We routinely use low-volume (2-L) polyethylene glycol electrolyte preparations such as Moviprep and Miralax in split-dose regimens, in which patients drink half of the preparation the day before the procedure and the other half the day of the procedure. In our experience, these are well tolerated by patients with a history of bariatric surgery and provide adequate colon cleansing before colonoscopy.
RATIONALE
Adequate bowel preparation by the ingestion of a cleansing agent is extremely important before colonoscopy: the quality of colon preparation affects the diagnostic accuracy and safety of the procedure, as inadequate bowel preparation has been associated with failure to detect polyps and with a higher rate of adverse events during the procedure.1–3
The most commonly used bowel preparations can be divided into high-volume (which require drinking at least 4 L of a cathartic solution) and low-volume (which require drinking about 2 L).4 Polyethylene glycol electrolyte solutions are among the most commonly used and are available in both high-volume (eg, Golytely, Nulytely) and low-volume (eg, Moviprep, Miralax) forms.
Other low-volume preparations include sodium picosulfate (Prepopik), magnesium citrate, and sodium phosphate tablets. However, these should be avoided in patients with renal insufficiency.4
Prices for bowel preparations vary. For example, the average reported wholesale price of Golytely is $24.56, Moviprep $81.17, and Miralax $10.08.4 However, the final cost depends on the patient’s insurance coverage. Generic formulations are available for some preparations.
After bariatric surgery, patients have a smaller stomach
After bariatric surgery, patients have significantly reduced stomach volume, due either to resection of a part of the stomach (such as in partial gastrectomy) or to diversion of the gastrointestinal (GI) tract to bypass most of the stomach (such as in Roux-en-Y gastric bypass). This causes early satiety with smaller amounts of food and leads to weight loss. However, this restriction in stomach volume also makes it more difficult for the patient to tolerate the intake of large volumes of fluids for bowel cleansing before colonoscopy.
Bariatric surgery patients may require colonoscopy for indications such as colorectal cancer screening, chronic diarrhea, or GI bleeding, all of which are commonly encountered during routine clinical practice.
Guidelines are available
Currently, there are no published data available to support the use of one preparation over another in patients with a history of bariatric surgery. However, for patients who have had bariatric surgery, guidelines from the US Multi-Society Task Force on Colorectal Cancer—endorsed by the three major American gastroenterology societies, ie, the American Gastroenterological Association, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy—recommend either a low-volume solution or, if a high-volume solution is used, extending the duration over which the preparation is consumed.5 In addition, it is recommended that patients consume sugar-free drinks and liquids to avoid dumping syndrome from high sugar content.6
The use of split-dose regimens is also strongly recommended for elective colonoscopy by the US Multi-Society Task Force on Colorectal Cancer.5
Our clinical experience has been in line with the above recommendations.
References
Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc 2012; 75:1197–1203.
Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015; 81:31–53.
Wexner SD, Beck DE, Baron TH, et al; American Society of Colon and Rectal Surgeons; American Society for Gastrointestinal Endoscopy; Society of American Gastrointestinal and Endoscopic Surgeons. A consensus document on bowel preparation before colonoscopy: prepared by a task force from the American Society of Colon and Rectal Surgeons (ASCRS), the American Society for Gastrointestinal Endoscopy (ASGE), and the Society of American Gastrointestinal and Endoscopic Surgerons (SAGES). Gastrointest Endosc 2006; 63:894–909.
ASGE Standards of Practice Committee; Saltzman JR, Cash BD, Pasha SF, et al. Bowel preparation before colonoscopy. Gastrointest Endosc 2015; 81:781–794.
Johnson DA, Barkun AN, Cohen LB, et al; US Multi-Society Task Force on Colorectal Cancer. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2014; 147:903–924.
Heber D, Greenway FL, Kaplan LM, Livingston E, Salvador J, Still C; Endocrine Society. Endocrine and nutritional management of the post-bariatric surgery patient: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2010; 95:4823–4843.
Zubin Arora, MD Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic
Gursimran Kochhar, MD Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic
Bo Shen, MD Section Head and The Ed and Joey Story Endowed Chair, Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic; Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Address: Bo Shen, MD, Department of Gastroenterology and Hepatology, A31, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; [email protected]
Zubin Arora, MD Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic
Gursimran Kochhar, MD Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic
Bo Shen, MD Section Head and The Ed and Joey Story Endowed Chair, Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic; Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Address: Bo Shen, MD, Department of Gastroenterology and Hepatology, A31, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; [email protected]
Author and Disclosure Information
Zubin Arora, MD Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic
Gursimran Kochhar, MD Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic
Bo Shen, MD Section Head and The Ed and Joey Story Endowed Chair, Department of Gastroenterology and Hepatology, Digestive Disease and Surgery Institute, Cleveland Clinic; Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Address: Bo Shen, MD, Department of Gastroenterology and Hepatology, A31, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; [email protected]
We routinely use low-volume (2-L) polyethylene glycol electrolyte preparations such as Moviprep and Miralax in split-dose regimens, in which patients drink half of the preparation the day before the procedure and the other half the day of the procedure. In our experience, these are well tolerated by patients with a history of bariatric surgery and provide adequate colon cleansing before colonoscopy.
RATIONALE
Adequate bowel preparation by the ingestion of a cleansing agent is extremely important before colonoscopy: the quality of colon preparation affects the diagnostic accuracy and safety of the procedure, as inadequate bowel preparation has been associated with failure to detect polyps and with a higher rate of adverse events during the procedure.1–3
The most commonly used bowel preparations can be divided into high-volume (which require drinking at least 4 L of a cathartic solution) and low-volume (which require drinking about 2 L).4 Polyethylene glycol electrolyte solutions are among the most commonly used and are available in both high-volume (eg, Golytely, Nulytely) and low-volume (eg, Moviprep, Miralax) forms.
Other low-volume preparations include sodium picosulfate (Prepopik), magnesium citrate, and sodium phosphate tablets. However, these should be avoided in patients with renal insufficiency.4
Prices for bowel preparations vary. For example, the average reported wholesale price of Golytely is $24.56, Moviprep $81.17, and Miralax $10.08.4 However, the final cost depends on the patient’s insurance coverage. Generic formulations are available for some preparations.
After bariatric surgery, patients have a smaller stomach
After bariatric surgery, patients have significantly reduced stomach volume, due either to resection of a part of the stomach (such as in partial gastrectomy) or to diversion of the gastrointestinal (GI) tract to bypass most of the stomach (such as in Roux-en-Y gastric bypass). This causes early satiety with smaller amounts of food and leads to weight loss. However, this restriction in stomach volume also makes it more difficult for the patient to tolerate the intake of large volumes of fluids for bowel cleansing before colonoscopy.
Bariatric surgery patients may require colonoscopy for indications such as colorectal cancer screening, chronic diarrhea, or GI bleeding, all of which are commonly encountered during routine clinical practice.
Guidelines are available
Currently, there are no published data available to support the use of one preparation over another in patients with a history of bariatric surgery. However, for patients who have had bariatric surgery, guidelines from the US Multi-Society Task Force on Colorectal Cancer—endorsed by the three major American gastroenterology societies, ie, the American Gastroenterological Association, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy—recommend either a low-volume solution or, if a high-volume solution is used, extending the duration over which the preparation is consumed.5 In addition, it is recommended that patients consume sugar-free drinks and liquids to avoid dumping syndrome from high sugar content.6
The use of split-dose regimens is also strongly recommended for elective colonoscopy by the US Multi-Society Task Force on Colorectal Cancer.5
Our clinical experience has been in line with the above recommendations.
We routinely use low-volume (2-L) polyethylene glycol electrolyte preparations such as Moviprep and Miralax in split-dose regimens, in which patients drink half of the preparation the day before the procedure and the other half the day of the procedure. In our experience, these are well tolerated by patients with a history of bariatric surgery and provide adequate colon cleansing before colonoscopy.
RATIONALE
Adequate bowel preparation by the ingestion of a cleansing agent is extremely important before colonoscopy: the quality of colon preparation affects the diagnostic accuracy and safety of the procedure, as inadequate bowel preparation has been associated with failure to detect polyps and with a higher rate of adverse events during the procedure.1–3
The most commonly used bowel preparations can be divided into high-volume (which require drinking at least 4 L of a cathartic solution) and low-volume (which require drinking about 2 L).4 Polyethylene glycol electrolyte solutions are among the most commonly used and are available in both high-volume (eg, Golytely, Nulytely) and low-volume (eg, Moviprep, Miralax) forms.
Other low-volume preparations include sodium picosulfate (Prepopik), magnesium citrate, and sodium phosphate tablets. However, these should be avoided in patients with renal insufficiency.4
Prices for bowel preparations vary. For example, the average reported wholesale price of Golytely is $24.56, Moviprep $81.17, and Miralax $10.08.4 However, the final cost depends on the patient’s insurance coverage. Generic formulations are available for some preparations.
After bariatric surgery, patients have a smaller stomach
After bariatric surgery, patients have significantly reduced stomach volume, due either to resection of a part of the stomach (such as in partial gastrectomy) or to diversion of the gastrointestinal (GI) tract to bypass most of the stomach (such as in Roux-en-Y gastric bypass). This causes early satiety with smaller amounts of food and leads to weight loss. However, this restriction in stomach volume also makes it more difficult for the patient to tolerate the intake of large volumes of fluids for bowel cleansing before colonoscopy.
Bariatric surgery patients may require colonoscopy for indications such as colorectal cancer screening, chronic diarrhea, or GI bleeding, all of which are commonly encountered during routine clinical practice.
Guidelines are available
Currently, there are no published data available to support the use of one preparation over another in patients with a history of bariatric surgery. However, for patients who have had bariatric surgery, guidelines from the US Multi-Society Task Force on Colorectal Cancer—endorsed by the three major American gastroenterology societies, ie, the American Gastroenterological Association, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy—recommend either a low-volume solution or, if a high-volume solution is used, extending the duration over which the preparation is consumed.5 In addition, it is recommended that patients consume sugar-free drinks and liquids to avoid dumping syndrome from high sugar content.6
The use of split-dose regimens is also strongly recommended for elective colonoscopy by the US Multi-Society Task Force on Colorectal Cancer.5
Our clinical experience has been in line with the above recommendations.
References
Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc 2012; 75:1197–1203.
Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015; 81:31–53.
Wexner SD, Beck DE, Baron TH, et al; American Society of Colon and Rectal Surgeons; American Society for Gastrointestinal Endoscopy; Society of American Gastrointestinal and Endoscopic Surgeons. A consensus document on bowel preparation before colonoscopy: prepared by a task force from the American Society of Colon and Rectal Surgeons (ASCRS), the American Society for Gastrointestinal Endoscopy (ASGE), and the Society of American Gastrointestinal and Endoscopic Surgerons (SAGES). Gastrointest Endosc 2006; 63:894–909.
ASGE Standards of Practice Committee; Saltzman JR, Cash BD, Pasha SF, et al. Bowel preparation before colonoscopy. Gastrointest Endosc 2015; 81:781–794.
Johnson DA, Barkun AN, Cohen LB, et al; US Multi-Society Task Force on Colorectal Cancer. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2014; 147:903–924.
Heber D, Greenway FL, Kaplan LM, Livingston E, Salvador J, Still C; Endocrine Society. Endocrine and nutritional management of the post-bariatric surgery patient: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2010; 95:4823–4843.
References
Chokshi RV, Hovis CE, Hollander T, Early DS, Wang JS. Prevalence of missed adenomas in patients with inadequate bowel preparation on screening colonoscopy. Gastrointest Endosc 2012; 75:1197–1203.
Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc 2015; 81:31–53.
Wexner SD, Beck DE, Baron TH, et al; American Society of Colon and Rectal Surgeons; American Society for Gastrointestinal Endoscopy; Society of American Gastrointestinal and Endoscopic Surgeons. A consensus document on bowel preparation before colonoscopy: prepared by a task force from the American Society of Colon and Rectal Surgeons (ASCRS), the American Society for Gastrointestinal Endoscopy (ASGE), and the Society of American Gastrointestinal and Endoscopic Surgerons (SAGES). Gastrointest Endosc 2006; 63:894–909.
ASGE Standards of Practice Committee; Saltzman JR, Cash BD, Pasha SF, et al. Bowel preparation before colonoscopy. Gastrointest Endosc 2015; 81:781–794.
Johnson DA, Barkun AN, Cohen LB, et al; US Multi-Society Task Force on Colorectal Cancer. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2014; 147:903–924.
Heber D, Greenway FL, Kaplan LM, Livingston E, Salvador J, Still C; Endocrine Society. Endocrine and nutritional management of the post-bariatric surgery patient: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2010; 95:4823–4843.
A 48-year-old Nicaraguan man underwent mag netic resonance imaging (MRI) 3 days after admission to a South Florida hospital for treatment of cellulitis of the right thigh with vancomycin. MRI had been ordered to evaluate for a possible drainable source of infection, as the clinical picture and duration of illness was worsening and longer than expected for typical uncomplicated cellulitis despite intravenous antibiotic therapy. The MRI showed multiple enlarged inguinal lymph nodes and cellulitis of the superficial soft tissues of the thigh without discrete drainable collections.
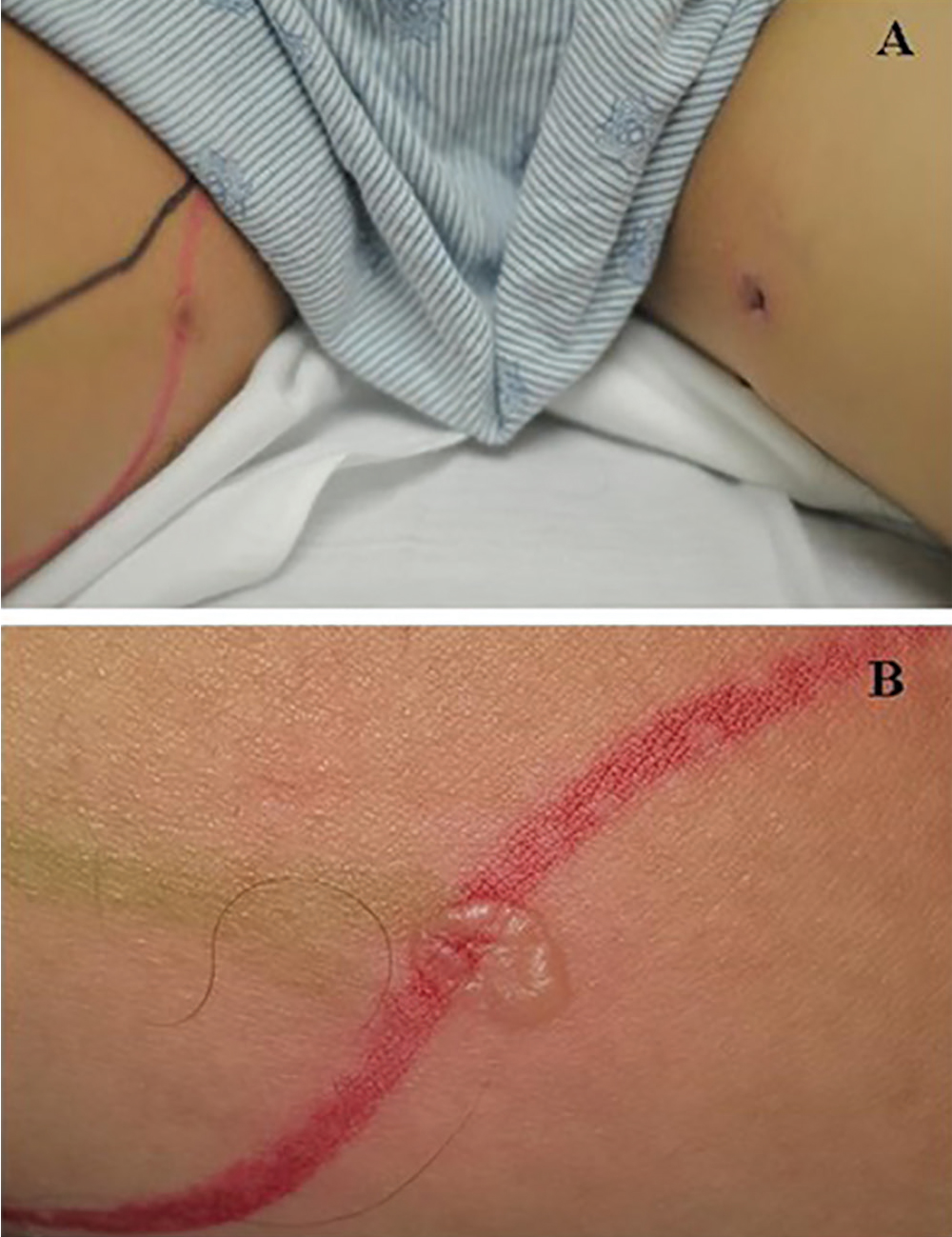
Figure 1. (A) Articulating 1-cm lesions developed after magnetic resonance imaging. The black and red tracings on the right inner thigh indicate the original area of cellulitis. (B) A bullous lesion with clear serous fluid on the right medial thigh.
After the procedure, the patient was noted to have a bullous lesion on each thigh, each lesion roughly 1 cm in diameter and filled with clear serous fluid (Figure 1). He reported that his legs had been pressed together before entering the MRI machine and that he had felt a burning sensation in both thighs during the test. Examination confirmed that the lesions indeed aligned with each other when he pressed his thighs together.
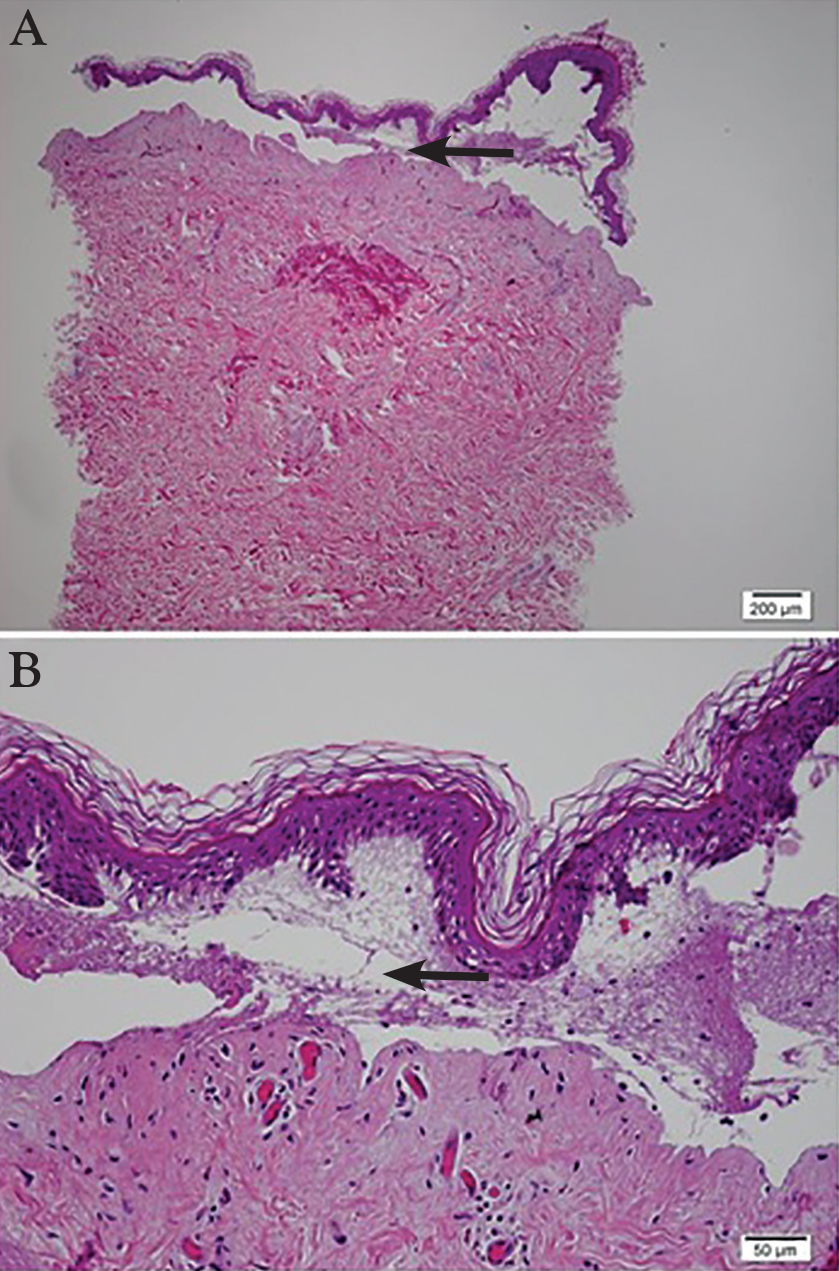
Study of a biopsy of one of the lesions revealed subepidermal cell blisters with focal epidermal necrosis and coagulative changes in the superficial dermis, consistent with a thermal injury (Figure 2).
HOW BURNS CAN OCCUR DURING MRI
Figure 2. Focal epidermal necrosis (arrows) and coagulative changes in the superficial dermis were consistent with thermal injury (hematoxylin and eosin; panel A magnification x 2.5; panel B magnification x 10).
Thermal burns are a potential cause of injury during MRI. Most have been observed in patients connected to external metal-containing monitoring devices, such as electrocardiogram leads and pulse oximeters.1,2 Thermal burns in patients unconnected to external devices have occurred when the patient’s body was touching radiofrequency coils3 or, as with our patient, when skin touches skin.2,4,5 Skin-to-skin contact during MRI can cause the scanner to emit high-power electromagnetic radiofrequency pulses that are conducted through the body, creating heat. Tissue loops are created at points of skin-to-skin contact, thus forming a closed conducting circuit. The current flowing through this circuit can produce second-degree burns.4
We believe that during placement in the scanner, our patient inadvertently moved his thighs together, forming a closed loop conduction circuit and resulting in a thermal burn.
This case illustrates the importance of correct positioning during MRI. The MRI technicians had taken standard precautions, placing a sheet over the patient and ensuring no direct contact with the radiofrequency transmitter receiver (MR unit). However, precautions against skin-to-skin contact were not taken, and the patient’s legs were not separated.
LESSONS LEARNED
Appropriate positioning prevents closed skin-to-skin loops, but this may be more challenging in a larger patient.6 While the patient is in the scanner, a “squeeze ball” alert system allows the patient to signal the technologist should unexpected distress or heating occur.6,7 A patient’s inability to utilize the squeeze ball contributes to the risk of a severe injury. Further, in this instance, there may have been a language barrier. Also, proximity of the anatomic skin-to-skin loop to the imaged body part (and therefore the center of the MRI coil) may have conferred risk related to field strength in this patient.
The MRI technologist, under supervision of a radiologist, is primarily responsible for positioning the patient to decrease the risk of this complication and for following institutional MRI safety protocols and professional guidelines.6–8 MRI technologist certification training highlights all aspects of safety, including skin-to-skin conducting loop prevention.7,8
References
Dempsey MF, Condon B. Thermal injuries associated with MRI. Clin Radiol 2001; 56:457–465.
Haik J, Daniel S, Tessone A, Orenstein A, Winkler E. MRI induced fourth-degree burn in an extremity, leading to amputation. Burns 2009; 35:294–296.
Friedstat J, Moore ME, Goverman J, Fagan SP. An unusual burn during routine magnetic resonance imaging. J Burn Care Res 2013; 34: e110–e111.
Eising EG, Hughes J, Nolte F, Jentzen W, Bockisch A. Burn injury by nuclear magnetic resonance imaging. Clin Imaging 2010; 34:293–297.
Landman A, Goldfarb S. Magnetic resonance-induced thermal burn. Ann Emerg Med 2008; 52:308–309.
Expert Panel on MR Safety; Kanal E, Barkovich AJ, Bell C, et al. ACR guidance document on MR safe practices: 2013. J Magn Reson Imaging 2013; 37:501–530.
Magnetic resonance safety. Radiol Technol 2010; 81:615–616.
A 48-year-old Nicaraguan man underwent mag netic resonance imaging (MRI) 3 days after admission to a South Florida hospital for treatment of cellulitis of the right thigh with vancomycin. MRI had been ordered to evaluate for a possible drainable source of infection, as the clinical picture and duration of illness was worsening and longer than expected for typical uncomplicated cellulitis despite intravenous antibiotic therapy. The MRI showed multiple enlarged inguinal lymph nodes and cellulitis of the superficial soft tissues of the thigh without discrete drainable collections.
Figure 1. (A) Articulating 1-cm lesions developed after magnetic resonance imaging. The black and red tracings on the right inner thigh indicate the original area of cellulitis. (B) A bullous lesion with clear serous fluid on the right medial thigh.
After the procedure, the patient was noted to have a bullous lesion on each thigh, each lesion roughly 1 cm in diameter and filled with clear serous fluid (Figure 1). He reported that his legs had been pressed together before entering the MRI machine and that he had felt a burning sensation in both thighs during the test. Examination confirmed that the lesions indeed aligned with each other when he pressed his thighs together.
Study of a biopsy of one of the lesions revealed subepidermal cell blisters with focal epidermal necrosis and coagulative changes in the superficial dermis, consistent with a thermal injury (Figure 2).
HOW BURNS CAN OCCUR DURING MRI
Figure 2. Focal epidermal necrosis (arrows) and coagulative changes in the superficial dermis were consistent with thermal injury (hematoxylin and eosin; panel A magnification x 2.5; panel B magnification x 10).
Thermal burns are a potential cause of injury during MRI. Most have been observed in patients connected to external metal-containing monitoring devices, such as electrocardiogram leads and pulse oximeters.1,2 Thermal burns in patients unconnected to external devices have occurred when the patient’s body was touching radiofrequency coils3 or, as with our patient, when skin touches skin.2,4,5 Skin-to-skin contact during MRI can cause the scanner to emit high-power electromagnetic radiofrequency pulses that are conducted through the body, creating heat. Tissue loops are created at points of skin-to-skin contact, thus forming a closed conducting circuit. The current flowing through this circuit can produce second-degree burns.4
We believe that during placement in the scanner, our patient inadvertently moved his thighs together, forming a closed loop conduction circuit and resulting in a thermal burn.
This case illustrates the importance of correct positioning during MRI. The MRI technicians had taken standard precautions, placing a sheet over the patient and ensuring no direct contact with the radiofrequency transmitter receiver (MR unit). However, precautions against skin-to-skin contact were not taken, and the patient’s legs were not separated.
LESSONS LEARNED
Appropriate positioning prevents closed skin-to-skin loops, but this may be more challenging in a larger patient.6 While the patient is in the scanner, a “squeeze ball” alert system allows the patient to signal the technologist should unexpected distress or heating occur.6,7 A patient’s inability to utilize the squeeze ball contributes to the risk of a severe injury. Further, in this instance, there may have been a language barrier. Also, proximity of the anatomic skin-to-skin loop to the imaged body part (and therefore the center of the MRI coil) may have conferred risk related to field strength in this patient.
The MRI technologist, under supervision of a radiologist, is primarily responsible for positioning the patient to decrease the risk of this complication and for following institutional MRI safety protocols and professional guidelines.6–8 MRI technologist certification training highlights all aspects of safety, including skin-to-skin conducting loop prevention.7,8
A 48-year-old Nicaraguan man underwent mag netic resonance imaging (MRI) 3 days after admission to a South Florida hospital for treatment of cellulitis of the right thigh with vancomycin. MRI had been ordered to evaluate for a possible drainable source of infection, as the clinical picture and duration of illness was worsening and longer than expected for typical uncomplicated cellulitis despite intravenous antibiotic therapy. The MRI showed multiple enlarged inguinal lymph nodes and cellulitis of the superficial soft tissues of the thigh without discrete drainable collections.
Figure 1. (A) Articulating 1-cm lesions developed after magnetic resonance imaging. The black and red tracings on the right inner thigh indicate the original area of cellulitis. (B) A bullous lesion with clear serous fluid on the right medial thigh.
After the procedure, the patient was noted to have a bullous lesion on each thigh, each lesion roughly 1 cm in diameter and filled with clear serous fluid (Figure 1). He reported that his legs had been pressed together before entering the MRI machine and that he had felt a burning sensation in both thighs during the test. Examination confirmed that the lesions indeed aligned with each other when he pressed his thighs together.
Study of a biopsy of one of the lesions revealed subepidermal cell blisters with focal epidermal necrosis and coagulative changes in the superficial dermis, consistent with a thermal injury (Figure 2).
HOW BURNS CAN OCCUR DURING MRI
Figure 2. Focal epidermal necrosis (arrows) and coagulative changes in the superficial dermis were consistent with thermal injury (hematoxylin and eosin; panel A magnification x 2.5; panel B magnification x 10).
Thermal burns are a potential cause of injury during MRI. Most have been observed in patients connected to external metal-containing monitoring devices, such as electrocardiogram leads and pulse oximeters.1,2 Thermal burns in patients unconnected to external devices have occurred when the patient’s body was touching radiofrequency coils3 or, as with our patient, when skin touches skin.2,4,5 Skin-to-skin contact during MRI can cause the scanner to emit high-power electromagnetic radiofrequency pulses that are conducted through the body, creating heat. Tissue loops are created at points of skin-to-skin contact, thus forming a closed conducting circuit. The current flowing through this circuit can produce second-degree burns.4
We believe that during placement in the scanner, our patient inadvertently moved his thighs together, forming a closed loop conduction circuit and resulting in a thermal burn.
This case illustrates the importance of correct positioning during MRI. The MRI technicians had taken standard precautions, placing a sheet over the patient and ensuring no direct contact with the radiofrequency transmitter receiver (MR unit). However, precautions against skin-to-skin contact were not taken, and the patient’s legs were not separated.
LESSONS LEARNED
Appropriate positioning prevents closed skin-to-skin loops, but this may be more challenging in a larger patient.6 While the patient is in the scanner, a “squeeze ball” alert system allows the patient to signal the technologist should unexpected distress or heating occur.6,7 A patient’s inability to utilize the squeeze ball contributes to the risk of a severe injury. Further, in this instance, there may have been a language barrier. Also, proximity of the anatomic skin-to-skin loop to the imaged body part (and therefore the center of the MRI coil) may have conferred risk related to field strength in this patient.
The MRI technologist, under supervision of a radiologist, is primarily responsible for positioning the patient to decrease the risk of this complication and for following institutional MRI safety protocols and professional guidelines.6–8 MRI technologist certification training highlights all aspects of safety, including skin-to-skin conducting loop prevention.7,8
References
Dempsey MF, Condon B. Thermal injuries associated with MRI. Clin Radiol 2001; 56:457–465.
Haik J, Daniel S, Tessone A, Orenstein A, Winkler E. MRI induced fourth-degree burn in an extremity, leading to amputation. Burns 2009; 35:294–296.
Friedstat J, Moore ME, Goverman J, Fagan SP. An unusual burn during routine magnetic resonance imaging. J Burn Care Res 2013; 34: e110–e111.
Eising EG, Hughes J, Nolte F, Jentzen W, Bockisch A. Burn injury by nuclear magnetic resonance imaging. Clin Imaging 2010; 34:293–297.
Landman A, Goldfarb S. Magnetic resonance-induced thermal burn. Ann Emerg Med 2008; 52:308–309.
Expert Panel on MR Safety; Kanal E, Barkovich AJ, Bell C, et al. ACR guidance document on MR safe practices: 2013. J Magn Reson Imaging 2013; 37:501–530.
Magnetic resonance safety. Radiol Technol 2010; 81:615–616.
Dempsey MF, Condon B. Thermal injuries associated with MRI. Clin Radiol 2001; 56:457–465.
Haik J, Daniel S, Tessone A, Orenstein A, Winkler E. MRI induced fourth-degree burn in an extremity, leading to amputation. Burns 2009; 35:294–296.
Friedstat J, Moore ME, Goverman J, Fagan SP. An unusual burn during routine magnetic resonance imaging. J Burn Care Res 2013; 34: e110–e111.
Eising EG, Hughes J, Nolte F, Jentzen W, Bockisch A. Burn injury by nuclear magnetic resonance imaging. Clin Imaging 2010; 34:293–297.
Landman A, Goldfarb S. Magnetic resonance-induced thermal burn. Ann Emerg Med 2008; 52:308–309.
Expert Panel on MR Safety; Kanal E, Barkovich AJ, Bell C, et al. ACR guidance document on MR safe practices: 2013. J Magn Reson Imaging 2013; 37:501–530.
Magnetic resonance safety. Radiol Technol 2010; 81:615–616.
SNOWMASS, COLO. – Mounting evidence attests to the value of noninvasive measurement of coronary flow reserve as a means of classifying cardiovascular risk in patients with stable coronary artery disease (CAD) more accurately than is possible via coronary angiography or measurement of fractional flow reserve, Marcelo F. Di Carli, MD, reported at the Annual Cardiovascular Conference at Snowmass.
“We use CFR [coronary flow reserve] as a way to exclude coronary disease. It’s a good practical measure of multivessel ischemic CAD. When the CFR is normal, you can with high confidence exclude the possibility of high-risk CAD,” according to Dr. Di Carli, executive director of the cardiovascular imaging program and chief of the division of nuclear medicine and molecular imaging at Brigham and Women’s Hospital, Boston.
Bruce Jancin/Frontline Medical News
Dr. Marcello di Carli
When the CFR is markedly low, however, a patient with stable CAD is at high risk for cardiovascular events, even if angiography shows no clinically significant stenosis, added Dr. Di Carli, who is also professor of radiology and medicine at Harvard Medical School, Boston.
Most recently, he and his coinvestigators utilized CFR to provide new insight into the paradox that women have a higher cardiovascular disease death rate than men, even though their prevalence of obstructive CAD is lower.
Their NIH-sponsored study included 329 consecutive patients with a left ventricular ejection fraction greater than 40% – 43% of them women – who underwent coronary angiography several days after noninvasive assessment of CFR via myocardial perfusion positron emission tomography. The women had a lower burden of angiographic CAD and a lower pretest clinical risk score than the men. Nevertheless, during a median of 3 years of follow-up, the women had an adjusted twofold greater risk of the composite endpoint of cardiovascular death, nonfatal MI, or heart failure.
This excess cardiovascular risk in women was independently associated with a very low CFR, defined as less than 1.6. Dr. Di Carli and his coinvestigators calculated that this impaired CFR mediated 40% of the excess risk in women. Thus, a low CFR represents a novel hidden biologic risk for ischemic heart disease (Circulation. 2017 Feb 7;135[6]:566-77).
CFR is defined as the ratio of absolute coronary flow or myocardial perfusion between drug-induced hyperemia and rest. It can be quantified noninvasively using positron emission tomography or MRI.
CFR integrates into a single measure the three components of CAD: the focal stenosis, the diffuse atherosclerotic plaque typically present to a varying degree throughout a target vessel, and microvascular dysfunction.
CFR is a measure of coronary physiology, as is invasive fractional flow reserve (FFR). However, FFR measures only the severity of stenosis and extent of diffuse disease; it doesn’t assess microvascular dysfunction. This is a limitation because it means FFR can give false-negative readings in patients without significant obstructive coronary disease who have severe microvascular dysfunction.
As for angiography, Dr. Di Carli continued, it’s now evident that this purely anatomic assessment is of limited value as a marker of clinical risk and is inadequate to guide management decisions in the setting of stable CAD. After all, angiographically guided revascularization has not reduced cardiovascular events in clinical trials comparing it with optimal medical therapy, as in the COURAGE and BARI-2D trials.
“It’s clear that there’s been a paradigm shift in how we manage patients with stable CAD. For many years the coronary angiogram was the cornerstone of what we did: how we understand the symptoms, the patient’s risk, and ultimately how we proceed with treatment. But there is no benefit in basing treatment solely on what the lesions look like anatomically. That’s why we’ve turned to functional testing of coronary physiology,” he said.
CFR has opened a window on the importance of microvascular dysfunction, which is present in about half of patients with stable CAD and has been shown to predict cardiovascular risk independent of whether or not severe obstructive disease is present.
In an earlier study, Dr. Di Carli and coworkers demonstrated that quantification of CFR enhances stratification for risk of cardiac death among diabetes patients (Circulation. 2012 Oct 9;126[15]:1858-68). The study included 2,783 patients, of whom 1,172 were diabetic, who underwent measurement of CFR and were subsequently followed for a median of 1.4 years, during which 137 cardiac deaths occurred.
Diabetes patients without known CAD who had a low CFR had a high cardiac death rate of 2.8%/year, similar to the 2.0%/year rate in nondiabetic patients with a history of acute MI or revascularization. On the other hand, diabetes patients with a normal CFR and without known CAD had a cardiac mortality rate of only 0.3%/year, comparable to the 0.5% rate in nondiabetics without known CAD who had preserved systolic function and a normal stress perfusion study.
In the future, CFR may aid in decision making as to whether an individual with stable CAD is best treated by percutaneous coronary intervention, surgical revascularization, or guideline-directed medical therapy. For example, if CFR indicates the presence of an isolated severe focal stenosis, and this is confirmed by angiography and FFR, PCI may be the best option, while diffuse disease as demonstrated by CFR may be better treated surgically or using optimal medical therapy. But this needs to be established in prospective clinical trials, added Dr. Di Carli.
He reported having no financial conflicts regarding his presentation.
SNOWMASS, COLO. – Mounting evidence attests to the value of noninvasive measurement of coronary flow reserve as a means of classifying cardiovascular risk in patients with stable coronary artery disease (CAD) more accurately than is possible via coronary angiography or measurement of fractional flow reserve, Marcelo F. Di Carli, MD, reported at the Annual Cardiovascular Conference at Snowmass.
“We use CFR [coronary flow reserve] as a way to exclude coronary disease. It’s a good practical measure of multivessel ischemic CAD. When the CFR is normal, you can with high confidence exclude the possibility of high-risk CAD,” according to Dr. Di Carli, executive director of the cardiovascular imaging program and chief of the division of nuclear medicine and molecular imaging at Brigham and Women’s Hospital, Boston.
Bruce Jancin/Frontline Medical News
Dr. Marcello di Carli
When the CFR is markedly low, however, a patient with stable CAD is at high risk for cardiovascular events, even if angiography shows no clinically significant stenosis, added Dr. Di Carli, who is also professor of radiology and medicine at Harvard Medical School, Boston.
Most recently, he and his coinvestigators utilized CFR to provide new insight into the paradox that women have a higher cardiovascular disease death rate than men, even though their prevalence of obstructive CAD is lower.
Their NIH-sponsored study included 329 consecutive patients with a left ventricular ejection fraction greater than 40% – 43% of them women – who underwent coronary angiography several days after noninvasive assessment of CFR via myocardial perfusion positron emission tomography. The women had a lower burden of angiographic CAD and a lower pretest clinical risk score than the men. Nevertheless, during a median of 3 years of follow-up, the women had an adjusted twofold greater risk of the composite endpoint of cardiovascular death, nonfatal MI, or heart failure.
This excess cardiovascular risk in women was independently associated with a very low CFR, defined as less than 1.6. Dr. Di Carli and his coinvestigators calculated that this impaired CFR mediated 40% of the excess risk in women. Thus, a low CFR represents a novel hidden biologic risk for ischemic heart disease (Circulation. 2017 Feb 7;135[6]:566-77).
CFR is defined as the ratio of absolute coronary flow or myocardial perfusion between drug-induced hyperemia and rest. It can be quantified noninvasively using positron emission tomography or MRI.
CFR integrates into a single measure the three components of CAD: the focal stenosis, the diffuse atherosclerotic plaque typically present to a varying degree throughout a target vessel, and microvascular dysfunction.
CFR is a measure of coronary physiology, as is invasive fractional flow reserve (FFR). However, FFR measures only the severity of stenosis and extent of diffuse disease; it doesn’t assess microvascular dysfunction. This is a limitation because it means FFR can give false-negative readings in patients without significant obstructive coronary disease who have severe microvascular dysfunction.
As for angiography, Dr. Di Carli continued, it’s now evident that this purely anatomic assessment is of limited value as a marker of clinical risk and is inadequate to guide management decisions in the setting of stable CAD. After all, angiographically guided revascularization has not reduced cardiovascular events in clinical trials comparing it with optimal medical therapy, as in the COURAGE and BARI-2D trials.
“It’s clear that there’s been a paradigm shift in how we manage patients with stable CAD. For many years the coronary angiogram was the cornerstone of what we did: how we understand the symptoms, the patient’s risk, and ultimately how we proceed with treatment. But there is no benefit in basing treatment solely on what the lesions look like anatomically. That’s why we’ve turned to functional testing of coronary physiology,” he said.
CFR has opened a window on the importance of microvascular dysfunction, which is present in about half of patients with stable CAD and has been shown to predict cardiovascular risk independent of whether or not severe obstructive disease is present.
In an earlier study, Dr. Di Carli and coworkers demonstrated that quantification of CFR enhances stratification for risk of cardiac death among diabetes patients (Circulation. 2012 Oct 9;126[15]:1858-68). The study included 2,783 patients, of whom 1,172 were diabetic, who underwent measurement of CFR and were subsequently followed for a median of 1.4 years, during which 137 cardiac deaths occurred.
Diabetes patients without known CAD who had a low CFR had a high cardiac death rate of 2.8%/year, similar to the 2.0%/year rate in nondiabetic patients with a history of acute MI or revascularization. On the other hand, diabetes patients with a normal CFR and without known CAD had a cardiac mortality rate of only 0.3%/year, comparable to the 0.5% rate in nondiabetics without known CAD who had preserved systolic function and a normal stress perfusion study.
In the future, CFR may aid in decision making as to whether an individual with stable CAD is best treated by percutaneous coronary intervention, surgical revascularization, or guideline-directed medical therapy. For example, if CFR indicates the presence of an isolated severe focal stenosis, and this is confirmed by angiography and FFR, PCI may be the best option, while diffuse disease as demonstrated by CFR may be better treated surgically or using optimal medical therapy. But this needs to be established in prospective clinical trials, added Dr. Di Carli.
He reported having no financial conflicts regarding his presentation.
SNOWMASS, COLO. – Mounting evidence attests to the value of noninvasive measurement of coronary flow reserve as a means of classifying cardiovascular risk in patients with stable coronary artery disease (CAD) more accurately than is possible via coronary angiography or measurement of fractional flow reserve, Marcelo F. Di Carli, MD, reported at the Annual Cardiovascular Conference at Snowmass.
“We use CFR [coronary flow reserve] as a way to exclude coronary disease. It’s a good practical measure of multivessel ischemic CAD. When the CFR is normal, you can with high confidence exclude the possibility of high-risk CAD,” according to Dr. Di Carli, executive director of the cardiovascular imaging program and chief of the division of nuclear medicine and molecular imaging at Brigham and Women’s Hospital, Boston.
Bruce Jancin/Frontline Medical News
Dr. Marcello di Carli
When the CFR is markedly low, however, a patient with stable CAD is at high risk for cardiovascular events, even if angiography shows no clinically significant stenosis, added Dr. Di Carli, who is also professor of radiology and medicine at Harvard Medical School, Boston.
Most recently, he and his coinvestigators utilized CFR to provide new insight into the paradox that women have a higher cardiovascular disease death rate than men, even though their prevalence of obstructive CAD is lower.
Their NIH-sponsored study included 329 consecutive patients with a left ventricular ejection fraction greater than 40% – 43% of them women – who underwent coronary angiography several days after noninvasive assessment of CFR via myocardial perfusion positron emission tomography. The women had a lower burden of angiographic CAD and a lower pretest clinical risk score than the men. Nevertheless, during a median of 3 years of follow-up, the women had an adjusted twofold greater risk of the composite endpoint of cardiovascular death, nonfatal MI, or heart failure.
This excess cardiovascular risk in women was independently associated with a very low CFR, defined as less than 1.6. Dr. Di Carli and his coinvestigators calculated that this impaired CFR mediated 40% of the excess risk in women. Thus, a low CFR represents a novel hidden biologic risk for ischemic heart disease (Circulation. 2017 Feb 7;135[6]:566-77).
CFR is defined as the ratio of absolute coronary flow or myocardial perfusion between drug-induced hyperemia and rest. It can be quantified noninvasively using positron emission tomography or MRI.
CFR integrates into a single measure the three components of CAD: the focal stenosis, the diffuse atherosclerotic plaque typically present to a varying degree throughout a target vessel, and microvascular dysfunction.
CFR is a measure of coronary physiology, as is invasive fractional flow reserve (FFR). However, FFR measures only the severity of stenosis and extent of diffuse disease; it doesn’t assess microvascular dysfunction. This is a limitation because it means FFR can give false-negative readings in patients without significant obstructive coronary disease who have severe microvascular dysfunction.
As for angiography, Dr. Di Carli continued, it’s now evident that this purely anatomic assessment is of limited value as a marker of clinical risk and is inadequate to guide management decisions in the setting of stable CAD. After all, angiographically guided revascularization has not reduced cardiovascular events in clinical trials comparing it with optimal medical therapy, as in the COURAGE and BARI-2D trials.
“It’s clear that there’s been a paradigm shift in how we manage patients with stable CAD. For many years the coronary angiogram was the cornerstone of what we did: how we understand the symptoms, the patient’s risk, and ultimately how we proceed with treatment. But there is no benefit in basing treatment solely on what the lesions look like anatomically. That’s why we’ve turned to functional testing of coronary physiology,” he said.
CFR has opened a window on the importance of microvascular dysfunction, which is present in about half of patients with stable CAD and has been shown to predict cardiovascular risk independent of whether or not severe obstructive disease is present.
In an earlier study, Dr. Di Carli and coworkers demonstrated that quantification of CFR enhances stratification for risk of cardiac death among diabetes patients (Circulation. 2012 Oct 9;126[15]:1858-68). The study included 2,783 patients, of whom 1,172 were diabetic, who underwent measurement of CFR and were subsequently followed for a median of 1.4 years, during which 137 cardiac deaths occurred.
Diabetes patients without known CAD who had a low CFR had a high cardiac death rate of 2.8%/year, similar to the 2.0%/year rate in nondiabetic patients with a history of acute MI or revascularization. On the other hand, diabetes patients with a normal CFR and without known CAD had a cardiac mortality rate of only 0.3%/year, comparable to the 0.5% rate in nondiabetics without known CAD who had preserved systolic function and a normal stress perfusion study.
In the future, CFR may aid in decision making as to whether an individual with stable CAD is best treated by percutaneous coronary intervention, surgical revascularization, or guideline-directed medical therapy. For example, if CFR indicates the presence of an isolated severe focal stenosis, and this is confirmed by angiography and FFR, PCI may be the best option, while diffuse disease as demonstrated by CFR may be better treated surgically or using optimal medical therapy. But this needs to be established in prospective clinical trials, added Dr. Di Carli.
He reported having no financial conflicts regarding his presentation.
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
References
Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
Salvatore Mangione, MD Associate Professor of Medicine, Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, PA
Address: Salvatore Mangione, MD, Sidney Kimmel Medical College of Thomas Jefferson University, Hamilton Building, 1001 Locust Street, Suite 309c, Philadelphia, PA 19107; [email protected]
Salvatore Mangione, MD Associate Professor of Medicine, Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, PA
Address: Salvatore Mangione, MD, Sidney Kimmel Medical College of Thomas Jefferson University, Hamilton Building, 1001 Locust Street, Suite 309c, Philadelphia, PA 19107; [email protected]
Author and Disclosure Information
Salvatore Mangione, MD Associate Professor of Medicine, Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, PA
Address: Salvatore Mangione, MD, Sidney Kimmel Medical College of Thomas Jefferson University, Hamilton Building, 1001 Locust Street, Suite 309c, Philadelphia, PA 19107; [email protected]
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
“... with the rapid extension of laboratory tests of greater accuracy, there is a tendency for some clinicians and hence for some students in reaching a diagnosis to rely more on laboratory reports and less on the history of the illness, the examination and behavior of the patient and clinical judgment. While in many cases laboratory findings are invaluable for reaching correct conclusions, the student should never be allowed to forget that it takes a man, not a machine, to understand a man.”
—Raymond B. Allen, MD, PhD, 19461
From Hippocrates onward, accurate diagnosis has always been the prerequisite for prognosis and treatment. Physicians typically diagnosed through astute interviewing, deductive reasoning, and skillful use of observation and touch. Then, in the past 250 years they added 2 more tools to their diagnostic skill set: percussion and auscultation, the dual foundation of bedside assessment. Intriguingly, both these skills were first envisioned by multifaceted minds: percussion by Leopold Auenbrugger, an Austrian music-lover who even wrote librettos for operas; and stethoscopy by René Laennec, a Breton flutist, poet, and dancer—not exactly the kind of doctors we tend to produce today.
Still, the point of this preamble is not to say that eclecticism may help creativity (it does), but to remind ourselves that it has only been for a century or so that physicians have been able to rely on laboratory and radiologic studies. In fact, the now ubiquitous and almost obligatory imaging tests (computed tomography, magnetic resonance imaging, positron-emission tomography, and ultrasonography) have been available to practitioners for only threescore years or less. Yet tests have become so dominant in our culture that it is hard to imagine a time when physicians could count only on their wit and senses.
CLINICAL SKILLS ARE STILL RELEVANT
Ironically, many studies tell us that history and bedside examination can still deliver most diagnoses.2,3 In fact, clinical skills can solve even the most perplexing dilemmas. In an automated analysis of the clinicopathologic conference cases presented in the New England Journal of Medicine,4 history and physical examination still yielded a correct diagnosis in 64% of those very challenging patients.
Bedside examination may be especially important in the hospital. In a study of inpatients,5 physical examination detected crucial findings in one-fourth of the cases and prompted management changes in many others. As the authors concluded, sick patients need careful examination, the more skilled the better.
Unfortunately, errors in physical examination are common. In a recent review of 208 cases, 63% of oversights were due to failure to perform an examination, while 25% were either missed or misinterpreted findings.6 These errors interfered with diagnosis in three-fourths of the cases, and with treatment in half.
Which brings us to the interesting observation by Kondo et al,7 who in this issue of the Journal report how the lowly physical examination proved more helpful than expensive magnetic resonance imaging in evaluating a perplexing case of refractory shoulder pain.
This is not an isolated instance. To get back to Laennec, whose stethoscope just turned 200, auscultation too can help the 21st-century physician. For example, posturally induced crackles, a recently discovered phenomenon, are the third-best predictor of outcome following myocardial infarction, immediately after the number of diseased vessels and pulmonary capillary wedge pressure.8
The time-honored art of observation can also yield new and important clues. From the earlobe crease of Dr. Frank, to the elfin face of Dr. Williams, there are lots of diseases out there waiting for our name—if only we could see them. As William Osler put it, “The whole art of medicine is in observation.”9
TECHNOLOGY: MASTER OR SERVANT?
But how can residents truly “observe” when they have to spend 40% of their time looking at computer screens and only 12% looking at people?10 To quote Osler again, “To educate the eye to see, the ear to hear, and the finger to feel takes time.”9 Yet time in medicine is at a premium. In a large national survey, the average ambulatory care visit to a general practitioner lasted 16 minutes,11 which makes it difficult to use inexpensive but time-consuming maneuvers. Detection of posturally induced crackles, for example, may require as much as 9 minutes, and a thorough breast examination up to 10.12 On the other hand, ordering tests costs little time to the physician but a huge sum to patients and society. Paradoxically, “tests” may be quite profitable for the medical-industrial complex. Hence the erosion of clinical skills.
Overreliance on diagnostic technology is particularly concerning when the cost of medicine has skyrocketed. The United States now spends $3.2 trillion a year for healthcare, and much of this money goes into technology.
In fact, high-tech might hurt us even more than in the pocket. It is a sad fact of modern medicine that when unguided by clinical skills, technology can take us down a rabbit hole, wherein tests beget tests, and where at the end there is usually a surgeon, often a lawyer, and sometimes even an undertaker. The literature is full of such cases, to the point that the risk of unnecessary tests has spawned a charming new acronym: VOMIT (victims of modern imaging technology).13
I’m not suggesting that we discard appropriate laboratory and radiologic testing. To the contrary. Yet contributions like those of Kondo et al remind us that even in today’s medicine, the bedside remains not only the royal road to diagnosis, but also the best filter for a more judicious and cost-effective use of technology.
That filter starts with history-taking (“Listen to the patient” said Osler, “he is telling you the diagnosis.”),9 and continues with the physical examination. In fact, the history typically guides the physical examination. Hence, when the patient’s symptoms point away from a particular organ, the examination of that organ may be reduced to a minimum. For instance, in neurologic patients whose history made certain findings unlikely, a Canadian group was able to cut in half the number of core items of their neurologic examination.14
Yet when the history flags a system, the clinician needs to go deeper into the examination. It’s very much what we do with laboratory tests, moving from screening tests to more advanced inquiries as we tailor our diagnostic studies to the patient’s presentation. For that we need validated maneuvers. Recent efforts in this direction have turned the art of physical examination into a science.15
Lastly, patients expect to be examined, and in fact they resent when this doesn’t happen.16 Lewis Thomas called touching our “real professional secret” and “the oldest and most effective art of doctors.”17 It may even have therapeutic value.
TEACHING BEDSIDE DIAGNOSIS
So, if bedside diagnosis is important, what can we do to rekindle it? Probably anything but continue in the old ways. Studies have consistently shown that auscultation does not improve with years of training, and that in fact attending physicians may be no more proficient than third-year medical students.18 Other areas of the examination have shown similarly depressing trends,19 thus suggesting that the traditional apprenticeship mode of learning from both faculty and senior trainees may not be helpful. In fact, it may be akin to Bruegel the Elder’s painting of the blind leading the blind, and all ending up in a ditch.
Advanced physical diagnosis courses have thus been advocated, and indeed implemented at many institutions, but usually as electives. Faculty development programs have also been recommended. Still, these interventions may not suffice.
Cutting the cord to technology by serving in a developing country
My hunch is that the rekindling of physical diagnosis may require extreme measures, like putting ourselves in a zero-tech, zero-tests environment. Years ago, I had that kind of cold-turkey experience when I spent a month in a remote Nepali clinic with neither electricity nor running water—and, of course, no cell phone and no Internet. In fact, my only tools were a translator, a stethoscope, and my brain and senses. It was both terrifying and instructive, very much like the time my uncle tried to teach me how to swim by suddenly throwing me into the Mediterranean.
Maybe we should offer that kind of “immersion” to our students. A senior rotation in a technology-depleted country might do a lot of good for a young medical mind. For one, it could remind students that physicians are not only the “natural attorneys of the poor,” as Virchow famously put it,20 but also the ultimate citizens of the world. To quote Dr. Osler again, “Distinctions of race, nationality, color, and creed are unknown within the portals of the temple of Æsculapius.”21 Such an experience might also foster empathy and tolerance for ambiguity, 2 other traits whose absence we lament in today’s medicine. More importantly, if preceded by an advanced physical diagnosis course, a rotation in a developing country could work miracles for honing bedside skills, especially if the students are accompanied by a faculty member who can be both inspiring and gifted in the art and science of bedside diagnosis.
Ultimately, this experience could remind our young that the art of medicine is much harder to acquire than the science, and that medicine is indeed a calling and not a trade. Osler said it too, and these are indeed provocative thoughts, but short of provocations and out-of-the-box ideas, the tail will continue to wag the dog. And in the end it will cost us more than money. It will cost us the art of medicine.
References
Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
References
Allen RB. Medical Education and the Changing Order: Studies of the New York Academy of Medicine, Committee on Medicine and the Changing Order. New York, NY: Commonwealth Fund, 1946.
Peterson MC, Holbrook JH, Von Hales D, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. West J Med 1992; 156:163–165.
Roshan M, Rao AP. A study on relative contributions of the history, physical examination and investigations in making medical diagnosis. J Assoc Physicians India 2000; 48:771–775.
Wagner MM, Bankowitz RA, McNeil M, Challinor SM, Janosky JE, Miller RA. The diagnostic importance of the history and physical examination as determined by the use of a medical decision support system. Proc Am Med Inform Assoc 1989: 139–144.
Reilly BM. Physical examination in the care of medical inpatients: an observational study. Lancet 2003; 362:1100–1105.
Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JPA. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.e3.
Kondo T, Ohira Y, Uehara T, Noda K, Ikusaka M. An unexpected cause of shoulder pain. Cleve Clin J Med 2017; 84:276–277.
Deguchi F, Hirakawa S, Gotoh K, Yagi Y, Ohshima S. Prognostic significance of posturally induced crackles. Long-term follow-up of patients after recovery from acute myocardial infarction. Chest 1993; 103:1457–1462.
Silverman ME, Murrary TJ, Bryan CS, eds. The Quotable Osler. Philadelphia, PA: Am Coll of Physicians; 2008.
Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med 2013; 28:1042–1047.
Blumenthal D, Causino N, Chang YC, et al. The duration of ambulatory visits to physicians. J Fam Pract 1999; 48:264–271.
Barton MB, Harris R, Fletcher SW. The rational clinical examination. Does this patient have breast cancer? The screening clinical breast examination: should it be done? How? JAMA 1999; 282:1270–1280.
Hayward R. VOMIT (victims of modern imaging technology)—an acronym for our times. BMJ 2003; 326:1273.
Moore FG, Chalk C. The essential neurologic examination: what should medical students be taught? Neurology 2009; 72:2020–2023.
Simel DL, Rennie D. The rational clinical examination: evidence-based clinical diagnosis. JAMA & Archives Journals. New York, NY: McGraw-Hill Education/Medical; 2009.
Kravitz RL, Callahan EJ. Patients’ perceptions of omitted examinations and tests: a qualitative analysis. J Gen Intern Med 2000; 15:38–45.
Thomas L. The Youngest Science: Notes of a Medicine Watcher. New York, NY: Viking Press, 1983.
Vukanovic-Criley JM, Criley S, Warde CM, et al. Competency in cardiac examination skills in medical students, trainees, physicians, and faculty: a multicenter study. Arch Intern Med 2006; 166:610–616.
Paauw DS, Wenrich MD, Curtis JR, Carline JD, Ramsey PG. Ability of primary care physicians to recognize physical findings associated with HIV infection. JAMA 1995; 274:1380–1382.
Brown TM, Fee E. Rudolf Carl Virchow: medical scientist, social reformer, role model. Am J Public Health 2006; 96:2104–2105.
Osler W. British medicine in Greater Britain. The Medical News 1897; 71:293–298.
Now that we can order MRI studies on a break from rounds walking to Starbucks, utilize portable ultrasounds to direct IV line placement, and use dual-energy CT to detect a gout attack that has not yet occurred, it seems like a romantic anachronism to extol the ongoing virtues of the seemingly lost art of the physical examination. Back “in the day,” the giants of medicine roamed the halls with their natural instruments of palpation and percussion and their skills in observation and auscultation. They were giants because they stood out then, just as skilled diagnosticians stand out today using an upgraded set of tools. Some physicians a few decades ago were able to recognize, describe, and diagnose late-stage endocarditis with a stethoscope, a magnifying glass, and an ophthalmoscope. The giants of today recognize the patient with endocarditis and document its presence using transesophageal echocardiography before the peripheral eponymous stigmata of Janeway and Osler appear or the blood cultures turn positive. The physical examination, history, diagnostic reasoning, and clinical technology are all essential for a blend that provides efficient and effective medical care. The blending is the challenge.
Clinicians are not created equal. We learn and prioritize our skills in different ways. But if we are not taught to value and trust the physical examination, if we don’t have the opportunity to see it influence patient management in positive ways, we may eschew it and instead indiscriminately use easily available laboratory and imaging tests—a more expensive and often misleading strategic approach. Today while in clinic, I saw a 54-year-old woman for evaluation of possible lupus who had arthritis of the hands and a high positive antinuclear antibody titer, but negative or normal results on other, previously ordered tests, including anti-DNA, rheumatoid factor, anti-cyclic citrullinated peptide, hepatitis C studies, complement levels, and another half-dozen immune serologic tests. On examination, she had typical nodular osteoarthritis of the proximal and distal interphalangeal joints of her hand with squaring of her thumbs. The antinuclear antibody was most likely associated with her previously diagnosed autoimmune thyroid disease.
In an editorial in this issue of the Journal, Dr. Salvatore Mangione, the author of a book on physical diagnosis,1 cites a recent study indicating that the most common recognized diagnostic error related to the physical examination is that the appropriate examination isn’t done.2 I would add to that my concerns over the new common custom of cutting and pasting the findings from earlier physical examinations into later progress notes in the electronic record. So much for the value of being able to recognize “changing murmurs” when diagnosing infectious endocarditis.
The apparent efficiency (reflected in length of stay) and availability of technology, as well as a lack of physician skill and time, are often cited as reasons for the demise of the physical examination. Yet this does not need to be the case. If I had trained with portable ultrasonography readily available to confirm or refute my impressions, my skills at detecting low-grade synovitis would surely be better than they are. With a gold standard at hand, which may be technology or at times a skilled mentor, our examinations can be refined if we want them to be.
But the issue of limited physician time must be addressed. Efficiency is a critical concept in preserving how we practice and perform the physical examination. When we know what we are looking for, we are more likely to find it if it is present, or to have confidence that it is not present. I am far more likely to recognize a loud pulmonic second heart sound if I suspect that the dyspneic patient I am examining has pulmonary hypertension associated with her scleroderma than if I am doing a perfunctory cardiac auscultation in a patient admitted with cellulitis. Appropriate focus provides power to the directed physical examination. If I am looking for the cause of unexplained fevers, I will do a purposeful axillary and epitrochlear lymph node examination. I am not mindlessly probing the flesh.
Nishigori and colleagues have written of the “hypothesis-driven” physical examination.3 Busy clinicians, they say, don’t have time to perform a head-to-toe, by-the-book physical examination. Instead, we should, by a dynamic process, formulate a differential diagnosis from the history and other initial information, and then perform the directed physical examination in earnest, looking for evidence to support or refute our diagnostic hypothesis—and thus redirect it. Plus, in a nice break from electronic charting, we can actually explain our thought processes to the patient as we perform the examination.
This approach makes sense to me as both intellectually satisfying and clinically efficient. And then we can consider which lab tests and technologic gadgetry we should order, while walking to get the café latte we ordered with our cell phone app.
New technology can support and not necessarily replace old habits.
References
Mangione S. Physical Diagnosis Secrets, 2nd ed. Philadelphia: Mosby/Elsevier, 2008.
Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JP. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.
Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Medical Teacher 2011; 33:410–417.
Now that we can order MRI studies on a break from rounds walking to Starbucks, utilize portable ultrasounds to direct IV line placement, and use dual-energy CT to detect a gout attack that has not yet occurred, it seems like a romantic anachronism to extol the ongoing virtues of the seemingly lost art of the physical examination. Back “in the day,” the giants of medicine roamed the halls with their natural instruments of palpation and percussion and their skills in observation and auscultation. They were giants because they stood out then, just as skilled diagnosticians stand out today using an upgraded set of tools. Some physicians a few decades ago were able to recognize, describe, and diagnose late-stage endocarditis with a stethoscope, a magnifying glass, and an ophthalmoscope. The giants of today recognize the patient with endocarditis and document its presence using transesophageal echocardiography before the peripheral eponymous stigmata of Janeway and Osler appear or the blood cultures turn positive. The physical examination, history, diagnostic reasoning, and clinical technology are all essential for a blend that provides efficient and effective medical care. The blending is the challenge.
Clinicians are not created equal. We learn and prioritize our skills in different ways. But if we are not taught to value and trust the physical examination, if we don’t have the opportunity to see it influence patient management in positive ways, we may eschew it and instead indiscriminately use easily available laboratory and imaging tests—a more expensive and often misleading strategic approach. Today while in clinic, I saw a 54-year-old woman for evaluation of possible lupus who had arthritis of the hands and a high positive antinuclear antibody titer, but negative or normal results on other, previously ordered tests, including anti-DNA, rheumatoid factor, anti-cyclic citrullinated peptide, hepatitis C studies, complement levels, and another half-dozen immune serologic tests. On examination, she had typical nodular osteoarthritis of the proximal and distal interphalangeal joints of her hand with squaring of her thumbs. The antinuclear antibody was most likely associated with her previously diagnosed autoimmune thyroid disease.
In an editorial in this issue of the Journal, Dr. Salvatore Mangione, the author of a book on physical diagnosis,1 cites a recent study indicating that the most common recognized diagnostic error related to the physical examination is that the appropriate examination isn’t done.2 I would add to that my concerns over the new common custom of cutting and pasting the findings from earlier physical examinations into later progress notes in the electronic record. So much for the value of being able to recognize “changing murmurs” when diagnosing infectious endocarditis.
The apparent efficiency (reflected in length of stay) and availability of technology, as well as a lack of physician skill and time, are often cited as reasons for the demise of the physical examination. Yet this does not need to be the case. If I had trained with portable ultrasonography readily available to confirm or refute my impressions, my skills at detecting low-grade synovitis would surely be better than they are. With a gold standard at hand, which may be technology or at times a skilled mentor, our examinations can be refined if we want them to be.
But the issue of limited physician time must be addressed. Efficiency is a critical concept in preserving how we practice and perform the physical examination. When we know what we are looking for, we are more likely to find it if it is present, or to have confidence that it is not present. I am far more likely to recognize a loud pulmonic second heart sound if I suspect that the dyspneic patient I am examining has pulmonary hypertension associated with her scleroderma than if I am doing a perfunctory cardiac auscultation in a patient admitted with cellulitis. Appropriate focus provides power to the directed physical examination. If I am looking for the cause of unexplained fevers, I will do a purposeful axillary and epitrochlear lymph node examination. I am not mindlessly probing the flesh.
Nishigori and colleagues have written of the “hypothesis-driven” physical examination.3 Busy clinicians, they say, don’t have time to perform a head-to-toe, by-the-book physical examination. Instead, we should, by a dynamic process, formulate a differential diagnosis from the history and other initial information, and then perform the directed physical examination in earnest, looking for evidence to support or refute our diagnostic hypothesis—and thus redirect it. Plus, in a nice break from electronic charting, we can actually explain our thought processes to the patient as we perform the examination.
This approach makes sense to me as both intellectually satisfying and clinically efficient. And then we can consider which lab tests and technologic gadgetry we should order, while walking to get the café latte we ordered with our cell phone app.
New technology can support and not necessarily replace old habits.
Now that we can order MRI studies on a break from rounds walking to Starbucks, utilize portable ultrasounds to direct IV line placement, and use dual-energy CT to detect a gout attack that has not yet occurred, it seems like a romantic anachronism to extol the ongoing virtues of the seemingly lost art of the physical examination. Back “in the day,” the giants of medicine roamed the halls with their natural instruments of palpation and percussion and their skills in observation and auscultation. They were giants because they stood out then, just as skilled diagnosticians stand out today using an upgraded set of tools. Some physicians a few decades ago were able to recognize, describe, and diagnose late-stage endocarditis with a stethoscope, a magnifying glass, and an ophthalmoscope. The giants of today recognize the patient with endocarditis and document its presence using transesophageal echocardiography before the peripheral eponymous stigmata of Janeway and Osler appear or the blood cultures turn positive. The physical examination, history, diagnostic reasoning, and clinical technology are all essential for a blend that provides efficient and effective medical care. The blending is the challenge.
Clinicians are not created equal. We learn and prioritize our skills in different ways. But if we are not taught to value and trust the physical examination, if we don’t have the opportunity to see it influence patient management in positive ways, we may eschew it and instead indiscriminately use easily available laboratory and imaging tests—a more expensive and often misleading strategic approach. Today while in clinic, I saw a 54-year-old woman for evaluation of possible lupus who had arthritis of the hands and a high positive antinuclear antibody titer, but negative or normal results on other, previously ordered tests, including anti-DNA, rheumatoid factor, anti-cyclic citrullinated peptide, hepatitis C studies, complement levels, and another half-dozen immune serologic tests. On examination, she had typical nodular osteoarthritis of the proximal and distal interphalangeal joints of her hand with squaring of her thumbs. The antinuclear antibody was most likely associated with her previously diagnosed autoimmune thyroid disease.
In an editorial in this issue of the Journal, Dr. Salvatore Mangione, the author of a book on physical diagnosis,1 cites a recent study indicating that the most common recognized diagnostic error related to the physical examination is that the appropriate examination isn’t done.2 I would add to that my concerns over the new common custom of cutting and pasting the findings from earlier physical examinations into later progress notes in the electronic record. So much for the value of being able to recognize “changing murmurs” when diagnosing infectious endocarditis.
The apparent efficiency (reflected in length of stay) and availability of technology, as well as a lack of physician skill and time, are often cited as reasons for the demise of the physical examination. Yet this does not need to be the case. If I had trained with portable ultrasonography readily available to confirm or refute my impressions, my skills at detecting low-grade synovitis would surely be better than they are. With a gold standard at hand, which may be technology or at times a skilled mentor, our examinations can be refined if we want them to be.
But the issue of limited physician time must be addressed. Efficiency is a critical concept in preserving how we practice and perform the physical examination. When we know what we are looking for, we are more likely to find it if it is present, or to have confidence that it is not present. I am far more likely to recognize a loud pulmonic second heart sound if I suspect that the dyspneic patient I am examining has pulmonary hypertension associated with her scleroderma than if I am doing a perfunctory cardiac auscultation in a patient admitted with cellulitis. Appropriate focus provides power to the directed physical examination. If I am looking for the cause of unexplained fevers, I will do a purposeful axillary and epitrochlear lymph node examination. I am not mindlessly probing the flesh.
Nishigori and colleagues have written of the “hypothesis-driven” physical examination.3 Busy clinicians, they say, don’t have time to perform a head-to-toe, by-the-book physical examination. Instead, we should, by a dynamic process, formulate a differential diagnosis from the history and other initial information, and then perform the directed physical examination in earnest, looking for evidence to support or refute our diagnostic hypothesis—and thus redirect it. Plus, in a nice break from electronic charting, we can actually explain our thought processes to the patient as we perform the examination.
This approach makes sense to me as both intellectually satisfying and clinically efficient. And then we can consider which lab tests and technologic gadgetry we should order, while walking to get the café latte we ordered with our cell phone app.
New technology can support and not necessarily replace old habits.
References
Mangione S. Physical Diagnosis Secrets, 2nd ed. Philadelphia: Mosby/Elsevier, 2008.
Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JP. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.
Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Medical Teacher 2011; 33:410–417.
References
Mangione S. Physical Diagnosis Secrets, 2nd ed. Philadelphia: Mosby/Elsevier, 2008.
Verghese A, Charlton B, Kassirer JP, Ramsey M, Ioannidis JP. Inadequacies of physical examination as a cause of medical errors and adverse events: a collection of vignettes. Am J Med 2015; 128:1322–1324.
Nishigori H, Masuda K, Kikukawa M, et al. A model teaching session for the hypothesis-driven physical examination. Medical Teacher 2011; 33:410–417.
A 43-year-old woman presented to the clinic complaining of bilateral ankle joint pain for 2 months. She denied a history of fever, weight loss, addictions, cough, or trauma. On physical examinatio, she had swelling of the ankle and wrist joints and digital clubbing (Figure 1). Active movement of the ankles and wrists was restricted due to pain. The examination was otherwise unremarkable.
Figure 1. Digital clubbing.
Radiography of both ankles showed a lamellar type periosteal reaction suggestive of periostitis (Figure 2). Computed tomography of the chest revealed a spiculated mass over the right lower lobe. Biopsy study of the mass was positive for squamous cell carcinoma. She was referred to the oncology center for further management.
FEATURES OF HYPERTROPHIC OSTEOARTHROPATHY
Figure 2. Radiography of the ankles showed a lamellar type of periosteal reaction (arrows).
Digital clubbing is one of the oldest signs in clinical medicine. It is characterized by bulbous enlargement of the terminal segments of the fingers and toes due to proliferation of subungual connective tissue. It usually appears as a painless finger deformity and is clinically appreciated as a loss of the normal angle between the nail bed and proximal nail fold.
Hypertrophic osteoarthropathy is a symptomatic form of clubbing associated with proliferative periostosis of the distal end of long tubular bones, commonly those adjacent to the wrist and ankle joints.1 The laminated appearance of these bones on radiography is due to the excess connective tissue secondary to new osteoid material deposited under the periosteum.
There is evidence to suggest that clubbing and hypertrophic osteoarthropathy represent different stages of the same disease process.2 In most cases, finger deformity is the first manifestation; as the disease progresses, periostosis becomes evident.
Hypertrophic osteoarthropathy can be classified as primary or secondary. The primary form, also known as primary pachydermoperiostosis, is rare and constitutes only 3% of all cases.3 The exact cause is not yet known; it occurs as a hereditary disease with autosomal dominant inheritance with variable penetrance. Congenital clubbing without periostosis is of no clinical significance.4
CONDITIONS ASSOCIATED WITH CLUBBING
Primary bronchogenic carcinoma is the most common cause of clubbing and hypertrophic osteoarthropathy. In one retrospective series, 4.5% of patients with lung cancer had radiologic evidence of hypertrophic osteoarthropathy.5 Other malignancies associated with this condition are mesothelioma, hepatocellular carcinoma, and certain types of gastrointestinal adenocarcinoma.
Other conditions associated with clubbing include:
Cardiovascular disease such as congenital cyanotic heart disease and infective endocarditis
Gastrointestinal conditions such as cirrhosis, primary sclerosing cholangitis, Crohn disease, and ulcerative colitis
Infections such as lung abscess and empyema.
Clubbing is generally bilaterally symmetrical. Asymmetric clubbing is rare and usually indicates impaired regional blood flow due to vascular disease. Unilateral clubbing or hypertrophic osteoarthropathy restricted to 1 upper limb can result from an anomaly of the aortic arch or from a subclavian or brachial artery aneurysm. Clubbing affecting predominantly the lower limbs has been reported in coarctation of aorta and patent ductus arteriosus.6 Rare cases of unidigital clubbing are reported in sarcoidosis.7
The importance of recognizing hypertrophic osteoarthropathy cannot be overemphasized. If any of the manifestations of the syndrome become evident in a previously healthy person, a thorough evaluation for an underlying disease should be done.
Clubbing should be differentiated from pseudoclubbing, which is seen in conditions such as hyperparathyroidism and scleroderma. The central mechanism for nail deformity in pseudoclubbing is acro-osteolysis with the resulting collapse of the subungual soft tissues. The important features differentiating it from true clubbing are preservation of the angle between the nail bed and proximal nail fold and asymmetric finger involvement.8
MANAGEMENT
The management of primary hypertrophic osteoarthropathy focuses on relieving the symptoms of periosteitis. Secondary forms require a detailed evaluation to rule out the underlying disease. In refractory cases, a bone-modifying agent (eg, zoledronic acid),9 octreotide,10 nonsteroidal anti-inflammatory drugs, or vagotomy11 may help.
References
Martínez-Lavín M, Matucci-Cerinic M, Jajic I, Pineda C. Hypertrophic osteoarthropathy: consensus on its definition, classification, assessment and diagnostic criteria. J Rheumatol 1993; 20:1386–1387.
Martínez-Lavín M. Digital clubbing and hypertrophic osteoarthropathy: a unifying hypothesis. J Rheumatol 1987; 14:6–8.
Jajic Z, Jajic I, Nemcic T. Primary hypertrophic osteoarthropathy: clinical, radiologic, and scintigraphic characteristics. Arch Med Res 2001; 32:136–142.
Walker HK, Hall WD, Hurst JW, eds. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990.
Izumi M, Takayama K, Yabuuchi H, Abe K, Nakanishi Y. Incidence of hypertrophic pulmonary osteoarthropathy associated with primary lung cancer. Respirology 2010; 15:809–812.
Anoop TM, George KC. Images in clinical medicine. Differential clubbing and cyanosis. N Engl J Med 2011; 364:666.
Singh A. Unidigital clubbing. Am J Med 2008; 121:e15.
Santiago MB, Lima I, Feitosa AC, Braz Ade S, Miranda LG. Pseudoclubbing: is it different from clubbing? Semin Arthritis Rheum 2009; 38:452–457.
Tachibana I, Gehi D, Rubin CD. Treatment of hypertrophic osteoarthropathy with underlying pulmonary adenocarcinoma using zoledronic acid. J Clin Rheumatol 2015; 21:333–334.
Birch E, Jenkins D, Noble S. Treatment of painful hypertrophic osteoarthropathy associated with non-small cell lung cancer with octreotide: a case report and review of the literature. BMJ Support Palliat Care 2011; 1:189–192.
Nguyen S, Hojjati M. Review of current therapies for secondary hypertrophic pulmonary osteoarthropathy. Clin Rheumatol 2011; 30:7–13.
A 43-year-old woman presented to the clinic complaining of bilateral ankle joint pain for 2 months. She denied a history of fever, weight loss, addictions, cough, or trauma. On physical examinatio, she had swelling of the ankle and wrist joints and digital clubbing (Figure 1). Active movement of the ankles and wrists was restricted due to pain. The examination was otherwise unremarkable.
Figure 1. Digital clubbing.
Radiography of both ankles showed a lamellar type periosteal reaction suggestive of periostitis (Figure 2). Computed tomography of the chest revealed a spiculated mass over the right lower lobe. Biopsy study of the mass was positive for squamous cell carcinoma. She was referred to the oncology center for further management.
FEATURES OF HYPERTROPHIC OSTEOARTHROPATHY
Figure 2. Radiography of the ankles showed a lamellar type of periosteal reaction (arrows).
Digital clubbing is one of the oldest signs in clinical medicine. It is characterized by bulbous enlargement of the terminal segments of the fingers and toes due to proliferation of subungual connective tissue. It usually appears as a painless finger deformity and is clinically appreciated as a loss of the normal angle between the nail bed and proximal nail fold.
Hypertrophic osteoarthropathy is a symptomatic form of clubbing associated with proliferative periostosis of the distal end of long tubular bones, commonly those adjacent to the wrist and ankle joints.1 The laminated appearance of these bones on radiography is due to the excess connective tissue secondary to new osteoid material deposited under the periosteum.
There is evidence to suggest that clubbing and hypertrophic osteoarthropathy represent different stages of the same disease process.2 In most cases, finger deformity is the first manifestation; as the disease progresses, periostosis becomes evident.
Hypertrophic osteoarthropathy can be classified as primary or secondary. The primary form, also known as primary pachydermoperiostosis, is rare and constitutes only 3% of all cases.3 The exact cause is not yet known; it occurs as a hereditary disease with autosomal dominant inheritance with variable penetrance. Congenital clubbing without periostosis is of no clinical significance.4
CONDITIONS ASSOCIATED WITH CLUBBING
Primary bronchogenic carcinoma is the most common cause of clubbing and hypertrophic osteoarthropathy. In one retrospective series, 4.5% of patients with lung cancer had radiologic evidence of hypertrophic osteoarthropathy.5 Other malignancies associated with this condition are mesothelioma, hepatocellular carcinoma, and certain types of gastrointestinal adenocarcinoma.
Other conditions associated with clubbing include:
Cardiovascular disease such as congenital cyanotic heart disease and infective endocarditis
Gastrointestinal conditions such as cirrhosis, primary sclerosing cholangitis, Crohn disease, and ulcerative colitis
Infections such as lung abscess and empyema.
Clubbing is generally bilaterally symmetrical. Asymmetric clubbing is rare and usually indicates impaired regional blood flow due to vascular disease. Unilateral clubbing or hypertrophic osteoarthropathy restricted to 1 upper limb can result from an anomaly of the aortic arch or from a subclavian or brachial artery aneurysm. Clubbing affecting predominantly the lower limbs has been reported in coarctation of aorta and patent ductus arteriosus.6 Rare cases of unidigital clubbing are reported in sarcoidosis.7
The importance of recognizing hypertrophic osteoarthropathy cannot be overemphasized. If any of the manifestations of the syndrome become evident in a previously healthy person, a thorough evaluation for an underlying disease should be done.
Clubbing should be differentiated from pseudoclubbing, which is seen in conditions such as hyperparathyroidism and scleroderma. The central mechanism for nail deformity in pseudoclubbing is acro-osteolysis with the resulting collapse of the subungual soft tissues. The important features differentiating it from true clubbing are preservation of the angle between the nail bed and proximal nail fold and asymmetric finger involvement.8
MANAGEMENT
The management of primary hypertrophic osteoarthropathy focuses on relieving the symptoms of periosteitis. Secondary forms require a detailed evaluation to rule out the underlying disease. In refractory cases, a bone-modifying agent (eg, zoledronic acid),9 octreotide,10 nonsteroidal anti-inflammatory drugs, or vagotomy11 may help.
A 43-year-old woman presented to the clinic complaining of bilateral ankle joint pain for 2 months. She denied a history of fever, weight loss, addictions, cough, or trauma. On physical examinatio, she had swelling of the ankle and wrist joints and digital clubbing (Figure 1). Active movement of the ankles and wrists was restricted due to pain. The examination was otherwise unremarkable.
Figure 1. Digital clubbing.
Radiography of both ankles showed a lamellar type periosteal reaction suggestive of periostitis (Figure 2). Computed tomography of the chest revealed a spiculated mass over the right lower lobe. Biopsy study of the mass was positive for squamous cell carcinoma. She was referred to the oncology center for further management.
FEATURES OF HYPERTROPHIC OSTEOARTHROPATHY
Figure 2. Radiography of the ankles showed a lamellar type of periosteal reaction (arrows).
Digital clubbing is one of the oldest signs in clinical medicine. It is characterized by bulbous enlargement of the terminal segments of the fingers and toes due to proliferation of subungual connective tissue. It usually appears as a painless finger deformity and is clinically appreciated as a loss of the normal angle between the nail bed and proximal nail fold.
Hypertrophic osteoarthropathy is a symptomatic form of clubbing associated with proliferative periostosis of the distal end of long tubular bones, commonly those adjacent to the wrist and ankle joints.1 The laminated appearance of these bones on radiography is due to the excess connective tissue secondary to new osteoid material deposited under the periosteum.
There is evidence to suggest that clubbing and hypertrophic osteoarthropathy represent different stages of the same disease process.2 In most cases, finger deformity is the first manifestation; as the disease progresses, periostosis becomes evident.
Hypertrophic osteoarthropathy can be classified as primary or secondary. The primary form, also known as primary pachydermoperiostosis, is rare and constitutes only 3% of all cases.3 The exact cause is not yet known; it occurs as a hereditary disease with autosomal dominant inheritance with variable penetrance. Congenital clubbing without periostosis is of no clinical significance.4
CONDITIONS ASSOCIATED WITH CLUBBING
Primary bronchogenic carcinoma is the most common cause of clubbing and hypertrophic osteoarthropathy. In one retrospective series, 4.5% of patients with lung cancer had radiologic evidence of hypertrophic osteoarthropathy.5 Other malignancies associated with this condition are mesothelioma, hepatocellular carcinoma, and certain types of gastrointestinal adenocarcinoma.
Other conditions associated with clubbing include:
Cardiovascular disease such as congenital cyanotic heart disease and infective endocarditis
Gastrointestinal conditions such as cirrhosis, primary sclerosing cholangitis, Crohn disease, and ulcerative colitis
Infections such as lung abscess and empyema.
Clubbing is generally bilaterally symmetrical. Asymmetric clubbing is rare and usually indicates impaired regional blood flow due to vascular disease. Unilateral clubbing or hypertrophic osteoarthropathy restricted to 1 upper limb can result from an anomaly of the aortic arch or from a subclavian or brachial artery aneurysm. Clubbing affecting predominantly the lower limbs has been reported in coarctation of aorta and patent ductus arteriosus.6 Rare cases of unidigital clubbing are reported in sarcoidosis.7
The importance of recognizing hypertrophic osteoarthropathy cannot be overemphasized. If any of the manifestations of the syndrome become evident in a previously healthy person, a thorough evaluation for an underlying disease should be done.
Clubbing should be differentiated from pseudoclubbing, which is seen in conditions such as hyperparathyroidism and scleroderma. The central mechanism for nail deformity in pseudoclubbing is acro-osteolysis with the resulting collapse of the subungual soft tissues. The important features differentiating it from true clubbing are preservation of the angle between the nail bed and proximal nail fold and asymmetric finger involvement.8
MANAGEMENT
The management of primary hypertrophic osteoarthropathy focuses on relieving the symptoms of periosteitis. Secondary forms require a detailed evaluation to rule out the underlying disease. In refractory cases, a bone-modifying agent (eg, zoledronic acid),9 octreotide,10 nonsteroidal anti-inflammatory drugs, or vagotomy11 may help.
References
Martínez-Lavín M, Matucci-Cerinic M, Jajic I, Pineda C. Hypertrophic osteoarthropathy: consensus on its definition, classification, assessment and diagnostic criteria. J Rheumatol 1993; 20:1386–1387.
Martínez-Lavín M. Digital clubbing and hypertrophic osteoarthropathy: a unifying hypothesis. J Rheumatol 1987; 14:6–8.
Jajic Z, Jajic I, Nemcic T. Primary hypertrophic osteoarthropathy: clinical, radiologic, and scintigraphic characteristics. Arch Med Res 2001; 32:136–142.
Walker HK, Hall WD, Hurst JW, eds. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990.
Izumi M, Takayama K, Yabuuchi H, Abe K, Nakanishi Y. Incidence of hypertrophic pulmonary osteoarthropathy associated with primary lung cancer. Respirology 2010; 15:809–812.
Anoop TM, George KC. Images in clinical medicine. Differential clubbing and cyanosis. N Engl J Med 2011; 364:666.
Singh A. Unidigital clubbing. Am J Med 2008; 121:e15.
Santiago MB, Lima I, Feitosa AC, Braz Ade S, Miranda LG. Pseudoclubbing: is it different from clubbing? Semin Arthritis Rheum 2009; 38:452–457.
Tachibana I, Gehi D, Rubin CD. Treatment of hypertrophic osteoarthropathy with underlying pulmonary adenocarcinoma using zoledronic acid. J Clin Rheumatol 2015; 21:333–334.
Birch E, Jenkins D, Noble S. Treatment of painful hypertrophic osteoarthropathy associated with non-small cell lung cancer with octreotide: a case report and review of the literature. BMJ Support Palliat Care 2011; 1:189–192.
Nguyen S, Hojjati M. Review of current therapies for secondary hypertrophic pulmonary osteoarthropathy. Clin Rheumatol 2011; 30:7–13.
References
Martínez-Lavín M, Matucci-Cerinic M, Jajic I, Pineda C. Hypertrophic osteoarthropathy: consensus on its definition, classification, assessment and diagnostic criteria. J Rheumatol 1993; 20:1386–1387.
Martínez-Lavín M. Digital clubbing and hypertrophic osteoarthropathy: a unifying hypothesis. J Rheumatol 1987; 14:6–8.
Jajic Z, Jajic I, Nemcic T. Primary hypertrophic osteoarthropathy: clinical, radiologic, and scintigraphic characteristics. Arch Med Res 2001; 32:136–142.
Walker HK, Hall WD, Hurst JW, eds. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990.
Izumi M, Takayama K, Yabuuchi H, Abe K, Nakanishi Y. Incidence of hypertrophic pulmonary osteoarthropathy associated with primary lung cancer. Respirology 2010; 15:809–812.
Anoop TM, George KC. Images in clinical medicine. Differential clubbing and cyanosis. N Engl J Med 2011; 364:666.
Singh A. Unidigital clubbing. Am J Med 2008; 121:e15.
Santiago MB, Lima I, Feitosa AC, Braz Ade S, Miranda LG. Pseudoclubbing: is it different from clubbing? Semin Arthritis Rheum 2009; 38:452–457.
Tachibana I, Gehi D, Rubin CD. Treatment of hypertrophic osteoarthropathy with underlying pulmonary adenocarcinoma using zoledronic acid. J Clin Rheumatol 2015; 21:333–334.
Birch E, Jenkins D, Noble S. Treatment of painful hypertrophic osteoarthropathy associated with non-small cell lung cancer with octreotide: a case report and review of the literature. BMJ Support Palliat Care 2011; 1:189–192.
Nguyen S, Hojjati M. Review of current therapies for secondary hypertrophic pulmonary osteoarthropathy. Clin Rheumatol 2011; 30:7–13.
Figure 3.
A 49-year-old man with a history of human immunodeficiency virus infection, untreated hepatitis C, endocarditis, and bilateral total hip arthroplasty (THA) presented to the ED with fever, chills, and a nonproductive cough, which he stated began 2 days prior. The patient was not able to walk due to worsening low back and bilateral leg pain.
Laboratory studies revealed leukocytosis with a left shift. Chest radiographs were negative for pneumonia. A magnetic resonance image (MRI) of the lumbar spine was obtained to evaluate for diskitis osteomyelitis. A radiograph of the pelvis was also obtained to evaluate the patient’s THAs, and a computed tomography scan (CT) of the abdomen and pelvis with contrast was obtained for further evaluation. Representative CT, radiographic, and MRI images are shown at left (Figures 1-3).
What is the suspected diagnosis?
Answer
The MRI of the lumbar spine demonstrated no evidence of diskitis osteomyelitis. However, T2-weighted axial images showed enlarged heterogeneous bilateral psoas muscles with bright signal, indicating the presence of fluid (white arrows, Figure 4).
Figure 4.
Figure 5.
On the pelvic radiographs, both femoral heads appeared off-center within the acetabular cups (red arrows, Figure 5).This eccentric positioning indicated wear of the polyethylene in the THAs that normally occupies the space between the acetabular cup and the femoral head. In addition, focal lucency in the right acetabulum indicated breakdown of the bone, a condition referred to as osteolysis (white asterisk, Figure 5).
An abdominopelvic CT scan with contrast was performed and confirmed the findings of polyethylene wear and osteolysis. The CT scan also demonstrated large bilateral hip joint effusions (white arrows, Figure 6), decompressed along distended bilateral iliopsoas bursae (red asterisks, Figure 6), and communicating with the bilateral psoas muscle collections (red arrows, Figure 6).
Osteolysis With Iliopsoas Bursitis
Bursae are fluid-filled sacs lined by synovial tissue located throughout the body to reduce friction at sites of movement between muscles, bones, and tendons. Bursitis develops when these sacs become inflamed and/or infected and fill with fluid. The iliopsoas bursa lies between the anterior capsule of the hip and the psoas tendon, iliacus tendon, and muscle fibers.1,2 This bursa frequently communicates with the hip joint.3,4 Iliopsoas bursal distension has been reported following THA in the setting of polyethylene wear,5 and aseptic bursitis is a commonly seen incidental finding at the time of revision surgery.6
Figure 6.
In this patient, long-standing polyethylene-induced synovitis had markedly expanded the hip joints and iliopsoas bursae, eventually resulting in superinfection, which accounted for the patient’s symptoms.
Treatment
Based on the imaging findings, interventional radiology services were contacted. The interventional radiologist drained the bilateral psoas abscesses. Cultures of the fluid were positive for both methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible S aureus (MSSA). The patient was admitted to the hospital for treatment of MRSA and MSSA with intravenous antibiotic therapy. He recovered from the infection and was discharged on hospital day 2, with instructions to follow up with an orthopedic surgeon to discuss eventual revision of the bilateral THAs.
References
1. Chandler SB. The iliopsoas bursa in man. Anatom Record. 1934;58(3),235-240. doi:10.1002/ar.1090580304. 2. Tatu L, Parratte B, Vuillier F, Diop M, Monnier G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg Radiol Anat. 2001;23(6):371-374. 3. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45(3):161-168. 4. Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57(3):413-415. 5. Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124(10):720-723. Epub 2004 Oct 23. doi:10.1007/s00402-004-0751-9. 6. Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29-32.
A 49-year-old man with multiple comorbidities presented with a 2-day history of fever and nonproductive cough.
A 49-year-old man with multiple comorbidities presented with a 2-day history of fever and nonproductive cough.
Figure 1.
Figure 2.
Figure 3.
A 49-year-old man with a history of human immunodeficiency virus infection, untreated hepatitis C, endocarditis, and bilateral total hip arthroplasty (THA) presented to the ED with fever, chills, and a nonproductive cough, which he stated began 2 days prior. The patient was not able to walk due to worsening low back and bilateral leg pain.
Laboratory studies revealed leukocytosis with a left shift. Chest radiographs were negative for pneumonia. A magnetic resonance image (MRI) of the lumbar spine was obtained to evaluate for diskitis osteomyelitis. A radiograph of the pelvis was also obtained to evaluate the patient’s THAs, and a computed tomography scan (CT) of the abdomen and pelvis with contrast was obtained for further evaluation. Representative CT, radiographic, and MRI images are shown at left (Figures 1-3).
What is the suspected diagnosis?
Answer
The MRI of the lumbar spine demonstrated no evidence of diskitis osteomyelitis. However, T2-weighted axial images showed enlarged heterogeneous bilateral psoas muscles with bright signal, indicating the presence of fluid (white arrows, Figure 4).
Figure 4.
Figure 5.
On the pelvic radiographs, both femoral heads appeared off-center within the acetabular cups (red arrows, Figure 5).This eccentric positioning indicated wear of the polyethylene in the THAs that normally occupies the space between the acetabular cup and the femoral head. In addition, focal lucency in the right acetabulum indicated breakdown of the bone, a condition referred to as osteolysis (white asterisk, Figure 5).
An abdominopelvic CT scan with contrast was performed and confirmed the findings of polyethylene wear and osteolysis. The CT scan also demonstrated large bilateral hip joint effusions (white arrows, Figure 6), decompressed along distended bilateral iliopsoas bursae (red asterisks, Figure 6), and communicating with the bilateral psoas muscle collections (red arrows, Figure 6).
Osteolysis With Iliopsoas Bursitis
Bursae are fluid-filled sacs lined by synovial tissue located throughout the body to reduce friction at sites of movement between muscles, bones, and tendons. Bursitis develops when these sacs become inflamed and/or infected and fill with fluid. The iliopsoas bursa lies between the anterior capsule of the hip and the psoas tendon, iliacus tendon, and muscle fibers.1,2 This bursa frequently communicates with the hip joint.3,4 Iliopsoas bursal distension has been reported following THA in the setting of polyethylene wear,5 and aseptic bursitis is a commonly seen incidental finding at the time of revision surgery.6
Figure 6.
In this patient, long-standing polyethylene-induced synovitis had markedly expanded the hip joints and iliopsoas bursae, eventually resulting in superinfection, which accounted for the patient’s symptoms.
Treatment
Based on the imaging findings, interventional radiology services were contacted. The interventional radiologist drained the bilateral psoas abscesses. Cultures of the fluid were positive for both methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible S aureus (MSSA). The patient was admitted to the hospital for treatment of MRSA and MSSA with intravenous antibiotic therapy. He recovered from the infection and was discharged on hospital day 2, with instructions to follow up with an orthopedic surgeon to discuss eventual revision of the bilateral THAs.
Figure 1.
Figure 2.
Figure 3.
A 49-year-old man with a history of human immunodeficiency virus infection, untreated hepatitis C, endocarditis, and bilateral total hip arthroplasty (THA) presented to the ED with fever, chills, and a nonproductive cough, which he stated began 2 days prior. The patient was not able to walk due to worsening low back and bilateral leg pain.
Laboratory studies revealed leukocytosis with a left shift. Chest radiographs were negative for pneumonia. A magnetic resonance image (MRI) of the lumbar spine was obtained to evaluate for diskitis osteomyelitis. A radiograph of the pelvis was also obtained to evaluate the patient’s THAs, and a computed tomography scan (CT) of the abdomen and pelvis with contrast was obtained for further evaluation. Representative CT, radiographic, and MRI images are shown at left (Figures 1-3).
What is the suspected diagnosis?
Answer
The MRI of the lumbar spine demonstrated no evidence of diskitis osteomyelitis. However, T2-weighted axial images showed enlarged heterogeneous bilateral psoas muscles with bright signal, indicating the presence of fluid (white arrows, Figure 4).
Figure 4.
Figure 5.
On the pelvic radiographs, both femoral heads appeared off-center within the acetabular cups (red arrows, Figure 5).This eccentric positioning indicated wear of the polyethylene in the THAs that normally occupies the space between the acetabular cup and the femoral head. In addition, focal lucency in the right acetabulum indicated breakdown of the bone, a condition referred to as osteolysis (white asterisk, Figure 5).
An abdominopelvic CT scan with contrast was performed and confirmed the findings of polyethylene wear and osteolysis. The CT scan also demonstrated large bilateral hip joint effusions (white arrows, Figure 6), decompressed along distended bilateral iliopsoas bursae (red asterisks, Figure 6), and communicating with the bilateral psoas muscle collections (red arrows, Figure 6).
Osteolysis With Iliopsoas Bursitis
Bursae are fluid-filled sacs lined by synovial tissue located throughout the body to reduce friction at sites of movement between muscles, bones, and tendons. Bursitis develops when these sacs become inflamed and/or infected and fill with fluid. The iliopsoas bursa lies between the anterior capsule of the hip and the psoas tendon, iliacus tendon, and muscle fibers.1,2 This bursa frequently communicates with the hip joint.3,4 Iliopsoas bursal distension has been reported following THA in the setting of polyethylene wear,5 and aseptic bursitis is a commonly seen incidental finding at the time of revision surgery.6
Figure 6.
In this patient, long-standing polyethylene-induced synovitis had markedly expanded the hip joints and iliopsoas bursae, eventually resulting in superinfection, which accounted for the patient’s symptoms.
Treatment
Based on the imaging findings, interventional radiology services were contacted. The interventional radiologist drained the bilateral psoas abscesses. Cultures of the fluid were positive for both methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-susceptible S aureus (MSSA). The patient was admitted to the hospital for treatment of MRSA and MSSA with intravenous antibiotic therapy. He recovered from the infection and was discharged on hospital day 2, with instructions to follow up with an orthopedic surgeon to discuss eventual revision of the bilateral THAs.
References
1. Chandler SB. The iliopsoas bursa in man. Anatom Record. 1934;58(3),235-240. doi:10.1002/ar.1090580304. 2. Tatu L, Parratte B, Vuillier F, Diop M, Monnier G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg Radiol Anat. 2001;23(6):371-374. 3. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45(3):161-168. 4. Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57(3):413-415. 5. Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124(10):720-723. Epub 2004 Oct 23. doi:10.1007/s00402-004-0751-9. 6. Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29-32.
References
1. Chandler SB. The iliopsoas bursa in man. Anatom Record. 1934;58(3),235-240. doi:10.1002/ar.1090580304. 2. Tatu L, Parratte B, Vuillier F, Diop M, Monnier G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg Radiol Anat. 2001;23(6):371-374. 3. Meaney JF, Cassar-Pullicino VN, Etherington R, Ritchie DA, McCall IW, Whitehouse GH. Ilio-psoas bursa enlargement. Clin Radiol. 1992;45(3):161-168. 4. Warren R, Kaye JJ, Salvati EA. Arthrographic demonstration of an enlarged iliopsoas bursa complicating osteoarthritis of the hip. A case report. J Bone Joint Surg Am. 1975;57(3):413-415. 5. Cheung YM, Gupte CM, Beverly MJ. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg. 2004;124(10):720-723. Epub 2004 Oct 23. doi:10.1007/s00402-004-0751-9. 6. Howie DW, Cain CM, Cornish BL. Pseudo-abscess of the psoas bursa in failed double-cup arthroplasty of the hip. J Bone Joint Surg Br. 1991;73:29-32.
Emergency Ultrasound: Identification of Aortic Dissection Using Limited Bedside Ultrasound
A case involving a 70-year-old woman presenting with acute chest pain highlights the utility of bedside ultrasound in rapidly diagnosing aortic dissection.
The diagnosis of aortic dissection is often challenging due to its various presentations and the frequent absence of classic findings. This high-morbidity and high-mortality condition may present with nonspecific chest, back, or abdominal pain, and is often associated with hypotension.1 Point-of-care (POC) ultrasound in the ED allows for rapid diagnosis of this time-sensitive disease.
Case
A 70-year-old woman presented to the ED for evaluation of acute sharp chest pain, which she stated began while she was exercising earlier that day. The pain was substernal and radiated to her upper back. The patient also described associated lightheadedness and dyspnea, but denied any focal weakness or paresthesias. Her vital signs were remarkable for a blood pressure of 90/31 mm Hg and a heart rate of 42 beats/min. A bedside ultrasound of the patient’s aortic root and abdominal aorta was performed to assess for evidence of aortic dissection.
Figure 1
Imaging Technique
To evaluate for aortic dissection using POC ultrasound, views of the aortic root and the abdominal aorta should be obtained with the patient in the supine position. The phased array (cardiac) probe is used to obtain the parasternal long axis (PSLA) view of the heart to visualize the aortic root. The PSLA view is obtained by placing the probe in the third or fourth intercostal space, adjacent to the left sternal border, with the probe parallel to the long axis of the left ventricle (Figure 1). The American Society of Echocardiography recommends measuring the aortic diameter at the sinus of Valsalva, but measurement of the largest visible portion of the aortic root may be more practical.2,3 Measurement of the aortic root diameter should occur at end diastole.2,3 Tricks for better visualization of the aortic root include tilting the probe tail 10° toward the patient’s right elbow (ie, aiming the probe footprint toward the patient’s left shoulder), or placing the patient in the left lateral decubitus position. Values greater than 4 cm indicate aortic root dilatation.4 Figure 2 demonstrates the PSLA view in our patient, showing the dilated aortic root, which measured roughly 5 cm.
Figure 2
The abdominal aorta is best visualized using a low-frequency curvilinear (abdominal) probe. The aorta should be visualized in the transverse plane from the diaphragm to its bifurcation by placing the probe in the epigastrium and slowly moving it inferiorly to the level of the umbilicus (Figure 3). The aorta can then be visualized in the longitudinal plane by rotating the probe clockwise until it is parallel with the long axis of the aorta (Figure 4). Visualization of an intimal flap is the most common sonographic finding associated with an abdominal aortic dissection. In our patient, an intimal flap was visualized in both the transverse and longitudinal views (Figures 5 and 6).
Figure 3
Discussion
Aortic dissection is a medical emergency—one that has a reported in-hospital mortality of 27.4%.1 Therefore, prompt diagnosis of an aortic dissection in the ED is crucial to improving patient outcomes. Traditionally, emergency physicians (EPs) have relied on aortography and contrast-enhanced computed tomography (CT) to diagnose aortic dissection. However, both of these modalities require a considerable length of time, injection of contrast material, and often transportation of the patient from the ED.
Point-of-care ultrasound provides a fast and noninvasive tool for the diagnosis of aortic dissection. Several recent case reports and case series have highlighted the utility of POC ultrasound to diagnose aortic dissection in the ED.5-7
Figure 4
As our case demonstrates, dilatation of the thoracic aorta and the presence of an intimal flap are indicators of aortic dissection. Evaluation of transthoracic and transabdominal ultrasound for aortic dissection shows that aortic root dilatation has a sensitivity of 77% and specificity of 95%, and visualization of an intimal flap has a sensitivity of 67% to 80% and a specificity of 99% to 100%.4,8-11 Therefore, a combination of a bedside transthoracic and transabdominal ultrasound provides a comprehensive bedside evaluation for aortic dissection.
Figure 5
Case Conclusion
After the results of the POC transthoracic and transabdominal ultrasound were reviewed, we promptly consulted the vascular surgery team. They performed a CT scan verifying a DeBakey type I aortic dissection involving both the ascending aorta and the descending aorta. The patient was subsequently taken to the operating room for definitive repair with a graft. She was discharged home on hospital day 9 in good condition.
Figure 6
Summary
Point-of-care ultrasound is a useful bedside tool for the rapid diagnosis of aortic dissection in the ED. The aortic root dilatation seen on the PSLA view and the presence of an intimal flap seen on either transthoracic or transabdominal views of the aorta are both highly sensitive for aortic dissection.
References
1. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. 2. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233-270. doi:10.1093/ehjci/jev014. 3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012;8(2):152-157. 4. Taylor RA, Oliva I, Van Tonder R, Elefteriades J, Dziura J, Moore CL. Point-of-care focused cardiac ultrasound for the assessment of thoracic aortic dimensions, dilation, and aneurysmal disease. Acad Emerg Med. 2012;19(2):244-247. doi:10.1111/j.1553-2712.2011.01279.x. 5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99. 6. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002;20(4):344-348. 7. Perkins AM, Liteplo A, Noble VE. Ultrasound diagnosis of type a aortic dissection. J Emerg Med. 2010;38(4):490-493. doi:10.1016/j.jemermed.2008.05.013. 8. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196. 9. Khandheria BK, Tajik AJ, Taylor CL, et al. Aortic dissection: review of value and limitations of two-dimensional echocardiography in a six-year experience. J Am Soc Echocardiogr. 1989;2(1):17-24. 10. Roudaut RP, Billes MA, Gosse P, et al. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988;11(8):553-562. 11. Victor MF, Mintz GS, Kotler MN, Wilson AR, Segal BL. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48(6):1155-1159.
A case involving a 70-year-old woman presenting with acute chest pain highlights the utility of bedside ultrasound in rapidly diagnosing aortic dissection.
A case involving a 70-year-old woman presenting with acute chest pain highlights the utility of bedside ultrasound in rapidly diagnosing aortic dissection.
The diagnosis of aortic dissection is often challenging due to its various presentations and the frequent absence of classic findings. This high-morbidity and high-mortality condition may present with nonspecific chest, back, or abdominal pain, and is often associated with hypotension.1 Point-of-care (POC) ultrasound in the ED allows for rapid diagnosis of this time-sensitive disease.
Case
A 70-year-old woman presented to the ED for evaluation of acute sharp chest pain, which she stated began while she was exercising earlier that day. The pain was substernal and radiated to her upper back. The patient also described associated lightheadedness and dyspnea, but denied any focal weakness or paresthesias. Her vital signs were remarkable for a blood pressure of 90/31 mm Hg and a heart rate of 42 beats/min. A bedside ultrasound of the patient’s aortic root and abdominal aorta was performed to assess for evidence of aortic dissection.
Figure 1
Imaging Technique
To evaluate for aortic dissection using POC ultrasound, views of the aortic root and the abdominal aorta should be obtained with the patient in the supine position. The phased array (cardiac) probe is used to obtain the parasternal long axis (PSLA) view of the heart to visualize the aortic root. The PSLA view is obtained by placing the probe in the third or fourth intercostal space, adjacent to the left sternal border, with the probe parallel to the long axis of the left ventricle (Figure 1). The American Society of Echocardiography recommends measuring the aortic diameter at the sinus of Valsalva, but measurement of the largest visible portion of the aortic root may be more practical.2,3 Measurement of the aortic root diameter should occur at end diastole.2,3 Tricks for better visualization of the aortic root include tilting the probe tail 10° toward the patient’s right elbow (ie, aiming the probe footprint toward the patient’s left shoulder), or placing the patient in the left lateral decubitus position. Values greater than 4 cm indicate aortic root dilatation.4 Figure 2 demonstrates the PSLA view in our patient, showing the dilated aortic root, which measured roughly 5 cm.
Figure 2
The abdominal aorta is best visualized using a low-frequency curvilinear (abdominal) probe. The aorta should be visualized in the transverse plane from the diaphragm to its bifurcation by placing the probe in the epigastrium and slowly moving it inferiorly to the level of the umbilicus (Figure 3). The aorta can then be visualized in the longitudinal plane by rotating the probe clockwise until it is parallel with the long axis of the aorta (Figure 4). Visualization of an intimal flap is the most common sonographic finding associated with an abdominal aortic dissection. In our patient, an intimal flap was visualized in both the transverse and longitudinal views (Figures 5 and 6).
Figure 3
Discussion
Aortic dissection is a medical emergency—one that has a reported in-hospital mortality of 27.4%.1 Therefore, prompt diagnosis of an aortic dissection in the ED is crucial to improving patient outcomes. Traditionally, emergency physicians (EPs) have relied on aortography and contrast-enhanced computed tomography (CT) to diagnose aortic dissection. However, both of these modalities require a considerable length of time, injection of contrast material, and often transportation of the patient from the ED.
Point-of-care ultrasound provides a fast and noninvasive tool for the diagnosis of aortic dissection. Several recent case reports and case series have highlighted the utility of POC ultrasound to diagnose aortic dissection in the ED.5-7
Figure 4
As our case demonstrates, dilatation of the thoracic aorta and the presence of an intimal flap are indicators of aortic dissection. Evaluation of transthoracic and transabdominal ultrasound for aortic dissection shows that aortic root dilatation has a sensitivity of 77% and specificity of 95%, and visualization of an intimal flap has a sensitivity of 67% to 80% and a specificity of 99% to 100%.4,8-11 Therefore, a combination of a bedside transthoracic and transabdominal ultrasound provides a comprehensive bedside evaluation for aortic dissection.
Figure 5
Case Conclusion
After the results of the POC transthoracic and transabdominal ultrasound were reviewed, we promptly consulted the vascular surgery team. They performed a CT scan verifying a DeBakey type I aortic dissection involving both the ascending aorta and the descending aorta. The patient was subsequently taken to the operating room for definitive repair with a graft. She was discharged home on hospital day 9 in good condition.
Figure 6
Summary
Point-of-care ultrasound is a useful bedside tool for the rapid diagnosis of aortic dissection in the ED. The aortic root dilatation seen on the PSLA view and the presence of an intimal flap seen on either transthoracic or transabdominal views of the aorta are both highly sensitive for aortic dissection.
The diagnosis of aortic dissection is often challenging due to its various presentations and the frequent absence of classic findings. This high-morbidity and high-mortality condition may present with nonspecific chest, back, or abdominal pain, and is often associated with hypotension.1 Point-of-care (POC) ultrasound in the ED allows for rapid diagnosis of this time-sensitive disease.
Case
A 70-year-old woman presented to the ED for evaluation of acute sharp chest pain, which she stated began while she was exercising earlier that day. The pain was substernal and radiated to her upper back. The patient also described associated lightheadedness and dyspnea, but denied any focal weakness or paresthesias. Her vital signs were remarkable for a blood pressure of 90/31 mm Hg and a heart rate of 42 beats/min. A bedside ultrasound of the patient’s aortic root and abdominal aorta was performed to assess for evidence of aortic dissection.
Figure 1
Imaging Technique
To evaluate for aortic dissection using POC ultrasound, views of the aortic root and the abdominal aorta should be obtained with the patient in the supine position. The phased array (cardiac) probe is used to obtain the parasternal long axis (PSLA) view of the heart to visualize the aortic root. The PSLA view is obtained by placing the probe in the third or fourth intercostal space, adjacent to the left sternal border, with the probe parallel to the long axis of the left ventricle (Figure 1). The American Society of Echocardiography recommends measuring the aortic diameter at the sinus of Valsalva, but measurement of the largest visible portion of the aortic root may be more practical.2,3 Measurement of the aortic root diameter should occur at end diastole.2,3 Tricks for better visualization of the aortic root include tilting the probe tail 10° toward the patient’s right elbow (ie, aiming the probe footprint toward the patient’s left shoulder), or placing the patient in the left lateral decubitus position. Values greater than 4 cm indicate aortic root dilatation.4 Figure 2 demonstrates the PSLA view in our patient, showing the dilated aortic root, which measured roughly 5 cm.
Figure 2
The abdominal aorta is best visualized using a low-frequency curvilinear (abdominal) probe. The aorta should be visualized in the transverse plane from the diaphragm to its bifurcation by placing the probe in the epigastrium and slowly moving it inferiorly to the level of the umbilicus (Figure 3). The aorta can then be visualized in the longitudinal plane by rotating the probe clockwise until it is parallel with the long axis of the aorta (Figure 4). Visualization of an intimal flap is the most common sonographic finding associated with an abdominal aortic dissection. In our patient, an intimal flap was visualized in both the transverse and longitudinal views (Figures 5 and 6).
Figure 3
Discussion
Aortic dissection is a medical emergency—one that has a reported in-hospital mortality of 27.4%.1 Therefore, prompt diagnosis of an aortic dissection in the ED is crucial to improving patient outcomes. Traditionally, emergency physicians (EPs) have relied on aortography and contrast-enhanced computed tomography (CT) to diagnose aortic dissection. However, both of these modalities require a considerable length of time, injection of contrast material, and often transportation of the patient from the ED.
Point-of-care ultrasound provides a fast and noninvasive tool for the diagnosis of aortic dissection. Several recent case reports and case series have highlighted the utility of POC ultrasound to diagnose aortic dissection in the ED.5-7
Figure 4
As our case demonstrates, dilatation of the thoracic aorta and the presence of an intimal flap are indicators of aortic dissection. Evaluation of transthoracic and transabdominal ultrasound for aortic dissection shows that aortic root dilatation has a sensitivity of 77% and specificity of 95%, and visualization of an intimal flap has a sensitivity of 67% to 80% and a specificity of 99% to 100%.4,8-11 Therefore, a combination of a bedside transthoracic and transabdominal ultrasound provides a comprehensive bedside evaluation for aortic dissection.
Figure 5
Case Conclusion
After the results of the POC transthoracic and transabdominal ultrasound were reviewed, we promptly consulted the vascular surgery team. They performed a CT scan verifying a DeBakey type I aortic dissection involving both the ascending aorta and the descending aorta. The patient was subsequently taken to the operating room for definitive repair with a graft. She was discharged home on hospital day 9 in good condition.
Figure 6
Summary
Point-of-care ultrasound is a useful bedside tool for the rapid diagnosis of aortic dissection in the ED. The aortic root dilatation seen on the PSLA view and the presence of an intimal flap seen on either transthoracic or transabdominal views of the aorta are both highly sensitive for aortic dissection.
References
1. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. 2. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233-270. doi:10.1093/ehjci/jev014. 3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012;8(2):152-157. 4. Taylor RA, Oliva I, Van Tonder R, Elefteriades J, Dziura J, Moore CL. Point-of-care focused cardiac ultrasound for the assessment of thoracic aortic dimensions, dilation, and aneurysmal disease. Acad Emerg Med. 2012;19(2):244-247. doi:10.1111/j.1553-2712.2011.01279.x. 5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99. 6. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002;20(4):344-348. 7. Perkins AM, Liteplo A, Noble VE. Ultrasound diagnosis of type a aortic dissection. J Emerg Med. 2010;38(4):490-493. doi:10.1016/j.jemermed.2008.05.013. 8. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196. 9. Khandheria BK, Tajik AJ, Taylor CL, et al. Aortic dissection: review of value and limitations of two-dimensional echocardiography in a six-year experience. J Am Soc Echocardiogr. 1989;2(1):17-24. 10. Roudaut RP, Billes MA, Gosse P, et al. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988;11(8):553-562. 11. Victor MF, Mintz GS, Kotler MN, Wilson AR, Segal BL. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48(6):1155-1159.
References
1. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. 2. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015;16(3):233-270. doi:10.1093/ehjci/jev014. 3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012;8(2):152-157. 4. Taylor RA, Oliva I, Van Tonder R, Elefteriades J, Dziura J, Moore CL. Point-of-care focused cardiac ultrasound for the assessment of thoracic aortic dimensions, dilation, and aneurysmal disease. Acad Emerg Med. 2012;19(2):244-247. doi:10.1111/j.1553-2712.2011.01279.x. 5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99. 6. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002;20(4):344-348. 7. Perkins AM, Liteplo A, Noble VE. Ultrasound diagnosis of type a aortic dissection. J Emerg Med. 2010;38(4):490-493. doi:10.1016/j.jemermed.2008.05.013. 8. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007;32(2):191-196. 9. Khandheria BK, Tajik AJ, Taylor CL, et al. Aortic dissection: review of value and limitations of two-dimensional echocardiography in a six-year experience. J Am Soc Echocardiogr. 1989;2(1):17-24. 10. Roudaut RP, Billes MA, Gosse P, et al. Accuracy of M-mode and two-dimensional echocardiography in the diagnosis of aortic dissection: an experience with 128 cases. Clin Cardiol. 1988;11(8):553-562. 11. Victor MF, Mintz GS, Kotler MN, Wilson AR, Segal BL. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48(6):1155-1159.
Arthrex Synergy MSK Ultrasound by Clarius is a new wireless ultrasound scanner that can connect to any iOS or Android device through a secure WiFi Direct connection. The scanner sets up the connection to an app on the device. Ultrasound and wireless technology have been around for decades, but combinations thereof have produced poor results. The main challenge has been to create and wirelessly transmit high-quality images without latency to a display while maintaining a reasonably sized transducer. Handheld ultrasound transducers scan effectively and process the scanned information in compact form. Recent advances in image processing and proprietary imaging algorithms now allow creation of high-resolution images comparable to those produced by most midrange or high-range machines costing $30,000 to $50,000. This new unit costs about $12,000. Ultrasound use has increased over the past decade. Numerous studies have found improved accuracy, efficacy, and outcomes of injections, and reduced pain, with ultrasound-guided injections over blind injections, and cost savings over magnetic resonance imaging.1-12
Three scanners are capable of targeting different tissue types and depths. We prefer the Synergy MSK Linear Ultrasound by Clarius, a linear transducer that can evaluate tissue to depths of 7 cm and use frequencies from 4 MHz to 13 MHz. Its battery holds a standby charge for 7 days and can be actively used for 45 minutes. The unit has a magnesium shell; with the battery removed, the unit can be completely immersed in liquid without being damaged, which allows for easy cleaning and, potentially, sterilization with a soak solution. Color Doppler (for blood-flow assessment) and proprietary advanced needle visualization technology will be available in June.
The app is simply controlled with typical smart-device gestures. Depth control requires a finger swipe, and zoom takes a pinch. Other controls, such as optimal gain and frequency settings, are automated. Images and videos can be stored on the device and uploaded either to the Clarius Cloud or to a PACS (picture archiving and communication system) device. New features will allow the device to use a Synergy arthroscopy tower (Arthrex) as its display for surgeons and anesthesiologists in the surgical suite.
This technology finally allows ultrasound to be used in the operating room without the hassles of cumbersome machines and the potential contamination by the sleeves covering the cord that connects the transducer and the base unit (Figure 1).
In addition, image viewing is easier with wireless technology, which works with all displays, including the same large 4K monitors used for arthroscopy. The current ultrasound systems’ fixed small screens, most less than 10 inches in size, need no longer be used.
Recent studies have demonstrated new ultrasound-guided surgical techniques for biceps tenodesis,4 anterolateral ligament reconstruction,13 medial patellofemoral ligament repair or reconstruction,14 and medial collateral ligament internal bracing.4
This small device can also be easily used on sports fields, as it can be carried in a pocket with a smart phone or tablet. With its 10- to 15-second start-up, it is readily available and allows for immediate evaluation of a player. No longer does a player need to be taken off the field for a radiograph. The same advantage of portability means the unit is appropriate for emergency department physicians and staff.
The simplicity of the device allows personnel to quickly assess patients and obtain central or peripheral intravenous access and nerve blocks without having to locate an ultrasound machine in a large, busy facility (Figure 2).
Surgical pearl: Overall, ultrasound is an imaging technology that has improved the accuracy and efficacy of injections. Wireless capability, portability, and versatility with high-resolution images improve this modality further and extend our reach into surgical, office, hospital, and sports settings. The ease, convenience, and reasonable price of high-resolution wireless ultrasound make it an attractive tool for physicians, nursing staff, athletic trainers, and physical therapists.
References
1. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63.
2. Finnoff JT, Hall MM, Adams E, et al. American Medical Society for Sports Medicine (AMSSM) position statement: interventional musculoskeletal ultrasound in sports medicine. Br J Sports Med. 2015;49(3):145-150.
3. Henkus HE, Cobben LP, Coerkamp EG, Nelissen RG, van Arkel ER. The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study. Arthroscopy. 2006;22(3):277-282.
4. Hirahara AM, Panero AJ. A guide to ultrasound of the shoulder, part 3: interventional and procedural uses. Am J Orthop. 2016;45(7):440-445.
5. Kang MN, Rizio L, Prybicien M, Middlemas DA, Blacksin MF. The accuracy of subacromial corticosteroid injections: a comparison of multiple methods. J Shoulder Elbow Surg. 2008;17(1 suppl):61S-66S.
6. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308-314.
7. Panero AJ, Hirahara AM. A guide to ultrasound of the shoulder, part 2: the diagnostic evaluation. Am J Orthop. 2016;45(4):233-238.
8. Partington PF, Broome GH. Diagnostic injection around the shoulder: hit and miss? A cadaveric study of injection accuracy. J Shoulder Elbow Surg. 1998;7(2):147-150.
9. Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of the subacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop. 2007;78(2):254-257.
10. Sethi PM, El Attrache N. Accuracy of intra-articular injection of the glenohumeral joint: a cadaveric study. Orthopedics. 2006;29(2):149-152.
11. Sivan M, Brown J, Brennan S, Bhakta B. A one-stop approach to the management of soft tissue and degenerative musculoskeletal conditions using clinic-based ultrasonography. Musculoskeletal Care. 2011;9(2):63-68.
12. Yamakado K. The targeting accuracy of subacromial injection to the shoulder: an arthrographic evaluation. Arthroscopy. 2002;18(8):887-891.
13. Hirahara AM, Andersen WJ. Ultrasound-guided percutaneous reconstruction of the anterolateral ligament: surgical technique and case report. Am J Orthop. 2016;45(7):418-422, 460.
14. Hirahara AM, Andersen WJ. Ultrasound-guided percutaneous repair of the medial patellofemoral ligament: surgical technique and outcomes. Am J Orthop. In press.
Authors’ Disclosure Statement: Dr. Hirahara reports that he receives consultant, royalty, and research support from Arthrex and is a medical advisor to Clarius Mobile Health. Mr. Andersen reports no actual or potential conflict of interest in relation to this article.
Authors’ Disclosure Statement: Dr. Hirahara reports that he receives consultant, royalty, and research support from Arthrex and is a medical advisor to Clarius Mobile Health. Mr. Andersen reports no actual or potential conflict of interest in relation to this article.
Author and Disclosure Information
Authors’ Disclosure Statement: Dr. Hirahara reports that he receives consultant, royalty, and research support from Arthrex and is a medical advisor to Clarius Mobile Health. Mr. Andersen reports no actual or potential conflict of interest in relation to this article.
Arthrex Synergy MSK Ultrasound by Clarius is a new wireless ultrasound scanner that can connect to any iOS or Android device through a secure WiFi Direct connection. The scanner sets up the connection to an app on the device. Ultrasound and wireless technology have been around for decades, but combinations thereof have produced poor results. The main challenge has been to create and wirelessly transmit high-quality images without latency to a display while maintaining a reasonably sized transducer. Handheld ultrasound transducers scan effectively and process the scanned information in compact form. Recent advances in image processing and proprietary imaging algorithms now allow creation of high-resolution images comparable to those produced by most midrange or high-range machines costing $30,000 to $50,000. This new unit costs about $12,000. Ultrasound use has increased over the past decade. Numerous studies have found improved accuracy, efficacy, and outcomes of injections, and reduced pain, with ultrasound-guided injections over blind injections, and cost savings over magnetic resonance imaging.1-12
Three scanners are capable of targeting different tissue types and depths. We prefer the Synergy MSK Linear Ultrasound by Clarius, a linear transducer that can evaluate tissue to depths of 7 cm and use frequencies from 4 MHz to 13 MHz. Its battery holds a standby charge for 7 days and can be actively used for 45 minutes. The unit has a magnesium shell; with the battery removed, the unit can be completely immersed in liquid without being damaged, which allows for easy cleaning and, potentially, sterilization with a soak solution. Color Doppler (for blood-flow assessment) and proprietary advanced needle visualization technology will be available in June.
The app is simply controlled with typical smart-device gestures. Depth control requires a finger swipe, and zoom takes a pinch. Other controls, such as optimal gain and frequency settings, are automated. Images and videos can be stored on the device and uploaded either to the Clarius Cloud or to a PACS (picture archiving and communication system) device. New features will allow the device to use a Synergy arthroscopy tower (Arthrex) as its display for surgeons and anesthesiologists in the surgical suite.
This technology finally allows ultrasound to be used in the operating room without the hassles of cumbersome machines and the potential contamination by the sleeves covering the cord that connects the transducer and the base unit (Figure 1).
In addition, image viewing is easier with wireless technology, which works with all displays, including the same large 4K monitors used for arthroscopy. The current ultrasound systems’ fixed small screens, most less than 10 inches in size, need no longer be used.
Recent studies have demonstrated new ultrasound-guided surgical techniques for biceps tenodesis,4 anterolateral ligament reconstruction,13 medial patellofemoral ligament repair or reconstruction,14 and medial collateral ligament internal bracing.4
This small device can also be easily used on sports fields, as it can be carried in a pocket with a smart phone or tablet. With its 10- to 15-second start-up, it is readily available and allows for immediate evaluation of a player. No longer does a player need to be taken off the field for a radiograph. The same advantage of portability means the unit is appropriate for emergency department physicians and staff.
The simplicity of the device allows personnel to quickly assess patients and obtain central or peripheral intravenous access and nerve blocks without having to locate an ultrasound machine in a large, busy facility (Figure 2).
Surgical pearl: Overall, ultrasound is an imaging technology that has improved the accuracy and efficacy of injections. Wireless capability, portability, and versatility with high-resolution images improve this modality further and extend our reach into surgical, office, hospital, and sports settings. The ease, convenience, and reasonable price of high-resolution wireless ultrasound make it an attractive tool for physicians, nursing staff, athletic trainers, and physical therapists.
Arthrex Synergy MSK Ultrasound by Clarius is a new wireless ultrasound scanner that can connect to any iOS or Android device through a secure WiFi Direct connection. The scanner sets up the connection to an app on the device. Ultrasound and wireless technology have been around for decades, but combinations thereof have produced poor results. The main challenge has been to create and wirelessly transmit high-quality images without latency to a display while maintaining a reasonably sized transducer. Handheld ultrasound transducers scan effectively and process the scanned information in compact form. Recent advances in image processing and proprietary imaging algorithms now allow creation of high-resolution images comparable to those produced by most midrange or high-range machines costing $30,000 to $50,000. This new unit costs about $12,000. Ultrasound use has increased over the past decade. Numerous studies have found improved accuracy, efficacy, and outcomes of injections, and reduced pain, with ultrasound-guided injections over blind injections, and cost savings over magnetic resonance imaging.1-12
Three scanners are capable of targeting different tissue types and depths. We prefer the Synergy MSK Linear Ultrasound by Clarius, a linear transducer that can evaluate tissue to depths of 7 cm and use frequencies from 4 MHz to 13 MHz. Its battery holds a standby charge for 7 days and can be actively used for 45 minutes. The unit has a magnesium shell; with the battery removed, the unit can be completely immersed in liquid without being damaged, which allows for easy cleaning and, potentially, sterilization with a soak solution. Color Doppler (for blood-flow assessment) and proprietary advanced needle visualization technology will be available in June.
The app is simply controlled with typical smart-device gestures. Depth control requires a finger swipe, and zoom takes a pinch. Other controls, such as optimal gain and frequency settings, are automated. Images and videos can be stored on the device and uploaded either to the Clarius Cloud or to a PACS (picture archiving and communication system) device. New features will allow the device to use a Synergy arthroscopy tower (Arthrex) as its display for surgeons and anesthesiologists in the surgical suite.
This technology finally allows ultrasound to be used in the operating room without the hassles of cumbersome machines and the potential contamination by the sleeves covering the cord that connects the transducer and the base unit (Figure 1).
In addition, image viewing is easier with wireless technology, which works with all displays, including the same large 4K monitors used for arthroscopy. The current ultrasound systems’ fixed small screens, most less than 10 inches in size, need no longer be used.
Recent studies have demonstrated new ultrasound-guided surgical techniques for biceps tenodesis,4 anterolateral ligament reconstruction,13 medial patellofemoral ligament repair or reconstruction,14 and medial collateral ligament internal bracing.4
This small device can also be easily used on sports fields, as it can be carried in a pocket with a smart phone or tablet. With its 10- to 15-second start-up, it is readily available and allows for immediate evaluation of a player. No longer does a player need to be taken off the field for a radiograph. The same advantage of portability means the unit is appropriate for emergency department physicians and staff.
The simplicity of the device allows personnel to quickly assess patients and obtain central or peripheral intravenous access and nerve blocks without having to locate an ultrasound machine in a large, busy facility (Figure 2).
Surgical pearl: Overall, ultrasound is an imaging technology that has improved the accuracy and efficacy of injections. Wireless capability, portability, and versatility with high-resolution images improve this modality further and extend our reach into surgical, office, hospital, and sports settings. The ease, convenience, and reasonable price of high-resolution wireless ultrasound make it an attractive tool for physicians, nursing staff, athletic trainers, and physical therapists.
References
1. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63.
2. Finnoff JT, Hall MM, Adams E, et al. American Medical Society for Sports Medicine (AMSSM) position statement: interventional musculoskeletal ultrasound in sports medicine. Br J Sports Med. 2015;49(3):145-150.
3. Henkus HE, Cobben LP, Coerkamp EG, Nelissen RG, van Arkel ER. The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study. Arthroscopy. 2006;22(3):277-282.
4. Hirahara AM, Panero AJ. A guide to ultrasound of the shoulder, part 3: interventional and procedural uses. Am J Orthop. 2016;45(7):440-445.
5. Kang MN, Rizio L, Prybicien M, Middlemas DA, Blacksin MF. The accuracy of subacromial corticosteroid injections: a comparison of multiple methods. J Shoulder Elbow Surg. 2008;17(1 suppl):61S-66S.
6. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308-314.
7. Panero AJ, Hirahara AM. A guide to ultrasound of the shoulder, part 2: the diagnostic evaluation. Am J Orthop. 2016;45(4):233-238.
8. Partington PF, Broome GH. Diagnostic injection around the shoulder: hit and miss? A cadaveric study of injection accuracy. J Shoulder Elbow Surg. 1998;7(2):147-150.
9. Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of the subacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop. 2007;78(2):254-257.
10. Sethi PM, El Attrache N. Accuracy of intra-articular injection of the glenohumeral joint: a cadaveric study. Orthopedics. 2006;29(2):149-152.
11. Sivan M, Brown J, Brennan S, Bhakta B. A one-stop approach to the management of soft tissue and degenerative musculoskeletal conditions using clinic-based ultrasonography. Musculoskeletal Care. 2011;9(2):63-68.
12. Yamakado K. The targeting accuracy of subacromial injection to the shoulder: an arthrographic evaluation. Arthroscopy. 2002;18(8):887-891.
13. Hirahara AM, Andersen WJ. Ultrasound-guided percutaneous reconstruction of the anterolateral ligament: surgical technique and case report. Am J Orthop. 2016;45(7):418-422, 460.
14. Hirahara AM, Andersen WJ. Ultrasound-guided percutaneous repair of the medial patellofemoral ligament: surgical technique and outcomes. Am J Orthop. In press.
References
1. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63.
2. Finnoff JT, Hall MM, Adams E, et al. American Medical Society for Sports Medicine (AMSSM) position statement: interventional musculoskeletal ultrasound in sports medicine. Br J Sports Med. 2015;49(3):145-150.
3. Henkus HE, Cobben LP, Coerkamp EG, Nelissen RG, van Arkel ER. The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study. Arthroscopy. 2006;22(3):277-282.
4. Hirahara AM, Panero AJ. A guide to ultrasound of the shoulder, part 3: interventional and procedural uses. Am J Orthop. 2016;45(7):440-445.
5. Kang MN, Rizio L, Prybicien M, Middlemas DA, Blacksin MF. The accuracy of subacromial corticosteroid injections: a comparison of multiple methods. J Shoulder Elbow Surg. 2008;17(1 suppl):61S-66S.
6. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308-314.
7. Panero AJ, Hirahara AM. A guide to ultrasound of the shoulder, part 2: the diagnostic evaluation. Am J Orthop. 2016;45(4):233-238.
8. Partington PF, Broome GH. Diagnostic injection around the shoulder: hit and miss? A cadaveric study of injection accuracy. J Shoulder Elbow Surg. 1998;7(2):147-150.
9. Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of the subacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop. 2007;78(2):254-257.
10. Sethi PM, El Attrache N. Accuracy of intra-articular injection of the glenohumeral joint: a cadaveric study. Orthopedics. 2006;29(2):149-152.
11. Sivan M, Brown J, Brennan S, Bhakta B. A one-stop approach to the management of soft tissue and degenerative musculoskeletal conditions using clinic-based ultrasonography. Musculoskeletal Care. 2011;9(2):63-68.
12. Yamakado K. The targeting accuracy of subacromial injection to the shoulder: an arthrographic evaluation. Arthroscopy. 2002;18(8):887-891.
13. Hirahara AM, Andersen WJ. Ultrasound-guided percutaneous reconstruction of the anterolateral ligament: surgical technique and case report. Am J Orthop. 2016;45(7):418-422, 460.
14. Hirahara AM, Andersen WJ. Ultrasound-guided percutaneous repair of the medial patellofemoral ligament: surgical technique and outcomes. Am J Orthop. In press.
A 58-year-old man with end-stage renal disease due to diabetic nephropathy was admitted with aggravated exertional dyspnea and intermittent chest pain for 1 week. He had been on hemodialysis for 15 years.
His blood pressure was 124/69 mm Hg, pulse 96 beats per minute, and temperature 35.8°C. On physical examination, he had bilateral diffuse crackles, elevated jugular venous pressure (9.5 cm H2O) with positive hepatojugular reflux, and apparent dependent pedal edema. The Kussmaul sign was not observed.
Cardiac enzymes were in the normal range (creatine kinase 73 U/L, troponin I 0.032 ng/mL), but the brain-natriuretic peptide level was elevated at 340 pg/mL. Other laboratory findings included calcium 9 mg/dL (reference range 8.4–10.2 mg/dL), inorganic phosphate 5 mg/dL (2.5–4.5 mg/dL), and intact parathyroid hormone 1,457 pg/mL (10–69 pg/mL).
Figure 1. Thoracic computed tomography revealed calcified pericardium with heart encasement in the coronal view (left) and sagittal view (right).
Electrocardiography showed sinus tachycardia with low voltage in diffuse leads and generalized flattening of the T wave. Chest radiography showed a bilateral reticulonodular pattern, mild costophrenic angle obliteration, and notable calcifications along the cardiac contour. Thoracic computed tomography showed a porcelain-like encasement of the heart (Figure 1). Transthoracic echocardiography showed thickened pericardium, pericardial calcification, and mild interventricular septal bounce in diastole, with no dyskinesia of ventricular wall motion. We decided not to perform an invasive hemodynamic assessment.
CAUSES OF PERICARDIAL CALCIFICATION
Pericardial calcification, abnormal calcium deposits in response to inflammation,1 has become more widely reported as the use of chest computed tomography has become more widespread. The common identifiable causes of pericardial calcification include recurrent or chronic pericarditis, radiation therapy for Hodgkin lymphoma or breast cancer, tuberculosis, and end-stage kidney disease.2,3 Other possible causes are retention of uremic metabolites, metastatic calcification induced by secondary hyperparathyroidism, and calcium-phosphate deposition induced by hyperphosphatemia.4
In chronic kidney disease, the amount of pericardial fluid and fibrinous pericardial deposition is thought to contribute to increased pericardial thickness and constriction. In some patients, pericardial calcification and thickening would lead to constrictive pericarditis, which could be confirmed by echocardiography and cardiac catheterization. About 25% to 50% of cases of pericardial calcification are complicated by constrictive pericarditis.5,6 Constrictive pericarditis occurs in up to 4% of patients with end-stage renal disease, even with successful dialysis.7
Partial clinical improvement may be obtained with intensive hemodialysis, strict volume control, and decreased catabolism in patients with multiple comorbidities.8 However, the definite treatment is total pericardiectomy, which reduces symptoms substantially and offers a favorable long-term outcome.7
SECONDARY HYPERPARATHYROIDISM
Secondary hyperparathyroidism is a common complication in patients with end-stage renal disease and is characterized by derangements in the homeostasis of calcium, phosphorus, and vitamin D.9
Because renal function is decreased, phosphate is retained and calcitriol synthesis is reduced, resulting in hypocalcemia, which induces parathyroid gland hyperplasia and parathyroid hormone secretion.10 Moreover, some patents with long-standing secondary hyperparathyroidism may develop tertiary hyperparathyroidism associated with autonomous parathyroid hormone secretion, hypercalcemia, and hyperphosphatemia.11
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group recommends screening for and managing secondary hyperparathyroidism in all patients with stage 3 chronic kidney disease (estimated glomerular filtration rate < 60 mL/min). In patients with stage 5 chronic kidney disease or on dialysis, the serum calcium and phosphorus levels should be monitored every 1 to 3 months and the parathyroid hormone levels every 3 to 6 months.12
According to KDIGO guidelines, the target level of calcium is less than 10.2 mg/dL, and the target phosphorus level is less than 4.6 mg/dL. The level of parathyroid hormone should be maintained at 2 to 9 times the upper limit of normal for the assay.
The management of secondary hyperparathyroidism includes a low-phosphorus diet, calcium-containing or calcium-free phosphate binders, a calcitriol supplement, and calcimimetics. If medical treatment fails and manifestations are significant, parathyroidectomy may be indicated.13
References
Alpert MA, Ravenscraft MD. Pericardial involvement in end-stage renal disease. Am J Med Sci 2003; 325:228–236.
Gowda RM, Boxt LM. Calcifications of the heart. Radiol Clin North Am 2004; 42:603–617.
Kleynberg RL, Kleynberg VM, Kleynberg LM, Farahmandian D. Chronic constrictive pericarditis in association with end-stage renal disease. Int J Nephrol 2011; 2011:469602.
Rao N, Crail S. Metastatic calcification and long-term hemodialysis. N Engl J Med 2013; 368:2415.
Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999; 100:1380–1386.
Bergman M, Vitrai J, Salman H. Constrictive pericarditis: a reminder of a not so rare disease. Eur J Intern Med 2006; 17:457–464.
Szabó G, Schmack B, Bulut C, et al. Constrictive pericarditis: risks, aetiologies and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg 2013; 44:1023–1028.
Feldman V, Dovrish Z, Weisenberg N, Neuman Y, Amital H. Uremic pericarditis. Isr Med Assoc J 2011; 13:256–257.
Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 2007; 71:31–38.
Martin KJ, Gonzalez EA. Metabolic bone disease in chronic kidney disease. J Am Soc Nephrol 2007; 18:875–885.
Kerby J, Rue LW, Blair H, Hudson S, Sellers MT, Diethelm AG. Operative treatment of tertiary hyperparathyroidism: a single-center experience. Ann Surg 1998; 227:878–886.
Kidney Disease: Improving Global Outcomes (KDIGO) CKDMBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease—mineral and bone disorder (CKD-MBD). Kidney Int Suppl 2009; 76:S1–130.
National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42(4 suppl 3):S1–201.
Hsiu-Chien Yang, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan; and Division of Nephrology, Department of Internal Medicine, Zuoying Branch of Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan
Chang-Han Lo, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Chun-Chi Chen, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Chia-Chao Wu, MD, PhD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Address: Chia-Chao Wu, MD PhD, Division of Nephrology, Department of Medicine, Tri-Service General Hospital, No. 325, Section 2, Cheng-Kung Road, Neihu 114, Taipei, Taiwan; [email protected]
Hsiu-Chien Yang, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan; and Division of Nephrology, Department of Internal Medicine, Zuoying Branch of Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan
Chang-Han Lo, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Chun-Chi Chen, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Chia-Chao Wu, MD, PhD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Address: Chia-Chao Wu, MD PhD, Division of Nephrology, Department of Medicine, Tri-Service General Hospital, No. 325, Section 2, Cheng-Kung Road, Neihu 114, Taipei, Taiwan; [email protected]
Author and Disclosure Information
Hsiu-Chien Yang, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan; and Division of Nephrology, Department of Internal Medicine, Zuoying Branch of Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan
Chang-Han Lo, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Chun-Chi Chen, MD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Chia-Chao Wu, MD, PhD Department of Internal Medicine, Division of Nephrology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
Address: Chia-Chao Wu, MD PhD, Division of Nephrology, Department of Medicine, Tri-Service General Hospital, No. 325, Section 2, Cheng-Kung Road, Neihu 114, Taipei, Taiwan; [email protected]
A 58-year-old man with end-stage renal disease due to diabetic nephropathy was admitted with aggravated exertional dyspnea and intermittent chest pain for 1 week. He had been on hemodialysis for 15 years.
His blood pressure was 124/69 mm Hg, pulse 96 beats per minute, and temperature 35.8°C. On physical examination, he had bilateral diffuse crackles, elevated jugular venous pressure (9.5 cm H2O) with positive hepatojugular reflux, and apparent dependent pedal edema. The Kussmaul sign was not observed.
Cardiac enzymes were in the normal range (creatine kinase 73 U/L, troponin I 0.032 ng/mL), but the brain-natriuretic peptide level was elevated at 340 pg/mL. Other laboratory findings included calcium 9 mg/dL (reference range 8.4–10.2 mg/dL), inorganic phosphate 5 mg/dL (2.5–4.5 mg/dL), and intact parathyroid hormone 1,457 pg/mL (10–69 pg/mL).
Figure 1. Thoracic computed tomography revealed calcified pericardium with heart encasement in the coronal view (left) and sagittal view (right).
Electrocardiography showed sinus tachycardia with low voltage in diffuse leads and generalized flattening of the T wave. Chest radiography showed a bilateral reticulonodular pattern, mild costophrenic angle obliteration, and notable calcifications along the cardiac contour. Thoracic computed tomography showed a porcelain-like encasement of the heart (Figure 1). Transthoracic echocardiography showed thickened pericardium, pericardial calcification, and mild interventricular septal bounce in diastole, with no dyskinesia of ventricular wall motion. We decided not to perform an invasive hemodynamic assessment.
CAUSES OF PERICARDIAL CALCIFICATION
Pericardial calcification, abnormal calcium deposits in response to inflammation,1 has become more widely reported as the use of chest computed tomography has become more widespread. The common identifiable causes of pericardial calcification include recurrent or chronic pericarditis, radiation therapy for Hodgkin lymphoma or breast cancer, tuberculosis, and end-stage kidney disease.2,3 Other possible causes are retention of uremic metabolites, metastatic calcification induced by secondary hyperparathyroidism, and calcium-phosphate deposition induced by hyperphosphatemia.4
In chronic kidney disease, the amount of pericardial fluid and fibrinous pericardial deposition is thought to contribute to increased pericardial thickness and constriction. In some patients, pericardial calcification and thickening would lead to constrictive pericarditis, which could be confirmed by echocardiography and cardiac catheterization. About 25% to 50% of cases of pericardial calcification are complicated by constrictive pericarditis.5,6 Constrictive pericarditis occurs in up to 4% of patients with end-stage renal disease, even with successful dialysis.7
Partial clinical improvement may be obtained with intensive hemodialysis, strict volume control, and decreased catabolism in patients with multiple comorbidities.8 However, the definite treatment is total pericardiectomy, which reduces symptoms substantially and offers a favorable long-term outcome.7
SECONDARY HYPERPARATHYROIDISM
Secondary hyperparathyroidism is a common complication in patients with end-stage renal disease and is characterized by derangements in the homeostasis of calcium, phosphorus, and vitamin D.9
Because renal function is decreased, phosphate is retained and calcitriol synthesis is reduced, resulting in hypocalcemia, which induces parathyroid gland hyperplasia and parathyroid hormone secretion.10 Moreover, some patents with long-standing secondary hyperparathyroidism may develop tertiary hyperparathyroidism associated with autonomous parathyroid hormone secretion, hypercalcemia, and hyperphosphatemia.11
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group recommends screening for and managing secondary hyperparathyroidism in all patients with stage 3 chronic kidney disease (estimated glomerular filtration rate < 60 mL/min). In patients with stage 5 chronic kidney disease or on dialysis, the serum calcium and phosphorus levels should be monitored every 1 to 3 months and the parathyroid hormone levels every 3 to 6 months.12
According to KDIGO guidelines, the target level of calcium is less than 10.2 mg/dL, and the target phosphorus level is less than 4.6 mg/dL. The level of parathyroid hormone should be maintained at 2 to 9 times the upper limit of normal for the assay.
The management of secondary hyperparathyroidism includes a low-phosphorus diet, calcium-containing or calcium-free phosphate binders, a calcitriol supplement, and calcimimetics. If medical treatment fails and manifestations are significant, parathyroidectomy may be indicated.13
A 58-year-old man with end-stage renal disease due to diabetic nephropathy was admitted with aggravated exertional dyspnea and intermittent chest pain for 1 week. He had been on hemodialysis for 15 years.
His blood pressure was 124/69 mm Hg, pulse 96 beats per minute, and temperature 35.8°C. On physical examination, he had bilateral diffuse crackles, elevated jugular venous pressure (9.5 cm H2O) with positive hepatojugular reflux, and apparent dependent pedal edema. The Kussmaul sign was not observed.
Cardiac enzymes were in the normal range (creatine kinase 73 U/L, troponin I 0.032 ng/mL), but the brain-natriuretic peptide level was elevated at 340 pg/mL. Other laboratory findings included calcium 9 mg/dL (reference range 8.4–10.2 mg/dL), inorganic phosphate 5 mg/dL (2.5–4.5 mg/dL), and intact parathyroid hormone 1,457 pg/mL (10–69 pg/mL).
Figure 1. Thoracic computed tomography revealed calcified pericardium with heart encasement in the coronal view (left) and sagittal view (right).
Electrocardiography showed sinus tachycardia with low voltage in diffuse leads and generalized flattening of the T wave. Chest radiography showed a bilateral reticulonodular pattern, mild costophrenic angle obliteration, and notable calcifications along the cardiac contour. Thoracic computed tomography showed a porcelain-like encasement of the heart (Figure 1). Transthoracic echocardiography showed thickened pericardium, pericardial calcification, and mild interventricular septal bounce in diastole, with no dyskinesia of ventricular wall motion. We decided not to perform an invasive hemodynamic assessment.
CAUSES OF PERICARDIAL CALCIFICATION
Pericardial calcification, abnormal calcium deposits in response to inflammation,1 has become more widely reported as the use of chest computed tomography has become more widespread. The common identifiable causes of pericardial calcification include recurrent or chronic pericarditis, radiation therapy for Hodgkin lymphoma or breast cancer, tuberculosis, and end-stage kidney disease.2,3 Other possible causes are retention of uremic metabolites, metastatic calcification induced by secondary hyperparathyroidism, and calcium-phosphate deposition induced by hyperphosphatemia.4
In chronic kidney disease, the amount of pericardial fluid and fibrinous pericardial deposition is thought to contribute to increased pericardial thickness and constriction. In some patients, pericardial calcification and thickening would lead to constrictive pericarditis, which could be confirmed by echocardiography and cardiac catheterization. About 25% to 50% of cases of pericardial calcification are complicated by constrictive pericarditis.5,6 Constrictive pericarditis occurs in up to 4% of patients with end-stage renal disease, even with successful dialysis.7
Partial clinical improvement may be obtained with intensive hemodialysis, strict volume control, and decreased catabolism in patients with multiple comorbidities.8 However, the definite treatment is total pericardiectomy, which reduces symptoms substantially and offers a favorable long-term outcome.7
SECONDARY HYPERPARATHYROIDISM
Secondary hyperparathyroidism is a common complication in patients with end-stage renal disease and is characterized by derangements in the homeostasis of calcium, phosphorus, and vitamin D.9
Because renal function is decreased, phosphate is retained and calcitriol synthesis is reduced, resulting in hypocalcemia, which induces parathyroid gland hyperplasia and parathyroid hormone secretion.10 Moreover, some patents with long-standing secondary hyperparathyroidism may develop tertiary hyperparathyroidism associated with autonomous parathyroid hormone secretion, hypercalcemia, and hyperphosphatemia.11
The Kidney Disease: Improving Global Outcomes (KDIGO) Work Group recommends screening for and managing secondary hyperparathyroidism in all patients with stage 3 chronic kidney disease (estimated glomerular filtration rate < 60 mL/min). In patients with stage 5 chronic kidney disease or on dialysis, the serum calcium and phosphorus levels should be monitored every 1 to 3 months and the parathyroid hormone levels every 3 to 6 months.12
According to KDIGO guidelines, the target level of calcium is less than 10.2 mg/dL, and the target phosphorus level is less than 4.6 mg/dL. The level of parathyroid hormone should be maintained at 2 to 9 times the upper limit of normal for the assay.
The management of secondary hyperparathyroidism includes a low-phosphorus diet, calcium-containing or calcium-free phosphate binders, a calcitriol supplement, and calcimimetics. If medical treatment fails and manifestations are significant, parathyroidectomy may be indicated.13
References
Alpert MA, Ravenscraft MD. Pericardial involvement in end-stage renal disease. Am J Med Sci 2003; 325:228–236.
Gowda RM, Boxt LM. Calcifications of the heart. Radiol Clin North Am 2004; 42:603–617.
Kleynberg RL, Kleynberg VM, Kleynberg LM, Farahmandian D. Chronic constrictive pericarditis in association with end-stage renal disease. Int J Nephrol 2011; 2011:469602.
Rao N, Crail S. Metastatic calcification and long-term hemodialysis. N Engl J Med 2013; 368:2415.
Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999; 100:1380–1386.
Bergman M, Vitrai J, Salman H. Constrictive pericarditis: a reminder of a not so rare disease. Eur J Intern Med 2006; 17:457–464.
Szabó G, Schmack B, Bulut C, et al. Constrictive pericarditis: risks, aetiologies and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg 2013; 44:1023–1028.
Feldman V, Dovrish Z, Weisenberg N, Neuman Y, Amital H. Uremic pericarditis. Isr Med Assoc J 2011; 13:256–257.
Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 2007; 71:31–38.
Martin KJ, Gonzalez EA. Metabolic bone disease in chronic kidney disease. J Am Soc Nephrol 2007; 18:875–885.
Kerby J, Rue LW, Blair H, Hudson S, Sellers MT, Diethelm AG. Operative treatment of tertiary hyperparathyroidism: a single-center experience. Ann Surg 1998; 227:878–886.
Kidney Disease: Improving Global Outcomes (KDIGO) CKDMBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease—mineral and bone disorder (CKD-MBD). Kidney Int Suppl 2009; 76:S1–130.
National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42(4 suppl 3):S1–201.
References
Alpert MA, Ravenscraft MD. Pericardial involvement in end-stage renal disease. Am J Med Sci 2003; 325:228–236.
Gowda RM, Boxt LM. Calcifications of the heart. Radiol Clin North Am 2004; 42:603–617.
Kleynberg RL, Kleynberg VM, Kleynberg LM, Farahmandian D. Chronic constrictive pericarditis in association with end-stage renal disease. Int J Nephrol 2011; 2011:469602.
Rao N, Crail S. Metastatic calcification and long-term hemodialysis. N Engl J Med 2013; 368:2415.
Ling LH, Oh JK, Schaff HV, et al. Constrictive pericarditis in the modern era: evolving clinical spectrum and impact on outcome after pericardiectomy. Circulation 1999; 100:1380–1386.
Bergman M, Vitrai J, Salman H. Constrictive pericarditis: a reminder of a not so rare disease. Eur J Intern Med 2006; 17:457–464.
Szabó G, Schmack B, Bulut C, et al. Constrictive pericarditis: risks, aetiologies and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg 2013; 44:1023–1028.
Feldman V, Dovrish Z, Weisenberg N, Neuman Y, Amital H. Uremic pericarditis. Isr Med Assoc J 2011; 13:256–257.
Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int 2007; 71:31–38.
Martin KJ, Gonzalez EA. Metabolic bone disease in chronic kidney disease. J Am Soc Nephrol 2007; 18:875–885.
Kerby J, Rue LW, Blair H, Hudson S, Sellers MT, Diethelm AG. Operative treatment of tertiary hyperparathyroidism: a single-center experience. Ann Surg 1998; 227:878–886.
Kidney Disease: Improving Global Outcomes (KDIGO) CKDMBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease—mineral and bone disorder (CKD-MBD). Kidney Int Suppl 2009; 76:S1–130.
National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42(4 suppl 3):S1–201.