It is estimated that there are 1.1 million people in the United States living with HIV and that 15% of those people do not know they have HIV. Although the number of new cases reported each year is decreasing, there were still 38,281 new diagnoses in 2017. New cases might be decreasing overall, but the incidence of HIV is rising in some groups including people aged 25-29 years old and American Indian/Alaska Native and Asian populations. In addition, HIV disproportionately affects men who have sex with men, black/African American populations, and Hispanic/Latino populations, according to the USPSTF statement.
Dr. Anne Sprogell and Dr. Neil Skolnik
Given the prevalence of HIV and rising new cases in certain groups, it is thought that preexposure prophylaxis (PrEP) is being underutilized. The CDC reported that, in 2015, 1.2 million people were candidates for PrEP, but in 2017, only 100,282 people were using PrEP. The USPSTF performed a meta-analysis of 12 RCTs comparing rates of HIV infection in groups treated with PrEP versus those treated with placebo or no treatment and found a risk ratio of 0.46 (95% confidence interval, 0.33-0.66) and absolute risk reduction of –2% (95% CI, –2.8% to –1.2%) after 4 months and 4 years.
With this epidemiologic data and the meta-analysis, the USPSTF offered the following recommendations.
Screening
In order to decrease the rates of transmission and incidence of HIV infection, we must appropriately identify those who would be good candidates for PrEP. That begins with taking a complete and thorough sexual and injection drug use history in a manner that does not make patients feel stigmatized or discriminated against. The USPSTF recommends screening for HIV infection in patients aged 15-65 years old, in younger and older patients who have increased risk factors, and all pregnant patients. PrEP is not an appropriate choice in those who have HIV because it can lead to drug resistance.
When screening for HIV and considering starting PrEP, it is recommended that clinicians also test for kidney function, hepatitis B and C, other STIs, and pregnancy. The USPSTF suggests that the following groups be considered for PrEP given the increased risk of HIV infection:
Men who have sex with men, are sexually active, and have one of these additional characteristics: a serodiscordant sex partner, inconsistent use of condoms during receptive or insertive anal sex, or infection with syphilis, gonorrhea, or chlamydia in the past 6 months.
Heterosexual men or women who are sexually active with one or more of these additional characteristics: a serodiscordant sex partner, inconsistent use of condoms during sex with a partner whose HIV status is unknown and who is at high risk, and infection with syphilis or gonorrhea in the past 6 months.
Patients who inject drugs with one or more of the following characteristics: shared use of drug injection equipment and risk of sexual acquisition (as in the categories above).
The USPSTF also notes that those who engage in transactional sex (for money, drugs, or housing) and transgender patients are at an increased risk of HIV infection.
Treatment
The only FDA approved treatment for the prevention HIV infection is once daily oral combined tenofovir disoproxil fumarate and emtricitabine; however, some studies have found that tenofovir disproxil fumarate monotherapy is also effective. Considering these trials, the CDC has suggested that tenofovir disoproxil fumarate monotherapy can be used as an alternative for men and women at high risk and those who inject drugs.
Tenofovir disoproxil fumarate/emtricitabine can also be used in pregnant patients, however the USPSTF notes that no PrEP trials included pregnant women. Additionally, tenofovir disoproxil fumarate/emtricitabine can be used in adolescents who weigh more than 35 kg. It is unknown how much time it takes to achieve protection against HIV infection after starting PrEP, and there is no clear timeline for how long patients should be on PrEP. Patients may discontinue medication because of preference, decreased risk of HIV exposure, or side effects.
Side effects include renal adverse events (serum creatinine rise), gastrointestinal adverse events (mostly nausea), and bone loss and increased fracture risk, although none were statistically significant when PrEP and placebo groups were compared. The USPSTF’s recommendations note that the effectiveness of PrEP is dependent on medication adherence.
While PrEP is an important part of preventing HIV, it is always important to counsel patients on other ways to reduce risk. The USPSTF notes that consistent condom use reduces the risk of HIV infection by around 80% in addition to reducing the risk of other STIs. All trials studied by the USPSTF for these recommendations included counseling on behavior, adherence, and condom use.
Bottom Line
It is estimated that 1.1 million Americans are living with HIV and 15% are unaware that they are positive for HIV. Overall cases of new HIV diagnoses are down, but they are rising in some groups. PrEP is an effective medication for reducing the risk of HIV infection, but is currently underutilized. Every patient should be screened for high-risk sexual behavior and drug use with a thorough history. Patients aged 15-65 years should be screened for HIV. If patients are negative for HIV, but participate in high-risk sexual behaviors and drug injection, they should be offered PrEP along with counseling on, medication adherence, condom use, and reduction of high-risk behaviors.
Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Sprogell is a second-year resident in the Family Medicine Residency Program at Abington Jefferson Health
Reference
Owens DK et al. “Preexposure prophylaxis for the prevention of HIV infection: US Preventive Services Task Force recommendation statement.” JAMA. 2019 Jun 11;321(22):2203-13.
It is estimated that there are 1.1 million people in the United States living with HIV and that 15% of those people do not know they have HIV. Although the number of new cases reported each year is decreasing, there were still 38,281 new diagnoses in 2017. New cases might be decreasing overall, but the incidence of HIV is rising in some groups including people aged 25-29 years old and American Indian/Alaska Native and Asian populations. In addition, HIV disproportionately affects men who have sex with men, black/African American populations, and Hispanic/Latino populations, according to the USPSTF statement.
Dr. Anne Sprogell and Dr. Neil Skolnik
Given the prevalence of HIV and rising new cases in certain groups, it is thought that preexposure prophylaxis (PrEP) is being underutilized. The CDC reported that, in 2015, 1.2 million people were candidates for PrEP, but in 2017, only 100,282 people were using PrEP. The USPSTF performed a meta-analysis of 12 RCTs comparing rates of HIV infection in groups treated with PrEP versus those treated with placebo or no treatment and found a risk ratio of 0.46 (95% confidence interval, 0.33-0.66) and absolute risk reduction of –2% (95% CI, –2.8% to –1.2%) after 4 months and 4 years.
With this epidemiologic data and the meta-analysis, the USPSTF offered the following recommendations.
Screening
In order to decrease the rates of transmission and incidence of HIV infection, we must appropriately identify those who would be good candidates for PrEP. That begins with taking a complete and thorough sexual and injection drug use history in a manner that does not make patients feel stigmatized or discriminated against. The USPSTF recommends screening for HIV infection in patients aged 15-65 years old, in younger and older patients who have increased risk factors, and all pregnant patients. PrEP is not an appropriate choice in those who have HIV because it can lead to drug resistance.
When screening for HIV and considering starting PrEP, it is recommended that clinicians also test for kidney function, hepatitis B and C, other STIs, and pregnancy. The USPSTF suggests that the following groups be considered for PrEP given the increased risk of HIV infection:
Men who have sex with men, are sexually active, and have one of these additional characteristics: a serodiscordant sex partner, inconsistent use of condoms during receptive or insertive anal sex, or infection with syphilis, gonorrhea, or chlamydia in the past 6 months.
Heterosexual men or women who are sexually active with one or more of these additional characteristics: a serodiscordant sex partner, inconsistent use of condoms during sex with a partner whose HIV status is unknown and who is at high risk, and infection with syphilis or gonorrhea in the past 6 months.
Patients who inject drugs with one or more of the following characteristics: shared use of drug injection equipment and risk of sexual acquisition (as in the categories above).
The USPSTF also notes that those who engage in transactional sex (for money, drugs, or housing) and transgender patients are at an increased risk of HIV infection.
Treatment
The only FDA approved treatment for the prevention HIV infection is once daily oral combined tenofovir disoproxil fumarate and emtricitabine; however, some studies have found that tenofovir disproxil fumarate monotherapy is also effective. Considering these trials, the CDC has suggested that tenofovir disoproxil fumarate monotherapy can be used as an alternative for men and women at high risk and those who inject drugs.
Tenofovir disoproxil fumarate/emtricitabine can also be used in pregnant patients, however the USPSTF notes that no PrEP trials included pregnant women. Additionally, tenofovir disoproxil fumarate/emtricitabine can be used in adolescents who weigh more than 35 kg. It is unknown how much time it takes to achieve protection against HIV infection after starting PrEP, and there is no clear timeline for how long patients should be on PrEP. Patients may discontinue medication because of preference, decreased risk of HIV exposure, or side effects.
Side effects include renal adverse events (serum creatinine rise), gastrointestinal adverse events (mostly nausea), and bone loss and increased fracture risk, although none were statistically significant when PrEP and placebo groups were compared. The USPSTF’s recommendations note that the effectiveness of PrEP is dependent on medication adherence.
While PrEP is an important part of preventing HIV, it is always important to counsel patients on other ways to reduce risk. The USPSTF notes that consistent condom use reduces the risk of HIV infection by around 80% in addition to reducing the risk of other STIs. All trials studied by the USPSTF for these recommendations included counseling on behavior, adherence, and condom use.
Bottom Line
It is estimated that 1.1 million Americans are living with HIV and 15% are unaware that they are positive for HIV. Overall cases of new HIV diagnoses are down, but they are rising in some groups. PrEP is an effective medication for reducing the risk of HIV infection, but is currently underutilized. Every patient should be screened for high-risk sexual behavior and drug use with a thorough history. Patients aged 15-65 years should be screened for HIV. If patients are negative for HIV, but participate in high-risk sexual behaviors and drug injection, they should be offered PrEP along with counseling on, medication adherence, condom use, and reduction of high-risk behaviors.
Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Sprogell is a second-year resident in the Family Medicine Residency Program at Abington Jefferson Health
Reference
Owens DK et al. “Preexposure prophylaxis for the prevention of HIV infection: US Preventive Services Task Force recommendation statement.” JAMA. 2019 Jun 11;321(22):2203-13.
It is estimated that there are 1.1 million people in the United States living with HIV and that 15% of those people do not know they have HIV. Although the number of new cases reported each year is decreasing, there were still 38,281 new diagnoses in 2017. New cases might be decreasing overall, but the incidence of HIV is rising in some groups including people aged 25-29 years old and American Indian/Alaska Native and Asian populations. In addition, HIV disproportionately affects men who have sex with men, black/African American populations, and Hispanic/Latino populations, according to the USPSTF statement.
Dr. Anne Sprogell and Dr. Neil Skolnik
Given the prevalence of HIV and rising new cases in certain groups, it is thought that preexposure prophylaxis (PrEP) is being underutilized. The CDC reported that, in 2015, 1.2 million people were candidates for PrEP, but in 2017, only 100,282 people were using PrEP. The USPSTF performed a meta-analysis of 12 RCTs comparing rates of HIV infection in groups treated with PrEP versus those treated with placebo or no treatment and found a risk ratio of 0.46 (95% confidence interval, 0.33-0.66) and absolute risk reduction of –2% (95% CI, –2.8% to –1.2%) after 4 months and 4 years.
With this epidemiologic data and the meta-analysis, the USPSTF offered the following recommendations.
Screening
In order to decrease the rates of transmission and incidence of HIV infection, we must appropriately identify those who would be good candidates for PrEP. That begins with taking a complete and thorough sexual and injection drug use history in a manner that does not make patients feel stigmatized or discriminated against. The USPSTF recommends screening for HIV infection in patients aged 15-65 years old, in younger and older patients who have increased risk factors, and all pregnant patients. PrEP is not an appropriate choice in those who have HIV because it can lead to drug resistance.
When screening for HIV and considering starting PrEP, it is recommended that clinicians also test for kidney function, hepatitis B and C, other STIs, and pregnancy. The USPSTF suggests that the following groups be considered for PrEP given the increased risk of HIV infection:
Men who have sex with men, are sexually active, and have one of these additional characteristics: a serodiscordant sex partner, inconsistent use of condoms during receptive or insertive anal sex, or infection with syphilis, gonorrhea, or chlamydia in the past 6 months.
Heterosexual men or women who are sexually active with one or more of these additional characteristics: a serodiscordant sex partner, inconsistent use of condoms during sex with a partner whose HIV status is unknown and who is at high risk, and infection with syphilis or gonorrhea in the past 6 months.
Patients who inject drugs with one or more of the following characteristics: shared use of drug injection equipment and risk of sexual acquisition (as in the categories above).
The USPSTF also notes that those who engage in transactional sex (for money, drugs, or housing) and transgender patients are at an increased risk of HIV infection.
Treatment
The only FDA approved treatment for the prevention HIV infection is once daily oral combined tenofovir disoproxil fumarate and emtricitabine; however, some studies have found that tenofovir disproxil fumarate monotherapy is also effective. Considering these trials, the CDC has suggested that tenofovir disoproxil fumarate monotherapy can be used as an alternative for men and women at high risk and those who inject drugs.
Tenofovir disoproxil fumarate/emtricitabine can also be used in pregnant patients, however the USPSTF notes that no PrEP trials included pregnant women. Additionally, tenofovir disoproxil fumarate/emtricitabine can be used in adolescents who weigh more than 35 kg. It is unknown how much time it takes to achieve protection against HIV infection after starting PrEP, and there is no clear timeline for how long patients should be on PrEP. Patients may discontinue medication because of preference, decreased risk of HIV exposure, or side effects.
Side effects include renal adverse events (serum creatinine rise), gastrointestinal adverse events (mostly nausea), and bone loss and increased fracture risk, although none were statistically significant when PrEP and placebo groups were compared. The USPSTF’s recommendations note that the effectiveness of PrEP is dependent on medication adherence.
While PrEP is an important part of preventing HIV, it is always important to counsel patients on other ways to reduce risk. The USPSTF notes that consistent condom use reduces the risk of HIV infection by around 80% in addition to reducing the risk of other STIs. All trials studied by the USPSTF for these recommendations included counseling on behavior, adherence, and condom use.
Bottom Line
It is estimated that 1.1 million Americans are living with HIV and 15% are unaware that they are positive for HIV. Overall cases of new HIV diagnoses are down, but they are rising in some groups. PrEP is an effective medication for reducing the risk of HIV infection, but is currently underutilized. Every patient should be screened for high-risk sexual behavior and drug use with a thorough history. Patients aged 15-65 years should be screened for HIV. If patients are negative for HIV, but participate in high-risk sexual behaviors and drug injection, they should be offered PrEP along with counseling on, medication adherence, condom use, and reduction of high-risk behaviors.
Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Sprogell is a second-year resident in the Family Medicine Residency Program at Abington Jefferson Health
Reference
Owens DK et al. “Preexposure prophylaxis for the prevention of HIV infection: US Preventive Services Task Force recommendation statement.” JAMA. 2019 Jun 11;321(22):2203-13.
Survivors of the 2013-2016 Ebola epidemic in West Africa had lingering health effects of the disease. These patients had a much greater mortality in the first year after discharge, compared with the general population. Among those survivors who died, the majority appear to have expired because of renal failure, according to the results of an assessment the by the Guinean national survivors’ monitoring program.
CDC/Athalia Christie
The Surveillance Active en Ceinture obtained data on 1,130 (89%) of survivors of Ebola virus disease who were discharged from Ebola treatment units in Guinea. Compared with the general Guinean population, survivors of Ebola virus showed a five times increased risk of mortality within a year of follow-up after discharge, according to a survey of patients’ medical records and patients’ relatives, reported researchers Mory Keita, MD, and colleagues.
After 1 year, the difference in mortality between Ebola survivors and the general population had disappeared, according to the study published online in the Lancet Infectious Diseases.
A total of 59 deaths were reported among the discharged survivors available for follow-up. Renal failure was the assumed cause in 37 (63%) of these patients based on a description of reported anuria. The exact date of death was unknown for 43 of the 59 deaths. Of the 16 initial survivors for whom an exact date of death was available, 5 died within a month of discharge from Ebola treatment units, an additional 3 died within 3 months of discharge, 4 died 3-12 months after discharge, and 4 died more than a year after discharge (up to 21 months).
Age and area of residence (urban vs. nonurban area) were independently and significantly associated with mortality, with patients of older age (55 years or greater) and those from nonurban areas being at greater risk. Patient sex was not associated with survival.
Those survivors who were hospitalized for 12 days or more had more than double the risk of death than did those hospitalized less than 12 days, which was a statistically significant association.
“Survivors’ monitoring programs should be strengthened and should not focus exclusively on testing of bodily fluids,” the authors advised. “Furthermore, our study provides preliminary evidence that survivors hospitalized for longer than 12 days with Ebola virus disease could be at particularly high risk of mortality and should be specifically targeted, and perhaps also evidence that renal function should be monitored,” Dr. Keita and colleagues concluded.
The study was funded by the World Health Organization, International Medical Corps, and the Guinean Red Cross. The authors reported that they had no conflicts
Survivors of the 2013-2016 Ebola epidemic in West Africa had lingering health effects of the disease. These patients had a much greater mortality in the first year after discharge, compared with the general population. Among those survivors who died, the majority appear to have expired because of renal failure, according to the results of an assessment the by the Guinean national survivors’ monitoring program.
CDC/Athalia Christie
The Surveillance Active en Ceinture obtained data on 1,130 (89%) of survivors of Ebola virus disease who were discharged from Ebola treatment units in Guinea. Compared with the general Guinean population, survivors of Ebola virus showed a five times increased risk of mortality within a year of follow-up after discharge, according to a survey of patients’ medical records and patients’ relatives, reported researchers Mory Keita, MD, and colleagues.
After 1 year, the difference in mortality between Ebola survivors and the general population had disappeared, according to the study published online in the Lancet Infectious Diseases.
A total of 59 deaths were reported among the discharged survivors available for follow-up. Renal failure was the assumed cause in 37 (63%) of these patients based on a description of reported anuria. The exact date of death was unknown for 43 of the 59 deaths. Of the 16 initial survivors for whom an exact date of death was available, 5 died within a month of discharge from Ebola treatment units, an additional 3 died within 3 months of discharge, 4 died 3-12 months after discharge, and 4 died more than a year after discharge (up to 21 months).
Age and area of residence (urban vs. nonurban area) were independently and significantly associated with mortality, with patients of older age (55 years or greater) and those from nonurban areas being at greater risk. Patient sex was not associated with survival.
Those survivors who were hospitalized for 12 days or more had more than double the risk of death than did those hospitalized less than 12 days, which was a statistically significant association.
“Survivors’ monitoring programs should be strengthened and should not focus exclusively on testing of bodily fluids,” the authors advised. “Furthermore, our study provides preliminary evidence that survivors hospitalized for longer than 12 days with Ebola virus disease could be at particularly high risk of mortality and should be specifically targeted, and perhaps also evidence that renal function should be monitored,” Dr. Keita and colleagues concluded.
The study was funded by the World Health Organization, International Medical Corps, and the Guinean Red Cross. The authors reported that they had no conflicts
Survivors of the 2013-2016 Ebola epidemic in West Africa had lingering health effects of the disease. These patients had a much greater mortality in the first year after discharge, compared with the general population. Among those survivors who died, the majority appear to have expired because of renal failure, according to the results of an assessment the by the Guinean national survivors’ monitoring program.
CDC/Athalia Christie
The Surveillance Active en Ceinture obtained data on 1,130 (89%) of survivors of Ebola virus disease who were discharged from Ebola treatment units in Guinea. Compared with the general Guinean population, survivors of Ebola virus showed a five times increased risk of mortality within a year of follow-up after discharge, according to a survey of patients’ medical records and patients’ relatives, reported researchers Mory Keita, MD, and colleagues.
After 1 year, the difference in mortality between Ebola survivors and the general population had disappeared, according to the study published online in the Lancet Infectious Diseases.
A total of 59 deaths were reported among the discharged survivors available for follow-up. Renal failure was the assumed cause in 37 (63%) of these patients based on a description of reported anuria. The exact date of death was unknown for 43 of the 59 deaths. Of the 16 initial survivors for whom an exact date of death was available, 5 died within a month of discharge from Ebola treatment units, an additional 3 died within 3 months of discharge, 4 died 3-12 months after discharge, and 4 died more than a year after discharge (up to 21 months).
Age and area of residence (urban vs. nonurban area) were independently and significantly associated with mortality, with patients of older age (55 years or greater) and those from nonurban areas being at greater risk. Patient sex was not associated with survival.
Those survivors who were hospitalized for 12 days or more had more than double the risk of death than did those hospitalized less than 12 days, which was a statistically significant association.
“Survivors’ monitoring programs should be strengthened and should not focus exclusively on testing of bodily fluids,” the authors advised. “Furthermore, our study provides preliminary evidence that survivors hospitalized for longer than 12 days with Ebola virus disease could be at particularly high risk of mortality and should be specifically targeted, and perhaps also evidence that renal function should be monitored,” Dr. Keita and colleagues concluded.
The study was funded by the World Health Organization, International Medical Corps, and the Guinean Red Cross. The authors reported that they had no conflicts
Key clinical point: Renal failure was the assumed cause of death in 63% of the survivors based on reported anuria.
Major finding: Ebola survivors in Guinea had a five times greater mortality in the first year after discharge, compared with the general population.
Study details: A postdischarge survey of 1,130 (89%) of the Ebola survivors and their relations in Guinea.
Disclosures: The study was funded by the World Health Organization, International Medical Corps, and the Guinean Red Cross. The authors reported that they had no conflicts.
Patients with viral hepatitis may live longer after treatment with direct-acting antiviral agents (DAAs), but their risk of extrahepatic causes of death may rise as a result, according to investigators.
Importantly, this increasing rate of extrahepatic mortality shouldn’t be seen as a causal link with DAA use, cautioned lead author Donghee Kim, MD, PhD, of Stanford (Calif.) University, and colleagues. Instead, the upward trend is more likely because of successful treatment with DAAs, which can increase lifespan, and with it, time for susceptibility to extrahepatic conditions.
This was just one finding from a retrospective study that used U.S. Census and National Center for Health Statistics mortality records to evaluate almost 28 million deaths that occurred between 2007 and 2017. The investigators looked for mortality trends among patients with common chronic liver diseases, including viral hepatitis, alcoholic liver disease (ALD), and nonalcoholic fatty liver disease (NAFLD), noting that each of these conditions is associated with extrahepatic complications. The study included deaths due to extrahepatic cancer, cardiovascular disease, and diabetes.
While the efficacy of therapy for viral hepatitis has improved markedly since 2014, treatments for ALD and NAFLD have remained static, the investigators noted.
“Unfortunately, there have been no significant breakthroughs in the treatment of [ALD] over the last 2 decades, resulting in an increase in estimated global mortality to 3.8%,” the investigators wrote in Gastroenterology.
“[NAFLD] is the most common chronic liver disease in the world,” they added. “The leading cause of death in individuals with NAFLD is cardiovascular disease, followed by extrahepatic malignancies, and then liver-related mortality. However, recent trends in ALD and NAFLD-related extrahepatic complications in comparison to viral hepatitis have not been studied.”
