User login
For MD-IQ use only
‘If only you knew’
Patient:
Alone in the Emergency Dept, breathless, I wait for you

“The Hospitalist will admit you” says the nurse, “she will come in a few.”
Muffled voices – masked faces bustle in & out of the room
Loud beeping machines & the rushed pace, fill me with gloom
You walk in the room, lean in to introduce
You tell me your name and what you will do
For a moment I’m more than a diagnosis, an H&P,
and then the fleeting connection passes, can’t you see?
You listen, seem hurried, but I think you care
Would you sit with me while my story I share?
Physician:
I do see you, I feel your fear & anguish
A moment to know you too, is all that I wish
How do I convince you that I truly care?
When, with all my tasks I have only minutes to spare
Patient:
You diligently ask questions from your checklist of H.P.I.,
Finalizing the diagnosis, when I hear your pager beep.
An admission awaits I know, but please sit by my side
Could we make our new-found meeting, a little more deep?
Physician:
The minute our day begins, it’s go-go-go
There isn’t a second to pause, inhale, or be slow
Missed lunch, it’s 6 p.m., bite to eat I dare?
My shift ended 3 hrs. back but I’m still here
Notes, DC summaries, calls to your PCP
Advocating for you, is more than a job to me.
Tirelessly I work, giving patients my all
Drained, exhausted yet, for you, standing tall
Our bond albeit short lived, is very important to me
Watching you get better each day, is fulfilling for me!
Patient:
You take time to ask about my family, about what I like to do
I tell you all about Beatles & my sweet grandkids
You sit & ask me “what matters most to you”
I reply: getting well for the wedding of my daughter “Sue”
Physician:
I sense loneliness engulfing you at times
Your fear and anxiety, I promise to help overcome
I will help you navigate this complex hospital stay
Together we will fight this virus or anything that comes our way
Each passing minute the line between doctor and patient disappears
That’s when we win over this virus, and hope replaces fear
Patient:
Every day you come see me, tell me my numbers are improving
I notice your warm and kind eyes behind that stifling mask
When they light up as you tell me I’m going home soon
I feel assured I mean more to you, than a mere task
Physician:
Each day I visit, together we hum “here comes the sun”
I too open up and share with you, my favorite Beatles song
Our visits cover much more than clinical medicine
True connection & mutual soul healing begins, before long.
Patient:
Today is the day, grateful to go home,
My body may be healed due to all the medicine & potions,
But my bruised soul was healed due to all your kind emotions.
Time to bid adieu Dear Doc – If I meet you at our local grocery store,
I promise I’ll remember those kind eyes, and wave
After all, you stood between me and death
I’m indebted to you, it’s my life that you did save!
Dr. Mehta is a hospitalist and director of quality and performance and patient experience at Vituity in Emeryville, Calif. She is chair of the SHM patient experience executive council and executive board member of the SHM San Francisco Bay Area chapter.
Patient:
Alone in the Emergency Dept, breathless, I wait for you
“The Hospitalist will admit you” says the nurse, “she will come in a few.”
Muffled voices – masked faces bustle in & out of the room
Loud beeping machines & the rushed pace, fill me with gloom
You walk in the room, lean in to introduce
You tell me your name and what you will do
For a moment I’m more than a diagnosis, an H&P,
and then the fleeting connection passes, can’t you see?
You listen, seem hurried, but I think you care
Would you sit with me while my story I share?
Physician:
I do see you, I feel your fear & anguish
A moment to know you too, is all that I wish
How do I convince you that I truly care?
When, with all my tasks I have only minutes to spare
Patient:
You diligently ask questions from your checklist of H.P.I.,
Finalizing the diagnosis, when I hear your pager beep.
An admission awaits I know, but please sit by my side
Could we make our new-found meeting, a little more deep?
Physician:
The minute our day begins, it’s go-go-go
There isn’t a second to pause, inhale, or be slow
Missed lunch, it’s 6 p.m., bite to eat I dare?
My shift ended 3 hrs. back but I’m still here
Notes, DC summaries, calls to your PCP
Advocating for you, is more than a job to me.
Tirelessly I work, giving patients my all
Drained, exhausted yet, for you, standing tall
Our bond albeit short lived, is very important to me
Watching you get better each day, is fulfilling for me!
Patient:
You take time to ask about my family, about what I like to do
I tell you all about Beatles & my sweet grandkids
You sit & ask me “what matters most to you”
I reply: getting well for the wedding of my daughter “Sue”
Physician:
I sense loneliness engulfing you at times
Your fear and anxiety, I promise to help overcome
I will help you navigate this complex hospital stay
Together we will fight this virus or anything that comes our way
Each passing minute the line between doctor and patient disappears
That’s when we win over this virus, and hope replaces fear
Patient:
Every day you come see me, tell me my numbers are improving
I notice your warm and kind eyes behind that stifling mask
When they light up as you tell me I’m going home soon
I feel assured I mean more to you, than a mere task
Physician:
Each day I visit, together we hum “here comes the sun”
I too open up and share with you, my favorite Beatles song
Our visits cover much more than clinical medicine
True connection & mutual soul healing begins, before long.
Patient:
Today is the day, grateful to go home,
My body may be healed due to all the medicine & potions,
But my bruised soul was healed due to all your kind emotions.
Time to bid adieu Dear Doc – If I meet you at our local grocery store,
I promise I’ll remember those kind eyes, and wave
After all, you stood between me and death
I’m indebted to you, it’s my life that you did save!
Dr. Mehta is a hospitalist and director of quality and performance and patient experience at Vituity in Emeryville, Calif. She is chair of the SHM patient experience executive council and executive board member of the SHM San Francisco Bay Area chapter.
Patient:
Alone in the Emergency Dept, breathless, I wait for you
“The Hospitalist will admit you” says the nurse, “she will come in a few.”
Muffled voices – masked faces bustle in & out of the room
Loud beeping machines & the rushed pace, fill me with gloom
You walk in the room, lean in to introduce
You tell me your name and what you will do
For a moment I’m more than a diagnosis, an H&P,
and then the fleeting connection passes, can’t you see?
You listen, seem hurried, but I think you care
Would you sit with me while my story I share?
Physician:
I do see you, I feel your fear & anguish
A moment to know you too, is all that I wish
How do I convince you that I truly care?
When, with all my tasks I have only minutes to spare
Patient:
You diligently ask questions from your checklist of H.P.I.,
Finalizing the diagnosis, when I hear your pager beep.
An admission awaits I know, but please sit by my side
Could we make our new-found meeting, a little more deep?
Physician:
The minute our day begins, it’s go-go-go
There isn’t a second to pause, inhale, or be slow
Missed lunch, it’s 6 p.m., bite to eat I dare?
My shift ended 3 hrs. back but I’m still here
Notes, DC summaries, calls to your PCP
Advocating for you, is more than a job to me.
Tirelessly I work, giving patients my all
Drained, exhausted yet, for you, standing tall
Our bond albeit short lived, is very important to me
Watching you get better each day, is fulfilling for me!
Patient:
You take time to ask about my family, about what I like to do
I tell you all about Beatles & my sweet grandkids
You sit & ask me “what matters most to you”
I reply: getting well for the wedding of my daughter “Sue”
Physician:
I sense loneliness engulfing you at times
Your fear and anxiety, I promise to help overcome
I will help you navigate this complex hospital stay
Together we will fight this virus or anything that comes our way
Each passing minute the line between doctor and patient disappears
That’s when we win over this virus, and hope replaces fear
Patient:
Every day you come see me, tell me my numbers are improving
I notice your warm and kind eyes behind that stifling mask
When they light up as you tell me I’m going home soon
I feel assured I mean more to you, than a mere task
Physician:
Each day I visit, together we hum “here comes the sun”
I too open up and share with you, my favorite Beatles song
Our visits cover much more than clinical medicine
True connection & mutual soul healing begins, before long.
Patient:
Today is the day, grateful to go home,
My body may be healed due to all the medicine & potions,
But my bruised soul was healed due to all your kind emotions.
Time to bid adieu Dear Doc – If I meet you at our local grocery store,
I promise I’ll remember those kind eyes, and wave
After all, you stood between me and death
I’m indebted to you, it’s my life that you did save!
Dr. Mehta is a hospitalist and director of quality and performance and patient experience at Vituity in Emeryville, Calif. She is chair of the SHM patient experience executive council and executive board member of the SHM San Francisco Bay Area chapter.
Musical instruments can throw skin out of tune
Violin and viola players can pay a price for the music they create: Many suffer from skin irritation and inflammation where the instruments touch their necks and upper bodies.

“These skin conditions are disfiguring, and they also carry so much psychological burden. Not only are these patients under constant pressure to perform at their maximum at all times, it really is troublesome when there is a barrier between you and performing art that you absolutely love,” lead author Henry Lim, an osteopathic medical student at the University of North Texas Health Science Center at Fort Worth, said in an interview.

The results of the literature review were presented in a poster at the Inaugural Symposium for Inflammatory Skin Disease.
Mr. Lim, who has a special interest in skin, said his own musical experience inspired the research. “Throughout my experience as a violinist, I faced many dermatologic issues because of my violin, and it affected my performance,” he said. “As time went on, I recognized that many other stringed instrumentalists were dealing with similar issues but chose to live with it because it came with the territory.”
One physician told Mr. Lim that he needed to quit in order to permanently treat his skin problems. He didn’t accept this answer and instead launched the literature review with colleagues Marshall Hall, MPH, also an osteopathic medical student with an interest in dermatology, and Sajid Surve, DO, codirector of the UNT Texas Center for Performing Arts Health.
Mr. Lim and colleagues evaluated 23 articles, which included case studies and literature reviews, about dermatitis in violinists, violists, cellists, bassists, guitarists and harpists. “Stringed instrumentalists are the highest at-risk population compared to performers who play other types of instruments,” Mr. Lim said.
The poster he presented at the meeting largely focuses on fiddler’s neck, which he defined as “simply dermatitis related to friction and allergic irritation from playing violin or viola.” Many people, he noted, are allergic to nickel, and the bracket that secures the violin’s chin rest “most often contains nickel. Even a very small concentration of nickel can cause massive reactions, and we found that the C string of a viola – the thickest, lowest-sounding string – contains a nickel concentration of up to 37%.”
Gold-coated strings are an alternative option, he said, but they’re more expensive.
Stringed instrumentalists may also be allergic to rosin applied to “bow hairs,” which is the hair – typically from horses – that is used to string bows, also described in the poster. “We found that there is an overall common allergy to the main ingredient called colophony,” Mr. Lim said. The legendary violin maker Antonio Stradivari “was rumored to have used colophony and another irritating ingredient called propolis in the wood varnish of his instruments. Because he was such a great influence on the art of violin crafting, his technique is still used in the modern era, which may be another contributing factor to the allergic reactions seen in stringed instrumentalists.”
(In the poster, the authors refer to one of the articles in the review, which described a violin maker allergic to colophony and propolis, who was treated with cetirizine, mild corticosteroids, and avoidance.)
What should dermatologists know about skin conditions in these musicians? Mr. Hall, one of the coauthors of the report, suggested they invite the patients to play their instruments during a visit. “The musicians may not understand that they are doing certain things with their movements, but looking from a clinical lens, we are able to see how their biomechanics and posture [are] contributing to their dermatitis,” he said.
Dr. Surve, the other coauthor, also suggested speaking to the patient’s teacher, coach, or mentor. “Keeping that person in the loop regarding what you are seeing and recommending will go a long way towards helping your patient,” he said. “If the teacher doesn’t understand or agree with what you’re trying to accomplish, they may try to undermine your plan of care. But if they are on board, they become a valuable tool for facilitating and reinforcing it.”
As for treatments, avoidance of the instruments is the most effective, but is simply not feasible for many musicians. “Certain interventions like creating a barrier between the musician and the instrument can reduce the risk of contact dermatitis without compromising the quality [of playing] as much,” Mr. Hall said. The poster reported that a handkerchief was used for this purpose in one case attributed to nickel sulfate in a 16-year-old .
Purchasing more expensive instrument materials to prevent reactions is another option, he said, and players can also purchase stands. But musicians may be resistant to any treatment that changes how the instruments sound or forces them to adjust the way they do things, he cautioned.
No funding for the study or author disclosures were reported.
Violin and viola players can pay a price for the music they create: Many suffer from skin irritation and inflammation where the instruments touch their necks and upper bodies.
“These skin conditions are disfiguring, and they also carry so much psychological burden. Not only are these patients under constant pressure to perform at their maximum at all times, it really is troublesome when there is a barrier between you and performing art that you absolutely love,” lead author Henry Lim, an osteopathic medical student at the University of North Texas Health Science Center at Fort Worth, said in an interview.
The results of the literature review were presented in a poster at the Inaugural Symposium for Inflammatory Skin Disease.
Mr. Lim, who has a special interest in skin, said his own musical experience inspired the research. “Throughout my experience as a violinist, I faced many dermatologic issues because of my violin, and it affected my performance,” he said. “As time went on, I recognized that many other stringed instrumentalists were dealing with similar issues but chose to live with it because it came with the territory.”
One physician told Mr. Lim that he needed to quit in order to permanently treat his skin problems. He didn’t accept this answer and instead launched the literature review with colleagues Marshall Hall, MPH, also an osteopathic medical student with an interest in dermatology, and Sajid Surve, DO, codirector of the UNT Texas Center for Performing Arts Health.
Mr. Lim and colleagues evaluated 23 articles, which included case studies and literature reviews, about dermatitis in violinists, violists, cellists, bassists, guitarists and harpists. “Stringed instrumentalists are the highest at-risk population compared to performers who play other types of instruments,” Mr. Lim said.
The poster he presented at the meeting largely focuses on fiddler’s neck, which he defined as “simply dermatitis related to friction and allergic irritation from playing violin or viola.” Many people, he noted, are allergic to nickel, and the bracket that secures the violin’s chin rest “most often contains nickel. Even a very small concentration of nickel can cause massive reactions, and we found that the C string of a viola – the thickest, lowest-sounding string – contains a nickel concentration of up to 37%.”
Gold-coated strings are an alternative option, he said, but they’re more expensive.
Stringed instrumentalists may also be allergic to rosin applied to “bow hairs,” which is the hair – typically from horses – that is used to string bows, also described in the poster. “We found that there is an overall common allergy to the main ingredient called colophony,” Mr. Lim said. The legendary violin maker Antonio Stradivari “was rumored to have used colophony and another irritating ingredient called propolis in the wood varnish of his instruments. Because he was such a great influence on the art of violin crafting, his technique is still used in the modern era, which may be another contributing factor to the allergic reactions seen in stringed instrumentalists.”
(In the poster, the authors refer to one of the articles in the review, which described a violin maker allergic to colophony and propolis, who was treated with cetirizine, mild corticosteroids, and avoidance.)
What should dermatologists know about skin conditions in these musicians? Mr. Hall, one of the coauthors of the report, suggested they invite the patients to play their instruments during a visit. “The musicians may not understand that they are doing certain things with their movements, but looking from a clinical lens, we are able to see how their biomechanics and posture [are] contributing to their dermatitis,” he said.
Dr. Surve, the other coauthor, also suggested speaking to the patient’s teacher, coach, or mentor. “Keeping that person in the loop regarding what you are seeing and recommending will go a long way towards helping your patient,” he said. “If the teacher doesn’t understand or agree with what you’re trying to accomplish, they may try to undermine your plan of care. But if they are on board, they become a valuable tool for facilitating and reinforcing it.”
As for treatments, avoidance of the instruments is the most effective, but is simply not feasible for many musicians. “Certain interventions like creating a barrier between the musician and the instrument can reduce the risk of contact dermatitis without compromising the quality [of playing] as much,” Mr. Hall said. The poster reported that a handkerchief was used for this purpose in one case attributed to nickel sulfate in a 16-year-old .
Purchasing more expensive instrument materials to prevent reactions is another option, he said, and players can also purchase stands. But musicians may be resistant to any treatment that changes how the instruments sound or forces them to adjust the way they do things, he cautioned.
No funding for the study or author disclosures were reported.
Violin and viola players can pay a price for the music they create: Many suffer from skin irritation and inflammation where the instruments touch their necks and upper bodies.
“These skin conditions are disfiguring, and they also carry so much psychological burden. Not only are these patients under constant pressure to perform at their maximum at all times, it really is troublesome when there is a barrier between you and performing art that you absolutely love,” lead author Henry Lim, an osteopathic medical student at the University of North Texas Health Science Center at Fort Worth, said in an interview.
The results of the literature review were presented in a poster at the Inaugural Symposium for Inflammatory Skin Disease.
Mr. Lim, who has a special interest in skin, said his own musical experience inspired the research. “Throughout my experience as a violinist, I faced many dermatologic issues because of my violin, and it affected my performance,” he said. “As time went on, I recognized that many other stringed instrumentalists were dealing with similar issues but chose to live with it because it came with the territory.”
One physician told Mr. Lim that he needed to quit in order to permanently treat his skin problems. He didn’t accept this answer and instead launched the literature review with colleagues Marshall Hall, MPH, also an osteopathic medical student with an interest in dermatology, and Sajid Surve, DO, codirector of the UNT Texas Center for Performing Arts Health.
Mr. Lim and colleagues evaluated 23 articles, which included case studies and literature reviews, about dermatitis in violinists, violists, cellists, bassists, guitarists and harpists. “Stringed instrumentalists are the highest at-risk population compared to performers who play other types of instruments,” Mr. Lim said.
The poster he presented at the meeting largely focuses on fiddler’s neck, which he defined as “simply dermatitis related to friction and allergic irritation from playing violin or viola.” Many people, he noted, are allergic to nickel, and the bracket that secures the violin’s chin rest “most often contains nickel. Even a very small concentration of nickel can cause massive reactions, and we found that the C string of a viola – the thickest, lowest-sounding string – contains a nickel concentration of up to 37%.”
Gold-coated strings are an alternative option, he said, but they’re more expensive.
Stringed instrumentalists may also be allergic to rosin applied to “bow hairs,” which is the hair – typically from horses – that is used to string bows, also described in the poster. “We found that there is an overall common allergy to the main ingredient called colophony,” Mr. Lim said. The legendary violin maker Antonio Stradivari “was rumored to have used colophony and another irritating ingredient called propolis in the wood varnish of his instruments. Because he was such a great influence on the art of violin crafting, his technique is still used in the modern era, which may be another contributing factor to the allergic reactions seen in stringed instrumentalists.”
(In the poster, the authors refer to one of the articles in the review, which described a violin maker allergic to colophony and propolis, who was treated with cetirizine, mild corticosteroids, and avoidance.)
What should dermatologists know about skin conditions in these musicians? Mr. Hall, one of the coauthors of the report, suggested they invite the patients to play their instruments during a visit. “The musicians may not understand that they are doing certain things with their movements, but looking from a clinical lens, we are able to see how their biomechanics and posture [are] contributing to their dermatitis,” he said.
Dr. Surve, the other coauthor, also suggested speaking to the patient’s teacher, coach, or mentor. “Keeping that person in the loop regarding what you are seeing and recommending will go a long way towards helping your patient,” he said. “If the teacher doesn’t understand or agree with what you’re trying to accomplish, they may try to undermine your plan of care. But if they are on board, they become a valuable tool for facilitating and reinforcing it.”
As for treatments, avoidance of the instruments is the most effective, but is simply not feasible for many musicians. “Certain interventions like creating a barrier between the musician and the instrument can reduce the risk of contact dermatitis without compromising the quality [of playing] as much,” Mr. Hall said. The poster reported that a handkerchief was used for this purpose in one case attributed to nickel sulfate in a 16-year-old .
Purchasing more expensive instrument materials to prevent reactions is another option, he said, and players can also purchase stands. But musicians may be resistant to any treatment that changes how the instruments sound or forces them to adjust the way they do things, he cautioned.
No funding for the study or author disclosures were reported.
FROM SISD 2021
Clinician practices to connect with patients
Background: As technology and medical advances improve patient care, physicians and patients have become more dissatisfied with their interactions and relationships. Practices are needed to improve the connection between physician and patient.
Study design: Mixed-methods.
Setting: Three diverse primary care settings (academic medical center, Veterans Affairs facility, federally qualified health center).
Synopsis: Initial evidence- and narrative-based practices were identified from a systematic literature review, clinical observations of primary care encounters, and qualitative discussions with physicians, patients, and nonmedical professionals. A three-round modified Delphi process was performed with experts representing different aspects of the patient-physician relationship.
Five recommended clinical practices were recognized to foster presence and meaningful connections with patients: 1. Prepare with intention (becoming familiar with the patient before you meet them); 2. Listen intently and completely (sit down, lean forward, and don’t interrupt, but listen); 3. Agree on what matters most (discover your patient’s goals and fit them into the visit); 4. Connect with the patient’s story (take notice of efforts by the patient and successes); 5. Explore emotional cues (be aware of your patient’s emotions). Limitations of this study include the use of convenience sampling for the qualitative research, lack of international diversity of the expert panelists, and the lack of validation of the five practices as a whole.
Bottom line: The five practices of prepare with intention, listen intently and completely, agree on what matters most, connect with the patient’s story, and explore emotional cues may improve the patient-physician connection.
Citation: Zulman DM et al. Practices to foster physician presence and connection with patients in the clinical encounter. JAMA. 2020;323(1):70-81.
Dr. Trammell-Velasquez is a hospitalist and associate professor of medicine at University of Texas Health, San Antonio.
Background: As technology and medical advances improve patient care, physicians and patients have become more dissatisfied with their interactions and relationships. Practices are needed to improve the connection between physician and patient.
Study design: Mixed-methods.
Setting: Three diverse primary care settings (academic medical center, Veterans Affairs facility, federally qualified health center).
Synopsis: Initial evidence- and narrative-based practices were identified from a systematic literature review, clinical observations of primary care encounters, and qualitative discussions with physicians, patients, and nonmedical professionals. A three-round modified Delphi process was performed with experts representing different aspects of the patient-physician relationship.
Five recommended clinical practices were recognized to foster presence and meaningful connections with patients: 1. Prepare with intention (becoming familiar with the patient before you meet them); 2. Listen intently and completely (sit down, lean forward, and don’t interrupt, but listen); 3. Agree on what matters most (discover your patient’s goals and fit them into the visit); 4. Connect with the patient’s story (take notice of efforts by the patient and successes); 5. Explore emotional cues (be aware of your patient’s emotions). Limitations of this study include the use of convenience sampling for the qualitative research, lack of international diversity of the expert panelists, and the lack of validation of the five practices as a whole.
Bottom line: The five practices of prepare with intention, listen intently and completely, agree on what matters most, connect with the patient’s story, and explore emotional cues may improve the patient-physician connection.
Citation: Zulman DM et al. Practices to foster physician presence and connection with patients in the clinical encounter. JAMA. 2020;323(1):70-81.
Dr. Trammell-Velasquez is a hospitalist and associate professor of medicine at University of Texas Health, San Antonio.
Background: As technology and medical advances improve patient care, physicians and patients have become more dissatisfied with their interactions and relationships. Practices are needed to improve the connection between physician and patient.
Study design: Mixed-methods.
Setting: Three diverse primary care settings (academic medical center, Veterans Affairs facility, federally qualified health center).
Synopsis: Initial evidence- and narrative-based practices were identified from a systematic literature review, clinical observations of primary care encounters, and qualitative discussions with physicians, patients, and nonmedical professionals. A three-round modified Delphi process was performed with experts representing different aspects of the patient-physician relationship.
Five recommended clinical practices were recognized to foster presence and meaningful connections with patients: 1. Prepare with intention (becoming familiar with the patient before you meet them); 2. Listen intently and completely (sit down, lean forward, and don’t interrupt, but listen); 3. Agree on what matters most (discover your patient’s goals and fit them into the visit); 4. Connect with the patient’s story (take notice of efforts by the patient and successes); 5. Explore emotional cues (be aware of your patient’s emotions). Limitations of this study include the use of convenience sampling for the qualitative research, lack of international diversity of the expert panelists, and the lack of validation of the five practices as a whole.
Bottom line: The five practices of prepare with intention, listen intently and completely, agree on what matters most, connect with the patient’s story, and explore emotional cues may improve the patient-physician connection.
Citation: Zulman DM et al. Practices to foster physician presence and connection with patients in the clinical encounter. JAMA. 2020;323(1):70-81.
Dr. Trammell-Velasquez is a hospitalist and associate professor of medicine at University of Texas Health, San Antonio.

COMMENT & CONTROVERSY
OBSTETRIC ANAL SPHINCTER INJURY: PREVENTION AND REPAIR
ROBERT L. BARBIERI, MD (EDITORIAL; MAY 2021)
Experience with warm perineal compresses and massage
I have been a midwife for 45 years. I have used warm compresses on the perineum my whole career. I don't need data to tell me it provides comfort. My patients do.
I don't do much massage of the perineum, only slightly while applying K-Y or another water-soluble gel.
A slow, controlled extension of the vertex and healthy tissue is the best way to prevent tears.
Karen Parker, MN, CNM
Ashland, Oregon
Dr. Barbieri responds
I thank Ms. Parker for her clinical recommendation: "Yes to warm compresses" and "Massage of the perineum?" Not so much.
Continue to: CESAREAN MYOMECTOMY...
CESAREAN MYOMECTOMY: SAFE OPERATION OR SURGICAL FOLLY?
ROBERT L. BARBIERI, MD (EDITORIAL; FEBRUARY 2021)
Timely comments on cesarean myomectomy
Dr. Barbieri's editorial on cesarean myomectomy is very timely, especially the quote from Dr. K.S.J. Olah: "The berating I received was severe and disproportionate to the crime. The rule was that myomectomy performed at cesarean section was not just frowned upon but expressly forbidden."
I had a very similar experience with panniculectomy and "tummy tuck" as a part of cesarean delivery (CD). Traditionally, a combination of a CD with any other surgical procedures (myomectomy, abdominoplasty, and so on) has not been accepted in the obstetric community. The main reason for such an opinion has been the unfounded fear of complications of combined procedures, including but not limited to infection, hematomas, and poor wound healing. None of these concerns have been supported by studies. Obvious advantages of combining a CD with other surgical procedures, including abdominoplasty, are obvious: the elimination of a second anesthesia, increased patient satisfaction, and no need for a second surgery.
We reviewed the outcomes in 52 patients who underwent a combination of CD with other procedures (such as panniculectomy, abdominoplasty, hernia repairs, myomectomies, and ovarian biopsies). The postsurgical outcomes included in the analysis were postsurgical fever and the presence of seromas, hematomas, and wound dehiscence.1 Twelve of our own patients had a panniculectomy during CD performed by a plastic surgeon. While the preoperative complications of panniculectomy may have been well described, there is a paucity of data in women who underwent the cosmetic procedure at the time of CD. We concluded that the performance of a panniculectomy and tummy tuck as part of a CD does not appear to increase surgical complications in patients with a high body mass index. Our preliminary results and call for further studies were received at the American College of Surgeons 2017 meeting in San Diego.2
Boris Petrikovsky, MD, PhD
Sunny Island Beach, Florida
References
1. Petrikovsky BM, Swancoat S, Zharov EV. Safety of panniculectomy during cesarean section: a prospective, non-randomized study. J Reprod Med. 2019;64:197-200.
2. Petrikovsky BM. Is the combination of panniculectomy and cesarean section safe? Scientific Poster Presentation-Obstetrics and Gynecology. J Am Coll Surg. 2017;225(4 suppl 2):E130.
Dr. Barbieri responds
I agree with Dr. Petrikovsky that advances in the field of obstetrical surgery have been inhibited by a tendency to criticize innovation. Less than 40 years ago, leaders in gynecology did not initially accept the application of minimally invasive gynecology surgical techniques to common gyn procedures including hysterectomy. Every surgical field is rapidly innovating. Obstetrical surgeons should be encouraged to pursue new approaches, as you are doing. We wish you success in your pioneering work.
Continue to: A CASE OF BV...
A CASE OF BV DURING PREGNANCY: BEST MANAGEMENT APPROACH
CALLIE FOX REEDER, MD, AND PATRICK DUFF, MD (ID CONSULT; FEBRUARY 2021)
Secnidazole for treatment of BV
The article by Drs. Reeder and Duff incorrectly states that there are no single-dose therapeutic options for bacterial vaginosis (BV) in the United States. Secnidazole 2 g single oral dose was approved by the US Food and Drug Administration (FDA) in 2017, and it is now included in the American College of Obstetricians and Gynecologists' (ACOG) clinical management guidelines for the treatment of BV in nonpregnant patients.
Secnidazole is not contraindicated in pregnancy. In a poster presented at the 2020 ACOG annual clinical meeting, we summarized results of the preclinical studies that were part of the FDA submission.1 There was no evidence of secnidazole toxicity in fertility and pre- and postnatal reproductive toxicology studies. In addition, there were no adverse developmental outcomes when secnidazole was administered orally to pregnant rats and rabbits during organogenesis at doses up to 4 times the clinical dose. These findings are consistent with the observation that no other preclinical studies, or experience from postmarketing use of secnidazole for approved indications, have suggested a risk of adverse effects when using secnidazole in pregnancy.
Steven E. Chavoustie, MD
North Miami, Florida
Reference
1. Pentikis H, Eder S, Kaufman G, Chavoustie S. Secnidazole, an approved single dose drug for bacterial vaginosis, does not cause reproductive toxicity in animals [16A]. Obstet Gynecol. 2020;135:12S.
Drs. Reeder and Duff respond
We are very appreciative of Dr. Chavoustie's interest in our article and for his thoughtful assessment of the role of single-dose secnidazole for the treatment of BV. As we noted in our article, this drug has been used extensively in Europe and Asia, but there is much less published experience with the drug in the United States. We pointed out the excellent results reported by Hillier and colleagues with 1-g and 2-g doses of this medication.1 Dr. Chavoustie is correct in stating that there is no risk of fetal harm based on animal data at up to 4 times the recommended human dose, although the manufacturer recommends discontinuing breastfeeding during, and for 96 hours after, treatment. According to www.goodrx.com, the cost of a single 2-g dose of secnidazole is $325; the cost of a 7-day course of metronidazole is approximately $16.
Reference
1. Hillier SL, Nyirjesy P, Waldbaum AS, et al. Secnidazole treatment of bacterial vaginosis: a randomized controlled trial. Obstet Gynecol. 2017;130:379-386.
Continue to: OPTIMIZING THE USE OF...
OPTIMIZING THE USE OF OXYTOCIN ON LABOR AND DELIVERY
ROBERT L. BARBIERI, MD (EDITORIAL; JANUARY 2021)
Vigilant labor progress aids in oxytocin optimization
I read with particular interest Dr. Barbieri's editorial on optimizing oxytocin infusion. This topic is relevant for my practice as I am the kind of physician described and I usually get upset when the oxytocin is not managed as I ordered.
In my opinion, several things need clarification. On our unit, the most significant point of controversy is the definition of tachysystole, mainly when we are using a tocodynamometer and not an internal transducer.
I contend that it is quite challenging to ascertain the effectiveness of any given labor pattern based only on the number of contractions. Although we joke about "pit to distress," the truth is that contractions need to be "effective," which to me means strong enough to induce cervical changes.
In my clinical practice, with a tocodynamometer, having 5 contractions that do not produce cervical changes (unless associated with abnormalities of the fetal heart rate tracing) is not a clinically relevant finding as we do not have a way to gauge the strength of such contractions.
I usually employ a mid-range oxytocin protocol, starting at 4 mU per minute and increasing by 4 mU every 20 minutes. Through 30 years of practicing obstetrics, I have found that this protocol renders excellent results in achieving an efficient labor pattern without jeopardizing fetal well-being.
On learning about oxytocin's pharmacokinetics, I still support Dr. Rhonda L. Perry and her colleagues' conclusion that, until we learn better about this aspect of oxytocin pharmacology, each woman is her own bioassay.1 Furthermore, we see this in our daily practice: some patients go into full efficient labor with oxytocin at 4 mU per minute while others at 30 mU per minute do zilch.
Based on the above, I think that optimization requires close vigilance of the labor and the fetal status at any given time, not determining an oxytocin rate of infusion or dosage.
We should be observant on evaluating labor progress, and we should not hesitate to use internal pressure catheters when needed to obtain a more accurate evaluation of the labor pattern.
By examining the patient's labor progress at regular intervals, we also optimize the oxytocin infusion by determining if the infusion is producing the expected cervical changes.
Tomas Hernandez-Mejia, MD
Pasco, Washington
Reference
1. Perry RL, Satin AJ, Barth WH, et al. The pharmacokinetics of oxytocin as they apply to labor induction. Am J Obstet Gynecol. 1996;174:1590-1593.
Dr. Barbieri responds
I thank Dr. Tomas Hernandez-Mejia for sharing his expertise in utilizing a higher dose of oxytocin to optimize labor and birth. Dr. Hernandez-Mejia's view is supported by the recent publication of a high-quality clinical trial showing that a high-dose oxytocin protocol (initial and incremental rate of 6 mIU/min) did not cause an increase in adverse perinatal outcomes compared with a standard-dose protocol (initial and incremental rate of 2 mIU/min) but slightly shortened the duration of labor.1 Based on this clinical trial, my conclusion is that the high-dose protocol, if appropriately monitored for excess uterine contractions and fetal heart rate pattern, is safe.
Reference
1. Son M, Roy A, Stetson BT, et al. High-dose compared with standard-dose oxytocin regimens to augment labor in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2021;137:991-998.
Continue to: PREGNANCY OF UNKNOWN...
PREGNANCY OF UNKNOWN LOCATION: EVIDENCE-BASED EVALUATION AND MANAGEMENT
IRIS G. INSOGNA, MD, AND PAULA C. BRADY, MD (AUGUST 2020)
I would like to thank Dr. Iris Insogna and Dr. Paula Brady for their very informative article on pregnancy of unknown location. However, please allow me to make a suggestion that will clarify terminology for all practicing ObGyns.
The medical literature uses the terms cornual pregnancy and interstitial pregnancy interchangeably, although they are actually very different conditions and have significant different implications. Clinicians are often confused about which is an intrauterine pregnancy and which is a true ectopic pregnancy. This confusion was addressed in a 2006 article in Fertility and Sterility, which explains that a cornual pregnancy refers to the implantation and development of a gestation in one of the upper and lateral portions of the uterus.1 This may occur in a rudimentary horn or in one horn of a septate or bicornuate uterus. Conversely, an interstitial pregnancy is a gestation that implants within the proximal, intramural portion of the fallopian tube that is enveloped by myometrium. Therefore, a cornual pregnancy is actually an intrauterine pregnancy, whereas an interstitial pregnancy is a true ectopic pregnancy.
I hope that all clinicians will read the article in Fertility and Sterility and adopt this terminology to avoid future confusion and misunderstandings.
Alan D. Rosen, MD
Houston, Texas
Reference
1. Malinowski A, Bates SK. Semantics and pitfalls in the diagnosis of cornual/interstitial pregnancy. Fertil Steril. 2006;86:1764.e11-1764.e14.
OBSTETRIC ANAL SPHINCTER INJURY: PREVENTION AND REPAIR
ROBERT L. BARBIERI, MD (EDITORIAL; MAY 2021)
Experience with warm perineal compresses and massage
I have been a midwife for 45 years. I have used warm compresses on the perineum my whole career. I don't need data to tell me it provides comfort. My patients do.
I don't do much massage of the perineum, only slightly while applying K-Y or another water-soluble gel.
A slow, controlled extension of the vertex and healthy tissue is the best way to prevent tears.
Karen Parker, MN, CNM
Ashland, Oregon
Dr. Barbieri responds
I thank Ms. Parker for her clinical recommendation: "Yes to warm compresses" and "Massage of the perineum?" Not so much.
Continue to: CESAREAN MYOMECTOMY...
CESAREAN MYOMECTOMY: SAFE OPERATION OR SURGICAL FOLLY?
ROBERT L. BARBIERI, MD (EDITORIAL; FEBRUARY 2021)
Timely comments on cesarean myomectomy
Dr. Barbieri's editorial on cesarean myomectomy is very timely, especially the quote from Dr. K.S.J. Olah: "The berating I received was severe and disproportionate to the crime. The rule was that myomectomy performed at cesarean section was not just frowned upon but expressly forbidden."
I had a very similar experience with panniculectomy and "tummy tuck" as a part of cesarean delivery (CD). Traditionally, a combination of a CD with any other surgical procedures (myomectomy, abdominoplasty, and so on) has not been accepted in the obstetric community. The main reason for such an opinion has been the unfounded fear of complications of combined procedures, including but not limited to infection, hematomas, and poor wound healing. None of these concerns have been supported by studies. Obvious advantages of combining a CD with other surgical procedures, including abdominoplasty, are obvious: the elimination of a second anesthesia, increased patient satisfaction, and no need for a second surgery.
We reviewed the outcomes in 52 patients who underwent a combination of CD with other procedures (such as panniculectomy, abdominoplasty, hernia repairs, myomectomies, and ovarian biopsies). The postsurgical outcomes included in the analysis were postsurgical fever and the presence of seromas, hematomas, and wound dehiscence.1 Twelve of our own patients had a panniculectomy during CD performed by a plastic surgeon. While the preoperative complications of panniculectomy may have been well described, there is a paucity of data in women who underwent the cosmetic procedure at the time of CD. We concluded that the performance of a panniculectomy and tummy tuck as part of a CD does not appear to increase surgical complications in patients with a high body mass index. Our preliminary results and call for further studies were received at the American College of Surgeons 2017 meeting in San Diego.2
Boris Petrikovsky, MD, PhD
Sunny Island Beach, Florida
References
1. Petrikovsky BM, Swancoat S, Zharov EV. Safety of panniculectomy during cesarean section: a prospective, non-randomized study. J Reprod Med. 2019;64:197-200.
2. Petrikovsky BM. Is the combination of panniculectomy and cesarean section safe? Scientific Poster Presentation-Obstetrics and Gynecology. J Am Coll Surg. 2017;225(4 suppl 2):E130.
Dr. Barbieri responds
I agree with Dr. Petrikovsky that advances in the field of obstetrical surgery have been inhibited by a tendency to criticize innovation. Less than 40 years ago, leaders in gynecology did not initially accept the application of minimally invasive gynecology surgical techniques to common gyn procedures including hysterectomy. Every surgical field is rapidly innovating. Obstetrical surgeons should be encouraged to pursue new approaches, as you are doing. We wish you success in your pioneering work.
Continue to: A CASE OF BV...
A CASE OF BV DURING PREGNANCY: BEST MANAGEMENT APPROACH
CALLIE FOX REEDER, MD, AND PATRICK DUFF, MD (ID CONSULT; FEBRUARY 2021)
Secnidazole for treatment of BV
The article by Drs. Reeder and Duff incorrectly states that there are no single-dose therapeutic options for bacterial vaginosis (BV) in the United States. Secnidazole 2 g single oral dose was approved by the US Food and Drug Administration (FDA) in 2017, and it is now included in the American College of Obstetricians and Gynecologists' (ACOG) clinical management guidelines for the treatment of BV in nonpregnant patients.
Secnidazole is not contraindicated in pregnancy. In a poster presented at the 2020 ACOG annual clinical meeting, we summarized results of the preclinical studies that were part of the FDA submission.1 There was no evidence of secnidazole toxicity in fertility and pre- and postnatal reproductive toxicology studies. In addition, there were no adverse developmental outcomes when secnidazole was administered orally to pregnant rats and rabbits during organogenesis at doses up to 4 times the clinical dose. These findings are consistent with the observation that no other preclinical studies, or experience from postmarketing use of secnidazole for approved indications, have suggested a risk of adverse effects when using secnidazole in pregnancy.
Steven E. Chavoustie, MD
North Miami, Florida
Reference
1. Pentikis H, Eder S, Kaufman G, Chavoustie S. Secnidazole, an approved single dose drug for bacterial vaginosis, does not cause reproductive toxicity in animals [16A]. Obstet Gynecol. 2020;135:12S.
Drs. Reeder and Duff respond
We are very appreciative of Dr. Chavoustie's interest in our article and for his thoughtful assessment of the role of single-dose secnidazole for the treatment of BV. As we noted in our article, this drug has been used extensively in Europe and Asia, but there is much less published experience with the drug in the United States. We pointed out the excellent results reported by Hillier and colleagues with 1-g and 2-g doses of this medication.1 Dr. Chavoustie is correct in stating that there is no risk of fetal harm based on animal data at up to 4 times the recommended human dose, although the manufacturer recommends discontinuing breastfeeding during, and for 96 hours after, treatment. According to www.goodrx.com, the cost of a single 2-g dose of secnidazole is $325; the cost of a 7-day course of metronidazole is approximately $16.
Reference
1. Hillier SL, Nyirjesy P, Waldbaum AS, et al. Secnidazole treatment of bacterial vaginosis: a randomized controlled trial. Obstet Gynecol. 2017;130:379-386.
Continue to: OPTIMIZING THE USE OF...
OPTIMIZING THE USE OF OXYTOCIN ON LABOR AND DELIVERY
ROBERT L. BARBIERI, MD (EDITORIAL; JANUARY 2021)
Vigilant labor progress aids in oxytocin optimization
I read with particular interest Dr. Barbieri's editorial on optimizing oxytocin infusion. This topic is relevant for my practice as I am the kind of physician described and I usually get upset when the oxytocin is not managed as I ordered.
In my opinion, several things need clarification. On our unit, the most significant point of controversy is the definition of tachysystole, mainly when we are using a tocodynamometer and not an internal transducer.
I contend that it is quite challenging to ascertain the effectiveness of any given labor pattern based only on the number of contractions. Although we joke about "pit to distress," the truth is that contractions need to be "effective," which to me means strong enough to induce cervical changes.
In my clinical practice, with a tocodynamometer, having 5 contractions that do not produce cervical changes (unless associated with abnormalities of the fetal heart rate tracing) is not a clinically relevant finding as we do not have a way to gauge the strength of such contractions.
I usually employ a mid-range oxytocin protocol, starting at 4 mU per minute and increasing by 4 mU every 20 minutes. Through 30 years of practicing obstetrics, I have found that this protocol renders excellent results in achieving an efficient labor pattern without jeopardizing fetal well-being.
On learning about oxytocin's pharmacokinetics, I still support Dr. Rhonda L. Perry and her colleagues' conclusion that, until we learn better about this aspect of oxytocin pharmacology, each woman is her own bioassay.1 Furthermore, we see this in our daily practice: some patients go into full efficient labor with oxytocin at 4 mU per minute while others at 30 mU per minute do zilch.
Based on the above, I think that optimization requires close vigilance of the labor and the fetal status at any given time, not determining an oxytocin rate of infusion or dosage.
We should be observant on evaluating labor progress, and we should not hesitate to use internal pressure catheters when needed to obtain a more accurate evaluation of the labor pattern.
By examining the patient's labor progress at regular intervals, we also optimize the oxytocin infusion by determining if the infusion is producing the expected cervical changes.
Tomas Hernandez-Mejia, MD
Pasco, Washington
Reference
1. Perry RL, Satin AJ, Barth WH, et al. The pharmacokinetics of oxytocin as they apply to labor induction. Am J Obstet Gynecol. 1996;174:1590-1593.
Dr. Barbieri responds
I thank Dr. Tomas Hernandez-Mejia for sharing his expertise in utilizing a higher dose of oxytocin to optimize labor and birth. Dr. Hernandez-Mejia's view is supported by the recent publication of a high-quality clinical trial showing that a high-dose oxytocin protocol (initial and incremental rate of 6 mIU/min) did not cause an increase in adverse perinatal outcomes compared with a standard-dose protocol (initial and incremental rate of 2 mIU/min) but slightly shortened the duration of labor.1 Based on this clinical trial, my conclusion is that the high-dose protocol, if appropriately monitored for excess uterine contractions and fetal heart rate pattern, is safe.
Reference
1. Son M, Roy A, Stetson BT, et al. High-dose compared with standard-dose oxytocin regimens to augment labor in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2021;137:991-998.
Continue to: PREGNANCY OF UNKNOWN...
PREGNANCY OF UNKNOWN LOCATION: EVIDENCE-BASED EVALUATION AND MANAGEMENT
IRIS G. INSOGNA, MD, AND PAULA C. BRADY, MD (AUGUST 2020)
I would like to thank Dr. Iris Insogna and Dr. Paula Brady for their very informative article on pregnancy of unknown location. However, please allow me to make a suggestion that will clarify terminology for all practicing ObGyns.
The medical literature uses the terms cornual pregnancy and interstitial pregnancy interchangeably, although they are actually very different conditions and have significant different implications. Clinicians are often confused about which is an intrauterine pregnancy and which is a true ectopic pregnancy. This confusion was addressed in a 2006 article in Fertility and Sterility, which explains that a cornual pregnancy refers to the implantation and development of a gestation in one of the upper and lateral portions of the uterus.1 This may occur in a rudimentary horn or in one horn of a septate or bicornuate uterus. Conversely, an interstitial pregnancy is a gestation that implants within the proximal, intramural portion of the fallopian tube that is enveloped by myometrium. Therefore, a cornual pregnancy is actually an intrauterine pregnancy, whereas an interstitial pregnancy is a true ectopic pregnancy.
I hope that all clinicians will read the article in Fertility and Sterility and adopt this terminology to avoid future confusion and misunderstandings.
Alan D. Rosen, MD
Houston, Texas
Reference
1. Malinowski A, Bates SK. Semantics and pitfalls in the diagnosis of cornual/interstitial pregnancy. Fertil Steril. 2006;86:1764.e11-1764.e14.
OBSTETRIC ANAL SPHINCTER INJURY: PREVENTION AND REPAIR
ROBERT L. BARBIERI, MD (EDITORIAL; MAY 2021)
Experience with warm perineal compresses and massage
I have been a midwife for 45 years. I have used warm compresses on the perineum my whole career. I don't need data to tell me it provides comfort. My patients do.
I don't do much massage of the perineum, only slightly while applying K-Y or another water-soluble gel.
A slow, controlled extension of the vertex and healthy tissue is the best way to prevent tears.
Karen Parker, MN, CNM
Ashland, Oregon
Dr. Barbieri responds
I thank Ms. Parker for her clinical recommendation: "Yes to warm compresses" and "Massage of the perineum?" Not so much.
Continue to: CESAREAN MYOMECTOMY...
CESAREAN MYOMECTOMY: SAFE OPERATION OR SURGICAL FOLLY?
ROBERT L. BARBIERI, MD (EDITORIAL; FEBRUARY 2021)
Timely comments on cesarean myomectomy
Dr. Barbieri's editorial on cesarean myomectomy is very timely, especially the quote from Dr. K.S.J. Olah: "The berating I received was severe and disproportionate to the crime. The rule was that myomectomy performed at cesarean section was not just frowned upon but expressly forbidden."
I had a very similar experience with panniculectomy and "tummy tuck" as a part of cesarean delivery (CD). Traditionally, a combination of a CD with any other surgical procedures (myomectomy, abdominoplasty, and so on) has not been accepted in the obstetric community. The main reason for such an opinion has been the unfounded fear of complications of combined procedures, including but not limited to infection, hematomas, and poor wound healing. None of these concerns have been supported by studies. Obvious advantages of combining a CD with other surgical procedures, including abdominoplasty, are obvious: the elimination of a second anesthesia, increased patient satisfaction, and no need for a second surgery.
We reviewed the outcomes in 52 patients who underwent a combination of CD with other procedures (such as panniculectomy, abdominoplasty, hernia repairs, myomectomies, and ovarian biopsies). The postsurgical outcomes included in the analysis were postsurgical fever and the presence of seromas, hematomas, and wound dehiscence.1 Twelve of our own patients had a panniculectomy during CD performed by a plastic surgeon. While the preoperative complications of panniculectomy may have been well described, there is a paucity of data in women who underwent the cosmetic procedure at the time of CD. We concluded that the performance of a panniculectomy and tummy tuck as part of a CD does not appear to increase surgical complications in patients with a high body mass index. Our preliminary results and call for further studies were received at the American College of Surgeons 2017 meeting in San Diego.2
Boris Petrikovsky, MD, PhD
Sunny Island Beach, Florida
References
1. Petrikovsky BM, Swancoat S, Zharov EV. Safety of panniculectomy during cesarean section: a prospective, non-randomized study. J Reprod Med. 2019;64:197-200.
2. Petrikovsky BM. Is the combination of panniculectomy and cesarean section safe? Scientific Poster Presentation-Obstetrics and Gynecology. J Am Coll Surg. 2017;225(4 suppl 2):E130.
Dr. Barbieri responds
I agree with Dr. Petrikovsky that advances in the field of obstetrical surgery have been inhibited by a tendency to criticize innovation. Less than 40 years ago, leaders in gynecology did not initially accept the application of minimally invasive gynecology surgical techniques to common gyn procedures including hysterectomy. Every surgical field is rapidly innovating. Obstetrical surgeons should be encouraged to pursue new approaches, as you are doing. We wish you success in your pioneering work.
Continue to: A CASE OF BV...
A CASE OF BV DURING PREGNANCY: BEST MANAGEMENT APPROACH
CALLIE FOX REEDER, MD, AND PATRICK DUFF, MD (ID CONSULT; FEBRUARY 2021)
Secnidazole for treatment of BV
The article by Drs. Reeder and Duff incorrectly states that there are no single-dose therapeutic options for bacterial vaginosis (BV) in the United States. Secnidazole 2 g single oral dose was approved by the US Food and Drug Administration (FDA) in 2017, and it is now included in the American College of Obstetricians and Gynecologists' (ACOG) clinical management guidelines for the treatment of BV in nonpregnant patients.
Secnidazole is not contraindicated in pregnancy. In a poster presented at the 2020 ACOG annual clinical meeting, we summarized results of the preclinical studies that were part of the FDA submission.1 There was no evidence of secnidazole toxicity in fertility and pre- and postnatal reproductive toxicology studies. In addition, there were no adverse developmental outcomes when secnidazole was administered orally to pregnant rats and rabbits during organogenesis at doses up to 4 times the clinical dose. These findings are consistent with the observation that no other preclinical studies, or experience from postmarketing use of secnidazole for approved indications, have suggested a risk of adverse effects when using secnidazole in pregnancy.
Steven E. Chavoustie, MD
North Miami, Florida
Reference
1. Pentikis H, Eder S, Kaufman G, Chavoustie S. Secnidazole, an approved single dose drug for bacterial vaginosis, does not cause reproductive toxicity in animals [16A]. Obstet Gynecol. 2020;135:12S.
Drs. Reeder and Duff respond
We are very appreciative of Dr. Chavoustie's interest in our article and for his thoughtful assessment of the role of single-dose secnidazole for the treatment of BV. As we noted in our article, this drug has been used extensively in Europe and Asia, but there is much less published experience with the drug in the United States. We pointed out the excellent results reported by Hillier and colleagues with 1-g and 2-g doses of this medication.1 Dr. Chavoustie is correct in stating that there is no risk of fetal harm based on animal data at up to 4 times the recommended human dose, although the manufacturer recommends discontinuing breastfeeding during, and for 96 hours after, treatment. According to www.goodrx.com, the cost of a single 2-g dose of secnidazole is $325; the cost of a 7-day course of metronidazole is approximately $16.
Reference
1. Hillier SL, Nyirjesy P, Waldbaum AS, et al. Secnidazole treatment of bacterial vaginosis: a randomized controlled trial. Obstet Gynecol. 2017;130:379-386.
Continue to: OPTIMIZING THE USE OF...
OPTIMIZING THE USE OF OXYTOCIN ON LABOR AND DELIVERY
ROBERT L. BARBIERI, MD (EDITORIAL; JANUARY 2021)
Vigilant labor progress aids in oxytocin optimization
I read with particular interest Dr. Barbieri's editorial on optimizing oxytocin infusion. This topic is relevant for my practice as I am the kind of physician described and I usually get upset when the oxytocin is not managed as I ordered.
In my opinion, several things need clarification. On our unit, the most significant point of controversy is the definition of tachysystole, mainly when we are using a tocodynamometer and not an internal transducer.
I contend that it is quite challenging to ascertain the effectiveness of any given labor pattern based only on the number of contractions. Although we joke about "pit to distress," the truth is that contractions need to be "effective," which to me means strong enough to induce cervical changes.
In my clinical practice, with a tocodynamometer, having 5 contractions that do not produce cervical changes (unless associated with abnormalities of the fetal heart rate tracing) is not a clinically relevant finding as we do not have a way to gauge the strength of such contractions.
I usually employ a mid-range oxytocin protocol, starting at 4 mU per minute and increasing by 4 mU every 20 minutes. Through 30 years of practicing obstetrics, I have found that this protocol renders excellent results in achieving an efficient labor pattern without jeopardizing fetal well-being.
On learning about oxytocin's pharmacokinetics, I still support Dr. Rhonda L. Perry and her colleagues' conclusion that, until we learn better about this aspect of oxytocin pharmacology, each woman is her own bioassay.1 Furthermore, we see this in our daily practice: some patients go into full efficient labor with oxytocin at 4 mU per minute while others at 30 mU per minute do zilch.
Based on the above, I think that optimization requires close vigilance of the labor and the fetal status at any given time, not determining an oxytocin rate of infusion or dosage.
We should be observant on evaluating labor progress, and we should not hesitate to use internal pressure catheters when needed to obtain a more accurate evaluation of the labor pattern.
By examining the patient's labor progress at regular intervals, we also optimize the oxytocin infusion by determining if the infusion is producing the expected cervical changes.
Tomas Hernandez-Mejia, MD
Pasco, Washington
Reference
1. Perry RL, Satin AJ, Barth WH, et al. The pharmacokinetics of oxytocin as they apply to labor induction. Am J Obstet Gynecol. 1996;174:1590-1593.
Dr. Barbieri responds
I thank Dr. Tomas Hernandez-Mejia for sharing his expertise in utilizing a higher dose of oxytocin to optimize labor and birth. Dr. Hernandez-Mejia's view is supported by the recent publication of a high-quality clinical trial showing that a high-dose oxytocin protocol (initial and incremental rate of 6 mIU/min) did not cause an increase in adverse perinatal outcomes compared with a standard-dose protocol (initial and incremental rate of 2 mIU/min) but slightly shortened the duration of labor.1 Based on this clinical trial, my conclusion is that the high-dose protocol, if appropriately monitored for excess uterine contractions and fetal heart rate pattern, is safe.
Reference
1. Son M, Roy A, Stetson BT, et al. High-dose compared with standard-dose oxytocin regimens to augment labor in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2021;137:991-998.
Continue to: PREGNANCY OF UNKNOWN...
PREGNANCY OF UNKNOWN LOCATION: EVIDENCE-BASED EVALUATION AND MANAGEMENT
IRIS G. INSOGNA, MD, AND PAULA C. BRADY, MD (AUGUST 2020)
I would like to thank Dr. Iris Insogna and Dr. Paula Brady for their very informative article on pregnancy of unknown location. However, please allow me to make a suggestion that will clarify terminology for all practicing ObGyns.
The medical literature uses the terms cornual pregnancy and interstitial pregnancy interchangeably, although they are actually very different conditions and have significant different implications. Clinicians are often confused about which is an intrauterine pregnancy and which is a true ectopic pregnancy. This confusion was addressed in a 2006 article in Fertility and Sterility, which explains that a cornual pregnancy refers to the implantation and development of a gestation in one of the upper and lateral portions of the uterus.1 This may occur in a rudimentary horn or in one horn of a septate or bicornuate uterus. Conversely, an interstitial pregnancy is a gestation that implants within the proximal, intramural portion of the fallopian tube that is enveloped by myometrium. Therefore, a cornual pregnancy is actually an intrauterine pregnancy, whereas an interstitial pregnancy is a true ectopic pregnancy.
I hope that all clinicians will read the article in Fertility and Sterility and adopt this terminology to avoid future confusion and misunderstandings.
Alan D. Rosen, MD
Houston, Texas
Reference
1. Malinowski A, Bates SK. Semantics and pitfalls in the diagnosis of cornual/interstitial pregnancy. Fertil Steril. 2006;86:1764.e11-1764.e14.
Top 12 tips for research success in fellowship and early academic faculty years
Congratulations! You have matched in a competitive medical subspecialty or you have secured your first faculty position. But what do you do now? Success in your early career – as a new fellow or a new attending – requires both hard work and perseverance. We present our top 12 tips for how to be successful as you transition into your new position.

Tip #1: Be kind to yourself
As you transition from medical resident to GI fellow or from GI fellow to first-time attending, it is important to recognize that you are going through a major career transition (not as major as fourth year to intern, but probably a close second). First and foremost, remember to be kind to yourself and set reasonable expectations. You need to allow yourself time to transition to a new role which may also be in a new city or state. Take care of yourself – don’t forget to exercise, eat well, and sleep. You are in the long game now. Work to get yourself in a routine that is sustainable. Block out time to exercise, explore your new city, meal plan, and pursue your interests outside of medicine.
Tip #2: Set up for success
Since you are going through this major life/career transition, it is really helpful if you can set yourself up for success by having some projects that are easily completed during this challenging time so that you can demonstrate success. If you have projects in different stages of development, you will always have something you can work on when some projects are delayed for reasons outside of your control. In particular, it is great to have a few papers ready to go during late fellowship so they are published during your first year as an academic attending! This will allow you to continue your research trajectory as you learn the ropes of your new position.
Tip #3: Ask for help
It turns out you cannot do everything on your own! Make sure you are getting help professionally and personally so that you are set up for success. It’s okay to feel overwhelmed or confused; we all do at some point or another. Fellowship and early academic faculty years are stressful and nobody expects you to do it alone. Chances are your mentors or cofellows have had similar struggles, and in opening up, this dialogue may help you both.
Tip #4: Write out your 5-year plan
You need to know where you are going before you can figure out how to get there. Take some time for “soul searching”: Think about where you would like to be in 5 years and work backward (along with help from your mentors; see Tip #5) to determine how best to get there. If you think a career in academia might be for you, it’s never too soon to start networking and involving yourself in research. If a specific institution or clinical position draws your attention, check out the current faculty. You can use their CVs as a roadmap of types of experiences and honors that should be on your radar throughout these 5 years. Remember that your 5-year plan is not written in stone – this is something that you should re-evaluate as your interests and priorities change throughout your career.
Tip #5: Develop your personal ‘Board of Directors’
Instead of trying to find the perfect mentor, we suggest you seek out a personal “Board of Directors” who can serve as your mentoring team. There will never be a single perfect mentor for you and it is likely that you will need separate mentors to help guide you on different aspects of your career. I personally have separate individuals serving as my clinical mentor, my research content mentor, my research methods mentor, my career mentor, and my personal/life mentor. Having multiple mentors allows you to maximize the impact of your different mentors’ strengths across each component of your career. Further, your mentors themselves may have past histories of collaboration that you may then leverage to buoy your own fledgling career. When deciding on who to choose as a mentor, it is important to talk to prior mentees about their experiences with a mentor to help you decide if you may be a good match.
Tip #6: Master the art of “Menteering”
Now that you have identified mentors, you need to do your part in nurturing this mentee-mentor relationship. Be an excellent mentee: Show up, stick to a timeline, bring ideas and enthusiasm, and make it easy for your mentor. Your mentors want to see you succeed and sometimes this requires you to help them help you. If you know your own learning style and how you like to interact, have that conversation with your mentor upfront (for example, you may need strict deadlines or you may prefer having more time to develop ideas). Having these conversations before you start a project or a relationship will help set the expectations and ensure effective communication with your mentor. If you find that your mentor is doing something that hinders your progress, such as asking for updates too often or not checking in enough, have a constructive conversation with them about how you feel. Come prepared for meetings with your mentor with an agenda and timeline. Be specific if there is something you need from your mentor and be respectful of their other commitments. For example, if you would like your mentor to review your grant application, let them know the grant deadline and find out when you need to get them a draft so that they will have time to provide meaningful feedback.
Tip #7: Identify sponsors
Equally, if not more important than your mentoring team, are sponsors. These are people in positions of power who will promote you and help push your career forward. Sponsors can be people more senior to you, cofellows, or even acquaintances in industry or pharmaceuticals. Your mentor may also be your sponsor, but not always. As early academic faculty, it is important to get your name out there with speaking engagements related to your clinical and research niche, and that is one way a sponsor can help bolster your career.
Tip #8: Develop your personal brand – what is on your T-shirt?
As medicine becomes more and more subspecialized, finding your brand is becoming increasingly important. A brand could be anything from your academic niche to social justice, or even social media utilization. Your brand should encompass what you are naturally excited by within your field. Finding your brand will not only distinguish you from your peers but will also provide you with expertise which you can then offer to your colleagues, near and far. Practice the “elevator pitch” of your personal brand so that you can effectively (and efficiently) describe yourself and your interests when meeting new people and networking.
Tip #9: Meet thought leaders in your field
Think of the top five or six most prominent and influential people in your area of clinical or research interest and introduce yourself. This can be done at a national meeting or simply over email, though in person is always best if possible. Although thought leaders are busy, in my experience, if you are persistent, you can always find a few minutes to make an introduction. I’ve shared cab rides just to get a few minutes of someone’s time. In my first few years on faculty, I met with most of the thought leaders in my field; some of these meetings led to fruitful collaborations and important introductions (see tip #7). Meet others at your career level too. They can be great to bounce ideas off, and they will be future leaders in the field. Inviting thought leaders to come to your institution to give talks (in-person or virtually) is another great way to show your interest in their work and also find time to introduce yourself.
Tip #10: Apply, apply, apply
Remember that feedback is a gift and the best way to receive feedback is to apply to as many opportunities as you can. Any successful person in GI will have a ‘CV of failures’ far longer than their actual CV documenting their successes. I applied to 8 grants before landing my first one, but I received invaluable feedback and improved my writing skills in the process. Success in fellowship and early faculty takes immense grit – work on building a thick skin and finding the learning opportunity within any outcome.
Tip #11: Don’t get sucked into the email abyss
It is easy to fill your time completing low priority, but easy to complete, tasks such as responding to emails. Time management is key and you need to make sure that you dedicate time to more time-consuming tasks – such as writing and developing projects/grants – that have a high reward. Dedicate time on your calendar for high-priority tasks and make sure you don’t open your email during this time. Turn off the email pop-up window and do emails at the end of the day (or whenever you are done writing and thinking). Limiting distractions will help get your creative juices flowing.
Tip #12: Don’t always say yes
In fact, don’t ever say yes to a career or research opportunity within the first 24 hours to allow yourself time to weigh the pros and cons of the commitment, to assess the timeline feasibility, and to decide it fits into your 5-year plan. You can say you need to talk to your mentor about it first. If you decide you cannot accept an opportunity, a great way to mitigate that is to simply say “I’d love to, but my mentor says no.” Act as a sponsor to someone else by suggesting a potential colleague who might be interested in the opportunity. As you accept more responsibilities, think about what you might be able to give up to give yourself time to be successful in this new opportunity (and not distract from yourself or your 5-year plan).
Conclusion
Success in research and early academic faculty years takes planning and determination. We hope these tips provide a broad outline for what to think about and how to approach planning your future career. First and foremost, you must put in the time to think about what you really want and what will make you happy in the long run. Academic success is a broad term that each of us defines differently. What does it mean to you? Once you figure that out, make your 5-year plan and run with it!
Dr. Rebello and Dr. Long are with section of gastroenterology at Boston Medical Center and Boston University. They have no conflicts to report.
Congratulations! You have matched in a competitive medical subspecialty or you have secured your first faculty position. But what do you do now? Success in your early career – as a new fellow or a new attending – requires both hard work and perseverance. We present our top 12 tips for how to be successful as you transition into your new position.
Tip #1: Be kind to yourself
As you transition from medical resident to GI fellow or from GI fellow to first-time attending, it is important to recognize that you are going through a major career transition (not as major as fourth year to intern, but probably a close second). First and foremost, remember to be kind to yourself and set reasonable expectations. You need to allow yourself time to transition to a new role which may also be in a new city or state. Take care of yourself – don’t forget to exercise, eat well, and sleep. You are in the long game now. Work to get yourself in a routine that is sustainable. Block out time to exercise, explore your new city, meal plan, and pursue your interests outside of medicine.
Tip #2: Set up for success
Since you are going through this major life/career transition, it is really helpful if you can set yourself up for success by having some projects that are easily completed during this challenging time so that you can demonstrate success. If you have projects in different stages of development, you will always have something you can work on when some projects are delayed for reasons outside of your control. In particular, it is great to have a few papers ready to go during late fellowship so they are published during your first year as an academic attending! This will allow you to continue your research trajectory as you learn the ropes of your new position.
Tip #3: Ask for help
It turns out you cannot do everything on your own! Make sure you are getting help professionally and personally so that you are set up for success. It’s okay to feel overwhelmed or confused; we all do at some point or another. Fellowship and early academic faculty years are stressful and nobody expects you to do it alone. Chances are your mentors or cofellows have had similar struggles, and in opening up, this dialogue may help you both.
Tip #4: Write out your 5-year plan
You need to know where you are going before you can figure out how to get there. Take some time for “soul searching”: Think about where you would like to be in 5 years and work backward (along with help from your mentors; see Tip #5) to determine how best to get there. If you think a career in academia might be for you, it’s never too soon to start networking and involving yourself in research. If a specific institution or clinical position draws your attention, check out the current faculty. You can use their CVs as a roadmap of types of experiences and honors that should be on your radar throughout these 5 years. Remember that your 5-year plan is not written in stone – this is something that you should re-evaluate as your interests and priorities change throughout your career.
Tip #5: Develop your personal ‘Board of Directors’
Instead of trying to find the perfect mentor, we suggest you seek out a personal “Board of Directors” who can serve as your mentoring team. There will never be a single perfect mentor for you and it is likely that you will need separate mentors to help guide you on different aspects of your career. I personally have separate individuals serving as my clinical mentor, my research content mentor, my research methods mentor, my career mentor, and my personal/life mentor. Having multiple mentors allows you to maximize the impact of your different mentors’ strengths across each component of your career. Further, your mentors themselves may have past histories of collaboration that you may then leverage to buoy your own fledgling career. When deciding on who to choose as a mentor, it is important to talk to prior mentees about their experiences with a mentor to help you decide if you may be a good match.
Tip #6: Master the art of “Menteering”
Now that you have identified mentors, you need to do your part in nurturing this mentee-mentor relationship. Be an excellent mentee: Show up, stick to a timeline, bring ideas and enthusiasm, and make it easy for your mentor. Your mentors want to see you succeed and sometimes this requires you to help them help you. If you know your own learning style and how you like to interact, have that conversation with your mentor upfront (for example, you may need strict deadlines or you may prefer having more time to develop ideas). Having these conversations before you start a project or a relationship will help set the expectations and ensure effective communication with your mentor. If you find that your mentor is doing something that hinders your progress, such as asking for updates too often or not checking in enough, have a constructive conversation with them about how you feel. Come prepared for meetings with your mentor with an agenda and timeline. Be specific if there is something you need from your mentor and be respectful of their other commitments. For example, if you would like your mentor to review your grant application, let them know the grant deadline and find out when you need to get them a draft so that they will have time to provide meaningful feedback.
Tip #7: Identify sponsors
Equally, if not more important than your mentoring team, are sponsors. These are people in positions of power who will promote you and help push your career forward. Sponsors can be people more senior to you, cofellows, or even acquaintances in industry or pharmaceuticals. Your mentor may also be your sponsor, but not always. As early academic faculty, it is important to get your name out there with speaking engagements related to your clinical and research niche, and that is one way a sponsor can help bolster your career.
Tip #8: Develop your personal brand – what is on your T-shirt?
As medicine becomes more and more subspecialized, finding your brand is becoming increasingly important. A brand could be anything from your academic niche to social justice, or even social media utilization. Your brand should encompass what you are naturally excited by within your field. Finding your brand will not only distinguish you from your peers but will also provide you with expertise which you can then offer to your colleagues, near and far. Practice the “elevator pitch” of your personal brand so that you can effectively (and efficiently) describe yourself and your interests when meeting new people and networking.
Tip #9: Meet thought leaders in your field
Think of the top five or six most prominent and influential people in your area of clinical or research interest and introduce yourself. This can be done at a national meeting or simply over email, though in person is always best if possible. Although thought leaders are busy, in my experience, if you are persistent, you can always find a few minutes to make an introduction. I’ve shared cab rides just to get a few minutes of someone’s time. In my first few years on faculty, I met with most of the thought leaders in my field; some of these meetings led to fruitful collaborations and important introductions (see tip #7). Meet others at your career level too. They can be great to bounce ideas off, and they will be future leaders in the field. Inviting thought leaders to come to your institution to give talks (in-person or virtually) is another great way to show your interest in their work and also find time to introduce yourself.
Tip #10: Apply, apply, apply
Remember that feedback is a gift and the best way to receive feedback is to apply to as many opportunities as you can. Any successful person in GI will have a ‘CV of failures’ far longer than their actual CV documenting their successes. I applied to 8 grants before landing my first one, but I received invaluable feedback and improved my writing skills in the process. Success in fellowship and early faculty takes immense grit – work on building a thick skin and finding the learning opportunity within any outcome.
Tip #11: Don’t get sucked into the email abyss
It is easy to fill your time completing low priority, but easy to complete, tasks such as responding to emails. Time management is key and you need to make sure that you dedicate time to more time-consuming tasks – such as writing and developing projects/grants – that have a high reward. Dedicate time on your calendar for high-priority tasks and make sure you don’t open your email during this time. Turn off the email pop-up window and do emails at the end of the day (or whenever you are done writing and thinking). Limiting distractions will help get your creative juices flowing.
Tip #12: Don’t always say yes
In fact, don’t ever say yes to a career or research opportunity within the first 24 hours to allow yourself time to weigh the pros and cons of the commitment, to assess the timeline feasibility, and to decide it fits into your 5-year plan. You can say you need to talk to your mentor about it first. If you decide you cannot accept an opportunity, a great way to mitigate that is to simply say “I’d love to, but my mentor says no.” Act as a sponsor to someone else by suggesting a potential colleague who might be interested in the opportunity. As you accept more responsibilities, think about what you might be able to give up to give yourself time to be successful in this new opportunity (and not distract from yourself or your 5-year plan).
Conclusion
Success in research and early academic faculty years takes planning and determination. We hope these tips provide a broad outline for what to think about and how to approach planning your future career. First and foremost, you must put in the time to think about what you really want and what will make you happy in the long run. Academic success is a broad term that each of us defines differently. What does it mean to you? Once you figure that out, make your 5-year plan and run with it!
Dr. Rebello and Dr. Long are with section of gastroenterology at Boston Medical Center and Boston University. They have no conflicts to report.
Congratulations! You have matched in a competitive medical subspecialty or you have secured your first faculty position. But what do you do now? Success in your early career – as a new fellow or a new attending – requires both hard work and perseverance. We present our top 12 tips for how to be successful as you transition into your new position.
Tip #1: Be kind to yourself
As you transition from medical resident to GI fellow or from GI fellow to first-time attending, it is important to recognize that you are going through a major career transition (not as major as fourth year to intern, but probably a close second). First and foremost, remember to be kind to yourself and set reasonable expectations. You need to allow yourself time to transition to a new role which may also be in a new city or state. Take care of yourself – don’t forget to exercise, eat well, and sleep. You are in the long game now. Work to get yourself in a routine that is sustainable. Block out time to exercise, explore your new city, meal plan, and pursue your interests outside of medicine.
Tip #2: Set up for success
Since you are going through this major life/career transition, it is really helpful if you can set yourself up for success by having some projects that are easily completed during this challenging time so that you can demonstrate success. If you have projects in different stages of development, you will always have something you can work on when some projects are delayed for reasons outside of your control. In particular, it is great to have a few papers ready to go during late fellowship so they are published during your first year as an academic attending! This will allow you to continue your research trajectory as you learn the ropes of your new position.
Tip #3: Ask for help
It turns out you cannot do everything on your own! Make sure you are getting help professionally and personally so that you are set up for success. It’s okay to feel overwhelmed or confused; we all do at some point or another. Fellowship and early academic faculty years are stressful and nobody expects you to do it alone. Chances are your mentors or cofellows have had similar struggles, and in opening up, this dialogue may help you both.
Tip #4: Write out your 5-year plan
You need to know where you are going before you can figure out how to get there. Take some time for “soul searching”: Think about where you would like to be in 5 years and work backward (along with help from your mentors; see Tip #5) to determine how best to get there. If you think a career in academia might be for you, it’s never too soon to start networking and involving yourself in research. If a specific institution or clinical position draws your attention, check out the current faculty. You can use their CVs as a roadmap of types of experiences and honors that should be on your radar throughout these 5 years. Remember that your 5-year plan is not written in stone – this is something that you should re-evaluate as your interests and priorities change throughout your career.
Tip #5: Develop your personal ‘Board of Directors’
Instead of trying to find the perfect mentor, we suggest you seek out a personal “Board of Directors” who can serve as your mentoring team. There will never be a single perfect mentor for you and it is likely that you will need separate mentors to help guide you on different aspects of your career. I personally have separate individuals serving as my clinical mentor, my research content mentor, my research methods mentor, my career mentor, and my personal/life mentor. Having multiple mentors allows you to maximize the impact of your different mentors’ strengths across each component of your career. Further, your mentors themselves may have past histories of collaboration that you may then leverage to buoy your own fledgling career. When deciding on who to choose as a mentor, it is important to talk to prior mentees about their experiences with a mentor to help you decide if you may be a good match.
Tip #6: Master the art of “Menteering”
Now that you have identified mentors, you need to do your part in nurturing this mentee-mentor relationship. Be an excellent mentee: Show up, stick to a timeline, bring ideas and enthusiasm, and make it easy for your mentor. Your mentors want to see you succeed and sometimes this requires you to help them help you. If you know your own learning style and how you like to interact, have that conversation with your mentor upfront (for example, you may need strict deadlines or you may prefer having more time to develop ideas). Having these conversations before you start a project or a relationship will help set the expectations and ensure effective communication with your mentor. If you find that your mentor is doing something that hinders your progress, such as asking for updates too often or not checking in enough, have a constructive conversation with them about how you feel. Come prepared for meetings with your mentor with an agenda and timeline. Be specific if there is something you need from your mentor and be respectful of their other commitments. For example, if you would like your mentor to review your grant application, let them know the grant deadline and find out when you need to get them a draft so that they will have time to provide meaningful feedback.
Tip #7: Identify sponsors
Equally, if not more important than your mentoring team, are sponsors. These are people in positions of power who will promote you and help push your career forward. Sponsors can be people more senior to you, cofellows, or even acquaintances in industry or pharmaceuticals. Your mentor may also be your sponsor, but not always. As early academic faculty, it is important to get your name out there with speaking engagements related to your clinical and research niche, and that is one way a sponsor can help bolster your career.
Tip #8: Develop your personal brand – what is on your T-shirt?
As medicine becomes more and more subspecialized, finding your brand is becoming increasingly important. A brand could be anything from your academic niche to social justice, or even social media utilization. Your brand should encompass what you are naturally excited by within your field. Finding your brand will not only distinguish you from your peers but will also provide you with expertise which you can then offer to your colleagues, near and far. Practice the “elevator pitch” of your personal brand so that you can effectively (and efficiently) describe yourself and your interests when meeting new people and networking.
Tip #9: Meet thought leaders in your field
Think of the top five or six most prominent and influential people in your area of clinical or research interest and introduce yourself. This can be done at a national meeting or simply over email, though in person is always best if possible. Although thought leaders are busy, in my experience, if you are persistent, you can always find a few minutes to make an introduction. I’ve shared cab rides just to get a few minutes of someone’s time. In my first few years on faculty, I met with most of the thought leaders in my field; some of these meetings led to fruitful collaborations and important introductions (see tip #7). Meet others at your career level too. They can be great to bounce ideas off, and they will be future leaders in the field. Inviting thought leaders to come to your institution to give talks (in-person or virtually) is another great way to show your interest in their work and also find time to introduce yourself.
Tip #10: Apply, apply, apply
Remember that feedback is a gift and the best way to receive feedback is to apply to as many opportunities as you can. Any successful person in GI will have a ‘CV of failures’ far longer than their actual CV documenting their successes. I applied to 8 grants before landing my first one, but I received invaluable feedback and improved my writing skills in the process. Success in fellowship and early faculty takes immense grit – work on building a thick skin and finding the learning opportunity within any outcome.
Tip #11: Don’t get sucked into the email abyss
It is easy to fill your time completing low priority, but easy to complete, tasks such as responding to emails. Time management is key and you need to make sure that you dedicate time to more time-consuming tasks – such as writing and developing projects/grants – that have a high reward. Dedicate time on your calendar for high-priority tasks and make sure you don’t open your email during this time. Turn off the email pop-up window and do emails at the end of the day (or whenever you are done writing and thinking). Limiting distractions will help get your creative juices flowing.
Tip #12: Don’t always say yes
In fact, don’t ever say yes to a career or research opportunity within the first 24 hours to allow yourself time to weigh the pros and cons of the commitment, to assess the timeline feasibility, and to decide it fits into your 5-year plan. You can say you need to talk to your mentor about it first. If you decide you cannot accept an opportunity, a great way to mitigate that is to simply say “I’d love to, but my mentor says no.” Act as a sponsor to someone else by suggesting a potential colleague who might be interested in the opportunity. As you accept more responsibilities, think about what you might be able to give up to give yourself time to be successful in this new opportunity (and not distract from yourself or your 5-year plan).
Conclusion
Success in research and early academic faculty years takes planning and determination. We hope these tips provide a broad outline for what to think about and how to approach planning your future career. First and foremost, you must put in the time to think about what you really want and what will make you happy in the long run. Academic success is a broad term that each of us defines differently. What does it mean to you? Once you figure that out, make your 5-year plan and run with it!
Dr. Rebello and Dr. Long are with section of gastroenterology at Boston Medical Center and Boston University. They have no conflicts to report.
Malignancy risk: Secukinumab shows long-term safety for psoriasis, PsA, ankylosing spondylitis
that included 49 clinical trials.

Secukinumab (Cosentyx), an interleukin-17A antagonist, is approved for several conditions: moderate to severe psoriasis in children and adults, PsA, ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis.
Although secukinumab has demonstrated safety and tolerability, data on long-term malignancy rates are limited, wrote Mark Lebwohl, MD, professor of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and coauthors.
In a study published in the British Journal of Dermatology, they analyzed the combined safety data from clinical trials and postmarketing surveillance. The study population included 10,685 patients with psoriasis, 2,523 patients with PsA, and 1,311 patients with ankylosing spondylitis who received at least one approved dose of secukinumab (300 mg or 150 mg). The maximum follow-up was 5 years. The exposure-adjusted incidence rate was defined as the incidence rates per 100 patient treatment-years (PTY). The cumulative exposure for patients with psoriasis, PsA, and AS was 16,482, 4,944, and 2,668 PTY, respectively, with average follow-up times of 1.54, 1.96, and 2.03 years, respectively.
The observed and the expected number of malignancies were comparable, with a standardized incidence ratio (SIR) for malignancy of 0.99 across all treatment indications, the researchers said. In further analysis of malignancy by indication, the SIR was 0.87, 1.16, and 1.61 for psoriasis, PsA, and AS, respectively.
Data from postmarketing surveillance showed similar results: The estimated crude cumulative incidence reporting rate per 100 PTY was 0.27 for malignancy across all indications. The cumulative exposure was 285,811 PTY.
The study findings were limited by several factors including the post hoc design, differences in clinical trial methodologies, and lack of controlling for confounding variables, such as smoking status and previous exposure to systemic and biologic treatments, the researchers noted. In addition, the analysis did not include postexposure follow-up data, or data on patients who discontinued clinical trials, they said.
Overall, the analysis is the largest to date and supports the low risk of malignancy in patients with psoriasis, PsA, and AS treated with secukinumab, the researchers noted.
However, “while this assessment provides a broader understanding of the safety of secukinumab and supports its long-term use in these chronic systemic inflammatory conditions, registry data are further warranted to fully understand the real-world effect of biologics on malignancy risk,” they concluded.
“Secukinumab is a relatively newer biologic, approved in 2015, and there is currently a lack of longer-term data on the incidence of malignancy in secukinumab-treated patients, so it’s important to look at the data we have so far on this topic so we can better understand the long-term risks and counsel our psoriasis and psoriatic arthritis patients,” Flavia Fedeles, MD, of the department of dermatology at Massachusetts General Hospital, Boston, said in an interview.
Dr. Fedeles, who was not involved with the study, said that she was not surprised by the study results. “Data reported in the past from phase 3 clinical trials of secukinumab compared with placebo did not show an increase in risk of malignancy, though at that time no long-term safety data or data from patients with history of malignancy was available,” she said. “This study is reassuring in that there wasn’t a signal of increased malignancy events up to 5 years of secukinumab treatment,” said Dr. Fedeles.

However, she noted that the study has a number of limitations, including the use of clinical trials data, which have stringent inclusion/exclusion criteria that can lead to selection bias, the use of postmarketing surveillance data, the post hoc nature of the analysis, and the fact that the sponsor of the trial was the manufacturer of secukinumab, which “potentially can lead to bias to this study.”
She added that “registry data are needed to fully understand the real-world long-term effect of secukinumab on malignancy risk.”
The study was funded by Novartis. Lead author Dr. Lebwohl disclosed participating in advisory boards and/or as an investigator and/or speaker and receiving grants and/or honoraria from multiple companies including Novartis. Several study coauthors are employees of Novartis.
Dr. Fedeles had no financial conflicts to disclose.
that included 49 clinical trials.
Secukinumab (Cosentyx), an interleukin-17A antagonist, is approved for several conditions: moderate to severe psoriasis in children and adults, PsA, ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis.
Although secukinumab has demonstrated safety and tolerability, data on long-term malignancy rates are limited, wrote Mark Lebwohl, MD, professor of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and coauthors.
In a study published in the British Journal of Dermatology, they analyzed the combined safety data from clinical trials and postmarketing surveillance. The study population included 10,685 patients with psoriasis, 2,523 patients with PsA, and 1,311 patients with ankylosing spondylitis who received at least one approved dose of secukinumab (300 mg or 150 mg). The maximum follow-up was 5 years. The exposure-adjusted incidence rate was defined as the incidence rates per 100 patient treatment-years (PTY). The cumulative exposure for patients with psoriasis, PsA, and AS was 16,482, 4,944, and 2,668 PTY, respectively, with average follow-up times of 1.54, 1.96, and 2.03 years, respectively.
The observed and the expected number of malignancies were comparable, with a standardized incidence ratio (SIR) for malignancy of 0.99 across all treatment indications, the researchers said. In further analysis of malignancy by indication, the SIR was 0.87, 1.16, and 1.61 for psoriasis, PsA, and AS, respectively.
Data from postmarketing surveillance showed similar results: The estimated crude cumulative incidence reporting rate per 100 PTY was 0.27 for malignancy across all indications. The cumulative exposure was 285,811 PTY.
The study findings were limited by several factors including the post hoc design, differences in clinical trial methodologies, and lack of controlling for confounding variables, such as smoking status and previous exposure to systemic and biologic treatments, the researchers noted. In addition, the analysis did not include postexposure follow-up data, or data on patients who discontinued clinical trials, they said.
Overall, the analysis is the largest to date and supports the low risk of malignancy in patients with psoriasis, PsA, and AS treated with secukinumab, the researchers noted.
However, “while this assessment provides a broader understanding of the safety of secukinumab and supports its long-term use in these chronic systemic inflammatory conditions, registry data are further warranted to fully understand the real-world effect of biologics on malignancy risk,” they concluded.
“Secukinumab is a relatively newer biologic, approved in 2015, and there is currently a lack of longer-term data on the incidence of malignancy in secukinumab-treated patients, so it’s important to look at the data we have so far on this topic so we can better understand the long-term risks and counsel our psoriasis and psoriatic arthritis patients,” Flavia Fedeles, MD, of the department of dermatology at Massachusetts General Hospital, Boston, said in an interview.
Dr. Fedeles, who was not involved with the study, said that she was not surprised by the study results. “Data reported in the past from phase 3 clinical trials of secukinumab compared with placebo did not show an increase in risk of malignancy, though at that time no long-term safety data or data from patients with history of malignancy was available,” she said. “This study is reassuring in that there wasn’t a signal of increased malignancy events up to 5 years of secukinumab treatment,” said Dr. Fedeles.
However, she noted that the study has a number of limitations, including the use of clinical trials data, which have stringent inclusion/exclusion criteria that can lead to selection bias, the use of postmarketing surveillance data, the post hoc nature of the analysis, and the fact that the sponsor of the trial was the manufacturer of secukinumab, which “potentially can lead to bias to this study.”
She added that “registry data are needed to fully understand the real-world long-term effect of secukinumab on malignancy risk.”
The study was funded by Novartis. Lead author Dr. Lebwohl disclosed participating in advisory boards and/or as an investigator and/or speaker and receiving grants and/or honoraria from multiple companies including Novartis. Several study coauthors are employees of Novartis.
Dr. Fedeles had no financial conflicts to disclose.
that included 49 clinical trials.
Secukinumab (Cosentyx), an interleukin-17A antagonist, is approved for several conditions: moderate to severe psoriasis in children and adults, PsA, ankylosing spondylitis (AS), and nonradiographic axial spondyloarthritis.
Although secukinumab has demonstrated safety and tolerability, data on long-term malignancy rates are limited, wrote Mark Lebwohl, MD, professor of dermatology at the Icahn School of Medicine at Mount Sinai, New York, and coauthors.
In a study published in the British Journal of Dermatology, they analyzed the combined safety data from clinical trials and postmarketing surveillance. The study population included 10,685 patients with psoriasis, 2,523 patients with PsA, and 1,311 patients with ankylosing spondylitis who received at least one approved dose of secukinumab (300 mg or 150 mg). The maximum follow-up was 5 years. The exposure-adjusted incidence rate was defined as the incidence rates per 100 patient treatment-years (PTY). The cumulative exposure for patients with psoriasis, PsA, and AS was 16,482, 4,944, and 2,668 PTY, respectively, with average follow-up times of 1.54, 1.96, and 2.03 years, respectively.
The observed and the expected number of malignancies were comparable, with a standardized incidence ratio (SIR) for malignancy of 0.99 across all treatment indications, the researchers said. In further analysis of malignancy by indication, the SIR was 0.87, 1.16, and 1.61 for psoriasis, PsA, and AS, respectively.
Data from postmarketing surveillance showed similar results: The estimated crude cumulative incidence reporting rate per 100 PTY was 0.27 for malignancy across all indications. The cumulative exposure was 285,811 PTY.
The study findings were limited by several factors including the post hoc design, differences in clinical trial methodologies, and lack of controlling for confounding variables, such as smoking status and previous exposure to systemic and biologic treatments, the researchers noted. In addition, the analysis did not include postexposure follow-up data, or data on patients who discontinued clinical trials, they said.
Overall, the analysis is the largest to date and supports the low risk of malignancy in patients with psoriasis, PsA, and AS treated with secukinumab, the researchers noted.
However, “while this assessment provides a broader understanding of the safety of secukinumab and supports its long-term use in these chronic systemic inflammatory conditions, registry data are further warranted to fully understand the real-world effect of biologics on malignancy risk,” they concluded.
“Secukinumab is a relatively newer biologic, approved in 2015, and there is currently a lack of longer-term data on the incidence of malignancy in secukinumab-treated patients, so it’s important to look at the data we have so far on this topic so we can better understand the long-term risks and counsel our psoriasis and psoriatic arthritis patients,” Flavia Fedeles, MD, of the department of dermatology at Massachusetts General Hospital, Boston, said in an interview.
Dr. Fedeles, who was not involved with the study, said that she was not surprised by the study results. “Data reported in the past from phase 3 clinical trials of secukinumab compared with placebo did not show an increase in risk of malignancy, though at that time no long-term safety data or data from patients with history of malignancy was available,” she said. “This study is reassuring in that there wasn’t a signal of increased malignancy events up to 5 years of secukinumab treatment,” said Dr. Fedeles.
However, she noted that the study has a number of limitations, including the use of clinical trials data, which have stringent inclusion/exclusion criteria that can lead to selection bias, the use of postmarketing surveillance data, the post hoc nature of the analysis, and the fact that the sponsor of the trial was the manufacturer of secukinumab, which “potentially can lead to bias to this study.”
She added that “registry data are needed to fully understand the real-world long-term effect of secukinumab on malignancy risk.”
The study was funded by Novartis. Lead author Dr. Lebwohl disclosed participating in advisory boards and/or as an investigator and/or speaker and receiving grants and/or honoraria from multiple companies including Novartis. Several study coauthors are employees of Novartis.
Dr. Fedeles had no financial conflicts to disclose.
FROM THE BRITISH JOURNAL OF DERMATOLOGY

A new world awaits us all
July is typically the month when new students/physicians arrive at academic medical centers, schools, and hospitals to begin the next phase of training. July also marks the beginning of practice for graduating fellows. In the post-COVID world, these settings will have changed dramatically from the past.

Community practices are consolidating rapidly, with many being acquired by private equity firms, hospitals, and health systems. Private equity made its first investment in GI in 2016, when Audax acquired Miami-based Gastro Health. It was announced this past May that Audax sold Gastro Health to Omers (a larger, Canadian PE firm), marking the first PE sale of a practice (second bite) (Newitt P. “Gastro Health sold to private equity company.” Becker’s GI & Endoscopy. 2021 May 19). The financial success of this model has not been lost on any community practice, so expect more such transactions.
Health systems are bouncing back from 2020, with balance sheets that are recovering quickly. But operating margins are still narrow so physician productivity is being pushed and burnout is a hot-button issue. Older workers are retiring at increasing rates, and low-wage workers are often reluctant to return to the workforce. Both trends increase Medicare and Medicaid rolls. As more patients enter government insurance programs, provider reimbursement falls. “Manage to Medicare” (bringing costs down to levels that are sustainable on Medicare rates) has again become a common goal. The historic reaction to these financial pressures has been to push commercial rates higher thru market consolidation and emphasize margin-producing services.
COVID has changed medicine. We will deliver care differently, and health inequities inherent in the current system will not be tolerable. We now can analyze population-level health outcomes by mining data from enormous databases containing both administrative and health records. Imagine the information we could derive by analyzing IBD populations scattered across multiple states, all cared for by 1,000 gastroenterologists working in a mega practice that uses a single electronic medical record. That might break down the town-gown barrier quickly.
John I. Allen, MD, MBA, AGAF
Editor in Chief
July is typically the month when new students/physicians arrive at academic medical centers, schools, and hospitals to begin the next phase of training. July also marks the beginning of practice for graduating fellows. In the post-COVID world, these settings will have changed dramatically from the past.
Community practices are consolidating rapidly, with many being acquired by private equity firms, hospitals, and health systems. Private equity made its first investment in GI in 2016, when Audax acquired Miami-based Gastro Health. It was announced this past May that Audax sold Gastro Health to Omers (a larger, Canadian PE firm), marking the first PE sale of a practice (second bite) (Newitt P. “Gastro Health sold to private equity company.” Becker’s GI & Endoscopy. 2021 May 19). The financial success of this model has not been lost on any community practice, so expect more such transactions.
Health systems are bouncing back from 2020, with balance sheets that are recovering quickly. But operating margins are still narrow so physician productivity is being pushed and burnout is a hot-button issue. Older workers are retiring at increasing rates, and low-wage workers are often reluctant to return to the workforce. Both trends increase Medicare and Medicaid rolls. As more patients enter government insurance programs, provider reimbursement falls. “Manage to Medicare” (bringing costs down to levels that are sustainable on Medicare rates) has again become a common goal. The historic reaction to these financial pressures has been to push commercial rates higher thru market consolidation and emphasize margin-producing services.
COVID has changed medicine. We will deliver care differently, and health inequities inherent in the current system will not be tolerable. We now can analyze population-level health outcomes by mining data from enormous databases containing both administrative and health records. Imagine the information we could derive by analyzing IBD populations scattered across multiple states, all cared for by 1,000 gastroenterologists working in a mega practice that uses a single electronic medical record. That might break down the town-gown barrier quickly.
John I. Allen, MD, MBA, AGAF
Editor in Chief
July is typically the month when new students/physicians arrive at academic medical centers, schools, and hospitals to begin the next phase of training. July also marks the beginning of practice for graduating fellows. In the post-COVID world, these settings will have changed dramatically from the past.
Community practices are consolidating rapidly, with many being acquired by private equity firms, hospitals, and health systems. Private equity made its first investment in GI in 2016, when Audax acquired Miami-based Gastro Health. It was announced this past May that Audax sold Gastro Health to Omers (a larger, Canadian PE firm), marking the first PE sale of a practice (second bite) (Newitt P. “Gastro Health sold to private equity company.” Becker’s GI & Endoscopy. 2021 May 19). The financial success of this model has not been lost on any community practice, so expect more such transactions.
Health systems are bouncing back from 2020, with balance sheets that are recovering quickly. But operating margins are still narrow so physician productivity is being pushed and burnout is a hot-button issue. Older workers are retiring at increasing rates, and low-wage workers are often reluctant to return to the workforce. Both trends increase Medicare and Medicaid rolls. As more patients enter government insurance programs, provider reimbursement falls. “Manage to Medicare” (bringing costs down to levels that are sustainable on Medicare rates) has again become a common goal. The historic reaction to these financial pressures has been to push commercial rates higher thru market consolidation and emphasize margin-producing services.
COVID has changed medicine. We will deliver care differently, and health inequities inherent in the current system will not be tolerable. We now can analyze population-level health outcomes by mining data from enormous databases containing both administrative and health records. Imagine the information we could derive by analyzing IBD populations scattered across multiple states, all cared for by 1,000 gastroenterologists working in a mega practice that uses a single electronic medical record. That might break down the town-gown barrier quickly.
John I. Allen, MD, MBA, AGAF
Editor in Chief

July 2021 - What's the diagnosis?
Answer: Erythropoietic protoporphyria.Figure B demonstrated massive cholestasis with brown deposits that represented protoporphyrin precipitates, which plugged the bile ducts and led to a cholestatic pattern of liver injury. Under polarized light, protoporhyrin precipitates produced Maltese crosses (Figure C), which are pathognomonic of erythropoietic protoporphyria (EPP). Porphyria is a rare group of inherited heme biosynthesis disorders. EPP is an uncommon type of porphyria and is secondary to a ferrochelatase (FECH) gene mutation, which results in deficient activity of the mitochondrial enzyme FECH.1
FECH catalyzes chelation of iron into proptoporphyrin IX to form heme. The inability of protoporphyrins to be transformed into heme inhibits hepatic elimination and results in hepatocyte accumulation of protoporphyrins, leading to protoporphyrin precipitation in bile canaliculi. Painful photosensitivity (Figure A) is the most common manifestation of EPP, beginning in childhood.2 Only a small proportion of patients with EPP develop liver dysfunction but the consequences can be severe.2 Therefore, therapeutic decisions are based on limited published experience without randomized, controlled data.2 One treatment method is to attempt to remove protoporphyrins from the blood via therapeutic plasma exchange.2Our patient underwent one session of therapeutic plasma exchange; however, after this initial course of treatment, the patient’s goals of care changed and she elected to enroll in hospice. Patients with severe liver dysfunction as a result of EPP require consideration of liver transplantation in the setting of fulminant hepatic failure. Liver transplantation does not cure EPP; the graft is at risk for similar EPP-related changes.1 Only bone marrow transplantation can correct the underlying enzymatic defect in FECH.1 Although physicians are often taught “common things are common,” this case highlights a rare complication of a rare disease such as porphyria is an often forgotten or missed condition. Vigilance should be kept for other rare conditions, especially ones with curative treatments or fatal consequences. In an era where the role of liver biopsy is often questioned in favor of prediction models or noninvasive testing, we must have a low threshold to safely perform a liver biopsy when the diagnosis is unclear or a patient is deteriorating.
The quiz authors disclosed no conflicts of interest.
References
1. Windon AL et al. Am J Transplant. 2018 Mar;18(3):745-9.
2. Pagano MB et al. J Clin Apher. 2012;27(6):336-41.
Answer: Erythropoietic protoporphyria.Figure B demonstrated massive cholestasis with brown deposits that represented protoporphyrin precipitates, which plugged the bile ducts and led to a cholestatic pattern of liver injury. Under polarized light, protoporhyrin precipitates produced Maltese crosses (Figure C), which are pathognomonic of erythropoietic protoporphyria (EPP). Porphyria is a rare group of inherited heme biosynthesis disorders. EPP is an uncommon type of porphyria and is secondary to a ferrochelatase (FECH) gene mutation, which results in deficient activity of the mitochondrial enzyme FECH.1
FECH catalyzes chelation of iron into proptoporphyrin IX to form heme. The inability of protoporphyrins to be transformed into heme inhibits hepatic elimination and results in hepatocyte accumulation of protoporphyrins, leading to protoporphyrin precipitation in bile canaliculi. Painful photosensitivity (Figure A) is the most common manifestation of EPP, beginning in childhood.2 Only a small proportion of patients with EPP develop liver dysfunction but the consequences can be severe.2 Therefore, therapeutic decisions are based on limited published experience without randomized, controlled data.2 One treatment method is to attempt to remove protoporphyrins from the blood via therapeutic plasma exchange.2Our patient underwent one session of therapeutic plasma exchange; however, after this initial course of treatment, the patient’s goals of care changed and she elected to enroll in hospice. Patients with severe liver dysfunction as a result of EPP require consideration of liver transplantation in the setting of fulminant hepatic failure. Liver transplantation does not cure EPP; the graft is at risk for similar EPP-related changes.1 Only bone marrow transplantation can correct the underlying enzymatic defect in FECH.1 Although physicians are often taught “common things are common,” this case highlights a rare complication of a rare disease such as porphyria is an often forgotten or missed condition. Vigilance should be kept for other rare conditions, especially ones with curative treatments or fatal consequences. In an era where the role of liver biopsy is often questioned in favor of prediction models or noninvasive testing, we must have a low threshold to safely perform a liver biopsy when the diagnosis is unclear or a patient is deteriorating.
The quiz authors disclosed no conflicts of interest.
References
1. Windon AL et al. Am J Transplant. 2018 Mar;18(3):745-9.
2. Pagano MB et al. J Clin Apher. 2012;27(6):336-41.
Answer: Erythropoietic protoporphyria.Figure B demonstrated massive cholestasis with brown deposits that represented protoporphyrin precipitates, which plugged the bile ducts and led to a cholestatic pattern of liver injury. Under polarized light, protoporhyrin precipitates produced Maltese crosses (Figure C), which are pathognomonic of erythropoietic protoporphyria (EPP). Porphyria is a rare group of inherited heme biosynthesis disorders. EPP is an uncommon type of porphyria and is secondary to a ferrochelatase (FECH) gene mutation, which results in deficient activity of the mitochondrial enzyme FECH.1
FECH catalyzes chelation of iron into proptoporphyrin IX to form heme. The inability of protoporphyrins to be transformed into heme inhibits hepatic elimination and results in hepatocyte accumulation of protoporphyrins, leading to protoporphyrin precipitation in bile canaliculi. Painful photosensitivity (Figure A) is the most common manifestation of EPP, beginning in childhood.2 Only a small proportion of patients with EPP develop liver dysfunction but the consequences can be severe.2 Therefore, therapeutic decisions are based on limited published experience without randomized, controlled data.2 One treatment method is to attempt to remove protoporphyrins from the blood via therapeutic plasma exchange.2Our patient underwent one session of therapeutic plasma exchange; however, after this initial course of treatment, the patient’s goals of care changed and she elected to enroll in hospice. Patients with severe liver dysfunction as a result of EPP require consideration of liver transplantation in the setting of fulminant hepatic failure. Liver transplantation does not cure EPP; the graft is at risk for similar EPP-related changes.1 Only bone marrow transplantation can correct the underlying enzymatic defect in FECH.1 Although physicians are often taught “common things are common,” this case highlights a rare complication of a rare disease such as porphyria is an often forgotten or missed condition. Vigilance should be kept for other rare conditions, especially ones with curative treatments or fatal consequences. In an era where the role of liver biopsy is often questioned in favor of prediction models or noninvasive testing, we must have a low threshold to safely perform a liver biopsy when the diagnosis is unclear or a patient is deteriorating.
The quiz authors disclosed no conflicts of interest.
References
1. Windon AL et al. Am J Transplant. 2018 Mar;18(3):745-9.
2. Pagano MB et al. J Clin Apher. 2012;27(6):336-41.
A 66-year-old White woman with tetralogy of Fallot status after remote pulmonic valve surgery, hypothyroidism, and previous cholecystectomy presented to her primary care provider with 2 days of constant, dull, right upper quadrant pain with nausea but without fever, association with meals, or association with defecation. Her home medications included low-dose aspirin and levothyroxine. Her physical examination revealed normal vital signs, a body mass index of 29 kg/m2, right upper quadrant tenderness to palpation without peritoneal signs, and normal bowel sounds. The remainder of her examination was normal.
The patient underwent an exhaustive evaluation beginning with laboratory tests, which revealed a normal complete blood count, basic metabolic panel, lipase, international normalized ratio, and urinalysis. Her liver function tests results showed aspartate aminotransferase 118 international IU/L, alanine aminotransferase 117 IU/L, alkaline phosphatase 147 IU/L, and total bilirubin 17.6 mg/dL, with a direct bilirubin of 11.9 mg/dL.
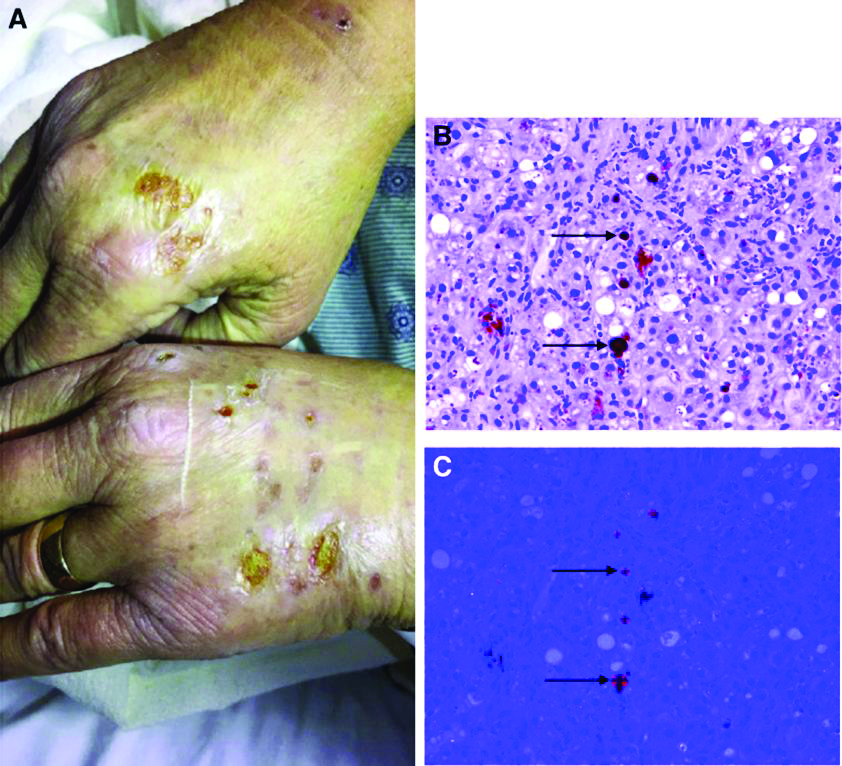
Her liver function tests were last checked 18 months prior and were normal. A liver ultrasound examination revealed cirrhotic morphology without ascites or hepatic or portal vein thrombosis. A magnetic resonance imaging study of the liver revealed morphologic changes of hepatic cirrhosis without portal hypertension, biliary dilation, or stricturing. Additionally, hepatitis A IgM, hepatitis B surface antigen, hepatitis B core IgM and IgG, hepatitis C antibody, ceruloplasmin, antinuclear antibody, anti-smooth muscle antibody, anti-liver-kidney-microsomal antibody, quantitative immunoglobulins, antimitochondrial antibody, alpha-1 antitrypsin phenotype, phosphatidylethanolamine, serum protein electrophoresis, and alpha fetoprotein were reassuring. Later, the patient reported sensitivity to the sun, described as a "sun allergy" with irritation on her hands (Figure A). Mentation remained normal; however, given progressive worsening hepatic function evidenced by international normalized ratio of 1.7 and bilirubin of 27.6 mg/dL, the patient was urgently admitted for expedited portal manometry with transjugular liver biopsy. The hepatic venous pressure gradient was 23 mm Hg. The liver biopsy images are shown in Figure B, C.
What's the diagnosis?
Britney Spears battles conservatorship for mental health protection
In a 24-minute statement, Ms. Spears told the judge overseeing the conservatorship that she wants it to end “without having to be evaluated.” She called the arrangement “abusive” and said she’s been “traumatized” and “in denial” despite the upbeat messages that she’s posted on Instagram during the past year, according to Reuters.
“I just want my life back,” she said. “I’m not here to be anyone’s slave.”
After the statement, the court recessed, and the audio transmission was stopped, Reuters reported. Full transcripts have been published by several news outlets, including this lightly edited version by Variety.
Ms. Spears’ statement came as a shock after years of silence about the conservatorship. Public speculation about the arrangement has resurfaced during the past year because of the #FreeBritney movement on social media, news reports of leaked court documents, and a 2021 documentary that showed she may feel trapped.
During the hearing, Ms. Spears spoke by phone to Los Angeles Superior Court Judge Brenda Penny about the court-approved arrangement that began in 2008 after she had a mental health breakdown. Judge Penny said Ms. Spears would need to submit a petition to the court to ask for the conservatorship to be terminated.
Under the terms of the conservatorship, Ms. Spears would have to demonstrate that she can take responsibility for her personal and financial affairs, Reuters reported. During the hearing, Judge Penny supported Ms. Spears for speaking out.
“I know it took a lot of courage for you to say everything you have to say today,” she said. “I want to let you know that the court does appreciate your coming on the line and sharing how you’re feeling.”
Ms. Spears, 39, said she wanted to get married again and have a baby but that she’s not allowed to go to the doctor to get a contraceptive device removed. She spoke up about her mental health and said doctors had put her on the drug lithium, which made her less able to function. Ms. Spears also said she was forced to perform in the past and is now required to attend numerous therapy sessions each week against her will.
“I’m not happy. I can’t sleep. I’m so angry, it’s insane,” she said. “And I’m depressed. I cry every day.”
Ms. Spears last spoke with the court in May 2019, but the hearing was closed to the public and her testimony was sealed. Ms. Spears recently said she wanted people to hear her thoughts.
“I feel ganged-up on and I feel bullied and I feel left out and alone,” she said. “I deserve to have the same rights as anybody does, by having a child, a family, any of those things, and more so.”
A version of this article first appeared on WebMD.com.
In a 24-minute statement, Ms. Spears told the judge overseeing the conservatorship that she wants it to end “without having to be evaluated.” She called the arrangement “abusive” and said she’s been “traumatized” and “in denial” despite the upbeat messages that she’s posted on Instagram during the past year, according to Reuters.
“I just want my life back,” she said. “I’m not here to be anyone’s slave.”
After the statement, the court recessed, and the audio transmission was stopped, Reuters reported. Full transcripts have been published by several news outlets, including this lightly edited version by Variety.
Ms. Spears’ statement came as a shock after years of silence about the conservatorship. Public speculation about the arrangement has resurfaced during the past year because of the #FreeBritney movement on social media, news reports of leaked court documents, and a 2021 documentary that showed she may feel trapped.
During the hearing, Ms. Spears spoke by phone to Los Angeles Superior Court Judge Brenda Penny about the court-approved arrangement that began in 2008 after she had a mental health breakdown. Judge Penny said Ms. Spears would need to submit a petition to the court to ask for the conservatorship to be terminated.
Under the terms of the conservatorship, Ms. Spears would have to demonstrate that she can take responsibility for her personal and financial affairs, Reuters reported. During the hearing, Judge Penny supported Ms. Spears for speaking out.
“I know it took a lot of courage for you to say everything you have to say today,” she said. “I want to let you know that the court does appreciate your coming on the line and sharing how you’re feeling.”
Ms. Spears, 39, said she wanted to get married again and have a baby but that she’s not allowed to go to the doctor to get a contraceptive device removed. She spoke up about her mental health and said doctors had put her on the drug lithium, which made her less able to function. Ms. Spears also said she was forced to perform in the past and is now required to attend numerous therapy sessions each week against her will.
“I’m not happy. I can’t sleep. I’m so angry, it’s insane,” she said. “And I’m depressed. I cry every day.”
Ms. Spears last spoke with the court in May 2019, but the hearing was closed to the public and her testimony was sealed. Ms. Spears recently said she wanted people to hear her thoughts.
“I feel ganged-up on and I feel bullied and I feel left out and alone,” she said. “I deserve to have the same rights as anybody does, by having a child, a family, any of those things, and more so.”
A version of this article first appeared on WebMD.com.
In a 24-minute statement, Ms. Spears told the judge overseeing the conservatorship that she wants it to end “without having to be evaluated.” She called the arrangement “abusive” and said she’s been “traumatized” and “in denial” despite the upbeat messages that she’s posted on Instagram during the past year, according to Reuters.
“I just want my life back,” she said. “I’m not here to be anyone’s slave.”
After the statement, the court recessed, and the audio transmission was stopped, Reuters reported. Full transcripts have been published by several news outlets, including this lightly edited version by Variety.
Ms. Spears’ statement came as a shock after years of silence about the conservatorship. Public speculation about the arrangement has resurfaced during the past year because of the #FreeBritney movement on social media, news reports of leaked court documents, and a 2021 documentary that showed she may feel trapped.
During the hearing, Ms. Spears spoke by phone to Los Angeles Superior Court Judge Brenda Penny about the court-approved arrangement that began in 2008 after she had a mental health breakdown. Judge Penny said Ms. Spears would need to submit a petition to the court to ask for the conservatorship to be terminated.
Under the terms of the conservatorship, Ms. Spears would have to demonstrate that she can take responsibility for her personal and financial affairs, Reuters reported. During the hearing, Judge Penny supported Ms. Spears for speaking out.
“I know it took a lot of courage for you to say everything you have to say today,” she said. “I want to let you know that the court does appreciate your coming on the line and sharing how you’re feeling.”
Ms. Spears, 39, said she wanted to get married again and have a baby but that she’s not allowed to go to the doctor to get a contraceptive device removed. She spoke up about her mental health and said doctors had put her on the drug lithium, which made her less able to function. Ms. Spears also said she was forced to perform in the past and is now required to attend numerous therapy sessions each week against her will.
“I’m not happy. I can’t sleep. I’m so angry, it’s insane,” she said. “And I’m depressed. I cry every day.”
Ms. Spears last spoke with the court in May 2019, but the hearing was closed to the public and her testimony was sealed. Ms. Spears recently said she wanted people to hear her thoughts.
“I feel ganged-up on and I feel bullied and I feel left out and alone,” she said. “I deserve to have the same rights as anybody does, by having a child, a family, any of those things, and more so.”
A version of this article first appeared on WebMD.com.
New! Spotlight on medical power couples: Their extraordinary lives
When people started dying from lethal anthrax spores sent through the mail in 2001, infectious disease expert Jeannette Guarner, MD, was called to Florida and Connecticut to analyze the bodies. She and her pathology team investigated how the bacteria had entered the victims and examined tissue samples from across the country to discern the scale of the attacks.

After conducting autopsies and identifying that inhalation anthrax had caused the deaths, Dr. Guarner rushed home to Atlanta just in time for Thanksgiving. Exhausted, the beloved family chef still managed to cook the big turkey that holiday, but she enlisted help with dessert.
“She returned home on Thanksgiving at like three in the morning,” recalls Carlos del Rio, MD. “She said to me, ‘In order for us to have Thanksgiving, you have to be in charge of the pies.’ When I told my daughter, she said, ‘This is going to be a disaster! If mom’s not cooking, this is not going to be good.’”
“It didn’t turn out that bad,” Dr. Guarner laughs. “There was dessert.”
As two of the top infectious disease experts in the country, Dr. Guarner and Dr. del Rio are no strangers to juggling their personal lives around disease outbreaks, last-minute travel, and pressing research.
Former director of the clinical laboratory at Mexico’s National Cancer Institute, Dr. Guarner worked for the Centers for Disease Control and Prevention for 10 years, where she played an integral part in the discovery of SARS. She and her team identified that a coronavirus was in cultures taken from a health care worker who died after working in Asia and determined through molecular testing that the virus was different from any other coronaviruses at the time.
Dr. Guarner went on to search for the novel virus in tissue samples and determine that it was SARS that had caused the damage. She is now a professor in the department of pathology and laboratory medicine at Emory University, Atlanta, medical director of the clinical laboratory at Emory University Hospital Midtown, and vice chair for faculty affairs.
Dr. Del Rio, who served as director of the National AIDS Council of Mexico, is a distinguished professor of medicine in Emory University’s division of infectious diseases and a professor of global health and epidemiology in the Rollins School of Public Health at Emory University. He is also co-director of the Emory Center for AIDS Research and co-principal investigator of the Emory-CDC HIV Clinical Trials Unit and the Emory Vaccine and Treatment Evaluation Unit.
Dr. Del Rio’s work in HIV prevention and care has made great strides, including developing the concept for the HIV Care Continuum, a public health model that outlines the stages that HIV patients go through, from diagnosis to achieving viral suppression. Dr. Del Rio, who is foreign secretary of the National Academy of Medicine, has also worked on emerging infections such as pandemic influenza and was a member of the WHO Influenza A (H1N1) Clinical Advisory Group and of the CDC Influenza A Task Force during the 2009 pandemic.
Dr. Del Rio and Dr. Guarner met during medical school in Mexico City. At first, the two carpooled to classes, but when Dr. Guarner fell ill with hepatitis A, Dr. del Rio brought Dr. Guarner the class notes so she wouldn’t fall behind. The study buddies later became a couple and married just before coming to the United States for residency.
With their expertise in infectious disease, Dr. del Rio and Dr. Guarner have worked collaboratively in the past, but the couple says they’ve always maintained separate professional identities.
“We try to create our own spaces,” Dr. del Rio said. “You try to keep your personal and professional identity independent as much as possible. You don’t want people to say, ‘Oh, you got this or you’re doing this because you are married to this other person.’ You want, to a certain degree, intellectual independence.”
This has been easier in some ways because Dr. del Rio and Dr. Guarner have different last names. Over the years they have frequently encountered people who had no idea that they are married.
“One time, we were both down in the lab and Jeanette was discussing a case, and she started teasing me or poking me, making fun,” recalls Dr. del Rio. “Some of the ID fellows were like, ‘Oh my God, who the hell is this woman?’ They didn’t realize she was my wife.”
Since the COVID-19 outbreak, both Dr. Guarner and Dr. del Rio have been involved in different ways with the pandemic. Dr. Del Rio has seen patients, conducted clinical trials, and given hundreds of local and national interviews about the virus. As a laboratory director, Dr. Guarner has validated tests for the diagnosis of COVID-19 and counseled staff on exposure concerns.
“An important aspect has also been to make sure that our laboratory technologists understand the disease and the need for the different protection elements we have had to use in the hospital,” she said. “In many ways I have had to scale down fears the techs have had when handling specimens from these patients.”
In their own words
What was one of your most surprising discoveries?
Jeannette: During the anthrax attacks, we received lots of tissues on live patients, particularly skin biopsies from different parts of the country where pathologists had concerns that there was anthrax. From New York, we received more than 50 skin biopsies and discovered that the necrotic lesions suspected of anthrax had Rickettsia in them. In other words, we discovered that rickettsialpox – a mite-borne infectious disease – was circulating in the city, which was unknown at the time.
Describe a challenge that you overcame:
Carlos: When I was appointed as director of the National AIDS Council of Mexico (CONASIDA), I was quite young, only 32 years old. I had to learn to listen to others who had expertise and institutional memory, to respect their opinions, and at the same time to push for change. A huge challenge was the role of the Catholic Church and conservative groups that were adamantly against condom promotion. Thus, I learned how to advance policies based in science without being confrontational.
Have you ever been famous for anything other than your work?
Jeannette: In 2017, a tree fell on our house during Hurricane Irma. It fell right on my husband’s office a few minutes after he left the room. Fortunately, I have always been small and flexible, and I crawled through the rubble to save our valuables before they were ruined by the rain. Later, a local Atlanta TV news crew was in the neighborhood reporting on the damage, and I told them to come to our house if they wanted to see real damage. That night, we were on the local news.
Power couple Paul and Mary Klotman
When Mary Klotman, MD, was offered an opportunity with the National Institutes of Health in 1991, Paul Klotman, MD, didn’t hesitate to resign his post at Duke University, Durham, N.C., and join his wife in Washington. Paul says he wanted to support Mary’s aspirations, even though it meant an uncertain track for his own career.

Fortunately for the Klotmans, the move proved instrumental for both of their careers and spurred one of their proudest scientific breakthroughs.
At NIH, Mary was a member of the Public Health Service and worked in the laboratory of tumor cell biology, and Paul became chief of the institute’s molecular medicine section in the laboratory of developmental biology. Together, their work led to the first animal model of HIV-associated nephropathy using transgenic techniques. The Klotmans and their team demonstrated that HIV resides in and evolves separately in kidney cells, a critical step in HIV-associated kidney disease.
“That’s where our longstanding collaboration around HIV-associated nephropathy started,” Mary says. “Paul and I have a passion for research, and we’ve had the same grant together for 25 years.”
After their successful stint at NIH, the Klotmans next climbed the ranks at the Icahn School of Medicine at Mount Sinai, where Paul started as chief of the nephrology division and became chair of medicine, and Mary became chief of infectious diseases and co-director of Mount Sinai’s Global Health and Emerging Pathogens Institute.
Today, Mary and Paul are the first – and only – married couple in the United States to lead separate medical schools. Mary is dean and vice chancellor for health affairs at Duke, and Paul is president and executive dean of Baylor College of Medicine, Houston.
Despite their 1,100-mile separation, the Klotmans manage their relationship in an unconventional way that some might balk at: Every Friday, one spouse hops on a plane and travels to the other for a date night and weekend.
“When we started this crazy lifestyle, we committed to being together every weekend,” says Mary. “And in 10 years – before COVID – we missed only one weekend together.”
The Klotmans say the scheduled time together places a hard end to each work week and enables them to truly enjoy their quality time.
“Friday at noon, I’m on the plane going to Durham, and I know that in 2 hours I’m going to have a date with my wife,” Paul said. “There are institutions that we’ve run into that think you have to be 7 days a week on site. But Duke and Baylor have been very supportive [of our situation].”
No doubt, the arrangement means a lot of time in the air for the couple. Paul says he travels about 150,000 miles every year by plane.
Having dual leadership positions in academic medicine has kept the Klotmans tightly connected, and the couple says their strong partnership has contributed to their success.
“It’s really been helpful having a deep understanding of our career paths, because we’ve been able to understand when one of us needed to be really focused on work and the other one would step back a bit with the kids and vice versa,” Mary said.
“There’s no question that we wouldn’t be in the positions we are in now if it weren’t for the fact that we’ve had each other,” Paul said.
In their own words
What is a little-known title that you have?
Paul: Purse-carrier for my wife. When she is honored at a national meeting or event, she often stands up and hands me her purse. I now make sure I have on an appropriate outfit that matches the purse.
Tell us about your children.
Mary: We had a very traumatic first pregnancy that we lost. Six years later, we adopted our first child, which was an amazing blessing. Our second son was Duke’s first successful frozen embryo transfer.
Describe a memorable moment in your relationship.
Paul: As we were leaving for our honeymoon, Mary’s dad handed me this booklet. It was the receipts for Mary’s medical school loans for the next 10 years. He said, “Congratulations, she’s all yours!”
A version of this article first appeared on Medscape.com.
When people started dying from lethal anthrax spores sent through the mail in 2001, infectious disease expert Jeannette Guarner, MD, was called to Florida and Connecticut to analyze the bodies. She and her pathology team investigated how the bacteria had entered the victims and examined tissue samples from across the country to discern the scale of the attacks.
After conducting autopsies and identifying that inhalation anthrax had caused the deaths, Dr. Guarner rushed home to Atlanta just in time for Thanksgiving. Exhausted, the beloved family chef still managed to cook the big turkey that holiday, but she enlisted help with dessert.
“She returned home on Thanksgiving at like three in the morning,” recalls Carlos del Rio, MD. “She said to me, ‘In order for us to have Thanksgiving, you have to be in charge of the pies.’ When I told my daughter, she said, ‘This is going to be a disaster! If mom’s not cooking, this is not going to be good.’”
“It didn’t turn out that bad,” Dr. Guarner laughs. “There was dessert.”
As two of the top infectious disease experts in the country, Dr. Guarner and Dr. del Rio are no strangers to juggling their personal lives around disease outbreaks, last-minute travel, and pressing research.
Former director of the clinical laboratory at Mexico’s National Cancer Institute, Dr. Guarner worked for the Centers for Disease Control and Prevention for 10 years, where she played an integral part in the discovery of SARS. She and her team identified that a coronavirus was in cultures taken from a health care worker who died after working in Asia and determined through molecular testing that the virus was different from any other coronaviruses at the time.
Dr. Guarner went on to search for the novel virus in tissue samples and determine that it was SARS that had caused the damage. She is now a professor in the department of pathology and laboratory medicine at Emory University, Atlanta, medical director of the clinical laboratory at Emory University Hospital Midtown, and vice chair for faculty affairs.
Dr. Del Rio, who served as director of the National AIDS Council of Mexico, is a distinguished professor of medicine in Emory University’s division of infectious diseases and a professor of global health and epidemiology in the Rollins School of Public Health at Emory University. He is also co-director of the Emory Center for AIDS Research and co-principal investigator of the Emory-CDC HIV Clinical Trials Unit and the Emory Vaccine and Treatment Evaluation Unit.
Dr. Del Rio’s work in HIV prevention and care has made great strides, including developing the concept for the HIV Care Continuum, a public health model that outlines the stages that HIV patients go through, from diagnosis to achieving viral suppression. Dr. Del Rio, who is foreign secretary of the National Academy of Medicine, has also worked on emerging infections such as pandemic influenza and was a member of the WHO Influenza A (H1N1) Clinical Advisory Group and of the CDC Influenza A Task Force during the 2009 pandemic.
Dr. Del Rio and Dr. Guarner met during medical school in Mexico City. At first, the two carpooled to classes, but when Dr. Guarner fell ill with hepatitis A, Dr. del Rio brought Dr. Guarner the class notes so she wouldn’t fall behind. The study buddies later became a couple and married just before coming to the United States for residency.
With their expertise in infectious disease, Dr. del Rio and Dr. Guarner have worked collaboratively in the past, but the couple says they’ve always maintained separate professional identities.
“We try to create our own spaces,” Dr. del Rio said. “You try to keep your personal and professional identity independent as much as possible. You don’t want people to say, ‘Oh, you got this or you’re doing this because you are married to this other person.’ You want, to a certain degree, intellectual independence.”
This has been easier in some ways because Dr. del Rio and Dr. Guarner have different last names. Over the years they have frequently encountered people who had no idea that they are married.
“One time, we were both down in the lab and Jeanette was discussing a case, and she started teasing me or poking me, making fun,” recalls Dr. del Rio. “Some of the ID fellows were like, ‘Oh my God, who the hell is this woman?’ They didn’t realize she was my wife.”
Since the COVID-19 outbreak, both Dr. Guarner and Dr. del Rio have been involved in different ways with the pandemic. Dr. Del Rio has seen patients, conducted clinical trials, and given hundreds of local and national interviews about the virus. As a laboratory director, Dr. Guarner has validated tests for the diagnosis of COVID-19 and counseled staff on exposure concerns.
“An important aspect has also been to make sure that our laboratory technologists understand the disease and the need for the different protection elements we have had to use in the hospital,” she said. “In many ways I have had to scale down fears the techs have had when handling specimens from these patients.”
In their own words
What was one of your most surprising discoveries?
Jeannette: During the anthrax attacks, we received lots of tissues on live patients, particularly skin biopsies from different parts of the country where pathologists had concerns that there was anthrax. From New York, we received more than 50 skin biopsies and discovered that the necrotic lesions suspected of anthrax had Rickettsia in them. In other words, we discovered that rickettsialpox – a mite-borne infectious disease – was circulating in the city, which was unknown at the time.
Describe a challenge that you overcame:
Carlos: When I was appointed as director of the National AIDS Council of Mexico (CONASIDA), I was quite young, only 32 years old. I had to learn to listen to others who had expertise and institutional memory, to respect their opinions, and at the same time to push for change. A huge challenge was the role of the Catholic Church and conservative groups that were adamantly against condom promotion. Thus, I learned how to advance policies based in science without being confrontational.
Have you ever been famous for anything other than your work?
Jeannette: In 2017, a tree fell on our house during Hurricane Irma. It fell right on my husband’s office a few minutes after he left the room. Fortunately, I have always been small and flexible, and I crawled through the rubble to save our valuables before they were ruined by the rain. Later, a local Atlanta TV news crew was in the neighborhood reporting on the damage, and I told them to come to our house if they wanted to see real damage. That night, we were on the local news.
Power couple Paul and Mary Klotman
When Mary Klotman, MD, was offered an opportunity with the National Institutes of Health in 1991, Paul Klotman, MD, didn’t hesitate to resign his post at Duke University, Durham, N.C., and join his wife in Washington. Paul says he wanted to support Mary’s aspirations, even though it meant an uncertain track for his own career.
Fortunately for the Klotmans, the move proved instrumental for both of their careers and spurred one of their proudest scientific breakthroughs.
At NIH, Mary was a member of the Public Health Service and worked in the laboratory of tumor cell biology, and Paul became chief of the institute’s molecular medicine section in the laboratory of developmental biology. Together, their work led to the first animal model of HIV-associated nephropathy using transgenic techniques. The Klotmans and their team demonstrated that HIV resides in and evolves separately in kidney cells, a critical step in HIV-associated kidney disease.
“That’s where our longstanding collaboration around HIV-associated nephropathy started,” Mary says. “Paul and I have a passion for research, and we’ve had the same grant together for 25 years.”
After their successful stint at NIH, the Klotmans next climbed the ranks at the Icahn School of Medicine at Mount Sinai, where Paul started as chief of the nephrology division and became chair of medicine, and Mary became chief of infectious diseases and co-director of Mount Sinai’s Global Health and Emerging Pathogens Institute.
Today, Mary and Paul are the first – and only – married couple in the United States to lead separate medical schools. Mary is dean and vice chancellor for health affairs at Duke, and Paul is president and executive dean of Baylor College of Medicine, Houston.
Despite their 1,100-mile separation, the Klotmans manage their relationship in an unconventional way that some might balk at: Every Friday, one spouse hops on a plane and travels to the other for a date night and weekend.
“When we started this crazy lifestyle, we committed to being together every weekend,” says Mary. “And in 10 years – before COVID – we missed only one weekend together.”
The Klotmans say the scheduled time together places a hard end to each work week and enables them to truly enjoy their quality time.
“Friday at noon, I’m on the plane going to Durham, and I know that in 2 hours I’m going to have a date with my wife,” Paul said. “There are institutions that we’ve run into that think you have to be 7 days a week on site. But Duke and Baylor have been very supportive [of our situation].”
No doubt, the arrangement means a lot of time in the air for the couple. Paul says he travels about 150,000 miles every year by plane.
Having dual leadership positions in academic medicine has kept the Klotmans tightly connected, and the couple says their strong partnership has contributed to their success.
“It’s really been helpful having a deep understanding of our career paths, because we’ve been able to understand when one of us needed to be really focused on work and the other one would step back a bit with the kids and vice versa,” Mary said.
“There’s no question that we wouldn’t be in the positions we are in now if it weren’t for the fact that we’ve had each other,” Paul said.
In their own words
What is a little-known title that you have?
Paul: Purse-carrier for my wife. When she is honored at a national meeting or event, she often stands up and hands me her purse. I now make sure I have on an appropriate outfit that matches the purse.
Tell us about your children.
Mary: We had a very traumatic first pregnancy that we lost. Six years later, we adopted our first child, which was an amazing blessing. Our second son was Duke’s first successful frozen embryo transfer.
Describe a memorable moment in your relationship.
Paul: As we were leaving for our honeymoon, Mary’s dad handed me this booklet. It was the receipts for Mary’s medical school loans for the next 10 years. He said, “Congratulations, she’s all yours!”
A version of this article first appeared on Medscape.com.
When people started dying from lethal anthrax spores sent through the mail in 2001, infectious disease expert Jeannette Guarner, MD, was called to Florida and Connecticut to analyze the bodies. She and her pathology team investigated how the bacteria had entered the victims and examined tissue samples from across the country to discern the scale of the attacks.
After conducting autopsies and identifying that inhalation anthrax had caused the deaths, Dr. Guarner rushed home to Atlanta just in time for Thanksgiving. Exhausted, the beloved family chef still managed to cook the big turkey that holiday, but she enlisted help with dessert.
“She returned home on Thanksgiving at like three in the morning,” recalls Carlos del Rio, MD. “She said to me, ‘In order for us to have Thanksgiving, you have to be in charge of the pies.’ When I told my daughter, she said, ‘This is going to be a disaster! If mom’s not cooking, this is not going to be good.’”
“It didn’t turn out that bad,” Dr. Guarner laughs. “There was dessert.”
As two of the top infectious disease experts in the country, Dr. Guarner and Dr. del Rio are no strangers to juggling their personal lives around disease outbreaks, last-minute travel, and pressing research.
Former director of the clinical laboratory at Mexico’s National Cancer Institute, Dr. Guarner worked for the Centers for Disease Control and Prevention for 10 years, where she played an integral part in the discovery of SARS. She and her team identified that a coronavirus was in cultures taken from a health care worker who died after working in Asia and determined through molecular testing that the virus was different from any other coronaviruses at the time.
Dr. Guarner went on to search for the novel virus in tissue samples and determine that it was SARS that had caused the damage. She is now a professor in the department of pathology and laboratory medicine at Emory University, Atlanta, medical director of the clinical laboratory at Emory University Hospital Midtown, and vice chair for faculty affairs.
Dr. Del Rio, who served as director of the National AIDS Council of Mexico, is a distinguished professor of medicine in Emory University’s division of infectious diseases and a professor of global health and epidemiology in the Rollins School of Public Health at Emory University. He is also co-director of the Emory Center for AIDS Research and co-principal investigator of the Emory-CDC HIV Clinical Trials Unit and the Emory Vaccine and Treatment Evaluation Unit.
Dr. Del Rio’s work in HIV prevention and care has made great strides, including developing the concept for the HIV Care Continuum, a public health model that outlines the stages that HIV patients go through, from diagnosis to achieving viral suppression. Dr. Del Rio, who is foreign secretary of the National Academy of Medicine, has also worked on emerging infections such as pandemic influenza and was a member of the WHO Influenza A (H1N1) Clinical Advisory Group and of the CDC Influenza A Task Force during the 2009 pandemic.
Dr. Del Rio and Dr. Guarner met during medical school in Mexico City. At first, the two carpooled to classes, but when Dr. Guarner fell ill with hepatitis A, Dr. del Rio brought Dr. Guarner the class notes so she wouldn’t fall behind. The study buddies later became a couple and married just before coming to the United States for residency.
With their expertise in infectious disease, Dr. del Rio and Dr. Guarner have worked collaboratively in the past, but the couple says they’ve always maintained separate professional identities.
“We try to create our own spaces,” Dr. del Rio said. “You try to keep your personal and professional identity independent as much as possible. You don’t want people to say, ‘Oh, you got this or you’re doing this because you are married to this other person.’ You want, to a certain degree, intellectual independence.”
This has been easier in some ways because Dr. del Rio and Dr. Guarner have different last names. Over the years they have frequently encountered people who had no idea that they are married.
“One time, we were both down in the lab and Jeanette was discussing a case, and she started teasing me or poking me, making fun,” recalls Dr. del Rio. “Some of the ID fellows were like, ‘Oh my God, who the hell is this woman?’ They didn’t realize she was my wife.”
Since the COVID-19 outbreak, both Dr. Guarner and Dr. del Rio have been involved in different ways with the pandemic. Dr. Del Rio has seen patients, conducted clinical trials, and given hundreds of local and national interviews about the virus. As a laboratory director, Dr. Guarner has validated tests for the diagnosis of COVID-19 and counseled staff on exposure concerns.
“An important aspect has also been to make sure that our laboratory technologists understand the disease and the need for the different protection elements we have had to use in the hospital,” she said. “In many ways I have had to scale down fears the techs have had when handling specimens from these patients.”
In their own words
What was one of your most surprising discoveries?
Jeannette: During the anthrax attacks, we received lots of tissues on live patients, particularly skin biopsies from different parts of the country where pathologists had concerns that there was anthrax. From New York, we received more than 50 skin biopsies and discovered that the necrotic lesions suspected of anthrax had Rickettsia in them. In other words, we discovered that rickettsialpox – a mite-borne infectious disease – was circulating in the city, which was unknown at the time.
Describe a challenge that you overcame:
Carlos: When I was appointed as director of the National AIDS Council of Mexico (CONASIDA), I was quite young, only 32 years old. I had to learn to listen to others who had expertise and institutional memory, to respect their opinions, and at the same time to push for change. A huge challenge was the role of the Catholic Church and conservative groups that were adamantly against condom promotion. Thus, I learned how to advance policies based in science without being confrontational.
Have you ever been famous for anything other than your work?
Jeannette: In 2017, a tree fell on our house during Hurricane Irma. It fell right on my husband’s office a few minutes after he left the room. Fortunately, I have always been small and flexible, and I crawled through the rubble to save our valuables before they were ruined by the rain. Later, a local Atlanta TV news crew was in the neighborhood reporting on the damage, and I told them to come to our house if they wanted to see real damage. That night, we were on the local news.
Power couple Paul and Mary Klotman
When Mary Klotman, MD, was offered an opportunity with the National Institutes of Health in 1991, Paul Klotman, MD, didn’t hesitate to resign his post at Duke University, Durham, N.C., and join his wife in Washington. Paul says he wanted to support Mary’s aspirations, even though it meant an uncertain track for his own career.
Fortunately for the Klotmans, the move proved instrumental for both of their careers and spurred one of their proudest scientific breakthroughs.
At NIH, Mary was a member of the Public Health Service and worked in the laboratory of tumor cell biology, and Paul became chief of the institute’s molecular medicine section in the laboratory of developmental biology. Together, their work led to the first animal model of HIV-associated nephropathy using transgenic techniques. The Klotmans and their team demonstrated that HIV resides in and evolves separately in kidney cells, a critical step in HIV-associated kidney disease.
“That’s where our longstanding collaboration around HIV-associated nephropathy started,” Mary says. “Paul and I have a passion for research, and we’ve had the same grant together for 25 years.”
After their successful stint at NIH, the Klotmans next climbed the ranks at the Icahn School of Medicine at Mount Sinai, where Paul started as chief of the nephrology division and became chair of medicine, and Mary became chief of infectious diseases and co-director of Mount Sinai’s Global Health and Emerging Pathogens Institute.
Today, Mary and Paul are the first – and only – married couple in the United States to lead separate medical schools. Mary is dean and vice chancellor for health affairs at Duke, and Paul is president and executive dean of Baylor College of Medicine, Houston.
Despite their 1,100-mile separation, the Klotmans manage their relationship in an unconventional way that some might balk at: Every Friday, one spouse hops on a plane and travels to the other for a date night and weekend.
“When we started this crazy lifestyle, we committed to being together every weekend,” says Mary. “And in 10 years – before COVID – we missed only one weekend together.”
The Klotmans say the scheduled time together places a hard end to each work week and enables them to truly enjoy their quality time.
“Friday at noon, I’m on the plane going to Durham, and I know that in 2 hours I’m going to have a date with my wife,” Paul said. “There are institutions that we’ve run into that think you have to be 7 days a week on site. But Duke and Baylor have been very supportive [of our situation].”
No doubt, the arrangement means a lot of time in the air for the couple. Paul says he travels about 150,000 miles every year by plane.
Having dual leadership positions in academic medicine has kept the Klotmans tightly connected, and the couple says their strong partnership has contributed to their success.
“It’s really been helpful having a deep understanding of our career paths, because we’ve been able to understand when one of us needed to be really focused on work and the other one would step back a bit with the kids and vice versa,” Mary said.
“There’s no question that we wouldn’t be in the positions we are in now if it weren’t for the fact that we’ve had each other,” Paul said.
In their own words
What is a little-known title that you have?
Paul: Purse-carrier for my wife. When she is honored at a national meeting or event, she often stands up and hands me her purse. I now make sure I have on an appropriate outfit that matches the purse.
Tell us about your children.
Mary: We had a very traumatic first pregnancy that we lost. Six years later, we adopted our first child, which was an amazing blessing. Our second son was Duke’s first successful frozen embryo transfer.
Describe a memorable moment in your relationship.
Paul: As we were leaving for our honeymoon, Mary’s dad handed me this booklet. It was the receipts for Mary’s medical school loans for the next 10 years. He said, “Congratulations, she’s all yours!”
A version of this article first appeared on Medscape.com.