User login
Life’s Essential 8: Higher scores extend health span
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. I’d like to talk with you about a recent report on
This study leveraged the UK Biobank and included more than 135,000 U.K. adults with a mean age of 55. The AHA metric was defined as including the following lifestyle behavioral factors:
- Not smoking.
- Regular physical activity.
- Healthy weight.
- Healthy diet.
- Healthy sleep (defined as an average of 7-9 hours nightly).
- Blood pressure in a healthy range.
- Blood glucose in a healthy range.
- Non-HDL cholesterol in a healthy range.
This study was just published in JAMA Internal Medicine. I’d like to acknowledge that I’m a coauthor of this study, along with my colleagues at Tulane.
We divided the study population into three groups: those with low, moderate, and high scores on the Life’s Essential 8 metric – low, moderate, and high cardiovascular health. Overall, the average life expectancy free of chronic disease was estimated to be age 50, with 25 additional years in men and 30 additional years in women.
We saw large differences across the Life’s Essential 8 metric group. Men with high cardiovascular health scores tended to have an additional 7 years of life expectancy free of chronic disease, compared with those who had poorer scores. In women, the difference was about 9.5 years between high scores and lower scores. Also, the number of years lived with chronic disease was compressed in those with high cardiovascular health scores. They tended to have fewer years living with those chronic diseases but more years living free of chronic diseases.
We were interested in how these results might differ by socioeconomic status, educational level, and income level, as well as the Townsend deprivation index. We were intrigued by the finding that the gain in life expectancy free of chronic disease was very similar across all socioeconomic strata – those with lower education and lower income gained as much in terms of chronic disease–free life expectancy as those who were in the higher socioeconomic strata.
Overall, the findings make a compelling case for the importance of lifestyle factors in extending health span and years free of chronic disease. It can be motivating to tell our patients that a healthy lifestyle not only extends life expectancy but also extends years of health free of chronic disease.
Nonetheless, we do have many disparities in life expectancy and health span. So it will be very important to population health to narrow those health disparities through education about the importance of lifestyle factors, more research on implementation of lifestyle factors and behaviors, and public policy to make a healthy lifestyle both affordable and accessible to all people across all of these socioeconomic groups.
Thank you so much for your attention.
JoAnn E. Manson, MD, DrPH, is professor of medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, Boston.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. I’d like to talk with you about a recent report on
This study leveraged the UK Biobank and included more than 135,000 U.K. adults with a mean age of 55. The AHA metric was defined as including the following lifestyle behavioral factors:
- Not smoking.
- Regular physical activity.
- Healthy weight.
- Healthy diet.
- Healthy sleep (defined as an average of 7-9 hours nightly).
- Blood pressure in a healthy range.
- Blood glucose in a healthy range.
- Non-HDL cholesterol in a healthy range.
This study was just published in JAMA Internal Medicine. I’d like to acknowledge that I’m a coauthor of this study, along with my colleagues at Tulane.
We divided the study population into three groups: those with low, moderate, and high scores on the Life’s Essential 8 metric – low, moderate, and high cardiovascular health. Overall, the average life expectancy free of chronic disease was estimated to be age 50, with 25 additional years in men and 30 additional years in women.
We saw large differences across the Life’s Essential 8 metric group. Men with high cardiovascular health scores tended to have an additional 7 years of life expectancy free of chronic disease, compared with those who had poorer scores. In women, the difference was about 9.5 years between high scores and lower scores. Also, the number of years lived with chronic disease was compressed in those with high cardiovascular health scores. They tended to have fewer years living with those chronic diseases but more years living free of chronic diseases.
We were interested in how these results might differ by socioeconomic status, educational level, and income level, as well as the Townsend deprivation index. We were intrigued by the finding that the gain in life expectancy free of chronic disease was very similar across all socioeconomic strata – those with lower education and lower income gained as much in terms of chronic disease–free life expectancy as those who were in the higher socioeconomic strata.
Overall, the findings make a compelling case for the importance of lifestyle factors in extending health span and years free of chronic disease. It can be motivating to tell our patients that a healthy lifestyle not only extends life expectancy but also extends years of health free of chronic disease.
Nonetheless, we do have many disparities in life expectancy and health span. So it will be very important to population health to narrow those health disparities through education about the importance of lifestyle factors, more research on implementation of lifestyle factors and behaviors, and public policy to make a healthy lifestyle both affordable and accessible to all people across all of these socioeconomic groups.
Thank you so much for your attention.
JoAnn E. Manson, MD, DrPH, is professor of medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, Boston.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. I’d like to talk with you about a recent report on
This study leveraged the UK Biobank and included more than 135,000 U.K. adults with a mean age of 55. The AHA metric was defined as including the following lifestyle behavioral factors:
- Not smoking.
- Regular physical activity.
- Healthy weight.
- Healthy diet.
- Healthy sleep (defined as an average of 7-9 hours nightly).
- Blood pressure in a healthy range.
- Blood glucose in a healthy range.
- Non-HDL cholesterol in a healthy range.
This study was just published in JAMA Internal Medicine. I’d like to acknowledge that I’m a coauthor of this study, along with my colleagues at Tulane.
We divided the study population into three groups: those with low, moderate, and high scores on the Life’s Essential 8 metric – low, moderate, and high cardiovascular health. Overall, the average life expectancy free of chronic disease was estimated to be age 50, with 25 additional years in men and 30 additional years in women.
We saw large differences across the Life’s Essential 8 metric group. Men with high cardiovascular health scores tended to have an additional 7 years of life expectancy free of chronic disease, compared with those who had poorer scores. In women, the difference was about 9.5 years between high scores and lower scores. Also, the number of years lived with chronic disease was compressed in those with high cardiovascular health scores. They tended to have fewer years living with those chronic diseases but more years living free of chronic diseases.
We were interested in how these results might differ by socioeconomic status, educational level, and income level, as well as the Townsend deprivation index. We were intrigued by the finding that the gain in life expectancy free of chronic disease was very similar across all socioeconomic strata – those with lower education and lower income gained as much in terms of chronic disease–free life expectancy as those who were in the higher socioeconomic strata.
Overall, the findings make a compelling case for the importance of lifestyle factors in extending health span and years free of chronic disease. It can be motivating to tell our patients that a healthy lifestyle not only extends life expectancy but also extends years of health free of chronic disease.
Nonetheless, we do have many disparities in life expectancy and health span. So it will be very important to population health to narrow those health disparities through education about the importance of lifestyle factors, more research on implementation of lifestyle factors and behaviors, and public policy to make a healthy lifestyle both affordable and accessible to all people across all of these socioeconomic groups.
Thank you so much for your attention.
JoAnn E. Manson, MD, DrPH, is professor of medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School, Boston.
A version of this article first appeared on Medscape.com.
What happens when newer weight loss meds are stopped?
Some of these medicines are approved for treating obesity (Wegovy), whereas others are approved for type 2 diabetes (Ozempic and Mounjaro). Tirzepatide (Mounjaro) has been fast-tracked for approval for weight loss by the U.S. Food and Drug Administration this year, and in the first of the series of studies looking at its effect on obesity, the SURMOUNT-1 trial, tirzepatide demonstrated a mean weight loss of around 22% in people without diabetes, spurring significant off-label use.
Our offices are full of patients who have taken these medications, with unprecedented improvements in their weight, cardiometabolic health, and quality of life. What happens when patients stop taking these medications? Or more importantly, why stop them?
Although these drugs are very effective for weight loss and treating diabetes, there can be adverse effects, primarily gastrointestinal, that limit treatment continuation. Nausea is the most common side effect and usually diminishes over time. Slow dose titration and dietary modification can minimize unwanted gastrointestinal side effects.
Drug-induced acute pancreatitis, a rare adverse event requiring patients to stop therapy, was seen in approximately 0.2% of people in clinical trials.
Medications effective but cost prohibitive?
Beyond adverse effects, patients may be forced to stop treatment because of medication cost, changes in insurance coverage, or issues with drug availability.
Two incretin therapies currently approved for treating obesity – liraglutide (Saxenda) and semaglutide (Wegovy) – cost around $1,400 per month. Insurance coverage and manufacturer discounts can make treatment affordable, but anti-obesity medicines aren’t covered by Medicare or by many employer-sponsored commercial plans.
Changes in employment or insurance coverage, or expiration of manufacturer copay cards, may require patients to stop or change therapies. The increased prescribing and overall expense of these drugs have prompted insurance plans and self-insured groups to consider whether providing coverage for these medications is sustainable.
Limited coverage has led to significant off-label prescribing of incretin therapies that aren’t approved for treating obesity (for instance, Ozempic and Mounjaro) and compounding pharmacies selling peptides that allegedly contain the active pharmaceutical ingredients. High demand for these medications has created significant supply shortages over the past year, causing many people to be without treatment for significant periods of time, as reported by this news organization.
Recently, I saw a patient who lost more than 30 pounds with semaglutide (Wegovy). She then changed employers and the medication was no longer covered. She gained back almost 10 pounds over 3 months and was prescribed tirzepatide (Mounjaro) off-label for weight loss by another provider, using a manufacturer discount card to make the medication affordable. The patient did well with the new regimen and lost about 20 pounds, but the pharmacy stopped filling the prescription when changes were made to the discount card. Afraid of regaining the weight, she came to see us as a new patient to discuss her options with her lack of coverage for anti-obesity medications.
Stopping equals weight regain
Obesity is a chronic disease like hypertension. It responds to treatment and when people stop taking these anti-obesity medications, this is generally associated with increased appetite and less satiety, and there is subsequent weight regain and a recurrence in excess weight-related complications.
The STEP-1 trial extension showed an initial mean body weight reduction of 17.3% with weekly semaglutide 2.4 mg over 1 year. On average, two-thirds of the weight lost was regained by participants within 1 year of stopping semaglutide and the study’s lifestyle intervention. Many of the improvements seen in cardiometabolic variables, like blood glucose and blood pressure, similarly reverted to baseline.
There are also 2-year data from the STEP-5 trial with semaglutide; 3-year data from the SCALE trial with liraglutide; and 5-year nonrandomized data with multiple agents that show durable, clinically significant weight loss from medical therapies for obesity.
These data together demonstrate that medications are effective for durable weight loss if they are continued. However, this is not how obesity is currently treated. Anti-obesity medications are prescribed to less than 3% of eligible people in the United States, and the average duration of therapy is less than 90 days. This treatment length isn’t sufficient to see the full benefits most medications offer and certainly doesn’t support long-term weight maintenance.
A recent study showed that, in addition to maintaining weight loss from medical therapies, incretin-containing anti-obesity medication regimens were effective for treating weight regain and facilitating healthier weight after bariatric surgery.
Chronic therapy is needed for weight maintenance because several neurohormonal changes occur owing to weight loss. Metabolic adaptation is the relative reduction in energy expenditure, below what would be expected, in people after weight loss. When this is combined with physiologic changes that increase appetite and decrease satiety, many people create a positive energy balance that results in weight regain. This has been observed in reality TV shows such as “The Biggest Loser”: It’s biology, not willpower.
Unfortunately, many people – including health care providers – don’t understand how these changes promote weight regain and patients are too often blamed when their weight goes back up after medications are stopped. This blame is greatly misinformed by weight-biased beliefs that people with obesity are lazy and lack self-control for weight loss or maintenance. Nobody would be surprised if someone’s blood pressure went up if their antihypertensive medications were stopped. Why do we think so differently when treating obesity?
The prevalence of obesity in the United States is over 40% and growing. We are fortunate to have new medications that on average lead to 15% or greater weight loss when combined with lifestyle modification.
However, these medications are expensive and the limited insurance coverage currently available may not improve. From a patient experience perspective, it’s distressing to have to discontinue treatments that have helped to achieve a healthier weight and then experience regain.
People need better access to evidence-based treatments for obesity, which include lifestyle interventions, anti-obesity medications, and bariatric procedures. Successful treatment of obesity should include a personalized, patient-centered approach that may require a combination of therapies, such as medications and surgery, for lasting weight control.
Dr. Almandoz is associate professor, department of internal medicine, division of endocrinology; medical director, weight wellness program, University of Texas Southwestern, Dallas. He disclosed ties with Novo Nordisk and Eli Lilly. Follow Dr. Almandoz on Twitter: @JaimeAlmandoz.
A version of this article originally appeared on Medscape.com.
Some of these medicines are approved for treating obesity (Wegovy), whereas others are approved for type 2 diabetes (Ozempic and Mounjaro). Tirzepatide (Mounjaro) has been fast-tracked for approval for weight loss by the U.S. Food and Drug Administration this year, and in the first of the series of studies looking at its effect on obesity, the SURMOUNT-1 trial, tirzepatide demonstrated a mean weight loss of around 22% in people without diabetes, spurring significant off-label use.
Our offices are full of patients who have taken these medications, with unprecedented improvements in their weight, cardiometabolic health, and quality of life. What happens when patients stop taking these medications? Or more importantly, why stop them?
Although these drugs are very effective for weight loss and treating diabetes, there can be adverse effects, primarily gastrointestinal, that limit treatment continuation. Nausea is the most common side effect and usually diminishes over time. Slow dose titration and dietary modification can minimize unwanted gastrointestinal side effects.
Drug-induced acute pancreatitis, a rare adverse event requiring patients to stop therapy, was seen in approximately 0.2% of people in clinical trials.
Medications effective but cost prohibitive?
Beyond adverse effects, patients may be forced to stop treatment because of medication cost, changes in insurance coverage, or issues with drug availability.
Two incretin therapies currently approved for treating obesity – liraglutide (Saxenda) and semaglutide (Wegovy) – cost around $1,400 per month. Insurance coverage and manufacturer discounts can make treatment affordable, but anti-obesity medicines aren’t covered by Medicare or by many employer-sponsored commercial plans.
