Background: Abdominal paracentesis is a commonly performed procedure, and with appropriate training, hospitalists can deliver similar outcomes when compared to interventional radiologists.
Study design: Position statement.
Setting: The Society of Hospital Medicine Point-of-Care Ultrasound (POCUS) Task Force developed these guidelines after reviewing available literature and voted on the appropriateness and consensus of a recommendation.
Synopsis: A total of 794 articles were screened, and 91 articles were included and incorporated into the recommendations. The 12 recommendations fall into three categories (clinical outcomes, technique, and training), and all 12 recommendations achieved consensus as strong recommendations.
To improve clinical outcomes, the authors recommended ultrasound guidance in performing paracentesis to reduce the risk of serious complications, to avoid attempting paracentesis with insufficient fluid, and to improve overall procedure success.
The authors advocated for several technique recommendations, including using the ultrasound to assess volume and location of intraperitoneal fluid, to identify the needle insertion site and confirm in multiple planes, to use color flow Doppler to identify abdominal wall vessels, to mark the insertion site immediately prior to the procedure, and to consider real-time ultrasound guidance.
When health care professionals are learning ultrasound-guided paracentesis, the authors recommended use of dedicated training sessions with simulation if available and that competency should be demonstrated before independently attempting the procedure.
Bottom line: These recommendations from SHM POCUS Task Force provides consensus guidelines on the use of ultrasound guidance when performing or learning abdominal paracentesis.
Citation: Cho J et al. Recommendations on the use of ultrasound guidance for adult abdominal paracentesis: A position statement of the Society of Hospital Medicine. 2019 Jan 2. doi: 10.12788/jhm.3095.
Dr. Schmit is an associate professor of medicine in the division of general and hospital medicine at UT Health San Antonio and a hospitalist at South Texas Veterans Health Care System, also in San Antonio.
Background: Abdominal paracentesis is a commonly performed procedure, and with appropriate training, hospitalists can deliver similar outcomes when compared to interventional radiologists.
Study design: Position statement.
Setting: The Society of Hospital Medicine Point-of-Care Ultrasound (POCUS) Task Force developed these guidelines after reviewing available literature and voted on the appropriateness and consensus of a recommendation.
Synopsis: A total of 794 articles were screened, and 91 articles were included and incorporated into the recommendations. The 12 recommendations fall into three categories (clinical outcomes, technique, and training), and all 12 recommendations achieved consensus as strong recommendations.
To improve clinical outcomes, the authors recommended ultrasound guidance in performing paracentesis to reduce the risk of serious complications, to avoid attempting paracentesis with insufficient fluid, and to improve overall procedure success.
The authors advocated for several technique recommendations, including using the ultrasound to assess volume and location of intraperitoneal fluid, to identify the needle insertion site and confirm in multiple planes, to use color flow Doppler to identify abdominal wall vessels, to mark the insertion site immediately prior to the procedure, and to consider real-time ultrasound guidance.
When health care professionals are learning ultrasound-guided paracentesis, the authors recommended use of dedicated training sessions with simulation if available and that competency should be demonstrated before independently attempting the procedure.
Bottom line: These recommendations from SHM POCUS Task Force provides consensus guidelines on the use of ultrasound guidance when performing or learning abdominal paracentesis.
Citation: Cho J et al. Recommendations on the use of ultrasound guidance for adult abdominal paracentesis: A position statement of the Society of Hospital Medicine. 2019 Jan 2. doi: 10.12788/jhm.3095.
Dr. Schmit is an associate professor of medicine in the division of general and hospital medicine at UT Health San Antonio and a hospitalist at South Texas Veterans Health Care System, also in San Antonio.
Background: Abdominal paracentesis is a commonly performed procedure, and with appropriate training, hospitalists can deliver similar outcomes when compared to interventional radiologists.
Study design: Position statement.
Setting: The Society of Hospital Medicine Point-of-Care Ultrasound (POCUS) Task Force developed these guidelines after reviewing available literature and voted on the appropriateness and consensus of a recommendation.
Synopsis: A total of 794 articles were screened, and 91 articles were included and incorporated into the recommendations. The 12 recommendations fall into three categories (clinical outcomes, technique, and training), and all 12 recommendations achieved consensus as strong recommendations.
To improve clinical outcomes, the authors recommended ultrasound guidance in performing paracentesis to reduce the risk of serious complications, to avoid attempting paracentesis with insufficient fluid, and to improve overall procedure success.
The authors advocated for several technique recommendations, including using the ultrasound to assess volume and location of intraperitoneal fluid, to identify the needle insertion site and confirm in multiple planes, to use color flow Doppler to identify abdominal wall vessels, to mark the insertion site immediately prior to the procedure, and to consider real-time ultrasound guidance.
When health care professionals are learning ultrasound-guided paracentesis, the authors recommended use of dedicated training sessions with simulation if available and that competency should be demonstrated before independently attempting the procedure.
Bottom line: These recommendations from SHM POCUS Task Force provides consensus guidelines on the use of ultrasound guidance when performing or learning abdominal paracentesis.
Citation: Cho J et al. Recommendations on the use of ultrasound guidance for adult abdominal paracentesis: A position statement of the Society of Hospital Medicine. 2019 Jan 2. doi: 10.12788/jhm.3095.
Dr. Schmit is an associate professor of medicine in the division of general and hospital medicine at UT Health San Antonio and a hospitalist at South Texas Veterans Health Care System, also in San Antonio.
A 50-year-old man with Crohn disease and psoriatic arthritis treated with infliximab and methotrexate presented to a tertiary care hospital with fever, cough, and chest discomfort. The symptoms had first appeared 2 weeks earlier, and he had gone to an urgent care center, where he was prescribed a 5-day course of azithromycin and a corticosteroid, but this had not relieved his symptoms.
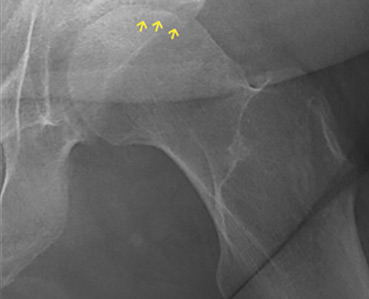
Figure 1. (A) An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).
He reported no recent travel, exposure to animals, or sick contacts. His temperature was 38.3°C (100.9°F). Results of the physical examination and initial laboratory testing were unremarkable. Chest computed tomography revealed prominent right hilar and mediastinal lymphadenopathy (Figure 1).
Bronchoscopy revealed edematous mucosa throughout, with minimal secretion. Specimens for bacterial, acid-fast bacillus, and fungal cultures were obtained from bronchoalveolar lavage. Endobronchial lymph node biopsy with ultrasonographic guidance revealed nonnecrotizing granuloma.
Bronchoalveolar lavage cultures showed no growth, but the patient’s serum histoplasma antigen was positive at 5.99 ng/dL (reference range: none detected), leading to the diagnosis of mediastinal granuloma due to histoplasmosis with possible dissemination. His immunosuppressant drugs were stopped, and oral itraconazole was started.
At a follow-up visit 2 months later, his serum antigen level had decreased to 0.68 ng/dL, and he had no symptoms whatsoever. At a visit 1 month after that, infliximab and methotrexate were restarted because of an exacerbation of Crohn disease. His oral itraconazole treatment was to be continued for at least 12 months, given the high suspicion for disseminated histoplasmosis while on immunosuppressant therapy.
DIFFERENTIAL DIAGNOSIS OF GRANULOMATOUS LUNG DISEASE AND LYMPHADENOPATHY
The differential diagnosis of granulomatous lung disease and lymphadenopathy is broad and includes noninfectious and infectious conditions.1
Noninfectious causes include lymphoma, sarcoidosis, inflammatory bowel disease, hypersensitivity pneumonia, side effects of drugs (eg, methotrexate, etanercept), rheumatoid nodules, vasculitis (eg, Churg-Strauss syndrome, granulomatosis with polyangiitis, primary amyloidosis, pneumoconiosis (eg, beryllium, cobalt), and Castleman disease.
There is concern that tumor necrosis factor antagonists may increase the risk of lymphoma, but a 2017 study found no evidence of this.2
Infectious conditions associated with granulomatous lung disease include tuberculosis, nontuberculous mycobacterial infection, fungal infection (eg, Cryptococcus, Coccidioides, Histoplasma, Blastomyces), brucellosis, tularemia (respiratory type B), parasitic infection (eg, Toxocara, Leishmania, Echinococcus, Schistosoma), and Whipple disease.
HISTOPLASMOSIS
Histoplasmosis, caused by infection with Histoplasma capsulatum, is the most prevalent endemic mycotic disease in the United States.3 The fungus is commonly found in the Ohio and Mississippi River valleys in the United States, and also in Central and South America and Asia.
Risk factors for histoplasmosis include living in or traveling to an endemic area, exposure to aerosolized soil that contains spores, and exposure to bats or birds and their droppings.4
Fewer than 5% of exposed individuals develop symptoms, which include fever, chills, headache, myalgia, anorexia, cough, and chest pain.5 Patients may experience symptoms shortly after exposure or may remain free of symptoms for years, with intermittent relapses of symptoms.6 Hilar or mediastinal lymphadenopathy is common in acute pulmonary histoplasmosis.7
The risk of disseminated histoplasmosis is greater in patients with reduced cell-mediated immunity, such as in human immunodeficiency virus infection, acquired immunodeficiency syndrome, solid-organ or bone marrow transplant, hematologic malignancies, immunosuppression (corticosteroids, disease-modifying antirheumatic drugs, and tumor necrosis factor antagonists), and congenital T-cell deficiencies.8
In a retrospective study, infliximab was the tumor necrosis factor antagonist most commonly associated with histoplasmosis.9 In a study of patients with rheumatoid arthritis, the disease-modifying drug most commonly associated was methotrexate.10
GOLD STANDARD FOR DIAGNOSIS
Isolation of H capsulatum from clinical specimens remains the gold standard for confirmation of histoplasmosis. The sensitivity of culture to detect H capsulatum depends on the clinical manifestations: it is 74% in patients with disseminated histoplasmosis, but only 42% in patients with acute pulmonary histoplasmosis.11 The serum histoplasma antigen test has a sensitivity of 91.8% in disseminated histoplasmosis, 87.5% in chronic pulmonary histoplasmosis, and 83% in acute pulmonary histoplasmosis.12
Urine testing for histoplasma antigen has generally proven to be slightly more sensitive than serum testing in all manifestations of histoplasmosis.13 Combining urine and serum testing increases the likelihood of antigen detection.
TREATMENT
Asymptomatic patients with mediastinal histoplasmosis do not require treatment. (Note: in some cases, lymphadenopathy is found incidentally, and biopsy is done to rule out malignancy.)
Standard treatment of symptomatic mediastinal histoplasmosis is oral itraconazole 200 mg, 3 times daily for 3 days, followed by 200 mg orally once or twice daily for 6 to 12 weeks.14
Although stopping immunosuppressant drugs is considered the standard of care in treating histoplasmosis in immunocompromised patients, there are no guidelines on when to resume them. However, a retrospective study of 98 cases of histoplasmosis in patients on tumor necrosis factor antagonists found that resuming immunosuppressants might be safe with close monitoring during the course of antifungal therapy.9 The role of long-term suppressive therapy with antifungal agents in patients on chronic immunosuppressive therapy is still unknown and needs further study.
TAKE-HOME MESSAGES
Histoplasmosis is the most prevalent endemic mycotic disease in the United States, and mediastinal lymphadenopathy is commonly seen in acute pulmonary histoplasmosis.
Histoplasmosis should be included in the differential diagnosis of granulomatous lung disease in patients from an endemic area or with a history of travel to an endemic area.
Immunosuppressive agents such as tumor necrosis factor antagonists and disease-modifying antirheumatic drugs can predispose to invasive fungal infection, including histoplasmosis.
While isolation of H capsulatum from culture remains the gold standard for the diagnosis of histoplasmosis, the histoplasma antigen tests (serum and urine) is more sensitive than culture.
References
Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician.” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev 2017; 26(145). doi:10.1183/16000617.0012-2017
Mercer LK, Galloway JB, Lunt M, et al. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2017; 76(3):497–503. doi:10.1136/annrheumdis-2016-209389
Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaoutis TE. Hospitalizations for endemic mycoses: a population-based national study. Clin Infect Dis 2006; 42(6):822–825. doi:10.1086/500405
Benedict K, Mody RK. Epidemiology of histoplasmosis outbreaks, United States, 1938–2013. Emerg Infect Dis 2016; 22(3):370–378. doi:10.3201/eid2203.151117
Wheat LJ. Diagnosis and management of histoplasmosis. Eur J Clin Microbiol Infect Dis 1989; 8(5):480–490. pmid:2502413
Goodwin RA Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980; 59(1):1–33. pmid:7356773
Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med 2004; 25(2):129–144. doi:10.1055/s-2004-824898
Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007; 86(3):162–169. doi:10.1097/md.0b013e3180679130
Vergidis P, Avery RK, Wheat LJ, et al. Histoplasmosis complicating tumor necrosis factor-a blocker therapy: a retrospective analysis of 98 cases. Clin Infect Dis 2015; 61(3):409–417. doi:10.1093/cid/civ299
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis 2011; 11:145. doi:10.1186/1471-2334-11-145
Hage CA, Ribes JA, Wengenack NL, et al. A multicenter evaluation of tests for diagnosis of histoplasmosis. Clin Infect Dis 2011; 53(5):448–454. doi:10.1093/cid/cir435
Azar MM, Hage CA. Laboratory diagnostics for histoplasmosis. J Clin Microbiol 2017; 55(6):1612–1620. doi:10.1128/JCM.02430-16
Swartzentruber S, Rhodes L, Kurkjian K, et al. Diagnosis of acute pulmonary histoplasmosis by antigen detection. Clin Infect Dis 2009; 49(12):1878–1882. doi:10.1086/648421
Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis 2007; 45(7):807–825. doi:10.1086/521259
Takaaki Kobayashi, MD Fellow, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Christine Cho, MD Associate, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Address: Takaaki Kobayashi, MD, Infectious Disease, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242; [email protected]
Takaaki Kobayashi, MD Fellow, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Christine Cho, MD Associate, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Address: Takaaki Kobayashi, MD, Infectious Disease, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242; [email protected]
Author and Disclosure Information
Takaaki Kobayashi, MD Fellow, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Christine Cho, MD Associate, Infectious Disease, University of Iowa Hospitals and Clinics, Iowa City, IA
Address: Takaaki Kobayashi, MD, Infectious Disease, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Iowa City, IA 52242; [email protected]
A 50-year-old man with Crohn disease and psoriatic arthritis treated with infliximab and methotrexate presented to a tertiary care hospital with fever, cough, and chest discomfort. The symptoms had first appeared 2 weeks earlier, and he had gone to an urgent care center, where he was prescribed a 5-day course of azithromycin and a corticosteroid, but this had not relieved his symptoms.
Figure 1. (A) An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).
He reported no recent travel, exposure to animals, or sick contacts. His temperature was 38.3°C (100.9°F). Results of the physical examination and initial laboratory testing were unremarkable. Chest computed tomography revealed prominent right hilar and mediastinal lymphadenopathy (Figure 1).
Bronchoscopy revealed edematous mucosa throughout, with minimal secretion. Specimens for bacterial, acid-fast bacillus, and fungal cultures were obtained from bronchoalveolar lavage. Endobronchial lymph node biopsy with ultrasonographic guidance revealed nonnecrotizing granuloma.
Bronchoalveolar lavage cultures showed no growth, but the patient’s serum histoplasma antigen was positive at 5.99 ng/dL (reference range: none detected), leading to the diagnosis of mediastinal granuloma due to histoplasmosis with possible dissemination. His immunosuppressant drugs were stopped, and oral itraconazole was started.
At a follow-up visit 2 months later, his serum antigen level had decreased to 0.68 ng/dL, and he had no symptoms whatsoever. At a visit 1 month after that, infliximab and methotrexate were restarted because of an exacerbation of Crohn disease. His oral itraconazole treatment was to be continued for at least 12 months, given the high suspicion for disseminated histoplasmosis while on immunosuppressant therapy.
DIFFERENTIAL DIAGNOSIS OF GRANULOMATOUS LUNG DISEASE AND LYMPHADENOPATHY
The differential diagnosis of granulomatous lung disease and lymphadenopathy is broad and includes noninfectious and infectious conditions.1
Noninfectious causes include lymphoma, sarcoidosis, inflammatory bowel disease, hypersensitivity pneumonia, side effects of drugs (eg, methotrexate, etanercept), rheumatoid nodules, vasculitis (eg, Churg-Strauss syndrome, granulomatosis with polyangiitis, primary amyloidosis, pneumoconiosis (eg, beryllium, cobalt), and Castleman disease.
There is concern that tumor necrosis factor antagonists may increase the risk of lymphoma, but a 2017 study found no evidence of this.2
Infectious conditions associated with granulomatous lung disease include tuberculosis, nontuberculous mycobacterial infection, fungal infection (eg, Cryptococcus, Coccidioides, Histoplasma, Blastomyces), brucellosis, tularemia (respiratory type B), parasitic infection (eg, Toxocara, Leishmania, Echinococcus, Schistosoma), and Whipple disease.
HISTOPLASMOSIS
Histoplasmosis, caused by infection with Histoplasma capsulatum, is the most prevalent endemic mycotic disease in the United States.3 The fungus is commonly found in the Ohio and Mississippi River valleys in the United States, and also in Central and South America and Asia.
Risk factors for histoplasmosis include living in or traveling to an endemic area, exposure to aerosolized soil that contains spores, and exposure to bats or birds and their droppings.4
Fewer than 5% of exposed individuals develop symptoms, which include fever, chills, headache, myalgia, anorexia, cough, and chest pain.5 Patients may experience symptoms shortly after exposure or may remain free of symptoms for years, with intermittent relapses of symptoms.6 Hilar or mediastinal lymphadenopathy is common in acute pulmonary histoplasmosis.7
The risk of disseminated histoplasmosis is greater in patients with reduced cell-mediated immunity, such as in human immunodeficiency virus infection, acquired immunodeficiency syndrome, solid-organ or bone marrow transplant, hematologic malignancies, immunosuppression (corticosteroids, disease-modifying antirheumatic drugs, and tumor necrosis factor antagonists), and congenital T-cell deficiencies.8
In a retrospective study, infliximab was the tumor necrosis factor antagonist most commonly associated with histoplasmosis.9 In a study of patients with rheumatoid arthritis, the disease-modifying drug most commonly associated was methotrexate.10
GOLD STANDARD FOR DIAGNOSIS
Isolation of H capsulatum from clinical specimens remains the gold standard for confirmation of histoplasmosis. The sensitivity of culture to detect H capsulatum depends on the clinical manifestations: it is 74% in patients with disseminated histoplasmosis, but only 42% in patients with acute pulmonary histoplasmosis.11 The serum histoplasma antigen test has a sensitivity of 91.8% in disseminated histoplasmosis, 87.5% in chronic pulmonary histoplasmosis, and 83% in acute pulmonary histoplasmosis.12
Urine testing for histoplasma antigen has generally proven to be slightly more sensitive than serum testing in all manifestations of histoplasmosis.13 Combining urine and serum testing increases the likelihood of antigen detection.
TREATMENT
Asymptomatic patients with mediastinal histoplasmosis do not require treatment. (Note: in some cases, lymphadenopathy is found incidentally, and biopsy is done to rule out malignancy.)
Standard treatment of symptomatic mediastinal histoplasmosis is oral itraconazole 200 mg, 3 times daily for 3 days, followed by 200 mg orally once or twice daily for 6 to 12 weeks.14
Although stopping immunosuppressant drugs is considered the standard of care in treating histoplasmosis in immunocompromised patients, there are no guidelines on when to resume them. However, a retrospective study of 98 cases of histoplasmosis in patients on tumor necrosis factor antagonists found that resuming immunosuppressants might be safe with close monitoring during the course of antifungal therapy.9 The role of long-term suppressive therapy with antifungal agents in patients on chronic immunosuppressive therapy is still unknown and needs further study.
TAKE-HOME MESSAGES
Histoplasmosis is the most prevalent endemic mycotic disease in the United States, and mediastinal lymphadenopathy is commonly seen in acute pulmonary histoplasmosis.
Histoplasmosis should be included in the differential diagnosis of granulomatous lung disease in patients from an endemic area or with a history of travel to an endemic area.
Immunosuppressive agents such as tumor necrosis factor antagonists and disease-modifying antirheumatic drugs can predispose to invasive fungal infection, including histoplasmosis.
While isolation of H capsulatum from culture remains the gold standard for the diagnosis of histoplasmosis, the histoplasma antigen tests (serum and urine) is more sensitive than culture.
A 50-year-old man with Crohn disease and psoriatic arthritis treated with infliximab and methotrexate presented to a tertiary care hospital with fever, cough, and chest discomfort. The symptoms had first appeared 2 weeks earlier, and he had gone to an urgent care center, where he was prescribed a 5-day course of azithromycin and a corticosteroid, but this had not relieved his symptoms.
Figure 1. (A) An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).
He reported no recent travel, exposure to animals, or sick contacts. His temperature was 38.3°C (100.9°F). Results of the physical examination and initial laboratory testing were unremarkable. Chest computed tomography revealed prominent right hilar and mediastinal lymphadenopathy (Figure 1).
Bronchoscopy revealed edematous mucosa throughout, with minimal secretion. Specimens for bacterial, acid-fast bacillus, and fungal cultures were obtained from bronchoalveolar lavage. Endobronchial lymph node biopsy with ultrasonographic guidance revealed nonnecrotizing granuloma.
Bronchoalveolar lavage cultures showed no growth, but the patient’s serum histoplasma antigen was positive at 5.99 ng/dL (reference range: none detected), leading to the diagnosis of mediastinal granuloma due to histoplasmosis with possible dissemination. His immunosuppressant drugs were stopped, and oral itraconazole was started.
At a follow-up visit 2 months later, his serum antigen level had decreased to 0.68 ng/dL, and he had no symptoms whatsoever. At a visit 1 month after that, infliximab and methotrexate were restarted because of an exacerbation of Crohn disease. His oral itraconazole treatment was to be continued for at least 12 months, given the high suspicion for disseminated histoplasmosis while on immunosuppressant therapy.
DIFFERENTIAL DIAGNOSIS OF GRANULOMATOUS LUNG DISEASE AND LYMPHADENOPATHY
The differential diagnosis of granulomatous lung disease and lymphadenopathy is broad and includes noninfectious and infectious conditions.1
Noninfectious causes include lymphoma, sarcoidosis, inflammatory bowel disease, hypersensitivity pneumonia, side effects of drugs (eg, methotrexate, etanercept), rheumatoid nodules, vasculitis (eg, Churg-Strauss syndrome, granulomatosis with polyangiitis, primary amyloidosis, pneumoconiosis (eg, beryllium, cobalt), and Castleman disease.
There is concern that tumor necrosis factor antagonists may increase the risk of lymphoma, but a 2017 study found no evidence of this.2
Infectious conditions associated with granulomatous lung disease include tuberculosis, nontuberculous mycobacterial infection, fungal infection (eg, Cryptococcus, Coccidioides, Histoplasma, Blastomyces), brucellosis, tularemia (respiratory type B), parasitic infection (eg, Toxocara, Leishmania, Echinococcus, Schistosoma), and Whipple disease.
HISTOPLASMOSIS
Histoplasmosis, caused by infection with Histoplasma capsulatum, is the most prevalent endemic mycotic disease in the United States.3 The fungus is commonly found in the Ohio and Mississippi River valleys in the United States, and also in Central and South America and Asia.
Risk factors for histoplasmosis include living in or traveling to an endemic area, exposure to aerosolized soil that contains spores, and exposure to bats or birds and their droppings.4
Fewer than 5% of exposed individuals develop symptoms, which include fever, chills, headache, myalgia, anorexia, cough, and chest pain.5 Patients may experience symptoms shortly after exposure or may remain free of symptoms for years, with intermittent relapses of symptoms.6 Hilar or mediastinal lymphadenopathy is common in acute pulmonary histoplasmosis.7
The risk of disseminated histoplasmosis is greater in patients with reduced cell-mediated immunity, such as in human immunodeficiency virus infection, acquired immunodeficiency syndrome, solid-organ or bone marrow transplant, hematologic malignancies, immunosuppression (corticosteroids, disease-modifying antirheumatic drugs, and tumor necrosis factor antagonists), and congenital T-cell deficiencies.8
In a retrospective study, infliximab was the tumor necrosis factor antagonist most commonly associated with histoplasmosis.9 In a study of patients with rheumatoid arthritis, the disease-modifying drug most commonly associated was methotrexate.10
GOLD STANDARD FOR DIAGNOSIS
Isolation of H capsulatum from clinical specimens remains the gold standard for confirmation of histoplasmosis. The sensitivity of culture to detect H capsulatum depends on the clinical manifestations: it is 74% in patients with disseminated histoplasmosis, but only 42% in patients with acute pulmonary histoplasmosis.11 The serum histoplasma antigen test has a sensitivity of 91.8% in disseminated histoplasmosis, 87.5% in chronic pulmonary histoplasmosis, and 83% in acute pulmonary histoplasmosis.12
Urine testing for histoplasma antigen has generally proven to be slightly more sensitive than serum testing in all manifestations of histoplasmosis.13 Combining urine and serum testing increases the likelihood of antigen detection.
TREATMENT
Asymptomatic patients with mediastinal histoplasmosis do not require treatment. (Note: in some cases, lymphadenopathy is found incidentally, and biopsy is done to rule out malignancy.)
Standard treatment of symptomatic mediastinal histoplasmosis is oral itraconazole 200 mg, 3 times daily for 3 days, followed by 200 mg orally once or twice daily for 6 to 12 weeks.14
Although stopping immunosuppressant drugs is considered the standard of care in treating histoplasmosis in immunocompromised patients, there are no guidelines on when to resume them. However, a retrospective study of 98 cases of histoplasmosis in patients on tumor necrosis factor antagonists found that resuming immunosuppressants might be safe with close monitoring during the course of antifungal therapy.9 The role of long-term suppressive therapy with antifungal agents in patients on chronic immunosuppressive therapy is still unknown and needs further study.
TAKE-HOME MESSAGES
Histoplasmosis is the most prevalent endemic mycotic disease in the United States, and mediastinal lymphadenopathy is commonly seen in acute pulmonary histoplasmosis.
Histoplasmosis should be included in the differential diagnosis of granulomatous lung disease in patients from an endemic area or with a history of travel to an endemic area.
Immunosuppressive agents such as tumor necrosis factor antagonists and disease-modifying antirheumatic drugs can predispose to invasive fungal infection, including histoplasmosis.
While isolation of H capsulatum from culture remains the gold standard for the diagnosis of histoplasmosis, the histoplasma antigen tests (serum and urine) is more sensitive than culture.
References
Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician.” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev 2017; 26(145). doi:10.1183/16000617.0012-2017
Mercer LK, Galloway JB, Lunt M, et al. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2017; 76(3):497–503. doi:10.1136/annrheumdis-2016-209389
Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaoutis TE. Hospitalizations for endemic mycoses: a population-based national study. Clin Infect Dis 2006; 42(6):822–825. doi:10.1086/500405
Benedict K, Mody RK. Epidemiology of histoplasmosis outbreaks, United States, 1938–2013. Emerg Infect Dis 2016; 22(3):370–378. doi:10.3201/eid2203.151117
Wheat LJ. Diagnosis and management of histoplasmosis. Eur J Clin Microbiol Infect Dis 1989; 8(5):480–490. pmid:2502413
Goodwin RA Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980; 59(1):1–33. pmid:7356773
Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med 2004; 25(2):129–144. doi:10.1055/s-2004-824898
Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007; 86(3):162–169. doi:10.1097/md.0b013e3180679130
Vergidis P, Avery RK, Wheat LJ, et al. Histoplasmosis complicating tumor necrosis factor-a blocker therapy: a retrospective analysis of 98 cases. Clin Infect Dis 2015; 61(3):409–417. doi:10.1093/cid/civ299
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis 2011; 11:145. doi:10.1186/1471-2334-11-145
Hage CA, Ribes JA, Wengenack NL, et al. A multicenter evaluation of tests for diagnosis of histoplasmosis. Clin Infect Dis 2011; 53(5):448–454. doi:10.1093/cid/cir435
Azar MM, Hage CA. Laboratory diagnostics for histoplasmosis. J Clin Microbiol 2017; 55(6):1612–1620. doi:10.1128/JCM.02430-16
Swartzentruber S, Rhodes L, Kurkjian K, et al. Diagnosis of acute pulmonary histoplasmosis by antigen detection. Clin Infect Dis 2009; 49(12):1878–1882. doi:10.1086/648421
Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis 2007; 45(7):807–825. doi:10.1086/521259
References
Ohshimo S, Guzman J, Costabel U, Bonella F. Differential diagnosis of granulomatous lung disease: clues and pitfalls: number 4 in the Series “Pathology for the clinician.” Edited by Peter Dorfmüller and Alberto Cavazza. Eur Respir Rev 2017; 26(145). doi:10.1183/16000617.0012-2017
Mercer LK, Galloway JB, Lunt M, et al. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2017; 76(3):497–503. doi:10.1136/annrheumdis-2016-209389
Chu JH, Feudtner C, Heydon K, Walsh TJ, Zaoutis TE. Hospitalizations for endemic mycoses: a population-based national study. Clin Infect Dis 2006; 42(6):822–825. doi:10.1086/500405
Benedict K, Mody RK. Epidemiology of histoplasmosis outbreaks, United States, 1938–2013. Emerg Infect Dis 2016; 22(3):370–378. doi:10.3201/eid2203.151117
Wheat LJ. Diagnosis and management of histoplasmosis. Eur J Clin Microbiol Infect Dis 1989; 8(5):480–490. pmid:2502413
Goodwin RA Jr, Shapiro JL, Thurman GH, Thurman SS, Des Prez RM. Disseminated histoplasmosis: clinical and pathologic correlations. Medicine (Baltimore) 1980; 59(1):1–33. pmid:7356773
Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, Loyd J. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med 2004; 25(2):129–144. doi:10.1055/s-2004-824898
Assi MA, Sandid MS, Baddour LM, Roberts GD, Walker RC. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore) 2007; 86(3):162–169. doi:10.1097/md.0b013e3180679130
Vergidis P, Avery RK, Wheat LJ, et al. Histoplasmosis complicating tumor necrosis factor-a blocker therapy: a retrospective analysis of 98 cases. Clin Infect Dis 2015; 61(3):409–417. doi:10.1093/cid/civ299
Olson TC, Bongartz T, Crowson CS, Roberts GD, Orenstein R, Matteson EL. Histoplasmosis infection in patients with rheumatoid arthritis, 1998–2009. BMC Infect Dis 2011; 11:145. doi:10.1186/1471-2334-11-145
Hage CA, Ribes JA, Wengenack NL, et al. A multicenter evaluation of tests for diagnosis of histoplasmosis. Clin Infect Dis 2011; 53(5):448–454. doi:10.1093/cid/cir435
Azar MM, Hage CA. Laboratory diagnostics for histoplasmosis. J Clin Microbiol 2017; 55(6):1612–1620. doi:10.1128/JCM.02430-16
Swartzentruber S, Rhodes L, Kurkjian K, et al. Diagnosis of acute pulmonary histoplasmosis by antigen detection. Clin Infect Dis 2009; 49(12):1878–1882. doi:10.1086/648421
Wheat LJ, Freifeld AG, Kleiman MB, et al; Infectious Diseases Society of America. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis 2007; 45(7):807–825. doi:10.1086/521259
No, they are not required or needed, but daily radiography and arterial blood gas testing are common practice: eg, 60% of intensive care unit (ICU) patients get daily radiographs,1 even though results provide low diagnostic yield and are unlikely to alter patient management compared with testing only when indicated.
The Choosing Wisely campaign,2 a collaborative effort of a number of professional societies, advises against ordering these diagnostic tests daily because routine testing increases risks to patients and burdens the healthcare system. Instead, testing is recommended only in response to a specific clinical question, or when the test results will affect the patient’s treatment.
CHEST RADIOGRAPHS: DAILY VS CLINICALLY INDICATED
Chest radiographs enable practitioners to monitor the position of endotracheal tubes and central venous catheters, evaluate fluid status, follow up on abnormal findings, detect complications of procedures (such as a pneumothorax), and identify otherwise undetected conditions.
And daily chest radiographs often detect abnormalities. A 1991 study by Hall et al3 of 538 chest radiographs in 74 patients on mechanical ventilation reported that 30% of daily routine chest radiographs disclosed a new but minor finding (eg, a small change in endotracheal tube position or a small infiltrate). The new findings were major in 13 (17.6%) of the 74 patients (95% confidence interval [CI] 9%–26%). These included findings that required an immediate diagnostic or therapeutic intervention (eg, endotracheal tube below the tracheal carina, malposition of a catheter, pneumothorax, large pleural effusion).
But most studies say daily radiographs are not needed. In a large prospective study published in 2006, Graat et al4 evaluated the clinical value of 2,457 routine chest radiographs in 754 patients in a combined surgical and medical ICU. Daily chest radiographs revealed new or unexpected findings in 5.8% of cases, but only 2.2% warranted a change in therapy. No differences were found between the medical and surgical patients. The authors concluded that daily routine radiographs in ICU patients seldom reveal unexpected, clinically relevant abnormalities, and those findings rarely require urgent intervention.
A 2010 meta-analysis of 8 studies (7,078 patients) by Oba and Zaza5 compared on-demand and daily routine strategies of performing chest radiographs. They estimated that eliminating daily routine chest radiographs would not affect death rates in the hospital (odds ratio [OR] 1.02, 95% CI 0.89–1.17, P = .78) or the ICU (OR 0.92, 95% CI 0.76–1.11, P = .4). They also found no significant differences in length of stay or duration of mechanical ventilation. This meta-analysis suggests that routine radiographs can be eliminated without adversely affecting outcomes in ICU patients.
A larger meta-analysis (9 trials, 39,358 radiographs, 9,611 patients) published in 2012 by Ganapathy et al6 also found no harm associated with restrictive radiography protocols. These investigators compared a daily chest radiography protocol against a protocol based on clinical indications. The primary outcome was the mortality rate in the ICU; secondary outcomes were the mortality rate in the hospital, the length of stay in the ICU, and duration of mechanical ventilation. They found no differences between routine and restrictive strategies in terms of ICU mortality (risk ratio [RR] 1.04, 95% CI 0.84–1.28, P = .72), hospital mortality (RR 0.98, 95% CI 0.68–1.41, P = .91), or other secondary outcomes.
Clinically indicated testing is better
The conclusion from these studies is that routine chest radiographs in patients undergoing mechanical ventilation does not improve patient outcomes, and thus, a clinically indicated protocol is preferred.
Furthermore, routine daily radiographs have adverse effects such as more cumulative radiation exposure to the patient7 and greater risk of accidental removal of devices (eg, catheters, tubes).8 Another concern is a higher risk of hospital-associated infections from bacterial spread from caregivers’ hands.9
Finally, daily radiographs increase the use of healthcare resources and expenditures. In a 2011 study, Gershengorn et al1 estimated that adopting a clinically indicated radiography strategy could save more than $144 million annually in the United States.
The ACR agrees. Appropriateness criteria published by the American College of Radiology (ACR) in 201510 recommend against routine daily chest radiographs in the ICU, in keeping with the findings of the critical care community. The ACR recommends an initial radiograph at admission to the ICU. However, follow-up radiographs should be obtained only for specific clinical indications, including a change in the patient’s clinical condition or to check for proper placement of endotracheal or nasogastric or orogastric tubes, pulmonary arterial catheters, central venous catheters, chest tubes, and other life-support devices.
Ultrasonography as an alternative
Ultrasonography is widely available and provides an alternative to chest radiography for detecting significant abnormalities in patients on mechanical ventilation without exposing them to radiation and using relatively fewer resources.
