User login
Bringing Back Kids in Cardiopulmonary Arrest
SAN FRANCISCO – Children in cardiopulmonary arrest require specialized resuscitation skills, and updated guidelines published late in 2010 contain some new recommendations, according to Dr. Marianne Gausche-Hill.
The recommended sequence for cardiopulmonary resuscitation (CPR) "has changed for all ages except for the newborn" to compressions, airway, breathing (CAB) – instead of airway, breathing, compressions (ABC) – when performed by a bystander. Emergency department (ED) providers usually will ventilate and do compressions simultaneously.
"If you’re doing bag mask [ventilation], the recommendation is just do your ventilations, and do compressions separately. If the patient has been intubated, you can do continued ventilations as you’re doing compressions," Dr. Gausche-Hill said at the annual meeting of the American College of Emergency Physicians.
In babies, if there is a single rescuer, chest compressions should be done using two fingers in the middle of the chest between the nipples (Circulation 2010;122:S862-75). With two rescuers, one can use the hand-encircling technique in which the thumbs are between the nipples and the rest of the fingers around the infant’s back, while the other does bag mask ventilation.
Compress the chest 1.5 inches in infants and 2 inches in children. Allow the chest to recoil between pushes and do at least 100 compressions per minute. "The key thing is to push hard and fast," said Dr. Gausche-Hill, professor of medicine at the University of California, Los Angeles. Do compressions for 2 minutes, then stop for no more than 10 seconds to check for a pulse. Mechanical devices for chest compressions have not been tested in children and should not be used in pediatric patients.

For a single rescuer, a ratio of compressions to ventilation of 30:2 is recommended, but for two rescuers in the ED the ratio is 15:2, with more emphasis on ventilation. Take care not to overventilate, she said.
"We overbag super amounts when we do resuscitation ventilation. You don’t need that much," she emphasized. "You want to squeeze the bag just until chest rise is initiated, and then begin the release phase." For children, this means about 10 breaths a minute. To avoid overbagging, a resuscitator can say "squeeze" as she squeezes the bag just until the chest starts to rise, then pause and say "release, release" to give time for the chest to recoil.
After beginning CPR, determine if the rhythm is shockable, and if so, use the defibrillator. Then do 2 minutes of CPR, give epinephrine, check the rhythm again, shock again. "It’s no more shock, shock, shock. You’re going to do 2 minutes of CPR in-between," she said.
The best option is a manual defibrillator with pediatric pads, she said, starting with 2 J and going up to 4 J if needed. But a dose even as high as 10 J is not harmful, according to Dr. Gausche-Hill. "If the patient is in persistent [ventricular fibrillation], I would strongly consider ramping it up, especially in the adolescent," she said. The new guidelines no longer require a pediatric attenuating device for an automated external defibrillator, and the standard automated external defibrillator can be used for any age (Circulation 2010;122:S876-908).

Cuffed endotracheal tubes (ETTs) are now preferred over the standard uncuffed tubes for intubation. "The bottom line is there’s no concern about cricoid pressure leading to necrosis. There’s no increased risk of subglottic stenosis by the use of these. That was really the main concern," she said. Cuffed ETTs are preferred in patients with poor lung compliance, a large glottic air leak, or high airway resistance. A randomized, controlled trial of 2,246 children found that those treated with a cuffed ETT did not have more postextubation stridor than those treated with an uncuffed ETT (4.4% vs. 4.7%) and were much less likely to need a tube exchange (2.1% vs. 30.8%) (Br. J. Anaesth. 2009;103:867-73). "Our PICU just says give it to everybody," she said. In pediatric patients, use a half-size smaller than their standard cuff size.
Cricoid pressure to present aspiration during intubation is not recommended in children, as it actually impedes the airway. Dr. Gausche-Hill prefers a jaw thrust or, in older kids, a little laryngeal manipulation.
In neonates, providing a lot of oxygen initially is harmful, leading to the creation of free radicals that may have an adverse neurologic effect (Circulation 2010;122:S909-19), but oxygen can be appropriate in older children, she said. "Bottom line is, give O2 100% and then back it down as quickly as you can," and aim to maintain an oxygen saturation of about 94%, said Dr. Gausche-Hill, who is also director of EMS and pediatric emergency medicine fellowships at Harbor-UCLA Medical Center in Torrance, Calif.

The guidelines now emphasize the use of capnography to monitor end-tidal CO2 to confirm endotracheal tube placement and assess the adequacy of CPR. With capnography, "you may see [return of spontaneous circulation] before you can even detect a pulse," she said.
Foreign body aspiration "is your worst nightmare in the ED because you know if you can’t get it out, the patient’s going to die. And we do know that kids just do this all the time," she said. More than 90% of patients with this condition are younger than 5 years. "You always begin with basic life support maneuvers if they’re still conscious. For the infant, it’s back blows and chest thrusts until the object is expelled or they become unconscious." For the conscious older child, start with the Heimlich maneuver. In unconscious children, progress to chest compressions; if the foreign body is esophageal, chest compressions may remove it.
If the foreign body is lodged deeper in the airway, use direct laryngoscopy and remove the object with Magill forceps in the pediatric size. Some recent surveys showed that "18% of EDs in the country do not have pediatric Magills. Look in your airway kit. Make sure you have them," she stressed.
Last, family presence during resuscitation attempts should be promoted, she said. Almost a dozen studies have shown that parents want that option and should be included in decision making when possible, she noted.
Dr. Gausche-Hill reported having no significant financial relationships to disclose.
SAN FRANCISCO – Children in cardiopulmonary arrest require specialized resuscitation skills, and updated guidelines published late in 2010 contain some new recommendations, according to Dr. Marianne Gausche-Hill.
The recommended sequence for cardiopulmonary resuscitation (CPR) "has changed for all ages except for the newborn" to compressions, airway, breathing (CAB) – instead of airway, breathing, compressions (ABC) – when performed by a bystander. Emergency department (ED) providers usually will ventilate and do compressions simultaneously.
"If you’re doing bag mask [ventilation], the recommendation is just do your ventilations, and do compressions separately. If the patient has been intubated, you can do continued ventilations as you’re doing compressions," Dr. Gausche-Hill said at the annual meeting of the American College of Emergency Physicians.
In babies, if there is a single rescuer, chest compressions should be done using two fingers in the middle of the chest between the nipples (Circulation 2010;122:S862-75). With two rescuers, one can use the hand-encircling technique in which the thumbs are between the nipples and the rest of the fingers around the infant’s back, while the other does bag mask ventilation.
Compress the chest 1.5 inches in infants and 2 inches in children. Allow the chest to recoil between pushes and do at least 100 compressions per minute. "The key thing is to push hard and fast," said Dr. Gausche-Hill, professor of medicine at the University of California, Los Angeles. Do compressions for 2 minutes, then stop for no more than 10 seconds to check for a pulse. Mechanical devices for chest compressions have not been tested in children and should not be used in pediatric patients.
For a single rescuer, a ratio of compressions to ventilation of 30:2 is recommended, but for two rescuers in the ED the ratio is 15:2, with more emphasis on ventilation. Take care not to overventilate, she said.
"We overbag super amounts when we do resuscitation ventilation. You don’t need that much," she emphasized. "You want to squeeze the bag just until chest rise is initiated, and then begin the release phase." For children, this means about 10 breaths a minute. To avoid overbagging, a resuscitator can say "squeeze" as she squeezes the bag just until the chest starts to rise, then pause and say "release, release" to give time for the chest to recoil.
After beginning CPR, determine if the rhythm is shockable, and if so, use the defibrillator. Then do 2 minutes of CPR, give epinephrine, check the rhythm again, shock again. "It’s no more shock, shock, shock. You’re going to do 2 minutes of CPR in-between," she said.
The best option is a manual defibrillator with pediatric pads, she said, starting with 2 J and going up to 4 J if needed. But a dose even as high as 10 J is not harmful, according to Dr. Gausche-Hill. "If the patient is in persistent [ventricular fibrillation], I would strongly consider ramping it up, especially in the adolescent," she said. The new guidelines no longer require a pediatric attenuating device for an automated external defibrillator, and the standard automated external defibrillator can be used for any age (Circulation 2010;122:S876-908).
Cuffed endotracheal tubes (ETTs) are now preferred over the standard uncuffed tubes for intubation. "The bottom line is there’s no concern about cricoid pressure leading to necrosis. There’s no increased risk of subglottic stenosis by the use of these. That was really the main concern," she said. Cuffed ETTs are preferred in patients with poor lung compliance, a large glottic air leak, or high airway resistance. A randomized, controlled trial of 2,246 children found that those treated with a cuffed ETT did not have more postextubation stridor than those treated with an uncuffed ETT (4.4% vs. 4.7%) and were much less likely to need a tube exchange (2.1% vs. 30.8%) (Br. J. Anaesth. 2009;103:867-73). "Our PICU just says give it to everybody," she said. In pediatric patients, use a half-size smaller than their standard cuff size.
Cricoid pressure to present aspiration during intubation is not recommended in children, as it actually impedes the airway. Dr. Gausche-Hill prefers a jaw thrust or, in older kids, a little laryngeal manipulation.
In neonates, providing a lot of oxygen initially is harmful, leading to the creation of free radicals that may have an adverse neurologic effect (Circulation 2010;122:S909-19), but oxygen can be appropriate in older children, she said. "Bottom line is, give O2 100% and then back it down as quickly as you can," and aim to maintain an oxygen saturation of about 94%, said Dr. Gausche-Hill, who is also director of EMS and pediatric emergency medicine fellowships at Harbor-UCLA Medical Center in Torrance, Calif.
The guidelines now emphasize the use of capnography to monitor end-tidal CO2 to confirm endotracheal tube placement and assess the adequacy of CPR. With capnography, "you may see [return of spontaneous circulation] before you can even detect a pulse," she said.
Foreign body aspiration "is your worst nightmare in the ED because you know if you can’t get it out, the patient’s going to die. And we do know that kids just do this all the time," she said. More than 90% of patients with this condition are younger than 5 years. "You always begin with basic life support maneuvers if they’re still conscious. For the infant, it’s back blows and chest thrusts until the object is expelled or they become unconscious." For the conscious older child, start with the Heimlich maneuver. In unconscious children, progress to chest compressions; if the foreign body is esophageal, chest compressions may remove it.
If the foreign body is lodged deeper in the airway, use direct laryngoscopy and remove the object with Magill forceps in the pediatric size. Some recent surveys showed that "18% of EDs in the country do not have pediatric Magills. Look in your airway kit. Make sure you have them," she stressed.
Last, family presence during resuscitation attempts should be promoted, she said. Almost a dozen studies have shown that parents want that option and should be included in decision making when possible, she noted.
Dr. Gausche-Hill reported having no significant financial relationships to disclose.
SAN FRANCISCO – Children in cardiopulmonary arrest require specialized resuscitation skills, and updated guidelines published late in 2010 contain some new recommendations, according to Dr. Marianne Gausche-Hill.
The recommended sequence for cardiopulmonary resuscitation (CPR) "has changed for all ages except for the newborn" to compressions, airway, breathing (CAB) – instead of airway, breathing, compressions (ABC) – when performed by a bystander. Emergency department (ED) providers usually will ventilate and do compressions simultaneously.
"If you’re doing bag mask [ventilation], the recommendation is just do your ventilations, and do compressions separately. If the patient has been intubated, you can do continued ventilations as you’re doing compressions," Dr. Gausche-Hill said at the annual meeting of the American College of Emergency Physicians.
In babies, if there is a single rescuer, chest compressions should be done using two fingers in the middle of the chest between the nipples (Circulation 2010;122:S862-75). With two rescuers, one can use the hand-encircling technique in which the thumbs are between the nipples and the rest of the fingers around the infant’s back, while the other does bag mask ventilation.
Compress the chest 1.5 inches in infants and 2 inches in children. Allow the chest to recoil between pushes and do at least 100 compressions per minute. "The key thing is to push hard and fast," said Dr. Gausche-Hill, professor of medicine at the University of California, Los Angeles. Do compressions for 2 minutes, then stop for no more than 10 seconds to check for a pulse. Mechanical devices for chest compressions have not been tested in children and should not be used in pediatric patients.
For a single rescuer, a ratio of compressions to ventilation of 30:2 is recommended, but for two rescuers in the ED the ratio is 15:2, with more emphasis on ventilation. Take care not to overventilate, she said.
"We overbag super amounts when we do resuscitation ventilation. You don’t need that much," she emphasized. "You want to squeeze the bag just until chest rise is initiated, and then begin the release phase." For children, this means about 10 breaths a minute. To avoid overbagging, a resuscitator can say "squeeze" as she squeezes the bag just until the chest starts to rise, then pause and say "release, release" to give time for the chest to recoil.
After beginning CPR, determine if the rhythm is shockable, and if so, use the defibrillator. Then do 2 minutes of CPR, give epinephrine, check the rhythm again, shock again. "It’s no more shock, shock, shock. You’re going to do 2 minutes of CPR in-between," she said.
The best option is a manual defibrillator with pediatric pads, she said, starting with 2 J and going up to 4 J if needed. But a dose even as high as 10 J is not harmful, according to Dr. Gausche-Hill. "If the patient is in persistent [ventricular fibrillation], I would strongly consider ramping it up, especially in the adolescent," she said. The new guidelines no longer require a pediatric attenuating device for an automated external defibrillator, and the standard automated external defibrillator can be used for any age (Circulation 2010;122:S876-908).
Cuffed endotracheal tubes (ETTs) are now preferred over the standard uncuffed tubes for intubation. "The bottom line is there’s no concern about cricoid pressure leading to necrosis. There’s no increased risk of subglottic stenosis by the use of these. That was really the main concern," she said. Cuffed ETTs are preferred in patients with poor lung compliance, a large glottic air leak, or high airway resistance. A randomized, controlled trial of 2,246 children found that those treated with a cuffed ETT did not have more postextubation stridor than those treated with an uncuffed ETT (4.4% vs. 4.7%) and were much less likely to need a tube exchange (2.1% vs. 30.8%) (Br. J. Anaesth. 2009;103:867-73). "Our PICU just says give it to everybody," she said. In pediatric patients, use a half-size smaller than their standard cuff size.
Cricoid pressure to present aspiration during intubation is not recommended in children, as it actually impedes the airway. Dr. Gausche-Hill prefers a jaw thrust or, in older kids, a little laryngeal manipulation.
In neonates, providing a lot of oxygen initially is harmful, leading to the creation of free radicals that may have an adverse neurologic effect (Circulation 2010;122:S909-19), but oxygen can be appropriate in older children, she said. "Bottom line is, give O2 100% and then back it down as quickly as you can," and aim to maintain an oxygen saturation of about 94%, said Dr. Gausche-Hill, who is also director of EMS and pediatric emergency medicine fellowships at Harbor-UCLA Medical Center in Torrance, Calif.
The guidelines now emphasize the use of capnography to monitor end-tidal CO2 to confirm endotracheal tube placement and assess the adequacy of CPR. With capnography, "you may see [return of spontaneous circulation] before you can even detect a pulse," she said.
Foreign body aspiration "is your worst nightmare in the ED because you know if you can’t get it out, the patient’s going to die. And we do know that kids just do this all the time," she said. More than 90% of patients with this condition are younger than 5 years. "You always begin with basic life support maneuvers if they’re still conscious. For the infant, it’s back blows and chest thrusts until the object is expelled or they become unconscious." For the conscious older child, start with the Heimlich maneuver. In unconscious children, progress to chest compressions; if the foreign body is esophageal, chest compressions may remove it.
If the foreign body is lodged deeper in the airway, use direct laryngoscopy and remove the object with Magill forceps in the pediatric size. Some recent surveys showed that "18% of EDs in the country do not have pediatric Magills. Look in your airway kit. Make sure you have them," she stressed.
Last, family presence during resuscitation attempts should be promoted, she said. Almost a dozen studies have shown that parents want that option and should be included in decision making when possible, she noted.
Dr. Gausche-Hill reported having no significant financial relationships to disclose.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Designer Drug ODs Call for Supportive Care and Education
Bath salts, spice, and nutmeg are more than common household items; they are also designer drugs that can send people to the emergency department.
While emergency department visits resulting from use of older drugs of abuse such as LSD and cocaine have gone up 29%-48% over the past decade, ED visits resulting from the use of nontraditional, emerging, and Web-based (NEW) drugs have increased by estimates ranging from 187%-5,846%, Dr. Mark B. Mycyk said at the annual meeting of the American College of Emergency Physicians.

The Internet has been a "huge source of information and a powerful influence on this rapidly evolving and changing epidemic," said Dr. Mycyk of Cook County Hospital in Chicago. Designer drugs are easily available from websites such as Silk Road, "the Amazon.com of some of these NEW drugs," he said, and anyone with access to a computer "can pretty much get almost anything delivered to their homes or dorm rooms or a post office box." According to one study, websites touting recreational drugs were a factor in 27% of new drug use in college-age students (Pediatrics 2002;109:e96).
"Cases we see in the ED are extreme ... cases where people end up with complications," Dr. Mycyk said. Emergency physicians may see patients who have used the following NEW drugs:
• Bath salts (methylenedioxypyrovalerone, MDPV). "Brand names" include Ivory Wave, Bliss, and White Lightning; also called Plant Food. Popularized in Australia, these are not the kind of bath salts you would buy at a home goods store, which cause only severe rhinitis if snorted. The type sold online and in "head shops" is a stimulant and hallucinogen that causes cardiovascular and psychiatric adverse effects. "Self-harm has become a common complication. ... People get so psychotic, they are actually getting aggressive and harming others," Dr. Mycyk said. MDPV also has "lots of other profound effects on human neurotransmitters that we still do not understand," and the drug is "so addictive that users say it provokes an almost-uncontrollable urge for another hit." The chemicals used to make "bath salts" were classified as schedule 1 substances in late October by the Drug Enforcement Agency.

• Spice. Also known as K2. This synthetic cannabinoid, developed for animal research, "has resulted in a number of ED visits, and some of these visits can be pretty prolonged, and we’ve seen some unanticipated complications," Dr. Mycyk said. K2 is "much more potent and powerful than natural marijuana, so the effects that we see are much more extreme." Symptoms include agitation, cardiovascular effects, and inappropriate affect (Clin. Toxicol. [Phila.] 2011;49:431-3). Several varieties are now illegal in the United States, but chemists can create "newer synthetic analogs, which look different from Spice and K2, and that way, they evade the legal authorities," he said.