Changes in employment or insurance coverage, or expiration of manufacturer copay cards, may require patients to stop or change therapies. The increased prescribing and overall expense of these drugs have prompted insurance plans and self-insured groups to consider whether providing coverage for these medications is sustainable.
Limited coverage has led to significant off-label prescribing of incretin therapies that aren’t approved for treating obesity (for instance, Ozempic and Mounjaro) and compounding pharmacies selling peptides that allegedly contain the active pharmaceutical ingredients. High demand for these medications has created significant supply shortages over the past year, causing many people to be without treatment for significant periods of time, as reported by this news organization.
Recently, I saw a patient who lost more than 30 pounds with semaglutide (Wegovy). She then changed employers and the medication was no longer covered. She gained back almost 10 pounds over 3 months and was prescribed tirzepatide (Mounjaro) off-label for weight loss by another provider, using a manufacturer discount card to make the medication affordable. The patient did well with the new regimen and lost about 20 pounds, but the pharmacy stopped filling the prescription when changes were made to the discount card. Afraid of regaining the weight, she came to see us as a new patient to discuss her options with her lack of coverage for anti-obesity medications.
Stopping equals weight regain
Obesity is a chronic disease like hypertension. It responds to treatment and when people stop taking these anti-obesity medications, this is generally associated with increased appetite and less satiety, and there is subsequent weight regain and a recurrence in excess weight-related complications.
The STEP-1 trial extension showed an initial mean body weight reduction of 17.3% with weekly semaglutide 2.4 mg over 1 year. On average, two-thirds of the weight lost was regained by participants within 1 year of stopping semaglutide and the study’s lifestyle intervention. Many of the improvements seen in cardiometabolic variables, like blood glucose and blood pressure, similarly reverted to baseline.
There are also 2-year data from the STEP-5 trial with semaglutide; 3-year data from the SCALE trial with liraglutide; and 5-year nonrandomized data with multiple agents that show durable, clinically significant weight loss from medical therapies for obesity.
These data together demonstrate that medications are effective for durable weight loss if they are continued. However, this is not how obesity is currently treated. Anti-obesity medications are prescribed to less than 3% of eligible people in the United States, and the average duration of therapy is less than 90 days. This treatment length isn’t sufficient to see the full benefits most medications offer and certainly doesn’t support long-term weight maintenance.
A recent study showed that, in addition to maintaining weight loss from medical therapies, incretin-containing anti-obesity medication regimens were effective for treating weight regain and facilitating healthier weight after bariatric surgery.
Chronic therapy is needed for weight maintenance because several neurohormonal changes occur owing to weight loss. Metabolic adaptation is the relative reduction in energy expenditure, below what would be expected, in people after weight loss. When this is combined with physiologic changes that increase appetite and decrease satiety, many people create a positive energy balance that results in weight regain. This has been observed in reality TV shows such as “The Biggest Loser”: It’s biology, not willpower.
Unfortunately, many people – including health care providers – don’t understand how these changes promote weight regain and patients are too often blamed when their weight goes back up after medications are stopped. This blame is greatly misinformed by weight-biased beliefs that people with obesity are lazy and lack self-control for weight loss or maintenance. Nobody would be surprised if someone’s blood pressure went up if their antihypertensive medications were stopped. Why do we think so differently when treating obesity?
The prevalence of obesity in the United States is over 40% and growing. We are fortunate to have new medications that on average lead to 15% or greater weight loss when combined with lifestyle modification.
However, these medications are expensive and the limited insurance coverage currently available may not improve. From a patient experience perspective, it’s distressing to have to discontinue treatments that have helped to achieve a healthier weight and then experience regain.
People need better access to evidence-based treatments for obesity, which include lifestyle interventions, anti-obesity medications, and bariatric procedures. Successful treatment of obesity should include a personalized, patient-centered approach that may require a combination of therapies, such as medications and surgery, for lasting weight control.
Dr. Almandoz is associate professor, department of internal medicine, division of endocrinology; medical director, weight wellness program, University of Texas Southwestern, Dallas. He disclosed ties with Novo Nordisk and Eli Lilly. Follow Dr. Almandoz on Twitter: @JaimeAlmandoz.
A version of this article originally appeared on Medscape.com.
Some of these medicines are approved for treating obesity (Wegovy), whereas others are approved for type 2 diabetes (Ozempic and Mounjaro). Tirzepatide (Mounjaro) has been fast-tracked for approval for weight loss by the U.S. Food and Drug Administration this year, and in the first of the series of studies looking at its effect on obesity, the SURMOUNT-1 trial, tirzepatide demonstrated a mean weight loss of around 22% in people without diabetes, spurring significant off-label use.
Our offices are full of patients who have taken these medications, with unprecedented improvements in their weight, cardiometabolic health, and quality of life. What happens when patients stop taking these medications? Or more importantly, why stop them?
Although these drugs are very effective for weight loss and treating diabetes, there can be adverse effects, primarily gastrointestinal, that limit treatment continuation. Nausea is the most common side effect and usually diminishes over time. Slow dose titration and dietary modification can minimize unwanted gastrointestinal side effects.
Drug-induced acute pancreatitis, a rare adverse event requiring patients to stop therapy, was seen in approximately 0.2% of people in clinical trials.
Medications effective but cost prohibitive?
Beyond adverse effects, patients may be forced to stop treatment because of medication cost, changes in insurance coverage, or issues with drug availability.
Two incretin therapies currently approved for treating obesity – liraglutide (Saxenda) and semaglutide (Wegovy) – cost around $1,400 per month. Insurance coverage and manufacturer discounts can make treatment affordable, but anti-obesity medicines aren’t covered by Medicare or by many employer-sponsored commercial plans.
Changes in employment or insurance coverage, or expiration of manufacturer copay cards, may require patients to stop or change therapies. The increased prescribing and overall expense of these drugs have prompted insurance plans and self-insured groups to consider whether providing coverage for these medications is sustainable.
Limited coverage has led to significant off-label prescribing of incretin therapies that aren’t approved for treating obesity (for instance, Ozempic and Mounjaro) and compounding pharmacies selling peptides that allegedly contain the active pharmaceutical ingredients. High demand for these medications has created significant supply shortages over the past year, causing many people to be without treatment for significant periods of time, as reported by this news organization.
Recently, I saw a patient who lost more than 30 pounds with semaglutide (Wegovy). She then changed employers and the medication was no longer covered. She gained back almost 10 pounds over 3 months and was prescribed tirzepatide (Mounjaro) off-label for weight loss by another provider, using a manufacturer discount card to make the medication affordable. The patient did well with the new regimen and lost about 20 pounds, but the pharmacy stopped filling the prescription when changes were made to the discount card. Afraid of regaining the weight, she came to see us as a new patient to discuss her options with her lack of coverage for anti-obesity medications.
Stopping equals weight regain
Obesity is a chronic disease like hypertension. It responds to treatment and when people stop taking these anti-obesity medications, this is generally associated with increased appetite and less satiety, and there is subsequent weight regain and a recurrence in excess weight-related complications.
The STEP-1 trial extension showed an initial mean body weight reduction of 17.3% with weekly semaglutide 2.4 mg over 1 year. On average, two-thirds of the weight lost was regained by participants within 1 year of stopping semaglutide and the study’s lifestyle intervention. Many of the improvements seen in cardiometabolic variables, like blood glucose and blood pressure, similarly reverted to baseline.
There are also 2-year data from the STEP-5 trial with semaglutide; 3-year data from the SCALE trial with liraglutide; and 5-year nonrandomized data with multiple agents that show durable, clinically significant weight loss from medical therapies for obesity.
These data together demonstrate that medications are effective for durable weight loss if they are continued. However, this is not how obesity is currently treated. Anti-obesity medications are prescribed to less than 3% of eligible people in the United States, and the average duration of therapy is less than 90 days. This treatment length isn’t sufficient to see the full benefits most medications offer and certainly doesn’t support long-term weight maintenance.
A recent study showed that, in addition to maintaining weight loss from medical therapies, incretin-containing anti-obesity medication regimens were effective for treating weight regain and facilitating healthier weight after bariatric surgery.
Chronic therapy is needed for weight maintenance because several neurohormonal changes occur owing to weight loss. Metabolic adaptation is the relative reduction in energy expenditure, below what would be expected, in people after weight loss. When this is combined with physiologic changes that increase appetite and decrease satiety, many people create a positive energy balance that results in weight regain. This has been observed in reality TV shows such as “The Biggest Loser”: It’s biology, not willpower.
Unfortunately, many people – including health care providers – don’t understand how these changes promote weight regain and patients are too often blamed when their weight goes back up after medications are stopped. This blame is greatly misinformed by weight-biased beliefs that people with obesity are lazy and lack self-control for weight loss or maintenance. Nobody would be surprised if someone’s blood pressure went up if their antihypertensive medications were stopped. Why do we think so differently when treating obesity?
The prevalence of obesity in the United States is over 40% and growing. We are fortunate to have new medications that on average lead to 15% or greater weight loss when combined with lifestyle modification.
However, these medications are expensive and the limited insurance coverage currently available may not improve. From a patient experience perspective, it’s distressing to have to discontinue treatments that have helped to achieve a healthier weight and then experience regain.
People need better access to evidence-based treatments for obesity, which include lifestyle interventions, anti-obesity medications, and bariatric procedures. Successful treatment of obesity should include a personalized, patient-centered approach that may require a combination of therapies, such as medications and surgery, for lasting weight control.
Dr. Almandoz is associate professor, department of internal medicine, division of endocrinology; medical director, weight wellness program, University of Texas Southwestern, Dallas. He disclosed ties with Novo Nordisk and Eli Lilly. Follow Dr. Almandoz on Twitter: @JaimeAlmandoz.
A version of this article originally appeared on Medscape.com.
The desk
Recently, Dr. Jeffrey Benabio (I don’t believe we’ve ever met), wrote an enjoyable commentary mourning the loss of letters – the wonderful paper-and-pen documents that were, for the vast majority of human history, the main method of long distance communication. Even today, he notes, there’s something special about a letter, with the time and human effort required to sit down and put pen to paper, seal it into an envelope, and entrust it to the post office.
In his piece, Dr. Benabio describes his work desk as “a small surface, perhaps just enough for the monitor and a mug ... it has no drawers. It is lean and immaculate, but it has no soul.”

With all due respect, I can’t do that. I need a desk to function. A REAL one.
I was 9 when I got my first desk, far more than a 4th-grader needed. My dad was an attorney and had an extra desk from a partner who’d retired. It was big and heavy and made of wood. It had three drawers on each side, one in the middle, and pull-outs on each side in case you needed even more writing space. I loved it. As the years went by I did homework, wrote short stories, and built models on it. I covered the pull-outs with stickers for starship controls, so on a whim I could jump to hyperspace. In 1984 a brand-new Apple Macintosh, with 128K of RAM showed up on it. I began using the computer to write college papers, but most of my work at the desk still involved books and handwriting.
My current home desk has been with me through college, medical school, residency, and fellowship, and it continues with me today.
At my office, though, is my main desk. Before 2013 I was in a small back office, with only room for a tiny three-drawer college desk.
But in 2013 I moved into my own office, for the first time in my career. Now it was time to bring in my real desk, waiting in storage since my Dad had retired.
This is my desk now. It’s huge. It’s heavy. My dad bought it when he started his law practice in 1968. It has eight drawers, and my Dad’s original leather blotter is on top. It came with his chrome and brass letter opener in the top drawer. It has space for my computer, writing pads, exam tools (for people who can’t get on the exam table across the hall), business cards, a few baubles from my kids, stapler, tape dispenser, pen cup, phone, coffee mug, and a million other things.
It takes up a lot of space, but I don’t mind. There’s a human comfort to it and the organized disorder on top of it.
Everyone practices medicine differently. What works for me isn’t going to work for another doctor, and definitely not for another specialty.
But here, the big desk is part of my personal style. Sitting there gets me into “doctor mode” each day. I hope the more casual surroundings make it comfortable for patients, too.
It’s part of the soul of my practice, and I wouldn’t have it any other way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, Dr. Jeffrey Benabio (I don’t believe we’ve ever met), wrote an enjoyable commentary mourning the loss of letters – the wonderful paper-and-pen documents that were, for the vast majority of human history, the main method of long distance communication. Even today, he notes, there’s something special about a letter, with the time and human effort required to sit down and put pen to paper, seal it into an envelope, and entrust it to the post office.
In his piece, Dr. Benabio describes his work desk as “a small surface, perhaps just enough for the monitor and a mug ... it has no drawers. It is lean and immaculate, but it has no soul.”
With all due respect, I can’t do that. I need a desk to function. A REAL one.
I was 9 when I got my first desk, far more than a 4th-grader needed. My dad was an attorney and had an extra desk from a partner who’d retired. It was big and heavy and made of wood. It had three drawers on each side, one in the middle, and pull-outs on each side in case you needed even more writing space. I loved it. As the years went by I did homework, wrote short stories, and built models on it. I covered the pull-outs with stickers for starship controls, so on a whim I could jump to hyperspace. In 1984 a brand-new Apple Macintosh, with 128K of RAM showed up on it. I began using the computer to write college papers, but most of my work at the desk still involved books and handwriting.
My current home desk has been with me through college, medical school, residency, and fellowship, and it continues with me today.
At my office, though, is my main desk. Before 2013 I was in a small back office, with only room for a tiny three-drawer college desk.
But in 2013 I moved into my own office, for the first time in my career. Now it was time to bring in my real desk, waiting in storage since my Dad had retired.
This is my desk now. It’s huge. It’s heavy. My dad bought it when he started his law practice in 1968. It has eight drawers, and my Dad’s original leather blotter is on top. It came with his chrome and brass letter opener in the top drawer. It has space for my computer, writing pads, exam tools (for people who can’t get on the exam table across the hall), business cards, a few baubles from my kids, stapler, tape dispenser, pen cup, phone, coffee mug, and a million other things.
It takes up a lot of space, but I don’t mind. There’s a human comfort to it and the organized disorder on top of it.
Everyone practices medicine differently. What works for me isn’t going to work for another doctor, and definitely not for another specialty.
But here, the big desk is part of my personal style. Sitting there gets me into “doctor mode” each day. I hope the more casual surroundings make it comfortable for patients, too.
It’s part of the soul of my practice, and I wouldn’t have it any other way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Recently, Dr. Jeffrey Benabio (I don’t believe we’ve ever met), wrote an enjoyable commentary mourning the loss of letters – the wonderful paper-and-pen documents that were, for the vast majority of human history, the main method of long distance communication. Even today, he notes, there’s something special about a letter, with the time and human effort required to sit down and put pen to paper, seal it into an envelope, and entrust it to the post office.
In his piece, Dr. Benabio describes his work desk as “a small surface, perhaps just enough for the monitor and a mug ... it has no drawers. It is lean and immaculate, but it has no soul.”
With all due respect, I can’t do that. I need a desk to function. A REAL one.
I was 9 when I got my first desk, far more than a 4th-grader needed. My dad was an attorney and had an extra desk from a partner who’d retired. It was big and heavy and made of wood. It had three drawers on each side, one in the middle, and pull-outs on each side in case you needed even more writing space. I loved it. As the years went by I did homework, wrote short stories, and built models on it. I covered the pull-outs with stickers for starship controls, so on a whim I could jump to hyperspace. In 1984 a brand-new Apple Macintosh, with 128K of RAM showed up on it. I began using the computer to write college papers, but most of my work at the desk still involved books and handwriting.
My current home desk has been with me through college, medical school, residency, and fellowship, and it continues with me today.
At my office, though, is my main desk. Before 2013 I was in a small back office, with only room for a tiny three-drawer college desk.
But in 2013 I moved into my own office, for the first time in my career. Now it was time to bring in my real desk, waiting in storage since my Dad had retired.
This is my desk now. It’s huge. It’s heavy. My dad bought it when he started his law practice in 1968. It has eight drawers, and my Dad’s original leather blotter is on top. It came with his chrome and brass letter opener in the top drawer. It has space for my computer, writing pads, exam tools (for people who can’t get on the exam table across the hall), business cards, a few baubles from my kids, stapler, tape dispenser, pen cup, phone, coffee mug, and a million other things.
It takes up a lot of space, but I don’t mind. There’s a human comfort to it and the organized disorder on top of it.
Everyone practices medicine differently. What works for me isn’t going to work for another doctor, and definitely not for another specialty.
But here, the big desk is part of my personal style. Sitting there gets me into “doctor mode” each day. I hope the more casual surroundings make it comfortable for patients, too.
It’s part of the soul of my practice, and I wouldn’t have it any other way.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Hydroxyurea underused in youth with sickle cell anemia
Even after endorsement in updated guidelines, hydroxyurea is substantially underused in youth with sickle cell anemia (SCA), new research indicates.
SCA can lead to pain crises, stroke, and early death. Hydroxyurea, an oral disease-modifying medication, can reduce the complications.
In 2014, the National Heart, Lung, and Blood Institute published revised guidelines that hydroxyurea should be offered as the primary therapy to all patients who were at least 9 months old and living with SCA, regardless of disease severity.
Low uptake even after guideline revision
Yet, a research team led by Sarah L. Reeves, PhD, MPH, with the Child Health Evaluation and Research Center at University of Michigan, Ann Arbor, found in their study of use in two sample states – Michigan and New York – that hydroxyurea use was low in children and adolescents enrolled in Medicaid and increased only slightly in Michigan and not at all in New York after the guideline revision.
After the guidelines were updated, the researchers observed that, on average, children and adolescents were getting the medication less than a third of the days in a year (32% maximum in the year with the highest uptake). The data were gathered from a study population that included 4,302 youths aged 1-17 years with SCA.
Findings were published online in JAMA Network Open.
‘A national issue’
Russell Ware, MD, PhD, chair of hematology translational research at Cincinnati Children’s Hospital, who was not part of the research, says that though data were gathered from Michigan and New York, “this is a national issue.”
Dr. Ware says the main problem is the way the health system describes the importance of hydroxyurea.
“There needs to be a realization that hydroxyurea is the standard of care for children with sickle cell anemia. It’s not just something they should take when they’re sick,” Dr. Ware said.
He added, “If you have diabetes, should you only take insulin if you’re really sick and hospitalized with a diabetic coma? Of course not.”
He said often providers aren’t giving a clear and consistent message to families.
“They’re not all sure they want to recommend it. They might offer it,” Dr. Ware said, which jeopardizes uptake. “Providers need to be more committed to it. They need to know how to dose it.”
Bad rap from past indications
Dr. Ware says hydroxyurea also gets a bad rap from use decades ago as a chemotherapeutic agent for cancer and then as an anti-HIV medication.
Now it’s used in a completely different way with SCA, but the fear of the association lingers.
“This label as a chemotherapeutic agent has really dogged hydroxyurea,” he said. “It’s a completely different mechanism. It’s a different dose. It’s a different purpose.”
The message to families should be more direct, he says: “Your child has sickle cell anemia and needs to be on disease-modifying therapy because this is a life-threatening disease.”
The underuse of this drug is particularly ironic, he says, as each capsule, taken daily, “costs about fifty cents.”
Medicaid support critical
Authors conclude that multifaceted interventions may be necessary to increase the number of filled prescriptions and use. They also point out that the interventions rely on states’ Medicaid support regarding hydroxyurea use. From 70% to 90% of young people with SCA are covered by Medicaid at some point, the researchers write.
“Variation may exist across states, as well as within states, in the coverage of hydroxyurea, outpatient visits, and associated lab monitoring,” they note.
The authors point to interventions in clinical trials that have had some success in hydroxyurea use.
Creary et al., for example, found that electronic directly observed therapy was associated with high adherence. That involved sending daily texts to patients to take hydroxyurea and patients recording and sending daily videos that show they took the medication.
The authors add that incorporating clinical pharmacists into the care team to provide education and support for families has been shown to be associated with successful outcomes for other chronic conditions – this approach may be particularly well suited to hydroxyurea given that this medication requires significant dosage monitoring.
Dr. Ware, however, says that solutions should focus on the health system more clearly communicating that hydroxyurea is the standard of care for all kids with SCA.
“We need to dispel these myths and these labels that are unfairly attributed to it. Then we’d probably do a lot better,” he said.
He added that children with SCA, “are a marginalized, neglected population of patients historically,” and addressing social determinants of health is also important in getting better uptake.
“Our pharmacy, for example, ships the drug to the families if they’re just getting a refill rather than making them drive all the way in,” Dr. Ware says.
Dr. Ware said given the interruption in doctor/patient relationships in the pandemic, the poor uptake of hydroxyurea could be even worse now.
The work was funded by the Agency for Healthcare Research and Quality and National Heart, Lung, and Blood Institute. Coauthor Dr. Green was the principal investigator of an NIH-funded trial of hydroxyurea in Uganda with a study drug provided by Siklos. No other author disclosures were reported. In addition to receiving research funding from the National Institutes of Health, Dr. Ware receives research donations from Bristol Myers Squibb, Addmedica, and Hemex Health. He is a medical adviser for Nova Laboratories and Octapharma, and serves on Data Safety Monitoring Boards for Novartis and Editas.
Even after endorsement in updated guidelines, hydroxyurea is substantially underused in youth with sickle cell anemia (SCA), new research indicates.
SCA can lead to pain crises, stroke, and early death. Hydroxyurea, an oral disease-modifying medication, can reduce the complications.
In 2014, the National Heart, Lung, and Blood Institute published revised guidelines that hydroxyurea should be offered as the primary therapy to all patients who were at least 9 months old and living with SCA, regardless of disease severity.
Low uptake even after guideline revision
Yet, a research team led by Sarah L. Reeves, PhD, MPH, with the Child Health Evaluation and Research Center at University of Michigan, Ann Arbor, found in their study of use in two sample states – Michigan and New York – that hydroxyurea use was low in children and adolescents enrolled in Medicaid and increased only slightly in Michigan and not at all in New York after the guideline revision.
After the guidelines were updated, the researchers observed that, on average, children and adolescents were getting the medication less than a third of the days in a year (32% maximum in the year with the highest uptake). The data were gathered from a study population that included 4,302 youths aged 1-17 years with SCA.
Findings were published online in JAMA Network Open.
‘A national issue’
Russell Ware, MD, PhD, chair of hematology translational research at Cincinnati Children’s Hospital, who was not part of the research, says that though data were gathered from Michigan and New York, “this is a national issue.”
Dr. Ware says the main problem is the way the health system describes the importance of hydroxyurea.
“There needs to be a realization that hydroxyurea is the standard of care for children with sickle cell anemia. It’s not just something they should take when they’re sick,” Dr. Ware said.
He added, “If you have diabetes, should you only take insulin if you’re really sick and hospitalized with a diabetic coma? Of course not.”
He said often providers aren’t giving a clear and consistent message to families.
“They’re not all sure they want to recommend it. They might offer it,” Dr. Ware said, which jeopardizes uptake. “Providers need to be more committed to it. They need to know how to dose it.”
Bad rap from past indications
Dr. Ware says hydroxyurea also gets a bad rap from use decades ago as a chemotherapeutic agent for cancer and then as an anti-HIV medication.
Now it’s used in a completely different way with SCA, but the fear of the association lingers.
“This label as a chemotherapeutic agent has really dogged hydroxyurea,” he said. “It’s a completely different mechanism. It’s a different dose. It’s a different purpose.”
The message to families should be more direct, he says: “Your child has sickle cell anemia and needs to be on disease-modifying therapy because this is a life-threatening disease.”
The underuse of this drug is particularly ironic, he says, as each capsule, taken daily, “costs about fifty cents.”
Medicaid support critical
Authors conclude that multifaceted interventions may be necessary to increase the number of filled prescriptions and use. They also point out that the interventions rely on states’ Medicaid support regarding hydroxyurea use. From 70% to 90% of young people with SCA are covered by Medicaid at some point, the researchers write.
“Variation may exist across states, as well as within states, in the coverage of hydroxyurea, outpatient visits, and associated lab monitoring,” they note.
The authors point to interventions in clinical trials that have had some success in hydroxyurea use.
Creary et al., for example, found that electronic directly observed therapy was associated with high adherence. That involved sending daily texts to patients to take hydroxyurea and patients recording and sending daily videos that show they took the medication.
The authors add that incorporating clinical pharmacists into the care team to provide education and support for families has been shown to be associated with successful outcomes for other chronic conditions – this approach may be particularly well suited to hydroxyurea given that this medication requires significant dosage monitoring.
Dr. Ware, however, says that solutions should focus on the health system more clearly communicating that hydroxyurea is the standard of care for all kids with SCA.
“We need to dispel these myths and these labels that are unfairly attributed to it. Then we’d probably do a lot better,” he said.
He added that children with SCA, “are a marginalized, neglected population of patients historically,” and addressing social determinants of health is also important in getting better uptake.
“Our pharmacy, for example, ships the drug to the families if they’re just getting a refill rather than making them drive all the way in,” Dr. Ware says.
Dr. Ware said given the interruption in doctor/patient relationships in the pandemic, the poor uptake of hydroxyurea could be even worse now.
The work was funded by the Agency for Healthcare Research and Quality and National Heart, Lung, and Blood Institute. Coauthor Dr. Green was the principal investigator of an NIH-funded trial of hydroxyurea in Uganda with a study drug provided by Siklos. No other author disclosures were reported. In addition to receiving research funding from the National Institutes of Health, Dr. Ware receives research donations from Bristol Myers Squibb, Addmedica, and Hemex Health. He is a medical adviser for Nova Laboratories and Octapharma, and serves on Data Safety Monitoring Boards for Novartis and Editas.
Even after endorsement in updated guidelines, hydroxyurea is substantially underused in youth with sickle cell anemia (SCA), new research indicates.
SCA can lead to pain crises, stroke, and early death. Hydroxyurea, an oral disease-modifying medication, can reduce the complications.
In 2014, the National Heart, Lung, and Blood Institute published revised guidelines that hydroxyurea should be offered as the primary therapy to all patients who were at least 9 months old and living with SCA, regardless of disease severity.
Low uptake even after guideline revision
Yet, a research team led by Sarah L. Reeves, PhD, MPH, with the Child Health Evaluation and Research Center at University of Michigan, Ann Arbor, found in their study of use in two sample states – Michigan and New York – that hydroxyurea use was low in children and adolescents enrolled in Medicaid and increased only slightly in Michigan and not at all in New York after the guideline revision.
After the guidelines were updated, the researchers observed that, on average, children and adolescents were getting the medication less than a third of the days in a year (32% maximum in the year with the highest uptake). The data were gathered from a study population that included 4,302 youths aged 1-17 years with SCA.
Findings were published online in JAMA Network Open.
‘A national issue’
Russell Ware, MD, PhD, chair of hematology translational research at Cincinnati Children’s Hospital, who was not part of the research, says that though data were gathered from Michigan and New York, “this is a national issue.”
Dr. Ware says the main problem is the way the health system describes the importance of hydroxyurea.
“There needs to be a realization that hydroxyurea is the standard of care for children with sickle cell anemia. It’s not just something they should take when they’re sick,” Dr. Ware said.
He added, “If you have diabetes, should you only take insulin if you’re really sick and hospitalized with a diabetic coma? Of course not.”
He said often providers aren’t giving a clear and consistent message to families.
“They’re not all sure they want to recommend it. They might offer it,” Dr. Ware said, which jeopardizes uptake. “Providers need to be more committed to it. They need to know how to dose it.”
Bad rap from past indications
Dr. Ware says hydroxyurea also gets a bad rap from use decades ago as a chemotherapeutic agent for cancer and then as an anti-HIV medication.
Now it’s used in a completely different way with SCA, but the fear of the association lingers.
“This label as a chemotherapeutic agent has really dogged hydroxyurea,” he said. “It’s a completely different mechanism. It’s a different dose. It’s a different purpose.”
The message to families should be more direct, he says: “Your child has sickle cell anemia and needs to be on disease-modifying therapy because this is a life-threatening disease.”
The underuse of this drug is particularly ironic, he says, as each capsule, taken daily, “costs about fifty cents.”
Medicaid support critical
Authors conclude that multifaceted interventions may be necessary to increase the number of filled prescriptions and use. They also point out that the interventions rely on states’ Medicaid support regarding hydroxyurea use. From 70% to 90% of young people with SCA are covered by Medicaid at some point, the researchers write.
“Variation may exist across states, as well as within states, in the coverage of hydroxyurea, outpatient visits, and associated lab monitoring,” they note.
The authors point to interventions in clinical trials that have had some success in hydroxyurea use.
Creary et al., for example, found that electronic directly observed therapy was associated with high adherence. That involved sending daily texts to patients to take hydroxyurea and patients recording and sending daily videos that show they took the medication.
The authors add that incorporating clinical pharmacists into the care team to provide education and support for families has been shown to be associated with successful outcomes for other chronic conditions – this approach may be particularly well suited to hydroxyurea given that this medication requires significant dosage monitoring.
Dr. Ware, however, says that solutions should focus on the health system more clearly communicating that hydroxyurea is the standard of care for all kids with SCA.
“We need to dispel these myths and these labels that are unfairly attributed to it. Then we’d probably do a lot better,” he said.
He added that children with SCA, “are a marginalized, neglected population of patients historically,” and addressing social determinants of health is also important in getting better uptake.
“Our pharmacy, for example, ships the drug to the families if they’re just getting a refill rather than making them drive all the way in,” Dr. Ware says.
Dr. Ware said given the interruption in doctor/patient relationships in the pandemic, the poor uptake of hydroxyurea could be even worse now.
The work was funded by the Agency for Healthcare Research and Quality and National Heart, Lung, and Blood Institute. Coauthor Dr. Green was the principal investigator of an NIH-funded trial of hydroxyurea in Uganda with a study drug provided by Siklos. No other author disclosures were reported. In addition to receiving research funding from the National Institutes of Health, Dr. Ware receives research donations from Bristol Myers Squibb, Addmedica, and Hemex Health. He is a medical adviser for Nova Laboratories and Octapharma, and serves on Data Safety Monitoring Boards for Novartis and Editas.
FROM JAMA NETWORK OPEN
Celebrity death finally solved – with locks of hair
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.

We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
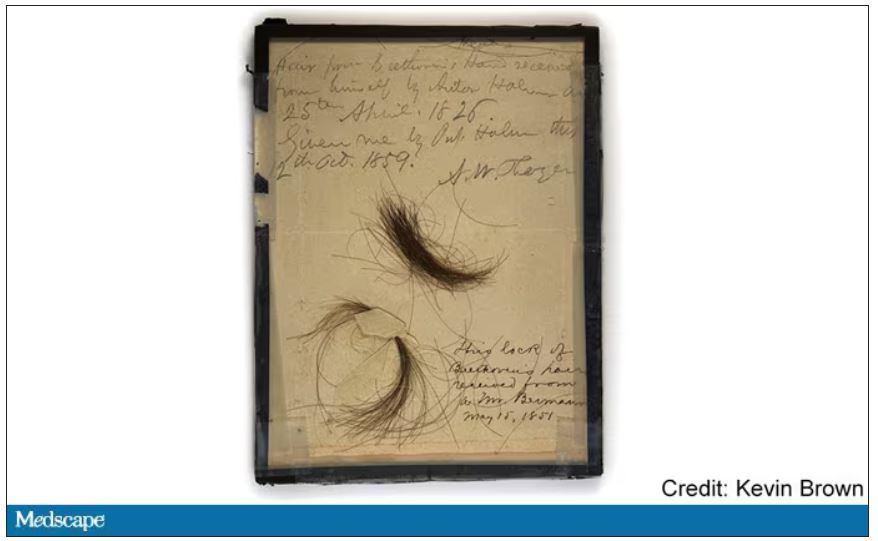
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
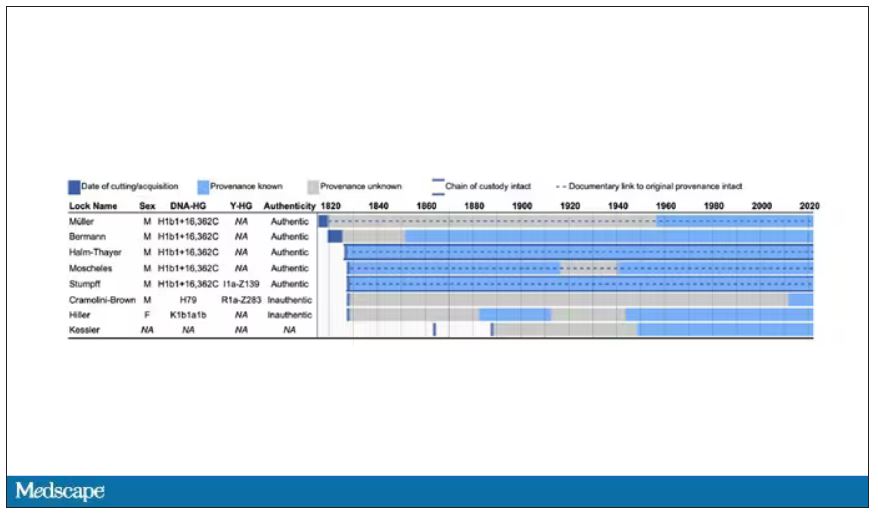
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
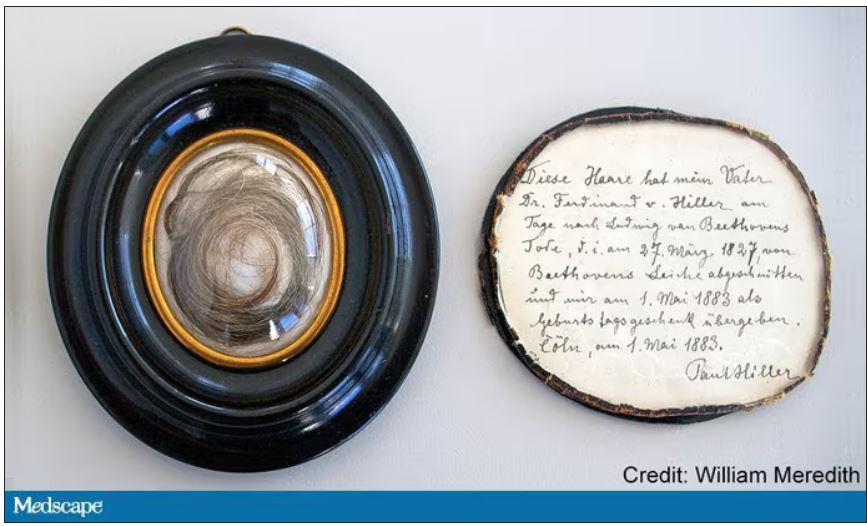
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
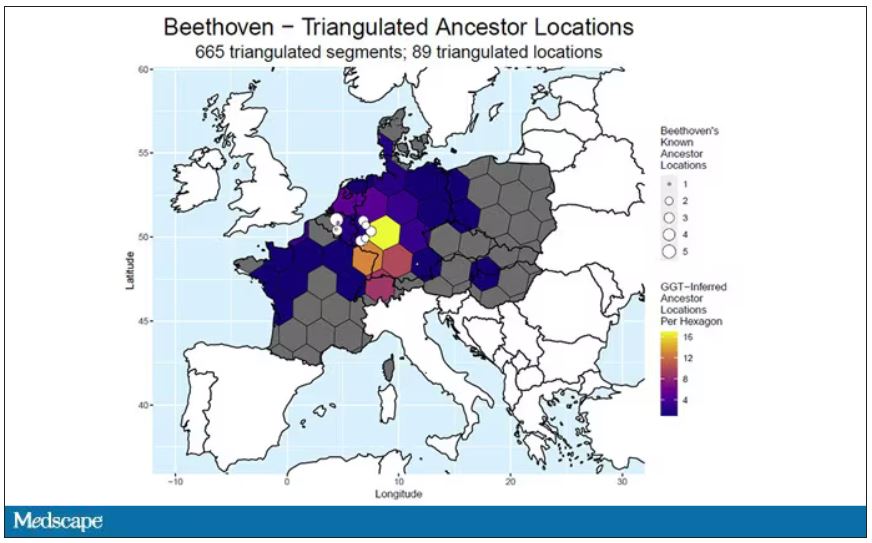
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Fast, cheap ... or accurate?
A recent study on the JAMA Network found that, .
Does this surprise anyone?
One of my friends, a pharmacist, has a sign in his home office: “Fast. Accurate. Cheap. You can’t have all 3.” A true statement. I’ve also seen it at car repair places, but they’re doctors in their own way.
The problem here is that physicians are increasingly squeezed for time. If your only revenue stream is seeing patients, and your expenses are going up (and whose aren’t?) then your options are to either raise your prices or see more patients.
Of course, raising prices in medicine can’t happen for most of us. We’re all tied into insurance contracts, which themselves are pegged to Medicare, as to how much we get paid. I mean, yes, you can raise your prices, but that doesn’t matter. The insurance company will still pay a predetermined amount set years ago, in better economic times, no matter what you charge.
So the only real option for most is to see more patients. Which means less time with each one. Which, inevitably, leads to more snap judgments, inappropriate prescriptions, and mistakes.
Patients may get Fast and Cheap, but Accurate gets sidelined. This is the nature of things. If you don’t have enough time to gather and process data, then you’re less likely to reach the right answer.
There’s also the fact that sometimes it’s easier for anyone to just take the path of least resistance. The patient wants an antibiotic, and you realize it’s going to take less time to hand them a script for one than to explain why they don’t need it for what’s probably a viral infection. Not only that, but then you run the risk of their giving you a bad Yelp review (“incompetent, refused to give me antibiotics when I obviously needed them, 1 star”) and who needs that? If you’re employed by a large health care system a bad online review will get you a talking-to by some nonmedical admin from marketing, saying you’re hurting the practice’s “brand.”
Years ago the satire site The Onion had an article about a doctor who specialized in “giving a shit” - assumedly where Accurate dominates. While none of us may intentionally rush through patients or do half-assed jobs, we also have to deal with pressures of time. There never seems to be enough in a workday.
Nowhere is this more true than in primary care, where the pressures of time, overhead, and a large patient volume intersect. There are patients to see, labs to review, phone calls to return, forms to complete, meetings to attend, samples to sign for ... and probably many other things I’ve left out.
The fact that this situation exists shouldn’t surprise anyone. People talk about “burnout” and “making health care better” but that just seems to be lip service. They give you a free subscription to a meditation app, phone access to a counselor, and a mandatory early morning meeting to discuss stress reduction. Of course, these things take time away from seeing patients, which sort of defeats the whole purpose. Unless you want to do them at home – taking time away from your family, or doing the taxes, or other things you have to do besides your day job.
This is not sustainable for patients, doctors, or the health care system as a whole. But right now the situation is only getting worse, and there aren’t any easy answers.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A recent study on the JAMA Network found that, .
Does this surprise anyone?
One of my friends, a pharmacist, has a sign in his home office: “Fast. Accurate. Cheap. You can’t have all 3.” A true statement. I’ve also seen it at car repair places, but they’re doctors in their own way.
The problem here is that physicians are increasingly squeezed for time. If your only revenue stream is seeing patients, and your expenses are going up (and whose aren’t?) then your options are to either raise your prices or see more patients.
Of course, raising prices in medicine can’t happen for most of us. We’re all tied into insurance contracts, which themselves are pegged to Medicare, as to how much we get paid. I mean, yes, you can raise your prices, but that doesn’t matter. The insurance company will still pay a predetermined amount set years ago, in better economic times, no matter what you charge.
So the only real option for most is to see more patients. Which means less time with each one. Which, inevitably, leads to more snap judgments, inappropriate prescriptions, and mistakes.
Patients may get Fast and Cheap, but Accurate gets sidelined. This is the nature of things. If you don’t have enough time to gather and process data, then you’re less likely to reach the right answer.
There’s also the fact that sometimes it’s easier for anyone to just take the path of least resistance. The patient wants an antibiotic, and you realize it’s going to take less time to hand them a script for one than to explain why they don’t need it for what’s probably a viral infection. Not only that, but then you run the risk of their giving you a bad Yelp review (“incompetent, refused to give me antibiotics when I obviously needed them, 1 star”) and who needs that? If you’re employed by a large health care system a bad online review will get you a talking-to by some nonmedical admin from marketing, saying you’re hurting the practice’s “brand.”
Years ago the satire site The Onion had an article about a doctor who specialized in “giving a shit” - assumedly where Accurate dominates. While none of us may intentionally rush through patients or do half-assed jobs, we also have to deal with pressures of time. There never seems to be enough in a workday.
Nowhere is this more true than in primary care, where the pressures of time, overhead, and a large patient volume intersect. There are patients to see, labs to review, phone calls to return, forms to complete, meetings to attend, samples to sign for ... and probably many other things I’ve left out.
The fact that this situation exists shouldn’t surprise anyone. People talk about “burnout” and “making health care better” but that just seems to be lip service. They give you a free subscription to a meditation app, phone access to a counselor, and a mandatory early morning meeting to discuss stress reduction. Of course, these things take time away from seeing patients, which sort of defeats the whole purpose. Unless you want to do them at home – taking time away from your family, or doing the taxes, or other things you have to do besides your day job.
This is not sustainable for patients, doctors, or the health care system as a whole. But right now the situation is only getting worse, and there aren’t any easy answers.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
A recent study on the JAMA Network found that, .
Does this surprise anyone?
One of my friends, a pharmacist, has a sign in his home office: “Fast. Accurate. Cheap. You can’t have all 3.” A true statement. I’ve also seen it at car repair places, but they’re doctors in their own way.
The problem here is that physicians are increasingly squeezed for time. If your only revenue stream is seeing patients, and your expenses are going up (and whose aren’t?) then your options are to either raise your prices or see more patients.
Of course, raising prices in medicine can’t happen for most of us. We’re all tied into insurance contracts, which themselves are pegged to Medicare, as to how much we get paid. I mean, yes, you can raise your prices, but that doesn’t matter. The insurance company will still pay a predetermined amount set years ago, in better economic times, no matter what you charge.
So the only real option for most is to see more patients. Which means less time with each one. Which, inevitably, leads to more snap judgments, inappropriate prescriptions, and mistakes.
Patients may get Fast and Cheap, but Accurate gets sidelined. This is the nature of things. If you don’t have enough time to gather and process data, then you’re less likely to reach the right answer.
There’s also the fact that sometimes it’s easier for anyone to just take the path of least resistance. The patient wants an antibiotic, and you realize it’s going to take less time to hand them a script for one than to explain why they don’t need it for what’s probably a viral infection. Not only that, but then you run the risk of their giving you a bad Yelp review (“incompetent, refused to give me antibiotics when I obviously needed them, 1 star”) and who needs that? If you’re employed by a large health care system a bad online review will get you a talking-to by some nonmedical admin from marketing, saying you’re hurting the practice’s “brand.”
Years ago the satire site The Onion had an article about a doctor who specialized in “giving a shit” - assumedly where Accurate dominates. While none of us may intentionally rush through patients or do half-assed jobs, we also have to deal with pressures of time. There never seems to be enough in a workday.
Nowhere is this more true than in primary care, where the pressures of time, overhead, and a large patient volume intersect. There are patients to see, labs to review, phone calls to return, forms to complete, meetings to attend, samples to sign for ... and probably many other things I’ve left out.
The fact that this situation exists shouldn’t surprise anyone. People talk about “burnout” and “making health care better” but that just seems to be lip service. They give you a free subscription to a meditation app, phone access to a counselor, and a mandatory early morning meeting to discuss stress reduction. Of course, these things take time away from seeing patients, which sort of defeats the whole purpose. Unless you want to do them at home – taking time away from your family, or doing the taxes, or other things you have to do besides your day job.
This is not sustainable for patients, doctors, or the health care system as a whole. But right now the situation is only getting worse, and there aren’t any easy answers.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
COVID can mimic prostate cancer symptoms
This patient has a strong likelihood of aggressive prostate cancer, right? If that same patient also presents with severe, burning bone pain with no precipitating trauma to the area and rest and over-the-counter painkillers are not helping, you’d think, “check for metastases,” right?
That patient was me in late January 2023.
As a research scientist member of the American Urological Association, I knew enough to know I had to consult my urologist ASAP.
With the above symptoms, I’ll admit I was scared. Fortunately, if that’s the right word, I was no stranger to a rapid, dramatic spike in PSA. In 2021 I was temporarily living in a new city, and I wanted to form a relationship with a good local urologist. The urologist that I was referred to gave me a thorough consultation, including a vigorous digital rectal exam (DRE) and sent me across the street for a blood draw.
To my shock, my PSA had spiked over 2 points, to 9.9 from 7.8 a few months earlier. I freaked. Had my 3-cm tumor burst out into an aggressive cancer? Research on PubMed provided an array of studies showing what could cause PSA to suddenly rise, including a DRE performed 72 hours before the blood draw.1 A week later, my PSA was back down to its normal 7.6.
But in January 2023, I had none of those previously reported experiences that could suddenly trigger a spike in PSA, like a DRE or riding on a thin bicycle seat for a few hours before the lab visit.
The COVID effect
I went back to PubMed and found a new circumstance that could cause a surge in PSA: COVID-19. A recent study2 of 91 men with benign prostatic hypertrophy by researchers in Turkey found that PSA spiked from 0 to 5 points during the COVID infection period and up to 2 points higher 3 months after the infection had cleared. I had tested positive for COVID-19 in mid-December 2022, 4 weeks before my 9.9 PSA reading.
Using Google translate, I communicated with the team in Turkey and found out that the PSA spike can last up to 6 months.
That study helps explain why my PSA dropped over 1.5 points to 8.5 just 2 weeks after the 9.9 reading, with the expectation that it would return to its previous normal of 7.8 within 6 months of infection with SARS-CoV-2. To be safe, my urologist scheduled another PSA test in May, along with an updated multiparametric MRI, which may be followed by an in-bore MRI-guided biopsy of the 3-cm tumor if the mass has enlarged.
COVID-19 pain
What about my burning bone pain in my upper right humerus and right rotator cuff that was not precipitated by trauma or strain? A radiograph found no evidence of metastasis, thank goodness. And my research showed that several studies3 have found that COVID-19 can cause burning musculoskeletal pain, including enthesopathy, which is what I had per the radiology report. So my PSA spike and searing pain were likely consequences of the infection.
To avoid the risk for a gross misdiagnosis after a radical spike in PSA, the informed urologist should ask the patient if he has had COVID-19 in the previous 6 months. Overlooking that question could lead to the wrong diagnostic decisions about a rapid jump in PSA or unexplained bone pain.
References
1. Bossens MM et al. Eur J Cancer. 1995;31A:682-5.
2. Cinislioglu AE et al. Urology. 2022;159:16-21.
3. Ciaffi J et al. Joint Bone Spine. 2021;88:105158.
Dr. Keller is founder of the Keller Research Institute, Jacksonville, Fla. He reported serving as a research scientist for the American Urological Association, serving on the advisory board of Active Surveillance Patient’s International, and serving on the boards of numerous nonprofit organizations.
A version of this article first appeared on Medscape.com.
This patient has a strong likelihood of aggressive prostate cancer, right? If that same patient also presents with severe, burning bone pain with no precipitating trauma to the area and rest and over-the-counter painkillers are not helping, you’d think, “check for metastases,” right?
That patient was me in late January 2023.
As a research scientist member of the American Urological Association, I knew enough to know I had to consult my urologist ASAP.
With the above symptoms, I’ll admit I was scared. Fortunately, if that’s the right word, I was no stranger to a rapid, dramatic spike in PSA. In 2021 I was temporarily living in a new city, and I wanted to form a relationship with a good local urologist. The urologist that I was referred to gave me a thorough consultation, including a vigorous digital rectal exam (DRE) and sent me across the street for a blood draw.
To my shock, my PSA had spiked over 2 points, to 9.9 from 7.8 a few months earlier. I freaked. Had my 3-cm tumor burst out into an aggressive cancer? Research on PubMed provided an array of studies showing what could cause PSA to suddenly rise, including a DRE performed 72 hours before the blood draw.1 A week later, my PSA was back down to its normal 7.6.
But in January 2023, I had none of those previously reported experiences that could suddenly trigger a spike in PSA, like a DRE or riding on a thin bicycle seat for a few hours before the lab visit.
The COVID effect
I went back to PubMed and found a new circumstance that could cause a surge in PSA: COVID-19. A recent study2 of 91 men with benign prostatic hypertrophy by researchers in Turkey found that PSA spiked from 0 to 5 points during the COVID infection period and up to 2 points higher 3 months after the infection had cleared. I had tested positive for COVID-19 in mid-December 2022, 4 weeks before my 9.9 PSA reading.
Using Google translate, I communicated with the team in Turkey and found out that the PSA spike can last up to 6 months.
That study helps explain why my PSA dropped over 1.5 points to 8.5 just 2 weeks after the 9.9 reading, with the expectation that it would return to its previous normal of 7.8 within 6 months of infection with SARS-CoV-2. To be safe, my urologist scheduled another PSA test in May, along with an updated multiparametric MRI, which may be followed by an in-bore MRI-guided biopsy of the 3-cm tumor if the mass has enlarged.
COVID-19 pain
What about my burning bone pain in my upper right humerus and right rotator cuff that was not precipitated by trauma or strain? A radiograph found no evidence of metastasis, thank goodness. And my research showed that several studies3 have found that COVID-19 can cause burning musculoskeletal pain, including enthesopathy, which is what I had per the radiology report. So my PSA spike and searing pain were likely consequences of the infection.
To avoid the risk for a gross misdiagnosis after a radical spike in PSA, the informed urologist should ask the patient if he has had COVID-19 in the previous 6 months. Overlooking that question could lead to the wrong diagnostic decisions about a rapid jump in PSA or unexplained bone pain.
References
1. Bossens MM et al. Eur J Cancer. 1995;31A:682-5.
2. Cinislioglu AE et al. Urology. 2022;159:16-21.
3. Ciaffi J et al. Joint Bone Spine. 2021;88:105158.
Dr. Keller is founder of the Keller Research Institute, Jacksonville, Fla. He reported serving as a research scientist for the American Urological Association, serving on the advisory board of Active Surveillance Patient’s International, and serving on the boards of numerous nonprofit organizations.
A version of this article first appeared on Medscape.com.
This patient has a strong likelihood of aggressive prostate cancer, right? If that same patient also presents with severe, burning bone pain with no precipitating trauma to the area and rest and over-the-counter painkillers are not helping, you’d think, “check for metastases,” right?
That patient was me in late January 2023.
As a research scientist member of the American Urological Association, I knew enough to know I had to consult my urologist ASAP.
With the above symptoms, I’ll admit I was scared. Fortunately, if that’s the right word, I was no stranger to a rapid, dramatic spike in PSA. In 2021 I was temporarily living in a new city, and I wanted to form a relationship with a good local urologist. The urologist that I was referred to gave me a thorough consultation, including a vigorous digital rectal exam (DRE) and sent me across the street for a blood draw.
To my shock, my PSA had spiked over 2 points, to 9.9 from 7.8 a few months earlier. I freaked. Had my 3-cm tumor burst out into an aggressive cancer? Research on PubMed provided an array of studies showing what could cause PSA to suddenly rise, including a DRE performed 72 hours before the blood draw.1 A week later, my PSA was back down to its normal 7.6.
But in January 2023, I had none of those previously reported experiences that could suddenly trigger a spike in PSA, like a DRE or riding on a thin bicycle seat for a few hours before the lab visit.
The COVID effect
I went back to PubMed and found a new circumstance that could cause a surge in PSA: COVID-19. A recent study2 of 91 men with benign prostatic hypertrophy by researchers in Turkey found that PSA spiked from 0 to 5 points during the COVID infection period and up to 2 points higher 3 months after the infection had cleared. I had tested positive for COVID-19 in mid-December 2022, 4 weeks before my 9.9 PSA reading.
Using Google translate, I communicated with the team in Turkey and found out that the PSA spike can last up to 6 months.
That study helps explain why my PSA dropped over 1.5 points to 8.5 just 2 weeks after the 9.9 reading, with the expectation that it would return to its previous normal of 7.8 within 6 months of infection with SARS-CoV-2. To be safe, my urologist scheduled another PSA test in May, along with an updated multiparametric MRI, which may be followed by an in-bore MRI-guided biopsy of the 3-cm tumor if the mass has enlarged.
COVID-19 pain
What about my burning bone pain in my upper right humerus and right rotator cuff that was not precipitated by trauma or strain? A radiograph found no evidence of metastasis, thank goodness. And my research showed that several studies3 have found that COVID-19 can cause burning musculoskeletal pain, including enthesopathy, which is what I had per the radiology report. So my PSA spike and searing pain were likely consequences of the infection.
To avoid the risk for a gross misdiagnosis after a radical spike in PSA, the informed urologist should ask the patient if he has had COVID-19 in the previous 6 months. Overlooking that question could lead to the wrong diagnostic decisions about a rapid jump in PSA or unexplained bone pain.
References
1. Bossens MM et al. Eur J Cancer. 1995;31A:682-5.
2. Cinislioglu AE et al. Urology. 2022;159:16-21.
3. Ciaffi J et al. Joint Bone Spine. 2021;88:105158.
Dr. Keller is founder of the Keller Research Institute, Jacksonville, Fla. He reported serving as a research scientist for the American Urological Association, serving on the advisory board of Active Surveillance Patient’s International, and serving on the boards of numerous nonprofit organizations.
A version of this article first appeared on Medscape.com.
Living kidney donors should receive money for their costs of donating
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at New York University’s Grossman School of Medicine in New York City.
We try very hard to get organ donation from those who die. That’s a commendable thing to do. I think doctors should always be discussing the opportunity to donate organs upon death, even in primary care settings.
It’s good to find out what people’s attitudes are. Let them learn about organ donation as something they can think about. Let them talk about it with family and friends and partners so that they know their wishes.
However, despite these efforts to encourage organ donation, we still have far fewer organs than we could use to transplant people, many people die on waiting lists because there are no organs to give them, and we’re in a situation where demand for organ transplant is actually increasing.
There is more capacity to do transplants both in the United States and elsewhere, and more people are living longer, so organ failure starts to become more common before, let’s say, terminal illness is really there. Now, we have more people who might benefit from organ transplant in an aging population.
One place to turn to help reduce the shortage of organs is to living donation. At least insofar as kidneys go, kidney donation from living persons has become a prominent source of organs for those who need kidneys – most of whom are surviving on dialysis, by the way, at a very high cost and often with a quality of life that they don’t find particularly easy to accept.
Transplant is far preferred, even though they have to take immunosuppression to keep those organ transplants going, and that has its own risks and side effects. They still get more mobility. They still are able to have a broader diet. They enjoy life far more than they do having to show up for dialysis three times a week for a couple of hours, every week, for every week that they live.
There is an interest in living kidney donation. One battle has been that, well, maybe we could get more kidneys if we just paid people to sell us their kidneys. That has been resisted, and I’ve been resistant to that idea, too, because I worry that it leads to exploitation.
The people who sell their kidneys are poor. They’re often in debt. They feel coerced by their circumstances, so they make a kidney sale. This happens in countries like India, where there are markets underground, and you see that it’s the poorest of the poor who do this, and they don’t really work their way out of debt. They just wind up without a kidney, help relieve their debt a little bit, and pretty soon, because they don’t have a job or an income except that sale of a kidney, they’re not much better off than they were before they started.
Also, people who sell kidneys for money are more likely not to admit to their own health problems, raising risks about the quality of organs. Then, of course, it puts doctors in a position to take out an organ for pay, even though it doesn’t benefit you, so that you can sell it. This raises some questions about whether that’s consistent with medical ethics.
A different idea has emerged. New York State Governor Kathy Hochul just signed legislation that allows living donors to be compensated for legitimate costs. That’s a little different matter. You’re not buying the organ, but you’re saying that if you experience health care problems due to complications from a donation, if you need money for transportation, if you lost money because you did this altruistically and you had to take time off from work and had expenses for a babysitter, restaurants, or other things, the state is going to try to create funds that will compensate you.
That, I think we should agree, is not a bad idea. You’re in a situation there where you don’t want to make people who are heroic, altruistic, and trying to help others by donating a kidney end up financially worse off.
I think there’s a difference between making someone financially whole after the decision to make a kidney available and creating a market where the poorest of the poor come forward to just sell because they see no other choice in terms of how to get rid of debts. I see these situations as not ethically equivalent, so I support efforts to try to compensate people who are our heroes. I don’t think we should ask them to financially suffer.
We’ll watch to see what happens as the New York state law comes into effect. By the way, New York is one of the states that really lags in the supply of organs for transplant, so this measure is particularly important for that state. Many other states should be considering this legislation as well.
It’s one thing to reward, if you will, donors by making sure they don’t suffer financial loss. It’s a very different thing to say, let’s have a free market and we’ll pay whoever it is that’s willing to sell us a kidney to do so. The former seems to me to be humane and just, whereas the latter risks exploitation.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at New York University’s Grossman School of Medicine in New York City.
We try very hard to get organ donation from those who die. That’s a commendable thing to do. I think doctors should always be discussing the opportunity to donate organs upon death, even in primary care settings.
It’s good to find out what people’s attitudes are. Let them learn about organ donation as something they can think about. Let them talk about it with family and friends and partners so that they know their wishes.
However, despite these efforts to encourage organ donation, we still have far fewer organs than we could use to transplant people, many people die on waiting lists because there are no organs to give them, and we’re in a situation where demand for organ transplant is actually increasing.
There is more capacity to do transplants both in the United States and elsewhere, and more people are living longer, so organ failure starts to become more common before, let’s say, terminal illness is really there. Now, we have more people who might benefit from organ transplant in an aging population.
One place to turn to help reduce the shortage of organs is to living donation. At least insofar as kidneys go, kidney donation from living persons has become a prominent source of organs for those who need kidneys – most of whom are surviving on dialysis, by the way, at a very high cost and often with a quality of life that they don’t find particularly easy to accept.
Transplant is far preferred, even though they have to take immunosuppression to keep those organ transplants going, and that has its own risks and side effects. They still get more mobility. They still are able to have a broader diet. They enjoy life far more than they do having to show up for dialysis three times a week for a couple of hours, every week, for every week that they live.
There is an interest in living kidney donation. One battle has been that, well, maybe we could get more kidneys if we just paid people to sell us their kidneys. That has been resisted, and I’ve been resistant to that idea, too, because I worry that it leads to exploitation.
The people who sell their kidneys are poor. They’re often in debt. They feel coerced by their circumstances, so they make a kidney sale. This happens in countries like India, where there are markets underground, and you see that it’s the poorest of the poor who do this, and they don’t really work their way out of debt. They just wind up without a kidney, help relieve their debt a little bit, and pretty soon, because they don’t have a job or an income except that sale of a kidney, they’re not much better off than they were before they started.
Also, people who sell kidneys for money are more likely not to admit to their own health problems, raising risks about the quality of organs. Then, of course, it puts doctors in a position to take out an organ for pay, even though it doesn’t benefit you, so that you can sell it. This raises some questions about whether that’s consistent with medical ethics.
A different idea has emerged. New York State Governor Kathy Hochul just signed legislation that allows living donors to be compensated for legitimate costs. That’s a little different matter. You’re not buying the organ, but you’re saying that if you experience health care problems due to complications from a donation, if you need money for transportation, if you lost money because you did this altruistically and you had to take time off from work and had expenses for a babysitter, restaurants, or other things, the state is going to try to create funds that will compensate you.
That, I think we should agree, is not a bad idea. You’re in a situation there where you don’t want to make people who are heroic, altruistic, and trying to help others by donating a kidney end up financially worse off.
I think there’s a difference between making someone financially whole after the decision to make a kidney available and creating a market where the poorest of the poor come forward to just sell because they see no other choice in terms of how to get rid of debts. I see these situations as not ethically equivalent, so I support efforts to try to compensate people who are our heroes. I don’t think we should ask them to financially suffer.
We’ll watch to see what happens as the New York state law comes into effect. By the way, New York is one of the states that really lags in the supply of organs for transplant, so this measure is particularly important for that state. Many other states should be considering this legislation as well.
It’s one thing to reward, if you will, donors by making sure they don’t suffer financial loss. It’s a very different thing to say, let’s have a free market and we’ll pay whoever it is that’s willing to sell us a kidney to do so. The former seems to me to be humane and just, whereas the latter risks exploitation.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the division of medical ethics at New York University’s Grossman School of Medicine in New York City.
We try very hard to get organ donation from those who die. That’s a commendable thing to do. I think doctors should always be discussing the opportunity to donate organs upon death, even in primary care settings.
It’s good to find out what people’s attitudes are. Let them learn about organ donation as something they can think about. Let them talk about it with family and friends and partners so that they know their wishes.
However, despite these efforts to encourage organ donation, we still have far fewer organs than we could use to transplant people, many people die on waiting lists because there are no organs to give them, and we’re in a situation where demand for organ transplant is actually increasing.
There is more capacity to do transplants both in the United States and elsewhere, and more people are living longer, so organ failure starts to become more common before, let’s say, terminal illness is really there. Now, we have more people who might benefit from organ transplant in an aging population.
One place to turn to help reduce the shortage of organs is to living donation. At least insofar as kidneys go, kidney donation from living persons has become a prominent source of organs for those who need kidneys – most of whom are surviving on dialysis, by the way, at a very high cost and often with a quality of life that they don’t find particularly easy to accept.
Transplant is far preferred, even though they have to take immunosuppression to keep those organ transplants going, and that has its own risks and side effects. They still get more mobility. They still are able to have a broader diet. They enjoy life far more than they do having to show up for dialysis three times a week for a couple of hours, every week, for every week that they live.
There is an interest in living kidney donation. One battle has been that, well, maybe we could get more kidneys if we just paid people to sell us their kidneys. That has been resisted, and I’ve been resistant to that idea, too, because I worry that it leads to exploitation.
The people who sell their kidneys are poor. They’re often in debt. They feel coerced by their circumstances, so they make a kidney sale. This happens in countries like India, where there are markets underground, and you see that it’s the poorest of the poor who do this, and they don’t really work their way out of debt. They just wind up without a kidney, help relieve their debt a little bit, and pretty soon, because they don’t have a job or an income except that sale of a kidney, they’re not much better off than they were before they started.
Also, people who sell kidneys for money are more likely not to admit to their own health problems, raising risks about the quality of organs. Then, of course, it puts doctors in a position to take out an organ for pay, even though it doesn’t benefit you, so that you can sell it. This raises some questions about whether that’s consistent with medical ethics.
A different idea has emerged. New York State Governor Kathy Hochul just signed legislation that allows living donors to be compensated for legitimate costs. That’s a little different matter. You’re not buying the organ, but you’re saying that if you experience health care problems due to complications from a donation, if you need money for transportation, if you lost money because you did this altruistically and you had to take time off from work and had expenses for a babysitter, restaurants, or other things, the state is going to try to create funds that will compensate you.
That, I think we should agree, is not a bad idea. You’re in a situation there where you don’t want to make people who are heroic, altruistic, and trying to help others by donating a kidney end up financially worse off.
I think there’s a difference between making someone financially whole after the decision to make a kidney available and creating a market where the poorest of the poor come forward to just sell because they see no other choice in terms of how to get rid of debts. I see these situations as not ethically equivalent, so I support efforts to try to compensate people who are our heroes. I don’t think we should ask them to financially suffer.
We’ll watch to see what happens as the New York state law comes into effect. By the way, New York is one of the states that really lags in the supply of organs for transplant, so this measure is particularly important for that state. Many other states should be considering this legislation as well.
It’s one thing to reward, if you will, donors by making sure they don’t suffer financial loss. It’s a very different thing to say, let’s have a free market and we’ll pay whoever it is that’s willing to sell us a kidney to do so. The former seems to me to be humane and just, whereas the latter risks exploitation.
A version of this article first appeared on Medscape.com.
Bruce Willis’ frontotemporal dementia is not your grandpa’s dementia
What is remarkable about the swamp that we call FTD is that it’s a somewhat rare and unusual type of dementia. We tend to characterize dementia as the erosion of memory, but FTD is more characterized by the loss of control over emotions and other cognitive functions. What›s especially tragic for performers like Mr. Willis is the loss of the verbal fluency required for delivering one’s lines.
Frontotemporal dementia
To this casual observer, Bruce Willis was an almost invincible force, vigorous, vital, one of the “immortals.” Alas, with his FTD diagnosis, we know that even a die-hard like Mr. Willis, now only 67 years of age, may have to endure years of progressive decline. If the disease follows its typical path, that will probably include slowly disconnecting and progressively losing emotional judgment and control as well as losing a reasonable understanding of what or why any of it is happening. He may also experience a progressive deterioration of the control of bodily functions and general health.
Most people with dementia lose their neurocognitive abilities through a number of different pathways, all of which result in brain shrinkage, disconnection, evident neuropathology, neurobehavioral expressions of loss, and forms of befuddlement. Alzheimer’s disease leads the list as the most common form of dementia, but vascular dementias; dementia with Lewy bodies; “mixed” dementias; dementias associated with Parkinson’s, Huntington’s, or other diseases; dementia rising from alcoholic or other brain poisoning, HIV, Lyme disease, or a host of other brain infections; or from traumatic encephalopathy (chronic or more current) may present at any active neurology clinic. These are what you might think of as your “grandpa’s dementia” – the common types often associated with old age.
FTD is a particularly interesting variant for several reasons. First, it usually arises in relatively young individuals, with initial symptoms emerging in one’s 50s or 60s. In most cases, there is no genetic and, with rare exception, any other explanation of origin – except that old medical standby, bad luck.
Second, FTD has little initial impact on a patient’s broader memory and associated cognitive abilities. The patient will stumble to come up with that next word and ultimately slow down their speech as their brain struggles with verbal fluency; they will struggle with translating their feelings and emotions into fast and appropriate actions expressed in their mind and their physical body while their memory will appear intact.
In all other dementias, cognitive losses can be profound, whereas social and emotional control and voluble speech production are generally better sustained. Imagine the impact that these struggles in verbal fluency and in emotional calibration and response must have for an established actor. By all reports, Mr. Willis vigorously pursued the work that he loved right up until the time of his dementia diagnosis, even as his colleagues would almost certainly have seen that he was struggling. Sadly, a lack of that type of self-awareness is an expected consequence of FTD.
The salience network and von Economo neurons
Third and most intriguing to a neuroscientific nerd like me is that patients with FTD experience an initial loss of a special population of cortical neurons located within the salience network in our brains, called the von Economo neurons. That salience network is designed to quickly read and evaluate our complex thoughts and emotions and via those Economo neurons, initiate appropriate neurologic and physical responses.
We share this special von Economo machinery with great apes, whales, elephants, and a handful of other especially social mammalian species.
When we see or hear or otherwise sense something that induces fear, alarm, or a potential reward, the salience network in our brain acts as a kind of gatekeeper. First, it assesses the emergent or changing situation, then it rapidly initiates an emotional and physical response. As I sit with a patient in obvious distress in my office, my salience network turns on an empathetic alarm. My brain and body immediately adjust to initiate appropriately sympathetic reactions. The von Economo neurons – those very neurons that have substantially died off in a brain with FTD – are the linchpins in this fast-response emotion and complex body signal-informed system.
Controlled emotional response is at the heart of our humanity. It’s a sad day when we lose it.
In other neurologic clinical conditions marked by the loss of specific brain cells, different forms of “disuse atrophy” are partly the cause. We don’t know whether that’s the case for FTD. Scientists have shown that specific forms of computerized brain exercises can sharply increase activity levels in the salience network which is linked to improvements in the regulatory control of the autonomic nervous system – one of the key response-mediating targets of the network’s von Economo neurons.
Interestingly, superagers who sustain body and brain health into their 90s (and beyond) die with a full complement of von Economo neurons operating happily in a still-vigorous salience network.
This neuroscientist can foresee a day when we routinely assess the integrity of this important brain system and more reliably maintain its good health. Keeping those very special neurons alive would have probably allowed Mr. Willis to sustain himself on the soundstage and on the grander stage of life for a long time to come. Alas, like so many things in medicine, there is promise. But at this moment for this famous patient, our current medical science appears to be a day late, and a dollar short.
Dr. Merzenichis is professor emeritus at the University of California, San Francisco, and a Kavli Laureate in Neuroscience. He reported conflicts of interest with the National Institutes of Health, Stronger Brains, and Posit Science.
A version of this article first appeared on Medscape.com.
What is remarkable about the swamp that we call FTD is that it’s a somewhat rare and unusual type of dementia. We tend to characterize dementia as the erosion of memory, but FTD is more characterized by the loss of control over emotions and other cognitive functions. What›s especially tragic for performers like Mr. Willis is the loss of the verbal fluency required for delivering one’s lines.
Frontotemporal dementia
To this casual observer, Bruce Willis was an almost invincible force, vigorous, vital, one of the “immortals.” Alas, with his FTD diagnosis, we know that even a die-hard like Mr. Willis, now only 67 years of age, may have to endure years of progressive decline. If the disease follows its typical path, that will probably include slowly disconnecting and progressively losing emotional judgment and control as well as losing a reasonable understanding of what or why any of it is happening. He may also experience a progressive deterioration of the control of bodily functions and general health.
Most people with dementia lose their neurocognitive abilities through a number of different pathways, all of which result in brain shrinkage, disconnection, evident neuropathology, neurobehavioral expressions of loss, and forms of befuddlement. Alzheimer’s disease leads the list as the most common form of dementia, but vascular dementias; dementia with Lewy bodies; “mixed” dementias; dementias associated with Parkinson’s, Huntington’s, or other diseases; dementia rising from alcoholic or other brain poisoning, HIV, Lyme disease, or a host of other brain infections; or from traumatic encephalopathy (chronic or more current) may present at any active neurology clinic. These are what you might think of as your “grandpa’s dementia” – the common types often associated with old age.
FTD is a particularly interesting variant for several reasons. First, it usually arises in relatively young individuals, with initial symptoms emerging in one’s 50s or 60s. In most cases, there is no genetic and, with rare exception, any other explanation of origin – except that old medical standby, bad luck.
Second, FTD has little initial impact on a patient’s broader memory and associated cognitive abilities. The patient will stumble to come up with that next word and ultimately slow down their speech as their brain struggles with verbal fluency; they will struggle with translating their feelings and emotions into fast and appropriate actions expressed in their mind and their physical body while their memory will appear intact.
In all other dementias, cognitive losses can be profound, whereas social and emotional control and voluble speech production are generally better sustained. Imagine the impact that these struggles in verbal fluency and in emotional calibration and response must have for an established actor. By all reports, Mr. Willis vigorously pursued the work that he loved right up until the time of his dementia diagnosis, even as his colleagues would almost certainly have seen that he was struggling. Sadly, a lack of that type of self-awareness is an expected consequence of FTD.
The salience network and von Economo neurons
Third and most intriguing to a neuroscientific nerd like me is that patients with FTD experience an initial loss of a special population of cortical neurons located within the salience network in our brains, called the von Economo neurons. That salience network is designed to quickly read and evaluate our complex thoughts and emotions and via those Economo neurons, initiate appropriate neurologic and physical responses.
We share this special von Economo machinery with great apes, whales, elephants, and a handful of other especially social mammalian species.
When we see or hear or otherwise sense something that induces fear, alarm, or a potential reward, the salience network in our brain acts as a kind of gatekeeper. First, it assesses the emergent or changing situation, then it rapidly initiates an emotional and physical response. As I sit with a patient in obvious distress in my office, my salience network turns on an empathetic alarm. My brain and body immediately adjust to initiate appropriately sympathetic reactions. The von Economo neurons – those very neurons that have substantially died off in a brain with FTD – are the linchpins in this fast-response emotion and complex body signal-informed system.
Controlled emotional response is at the heart of our humanity. It’s a sad day when we lose it.
In other neurologic clinical conditions marked by the loss of specific brain cells, different forms of “disuse atrophy” are partly the cause. We don’t know whether that’s the case for FTD. Scientists have shown that specific forms of computerized brain exercises can sharply increase activity levels in the salience network which is linked to improvements in the regulatory control of the autonomic nervous system – one of the key response-mediating targets of the network’s von Economo neurons.
Interestingly, superagers who sustain body and brain health into their 90s (and beyond) die with a full complement of von Economo neurons operating happily in a still-vigorous salience network.
This neuroscientist can foresee a day when we routinely assess the integrity of this important brain system and more reliably maintain its good health. Keeping those very special neurons alive would have probably allowed Mr. Willis to sustain himself on the soundstage and on the grander stage of life for a long time to come. Alas, like so many things in medicine, there is promise. But at this moment for this famous patient, our current medical science appears to be a day late, and a dollar short.
Dr. Merzenichis is professor emeritus at the University of California, San Francisco, and a Kavli Laureate in Neuroscience. He reported conflicts of interest with the National Institutes of Health, Stronger Brains, and Posit Science.
A version of this article first appeared on Medscape.com.
What is remarkable about the swamp that we call FTD is that it’s a somewhat rare and unusual type of dementia. We tend to characterize dementia as the erosion of memory, but FTD is more characterized by the loss of control over emotions and other cognitive functions. What›s especially tragic for performers like Mr. Willis is the loss of the verbal fluency required for delivering one’s lines.
Frontotemporal dementia
To this casual observer, Bruce Willis was an almost invincible force, vigorous, vital, one of the “immortals.” Alas, with his FTD diagnosis, we know that even a die-hard like Mr. Willis, now only 67 years of age, may have to endure years of progressive decline. If the disease follows its typical path, that will probably include slowly disconnecting and progressively losing emotional judgment and control as well as losing a reasonable understanding of what or why any of it is happening. He may also experience a progressive deterioration of the control of bodily functions and general health.
Most people with dementia lose their neurocognitive abilities through a number of different pathways, all of which result in brain shrinkage, disconnection, evident neuropathology, neurobehavioral expressions of loss, and forms of befuddlement. Alzheimer’s disease leads the list as the most common form of dementia, but vascular dementias; dementia with Lewy bodies; “mixed” dementias; dementias associated with Parkinson’s, Huntington’s, or other diseases; dementia rising from alcoholic or other brain poisoning, HIV, Lyme disease, or a host of other brain infections; or from traumatic encephalopathy (chronic or more current) may present at any active neurology clinic. These are what you might think of as your “grandpa’s dementia” – the common types often associated with old age.
FTD is a particularly interesting variant for several reasons. First, it usually arises in relatively young individuals, with initial symptoms emerging in one’s 50s or 60s. In most cases, there is no genetic and, with rare exception, any other explanation of origin – except that old medical standby, bad luck.
Second, FTD has little initial impact on a patient’s broader memory and associated cognitive abilities. The patient will stumble to come up with that next word and ultimately slow down their speech as their brain struggles with verbal fluency; they will struggle with translating their feelings and emotions into fast and appropriate actions expressed in their mind and their physical body while their memory will appear intact.
In all other dementias, cognitive losses can be profound, whereas social and emotional control and voluble speech production are generally better sustained. Imagine the impact that these struggles in verbal fluency and in emotional calibration and response must have for an established actor. By all reports, Mr. Willis vigorously pursued the work that he loved right up until the time of his dementia diagnosis, even as his colleagues would almost certainly have seen that he was struggling. Sadly, a lack of that type of self-awareness is an expected consequence of FTD.
The salience network and von Economo neurons
Third and most intriguing to a neuroscientific nerd like me is that patients with FTD experience an initial loss of a special population of cortical neurons located within the salience network in our brains, called the von Economo neurons. That salience network is designed to quickly read and evaluate our complex thoughts and emotions and via those Economo neurons, initiate appropriate neurologic and physical responses.
We share this special von Economo machinery with great apes, whales, elephants, and a handful of other especially social mammalian species.
When we see or hear or otherwise sense something that induces fear, alarm, or a potential reward, the salience network in our brain acts as a kind of gatekeeper. First, it assesses the emergent or changing situation, then it rapidly initiates an emotional and physical response. As I sit with a patient in obvious distress in my office, my salience network turns on an empathetic alarm. My brain and body immediately adjust to initiate appropriately sympathetic reactions. The von Economo neurons – those very neurons that have substantially died off in a brain with FTD – are the linchpins in this fast-response emotion and complex body signal-informed system.
Controlled emotional response is at the heart of our humanity. It’s a sad day when we lose it.
In other neurologic clinical conditions marked by the loss of specific brain cells, different forms of “disuse atrophy” are partly the cause. We don’t know whether that’s the case for FTD. Scientists have shown that specific forms of computerized brain exercises can sharply increase activity levels in the salience network which is linked to improvements in the regulatory control of the autonomic nervous system – one of the key response-mediating targets of the network’s von Economo neurons.
Interestingly, superagers who sustain body and brain health into their 90s (and beyond) die with a full complement of von Economo neurons operating happily in a still-vigorous salience network.
This neuroscientist can foresee a day when we routinely assess the integrity of this important brain system and more reliably maintain its good health. Keeping those very special neurons alive would have probably allowed Mr. Willis to sustain himself on the soundstage and on the grander stage of life for a long time to come. Alas, like so many things in medicine, there is promise. But at this moment for this famous patient, our current medical science appears to be a day late, and a dollar short.
Dr. Merzenichis is professor emeritus at the University of California, San Francisco, and a Kavli Laureate in Neuroscience. He reported conflicts of interest with the National Institutes of Health, Stronger Brains, and Posit Science.
A version of this article first appeared on Medscape.com.
What’s the ‘secret sauce’ to help patients move more?
“Just Do It” is a cute marketing slogan. But let’s face it: Clinically, it doesn’t work well. Most people just don’t exercise. according to recent data from the Centers for Disease Control and Prevention.
Furthermore, when surveyed about aerobic exercise and strength training, only 24.6% meet these weekly recommendations. These low rates of physical activity are alarming, given the immense benefits of exercise in improving mental and physical health and well-being.
Many people know that exercise is good for them but struggle to go workout consistently. I know firsthand how challenging this can be. In addition to being an integrative obesity specialist, I have gone from 0 minutes of physical activity in 2014 to becoming a fitness enthusiast who’s run more than 5,300 miles over 8 years. I know that as doctors and clinicians, we can profoundly influence our patients’ exercise journey.
Here are five tips to help motivate your patients make the change from “I Won’t Do It” to “I’m Doing It.”
Tip 1: ‘[Clinician], heal thyself’
Data don’t lie. Doctors who move more are more likely to counsel patients on exercise. I’ve been the doctor on both sides of the exercise spectrum. At my heaviest weight and lowest physical activity level, I felt hypocritical counseling patients on exercise.
If and when I counseled my patients on exercise, it was very directive and impersonal. When I started running consistently, I went to the opposite end of the spectrum. In my running zeal, it took a while for me to understand that not everyone wants to run dozens of miles a week. Shocking! Some people can’t handle intense workouts. The “I did it so you can too” perspective wasn’t helpful for long-term change in most patients.
What has been beneficial is recalling the obstacles and emotions I had (and still have) with staying consistent with physical activity. When physicians and clinicians move regularly, we’re more equipped to give our patients genuine counseling based on practicality rather than theory.
Now that self-reflection has been addressed, let’s get to patient counseling.
Tip 2: Motivate, don’t berate
Lectures on why patients should exercise are less helpful than asking, “Why aren›t you able to exercise more often?”
Asking open-ended questions is essential in motivational interviewing. Motivational interviewing promotes behavioral change through collaborative conversation.
Instead of telling the patient what to do, motivational interviewing seeks to establish a person’s why and create an effective plan based on their motivation. Asking open-ended questions is also helpful in determining any challenges to regular exercise, rather than calling these challenges “excuses,” which can be counterproductive.
I encourage patients to embrace challenges as opportunities for improvement. If they say: “I can’t find time to work out,” I suggest that they create time to work out by walking 10-15 minutes during lunch or after dinner. The information gleaned from open-ended questions helps set practical SMARTER goals, which we will discuss next.
Tip 3: Set SMARTER goals
After assessing the patient’s motivation and barriers, use this information to transform their desire to change into an actionable plan through a SMARTER goal. SMARTER stands for Specific, Measurable, Attainable, Relevant, Time-Sensitive, Enjoyable, and Rewarding. Practical goals have each of these components. That’s why “Just Do It” or even “Exercise 150 minutes a week” isn’t a clear path for actionable change. SMARTER goals go beyond what to do and help people personalize how to change.
For example, the SMARTER version of “exercise 150 minutes a week” for a busy person who works 50 hours a week may look like this: “My goal is to incorporate 150 minutes of physical activity through 60 minutes of aerobic exercise Monday through Friday (20-minute lunch walks) and 90 minutes of combination resistance training on the weekend (two 45-minute sessions) while listening to my favorite music. To meet my goal, I will reward myself by calling a friend to catch up or buy myself a new workout outfit.”
Exercise prescriptions are another helpful way to empower patients with a realistic exercise strategy. In my practice, I developed my own exercise prescription which focuses on overcoming time barriers to exercise and finding personally enjoyable exercises. To enhance self-directed physical activity, I›ve found it useful to have patients complete part of the “exercise prescription” on their own before or after their visit.
Tip 4: Use accountability tools
Making a SMARTER goal is one thing, but sticking with it takes regular reinforcement. Even with the best plan, once patients leave the office, there are many distractions from their goals. Accountability is the secret sauce to cultivating consistency. Fitness trackers are an affordable form of accountability. Studies show that wearing a fitness tracker can help people get up to 40 minutes of extra walking, compared with people who don’t wear trackers.
Additionally, clinicians can use different ways to offer exercise accountability. For example, more frequent check-ins, individually or in groups, can be helpful. The increase in telehealth has made interval visits easier. Reimbursement and time can limit clinician-level accountability, however. Other options are referring patients to online support groups or programs sponsored by the government or organizations. For years, I coled a Walk With a Doc chapter in Richmond, Va. There are chapters throughout the country.
Tip 5: Prepare and PLAN for setbacks
Breaking news: Most plans don’t go quite as envisioned. Accounting for the potential of setbacks early on helps patients set realistic expectations. As physicians and clinicians, we can help our patients anticipate a few likely obstacles. This may lessen the impact when a setback occurs. Also, it’s helpful to have the patient prepare for a setback with a PLAN for recovering quickly. PLAN stands for Ponder what happened; Learn from it; Adjust the original goal; Now get back on track. Getting back on track as soon as possible is important to keep patients motivated and prevent muscle deconditioning.
Exercise is medicine. Physical inactivity is a leading contributor to many preventable diseases. Although the physical activity statistics are disappointing, improvement is possible. Many systemic changes are needed to increase physical activity on a population level.
While waiting for more extensive changes, we have the power to equip patients with personalized, actionable tools for improving and maintaining physical activity.
We can transform one person at a time through our clinical encounters. Let’s use effective tools to help patients shift from “I Won’t Do It” to “I’m Doing It.”
Sylvia Gonsahn-Bollie, MD, DipABOM, is an integrative obesity specialist focused on individualized solutions for emotional and biological overeating. Her bestselling book, “Embrace You: Your Guide to Transforming Weight Loss Misconceptions Into Lifelong Wellness,” was Healthline.com’s Best Overall Weight Loss Book of 2022 and one of Livestrong.com’s 8 Best Weight-Loss Books to Read in 2022. She reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
“Just Do It” is a cute marketing slogan. But let’s face it: Clinically, it doesn’t work well. Most people just don’t exercise. according to recent data from the Centers for Disease Control and Prevention.
Furthermore, when surveyed about aerobic exercise and strength training, only 24.6% meet these weekly recommendations. These low rates of physical activity are alarming, given the immense benefits of exercise in improving mental and physical health and well-being.
Many people know that exercise is good for them but struggle to go workout consistently. I know firsthand how challenging this can be. In addition to being an integrative obesity specialist, I have gone from 0 minutes of physical activity in 2014 to becoming a fitness enthusiast who’s run more than 5,300 miles over 8 years. I know that as doctors and clinicians, we can profoundly influence our patients’ exercise journey.
Here are five tips to help motivate your patients make the change from “I Won’t Do It” to “I’m Doing It.”
Tip 1: ‘[Clinician], heal thyself’
Data don’t lie. Doctors who move more are more likely to counsel patients on exercise. I’ve been the doctor on both sides of the exercise spectrum. At my heaviest weight and lowest physical activity level, I felt hypocritical counseling patients on exercise.
If and when I counseled my patients on exercise, it was very directive and impersonal. When I started running consistently, I went to the opposite end of the spectrum. In my running zeal, it took a while for me to understand that not everyone wants to run dozens of miles a week. Shocking! Some people can’t handle intense workouts. The “I did it so you can too” perspective wasn’t helpful for long-term change in most patients.
What has been beneficial is recalling the obstacles and emotions I had (and still have) with staying consistent with physical activity. When physicians and clinicians move regularly, we’re more equipped to give our patients genuine counseling based on practicality rather than theory.
Now that self-reflection has been addressed, let’s get to patient counseling.
Tip 2: Motivate, don’t berate
Lectures on why patients should exercise are less helpful than asking, “Why aren›t you able to exercise more often?”
Asking open-ended questions is essential in motivational interviewing. Motivational interviewing promotes behavioral change through collaborative conversation.
Instead of telling the patient what to do, motivational interviewing seeks to establish a person’s why and create an effective plan based on their motivation. Asking open-ended questions is also helpful in determining any challenges to regular exercise, rather than calling these challenges “excuses,” which can be counterproductive.
I encourage patients to embrace challenges as opportunities for improvement. If they say: “I can’t find time to work out,” I suggest that they create time to work out by walking 10-15 minutes during lunch or after dinner. The information gleaned from open-ended questions helps set practical SMARTER goals, which we will discuss next.
Tip 3: Set SMARTER goals
After assessing the patient’s motivation and barriers, use this information to transform their desire to change into an actionable plan through a SMARTER goal. SMARTER stands for Specific, Measurable, Attainable, Relevant, Time-Sensitive, Enjoyable, and Rewarding. Practical goals have each of these components. That’s why “Just Do It” or even “Exercise 150 minutes a week” isn’t a clear path for actionable change. SMARTER goals go beyond what to do and help people personalize how to change.
For example, the SMARTER version of “exercise 150 minutes a week” for a busy person who works 50 hours a week may look like this: “My goal is to incorporate 150 minutes of physical activity through 60 minutes of aerobic exercise Monday through Friday (20-minute lunch walks) and 90 minutes of combination resistance training on the weekend (two 45-minute sessions) while listening to my favorite music. To meet my goal, I will reward myself by calling a friend to catch up or buy myself a new workout outfit.”
Exercise prescriptions are another helpful way to empower patients with a realistic exercise strategy. In my practice, I developed my own exercise prescription which focuses on overcoming time barriers to exercise and finding personally enjoyable exercises. To enhance self-directed physical activity, I›ve found it useful to have patients complete part of the “exercise prescription” on their own before or after their visit.
Tip 4: Use accountability tools
Making a SMARTER goal is one thing, but sticking with it takes regular reinforcement. Even with the best plan, once patients leave the office, there are many distractions from their goals. Accountability is the secret sauce to cultivating consistency. Fitness trackers are an affordable form of accountability. Studies show that wearing a fitness tracker can help people get up to 40 minutes of extra walking, compared with people who don’t wear trackers.
Additionally, clinicians can use different ways to offer exercise accountability. For example, more frequent check-ins, individually or in groups, can be helpful. The increase in telehealth has made interval visits easier. Reimbursement and time can limit clinician-level accountability, however. Other options are referring patients to online support groups or programs sponsored by the government or organizations. For years, I coled a Walk With a Doc chapter in Richmond, Va. There are chapters throughout the country.
Tip 5: Prepare and PLAN for setbacks
Breaking news: Most plans don’t go quite as envisioned. Accounting for the potential of setbacks early on helps patients set realistic expectations. As physicians and clinicians, we can help our patients anticipate a few likely obstacles. This may lessen the impact when a setback occurs. Also, it’s helpful to have the patient prepare for a setback with a PLAN for recovering quickly. PLAN stands for Ponder what happened; Learn from it; Adjust the original goal; Now get back on track. Getting back on track as soon as possible is important to keep patients motivated and prevent muscle deconditioning.
Exercise is medicine. Physical inactivity is a leading contributor to many preventable diseases. Although the physical activity statistics are disappointing, improvement is possible. Many systemic changes are needed to increase physical activity on a population level.
While waiting for more extensive changes, we have the power to equip patients with personalized, actionable tools for improving and maintaining physical activity.
We can transform one person at a time through our clinical encounters. Let’s use effective tools to help patients shift from “I Won’t Do It” to “I’m Doing It.”
Sylvia Gonsahn-Bollie, MD, DipABOM, is an integrative obesity specialist focused on individualized solutions for emotional and biological overeating. Her bestselling book, “Embrace You: Your Guide to Transforming Weight Loss Misconceptions Into Lifelong Wellness,” was Healthline.com’s Best Overall Weight Loss Book of 2022 and one of Livestrong.com’s 8 Best Weight-Loss Books to Read in 2022. She reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
“Just Do It” is a cute marketing slogan. But let’s face it: Clinically, it doesn’t work well. Most people just don’t exercise. according to recent data from the Centers for Disease Control and Prevention.
Furthermore, when surveyed about aerobic exercise and strength training, only 24.6% meet these weekly recommendations. These low rates of physical activity are alarming, given the immense benefits of exercise in improving mental and physical health and well-being.
Many people know that exercise is good for them but struggle to go workout consistently. I know firsthand how challenging this can be. In addition to being an integrative obesity specialist, I have gone from 0 minutes of physical activity in 2014 to becoming a fitness enthusiast who’s run more than 5,300 miles over 8 years. I know that as doctors and clinicians, we can profoundly influence our patients’ exercise journey.
Here are five tips to help motivate your patients make the change from “I Won’t Do It” to “I’m Doing It.”
Tip 1: ‘[Clinician], heal thyself’
Data don’t lie. Doctors who move more are more likely to counsel patients on exercise. I’ve been the doctor on both sides of the exercise spectrum. At my heaviest weight and lowest physical activity level, I felt hypocritical counseling patients on exercise.
If and when I counseled my patients on exercise, it was very directive and impersonal. When I started running consistently, I went to the opposite end of the spectrum. In my running zeal, it took a while for me to understand that not everyone wants to run dozens of miles a week. Shocking! Some people can’t handle intense workouts. The “I did it so you can too” perspective wasn’t helpful for long-term change in most patients.
What has been beneficial is recalling the obstacles and emotions I had (and still have) with staying consistent with physical activity. When physicians and clinicians move regularly, we’re more equipped to give our patients genuine counseling based on practicality rather than theory.
Now that self-reflection has been addressed, let’s get to patient counseling.
Tip 2: Motivate, don’t berate
Lectures on why patients should exercise are less helpful than asking, “Why aren›t you able to exercise more often?”
Asking open-ended questions is essential in motivational interviewing. Motivational interviewing promotes behavioral change through collaborative conversation.
Instead of telling the patient what to do, motivational interviewing seeks to establish a person’s why and create an effective plan based on their motivation. Asking open-ended questions is also helpful in determining any challenges to regular exercise, rather than calling these challenges “excuses,” which can be counterproductive.
I encourage patients to embrace challenges as opportunities for improvement. If they say: “I can’t find time to work out,” I suggest that they create time to work out by walking 10-15 minutes during lunch or after dinner. The information gleaned from open-ended questions helps set practical SMARTER goals, which we will discuss next.
Tip 3: Set SMARTER goals
After assessing the patient’s motivation and barriers, use this information to transform their desire to change into an actionable plan through a SMARTER goal. SMARTER stands for Specific, Measurable, Attainable, Relevant, Time-Sensitive, Enjoyable, and Rewarding. Practical goals have each of these components. That’s why “Just Do It” or even “Exercise 150 minutes a week” isn’t a clear path for actionable change. SMARTER goals go beyond what to do and help people personalize how to change.
For example, the SMARTER version of “exercise 150 minutes a week” for a busy person who works 50 hours a week may look like this: “My goal is to incorporate 150 minutes of physical activity through 60 minutes of aerobic exercise Monday through Friday (20-minute lunch walks) and 90 minutes of combination resistance training on the weekend (two 45-minute sessions) while listening to my favorite music. To meet my goal, I will reward myself by calling a friend to catch up or buy myself a new workout outfit.”
Exercise prescriptions are another helpful way to empower patients with a realistic exercise strategy. In my practice, I developed my own exercise prescription which focuses on overcoming time barriers to exercise and finding personally enjoyable exercises. To enhance self-directed physical activity, I›ve found it useful to have patients complete part of the “exercise prescription” on their own before or after their visit.
Tip 4: Use accountability tools
Making a SMARTER goal is one thing, but sticking with it takes regular reinforcement. Even with the best plan, once patients leave the office, there are many distractions from their goals. Accountability is the secret sauce to cultivating consistency. Fitness trackers are an affordable form of accountability. Studies show that wearing a fitness tracker can help people get up to 40 minutes of extra walking, compared with people who don’t wear trackers.
Additionally, clinicians can use different ways to offer exercise accountability. For example, more frequent check-ins, individually or in groups, can be helpful. The increase in telehealth has made interval visits easier. Reimbursement and time can limit clinician-level accountability, however. Other options are referring patients to online support groups or programs sponsored by the government or organizations. For years, I coled a Walk With a Doc chapter in Richmond, Va. There are chapters throughout the country.
Tip 5: Prepare and PLAN for setbacks
Breaking news: Most plans don’t go quite as envisioned. Accounting for the potential of setbacks early on helps patients set realistic expectations. As physicians and clinicians, we can help our patients anticipate a few likely obstacles. This may lessen the impact when a setback occurs. Also, it’s helpful to have the patient prepare for a setback with a PLAN for recovering quickly. PLAN stands for Ponder what happened; Learn from it; Adjust the original goal; Now get back on track. Getting back on track as soon as possible is important to keep patients motivated and prevent muscle deconditioning.
Exercise is medicine. Physical inactivity is a leading contributor to many preventable diseases. Although the physical activity statistics are disappointing, improvement is possible. Many systemic changes are needed to increase physical activity on a population level.
While waiting for more extensive changes, we have the power to equip patients with personalized, actionable tools for improving and maintaining physical activity.
We can transform one person at a time through our clinical encounters. Let’s use effective tools to help patients shift from “I Won’t Do It” to “I’m Doing It.”
Sylvia Gonsahn-Bollie, MD, DipABOM, is an integrative obesity specialist focused on individualized solutions for emotional and biological overeating. Her bestselling book, “Embrace You: Your Guide to Transforming Weight Loss Misconceptions Into Lifelong Wellness,” was Healthline.com’s Best Overall Weight Loss Book of 2022 and one of Livestrong.com’s 8 Best Weight-Loss Books to Read in 2022. She reported no conflicts of interest.
A version of this article first appeared on Medscape.com.