A 2012 meta-analysis (8 studies, 1,048 patients) found that bedside ultrasonography reliably detects pneumothorax.11 It can also provide a rapid diagnosis of the cause of acute respiratory failure such as pneumonia or pulmonary edema.12 Ultrasonography, with the appropriate expertise, can also confirm the position of an endotracheal tube13 or central venous catheter.14
ARTERIAL BLOOD GAS TESTING: DAILY VS CLINICALLY INDICATED
Arterial blood gas testing has value for managing patients undergoing mechanical ventilation, and it is one of the most commonly performed diagnostic tests in the ICU. It provides reliable information about the patient’s oxygenation and acid-base status. It is commonly requested when changing ventilator settings.
Downsides. Arterial blood gas measurements account for 10% to 20% of the cost incurred during ICU stay.15 In addition, they require an arterial puncture—an invasive procedure associated with potentially serious complications such as occlusion of the artery, digital embolization leading to digital ischemia, local infection, pseudoaneurysm, hematoma, bleeding, and skin necrosis.
Is daily testing needed?
Guidelines say no. The 2013 American Association for Respiratory Care16 guidelines suggest that arterial blood gas testing should be based on the clinical assessment of the patient. They recommend blood gas analysis to evaluate the patient’s ventilatory status (reflected by the partial pressure of arterial carbon dioxide [PaCO2], acid-base status (reflected by pH), arterial oxygenation (partial pressure of arterial oxygen [PaO2] and oxyhemoglobin saturation), oxygen-carrying capacity, and whether the patient likely has an intrapulmonary shunt. They state that testing is useful to quantify the response to therapeutic or diagnostic interventions such as cardiopulmonary exercise testing, to monitor severity and progression of documented disease, and to assess the adequacy of circulatory response.
Studies agree
The ACR recommendation to test “as clinically indicated” is supported by studies showing that patient outcomes are not inferior for arterial blood gas testing when clinically indicated instead of daily, and that this practice is associated with fewer complications, less resource use, and reduced overall patient care costs.
A 2015 study compared the efficacy and safety of obtaining arterial blood gases based on clinical assessment vs daily in 300 critically ill patients.17 Overall, fewer samples were obtained per patient in the clinical assessment group than in the daily group (all patients 3.7 vs 5.5; ventilated patients 2.03 vs 6.12; P < .001 for both). In ventilated patients, there was a 60% decrease in arterial blood gas orders without affecting patient outcomes and safety, including a lower risk of complications and overall cost of care.
In another study, Martinez-Balzano et al18 evaluated the effect of guidelines they developed to optimize the use of arterial blood gas testing in their ICUs. These guidelines encouraged testing of arterial blood gases after an acute respiratory event or for a rational clinical concern, and discouraged testing for routine surveillance, after planned changes of positive end-expiratory pressure or inspired oxygen fraction on mechanical ventilation, for spontaneous breathing trials, or when a disorder was not suspected.
Compared with data collected before implementation, these guidelines reduced the number of arterial blood gas tests by 821.5 per month (41.5%), or approximately 1 test per patient per mechanical-ventilation day for each month (43.1%; P < .001). Appropriately indicated testing rose to 83.4% from a baseline of 67.5% (P = .002). Additionally, this approach was associated with saving 49 liters of blood, reducing ICU costs by $39,432, and freeing up 1,643 staff work hours for other tasks. There were no significant differences in days on mechanical ventilation, severity of illness, or mortality between the 2 periods.18
Extubation effects. Routine arterial blood gas testing has not been shown to affect extubation decisions in patients on mechanical ventilation. In a study of 83 patients who completed a spontaneous breathing trial (total of 100 trials), Salam et al19 found arterial blood gas values obtained during the trial did not change the extubation decision in 93% of the cases.
In a study of 54 extubations in 52 patients,20 65% of the extubations were performed without obtaining an arterial blood gas test after the patient completed a trial of spontaneous breathing. The extubation success rate was 94% for the entire group, and it was the same regardless of whether testing was done (94.7% vs 94.3%, respectively).
Alternatives to arterial blood gases
There are less-invasive means to obtain the information that comes from an arterial blood gas test.
Pulse oximetry is a rapid noninvasive tool that provides continuous assessment of peripheral arterial oxygen saturation as a surrogate marker for tissue arterial oxygenation. However, it cannot measure PaO2 or PaCO2.21
Transcutaneous carbon dioxide (PTCO2) monitoring is another continuous noninvasive alternative. The newer PTCO2 devices are useful in patients with acute respiratory failure and in critically ill patients on vasopressors or vasodilators. Studies have shown good correlation between PTCO2 and PaCO2.22,23
End-tidal carbon dioxide (PetCO2) is another alternative to estimate PaCO2. It can also be used to confirm endotracheal tube placement, during transportation, during procedures in which the patient is under conscious sedation, and to monitor the effectiveness of cardiopulmonary resuscitation and return of circulation after cardiac arrest. PetCO2 measurements are not as accurate as arterial blood gas testing owing to a difference of approximately 2 to 5 mm Hg between PaCO2 and PetCO2 in normal lungs due to alveolar dead space. This difference may be much higher depending on the clinical condition and the degree of alveolar dead space.21,24,25
Venous blood gases, which can be obtained from a peripheral or central venous catheter, are adequate to assess pH and partial pressure of carbon dioxide (PCO2) in hemodynamically stable patients. Walkey et al26 found that the accuracy of venous blood gas measurement to predict arterial blood gases was 90%. They recommended adjusting the venous pH up by 0.05 and the PCO2 down by 5 mm Hg to account for the positive bias of venous blood gases. A limitation of this method is that the values are not reliable in patients who are in shock.
These alternatives can be used as a substitute for daily arterial blood gases. However, in certain clinical scenarios, arterial blood gas measurement remains a necessary and useful clinical tool.
TAKE-HOME MESSAGE
Most scientific evidence suggests that chest radiographs and arterial blood gas measurement in patients undergoing mechanical ventilation—and critically ill, in general—are best done when clinically indicated rather than routinely on a daily basis. This will reduce cost and harm to patients that may result from these unnecessary tests and not adversely affect outcomes.
References
Gershengorn HB, Wunsch H, Scales DC, Rubenfeld GD. Trends in use of daily chest radiographs among US adults receiving mechanical ventilation. JAMA Netw Open 2018; 1(4):e181119. doi:10.1001/jamanetworkopen.2018.1119
Hall JB, White SR, Karrison T. Efficacy of daily routine chest radiographs in intubated, mechanically ventilated patients. Crit Care Med 1991; 19(5):689–693. pmid:2026031
Graat ME, Choi G, Wolthuis EK, et al. The clinical value of daily routine chest radiographs in a mixed medical-surgical intensive care unit is low. Crit Care 2006; 10(1):R11. doi:10.1186/cc3955
Oba Y, Zaza T. Abandoning daily routine chest radiography in the intensive care unit: meta-analysis. Radiology 2010; 255(2):386–395. doi:10.1148/radiol.10090946
Ganapathy A, Adhikari NK, Spiegelman J, Scales DC. Routine chest x-rays in intensive care units: a systematic review and meta-analysis. Crit Care 2012; 16(2):R68. doi:10.1186/cc11321
Krishnan S, Moghekar A, Duggal A, et al. Radiation exposure in the medical ICU: predictors and characteristics. Chest 2018; 153(5):1160–1168. doi:10.1016/j.chest.2018.01.019
Hejblum G, Chalumeau-Lemoine L, Ioos V, et al. Comparison of routine and on-demand prescription of chest radiographs in mechanically ventilated adults: a multicentre, cluster-randomised, two-period crossover study. Lancet 2009; 374(9702):1687–1693. doi:10.1016/S0140-6736(09)61459-8
Levin PD, Shatz O, Sviri S, et al. Contamination of portable radiograph equipment with resistant bacteria in the ICU. Chest 2009; 136(2):426–432. doi:10.1378/chest.09-0049
Suh RD, Genshaft SJ, Kirsch J, et al. ACR Appropriateness Criteria® Intensive Care Unit Patients. J Thorac Imaging 2015; 30(6):W63–W65. doi:10.1097/RTI.0000000000000174
Alrajhi K, Woo MY, Vaillancourt C. Test characteristics of ultrasonography for the detection of pneumothorax: a systematic review and meta-analysis. Chest 2012; 141(3):703–708. doi:10.1378/chest.11-0131
Lichetenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008; 134(1):117–125. doi:10.1378/chest.07-2800
Das SK, Choupoo NS, Haldar R, Lahkar A. Transtracheal ultrasound for verification of endotracheal tube placement: a systematic review and meta-analysis. Can J Anaesth 2015; 62(4):413–423. doi:10.1007/s12630-014-0301-z
Ablordeppey EA, Drewry AM, Beyer AB, et al. Diagnostic accuracy of central venous catheter confirmation by bedside ultrasound versus chest radiography in critically ill patients: a systematic review and meta-analysis. Crit Care Med 2017; 45(4):715–724. doi:10.1097/CCM.0000000000002188
DellaVolpe JD, Chakraborti C, Cerreta K, et al. Effects of implementing a protocol for arterial blood gas use on ordering practices and diagnostic yield. Healthc (Amst) 2014; 2(2):130–135. doi:10.1016/j.hjdsi.2013.09.006
Davis MD, Walsh BK, Sittig SE, Restrepo RD. AARC clinical practice guideline: blood gas analysis and hemoximetry. Respir Care 2013; 58(10):1694–1703. doi:10.4187/respcare.02786
Blum FE, Lund ET, Hall HA, Tachauer AD, Chedrawy EG, Zilberstein J. Reevaluation of the utilization of arterial blood gas analysis in the intensive care unit: effects on patient safety and patient outcome. J Crit Care 2015; 30(2):438.e1–e5. doi:10.1016/j.jcrc.2014.10.025
Martínez-Balzano CD, Oliveira P, O’Rourke M, Hills L, Sosa AF; Critical Care Operations Committee of the UMass Memorial Healthcare Center. An educational intervention optimizes the use of arterial blood gas determinations across ICUs from different specialties: a quality-improvement study. Chest 2017; 151(3):579–585. doi:10.1016/j.chest.2016.10.035
Salam A, Smina M, Gada P, et al. The effect of arterial blood gas values on extubation decisions. Respir Care 2003; 48(11):1033–1037. pmid:14585115
Pawson SR, DePriest JL. Are blood gases necessary in mechanically ventilated patients who have successfully completed a spontaneous breathing trial? Respir Care 2004; 49(11):1316–1319. pmid:15507165
Soubani AO. Noninvasive monitoring of oxygen and carbon dioxide. Am J Emerg Med 2001; 19(2):141–146. doi:10.1053/ajem.2001.21353
Nicolini A, Ferrari MB. Evaluation of a transcutaneous carbon dioxide monitor in patients with acute respiratory failure. Ann Thorac Med 2011; 6(4):217–220. doi:10.4103/1817-1737.84776
Bendjelid K, Schütz N, Stotz M, Gerard I, Suter PM, Romand JA. Transcutaneous PCO2 monitoring in critically ill adults: clinical evaluation of a new sensor. Crit Care Med 2005; 33(10):2203–2206. pmid:16215371
Huttmann SE, Windisch W, Storre JH. Techniques for the measurement and monitoring of carbon dioxide in the blood. Ann Am Thorac Soc 2014; 11(4):645–652. doi:10.1513/AnnalsATS.201311-387FR
McSwain SD, Hamel DS, Smith PB, et al. End-tidal and arterial carbon dioxide measurements correlate across all levels of physiologic dead space. Respir Care 2010; 55(3):288–293. pmid:20196877
Walkey AJ, Farber HW, O'Donnell C, Cabral H, Eagan JS, Philippides GJ. The accuracy of the central venous blood gas for acid-base monitoring. J Intensive Care Med 2010; 25(2):104–110. doi:10.1177/0885066609356164
Shyam Ganti, MD Division of Pulmonary, Critical Care, and Sleep Medicine, Wayne State University School of Medicine, Detroit, MI
Ravinder D. Bhanot, MD Division of Pulmonary and Critical Care, Ascension St. Mary’s, Saginaw, MI
Jasleen Kaur, MD Department of Internal Medicine, Wayne State University School of Medicine, Detroit, MI
Cassondra Cramer-Bour, MD Department of Medicine, Boston University School of Medicine, Boston, MA
Ayman O. Soubani, MD Professor of Medicine, Wayne State University School of Medicine; Medical Director, Medical ICU, Harper University Hospital; Service Chief, Pulmonary and Critical Care, and Medical Director, Critical Care Service, Karmanos Cancer Center; Division of Pulmonary, Critical Care and Sleep Medicine, Wayne State University School of Medicine, Detroit, MI
Address: Ayman O. Soubani, MD, Division of Pulmonary, Critical Care and Sleep Medicine. Wayne State University School of Medicine, 3990 John R-3 Hudson, Detroit, MI 48201; [email protected]
Shyam Ganti, MD Division of Pulmonary, Critical Care, and Sleep Medicine, Wayne State University School of Medicine, Detroit, MI
Ravinder D. Bhanot, MD Division of Pulmonary and Critical Care, Ascension St. Mary’s, Saginaw, MI
Jasleen Kaur, MD Department of Internal Medicine, Wayne State University School of Medicine, Detroit, MI
Cassondra Cramer-Bour, MD Department of Medicine, Boston University School of Medicine, Boston, MA
Ayman O. Soubani, MD Professor of Medicine, Wayne State University School of Medicine; Medical Director, Medical ICU, Harper University Hospital; Service Chief, Pulmonary and Critical Care, and Medical Director, Critical Care Service, Karmanos Cancer Center; Division of Pulmonary, Critical Care and Sleep Medicine, Wayne State University School of Medicine, Detroit, MI
Address: Ayman O. Soubani, MD, Division of Pulmonary, Critical Care and Sleep Medicine. Wayne State University School of Medicine, 3990 John R-3 Hudson, Detroit, MI 48201; [email protected]
Author and Disclosure Information
Shyam Ganti, MD Division of Pulmonary, Critical Care, and Sleep Medicine, Wayne State University School of Medicine, Detroit, MI
Ravinder D. Bhanot, MD Division of Pulmonary and Critical Care, Ascension St. Mary’s, Saginaw, MI
Jasleen Kaur, MD Department of Internal Medicine, Wayne State University School of Medicine, Detroit, MI
Cassondra Cramer-Bour, MD Department of Medicine, Boston University School of Medicine, Boston, MA
Ayman O. Soubani, MD Professor of Medicine, Wayne State University School of Medicine; Medical Director, Medical ICU, Harper University Hospital; Service Chief, Pulmonary and Critical Care, and Medical Director, Critical Care Service, Karmanos Cancer Center; Division of Pulmonary, Critical Care and Sleep Medicine, Wayne State University School of Medicine, Detroit, MI
Address: Ayman O. Soubani, MD, Division of Pulmonary, Critical Care and Sleep Medicine. Wayne State University School of Medicine, 3990 John R-3 Hudson, Detroit, MI 48201; [email protected]
No, they are not required or needed, but daily radiography and arterial blood gas testing are common practice: eg, 60% of intensive care unit (ICU) patients get daily radiographs,1 even though results provide low diagnostic yield and are unlikely to alter patient management compared with testing only when indicated.
The Choosing Wisely campaign,2 a collaborative effort of a number of professional societies, advises against ordering these diagnostic tests daily because routine testing increases risks to patients and burdens the healthcare system. Instead, testing is recommended only in response to a specific clinical question, or when the test results will affect the patient’s treatment.
CHEST RADIOGRAPHS: DAILY VS CLINICALLY INDICATED
Chest radiographs enable practitioners to monitor the position of endotracheal tubes and central venous catheters, evaluate fluid status, follow up on abnormal findings, detect complications of procedures (such as a pneumothorax), and identify otherwise undetected conditions.
And daily chest radiographs often detect abnormalities. A 1991 study by Hall et al3 of 538 chest radiographs in 74 patients on mechanical ventilation reported that 30% of daily routine chest radiographs disclosed a new but minor finding (eg, a small change in endotracheal tube position or a small infiltrate). The new findings were major in 13 (17.6%) of the 74 patients (95% confidence interval [CI] 9%–26%). These included findings that required an immediate diagnostic or therapeutic intervention (eg, endotracheal tube below the tracheal carina, malposition of a catheter, pneumothorax, large pleural effusion).
But most studies say daily radiographs are not needed. In a large prospective study published in 2006, Graat et al4 evaluated the clinical value of 2,457 routine chest radiographs in 754 patients in a combined surgical and medical ICU. Daily chest radiographs revealed new or unexpected findings in 5.8% of cases, but only 2.2% warranted a change in therapy. No differences were found between the medical and surgical patients. The authors concluded that daily routine radiographs in ICU patients seldom reveal unexpected, clinically relevant abnormalities, and those findings rarely require urgent intervention.
A 2010 meta-analysis of 8 studies (7,078 patients) by Oba and Zaza5 compared on-demand and daily routine strategies of performing chest radiographs. They estimated that eliminating daily routine chest radiographs would not affect death rates in the hospital (odds ratio [OR] 1.02, 95% CI 0.89–1.17, P = .78) or the ICU (OR 0.92, 95% CI 0.76–1.11, P = .4). They also found no significant differences in length of stay or duration of mechanical ventilation. This meta-analysis suggests that routine radiographs can be eliminated without adversely affecting outcomes in ICU patients.
A larger meta-analysis (9 trials, 39,358 radiographs, 9,611 patients) published in 2012 by Ganapathy et al6 also found no harm associated with restrictive radiography protocols. These investigators compared a daily chest radiography protocol against a protocol based on clinical indications. The primary outcome was the mortality rate in the ICU; secondary outcomes were the mortality rate in the hospital, the length of stay in the ICU, and duration of mechanical ventilation. They found no differences between routine and restrictive strategies in terms of ICU mortality (risk ratio [RR] 1.04, 95% CI 0.84–1.28, P = .72), hospital mortality (RR 0.98, 95% CI 0.68–1.41, P = .91), or other secondary outcomes.
Clinically indicated testing is better
The conclusion from these studies is that routine chest radiographs in patients undergoing mechanical ventilation does not improve patient outcomes, and thus, a clinically indicated protocol is preferred.
Furthermore, routine daily radiographs have adverse effects such as more cumulative radiation exposure to the patient7 and greater risk of accidental removal of devices (eg, catheters, tubes).8 Another concern is a higher risk of hospital-associated infections from bacterial spread from caregivers’ hands.9
Finally, daily radiographs increase the use of healthcare resources and expenditures. In a 2011 study, Gershengorn et al1 estimated that adopting a clinically indicated radiography strategy could save more than $144 million annually in the United States.
The ACR agrees. Appropriateness criteria published by the American College of Radiology (ACR) in 201510 recommend against routine daily chest radiographs in the ICU, in keeping with the findings of the critical care community. The ACR recommends an initial radiograph at admission to the ICU. However, follow-up radiographs should be obtained only for specific clinical indications, including a change in the patient’s clinical condition or to check for proper placement of endotracheal or nasogastric or orogastric tubes, pulmonary arterial catheters, central venous catheters, chest tubes, and other life-support devices.
Ultrasonography as an alternative
Ultrasonography is widely available and provides an alternative to chest radiography for detecting significant abnormalities in patients on mechanical ventilation without exposing them to radiation and using relatively fewer resources.
A 2012 meta-analysis (8 studies, 1,048 patients) found that bedside ultrasonography reliably detects pneumothorax.11 It can also provide a rapid diagnosis of the cause of acute respiratory failure such as pneumonia or pulmonary edema.12 Ultrasonography, with the appropriate expertise, can also confirm the position of an endotracheal tube13 or central venous catheter.14
ARTERIAL BLOOD GAS TESTING: DAILY VS CLINICALLY INDICATED
Arterial blood gas testing has value for managing patients undergoing mechanical ventilation, and it is one of the most commonly performed diagnostic tests in the ICU. It provides reliable information about the patient’s oxygenation and acid-base status. It is commonly requested when changing ventilator settings.
Downsides. Arterial blood gas measurements account for 10% to 20% of the cost incurred during ICU stay.15 In addition, they require an arterial puncture—an invasive procedure associated with potentially serious complications such as occlusion of the artery, digital embolization leading to digital ischemia, local infection, pseudoaneurysm, hematoma, bleeding, and skin necrosis.
Is daily testing needed?
Guidelines say no. The 2013 American Association for Respiratory Care16 guidelines suggest that arterial blood gas testing should be based on the clinical assessment of the patient. They recommend blood gas analysis to evaluate the patient’s ventilatory status (reflected by the partial pressure of arterial carbon dioxide [PaCO2], acid-base status (reflected by pH), arterial oxygenation (partial pressure of arterial oxygen [PaO2] and oxyhemoglobin saturation), oxygen-carrying capacity, and whether the patient likely has an intrapulmonary shunt. They state that testing is useful to quantify the response to therapeutic or diagnostic interventions such as cardiopulmonary exercise testing, to monitor severity and progression of documented disease, and to assess the adequacy of circulatory response.
Studies agree
The ACR recommendation to test “as clinically indicated” is supported by studies showing that patient outcomes are not inferior for arterial blood gas testing when clinically indicated instead of daily, and that this practice is associated with fewer complications, less resource use, and reduced overall patient care costs.
A 2015 study compared the efficacy and safety of obtaining arterial blood gases based on clinical assessment vs daily in 300 critically ill patients.17 Overall, fewer samples were obtained per patient in the clinical assessment group than in the daily group (all patients 3.7 vs 5.5; ventilated patients 2.03 vs 6.12; P < .001 for both). In ventilated patients, there was a 60% decrease in arterial blood gas orders without affecting patient outcomes and safety, including a lower risk of complications and overall cost of care.
In another study, Martinez-Balzano et al18 evaluated the effect of guidelines they developed to optimize the use of arterial blood gas testing in their ICUs. These guidelines encouraged testing of arterial blood gases after an acute respiratory event or for a rational clinical concern, and discouraged testing for routine surveillance, after planned changes of positive end-expiratory pressure or inspired oxygen fraction on mechanical ventilation, for spontaneous breathing trials, or when a disorder was not suspected.
Compared with data collected before implementation, these guidelines reduced the number of arterial blood gas tests by 821.5 per month (41.5%), or approximately 1 test per patient per mechanical-ventilation day for each month (43.1%; P < .001). Appropriately indicated testing rose to 83.4% from a baseline of 67.5% (P = .002). Additionally, this approach was associated with saving 49 liters of blood, reducing ICU costs by $39,432, and freeing up 1,643 staff work hours for other tasks. There were no significant differences in days on mechanical ventilation, severity of illness, or mortality between the 2 periods.18
Extubation effects. Routine arterial blood gas testing has not been shown to affect extubation decisions in patients on mechanical ventilation. In a study of 83 patients who completed a spontaneous breathing trial (total of 100 trials), Salam et al19 found arterial blood gas values obtained during the trial did not change the extubation decision in 93% of the cases.
In a study of 54 extubations in 52 patients,20 65% of the extubations were performed without obtaining an arterial blood gas test after the patient completed a trial of spontaneous breathing. The extubation success rate was 94% for the entire group, and it was the same regardless of whether testing was done (94.7% vs 94.3%, respectively).
Alternatives to arterial blood gases
There are less-invasive means to obtain the information that comes from an arterial blood gas test.
Pulse oximetry is a rapid noninvasive tool that provides continuous assessment of peripheral arterial oxygen saturation as a surrogate marker for tissue arterial oxygenation. However, it cannot measure PaO2 or PaCO2.21
Transcutaneous carbon dioxide (PTCO2) monitoring is another continuous noninvasive alternative. The newer PTCO2 devices are useful in patients with acute respiratory failure and in critically ill patients on vasopressors or vasodilators. Studies have shown good correlation between PTCO2 and PaCO2.22,23
End-tidal carbon dioxide (PetCO2) is another alternative to estimate PaCO2. It can also be used to confirm endotracheal tube placement, during transportation, during procedures in which the patient is under conscious sedation, and to monitor the effectiveness of cardiopulmonary resuscitation and return of circulation after cardiac arrest. PetCO2 measurements are not as accurate as arterial blood gas testing owing to a difference of approximately 2 to 5 mm Hg between PaCO2 and PetCO2 in normal lungs due to alveolar dead space. This difference may be much higher depending on the clinical condition and the degree of alveolar dead space.21,24,25
Venous blood gases, which can be obtained from a peripheral or central venous catheter, are adequate to assess pH and partial pressure of carbon dioxide (PCO2) in hemodynamically stable patients. Walkey et al26 found that the accuracy of venous blood gas measurement to predict arterial blood gases was 90%. They recommended adjusting the venous pH up by 0.05 and the PCO2 down by 5 mm Hg to account for the positive bias of venous blood gases. A limitation of this method is that the values are not reliable in patients who are in shock.
These alternatives can be used as a substitute for daily arterial blood gases. However, in certain clinical scenarios, arterial blood gas measurement remains a necessary and useful clinical tool.
TAKE-HOME MESSAGE
Most scientific evidence suggests that chest radiographs and arterial blood gas measurement in patients undergoing mechanical ventilation—and critically ill, in general—are best done when clinically indicated rather than routinely on a daily basis. This will reduce cost and harm to patients that may result from these unnecessary tests and not adversely affect outcomes.
No, they are not required or needed, but daily radiography and arterial blood gas testing are common practice: eg, 60% of intensive care unit (ICU) patients get daily radiographs,1 even though results provide low diagnostic yield and are unlikely to alter patient management compared with testing only when indicated.
The Choosing Wisely campaign,2 a collaborative effort of a number of professional societies, advises against ordering these diagnostic tests daily because routine testing increases risks to patients and burdens the healthcare system. Instead, testing is recommended only in response to a specific clinical question, or when the test results will affect the patient’s treatment.
CHEST RADIOGRAPHS: DAILY VS CLINICALLY INDICATED
Chest radiographs enable practitioners to monitor the position of endotracheal tubes and central venous catheters, evaluate fluid status, follow up on abnormal findings, detect complications of procedures (such as a pneumothorax), and identify otherwise undetected conditions.
And daily chest radiographs often detect abnormalities. A 1991 study by Hall et al3 of 538 chest radiographs in 74 patients on mechanical ventilation reported that 30% of daily routine chest radiographs disclosed a new but minor finding (eg, a small change in endotracheal tube position or a small infiltrate). The new findings were major in 13 (17.6%) of the 74 patients (95% confidence interval [CI] 9%–26%). These included findings that required an immediate diagnostic or therapeutic intervention (eg, endotracheal tube below the tracheal carina, malposition of a catheter, pneumothorax, large pleural effusion).
But most studies say daily radiographs are not needed. In a large prospective study published in 2006, Graat et al4 evaluated the clinical value of 2,457 routine chest radiographs in 754 patients in a combined surgical and medical ICU. Daily chest radiographs revealed new or unexpected findings in 5.8% of cases, but only 2.2% warranted a change in therapy. No differences were found between the medical and surgical patients. The authors concluded that daily routine radiographs in ICU patients seldom reveal unexpected, clinically relevant abnormalities, and those findings rarely require urgent intervention.
A 2010 meta-analysis of 8 studies (7,078 patients) by Oba and Zaza5 compared on-demand and daily routine strategies of performing chest radiographs. They estimated that eliminating daily routine chest radiographs would not affect death rates in the hospital (odds ratio [OR] 1.02, 95% CI 0.89–1.17, P = .78) or the ICU (OR 0.92, 95% CI 0.76–1.11, P = .4). They also found no significant differences in length of stay or duration of mechanical ventilation. This meta-analysis suggests that routine radiographs can be eliminated without adversely affecting outcomes in ICU patients.
A larger meta-analysis (9 trials, 39,358 radiographs, 9,611 patients) published in 2012 by Ganapathy et al6 also found no harm associated with restrictive radiography protocols. These investigators compared a daily chest radiography protocol against a protocol based on clinical indications. The primary outcome was the mortality rate in the ICU; secondary outcomes were the mortality rate in the hospital, the length of stay in the ICU, and duration of mechanical ventilation. They found no differences between routine and restrictive strategies in terms of ICU mortality (risk ratio [RR] 1.04, 95% CI 0.84–1.28, P = .72), hospital mortality (RR 0.98, 95% CI 0.68–1.41, P = .91), or other secondary outcomes.
Clinically indicated testing is better
The conclusion from these studies is that routine chest radiographs in patients undergoing mechanical ventilation does not improve patient outcomes, and thus, a clinically indicated protocol is preferred.
Furthermore, routine daily radiographs have adverse effects such as more cumulative radiation exposure to the patient7 and greater risk of accidental removal of devices (eg, catheters, tubes).8 Another concern is a higher risk of hospital-associated infections from bacterial spread from caregivers’ hands.9
Finally, daily radiographs increase the use of healthcare resources and expenditures. In a 2011 study, Gershengorn et al1 estimated that adopting a clinically indicated radiography strategy could save more than $144 million annually in the United States.
The ACR agrees. Appropriateness criteria published by the American College of Radiology (ACR) in 201510 recommend against routine daily chest radiographs in the ICU, in keeping with the findings of the critical care community. The ACR recommends an initial radiograph at admission to the ICU. However, follow-up radiographs should be obtained only for specific clinical indications, including a change in the patient’s clinical condition or to check for proper placement of endotracheal or nasogastric or orogastric tubes, pulmonary arterial catheters, central venous catheters, chest tubes, and other life-support devices.
Ultrasonography as an alternative
Ultrasonography is widely available and provides an alternative to chest radiography for detecting significant abnormalities in patients on mechanical ventilation without exposing them to radiation and using relatively fewer resources.
A 2012 meta-analysis (8 studies, 1,048 patients) found that bedside ultrasonography reliably detects pneumothorax.11 It can also provide a rapid diagnosis of the cause of acute respiratory failure such as pneumonia or pulmonary edema.12 Ultrasonography, with the appropriate expertise, can also confirm the position of an endotracheal tube13 or central venous catheter.14
ARTERIAL BLOOD GAS TESTING: DAILY VS CLINICALLY INDICATED
Arterial blood gas testing has value for managing patients undergoing mechanical ventilation, and it is one of the most commonly performed diagnostic tests in the ICU. It provides reliable information about the patient’s oxygenation and acid-base status. It is commonly requested when changing ventilator settings.
Downsides. Arterial blood gas measurements account for 10% to 20% of the cost incurred during ICU stay.15 In addition, they require an arterial puncture—an invasive procedure associated with potentially serious complications such as occlusion of the artery, digital embolization leading to digital ischemia, local infection, pseudoaneurysm, hematoma, bleeding, and skin necrosis.
Is daily testing needed?
Guidelines say no. The 2013 American Association for Respiratory Care16 guidelines suggest that arterial blood gas testing should be based on the clinical assessment of the patient. They recommend blood gas analysis to evaluate the patient’s ventilatory status (reflected by the partial pressure of arterial carbon dioxide [PaCO2], acid-base status (reflected by pH), arterial oxygenation (partial pressure of arterial oxygen [PaO2] and oxyhemoglobin saturation), oxygen-carrying capacity, and whether the patient likely has an intrapulmonary shunt. They state that testing is useful to quantify the response to therapeutic or diagnostic interventions such as cardiopulmonary exercise testing, to monitor severity and progression of documented disease, and to assess the adequacy of circulatory response.
Studies agree
The ACR recommendation to test “as clinically indicated” is supported by studies showing that patient outcomes are not inferior for arterial blood gas testing when clinically indicated instead of daily, and that this practice is associated with fewer complications, less resource use, and reduced overall patient care costs.
A 2015 study compared the efficacy and safety of obtaining arterial blood gases based on clinical assessment vs daily in 300 critically ill patients.17 Overall, fewer samples were obtained per patient in the clinical assessment group than in the daily group (all patients 3.7 vs 5.5; ventilated patients 2.03 vs 6.12; P < .001 for both). In ventilated patients, there was a 60% decrease in arterial blood gas orders without affecting patient outcomes and safety, including a lower risk of complications and overall cost of care.
In another study, Martinez-Balzano et al18 evaluated the effect of guidelines they developed to optimize the use of arterial blood gas testing in their ICUs. These guidelines encouraged testing of arterial blood gases after an acute respiratory event or for a rational clinical concern, and discouraged testing for routine surveillance, after planned changes of positive end-expiratory pressure or inspired oxygen fraction on mechanical ventilation, for spontaneous breathing trials, or when a disorder was not suspected.
Compared with data collected before implementation, these guidelines reduced the number of arterial blood gas tests by 821.5 per month (41.5%), or approximately 1 test per patient per mechanical-ventilation day for each month (43.1%; P < .001). Appropriately indicated testing rose to 83.4% from a baseline of 67.5% (P = .002). Additionally, this approach was associated with saving 49 liters of blood, reducing ICU costs by $39,432, and freeing up 1,643 staff work hours for other tasks. There were no significant differences in days on mechanical ventilation, severity of illness, or mortality between the 2 periods.18
Extubation effects. Routine arterial blood gas testing has not been shown to affect extubation decisions in patients on mechanical ventilation. In a study of 83 patients who completed a spontaneous breathing trial (total of 100 trials), Salam et al19 found arterial blood gas values obtained during the trial did not change the extubation decision in 93% of the cases.
In a study of 54 extubations in 52 patients,20 65% of the extubations were performed without obtaining an arterial blood gas test after the patient completed a trial of spontaneous breathing. The extubation success rate was 94% for the entire group, and it was the same regardless of whether testing was done (94.7% vs 94.3%, respectively).
Alternatives to arterial blood gases
There are less-invasive means to obtain the information that comes from an arterial blood gas test.
Pulse oximetry is a rapid noninvasive tool that provides continuous assessment of peripheral arterial oxygen saturation as a surrogate marker for tissue arterial oxygenation. However, it cannot measure PaO2 or PaCO2.21
Transcutaneous carbon dioxide (PTCO2) monitoring is another continuous noninvasive alternative. The newer PTCO2 devices are useful in patients with acute respiratory failure and in critically ill patients on vasopressors or vasodilators. Studies have shown good correlation between PTCO2 and PaCO2.22,23
End-tidal carbon dioxide (PetCO2) is another alternative to estimate PaCO2. It can also be used to confirm endotracheal tube placement, during transportation, during procedures in which the patient is under conscious sedation, and to monitor the effectiveness of cardiopulmonary resuscitation and return of circulation after cardiac arrest. PetCO2 measurements are not as accurate as arterial blood gas testing owing to a difference of approximately 2 to 5 mm Hg between PaCO2 and PetCO2 in normal lungs due to alveolar dead space. This difference may be much higher depending on the clinical condition and the degree of alveolar dead space.21,24,25
Venous blood gases, which can be obtained from a peripheral or central venous catheter, are adequate to assess pH and partial pressure of carbon dioxide (PCO2) in hemodynamically stable patients. Walkey et al26 found that the accuracy of venous blood gas measurement to predict arterial blood gases was 90%. They recommended adjusting the venous pH up by 0.05 and the PCO2 down by 5 mm Hg to account for the positive bias of venous blood gases. A limitation of this method is that the values are not reliable in patients who are in shock.
These alternatives can be used as a substitute for daily arterial blood gases. However, in certain clinical scenarios, arterial blood gas measurement remains a necessary and useful clinical tool.
TAKE-HOME MESSAGE
Most scientific evidence suggests that chest radiographs and arterial blood gas measurement in patients undergoing mechanical ventilation—and critically ill, in general—are best done when clinically indicated rather than routinely on a daily basis. This will reduce cost and harm to patients that may result from these unnecessary tests and not adversely affect outcomes.
References
Gershengorn HB, Wunsch H, Scales DC, Rubenfeld GD. Trends in use of daily chest radiographs among US adults receiving mechanical ventilation. JAMA Netw Open 2018; 1(4):e181119. doi:10.1001/jamanetworkopen.2018.1119
Hall JB, White SR, Karrison T. Efficacy of daily routine chest radiographs in intubated, mechanically ventilated patients. Crit Care Med 1991; 19(5):689–693. pmid:2026031
Graat ME, Choi G, Wolthuis EK, et al. The clinical value of daily routine chest radiographs in a mixed medical-surgical intensive care unit is low. Crit Care 2006; 10(1):R11. doi:10.1186/cc3955
Oba Y, Zaza T. Abandoning daily routine chest radiography in the intensive care unit: meta-analysis. Radiology 2010; 255(2):386–395. doi:10.1148/radiol.10090946
Ganapathy A, Adhikari NK, Spiegelman J, Scales DC. Routine chest x-rays in intensive care units: a systematic review and meta-analysis. Crit Care 2012; 16(2):R68. doi:10.1186/cc11321
Krishnan S, Moghekar A, Duggal A, et al. Radiation exposure in the medical ICU: predictors and characteristics. Chest 2018; 153(5):1160–1168. doi:10.1016/j.chest.2018.01.019
Hejblum G, Chalumeau-Lemoine L, Ioos V, et al. Comparison of routine and on-demand prescription of chest radiographs in mechanically ventilated adults: a multicentre, cluster-randomised, two-period crossover study. Lancet 2009; 374(9702):1687–1693. doi:10.1016/S0140-6736(09)61459-8
Levin PD, Shatz O, Sviri S, et al. Contamination of portable radiograph equipment with resistant bacteria in the ICU. Chest 2009; 136(2):426–432. doi:10.1378/chest.09-0049
Suh RD, Genshaft SJ, Kirsch J, et al. ACR Appropriateness Criteria® Intensive Care Unit Patients. J Thorac Imaging 2015; 30(6):W63–W65. doi:10.1097/RTI.0000000000000174
Alrajhi K, Woo MY, Vaillancourt C. Test characteristics of ultrasonography for the detection of pneumothorax: a systematic review and meta-analysis. Chest 2012; 141(3):703–708. doi:10.1378/chest.11-0131
Lichetenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008; 134(1):117–125. doi:10.1378/chest.07-2800
Das SK, Choupoo NS, Haldar R, Lahkar A. Transtracheal ultrasound for verification of endotracheal tube placement: a systematic review and meta-analysis. Can J Anaesth 2015; 62(4):413–423. doi:10.1007/s12630-014-0301-z
Ablordeppey EA, Drewry AM, Beyer AB, et al. Diagnostic accuracy of central venous catheter confirmation by bedside ultrasound versus chest radiography in critically ill patients: a systematic review and meta-analysis. Crit Care Med 2017; 45(4):715–724. doi:10.1097/CCM.0000000000002188
DellaVolpe JD, Chakraborti C, Cerreta K, et al. Effects of implementing a protocol for arterial blood gas use on ordering practices and diagnostic yield. Healthc (Amst) 2014; 2(2):130–135. doi:10.1016/j.hjdsi.2013.09.006
Davis MD, Walsh BK, Sittig SE, Restrepo RD. AARC clinical practice guideline: blood gas analysis and hemoximetry. Respir Care 2013; 58(10):1694–1703. doi:10.4187/respcare.02786
Blum FE, Lund ET, Hall HA, Tachauer AD, Chedrawy EG, Zilberstein J. Reevaluation of the utilization of arterial blood gas analysis in the intensive care unit: effects on patient safety and patient outcome. J Crit Care 2015; 30(2):438.e1–e5. doi:10.1016/j.jcrc.2014.10.025
Martínez-Balzano CD, Oliveira P, O’Rourke M, Hills L, Sosa AF; Critical Care Operations Committee of the UMass Memorial Healthcare Center. An educational intervention optimizes the use of arterial blood gas determinations across ICUs from different specialties: a quality-improvement study. Chest 2017; 151(3):579–585. doi:10.1016/j.chest.2016.10.035
Salam A, Smina M, Gada P, et al. The effect of arterial blood gas values on extubation decisions. Respir Care 2003; 48(11):1033–1037. pmid:14585115
Pawson SR, DePriest JL. Are blood gases necessary in mechanically ventilated patients who have successfully completed a spontaneous breathing trial? Respir Care 2004; 49(11):1316–1319. pmid:15507165
Soubani AO. Noninvasive monitoring of oxygen and carbon dioxide. Am J Emerg Med 2001; 19(2):141–146. doi:10.1053/ajem.2001.21353
Nicolini A, Ferrari MB. Evaluation of a transcutaneous carbon dioxide monitor in patients with acute respiratory failure. Ann Thorac Med 2011; 6(4):217–220. doi:10.4103/1817-1737.84776
Bendjelid K, Schütz N, Stotz M, Gerard I, Suter PM, Romand JA. Transcutaneous PCO2 monitoring in critically ill adults: clinical evaluation of a new sensor. Crit Care Med 2005; 33(10):2203–2206. pmid:16215371
Huttmann SE, Windisch W, Storre JH. Techniques for the measurement and monitoring of carbon dioxide in the blood. Ann Am Thorac Soc 2014; 11(4):645–652. doi:10.1513/AnnalsATS.201311-387FR
McSwain SD, Hamel DS, Smith PB, et al. End-tidal and arterial carbon dioxide measurements correlate across all levels of physiologic dead space. Respir Care 2010; 55(3):288–293. pmid:20196877
Walkey AJ, Farber HW, O'Donnell C, Cabral H, Eagan JS, Philippides GJ. The accuracy of the central venous blood gas for acid-base monitoring. J Intensive Care Med 2010; 25(2):104–110. doi:10.1177/0885066609356164
References
Gershengorn HB, Wunsch H, Scales DC, Rubenfeld GD. Trends in use of daily chest radiographs among US adults receiving mechanical ventilation. JAMA Netw Open 2018; 1(4):e181119. doi:10.1001/jamanetworkopen.2018.1119
Hall JB, White SR, Karrison T. Efficacy of daily routine chest radiographs in intubated, mechanically ventilated patients. Crit Care Med 1991; 19(5):689–693. pmid:2026031
Graat ME, Choi G, Wolthuis EK, et al. The clinical value of daily routine chest radiographs in a mixed medical-surgical intensive care unit is low. Crit Care 2006; 10(1):R11. doi:10.1186/cc3955
Oba Y, Zaza T. Abandoning daily routine chest radiography in the intensive care unit: meta-analysis. Radiology 2010; 255(2):386–395. doi:10.1148/radiol.10090946
Ganapathy A, Adhikari NK, Spiegelman J, Scales DC. Routine chest x-rays in intensive care units: a systematic review and meta-analysis. Crit Care 2012; 16(2):R68. doi:10.1186/cc11321
Krishnan S, Moghekar A, Duggal A, et al. Radiation exposure in the medical ICU: predictors and characteristics. Chest 2018; 153(5):1160–1168. doi:10.1016/j.chest.2018.01.019
Hejblum G, Chalumeau-Lemoine L, Ioos V, et al. Comparison of routine and on-demand prescription of chest radiographs in mechanically ventilated adults: a multicentre, cluster-randomised, two-period crossover study. Lancet 2009; 374(9702):1687–1693. doi:10.1016/S0140-6736(09)61459-8
Levin PD, Shatz O, Sviri S, et al. Contamination of portable radiograph equipment with resistant bacteria in the ICU. Chest 2009; 136(2):426–432. doi:10.1378/chest.09-0049
Suh RD, Genshaft SJ, Kirsch J, et al. ACR Appropriateness Criteria® Intensive Care Unit Patients. J Thorac Imaging 2015; 30(6):W63–W65. doi:10.1097/RTI.0000000000000174
Alrajhi K, Woo MY, Vaillancourt C. Test characteristics of ultrasonography for the detection of pneumothorax: a systematic review and meta-analysis. Chest 2012; 141(3):703–708. doi:10.1378/chest.11-0131
Lichetenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008; 134(1):117–125. doi:10.1378/chest.07-2800
Das SK, Choupoo NS, Haldar R, Lahkar A. Transtracheal ultrasound for verification of endotracheal tube placement: a systematic review and meta-analysis. Can J Anaesth 2015; 62(4):413–423. doi:10.1007/s12630-014-0301-z
Ablordeppey EA, Drewry AM, Beyer AB, et al. Diagnostic accuracy of central venous catheter confirmation by bedside ultrasound versus chest radiography in critically ill patients: a systematic review and meta-analysis. Crit Care Med 2017; 45(4):715–724. doi:10.1097/CCM.0000000000002188
DellaVolpe JD, Chakraborti C, Cerreta K, et al. Effects of implementing a protocol for arterial blood gas use on ordering practices and diagnostic yield. Healthc (Amst) 2014; 2(2):130–135. doi:10.1016/j.hjdsi.2013.09.006
Davis MD, Walsh BK, Sittig SE, Restrepo RD. AARC clinical practice guideline: blood gas analysis and hemoximetry. Respir Care 2013; 58(10):1694–1703. doi:10.4187/respcare.02786
Blum FE, Lund ET, Hall HA, Tachauer AD, Chedrawy EG, Zilberstein J. Reevaluation of the utilization of arterial blood gas analysis in the intensive care unit: effects on patient safety and patient outcome. J Crit Care 2015; 30(2):438.e1–e5. doi:10.1016/j.jcrc.2014.10.025
Martínez-Balzano CD, Oliveira P, O’Rourke M, Hills L, Sosa AF; Critical Care Operations Committee of the UMass Memorial Healthcare Center. An educational intervention optimizes the use of arterial blood gas determinations across ICUs from different specialties: a quality-improvement study. Chest 2017; 151(3):579–585. doi:10.1016/j.chest.2016.10.035
Salam A, Smina M, Gada P, et al. The effect of arterial blood gas values on extubation decisions. Respir Care 2003; 48(11):1033–1037. pmid:14585115
Pawson SR, DePriest JL. Are blood gases necessary in mechanically ventilated patients who have successfully completed a spontaneous breathing trial? Respir Care 2004; 49(11):1316–1319. pmid:15507165
Soubani AO. Noninvasive monitoring of oxygen and carbon dioxide. Am J Emerg Med 2001; 19(2):141–146. doi:10.1053/ajem.2001.21353
Nicolini A, Ferrari MB. Evaluation of a transcutaneous carbon dioxide monitor in patients with acute respiratory failure. Ann Thorac Med 2011; 6(4):217–220. doi:10.4103/1817-1737.84776
Bendjelid K, Schütz N, Stotz M, Gerard I, Suter PM, Romand JA. Transcutaneous PCO2 monitoring in critically ill adults: clinical evaluation of a new sensor. Crit Care Med 2005; 33(10):2203–2206. pmid:16215371
Huttmann SE, Windisch W, Storre JH. Techniques for the measurement and monitoring of carbon dioxide in the blood. Ann Am Thorac Soc 2014; 11(4):645–652. doi:10.1513/AnnalsATS.201311-387FR
McSwain SD, Hamel DS, Smith PB, et al. End-tidal and arterial carbon dioxide measurements correlate across all levels of physiologic dead space. Respir Care 2010; 55(3):288–293. pmid:20196877
Walkey AJ, Farber HW, O'Donnell C, Cabral H, Eagan JS, Philippides GJ. The accuracy of the central venous blood gas for acid-base monitoring. J Intensive Care Med 2010; 25(2):104–110. doi:10.1177/0885066609356164
An 18-year-old man without any significant medical history was transferred from another hospital for higher-level care after presenting with unremitting chest pain. He had been in his usual state of good health until 7 days before presentation, when he developed mild rhinorrhea and a sore throat, but not a cough. He went to an outpatient clinic, where a rapid test for group A streptococci was done; the result was negative, and he was sent home on supportive measures.
On the day of admission, he awoke with severe, pressure-like, midsternal, nonradiating pain, which he rated 10 on a scale of 10. The pain intensified in the supine position and improved with sitting. A complete review of systems was otherwise negative. He denied having had similar symptoms in the past, as well as sick contacts, recent travel, toxin exposure, illicit substance abuse, pets at home, or tick bites. His family history was negative for cardiac arrhythmias, premature coronary artery disease, thoracic aneurysms or dissection, and infiltrative disorders. His surgical and social histories were unremarkable. He said he had no drug allergies.
Figure 1. The patient’s electrocardiogram on presentation shows ST-segment elevation (arrows) over the lateral and inferior distribution (V4–V6, II, III, and aVF).
An electrocardiogram was obtained (Figure 1). His troponin I level was 7.0 ng/mL (reference range < 0.04 ng/mL).
On examination, his temperature was 38.1°C (100.6°F), heart rate 101 beats per minute, blood pressure 142/78 mm Hg, respiratory rate 16 breaths per minute, and oxygen saturation 98% on room air. He appeared anxious but was in no acute distress. Neck examination showed no elevation in jugular venous pulsation, bruits, thyromegaly, or lymphadenopathy. Cardiac examination revealed tachycardia without murmurs, rubs, or gallops. Lungs were clear to auscultation. Examination of all 4 extremities found 2+ pulses (on a scale of 0 to 4+) throughout and no cyanosis, clubbing, or edema. Abdominal, neurologic, and dermatologic examinations were unremarkable.
Further blood testing revealed the following:
Troponin I (3 hours after the first level) 15.5 ng/mL
B-type natriuretic peptide 200 mg/dL (reference range 0–100 mg/dL)
C-reactive protein 0.9 mg/dL (reference range 0.0–0.8 mg/dL)
Erythrocyte sedimentation rate 10 mm/h (reference range < 15 mm/h).
Metabolic and hematologic assessments were unremarkable. A toxicology screen for drugs of abuse was negative. Viral serologic testing was not done.
A chest radiograph showed no acute cardiopulmonary processes.
Given his presenting symptoms, persistent tachycardia, rapidly rising troponin I level, and electrocardiogram showing diffuse ST elevation, he was taken for urgent cardiac catheterization. Coronary angiography revealed no evidence of atherosclerotic disease, acute thrombosis, dissection, or aneurysm. Echocardiography 2 hours after the procedure showed a normal ejection fraction and no regional wall-motion abnormalities or valvular heart disease.
FURTHER TESTING
1. Which test should be done next to further evaluate this patient’s chest pain?
Serum viral serologic testing
Serum free light chain assay
Nuclear myocardial perfusion study
Cardiac magnetic resonance imaging (MRI)
Endomyocardial biopsy
In this patient without ischemic coronary disease or valvular heart disease, the recent upper respiratory tract prodrome, active positional chest pain, and diffuse electrocardiographic changes raise the possibility of myocarditis with pericardial involvement.
Viral serologic tests
Viral serologic tests are often obtained in the workup of myocarditis as a noninvasive means of detecting an infectious cause.
However, this approach has several problems. First, a positive serologic result is a signal of the peripheral immune response to a pathogen but does not necessarily indicate active myocardial inflammation. Additionally, circulating immunoglobulin G against cardiotropic viruses is commonly found, even in the absence of myocarditis.1 This is often the result of a high prevalence and exposure to these viruses in the general population. Further, trials have shown no correlation between serologic results and organisms identified by endomyocardial biopsy.2
Thus, serologic testing seems to be of limited utility, reserved for testing for infection with Borrelia burgdorferi (Lyme disease) in endemic areas, hepatitis C virus, human immunodeficiency virus in patients at high risk, Rickettsia conorii, and Rickettsia rickettsii.3
Serum free light chain testing for amyloidosis
Serum free light chain testing is replacing serum and urine protein electrophoresis in the workup of cardiac amyloidosis,4 as electrophoresis has poor sensitivity.4,5
Cardiac amyloidosis often affects older persons, although in rare cases it can affect young patients who carry mutations in the transthyretin gene (ATTR amyloidosis).6 This diagnosis is unlikely in our patient, as he has no other affected organ systems (amyloidosis often affects the renal and neurologic systems), normal QRS voltages on electrocardiography (which are often but not always low in amyloidosis), and no left ventricular hypertrophy or diastolic dysfunction on echocardiography (which are often seen in amyloidosis).4
Nuclear perfusion imaging for sarcoidosis
Nuclear imaging has a limited role in evaluating myocarditis,3 but positron-emission tomography with fluorine-18 fluorodeoxyglucose has a diagnostic role in sarcoidosis, an immune-mediated cause of myocarditis.7
Based on the acuity of the patient’s presentation, preceded by upper respiratory tract symptoms, sarcoidosis is less likely. Sarcoidosis is difficult to diagnose, although when it is the cause of myocarditis, some clues exist, as patients usually present with heart failure symptoms, a second- or third-degree atrioventricular block, or a dilated left ventricle on echocardiography.3 All of these were absent in our patient.
Cardiac MRI
Cardiac MRI has undergone many advances, making it an extremely useful noninvasive test. It has excellent utility as a stand-alone test in diagnosing myocarditis and has synergistic value when combined with endomyocardial biopsy.8 It is indicated in hemodynamically stable patients with a clinical suspicion of myocarditis, persistent symptoms, absence of heart failure, and when imaging findings will change management. It is particularly useful to help elucidate a cause and guide tailored therapy.9 Therefore, it is a reasonable next step in the diagnostic pathway for this patient.10
Cardiac MRI also allows for concurrent assessment of scar. In myocardial infarction, the late gadolinium enhancement is subendocardial or transmural. In myocarditis, the pattern differs, being found in the subepicardial lateral free wall (in most patients with parvovirus B19) and mid-myocardial septum (in most patients with herpesvirus 6).9,11 Cardiac MRI also confers prognostic information for patients with suspected myocarditis.12
The Lake Louise criteria9 for the diagnosis of myocarditis require 2 of the following:
Evidence of myocardial edema
Increased ratio of early gadolinium enhancement between myocardium and skeletal muscle (indicates hyperemia)
At least 1 focal lesion with nonischemic late gadolinium enhancement (indicates cardiac myocyte injury or scarring).
The Lake Louise criteria may be replaced by T1 and T2 mapping, which was found to be considerably better for diagnosing myocarditis when the 2 were compared.9,13,14
Endomyocardial biopsy
Endomyocardial biopsy should not be delayed while waiting for cardiac MRI in patients who are hemodynamically unstable or present with life-threatening features (ventricular arrhythmia, left ventricular failure, or resuscitation after sudden cardiac death).3,10
The indications for endomyocardial biopsy have been highly debated. The 2013 guidelines from the European Society of Cardiology (ESC) recommending endomyocardial biopsy in all clinically suspected cases of myocarditis have only heightened the controversy.3 The American Heart Association (AHA) guidelines reserve biopsy for patients with suspected myocarditis who have acute or subacute heart failure symptoms or who do not respond to standard medical therapy.15 Other reasonable indications may include the following: myocarditis with life-threatening ventricular arrhythmias, suspicion of giant cell myocarditis, necrotizing eosinophilic myocarditis, or cardiac sarcoidosis.16
Endomyocardial biopsy is the only way to make a definitive diagnosis of myocarditis.3 However, given the patchy distribution of myocardial involvement, a negative result does not rule out myocarditis. The diagnostic utility can be improved by increasing the number of samples taken (at least 3 but up to 10), obtaining samples from both ventricles, and using cardiac MRI data to determine which sites to biopsy.3,13,17,18
Noninvasive testing such as cardiac MRI does not distinguish cell type or etiology (viral vs nonviral).3 Further, endomyocardial biopsy must be performed before immunosuppressive therapy can be safely started.3,16 At experienced centers, the complication rate is 0% to 0.8%.3 The addition of immunohistochemical testing and viral genomic detection by polymerase chain reaction testing have increased the sensitivity of this technique.19 Finally, endomyocardial biopsy can help rule out some of the other possibilities in the differential diagnosis for myocarditis, including infiltrative and storage diseases, and possibly cardiac tumors.3
Of additional note, the diffuse ST-segment elevation seen on the patient’s electrocardiogram (Figure 1) is indicative of subepicardial inflammation. Since the distribution involves more than one epicardial coronary territory, this helps to differentiate the changes from those that occur with myocardial infarction.20
CASE CONTINUED
Figure 2. Cardiac magnetic resonance imaging shows areas of patchy subepicardial late gadolinium enhancement (arrows).
The patient underwent cardiac MRI, which showed myocardial edema and patchy areas of late gadolinium enhancement, raising suspicion for myocarditis (Figure 2).
Causes of myocarditis are numerous (Table 1),3,21,22 but viral and postinfectious etiologies remain the most common causes of acute myocarditis.23
2. What is the most likely causative infectious agent?
Parvovirus B19
Coxsackievirus B
Adenovirus species
Human herpesvirus 6
Staphylococcus aureus
Corynebacterium diphtheria
Trypanosoma cruzi
Influenza H1/N1
INFECTIOUS CAUSES OF MYOCARDITIS
Coxsackievirus B was the agent most often linked to this condition from the 1950s through the 1990s. However, in the last 2 decades, adenovirus species and human herpesvirus 6 have been increasingly encountered, and recently, parvovirus B19 has been credited as the most common culprit,11,23 at least in the Western world. In developing nations, T cruzi and C diphtheria are the most common offenders.21
S aureus is a common cause of endocarditis, but it rarely plays a role in myocarditis. When it does, the myocarditis is often the sequela of profound bacteremia. This was much more common before antibiotics were invented.24,25
Influenza H1/N1 is not among the most common causes of viral myocarditis, but it should be considered during flu season, given its ability to result in fulminant myocarditis.3,26
TREATMENT FOR MYOCARDITIS
3. Which treatment is the most appropriate at this time?
Intravenous immunoglobulin
Interferon beta
Acyclovir
Prednisone
Colchicine
Treatment for myocarditis depends on the cause but always includes supportive care to address the constellation of presenting symptoms. Standard therapies for tachy- or bradyarrhythmias, heart failure, and hemodynamic derangement should be started.
Supportive care
In patients with severe left ventricular dysfunction, an implantable cardiac electronic device, left ventricular assist device, or heart transplant may ultimately be needed. However, if possible these should be deferred for several months to determine response to treatment, since the myocardium can possibly recover.16
Diuretics, beta-blockers, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists should be given as part of guideline-directed medical therapy for patients with heart failure and reduced ejection fraction.3,27 However, whether and how the patient should be weaned from these agents after disease recovery are unknown.3
Intravenous immunoglobulin
Intravenous immunoglobulin in high doses has had mixed results. Its efficacy is well documented in children,21 but limited supportive data are available in adults.3 As such, recent ESC guidelines do not provide recommendations regarding its use in adults.3
Interferon beta
Interferon beta has shown promise in improving New York Heart Association class and left ventricular ejection fraction.3 This is attributed to its effects on eliminating adenoviral species and enteroviruses. Treatment of enteroviral organisms in particular has been associated with improved 10-year prognosis.3 Interferon beta also has in vitro data showing efficacy at diminishing apoptosis from parvovirus B19.28
Nucleoside analogues
Empiric treatment with nucleoside analogues (acyclovir, ganciclovir, and valacyclovir) has been tried for patients in whom human herpesvirus is suspected as the causative organism, although with unconfirmed effects.3 Consultation with an infectious disease specialist is recommended before starting these agents, and biopsy is often needed beforehand.3
Immunosuppressive agents
Immunosuppressive agents such as prednisone, azathioprine, and cyclosporine can be used in cases of biopsy-proven disease with manifestations of severe heart failure, especially if biopsy results reveal sarcoidosis, giant cell myocarditis, or necrotizing eosinophilic myocarditis. Although the results were neutral in the Myocarditis Treatment Trial,29 the cause of myocarditis in this trial was unknown. Therapy with such agents should be initiated after active infection is ruled out, which also would require a biopsy.
Colchicine
Mechanisms of chest pain in myocarditis include associated pericarditis and coronary artery vasospasm.3,23 Our patient’s chest pain changed when he changed position, possibly indicating associated pericarditis. In myocarditis with accompanying pericarditis symptoms, colchicine (1–2 mg as an initial dose and then 0.6 mg daily for up to 3 months) can be helpful in alleviating symptoms.21,30 Thus, starting this agent in a patient who presents with myocarditis in absence of heart failure, arrhythmias, or left ventricular dysfunction is prudent.
Colchicine is used mainly to address the pain associated with pericarditis. For patients who present with pericarditis without myocarditis, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, with the addition of colchicine leading to faster symptom resolution.30 The benefit of colchicine for isolated myocarditis is not well established, with only limited data showing some clinical effects.31
CASE CONTINUED
The patient was given colchicine 1.2 mg on the first day and then 0.6 mg daily. Within 2 days, his chest pain had resolved. He did not receive any immunosuppressive agents.
DISCHARGE INSTRUCTIONS
4. Before discharge, this patient should be instructed to do which of the following?
Take over-the-counter NSAIDs to supplement the effects of colchicine
Avoid competitive sports and athletics for at least 6 months
Call to schedule repeat cardiac MRI
No further instruction is needed
NSAIDs are used by themselves or in combination with colchicine in the treatment of pericarditis, but their use may be associated with worse outcomes in myocarditis.3,21 Thus, their use is not recommended in most cases.3
Excessive physical activity should be avoided for at least 6 months after the clinical syndrome resolves. This recommendation is included in the most recent ESC guidelines but is based mainly on expert opinion and murine models with coxsackievirus B.3 Periodic reassessment is indicated with exercise stress testing before return to strenuous activity.3,16,32 Testing should look for exercise tolerance, and exercise electrocardiography also helps to evaluate for clinically relevant arrythmias.
Cardiac MRI can help clarify the prognosis in myocarditis, but the role of repeat testing in guiding therapy is limited.3 Indications for repeat cardiac MRI include presence of 0 or 1 of the Lake Louise criteria (recall that 2 are necessary to make the diagnosis) with recurrence of symptoms and a high suspicion for myocardial inflammation.3,9 Repeat cardiac MRI was not performed for our patient.
CASE CONCLUDED
The patient was evaluated in the cardiology clinic within 1 week of discharge. At that time, he was in sinus tachycardia with a heart rate of 102 bpm, and he was instructed to avoid any exercise until further notice.
At 6-month follow-up, the sinus tachycardia had resolved. However, because persistent tachycardia had been noted at the first postdischarge visit, and in view of the extent of myocardial involvement, he underwent exercise treadmill testing to evaluate for ventricular arrhythmias. The study did show premature ventricular complexes and 1 ventricular couplet at submaximal exercise levels. As this indicated a higher risk of exercise-induced arrhythmias, he was asked to continue normal activity levels but to abstain from exercise until the next evaluation.
During his 1-year follow-up, a repeat treadmill test showed no ventricular ectopy. Holter monitoring was ordered and showed no premature ventricular complexes, supraventricular arrhythmias, or atrioventricular block within the 48-hour period.
At his 2-year evaluation, he had returned to playing basketball and soccer on weekends and reported no recurrence of his initial symptoms.
KEY POINTS
Figure 3. Our suggested approach to suspected acute myocarditis.Cardiac MRI has emerged as an excellent noninvasive imaging modality for the diagnosis of myocarditis.
Treatment of myocarditis depends on the cause and severity of the patient’s presentation, spanning the spectrum from conservative care to immunosuppressive agents and even heart failure therapy.
Excessive physical activity should be avoided for the first 6 months after disease diagnosis and treatment.
If myocarditis is associated with pericardial involvement, colchicine is the agent of choice, and NSAIDs should be avoided.
Our suggested strategy for approaching myocarditis is shown in Figure 3.
Mahfoud F, Gärtner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011; 32(7):897–903. doi:10.1093/eurheartj/ehq493
Caforio AL, Pankuweit S, Arbustini E, et al; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013; 34(33):2636–2648, 2648a–2648d. doi:10.1093/eurheartj/eht210
Donnelly JP, Hanna M. Cardiac amyloidosis: an update on diagnosis and treatment. Cleve Clin J Med 2017; 84(12 suppl 3):12–26. doi:10.3949/ccjm.84.s3.02
Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28(1):10–21. doi:10.1016/j.tcm.2017.07.004
Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol 2015; 66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
Blankstein R, Osborne M, Naya M, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014; 63(4):329–336. doi:10.1016/j.jacc.2013.09.022
Baccouche H, Mahrholtz H, Meinhardt G, et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009; 30(23):2869–2879. doi:10.1093/eurheartj/ehp328
Friedrich MG, Sechtem U, Schulz-Menger J, et al; International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009; 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012; 59(9):779–792. doi:10.1016/j.jacc.2011.09.074
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006; 114(15):1581–1590. doi:10.1161/CIRCULATIONAHA.105.606509
Gräni C, Eichhorn C, Bière L, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017; 70(16):1964–1976. doi:10.1016/j.jacc.2017.08.050
Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-Trial. J Am Coll Cardiol 2016; 67(15):1800–1811. doi:10.1016/j.jacc.2016.02.013
Gannon MP, Schaub E, Griens CL, Saba SG. State of the art: evaluation and prognostication of myocarditis using cardiac MRI. J Magn Reson Imaging 2019; 49(7):e122–e131. doi:10.1002/jmri.26611
Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007; 28(24):3076–3093. doi:10.1093/eurheartj/ehm456
Sinagra G, Anzini M, Pereira NL, et al. Myocarditis in clinical practice. Mayo Clin Proc 2016; 91(9):1256–1266. doi:10.1016/j.mayocp.2016.05.013
Cooper LT, Baughman KL, Feldman AM, et al; American Heart Association; American College of Cardiology; European Society of Cardiology. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007; 116(19):2216–2233. doi:10.1161/CIRCULATIONAHA.107.186093
Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012; 21(4):245–274. doi:10.1016/j.carpath.2011.10.001
Alraies MC, Klein AL. Should we still use electrocardiography to diagnose pericardial disease? Cleve Clin J Med 2013; 80(2):97–100. doi:10.3949/ccjm.80a.11144
Wasi F, Shuter J. Primary bacterial infection of the myocardium. Front Biosci 2003; 8:s228–s231. pmid:12700039
Al-Amoodi M, Rao K, Rao S, Brewer JH, Magalski A, Chhatriwalla AK. Fulminant myocarditis due to H1N1 influenza. Circ Heart Fail 2010; 3(3):e7–e9. doi:10.1161/CIRCHEARTFAILURE.110.938506
Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2016; 68(13):1476–1488. doi:10.1016/j.jacc.2016.05.011
Schmidt-Lucke C, Spillmann F, Bock T, et al. Interferon beta modulates endothelial damage in patients with cardiac persistence of human parvovirus b19 infection. J Infect Dis 2010; 201(6):936–945. doi:10.1086/650700
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosuppressive therapy for myocarditis: the Myocarditis Treatment Trial Investigators. N Engl J Med 1995; 333(5):269–275. doi:10.1056/NEJM199508033330501
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005; 112(13):2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738
Morgenstern D, Lisko J, Boniface NC, Mikolich BM, Mikolich JR. Myocarditis and colchicine: a new perspective from cardiac MRI. J Cardiovasc Magn Reson 2016; 18(suppl 1):0100.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015; 66(21):2343–2349. doi:10.1016/j.jacc.2015.09.032
Amir Farid, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Neil Beri, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
David Torres-Barba, MD, PhD Department of Cardiology, University of California San Diego
Charles Whitcomb, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Address: David Torres-Barba, MD, PhD, Department of Internal Medicine, University of California, Davis, 4150 V. Street, Sacramento, CA 95817; [email protected]
Amir Farid, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Neil Beri, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
David Torres-Barba, MD, PhD Department of Cardiology, University of California San Diego
Charles Whitcomb, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Address: David Torres-Barba, MD, PhD, Department of Internal Medicine, University of California, Davis, 4150 V. Street, Sacramento, CA 95817; [email protected]
Author and Disclosure Information
Amir Farid, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Neil Beri, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
David Torres-Barba, MD, PhD Department of Cardiology, University of California San Diego
Charles Whitcomb, MD Department of Cardiology, University of California Davis Medical Center, Sacramento
Address: David Torres-Barba, MD, PhD, Department of Internal Medicine, University of California, Davis, 4150 V. Street, Sacramento, CA 95817; [email protected]
An 18-year-old man without any significant medical history was transferred from another hospital for higher-level care after presenting with unremitting chest pain. He had been in his usual state of good health until 7 days before presentation, when he developed mild rhinorrhea and a sore throat, but not a cough. He went to an outpatient clinic, where a rapid test for group A streptococci was done; the result was negative, and he was sent home on supportive measures.
On the day of admission, he awoke with severe, pressure-like, midsternal, nonradiating pain, which he rated 10 on a scale of 10. The pain intensified in the supine position and improved with sitting. A complete review of systems was otherwise negative. He denied having had similar symptoms in the past, as well as sick contacts, recent travel, toxin exposure, illicit substance abuse, pets at home, or tick bites. His family history was negative for cardiac arrhythmias, premature coronary artery disease, thoracic aneurysms or dissection, and infiltrative disorders. His surgical and social histories were unremarkable. He said he had no drug allergies.
Figure 1. The patient’s electrocardiogram on presentation shows ST-segment elevation (arrows) over the lateral and inferior distribution (V4–V6, II, III, and aVF).
An electrocardiogram was obtained (Figure 1). His troponin I level was 7.0 ng/mL (reference range < 0.04 ng/mL).
On examination, his temperature was 38.1°C (100.6°F), heart rate 101 beats per minute, blood pressure 142/78 mm Hg, respiratory rate 16 breaths per minute, and oxygen saturation 98% on room air. He appeared anxious but was in no acute distress. Neck examination showed no elevation in jugular venous pulsation, bruits, thyromegaly, or lymphadenopathy. Cardiac examination revealed tachycardia without murmurs, rubs, or gallops. Lungs were clear to auscultation. Examination of all 4 extremities found 2+ pulses (on a scale of 0 to 4+) throughout and no cyanosis, clubbing, or edema. Abdominal, neurologic, and dermatologic examinations were unremarkable.
Further blood testing revealed the following:
Troponin I (3 hours after the first level) 15.5 ng/mL
B-type natriuretic peptide 200 mg/dL (reference range 0–100 mg/dL)
C-reactive protein 0.9 mg/dL (reference range 0.0–0.8 mg/dL)
Erythrocyte sedimentation rate 10 mm/h (reference range < 15 mm/h).
Metabolic and hematologic assessments were unremarkable. A toxicology screen for drugs of abuse was negative. Viral serologic testing was not done.
A chest radiograph showed no acute cardiopulmonary processes.
Given his presenting symptoms, persistent tachycardia, rapidly rising troponin I level, and electrocardiogram showing diffuse ST elevation, he was taken for urgent cardiac catheterization. Coronary angiography revealed no evidence of atherosclerotic disease, acute thrombosis, dissection, or aneurysm. Echocardiography 2 hours after the procedure showed a normal ejection fraction and no regional wall-motion abnormalities or valvular heart disease.
FURTHER TESTING
1. Which test should be done next to further evaluate this patient’s chest pain?
Serum viral serologic testing
Serum free light chain assay
Nuclear myocardial perfusion study
Cardiac magnetic resonance imaging (MRI)
Endomyocardial biopsy
In this patient without ischemic coronary disease or valvular heart disease, the recent upper respiratory tract prodrome, active positional chest pain, and diffuse electrocardiographic changes raise the possibility of myocarditis with pericardial involvement.
Viral serologic tests
Viral serologic tests are often obtained in the workup of myocarditis as a noninvasive means of detecting an infectious cause.
However, this approach has several problems. First, a positive serologic result is a signal of the peripheral immune response to a pathogen but does not necessarily indicate active myocardial inflammation. Additionally, circulating immunoglobulin G against cardiotropic viruses is commonly found, even in the absence of myocarditis.1 This is often the result of a high prevalence and exposure to these viruses in the general population. Further, trials have shown no correlation between serologic results and organisms identified by endomyocardial biopsy.2
Thus, serologic testing seems to be of limited utility, reserved for testing for infection with Borrelia burgdorferi (Lyme disease) in endemic areas, hepatitis C virus, human immunodeficiency virus in patients at high risk, Rickettsia conorii, and Rickettsia rickettsii.3
Serum free light chain testing for amyloidosis
Serum free light chain testing is replacing serum and urine protein electrophoresis in the workup of cardiac amyloidosis,4 as electrophoresis has poor sensitivity.4,5
Cardiac amyloidosis often affects older persons, although in rare cases it can affect young patients who carry mutations in the transthyretin gene (ATTR amyloidosis).6 This diagnosis is unlikely in our patient, as he has no other affected organ systems (amyloidosis often affects the renal and neurologic systems), normal QRS voltages on electrocardiography (which are often but not always low in amyloidosis), and no left ventricular hypertrophy or diastolic dysfunction on echocardiography (which are often seen in amyloidosis).4
Nuclear perfusion imaging for sarcoidosis
Nuclear imaging has a limited role in evaluating myocarditis,3 but positron-emission tomography with fluorine-18 fluorodeoxyglucose has a diagnostic role in sarcoidosis, an immune-mediated cause of myocarditis.7
Based on the acuity of the patient’s presentation, preceded by upper respiratory tract symptoms, sarcoidosis is less likely. Sarcoidosis is difficult to diagnose, although when it is the cause of myocarditis, some clues exist, as patients usually present with heart failure symptoms, a second- or third-degree atrioventricular block, or a dilated left ventricle on echocardiography.3 All of these were absent in our patient.
