User login
Cosmetic Corner: Dermatologists Weigh in on OTC Hair Restoration
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC hair restoration products. Consideration must be given to:
- Glytone by Ducray
- Rogaine Unscented Foam 5% and Rogaine Extra Strength Solution
- Toppik
- Triple Moisture Deep Recovery Hair Mask
- Viviscal
Cutis invites readers to send us their recommendations. Antiperspirants, stretch mark therapies, exfoliators, and hair removal products will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC hair restoration products. Consideration must be given to:
- Glytone by Ducray
- Rogaine Unscented Foam 5% and Rogaine Extra Strength Solution
- Toppik
- Triple Moisture Deep Recovery Hair Mask
- Viviscal
Cutis invites readers to send us their recommendations. Antiperspirants, stretch mark therapies, exfoliators, and hair removal products will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC hair restoration products. Consideration must be given to:
- Glytone by Ducray
- Rogaine Unscented Foam 5% and Rogaine Extra Strength Solution
- Toppik
- Triple Moisture Deep Recovery Hair Mask
- Viviscal
Cutis invites readers to send us their recommendations. Antiperspirants, stretch mark therapies, exfoliators, and hair removal products will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

A consistent approach drives optimal scarring alopecia treatment
DENVER – To limit the progression of scarring alopecia, Dr. Jeff Donovan makes it a point to ask his patients about symptoms and shedding, and he always performs a thorough scalp examination to record the affected sites and signs of the condition.
"Everything on the history potentially may be important, but always ask about symptoms of itching, burning, pain, tenderness, and shedding," Dr. Donovan of the department of dermatology at the University of Toronto advised at the annual meeting of the American Academy of Dermatology.

Upon examination, he continued, document sites and signs by considering the following questions: Where is the hair loss – frontal, top, or occipital? Can you still see the follicular ostia? Is there erythema of the scalp? Is there perifollicular erythema or scale, crusting, pustules, or loss of eyebrow or body hair?
"When you perform dermoscopy of the normal scalp, one can see that the hairs are similar in ‘caliber’ (no miniaturization suggestive of androgenetic alopecia), and there are no changes around the hair follicles or between the hair follicles," Dr. Donovan said. "In scarring alopecia, a variety of findings may be present which help point to the correct diagnosis."
A 4-mm punch biopsy is helpful to confirm the diagnosis and is recommended in areas of early active disease, including areas that may have primary morphologic features, areas with a positive pull test (if possible), or areas that are symptomatic (if needed). "Diagnosing a hair disease with a biopsy requires a hair to be present in the biopsy," he noted. "Biopsies of completely scarred areas are not helpful." In scarring alopecias, inflammatory infiltrates are found in the upper parts of the hair follicle, which destroys hair follicle stem cells. "It’s this destruction of stem cells which ultimately leads to permanent hair loss," Dr. Donovan said.
Lichen planopilaris, a common form of scarring alopecia, typically occurs in middle age and is twice as common in women as in men. It most often affects the central scalp but may be present in other sites in up to half of cases. Key symptoms of lichen planopilaris (LPP) include hair loss, scalp pruritus, and pain/tenderness, often a burning sensation at the site of hair loss. On dermoscopy, most LPP cases appear as reduced hair density with scalp erythema and perifollicular scale, also called peripilar casts.

The goal of LPP treatment is to reduce symptoms and shedding and to stop the disease from occurring in new sites. "Regrowth is not possible in most scarring alopecias," said Dr. Donovan, who leads the University of Toronto’s program in hair transplantation and hair loss. "Treatments help to halt the underlying disease process. Disease activity may recur."
Treatment options for localized/limited LPP include intralesional triamcinolone acetonide and/or several treatments at home, including 0.05% clobetasol propionate lotion or foam, clobetasol propionate shampoo to help decrease itching and burning, fluocinolone acetonide oil one time per week to help with removal of scales, and topical 0.1% tacrolimus ointment (or compounded lotion) as needed.
Systemic treatment of LPP is also an option, and he said he relies on the dermatopathology report to guide his treatment decisions. If biopsy reveals minimal lymphocytic infiltrate, Dr. Donovan said he recommends doxycycline 100 mg b.i.d. as his first-line approach. If biopsy reveals moderate lymphocytic infiltrate, he turns to hydroxychloroquine 6 mg/kg.

His recommended second-line systemic treatment is mycophenolate mofetil 500 mg b.i.d. for 1 month, then 1,000 mg b.i.d. thereafter. Third-line systemic treatment options include cyclosporine 3-5 mg/kg per day and retinoids such as isotretinoin, but fewer than 20% of patients benefit from retinoids, he said. Once the disease becomes quiet, hair transplant surgery can sometimes be an option to restore hair density.
Dr. Donovan disclosed that he is the cofounder of Okavana Laboratories, a privately held company devoted to hair.
DENVER – To limit the progression of scarring alopecia, Dr. Jeff Donovan makes it a point to ask his patients about symptoms and shedding, and he always performs a thorough scalp examination to record the affected sites and signs of the condition.
"Everything on the history potentially may be important, but always ask about symptoms of itching, burning, pain, tenderness, and shedding," Dr. Donovan of the department of dermatology at the University of Toronto advised at the annual meeting of the American Academy of Dermatology.
Upon examination, he continued, document sites and signs by considering the following questions: Where is the hair loss – frontal, top, or occipital? Can you still see the follicular ostia? Is there erythema of the scalp? Is there perifollicular erythema or scale, crusting, pustules, or loss of eyebrow or body hair?
"When you perform dermoscopy of the normal scalp, one can see that the hairs are similar in ‘caliber’ (no miniaturization suggestive of androgenetic alopecia), and there are no changes around the hair follicles or between the hair follicles," Dr. Donovan said. "In scarring alopecia, a variety of findings may be present which help point to the correct diagnosis."
A 4-mm punch biopsy is helpful to confirm the diagnosis and is recommended in areas of early active disease, including areas that may have primary morphologic features, areas with a positive pull test (if possible), or areas that are symptomatic (if needed). "Diagnosing a hair disease with a biopsy requires a hair to be present in the biopsy," he noted. "Biopsies of completely scarred areas are not helpful." In scarring alopecias, inflammatory infiltrates are found in the upper parts of the hair follicle, which destroys hair follicle stem cells. "It’s this destruction of stem cells which ultimately leads to permanent hair loss," Dr. Donovan said.
Lichen planopilaris, a common form of scarring alopecia, typically occurs in middle age and is twice as common in women as in men. It most often affects the central scalp but may be present in other sites in up to half of cases. Key symptoms of lichen planopilaris (LPP) include hair loss, scalp pruritus, and pain/tenderness, often a burning sensation at the site of hair loss. On dermoscopy, most LPP cases appear as reduced hair density with scalp erythema and perifollicular scale, also called peripilar casts.
The goal of LPP treatment is to reduce symptoms and shedding and to stop the disease from occurring in new sites. "Regrowth is not possible in most scarring alopecias," said Dr. Donovan, who leads the University of Toronto’s program in hair transplantation and hair loss. "Treatments help to halt the underlying disease process. Disease activity may recur."
Treatment options for localized/limited LPP include intralesional triamcinolone acetonide and/or several treatments at home, including 0.05% clobetasol propionate lotion or foam, clobetasol propionate shampoo to help decrease itching and burning, fluocinolone acetonide oil one time per week to help with removal of scales, and topical 0.1% tacrolimus ointment (or compounded lotion) as needed.
Systemic treatment of LPP is also an option, and he said he relies on the dermatopathology report to guide his treatment decisions. If biopsy reveals minimal lymphocytic infiltrate, Dr. Donovan said he recommends doxycycline 100 mg b.i.d. as his first-line approach. If biopsy reveals moderate lymphocytic infiltrate, he turns to hydroxychloroquine 6 mg/kg.
His recommended second-line systemic treatment is mycophenolate mofetil 500 mg b.i.d. for 1 month, then 1,000 mg b.i.d. thereafter. Third-line systemic treatment options include cyclosporine 3-5 mg/kg per day and retinoids such as isotretinoin, but fewer than 20% of patients benefit from retinoids, he said. Once the disease becomes quiet, hair transplant surgery can sometimes be an option to restore hair density.
Dr. Donovan disclosed that he is the cofounder of Okavana Laboratories, a privately held company devoted to hair.
