User login
Hospitals Failing to Address Patient Boarding in the ED
Hospital flow inefficiencies are the real culprit behind patient boarding in the emergency department, according to a report in Health Affairs released on Aug. 6.
Most hospitals have implemented just two of nine measures proven to reduce ED boarding, according to the report. "Boarding" (keeping admitted patients in hallway beds in the emergency department for more than 2-4 hours because an inpatient bed is not available) has been shown to increase in-hospital mortality and length of stay (Acad. Emerg. Med. 2011;18:1324-9). The practice also reduces hospital income, increases patients’ risk for hospital-acquired infections, and contributes to lapses in routine care and medications.
Proven strategies to address the problem "are grossly underused," wrote Dr. Elaine Rabin, of Mount Sinai School of Medicine in New York, and her coauthors (Health Affairs 2012 Aug. 6 [doi:10.1377/hlthaff.2011.0786]).
The problem has escalated over the last decade. A 2001 survey "found that one in five patients in U.S. emergency departments were boarding, and three in four emergency departments were boarding at least two inpatients" (Ann. Emerg. Med. 2003;42:167-72). A 2003 report "found that nine out of ten hospitals reported some degree of boarding," with 20% of hospitals boarding patients for an average of 8 hours. Most recently, a 2010 survey showed that 85% of hospitals had boarded patients the previous week (Acad. Emerg. Med. 2010;17[suppl s1]:s90; abstract 260).
Boarding substantially reduces ED capacity. In a study done at one community hospital in Pennsylvania, moving patients who were admitted from the ED to inpatient beds within 2 hours would have increased ED capacity by 10,397 hours (433 days) over the 1-year study period (Acad. Emerg. Med. 2007;14:332-7).
Nowhere to Go
"Crowding is not an emergency department–based problem. Rather, it is a symptom of dysfunction in interrelated parts of the broader health care system," wrote Dr. Rabin and her coauthors.
Although it is commonly believed that "crowding results from uninsured patients’ seeking nonemergency care in the emergency department," studies have shown that "the main driver of emergency department crowding is patient outflow obstruction: an inability to move admitted patients to inpatient beds in a timely manner," they wrote.
Another assumption is that hospitals are swamped with too many patients, but boarding actually begins when a hospital is at 80%-85% of capacity, "partly because specified bed types ... fill earlier than other types," Dr. Rabin and her colleagues said. The common practice of reserving inpatient beds for specified categories of patients, such as postelective procedure patients or isolation cases, or to maintain a "geographic" bed plan (similar patients grouped together to match specialized nurses with patients), can mean that patients linger in the ED despite available beds. "Introducing some flexibility in the geographic pooling of beds decreased emergency department boarding times" by 50% and increased hospital revenue by 1% at one hospital (Oper. Res. 2009;57:261-73).
Bottom Line
ED crowding and boarding may substantially reduce hospital income; for example, in the 2007 study of the Pennsylvania community hospital, boarding resulted in an estimated loss of almost $4 million in net revenue.
But exactly how much revenue might be lost because of ED crowding is still under debate; ED patients are more likely to be uninsured than are elective admissions, so crowding may have the unintended effect of reducing the number of patients who can’t pay for care. In addition, the tasks involved in assessing and stabilizing ED patients are reimbursed at a lower rate, compared with scheduled surgical procedures.
On the other hand, "low patient satisfaction related to long wait times and boarding may also drive well-reimbursed business away," the authors pointed out.
Strategies That Work
Addressing the bottlenecks does not have to mean adding beds. On the contrary, "improved use of existing beds should be the first-line strategy," Dr. Rabin and her coauthors said.
Evidence supports the use of these nine measures:
"Boarding is a systemwide problem."
• Moving ED hall patients to inpatient hallways. Patients prefer the quieter hallways, the nurse-patient ratio is usually lower, and the ED reclaims the beds for more incoming patients.
• Smoothing surgical schedules. By decreasing demand at peak times, this measure alone has been shown to "nearly eliminate boarding" at some hospitals, according to the report.
• Scheduling cardiac catheterizations for early in the day.
• Actively managing bed use. Approaches include making information on free beds quickly available via a computerized system, and use of a bed coordinator or "bed czar."
• Setting up a discharge lounge. Patients can be moved out of their beds into another area to await the completion of their discharge paperwork.
• Planning for discharge at time of admission. Making early arrangements for patients who will need outpatient placement in a nursing home or rehabilitation facility can speed their discharge by as much as 22 hours (J. Hosp. Med. 2009;4:226-33).
• Monitoring room-cleaning turnaround times. Cleaning staff should be held accountable for prompt work.
• Simplifying the steps needed to admit patients.
• Performing "reverse triage." During peak times, patients who have the least need for a bed can be discharged.
The most commonly adopted of these nine proven measures are actively managing bed use (quickly available bed information, 66% of hospitals; bed coordinator, 51%) and smoothing surgical schedules (58%).
Taking action to reduce boarding requires "a clear commitment by hospital leadership to overcome operations barriers across departments," Dr. Rabin and her coauthors said.

"Boarding is a systemwide problem, and successful responses require the endorsement of hospital leaders. ... If continued education of hospital managers and the public does not result in change, enhanced regulation will be necessary to protect patients," they concluded.
All of the authors are members of the Emergency Department Crowding Interest Group of the Society for Academic Emergency Medicine. No disclosures were reported.
Hospital flow inefficiencies are the real culprit behind patient boarding in the emergency department, according to a report in Health Affairs released on Aug. 6.
Most hospitals have implemented just two of nine measures proven to reduce ED boarding, according to the report. "Boarding" (keeping admitted patients in hallway beds in the emergency department for more than 2-4 hours because an inpatient bed is not available) has been shown to increase in-hospital mortality and length of stay (Acad. Emerg. Med. 2011;18:1324-9). The practice also reduces hospital income, increases patients’ risk for hospital-acquired infections, and contributes to lapses in routine care and medications.
Proven strategies to address the problem "are grossly underused," wrote Dr. Elaine Rabin, of Mount Sinai School of Medicine in New York, and her coauthors (Health Affairs 2012 Aug. 6 [doi:10.1377/hlthaff.2011.0786]).
The problem has escalated over the last decade. A 2001 survey "found that one in five patients in U.S. emergency departments were boarding, and three in four emergency departments were boarding at least two inpatients" (Ann. Emerg. Med. 2003;42:167-72). A 2003 report "found that nine out of ten hospitals reported some degree of boarding," with 20% of hospitals boarding patients for an average of 8 hours. Most recently, a 2010 survey showed that 85% of hospitals had boarded patients the previous week (Acad. Emerg. Med. 2010;17[suppl s1]:s90; abstract 260).
Boarding substantially reduces ED capacity. In a study done at one community hospital in Pennsylvania, moving patients who were admitted from the ED to inpatient beds within 2 hours would have increased ED capacity by 10,397 hours (433 days) over the 1-year study period (Acad. Emerg. Med. 2007;14:332-7).
Nowhere to Go
"Crowding is not an emergency department–based problem. Rather, it is a symptom of dysfunction in interrelated parts of the broader health care system," wrote Dr. Rabin and her coauthors.
Although it is commonly believed that "crowding results from uninsured patients’ seeking nonemergency care in the emergency department," studies have shown that "the main driver of emergency department crowding is patient outflow obstruction: an inability to move admitted patients to inpatient beds in a timely manner," they wrote.
Another assumption is that hospitals are swamped with too many patients, but boarding actually begins when a hospital is at 80%-85% of capacity, "partly because specified bed types ... fill earlier than other types," Dr. Rabin and her colleagues said. The common practice of reserving inpatient beds for specified categories of patients, such as postelective procedure patients or isolation cases, or to maintain a "geographic" bed plan (similar patients grouped together to match specialized nurses with patients), can mean that patients linger in the ED despite available beds. "Introducing some flexibility in the geographic pooling of beds decreased emergency department boarding times" by 50% and increased hospital revenue by 1% at one hospital (Oper. Res. 2009;57:261-73).
Bottom Line
ED crowding and boarding may substantially reduce hospital income; for example, in the 2007 study of the Pennsylvania community hospital, boarding resulted in an estimated loss of almost $4 million in net revenue.
But exactly how much revenue might be lost because of ED crowding is still under debate; ED patients are more likely to be uninsured than are elective admissions, so crowding may have the unintended effect of reducing the number of patients who can’t pay for care. In addition, the tasks involved in assessing and stabilizing ED patients are reimbursed at a lower rate, compared with scheduled surgical procedures.
On the other hand, "low patient satisfaction related to long wait times and boarding may also drive well-reimbursed business away," the authors pointed out.
Strategies That Work
Addressing the bottlenecks does not have to mean adding beds. On the contrary, "improved use of existing beds should be the first-line strategy," Dr. Rabin and her coauthors said.
Evidence supports the use of these nine measures:
"Boarding is a systemwide problem."
• Moving ED hall patients to inpatient hallways. Patients prefer the quieter hallways, the nurse-patient ratio is usually lower, and the ED reclaims the beds for more incoming patients.
• Smoothing surgical schedules. By decreasing demand at peak times, this measure alone has been shown to "nearly eliminate boarding" at some hospitals, according to the report.
• Scheduling cardiac catheterizations for early in the day.
• Actively managing bed use. Approaches include making information on free beds quickly available via a computerized system, and use of a bed coordinator or "bed czar."
• Setting up a discharge lounge. Patients can be moved out of their beds into another area to await the completion of their discharge paperwork.
• Planning for discharge at time of admission. Making early arrangements for patients who will need outpatient placement in a nursing home or rehabilitation facility can speed their discharge by as much as 22 hours (J. Hosp. Med. 2009;4:226-33).
• Monitoring room-cleaning turnaround times. Cleaning staff should be held accountable for prompt work.
• Simplifying the steps needed to admit patients.
• Performing "reverse triage." During peak times, patients who have the least need for a bed can be discharged.
The most commonly adopted of these nine proven measures are actively managing bed use (quickly available bed information, 66% of hospitals; bed coordinator, 51%) and smoothing surgical schedules (58%).
Taking action to reduce boarding requires "a clear commitment by hospital leadership to overcome operations barriers across departments," Dr. Rabin and her coauthors said.
"Boarding is a systemwide problem, and successful responses require the endorsement of hospital leaders. ... If continued education of hospital managers and the public does not result in change, enhanced regulation will be necessary to protect patients," they concluded.
All of the authors are members of the Emergency Department Crowding Interest Group of the Society for Academic Emergency Medicine. No disclosures were reported.
Hospital flow inefficiencies are the real culprit behind patient boarding in the emergency department, according to a report in Health Affairs released on Aug. 6.
Most hospitals have implemented just two of nine measures proven to reduce ED boarding, according to the report. "Boarding" (keeping admitted patients in hallway beds in the emergency department for more than 2-4 hours because an inpatient bed is not available) has been shown to increase in-hospital mortality and length of stay (Acad. Emerg. Med. 2011;18:1324-9). The practice also reduces hospital income, increases patients’ risk for hospital-acquired infections, and contributes to lapses in routine care and medications.
Proven strategies to address the problem "are grossly underused," wrote Dr. Elaine Rabin, of Mount Sinai School of Medicine in New York, and her coauthors (Health Affairs 2012 Aug. 6 [doi:10.1377/hlthaff.2011.0786]).
The problem has escalated over the last decade. A 2001 survey "found that one in five patients in U.S. emergency departments were boarding, and three in four emergency departments were boarding at least two inpatients" (Ann. Emerg. Med. 2003;42:167-72). A 2003 report "found that nine out of ten hospitals reported some degree of boarding," with 20% of hospitals boarding patients for an average of 8 hours. Most recently, a 2010 survey showed that 85% of hospitals had boarded patients the previous week (Acad. Emerg. Med. 2010;17[suppl s1]:s90; abstract 260).
Boarding substantially reduces ED capacity. In a study done at one community hospital in Pennsylvania, moving patients who were admitted from the ED to inpatient beds within 2 hours would have increased ED capacity by 10,397 hours (433 days) over the 1-year study period (Acad. Emerg. Med. 2007;14:332-7).
Nowhere to Go
"Crowding is not an emergency department–based problem. Rather, it is a symptom of dysfunction in interrelated parts of the broader health care system," wrote Dr. Rabin and her coauthors.
Although it is commonly believed that "crowding results from uninsured patients’ seeking nonemergency care in the emergency department," studies have shown that "the main driver of emergency department crowding is patient outflow obstruction: an inability to move admitted patients to inpatient beds in a timely manner," they wrote.
Another assumption is that hospitals are swamped with too many patients, but boarding actually begins when a hospital is at 80%-85% of capacity, "partly because specified bed types ... fill earlier than other types," Dr. Rabin and her colleagues said. The common practice of reserving inpatient beds for specified categories of patients, such as postelective procedure patients or isolation cases, or to maintain a "geographic" bed plan (similar patients grouped together to match specialized nurses with patients), can mean that patients linger in the ED despite available beds. "Introducing some flexibility in the geographic pooling of beds decreased emergency department boarding times" by 50% and increased hospital revenue by 1% at one hospital (Oper. Res. 2009;57:261-73).
Bottom Line
ED crowding and boarding may substantially reduce hospital income; for example, in the 2007 study of the Pennsylvania community hospital, boarding resulted in an estimated loss of almost $4 million in net revenue.
But exactly how much revenue might be lost because of ED crowding is still under debate; ED patients are more likely to be uninsured than are elective admissions, so crowding may have the unintended effect of reducing the number of patients who can’t pay for care. In addition, the tasks involved in assessing and stabilizing ED patients are reimbursed at a lower rate, compared with scheduled surgical procedures.
On the other hand, "low patient satisfaction related to long wait times and boarding may also drive well-reimbursed business away," the authors pointed out.
Strategies That Work
Addressing the bottlenecks does not have to mean adding beds. On the contrary, "improved use of existing beds should be the first-line strategy," Dr. Rabin and her coauthors said.
Evidence supports the use of these nine measures:
"Boarding is a systemwide problem."
• Moving ED hall patients to inpatient hallways. Patients prefer the quieter hallways, the nurse-patient ratio is usually lower, and the ED reclaims the beds for more incoming patients.
• Smoothing surgical schedules. By decreasing demand at peak times, this measure alone has been shown to "nearly eliminate boarding" at some hospitals, according to the report.
• Scheduling cardiac catheterizations for early in the day.
• Actively managing bed use. Approaches include making information on free beds quickly available via a computerized system, and use of a bed coordinator or "bed czar."
• Setting up a discharge lounge. Patients can be moved out of their beds into another area to await the completion of their discharge paperwork.
• Planning for discharge at time of admission. Making early arrangements for patients who will need outpatient placement in a nursing home or rehabilitation facility can speed their discharge by as much as 22 hours (J. Hosp. Med. 2009;4:226-33).
• Monitoring room-cleaning turnaround times. Cleaning staff should be held accountable for prompt work.
• Simplifying the steps needed to admit patients.
• Performing "reverse triage." During peak times, patients who have the least need for a bed can be discharged.
The most commonly adopted of these nine proven measures are actively managing bed use (quickly available bed information, 66% of hospitals; bed coordinator, 51%) and smoothing surgical schedules (58%).
Taking action to reduce boarding requires "a clear commitment by hospital leadership to overcome operations barriers across departments," Dr. Rabin and her coauthors said.
"Boarding is a systemwide problem, and successful responses require the endorsement of hospital leaders. ... If continued education of hospital managers and the public does not result in change, enhanced regulation will be necessary to protect patients," they concluded.
All of the authors are members of the Emergency Department Crowding Interest Group of the Society for Academic Emergency Medicine. No disclosures were reported.
FROM HEALTH AFFAIRS

Nighttime Air Filter Boosts Asthmatics' Quality of Life
A device that provides cooled, filtered airflow while patients sleep improved quality of life in patients with atopic asthma, according to the findings of randomized controlled trial conducted in six European countries.
The benefits of treatment with the device, Protexo, developed by Airsonett, seemed "greatest in patients with a combination of high asthma intensity and poor asthma control, who represent a significant area of unmet need," said Dr. Robert J. Boyle of the pediatrics department at Imperial College London, and his coinvestigators.
A total of 312 patients with atopic asthma were randomized to use the device, which filters and cools the air near the user’s nighttime breathing zone, or an identical placebo device. The active therapy arm received temperature-controlled laminar airflow (TLA) treatment, which is proposed to decrease exposure to allergens.
The primary end point of the phase III study was an improvement of at least 0.5 points on the Asthma Quality of Life Questionnaire. Secondary end points included fractional exhaled nitric oxide (FENO); IgE levels and blood eosinophil count; and airflow obstruction as measured by forced expiratory volume in 1 second (FEV1), forced expiratory flow at 50% of vital capacity (FEF50), and peak expiratory flow (PEF). Subgroup analyses were done by age, treatment intensity at baseline, symptom control at baseline, and a combination of treatment intensity and symptom control (Thorax 2011 [doi:10.1136/thoraxjnl-2011-200665).
Participants were enrolled between April 2008 and February 2009, and the two groups had similar demographic and clinical characteristics at baseline. Patients were aged 7-70 years (mean 24 years), had a history of asthma for at least 1 year (mean approximately 13 years), had a demonstrated allergy to pets or dust mites, and were on daily corticosteroids. A little over half of the participants were male. Patients continued using asthma medications as needed during the study and underwent medical assessment at 1, 3, 6, 9 and 12 months.
Of the active treatment group, 76% reached the primary end point at 1 year, compared with 61% of the placebo group, a significant difference (95% confidence interval 3%-27%, P = .02). Findings were similar for the subgroup analysis of patients aged 12 years and older (74% vs. 60%; 95% CI 1%-28%, P = .06). The greatest difference was seen in TLA recipients who had both high treatment intensity and low symptom control at baseline, compared with similar patients who received placebo (75% vs. 50%; 95% CI 4%-47%, P = .009).
Regarding the secondary outcomes, use of the treatment device was linked to a greater decrease in FENO, with a mean difference of –7.1 parts per billion, compared with use of the placebo device (95% CI –13.6 to –0.7, P = .03). The treatment group also saw a smaller increase in cat-specific IgE levels relative to baseline, compared with the placebo group (8% vs. 35%), and smaller increases in IgE levels specific to dust mites and dog allergens (differences not significant). No significant differences were found between groups in total IgE level change, eosinophil count, FEV1, FEF50, or PEF. There also were no differences in medication use or exacerbation rates.
Although previous studies have found no benefit to avoiding allergens in asthma, this study "found that exposure control using TLA treatment at night has an impact on overall asthma-related quality of life," Dr. Boyle and his colleagues wrote. The researchers theorized that "the reason that nocturnal TLA is successful where so many other approaches have failed may be the profound reduction in inhaled aeroallergen exposure." They suggested that "the clinical effects of TLA can be explained by its ability to break the persistent body convection and thereby reduce aeroallergen exposure."
Because the patient cohort encompassed a wide range of ages and residents of several countries, the authors said that "the clinical effects of nocturnal TLA treatment appear to be applicable to a broad patient group." However, they noted that it may be of most benefit in "patients with uncontrolled atopic asthma despite high treatment intensity, where guidelines recommend stepping up treatment."
There were no treatment-related adverse events in either group.
The study was funded by Airsonett. The researchers reported having no other financial conflicts.
A device that provides cooled, filtered airflow while patients sleep improved quality of life in patients with atopic asthma, according to the findings of randomized controlled trial conducted in six European countries.
The benefits of treatment with the device, Protexo, developed by Airsonett, seemed "greatest in patients with a combination of high asthma intensity and poor asthma control, who represent a significant area of unmet need," said Dr. Robert J. Boyle of the pediatrics department at Imperial College London, and his coinvestigators.
A total of 312 patients with atopic asthma were randomized to use the device, which filters and cools the air near the user’s nighttime breathing zone, or an identical placebo device. The active therapy arm received temperature-controlled laminar airflow (TLA) treatment, which is proposed to decrease exposure to allergens.
The primary end point of the phase III study was an improvement of at least 0.5 points on the Asthma Quality of Life Questionnaire. Secondary end points included fractional exhaled nitric oxide (FENO); IgE levels and blood eosinophil count; and airflow obstruction as measured by forced expiratory volume in 1 second (FEV1), forced expiratory flow at 50% of vital capacity (FEF50), and peak expiratory flow (PEF). Subgroup analyses were done by age, treatment intensity at baseline, symptom control at baseline, and a combination of treatment intensity and symptom control (Thorax 2011 [doi:10.1136/thoraxjnl-2011-200665).
Participants were enrolled between April 2008 and February 2009, and the two groups had similar demographic and clinical characteristics at baseline. Patients were aged 7-70 years (mean 24 years), had a history of asthma for at least 1 year (mean approximately 13 years), had a demonstrated allergy to pets or dust mites, and were on daily corticosteroids. A little over half of the participants were male. Patients continued using asthma medications as needed during the study and underwent medical assessment at 1, 3, 6, 9 and 12 months.
Of the active treatment group, 76% reached the primary end point at 1 year, compared with 61% of the placebo group, a significant difference (95% confidence interval 3%-27%, P = .02). Findings were similar for the subgroup analysis of patients aged 12 years and older (74% vs. 60%; 95% CI 1%-28%, P = .06). The greatest difference was seen in TLA recipients who had both high treatment intensity and low symptom control at baseline, compared with similar patients who received placebo (75% vs. 50%; 95% CI 4%-47%, P = .009).
Regarding the secondary outcomes, use of the treatment device was linked to a greater decrease in FENO, with a mean difference of –7.1 parts per billion, compared with use of the placebo device (95% CI –13.6 to –0.7, P = .03). The treatment group also saw a smaller increase in cat-specific IgE levels relative to baseline, compared with the placebo group (8% vs. 35%), and smaller increases in IgE levels specific to dust mites and dog allergens (differences not significant). No significant differences were found between groups in total IgE level change, eosinophil count, FEV1, FEF50, or PEF. There also were no differences in medication use or exacerbation rates.
Although previous studies have found no benefit to avoiding allergens in asthma, this study "found that exposure control using TLA treatment at night has an impact on overall asthma-related quality of life," Dr. Boyle and his colleagues wrote. The researchers theorized that "the reason that nocturnal TLA is successful where so many other approaches have failed may be the profound reduction in inhaled aeroallergen exposure." They suggested that "the clinical effects of TLA can be explained by its ability to break the persistent body convection and thereby reduce aeroallergen exposure."
Because the patient cohort encompassed a wide range of ages and residents of several countries, the authors said that "the clinical effects of nocturnal TLA treatment appear to be applicable to a broad patient group." However, they noted that it may be of most benefit in "patients with uncontrolled atopic asthma despite high treatment intensity, where guidelines recommend stepping up treatment."
There were no treatment-related adverse events in either group.
The study was funded by Airsonett. The researchers reported having no other financial conflicts.
A device that provides cooled, filtered airflow while patients sleep improved quality of life in patients with atopic asthma, according to the findings of randomized controlled trial conducted in six European countries.
The benefits of treatment with the device, Protexo, developed by Airsonett, seemed "greatest in patients with a combination of high asthma intensity and poor asthma control, who represent a significant area of unmet need," said Dr. Robert J. Boyle of the pediatrics department at Imperial College London, and his coinvestigators.
A total of 312 patients with atopic asthma were randomized to use the device, which filters and cools the air near the user’s nighttime breathing zone, or an identical placebo device. The active therapy arm received temperature-controlled laminar airflow (TLA) treatment, which is proposed to decrease exposure to allergens.
The primary end point of the phase III study was an improvement of at least 0.5 points on the Asthma Quality of Life Questionnaire. Secondary end points included fractional exhaled nitric oxide (FENO); IgE levels and blood eosinophil count; and airflow obstruction as measured by forced expiratory volume in 1 second (FEV1), forced expiratory flow at 50% of vital capacity (FEF50), and peak expiratory flow (PEF). Subgroup analyses were done by age, treatment intensity at baseline, symptom control at baseline, and a combination of treatment intensity and symptom control (Thorax 2011 [doi:10.1136/thoraxjnl-2011-200665).
Participants were enrolled between April 2008 and February 2009, and the two groups had similar demographic and clinical characteristics at baseline. Patients were aged 7-70 years (mean 24 years), had a history of asthma for at least 1 year (mean approximately 13 years), had a demonstrated allergy to pets or dust mites, and were on daily corticosteroids. A little over half of the participants were male. Patients continued using asthma medications as needed during the study and underwent medical assessment at 1, 3, 6, 9 and 12 months.
Of the active treatment group, 76% reached the primary end point at 1 year, compared with 61% of the placebo group, a significant difference (95% confidence interval 3%-27%, P = .02). Findings were similar for the subgroup analysis of patients aged 12 years and older (74% vs. 60%; 95% CI 1%-28%, P = .06). The greatest difference was seen in TLA recipients who had both high treatment intensity and low symptom control at baseline, compared with similar patients who received placebo (75% vs. 50%; 95% CI 4%-47%, P = .009).
Regarding the secondary outcomes, use of the treatment device was linked to a greater decrease in FENO, with a mean difference of –7.1 parts per billion, compared with use of the placebo device (95% CI –13.6 to –0.7, P = .03). The treatment group also saw a smaller increase in cat-specific IgE levels relative to baseline, compared with the placebo group (8% vs. 35%), and smaller increases in IgE levels specific to dust mites and dog allergens (differences not significant). No significant differences were found between groups in total IgE level change, eosinophil count, FEV1, FEF50, or PEF. There also were no differences in medication use or exacerbation rates.
Although previous studies have found no benefit to avoiding allergens in asthma, this study "found that exposure control using TLA treatment at night has an impact on overall asthma-related quality of life," Dr. Boyle and his colleagues wrote. The researchers theorized that "the reason that nocturnal TLA is successful where so many other approaches have failed may be the profound reduction in inhaled aeroallergen exposure." They suggested that "the clinical effects of TLA can be explained by its ability to break the persistent body convection and thereby reduce aeroallergen exposure."
Because the patient cohort encompassed a wide range of ages and residents of several countries, the authors said that "the clinical effects of nocturnal TLA treatment appear to be applicable to a broad patient group." However, they noted that it may be of most benefit in "patients with uncontrolled atopic asthma despite high treatment intensity, where guidelines recommend stepping up treatment."
There were no treatment-related adverse events in either group.
The study was funded by Airsonett. The researchers reported having no other financial conflicts.
FROM THORAX
Major Finding: A total of 76% of the treatment group improved by at least 0.5 points on the Asthma Quality of Life Questionnaire, compared with 61% of the placebo group, a significant difference.
Data Source: Randomized, controlled, double-blind study of 312 patients with atopic asthma.
Disclosures: The study was funded by Airsonett. The researchers reported having no other financial conflicts.
Bringing Back Kids in Cardiopulmonary Arrest
SAN FRANCISCO – Children in cardiopulmonary arrest require specialized resuscitation skills, and updated guidelines published late in 2010 contain some new recommendations, according to Dr. Marianne Gausche-Hill.
The recommended sequence for cardiopulmonary resuscitation (CPR) "has changed for all ages except for the newborn" to compressions, airway, breathing (CAB) – instead of airway, breathing, compressions (ABC) – when performed by a bystander. Emergency department (ED) providers usually will ventilate and do compressions simultaneously.
"If you’re doing bag mask [ventilation], the recommendation is just do your ventilations, and do compressions separately. If the patient has been intubated, you can do continued ventilations as you’re doing compressions," Dr. Gausche-Hill said at the annual meeting of the American College of Emergency Physicians.
In babies, if there is a single rescuer, chest compressions should be done using two fingers in the middle of the chest between the nipples (Circulation 2010;122:S862-75). With two rescuers, one can use the hand-encircling technique in which the thumbs are between the nipples and the rest of the fingers around the infant’s back, while the other does bag mask ventilation.
Compress the chest 1.5 inches in infants and 2 inches in children. Allow the chest to recoil between pushes and do at least 100 compressions per minute. "The key thing is to push hard and fast," said Dr. Gausche-Hill, professor of medicine at the University of California, Los Angeles. Do compressions for 2 minutes, then stop for no more than 10 seconds to check for a pulse. Mechanical devices for chest compressions have not been tested in children and should not be used in pediatric patients.

For a single rescuer, a ratio of compressions to ventilation of 30:2 is recommended, but for two rescuers in the ED the ratio is 15:2, with more emphasis on ventilation. Take care not to overventilate, she said.
"We overbag super amounts when we do resuscitation ventilation. You don’t need that much," she emphasized. "You want to squeeze the bag just until chest rise is initiated, and then begin the release phase." For children, this means about 10 breaths a minute. To avoid overbagging, a resuscitator can say "squeeze" as she squeezes the bag just until the chest starts to rise, then pause and say "release, release" to give time for the chest to recoil.
After beginning CPR, determine if the rhythm is shockable, and if so, use the defibrillator. Then do 2 minutes of CPR, give epinephrine, check the rhythm again, shock again. "It’s no more shock, shock, shock. You’re going to do 2 minutes of CPR in-between," she said.
The best option is a manual defibrillator with pediatric pads, she said, starting with 2 J and going up to 4 J if needed. But a dose even as high as 10 J is not harmful, according to Dr. Gausche-Hill. "If the patient is in persistent [ventricular fibrillation], I would strongly consider ramping it up, especially in the adolescent," she said. The new guidelines no longer require a pediatric attenuating device for an automated external defibrillator, and the standard automated external defibrillator can be used for any age (Circulation 2010;122:S876-908).

Cuffed endotracheal tubes (ETTs) are now preferred over the standard uncuffed tubes for intubation. "The bottom line is there’s no concern about cricoid pressure leading to necrosis. There’s no increased risk of subglottic stenosis by the use of these. That was really the main concern," she said. Cuffed ETTs are preferred in patients with poor lung compliance, a large glottic air leak, or high airway resistance. A randomized, controlled trial of 2,246 children found that those treated with a cuffed ETT did not have more postextubation stridor than those treated with an uncuffed ETT (4.4% vs. 4.7%) and were much less likely to need a tube exchange (2.1% vs. 30.8%) (Br. J. Anaesth. 2009;103:867-73). "Our PICU just says give it to everybody," she said. In pediatric patients, use a half-size smaller than their standard cuff size.
Cricoid pressure to present aspiration during intubation is not recommended in children, as it actually impedes the airway. Dr. Gausche-Hill prefers a jaw thrust or, in older kids, a little laryngeal manipulation.
In neonates, providing a lot of oxygen initially is harmful, leading to the creation of free radicals that may have an adverse neurologic effect (Circulation 2010;122:S909-19), but oxygen can be appropriate in older children, she said. "Bottom line is, give O2 100% and then back it down as quickly as you can," and aim to maintain an oxygen saturation of about 94%, said Dr. Gausche-Hill, who is also director of EMS and pediatric emergency medicine fellowships at Harbor-UCLA Medical Center in Torrance, Calif.

The guidelines now emphasize the use of capnography to monitor end-tidal CO2 to confirm endotracheal tube placement and assess the adequacy of CPR. With capnography, "you may see [return of spontaneous circulation] before you can even detect a pulse," she said.
Foreign body aspiration "is your worst nightmare in the ED because you know if you can’t get it out, the patient’s going to die. And we do know that kids just do this all the time," she said. More than 90% of patients with this condition are younger than 5 years. "You always begin with basic life support maneuvers if they’re still conscious. For the infant, it’s back blows and chest thrusts until the object is expelled or they become unconscious." For the conscious older child, start with the Heimlich maneuver. In unconscious children, progress to chest compressions; if the foreign body is esophageal, chest compressions may remove it.
If the foreign body is lodged deeper in the airway, use direct laryngoscopy and remove the object with Magill forceps in the pediatric size. Some recent surveys showed that "18% of EDs in the country do not have pediatric Magills. Look in your airway kit. Make sure you have them," she stressed.
Last, family presence during resuscitation attempts should be promoted, she said. Almost a dozen studies have shown that parents want that option and should be included in decision making when possible, she noted.
Dr. Gausche-Hill reported having no significant financial relationships to disclose.
SAN FRANCISCO – Children in cardiopulmonary arrest require specialized resuscitation skills, and updated guidelines published late in 2010 contain some new recommendations, according to Dr. Marianne Gausche-Hill.
The recommended sequence for cardiopulmonary resuscitation (CPR) "has changed for all ages except for the newborn" to compressions, airway, breathing (CAB) – instead of airway, breathing, compressions (ABC) – when performed by a bystander. Emergency department (ED) providers usually will ventilate and do compressions simultaneously.
"If you’re doing bag mask [ventilation], the recommendation is just do your ventilations, and do compressions separately. If the patient has been intubated, you can do continued ventilations as you’re doing compressions," Dr. Gausche-Hill said at the annual meeting of the American College of Emergency Physicians.
In babies, if there is a single rescuer, chest compressions should be done using two fingers in the middle of the chest between the nipples (Circulation 2010;122:S862-75). With two rescuers, one can use the hand-encircling technique in which the thumbs are between the nipples and the rest of the fingers around the infant’s back, while the other does bag mask ventilation.
Compress the chest 1.5 inches in infants and 2 inches in children. Allow the chest to recoil between pushes and do at least 100 compressions per minute. "The key thing is to push hard and fast," said Dr. Gausche-Hill, professor of medicine at the University of California, Los Angeles. Do compressions for 2 minutes, then stop for no more than 10 seconds to check for a pulse. Mechanical devices for chest compressions have not been tested in children and should not be used in pediatric patients.
For a single rescuer, a ratio of compressions to ventilation of 30:2 is recommended, but for two rescuers in the ED the ratio is 15:2, with more emphasis on ventilation. Take care not to overventilate, she said.
"We overbag super amounts when we do resuscitation ventilation. You don’t need that much," she emphasized. "You want to squeeze the bag just until chest rise is initiated, and then begin the release phase." For children, this means about 10 breaths a minute. To avoid overbagging, a resuscitator can say "squeeze" as she squeezes the bag just until the chest starts to rise, then pause and say "release, release" to give time for the chest to recoil.
After beginning CPR, determine if the rhythm is shockable, and if so, use the defibrillator. Then do 2 minutes of CPR, give epinephrine, check the rhythm again, shock again. "It’s no more shock, shock, shock. You’re going to do 2 minutes of CPR in-between," she said.
The best option is a manual defibrillator with pediatric pads, she said, starting with 2 J and going up to 4 J if needed. But a dose even as high as 10 J is not harmful, according to Dr. Gausche-Hill. "If the patient is in persistent [ventricular fibrillation], I would strongly consider ramping it up, especially in the adolescent," she said. The new guidelines no longer require a pediatric attenuating device for an automated external defibrillator, and the standard automated external defibrillator can be used for any age (Circulation 2010;122:S876-908).
Cuffed endotracheal tubes (ETTs) are now preferred over the standard uncuffed tubes for intubation. "The bottom line is there’s no concern about cricoid pressure leading to necrosis. There’s no increased risk of subglottic stenosis by the use of these. That was really the main concern," she said. Cuffed ETTs are preferred in patients with poor lung compliance, a large glottic air leak, or high airway resistance. A randomized, controlled trial of 2,246 children found that those treated with a cuffed ETT did not have more postextubation stridor than those treated with an uncuffed ETT (4.4% vs. 4.7%) and were much less likely to need a tube exchange (2.1% vs. 30.8%) (Br. J. Anaesth. 2009;103:867-73). "Our PICU just says give it to everybody," she said. In pediatric patients, use a half-size smaller than their standard cuff size.
Cricoid pressure to present aspiration during intubation is not recommended in children, as it actually impedes the airway. Dr. Gausche-Hill prefers a jaw thrust or, in older kids, a little laryngeal manipulation.
In neonates, providing a lot of oxygen initially is harmful, leading to the creation of free radicals that may have an adverse neurologic effect (Circulation 2010;122:S909-19), but oxygen can be appropriate in older children, she said. "Bottom line is, give O2 100% and then back it down as quickly as you can," and aim to maintain an oxygen saturation of about 94%, said Dr. Gausche-Hill, who is also director of EMS and pediatric emergency medicine fellowships at Harbor-UCLA Medical Center in Torrance, Calif.
The guidelines now emphasize the use of capnography to monitor end-tidal CO2 to confirm endotracheal tube placement and assess the adequacy of CPR. With capnography, "you may see [return of spontaneous circulation] before you can even detect a pulse," she said.
Foreign body aspiration "is your worst nightmare in the ED because you know if you can’t get it out, the patient’s going to die. And we do know that kids just do this all the time," she said. More than 90% of patients with this condition are younger than 5 years. "You always begin with basic life support maneuvers if they’re still conscious. For the infant, it’s back blows and chest thrusts until the object is expelled or they become unconscious." For the conscious older child, start with the Heimlich maneuver. In unconscious children, progress to chest compressions; if the foreign body is esophageal, chest compressions may remove it.
If the foreign body is lodged deeper in the airway, use direct laryngoscopy and remove the object with Magill forceps in the pediatric size. Some recent surveys showed that "18% of EDs in the country do not have pediatric Magills. Look in your airway kit. Make sure you have them," she stressed.
Last, family presence during resuscitation attempts should be promoted, she said. Almost a dozen studies have shown that parents want that option and should be included in decision making when possible, she noted.
Dr. Gausche-Hill reported having no significant financial relationships to disclose.
SAN FRANCISCO – Children in cardiopulmonary arrest require specialized resuscitation skills, and updated guidelines published late in 2010 contain some new recommendations, according to Dr. Marianne Gausche-Hill.
The recommended sequence for cardiopulmonary resuscitation (CPR) "has changed for all ages except for the newborn" to compressions, airway, breathing (CAB) – instead of airway, breathing, compressions (ABC) – when performed by a bystander. Emergency department (ED) providers usually will ventilate and do compressions simultaneously.
"If you’re doing bag mask [ventilation], the recommendation is just do your ventilations, and do compressions separately. If the patient has been intubated, you can do continued ventilations as you’re doing compressions," Dr. Gausche-Hill said at the annual meeting of the American College of Emergency Physicians.
In babies, if there is a single rescuer, chest compressions should be done using two fingers in the middle of the chest between the nipples (Circulation 2010;122:S862-75). With two rescuers, one can use the hand-encircling technique in which the thumbs are between the nipples and the rest of the fingers around the infant’s back, while the other does bag mask ventilation.
Compress the chest 1.5 inches in infants and 2 inches in children. Allow the chest to recoil between pushes and do at least 100 compressions per minute. "The key thing is to push hard and fast," said Dr. Gausche-Hill, professor of medicine at the University of California, Los Angeles. Do compressions for 2 minutes, then stop for no more than 10 seconds to check for a pulse. Mechanical devices for chest compressions have not been tested in children and should not be used in pediatric patients.
For a single rescuer, a ratio of compressions to ventilation of 30:2 is recommended, but for two rescuers in the ED the ratio is 15:2, with more emphasis on ventilation. Take care not to overventilate, she said.
"We overbag super amounts when we do resuscitation ventilation. You don’t need that much," she emphasized. "You want to squeeze the bag just until chest rise is initiated, and then begin the release phase." For children, this means about 10 breaths a minute. To avoid overbagging, a resuscitator can say "squeeze" as she squeezes the bag just until the chest starts to rise, then pause and say "release, release" to give time for the chest to recoil.
After beginning CPR, determine if the rhythm is shockable, and if so, use the defibrillator. Then do 2 minutes of CPR, give epinephrine, check the rhythm again, shock again. "It’s no more shock, shock, shock. You’re going to do 2 minutes of CPR in-between," she said.
The best option is a manual defibrillator with pediatric pads, she said, starting with 2 J and going up to 4 J if needed. But a dose even as high as 10 J is not harmful, according to Dr. Gausche-Hill. "If the patient is in persistent [ventricular fibrillation], I would strongly consider ramping it up, especially in the adolescent," she said. The new guidelines no longer require a pediatric attenuating device for an automated external defibrillator, and the standard automated external defibrillator can be used for any age (Circulation 2010;122:S876-908).
Cuffed endotracheal tubes (ETTs) are now preferred over the standard uncuffed tubes for intubation. "The bottom line is there’s no concern about cricoid pressure leading to necrosis. There’s no increased risk of subglottic stenosis by the use of these. That was really the main concern," she said. Cuffed ETTs are preferred in patients with poor lung compliance, a large glottic air leak, or high airway resistance. A randomized, controlled trial of 2,246 children found that those treated with a cuffed ETT did not have more postextubation stridor than those treated with an uncuffed ETT (4.4% vs. 4.7%) and were much less likely to need a tube exchange (2.1% vs. 30.8%) (Br. J. Anaesth. 2009;103:867-73). "Our PICU just says give it to everybody," she said. In pediatric patients, use a half-size smaller than their standard cuff size.
Cricoid pressure to present aspiration during intubation is not recommended in children, as it actually impedes the airway. Dr. Gausche-Hill prefers a jaw thrust or, in older kids, a little laryngeal manipulation.
In neonates, providing a lot of oxygen initially is harmful, leading to the creation of free radicals that may have an adverse neurologic effect (Circulation 2010;122:S909-19), but oxygen can be appropriate in older children, she said. "Bottom line is, give O2 100% and then back it down as quickly as you can," and aim to maintain an oxygen saturation of about 94%, said Dr. Gausche-Hill, who is also director of EMS and pediatric emergency medicine fellowships at Harbor-UCLA Medical Center in Torrance, Calif.
The guidelines now emphasize the use of capnography to monitor end-tidal CO2 to confirm endotracheal tube placement and assess the adequacy of CPR. With capnography, "you may see [return of spontaneous circulation] before you can even detect a pulse," she said.
Foreign body aspiration "is your worst nightmare in the ED because you know if you can’t get it out, the patient’s going to die. And we do know that kids just do this all the time," she said. More than 90% of patients with this condition are younger than 5 years. "You always begin with basic life support maneuvers if they’re still conscious. For the infant, it’s back blows and chest thrusts until the object is expelled or they become unconscious." For the conscious older child, start with the Heimlich maneuver. In unconscious children, progress to chest compressions; if the foreign body is esophageal, chest compressions may remove it.
If the foreign body is lodged deeper in the airway, use direct laryngoscopy and remove the object with Magill forceps in the pediatric size. Some recent surveys showed that "18% of EDs in the country do not have pediatric Magills. Look in your airway kit. Make sure you have them," she stressed.
Last, family presence during resuscitation attempts should be promoted, she said. Almost a dozen studies have shown that parents want that option and should be included in decision making when possible, she noted.
Dr. Gausche-Hill reported having no significant financial relationships to disclose.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Designer Drug ODs Call for Supportive Care and Education
Bath salts, spice, and nutmeg are more than common household items; they are also designer drugs that can send people to the emergency department.
While emergency department visits resulting from use of older drugs of abuse such as LSD and cocaine have gone up 29%-48% over the past decade, ED visits resulting from the use of nontraditional, emerging, and Web-based (NEW) drugs have increased by estimates ranging from 187%-5,846%, Dr. Mark B. Mycyk said at the annual meeting of the American College of Emergency Physicians.

The Internet has been a "huge source of information and a powerful influence on this rapidly evolving and changing epidemic," said Dr. Mycyk of Cook County Hospital in Chicago. Designer drugs are easily available from websites such as Silk Road, "the Amazon.com of some of these NEW drugs," he said, and anyone with access to a computer "can pretty much get almost anything delivered to their homes or dorm rooms or a post office box." According to one study, websites touting recreational drugs were a factor in 27% of new drug use in college-age students (Pediatrics 2002;109:e96).
"Cases we see in the ED are extreme ... cases where people end up with complications," Dr. Mycyk said. Emergency physicians may see patients who have used the following NEW drugs:
• Bath salts (methylenedioxypyrovalerone, MDPV). "Brand names" include Ivory Wave, Bliss, and White Lightning; also called Plant Food. Popularized in Australia, these are not the kind of bath salts you would buy at a home goods store, which cause only severe rhinitis if snorted. The type sold online and in "head shops" is a stimulant and hallucinogen that causes cardiovascular and psychiatric adverse effects. "Self-harm has become a common complication. ... People get so psychotic, they are actually getting aggressive and harming others," Dr. Mycyk said. MDPV also has "lots of other profound effects on human neurotransmitters that we still do not understand," and the drug is "so addictive that users say it provokes an almost-uncontrollable urge for another hit." The chemicals used to make "bath salts" were classified as schedule 1 substances in late October by the Drug Enforcement Agency.

• Spice. Also known as K2. This synthetic cannabinoid, developed for animal research, "has resulted in a number of ED visits, and some of these visits can be pretty prolonged, and we’ve seen some unanticipated complications," Dr. Mycyk said. K2 is "much more potent and powerful than natural marijuana, so the effects that we see are much more extreme." Symptoms include agitation, cardiovascular effects, and inappropriate affect (Clin. Toxicol. [Phila.] 2011;49:431-3). Several varieties are now illegal in the United States, but chemists can create "newer synthetic analogs, which look different from Spice and K2, and that way, they evade the legal authorities," he said.

• Meow-Meow (mephedrone, 4-methylmethcathinone). Other street names include Drone, Bubble, and MCAT. This synthetic cathinone, derived from an African shrub, is a stimulant and sympathomimetic agent. Its effects and structure are similar to those of ephedra and amphetamine. Symptoms of Meow-Meow use include seizures, agitation, tachycardia, hypertension, and hyperthermia (Toxicol. Lett. 2011;201:191-5).
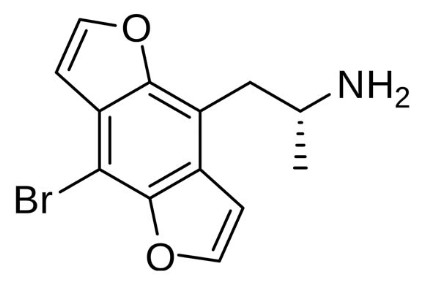
• Bromo-DragonFLY (bromo-benzodifuranyl-isopropylamine). Adverse effects of this designer drug include hallucinations, seizures, vomiting, and intense vasoconstriction with resulting ischemia in fingers and toes. The drug has "hallucinogenic, Ecstasy-like properties" and is a serotoninergic receptor agonist. The name derives from the resemblance its chemical structure has to a dragonfly.
• Nutmeg. At doses as high as 50 g, the common spice nutmeg has hallucinogenic properties. "When we see nutmeg users in the ED, we’re seeing a small proportion who took an extremely large dose or have an unanticipated complication from it," Dr. Mycyk said. In one case series of 119 patients, the most common symptoms were tachycardia, palpitations, and agitation. The researchers found that "clinical effects from ingestion can be significant and can require medical intervention" (Clin. Toxicol. [Phila.] 2011;49:177-80).
• Salvia. Street names of the salvia divinorum plant include Diviner’s Sage, Shepherdess, and Sally D. Related to mint, salvia has hallucinogenic and psychotomimetic properties. Symptoms include agitation and neurologic, cardiovascular, and gastrointestinal effects. The herb can be made into a tea; fresh leaves can be chewed; or leaves can be dried and then smoked, snorted, or injected. The drug has not been well studied, but one group of researchers analyzed YouTube videos of salvia users to study its effects (Drug Alcohol Depend. 2010;108:138-40).

• Snakebite. The venom of the naja naja snake, or Indian cobra, contains neurotoxins that can have opiate-like effects on the central nervous system. The venom can cause blackouts and feelings of well-being and lethargy in people who deliberately have themselves bitten by a cobra (Subst. Abus. 2011;32:43-6). "It boggles my mind what people will do to get high," Dr. Mycyk said.
• Buprenorphine (Suboxone). Clinically used for opioid dependence, this drug is smuggled into prisons by being crushed into a paste that is applied to a drawing or card, or hidden under stamps. A recent study found that 12% of drug contraband in Massachusetts prisons is buprenorphine (Curr. Drug Abuse Rev. 2011;4:28-41). Buprenorphine intoxication causes mild euphoria, somnolence, and possible respiratory depression; laboratory and toxicology screens for illicit drugs would be negative.
Diagnosis
Hospital-based drug screens don’t detect most of the new and evolving designer drugs that result in emergency department visits. "A lot of hospitals have invested in expanded drug-screening panels, but these hospital machines cannot keep up with the creative chemists and users out there," Dr. Mycyk said. So "tox testing is not that helpful for some of these NEW drugs. In fact, it might falsely reassure you."
So, to make the diagnosis, "if the patient is conscious, ask them. Know their language, know the slang. They will tell you. ... They are frightened, and they don’t want to die."
If the patient is delirious or has altered mental status, examine his or her belongings carefully. "Completely examine your patient’s belongings, and you will probably find your answer." Check the small pocket in jeans, Dr. Mycyk suggested. "I’ve been surprised how often I find drug contraband in that small pocket."
Accessing one of the "drug partisan sites" – such as erowid.org, lycaeum.org, shroomery.org, and talktofrank.com – also can be useful if you want to figure out what your patient has taken. However, while it might be helpful to know the agent, focus on symptoms and "treat the patient; don’t treat the product," he said.
Treatment
Deaths from NEW drug abuse most commonly occur due to dysrhythmias, hyperthermia, or metabolic complications. There are no antidotes for any of these NEW drugs, but "symptom-based, goal-directed, supportive therapy will save most of these patients’ lives."
Use common sense, and trust your instincts, Dr. Mycyk said. Get an electrolyte panel if the patient is persistently symptomatic. If a patient is tachycardic and having palpitations, getting an ECG may be appropriate. If they’re overly agitated, it is safe to use benzodiazepines. If they’re dehydrated, give them IV fluids, he said.
It is important to get complete vital signs on these patients, and the most important vital sign is temperature, as elevated body temperature is the best predictor of death in the ED. Degree of tachycardia or tachypnea is not as concerning, he said.
For most of these patients, brief ED observation is fine. However, some of the NEW drugs have long duration of activity; for example, the effects of buprenorphine can last 24-37 hours, so admission might be considered.
All patients with an ED visit for drug use should have counseling before discharge. Simple ED counseling can help, Dr. Mycyk said. "They think a lot of this stuff is safe, and we just need to remind them that it is not safe."
Dr. Mycyk had no significant financial relationships to disclose.
Bath salts, spice, and nutmeg are more than common household items; they are also designer drugs that can send people to the emergency department.
While emergency department visits resulting from use of older drugs of abuse such as LSD and cocaine have gone up 29%-48% over the past decade, ED visits resulting from the use of nontraditional, emerging, and Web-based (NEW) drugs have increased by estimates ranging from 187%-5,846%, Dr. Mark B. Mycyk said at the annual meeting of the American College of Emergency Physicians.
The Internet has been a "huge source of information and a powerful influence on this rapidly evolving and changing epidemic," said Dr. Mycyk of Cook County Hospital in Chicago. Designer drugs are easily available from websites such as Silk Road, "the Amazon.com of some of these NEW drugs," he said, and anyone with access to a computer "can pretty much get almost anything delivered to their homes or dorm rooms or a post office box." According to one study, websites touting recreational drugs were a factor in 27% of new drug use in college-age students (Pediatrics 2002;109:e96).
"Cases we see in the ED are extreme ... cases where people end up with complications," Dr. Mycyk said. Emergency physicians may see patients who have used the following NEW drugs:
• Bath salts (methylenedioxypyrovalerone, MDPV). "Brand names" include Ivory Wave, Bliss, and White Lightning; also called Plant Food. Popularized in Australia, these are not the kind of bath salts you would buy at a home goods store, which cause only severe rhinitis if snorted. The type sold online and in "head shops" is a stimulant and hallucinogen that causes cardiovascular and psychiatric adverse effects. "Self-harm has become a common complication. ... People get so psychotic, they are actually getting aggressive and harming others," Dr. Mycyk said. MDPV also has "lots of other profound effects on human neurotransmitters that we still do not understand," and the drug is "so addictive that users say it provokes an almost-uncontrollable urge for another hit." The chemicals used to make "bath salts" were classified as schedule 1 substances in late October by the Drug Enforcement Agency.
• Spice. Also known as K2. This synthetic cannabinoid, developed for animal research, "has resulted in a number of ED visits, and some of these visits can be pretty prolonged, and we’ve seen some unanticipated complications," Dr. Mycyk said. K2 is "much more potent and powerful than natural marijuana, so the effects that we see are much more extreme." Symptoms include agitation, cardiovascular effects, and inappropriate affect (Clin. Toxicol. [Phila.] 2011;49:431-3). Several varieties are now illegal in the United States, but chemists can create "newer synthetic analogs, which look different from Spice and K2, and that way, they evade the legal authorities," he said.
• Meow-Meow (mephedrone, 4-methylmethcathinone). Other street names include Drone, Bubble, and MCAT. This synthetic cathinone, derived from an African shrub, is a stimulant and sympathomimetic agent. Its effects and structure are similar to those of ephedra and amphetamine. Symptoms of Meow-Meow use include seizures, agitation, tachycardia, hypertension, and hyperthermia (Toxicol. Lett. 2011;201:191-5).
• Bromo-DragonFLY (bromo-benzodifuranyl-isopropylamine). Adverse effects of this designer drug include hallucinations, seizures, vomiting, and intense vasoconstriction with resulting ischemia in fingers and toes. The drug has "hallucinogenic, Ecstasy-like properties" and is a serotoninergic receptor agonist. The name derives from the resemblance its chemical structure has to a dragonfly.
• Nutmeg. At doses as high as 50 g, the common spice nutmeg has hallucinogenic properties. "When we see nutmeg users in the ED, we’re seeing a small proportion who took an extremely large dose or have an unanticipated complication from it," Dr. Mycyk said. In one case series of 119 patients, the most common symptoms were tachycardia, palpitations, and agitation. The researchers found that "clinical effects from ingestion can be significant and can require medical intervention" (Clin. Toxicol. [Phila.] 2011;49:177-80).
• Salvia. Street names of the salvia divinorum plant include Diviner’s Sage, Shepherdess, and Sally D. Related to mint, salvia has hallucinogenic and psychotomimetic properties. Symptoms include agitation and neurologic, cardiovascular, and gastrointestinal effects. The herb can be made into a tea; fresh leaves can be chewed; or leaves can be dried and then smoked, snorted, or injected. The drug has not been well studied, but one group of researchers analyzed YouTube videos of salvia users to study its effects (Drug Alcohol Depend. 2010;108:138-40).
• Snakebite. The venom of the naja naja snake, or Indian cobra, contains neurotoxins that can have opiate-like effects on the central nervous system. The venom can cause blackouts and feelings of well-being and lethargy in people who deliberately have themselves bitten by a cobra (Subst. Abus. 2011;32:43-6). "It boggles my mind what people will do to get high," Dr. Mycyk said.
• Buprenorphine (Suboxone). Clinically used for opioid dependence, this drug is smuggled into prisons by being crushed into a paste that is applied to a drawing or card, or hidden under stamps. A recent study found that 12% of drug contraband in Massachusetts prisons is buprenorphine (Curr. Drug Abuse Rev. 2011;4:28-41). Buprenorphine intoxication causes mild euphoria, somnolence, and possible respiratory depression; laboratory and toxicology screens for illicit drugs would be negative.
Diagnosis
Hospital-based drug screens don’t detect most of the new and evolving designer drugs that result in emergency department visits. "A lot of hospitals have invested in expanded drug-screening panels, but these hospital machines cannot keep up with the creative chemists and users out there," Dr. Mycyk said. So "tox testing is not that helpful for some of these NEW drugs. In fact, it might falsely reassure you."
So, to make the diagnosis, "if the patient is conscious, ask them. Know their language, know the slang. They will tell you. ... They are frightened, and they don’t want to die."
If the patient is delirious or has altered mental status, examine his or her belongings carefully. "Completely examine your patient’s belongings, and you will probably find your answer." Check the small pocket in jeans, Dr. Mycyk suggested. "I’ve been surprised how often I find drug contraband in that small pocket."
Accessing one of the "drug partisan sites" – such as erowid.org, lycaeum.org, shroomery.org, and talktofrank.com – also can be useful if you want to figure out what your patient has taken. However, while it might be helpful to know the agent, focus on symptoms and "treat the patient; don’t treat the product," he said.
Treatment
Deaths from NEW drug abuse most commonly occur due to dysrhythmias, hyperthermia, or metabolic complications. There are no antidotes for any of these NEW drugs, but "symptom-based, goal-directed, supportive therapy will save most of these patients’ lives."
Use common sense, and trust your instincts, Dr. Mycyk said. Get an electrolyte panel if the patient is persistently symptomatic. If a patient is tachycardic and having palpitations, getting an ECG may be appropriate. If they’re overly agitated, it is safe to use benzodiazepines. If they’re dehydrated, give them IV fluids, he said.
It is important to get complete vital signs on these patients, and the most important vital sign is temperature, as elevated body temperature is the best predictor of death in the ED. Degree of tachycardia or tachypnea is not as concerning, he said.
For most of these patients, brief ED observation is fine. However, some of the NEW drugs have long duration of activity; for example, the effects of buprenorphine can last 24-37 hours, so admission might be considered.
All patients with an ED visit for drug use should have counseling before discharge. Simple ED counseling can help, Dr. Mycyk said. "They think a lot of this stuff is safe, and we just need to remind them that it is not safe."
Dr. Mycyk had no significant financial relationships to disclose.
Bath salts, spice, and nutmeg are more than common household items; they are also designer drugs that can send people to the emergency department.
While emergency department visits resulting from use of older drugs of abuse such as LSD and cocaine have gone up 29%-48% over the past decade, ED visits resulting from the use of nontraditional, emerging, and Web-based (NEW) drugs have increased by estimates ranging from 187%-5,846%, Dr. Mark B. Mycyk said at the annual meeting of the American College of Emergency Physicians.
The Internet has been a "huge source of information and a powerful influence on this rapidly evolving and changing epidemic," said Dr. Mycyk of Cook County Hospital in Chicago. Designer drugs are easily available from websites such as Silk Road, "the Amazon.com of some of these NEW drugs," he said, and anyone with access to a computer "can pretty much get almost anything delivered to their homes or dorm rooms or a post office box." According to one study, websites touting recreational drugs were a factor in 27% of new drug use in college-age students (Pediatrics 2002;109:e96).
"Cases we see in the ED are extreme ... cases where people end up with complications," Dr. Mycyk said. Emergency physicians may see patients who have used the following NEW drugs:
• Bath salts (methylenedioxypyrovalerone, MDPV). "Brand names" include Ivory Wave, Bliss, and White Lightning; also called Plant Food. Popularized in Australia, these are not the kind of bath salts you would buy at a home goods store, which cause only severe rhinitis if snorted. The type sold online and in "head shops" is a stimulant and hallucinogen that causes cardiovascular and psychiatric adverse effects. "Self-harm has become a common complication. ... People get so psychotic, they are actually getting aggressive and harming others," Dr. Mycyk said. MDPV also has "lots of other profound effects on human neurotransmitters that we still do not understand," and the drug is "so addictive that users say it provokes an almost-uncontrollable urge for another hit." The chemicals used to make "bath salts" were classified as schedule 1 substances in late October by the Drug Enforcement Agency.
• Spice. Also known as K2. This synthetic cannabinoid, developed for animal research, "has resulted in a number of ED visits, and some of these visits can be pretty prolonged, and we’ve seen some unanticipated complications," Dr. Mycyk said. K2 is "much more potent and powerful than natural marijuana, so the effects that we see are much more extreme." Symptoms include agitation, cardiovascular effects, and inappropriate affect (Clin. Toxicol. [Phila.] 2011;49:431-3). Several varieties are now illegal in the United States, but chemists can create "newer synthetic analogs, which look different from Spice and K2, and that way, they evade the legal authorities," he said.
• Meow-Meow (mephedrone, 4-methylmethcathinone). Other street names include Drone, Bubble, and MCAT. This synthetic cathinone, derived from an African shrub, is a stimulant and sympathomimetic agent. Its effects and structure are similar to those of ephedra and amphetamine. Symptoms of Meow-Meow use include seizures, agitation, tachycardia, hypertension, and hyperthermia (Toxicol. Lett. 2011;201:191-5).
• Bromo-DragonFLY (bromo-benzodifuranyl-isopropylamine). Adverse effects of this designer drug include hallucinations, seizures, vomiting, and intense vasoconstriction with resulting ischemia in fingers and toes. The drug has "hallucinogenic, Ecstasy-like properties" and is a serotoninergic receptor agonist. The name derives from the resemblance its chemical structure has to a dragonfly.
• Nutmeg. At doses as high as 50 g, the common spice nutmeg has hallucinogenic properties. "When we see nutmeg users in the ED, we’re seeing a small proportion who took an extremely large dose or have an unanticipated complication from it," Dr. Mycyk said. In one case series of 119 patients, the most common symptoms were tachycardia, palpitations, and agitation. The researchers found that "clinical effects from ingestion can be significant and can require medical intervention" (Clin. Toxicol. [Phila.] 2011;49:177-80).
• Salvia. Street names of the salvia divinorum plant include Diviner’s Sage, Shepherdess, and Sally D. Related to mint, salvia has hallucinogenic and psychotomimetic properties. Symptoms include agitation and neurologic, cardiovascular, and gastrointestinal effects. The herb can be made into a tea; fresh leaves can be chewed; or leaves can be dried and then smoked, snorted, or injected. The drug has not been well studied, but one group of researchers analyzed YouTube videos of salvia users to study its effects (Drug Alcohol Depend. 2010;108:138-40).
• Snakebite. The venom of the naja naja snake, or Indian cobra, contains neurotoxins that can have opiate-like effects on the central nervous system. The venom can cause blackouts and feelings of well-being and lethargy in people who deliberately have themselves bitten by a cobra (Subst. Abus. 2011;32:43-6). "It boggles my mind what people will do to get high," Dr. Mycyk said.
• Buprenorphine (Suboxone). Clinically used for opioid dependence, this drug is smuggled into prisons by being crushed into a paste that is applied to a drawing or card, or hidden under stamps. A recent study found that 12% of drug contraband in Massachusetts prisons is buprenorphine (Curr. Drug Abuse Rev. 2011;4:28-41). Buprenorphine intoxication causes mild euphoria, somnolence, and possible respiratory depression; laboratory and toxicology screens for illicit drugs would be negative.
Diagnosis
Hospital-based drug screens don’t detect most of the new and evolving designer drugs that result in emergency department visits. "A lot of hospitals have invested in expanded drug-screening panels, but these hospital machines cannot keep up with the creative chemists and users out there," Dr. Mycyk said. So "tox testing is not that helpful for some of these NEW drugs. In fact, it might falsely reassure you."
So, to make the diagnosis, "if the patient is conscious, ask them. Know their language, know the slang. They will tell you. ... They are frightened, and they don’t want to die."
If the patient is delirious or has altered mental status, examine his or her belongings carefully. "Completely examine your patient’s belongings, and you will probably find your answer." Check the small pocket in jeans, Dr. Mycyk suggested. "I’ve been surprised how often I find drug contraband in that small pocket."
Accessing one of the "drug partisan sites" – such as erowid.org, lycaeum.org, shroomery.org, and talktofrank.com – also can be useful if you want to figure out what your patient has taken. However, while it might be helpful to know the agent, focus on symptoms and "treat the patient; don’t treat the product," he said.
Treatment
Deaths from NEW drug abuse most commonly occur due to dysrhythmias, hyperthermia, or metabolic complications. There are no antidotes for any of these NEW drugs, but "symptom-based, goal-directed, supportive therapy will save most of these patients’ lives."
Use common sense, and trust your instincts, Dr. Mycyk said. Get an electrolyte panel if the patient is persistently symptomatic. If a patient is tachycardic and having palpitations, getting an ECG may be appropriate. If they’re overly agitated, it is safe to use benzodiazepines. If they’re dehydrated, give them IV fluids, he said.
It is important to get complete vital signs on these patients, and the most important vital sign is temperature, as elevated body temperature is the best predictor of death in the ED. Degree of tachycardia or tachypnea is not as concerning, he said.
For most of these patients, brief ED observation is fine. However, some of the NEW drugs have long duration of activity; for example, the effects of buprenorphine can last 24-37 hours, so admission might be considered.
All patients with an ED visit for drug use should have counseling before discharge. Simple ED counseling can help, Dr. Mycyk said. "They think a lot of this stuff is safe, and we just need to remind them that it is not safe."
Dr. Mycyk had no significant financial relationships to disclose.
Staffing Crucial to HIV Testing in the ED
Of the more than 1 million HIV-positive patients in the United States, approximately 21% are undiagnosed, as more than 50,000 new infections occur annually. The emergency department is recognized as an important point of access to HIV testing for many patients.
In 2006, the Centers for Disease Control and Prevention recommended that HIV testing be incorporated into routine medical care, including emergency care and, in 2007, the American College of Emergency Physicians agreed, saying in a policy statement that HIV testing in the emergency department "should be available in an expeditious and efficient fashion similar to testing and results for other conditions."
Although HIV testing in EDs has become more common since the CDC and ACEP recommendations were made, controversies about and obstacles to such testing remain.
Perceptions of Testing
In a 2007 study of the perceived benefits and disadvantages of HIV testing in the ED, researchers did a structured evaluation of opinions gathered from 98 experts from 42 institutions who attended the 2007 conference of the National Emergency Department HIV Testing Consortium in Baltimore (Ann. Emerg. Med. 2011;58:S151-9).
The expert opinions were organized using a subjective analytic planning tool called SWOT (strengths, weaknesses, opportunities, threats) by the researchers, led by Aleksandar Kecojevic of Johns Hopkins University, Baltimore.
The identified strengths of HIV testing in the ED were the high volume of ED visits (110 million annually) and the high prevalence of HIV in the ED patient population (cited by 19.6% of the experts). Access to an underserved patient population was cited by 16.1%. Other strengths included the availability of testing around the clock (11.7%) and the chance for earlier diagnosis (8.1%).
A total of 23.2% of the experts identified the additional strain on ED staff and resources as the biggest weakness of the approach. Inadequate privacy for testing in the ED was mentioned by 13%.
The opportunity to reduce the stigma of HIV was cited by 26.8% of the experts and better surveillance of disease rates and transmission networks by 18.4%. The threat category included lack of funding and other resources (44%), and diversion of resources and staff from the emergency department’s primary mission of acute care (13.4%).
Increasing Rates of Testing
Despite the barriers to HIV testing in EDs, the rates have increased substantially since the testing recommendations were published.
A 1996 survey found that about 50% of academic EDs tested for HIV after suspected exposure. In 2006, a survey found that a similar 57% of academic EDs did some rapid HIV testing, but only 4% did so routinely. Only 3 years later, in 2009, a cross-sectional survey of medical providers by Dr. Richard E. Rothman and his colleagues found that 82% of EDs conducted HIV testing (Ann. Emerg. Med. 2011;58[suppl]:S3-9).
However, only 22% did so as part of a routine HIV testing program, and 18% did no testing at all, according to Dr. Rothman of Johns Hopkins University, Baltimore, and his coinvestigators.
The survey included 338 academic, nonacademic, and community hospitals from urban and rural areas across the country. Survey respondents included ED directors and chairs, HIV program directors, nurses, and ED social workers.
Of the 22% of EDs that reported routine HIV screening, 85% were in urban areas and 65% were in academic hospitals. Most of the 18% that did no testing were small community hospitals. Of large hospitals with more than 100,000 visits a year, 91% offered HIV testing and more than half had routine HIV testing programs. More than 80% of the screening programs had been in place for less than 3 years, and about a third had existed for less than a year.
"These results represent a recent increase in the availability of HIV testing in U.S. EDs and a steady increase in HIV screening," Dr. Rothman and his colleagues concluded.
Overall, EDs in academic hospitals implement HIV testing at a higher rate than do those in community hospitals, according to a 2007 cross-sectional survey by Dr. Jason S. Haukoos and his colleagues, which found significant differences in testing rates (Ann. Emerg. Med. 2011;58[suppl]:S10-16).
Their survey included ED administrators, emergency physicians, and other health care staff at 99 academic EDs and 150 community institutions. They found that 65% of academic EDs offered testing, compared with 50% of community hospitals; more academic institutions tested without charging patients (34% vs. 7%) and received funding for testing (15% vs. 2%), said Dr. Haukoos of Denver Health Medical Center and his colleagues.
Diagnostic testing was offered most widely (73% of academic EDs, 63% of community EDs). Nontargeted screening was performed at 16% of academic institutions, compared with only 5% of community EDs.
"There remain substantial differences related to HIV testing between academic and community institutions, and a substantial proportion of institutions still do not provide some form of HIV testing," the authors said.
Staffing for Testing Programs
Having enough personnel with the right training is the key to implementing any HIV testing program in the ED. The Universal Screening for HIV Infection in the Emergency Room (USHER) trial compared HIV testing offered by supplemental HIV counselors to testing offered by ED providers. The objective of the trial was to determine whether testing rates were higher when offered by existing ED providers or by additional staff such as counselors and social workers (Ann. Emerg. Med. 2011;58[suppl]:S126-132).