• Meow-Meow (mephedrone, 4-methylmethcathinone). Other street names include Drone, Bubble, and MCAT. This synthetic cathinone, derived from an African shrub, is a stimulant and sympathomimetic agent. Its effects and structure are similar to those of ephedra and amphetamine. Symptoms of Meow-Meow use include seizures, agitation, tachycardia, hypertension, and hyperthermia (Toxicol. Lett. 2011;201:191-5).
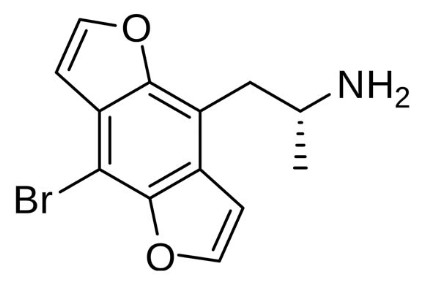
• Bromo-DragonFLY (bromo-benzodifuranyl-isopropylamine). Adverse effects of this designer drug include hallucinations, seizures, vomiting, and intense vasoconstriction with resulting ischemia in fingers and toes. The drug has "hallucinogenic, Ecstasy-like properties" and is a serotoninergic receptor agonist. The name derives from the resemblance its chemical structure has to a dragonfly.
• Nutmeg. At doses as high as 50 g, the common spice nutmeg has hallucinogenic properties. "When we see nutmeg users in the ED, we’re seeing a small proportion who took an extremely large dose or have an unanticipated complication from it," Dr. Mycyk said. In one case series of 119 patients, the most common symptoms were tachycardia, palpitations, and agitation. The researchers found that "clinical effects from ingestion can be significant and can require medical intervention" (Clin. Toxicol. [Phila.] 2011;49:177-80).
• Salvia. Street names of the salvia divinorum plant include Diviner’s Sage, Shepherdess, and Sally D. Related to mint, salvia has hallucinogenic and psychotomimetic properties. Symptoms include agitation and neurologic, cardiovascular, and gastrointestinal effects. The herb can be made into a tea; fresh leaves can be chewed; or leaves can be dried and then smoked, snorted, or injected. The drug has not been well studied, but one group of researchers analyzed YouTube videos of salvia users to study its effects (Drug Alcohol Depend. 2010;108:138-40).

• Snakebite. The venom of the naja naja snake, or Indian cobra, contains neurotoxins that can have opiate-like effects on the central nervous system. The venom can cause blackouts and feelings of well-being and lethargy in people who deliberately have themselves bitten by a cobra (Subst. Abus. 2011;32:43-6). "It boggles my mind what people will do to get high," Dr. Mycyk said.
• Buprenorphine (Suboxone). Clinically used for opioid dependence, this drug is smuggled into prisons by being crushed into a paste that is applied to a drawing or card, or hidden under stamps. A recent study found that 12% of drug contraband in Massachusetts prisons is buprenorphine (Curr. Drug Abuse Rev. 2011;4:28-41). Buprenorphine intoxication causes mild euphoria, somnolence, and possible respiratory depression; laboratory and toxicology screens for illicit drugs would be negative.
Diagnosis
Hospital-based drug screens don’t detect most of the new and evolving designer drugs that result in emergency department visits. "A lot of hospitals have invested in expanded drug-screening panels, but these hospital machines cannot keep up with the creative chemists and users out there," Dr. Mycyk said. So "tox testing is not that helpful for some of these NEW drugs. In fact, it might falsely reassure you."
So, to make the diagnosis, "if the patient is conscious, ask them. Know their language, know the slang. They will tell you. ... They are frightened, and they don’t want to die."
If the patient is delirious or has altered mental status, examine his or her belongings carefully. "Completely examine your patient’s belongings, and you will probably find your answer." Check the small pocket in jeans, Dr. Mycyk suggested. "I’ve been surprised how often I find drug contraband in that small pocket."
Accessing one of the "drug partisan sites" – such as erowid.org, lycaeum.org, shroomery.org, and talktofrank.com – also can be useful if you want to figure out what your patient has taken. However, while it might be helpful to know the agent, focus on symptoms and "treat the patient; don’t treat the product," he said.
Treatment
Deaths from NEW drug abuse most commonly occur due to dysrhythmias, hyperthermia, or metabolic complications. There are no antidotes for any of these NEW drugs, but "symptom-based, goal-directed, supportive therapy will save most of these patients’ lives."
Use common sense, and trust your instincts, Dr. Mycyk said. Get an electrolyte panel if the patient is persistently symptomatic. If a patient is tachycardic and having palpitations, getting an ECG may be appropriate. If they’re overly agitated, it is safe to use benzodiazepines. If they’re dehydrated, give them IV fluids, he said.
It is important to get complete vital signs on these patients, and the most important vital sign is temperature, as elevated body temperature is the best predictor of death in the ED. Degree of tachycardia or tachypnea is not as concerning, he said.
For most of these patients, brief ED observation is fine. However, some of the NEW drugs have long duration of activity; for example, the effects of buprenorphine can last 24-37 hours, so admission might be considered.
All patients with an ED visit for drug use should have counseling before discharge. Simple ED counseling can help, Dr. Mycyk said. "They think a lot of this stuff is safe, and we just need to remind them that it is not safe."
Dr. Mycyk had no significant financial relationships to disclose.
Bath salts, spice, and nutmeg are more than common household items; they are also designer drugs that can send people to the emergency department.
While emergency department visits resulting from use of older drugs of abuse such as LSD and cocaine have gone up 29%-48% over the past decade, ED visits resulting from the use of nontraditional, emerging, and Web-based (NEW) drugs have increased by estimates ranging from 187%-5,846%, Dr. Mark B. Mycyk said at the annual meeting of the American College of Emergency Physicians.
The Internet has been a "huge source of information and a powerful influence on this rapidly evolving and changing epidemic," said Dr. Mycyk of Cook County Hospital in Chicago. Designer drugs are easily available from websites such as Silk Road, "the Amazon.com of some of these NEW drugs," he said, and anyone with access to a computer "can pretty much get almost anything delivered to their homes or dorm rooms or a post office box." According to one study, websites touting recreational drugs were a factor in 27% of new drug use in college-age students (Pediatrics 2002;109:e96).
"Cases we see in the ED are extreme ... cases where people end up with complications," Dr. Mycyk said. Emergency physicians may see patients who have used the following NEW drugs:
• Bath salts (methylenedioxypyrovalerone, MDPV). "Brand names" include Ivory Wave, Bliss, and White Lightning; also called Plant Food. Popularized in Australia, these are not the kind of bath salts you would buy at a home goods store, which cause only severe rhinitis if snorted. The type sold online and in "head shops" is a stimulant and hallucinogen that causes cardiovascular and psychiatric adverse effects. "Self-harm has become a common complication. ... People get so psychotic, they are actually getting aggressive and harming others," Dr. Mycyk said. MDPV also has "lots of other profound effects on human neurotransmitters that we still do not understand," and the drug is "so addictive that users say it provokes an almost-uncontrollable urge for another hit." The chemicals used to make "bath salts" were classified as schedule 1 substances in late October by the Drug Enforcement Agency.
• Spice. Also known as K2. This synthetic cannabinoid, developed for animal research, "has resulted in a number of ED visits, and some of these visits can be pretty prolonged, and we’ve seen some unanticipated complications," Dr. Mycyk said. K2 is "much more potent and powerful than natural marijuana, so the effects that we see are much more extreme." Symptoms include agitation, cardiovascular effects, and inappropriate affect (Clin. Toxicol. [Phila.] 2011;49:431-3). Several varieties are now illegal in the United States, but chemists can create "newer synthetic analogs, which look different from Spice and K2, and that way, they evade the legal authorities," he said.
• Meow-Meow (mephedrone, 4-methylmethcathinone). Other street names include Drone, Bubble, and MCAT. This synthetic cathinone, derived from an African shrub, is a stimulant and sympathomimetic agent. Its effects and structure are similar to those of ephedra and amphetamine. Symptoms of Meow-Meow use include seizures, agitation, tachycardia, hypertension, and hyperthermia (Toxicol. Lett. 2011;201:191-5).
• Bromo-DragonFLY (bromo-benzodifuranyl-isopropylamine). Adverse effects of this designer drug include hallucinations, seizures, vomiting, and intense vasoconstriction with resulting ischemia in fingers and toes. The drug has "hallucinogenic, Ecstasy-like properties" and is a serotoninergic receptor agonist. The name derives from the resemblance its chemical structure has to a dragonfly.
• Nutmeg. At doses as high as 50 g, the common spice nutmeg has hallucinogenic properties. "When we see nutmeg users in the ED, we’re seeing a small proportion who took an extremely large dose or have an unanticipated complication from it," Dr. Mycyk said. In one case series of 119 patients, the most common symptoms were tachycardia, palpitations, and agitation. The researchers found that "clinical effects from ingestion can be significant and can require medical intervention" (Clin. Toxicol. [Phila.] 2011;49:177-80).
• Salvia. Street names of the salvia divinorum plant include Diviner’s Sage, Shepherdess, and Sally D. Related to mint, salvia has hallucinogenic and psychotomimetic properties. Symptoms include agitation and neurologic, cardiovascular, and gastrointestinal effects. The herb can be made into a tea; fresh leaves can be chewed; or leaves can be dried and then smoked, snorted, or injected. The drug has not been well studied, but one group of researchers analyzed YouTube videos of salvia users to study its effects (Drug Alcohol Depend. 2010;108:138-40).
• Snakebite. The venom of the naja naja snake, or Indian cobra, contains neurotoxins that can have opiate-like effects on the central nervous system. The venom can cause blackouts and feelings of well-being and lethargy in people who deliberately have themselves bitten by a cobra (Subst. Abus. 2011;32:43-6). "It boggles my mind what people will do to get high," Dr. Mycyk said.
• Buprenorphine (Suboxone). Clinically used for opioid dependence, this drug is smuggled into prisons by being crushed into a paste that is applied to a drawing or card, or hidden under stamps. A recent study found that 12% of drug contraband in Massachusetts prisons is buprenorphine (Curr. Drug Abuse Rev. 2011;4:28-41). Buprenorphine intoxication causes mild euphoria, somnolence, and possible respiratory depression; laboratory and toxicology screens for illicit drugs would be negative.
Diagnosis
Hospital-based drug screens don’t detect most of the new and evolving designer drugs that result in emergency department visits. "A lot of hospitals have invested in expanded drug-screening panels, but these hospital machines cannot keep up with the creative chemists and users out there," Dr. Mycyk said. So "tox testing is not that helpful for some of these NEW drugs. In fact, it might falsely reassure you."
So, to make the diagnosis, "if the patient is conscious, ask them. Know their language, know the slang. They will tell you. ... They are frightened, and they don’t want to die."
If the patient is delirious or has altered mental status, examine his or her belongings carefully. "Completely examine your patient’s belongings, and you will probably find your answer." Check the small pocket in jeans, Dr. Mycyk suggested. "I’ve been surprised how often I find drug contraband in that small pocket."
Accessing one of the "drug partisan sites" – such as erowid.org, lycaeum.org, shroomery.org, and talktofrank.com – also can be useful if you want to figure out what your patient has taken. However, while it might be helpful to know the agent, focus on symptoms and "treat the patient; don’t treat the product," he said.
Treatment
Deaths from NEW drug abuse most commonly occur due to dysrhythmias, hyperthermia, or metabolic complications. There are no antidotes for any of these NEW drugs, but "symptom-based, goal-directed, supportive therapy will save most of these patients’ lives."
Use common sense, and trust your instincts, Dr. Mycyk said. Get an electrolyte panel if the patient is persistently symptomatic. If a patient is tachycardic and having palpitations, getting an ECG may be appropriate. If they’re overly agitated, it is safe to use benzodiazepines. If they’re dehydrated, give them IV fluids, he said.
It is important to get complete vital signs on these patients, and the most important vital sign is temperature, as elevated body temperature is the best predictor of death in the ED. Degree of tachycardia or tachypnea is not as concerning, he said.
For most of these patients, brief ED observation is fine. However, some of the NEW drugs have long duration of activity; for example, the effects of buprenorphine can last 24-37 hours, so admission might be considered.
All patients with an ED visit for drug use should have counseling before discharge. Simple ED counseling can help, Dr. Mycyk said. "They think a lot of this stuff is safe, and we just need to remind them that it is not safe."
Dr. Mycyk had no significant financial relationships to disclose.
Bath salts, spice, and nutmeg are more than common household items; they are also designer drugs that can send people to the emergency department.
While emergency department visits resulting from use of older drugs of abuse such as LSD and cocaine have gone up 29%-48% over the past decade, ED visits resulting from the use of nontraditional, emerging, and Web-based (NEW) drugs have increased by estimates ranging from 187%-5,846%, Dr. Mark B. Mycyk said at the annual meeting of the American College of Emergency Physicians.
The Internet has been a "huge source of information and a powerful influence on this rapidly evolving and changing epidemic," said Dr. Mycyk of Cook County Hospital in Chicago. Designer drugs are easily available from websites such as Silk Road, "the Amazon.com of some of these NEW drugs," he said, and anyone with access to a computer "can pretty much get almost anything delivered to their homes or dorm rooms or a post office box." According to one study, websites touting recreational drugs were a factor in 27% of new drug use in college-age students (Pediatrics 2002;109:e96).
"Cases we see in the ED are extreme ... cases where people end up with complications," Dr. Mycyk said. Emergency physicians may see patients who have used the following NEW drugs:
• Bath salts (methylenedioxypyrovalerone, MDPV). "Brand names" include Ivory Wave, Bliss, and White Lightning; also called Plant Food. Popularized in Australia, these are not the kind of bath salts you would buy at a home goods store, which cause only severe rhinitis if snorted. The type sold online and in "head shops" is a stimulant and hallucinogen that causes cardiovascular and psychiatric adverse effects. "Self-harm has become a common complication. ... People get so psychotic, they are actually getting aggressive and harming others," Dr. Mycyk said. MDPV also has "lots of other profound effects on human neurotransmitters that we still do not understand," and the drug is "so addictive that users say it provokes an almost-uncontrollable urge for another hit." The chemicals used to make "bath salts" were classified as schedule 1 substances in late October by the Drug Enforcement Agency.
• Spice. Also known as K2. This synthetic cannabinoid, developed for animal research, "has resulted in a number of ED visits, and some of these visits can be pretty prolonged, and we’ve seen some unanticipated complications," Dr. Mycyk said. K2 is "much more potent and powerful than natural marijuana, so the effects that we see are much more extreme." Symptoms include agitation, cardiovascular effects, and inappropriate affect (Clin. Toxicol. [Phila.] 2011;49:431-3). Several varieties are now illegal in the United States, but chemists can create "newer synthetic analogs, which look different from Spice and K2, and that way, they evade the legal authorities," he said.
• Meow-Meow (mephedrone, 4-methylmethcathinone). Other street names include Drone, Bubble, and MCAT. This synthetic cathinone, derived from an African shrub, is a stimulant and sympathomimetic agent. Its effects and structure are similar to those of ephedra and amphetamine. Symptoms of Meow-Meow use include seizures, agitation, tachycardia, hypertension, and hyperthermia (Toxicol. Lett. 2011;201:191-5).
• Bromo-DragonFLY (bromo-benzodifuranyl-isopropylamine). Adverse effects of this designer drug include hallucinations, seizures, vomiting, and intense vasoconstriction with resulting ischemia in fingers and toes. The drug has "hallucinogenic, Ecstasy-like properties" and is a serotoninergic receptor agonist. The name derives from the resemblance its chemical structure has to a dragonfly.
• Nutmeg. At doses as high as 50 g, the common spice nutmeg has hallucinogenic properties. "When we see nutmeg users in the ED, we’re seeing a small proportion who took an extremely large dose or have an unanticipated complication from it," Dr. Mycyk said. In one case series of 119 patients, the most common symptoms were tachycardia, palpitations, and agitation. The researchers found that "clinical effects from ingestion can be significant and can require medical intervention" (Clin. Toxicol. [Phila.] 2011;49:177-80).
• Salvia. Street names of the salvia divinorum plant include Diviner’s Sage, Shepherdess, and Sally D. Related to mint, salvia has hallucinogenic and psychotomimetic properties. Symptoms include agitation and neurologic, cardiovascular, and gastrointestinal effects. The herb can be made into a tea; fresh leaves can be chewed; or leaves can be dried and then smoked, snorted, or injected. The drug has not been well studied, but one group of researchers analyzed YouTube videos of salvia users to study its effects (Drug Alcohol Depend. 2010;108:138-40).
• Snakebite. The venom of the naja naja snake, or Indian cobra, contains neurotoxins that can have opiate-like effects on the central nervous system. The venom can cause blackouts and feelings of well-being and lethargy in people who deliberately have themselves bitten by a cobra (Subst. Abus. 2011;32:43-6). "It boggles my mind what people will do to get high," Dr. Mycyk said.
• Buprenorphine (Suboxone). Clinically used for opioid dependence, this drug is smuggled into prisons by being crushed into a paste that is applied to a drawing or card, or hidden under stamps. A recent study found that 12% of drug contraband in Massachusetts prisons is buprenorphine (Curr. Drug Abuse Rev. 2011;4:28-41). Buprenorphine intoxication causes mild euphoria, somnolence, and possible respiratory depression; laboratory and toxicology screens for illicit drugs would be negative.
Diagnosis
Hospital-based drug screens don’t detect most of the new and evolving designer drugs that result in emergency department visits. "A lot of hospitals have invested in expanded drug-screening panels, but these hospital machines cannot keep up with the creative chemists and users out there," Dr. Mycyk said. So "tox testing is not that helpful for some of these NEW drugs. In fact, it might falsely reassure you."
So, to make the diagnosis, "if the patient is conscious, ask them. Know their language, know the slang. They will tell you. ... They are frightened, and they don’t want to die."
If the patient is delirious or has altered mental status, examine his or her belongings carefully. "Completely examine your patient’s belongings, and you will probably find your answer." Check the small pocket in jeans, Dr. Mycyk suggested. "I’ve been surprised how often I find drug contraband in that small pocket."
Accessing one of the "drug partisan sites" – such as erowid.org, lycaeum.org, shroomery.org, and talktofrank.com – also can be useful if you want to figure out what your patient has taken. However, while it might be helpful to know the agent, focus on symptoms and "treat the patient; don’t treat the product," he said.
Treatment
Deaths from NEW drug abuse most commonly occur due to dysrhythmias, hyperthermia, or metabolic complications. There are no antidotes for any of these NEW drugs, but "symptom-based, goal-directed, supportive therapy will save most of these patients’ lives."
Use common sense, and trust your instincts, Dr. Mycyk said. Get an electrolyte panel if the patient is persistently symptomatic. If a patient is tachycardic and having palpitations, getting an ECG may be appropriate. If they’re overly agitated, it is safe to use benzodiazepines. If they’re dehydrated, give them IV fluids, he said.
It is important to get complete vital signs on these patients, and the most important vital sign is temperature, as elevated body temperature is the best predictor of death in the ED. Degree of tachycardia or tachypnea is not as concerning, he said.
For most of these patients, brief ED observation is fine. However, some of the NEW drugs have long duration of activity; for example, the effects of buprenorphine can last 24-37 hours, so admission might be considered.
All patients with an ED visit for drug use should have counseling before discharge. Simple ED counseling can help, Dr. Mycyk said. "They think a lot of this stuff is safe, and we just need to remind them that it is not safe."
Dr. Mycyk had no significant financial relationships to disclose.
SAVE Helps Manage Septic Shock
SAN FRANCISCO – To save a patient in septic shock, think SAVE.
The acronym stands for Suspicion, Act, Ventilation/oxygenation, and Evaluate the goals, Dr. Robert J. Vissers said at the annual meeting of the American College of Emergency Physicians.
He adapted the SAVE acronym from the 2011 Critical Points continuing medical education course for emergency physicians.
Suspicion starts with recognizing systemic inflammatory response syndrome (SIRS), which combined with an infection constitutes sepsis. Patients have SIRS if they have at least two of the following: temperature higher than 38° C or below 36° C; heart rate faster than 90 beats per minute; white blood cell count over 12,000 or less than 4,000 cells/mcL or with greater than 10% bands (immature forms); and a respiratory rate over 20 breaths per minute or, on blood gas, a partial pressure of carbon dioxide less than 32 mm Hg.
Patients with sepsis and organ dysfunction, hypoperfusion, or hypotension have severe sepsis and are considered to have septic shock if the hypotension or hypoperfusion is refractory to fluid resuscitation, said Dr. Vissers, chief of emergency medicine at Legacy Emanuel Hospital, Portland, Ore.
The shock index – the ratio of heart rate divided by systolic blood pressure – is a simple calculation that can help fuel or allay suspicion of septic shock, he said. A normal ratio is 0.5-0.7. A ratio of 1.0 or greater may predict uncompensated shock.
Lactate levels also help stratify patients. A lactate level greater than 2 mmol/L has been associated with increased risk of sepsis and death and indicates end-organ dysfunction, he said. Lactate levels greater than 4 mmol/L are associated with a 25% risk of death.
The second step in SAVE is to act by perfusing the patient and giving the right antibiotics.
Fill the patient’s "tank" by aggressively giving fluids in serial 500- to 1,000-mL boluses of normal saline, he said. Often, 50-60 mL/kg are needed. "The fluids are about a liter every 30 minutes, if you think you’ve got someone with severe sepsis or septic shock. Four to six liters is not unusual before you fill the tank," he said.
Early goals in perfusion should be a mean arterial pressure greater than 65 mm Hg, urine output greater than 0.5 mL/kg per hour, and signs of clinical improvement such as waking up.
Tighten the patient’s perfusion "hose" by administering pressors when the "tank" is full and central venous pressure measures 8-12 mm Hg or ultrasound assessment of the inferior vena cava (IVC) shows greater than a 50% collapse of the IVC on breathing, which is suggestive of a central venous pressure less than 8 mm Hg.
"It’s easy to take the ultrasound, slap it on the IVC. When they breathe in, if the IVC is collapsing, they need more fluid," Dr. Vissers said.
Use norepinephrine or dopamine; there’s no evidence that one pressor is better than another, he said. The perfusion goals at this point would be a mean arterial pressure less than 65 mm Hg, central venous oxygen saturation greater than 70%, and lactate clearance equivalent to central venous oxygen saturation. Greater than a 10% clearance in lactate improves the chance of survival.
Delay in antibiotics is associated with significantly higher mortality, so aim to give antibiotics within an hour of triage or diagnosis. Giving inappropriate antibiotics increases the risk of death two- to fivefold.
If the infection has an unknown source, treat with vancomycin plus piperacillin-tazobactam, ticarcillin-clavulanate, ceftriaxone, cefotaxime, imipenem, or meropenem. If the source is unknown and there’s a risk for pseudomonas infection, give three antibiotics – vancomycin plus two of the following categories: piperacillin-tazobactam or ticarcillin-clavulanate; ciprofloxacin; gentamicin; ceftazidime or cefepime; and imipenem or meropenem.
Early initiation of mechanical ventilation/oxygenation is the third part of SAVE. Septic shock makes breathing harder, which can lead to hypoxia and acidosis and produces a 50% chance of adult respiratory distress syndrome. To reduce potential lung damage, Dr. Vissers recommended these ventilator settings: a low tidal volume of 6 cc/kg of ideal body weight and plateau pressure less than 30 cm H2O.
Last, evaluate the goals to SAVE a patient in septic shock. If lactate does not decrease by 10% or central venous oxygen saturation is less than 70% and the hemoglobin level is less than 7 g/dL, transfuse packed red blood cells. If the mean arterial pressure is less than 65 mm Hg despite optimal fluids and a pressor, consider giving IV hydrocortisone 100 mg and packed red blood cells if the hemoglobin is less than 10 g/dL. If the mean arterial pressure is greater than 65 mm Hg but the patient is still underperfused, consider giving inotropic dobutamine.
Some basic steps in the emergency department can help improve outcomes beyond the hospital, Dr. Vissers added. Elevate the head of the patient’s bed by 30-45 degrees. Decompress the stomach with an orogastric tube, and use sterile technique with any procedures.
Dr. Vissers said he has no relevant conflicts of interest.
SAN FRANCISCO – To save a patient in septic shock, think SAVE.
The acronym stands for Suspicion, Act, Ventilation/oxygenation, and Evaluate the goals, Dr. Robert J. Vissers said at the annual meeting of the American College of Emergency Physicians.
He adapted the SAVE acronym from the 2011 Critical Points continuing medical education course for emergency physicians.
Suspicion starts with recognizing systemic inflammatory response syndrome (SIRS), which combined with an infection constitutes sepsis. Patients have SIRS if they have at least two of the following: temperature higher than 38° C or below 36° C; heart rate faster than 90 beats per minute; white blood cell count over 12,000 or less than 4,000 cells/mcL or with greater than 10% bands (immature forms); and a respiratory rate over 20 breaths per minute or, on blood gas, a partial pressure of carbon dioxide less than 32 mm Hg.
Patients with sepsis and organ dysfunction, hypoperfusion, or hypotension have severe sepsis and are considered to have septic shock if the hypotension or hypoperfusion is refractory to fluid resuscitation, said Dr. Vissers, chief of emergency medicine at Legacy Emanuel Hospital, Portland, Ore.
The shock index – the ratio of heart rate divided by systolic blood pressure – is a simple calculation that can help fuel or allay suspicion of septic shock, he said. A normal ratio is 0.5-0.7. A ratio of 1.0 or greater may predict uncompensated shock.
Lactate levels also help stratify patients. A lactate level greater than 2 mmol/L has been associated with increased risk of sepsis and death and indicates end-organ dysfunction, he said. Lactate levels greater than 4 mmol/L are associated with a 25% risk of death.
The second step in SAVE is to act by perfusing the patient and giving the right antibiotics.
Fill the patient’s "tank" by aggressively giving fluids in serial 500- to 1,000-mL boluses of normal saline, he said. Often, 50-60 mL/kg are needed. "The fluids are about a liter every 30 minutes, if you think you’ve got someone with severe sepsis or septic shock. Four to six liters is not unusual before you fill the tank," he said.
Early goals in perfusion should be a mean arterial pressure greater than 65 mm Hg, urine output greater than 0.5 mL/kg per hour, and signs of clinical improvement such as waking up.
Tighten the patient’s perfusion "hose" by administering pressors when the "tank" is full and central venous pressure measures 8-12 mm Hg or ultrasound assessment of the inferior vena cava (IVC) shows greater than a 50% collapse of the IVC on breathing, which is suggestive of a central venous pressure less than 8 mm Hg.
"It’s easy to take the ultrasound, slap it on the IVC. When they breathe in, if the IVC is collapsing, they need more fluid," Dr. Vissers said.
Use norepinephrine or dopamine; there’s no evidence that one pressor is better than another, he said. The perfusion goals at this point would be a mean arterial pressure less than 65 mm Hg, central venous oxygen saturation greater than 70%, and lactate clearance equivalent to central venous oxygen saturation. Greater than a 10% clearance in lactate improves the chance of survival.
Delay in antibiotics is associated with significantly higher mortality, so aim to give antibiotics within an hour of triage or diagnosis. Giving inappropriate antibiotics increases the risk of death two- to fivefold.
If the infection has an unknown source, treat with vancomycin plus piperacillin-tazobactam, ticarcillin-clavulanate, ceftriaxone, cefotaxime, imipenem, or meropenem. If the source is unknown and there’s a risk for pseudomonas infection, give three antibiotics – vancomycin plus two of the following categories: piperacillin-tazobactam or ticarcillin-clavulanate; ciprofloxacin; gentamicin; ceftazidime or cefepime; and imipenem or meropenem.
Early initiation of mechanical ventilation/oxygenation is the third part of SAVE. Septic shock makes breathing harder, which can lead to hypoxia and acidosis and produces a 50% chance of adult respiratory distress syndrome. To reduce potential lung damage, Dr. Vissers recommended these ventilator settings: a low tidal volume of 6 cc/kg of ideal body weight and plateau pressure less than 30 cm H2O.
Last, evaluate the goals to SAVE a patient in septic shock. If lactate does not decrease by 10% or central venous oxygen saturation is less than 70% and the hemoglobin level is less than 7 g/dL, transfuse packed red blood cells. If the mean arterial pressure is less than 65 mm Hg despite optimal fluids and a pressor, consider giving IV hydrocortisone 100 mg and packed red blood cells if the hemoglobin is less than 10 g/dL. If the mean arterial pressure is greater than 65 mm Hg but the patient is still underperfused, consider giving inotropic dobutamine.
Some basic steps in the emergency department can help improve outcomes beyond the hospital, Dr. Vissers added. Elevate the head of the patient’s bed by 30-45 degrees. Decompress the stomach with an orogastric tube, and use sterile technique with any procedures.
Dr. Vissers said he has no relevant conflicts of interest.
SAN FRANCISCO – To save a patient in septic shock, think SAVE.
The acronym stands for Suspicion, Act, Ventilation/oxygenation, and Evaluate the goals, Dr. Robert J. Vissers said at the annual meeting of the American College of Emergency Physicians.
He adapted the SAVE acronym from the 2011 Critical Points continuing medical education course for emergency physicians.
Suspicion starts with recognizing systemic inflammatory response syndrome (SIRS), which combined with an infection constitutes sepsis. Patients have SIRS if they have at least two of the following: temperature higher than 38° C or below 36° C; heart rate faster than 90 beats per minute; white blood cell count over 12,000 or less than 4,000 cells/mcL or with greater than 10% bands (immature forms); and a respiratory rate over 20 breaths per minute or, on blood gas, a partial pressure of carbon dioxide less than 32 mm Hg.
Patients with sepsis and organ dysfunction, hypoperfusion, or hypotension have severe sepsis and are considered to have septic shock if the hypotension or hypoperfusion is refractory to fluid resuscitation, said Dr. Vissers, chief of emergency medicine at Legacy Emanuel Hospital, Portland, Ore.
The shock index – the ratio of heart rate divided by systolic blood pressure – is a simple calculation that can help fuel or allay suspicion of septic shock, he said. A normal ratio is 0.5-0.7. A ratio of 1.0 or greater may predict uncompensated shock.
Lactate levels also help stratify patients. A lactate level greater than 2 mmol/L has been associated with increased risk of sepsis and death and indicates end-organ dysfunction, he said. Lactate levels greater than 4 mmol/L are associated with a 25% risk of death.
The second step in SAVE is to act by perfusing the patient and giving the right antibiotics.
Fill the patient’s "tank" by aggressively giving fluids in serial 500- to 1,000-mL boluses of normal saline, he said. Often, 50-60 mL/kg are needed. "The fluids are about a liter every 30 minutes, if you think you’ve got someone with severe sepsis or septic shock. Four to six liters is not unusual before you fill the tank," he said.
Early goals in perfusion should be a mean arterial pressure greater than 65 mm Hg, urine output greater than 0.5 mL/kg per hour, and signs of clinical improvement such as waking up.
Tighten the patient’s perfusion "hose" by administering pressors when the "tank" is full and central venous pressure measures 8-12 mm Hg or ultrasound assessment of the inferior vena cava (IVC) shows greater than a 50% collapse of the IVC on breathing, which is suggestive of a central venous pressure less than 8 mm Hg.
"It’s easy to take the ultrasound, slap it on the IVC. When they breathe in, if the IVC is collapsing, they need more fluid," Dr. Vissers said.
Use norepinephrine or dopamine; there’s no evidence that one pressor is better than another, he said. The perfusion goals at this point would be a mean arterial pressure less than 65 mm Hg, central venous oxygen saturation greater than 70%, and lactate clearance equivalent to central venous oxygen saturation. Greater than a 10% clearance in lactate improves the chance of survival.
Delay in antibiotics is associated with significantly higher mortality, so aim to give antibiotics within an hour of triage or diagnosis. Giving inappropriate antibiotics increases the risk of death two- to fivefold.
If the infection has an unknown source, treat with vancomycin plus piperacillin-tazobactam, ticarcillin-clavulanate, ceftriaxone, cefotaxime, imipenem, or meropenem. If the source is unknown and there’s a risk for pseudomonas infection, give three antibiotics – vancomycin plus two of the following categories: piperacillin-tazobactam or ticarcillin-clavulanate; ciprofloxacin; gentamicin; ceftazidime or cefepime; and imipenem or meropenem.
Early initiation of mechanical ventilation/oxygenation is the third part of SAVE. Septic shock makes breathing harder, which can lead to hypoxia and acidosis and produces a 50% chance of adult respiratory distress syndrome. To reduce potential lung damage, Dr. Vissers recommended these ventilator settings: a low tidal volume of 6 cc/kg of ideal body weight and plateau pressure less than 30 cm H2O.
Last, evaluate the goals to SAVE a patient in septic shock. If lactate does not decrease by 10% or central venous oxygen saturation is less than 70% and the hemoglobin level is less than 7 g/dL, transfuse packed red blood cells. If the mean arterial pressure is less than 65 mm Hg despite optimal fluids and a pressor, consider giving IV hydrocortisone 100 mg and packed red blood cells if the hemoglobin is less than 10 g/dL. If the mean arterial pressure is greater than 65 mm Hg but the patient is still underperfused, consider giving inotropic dobutamine.
Some basic steps in the emergency department can help improve outcomes beyond the hospital, Dr. Vissers added. Elevate the head of the patient’s bed by 30-45 degrees. Decompress the stomach with an orogastric tube, and use sterile technique with any procedures.
Dr. Vissers said he has no relevant conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Lower Blood Pressure Slowly in Hypertensive Emergency
SAN FRANCISCO – Rapidly lowering blood pressure in patients who are having a hypertensive emergency or hypertensive urgency isn’t necessary and may be harmful, except in the case of aortic dissection.
Lower blood pressure gradually in the emergency department to maintain cerebral perfusion within acceptable limits, Dr. Michael J. Bresler advised at the annual meeting of the American College of Emergency Physicians. For most patients, don’t push diastolic blood pressure down below 110 mm Hg, he added.
Hypertensive emergencies should be treated with IV medications, said Dr. Bresler of Stanford (Calif.) University. It’s not an emergency unless acute high blood pressure is causing end-organ damage, usually to the brain, heart, or kidneys. Blood pressure usually measures above 220 mm Hg systolic or 130 mm Hg diastolic in hypertensive emergencies.
Hypertensive urgency consists of blood pressure greater than 220 mm Hg systolic or 120 mm Hg diastolic but without acute organ failure or acute symptoms directly attributable to the blood pressure elevation. Physicians may opt to treat hypertensive urgency with oral medications in the ED, but usually the patient gets a prescription for outpatient therapy, he said.
Patients with elevated blood pressure greater than 140 mm Hg systolic or 90 mm Hg diastolic do not have urgent or emergent hypertension, but should be referred for further evaluation. Physicians may choose to write a prescription for outpatient antihypertensive therapy, but treatment in the ED is not warranted, Dr. Bresler said.
"It’s not the numbers that count" in assessing hypertension in the ED, he said. "It’s whether the patient has an acute problem from the blood pressure."
When choosing antihypertensive therapy, some medications are more suitable for the ED than are others.
The most commonly used antihypertensive in emergency medicine is nitroprusside, a parenteral vasodilator that’s very effective and has a very short half-life. The drug has disadvantages, however. It’s unstable in UV light, and so must be wrapped, and it metabolizes to cyanide/thiocyanate. Nitroprusside can cause orthostatic hypotension, is toxic at higher doses and potentially toxic to fetuses, increases intracranial pressure, and can cause tissue necrosis if there’s extravasation.
Nitroglycerin, another parenteral vasodilator, is good for patients with heart failure and angina, but it’s not a good drug for hypertensive crisis, Dr. Bresler said.
Among calcium channel blockers, the most useful for blood pressure control in the emergency department are IV nicardipine or IV clevidipine. These drugs are as effective as nitroprusside without the cyanide/thiocyanate toxicity. They are not light sensitive and so don’t need a foil wrap. Rate adjustments are required about a third as often as with nitroprusside. The IV calcium channel blockers don’t need an arterial line and don’t cause intracerebral vasodilation, which can lead to edema.
"Many of us are switching to nicardipine instead of nitroprusside," Dr. Bresler said.
Among beta-blockers, his top picks for emergency medicine are IV labetalol (which also is an alpha-blocker), oral or IV metoprolol, or IV esmolol, a short-acting cardioselective agent. In patients with coronary artery disease or with anxiety, beta-blockers are a good choice, he said. For oral therapy, the long-acting preparations are best.
ACE inhibitors are especially helpful for hypertension in patients with diabetes, renal failure, or heart failure. The most useful for emergency departments is IV enalapril, he said. But 1 in 2,000 patients who are treated with an ACE inhibitor will develop angioedema, and 1 in 10 will develop cough.
Angiotension II receptor blockers (ARBs) such as losartan, valsartan, or irbesartan are as effective as ACE inhibitors and have fewer side effects. Angioedema is rare, and the drugs do not cause cough. "I think as these become generic, they will replace ACE inhibitors," Dr. Bresler said.
Like ARBs, direct renin inhibitors such as aliskiren are similar in efficacy to ACE inhibitors with fewer side effects.
Hypertensive urgency also could be treated with oral clonidine, an alpha2 adrenergic agonist.
Diuretics have no role in treating high blood pressure in the ED, but are a mainstay of outpatient therapy, he said. Diuretics are inexpensive and are at least as effective as ACE inhibitors or calcium channel blockers, but most hypertensive patients will require other medications in addition to diuretics.
Dr. Bresler said he has no relevant conflicts of interest.
SAN FRANCISCO – Rapidly lowering blood pressure in patients who are having a hypertensive emergency or hypertensive urgency isn’t necessary and may be harmful, except in the case of aortic dissection.
Lower blood pressure gradually in the emergency department to maintain cerebral perfusion within acceptable limits, Dr. Michael J. Bresler advised at the annual meeting of the American College of Emergency Physicians. For most patients, don’t push diastolic blood pressure down below 110 mm Hg, he added.
Hypertensive emergencies should be treated with IV medications, said Dr. Bresler of Stanford (Calif.) University. It’s not an emergency unless acute high blood pressure is causing end-organ damage, usually to the brain, heart, or kidneys. Blood pressure usually measures above 220 mm Hg systolic or 130 mm Hg diastolic in hypertensive emergencies.
Hypertensive urgency consists of blood pressure greater than 220 mm Hg systolic or 120 mm Hg diastolic but without acute organ failure or acute symptoms directly attributable to the blood pressure elevation. Physicians may opt to treat hypertensive urgency with oral medications in the ED, but usually the patient gets a prescription for outpatient therapy, he said.
Patients with elevated blood pressure greater than 140 mm Hg systolic or 90 mm Hg diastolic do not have urgent or emergent hypertension, but should be referred for further evaluation. Physicians may choose to write a prescription for outpatient antihypertensive therapy, but treatment in the ED is not warranted, Dr. Bresler said.
"It’s not the numbers that count" in assessing hypertension in the ED, he said. "It’s whether the patient has an acute problem from the blood pressure."
When choosing antihypertensive therapy, some medications are more suitable for the ED than are others.
The most commonly used antihypertensive in emergency medicine is nitroprusside, a parenteral vasodilator that’s very effective and has a very short half-life. The drug has disadvantages, however. It’s unstable in UV light, and so must be wrapped, and it metabolizes to cyanide/thiocyanate. Nitroprusside can cause orthostatic hypotension, is toxic at higher doses and potentially toxic to fetuses, increases intracranial pressure, and can cause tissue necrosis if there’s extravasation.
Nitroglycerin, another parenteral vasodilator, is good for patients with heart failure and angina, but it’s not a good drug for hypertensive crisis, Dr. Bresler said.
Among calcium channel blockers, the most useful for blood pressure control in the emergency department are IV nicardipine or IV clevidipine. These drugs are as effective as nitroprusside without the cyanide/thiocyanate toxicity. They are not light sensitive and so don’t need a foil wrap. Rate adjustments are required about a third as often as with nitroprusside. The IV calcium channel blockers don’t need an arterial line and don’t cause intracerebral vasodilation, which can lead to edema.
"Many of us are switching to nicardipine instead of nitroprusside," Dr. Bresler said.
Among beta-blockers, his top picks for emergency medicine are IV labetalol (which also is an alpha-blocker), oral or IV metoprolol, or IV esmolol, a short-acting cardioselective agent. In patients with coronary artery disease or with anxiety, beta-blockers are a good choice, he said. For oral therapy, the long-acting preparations are best.
ACE inhibitors are especially helpful for hypertension in patients with diabetes, renal failure, or heart failure. The most useful for emergency departments is IV enalapril, he said. But 1 in 2,000 patients who are treated with an ACE inhibitor will develop angioedema, and 1 in 10 will develop cough.
Angiotension II receptor blockers (ARBs) such as losartan, valsartan, or irbesartan are as effective as ACE inhibitors and have fewer side effects. Angioedema is rare, and the drugs do not cause cough. "I think as these become generic, they will replace ACE inhibitors," Dr. Bresler said.
Like ARBs, direct renin inhibitors such as aliskiren are similar in efficacy to ACE inhibitors with fewer side effects.
Hypertensive urgency also could be treated with oral clonidine, an alpha2 adrenergic agonist.
Diuretics have no role in treating high blood pressure in the ED, but are a mainstay of outpatient therapy, he said. Diuretics are inexpensive and are at least as effective as ACE inhibitors or calcium channel blockers, but most hypertensive patients will require other medications in addition to diuretics.
Dr. Bresler said he has no relevant conflicts of interest.
SAN FRANCISCO – Rapidly lowering blood pressure in patients who are having a hypertensive emergency or hypertensive urgency isn’t necessary and may be harmful, except in the case of aortic dissection.
Lower blood pressure gradually in the emergency department to maintain cerebral perfusion within acceptable limits, Dr. Michael J. Bresler advised at the annual meeting of the American College of Emergency Physicians. For most patients, don’t push diastolic blood pressure down below 110 mm Hg, he added.
Hypertensive emergencies should be treated with IV medications, said Dr. Bresler of Stanford (Calif.) University. It’s not an emergency unless acute high blood pressure is causing end-organ damage, usually to the brain, heart, or kidneys. Blood pressure usually measures above 220 mm Hg systolic or 130 mm Hg diastolic in hypertensive emergencies.
Hypertensive urgency consists of blood pressure greater than 220 mm Hg systolic or 120 mm Hg diastolic but without acute organ failure or acute symptoms directly attributable to the blood pressure elevation. Physicians may opt to treat hypertensive urgency with oral medications in the ED, but usually the patient gets a prescription for outpatient therapy, he said.
Patients with elevated blood pressure greater than 140 mm Hg systolic or 90 mm Hg diastolic do not have urgent or emergent hypertension, but should be referred for further evaluation. Physicians may choose to write a prescription for outpatient antihypertensive therapy, but treatment in the ED is not warranted, Dr. Bresler said.
"It’s not the numbers that count" in assessing hypertension in the ED, he said. "It’s whether the patient has an acute problem from the blood pressure."
When choosing antihypertensive therapy, some medications are more suitable for the ED than are others.
The most commonly used antihypertensive in emergency medicine is nitroprusside, a parenteral vasodilator that’s very effective and has a very short half-life. The drug has disadvantages, however. It’s unstable in UV light, and so must be wrapped, and it metabolizes to cyanide/thiocyanate. Nitroprusside can cause orthostatic hypotension, is toxic at higher doses and potentially toxic to fetuses, increases intracranial pressure, and can cause tissue necrosis if there’s extravasation.
Nitroglycerin, another parenteral vasodilator, is good for patients with heart failure and angina, but it’s not a good drug for hypertensive crisis, Dr. Bresler said.
Among calcium channel blockers, the most useful for blood pressure control in the emergency department are IV nicardipine or IV clevidipine. These drugs are as effective as nitroprusside without the cyanide/thiocyanate toxicity. They are not light sensitive and so don’t need a foil wrap. Rate adjustments are required about a third as often as with nitroprusside. The IV calcium channel blockers don’t need an arterial line and don’t cause intracerebral vasodilation, which can lead to edema.
"Many of us are switching to nicardipine instead of nitroprusside," Dr. Bresler said.
Among beta-blockers, his top picks for emergency medicine are IV labetalol (which also is an alpha-blocker), oral or IV metoprolol, or IV esmolol, a short-acting cardioselective agent. In patients with coronary artery disease or with anxiety, beta-blockers are a good choice, he said. For oral therapy, the long-acting preparations are best.
ACE inhibitors are especially helpful for hypertension in patients with diabetes, renal failure, or heart failure. The most useful for emergency departments is IV enalapril, he said. But 1 in 2,000 patients who are treated with an ACE inhibitor will develop angioedema, and 1 in 10 will develop cough.
Angiotension II receptor blockers (ARBs) such as losartan, valsartan, or irbesartan are as effective as ACE inhibitors and have fewer side effects. Angioedema is rare, and the drugs do not cause cough. "I think as these become generic, they will replace ACE inhibitors," Dr. Bresler said.
Like ARBs, direct renin inhibitors such as aliskiren are similar in efficacy to ACE inhibitors with fewer side effects.
Hypertensive urgency also could be treated with oral clonidine, an alpha2 adrenergic agonist.
Diuretics have no role in treating high blood pressure in the ED, but are a mainstay of outpatient therapy, he said. Diuretics are inexpensive and are at least as effective as ACE inhibitors or calcium channel blockers, but most hypertensive patients will require other medications in addition to diuretics.
Dr. Bresler said he has no relevant conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Trauma CT Saves Lives - If Scans Are Read in Time
SAN FRANCISCO – With radiology assistance often taking hours, more physicians should know the basics of reading a trauma CT to identify injuries that require immediate action, Dr. Andrew D. Perron said.
"At 3 a.m., I have to know without calling someone whether I need to get moving," said Dr. Perron, an emergency physician at Maine Medical Center, Portland. It is crucial to be able to identify which diagnoses could kill a patient within an hour, so focus on detecting a handful of potentially life-threatening injuries in the head, chest, abdomen, and pelvis, he said at the Scientific Assembly of the American College of Emergency Physicians.

For trauma victims, CT scans have become almost automatic. Currently in the United States, 60-70 million CT scans are conducted each year, compared with only 3 million in 1980, Dr. Perron said. A quarter of the scans are of the head.
When reading a CT of the head, look for epidural hematoma, subdural hematoma, skull fracture, contusions, head pressure and shift, and neck injuries. An epidural hematoma will be lens shaped and does not cross the sutures. A clot will appear as bright white on the scan; if an area is on its way to clotting, it will be gray. Epidural hematomas have low mortality if the patient is treated before he or she loses consciousness.
Subdural hematomas are sickle-shaped and do cross the sutures but not the midline. Subdurals have an 80% mortality rate. Even if a neurosurgeon suctions out the clot, the brain may not recover, Dr. Perron said.
Any area of the skull can sustain a fracture, but skull fractures sometimes aren’t readily visible on plain film or CT. The give-away on imaging is if there is blood instead of air in the mastoid cells, he said.
Although brain contusions are not readily treatable, it is important to know they are there, Dr. Perron said. A contusion will appear as a high-density area on the scan. They commonly result from a sudden deceleration, as in a motor vehicle collision. CT scans can be used to show high pressure within the skull, but there is divergence in the literature about CT’s true utility for these cases, Dr. Perron said.
In the neck, look for fracture and dislocation. CT is 98% sensitive for neck fractures and is especially good for diagnosing fractures located either high or low in the neck. Vertebral body fractures are the most common and account for about a third of neck fractures. Axial views provide the most data on the state of the spinal canal, but a coronal view is easier to read if the physician is more experienced with plain x-rays.
Dislocation is most common, but easier to miss, at C5-6 and C6-7. Dislocations are usually accompanied by torn ligaments. The injury comes from a rotational deceleration in most cases. Vascular injury can occur with dislocation or subluxation, with an attendant risk for dissection. An angiogram should be considered for patients with a C1-3 fracture and subluxation or fracture of the foramen transversarium.
In the chest, the main concerns are aortic injury, pneumothorax, and hemothorax. Like contusions, aortic injuries often are caused by sudden deceleration. Most patients with an aortic injury die in the field. If they survive to the hospital and are scanned, leaking contrast material seen on imaging indicates a ruptured aorta, Dr. Perron said.
A chest x-ray can miss a small pneumothorax, but they are easy to see on CT, with a black space demonstrating where air is outside the lung. A hemothorax cannot be detected by x-ray until at least 250 cc of blood has accumulated, but CT is more sensitive for these as well.
The spleen, liver, kidneys, pancreas, and blood in the abdomen are the areas of greatest concern in abdominal trauma. When scanning the abdomen, Dr. Perron generally uses intravenous contrast because it helps identify the major blood vessels and shows active bleeding. He starts with a supine and coronal view, as axial orientations are more difficult to read.
There should never be blood visible in the middle of the spleen. The liver has more vascularity on a normal view. Lacerations are the most common injury in the liver, and lacerations to the kidneys are also often seen. CT may detect an absence of blood flow to the liver or kidney, indicating severe injury. The main issue with these organs is to be sure they are in one piece and functioning.
The sensitivity of CT is only 68% for pancreatic injuries. This pancreas can be damaged when it is compressed against the spine, which may occur in a bicycle- or sports-related impact. CT can be used to spot active bleeding; the active extravasation of IV contrast is the hallmark, but it may be subtle.
In the pelvis, fractures and other bony injuries and free fluid are the biggest concerns. Pelvic fractures, which are generally easy to see on imaging, suggest that the body sustained a large amount of force. Free fluid in the pelvis can indicate a solid organ injury, a mesenteric injury, a bowel injury, or even a preexisting condition such as ascites.
Dr. Perron reported no conflicts of interest.
SAN FRANCISCO – With radiology assistance often taking hours, more physicians should know the basics of reading a trauma CT to identify injuries that require immediate action, Dr. Andrew D. Perron said.
"At 3 a.m., I have to know without calling someone whether I need to get moving," said Dr. Perron, an emergency physician at Maine Medical Center, Portland. It is crucial to be able to identify which diagnoses could kill a patient within an hour, so focus on detecting a handful of potentially life-threatening injuries in the head, chest, abdomen, and pelvis, he said at the Scientific Assembly of the American College of Emergency Physicians.
For trauma victims, CT scans have become almost automatic. Currently in the United States, 60-70 million CT scans are conducted each year, compared with only 3 million in 1980, Dr. Perron said. A quarter of the scans are of the head.
When reading a CT of the head, look for epidural hematoma, subdural hematoma, skull fracture, contusions, head pressure and shift, and neck injuries. An epidural hematoma will be lens shaped and does not cross the sutures. A clot will appear as bright white on the scan; if an area is on its way to clotting, it will be gray. Epidural hematomas have low mortality if the patient is treated before he or she loses consciousness.
Subdural hematomas are sickle-shaped and do cross the sutures but not the midline. Subdurals have an 80% mortality rate. Even if a neurosurgeon suctions out the clot, the brain may not recover, Dr. Perron said.
Any area of the skull can sustain a fracture, but skull fractures sometimes aren’t readily visible on plain film or CT. The give-away on imaging is if there is blood instead of air in the mastoid cells, he said.
Although brain contusions are not readily treatable, it is important to know they are there, Dr. Perron said. A contusion will appear as a high-density area on the scan. They commonly result from a sudden deceleration, as in a motor vehicle collision. CT scans can be used to show high pressure within the skull, but there is divergence in the literature about CT’s true utility for these cases, Dr. Perron said.
In the neck, look for fracture and dislocation. CT is 98% sensitive for neck fractures and is especially good for diagnosing fractures located either high or low in the neck. Vertebral body fractures are the most common and account for about a third of neck fractures. Axial views provide the most data on the state of the spinal canal, but a coronal view is easier to read if the physician is more experienced with plain x-rays.
Dislocation is most common, but easier to miss, at C5-6 and C6-7. Dislocations are usually accompanied by torn ligaments. The injury comes from a rotational deceleration in most cases. Vascular injury can occur with dislocation or subluxation, with an attendant risk for dissection. An angiogram should be considered for patients with a C1-3 fracture and subluxation or fracture of the foramen transversarium.
In the chest, the main concerns are aortic injury, pneumothorax, and hemothorax. Like contusions, aortic injuries often are caused by sudden deceleration. Most patients with an aortic injury die in the field. If they survive to the hospital and are scanned, leaking contrast material seen on imaging indicates a ruptured aorta, Dr. Perron said.
A chest x-ray can miss a small pneumothorax, but they are easy to see on CT, with a black space demonstrating where air is outside the lung. A hemothorax cannot be detected by x-ray until at least 250 cc of blood has accumulated, but CT is more sensitive for these as well.
The spleen, liver, kidneys, pancreas, and blood in the abdomen are the areas of greatest concern in abdominal trauma. When scanning the abdomen, Dr. Perron generally uses intravenous contrast because it helps identify the major blood vessels and shows active bleeding. He starts with a supine and coronal view, as axial orientations are more difficult to read.
There should never be blood visible in the middle of the spleen. The liver has more vascularity on a normal view. Lacerations are the most common injury in the liver, and lacerations to the kidneys are also often seen. CT may detect an absence of blood flow to the liver or kidney, indicating severe injury. The main issue with these organs is to be sure they are in one piece and functioning.
The sensitivity of CT is only 68% for pancreatic injuries. This pancreas can be damaged when it is compressed against the spine, which may occur in a bicycle- or sports-related impact. CT can be used to spot active bleeding; the active extravasation of IV contrast is the hallmark, but it may be subtle.
In the pelvis, fractures and other bony injuries and free fluid are the biggest concerns. Pelvic fractures, which are generally easy to see on imaging, suggest that the body sustained a large amount of force. Free fluid in the pelvis can indicate a solid organ injury, a mesenteric injury, a bowel injury, or even a preexisting condition such as ascites.
Dr. Perron reported no conflicts of interest.
