User login
Official Newspaper of the American College of Surgeons
January Hot Threads in ACS Communities
Want to know what your colleagues are talking about? Here are the top discussion threads in ACS Communities (all from the General Surgery community):
1. A lap appy ain’t always easy ...
3. Privileging
4. Malpractice moles
5. Safe laparoscopic entry
6. Is PID a general surgery problem?
7. Family debriefing after surgery
8. Peer-to-peer review
9. What should I do?
10. CT colonography
To join communities, log in to ACS Communities at http://acscommunities.facs.org/home, go to “Browse All Communities” near the top of any page, and click the blue “Join” button next to the community you’d like to join. If you have any questions, please send them to [email protected].
Want to know what your colleagues are talking about? Here are the top discussion threads in ACS Communities (all from the General Surgery community):
1. A lap appy ain’t always easy ...
3. Privileging
4. Malpractice moles
5. Safe laparoscopic entry
6. Is PID a general surgery problem?
7. Family debriefing after surgery
8. Peer-to-peer review
9. What should I do?
10. CT colonography
To join communities, log in to ACS Communities at http://acscommunities.facs.org/home, go to “Browse All Communities” near the top of any page, and click the blue “Join” button next to the community you’d like to join. If you have any questions, please send them to [email protected].
Want to know what your colleagues are talking about? Here are the top discussion threads in ACS Communities (all from the General Surgery community):
1. A lap appy ain’t always easy ...
3. Privileging
4. Malpractice moles
5. Safe laparoscopic entry
6. Is PID a general surgery problem?
7. Family debriefing after surgery
8. Peer-to-peer review
9. What should I do?
10. CT colonography
To join communities, log in to ACS Communities at http://acscommunities.facs.org/home, go to “Browse All Communities” near the top of any page, and click the blue “Join” button next to the community you’d like to join. If you have any questions, please send them to [email protected].
LMWH trumps unfractionated heparin in reducing posttrauma thrombotic events
HOLLYWOOD, FLA. – Low-molecular-weight heparin (LMWH) decreased the risk of venous thromboembolism in trauma patients significantly more than did unfractionated heparin, a large state database review has found.
It also was associated with a 37% decrease in overall mortality, compared with unfractionated heparin, Benjamin Jacobs, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.

He extracted data describing thromboembolism prophylaxis among 37,868 trauma patients included in the Michigan Trauma Quality Improvement Program from 2012 to 2014. The patients were treated at 23 hospitals around the state. They received either unfractionated or LMWH as their only clot-preventing protocol.
The primary outcomes of the study were reductions in the risk of venous thromboembolism (VTE), deep vein thrombosis (DVT), pulmonary thrombosis (PT), and mortality.
LMWH was given at either 40 mg every day or 30 mg twice a day. The comparator was unfractionated heparin at 5,000 U either two or three times a day.
The preferred method was LMWH, which 83% of patients received, compared with 17% who got the unfractionated heparin. Most patients who got LMWH received the 40 mg/day dose (70%). Most who got unfractionated heparin received 5,000 U three times a day (87%).
Both types of heparin reduced the risk of all thromboembolic outcomes, and both doses of LMWH significantly reduced the risks. However, the 40 mg/day dose was significantly more effective than the twice-daily 30-mg dose in reducing the risk of VTE and DVT. Risk reductions for PT and mortality were not significantly different between the doses.
Overall, compared with unfractionated heparin, LMWH decreased the risk of VTE by 33%; of PT by 48%; and of DVT by 27%. It also conferred a significant mortality benefit, reducing the risk of death by 37%, compared with the unfractionated type
When Dr. Jacobs grouped the patients according to Injury Severity Score (ISS), he saw a consistently higher benefit among patients with lower scores. For example, LMWH significantly reduced the risk of PT by 59% in patients with an ISS of 5-14. In those with an ISS of 25 or higher, the drug was associated with a 20% increased risk, although that wasn’t statistically significant.
There was a similar finding in DVT. LMWH reduced the risk by 18% in those with an ISS of 5-15, and by 50% among those with an score of 16-24 – both significant reductions. Among those with an ISS of at least 25, the risk was 18% higher, although, again, it was not a significant finding.
Curiously, the mortality benefit was stronger among sicker patients. The benefit was nonsignificant among those with an ISS of less than 25 but for those above 25, the mortality risk reduction was a significant 45%.
Dr Jacobs had no financial disclosures.
[email protected]
On Twitter @alz_gal
HOLLYWOOD, FLA. – Low-molecular-weight heparin (LMWH) decreased the risk of venous thromboembolism in trauma patients significantly more than did unfractionated heparin, a large state database review has found.
It also was associated with a 37% decrease in overall mortality, compared with unfractionated heparin, Benjamin Jacobs, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
He extracted data describing thromboembolism prophylaxis among 37,868 trauma patients included in the Michigan Trauma Quality Improvement Program from 2012 to 2014. The patients were treated at 23 hospitals around the state. They received either unfractionated or LMWH as their only clot-preventing protocol.
The primary outcomes of the study were reductions in the risk of venous thromboembolism (VTE), deep vein thrombosis (DVT), pulmonary thrombosis (PT), and mortality.
LMWH was given at either 40 mg every day or 30 mg twice a day. The comparator was unfractionated heparin at 5,000 U either two or three times a day.
The preferred method was LMWH, which 83% of patients received, compared with 17% who got the unfractionated heparin. Most patients who got LMWH received the 40 mg/day dose (70%). Most who got unfractionated heparin received 5,000 U three times a day (87%).
Both types of heparin reduced the risk of all thromboembolic outcomes, and both doses of LMWH significantly reduced the risks. However, the 40 mg/day dose was significantly more effective than the twice-daily 30-mg dose in reducing the risk of VTE and DVT. Risk reductions for PT and mortality were not significantly different between the doses.
Overall, compared with unfractionated heparin, LMWH decreased the risk of VTE by 33%; of PT by 48%; and of DVT by 27%. It also conferred a significant mortality benefit, reducing the risk of death by 37%, compared with the unfractionated type
When Dr. Jacobs grouped the patients according to Injury Severity Score (ISS), he saw a consistently higher benefit among patients with lower scores. For example, LMWH significantly reduced the risk of PT by 59% in patients with an ISS of 5-14. In those with an ISS of 25 or higher, the drug was associated with a 20% increased risk, although that wasn’t statistically significant.
There was a similar finding in DVT. LMWH reduced the risk by 18% in those with an ISS of 5-15, and by 50% among those with an score of 16-24 – both significant reductions. Among those with an ISS of at least 25, the risk was 18% higher, although, again, it was not a significant finding.
Curiously, the mortality benefit was stronger among sicker patients. The benefit was nonsignificant among those with an ISS of less than 25 but for those above 25, the mortality risk reduction was a significant 45%.
Dr Jacobs had no financial disclosures.
[email protected]
On Twitter @alz_gal
HOLLYWOOD, FLA. – Low-molecular-weight heparin (LMWH) decreased the risk of venous thromboembolism in trauma patients significantly more than did unfractionated heparin, a large state database review has found.
It also was associated with a 37% decrease in overall mortality, compared with unfractionated heparin, Benjamin Jacobs, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
He extracted data describing thromboembolism prophylaxis among 37,868 trauma patients included in the Michigan Trauma Quality Improvement Program from 2012 to 2014. The patients were treated at 23 hospitals around the state. They received either unfractionated or LMWH as their only clot-preventing protocol.
The primary outcomes of the study were reductions in the risk of venous thromboembolism (VTE), deep vein thrombosis (DVT), pulmonary thrombosis (PT), and mortality.
LMWH was given at either 40 mg every day or 30 mg twice a day. The comparator was unfractionated heparin at 5,000 U either two or three times a day.
The preferred method was LMWH, which 83% of patients received, compared with 17% who got the unfractionated heparin. Most patients who got LMWH received the 40 mg/day dose (70%). Most who got unfractionated heparin received 5,000 U three times a day (87%).
Both types of heparin reduced the risk of all thromboembolic outcomes, and both doses of LMWH significantly reduced the risks. However, the 40 mg/day dose was significantly more effective than the twice-daily 30-mg dose in reducing the risk of VTE and DVT. Risk reductions for PT and mortality were not significantly different between the doses.
Overall, compared with unfractionated heparin, LMWH decreased the risk of VTE by 33%; of PT by 48%; and of DVT by 27%. It also conferred a significant mortality benefit, reducing the risk of death by 37%, compared with the unfractionated type
When Dr. Jacobs grouped the patients according to Injury Severity Score (ISS), he saw a consistently higher benefit among patients with lower scores. For example, LMWH significantly reduced the risk of PT by 59% in patients with an ISS of 5-14. In those with an ISS of 25 or higher, the drug was associated with a 20% increased risk, although that wasn’t statistically significant.
There was a similar finding in DVT. LMWH reduced the risk by 18% in those with an ISS of 5-15, and by 50% among those with an score of 16-24 – both significant reductions. Among those with an ISS of at least 25, the risk was 18% higher, although, again, it was not a significant finding.
Curiously, the mortality benefit was stronger among sicker patients. The benefit was nonsignificant among those with an ISS of less than 25 but for those above 25, the mortality risk reduction was a significant 45%.
Dr Jacobs had no financial disclosures.
[email protected]
On Twitter @alz_gal
AT THE EAST ANNUAL SCIENTIFIC ASSEMBLY
Key clinical point:
Major finding: Overall mortality was reduced by 37% with LMWH, compared with unfractionated heparin.
Data source: The review comprised 37,868 patients included in the Michigan Trauma Quality Improvement Program.
Disclosures: Dr. Jacobs had no financial disclosures.
Screen opioid users for depression, study recommends
Depression combined with chronic opioid analgesic use involves more symptoms and comorbidities than depression without chronic opioid use, according to a study of Department of Veterans Affairs patients seen between 2000 and 2012.
“Screening and treatment of depression in non–cancer pain patients may limit risk of persistent mood disorder and subsequent suicidal ideation,” wrote Jeffrey F. Scherrer, PhD, and his coauthors. “Opioid prescribing for pain management should be coupled with careful screening and treatment of emerging depression.”
“Eligible patients were cancer free, HIV free. ... Because we were interested in characterizing severity of new-onset [new depression episodes] and not predictors of NDE, we measured incident substance use and psychiatric comorbidities that occurred at the same time or after NDE. Therefore, eligible patients were free of psychiatric and substance use disorders before NDE. Patients whose opioid use began after NDE and patients without NDE in follow-up were excluded,” wrote Dr. Scherrer of Saint Louis University and his coauthors (J Affect Disord. 2017 Mar 1;210:125-9).
This process left the researchers with a sample size of 4,758 patients. Of those, 4,314 developed NDE without receiving an opioid, while the remaining 444 developed NDE after opioid use of more than 90 days.
Looking at raw figures prior to the application of inverse probability of treatment weighting (IPTW), the opioid use group was more likely than was the nonopioid use group to have comorbid posttraumatic stress disorder (17.3% vs. 11.9%), opioid (4.3% vs. 0.5%) and other drug abuse/dependence (11.3% vs. 4.8%), all pain-related conditions, obesity (48.2% vs. 37.4%), and nicotine abuse/dependence (52.5% vs. 30.5%). The further calculations were made “to assess whether differences between the groups were irrespective of pain-related variables.”
With IPTW adjustments made, the differences in pain-related comorbidities went away. Opioid-using patients had higher depression severity as measured by Patient Health Questionnaire–9 scores (P = .012). They also were more likely to have had antidepressant treatment for at least 12 weeks (P less than .0001). Nonopioid use patients were more likely to have anxiety disorders other than PTSD (P = .014).
Dr. Scherrer had no conflicts of interest. The study received funding support from the National Institute of Mental Health. The views reflected in the article are those of the authors and not necessarily those of the VA, the researchers reported.
Depression combined with chronic opioid analgesic use involves more symptoms and comorbidities than depression without chronic opioid use, according to a study of Department of Veterans Affairs patients seen between 2000 and 2012.
“Screening and treatment of depression in non–cancer pain patients may limit risk of persistent mood disorder and subsequent suicidal ideation,” wrote Jeffrey F. Scherrer, PhD, and his coauthors. “Opioid prescribing for pain management should be coupled with careful screening and treatment of emerging depression.”
“Eligible patients were cancer free, HIV free. ... Because we were interested in characterizing severity of new-onset [new depression episodes] and not predictors of NDE, we measured incident substance use and psychiatric comorbidities that occurred at the same time or after NDE. Therefore, eligible patients were free of psychiatric and substance use disorders before NDE. Patients whose opioid use began after NDE and patients without NDE in follow-up were excluded,” wrote Dr. Scherrer of Saint Louis University and his coauthors (J Affect Disord. 2017 Mar 1;210:125-9).
This process left the researchers with a sample size of 4,758 patients. Of those, 4,314 developed NDE without receiving an opioid, while the remaining 444 developed NDE after opioid use of more than 90 days.
Looking at raw figures prior to the application of inverse probability of treatment weighting (IPTW), the opioid use group was more likely than was the nonopioid use group to have comorbid posttraumatic stress disorder (17.3% vs. 11.9%), opioid (4.3% vs. 0.5%) and other drug abuse/dependence (11.3% vs. 4.8%), all pain-related conditions, obesity (48.2% vs. 37.4%), and nicotine abuse/dependence (52.5% vs. 30.5%). The further calculations were made “to assess whether differences between the groups were irrespective of pain-related variables.”
With IPTW adjustments made, the differences in pain-related comorbidities went away. Opioid-using patients had higher depression severity as measured by Patient Health Questionnaire–9 scores (P = .012). They also were more likely to have had antidepressant treatment for at least 12 weeks (P less than .0001). Nonopioid use patients were more likely to have anxiety disorders other than PTSD (P = .014).
Dr. Scherrer had no conflicts of interest. The study received funding support from the National Institute of Mental Health. The views reflected in the article are those of the authors and not necessarily those of the VA, the researchers reported.
Depression combined with chronic opioid analgesic use involves more symptoms and comorbidities than depression without chronic opioid use, according to a study of Department of Veterans Affairs patients seen between 2000 and 2012.
“Screening and treatment of depression in non–cancer pain patients may limit risk of persistent mood disorder and subsequent suicidal ideation,” wrote Jeffrey F. Scherrer, PhD, and his coauthors. “Opioid prescribing for pain management should be coupled with careful screening and treatment of emerging depression.”
“Eligible patients were cancer free, HIV free. ... Because we were interested in characterizing severity of new-onset [new depression episodes] and not predictors of NDE, we measured incident substance use and psychiatric comorbidities that occurred at the same time or after NDE. Therefore, eligible patients were free of psychiatric and substance use disorders before NDE. Patients whose opioid use began after NDE and patients without NDE in follow-up were excluded,” wrote Dr. Scherrer of Saint Louis University and his coauthors (J Affect Disord. 2017 Mar 1;210:125-9).
This process left the researchers with a sample size of 4,758 patients. Of those, 4,314 developed NDE without receiving an opioid, while the remaining 444 developed NDE after opioid use of more than 90 days.
Looking at raw figures prior to the application of inverse probability of treatment weighting (IPTW), the opioid use group was more likely than was the nonopioid use group to have comorbid posttraumatic stress disorder (17.3% vs. 11.9%), opioid (4.3% vs. 0.5%) and other drug abuse/dependence (11.3% vs. 4.8%), all pain-related conditions, obesity (48.2% vs. 37.4%), and nicotine abuse/dependence (52.5% vs. 30.5%). The further calculations were made “to assess whether differences between the groups were irrespective of pain-related variables.”
With IPTW adjustments made, the differences in pain-related comorbidities went away. Opioid-using patients had higher depression severity as measured by Patient Health Questionnaire–9 scores (P = .012). They also were more likely to have had antidepressant treatment for at least 12 weeks (P less than .0001). Nonopioid use patients were more likely to have anxiety disorders other than PTSD (P = .014).
Dr. Scherrer had no conflicts of interest. The study received funding support from the National Institute of Mental Health. The views reflected in the article are those of the authors and not necessarily those of the VA, the researchers reported.
New data signal paradigm shift in FMD and arterial disease
CHICAGO – New data have shown that fibromuscular dysplasia is associated with high rates of dissection and/or aneurysm, and emerging recommendations call for routine imaging early on in the diagnosis of FMD to monitor for these vascular events, a researcher who developed those recommendations reported at a symposium on vascular surgery sponsored by Northwestern University.
“Given the very high rate of aneurysms in this population, it is now recommended that all patients with FMD should undergo at least one-time head-to pelvis imaging with CT angiography or MR angiography to screen for the presence of an aneurysm or to identify other areas of FMD involvement,” said Daniella Kadian-Dodov, MD, of Icahn School of Medicine at Mount Sinai in New York (J Am Coll Cardiol. 2016;68:176-85).

First described in 1938, FMD is a non-atherosclerotic, noninflammatory disease that had been thought to be a rare cause of renovascular hypertension with a classic “string-of-beads” appearance upon imaging, Dr. Kadian-Dodov noted. However, recent data from the Fibromuscular Dysplasia Society of America–sponsored U.S. registry has changed that thinking. “We now know it occurs more frequently in the carotid and renal arteries, although it has been observed in almost every artery,” she said. “The pathogenesis is still unknown but up to 10% of cases are familial.”
And manifestations of disease now extend beyond the “string-of-beads” appearance to include aneurysm, dissection, and arterial tortuosity, she said (Circulation. 2012;125:3182-90; Circulation. 2014;129:1048-78; J Am Coll Cardiol. 2016;68:176-85). The classification system for FMD has also undergone a recent change, according to Dr. Kadian-Dodov. “Traditionally, a histopathologic scheme was used to classify FMD,” she said. “Nowadays, fewer and fewer patients are undergoing surgical procedures, so the classification has changed to an angiographic system,” the most common of which is the American Heart Association system adopted in 2014 that distinguishes between multifocal, characterized by the classic “string-of-beads” appearance, and focal FMD with a single area of stenosis.
But the diagnosis of either variant of FMD is not exclusive. “Patients may have multiple areas of disease involvement and the same patient may have both focal and multifocal FMD findings,” Dr. Kadian-Dodov said.
The U.S. registry has helped clarify the thinking on FMD, Dr. Kadian-Dodov said. More than 1,400 patients are in the registry, 90% of whom are women with multifocal disease. The average age of onset of symptoms is 47 years, but 52 is the average age for diagnosis. “So these patients are experiencing several years delay to FMD diagnosis,” she said.
Manifestations depend on the vascular bed involved. “In the case of cervical artery FMD, headaches and pulsatile tinnitus are commonly reported, whereas with renal artery involvement hypertension is the most common symptom,” she said. A recent analysis showed 41.7% of the FMD population have either aneurysm and dissection or both (J Am Coll Cardiol. 2016;68:176-185).
But no specific guidelines for treatment of FMD yet exist, Dr. Kadian-Dodov said. “General guidelines should be applied for the management of dissection and aneurysm in patients with FMD,” she said. For patients with arterial dissection, that means conservative therapy comprising either anticoagulation or antiplatelet agents for 3-6 months followed by daily low-dose aspirin therapy. “Revascularization is rarely required for these patients,” she said. “Endovascular or surgical modalities should be reserved for those with continued ischemia despite conservative management or more complicated pseudoaneurysm formations.”
Daily aspirin therapy is likewise the recommendation for patients with cervical artery multifocal or focal FMD involvement without dissection or aneurysms. “We follow up with imaging every 6 months for 2 years,” Dr. Kadian-Dodov said. “If they’re stable, we switch over to annual surveillance; and if the patient has an aneurysm or dissection, that might alter the imaging and surveillance program.”
During angioplasty, determining the severity of stenosis upon visual inspection is difficult, especially in multifocal FMD. She advised measuring the gradient across the area of FMD involvement with a pressure wire to determine if angioplasty has adequately treated the lesion. “You should see obliteration of the gradient with successful treatment; you don’t have to target your therapy to a perfect angiographic result,” she said.
In patients with FMD and hypertension, she recommended renal artery angioplasty for hypertension of less than 5 years duration or in resistant or labile hypertension. “In this setting, stents are only reserved for complicated or refractory cases; angioplasty alone is sufficient,” Dr. Kadian-Dodov said. Cure rates decline with age, and hypertension in focal disease has a higher cure rate than does multifocal disease, she said (Hypertension. 2010;56:525-32).
Dr. Kadian-Dodov had no relevant financial relationships to disclose.
CHICAGO – New data have shown that fibromuscular dysplasia is associated with high rates of dissection and/or aneurysm, and emerging recommendations call for routine imaging early on in the diagnosis of FMD to monitor for these vascular events, a researcher who developed those recommendations reported at a symposium on vascular surgery sponsored by Northwestern University.
“Given the very high rate of aneurysms in this population, it is now recommended that all patients with FMD should undergo at least one-time head-to pelvis imaging with CT angiography or MR angiography to screen for the presence of an aneurysm or to identify other areas of FMD involvement,” said Daniella Kadian-Dodov, MD, of Icahn School of Medicine at Mount Sinai in New York (J Am Coll Cardiol. 2016;68:176-85).
First described in 1938, FMD is a non-atherosclerotic, noninflammatory disease that had been thought to be a rare cause of renovascular hypertension with a classic “string-of-beads” appearance upon imaging, Dr. Kadian-Dodov noted. However, recent data from the Fibromuscular Dysplasia Society of America–sponsored U.S. registry has changed that thinking. “We now know it occurs more frequently in the carotid and renal arteries, although it has been observed in almost every artery,” she said. “The pathogenesis is still unknown but up to 10% of cases are familial.”
And manifestations of disease now extend beyond the “string-of-beads” appearance to include aneurysm, dissection, and arterial tortuosity, she said (Circulation. 2012;125:3182-90; Circulation. 2014;129:1048-78; J Am Coll Cardiol. 2016;68:176-85). The classification system for FMD has also undergone a recent change, according to Dr. Kadian-Dodov. “Traditionally, a histopathologic scheme was used to classify FMD,” she said. “Nowadays, fewer and fewer patients are undergoing surgical procedures, so the classification has changed to an angiographic system,” the most common of which is the American Heart Association system adopted in 2014 that distinguishes between multifocal, characterized by the classic “string-of-beads” appearance, and focal FMD with a single area of stenosis.
But the diagnosis of either variant of FMD is not exclusive. “Patients may have multiple areas of disease involvement and the same patient may have both focal and multifocal FMD findings,” Dr. Kadian-Dodov said.
The U.S. registry has helped clarify the thinking on FMD, Dr. Kadian-Dodov said. More than 1,400 patients are in the registry, 90% of whom are women with multifocal disease. The average age of onset of symptoms is 47 years, but 52 is the average age for diagnosis. “So these patients are experiencing several years delay to FMD diagnosis,” she said.
Manifestations depend on the vascular bed involved. “In the case of cervical artery FMD, headaches and pulsatile tinnitus are commonly reported, whereas with renal artery involvement hypertension is the most common symptom,” she said. A recent analysis showed 41.7% of the FMD population have either aneurysm and dissection or both (J Am Coll Cardiol. 2016;68:176-185).
But no specific guidelines for treatment of FMD yet exist, Dr. Kadian-Dodov said. “General guidelines should be applied for the management of dissection and aneurysm in patients with FMD,” she said. For patients with arterial dissection, that means conservative therapy comprising either anticoagulation or antiplatelet agents for 3-6 months followed by daily low-dose aspirin therapy. “Revascularization is rarely required for these patients,” she said. “Endovascular or surgical modalities should be reserved for those with continued ischemia despite conservative management or more complicated pseudoaneurysm formations.”
Daily aspirin therapy is likewise the recommendation for patients with cervical artery multifocal or focal FMD involvement without dissection or aneurysms. “We follow up with imaging every 6 months for 2 years,” Dr. Kadian-Dodov said. “If they’re stable, we switch over to annual surveillance; and if the patient has an aneurysm or dissection, that might alter the imaging and surveillance program.”
During angioplasty, determining the severity of stenosis upon visual inspection is difficult, especially in multifocal FMD. She advised measuring the gradient across the area of FMD involvement with a pressure wire to determine if angioplasty has adequately treated the lesion. “You should see obliteration of the gradient with successful treatment; you don’t have to target your therapy to a perfect angiographic result,” she said.
In patients with FMD and hypertension, she recommended renal artery angioplasty for hypertension of less than 5 years duration or in resistant or labile hypertension. “In this setting, stents are only reserved for complicated or refractory cases; angioplasty alone is sufficient,” Dr. Kadian-Dodov said. Cure rates decline with age, and hypertension in focal disease has a higher cure rate than does multifocal disease, she said (Hypertension. 2010;56:525-32).
Dr. Kadian-Dodov had no relevant financial relationships to disclose.
CHICAGO – New data have shown that fibromuscular dysplasia is associated with high rates of dissection and/or aneurysm, and emerging recommendations call for routine imaging early on in the diagnosis of FMD to monitor for these vascular events, a researcher who developed those recommendations reported at a symposium on vascular surgery sponsored by Northwestern University.
“Given the very high rate of aneurysms in this population, it is now recommended that all patients with FMD should undergo at least one-time head-to pelvis imaging with CT angiography or MR angiography to screen for the presence of an aneurysm or to identify other areas of FMD involvement,” said Daniella Kadian-Dodov, MD, of Icahn School of Medicine at Mount Sinai in New York (J Am Coll Cardiol. 2016;68:176-85).
First described in 1938, FMD is a non-atherosclerotic, noninflammatory disease that had been thought to be a rare cause of renovascular hypertension with a classic “string-of-beads” appearance upon imaging, Dr. Kadian-Dodov noted. However, recent data from the Fibromuscular Dysplasia Society of America–sponsored U.S. registry has changed that thinking. “We now know it occurs more frequently in the carotid and renal arteries, although it has been observed in almost every artery,” she said. “The pathogenesis is still unknown but up to 10% of cases are familial.”
And manifestations of disease now extend beyond the “string-of-beads” appearance to include aneurysm, dissection, and arterial tortuosity, she said (Circulation. 2012;125:3182-90; Circulation. 2014;129:1048-78; J Am Coll Cardiol. 2016;68:176-85). The classification system for FMD has also undergone a recent change, according to Dr. Kadian-Dodov. “Traditionally, a histopathologic scheme was used to classify FMD,” she said. “Nowadays, fewer and fewer patients are undergoing surgical procedures, so the classification has changed to an angiographic system,” the most common of which is the American Heart Association system adopted in 2014 that distinguishes between multifocal, characterized by the classic “string-of-beads” appearance, and focal FMD with a single area of stenosis.
But the diagnosis of either variant of FMD is not exclusive. “Patients may have multiple areas of disease involvement and the same patient may have both focal and multifocal FMD findings,” Dr. Kadian-Dodov said.
The U.S. registry has helped clarify the thinking on FMD, Dr. Kadian-Dodov said. More than 1,400 patients are in the registry, 90% of whom are women with multifocal disease. The average age of onset of symptoms is 47 years, but 52 is the average age for diagnosis. “So these patients are experiencing several years delay to FMD diagnosis,” she said.
Manifestations depend on the vascular bed involved. “In the case of cervical artery FMD, headaches and pulsatile tinnitus are commonly reported, whereas with renal artery involvement hypertension is the most common symptom,” she said. A recent analysis showed 41.7% of the FMD population have either aneurysm and dissection or both (J Am Coll Cardiol. 2016;68:176-185).
But no specific guidelines for treatment of FMD yet exist, Dr. Kadian-Dodov said. “General guidelines should be applied for the management of dissection and aneurysm in patients with FMD,” she said. For patients with arterial dissection, that means conservative therapy comprising either anticoagulation or antiplatelet agents for 3-6 months followed by daily low-dose aspirin therapy. “Revascularization is rarely required for these patients,” she said. “Endovascular or surgical modalities should be reserved for those with continued ischemia despite conservative management or more complicated pseudoaneurysm formations.”
Daily aspirin therapy is likewise the recommendation for patients with cervical artery multifocal or focal FMD involvement without dissection or aneurysms. “We follow up with imaging every 6 months for 2 years,” Dr. Kadian-Dodov said. “If they’re stable, we switch over to annual surveillance; and if the patient has an aneurysm or dissection, that might alter the imaging and surveillance program.”
During angioplasty, determining the severity of stenosis upon visual inspection is difficult, especially in multifocal FMD. She advised measuring the gradient across the area of FMD involvement with a pressure wire to determine if angioplasty has adequately treated the lesion. “You should see obliteration of the gradient with successful treatment; you don’t have to target your therapy to a perfect angiographic result,” she said.
In patients with FMD and hypertension, she recommended renal artery angioplasty for hypertension of less than 5 years duration or in resistant or labile hypertension. “In this setting, stents are only reserved for complicated or refractory cases; angioplasty alone is sufficient,” Dr. Kadian-Dodov said. Cure rates decline with age, and hypertension in focal disease has a higher cure rate than does multifocal disease, she said (Hypertension. 2010;56:525-32).
Dr. Kadian-Dodov had no relevant financial relationships to disclose.
Key clinical point: Fibromuscular dysplasia was thought to be a rare cause of renovascular hypertension, but new data has challenged this thinking.
Major finding: FMD accounts for 15%-20% of patients with spontaneous carotid or vertebral artery dissection and 45%-86% of patients with spontaneous coronary artery dissection.
Data source: U.S. Registry for FMD maintained by the Fibromuscular Dystrophy Society of America.
Disclosures: Dr. Kadian-Dodov reported having no financial disclosures.
Senate, House take first step toward repealing ACA
With a Jan. 12 early morning procedural passed on party lines, the Senate has set the stage for the repeal of the revenue aspects of the Affordable Care Act. The House of Representatives passed similar legislation Jan. 13.*
Republicans will be using the budget reconciliation process, which will allow them to move forward with repealing certain provisions of the health care reform law without any Democratic support, although passage of any replacement will require some bipartisan support as Republicans do not have the required 60 votes to guarantee passage in the Senate.
The budget resolutions contain no details about what could be repealed or whether there will be a replacement, but it does direct the key committees to write draft legislation by Jan. 27.

Senate Republicans “plan to rescue those trapped in a failing system, to replace that system with a functional market, or markets, and then repeal Obamacare for good,” he said.
Sen. Alexander said the process will come in three parts. The first will protect the 11 million people who have purchased health insurance through the exchanges so that they don’t lose coverage.
“Second, we will build better systems providing Americans with more choices that cost less,” he said. “Note I say systems, not one system. If anyone is expecting [Senate Majority Leader Mitch] McConnell [R-Ky.] to roll a wheelbarrow on the Senate floor with a comprehensive Republican health care plan, they’re going to be waiting a long time because we don’t believe in that. We don’t want to replace a failed Obamacare federal system with another failed federal system.”
The last part will be to repeal what remains of the law after the new plan is in place.
Sen. Alexander reiterated that any future bill will keep the ban on coverage denials for preexisting conditions and the allowance of coverage of children up to the age of 26 who are on their parents’ plans.
He stated that this reform effort will not address Medicare reform, which will be the subject of separate legislative action.
*This story was updated Jan. 13 at 4:30 pm.

With a Jan. 12 early morning procedural passed on party lines, the Senate has set the stage for the repeal of the revenue aspects of the Affordable Care Act. The House of Representatives passed similar legislation Jan. 13.*
Republicans will be using the budget reconciliation process, which will allow them to move forward with repealing certain provisions of the health care reform law without any Democratic support, although passage of any replacement will require some bipartisan support as Republicans do not have the required 60 votes to guarantee passage in the Senate.
The budget resolutions contain no details about what could be repealed or whether there will be a replacement, but it does direct the key committees to write draft legislation by Jan. 27.
Senate Republicans “plan to rescue those trapped in a failing system, to replace that system with a functional market, or markets, and then repeal Obamacare for good,” he said.
Sen. Alexander said the process will come in three parts. The first will protect the 11 million people who have purchased health insurance through the exchanges so that they don’t lose coverage.
“Second, we will build better systems providing Americans with more choices that cost less,” he said. “Note I say systems, not one system. If anyone is expecting [Senate Majority Leader Mitch] McConnell [R-Ky.] to roll a wheelbarrow on the Senate floor with a comprehensive Republican health care plan, they’re going to be waiting a long time because we don’t believe in that. We don’t want to replace a failed Obamacare federal system with another failed federal system.”
The last part will be to repeal what remains of the law after the new plan is in place.
Sen. Alexander reiterated that any future bill will keep the ban on coverage denials for preexisting conditions and the allowance of coverage of children up to the age of 26 who are on their parents’ plans.
He stated that this reform effort will not address Medicare reform, which will be the subject of separate legislative action.
*This story was updated Jan. 13 at 4:30 pm.
With a Jan. 12 early morning procedural passed on party lines, the Senate has set the stage for the repeal of the revenue aspects of the Affordable Care Act. The House of Representatives passed similar legislation Jan. 13.*
Republicans will be using the budget reconciliation process, which will allow them to move forward with repealing certain provisions of the health care reform law without any Democratic support, although passage of any replacement will require some bipartisan support as Republicans do not have the required 60 votes to guarantee passage in the Senate.
The budget resolutions contain no details about what could be repealed or whether there will be a replacement, but it does direct the key committees to write draft legislation by Jan. 27.
Senate Republicans “plan to rescue those trapped in a failing system, to replace that system with a functional market, or markets, and then repeal Obamacare for good,” he said.
Sen. Alexander said the process will come in three parts. The first will protect the 11 million people who have purchased health insurance through the exchanges so that they don’t lose coverage.
“Second, we will build better systems providing Americans with more choices that cost less,” he said. “Note I say systems, not one system. If anyone is expecting [Senate Majority Leader Mitch] McConnell [R-Ky.] to roll a wheelbarrow on the Senate floor with a comprehensive Republican health care plan, they’re going to be waiting a long time because we don’t believe in that. We don’t want to replace a failed Obamacare federal system with another failed federal system.”
The last part will be to repeal what remains of the law after the new plan is in place.
Sen. Alexander reiterated that any future bill will keep the ban on coverage denials for preexisting conditions and the allowance of coverage of children up to the age of 26 who are on their parents’ plans.
He stated that this reform effort will not address Medicare reform, which will be the subject of separate legislative action.
*This story was updated Jan. 13 at 4:30 pm.
LAA closure during cardiac surgery cuts late mortality
NEW ORLEANS – Surgical left atrial appendage closure at the time of open heart surgery in patients with atrial fibrillation doesn’t decrease patients’ early or late risk of stroke, but it does substantially reduce their risk of late mortality, Masahiko Ando, MD, reported at the American Heart Association scientific sessions.
Solid evidence demonstrates that percutaneous left atrial appendage (LAA) closure using the Watchman or other devices in patients with atrial fibrillation offers a potential alternative to lifelong oral anticoagulation.
In contrast, even though surgical LAA closure at the time of cardiac surgery is commonly done, the data as to its long-term impact are scanty. This was the impetus for Dr. Ando and his coinvestigators at Massachusetts General Hospital in Boston to perform a comprehensive systematic review of the medical literature. They also conducted a meta-analysis that involved 7,466 patients who underwent open-heart surgery with or without surgical LAA closure in 12 studies, 3 of which were randomized controlled trials, 2 propensity-matched comparisons, and the rest cohort studies.
At 30-day follow-up, LAA closure was not associated with any significant effect on the risks of stroke, death, reexploration for bleeding, or postoperative atrial fibrillation.
At the latest follow-up in the studies, however, surgical LAA closure was associated with a highly significant 36% reduction in mortality risk compared with the no–LAA-closure control group. This remained the case even after statistical adjustment for demographics, type of cardiac surgery, and the form of preoperative atrial fibrillation.
“Given that we generally add LAA closure to those who have a higher risk of embolization, which could have negatively affected the efficacy of LAA closure, this preventive effect of LAA closure on late mortality cannot be ignored,” said Dr. Ando.
The most likely explanation for the improved survival in surgical LAA closure recipients, he continued, is that the procedure enabled them to avoid aggressive lifelong oral anticoagulation, with its attendant risks.
Dr. Ando reported having no financial conflicts regarding his study.
NEW ORLEANS – Surgical left atrial appendage closure at the time of open heart surgery in patients with atrial fibrillation doesn’t decrease patients’ early or late risk of stroke, but it does substantially reduce their risk of late mortality, Masahiko Ando, MD, reported at the American Heart Association scientific sessions.
Solid evidence demonstrates that percutaneous left atrial appendage (LAA) closure using the Watchman or other devices in patients with atrial fibrillation offers a potential alternative to lifelong oral anticoagulation.
In contrast, even though surgical LAA closure at the time of cardiac surgery is commonly done, the data as to its long-term impact are scanty. This was the impetus for Dr. Ando and his coinvestigators at Massachusetts General Hospital in Boston to perform a comprehensive systematic review of the medical literature. They also conducted a meta-analysis that involved 7,466 patients who underwent open-heart surgery with or without surgical LAA closure in 12 studies, 3 of which were randomized controlled trials, 2 propensity-matched comparisons, and the rest cohort studies.
At 30-day follow-up, LAA closure was not associated with any significant effect on the risks of stroke, death, reexploration for bleeding, or postoperative atrial fibrillation.
At the latest follow-up in the studies, however, surgical LAA closure was associated with a highly significant 36% reduction in mortality risk compared with the no–LAA-closure control group. This remained the case even after statistical adjustment for demographics, type of cardiac surgery, and the form of preoperative atrial fibrillation.
“Given that we generally add LAA closure to those who have a higher risk of embolization, which could have negatively affected the efficacy of LAA closure, this preventive effect of LAA closure on late mortality cannot be ignored,” said Dr. Ando.
The most likely explanation for the improved survival in surgical LAA closure recipients, he continued, is that the procedure enabled them to avoid aggressive lifelong oral anticoagulation, with its attendant risks.
Dr. Ando reported having no financial conflicts regarding his study.
NEW ORLEANS – Surgical left atrial appendage closure at the time of open heart surgery in patients with atrial fibrillation doesn’t decrease patients’ early or late risk of stroke, but it does substantially reduce their risk of late mortality, Masahiko Ando, MD, reported at the American Heart Association scientific sessions.
Solid evidence demonstrates that percutaneous left atrial appendage (LAA) closure using the Watchman or other devices in patients with atrial fibrillation offers a potential alternative to lifelong oral anticoagulation.
In contrast, even though surgical LAA closure at the time of cardiac surgery is commonly done, the data as to its long-term impact are scanty. This was the impetus for Dr. Ando and his coinvestigators at Massachusetts General Hospital in Boston to perform a comprehensive systematic review of the medical literature. They also conducted a meta-analysis that involved 7,466 patients who underwent open-heart surgery with or without surgical LAA closure in 12 studies, 3 of which were randomized controlled trials, 2 propensity-matched comparisons, and the rest cohort studies.
At 30-day follow-up, LAA closure was not associated with any significant effect on the risks of stroke, death, reexploration for bleeding, or postoperative atrial fibrillation.
At the latest follow-up in the studies, however, surgical LAA closure was associated with a highly significant 36% reduction in mortality risk compared with the no–LAA-closure control group. This remained the case even after statistical adjustment for demographics, type of cardiac surgery, and the form of preoperative atrial fibrillation.
“Given that we generally add LAA closure to those who have a higher risk of embolization, which could have negatively affected the efficacy of LAA closure, this preventive effect of LAA closure on late mortality cannot be ignored,” said Dr. Ando.
The most likely explanation for the improved survival in surgical LAA closure recipients, he continued, is that the procedure enabled them to avoid aggressive lifelong oral anticoagulation, with its attendant risks.
Dr. Ando reported having no financial conflicts regarding his study.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: Late mortality risk was reduced by 36% in patients with atrial fibrillation who underwent surgical LAA closure during open heart surgery, compared with those who did not.
Data source: This meta-analysis included 12 published studies and 7,466 patients who either did or did not undergo surgical LAA closure during open heart surgery.
Disclosures: The study presenter reported having no financial conflicts.
Surgical discharge data highlight stewardship need at transition
NEW ORLEANS – Most antibiotic prescriptions written at the time of patient discharge at an academic hospital were inappropriate, according to a retrospective review of 2014 discharge data.
These drugs were prescribed despite the existence of a robust inpatient antibiotic stewardship program (ASP) at the hospital, Sarah Scarpato, MD, reported at IDWeek, an annual scientific meeting on infectious diseases.
Of 9,750 prescriptions written during the study year, 86% were for oral antibiotics and 14% were for outpatient parenteral antibiotic therapy. Among a random sample of 150 patients discharged on antibiotics, 22.7% had no clinical indication of infection, 13% received an antibiotic with inappropriate spectrum of activity, 17% received an incorrect dose, 55% received an antibiotic course that was too long, and 7.3% received a course that was too short, Dr. Scarpato said at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
A total of 57.7% of surgical patients and 57.6% of medical patients received an antibiotic prescription that was inappropriate.
“A whopping 70% of prescriptions had at least one error in drug choice, dose, indication, or duration,” she said.
“The most common scenarios in which an antibiotic use was not indicated were prolonged surgical prophylaxis and prolonged prophylaxis in patients who had neutropenic fever during their hospitalization but were no longer neutropenic on discharge. The most common infectious indications were consistent with previous data, with genitourinary, respiratory, and skin and soft tissue being the most common, followed by gastrointestinal,” Dr. Scarpato of the Hospital of the University of Pennsylvania, Philadelphia, said.
In addition, she noted, “100% of patients discharged from cardiothoracic surgery, ear/nose/throat surgery, oral and maxillofacial surgery, neurosurgery, and neurology had at least one error. Oncology was the medical service with the highest rate of inappropriate prescriptions at 80%. The rest, including infectious diseases, had error rates between 40% and 60%.”
Also in line with previous data, fluoroquinolones were the most commonly prescribed antibiotics, accounting for 23.5%, followed by cephalosporins, penicillins, trimethoprim-sulfamethoxazole, and metronidazole.
“Antibiotic prescription in the absence of an acceptable indication and inappropriate duration accounted for the vast majority – 76% – of inappropriate prescriptions,” Dr. Scarpato said, noting that this may be because of a failure by physicians to account for antibiotics given as an inpatient, a lack of familiarity with a patient’s course because of hand-offs, the writing of a prescription with a given duration expecting discharge on a different day, or a lack of familiarity with recommended treatment durations.
“On average, we saw an excess of 3.8 days of unnecessary antibiotics per patient,” she said. The range, however, was 18 days too few to 36 days too many. Further, readmission rates at days 7 and 30 were 6.4% and 19.4%, respectively, for patients discharged on antibiotics, compared with 3.70% and 13.79% hospital wide. The respective rates among those discharged on outpatient parenteral antibiotic therapy were 5.6% and 16.4%, compared with 6.5% and 19.9% among those on oral antibiotic therapy.
The higher rates among those on oral vs. parenteral therapy may be because patients on outpatient parenteral antibiotic therapy are followed closely by a team of infectious disease physicians and pharmacists, while those discharged on oral therapy are not routinely monitored, or it may reflect an unintended consequence of switching from parenteral to oral therapy at discharge, Dr. Scarpato said.
Transitions of care are vulnerable times for patients, she said, noting that “nearly a quarter of patients suffer an adverse event from an error in transition of care during hospital discharge, and up to half of those who suffer an adverse drug reaction at discharge are prescribed an antibiotic.”
Though limited by the retrospective and descriptive nature of the study, and the single-center design, the findings demonstrate “a significant and unmet need for antimicrobial stewardship at transition in care, even at institutions such as ours that have a substantial inpatient ASP,” Dr. Scarpato concluded.
Dr. Scarpato reported having no conflicts of interest.
NEW ORLEANS – Most antibiotic prescriptions written at the time of patient discharge at an academic hospital were inappropriate, according to a retrospective review of 2014 discharge data.
These drugs were prescribed despite the existence of a robust inpatient antibiotic stewardship program (ASP) at the hospital, Sarah Scarpato, MD, reported at IDWeek, an annual scientific meeting on infectious diseases.
Of 9,750 prescriptions written during the study year, 86% were for oral antibiotics and 14% were for outpatient parenteral antibiotic therapy. Among a random sample of 150 patients discharged on antibiotics, 22.7% had no clinical indication of infection, 13% received an antibiotic with inappropriate spectrum of activity, 17% received an incorrect dose, 55% received an antibiotic course that was too long, and 7.3% received a course that was too short, Dr. Scarpato said at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
A total of 57.7% of surgical patients and 57.6% of medical patients received an antibiotic prescription that was inappropriate.
“A whopping 70% of prescriptions had at least one error in drug choice, dose, indication, or duration,” she said.
“The most common scenarios in which an antibiotic use was not indicated were prolonged surgical prophylaxis and prolonged prophylaxis in patients who had neutropenic fever during their hospitalization but were no longer neutropenic on discharge. The most common infectious indications were consistent with previous data, with genitourinary, respiratory, and skin and soft tissue being the most common, followed by gastrointestinal,” Dr. Scarpato of the Hospital of the University of Pennsylvania, Philadelphia, said.
In addition, she noted, “100% of patients discharged from cardiothoracic surgery, ear/nose/throat surgery, oral and maxillofacial surgery, neurosurgery, and neurology had at least one error. Oncology was the medical service with the highest rate of inappropriate prescriptions at 80%. The rest, including infectious diseases, had error rates between 40% and 60%.”
Also in line with previous data, fluoroquinolones were the most commonly prescribed antibiotics, accounting for 23.5%, followed by cephalosporins, penicillins, trimethoprim-sulfamethoxazole, and metronidazole.
“Antibiotic prescription in the absence of an acceptable indication and inappropriate duration accounted for the vast majority – 76% – of inappropriate prescriptions,” Dr. Scarpato said, noting that this may be because of a failure by physicians to account for antibiotics given as an inpatient, a lack of familiarity with a patient’s course because of hand-offs, the writing of a prescription with a given duration expecting discharge on a different day, or a lack of familiarity with recommended treatment durations.
“On average, we saw an excess of 3.8 days of unnecessary antibiotics per patient,” she said. The range, however, was 18 days too few to 36 days too many. Further, readmission rates at days 7 and 30 were 6.4% and 19.4%, respectively, for patients discharged on antibiotics, compared with 3.70% and 13.79% hospital wide. The respective rates among those discharged on outpatient parenteral antibiotic therapy were 5.6% and 16.4%, compared with 6.5% and 19.9% among those on oral antibiotic therapy.
The higher rates among those on oral vs. parenteral therapy may be because patients on outpatient parenteral antibiotic therapy are followed closely by a team of infectious disease physicians and pharmacists, while those discharged on oral therapy are not routinely monitored, or it may reflect an unintended consequence of switching from parenteral to oral therapy at discharge, Dr. Scarpato said.
Transitions of care are vulnerable times for patients, she said, noting that “nearly a quarter of patients suffer an adverse event from an error in transition of care during hospital discharge, and up to half of those who suffer an adverse drug reaction at discharge are prescribed an antibiotic.”
Though limited by the retrospective and descriptive nature of the study, and the single-center design, the findings demonstrate “a significant and unmet need for antimicrobial stewardship at transition in care, even at institutions such as ours that have a substantial inpatient ASP,” Dr. Scarpato concluded.
Dr. Scarpato reported having no conflicts of interest.
NEW ORLEANS – Most antibiotic prescriptions written at the time of patient discharge at an academic hospital were inappropriate, according to a retrospective review of 2014 discharge data.
These drugs were prescribed despite the existence of a robust inpatient antibiotic stewardship program (ASP) at the hospital, Sarah Scarpato, MD, reported at IDWeek, an annual scientific meeting on infectious diseases.
Of 9,750 prescriptions written during the study year, 86% were for oral antibiotics and 14% were for outpatient parenteral antibiotic therapy. Among a random sample of 150 patients discharged on antibiotics, 22.7% had no clinical indication of infection, 13% received an antibiotic with inappropriate spectrum of activity, 17% received an incorrect dose, 55% received an antibiotic course that was too long, and 7.3% received a course that was too short, Dr. Scarpato said at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
A total of 57.7% of surgical patients and 57.6% of medical patients received an antibiotic prescription that was inappropriate.
“A whopping 70% of prescriptions had at least one error in drug choice, dose, indication, or duration,” she said.
“The most common scenarios in which an antibiotic use was not indicated were prolonged surgical prophylaxis and prolonged prophylaxis in patients who had neutropenic fever during their hospitalization but were no longer neutropenic on discharge. The most common infectious indications were consistent with previous data, with genitourinary, respiratory, and skin and soft tissue being the most common, followed by gastrointestinal,” Dr. Scarpato of the Hospital of the University of Pennsylvania, Philadelphia, said.
In addition, she noted, “100% of patients discharged from cardiothoracic surgery, ear/nose/throat surgery, oral and maxillofacial surgery, neurosurgery, and neurology had at least one error. Oncology was the medical service with the highest rate of inappropriate prescriptions at 80%. The rest, including infectious diseases, had error rates between 40% and 60%.”
Also in line with previous data, fluoroquinolones were the most commonly prescribed antibiotics, accounting for 23.5%, followed by cephalosporins, penicillins, trimethoprim-sulfamethoxazole, and metronidazole.
“Antibiotic prescription in the absence of an acceptable indication and inappropriate duration accounted for the vast majority – 76% – of inappropriate prescriptions,” Dr. Scarpato said, noting that this may be because of a failure by physicians to account for antibiotics given as an inpatient, a lack of familiarity with a patient’s course because of hand-offs, the writing of a prescription with a given duration expecting discharge on a different day, or a lack of familiarity with recommended treatment durations.
“On average, we saw an excess of 3.8 days of unnecessary antibiotics per patient,” she said. The range, however, was 18 days too few to 36 days too many. Further, readmission rates at days 7 and 30 were 6.4% and 19.4%, respectively, for patients discharged on antibiotics, compared with 3.70% and 13.79% hospital wide. The respective rates among those discharged on outpatient parenteral antibiotic therapy were 5.6% and 16.4%, compared with 6.5% and 19.9% among those on oral antibiotic therapy.
The higher rates among those on oral vs. parenteral therapy may be because patients on outpatient parenteral antibiotic therapy are followed closely by a team of infectious disease physicians and pharmacists, while those discharged on oral therapy are not routinely monitored, or it may reflect an unintended consequence of switching from parenteral to oral therapy at discharge, Dr. Scarpato said.
Transitions of care are vulnerable times for patients, she said, noting that “nearly a quarter of patients suffer an adverse event from an error in transition of care during hospital discharge, and up to half of those who suffer an adverse drug reaction at discharge are prescribed an antibiotic.”
Though limited by the retrospective and descriptive nature of the study, and the single-center design, the findings demonstrate “a significant and unmet need for antimicrobial stewardship at transition in care, even at institutions such as ours that have a substantial inpatient ASP,” Dr. Scarpato concluded.
Dr. Scarpato reported having no conflicts of interest.
AT IDWEEK 2016
Key clinical point:
Major finding: 70% of prescriptions had at least one error in drug choice, dose, indication, or duration.
Data source: A review of discharge data for 150 patients at an academic hospital.
Disclosures: Dr. Scarpato reported having no conflicts of interest.
Older adults can sustain asymptomatic cervical fractures
HOLLYWOOD, FLA. –
The 4-year review found that 21% of older patients with a confirmed C-spine fracture reported no pain on history or physical exam, and that 76% of these fractures needed treatment – twin findings suggesting that asymptomatic neck fractures may be undiagnosed and untreated in this population.
The 183-patient study also found no significant pain differences between age groups: The silent injuries were just as common among 55-year-olds as among 65-year-olds, Christopher Healey, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
“I guess we can say, ‘55 is the new 65,’ when it comes to this injury,” said Dr. Healey of the Iowa Methodist Medical Center, Des Moines. “In our study the rate of a pain-free neck fracture in 55-year-olds was equivalent to that in their older counterpoints, so they also represent a group at increased risk.”
Dr. Healey and his colleagues conducted a 4-year review of trauma patients aged 55 years and older who were treated for a C-spine fracture. All of the patients had a Glasgow Coma

There were no differences in the mechanism of injury between the pain-free and pain-positive groups. The most common source of injury was a fall from the person’s own height (39% vs. 49%), followed by a high fall (21% vs. 19%). Motor vehicle crashes came in third (37% vs. 30%), with other methods of injury accounting for about 3% of each group.
The level of fracture was widely dispersed among both groups and not associated with pain. Asymptomatic fractures occurred at C1 and C2 vertabrae (about 13%); C3 (26%); C4 (10%); C5 (12%); and C6 and C7 (30%).
Perhaps surprisingly, patients who didn’t report pain had significantly higher Injury Severity Scores (15 vs. 10). They were also significantly more likely to have injuries to other body regions (71% vs. 47%), including the head (22% vs. 16%), thorax/abdomen (39% vs. 20%), and extremities (33% vs. 20%).
A third of those with a pain-free fracture had breaks at multiple levels. Their hospital stays were significantly longer than were those of patients with painful fractures (7 vs. 5 days).
These findings of more severe injuries in the asymptomatic group led Dr. Healey to suggest that distracting pain might be playing a part in the phenomenon.
When the group was split into 10-year age increments, asymptomatic fractures occurred in about 20% of each group from 55-64 years up to 85 years and older.
The majority of both groups required treatment (91% with pain; 76% asymptomatic), Dr. Healey said. The most common treatment in each group was a cervical collar (61% with pain vs. 46% asymptomatic ). A cervical-thoracic-lumbar-sacral orthosis brace was used in 8% of those with pain and 11% of the asymptomatic patients.
Invasive procedures were performed in just as many of the asymptomatic patients as in those who had pain. These included vertebral fusion (11% asymptomatic vs. 9% with pain) and cervical halo (8% vs. 13%).
The lesson here, Dr. Healey concluded, is that pain is not always a reliable indicator of neck injury in older patients. “Older adults can break their neck and have no pain at all. This is concerning, because the presence or absence of neck pain is a major component in many clearance protocols for C-spine trauma. This begs the question whether we should be treating our older patients by general adult guidelines. I would advocate the development of trauma guidelines that are specific for the older or geriatric patient.”
Dr. Healey had no financial disclosures.
HOLLYWOOD, FLA. –
The 4-year review found that 21% of older patients with a confirmed C-spine fracture reported no pain on history or physical exam, and that 76% of these fractures needed treatment – twin findings suggesting that asymptomatic neck fractures may be undiagnosed and untreated in this population.
The 183-patient study also found no significant pain differences between age groups: The silent injuries were just as common among 55-year-olds as among 65-year-olds, Christopher Healey, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
“I guess we can say, ‘55 is the new 65,’ when it comes to this injury,” said Dr. Healey of the Iowa Methodist Medical Center, Des Moines. “In our study the rate of a pain-free neck fracture in 55-year-olds was equivalent to that in their older counterpoints, so they also represent a group at increased risk.”
Dr. Healey and his colleagues conducted a 4-year review of trauma patients aged 55 years and older who were treated for a C-spine fracture. All of the patients had a Glasgow Coma
There were no differences in the mechanism of injury between the pain-free and pain-positive groups. The most common source of injury was a fall from the person’s own height (39% vs. 49%), followed by a high fall (21% vs. 19%). Motor vehicle crashes came in third (37% vs. 30%), with other methods of injury accounting for about 3% of each group.
The level of fracture was widely dispersed among both groups and not associated with pain. Asymptomatic fractures occurred at C1 and C2 vertabrae (about 13%); C3 (26%); C4 (10%); C5 (12%); and C6 and C7 (30%).
Perhaps surprisingly, patients who didn’t report pain had significantly higher Injury Severity Scores (15 vs. 10). They were also significantly more likely to have injuries to other body regions (71% vs. 47%), including the head (22% vs. 16%), thorax/abdomen (39% vs. 20%), and extremities (33% vs. 20%).
A third of those with a pain-free fracture had breaks at multiple levels. Their hospital stays were significantly longer than were those of patients with painful fractures (7 vs. 5 days).
These findings of more severe injuries in the asymptomatic group led Dr. Healey to suggest that distracting pain might be playing a part in the phenomenon.
When the group was split into 10-year age increments, asymptomatic fractures occurred in about 20% of each group from 55-64 years up to 85 years and older.
The majority of both groups required treatment (91% with pain; 76% asymptomatic), Dr. Healey said. The most common treatment in each group was a cervical collar (61% with pain vs. 46% asymptomatic ). A cervical-thoracic-lumbar-sacral orthosis brace was used in 8% of those with pain and 11% of the asymptomatic patients.
Invasive procedures were performed in just as many of the asymptomatic patients as in those who had pain. These included vertebral fusion (11% asymptomatic vs. 9% with pain) and cervical halo (8% vs. 13%).
The lesson here, Dr. Healey concluded, is that pain is not always a reliable indicator of neck injury in older patients. “Older adults can break their neck and have no pain at all. This is concerning, because the presence or absence of neck pain is a major component in many clearance protocols for C-spine trauma. This begs the question whether we should be treating our older patients by general adult guidelines. I would advocate the development of trauma guidelines that are specific for the older or geriatric patient.”
Dr. Healey had no financial disclosures.
HOLLYWOOD, FLA. –
The 4-year review found that 21% of older patients with a confirmed C-spine fracture reported no pain on history or physical exam, and that 76% of these fractures needed treatment – twin findings suggesting that asymptomatic neck fractures may be undiagnosed and untreated in this population.
The 183-patient study also found no significant pain differences between age groups: The silent injuries were just as common among 55-year-olds as among 65-year-olds, Christopher Healey, MD, said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
“I guess we can say, ‘55 is the new 65,’ when it comes to this injury,” said Dr. Healey of the Iowa Methodist Medical Center, Des Moines. “In our study the rate of a pain-free neck fracture in 55-year-olds was equivalent to that in their older counterpoints, so they also represent a group at increased risk.”
Dr. Healey and his colleagues conducted a 4-year review of trauma patients aged 55 years and older who were treated for a C-spine fracture. All of the patients had a Glasgow Coma
There were no differences in the mechanism of injury between the pain-free and pain-positive groups. The most common source of injury was a fall from the person’s own height (39% vs. 49%), followed by a high fall (21% vs. 19%). Motor vehicle crashes came in third (37% vs. 30%), with other methods of injury accounting for about 3% of each group.
The level of fracture was widely dispersed among both groups and not associated with pain. Asymptomatic fractures occurred at C1 and C2 vertabrae (about 13%); C3 (26%); C4 (10%); C5 (12%); and C6 and C7 (30%).
Perhaps surprisingly, patients who didn’t report pain had significantly higher Injury Severity Scores (15 vs. 10). They were also significantly more likely to have injuries to other body regions (71% vs. 47%), including the head (22% vs. 16%), thorax/abdomen (39% vs. 20%), and extremities (33% vs. 20%).
A third of those with a pain-free fracture had breaks at multiple levels. Their hospital stays were significantly longer than were those of patients with painful fractures (7 vs. 5 days).
These findings of more severe injuries in the asymptomatic group led Dr. Healey to suggest that distracting pain might be playing a part in the phenomenon.
When the group was split into 10-year age increments, asymptomatic fractures occurred in about 20% of each group from 55-64 years up to 85 years and older.
The majority of both groups required treatment (91% with pain; 76% asymptomatic), Dr. Healey said. The most common treatment in each group was a cervical collar (61% with pain vs. 46% asymptomatic ). A cervical-thoracic-lumbar-sacral orthosis brace was used in 8% of those with pain and 11% of the asymptomatic patients.
Invasive procedures were performed in just as many of the asymptomatic patients as in those who had pain. These included vertebral fusion (11% asymptomatic vs. 9% with pain) and cervical halo (8% vs. 13%).
The lesson here, Dr. Healey concluded, is that pain is not always a reliable indicator of neck injury in older patients. “Older adults can break their neck and have no pain at all. This is concerning, because the presence or absence of neck pain is a major component in many clearance protocols for C-spine trauma. This begs the question whether we should be treating our older patients by general adult guidelines. I would advocate the development of trauma guidelines that are specific for the older or geriatric patient.”
Dr. Healey had no financial disclosures.
Key clinical point: Older trauma patients can present with pain-free cervical fractures. Major finding: Cervical fractures were asymptomatic in 21% of the study group; of these, 76% required treatment.
Data source: The 4-year retrospective study comprised 183 older patients with confirmed cervical fractures.
Disclosures: Dr. Healey had no financial disclosures.
Study: Docs could see financial losses under partial ACA repeal
An expected partial repeal of the Affordable Care Act would hit physicians’ bottom line, according to a new analysis from the Urban Institute.
Analysts using the vetoed January 2016 budget reconciliation bill as the basis for their projections estimate that the partial repeal could result in as many as 29.8 million Americans losing coverage through the elimination of the Medicaid expansion, the individual and employer mandates, and the insurance marketplace premium tax credits and cost-sharing reductions. In addition, there would be a surge in uncompensated care.
“The coverage losses would in turn decrease revenues for providers of all types,” the report states. “Providers’ variable costs would also decrease, but their fixed costs would not.”
The Urban Institute estimates that spending by insurers (public and private) and households on health care delivered to the nonelderly would decrease by $145.8 billion in 2019 and $1.7 trillion between 2019 and 2028. 
The increase in the uninsured would cause a spike of $88 billion in uncompensated care ($26.4 billion in hospital care, $11.9 billion in physician office care, $33.6 billion in other services, and $18.0 billion in prescription drugs), reaching $1.1 trillion between 2019 and 2028. At the same time, federal funding for uncompensated care would increase no more than $3.2 billion in 2019 and no more than $35 billion from 2019 and 2028, analysts state.
“There is no clear source of funding for the remainder,” the report notes. “If federal, state, and local governments do not allocate more funding for this care, the financial burden would fall on health care providers. Large increases in unmet need for the uninsured are likely because the additional costs would require a fourfold increase in provider funding of uncompensated care from current levels.”
Congressional Republicans plan to use the budget reconciliation process to partially repeal the revenue generating aspects of the ACA, a process that allows the repeal to go through with a simple majority in the Senate. However, repeal of the health care reform law’s other parts would require at least 60 votes in the Senate, requiring at least eight Democrats to side with the Republican majority, assuming none in the majority go against the party.
The Trump administration has signaled that it plans to maintain certain aspects of the ACA, including the ability for parents to cover children up to age 26 and the ban on denial of coverage for preexisting conditions.
Research for the report was funded by the Robert Wood Johnson Foundation.
This article was updated January 20, 2017 and February 9, 2017.
An expected partial repeal of the Affordable Care Act would hit physicians’ bottom line, according to a new analysis from the Urban Institute.
Analysts using the vetoed January 2016 budget reconciliation bill as the basis for their projections estimate that the partial repeal could result in as many as 29.8 million Americans losing coverage through the elimination of the Medicaid expansion, the individual and employer mandates, and the insurance marketplace premium tax credits and cost-sharing reductions. In addition, there would be a surge in uncompensated care.
“The coverage losses would in turn decrease revenues for providers of all types,” the report states. “Providers’ variable costs would also decrease, but their fixed costs would not.”
The Urban Institute estimates that spending by insurers (public and private) and households on health care delivered to the nonelderly would decrease by $145.8 billion in 2019 and $1.7 trillion between 2019 and 2028.
The increase in the uninsured would cause a spike of $88 billion in uncompensated care ($26.4 billion in hospital care, $11.9 billion in physician office care, $33.6 billion in other services, and $18.0 billion in prescription drugs), reaching $1.1 trillion between 2019 and 2028. At the same time, federal funding for uncompensated care would increase no more than $3.2 billion in 2019 and no more than $35 billion from 2019 and 2028, analysts state.
“There is no clear source of funding for the remainder,” the report notes. “If federal, state, and local governments do not allocate more funding for this care, the financial burden would fall on health care providers. Large increases in unmet need for the uninsured are likely because the additional costs would require a fourfold increase in provider funding of uncompensated care from current levels.”
Congressional Republicans plan to use the budget reconciliation process to partially repeal the revenue generating aspects of the ACA, a process that allows the repeal to go through with a simple majority in the Senate. However, repeal of the health care reform law’s other parts would require at least 60 votes in the Senate, requiring at least eight Democrats to side with the Republican majority, assuming none in the majority go against the party.
The Trump administration has signaled that it plans to maintain certain aspects of the ACA, including the ability for parents to cover children up to age 26 and the ban on denial of coverage for preexisting conditions.
Research for the report was funded by the Robert Wood Johnson Foundation.
This article was updated January 20, 2017 and February 9, 2017.
An expected partial repeal of the Affordable Care Act would hit physicians’ bottom line, according to a new analysis from the Urban Institute.
Analysts using the vetoed January 2016 budget reconciliation bill as the basis for their projections estimate that the partial repeal could result in as many as 29.8 million Americans losing coverage through the elimination of the Medicaid expansion, the individual and employer mandates, and the insurance marketplace premium tax credits and cost-sharing reductions. In addition, there would be a surge in uncompensated care.
“The coverage losses would in turn decrease revenues for providers of all types,” the report states. “Providers’ variable costs would also decrease, but their fixed costs would not.”
The Urban Institute estimates that spending by insurers (public and private) and households on health care delivered to the nonelderly would decrease by $145.8 billion in 2019 and $1.7 trillion between 2019 and 2028.
The increase in the uninsured would cause a spike of $88 billion in uncompensated care ($26.4 billion in hospital care, $11.9 billion in physician office care, $33.6 billion in other services, and $18.0 billion in prescription drugs), reaching $1.1 trillion between 2019 and 2028. At the same time, federal funding for uncompensated care would increase no more than $3.2 billion in 2019 and no more than $35 billion from 2019 and 2028, analysts state.
“There is no clear source of funding for the remainder,” the report notes. “If federal, state, and local governments do not allocate more funding for this care, the financial burden would fall on health care providers. Large increases in unmet need for the uninsured are likely because the additional costs would require a fourfold increase in provider funding of uncompensated care from current levels.”
Congressional Republicans plan to use the budget reconciliation process to partially repeal the revenue generating aspects of the ACA, a process that allows the repeal to go through with a simple majority in the Senate. However, repeal of the health care reform law’s other parts would require at least 60 votes in the Senate, requiring at least eight Democrats to side with the Republican majority, assuming none in the majority go against the party.
The Trump administration has signaled that it plans to maintain certain aspects of the ACA, including the ability for parents to cover children up to age 26 and the ban on denial of coverage for preexisting conditions.
Research for the report was funded by the Robert Wood Johnson Foundation.
This article was updated January 20, 2017 and February 9, 2017.
Survey: Docs see health care improvements as unlikely in 2017
Physicians appear to be quite pessimistic about the chances for improving health care quality, costs, and access in 2017, according to a survey conducted by InCrowd, a market insights technology firm.
Of the 150 physicians who responded to the 3-minute “mobile microsurvey” conducted on Dec. 4, 2016, 70% said it was unlikely that the cost of health care would improve under the incoming Trump administration, 69% said it was unlikely that access to care would improve, and 60% said it was unlikely that the quality of health care would improve, InCrowd reported.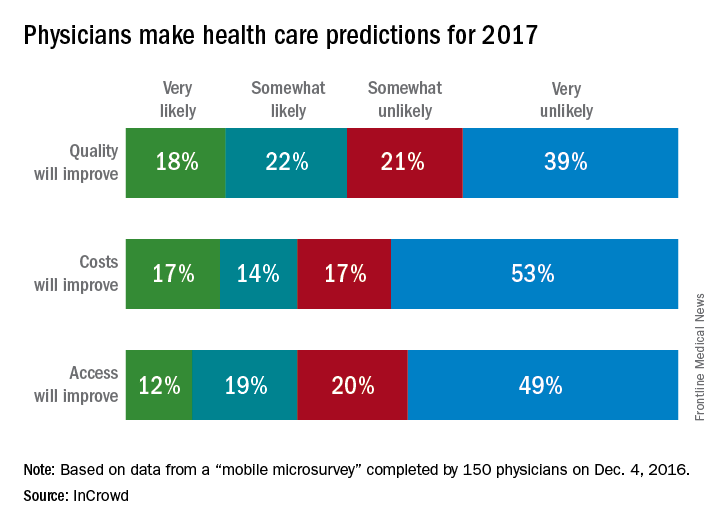
Physicians appear to be quite pessimistic about the chances for improving health care quality, costs, and access in 2017, according to a survey conducted by InCrowd, a market insights technology firm.
Of the 150 physicians who responded to the 3-minute “mobile microsurvey” conducted on Dec. 4, 2016, 70% said it was unlikely that the cost of health care would improve under the incoming Trump administration, 69% said it was unlikely that access to care would improve, and 60% said it was unlikely that the quality of health care would improve, InCrowd reported.
Physicians appear to be quite pessimistic about the chances for improving health care quality, costs, and access in 2017, according to a survey conducted by InCrowd, a market insights technology firm.
Of the 150 physicians who responded to the 3-minute “mobile microsurvey” conducted on Dec. 4, 2016, 70% said it was unlikely that the cost of health care would improve under the incoming Trump administration, 69% said it was unlikely that access to care would improve, and 60% said it was unlikely that the quality of health care would improve, InCrowd reported.