"Routine, voluntary HIV testing was completed more than twice as frequently when personnel were dedicated specifically to this task," reported Dr. Rochelle P. Walensky of Massachusetts General Hospital, Boston, and her colleagues.
In this 2007-2008 randomized controlled trial, 2,446 ED patients were randomized to the counselor arm and 2,409 to the ED provider arm. A total of 80% of patients in the counselor arm were offered testing vs. 36% of those in the provider arm. In the provider arm, the offer rate declined with increasing age of the patient and declined over the course of the study (from 76% at 2 months to 25% at 17 months). "Testing attrition over time [in the provider arm] may be due to waning enthusiasm for the program in the face of patient acuity and other clinical duties," Dr. Walensky and her coauthors suggested.
A comparable proportion of patients accepted testing when it was offered (71% in the counselor arm and 75% in the provider arm), for an overall testing rate of 57% in the counselor arm and 27% in the provider arm.
"Although HIV counselor time certainly costs less than that of ED providers, the cost of additional trained personnel is not trivial." However, "without such resources, rapid HIV testing in this setting is most likely diagnostic and not truly routine," they concluded.
In another 2007-2008 study of six EDs that had HIV screening programs in place for at least 6 months, Gretchen Williams Torres and her coinvestigators found that "several sites had 1 or more staff individuals, generally an emergency physician or nurse, who took ownership of the screening program" (Ann. Emerg. Med. 2011;58[suppl]:S104-13).
Testing was done by supplemental staff at four hospitals and by existing ED staff at two. Costs were higher at the two EDs in which supplemental staff was used to implement the programs, at $10,200-$12,300, compared with $3,400-$8,600 when ED providers added it to their tasks, wrote Ms. Torres of the University of Chicago and her coauthors.
The six study institutions were a public hospital and a for-profit hospital in the South, two nonprofits in the Midwest, a public hospital in the West, and a public hospital in the Northeast. All were teaching hospitals, with a median of 37.5 ED beds. Two of the EDs did targeted screening of higher-risk patients, three screened some patients regardless of risk, and one screened all patients (universal screening).
Yet "none of the EDs were able to test more than 10% of the patients presenting for care," with a median of 4.7% of patients tested. EDs with targeted programs tested 2%-3% of their patients, those with nontargeted programs tested 5%-8%, and the hospital with universal screening tested 7% (while that institution offered screening to 97% of its patients, most declined the test).
In a report of a 2009 pilot program at an urban academic ED, the investigators found that the success of the program was dependent on "a core group of coordinators, involvement and support from administration, and broad buy-in from faculty and staff," including "ED technicians, nurses, and physician extenders and emergency physicians" (Ann. Emerg. Med. 2011;58[suppl]:S44-8).
The program required a commitment from staff to perform the tasks necessary "for patient recruitment, specimen collection and processing, result notification, posttest counseling, and data entry," said Dr. Bryn E. Mumma of the University of Pittsburgh and her colleagues.
"Finding someone with time to enroll patients and collect the OraSure specimen without compromising patient care or ED flow was the most significant barrier to universal screening in our pilot program," they said.
Providing HIV screening in the ED setting serves a hard-to-reach population, and much progress has been made in adding routine HIV testing to ED visits. However, the lack of available dedicated staff, inadequate funding, and other obstacles will continue to hamper future efforts.
Mr. Kecojevic had no disclosures. Dr. Rothman received funding from the Maryland Department of Health and Mental Hygiene. Dr. Haukoos received an award from the Agency for Healthcare Research and Quality, support from the CDC, and an unrestricted grant from Abbott Laboratories. Dr. Walensky received the Doris Duke Charitable Foundation Clinical Scientist Development Award, and her study had support from the National Institute of Mental Health. Ms. Torres’ study was funding by the CDC and the Health Research and Educational Trust of the American Hospital Association. The Allegheny County Health Department provided the OraSure tests and processing for Dr. Mumma’s study.
Of the more than 1 million HIV-positive patients in the United States, approximately 21% are undiagnosed, as more than 50,000 new infections occur annually. The emergency department is recognized as an important point of access to HIV testing for many patients.
In 2006, the Centers for Disease Control and Prevention recommended that HIV testing be incorporated into routine medical care, including emergency care and, in 2007, the American College of Emergency Physicians agreed, saying in a policy statement that HIV testing in the emergency department "should be available in an expeditious and efficient fashion similar to testing and results for other conditions."
Although HIV testing in EDs has become more common since the CDC and ACEP recommendations were made, controversies about and obstacles to such testing remain.
Perceptions of Testing
In a 2007 study of the perceived benefits and disadvantages of HIV testing in the ED, researchers did a structured evaluation of opinions gathered from 98 experts from 42 institutions who attended the 2007 conference of the National Emergency Department HIV Testing Consortium in Baltimore (Ann. Emerg. Med. 2011;58:S151-9).
The expert opinions were organized using a subjective analytic planning tool called SWOT (strengths, weaknesses, opportunities, threats) by the researchers, led by Aleksandar Kecojevic of Johns Hopkins University, Baltimore.
The identified strengths of HIV testing in the ED were the high volume of ED visits (110 million annually) and the high prevalence of HIV in the ED patient population (cited by 19.6% of the experts). Access to an underserved patient population was cited by 16.1%. Other strengths included the availability of testing around the clock (11.7%) and the chance for earlier diagnosis (8.1%).
A total of 23.2% of the experts identified the additional strain on ED staff and resources as the biggest weakness of the approach. Inadequate privacy for testing in the ED was mentioned by 13%.
The opportunity to reduce the stigma of HIV was cited by 26.8% of the experts and better surveillance of disease rates and transmission networks by 18.4%. The threat category included lack of funding and other resources (44%), and diversion of resources and staff from the emergency department’s primary mission of acute care (13.4%).
Increasing Rates of Testing
Despite the barriers to HIV testing in EDs, the rates have increased substantially since the testing recommendations were published.
A 1996 survey found that about 50% of academic EDs tested for HIV after suspected exposure. In 2006, a survey found that a similar 57% of academic EDs did some rapid HIV testing, but only 4% did so routinely. Only 3 years later, in 2009, a cross-sectional survey of medical providers by Dr. Richard E. Rothman and his colleagues found that 82% of EDs conducted HIV testing (Ann. Emerg. Med. 2011;58[suppl]:S3-9).
However, only 22% did so as part of a routine HIV testing program, and 18% did no testing at all, according to Dr. Rothman of Johns Hopkins University, Baltimore, and his coinvestigators.
The survey included 338 academic, nonacademic, and community hospitals from urban and rural areas across the country. Survey respondents included ED directors and chairs, HIV program directors, nurses, and ED social workers.
Of the 22% of EDs that reported routine HIV screening, 85% were in urban areas and 65% were in academic hospitals. Most of the 18% that did no testing were small community hospitals. Of large hospitals with more than 100,000 visits a year, 91% offered HIV testing and more than half had routine HIV testing programs. More than 80% of the screening programs had been in place for less than 3 years, and about a third had existed for less than a year.
"These results represent a recent increase in the availability of HIV testing in U.S. EDs and a steady increase in HIV screening," Dr. Rothman and his colleagues concluded.
Overall, EDs in academic hospitals implement HIV testing at a higher rate than do those in community hospitals, according to a 2007 cross-sectional survey by Dr. Jason S. Haukoos and his colleagues, which found significant differences in testing rates (Ann. Emerg. Med. 2011;58[suppl]:S10-16).
Their survey included ED administrators, emergency physicians, and other health care staff at 99 academic EDs and 150 community institutions. They found that 65% of academic EDs offered testing, compared with 50% of community hospitals; more academic institutions tested without charging patients (34% vs. 7%) and received funding for testing (15% vs. 2%), said Dr. Haukoos of Denver Health Medical Center and his colleagues.
Diagnostic testing was offered most widely (73% of academic EDs, 63% of community EDs). Nontargeted screening was performed at 16% of academic institutions, compared with only 5% of community EDs.
"There remain substantial differences related to HIV testing between academic and community institutions, and a substantial proportion of institutions still do not provide some form of HIV testing," the authors said.
Staffing for Testing Programs
Having enough personnel with the right training is the key to implementing any HIV testing program in the ED. The Universal Screening for HIV Infection in the Emergency Room (USHER) trial compared HIV testing offered by supplemental HIV counselors to testing offered by ED providers. The objective of the trial was to determine whether testing rates were higher when offered by existing ED providers or by additional staff such as counselors and social workers (Ann. Emerg. Med. 2011;58[suppl]:S126-132).
"Routine, voluntary HIV testing was completed more than twice as frequently when personnel were dedicated specifically to this task," reported Dr. Rochelle P. Walensky of Massachusetts General Hospital, Boston, and her colleagues.
In this 2007-2008 randomized controlled trial, 2,446 ED patients were randomized to the counselor arm and 2,409 to the ED provider arm. A total of 80% of patients in the counselor arm were offered testing vs. 36% of those in the provider arm. In the provider arm, the offer rate declined with increasing age of the patient and declined over the course of the study (from 76% at 2 months to 25% at 17 months). "Testing attrition over time [in the provider arm] may be due to waning enthusiasm for the program in the face of patient acuity and other clinical duties," Dr. Walensky and her coauthors suggested.
A comparable proportion of patients accepted testing when it was offered (71% in the counselor arm and 75% in the provider arm), for an overall testing rate of 57% in the counselor arm and 27% in the provider arm.
"Although HIV counselor time certainly costs less than that of ED providers, the cost of additional trained personnel is not trivial." However, "without such resources, rapid HIV testing in this setting is most likely diagnostic and not truly routine," they concluded.
In another 2007-2008 study of six EDs that had HIV screening programs in place for at least 6 months, Gretchen Williams Torres and her coinvestigators found that "several sites had 1 or more staff individuals, generally an emergency physician or nurse, who took ownership of the screening program" (Ann. Emerg. Med. 2011;58[suppl]:S104-13).
Testing was done by supplemental staff at four hospitals and by existing ED staff at two. Costs were higher at the two EDs in which supplemental staff was used to implement the programs, at $10,200-$12,300, compared with $3,400-$8,600 when ED providers added it to their tasks, wrote Ms. Torres of the University of Chicago and her coauthors.
The six study institutions were a public hospital and a for-profit hospital in the South, two nonprofits in the Midwest, a public hospital in the West, and a public hospital in the Northeast. All were teaching hospitals, with a median of 37.5 ED beds. Two of the EDs did targeted screening of higher-risk patients, three screened some patients regardless of risk, and one screened all patients (universal screening).
Yet "none of the EDs were able to test more than 10% of the patients presenting for care," with a median of 4.7% of patients tested. EDs with targeted programs tested 2%-3% of their patients, those with nontargeted programs tested 5%-8%, and the hospital with universal screening tested 7% (while that institution offered screening to 97% of its patients, most declined the test).
In a report of a 2009 pilot program at an urban academic ED, the investigators found that the success of the program was dependent on "a core group of coordinators, involvement and support from administration, and broad buy-in from faculty and staff," including "ED technicians, nurses, and physician extenders and emergency physicians" (Ann. Emerg. Med. 2011;58[suppl]:S44-8).
The program required a commitment from staff to perform the tasks necessary "for patient recruitment, specimen collection and processing, result notification, posttest counseling, and data entry," said Dr. Bryn E. Mumma of the University of Pittsburgh and her colleagues.
"Finding someone with time to enroll patients and collect the OraSure specimen without compromising patient care or ED flow was the most significant barrier to universal screening in our pilot program," they said.
Providing HIV screening in the ED setting serves a hard-to-reach population, and much progress has been made in adding routine HIV testing to ED visits. However, the lack of available dedicated staff, inadequate funding, and other obstacles will continue to hamper future efforts.
Mr. Kecojevic had no disclosures. Dr. Rothman received funding from the Maryland Department of Health and Mental Hygiene. Dr. Haukoos received an award from the Agency for Healthcare Research and Quality, support from the CDC, and an unrestricted grant from Abbott Laboratories. Dr. Walensky received the Doris Duke Charitable Foundation Clinical Scientist Development Award, and her study had support from the National Institute of Mental Health. Ms. Torres’ study was funding by the CDC and the Health Research and Educational Trust of the American Hospital Association. The Allegheny County Health Department provided the OraSure tests and processing for Dr. Mumma’s study.
Of the more than 1 million HIV-positive patients in the United States, approximately 21% are undiagnosed, as more than 50,000 new infections occur annually. The emergency department is recognized as an important point of access to HIV testing for many patients.
In 2006, the Centers for Disease Control and Prevention recommended that HIV testing be incorporated into routine medical care, including emergency care and, in 2007, the American College of Emergency Physicians agreed, saying in a policy statement that HIV testing in the emergency department "should be available in an expeditious and efficient fashion similar to testing and results for other conditions."
Although HIV testing in EDs has become more common since the CDC and ACEP recommendations were made, controversies about and obstacles to such testing remain.
Perceptions of Testing
In a 2007 study of the perceived benefits and disadvantages of HIV testing in the ED, researchers did a structured evaluation of opinions gathered from 98 experts from 42 institutions who attended the 2007 conference of the National Emergency Department HIV Testing Consortium in Baltimore (Ann. Emerg. Med. 2011;58:S151-9).
The expert opinions were organized using a subjective analytic planning tool called SWOT (strengths, weaknesses, opportunities, threats) by the researchers, led by Aleksandar Kecojevic of Johns Hopkins University, Baltimore.
The identified strengths of HIV testing in the ED were the high volume of ED visits (110 million annually) and the high prevalence of HIV in the ED patient population (cited by 19.6% of the experts). Access to an underserved patient population was cited by 16.1%. Other strengths included the availability of testing around the clock (11.7%) and the chance for earlier diagnosis (8.1%).
A total of 23.2% of the experts identified the additional strain on ED staff and resources as the biggest weakness of the approach. Inadequate privacy for testing in the ED was mentioned by 13%.
The opportunity to reduce the stigma of HIV was cited by 26.8% of the experts and better surveillance of disease rates and transmission networks by 18.4%. The threat category included lack of funding and other resources (44%), and diversion of resources and staff from the emergency department’s primary mission of acute care (13.4%).
Increasing Rates of Testing
Despite the barriers to HIV testing in EDs, the rates have increased substantially since the testing recommendations were published.
A 1996 survey found that about 50% of academic EDs tested for HIV after suspected exposure. In 2006, a survey found that a similar 57% of academic EDs did some rapid HIV testing, but only 4% did so routinely. Only 3 years later, in 2009, a cross-sectional survey of medical providers by Dr. Richard E. Rothman and his colleagues found that 82% of EDs conducted HIV testing (Ann. Emerg. Med. 2011;58[suppl]:S3-9).
However, only 22% did so as part of a routine HIV testing program, and 18% did no testing at all, according to Dr. Rothman of Johns Hopkins University, Baltimore, and his coinvestigators.
The survey included 338 academic, nonacademic, and community hospitals from urban and rural areas across the country. Survey respondents included ED directors and chairs, HIV program directors, nurses, and ED social workers.
Of the 22% of EDs that reported routine HIV screening, 85% were in urban areas and 65% were in academic hospitals. Most of the 18% that did no testing were small community hospitals. Of large hospitals with more than 100,000 visits a year, 91% offered HIV testing and more than half had routine HIV testing programs. More than 80% of the screening programs had been in place for less than 3 years, and about a third had existed for less than a year.
"These results represent a recent increase in the availability of HIV testing in U.S. EDs and a steady increase in HIV screening," Dr. Rothman and his colleagues concluded.
Overall, EDs in academic hospitals implement HIV testing at a higher rate than do those in community hospitals, according to a 2007 cross-sectional survey by Dr. Jason S. Haukoos and his colleagues, which found significant differences in testing rates (Ann. Emerg. Med. 2011;58[suppl]:S10-16).
Their survey included ED administrators, emergency physicians, and other health care staff at 99 academic EDs and 150 community institutions. They found that 65% of academic EDs offered testing, compared with 50% of community hospitals; more academic institutions tested without charging patients (34% vs. 7%) and received funding for testing (15% vs. 2%), said Dr. Haukoos of Denver Health Medical Center and his colleagues.
Diagnostic testing was offered most widely (73% of academic EDs, 63% of community EDs). Nontargeted screening was performed at 16% of academic institutions, compared with only 5% of community EDs.
"There remain substantial differences related to HIV testing between academic and community institutions, and a substantial proportion of institutions still do not provide some form of HIV testing," the authors said.
Staffing for Testing Programs
Having enough personnel with the right training is the key to implementing any HIV testing program in the ED. The Universal Screening for HIV Infection in the Emergency Room (USHER) trial compared HIV testing offered by supplemental HIV counselors to testing offered by ED providers. The objective of the trial was to determine whether testing rates were higher when offered by existing ED providers or by additional staff such as counselors and social workers (Ann. Emerg. Med. 2011;58[suppl]:S126-132).
"Routine, voluntary HIV testing was completed more than twice as frequently when personnel were dedicated specifically to this task," reported Dr. Rochelle P. Walensky of Massachusetts General Hospital, Boston, and her colleagues.
In this 2007-2008 randomized controlled trial, 2,446 ED patients were randomized to the counselor arm and 2,409 to the ED provider arm. A total of 80% of patients in the counselor arm were offered testing vs. 36% of those in the provider arm. In the provider arm, the offer rate declined with increasing age of the patient and declined over the course of the study (from 76% at 2 months to 25% at 17 months). "Testing attrition over time [in the provider arm] may be due to waning enthusiasm for the program in the face of patient acuity and other clinical duties," Dr. Walensky and her coauthors suggested.
A comparable proportion of patients accepted testing when it was offered (71% in the counselor arm and 75% in the provider arm), for an overall testing rate of 57% in the counselor arm and 27% in the provider arm.
"Although HIV counselor time certainly costs less than that of ED providers, the cost of additional trained personnel is not trivial." However, "without such resources, rapid HIV testing in this setting is most likely diagnostic and not truly routine," they concluded.
In another 2007-2008 study of six EDs that had HIV screening programs in place for at least 6 months, Gretchen Williams Torres and her coinvestigators found that "several sites had 1 or more staff individuals, generally an emergency physician or nurse, who took ownership of the screening program" (Ann. Emerg. Med. 2011;58[suppl]:S104-13).
Testing was done by supplemental staff at four hospitals and by existing ED staff at two. Costs were higher at the two EDs in which supplemental staff was used to implement the programs, at $10,200-$12,300, compared with $3,400-$8,600 when ED providers added it to their tasks, wrote Ms. Torres of the University of Chicago and her coauthors.
The six study institutions were a public hospital and a for-profit hospital in the South, two nonprofits in the Midwest, a public hospital in the West, and a public hospital in the Northeast. All were teaching hospitals, with a median of 37.5 ED beds. Two of the EDs did targeted screening of higher-risk patients, three screened some patients regardless of risk, and one screened all patients (universal screening).
Yet "none of the EDs were able to test more than 10% of the patients presenting for care," with a median of 4.7% of patients tested. EDs with targeted programs tested 2%-3% of their patients, those with nontargeted programs tested 5%-8%, and the hospital with universal screening tested 7% (while that institution offered screening to 97% of its patients, most declined the test).
In a report of a 2009 pilot program at an urban academic ED, the investigators found that the success of the program was dependent on "a core group of coordinators, involvement and support from administration, and broad buy-in from faculty and staff," including "ED technicians, nurses, and physician extenders and emergency physicians" (Ann. Emerg. Med. 2011;58[suppl]:S44-8).
The program required a commitment from staff to perform the tasks necessary "for patient recruitment, specimen collection and processing, result notification, posttest counseling, and data entry," said Dr. Bryn E. Mumma of the University of Pittsburgh and her colleagues.
"Finding someone with time to enroll patients and collect the OraSure specimen without compromising patient care or ED flow was the most significant barrier to universal screening in our pilot program," they said.
Providing HIV screening in the ED setting serves a hard-to-reach population, and much progress has been made in adding routine HIV testing to ED visits. However, the lack of available dedicated staff, inadequate funding, and other obstacles will continue to hamper future efforts.
Mr. Kecojevic had no disclosures. Dr. Rothman received funding from the Maryland Department of Health and Mental Hygiene. Dr. Haukoos received an award from the Agency for Healthcare Research and Quality, support from the CDC, and an unrestricted grant from Abbott Laboratories. Dr. Walensky received the Doris Duke Charitable Foundation Clinical Scientist Development Award, and her study had support from the National Institute of Mental Health. Ms. Torres’ study was funding by the CDC and the Health Research and Educational Trust of the American Hospital Association. The Allegheny County Health Department provided the OraSure tests and processing for Dr. Mumma’s study.
FROM THE ANNALS OF EMERGENCY MEDICINE
Required Rural Rotations Influence Job Choice After Graduation
Increasing the number of residency programs that require rotations in rural areas would help address the shortage of emergency physicians who choose to work in rural U.S. emergency departments, according to a survey of 2,380 graduates of 111 residency training programs.
Based on the findings of their nationwide July-December 2009 survey, "exposure to rural emergency department (ED) rotations may positively enhance rural recruitment after graduation," wrote Dr. Brad E. Talley of the department of emergency medicine at Denver Health Medical Center, and his coauthors.
The investigators surveyed the program directors of all 126 emergency medicine residency training programs recognized by the Accreditation Council for Graduate Medical Education, with the exception of military programs and those started after 2006. Of the 111 programs that provided complete responses, only 6 (5%) required residents to have a rotation in a rural area. Of the remainder, 16 (14%) offered residents rural rotations at predesignated sites as an elective, 76 (69%) offered rural rotations as an elective but students were required to find their own site, and 13 (12%) offered no opportunity for a rural rotation.
Programs that required rural rotations had a significantly greater percentage of residents who later chose to start their careers in rural areas (22%) than did programs with electives at predesignated sites (7%), programs with electives at student-selected sites (6%), and programs with no rural rotations (7%), Dr. Talley and his coinvestigators reported.
Overall, 7% of residents took jobs in rural areas after completing their training programs (Acad. Emerg. Med. 2011;18:297-300).
A total of 197 students completed a rural rotation, and 111 of these were from the six programs that required them. In comparison, only 86 students from the 92 programs that offered rural rotations as electives chose to train in a rural location.
Of residents in programs with elective rotations, more chose a rural rotation if a predesignated site was offered (7% vs. 4% without predesignated sites).
When categorized by geographic area, a high of 19% of residents in programs in the East South Central part of the United States chose rural positions after graduation, compared with only 2% of residents who trained in the Pacific part of the country. Although students in programs located in states with high rural populations (according to U.S. Census Bureau statistics) were more likely to have completed a rural rotation, a program’s geographic area was not associated with the probability of its residents working in a rural hospital after graduation.
The low percentage of programs offering rural rotations may be due to funding patterns and resident preferences. While acknowledging that rural hospitals may have fewer resources, Dr. Talley and his colleagues noted that practicing in a rural ED "requires a unique skill set" that students without such an experience may not acquire. And despite previous criticisms, "rural EDs can provide adequate patient volume and experience to support [emergency medicine] resident education," they added.
Emergency physicians are in short supply, especially in rural areas (Ann. Emerg. Med. 2009;54:349-59). As this study "found that exposure to rural [emergency medicine] rotations through required rotations was associated with subsequent resident job selection in rural areas," increasing the number of programs that require rural rotations may be an important strategy to help alleviate the shortage, according to Dr. Talley and his colleagues.
Future studies are needed to determine the costs of such an approach, which may be prohibitive, they wrote.
Limitations of the study include the lack of data from the 15 program directors who did not participate. In addition, the researchers did not provide survey respondents with a standard definition of "rural."
The authors did not have any conflicts of interest to report.
Increasing the number of residency programs that require rotations in rural areas would help address the shortage of emergency physicians who choose to work in rural U.S. emergency departments, according to a survey of 2,380 graduates of 111 residency training programs.
Based on the findings of their nationwide July-December 2009 survey, "exposure to rural emergency department (ED) rotations may positively enhance rural recruitment after graduation," wrote Dr. Brad E. Talley of the department of emergency medicine at Denver Health Medical Center, and his coauthors.
The investigators surveyed the program directors of all 126 emergency medicine residency training programs recognized by the Accreditation Council for Graduate Medical Education, with the exception of military programs and those started after 2006. Of the 111 programs that provided complete responses, only 6 (5%) required residents to have a rotation in a rural area. Of the remainder, 16 (14%) offered residents rural rotations at predesignated sites as an elective, 76 (69%) offered rural rotations as an elective but students were required to find their own site, and 13 (12%) offered no opportunity for a rural rotation.
Programs that required rural rotations had a significantly greater percentage of residents who later chose to start their careers in rural areas (22%) than did programs with electives at predesignated sites (7%), programs with electives at student-selected sites (6%), and programs with no rural rotations (7%), Dr. Talley and his coinvestigators reported.
Overall, 7% of residents took jobs in rural areas after completing their training programs (Acad. Emerg. Med. 2011;18:297-300).
A total of 197 students completed a rural rotation, and 111 of these were from the six programs that required them. In comparison, only 86 students from the 92 programs that offered rural rotations as electives chose to train in a rural location.
Of residents in programs with elective rotations, more chose a rural rotation if a predesignated site was offered (7% vs. 4% without predesignated sites).
When categorized by geographic area, a high of 19% of residents in programs in the East South Central part of the United States chose rural positions after graduation, compared with only 2% of residents who trained in the Pacific part of the country. Although students in programs located in states with high rural populations (according to U.S. Census Bureau statistics) were more likely to have completed a rural rotation, a program’s geographic area was not associated with the probability of its residents working in a rural hospital after graduation.
The low percentage of programs offering rural rotations may be due to funding patterns and resident preferences. While acknowledging that rural hospitals may have fewer resources, Dr. Talley and his colleagues noted that practicing in a rural ED "requires a unique skill set" that students without such an experience may not acquire. And despite previous criticisms, "rural EDs can provide adequate patient volume and experience to support [emergency medicine] resident education," they added.
Emergency physicians are in short supply, especially in rural areas (Ann. Emerg. Med. 2009;54:349-59). As this study "found that exposure to rural [emergency medicine] rotations through required rotations was associated with subsequent resident job selection in rural areas," increasing the number of programs that require rural rotations may be an important strategy to help alleviate the shortage, according to Dr. Talley and his colleagues.
Future studies are needed to determine the costs of such an approach, which may be prohibitive, they wrote.
Limitations of the study include the lack of data from the 15 program directors who did not participate. In addition, the researchers did not provide survey respondents with a standard definition of "rural."
The authors did not have any conflicts of interest to report.
Increasing the number of residency programs that require rotations in rural areas would help address the shortage of emergency physicians who choose to work in rural U.S. emergency departments, according to a survey of 2,380 graduates of 111 residency training programs.
Based on the findings of their nationwide July-December 2009 survey, "exposure to rural emergency department (ED) rotations may positively enhance rural recruitment after graduation," wrote Dr. Brad E. Talley of the department of emergency medicine at Denver Health Medical Center, and his coauthors.
The investigators surveyed the program directors of all 126 emergency medicine residency training programs recognized by the Accreditation Council for Graduate Medical Education, with the exception of military programs and those started after 2006. Of the 111 programs that provided complete responses, only 6 (5%) required residents to have a rotation in a rural area. Of the remainder, 16 (14%) offered residents rural rotations at predesignated sites as an elective, 76 (69%) offered rural rotations as an elective but students were required to find their own site, and 13 (12%) offered no opportunity for a rural rotation.
Programs that required rural rotations had a significantly greater percentage of residents who later chose to start their careers in rural areas (22%) than did programs with electives at predesignated sites (7%), programs with electives at student-selected sites (6%), and programs with no rural rotations (7%), Dr. Talley and his coinvestigators reported.
Overall, 7% of residents took jobs in rural areas after completing their training programs (Acad. Emerg. Med. 2011;18:297-300).
A total of 197 students completed a rural rotation, and 111 of these were from the six programs that required them. In comparison, only 86 students from the 92 programs that offered rural rotations as electives chose to train in a rural location.
Of residents in programs with elective rotations, more chose a rural rotation if a predesignated site was offered (7% vs. 4% without predesignated sites).
When categorized by geographic area, a high of 19% of residents in programs in the East South Central part of the United States chose rural positions after graduation, compared with only 2% of residents who trained in the Pacific part of the country. Although students in programs located in states with high rural populations (according to U.S. Census Bureau statistics) were more likely to have completed a rural rotation, a program’s geographic area was not associated with the probability of its residents working in a rural hospital after graduation.
The low percentage of programs offering rural rotations may be due to funding patterns and resident preferences. While acknowledging that rural hospitals may have fewer resources, Dr. Talley and his colleagues noted that practicing in a rural ED "requires a unique skill set" that students without such an experience may not acquire. And despite previous criticisms, "rural EDs can provide adequate patient volume and experience to support [emergency medicine] resident education," they added.
Emergency physicians are in short supply, especially in rural areas (Ann. Emerg. Med. 2009;54:349-59). As this study "found that exposure to rural [emergency medicine] rotations through required rotations was associated with subsequent resident job selection in rural areas," increasing the number of programs that require rural rotations may be an important strategy to help alleviate the shortage, according to Dr. Talley and his colleagues.
Future studies are needed to determine the costs of such an approach, which may be prohibitive, they wrote.
Limitations of the study include the lack of data from the 15 program directors who did not participate. In addition, the researchers did not provide survey respondents with a standard definition of "rural."
The authors did not have any conflicts of interest to report.
FROM ACADEMIC EMERGENCY MEDICINE
Undiagnosed OSA Common in Hospitalized Patients, May Increase Risk of Complications
VANCOUVER, B.C. – A significant number of hospitalized patients are at high risk for obstructive sleep apnea, but few have been evaluated for OSA, Dr. Sunita Kumar reported at the annual meeting of the American College of Chest Physicians.
Because OSA has been shown to increase the risk of adverse outcomes such as stroke and heart failure, screening inpatients might help prevent complications. However, Dr. Kumar noted, the diagnosis and treatment of OSA in hospitalized patients have not been shown to affect outcomes.
Of 195 inpatients surveyed over a 24-hour period at Loyola University Medical Center in Maywood, Ill., 157 (81%) were found to be at high risk for OSA. Of those, 41 had undergone a previous sleep study, and of the 41 patients who had been evaluated, 31 were found to have OSA, said Dr. Kumar of the Division of Pulmonary and Critical Care Medicine at Loyola.
In comparison, 5% of the general population is estimated to have sleep apnea.
The patients had a mean age of 62 years, and 82% were older than 50 years. Their mean body mass index was 28 kg/m2, with 14% having a BMI over 35. More than half (59%) were men. Of the 31 patients with a previous diagnosis of OSA, 17 were using continuous positive airway pressure (CPAP), 1 had undergone surgery, and 13 were not receiving treatment, generally because of nontolerance of CPAP.
The patients were screened using the STOP-BANG questionnaire, which has high sensitivity for detecting a high risk of sleep apnea but is not very specific, Dr. Kumar reported. It has also not been validated in inpatients, she said, which was a limitation of the study. However, the STOP-BANG (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender) questionnaire has been reported to be of high quality for predicting OSA (Can. J. Anaesth. 2010;57:423-38). When these patients were evaluated using only the STOP portion of the survey, 65% were found to be at high risk.
The few previous studies that looked at OSA in hospitalized patients found the prevalence to be as high as 77% (J. Clin. Sleep Med. 2008;4:105-10; Sleep Breath. 2008;12:229-34).
The take-home point of the recent study might be that it is safer to make a presumptive diagnosis of OSA in inpatients, commented session moderator Dr. Rochelle Goldberg, president and chief medical officer of the American Sleep Apnea Association.
Also at the session, Dr. Dennis Auckley presented his study on the frequency of complications in 217 hospitalized patients divided into three groups: those with known OSA (36 patients, 17%), those determined to be at high risk using the STOP and Berlin questionnaires (106 patients, 49%), and those at low risk (75 patients, 35%) based on the questionnaires.
The patients’ mean age was 50 years. Those with known OSA had a mean BMI of 44, the high-risk patients had a mean BMI of 32, and the low-risk patients had a mean BMI of 28.
Dr. Auckley of Case Western Reserve University in Cleveland and his colleagues undertook their 4-month, prospective observational study to further explore earlier findings that patients with OSA experience more adverse outcomes in the perioperative setting (Chest 2008;133:1128-34).
In their study, 38% of those with diagnosed OSA, 22% of those at high risk, and 14% of the low-risk patients experienced complications. Hypoxemia was the most frequent complication. The difference in complication rate between the known OSA patients and the low-risk patients was significant, even after researchers controlled for age, diagnosis, and comorbidities.
Patients with sleep apnea more commonly experience complications, especially hypoxemia, while hospitalized, Dr. Auckley concluded. The questionnaires have not been validated in hospitalized patients, and the patients were not monitored by oximetry, which were two limitations of the study, he noted.
Dr. Kumar reported that she had no relevant financial conflicts. Dr. Auckley disclosed support from ResMed Corp., and Cephalon Inc., and has received equipment from Cleveland Medical Devices Inc. His current study received no funding.
VANCOUVER, B.C. – A significant number of hospitalized patients are at high risk for obstructive sleep apnea, but few have been evaluated for OSA, Dr. Sunita Kumar reported at the annual meeting of the American College of Chest Physicians.
Because OSA has been shown to increase the risk of adverse outcomes such as stroke and heart failure, screening inpatients might help prevent complications. However, Dr. Kumar noted, the diagnosis and treatment of OSA in hospitalized patients have not been shown to affect outcomes.
Of 195 inpatients surveyed over a 24-hour period at Loyola University Medical Center in Maywood, Ill., 157 (81%) were found to be at high risk for OSA. Of those, 41 had undergone a previous sleep study, and of the 41 patients who had been evaluated, 31 were found to have OSA, said Dr. Kumar of the Division of Pulmonary and Critical Care Medicine at Loyola.
In comparison, 5% of the general population is estimated to have sleep apnea.
The patients had a mean age of 62 years, and 82% were older than 50 years. Their mean body mass index was 28 kg/m2, with 14% having a BMI over 35. More than half (59%) were men. Of the 31 patients with a previous diagnosis of OSA, 17 were using continuous positive airway pressure (CPAP), 1 had undergone surgery, and 13 were not receiving treatment, generally because of nontolerance of CPAP.
The patients were screened using the STOP-BANG questionnaire, which has high sensitivity for detecting a high risk of sleep apnea but is not very specific, Dr. Kumar reported. It has also not been validated in inpatients, she said, which was a limitation of the study. However, the STOP-BANG (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender) questionnaire has been reported to be of high quality for predicting OSA (Can. J. Anaesth. 2010;57:423-38). When these patients were evaluated using only the STOP portion of the survey, 65% were found to be at high risk.
The few previous studies that looked at OSA in hospitalized patients found the prevalence to be as high as 77% (J. Clin. Sleep Med. 2008;4:105-10; Sleep Breath. 2008;12:229-34).
The take-home point of the recent study might be that it is safer to make a presumptive diagnosis of OSA in inpatients, commented session moderator Dr. Rochelle Goldberg, president and chief medical officer of the American Sleep Apnea Association.
Also at the session, Dr. Dennis Auckley presented his study on the frequency of complications in 217 hospitalized patients divided into three groups: those with known OSA (36 patients, 17%), those determined to be at high risk using the STOP and Berlin questionnaires (106 patients, 49%), and those at low risk (75 patients, 35%) based on the questionnaires.
The patients’ mean age was 50 years. Those with known OSA had a mean BMI of 44, the high-risk patients had a mean BMI of 32, and the low-risk patients had a mean BMI of 28.
Dr. Auckley of Case Western Reserve University in Cleveland and his colleagues undertook their 4-month, prospective observational study to further explore earlier findings that patients with OSA experience more adverse outcomes in the perioperative setting (Chest 2008;133:1128-34).
In their study, 38% of those with diagnosed OSA, 22% of those at high risk, and 14% of the low-risk patients experienced complications. Hypoxemia was the most frequent complication. The difference in complication rate between the known OSA patients and the low-risk patients was significant, even after researchers controlled for age, diagnosis, and comorbidities.
Patients with sleep apnea more commonly experience complications, especially hypoxemia, while hospitalized, Dr. Auckley concluded. The questionnaires have not been validated in hospitalized patients, and the patients were not monitored by oximetry, which were two limitations of the study, he noted.
Dr. Kumar reported that she had no relevant financial conflicts. Dr. Auckley disclosed support from ResMed Corp., and Cephalon Inc., and has received equipment from Cleveland Medical Devices Inc. His current study received no funding.
VANCOUVER, B.C. – A significant number of hospitalized patients are at high risk for obstructive sleep apnea, but few have been evaluated for OSA, Dr. Sunita Kumar reported at the annual meeting of the American College of Chest Physicians.
Because OSA has been shown to increase the risk of adverse outcomes such as stroke and heart failure, screening inpatients might help prevent complications. However, Dr. Kumar noted, the diagnosis and treatment of OSA in hospitalized patients have not been shown to affect outcomes.
Of 195 inpatients surveyed over a 24-hour period at Loyola University Medical Center in Maywood, Ill., 157 (81%) were found to be at high risk for OSA. Of those, 41 had undergone a previous sleep study, and of the 41 patients who had been evaluated, 31 were found to have OSA, said Dr. Kumar of the Division of Pulmonary and Critical Care Medicine at Loyola.
In comparison, 5% of the general population is estimated to have sleep apnea.
The patients had a mean age of 62 years, and 82% were older than 50 years. Their mean body mass index was 28 kg/m2, with 14% having a BMI over 35. More than half (59%) were men. Of the 31 patients with a previous diagnosis of OSA, 17 were using continuous positive airway pressure (CPAP), 1 had undergone surgery, and 13 were not receiving treatment, generally because of nontolerance of CPAP.
The patients were screened using the STOP-BANG questionnaire, which has high sensitivity for detecting a high risk of sleep apnea but is not very specific, Dr. Kumar reported. It has also not been validated in inpatients, she said, which was a limitation of the study. However, the STOP-BANG (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender) questionnaire has been reported to be of high quality for predicting OSA (Can. J. Anaesth. 2010;57:423-38). When these patients were evaluated using only the STOP portion of the survey, 65% were found to be at high risk.
The few previous studies that looked at OSA in hospitalized patients found the prevalence to be as high as 77% (J. Clin. Sleep Med. 2008;4:105-10; Sleep Breath. 2008;12:229-34).
The take-home point of the recent study might be that it is safer to make a presumptive diagnosis of OSA in inpatients, commented session moderator Dr. Rochelle Goldberg, president and chief medical officer of the American Sleep Apnea Association.
Also at the session, Dr. Dennis Auckley presented his study on the frequency of complications in 217 hospitalized patients divided into three groups: those with known OSA (36 patients, 17%), those determined to be at high risk using the STOP and Berlin questionnaires (106 patients, 49%), and those at low risk (75 patients, 35%) based on the questionnaires.
The patients’ mean age was 50 years. Those with known OSA had a mean BMI of 44, the high-risk patients had a mean BMI of 32, and the low-risk patients had a mean BMI of 28.
Dr. Auckley of Case Western Reserve University in Cleveland and his colleagues undertook their 4-month, prospective observational study to further explore earlier findings that patients with OSA experience more adverse outcomes in the perioperative setting (Chest 2008;133:1128-34).
In their study, 38% of those with diagnosed OSA, 22% of those at high risk, and 14% of the low-risk patients experienced complications. Hypoxemia was the most frequent complication. The difference in complication rate between the known OSA patients and the low-risk patients was significant, even after researchers controlled for age, diagnosis, and comorbidities.
Patients with sleep apnea more commonly experience complications, especially hypoxemia, while hospitalized, Dr. Auckley concluded. The questionnaires have not been validated in hospitalized patients, and the patients were not monitored by oximetry, which were two limitations of the study, he noted.
Dr. Kumar reported that she had no relevant financial conflicts. Dr. Auckley disclosed support from ResMed Corp., and Cephalon Inc., and has received equipment from Cleveland Medical Devices Inc. His current study received no funding.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Undiagnosed OSA Common in Hospitalized Patients, May Increase Risk of Complications
VANCOUVER, B.C. – A significant number of hospitalized patients are at high risk for obstructive sleep apnea, but few have been evaluated for OSA, Dr. Sunita Kumar reported at the annual meeting of the American College of Chest Physicians.
Because OSA has been shown to increase the risk of adverse outcomes such as stroke and heart failure, screening inpatients might help prevent complications. However, Dr. Kumar noted, the diagnosis and treatment of OSA in hospitalized patients have not been shown to affect outcomes.
Of 195 inpatients surveyed over a 24-hour period at Loyola University Medical Center in Maywood, Ill., 157 (81%) were found to be at high risk for OSA. Of those, 41 had undergone a previous sleep study, and of the 41 patients who had been evaluated, 31 were found to have OSA, said Dr. Kumar of the Division of Pulmonary and Critical Care Medicine at Loyola.
In comparison, 5% of the general population is estimated to have sleep apnea.
The patients had a mean age of 62 years, and 82% were older than 50 years. Their mean body mass index was 28 kg/m2, with 14% having a BMI over 35. More than half (59%) were men. Of the 31 patients with a previous diagnosis of OSA, 17 were using continuous positive airway pressure (CPAP), 1 had undergone surgery, and 13 were not receiving treatment, generally because of nontolerance of CPAP.
The patients were screened using the STOP-BANG questionnaire, which has high sensitivity for detecting a high risk of sleep apnea but is not very specific, Dr. Kumar reported. It has also not been validated in inpatients, she said, which was a limitation of the study. However, the STOP-BANG (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender) questionnaire has been reported to be of high quality for predicting OSA (Can. J. Anaesth. 2010;57:423-38). When these patients were evaluated using only the STOP portion of the survey, 65% were found to be at high risk.
The few previous studies that looked at OSA in hospitalized patients found the prevalence to be as high as 77% (J. Clin. Sleep Med. 2008;4:105-10; Sleep Breath. 2008;12:229-34).
The take-home point of the recent study might be that it is safer to make a presumptive diagnosis of OSA in inpatients, commented session moderator Dr. Rochelle Goldberg, president and chief medical officer of the American Sleep Apnea Association.
Also at the session, Dr. Dennis Auckley presented his study on the frequency of complications in 217 hospitalized patients divided into three groups: those with known OSA (36 patients, 17%), those determined to be at high risk using the STOP and Berlin questionnaires (106 patients, 49%), and those at low risk (75 patients, 35%) based on the questionnaires.
The patients’ mean age was 50 years. Those with known OSA had a mean BMI of 44, the high-risk patients had a mean BMI of 32, and the low-risk patients had a mean BMI of 28.
Dr. Auckley of Case Western Reserve University in Cleveland and his colleagues undertook their 4-month, prospective observational study to further explore earlier findings that patients with OSA experience more adverse outcomes in the perioperative setting (Chest 2008;133:1128-34).
In their study, 38% of those with diagnosed OSA, 22% of those at high risk, and 14% of the low-risk patients experienced complications. Hypoxemia was the most frequent complication. The difference in complication rate between the known OSA patients and the low-risk patients was significant, even after researchers controlled for age, diagnosis, and comorbidities.
Patients with sleep apnea more commonly experience complications, especially hypoxemia, while hospitalized, Dr. Auckley concluded. The questionnaires have not been validated in hospitalized patients, and the patients were not monitored by oximetry, which were two limitations of the study, he noted.
Dr. Kumar reported that she had no relevant financial conflicts. Dr. Auckley disclosed support from ResMed Corp., and Cephalon Inc., and has received equipment from Cleveland Medical Devices Inc. His current study received no funding.
VANCOUVER, B.C. – A significant number of hospitalized patients are at high risk for obstructive sleep apnea, but few have been evaluated for OSA, Dr. Sunita Kumar reported at the annual meeting of the American College of Chest Physicians.
Because OSA has been shown to increase the risk of adverse outcomes such as stroke and heart failure, screening inpatients might help prevent complications. However, Dr. Kumar noted, the diagnosis and treatment of OSA in hospitalized patients have not been shown to affect outcomes.
Of 195 inpatients surveyed over a 24-hour period at Loyola University Medical Center in Maywood, Ill., 157 (81%) were found to be at high risk for OSA. Of those, 41 had undergone a previous sleep study, and of the 41 patients who had been evaluated, 31 were found to have OSA, said Dr. Kumar of the Division of Pulmonary and Critical Care Medicine at Loyola.
In comparison, 5% of the general population is estimated to have sleep apnea.
The patients had a mean age of 62 years, and 82% were older than 50 years. Their mean body mass index was 28 kg/m2, with 14% having a BMI over 35. More than half (59%) were men. Of the 31 patients with a previous diagnosis of OSA, 17 were using continuous positive airway pressure (CPAP), 1 had undergone surgery, and 13 were not receiving treatment, generally because of nontolerance of CPAP.
The patients were screened using the STOP-BANG questionnaire, which has high sensitivity for detecting a high risk of sleep apnea but is not very specific, Dr. Kumar reported. It has also not been validated in inpatients, she said, which was a limitation of the study. However, the STOP-BANG (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender) questionnaire has been reported to be of high quality for predicting OSA (Can. J. Anaesth. 2010;57:423-38). When these patients were evaluated using only the STOP portion of the survey, 65% were found to be at high risk.
The few previous studies that looked at OSA in hospitalized patients found the prevalence to be as high as 77% (J. Clin. Sleep Med. 2008;4:105-10; Sleep Breath. 2008;12:229-34).
The take-home point of the recent study might be that it is safer to make a presumptive diagnosis of OSA in inpatients, commented session moderator Dr. Rochelle Goldberg, president and chief medical officer of the American Sleep Apnea Association.
Also at the session, Dr. Dennis Auckley presented his study on the frequency of complications in 217 hospitalized patients divided into three groups: those with known OSA (36 patients, 17%), those determined to be at high risk using the STOP and Berlin questionnaires (106 patients, 49%), and those at low risk (75 patients, 35%) based on the questionnaires.
The patients’ mean age was 50 years. Those with known OSA had a mean BMI of 44, the high-risk patients had a mean BMI of 32, and the low-risk patients had a mean BMI of 28.
Dr. Auckley of Case Western Reserve University in Cleveland and his colleagues undertook their 4-month, prospective observational study to further explore earlier findings that patients with OSA experience more adverse outcomes in the perioperative setting (Chest 2008;133:1128-34).
In their study, 38% of those with diagnosed OSA, 22% of those at high risk, and 14% of the low-risk patients experienced complications. Hypoxemia was the most frequent complication. The difference in complication rate between the known OSA patients and the low-risk patients was significant, even after researchers controlled for age, diagnosis, and comorbidities.
Patients with sleep apnea more commonly experience complications, especially hypoxemia, while hospitalized, Dr. Auckley concluded. The questionnaires have not been validated in hospitalized patients, and the patients were not monitored by oximetry, which were two limitations of the study, he noted.
Dr. Kumar reported that she had no relevant financial conflicts. Dr. Auckley disclosed support from ResMed Corp., and Cephalon Inc., and has received equipment from Cleveland Medical Devices Inc. His current study received no funding.
VANCOUVER, B.C. – A significant number of hospitalized patients are at high risk for obstructive sleep apnea, but few have been evaluated for OSA, Dr. Sunita Kumar reported at the annual meeting of the American College of Chest Physicians.
Because OSA has been shown to increase the risk of adverse outcomes such as stroke and heart failure, screening inpatients might help prevent complications. However, Dr. Kumar noted, the diagnosis and treatment of OSA in hospitalized patients have not been shown to affect outcomes.
Of 195 inpatients surveyed over a 24-hour period at Loyola University Medical Center in Maywood, Ill., 157 (81%) were found to be at high risk for OSA. Of those, 41 had undergone a previous sleep study, and of the 41 patients who had been evaluated, 31 were found to have OSA, said Dr. Kumar of the Division of Pulmonary and Critical Care Medicine at Loyola.
In comparison, 5% of the general population is estimated to have sleep apnea.
The patients had a mean age of 62 years, and 82% were older than 50 years. Their mean body mass index was 28 kg/m2, with 14% having a BMI over 35. More than half (59%) were men. Of the 31 patients with a previous diagnosis of OSA, 17 were using continuous positive airway pressure (CPAP), 1 had undergone surgery, and 13 were not receiving treatment, generally because of nontolerance of CPAP.
The patients were screened using the STOP-BANG questionnaire, which has high sensitivity for detecting a high risk of sleep apnea but is not very specific, Dr. Kumar reported. It has also not been validated in inpatients, she said, which was a limitation of the study. However, the STOP-BANG (snoring, tiredness, observed apnea, high blood pressure, body mass index, age, neck circumference, and gender) questionnaire has been reported to be of high quality for predicting OSA (Can. J. Anaesth. 2010;57:423-38). When these patients were evaluated using only the STOP portion of the survey, 65% were found to be at high risk.
The few previous studies that looked at OSA in hospitalized patients found the prevalence to be as high as 77% (J. Clin. Sleep Med. 2008;4:105-10; Sleep Breath. 2008;12:229-34).
The take-home point of the recent study might be that it is safer to make a presumptive diagnosis of OSA in inpatients, commented session moderator Dr. Rochelle Goldberg, president and chief medical officer of the American Sleep Apnea Association.
Also at the session, Dr. Dennis Auckley presented his study on the frequency of complications in 217 hospitalized patients divided into three groups: those with known OSA (36 patients, 17%), those determined to be at high risk using the STOP and Berlin questionnaires (106 patients, 49%), and those at low risk (75 patients, 35%) based on the questionnaires.
The patients’ mean age was 50 years. Those with known OSA had a mean BMI of 44, the high-risk patients had a mean BMI of 32, and the low-risk patients had a mean BMI of 28.
Dr. Auckley of Case Western Reserve University in Cleveland and his colleagues undertook their 4-month, prospective observational study to further explore earlier findings that patients with OSA experience more adverse outcomes in the perioperative setting (Chest 2008;133:1128-34).
In their study, 38% of those with diagnosed OSA, 22% of those at high risk, and 14% of the low-risk patients experienced complications. Hypoxemia was the most frequent complication. The difference in complication rate between the known OSA patients and the low-risk patients was significant, even after researchers controlled for age, diagnosis, and comorbidities.
Patients with sleep apnea more commonly experience complications, especially hypoxemia, while hospitalized, Dr. Auckley concluded. The questionnaires have not been validated in hospitalized patients, and the patients were not monitored by oximetry, which were two limitations of the study, he noted.
Dr. Kumar reported that she had no relevant financial conflicts. Dr. Auckley disclosed support from ResMed Corp., and Cephalon Inc., and has received equipment from Cleveland Medical Devices Inc. His current study received no funding.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS
Brain Exercises Fail To Improve Memory, Cognitive Function
“Brain training” does not improve general cognitive function, according to a 6-week trial of more than 11,000 participants.
The study results “provide no evidence for any generalized improvements in cognitive function following brain training in a large sample of healthy adults,” Adrian M. Owen and his colleagues reported.
The participants were divided into three groups: the experimental group 1 (4,678 subjects), which did six tasks emphasizing reasoning, planning, and problem solving; experimental group 2 (4,014 subjects), which practiced six tasks focusing on short-term memory, attention, visuospatial processing, and mathematics; and a control group (2,738 subjects), which answered various research questions using the Internet, said Mr. Owen of the Medical Research Council Cognition and Brain Sciences Unit, Cambridge, England, and his colleagues.
The participants were assessed before and after the intervention using benchmarking tests that measuring reasoning, verbal short-term memory, spatial working memory, and paired-associates learning.
All three groups improved on the tasks they had been assigned topractic the trial (effectstintervention improvementson the beh smaller (effect sizes: 0.01-0.22 for all groups).
No relationship was seen between number of training sessions performed or age of participants and postintervention benchmarking test scores. The scores on two tests reflected small gender differences.
Although participants improved at their assigned tasks, “training-related improvements may not even generalize to other tasks that use similar cognitive functions,” the researchers said (Nature 2010 Apr. 20 [doi: 10.1038/nature09042
The authors reported no financial conflicts of interest.
My Take
Credible Study on Complex Question
The notion of exercising the mind to reduce its deterioration is popular in the world of Alzheimer's disease.
Do more crossword puzzles and you will slow the progression of dementia. But is it true? Epidemiological studies have shown mixed results, possibly reflecting presymptomatic-stage disease, confounding medical issues, and medications influencing outcomes. Functional brain imaging studies show activation of prefrontal cortices during the early attentional practice stage that diminishes and ultimately vanishes as any skill becomes automatic (Proc. Natl. Acad. Sci. USA 1998;95:853-60).
Cognitive tasks, in contrast to sensorimotor tasks, rely on the integration of multiple brain regions that are geographically distant and serve different functions. Because a related, nonidentical task might use this network, it is conceivable that related tasks may be performed with greater facility and dexterity.
Given the effort required to achieve even a “simple” practice effect, studies such as that of Adrian M. Owen and his colleagues that fail to show any major translational skill differences after a mere 6 weeks of “brain exercises” that sound far less grueling than the practice of professional musicians and athletes are certainly credible.
RICHARD J. CASELLI, M.D., is a professor of neurology at the Mayo Clinic Arizona, Scottsdale. He has no financial conflicts of interest related to this subject.
{kind=link}
“Brain training” does not improve general cognitive function, according to a 6-week trial of more than 11,000 participants.
The study results “provide no evidence for any generalized improvements in cognitive function following brain training in a large sample of healthy adults,” Adrian M. Owen and his colleagues reported.
The participants were divided into three groups: the experimental group 1 (4,678 subjects), which did six tasks emphasizing reasoning, planning, and problem solving; experimental group 2 (4,014 subjects), which practiced six tasks focusing on short-term memory, attention, visuospatial processing, and mathematics; and a control group (2,738 subjects), which answered various research questions using the Internet, said Mr. Owen of the Medical Research Council Cognition and Brain Sciences Unit, Cambridge, England, and his colleagues.
The participants were assessed before and after the intervention using benchmarking tests that measuring reasoning, verbal short-term memory, spatial working memory, and paired-associates learning.
All three groups improved on the tasks they had been assigned topractic the trial (effectstintervention improvementson the beh smaller (effect sizes: 0.01-0.22 for all groups).
No relationship was seen between number of training sessions performed or age of participants and postintervention benchmarking test scores. The scores on two tests reflected small gender differences.
Although participants improved at their assigned tasks, “training-related improvements may not even generalize to other tasks that use similar cognitive functions,” the researchers said (Nature 2010 Apr. 20 [doi: 10.1038/nature09042
The authors reported no financial conflicts of interest.
My Take
Credible Study on Complex Question
The notion of exercising the mind to reduce its deterioration is popular in the world of Alzheimer's disease.
Do more crossword puzzles and you will slow the progression of dementia. But is it true? Epidemiological studies have shown mixed results, possibly reflecting presymptomatic-stage disease, confounding medical issues, and medications influencing outcomes. Functional brain imaging studies show activation of prefrontal cortices during the early attentional practice stage that diminishes and ultimately vanishes as any skill becomes automatic (Proc. Natl. Acad. Sci. USA 1998;95:853-60).
Cognitive tasks, in contrast to sensorimotor tasks, rely on the integration of multiple brain regions that are geographically distant and serve different functions. Because a related, nonidentical task might use this network, it is conceivable that related tasks may be performed with greater facility and dexterity.
Given the effort required to achieve even a “simple” practice effect, studies such as that of Adrian M. Owen and his colleagues that fail to show any major translational skill differences after a mere 6 weeks of “brain exercises” that sound far less grueling than the practice of professional musicians and athletes are certainly credible.
RICHARD J. CASELLI, M.D., is a professor of neurology at the Mayo Clinic Arizona, Scottsdale. He has no financial conflicts of interest related to this subject.
“Brain training” does not improve general cognitive function, according to a 6-week trial of more than 11,000 participants.
The study results “provide no evidence for any generalized improvements in cognitive function following brain training in a large sample of healthy adults,” Adrian M. Owen and his colleagues reported.
The participants were divided into three groups: the experimental group 1 (4,678 subjects), which did six tasks emphasizing reasoning, planning, and problem solving; experimental group 2 (4,014 subjects), which practiced six tasks focusing on short-term memory, attention, visuospatial processing, and mathematics; and a control group (2,738 subjects), which answered various research questions using the Internet, said Mr. Owen of the Medical Research Council Cognition and Brain Sciences Unit, Cambridge, England, and his colleagues.
The participants were assessed before and after the intervention using benchmarking tests that measuring reasoning, verbal short-term memory, spatial working memory, and paired-associates learning.
All three groups improved on the tasks they had been assigned topractic the trial (effectstintervention improvementson the beh smaller (effect sizes: 0.01-0.22 for all groups).
No relationship was seen between number of training sessions performed or age of participants and postintervention benchmarking test scores. The scores on two tests reflected small gender differences.
Although participants improved at their assigned tasks, “training-related improvements may not even generalize to other tasks that use similar cognitive functions,” the researchers said (Nature 2010 Apr. 20 [doi: 10.1038/nature09042
The authors reported no financial conflicts of interest.
My Take
Credible Study on Complex Question
The notion of exercising the mind to reduce its deterioration is popular in the world of Alzheimer's disease.
Do more crossword puzzles and you will slow the progression of dementia. But is it true? Epidemiological studies have shown mixed results, possibly reflecting presymptomatic-stage disease, confounding medical issues, and medications influencing outcomes. Functional brain imaging studies show activation of prefrontal cortices during the early attentional practice stage that diminishes and ultimately vanishes as any skill becomes automatic (Proc. Natl. Acad. Sci. USA 1998;95:853-60).
Cognitive tasks, in contrast to sensorimotor tasks, rely on the integration of multiple brain regions that are geographically distant and serve different functions. Because a related, nonidentical task might use this network, it is conceivable that related tasks may be performed with greater facility and dexterity.
Given the effort required to achieve even a “simple” practice effect, studies such as that of Adrian M. Owen and his colleagues that fail to show any major translational skill differences after a mere 6 weeks of “brain exercises” that sound far less grueling than the practice of professional musicians and athletes are certainly credible.
RICHARD J. CASELLI, M.D., is a professor of neurology at the Mayo Clinic Arizona, Scottsdale. He has no financial conflicts of interest related to this subject.
Brain Training Exercises Fail to Boost Cognitive Function
“Brain training” does not improve general cognitive function, according to a 6-week trial of more than 11,000 participants.
The study results “provide no evidence for any generalized improvements in cognitive function following brain training in a large sample of healthy adults,” Adrian M. Owen and his colleagues reported.
The participants were divided into three groups: experimental group 1 (4,678 subjects), which did six tasks emphasizing reasoning, planning, and problem solving; experimental group 2 (4,014 subjects), which practiced six tasks focusing on short-term memory, attention, visuospatial processing, and math; and a control group (2,738 subjects), which answered various questions using the Internet. The groups were matched in size initially, but more of the control group members dropped out before the final assessment. Participants were recruited from viewers of a British science TV show.
The tasks given to group 2 were considered to be most like those of commercially available “brain training” programs, said Mr. Owen of the Medical Research Council Cognition and Brain Sciences Unit, Cambridge, England, and his colleagues.
The participants were assessed before and after the intervention using benchmarking tests that measured reasoning, verbal short-term memory, spatial working memory, and paired-associates learning. These validated cognitive assessment tools (available at www.cambridgebrainsciences.com
Participants completed an average of 24 training sessions over the 6-week period (range, 1-188). The tasks were performed for a minimum of 10 minutes a day, three times a week.
All three groups improved on the tasks they had been assigned to practice (effect sizes: group 1, 0.73-1.63; group 2, 0.72-0.97; controls, 0.33). However, postintervention improvements on the benchmarking tests were much smaller (effect sizes: 0.01-0.22 for all groups).
The control group improved slightly more than the experimental groups on two measures.
The groups were similar in age (average, 39-40 years) and gender (each group had 4-5 times as many female participants). No relationship was seen between number of training sessions performed or age of participants and postintervention benchmarking test scores. The scores on two tests reflected small gender differences.
Although participants improved at their assigned tasks, “training-related improvements may not even generalize to other tasks that use similar cognitive functions,” the researchers said (Nature 2010 April 20 [doi:10.1038/nature09042]).
“Six weeks of regular computerized brain training confers no greater benefit than simply answering general knowledge questions using the Internet,” the study authors concluded.
Disclosures: The authors reported having no conflicts.
My Take
A Credible Study on a Complex Question
The notion of exercising the mind to reduce its deterioration is popular in the world of Alzheimer's disease: Do more crossword puzzles, and you will slow the progression of dementia. But is it true? Epidemiological studies have shown mixed results, possibly reflecting presymptomatic-stage disease, confounding medical issues, and medications influencing outcomes.
Most people “exercise” their brain during their daily activities whether they conceptualize it in this way or not. The term “brain training” implies some kind of special activity that the term “practice” lacks, but acquiring any new skill requires enhanced attention, and with increasing task familiarity comes greater automaticity and increasing dexterity.
Functional brain imaging studies show activation of prefrontal cortices during the early attentional practice stage that diminishes and ultimately vanishes as any skill becomes automatic (Proc. Natl. Acad. Sci. USA 1998;95:853-60).
Cognitive tasks, in contrast to sensorimotor tasks, rely on the integration of multiple brain regions that are geographically distant and serve different functions. Because a related, nonidentical task might use this network, it is conceivable that related tasks may be performed with greater facility and dexterity.
The background of the question is complex, but given the effort required to achieve even a “simple” practice effect, studies such as that of Adrian M. Owen and his colleagues that fail to show any major translational skill differences after a mere 6 weeks of “brain exercises” that sound far less grueling than the practice of professional musicians and athletes are certainly credible.
RICHARD J. CASELLI, M.D., is a professor of neurology at the Mayo Clinic Arizona, Scottsdale. He has no financial conflicts of interest related to this subject.
{kind=link}
“Brain training” does not improve general cognitive function, according to a 6-week trial of more than 11,000 participants.
The study results “provide no evidence for any generalized improvements in cognitive function following brain training in a large sample of healthy adults,” Adrian M. Owen and his colleagues reported.
The participants were divided into three groups: experimental group 1 (4,678 subjects), which did six tasks emphasizing reasoning, planning, and problem solving; experimental group 2 (4,014 subjects), which practiced six tasks focusing on short-term memory, attention, visuospatial processing, and math; and a control group (2,738 subjects), which answered various questions using the Internet. The groups were matched in size initially, but more of the control group members dropped out before the final assessment. Participants were recruited from viewers of a British science TV show.
The tasks given to group 2 were considered to be most like those of commercially available “brain training” programs, said Mr. Owen of the Medical Research Council Cognition and Brain Sciences Unit, Cambridge, England, and his colleagues.
The participants were assessed before and after the intervention using benchmarking tests that measured reasoning, verbal short-term memory, spatial working memory, and paired-associates learning. These validated cognitive assessment tools (available at www.cambridgebrainsciences.com
Participants completed an average of 24 training sessions over the 6-week period (range, 1-188). The tasks were performed for a minimum of 10 minutes a day, three times a week.
All three groups improved on the tasks they had been assigned to practice (effect sizes: group 1, 0.73-1.63; group 2, 0.72-0.97; controls, 0.33). However, postintervention improvements on the benchmarking tests were much smaller (effect sizes: 0.01-0.22 for all groups).
The control group improved slightly more than the experimental groups on two measures.
The groups were similar in age (average, 39-40 years) and gender (each group had 4-5 times as many female participants). No relationship was seen between number of training sessions performed or age of participants and postintervention benchmarking test scores. The scores on two tests reflected small gender differences.
Although participants improved at their assigned tasks, “training-related improvements may not even generalize to other tasks that use similar cognitive functions,” the researchers said (Nature 2010 April 20 [doi:10.1038/nature09042]).
“Six weeks of regular computerized brain training confers no greater benefit than simply answering general knowledge questions using the Internet,” the study authors concluded.
Disclosures: The authors reported having no conflicts.
My Take
A Credible Study on a Complex Question
The notion of exercising the mind to reduce its deterioration is popular in the world of Alzheimer's disease: Do more crossword puzzles, and you will slow the progression of dementia. But is it true? Epidemiological studies have shown mixed results, possibly reflecting presymptomatic-stage disease, confounding medical issues, and medications influencing outcomes.
Most people “exercise” their brain during their daily activities whether they conceptualize it in this way or not. The term “brain training” implies some kind of special activity that the term “practice” lacks, but acquiring any new skill requires enhanced attention, and with increasing task familiarity comes greater automaticity and increasing dexterity.
Functional brain imaging studies show activation of prefrontal cortices during the early attentional practice stage that diminishes and ultimately vanishes as any skill becomes automatic (Proc. Natl. Acad. Sci. USA 1998;95:853-60).
Cognitive tasks, in contrast to sensorimotor tasks, rely on the integration of multiple brain regions that are geographically distant and serve different functions. Because a related, nonidentical task might use this network, it is conceivable that related tasks may be performed with greater facility and dexterity.
The background of the question is complex, but given the effort required to achieve even a “simple” practice effect, studies such as that of Adrian M. Owen and his colleagues that fail to show any major translational skill differences after a mere 6 weeks of “brain exercises” that sound far less grueling than the practice of professional musicians and athletes are certainly credible.
RICHARD J. CASELLI, M.D., is a professor of neurology at the Mayo Clinic Arizona, Scottsdale. He has no financial conflicts of interest related to this subject.
“Brain training” does not improve general cognitive function, according to a 6-week trial of more than 11,000 participants.
The study results “provide no evidence for any generalized improvements in cognitive function following brain training in a large sample of healthy adults,” Adrian M. Owen and his colleagues reported.
The participants were divided into three groups: experimental group 1 (4,678 subjects), which did six tasks emphasizing reasoning, planning, and problem solving; experimental group 2 (4,014 subjects), which practiced six tasks focusing on short-term memory, attention, visuospatial processing, and math; and a control group (2,738 subjects), which answered various questions using the Internet. The groups were matched in size initially, but more of the control group members dropped out before the final assessment. Participants were recruited from viewers of a British science TV show.
The tasks given to group 2 were considered to be most like those of commercially available “brain training” programs, said Mr. Owen of the Medical Research Council Cognition and Brain Sciences Unit, Cambridge, England, and his colleagues.
The participants were assessed before and after the intervention using benchmarking tests that measured reasoning, verbal short-term memory, spatial working memory, and paired-associates learning. These validated cognitive assessment tools (available at www.cambridgebrainsciences.com
Participants completed an average of 24 training sessions over the 6-week period (range, 1-188). The tasks were performed for a minimum of 10 minutes a day, three times a week.
All three groups improved on the tasks they had been assigned to practice (effect sizes: group 1, 0.73-1.63; group 2, 0.72-0.97; controls, 0.33). However, postintervention improvements on the benchmarking tests were much smaller (effect sizes: 0.01-0.22 for all groups).
The control group improved slightly more than the experimental groups on two measures.
The groups were similar in age (average, 39-40 years) and gender (each group had 4-5 times as many female participants). No relationship was seen between number of training sessions performed or age of participants and postintervention benchmarking test scores. The scores on two tests reflected small gender differences.
Although participants improved at their assigned tasks, “training-related improvements may not even generalize to other tasks that use similar cognitive functions,” the researchers said (Nature 2010 April 20 [doi:10.1038/nature09042]).
“Six weeks of regular computerized brain training confers no greater benefit than simply answering general knowledge questions using the Internet,” the study authors concluded.
Disclosures: The authors reported having no conflicts.
My Take
A Credible Study on a Complex Question
The notion of exercising the mind to reduce its deterioration is popular in the world of Alzheimer's disease: Do more crossword puzzles, and you will slow the progression of dementia. But is it true? Epidemiological studies have shown mixed results, possibly reflecting presymptomatic-stage disease, confounding medical issues, and medications influencing outcomes.
Most people “exercise” their brain during their daily activities whether they conceptualize it in this way or not. The term “brain training” implies some kind of special activity that the term “practice” lacks, but acquiring any new skill requires enhanced attention, and with increasing task familiarity comes greater automaticity and increasing dexterity.
Functional brain imaging studies show activation of prefrontal cortices during the early attentional practice stage that diminishes and ultimately vanishes as any skill becomes automatic (Proc. Natl. Acad. Sci. USA 1998;95:853-60).
Cognitive tasks, in contrast to sensorimotor tasks, rely on the integration of multiple brain regions that are geographically distant and serve different functions. Because a related, nonidentical task might use this network, it is conceivable that related tasks may be performed with greater facility and dexterity.
The background of the question is complex, but given the effort required to achieve even a “simple” practice effect, studies such as that of Adrian M. Owen and his colleagues that fail to show any major translational skill differences after a mere 6 weeks of “brain exercises” that sound far less grueling than the practice of professional musicians and athletes are certainly credible.
RICHARD J. CASELLI, M.D., is a professor of neurology at the Mayo Clinic Arizona, Scottsdale. He has no financial conflicts of interest related to this subject.