DENVER – To limit the progression of scarring alopecia, Dr. Jeff Donovan makes it a point to ask his patients about symptoms and shedding, and he always performs a thorough scalp examination to record the affected sites and signs of the condition.
"Everything on the history potentially may be important, but always ask about symptoms of itching, burning, pain, tenderness, and shedding," Dr. Donovan of the department of dermatology at the University of Toronto advised at the annual meeting of the American Academy of Dermatology.
Upon examination, he continued, document sites and signs by considering the following questions: Where is the hair loss – frontal, top, or occipital? Can you still see the follicular ostia? Is there erythema of the scalp? Is there perifollicular erythema or scale, crusting, pustules, or loss of eyebrow or body hair?
"When you perform dermoscopy of the normal scalp, one can see that the hairs are similar in ‘caliber’ (no miniaturization suggestive of androgenetic alopecia), and there are no changes around the hair follicles or between the hair follicles," Dr. Donovan said. "In scarring alopecia, a variety of findings may be present which help point to the correct diagnosis."
A 4-mm punch biopsy is helpful to confirm the diagnosis and is recommended in areas of early active disease, including areas that may have primary morphologic features, areas with a positive pull test (if possible), or areas that are symptomatic (if needed). "Diagnosing a hair disease with a biopsy requires a hair to be present in the biopsy," he noted. "Biopsies of completely scarred areas are not helpful." In scarring alopecias, inflammatory infiltrates are found in the upper parts of the hair follicle, which destroys hair follicle stem cells. "It’s this destruction of stem cells which ultimately leads to permanent hair loss," Dr. Donovan said.
Lichen planopilaris, a common form of scarring alopecia, typically occurs in middle age and is twice as common in women as in men. It most often affects the central scalp but may be present in other sites in up to half of cases. Key symptoms of lichen planopilaris (LPP) include hair loss, scalp pruritus, and pain/tenderness, often a burning sensation at the site of hair loss. On dermoscopy, most LPP cases appear as reduced hair density with scalp erythema and perifollicular scale, also called peripilar casts.
The goal of LPP treatment is to reduce symptoms and shedding and to stop the disease from occurring in new sites. "Regrowth is not possible in most scarring alopecias," said Dr. Donovan, who leads the University of Toronto’s program in hair transplantation and hair loss. "Treatments help to halt the underlying disease process. Disease activity may recur."
Treatment options for localized/limited LPP include intralesional triamcinolone acetonide and/or several treatments at home, including 0.05% clobetasol propionate lotion or foam, clobetasol propionate shampoo to help decrease itching and burning, fluocinolone acetonide oil one time per week to help with removal of scales, and topical 0.1% tacrolimus ointment (or compounded lotion) as needed.
Systemic treatment of LPP is also an option, and he said he relies on the dermatopathology report to guide his treatment decisions. If biopsy reveals minimal lymphocytic infiltrate, Dr. Donovan said he recommends doxycycline 100 mg b.i.d. as his first-line approach. If biopsy reveals moderate lymphocytic infiltrate, he turns to hydroxychloroquine 6 mg/kg.
His recommended second-line systemic treatment is mycophenolate mofetil 500 mg b.i.d. for 1 month, then 1,000 mg b.i.d. thereafter. Third-line systemic treatment options include cyclosporine 3-5 mg/kg per day and retinoids such as isotretinoin, but fewer than 20% of patients benefit from retinoids, he said. Once the disease becomes quiet, hair transplant surgery can sometimes be an option to restore hair density.
Dr. Donovan disclosed that he is the cofounder of Okavana Laboratories, a privately held company devoted to hair.
AT THE AAD ANNUAL MEETING

AAD 2014 sessions offer something for everyone
The American Academy’s 2014 annual meeting in Denver will feature new CME sessions and updates on the latest dermatology research.
This year’s program features expert commentary on key issues in medical dermatology, including "Melanoma Multidisciplinary Care 2014: What You Need to Know" on Sunday, March 23, from 1 p.m. to 3 p.m. in Room 705/707 and "Dermatologic Manifestations of New Oncology Drugs," also on Sunday, March 23, from 1 p.m. to 3 p.m. in the Mile High Ballroom 3B. Looking for the latest in aesthetic dermatology? Check out the "Advanced Botulinum Toxin" live demonstration session on Saturday, March 22, from 2 p.m. to 5 p.m. in the Bellco Theater.
There will be expert sessions on pregnancy dermatoses, cutaneous T-cell lymphoma, pediatric dermatology, skin of color, and the latest on treatments for hair and nail conditions. The full scientific session list is available online.
A series of practice management lectures includes topics such as "How to Have an Unforgettably Positive Office Visit" on Saturday, March 22, from 10:00 a.m. to 12:00 p.m. in Room 709/7111 and "Hot Buttons: Recognizing What Sets You Off and Managing Your Triggers" on Sunday, March 23, from 1:00 p.m. to 3:00 p.m. in Room 702.
There is also a mobile device app that meeting attendees can download that contains session schedules, exhibitor and attendee lists, and more.
Can’t attend the meeting? Visit www.eDermatologyNews.com for live conference coverage.
On Twitter @Sknews
The American Academy’s 2014 annual meeting in Denver will feature new CME sessions and updates on the latest dermatology research.
This year’s program features expert commentary on key issues in medical dermatology, including "Melanoma Multidisciplinary Care 2014: What You Need to Know" on Sunday, March 23, from 1 p.m. to 3 p.m. in Room 705/707 and "Dermatologic Manifestations of New Oncology Drugs," also on Sunday, March 23, from 1 p.m. to 3 p.m. in the Mile High Ballroom 3B. Looking for the latest in aesthetic dermatology? Check out the "Advanced Botulinum Toxin" live demonstration session on Saturday, March 22, from 2 p.m. to 5 p.m. in the Bellco Theater.
There will be expert sessions on pregnancy dermatoses, cutaneous T-cell lymphoma, pediatric dermatology, skin of color, and the latest on treatments for hair and nail conditions. The full scientific session list is available online.
A series of practice management lectures includes topics such as "How to Have an Unforgettably Positive Office Visit" on Saturday, March 22, from 10:00 a.m. to 12:00 p.m. in Room 709/7111 and "Hot Buttons: Recognizing What Sets You Off and Managing Your Triggers" on Sunday, March 23, from 1:00 p.m. to 3:00 p.m. in Room 702.
There is also a mobile device app that meeting attendees can download that contains session schedules, exhibitor and attendee lists, and more.
Can’t attend the meeting? Visit www.eDermatologyNews.com for live conference coverage.
On Twitter @Sknews
The American Academy’s 2014 annual meeting in Denver will feature new CME sessions and updates on the latest dermatology research.
This year’s program features expert commentary on key issues in medical dermatology, including "Melanoma Multidisciplinary Care 2014: What You Need to Know" on Sunday, March 23, from 1 p.m. to 3 p.m. in Room 705/707 and "Dermatologic Manifestations of New Oncology Drugs," also on Sunday, March 23, from 1 p.m. to 3 p.m. in the Mile High Ballroom 3B. Looking for the latest in aesthetic dermatology? Check out the "Advanced Botulinum Toxin" live demonstration session on Saturday, March 22, from 2 p.m. to 5 p.m. in the Bellco Theater.
There will be expert sessions on pregnancy dermatoses, cutaneous T-cell lymphoma, pediatric dermatology, skin of color, and the latest on treatments for hair and nail conditions. The full scientific session list is available online.
A series of practice management lectures includes topics such as "How to Have an Unforgettably Positive Office Visit" on Saturday, March 22, from 10:00 a.m. to 12:00 p.m. in Room 709/7111 and "Hot Buttons: Recognizing What Sets You Off and Managing Your Triggers" on Sunday, March 23, from 1:00 p.m. to 3:00 p.m. in Room 702.
There is also a mobile device app that meeting attendees can download that contains session schedules, exhibitor and attendee lists, and more.
Can’t attend the meeting? Visit www.eDermatologyNews.com for live conference coverage.
On Twitter @Sknews
Cosmetic Corner: Dermatologists Weigh in on OTC Antifungals
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC antifungal products. Consideration must be given to:
Cutis invites readers to send us their recommendations. Antiperspirants and OTC hair restoration products will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC antifungal products. Consideration must be given to:
Cutis invites readers to send us their recommendations. Antiperspirants and OTC hair restoration products will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on the top OTC antifungal products. Consideration must be given to:
Cutis invites readers to send us their recommendations. Antiperspirants and OTC hair restoration products will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

VIDEO: New and upcoming topical antifungals
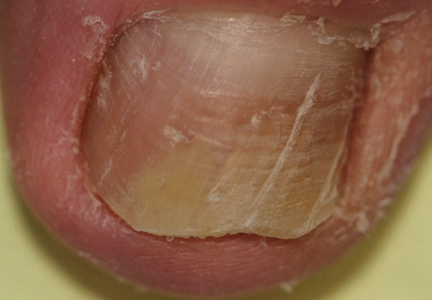
PALM BEACH, ARUBA – Systemic therapy is currently the standard of treatment for onychomycosis, but Dr. David Pariser discusses several new topical antifungals – efinaconazole, tavaborole, and luliconazole – that may be available in the next year to improve therapy options for patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PALM BEACH, ARUBA – Systemic therapy is currently the standard of treatment for onychomycosis, but Dr. David Pariser discusses several new topical antifungals – efinaconazole, tavaborole, and luliconazole – that may be available in the next year to improve therapy options for patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PALM BEACH, ARUBA – Systemic therapy is currently the standard of treatment for onychomycosis, but Dr. David Pariser discusses several new topical antifungals – efinaconazole, tavaborole, and luliconazole – that may be available in the next year to improve therapy options for patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE CARIBBEAN DERMATOLOGY SYMPOSIUM
VIDEO: Coffee Break 1: What did you learn at the meeting?
WAIKOLOA, HAWAII – Our editor, Heidi Splete, catches up with attendees at the SDEF Hawaii Dermatology Seminar to find out what they learned at the meeting that they will take back to their practices.
During a coffee break video interview, doctors said they enjoyed presentations on the need to treat onychomycosis aggressively in patients with diabetes; diet and acne; and recent trends in the use of systemic biologic therapies for psoriasis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAIKOLOA, HAWAII – Our editor, Heidi Splete, catches up with attendees at the SDEF Hawaii Dermatology Seminar to find out what they learned at the meeting that they will take back to their practices.
During a coffee break video interview, doctors said they enjoyed presentations on the need to treat onychomycosis aggressively in patients with diabetes; diet and acne; and recent trends in the use of systemic biologic therapies for psoriasis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAIKOLOA, HAWAII – Our editor, Heidi Splete, catches up with attendees at the SDEF Hawaii Dermatology Seminar to find out what they learned at the meeting that they will take back to their practices.
During a coffee break video interview, doctors said they enjoyed presentations on the need to treat onychomycosis aggressively in patients with diabetes; diet and acne; and recent trends in the use of systemic biologic therapies for psoriasis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

VIDEO: Investigational topical antifungals target onychomycosis
WAIKOLA, HAWAII – Two topical antifungals that are designed to treat onychomycosis may reach the U.S. market within the next year, according to nail expert Dr. Phoebe Rich.
"It’s very exciting that we finally have some new medications for onychomycosis," said Dr. Rich of Oregon Dermatology and Research Center, Portland. She spoke with us about the two agents – tavaborole and efinaconazole – in a video interview during the SDEF Hawaii Dermatology Seminar.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAIKOLA, HAWAII – Two topical antifungals that are designed to treat onychomycosis may reach the U.S. market within the next year, according to nail expert Dr. Phoebe Rich.
"It’s very exciting that we finally have some new medications for onychomycosis," said Dr. Rich of Oregon Dermatology and Research Center, Portland. She spoke with us about the two agents – tavaborole and efinaconazole – in a video interview during the SDEF Hawaii Dermatology Seminar.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAIKOLA, HAWAII – Two topical antifungals that are designed to treat onychomycosis may reach the U.S. market within the next year, according to nail expert Dr. Phoebe Rich.
"It’s very exciting that we finally have some new medications for onychomycosis," said Dr. Rich of Oregon Dermatology and Research Center, Portland. She spoke with us about the two agents – tavaborole and efinaconazole – in a video interview during the SDEF Hawaii Dermatology Seminar.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR