group experienced mild injection site reactions.
Etrolizumab works by inhibiting the interaction of alpha-4 beta-7 integrin with mucosal addressin cell adhesion molecule-1. This action inhibits the movement of immune cells into the intestine while avoiding the broad immunosuppressive effects of other antibodies.
Genentech sponsored the study. Dr. Vermeire had no financial ties with the company, although she disclosed relationships with other pharmaceutical companies. The coauthors also had multiple relationships with drug manufacturers, including Genentech.
On Twitter @Alz_Gal
FROM THE LANCET
Key clinical point: The investigational antibody etrolizumab was linked to clinical remission in some patients with treatment-resistant ulcerative colitis.
Major finding: By 10 weeks, clinical remission had occurred in 21% of the 100-mg group, 10% of the 300-mg group, and in none of the placebo group.
Data source: The phase II placebo-controlled trial involved 124 patients.
Disclosures: Genentech sponsored the study. Dr. Vermeire had no financial ties with the company although she disclosed relationships with other pharmaceutical companies. The coauthors also had multiple relationships with drug manufacturers, including Genentech.
Cochrane Review: Supplementation reduced deaths in zinc-deficient children
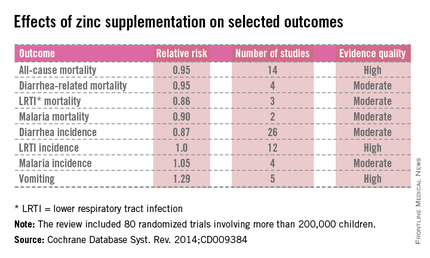
For children who have a zinc deficiency, supplementation significantly reduced their overall risk of death as well as risk of death from diarrhea and lower respiratory tract infection, based on a Cochrane Review of 80 randomized controlled trials that included more than 200,000 children aged 6 months to 12 years.
Most of the studies in the review were conducted in countries with impoverished populations – South and Central America, Africa, and Asia – although a few were conducted in impoverished communities in developed countries, including the United States, wrote Evan Mayo-Wilson, Ph.D., an epidemiologist at the Johns Hopkins University Bloomberg School of Public Health, Baltimore, and his colleagues (Cochrane Database Syst. Rev. 2014;CD009384 [doi:10.1002/14651858.CD009384.pub2]).
"At both national and individual levels, zinc deficiency and its consequences are linked to poverty. Firstly, foods from animal sources, which are rich in zinc, are often expensive. Particularly in low- and middle-income countries, poor individuals may primarily eat foods such as cereals, grains, and legumes. These foods have relatively low concentrations of zinc; they also have relatively high concentrations of fiber and phytate molecules, which reduce zinc absorption by the intestine," they said.
The review also found that "zinc supplementation may have a very small effect on growth, but eating more calories would probably have a larger effect for many malnourished children," wrote Dr. Mayo-Wilson and his colleagues.
Also, water-borne illnesses common in Third World countries cause diarrhea that impairs intestinal zinc absorption.
The studies looked at orally administered zinc given as a supplement, regardless of compound, formulation, dose, duration, or frequency. Comparators were placebo, wait-list controls, or populations with no intervention. Hospitalized children and children with chronic diseases or conditions were excluded as were those using food fortification or intake, sprinkles, and therapeutic interventions.
Risk reductions for mortality ranged from 5% to 14%. The only significant disease reduction occurred with all-cause diarrhea.
Zinc possibly reduced the risks of death from malaria and the incidence of malaria and lower respiratory tract infection, but the authors said those findings were "imprecise."
Although zinc slightly increased the incidence of vomiting, "in our opinion, the benefits of preventive zinc supplementation outweigh the harms in areas where the risk of zinc deficiency is relatively high," the authors said.
No author disclosures were listed in the paper.
On Twitter @alz_gal
For children who have a zinc deficiency, supplementation significantly reduced their overall risk of death as well as risk of death from diarrhea and lower respiratory tract infection, based on a Cochrane Review of 80 randomized controlled trials that included more than 200,000 children aged 6 months to 12 years.
Most of the studies in the review were conducted in countries with impoverished populations – South and Central America, Africa, and Asia – although a few were conducted in impoverished communities in developed countries, including the United States, wrote Evan Mayo-Wilson, Ph.D., an epidemiologist at the Johns Hopkins University Bloomberg School of Public Health, Baltimore, and his colleagues (Cochrane Database Syst. Rev. 2014;CD009384 [doi:10.1002/14651858.CD009384.pub2]).
"At both national and individual levels, zinc deficiency and its consequences are linked to poverty. Firstly, foods from animal sources, which are rich in zinc, are often expensive. Particularly in low- and middle-income countries, poor individuals may primarily eat foods such as cereals, grains, and legumes. These foods have relatively low concentrations of zinc; they also have relatively high concentrations of fiber and phytate molecules, which reduce zinc absorption by the intestine," they said.
The review also found that "zinc supplementation may have a very small effect on growth, but eating more calories would probably have a larger effect for many malnourished children," wrote Dr. Mayo-Wilson and his colleagues.
Also, water-borne illnesses common in Third World countries cause diarrhea that impairs intestinal zinc absorption.
The studies looked at orally administered zinc given as a supplement, regardless of compound, formulation, dose, duration, or frequency. Comparators were placebo, wait-list controls, or populations with no intervention. Hospitalized children and children with chronic diseases or conditions were excluded as were those using food fortification or intake, sprinkles, and therapeutic interventions.
Risk reductions for mortality ranged from 5% to 14%. The only significant disease reduction occurred with all-cause diarrhea.
Zinc possibly reduced the risks of death from malaria and the incidence of malaria and lower respiratory tract infection, but the authors said those findings were "imprecise."
Although zinc slightly increased the incidence of vomiting, "in our opinion, the benefits of preventive zinc supplementation outweigh the harms in areas where the risk of zinc deficiency is relatively high," the authors said.
No author disclosures were listed in the paper.
On Twitter @alz_gal
For children who have a zinc deficiency, supplementation significantly reduced their overall risk of death as well as risk of death from diarrhea and lower respiratory tract infection, based on a Cochrane Review of 80 randomized controlled trials that included more than 200,000 children aged 6 months to 12 years.
Most of the studies in the review were conducted in countries with impoverished populations – South and Central America, Africa, and Asia – although a few were conducted in impoverished communities in developed countries, including the United States, wrote Evan Mayo-Wilson, Ph.D., an epidemiologist at the Johns Hopkins University Bloomberg School of Public Health, Baltimore, and his colleagues (Cochrane Database Syst. Rev. 2014;CD009384 [doi:10.1002/14651858.CD009384.pub2]).
"At both national and individual levels, zinc deficiency and its consequences are linked to poverty. Firstly, foods from animal sources, which are rich in zinc, are often expensive. Particularly in low- and middle-income countries, poor individuals may primarily eat foods such as cereals, grains, and legumes. These foods have relatively low concentrations of zinc; they also have relatively high concentrations of fiber and phytate molecules, which reduce zinc absorption by the intestine," they said.
The review also found that "zinc supplementation may have a very small effect on growth, but eating more calories would probably have a larger effect for many malnourished children," wrote Dr. Mayo-Wilson and his colleagues.
Also, water-borne illnesses common in Third World countries cause diarrhea that impairs intestinal zinc absorption.
The studies looked at orally administered zinc given as a supplement, regardless of compound, formulation, dose, duration, or frequency. Comparators were placebo, wait-list controls, or populations with no intervention. Hospitalized children and children with chronic diseases or conditions were excluded as were those using food fortification or intake, sprinkles, and therapeutic interventions.
Risk reductions for mortality ranged from 5% to 14%. The only significant disease reduction occurred with all-cause diarrhea.
Zinc possibly reduced the risks of death from malaria and the incidence of malaria and lower respiratory tract infection, but the authors said those findings were "imprecise."
Although zinc slightly increased the incidence of vomiting, "in our opinion, the benefits of preventive zinc supplementation outweigh the harms in areas where the risk of zinc deficiency is relatively high," the authors said.
No author disclosures were listed in the paper.
On Twitter @alz_gal
FROM THE COCHRANE REVIEW
Key clinical point: Zinc supplements reduced the risk of death and some diseases for children who were deficient in the mineral.
Major finding: Zinc supplementation reduced the overall risk of death by 5% and the incidence of diarrhea by 13%.
Data source: The Cochrane Review comprised 80 studies of 205,401 children.
Disclosures: No author disclosures were listed in the paper.
Alteplase uses fewer resources to manage CVC occlusion
Clearing an occluded central venous catheter with alteplase is just as effective as replacing the line, but costs significantly less.
A large, retrospective, industry-funded study has concluded that treatment with alteplase costs about $1,400 less than replacing the line. Differences in radiologic, nursing, and surgical costs accounted for most of that, Frank R. Ernst, Pharm.D., and his colleagues wrote online in the Journal of Hospital Medicine (J. Hosp. Med. 2014 May 14 [doi: 10.1002/jhm.2208]).
The additional finding that length of stay was not a main cost driver lends credence to the idea that alteplase could be a good choice whether patients only need line clearance, or are already in the hospital for other reasons, wrote Dr. Ernst of Premier Research Services, Charlotte, N.C., and his coauthors.
"If patients are admitted for a noncardiovascular condition and have central venous catheter occlusion, using alteplase to clear the ... occlusion, along with implementing strategies to manage the underlying disease to reduce the length of stay, becomes a powerful opportunity to impact cost," the investigators wrote.
"Among patients who may come to the hospital for just the ... occlusion, the length of stay should be short. There may be no significant opportunity to reduce the length of stay in those cases, but opportunities to decrease core hospital resource utilization with alteplase make this approach beneficial if the patient can tolerate it."
The retrospective study comprised data on 34,579 patients who had been treated for a central venous catheter (CVC) occlusion. Of these, 33,551 were treated with 2 mg alteplase. The other 1,028 had the CVC replaced.
More than half of the cohort were older than 65 years, but patients who got alteplase were an average of 2 years younger than those who had surgery (63 vs. 65 years). Significantly more of those in the alteplase group had serious comorbidities, including chronic obstructive pulmonary disease, liver and renal disease, and diabetes with complications. Catheter replacements were more commonly done in teaching hospitals than in nonteaching hospitals (58% vs. 42%). Larger hospitals also did more replacements: up to 42% of those with 300 or more beds, but no more than 12% for those with 299 or fewer beds.
After adjustment for baseline characteristics, the daily charge for patients treated with alteplase was $317 less than for those who had the line replaced. This translated to an average savings of $1,419 per patient.
Those savings accrued in different departments, and for different periods, the authors said. For example, in the preocclusion period, cardiology/electrocardiography costs were lower for those in the replacement group – but in the postocclusion period, they were lower in the alteplase group. Many other hospital charges were also lower for the replacement group during the preocclusion period (lab, nursing, surgical, pharmacy, radiology, and intensive care costs), but higher in the postocclusion period.
In an unadjusted analysis of readmissions, there were no statistically significant differences between groups in either the 30- or 90-day rates. Neither diagnoses of heart failure, heart attack, nor cancer altered this finding.
The authors, one of whom is Dr. Alpesh N. Amin, an adviser to Hospitalist News, noted that the findings are limited by the issues inherent in every retrospective database study, including an inability to access the clinical information that would have affected decision-making.
Genentech, which markets alteplase, funded the study. Dr. Ernst is an employee of Premier, which Genentech contracted to perform the study. Several of the coauthors reported financial relationships with Genentech.
Clearing an occluded central venous catheter with alteplase is just as effective as replacing the line, but costs significantly less.
A large, retrospective, industry-funded study has concluded that treatment with alteplase costs about $1,400 less than replacing the line. Differences in radiologic, nursing, and surgical costs accounted for most of that, Frank R. Ernst, Pharm.D., and his colleagues wrote online in the Journal of Hospital Medicine (J. Hosp. Med. 2014 May 14 [doi: 10.1002/jhm.2208]).
The additional finding that length of stay was not a main cost driver lends credence to the idea that alteplase could be a good choice whether patients only need line clearance, or are already in the hospital for other reasons, wrote Dr. Ernst of Premier Research Services, Charlotte, N.C., and his coauthors.
"If patients are admitted for a noncardiovascular condition and have central venous catheter occlusion, using alteplase to clear the ... occlusion, along with implementing strategies to manage the underlying disease to reduce the length of stay, becomes a powerful opportunity to impact cost," the investigators wrote.
"Among patients who may come to the hospital for just the ... occlusion, the length of stay should be short. There may be no significant opportunity to reduce the length of stay in those cases, but opportunities to decrease core hospital resource utilization with alteplase make this approach beneficial if the patient can tolerate it."
The retrospective study comprised data on 34,579 patients who had been treated for a central venous catheter (CVC) occlusion. Of these, 33,551 were treated with 2 mg alteplase. The other 1,028 had the CVC replaced.
More than half of the cohort were older than 65 years, but patients who got alteplase were an average of 2 years younger than those who had surgery (63 vs. 65 years). Significantly more of those in the alteplase group had serious comorbidities, including chronic obstructive pulmonary disease, liver and renal disease, and diabetes with complications. Catheter replacements were more commonly done in teaching hospitals than in nonteaching hospitals (58% vs. 42%). Larger hospitals also did more replacements: up to 42% of those with 300 or more beds, but no more than 12% for those with 299 or fewer beds.
After adjustment for baseline characteristics, the daily charge for patients treated with alteplase was $317 less than for those who had the line replaced. This translated to an average savings of $1,419 per patient.
Those savings accrued in different departments, and for different periods, the authors said. For example, in the preocclusion period, cardiology/electrocardiography costs were lower for those in the replacement group – but in the postocclusion period, they were lower in the alteplase group. Many other hospital charges were also lower for the replacement group during the preocclusion period (lab, nursing, surgical, pharmacy, radiology, and intensive care costs), but higher in the postocclusion period.
In an unadjusted analysis of readmissions, there were no statistically significant differences between groups in either the 30- or 90-day rates. Neither diagnoses of heart failure, heart attack, nor cancer altered this finding.
The authors, one of whom is Dr. Alpesh N. Amin, an adviser to Hospitalist News, noted that the findings are limited by the issues inherent in every retrospective database study, including an inability to access the clinical information that would have affected decision-making.
Genentech, which markets alteplase, funded the study. Dr. Ernst is an employee of Premier, which Genentech contracted to perform the study. Several of the coauthors reported financial relationships with Genentech.
Clearing an occluded central venous catheter with alteplase is just as effective as replacing the line, but costs significantly less.
A large, retrospective, industry-funded study has concluded that treatment with alteplase costs about $1,400 less than replacing the line. Differences in radiologic, nursing, and surgical costs accounted for most of that, Frank R. Ernst, Pharm.D., and his colleagues wrote online in the Journal of Hospital Medicine (J. Hosp. Med. 2014 May 14 [doi: 10.1002/jhm.2208]).
The additional finding that length of stay was not a main cost driver lends credence to the idea that alteplase could be a good choice whether patients only need line clearance, or are already in the hospital for other reasons, wrote Dr. Ernst of Premier Research Services, Charlotte, N.C., and his coauthors.
"If patients are admitted for a noncardiovascular condition and have central venous catheter occlusion, using alteplase to clear the ... occlusion, along with implementing strategies to manage the underlying disease to reduce the length of stay, becomes a powerful opportunity to impact cost," the investigators wrote.
"Among patients who may come to the hospital for just the ... occlusion, the length of stay should be short. There may be no significant opportunity to reduce the length of stay in those cases, but opportunities to decrease core hospital resource utilization with alteplase make this approach beneficial if the patient can tolerate it."
The retrospective study comprised data on 34,579 patients who had been treated for a central venous catheter (CVC) occlusion. Of these, 33,551 were treated with 2 mg alteplase. The other 1,028 had the CVC replaced.
More than half of the cohort were older than 65 years, but patients who got alteplase were an average of 2 years younger than those who had surgery (63 vs. 65 years). Significantly more of those in the alteplase group had serious comorbidities, including chronic obstructive pulmonary disease, liver and renal disease, and diabetes with complications. Catheter replacements were more commonly done in teaching hospitals than in nonteaching hospitals (58% vs. 42%). Larger hospitals also did more replacements: up to 42% of those with 300 or more beds, but no more than 12% for those with 299 or fewer beds.
After adjustment for baseline characteristics, the daily charge for patients treated with alteplase was $317 less than for those who had the line replaced. This translated to an average savings of $1,419 per patient.
Those savings accrued in different departments, and for different periods, the authors said. For example, in the preocclusion period, cardiology/electrocardiography costs were lower for those in the replacement group – but in the postocclusion period, they were lower in the alteplase group. Many other hospital charges were also lower for the replacement group during the preocclusion period (lab, nursing, surgical, pharmacy, radiology, and intensive care costs), but higher in the postocclusion period.
In an unadjusted analysis of readmissions, there were no statistically significant differences between groups in either the 30- or 90-day rates. Neither diagnoses of heart failure, heart attack, nor cancer altered this finding.
The authors, one of whom is Dr. Alpesh N. Amin, an adviser to Hospitalist News, noted that the findings are limited by the issues inherent in every retrospective database study, including an inability to access the clinical information that would have affected decision-making.
Genentech, which markets alteplase, funded the study. Dr. Ernst is an employee of Premier, which Genentech contracted to perform the study. Several of the coauthors reported financial relationships with Genentech.
FROM THE JOURNAL OF HOSPITAL MEDICINE
Key clinical point: It may be more cost effective to treat central venous catheter occlusion with alteplase rather than line replacement.
Major finding: Clearing a blocked CVC with 2 mg alteplase saved an average of $1,419 per patient, compared with replacing the line.
Data source: The retrospective database study comprised 34,579 patients.
Disclosures: Genentech, which markets alteplase, funded the study. Dr. Ernst is an employee of Premier, which Genentech contracted to perform the study. Several of the coauthors reported financial relationships with Genentech.
Pasireotide decreases incidence of postoperative fistula
The somatostatin analogue pasireotide reduced postoperative pancreatic fistula leak or abscess by 56%, compared with placebo, a randomized study has determined.
Pasireotide (Signifor) was effective after both pancreaticoduodenectomy and distal pancreatectomy, whether or not the pancreatic duct was dilated, Dr. Peter J. Allen and his colleagues wrote in the May 21 issue of the New England Journal of Medicine (N. Engl. J. Med. 2014;370:2014-22).
In those patients who did develop fistulas or leaks, pasireotide was associated with fewer grade 3 occurrences.
"These results suggest that ... not only were many leaks and fistulas prevented, but when they did occur they were less clinically relevant," wrote Dr. Allen of the Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
The study randomized 300 patients to subcutaneous injections of either placebo or pasireotide twice daily for 7 days after pancreatic surgery. The primary endpoint was the development of a pancreatic leak, fistula, or abscess of at least grade 3. Secondary endpoints included the overall rate of pancreatic complications (all grades) and the rate of grade B or grade C pancreatic fistula.
Patients were a mean of 64 years old. Most (73%) underwent a pancreaticoduodenectomy. The average length of stay for these patients was about 10 days. The active group received 900 mcg of pasireotide subcutaneously twice daily for 7 days, beginning on the morning of surgery.
Mean postoperative serum glucose levels were significantly higher in patients taking pasireotide (258 mg/dL vs. 215 mg/dL). Readmission occurred in significantly fewer pasireotide patients (17% vs. 29%).
Significantly fewer of those taking the active drug were able to finish the entire course of 14 doses (76% vs. 86% given placebo). The lower completion rate was mostly due to nausea and vomiting, which caused 26 patients in the active group and 3 in the placebo group to withdraw from the study.
A leak or fistula of grade 3 or higher developed in 45 patients. The outcome was significantly less common among those taking pasireotide than among those on placebo (9% vs. 21%; relative risk, 0.44). "This corresponded to an absolute risk reduction of 11.7 percentage points," with a number needed to treat of 8, the investigators said.
Pasireotide was significantly more effective than placebo in surgical subgroups, including pancreaticoduodenectomy (RR, 0.49) and distal pancreatectomy (RR, 0.32). The effect was also positive whether the pancreatic duct was dilated (RR, 0.11) or nondilated (RR, 0.55).
The secondary outcome (grade B or C postoperative fistula) occurred in 37 patients (12%). In the pasireotide group, there were 12 grade B fistulas and no grade C fistulas. In the placebo group, there were 20 grade B and 5 grade C fistulas.
Overall 60-day mortality was 0.7% (one death in each treatment group). Grade 3 and 4 complications were common, occurring in 92% of the pasireotide group and 90% of the placebo group. Most of these were expected postoperative serum abnormalities.
The investigators said that the other approved somatostatin analogue, octreotide, has not been clearly associated with pancreatic leak reduction. They suggested that pasireotide may be more effective because it has a longer half-life and binds to four of the five somatostatin-receptor subtypes, rather than just two, as octreotide does.
They added that the octreotide studies were conducted before 2005, when there was no consistent definition of postoperative pancreatic fistula. Therefore, they concluded, the extant data cannot be used to identify octreotide efficacy in this application.
Pasireotide, which is made by Novartis Pharmaceuticals, is currently approved as an injection for the treatment of Cushing’s disease patients who cannot be helped through surgery.
Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
The somatostatin analogue pasireotide reduced postoperative pancreatic fistula leak or abscess by 56%, compared with placebo, a randomized study has determined.
Pasireotide (Signifor) was effective after both pancreaticoduodenectomy and distal pancreatectomy, whether or not the pancreatic duct was dilated, Dr. Peter J. Allen and his colleagues wrote in the May 21 issue of the New England Journal of Medicine (N. Engl. J. Med. 2014;370:2014-22).
In those patients who did develop fistulas or leaks, pasireotide was associated with fewer grade 3 occurrences.
"These results suggest that ... not only were many leaks and fistulas prevented, but when they did occur they were less clinically relevant," wrote Dr. Allen of the Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
The study randomized 300 patients to subcutaneous injections of either placebo or pasireotide twice daily for 7 days after pancreatic surgery. The primary endpoint was the development of a pancreatic leak, fistula, or abscess of at least grade 3. Secondary endpoints included the overall rate of pancreatic complications (all grades) and the rate of grade B or grade C pancreatic fistula.
Patients were a mean of 64 years old. Most (73%) underwent a pancreaticoduodenectomy. The average length of stay for these patients was about 10 days. The active group received 900 mcg of pasireotide subcutaneously twice daily for 7 days, beginning on the morning of surgery.
Mean postoperative serum glucose levels were significantly higher in patients taking pasireotide (258 mg/dL vs. 215 mg/dL). Readmission occurred in significantly fewer pasireotide patients (17% vs. 29%).
Significantly fewer of those taking the active drug were able to finish the entire course of 14 doses (76% vs. 86% given placebo). The lower completion rate was mostly due to nausea and vomiting, which caused 26 patients in the active group and 3 in the placebo group to withdraw from the study.
A leak or fistula of grade 3 or higher developed in 45 patients. The outcome was significantly less common among those taking pasireotide than among those on placebo (9% vs. 21%; relative risk, 0.44). "This corresponded to an absolute risk reduction of 11.7 percentage points," with a number needed to treat of 8, the investigators said.
Pasireotide was significantly more effective than placebo in surgical subgroups, including pancreaticoduodenectomy (RR, 0.49) and distal pancreatectomy (RR, 0.32). The effect was also positive whether the pancreatic duct was dilated (RR, 0.11) or nondilated (RR, 0.55).
The secondary outcome (grade B or C postoperative fistula) occurred in 37 patients (12%). In the pasireotide group, there were 12 grade B fistulas and no grade C fistulas. In the placebo group, there were 20 grade B and 5 grade C fistulas.
Overall 60-day mortality was 0.7% (one death in each treatment group). Grade 3 and 4 complications were common, occurring in 92% of the pasireotide group and 90% of the placebo group. Most of these were expected postoperative serum abnormalities.
The investigators said that the other approved somatostatin analogue, octreotide, has not been clearly associated with pancreatic leak reduction. They suggested that pasireotide may be more effective because it has a longer half-life and binds to four of the five somatostatin-receptor subtypes, rather than just two, as octreotide does.
They added that the octreotide studies were conducted before 2005, when there was no consistent definition of postoperative pancreatic fistula. Therefore, they concluded, the extant data cannot be used to identify octreotide efficacy in this application.
Pasireotide, which is made by Novartis Pharmaceuticals, is currently approved as an injection for the treatment of Cushing’s disease patients who cannot be helped through surgery.
Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
The somatostatin analogue pasireotide reduced postoperative pancreatic fistula leak or abscess by 56%, compared with placebo, a randomized study has determined.
Pasireotide (Signifor) was effective after both pancreaticoduodenectomy and distal pancreatectomy, whether or not the pancreatic duct was dilated, Dr. Peter J. Allen and his colleagues wrote in the May 21 issue of the New England Journal of Medicine (N. Engl. J. Med. 2014;370:2014-22).
In those patients who did develop fistulas or leaks, pasireotide was associated with fewer grade 3 occurrences.
"These results suggest that ... not only were many leaks and fistulas prevented, but when they did occur they were less clinically relevant," wrote Dr. Allen of the Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
The study randomized 300 patients to subcutaneous injections of either placebo or pasireotide twice daily for 7 days after pancreatic surgery. The primary endpoint was the development of a pancreatic leak, fistula, or abscess of at least grade 3. Secondary endpoints included the overall rate of pancreatic complications (all grades) and the rate of grade B or grade C pancreatic fistula.
Patients were a mean of 64 years old. Most (73%) underwent a pancreaticoduodenectomy. The average length of stay for these patients was about 10 days. The active group received 900 mcg of pasireotide subcutaneously twice daily for 7 days, beginning on the morning of surgery.
Mean postoperative serum glucose levels were significantly higher in patients taking pasireotide (258 mg/dL vs. 215 mg/dL). Readmission occurred in significantly fewer pasireotide patients (17% vs. 29%).
Significantly fewer of those taking the active drug were able to finish the entire course of 14 doses (76% vs. 86% given placebo). The lower completion rate was mostly due to nausea and vomiting, which caused 26 patients in the active group and 3 in the placebo group to withdraw from the study.
A leak or fistula of grade 3 or higher developed in 45 patients. The outcome was significantly less common among those taking pasireotide than among those on placebo (9% vs. 21%; relative risk, 0.44). "This corresponded to an absolute risk reduction of 11.7 percentage points," with a number needed to treat of 8, the investigators said.
Pasireotide was significantly more effective than placebo in surgical subgroups, including pancreaticoduodenectomy (RR, 0.49) and distal pancreatectomy (RR, 0.32). The effect was also positive whether the pancreatic duct was dilated (RR, 0.11) or nondilated (RR, 0.55).
The secondary outcome (grade B or C postoperative fistula) occurred in 37 patients (12%). In the pasireotide group, there were 12 grade B fistulas and no grade C fistulas. In the placebo group, there were 20 grade B and 5 grade C fistulas.
Overall 60-day mortality was 0.7% (one death in each treatment group). Grade 3 and 4 complications were common, occurring in 92% of the pasireotide group and 90% of the placebo group. Most of these were expected postoperative serum abnormalities.
The investigators said that the other approved somatostatin analogue, octreotide, has not been clearly associated with pancreatic leak reduction. They suggested that pasireotide may be more effective because it has a longer half-life and binds to four of the five somatostatin-receptor subtypes, rather than just two, as octreotide does.
They added that the octreotide studies were conducted before 2005, when there was no consistent definition of postoperative pancreatic fistula. Therefore, they concluded, the extant data cannot be used to identify octreotide efficacy in this application.
Pasireotide, which is made by Novartis Pharmaceuticals, is currently approved as an injection for the treatment of Cushing’s disease patients who cannot be helped through surgery.
Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
FROM NEJM
Key clinical point: Pasireotide reduced the incidence of postoperative pancreatic fistula, leak, or abscess.
Major finding: Compared with placebo, pasireotide reduced the rate of fistula, leak, or abscess by 56%.
Data source: The randomized, placebo-controlled study included 300 patients.
Disclosures: Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
Breast cancer fear contributes to prophylactic mastectomy rate
Fear seems to be a major driver of contralateral prophylactic mastectomy after initial breast cancer surgery.
Almost two-thirds of those who had the procedure had no clinical indication for it, Sarah T. Hawley, Ph.D., and her colleagues wrote in the May 21 online issue of JAMA Surgery (doi:10.1001/jamasurg.2013.5689). The women choosing contralateral prophylactic mastectomy (CPM) for which there was no clinical indication were more highly educated than were those who didn’t elect the surgery, more likely to be white, and two to four times more likely to be worried about a recurrence.

Fear of recurrence was a "powerful nonclinical factor" in the analysis, wrote Dr. Hawley of the University of Michigan, Ann Arbor – and education may be the best way to overcome it.
"A patient’s decision to undergo contralateral prophylactic mastectomy based on a strong fear of recurrence in the absence of clinical indications presents an important clinical challenge for surgeons," she and her colleagues wrote. "Growing literature supports the notion that patients have a difficult time assessing and interpreting their own risk and that fear and anxiety related to disease recurrence often supersede accurate risk perceptions to drive health decisions."
Dr. Hawley and her coinvestigators extracted their data from the Surveillance, Epidemiology, and End Results (SEER) registries for Los Angeles and Detroit. They included records from 1,447 women aged 20-79 years who had been diagnosed with a first incident primary ductal carcinoma in situ or invasive breast cancer of stages I-IIIa.
About half of the sample was white; 21% was black, and 30% Hispanic. Other groups made up the balance. More than half (59%) had achieved some college-level education.
About half the respondents (57%) underwent breast-conserving surgery (BCS). Other surgical treatments included unilateral mastectomy (UM; 34%), and contralateral prophylactic mastectomy (8%).
CPM was pondered more frequently than it was an executed, the investigators said, with 19% of the entire sample considering it "strongly or very strongly."
Most of the women who had CPM said that they did it to prevent recurrence, with 78% citing that worry as a very important driver of their decision. However, the authors said, of the 106 women who underwent CPM, only 31% had clinical indications, while the majority (67%) did not.
A multivariate analysis determined the relationships between patient characteristics and breast surgery,
Those with some college-level education were five times more likely to have CPM than UM, and four times more likely to have that than BCS. Those with high worry were almost three times more likely to have CPM than UM, and four times more likely to have CPM than BCS.
Women who had positive genetic testing were 10 times more likely to have contralateral prophylactic mastectomy than unilateral mastectomy, and 19 times more likely to have CPM than BCS. But those with negative results were still twice as likely to have the CPM as either of the other surgeries.
Having at least two close relatives with breast or ovarian cancer also significantly increased the likelihood of a CMP vs. UM (relative risk = 5) or BCS (RR = 4). Having had a diagnostic MRI doubled the chance of having CPM, compared with the other surgeries.
"Our results provide evidence that decisions about CPM represent a clear case in which better strategies to increase patient knowledge about their own risk of developing contralateral cancer as well as the net benefit of treatment are needed and should be made only after patients are accurately informed about these issues," Dr. Hawley and her coauthors said, adding that such patients need to clearly understand the consequences of CMP, "including lengthy recovery time and increased risk for serious operative complications."
The National Institutes of Health and the University of Michigan supported the study. Neither Dr. Hawley nor her coauthors had any financial disclosures.
On Twitter @alz_gal
Decisions about breast cancer surgery are often done when emotions run high, and when real comprehension of the long-term effects might be difficult, Dr. Shoshana Rosenberg wrote in an accompanying editorial.
"Anxiety and fear hamper optimal decision making, and greater psychological and emotional support may prove valuable in this situation."
Treatment decisions built on fear put surgeons in a tough spot, forcing them to balance their clinical knowledge of recurrence and surgical risk against the need to respect patients’ own desires. "While CPM might be considered overtreating women without clinical indications, it might still be the right choice for some women for risks reduction, cosmetic, and/or emotional reasons."
The earlier education about these issues, commences, the better incorporated it can become into this journey.
"Not only should the pros and cons of different treatment options be communicated, but there needs to be consideration of the patient’s personal circumstances and perceptions, all the while addressing anxiety and concerns about breast cancer recurrence. ... Finding balance around this issue, like the decision process itself, should be a goal shared by patients and clinicians alike."
Dr. Rosenberg is a research fellow at the Dana Farber Cancer Institute, Boston. She had no financial disclosures.
Decisions about breast cancer surgery are often done when emotions run high, and when real comprehension of the long-term effects might be difficult, Dr. Shoshana Rosenberg wrote in an accompanying editorial.
"Anxiety and fear hamper optimal decision making, and greater psychological and emotional support may prove valuable in this situation."
Treatment decisions built on fear put surgeons in a tough spot, forcing them to balance their clinical knowledge of recurrence and surgical risk against the need to respect patients’ own desires. "While CPM might be considered overtreating women without clinical indications, it might still be the right choice for some women for risks reduction, cosmetic, and/or emotional reasons."
The earlier education about these issues, commences, the better incorporated it can become into this journey.
"Not only should the pros and cons of different treatment options be communicated, but there needs to be consideration of the patient’s personal circumstances and perceptions, all the while addressing anxiety and concerns about breast cancer recurrence. ... Finding balance around this issue, like the decision process itself, should be a goal shared by patients and clinicians alike."
Dr. Rosenberg is a research fellow at the Dana Farber Cancer Institute, Boston. She had no financial disclosures.
Decisions about breast cancer surgery are often done when emotions run high, and when real comprehension of the long-term effects might be difficult, Dr. Shoshana Rosenberg wrote in an accompanying editorial.
"Anxiety and fear hamper optimal decision making, and greater psychological and emotional support may prove valuable in this situation."
Treatment decisions built on fear put surgeons in a tough spot, forcing them to balance their clinical knowledge of recurrence and surgical risk against the need to respect patients’ own desires. "While CPM might be considered overtreating women without clinical indications, it might still be the right choice for some women for risks reduction, cosmetic, and/or emotional reasons."
The earlier education about these issues, commences, the better incorporated it can become into this journey.
"Not only should the pros and cons of different treatment options be communicated, but there needs to be consideration of the patient’s personal circumstances and perceptions, all the while addressing anxiety and concerns about breast cancer recurrence. ... Finding balance around this issue, like the decision process itself, should be a goal shared by patients and clinicians alike."
Dr. Rosenberg is a research fellow at the Dana Farber Cancer Institute, Boston. She had no financial disclosures.
Fear seems to be a major driver of contralateral prophylactic mastectomy after initial breast cancer surgery.
Almost two-thirds of those who had the procedure had no clinical indication for it, Sarah T. Hawley, Ph.D., and her colleagues wrote in the May 21 online issue of JAMA Surgery (doi:10.1001/jamasurg.2013.5689). The women choosing contralateral prophylactic mastectomy (CPM) for which there was no clinical indication were more highly educated than were those who didn’t elect the surgery, more likely to be white, and two to four times more likely to be worried about a recurrence.
Fear of recurrence was a "powerful nonclinical factor" in the analysis, wrote Dr. Hawley of the University of Michigan, Ann Arbor – and education may be the best way to overcome it.
"A patient’s decision to undergo contralateral prophylactic mastectomy based on a strong fear of recurrence in the absence of clinical indications presents an important clinical challenge for surgeons," she and her colleagues wrote. "Growing literature supports the notion that patients have a difficult time assessing and interpreting their own risk and that fear and anxiety related to disease recurrence often supersede accurate risk perceptions to drive health decisions."
Dr. Hawley and her coinvestigators extracted their data from the Surveillance, Epidemiology, and End Results (SEER) registries for Los Angeles and Detroit. They included records from 1,447 women aged 20-79 years who had been diagnosed with a first incident primary ductal carcinoma in situ or invasive breast cancer of stages I-IIIa.
About half of the sample was white; 21% was black, and 30% Hispanic. Other groups made up the balance. More than half (59%) had achieved some college-level education.
About half the respondents (57%) underwent breast-conserving surgery (BCS). Other surgical treatments included unilateral mastectomy (UM; 34%), and contralateral prophylactic mastectomy (8%).
CPM was pondered more frequently than it was an executed, the investigators said, with 19% of the entire sample considering it "strongly or very strongly."
Most of the women who had CPM said that they did it to prevent recurrence, with 78% citing that worry as a very important driver of their decision. However, the authors said, of the 106 women who underwent CPM, only 31% had clinical indications, while the majority (67%) did not.
A multivariate analysis determined the relationships between patient characteristics and breast surgery,
Those with some college-level education were five times more likely to have CPM than UM, and four times more likely to have that than BCS. Those with high worry were almost three times more likely to have CPM than UM, and four times more likely to have CPM than BCS.
Women who had positive genetic testing were 10 times more likely to have contralateral prophylactic mastectomy than unilateral mastectomy, and 19 times more likely to have CPM than BCS. But those with negative results were still twice as likely to have the CPM as either of the other surgeries.
Having at least two close relatives with breast or ovarian cancer also significantly increased the likelihood of a CMP vs. UM (relative risk = 5) or BCS (RR = 4). Having had a diagnostic MRI doubled the chance of having CPM, compared with the other surgeries.
"Our results provide evidence that decisions about CPM represent a clear case in which better strategies to increase patient knowledge about their own risk of developing contralateral cancer as well as the net benefit of treatment are needed and should be made only after patients are accurately informed about these issues," Dr. Hawley and her coauthors said, adding that such patients need to clearly understand the consequences of CMP, "including lengthy recovery time and increased risk for serious operative complications."
The National Institutes of Health and the University of Michigan supported the study. Neither Dr. Hawley nor her coauthors had any financial disclosures.
On Twitter @alz_gal
Fear seems to be a major driver of contralateral prophylactic mastectomy after initial breast cancer surgery.
Almost two-thirds of those who had the procedure had no clinical indication for it, Sarah T. Hawley, Ph.D., and her colleagues wrote in the May 21 online issue of JAMA Surgery (doi:10.1001/jamasurg.2013.5689). The women choosing contralateral prophylactic mastectomy (CPM) for which there was no clinical indication were more highly educated than were those who didn’t elect the surgery, more likely to be white, and two to four times more likely to be worried about a recurrence.
Fear of recurrence was a "powerful nonclinical factor" in the analysis, wrote Dr. Hawley of the University of Michigan, Ann Arbor – and education may be the best way to overcome it.
"A patient’s decision to undergo contralateral prophylactic mastectomy based on a strong fear of recurrence in the absence of clinical indications presents an important clinical challenge for surgeons," she and her colleagues wrote. "Growing literature supports the notion that patients have a difficult time assessing and interpreting their own risk and that fear and anxiety related to disease recurrence often supersede accurate risk perceptions to drive health decisions."
Dr. Hawley and her coinvestigators extracted their data from the Surveillance, Epidemiology, and End Results (SEER) registries for Los Angeles and Detroit. They included records from 1,447 women aged 20-79 years who had been diagnosed with a first incident primary ductal carcinoma in situ or invasive breast cancer of stages I-IIIa.
About half of the sample was white; 21% was black, and 30% Hispanic. Other groups made up the balance. More than half (59%) had achieved some college-level education.
About half the respondents (57%) underwent breast-conserving surgery (BCS). Other surgical treatments included unilateral mastectomy (UM; 34%), and contralateral prophylactic mastectomy (8%).
CPM was pondered more frequently than it was an executed, the investigators said, with 19% of the entire sample considering it "strongly or very strongly."
Most of the women who had CPM said that they did it to prevent recurrence, with 78% citing that worry as a very important driver of their decision. However, the authors said, of the 106 women who underwent CPM, only 31% had clinical indications, while the majority (67%) did not.
A multivariate analysis determined the relationships between patient characteristics and breast surgery,
Those with some college-level education were five times more likely to have CPM than UM, and four times more likely to have that than BCS. Those with high worry were almost three times more likely to have CPM than UM, and four times more likely to have CPM than BCS.
Women who had positive genetic testing were 10 times more likely to have contralateral prophylactic mastectomy than unilateral mastectomy, and 19 times more likely to have CPM than BCS. But those with negative results were still twice as likely to have the CPM as either of the other surgeries.
Having at least two close relatives with breast or ovarian cancer also significantly increased the likelihood of a CMP vs. UM (relative risk = 5) or BCS (RR = 4). Having had a diagnostic MRI doubled the chance of having CPM, compared with the other surgeries.
"Our results provide evidence that decisions about CPM represent a clear case in which better strategies to increase patient knowledge about their own risk of developing contralateral cancer as well as the net benefit of treatment are needed and should be made only after patients are accurately informed about these issues," Dr. Hawley and her coauthors said, adding that such patients need to clearly understand the consequences of CMP, "including lengthy recovery time and increased risk for serious operative complications."
The National Institutes of Health and the University of Michigan supported the study. Neither Dr. Hawley nor her coauthors had any financial disclosures.
On Twitter @alz_gal
FROM JAMA SURGERY
Key clinical point: Fear of breast cancer recurrence results in many unnecessary contralateral prophylactic mastectomies.
Major finding: Women with high worry levels about recurrence were almost three times more likely to have contralateral prophylactic mastectomy than unilateral mastectomy, and four times more likely to have it than breast-conserving surgery.
Data source: The database review comprised 1,447 women.
Disclosures: The National Institutes of Health and University of Michigan funded the studies. None of the authors had any financial disclosures.

Lesion length, number correspond to neuromyelitis optica Dx
PHILADELPHIA – Magnetic resonance imaging of the optic nerve may help differentiate the causes of a first optic neuritis event, a study at Johns Hopkins University showed.
Optic neuritis can be a presenting symptom of both neuromyelitis optica and multiple sclerosis, Maureen Mealy, M.S.C.N., said at the annual meeting of the American Academy of Neurology. Serum antibodies can differentiate the two disorders as root causes. But early in the neuromyelitis optica (NMO) disease process, less than 20% of patients are positive for NMO immunoglobulin.
"It would be helpful if we could know whether the first incidence of optic neuritis was the presenting symptom of MS or NMO," said Ms. Mealy, clinical manager of the Johns Hopkins Transverse Myelitis Center and Neuromyelitis Optica Clinic, Baltimore.
To investigate the usefulness of MRI as a possible diagnostic tool, Ms. Mealy and her colleagues reviewed the records of 52 patients who presented with optic neuritis. Of these, 26 were later found to have NMO and 26 to have MS. The incident was a first event in 35% of the NMO patients and 61% of the MS patients.
Those with MS were a median of 32 years old, while those with NMO were a median of 36 years. At the time of the MRI, a test for NMO IgG was positive in 54% of those with NMO. None of the MS patients were positive for the antibody. Ms. Mealy noted that positive antibodies were more common among this NMO group than what is normally found in published studies, probably because the patients were seen at a major regional referral center.
The MRI was performed within 30 days of symptom onset. Investigators looked at some very specific regions of the optic nerve, Ms. Mealy said: the retrobulbar, canalicular, and prechiasmal segments; the chiasm; and the optic tract extending into the brain. Neuroradiologists measured the length of each lesion, and also scored each lesion by the number of involved segments. "There were a total of nine segments examined in each image – two retrobulbar, two canalicular, two prechiasmal, the chiasm, and the two optic tracts," she said.
Lesions were significantly longer among patients with NMO than among those with MS (30.5 vs. 13.5 mm). In addition, NMO-related events were significantly more likely to have multisegment lesions. Most MS-related events (19) had only one segment involved, whereas just 6 NMO events had only one segment involved. Eleven NMO events had three segments involved, two had four segments, and four had five or more segments. "There were no MS events with three or more involved segments," said Ms. Mealy, a multiple sclerosis certified nurse.
NMO-associated lesions were also more likely to be bilateral (25% vs. 0% MS lesions), and to involve the optic chiasm (25% vs. 7%) and optic tracts (18% vs. 4%).
MS lesions were more likely to be localized anteriorly in the retrobulbar and/or canalicular optic nerve (70% vs. 36% in NMO). "In contrast, 64% of NMO lesions involved the posterior pathways," she noted. "It seems that a long or extensive lesion that occurs more posteriorly could be an early biomarker for NMO."
She cautioned that the neuroradiologists were not blinded when reading the MRIs. This adds to the necessity for prospective blinded studies before imaging can be used as a predictor or diagnostic tool, she said.
Ms. Mealy said she had no financial disclosures.
On Twitter @Alz_Gal
PHILADELPHIA – Magnetic resonance imaging of the optic nerve may help differentiate the causes of a first optic neuritis event, a study at Johns Hopkins University showed.
Optic neuritis can be a presenting symptom of both neuromyelitis optica and multiple sclerosis, Maureen Mealy, M.S.C.N., said at the annual meeting of the American Academy of Neurology. Serum antibodies can differentiate the two disorders as root causes. But early in the neuromyelitis optica (NMO) disease process, less than 20% of patients are positive for NMO immunoglobulin.
"It would be helpful if we could know whether the first incidence of optic neuritis was the presenting symptom of MS or NMO," said Ms. Mealy, clinical manager of the Johns Hopkins Transverse Myelitis Center and Neuromyelitis Optica Clinic, Baltimore.
To investigate the usefulness of MRI as a possible diagnostic tool, Ms. Mealy and her colleagues reviewed the records of 52 patients who presented with optic neuritis. Of these, 26 were later found to have NMO and 26 to have MS. The incident was a first event in 35% of the NMO patients and 61% of the MS patients.
Those with MS were a median of 32 years old, while those with NMO were a median of 36 years. At the time of the MRI, a test for NMO IgG was positive in 54% of those with NMO. None of the MS patients were positive for the antibody. Ms. Mealy noted that positive antibodies were more common among this NMO group than what is normally found in published studies, probably because the patients were seen at a major regional referral center.
The MRI was performed within 30 days of symptom onset. Investigators looked at some very specific regions of the optic nerve, Ms. Mealy said: the retrobulbar, canalicular, and prechiasmal segments; the chiasm; and the optic tract extending into the brain. Neuroradiologists measured the length of each lesion, and also scored each lesion by the number of involved segments. "There were a total of nine segments examined in each image – two retrobulbar, two canalicular, two prechiasmal, the chiasm, and the two optic tracts," she said.
Lesions were significantly longer among patients with NMO than among those with MS (30.5 vs. 13.5 mm). In addition, NMO-related events were significantly more likely to have multisegment lesions. Most MS-related events (19) had only one segment involved, whereas just 6 NMO events had only one segment involved. Eleven NMO events had three segments involved, two had four segments, and four had five or more segments. "There were no MS events with three or more involved segments," said Ms. Mealy, a multiple sclerosis certified nurse.
NMO-associated lesions were also more likely to be bilateral (25% vs. 0% MS lesions), and to involve the optic chiasm (25% vs. 7%) and optic tracts (18% vs. 4%).
MS lesions were more likely to be localized anteriorly in the retrobulbar and/or canalicular optic nerve (70% vs. 36% in NMO). "In contrast, 64% of NMO lesions involved the posterior pathways," she noted. "It seems that a long or extensive lesion that occurs more posteriorly could be an early biomarker for NMO."
She cautioned that the neuroradiologists were not blinded when reading the MRIs. This adds to the necessity for prospective blinded studies before imaging can be used as a predictor or diagnostic tool, she said.
Ms. Mealy said she had no financial disclosures.
On Twitter @Alz_Gal
PHILADELPHIA – Magnetic resonance imaging of the optic nerve may help differentiate the causes of a first optic neuritis event, a study at Johns Hopkins University showed.
Optic neuritis can be a presenting symptom of both neuromyelitis optica and multiple sclerosis, Maureen Mealy, M.S.C.N., said at the annual meeting of the American Academy of Neurology. Serum antibodies can differentiate the two disorders as root causes. But early in the neuromyelitis optica (NMO) disease process, less than 20% of patients are positive for NMO immunoglobulin.
"It would be helpful if we could know whether the first incidence of optic neuritis was the presenting symptom of MS or NMO," said Ms. Mealy, clinical manager of the Johns Hopkins Transverse Myelitis Center and Neuromyelitis Optica Clinic, Baltimore.
To investigate the usefulness of MRI as a possible diagnostic tool, Ms. Mealy and her colleagues reviewed the records of 52 patients who presented with optic neuritis. Of these, 26 were later found to have NMO and 26 to have MS. The incident was a first event in 35% of the NMO patients and 61% of the MS patients.
Those with MS were a median of 32 years old, while those with NMO were a median of 36 years. At the time of the MRI, a test for NMO IgG was positive in 54% of those with NMO. None of the MS patients were positive for the antibody. Ms. Mealy noted that positive antibodies were more common among this NMO group than what is normally found in published studies, probably because the patients were seen at a major regional referral center.
The MRI was performed within 30 days of symptom onset. Investigators looked at some very specific regions of the optic nerve, Ms. Mealy said: the retrobulbar, canalicular, and prechiasmal segments; the chiasm; and the optic tract extending into the brain. Neuroradiologists measured the length of each lesion, and also scored each lesion by the number of involved segments. "There were a total of nine segments examined in each image – two retrobulbar, two canalicular, two prechiasmal, the chiasm, and the two optic tracts," she said.
Lesions were significantly longer among patients with NMO than among those with MS (30.5 vs. 13.5 mm). In addition, NMO-related events were significantly more likely to have multisegment lesions. Most MS-related events (19) had only one segment involved, whereas just 6 NMO events had only one segment involved. Eleven NMO events had three segments involved, two had four segments, and four had five or more segments. "There were no MS events with three or more involved segments," said Ms. Mealy, a multiple sclerosis certified nurse.
NMO-associated lesions were also more likely to be bilateral (25% vs. 0% MS lesions), and to involve the optic chiasm (25% vs. 7%) and optic tracts (18% vs. 4%).
MS lesions were more likely to be localized anteriorly in the retrobulbar and/or canalicular optic nerve (70% vs. 36% in NMO). "In contrast, 64% of NMO lesions involved the posterior pathways," she noted. "It seems that a long or extensive lesion that occurs more posteriorly could be an early biomarker for NMO."
She cautioned that the neuroradiologists were not blinded when reading the MRIs. This adds to the necessity for prospective blinded studies before imaging can be used as a predictor or diagnostic tool, she said.
Ms. Mealy said she had no financial disclosures.
On Twitter @Alz_Gal
AT THE AAN 2014 ANNUAL MEETING
Key clinical point: Patients who present with optic neuritis and have multisegment lesions on MRI, particularly involving posterior pathways of the optic nerve, may be more likely to have NMO than MS.
Major finding: Optic nerve lesions associated with neuromyelitis optica were a mean of 30.5 mm long, compared with 13.5 mm for lesions associated with multiple sclerosis.
Data source: A retrospective study of 52 patients.
Disclosures: Ms. Mealy said she had no financial disclosures.

For smokers, prenatal vitamin C improves infants’ lung function
Daily vitamin C during smokers’ pregnancies significantly improved the lung function of their infants at birth and reduced the incidence of wheezing during the first year of life, compared with infants of smokers who weren’t exposed to the vitamin.
Those infants had significantly poorer respiratory outcomes, both at birth and 1 year, according to Dr. Cindy McEvoy and colleagues. The study was presented at an international conference of the American Thoracic Society and simultaneously published in the May 18 issue ofthe Journal of the American Medical Association.

While it’s not entirely clear how vitamin C influences prenatal lung development, there are tantalizing hints, wrote Dr. McEvoy of the Oregon Health and Science University, Portland, and her coinvestigators. "Supplemental vitamin C may act by blocking formation of reactive oxygen species, which stimulate abnormal patterns of airway cell proliferation, resulting in narrowed airways and abnormal airway geometry," they said.
Dr. McEvoy and her team randomized 179 pregnant smokers to either placebo or 500 mg vitamin C daily from week 16 of pregnancy. At birth, they examined two respiratory function measures: the ratio of time to peak expiratory flow/expiratory time (TPTEF:TE) and passive respiratory compliance per kg (Crs/kg). They also compared the incidences of wheezing during the first year. A control group of 76 infants from nonsmokers provided a comparator (JAMA 2014 May 18 [doi:10.1001/jama.2014.5217]).
The women were a mean age of 26 years at baseline. Most were white (about 85%), and 20% had at least some college education. In the placebo group, 36% smoked at least 10 cigarettes a day; in the active group, 41% smoked that many. All smoking mothers were offered the chance to participate in a smoking cessation program; 10% were able to stop.
At birth, infants exposed to vitamin C had significantly better lung function than nonexposed infants on both measures. The TPTEF:TE was 10% better in the exposed group (0.383 vs. 0.345) – similar to the ratio in the comparator group of infants from nonsmoking mothers. The Crs/kg was also significantly better (11%) in the vitamin C group (1.32 vs. 1.20 mL/cmH20/kg).
Almost all of the babies had 1-year follow-up (92%). At that time, the incidence of wheezing during the first year was 21% in the treated group and 40% in the placebo group (adjusted relative risk, 0.56). However, the authors noted, there was no between-group difference in the other lung function measures at 1 year.
A subgroup of 173 mothers was genotyped for two polymorphisms that are strongly associated with a lifelong risk of nicotine addiction, lung cancer, and chronic obstructive pulmonary disease.
The infants of mothers who were heterozygous for one of those (rs16969968), experienced the largest benefit from vitamin C exposure. The incidence of wheezing through 1 year in these infants was 14%, compared with 48% among those randomized to placebo.
The National Heart, Lung, and Blood Institute sponsored the study. Neither Dr. McEvoy nor any of her coauthors had any financial disclosures.
Quitting is the best way for smokers to protect their unborn babies against the harms of tobacco.
But unfortunately, quitting doesn’t always happen. Thus, the finding that vitamin C may offer babies some protection against the harms of tobacco is heartening news. Although the improvement over placebo was rather small (10%), it could have a profound effect.
"Small population-level changes in lung function may lead to significant public health benefits, and the improvements in lung function reported here could be associated with future benefit."
The study was well designed and well executed, and the 1-year endpoints intriguing. However, there is no evidence that vitamin C fully prevents or reverses the effects of maternal smoking during gestation. Thus, prenatal treatment should never be seen as a panacea.
"Achieving smoking cessation should be the primary goal for women who smoke and who intend to become pregnant. By preventing her developing fetus and newborn infant from becoming exposed to tobacco smoke, a pregnant woman can do more for the respiratory health and overall health of her child than any amount of vitamin C may be able to accomplish."
Graham L. Hall, Ph.D., is head of pediatric respiratory physiology and research at the Telethon Kids Institute, University of Western Australia, West Perth. These remarks were taken from his accompanying editorial (JAMA 2014 May 18 [doi:10.1001/jama.2014.5218]).
Quitting is the best way for smokers to protect their unborn babies against the harms of tobacco.
But unfortunately, quitting doesn’t always happen. Thus, the finding that vitamin C may offer babies some protection against the harms of tobacco is heartening news. Although the improvement over placebo was rather small (10%), it could have a profound effect.
"Small population-level changes in lung function may lead to significant public health benefits, and the improvements in lung function reported here could be associated with future benefit."
The study was well designed and well executed, and the 1-year endpoints intriguing. However, there is no evidence that vitamin C fully prevents or reverses the effects of maternal smoking during gestation. Thus, prenatal treatment should never be seen as a panacea.
"Achieving smoking cessation should be the primary goal for women who smoke and who intend to become pregnant. By preventing her developing fetus and newborn infant from becoming exposed to tobacco smoke, a pregnant woman can do more for the respiratory health and overall health of her child than any amount of vitamin C may be able to accomplish."
Graham L. Hall, Ph.D., is head of pediatric respiratory physiology and research at the Telethon Kids Institute, University of Western Australia, West Perth. These remarks were taken from his accompanying editorial (JAMA 2014 May 18 [doi:10.1001/jama.2014.5218]).
Quitting is the best way for smokers to protect their unborn babies against the harms of tobacco.
But unfortunately, quitting doesn’t always happen. Thus, the finding that vitamin C may offer babies some protection against the harms of tobacco is heartening news. Although the improvement over placebo was rather small (10%), it could have a profound effect.
"Small population-level changes in lung function may lead to significant public health benefits, and the improvements in lung function reported here could be associated with future benefit."
The study was well designed and well executed, and the 1-year endpoints intriguing. However, there is no evidence that vitamin C fully prevents or reverses the effects of maternal smoking during gestation. Thus, prenatal treatment should never be seen as a panacea.
"Achieving smoking cessation should be the primary goal for women who smoke and who intend to become pregnant. By preventing her developing fetus and newborn infant from becoming exposed to tobacco smoke, a pregnant woman can do more for the respiratory health and overall health of her child than any amount of vitamin C may be able to accomplish."
Graham L. Hall, Ph.D., is head of pediatric respiratory physiology and research at the Telethon Kids Institute, University of Western Australia, West Perth. These remarks were taken from his accompanying editorial (JAMA 2014 May 18 [doi:10.1001/jama.2014.5218]).
Daily vitamin C during smokers’ pregnancies significantly improved the lung function of their infants at birth and reduced the incidence of wheezing during the first year of life, compared with infants of smokers who weren’t exposed to the vitamin.
Those infants had significantly poorer respiratory outcomes, both at birth and 1 year, according to Dr. Cindy McEvoy and colleagues. The study was presented at an international conference of the American Thoracic Society and simultaneously published in the May 18 issue ofthe Journal of the American Medical Association.
While it’s not entirely clear how vitamin C influences prenatal lung development, there are tantalizing hints, wrote Dr. McEvoy of the Oregon Health and Science University, Portland, and her coinvestigators. "Supplemental vitamin C may act by blocking formation of reactive oxygen species, which stimulate abnormal patterns of airway cell proliferation, resulting in narrowed airways and abnormal airway geometry," they said.
Dr. McEvoy and her team randomized 179 pregnant smokers to either placebo or 500 mg vitamin C daily from week 16 of pregnancy. At birth, they examined two respiratory function measures: the ratio of time to peak expiratory flow/expiratory time (TPTEF:TE) and passive respiratory compliance per kg (Crs/kg). They also compared the incidences of wheezing during the first year. A control group of 76 infants from nonsmokers provided a comparator (JAMA 2014 May 18 [doi:10.1001/jama.2014.5217]).
The women were a mean age of 26 years at baseline. Most were white (about 85%), and 20% had at least some college education. In the placebo group, 36% smoked at least 10 cigarettes a day; in the active group, 41% smoked that many. All smoking mothers were offered the chance to participate in a smoking cessation program; 10% were able to stop.
At birth, infants exposed to vitamin C had significantly better lung function than nonexposed infants on both measures. The TPTEF:TE was 10% better in the exposed group (0.383 vs. 0.345) – similar to the ratio in the comparator group of infants from nonsmoking mothers. The Crs/kg was also significantly better (11%) in the vitamin C group (1.32 vs. 1.20 mL/cmH20/kg).
Almost all of the babies had 1-year follow-up (92%). At that time, the incidence of wheezing during the first year was 21% in the treated group and 40% in the placebo group (adjusted relative risk, 0.56). However, the authors noted, there was no between-group difference in the other lung function measures at 1 year.
A subgroup of 173 mothers was genotyped for two polymorphisms that are strongly associated with a lifelong risk of nicotine addiction, lung cancer, and chronic obstructive pulmonary disease.
The infants of mothers who were heterozygous for one of those (rs16969968), experienced the largest benefit from vitamin C exposure. The incidence of wheezing through 1 year in these infants was 14%, compared with 48% among those randomized to placebo.
The National Heart, Lung, and Blood Institute sponsored the study. Neither Dr. McEvoy nor any of her coauthors had any financial disclosures.
Daily vitamin C during smokers’ pregnancies significantly improved the lung function of their infants at birth and reduced the incidence of wheezing during the first year of life, compared with infants of smokers who weren’t exposed to the vitamin.
Those infants had significantly poorer respiratory outcomes, both at birth and 1 year, according to Dr. Cindy McEvoy and colleagues. The study was presented at an international conference of the American Thoracic Society and simultaneously published in the May 18 issue ofthe Journal of the American Medical Association.
While it’s not entirely clear how vitamin C influences prenatal lung development, there are tantalizing hints, wrote Dr. McEvoy of the Oregon Health and Science University, Portland, and her coinvestigators. "Supplemental vitamin C may act by blocking formation of reactive oxygen species, which stimulate abnormal patterns of airway cell proliferation, resulting in narrowed airways and abnormal airway geometry," they said.
Dr. McEvoy and her team randomized 179 pregnant smokers to either placebo or 500 mg vitamin C daily from week 16 of pregnancy. At birth, they examined two respiratory function measures: the ratio of time to peak expiratory flow/expiratory time (TPTEF:TE) and passive respiratory compliance per kg (Crs/kg). They also compared the incidences of wheezing during the first year. A control group of 76 infants from nonsmokers provided a comparator (JAMA 2014 May 18 [doi:10.1001/jama.2014.5217]).
The women were a mean age of 26 years at baseline. Most were white (about 85%), and 20% had at least some college education. In the placebo group, 36% smoked at least 10 cigarettes a day; in the active group, 41% smoked that many. All smoking mothers were offered the chance to participate in a smoking cessation program; 10% were able to stop.
At birth, infants exposed to vitamin C had significantly better lung function than nonexposed infants on both measures. The TPTEF:TE was 10% better in the exposed group (0.383 vs. 0.345) – similar to the ratio in the comparator group of infants from nonsmoking mothers. The Crs/kg was also significantly better (11%) in the vitamin C group (1.32 vs. 1.20 mL/cmH20/kg).
Almost all of the babies had 1-year follow-up (92%). At that time, the incidence of wheezing during the first year was 21% in the treated group and 40% in the placebo group (adjusted relative risk, 0.56). However, the authors noted, there was no between-group difference in the other lung function measures at 1 year.
A subgroup of 173 mothers was genotyped for two polymorphisms that are strongly associated with a lifelong risk of nicotine addiction, lung cancer, and chronic obstructive pulmonary disease.
The infants of mothers who were heterozygous for one of those (rs16969968), experienced the largest benefit from vitamin C exposure. The incidence of wheezing through 1 year in these infants was 14%, compared with 48% among those randomized to placebo.
The National Heart, Lung, and Blood Institute sponsored the study. Neither Dr. McEvoy nor any of her coauthors had any financial disclosures.
FROM ATS 2014
Key clinical point: Giving Vitamin C to pregnant smokers may improve newborns’ lung health.
Major finding: Lung function at birth was about 10% better in infants’ of smokers 500 mg vitamin C daily during pregnancy, compared to those who did not. The incidence of wheezing during the first year was 21% in the treated group vs. 40% in the placebo group.
Data source: A randomized, placebo-controlled study of 179 pregnant smokers.
Disclosures: The National Heart, Lung, and Blood Institute funded the study. None of the authors had financial disclosures.