The results of the current study supported the positive impact of DAAs, which began to see widespread use in 2014. Age-standardized mortality among patients with hepatitis C virus rose until 2014 (2.2% per year) and dropped thereafter (–6.5% per year). Mortality among those with hepatitis B virus steadily decreased over the study period (–1.2% per year).
Of note, while deaths because of HCV-related liver disease dropped from 2014 to 2017, extrahepatic causes of death didn’t follow suit. Age-standardized mortality for cardiovascular disease and diabetes increased at average annual rates of 1.9% and 3.3%, respectively, while the rate of extrahepatic cancer-related deaths held steady.
“The widespread use, higher efficacy and durable response to DAA agents in individuals with HCV infection may have resulted in a paradigm shift in the clinical progression of coexisting disease entities following response to DAA agents in the virus-free environment,” the investigators wrote. “These findings suggest assessment and identification of risk and risk factors for extrahepatic cancer, cardiovascular disease, and diabetes in individuals who have been successfully treated and cured of HCV infection.”
In sharp contrast with the viral hepatitis findings, mortality rates among patients with ALD and NAFLD increased at an accelerating rate over the 11-year study period.
Among patients with ALD, all-cause mortality increased by an average of 3.4% per year, at a higher rate in the second half of the study than the first (4.6% vs 2.1%). Liver disease–related mortality rose at a similar, accelerating rate. In the same group, deaths due to cardiovascular disease increased at an average annual rate of 2.1%, which was accelerating, while extrahepatic cancer-related deaths increased at a more constant rate of 3.6%.
For patients with NAFLD, all-cause mortality increased by 8.1% per year, accelerating from 6.1% in the first half of the study to 11.2% in the second. Deaths from liver disease increased at an average rate of 12.6% per year, while extrahepatic deaths increased significantly for all three included types: cardiovascular disease (2.0%), extrahepatic cancer (15.1%), and diabetes (9.7%).
Concerning the worsening rates of mortality among patients with ALD and NAFLD, the investigators cited a lack of progress in treatments, and suggested that “the quest for newer therapies must remain the cornerstone in our efforts.”
The investigators reported no external funding or conflicts of interest.
Chronic liver disease is one of the leading causes of death in the United States. Whereas mortality from other causes (e.g., heart disease and cancer) has declined, age-adjusted mortality from chronic liver disease has continued to increase. There have been a few major advances in the treatment of several chronic liver diseases in recent years. These include nucleos(t)ide analogues for hepatitis B virus (HBV) and direct-acting antiviral agents for the treatment of hepatitis C virus infection (HCV). Many studies show that these treatments are highly effective in improving patient outcomes, including patient survival. However, whether these individual-level benefits have translated into population-level improvements remains unclear.
Dr. Fasiha Kanwal
This study used the U.S. Census and the National Center for Health Statistics mortality records from over an 11-year period to examine population level changes in overall mortality, including mortality from liver- and nonliver (extrahepatic) complications of viral hepatitis, alcoholic liver disease, and nonalcoholic liver disease in the United States.
Overall, the results were mixed; they were encouraging for viral hepatitis but concerning for alcoholic and nonalcoholic liver disease. Specifically, all-cause mortality from HCV was on an upward trajectory in the first 7 years (from 2007 to 2014) but the trend shifted from 2014 onward. Importantly, this inflection point coincided with the timing of the new HCV treatments. Most of this positive shift post 2014 was related to a strong downward trend in liver-related mortality. In contrast, upward trends in mortality related to extrahepatic causes (such as cardiovascular mortality) continued unabated. The authors found similar results for HBV. The story, however, was different for alcohol and nonalcohol-related liver disease – both conditions lacking effective treatments; liver-related mortality for both continued to increase during the study period.
Although we cannot make causal inferences from this study, overall, the results are good news. They suggest that HBV and HCV treatments have reached enough infected people to result in tangible improvements in the burden of chronic liver disease. We may now need to shift the focus of secondary prevention efforts from liver to nonliver (extrahepatic) morbidity in the newer cohorts of patients with treated HCV and HBV.
Fasiha Kanwal, MD, MSHS, is an investigator in the clinical epidemiology and comparative effectiveness program for the Center for Innovations in Quality, Effectiveness, and Safety in collaboration with the Michael E. DeBakey VA Medical Center, as well as an associate professor of medicine in gastroenterology and hepatology at Baylor College of Medicine in Houston. She has no conflicts of interest.
Chronic liver disease is one of the leading causes of death in the United States. Whereas mortality from other causes (e.g., heart disease and cancer) has declined, age-adjusted mortality from chronic liver disease has continued to increase. There have been a few major advances in the treatment of several chronic liver diseases in recent years. These include nucleos(t)ide analogues for hepatitis B virus (HBV) and direct-acting antiviral agents for the treatment of hepatitis C virus infection (HCV). Many studies show that these treatments are highly effective in improving patient outcomes, including patient survival. However, whether these individual-level benefits have translated into population-level improvements remains unclear.
Dr. Fasiha Kanwal
This study used the U.S. Census and the National Center for Health Statistics mortality records from over an 11-year period to examine population level changes in overall mortality, including mortality from liver- and nonliver (extrahepatic) complications of viral hepatitis, alcoholic liver disease, and nonalcoholic liver disease in the United States.
Overall, the results were mixed; they were encouraging for viral hepatitis but concerning for alcoholic and nonalcoholic liver disease. Specifically, all-cause mortality from HCV was on an upward trajectory in the first 7 years (from 2007 to 2014) but the trend shifted from 2014 onward. Importantly, this inflection point coincided with the timing of the new HCV treatments. Most of this positive shift post 2014 was related to a strong downward trend in liver-related mortality. In contrast, upward trends in mortality related to extrahepatic causes (such as cardiovascular mortality) continued unabated. The authors found similar results for HBV. The story, however, was different for alcohol and nonalcohol-related liver disease – both conditions lacking effective treatments; liver-related mortality for both continued to increase during the study period.
Although we cannot make causal inferences from this study, overall, the results are good news. They suggest that HBV and HCV treatments have reached enough infected people to result in tangible improvements in the burden of chronic liver disease. We may now need to shift the focus of secondary prevention efforts from liver to nonliver (extrahepatic) morbidity in the newer cohorts of patients with treated HCV and HBV.
Fasiha Kanwal, MD, MSHS, is an investigator in the clinical epidemiology and comparative effectiveness program for the Center for Innovations in Quality, Effectiveness, and Safety in collaboration with the Michael E. DeBakey VA Medical Center, as well as an associate professor of medicine in gastroenterology and hepatology at Baylor College of Medicine in Houston. She has no conflicts of interest.
Body
Chronic liver disease is one of the leading causes of death in the United States. Whereas mortality from other causes (e.g., heart disease and cancer) has declined, age-adjusted mortality from chronic liver disease has continued to increase. There have been a few major advances in the treatment of several chronic liver diseases in recent years. These include nucleos(t)ide analogues for hepatitis B virus (HBV) and direct-acting antiviral agents for the treatment of hepatitis C virus infection (HCV). Many studies show that these treatments are highly effective in improving patient outcomes, including patient survival. However, whether these individual-level benefits have translated into population-level improvements remains unclear.
Dr. Fasiha Kanwal
This study used the U.S. Census and the National Center for Health Statistics mortality records from over an 11-year period to examine population level changes in overall mortality, including mortality from liver- and nonliver (extrahepatic) complications of viral hepatitis, alcoholic liver disease, and nonalcoholic liver disease in the United States.
Overall, the results were mixed; they were encouraging for viral hepatitis but concerning for alcoholic and nonalcoholic liver disease. Specifically, all-cause mortality from HCV was on an upward trajectory in the first 7 years (from 2007 to 2014) but the trend shifted from 2014 onward. Importantly, this inflection point coincided with the timing of the new HCV treatments. Most of this positive shift post 2014 was related to a strong downward trend in liver-related mortality. In contrast, upward trends in mortality related to extrahepatic causes (such as cardiovascular mortality) continued unabated. The authors found similar results for HBV. The story, however, was different for alcohol and nonalcohol-related liver disease – both conditions lacking effective treatments; liver-related mortality for both continued to increase during the study period.
Although we cannot make causal inferences from this study, overall, the results are good news. They suggest that HBV and HCV treatments have reached enough infected people to result in tangible improvements in the burden of chronic liver disease. We may now need to shift the focus of secondary prevention efforts from liver to nonliver (extrahepatic) morbidity in the newer cohorts of patients with treated HCV and HBV.
Fasiha Kanwal, MD, MSHS, is an investigator in the clinical epidemiology and comparative effectiveness program for the Center for Innovations in Quality, Effectiveness, and Safety in collaboration with the Michael E. DeBakey VA Medical Center, as well as an associate professor of medicine in gastroenterology and hepatology at Baylor College of Medicine in Houston. She has no conflicts of interest.
Title
Nonliver diseases such as heart disease and cancer should take more focus
Nonliver diseases such as heart disease and cancer should take more focus
Patients with viral hepatitis may live longer after treatment with direct-acting antiviral agents (DAAs), but their risk of extrahepatic causes of death may rise as a result, according to investigators.
Importantly, this increasing rate of extrahepatic mortality shouldn’t be seen as a causal link with DAA use, cautioned lead author Donghee Kim, MD, PhD, of Stanford (Calif.) University, and colleagues. Instead, the upward trend is more likely because of successful treatment with DAAs, which can increase lifespan, and with it, time for susceptibility to extrahepatic conditions.
This was just one finding from a retrospective study that used U.S. Census and National Center for Health Statistics mortality records to evaluate almost 28 million deaths that occurred between 2007 and 2017. The investigators looked for mortality trends among patients with common chronic liver diseases, including viral hepatitis, alcoholic liver disease (ALD), and nonalcoholic fatty liver disease (NAFLD), noting that each of these conditions is associated with extrahepatic complications. The study included deaths due to extrahepatic cancer, cardiovascular disease, and diabetes.
While the efficacy of therapy for viral hepatitis has improved markedly since 2014, treatments for ALD and NAFLD have remained static, the investigators noted.
“Unfortunately, there have been no significant breakthroughs in the treatment of [ALD] over the last 2 decades, resulting in an increase in estimated global mortality to 3.8%,” the investigators wrote in Gastroenterology.
“[NAFLD] is the most common chronic liver disease in the world,” they added. “The leading cause of death in individuals with NAFLD is cardiovascular disease, followed by extrahepatic malignancies, and then liver-related mortality. However, recent trends in ALD and NAFLD-related extrahepatic complications in comparison to viral hepatitis have not been studied.”
The results of the current study supported the positive impact of DAAs, which began to see widespread use in 2014. Age-standardized mortality among patients with hepatitis C virus rose until 2014 (2.2% per year) and dropped thereafter (–6.5% per year). Mortality among those with hepatitis B virus steadily decreased over the study period (–1.2% per year).
Of note, while deaths because of HCV-related liver disease dropped from 2014 to 2017, extrahepatic causes of death didn’t follow suit. Age-standardized mortality for cardiovascular disease and diabetes increased at average annual rates of 1.9% and 3.3%, respectively, while the rate of extrahepatic cancer-related deaths held steady.
“The widespread use, higher efficacy and durable response to DAA agents in individuals with HCV infection may have resulted in a paradigm shift in the clinical progression of coexisting disease entities following response to DAA agents in the virus-free environment,” the investigators wrote. “These findings suggest assessment and identification of risk and risk factors for extrahepatic cancer, cardiovascular disease, and diabetes in individuals who have been successfully treated and cured of HCV infection.”
In sharp contrast with the viral hepatitis findings, mortality rates among patients with ALD and NAFLD increased at an accelerating rate over the 11-year study period.
Among patients with ALD, all-cause mortality increased by an average of 3.4% per year, at a higher rate in the second half of the study than the first (4.6% vs 2.1%). Liver disease–related mortality rose at a similar, accelerating rate. In the same group, deaths due to cardiovascular disease increased at an average annual rate of 2.1%, which was accelerating, while extrahepatic cancer-related deaths increased at a more constant rate of 3.6%.
For patients with NAFLD, all-cause mortality increased by 8.1% per year, accelerating from 6.1% in the first half of the study to 11.2% in the second. Deaths from liver disease increased at an average rate of 12.6% per year, while extrahepatic deaths increased significantly for all three included types: cardiovascular disease (2.0%), extrahepatic cancer (15.1%), and diabetes (9.7%).
Concerning the worsening rates of mortality among patients with ALD and NAFLD, the investigators cited a lack of progress in treatments, and suggested that “the quest for newer therapies must remain the cornerstone in our efforts.”
The investigators reported no external funding or conflicts of interest.
Patients with viral hepatitis may live longer after treatment with direct-acting antiviral agents (DAAs), but their risk of extrahepatic causes of death may rise as a result, according to investigators.
Importantly, this increasing rate of extrahepatic mortality shouldn’t be seen as a causal link with DAA use, cautioned lead author Donghee Kim, MD, PhD, of Stanford (Calif.) University, and colleagues. Instead, the upward trend is more likely because of successful treatment with DAAs, which can increase lifespan, and with it, time for susceptibility to extrahepatic conditions.
This was just one finding from a retrospective study that used U.S. Census and National Center for Health Statistics mortality records to evaluate almost 28 million deaths that occurred between 2007 and 2017. The investigators looked for mortality trends among patients with common chronic liver diseases, including viral hepatitis, alcoholic liver disease (ALD), and nonalcoholic fatty liver disease (NAFLD), noting that each of these conditions is associated with extrahepatic complications. The study included deaths due to extrahepatic cancer, cardiovascular disease, and diabetes.
While the efficacy of therapy for viral hepatitis has improved markedly since 2014, treatments for ALD and NAFLD have remained static, the investigators noted.
“Unfortunately, there have been no significant breakthroughs in the treatment of [ALD] over the last 2 decades, resulting in an increase in estimated global mortality to 3.8%,” the investigators wrote in Gastroenterology.
“[NAFLD] is the most common chronic liver disease in the world,” they added. “The leading cause of death in individuals with NAFLD is cardiovascular disease, followed by extrahepatic malignancies, and then liver-related mortality. However, recent trends in ALD and NAFLD-related extrahepatic complications in comparison to viral hepatitis have not been studied.”
The results of the current study supported the positive impact of DAAs, which began to see widespread use in 2014. Age-standardized mortality among patients with hepatitis C virus rose until 2014 (2.2% per year) and dropped thereafter (–6.5% per year). Mortality among those with hepatitis B virus steadily decreased over the study period (–1.2% per year).
Of note, while deaths because of HCV-related liver disease dropped from 2014 to 2017, extrahepatic causes of death didn’t follow suit. Age-standardized mortality for cardiovascular disease and diabetes increased at average annual rates of 1.9% and 3.3%, respectively, while the rate of extrahepatic cancer-related deaths held steady.
“The widespread use, higher efficacy and durable response to DAA agents in individuals with HCV infection may have resulted in a paradigm shift in the clinical progression of coexisting disease entities following response to DAA agents in the virus-free environment,” the investigators wrote. “These findings suggest assessment and identification of risk and risk factors for extrahepatic cancer, cardiovascular disease, and diabetes in individuals who have been successfully treated and cured of HCV infection.”
In sharp contrast with the viral hepatitis findings, mortality rates among patients with ALD and NAFLD increased at an accelerating rate over the 11-year study period.
Among patients with ALD, all-cause mortality increased by an average of 3.4% per year, at a higher rate in the second half of the study than the first (4.6% vs 2.1%). Liver disease–related mortality rose at a similar, accelerating rate. In the same group, deaths due to cardiovascular disease increased at an average annual rate of 2.1%, which was accelerating, while extrahepatic cancer-related deaths increased at a more constant rate of 3.6%.
For patients with NAFLD, all-cause mortality increased by 8.1% per year, accelerating from 6.1% in the first half of the study to 11.2% in the second. Deaths from liver disease increased at an average rate of 12.6% per year, while extrahepatic deaths increased significantly for all three included types: cardiovascular disease (2.0%), extrahepatic cancer (15.1%), and diabetes (9.7%).
Concerning the worsening rates of mortality among patients with ALD and NAFLD, the investigators cited a lack of progress in treatments, and suggested that “the quest for newer therapies must remain the cornerstone in our efforts.”
The investigators reported no external funding or conflicts of interest.
Fleas of the order Siphonaptera are insects that feed on the blood of a mammalian host. They have no wings but jump to near 150 times their body lengths to reach potential hosts.1 An epidemiologic survey performed in 2016 demonstrated that 96% of fleas in the United States are cat fleas (Ctenocephalidesfelis).2 The bites often present as pruritic, nonfollicular-based, excoriated papules; papular urticaria; or vesiculobullous lesions distributed across the lower legs. Antihistamines and topical steroids may be helpful for symptomatic relief, but flea eradication is key.
Figure 1. Characteristic pronotal and genal combs in a cat flea (Ctenocephalides felis)
Figure 2. A, Male cat flea (Ctenocephalides felis). B, Female cat flea.
Identification
Ctenocephalides fleas, including the common cat flea and the dog flea, have a characteristic pronotal comb that resembles a mane of hair (Figure 1) and genal comb that resembles a mustache. Compared to the dog flea (Ctenocephalides canis), cat fleas have a flatter head and fewer hair-bearing notches on the dorsal hind tibia (the dog flea has 8 notches and the cat flea has 6 notches)(Figure 2).
Flea Prevention and Eradication
Effective management of flea bites requires avoidance of infested areas and eradication of fleas from the home and pets. Home treatment should be performed by a qualified specialist and a veterinarian should treat the pet, but the dermatologist must be knowledgeable about treatment options. Flea pupae can lie dormant between floorboards for extended periods of time and hatch rapidly when new tenants enter a house or apartment. Insecticidal dusts and spray formulations frequently are used to treat infested homes. It also is important to reduce flea egg numbers by vacuuming carpets and areas where pets sleep.3 Rodents often introduce fleas to households and pets, so eliminating them from the area may play an important role in flea control. Consulting with a veterinarian is important, as treatment directed at pets is critical to control flea populations. Oral agents, including fluralaner, afoxolaner, sarolaner, and spinosad, can reduce flea populations on animals by as much as 99.3% after 7 days.4,5 Fast-acting pulicidal agents, such as the combination of dinotefuran and fipronil, demonstrate curative activity as soon as 3 hours after treatment, which also may prevent reinfestation for as long as 6 weeks after treatment.6
Vector-Borne Disease
Fleas living on animals in close contact with humans, such as cats and dogs, can transmit zoonotic pathogens. Around 12,000 outpatients and 500 inpatients are diagnosed with cat scratch disease, a form of bartonellosis, annually. Ctenocephalides felis transmits Bartonella henselae from cat-to-cat and often cat-to-human through infected flea feces, causing a primary inoculation lesion and lymphadenitis. Of 3011 primary care providers surveyed from 2014 to 2015, 37.2% had treated at least 1 patient with cat scratch disease, yet knowledge gaps remain regarding the proper treatment and preventative measures for the disease.7 Current recommendations for the treatment of lymphadenitis caused by B henselae include a 5-day course of oral azithromycin.8 The preferred dosing regimen in adults is 500 mg on day 1 and 250 mg on days 2 through 5. Pediatric patients weighing less than 45.5 kg should receive 10 mg/kg on day 1 and 5 mg/kg on days 2 through 5.8 Additionally, less than one-third of the primary care providers surveyed from 2014 to 2015 said they would discuss the importance of pet flea control with immunocompromised patients who own cats, despite evidence implicating fleas in disease transmission.7 Pet-directed topical therapy with agents such as selamectin prescribed by a qualified veterinarian can prevent transmission of B henselae in cats exposed to fleas infected with the bacteria,9 which supports the importance of patient education and flea control, especially in pets owned by immunocompromised patients. Patients who are immunocompromised are at increased risk for persistent or disseminated bartonellosis, including endocarditis, in addition to cat scratch disease. Although arriving at a diagnosis may be difficult, one study found that bartonellosis in 13 renal transplant recipients was best diagnosed using both serology and polymerase chain reaction via DNA extraction of tissue specimens.10 These findings may enhance diagnostic yield for similar patients when bartonellosis is suspected.
Flea-borne typhus is endemic to Texas and Southern California.11,12 Evidence suggests that the pathogenic bacteria, Rickettsia typhi and Rickettsia felis, also commonly infect fleas in the Great Plains area.13 Opossums carry R felis, and the fleas transmit murine or endemic typhus. A retrospective case series in Texas identified 11 cases of fatal flea-borne typhus from 1985 to 2015.11 More than half of the patients reported contact with animals or fleas prior to the illness. Patients with typhus may present with fever, nausea, vomiting, rash (macular, maculopapular, papular, petechial, or morbilliform), respiratory or neurologic symptoms, thrombocytopenia, and elevated hepatic liver enzymes. Unfortunately, there often is a notable delay in initiation of treatment with the appropriate class of antibiotics—tetracyclines—and such delays can prove fatal.11 The current recommendation for nonpregnant adults is oral doxycycline 100 mg twice daily continued 48 hours after the patient becomes afebrile or for 7 days, whichever therapy duration is longer.14 Because of the consequences of delayed treatment, it is important for clinicians to consider a diagnosis of vector-borne illness in a febrile patient with other associated gastrointestinal, cutaneous, respiratory, or neurologic symptoms, especially if they have animal or flea exposures. Flea control and exposure awareness remains paramount in preventing and treating this illness.
Yersinia pestis causes the plague, an important re-emerging disease that causes infection through flea bites, inhalation, or ingestion.15 From 2000 to 2009, 56 cases and 7 deaths in the United States—New Mexico, Arizona, Colorado, California, and Texas—and 21,725 cases and 1612 deaths worldwide were attributed to Y pestis. Most patients present with the bubonic form of the disease, with fever and an enlarging painful femoral or inguinal lymph node due to leg flea bites.16 Other forms of disease, including septicemic and pneumonic plague, are less common but relevant, as one-third of cases in the United States present with septicemia.15,17,18 Although molecular diagnosis and immunohistochemistry play important roles, the diagnosis of Y pestis infection often is still accomplished with culture. A 2012 survey of 392 strains from 17 countries demonstrated that Y pestis remained susceptible to the antibiotics currently used to treat the disease, including doxycycline, streptomycin, gentamicin, tetracycline, trimethoprim-sulfamethoxazole, and ciprofloxacin.19
Human infection with Dipylidium caninum, a dog tapeworm, has been reported after suspected accidental ingestion of cat fleas carrying the parasite.20 Children, who may present with diarrhea or white worms in their feces, are more susceptible to the infection, perhaps due to accidental flea consumption while being licked by the pet.20,21
Conclusion
Cat fleas may act as a pruritic nuisance for pet owners and even deliver deadly pathogens to immunocompromised patients. Providers can minimize their impact by educating patients on flea prevention and eradication as well as astutely recognizing and treating flea-borne diseases.
References
Cadiergues MC. A comparison of jump performances of the dog flea, Ctenocephalides canis (Curtis, 1826) and the cat flea, Ctenocephalides felis (Bouché, 1835). Vet Parasitol. 2000;92:239-241.
Blagburn B, Butler J, Land T, et al. Who’s who and where: prevalence of Ctenocephalides felis and Ctenocephalides canis in shelter dogs and cats in the United States. Presented at: American Association of Veterinary Parasitologists 61st Annual Meeting; August 6-9, 2016; San Antonio, TX. P9.
Bitam I, Dittmar K, Parola P, et al. Fleas and flea-borne diseases. Int J Infect Dis. 2010;14:E667-E676.
Dryden MW, Canfield MS, Niedfeldt E, et al. Evaluation of sarolaner and spinosad oral treatments to eliminate fleas, reduce dermatologic lesions and minimize pruritus in naturally infested dogs in west Central Florida, USA. Parasit Vectors. 2017;10:389.
Dryden MW, Canfield MS, Kalosy K, et al. Evaluation of fluralaner and afoxolaner treatments to control flea populations, reduce pruritus and minimize dermatologic lesions in naturally infested dogs in private residences in west Central Florida, USA. Parasit Vectors. 2016;9:365.
Delcombel R, Karembe H, Nare B, et al. Synergy between dinotefuran and fipronil against the cat flea (Ctenocephalides felis): improved onset of action and residual speed of kill in adult cats. Parasit Vectors. 2017;10:341.
Nelson CA, Moore AR, Perea AE, et al. Cat scratch disease: U.S. clinicians’ experience and knowledge. Zoonoses Public Health. 2018;65:67-73.
Spach DH, Kaplan SL. Treatment of cat scratch disease. UpToDate. https://www.uptodate.com/contents/treatment-of-cat-scratch-disease?search=treatment%20of%20cat%20scratch&source=search_result&selectedTitle=1~59&usage_type=default&display_rank=1.Updated June 12, 2019. Accessed August 15, 2019.
Bouhsira E, Franc M, Lienard E, et al. The efficacy of a selamectin (Stronghold®) spot on treatment in the prevention of Bartonella henselae transmission by Ctenocephalides felis in cats, using a new high-challenge model. Parasitol Res. 2015;114:1045-1050.
Shamekhi Amiri F. Bartonellosis in chronic kidney disease: an unrecognized and unsuspected diagnosis. Ther Apher Dial. 2017;21:430-440.
Pieracci EG, Evert N, Drexler NA, et al. Fatal flea-borne typhus in Texas: a retrospective case series, 1985-2015. American J Trop Med Hyg. 2017;96:1088-1093.
Maina AN, Fogarty C, Krueger L, et al. Rickettsial infections among Ctenocephalides felis and host animals during a flea-borne rickettsioses outbreak in Orange County, California. PLoS One. 2016;11:e0160604.
Noden BH, Davidson S, Smith JL, et al. First detection of Rickettsia typhi and Rickettsia felis in fleas collected from client-owned companion animals in the Southern Great Plains. J Med Entomol. 2017;54:1093-1097.
Sexton DJ. Murine typhus. UpToDate. https://www.uptodate.com/contents/murine-typhus?search=diagnosis-and-treatment-of-murine-typhus&source=search_result&selectedTitle=1~21&usage_type=default&display_rank=1. Updated January 17, 2019. Accessed August 15, 2019.
Riehm JM, Löscher T. Human plague and pneumonic plague: pathogenicity, epidemiology, clinical presentations and therapy [in German]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2015;58:721-729.
Butler T. Plague gives surprises in the first decade of the 21st century in the United States and worldwide. Am J Trop Med Hyg. 2013;89:788-793.
Gould LH, Pape J, Ettestad P, Griffith KS, et al. Dog-associated risk factors for human plague. Zoonoses Public Health. 2008;55:448-454.
Margolis DA, Burns J, Reed SL, et al. Septicemic plague in a community hospital in California. Am J Trop Med Hyg. 2008;78:868-871.
Urich SK, Chalcraft L, Schriefer ME, et al. Lack of antimicrobial resistance in Yersinia pestis isolates from 17 countries in the Americas, Africa, and Asia. Antimicrob Agents Chemother. 2012;56:555-558.
Jiang P, Zhang X, Liu RD, et al. A human case of zoonotic dog tapeworm, Dipylidium caninum (Eucestoda: Dilepidiidae), in China. Korean J Parasitol. 2017;55:61-64.
Roberts LS, Janovy J Jr, eds. Foundations of Parasitology. 8th ed. New York, NY: McGraw-Hill; 2009.
Fleas of the order Siphonaptera are insects that feed on the blood of a mammalian host. They have no wings but jump to near 150 times their body lengths to reach potential hosts.1 An epidemiologic survey performed in 2016 demonstrated that 96% of fleas in the United States are cat fleas (Ctenocephalidesfelis).2 The bites often present as pruritic, nonfollicular-based, excoriated papules; papular urticaria; or vesiculobullous lesions distributed across the lower legs. Antihistamines and topical steroids may be helpful for symptomatic relief, but flea eradication is key.
Figure 1. Characteristic pronotal and genal combs in a cat flea (Ctenocephalides felis)
Figure 2. A, Male cat flea (Ctenocephalides felis). B, Female cat flea.
Identification
Ctenocephalides fleas, including the common cat flea and the dog flea, have a characteristic pronotal comb that resembles a mane of hair (Figure 1) and genal comb that resembles a mustache. Compared to the dog flea (Ctenocephalides canis), cat fleas have a flatter head and fewer hair-bearing notches on the dorsal hind tibia (the dog flea has 8 notches and the cat flea has 6 notches)(Figure 2).
Flea Prevention and Eradication
Effective management of flea bites requires avoidance of infested areas and eradication of fleas from the home and pets. Home treatment should be performed by a qualified specialist and a veterinarian should treat the pet, but the dermatologist must be knowledgeable about treatment options. Flea pupae can lie dormant between floorboards for extended periods of time and hatch rapidly when new tenants enter a house or apartment. Insecticidal dusts and spray formulations frequently are used to treat infested homes. It also is important to reduce flea egg numbers by vacuuming carpets and areas where pets sleep.3 Rodents often introduce fleas to households and pets, so eliminating them from the area may play an important role in flea control. Consulting with a veterinarian is important, as treatment directed at pets is critical to control flea populations. Oral agents, including fluralaner, afoxolaner, sarolaner, and spinosad, can reduce flea populations on animals by as much as 99.3% after 7 days.4,5 Fast-acting pulicidal agents, such as the combination of dinotefuran and fipronil, demonstrate curative activity as soon as 3 hours after treatment, which also may prevent reinfestation for as long as 6 weeks after treatment.6
Vector-Borne Disease
Fleas living on animals in close contact with humans, such as cats and dogs, can transmit zoonotic pathogens. Around 12,000 outpatients and 500 inpatients are diagnosed with cat scratch disease, a form of bartonellosis, annually. Ctenocephalides felis transmits Bartonella henselae from cat-to-cat and often cat-to-human through infected flea feces, causing a primary inoculation lesion and lymphadenitis. Of 3011 primary care providers surveyed from 2014 to 2015, 37.2% had treated at least 1 patient with cat scratch disease, yet knowledge gaps remain regarding the proper treatment and preventative measures for the disease.7 Current recommendations for the treatment of lymphadenitis caused by B henselae include a 5-day course of oral azithromycin.8 The preferred dosing regimen in adults is 500 mg on day 1 and 250 mg on days 2 through 5. Pediatric patients weighing less than 45.5 kg should receive 10 mg/kg on day 1 and 5 mg/kg on days 2 through 5.8 Additionally, less than one-third of the primary care providers surveyed from 2014 to 2015 said they would discuss the importance of pet flea control with immunocompromised patients who own cats, despite evidence implicating fleas in disease transmission.7 Pet-directed topical therapy with agents such as selamectin prescribed by a qualified veterinarian can prevent transmission of B henselae in cats exposed to fleas infected with the bacteria,9 which supports the importance of patient education and flea control, especially in pets owned by immunocompromised patients. Patients who are immunocompromised are at increased risk for persistent or disseminated bartonellosis, including endocarditis, in addition to cat scratch disease. Although arriving at a diagnosis may be difficult, one study found that bartonellosis in 13 renal transplant recipients was best diagnosed using both serology and polymerase chain reaction via DNA extraction of tissue specimens.10 These findings may enhance diagnostic yield for similar patients when bartonellosis is suspected.
Flea-borne typhus is endemic to Texas and Southern California.11,12 Evidence suggests that the pathogenic bacteria, Rickettsia typhi and Rickettsia felis, also commonly infect fleas in the Great Plains area.13 Opossums carry R felis, and the fleas transmit murine or endemic typhus. A retrospective case series in Texas identified 11 cases of fatal flea-borne typhus from 1985 to 2015.11 More than half of the patients reported contact with animals or fleas prior to the illness. Patients with typhus may present with fever, nausea, vomiting, rash (macular, maculopapular, papular, petechial, or morbilliform), respiratory or neurologic symptoms, thrombocytopenia, and elevated hepatic liver enzymes. Unfortunately, there often is a notable delay in initiation of treatment with the appropriate class of antibiotics—tetracyclines—and such delays can prove fatal.11 The current recommendation for nonpregnant adults is oral doxycycline 100 mg twice daily continued 48 hours after the patient becomes afebrile or for 7 days, whichever therapy duration is longer.14 Because of the consequences of delayed treatment, it is important for clinicians to consider a diagnosis of vector-borne illness in a febrile patient with other associated gastrointestinal, cutaneous, respiratory, or neurologic symptoms, especially if they have animal or flea exposures. Flea control and exposure awareness remains paramount in preventing and treating this illness.
Yersinia pestis causes the plague, an important re-emerging disease that causes infection through flea bites, inhalation, or ingestion.15 From 2000 to 2009, 56 cases and 7 deaths in the United States—New Mexico, Arizona, Colorado, California, and Texas—and 21,725 cases and 1612 deaths worldwide were attributed to Y pestis. Most patients present with the bubonic form of the disease, with fever and an enlarging painful femoral or inguinal lymph node due to leg flea bites.16 Other forms of disease, including septicemic and pneumonic plague, are less common but relevant, as one-third of cases in the United States present with septicemia.15,17,18 Although molecular diagnosis and immunohistochemistry play important roles, the diagnosis of Y pestis infection often is still accomplished with culture. A 2012 survey of 392 strains from 17 countries demonstrated that Y pestis remained susceptible to the antibiotics currently used to treat the disease, including doxycycline, streptomycin, gentamicin, tetracycline, trimethoprim-sulfamethoxazole, and ciprofloxacin.19
Human infection with Dipylidium caninum, a dog tapeworm, has been reported after suspected accidental ingestion of cat fleas carrying the parasite.20 Children, who may present with diarrhea or white worms in their feces, are more susceptible to the infection, perhaps due to accidental flea consumption while being licked by the pet.20,21
Conclusion
Cat fleas may act as a pruritic nuisance for pet owners and even deliver deadly pathogens to immunocompromised patients. Providers can minimize their impact by educating patients on flea prevention and eradication as well as astutely recognizing and treating flea-borne diseases.
Fleas of the order Siphonaptera are insects that feed on the blood of a mammalian host. They have no wings but jump to near 150 times their body lengths to reach potential hosts.1 An epidemiologic survey performed in 2016 demonstrated that 96% of fleas in the United States are cat fleas (Ctenocephalidesfelis).2 The bites often present as pruritic, nonfollicular-based, excoriated papules; papular urticaria; or vesiculobullous lesions distributed across the lower legs. Antihistamines and topical steroids may be helpful for symptomatic relief, but flea eradication is key.
Figure 1. Characteristic pronotal and genal combs in a cat flea (Ctenocephalides felis)
Figure 2. A, Male cat flea (Ctenocephalides felis). B, Female cat flea.
Identification
Ctenocephalides fleas, including the common cat flea and the dog flea, have a characteristic pronotal comb that resembles a mane of hair (Figure 1) and genal comb that resembles a mustache. Compared to the dog flea (Ctenocephalides canis), cat fleas have a flatter head and fewer hair-bearing notches on the dorsal hind tibia (the dog flea has 8 notches and the cat flea has 6 notches)(Figure 2).
Flea Prevention and Eradication
Effective management of flea bites requires avoidance of infested areas and eradication of fleas from the home and pets. Home treatment should be performed by a qualified specialist and a veterinarian should treat the pet, but the dermatologist must be knowledgeable about treatment options. Flea pupae can lie dormant between floorboards for extended periods of time and hatch rapidly when new tenants enter a house or apartment. Insecticidal dusts and spray formulations frequently are used to treat infested homes. It also is important to reduce flea egg numbers by vacuuming carpets and areas where pets sleep.3 Rodents often introduce fleas to households and pets, so eliminating them from the area may play an important role in flea control. Consulting with a veterinarian is important, as treatment directed at pets is critical to control flea populations. Oral agents, including fluralaner, afoxolaner, sarolaner, and spinosad, can reduce flea populations on animals by as much as 99.3% after 7 days.4,5 Fast-acting pulicidal agents, such as the combination of dinotefuran and fipronil, demonstrate curative activity as soon as 3 hours after treatment, which also may prevent reinfestation for as long as 6 weeks after treatment.6
Vector-Borne Disease
Fleas living on animals in close contact with humans, such as cats and dogs, can transmit zoonotic pathogens. Around 12,000 outpatients and 500 inpatients are diagnosed with cat scratch disease, a form of bartonellosis, annually. Ctenocephalides felis transmits Bartonella henselae from cat-to-cat and often cat-to-human through infected flea feces, causing a primary inoculation lesion and lymphadenitis. Of 3011 primary care providers surveyed from 2014 to 2015, 37.2% had treated at least 1 patient with cat scratch disease, yet knowledge gaps remain regarding the proper treatment and preventative measures for the disease.7 Current recommendations for the treatment of lymphadenitis caused by B henselae include a 5-day course of oral azithromycin.8 The preferred dosing regimen in adults is 500 mg on day 1 and 250 mg on days 2 through 5. Pediatric patients weighing less than 45.5 kg should receive 10 mg/kg on day 1 and 5 mg/kg on days 2 through 5.8 Additionally, less than one-third of the primary care providers surveyed from 2014 to 2015 said they would discuss the importance of pet flea control with immunocompromised patients who own cats, despite evidence implicating fleas in disease transmission.7 Pet-directed topical therapy with agents such as selamectin prescribed by a qualified veterinarian can prevent transmission of B henselae in cats exposed to fleas infected with the bacteria,9 which supports the importance of patient education and flea control, especially in pets owned by immunocompromised patients. Patients who are immunocompromised are at increased risk for persistent or disseminated bartonellosis, including endocarditis, in addition to cat scratch disease. Although arriving at a diagnosis may be difficult, one study found that bartonellosis in 13 renal transplant recipients was best diagnosed using both serology and polymerase chain reaction via DNA extraction of tissue specimens.10 These findings may enhance diagnostic yield for similar patients when bartonellosis is suspected.
Flea-borne typhus is endemic to Texas and Southern California.11,12 Evidence suggests that the pathogenic bacteria, Rickettsia typhi and Rickettsia felis, also commonly infect fleas in the Great Plains area.13 Opossums carry R felis, and the fleas transmit murine or endemic typhus. A retrospective case series in Texas identified 11 cases of fatal flea-borne typhus from 1985 to 2015.11 More than half of the patients reported contact with animals or fleas prior to the illness. Patients with typhus may present with fever, nausea, vomiting, rash (macular, maculopapular, papular, petechial, or morbilliform), respiratory or neurologic symptoms, thrombocytopenia, and elevated hepatic liver enzymes. Unfortunately, there often is a notable delay in initiation of treatment with the appropriate class of antibiotics—tetracyclines—and such delays can prove fatal.11 The current recommendation for nonpregnant adults is oral doxycycline 100 mg twice daily continued 48 hours after the patient becomes afebrile or for 7 days, whichever therapy duration is longer.14 Because of the consequences of delayed treatment, it is important for clinicians to consider a diagnosis of vector-borne illness in a febrile patient with other associated gastrointestinal, cutaneous, respiratory, or neurologic symptoms, especially if they have animal or flea exposures. Flea control and exposure awareness remains paramount in preventing and treating this illness.
Yersinia pestis causes the plague, an important re-emerging disease that causes infection through flea bites, inhalation, or ingestion.15 From 2000 to 2009, 56 cases and 7 deaths in the United States—New Mexico, Arizona, Colorado, California, and Texas—and 21,725 cases and 1612 deaths worldwide were attributed to Y pestis. Most patients present with the bubonic form of the disease, with fever and an enlarging painful femoral or inguinal lymph node due to leg flea bites.16 Other forms of disease, including septicemic and pneumonic plague, are less common but relevant, as one-third of cases in the United States present with septicemia.15,17,18 Although molecular diagnosis and immunohistochemistry play important roles, the diagnosis of Y pestis infection often is still accomplished with culture. A 2012 survey of 392 strains from 17 countries demonstrated that Y pestis remained susceptible to the antibiotics currently used to treat the disease, including doxycycline, streptomycin, gentamicin, tetracycline, trimethoprim-sulfamethoxazole, and ciprofloxacin.19
Human infection with Dipylidium caninum, a dog tapeworm, has been reported after suspected accidental ingestion of cat fleas carrying the parasite.20 Children, who may present with diarrhea or white worms in their feces, are more susceptible to the infection, perhaps due to accidental flea consumption while being licked by the pet.20,21
Conclusion
Cat fleas may act as a pruritic nuisance for pet owners and even deliver deadly pathogens to immunocompromised patients. Providers can minimize their impact by educating patients on flea prevention and eradication as well as astutely recognizing and treating flea-borne diseases.
References
Cadiergues MC. A comparison of jump performances of the dog flea, Ctenocephalides canis (Curtis, 1826) and the cat flea, Ctenocephalides felis (Bouché, 1835). Vet Parasitol. 2000;92:239-241.
Blagburn B, Butler J, Land T, et al. Who’s who and where: prevalence of Ctenocephalides felis and Ctenocephalides canis in shelter dogs and cats in the United States. Presented at: American Association of Veterinary Parasitologists 61st Annual Meeting; August 6-9, 2016; San Antonio, TX. P9.
Bitam I, Dittmar K, Parola P, et al. Fleas and flea-borne diseases. Int J Infect Dis. 2010;14:E667-E676.
Dryden MW, Canfield MS, Niedfeldt E, et al. Evaluation of sarolaner and spinosad oral treatments to eliminate fleas, reduce dermatologic lesions and minimize pruritus in naturally infested dogs in west Central Florida, USA. Parasit Vectors. 2017;10:389.
Dryden MW, Canfield MS, Kalosy K, et al. Evaluation of fluralaner and afoxolaner treatments to control flea populations, reduce pruritus and minimize dermatologic lesions in naturally infested dogs in private residences in west Central Florida, USA. Parasit Vectors. 2016;9:365.
Delcombel R, Karembe H, Nare B, et al. Synergy between dinotefuran and fipronil against the cat flea (Ctenocephalides felis): improved onset of action and residual speed of kill in adult cats. Parasit Vectors. 2017;10:341.
Nelson CA, Moore AR, Perea AE, et al. Cat scratch disease: U.S. clinicians’ experience and knowledge. Zoonoses Public Health. 2018;65:67-73.
Spach DH, Kaplan SL. Treatment of cat scratch disease. UpToDate. https://www.uptodate.com/contents/treatment-of-cat-scratch-disease?search=treatment%20of%20cat%20scratch&source=search_result&selectedTitle=1~59&usage_type=default&display_rank=1.Updated June 12, 2019. Accessed August 15, 2019.
Bouhsira E, Franc M, Lienard E, et al. The efficacy of a selamectin (Stronghold®) spot on treatment in the prevention of Bartonella henselae transmission by Ctenocephalides felis in cats, using a new high-challenge model. Parasitol Res. 2015;114:1045-1050.
Shamekhi Amiri F. Bartonellosis in chronic kidney disease: an unrecognized and unsuspected diagnosis. Ther Apher Dial. 2017;21:430-440.
Pieracci EG, Evert N, Drexler NA, et al. Fatal flea-borne typhus in Texas: a retrospective case series, 1985-2015. American J Trop Med Hyg. 2017;96:1088-1093.
Maina AN, Fogarty C, Krueger L, et al. Rickettsial infections among Ctenocephalides felis and host animals during a flea-borne rickettsioses outbreak in Orange County, California. PLoS One. 2016;11:e0160604.
Noden BH, Davidson S, Smith JL, et al. First detection of Rickettsia typhi and Rickettsia felis in fleas collected from client-owned companion animals in the Southern Great Plains. J Med Entomol. 2017;54:1093-1097.
Sexton DJ. Murine typhus. UpToDate. https://www.uptodate.com/contents/murine-typhus?search=diagnosis-and-treatment-of-murine-typhus&source=search_result&selectedTitle=1~21&usage_type=default&display_rank=1. Updated January 17, 2019. Accessed August 15, 2019.
Riehm JM, Löscher T. Human plague and pneumonic plague: pathogenicity, epidemiology, clinical presentations and therapy [in German]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2015;58:721-729.
Butler T. Plague gives surprises in the first decade of the 21st century in the United States and worldwide. Am J Trop Med Hyg. 2013;89:788-793.
Gould LH, Pape J, Ettestad P, Griffith KS, et al. Dog-associated risk factors for human plague. Zoonoses Public Health. 2008;55:448-454.
Margolis DA, Burns J, Reed SL, et al. Septicemic plague in a community hospital in California. Am J Trop Med Hyg. 2008;78:868-871.
Urich SK, Chalcraft L, Schriefer ME, et al. Lack of antimicrobial resistance in Yersinia pestis isolates from 17 countries in the Americas, Africa, and Asia. Antimicrob Agents Chemother. 2012;56:555-558.
Jiang P, Zhang X, Liu RD, et al. A human case of zoonotic dog tapeworm, Dipylidium caninum (Eucestoda: Dilepidiidae), in China. Korean J Parasitol. 2017;55:61-64.
Roberts LS, Janovy J Jr, eds. Foundations of Parasitology. 8th ed. New York, NY: McGraw-Hill; 2009.
References
Cadiergues MC. A comparison of jump performances of the dog flea, Ctenocephalides canis (Curtis, 1826) and the cat flea, Ctenocephalides felis (Bouché, 1835). Vet Parasitol. 2000;92:239-241.
Blagburn B, Butler J, Land T, et al. Who’s who and where: prevalence of Ctenocephalides felis and Ctenocephalides canis in shelter dogs and cats in the United States. Presented at: American Association of Veterinary Parasitologists 61st Annual Meeting; August 6-9, 2016; San Antonio, TX. P9.
Bitam I, Dittmar K, Parola P, et al. Fleas and flea-borne diseases. Int J Infect Dis. 2010;14:E667-E676.
Dryden MW, Canfield MS, Niedfeldt E, et al. Evaluation of sarolaner and spinosad oral treatments to eliminate fleas, reduce dermatologic lesions and minimize pruritus in naturally infested dogs in west Central Florida, USA. Parasit Vectors. 2017;10:389.
Dryden MW, Canfield MS, Kalosy K, et al. Evaluation of fluralaner and afoxolaner treatments to control flea populations, reduce pruritus and minimize dermatologic lesions in naturally infested dogs in private residences in west Central Florida, USA. Parasit Vectors. 2016;9:365.
Delcombel R, Karembe H, Nare B, et al. Synergy between dinotefuran and fipronil against the cat flea (Ctenocephalides felis): improved onset of action and residual speed of kill in adult cats. Parasit Vectors. 2017;10:341.
Nelson CA, Moore AR, Perea AE, et al. Cat scratch disease: U.S. clinicians’ experience and knowledge. Zoonoses Public Health. 2018;65:67-73.
Spach DH, Kaplan SL. Treatment of cat scratch disease. UpToDate. https://www.uptodate.com/contents/treatment-of-cat-scratch-disease?search=treatment%20of%20cat%20scratch&source=search_result&selectedTitle=1~59&usage_type=default&display_rank=1.Updated June 12, 2019. Accessed August 15, 2019.
Bouhsira E, Franc M, Lienard E, et al. The efficacy of a selamectin (Stronghold®) spot on treatment in the prevention of Bartonella henselae transmission by Ctenocephalides felis in cats, using a new high-challenge model. Parasitol Res. 2015;114:1045-1050.
Shamekhi Amiri F. Bartonellosis in chronic kidney disease: an unrecognized and unsuspected diagnosis. Ther Apher Dial. 2017;21:430-440.
Pieracci EG, Evert N, Drexler NA, et al. Fatal flea-borne typhus in Texas: a retrospective case series, 1985-2015. American J Trop Med Hyg. 2017;96:1088-1093.
Maina AN, Fogarty C, Krueger L, et al. Rickettsial infections among Ctenocephalides felis and host animals during a flea-borne rickettsioses outbreak in Orange County, California. PLoS One. 2016;11:e0160604.
Noden BH, Davidson S, Smith JL, et al. First detection of Rickettsia typhi and Rickettsia felis in fleas collected from client-owned companion animals in the Southern Great Plains. J Med Entomol. 2017;54:1093-1097.
Sexton DJ. Murine typhus. UpToDate. https://www.uptodate.com/contents/murine-typhus?search=diagnosis-and-treatment-of-murine-typhus&source=search_result&selectedTitle=1~21&usage_type=default&display_rank=1. Updated January 17, 2019. Accessed August 15, 2019.
Riehm JM, Löscher T. Human plague and pneumonic plague: pathogenicity, epidemiology, clinical presentations and therapy [in German]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2015;58:721-729.
Butler T. Plague gives surprises in the first decade of the 21st century in the United States and worldwide. Am J Trop Med Hyg. 2013;89:788-793.
Gould LH, Pape J, Ettestad P, Griffith KS, et al. Dog-associated risk factors for human plague. Zoonoses Public Health. 2008;55:448-454.
Margolis DA, Burns J, Reed SL, et al. Septicemic plague in a community hospital in California. Am J Trop Med Hyg. 2008;78:868-871.
Urich SK, Chalcraft L, Schriefer ME, et al. Lack of antimicrobial resistance in Yersinia pestis isolates from 17 countries in the Americas, Africa, and Asia. Antimicrob Agents Chemother. 2012;56:555-558.
Jiang P, Zhang X, Liu RD, et al. A human case of zoonotic dog tapeworm, Dipylidium caninum (Eucestoda: Dilepidiidae), in China. Korean J Parasitol. 2017;55:61-64.
Roberts LS, Janovy J Jr, eds. Foundations of Parasitology. 8th ed. New York, NY: McGraw-Hill; 2009.
The measles outbreak in New York City, the largest in the nation this year, has officially ended, Mayor Bill de Blasio and city health officials announced Sept. 3.
CDC/ Cynthia S. Goldsmith; William Bellini, Ph.D.
“Ending the measles outbreak required extensive collaboration with community organizations and Jewish leaders. They helped encourage vaccinations and achieve record immunization levels in parts of Brooklyn,” Mayor de Blasio said in a written statement. “As we head back to school this week, we just remain vigilant. To keep our children and communities safe, I urge all New Yorkers to get vaccinated. It’s the best defense we have.”
A measles outbreak is considered to be over when 42 days, or two incubation periods, have elapsed since the last affected persons in the area were no longer infectious. “That time period has now passed for the people most recently infected with measles and reported,” the city health department said in the statement.
Since the outbreak began in October of last year, 654 individuals were diagnosed with measles in the five boroughs of New York, although 72% occurred in the Williamsburg neighborhood of Brooklyn. Of those 654 cases, there have been 52 hospitalizations and 16 admissions to intensive care, according to the health department. The majority of affected people were under 18 years of age (80%), and most were either unvaccinated (73%) or incompletely vaccinated (7%).
The end of the measles outbreak also brings an end to the public health emergency that was declared on April 9 for parts of Brooklyn, the statement noted.
“Vaccination coverage has increased significantly since the emergency order, which has been supported by community-led efforts. We are grateful to the New Yorkers who shared the truth about vaccines and protected the health of their friends and neighbors through this outbreak,” city health commissioner Dr. Oxiris Barbot said in the statement.
The measles outbreak in New York City, the largest in the nation this year, has officially ended, Mayor Bill de Blasio and city health officials announced Sept. 3.
CDC/ Cynthia S. Goldsmith; William Bellini, Ph.D.
“Ending the measles outbreak required extensive collaboration with community organizations and Jewish leaders. They helped encourage vaccinations and achieve record immunization levels in parts of Brooklyn,” Mayor de Blasio said in a written statement. “As we head back to school this week, we just remain vigilant. To keep our children and communities safe, I urge all New Yorkers to get vaccinated. It’s the best defense we have.”
A measles outbreak is considered to be over when 42 days, or two incubation periods, have elapsed since the last affected persons in the area were no longer infectious. “That time period has now passed for the people most recently infected with measles and reported,” the city health department said in the statement.
Since the outbreak began in October of last year, 654 individuals were diagnosed with measles in the five boroughs of New York, although 72% occurred in the Williamsburg neighborhood of Brooklyn. Of those 654 cases, there have been 52 hospitalizations and 16 admissions to intensive care, according to the health department. The majority of affected people were under 18 years of age (80%), and most were either unvaccinated (73%) or incompletely vaccinated (7%).
The end of the measles outbreak also brings an end to the public health emergency that was declared on April 9 for parts of Brooklyn, the statement noted.
“Vaccination coverage has increased significantly since the emergency order, which has been supported by community-led efforts. We are grateful to the New Yorkers who shared the truth about vaccines and protected the health of their friends and neighbors through this outbreak,” city health commissioner Dr. Oxiris Barbot said in the statement.
The measles outbreak in New York City, the largest in the nation this year, has officially ended, Mayor Bill de Blasio and city health officials announced Sept. 3.
CDC/ Cynthia S. Goldsmith; William Bellini, Ph.D.
“Ending the measles outbreak required extensive collaboration with community organizations and Jewish leaders. They helped encourage vaccinations and achieve record immunization levels in parts of Brooklyn,” Mayor de Blasio said in a written statement. “As we head back to school this week, we just remain vigilant. To keep our children and communities safe, I urge all New Yorkers to get vaccinated. It’s the best defense we have.”
A measles outbreak is considered to be over when 42 days, or two incubation periods, have elapsed since the last affected persons in the area were no longer infectious. “That time period has now passed for the people most recently infected with measles and reported,” the city health department said in the statement.
Since the outbreak began in October of last year, 654 individuals were diagnosed with measles in the five boroughs of New York, although 72% occurred in the Williamsburg neighborhood of Brooklyn. Of those 654 cases, there have been 52 hospitalizations and 16 admissions to intensive care, according to the health department. The majority of affected people were under 18 years of age (80%), and most were either unvaccinated (73%) or incompletely vaccinated (7%).
The end of the measles outbreak also brings an end to the public health emergency that was declared on April 9 for parts of Brooklyn, the statement noted.
“Vaccination coverage has increased significantly since the emergency order, which has been supported by community-led efforts. We are grateful to the New Yorkers who shared the truth about vaccines and protected the health of their friends and neighbors through this outbreak,” city health commissioner Dr. Oxiris Barbot said in the statement.
A 50-year-old man with Crohn disease and psoriatic arthritis treated with infliximab and methotrexate presented to a tertiary care hospital with fever, cough, and chest discomfort. The symptoms had first appeared 2 weeks earlier, and he had gone to an urgent care center, where he was prescribed a 5-day course of azithromycin and a corticosteroid, but this had not relieved his symptoms.
Figure 1. (A) An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).
He reported no recent travel, exposure to animals, or sick contacts. His temperature was 38.3°C (100.9°F). Results of the physical examination and initial laboratory testing were unremarkable. Chest computed tomography revealed prominent right hilar and mediastinal lymphadenopathy (Figure 1).
Bronchoscopy revealed edematous mucosa throughout, with minimal secretion. Specimens for bacterial, acid-fast bacillus, and fungal cultures were obtained from bronchoalveolar lavage. Endobronchial lymph node biopsy with ultrasonographic guidance revealed nonnecrotizing granuloma.
Bronchoalveolar lavage cultures showed no growth, but the patient’s serum histoplasma antigen was positive at 5.99 ng/dL (reference range: none detected), leading to the diagnosis of mediastinal granuloma due to histoplasmosis with possible dissemination. His immunosuppressant drugs were stopped, and oral itraconazole was started.
At a follow-up visit 2 months later, his serum antigen level had decreased to 0.68 ng/dL, and he had no symptoms whatsoever. At a visit 1 month after that, infliximab and methotrexate were restarted because of an exacerbation of Crohn disease. His oral itraconazole treatment was to be continued for at least 12 months, given the high suspicion for disseminated histoplasmosis while on immunosuppressant therapy.
DIFFERENTIAL DIAGNOSIS OF GRANULOMATOUS LUNG DISEASE AND LYMPHADENOPATHY
The differential diagnosis of granulomatous lung disease and lymphadenopathy is broad and includes noninfectious and infectious conditions.1
Noninfectious causes include lymphoma, sarcoidosis, inflammatory bowel disease, hypersensitivity pneumonia, side effects of drugs (eg, methotrexate, etanercept), rheumatoid nodules, vasculitis (eg, Churg-Strauss syndrome, granulomatosis with polyangiitis, primary amyloidosis, pneumoconiosis (eg, beryllium, cobalt), and Castleman disease.
There is concern that tumor necrosis factor antagonists may increase the risk of lymphoma, but a 2017 study found no evidence of this.2
Infectious conditions associated with granulomatous lung disease include tuberculosis, nontuberculous mycobacterial infection, fungal infection (eg, Cryptococcus, Coccidioides, Histoplasma, Blastomyces), brucellosis, tularemia (respiratory type B), parasitic infection (eg, Toxocara, Leishmania, Echinococcus, Schistosoma), and Whipple disease.
HISTOPLASMOSIS
Histoplasmosis, caused by infection with Histoplasma capsulatum, is the most prevalent endemic mycotic disease in the United States.3 The fungus is commonly found in the Ohio and Mississippi River valleys in the United States, and also in Central and South America and Asia.
Risk factors for histoplasmosis include living in or traveling to an endemic area, exposure to aerosolized soil that contains spores, and exposure to bats or birds and their droppings.4
Fewer than 5% of exposed individuals develop symptoms, which include fever, chills, headache, myalgia, anorexia, cough, and chest pain.5 Patients may experience symptoms shortly after exposure or may remain free of symptoms for years, with intermittent relapses of symptoms.6 Hilar or mediastinal lymphadenopathy is common in acute pulmonary histoplasmosis.7
The risk of disseminated histoplasmosis is greater in patients with reduced cell-mediated immunity, such as in human immunodeficiency virus infection, acquired immunodeficiency syndrome, solid-organ or bone marrow transplant, hematologic malignancies, immunosuppression (corticosteroids, disease-modifying antirheumatic drugs, and tumor necrosis factor antagonists), and congenital T-cell deficiencies.8
In a retrospective study, infliximab was the tumor necrosis factor antagonist most commonly associated with histoplasmosis.9 In a study of patients with rheumatoid arthritis, the disease-modifying drug most commonly associated was methotrexate.10
GOLD STANDARD FOR DIAGNOSIS
Isolation of H capsulatum from clinical specimens remains the gold standard for confirmation of histoplasmosis. The sensitivity of culture to detect H capsulatum depends on the clinical manifestations: it is 74% in patients with disseminated histoplasmosis, but only 42% in patients with acute pulmonary histoplasmosis.11 The serum histoplasma antigen test has a sensitivity of 91.8% in disseminated histoplasmosis, 87.5% in chronic pulmonary histoplasmosis, and 83% in acute pulmonary histoplasmosis.12
Urine testing for histoplasma antigen has generally proven to be slightly more sensitive than serum testing in all manifestations of histoplasmosis.13 Combining urine and serum testing increases the likelihood of antigen detection.
TREATMENT
Asymptomatic patients with mediastinal histoplasmosis do not require treatment. (Note: in some cases, lymphadenopathy is found incidentally, and biopsy is done to rule out malignancy.)
Standard treatment of symptomatic mediastinal histoplasmosis is oral itraconazole 200 mg, 3 times daily for 3 days, followed by 200 mg orally once or twice daily for 6 to 12 weeks.14
Although stopping immunosuppressant drugs is considered the standard of care in treating histoplasmosis in immunocompromised patients, there are no guidelines on when to resume them. However, a retrospective study of 98 cases of histoplasmosis in patients on tumor necrosis factor antagonists found that resuming immunosuppressants might be safe with close monitoring during the course of antifungal therapy.9 The role of long-term suppressive therapy with antifungal agents in patients on chronic immunosuppressive therapy is still unknown and needs further study.
TAKE-HOME MESSAGES
Histoplasmosis is the most prevalent endemic mycotic disease in the United States, and mediastinal lymphadenopathy is commonly seen in acute pulmonary histoplasmosis.
Histoplasmosis should be included in the differential diagnosis of granulomatous lung disease in patients from an endemic area or with a history of travel to an endemic area.
Immunosuppressive agents such as tumor necrosis factor antagonists and disease-modifying antirheumatic drugs can predispose to invasive fungal infection, including histoplasmosis.
While isolation of H capsulatum from culture remains the gold standard for the diagnosis of histoplasmosis, the histoplasma antigen tests (serum and urine) is more sensitive than culture.
References
Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician.” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev 2017; 26(145). doi:10.1183/16000617.0012-2017
Mercer LK, Galloway JB, Lunt M, et al. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2017; 76(3):497–503. doi:10.1136/annrheumdis-2016-209389
Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaoutis TE. Hospitalizations for endemic mycoses: a population-based national study. Clin Infect Dis 2006; 42(6):822–825. doi:10.1086/500405
Benedict K, Mody RK. Epidemiology of histoplasmosis outbreaks, United States, 1938–2013. Emerg Infect Dis 2016; 22(3):370–378. doi:10.3201/eid2203.151117
Wheat LJ. Diagnosis and management of histoplasmosis. Eur J Clin Microbiol Infect Dis 1989; 8(5):480–490. pmid:2502413
Goodwin RA Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980; 59(1):1–33. pmid:7356773
Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med 2004; 25(2):129–144. doi:10.1055/s-2004-824898
Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007; 86(3):162–169. doi:10.1097/md.0b013e3180679130
Vergidis P, Avery RK, Wheat LJ, et al. Histoplasmosis complicating tumor necrosis factor-a blocker therapy: a retrospective analysis of 98 cases. Clin Infect Dis 2015; 61(3):409–417. doi:10.1093/cid/civ299
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis 2011; 11:145. doi:10.1186/1471-2334-11-145
Hage CA, Ribes JA, Wengenack NL, et al. A multicenter evaluation of tests for diagnosis of histoplasmosis. Clin Infect Dis 2011; 53(5):448–454. doi:10.1093/cid/cir435
Azar MM, Hage CA. Laboratory diagnostics for histoplasmosis. J Clin Microbiol 2017; 55(6):1612–1620. doi:10.1128/JCM.02430-16
Swartzentruber S, Rhodes L, Kurkjian K, et al. Diagnosis of acute pulmonary histoplasmosis by antigen detection. Clin Infect Dis 2009; 49(12):1878–1882. doi:10.1086/648421
Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis 2007; 45(7):807–825. doi:10.1086/521259
Takaaki Kobayashi, MD Fellow, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Christine Cho, MD Associate, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Address: Takaaki Kobayashi, MD, Infectious Disease, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242; [email protected]
Takaaki Kobayashi, MD Fellow, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Christine Cho, MD Associate, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Address: Takaaki Kobayashi, MD, Infectious Disease, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242; [email protected]
Author and Disclosure Information
Takaaki Kobayashi, MD Fellow, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Christine Cho, MD Associate, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Address: Takaaki Kobayashi, MD, Infectious Disease, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242; [email protected]
A 50-year-old man with Crohn disease and psoriatic arthritis treated with infliximab and methotrexate presented to a tertiary care hospital with fever, cough, and chest discomfort. The symptoms had first appeared 2 weeks earlier, and he had gone to an urgent care center, where he was prescribed a 5-day course of azithromycin and a corticosteroid, but this had not relieved his symptoms.
Figure 1. (A) An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).
He reported no recent travel, exposure to animals, or sick contacts. His temperature was 38.3°C (100.9°F). Results of the physical examination and initial laboratory testing were unremarkable. Chest computed tomography revealed prominent right hilar and mediastinal lymphadenopathy (Figure 1).
Bronchoscopy revealed edematous mucosa throughout, with minimal secretion. Specimens for bacterial, acid-fast bacillus, and fungal cultures were obtained from bronchoalveolar lavage. Endobronchial lymph node biopsy with ultrasonographic guidance revealed nonnecrotizing granuloma.
Bronchoalveolar lavage cultures showed no growth, but the patient’s serum histoplasma antigen was positive at 5.99 ng/dL (reference range: none detected), leading to the diagnosis of mediastinal granuloma due to histoplasmosis with possible dissemination. His immunosuppressant drugs were stopped, and oral itraconazole was started.
At a follow-up visit 2 months later, his serum antigen level had decreased to 0.68 ng/dL, and he had no symptoms whatsoever. At a visit 1 month after that, infliximab and methotrexate were restarted because of an exacerbation of Crohn disease. His oral itraconazole treatment was to be continued for at least 12 months, given the high suspicion for disseminated histoplasmosis while on immunosuppressant therapy.
DIFFERENTIAL DIAGNOSIS OF GRANULOMATOUS LUNG DISEASE AND LYMPHADENOPATHY
The differential diagnosis of granulomatous lung disease and lymphadenopathy is broad and includes noninfectious and infectious conditions.1
Noninfectious causes include lymphoma, sarcoidosis, inflammatory bowel disease, hypersensitivity pneumonia, side effects of drugs (eg, methotrexate, etanercept), rheumatoid nodules, vasculitis (eg, Churg-Strauss syndrome, granulomatosis with polyangiitis, primary amyloidosis, pneumoconiosis (eg, beryllium, cobalt), and Castleman disease.
There is concern that tumor necrosis factor antagonists may increase the risk of lymphoma, but a 2017 study found no evidence of this.2
Infectious conditions associated with granulomatous lung disease include tuberculosis, nontuberculous mycobacterial infection, fungal infection (eg, Cryptococcus, Coccidioides, Histoplasma, Blastomyces), brucellosis, tularemia (respiratory type B), parasitic infection (eg, Toxocara, Leishmania, Echinococcus, Schistosoma), and Whipple disease.
HISTOPLASMOSIS
Histoplasmosis, caused by infection with Histoplasma capsulatum, is the most prevalent endemic mycotic disease in the United States.3 The fungus is commonly found in the Ohio and Mississippi River valleys in the United States, and also in Central and South America and Asia.
Risk factors for histoplasmosis include living in or traveling to an endemic area, exposure to aerosolized soil that contains spores, and exposure to bats or birds and their droppings.4
Fewer than 5% of exposed individuals develop symptoms, which include fever, chills, headache, myalgia, anorexia, cough, and chest pain.5 Patients may experience symptoms shortly after exposure or may remain free of symptoms for years, with intermittent relapses of symptoms.6 Hilar or mediastinal lymphadenopathy is common in acute pulmonary histoplasmosis.7
The risk of disseminated histoplasmosis is greater in patients with reduced cell-mediated immunity, such as in human immunodeficiency virus infection, acquired immunodeficiency syndrome, solid-organ or bone marrow transplant, hematologic malignancies, immunosuppression (corticosteroids, disease-modifying antirheumatic drugs, and tumor necrosis factor antagonists), and congenital T-cell deficiencies.8
In a retrospective study, infliximab was the tumor necrosis factor antagonist most commonly associated with histoplasmosis.9 In a study of patients with rheumatoid arthritis, the disease-modifying drug most commonly associated was methotrexate.10
GOLD STANDARD FOR DIAGNOSIS
Isolation of H capsulatum from clinical specimens remains the gold standard for confirmation of histoplasmosis. The sensitivity of culture to detect H capsulatum depends on the clinical manifestations: it is 74% in patients with disseminated histoplasmosis, but only 42% in patients with acute pulmonary histoplasmosis.11 The serum histoplasma antigen test has a sensitivity of 91.8% in disseminated histoplasmosis, 87.5% in chronic pulmonary histoplasmosis, and 83% in acute pulmonary histoplasmosis.12
Urine testing for histoplasma antigen has generally proven to be slightly more sensitive than serum testing in all manifestations of histoplasmosis.13 Combining urine and serum testing increases the likelihood of antigen detection.
TREATMENT
Asymptomatic patients with mediastinal histoplasmosis do not require treatment. (Note: in some cases, lymphadenopathy is found incidentally, and biopsy is done to rule out malignancy.)
Standard treatment of symptomatic mediastinal histoplasmosis is oral itraconazole 200 mg, 3 times daily for 3 days, followed by 200 mg orally once or twice daily for 6 to 12 weeks.14
Although stopping immunosuppressant drugs is considered the standard of care in treating histoplasmosis in immunocompromised patients, there are no guidelines on when to resume them. However, a retrospective study of 98 cases of histoplasmosis in patients on tumor necrosis factor antagonists found that resuming immunosuppressants might be safe with close monitoring during the course of antifungal therapy.9 The role of long-term suppressive therapy with antifungal agents in patients on chronic immunosuppressive therapy is still unknown and needs further study.
TAKE-HOME MESSAGES
Histoplasmosis is the most prevalent endemic mycotic disease in the United States, and mediastinal lymphadenopathy is commonly seen in acute pulmonary histoplasmosis.
Histoplasmosis should be included in the differential diagnosis of granulomatous lung disease in patients from an endemic area or with a history of travel to an endemic area.
Immunosuppressive agents such as tumor necrosis factor antagonists and disease-modifying antirheumatic drugs can predispose to invasive fungal infection, including histoplasmosis.
While isolation of H capsulatum from culture remains the gold standard for the diagnosis of histoplasmosis, the histoplasma antigen tests (serum and urine) is more sensitive than culture.
A 50-year-old man with Crohn disease and psoriatic arthritis treated with infliximab and methotrexate presented to a tertiary care hospital with fever, cough, and chest discomfort. The symptoms had first appeared 2 weeks earlier, and he had gone to an urgent care center, where he was prescribed a 5-day course of azithromycin and a corticosteroid, but this had not relieved his symptoms.
Figure 1. (A) An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).
He reported no recent travel, exposure to animals, or sick contacts. His temperature was 38.3°C (100.9°F). Results of the physical examination and initial laboratory testing were unremarkable. Chest computed tomography revealed prominent right hilar and mediastinal lymphadenopathy (Figure 1).
Bronchoscopy revealed edematous mucosa throughout, with minimal secretion. Specimens for bacterial, acid-fast bacillus, and fungal cultures were obtained from bronchoalveolar lavage. Endobronchial lymph node biopsy with ultrasonographic guidance revealed nonnecrotizing granuloma.
Bronchoalveolar lavage cultures showed no growth, but the patient’s serum histoplasma antigen was positive at 5.99 ng/dL (reference range: none detected), leading to the diagnosis of mediastinal granuloma due to histoplasmosis with possible dissemination. His immunosuppressant drugs were stopped, and oral itraconazole was started.
At a follow-up visit 2 months later, his serum antigen level had decreased to 0.68 ng/dL, and he had no symptoms whatsoever. At a visit 1 month after that, infliximab and methotrexate were restarted because of an exacerbation of Crohn disease. His oral itraconazole treatment was to be continued for at least 12 months, given the high suspicion for disseminated histoplasmosis while on immunosuppressant therapy.
DIFFERENTIAL DIAGNOSIS OF GRANULOMATOUS LUNG DISEASE AND LYMPHADENOPATHY
The differential diagnosis of granulomatous lung disease and lymphadenopathy is broad and includes noninfectious and infectious conditions.1
Noninfectious causes include lymphoma, sarcoidosis, inflammatory bowel disease, hypersensitivity pneumonia, side effects of drugs (eg, methotrexate, etanercept), rheumatoid nodules, vasculitis (eg, Churg-Strauss syndrome, granulomatosis with polyangiitis, primary amyloidosis, pneumoconiosis (eg, beryllium, cobalt), and Castleman disease.
There is concern that tumor necrosis factor antagonists may increase the risk of lymphoma, but a 2017 study found no evidence of this.2
Infectious conditions associated with granulomatous lung disease include tuberculosis, nontuberculous mycobacterial infection, fungal infection (eg, Cryptococcus, Coccidioides, Histoplasma, Blastomyces), brucellosis, tularemia (respiratory type B), parasitic infection (eg, Toxocara, Leishmania, Echinococcus, Schistosoma), and Whipple disease.
HISTOPLASMOSIS
Histoplasmosis, caused by infection with Histoplasma capsulatum, is the most prevalent endemic mycotic disease in the United States.3 The fungus is commonly found in the Ohio and Mississippi River valleys in the United States, and also in Central and South America and Asia.
Risk factors for histoplasmosis include living in or traveling to an endemic area, exposure to aerosolized soil that contains spores, and exposure to bats or birds and their droppings.4
Fewer than 5% of exposed individuals develop symptoms, which include fever, chills, headache, myalgia, anorexia, cough, and chest pain.5 Patients may experience symptoms shortly after exposure or may remain free of symptoms for years, with intermittent relapses of symptoms.6 Hilar or mediastinal lymphadenopathy is common in acute pulmonary histoplasmosis.7
The risk of disseminated histoplasmosis is greater in patients with reduced cell-mediated immunity, such as in human immunodeficiency virus infection, acquired immunodeficiency syndrome, solid-organ or bone marrow transplant, hematologic malignancies, immunosuppression (corticosteroids, disease-modifying antirheumatic drugs, and tumor necrosis factor antagonists), and congenital T-cell deficiencies.8
In a retrospective study, infliximab was the tumor necrosis factor antagonist most commonly associated with histoplasmosis.9 In a study of patients with rheumatoid arthritis, the disease-modifying drug most commonly associated was methotrexate.10
GOLD STANDARD FOR DIAGNOSIS
Isolation of H capsulatum from clinical specimens remains the gold standard for confirmation of histoplasmosis. The sensitivity of culture to detect H capsulatum depends on the clinical manifestations: it is 74% in patients with disseminated histoplasmosis, but only 42% in patients with acute pulmonary histoplasmosis.11 The serum histoplasma antigen test has a sensitivity of 91.8% in disseminated histoplasmosis, 87.5% in chronic pulmonary histoplasmosis, and 83% in acute pulmonary histoplasmosis.12
Urine testing for histoplasma antigen has generally proven to be slightly more sensitive than serum testing in all manifestations of histoplasmosis.13 Combining urine and serum testing increases the likelihood of antigen detection.
TREATMENT
Asymptomatic patients with mediastinal histoplasmosis do not require treatment. (Note: in some cases, lymphadenopathy is found incidentally, and biopsy is done to rule out malignancy.)
Standard treatment of symptomatic mediastinal histoplasmosis is oral itraconazole 200 mg, 3 times daily for 3 days, followed by 200 mg orally once or twice daily for 6 to 12 weeks.14
Although stopping immunosuppressant drugs is considered the standard of care in treating histoplasmosis in immunocompromised patients, there are no guidelines on when to resume them. However, a retrospective study of 98 cases of histoplasmosis in patients on tumor necrosis factor antagonists found that resuming immunosuppressants might be safe with close monitoring during the course of antifungal therapy.9 The role of long-term suppressive therapy with antifungal agents in patients on chronic immunosuppressive therapy is still unknown and needs further study.
TAKE-HOME MESSAGES
Histoplasmosis is the most prevalent endemic mycotic disease in the United States, and mediastinal lymphadenopathy is commonly seen in acute pulmonary histoplasmosis.
Histoplasmosis should be included in the differential diagnosis of granulomatous lung disease in patients from an endemic area or with a history of travel to an endemic area.
Immunosuppressive agents such as tumor necrosis factor antagonists and disease-modifying antirheumatic drugs can predispose to invasive fungal infection, including histoplasmosis.
While isolation of H capsulatum from culture remains the gold standard for the diagnosis of histoplasmosis, the histoplasma antigen tests (serum and urine) is more sensitive than culture.
References
Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician.” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev 2017; 26(145). doi:10.1183/16000617.0012-2017
Mercer LK, Galloway JB, Lunt M, et al. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2017; 76(3):497–503. doi:10.1136/annrheumdis-2016-209389
Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaoutis TE. Hospitalizations for endemic mycoses: a population-based national study. Clin Infect Dis 2006; 42(6):822–825. doi:10.1086/500405
Benedict K, Mody RK. Epidemiology of histoplasmosis outbreaks, United States, 1938–2013. Emerg Infect Dis 2016; 22(3):370–378. doi:10.3201/eid2203.151117
Wheat LJ. Diagnosis and management of histoplasmosis. Eur J Clin Microbiol Infect Dis 1989; 8(5):480–490. pmid:2502413
Goodwin RA Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980; 59(1):1–33. pmid:7356773
Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med 2004; 25(2):129–144. doi:10.1055/s-2004-824898
Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007; 86(3):162–169. doi:10.1097/md.0b013e3180679130
Vergidis P, Avery RK, Wheat LJ, et al. Histoplasmosis complicating tumor necrosis factor-a blocker therapy: a retrospective analysis of 98 cases. Clin Infect Dis 2015; 61(3):409–417. doi:10.1093/cid/civ299
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis 2011; 11:145. doi:10.1186/1471-2334-11-145
Hage CA, Ribes JA, Wengenack NL, et al. A multicenter evaluation of tests for diagnosis of histoplasmosis. Clin Infect Dis 2011; 53(5):448–454. doi:10.1093/cid/cir435
Azar MM, Hage CA. Laboratory diagnostics for histoplasmosis. J Clin Microbiol 2017; 55(6):1612–1620. doi:10.1128/JCM.02430-16
Swartzentruber S, Rhodes L, Kurkjian K, et al. Diagnosis of acute pulmonary histoplasmosis by antigen detection. Clin Infect Dis 2009; 49(12):1878–1882. doi:10.1086/648421
Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis 2007; 45(7):807–825. doi:10.1086/521259
References
Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician.” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev 2017; 26(145). doi:10.1183/16000617.0012-2017
Mercer LK, Galloway JB, Lunt M, et al. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2017; 76(3):497–503. doi:10.1136/annrheumdis-2016-209389
Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaoutis TE. Hospitalizations for endemic mycoses: a population-based national study. Clin Infect Dis 2006; 42(6):822–825. doi:10.1086/500405
Benedict K, Mody RK. Epidemiology of histoplasmosis outbreaks, United States, 1938–2013. Emerg Infect Dis 2016; 22(3):370–378. doi:10.3201/eid2203.151117
Wheat LJ. Diagnosis and management of histoplasmosis. Eur J Clin Microbiol Infect Dis 1989; 8(5):480–490. pmid:2502413
Goodwin RA Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980; 59(1):1–33. pmid:7356773
Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med 2004; 25(2):129–144. doi:10.1055/s-2004-824898
Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007; 86(3):162–169. doi:10.1097/md.0b013e3180679130
Vergidis P, Avery RK, Wheat LJ, et al. Histoplasmosis complicating tumor necrosis factor-a blocker therapy: a retrospective analysis of 98 cases. Clin Infect Dis 2015; 61(3):409–417. doi:10.1093/cid/civ299
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis 2011; 11:145. doi:10.1186/1471-2334-11-145
Hage CA, Ribes JA, Wengenack NL, et al. A multicenter evaluation of tests for diagnosis of histoplasmosis. Clin Infect Dis 2011; 53(5):448–454. doi:10.1093/cid/cir435
Azar MM, Hage CA. Laboratory diagnostics for histoplasmosis. J Clin Microbiol 2017; 55(6):1612–1620. doi:10.1128/JCM.02430-16
Swartzentruber S, Rhodes L, Kurkjian K, et al. Diagnosis of acute pulmonary histoplasmosis by antigen detection. Clin Infect Dis 2009; 49(12):1878–1882. doi:10.1086/648421
Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis 2007; 45(7):807–825. doi:10.1086/521259
An 18-year-old man without any significant medical history was transferred from another hospital for higher-level care after presenting with unremitting chest pain. He had been in his usual state of good health until 7 days before presentation, when he developed mild rhinorrhea and a sore throat, but not a cough. He went to an outpatient clinic, where a rapid test for group A streptococci was done; the result was negative, and he was sent home on supportive measures.
On the day of admission, he awoke with severe, pressure-like, midsternal, nonradiating pain, which he rated 10 on a scale of 10. The pain intensified in the supine position and improved with sitting. A complete review of systems was otherwise negative. He denied having had similar symptoms in the past, as well as sick contacts, recent travel, toxin exposure, illicit substance abuse, pets at home, or tick bites. His family history was negative for cardiac arrhythmias, premature coronary artery disease, thoracic aneurysms or dissection, and infiltrative disorders. His surgical and social histories were unremarkable. He said he had no drug allergies.
Figure 1. The patient’s electrocardiogram on presentation shows ST-segment elevation (arrows) over the lateral and inferior distribution (V4–V6, II, III, and aVF).
An electrocardiogram was obtained (Figure 1). His troponin I level was 7.0 ng/mL (reference range < 0.04 ng/mL).
On examination, his temperature was 38.1°C (100.6°F), heart rate 101 beats per minute, blood pressure 142/78 mm Hg, respiratory rate 16 breaths per minute, and oxygen saturation 98% on room air. He appeared anxious but was in no acute distress. Neck examination showed no elevation in jugular venous pulsation, bruits, thyromegaly, or lymphadenopathy. Cardiac examination revealed tachycardia without murmurs, rubs, or gallops. Lungs were clear to auscultation. Examination of all 4 extremities found 2+ pulses (on a scale of 0 to 4+) throughout and no cyanosis, clubbing, or edema. Abdominal, neurologic, and dermatologic examinations were unremarkable.
Further blood testing revealed the following:
Troponin I (3 hours after the first level) 15.5 ng/mL
B-type natriuretic peptide 200 mg/dL (reference range 0–100 mg/dL)
C-reactive protein 0.9 mg/dL (reference range 0.0–0.8 mg/dL)
Erythrocyte sedimentation rate 10 mm/h (reference range < 15 mm/h).
Metabolic and hematologic assessments were unremarkable. A toxicology screen for drugs of abuse was negative. Viral serologic testing was not done.
A chest radiograph showed no acute cardiopulmonary processes.
Given his presenting symptoms, persistent tachycardia, rapidly rising troponin I level, and electrocardiogram showing diffuse ST elevation, he was taken for urgent cardiac catheterization. Coronary angiography revealed no evidence of atherosclerotic disease, acute thrombosis, dissection, or aneurysm. Echocardiography 2 hours after the procedure showed a normal ejection fraction and no regional wall-motion abnormalities or valvular heart disease.
FURTHER TESTING
1. Which test should be done next to further evaluate this patient’s chest pain?
Serum viral serologic testing
Serum free light chain assay
Nuclear myocardial perfusion study
Cardiac magnetic resonance imaging (MRI)
Endomyocardial biopsy
In this patient without ischemic coronary disease or valvular heart disease, the recent upper respiratory tract prodrome, active positional chest pain, and diffuse electrocardiographic changes raise the possibility of myocarditis with pericardial involvement.
Viral serologic tests
Viral serologic tests are often obtained in the workup of myocarditis as a noninvasive means of detecting an infectious cause.
However, this approach has several problems. First, a positive serologic result is a signal of the peripheral immune response to a pathogen but does not necessarily indicate active myocardial inflammation. Additionally, circulating immunoglobulin G against cardiotropic viruses is commonly found, even in the absence of myocarditis.1 This is often the result of a high prevalence and exposure to these viruses in the general population. Further, trials have shown no correlation between serologic results and organisms identified by endomyocardial biopsy.2
Thus, serologic testing seems to be of limited utility, reserved for testing for infection with Borrelia burgdorferi (Lyme disease) in endemic areas, hepatitis C virus, human immunodeficiency virus in patients at high risk, Rickettsia conorii, and Rickettsia rickettsii.3
Serum free light chain testing for amyloidosis
Serum free light chain testing is replacing serum and urine protein electrophoresis in the workup of cardiac amyloidosis,4 as electrophoresis has poor sensitivity.4,5
Cardiac amyloidosis often affects older persons, although in rare cases it can affect young patients who carry mutations in the transthyretin gene (ATTR amyloidosis).6 This diagnosis is unlikely in our patient, as he has no other affected organ systems (amyloidosis often affects the renal and neurologic systems), normal QRS voltages on electrocardiography (which are often but not always low in amyloidosis), and no left ventricular hypertrophy or diastolic dysfunction on echocardiography (which are often seen in amyloidosis).4
Nuclear perfusion imaging for sarcoidosis
Nuclear imaging has a limited role in evaluating myocarditis,3 but positron-emission tomography with fluorine-18 fluorodeoxyglucose has a diagnostic role in sarcoidosis, an immune-mediated cause of myocarditis.7
Based on the acuity of the patient’s presentation, preceded by upper respiratory tract symptoms, sarcoidosis is less likely. Sarcoidosis is difficult to diagnose, although when it is the cause of myocarditis, some clues exist, as patients usually present with heart failure symptoms, a second- or third-degree atrioventricular block, or a dilated left ventricle on echocardiography.3 All of these were absent in our patient.
Cardiac MRI
Cardiac MRI has undergone many advances, making it an extremely useful noninvasive test. It has excellent utility as a stand-alone test in diagnosing myocarditis and has synergistic value when combined with endomyocardial biopsy.8 It is indicated in hemodynamically stable patients with a clinical suspicion of myocarditis, persistent symptoms, absence of heart failure, and when imaging findings will change management. It is particularly useful to help elucidate a cause and guide tailored therapy.9 Therefore, it is a reasonable next step in the diagnostic pathway for this patient.10
Cardiac MRI also allows for concurrent assessment of scar. In myocardial infarction, the late gadolinium enhancement is subendocardial or transmural. In myocarditis, the pattern differs, being found in the subepicardial lateral free wall (in most patients with parvovirus B19) and mid-myocardial septum (in most patients with herpesvirus 6).9,11 Cardiac MRI also confers prognostic information for patients with suspected myocarditis.12
The Lake Louise criteria9 for the diagnosis of myocarditis require 2 of the following:
Evidence of myocardial edema
Increased ratio of early gadolinium enhancement between myocardium and skeletal muscle (indicates hyperemia)
At least 1 focal lesion with nonischemic late gadolinium enhancement (indicates cardiac myocyte injury or scarring).
The Lake Louise criteria may be replaced by T1 and T2 mapping, which was found to be considerably better for diagnosing myocarditis when the 2 were compared.9,13,14
Endomyocardial biopsy
Endomyocardial biopsy should not be delayed while waiting for cardiac MRI in patients who are hemodynamically unstable or present with life-threatening features (ventricular arrhythmia, left ventricular failure, or resuscitation after sudden cardiac death).3,10
The indications for endomyocardial biopsy have been highly debated. The 2013 guidelines from the European Society of Cardiology (ESC) recommending endomyocardial biopsy in all clinically suspected cases of myocarditis have only heightened the controversy.3 The American Heart Association (AHA) guidelines reserve biopsy for patients with suspected myocarditis who have acute or subacute heart failure symptoms or who do not respond to standard medical therapy.15 Other reasonable indications may include the following: myocarditis with life-threatening ventricular arrhythmias, suspicion of giant cell myocarditis, necrotizing eosinophilic myocarditis, or cardiac sarcoidosis.16
Endomyocardial biopsy is the only way to make a definitive diagnosis of myocarditis.3 However, given the patchy distribution of myocardial involvement, a negative result does not rule out myocarditis. The diagnostic utility can be improved by increasing the number of samples taken (at least 3 but up to 10), obtaining samples from both ventricles, and using cardiac MRI data to determine which sites to biopsy.3,13,17,18
Noninvasive testing such as cardiac MRI does not distinguish cell type or etiology (viral vs nonviral).3 Further, endomyocardial biopsy must be performed before immunosuppressive therapy can be safely started.3,16 At experienced centers, the complication rate is 0% to 0.8%.3 The addition of immunohistochemical testing and viral genomic detection by polymerase chain reaction testing have increased the sensitivity of this technique.19 Finally, endomyocardial biopsy can help rule out some of the other possibilities in the differential diagnosis for myocarditis, including infiltrative and storage diseases, and possibly cardiac tumors.3
Of additional note, the diffuse ST-segment elevation seen on the patient’s electrocardiogram (Figure 1) is indicative of subepicardial inflammation. Since the distribution involves more than one epicardial coronary territory, this helps to differentiate the changes from those that occur with myocardial infarction.20
CASE CONTINUED
Figure 2. Cardiac magnetic resonance imaging shows areas of patchy subepicardial late gadolinium enhancement (arrows).
The patient underwent cardiac MRI, which showed myocardial edema and patchy areas of late gadolinium enhancement, raising suspicion for myocarditis (Figure 2).
Causes of myocarditis are numerous (Table 1),3,21,22 but viral and postinfectious etiologies remain the most common causes of acute myocarditis.23
2. What is the most likely causative infectious agent?
Parvovirus B19
Coxsackievirus B
Adenovirus species
Human herpesvirus 6
Staphylococcus aureus
Corynebacterium diphtheria
Trypanosoma cruzi
Influenza H1/N1
INFECTIOUS CAUSES OF MYOCARDITIS
Coxsackievirus B was the agent most often linked to this condition from the 1950s through the 1990s. However, in the last 2 decades, adenovirus species and human herpesvirus 6 have been increasingly encountered, and recently, parvovirus B19 has been credited as the most common culprit,11,23 at least in the Western world. In developing nations, T cruzi and C diphtheria are the most common offenders.21
S aureus is a common cause of endocarditis, but it rarely plays a role in myocarditis. When it does, the myocarditis is often the sequela of profound bacteremia. This was much more common before antibiotics were invented.24,25
Influenza H1/N1 is not among the most common causes of viral myocarditis, but it should be considered during flu season, given its ability to result in fulminant myocarditis.3,26
TREATMENT FOR MYOCARDITIS
3. Which treatment is the most appropriate at this time?
Intravenous immunoglobulin
Interferon beta
Acyclovir
Prednisone
Colchicine
Treatment for myocarditis depends on the cause but always includes supportive care to address the constellation of presenting symptoms. Standard therapies for tachy- or bradyarrhythmias, heart failure, and hemodynamic derangement should be started.
Supportive care
In patients with severe left ventricular dysfunction, an implantable cardiac electronic device, left ventricular assist device, or heart transplant may ultimately be needed. However, if possible these should be deferred for several months to determine response to treatment, since the myocardium can possibly recover.16
Diuretics, beta-blockers, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists should be given as part of guideline-directed medical therapy for patients with heart failure and reduced ejection fraction.3,27 However, whether and how the patient should be weaned from these agents after disease recovery are unknown.3
Intravenous immunoglobulin
Intravenous immunoglobulin in high doses has had mixed results. Its efficacy is well documented in children,21 but limited supportive data are available in adults.3 As such, recent ESC guidelines do not provide recommendations regarding its use in adults.3
Interferon beta
Interferon beta has shown promise in improving New York Heart Association class and left ventricular ejection fraction.3 This is attributed to its effects on eliminating adenoviral species and enteroviruses. Treatment of enteroviral organisms in particular has been associated with improved 10-year prognosis.3 Interferon beta also has in vitro data showing efficacy at diminishing apoptosis from parvovirus B19.28
Nucleoside analogues
Empiric treatment with nucleoside analogues (acyclovir, ganciclovir, and valacyclovir) has been tried for patients in whom human herpesvirus is suspected as the causative organism, although with unconfirmed effects.3 Consultation with an infectious disease specialist is recommended before starting these agents, and biopsy is often needed beforehand.3
Immunosuppressive agents
Immunosuppressive agents such as prednisone, azathioprine, and cyclosporine can be used in cases of biopsy-proven disease with manifestations of severe heart failure, especially if biopsy results reveal sarcoidosis, giant cell myocarditis, or necrotizing eosinophilic myocarditis. Although the results were neutral in the Myocarditis Treatment Trial,29 the cause of myocarditis in this trial was unknown. Therapy with such agents should be initiated after active infection is ruled out, which also would require a biopsy.
Colchicine
Mechanisms of chest pain in myocarditis include associated pericarditis and coronary artery vasospasm.3,23 Our patient’s chest pain changed when he changed position, possibly indicating associated pericarditis. In myocarditis with accompanying pericarditis symptoms, colchicine (1–2 mg as an initial dose and then 0.6 mg daily for up to 3 months) can be helpful in alleviating symptoms.21,30 Thus, starting this agent in a patient who presents with myocarditis in absence of heart failure, arrhythmias, or left ventricular dysfunction is prudent.
Colchicine is used mainly to address the pain associated with pericarditis. For patients who present with pericarditis without myocarditis, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, with the addition of colchicine leading to faster symptom resolution.30 The benefit of colchicine for isolated myocarditis is not well established, with only limited data showing some clinical effects.31
CASE CONTINUED
The patient was given colchicine 1.2 mg on the first day and then 0.6 mg daily. Within 2 days, his chest pain had resolved. He did not receive any immunosuppressive agents.
DISCHARGE INSTRUCTIONS
4. Before discharge, this patient should be instructed to do which of the following?
Take over-the-counter NSAIDs to supplement the effects of colchicine
Avoid competitive sports and athletics for at least 6 months
Call to schedule repeat cardiac MRI
No further instruction is needed
NSAIDs are used by themselves or in combination with colchicine in the treatment of pericarditis, but their use may be associated with worse outcomes in myocarditis.3,21 Thus, their use is not recommended in most cases.3
Excessive physical activity should be avoided for at least 6 months after the clinical syndrome resolves. This recommendation is included in the most recent ESC guidelines but is based mainly on expert opinion and murine models with coxsackievirus B.3 Periodic reassessment is indicated with exercise stress testing before return to strenuous activity.3,16,32 Testing should look for exercise tolerance, and exercise electrocardiography also helps to evaluate for clinically relevant arrythmias.
Cardiac MRI can help clarify the prognosis in myocarditis, but the role of repeat testing in guiding therapy is limited.3 Indications for repeat cardiac MRI include presence of 0 or 1 of the Lake Louise criteria (recall that 2 are necessary to make the diagnosis) with recurrence of symptoms and a high suspicion for myocardial inflammation.3,9 Repeat cardiac MRI was not performed for our patient.
CASE CONCLUDED
The patient was evaluated in the cardiology clinic within 1 week of discharge. At that time, he was in sinus tachycardia with a heart rate of 102 bpm, and he was instructed to avoid any exercise until further notice.
At 6-month follow-up, the sinus tachycardia had resolved. However, because persistent tachycardia had been noted at the first postdischarge visit, and in view of the extent of myocardial involvement, he underwent exercise treadmill testing to evaluate for ventricular arrhythmias. The study did show premature ventricular complexes and 1 ventricular couplet at submaximal exercise levels. As this indicated a higher risk of exercise-induced arrhythmias, he was asked to continue normal activity levels but to abstain from exercise until the next evaluation.
During his 1-year follow-up, a repeat treadmill test showed no ventricular ectopy. Holter monitoring was ordered and showed no premature ventricular complexes, supraventricular arrhythmias, or atrioventricular block within the 48-hour period.
At his 2-year evaluation, he had returned to playing basketball and soccer on weekends and reported no recurrence of his initial symptoms.
KEY POINTS
Figure 3. Our suggested approach to suspected acute myocarditis.Cardiac MRI has emerged as an excellent noninvasive imaging modality for the diagnosis of myocarditis.
Treatment of myocarditis depends on the cause and severity of the patient’s presentation, spanning the spectrum from conservative care to immunosuppressive agents and even heart failure therapy.
Excessive physical activity should be avoided for the first 6 months after disease diagnosis and treatment.
If myocarditis is associated with pericardial involvement, colchicine is the agent of choice, and NSAIDs should be avoided.
Our suggested strategy for approaching myocarditis is shown in Figure 3.
Mahfoud F, Gärtner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011; 32(7):897–903. doi:10.1093/eurheartj/ehq493
Caforio AL, Pankuweit S, Arbustini E, et al; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013; 34(33):2636–2648, 2648a–2648d. doi:10.1093/eurheartj/eht210
Donnelly JP, Hanna M. Cardiac amyloidosis: an update on diagnosis and treatment. Cleve Clin J Med 2017; 84(12 suppl 3):12–26. doi:10.3949/ccjm.84.s3.02
Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28(1):10–21. doi:10.1016/j.tcm.2017.07.004
Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol 2015; 66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
Blankstein R, Osborne M, Naya M, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014; 63(4):329–336. doi:10.1016/j.jacc.2013.09.022
Baccouche H, Mahrholtz H, Meinhardt G, et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009; 30(23):2869–2879. doi:10.1093/eurheartj/ehp328
Friedrich MG, Sechtem U, Schulz-Menger J, et al; International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009; 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012; 59(9):779–792. doi:10.1016/j.jacc.2011.09.074
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006; 114(15):1581–1590. doi:10.1161/CIRCULATIONAHA.105.606509
Gräni C, Eichhorn C, Bière L, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017; 70(16):1964–1976. doi:10.1016/j.jacc.2017.08.050
Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-Trial. J Am Coll Cardiol 2016; 67(15):1800–1811. doi:10.1016/j.jacc.2016.02.013
Gannon MP, Schaub E, Griens CL, Saba SG. State of the art: evaluation and prognostication of myocarditis using cardiac MRI. J Magn Reson Imaging 2019; 49(7):e122–e131. doi:10.1002/jmri.26611
Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007; 28(24):3076–3093. doi:10.1093/eurheartj/ehm456
Sinagra G, Anzini M, Pereira NL, et al. Myocarditis in clinical practice. Mayo Clin Proc 2016; 91(9):1256–1266. doi:10.1016/j.mayocp.2016.05.013
Cooper LT, Baughman KL, Feldman AM, et al; American Heart Association; American College of Cardiology; European Society of Cardiology. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007; 116(19):2216–2233. doi:10.1161/CIRCULATIONAHA.107.186093
Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012; 21(4):245–274. doi:10.1016/j.carpath.2011.10.001
Alraies MC, Klein AL. Should we still use electrocardiography to diagnose pericardial disease? Cleve Clin J Med 2013; 80(2):97–100. doi:10.3949/ccjm.80a.11144
Wasi F, Shuter J. Primary bacterial infection of the myocardium. Front Biosci 2003; 8:s228–s231. pmid:12700039
Al-Amoodi M, Rao K, Rao S, Brewer JH, Magalski A, Chhatriwalla AK. Fulminant myocarditis due to H1N1 influenza. Circ Heart Fail 2010; 3(3):e7–e9. doi:10.1161/CIRCHEARTFAILURE.110.938506
Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2016; 68(13):1476–1488. doi:10.1016/j.jacc.2016.05.011
Schmidt-Lucke C, Spillmann F, Bock T, et al. Interferon beta modulates endothelial damage in patients with cardiac persistence of human parvovirus b19 infection. J Infect Dis 2010; 201(6):936–945. doi:10.1086/650700
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosuppressive therapy for myocarditis: the Myocarditis Treatment Trial Investigators. N Engl J Med 1995; 333(5):269–275. doi:10.1056/NEJM199508033330501
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005; 112(13):2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738
Morgenstern D, Lisko J, Boniface NC, Mikolich BM, Mikolich JR. Myocarditis and colchicine: a new perspective from cardiac MRI. J Cardiovasc Magn Reson 2016; 18(suppl 1):0100.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015; 66(21):2343–2349. doi:10.1016/j.jacc.2015.09.032
Amir Farid, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Neil Beri, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
David Torres-Barba, MD, PhD Department of Cardiology, University of California San Diego
Charles Whitcomb, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Address: David Torres-Barba, MD, PhD, Department of Internal Medicine, University of California, Davis, 4150 V. Street, Sacramento, CA 95817; [email protected]
Amir Farid, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Neil Beri, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
David Torres-Barba, MD, PhD Department of Cardiology, University of California San Diego
Charles Whitcomb, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Address: David Torres-Barba, MD, PhD, Department of Internal Medicine, University of California, Davis, 4150 V. Street, Sacramento, CA 95817; [email protected]
Author and Disclosure Information
Amir Farid, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Neil Beri, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
David Torres-Barba, MD, PhD Department of Cardiology, University of California San Diego
Charles Whitcomb, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Address: David Torres-Barba, MD, PhD, Department of Internal Medicine, University of California, Davis, 4150 V. Street, Sacramento, CA 95817; [email protected]
An 18-year-old man without any significant medical history was transferred from another hospital for higher-level care after presenting with unremitting chest pain. He had been in his usual state of good health until 7 days before presentation, when he developed mild rhinorrhea and a sore throat, but not a cough. He went to an outpatient clinic, where a rapid test for group A streptococci was done; the result was negative, and he was sent home on supportive measures.
On the day of admission, he awoke with severe, pressure-like, midsternal, nonradiating pain, which he rated 10 on a scale of 10. The pain intensified in the supine position and improved with sitting. A complete review of systems was otherwise negative. He denied having had similar symptoms in the past, as well as sick contacts, recent travel, toxin exposure, illicit substance abuse, pets at home, or tick bites. His family history was negative for cardiac arrhythmias, premature coronary artery disease, thoracic aneurysms or dissection, and infiltrative disorders. His surgical and social histories were unremarkable. He said he had no drug allergies.
Figure 1. The patient’s electrocardiogram on presentation shows ST-segment elevation (arrows) over the lateral and inferior distribution (V4–V6, II, III, and aVF).
An electrocardiogram was obtained (Figure 1). His troponin I level was 7.0 ng/mL (reference range < 0.04 ng/mL).
On examination, his temperature was 38.1°C (100.6°F), heart rate 101 beats per minute, blood pressure 142/78 mm Hg, respiratory rate 16 breaths per minute, and oxygen saturation 98% on room air. He appeared anxious but was in no acute distress. Neck examination showed no elevation in jugular venous pulsation, bruits, thyromegaly, or lymphadenopathy. Cardiac examination revealed tachycardia without murmurs, rubs, or gallops. Lungs were clear to auscultation. Examination of all 4 extremities found 2+ pulses (on a scale of 0 to 4+) throughout and no cyanosis, clubbing, or edema. Abdominal, neurologic, and dermatologic examinations were unremarkable.
Further blood testing revealed the following:
Troponin I (3 hours after the first level) 15.5 ng/mL
B-type natriuretic peptide 200 mg/dL (reference range 0–100 mg/dL)
C-reactive protein 0.9 mg/dL (reference range 0.0–0.8 mg/dL)
Erythrocyte sedimentation rate 10 mm/h (reference range < 15 mm/h).
Metabolic and hematologic assessments were unremarkable. A toxicology screen for drugs of abuse was negative. Viral serologic testing was not done.
A chest radiograph showed no acute cardiopulmonary processes.
Given his presenting symptoms, persistent tachycardia, rapidly rising troponin I level, and electrocardiogram showing diffuse ST elevation, he was taken for urgent cardiac catheterization. Coronary angiography revealed no evidence of atherosclerotic disease, acute thrombosis, dissection, or aneurysm. Echocardiography 2 hours after the procedure showed a normal ejection fraction and no regional wall-motion abnormalities or valvular heart disease.
FURTHER TESTING
1. Which test should be done next to further evaluate this patient’s chest pain?
Serum viral serologic testing
Serum free light chain assay
Nuclear myocardial perfusion study
Cardiac magnetic resonance imaging (MRI)
Endomyocardial biopsy
In this patient without ischemic coronary disease or valvular heart disease, the recent upper respiratory tract prodrome, active positional chest pain, and diffuse electrocardiographic changes raise the possibility of myocarditis with pericardial involvement.
Viral serologic tests
Viral serologic tests are often obtained in the workup of myocarditis as a noninvasive means of detecting an infectious cause.
However, this approach has several problems. First, a positive serologic result is a signal of the peripheral immune response to a pathogen but does not necessarily indicate active myocardial inflammation. Additionally, circulating immunoglobulin G against cardiotropic viruses is commonly found, even in the absence of myocarditis.1 This is often the result of a high prevalence and exposure to these viruses in the general population. Further, trials have shown no correlation between serologic results and organisms identified by endomyocardial biopsy.2
Thus, serologic testing seems to be of limited utility, reserved for testing for infection with Borrelia burgdorferi (Lyme disease) in endemic areas, hepatitis C virus, human immunodeficiency virus in patients at high risk, Rickettsia conorii, and Rickettsia rickettsii.3
Serum free light chain testing for amyloidosis
Serum free light chain testing is replacing serum and urine protein electrophoresis in the workup of cardiac amyloidosis,4 as electrophoresis has poor sensitivity.4,5
Cardiac amyloidosis often affects older persons, although in rare cases it can affect young patients who carry mutations in the transthyretin gene (ATTR amyloidosis).6 This diagnosis is unlikely in our patient, as he has no other affected organ systems (amyloidosis often affects the renal and neurologic systems), normal QRS voltages on electrocardiography (which are often but not always low in amyloidosis), and no left ventricular hypertrophy or diastolic dysfunction on echocardiography (which are often seen in amyloidosis).4
Nuclear perfusion imaging for sarcoidosis
Nuclear imaging has a limited role in evaluating myocarditis,3 but positron-emission tomography with fluorine-18 fluorodeoxyglucose has a diagnostic role in sarcoidosis, an immune-mediated cause of myocarditis.7
Based on the acuity of the patient’s presentation, preceded by upper respiratory tract symptoms, sarcoidosis is less likely. Sarcoidosis is difficult to diagnose, although when it is the cause of myocarditis, some clues exist, as patients usually present with heart failure symptoms, a second- or third-degree atrioventricular block, or a dilated left ventricle on echocardiography.3 All of these were absent in our patient.
Cardiac MRI
Cardiac MRI has undergone many advances, making it an extremely useful noninvasive test. It has excellent utility as a stand-alone test in diagnosing myocarditis and has synergistic value when combined with endomyocardial biopsy.8 It is indicated in hemodynamically stable patients with a clinical suspicion of myocarditis, persistent symptoms, absence of heart failure, and when imaging findings will change management. It is particularly useful to help elucidate a cause and guide tailored therapy.9 Therefore, it is a reasonable next step in the diagnostic pathway for this patient.10
Cardiac MRI also allows for concurrent assessment of scar. In myocardial infarction, the late gadolinium enhancement is subendocardial or transmural. In myocarditis, the pattern differs, being found in the subepicardial lateral free wall (in most patients with parvovirus B19) and mid-myocardial septum (in most patients with herpesvirus 6).9,11 Cardiac MRI also confers prognostic information for patients with suspected myocarditis.12
The Lake Louise criteria9 for the diagnosis of myocarditis require 2 of the following:
Evidence of myocardial edema
Increased ratio of early gadolinium enhancement between myocardium and skeletal muscle (indicates hyperemia)
At least 1 focal lesion with nonischemic late gadolinium enhancement (indicates cardiac myocyte injury or scarring).
The Lake Louise criteria may be replaced by T1 and T2 mapping, which was found to be considerably better for diagnosing myocarditis when the 2 were compared.9,13,14
Endomyocardial biopsy
Endomyocardial biopsy should not be delayed while waiting for cardiac MRI in patients who are hemodynamically unstable or present with life-threatening features (ventricular arrhythmia, left ventricular failure, or resuscitation after sudden cardiac death).3,10
The indications for endomyocardial biopsy have been highly debated. The 2013 guidelines from the European Society of Cardiology (ESC) recommending endomyocardial biopsy in all clinically suspected cases of myocarditis have only heightened the controversy.3 The American Heart Association (AHA) guidelines reserve biopsy for patients with suspected myocarditis who have acute or subacute heart failure symptoms or who do not respond to standard medical therapy.15 Other reasonable indications may include the following: myocarditis with life-threatening ventricular arrhythmias, suspicion of giant cell myocarditis, necrotizing eosinophilic myocarditis, or cardiac sarcoidosis.16
Endomyocardial biopsy is the only way to make a definitive diagnosis of myocarditis.3 However, given the patchy distribution of myocardial involvement, a negative result does not rule out myocarditis. The diagnostic utility can be improved by increasing the number of samples taken (at least 3 but up to 10), obtaining samples from both ventricles, and using cardiac MRI data to determine which sites to biopsy.3,13,17,18
Noninvasive testing such as cardiac MRI does not distinguish cell type or etiology (viral vs nonviral).3 Further, endomyocardial biopsy must be performed before immunosuppressive therapy can be safely started.3,16 At experienced centers, the complication rate is 0% to 0.8%.3 The addition of immunohistochemical testing and viral genomic detection by polymerase chain reaction testing have increased the sensitivity of this technique.19 Finally, endomyocardial biopsy can help rule out some of the other possibilities in the differential diagnosis for myocarditis, including infiltrative and storage diseases, and possibly cardiac tumors.3
Of additional note, the diffuse ST-segment elevation seen on the patient’s electrocardiogram (Figure 1) is indicative of subepicardial inflammation. Since the distribution involves more than one epicardial coronary territory, this helps to differentiate the changes from those that occur with myocardial infarction.20
CASE CONTINUED
Figure 2. Cardiac magnetic resonance imaging shows areas of patchy subepicardial late gadolinium enhancement (arrows).
The patient underwent cardiac MRI, which showed myocardial edema and patchy areas of late gadolinium enhancement, raising suspicion for myocarditis (Figure 2).
Causes of myocarditis are numerous (Table 1),3,21,22 but viral and postinfectious etiologies remain the most common causes of acute myocarditis.23
2. What is the most likely causative infectious agent?
Parvovirus B19
Coxsackievirus B
Adenovirus species
Human herpesvirus 6
Staphylococcus aureus
Corynebacterium diphtheria
Trypanosoma cruzi
Influenza H1/N1
INFECTIOUS CAUSES OF MYOCARDITIS
Coxsackievirus B was the agent most often linked to this condition from the 1950s through the 1990s. However, in the last 2 decades, adenovirus species and human herpesvirus 6 have been increasingly encountered, and recently, parvovirus B19 has been credited as the most common culprit,11,23 at least in the Western world. In developing nations, T cruzi and C diphtheria are the most common offenders.21
S aureus is a common cause of endocarditis, but it rarely plays a role in myocarditis. When it does, the myocarditis is often the sequela of profound bacteremia. This was much more common before antibiotics were invented.24,25
Influenza H1/N1 is not among the most common causes of viral myocarditis, but it should be considered during flu season, given its ability to result in fulminant myocarditis.3,26
TREATMENT FOR MYOCARDITIS
3. Which treatment is the most appropriate at this time?
Intravenous immunoglobulin
Interferon beta
Acyclovir
Prednisone
Colchicine
Treatment for myocarditis depends on the cause but always includes supportive care to address the constellation of presenting symptoms. Standard therapies for tachy- or bradyarrhythmias, heart failure, and hemodynamic derangement should be started.
Supportive care
In patients with severe left ventricular dysfunction, an implantable cardiac electronic device, left ventricular assist device, or heart transplant may ultimately be needed. However, if possible these should be deferred for several months to determine response to treatment, since the myocardium can possibly recover.16
Diuretics, beta-blockers, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists should be given as part of guideline-directed medical therapy for patients with heart failure and reduced ejection fraction.3,27 However, whether and how the patient should be weaned from these agents after disease recovery are unknown.3
Intravenous immunoglobulin
Intravenous immunoglobulin in high doses has had mixed results. Its efficacy is well documented in children,21 but limited supportive data are available in adults.3 As such, recent ESC guidelines do not provide recommendations regarding its use in adults.3
Interferon beta
Interferon beta has shown promise in improving New York Heart Association class and left ventricular ejection fraction.3 This is attributed to its effects on eliminating adenoviral species and enteroviruses. Treatment of enteroviral organisms in particular has been associated with improved 10-year prognosis.3 Interferon beta also has in vitro data showing efficacy at diminishing apoptosis from parvovirus B19.28
Nucleoside analogues
Empiric treatment with nucleoside analogues (acyclovir, ganciclovir, and valacyclovir) has been tried for patients in whom human herpesvirus is suspected as the causative organism, although with unconfirmed effects.3 Consultation with an infectious disease specialist is recommended before starting these agents, and biopsy is often needed beforehand.3
Immunosuppressive agents
Immunosuppressive agents such as prednisone, azathioprine, and cyclosporine can be used in cases of biopsy-proven disease with manifestations of severe heart failure, especially if biopsy results reveal sarcoidosis, giant cell myocarditis, or necrotizing eosinophilic myocarditis. Although the results were neutral in the Myocarditis Treatment Trial,29 the cause of myocarditis in this trial was unknown. Therapy with such agents should be initiated after active infection is ruled out, which also would require a biopsy.
Colchicine
Mechanisms of chest pain in myocarditis include associated pericarditis and coronary artery vasospasm.3,23 Our patient’s chest pain changed when he changed position, possibly indicating associated pericarditis. In myocarditis with accompanying pericarditis symptoms, colchicine (1–2 mg as an initial dose and then 0.6 mg daily for up to 3 months) can be helpful in alleviating symptoms.21,30 Thus, starting this agent in a patient who presents with myocarditis in absence of heart failure, arrhythmias, or left ventricular dysfunction is prudent.
Colchicine is used mainly to address the pain associated with pericarditis. For patients who present with pericarditis without myocarditis, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, with the addition of colchicine leading to faster symptom resolution.30 The benefit of colchicine for isolated myocarditis is not well established, with only limited data showing some clinical effects.31
CASE CONTINUED
The patient was given colchicine 1.2 mg on the first day and then 0.6 mg daily. Within 2 days, his chest pain had resolved. He did not receive any immunosuppressive agents.
DISCHARGE INSTRUCTIONS
4. Before discharge, this patient should be instructed to do which of the following?
Take over-the-counter NSAIDs to supplement the effects of colchicine
Avoid competitive sports and athletics for at least 6 months
Call to schedule repeat cardiac MRI
No further instruction is needed
NSAIDs are used by themselves or in combination with colchicine in the treatment of pericarditis, but their use may be associated with worse outcomes in myocarditis.3,21 Thus, their use is not recommended in most cases.3
Excessive physical activity should be avoided for at least 6 months after the clinical syndrome resolves. This recommendation is included in the most recent ESC guidelines but is based mainly on expert opinion and murine models with coxsackievirus B.3 Periodic reassessment is indicated with exercise stress testing before return to strenuous activity.3,16,32 Testing should look for exercise tolerance, and exercise electrocardiography also helps to evaluate for clinically relevant arrythmias.
Cardiac MRI can help clarify the prognosis in myocarditis, but the role of repeat testing in guiding therapy is limited.3 Indications for repeat cardiac MRI include presence of 0 or 1 of the Lake Louise criteria (recall that 2 are necessary to make the diagnosis) with recurrence of symptoms and a high suspicion for myocardial inflammation.3,9 Repeat cardiac MRI was not performed for our patient.
CASE CONCLUDED
The patient was evaluated in the cardiology clinic within 1 week of discharge. At that time, he was in sinus tachycardia with a heart rate of 102 bpm, and he was instructed to avoid any exercise until further notice.
At 6-month follow-up, the sinus tachycardia had resolved. However, because persistent tachycardia had been noted at the first postdischarge visit, and in view of the extent of myocardial involvement, he underwent exercise treadmill testing to evaluate for ventricular arrhythmias. The study did show premature ventricular complexes and 1 ventricular couplet at submaximal exercise levels. As this indicated a higher risk of exercise-induced arrhythmias, he was asked to continue normal activity levels but to abstain from exercise until the next evaluation.
During his 1-year follow-up, a repeat treadmill test showed no ventricular ectopy. Holter monitoring was ordered and showed no premature ventricular complexes, supraventricular arrhythmias, or atrioventricular block within the 48-hour period.
At his 2-year evaluation, he had returned to playing basketball and soccer on weekends and reported no recurrence of his initial symptoms.
KEY POINTS
Figure 3. Our suggested approach to suspected acute myocarditis.Cardiac MRI has emerged as an excellent noninvasive imaging modality for the diagnosis of myocarditis.
Treatment of myocarditis depends on the cause and severity of the patient’s presentation, spanning the spectrum from conservative care to immunosuppressive agents and even heart failure therapy.
Excessive physical activity should be avoided for the first 6 months after disease diagnosis and treatment.
If myocarditis is associated with pericardial involvement, colchicine is the agent of choice, and NSAIDs should be avoided.
Our suggested strategy for approaching myocarditis is shown in Figure 3.
An 18-year-old man without any significant medical history was transferred from another hospital for higher-level care after presenting with unremitting chest pain. He had been in his usual state of good health until 7 days before presentation, when he developed mild rhinorrhea and a sore throat, but not a cough. He went to an outpatient clinic, where a rapid test for group A streptococci was done; the result was negative, and he was sent home on supportive measures.
On the day of admission, he awoke with severe, pressure-like, midsternal, nonradiating pain, which he rated 10 on a scale of 10. The pain intensified in the supine position and improved with sitting. A complete review of systems was otherwise negative. He denied having had similar symptoms in the past, as well as sick contacts, recent travel, toxin exposure, illicit substance abuse, pets at home, or tick bites. His family history was negative for cardiac arrhythmias, premature coronary artery disease, thoracic aneurysms or dissection, and infiltrative disorders. His surgical and social histories were unremarkable. He said he had no drug allergies.
Figure 1. The patient’s electrocardiogram on presentation shows ST-segment elevation (arrows) over the lateral and inferior distribution (V4–V6, II, III, and aVF).
An electrocardiogram was obtained (Figure 1). His troponin I level was 7.0 ng/mL (reference range < 0.04 ng/mL).
On examination, his temperature was 38.1°C (100.6°F), heart rate 101 beats per minute, blood pressure 142/78 mm Hg, respiratory rate 16 breaths per minute, and oxygen saturation 98% on room air. He appeared anxious but was in no acute distress. Neck examination showed no elevation in jugular venous pulsation, bruits, thyromegaly, or lymphadenopathy. Cardiac examination revealed tachycardia without murmurs, rubs, or gallops. Lungs were clear to auscultation. Examination of all 4 extremities found 2+ pulses (on a scale of 0 to 4+) throughout and no cyanosis, clubbing, or edema. Abdominal, neurologic, and dermatologic examinations were unremarkable.
Further blood testing revealed the following:
Troponin I (3 hours after the first level) 15.5 ng/mL
B-type natriuretic peptide 200 mg/dL (reference range 0–100 mg/dL)
C-reactive protein 0.9 mg/dL (reference range 0.0–0.8 mg/dL)
Erythrocyte sedimentation rate 10 mm/h (reference range < 15 mm/h).
Metabolic and hematologic assessments were unremarkable. A toxicology screen for drugs of abuse was negative. Viral serologic testing was not done.
A chest radiograph showed no acute cardiopulmonary processes.
Given his presenting symptoms, persistent tachycardia, rapidly rising troponin I level, and electrocardiogram showing diffuse ST elevation, he was taken for urgent cardiac catheterization. Coronary angiography revealed no evidence of atherosclerotic disease, acute thrombosis, dissection, or aneurysm. Echocardiography 2 hours after the procedure showed a normal ejection fraction and no regional wall-motion abnormalities or valvular heart disease.
FURTHER TESTING
1. Which test should be done next to further evaluate this patient’s chest pain?
Serum viral serologic testing
Serum free light chain assay
Nuclear myocardial perfusion study
Cardiac magnetic resonance imaging (MRI)
Endomyocardial biopsy
In this patient without ischemic coronary disease or valvular heart disease, the recent upper respiratory tract prodrome, active positional chest pain, and diffuse electrocardiographic changes raise the possibility of myocarditis with pericardial involvement.
Viral serologic tests
Viral serologic tests are often obtained in the workup of myocarditis as a noninvasive means of detecting an infectious cause.
However, this approach has several problems. First, a positive serologic result is a signal of the peripheral immune response to a pathogen but does not necessarily indicate active myocardial inflammation. Additionally, circulating immunoglobulin G against cardiotropic viruses is commonly found, even in the absence of myocarditis.1 This is often the result of a high prevalence and exposure to these viruses in the general population. Further, trials have shown no correlation between serologic results and organisms identified by endomyocardial biopsy.2
Thus, serologic testing seems to be of limited utility, reserved for testing for infection with Borrelia burgdorferi (Lyme disease) in endemic areas, hepatitis C virus, human immunodeficiency virus in patients at high risk, Rickettsia conorii, and Rickettsia rickettsii.3
Serum free light chain testing for amyloidosis
Serum free light chain testing is replacing serum and urine protein electrophoresis in the workup of cardiac amyloidosis,4 as electrophoresis has poor sensitivity.4,5
Cardiac amyloidosis often affects older persons, although in rare cases it can affect young patients who carry mutations in the transthyretin gene (ATTR amyloidosis).6 This diagnosis is unlikely in our patient, as he has no other affected organ systems (amyloidosis often affects the renal and neurologic systems), normal QRS voltages on electrocardiography (which are often but not always low in amyloidosis), and no left ventricular hypertrophy or diastolic dysfunction on echocardiography (which are often seen in amyloidosis).4
Nuclear perfusion imaging for sarcoidosis
Nuclear imaging has a limited role in evaluating myocarditis,3 but positron-emission tomography with fluorine-18 fluorodeoxyglucose has a diagnostic role in sarcoidosis, an immune-mediated cause of myocarditis.7
Based on the acuity of the patient’s presentation, preceded by upper respiratory tract symptoms, sarcoidosis is less likely. Sarcoidosis is difficult to diagnose, although when it is the cause of myocarditis, some clues exist, as patients usually present with heart failure symptoms, a second- or third-degree atrioventricular block, or a dilated left ventricle on echocardiography.3 All of these were absent in our patient.
Cardiac MRI
Cardiac MRI has undergone many advances, making it an extremely useful noninvasive test. It has excellent utility as a stand-alone test in diagnosing myocarditis and has synergistic value when combined with endomyocardial biopsy.8 It is indicated in hemodynamically stable patients with a clinical suspicion of myocarditis, persistent symptoms, absence of heart failure, and when imaging findings will change management. It is particularly useful to help elucidate a cause and guide tailored therapy.9 Therefore, it is a reasonable next step in the diagnostic pathway for this patient.10
Cardiac MRI also allows for concurrent assessment of scar. In myocardial infarction, the late gadolinium enhancement is subendocardial or transmural. In myocarditis, the pattern differs, being found in the subepicardial lateral free wall (in most patients with parvovirus B19) and mid-myocardial septum (in most patients with herpesvirus 6).9,11 Cardiac MRI also confers prognostic information for patients with suspected myocarditis.12
The Lake Louise criteria9 for the diagnosis of myocarditis require 2 of the following:
Evidence of myocardial edema
Increased ratio of early gadolinium enhancement between myocardium and skeletal muscle (indicates hyperemia)
At least 1 focal lesion with nonischemic late gadolinium enhancement (indicates cardiac myocyte injury or scarring).
The Lake Louise criteria may be replaced by T1 and T2 mapping, which was found to be considerably better for diagnosing myocarditis when the 2 were compared.9,13,14
Endomyocardial biopsy
Endomyocardial biopsy should not be delayed while waiting for cardiac MRI in patients who are hemodynamically unstable or present with life-threatening features (ventricular arrhythmia, left ventricular failure, or resuscitation after sudden cardiac death).3,10
The indications for endomyocardial biopsy have been highly debated. The 2013 guidelines from the European Society of Cardiology (ESC) recommending endomyocardial biopsy in all clinically suspected cases of myocarditis have only heightened the controversy.3 The American Heart Association (AHA) guidelines reserve biopsy for patients with suspected myocarditis who have acute or subacute heart failure symptoms or who do not respond to standard medical therapy.15 Other reasonable indications may include the following: myocarditis with life-threatening ventricular arrhythmias, suspicion of giant cell myocarditis, necrotizing eosinophilic myocarditis, or cardiac sarcoidosis.16
Endomyocardial biopsy is the only way to make a definitive diagnosis of myocarditis.3 However, given the patchy distribution of myocardial involvement, a negative result does not rule out myocarditis. The diagnostic utility can be improved by increasing the number of samples taken (at least 3 but up to 10), obtaining samples from both ventricles, and using cardiac MRI data to determine which sites to biopsy.3,13,17,18
Noninvasive testing such as cardiac MRI does not distinguish cell type or etiology (viral vs nonviral).3 Further, endomyocardial biopsy must be performed before immunosuppressive therapy can be safely started.3,16 At experienced centers, the complication rate is 0% to 0.8%.3 The addition of immunohistochemical testing and viral genomic detection by polymerase chain reaction testing have increased the sensitivity of this technique.19 Finally, endomyocardial biopsy can help rule out some of the other possibilities in the differential diagnosis for myocarditis, including infiltrative and storage diseases, and possibly cardiac tumors.3
Of additional note, the diffuse ST-segment elevation seen on the patient’s electrocardiogram (Figure 1) is indicative of subepicardial inflammation. Since the distribution involves more than one epicardial coronary territory, this helps to differentiate the changes from those that occur with myocardial infarction.20
CASE CONTINUED
Figure 2. Cardiac magnetic resonance imaging shows areas of patchy subepicardial late gadolinium enhancement (arrows).
The patient underwent cardiac MRI, which showed myocardial edema and patchy areas of late gadolinium enhancement, raising suspicion for myocarditis (Figure 2).
Causes of myocarditis are numerous (Table 1),3,21,22 but viral and postinfectious etiologies remain the most common causes of acute myocarditis.23
2. What is the most likely causative infectious agent?
Parvovirus B19
Coxsackievirus B
Adenovirus species
Human herpesvirus 6
Staphylococcus aureus
Corynebacterium diphtheria
Trypanosoma cruzi
Influenza H1/N1
INFECTIOUS CAUSES OF MYOCARDITIS
Coxsackievirus B was the agent most often linked to this condition from the 1950s through the 1990s. However, in the last 2 decades, adenovirus species and human herpesvirus 6 have been increasingly encountered, and recently, parvovirus B19 has been credited as the most common culprit,11,23 at least in the Western world. In developing nations, T cruzi and C diphtheria are the most common offenders.21
S aureus is a common cause of endocarditis, but it rarely plays a role in myocarditis. When it does, the myocarditis is often the sequela of profound bacteremia. This was much more common before antibiotics were invented.24,25
Influenza H1/N1 is not among the most common causes of viral myocarditis, but it should be considered during flu season, given its ability to result in fulminant myocarditis.3,26
TREATMENT FOR MYOCARDITIS
3. Which treatment is the most appropriate at this time?
Intravenous immunoglobulin
Interferon beta
Acyclovir
Prednisone
Colchicine
Treatment for myocarditis depends on the cause but always includes supportive care to address the constellation of presenting symptoms. Standard therapies for tachy- or bradyarrhythmias, heart failure, and hemodynamic derangement should be started.
Supportive care
In patients with severe left ventricular dysfunction, an implantable cardiac electronic device, left ventricular assist device, or heart transplant may ultimately be needed. However, if possible these should be deferred for several months to determine response to treatment, since the myocardium can possibly recover.16
Diuretics, beta-blockers, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists should be given as part of guideline-directed medical therapy for patients with heart failure and reduced ejection fraction.3,27 However, whether and how the patient should be weaned from these agents after disease recovery are unknown.3
Intravenous immunoglobulin
Intravenous immunoglobulin in high doses has had mixed results. Its efficacy is well documented in children,21 but limited supportive data are available in adults.3 As such, recent ESC guidelines do not provide recommendations regarding its use in adults.3
Interferon beta
Interferon beta has shown promise in improving New York Heart Association class and left ventricular ejection fraction.3 This is attributed to its effects on eliminating adenoviral species and enteroviruses. Treatment of enteroviral organisms in particular has been associated with improved 10-year prognosis.3 Interferon beta also has in vitro data showing efficacy at diminishing apoptosis from parvovirus B19.28
Nucleoside analogues
Empiric treatment with nucleoside analogues (acyclovir, ganciclovir, and valacyclovir) has been tried for patients in whom human herpesvirus is suspected as the causative organism, although with unconfirmed effects.3 Consultation with an infectious disease specialist is recommended before starting these agents, and biopsy is often needed beforehand.3
Immunosuppressive agents
Immunosuppressive agents such as prednisone, azathioprine, and cyclosporine can be used in cases of biopsy-proven disease with manifestations of severe heart failure, especially if biopsy results reveal sarcoidosis, giant cell myocarditis, or necrotizing eosinophilic myocarditis. Although the results were neutral in the Myocarditis Treatment Trial,29 the cause of myocarditis in this trial was unknown. Therapy with such agents should be initiated after active infection is ruled out, which also would require a biopsy.
Colchicine
Mechanisms of chest pain in myocarditis include associated pericarditis and coronary artery vasospasm.3,23 Our patient’s chest pain changed when he changed position, possibly indicating associated pericarditis. In myocarditis with accompanying pericarditis symptoms, colchicine (1–2 mg as an initial dose and then 0.6 mg daily for up to 3 months) can be helpful in alleviating symptoms.21,30 Thus, starting this agent in a patient who presents with myocarditis in absence of heart failure, arrhythmias, or left ventricular dysfunction is prudent.
Colchicine is used mainly to address the pain associated with pericarditis. For patients who present with pericarditis without myocarditis, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, with the addition of colchicine leading to faster symptom resolution.30 The benefit of colchicine for isolated myocarditis is not well established, with only limited data showing some clinical effects.31
CASE CONTINUED
The patient was given colchicine 1.2 mg on the first day and then 0.6 mg daily. Within 2 days, his chest pain had resolved. He did not receive any immunosuppressive agents.
DISCHARGE INSTRUCTIONS
4. Before discharge, this patient should be instructed to do which of the following?
Take over-the-counter NSAIDs to supplement the effects of colchicine
Avoid competitive sports and athletics for at least 6 months
Call to schedule repeat cardiac MRI
No further instruction is needed
NSAIDs are used by themselves or in combination with colchicine in the treatment of pericarditis, but their use may be associated with worse outcomes in myocarditis.3,21 Thus, their use is not recommended in most cases.3
Excessive physical activity should be avoided for at least 6 months after the clinical syndrome resolves. This recommendation is included in the most recent ESC guidelines but is based mainly on expert opinion and murine models with coxsackievirus B.3 Periodic reassessment is indicated with exercise stress testing before return to strenuous activity.3,16,32 Testing should look for exercise tolerance, and exercise electrocardiography also helps to evaluate for clinically relevant arrythmias.
Cardiac MRI can help clarify the prognosis in myocarditis, but the role of repeat testing in guiding therapy is limited.3 Indications for repeat cardiac MRI include presence of 0 or 1 of the Lake Louise criteria (recall that 2 are necessary to make the diagnosis) with recurrence of symptoms and a high suspicion for myocardial inflammation.3,9 Repeat cardiac MRI was not performed for our patient.
CASE CONCLUDED
The patient was evaluated in the cardiology clinic within 1 week of discharge. At that time, he was in sinus tachycardia with a heart rate of 102 bpm, and he was instructed to avoid any exercise until further notice.
At 6-month follow-up, the sinus tachycardia had resolved. However, because persistent tachycardia had been noted at the first postdischarge visit, and in view of the extent of myocardial involvement, he underwent exercise treadmill testing to evaluate for ventricular arrhythmias. The study did show premature ventricular complexes and 1 ventricular couplet at submaximal exercise levels. As this indicated a higher risk of exercise-induced arrhythmias, he was asked to continue normal activity levels but to abstain from exercise until the next evaluation.
During his 1-year follow-up, a repeat treadmill test showed no ventricular ectopy. Holter monitoring was ordered and showed no premature ventricular complexes, supraventricular arrhythmias, or atrioventricular block within the 48-hour period.
At his 2-year evaluation, he had returned to playing basketball and soccer on weekends and reported no recurrence of his initial symptoms.
KEY POINTS
Figure 3. Our suggested approach to suspected acute myocarditis.Cardiac MRI has emerged as an excellent noninvasive imaging modality for the diagnosis of myocarditis.
Treatment of myocarditis depends on the cause and severity of the patient’s presentation, spanning the spectrum from conservative care to immunosuppressive agents and even heart failure therapy.
Excessive physical activity should be avoided for the first 6 months after disease diagnosis and treatment.
If myocarditis is associated with pericardial involvement, colchicine is the agent of choice, and NSAIDs should be avoided.
Our suggested strategy for approaching myocarditis is shown in Figure 3.
Mahfoud F, Gärtner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011; 32(7):897–903. doi:10.1093/eurheartj/ehq493
Caforio AL, Pankuweit S, Arbustini E, et al; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013; 34(33):2636–2648, 2648a–2648d. doi:10.1093/eurheartj/eht210
Donnelly JP, Hanna M. Cardiac amyloidosis: an update on diagnosis and treatment. Cleve Clin J Med 2017; 84(12 suppl 3):12–26. doi:10.3949/ccjm.84.s3.02
Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28(1):10–21. doi:10.1016/j.tcm.2017.07.004
Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol 2015; 66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
Blankstein R, Osborne M, Naya M, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014; 63(4):329–336. doi:10.1016/j.jacc.2013.09.022
Baccouche H, Mahrholtz H, Meinhardt G, et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009; 30(23):2869–2879. doi:10.1093/eurheartj/ehp328
Friedrich MG, Sechtem U, Schulz-Menger J, et al; International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009; 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012; 59(9):779–792. doi:10.1016/j.jacc.2011.09.074
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006; 114(15):1581–1590. doi:10.1161/CIRCULATIONAHA.105.606509
Gräni C, Eichhorn C, Bière L, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017; 70(16):1964–1976. doi:10.1016/j.jacc.2017.08.050
Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-Trial. J Am Coll Cardiol 2016; 67(15):1800–1811. doi:10.1016/j.jacc.2016.02.013
Gannon MP, Schaub E, Griens CL, Saba SG. State of the art: evaluation and prognostication of myocarditis using cardiac MRI. J Magn Reson Imaging 2019; 49(7):e122–e131. doi:10.1002/jmri.26611
Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007; 28(24):3076–3093. doi:10.1093/eurheartj/ehm456
Sinagra G, Anzini M, Pereira NL, et al. Myocarditis in clinical practice. Mayo Clin Proc 2016; 91(9):1256–1266. doi:10.1016/j.mayocp.2016.05.013
Cooper LT, Baughman KL, Feldman AM, et al; American Heart Association; American College of Cardiology; European Society of Cardiology. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007; 116(19):2216–2233. doi:10.1161/CIRCULATIONAHA.107.186093
Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012; 21(4):245–274. doi:10.1016/j.carpath.2011.10.001
Alraies MC, Klein AL. Should we still use electrocardiography to diagnose pericardial disease? Cleve Clin J Med 2013; 80(2):97–100. doi:10.3949/ccjm.80a.11144
Wasi F, Shuter J. Primary bacterial infection of the myocardium. Front Biosci 2003; 8:s228–s231. pmid:12700039
Al-Amoodi M, Rao K, Rao S, Brewer JH, Magalski A, Chhatriwalla AK. Fulminant myocarditis due to H1N1 influenza. Circ Heart Fail 2010; 3(3):e7–e9. doi:10.1161/CIRCHEARTFAILURE.110.938506
Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2016; 68(13):1476–1488. doi:10.1016/j.jacc.2016.05.011
Schmidt-Lucke C, Spillmann F, Bock T, et al. Interferon beta modulates endothelial damage in patients with cardiac persistence of human parvovirus b19 infection. J Infect Dis 2010; 201(6):936–945. doi:10.1086/650700
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosuppressive therapy for myocarditis: the Myocarditis Treatment Trial Investigators. N Engl J Med 1995; 333(5):269–275. doi:10.1056/NEJM199508033330501
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005; 112(13):2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738
Morgenstern D, Lisko J, Boniface NC, Mikolich BM, Mikolich JR. Myocarditis and colchicine: a new perspective from cardiac MRI. J Cardiovasc Magn Reson 2016; 18(suppl 1):0100.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015; 66(21):2343–2349. doi:10.1016/j.jacc.2015.09.032
Mahfoud F, Gärtner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011; 32(7):897–903. doi:10.1093/eurheartj/ehq493
Caforio AL, Pankuweit S, Arbustini E, et al; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013; 34(33):2636–2648, 2648a–2648d. doi:10.1093/eurheartj/eht210
Donnelly JP, Hanna M. Cardiac amyloidosis: an update on diagnosis and treatment. Cleve Clin J Med 2017; 84(12 suppl 3):12–26. doi:10.3949/ccjm.84.s3.02
Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28(1):10–21. doi:10.1016/j.tcm.2017.07.004
Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol 2015; 66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
Blankstein R, Osborne M, Naya M, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014; 63(4):329–336. doi:10.1016/j.jacc.2013.09.022
Baccouche H, Mahrholtz H, Meinhardt G, et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009; 30(23):2869–2879. doi:10.1093/eurheartj/ehp328
Friedrich MG, Sechtem U, Schulz-Menger J, et al; International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009; 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012; 59(9):779–792. doi:10.1016/j.jacc.2011.09.074
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006; 114(15):1581–1590. doi:10.1161/CIRCULATIONAHA.105.606509
Gräni C, Eichhorn C, Bière L, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017; 70(16):1964–1976. doi:10.1016/j.jacc.2017.08.050
Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-Trial. J Am Coll Cardiol 2016; 67(15):1800–1811. doi:10.1016/j.jacc.2016.02.013
Gannon MP, Schaub E, Griens CL, Saba SG. State of the art: evaluation and prognostication of myocarditis using cardiac MRI. J Magn Reson Imaging 2019; 49(7):e122–e131. doi:10.1002/jmri.26611
Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007; 28(24):3076–3093. doi:10.1093/eurheartj/ehm456
Sinagra G, Anzini M, Pereira NL, et al. Myocarditis in clinical practice. Mayo Clin Proc 2016; 91(9):1256–1266. doi:10.1016/j.mayocp.2016.05.013
Cooper LT, Baughman KL, Feldman AM, et al; American Heart Association; American College of Cardiology; European Society of Cardiology. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007; 116(19):2216–2233. doi:10.1161/CIRCULATIONAHA.107.186093
Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012; 21(4):245–274. doi:10.1016/j.carpath.2011.10.001
Alraies MC, Klein AL. Should we still use electrocardiography to diagnose pericardial disease? Cleve Clin J Med 2013; 80(2):97–100. doi:10.3949/ccjm.80a.11144
Wasi F, Shuter J. Primary bacterial infection of the myocardium. Front Biosci 2003; 8:s228–s231. pmid:12700039
Al-Amoodi M, Rao K, Rao S, Brewer JH, Magalski A, Chhatriwalla AK. Fulminant myocarditis due to H1N1 influenza. Circ Heart Fail 2010; 3(3):e7–e9. doi:10.1161/CIRCHEARTFAILURE.110.938506
Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2016; 68(13):1476–1488. doi:10.1016/j.jacc.2016.05.011
Schmidt-Lucke C, Spillmann F, Bock T, et al. Interferon beta modulates endothelial damage in patients with cardiac persistence of human parvovirus b19 infection. J Infect Dis 2010; 201(6):936–945. doi:10.1086/650700
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosuppressive therapy for myocarditis: the Myocarditis Treatment Trial Investigators. N Engl J Med 1995; 333(5):269–275. doi:10.1056/NEJM199508033330501
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005; 112(13):2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738
Morgenstern D, Lisko J, Boniface NC, Mikolich BM, Mikolich JR. Myocarditis and colchicine: a new perspective from cardiac MRI. J Cardiovasc Magn Reson 2016; 18(suppl 1):0100.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015; 66(21):2343–2349. doi:10.1016/j.jacc.2015.09.032
A new study has reaffirmed that, as methicillin‐sensitive Staphylococcus aureus (MSSA) remains the most common skin infection in pediatric atopic dermatitis (AD) patients, first‐generation cephalosporins remain the appropriate empiric therapy.
“Clindamycin, tetracyclines, or TMP‐SMX can be considered in patients suspected to have, or with a history of, MRSA [methicillin‐resistant S. aureus] infection,” wrote Cristopher C. Briscoe, MD, of the Washington University School of Medicine in St. Louis, Missouri, and his coauthors. The study was published in Pediatric Dermatology.
To determine the optimal empiric antibiotic for pediatric AD patients with skin infections, the researchers analyzed skin cultures from 106 patients seen at Saint Louis Children’s Hospital (SLCH). The results were also compared to cultures from pediatric patients who presented at the SLCH emergency department (ED) with S. aureus skin abscesses.
Of the 170 cultures that grew S. aureus, 130 (77.8%) grew MSSA, and 37 (22.2%) grew MRSA. Three of the cultures grew both. The prevalence of MRSA in the cohort differed from the prevalence in the ED patients (44%). The prevalence of either infection did not differ significantly by age, sex or race, though the average number of cultures in African American patients topped the average for Caucasian patients (1.8 vs. 1.2, P less than .003).
All patients with MSSA – in both the cohort and the ED – proved 100% susceptible to cefazolin. Cohort patients with MSSA saw lower susceptibility to doxycycline compared to the ED patients (89.4% vs. 97%), as did MRSA cohort patients to trimethoprim‐sulfamethoxazole (92% vs. 98%).
“When a patient with AD walks into your office and looks like they have an infection of their eczema, your go-to antibiotic is going to be one that targets MSSA,” said coauthor Carrie Coughlin, MD, of the Washington University School of Medicine in an interview. “You’ll still do a culture to prove or disprove that assumption, but it gives you a guide to help make that patient better in the short term while you work things up.”
“Also, remember that MSSA is not ‘better’ to have than MRSA,” she added. “You can now see some of the virulence factors from MRSA strains in MSSA strains, so treating both of them is important.”
The authors acknowledged their study’s limitations, including the limited generalizability of a single-center design and a lack of information as to the body sites from which the cultures were obtained. They were also unable to reliably determine prior antibiotic exposure, noting that “future work could examine whether prior exposure differed significantly in the MRSA and MSSA groups.”
The study was funded by grants from the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
A new study has reaffirmed that, as methicillin‐sensitive Staphylococcus aureus (MSSA) remains the most common skin infection in pediatric atopic dermatitis (AD) patients, first‐generation cephalosporins remain the appropriate empiric therapy.
“Clindamycin, tetracyclines, or TMP‐SMX can be considered in patients suspected to have, or with a history of, MRSA [methicillin‐resistant S. aureus] infection,” wrote Cristopher C. Briscoe, MD, of the Washington University School of Medicine in St. Louis, Missouri, and his coauthors. The study was published in Pediatric Dermatology.
To determine the optimal empiric antibiotic for pediatric AD patients with skin infections, the researchers analyzed skin cultures from 106 patients seen at Saint Louis Children’s Hospital (SLCH). The results were also compared to cultures from pediatric patients who presented at the SLCH emergency department (ED) with S. aureus skin abscesses.
Of the 170 cultures that grew S. aureus, 130 (77.8%) grew MSSA, and 37 (22.2%) grew MRSA. Three of the cultures grew both. The prevalence of MRSA in the cohort differed from the prevalence in the ED patients (44%). The prevalence of either infection did not differ significantly by age, sex or race, though the average number of cultures in African American patients topped the average for Caucasian patients (1.8 vs. 1.2, P less than .003).
All patients with MSSA – in both the cohort and the ED – proved 100% susceptible to cefazolin. Cohort patients with MSSA saw lower susceptibility to doxycycline compared to the ED patients (89.4% vs. 97%), as did MRSA cohort patients to trimethoprim‐sulfamethoxazole (92% vs. 98%).
“When a patient with AD walks into your office and looks like they have an infection of their eczema, your go-to antibiotic is going to be one that targets MSSA,” said coauthor Carrie Coughlin, MD, of the Washington University School of Medicine in an interview. “You’ll still do a culture to prove or disprove that assumption, but it gives you a guide to help make that patient better in the short term while you work things up.”
“Also, remember that MSSA is not ‘better’ to have than MRSA,” she added. “You can now see some of the virulence factors from MRSA strains in MSSA strains, so treating both of them is important.”
The authors acknowledged their study’s limitations, including the limited generalizability of a single-center design and a lack of information as to the body sites from which the cultures were obtained. They were also unable to reliably determine prior antibiotic exposure, noting that “future work could examine whether prior exposure differed significantly in the MRSA and MSSA groups.”
The study was funded by grants from the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
A new study has reaffirmed that, as methicillin‐sensitive Staphylococcus aureus (MSSA) remains the most common skin infection in pediatric atopic dermatitis (AD) patients, first‐generation cephalosporins remain the appropriate empiric therapy.
“Clindamycin, tetracyclines, or TMP‐SMX can be considered in patients suspected to have, or with a history of, MRSA [methicillin‐resistant S. aureus] infection,” wrote Cristopher C. Briscoe, MD, of the Washington University School of Medicine in St. Louis, Missouri, and his coauthors. The study was published in Pediatric Dermatology.
To determine the optimal empiric antibiotic for pediatric AD patients with skin infections, the researchers analyzed skin cultures from 106 patients seen at Saint Louis Children’s Hospital (SLCH). The results were also compared to cultures from pediatric patients who presented at the SLCH emergency department (ED) with S. aureus skin abscesses.
Of the 170 cultures that grew S. aureus, 130 (77.8%) grew MSSA, and 37 (22.2%) grew MRSA. Three of the cultures grew both. The prevalence of MRSA in the cohort differed from the prevalence in the ED patients (44%). The prevalence of either infection did not differ significantly by age, sex or race, though the average number of cultures in African American patients topped the average for Caucasian patients (1.8 vs. 1.2, P less than .003).
All patients with MSSA – in both the cohort and the ED – proved 100% susceptible to cefazolin. Cohort patients with MSSA saw lower susceptibility to doxycycline compared to the ED patients (89.4% vs. 97%), as did MRSA cohort patients to trimethoprim‐sulfamethoxazole (92% vs. 98%).
“When a patient with AD walks into your office and looks like they have an infection of their eczema, your go-to antibiotic is going to be one that targets MSSA,” said coauthor Carrie Coughlin, MD, of the Washington University School of Medicine in an interview. “You’ll still do a culture to prove or disprove that assumption, but it gives you a guide to help make that patient better in the short term while you work things up.”
“Also, remember that MSSA is not ‘better’ to have than MRSA,” she added. “You can now see some of the virulence factors from MRSA strains in MSSA strains, so treating both of them is important.”
The authors acknowledged their study’s limitations, including the limited generalizability of a single-center design and a lack of information as to the body sites from which the cultures were obtained. They were also unable to reliably determine prior antibiotic exposure, noting that “future work could examine whether prior exposure differed significantly in the MRSA and MSSA groups.”
The study was funded by grants from the Agency for Healthcare Research and Quality. The authors reported no conflicts of interest.
Parents who accepted, denied, or partially accepted participation in the Dutch National Immunization Program reached their decisions through different methods, according to Kim A.G.J. Romijnders of the National Institute for Public Health and the Environment in Bilthoven, the Netherlands, and associates.
MarianVejcik/Getty Images
For the study published in Vaccine, the investigators conducted a series of 12 focus groups: 3 with accepters (n = 19), 3 with deniers (n =12), and 6 with partial accepters (n =24); in the partial accepters groups, there were three groups with parents delaying vaccination and three with parents refusing some vaccinations. Three-quarters of participants were women, the average age was 39 years, and 96% had at least university education. Parents were asked about their knowledge, attitudes, deliberation, and information needs regarding childhood vaccination.
Vaccine accepters regarded the decision to vaccinate their children as self-evident, but deniers and partial accepters reported conducting extensive deliberation on the pros and cons of vaccination. Deniers and partial accepters, in general, perceived fewer risks of vaccine-preventable diseases, more risks of vaccine side effects, less social support from their environment, less trust in child welfare centers, and provided less information than accepters.
The investigators noted that vaccine deniers tended to rely on anecdotal evidence, while the deliberation that partial accepters undertook was both time consuming and difficult. This process alienated them from their child vaccine provider, with trust being lost when the provider either refused or was unable to answer questions. Partial accepters also reported a lack of social support from friends, family, and providers regarding partial vaccine acceptance.
“The findings can facilitate informed decision making among parents by promoting an open dialogue at the [child welfare center], and improving the type and form of information presented. An open dialogue between parents and [child vaccine providers] may increase deliberation among parents, strengthen positive attitudes, prevent misperceptions, and resolve decisional conflict,” the investigators concluded.
The study was supported by the Dutch National Institute for Public Health and the Environment; the authors reported no conflicts of interest.
Parents who accepted, denied, or partially accepted participation in the Dutch National Immunization Program reached their decisions through different methods, according to Kim A.G.J. Romijnders of the National Institute for Public Health and the Environment in Bilthoven, the Netherlands, and associates.
MarianVejcik/Getty Images
For the study published in Vaccine, the investigators conducted a series of 12 focus groups: 3 with accepters (n = 19), 3 with deniers (n =12), and 6 with partial accepters (n =24); in the partial accepters groups, there were three groups with parents delaying vaccination and three with parents refusing some vaccinations. Three-quarters of participants were women, the average age was 39 years, and 96% had at least university education. Parents were asked about their knowledge, attitudes, deliberation, and information needs regarding childhood vaccination.
Vaccine accepters regarded the decision to vaccinate their children as self-evident, but deniers and partial accepters reported conducting extensive deliberation on the pros and cons of vaccination. Deniers and partial accepters, in general, perceived fewer risks of vaccine-preventable diseases, more risks of vaccine side effects, less social support from their environment, less trust in child welfare centers, and provided less information than accepters.
The investigators noted that vaccine deniers tended to rely on anecdotal evidence, while the deliberation that partial accepters undertook was both time consuming and difficult. This process alienated them from their child vaccine provider, with trust being lost when the provider either refused or was unable to answer questions. Partial accepters also reported a lack of social support from friends, family, and providers regarding partial vaccine acceptance.
“The findings can facilitate informed decision making among parents by promoting an open dialogue at the [child welfare center], and improving the type and form of information presented. An open dialogue between parents and [child vaccine providers] may increase deliberation among parents, strengthen positive attitudes, prevent misperceptions, and resolve decisional conflict,” the investigators concluded.
The study was supported by the Dutch National Institute for Public Health and the Environment; the authors reported no conflicts of interest.
Parents who accepted, denied, or partially accepted participation in the Dutch National Immunization Program reached their decisions through different methods, according to Kim A.G.J. Romijnders of the National Institute for Public Health and the Environment in Bilthoven, the Netherlands, and associates.
MarianVejcik/Getty Images
For the study published in Vaccine, the investigators conducted a series of 12 focus groups: 3 with accepters (n = 19), 3 with deniers (n =12), and 6 with partial accepters (n =24); in the partial accepters groups, there were three groups with parents delaying vaccination and three with parents refusing some vaccinations. Three-quarters of participants were women, the average age was 39 years, and 96% had at least university education. Parents were asked about their knowledge, attitudes, deliberation, and information needs regarding childhood vaccination.
Vaccine accepters regarded the decision to vaccinate their children as self-evident, but deniers and partial accepters reported conducting extensive deliberation on the pros and cons of vaccination. Deniers and partial accepters, in general, perceived fewer risks of vaccine-preventable diseases, more risks of vaccine side effects, less social support from their environment, less trust in child welfare centers, and provided less information than accepters.
The investigators noted that vaccine deniers tended to rely on anecdotal evidence, while the deliberation that partial accepters undertook was both time consuming and difficult. This process alienated them from their child vaccine provider, with trust being lost when the provider either refused or was unable to answer questions. Partial accepters also reported a lack of social support from friends, family, and providers regarding partial vaccine acceptance.
“The findings can facilitate informed decision making among parents by promoting an open dialogue at the [child welfare center], and improving the type and form of information presented. An open dialogue between parents and [child vaccine providers] may increase deliberation among parents, strengthen positive attitudes, prevent misperceptions, and resolve decisional conflict,” the investigators concluded.
The study was supported by the Dutch National Institute for Public Health and the Environment; the authors reported no conflicts of interest.
The Food and Drug Administration has warned that certain hepatitis C virus medications have led to rare instances of worsening liver function or liver failure.
Many of the affected patients had signs or symptoms of moderate to severe liver impairment (Child-Pugh class B or C), and given that these medications – glecaprevir/pibrentasvir (Mavyret), elbasvir/grazoprevir (Zepatier), and sofosbuvir/velpatasvir/voxilaprevir (Vosevi) – are not indicated for such patients, they should not have been prescribed in the first place, the FDA noted in the drug safety communication. Some cases had other preexisting risk factors, such as liver cancer, alcohol abuse, or serious medical illnesses associated with liver problems.
In most cases, impairment or decompensation occurred within the first 4 weeks of starting treatment, and symptoms resolved or new-onset worsening of liver function improved after stopping. These medicines have been widely used and, among patients with no or mild liver impairment, have been shown to be safe and effective.
Health care professionals should continue prescribing these medicines as indicated; they should assess patients at baseline for severity of liver disease and other risk factors and closely monitor these patients after for signs and symptoms of worsening liver function. Patients should be aware that the risk of injury is rare and continue taking prescribed medicines; if they develop fatigue, weakness, loss of appetite, nausea and vomiting, yellow eyes or skin, or light-colored stools, they should talk with their health care professional but should continue taking the medications in question until instructed to do otherwise.
The full communication is available on the FDA website and includes more facts about these drugs and information for patients and health care professionals.
The Food and Drug Administration has warned that certain hepatitis C virus medications have led to rare instances of worsening liver function or liver failure.
Many of the affected patients had signs or symptoms of moderate to severe liver impairment (Child-Pugh class B or C), and given that these medications – glecaprevir/pibrentasvir (Mavyret), elbasvir/grazoprevir (Zepatier), and sofosbuvir/velpatasvir/voxilaprevir (Vosevi) – are not indicated for such patients, they should not have been prescribed in the first place, the FDA noted in the drug safety communication. Some cases had other preexisting risk factors, such as liver cancer, alcohol abuse, or serious medical illnesses associated with liver problems.
In most cases, impairment or decompensation occurred within the first 4 weeks of starting treatment, and symptoms resolved or new-onset worsening of liver function improved after stopping. These medicines have been widely used and, among patients with no or mild liver impairment, have been shown to be safe and effective.
Health care professionals should continue prescribing these medicines as indicated; they should assess patients at baseline for severity of liver disease and other risk factors and closely monitor these patients after for signs and symptoms of worsening liver function. Patients should be aware that the risk of injury is rare and continue taking prescribed medicines; if they develop fatigue, weakness, loss of appetite, nausea and vomiting, yellow eyes or skin, or light-colored stools, they should talk with their health care professional but should continue taking the medications in question until instructed to do otherwise.
The full communication is available on the FDA website and includes more facts about these drugs and information for patients and health care professionals.
The Food and Drug Administration has warned that certain hepatitis C virus medications have led to rare instances of worsening liver function or liver failure.
Many of the affected patients had signs or symptoms of moderate to severe liver impairment (Child-Pugh class B or C), and given that these medications – glecaprevir/pibrentasvir (Mavyret), elbasvir/grazoprevir (Zepatier), and sofosbuvir/velpatasvir/voxilaprevir (Vosevi) – are not indicated for such patients, they should not have been prescribed in the first place, the FDA noted in the drug safety communication. Some cases had other preexisting risk factors, such as liver cancer, alcohol abuse, or serious medical illnesses associated with liver problems.
In most cases, impairment or decompensation occurred within the first 4 weeks of starting treatment, and symptoms resolved or new-onset worsening of liver function improved after stopping. These medicines have been widely used and, among patients with no or mild liver impairment, have been shown to be safe and effective.
Health care professionals should continue prescribing these medicines as indicated; they should assess patients at baseline for severity of liver disease and other risk factors and closely monitor these patients after for signs and symptoms of worsening liver function. Patients should be aware that the risk of injury is rare and continue taking prescribed medicines; if they develop fatigue, weakness, loss of appetite, nausea and vomiting, yellow eyes or skin, or light-colored stools, they should talk with their health care professional but should continue taking the medications in question until instructed to do otherwise.
The full communication is available on the FDA website and includes more facts about these drugs and information for patients and health care professionals.




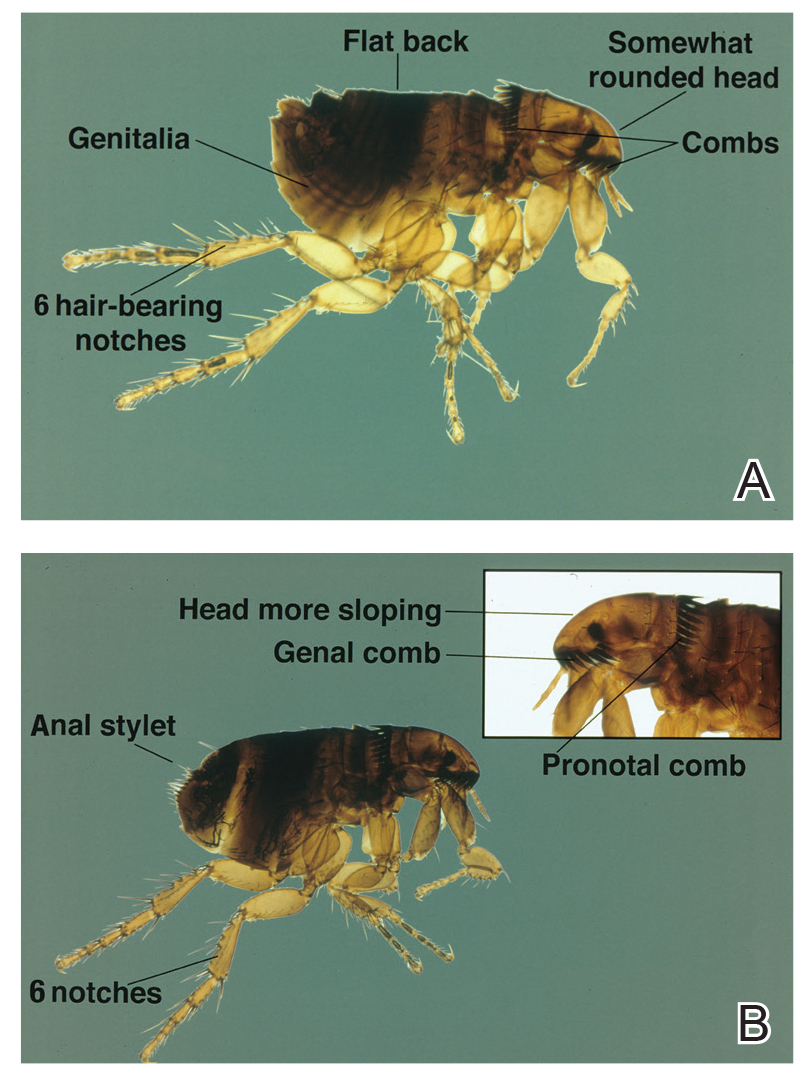


 An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).")
 over the lateral and inferior distribution (V4–V6, II, III, and aVF).")
.")