Cardiac MRI
Cardiac MRI has undergone many advances, making it an extremely useful noninvasive test. It has excellent utility as a stand-alone test in diagnosing myocarditis and has synergistic value when combined with endomyocardial biopsy.8 It is indicated in hemodynamically stable patients with a clinical suspicion of myocarditis, persistent symptoms, absence of heart failure, and when imaging findings will change management. It is particularly useful to help elucidate a cause and guide tailored therapy.9 Therefore, it is a reasonable next step in the diagnostic pathway for this patient.10
Cardiac MRI also allows for concurrent assessment of scar. In myocardial infarction, the late gadolinium enhancement is subendocardial or transmural. In myocarditis, the pattern differs, being found in the subepicardial lateral free wall (in most patients with parvovirus B19) and mid-myocardial septum (in most patients with herpesvirus 6).9,11 Cardiac MRI also confers prognostic information for patients with suspected myocarditis.12
The Lake Louise criteria9 for the diagnosis of myocarditis require 2 of the following:
Evidence of myocardial edema
Increased ratio of early gadolinium enhancement between myocardium and skeletal muscle (indicates hyperemia)
At least 1 focal lesion with nonischemic late gadolinium enhancement (indicates cardiac myocyte injury or scarring).
The Lake Louise criteria may be replaced by T1 and T2 mapping, which was found to be considerably better for diagnosing myocarditis when the 2 were compared.9,13,14
Endomyocardial biopsy
Endomyocardial biopsy should not be delayed while waiting for cardiac MRI in patients who are hemodynamically unstable or present with life-threatening features (ventricular arrhythmia, left ventricular failure, or resuscitation after sudden cardiac death).3,10
The indications for endomyocardial biopsy have been highly debated. The 2013 guidelines from the European Society of Cardiology (ESC) recommending endomyocardial biopsy in all clinically suspected cases of myocarditis have only heightened the controversy.3 The American Heart Association (AHA) guidelines reserve biopsy for patients with suspected myocarditis who have acute or subacute heart failure symptoms or who do not respond to standard medical therapy.15 Other reasonable indications may include the following: myocarditis with life-threatening ventricular arrhythmias, suspicion of giant cell myocarditis, necrotizing eosinophilic myocarditis, or cardiac sarcoidosis.16
Endomyocardial biopsy is the only way to make a definitive diagnosis of myocarditis.3 However, given the patchy distribution of myocardial involvement, a negative result does not rule out myocarditis. The diagnostic utility can be improved by increasing the number of samples taken (at least 3 but up to 10), obtaining samples from both ventricles, and using cardiac MRI data to determine which sites to biopsy.3,13,17,18
Noninvasive testing such as cardiac MRI does not distinguish cell type or etiology (viral vs nonviral).3 Further, endomyocardial biopsy must be performed before immunosuppressive therapy can be safely started.3,16 At experienced centers, the complication rate is 0% to 0.8%.3 The addition of immunohistochemical testing and viral genomic detection by polymerase chain reaction testing have increased the sensitivity of this technique.19 Finally, endomyocardial biopsy can help rule out some of the other possibilities in the differential diagnosis for myocarditis, including infiltrative and storage diseases, and possibly cardiac tumors.3
Of additional note, the diffuse ST-segment elevation seen on the patient’s electrocardiogram (Figure 1) is indicative of subepicardial inflammation. Since the distribution involves more than one epicardial coronary territory, this helps to differentiate the changes from those that occur with myocardial infarction.20
CASE CONTINUED
Figure 2. Cardiac magnetic resonance imaging shows areas of patchy subepicardial late gadolinium enhancement (arrows).
The patient underwent cardiac MRI, which showed myocardial edema and patchy areas of late gadolinium enhancement, raising suspicion for myocarditis (Figure 2).
Causes of myocarditis are numerous (Table 1),3,21,22 but viral and postinfectious etiologies remain the most common causes of acute myocarditis.23
2. What is the most likely causative infectious agent?
Parvovirus B19
Coxsackievirus B
Adenovirus species
Human herpesvirus 6
Staphylococcus aureus
Corynebacterium diphtheria
Trypanosoma cruzi
Influenza H1/N1
INFECTIOUS CAUSES OF MYOCARDITIS
Coxsackievirus B was the agent most often linked to this condition from the 1950s through the 1990s. However, in the last 2 decades, adenovirus species and human herpesvirus 6 have been increasingly encountered, and recently, parvovirus B19 has been credited as the most common culprit,11,23 at least in the Western world. In developing nations, T cruzi and C diphtheria are the most common offenders.21
S aureus is a common cause of endocarditis, but it rarely plays a role in myocarditis. When it does, the myocarditis is often the sequela of profound bacteremia. This was much more common before antibiotics were invented.24,25
Influenza H1/N1 is not among the most common causes of viral myocarditis, but it should be considered during flu season, given its ability to result in fulminant myocarditis.3,26
TREATMENT FOR MYOCARDITIS
3. Which treatment is the most appropriate at this time?
Intravenous immunoglobulin
Interferon beta
Acyclovir
Prednisone
Colchicine
Treatment for myocarditis depends on the cause but always includes supportive care to address the constellation of presenting symptoms. Standard therapies for tachy- or bradyarrhythmias, heart failure, and hemodynamic derangement should be started.
Supportive care
In patients with severe left ventricular dysfunction, an implantable cardiac electronic device, left ventricular assist device, or heart transplant may ultimately be needed. However, if possible these should be deferred for several months to determine response to treatment, since the myocardium can possibly recover.16
Diuretics, beta-blockers, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists should be given as part of guideline-directed medical therapy for patients with heart failure and reduced ejection fraction.3,27 However, whether and how the patient should be weaned from these agents after disease recovery are unknown.3
Intravenous immunoglobulin
Intravenous immunoglobulin in high doses has had mixed results. Its efficacy is well documented in children,21 but limited supportive data are available in adults.3 As such, recent ESC guidelines do not provide recommendations regarding its use in adults.3
Interferon beta
Interferon beta has shown promise in improving New York Heart Association class and left ventricular ejection fraction.3 This is attributed to its effects on eliminating adenoviral species and enteroviruses. Treatment of enteroviral organisms in particular has been associated with improved 10-year prognosis.3 Interferon beta also has in vitro data showing efficacy at diminishing apoptosis from parvovirus B19.28
Nucleoside analogues
Empiric treatment with nucleoside analogues (acyclovir, ganciclovir, and valacyclovir) has been tried for patients in whom human herpesvirus is suspected as the causative organism, although with unconfirmed effects.3 Consultation with an infectious disease specialist is recommended before starting these agents, and biopsy is often needed beforehand.3
Immunosuppressive agents
Immunosuppressive agents such as prednisone, azathioprine, and cyclosporine can be used in cases of biopsy-proven disease with manifestations of severe heart failure, especially if biopsy results reveal sarcoidosis, giant cell myocarditis, or necrotizing eosinophilic myocarditis. Although the results were neutral in the Myocarditis Treatment Trial,29 the cause of myocarditis in this trial was unknown. Therapy with such agents should be initiated after active infection is ruled out, which also would require a biopsy.
Colchicine
Mechanisms of chest pain in myocarditis include associated pericarditis and coronary artery vasospasm.3,23 Our patient’s chest pain changed when he changed position, possibly indicating associated pericarditis. In myocarditis with accompanying pericarditis symptoms, colchicine (1–2 mg as an initial dose and then 0.6 mg daily for up to 3 months) can be helpful in alleviating symptoms.21,30 Thus, starting this agent in a patient who presents with myocarditis in absence of heart failure, arrhythmias, or left ventricular dysfunction is prudent.
Colchicine is used mainly to address the pain associated with pericarditis. For patients who present with pericarditis without myocarditis, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, with the addition of colchicine leading to faster symptom resolution.30 The benefit of colchicine for isolated myocarditis is not well established, with only limited data showing some clinical effects.31
CASE CONTINUED
The patient was given colchicine 1.2 mg on the first day and then 0.6 mg daily. Within 2 days, his chest pain had resolved. He did not receive any immunosuppressive agents.
DISCHARGE INSTRUCTIONS
4. Before discharge, this patient should be instructed to do which of the following?
Take over-the-counter NSAIDs to supplement the effects of colchicine
Avoid competitive sports and athletics for at least 6 months
Call to schedule repeat cardiac MRI
No further instruction is needed
NSAIDs are used by themselves or in combination with colchicine in the treatment of pericarditis, but their use may be associated with worse outcomes in myocarditis.3,21 Thus, their use is not recommended in most cases.3
Excessive physical activity should be avoided for at least 6 months after the clinical syndrome resolves. This recommendation is included in the most recent ESC guidelines but is based mainly on expert opinion and murine models with coxsackievirus B.3 Periodic reassessment is indicated with exercise stress testing before return to strenuous activity.3,16,32 Testing should look for exercise tolerance, and exercise electrocardiography also helps to evaluate for clinically relevant arrythmias.
Cardiac MRI can help clarify the prognosis in myocarditis, but the role of repeat testing in guiding therapy is limited.3 Indications for repeat cardiac MRI include presence of 0 or 1 of the Lake Louise criteria (recall that 2 are necessary to make the diagnosis) with recurrence of symptoms and a high suspicion for myocardial inflammation.3,9 Repeat cardiac MRI was not performed for our patient.
CASE CONCLUDED
The patient was evaluated in the cardiology clinic within 1 week of discharge. At that time, he was in sinus tachycardia with a heart rate of 102 bpm, and he was instructed to avoid any exercise until further notice.
At 6-month follow-up, the sinus tachycardia had resolved. However, because persistent tachycardia had been noted at the first postdischarge visit, and in view of the extent of myocardial involvement, he underwent exercise treadmill testing to evaluate for ventricular arrhythmias. The study did show premature ventricular complexes and 1 ventricular couplet at submaximal exercise levels. As this indicated a higher risk of exercise-induced arrhythmias, he was asked to continue normal activity levels but to abstain from exercise until the next evaluation.
During his 1-year follow-up, a repeat treadmill test showed no ventricular ectopy. Holter monitoring was ordered and showed no premature ventricular complexes, supraventricular arrhythmias, or atrioventricular block within the 48-hour period.
At his 2-year evaluation, he had returned to playing basketball and soccer on weekends and reported no recurrence of his initial symptoms.
KEY POINTS
Figure 3. Our suggested approach to suspected acute myocarditis.Cardiac MRI has emerged as an excellent noninvasive imaging modality for the diagnosis of myocarditis.
Treatment of myocarditis depends on the cause and severity of the patient’s presentation, spanning the spectrum from conservative care to immunosuppressive agents and even heart failure therapy.
Excessive physical activity should be avoided for the first 6 months after disease diagnosis and treatment.
If myocarditis is associated with pericardial involvement, colchicine is the agent of choice, and NSAIDs should be avoided.
Our suggested strategy for approaching myocarditis is shown in Figure 3.
An 18-year-old man without any significant medical history was transferred from another hospital for higher-level care after presenting with unremitting chest pain. He had been in his usual state of good health until 7 days before presentation, when he developed mild rhinorrhea and a sore throat, but not a cough. He went to an outpatient clinic, where a rapid test for group A streptococci was done; the result was negative, and he was sent home on supportive measures.
On the day of admission, he awoke with severe, pressure-like, midsternal, nonradiating pain, which he rated 10 on a scale of 10. The pain intensified in the supine position and improved with sitting. A complete review of systems was otherwise negative. He denied having had similar symptoms in the past, as well as sick contacts, recent travel, toxin exposure, illicit substance abuse, pets at home, or tick bites. His family history was negative for cardiac arrhythmias, premature coronary artery disease, thoracic aneurysms or dissection, and infiltrative disorders. His surgical and social histories were unremarkable. He said he had no drug allergies.
Figure 1. The patient’s electrocardiogram on presentation shows ST-segment elevation (arrows) over the lateral and inferior distribution (V4–V6, II, III, and aVF).
An electrocardiogram was obtained (Figure 1). His troponin I level was 7.0 ng/mL (reference range < 0.04 ng/mL).
On examination, his temperature was 38.1°C (100.6°F), heart rate 101 beats per minute, blood pressure 142/78 mm Hg, respiratory rate 16 breaths per minute, and oxygen saturation 98% on room air. He appeared anxious but was in no acute distress. Neck examination showed no elevation in jugular venous pulsation, bruits, thyromegaly, or lymphadenopathy. Cardiac examination revealed tachycardia without murmurs, rubs, or gallops. Lungs were clear to auscultation. Examination of all 4 extremities found 2+ pulses (on a scale of 0 to 4+) throughout and no cyanosis, clubbing, or edema. Abdominal, neurologic, and dermatologic examinations were unremarkable.
Further blood testing revealed the following:
Troponin I (3 hours after the first level) 15.5 ng/mL
B-type natriuretic peptide 200 mg/dL (reference range 0–100 mg/dL)
C-reactive protein 0.9 mg/dL (reference range 0.0–0.8 mg/dL)
Erythrocyte sedimentation rate 10 mm/h (reference range < 15 mm/h).
Metabolic and hematologic assessments were unremarkable. A toxicology screen for drugs of abuse was negative. Viral serologic testing was not done.
A chest radiograph showed no acute cardiopulmonary processes.
Given his presenting symptoms, persistent tachycardia, rapidly rising troponin I level, and electrocardiogram showing diffuse ST elevation, he was taken for urgent cardiac catheterization. Coronary angiography revealed no evidence of atherosclerotic disease, acute thrombosis, dissection, or aneurysm. Echocardiography 2 hours after the procedure showed a normal ejection fraction and no regional wall-motion abnormalities or valvular heart disease.
FURTHER TESTING
1. Which test should be done next to further evaluate this patient’s chest pain?
Serum viral serologic testing
Serum free light chain assay
Nuclear myocardial perfusion study
Cardiac magnetic resonance imaging (MRI)
Endomyocardial biopsy
In this patient without ischemic coronary disease or valvular heart disease, the recent upper respiratory tract prodrome, active positional chest pain, and diffuse electrocardiographic changes raise the possibility of myocarditis with pericardial involvement.
Viral serologic tests
Viral serologic tests are often obtained in the workup of myocarditis as a noninvasive means of detecting an infectious cause.
However, this approach has several problems. First, a positive serologic result is a signal of the peripheral immune response to a pathogen but does not necessarily indicate active myocardial inflammation. Additionally, circulating immunoglobulin G against cardiotropic viruses is commonly found, even in the absence of myocarditis.1 This is often the result of a high prevalence and exposure to these viruses in the general population. Further, trials have shown no correlation between serologic results and organisms identified by endomyocardial biopsy.2
Thus, serologic testing seems to be of limited utility, reserved for testing for infection with Borrelia burgdorferi (Lyme disease) in endemic areas, hepatitis C virus, human immunodeficiency virus in patients at high risk, Rickettsia conorii, and Rickettsia rickettsii.3
Serum free light chain testing for amyloidosis
Serum free light chain testing is replacing serum and urine protein electrophoresis in the workup of cardiac amyloidosis,4 as electrophoresis has poor sensitivity.4,5
Cardiac amyloidosis often affects older persons, although in rare cases it can affect young patients who carry mutations in the transthyretin gene (ATTR amyloidosis).6 This diagnosis is unlikely in our patient, as he has no other affected organ systems (amyloidosis often affects the renal and neurologic systems), normal QRS voltages on electrocardiography (which are often but not always low in amyloidosis), and no left ventricular hypertrophy or diastolic dysfunction on echocardiography (which are often seen in amyloidosis).4
Nuclear perfusion imaging for sarcoidosis
Nuclear imaging has a limited role in evaluating myocarditis,3 but positron-emission tomography with fluorine-18 fluorodeoxyglucose has a diagnostic role in sarcoidosis, an immune-mediated cause of myocarditis.7
Based on the acuity of the patient’s presentation, preceded by upper respiratory tract symptoms, sarcoidosis is less likely. Sarcoidosis is difficult to diagnose, although when it is the cause of myocarditis, some clues exist, as patients usually present with heart failure symptoms, a second- or third-degree atrioventricular block, or a dilated left ventricle on echocardiography.3 All of these were absent in our patient.
Cardiac MRI
Cardiac MRI has undergone many advances, making it an extremely useful noninvasive test. It has excellent utility as a stand-alone test in diagnosing myocarditis and has synergistic value when combined with endomyocardial biopsy.8 It is indicated in hemodynamically stable patients with a clinical suspicion of myocarditis, persistent symptoms, absence of heart failure, and when imaging findings will change management. It is particularly useful to help elucidate a cause and guide tailored therapy.9 Therefore, it is a reasonable next step in the diagnostic pathway for this patient.10
Cardiac MRI also allows for concurrent assessment of scar. In myocardial infarction, the late gadolinium enhancement is subendocardial or transmural. In myocarditis, the pattern differs, being found in the subepicardial lateral free wall (in most patients with parvovirus B19) and mid-myocardial septum (in most patients with herpesvirus 6).9,11 Cardiac MRI also confers prognostic information for patients with suspected myocarditis.12
The Lake Louise criteria9 for the diagnosis of myocarditis require 2 of the following:
Evidence of myocardial edema
Increased ratio of early gadolinium enhancement between myocardium and skeletal muscle (indicates hyperemia)
At least 1 focal lesion with nonischemic late gadolinium enhancement (indicates cardiac myocyte injury or scarring).
The Lake Louise criteria may be replaced by T1 and T2 mapping, which was found to be considerably better for diagnosing myocarditis when the 2 were compared.9,13,14
Endomyocardial biopsy
Endomyocardial biopsy should not be delayed while waiting for cardiac MRI in patients who are hemodynamically unstable or present with life-threatening features (ventricular arrhythmia, left ventricular failure, or resuscitation after sudden cardiac death).3,10
The indications for endomyocardial biopsy have been highly debated. The 2013 guidelines from the European Society of Cardiology (ESC) recommending endomyocardial biopsy in all clinically suspected cases of myocarditis have only heightened the controversy.3 The American Heart Association (AHA) guidelines reserve biopsy for patients with suspected myocarditis who have acute or subacute heart failure symptoms or who do not respond to standard medical therapy.15 Other reasonable indications may include the following: myocarditis with life-threatening ventricular arrhythmias, suspicion of giant cell myocarditis, necrotizing eosinophilic myocarditis, or cardiac sarcoidosis.16
Endomyocardial biopsy is the only way to make a definitive diagnosis of myocarditis.3 However, given the patchy distribution of myocardial involvement, a negative result does not rule out myocarditis. The diagnostic utility can be improved by increasing the number of samples taken (at least 3 but up to 10), obtaining samples from both ventricles, and using cardiac MRI data to determine which sites to biopsy.3,13,17,18
Noninvasive testing such as cardiac MRI does not distinguish cell type or etiology (viral vs nonviral).3 Further, endomyocardial biopsy must be performed before immunosuppressive therapy can be safely started.3,16 At experienced centers, the complication rate is 0% to 0.8%.3 The addition of immunohistochemical testing and viral genomic detection by polymerase chain reaction testing have increased the sensitivity of this technique.19 Finally, endomyocardial biopsy can help rule out some of the other possibilities in the differential diagnosis for myocarditis, including infiltrative and storage diseases, and possibly cardiac tumors.3
Of additional note, the diffuse ST-segment elevation seen on the patient’s electrocardiogram (Figure 1) is indicative of subepicardial inflammation. Since the distribution involves more than one epicardial coronary territory, this helps to differentiate the changes from those that occur with myocardial infarction.20
CASE CONTINUED
Figure 2. Cardiac magnetic resonance imaging shows areas of patchy subepicardial late gadolinium enhancement (arrows).
The patient underwent cardiac MRI, which showed myocardial edema and patchy areas of late gadolinium enhancement, raising suspicion for myocarditis (Figure 2).
Causes of myocarditis are numerous (Table 1),3,21,22 but viral and postinfectious etiologies remain the most common causes of acute myocarditis.23
2. What is the most likely causative infectious agent?
Parvovirus B19
Coxsackievirus B
Adenovirus species
Human herpesvirus 6
Staphylococcus aureus
Corynebacterium diphtheria
Trypanosoma cruzi
Influenza H1/N1
INFECTIOUS CAUSES OF MYOCARDITIS
Coxsackievirus B was the agent most often linked to this condition from the 1950s through the 1990s. However, in the last 2 decades, adenovirus species and human herpesvirus 6 have been increasingly encountered, and recently, parvovirus B19 has been credited as the most common culprit,11,23 at least in the Western world. In developing nations, T cruzi and C diphtheria are the most common offenders.21
S aureus is a common cause of endocarditis, but it rarely plays a role in myocarditis. When it does, the myocarditis is often the sequela of profound bacteremia. This was much more common before antibiotics were invented.24,25
Influenza H1/N1 is not among the most common causes of viral myocarditis, but it should be considered during flu season, given its ability to result in fulminant myocarditis.3,26
TREATMENT FOR MYOCARDITIS
3. Which treatment is the most appropriate at this time?
Intravenous immunoglobulin
Interferon beta
Acyclovir
Prednisone
Colchicine
Treatment for myocarditis depends on the cause but always includes supportive care to address the constellation of presenting symptoms. Standard therapies for tachy- or bradyarrhythmias, heart failure, and hemodynamic derangement should be started.
Supportive care
In patients with severe left ventricular dysfunction, an implantable cardiac electronic device, left ventricular assist device, or heart transplant may ultimately be needed. However, if possible these should be deferred for several months to determine response to treatment, since the myocardium can possibly recover.16
Diuretics, beta-blockers, angiotensin II receptor blockers, angiotensin-converting enzyme inhibitors, and aldosterone antagonists should be given as part of guideline-directed medical therapy for patients with heart failure and reduced ejection fraction.3,27 However, whether and how the patient should be weaned from these agents after disease recovery are unknown.3
Intravenous immunoglobulin
Intravenous immunoglobulin in high doses has had mixed results. Its efficacy is well documented in children,21 but limited supportive data are available in adults.3 As such, recent ESC guidelines do not provide recommendations regarding its use in adults.3
Interferon beta
Interferon beta has shown promise in improving New York Heart Association class and left ventricular ejection fraction.3 This is attributed to its effects on eliminating adenoviral species and enteroviruses. Treatment of enteroviral organisms in particular has been associated with improved 10-year prognosis.3 Interferon beta also has in vitro data showing efficacy at diminishing apoptosis from parvovirus B19.28
Nucleoside analogues
Empiric treatment with nucleoside analogues (acyclovir, ganciclovir, and valacyclovir) has been tried for patients in whom human herpesvirus is suspected as the causative organism, although with unconfirmed effects.3 Consultation with an infectious disease specialist is recommended before starting these agents, and biopsy is often needed beforehand.3
Immunosuppressive agents
Immunosuppressive agents such as prednisone, azathioprine, and cyclosporine can be used in cases of biopsy-proven disease with manifestations of severe heart failure, especially if biopsy results reveal sarcoidosis, giant cell myocarditis, or necrotizing eosinophilic myocarditis. Although the results were neutral in the Myocarditis Treatment Trial,29 the cause of myocarditis in this trial was unknown. Therapy with such agents should be initiated after active infection is ruled out, which also would require a biopsy.
Colchicine
Mechanisms of chest pain in myocarditis include associated pericarditis and coronary artery vasospasm.3,23 Our patient’s chest pain changed when he changed position, possibly indicating associated pericarditis. In myocarditis with accompanying pericarditis symptoms, colchicine (1–2 mg as an initial dose and then 0.6 mg daily for up to 3 months) can be helpful in alleviating symptoms.21,30 Thus, starting this agent in a patient who presents with myocarditis in absence of heart failure, arrhythmias, or left ventricular dysfunction is prudent.
Colchicine is used mainly to address the pain associated with pericarditis. For patients who present with pericarditis without myocarditis, nonsteroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment, with the addition of colchicine leading to faster symptom resolution.30 The benefit of colchicine for isolated myocarditis is not well established, with only limited data showing some clinical effects.31
CASE CONTINUED
The patient was given colchicine 1.2 mg on the first day and then 0.6 mg daily. Within 2 days, his chest pain had resolved. He did not receive any immunosuppressive agents.
DISCHARGE INSTRUCTIONS
4. Before discharge, this patient should be instructed to do which of the following?
Take over-the-counter NSAIDs to supplement the effects of colchicine
Avoid competitive sports and athletics for at least 6 months
Call to schedule repeat cardiac MRI
No further instruction is needed
NSAIDs are used by themselves or in combination with colchicine in the treatment of pericarditis, but their use may be associated with worse outcomes in myocarditis.3,21 Thus, their use is not recommended in most cases.3
Excessive physical activity should be avoided for at least 6 months after the clinical syndrome resolves. This recommendation is included in the most recent ESC guidelines but is based mainly on expert opinion and murine models with coxsackievirus B.3 Periodic reassessment is indicated with exercise stress testing before return to strenuous activity.3,16,32 Testing should look for exercise tolerance, and exercise electrocardiography also helps to evaluate for clinically relevant arrythmias.
Cardiac MRI can help clarify the prognosis in myocarditis, but the role of repeat testing in guiding therapy is limited.3 Indications for repeat cardiac MRI include presence of 0 or 1 of the Lake Louise criteria (recall that 2 are necessary to make the diagnosis) with recurrence of symptoms and a high suspicion for myocardial inflammation.3,9 Repeat cardiac MRI was not performed for our patient.
CASE CONCLUDED
The patient was evaluated in the cardiology clinic within 1 week of discharge. At that time, he was in sinus tachycardia with a heart rate of 102 bpm, and he was instructed to avoid any exercise until further notice.
At 6-month follow-up, the sinus tachycardia had resolved. However, because persistent tachycardia had been noted at the first postdischarge visit, and in view of the extent of myocardial involvement, he underwent exercise treadmill testing to evaluate for ventricular arrhythmias. The study did show premature ventricular complexes and 1 ventricular couplet at submaximal exercise levels. As this indicated a higher risk of exercise-induced arrhythmias, he was asked to continue normal activity levels but to abstain from exercise until the next evaluation.
During his 1-year follow-up, a repeat treadmill test showed no ventricular ectopy. Holter monitoring was ordered and showed no premature ventricular complexes, supraventricular arrhythmias, or atrioventricular block within the 48-hour period.
At his 2-year evaluation, he had returned to playing basketball and soccer on weekends and reported no recurrence of his initial symptoms.
KEY POINTS
Figure 3. Our suggested approach to suspected acute myocarditis.Cardiac MRI has emerged as an excellent noninvasive imaging modality for the diagnosis of myocarditis.
Treatment of myocarditis depends on the cause and severity of the patient’s presentation, spanning the spectrum from conservative care to immunosuppressive agents and even heart failure therapy.
Excessive physical activity should be avoided for the first 6 months after disease diagnosis and treatment.
If myocarditis is associated with pericardial involvement, colchicine is the agent of choice, and NSAIDs should be avoided.
Our suggested strategy for approaching myocarditis is shown in Figure 3.
Mahfoud F, Gärtner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011; 32(7):897–903. doi:10.1093/eurheartj/ehq493
Caforio AL, Pankuweit S, Arbustini E, et al; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013; 34(33):2636–2648, 2648a–2648d. doi:10.1093/eurheartj/eht210
Donnelly JP, Hanna M. Cardiac amyloidosis: an update on diagnosis and treatment. Cleve Clin J Med 2017; 84(12 suppl 3):12–26. doi:10.3949/ccjm.84.s3.02
Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28(1):10–21. doi:10.1016/j.tcm.2017.07.004
Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol 2015; 66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
Blankstein R, Osborne M, Naya M, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014; 63(4):329–336. doi:10.1016/j.jacc.2013.09.022
Baccouche H, Mahrholtz H, Meinhardt G, et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009; 30(23):2869–2879. doi:10.1093/eurheartj/ehp328
Friedrich MG, Sechtem U, Schulz-Menger J, et al; International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009; 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012; 59(9):779–792. doi:10.1016/j.jacc.2011.09.074
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006; 114(15):1581–1590. doi:10.1161/CIRCULATIONAHA.105.606509
Gräni C, Eichhorn C, Bière L, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017; 70(16):1964–1976. doi:10.1016/j.jacc.2017.08.050
Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-Trial. J Am Coll Cardiol 2016; 67(15):1800–1811. doi:10.1016/j.jacc.2016.02.013
Gannon MP, Schaub E, Griens CL, Saba SG. State of the art: evaluation and prognostication of myocarditis using cardiac MRI. J Magn Reson Imaging 2019; 49(7):e122–e131. doi:10.1002/jmri.26611
Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007; 28(24):3076–3093. doi:10.1093/eurheartj/ehm456
Sinagra G, Anzini M, Pereira NL, et al. Myocarditis in clinical practice. Mayo Clin Proc 2016; 91(9):1256–1266. doi:10.1016/j.mayocp.2016.05.013
Cooper LT, Baughman KL, Feldman AM, et al; American Heart Association; American College of Cardiology; European Society of Cardiology. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007; 116(19):2216–2233. doi:10.1161/CIRCULATIONAHA.107.186093
Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012; 21(4):245–274. doi:10.1016/j.carpath.2011.10.001
Alraies MC, Klein AL. Should we still use electrocardiography to diagnose pericardial disease? Cleve Clin J Med 2013; 80(2):97–100. doi:10.3949/ccjm.80a.11144
Wasi F, Shuter J. Primary bacterial infection of the myocardium. Front Biosci 2003; 8:s228–s231. pmid:12700039
Al-Amoodi M, Rao K, Rao S, Brewer JH, Magalski A, Chhatriwalla AK. Fulminant myocarditis due to H1N1 influenza. Circ Heart Fail 2010; 3(3):e7–e9. doi:10.1161/CIRCHEARTFAILURE.110.938506
Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2016; 68(13):1476–1488. doi:10.1016/j.jacc.2016.05.011
Schmidt-Lucke C, Spillmann F, Bock T, et al. Interferon beta modulates endothelial damage in patients with cardiac persistence of human parvovirus b19 infection. J Infect Dis 2010; 201(6):936–945. doi:10.1086/650700
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosuppressive therapy for myocarditis: the Myocarditis Treatment Trial Investigators. N Engl J Med 1995; 333(5):269–275. doi:10.1056/NEJM199508033330501
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005; 112(13):2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738
Morgenstern D, Lisko J, Boniface NC, Mikolich BM, Mikolich JR. Myocarditis and colchicine: a new perspective from cardiac MRI. J Cardiovasc Magn Reson 2016; 18(suppl 1):0100.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015; 66(21):2343–2349. doi:10.1016/j.jacc.2015.09.032
Mahfoud F, Gärtner B, Kindermann M, et al. Virus serology in patients with suspected myocarditis: utility or futility? Eur Heart J 2011; 32(7):897–903. doi:10.1093/eurheartj/ehq493
Caforio AL, Pankuweit S, Arbustini E, et al; European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013; 34(33):2636–2648, 2648a–2648d. doi:10.1093/eurheartj/eht210
Donnelly JP, Hanna M. Cardiac amyloidosis: an update on diagnosis and treatment. Cleve Clin J Med 2017; 84(12 suppl 3):12–26. doi:10.3949/ccjm.84.s3.02
Siddiqi OK, Ruberg FL. Cardiac amyloidosis: an update on pathophysiology, diagnosis, and treatment. Trends Cardiovasc Med 2018; 28(1):10–21. doi:10.1016/j.tcm.2017.07.004
Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol 2015; 66(21):2451–2466. doi:10.1016/j.jacc.2015.09.075
Blankstein R, Osborne M, Naya M, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014; 63(4):329–336. doi:10.1016/j.jacc.2013.09.022
Baccouche H, Mahrholtz H, Meinhardt G, et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009; 30(23):2869–2879. doi:10.1093/eurheartj/ehp328
Friedrich MG, Sechtem U, Schulz-Menger J, et al; International Consensus Group on Cardiovascular Magnetic Resonance in Myocarditis. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009; 53(17):1475–1487. doi:10.1016/j.jacc.2009.02.007
Kindermann I, Barth C, Mahfoud F, et al. Update on myocarditis. J Am Coll Cardiol 2012; 59(9):779–792. doi:10.1016/j.jacc.2011.09.074
Mahrholdt H, Wagner A, Deluigi CC, et al. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation 2006; 114(15):1581–1590. doi:10.1161/CIRCULATIONAHA.105.606509
Gräni C, Eichhorn C, Bière L, et al. Prognostic value of cardiac magnetic resonance tissue characterization in risk stratifying patients with suspected myocarditis. J Am Coll Cardiol 2017; 70(16):1964–1976. doi:10.1016/j.jacc.2017.08.050
Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: the MyoRacer-Trial. J Am Coll Cardiol 2016; 67(15):1800–1811. doi:10.1016/j.jacc.2016.02.013
Gannon MP, Schaub E, Griens CL, Saba SG. State of the art: evaluation and prognostication of myocarditis using cardiac MRI. J Magn Reson Imaging 2019; 49(7):e122–e131. doi:10.1002/jmri.26611
Cooper LT, Baughman KL, Feldman AM, et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. Eur Heart J 2007; 28(24):3076–3093. doi:10.1093/eurheartj/ehm456
Sinagra G, Anzini M, Pereira NL, et al. Myocarditis in clinical practice. Mayo Clin Proc 2016; 91(9):1256–1266. doi:10.1016/j.mayocp.2016.05.013
Cooper LT, Baughman KL, Feldman AM, et al; American Heart Association; American College of Cardiology; European Society of Cardiology. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation 2007; 116(19):2216–2233. doi:10.1161/CIRCULATIONAHA.107.186093
Leone O, Veinot JP, Angelini A, et al. 2011 consensus statement on endomyocardial biopsy from the Association for European Cardiovascular Pathology and the Society for Cardiovascular Pathology. Cardiovasc Pathol 2012; 21(4):245–274. doi:10.1016/j.carpath.2011.10.001
Alraies MC, Klein AL. Should we still use electrocardiography to diagnose pericardial disease? Cleve Clin J Med 2013; 80(2):97–100. doi:10.3949/ccjm.80a.11144
Wasi F, Shuter J. Primary bacterial infection of the myocardium. Front Biosci 2003; 8:s228–s231. pmid:12700039
Al-Amoodi M, Rao K, Rao S, Brewer JH, Magalski A, Chhatriwalla AK. Fulminant myocarditis due to H1N1 influenza. Circ Heart Fail 2010; 3(3):e7–e9. doi:10.1161/CIRCHEARTFAILURE.110.938506
Yancy CW, Jessup M, Bozkurt B, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol 2016; 68(13):1476–1488. doi:10.1016/j.jacc.2016.05.011
Schmidt-Lucke C, Spillmann F, Bock T, et al. Interferon beta modulates endothelial damage in patients with cardiac persistence of human parvovirus b19 infection. J Infect Dis 2010; 201(6):936–945. doi:10.1086/650700
Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial of immunosuppressive therapy for myocarditis: the Myocarditis Treatment Trial Investigators. N Engl J Med 1995; 333(5):269–275. doi:10.1056/NEJM199508033330501
Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the COlchicine for acute PEricarditis (COPE) trial. Circulation 2005; 112(13):2012–2016. doi:10.1161/CIRCULATIONAHA.105.542738
Morgenstern D, Lisko J, Boniface NC, Mikolich BM, Mikolich JR. Myocarditis and colchicine: a new perspective from cardiac MRI. J Cardiovasc Magn Reson 2016; 18(suppl 1):0100.
Maron BJ, Zipes DP, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: preamble, principles, and general considerations: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol 2015; 66(21):2343–2349. doi:10.1016/j.jacc.2015.09.032
Biologics improved coronary inflammation as well as psoriasis symptoms, according to data from the perivascular fat attenuation index in 134 adults identified using coronary CT angiography.
Oxford Academic Cardiovascular CT Core Lab and Lab of Inflammation and Cardiometabolic Diseases at NHLBI
Coronary CT angiography image of the coronary arteries depicting the perivascular fat attenuation index before and after biologic therapy at 1-year follow-up for patients with excellent response to biologic therapy.
“The perivascular fat attenuation index [FAI] is a [CT]-based, novel, noninvasive imaging technique that allows for direct visualization and quantification of coronary inflammation using differential mapping of attenuation gradients in pericoronary fat,” wrote Youssef A. Elnabawi, MD, of the National Heart, Lung, and Blood Institute and colleagues. Biologics have been associated with reduced noncalcified coronary plaques in psoriasis patients, which suggests possible reduction in coronary inflammation as well.
In a study published in JAMA Cardiology, the researchers analyzed data from 134 adults with moderate to severe psoriasis who received no biologic therapy for at least 3 months before starting the study. Of these, 52 chose not to receive biologics, and served as controls while being treated with topical or light therapies. The participants are part of the Psoriasis Atherosclerosis Cardiometabolic Initiative, an ongoing, prospective cohort study. The average age of the patients was 51 years, and 63% were male.
The 82 patients given biologics received anti–tumor necrosis factor–alpha, anti–interleukin-12/23, or anti-IL-17 for 1 year. Overall, patients on biologics showed a significant decrease in FAI from a median of –71.22 Hounsfield units (HU) at baseline to a median of –76.06 at 1 year. These patients also showed significant improvement in Psoriasis Area and Severity Index scores, from a median of 7.7 at baseline to a median of 3.2 at 1 year. The control patients not on biologics showed no significant changes in FAI, with a median of –71.98 HU at baseline and –72.66 HU at 1 year.
The changes were consistent among the various biologics used, and The median FAI for patients on anti–tumor necrosis factor–alpha changed from –71.25 at baseline to –75.49 at 1 year; median FAI for both IL-12/23 and anti-IL-17 treatment groups changed from –71.18 HU at baseline to –76.92 at 1 year.
In addition, only patients treated with biologics showed a significant reduction in median C-reactive protein levels from baseline (2.2 mg/L vs. 1.3 mg/L). The changes in FAI were not associated with the presence of coronary plaques, the researchers noted.
The study findings were limited by several factors, including the observational design, small size, and lack of data on cardiovascular endpoints. “Future studies will be needed to explore whether the residual CV risk detected by perivascular FAI can be attenuated using targeted anti-inflammatory interventions,” they wrote.
However, the results suggest that biologics impact coronary vasculature at the microenvironmental level, and that FAI can be a noninvasive, cost-effective way to stratify patients at increased risk for cardiovascular disease, the researchers noted.
“We believe that the strength of perivascular FAI in risk stratifying patients with increased coronary inflammation will allow for better identification of patients at increased risk of future myocardial events that are not captured by traditional CV risk factors,” they wrote.
The study was funded by the National Institutes of Health, several research foundations, Elsevier, Colgate-Palmolive, and Genentech. Dr. Elnabawi had no financial conflicts to disclose; several coauthors reported relationships with multiple companies. One coauthor disclosed a pending and licensed patent to a novel tool for cardiovascular risk stratification based on the CT attenuation of perivascular tissue (OxScore) and a pending and licensed patent to perivascular texture index.
Biologics improved coronary inflammation as well as psoriasis symptoms, according to data from the perivascular fat attenuation index in 134 adults identified using coronary CT angiography.
Oxford Academic Cardiovascular CT Core Lab and Lab of Inflammation and Cardiometabolic Diseases at NHLBI
Coronary CT angiography image of the coronary arteries depicting the perivascular fat attenuation index before and after biologic therapy at 1-year follow-up for patients with excellent response to biologic therapy.
“The perivascular fat attenuation index [FAI] is a [CT]-based, novel, noninvasive imaging technique that allows for direct visualization and quantification of coronary inflammation using differential mapping of attenuation gradients in pericoronary fat,” wrote Youssef A. Elnabawi, MD, of the National Heart, Lung, and Blood Institute and colleagues. Biologics have been associated with reduced noncalcified coronary plaques in psoriasis patients, which suggests possible reduction in coronary inflammation as well.
In a study published in JAMA Cardiology, the researchers analyzed data from 134 adults with moderate to severe psoriasis who received no biologic therapy for at least 3 months before starting the study. Of these, 52 chose not to receive biologics, and served as controls while being treated with topical or light therapies. The participants are part of the Psoriasis Atherosclerosis Cardiometabolic Initiative, an ongoing, prospective cohort study. The average age of the patients was 51 years, and 63% were male.
The 82 patients given biologics received anti–tumor necrosis factor–alpha, anti–interleukin-12/23, or anti-IL-17 for 1 year. Overall, patients on biologics showed a significant decrease in FAI from a median of –71.22 Hounsfield units (HU) at baseline to a median of –76.06 at 1 year. These patients also showed significant improvement in Psoriasis Area and Severity Index scores, from a median of 7.7 at baseline to a median of 3.2 at 1 year. The control patients not on biologics showed no significant changes in FAI, with a median of –71.98 HU at baseline and –72.66 HU at 1 year.
The changes were consistent among the various biologics used, and The median FAI for patients on anti–tumor necrosis factor–alpha changed from –71.25 at baseline to –75.49 at 1 year; median FAI for both IL-12/23 and anti-IL-17 treatment groups changed from –71.18 HU at baseline to –76.92 at 1 year.
In addition, only patients treated with biologics showed a significant reduction in median C-reactive protein levels from baseline (2.2 mg/L vs. 1.3 mg/L). The changes in FAI were not associated with the presence of coronary plaques, the researchers noted.
The study findings were limited by several factors, including the observational design, small size, and lack of data on cardiovascular endpoints. “Future studies will be needed to explore whether the residual CV risk detected by perivascular FAI can be attenuated using targeted anti-inflammatory interventions,” they wrote.
However, the results suggest that biologics impact coronary vasculature at the microenvironmental level, and that FAI can be a noninvasive, cost-effective way to stratify patients at increased risk for cardiovascular disease, the researchers noted.
“We believe that the strength of perivascular FAI in risk stratifying patients with increased coronary inflammation will allow for better identification of patients at increased risk of future myocardial events that are not captured by traditional CV risk factors,” they wrote.
The study was funded by the National Institutes of Health, several research foundations, Elsevier, Colgate-Palmolive, and Genentech. Dr. Elnabawi had no financial conflicts to disclose; several coauthors reported relationships with multiple companies. One coauthor disclosed a pending and licensed patent to a novel tool for cardiovascular risk stratification based on the CT attenuation of perivascular tissue (OxScore) and a pending and licensed patent to perivascular texture index.
Biologics improved coronary inflammation as well as psoriasis symptoms, according to data from the perivascular fat attenuation index in 134 adults identified using coronary CT angiography.
Oxford Academic Cardiovascular CT Core Lab and Lab of Inflammation and Cardiometabolic Diseases at NHLBI
Coronary CT angiography image of the coronary arteries depicting the perivascular fat attenuation index before and after biologic therapy at 1-year follow-up for patients with excellent response to biologic therapy.
“The perivascular fat attenuation index [FAI] is a [CT]-based, novel, noninvasive imaging technique that allows for direct visualization and quantification of coronary inflammation using differential mapping of attenuation gradients in pericoronary fat,” wrote Youssef A. Elnabawi, MD, of the National Heart, Lung, and Blood Institute and colleagues. Biologics have been associated with reduced noncalcified coronary plaques in psoriasis patients, which suggests possible reduction in coronary inflammation as well.
In a study published in JAMA Cardiology, the researchers analyzed data from 134 adults with moderate to severe psoriasis who received no biologic therapy for at least 3 months before starting the study. Of these, 52 chose not to receive biologics, and served as controls while being treated with topical or light therapies. The participants are part of the Psoriasis Atherosclerosis Cardiometabolic Initiative, an ongoing, prospective cohort study. The average age of the patients was 51 years, and 63% were male.
The 82 patients given biologics received anti–tumor necrosis factor–alpha, anti–interleukin-12/23, or anti-IL-17 for 1 year. Overall, patients on biologics showed a significant decrease in FAI from a median of –71.22 Hounsfield units (HU) at baseline to a median of –76.06 at 1 year. These patients also showed significant improvement in Psoriasis Area and Severity Index scores, from a median of 7.7 at baseline to a median of 3.2 at 1 year. The control patients not on biologics showed no significant changes in FAI, with a median of –71.98 HU at baseline and –72.66 HU at 1 year.
The changes were consistent among the various biologics used, and The median FAI for patients on anti–tumor necrosis factor–alpha changed from –71.25 at baseline to –75.49 at 1 year; median FAI for both IL-12/23 and anti-IL-17 treatment groups changed from –71.18 HU at baseline to –76.92 at 1 year.
In addition, only patients treated with biologics showed a significant reduction in median C-reactive protein levels from baseline (2.2 mg/L vs. 1.3 mg/L). The changes in FAI were not associated with the presence of coronary plaques, the researchers noted.
The study findings were limited by several factors, including the observational design, small size, and lack of data on cardiovascular endpoints. “Future studies will be needed to explore whether the residual CV risk detected by perivascular FAI can be attenuated using targeted anti-inflammatory interventions,” they wrote.
However, the results suggest that biologics impact coronary vasculature at the microenvironmental level, and that FAI can be a noninvasive, cost-effective way to stratify patients at increased risk for cardiovascular disease, the researchers noted.
“We believe that the strength of perivascular FAI in risk stratifying patients with increased coronary inflammation will allow for better identification of patients at increased risk of future myocardial events that are not captured by traditional CV risk factors,” they wrote.
The study was funded by the National Institutes of Health, several research foundations, Elsevier, Colgate-Palmolive, and Genentech. Dr. Elnabawi had no financial conflicts to disclose; several coauthors reported relationships with multiple companies. One coauthor disclosed a pending and licensed patent to a novel tool for cardiovascular risk stratification based on the CT attenuation of perivascular tissue (OxScore) and a pending and licensed patent to perivascular texture index.
Prompt diagnois of infective endocarditis is critical. Potential consequences of missed or delayed diagnosis, including heart failure, stroke, intracardiac abscess, conduction delays, prosthesis dysfunction, and cerebral emboli, are often catastrophic. Echocardiography is the test used most frequently to evaluate for infective endocarditis, but it misses the diagnosis in almost one-third of cases, and even more often if the patient has a prosthetic valve.
But now, several sophisticated imaging tests are available that complement echocardiography in diagnosing and assessing infective endocarditis; these include 4-dimensional computed tomography (4D CT), fluorodeoxyglucose positron emission tomography (FDG-PET), and leukocyte scintigraphy. These tests have greatly improved our ability not only to diagnose infective endocarditis, but also to determine the extent and spread of infection, and they aid in perioperative assessment. Abnormal findings on these tests have been incorporated into the European Society of Cardiology’s 2015 modified diagnostic criteria for infective endocarditis.1
This article details the indications, advantages, and limitations of the various imaging tests for diagnosing and evaluating infective endocarditis (Table 1).
INFECTIVE ENDOCARDITIS IS DIFFICULT TO DIAGNOSE AND TREAT
Infective endocarditis is difficult to diagnose and treat. Clinical and imaging clues can be subtle, and the diagnosis requires a high level of suspicion and visualization of cardiac structures.
Further, the incidence of infective endocarditis is on the rise in the United States, particularly in women and young adults, likely due to intravenous drug use.2,3
ECHOCARDIOGRAPHY HAS AN IMPORTANT ROLE, BUT IS LIMITED
Echocardiography remains the most commonly performed study for diagnosing infective endocarditis, as it is fast, widely accessible, and less expensive than other imaging tests.
Transthoracic echocardiography (TTE) is often the first choice for testing. However, its sensitivity is only about 70% for detecting vegetations on native valves and 50% for detecting vegetations on prosthetic valves.1 It is inherently constrained by the limited number of views by which a comprehensive external evaluation of the heart can be achieved. Using a 2-dimensional instrument to view a 3-dimensional object is difficult, and depending on several factors, it can be hard to see vegetations and abscesses that are associated with infective endocarditis. Further, TTE is impeded by obesity and by hyperinflated lungs from obstructive pulmonary disease or mechanical ventilation. It has poor sensitivity for detecting small vegetations and for detecting vegetations and paravalvular complications in patients who have a prosthetic valve or a cardiac implanted electronic device.
Transesophageal echocardiography (TEE) is the recommended first-line imaging test for patients with prosthetic valves and no contraindications to the test. Otherwise, it should be done after TTE if the results of TTE are negative but clinical suspicion for infective endocarditis remains high (eg, because the patient uses intravenous drugs). But although TEE has a higher sensitivity than TTE (up to 96% for vegetations on native valves and 92% for those on prosthetic valves, if performed by an experienced sonographer), it can still miss infective endocarditis. Also, TEE does not provide a significant advantage over TTE in patients who have a cardiac implanted electronic device.1,4,5
Regardless of whether TTE or TEE is used, they are estimated to miss up to 30% of cases of infective endocarditis and its sequelae.4 False-negative findings are likelier in patients who have preexisting severe valvular lesions, prosthetic valves, cardiac implanted electronic devices, small vegetations, or abscesses, or if a vegetation has already broken free and embolized. Furthermore, distinguishing between vegetations and thrombi, cardiac tumors, and myxomatous changes using echocardiography is difficult.
CARDIAC CT
For patients who have inconclusive results on echocardiography, contraindications to TEE, or poor sonic windows, cardiac CT can be an excellent alternative. It is especially useful in the setting of a prosthetic valve.
Synchronized (“gated”) with the patient’s heart rate and rhythm, CT machines can acquire images during diastole, reducing motion artifact, and can create 3D images of the heart. In addition, newer machines can acquire several images at different points in the heart cycle to add a fourth dimension—time. The resulting 4D images play like short video loops of the beating heart and allow noninvasive assessment of cardiac anatomy with remarkable detail and resolution.
4D CT is increasingly being used in infective endocarditis, and growing evidence indicates that its accuracy is similar to that of TEE in the preoperative evaluation of patients with aortic prosthetic valve endocarditis.6 In a study of 28 patients, complementary use of CT angiography led to a change in treatment strategy in 7 (25%) compared with routine clinical workup.7 Several studies have found no difference between 4D CT and preoperative TEE in detecting pseudoaneurysm, abscess, or valve dehiscence. TEE and 4D CT also have similar sensitivities for detecting infective endocarditis in native and prosthetic valves.8,9
Figure 1A. Transesophageal echocardiography in a 73-year-old man with a bioprosthetic aortic valve who presented with 2 months of fevers, chills, and night sweats. He had several negative blood cultures and 2 negative transesophageal echocardiograms over 1 month. No mass, vegetation, paravalvular abscess, or significant valve dysfunction was noted.
Figure 1B. Cardiac computed tomographic (CT) angiography with iodinated contrast, including 4D reconstruction, in the same patient, however, shows an 11-mm vegetation on the bioprosthetic aortic valve leaflets (arrow).
Figure 1C. Fluorodeoxyglucose positron emission tomography (FDG-PET) in the same patient confirms the diagnosis, showing a 13-mm hypermetabolic focus on the prosthetic valve (arrow), yielding the diagnosis of infectious endocarditis.
Coupled with CT angiography, 4D CT is also an excellent noninvasive way to perioperatively evaluate the coronary arteries without the risks associated with catheterization in those requiring nonemergency surgery (Figure 1A, B, and C).
4D CT performs well for detecting abscess and pseudoaneurysm but has slightly lower sensitivity for vegetations than TEE (91% vs 99%).9
Gated CT, PET, or both may be useful in cases of suspected prosthetic aortic valve endocarditis when TEE is negative. Pseudoaneurysms are not well visualized with TEE, and the atrial mitral curtain area is often thickened on TEE in cases of aortic prosthetic valve infective endocarditis that do not definitely involve abscesses. Gated CT and PET show this area better.8 This information is important in cases in which a surgeon may be unconvinced that the patient has prosthetic valve endocarditis.
Limitations of 4D cardiac CT
4D CT with or without angiography has limitations. It requires a wide-volume scanner and an experienced reader.
Patients with irregular heart rhythms or uncontrolled tachycardia pose technical problems for image acquisition. Cardiac CT is typically gated (ie, images are obtained within a defined time period) to acquire images during diastole. Ideally, images are acquired when the heart is in mid to late diastole, a time of minimal cardiac motion, so that motion artifact is minimized. To estimate the timing of image acquisition, the cardiac cycle must be predictable, and its duration should be as long as possible. Tachycardia or irregular rhythms such as frequent ectopic beats or atrial fibrillation make acquisition timing difficult, and thus make it nearly impossible to accurately obtain images when the heart is at minimum motion, limiting assessment of cardiac structures or the coronary tree.4,10
Extensive coronary calcification can hinder assessment of the coronary tree by CT coronary angiography.
Contrast exposure may limit the use of CT in some patients (eg, those with contrast allergies or renal dysfunction). However, modern scanners allow for much smaller contrast boluses without decreasing sensitivity.
4D CT involves radiation exposure, especially when done with angiography, although modern scanners have greatly reduced exposure. The average radiation dose in CT coronary angiography is 2.9 to 5.9 mSv11 compared with 7 mSv in diagnostic cardiac catheterization (without angioplasty or stenting) or 16 mSv in routine CT of the abdomen and pelvis with contrast.12,13 In view of the morbidity and mortality risks associated with infective endocarditis, especially if the diagnosis is delayed, this small radiation exposure may be justifiable.
Bottom line for cardiac CT
4D CT is an excellent alternative to echocardiography for select patients. Clinicians should strongly consider this study in the following situations:
Patients with a prosthetic valve
Patients who are strongly suspected of having infective endocarditis but who have a poor sonic window on TTE or TEE, as can occur with chronic obstructive lung disease, morbid obesity, or previous thoracic or cardiovascular surgery
Patients who meet clinical indications for TEE, such as having a prosthetic valve or a high suspicion for native valve infective endocarditis with negative TTE, but who have contraindications to TEE
As an alternative to TEE for preoperative evaluation in patients with known infective endocarditis.
Patients with tachycardia or irregular heart rhythms are not good candidates for this test.
FDG-PET AND LEUKOCYTE SCINTIGRAPHY
FDG-PET and leukocyte scintigraphy are other options for diagnosing infective endocarditis and determining the presence and extent of intra- and extracardiac infection. They are more sensitive than echocardiography for detecting infection of cardiac implanted electronic devices such as ventricular assist devices, pacemakers, implanted cardiac defibrillators, and cardiac resynchronization therapy devices.14–16
The utility of FDG-PET is founded on the uptake of 18F-fluorodeoxyglucose by cells, with higher uptake taking place in cells with higher metabolic activity (such as in areas of inflammation). Similarly, leukocyte scintigraphy relies on the use of radiolabeled leukocytes (ie, leukocytes previously extracted from the patient, labelled, and re-introduced into the patient) to allow for localization of inflamed tissue.
The most significant contribution of FDG-PET may be the ability to detect infective endocarditis early, when echocardiography is initially negative. When abnormal FDG uptake was included in the modified Duke criteria, it increased the sensitivity to 97% for detecting infective endocarditis on admission, leading some to propose its incorporation as a major criterion.17 In patients with prosthetic valves and suspected infective endocarditis, FDG-PET was found in one study to have a sensitivity of up to 91% and a specificity of up to 95%.18
Both FDG-PET and leukocyte scintigraphy have a high sensitivity, specificity, and negative predictive value for cardiac implanted electronic device infection, and should be strongly considered in patients in whom it is suspected but who have negative or inconclusive findings on echocardiography.14,15
In addition, a common conundrum faced by clinicians with use of echocardiography is the difficulty of differentiating thrombus from infected vegetation on valves or device lead wires. Some evidence indicates that FDG-PET may help to discriminate between vegetation and thrombus, although more rigorous studies are needed before its use for that purpose can be recommended.19
Limitations of nuclear studies
Both FDG-PET and leukocyte scintigraphy perform poorly for detecting native-valve infective endocarditis. In a study in which 90% of the patients had native-valve infective endocarditis according to the Duke criteria, FDG-PET had a specificity of 93% but a sensitivity of only 39%.20
Both studies can be cumbersome, laborious, and time-consuming for patients. FDG-PET requires a fasting or glucose-restricted diet before testing, and the test itself can be complicated by development of hyperglycemia, although this is rare.
While FDG-PET is most effective in detecting infections of prosthetic valves and cardiac implanted electronic devices, the results can be falsely positive in patients with a history of recent cardiac surgery (due to ongoing tissue healing), as well as maladies other than infective endocarditis that lead to inflammation, such as vasculitis or malignancy. Similarly, for unclear reasons, leukocyte scintigraphy can yield false-negative results in patients with enterococcal or candidal infective endocarditis.21
FDG-PET and leukocyte scintigraphy are more expensive than TEE and cardiac CT22 and are not widely available.
Both tests entail radiation exposure, with the average dose ranging from 7 to 14 mSv. However, this is less than the average amount acquired during percutaneous coronary intervention (16 mSv), and overlaps with the amount in chest CT with contrast when assessing for pulmonary embolism (7 to 9 mSv). Lower doses are possible with optimized protocols.12,13,15,23
Bottom line for nuclear studies
Figure 2. Suggested algorithm for evaluating suspected infective endocarditis with negative or inconclusive results on echocardiography.
FDG-PET and leukocyte scintigraphy are especially useful for patients with a prosthetic valve or cardiac implanted electronic device. However, limitations must be kept in mind.
A suggested algorithm for testing with nuclear imaging is shown in Figure 2.1,4
CEREBRAL MAGNETIC RESONANCE IMAGING
Cerebral magnetic resonance imaging (MRI) is more sensitive than cerebral CT for detecting emboli in the brain. According to American Heart Association guidelines, cerebral MRI should be done in patients with known or suspected infective endocarditis and neurologic impairment, defined as headaches, meningeal symptoms, or neurologic deficits. It is also often used in neurologically asymptomatic patients with infective endocarditis who have indications for valve surgery to assess for mycotic aneurysms, which are associated with increased intracranial bleeding during surgery.
MRI use in other asymptomatic patients remains controversial.24 In cases with high clinical suspicion for infective endocarditis and no findings on echocardiography, cerebral MRI can increase the sensitivity of the Duke criteria by adding a minor criterion. Some have argued that, in patients with definite infective endocarditis, detecting silent cerebral complications can lead to management changes. However, more studies are needed to determine if there is indeed a group of neurologically asymptomatic infective endocarditis patients for whom cerebral MRI leads to improved outcomes.
Limitations of cerebral MRI
Cerebral MRI cannot be used in patients with non-MRI-compatible implanted hardware.
Gadolinium, the contrast agent typically used, can cause nephrogenic systemic fibrosis in patients who have poor renal function. This rare but serious adverse effect is characterized by irreversible systemic fibrosis affecting skin, muscles, and even visceral tissue such as lungs. The American College of Radiology allows for gadolinium use in patients without acute kidney injury and patients with stable chronic kidney disease with a glomerular filtration rate of at least 30 mL/min/1.73 m2. Its use should be avoided in patients with renal failure on replacement therapy, with advanced chronic kidney disease (glomerular filtration rate < 30 mL/min/1.73 m2), or with acute kidney injury, even if they do not need renal replacement therapy.25
Concerns have also been raised about gadolinium retention in the brain, even in patients with normal renal function.26–28 Thus far, no conclusive clinical adverse effects of retention have been found, although more study is warranted. Nevertheless, the US Food and Drug Administration now requires a black-box warning about this possibility and advises clinicians to counsel patients appropriately.
Bottom line on cerebral MRI
Cerebral MRI should be obtained when a patient presents with definite or possible infective endocarditis with neurologic impairment, such as new headaches, meningismus, or focal neurologic deficits. Routine brain MRI in patients with confirmed infective endocarditis without neurologic symptoms, or those without definite infective endocarditis, is discouraged.
CARDIAC MRI
Cardiac MRI, typically obtained with gadolinium contrast, allows for better 3D assessment of cardiac structures and morphology than echocardiography or CT, and can detect infiltrative cardiac disease, myopericarditis, and much more. It is increasingly used in the field of structural cardiology, but its role for evaluating infective endocarditis remains unclear.
Cardiac MRI does not appear to be better than echocardiography for diagnosing infective endocarditis. However, it may prove helpful in the evaluation of patients known to have infective endocarditis but who cannot be properly evaluated for disease extent because of poor image quality on echocardiography and contraindications to CT.1,29 Its role is limited in patients with cardiac implanted electronic devices, as most devices are incompatible with MRI use, although newer devices obviate this concern. But even for devices that are MRI-compatible, results are diminished due to an eclipsing effect, wherein the device parts can make it hard to see structures clearly because the “brightness” basically eclipses the surrounding area.4
Concerns regarding use of gadolinium as described above need also be considered.
The role of cardiac MRI in diagnosing and managing infective endocarditis may evolve, but at present, the 2017 American College of Cardiology and American Heart Association appropriate-use criteria discourage its use for these purposes.16
Bottom line for cardiac MRI
Cardiac MRI to evaluate a patient for suspected infective endocarditis is not recommended due to lack of superiority compared with echocardiography or CT, and the risk of nephrogenic systemic fibrosis from gadolinium in patients with renal compromise.
References
Habib G, Lancellotti P, Antunes MJ, et al; ESC Scientific Document Group. 2015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015; 36(44):3075–3128. doi:10.1093/eurheartj/ehv319
Durante-Mangoni E, Bradley S, Selton-Suty C, et al; International Collaboration on Endocarditis Prospective Cohort Study Group. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 2008; 168(19):2095–2103. doi:10.1001/archinte.168.19.2095
Wurcel AG, Anderson JE, Chui KK, et al. Increasing infectious endocarditis admissions among young people who inject drugs. Open Forum Infect Dis 2016; 3(3):ofw157. doi:10.1093/ofid/ofw157
Gomes A, Glaudemans AW, Touw DJ, et al. Diagnostic value of imaging in infective endocarditis: a systematic review. Lancet Infect Dis 2017; 17(1):e1–e14. doi:10.1016/S1473-3099(16)30141-4
Cahill TJ, Baddour LM, Habib G, et al. Challenges in infective endocarditis. J Am Coll Cardiol 2017; 69(3):325–344. doi:10.1016/j.jacc.2016.10.066
Fagman E, Perrotta S, Bech-Hanssen O, et al. ECG-gated computed tomography: a new role for patients with suspected aortic prosthetic valve endocarditis. Eur Radiol 2012; 22(11):2407–2414. doi:10.1007/s00330-012-2491-5
Habets J, Tanis W, van Herwerden LA, et al. Cardiac computed tomography angiography results in diagnostic and therapeutic change in prosthetic heart valve endocarditis. Int J Cardiovasc Imaging 2014; 30(2):377–387. doi:10.1007/s10554-013-0335-2
Koneru S, Huang SS, Oldan J, et al. Role of preoperative cardiac CT in the evaluation of infective endocarditis: comparison with transesophageal echocardiography and surgical findings. Cardiovasc Diagn Ther 2018; 8(4):439–449. doi:10.21037/cdt.2018.07.07
Koo HJ, Yang DH, Kang J, et al. Demonstration of infective endocarditis by cardiac CT and transoesophageal echocardiography: comparison with intra-operative findings. Eur Heart J Cardiovasc Imaging 2018; 19(2):199–207. doi:10.1093/ehjci/jex010
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol 2009; 53(5):436–444. doi:10.1016/j.jacc.2008.01.077
Castellano IA, Nicol ED, Bull RK, Roobottom CA, Williams MC, Harden SP. A prospective national survey of coronary CT angiography radiation doses in the United Kingdom. J Cardiovasc Comput Tomogr 2017; 11(4):268–273. doi:10.1016/j.jcct.2017.05.002
Mettler FA Jr, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008; 248(1):254–263. doi:10.1148/radiol.2481071451
Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med 2009; 169(22):2078–2086. doi:10.1001/archinternmed.2009.427
Ploux S, Riviere A, Amraoui S, et al. Positron emission tomography in patients with suspected pacing system infections may play a critical role in difficult cases. Heart Rhythm 2011; 8(9):1478–1481. doi:10.1016/j.hrthm.2011.03.062
Sarrazin J, Philippon F, Tessier M, et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J Am Coll Cardiol 2012; 59(18):1616–1625. doi:10.1016/j.jacc.2011.11.059
Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P; Rating Panel Members; Appropriate Use Criteria Task Force. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate use criteria for multimodality imaging in valvular heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Nucl Cardiol 2017; 24(6):2043–2063. doi:10.1007/s12350-017-1070-1
Saby L, Laas O, Habib G, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol 2013; 61(23):2374–2382. doi:10.1016/j.jacc.2013.01.092
Swart LE, Gomes A, Scholtens AM, et al. Improving the diagnostic performance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography in prosthetic heart valve endocarditis. Circulation 2018; 138(14):1412–1427. doi:10.1161/CIRCULATIONAHA.118.035032
Graziosi M, Nanni C, Lorenzini M, et al. Role of 18F-FDG PET/CT in the diagnosis of infective endocarditis in patients with an implanted cardiac device: a prospective study. Eur J Nucl Med Mol Imaging 2014; 41(8):1617–1623. doi:10.1007/s00259-014-2773-z
Kouijzer IJ, Vos FJ, Janssen MJ, van Dijk AP, Oyen WJ, Bleeker-Rovers CP. The value of 18F-FDG PET/CT in diagnosing infectious endocarditis. Eur J Nucl Med Mol Imaging 2013; 40(7):1102–1107. doi:10.1007/s00259-013-2376-0
Wong D, Rubinshtein R, Keynan Y. Alternative cardiac imaging modalities to echocardiography for the diagnosis of infective endocarditis. Am J Cardiol 2016; 118(9):1410–1418. doi:10.1016/j.amjcard.2016.07.053
Vos FJ, Bleeker-Rovers CP, Kullberg BJ, Adang EM, Oyen WJ. Cost-effectiveness of routine (18)F-FDG PET/CT in high-risk patients with gram-positive bacteremia. J Nucl Med 2011; 52(11):1673–1678. doi:10.2967/jnumed.111.089714
McCollough CH, Bushberg JT, Fletcher JG, Eckel LJ. Answers to common questions about the use and safety of CT scans. Mayo Clin Proc 2015; 90(10):1380–1392. doi:10.1016/j.mayocp.2015.07.011
Duval X, Iung B, Klein I, et al; IMAGE (Resonance Magnetic Imaging at the Acute Phase of Endocarditis) Study Group. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med 2010; 152(8):497–504, W175. doi:10.7326/0003-4819-152-8-201004200-00006
Kanda T, Fukusato T, Matsuda M, et al. Gadolinium-based contrast agent accumulates in the brain even in subjects without severe renal dysfunction: evaluation of autopsy brain specimens with inductively coupled plasma mass spectroscopy. Radiology 2015; 276(1):228–232. doi:10.1148/radiol.2015142690
McDonald RJ, McDonald JS, Kallmes DF, et al. Intracranial gadolinium deposition after contrast-enhanced MR imaging. Radiology 2015; 275(3):772–782. doi:10.1148/radiol.15150025
Kanda T, Ishii K, Kawaguchi H, Kitajima K, Takenaka D. High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose of a gadolinium-based contrast material. Radiology 2014; 270(3):834–841. doi:10.1148/radiol.13131669
Expert Panel on Pediatric Imaging; Hayes LL, Palasis S, Bartel TB, et al. ACR appropriateness criteria headache-child. J Am Coll Radiol 2018; 15(5S):S78–S90. doi:10.1016/j.jacr.2018.03.017
Nkemdilim Mgbojikwe, MD Assistant Professor of Medicine, Johns Hopkins University School of Medicine; Assistant Director of Clinical Operations, Hospitalist Program, The Johns Hopkins Hospital, Baltimore, MD
Steven R. Jones, MD Associate Professor of Medicine, Johns Hopkins University School of Medicine; Director, Inpatient Cardiology, Johns Hopkins Heart and Vascular Institute, Baltimore, MD
Thorsten M. Leucker, MD, PhD Assistant Professor of Medicine, Division of Cardiology, Department of Medicine, Johns Hopkins University School of Medicine; Director of Basic and Translational Vascular Biology Research within the Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, Baltimore, MD
Daniel J. Brotman, MD Professor of Medicine, Johns Hopkins University School of Medicine; Director, Hospitalist Program, The Johns Hopkins Hospital, Baltimore, MD
Address: Nkemdilim Mgbojikwe, MD, Hospitalist Program, Division of General Internal Medicine, Johns Hopkins Hospital, 600 N. Wolfe Street/ Meyer 8-134B, Baltimore, MD 21287; [email protected]
Dr. Brotman has disclosed consulting for Portola Pharmaceuticals.
Nkemdilim Mgbojikwe, MD Assistant Professor of Medicine, Johns Hopkins University School of Medicine; Assistant Director of Clinical Operations, Hospitalist Program, The Johns Hopkins Hospital, Baltimore, MD
Steven R. Jones, MD Associate Professor of Medicine, Johns Hopkins University School of Medicine; Director, Inpatient Cardiology, Johns Hopkins Heart and Vascular Institute, Baltimore, MD
Thorsten M. Leucker, MD, PhD Assistant Professor of Medicine, Division of Cardiology, Department of Medicine, Johns Hopkins University School of Medicine; Director of Basic and Translational Vascular Biology Research within the Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, Baltimore, MD
Daniel J. Brotman, MD Professor of Medicine, Johns Hopkins University School of Medicine; Director, Hospitalist Program, The Johns Hopkins Hospital, Baltimore, MD
Address: Nkemdilim Mgbojikwe, MD, Hospitalist Program, Division of General Internal Medicine, Johns Hopkins Hospital, 600 N. Wolfe Street/ Meyer 8-134B, Baltimore, MD 21287; [email protected]
Dr. Brotman has disclosed consulting for Portola Pharmaceuticals.
Author and Disclosure Information
Nkemdilim Mgbojikwe, MD Assistant Professor of Medicine, Johns Hopkins University School of Medicine; Assistant Director of Clinical Operations, Hospitalist Program, The Johns Hopkins Hospital, Baltimore, MD
Steven R. Jones, MD Associate Professor of Medicine, Johns Hopkins University School of Medicine; Director, Inpatient Cardiology, Johns Hopkins Heart and Vascular Institute, Baltimore, MD
Thorsten M. Leucker, MD, PhD Assistant Professor of Medicine, Division of Cardiology, Department of Medicine, Johns Hopkins University School of Medicine; Director of Basic and Translational Vascular Biology Research within the Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, Baltimore, MD
Daniel J. Brotman, MD Professor of Medicine, Johns Hopkins University School of Medicine; Director, Hospitalist Program, The Johns Hopkins Hospital, Baltimore, MD
Address: Nkemdilim Mgbojikwe, MD, Hospitalist Program, Division of General Internal Medicine, Johns Hopkins Hospital, 600 N. Wolfe Street/ Meyer 8-134B, Baltimore, MD 21287; [email protected]
Dr. Brotman has disclosed consulting for Portola Pharmaceuticals.
Prompt diagnois of infective endocarditis is critical. Potential consequences of missed or delayed diagnosis, including heart failure, stroke, intracardiac abscess, conduction delays, prosthesis dysfunction, and cerebral emboli, are often catastrophic. Echocardiography is the test used most frequently to evaluate for infective endocarditis, but it misses the diagnosis in almost one-third of cases, and even more often if the patient has a prosthetic valve.
But now, several sophisticated imaging tests are available that complement echocardiography in diagnosing and assessing infective endocarditis; these include 4-dimensional computed tomography (4D CT), fluorodeoxyglucose positron emission tomography (FDG-PET), and leukocyte scintigraphy. These tests have greatly improved our ability not only to diagnose infective endocarditis, but also to determine the extent and spread of infection, and they aid in perioperative assessment. Abnormal findings on these tests have been incorporated into the European Society of Cardiology’s 2015 modified diagnostic criteria for infective endocarditis.1
This article details the indications, advantages, and limitations of the various imaging tests for diagnosing and evaluating infective endocarditis (Table 1).
INFECTIVE ENDOCARDITIS IS DIFFICULT TO DIAGNOSE AND TREAT
Infective endocarditis is difficult to diagnose and treat. Clinical and imaging clues can be subtle, and the diagnosis requires a high level of suspicion and visualization of cardiac structures.
Further, the incidence of infective endocarditis is on the rise in the United States, particularly in women and young adults, likely due to intravenous drug use.2,3
ECHOCARDIOGRAPHY HAS AN IMPORTANT ROLE, BUT IS LIMITED
Echocardiography remains the most commonly performed study for diagnosing infective endocarditis, as it is fast, widely accessible, and less expensive than other imaging tests.
Transthoracic echocardiography (TTE) is often the first choice for testing. However, its sensitivity is only about 70% for detecting vegetations on native valves and 50% for detecting vegetations on prosthetic valves.1 It is inherently constrained by the limited number of views by which a comprehensive external evaluation of the heart can be achieved. Using a 2-dimensional instrument to view a 3-dimensional object is difficult, and depending on several factors, it can be hard to see vegetations and abscesses that are associated with infective endocarditis. Further, TTE is impeded by obesity and by hyperinflated lungs from obstructive pulmonary disease or mechanical ventilation. It has poor sensitivity for detecting small vegetations and for detecting vegetations and paravalvular complications in patients who have a prosthetic valve or a cardiac implanted electronic device.
Transesophageal echocardiography (TEE) is the recommended first-line imaging test for patients with prosthetic valves and no contraindications to the test. Otherwise, it should be done after TTE if the results of TTE are negative but clinical suspicion for infective endocarditis remains high (eg, because the patient uses intravenous drugs). But although TEE has a higher sensitivity than TTE (up to 96% for vegetations on native valves and 92% for those on prosthetic valves, if performed by an experienced sonographer), it can still miss infective endocarditis. Also, TEE does not provide a significant advantage over TTE in patients who have a cardiac implanted electronic device.1,4,5
Regardless of whether TTE or TEE is used, they are estimated to miss up to 30% of cases of infective endocarditis and its sequelae.4 False-negative findings are likelier in patients who have preexisting severe valvular lesions, prosthetic valves, cardiac implanted electronic devices, small vegetations, or abscesses, or if a vegetation has already broken free and embolized. Furthermore, distinguishing between vegetations and thrombi, cardiac tumors, and myxomatous changes using echocardiography is difficult.
CARDIAC CT
For patients who have inconclusive results on echocardiography, contraindications to TEE, or poor sonic windows, cardiac CT can be an excellent alternative. It is especially useful in the setting of a prosthetic valve.
Synchronized (“gated”) with the patient’s heart rate and rhythm, CT machines can acquire images during diastole, reducing motion artifact, and can create 3D images of the heart. In addition, newer machines can acquire several images at different points in the heart cycle to add a fourth dimension—time. The resulting 4D images play like short video loops of the beating heart and allow noninvasive assessment of cardiac anatomy with remarkable detail and resolution.
4D CT is increasingly being used in infective endocarditis, and growing evidence indicates that its accuracy is similar to that of TEE in the preoperative evaluation of patients with aortic prosthetic valve endocarditis.6 In a study of 28 patients, complementary use of CT angiography led to a change in treatment strategy in 7 (25%) compared with routine clinical workup.7 Several studies have found no difference between 4D CT and preoperative TEE in detecting pseudoaneurysm, abscess, or valve dehiscence. TEE and 4D CT also have similar sensitivities for detecting infective endocarditis in native and prosthetic valves.8,9
Figure 1A. Transesophageal echocardiography in a 73-year-old man with a bioprosthetic aortic valve who presented with 2 months of fevers, chills, and night sweats. He had several negative blood cultures and 2 negative transesophageal echocardiograms over 1 month. No mass, vegetation, paravalvular abscess, or significant valve dysfunction was noted.
Figure 1B. Cardiac computed tomographic (CT) angiography with iodinated contrast, including 4D reconstruction, in the same patient, however, shows an 11-mm vegetation on the bioprosthetic aortic valve leaflets (arrow).
Figure 1C. Fluorodeoxyglucose positron emission tomography (FDG-PET) in the same patient confirms the diagnosis, showing a 13-mm hypermetabolic focus on the prosthetic valve (arrow), yielding the diagnosis of infectious endocarditis.
Coupled with CT angiography, 4D CT is also an excellent noninvasive way to perioperatively evaluate the coronary arteries without the risks associated with catheterization in those requiring nonemergency surgery (Figure 1A, B, and C).
4D CT performs well for detecting abscess and pseudoaneurysm but has slightly lower sensitivity for vegetations than TEE (91% vs 99%).9
Gated CT, PET, or both may be useful in cases of suspected prosthetic aortic valve endocarditis when TEE is negative. Pseudoaneurysms are not well visualized with TEE, and the atrial mitral curtain area is often thickened on TEE in cases of aortic prosthetic valve infective endocarditis that do not definitely involve abscesses. Gated CT and PET show this area better.8 This information is important in cases in which a surgeon may be unconvinced that the patient has prosthetic valve endocarditis.
Limitations of 4D cardiac CT
4D CT with or without angiography has limitations. It requires a wide-volume scanner and an experienced reader.
Patients with irregular heart rhythms or uncontrolled tachycardia pose technical problems for image acquisition. Cardiac CT is typically gated (ie, images are obtained within a defined time period) to acquire images during diastole. Ideally, images are acquired when the heart is in mid to late diastole, a time of minimal cardiac motion, so that motion artifact is minimized. To estimate the timing of image acquisition, the cardiac cycle must be predictable, and its duration should be as long as possible. Tachycardia or irregular rhythms such as frequent ectopic beats or atrial fibrillation make acquisition timing difficult, and thus make it nearly impossible to accurately obtain images when the heart is at minimum motion, limiting assessment of cardiac structures or the coronary tree.4,10
Extensive coronary calcification can hinder assessment of the coronary tree by CT coronary angiography.
Contrast exposure may limit the use of CT in some patients (eg, those with contrast allergies or renal dysfunction). However, modern scanners allow for much smaller contrast boluses without decreasing sensitivity.
4D CT involves radiation exposure, especially when done with angiography, although modern scanners have greatly reduced exposure. The average radiation dose in CT coronary angiography is 2.9 to 5.9 mSv11 compared with 7 mSv in diagnostic cardiac catheterization (without angioplasty or stenting) or 16 mSv in routine CT of the abdomen and pelvis with contrast.12,13 In view of the morbidity and mortality risks associated with infective endocarditis, especially if the diagnosis is delayed, this small radiation exposure may be justifiable.
Bottom line for cardiac CT
4D CT is an excellent alternative to echocardiography for select patients. Clinicians should strongly consider this study in the following situations:
Patients with a prosthetic valve
Patients who are strongly suspected of having infective endocarditis but who have a poor sonic window on TTE or TEE, as can occur with chronic obstructive lung disease, morbid obesity, or previous thoracic or cardiovascular surgery
Patients who meet clinical indications for TEE, such as having a prosthetic valve or a high suspicion for native valve infective endocarditis with negative TTE, but who have contraindications to TEE
As an alternative to TEE for preoperative evaluation in patients with known infective endocarditis.
Patients with tachycardia or irregular heart rhythms are not good candidates for this test.
FDG-PET AND LEUKOCYTE SCINTIGRAPHY
FDG-PET and leukocyte scintigraphy are other options for diagnosing infective endocarditis and determining the presence and extent of intra- and extracardiac infection. They are more sensitive than echocardiography for detecting infection of cardiac implanted electronic devices such as ventricular assist devices, pacemakers, implanted cardiac defibrillators, and cardiac resynchronization therapy devices.14–16
The utility of FDG-PET is founded on the uptake of 18F-fluorodeoxyglucose by cells, with higher uptake taking place in cells with higher metabolic activity (such as in areas of inflammation). Similarly, leukocyte scintigraphy relies on the use of radiolabeled leukocytes (ie, leukocytes previously extracted from the patient, labelled, and re-introduced into the patient) to allow for localization of inflamed tissue.
The most significant contribution of FDG-PET may be the ability to detect infective endocarditis early, when echocardiography is initially negative. When abnormal FDG uptake was included in the modified Duke criteria, it increased the sensitivity to 97% for detecting infective endocarditis on admission, leading some to propose its incorporation as a major criterion.17 In patients with prosthetic valves and suspected infective endocarditis, FDG-PET was found in one study to have a sensitivity of up to 91% and a specificity of up to 95%.18
Both FDG-PET and leukocyte scintigraphy have a high sensitivity, specificity, and negative predictive value for cardiac implanted electronic device infection, and should be strongly considered in patients in whom it is suspected but who have negative or inconclusive findings on echocardiography.14,15
In addition, a common conundrum faced by clinicians with use of echocardiography is the difficulty of differentiating thrombus from infected vegetation on valves or device lead wires. Some evidence indicates that FDG-PET may help to discriminate between vegetation and thrombus, although more rigorous studies are needed before its use for that purpose can be recommended.19
Limitations of nuclear studies
Both FDG-PET and leukocyte scintigraphy perform poorly for detecting native-valve infective endocarditis. In a study in which 90% of the patients had native-valve infective endocarditis according to the Duke criteria, FDG-PET had a specificity of 93% but a sensitivity of only 39%.20
Both studies can be cumbersome, laborious, and time-consuming for patients. FDG-PET requires a fasting or glucose-restricted diet before testing, and the test itself can be complicated by development of hyperglycemia, although this is rare.
While FDG-PET is most effective in detecting infections of prosthetic valves and cardiac implanted electronic devices, the results can be falsely positive in patients with a history of recent cardiac surgery (due to ongoing tissue healing), as well as maladies other than infective endocarditis that lead to inflammation, such as vasculitis or malignancy. Similarly, for unclear reasons, leukocyte scintigraphy can yield false-negative results in patients with enterococcal or candidal infective endocarditis.21
FDG-PET and leukocyte scintigraphy are more expensive than TEE and cardiac CT22 and are not widely available.
Both tests entail radiation exposure, with the average dose ranging from 7 to 14 mSv. However, this is less than the average amount acquired during percutaneous coronary intervention (16 mSv), and overlaps with the amount in chest CT with contrast when assessing for pulmonary embolism (7 to 9 mSv). Lower doses are possible with optimized protocols.12,13,15,23
Bottom line for nuclear studies
Figure 2. Suggested algorithm for evaluating suspected infective endocarditis with negative or inconclusive results on echocardiography.
FDG-PET and leukocyte scintigraphy are especially useful for patients with a prosthetic valve or cardiac implanted electronic device. However, limitations must be kept in mind.
A suggested algorithm for testing with nuclear imaging is shown in Figure 2.1,4
CEREBRAL MAGNETIC RESONANCE IMAGING
Cerebral magnetic resonance imaging (MRI) is more sensitive than cerebral CT for detecting emboli in the brain. According to American Heart Association guidelines, cerebral MRI should be done in patients with known or suspected infective endocarditis and neurologic impairment, defined as headaches, meningeal symptoms, or neurologic deficits. It is also often used in neurologically asymptomatic patients with infective endocarditis who have indications for valve surgery to assess for mycotic aneurysms, which are associated with increased intracranial bleeding during surgery.
MRI use in other asymptomatic patients remains controversial.24 In cases with high clinical suspicion for infective endocarditis and no findings on echocardiography, cerebral MRI can increase the sensitivity of the Duke criteria by adding a minor criterion. Some have argued that, in patients with definite infective endocarditis, detecting silent cerebral complications can lead to management changes. However, more studies are needed to determine if there is indeed a group of neurologically asymptomatic infective endocarditis patients for whom cerebral MRI leads to improved outcomes.
Limitations of cerebral MRI
Cerebral MRI cannot be used in patients with non-MRI-compatible implanted hardware.
Gadolinium, the contrast agent typically used, can cause nephrogenic systemic fibrosis in patients who have poor renal function. This rare but serious adverse effect is characterized by irreversible systemic fibrosis affecting skin, muscles, and even visceral tissue such as lungs. The American College of Radiology allows for gadolinium use in patients without acute kidney injury and patients with stable chronic kidney disease with a glomerular filtration rate of at least 30 mL/min/1.73 m2. Its use should be avoided in patients with renal failure on replacement therapy, with advanced chronic kidney disease (glomerular filtration rate < 30 mL/min/1.73 m2), or with acute kidney injury, even if they do not need renal replacement therapy.25
Concerns have also been raised about gadolinium retention in the brain, even in patients with normal renal function.26–28 Thus far, no conclusive clinical adverse effects of retention have been found, although more study is warranted. Nevertheless, the US Food and Drug Administration now requires a black-box warning about this possibility and advises clinicians to counsel patients appropriately.
Bottom line on cerebral MRI
Cerebral MRI should be obtained when a patient presents with definite or possible infective endocarditis with neurologic impairment, such as new headaches, meningismus, or focal neurologic deficits. Routine brain MRI in patients with confirmed infective endocarditis without neurologic symptoms, or those without definite infective endocarditis, is discouraged.
CARDIAC MRI
Cardiac MRI, typically obtained with gadolinium contrast, allows for better 3D assessment of cardiac structures and morphology than echocardiography or CT, and can detect infiltrative cardiac disease, myopericarditis, and much more. It is increasingly used in the field of structural cardiology, but its role for evaluating infective endocarditis remains unclear.
Cardiac MRI does not appear to be better than echocardiography for diagnosing infective endocarditis. However, it may prove helpful in the evaluation of patients known to have infective endocarditis but who cannot be properly evaluated for disease extent because of poor image quality on echocardiography and contraindications to CT.1,29 Its role is limited in patients with cardiac implanted electronic devices, as most devices are incompatible with MRI use, although newer devices obviate this concern. But even for devices that are MRI-compatible, results are diminished due to an eclipsing effect, wherein the device parts can make it hard to see structures clearly because the “brightness” basically eclipses the surrounding area.4
Concerns regarding use of gadolinium as described above need also be considered.
The role of cardiac MRI in diagnosing and managing infective endocarditis may evolve, but at present, the 2017 American College of Cardiology and American Heart Association appropriate-use criteria discourage its use for these purposes.16
Bottom line for cardiac MRI
Cardiac MRI to evaluate a patient for suspected infective endocarditis is not recommended due to lack of superiority compared with echocardiography or CT, and the risk of nephrogenic systemic fibrosis from gadolinium in patients with renal compromise.
Prompt diagnois of infective endocarditis is critical. Potential consequences of missed or delayed diagnosis, including heart failure, stroke, intracardiac abscess, conduction delays, prosthesis dysfunction, and cerebral emboli, are often catastrophic. Echocardiography is the test used most frequently to evaluate for infective endocarditis, but it misses the diagnosis in almost one-third of cases, and even more often if the patient has a prosthetic valve.
But now, several sophisticated imaging tests are available that complement echocardiography in diagnosing and assessing infective endocarditis; these include 4-dimensional computed tomography (4D CT), fluorodeoxyglucose positron emission tomography (FDG-PET), and leukocyte scintigraphy. These tests have greatly improved our ability not only to diagnose infective endocarditis, but also to determine the extent and spread of infection, and they aid in perioperative assessment. Abnormal findings on these tests have been incorporated into the European Society of Cardiology’s 2015 modified diagnostic criteria for infective endocarditis.1
This article details the indications, advantages, and limitations of the various imaging tests for diagnosing and evaluating infective endocarditis (Table 1).
INFECTIVE ENDOCARDITIS IS DIFFICULT TO DIAGNOSE AND TREAT
Infective endocarditis is difficult to diagnose and treat. Clinical and imaging clues can be subtle, and the diagnosis requires a high level of suspicion and visualization of cardiac structures.
Further, the incidence of infective endocarditis is on the rise in the United States, particularly in women and young adults, likely due to intravenous drug use.2,3
ECHOCARDIOGRAPHY HAS AN IMPORTANT ROLE, BUT IS LIMITED
Echocardiography remains the most commonly performed study for diagnosing infective endocarditis, as it is fast, widely accessible, and less expensive than other imaging tests.
Transthoracic echocardiography (TTE) is often the first choice for testing. However, its sensitivity is only about 70% for detecting vegetations on native valves and 50% for detecting vegetations on prosthetic valves.1 It is inherently constrained by the limited number of views by which a comprehensive external evaluation of the heart can be achieved. Using a 2-dimensional instrument to view a 3-dimensional object is difficult, and depending on several factors, it can be hard to see vegetations and abscesses that are associated with infective endocarditis. Further, TTE is impeded by obesity and by hyperinflated lungs from obstructive pulmonary disease or mechanical ventilation. It has poor sensitivity for detecting small vegetations and for detecting vegetations and paravalvular complications in patients who have a prosthetic valve or a cardiac implanted electronic device.
Transesophageal echocardiography (TEE) is the recommended first-line imaging test for patients with prosthetic valves and no contraindications to the test. Otherwise, it should be done after TTE if the results of TTE are negative but clinical suspicion for infective endocarditis remains high (eg, because the patient uses intravenous drugs). But although TEE has a higher sensitivity than TTE (up to 96% for vegetations on native valves and 92% for those on prosthetic valves, if performed by an experienced sonographer), it can still miss infective endocarditis. Also, TEE does not provide a significant advantage over TTE in patients who have a cardiac implanted electronic device.1,4,5
Regardless of whether TTE or TEE is used, they are estimated to miss up to 30% of cases of infective endocarditis and its sequelae.4 False-negative findings are likelier in patients who have preexisting severe valvular lesions, prosthetic valves, cardiac implanted electronic devices, small vegetations, or abscesses, or if a vegetation has already broken free and embolized. Furthermore, distinguishing between vegetations and thrombi, cardiac tumors, and myxomatous changes using echocardiography is difficult.
CARDIAC CT
For patients who have inconclusive results on echocardiography, contraindications to TEE, or poor sonic windows, cardiac CT can be an excellent alternative. It is especially useful in the setting of a prosthetic valve.
Synchronized (“gated”) with the patient’s heart rate and rhythm, CT machines can acquire images during diastole, reducing motion artifact, and can create 3D images of the heart. In addition, newer machines can acquire several images at different points in the heart cycle to add a fourth dimension—time. The resulting 4D images play like short video loops of the beating heart and allow noninvasive assessment of cardiac anatomy with remarkable detail and resolution.
4D CT is increasingly being used in infective endocarditis, and growing evidence indicates that its accuracy is similar to that of TEE in the preoperative evaluation of patients with aortic prosthetic valve endocarditis.6 In a study of 28 patients, complementary use of CT angiography led to a change in treatment strategy in 7 (25%) compared with routine clinical workup.7 Several studies have found no difference between 4D CT and preoperative TEE in detecting pseudoaneurysm, abscess, or valve dehiscence. TEE and 4D CT also have similar sensitivities for detecting infective endocarditis in native and prosthetic valves.8,9
Figure 1A. Transesophageal echocardiography in a 73-year-old man with a bioprosthetic aortic valve who presented with 2 months of fevers, chills, and night sweats. He had several negative blood cultures and 2 negative transesophageal echocardiograms over 1 month. No mass, vegetation, paravalvular abscess, or significant valve dysfunction was noted.
Figure 1B. Cardiac computed tomographic (CT) angiography with iodinated contrast, including 4D reconstruction, in the same patient, however, shows an 11-mm vegetation on the bioprosthetic aortic valve leaflets (arrow).
Figure 1C. Fluorodeoxyglucose positron emission tomography (FDG-PET) in the same patient confirms the diagnosis, showing a 13-mm hypermetabolic focus on the prosthetic valve (arrow), yielding the diagnosis of infectious endocarditis.
Coupled with CT angiography, 4D CT is also an excellent noninvasive way to perioperatively evaluate the coronary arteries without the risks associated with catheterization in those requiring nonemergency surgery (Figure 1A, B, and C).
4D CT performs well for detecting abscess and pseudoaneurysm but has slightly lower sensitivity for vegetations than TEE (91% vs 99%).9
Gated CT, PET, or both may be useful in cases of suspected prosthetic aortic valve endocarditis when TEE is negative. Pseudoaneurysms are not well visualized with TEE, and the atrial mitral curtain area is often thickened on TEE in cases of aortic prosthetic valve infective endocarditis that do not definitely involve abscesses. Gated CT and PET show this area better.8 This information is important in cases in which a surgeon may be unconvinced that the patient has prosthetic valve endocarditis.
Limitations of 4D cardiac CT
4D CT with or without angiography has limitations. It requires a wide-volume scanner and an experienced reader.
Patients with irregular heart rhythms or uncontrolled tachycardia pose technical problems for image acquisition. Cardiac CT is typically gated (ie, images are obtained within a defined time period) to acquire images during diastole. Ideally, images are acquired when the heart is in mid to late diastole, a time of minimal cardiac motion, so that motion artifact is minimized. To estimate the timing of image acquisition, the cardiac cycle must be predictable, and its duration should be as long as possible. Tachycardia or irregular rhythms such as frequent ectopic beats or atrial fibrillation make acquisition timing difficult, and thus make it nearly impossible to accurately obtain images when the heart is at minimum motion, limiting assessment of cardiac structures or the coronary tree.4,10
Extensive coronary calcification can hinder assessment of the coronary tree by CT coronary angiography.
Contrast exposure may limit the use of CT in some patients (eg, those with contrast allergies or renal dysfunction). However, modern scanners allow for much smaller contrast boluses without decreasing sensitivity.
4D CT involves radiation exposure, especially when done with angiography, although modern scanners have greatly reduced exposure. The average radiation dose in CT coronary angiography is 2.9 to 5.9 mSv11 compared with 7 mSv in diagnostic cardiac catheterization (without angioplasty or stenting) or 16 mSv in routine CT of the abdomen and pelvis with contrast.12,13 In view of the morbidity and mortality risks associated with infective endocarditis, especially if the diagnosis is delayed, this small radiation exposure may be justifiable.
Bottom line for cardiac CT
4D CT is an excellent alternative to echocardiography for select patients. Clinicians should strongly consider this study in the following situations:
Patients with a prosthetic valve
Patients who are strongly suspected of having infective endocarditis but who have a poor sonic window on TTE or TEE, as can occur with chronic obstructive lung disease, morbid obesity, or previous thoracic or cardiovascular surgery
Patients who meet clinical indications for TEE, such as having a prosthetic valve or a high suspicion for native valve infective endocarditis with negative TTE, but who have contraindications to TEE
As an alternative to TEE for preoperative evaluation in patients with known infective endocarditis.
Patients with tachycardia or irregular heart rhythms are not good candidates for this test.
FDG-PET AND LEUKOCYTE SCINTIGRAPHY
FDG-PET and leukocyte scintigraphy are other options for diagnosing infective endocarditis and determining the presence and extent of intra- and extracardiac infection. They are more sensitive than echocardiography for detecting infection of cardiac implanted electronic devices such as ventricular assist devices, pacemakers, implanted cardiac defibrillators, and cardiac resynchronization therapy devices.14–16
The utility of FDG-PET is founded on the uptake of 18F-fluorodeoxyglucose by cells, with higher uptake taking place in cells with higher metabolic activity (such as in areas of inflammation). Similarly, leukocyte scintigraphy relies on the use of radiolabeled leukocytes (ie, leukocytes previously extracted from the patient, labelled, and re-introduced into the patient) to allow for localization of inflamed tissue.
The most significant contribution of FDG-PET may be the ability to detect infective endocarditis early, when echocardiography is initially negative. When abnormal FDG uptake was included in the modified Duke criteria, it increased the sensitivity to 97% for detecting infective endocarditis on admission, leading some to propose its incorporation as a major criterion.17 In patients with prosthetic valves and suspected infective endocarditis, FDG-PET was found in one study to have a sensitivity of up to 91% and a specificity of up to 95%.18
Both FDG-PET and leukocyte scintigraphy have a high sensitivity, specificity, and negative predictive value for cardiac implanted electronic device infection, and should be strongly considered in patients in whom it is suspected but who have negative or inconclusive findings on echocardiography.14,15
In addition, a common conundrum faced by clinicians with use of echocardiography is the difficulty of differentiating thrombus from infected vegetation on valves or device lead wires. Some evidence indicates that FDG-PET may help to discriminate between vegetation and thrombus, although more rigorous studies are needed before its use for that purpose can be recommended.19
Limitations of nuclear studies
Both FDG-PET and leukocyte scintigraphy perform poorly for detecting native-valve infective endocarditis. In a study in which 90% of the patients had native-valve infective endocarditis according to the Duke criteria, FDG-PET had a specificity of 93% but a sensitivity of only 39%.20
Both studies can be cumbersome, laborious, and time-consuming for patients. FDG-PET requires a fasting or glucose-restricted diet before testing, and the test itself can be complicated by development of hyperglycemia, although this is rare.
While FDG-PET is most effective in detecting infections of prosthetic valves and cardiac implanted electronic devices, the results can be falsely positive in patients with a history of recent cardiac surgery (due to ongoing tissue healing), as well as maladies other than infective endocarditis that lead to inflammation, such as vasculitis or malignancy. Similarly, for unclear reasons, leukocyte scintigraphy can yield false-negative results in patients with enterococcal or candidal infective endocarditis.21
FDG-PET and leukocyte scintigraphy are more expensive than TEE and cardiac CT22 and are not widely available.
Both tests entail radiation exposure, with the average dose ranging from 7 to 14 mSv. However, this is less than the average amount acquired during percutaneous coronary intervention (16 mSv), and overlaps with the amount in chest CT with contrast when assessing for pulmonary embolism (7 to 9 mSv). Lower doses are possible with optimized protocols.12,13,15,23
Bottom line for nuclear studies
Figure 2. Suggested algorithm for evaluating suspected infective endocarditis with negative or inconclusive results on echocardiography.
FDG-PET and leukocyte scintigraphy are especially useful for patients with a prosthetic valve or cardiac implanted electronic device. However, limitations must be kept in mind.
A suggested algorithm for testing with nuclear imaging is shown in Figure 2.1,4
CEREBRAL MAGNETIC RESONANCE IMAGING
Cerebral magnetic resonance imaging (MRI) is more sensitive than cerebral CT for detecting emboli in the brain. According to American Heart Association guidelines, cerebral MRI should be done in patients with known or suspected infective endocarditis and neurologic impairment, defined as headaches, meningeal symptoms, or neurologic deficits. It is also often used in neurologically asymptomatic patients with infective endocarditis who have indications for valve surgery to assess for mycotic aneurysms, which are associated with increased intracranial bleeding during surgery.
MRI use in other asymptomatic patients remains controversial.24 In cases with high clinical suspicion for infective endocarditis and no findings on echocardiography, cerebral MRI can increase the sensitivity of the Duke criteria by adding a minor criterion. Some have argued that, in patients with definite infective endocarditis, detecting silent cerebral complications can lead to management changes. However, more studies are needed to determine if there is indeed a group of neurologically asymptomatic infective endocarditis patients for whom cerebral MRI leads to improved outcomes.
Limitations of cerebral MRI
Cerebral MRI cannot be used in patients with non-MRI-compatible implanted hardware.
Gadolinium, the contrast agent typically used, can cause nephrogenic systemic fibrosis in patients who have poor renal function. This rare but serious adverse effect is characterized by irreversible systemic fibrosis affecting skin, muscles, and even visceral tissue such as lungs. The American College of Radiology allows for gadolinium use in patients without acute kidney injury and patients with stable chronic kidney disease with a glomerular filtration rate of at least 30 mL/min/1.73 m2. Its use should be avoided in patients with renal failure on replacement therapy, with advanced chronic kidney disease (glomerular filtration rate < 30 mL/min/1.73 m2), or with acute kidney injury, even if they do not need renal replacement therapy.25
Concerns have also been raised about gadolinium retention in the brain, even in patients with normal renal function.26–28 Thus far, no conclusive clinical adverse effects of retention have been found, although more study is warranted. Nevertheless, the US Food and Drug Administration now requires a black-box warning about this possibility and advises clinicians to counsel patients appropriately.
Bottom line on cerebral MRI
Cerebral MRI should be obtained when a patient presents with definite or possible infective endocarditis with neurologic impairment, such as new headaches, meningismus, or focal neurologic deficits. Routine brain MRI in patients with confirmed infective endocarditis without neurologic symptoms, or those without definite infective endocarditis, is discouraged.
CARDIAC MRI
Cardiac MRI, typically obtained with gadolinium contrast, allows for better 3D assessment of cardiac structures and morphology than echocardiography or CT, and can detect infiltrative cardiac disease, myopericarditis, and much more. It is increasingly used in the field of structural cardiology, but its role for evaluating infective endocarditis remains unclear.
Cardiac MRI does not appear to be better than echocardiography for diagnosing infective endocarditis. However, it may prove helpful in the evaluation of patients known to have infective endocarditis but who cannot be properly evaluated for disease extent because of poor image quality on echocardiography and contraindications to CT.1,29 Its role is limited in patients with cardiac implanted electronic devices, as most devices are incompatible with MRI use, although newer devices obviate this concern. But even for devices that are MRI-compatible, results are diminished due to an eclipsing effect, wherein the device parts can make it hard to see structures clearly because the “brightness” basically eclipses the surrounding area.4
Concerns regarding use of gadolinium as described above need also be considered.
The role of cardiac MRI in diagnosing and managing infective endocarditis may evolve, but at present, the 2017 American College of Cardiology and American Heart Association appropriate-use criteria discourage its use for these purposes.16
Bottom line for cardiac MRI
Cardiac MRI to evaluate a patient for suspected infective endocarditis is not recommended due to lack of superiority compared with echocardiography or CT, and the risk of nephrogenic systemic fibrosis from gadolinium in patients with renal compromise.
References
Habib G, Lancellotti P, Antunes MJ, et al; ESC Scientific Document Group. 2015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015; 36(44):3075–3128. doi:10.1093/eurheartj/ehv319
Durante-Mangoni E, Bradley S, Selton-Suty C, et al; International Collaboration on Endocarditis Prospective Cohort Study Group. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 2008; 168(19):2095–2103. doi:10.1001/archinte.168.19.2095
Wurcel AG, Anderson JE, Chui KK, et al. Increasing infectious endocarditis admissions among young people who inject drugs. Open Forum Infect Dis 2016; 3(3):ofw157. doi:10.1093/ofid/ofw157
Gomes A, Glaudemans AW, Touw DJ, et al. Diagnostic value of imaging in infective endocarditis: a systematic review. Lancet Infect Dis 2017; 17(1):e1–e14. doi:10.1016/S1473-3099(16)30141-4
Cahill TJ, Baddour LM, Habib G, et al. Challenges in infective endocarditis. J Am Coll Cardiol 2017; 69(3):325–344. doi:10.1016/j.jacc.2016.10.066
Fagman E, Perrotta S, Bech-Hanssen O, et al. ECG-gated computed tomography: a new role for patients with suspected aortic prosthetic valve endocarditis. Eur Radiol 2012; 22(11):2407–2414. doi:10.1007/s00330-012-2491-5
Habets J, Tanis W, van Herwerden LA, et al. Cardiac computed tomography angiography results in diagnostic and therapeutic change in prosthetic heart valve endocarditis. Int J Cardiovasc Imaging 2014; 30(2):377–387. doi:10.1007/s10554-013-0335-2
Koneru S, Huang SS, Oldan J, et al. Role of preoperative cardiac CT in the evaluation of infective endocarditis: comparison with transesophageal echocardiography and surgical findings. Cardiovasc Diagn Ther 2018; 8(4):439–449. doi:10.21037/cdt.2018.07.07
Koo HJ, Yang DH, Kang J, et al. Demonstration of infective endocarditis by cardiac CT and transoesophageal echocardiography: comparison with intra-operative findings. Eur Heart J Cardiovasc Imaging 2018; 19(2):199–207. doi:10.1093/ehjci/jex010
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol 2009; 53(5):436–444. doi:10.1016/j.jacc.2008.01.077
Castellano IA, Nicol ED, Bull RK, Roobottom CA, Williams MC, Harden SP. A prospective national survey of coronary CT angiography radiation doses in the United Kingdom. J Cardiovasc Comput Tomogr 2017; 11(4):268–273. doi:10.1016/j.jcct.2017.05.002
Mettler FA Jr, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008; 248(1):254–263. doi:10.1148/radiol.2481071451
Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med 2009; 169(22):2078–2086. doi:10.1001/archinternmed.2009.427
Ploux S, Riviere A, Amraoui S, et al. Positron emission tomography in patients with suspected pacing system infections may play a critical role in difficult cases. Heart Rhythm 2011; 8(9):1478–1481. doi:10.1016/j.hrthm.2011.03.062
Sarrazin J, Philippon F, Tessier M, et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J Am Coll Cardiol 2012; 59(18):1616–1625. doi:10.1016/j.jacc.2011.11.059
Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P; Rating Panel Members; Appropriate Use Criteria Task Force. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate use criteria for multimodality imaging in valvular heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Nucl Cardiol 2017; 24(6):2043–2063. doi:10.1007/s12350-017-1070-1
Saby L, Laas O, Habib G, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol 2013; 61(23):2374–2382. doi:10.1016/j.jacc.2013.01.092
Swart LE, Gomes A, Scholtens AM, et al. Improving the diagnostic performance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography in prosthetic heart valve endocarditis. Circulation 2018; 138(14):1412–1427. doi:10.1161/CIRCULATIONAHA.118.035032
Graziosi M, Nanni C, Lorenzini M, et al. Role of 18F-FDG PET/CT in the diagnosis of infective endocarditis in patients with an implanted cardiac device: a prospective study. Eur J Nucl Med Mol Imaging 2014; 41(8):1617–1623. doi:10.1007/s00259-014-2773-z
Kouijzer IJ, Vos FJ, Janssen MJ, van Dijk AP, Oyen WJ, Bleeker-Rovers CP. The value of 18F-FDG PET/CT in diagnosing infectious endocarditis. Eur J Nucl Med Mol Imaging 2013; 40(7):1102–1107. doi:10.1007/s00259-013-2376-0
Wong D, Rubinshtein R, Keynan Y. Alternative cardiac imaging modalities to echocardiography for the diagnosis of infective endocarditis. Am J Cardiol 2016; 118(9):1410–1418. doi:10.1016/j.amjcard.2016.07.053
Vos FJ, Bleeker-Rovers CP, Kullberg BJ, Adang EM, Oyen WJ. Cost-effectiveness of routine (18)F-FDG PET/CT in high-risk patients with gram-positive bacteremia. J Nucl Med 2011; 52(11):1673–1678. doi:10.2967/jnumed.111.089714
McCollough CH, Bushberg JT, Fletcher JG, Eckel LJ. Answers to common questions about the use and safety of CT scans. Mayo Clin Proc 2015; 90(10):1380–1392. doi:10.1016/j.mayocp.2015.07.011
Duval X, Iung B, Klein I, et al; IMAGE (Resonance Magnetic Imaging at the Acute Phase of Endocarditis) Study Group. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med 2010; 152(8):497–504, W175. doi:10.7326/0003-4819-152-8-201004200-00006
Kanda T, Fukusato T, Matsuda M, et al. Gadolinium-based contrast agent accumulates in the brain even in subjects without severe renal dysfunction: evaluation of autopsy brain specimens with inductively coupled plasma mass spectroscopy. Radiology 2015; 276(1):228–232. doi:10.1148/radiol.2015142690
McDonald RJ, McDonald JS, Kallmes DF, et al. Intracranial gadolinium deposition after contrast-enhanced MR imaging. Radiology 2015; 275(3):772–782. doi:10.1148/radiol.15150025
Kanda T, Ishii K, Kawaguchi H, Kitajima K, Takenaka D. High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose of a gadolinium-based contrast material. Radiology 2014; 270(3):834–841. doi:10.1148/radiol.13131669
Expert Panel on Pediatric Imaging; Hayes LL, Palasis S, Bartel TB, et al. ACR appropriateness criteria headache-child. J Am Coll Radiol 2018; 15(5S):S78–S90. doi:10.1016/j.jacr.2018.03.017
References
Habib G, Lancellotti P, Antunes MJ, et al; ESC Scientific Document Group. 2015 ESC guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015; 36(44):3075–3128. doi:10.1093/eurheartj/ehv319
Durante-Mangoni E, Bradley S, Selton-Suty C, et al; International Collaboration on Endocarditis Prospective Cohort Study Group. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 2008; 168(19):2095–2103. doi:10.1001/archinte.168.19.2095
Wurcel AG, Anderson JE, Chui KK, et al. Increasing infectious endocarditis admissions among young people who inject drugs. Open Forum Infect Dis 2016; 3(3):ofw157. doi:10.1093/ofid/ofw157
Gomes A, Glaudemans AW, Touw DJ, et al. Diagnostic value of imaging in infective endocarditis: a systematic review. Lancet Infect Dis 2017; 17(1):e1–e14. doi:10.1016/S1473-3099(16)30141-4
Cahill TJ, Baddour LM, Habib G, et al. Challenges in infective endocarditis. J Am Coll Cardiol 2017; 69(3):325–344. doi:10.1016/j.jacc.2016.10.066
Fagman E, Perrotta S, Bech-Hanssen O, et al. ECG-gated computed tomography: a new role for patients with suspected aortic prosthetic valve endocarditis. Eur Radiol 2012; 22(11):2407–2414. doi:10.1007/s00330-012-2491-5
Habets J, Tanis W, van Herwerden LA, et al. Cardiac computed tomography angiography results in diagnostic and therapeutic change in prosthetic heart valve endocarditis. Int J Cardiovasc Imaging 2014; 30(2):377–387. doi:10.1007/s10554-013-0335-2
Koneru S, Huang SS, Oldan J, et al. Role of preoperative cardiac CT in the evaluation of infective endocarditis: comparison with transesophageal echocardiography and surgical findings. Cardiovasc Diagn Ther 2018; 8(4):439–449. doi:10.21037/cdt.2018.07.07
Koo HJ, Yang DH, Kang J, et al. Demonstration of infective endocarditis by cardiac CT and transoesophageal echocardiography: comparison with intra-operative findings. Eur Heart J Cardiovasc Imaging 2018; 19(2):199–207. doi:10.1093/ehjci/jex010
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol 2009; 53(5):436–444. doi:10.1016/j.jacc.2008.01.077
Castellano IA, Nicol ED, Bull RK, Roobottom CA, Williams MC, Harden SP. A prospective national survey of coronary CT angiography radiation doses in the United Kingdom. J Cardiovasc Comput Tomogr 2017; 11(4):268–273. doi:10.1016/j.jcct.2017.05.002
Mettler FA Jr, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008; 248(1):254–263. doi:10.1148/radiol.2481071451
Smith-Bindman R, Lipson J, Marcus R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer. Arch Intern Med 2009; 169(22):2078–2086. doi:10.1001/archinternmed.2009.427
Ploux S, Riviere A, Amraoui S, et al. Positron emission tomography in patients with suspected pacing system infections may play a critical role in difficult cases. Heart Rhythm 2011; 8(9):1478–1481. doi:10.1016/j.hrthm.2011.03.062
Sarrazin J, Philippon F, Tessier M, et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J Am Coll Cardiol 2012; 59(18):1616–1625. doi:10.1016/j.jacc.2011.11.059
Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P; Rating Panel Members; Appropriate Use Criteria Task Force. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate use criteria for multimodality imaging in valvular heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Nucl Cardiol 2017; 24(6):2043–2063. doi:10.1007/s12350-017-1070-1
Saby L, Laas O, Habib G, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol 2013; 61(23):2374–2382. doi:10.1016/j.jacc.2013.01.092
Swart LE, Gomes A, Scholtens AM, et al. Improving the diagnostic performance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography in prosthetic heart valve endocarditis. Circulation 2018; 138(14):1412–1427. doi:10.1161/CIRCULATIONAHA.118.035032
Graziosi M, Nanni C, Lorenzini M, et al. Role of 18F-FDG PET/CT in the diagnosis of infective endocarditis in patients with an implanted cardiac device: a prospective study. Eur J Nucl Med Mol Imaging 2014; 41(8):1617–1623. doi:10.1007/s00259-014-2773-z
Kouijzer IJ, Vos FJ, Janssen MJ, van Dijk AP, Oyen WJ, Bleeker-Rovers CP. The value of 18F-FDG PET/CT in diagnosing infectious endocarditis. Eur J Nucl Med Mol Imaging 2013; 40(7):1102–1107. doi:10.1007/s00259-013-2376-0
Wong D, Rubinshtein R, Keynan Y. Alternative cardiac imaging modalities to echocardiography for the diagnosis of infective endocarditis. Am J Cardiol 2016; 118(9):1410–1418. doi:10.1016/j.amjcard.2016.07.053
Vos FJ, Bleeker-Rovers CP, Kullberg BJ, Adang EM, Oyen WJ. Cost-effectiveness of routine (18)F-FDG PET/CT in high-risk patients with gram-positive bacteremia. J Nucl Med 2011; 52(11):1673–1678. doi:10.2967/jnumed.111.089714
McCollough CH, Bushberg JT, Fletcher JG, Eckel LJ. Answers to common questions about the use and safety of CT scans. Mayo Clin Proc 2015; 90(10):1380–1392. doi:10.1016/j.mayocp.2015.07.011
Duval X, Iung B, Klein I, et al; IMAGE (Resonance Magnetic Imaging at the Acute Phase of Endocarditis) Study Group. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med 2010; 152(8):497–504, W175. doi:10.7326/0003-4819-152-8-201004200-00006
Kanda T, Fukusato T, Matsuda M, et al. Gadolinium-based contrast agent accumulates in the brain even in subjects without severe renal dysfunction: evaluation of autopsy brain specimens with inductively coupled plasma mass spectroscopy. Radiology 2015; 276(1):228–232. doi:10.1148/radiol.2015142690
McDonald RJ, McDonald JS, Kallmes DF, et al. Intracranial gadolinium deposition after contrast-enhanced MR imaging. Radiology 2015; 275(3):772–782. doi:10.1148/radiol.15150025
Kanda T, Ishii K, Kawaguchi H, Kitajima K, Takenaka D. High signal intensity in the dentate nucleus and globus pallidus on unenhanced T1-weighted MR images: relationship with increasing cumulative dose of a gadolinium-based contrast material. Radiology 2014; 270(3):834–841. doi:10.1148/radiol.13131669
Expert Panel on Pediatric Imaging; Hayes LL, Palasis S, Bartel TB, et al. ACR appropriateness criteria headache-child. J Am Coll Radiol 2018; 15(5S):S78–S90. doi:10.1016/j.jacr.2018.03.017
Echocardiography can produce false-negative results in native-valve infective endocarditis and is even less sensitive in patients with a prosthetic valve or cardiac implanted electronic device.
4D CT is a reasonable alternative to transesophageal echocardiography. It can also be used as a second test if echocardiography is inconclusive. Coupled with angiography, it also provides a noninvasive method to evaluate coronary arteries perioperatively.
Nuclear imaging tests—FDG-PET and leukocyte scintigraphy—increase the sensitivity of the Duke criteria for diagnosing infective endocarditis. They should be considered for evaluating suspected infective endocarditis in all patients who have a prosthetic valve or cardiac implanted electronic device, and whenever echocardiography is inconclusive and clinical suspicion remains high.
Disallow All Ads
Content Gating
No Gating (article Unlocked/Free)
Alternative CME
Disqus Comments
Default
Gate On Date
Un-Gate On Date
Consolidated Pubs: Do Not Show Source Publication Logo
The costs of medical care in the United States are clearly out of line with those in other high-income countries. In a recent analysis,1 Papanicolas et al noted that despite comparable utilization of services, costs were far higher in the United States. Notably high were our administrative costs (accounting for almost 8% of spending), our use of imaging studies, and the cost of those studies. While many clinicians are troubled by the seemingly massive growth of administrative personnel and functions and would like to significantly shrink both, the path to reducing costs of imaging (and of testing in general) is fraught with potholes related to clinical care.
In a study from the University of Pennsylvania,2 Sedrak et al surveyed residents about their lab test ordering practices. Almost all responders recognized that they ordered “unnecessary tests.” The authors of the paper probed to understand why, and strikingly, the more common responses were the same that my resident peers and I would have given 4 decades ago: the culture of the system (“We don’t want to miss anything or be asked on rounds for data that hadn’t been checked”), the lack of transparency of cost of the tests, and the lack of role-modeling by teaching staff. There has been hope that the last of these would be resolved by increased visibility of subspecialists in hospital medicine, well-versed in the nuances of system-based practice. And the Society of Hospital Medicine, along with the American College of Physicians and others, has pushed hard to promote choosing wisely when ordering diagnostic studies. But we have a way to go.
Lab tests represent a small fraction of healthcare costs. Imaging tests, especially advanced and complex imaging studies, comprise a far greater fraction of healthcare costs. And here is the challenge: developers of new imaging modalities are now able to design and refine specific tests that are good enough to become the gold standard for diagnosis and staging of specific diseases—great for clinical care, bad for cost savings. One need only review a few new guidelines or clinical research protocols to appreciate the successful integration of these tests into clinical practice. Some tests are supplanting the need for aggressive biopsies, angiography, or a series of alternative imaging tests. This is potentially good for patients, but many of these tests are strikingly expensive and are being adopted for use prior to full vetting of their utility and limitations in large clinical studies; the cost of the tests can be an impediment to conducting a series of clinical studies that include appropriate patient subsets. The increasingly proposed use of positron emission tomography in patients with suspected malignancy, inflammation, or infection is a great example of a useful test that we are still learning how best to interpret in several conditions.
In this issue of the Journal, two testing scenarios are discussed. Lacy et al address the question of when patients with pyelonephritis should receive imaging studies. There are data to guide this decision process, but as noted in the study by Sedrak et al,2 there are forces at work that challenge the clinician to bypass the rational guidelines—not the least of which are the desire for efficiency (don’t take the chance that the test may be required later and delay discharge from the hospital or observation area) and greater surety in the clinical diagnosis. Although fear of litigation was not high on Sedrak’s list of reasons for ordering more “unnecessary” tests, I posit that a decrease in the confidence placed on clinical diagnosis drives a significant amount of imaging, in conjunction with the desire for shorter hospital stays.
The second paper, by Mgbojikwe et al, relates to the issue of which advanced technology should be ordered, and when. They review the limitations of traditional (echocardiographic) diagnosis and staging of infective endocarditis, and discuss the strengths and limitations of several advanced imaging tools in the setting of suspected or known infectious endocarditis. I suspect that in most medical centers the decisions to utilize these tests will rest with the infectious disease, cardiology, and cardiothoracic surgery consultants. But it is worth being aware of how the diagnostic and staging strategies are evolving, and of the limitations to these studies.
We have come a long way from diagnosing bacterial endocarditis with a valve abscess on the basis of finding changing murmurs, a Roth spot, a palpable spleen tip, new conduction abnormalities on the ECG, and documented daily afternoon fevers. Performing that physical examination is cheap but not highly reproducible. The new testing algorithms are not cheap but, hopefully, will offer superior sensitivity and specificity. Used correctly—and we likely have a way to go to learn what that means—these pictures may well be worth the cost.
Although someone still has to suspect the diagnosis of endocarditis.
References
Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA 2018; 319(10):1024–1039. doi:10.1001/jama.2018.1150
Sedrak MS, Patel MS, Ziemba JB, et al. Residents’ self-report on why they order perceived unnecessary inpatient laboratory tests. J Hosp Med 2016; 11(12):869–872. doi:10.1002/jhm.2645
The costs of medical care in the United States are clearly out of line with those in other high-income countries. In a recent analysis,1 Papanicolas et al noted that despite comparable utilization of services, costs were far higher in the United States. Notably high were our administrative costs (accounting for almost 8% of spending), our use of imaging studies, and the cost of those studies. While many clinicians are troubled by the seemingly massive growth of administrative personnel and functions and would like to significantly shrink both, the path to reducing costs of imaging (and of testing in general) is fraught with potholes related to clinical care.
In a study from the University of Pennsylvania,2 Sedrak et al surveyed residents about their lab test ordering practices. Almost all responders recognized that they ordered “unnecessary tests.” The authors of the paper probed to understand why, and strikingly, the more common responses were the same that my resident peers and I would have given 4 decades ago: the culture of the system (“We don’t want to miss anything or be asked on rounds for data that hadn’t been checked”), the lack of transparency of cost of the tests, and the lack of role-modeling by teaching staff. There has been hope that the last of these would be resolved by increased visibility of subspecialists in hospital medicine, well-versed in the nuances of system-based practice. And the Society of Hospital Medicine, along with the American College of Physicians and others, has pushed hard to promote choosing wisely when ordering diagnostic studies. But we have a way to go.
Lab tests represent a small fraction of healthcare costs. Imaging tests, especially advanced and complex imaging studies, comprise a far greater fraction of healthcare costs. And here is the challenge: developers of new imaging modalities are now able to design and refine specific tests that are good enough to become the gold standard for diagnosis and staging of specific diseases—great for clinical care, bad for cost savings. One need only review a few new guidelines or clinical research protocols to appreciate the successful integration of these tests into clinical practice. Some tests are supplanting the need for aggressive biopsies, angiography, or a series of alternative imaging tests. This is potentially good for patients, but many of these tests are strikingly expensive and are being adopted for use prior to full vetting of their utility and limitations in large clinical studies; the cost of the tests can be an impediment to conducting a series of clinical studies that include appropriate patient subsets. The increasingly proposed use of positron emission tomography in patients with suspected malignancy, inflammation, or infection is a great example of a useful test that we are still learning how best to interpret in several conditions.
In this issue of the Journal, two testing scenarios are discussed. Lacy et al address the question of when patients with pyelonephritis should receive imaging studies. There are data to guide this decision process, but as noted in the study by Sedrak et al,2 there are forces at work that challenge the clinician to bypass the rational guidelines—not the least of which are the desire for efficiency (don’t take the chance that the test may be required later and delay discharge from the hospital or observation area) and greater surety in the clinical diagnosis. Although fear of litigation was not high on Sedrak’s list of reasons for ordering more “unnecessary” tests, I posit that a decrease in the confidence placed on clinical diagnosis drives a significant amount of imaging, in conjunction with the desire for shorter hospital stays.
The second paper, by Mgbojikwe et al, relates to the issue of which advanced technology should be ordered, and when. They review the limitations of traditional (echocardiographic) diagnosis and staging of infective endocarditis, and discuss the strengths and limitations of several advanced imaging tools in the setting of suspected or known infectious endocarditis. I suspect that in most medical centers the decisions to utilize these tests will rest with the infectious disease, cardiology, and cardiothoracic surgery consultants. But it is worth being aware of how the diagnostic and staging strategies are evolving, and of the limitations to these studies.
We have come a long way from diagnosing bacterial endocarditis with a valve abscess on the basis of finding changing murmurs, a Roth spot, a palpable spleen tip, new conduction abnormalities on the ECG, and documented daily afternoon fevers. Performing that physical examination is cheap but not highly reproducible. The new testing algorithms are not cheap but, hopefully, will offer superior sensitivity and specificity. Used correctly—and we likely have a way to go to learn what that means—these pictures may well be worth the cost.
Although someone still has to suspect the diagnosis of endocarditis.
The costs of medical care in the United States are clearly out of line with those in other high-income countries. In a recent analysis,1 Papanicolas et al noted that despite comparable utilization of services, costs were far higher in the United States. Notably high were our administrative costs (accounting for almost 8% of spending), our use of imaging studies, and the cost of those studies. While many clinicians are troubled by the seemingly massive growth of administrative personnel and functions and would like to significantly shrink both, the path to reducing costs of imaging (and of testing in general) is fraught with potholes related to clinical care.
In a study from the University of Pennsylvania,2 Sedrak et al surveyed residents about their lab test ordering practices. Almost all responders recognized that they ordered “unnecessary tests.” The authors of the paper probed to understand why, and strikingly, the more common responses were the same that my resident peers and I would have given 4 decades ago: the culture of the system (“We don’t want to miss anything or be asked on rounds for data that hadn’t been checked”), the lack of transparency of cost of the tests, and the lack of role-modeling by teaching staff. There has been hope that the last of these would be resolved by increased visibility of subspecialists in hospital medicine, well-versed in the nuances of system-based practice. And the Society of Hospital Medicine, along with the American College of Physicians and others, has pushed hard to promote choosing wisely when ordering diagnostic studies. But we have a way to go.
Lab tests represent a small fraction of healthcare costs. Imaging tests, especially advanced and complex imaging studies, comprise a far greater fraction of healthcare costs. And here is the challenge: developers of new imaging modalities are now able to design and refine specific tests that are good enough to become the gold standard for diagnosis and staging of specific diseases—great for clinical care, bad for cost savings. One need only review a few new guidelines or clinical research protocols to appreciate the successful integration of these tests into clinical practice. Some tests are supplanting the need for aggressive biopsies, angiography, or a series of alternative imaging tests. This is potentially good for patients, but many of these tests are strikingly expensive and are being adopted for use prior to full vetting of their utility and limitations in large clinical studies; the cost of the tests can be an impediment to conducting a series of clinical studies that include appropriate patient subsets. The increasingly proposed use of positron emission tomography in patients with suspected malignancy, inflammation, or infection is a great example of a useful test that we are still learning how best to interpret in several conditions.
In this issue of the Journal, two testing scenarios are discussed. Lacy et al address the question of when patients with pyelonephritis should receive imaging studies. There are data to guide this decision process, but as noted in the study by Sedrak et al,2 there are forces at work that challenge the clinician to bypass the rational guidelines—not the least of which are the desire for efficiency (don’t take the chance that the test may be required later and delay discharge from the hospital or observation area) and greater surety in the clinical diagnosis. Although fear of litigation was not high on Sedrak’s list of reasons for ordering more “unnecessary” tests, I posit that a decrease in the confidence placed on clinical diagnosis drives a significant amount of imaging, in conjunction with the desire for shorter hospital stays.
The second paper, by Mgbojikwe et al, relates to the issue of which advanced technology should be ordered, and when. They review the limitations of traditional (echocardiographic) diagnosis and staging of infective endocarditis, and discuss the strengths and limitations of several advanced imaging tools in the setting of suspected or known infectious endocarditis. I suspect that in most medical centers the decisions to utilize these tests will rest with the infectious disease, cardiology, and cardiothoracic surgery consultants. But it is worth being aware of how the diagnostic and staging strategies are evolving, and of the limitations to these studies.
We have come a long way from diagnosing bacterial endocarditis with a valve abscess on the basis of finding changing murmurs, a Roth spot, a palpable spleen tip, new conduction abnormalities on the ECG, and documented daily afternoon fevers. Performing that physical examination is cheap but not highly reproducible. The new testing algorithms are not cheap but, hopefully, will offer superior sensitivity and specificity. Used correctly—and we likely have a way to go to learn what that means—these pictures may well be worth the cost.
Although someone still has to suspect the diagnosis of endocarditis.
References
Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA 2018; 319(10):1024–1039. doi:10.1001/jama.2018.1150
Sedrak MS, Patel MS, Ziemba JB, et al. Residents’ self-report on why they order perceived unnecessary inpatient laboratory tests. J Hosp Med 2016; 11(12):869–872. doi:10.1002/jhm.2645
References
Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA 2018; 319(10):1024–1039. doi:10.1001/jama.2018.1150
Sedrak MS, Patel MS, Ziemba JB, et al. Residents’ self-report on why they order perceived unnecessary inpatient laboratory tests. J Hosp Med 2016; 11(12):869–872. doi:10.1002/jhm.2645
A 45-year-old woman with a history of multiple organ transplants presented with a 1-month history of anterior left hip pain with insidious onset. Although she was able to perform activities of daily living, she reported increasing difficulty with weight-bearing activities.
Figure 1. On plain radiography, a subchondral radiolucent line (arrows) was seen on internal rotation of the hip (A), and more clearly on external rotation (B) (arrows).
Physical examination of the left hip elicited pain on passive movement, particularly on internal rotation. Plain radiography of the left hip (Figure 1) revealed a subchondral radiolucent line in the femoral head, representing subchondral collapse. This radiographic sign, referred to as the “crescent sign,” is seen in advanced stages of osteonecrosis of the femoral head. Recognition of this subtle radiographic sign is important because it represents considerable subchondral necrosis and collapse, and indicates that further collapse is likely.1
RISK FACTORS
Osteonecrosis of the hip is caused by prolonged interruption of blood flow to the femoral head.2 While idiopathic osteonecrosis is not uncommon, the condition is often associated with alcohol abuse or, as in our patient, long-term corticosteroid use after organ transplant.3 Corticosteroid use is also the most frequently reported risk factor for multifocal osteonecrosis.
Less common risk factors include systemic lupus erythematosus, antiphospholipid antibodies, coagulopathies, sickle cell disease, Gaucher disease, trauma, and external-beam therapy.
Young age is also associated with osteonecrosis, as nearly 75% of patients are between age 30 and 60.4
APPROACH TO DIAGNOSIS
Our patient had a typical clinical presentation of this disease: she was relatively young, was on long-term corticosteroids, and had acute anterior groin pain followed by progressive functional impairment.
The diagnostic evaluation consists of a detailed history, with attention to specific risk factors, and a thorough clinical examination followed by imaging, usually with plain radiography. However, plain radiographs are often unremarkable when the condition is in the early stages. In such cases, magnetic resonance imaging is recommended if clinical suspicion for osteonecrosis is high. It is far more sensitive (> 99%) and specific (> 99%) than plain radiography, and it detects early changes in the femoral head such as focal lesions and bone marrow edema.5
TREATMENT OPTIONS
Treatment of osteonecrosis is surgical and depends on the stage of disease.6
Joint preservation may be an option for small to medium-sized lesions before subchondral collapse has occurred; options include core decompression, bone grafting, and femoral osteotomy to preserve the native femoral head. These procedures have a higher success rate in young patients.
Subchondral collapse usually warrants hip replacement.
OUR PATIENT’S TREATMENT
Figure 2. Inspection of the femoral head confirmed palpable chondral softening and necrosis.
Our patient underwent total arthroplasty of the left hip. Macroscopic inspection and palpation of the femoral head demonstrated chondral softening. Anatomic specimens (Figure 2) showed the distinct correlation between radiographic images and subchondral collapse secondary to the underlying necrotic bone in the femoral head.
Shah KN, Racine J, Jones LC, Aaron RK. Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med 2015; 8(3):201–209. doi:10.1007/s12178-015-9277-8
Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World J Orthop 2015; 6(8):590–601. doi:10.5312/wjo.v6.i8.590
Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum 2002; 32(2):94–124. pmid:12430099
Pierce TP, Jauregui JJ, Cherian JJ, Elmallah RK, Mont MA. Imaging evaluation of patients with osteonecrosis of the femoral head. Curr Rev Musculoskelet Med 2015; 8(3):221–227. doi:10.1007/s12178-015-9279-6
Chughtai M, Piuzzi NS, Khlopas A, Jones LC, Goodman SB, Mont MA. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Joint J 2017; 99-B(10):1267–1279. doi:10.1302/0301-620X.99B10.BJJ-2017-0233.R2
Nicolas S. Piuzzi, MD Associate Staff, Adult Joint Reconstruction, Department of Orthopaedic Surgery, Cleveland Clinic
Hiba K. Anis, MD Research Fellow, Department of Orthopaedic Surgery, Cleveland Clinic
George F. Muschler, MD Department of Orthopaedic Surgery, Cleveland Clinic; Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Address: Nicolas S. Piuzzi, MD, Department of Orthopaedic Surgery, A41, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; [email protected]
osteonecrosis, hip, femur, steroids, glucocorticoids, corticosteroids, prednisone, side effect, osteoporosis, bone loss, osteopenia, crescent sign, organ transplant, arthroplasty, hip replacement, Nicolas Piuzzi, Hiba Anis, George Muschler
Nicolas S. Piuzzi, MD Associate Staff, Adult Joint Reconstruction, Department of Orthopaedic Surgery, Cleveland Clinic
Hiba K. Anis, MD Research Fellow, Department of Orthopaedic Surgery, Cleveland Clinic
George F. Muschler, MD Department of Orthopaedic Surgery, Cleveland Clinic; Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Address: Nicolas S. Piuzzi, MD, Department of Orthopaedic Surgery, A41, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; [email protected]
Author and Disclosure Information
Nicolas S. Piuzzi, MD Associate Staff, Adult Joint Reconstruction, Department of Orthopaedic Surgery, Cleveland Clinic
Hiba K. Anis, MD Research Fellow, Department of Orthopaedic Surgery, Cleveland Clinic
George F. Muschler, MD Department of Orthopaedic Surgery, Cleveland Clinic; Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Address: Nicolas S. Piuzzi, MD, Department of Orthopaedic Surgery, A41, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; [email protected]
A 45-year-old woman with a history of multiple organ transplants presented with a 1-month history of anterior left hip pain with insidious onset. Although she was able to perform activities of daily living, she reported increasing difficulty with weight-bearing activities.
Figure 1. On plain radiography, a subchondral radiolucent line (arrows) was seen on internal rotation of the hip (A), and more clearly on external rotation (B) (arrows).
Physical examination of the left hip elicited pain on passive movement, particularly on internal rotation. Plain radiography of the left hip (Figure 1) revealed a subchondral radiolucent line in the femoral head, representing subchondral collapse. This radiographic sign, referred to as the “crescent sign,” is seen in advanced stages of osteonecrosis of the femoral head. Recognition of this subtle radiographic sign is important because it represents considerable subchondral necrosis and collapse, and indicates that further collapse is likely.1
RISK FACTORS
Osteonecrosis of the hip is caused by prolonged interruption of blood flow to the femoral head.2 While idiopathic osteonecrosis is not uncommon, the condition is often associated with alcohol abuse or, as in our patient, long-term corticosteroid use after organ transplant.3 Corticosteroid use is also the most frequently reported risk factor for multifocal osteonecrosis.
Less common risk factors include systemic lupus erythematosus, antiphospholipid antibodies, coagulopathies, sickle cell disease, Gaucher disease, trauma, and external-beam therapy.
Young age is also associated with osteonecrosis, as nearly 75% of patients are between age 30 and 60.4
APPROACH TO DIAGNOSIS
Our patient had a typical clinical presentation of this disease: she was relatively young, was on long-term corticosteroids, and had acute anterior groin pain followed by progressive functional impairment.
The diagnostic evaluation consists of a detailed history, with attention to specific risk factors, and a thorough clinical examination followed by imaging, usually with plain radiography. However, plain radiographs are often unremarkable when the condition is in the early stages. In such cases, magnetic resonance imaging is recommended if clinical suspicion for osteonecrosis is high. It is far more sensitive (> 99%) and specific (> 99%) than plain radiography, and it detects early changes in the femoral head such as focal lesions and bone marrow edema.5
TREATMENT OPTIONS
Treatment of osteonecrosis is surgical and depends on the stage of disease.6
Joint preservation may be an option for small to medium-sized lesions before subchondral collapse has occurred; options include core decompression, bone grafting, and femoral osteotomy to preserve the native femoral head. These procedures have a higher success rate in young patients.
Subchondral collapse usually warrants hip replacement.
OUR PATIENT’S TREATMENT
Figure 2. Inspection of the femoral head confirmed palpable chondral softening and necrosis.
Our patient underwent total arthroplasty of the left hip. Macroscopic inspection and palpation of the femoral head demonstrated chondral softening. Anatomic specimens (Figure 2) showed the distinct correlation between radiographic images and subchondral collapse secondary to the underlying necrotic bone in the femoral head.
A 45-year-old woman with a history of multiple organ transplants presented with a 1-month history of anterior left hip pain with insidious onset. Although she was able to perform activities of daily living, she reported increasing difficulty with weight-bearing activities.
Figure 1. On plain radiography, a subchondral radiolucent line (arrows) was seen on internal rotation of the hip (A), and more clearly on external rotation (B) (arrows).
Physical examination of the left hip elicited pain on passive movement, particularly on internal rotation. Plain radiography of the left hip (Figure 1) revealed a subchondral radiolucent line in the femoral head, representing subchondral collapse. This radiographic sign, referred to as the “crescent sign,” is seen in advanced stages of osteonecrosis of the femoral head. Recognition of this subtle radiographic sign is important because it represents considerable subchondral necrosis and collapse, and indicates that further collapse is likely.1
RISK FACTORS
Osteonecrosis of the hip is caused by prolonged interruption of blood flow to the femoral head.2 While idiopathic osteonecrosis is not uncommon, the condition is often associated with alcohol abuse or, as in our patient, long-term corticosteroid use after organ transplant.3 Corticosteroid use is also the most frequently reported risk factor for multifocal osteonecrosis.
Less common risk factors include systemic lupus erythematosus, antiphospholipid antibodies, coagulopathies, sickle cell disease, Gaucher disease, trauma, and external-beam therapy.
Young age is also associated with osteonecrosis, as nearly 75% of patients are between age 30 and 60.4
APPROACH TO DIAGNOSIS
Our patient had a typical clinical presentation of this disease: she was relatively young, was on long-term corticosteroids, and had acute anterior groin pain followed by progressive functional impairment.
The diagnostic evaluation consists of a detailed history, with attention to specific risk factors, and a thorough clinical examination followed by imaging, usually with plain radiography. However, plain radiographs are often unremarkable when the condition is in the early stages. In such cases, magnetic resonance imaging is recommended if clinical suspicion for osteonecrosis is high. It is far more sensitive (> 99%) and specific (> 99%) than plain radiography, and it detects early changes in the femoral head such as focal lesions and bone marrow edema.5
TREATMENT OPTIONS
Treatment of osteonecrosis is surgical and depends on the stage of disease.6
Joint preservation may be an option for small to medium-sized lesions before subchondral collapse has occurred; options include core decompression, bone grafting, and femoral osteotomy to preserve the native femoral head. These procedures have a higher success rate in young patients.
Subchondral collapse usually warrants hip replacement.
OUR PATIENT’S TREATMENT
Figure 2. Inspection of the femoral head confirmed palpable chondral softening and necrosis.
Our patient underwent total arthroplasty of the left hip. Macroscopic inspection and palpation of the femoral head demonstrated chondral softening. Anatomic specimens (Figure 2) showed the distinct correlation between radiographic images and subchondral collapse secondary to the underlying necrotic bone in the femoral head.
Shah KN, Racine J, Jones LC, Aaron RK. Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med 2015; 8(3):201–209. doi:10.1007/s12178-015-9277-8
Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World J Orthop 2015; 6(8):590–601. doi:10.5312/wjo.v6.i8.590
Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum 2002; 32(2):94–124. pmid:12430099
Pierce TP, Jauregui JJ, Cherian JJ, Elmallah RK, Mont MA. Imaging evaluation of patients with osteonecrosis of the femoral head. Curr Rev Musculoskelet Med 2015; 8(3):221–227. doi:10.1007/s12178-015-9279-6
Chughtai M, Piuzzi NS, Khlopas A, Jones LC, Goodman SB, Mont MA. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Joint J 2017; 99-B(10):1267–1279. doi:10.1302/0301-620X.99B10.BJJ-2017-0233.R2
Shah KN, Racine J, Jones LC, Aaron RK. Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med 2015; 8(3):201–209. doi:10.1007/s12178-015-9277-8
Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World J Orthop 2015; 6(8):590–601. doi:10.5312/wjo.v6.i8.590
Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum 2002; 32(2):94–124. pmid:12430099
Pierce TP, Jauregui JJ, Cherian JJ, Elmallah RK, Mont MA. Imaging evaluation of patients with osteonecrosis of the femoral head. Curr Rev Musculoskelet Med 2015; 8(3):221–227. doi:10.1007/s12178-015-9279-6
Chughtai M, Piuzzi NS, Khlopas A, Jones LC, Goodman SB, Mont MA. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Joint J 2017; 99-B(10):1267–1279. doi:10.1302/0301-620X.99B10.BJJ-2017-0233.R2
Osteonecrosis of the femoral head with subchondral collapse
Display Headline
Osteonecrosis of the femoral head with subchondral collapse
Legacy Keywords
osteonecrosis, hip, femur, steroids, glucocorticoids, corticosteroids, prednisone, side effect, osteoporosis, bone loss, osteopenia, crescent sign, organ transplant, arthroplasty, hip replacement, Nicolas Piuzzi, Hiba Anis, George Muschler
Legacy Keywords
osteonecrosis, hip, femur, steroids, glucocorticoids, corticosteroids, prednisone, side effect, osteoporosis, bone loss, osteopenia, crescent sign, organ transplant, arthroplasty, hip replacement, Nicolas Piuzzi, Hiba Anis, George Muschler
A previously healthy 44-year-old woman presents to the emergency department with 1 day of fever, flank pain, dysuria, and persistent nausea and vomiting. Her temperature is 38.7°C (101.7°F), heart rate 102 beats per minute, and blood pressure 120/70 mm Hg. She has costovertebral angle tenderness. Laboratory testing reveals mild leukocytosis and a normal serum creatinine level; urinalysis shows leukocytes, as well as leukocyte esterase and nitrites. She has no personal or family history of nephrolithiasis. Urine cultures are obtained, and she is started on intravenous antibiotics and intravenous hydration to treat pyelonephritis.
Is imaging indicated at this point? And if so, which study is recommended?
KEY FEATURES
Acute pyelonephritis, infection of the renal parenchyma and collecting system, most often results from an ascending infection of the lower urinary tract. It is estimated to account for 250,000 office visits and 200,000 hospital admissions each year in the United States.1
Lower urinary tract symptoms such as urinary frequency, urgency, and dysuria accompanied by fever, nausea, vomiting, and flank pain raise suspicion for acute pyelonephritis. Flank pain is a key, nearly universal feature of upper urinary tract infection in patients without diabetes, though it may be absent in up to 50% of patients with diabetes.2
Additional findings include costovertebral angle tenderness on physical examination and leukocytosis, pyuria, and bacteriuria on laboratory studies.
PREDICTING THE NEED FOR EARLY IMAGING
Figure 1. Pathway for considering imaging in acute pyelonephritis. The recommended imaging study is computed tomography of the abdomen and pelvis with contrast, or computed tomography without and with contrast. The choice may be tailored to the patient’s clinical condition.
The primary goal of imaging in acute pyelonephritis is to identify significant complications (eg, gas-forming infection, abscess formation, urinary obstruction) that may necessitate a change in management. Risk of complications is higher in patients with diabetes, compromised immunity, a recent urologic procedure, or a history of urolithiasis. Patients without these risk factors usually do not need imaging unless fever or leukocytosis persists 72 hours after the start of antibiotics. Figure 1 offers guidance on deciding when imaging is needed in these patients.
Though guidelines state that imaging is inappropriate in most patients with pyelonephritis,2–4 it is nevertheless often done for diagnosis or identification of complications, which have been reported in more than two-thirds of patients.2–4
Acute pyelonephritis is generally classified as complicated or uncomplicated, though different definitions exist with regard to these classifications. The American College of Radiology’s Appropriateness Criteria2 consider patients with diabetes, immune compromise, a history of urolithiasis, or anatomic abnormality to be at highest risk for complications, and therefore recommend early imaging to assess for hydronephrosis, pyonephrosis, emphysematous pyelonephritis, and intrinsic or perinephric abscess.2
A clinical rule for predicting the need for imaging in acute pyelonephritis was developed and validated in an emergency department population in the Netherlands.3 The study suggested that restricting early imaging to patients with a history of urolithiasis, a urine pH of 7.0 or higher, or renal insufficiency—defined as a glomerular filtration rate (GFR) of 40 mL/min/1.73m2 or lower as estimated by the Modification of Diet in Renal Disease formula—would provide a negative predictive value of 94% to 100% for detection of an urgent urologic disorder (pyonephrosis, renal abscess, or urolithiasis). This high negative predictive value highlights that an absence of these signs and symptoms can safely identify patients who do not need renal imaging.
The positive predictive value was less useful, as only 5% to 23% of patients who had at least 1 risk factor went on to have urgent urologic risk factors.3
Implementation of this prediction rule would have resulted in a relative reduction in imaging of 40% and an absolute reduction of 28%. Of note, use of reduced GFR in this prediction rule is not clearly validated for patients with chronic kidney disease, as the previous GFR for most patients in this study was unknown.3
Based on these data, initial imaging is recommended in patients with diabetes, immune compromise, a history of urolithiasis, anatomic abnormality, a urine pH 7.0 or higher, or a GFR 40 mL/min or lower in a patient with no history of significant renal dysfunction. Early imaging would also be reasonable in patients with a complex clinical presentation, early recurrence of symptoms after treatment, clinical decompensation, or critical illness.
TREATMENT FAILURE
In a retrospective review of 62 patients hospitalized for acute renal infection, Soulen et al5 found that the most reliable indicator of complicated acute pyelonephritis was the persistence of fever and leukocytosis at 72 hours. And another small prospective study of patients with uncomplicated pyelonephritis reported a time to defervescence of no more than 4 days.6
In accordance with the Appropriateness Criteria2 and based on the best available evidence, imaging is recommended in all patients who remain febrile or have persistent leukocytosis after 72 hours of antibiotic therapy. In such cases, there should be high suspicion for a complication requiring treatment.
OPTIONS FOR IMAGING
Computed tomography
Computed tomography (CT) of the abdomen and pelvis with contrast is considered the study of choice in complicated acute pyelonephritis. CT can detect focal parenchymal abnormalities, emphysematous changes, and anatomic anomalies, and can also define the extent of disease. It can also detect perinephric fluid collections and abscesses that necessitate a change in management.2,5
A retrospective study in 2017 found that contrast-enhanced CT done without the usual noncontrast and excretory phases had an accuracy of 90% to 92% for pyelonephritis and 96% to 99% for urolithiasis, suggesting that reduction in radiation exposure through use of only the contrast-enhanced phase of CT imaging may be reasonable.7
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is increasingly acknowledged as effective in the evaluation of renal pathology, including the diagnosis of pyelonephritis; but it lacks the level of evidence that CT provides for detecting renal abscesses, calculi, and emphysematous pyelonephritis.2,8,9
Though it is more costly and time-consuming than CT with contrast enhancement, MRI is nevertheless the imaging study of choice if iodinated contrast or ionizing radiation must be avoided.
MRI typically involves a precontrast phase and a gadolinium contrast-enhanced phase, though there are data to support diffusion-weighted MRI when exposure to gadolinium poses a risk to the patient, such as in pregnancy or renal impairment (particularly when the estimated GFR is < 30 mL/min/1.73 m2).10
Ultrasonography
Conventional ultrasonography is appealing due to its relatively low cost, its availability and portability, and the lack of radiation and contrast exposure. It is most helpful in detecting hydronephrosis and pyonephrosis rather than intrarenal or perinephric abscess.2,9
Color and power Doppler ultrasonography may improve testing characteristics but not to the level of CT; in one study, sensitivity for detection of pyelonephritis was 33.3% with ultrasonography vs 81.0% with CT.11
Recent studies of ultrasonography with contrast enhancement show promising results,2 and it may ultimately prove to have a similar efficacy with lower risk for patients, but this has not been validated in large studies, and its availability remains limited.
Ultrasonography should be considered for patients in whom obstruction (with resulting hydronephrosis or pyonephrosis) is a primary concern, particularly when contrast exposure or radiation is contraindicated and MRI is unavailable.2
Abdominal radiography
While emphysematous pyelonephritis or a large staghorn calculus may be seen on abdominal radiography, it is not recommended for the assessment of complications in acute pyelonephritis because it lacks sensitivity.2
RETURN TO THE CASE SCENARIO
The patient in our case scenario meets the clinical criteria for uncomplicated pyelonephritis and is therefore not a candidate for imaging. Intravenous antibiotics should be started and should lead to rapid improvement in her condition.
Acknowledgment: The authors would like to thank Dr. Lisa Blacklock for her review of the radiology section of this paper.
References
Foxman B, Klemstine KL, Brown PD. Acute pyelonephritis in US hospitals in 1997: hospitalization and in-hospital mortality. Ann Epidemiol 2003; 13(2):144–150. pmid:12559674
Expert Panel on Urologic Imaging: Nikolaidis P, Dogra VS, Goldfarb S, et al. ACR appropriateness criteria acute pyelonephritis. J Am Coll Radiol 2018; 15(11S):S232–S239. doi:10.1016/j.jacr.2018.09.011
van Nieuwkoop C, Hoppe BP, Bonten TN, et al. Predicting the need for radiologic imaging in adults with febrile urinary tract infection. Clin Infect Dis 2010; 51(11):1266–1272. doi:10.1086/657071
Kim Y, Seo MR, Kim SJ, et al. Usefulness of blood cultures and radiologic imaging studies in the management of patients with community-acquired acute pyelonephritis. Infect Chemother 2017; 49(1):22–30. doi:10.3947/ic.2017.49.1.22
Soulen MC, Fishman EK, Goldman SM, Gatewood OM. Bacterial renal infection: role of CT. Radiology 1989; 171(3):703–707. doi:10.1148/radiology.171.3.2655002
June CH, Browning MD, Smith LP, et al. Ultrasonography and computed tomography in severe urinary tract infection. Arch Intern Med 1985; 145(5):841–845. pmid:3888134
Taniguchi LS, Torres US, Souza SM, Torres LR, D’Ippolito G. Are the unenhanced and excretory CT phases necessary for the evaluation of acute pyelonephritis? Acta Radiol 2017; 58(5):634–640. doi:10.1177/0284185116665424
Rathod SB, Kumbhar SS, Nanivadekar A, Aman K. Role of diffusion-weighted MRI in acute pyelonephritis: a prospective study. Acta Radiol 2015; 56(2):244–249. doi:10.1177/0284185114520862
Stunell H, Buckley O, Feeney J, Geoghegan T, Browne RF, Torreggiani WC. Imaging of acute pyelonephritis in the adult. Eur Radiol 2007; 17(7):1820–1828.
Yoo JM, Koh JS, Han CH, et al. Diagnosing acute pyelonephritis with CT, Tc-DMSA SPECT, and Doppler ultrasound: a comparative study. Korean J Urol 2010; 51(4):260–265. doi:10.4111/kju.2010.51.4.260
Mary E. Lacy, MD Assistant Professor, Department of Internal Medicine, University of New Mexico School of Medicine, Albuquerque, NM
Navneet Sidhu, MD Department Head, Hospitalist Medicine, Langley Memorial Hospital, Fraser Health, Langley, BC, Canada
Justin Miller, MD Assistant Professor, Department of Internal Medicine, University of New Mexico School of Medicine, Albuquerque, NM
Address: Mary E. Lacy, MD, Department of Internal Medicine, University of New Mexico School of Medicine, MSC 10-550, University of NM SOM, Albuquerque, NM 87131; [email protected]
Mary E. Lacy, MD Assistant Professor, Department of Internal Medicine, University of New Mexico School of Medicine, Albuquerque, NM
Navneet Sidhu, MD Department Head, Hospitalist Medicine, Langley Memorial Hospital, Fraser Health, Langley, BC, Canada
Justin Miller, MD Assistant Professor, Department of Internal Medicine, University of New Mexico School of Medicine, Albuquerque, NM
Address: Mary E. Lacy, MD, Department of Internal Medicine, University of New Mexico School of Medicine, MSC 10-550, University of NM SOM, Albuquerque, NM 87131; [email protected]
Author and Disclosure Information
Mary E. Lacy, MD Assistant Professor, Department of Internal Medicine, University of New Mexico School of Medicine, Albuquerque, NM
Navneet Sidhu, MD Department Head, Hospitalist Medicine, Langley Memorial Hospital, Fraser Health, Langley, BC, Canada
Justin Miller, MD Assistant Professor, Department of Internal Medicine, University of New Mexico School of Medicine, Albuquerque, NM
Address: Mary E. Lacy, MD, Department of Internal Medicine, University of New Mexico School of Medicine, MSC 10-550, University of NM SOM, Albuquerque, NM 87131; [email protected]
A previously healthy 44-year-old woman presents to the emergency department with 1 day of fever, flank pain, dysuria, and persistent nausea and vomiting. Her temperature is 38.7°C (101.7°F), heart rate 102 beats per minute, and blood pressure 120/70 mm Hg. She has costovertebral angle tenderness. Laboratory testing reveals mild leukocytosis and a normal serum creatinine level; urinalysis shows leukocytes, as well as leukocyte esterase and nitrites. She has no personal or family history of nephrolithiasis. Urine cultures are obtained, and she is started on intravenous antibiotics and intravenous hydration to treat pyelonephritis.
Is imaging indicated at this point? And if so, which study is recommended?
KEY FEATURES
Acute pyelonephritis, infection of the renal parenchyma and collecting system, most often results from an ascending infection of the lower urinary tract. It is estimated to account for 250,000 office visits and 200,000 hospital admissions each year in the United States.1
Lower urinary tract symptoms such as urinary frequency, urgency, and dysuria accompanied by fever, nausea, vomiting, and flank pain raise suspicion for acute pyelonephritis. Flank pain is a key, nearly universal feature of upper urinary tract infection in patients without diabetes, though it may be absent in up to 50% of patients with diabetes.2
Additional findings include costovertebral angle tenderness on physical examination and leukocytosis, pyuria, and bacteriuria on laboratory studies.
PREDICTING THE NEED FOR EARLY IMAGING
Figure 1. Pathway for considering imaging in acute pyelonephritis. The recommended imaging study is computed tomography of the abdomen and pelvis with contrast, or computed tomography without and with contrast. The choice may be tailored to the patient’s clinical condition.
The primary goal of imaging in acute pyelonephritis is to identify significant complications (eg, gas-forming infection, abscess formation, urinary obstruction) that may necessitate a change in management. Risk of complications is higher in patients with diabetes, compromised immunity, a recent urologic procedure, or a history of urolithiasis. Patients without these risk factors usually do not need imaging unless fever or leukocytosis persists 72 hours after the start of antibiotics. Figure 1 offers guidance on deciding when imaging is needed in these patients.
Though guidelines state that imaging is inappropriate in most patients with pyelonephritis,2–4 it is nevertheless often done for diagnosis or identification of complications, which have been reported in more than two-thirds of patients.2–4
Acute pyelonephritis is generally classified as complicated or uncomplicated, though different definitions exist with regard to these classifications. The American College of Radiology’s Appropriateness Criteria2 consider patients with diabetes, immune compromise, a history of urolithiasis, or anatomic abnormality to be at highest risk for complications, and therefore recommend early imaging to assess for hydronephrosis, pyonephrosis, emphysematous pyelonephritis, and intrinsic or perinephric abscess.2
A clinical rule for predicting the need for imaging in acute pyelonephritis was developed and validated in an emergency department population in the Netherlands.3 The study suggested that restricting early imaging to patients with a history of urolithiasis, a urine pH of 7.0 or higher, or renal insufficiency—defined as a glomerular filtration rate (GFR) of 40 mL/min/1.73m2 or lower as estimated by the Modification of Diet in Renal Disease formula—would provide a negative predictive value of 94% to 100% for detection of an urgent urologic disorder (pyonephrosis, renal abscess, or urolithiasis). This high negative predictive value highlights that an absence of these signs and symptoms can safely identify patients who do not need renal imaging.
The positive predictive value was less useful, as only 5% to 23% of patients who had at least 1 risk factor went on to have urgent urologic risk factors.3
Implementation of this prediction rule would have resulted in a relative reduction in imaging of 40% and an absolute reduction of 28%. Of note, use of reduced GFR in this prediction rule is not clearly validated for patients with chronic kidney disease, as the previous GFR for most patients in this study was unknown.3
Based on these data, initial imaging is recommended in patients with diabetes, immune compromise, a history of urolithiasis, anatomic abnormality, a urine pH 7.0 or higher, or a GFR 40 mL/min or lower in a patient with no history of significant renal dysfunction. Early imaging would also be reasonable in patients with a complex clinical presentation, early recurrence of symptoms after treatment, clinical decompensation, or critical illness.
TREATMENT FAILURE
In a retrospective review of 62 patients hospitalized for acute renal infection, Soulen et al5 found that the most reliable indicator of complicated acute pyelonephritis was the persistence of fever and leukocytosis at 72 hours. And another small prospective study of patients with uncomplicated pyelonephritis reported a time to defervescence of no more than 4 days.6
In accordance with the Appropriateness Criteria2 and based on the best available evidence, imaging is recommended in all patients who remain febrile or have persistent leukocytosis after 72 hours of antibiotic therapy. In such cases, there should be high suspicion for a complication requiring treatment.
OPTIONS FOR IMAGING
Computed tomography
Computed tomography (CT) of the abdomen and pelvis with contrast is considered the study of choice in complicated acute pyelonephritis. CT can detect focal parenchymal abnormalities, emphysematous changes, and anatomic anomalies, and can also define the extent of disease. It can also detect perinephric fluid collections and abscesses that necessitate a change in management.2,5
A retrospective study in 2017 found that contrast-enhanced CT done without the usual noncontrast and excretory phases had an accuracy of 90% to 92% for pyelonephritis and 96% to 99% for urolithiasis, suggesting that reduction in radiation exposure through use of only the contrast-enhanced phase of CT imaging may be reasonable.7
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is increasingly acknowledged as effective in the evaluation of renal pathology, including the diagnosis of pyelonephritis; but it lacks the level of evidence that CT provides for detecting renal abscesses, calculi, and emphysematous pyelonephritis.2,8,9
Though it is more costly and time-consuming than CT with contrast enhancement, MRI is nevertheless the imaging study of choice if iodinated contrast or ionizing radiation must be avoided.
MRI typically involves a precontrast phase and a gadolinium contrast-enhanced phase, though there are data to support diffusion-weighted MRI when exposure to gadolinium poses a risk to the patient, such as in pregnancy or renal impairment (particularly when the estimated GFR is < 30 mL/min/1.73 m2).10
Ultrasonography
Conventional ultrasonography is appealing due to its relatively low cost, its availability and portability, and the lack of radiation and contrast exposure. It is most helpful in detecting hydronephrosis and pyonephrosis rather than intrarenal or perinephric abscess.2,9
Color and power Doppler ultrasonography may improve testing characteristics but not to the level of CT; in one study, sensitivity for detection of pyelonephritis was 33.3% with ultrasonography vs 81.0% with CT.11
Recent studies of ultrasonography with contrast enhancement show promising results,2 and it may ultimately prove to have a similar efficacy with lower risk for patients, but this has not been validated in large studies, and its availability remains limited.
Ultrasonography should be considered for patients in whom obstruction (with resulting hydronephrosis or pyonephrosis) is a primary concern, particularly when contrast exposure or radiation is contraindicated and MRI is unavailable.2
Abdominal radiography
While emphysematous pyelonephritis or a large staghorn calculus may be seen on abdominal radiography, it is not recommended for the assessment of complications in acute pyelonephritis because it lacks sensitivity.2
RETURN TO THE CASE SCENARIO
The patient in our case scenario meets the clinical criteria for uncomplicated pyelonephritis and is therefore not a candidate for imaging. Intravenous antibiotics should be started and should lead to rapid improvement in her condition.
Acknowledgment: The authors would like to thank Dr. Lisa Blacklock for her review of the radiology section of this paper.
A previously healthy 44-year-old woman presents to the emergency department with 1 day of fever, flank pain, dysuria, and persistent nausea and vomiting. Her temperature is 38.7°C (101.7°F), heart rate 102 beats per minute, and blood pressure 120/70 mm Hg. She has costovertebral angle tenderness. Laboratory testing reveals mild leukocytosis and a normal serum creatinine level; urinalysis shows leukocytes, as well as leukocyte esterase and nitrites. She has no personal or family history of nephrolithiasis. Urine cultures are obtained, and she is started on intravenous antibiotics and intravenous hydration to treat pyelonephritis.
Is imaging indicated at this point? And if so, which study is recommended?
KEY FEATURES
Acute pyelonephritis, infection of the renal parenchyma and collecting system, most often results from an ascending infection of the lower urinary tract. It is estimated to account for 250,000 office visits and 200,000 hospital admissions each year in the United States.1
Lower urinary tract symptoms such as urinary frequency, urgency, and dysuria accompanied by fever, nausea, vomiting, and flank pain raise suspicion for acute pyelonephritis. Flank pain is a key, nearly universal feature of upper urinary tract infection in patients without diabetes, though it may be absent in up to 50% of patients with diabetes.2
Additional findings include costovertebral angle tenderness on physical examination and leukocytosis, pyuria, and bacteriuria on laboratory studies.
PREDICTING THE NEED FOR EARLY IMAGING
Figure 1. Pathway for considering imaging in acute pyelonephritis. The recommended imaging study is computed tomography of the abdomen and pelvis with contrast, or computed tomography without and with contrast. The choice may be tailored to the patient’s clinical condition.
The primary goal of imaging in acute pyelonephritis is to identify significant complications (eg, gas-forming infection, abscess formation, urinary obstruction) that may necessitate a change in management. Risk of complications is higher in patients with diabetes, compromised immunity, a recent urologic procedure, or a history of urolithiasis. Patients without these risk factors usually do not need imaging unless fever or leukocytosis persists 72 hours after the start of antibiotics. Figure 1 offers guidance on deciding when imaging is needed in these patients.
Though guidelines state that imaging is inappropriate in most patients with pyelonephritis,2–4 it is nevertheless often done for diagnosis or identification of complications, which have been reported in more than two-thirds of patients.2–4
Acute pyelonephritis is generally classified as complicated or uncomplicated, though different definitions exist with regard to these classifications. The American College of Radiology’s Appropriateness Criteria2 consider patients with diabetes, immune compromise, a history of urolithiasis, or anatomic abnormality to be at highest risk for complications, and therefore recommend early imaging to assess for hydronephrosis, pyonephrosis, emphysematous pyelonephritis, and intrinsic or perinephric abscess.2
A clinical rule for predicting the need for imaging in acute pyelonephritis was developed and validated in an emergency department population in the Netherlands.3 The study suggested that restricting early imaging to patients with a history of urolithiasis, a urine pH of 7.0 or higher, or renal insufficiency—defined as a glomerular filtration rate (GFR) of 40 mL/min/1.73m2 or lower as estimated by the Modification of Diet in Renal Disease formula—would provide a negative predictive value of 94% to 100% for detection of an urgent urologic disorder (pyonephrosis, renal abscess, or urolithiasis). This high negative predictive value highlights that an absence of these signs and symptoms can safely identify patients who do not need renal imaging.
The positive predictive value was less useful, as only 5% to 23% of patients who had at least 1 risk factor went on to have urgent urologic risk factors.3
Implementation of this prediction rule would have resulted in a relative reduction in imaging of 40% and an absolute reduction of 28%. Of note, use of reduced GFR in this prediction rule is not clearly validated for patients with chronic kidney disease, as the previous GFR for most patients in this study was unknown.3
Based on these data, initial imaging is recommended in patients with diabetes, immune compromise, a history of urolithiasis, anatomic abnormality, a urine pH 7.0 or higher, or a GFR 40 mL/min or lower in a patient with no history of significant renal dysfunction. Early imaging would also be reasonable in patients with a complex clinical presentation, early recurrence of symptoms after treatment, clinical decompensation, or critical illness.
TREATMENT FAILURE
In a retrospective review of 62 patients hospitalized for acute renal infection, Soulen et al5 found that the most reliable indicator of complicated acute pyelonephritis was the persistence of fever and leukocytosis at 72 hours. And another small prospective study of patients with uncomplicated pyelonephritis reported a time to defervescence of no more than 4 days.6
In accordance with the Appropriateness Criteria2 and based on the best available evidence, imaging is recommended in all patients who remain febrile or have persistent leukocytosis after 72 hours of antibiotic therapy. In such cases, there should be high suspicion for a complication requiring treatment.
OPTIONS FOR IMAGING
Computed tomography
Computed tomography (CT) of the abdomen and pelvis with contrast is considered the study of choice in complicated acute pyelonephritis. CT can detect focal parenchymal abnormalities, emphysematous changes, and anatomic anomalies, and can also define the extent of disease. It can also detect perinephric fluid collections and abscesses that necessitate a change in management.2,5
A retrospective study in 2017 found that contrast-enhanced CT done without the usual noncontrast and excretory phases had an accuracy of 90% to 92% for pyelonephritis and 96% to 99% for urolithiasis, suggesting that reduction in radiation exposure through use of only the contrast-enhanced phase of CT imaging may be reasonable.7
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is increasingly acknowledged as effective in the evaluation of renal pathology, including the diagnosis of pyelonephritis; but it lacks the level of evidence that CT provides for detecting renal abscesses, calculi, and emphysematous pyelonephritis.2,8,9
Though it is more costly and time-consuming than CT with contrast enhancement, MRI is nevertheless the imaging study of choice if iodinated contrast or ionizing radiation must be avoided.
MRI typically involves a precontrast phase and a gadolinium contrast-enhanced phase, though there are data to support diffusion-weighted MRI when exposure to gadolinium poses a risk to the patient, such as in pregnancy or renal impairment (particularly when the estimated GFR is < 30 mL/min/1.73 m2).10
Ultrasonography
Conventional ultrasonography is appealing due to its relatively low cost, its availability and portability, and the lack of radiation and contrast exposure. It is most helpful in detecting hydronephrosis and pyonephrosis rather than intrarenal or perinephric abscess.2,9
Color and power Doppler ultrasonography may improve testing characteristics but not to the level of CT; in one study, sensitivity for detection of pyelonephritis was 33.3% with ultrasonography vs 81.0% with CT.11
Recent studies of ultrasonography with contrast enhancement show promising results,2 and it may ultimately prove to have a similar efficacy with lower risk for patients, but this has not been validated in large studies, and its availability remains limited.
Ultrasonography should be considered for patients in whom obstruction (with resulting hydronephrosis or pyonephrosis) is a primary concern, particularly when contrast exposure or radiation is contraindicated and MRI is unavailable.2
Abdominal radiography
While emphysematous pyelonephritis or a large staghorn calculus may be seen on abdominal radiography, it is not recommended for the assessment of complications in acute pyelonephritis because it lacks sensitivity.2
RETURN TO THE CASE SCENARIO
The patient in our case scenario meets the clinical criteria for uncomplicated pyelonephritis and is therefore not a candidate for imaging. Intravenous antibiotics should be started and should lead to rapid improvement in her condition.
Acknowledgment: The authors would like to thank Dr. Lisa Blacklock for her review of the radiology section of this paper.
References
Foxman B, Klemstine KL, Brown PD. Acute pyelonephritis in US hospitals in 1997: hospitalization and in-hospital mortality. Ann Epidemiol 2003; 13(2):144–150. pmid:12559674
Expert Panel on Urologic Imaging: Nikolaidis P, Dogra VS, Goldfarb S, et al. ACR appropriateness criteria acute pyelonephritis. J Am Coll Radiol 2018; 15(11S):S232–S239. doi:10.1016/j.jacr.2018.09.011
van Nieuwkoop C, Hoppe BP, Bonten TN, et al. Predicting the need for radiologic imaging in adults with febrile urinary tract infection. Clin Infect Dis 2010; 51(11):1266–1272. doi:10.1086/657071
Kim Y, Seo MR, Kim SJ, et al. Usefulness of blood cultures and radiologic imaging studies in the management of patients with community-acquired acute pyelonephritis. Infect Chemother 2017; 49(1):22–30. doi:10.3947/ic.2017.49.1.22
Soulen MC, Fishman EK, Goldman SM, Gatewood OM. Bacterial renal infection: role of CT. Radiology 1989; 171(3):703–707. doi:10.1148/radiology.171.3.2655002
June CH, Browning MD, Smith LP, et al. Ultrasonography and computed tomography in severe urinary tract infection. Arch Intern Med 1985; 145(5):841–845. pmid:3888134
Taniguchi LS, Torres US, Souza SM, Torres LR, D’Ippolito G. Are the unenhanced and excretory CT phases necessary for the evaluation of acute pyelonephritis? Acta Radiol 2017; 58(5):634–640. doi:10.1177/0284185116665424
Rathod SB, Kumbhar SS, Nanivadekar A, Aman K. Role of diffusion-weighted MRI in acute pyelonephritis: a prospective study. Acta Radiol 2015; 56(2):244–249. doi:10.1177/0284185114520862
Stunell H, Buckley O, Feeney J, Geoghegan T, Browne RF, Torreggiani WC. Imaging of acute pyelonephritis in the adult. Eur Radiol 2007; 17(7):1820–1828.
Yoo JM, Koh JS, Han CH, et al. Diagnosing acute pyelonephritis with CT, Tc-DMSA SPECT, and Doppler ultrasound: a comparative study. Korean J Urol 2010; 51(4):260–265. doi:10.4111/kju.2010.51.4.260
References
Foxman B, Klemstine KL, Brown PD. Acute pyelonephritis in US hospitals in 1997: hospitalization and in-hospital mortality. Ann Epidemiol 2003; 13(2):144–150. pmid:12559674
Expert Panel on Urologic Imaging: Nikolaidis P, Dogra VS, Goldfarb S, et al. ACR appropriateness criteria acute pyelonephritis. J Am Coll Radiol 2018; 15(11S):S232–S239. doi:10.1016/j.jacr.2018.09.011
van Nieuwkoop C, Hoppe BP, Bonten TN, et al. Predicting the need for radiologic imaging in adults with febrile urinary tract infection. Clin Infect Dis 2010; 51(11):1266–1272. doi:10.1086/657071
Kim Y, Seo MR, Kim SJ, et al. Usefulness of blood cultures and radiologic imaging studies in the management of patients with community-acquired acute pyelonephritis. Infect Chemother 2017; 49(1):22–30. doi:10.3947/ic.2017.49.1.22
Soulen MC, Fishman EK, Goldman SM, Gatewood OM. Bacterial renal infection: role of CT. Radiology 1989; 171(3):703–707. doi:10.1148/radiology.171.3.2655002
June CH, Browning MD, Smith LP, et al. Ultrasonography and computed tomography in severe urinary tract infection. Arch Intern Med 1985; 145(5):841–845. pmid:3888134
Taniguchi LS, Torres US, Souza SM, Torres LR, D’Ippolito G. Are the unenhanced and excretory CT phases necessary for the evaluation of acute pyelonephritis? Acta Radiol 2017; 58(5):634–640. doi:10.1177/0284185116665424
Rathod SB, Kumbhar SS, Nanivadekar A, Aman K. Role of diffusion-weighted MRI in acute pyelonephritis: a prospective study. Acta Radiol 2015; 56(2):244–249. doi:10.1177/0284185114520862
Stunell H, Buckley O, Feeney J, Geoghegan T, Browne RF, Torreggiani WC. Imaging of acute pyelonephritis in the adult. Eur Radiol 2007; 17(7):1820–1828.
Yoo JM, Koh JS, Han CH, et al. Diagnosing acute pyelonephritis with CT, Tc-DMSA SPECT, and Doppler ultrasound: a comparative study. Korean J Urol 2010; 51(4):260–265. doi:10.4111/kju.2010.51.4.260
The Food and Drug Administration has approved gadobutrol (Gadavist) injections, for use in conjunction with magnetic resonance angiography (MRA), to evaluate known or suspected supra-aortic or renal artery disease in adult and pediatric patients.
Olivier Le Moal/Getty Images
Approval was based on a pair of open-label, phase 3 studies in which the efficacy of gadobutrol was assessed, based on visualization and performance for distinguishing between normal and abnormal anatomy. MRA with gadobutrol improved visualization by 88%-98%, compared with unenhanced MRA, in which visualization was improved by 24%-82%. Sensitivity and specificity were noninferior to unenhanced MRA.
Gadobutrol was previously indicated for use in diagnostic MRI in both adults and children to detect areas with disrupted blood-brain barrier and/or abnormal vascularity of the central nervous system, and for MRI of the breast to assess the presence and extent of malignant breast disease. The safety profile in the two current trials matched data previously gathered, with the most common adverse events including headache, nausea, and dizziness.
“Until now, no contrast agents were FDA approved for use with MRA of the supra-aortic arteries. With FDA’s action, radiologists now have an approved MRA contrast agent to help visualize supra-aortic arteries in patients with known or suspected supra-aortic arterial disease, including conditions such as prior stroke or transient ischemic attack,” Elias Melhem, MD, chair of the department of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, said in the press release.
The Food and Drug Administration has approved gadobutrol (Gadavist) injections, for use in conjunction with magnetic resonance angiography (MRA), to evaluate known or suspected supra-aortic or renal artery disease in adult and pediatric patients.
Olivier Le Moal/Getty Images
Approval was based on a pair of open-label, phase 3 studies in which the efficacy of gadobutrol was assessed, based on visualization and performance for distinguishing between normal and abnormal anatomy. MRA with gadobutrol improved visualization by 88%-98%, compared with unenhanced MRA, in which visualization was improved by 24%-82%. Sensitivity and specificity were noninferior to unenhanced MRA.
Gadobutrol was previously indicated for use in diagnostic MRI in both adults and children to detect areas with disrupted blood-brain barrier and/or abnormal vascularity of the central nervous system, and for MRI of the breast to assess the presence and extent of malignant breast disease. The safety profile in the two current trials matched data previously gathered, with the most common adverse events including headache, nausea, and dizziness.
“Until now, no contrast agents were FDA approved for use with MRA of the supra-aortic arteries. With FDA’s action, radiologists now have an approved MRA contrast agent to help visualize supra-aortic arteries in patients with known or suspected supra-aortic arterial disease, including conditions such as prior stroke or transient ischemic attack,” Elias Melhem, MD, chair of the department of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, said in the press release.
The Food and Drug Administration has approved gadobutrol (Gadavist) injections, for use in conjunction with magnetic resonance angiography (MRA), to evaluate known or suspected supra-aortic or renal artery disease in adult and pediatric patients.
Olivier Le Moal/Getty Images
Approval was based on a pair of open-label, phase 3 studies in which the efficacy of gadobutrol was assessed, based on visualization and performance for distinguishing between normal and abnormal anatomy. MRA with gadobutrol improved visualization by 88%-98%, compared with unenhanced MRA, in which visualization was improved by 24%-82%. Sensitivity and specificity were noninferior to unenhanced MRA.
Gadobutrol was previously indicated for use in diagnostic MRI in both adults and children to detect areas with disrupted blood-brain barrier and/or abnormal vascularity of the central nervous system, and for MRI of the breast to assess the presence and extent of malignant breast disease. The safety profile in the two current trials matched data previously gathered, with the most common adverse events including headache, nausea, and dizziness.
“Until now, no contrast agents were FDA approved for use with MRA of the supra-aortic arteries. With FDA’s action, radiologists now have an approved MRA contrast agent to help visualize supra-aortic arteries in patients with known or suspected supra-aortic arterial disease, including conditions such as prior stroke or transient ischemic attack,” Elias Melhem, MD, chair of the department of diagnostic radiology and nuclear medicine at the University of Maryland, Baltimore, said in the press release.

 An enlarged lymph node (2.4 cm × 2.0 cm) at the bifurcation of the bronchus intermedius. (B) An enlarged inferior mediastinal lymph node (2.0 cm × 5.4 cm).")
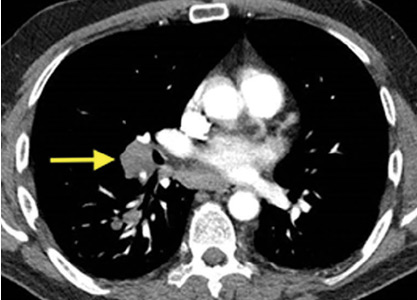

 over the lateral and inferior distribution (V4–V6, II, III, and aVF).")
.")




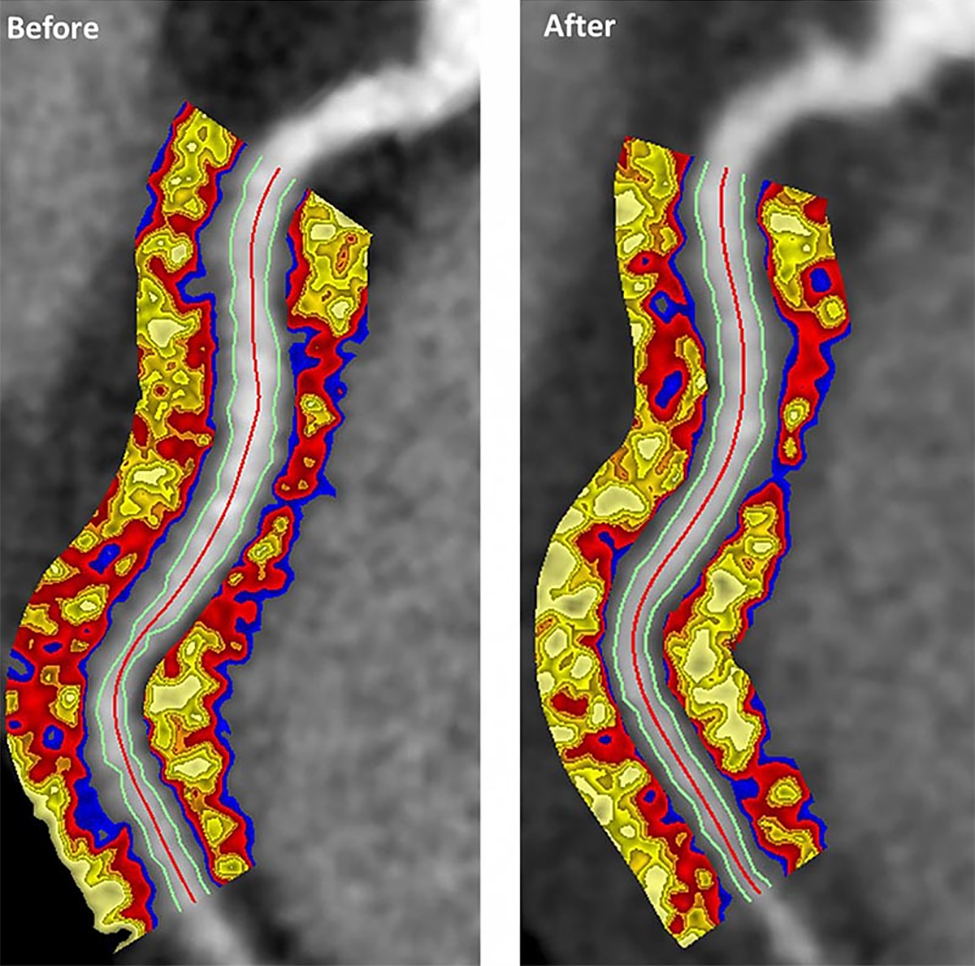


 angiography with iodinated contrast, including 4D reconstruc-tion, in the same patient, however, shows an 11-mm vegetation on the bioprosthetic aortic valve leaflets (arrow).")
 in the same patient confirms the diagnosis, showing a 13-mm hypermetabolic focus on the prosthetic valve (arrow), yielding the diagnosis of infectious endocarditis.")

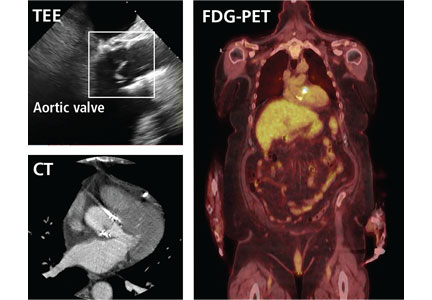


 was seen on internal rotation of the hip (A), and more clearly on external rotation (B) (arrows).")