SAN FRANCISCO – With radiology assistance often taking hours, more physicians should know the basics of reading a trauma CT to identify injuries that require immediate action, Dr. Andrew D. Perron said.
"At 3 a.m., I have to know without calling someone whether I need to get moving," said Dr. Perron, an emergency physician at Maine Medical Center, Portland. It is crucial to be able to identify which diagnoses could kill a patient within an hour, so focus on detecting a handful of potentially life-threatening injuries in the head, chest, abdomen, and pelvis, he said at the Scientific Assembly of the American College of Emergency Physicians.
For trauma victims, CT scans have become almost automatic. Currently in the United States, 60-70 million CT scans are conducted each year, compared with only 3 million in 1980, Dr. Perron said. A quarter of the scans are of the head.
When reading a CT of the head, look for epidural hematoma, subdural hematoma, skull fracture, contusions, head pressure and shift, and neck injuries. An epidural hematoma will be lens shaped and does not cross the sutures. A clot will appear as bright white on the scan; if an area is on its way to clotting, it will be gray. Epidural hematomas have low mortality if the patient is treated before he or she loses consciousness.
Subdural hematomas are sickle-shaped and do cross the sutures but not the midline. Subdurals have an 80% mortality rate. Even if a neurosurgeon suctions out the clot, the brain may not recover, Dr. Perron said.
Any area of the skull can sustain a fracture, but skull fractures sometimes aren’t readily visible on plain film or CT. The give-away on imaging is if there is blood instead of air in the mastoid cells, he said.
Although brain contusions are not readily treatable, it is important to know they are there, Dr. Perron said. A contusion will appear as a high-density area on the scan. They commonly result from a sudden deceleration, as in a motor vehicle collision. CT scans can be used to show high pressure within the skull, but there is divergence in the literature about CT’s true utility for these cases, Dr. Perron said.
In the neck, look for fracture and dislocation. CT is 98% sensitive for neck fractures and is especially good for diagnosing fractures located either high or low in the neck. Vertebral body fractures are the most common and account for about a third of neck fractures. Axial views provide the most data on the state of the spinal canal, but a coronal view is easier to read if the physician is more experienced with plain x-rays.
Dislocation is most common, but easier to miss, at C5-6 and C6-7. Dislocations are usually accompanied by torn ligaments. The injury comes from a rotational deceleration in most cases. Vascular injury can occur with dislocation or subluxation, with an attendant risk for dissection. An angiogram should be considered for patients with a C1-3 fracture and subluxation or fracture of the foramen transversarium.
In the chest, the main concerns are aortic injury, pneumothorax, and hemothorax. Like contusions, aortic injuries often are caused by sudden deceleration. Most patients with an aortic injury die in the field. If they survive to the hospital and are scanned, leaking contrast material seen on imaging indicates a ruptured aorta, Dr. Perron said.
A chest x-ray can miss a small pneumothorax, but they are easy to see on CT, with a black space demonstrating where air is outside the lung. A hemothorax cannot be detected by x-ray until at least 250 cc of blood has accumulated, but CT is more sensitive for these as well.
The spleen, liver, kidneys, pancreas, and blood in the abdomen are the areas of greatest concern in abdominal trauma. When scanning the abdomen, Dr. Perron generally uses intravenous contrast because it helps identify the major blood vessels and shows active bleeding. He starts with a supine and coronal view, as axial orientations are more difficult to read.
There should never be blood visible in the middle of the spleen. The liver has more vascularity on a normal view. Lacerations are the most common injury in the liver, and lacerations to the kidneys are also often seen. CT may detect an absence of blood flow to the liver or kidney, indicating severe injury. The main issue with these organs is to be sure they are in one piece and functioning.
The sensitivity of CT is only 68% for pancreatic injuries. This pancreas can be damaged when it is compressed against the spine, which may occur in a bicycle- or sports-related impact. CT can be used to spot active bleeding; the active extravasation of IV contrast is the hallmark, but it may be subtle.
In the pelvis, fractures and other bony injuries and free fluid are the biggest concerns. Pelvic fractures, which are generally easy to see on imaging, suggest that the body sustained a large amount of force. Free fluid in the pelvis can indicate a solid organ injury, a mesenteric injury, a bowel injury, or even a preexisting condition such as ascites.
Dr. Perron reported no conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
'C for Compressions' Usurps 'A for Airway'
SAN FRANCISCO – The alphabet is changing for critical care of patients in cardiac arrest.
"A is for airway" is no longer at the top of the list. The ABCs (airway, breathing, and circulation) of cardiopulmonary resuscitation have been replaced by an emphasis on CAB – compressions, airway, and breathing, in that order.
The American Heart Association promotes the "CPR is as easy as C-A-B" slogan, and the key to success in treating cardiac arrest is high-quality, uninterrupted chest compressions, Dr. Robert J. Vissers said at the annual meeting of the American College of Emergency Physicians.
"Airway may not always come first" if the patient has lost perfusion and circulation, said Dr. Vissers, chief of emergency medicine at Legacy Emanuel Medical Center, Portland, Ore. "It’s hard for me to say, because I’m an airway guy."
While "C" stands for compressions, it also serves to remind physicians to attend to cardioversion, capnography, cooling, and catheterization, if needed. Dr. Vissers addressed each of these in more detail. "These are the things that recently have led to pretty substantial improvements in the outcomes of these patients," he said.
Compressions. With high-quality, uninterrupted chest compressions, the patient gets good passive ventilation, which may be superior to positive pressure ventilation in these situations. Aim for 30 compressions per breath. Consider creating a supraglottic airway without interrupting the CPR, he said.
Put some muscle into it to maintain compressions 2 inches in depth with full recoil, at a rate of 100 compressions per minute. If more than one person is available, take turns applying compressions to reduce fatigue. Monitor the patient closely with end-tidal capnography. (See below.)
Proper compressions restore cerebral and coronary perfusion. Sustained coronary perfusion pressure is critical to successful defibrillation.
Cardioversion. The first 4 minutes after cardiac arrest provide the greatest chance of successful cardioversion (defibrillation). If more than 4 minutes have elapsed, reperfuse the myocardium with a few minutes of chest compressions before applying shock. Wait 2 minutes after defibrillation to check the pulse, and maintain compressions during that time.
The traditional admonition to "clear!" before shocking may not be necessary, Dr. Vissers said. Studies have shown that no appreciable electrical current reaches the people applying compressions if they are wearing gloves and a biphasic defibrillator is used for cardioversion.
Capnography. Confirm proper tube placement for capnography, which helps assess the quality of the CPR and identify return of spontaneous circulation without checking pulses. Capnography readings also help predict outcome.
"I think capnography is one of the most underutilized tools that we have for the critically ill patient," Dr. Vissers said.
High-quality compressions and coronary perfusion pressures correlate with end-tidal carbon dioxide (ETCO2) levels of 20-25 mm Hg on capnography. A sudden rise in ETCO2 suggests return of spontaneous circulation and is more sensitive than manual pulse checks. If ETCO2 readings persistently stay below 10 mm Hg, return of spontaneous circulation is unlikely. In studies, an ETCO2 less than 10 mm Hg after 20 minutes of compressions was associated with zero chance of return of spontaneous circulation.
Cooling. For unconscious adults who went into cardiac arrest outside of hospital care, cooling the body to 32-34° C for 12-24 hours improves chances of a good outcome, Dr. Vissers said. Applying ice packs to the groin, axilla, and neck will cool the body about 0.2-1° C per hour. The best cooling method may be cooling blankets that circulate cooled water through material designed to promote heat exchange. The blankets cool a body on average by 1-1.5° C per hour.
Used in combination, the ice packs can be removed when the body temperature reaches 33° C and the blankets left on to maintain the cool temperature for 12-24 hours. "That works very well," he said. Cooled normal saline infusions or cooling catheters also are options for cooling a body after cardiac arrest.
Of every 4-13 patients cooled after cardiac arrest, 1 will leave the hospital neurologically intact, he said.
Catheterization. Early percutaneous coronary intervention benefits patients with cardiac arrest, even those without ST-segment elevation MI, studies suggest. Consider transferring the patient for cardiac catheterization. It’s okay to cool the body and then transfer for catheterization. This may become a more common model as care after cardiac arrest becomes more regionalized, he said.
Dr. Vissers said he has no relevant conflicts of interest.
cardiopulmonary resuscitation CPR, chest compressions, cardioversion defibrillation, capnography
SAN FRANCISCO – The alphabet is changing for critical care of patients in cardiac arrest.
"A is for airway" is no longer at the top of the list. The ABCs (airway, breathing, and circulation) of cardiopulmonary resuscitation have been replaced by an emphasis on CAB – compressions, airway, and breathing, in that order.
The American Heart Association promotes the "CPR is as easy as C-A-B" slogan, and the key to success in treating cardiac arrest is high-quality, uninterrupted chest compressions, Dr. Robert J. Vissers said at the annual meeting of the American College of Emergency Physicians.
"Airway may not always come first" if the patient has lost perfusion and circulation, said Dr. Vissers, chief of emergency medicine at Legacy Emanuel Medical Center, Portland, Ore. "It’s hard for me to say, because I’m an airway guy."
While "C" stands for compressions, it also serves to remind physicians to attend to cardioversion, capnography, cooling, and catheterization, if needed. Dr. Vissers addressed each of these in more detail. "These are the things that recently have led to pretty substantial improvements in the outcomes of these patients," he said.
Compressions. With high-quality, uninterrupted chest compressions, the patient gets good passive ventilation, which may be superior to positive pressure ventilation in these situations. Aim for 30 compressions per breath. Consider creating a supraglottic airway without interrupting the CPR, he said.
Put some muscle into it to maintain compressions 2 inches in depth with full recoil, at a rate of 100 compressions per minute. If more than one person is available, take turns applying compressions to reduce fatigue. Monitor the patient closely with end-tidal capnography. (See below.)
Proper compressions restore cerebral and coronary perfusion. Sustained coronary perfusion pressure is critical to successful defibrillation.
Cardioversion. The first 4 minutes after cardiac arrest provide the greatest chance of successful cardioversion (defibrillation). If more than 4 minutes have elapsed, reperfuse the myocardium with a few minutes of chest compressions before applying shock. Wait 2 minutes after defibrillation to check the pulse, and maintain compressions during that time.
The traditional admonition to "clear!" before shocking may not be necessary, Dr. Vissers said. Studies have shown that no appreciable electrical current reaches the people applying compressions if they are wearing gloves and a biphasic defibrillator is used for cardioversion.
Capnography. Confirm proper tube placement for capnography, which helps assess the quality of the CPR and identify return of spontaneous circulation without checking pulses. Capnography readings also help predict outcome.
"I think capnography is one of the most underutilized tools that we have for the critically ill patient," Dr. Vissers said.
High-quality compressions and coronary perfusion pressures correlate with end-tidal carbon dioxide (ETCO2) levels of 20-25 mm Hg on capnography. A sudden rise in ETCO2 suggests return of spontaneous circulation and is more sensitive than manual pulse checks. If ETCO2 readings persistently stay below 10 mm Hg, return of spontaneous circulation is unlikely. In studies, an ETCO2 less than 10 mm Hg after 20 minutes of compressions was associated with zero chance of return of spontaneous circulation.
Cooling. For unconscious adults who went into cardiac arrest outside of hospital care, cooling the body to 32-34° C for 12-24 hours improves chances of a good outcome, Dr. Vissers said. Applying ice packs to the groin, axilla, and neck will cool the body about 0.2-1° C per hour. The best cooling method may be cooling blankets that circulate cooled water through material designed to promote heat exchange. The blankets cool a body on average by 1-1.5° C per hour.
Used in combination, the ice packs can be removed when the body temperature reaches 33° C and the blankets left on to maintain the cool temperature for 12-24 hours. "That works very well," he said. Cooled normal saline infusions or cooling catheters also are options for cooling a body after cardiac arrest.
Of every 4-13 patients cooled after cardiac arrest, 1 will leave the hospital neurologically intact, he said.
Catheterization. Early percutaneous coronary intervention benefits patients with cardiac arrest, even those without ST-segment elevation MI, studies suggest. Consider transferring the patient for cardiac catheterization. It’s okay to cool the body and then transfer for catheterization. This may become a more common model as care after cardiac arrest becomes more regionalized, he said.
Dr. Vissers said he has no relevant conflicts of interest.
SAN FRANCISCO – The alphabet is changing for critical care of patients in cardiac arrest.
"A is for airway" is no longer at the top of the list. The ABCs (airway, breathing, and circulation) of cardiopulmonary resuscitation have been replaced by an emphasis on CAB – compressions, airway, and breathing, in that order.
The American Heart Association promotes the "CPR is as easy as C-A-B" slogan, and the key to success in treating cardiac arrest is high-quality, uninterrupted chest compressions, Dr. Robert J. Vissers said at the annual meeting of the American College of Emergency Physicians.
"Airway may not always come first" if the patient has lost perfusion and circulation, said Dr. Vissers, chief of emergency medicine at Legacy Emanuel Medical Center, Portland, Ore. "It’s hard for me to say, because I’m an airway guy."
While "C" stands for compressions, it also serves to remind physicians to attend to cardioversion, capnography, cooling, and catheterization, if needed. Dr. Vissers addressed each of these in more detail. "These are the things that recently have led to pretty substantial improvements in the outcomes of these patients," he said.
Compressions. With high-quality, uninterrupted chest compressions, the patient gets good passive ventilation, which may be superior to positive pressure ventilation in these situations. Aim for 30 compressions per breath. Consider creating a supraglottic airway without interrupting the CPR, he said.
Put some muscle into it to maintain compressions 2 inches in depth with full recoil, at a rate of 100 compressions per minute. If more than one person is available, take turns applying compressions to reduce fatigue. Monitor the patient closely with end-tidal capnography. (See below.)
Proper compressions restore cerebral and coronary perfusion. Sustained coronary perfusion pressure is critical to successful defibrillation.
Cardioversion. The first 4 minutes after cardiac arrest provide the greatest chance of successful cardioversion (defibrillation). If more than 4 minutes have elapsed, reperfuse the myocardium with a few minutes of chest compressions before applying shock. Wait 2 minutes after defibrillation to check the pulse, and maintain compressions during that time.
The traditional admonition to "clear!" before shocking may not be necessary, Dr. Vissers said. Studies have shown that no appreciable electrical current reaches the people applying compressions if they are wearing gloves and a biphasic defibrillator is used for cardioversion.
Capnography. Confirm proper tube placement for capnography, which helps assess the quality of the CPR and identify return of spontaneous circulation without checking pulses. Capnography readings also help predict outcome.
"I think capnography is one of the most underutilized tools that we have for the critically ill patient," Dr. Vissers said.
High-quality compressions and coronary perfusion pressures correlate with end-tidal carbon dioxide (ETCO2) levels of 20-25 mm Hg on capnography. A sudden rise in ETCO2 suggests return of spontaneous circulation and is more sensitive than manual pulse checks. If ETCO2 readings persistently stay below 10 mm Hg, return of spontaneous circulation is unlikely. In studies, an ETCO2 less than 10 mm Hg after 20 minutes of compressions was associated with zero chance of return of spontaneous circulation.
Cooling. For unconscious adults who went into cardiac arrest outside of hospital care, cooling the body to 32-34° C for 12-24 hours improves chances of a good outcome, Dr. Vissers said. Applying ice packs to the groin, axilla, and neck will cool the body about 0.2-1° C per hour. The best cooling method may be cooling blankets that circulate cooled water through material designed to promote heat exchange. The blankets cool a body on average by 1-1.5° C per hour.
Used in combination, the ice packs can be removed when the body temperature reaches 33° C and the blankets left on to maintain the cool temperature for 12-24 hours. "That works very well," he said. Cooled normal saline infusions or cooling catheters also are options for cooling a body after cardiac arrest.
Of every 4-13 patients cooled after cardiac arrest, 1 will leave the hospital neurologically intact, he said.
Catheterization. Early percutaneous coronary intervention benefits patients with cardiac arrest, even those without ST-segment elevation MI, studies suggest. Consider transferring the patient for cardiac catheterization. It’s okay to cool the body and then transfer for catheterization. This may become a more common model as care after cardiac arrest becomes more regionalized, he said.
Dr. Vissers said he has no relevant conflicts of interest.
cardiopulmonary resuscitation CPR, chest compressions, cardioversion defibrillation, capnography
cardiopulmonary resuscitation CPR, chest compressions, cardioversion defibrillation, capnography
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Defensive Medicine Factors Into Cardiac Admissions
SAN FRANCISCO – Liability concerns may drive emergency physicians’ decisions regarding patients with possible cardiac conditions, based on the results of two studies presented at the Scientific Assembly of the American College of Emergency Physicians.
Many emergency physicians weighed legal concerns more heavily than actual risk when considering whether to admit a patient for acute coronary syndrome, concluded Dr. David H. Newman and his colleagues.
The conclusion was based on an observational, matched-pairs survey conducted at the emergency departments of St. Luke’s Hospital and Roosevelt Hospital in New York. Patients who were admitted "primarily for acute coronary syndrome" were surveyed after they had discussed their admission with the physician. The admitting doctor also completed a survey after communicating with the patient.
Both were asked whether risk and prognosis were discussed, as well as about the perceived potential benefits of admission and perceived primary purpose of admission.
"Doctors and patients in the emergency department are communicating poorly about the risks of death and heart attack, and this is something we need to fix."
When asked to place themselves in the same position as the patient they had just evaluated, physicians often said that they would not have chosen admission for themselves but had admitted the patient, said Dr. Newman, director of clinical research in the department of emergency medicine at Mount Sinai School of Medicine in New York.
During the 18 months of the study, 849 surveys were completed. All patients had primary or secondary complaints of chest pain. Just over half were men. One-third were black, 24% were Hispanic, 23% were white, and 19% were "other" or did not report a race. The largest proportion had attended some high school or graduated (39%), 25% had attended college, 14% had a bachelor’s degree, and 15% had a graduate or professional degree (Ann. Emerg. Med. 2011;58:S210).
Dr. Newman said in an interview that he and his colleagues were surprised to see that education level was not strongly correlated with risk communication or with agreement between the physician and the patient about true risk.
In a post hoc analysis, the authors calculated a mean risk of less than 5% for death, myocardial infarction, or revascularization within 30 days.
The physicians, however, estimated a mean risk for these outcomes of 15%, and patients estimated their risk at 33%.
One-third of patients and 48% of physicians said that coronary risk (the main reason for admission) had not been part of their discussion about admitting the patient. When coronary risk was discussed, agreement between the physician and the patient about the patient’s level of risk was 0.38 (about 40% more likely to agree, compared with random chance).
In 11% of cases, physicians said that concern about liability was one of the reasons for admission. That concern likely represents millions of dollars in health care spending, Dr. Newman said.
In 27% of the cases, the doctor reported that if they were a patient with the same risk, they would not stay overnight.
The results hint that "something is affecting patients’ decision to stay even when someone with a theoretically much more complete understanding of the risks – the doctor – would not stay," Dr. Newman said.
"It is possible that physicians do not recognize the degree to which legal concerns affect these conversations, or perhaps other system pressures [such as] financial incentives, crowding, resource utilization, [or] time are affecting this conversation," he said. "What we can say with confidence is this: Doctors and patients in the emergency department are communicating poorly about the risks of death and heart attack, and this is something we need to fix."
In another study, Dr. Patrick J. Lenehan of Morristown (N.J.) Hospital and colleagues found that a decreasing number of congestive heart failure patients were discharged from the emergency department in 1996-2010.
"It is possible that physicians do not recognize the degree to which legal concerns affect these conversations."
The authors retrospectively reviewed emergency department visits to 27 suburban, urban, and rural New York and New Jersey hospitals. The facilities had 18,000-72,000 annual visits. Using ICD9 codes, the researched identified patients who had likely CHF. This group included those who had CHF, heart failure, or pulmonary edema as a primary diagnosis, or as a secondary diagnosis if the primary was shortness of breath or dyspnea (Ann. Emerg. Med. 2011;58:S237).
Of 6.6 million emergency department visits, 82,230 (1%) were for CHF. Half of the patients were women, and their mean age was 72 years. The authors found that there was a 63% decrease in the number of patients discharged from 1996 to 2010. In 1996, 24% were discharged. By 2010, only 9% were discharged.
The pattern was the same for male and female patients. Given that there has been no increase in the mean patient age, the difference in discharges is not likely the result of an aging population, the authors said.
The "trend is mainly due to increasing concerns about medical malpractice litigation," they suggested.
The two studies indicate an ongoing crisis and the need to enact liability reform, said Dr. David Seaberg, ACEP president. "The rapidly rising tide of patients coupled with increasing hospital admissions from the emergency department will create pressure on the health system that is not sustainable," Dr. Seaberg said in a statement. "Liability reform could relieve some of that pressure and bring down costs."
No conflicts of interest were reported.
SAN FRANCISCO – Liability concerns may drive emergency physicians’ decisions regarding patients with possible cardiac conditions, based on the results of two studies presented at the Scientific Assembly of the American College of Emergency Physicians.
Many emergency physicians weighed legal concerns more heavily than actual risk when considering whether to admit a patient for acute coronary syndrome, concluded Dr. David H. Newman and his colleagues.
The conclusion was based on an observational, matched-pairs survey conducted at the emergency departments of St. Luke’s Hospital and Roosevelt Hospital in New York. Patients who were admitted "primarily for acute coronary syndrome" were surveyed after they had discussed their admission with the physician. The admitting doctor also completed a survey after communicating with the patient.
Both were asked whether risk and prognosis were discussed, as well as about the perceived potential benefits of admission and perceived primary purpose of admission.
"Doctors and patients in the emergency department are communicating poorly about the risks of death and heart attack, and this is something we need to fix."
When asked to place themselves in the same position as the patient they had just evaluated, physicians often said that they would not have chosen admission for themselves but had admitted the patient, said Dr. Newman, director of clinical research in the department of emergency medicine at Mount Sinai School of Medicine in New York.
During the 18 months of the study, 849 surveys were completed. All patients had primary or secondary complaints of chest pain. Just over half were men. One-third were black, 24% were Hispanic, 23% were white, and 19% were "other" or did not report a race. The largest proportion had attended some high school or graduated (39%), 25% had attended college, 14% had a bachelor’s degree, and 15% had a graduate or professional degree (Ann. Emerg. Med. 2011;58:S210).
Dr. Newman said in an interview that he and his colleagues were surprised to see that education level was not strongly correlated with risk communication or with agreement between the physician and the patient about true risk.
In a post hoc analysis, the authors calculated a mean risk of less than 5% for death, myocardial infarction, or revascularization within 30 days.
The physicians, however, estimated a mean risk for these outcomes of 15%, and patients estimated their risk at 33%.
One-third of patients and 48% of physicians said that coronary risk (the main reason for admission) had not been part of their discussion about admitting the patient. When coronary risk was discussed, agreement between the physician and the patient about the patient’s level of risk was 0.38 (about 40% more likely to agree, compared with random chance).
In 11% of cases, physicians said that concern about liability was one of the reasons for admission. That concern likely represents millions of dollars in health care spending, Dr. Newman said.
In 27% of the cases, the doctor reported that if they were a patient with the same risk, they would not stay overnight.
The results hint that "something is affecting patients’ decision to stay even when someone with a theoretically much more complete understanding of the risks – the doctor – would not stay," Dr. Newman said.
"It is possible that physicians do not recognize the degree to which legal concerns affect these conversations, or perhaps other system pressures [such as] financial incentives, crowding, resource utilization, [or] time are affecting this conversation," he said. "What we can say with confidence is this: Doctors and patients in the emergency department are communicating poorly about the risks of death and heart attack, and this is something we need to fix."
In another study, Dr. Patrick J. Lenehan of Morristown (N.J.) Hospital and colleagues found that a decreasing number of congestive heart failure patients were discharged from the emergency department in 1996-2010.
"It is possible that physicians do not recognize the degree to which legal concerns affect these conversations."
The authors retrospectively reviewed emergency department visits to 27 suburban, urban, and rural New York and New Jersey hospitals. The facilities had 18,000-72,000 annual visits. Using ICD9 codes, the researched identified patients who had likely CHF. This group included those who had CHF, heart failure, or pulmonary edema as a primary diagnosis, or as a secondary diagnosis if the primary was shortness of breath or dyspnea (Ann. Emerg. Med. 2011;58:S237).
Of 6.6 million emergency department visits, 82,230 (1%) were for CHF. Half of the patients were women, and their mean age was 72 years. The authors found that there was a 63% decrease in the number of patients discharged from 1996 to 2010. In 1996, 24% were discharged. By 2010, only 9% were discharged.
The pattern was the same for male and female patients. Given that there has been no increase in the mean patient age, the difference in discharges is not likely the result of an aging population, the authors said.
The "trend is mainly due to increasing concerns about medical malpractice litigation," they suggested.
The two studies indicate an ongoing crisis and the need to enact liability reform, said Dr. David Seaberg, ACEP president. "The rapidly rising tide of patients coupled with increasing hospital admissions from the emergency department will create pressure on the health system that is not sustainable," Dr. Seaberg said in a statement. "Liability reform could relieve some of that pressure and bring down costs."
No conflicts of interest were reported.
SAN FRANCISCO – Liability concerns may drive emergency physicians’ decisions regarding patients with possible cardiac conditions, based on the results of two studies presented at the Scientific Assembly of the American College of Emergency Physicians.
Many emergency physicians weighed legal concerns more heavily than actual risk when considering whether to admit a patient for acute coronary syndrome, concluded Dr. David H. Newman and his colleagues.
The conclusion was based on an observational, matched-pairs survey conducted at the emergency departments of St. Luke’s Hospital and Roosevelt Hospital in New York. Patients who were admitted "primarily for acute coronary syndrome" were surveyed after they had discussed their admission with the physician. The admitting doctor also completed a survey after communicating with the patient.
Both were asked whether risk and prognosis were discussed, as well as about the perceived potential benefits of admission and perceived primary purpose of admission.
"Doctors and patients in the emergency department are communicating poorly about the risks of death and heart attack, and this is something we need to fix."
When asked to place themselves in the same position as the patient they had just evaluated, physicians often said that they would not have chosen admission for themselves but had admitted the patient, said Dr. Newman, director of clinical research in the department of emergency medicine at Mount Sinai School of Medicine in New York.
During the 18 months of the study, 849 surveys were completed. All patients had primary or secondary complaints of chest pain. Just over half were men. One-third were black, 24% were Hispanic, 23% were white, and 19% were "other" or did not report a race. The largest proportion had attended some high school or graduated (39%), 25% had attended college, 14% had a bachelor’s degree, and 15% had a graduate or professional degree (Ann. Emerg. Med. 2011;58:S210).
Dr. Newman said in an interview that he and his colleagues were surprised to see that education level was not strongly correlated with risk communication or with agreement between the physician and the patient about true risk.
In a post hoc analysis, the authors calculated a mean risk of less than 5% for death, myocardial infarction, or revascularization within 30 days.
The physicians, however, estimated a mean risk for these outcomes of 15%, and patients estimated their risk at 33%.
One-third of patients and 48% of physicians said that coronary risk (the main reason for admission) had not been part of their discussion about admitting the patient. When coronary risk was discussed, agreement between the physician and the patient about the patient’s level of risk was 0.38 (about 40% more likely to agree, compared with random chance).
In 11% of cases, physicians said that concern about liability was one of the reasons for admission. That concern likely represents millions of dollars in health care spending, Dr. Newman said.
In 27% of the cases, the doctor reported that if they were a patient with the same risk, they would not stay overnight.
The results hint that "something is affecting patients’ decision to stay even when someone with a theoretically much more complete understanding of the risks – the doctor – would not stay," Dr. Newman said.
"It is possible that physicians do not recognize the degree to which legal concerns affect these conversations, or perhaps other system pressures [such as] financial incentives, crowding, resource utilization, [or] time are affecting this conversation," he said. "What we can say with confidence is this: Doctors and patients in the emergency department are communicating poorly about the risks of death and heart attack, and this is something we need to fix."
In another study, Dr. Patrick J. Lenehan of Morristown (N.J.) Hospital and colleagues found that a decreasing number of congestive heart failure patients were discharged from the emergency department in 1996-2010.
"It is possible that physicians do not recognize the degree to which legal concerns affect these conversations."
The authors retrospectively reviewed emergency department visits to 27 suburban, urban, and rural New York and New Jersey hospitals. The facilities had 18,000-72,000 annual visits. Using ICD9 codes, the researched identified patients who had likely CHF. This group included those who had CHF, heart failure, or pulmonary edema as a primary diagnosis, or as a secondary diagnosis if the primary was shortness of breath or dyspnea (Ann. Emerg. Med. 2011;58:S237).
Of 6.6 million emergency department visits, 82,230 (1%) were for CHF. Half of the patients were women, and their mean age was 72 years. The authors found that there was a 63% decrease in the number of patients discharged from 1996 to 2010. In 1996, 24% were discharged. By 2010, only 9% were discharged.
The pattern was the same for male and female patients. Given that there has been no increase in the mean patient age, the difference in discharges is not likely the result of an aging population, the authors said.
The "trend is mainly due to increasing concerns about medical malpractice litigation," they suggested.
The two studies indicate an ongoing crisis and the need to enact liability reform, said Dr. David Seaberg, ACEP president. "The rapidly rising tide of patients coupled with increasing hospital admissions from the emergency department will create pressure on the health system that is not sustainable," Dr. Seaberg said in a statement. "Liability reform could relieve some of that pressure and bring down costs."
No conflicts of interest were reported.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Be Prepared for Troublesome Tattoos, Problematic Piercings
SAN FRANCISCO – Body modifications are all the rage, so physicians need to know that troublesome tattoos can interfere with MRIs, and should keep a pair of pliers handy to deal with problematic piercings.
Approximately 36% of Americans aged 25-29 years have one or more tattoos. Piercings are most common among 16- to 20-year-olds, 47% of whom have rings, anchors, studs, or other metallic objects poking through various body parts. Some 10% of Americans aged 12-15 years and 27% of people aged 21-25 years have body piercings, Dr. Rachel L. Chin said at the annual meeting of the American College of Emergency Physicians.
Patients aren’t the only ones favoring the fashion.

"I don’t think I can name a single night nurse who doesn’t have more than one piercing other than in the ear," said Dr. Chin of San Francisco General Hospital and a professor of emergency medicine at the University of California, San Francisco.
Tattoo pigments may contain heavy metals and iron that act as conductors during MRI and can cause a burning sensation and intense pain. Although a 2002 survey of 1,032 patients with tattoos who underwent MRI reported no serious soft-tissue reactions or adverse events, the popularity of tattoos has grown astronomically in the past decade, and there now are many case reports of severe burning associated with tattoos and MRI, Dr. Chin said.
If this happens, apply a cool compress or ice packs, she suggested.
It’s difficult to know what’s in an individual’s tattoo. There are no federal regulations of tattoo pigments or studios that offer tattoos, and international pigment suppliers rarely produce lists of ingredients. Tattoo artists also may mix their own colors, and some use printer’s ink or automobile paint, she said. Most tattoo artists have had no formal training in anatomy, infection control, or universal precautions.
The Red Cross prohibits blood donations from anyone who has gotten a tattoo or piercing in the past 12 months unless the tattoo was applied by a studio certified by the Association of Professional Piercers or the Alliance of Professional Tattooists.
Tattoo recipients may show up with another common problem: infection. One study of 766 college students found that tattoos were associated with infection in 45%, local skin reactions in 39%, and hepatitis in two cases (Clin. Nurs. Res. 1999;8:368-85). Infection with hepatitis B and C, HIV, Pseudomonas, Staphylococcus, tetanus, and syphilis have been associated with tattoos. Tattoos from unlicensed artists were associated with outbreaks of methicillin-resistant S. aureus in Ohio, Kentucky, and Vermont.
Tattoo infections can be deadly. If you see a febrile patient with a recent tattoo and no other source of infection, consider the possibility of infective endocarditis, Dr. Chin said.
Another body modification technique called scarification is legal in some states, and regulations of shops vary by county or city. Customers may be branded using an electrocautery knife or may undergo scarring via a chemical burn, a tattoo gun without ink, or a scalpel to remove the outer layer of skin tissue. The design result relies solely on how well the body scars.
Piercing is a common practice in many cultures. In the United States, it most often involves rings in the earlobes, but rings, posts, rods, and dermal anchors are increasingly frequent in other body parts, including the nose, tongue, eyelid, lips, ear cartilage, nipples, belly, genitals, and more. When pop artist Lady Gaga showed up at the Grammy Awards sporting subdermal implants on her forehead, some fans began copying her.
One survey of 225 adolescents with piercings who were seen at an urban hospital found associated infection in 74%, bleeding in 30%, allergic reactions in 26%, and keloids in 19%, Dr. Chin said.
The upper ear cartilage is largely avascular, and thus prone to poor healing and more serious infection from piercing. In such cases, treat infection for staphylococcus or streptococcus infection (as well as methicillin-resistant S. aureus, if it’s a significant infection in your geographical area), but if the patient doesn’t improve after a few days of treatment, switch to ciprofloxacin and assess for Pseudomonas aeruginosa infection, she advised.
Tongue piercings can chip or fracture teeth and significantly increase the risk for gingival recession requiring gum surgery. Aspiration of tongue piercings have been reported during contact sports. Tongue piercings also have been associated with blood-borne infections (such as hepatitis and HIV), endocarditis, significant blood loss, and lingering pain, including trigeminal neuralgia.
Systemic infections that have been seen from body piercings include tetanus, acute poststreptococcal glomerulonephritis, streptococcal septicemia, staphylococcal toxic shock syndrome, and pseudomonal abscesses.
Any piercing can cause a traumatic laceration, which may be sutured just like any other laceration, she said.
Some penile piercings can lead to paraphimosis, and without prompt treatment the tissue ischemia may cause gangrene and autoamputation of the distal penis. Urethral injuries, infections, prolonged priapism, and recurrent condyloma acuminatum are other risks from male genital piercing. Female genital piercings increase the risk for vaginal lacerations, sexually transmitted diseases, and urinary tract infections.

Remind any patients with genital piercings to use condoms for any sexual contact, and to be aware that condoms may be torn by the body jewelry, Dr. Chin said.
Learn how to remove the most common kinds of body piercing jewelry, she suggested. These include barbell studs, labret studs, and bead rings, which may be removed by unscrewing and/or pulling on parts of the jewelry. A captive bead ring is most easily removed using ring expanding pliers or external snap ring pliers.
Pearling is another body modification technique in which small objects of various materials are placed beneath the skin of the penis, hands, or other body parts. The risks and healing characteristics are similar to those of any subdermal implants, and rejection can occur but is rare. Migration of the implanted material is common, however, both during and after healing.
At Dr. Chin’s institution, it’s not uncommon to see problematic penis rings, in which a metal ring that the patient has placed over his penis to keep an erection becomes stuck and interferes with blood flow. "We call the fire department" to come cut off the ring, she said. These patients can’t be given too much sedation, because the room must be free of excess oxygen when the fire department’s saw sends sparks flying.
If you see this problem and your fire department won’t come, call the orthopedics department. "They have the right tools" for the job, she said.
Dr. Chin said she has no relevant conflicts of interest.
SAN FRANCISCO – Body modifications are all the rage, so physicians need to know that troublesome tattoos can interfere with MRIs, and should keep a pair of pliers handy to deal with problematic piercings.
Approximately 36% of Americans aged 25-29 years have one or more tattoos. Piercings are most common among 16- to 20-year-olds, 47% of whom have rings, anchors, studs, or other metallic objects poking through various body parts. Some 10% of Americans aged 12-15 years and 27% of people aged 21-25 years have body piercings, Dr. Rachel L. Chin said at the annual meeting of the American College of Emergency Physicians.
Patients aren’t the only ones favoring the fashion.
"I don’t think I can name a single night nurse who doesn’t have more than one piercing other than in the ear," said Dr. Chin of San Francisco General Hospital and a professor of emergency medicine at the University of California, San Francisco.
Tattoo pigments may contain heavy metals and iron that act as conductors during MRI and can cause a burning sensation and intense pain. Although a 2002 survey of 1,032 patients with tattoos who underwent MRI reported no serious soft-tissue reactions or adverse events, the popularity of tattoos has grown astronomically in the past decade, and there now are many case reports of severe burning associated with tattoos and MRI, Dr. Chin said.
If this happens, apply a cool compress or ice packs, she suggested.
It’s difficult to know what’s in an individual’s tattoo. There are no federal regulations of tattoo pigments or studios that offer tattoos, and international pigment suppliers rarely produce lists of ingredients. Tattoo artists also may mix their own colors, and some use printer’s ink or automobile paint, she said. Most tattoo artists have had no formal training in anatomy, infection control, or universal precautions.
The Red Cross prohibits blood donations from anyone who has gotten a tattoo or piercing in the past 12 months unless the tattoo was applied by a studio certified by the Association of Professional Piercers or the Alliance of Professional Tattooists.
Tattoo recipients may show up with another common problem: infection. One study of 766 college students found that tattoos were associated with infection in 45%, local skin reactions in 39%, and hepatitis in two cases (Clin. Nurs. Res. 1999;8:368-85). Infection with hepatitis B and C, HIV, Pseudomonas, Staphylococcus, tetanus, and syphilis have been associated with tattoos. Tattoos from unlicensed artists were associated with outbreaks of methicillin-resistant S. aureus in Ohio, Kentucky, and Vermont.
Tattoo infections can be deadly. If you see a febrile patient with a recent tattoo and no other source of infection, consider the possibility of infective endocarditis, Dr. Chin said.
Another body modification technique called scarification is legal in some states, and regulations of shops vary by county or city. Customers may be branded using an electrocautery knife or may undergo scarring via a chemical burn, a tattoo gun without ink, or a scalpel to remove the outer layer of skin tissue. The design result relies solely on how well the body scars.
Piercing is a common practice in many cultures. In the United States, it most often involves rings in the earlobes, but rings, posts, rods, and dermal anchors are increasingly frequent in other body parts, including the nose, tongue, eyelid, lips, ear cartilage, nipples, belly, genitals, and more. When pop artist Lady Gaga showed up at the Grammy Awards sporting subdermal implants on her forehead, some fans began copying her.
One survey of 225 adolescents with piercings who were seen at an urban hospital found associated infection in 74%, bleeding in 30%, allergic reactions in 26%, and keloids in 19%, Dr. Chin said.
The upper ear cartilage is largely avascular, and thus prone to poor healing and more serious infection from piercing. In such cases, treat infection for staphylococcus or streptococcus infection (as well as methicillin-resistant S. aureus, if it’s a significant infection in your geographical area), but if the patient doesn’t improve after a few days of treatment, switch to ciprofloxacin and assess for Pseudomonas aeruginosa infection, she advised.
Tongue piercings can chip or fracture teeth and significantly increase the risk for gingival recession requiring gum surgery. Aspiration of tongue piercings have been reported during contact sports. Tongue piercings also have been associated with blood-borne infections (such as hepatitis and HIV), endocarditis, significant blood loss, and lingering pain, including trigeminal neuralgia.
Systemic infections that have been seen from body piercings include tetanus, acute poststreptococcal glomerulonephritis, streptococcal septicemia, staphylococcal toxic shock syndrome, and pseudomonal abscesses.
Any piercing can cause a traumatic laceration, which may be sutured just like any other laceration, she said.
Some penile piercings can lead to paraphimosis, and without prompt treatment the tissue ischemia may cause gangrene and autoamputation of the distal penis. Urethral injuries, infections, prolonged priapism, and recurrent condyloma acuminatum are other risks from male genital piercing. Female genital piercings increase the risk for vaginal lacerations, sexually transmitted diseases, and urinary tract infections.
Remind any patients with genital piercings to use condoms for any sexual contact, and to be aware that condoms may be torn by the body jewelry, Dr. Chin said.
Learn how to remove the most common kinds of body piercing jewelry, she suggested. These include barbell studs, labret studs, and bead rings, which may be removed by unscrewing and/or pulling on parts of the jewelry. A captive bead ring is most easily removed using ring expanding pliers or external snap ring pliers.
Pearling is another body modification technique in which small objects of various materials are placed beneath the skin of the penis, hands, or other body parts. The risks and healing characteristics are similar to those of any subdermal implants, and rejection can occur but is rare. Migration of the implanted material is common, however, both during and after healing.
At Dr. Chin’s institution, it’s not uncommon to see problematic penis rings, in which a metal ring that the patient has placed over his penis to keep an erection becomes stuck and interferes with blood flow. "We call the fire department" to come cut off the ring, she said. These patients can’t be given too much sedation, because the room must be free of excess oxygen when the fire department’s saw sends sparks flying.
If you see this problem and your fire department won’t come, call the orthopedics department. "They have the right tools" for the job, she said.
Dr. Chin said she has no relevant conflicts of interest.
SAN FRANCISCO – Body modifications are all the rage, so physicians need to know that troublesome tattoos can interfere with MRIs, and should keep a pair of pliers handy to deal with problematic piercings.
Approximately 36% of Americans aged 25-29 years have one or more tattoos. Piercings are most common among 16- to 20-year-olds, 47% of whom have rings, anchors, studs, or other metallic objects poking through various body parts. Some 10% of Americans aged 12-15 years and 27% of people aged 21-25 years have body piercings, Dr. Rachel L. Chin said at the annual meeting of the American College of Emergency Physicians.
Patients aren’t the only ones favoring the fashion.
"I don’t think I can name a single night nurse who doesn’t have more than one piercing other than in the ear," said Dr. Chin of San Francisco General Hospital and a professor of emergency medicine at the University of California, San Francisco.
Tattoo pigments may contain heavy metals and iron that act as conductors during MRI and can cause a burning sensation and intense pain. Although a 2002 survey of 1,032 patients with tattoos who underwent MRI reported no serious soft-tissue reactions or adverse events, the popularity of tattoos has grown astronomically in the past decade, and there now are many case reports of severe burning associated with tattoos and MRI, Dr. Chin said.
If this happens, apply a cool compress or ice packs, she suggested.
It’s difficult to know what’s in an individual’s tattoo. There are no federal regulations of tattoo pigments or studios that offer tattoos, and international pigment suppliers rarely produce lists of ingredients. Tattoo artists also may mix their own colors, and some use printer’s ink or automobile paint, she said. Most tattoo artists have had no formal training in anatomy, infection control, or universal precautions.
The Red Cross prohibits blood donations from anyone who has gotten a tattoo or piercing in the past 12 months unless the tattoo was applied by a studio certified by the Association of Professional Piercers or the Alliance of Professional Tattooists.
Tattoo recipients may show up with another common problem: infection. One study of 766 college students found that tattoos were associated with infection in 45%, local skin reactions in 39%, and hepatitis in two cases (Clin. Nurs. Res. 1999;8:368-85). Infection with hepatitis B and C, HIV, Pseudomonas, Staphylococcus, tetanus, and syphilis have been associated with tattoos. Tattoos from unlicensed artists were associated with outbreaks of methicillin-resistant S. aureus in Ohio, Kentucky, and Vermont.
Tattoo infections can be deadly. If you see a febrile patient with a recent tattoo and no other source of infection, consider the possibility of infective endocarditis, Dr. Chin said.
Another body modification technique called scarification is legal in some states, and regulations of shops vary by county or city. Customers may be branded using an electrocautery knife or may undergo scarring via a chemical burn, a tattoo gun without ink, or a scalpel to remove the outer layer of skin tissue. The design result relies solely on how well the body scars.
Piercing is a common practice in many cultures. In the United States, it most often involves rings in the earlobes, but rings, posts, rods, and dermal anchors are increasingly frequent in other body parts, including the nose, tongue, eyelid, lips, ear cartilage, nipples, belly, genitals, and more. When pop artist Lady Gaga showed up at the Grammy Awards sporting subdermal implants on her forehead, some fans began copying her.
One survey of 225 adolescents with piercings who were seen at an urban hospital found associated infection in 74%, bleeding in 30%, allergic reactions in 26%, and keloids in 19%, Dr. Chin said.
The upper ear cartilage is largely avascular, and thus prone to poor healing and more serious infection from piercing. In such cases, treat infection for staphylococcus or streptococcus infection (as well as methicillin-resistant S. aureus, if it’s a significant infection in your geographical area), but if the patient doesn’t improve after a few days of treatment, switch to ciprofloxacin and assess for Pseudomonas aeruginosa infection, she advised.
Tongue piercings can chip or fracture teeth and significantly increase the risk for gingival recession requiring gum surgery. Aspiration of tongue piercings have been reported during contact sports. Tongue piercings also have been associated with blood-borne infections (such as hepatitis and HIV), endocarditis, significant blood loss, and lingering pain, including trigeminal neuralgia.
Systemic infections that have been seen from body piercings include tetanus, acute poststreptococcal glomerulonephritis, streptococcal septicemia, staphylococcal toxic shock syndrome, and pseudomonal abscesses.
Any piercing can cause a traumatic laceration, which may be sutured just like any other laceration, she said.
Some penile piercings can lead to paraphimosis, and without prompt treatment the tissue ischemia may cause gangrene and autoamputation of the distal penis. Urethral injuries, infections, prolonged priapism, and recurrent condyloma acuminatum are other risks from male genital piercing. Female genital piercings increase the risk for vaginal lacerations, sexually transmitted diseases, and urinary tract infections.
Remind any patients with genital piercings to use condoms for any sexual contact, and to be aware that condoms may be torn by the body jewelry, Dr. Chin said.
Learn how to remove the most common kinds of body piercing jewelry, she suggested. These include barbell studs, labret studs, and bead rings, which may be removed by unscrewing and/or pulling on parts of the jewelry. A captive bead ring is most easily removed using ring expanding pliers or external snap ring pliers.
Pearling is another body modification technique in which small objects of various materials are placed beneath the skin of the penis, hands, or other body parts. The risks and healing characteristics are similar to those of any subdermal implants, and rejection can occur but is rare. Migration of the implanted material is common, however, both during and after healing.
At Dr. Chin’s institution, it’s not uncommon to see problematic penis rings, in which a metal ring that the patient has placed over his penis to keep an erection becomes stuck and interferes with blood flow. "We call the fire department" to come cut off the ring, she said. These patients can’t be given too much sedation, because the room must be free of excess oxygen when the fire department’s saw sends sparks flying.
If you see this problem and your fire department won’t come, call the orthopedics department. "They have the right tools" for the job, she said.
Dr. Chin said she has no relevant conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Dispel Myths to Recognize Child Abuse
SAN FRANCISCO – The color of a bruise indicates its age. You’ll almost always see bruising when a child has a fracture. Sexual abuse leaves behind physical exam findings.
These are all myths that can get in the way of physicians recognizing abuse of an infant or child. Physicians are required by law to report all suspicions of nonaccidental trauma, a catch-all term for child abuse, shaken baby syndrome, and battered-child syndrome.

Physicians can meet that obligation by ignoring these myths, recognizing red flags for nonaccidental trauma, and being familiar with signs of accidental trauma or medical conditions that can mimic the physical findings of nonaccidental trauma, Dr. Maureen D. McCollough said at the annual meeting of the American College of Emergency Physicians.
Myth: The age of bruises can be accurately determined by their color – red, purple, yellow, green, or brown. In reality, there is no predictable order or chronology of color in bruising, and even in the same person bruises of similar ages may have different colors, said Dr. McCollough of the University of Southern California, Los Angeles, and director of pediatric emergency medicine at Los Angeles County USC Medical Center.
Studies have shown poor interobserver reliability in assessing bruise coloring and poor physician accuracy in characterizing coloring.
Red flags of suspicion should go up if you see multiple bruises or lacerations, or see them in unusual locations. Accidental toddler tumbles can produce multiple bruises, but generally these are on bony prominences. Unusual locations for pediatric bruising include the lower back, buttocks, cheeks, ears, or neck. Bruising anywhere in an infant who is not yet mobile is suspicious.
"Remember, if you don’t cruise, you don’t bruise," she said.
Be suspicious if the pattern of the marks, bruises, or lacerations remind you of an object like a hand, hairbrush, belt, or buckle. Bruises around wrists or extremities may be from the child being tied up. Tight elastic socks can leave a mark around an infant’s leg that mimics this, in which case the parent should be able to provide a sock with dimensions that match the bruising.
Visible injuries around a baby’s mouth or frenulum should raise a red flag for forced feeding. Genital injuries may indicate forced toilet training. Hair pulling produces characteristic marks of traumatic alopecia – an incompletely bald child with diffuse alopecia, broken hairs, and no loose hairs at the periphery.
A wide variety of problems can mimic the visual signs of nonaccidental bruising, including dermal melanosis, vitamin K deficiency, leukemia, hemophilia, millipede secretions, Ehlers-Danlos syndrome, dermatitis, lice, and more.
An equally impressive array of events can mimic the look of abusive burns, bullae, and erythema. These include the cultural practices of coining, cupping, spooning, or moxibustion, skin infections, allergic reactions, herpes or varicella infection, diaper dermatitis, impetigo, and more.
Accidental burns usually have a typical "splash" pattern if liquid is involved, or a child who grasps something hot will have burns on the volar aspect of the fingers and palm. Accidental cigarette burns usually have a streaky appearance.
If there are no splash marks, or there is a sharp line of demarcation, or burns are limited to the perineum, consider that the child may have been forcibly immersed in something hot. Intentional cigarette burns tend to be similar in size – often 5-mm circles – and create injuries from bullae to deep craters that scab over. These usually are on the palms or soles but can be anywhere on the body. Again, be suspicious if you see a burn mark that looks like an object, such as a radiator or an iron.
Myth: Fractures usually are associated with overlying bruising. In fact, children with inflicted skeletal fractures often have no associated bruising. Bruising is present in only 43% of skull fractures and less than 20% of lower extremity fractures in cases of abuse, Dr. McCollough said.
Infants who can’t walk shouldn’t fracture. Spiral fractures caused by the twisting of a long bone such as the femur suggest nonaccidental trauma. Toddler spiral fractures of the tibia, on the other hand, are very common, caused when a leg is trapped under the body during a fall, such as getting a leg caught in a couch. "This is not abuse," she said.
Raise the red flags when you see swelling of a body part that is out of proportion to a described injury; this may indicate an underlying fracture. A diaphyseal (midshaft) fracture in a child less than 3 years old is suspect, and metaphyseal or epiphyseal fractures beyond the newborn period (also called corner fractures or bucket handle fractures) are virtually diagnostic of abuse.
The posterior ribs are the most common area of nonaccidental rib fractures.
Suspect head injuries and possible abuse if the child has unexplained seizures, vomiting, changes in neurological or mental status, or large scalp hematomas. Be suspicious if the parents’ explanation changes over time, if there is intracranial bleeds after "minimal" trauma, or if you find retinal hemorrhages outside of the newborn period, she said.
Myth: Sexual abuse leaves physical findings. More myths: A colposcope is needed to detect sexual abuse, and some girls are born without hymens.
Although hymens come in a wide variety of shapes and sizes, a study of more than 1,100 newborn girls showed that all of them had one, she noted. Reviews of cases of sexual abuse show that physical exam findings of pediatric sexual abuse are rare because the tissue is very elastic and heals quickly.
Physical evidence will be more likely if force was used, if the child resisted, if there are great differences in the sizes and ages of the perpetrator and victim, and if a foreign object was forced into the mouth, vagina, or anus. Bruising or bite marks on a child’s penis may suggest nonaccidental trauma from forced toilet training.
When you see visible clues to what may be abuse, photograph or draw what you see and include something in the image to show size or scale. Don’t just rely on written notes, she said.
SAN FRANCISCO – The color of a bruise indicates its age. You’ll almost always see bruising when a child has a fracture. Sexual abuse leaves behind physical exam findings.
These are all myths that can get in the way of physicians recognizing abuse of an infant or child. Physicians are required by law to report all suspicions of nonaccidental trauma, a catch-all term for child abuse, shaken baby syndrome, and battered-child syndrome.
Physicians can meet that obligation by ignoring these myths, recognizing red flags for nonaccidental trauma, and being familiar with signs of accidental trauma or medical conditions that can mimic the physical findings of nonaccidental trauma, Dr. Maureen D. McCollough said at the annual meeting of the American College of Emergency Physicians.
Myth: The age of bruises can be accurately determined by their color – red, purple, yellow, green, or brown. In reality, there is no predictable order or chronology of color in bruising, and even in the same person bruises of similar ages may have different colors, said Dr. McCollough of the University of Southern California, Los Angeles, and director of pediatric emergency medicine at Los Angeles County USC Medical Center.
Studies have shown poor interobserver reliability in assessing bruise coloring and poor physician accuracy in characterizing coloring.
Red flags of suspicion should go up if you see multiple bruises or lacerations, or see them in unusual locations. Accidental toddler tumbles can produce multiple bruises, but generally these are on bony prominences. Unusual locations for pediatric bruising include the lower back, buttocks, cheeks, ears, or neck. Bruising anywhere in an infant who is not yet mobile is suspicious.
"Remember, if you don’t cruise, you don’t bruise," she said.
Be suspicious if the pattern of the marks, bruises, or lacerations remind you of an object like a hand, hairbrush, belt, or buckle. Bruises around wrists or extremities may be from the child being tied up. Tight elastic socks can leave a mark around an infant’s leg that mimics this, in which case the parent should be able to provide a sock with dimensions that match the bruising.
Visible injuries around a baby’s mouth or frenulum should raise a red flag for forced feeding. Genital injuries may indicate forced toilet training. Hair pulling produces characteristic marks of traumatic alopecia – an incompletely bald child with diffuse alopecia, broken hairs, and no loose hairs at the periphery.
A wide variety of problems can mimic the visual signs of nonaccidental bruising, including dermal melanosis, vitamin K deficiency, leukemia, hemophilia, millipede secretions, Ehlers-Danlos syndrome, dermatitis, lice, and more.
An equally impressive array of events can mimic the look of abusive burns, bullae, and erythema. These include the cultural practices of coining, cupping, spooning, or moxibustion, skin infections, allergic reactions, herpes or varicella infection, diaper dermatitis, impetigo, and more.
Accidental burns usually have a typical "splash" pattern if liquid is involved, or a child who grasps something hot will have burns on the volar aspect of the fingers and palm. Accidental cigarette burns usually have a streaky appearance.
If there are no splash marks, or there is a sharp line of demarcation, or burns are limited to the perineum, consider that the child may have been forcibly immersed in something hot. Intentional cigarette burns tend to be similar in size – often 5-mm circles – and create injuries from bullae to deep craters that scab over. These usually are on the palms or soles but can be anywhere on the body. Again, be suspicious if you see a burn mark that looks like an object, such as a radiator or an iron.
Myth: Fractures usually are associated with overlying bruising. In fact, children with inflicted skeletal fractures often have no associated bruising. Bruising is present in only 43% of skull fractures and less than 20% of lower extremity fractures in cases of abuse, Dr. McCollough said.
Infants who can’t walk shouldn’t fracture. Spiral fractures caused by the twisting of a long bone such as the femur suggest nonaccidental trauma. Toddler spiral fractures of the tibia, on the other hand, are very common, caused when a leg is trapped under the body during a fall, such as getting a leg caught in a couch. "This is not abuse," she said.
Raise the red flags when you see swelling of a body part that is out of proportion to a described injury; this may indicate an underlying fracture. A diaphyseal (midshaft) fracture in a child less than 3 years old is suspect, and metaphyseal or epiphyseal fractures beyond the newborn period (also called corner fractures or bucket handle fractures) are virtually diagnostic of abuse.
The posterior ribs are the most common area of nonaccidental rib fractures.
Suspect head injuries and possible abuse if the child has unexplained seizures, vomiting, changes in neurological or mental status, or large scalp hematomas. Be suspicious if the parents’ explanation changes over time, if there is intracranial bleeds after "minimal" trauma, or if you find retinal hemorrhages outside of the newborn period, she said.
Myth: Sexual abuse leaves physical findings. More myths: A colposcope is needed to detect sexual abuse, and some girls are born without hymens.
Although hymens come in a wide variety of shapes and sizes, a study of more than 1,100 newborn girls showed that all of them had one, she noted. Reviews of cases of sexual abuse show that physical exam findings of pediatric sexual abuse are rare because the tissue is very elastic and heals quickly.
Physical evidence will be more likely if force was used, if the child resisted, if there are great differences in the sizes and ages of the perpetrator and victim, and if a foreign object was forced into the mouth, vagina, or anus. Bruising or bite marks on a child’s penis may suggest nonaccidental trauma from forced toilet training.
When you see visible clues to what may be abuse, photograph or draw what you see and include something in the image to show size or scale. Don’t just rely on written notes, she said.
SAN FRANCISCO – The color of a bruise indicates its age. You’ll almost always see bruising when a child has a fracture. Sexual abuse leaves behind physical exam findings.
These are all myths that can get in the way of physicians recognizing abuse of an infant or child. Physicians are required by law to report all suspicions of nonaccidental trauma, a catch-all term for child abuse, shaken baby syndrome, and battered-child syndrome.
Physicians can meet that obligation by ignoring these myths, recognizing red flags for nonaccidental trauma, and being familiar with signs of accidental trauma or medical conditions that can mimic the physical findings of nonaccidental trauma, Dr. Maureen D. McCollough said at the annual meeting of the American College of Emergency Physicians.
Myth: The age of bruises can be accurately determined by their color – red, purple, yellow, green, or brown. In reality, there is no predictable order or chronology of color in bruising, and even in the same person bruises of similar ages may have different colors, said Dr. McCollough of the University of Southern California, Los Angeles, and director of pediatric emergency medicine at Los Angeles County USC Medical Center.
Studies have shown poor interobserver reliability in assessing bruise coloring and poor physician accuracy in characterizing coloring.
Red flags of suspicion should go up if you see multiple bruises or lacerations, or see them in unusual locations. Accidental toddler tumbles can produce multiple bruises, but generally these are on bony prominences. Unusual locations for pediatric bruising include the lower back, buttocks, cheeks, ears, or neck. Bruising anywhere in an infant who is not yet mobile is suspicious.
"Remember, if you don’t cruise, you don’t bruise," she said.
Be suspicious if the pattern of the marks, bruises, or lacerations remind you of an object like a hand, hairbrush, belt, or buckle. Bruises around wrists or extremities may be from the child being tied up. Tight elastic socks can leave a mark around an infant’s leg that mimics this, in which case the parent should be able to provide a sock with dimensions that match the bruising.
Visible injuries around a baby’s mouth or frenulum should raise a red flag for forced feeding. Genital injuries may indicate forced toilet training. Hair pulling produces characteristic marks of traumatic alopecia – an incompletely bald child with diffuse alopecia, broken hairs, and no loose hairs at the periphery.
A wide variety of problems can mimic the visual signs of nonaccidental bruising, including dermal melanosis, vitamin K deficiency, leukemia, hemophilia, millipede secretions, Ehlers-Danlos syndrome, dermatitis, lice, and more.
An equally impressive array of events can mimic the look of abusive burns, bullae, and erythema. These include the cultural practices of coining, cupping, spooning, or moxibustion, skin infections, allergic reactions, herpes or varicella infection, diaper dermatitis, impetigo, and more.
Accidental burns usually have a typical "splash" pattern if liquid is involved, or a child who grasps something hot will have burns on the volar aspect of the fingers and palm. Accidental cigarette burns usually have a streaky appearance.
If there are no splash marks, or there is a sharp line of demarcation, or burns are limited to the perineum, consider that the child may have been forcibly immersed in something hot. Intentional cigarette burns tend to be similar in size – often 5-mm circles – and create injuries from bullae to deep craters that scab over. These usually are on the palms or soles but can be anywhere on the body. Again, be suspicious if you see a burn mark that looks like an object, such as a radiator or an iron.
Myth: Fractures usually are associated with overlying bruising. In fact, children with inflicted skeletal fractures often have no associated bruising. Bruising is present in only 43% of skull fractures and less than 20% of lower extremity fractures in cases of abuse, Dr. McCollough said.
Infants who can’t walk shouldn’t fracture. Spiral fractures caused by the twisting of a long bone such as the femur suggest nonaccidental trauma. Toddler spiral fractures of the tibia, on the other hand, are very common, caused when a leg is trapped under the body during a fall, such as getting a leg caught in a couch. "This is not abuse," she said.
Raise the red flags when you see swelling of a body part that is out of proportion to a described injury; this may indicate an underlying fracture. A diaphyseal (midshaft) fracture in a child less than 3 years old is suspect, and metaphyseal or epiphyseal fractures beyond the newborn period (also called corner fractures or bucket handle fractures) are virtually diagnostic of abuse.
The posterior ribs are the most common area of nonaccidental rib fractures.
Suspect head injuries and possible abuse if the child has unexplained seizures, vomiting, changes in neurological or mental status, or large scalp hematomas. Be suspicious if the parents’ explanation changes over time, if there is intracranial bleeds after "minimal" trauma, or if you find retinal hemorrhages outside of the newborn period, she said.
Myth: Sexual abuse leaves physical findings. More myths: A colposcope is needed to detect sexual abuse, and some girls are born without hymens.
Although hymens come in a wide variety of shapes and sizes, a study of more than 1,100 newborn girls showed that all of them had one, she noted. Reviews of cases of sexual abuse show that physical exam findings of pediatric sexual abuse are rare because the tissue is very elastic and heals quickly.
Physical evidence will be more likely if force was used, if the child resisted, if there are great differences in the sizes and ages of the perpetrator and victim, and if a foreign object was forced into the mouth, vagina, or anus. Bruising or bite marks on a child’s penis may suggest nonaccidental trauma from forced toilet training.
When you see visible clues to what may be abuse, photograph or draw what you see and include something in the image to show size or scale. Don’t just rely on written notes, she said.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Simple Leg Raise Assesses 'Tank' in Septic Shock
SAN FRANCISCO – Before reaching for vasopressors to treat a patient in septic shock, physicians want to know that the patient has received enough fluid. Two traditional ways of assessing the patient’s "tank" both have limitations, but a relatively simple bedside procedure can predict the need for a fluid bolus.
Observing respiratory variations in arterial wave form analysis while health care workers raise a supine patient’s legs into a sitting position helps assess the volume status, also known as the pre-load or "the tank," in a patient with septic shock, Dr. Peter M. C. DeBlieux said at the annual meeting of the American College of Emergency Physicians.
"What that requires is a simple arterial line placed in either the radial or femoral artery, and then that’s transduced" and observed on a monitor with the heart rate, he said. Changes greater than 12%-15% in the pulse amplitude of the arterial wave form during either physiologic or mechanical breathing predicts that the patient would benefit from a fluid bolus, said Dr. DeBlieux, professor of medicine at Louisiana State University and professor of surgery at Tulane University, both in New Orleans.
This is more easily seen by raising the legs of a supine patient with septic shock. The patient’s head may be at a 45-degree angle, but the legs should start flat on the table. Two health care workers on either side of the bed should raise the patient’s legs to 90-degree angles at the hips and knees, as if the patient was in a sitting position, while observing the arterial tracing. If the arterial tracing shows at least a 12%-15% increase in pulse pressure, that warrants a fluid bolus.
"It’s a pretty simple thing to do at the bedside that changes management," he said.
Previously, volume status in patients with septic shock has been assessed by central venous pressure monitoring. Bedside ultrasound also has been used, focusing on the inferior vena cava and the collapsibility of the vena cava during normal respiratory cycles. A collapse of 20%-50% indicates that a fluid bolus would be beneficial. Both of these measures can give false elevations, however, if the patient has preexisting acute or chronic heart or lung disease.
Although an elevated central venous pressure (CVP) or collapsing inferior vena cava (IVC) on ultrasound during respiration indicated the need for a fluid bolus, "once the CVP is elevated or if you have a plethoric IVC, you’re left scratching your head," Dr. DeBlieux said. "Remember that any cardiac or pulmonary dysfunction gets immediately transmitted to the great vein," so the CVP may be high, or the IVC may look plethoric on ultrasound, but the patient may still need a fluid bolus.
"You would say that the tank is full, but you don’t know. I don’t know. We don’t know," he said.
Managing the tank corresponds with the first of three steps in the Surviving Sepsis Campaign's perfusion goals in early goal-directed therapy in acute care of septic shock. Dr. DeBlieux and some other educators refer to these as the tank, the hose and the pump for teaching purposes.
The tank goal is a CVP of 8-12 mm Hg through treatment with serial crystalloid fluid infusions.
The hose is marked by systemic vascular resistance. After addressing the tank, if the mean arterial blood pressure is lower than 65 mmHg, administer norepinephrine, dopamine or epinephrine to bring it up to 65 mm Hg. The medical literature supports any one of those three choices, but norepinephrine will produce fewer tachyarrhythmic events, he said.
In reality, managing the tank and hose may happen simultaneously because physicians may not want to wait for hours until the CVP gets to goal before administering vasopressors, he added.
The pump reflects oxygen delivery and utilization. After addressing the tank and hose, if the lactate level is greater than 4 mmol and central venous oxygen saturation (ScvO2) is less than 70%, consider giving dobutamine in the setting of left ventricular dysfunction, start invasive mechanical ventilation, and/or blood transfusion if the hemoglobin/hematocrit is less than 10/30 within 6 hours.
Dr. DeBlieux said he has no relevant conflicts of interest.
SAN FRANCISCO – Before reaching for vasopressors to treat a patient in septic shock, physicians want to know that the patient has received enough fluid. Two traditional ways of assessing the patient’s "tank" both have limitations, but a relatively simple bedside procedure can predict the need for a fluid bolus.
Observing respiratory variations in arterial wave form analysis while health care workers raise a supine patient’s legs into a sitting position helps assess the volume status, also known as the pre-load or "the tank," in a patient with septic shock, Dr. Peter M. C. DeBlieux said at the annual meeting of the American College of Emergency Physicians.
"What that requires is a simple arterial line placed in either the radial or femoral artery, and then that’s transduced" and observed on a monitor with the heart rate, he said. Changes greater than 12%-15% in the pulse amplitude of the arterial wave form during either physiologic or mechanical breathing predicts that the patient would benefit from a fluid bolus, said Dr. DeBlieux, professor of medicine at Louisiana State University and professor of surgery at Tulane University, both in New Orleans.
This is more easily seen by raising the legs of a supine patient with septic shock. The patient’s head may be at a 45-degree angle, but the legs should start flat on the table. Two health care workers on either side of the bed should raise the patient’s legs to 90-degree angles at the hips and knees, as if the patient was in a sitting position, while observing the arterial tracing. If the arterial tracing shows at least a 12%-15% increase in pulse pressure, that warrants a fluid bolus.
"It’s a pretty simple thing to do at the bedside that changes management," he said.
Previously, volume status in patients with septic shock has been assessed by central venous pressure monitoring. Bedside ultrasound also has been used, focusing on the inferior vena cava and the collapsibility of the vena cava during normal respiratory cycles. A collapse of 20%-50% indicates that a fluid bolus would be beneficial. Both of these measures can give false elevations, however, if the patient has preexisting acute or chronic heart or lung disease.
Although an elevated central venous pressure (CVP) or collapsing inferior vena cava (IVC) on ultrasound during respiration indicated the need for a fluid bolus, "once the CVP is elevated or if you have a plethoric IVC, you’re left scratching your head," Dr. DeBlieux said. "Remember that any cardiac or pulmonary dysfunction gets immediately transmitted to the great vein," so the CVP may be high, or the IVC may look plethoric on ultrasound, but the patient may still need a fluid bolus.
"You would say that the tank is full, but you don’t know. I don’t know. We don’t know," he said.
Managing the tank corresponds with the first of three steps in the Surviving Sepsis Campaign's perfusion goals in early goal-directed therapy in acute care of septic shock. Dr. DeBlieux and some other educators refer to these as the tank, the hose and the pump for teaching purposes.
The tank goal is a CVP of 8-12 mm Hg through treatment with serial crystalloid fluid infusions.
The hose is marked by systemic vascular resistance. After addressing the tank, if the mean arterial blood pressure is lower than 65 mmHg, administer norepinephrine, dopamine or epinephrine to bring it up to 65 mm Hg. The medical literature supports any one of those three choices, but norepinephrine will produce fewer tachyarrhythmic events, he said.
In reality, managing the tank and hose may happen simultaneously because physicians may not want to wait for hours until the CVP gets to goal before administering vasopressors, he added.
The pump reflects oxygen delivery and utilization. After addressing the tank and hose, if the lactate level is greater than 4 mmol and central venous oxygen saturation (ScvO2) is less than 70%, consider giving dobutamine in the setting of left ventricular dysfunction, start invasive mechanical ventilation, and/or blood transfusion if the hemoglobin/hematocrit is less than 10/30 within 6 hours.
Dr. DeBlieux said he has no relevant conflicts of interest.
SAN FRANCISCO – Before reaching for vasopressors to treat a patient in septic shock, physicians want to know that the patient has received enough fluid. Two traditional ways of assessing the patient’s "tank" both have limitations, but a relatively simple bedside procedure can predict the need for a fluid bolus.
Observing respiratory variations in arterial wave form analysis while health care workers raise a supine patient’s legs into a sitting position helps assess the volume status, also known as the pre-load or "the tank," in a patient with septic shock, Dr. Peter M. C. DeBlieux said at the annual meeting of the American College of Emergency Physicians.
"What that requires is a simple arterial line placed in either the radial or femoral artery, and then that’s transduced" and observed on a monitor with the heart rate, he said. Changes greater than 12%-15% in the pulse amplitude of the arterial wave form during either physiologic or mechanical breathing predicts that the patient would benefit from a fluid bolus, said Dr. DeBlieux, professor of medicine at Louisiana State University and professor of surgery at Tulane University, both in New Orleans.
This is more easily seen by raising the legs of a supine patient with septic shock. The patient’s head may be at a 45-degree angle, but the legs should start flat on the table. Two health care workers on either side of the bed should raise the patient’s legs to 90-degree angles at the hips and knees, as if the patient was in a sitting position, while observing the arterial tracing. If the arterial tracing shows at least a 12%-15% increase in pulse pressure, that warrants a fluid bolus.
"It’s a pretty simple thing to do at the bedside that changes management," he said.
Previously, volume status in patients with septic shock has been assessed by central venous pressure monitoring. Bedside ultrasound also has been used, focusing on the inferior vena cava and the collapsibility of the vena cava during normal respiratory cycles. A collapse of 20%-50% indicates that a fluid bolus would be beneficial. Both of these measures can give false elevations, however, if the patient has preexisting acute or chronic heart or lung disease.
Although an elevated central venous pressure (CVP) or collapsing inferior vena cava (IVC) on ultrasound during respiration indicated the need for a fluid bolus, "once the CVP is elevated or if you have a plethoric IVC, you’re left scratching your head," Dr. DeBlieux said. "Remember that any cardiac or pulmonary dysfunction gets immediately transmitted to the great vein," so the CVP may be high, or the IVC may look plethoric on ultrasound, but the patient may still need a fluid bolus.
"You would say that the tank is full, but you don’t know. I don’t know. We don’t know," he said.
Managing the tank corresponds with the first of three steps in the Surviving Sepsis Campaign's perfusion goals in early goal-directed therapy in acute care of septic shock. Dr. DeBlieux and some other educators refer to these as the tank, the hose and the pump for teaching purposes.
The tank goal is a CVP of 8-12 mm Hg through treatment with serial crystalloid fluid infusions.
The hose is marked by systemic vascular resistance. After addressing the tank, if the mean arterial blood pressure is lower than 65 mmHg, administer norepinephrine, dopamine or epinephrine to bring it up to 65 mm Hg. The medical literature supports any one of those three choices, but norepinephrine will produce fewer tachyarrhythmic events, he said.
In reality, managing the tank and hose may happen simultaneously because physicians may not want to wait for hours until the CVP gets to goal before administering vasopressors, he added.
The pump reflects oxygen delivery and utilization. After addressing the tank and hose, if the lactate level is greater than 4 mmol and central venous oxygen saturation (ScvO2) is less than 70%, consider giving dobutamine in the setting of left ventricular dysfunction, start invasive mechanical ventilation, and/or blood transfusion if the hemoglobin/hematocrit is less than 10/30 within 6 hours.
Dr. DeBlieux said he has no relevant conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS