User login
For MD-IQ use only
Can overweight docs really give credible weight loss advice?
Kevin Gendreau, MD, a weight loss doctor at Southcoast Health in Fall River, Maine, lets patients know that he was once obese. He says this knowledge inspires and motivates them to lose weight.

After dropping 125 pounds over 18 months, “I can relate to their binges, hardships, and plateaus on a very personal level,” he says.
Peminda Cabandugama, MD, an endocrinologist and obesity medicine specialist at Truman Medical Center at the University of Missouri-Kansas City, has weighed between 180 and 240 pounds in the past decade. He now weighs 225 pounds and has a healthy lifestyle.
“I have had patients come to me saying, ‘I used to see a different weight loss doctor who was not heavy. But how can he understand what I’m going through?’” he says.
Dr. Cabandugama shares his weight loss struggles with patients “to dispel this myth that weight management is as simple as just eating too much and not exercising. It involves a smorgasbord of emotions and hormones, some within and outside of our control. I hope that sharing this allows me to connect more with my patients so that they know that even their health care professional goes through the same challenges that they do.”
“Patients are more likely to make behavior changes when doctors are supportive and have had similar experiences and talk about their stories,” says Wendy Bennett, MD, an obesity researcher and associate professor of medicine at Johns Hopkins University in Baltimore.
Do patients respect overweight doctors?
While Dr. Gendreau and Dr. Cabandugama have lost weight,
Doctors sometimes have biased attitudes toward overweight patients, but few studies have looked at whether patients have biases towards overweight doctors. The results vary and may depend on whether or not the patients are overweight.
A random online survey of 358 participants suggested that regardless of their own weight, people had biases about doctor weight gain. They viewed the overweight or obese doctors as less trustworthy and credible, which could lead the participants to reject their medical advice and change doctors.
“Patients expect doctors who are providing health care to be doing everything they can to take care of their own health and well-being,” says Pamela Peeke, MD, an assistant clinical professor of medicine at the University of Maryland in Baltimore.
“I am a physician who believes you have to walk the talk — that the best teachers are those who live it,” she says.
Still, “I don’t think based on this one experimental study that we can conclude that overweight physicians are harming patients’ efforts to change their behavior,” notes Dr. Bennett, who was not involved in the study.
“I think that patients do often want to connect with their physicians on more personal levels, but without the story behind where the advice is coming from, patients may struggle to trust a provider who seems to be contradicting the messages,” she says.
A study that Dr. Bennett helped lead suggests that patients are not biased against overweight doctors if they themselves need to lose weight. A national survey of 600 overweight patients showed that 87% trusted diet advice from overweight primary care doctors, compared to 77% who trusted diet advice from doctors who had a healthy weight.
“This shows that patients were more trusting of physicians who are more like them, which can lead to better relationships. We know from the studies on race that patients are often more trusting of physicians from the same race as them,” says Dr. Bennett.
Dr. Gendreau says that when he was severely obese, some patients questioned whether to trust his weight loss advice.
“It was very awkward when they turned to me and said, ‘What about you?’ I would respond that it’s my job to inform them about the risks to their health,” he says.
Nearly half (48%) of doctors said they are trying to lose weight, according to the 2021 Medscape Physician Lifestyle and Happiness Report. As a result, many doctors may end up in the position of seemingly advising to “do what I say, not what I do.”
Nearly three in five Americans are trying to lose weight, according to Gelesis poll results released in December 2020.
Should doctors pay more attention to wellness?
Doctors have an ethical duty to maintain their own health and wellness so they can provide safe and effective medical care. If they don’t have a healthy lifestyle, they need to make adjustments, the American Medical Association Code of Ethics advises.
Dr. Peeke agrees with the AMA. “We signed on to do this — we have to go out of our way to carve out time, even if it’s just 15 minutes where we hide away and eat that healthy lunch that we brought with us,” she says.
Dr. Gendreau suggests busy doctors do what he did.
“I started by bringing healthy snacks — small Ziploc bags filled with mixed nuts and berries — and expanded from there. This way, if I got hungry or stressed between patients, I would have easy access to something nutritious,” he says.
He and Dr. Peeke also suggest making protein shakes or berry smoothies that are low in sugar.
“These can keep you full for hours as you sip them between patients,” says Dr. Gendreau.
Convincing busy doctors to make lifestyle changes may be challenging. Sixty-five percent of those who responded to the Physician Lifestyle and Happiness Report say that they sometimes, rarely, or never focus on their health and wellness. Only 45% said they are eating healthy, and 65% said they exercise.
“Self-care isn’t a priority for most physicians because we are taught to take care of others and to put them first,” says Dr. Gendreau. “Like many doctors, I had so many other priorities — family, friends, career. Also, my last year of medical school was so difficult that my priority was finishing. I pushed my health to the side and told myself that I could fix this later.”
Only about one in five medical schools require students to take a nutrition course, according to David Eisenberg, MD, an adjunct associate professor of nutrition at the Harvard T.H. Chan School of Public Health, Boston.
“I didn’t get one ounce of nutrition training, which is the reason I became a Pew Foundation scholar in nutrition and metabolism. I had to go outside of my traditional training,” says Dr. Peeke.
“Physicians are not adequately trained to do the behavioral counseling and motivational interviewing that is needed,” says Dr. Bennett. “We do a good job of diagnosing obesity based on body mass index and understanding the relationship with future health conditions. But most doctors struggle with both a lack of time and the skill set to make significant behavior changes.”
“Medical school curriculum is focused so heavily on the pathology and pathophysiology of obesity, rather than how to prevent it with the appropriate diet and exercise regimen,” Dr. Gendreau says. “My physician patients often tell me that their own education in the field of nutrition is lacking, which can affect their weight loss journey and what they teach their patients.”
Dr. Gendreau, crediting his own weight loss journey as well as his obesity medicine fellowship, says his confidence in discussing weight loss with patients has soared.
Reframing obesity as a chronic disease
Rather than criticizing overweight people, including doctors, for their personal health choices, a better approach is to think of weight or obesity as a chronic illness, says Dr. Bennett.
“If we understand that obesity is a chronic health condition that people are struggling with, we can empathize with them,” she says, recommending that more providers share their weight loss journeys with patients they give lifestyle advice to, which may help address and repair potential biases.
A version of this article first appeared on WebMD.com.
Kevin Gendreau, MD, a weight loss doctor at Southcoast Health in Fall River, Maine, lets patients know that he was once obese. He says this knowledge inspires and motivates them to lose weight.
After dropping 125 pounds over 18 months, “I can relate to their binges, hardships, and plateaus on a very personal level,” he says.
Peminda Cabandugama, MD, an endocrinologist and obesity medicine specialist at Truman Medical Center at the University of Missouri-Kansas City, has weighed between 180 and 240 pounds in the past decade. He now weighs 225 pounds and has a healthy lifestyle.
“I have had patients come to me saying, ‘I used to see a different weight loss doctor who was not heavy. But how can he understand what I’m going through?’” he says.
Dr. Cabandugama shares his weight loss struggles with patients “to dispel this myth that weight management is as simple as just eating too much and not exercising. It involves a smorgasbord of emotions and hormones, some within and outside of our control. I hope that sharing this allows me to connect more with my patients so that they know that even their health care professional goes through the same challenges that they do.”
“Patients are more likely to make behavior changes when doctors are supportive and have had similar experiences and talk about their stories,” says Wendy Bennett, MD, an obesity researcher and associate professor of medicine at Johns Hopkins University in Baltimore.
Do patients respect overweight doctors?
While Dr. Gendreau and Dr. Cabandugama have lost weight,
Doctors sometimes have biased attitudes toward overweight patients, but few studies have looked at whether patients have biases towards overweight doctors. The results vary and may depend on whether or not the patients are overweight.
A random online survey of 358 participants suggested that regardless of their own weight, people had biases about doctor weight gain. They viewed the overweight or obese doctors as less trustworthy and credible, which could lead the participants to reject their medical advice and change doctors.
“Patients expect doctors who are providing health care to be doing everything they can to take care of their own health and well-being,” says Pamela Peeke, MD, an assistant clinical professor of medicine at the University of Maryland in Baltimore.
“I am a physician who believes you have to walk the talk — that the best teachers are those who live it,” she says.
Still, “I don’t think based on this one experimental study that we can conclude that overweight physicians are harming patients’ efforts to change their behavior,” notes Dr. Bennett, who was not involved in the study.
“I think that patients do often want to connect with their physicians on more personal levels, but without the story behind where the advice is coming from, patients may struggle to trust a provider who seems to be contradicting the messages,” she says.
A study that Dr. Bennett helped lead suggests that patients are not biased against overweight doctors if they themselves need to lose weight. A national survey of 600 overweight patients showed that 87% trusted diet advice from overweight primary care doctors, compared to 77% who trusted diet advice from doctors who had a healthy weight.
“This shows that patients were more trusting of physicians who are more like them, which can lead to better relationships. We know from the studies on race that patients are often more trusting of physicians from the same race as them,” says Dr. Bennett.
Dr. Gendreau says that when he was severely obese, some patients questioned whether to trust his weight loss advice.
“It was very awkward when they turned to me and said, ‘What about you?’ I would respond that it’s my job to inform them about the risks to their health,” he says.
Nearly half (48%) of doctors said they are trying to lose weight, according to the 2021 Medscape Physician Lifestyle and Happiness Report. As a result, many doctors may end up in the position of seemingly advising to “do what I say, not what I do.”
Nearly three in five Americans are trying to lose weight, according to Gelesis poll results released in December 2020.
Should doctors pay more attention to wellness?
Doctors have an ethical duty to maintain their own health and wellness so they can provide safe and effective medical care. If they don’t have a healthy lifestyle, they need to make adjustments, the American Medical Association Code of Ethics advises.
Dr. Peeke agrees with the AMA. “We signed on to do this — we have to go out of our way to carve out time, even if it’s just 15 minutes where we hide away and eat that healthy lunch that we brought with us,” she says.
Dr. Gendreau suggests busy doctors do what he did.
“I started by bringing healthy snacks — small Ziploc bags filled with mixed nuts and berries — and expanded from there. This way, if I got hungry or stressed between patients, I would have easy access to something nutritious,” he says.
He and Dr. Peeke also suggest making protein shakes or berry smoothies that are low in sugar.
“These can keep you full for hours as you sip them between patients,” says Dr. Gendreau.
Convincing busy doctors to make lifestyle changes may be challenging. Sixty-five percent of those who responded to the Physician Lifestyle and Happiness Report say that they sometimes, rarely, or never focus on their health and wellness. Only 45% said they are eating healthy, and 65% said they exercise.
“Self-care isn’t a priority for most physicians because we are taught to take care of others and to put them first,” says Dr. Gendreau. “Like many doctors, I had so many other priorities — family, friends, career. Also, my last year of medical school was so difficult that my priority was finishing. I pushed my health to the side and told myself that I could fix this later.”
Only about one in five medical schools require students to take a nutrition course, according to David Eisenberg, MD, an adjunct associate professor of nutrition at the Harvard T.H. Chan School of Public Health, Boston.
“I didn’t get one ounce of nutrition training, which is the reason I became a Pew Foundation scholar in nutrition and metabolism. I had to go outside of my traditional training,” says Dr. Peeke.
“Physicians are not adequately trained to do the behavioral counseling and motivational interviewing that is needed,” says Dr. Bennett. “We do a good job of diagnosing obesity based on body mass index and understanding the relationship with future health conditions. But most doctors struggle with both a lack of time and the skill set to make significant behavior changes.”
“Medical school curriculum is focused so heavily on the pathology and pathophysiology of obesity, rather than how to prevent it with the appropriate diet and exercise regimen,” Dr. Gendreau says. “My physician patients often tell me that their own education in the field of nutrition is lacking, which can affect their weight loss journey and what they teach their patients.”
Dr. Gendreau, crediting his own weight loss journey as well as his obesity medicine fellowship, says his confidence in discussing weight loss with patients has soared.
Reframing obesity as a chronic disease
Rather than criticizing overweight people, including doctors, for their personal health choices, a better approach is to think of weight or obesity as a chronic illness, says Dr. Bennett.
“If we understand that obesity is a chronic health condition that people are struggling with, we can empathize with them,” she says, recommending that more providers share their weight loss journeys with patients they give lifestyle advice to, which may help address and repair potential biases.
A version of this article first appeared on WebMD.com.
Kevin Gendreau, MD, a weight loss doctor at Southcoast Health in Fall River, Maine, lets patients know that he was once obese. He says this knowledge inspires and motivates them to lose weight.
After dropping 125 pounds over 18 months, “I can relate to their binges, hardships, and plateaus on a very personal level,” he says.
Peminda Cabandugama, MD, an endocrinologist and obesity medicine specialist at Truman Medical Center at the University of Missouri-Kansas City, has weighed between 180 and 240 pounds in the past decade. He now weighs 225 pounds and has a healthy lifestyle.
“I have had patients come to me saying, ‘I used to see a different weight loss doctor who was not heavy. But how can he understand what I’m going through?’” he says.
Dr. Cabandugama shares his weight loss struggles with patients “to dispel this myth that weight management is as simple as just eating too much and not exercising. It involves a smorgasbord of emotions and hormones, some within and outside of our control. I hope that sharing this allows me to connect more with my patients so that they know that even their health care professional goes through the same challenges that they do.”
“Patients are more likely to make behavior changes when doctors are supportive and have had similar experiences and talk about their stories,” says Wendy Bennett, MD, an obesity researcher and associate professor of medicine at Johns Hopkins University in Baltimore.
Do patients respect overweight doctors?
While Dr. Gendreau and Dr. Cabandugama have lost weight,
Doctors sometimes have biased attitudes toward overweight patients, but few studies have looked at whether patients have biases towards overweight doctors. The results vary and may depend on whether or not the patients are overweight.
A random online survey of 358 participants suggested that regardless of their own weight, people had biases about doctor weight gain. They viewed the overweight or obese doctors as less trustworthy and credible, which could lead the participants to reject their medical advice and change doctors.
“Patients expect doctors who are providing health care to be doing everything they can to take care of their own health and well-being,” says Pamela Peeke, MD, an assistant clinical professor of medicine at the University of Maryland in Baltimore.
“I am a physician who believes you have to walk the talk — that the best teachers are those who live it,” she says.
Still, “I don’t think based on this one experimental study that we can conclude that overweight physicians are harming patients’ efforts to change their behavior,” notes Dr. Bennett, who was not involved in the study.
“I think that patients do often want to connect with their physicians on more personal levels, but without the story behind where the advice is coming from, patients may struggle to trust a provider who seems to be contradicting the messages,” she says.
A study that Dr. Bennett helped lead suggests that patients are not biased against overweight doctors if they themselves need to lose weight. A national survey of 600 overweight patients showed that 87% trusted diet advice from overweight primary care doctors, compared to 77% who trusted diet advice from doctors who had a healthy weight.
“This shows that patients were more trusting of physicians who are more like them, which can lead to better relationships. We know from the studies on race that patients are often more trusting of physicians from the same race as them,” says Dr. Bennett.
Dr. Gendreau says that when he was severely obese, some patients questioned whether to trust his weight loss advice.
“It was very awkward when they turned to me and said, ‘What about you?’ I would respond that it’s my job to inform them about the risks to their health,” he says.
Nearly half (48%) of doctors said they are trying to lose weight, according to the 2021 Medscape Physician Lifestyle and Happiness Report. As a result, many doctors may end up in the position of seemingly advising to “do what I say, not what I do.”
Nearly three in five Americans are trying to lose weight, according to Gelesis poll results released in December 2020.
Should doctors pay more attention to wellness?
Doctors have an ethical duty to maintain their own health and wellness so they can provide safe and effective medical care. If they don’t have a healthy lifestyle, they need to make adjustments, the American Medical Association Code of Ethics advises.
Dr. Peeke agrees with the AMA. “We signed on to do this — we have to go out of our way to carve out time, even if it’s just 15 minutes where we hide away and eat that healthy lunch that we brought with us,” she says.
Dr. Gendreau suggests busy doctors do what he did.
“I started by bringing healthy snacks — small Ziploc bags filled with mixed nuts and berries — and expanded from there. This way, if I got hungry or stressed between patients, I would have easy access to something nutritious,” he says.
He and Dr. Peeke also suggest making protein shakes or berry smoothies that are low in sugar.
“These can keep you full for hours as you sip them between patients,” says Dr. Gendreau.
Convincing busy doctors to make lifestyle changes may be challenging. Sixty-five percent of those who responded to the Physician Lifestyle and Happiness Report say that they sometimes, rarely, or never focus on their health and wellness. Only 45% said they are eating healthy, and 65% said they exercise.
“Self-care isn’t a priority for most physicians because we are taught to take care of others and to put them first,” says Dr. Gendreau. “Like many doctors, I had so many other priorities — family, friends, career. Also, my last year of medical school was so difficult that my priority was finishing. I pushed my health to the side and told myself that I could fix this later.”
Only about one in five medical schools require students to take a nutrition course, according to David Eisenberg, MD, an adjunct associate professor of nutrition at the Harvard T.H. Chan School of Public Health, Boston.
“I didn’t get one ounce of nutrition training, which is the reason I became a Pew Foundation scholar in nutrition and metabolism. I had to go outside of my traditional training,” says Dr. Peeke.
“Physicians are not adequately trained to do the behavioral counseling and motivational interviewing that is needed,” says Dr. Bennett. “We do a good job of diagnosing obesity based on body mass index and understanding the relationship with future health conditions. But most doctors struggle with both a lack of time and the skill set to make significant behavior changes.”
“Medical school curriculum is focused so heavily on the pathology and pathophysiology of obesity, rather than how to prevent it with the appropriate diet and exercise regimen,” Dr. Gendreau says. “My physician patients often tell me that their own education in the field of nutrition is lacking, which can affect their weight loss journey and what they teach their patients.”
Dr. Gendreau, crediting his own weight loss journey as well as his obesity medicine fellowship, says his confidence in discussing weight loss with patients has soared.
Reframing obesity as a chronic disease
Rather than criticizing overweight people, including doctors, for their personal health choices, a better approach is to think of weight or obesity as a chronic illness, says Dr. Bennett.
“If we understand that obesity is a chronic health condition that people are struggling with, we can empathize with them,” she says, recommending that more providers share their weight loss journeys with patients they give lifestyle advice to, which may help address and repair potential biases.
A version of this article first appeared on WebMD.com.
OSA in women: Different symptoms, risks and consequences
The reported prevalence and severity of obstructive sleep apnea in women is lower, compared with men, but the consequences of the disease are “at least the same, if not worse,” with women appearing to have greater susceptibility to adverse OSA-related cardiovascular consequences – particularly as it pertains to endothelial dysfunction, Reena Mehra, MD, MS, said at the virtual annual meeting of the Associated Professional Sleep Societies.
Women more so than men have endothelial dysfunction associated with OSA, “suggesting there is an enhanced sensitivity of the female vascular endothelium to intermittent hypoxia,” said Dr. Mehra, director of sleep disorders research at the Cleveland Clinic and professor of medicine at Case Western Reserve University, also in Cleveland.
Sex-specific differences in the anatomic and physiological characteristics of the upper airway, in fat distribution and in respiratory stability as they relate to OSA have been documented for some time – and today, these and other differences relating to the diagnosis, treatment, and consequences of sleep apnea continue to be studied and elucidated, said Dr. Mehra, Anita Rajagopal, MD, and Chitra Lal, MD, in a session on OSA in women. Each spoke about the breath and implications of these differences, and of increasing recognition of the significance of OSA in women.
Likely underdiagnosis
Epidemiologic studies have suggested a three- to fivefold higher prevalence of OSA in men than in women in the general population. But it has also been estimated that 17%-25% of women have sleep apnea, and the prevalence reported in various studies has generally increased with time, said Dr. Rajagopal, department medical director for sleep medicine at Community Physician Network in Indianapolis, and medical director of the Community Health Network Sleep/Wake Disorders Center, also in Indianapolis.
One population-based study in Sweden, reported in 2013, found OSA (defined as an apnea-hypopnea index [AHI] ≥5) in 50% of women aged 20-70, she noted.
It’s quite possible women are being misdiagnosed or underdiagnosed because of their reporting of different symptoms, Dr. Rajagopal said. The Epworth Sleepiness Scale, commonly used to screen for OSA, has not been validated for use in women and has not been strongly associated with daytime sleepiness in women in population-based studies, she said, noting that women who report similar levels of daytime sleepiness to men are less likely to have an ESS score greater than 10.
“We shouldn’t rule out obstructive sleep apnea in women with a low ESS,” Dr. Rajagopal said in an interview after the meeting. Attentiveness to the symptoms more often reported by women – generalized daytime fatigue/lack of energy, insomnia, morning headaches, mood disturbances, and nightmares – is important, as is performance of overnight polysomnography when a home sleep study is negative and there is clinical suspicion of OSA.Respiratory disturbances in women are frequently associated with arousals – which induce less ventilatory instability in women than in men – rather than oxygen desaturations, leading to underestimation of OSA on home sleep testing. Insomnia associated with OSA in women may also increase the likelihood of a false negative result, Dr. Rajagopal said at the meeting.
“It’s really important [in sleep testing] to consider your AHI values in women,” she said. “The AHI value may not provide a true indication of the degree of sleep fragmentation being experienced by patients.” That OSA symptoms manifest in women with lower AHIs has been elucidated in research showing, for instance, that those with an AHI of 2-5 per hour have a similar level of symptoms to men with an AHI of at least 15 per hour, she said.
Women tend to have a clustering of apnea during REM sleep, and it’s possible that “the long-term effects of REM disruption contribute to greater symptomatology at lower AHI values in women compared to men,” Dr. Rajagopal said.
Also at play are when it comes to testing and diagnosis are several other key sex differences, she said. For one, the upper airways in women are less collapsible and more stable during sleep (most evident during non-REM sleep), and respiratory events during sleep are less frequently associated with complete upper airway collapse.
Women also have shorter apneic episodes, but “the longest apneas are associated with a more severe oxygen desaturation,” she said. Moreover, they have more episodes of upper airway resistance during sleep, which in and of itself “has been shown to produce clinical symptoms such as daytime fatigue and clinical depression.”
In her presentation, Dr. Mehra similarly commented on a likely underdiagnosis of OSA in women. In addition to differing symptoms, including palpitations, “women are less likely to have arousals, and have a lesser degree of nocturnal hypoxia compared to men ... perhaps leading to even more of an underdiagnosis.”
Unique consequences
Differences in upper airway physiology and other sex-specific differences impacting OSA susceptibility are at least partly attributable to sex hormones, said Dr. Mehra and Dr. Lal, associate professor of medicine at the Medical University of South Carolina, Charleston.
A significant increase in prevalence is seen after menopause, and research has shown that each additional year in menopause is associated with a greater AHI – a “dose-response effect,” Dr. Lal said. An inverse association between hormone replacement therapy and OSA severity has been seen in epidemiological studies including the Sleep Heart Health Study, Dr. Mehra said. But in prospective studies, Dr. Lal noted, hormone replacement therapy has not been shown to decrease AHI.
Experimental and clinical studies suggest that the vascular endothelium is influenced by sex hormones, Dr. Mehra said. Estrogen is known to improve endothelial function by inducing increased nitric oxide bioavailability – important in the setting of hypoxemia, which leads to reduced bioavailability of nitric oxide. “Alterations of sex-specific hormones in OSA may represent a key factor in increasing vulnerability to vascular dysfunction,” Dr. Mehra added.
The Sleep Heart Health Study also documented sex-specific differences, showing a graded increase of troponin with increasing OSA severity category as well as an increase in left ventricular mass thickness, and a 30% increased risk of heart failure or death in women with moderate/severe OSA, compared with women without OSA or with mild OSA, Dr. Mehra said. These findings were not observed in men.
The dominance of REM-related OSA in women raises risk because sleep disturbances during REM sleep are associated with adverse cardiometabolic outcomes including prevalent and incident hypertension, Dr. Mehra noted. “REM-related OSA may also adversely impact glucose metabolism,” she said, “even in the absence of non-REM obstructive sleep apnea.”
Regarding OSA treatment and responsivity, Dr. Mehra said that preliminary, post hoc data from a randomized, controlled trial of the impact of continuous positive airway pressure (CPAP) therapy on cardiovascular biomarkers showed a sex-specific effect. “There were differences in men versus women in terms of responsiveness with regards to biomarkers of inflammation and oxidative stress ... with reductions from CPAP observed in women but not in men,” said Dr. Mehra, a co-investigator of the study.
The data suggests, she said that “these biomarkers may be more responsive to treatment and a reversal of sleep apnea pathophysiology in women.”
Women also appear to respond better than men to upper airway nerve stimulation (UAS), she said, referring to an international registry study showing a 3.6-fold higher odds of responsiveness to the therapy relative to men. Women in the study were 60% less likely to be approved by insurance for UAS, however, making it “a public policy issue, said Dr. Mehra, a coinvestigator.
Dr. Rajagopal, Dr. Mehra, and Dr. Lal all reported that they had no potential conflicts of interest.
The reported prevalence and severity of obstructive sleep apnea in women is lower, compared with men, but the consequences of the disease are “at least the same, if not worse,” with women appearing to have greater susceptibility to adverse OSA-related cardiovascular consequences – particularly as it pertains to endothelial dysfunction, Reena Mehra, MD, MS, said at the virtual annual meeting of the Associated Professional Sleep Societies.
Women more so than men have endothelial dysfunction associated with OSA, “suggesting there is an enhanced sensitivity of the female vascular endothelium to intermittent hypoxia,” said Dr. Mehra, director of sleep disorders research at the Cleveland Clinic and professor of medicine at Case Western Reserve University, also in Cleveland.
Sex-specific differences in the anatomic and physiological characteristics of the upper airway, in fat distribution and in respiratory stability as they relate to OSA have been documented for some time – and today, these and other differences relating to the diagnosis, treatment, and consequences of sleep apnea continue to be studied and elucidated, said Dr. Mehra, Anita Rajagopal, MD, and Chitra Lal, MD, in a session on OSA in women. Each spoke about the breath and implications of these differences, and of increasing recognition of the significance of OSA in women.
Likely underdiagnosis
Epidemiologic studies have suggested a three- to fivefold higher prevalence of OSA in men than in women in the general population. But it has also been estimated that 17%-25% of women have sleep apnea, and the prevalence reported in various studies has generally increased with time, said Dr. Rajagopal, department medical director for sleep medicine at Community Physician Network in Indianapolis, and medical director of the Community Health Network Sleep/Wake Disorders Center, also in Indianapolis.
One population-based study in Sweden, reported in 2013, found OSA (defined as an apnea-hypopnea index [AHI] ≥5) in 50% of women aged 20-70, she noted.
It’s quite possible women are being misdiagnosed or underdiagnosed because of their reporting of different symptoms, Dr. Rajagopal said. The Epworth Sleepiness Scale, commonly used to screen for OSA, has not been validated for use in women and has not been strongly associated with daytime sleepiness in women in population-based studies, she said, noting that women who report similar levels of daytime sleepiness to men are less likely to have an ESS score greater than 10.
“We shouldn’t rule out obstructive sleep apnea in women with a low ESS,” Dr. Rajagopal said in an interview after the meeting. Attentiveness to the symptoms more often reported by women – generalized daytime fatigue/lack of energy, insomnia, morning headaches, mood disturbances, and nightmares – is important, as is performance of overnight polysomnography when a home sleep study is negative and there is clinical suspicion of OSA.Respiratory disturbances in women are frequently associated with arousals – which induce less ventilatory instability in women than in men – rather than oxygen desaturations, leading to underestimation of OSA on home sleep testing. Insomnia associated with OSA in women may also increase the likelihood of a false negative result, Dr. Rajagopal said at the meeting.
“It’s really important [in sleep testing] to consider your AHI values in women,” she said. “The AHI value may not provide a true indication of the degree of sleep fragmentation being experienced by patients.” That OSA symptoms manifest in women with lower AHIs has been elucidated in research showing, for instance, that those with an AHI of 2-5 per hour have a similar level of symptoms to men with an AHI of at least 15 per hour, she said.
Women tend to have a clustering of apnea during REM sleep, and it’s possible that “the long-term effects of REM disruption contribute to greater symptomatology at lower AHI values in women compared to men,” Dr. Rajagopal said.
Also at play are when it comes to testing and diagnosis are several other key sex differences, she said. For one, the upper airways in women are less collapsible and more stable during sleep (most evident during non-REM sleep), and respiratory events during sleep are less frequently associated with complete upper airway collapse.
Women also have shorter apneic episodes, but “the longest apneas are associated with a more severe oxygen desaturation,” she said. Moreover, they have more episodes of upper airway resistance during sleep, which in and of itself “has been shown to produce clinical symptoms such as daytime fatigue and clinical depression.”
In her presentation, Dr. Mehra similarly commented on a likely underdiagnosis of OSA in women. In addition to differing symptoms, including palpitations, “women are less likely to have arousals, and have a lesser degree of nocturnal hypoxia compared to men ... perhaps leading to even more of an underdiagnosis.”
Unique consequences
Differences in upper airway physiology and other sex-specific differences impacting OSA susceptibility are at least partly attributable to sex hormones, said Dr. Mehra and Dr. Lal, associate professor of medicine at the Medical University of South Carolina, Charleston.
A significant increase in prevalence is seen after menopause, and research has shown that each additional year in menopause is associated with a greater AHI – a “dose-response effect,” Dr. Lal said. An inverse association between hormone replacement therapy and OSA severity has been seen in epidemiological studies including the Sleep Heart Health Study, Dr. Mehra said. But in prospective studies, Dr. Lal noted, hormone replacement therapy has not been shown to decrease AHI.
Experimental and clinical studies suggest that the vascular endothelium is influenced by sex hormones, Dr. Mehra said. Estrogen is known to improve endothelial function by inducing increased nitric oxide bioavailability – important in the setting of hypoxemia, which leads to reduced bioavailability of nitric oxide. “Alterations of sex-specific hormones in OSA may represent a key factor in increasing vulnerability to vascular dysfunction,” Dr. Mehra added.
The Sleep Heart Health Study also documented sex-specific differences, showing a graded increase of troponin with increasing OSA severity category as well as an increase in left ventricular mass thickness, and a 30% increased risk of heart failure or death in women with moderate/severe OSA, compared with women without OSA or with mild OSA, Dr. Mehra said. These findings were not observed in men.
The dominance of REM-related OSA in women raises risk because sleep disturbances during REM sleep are associated with adverse cardiometabolic outcomes including prevalent and incident hypertension, Dr. Mehra noted. “REM-related OSA may also adversely impact glucose metabolism,” she said, “even in the absence of non-REM obstructive sleep apnea.”
Regarding OSA treatment and responsivity, Dr. Mehra said that preliminary, post hoc data from a randomized, controlled trial of the impact of continuous positive airway pressure (CPAP) therapy on cardiovascular biomarkers showed a sex-specific effect. “There were differences in men versus women in terms of responsiveness with regards to biomarkers of inflammation and oxidative stress ... with reductions from CPAP observed in women but not in men,” said Dr. Mehra, a co-investigator of the study.
The data suggests, she said that “these biomarkers may be more responsive to treatment and a reversal of sleep apnea pathophysiology in women.”
Women also appear to respond better than men to upper airway nerve stimulation (UAS), she said, referring to an international registry study showing a 3.6-fold higher odds of responsiveness to the therapy relative to men. Women in the study were 60% less likely to be approved by insurance for UAS, however, making it “a public policy issue, said Dr. Mehra, a coinvestigator.
Dr. Rajagopal, Dr. Mehra, and Dr. Lal all reported that they had no potential conflicts of interest.
The reported prevalence and severity of obstructive sleep apnea in women is lower, compared with men, but the consequences of the disease are “at least the same, if not worse,” with women appearing to have greater susceptibility to adverse OSA-related cardiovascular consequences – particularly as it pertains to endothelial dysfunction, Reena Mehra, MD, MS, said at the virtual annual meeting of the Associated Professional Sleep Societies.
Women more so than men have endothelial dysfunction associated with OSA, “suggesting there is an enhanced sensitivity of the female vascular endothelium to intermittent hypoxia,” said Dr. Mehra, director of sleep disorders research at the Cleveland Clinic and professor of medicine at Case Western Reserve University, also in Cleveland.
Sex-specific differences in the anatomic and physiological characteristics of the upper airway, in fat distribution and in respiratory stability as they relate to OSA have been documented for some time – and today, these and other differences relating to the diagnosis, treatment, and consequences of sleep apnea continue to be studied and elucidated, said Dr. Mehra, Anita Rajagopal, MD, and Chitra Lal, MD, in a session on OSA in women. Each spoke about the breath and implications of these differences, and of increasing recognition of the significance of OSA in women.
Likely underdiagnosis
Epidemiologic studies have suggested a three- to fivefold higher prevalence of OSA in men than in women in the general population. But it has also been estimated that 17%-25% of women have sleep apnea, and the prevalence reported in various studies has generally increased with time, said Dr. Rajagopal, department medical director for sleep medicine at Community Physician Network in Indianapolis, and medical director of the Community Health Network Sleep/Wake Disorders Center, also in Indianapolis.
One population-based study in Sweden, reported in 2013, found OSA (defined as an apnea-hypopnea index [AHI] ≥5) in 50% of women aged 20-70, she noted.
It’s quite possible women are being misdiagnosed or underdiagnosed because of their reporting of different symptoms, Dr. Rajagopal said. The Epworth Sleepiness Scale, commonly used to screen for OSA, has not been validated for use in women and has not been strongly associated with daytime sleepiness in women in population-based studies, she said, noting that women who report similar levels of daytime sleepiness to men are less likely to have an ESS score greater than 10.
“We shouldn’t rule out obstructive sleep apnea in women with a low ESS,” Dr. Rajagopal said in an interview after the meeting. Attentiveness to the symptoms more often reported by women – generalized daytime fatigue/lack of energy, insomnia, morning headaches, mood disturbances, and nightmares – is important, as is performance of overnight polysomnography when a home sleep study is negative and there is clinical suspicion of OSA.Respiratory disturbances in women are frequently associated with arousals – which induce less ventilatory instability in women than in men – rather than oxygen desaturations, leading to underestimation of OSA on home sleep testing. Insomnia associated with OSA in women may also increase the likelihood of a false negative result, Dr. Rajagopal said at the meeting.
“It’s really important [in sleep testing] to consider your AHI values in women,” she said. “The AHI value may not provide a true indication of the degree of sleep fragmentation being experienced by patients.” That OSA symptoms manifest in women with lower AHIs has been elucidated in research showing, for instance, that those with an AHI of 2-5 per hour have a similar level of symptoms to men with an AHI of at least 15 per hour, she said.
Women tend to have a clustering of apnea during REM sleep, and it’s possible that “the long-term effects of REM disruption contribute to greater symptomatology at lower AHI values in women compared to men,” Dr. Rajagopal said.
Also at play are when it comes to testing and diagnosis are several other key sex differences, she said. For one, the upper airways in women are less collapsible and more stable during sleep (most evident during non-REM sleep), and respiratory events during sleep are less frequently associated with complete upper airway collapse.
Women also have shorter apneic episodes, but “the longest apneas are associated with a more severe oxygen desaturation,” she said. Moreover, they have more episodes of upper airway resistance during sleep, which in and of itself “has been shown to produce clinical symptoms such as daytime fatigue and clinical depression.”
In her presentation, Dr. Mehra similarly commented on a likely underdiagnosis of OSA in women. In addition to differing symptoms, including palpitations, “women are less likely to have arousals, and have a lesser degree of nocturnal hypoxia compared to men ... perhaps leading to even more of an underdiagnosis.”
Unique consequences
Differences in upper airway physiology and other sex-specific differences impacting OSA susceptibility are at least partly attributable to sex hormones, said Dr. Mehra and Dr. Lal, associate professor of medicine at the Medical University of South Carolina, Charleston.
A significant increase in prevalence is seen after menopause, and research has shown that each additional year in menopause is associated with a greater AHI – a “dose-response effect,” Dr. Lal said. An inverse association between hormone replacement therapy and OSA severity has been seen in epidemiological studies including the Sleep Heart Health Study, Dr. Mehra said. But in prospective studies, Dr. Lal noted, hormone replacement therapy has not been shown to decrease AHI.
Experimental and clinical studies suggest that the vascular endothelium is influenced by sex hormones, Dr. Mehra said. Estrogen is known to improve endothelial function by inducing increased nitric oxide bioavailability – important in the setting of hypoxemia, which leads to reduced bioavailability of nitric oxide. “Alterations of sex-specific hormones in OSA may represent a key factor in increasing vulnerability to vascular dysfunction,” Dr. Mehra added.
The Sleep Heart Health Study also documented sex-specific differences, showing a graded increase of troponin with increasing OSA severity category as well as an increase in left ventricular mass thickness, and a 30% increased risk of heart failure or death in women with moderate/severe OSA, compared with women without OSA or with mild OSA, Dr. Mehra said. These findings were not observed in men.
The dominance of REM-related OSA in women raises risk because sleep disturbances during REM sleep are associated with adverse cardiometabolic outcomes including prevalent and incident hypertension, Dr. Mehra noted. “REM-related OSA may also adversely impact glucose metabolism,” she said, “even in the absence of non-REM obstructive sleep apnea.”
Regarding OSA treatment and responsivity, Dr. Mehra said that preliminary, post hoc data from a randomized, controlled trial of the impact of continuous positive airway pressure (CPAP) therapy on cardiovascular biomarkers showed a sex-specific effect. “There were differences in men versus women in terms of responsiveness with regards to biomarkers of inflammation and oxidative stress ... with reductions from CPAP observed in women but not in men,” said Dr. Mehra, a co-investigator of the study.
The data suggests, she said that “these biomarkers may be more responsive to treatment and a reversal of sleep apnea pathophysiology in women.”
Women also appear to respond better than men to upper airway nerve stimulation (UAS), she said, referring to an international registry study showing a 3.6-fold higher odds of responsiveness to the therapy relative to men. Women in the study were 60% less likely to be approved by insurance for UAS, however, making it “a public policy issue, said Dr. Mehra, a coinvestigator.
Dr. Rajagopal, Dr. Mehra, and Dr. Lal all reported that they had no potential conflicts of interest.
FROM SLEEP 2021
Malpractice claims from the COVID-19 pandemic: More questions than answers
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
The pandemic has raised pressing questions around preventive measures, vaccines, and safe treatment, but it has also obscured one key lingering uncertainty for medical professionals: Where are all the medical malpractice claims?
A variety of factors create a cloud of uncertainty around when, if ever, we will see the claims we expected from care provided just before the pandemic, much less claims deriving from care during the pandemic of both COVID-19 and non–COVID-19 patients.
Malpractice claims take time to surface
We won’t know until 2022 or later whether there will be an increase in claims related to the pandemic. When a medical error occurs, it’s not like an automobile accident. Everybody nearby knows when there’s been an automobile accident because they hear screeching tires, a loud crash, and then sirens. But when a medical error occurs, generally speaking, neither the doctor nor the patient immediately knows that something is amiss. It can take months or years for people to realize that something untoward has occurred.
Claims from medical errors that occurred before the pandemic bring additional uncertainties. In 2020, we saw fewer than expected overall claims filed from events occurring 18-24 months before the pandemic. In total, 20% fewer claims were filed than in 2019. This may have had to do with courts shutting down, people being reluctant to meet with attorneys to discuss a claim, and/or lawyers working from home. We may see these claims filed later than expected, or maybe we won’t see them at all.
But without a doubt, pandemic-related claims will be filed. The pandemic’s impact on physicians increases the risk of claims. Burnout is a major cause of medical errors, and a recent study found that out of 60 countries, U.S. health care providers showed the highest rates of burnout. We’re concerned about the stress affecting physicians’ performance – not just the physical stress of the demands put on them while treating COVID-19 patients, but all of the worry. For instance, a lot of doctors at the start of this pandemic stayed at hotels because they didn’t want to bring the virus home to their families – if they got exposed. Those sorts of stressors from life disruptions, on top of the stress of treating COVID-19 patients and the stress of treating non–COVID-19 patients within overtaxed health care systems, contribute to the possibilities for error.
Immunity protections are not fail-safe
And while health care providers have medical liability protections during the pandemic, these protections may not prevent claims. Health care provider pandemic-related liability laws vary from state to state, and they will be tested in the courts as to whether they’re constitutional. For example, there is pending legislation in New York state that would repeal the provider protections created there at the start of the pandemic. Further, some expert witnesses will couch their statements in terms of what it takes to get around one of these statutes. Therefore, physicians do have reason for concern, even in states with strong liability protections.
The following case example, which is one of about 40 COVID-19–related claims made against our members so far, is a poster child for why these protections are necessary: A quadriplegic patient with COVID-19 had reached the point of organ failure before he reached the ED. There was really nothing medical science could do for him at that point, in terms of a chance at recovery. Therefore, the patient’s physician and conservator placed him in assisted living for palliative care. This was a sad but reasonable decision during a pandemic, with hospital beds needed for patients with a shot at surviving. Following that patient’s death, the physician is being sued.
Defending claims regarding treatment vs. regarding infection control
We are very confident in our ability to protect our members against claims where they are being sued over the treatment of the disease. Claims arising out of treatment are not concerning to us because there is no cure for COVID-19 – one can only treat the symptoms as the virus runs its course.
On the other hand, suits harder to defend would be those that revolve around transmitting the disease because providers didn’t follow guidelines from the Centers for Disease Control and Prevention or there wasn’t enough personal protective equipment. That’s why we stress the importance of following CDC guidelines, and why we’ve taken proactive steps to communicate with the entire medical community throughout the pandemic as part of our commitment to serve those who provide care.
Mr. White is chief operating officer at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
The pandemic has raised pressing questions around preventive measures, vaccines, and safe treatment, but it has also obscured one key lingering uncertainty for medical professionals: Where are all the medical malpractice claims?
A variety of factors create a cloud of uncertainty around when, if ever, we will see the claims we expected from care provided just before the pandemic, much less claims deriving from care during the pandemic of both COVID-19 and non–COVID-19 patients.
Malpractice claims take time to surface
We won’t know until 2022 or later whether there will be an increase in claims related to the pandemic. When a medical error occurs, it’s not like an automobile accident. Everybody nearby knows when there’s been an automobile accident because they hear screeching tires, a loud crash, and then sirens. But when a medical error occurs, generally speaking, neither the doctor nor the patient immediately knows that something is amiss. It can take months or years for people to realize that something untoward has occurred.
Claims from medical errors that occurred before the pandemic bring additional uncertainties. In 2020, we saw fewer than expected overall claims filed from events occurring 18-24 months before the pandemic. In total, 20% fewer claims were filed than in 2019. This may have had to do with courts shutting down, people being reluctant to meet with attorneys to discuss a claim, and/or lawyers working from home. We may see these claims filed later than expected, or maybe we won’t see them at all.
But without a doubt, pandemic-related claims will be filed. The pandemic’s impact on physicians increases the risk of claims. Burnout is a major cause of medical errors, and a recent study found that out of 60 countries, U.S. health care providers showed the highest rates of burnout. We’re concerned about the stress affecting physicians’ performance – not just the physical stress of the demands put on them while treating COVID-19 patients, but all of the worry. For instance, a lot of doctors at the start of this pandemic stayed at hotels because they didn’t want to bring the virus home to their families – if they got exposed. Those sorts of stressors from life disruptions, on top of the stress of treating COVID-19 patients and the stress of treating non–COVID-19 patients within overtaxed health care systems, contribute to the possibilities for error.
Immunity protections are not fail-safe
And while health care providers have medical liability protections during the pandemic, these protections may not prevent claims. Health care provider pandemic-related liability laws vary from state to state, and they will be tested in the courts as to whether they’re constitutional. For example, there is pending legislation in New York state that would repeal the provider protections created there at the start of the pandemic. Further, some expert witnesses will couch their statements in terms of what it takes to get around one of these statutes. Therefore, physicians do have reason for concern, even in states with strong liability protections.
The following case example, which is one of about 40 COVID-19–related claims made against our members so far, is a poster child for why these protections are necessary: A quadriplegic patient with COVID-19 had reached the point of organ failure before he reached the ED. There was really nothing medical science could do for him at that point, in terms of a chance at recovery. Therefore, the patient’s physician and conservator placed him in assisted living for palliative care. This was a sad but reasonable decision during a pandemic, with hospital beds needed for patients with a shot at surviving. Following that patient’s death, the physician is being sued.
Defending claims regarding treatment vs. regarding infection control
We are very confident in our ability to protect our members against claims where they are being sued over the treatment of the disease. Claims arising out of treatment are not concerning to us because there is no cure for COVID-19 – one can only treat the symptoms as the virus runs its course.
On the other hand, suits harder to defend would be those that revolve around transmitting the disease because providers didn’t follow guidelines from the Centers for Disease Control and Prevention or there wasn’t enough personal protective equipment. That’s why we stress the importance of following CDC guidelines, and why we’ve taken proactive steps to communicate with the entire medical community throughout the pandemic as part of our commitment to serve those who provide care.
Mr. White is chief operating officer at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
The pandemic has raised pressing questions around preventive measures, vaccines, and safe treatment, but it has also obscured one key lingering uncertainty for medical professionals: Where are all the medical malpractice claims?
A variety of factors create a cloud of uncertainty around when, if ever, we will see the claims we expected from care provided just before the pandemic, much less claims deriving from care during the pandemic of both COVID-19 and non–COVID-19 patients.
Malpractice claims take time to surface
We won’t know until 2022 or later whether there will be an increase in claims related to the pandemic. When a medical error occurs, it’s not like an automobile accident. Everybody nearby knows when there’s been an automobile accident because they hear screeching tires, a loud crash, and then sirens. But when a medical error occurs, generally speaking, neither the doctor nor the patient immediately knows that something is amiss. It can take months or years for people to realize that something untoward has occurred.
Claims from medical errors that occurred before the pandemic bring additional uncertainties. In 2020, we saw fewer than expected overall claims filed from events occurring 18-24 months before the pandemic. In total, 20% fewer claims were filed than in 2019. This may have had to do with courts shutting down, people being reluctant to meet with attorneys to discuss a claim, and/or lawyers working from home. We may see these claims filed later than expected, or maybe we won’t see them at all.
But without a doubt, pandemic-related claims will be filed. The pandemic’s impact on physicians increases the risk of claims. Burnout is a major cause of medical errors, and a recent study found that out of 60 countries, U.S. health care providers showed the highest rates of burnout. We’re concerned about the stress affecting physicians’ performance – not just the physical stress of the demands put on them while treating COVID-19 patients, but all of the worry. For instance, a lot of doctors at the start of this pandemic stayed at hotels because they didn’t want to bring the virus home to their families – if they got exposed. Those sorts of stressors from life disruptions, on top of the stress of treating COVID-19 patients and the stress of treating non–COVID-19 patients within overtaxed health care systems, contribute to the possibilities for error.
Immunity protections are not fail-safe
And while health care providers have medical liability protections during the pandemic, these protections may not prevent claims. Health care provider pandemic-related liability laws vary from state to state, and they will be tested in the courts as to whether they’re constitutional. For example, there is pending legislation in New York state that would repeal the provider protections created there at the start of the pandemic. Further, some expert witnesses will couch their statements in terms of what it takes to get around one of these statutes. Therefore, physicians do have reason for concern, even in states with strong liability protections.
The following case example, which is one of about 40 COVID-19–related claims made against our members so far, is a poster child for why these protections are necessary: A quadriplegic patient with COVID-19 had reached the point of organ failure before he reached the ED. There was really nothing medical science could do for him at that point, in terms of a chance at recovery. Therefore, the patient’s physician and conservator placed him in assisted living for palliative care. This was a sad but reasonable decision during a pandemic, with hospital beds needed for patients with a shot at surviving. Following that patient’s death, the physician is being sued.
Defending claims regarding treatment vs. regarding infection control
We are very confident in our ability to protect our members against claims where they are being sued over the treatment of the disease. Claims arising out of treatment are not concerning to us because there is no cure for COVID-19 – one can only treat the symptoms as the virus runs its course.
On the other hand, suits harder to defend would be those that revolve around transmitting the disease because providers didn’t follow guidelines from the Centers for Disease Control and Prevention or there wasn’t enough personal protective equipment. That’s why we stress the importance of following CDC guidelines, and why we’ve taken proactive steps to communicate with the entire medical community throughout the pandemic as part of our commitment to serve those who provide care.
Mr. White is chief operating officer at The Doctors Company. The guidelines suggested here are not rules, do not constitute legal advice, and do not ensure a successful outcome. The ultimate decision regarding the appropriateness of any treatment must be made by each health care provider considering the circumstances of the individual situation and in accordance with the laws of the jurisdiction in which the care is rendered.
Network meta-analysis ranks first-line H. pylori regimens
A network meta-analysis of current first-line dual, triple, and quadruple therapies for Helicobacter pylori infection found that vonoprazan triple therapy was most effective, while standard triple therapy of a proton pump inhibitor (PPI), amoxicillin, and clarithromycin was least effective. Levofloxacin-containing triple therapy performed best in Western countries and West Asia, while reverse hybrid therapy was most effective in East Asia.
The results “[suggest that] a new approach concerning H. pylori treatment is now needed and that the time for transitioning from trial and error to antimicrobial stewardship [of H. pylori infection] has arrived,” wrote Theodore Rokkas, PhD, MD, of the European University of Cyprus in Engomi, and colleagues. Their study was published in Gastroenterology.
H. pylori infection is the primary cause of gastritis, peptic ulcer disease, gastric mucosa–associated lymphoid tissue lymphoma, and gastric cancer.
Since H. pylori infection was first recognized, physicians have employed a range of drugs in double, triple, and quadruple combinations to combat it.
Despite those efforts, treatment success is lower than with many other infectious diseases. A newcomer is the potassium-competing acid blocker vonoprazan, which increases efficacy of amoxicillin combination therapies and has, thereby, generated renewed interest in all combination therapies, according to the study authors. Vonoprazan is currently available in some Asian countries, but not the United States or Europe.
Current guidelines for H. pylori treatment relied on randomized controlled trials and relevant pair-wise meta-analyses, but no previous pairwise analysis has included all currently available medications, the authors noted. Network meta-analyses can help fill this evidence gap: They incorporate both direct and indirect evidence from a collection of randomized controlled trials to estimate the comparative effectiveness of three or more regimens.
The researchers conducted a network meta-analysis that included 68 randomized, controlled trials totaling 22,975 patients. The following regimens were included in the analysis: Concomitant quadruple bismuth treatment (bismuth quadruple therapy), concomitant quadruple nonbismuth treatment (nonbismuth quadruple therapy), high-dose amoxicillin double treatment (Amox-dual therapy), levofloxacin-containing treatment (Levo-therapy), reverse hybrid therapy (R-hybrid therapy), sequential quadruple treatment (sequential therapy), standard triple treatment (triple therapy), and vonoprazan-containing therapy (Vono-triple therapy).
Statistically significant results were found with Vono-triple therapy versus triple therapy (odds ratio, 3.80; 95% confidence interval, 1.62-8.94), sequential therapy versus triple therapy (OR, 1.79; 95% CI, 1.26-2.53), nonbismuth quadruple therapy versus triple therapy (OR, 2.08; 95% CI, 1.45-2.98), bismuth quadruple therapy versus triple therapy (OR, 1.47; 95% CI, 1.02-2.11), and Levo-therapy versus triple therapy (OR, 1.79; 95% CI, 1.26-2.53).
In the overall data, mean cure rates greater than 90% were seen only in Vono-triple therapy (91.4%; 95% CI, 88.5-93.5%) and R-hybrid therapy (93.6%; 95% CI, 90.4-96.8%). Cure rates were lower for Nonbismuth quadruple therapy (84.3%; 95% CI, 82.7-85.8%), Levo-therapy (83.8%; 95% CI, 82.1-85.4%), Sequential therapy (83.7%; 95% CI, 82.7-84.7%), bismuth quadruple therapy (81.3%; 95% CI, 79.5-83.1%), Amox-dual therapy (80.2%; 75.3%-84.4%), and triple therapy (75.7%; 95% CI, 74.9-76.4%). Levo-therapy performed best in Western countries (88.5%; 95% CI, 86.5-90.5%) and West Asia (88.4%; 95% CI, 84.6-91.1%). R-hybrid therapy performed best in East Asia (93.6%; 95% CI, 90.4-96.8%).
A surface under the cumulative ranking (SUCRA) value, which represents the efficacy of the intervention compared to an ideal intervention, was 92.4% for Vono-triple therapy. The second highest SUCRA value was for 68.8% for nonbismuth quadruple therapy. The SUCRA value of standard triple therapy was 4.7%.
A key limitation to the study is that Vono-triple therapy was tested only in Japan, and requires additional study in other geographic regions.
The study received support from the Department of Veteran Affairs. The authors have consulted for and received research funding from various pharmaceutical companies.
A network meta-analysis of current first-line dual, triple, and quadruple therapies for Helicobacter pylori infection found that vonoprazan triple therapy was most effective, while standard triple therapy of a proton pump inhibitor (PPI), amoxicillin, and clarithromycin was least effective. Levofloxacin-containing triple therapy performed best in Western countries and West Asia, while reverse hybrid therapy was most effective in East Asia.
The results “[suggest that] a new approach concerning H. pylori treatment is now needed and that the time for transitioning from trial and error to antimicrobial stewardship [of H. pylori infection] has arrived,” wrote Theodore Rokkas, PhD, MD, of the European University of Cyprus in Engomi, and colleagues. Their study was published in Gastroenterology.
H. pylori infection is the primary cause of gastritis, peptic ulcer disease, gastric mucosa–associated lymphoid tissue lymphoma, and gastric cancer.
Since H. pylori infection was first recognized, physicians have employed a range of drugs in double, triple, and quadruple combinations to combat it.
Despite those efforts, treatment success is lower than with many other infectious diseases. A newcomer is the potassium-competing acid blocker vonoprazan, which increases efficacy of amoxicillin combination therapies and has, thereby, generated renewed interest in all combination therapies, according to the study authors. Vonoprazan is currently available in some Asian countries, but not the United States or Europe.
Current guidelines for H. pylori treatment relied on randomized controlled trials and relevant pair-wise meta-analyses, but no previous pairwise analysis has included all currently available medications, the authors noted. Network meta-analyses can help fill this evidence gap: They incorporate both direct and indirect evidence from a collection of randomized controlled trials to estimate the comparative effectiveness of three or more regimens.
The researchers conducted a network meta-analysis that included 68 randomized, controlled trials totaling 22,975 patients. The following regimens were included in the analysis: Concomitant quadruple bismuth treatment (bismuth quadruple therapy), concomitant quadruple nonbismuth treatment (nonbismuth quadruple therapy), high-dose amoxicillin double treatment (Amox-dual therapy), levofloxacin-containing treatment (Levo-therapy), reverse hybrid therapy (R-hybrid therapy), sequential quadruple treatment (sequential therapy), standard triple treatment (triple therapy), and vonoprazan-containing therapy (Vono-triple therapy).
Statistically significant results were found with Vono-triple therapy versus triple therapy (odds ratio, 3.80; 95% confidence interval, 1.62-8.94), sequential therapy versus triple therapy (OR, 1.79; 95% CI, 1.26-2.53), nonbismuth quadruple therapy versus triple therapy (OR, 2.08; 95% CI, 1.45-2.98), bismuth quadruple therapy versus triple therapy (OR, 1.47; 95% CI, 1.02-2.11), and Levo-therapy versus triple therapy (OR, 1.79; 95% CI, 1.26-2.53).
In the overall data, mean cure rates greater than 90% were seen only in Vono-triple therapy (91.4%; 95% CI, 88.5-93.5%) and R-hybrid therapy (93.6%; 95% CI, 90.4-96.8%). Cure rates were lower for Nonbismuth quadruple therapy (84.3%; 95% CI, 82.7-85.8%), Levo-therapy (83.8%; 95% CI, 82.1-85.4%), Sequential therapy (83.7%; 95% CI, 82.7-84.7%), bismuth quadruple therapy (81.3%; 95% CI, 79.5-83.1%), Amox-dual therapy (80.2%; 75.3%-84.4%), and triple therapy (75.7%; 95% CI, 74.9-76.4%). Levo-therapy performed best in Western countries (88.5%; 95% CI, 86.5-90.5%) and West Asia (88.4%; 95% CI, 84.6-91.1%). R-hybrid therapy performed best in East Asia (93.6%; 95% CI, 90.4-96.8%).
A surface under the cumulative ranking (SUCRA) value, which represents the efficacy of the intervention compared to an ideal intervention, was 92.4% for Vono-triple therapy. The second highest SUCRA value was for 68.8% for nonbismuth quadruple therapy. The SUCRA value of standard triple therapy was 4.7%.
A key limitation to the study is that Vono-triple therapy was tested only in Japan, and requires additional study in other geographic regions.
The study received support from the Department of Veteran Affairs. The authors have consulted for and received research funding from various pharmaceutical companies.
A network meta-analysis of current first-line dual, triple, and quadruple therapies for Helicobacter pylori infection found that vonoprazan triple therapy was most effective, while standard triple therapy of a proton pump inhibitor (PPI), amoxicillin, and clarithromycin was least effective. Levofloxacin-containing triple therapy performed best in Western countries and West Asia, while reverse hybrid therapy was most effective in East Asia.
The results “[suggest that] a new approach concerning H. pylori treatment is now needed and that the time for transitioning from trial and error to antimicrobial stewardship [of H. pylori infection] has arrived,” wrote Theodore Rokkas, PhD, MD, of the European University of Cyprus in Engomi, and colleagues. Their study was published in Gastroenterology.
H. pylori infection is the primary cause of gastritis, peptic ulcer disease, gastric mucosa–associated lymphoid tissue lymphoma, and gastric cancer.
Since H. pylori infection was first recognized, physicians have employed a range of drugs in double, triple, and quadruple combinations to combat it.
Despite those efforts, treatment success is lower than with many other infectious diseases. A newcomer is the potassium-competing acid blocker vonoprazan, which increases efficacy of amoxicillin combination therapies and has, thereby, generated renewed interest in all combination therapies, according to the study authors. Vonoprazan is currently available in some Asian countries, but not the United States or Europe.
Current guidelines for H. pylori treatment relied on randomized controlled trials and relevant pair-wise meta-analyses, but no previous pairwise analysis has included all currently available medications, the authors noted. Network meta-analyses can help fill this evidence gap: They incorporate both direct and indirect evidence from a collection of randomized controlled trials to estimate the comparative effectiveness of three or more regimens.
The researchers conducted a network meta-analysis that included 68 randomized, controlled trials totaling 22,975 patients. The following regimens were included in the analysis: Concomitant quadruple bismuth treatment (bismuth quadruple therapy), concomitant quadruple nonbismuth treatment (nonbismuth quadruple therapy), high-dose amoxicillin double treatment (Amox-dual therapy), levofloxacin-containing treatment (Levo-therapy), reverse hybrid therapy (R-hybrid therapy), sequential quadruple treatment (sequential therapy), standard triple treatment (triple therapy), and vonoprazan-containing therapy (Vono-triple therapy).
Statistically significant results were found with Vono-triple therapy versus triple therapy (odds ratio, 3.80; 95% confidence interval, 1.62-8.94), sequential therapy versus triple therapy (OR, 1.79; 95% CI, 1.26-2.53), nonbismuth quadruple therapy versus triple therapy (OR, 2.08; 95% CI, 1.45-2.98), bismuth quadruple therapy versus triple therapy (OR, 1.47; 95% CI, 1.02-2.11), and Levo-therapy versus triple therapy (OR, 1.79; 95% CI, 1.26-2.53).
In the overall data, mean cure rates greater than 90% were seen only in Vono-triple therapy (91.4%; 95% CI, 88.5-93.5%) and R-hybrid therapy (93.6%; 95% CI, 90.4-96.8%). Cure rates were lower for Nonbismuth quadruple therapy (84.3%; 95% CI, 82.7-85.8%), Levo-therapy (83.8%; 95% CI, 82.1-85.4%), Sequential therapy (83.7%; 95% CI, 82.7-84.7%), bismuth quadruple therapy (81.3%; 95% CI, 79.5-83.1%), Amox-dual therapy (80.2%; 75.3%-84.4%), and triple therapy (75.7%; 95% CI, 74.9-76.4%). Levo-therapy performed best in Western countries (88.5%; 95% CI, 86.5-90.5%) and West Asia (88.4%; 95% CI, 84.6-91.1%). R-hybrid therapy performed best in East Asia (93.6%; 95% CI, 90.4-96.8%).
A surface under the cumulative ranking (SUCRA) value, which represents the efficacy of the intervention compared to an ideal intervention, was 92.4% for Vono-triple therapy. The second highest SUCRA value was for 68.8% for nonbismuth quadruple therapy. The SUCRA value of standard triple therapy was 4.7%.
A key limitation to the study is that Vono-triple therapy was tested only in Japan, and requires additional study in other geographic regions.
The study received support from the Department of Veteran Affairs. The authors have consulted for and received research funding from various pharmaceutical companies.
FROM GASTROENTEROLOGY
Limited English proficiency linked with less health care in U.S.
Jessica Himmelstein, MD, a Harvard research fellow and primary care physician at Cambridge Health Alliance in Cambridge, Mass., led a study of more than 120,000 adults published July 6, 2021. The study population included 17,776 Hispanic adults with limited English proficiency, 14,936 Hispanic adults proficient in English and 87,834 non-Hispanic, English-proficient adults.
Researchers compared several measures of care usage from information in the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey from 1998 to 2018.
They found that, in adjusted analyses, total use of care per capita from 2014-2018, measured by health care expenditures, was $1,463 lower (98% confidence interval, $1,030-$1,897), or 35% lower for primary-Spanish speakers than for Hispanic adults who were English proficient and $2,802 lower (98% CI, $2,356-$3,247), or 42% lower versus non-Hispanic adults who were English proficient.
Spanish speakers also had 36% fewer outpatient visits and 48% fewer prescription medications than non-Hispanic adults, and 35% fewer outpatient visits and 37% fewer prescription medications than English-proficient Hispanic adults.
Even when accounting for differences in health, age, sex, income and insurance, adults with language barriers fared worse.
Gaps span all types of care
The services that those with limited English skills are missing are “the types of care people need to lead a healthy life,” from routine visits and medications to urgent or emergency care, Dr. Himmelstein said in an interview.
She said the gaps were greater in outpatient care and in medication use, compared with emergency department visits and inpatient care, but the inequities were present in all the categories she and her coinvestigators studied.
Underlying causes for having less care may include that people who struggle with English may not feel comfortable accessing the health system or may feel unwelcome or discriminated against.
“An undercurrent of biases, including racism, could also be contributing,” she said.
The data show that, despite several federal policy changes aimed at promoting language services in hospitals and clinics, several language-based disparities have not improved over 2 decades.
Some of the changes have included an executive order in 2000 requiring interpreters to be available in federally funded health facilities. In 2010, the Affordable Care Act enhanced the definition of meaningful access to language services and setting standards for qualified interpreters.
Gap widened over 2 decades
The adjusted gap in annual health care expenditures per capita between adults with limited English skills and non-Hispanic, English-proficient adults widened by $1,596 (98% CI, $837-$2,356) between 1999-2000 and 2017-2018, after accounting for inflation.
Dr. Himmelstein said that though this study period predated COVID-19, its findings may help explain the disproportionate burden the pandemic placed on the Hispanic population.
“This is a community that traditionally wasn’t getting access to care and then suddenly something like COVID-19 comes and they were even more devastated,” she noted.
Telehealth, which proved an important way to access care during the pandemic, also added a degree of communication difficulty for those with fewer English skills, she said.
Many of the telehealth changes are here to stay, and it will be important to ask: “Are we ensuring equity in telehealth use for individuals who face language barriers?” Dr. Himmelstein said.

Olga Garcia-Bedoya, MD, an associate professor at University of Illinois at Chicago’s department of medicine and medical director of UIC’s Institute for Minority Health Research, said having access to interpreters with high accuracy is key to narrowing the gaps.
“The literature is very clear that access to professional medical interpreters is associated with decreased health disparities for patients with limited English proficiency,” she said.
More cultural training for clinicians is needed surrounding beliefs about illness and that some care may be declined not because of a person’s limited English proficiency, but because their beliefs may keep them from getting care, Dr. Garcia-Bedoya added. When it comes to getting a flu shot, for example, sometimes belief systems, rather than English proficiency, keep people from accessing care.
What can be done?
Addressing barriers caused by lack of English proficiency will likely take change in policies, including one related reimbursement for medical interpreters, Dr. Himmelstein said.
Currently, only 15 states’ Medicaid programs or Children’s Health Insurance Programs reimburse providers for language services, the paper notes, and neither Medicare nor private insurers routinely pay for those services.
Recruiting bilingual providers and staff at health care facilities and in medical and nursing schools will also be important to narrow the gaps, Dr. Himmelstein said.
Strengthening standards for interpreters also will help. “Currently such standards vary by state or by institution and are not necessarily enforced,” she explained.
It will also be important to make sure patients know that they are entitled by law to care, free of discriminatory practices and to have certain language services including qualified interpreters, Dr. Himmelstein said.
Dr. Garcia-Bedoya said changes need to come from health systems working in combination with clinicians, providing resources so that quality interpreters can be accessed and making sure that equipment supports clear communication in telehealth. Patients’ language preferences should also be noted as soon as they make the appointment.
The findings of the study may have large significance as one in seven people in the United States speak Spanish at home, and 25 million people in the United States have limited English proficiency, the authors noted.
Dr. Himmelstein receives funding support from an Institutional National Research Service Award. Dr. Garcia-Bedoya reports no relevant financial relationships.
Jessica Himmelstein, MD, a Harvard research fellow and primary care physician at Cambridge Health Alliance in Cambridge, Mass., led a study of more than 120,000 adults published July 6, 2021. The study population included 17,776 Hispanic adults with limited English proficiency, 14,936 Hispanic adults proficient in English and 87,834 non-Hispanic, English-proficient adults.
Researchers compared several measures of care usage from information in the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey from 1998 to 2018.
They found that, in adjusted analyses, total use of care per capita from 2014-2018, measured by health care expenditures, was $1,463 lower (98% confidence interval, $1,030-$1,897), or 35% lower for primary-Spanish speakers than for Hispanic adults who were English proficient and $2,802 lower (98% CI, $2,356-$3,247), or 42% lower versus non-Hispanic adults who were English proficient.
Spanish speakers also had 36% fewer outpatient visits and 48% fewer prescription medications than non-Hispanic adults, and 35% fewer outpatient visits and 37% fewer prescription medications than English-proficient Hispanic adults.
Even when accounting for differences in health, age, sex, income and insurance, adults with language barriers fared worse.
Gaps span all types of care
The services that those with limited English skills are missing are “the types of care people need to lead a healthy life,” from routine visits and medications to urgent or emergency care, Dr. Himmelstein said in an interview.
She said the gaps were greater in outpatient care and in medication use, compared with emergency department visits and inpatient care, but the inequities were present in all the categories she and her coinvestigators studied.
Underlying causes for having less care may include that people who struggle with English may not feel comfortable accessing the health system or may feel unwelcome or discriminated against.
“An undercurrent of biases, including racism, could also be contributing,” she said.
The data show that, despite several federal policy changes aimed at promoting language services in hospitals and clinics, several language-based disparities have not improved over 2 decades.
Some of the changes have included an executive order in 2000 requiring interpreters to be available in federally funded health facilities. In 2010, the Affordable Care Act enhanced the definition of meaningful access to language services and setting standards for qualified interpreters.
Gap widened over 2 decades
The adjusted gap in annual health care expenditures per capita between adults with limited English skills and non-Hispanic, English-proficient adults widened by $1,596 (98% CI, $837-$2,356) between 1999-2000 and 2017-2018, after accounting for inflation.
Dr. Himmelstein said that though this study period predated COVID-19, its findings may help explain the disproportionate burden the pandemic placed on the Hispanic population.
“This is a community that traditionally wasn’t getting access to care and then suddenly something like COVID-19 comes and they were even more devastated,” she noted.
Telehealth, which proved an important way to access care during the pandemic, also added a degree of communication difficulty for those with fewer English skills, she said.
Many of the telehealth changes are here to stay, and it will be important to ask: “Are we ensuring equity in telehealth use for individuals who face language barriers?” Dr. Himmelstein said.
Olga Garcia-Bedoya, MD, an associate professor at University of Illinois at Chicago’s department of medicine and medical director of UIC’s Institute for Minority Health Research, said having access to interpreters with high accuracy is key to narrowing the gaps.
“The literature is very clear that access to professional medical interpreters is associated with decreased health disparities for patients with limited English proficiency,” she said.
More cultural training for clinicians is needed surrounding beliefs about illness and that some care may be declined not because of a person’s limited English proficiency, but because their beliefs may keep them from getting care, Dr. Garcia-Bedoya added. When it comes to getting a flu shot, for example, sometimes belief systems, rather than English proficiency, keep people from accessing care.
What can be done?
Addressing barriers caused by lack of English proficiency will likely take change in policies, including one related reimbursement for medical interpreters, Dr. Himmelstein said.
Currently, only 15 states’ Medicaid programs or Children’s Health Insurance Programs reimburse providers for language services, the paper notes, and neither Medicare nor private insurers routinely pay for those services.
Recruiting bilingual providers and staff at health care facilities and in medical and nursing schools will also be important to narrow the gaps, Dr. Himmelstein said.
Strengthening standards for interpreters also will help. “Currently such standards vary by state or by institution and are not necessarily enforced,” she explained.
It will also be important to make sure patients know that they are entitled by law to care, free of discriminatory practices and to have certain language services including qualified interpreters, Dr. Himmelstein said.
Dr. Garcia-Bedoya said changes need to come from health systems working in combination with clinicians, providing resources so that quality interpreters can be accessed and making sure that equipment supports clear communication in telehealth. Patients’ language preferences should also be noted as soon as they make the appointment.
The findings of the study may have large significance as one in seven people in the United States speak Spanish at home, and 25 million people in the United States have limited English proficiency, the authors noted.
Dr. Himmelstein receives funding support from an Institutional National Research Service Award. Dr. Garcia-Bedoya reports no relevant financial relationships.
Jessica Himmelstein, MD, a Harvard research fellow and primary care physician at Cambridge Health Alliance in Cambridge, Mass., led a study of more than 120,000 adults published July 6, 2021. The study population included 17,776 Hispanic adults with limited English proficiency, 14,936 Hispanic adults proficient in English and 87,834 non-Hispanic, English-proficient adults.
Researchers compared several measures of care usage from information in the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey from 1998 to 2018.
They found that, in adjusted analyses, total use of care per capita from 2014-2018, measured by health care expenditures, was $1,463 lower (98% confidence interval, $1,030-$1,897), or 35% lower for primary-Spanish speakers than for Hispanic adults who were English proficient and $2,802 lower (98% CI, $2,356-$3,247), or 42% lower versus non-Hispanic adults who were English proficient.
Spanish speakers also had 36% fewer outpatient visits and 48% fewer prescription medications than non-Hispanic adults, and 35% fewer outpatient visits and 37% fewer prescription medications than English-proficient Hispanic adults.
Even when accounting for differences in health, age, sex, income and insurance, adults with language barriers fared worse.
Gaps span all types of care
The services that those with limited English skills are missing are “the types of care people need to lead a healthy life,” from routine visits and medications to urgent or emergency care, Dr. Himmelstein said in an interview.
She said the gaps were greater in outpatient care and in medication use, compared with emergency department visits and inpatient care, but the inequities were present in all the categories she and her coinvestigators studied.
Underlying causes for having less care may include that people who struggle with English may not feel comfortable accessing the health system or may feel unwelcome or discriminated against.
“An undercurrent of biases, including racism, could also be contributing,” she said.
The data show that, despite several federal policy changes aimed at promoting language services in hospitals and clinics, several language-based disparities have not improved over 2 decades.
Some of the changes have included an executive order in 2000 requiring interpreters to be available in federally funded health facilities. In 2010, the Affordable Care Act enhanced the definition of meaningful access to language services and setting standards for qualified interpreters.
Gap widened over 2 decades
The adjusted gap in annual health care expenditures per capita between adults with limited English skills and non-Hispanic, English-proficient adults widened by $1,596 (98% CI, $837-$2,356) between 1999-2000 and 2017-2018, after accounting for inflation.
Dr. Himmelstein said that though this study period predated COVID-19, its findings may help explain the disproportionate burden the pandemic placed on the Hispanic population.
“This is a community that traditionally wasn’t getting access to care and then suddenly something like COVID-19 comes and they were even more devastated,” she noted.
Telehealth, which proved an important way to access care during the pandemic, also added a degree of communication difficulty for those with fewer English skills, she said.
Many of the telehealth changes are here to stay, and it will be important to ask: “Are we ensuring equity in telehealth use for individuals who face language barriers?” Dr. Himmelstein said.
Olga Garcia-Bedoya, MD, an associate professor at University of Illinois at Chicago’s department of medicine and medical director of UIC’s Institute for Minority Health Research, said having access to interpreters with high accuracy is key to narrowing the gaps.
“The literature is very clear that access to professional medical interpreters is associated with decreased health disparities for patients with limited English proficiency,” she said.
More cultural training for clinicians is needed surrounding beliefs about illness and that some care may be declined not because of a person’s limited English proficiency, but because their beliefs may keep them from getting care, Dr. Garcia-Bedoya added. When it comes to getting a flu shot, for example, sometimes belief systems, rather than English proficiency, keep people from accessing care.
What can be done?
Addressing barriers caused by lack of English proficiency will likely take change in policies, including one related reimbursement for medical interpreters, Dr. Himmelstein said.
Currently, only 15 states’ Medicaid programs or Children’s Health Insurance Programs reimburse providers for language services, the paper notes, and neither Medicare nor private insurers routinely pay for those services.
Recruiting bilingual providers and staff at health care facilities and in medical and nursing schools will also be important to narrow the gaps, Dr. Himmelstein said.
Strengthening standards for interpreters also will help. “Currently such standards vary by state or by institution and are not necessarily enforced,” she explained.
It will also be important to make sure patients know that they are entitled by law to care, free of discriminatory practices and to have certain language services including qualified interpreters, Dr. Himmelstein said.
Dr. Garcia-Bedoya said changes need to come from health systems working in combination with clinicians, providing resources so that quality interpreters can be accessed and making sure that equipment supports clear communication in telehealth. Patients’ language preferences should also be noted as soon as they make the appointment.
The findings of the study may have large significance as one in seven people in the United States speak Spanish at home, and 25 million people in the United States have limited English proficiency, the authors noted.
Dr. Himmelstein receives funding support from an Institutional National Research Service Award. Dr. Garcia-Bedoya reports no relevant financial relationships.
FROM HEALTH AFFAIRS
Married docs remove girl’s lethal facial tumor in ‘excruciatingly difficult’ procedure
In 2019, doctors in London saw a 5-year old girl from rural Ethiopia with an enormous tumor extending from her cheek to her lower jaw. Her name was Negalem and the tumor was a vascular malformation, a life-threatening web of tangled blood vessels.
Surgery to remove it was impossible, the doctors told the foundation advocating for the girl. The child would never make it off the operating table. After a closer examination, the London group still declined to do the procedure, but told the child’s parents and advocates that if anyone was going to attempt this, they’d need to get the little girl to New York.
In New York City, on 64th St. in Manhattan, is the Vascular Birthmark Institute, founded by Milton Waner, MD, who has exclusively treated hemangiomas and vascular malformations for the last 30 years. “I’m the only person in the [United] States whose practice is exclusively [treating] vascular anomalies,” Dr. Waner said in an interview.
Dr. Waner has assembled a multidisciplinary team of experts at the institute’s offices in Lenox Hill – including his wife Teresa O, MD, a facial plastic and reconstructive surgeon and neurospecialist. “People often ask how the hell do you spend so much time with your spouse?” Dr. Waner says. “We work extremely well together. We complement each other.”
Dr. O and Dr. Waner each manage half of the cases at VBI. And in January they received an email about Negalem. After corresponding with the child’s advocate and reviewing images,
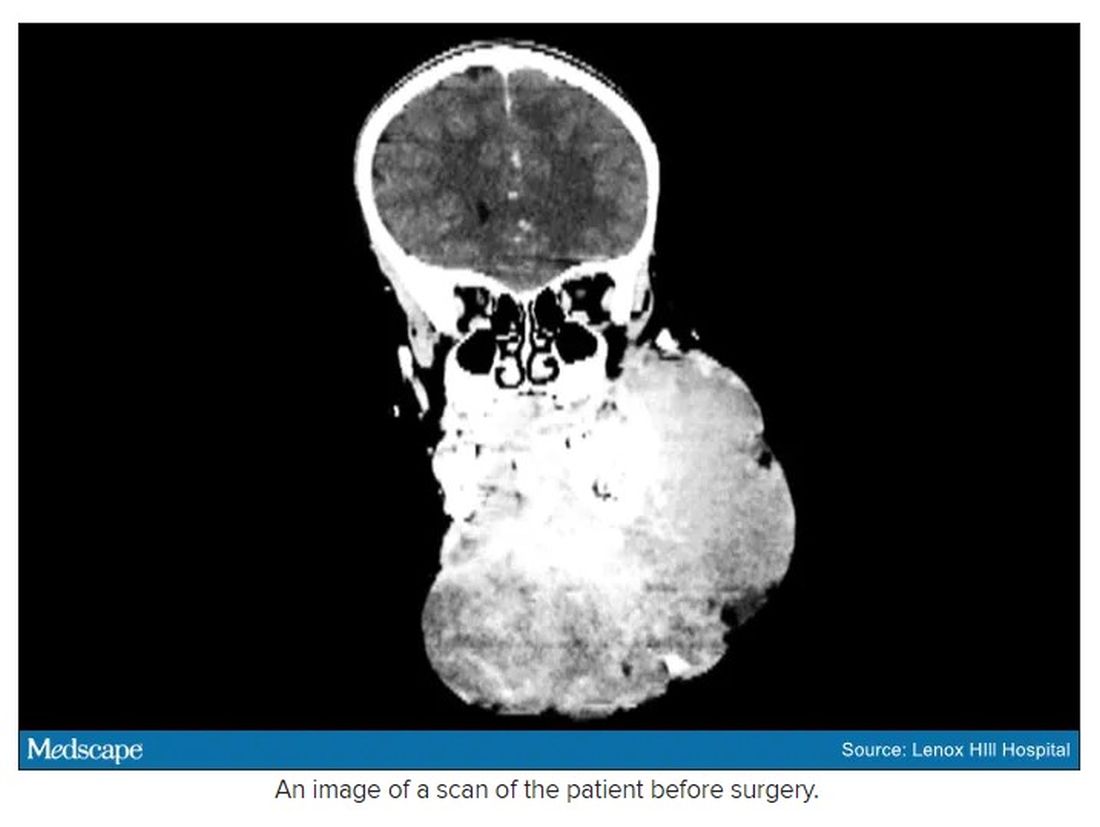
The challenge with vascular malformations in children, Dr. Waner said, is that they have a fraction of the blood an adult has. Where adults have an average of 5 L of blood, a child this age has only 1 L. To lose 200 or 300 mL of blood, “that’s 20% or 30% of their blood volume,” Dr. Waner said. So the removal of such a mass, which requires a meticulous dissection around many blood vessels, carries a high risk of the child bleeding out.
There were some logistical hurdles, but the patient arrived in Manhattan in mid-June, at no cost to her family. The medical visa was organized by a volunteer who also work for USAID. Healing the Children Northeast paid for her travel and the Waner Kids Foundation paid for her hotel stay. Lenox Hill Hospital and Northwell Health covered all hospital costs and postsurgery care. And Dr. O and Dr. Waner did the planning, consult visits, and procedure pro bono.
The surgery was possible because of the generosity of several organizations, but the two surgeons still had a limited time to remove the mass. Under different circumstances, and with the luxury of more time, the patient would have undergone several rounds of sclerotherapy. This procedure, done by interventional radiologists, involves injecting a toxin into the blood vessels, which causes them to clot. Done prior to surgery it can help limit bleeding risk.
On June 23, the morning of the surgery, the patient underwent one round of sclerotherapy. However, it didn’t have the intended effect, Dr. Waner said, “because the lesion was just so massive.”
The team had planned several of their moves ahead of time. But this isn’t the sort of surgery you’d find in a textbook. Because it’s such a unique field, Dr. Waner and Dr. O have developed many of their own techniques along the way. This patient was much like the cases they treat every day, only “several orders of magnitudes greater,” Dr. Waner said. “On a scale of 1 to 10 she was a 12.”
The morning of the surgery, “I was very apprehensive,” Dr. Waner recalled. He vividly remembers the girl’s father repeatedly kissing her to say goodbye as she lay on the operating table, fully aware that this procedure was a life-threatening one. And from the beginning there were challenges, like getting her under anesthesia when the anatomy of her mouth, deformed by the tumor, didn’t allow the anesthesiologists to use their typical tubing. Then, once the skin was removed, it became clear how dilated and tangled the involved blood vessels were. There were many vital structures tangled in the anomaly. “The jugular vein was right there. The carotid artery was right there,” Dr. Waner said. It was extremely difficult to delineate and preserve them, he said.
“That’s why we really took our time. We just went very slowly and deliberately,” Dr. O said. The blood vessels were so dilated that their only option was to move painstakingly slow – otherwise a small nick could be devastating.
But even with the slow pace the surgery was “excruciatingly difficult,” Dr. Waner said. And early on in the dissection he wasn’t quite sure they’d make it out. The sclerotherapy hadn’t done much to prevent bleeding. “At one point every millimeter or 2 that we advanced we got into some bleeding,” Dr. Waner said. “Brisk bleeding.”
Once they got into the surgery they also realized that the growth had adhered to the jaw bone. “There were vessels traversing into the bone, which were hard to control,” Dr. O said.
But finally, both doctors realized they’d be able to remove it. With the lesion removed they began the work of reconstruction and reanimation.
The child’s jaw and cheek bone had grown beyond their normal size to support the growth. They had to shave them down to achieve facial symmetry. The tumor had also inhibited much of the child’s facial nerve control. With it gone, Dr. O began the work of finding all the facial nerve branches and assembling them to reanimate the child’s face.
Before medicine, Dr. O trained as an architect, which, according to Dr. Waner, has equipped her with very good spatial awareness – a valuable skill in the surgical reconstruction phase. After seeing a lecture by Dr. Waner, she immediately saw a fit for her unique interest and skill set. She did fellowship training with Dr. Waner in vascular anomalies, and then went on to specialize in facial nerve reanimation. The proof of Dr. O’s expertise is Negalem’s new, beautiful smile, Dr. Waner said.
The surgery drew out over 8 hours, as long as a day of surgeries for the two doctors. When Dr. O finally walked into the waiting room to inform the family of the success, the first words out of the father’s mouth were: “Is my daughter alive?”
A growth like Negalem had is not compatible with a normal life. Dr. Waner’s mantra is that every child has the right to look normal. But this case went beyond aesthetics. If the growth hadn’t been removed, the child was expected to live only 4-6 more years, Dr. Waner said. Without the surgery, she could have suffocated, starved without the ability to swallow, or suffered a fatal bleed.

Dr. O and Dr. Waner are uniquely equipped to do this kind of work, but both are adamant that treating vascular anomalies is a multidisciplinary, multimodal approach. Specialties in anesthesiology, radiology, lasers, facial nerves – they are all critical to these procedures. And often patients with these kinds of lesions require medical and radiologic interventions in addition to surgery. In this particular case, from logistics to post op, “it was a lot of teamwork,” Dr. O said, “a lot of international teams coming together.”
Though extremely difficult, “in the end the result was exactly what we wanted,” Dr. Waner said. Negalem can live a normal life. And as for the surgical duo, both feel very fortunate to do this work. Dr. O said, “I’m honored to have found this specialty and to be able to train with and work with Milton. I’m so happy to do what I do every day.”
A version of this article first appeared on Medscape.com.
In 2019, doctors in London saw a 5-year old girl from rural Ethiopia with an enormous tumor extending from her cheek to her lower jaw. Her name was Negalem and the tumor was a vascular malformation, a life-threatening web of tangled blood vessels.
Surgery to remove it was impossible, the doctors told the foundation advocating for the girl. The child would never make it off the operating table. After a closer examination, the London group still declined to do the procedure, but told the child’s parents and advocates that if anyone was going to attempt this, they’d need to get the little girl to New York.
In New York City, on 64th St. in Manhattan, is the Vascular Birthmark Institute, founded by Milton Waner, MD, who has exclusively treated hemangiomas and vascular malformations for the last 30 years. “I’m the only person in the [United] States whose practice is exclusively [treating] vascular anomalies,” Dr. Waner said in an interview.
Dr. Waner has assembled a multidisciplinary team of experts at the institute’s offices in Lenox Hill – including his wife Teresa O, MD, a facial plastic and reconstructive surgeon and neurospecialist. “People often ask how the hell do you spend so much time with your spouse?” Dr. Waner says. “We work extremely well together. We complement each other.”
Dr. O and Dr. Waner each manage half of the cases at VBI. And in January they received an email about Negalem. After corresponding with the child’s advocate and reviewing images,
The challenge with vascular malformations in children, Dr. Waner said, is that they have a fraction of the blood an adult has. Where adults have an average of 5 L of blood, a child this age has only 1 L. To lose 200 or 300 mL of blood, “that’s 20% or 30% of their blood volume,” Dr. Waner said. So the removal of such a mass, which requires a meticulous dissection around many blood vessels, carries a high risk of the child bleeding out.
There were some logistical hurdles, but the patient arrived in Manhattan in mid-June, at no cost to her family. The medical visa was organized by a volunteer who also work for USAID. Healing the Children Northeast paid for her travel and the Waner Kids Foundation paid for her hotel stay. Lenox Hill Hospital and Northwell Health covered all hospital costs and postsurgery care. And Dr. O and Dr. Waner did the planning, consult visits, and procedure pro bono.
The surgery was possible because of the generosity of several organizations, but the two surgeons still had a limited time to remove the mass. Under different circumstances, and with the luxury of more time, the patient would have undergone several rounds of sclerotherapy. This procedure, done by interventional radiologists, involves injecting a toxin into the blood vessels, which causes them to clot. Done prior to surgery it can help limit bleeding risk.
On June 23, the morning of the surgery, the patient underwent one round of sclerotherapy. However, it didn’t have the intended effect, Dr. Waner said, “because the lesion was just so massive.”
The team had planned several of their moves ahead of time. But this isn’t the sort of surgery you’d find in a textbook. Because it’s such a unique field, Dr. Waner and Dr. O have developed many of their own techniques along the way. This patient was much like the cases they treat every day, only “several orders of magnitudes greater,” Dr. Waner said. “On a scale of 1 to 10 she was a 12.”
The morning of the surgery, “I was very apprehensive,” Dr. Waner recalled. He vividly remembers the girl’s father repeatedly kissing her to say goodbye as she lay on the operating table, fully aware that this procedure was a life-threatening one. And from the beginning there were challenges, like getting her under anesthesia when the anatomy of her mouth, deformed by the tumor, didn’t allow the anesthesiologists to use their typical tubing. Then, once the skin was removed, it became clear how dilated and tangled the involved blood vessels were. There were many vital structures tangled in the anomaly. “The jugular vein was right there. The carotid artery was right there,” Dr. Waner said. It was extremely difficult to delineate and preserve them, he said.
“That’s why we really took our time. We just went very slowly and deliberately,” Dr. O said. The blood vessels were so dilated that their only option was to move painstakingly slow – otherwise a small nick could be devastating.
But even with the slow pace the surgery was “excruciatingly difficult,” Dr. Waner said. And early on in the dissection he wasn’t quite sure they’d make it out. The sclerotherapy hadn’t done much to prevent bleeding. “At one point every millimeter or 2 that we advanced we got into some bleeding,” Dr. Waner said. “Brisk bleeding.”
Once they got into the surgery they also realized that the growth had adhered to the jaw bone. “There were vessels traversing into the bone, which were hard to control,” Dr. O said.
But finally, both doctors realized they’d be able to remove it. With the lesion removed they began the work of reconstruction and reanimation.
The child’s jaw and cheek bone had grown beyond their normal size to support the growth. They had to shave them down to achieve facial symmetry. The tumor had also inhibited much of the child’s facial nerve control. With it gone, Dr. O began the work of finding all the facial nerve branches and assembling them to reanimate the child’s face.
Before medicine, Dr. O trained as an architect, which, according to Dr. Waner, has equipped her with very good spatial awareness – a valuable skill in the surgical reconstruction phase. After seeing a lecture by Dr. Waner, she immediately saw a fit for her unique interest and skill set. She did fellowship training with Dr. Waner in vascular anomalies, and then went on to specialize in facial nerve reanimation. The proof of Dr. O’s expertise is Negalem’s new, beautiful smile, Dr. Waner said.
The surgery drew out over 8 hours, as long as a day of surgeries for the two doctors. When Dr. O finally walked into the waiting room to inform the family of the success, the first words out of the father’s mouth were: “Is my daughter alive?”
A growth like Negalem had is not compatible with a normal life. Dr. Waner’s mantra is that every child has the right to look normal. But this case went beyond aesthetics. If the growth hadn’t been removed, the child was expected to live only 4-6 more years, Dr. Waner said. Without the surgery, she could have suffocated, starved without the ability to swallow, or suffered a fatal bleed.
Dr. O and Dr. Waner are uniquely equipped to do this kind of work, but both are adamant that treating vascular anomalies is a multidisciplinary, multimodal approach. Specialties in anesthesiology, radiology, lasers, facial nerves – they are all critical to these procedures. And often patients with these kinds of lesions require medical and radiologic interventions in addition to surgery. In this particular case, from logistics to post op, “it was a lot of teamwork,” Dr. O said, “a lot of international teams coming together.”
Though extremely difficult, “in the end the result was exactly what we wanted,” Dr. Waner said. Negalem can live a normal life. And as for the surgical duo, both feel very fortunate to do this work. Dr. O said, “I’m honored to have found this specialty and to be able to train with and work with Milton. I’m so happy to do what I do every day.”
A version of this article first appeared on Medscape.com.
In 2019, doctors in London saw a 5-year old girl from rural Ethiopia with an enormous tumor extending from her cheek to her lower jaw. Her name was Negalem and the tumor was a vascular malformation, a life-threatening web of tangled blood vessels.
Surgery to remove it was impossible, the doctors told the foundation advocating for the girl. The child would never make it off the operating table. After a closer examination, the London group still declined to do the procedure, but told the child’s parents and advocates that if anyone was going to attempt this, they’d need to get the little girl to New York.
In New York City, on 64th St. in Manhattan, is the Vascular Birthmark Institute, founded by Milton Waner, MD, who has exclusively treated hemangiomas and vascular malformations for the last 30 years. “I’m the only person in the [United] States whose practice is exclusively [treating] vascular anomalies,” Dr. Waner said in an interview.
Dr. Waner has assembled a multidisciplinary team of experts at the institute’s offices in Lenox Hill – including his wife Teresa O, MD, a facial plastic and reconstructive surgeon and neurospecialist. “People often ask how the hell do you spend so much time with your spouse?” Dr. Waner says. “We work extremely well together. We complement each other.”
Dr. O and Dr. Waner each manage half of the cases at VBI. And in January they received an email about Negalem. After corresponding with the child’s advocate and reviewing images,
The challenge with vascular malformations in children, Dr. Waner said, is that they have a fraction of the blood an adult has. Where adults have an average of 5 L of blood, a child this age has only 1 L. To lose 200 or 300 mL of blood, “that’s 20% or 30% of their blood volume,” Dr. Waner said. So the removal of such a mass, which requires a meticulous dissection around many blood vessels, carries a high risk of the child bleeding out.
There were some logistical hurdles, but the patient arrived in Manhattan in mid-June, at no cost to her family. The medical visa was organized by a volunteer who also work for USAID. Healing the Children Northeast paid for her travel and the Waner Kids Foundation paid for her hotel stay. Lenox Hill Hospital and Northwell Health covered all hospital costs and postsurgery care. And Dr. O and Dr. Waner did the planning, consult visits, and procedure pro bono.
The surgery was possible because of the generosity of several organizations, but the two surgeons still had a limited time to remove the mass. Under different circumstances, and with the luxury of more time, the patient would have undergone several rounds of sclerotherapy. This procedure, done by interventional radiologists, involves injecting a toxin into the blood vessels, which causes them to clot. Done prior to surgery it can help limit bleeding risk.
On June 23, the morning of the surgery, the patient underwent one round of sclerotherapy. However, it didn’t have the intended effect, Dr. Waner said, “because the lesion was just so massive.”
The team had planned several of their moves ahead of time. But this isn’t the sort of surgery you’d find in a textbook. Because it’s such a unique field, Dr. Waner and Dr. O have developed many of their own techniques along the way. This patient was much like the cases they treat every day, only “several orders of magnitudes greater,” Dr. Waner said. “On a scale of 1 to 10 she was a 12.”
The morning of the surgery, “I was very apprehensive,” Dr. Waner recalled. He vividly remembers the girl’s father repeatedly kissing her to say goodbye as she lay on the operating table, fully aware that this procedure was a life-threatening one. And from the beginning there were challenges, like getting her under anesthesia when the anatomy of her mouth, deformed by the tumor, didn’t allow the anesthesiologists to use their typical tubing. Then, once the skin was removed, it became clear how dilated and tangled the involved blood vessels were. There were many vital structures tangled in the anomaly. “The jugular vein was right there. The carotid artery was right there,” Dr. Waner said. It was extremely difficult to delineate and preserve them, he said.
“That’s why we really took our time. We just went very slowly and deliberately,” Dr. O said. The blood vessels were so dilated that their only option was to move painstakingly slow – otherwise a small nick could be devastating.
But even with the slow pace the surgery was “excruciatingly difficult,” Dr. Waner said. And early on in the dissection he wasn’t quite sure they’d make it out. The sclerotherapy hadn’t done much to prevent bleeding. “At one point every millimeter or 2 that we advanced we got into some bleeding,” Dr. Waner said. “Brisk bleeding.”
Once they got into the surgery they also realized that the growth had adhered to the jaw bone. “There were vessels traversing into the bone, which were hard to control,” Dr. O said.
But finally, both doctors realized they’d be able to remove it. With the lesion removed they began the work of reconstruction and reanimation.
The child’s jaw and cheek bone had grown beyond their normal size to support the growth. They had to shave them down to achieve facial symmetry. The tumor had also inhibited much of the child’s facial nerve control. With it gone, Dr. O began the work of finding all the facial nerve branches and assembling them to reanimate the child’s face.
Before medicine, Dr. O trained as an architect, which, according to Dr. Waner, has equipped her with very good spatial awareness – a valuable skill in the surgical reconstruction phase. After seeing a lecture by Dr. Waner, she immediately saw a fit for her unique interest and skill set. She did fellowship training with Dr. Waner in vascular anomalies, and then went on to specialize in facial nerve reanimation. The proof of Dr. O’s expertise is Negalem’s new, beautiful smile, Dr. Waner said.
The surgery drew out over 8 hours, as long as a day of surgeries for the two doctors. When Dr. O finally walked into the waiting room to inform the family of the success, the first words out of the father’s mouth were: “Is my daughter alive?”
A growth like Negalem had is not compatible with a normal life. Dr. Waner’s mantra is that every child has the right to look normal. But this case went beyond aesthetics. If the growth hadn’t been removed, the child was expected to live only 4-6 more years, Dr. Waner said. Without the surgery, she could have suffocated, starved without the ability to swallow, or suffered a fatal bleed.
Dr. O and Dr. Waner are uniquely equipped to do this kind of work, but both are adamant that treating vascular anomalies is a multidisciplinary, multimodal approach. Specialties in anesthesiology, radiology, lasers, facial nerves – they are all critical to these procedures. And often patients with these kinds of lesions require medical and radiologic interventions in addition to surgery. In this particular case, from logistics to post op, “it was a lot of teamwork,” Dr. O said, “a lot of international teams coming together.”
Though extremely difficult, “in the end the result was exactly what we wanted,” Dr. Waner said. Negalem can live a normal life. And as for the surgical duo, both feel very fortunate to do this work. Dr. O said, “I’m honored to have found this specialty and to be able to train with and work with Milton. I’m so happy to do what I do every day.”
A version of this article first appeared on Medscape.com.
Finding room for hope
Dear colleagues,
I’m thrilled to introduce the August edition of The New Gastroenterologist, which features an excellent line-up of articles! Summer has been in full swing, and gradually, we eased into aspects of our prepandemic routine. The fear, caution, and isolation that characterized the last year and a half was less pervasive, and the ability to reconnect in person felt both refreshing and liberating. While new threats of variants and rising infection rates have emerged, there is hope that, with the availability of vaccines, the worst of the pandemic may still be behind us.

One of the most difficult aspects of treating patients with inflammatory bowel disease is acute pain management. Dr. Jami Kinnucan and Dr. Mehwish Ahmed (University of Michigan) outline an expert approach on differentiating between visceral and somatic pain and how to manage each accordingly.
The diagnosis of microscopic colitis can be elusive because colonic mucosa typically appears endoscopically normal and the pathognomonic findings are histologic. Management can also be challenging given the frequently relapsing and remitting nature of its clinical course. The “In Focus” feature for August, written by Dr. June Tome, Dr. Amrit Kamboj, and Dr. Darrell Pardi (Mayo Clinic), is an absolute must-read as it provides a detailed review on the diagnosis, management, and therapeutic options for microscopic colitis.
As gastroenterologists, we are often asked to place percutaneous endoscopic gastrostomy (PEG) tubes. This can be a difficult situation to navigate especially when the indication or timing of placement seems questionable. In our ethics case for this quarter, Dr. David Seres and Dr. Jane Cowan (Columbia University) unpack the ethical considerations of PEG tube placement in order to facilitate discharge to subacute nursing facilities.
Months in quarantine have incited many to crave larger living spaces, lending to a chaotic housing market. Jon Solitro (FinancialMD) offers sound financial advice for physicians interested purchasing a home – including factors to consider when choosing a home, how much to spend, and whether or not to consider a doctor’s loan.
Success in research can be particularly difficult for fellows and early career gastroenterologists as they juggle the many responsibilities inherent to busy training programs or adjust to independent practice. Dr. Dionne Rebello and Dr. Michelle Long (Boston University) compile a list of incredibly helpful tips on how to optimize productivity. For those interested in ways to harness experiences in clinical medicine into health technology, Dr. Simon Matthews (Johns Hopkins) discusses his role as chief medical officer in a health tech start-up in our postfellowship pathways section.
Lastly, our DHPA Private Practice Perspectives article, written by Dr. George Dickstein (Greater Boston Gastroenterology), nicely summarizes lessons learned from the pandemic and how a practice can be adequately prepared for a post-pandemic surge of procedures.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]) or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor in Chief
Assistant Professor of Medicine, University of Chicago, Section of Gastroenterology, Hepatology & Nutrition
Dear colleagues,
I’m thrilled to introduce the August edition of The New Gastroenterologist, which features an excellent line-up of articles! Summer has been in full swing, and gradually, we eased into aspects of our prepandemic routine. The fear, caution, and isolation that characterized the last year and a half was less pervasive, and the ability to reconnect in person felt both refreshing and liberating. While new threats of variants and rising infection rates have emerged, there is hope that, with the availability of vaccines, the worst of the pandemic may still be behind us.
One of the most difficult aspects of treating patients with inflammatory bowel disease is acute pain management. Dr. Jami Kinnucan and Dr. Mehwish Ahmed (University of Michigan) outline an expert approach on differentiating between visceral and somatic pain and how to manage each accordingly.
The diagnosis of microscopic colitis can be elusive because colonic mucosa typically appears endoscopically normal and the pathognomonic findings are histologic. Management can also be challenging given the frequently relapsing and remitting nature of its clinical course. The “In Focus” feature for August, written by Dr. June Tome, Dr. Amrit Kamboj, and Dr. Darrell Pardi (Mayo Clinic), is an absolute must-read as it provides a detailed review on the diagnosis, management, and therapeutic options for microscopic colitis.
As gastroenterologists, we are often asked to place percutaneous endoscopic gastrostomy (PEG) tubes. This can be a difficult situation to navigate especially when the indication or timing of placement seems questionable. In our ethics case for this quarter, Dr. David Seres and Dr. Jane Cowan (Columbia University) unpack the ethical considerations of PEG tube placement in order to facilitate discharge to subacute nursing facilities.
Months in quarantine have incited many to crave larger living spaces, lending to a chaotic housing market. Jon Solitro (FinancialMD) offers sound financial advice for physicians interested purchasing a home – including factors to consider when choosing a home, how much to spend, and whether or not to consider a doctor’s loan.
Success in research can be particularly difficult for fellows and early career gastroenterologists as they juggle the many responsibilities inherent to busy training programs or adjust to independent practice. Dr. Dionne Rebello and Dr. Michelle Long (Boston University) compile a list of incredibly helpful tips on how to optimize productivity. For those interested in ways to harness experiences in clinical medicine into health technology, Dr. Simon Matthews (Johns Hopkins) discusses his role as chief medical officer in a health tech start-up in our postfellowship pathways section.
Lastly, our DHPA Private Practice Perspectives article, written by Dr. George Dickstein (Greater Boston Gastroenterology), nicely summarizes lessons learned from the pandemic and how a practice can be adequately prepared for a post-pandemic surge of procedures.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]) or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor in Chief
Assistant Professor of Medicine, University of Chicago, Section of Gastroenterology, Hepatology & Nutrition
Dear colleagues,
I’m thrilled to introduce the August edition of The New Gastroenterologist, which features an excellent line-up of articles! Summer has been in full swing, and gradually, we eased into aspects of our prepandemic routine. The fear, caution, and isolation that characterized the last year and a half was less pervasive, and the ability to reconnect in person felt both refreshing and liberating. While new threats of variants and rising infection rates have emerged, there is hope that, with the availability of vaccines, the worst of the pandemic may still be behind us.
One of the most difficult aspects of treating patients with inflammatory bowel disease is acute pain management. Dr. Jami Kinnucan and Dr. Mehwish Ahmed (University of Michigan) outline an expert approach on differentiating between visceral and somatic pain and how to manage each accordingly.
The diagnosis of microscopic colitis can be elusive because colonic mucosa typically appears endoscopically normal and the pathognomonic findings are histologic. Management can also be challenging given the frequently relapsing and remitting nature of its clinical course. The “In Focus” feature for August, written by Dr. June Tome, Dr. Amrit Kamboj, and Dr. Darrell Pardi (Mayo Clinic), is an absolute must-read as it provides a detailed review on the diagnosis, management, and therapeutic options for microscopic colitis.
As gastroenterologists, we are often asked to place percutaneous endoscopic gastrostomy (PEG) tubes. This can be a difficult situation to navigate especially when the indication or timing of placement seems questionable. In our ethics case for this quarter, Dr. David Seres and Dr. Jane Cowan (Columbia University) unpack the ethical considerations of PEG tube placement in order to facilitate discharge to subacute nursing facilities.
Months in quarantine have incited many to crave larger living spaces, lending to a chaotic housing market. Jon Solitro (FinancialMD) offers sound financial advice for physicians interested purchasing a home – including factors to consider when choosing a home, how much to spend, and whether or not to consider a doctor’s loan.
Success in research can be particularly difficult for fellows and early career gastroenterologists as they juggle the many responsibilities inherent to busy training programs or adjust to independent practice. Dr. Dionne Rebello and Dr. Michelle Long (Boston University) compile a list of incredibly helpful tips on how to optimize productivity. For those interested in ways to harness experiences in clinical medicine into health technology, Dr. Simon Matthews (Johns Hopkins) discusses his role as chief medical officer in a health tech start-up in our postfellowship pathways section.
Lastly, our DHPA Private Practice Perspectives article, written by Dr. George Dickstein (Greater Boston Gastroenterology), nicely summarizes lessons learned from the pandemic and how a practice can be adequately prepared for a post-pandemic surge of procedures.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]) or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor in Chief
Assistant Professor of Medicine, University of Chicago, Section of Gastroenterology, Hepatology & Nutrition

August 2021 – ICYMI
Gastroenterology
May 2021
Understanding GI Twitter and its major contributors. Elfanagely Y et al. Gastroenterology. 2021 May;160(6):1917-21. doi: 10.1053/j.gastro.2021.01.232.
Long-term safety of fecal microbiota transplantation for recurrent Clostridioides difficile infection. Saha S et al. Gastroenterology. 2021 May;160(6):1961-9.e3. doi: 10.1053/j.gastro.2021.01.010.
How to incorporate health equity training into gastroenterology and hepatology fellowships. Lee-Allen J, Shah BJ. Gastroenterology. 2021 May;160(6):1924-8. doi: 10.1053/j.gastro.2021.03.018.
Functional dyspepsia and gastroparesis in tertiary care are interchangeable syndromes with common clinical and pathologic features. Pasricha PJ et al. Gastroenterology. 2021 May;160(6):2006-17. doi: 10.1053/j.gastro.2021.01.230.
June 2021
How to manage the large nonpedunculated colorectal polyp. Shahidi N, Bourke MJ. Gastroenterology. 2021 Jun;160(7):2239-43.e1. doi: 10.1053/j.gastro.2021.04.029.
Mortality, reoperation, and hospital stay within 90 days of primary and secondary antireflux surgery in a population-based multinational study. Yanes M et al. Gastroenterology. 2021 Jun;160(7):2283-90. doi: 10.1053/j.gastro.2021.02.022.
Endoscopic submucosal dissection in north america: A large prospective multicenter study. Draganov PV et al. Gastroenterology. 2021 Jun;160(7):2317-27.e2. doi: 10.1053/j.gastro.2021.02.036.
July 2021
Gluten degradation, pharmacokinetics, safety, and tolerability of TAK-062, an engineered enzyme to treat celiac disease. Pultz IG et al. Gastroenterology. 2021 Jul;161(1):81-93.e3. doi: 10.1053/j.gastro.2021.03.019.
Paternal exposure to immunosuppressive and/or biologic agents and birth outcomes in patients with immune-mediated inflammatory diseases. Meserve J et al. Gastroenterology. 2021 Jul;161(1):107-115.e3. doi: 10.1053/j.gastro.2021.03.020.
Ethnicity associations with food sensitization are mediated by gut microbiota development in the first year of life. Tun Hm et al. Gastroenterology. 2021 Jul;161(1):94-106. doi: 10.1053/j.gastro.2021.03.016.
How to incorporate bariatric training into your fellowship program. Jirapinyo P, Thompson CC. Gastroenterology. 2019 Jul;157(1):9-13. doi: 10.1053/j.gastro.2019.05.034.
CGH
May 2021
Intestinal failure: What all gastroenterologists should know. Jansson-Knodell CL et al. Clin Gastroenterol Hepatol. 2021 May;19(5):885-8. doi: 10.1016/j.cgh.2021.01.038.
When and how to use endoscopic tattooing in the colon: An international Delphi agreement. Medina-Prado L et al. Clin Gastroenterol Hepatol. 2021 May;19(5):1038-50. doi: 10.1016/j.cgh.2021.01.024.
Five-year outcomes of endoscopic sleeve gastroplasty for the treatment of obesity. Sharaiha RZ et al. Clin Gastroenterol Hepatol. 2021 May;19(5):1051-57.e2. doi: 10.1016/j.cgh.2020.09.055.
June 2021
GA Clinical Practice Update on management of bleeding gastric varices: Expert review. Henry Z et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1098-107.e1. doi: 10.1016/j.cgh.2021.01.027.
Inter- and intra-individual variation, and limited prognostic utility, of serum alkaline phosphatase in a trial of patients with primary sclerosing cholangitis
Palak J. Trivedi PJ et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1248-57. doi: 10.1016/j.cgh.2020.07.032.
Low-fat, high-fiber diet reduces markers of inflammation and dysbiosis and improves quality of life in patients with ulcerative colitis. Julia Fritsch J et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1189-99.e30. doi: 10.1016/j.cgh.2020.05.026.
July 2021
Scoping out a better parental leave policy for gastroenterology fellows. Wegermann K. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1307-9. doi: 10.1016/j.cgh.2021.01.040.
An impetus for change: How COVID-19 will transform the delivery of GI health care. Leiman DA et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1310-1313. doi: 10.1016/j.cgh.2021.03.042.
Untangling nonerosive reflux disease from functional heartburn. Patel D et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1314-26. doi: 10.1016/j.cgh.2020.03.057.
AGA Clinical Practice Update on chemoprevention for colorectal neoplasia: Expert review. Liang PS et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1327-36. doi: 10.1016/j.cgh.2021.02.014.
CMGH
Drug inhibition of SARS-CoV-2 replication in human pluripotent stem cell–derived intestinal organoids. Krüger J et al. Cell Mol Gastroenterol Hepatol. 2021;11(4):935-48. doi: 10.1016/j.jcmgh.2020.11.003.
TIGE
Virtual interviews during the COVID-19 Pandemic: A survey of advanced endoscopy fellowship applicants and programs. Amrit K. Kamboj AK et al. Tech Innov Gastrointest Endosc. 2021;23(2):159-68. doi: 10.1016/j.tige.2021.02.001.
Triage of general gastrointestinal endoscopic procedures during the COVID-19 pandemic: Results from a national Delphi consensus panel. Feuerstein JD et al. Tech Innov Gastrointest Endosc. 2021;23(2):113-21. doi: 10.1016/j.tige.2020.12.005.
Development of a scoring system to predict a positive diagnosis on video capsule endoscopy for suspected small bowel bleeding. Marya NB et al. Tech Innov Gastrointest Endosc. 2021;22(4):178-84. doi: 10.1016/j.tige.2020.06.001.
Gastroenterology
May 2021
Understanding GI Twitter and its major contributors. Elfanagely Y et al. Gastroenterology. 2021 May;160(6):1917-21. doi: 10.1053/j.gastro.2021.01.232.
Long-term safety of fecal microbiota transplantation for recurrent Clostridioides difficile infection. Saha S et al. Gastroenterology. 2021 May;160(6):1961-9.e3. doi: 10.1053/j.gastro.2021.01.010.
How to incorporate health equity training into gastroenterology and hepatology fellowships. Lee-Allen J, Shah BJ. Gastroenterology. 2021 May;160(6):1924-8. doi: 10.1053/j.gastro.2021.03.018.
Functional dyspepsia and gastroparesis in tertiary care are interchangeable syndromes with common clinical and pathologic features. Pasricha PJ et al. Gastroenterology. 2021 May;160(6):2006-17. doi: 10.1053/j.gastro.2021.01.230.
June 2021
How to manage the large nonpedunculated colorectal polyp. Shahidi N, Bourke MJ. Gastroenterology. 2021 Jun;160(7):2239-43.e1. doi: 10.1053/j.gastro.2021.04.029.
Mortality, reoperation, and hospital stay within 90 days of primary and secondary antireflux surgery in a population-based multinational study. Yanes M et al. Gastroenterology. 2021 Jun;160(7):2283-90. doi: 10.1053/j.gastro.2021.02.022.
Endoscopic submucosal dissection in north america: A large prospective multicenter study. Draganov PV et al. Gastroenterology. 2021 Jun;160(7):2317-27.e2. doi: 10.1053/j.gastro.2021.02.036.
July 2021
Gluten degradation, pharmacokinetics, safety, and tolerability of TAK-062, an engineered enzyme to treat celiac disease. Pultz IG et al. Gastroenterology. 2021 Jul;161(1):81-93.e3. doi: 10.1053/j.gastro.2021.03.019.
Paternal exposure to immunosuppressive and/or biologic agents and birth outcomes in patients with immune-mediated inflammatory diseases. Meserve J et al. Gastroenterology. 2021 Jul;161(1):107-115.e3. doi: 10.1053/j.gastro.2021.03.020.
Ethnicity associations with food sensitization are mediated by gut microbiota development in the first year of life. Tun Hm et al. Gastroenterology. 2021 Jul;161(1):94-106. doi: 10.1053/j.gastro.2021.03.016.
How to incorporate bariatric training into your fellowship program. Jirapinyo P, Thompson CC. Gastroenterology. 2019 Jul;157(1):9-13. doi: 10.1053/j.gastro.2019.05.034.
CGH
May 2021
Intestinal failure: What all gastroenterologists should know. Jansson-Knodell CL et al. Clin Gastroenterol Hepatol. 2021 May;19(5):885-8. doi: 10.1016/j.cgh.2021.01.038.
When and how to use endoscopic tattooing in the colon: An international Delphi agreement. Medina-Prado L et al. Clin Gastroenterol Hepatol. 2021 May;19(5):1038-50. doi: 10.1016/j.cgh.2021.01.024.
Five-year outcomes of endoscopic sleeve gastroplasty for the treatment of obesity. Sharaiha RZ et al. Clin Gastroenterol Hepatol. 2021 May;19(5):1051-57.e2. doi: 10.1016/j.cgh.2020.09.055.
June 2021
GA Clinical Practice Update on management of bleeding gastric varices: Expert review. Henry Z et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1098-107.e1. doi: 10.1016/j.cgh.2021.01.027.
Inter- and intra-individual variation, and limited prognostic utility, of serum alkaline phosphatase in a trial of patients with primary sclerosing cholangitis
Palak J. Trivedi PJ et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1248-57. doi: 10.1016/j.cgh.2020.07.032.
Low-fat, high-fiber diet reduces markers of inflammation and dysbiosis and improves quality of life in patients with ulcerative colitis. Julia Fritsch J et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1189-99.e30. doi: 10.1016/j.cgh.2020.05.026.
July 2021
Scoping out a better parental leave policy for gastroenterology fellows. Wegermann K. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1307-9. doi: 10.1016/j.cgh.2021.01.040.
An impetus for change: How COVID-19 will transform the delivery of GI health care. Leiman DA et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1310-1313. doi: 10.1016/j.cgh.2021.03.042.
Untangling nonerosive reflux disease from functional heartburn. Patel D et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1314-26. doi: 10.1016/j.cgh.2020.03.057.
AGA Clinical Practice Update on chemoprevention for colorectal neoplasia: Expert review. Liang PS et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1327-36. doi: 10.1016/j.cgh.2021.02.014.
CMGH
Drug inhibition of SARS-CoV-2 replication in human pluripotent stem cell–derived intestinal organoids. Krüger J et al. Cell Mol Gastroenterol Hepatol. 2021;11(4):935-48. doi: 10.1016/j.jcmgh.2020.11.003.
TIGE
Virtual interviews during the COVID-19 Pandemic: A survey of advanced endoscopy fellowship applicants and programs. Amrit K. Kamboj AK et al. Tech Innov Gastrointest Endosc. 2021;23(2):159-68. doi: 10.1016/j.tige.2021.02.001.
Triage of general gastrointestinal endoscopic procedures during the COVID-19 pandemic: Results from a national Delphi consensus panel. Feuerstein JD et al. Tech Innov Gastrointest Endosc. 2021;23(2):113-21. doi: 10.1016/j.tige.2020.12.005.
Development of a scoring system to predict a positive diagnosis on video capsule endoscopy for suspected small bowel bleeding. Marya NB et al. Tech Innov Gastrointest Endosc. 2021;22(4):178-84. doi: 10.1016/j.tige.2020.06.001.
Gastroenterology
May 2021
Understanding GI Twitter and its major contributors. Elfanagely Y et al. Gastroenterology. 2021 May;160(6):1917-21. doi: 10.1053/j.gastro.2021.01.232.
Long-term safety of fecal microbiota transplantation for recurrent Clostridioides difficile infection. Saha S et al. Gastroenterology. 2021 May;160(6):1961-9.e3. doi: 10.1053/j.gastro.2021.01.010.
How to incorporate health equity training into gastroenterology and hepatology fellowships. Lee-Allen J, Shah BJ. Gastroenterology. 2021 May;160(6):1924-8. doi: 10.1053/j.gastro.2021.03.018.
Functional dyspepsia and gastroparesis in tertiary care are interchangeable syndromes with common clinical and pathologic features. Pasricha PJ et al. Gastroenterology. 2021 May;160(6):2006-17. doi: 10.1053/j.gastro.2021.01.230.
June 2021
How to manage the large nonpedunculated colorectal polyp. Shahidi N, Bourke MJ. Gastroenterology. 2021 Jun;160(7):2239-43.e1. doi: 10.1053/j.gastro.2021.04.029.
Mortality, reoperation, and hospital stay within 90 days of primary and secondary antireflux surgery in a population-based multinational study. Yanes M et al. Gastroenterology. 2021 Jun;160(7):2283-90. doi: 10.1053/j.gastro.2021.02.022.
Endoscopic submucosal dissection in north america: A large prospective multicenter study. Draganov PV et al. Gastroenterology. 2021 Jun;160(7):2317-27.e2. doi: 10.1053/j.gastro.2021.02.036.
July 2021
Gluten degradation, pharmacokinetics, safety, and tolerability of TAK-062, an engineered enzyme to treat celiac disease. Pultz IG et al. Gastroenterology. 2021 Jul;161(1):81-93.e3. doi: 10.1053/j.gastro.2021.03.019.
Paternal exposure to immunosuppressive and/or biologic agents and birth outcomes in patients with immune-mediated inflammatory diseases. Meserve J et al. Gastroenterology. 2021 Jul;161(1):107-115.e3. doi: 10.1053/j.gastro.2021.03.020.
Ethnicity associations with food sensitization are mediated by gut microbiota development in the first year of life. Tun Hm et al. Gastroenterology. 2021 Jul;161(1):94-106. doi: 10.1053/j.gastro.2021.03.016.
How to incorporate bariatric training into your fellowship program. Jirapinyo P, Thompson CC. Gastroenterology. 2019 Jul;157(1):9-13. doi: 10.1053/j.gastro.2019.05.034.
CGH
May 2021
Intestinal failure: What all gastroenterologists should know. Jansson-Knodell CL et al. Clin Gastroenterol Hepatol. 2021 May;19(5):885-8. doi: 10.1016/j.cgh.2021.01.038.
When and how to use endoscopic tattooing in the colon: An international Delphi agreement. Medina-Prado L et al. Clin Gastroenterol Hepatol. 2021 May;19(5):1038-50. doi: 10.1016/j.cgh.2021.01.024.
Five-year outcomes of endoscopic sleeve gastroplasty for the treatment of obesity. Sharaiha RZ et al. Clin Gastroenterol Hepatol. 2021 May;19(5):1051-57.e2. doi: 10.1016/j.cgh.2020.09.055.
June 2021
GA Clinical Practice Update on management of bleeding gastric varices: Expert review. Henry Z et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1098-107.e1. doi: 10.1016/j.cgh.2021.01.027.
Inter- and intra-individual variation, and limited prognostic utility, of serum alkaline phosphatase in a trial of patients with primary sclerosing cholangitis
Palak J. Trivedi PJ et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1248-57. doi: 10.1016/j.cgh.2020.07.032.
Low-fat, high-fiber diet reduces markers of inflammation and dysbiosis and improves quality of life in patients with ulcerative colitis. Julia Fritsch J et al. Clin Gastroenterol Hepatol. 2021 Jun;19(6):1189-99.e30. doi: 10.1016/j.cgh.2020.05.026.
July 2021
Scoping out a better parental leave policy for gastroenterology fellows. Wegermann K. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1307-9. doi: 10.1016/j.cgh.2021.01.040.
An impetus for change: How COVID-19 will transform the delivery of GI health care. Leiman DA et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1310-1313. doi: 10.1016/j.cgh.2021.03.042.
Untangling nonerosive reflux disease from functional heartburn. Patel D et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1314-26. doi: 10.1016/j.cgh.2020.03.057.
AGA Clinical Practice Update on chemoprevention for colorectal neoplasia: Expert review. Liang PS et al. Clin Gastroenterol Hepatol. 2021 Jul;19(7):1327-36. doi: 10.1016/j.cgh.2021.02.014.
CMGH
Drug inhibition of SARS-CoV-2 replication in human pluripotent stem cell–derived intestinal organoids. Krüger J et al. Cell Mol Gastroenterol Hepatol. 2021;11(4):935-48. doi: 10.1016/j.jcmgh.2020.11.003.
TIGE
Virtual interviews during the COVID-19 Pandemic: A survey of advanced endoscopy fellowship applicants and programs. Amrit K. Kamboj AK et al. Tech Innov Gastrointest Endosc. 2021;23(2):159-68. doi: 10.1016/j.tige.2021.02.001.
Triage of general gastrointestinal endoscopic procedures during the COVID-19 pandemic: Results from a national Delphi consensus panel. Feuerstein JD et al. Tech Innov Gastrointest Endosc. 2021;23(2):113-21. doi: 10.1016/j.tige.2020.12.005.
Development of a scoring system to predict a positive diagnosis on video capsule endoscopy for suspected small bowel bleeding. Marya NB et al. Tech Innov Gastrointest Endosc. 2021;22(4):178-84. doi: 10.1016/j.tige.2020.06.001.
Clostridioides difficile: Two sets of guidelines disagree
With two sets of Clostridioides difficile recommendations being published within a month of each other, clinicians may find themselves trying to reconcile some of the conflicts between the two guidelines.
The first set, published June 1 by the American College of Gastroenterology, focuses on fecal microbiota transplantation (FMT) and the antibiotic vancomycin. The second, published June 24 by the Infectious Diseases Society of America and Society for Healthcare Epidemiology of America, drives a shift in treatment for initial episodes and short-term recurrence from vancomycin to fidaxomicin and, in some cases, adding on the monoclonal antibody bezlotoxumab, both made by Merck.
The updates are timely because researchers are now recognizing that C. difficile can colonize people without causing symptoms, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, said in an interview. He was not involved in writing either set of guidelines. “C. diff infection was a hospital-type infection, but we’re now seeing it in up to approximately 35%-50% of patients coming from the community, so it’s a big concern.”
Although the guidelines agree on which treatments are effective, the recommendations give the options a different emphasis.
Infectious disease specialist Stuart Johnson, MD, professor of medicine at Loyola University Medical Center in Maywood, Ill., and a physician researcher at Edward Hines Jr. Veterans Affairs Hospital in Hines, Ill., is the first author in the IDSA/SHEA guidelines. He told this news organization that one reason the two sets of recommendations may diverge in emphasis for initial and recurrent C. difficile is that “everyone has a different way of looking at things.” Compared with infectious disease specialists like him, he said, gastroenterologists “for the most part see the world a little different and have their own bent on things.”
The differences between the two guidelines relate to the first-line therapy for people with an initial or recurrent C. difficile episode. For an initial episode, the IDSA/SHEA authors conditionally recommend fidaxomicin as first preferred choice over vancomycin, with a moderate certainty of evidence. They noted that implementing this recommendation depends on “available resources,” a reference to the higher cost and difficulty of access associated with fidaxomicin.
Gastroenterologist Monika Fischer, MD, an associate professor of medicine at Indiana University, Indianapolis, is one of the authors of the ACG guidelines. She told this news organization that the cost difference between fidaxomicin and vancomycin is considerable and finds the choice to foreground fidaxomicin puzzling. “They did not reference any new data compared to those we have published.” Their recommendation may make sense in terms of efficacy, but real-world demands require attention to cost and reimbursement. “They themselves state this in their recommendations,” she noted.
Dr. Fischer cited a ballpark of about $100 for a course of vancomycin, compared with about $3,000 for a course of fidaxomicin. The IDSA/SHEA guidelines do cite vancomycin as an acceptable alternative. According to Dr. Fischer, the ACG guidelines authors discussed fidaxomicin and concluded that there just wasn’t enough evidence to justify favoring this antibiotic over vancomycin, given the cost-benefit imbalance. The ACG guidelines call for a standard course of oral vancomycin for a first, nonsevere C. difficile episode, listing oral fidaxomicin or oral metronidazole as alternatives.
For a recurrence, the IDSA/SHEA authors also favor fidaxomicin in a conditional recommendation over a standard course of vancomycin. For multiple recurrences, a tapered and pulsed vancomycin regimen, vancomycin followed by rifaximin, or FMT are also options.
Dr. David Johnson said that these recommendations favoring fidaxomicin are “surprising,” and that lower costs of vancomycin outweigh the benefit of fidaxomicin, given more-or-less comparable data on cure rates.
In contrast, the ACG guidelines recommend that an initial recurrence be treated with a tapering dose of vancomycin, and call for FMT for patients who are eligible and who experience a second or more C. difficile recurrences after a round of pulsed vancomycin.
Dr. Stuart Johnson said that FMT carries its own special set of issues. “If you don’t have a donor program set up, you have to rely on a stool bank,” noting that one widely used stool bank “basically had to stop making the product because of the coronavirus.” Costs for FMT products have doubled in recent years, and because Food and Drug Administration approval of the therapy is lacking, insurance does not cover it.
Dr. David Johnson also said that he is not “terribly happy” about the ACG recommendation for vancomycin prophylaxis. “It may help, but it also can have off-target effects against colonic bacterial flora, so we would not agree with that recommendation.”
The IDSA/SHEA authors also conditionally recommend bezlotoxumab, on very low certainty of evidence, as a cotherapy with standard of care antibiotics for recurrence prevention in patients with an episode in the last 6 months, particularly for patients at high recurrence risk “where logistics is not an issue.” The FDA has warned that this monoclonal antibody should be used with great care in patients with heart failure and only when benefits outweigh risks.
The ACG guidelines conditionally recommend considering bezlotoxumab to prevent recurrence in patients with specific risk factors, including age over 65 years and severe presentation. The IDSA/SHEA guidelines expand this population to anyone with a recurrence within 6 months, Dr. Fischer pointed out.
The antibody treatment “does offer another 10% absolute reduction in recurrent C. diff disease,” said Dr. Stuart Johnson, which is a “helpful option and primarily for people who have had recurrent C. diff already.” In general, he said, for both drugs, “access is still something we have to work with.”
In a commentary on the ACG guidelines, Dr. David Johnson wrote that there is good evidence that bezlotoxumab prevents relapse, especially in patients with specific risk factors. The hitch is the $4,500 price tag for a 1,000-mg vial, with a recommended dose of 10 mg/kg.
Dr. Stuart Johnson agreed that the costs of the fidaxomicin and bezlotoxumab are important considerations. In addition, there are logistical issues with using the antibody because most hospitals don’t offer infusions, which pushes patients to infusion centers.
Regardless, he added, “we’re happy that we have new options.”
Dr. Fischer, Dr. Stuart Johnson, and Dr. David Johnson reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
With two sets of Clostridioides difficile recommendations being published within a month of each other, clinicians may find themselves trying to reconcile some of the conflicts between the two guidelines.
The first set, published June 1 by the American College of Gastroenterology, focuses on fecal microbiota transplantation (FMT) and the antibiotic vancomycin. The second, published June 24 by the Infectious Diseases Society of America and Society for Healthcare Epidemiology of America, drives a shift in treatment for initial episodes and short-term recurrence from vancomycin to fidaxomicin and, in some cases, adding on the monoclonal antibody bezlotoxumab, both made by Merck.
The updates are timely because researchers are now recognizing that C. difficile can colonize people without causing symptoms, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, said in an interview. He was not involved in writing either set of guidelines. “C. diff infection was a hospital-type infection, but we’re now seeing it in up to approximately 35%-50% of patients coming from the community, so it’s a big concern.”
Although the guidelines agree on which treatments are effective, the recommendations give the options a different emphasis.
Infectious disease specialist Stuart Johnson, MD, professor of medicine at Loyola University Medical Center in Maywood, Ill., and a physician researcher at Edward Hines Jr. Veterans Affairs Hospital in Hines, Ill., is the first author in the IDSA/SHEA guidelines. He told this news organization that one reason the two sets of recommendations may diverge in emphasis for initial and recurrent C. difficile is that “everyone has a different way of looking at things.” Compared with infectious disease specialists like him, he said, gastroenterologists “for the most part see the world a little different and have their own bent on things.”
The differences between the two guidelines relate to the first-line therapy for people with an initial or recurrent C. difficile episode. For an initial episode, the IDSA/SHEA authors conditionally recommend fidaxomicin as first preferred choice over vancomycin, with a moderate certainty of evidence. They noted that implementing this recommendation depends on “available resources,” a reference to the higher cost and difficulty of access associated with fidaxomicin.
Gastroenterologist Monika Fischer, MD, an associate professor of medicine at Indiana University, Indianapolis, is one of the authors of the ACG guidelines. She told this news organization that the cost difference between fidaxomicin and vancomycin is considerable and finds the choice to foreground fidaxomicin puzzling. “They did not reference any new data compared to those we have published.” Their recommendation may make sense in terms of efficacy, but real-world demands require attention to cost and reimbursement. “They themselves state this in their recommendations,” she noted.
Dr. Fischer cited a ballpark of about $100 for a course of vancomycin, compared with about $3,000 for a course of fidaxomicin. The IDSA/SHEA guidelines do cite vancomycin as an acceptable alternative. According to Dr. Fischer, the ACG guidelines authors discussed fidaxomicin and concluded that there just wasn’t enough evidence to justify favoring this antibiotic over vancomycin, given the cost-benefit imbalance. The ACG guidelines call for a standard course of oral vancomycin for a first, nonsevere C. difficile episode, listing oral fidaxomicin or oral metronidazole as alternatives.
For a recurrence, the IDSA/SHEA authors also favor fidaxomicin in a conditional recommendation over a standard course of vancomycin. For multiple recurrences, a tapered and pulsed vancomycin regimen, vancomycin followed by rifaximin, or FMT are also options.
Dr. David Johnson said that these recommendations favoring fidaxomicin are “surprising,” and that lower costs of vancomycin outweigh the benefit of fidaxomicin, given more-or-less comparable data on cure rates.
In contrast, the ACG guidelines recommend that an initial recurrence be treated with a tapering dose of vancomycin, and call for FMT for patients who are eligible and who experience a second or more C. difficile recurrences after a round of pulsed vancomycin.
Dr. Stuart Johnson said that FMT carries its own special set of issues. “If you don’t have a donor program set up, you have to rely on a stool bank,” noting that one widely used stool bank “basically had to stop making the product because of the coronavirus.” Costs for FMT products have doubled in recent years, and because Food and Drug Administration approval of the therapy is lacking, insurance does not cover it.
Dr. David Johnson also said that he is not “terribly happy” about the ACG recommendation for vancomycin prophylaxis. “It may help, but it also can have off-target effects against colonic bacterial flora, so we would not agree with that recommendation.”
The IDSA/SHEA authors also conditionally recommend bezlotoxumab, on very low certainty of evidence, as a cotherapy with standard of care antibiotics for recurrence prevention in patients with an episode in the last 6 months, particularly for patients at high recurrence risk “where logistics is not an issue.” The FDA has warned that this monoclonal antibody should be used with great care in patients with heart failure and only when benefits outweigh risks.
The ACG guidelines conditionally recommend considering bezlotoxumab to prevent recurrence in patients with specific risk factors, including age over 65 years and severe presentation. The IDSA/SHEA guidelines expand this population to anyone with a recurrence within 6 months, Dr. Fischer pointed out.
The antibody treatment “does offer another 10% absolute reduction in recurrent C. diff disease,” said Dr. Stuart Johnson, which is a “helpful option and primarily for people who have had recurrent C. diff already.” In general, he said, for both drugs, “access is still something we have to work with.”
In a commentary on the ACG guidelines, Dr. David Johnson wrote that there is good evidence that bezlotoxumab prevents relapse, especially in patients with specific risk factors. The hitch is the $4,500 price tag for a 1,000-mg vial, with a recommended dose of 10 mg/kg.
Dr. Stuart Johnson agreed that the costs of the fidaxomicin and bezlotoxumab are important considerations. In addition, there are logistical issues with using the antibody because most hospitals don’t offer infusions, which pushes patients to infusion centers.
Regardless, he added, “we’re happy that we have new options.”
Dr. Fischer, Dr. Stuart Johnson, and Dr. David Johnson reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
With two sets of Clostridioides difficile recommendations being published within a month of each other, clinicians may find themselves trying to reconcile some of the conflicts between the two guidelines.
The first set, published June 1 by the American College of Gastroenterology, focuses on fecal microbiota transplantation (FMT) and the antibiotic vancomycin. The second, published June 24 by the Infectious Diseases Society of America and Society for Healthcare Epidemiology of America, drives a shift in treatment for initial episodes and short-term recurrence from vancomycin to fidaxomicin and, in some cases, adding on the monoclonal antibody bezlotoxumab, both made by Merck.
The updates are timely because researchers are now recognizing that C. difficile can colonize people without causing symptoms, David Johnson, MD, professor of medicine and chief of gastroenterology at the Eastern Virginia School of Medicine, Norfolk, said in an interview. He was not involved in writing either set of guidelines. “C. diff infection was a hospital-type infection, but we’re now seeing it in up to approximately 35%-50% of patients coming from the community, so it’s a big concern.”
Although the guidelines agree on which treatments are effective, the recommendations give the options a different emphasis.
Infectious disease specialist Stuart Johnson, MD, professor of medicine at Loyola University Medical Center in Maywood, Ill., and a physician researcher at Edward Hines Jr. Veterans Affairs Hospital in Hines, Ill., is the first author in the IDSA/SHEA guidelines. He told this news organization that one reason the two sets of recommendations may diverge in emphasis for initial and recurrent C. difficile is that “everyone has a different way of looking at things.” Compared with infectious disease specialists like him, he said, gastroenterologists “for the most part see the world a little different and have their own bent on things.”
The differences between the two guidelines relate to the first-line therapy for people with an initial or recurrent C. difficile episode. For an initial episode, the IDSA/SHEA authors conditionally recommend fidaxomicin as first preferred choice over vancomycin, with a moderate certainty of evidence. They noted that implementing this recommendation depends on “available resources,” a reference to the higher cost and difficulty of access associated with fidaxomicin.
Gastroenterologist Monika Fischer, MD, an associate professor of medicine at Indiana University, Indianapolis, is one of the authors of the ACG guidelines. She told this news organization that the cost difference between fidaxomicin and vancomycin is considerable and finds the choice to foreground fidaxomicin puzzling. “They did not reference any new data compared to those we have published.” Their recommendation may make sense in terms of efficacy, but real-world demands require attention to cost and reimbursement. “They themselves state this in their recommendations,” she noted.
Dr. Fischer cited a ballpark of about $100 for a course of vancomycin, compared with about $3,000 for a course of fidaxomicin. The IDSA/SHEA guidelines do cite vancomycin as an acceptable alternative. According to Dr. Fischer, the ACG guidelines authors discussed fidaxomicin and concluded that there just wasn’t enough evidence to justify favoring this antibiotic over vancomycin, given the cost-benefit imbalance. The ACG guidelines call for a standard course of oral vancomycin for a first, nonsevere C. difficile episode, listing oral fidaxomicin or oral metronidazole as alternatives.
For a recurrence, the IDSA/SHEA authors also favor fidaxomicin in a conditional recommendation over a standard course of vancomycin. For multiple recurrences, a tapered and pulsed vancomycin regimen, vancomycin followed by rifaximin, or FMT are also options.
Dr. David Johnson said that these recommendations favoring fidaxomicin are “surprising,” and that lower costs of vancomycin outweigh the benefit of fidaxomicin, given more-or-less comparable data on cure rates.
In contrast, the ACG guidelines recommend that an initial recurrence be treated with a tapering dose of vancomycin, and call for FMT for patients who are eligible and who experience a second or more C. difficile recurrences after a round of pulsed vancomycin.
Dr. Stuart Johnson said that FMT carries its own special set of issues. “If you don’t have a donor program set up, you have to rely on a stool bank,” noting that one widely used stool bank “basically had to stop making the product because of the coronavirus.” Costs for FMT products have doubled in recent years, and because Food and Drug Administration approval of the therapy is lacking, insurance does not cover it.
Dr. David Johnson also said that he is not “terribly happy” about the ACG recommendation for vancomycin prophylaxis. “It may help, but it also can have off-target effects against colonic bacterial flora, so we would not agree with that recommendation.”
The IDSA/SHEA authors also conditionally recommend bezlotoxumab, on very low certainty of evidence, as a cotherapy with standard of care antibiotics for recurrence prevention in patients with an episode in the last 6 months, particularly for patients at high recurrence risk “where logistics is not an issue.” The FDA has warned that this monoclonal antibody should be used with great care in patients with heart failure and only when benefits outweigh risks.
The ACG guidelines conditionally recommend considering bezlotoxumab to prevent recurrence in patients with specific risk factors, including age over 65 years and severe presentation. The IDSA/SHEA guidelines expand this population to anyone with a recurrence within 6 months, Dr. Fischer pointed out.
The antibody treatment “does offer another 10% absolute reduction in recurrent C. diff disease,” said Dr. Stuart Johnson, which is a “helpful option and primarily for people who have had recurrent C. diff already.” In general, he said, for both drugs, “access is still something we have to work with.”
In a commentary on the ACG guidelines, Dr. David Johnson wrote that there is good evidence that bezlotoxumab prevents relapse, especially in patients with specific risk factors. The hitch is the $4,500 price tag for a 1,000-mg vial, with a recommended dose of 10 mg/kg.
Dr. Stuart Johnson agreed that the costs of the fidaxomicin and bezlotoxumab are important considerations. In addition, there are logistical issues with using the antibody because most hospitals don’t offer infusions, which pushes patients to infusion centers.
Regardless, he added, “we’re happy that we have new options.”
Dr. Fischer, Dr. Stuart Johnson, and Dr. David Johnson reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
2021 Update on abnormal uterine bleeding
Abnormal uterine bleeding (AUB) continues to be a top-10 reason why women present for gynecologic care, which makes keeping up with clinical therapies important. Over the past year, we have learned a tremendous amount about elagolix with hormonal add-back therapy for the treatment of bleeding associated with uterine fibroids. In this Update, we provide an overview from 3 randomized clinical trials on the recent US Food and Drug Administration (FDA)-approved drug, elagolix with hormonal add-back therapy (approved May 29, 2020). In addition, we review the data on the Cerene cryotherapy device (Channel Medsystems), as one might rightly ask, do we need another endometrial ablation device? We will address that question, as this device has some unique features that gynecologists should be aware of. Last, we review a study on the importance of considering quality of life in patients with uterine fibroids, which provides sobering information on the psychosocial aspects of uterine fibroids that all clinicians who care for such patients should be aware of.
Endometrial ablation with a new cryotherapy device: Is less more?
Curlin HL, Cintron LC, Anderson TL. A prospective, multicenter, clinical trial evaluating the safety and effectiveness of the Cerene device to treat heavy menstrual bleeding. J Minim Invasive Gynecol. 2021;28:899-908.
The phrase “less is more,” in the world of architecture and design, is often associated with Ludwig Mies van der Rohe (1886–1969). One could argue that this principle is one key advantage with the addition of yet another non-resectoscopic endometrial ablation device. The Cerene cryotherapy device, FDA approved in 2019, is presented as a simple, disposable device for in-office use that takes advantage of natural cryoanesthesia and results in less tissue destruction than many other ablation methods.
Device reduces bleeding and permits greater ability for future evaluation
Recently, Curlin and colleagues conducted a prospective, multicenter clinical trial to evaluate the safety and efficacy of the Cerene device in reducing menstrual blood loss.1 They followed 230 patients over 12 months and found that 81% (77% with intention-to-treat analysis) met the primary end point of a pictorial blood loss assessment chart (PBLAC) score of 75 or lower. Clinically, this translated to 44% of patients experiencing light bleeding; 27%, eumenorrhea; and 10%, amenorrhea. This is clearly “less” in terms of the rate of amenorrhea in most endometrial ablation studies. However, this also may translate into “more” ability to evaluate the endometrial cavity in the future, as 97% of the patients were able to undergo hysteroscopy at the 12-month mark and, of those, 93% were able to have the entire endometrial cavity assessed.
Further, of 97 patients who had a tubal sterilization, none had symptoms or evidence of postablation tubal sterilization syndrome. Three patients were unable to undergo hysteroscopy due to pain intolerance (2) or cervical stenosis (1). This is important because some gynecologists have expressed concern over intrauterine synechiae, which may result in scarring and associated future difficulty in assessing the endometrium for possible cancer.
Details about the device
The Cerene device is a single use, disposable device that uses cryothermal energy from nitrous oxide that results in a liquid-to-gas phase change within a polyurethane balloon (resulting in a temperature of -86°C) and delivered through a 6-mm sheath. It may be used in uterine cavities that measure between 2.5 and 6.5 cm in length, corresponding to approximately 10 cm in a uterine sound measurement. Treatment time is 2.5 minutes of nitrous oxide flow.
As mentioned, another benefit claimed is that the Cerene device’s cryoanalgesia properties enable the procedure to be more tolerated in the office setting. Of the 230 patients studied in the Curlin trial, no procedures were performed under general anesthesia.1 Medications used included paracervical block (PCB) only (8%), PCB plus nonsteroidal anti-inflammatory drugs (19.8%), PCB plus oral narcotics/anxiolytics (69%), and PCB plus intravenous sedation (2.9%), showing that this device is ideally suited for in-office use.
The rate of serious adverse events was 2.5% (7 total events in 6 patients within 12 months). All serious adverse events were reviewed by a Clinical Events Committee and none were deemed to be device-related events.
Long-term outcomes remain to be seen
For physicians and patients who worry about the ability to access the endometrial cavity in the future, less may be more. It will be interesting to see what the long-term outcomes show with use of the Cerene cryotherapy device, and whether a lower amenorrhea rate will translate into a higher repeat intervention rate or not. Of course, not all are minimalists. As the architect Robert Venturi (1925–2018) was quoted as saying, “Less is a bore.”
The new Cerene cryotherapy endometrial ablation method meets the FDA’s target for reduction of menstrual blood loss, but it has a slightly lower amenorrhea rate than other devices. Its most significant features are the potential for improved analgesia for in-office use and the possibility that there may be less scarring of the endometrial cavity for future assessment if needed.
Continue to: QoL assessment in women with fibroids is useful in evaluating treatment success...
QoL assessment in women with fibroids is useful in evaluating treatment success
Go VAA, Thomas MC, Singh B, et al. A systematic review of the psychosocial impact of fibroids before and after treatment. Am J Obstet Gynecol. 2020;223:674- 708.e8.
In many studies that assess AUB, the primary emphasis generally is placed on quantitation of menstrual bleeding by using PBLAC and alkaline hematin scores. In a systematic review, Go and colleagues argue the case for the importance of measuring the psychosocial impact of abnormal bleeding, emphasizing the concerning finding that many women with fibroids report lower vitality and lower social function scores than women with breast cancer.2
Fibroids associated with inconvenience—and anxiety
The authors analyzed and reviewed 18 randomized trials and 39 observational studies after screening 3,625 records from electronic database searches, with the goal to include only studies with validated quality of life (QoL) questionnaires that were administered both before and after treatment. A highlighted aspect of the reviewed studies was that “control” and “concern” subscales were most affected by fibroids, noting the inconvenience and anxiety that are related to the unpredictable onset and intensity of menses and the feeling of loss of control over one’s health and future.
This systematic review is important because although previous research has shown that fibroids significantly affect QoL, the psychosocial burden of fibroid symptoms had not been compared across different QoL instruments for both disease-specific and general validated health subscales.
Disability levels with fibroids are similar to those with other chronic diseases
Go and colleagues further reported that uterine fibroids have considerable psychosocial impact and lead to poor overall QoL physically and emotionally, with diminished sexual function and increased urinary or defecatory issues. Women with fibroids experienced a level of disability that was similar to that seen in other chronic diseases, and their vitality scores were lower than those associated with heart disease, diabetes, and as mentioned, breast cancer.
The authors concluded that “although objective clinical measures are important to establish a comprehensive understanding of health status, patient reported QoL outcomes play a critical role in evaluating success of a therapy.” They suggested that a larger emphasis on patient-centered care may help to mitigate the psychosocial effects of fibroids.
The study by Go and colleagues highlights the significant psychosocial aspects of the heavy menstrual bleeding associated with fibroids, and the authors found that many women with fibroids score in the range of those with other significant diseases, such as breast cancer and diabetes.
We have noted the trend of including QoL in research, and Go and colleagues make an excellent and compelling argument for this trend using quantitative analysis. It is important to consider this not only in our design of future research but also, and perhaps more importantly, in our clinical care of women as we try to better understand what they are experiencing.
Continue to: What have we learned over the past year about elagolix for uterine fibroids?...
What have we learned over the past year about elagolix for uterine fibroids?
Schlaff WD, Ackerman RT, Al-Hendy A, et al. Elagolix for heavy menstrual bleeding in women with uterine fibroids. N Engl J Med. 2020;382:328-340.
Simon JA, Al-Hendy A, Archer DF, et al. Elagolix treatment for up to 12 months in women with heavy menstrual bleeding and uterine leiomyomas. Obstet Gynecol. 2020;135:1313-1326.
Al-Hendy A, Bradley L, Owens CD, et al. Predictors of response for elagolix with add-back therapy in women with heavy menstrual bleeding associated with uterine fibroids. Am J Obstet Gynecol. 2021:224-72.e1-72.e50.
Data from the Elaris UF-1 and UF-2 6-month, phase 3 trials3 and the results of the Elaris UF-EXTEND trial with a 6-month extension (totaling 12 months of use)4 were published in 2020, and the 12-month results were discussed in OBG Management (2020;32[7]:35, 39-40). An additional data analysis from the same researchers assessed the effect of elagolix with hormonal add-back therapy in a number of patient subgroups.5 These 3 publications have added to our knowledge of this therapy, and it is worth reviewing them in this context
Design of the elagolix plus hormonal add-back therapy trials
The initial UF-1 and UF-2 trials were 2 identical, double-blind, randomized, placebo-controlled, 6-month, phase 3 trials designed to evaluate the safety and efficacy of elagolix and hormonal add-back therapy.3 UF-1 was conducted at 76 sites in the United States from December 2015 through December 2018, whereas UF-2 was conducted at 77 sites in the United States and Canada from February 2016 through January 2019; the trials were registered separately. Both trials had a 2:1:1 randomization of elagolix (300 mg twice daily) with hormonal add-back therapy (estradiol 1 mg and norethindrone acetate 0.5 mg daily), elagolix alone (300 mg twice daily), or placebo.
In the 6-month studies, the primary end point was both menstrual blood loss of less than 80 mL and at least a 50% reduction of menstrual blood loss as measured by the alkaline hematin method.3 Among several secondary end points was the assessment of QoL using the Uterine Fibroid Symptom QoL questionnaire (UFS-QoL).
Trial results. In UF-1, 68.5% of 206 women, and in UF-2, 76.5% of 189 women, respectively, taking elagolix with add-back therapy met the primary objective. Among women taking elagolix alone, in UF-1, 84.1% of 104 women, and in UF-2, 77% of 95 women, respectively, met criteria. There was improvement in UFS-QoL scores in women receiving elagolix plus add-back therapy with a reduction of symptom severity of -33.2 in UF-1 and -41.4 in UF-2, as compared with the placebo-treated groups (-10.3 and -7.7, respectively).
Adverse effects. Elagolix was associated with a low incidence of serious adverse effects, and the addition of hormonal add-back therapy attenuated the decreases in bone mineral density observed with elagolix alone. In both UF-1 and UF-2 trials, bone mineral density did not differ significantly in the groups of women who received elagolix with hormonal addback therapy versus placebo.
The extension trial results
Of note, in the 12-month study (6-month extension), the authors reported that 87.9% of the women taking elagolix with hormonal add-back therapy met the primary objective.4 Among the women taking elagolix alone, 89.4% met the primary objective.
In a review of the AbbVie-funded extension study, the editorial comments in the Obstetrical and Gynecological Survey expressed concern over the high proportion of data loss, comparing the number of patients joining the extended trial, patients who completed an additional 6 months of treatment, and patients who completed the posttreatment follow-up period of “up to 12 months.”6 Approximately one-third of patients were lost between initial enrollment to the subset who completed follow-up. There was concern that “losses of that magnitude pose a serious threat to validity.”6
Effectiveness in subgroups
Al-Hendy and colleagues analyzed data from the Elaris UF-1 and UF-2 trials to see if the outcomes for elagolix with hormonal addback therapy demonstrated safety and efficacy in subgroups of patients of varying ages, races and ethnicities, baseline menstrual blood loss, body mass indices, fibroid location, and uterine and fibroid volume.5
Results. In all subgroups, they found a statistically significant reduction in blood loss in mean menstrual blood loss volume for those treated with elagolix plus hormonal addback therapy compared with those treated with placebo. As well, in terms of QoL, among all subgroups, the mean change in symptom severity score as well as health-related QoL total score from baseline to month 6 was statistically significantly greater than the mean change in the placebo group.
The bottom line
Elagolix with hormonal add-back therapy appears to be a safe and effective method to reduce menstrual blood loss associated with uterine fibroids. It also has a favorable effect on QoL and appears to have benefits in subgroups of women of varying ages, races and ethnicities, baseline menstrual blood loss, body mass indices, fibroid location, and uterine and fibroid volume. ●
Elagolix plus hormonal add-back therapy provides several advantages to fibroid care, including a pill form that, as a gonadotropin-releasing hormone (GnRH) antagonist, provides much quicker action than GnRH agonists. The hormonal add-back feature seems to improve QoL measures and has a favorable reported bleeding reduction rate. It also appears to be reasonably safe. Although the studies reviewed here may have some weaknesses, it helps to have another therapy to offer to women who have blood loss associated with fibroids. Deciding on the drug’s optimal clinical use has not been fully explored, as it may be a short-term solution to a long-term problem and may not be ideal for all patients with fibroids. Elagolix and hormonal add-back therapy may be advantageous for patients who need to stop bleeding quickly and are trying to decide about their reproductive plans, for patients close to menopause who need a therapy to bridge this gap, and for patients trying to obtain relief between pregnancies.
- Curlin HL, Cintron LC, Anderson TL. A prospective, multicenter, clinical trial evaluating the safety and effectiveness of the Cerene device to treat heavy menstrual bleeding. J Minim Invasive Gynecol. 2021;28:899-908.
- Go VAA, Thomas MC, Singh B, et al. A systematic review of the psychosocial impact of fibroids before and after treatment. Am J Obstet Gynecol. 2020;223:674-708.e8.
- Schlaff WD, Ackerman RT, Al-Hendy A, et al. Elagolix for heavy menstrual bleeding in women with uterine fibroids. N Engl J Med. 2020;382:328-340.
- Simon JA, Al-Hendy A, Archer DF, et al. Elagolix treatment for up to 12 months in women with heavy menstrual bleeding and uterine leiomyomas. Obstet Gynecol. 2020;135:1313-1326.
- Al-Hendy A, Bradley L, Owens CD, et al. Predictors of response for elagolix with add-back therapy in women with heavy menstrual bleeding associated with uterine fibroids. Am J Obstet Gynecol. 2021:224-72.e1-72.e50.
- Obstetrical & Gynecological Survey. 2020;75:545-547.

Howard T. Sharp, MD
Dr. Sharp is Jon M. Huntsman Presidential Endowed Professor, Vice Chair for Clinical Activities and Quality, Department of Obstetrics and Gynecology, University of Utah Health, Salt Lake City, Utah.
Marisa R. Adelman, MD
Dr. Adelman is Associate Professor, Department of Obstetrics and Gynecology, University of Utah Health.
Dr. Sharp reports being an author and editor and receiving royalties from UpToDate, Inc. Dr. Adelman reports no financial relationships relevant to this article.
Howard T. Sharp, MD
Dr. Sharp is Jon M. Huntsman Presidential Endowed Professor, Vice Chair for Clinical Activities and Quality, Department of Obstetrics and Gynecology, University of Utah Health, Salt Lake City, Utah.
Marisa R. Adelman, MD
Dr. Adelman is Associate Professor, Department of Obstetrics and Gynecology, University of Utah Health.
Dr. Sharp reports being an author and editor and receiving royalties from UpToDate, Inc. Dr. Adelman reports no financial relationships relevant to this article.
Howard T. Sharp, MD
Dr. Sharp is Jon M. Huntsman Presidential Endowed Professor, Vice Chair for Clinical Activities and Quality, Department of Obstetrics and Gynecology, University of Utah Health, Salt Lake City, Utah.
Marisa R. Adelman, MD
Dr. Adelman is Associate Professor, Department of Obstetrics and Gynecology, University of Utah Health.
Dr. Sharp reports being an author and editor and receiving royalties from UpToDate, Inc. Dr. Adelman reports no financial relationships relevant to this article.
Abnormal uterine bleeding (AUB) continues to be a top-10 reason why women present for gynecologic care, which makes keeping up with clinical therapies important. Over the past year, we have learned a tremendous amount about elagolix with hormonal add-back therapy for the treatment of bleeding associated with uterine fibroids. In this Update, we provide an overview from 3 randomized clinical trials on the recent US Food and Drug Administration (FDA)-approved drug, elagolix with hormonal add-back therapy (approved May 29, 2020). In addition, we review the data on the Cerene cryotherapy device (Channel Medsystems), as one might rightly ask, do we need another endometrial ablation device? We will address that question, as this device has some unique features that gynecologists should be aware of. Last, we review a study on the importance of considering quality of life in patients with uterine fibroids, which provides sobering information on the psychosocial aspects of uterine fibroids that all clinicians who care for such patients should be aware of.
Endometrial ablation with a new cryotherapy device: Is less more?
Curlin HL, Cintron LC, Anderson TL. A prospective, multicenter, clinical trial evaluating the safety and effectiveness of the Cerene device to treat heavy menstrual bleeding. J Minim Invasive Gynecol. 2021;28:899-908.
The phrase “less is more,” in the world of architecture and design, is often associated with Ludwig Mies van der Rohe (1886–1969). One could argue that this principle is one key advantage with the addition of yet another non-resectoscopic endometrial ablation device. The Cerene cryotherapy device, FDA approved in 2019, is presented as a simple, disposable device for in-office use that takes advantage of natural cryoanesthesia and results in less tissue destruction than many other ablation methods.
Device reduces bleeding and permits greater ability for future evaluation
Recently, Curlin and colleagues conducted a prospective, multicenter clinical trial to evaluate the safety and efficacy of the Cerene device in reducing menstrual blood loss.1 They followed 230 patients over 12 months and found that 81% (77% with intention-to-treat analysis) met the primary end point of a pictorial blood loss assessment chart (PBLAC) score of 75 or lower. Clinically, this translated to 44% of patients experiencing light bleeding; 27%, eumenorrhea; and 10%, amenorrhea. This is clearly “less” in terms of the rate of amenorrhea in most endometrial ablation studies. However, this also may translate into “more” ability to evaluate the endometrial cavity in the future, as 97% of the patients were able to undergo hysteroscopy at the 12-month mark and, of those, 93% were able to have the entire endometrial cavity assessed.
Further, of 97 patients who had a tubal sterilization, none had symptoms or evidence of postablation tubal sterilization syndrome. Three patients were unable to undergo hysteroscopy due to pain intolerance (2) or cervical stenosis (1). This is important because some gynecologists have expressed concern over intrauterine synechiae, which may result in scarring and associated future difficulty in assessing the endometrium for possible cancer.
Details about the device
The Cerene device is a single use, disposable device that uses cryothermal energy from nitrous oxide that results in a liquid-to-gas phase change within a polyurethane balloon (resulting in a temperature of -86°C) and delivered through a 6-mm sheath. It may be used in uterine cavities that measure between 2.5 and 6.5 cm in length, corresponding to approximately 10 cm in a uterine sound measurement. Treatment time is 2.5 minutes of nitrous oxide flow.
As mentioned, another benefit claimed is that the Cerene device’s cryoanalgesia properties enable the procedure to be more tolerated in the office setting. Of the 230 patients studied in the Curlin trial, no procedures were performed under general anesthesia.1 Medications used included paracervical block (PCB) only (8%), PCB plus nonsteroidal anti-inflammatory drugs (19.8%), PCB plus oral narcotics/anxiolytics (69%), and PCB plus intravenous sedation (2.9%), showing that this device is ideally suited for in-office use.
The rate of serious adverse events was 2.5% (7 total events in 6 patients within 12 months). All serious adverse events were reviewed by a Clinical Events Committee and none were deemed to be device-related events.
Long-term outcomes remain to be seen
For physicians and patients who worry about the ability to access the endometrial cavity in the future, less may be more. It will be interesting to see what the long-term outcomes show with use of the Cerene cryotherapy device, and whether a lower amenorrhea rate will translate into a higher repeat intervention rate or not. Of course, not all are minimalists. As the architect Robert Venturi (1925–2018) was quoted as saying, “Less is a bore.”
The new Cerene cryotherapy endometrial ablation method meets the FDA’s target for reduction of menstrual blood loss, but it has a slightly lower amenorrhea rate than other devices. Its most significant features are the potential for improved analgesia for in-office use and the possibility that there may be less scarring of the endometrial cavity for future assessment if needed.
Continue to: QoL assessment in women with fibroids is useful in evaluating treatment success...
QoL assessment in women with fibroids is useful in evaluating treatment success
Go VAA, Thomas MC, Singh B, et al. A systematic review of the psychosocial impact of fibroids before and after treatment. Am J Obstet Gynecol. 2020;223:674- 708.e8.
In many studies that assess AUB, the primary emphasis generally is placed on quantitation of menstrual bleeding by using PBLAC and alkaline hematin scores. In a systematic review, Go and colleagues argue the case for the importance of measuring the psychosocial impact of abnormal bleeding, emphasizing the concerning finding that many women with fibroids report lower vitality and lower social function scores than women with breast cancer.2
Fibroids associated with inconvenience—and anxiety
The authors analyzed and reviewed 18 randomized trials and 39 observational studies after screening 3,625 records from electronic database searches, with the goal to include only studies with validated quality of life (QoL) questionnaires that were administered both before and after treatment. A highlighted aspect of the reviewed studies was that “control” and “concern” subscales were most affected by fibroids, noting the inconvenience and anxiety that are related to the unpredictable onset and intensity of menses and the feeling of loss of control over one’s health and future.
This systematic review is important because although previous research has shown that fibroids significantly affect QoL, the psychosocial burden of fibroid symptoms had not been compared across different QoL instruments for both disease-specific and general validated health subscales.
Disability levels with fibroids are similar to those with other chronic diseases
Go and colleagues further reported that uterine fibroids have considerable psychosocial impact and lead to poor overall QoL physically and emotionally, with diminished sexual function and increased urinary or defecatory issues. Women with fibroids experienced a level of disability that was similar to that seen in other chronic diseases, and their vitality scores were lower than those associated with heart disease, diabetes, and as mentioned, breast cancer.
The authors concluded that “although objective clinical measures are important to establish a comprehensive understanding of health status, patient reported QoL outcomes play a critical role in evaluating success of a therapy.” They suggested that a larger emphasis on patient-centered care may help to mitigate the psychosocial effects of fibroids.
The study by Go and colleagues highlights the significant psychosocial aspects of the heavy menstrual bleeding associated with fibroids, and the authors found that many women with fibroids score in the range of those with other significant diseases, such as breast cancer and diabetes.
We have noted the trend of including QoL in research, and Go and colleagues make an excellent and compelling argument for this trend using quantitative analysis. It is important to consider this not only in our design of future research but also, and perhaps more importantly, in our clinical care of women as we try to better understand what they are experiencing.
Continue to: What have we learned over the past year about elagolix for uterine fibroids?...
What have we learned over the past year about elagolix for uterine fibroids?
Schlaff WD, Ackerman RT, Al-Hendy A, et al. Elagolix for heavy menstrual bleeding in women with uterine fibroids. N Engl J Med. 2020;382:328-340.
Simon JA, Al-Hendy A, Archer DF, et al. Elagolix treatment for up to 12 months in women with heavy menstrual bleeding and uterine leiomyomas. Obstet Gynecol. 2020;135:1313-1326.
Al-Hendy A, Bradley L, Owens CD, et al. Predictors of response for elagolix with add-back therapy in women with heavy menstrual bleeding associated with uterine fibroids. Am J Obstet Gynecol. 2021:224-72.e1-72.e50.
Data from the Elaris UF-1 and UF-2 6-month, phase 3 trials3 and the results of the Elaris UF-EXTEND trial with a 6-month extension (totaling 12 months of use)4 were published in 2020, and the 12-month results were discussed in OBG Management (2020;32[7]:35, 39-40). An additional data analysis from the same researchers assessed the effect of elagolix with hormonal add-back therapy in a number of patient subgroups.5 These 3 publications have added to our knowledge of this therapy, and it is worth reviewing them in this context
Design of the elagolix plus hormonal add-back therapy trials
The initial UF-1 and UF-2 trials were 2 identical, double-blind, randomized, placebo-controlled, 6-month, phase 3 trials designed to evaluate the safety and efficacy of elagolix and hormonal add-back therapy.3 UF-1 was conducted at 76 sites in the United States from December 2015 through December 2018, whereas UF-2 was conducted at 77 sites in the United States and Canada from February 2016 through January 2019; the trials were registered separately. Both trials had a 2:1:1 randomization of elagolix (300 mg twice daily) with hormonal add-back therapy (estradiol 1 mg and norethindrone acetate 0.5 mg daily), elagolix alone (300 mg twice daily), or placebo.
In the 6-month studies, the primary end point was both menstrual blood loss of less than 80 mL and at least a 50% reduction of menstrual blood loss as measured by the alkaline hematin method.3 Among several secondary end points was the assessment of QoL using the Uterine Fibroid Symptom QoL questionnaire (UFS-QoL).
Trial results. In UF-1, 68.5% of 206 women, and in UF-2, 76.5% of 189 women, respectively, taking elagolix with add-back therapy met the primary objective. Among women taking elagolix alone, in UF-1, 84.1% of 104 women, and in UF-2, 77% of 95 women, respectively, met criteria. There was improvement in UFS-QoL scores in women receiving elagolix plus add-back therapy with a reduction of symptom severity of -33.2 in UF-1 and -41.4 in UF-2, as compared with the placebo-treated groups (-10.3 and -7.7, respectively).
Adverse effects. Elagolix was associated with a low incidence of serious adverse effects, and the addition of hormonal add-back therapy attenuated the decreases in bone mineral density observed with elagolix alone. In both UF-1 and UF-2 trials, bone mineral density did not differ significantly in the groups of women who received elagolix with hormonal addback therapy versus placebo.
The extension trial results
Of note, in the 12-month study (6-month extension), the authors reported that 87.9% of the women taking elagolix with hormonal add-back therapy met the primary objective.4 Among the women taking elagolix alone, 89.4% met the primary objective.
In a review of the AbbVie-funded extension study, the editorial comments in the Obstetrical and Gynecological Survey expressed concern over the high proportion of data loss, comparing the number of patients joining the extended trial, patients who completed an additional 6 months of treatment, and patients who completed the posttreatment follow-up period of “up to 12 months.”6 Approximately one-third of patients were lost between initial enrollment to the subset who completed follow-up. There was concern that “losses of that magnitude pose a serious threat to validity.”6
Effectiveness in subgroups
Al-Hendy and colleagues analyzed data from the Elaris UF-1 and UF-2 trials to see if the outcomes for elagolix with hormonal addback therapy demonstrated safety and efficacy in subgroups of patients of varying ages, races and ethnicities, baseline menstrual blood loss, body mass indices, fibroid location, and uterine and fibroid volume.5
Results. In all subgroups, they found a statistically significant reduction in blood loss in mean menstrual blood loss volume for those treated with elagolix plus hormonal addback therapy compared with those treated with placebo. As well, in terms of QoL, among all subgroups, the mean change in symptom severity score as well as health-related QoL total score from baseline to month 6 was statistically significantly greater than the mean change in the placebo group.
The bottom line
Elagolix with hormonal add-back therapy appears to be a safe and effective method to reduce menstrual blood loss associated with uterine fibroids. It also has a favorable effect on QoL and appears to have benefits in subgroups of women of varying ages, races and ethnicities, baseline menstrual blood loss, body mass indices, fibroid location, and uterine and fibroid volume. ●
Elagolix plus hormonal add-back therapy provides several advantages to fibroid care, including a pill form that, as a gonadotropin-releasing hormone (GnRH) antagonist, provides much quicker action than GnRH agonists. The hormonal add-back feature seems to improve QoL measures and has a favorable reported bleeding reduction rate. It also appears to be reasonably safe. Although the studies reviewed here may have some weaknesses, it helps to have another therapy to offer to women who have blood loss associated with fibroids. Deciding on the drug’s optimal clinical use has not been fully explored, as it may be a short-term solution to a long-term problem and may not be ideal for all patients with fibroids. Elagolix and hormonal add-back therapy may be advantageous for patients who need to stop bleeding quickly and are trying to decide about their reproductive plans, for patients close to menopause who need a therapy to bridge this gap, and for patients trying to obtain relief between pregnancies.
Abnormal uterine bleeding (AUB) continues to be a top-10 reason why women present for gynecologic care, which makes keeping up with clinical therapies important. Over the past year, we have learned a tremendous amount about elagolix with hormonal add-back therapy for the treatment of bleeding associated with uterine fibroids. In this Update, we provide an overview from 3 randomized clinical trials on the recent US Food and Drug Administration (FDA)-approved drug, elagolix with hormonal add-back therapy (approved May 29, 2020). In addition, we review the data on the Cerene cryotherapy device (Channel Medsystems), as one might rightly ask, do we need another endometrial ablation device? We will address that question, as this device has some unique features that gynecologists should be aware of. Last, we review a study on the importance of considering quality of life in patients with uterine fibroids, which provides sobering information on the psychosocial aspects of uterine fibroids that all clinicians who care for such patients should be aware of.
Endometrial ablation with a new cryotherapy device: Is less more?
Curlin HL, Cintron LC, Anderson TL. A prospective, multicenter, clinical trial evaluating the safety and effectiveness of the Cerene device to treat heavy menstrual bleeding. J Minim Invasive Gynecol. 2021;28:899-908.
The phrase “less is more,” in the world of architecture and design, is often associated with Ludwig Mies van der Rohe (1886–1969). One could argue that this principle is one key advantage with the addition of yet another non-resectoscopic endometrial ablation device. The Cerene cryotherapy device, FDA approved in 2019, is presented as a simple, disposable device for in-office use that takes advantage of natural cryoanesthesia and results in less tissue destruction than many other ablation methods.
Device reduces bleeding and permits greater ability for future evaluation
Recently, Curlin and colleagues conducted a prospective, multicenter clinical trial to evaluate the safety and efficacy of the Cerene device in reducing menstrual blood loss.1 They followed 230 patients over 12 months and found that 81% (77% with intention-to-treat analysis) met the primary end point of a pictorial blood loss assessment chart (PBLAC) score of 75 or lower. Clinically, this translated to 44% of patients experiencing light bleeding; 27%, eumenorrhea; and 10%, amenorrhea. This is clearly “less” in terms of the rate of amenorrhea in most endometrial ablation studies. However, this also may translate into “more” ability to evaluate the endometrial cavity in the future, as 97% of the patients were able to undergo hysteroscopy at the 12-month mark and, of those, 93% were able to have the entire endometrial cavity assessed.
Further, of 97 patients who had a tubal sterilization, none had symptoms or evidence of postablation tubal sterilization syndrome. Three patients were unable to undergo hysteroscopy due to pain intolerance (2) or cervical stenosis (1). This is important because some gynecologists have expressed concern over intrauterine synechiae, which may result in scarring and associated future difficulty in assessing the endometrium for possible cancer.
Details about the device
The Cerene device is a single use, disposable device that uses cryothermal energy from nitrous oxide that results in a liquid-to-gas phase change within a polyurethane balloon (resulting in a temperature of -86°C) and delivered through a 6-mm sheath. It may be used in uterine cavities that measure between 2.5 and 6.5 cm in length, corresponding to approximately 10 cm in a uterine sound measurement. Treatment time is 2.5 minutes of nitrous oxide flow.
As mentioned, another benefit claimed is that the Cerene device’s cryoanalgesia properties enable the procedure to be more tolerated in the office setting. Of the 230 patients studied in the Curlin trial, no procedures were performed under general anesthesia.1 Medications used included paracervical block (PCB) only (8%), PCB plus nonsteroidal anti-inflammatory drugs (19.8%), PCB plus oral narcotics/anxiolytics (69%), and PCB plus intravenous sedation (2.9%), showing that this device is ideally suited for in-office use.
The rate of serious adverse events was 2.5% (7 total events in 6 patients within 12 months). All serious adverse events were reviewed by a Clinical Events Committee and none were deemed to be device-related events.
Long-term outcomes remain to be seen
For physicians and patients who worry about the ability to access the endometrial cavity in the future, less may be more. It will be interesting to see what the long-term outcomes show with use of the Cerene cryotherapy device, and whether a lower amenorrhea rate will translate into a higher repeat intervention rate or not. Of course, not all are minimalists. As the architect Robert Venturi (1925–2018) was quoted as saying, “Less is a bore.”
The new Cerene cryotherapy endometrial ablation method meets the FDA’s target for reduction of menstrual blood loss, but it has a slightly lower amenorrhea rate than other devices. Its most significant features are the potential for improved analgesia for in-office use and the possibility that there may be less scarring of the endometrial cavity for future assessment if needed.
Continue to: QoL assessment in women with fibroids is useful in evaluating treatment success...
QoL assessment in women with fibroids is useful in evaluating treatment success
Go VAA, Thomas MC, Singh B, et al. A systematic review of the psychosocial impact of fibroids before and after treatment. Am J Obstet Gynecol. 2020;223:674- 708.e8.
In many studies that assess AUB, the primary emphasis generally is placed on quantitation of menstrual bleeding by using PBLAC and alkaline hematin scores. In a systematic review, Go and colleagues argue the case for the importance of measuring the psychosocial impact of abnormal bleeding, emphasizing the concerning finding that many women with fibroids report lower vitality and lower social function scores than women with breast cancer.2
Fibroids associated with inconvenience—and anxiety
The authors analyzed and reviewed 18 randomized trials and 39 observational studies after screening 3,625 records from electronic database searches, with the goal to include only studies with validated quality of life (QoL) questionnaires that were administered both before and after treatment. A highlighted aspect of the reviewed studies was that “control” and “concern” subscales were most affected by fibroids, noting the inconvenience and anxiety that are related to the unpredictable onset and intensity of menses and the feeling of loss of control over one’s health and future.
This systematic review is important because although previous research has shown that fibroids significantly affect QoL, the psychosocial burden of fibroid symptoms had not been compared across different QoL instruments for both disease-specific and general validated health subscales.
Disability levels with fibroids are similar to those with other chronic diseases
Go and colleagues further reported that uterine fibroids have considerable psychosocial impact and lead to poor overall QoL physically and emotionally, with diminished sexual function and increased urinary or defecatory issues. Women with fibroids experienced a level of disability that was similar to that seen in other chronic diseases, and their vitality scores were lower than those associated with heart disease, diabetes, and as mentioned, breast cancer.
The authors concluded that “although objective clinical measures are important to establish a comprehensive understanding of health status, patient reported QoL outcomes play a critical role in evaluating success of a therapy.” They suggested that a larger emphasis on patient-centered care may help to mitigate the psychosocial effects of fibroids.
The study by Go and colleagues highlights the significant psychosocial aspects of the heavy menstrual bleeding associated with fibroids, and the authors found that many women with fibroids score in the range of those with other significant diseases, such as breast cancer and diabetes.
We have noted the trend of including QoL in research, and Go and colleagues make an excellent and compelling argument for this trend using quantitative analysis. It is important to consider this not only in our design of future research but also, and perhaps more importantly, in our clinical care of women as we try to better understand what they are experiencing.
Continue to: What have we learned over the past year about elagolix for uterine fibroids?...
What have we learned over the past year about elagolix for uterine fibroids?
Schlaff WD, Ackerman RT, Al-Hendy A, et al. Elagolix for heavy menstrual bleeding in women with uterine fibroids. N Engl J Med. 2020;382:328-340.
Simon JA, Al-Hendy A, Archer DF, et al. Elagolix treatment for up to 12 months in women with heavy menstrual bleeding and uterine leiomyomas. Obstet Gynecol. 2020;135:1313-1326.
Al-Hendy A, Bradley L, Owens CD, et al. Predictors of response for elagolix with add-back therapy in women with heavy menstrual bleeding associated with uterine fibroids. Am J Obstet Gynecol. 2021:224-72.e1-72.e50.
Data from the Elaris UF-1 and UF-2 6-month, phase 3 trials3 and the results of the Elaris UF-EXTEND trial with a 6-month extension (totaling 12 months of use)4 were published in 2020, and the 12-month results were discussed in OBG Management (2020;32[7]:35, 39-40). An additional data analysis from the same researchers assessed the effect of elagolix with hormonal add-back therapy in a number of patient subgroups.5 These 3 publications have added to our knowledge of this therapy, and it is worth reviewing them in this context
Design of the elagolix plus hormonal add-back therapy trials
The initial UF-1 and UF-2 trials were 2 identical, double-blind, randomized, placebo-controlled, 6-month, phase 3 trials designed to evaluate the safety and efficacy of elagolix and hormonal add-back therapy.3 UF-1 was conducted at 76 sites in the United States from December 2015 through December 2018, whereas UF-2 was conducted at 77 sites in the United States and Canada from February 2016 through January 2019; the trials were registered separately. Both trials had a 2:1:1 randomization of elagolix (300 mg twice daily) with hormonal add-back therapy (estradiol 1 mg and norethindrone acetate 0.5 mg daily), elagolix alone (300 mg twice daily), or placebo.
In the 6-month studies, the primary end point was both menstrual blood loss of less than 80 mL and at least a 50% reduction of menstrual blood loss as measured by the alkaline hematin method.3 Among several secondary end points was the assessment of QoL using the Uterine Fibroid Symptom QoL questionnaire (UFS-QoL).
Trial results. In UF-1, 68.5% of 206 women, and in UF-2, 76.5% of 189 women, respectively, taking elagolix with add-back therapy met the primary objective. Among women taking elagolix alone, in UF-1, 84.1% of 104 women, and in UF-2, 77% of 95 women, respectively, met criteria. There was improvement in UFS-QoL scores in women receiving elagolix plus add-back therapy with a reduction of symptom severity of -33.2 in UF-1 and -41.4 in UF-2, as compared with the placebo-treated groups (-10.3 and -7.7, respectively).
Adverse effects. Elagolix was associated with a low incidence of serious adverse effects, and the addition of hormonal add-back therapy attenuated the decreases in bone mineral density observed with elagolix alone. In both UF-1 and UF-2 trials, bone mineral density did not differ significantly in the groups of women who received elagolix with hormonal addback therapy versus placebo.
The extension trial results
Of note, in the 12-month study (6-month extension), the authors reported that 87.9% of the women taking elagolix with hormonal add-back therapy met the primary objective.4 Among the women taking elagolix alone, 89.4% met the primary objective.
In a review of the AbbVie-funded extension study, the editorial comments in the Obstetrical and Gynecological Survey expressed concern over the high proportion of data loss, comparing the number of patients joining the extended trial, patients who completed an additional 6 months of treatment, and patients who completed the posttreatment follow-up period of “up to 12 months.”6 Approximately one-third of patients were lost between initial enrollment to the subset who completed follow-up. There was concern that “losses of that magnitude pose a serious threat to validity.”6
Effectiveness in subgroups
Al-Hendy and colleagues analyzed data from the Elaris UF-1 and UF-2 trials to see if the outcomes for elagolix with hormonal addback therapy demonstrated safety and efficacy in subgroups of patients of varying ages, races and ethnicities, baseline menstrual blood loss, body mass indices, fibroid location, and uterine and fibroid volume.5
Results. In all subgroups, they found a statistically significant reduction in blood loss in mean menstrual blood loss volume for those treated with elagolix plus hormonal addback therapy compared with those treated with placebo. As well, in terms of QoL, among all subgroups, the mean change in symptom severity score as well as health-related QoL total score from baseline to month 6 was statistically significantly greater than the mean change in the placebo group.
The bottom line
Elagolix with hormonal add-back therapy appears to be a safe and effective method to reduce menstrual blood loss associated with uterine fibroids. It also has a favorable effect on QoL and appears to have benefits in subgroups of women of varying ages, races and ethnicities, baseline menstrual blood loss, body mass indices, fibroid location, and uterine and fibroid volume. ●
Elagolix plus hormonal add-back therapy provides several advantages to fibroid care, including a pill form that, as a gonadotropin-releasing hormone (GnRH) antagonist, provides much quicker action than GnRH agonists. The hormonal add-back feature seems to improve QoL measures and has a favorable reported bleeding reduction rate. It also appears to be reasonably safe. Although the studies reviewed here may have some weaknesses, it helps to have another therapy to offer to women who have blood loss associated with fibroids. Deciding on the drug’s optimal clinical use has not been fully explored, as it may be a short-term solution to a long-term problem and may not be ideal for all patients with fibroids. Elagolix and hormonal add-back therapy may be advantageous for patients who need to stop bleeding quickly and are trying to decide about their reproductive plans, for patients close to menopause who need a therapy to bridge this gap, and for patients trying to obtain relief between pregnancies.
- Curlin HL, Cintron LC, Anderson TL. A prospective, multicenter, clinical trial evaluating the safety and effectiveness of the Cerene device to treat heavy menstrual bleeding. J Minim Invasive Gynecol. 2021;28:899-908.
- Go VAA, Thomas MC, Singh B, et al. A systematic review of the psychosocial impact of fibroids before and after treatment. Am J Obstet Gynecol. 2020;223:674-708.e8.
- Schlaff WD, Ackerman RT, Al-Hendy A, et al. Elagolix for heavy menstrual bleeding in women with uterine fibroids. N Engl J Med. 2020;382:328-340.
- Simon JA, Al-Hendy A, Archer DF, et al. Elagolix treatment for up to 12 months in women with heavy menstrual bleeding and uterine leiomyomas. Obstet Gynecol. 2020;135:1313-1326.
- Al-Hendy A, Bradley L, Owens CD, et al. Predictors of response for elagolix with add-back therapy in women with heavy menstrual bleeding associated with uterine fibroids. Am J Obstet Gynecol. 2021:224-72.e1-72.e50.
- Obstetrical & Gynecological Survey. 2020;75:545-547.
- Curlin HL, Cintron LC, Anderson TL. A prospective, multicenter, clinical trial evaluating the safety and effectiveness of the Cerene device to treat heavy menstrual bleeding. J Minim Invasive Gynecol. 2021;28:899-908.
- Go VAA, Thomas MC, Singh B, et al. A systematic review of the psychosocial impact of fibroids before and after treatment. Am J Obstet Gynecol. 2020;223:674-708.e8.
- Schlaff WD, Ackerman RT, Al-Hendy A, et al. Elagolix for heavy menstrual bleeding in women with uterine fibroids. N Engl J Med. 2020;382:328-340.
- Simon JA, Al-Hendy A, Archer DF, et al. Elagolix treatment for up to 12 months in women with heavy menstrual bleeding and uterine leiomyomas. Obstet Gynecol. 2020;135:1313-1326.
- Al-Hendy A, Bradley L, Owens CD, et al. Predictors of response for elagolix with add-back therapy in women with heavy menstrual bleeding associated with uterine fibroids. Am J Obstet Gynecol. 2021:224-72.e1-72.e50.
- Obstetrical & Gynecological Survey. 2020;75:545-547.
