User login
Subcutaneous Immunotherapy Promises Better Life For Cancer Patients
The possibility is being driven by the development of subcutaneous formulations of commonly used immune checkpoint inhibitors for non–small cell lung cancer (NSCLC) and other indications, including pembrolizumab, nivolumab, durvalumab, atezolizumab, and amivantamab.
Instead of waiting anywhere from 30 minutes to several hours for infusions into their veins, patients would spend just a few minutes being injected under the loose skin of their abdomens or thighs. Clinicians would save time and money, and patients would leave the clinic much sooner than normal. The ease of subcutaneous injections also opens up an opportunity for home treatment, a potential boon for people who don’t want to spend their remaining time on hospital visits.
“In the future, I hope we can deliver these medicines at home,” said Hazel O’Sullivan, MBBCh, a medical lung cancer oncologist at Cork University, Ireland, who explained the issues during a session at the 2024 European Lung Cancer Congress.
She was the discussant on two studies at the meeting that highlighted the latest developments in the field, the IMscin002 study of subcutaneous atezolizumab and the PALOMA study of subcutaneous amivantamab, both mostly in NSCLC patients.
Subcutaneous atezolizumab was approved recently in Europe after its maker, Genentech/Roche, made a convincing case that its pharmacokinetics, efficacy, and safety are comparable to the intravenous (IV) version. The U.S. Food and Drug Administration is considering approval; Genentech/Roche anticipates a decision in 2024.
IMscin002 randomized 179 stage 2-4 NSCLC patients evenly to IV or subcutaneous atezolizumab for the first three cycles, then switched them for three more cycles.
Participants were then asked what version they preferred and what they wanted to continue with.
Seventy-one percent said they liked the subcutaneous version better and 80% opted to continue with it. Their main reasons were because they spent less time in the clinic and it was more comfortable.
When asked about the potential for home administration, presenter Federico Cappuzzo, MD, PhD, a medical lung cancer oncologist in Rome, said that it could be “an important option in the future,” particularly in isolated areas far away from hospitals.
The authors of new research are currently evaluating whether home administration is possible. Nurses are administering atezolizumab to patients in their homes with telemedicine monitoring.
The other subcutaneous study presented at the meeting, the PALOMA trial with amivantamab, had only 19 subjects. Administration took no more than 10 minutes, versus potentially hours, especially for the first dose. Subcutaneous amivantamab was given once a month, versus every 2 weeks for the IV formulation, during the maintenance phase of treatment.
The take-home from PALOMA is that the risk of infusion reactions is lower with subcutaneous administration (16% versus 67%) but the risk of mostly mild skin rashes is higher (79% versus 36%).
Investigation is ongoing to confirm safety, pharmacokinetic, and efficacy equivalence with the IV formulation, including in combination with other medications.
When asked about home administration of amivantamab, PALOMA lead investigator Natasha Leighl, MD, a lung, and breast cancer medical oncologist at the University of Toronto, stated that patients probably need to be watched in the clinic for the first 4 months.
The atezolizumab study was funded by maker Genentech/Roche. The amivantamab study was funded by its maker, Janssen. The amivantamab investigator, Dr. Leighl, reported grants, honoraria, and travel payments from Janssen. Dr. Cappuzzo, the investigator on the atezolizumab study, reported speaker and adviser payments from Genentech/Roche. The discussant, Dr. O’Sullivan, wasn’t involved with either company but reported payments from Amgen and AstraZeneca and travel costs covered by Takeda.
The possibility is being driven by the development of subcutaneous formulations of commonly used immune checkpoint inhibitors for non–small cell lung cancer (NSCLC) and other indications, including pembrolizumab, nivolumab, durvalumab, atezolizumab, and amivantamab.
Instead of waiting anywhere from 30 minutes to several hours for infusions into their veins, patients would spend just a few minutes being injected under the loose skin of their abdomens or thighs. Clinicians would save time and money, and patients would leave the clinic much sooner than normal. The ease of subcutaneous injections also opens up an opportunity for home treatment, a potential boon for people who don’t want to spend their remaining time on hospital visits.
“In the future, I hope we can deliver these medicines at home,” said Hazel O’Sullivan, MBBCh, a medical lung cancer oncologist at Cork University, Ireland, who explained the issues during a session at the 2024 European Lung Cancer Congress.
She was the discussant on two studies at the meeting that highlighted the latest developments in the field, the IMscin002 study of subcutaneous atezolizumab and the PALOMA study of subcutaneous amivantamab, both mostly in NSCLC patients.
Subcutaneous atezolizumab was approved recently in Europe after its maker, Genentech/Roche, made a convincing case that its pharmacokinetics, efficacy, and safety are comparable to the intravenous (IV) version. The U.S. Food and Drug Administration is considering approval; Genentech/Roche anticipates a decision in 2024.
IMscin002 randomized 179 stage 2-4 NSCLC patients evenly to IV or subcutaneous atezolizumab for the first three cycles, then switched them for three more cycles.
Participants were then asked what version they preferred and what they wanted to continue with.
Seventy-one percent said they liked the subcutaneous version better and 80% opted to continue with it. Their main reasons were because they spent less time in the clinic and it was more comfortable.
When asked about the potential for home administration, presenter Federico Cappuzzo, MD, PhD, a medical lung cancer oncologist in Rome, said that it could be “an important option in the future,” particularly in isolated areas far away from hospitals.
The authors of new research are currently evaluating whether home administration is possible. Nurses are administering atezolizumab to patients in their homes with telemedicine monitoring.
The other subcutaneous study presented at the meeting, the PALOMA trial with amivantamab, had only 19 subjects. Administration took no more than 10 minutes, versus potentially hours, especially for the first dose. Subcutaneous amivantamab was given once a month, versus every 2 weeks for the IV formulation, during the maintenance phase of treatment.
The take-home from PALOMA is that the risk of infusion reactions is lower with subcutaneous administration (16% versus 67%) but the risk of mostly mild skin rashes is higher (79% versus 36%).
Investigation is ongoing to confirm safety, pharmacokinetic, and efficacy equivalence with the IV formulation, including in combination with other medications.
When asked about home administration of amivantamab, PALOMA lead investigator Natasha Leighl, MD, a lung, and breast cancer medical oncologist at the University of Toronto, stated that patients probably need to be watched in the clinic for the first 4 months.
The atezolizumab study was funded by maker Genentech/Roche. The amivantamab study was funded by its maker, Janssen. The amivantamab investigator, Dr. Leighl, reported grants, honoraria, and travel payments from Janssen. Dr. Cappuzzo, the investigator on the atezolizumab study, reported speaker and adviser payments from Genentech/Roche. The discussant, Dr. O’Sullivan, wasn’t involved with either company but reported payments from Amgen and AstraZeneca and travel costs covered by Takeda.
The possibility is being driven by the development of subcutaneous formulations of commonly used immune checkpoint inhibitors for non–small cell lung cancer (NSCLC) and other indications, including pembrolizumab, nivolumab, durvalumab, atezolizumab, and amivantamab.
Instead of waiting anywhere from 30 minutes to several hours for infusions into their veins, patients would spend just a few minutes being injected under the loose skin of their abdomens or thighs. Clinicians would save time and money, and patients would leave the clinic much sooner than normal. The ease of subcutaneous injections also opens up an opportunity for home treatment, a potential boon for people who don’t want to spend their remaining time on hospital visits.
“In the future, I hope we can deliver these medicines at home,” said Hazel O’Sullivan, MBBCh, a medical lung cancer oncologist at Cork University, Ireland, who explained the issues during a session at the 2024 European Lung Cancer Congress.
She was the discussant on two studies at the meeting that highlighted the latest developments in the field, the IMscin002 study of subcutaneous atezolizumab and the PALOMA study of subcutaneous amivantamab, both mostly in NSCLC patients.
Subcutaneous atezolizumab was approved recently in Europe after its maker, Genentech/Roche, made a convincing case that its pharmacokinetics, efficacy, and safety are comparable to the intravenous (IV) version. The U.S. Food and Drug Administration is considering approval; Genentech/Roche anticipates a decision in 2024.
IMscin002 randomized 179 stage 2-4 NSCLC patients evenly to IV or subcutaneous atezolizumab for the first three cycles, then switched them for three more cycles.
Participants were then asked what version they preferred and what they wanted to continue with.
Seventy-one percent said they liked the subcutaneous version better and 80% opted to continue with it. Their main reasons were because they spent less time in the clinic and it was more comfortable.
When asked about the potential for home administration, presenter Federico Cappuzzo, MD, PhD, a medical lung cancer oncologist in Rome, said that it could be “an important option in the future,” particularly in isolated areas far away from hospitals.
The authors of new research are currently evaluating whether home administration is possible. Nurses are administering atezolizumab to patients in their homes with telemedicine monitoring.
The other subcutaneous study presented at the meeting, the PALOMA trial with amivantamab, had only 19 subjects. Administration took no more than 10 minutes, versus potentially hours, especially for the first dose. Subcutaneous amivantamab was given once a month, versus every 2 weeks for the IV formulation, during the maintenance phase of treatment.
The take-home from PALOMA is that the risk of infusion reactions is lower with subcutaneous administration (16% versus 67%) but the risk of mostly mild skin rashes is higher (79% versus 36%).
Investigation is ongoing to confirm safety, pharmacokinetic, and efficacy equivalence with the IV formulation, including in combination with other medications.
When asked about home administration of amivantamab, PALOMA lead investigator Natasha Leighl, MD, a lung, and breast cancer medical oncologist at the University of Toronto, stated that patients probably need to be watched in the clinic for the first 4 months.
The atezolizumab study was funded by maker Genentech/Roche. The amivantamab study was funded by its maker, Janssen. The amivantamab investigator, Dr. Leighl, reported grants, honoraria, and travel payments from Janssen. Dr. Cappuzzo, the investigator on the atezolizumab study, reported speaker and adviser payments from Genentech/Roche. The discussant, Dr. O’Sullivan, wasn’t involved with either company but reported payments from Amgen and AstraZeneca and travel costs covered by Takeda.
FROM ELCC 2024
Lung Cancer Screening Unveils Hidden Health Risks
The reason is because the low-dose CT scans used for screening cover the lower neck down to the upper abdomen, revealing far more anatomy than simply the lungs.
In fact, lung cancer screening can provide information on three of the top 10 causes of death worldwide: ischemic heart disease, chronic obstructive pulmonary disease, and, of course, lung cancer.
With lung cancer screening, “we are basically targeting many birds with one low-dose stone,” explained Jelena Spasic MD, PhD, at the European Lung Cancer Congress (ELCC) 2024.
Dr. Spasic, a medical oncologist at the Institute for Oncology and Radiology of Serbia in Belgrade, was the discussant on a study that gave an indication on just how useful screening can be for other diseases.
The study, dubbed 4-IN-THE-LUNG-RUN trial (4ITLR), is an ongoing prospective trial in six European countries that is using lung cancer screening scans to also look for coronary artery calcifications, a marker of atherosclerosis.
Usually, coronary calcifications are considered incidental findings on lung cancer screenings and reported to subjects’ physicians for heart disease risk assessment.
The difference in 4ITLR is that investigators are actively looking for the lesions and quantifying the extent of calcifications.
It’s made possible by the artificial intelligence-based software being used to read the scans. In addition to generating reports on lung nodules, it also automatically calculates an Agatston score, a quantification of the degree of coronary artery calcification for each subject.
At the meeting, which was organized by the European Society for Clinical Oncology, 4ITLR investigator Daiwei Han, MD, PhD, a research associate at the Institute for Diagnostic Accuracy in Groningen, the Netherlands, reported outcomes in the first 2487 of the 24,000 planned subjects.
To be eligible for screening, participants had to be 60-79 years old and either current smokers, past smokers who had quit within 10 years, or people with a 35 or more pack-year history. The median age in the study was 68.1 years.
Overall, 53% of subjects had Agatston scores of 100 or more, indicating the need for treatment to prevent active coronary artery disease, Dr. Han said.
Fifteen percent were at high risk for heart disease with scores of 400-999, indicating extensive coronary artery calcification, and 16.2% were at very high risk, with scores of 1000 or higher. The information is being shared with participants’ physicians.
The risk of heart disease was far higher in men, who made up 56% of the study population. While women had a median Agatston score of 61, the median score for men was 211.1.
The findings illustrate the potential of dedicated cardiovascular screening within lung cancer screening programs, Dr. Han said, noting that 4ITLR will also incorporate COPD risk assessment.
The study also shows the increased impact lung cancer screening programs could have if greater use were made of the CT images to look for other diseases, Dr. Spasic said.
4ITLR is funded by the European Union’s Horizon 2020 Program. Dr. Spasic and Dr. Han didn’t have any relevant disclosures.
The reason is because the low-dose CT scans used for screening cover the lower neck down to the upper abdomen, revealing far more anatomy than simply the lungs.
In fact, lung cancer screening can provide information on three of the top 10 causes of death worldwide: ischemic heart disease, chronic obstructive pulmonary disease, and, of course, lung cancer.
With lung cancer screening, “we are basically targeting many birds with one low-dose stone,” explained Jelena Spasic MD, PhD, at the European Lung Cancer Congress (ELCC) 2024.
Dr. Spasic, a medical oncologist at the Institute for Oncology and Radiology of Serbia in Belgrade, was the discussant on a study that gave an indication on just how useful screening can be for other diseases.
The study, dubbed 4-IN-THE-LUNG-RUN trial (4ITLR), is an ongoing prospective trial in six European countries that is using lung cancer screening scans to also look for coronary artery calcifications, a marker of atherosclerosis.
Usually, coronary calcifications are considered incidental findings on lung cancer screenings and reported to subjects’ physicians for heart disease risk assessment.
The difference in 4ITLR is that investigators are actively looking for the lesions and quantifying the extent of calcifications.
It’s made possible by the artificial intelligence-based software being used to read the scans. In addition to generating reports on lung nodules, it also automatically calculates an Agatston score, a quantification of the degree of coronary artery calcification for each subject.
At the meeting, which was organized by the European Society for Clinical Oncology, 4ITLR investigator Daiwei Han, MD, PhD, a research associate at the Institute for Diagnostic Accuracy in Groningen, the Netherlands, reported outcomes in the first 2487 of the 24,000 planned subjects.
To be eligible for screening, participants had to be 60-79 years old and either current smokers, past smokers who had quit within 10 years, or people with a 35 or more pack-year history. The median age in the study was 68.1 years.
Overall, 53% of subjects had Agatston scores of 100 or more, indicating the need for treatment to prevent active coronary artery disease, Dr. Han said.
Fifteen percent were at high risk for heart disease with scores of 400-999, indicating extensive coronary artery calcification, and 16.2% were at very high risk, with scores of 1000 or higher. The information is being shared with participants’ physicians.
The risk of heart disease was far higher in men, who made up 56% of the study population. While women had a median Agatston score of 61, the median score for men was 211.1.
The findings illustrate the potential of dedicated cardiovascular screening within lung cancer screening programs, Dr. Han said, noting that 4ITLR will also incorporate COPD risk assessment.
The study also shows the increased impact lung cancer screening programs could have if greater use were made of the CT images to look for other diseases, Dr. Spasic said.
4ITLR is funded by the European Union’s Horizon 2020 Program. Dr. Spasic and Dr. Han didn’t have any relevant disclosures.
The reason is because the low-dose CT scans used for screening cover the lower neck down to the upper abdomen, revealing far more anatomy than simply the lungs.
In fact, lung cancer screening can provide information on three of the top 10 causes of death worldwide: ischemic heart disease, chronic obstructive pulmonary disease, and, of course, lung cancer.
With lung cancer screening, “we are basically targeting many birds with one low-dose stone,” explained Jelena Spasic MD, PhD, at the European Lung Cancer Congress (ELCC) 2024.
Dr. Spasic, a medical oncologist at the Institute for Oncology and Radiology of Serbia in Belgrade, was the discussant on a study that gave an indication on just how useful screening can be for other diseases.
The study, dubbed 4-IN-THE-LUNG-RUN trial (4ITLR), is an ongoing prospective trial in six European countries that is using lung cancer screening scans to also look for coronary artery calcifications, a marker of atherosclerosis.
Usually, coronary calcifications are considered incidental findings on lung cancer screenings and reported to subjects’ physicians for heart disease risk assessment.
The difference in 4ITLR is that investigators are actively looking for the lesions and quantifying the extent of calcifications.
It’s made possible by the artificial intelligence-based software being used to read the scans. In addition to generating reports on lung nodules, it also automatically calculates an Agatston score, a quantification of the degree of coronary artery calcification for each subject.
At the meeting, which was organized by the European Society for Clinical Oncology, 4ITLR investigator Daiwei Han, MD, PhD, a research associate at the Institute for Diagnostic Accuracy in Groningen, the Netherlands, reported outcomes in the first 2487 of the 24,000 planned subjects.
To be eligible for screening, participants had to be 60-79 years old and either current smokers, past smokers who had quit within 10 years, or people with a 35 or more pack-year history. The median age in the study was 68.1 years.
Overall, 53% of subjects had Agatston scores of 100 or more, indicating the need for treatment to prevent active coronary artery disease, Dr. Han said.
Fifteen percent were at high risk for heart disease with scores of 400-999, indicating extensive coronary artery calcification, and 16.2% were at very high risk, with scores of 1000 or higher. The information is being shared with participants’ physicians.
The risk of heart disease was far higher in men, who made up 56% of the study population. While women had a median Agatston score of 61, the median score for men was 211.1.
The findings illustrate the potential of dedicated cardiovascular screening within lung cancer screening programs, Dr. Han said, noting that 4ITLR will also incorporate COPD risk assessment.
The study also shows the increased impact lung cancer screening programs could have if greater use were made of the CT images to look for other diseases, Dr. Spasic said.
4ITLR is funded by the European Union’s Horizon 2020 Program. Dr. Spasic and Dr. Han didn’t have any relevant disclosures.
FROM ELCC 2024
VA to Expand Cancer Prevention Services
The US Department of Veterans Affairs (VA) announced plans to expand preventive services, health care, and benefits for veterans with cancer.
Urethral cancers are set to be added to the list of > 300 conditions considered presumptive under the Sergeant First Class Heath Robinson Honoring our Promise to Address Comprehensive Toxics (PACT) Act of 2022. Veterans deployed to Iraq, Afghanistan, Somalia, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, Uzbekistan, and the entire Southwest Asia theater will not need to prove their service caused their urethral cancer in order to receive treatment for it. Additionally, the VA plans to evaluate whether there is a relationship between urinary bladder and ureteral cancers and toxic exposures for these veterans, and determine whether these conditions are presumptive. The VA has already screened > 5 million veterans for toxic exposures under the PACT Act, as part of an ongoing mission to expand cancer care services.
The VA is also set to expand access to screening programs in 2024 by providing:
- genetic testing to every veteran who may need it;
- lung cancer screening programs to every VA medical center; and
- home tests for colorectal cancer to > 1 million veterans nationwide.
The VA continues to expand the reach of smoking cessation services, with ≥ 6 additional sites added to the Quit VET eReferral program by the end of 2024, and a new pilot program to integrate smoking cessation services into lung cancer screening.
The VA has already taken steps to build on the Biden-Harris Administration Cancer Moonshot program, which has the goals of preventing ≥ 4 million cancer deaths by 2047 and to improve the experience of individuals with cancer. For instance, it has prioritized claims processing for veterans with cancer and expanded cancer risk assessments and mammograms to veterans aged < 40 years, regardless of age, symptoms, family history, or whether they are enrolled in VA health care. In September, the VA and the National Cancer Institute announced a data-sharing collaboration to better understand and treat cancer among veterans.
“VA is planting the seeds for the future of cancer care,” said VHA Under Secretary for Health Shereef Elnahal, MD. “By investing in screenings, expanding access, and embracing cutting-edge technologies, VA is revolutionizing cancer care delivery, providing the best care possible to our nation’s heroes.”
The US Department of Veterans Affairs (VA) announced plans to expand preventive services, health care, and benefits for veterans with cancer.
Urethral cancers are set to be added to the list of > 300 conditions considered presumptive under the Sergeant First Class Heath Robinson Honoring our Promise to Address Comprehensive Toxics (PACT) Act of 2022. Veterans deployed to Iraq, Afghanistan, Somalia, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, Uzbekistan, and the entire Southwest Asia theater will not need to prove their service caused their urethral cancer in order to receive treatment for it. Additionally, the VA plans to evaluate whether there is a relationship between urinary bladder and ureteral cancers and toxic exposures for these veterans, and determine whether these conditions are presumptive. The VA has already screened > 5 million veterans for toxic exposures under the PACT Act, as part of an ongoing mission to expand cancer care services.
The VA is also set to expand access to screening programs in 2024 by providing:
- genetic testing to every veteran who may need it;
- lung cancer screening programs to every VA medical center; and
- home tests for colorectal cancer to > 1 million veterans nationwide.
The VA continues to expand the reach of smoking cessation services, with ≥ 6 additional sites added to the Quit VET eReferral program by the end of 2024, and a new pilot program to integrate smoking cessation services into lung cancer screening.
The VA has already taken steps to build on the Biden-Harris Administration Cancer Moonshot program, which has the goals of preventing ≥ 4 million cancer deaths by 2047 and to improve the experience of individuals with cancer. For instance, it has prioritized claims processing for veterans with cancer and expanded cancer risk assessments and mammograms to veterans aged < 40 years, regardless of age, symptoms, family history, or whether they are enrolled in VA health care. In September, the VA and the National Cancer Institute announced a data-sharing collaboration to better understand and treat cancer among veterans.
“VA is planting the seeds for the future of cancer care,” said VHA Under Secretary for Health Shereef Elnahal, MD. “By investing in screenings, expanding access, and embracing cutting-edge technologies, VA is revolutionizing cancer care delivery, providing the best care possible to our nation’s heroes.”
The US Department of Veterans Affairs (VA) announced plans to expand preventive services, health care, and benefits for veterans with cancer.
Urethral cancers are set to be added to the list of > 300 conditions considered presumptive under the Sergeant First Class Heath Robinson Honoring our Promise to Address Comprehensive Toxics (PACT) Act of 2022. Veterans deployed to Iraq, Afghanistan, Somalia, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, Uzbekistan, and the entire Southwest Asia theater will not need to prove their service caused their urethral cancer in order to receive treatment for it. Additionally, the VA plans to evaluate whether there is a relationship between urinary bladder and ureteral cancers and toxic exposures for these veterans, and determine whether these conditions are presumptive. The VA has already screened > 5 million veterans for toxic exposures under the PACT Act, as part of an ongoing mission to expand cancer care services.
The VA is also set to expand access to screening programs in 2024 by providing:
- genetic testing to every veteran who may need it;
- lung cancer screening programs to every VA medical center; and
- home tests for colorectal cancer to > 1 million veterans nationwide.
The VA continues to expand the reach of smoking cessation services, with ≥ 6 additional sites added to the Quit VET eReferral program by the end of 2024, and a new pilot program to integrate smoking cessation services into lung cancer screening.
The VA has already taken steps to build on the Biden-Harris Administration Cancer Moonshot program, which has the goals of preventing ≥ 4 million cancer deaths by 2047 and to improve the experience of individuals with cancer. For instance, it has prioritized claims processing for veterans with cancer and expanded cancer risk assessments and mammograms to veterans aged < 40 years, regardless of age, symptoms, family history, or whether they are enrolled in VA health care. In September, the VA and the National Cancer Institute announced a data-sharing collaboration to better understand and treat cancer among veterans.
“VA is planting the seeds for the future of cancer care,” said VHA Under Secretary for Health Shereef Elnahal, MD. “By investing in screenings, expanding access, and embracing cutting-edge technologies, VA is revolutionizing cancer care delivery, providing the best care possible to our nation’s heroes.”
Upfront Low-Dose Radiation Improves Advanced SCLC Outcomes
The analysis, presented at the 2024 European Lung Cancer Congress, revealed that low-dose radiation improved patients’ median progression-free and overall survival compared with standard first-line treatment, reported in a 2019 trial, lead author Yan Zhang, MD, reported.
The standard first-line treatment results came from the 2019 CASPIAN trial, which found that patients receiving the first-line regimen had a median progression-free survival of 5 months and a median overall survival of 13 months, with 54% of patient alive at 1 year.
The latest data, which included a small cohort of 30 patients, revealed that adding low-dose radiation to the standard first-line therapy led to a higher median progression-free survival of 8.3 months and extended median overall survival beyond the study follow-up period of 17.3 months. Overall, 66% of patients were alive at 1 year.
These are “promising” improvements over CASPIAN, Dr. Zhang, a lung cancer medical oncologist at Sichuan University, Chengdu, China, said at the Congress, which was organized by the European Society for Medical Oncology.
Study discussant Gerry Hanna, PhD, MBBS, a radiation oncologist at Belfast City Hospital, Belfast, Northern Ireland, agreed. Although there were just 30 patients, “you cannot deny these are [strong] results in terms of extensive-stage small cell cancer,” Dr. Hanna said.
Although standard first-line treatment of extensive-stage SCLC is durvalumab plus etoposide-platinum chemotherapy, the benefits aren’t durable for many patients.
This problem led Dr. Zhang and his colleagues to look for ways to improve outcomes. Because the CASPIAN trial did not include radiation to the primary tumor, it seemed a logical strategy to explore.
In the current single-arm study, Dr. Zhang and his team added 15 Gy radiation in five fractions to the primary lung tumors of 30 patients during the first cycle of durvalumab plus etoposide-platinum.
Subjects received 1500 mg of durvalumab plus etoposide-platinum every 3 weeks for four cycles. Low-dose radiation to the primary tumor was delivered over 5 days at the start of treatment. Patients then continued with durvalumab maintenance every 4 weeks until progression or intolerable toxicity.
Six patients (20%) had liver metastases at the baseline, and three (10%) had brain metastases. Over half had prophylactic cranial radiation. Performance scores were 0-1, and all but one of the participants were men.
Six- and 12-month progression-free survival rates were 57% and 40%, respectively. Overall survival was 90% at 6 months and 66% at 12 months. Median overall survival was 13 months in the CASPIAN trial but not reached in Dr. Zhang’s trial after a median follow-up of 17.3 months, with the earliest deaths occurring at 10.8 months.
Grade 3 treatment-related adverse events occurred in 80% of patients, most frequently hematologic toxicities. Five patients (16.7%) had severe adverse reactions to radiation. Although the overall dose of radiation was low, at 3 Gy each, the fractions were on the large side.
Hanna wanted more information on the radiotoxicity issue, but even so, he said that adding low-dose radiation to our durvalumab-chemotherapy doublet warrants further investigation.
Both Dr. Hanna and Dr. Zhang thought that instead of killing cancer cells directly, the greatest benefit of upfront radiation, and the peritumoral inflammation it causes, is to augment durvalumab’s effect.
Overall, Dr. Hanna stressed that we haven’t had results like these before in a SCLC study, particularly for novel agents, let alone radiation.
The study was funded by AstraZeneca, maker of durvalumab. Dr. Zhang and Dr. Hanna didn’t have any relevant disclosures.
A version of this article appeared on Medscape.com.
The analysis, presented at the 2024 European Lung Cancer Congress, revealed that low-dose radiation improved patients’ median progression-free and overall survival compared with standard first-line treatment, reported in a 2019 trial, lead author Yan Zhang, MD, reported.
The standard first-line treatment results came from the 2019 CASPIAN trial, which found that patients receiving the first-line regimen had a median progression-free survival of 5 months and a median overall survival of 13 months, with 54% of patient alive at 1 year.
The latest data, which included a small cohort of 30 patients, revealed that adding low-dose radiation to the standard first-line therapy led to a higher median progression-free survival of 8.3 months and extended median overall survival beyond the study follow-up period of 17.3 months. Overall, 66% of patients were alive at 1 year.
These are “promising” improvements over CASPIAN, Dr. Zhang, a lung cancer medical oncologist at Sichuan University, Chengdu, China, said at the Congress, which was organized by the European Society for Medical Oncology.
Study discussant Gerry Hanna, PhD, MBBS, a radiation oncologist at Belfast City Hospital, Belfast, Northern Ireland, agreed. Although there were just 30 patients, “you cannot deny these are [strong] results in terms of extensive-stage small cell cancer,” Dr. Hanna said.
Although standard first-line treatment of extensive-stage SCLC is durvalumab plus etoposide-platinum chemotherapy, the benefits aren’t durable for many patients.
This problem led Dr. Zhang and his colleagues to look for ways to improve outcomes. Because the CASPIAN trial did not include radiation to the primary tumor, it seemed a logical strategy to explore.
In the current single-arm study, Dr. Zhang and his team added 15 Gy radiation in five fractions to the primary lung tumors of 30 patients during the first cycle of durvalumab plus etoposide-platinum.
Subjects received 1500 mg of durvalumab plus etoposide-platinum every 3 weeks for four cycles. Low-dose radiation to the primary tumor was delivered over 5 days at the start of treatment. Patients then continued with durvalumab maintenance every 4 weeks until progression or intolerable toxicity.
Six patients (20%) had liver metastases at the baseline, and three (10%) had brain metastases. Over half had prophylactic cranial radiation. Performance scores were 0-1, and all but one of the participants were men.
Six- and 12-month progression-free survival rates were 57% and 40%, respectively. Overall survival was 90% at 6 months and 66% at 12 months. Median overall survival was 13 months in the CASPIAN trial but not reached in Dr. Zhang’s trial after a median follow-up of 17.3 months, with the earliest deaths occurring at 10.8 months.
Grade 3 treatment-related adverse events occurred in 80% of patients, most frequently hematologic toxicities. Five patients (16.7%) had severe adverse reactions to radiation. Although the overall dose of radiation was low, at 3 Gy each, the fractions were on the large side.
Hanna wanted more information on the radiotoxicity issue, but even so, he said that adding low-dose radiation to our durvalumab-chemotherapy doublet warrants further investigation.
Both Dr. Hanna and Dr. Zhang thought that instead of killing cancer cells directly, the greatest benefit of upfront radiation, and the peritumoral inflammation it causes, is to augment durvalumab’s effect.
Overall, Dr. Hanna stressed that we haven’t had results like these before in a SCLC study, particularly for novel agents, let alone radiation.
The study was funded by AstraZeneca, maker of durvalumab. Dr. Zhang and Dr. Hanna didn’t have any relevant disclosures.
A version of this article appeared on Medscape.com.
The analysis, presented at the 2024 European Lung Cancer Congress, revealed that low-dose radiation improved patients’ median progression-free and overall survival compared with standard first-line treatment, reported in a 2019 trial, lead author Yan Zhang, MD, reported.
The standard first-line treatment results came from the 2019 CASPIAN trial, which found that patients receiving the first-line regimen had a median progression-free survival of 5 months and a median overall survival of 13 months, with 54% of patient alive at 1 year.
The latest data, which included a small cohort of 30 patients, revealed that adding low-dose radiation to the standard first-line therapy led to a higher median progression-free survival of 8.3 months and extended median overall survival beyond the study follow-up period of 17.3 months. Overall, 66% of patients were alive at 1 year.
These are “promising” improvements over CASPIAN, Dr. Zhang, a lung cancer medical oncologist at Sichuan University, Chengdu, China, said at the Congress, which was organized by the European Society for Medical Oncology.
Study discussant Gerry Hanna, PhD, MBBS, a radiation oncologist at Belfast City Hospital, Belfast, Northern Ireland, agreed. Although there were just 30 patients, “you cannot deny these are [strong] results in terms of extensive-stage small cell cancer,” Dr. Hanna said.
Although standard first-line treatment of extensive-stage SCLC is durvalumab plus etoposide-platinum chemotherapy, the benefits aren’t durable for many patients.
This problem led Dr. Zhang and his colleagues to look for ways to improve outcomes. Because the CASPIAN trial did not include radiation to the primary tumor, it seemed a logical strategy to explore.
In the current single-arm study, Dr. Zhang and his team added 15 Gy radiation in five fractions to the primary lung tumors of 30 patients during the first cycle of durvalumab plus etoposide-platinum.
Subjects received 1500 mg of durvalumab plus etoposide-platinum every 3 weeks for four cycles. Low-dose radiation to the primary tumor was delivered over 5 days at the start of treatment. Patients then continued with durvalumab maintenance every 4 weeks until progression or intolerable toxicity.
Six patients (20%) had liver metastases at the baseline, and three (10%) had brain metastases. Over half had prophylactic cranial radiation. Performance scores were 0-1, and all but one of the participants were men.
Six- and 12-month progression-free survival rates were 57% and 40%, respectively. Overall survival was 90% at 6 months and 66% at 12 months. Median overall survival was 13 months in the CASPIAN trial but not reached in Dr. Zhang’s trial after a median follow-up of 17.3 months, with the earliest deaths occurring at 10.8 months.
Grade 3 treatment-related adverse events occurred in 80% of patients, most frequently hematologic toxicities. Five patients (16.7%) had severe adverse reactions to radiation. Although the overall dose of radiation was low, at 3 Gy each, the fractions were on the large side.
Hanna wanted more information on the radiotoxicity issue, but even so, he said that adding low-dose radiation to our durvalumab-chemotherapy doublet warrants further investigation.
Both Dr. Hanna and Dr. Zhang thought that instead of killing cancer cells directly, the greatest benefit of upfront radiation, and the peritumoral inflammation it causes, is to augment durvalumab’s effect.
Overall, Dr. Hanna stressed that we haven’t had results like these before in a SCLC study, particularly for novel agents, let alone radiation.
The study was funded by AstraZeneca, maker of durvalumab. Dr. Zhang and Dr. Hanna didn’t have any relevant disclosures.
A version of this article appeared on Medscape.com.
FROM ELCC 2024
Most Cancer Trial Centers Located Closer to White, Affluent Populations
This inequity may be potentiating the underrepresentation of racially minoritized and socioeconomically disadvantaged populations in clinical trials, suggesting that employment of satellite hospitals is needed to expand access to investigational therapies, reported lead author Hassal Lee, MD, PhD, of Cold Spring Harbor Laboratory, Cold Spring Harbor, New York, and colleagues.
“Minoritized and socioeconomically disadvantaged populations are underrepresented in clinical trials,” the investigators wrote in JAMA Oncology. “This may reduce the generalizability of trial results and propagate health disparities. Contributors to inequitable trial participation include individual-level factors and structural factors.”
Specifically, travel time to trial centers, as well as socioeconomic deprivation, can reduce likelihood of trial participation.
“Data on these parameters and population data on self-identified race exist, but their interrelation with clinical research facilities has not been systematically analyzed,” they wrote.
To try to draw comparisons between the distribution of patients of different races and socioeconomic statuses and the locations of clinical research facilities, Dr. Lee and colleagues aggregated data from the US Census, National Trial registry, Nature Index of Cancer Research Health Institutions, OpenStreetMap, National Cancer Institute–designated Cancer Centers list, and National Homeland Infrastructure Foundation. They then characterized catchment population demographics within 30-, 60-, and 120-minute driving commute times of all US hospitals, along with a more focused look at centers capable of conducting phase 1, phase 2, and phase 3 trials.
These efforts revealed broad geographic inequity.The 78 major centers that conduct 94% of all US cancer trials are located within 30 minutes of populations that have a 10.1% higher proportion of self-identified White individuals than the average US county, and a median income $18,900 higher than average (unpaired mean differences).
The publication also includes several maps characterizing racial and socioeconomic demographics within various catchment areas. For example, centers in New York City, Houston, and Chicago have the most diverse catchment populations within a 30-minute commute. Maps of all cities in the United States with populations greater than 500,000 are available in a supplementary index.
“This study indicates that geographical population distributions may present barriers to equitable clinical trial access and that data are available to proactively strategize about reduction of such barriers,” Dr. Lee and colleagues wrote.
The findings call attention to modifiable socioeconomic factors associated with trial participation, they added, like financial toxicity and affordable transportation, noting that ethnic and racial groups consent to trials at similar rates after controlling for income.
In addition, Dr. Lee and colleagues advised clinical trial designers to enlist satellite hospitals to increase participant diversity, since long commutes exacerbate “socioeconomic burdens associated with clinical trial participation,” with trial participation decreasing as commute time increases.
“Existing clinical trial centers may build collaborative efforts with nearby hospitals closer to underrepresented populations or set up community centers to support new collaborative networks to improve geographical access equity,” they wrote. “Methodologically, our approach is transferable to any country, region, or global effort with sufficient source data and can inform decision-making along the continuum of cancer care, from screening to implementing specialist care.”
A coauthor disclosed relationships with Flagship Therapeutics, Leidos Holding Ltd, Pershing Square Foundation, and others.
This inequity may be potentiating the underrepresentation of racially minoritized and socioeconomically disadvantaged populations in clinical trials, suggesting that employment of satellite hospitals is needed to expand access to investigational therapies, reported lead author Hassal Lee, MD, PhD, of Cold Spring Harbor Laboratory, Cold Spring Harbor, New York, and colleagues.
“Minoritized and socioeconomically disadvantaged populations are underrepresented in clinical trials,” the investigators wrote in JAMA Oncology. “This may reduce the generalizability of trial results and propagate health disparities. Contributors to inequitable trial participation include individual-level factors and structural factors.”
Specifically, travel time to trial centers, as well as socioeconomic deprivation, can reduce likelihood of trial participation.
“Data on these parameters and population data on self-identified race exist, but their interrelation with clinical research facilities has not been systematically analyzed,” they wrote.
To try to draw comparisons between the distribution of patients of different races and socioeconomic statuses and the locations of clinical research facilities, Dr. Lee and colleagues aggregated data from the US Census, National Trial registry, Nature Index of Cancer Research Health Institutions, OpenStreetMap, National Cancer Institute–designated Cancer Centers list, and National Homeland Infrastructure Foundation. They then characterized catchment population demographics within 30-, 60-, and 120-minute driving commute times of all US hospitals, along with a more focused look at centers capable of conducting phase 1, phase 2, and phase 3 trials.
These efforts revealed broad geographic inequity.The 78 major centers that conduct 94% of all US cancer trials are located within 30 minutes of populations that have a 10.1% higher proportion of self-identified White individuals than the average US county, and a median income $18,900 higher than average (unpaired mean differences).
The publication also includes several maps characterizing racial and socioeconomic demographics within various catchment areas. For example, centers in New York City, Houston, and Chicago have the most diverse catchment populations within a 30-minute commute. Maps of all cities in the United States with populations greater than 500,000 are available in a supplementary index.
“This study indicates that geographical population distributions may present barriers to equitable clinical trial access and that data are available to proactively strategize about reduction of such barriers,” Dr. Lee and colleagues wrote.
The findings call attention to modifiable socioeconomic factors associated with trial participation, they added, like financial toxicity and affordable transportation, noting that ethnic and racial groups consent to trials at similar rates after controlling for income.
In addition, Dr. Lee and colleagues advised clinical trial designers to enlist satellite hospitals to increase participant diversity, since long commutes exacerbate “socioeconomic burdens associated with clinical trial participation,” with trial participation decreasing as commute time increases.
“Existing clinical trial centers may build collaborative efforts with nearby hospitals closer to underrepresented populations or set up community centers to support new collaborative networks to improve geographical access equity,” they wrote. “Methodologically, our approach is transferable to any country, region, or global effort with sufficient source data and can inform decision-making along the continuum of cancer care, from screening to implementing specialist care.”
A coauthor disclosed relationships with Flagship Therapeutics, Leidos Holding Ltd, Pershing Square Foundation, and others.
This inequity may be potentiating the underrepresentation of racially minoritized and socioeconomically disadvantaged populations in clinical trials, suggesting that employment of satellite hospitals is needed to expand access to investigational therapies, reported lead author Hassal Lee, MD, PhD, of Cold Spring Harbor Laboratory, Cold Spring Harbor, New York, and colleagues.
“Minoritized and socioeconomically disadvantaged populations are underrepresented in clinical trials,” the investigators wrote in JAMA Oncology. “This may reduce the generalizability of trial results and propagate health disparities. Contributors to inequitable trial participation include individual-level factors and structural factors.”
Specifically, travel time to trial centers, as well as socioeconomic deprivation, can reduce likelihood of trial participation.
“Data on these parameters and population data on self-identified race exist, but their interrelation with clinical research facilities has not been systematically analyzed,” they wrote.
To try to draw comparisons between the distribution of patients of different races and socioeconomic statuses and the locations of clinical research facilities, Dr. Lee and colleagues aggregated data from the US Census, National Trial registry, Nature Index of Cancer Research Health Institutions, OpenStreetMap, National Cancer Institute–designated Cancer Centers list, and National Homeland Infrastructure Foundation. They then characterized catchment population demographics within 30-, 60-, and 120-minute driving commute times of all US hospitals, along with a more focused look at centers capable of conducting phase 1, phase 2, and phase 3 trials.
These efforts revealed broad geographic inequity.The 78 major centers that conduct 94% of all US cancer trials are located within 30 minutes of populations that have a 10.1% higher proportion of self-identified White individuals than the average US county, and a median income $18,900 higher than average (unpaired mean differences).
The publication also includes several maps characterizing racial and socioeconomic demographics within various catchment areas. For example, centers in New York City, Houston, and Chicago have the most diverse catchment populations within a 30-minute commute. Maps of all cities in the United States with populations greater than 500,000 are available in a supplementary index.
“This study indicates that geographical population distributions may present barriers to equitable clinical trial access and that data are available to proactively strategize about reduction of such barriers,” Dr. Lee and colleagues wrote.
The findings call attention to modifiable socioeconomic factors associated with trial participation, they added, like financial toxicity and affordable transportation, noting that ethnic and racial groups consent to trials at similar rates after controlling for income.
In addition, Dr. Lee and colleagues advised clinical trial designers to enlist satellite hospitals to increase participant diversity, since long commutes exacerbate “socioeconomic burdens associated with clinical trial participation,” with trial participation decreasing as commute time increases.
“Existing clinical trial centers may build collaborative efforts with nearby hospitals closer to underrepresented populations or set up community centers to support new collaborative networks to improve geographical access equity,” they wrote. “Methodologically, our approach is transferable to any country, region, or global effort with sufficient source data and can inform decision-making along the continuum of cancer care, from screening to implementing specialist care.”
A coauthor disclosed relationships with Flagship Therapeutics, Leidos Holding Ltd, Pershing Square Foundation, and others.
FROM JAMA ONCOLOGY
New Drug Approvals Are the Wrong Metric for Cancer Policy
How should we define success in cancer policy — what should the endpoint be?
It’s debatable. Is it fewer cancer deaths? Perhaps improved access to therapies or a reduction in disparities?
One thing I know with certainty: The number of new cancer drugs approved by the US Food and Drug Administration (FDA) is not and should not be our primary endpoint in and of itself.
I’ll go a step further: It is not even a surrogate marker for success.
Unfortunately, a new drug approval does not necessarily mean improved patient outcomes. In fact, the majority of cancer drugs approved these days improve neither survival nor quality of life. Our previous work has shown better mortality outcomes in other high-income countries that have not approved or do not fund several cancer drugs that the FDA has approved.
Even if a drug has a meaningful benefit, at an average cost of more than $250,000 per year, if a new drug cannot reach patients because of access or cost issues, it’s meaningless.
However, regulators and media celebrate the number (and speed) of drug approvals every year as if it were a marker of success in and of itself. But approving more drugs should not be the goal; improving outcomes should. The FDA’s current approach is akin to a university celebrating its graduation rate by lowering the requirements to pass.
When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine ‘ending cancer as we know it’ is premature and even embarrassing.
This is exactly what the FDA has been doing with our regulatory standards for drug approval. They have gradually lowered the requirements for approval from two randomized trials to one randomized trial, then further to one randomized trial with a surrogate endpoint. In many instances, they have gone even further, demanding merely single-arm trials. They’ve also gone from requiring overall survival benefits to celebrating nondetrimental effects on overall survival. It’s no wonder that we approve more drugs today than we did in the past — the bar for approval is pretty low nowadays.
In 2019, our lab found an interesting phenomenon: The number of approvals based on surrogate endpoints has been increasing while the number of accelerated approvals has been decreasing. This made no sense at first, because you’d think surrogate-based approvals and accelerated approvals would be collinear. However, we realized that the recent approvals based on surrogate endpoints were regular approvals instead of accelerated approvals, which explained the phenomenon. Not only is the FDA approving more drugs on the basis of lower levels of evidence, but the agency is also offering regular instead of accelerated approval, thereby removing the safety net of a confirmatory trial.
Nearly everybody sees this as a cause for celebration. Pharma celebrates record profits, regulators celebrate record numbers of drug approvals, insurance companies celebrate because they can pass these costs on as insurance premiums and make even more money, and physicians and patients celebrate access to the shiniest, sexiest new cancer drug.
Everybody is happy in this system. The only problem is that patient outcomes don’t improve, resources are taken away from other priorities, and society suffers a net harm.
When you contrast this celebration with the reality on the ground, the difference is stark and sobering. In our clinics, patients lack access to even old chemotherapeutic drugs that are already generic and cheap but make a meaningful difference in patient outcomes. Citing a current lack of incentives, several generic cancer drug manufacturers have stopped making these drugs; the US supply now relies heavily on importing them from emerging economies such as India. When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine “ending cancer as we know it” is premature and even embarrassing.
5-Fluorouracil, methotrexate, and the platinums are backbones of cancer treatment. Cisplatin and carboplatin are not drugs we use with the hope of improving survival by a couple of months; these drugs are the difference between life and death for patients with testicular and ovarian cancers. In a survey of 948 global oncologists, these were considered among the most essential cancer drugs by oncologists in high-income and low- and middle-income countries alike. Although oncologists in low- and middle-income countries sometimes argue that even these cheap generic drugs may be unaffordable to their patients, they usually remain available; access is a function of both availability and affordability. However, the shortage situation in the US is unique in that availability — rather than affordability — is impacting access.
Our profit-over-patients policy has landed us in a terrible paradox.
Generic drugs are cheap, and any industrialized country can manufacture them. This is why so few companies actually do so; the profit margins are low and companies have little incentive to produce them, despite their benefit. Meanwhile, the FDA is approving and offering access to new shiny molecules that cost more than $15,000 per month yet offer less than a month of progression-free survival benefit and no overall survival benefit (see margetuximab in breast cancer). We have a literal fatal attraction to everything new and shiny.
This is a clear misalignment of priorities in US cancer drug policy. Our profit-over-patients policy has landed us in a terrible paradox: If a drug is cheap and meaningful, it won’t be available, but if it is marginal and expensive, we will do everything to ensure patients can get it. It’s no wonder that patients on Medicaid are disproportionately affected by these drug shortages. Unless all patients have easy access to cisplatin, carboplatin, and 5-fluorouracil, it is frankly embarrassing to celebrate the number of new cancer drugs approved each year.
We all have a responsibility in this — policymakers and lawmakers, regulators and payers, manufacturers and distributors, the American Society of Clinical Oncology and other oncology societies, and physicians and patients. This is where our advocacy work should focus. The primary endpoint of our cancer policy should not be how many new treatments we can approve or how many expensive drugs a rich person with the best insurance can get at a leading cancer center. The true measure of our civilization is how it treats its most vulnerable members.
Dr. Gyawali has disclosed the following relevant financial relationship: Received consulting fees from Vivio Health.
Dr. Gyawali is an associate professor in the Departments of Oncology and Public Health Sciences and a scientist in the Division of Cancer Care and Epidemiology at Queen’s University in Kingston, Ontario, Canada, and is also affiliated faculty at the Program on Regulation, Therapeutics, and Law in the Department of Medicine at Brigham and Women’s Hospital in Boston. His clinical and research interests revolve around cancer policy, global oncology, evidence-based oncology, financial toxicities of cancer treatment, clinical trial methods, and supportive care. He tweets at @oncology_bg.
A version of this article appeared on Medscape.com.
How should we define success in cancer policy — what should the endpoint be?
It’s debatable. Is it fewer cancer deaths? Perhaps improved access to therapies or a reduction in disparities?
One thing I know with certainty: The number of new cancer drugs approved by the US Food and Drug Administration (FDA) is not and should not be our primary endpoint in and of itself.
I’ll go a step further: It is not even a surrogate marker for success.
Unfortunately, a new drug approval does not necessarily mean improved patient outcomes. In fact, the majority of cancer drugs approved these days improve neither survival nor quality of life. Our previous work has shown better mortality outcomes in other high-income countries that have not approved or do not fund several cancer drugs that the FDA has approved.
Even if a drug has a meaningful benefit, at an average cost of more than $250,000 per year, if a new drug cannot reach patients because of access or cost issues, it’s meaningless.
However, regulators and media celebrate the number (and speed) of drug approvals every year as if it were a marker of success in and of itself. But approving more drugs should not be the goal; improving outcomes should. The FDA’s current approach is akin to a university celebrating its graduation rate by lowering the requirements to pass.
When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine ‘ending cancer as we know it’ is premature and even embarrassing.
This is exactly what the FDA has been doing with our regulatory standards for drug approval. They have gradually lowered the requirements for approval from two randomized trials to one randomized trial, then further to one randomized trial with a surrogate endpoint. In many instances, they have gone even further, demanding merely single-arm trials. They’ve also gone from requiring overall survival benefits to celebrating nondetrimental effects on overall survival. It’s no wonder that we approve more drugs today than we did in the past — the bar for approval is pretty low nowadays.
In 2019, our lab found an interesting phenomenon: The number of approvals based on surrogate endpoints has been increasing while the number of accelerated approvals has been decreasing. This made no sense at first, because you’d think surrogate-based approvals and accelerated approvals would be collinear. However, we realized that the recent approvals based on surrogate endpoints were regular approvals instead of accelerated approvals, which explained the phenomenon. Not only is the FDA approving more drugs on the basis of lower levels of evidence, but the agency is also offering regular instead of accelerated approval, thereby removing the safety net of a confirmatory trial.
Nearly everybody sees this as a cause for celebration. Pharma celebrates record profits, regulators celebrate record numbers of drug approvals, insurance companies celebrate because they can pass these costs on as insurance premiums and make even more money, and physicians and patients celebrate access to the shiniest, sexiest new cancer drug.
Everybody is happy in this system. The only problem is that patient outcomes don’t improve, resources are taken away from other priorities, and society suffers a net harm.
When you contrast this celebration with the reality on the ground, the difference is stark and sobering. In our clinics, patients lack access to even old chemotherapeutic drugs that are already generic and cheap but make a meaningful difference in patient outcomes. Citing a current lack of incentives, several generic cancer drug manufacturers have stopped making these drugs; the US supply now relies heavily on importing them from emerging economies such as India. When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine “ending cancer as we know it” is premature and even embarrassing.
5-Fluorouracil, methotrexate, and the platinums are backbones of cancer treatment. Cisplatin and carboplatin are not drugs we use with the hope of improving survival by a couple of months; these drugs are the difference between life and death for patients with testicular and ovarian cancers. In a survey of 948 global oncologists, these were considered among the most essential cancer drugs by oncologists in high-income and low- and middle-income countries alike. Although oncologists in low- and middle-income countries sometimes argue that even these cheap generic drugs may be unaffordable to their patients, they usually remain available; access is a function of both availability and affordability. However, the shortage situation in the US is unique in that availability — rather than affordability — is impacting access.
Our profit-over-patients policy has landed us in a terrible paradox.
Generic drugs are cheap, and any industrialized country can manufacture them. This is why so few companies actually do so; the profit margins are low and companies have little incentive to produce them, despite their benefit. Meanwhile, the FDA is approving and offering access to new shiny molecules that cost more than $15,000 per month yet offer less than a month of progression-free survival benefit and no overall survival benefit (see margetuximab in breast cancer). We have a literal fatal attraction to everything new and shiny.
This is a clear misalignment of priorities in US cancer drug policy. Our profit-over-patients policy has landed us in a terrible paradox: If a drug is cheap and meaningful, it won’t be available, but if it is marginal and expensive, we will do everything to ensure patients can get it. It’s no wonder that patients on Medicaid are disproportionately affected by these drug shortages. Unless all patients have easy access to cisplatin, carboplatin, and 5-fluorouracil, it is frankly embarrassing to celebrate the number of new cancer drugs approved each year.
We all have a responsibility in this — policymakers and lawmakers, regulators and payers, manufacturers and distributors, the American Society of Clinical Oncology and other oncology societies, and physicians and patients. This is where our advocacy work should focus. The primary endpoint of our cancer policy should not be how many new treatments we can approve or how many expensive drugs a rich person with the best insurance can get at a leading cancer center. The true measure of our civilization is how it treats its most vulnerable members.
Dr. Gyawali has disclosed the following relevant financial relationship: Received consulting fees from Vivio Health.
Dr. Gyawali is an associate professor in the Departments of Oncology and Public Health Sciences and a scientist in the Division of Cancer Care and Epidemiology at Queen’s University in Kingston, Ontario, Canada, and is also affiliated faculty at the Program on Regulation, Therapeutics, and Law in the Department of Medicine at Brigham and Women’s Hospital in Boston. His clinical and research interests revolve around cancer policy, global oncology, evidence-based oncology, financial toxicities of cancer treatment, clinical trial methods, and supportive care. He tweets at @oncology_bg.
A version of this article appeared on Medscape.com.
How should we define success in cancer policy — what should the endpoint be?
It’s debatable. Is it fewer cancer deaths? Perhaps improved access to therapies or a reduction in disparities?
One thing I know with certainty: The number of new cancer drugs approved by the US Food and Drug Administration (FDA) is not and should not be our primary endpoint in and of itself.
I’ll go a step further: It is not even a surrogate marker for success.
Unfortunately, a new drug approval does not necessarily mean improved patient outcomes. In fact, the majority of cancer drugs approved these days improve neither survival nor quality of life. Our previous work has shown better mortality outcomes in other high-income countries that have not approved or do not fund several cancer drugs that the FDA has approved.
Even if a drug has a meaningful benefit, at an average cost of more than $250,000 per year, if a new drug cannot reach patients because of access or cost issues, it’s meaningless.
However, regulators and media celebrate the number (and speed) of drug approvals every year as if it were a marker of success in and of itself. But approving more drugs should not be the goal; improving outcomes should. The FDA’s current approach is akin to a university celebrating its graduation rate by lowering the requirements to pass.
When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine ‘ending cancer as we know it’ is premature and even embarrassing.
This is exactly what the FDA has been doing with our regulatory standards for drug approval. They have gradually lowered the requirements for approval from two randomized trials to one randomized trial, then further to one randomized trial with a surrogate endpoint. In many instances, they have gone even further, demanding merely single-arm trials. They’ve also gone from requiring overall survival benefits to celebrating nondetrimental effects on overall survival. It’s no wonder that we approve more drugs today than we did in the past — the bar for approval is pretty low nowadays.
In 2019, our lab found an interesting phenomenon: The number of approvals based on surrogate endpoints has been increasing while the number of accelerated approvals has been decreasing. This made no sense at first, because you’d think surrogate-based approvals and accelerated approvals would be collinear. However, we realized that the recent approvals based on surrogate endpoints were regular approvals instead of accelerated approvals, which explained the phenomenon. Not only is the FDA approving more drugs on the basis of lower levels of evidence, but the agency is also offering regular instead of accelerated approval, thereby removing the safety net of a confirmatory trial.
Nearly everybody sees this as a cause for celebration. Pharma celebrates record profits, regulators celebrate record numbers of drug approvals, insurance companies celebrate because they can pass these costs on as insurance premiums and make even more money, and physicians and patients celebrate access to the shiniest, sexiest new cancer drug.
Everybody is happy in this system. The only problem is that patient outcomes don’t improve, resources are taken away from other priorities, and society suffers a net harm.
When you contrast this celebration with the reality on the ground, the difference is stark and sobering. In our clinics, patients lack access to even old chemotherapeutic drugs that are already generic and cheap but make a meaningful difference in patient outcomes. Citing a current lack of incentives, several generic cancer drug manufacturers have stopped making these drugs; the US supply now relies heavily on importing them from emerging economies such as India. When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine “ending cancer as we know it” is premature and even embarrassing.
5-Fluorouracil, methotrexate, and the platinums are backbones of cancer treatment. Cisplatin and carboplatin are not drugs we use with the hope of improving survival by a couple of months; these drugs are the difference between life and death for patients with testicular and ovarian cancers. In a survey of 948 global oncologists, these were considered among the most essential cancer drugs by oncologists in high-income and low- and middle-income countries alike. Although oncologists in low- and middle-income countries sometimes argue that even these cheap generic drugs may be unaffordable to their patients, they usually remain available; access is a function of both availability and affordability. However, the shortage situation in the US is unique in that availability — rather than affordability — is impacting access.
Our profit-over-patients policy has landed us in a terrible paradox.
Generic drugs are cheap, and any industrialized country can manufacture them. This is why so few companies actually do so; the profit margins are low and companies have little incentive to produce them, despite their benefit. Meanwhile, the FDA is approving and offering access to new shiny molecules that cost more than $15,000 per month yet offer less than a month of progression-free survival benefit and no overall survival benefit (see margetuximab in breast cancer). We have a literal fatal attraction to everything new and shiny.
This is a clear misalignment of priorities in US cancer drug policy. Our profit-over-patients policy has landed us in a terrible paradox: If a drug is cheap and meaningful, it won’t be available, but if it is marginal and expensive, we will do everything to ensure patients can get it. It’s no wonder that patients on Medicaid are disproportionately affected by these drug shortages. Unless all patients have easy access to cisplatin, carboplatin, and 5-fluorouracil, it is frankly embarrassing to celebrate the number of new cancer drugs approved each year.
We all have a responsibility in this — policymakers and lawmakers, regulators and payers, manufacturers and distributors, the American Society of Clinical Oncology and other oncology societies, and physicians and patients. This is where our advocacy work should focus. The primary endpoint of our cancer policy should not be how many new treatments we can approve or how many expensive drugs a rich person with the best insurance can get at a leading cancer center. The true measure of our civilization is how it treats its most vulnerable members.
Dr. Gyawali has disclosed the following relevant financial relationship: Received consulting fees from Vivio Health.
Dr. Gyawali is an associate professor in the Departments of Oncology and Public Health Sciences and a scientist in the Division of Cancer Care and Epidemiology at Queen’s University in Kingston, Ontario, Canada, and is also affiliated faculty at the Program on Regulation, Therapeutics, and Law in the Department of Medicine at Brigham and Women’s Hospital in Boston. His clinical and research interests revolve around cancer policy, global oncology, evidence-based oncology, financial toxicities of cancer treatment, clinical trial methods, and supportive care. He tweets at @oncology_bg.
A version of this article appeared on Medscape.com.
Extraordinary Patients Inspired Father of Cancer Immunotherapy
His pioneering research established interleukin-2 (IL-2) as the first U.S. Food and Drug Administration–approved cancer immunotherapy in 1992.
To recognize his trailblazing work and other achievements, the American Association for Cancer Research (AACR) will award Dr. Rosenberg with the 2024 AACR Award for Lifetime Achievement in Cancer Research at its annual meeting in April.

Dr. Rosenberg, a senior investigator for the Center for Cancer Research at the National Cancer Institute (NCI), and chief of the NCI Surgery Branch, shared the history behind his novel research and the patient stories that inspired his discoveries, during an interview.
Tell us a little about yourself and where you grew up.
Dr. Rosenberg: I grew up in the Bronx. My parents both immigrated to the United States from Poland as teenagers.
As a young boy, did you always want to become a doctor?
Dr. Rosenberg: I think some defining moments on why I decided to go into medicine occurred when I was 6 or 7 years old. The second world war was over, and many of the horrors of the Holocaust became apparent to me. I was brought up as an Orthodox Jew. My parents were quite religious, and I remember postcards coming in one after another about relatives that had died in the death camps. That had a profound influence on me.
How did that experience impact your aspirations?
Dr. Rosenberg: It was an example to me of how evil certain people and groups can be toward one another. I decided at that point, that I wanted to do something good for people, and medicine seemed the most likely way to do that. But also, I was developing a broad scientific interest. I ended up at the Bronx High School of Science and knew that I not only wanted to practice the medicine of today, but I wanted to play a role in helping develop the medicine.
What led to your interest in cancer treatment?
Dr. Rosenberg: Well, as a medical student and resident, it became clear that the field of cancer needed major improvement. We had three major ways to treat cancer: surgery, radiation therapy, and chemotherapy. That could cure about half of the people [who] had cancer. But despite the best application of those three specialties, there were over 600,000 deaths from cancer each year in the United States alone. It was clear to me that new approaches were needed, and I became very interested in taking advantage of the body’s immune system as a source of information to try to make progress.
Were there patients who inspired your research?
Dr. Rosenberg: There were two patients that I saw early in my career that impressed me a great deal. One was a patient that I saw when working in the emergency ward as a resident. A patient came in with right upper quadrant pain that looked like a gallbladder attack. That’s what it was. But when I went through his chart, I saw that he had been at that hospital 12 years earlier with a metastatic gastric cancer. The surgeons had operated. They saw tumor had spread to the liver and could not be removed. They closed the belly, not expecting him to survive. Yet he kept showing up for follow-up visits.
Here he was 12 years later. When I helped operate to take out his gallbladder, there was no evidence of any cancer. The cancer had disappeared in the absence of any external treatment. One of the rarest events in medicine, the spontaneous regression of a cancer. Somehow his body had learned how to destroy the tumor.
Was the second patient’s case as impressive?
Dr. Rosenberg: This patient had received a kidney transplant from a gentleman who died in an auto accident. [The donor’s] kidney contained a cancer deposit, a kidney cancer, unbeknownst to the transplant surgeons. [When the kidney was transplanted], the recipient developed widespread metastatic kidney cancer.
[The recipient] was on immunosuppressive drugs, and so the drugs had to be stopped. [When the immunosuppressive drugs were stopped], the patient’s body rejected the kidney and his cancer disappeared.
That showed me that, in fact, if you could stimulate a strong enough immune reaction, in this case, an [allogeneic] reaction, against foreign tissues from a different individual, that you could make large vascularized, invasive cancers disappear based on immune reactivities. Those were clues that led me toward studying the immune system’s impact on cancer.
From there, how did your work evolve?
Dr. Rosenberg: As chief of the surgery branch at NIH, I began doing research. It was very difficult to manipulate immune cells in the laboratory. They wouldn’t stay alive. But I tried to study immune reactions in patients with cancer to see if there was such a thing as an immune reaction against the cancer. There was no such thing known at the time. There were no cancer antigens and no known immune reactions against the disease in the human.
Around this time, investigators were publishing studies about interleukin-2 (IL-2), or white blood cells known as leukocytes. How did interleukin-2 further your research?
Dr. Rosenberg: The advent of interleukin-2 enabled scientists to grow lymphocytes outside the body. [This] enabled us to grow t-lymphocytes, which are some of the major warriors of the immune system against foreign tissue. After [studying] 66 patients in which we studied interleukin-2 and cells that would develop from it, we finally saw a disappearance of melanoma in a patient that received interleukin-2. And we went on to treat hundreds of patients with that hormone, interleukin-2. In fact, interleukin-2 became the first immunotherapy ever approved by the Food and Drug Administration for the treatment of cancer in humans.
How did this finding impact your future discoveries?
Dr. Rosenberg: [It] led to studies of the mechanism of action of interleukin-2 and to do that, we identified a kind of cell called a tumor infiltrating lymphocyte. What better place, intuitively to look for cells doing battle against the cancer than within the cancer itself?
In 1988, we demonstrated for the first time that transfer of lymphocytes with antitumor activity could cause the regression of melanoma. This was a living drug obtained from melanoma deposits that could be grown outside the body and then readministered to the patient under suitable conditions. Interestingly, [in February the FDA approved that drug as treatment for patients with melanoma]. A company developed it to the point where in multi-institutional studies, they reproduced our results.
And we’ve now emphasized the value of using T cell therapy, t cell transfer, for the treatment of patients with the common solid cancers, the cancers that start anywhere from the colon up through the intestine, the stomach, the pancreas, and the esophagus. Solid tumors such as ovarian cancer, uterine cancer and so on, are also potentially susceptible to this T cell therapy.
We’ve published several papers showing in isolated patients that you could cause major regressions, if not complete regressions, of these solid cancers in the liver, in the breast, the cervix, the colon. That’s a major aspect of what we’re doing now.
I think immunotherapy has come to be recognized as a major fourth arm that can be used to attack cancers, adding to surgery, radiation, and chemotherapy.
What guidance would you have for other physician-investigators or young doctors who want to follow in your path?
Dr. Rosenberg: You have to have a broad base of knowledge. You have to be willing to immerse yourself in a problem so that your mind is working on it when you’re doing things where you can only think. [When] you’re taking a shower, [or] waiting at a red light, your mind is working on this problem because you’re immersed in trying to understand it.
You need to have a laser focus on the goals that you have and not get sidetracked by issues that may be interesting but not directly related to the goals that you’re attempting to achieve.
His pioneering research established interleukin-2 (IL-2) as the first U.S. Food and Drug Administration–approved cancer immunotherapy in 1992.
To recognize his trailblazing work and other achievements, the American Association for Cancer Research (AACR) will award Dr. Rosenberg with the 2024 AACR Award for Lifetime Achievement in Cancer Research at its annual meeting in April.
Dr. Rosenberg, a senior investigator for the Center for Cancer Research at the National Cancer Institute (NCI), and chief of the NCI Surgery Branch, shared the history behind his novel research and the patient stories that inspired his discoveries, during an interview.
Tell us a little about yourself and where you grew up.
Dr. Rosenberg: I grew up in the Bronx. My parents both immigrated to the United States from Poland as teenagers.
As a young boy, did you always want to become a doctor?
Dr. Rosenberg: I think some defining moments on why I decided to go into medicine occurred when I was 6 or 7 years old. The second world war was over, and many of the horrors of the Holocaust became apparent to me. I was brought up as an Orthodox Jew. My parents were quite religious, and I remember postcards coming in one after another about relatives that had died in the death camps. That had a profound influence on me.
How did that experience impact your aspirations?
Dr. Rosenberg: It was an example to me of how evil certain people and groups can be toward one another. I decided at that point, that I wanted to do something good for people, and medicine seemed the most likely way to do that. But also, I was developing a broad scientific interest. I ended up at the Bronx High School of Science and knew that I not only wanted to practice the medicine of today, but I wanted to play a role in helping develop the medicine.
What led to your interest in cancer treatment?
Dr. Rosenberg: Well, as a medical student and resident, it became clear that the field of cancer needed major improvement. We had three major ways to treat cancer: surgery, radiation therapy, and chemotherapy. That could cure about half of the people [who] had cancer. But despite the best application of those three specialties, there were over 600,000 deaths from cancer each year in the United States alone. It was clear to me that new approaches were needed, and I became very interested in taking advantage of the body’s immune system as a source of information to try to make progress.
Were there patients who inspired your research?
Dr. Rosenberg: There were two patients that I saw early in my career that impressed me a great deal. One was a patient that I saw when working in the emergency ward as a resident. A patient came in with right upper quadrant pain that looked like a gallbladder attack. That’s what it was. But when I went through his chart, I saw that he had been at that hospital 12 years earlier with a metastatic gastric cancer. The surgeons had operated. They saw tumor had spread to the liver and could not be removed. They closed the belly, not expecting him to survive. Yet he kept showing up for follow-up visits.
Here he was 12 years later. When I helped operate to take out his gallbladder, there was no evidence of any cancer. The cancer had disappeared in the absence of any external treatment. One of the rarest events in medicine, the spontaneous regression of a cancer. Somehow his body had learned how to destroy the tumor.
Was the second patient’s case as impressive?
Dr. Rosenberg: This patient had received a kidney transplant from a gentleman who died in an auto accident. [The donor’s] kidney contained a cancer deposit, a kidney cancer, unbeknownst to the transplant surgeons. [When the kidney was transplanted], the recipient developed widespread metastatic kidney cancer.
[The recipient] was on immunosuppressive drugs, and so the drugs had to be stopped. [When the immunosuppressive drugs were stopped], the patient’s body rejected the kidney and his cancer disappeared.
That showed me that, in fact, if you could stimulate a strong enough immune reaction, in this case, an [allogeneic] reaction, against foreign tissues from a different individual, that you could make large vascularized, invasive cancers disappear based on immune reactivities. Those were clues that led me toward studying the immune system’s impact on cancer.
From there, how did your work evolve?
Dr. Rosenberg: As chief of the surgery branch at NIH, I began doing research. It was very difficult to manipulate immune cells in the laboratory. They wouldn’t stay alive. But I tried to study immune reactions in patients with cancer to see if there was such a thing as an immune reaction against the cancer. There was no such thing known at the time. There were no cancer antigens and no known immune reactions against the disease in the human.
Around this time, investigators were publishing studies about interleukin-2 (IL-2), or white blood cells known as leukocytes. How did interleukin-2 further your research?
Dr. Rosenberg: The advent of interleukin-2 enabled scientists to grow lymphocytes outside the body. [This] enabled us to grow t-lymphocytes, which are some of the major warriors of the immune system against foreign tissue. After [studying] 66 patients in which we studied interleukin-2 and cells that would develop from it, we finally saw a disappearance of melanoma in a patient that received interleukin-2. And we went on to treat hundreds of patients with that hormone, interleukin-2. In fact, interleukin-2 became the first immunotherapy ever approved by the Food and Drug Administration for the treatment of cancer in humans.
How did this finding impact your future discoveries?
Dr. Rosenberg: [It] led to studies of the mechanism of action of interleukin-2 and to do that, we identified a kind of cell called a tumor infiltrating lymphocyte. What better place, intuitively to look for cells doing battle against the cancer than within the cancer itself?
In 1988, we demonstrated for the first time that transfer of lymphocytes with antitumor activity could cause the regression of melanoma. This was a living drug obtained from melanoma deposits that could be grown outside the body and then readministered to the patient under suitable conditions. Interestingly, [in February the FDA approved that drug as treatment for patients with melanoma]. A company developed it to the point where in multi-institutional studies, they reproduced our results.
And we’ve now emphasized the value of using T cell therapy, t cell transfer, for the treatment of patients with the common solid cancers, the cancers that start anywhere from the colon up through the intestine, the stomach, the pancreas, and the esophagus. Solid tumors such as ovarian cancer, uterine cancer and so on, are also potentially susceptible to this T cell therapy.
We’ve published several papers showing in isolated patients that you could cause major regressions, if not complete regressions, of these solid cancers in the liver, in the breast, the cervix, the colon. That’s a major aspect of what we’re doing now.
I think immunotherapy has come to be recognized as a major fourth arm that can be used to attack cancers, adding to surgery, radiation, and chemotherapy.
What guidance would you have for other physician-investigators or young doctors who want to follow in your path?
Dr. Rosenberg: You have to have a broad base of knowledge. You have to be willing to immerse yourself in a problem so that your mind is working on it when you’re doing things where you can only think. [When] you’re taking a shower, [or] waiting at a red light, your mind is working on this problem because you’re immersed in trying to understand it.
You need to have a laser focus on the goals that you have and not get sidetracked by issues that may be interesting but not directly related to the goals that you’re attempting to achieve.
His pioneering research established interleukin-2 (IL-2) as the first U.S. Food and Drug Administration–approved cancer immunotherapy in 1992.
To recognize his trailblazing work and other achievements, the American Association for Cancer Research (AACR) will award Dr. Rosenberg with the 2024 AACR Award for Lifetime Achievement in Cancer Research at its annual meeting in April.
Dr. Rosenberg, a senior investigator for the Center for Cancer Research at the National Cancer Institute (NCI), and chief of the NCI Surgery Branch, shared the history behind his novel research and the patient stories that inspired his discoveries, during an interview.
Tell us a little about yourself and where you grew up.
Dr. Rosenberg: I grew up in the Bronx. My parents both immigrated to the United States from Poland as teenagers.
As a young boy, did you always want to become a doctor?
Dr. Rosenberg: I think some defining moments on why I decided to go into medicine occurred when I was 6 or 7 years old. The second world war was over, and many of the horrors of the Holocaust became apparent to me. I was brought up as an Orthodox Jew. My parents were quite religious, and I remember postcards coming in one after another about relatives that had died in the death camps. That had a profound influence on me.
How did that experience impact your aspirations?
Dr. Rosenberg: It was an example to me of how evil certain people and groups can be toward one another. I decided at that point, that I wanted to do something good for people, and medicine seemed the most likely way to do that. But also, I was developing a broad scientific interest. I ended up at the Bronx High School of Science and knew that I not only wanted to practice the medicine of today, but I wanted to play a role in helping develop the medicine.
What led to your interest in cancer treatment?
Dr. Rosenberg: Well, as a medical student and resident, it became clear that the field of cancer needed major improvement. We had three major ways to treat cancer: surgery, radiation therapy, and chemotherapy. That could cure about half of the people [who] had cancer. But despite the best application of those three specialties, there were over 600,000 deaths from cancer each year in the United States alone. It was clear to me that new approaches were needed, and I became very interested in taking advantage of the body’s immune system as a source of information to try to make progress.
Were there patients who inspired your research?
Dr. Rosenberg: There were two patients that I saw early in my career that impressed me a great deal. One was a patient that I saw when working in the emergency ward as a resident. A patient came in with right upper quadrant pain that looked like a gallbladder attack. That’s what it was. But when I went through his chart, I saw that he had been at that hospital 12 years earlier with a metastatic gastric cancer. The surgeons had operated. They saw tumor had spread to the liver and could not be removed. They closed the belly, not expecting him to survive. Yet he kept showing up for follow-up visits.
Here he was 12 years later. When I helped operate to take out his gallbladder, there was no evidence of any cancer. The cancer had disappeared in the absence of any external treatment. One of the rarest events in medicine, the spontaneous regression of a cancer. Somehow his body had learned how to destroy the tumor.
Was the second patient’s case as impressive?
Dr. Rosenberg: This patient had received a kidney transplant from a gentleman who died in an auto accident. [The donor’s] kidney contained a cancer deposit, a kidney cancer, unbeknownst to the transplant surgeons. [When the kidney was transplanted], the recipient developed widespread metastatic kidney cancer.
[The recipient] was on immunosuppressive drugs, and so the drugs had to be stopped. [When the immunosuppressive drugs were stopped], the patient’s body rejected the kidney and his cancer disappeared.
That showed me that, in fact, if you could stimulate a strong enough immune reaction, in this case, an [allogeneic] reaction, against foreign tissues from a different individual, that you could make large vascularized, invasive cancers disappear based on immune reactivities. Those were clues that led me toward studying the immune system’s impact on cancer.
From there, how did your work evolve?
Dr. Rosenberg: As chief of the surgery branch at NIH, I began doing research. It was very difficult to manipulate immune cells in the laboratory. They wouldn’t stay alive. But I tried to study immune reactions in patients with cancer to see if there was such a thing as an immune reaction against the cancer. There was no such thing known at the time. There were no cancer antigens and no known immune reactions against the disease in the human.
Around this time, investigators were publishing studies about interleukin-2 (IL-2), or white blood cells known as leukocytes. How did interleukin-2 further your research?
Dr. Rosenberg: The advent of interleukin-2 enabled scientists to grow lymphocytes outside the body. [This] enabled us to grow t-lymphocytes, which are some of the major warriors of the immune system against foreign tissue. After [studying] 66 patients in which we studied interleukin-2 and cells that would develop from it, we finally saw a disappearance of melanoma in a patient that received interleukin-2. And we went on to treat hundreds of patients with that hormone, interleukin-2. In fact, interleukin-2 became the first immunotherapy ever approved by the Food and Drug Administration for the treatment of cancer in humans.
How did this finding impact your future discoveries?
Dr. Rosenberg: [It] led to studies of the mechanism of action of interleukin-2 and to do that, we identified a kind of cell called a tumor infiltrating lymphocyte. What better place, intuitively to look for cells doing battle against the cancer than within the cancer itself?
In 1988, we demonstrated for the first time that transfer of lymphocytes with antitumor activity could cause the regression of melanoma. This was a living drug obtained from melanoma deposits that could be grown outside the body and then readministered to the patient under suitable conditions. Interestingly, [in February the FDA approved that drug as treatment for patients with melanoma]. A company developed it to the point where in multi-institutional studies, they reproduced our results.
And we’ve now emphasized the value of using T cell therapy, t cell transfer, for the treatment of patients with the common solid cancers, the cancers that start anywhere from the colon up through the intestine, the stomach, the pancreas, and the esophagus. Solid tumors such as ovarian cancer, uterine cancer and so on, are also potentially susceptible to this T cell therapy.
We’ve published several papers showing in isolated patients that you could cause major regressions, if not complete regressions, of these solid cancers in the liver, in the breast, the cervix, the colon. That’s a major aspect of what we’re doing now.
I think immunotherapy has come to be recognized as a major fourth arm that can be used to attack cancers, adding to surgery, radiation, and chemotherapy.
What guidance would you have for other physician-investigators or young doctors who want to follow in your path?
Dr. Rosenberg: You have to have a broad base of knowledge. You have to be willing to immerse yourself in a problem so that your mind is working on it when you’re doing things where you can only think. [When] you’re taking a shower, [or] waiting at a red light, your mind is working on this problem because you’re immersed in trying to understand it.
You need to have a laser focus on the goals that you have and not get sidetracked by issues that may be interesting but not directly related to the goals that you’re attempting to achieve.
Why a New Inhalable Lung Cancer Treatment Is So Promising
Cells in the human body chat with each other all the time. One major way they communicate is by releasing tiny spheres called exosomes. These carry fats, proteins, and genetic material that help regulate everything from pregnancy and immune responses to heart health and kidney function.
“Exosomes work like text messages between cells , sending and receiving information,” said lead researcher Ke Cheng, PhD, professor of biomedical engineering at Columbia. “The significance of this study is that exosomes can bring mRNA-based treatment to lung cancer cells locally, unlike systemic chemotherapy that can have side effects throughout the body. And inhalation is totally noninvasive. You don’t need a nurse to use an IV needle to pierce your skin.”
Dr. Cheng expects a human trial could launch within 5 years. For now, his study is attracting attention because it marks an advance in three areas of intense interest by researchers and biotech companies alike: Therapeutic uses of exosomes, inhalable treatments for lung conditions, and the safe delivery of powerful interleukin-12 (IL-12) immunotherapy.
Inside the Study
Dr. Cheng, who has been developing exosome and stem cell therapies for more than 15 years, and his lab team focused on lung cancer because the disease, often detected in later stages, “has a huge mortality rate,” he said. “Therapies have been suboptimal and leave the organ so damaged.”
He wanted to explore new alternatives to systemic treatments. Most are given intravenously, but Dr. Cheng thinks exosomes — also called extracellular vesicles (EVs) — could change that.
“One of the advantages of exosomes is that they are naturally secreted by the body or cultured cells,” he noted. “They have low toxicity and have multiple ways of getting their message into cells.”
The scientists borrowed an approach that captured public attention during the pandemic: Using messenger RNA, which directs cells to make proteins for tasks — including boosting immune response.
IL-12 has shown promise against cancer for decades, but early human trials triggered serious side effects and several deaths. Researchers are now trying new delivery methods that target tumor cells without affecting healthy tissue. Dr. Cheng’s team took a new approach, inserting mRNA for IL-12 into exosomes.
One aim of the study was to compare the effectiveness of inhaled exosomes vs inhaled liposomes, engineered fat droplets also under investigation as drug carriers. The team’s question: Which would work better at introducing IL-12 to the lungs to affect cancer, without triggering side effects?
After lab mice inhaled the particles through the nose, the researchers found that exosomes delivered more mRNA into cancer cells in the lungs and fought lung cancer with few side effects. Three days after treatment, researchers saw an influx of cancer-fighting T cells within tumors — with higher levels for exosome-based treatment. Plus, the exosomes led to more cancer-destroying nature killer cells and more monocytes, a sign of immune-system activation.
Researchers also found the treatment acted as a vaccine, training the immune system to battle newly introduced cancers. Little of the exosome-delivered drug escaped into the bloodstream, and the study found minimal side effects. Inhalation didn’t affect normal breathing, Dr. Cheng added.
The study’s use of inhaled exosomes makes it significant, said Raghu Kalluri, MD, PhD, professor and chair of the Department of Cancer Biology at MD Anderson Cancer Center. “This is an interesting study that explores the inhalable delivery of engineered EVs for the treatment of lung cancer and offers insights into focused delivery of EV-based drugs…with implications for diseases beyond cancer,” he said. Dr. Kalluri is also an exosome researcher.
New Frontiers
Once seen as a “quirky biological phenomenon” or just cellular trash, exosomes are now the subject of intense medical research for their potential as drug carriers, as treatments in their own right for everything from wound healing and pneumonia to heart attacks and bowel disorders, and as measurable biological markers that could lead to new tests for cancer and other conditions. One exosome-based prostate cancer test, the ExoDx Prostate Test, is already on the market.
The explosion in exosome research — the number of published studies has grown from just a handful in the early 1980s to more than 9000 — spotlights a particular focus on cancer. According to a 2021 paper in Annals of Oncology, clinical trials for exosomes in cancer treatments and tests far out-paces those for diabetes, heart disease, or neurologic conditions. Currently, 52 clinical trials using exosomes in cancer diagnosis or treatment have been completed, are underway, or are looking for participants, according to clinicaltrials.gov.
Dr. Cheng’s approach could also be used to deliver other drugs to the lungs and other organs via inhalation. “We’re testing inhalation for a different type of lung disease, acute lung injury,” Dr. Cheng said. Other potential targets include lung disorders like pulmonary hypertension. Inhaled exosomes could potentially reach the brain via the olfactory bulb or the heart as it receives oxygenated blood from the lungs.
Breathing in Medicine
So far, inhalable cancer treatments are not available outside research studies in the United States or Europe , said Remi Rosiere, PhD, a lecturer at the Université libre de Bruxelles in Brussels, Belgium, and chief scientific officer of InhaTarget Therapeutics, a company developing its own inhaled treatments for severe respiratory diseases. “Oncologists are very interested,” he said. “If you concentrate the drug on the tumor site, you can avoid distribution to the body.”
Early research into inhalable chemotherapy began in the 1960s but was unsuccessful because breathing equipment dispersed toxic cancer drugs into the air or delivered only small amounts to the lungs, he said.
New delivery techniques aim to change that. Dr. Rosiere’s company is starting a human trial of a dry powder inhaler with the chemotherapy drug cisplatin for lung cancer. Also in the pipeline is an immunotherapy treatment for lung cancer inserted in lipid nanoparticles, which are tiny fat particles similar to liposomes.
He said Dr. Cheng’s study shows the advantages of sending in exosomes. “The data are very persuasive,” Dr. Rosier said of the study. “Exosomes have a good safety profile and are able to remain in the lung for quite a long time. This prolongs exposure to the drug for greater effectiveness, without causing toxicities.”
Getting from a mouse study to a human trial will take time. “You need to understand this is very early stage,” Dr. Rosiere added. “There will be many challenges to overcome.”
One is purely practical: If the drug approaches human trials, he said, regulators will ask whether the exosomes can be produced in large quantities to meet the huge demand for new lung cancer treatments. “Lung cancer is the number one fatal cancer in the world,” Dr. Rosiere said.
A New Route for ‘Powerful’ Cancer Treatment
Meanwhile, the Columbia University study showed that inhalable exosomes are a unique delivery method for IL-12 — and could help solve a major problem that’s plagued this promising cancer treatment for decades.
Called “one of the most powerful immunotherapy agents ever discovered” in a 2022 literature review, IL-12 showed serious side effects that stalled research in the 1980s , sparking an ongoing search for new delivery methods that continues today. In 2022 and 2023, Big Pharma companies including AstraZenca, Moderna, and Bristol Myers Squib reduced their involvement with IL-12 treatment research, leaving the field open to smaller biotech companies working on a variety of drug-delivery approaches that could make IL-12 safe and effective in humans.
These include injecting it directly into tumors, encasing it in various types of particles, masking the drug so it is activated only in cancer cells, and using IL-12 mRNA, which essentially turns tumor cells into IL-12–producing factories. Another IL-12 mRNA drug, from Pittsburgh-based Krystal Biotech, received a fast-track designation from the US Food and Drug Administration in February 2024 for an inhaled lung cancer treatment that packages mRNA for IL-12 and IL-2 inside an engineered virus.
And of course, there is Dr. Cheng’s inhalable treatment, culminating decades of work across three burgeoning fields.
A version of this article appeared on Medscape.com.
Cells in the human body chat with each other all the time. One major way they communicate is by releasing tiny spheres called exosomes. These carry fats, proteins, and genetic material that help regulate everything from pregnancy and immune responses to heart health and kidney function.
“Exosomes work like text messages between cells , sending and receiving information,” said lead researcher Ke Cheng, PhD, professor of biomedical engineering at Columbia. “The significance of this study is that exosomes can bring mRNA-based treatment to lung cancer cells locally, unlike systemic chemotherapy that can have side effects throughout the body. And inhalation is totally noninvasive. You don’t need a nurse to use an IV needle to pierce your skin.”
Dr. Cheng expects a human trial could launch within 5 years. For now, his study is attracting attention because it marks an advance in three areas of intense interest by researchers and biotech companies alike: Therapeutic uses of exosomes, inhalable treatments for lung conditions, and the safe delivery of powerful interleukin-12 (IL-12) immunotherapy.
Inside the Study
Dr. Cheng, who has been developing exosome and stem cell therapies for more than 15 years, and his lab team focused on lung cancer because the disease, often detected in later stages, “has a huge mortality rate,” he said. “Therapies have been suboptimal and leave the organ so damaged.”
He wanted to explore new alternatives to systemic treatments. Most are given intravenously, but Dr. Cheng thinks exosomes — also called extracellular vesicles (EVs) — could change that.
“One of the advantages of exosomes is that they are naturally secreted by the body or cultured cells,” he noted. “They have low toxicity and have multiple ways of getting their message into cells.”
The scientists borrowed an approach that captured public attention during the pandemic: Using messenger RNA, which directs cells to make proteins for tasks — including boosting immune response.
IL-12 has shown promise against cancer for decades, but early human trials triggered serious side effects and several deaths. Researchers are now trying new delivery methods that target tumor cells without affecting healthy tissue. Dr. Cheng’s team took a new approach, inserting mRNA for IL-12 into exosomes.
One aim of the study was to compare the effectiveness of inhaled exosomes vs inhaled liposomes, engineered fat droplets also under investigation as drug carriers. The team’s question: Which would work better at introducing IL-12 to the lungs to affect cancer, without triggering side effects?
After lab mice inhaled the particles through the nose, the researchers found that exosomes delivered more mRNA into cancer cells in the lungs and fought lung cancer with few side effects. Three days after treatment, researchers saw an influx of cancer-fighting T cells within tumors — with higher levels for exosome-based treatment. Plus, the exosomes led to more cancer-destroying nature killer cells and more monocytes, a sign of immune-system activation.
Researchers also found the treatment acted as a vaccine, training the immune system to battle newly introduced cancers. Little of the exosome-delivered drug escaped into the bloodstream, and the study found minimal side effects. Inhalation didn’t affect normal breathing, Dr. Cheng added.
The study’s use of inhaled exosomes makes it significant, said Raghu Kalluri, MD, PhD, professor and chair of the Department of Cancer Biology at MD Anderson Cancer Center. “This is an interesting study that explores the inhalable delivery of engineered EVs for the treatment of lung cancer and offers insights into focused delivery of EV-based drugs…with implications for diseases beyond cancer,” he said. Dr. Kalluri is also an exosome researcher.
New Frontiers
Once seen as a “quirky biological phenomenon” or just cellular trash, exosomes are now the subject of intense medical research for their potential as drug carriers, as treatments in their own right for everything from wound healing and pneumonia to heart attacks and bowel disorders, and as measurable biological markers that could lead to new tests for cancer and other conditions. One exosome-based prostate cancer test, the ExoDx Prostate Test, is already on the market.
The explosion in exosome research — the number of published studies has grown from just a handful in the early 1980s to more than 9000 — spotlights a particular focus on cancer. According to a 2021 paper in Annals of Oncology, clinical trials for exosomes in cancer treatments and tests far out-paces those for diabetes, heart disease, or neurologic conditions. Currently, 52 clinical trials using exosomes in cancer diagnosis or treatment have been completed, are underway, or are looking for participants, according to clinicaltrials.gov.
Dr. Cheng’s approach could also be used to deliver other drugs to the lungs and other organs via inhalation. “We’re testing inhalation for a different type of lung disease, acute lung injury,” Dr. Cheng said. Other potential targets include lung disorders like pulmonary hypertension. Inhaled exosomes could potentially reach the brain via the olfactory bulb or the heart as it receives oxygenated blood from the lungs.
Breathing in Medicine
So far, inhalable cancer treatments are not available outside research studies in the United States or Europe , said Remi Rosiere, PhD, a lecturer at the Université libre de Bruxelles in Brussels, Belgium, and chief scientific officer of InhaTarget Therapeutics, a company developing its own inhaled treatments for severe respiratory diseases. “Oncologists are very interested,” he said. “If you concentrate the drug on the tumor site, you can avoid distribution to the body.”
Early research into inhalable chemotherapy began in the 1960s but was unsuccessful because breathing equipment dispersed toxic cancer drugs into the air or delivered only small amounts to the lungs, he said.
New delivery techniques aim to change that. Dr. Rosiere’s company is starting a human trial of a dry powder inhaler with the chemotherapy drug cisplatin for lung cancer. Also in the pipeline is an immunotherapy treatment for lung cancer inserted in lipid nanoparticles, which are tiny fat particles similar to liposomes.
He said Dr. Cheng’s study shows the advantages of sending in exosomes. “The data are very persuasive,” Dr. Rosier said of the study. “Exosomes have a good safety profile and are able to remain in the lung for quite a long time. This prolongs exposure to the drug for greater effectiveness, without causing toxicities.”
Getting from a mouse study to a human trial will take time. “You need to understand this is very early stage,” Dr. Rosiere added. “There will be many challenges to overcome.”
One is purely practical: If the drug approaches human trials, he said, regulators will ask whether the exosomes can be produced in large quantities to meet the huge demand for new lung cancer treatments. “Lung cancer is the number one fatal cancer in the world,” Dr. Rosiere said.
A New Route for ‘Powerful’ Cancer Treatment
Meanwhile, the Columbia University study showed that inhalable exosomes are a unique delivery method for IL-12 — and could help solve a major problem that’s plagued this promising cancer treatment for decades.
Called “one of the most powerful immunotherapy agents ever discovered” in a 2022 literature review, IL-12 showed serious side effects that stalled research in the 1980s , sparking an ongoing search for new delivery methods that continues today. In 2022 and 2023, Big Pharma companies including AstraZenca, Moderna, and Bristol Myers Squib reduced their involvement with IL-12 treatment research, leaving the field open to smaller biotech companies working on a variety of drug-delivery approaches that could make IL-12 safe and effective in humans.
These include injecting it directly into tumors, encasing it in various types of particles, masking the drug so it is activated only in cancer cells, and using IL-12 mRNA, which essentially turns tumor cells into IL-12–producing factories. Another IL-12 mRNA drug, from Pittsburgh-based Krystal Biotech, received a fast-track designation from the US Food and Drug Administration in February 2024 for an inhaled lung cancer treatment that packages mRNA for IL-12 and IL-2 inside an engineered virus.
And of course, there is Dr. Cheng’s inhalable treatment, culminating decades of work across three burgeoning fields.
A version of this article appeared on Medscape.com.
Cells in the human body chat with each other all the time. One major way they communicate is by releasing tiny spheres called exosomes. These carry fats, proteins, and genetic material that help regulate everything from pregnancy and immune responses to heart health and kidney function.
“Exosomes work like text messages between cells , sending and receiving information,” said lead researcher Ke Cheng, PhD, professor of biomedical engineering at Columbia. “The significance of this study is that exosomes can bring mRNA-based treatment to lung cancer cells locally, unlike systemic chemotherapy that can have side effects throughout the body. And inhalation is totally noninvasive. You don’t need a nurse to use an IV needle to pierce your skin.”
Dr. Cheng expects a human trial could launch within 5 years. For now, his study is attracting attention because it marks an advance in three areas of intense interest by researchers and biotech companies alike: Therapeutic uses of exosomes, inhalable treatments for lung conditions, and the safe delivery of powerful interleukin-12 (IL-12) immunotherapy.
Inside the Study
Dr. Cheng, who has been developing exosome and stem cell therapies for more than 15 years, and his lab team focused on lung cancer because the disease, often detected in later stages, “has a huge mortality rate,” he said. “Therapies have been suboptimal and leave the organ so damaged.”
He wanted to explore new alternatives to systemic treatments. Most are given intravenously, but Dr. Cheng thinks exosomes — also called extracellular vesicles (EVs) — could change that.
“One of the advantages of exosomes is that they are naturally secreted by the body or cultured cells,” he noted. “They have low toxicity and have multiple ways of getting their message into cells.”
The scientists borrowed an approach that captured public attention during the pandemic: Using messenger RNA, which directs cells to make proteins for tasks — including boosting immune response.
IL-12 has shown promise against cancer for decades, but early human trials triggered serious side effects and several deaths. Researchers are now trying new delivery methods that target tumor cells without affecting healthy tissue. Dr. Cheng’s team took a new approach, inserting mRNA for IL-12 into exosomes.
One aim of the study was to compare the effectiveness of inhaled exosomes vs inhaled liposomes, engineered fat droplets also under investigation as drug carriers. The team’s question: Which would work better at introducing IL-12 to the lungs to affect cancer, without triggering side effects?
After lab mice inhaled the particles through the nose, the researchers found that exosomes delivered more mRNA into cancer cells in the lungs and fought lung cancer with few side effects. Three days after treatment, researchers saw an influx of cancer-fighting T cells within tumors — with higher levels for exosome-based treatment. Plus, the exosomes led to more cancer-destroying nature killer cells and more monocytes, a sign of immune-system activation.
Researchers also found the treatment acted as a vaccine, training the immune system to battle newly introduced cancers. Little of the exosome-delivered drug escaped into the bloodstream, and the study found minimal side effects. Inhalation didn’t affect normal breathing, Dr. Cheng added.
The study’s use of inhaled exosomes makes it significant, said Raghu Kalluri, MD, PhD, professor and chair of the Department of Cancer Biology at MD Anderson Cancer Center. “This is an interesting study that explores the inhalable delivery of engineered EVs for the treatment of lung cancer and offers insights into focused delivery of EV-based drugs…with implications for diseases beyond cancer,” he said. Dr. Kalluri is also an exosome researcher.
New Frontiers
Once seen as a “quirky biological phenomenon” or just cellular trash, exosomes are now the subject of intense medical research for their potential as drug carriers, as treatments in their own right for everything from wound healing and pneumonia to heart attacks and bowel disorders, and as measurable biological markers that could lead to new tests for cancer and other conditions. One exosome-based prostate cancer test, the ExoDx Prostate Test, is already on the market.
The explosion in exosome research — the number of published studies has grown from just a handful in the early 1980s to more than 9000 — spotlights a particular focus on cancer. According to a 2021 paper in Annals of Oncology, clinical trials for exosomes in cancer treatments and tests far out-paces those for diabetes, heart disease, or neurologic conditions. Currently, 52 clinical trials using exosomes in cancer diagnosis or treatment have been completed, are underway, or are looking for participants, according to clinicaltrials.gov.
Dr. Cheng’s approach could also be used to deliver other drugs to the lungs and other organs via inhalation. “We’re testing inhalation for a different type of lung disease, acute lung injury,” Dr. Cheng said. Other potential targets include lung disorders like pulmonary hypertension. Inhaled exosomes could potentially reach the brain via the olfactory bulb or the heart as it receives oxygenated blood from the lungs.
Breathing in Medicine
So far, inhalable cancer treatments are not available outside research studies in the United States or Europe , said Remi Rosiere, PhD, a lecturer at the Université libre de Bruxelles in Brussels, Belgium, and chief scientific officer of InhaTarget Therapeutics, a company developing its own inhaled treatments for severe respiratory diseases. “Oncologists are very interested,” he said. “If you concentrate the drug on the tumor site, you can avoid distribution to the body.”
Early research into inhalable chemotherapy began in the 1960s but was unsuccessful because breathing equipment dispersed toxic cancer drugs into the air or delivered only small amounts to the lungs, he said.
New delivery techniques aim to change that. Dr. Rosiere’s company is starting a human trial of a dry powder inhaler with the chemotherapy drug cisplatin for lung cancer. Also in the pipeline is an immunotherapy treatment for lung cancer inserted in lipid nanoparticles, which are tiny fat particles similar to liposomes.
He said Dr. Cheng’s study shows the advantages of sending in exosomes. “The data are very persuasive,” Dr. Rosier said of the study. “Exosomes have a good safety profile and are able to remain in the lung for quite a long time. This prolongs exposure to the drug for greater effectiveness, without causing toxicities.”
Getting from a mouse study to a human trial will take time. “You need to understand this is very early stage,” Dr. Rosiere added. “There will be many challenges to overcome.”
One is purely practical: If the drug approaches human trials, he said, regulators will ask whether the exosomes can be produced in large quantities to meet the huge demand for new lung cancer treatments. “Lung cancer is the number one fatal cancer in the world,” Dr. Rosiere said.
A New Route for ‘Powerful’ Cancer Treatment
Meanwhile, the Columbia University study showed that inhalable exosomes are a unique delivery method for IL-12 — and could help solve a major problem that’s plagued this promising cancer treatment for decades.
Called “one of the most powerful immunotherapy agents ever discovered” in a 2022 literature review, IL-12 showed serious side effects that stalled research in the 1980s , sparking an ongoing search for new delivery methods that continues today. In 2022 and 2023, Big Pharma companies including AstraZenca, Moderna, and Bristol Myers Squib reduced their involvement with IL-12 treatment research, leaving the field open to smaller biotech companies working on a variety of drug-delivery approaches that could make IL-12 safe and effective in humans.
These include injecting it directly into tumors, encasing it in various types of particles, masking the drug so it is activated only in cancer cells, and using IL-12 mRNA, which essentially turns tumor cells into IL-12–producing factories. Another IL-12 mRNA drug, from Pittsburgh-based Krystal Biotech, received a fast-track designation from the US Food and Drug Administration in February 2024 for an inhaled lung cancer treatment that packages mRNA for IL-12 and IL-2 inside an engineered virus.
And of course, there is Dr. Cheng’s inhalable treatment, culminating decades of work across three burgeoning fields.
A version of this article appeared on Medscape.com.
FROM NATURE NANOTECHNOLOGY
Cancer Data Trends 2024: Lung Cancer
1. Wolf AMD, Oeffinger KC, Shih TYC, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin. 2023;10.3322/caac.21811. doi:10.3322/caac.21811
2. US Department of Veterans Affairs. VA promotes high-quality, patient-centered lung cancer screening for veterans. Published June 15, 2023. Accessed December 18, 2023. http://www.hsrd.research.va.gov/impacts/lcs.cfm
3. Navuluri N, Morrison S, Green CL, et al. Racial disparities in lung cancer screening among veterans, 2013 to 2021. JAMA Netw Open. 2023;6(6):e2318795. doi:10.1001/jamanetworkopen.2023.18795
4. Bruno DS, Hess LM, Li X, Su EW, Patel M. Disparities in biomarker testing and clinical trial enrollment among patients with lung, breast, or colorectal cancers in the United States. JCO Precis Oncol. 2022;6:e2100427. doi:10.1200/PO.21.00427
5. Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in lung carcinoma from the VA National Precision Oncology Program. Semin Oncol. 2022;S0093-7754(22)00054-9. doi:10.1053/j.seminoncol.2022.06.014
6. Williams CD, Allo MA, Gu L, Vashistha V, Press A, Kelley M. Health outcomes and healthcare resource utilization among veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS One. 2023;18(2):e0282020. doi:10.1371/journal.pone.0282020
7. US Food and Drug Administration. Oncology (cancer)/hematologic malignancies approval notifications. Updated December 15, 2023. Accessed December 18, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications
8. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
1. Wolf AMD, Oeffinger KC, Shih TYC, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin. 2023;10.3322/caac.21811. doi:10.3322/caac.21811
2. US Department of Veterans Affairs. VA promotes high-quality, patient-centered lung cancer screening for veterans. Published June 15, 2023. Accessed December 18, 2023. http://www.hsrd.research.va.gov/impacts/lcs.cfm
3. Navuluri N, Morrison S, Green CL, et al. Racial disparities in lung cancer screening among veterans, 2013 to 2021. JAMA Netw Open. 2023;6(6):e2318795. doi:10.1001/jamanetworkopen.2023.18795
4. Bruno DS, Hess LM, Li X, Su EW, Patel M. Disparities in biomarker testing and clinical trial enrollment among patients with lung, breast, or colorectal cancers in the United States. JCO Precis Oncol. 2022;6:e2100427. doi:10.1200/PO.21.00427
5. Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in lung carcinoma from the VA National Precision Oncology Program. Semin Oncol. 2022;S0093-7754(22)00054-9. doi:10.1053/j.seminoncol.2022.06.014
6. Williams CD, Allo MA, Gu L, Vashistha V, Press A, Kelley M. Health outcomes and healthcare resource utilization among veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS One. 2023;18(2):e0282020. doi:10.1371/journal.pone.0282020
7. US Food and Drug Administration. Oncology (cancer)/hematologic malignancies approval notifications. Updated December 15, 2023. Accessed December 18, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications
8. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
1. Wolf AMD, Oeffinger KC, Shih TYC, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA Cancer J Clin. 2023;10.3322/caac.21811. doi:10.3322/caac.21811
2. US Department of Veterans Affairs. VA promotes high-quality, patient-centered lung cancer screening for veterans. Published June 15, 2023. Accessed December 18, 2023. http://www.hsrd.research.va.gov/impacts/lcs.cfm
3. Navuluri N, Morrison S, Green CL, et al. Racial disparities in lung cancer screening among veterans, 2013 to 2021. JAMA Netw Open. 2023;6(6):e2318795. doi:10.1001/jamanetworkopen.2023.18795
4. Bruno DS, Hess LM, Li X, Su EW, Patel M. Disparities in biomarker testing and clinical trial enrollment among patients with lung, breast, or colorectal cancers in the United States. JCO Precis Oncol. 2022;6:e2100427. doi:10.1200/PO.21.00427
5. Jalal SI, Guo A, Ahmed S, Kelley MJ. Analysis of actionable genetic alterations in lung carcinoma from the VA National Precision Oncology Program. Semin Oncol. 2022;S0093-7754(22)00054-9. doi:10.1053/j.seminoncol.2022.06.014
6. Williams CD, Allo MA, Gu L, Vashistha V, Press A, Kelley M. Health outcomes and healthcare resource utilization among veterans with stage IV non-small cell lung cancer treated with second-line chemotherapy versus immunotherapy. PLoS One. 2023;18(2):e0282020. doi:10.1371/journal.pone.0282020
7. US Food and Drug Administration. Oncology (cancer)/hematologic malignancies approval notifications. Updated December 15, 2023. Accessed December 18, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications
8. Paz-Ares L, Chen Y, Reinmuth N, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open. 2022;7(2):100408. doi:10.1016/j.esmoop.2022.100408
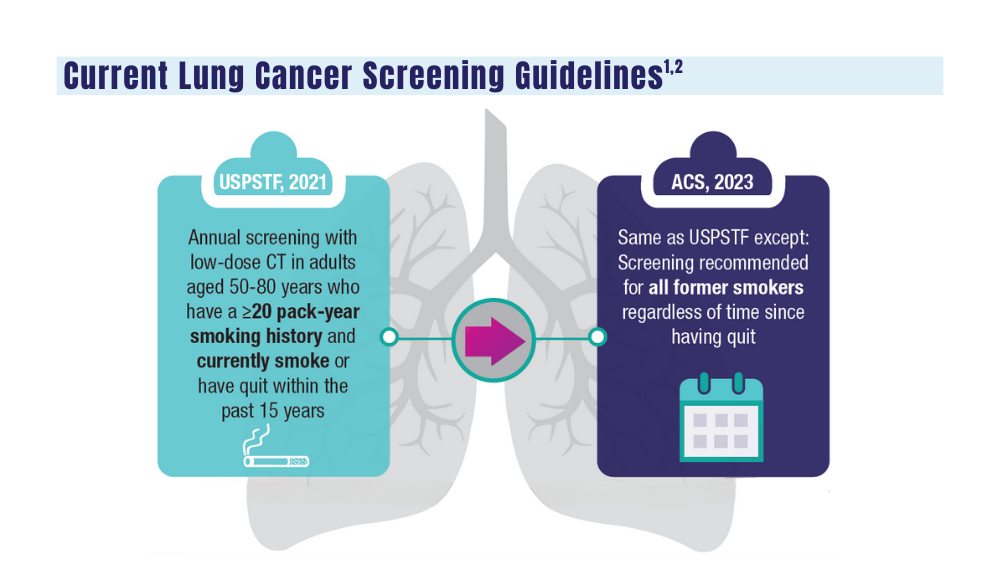
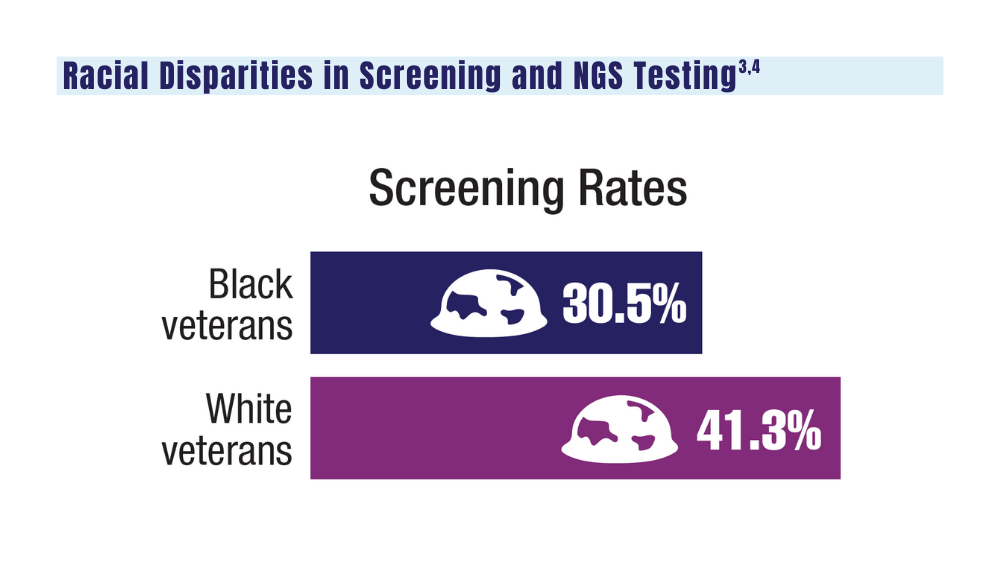
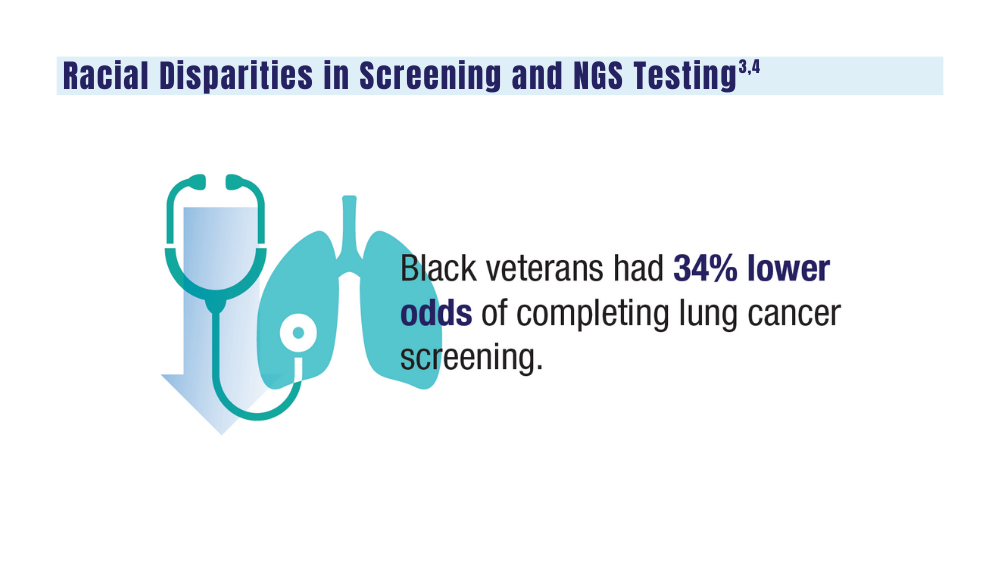
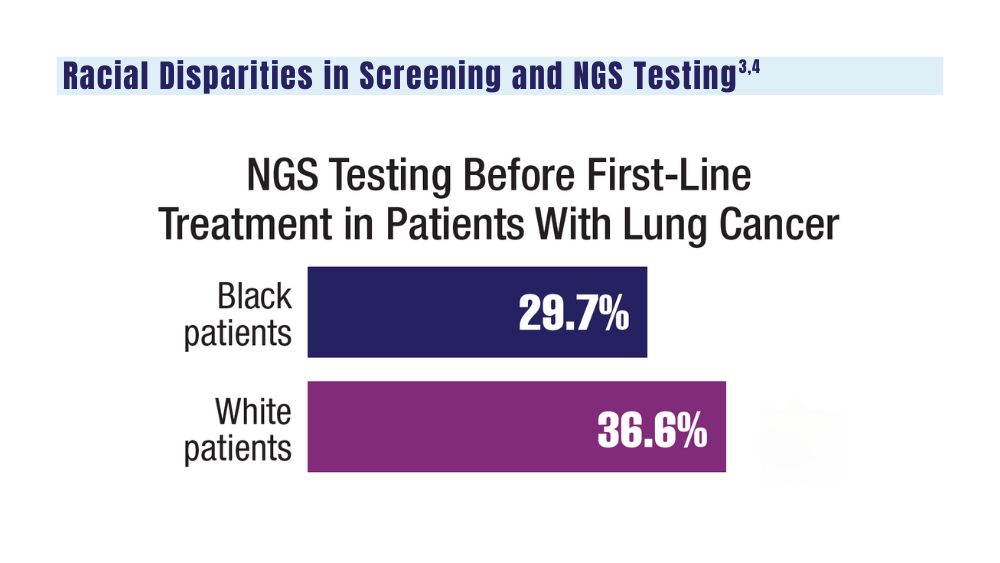
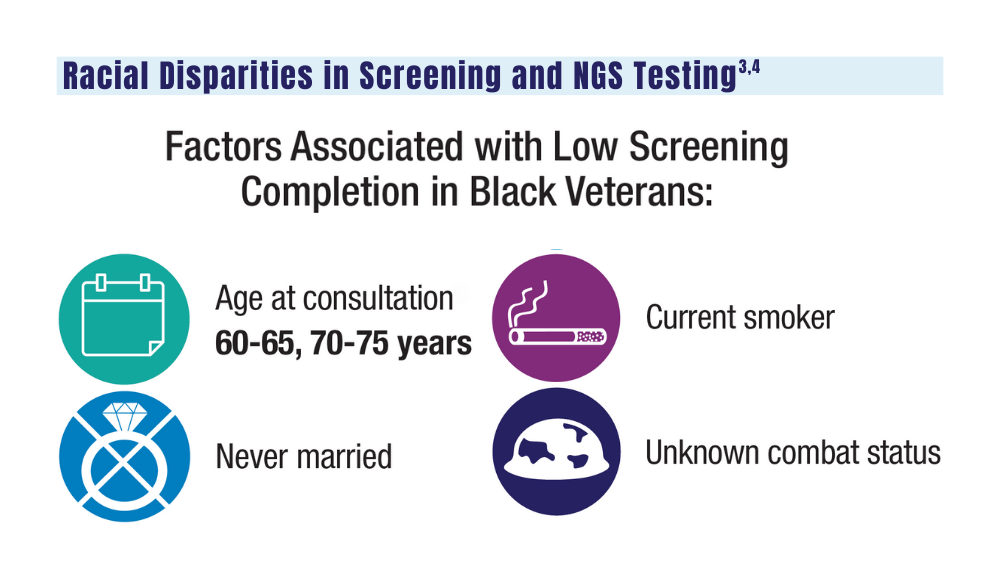
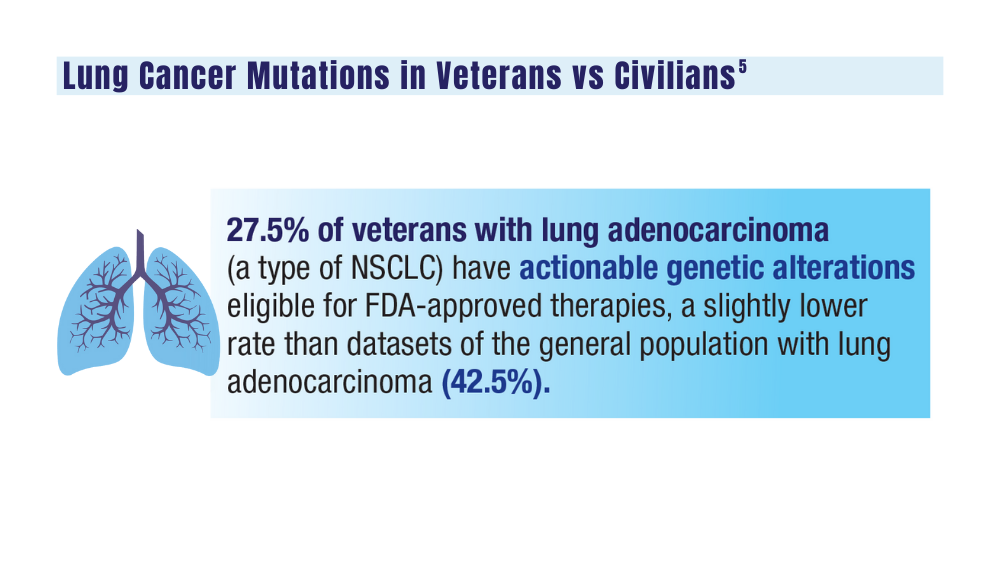
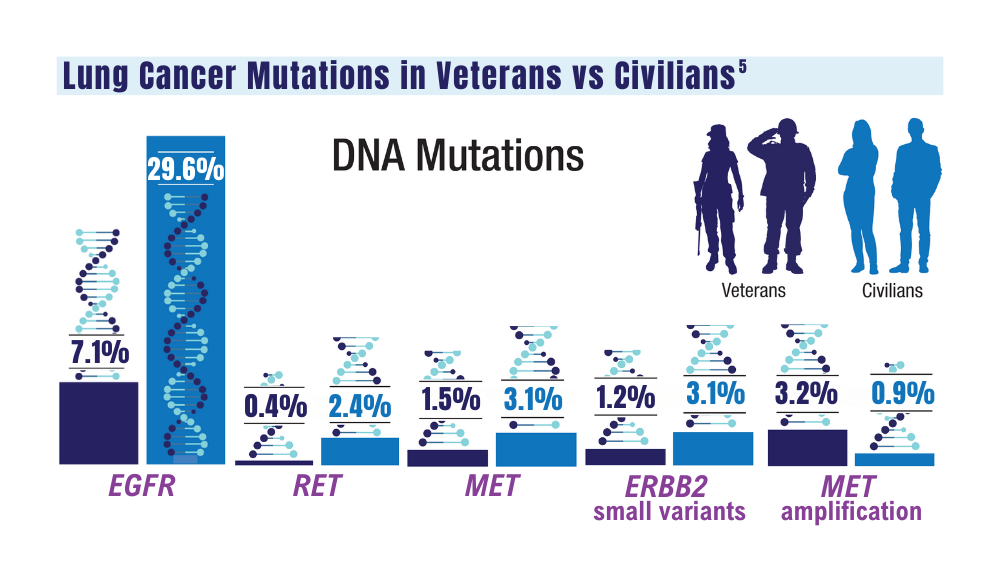
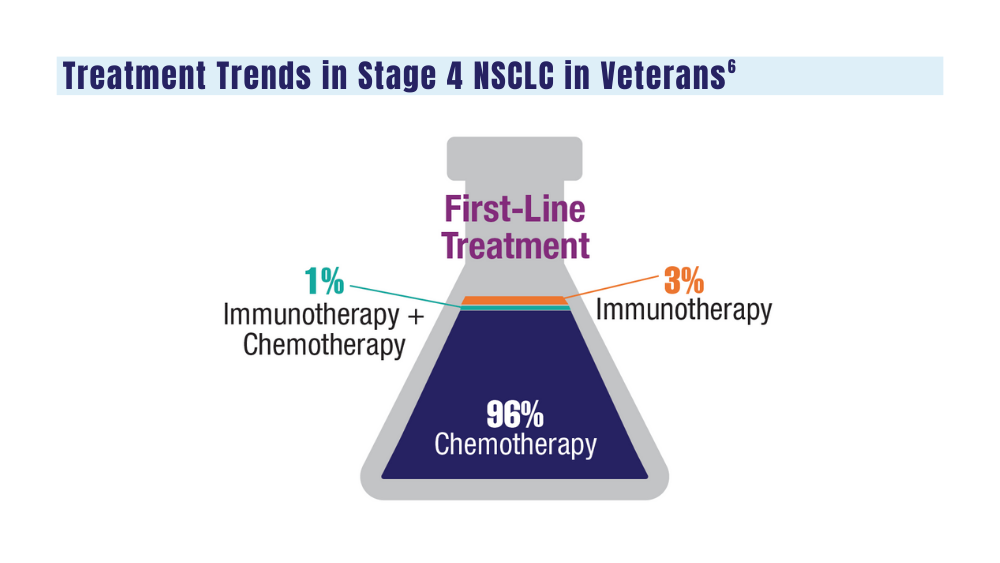
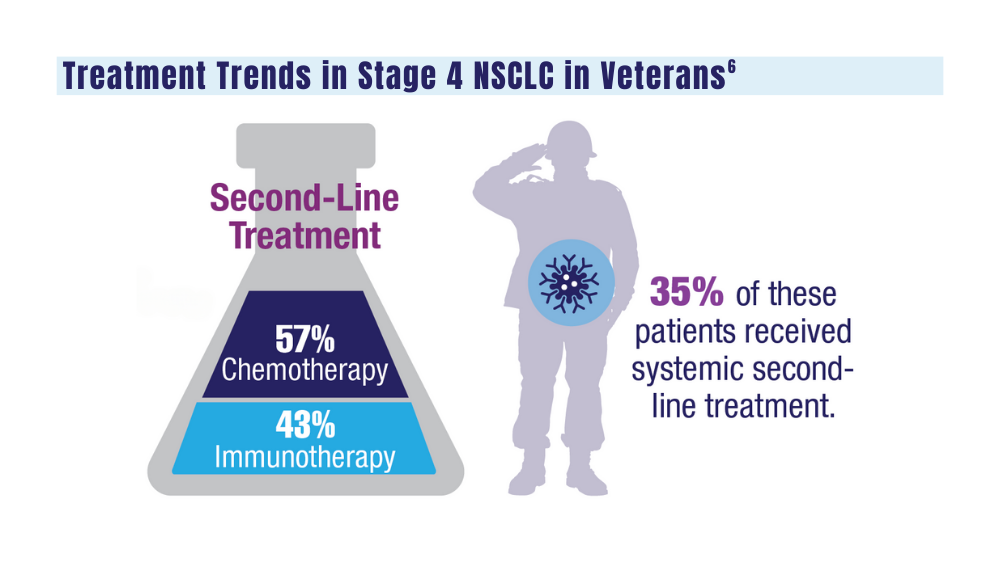
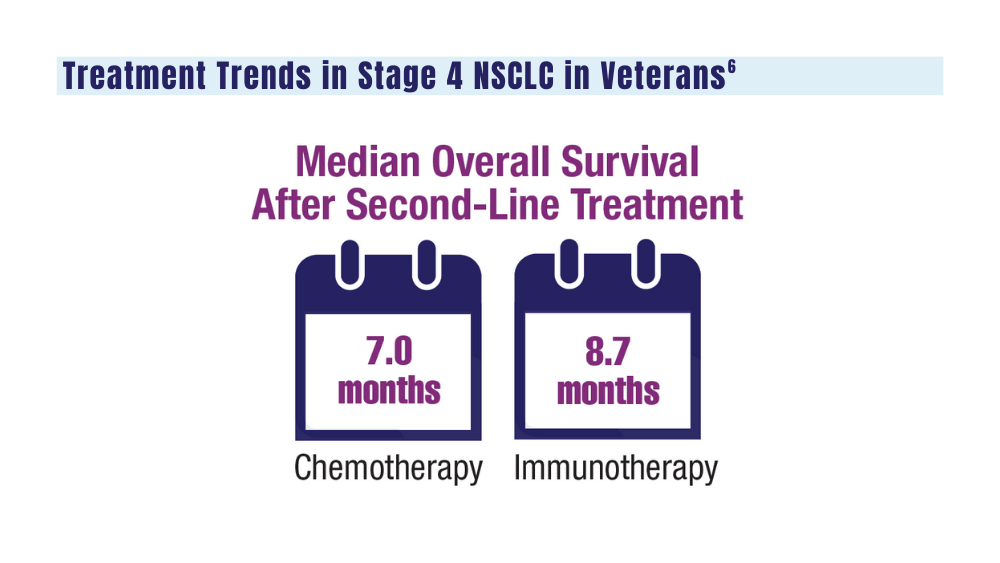
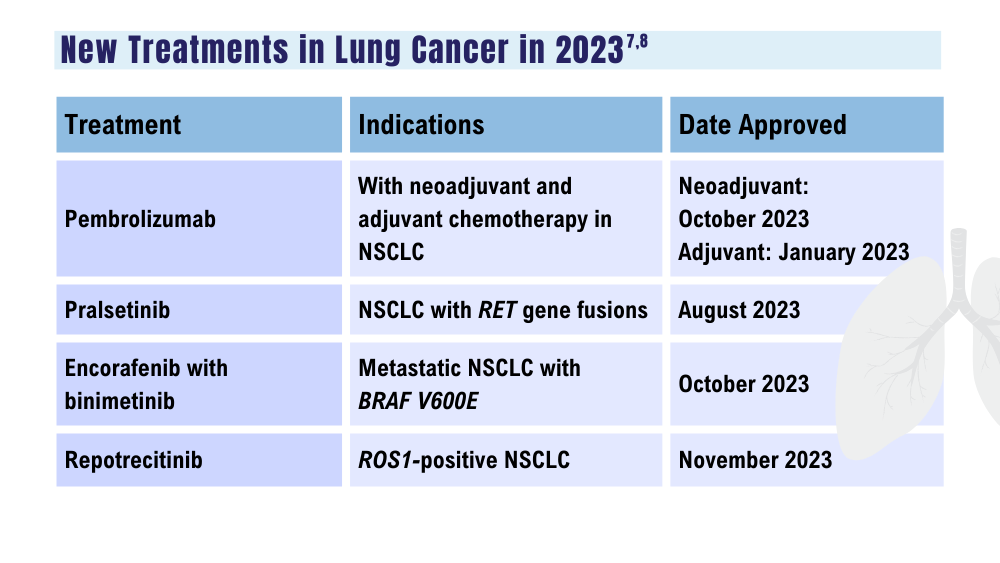
Cancer Data Trends 2024

The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure