User login
Differences in right vs. left colon in Black vs. White individuals
The right colon appears to age faster in Black people than in White people, perhaps explaining the higher prevalence of right-side colon cancer among Black Americans, according to results from a biopsy study.
The findings were published online Dec. 30 in the Journal of the National Cancer Institute.
For the study, investigators analyzed colon biopsy specimens from 128 individuals who underwent routine colorectal screening.
The researchers compared DNA methylation levels in right and left colon biopsy samples from the same patient. They then assigned epigenetic ages to the tissue samples using the Hovarth clock, which estimates tissue age on the basis of DNA methylation.
DNA methylation is influenced by age and environmental exposures. Aberrant DNA methylation is a hallmark of colorectal cancer, the researchers explained.
The epigenetic age of the right colon of the 88 Black patients was 1.51 years ahead of their left colon; the right colon of the 44 White patients was epigenetically 1.93 years younger than their left colon.
The right colon was epigenetically older than the left colon in 60.2% of Black patients; it was younger in more than 70% of White patients.
A unique pattern of DNA hypermethylation was found in the right colon of Black patients.
“Our results provide biological plausibility for the observed relative preponderance of right colon cancer and younger age of onset in African Americans as compared to European Americans,” wrote the investigators, led by Matthew Devall, PhD, a research associate at the Center for Public Health Genomics at the University of Virginia, Charlottesville.
“Side-specific colonic epigenetic aging may be a promising marker to guide interventions to reduce CRC [colorectal cancer] burden,” they suggested.
If these findings are “corroborated in African Americans in future studies, these results could potentially explain racial differences in the site predilection of colorectal cancers,” Amit Joshi, MBBS, PhD, and Andrew Chan, MD, gastrointestinal molecular epidemiologists at Harvard Medical School, Boston, wrote in an accompanying editorial.
However, “it is not clear if the higher epigenetic aging measured using the Horvath clock ... directly translates to a higher risk of colorectal cancer,” they noted.
Some differences between the Black patients and the White patients in the study could explain the methylation differences, they pointed out. A higher proportion of Black patients smoked (37.5% vs. 15%), and Black patients were younger (median age, 55.5 years, vs. 61.7 years). In addition, the study included more Black women than White women (67% vs. 58%), and body mass indexes were higher for Black patients than White patients (31.36 kg/m2 vs 28.29 kg/m2).
“One or more of these factors, or others that were not measured, may be linked to differential methylation in the right compared with left colon,” the editorialists wrote.
Even so, among the Black patients, almost 70% of differentially methylated positions in the right colon were hypermethylated, compared to less than half in the left colon. These included positions previously associated with colorectal cancer, aging, and ancestry, “suggesting a role for genetic variation in contributing to DNA methylation differences in AA right colon,” the investigators said.
The work was supported the National Cancer Institute Cancer, the Case Comprehensive Cancer Center, and the University of Virginia Cancer Center. The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The right colon appears to age faster in Black people than in White people, perhaps explaining the higher prevalence of right-side colon cancer among Black Americans, according to results from a biopsy study.
The findings were published online Dec. 30 in the Journal of the National Cancer Institute.
For the study, investigators analyzed colon biopsy specimens from 128 individuals who underwent routine colorectal screening.
The researchers compared DNA methylation levels in right and left colon biopsy samples from the same patient. They then assigned epigenetic ages to the tissue samples using the Hovarth clock, which estimates tissue age on the basis of DNA methylation.
DNA methylation is influenced by age and environmental exposures. Aberrant DNA methylation is a hallmark of colorectal cancer, the researchers explained.
The epigenetic age of the right colon of the 88 Black patients was 1.51 years ahead of their left colon; the right colon of the 44 White patients was epigenetically 1.93 years younger than their left colon.
The right colon was epigenetically older than the left colon in 60.2% of Black patients; it was younger in more than 70% of White patients.
A unique pattern of DNA hypermethylation was found in the right colon of Black patients.
“Our results provide biological plausibility for the observed relative preponderance of right colon cancer and younger age of onset in African Americans as compared to European Americans,” wrote the investigators, led by Matthew Devall, PhD, a research associate at the Center for Public Health Genomics at the University of Virginia, Charlottesville.
“Side-specific colonic epigenetic aging may be a promising marker to guide interventions to reduce CRC [colorectal cancer] burden,” they suggested.
If these findings are “corroborated in African Americans in future studies, these results could potentially explain racial differences in the site predilection of colorectal cancers,” Amit Joshi, MBBS, PhD, and Andrew Chan, MD, gastrointestinal molecular epidemiologists at Harvard Medical School, Boston, wrote in an accompanying editorial.
However, “it is not clear if the higher epigenetic aging measured using the Horvath clock ... directly translates to a higher risk of colorectal cancer,” they noted.
Some differences between the Black patients and the White patients in the study could explain the methylation differences, they pointed out. A higher proportion of Black patients smoked (37.5% vs. 15%), and Black patients were younger (median age, 55.5 years, vs. 61.7 years). In addition, the study included more Black women than White women (67% vs. 58%), and body mass indexes were higher for Black patients than White patients (31.36 kg/m2 vs 28.29 kg/m2).
“One or more of these factors, or others that were not measured, may be linked to differential methylation in the right compared with left colon,” the editorialists wrote.
Even so, among the Black patients, almost 70% of differentially methylated positions in the right colon were hypermethylated, compared to less than half in the left colon. These included positions previously associated with colorectal cancer, aging, and ancestry, “suggesting a role for genetic variation in contributing to DNA methylation differences in AA right colon,” the investigators said.
The work was supported the National Cancer Institute Cancer, the Case Comprehensive Cancer Center, and the University of Virginia Cancer Center. The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The right colon appears to age faster in Black people than in White people, perhaps explaining the higher prevalence of right-side colon cancer among Black Americans, according to results from a biopsy study.
The findings were published online Dec. 30 in the Journal of the National Cancer Institute.
For the study, investigators analyzed colon biopsy specimens from 128 individuals who underwent routine colorectal screening.
The researchers compared DNA methylation levels in right and left colon biopsy samples from the same patient. They then assigned epigenetic ages to the tissue samples using the Hovarth clock, which estimates tissue age on the basis of DNA methylation.
DNA methylation is influenced by age and environmental exposures. Aberrant DNA methylation is a hallmark of colorectal cancer, the researchers explained.
The epigenetic age of the right colon of the 88 Black patients was 1.51 years ahead of their left colon; the right colon of the 44 White patients was epigenetically 1.93 years younger than their left colon.
The right colon was epigenetically older than the left colon in 60.2% of Black patients; it was younger in more than 70% of White patients.
A unique pattern of DNA hypermethylation was found in the right colon of Black patients.
“Our results provide biological plausibility for the observed relative preponderance of right colon cancer and younger age of onset in African Americans as compared to European Americans,” wrote the investigators, led by Matthew Devall, PhD, a research associate at the Center for Public Health Genomics at the University of Virginia, Charlottesville.
“Side-specific colonic epigenetic aging may be a promising marker to guide interventions to reduce CRC [colorectal cancer] burden,” they suggested.
If these findings are “corroborated in African Americans in future studies, these results could potentially explain racial differences in the site predilection of colorectal cancers,” Amit Joshi, MBBS, PhD, and Andrew Chan, MD, gastrointestinal molecular epidemiologists at Harvard Medical School, Boston, wrote in an accompanying editorial.
However, “it is not clear if the higher epigenetic aging measured using the Horvath clock ... directly translates to a higher risk of colorectal cancer,” they noted.
Some differences between the Black patients and the White patients in the study could explain the methylation differences, they pointed out. A higher proportion of Black patients smoked (37.5% vs. 15%), and Black patients were younger (median age, 55.5 years, vs. 61.7 years). In addition, the study included more Black women than White women (67% vs. 58%), and body mass indexes were higher for Black patients than White patients (31.36 kg/m2 vs 28.29 kg/m2).
“One or more of these factors, or others that were not measured, may be linked to differential methylation in the right compared with left colon,” the editorialists wrote.
Even so, among the Black patients, almost 70% of differentially methylated positions in the right colon were hypermethylated, compared to less than half in the left colon. These included positions previously associated with colorectal cancer, aging, and ancestry, “suggesting a role for genetic variation in contributing to DNA methylation differences in AA right colon,” the investigators said.
The work was supported the National Cancer Institute Cancer, the Case Comprehensive Cancer Center, and the University of Virginia Cancer Center. The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Racial, ethnic disparities in maternal mortality, morbidity persist
Racial and ethnic disparities in maternal and infant outcomes persist in the United States, with Black women being 3-4 times more likely to die of pregnancy-related causes, compared with Latina and non-Latina white women, Elizabeth Howell, MD, said in a presentation at the 2020 virtual meeting of the American College of Obstetricians and Gynecologists.
Location matters, too, and ethnic disparities appear to transcend class, said Dr. Howell of Penn Medicine, Philadelphia. In New York City, for example, Black women are 8-12 times more likely to die than white women regardless of educational attainment.
Dr. Howell cited the definitions of health equity and health disparities as defined by Paula Braveman, MD, in 2014 in the journal Public Health Reports, as follows: “Health equity means social justice in health (i.e., no one is denied the possibility to be healthy for belonging to a group that has historically been economically/socially disadvantaged. Health disparities are the metric we use to measure progress toward achieving health equity.”
Structural racism and discrimination contribute to disparities in maternal and infant morbidity and mortality in several ways, she said. Patient factors include sociodemographics, age, education, poverty, insurance, marital status, language, and literacy. In addition, a patient’s knowledge, beliefs, and health behaviors, as well as stress and self-efficacy are involved. Community factors such as crime, poverty, and community support play a role.
“These factors contribute to the health status of a woman when she becomes pregnant,” Dr. Howell said. “These factors contribute as the woman goes through the health system.”
Then provider factors that impact maternal and infant morbidity and mortality include knowledge, experience, implicit bias, cultural humility, and communication; these factors affect the quality and delivery of neonatal care, and can impact outcomes, Dr. Howell said.
“It is really important to note that many of these pregnancy-related deaths are thought to be preventable,” she said. “They are often caused by delays in diagnosis, problems with communication, and other system failures. Site care has received a great deal of attention” in recent years, the ob.gyn. noted.
How hospital quality contributes to health disparities
Dr. Howell shared data from a pair of National Institutes of Health–funded parallel group studies she conducted at New York City hospitals to investigate the contribution of hospital quality to health disparities in severe maternal morbidity and very preterm birth (prior to 32 weeks).
The researchers used vital statistics linked with discharge abstracts for all New York City deliveries between 2011-2013 and 2010-2014. They conducted a logistic regression analysis and ranked hospitals based on metrics of severe maternal morbidity and very preterm birth, and assessed differences by race in each delivery location.
Overall, Black women were almost three times as likely and Latina women were almost twice as likely as White women to experience some type of severe maternal morbidity, with rates of 4.2%, 2.7%, and 1.5%, respectively.
The researchers also ranked hospitals, and found a wide variation; women delivering in the lowest-ranked hospitals had six times the rate of severe maternal morbidity. They also conducted a simulation/thought exercise and determined that the hospital of delivery accounted for approximately 48% of the disparity in severe maternal morbidity between Black and White women.
Results were similar in the parallel study of very preterm birth rates in New York City hospitals, which were 32%, 28%, and 23% for Black, Latina, and White women, respectively.
The researchers also conducted interviews with personnel including chief medical officers, neonatal ICU directors, nurses, and respiratory therapists. The final phase of the research, which is ongoing, is the dissemination of the information, said Dr. Howell.
Overall, the high-performing hospitals were more likely to focus on standards and standardized care, stronger nurse/physician communication, greater awareness of the potential impact of racism on care, and greater sharing of performance data.
Women who participated in focus groups reported a range of experiences, but women of color were likely to report poor communication, feeling traumatized, and not being heard.
Study implications
Dr. Howell discussed the implications of her study in a question and answer session. “It is incredibly important for us to think about all the levers that we have to address disparities.”
“It is a complex web of factors, but quality of care is one of those mechanisms, and it is something we can do something about,” she noted.
In response to a question about whether women should know the rates of adverse outcomes at various hospitals, she said, “I think we have a responsibility to come up with quality of care measures that are informative to the women we care for.”
Much of obstetric quality issues focus on overuse of resources, “but that doesn’t help us reduce disparities,” she said.
Dr. Howell had no financial conflicts to disclose.
Racial and ethnic disparities in maternal and infant outcomes persist in the United States, with Black women being 3-4 times more likely to die of pregnancy-related causes, compared with Latina and non-Latina white women, Elizabeth Howell, MD, said in a presentation at the 2020 virtual meeting of the American College of Obstetricians and Gynecologists.
Location matters, too, and ethnic disparities appear to transcend class, said Dr. Howell of Penn Medicine, Philadelphia. In New York City, for example, Black women are 8-12 times more likely to die than white women regardless of educational attainment.
Dr. Howell cited the definitions of health equity and health disparities as defined by Paula Braveman, MD, in 2014 in the journal Public Health Reports, as follows: “Health equity means social justice in health (i.e., no one is denied the possibility to be healthy for belonging to a group that has historically been economically/socially disadvantaged. Health disparities are the metric we use to measure progress toward achieving health equity.”
Structural racism and discrimination contribute to disparities in maternal and infant morbidity and mortality in several ways, she said. Patient factors include sociodemographics, age, education, poverty, insurance, marital status, language, and literacy. In addition, a patient’s knowledge, beliefs, and health behaviors, as well as stress and self-efficacy are involved. Community factors such as crime, poverty, and community support play a role.
“These factors contribute to the health status of a woman when she becomes pregnant,” Dr. Howell said. “These factors contribute as the woman goes through the health system.”
Then provider factors that impact maternal and infant morbidity and mortality include knowledge, experience, implicit bias, cultural humility, and communication; these factors affect the quality and delivery of neonatal care, and can impact outcomes, Dr. Howell said.
“It is really important to note that many of these pregnancy-related deaths are thought to be preventable,” she said. “They are often caused by delays in diagnosis, problems with communication, and other system failures. Site care has received a great deal of attention” in recent years, the ob.gyn. noted.
How hospital quality contributes to health disparities
Dr. Howell shared data from a pair of National Institutes of Health–funded parallel group studies she conducted at New York City hospitals to investigate the contribution of hospital quality to health disparities in severe maternal morbidity and very preterm birth (prior to 32 weeks).
The researchers used vital statistics linked with discharge abstracts for all New York City deliveries between 2011-2013 and 2010-2014. They conducted a logistic regression analysis and ranked hospitals based on metrics of severe maternal morbidity and very preterm birth, and assessed differences by race in each delivery location.
Overall, Black women were almost three times as likely and Latina women were almost twice as likely as White women to experience some type of severe maternal morbidity, with rates of 4.2%, 2.7%, and 1.5%, respectively.
The researchers also ranked hospitals, and found a wide variation; women delivering in the lowest-ranked hospitals had six times the rate of severe maternal morbidity. They also conducted a simulation/thought exercise and determined that the hospital of delivery accounted for approximately 48% of the disparity in severe maternal morbidity between Black and White women.
Results were similar in the parallel study of very preterm birth rates in New York City hospitals, which were 32%, 28%, and 23% for Black, Latina, and White women, respectively.
The researchers also conducted interviews with personnel including chief medical officers, neonatal ICU directors, nurses, and respiratory therapists. The final phase of the research, which is ongoing, is the dissemination of the information, said Dr. Howell.
Overall, the high-performing hospitals were more likely to focus on standards and standardized care, stronger nurse/physician communication, greater awareness of the potential impact of racism on care, and greater sharing of performance data.
Women who participated in focus groups reported a range of experiences, but women of color were likely to report poor communication, feeling traumatized, and not being heard.
Study implications
Dr. Howell discussed the implications of her study in a question and answer session. “It is incredibly important for us to think about all the levers that we have to address disparities.”
“It is a complex web of factors, but quality of care is one of those mechanisms, and it is something we can do something about,” she noted.
In response to a question about whether women should know the rates of adverse outcomes at various hospitals, she said, “I think we have a responsibility to come up with quality of care measures that are informative to the women we care for.”
Much of obstetric quality issues focus on overuse of resources, “but that doesn’t help us reduce disparities,” she said.
Dr. Howell had no financial conflicts to disclose.
Racial and ethnic disparities in maternal and infant outcomes persist in the United States, with Black women being 3-4 times more likely to die of pregnancy-related causes, compared with Latina and non-Latina white women, Elizabeth Howell, MD, said in a presentation at the 2020 virtual meeting of the American College of Obstetricians and Gynecologists.
Location matters, too, and ethnic disparities appear to transcend class, said Dr. Howell of Penn Medicine, Philadelphia. In New York City, for example, Black women are 8-12 times more likely to die than white women regardless of educational attainment.
Dr. Howell cited the definitions of health equity and health disparities as defined by Paula Braveman, MD, in 2014 in the journal Public Health Reports, as follows: “Health equity means social justice in health (i.e., no one is denied the possibility to be healthy for belonging to a group that has historically been economically/socially disadvantaged. Health disparities are the metric we use to measure progress toward achieving health equity.”
Structural racism and discrimination contribute to disparities in maternal and infant morbidity and mortality in several ways, she said. Patient factors include sociodemographics, age, education, poverty, insurance, marital status, language, and literacy. In addition, a patient’s knowledge, beliefs, and health behaviors, as well as stress and self-efficacy are involved. Community factors such as crime, poverty, and community support play a role.
“These factors contribute to the health status of a woman when she becomes pregnant,” Dr. Howell said. “These factors contribute as the woman goes through the health system.”
Then provider factors that impact maternal and infant morbidity and mortality include knowledge, experience, implicit bias, cultural humility, and communication; these factors affect the quality and delivery of neonatal care, and can impact outcomes, Dr. Howell said.
“It is really important to note that many of these pregnancy-related deaths are thought to be preventable,” she said. “They are often caused by delays in diagnosis, problems with communication, and other system failures. Site care has received a great deal of attention” in recent years, the ob.gyn. noted.
How hospital quality contributes to health disparities
Dr. Howell shared data from a pair of National Institutes of Health–funded parallel group studies she conducted at New York City hospitals to investigate the contribution of hospital quality to health disparities in severe maternal morbidity and very preterm birth (prior to 32 weeks).
The researchers used vital statistics linked with discharge abstracts for all New York City deliveries between 2011-2013 and 2010-2014. They conducted a logistic regression analysis and ranked hospitals based on metrics of severe maternal morbidity and very preterm birth, and assessed differences by race in each delivery location.
Overall, Black women were almost three times as likely and Latina women were almost twice as likely as White women to experience some type of severe maternal morbidity, with rates of 4.2%, 2.7%, and 1.5%, respectively.
The researchers also ranked hospitals, and found a wide variation; women delivering in the lowest-ranked hospitals had six times the rate of severe maternal morbidity. They also conducted a simulation/thought exercise and determined that the hospital of delivery accounted for approximately 48% of the disparity in severe maternal morbidity between Black and White women.
Results were similar in the parallel study of very preterm birth rates in New York City hospitals, which were 32%, 28%, and 23% for Black, Latina, and White women, respectively.
The researchers also conducted interviews with personnel including chief medical officers, neonatal ICU directors, nurses, and respiratory therapists. The final phase of the research, which is ongoing, is the dissemination of the information, said Dr. Howell.
Overall, the high-performing hospitals were more likely to focus on standards and standardized care, stronger nurse/physician communication, greater awareness of the potential impact of racism on care, and greater sharing of performance data.
Women who participated in focus groups reported a range of experiences, but women of color were likely to report poor communication, feeling traumatized, and not being heard.
Study implications
Dr. Howell discussed the implications of her study in a question and answer session. “It is incredibly important for us to think about all the levers that we have to address disparities.”
“It is a complex web of factors, but quality of care is one of those mechanisms, and it is something we can do something about,” she noted.
In response to a question about whether women should know the rates of adverse outcomes at various hospitals, she said, “I think we have a responsibility to come up with quality of care measures that are informative to the women we care for.”
Much of obstetric quality issues focus on overuse of resources, “but that doesn’t help us reduce disparities,” she said.
Dr. Howell had no financial conflicts to disclose.
FROM ACOG 2020
Rural Residency Curricula: Potential Target for Improved Access to Care?
To the Editor:
There is an irrefutable trend toward urban dermatology practice in the United States, leading to growing problems with rural access to care. The provision of rural clinical experiences and telehealth in dermatology residency training might increase the likelihood of trainees establishing a rural practice.
In 2017, the American Academy of Dermatology released an updated statement supporting direct patient access to board-certified dermatologists in an effort to reduce morbidity and mortality associated with skin disease.1 Twenty percent of the US population lives in a rural and medically underserved location, yet these areas remain largely underserved, in part because of an irrefutable trend toward urban dermatology practice.2-4 Successful approaches to improving rural access to dermatology care are poorly defined in the literature.
Several variables have been shown to influence a young physician’s decision to establish a clinical practice in geographically isolated areas, including rural upbringing, longitudinal rural clinical experiences during medical training, and family influences.5 Location of residency training is an additional variable that impacts practice location, though migration following dermatology residency is a complex phenomenon. However, training location does not guarantee retention of dermatology graduates in any particular geographic area.6 Practice incentives and stipends might encourage rural dermatology practice, yet these programs are underfunded. Last, telemedicine in dermatology (including teledermatology and teledermoscopy), though not always an ideal substitute for a live visit, can improve access to care in geographically isolated or underserved areas in general.7-9
Focused recruitment of medical students interested in rural dermatology practice to accredited dermatology residency programs aligned with this goal represents another approach to improve geographic diversity in the field of dermatology. Online access to this information would be useful for both applicants and their mentors.
We assessed viewable online curricula related to rural dermatology and telemedicine experiences at all Accreditation Council for Graduate Medical Education (ACGME)–accredited residency programs. Telemedicine experiences at Veterans Health Administration (VHA) health systems also were assessed.
Methods
This study was exempt from review by the institutional review board at the University of Minnesota (Minneapolis, Minnesota)(IRB #STUDY00004915) because no human subjects were involved. Online curricula of all ACGME-accredited dermatology residency programs in the United States and Puerto Rico were reviewed from November to December 2018. The following information was recorded: specialized “rural-track” training; optional elective time in rural settings; teledermatology training; and teledermoscopy training.
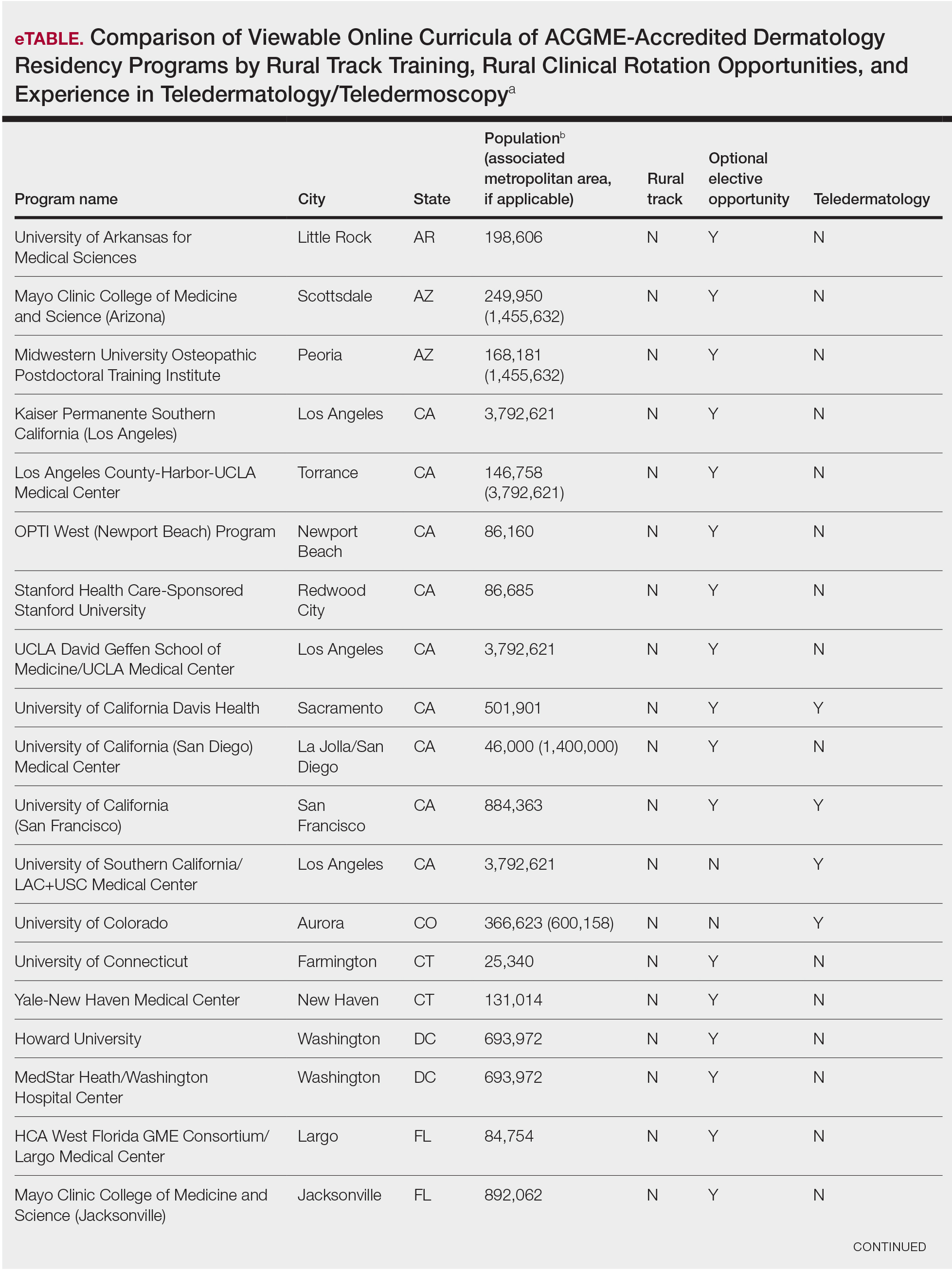
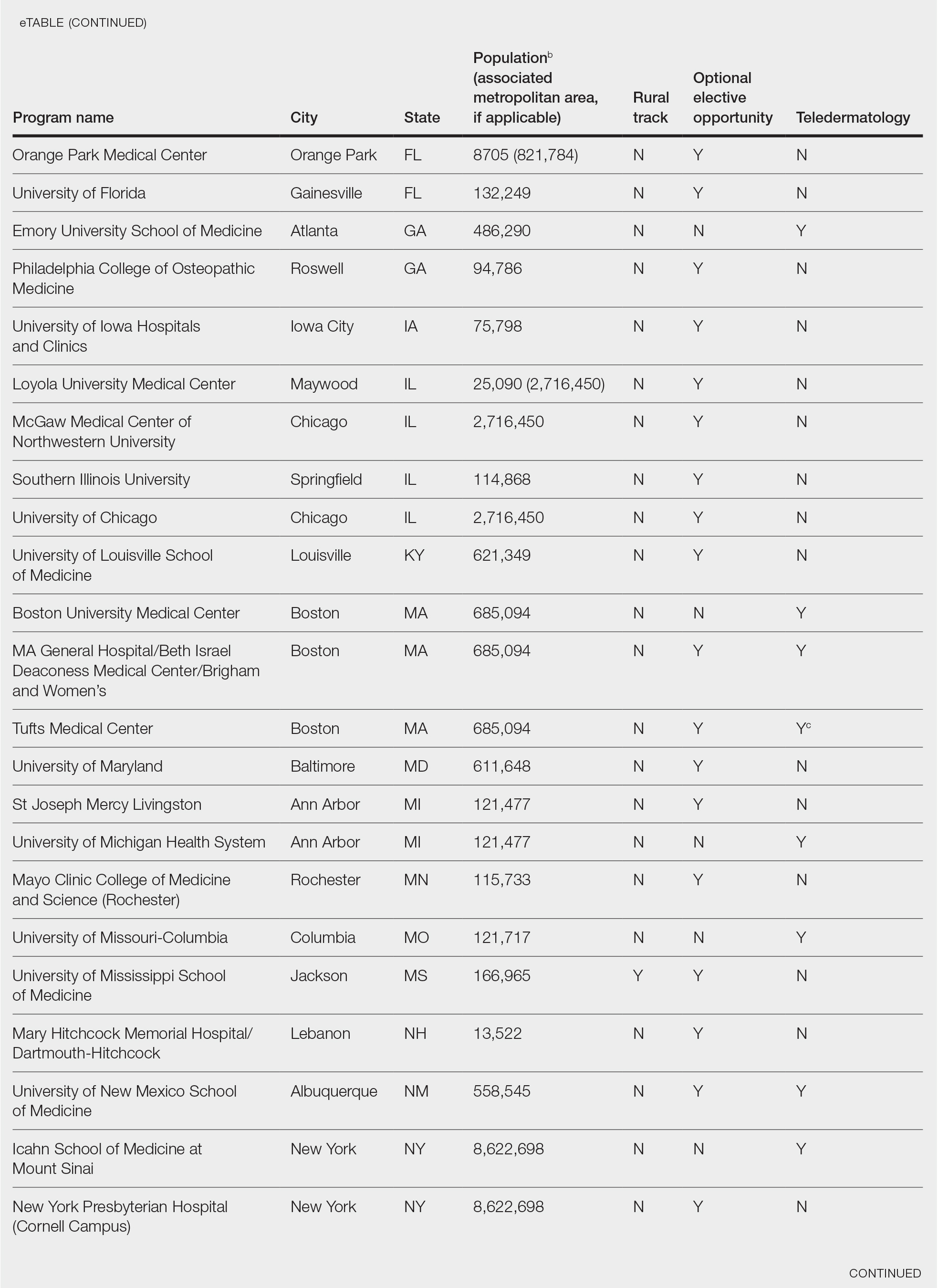
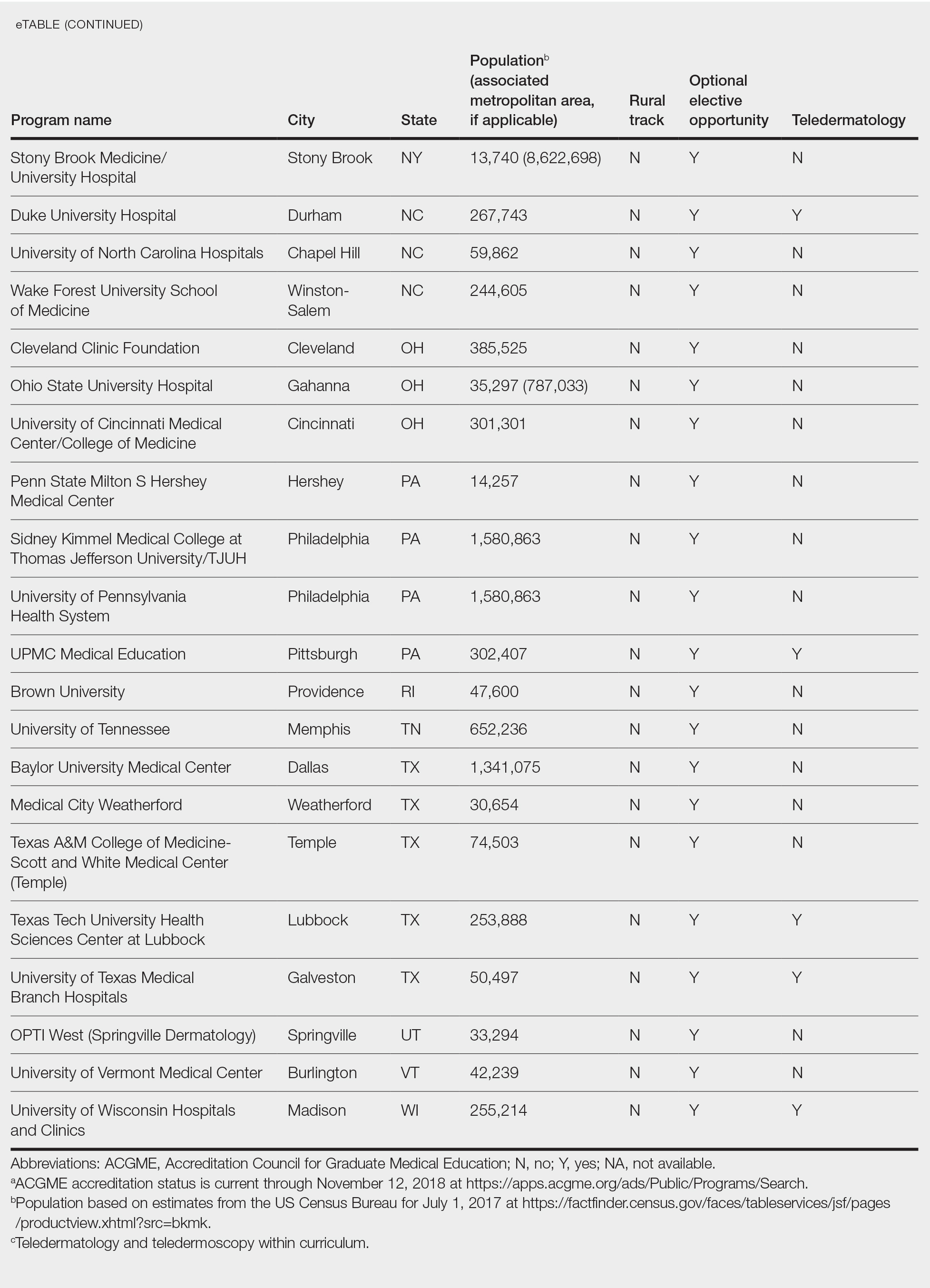
Additionally, population density at each program’s primary location was determined using US Census Bureau data and with consideration to communities contained within particular Metropolitan Statistical Areas (MSAs)(eTable). Data were obtained from the VHA system to assess teledermatology services at VHA locations affiliated with residency programs.
Results
Of 154 dermatology residency programs identified in the United States and Puerto Rico, 142 were accredited at the time of data collection. Fifteen (10%) were based in communities of 50,000 individuals or fewer that were not near a large metropolitan area. One program (<1%) offered a specific rural track. Fifty-six programs (39%) cited optional rotations or clinical electives, or both, that could be utilized for a rural experience. Eighteen (12%) offered teledermatology experiences and 1 (<1%) offered teledermoscopy during training. Fifty-three programs (37%) offered a rotation at a VHA hospital that had an active teledermatology service.
Comment
Program websites are a free and easily accessible means of acquiring relevant information. The paucity of readily available data on rural dermatology and teledermatology opportunities is unfortunate and a detriment to dermatology residency applicants interested in rural practice, which may result in a missed opportunity to foster a true passion for rural medicine. A brief comment on a website can be impactful, leading to a postgraduate year 4 dermatology elective rotation at a prospective fellowship training site or a rural dermatology experience.
The paucity of dermatologists working directly in rural areas has led to development of teledermatology initiatives to reach deeply into underserved regions. One of the largest providers of teledermatology is the VHA, which standardized its teledermatology efforts in 2012 and provides remarkable educational opportunities for dermatology residents. However, many residency program and VHA websites provide no information about the participation of dermatology residents in the provision of teledermatology services.
A limitation of this study is that it is based on online published curricula. Dermatology residency programs with excellent rural curricula that are not published online might exist.
Residency program directors with an interest in geographic diversity are encouraged to provide rural and teledermatology opportunities and to update these offerings on their websites, which is a simple modifiable strategy that can impact the rural dermatology care gap by recruiting students interested in filling this role. These efforts should be studied to determine whether this strategy impacts resident selection as well as whether focused rural and telemedicine exposure during training increases the likelihood of establishing a rural dermatology practice in the future.
- American Academy of Dermatology. Position statement on access to specialty care and direct access to dermatologic care. Revised May 20, 2017. Accessed December 13, 2020. https://server.aad.org/forms/Policies/Uploads/PS/PS-Access%20to%20Specialty%20Care%20and%20Direct%20Access%20to%20Dermatologic%20Care.pdf
- Dill MJ, Salsberg ES. The Complexities of Physician Supply and Demand: Projections Through 2025. Center for Workforce Studies, Association of American Medical Colleges (AAMC); November 2008. Accessed December 13, 2020. http://innovationlabs.com/pa_future/1/background_docs/AAMC%20Complexities%20of%20physician%20demand,%202008.pdf
- Glazer AM, Rigel DS. Analysis of trends in geographic distribution of US dermatology workforce density. JAMA Dermatol. 2017;153:472-473.
- Yoo JY, Rigel DS. Trends in dermatology: geographic density of US dermatologists. Arch Dermatol. 2010;146:779.
- Feng H, Berk-Krauss J, Feng PW, et al. Comparison of dermatologist density between urban and rural counties in the United States. JAMA Dermatol. 2018;154:1265-1271.
- Landow SM, Oh DH, Weinstock MA. Teledermatology within the Veterans Health Administration, 2002-2014. Telemed J E Health. 2015;21:769-773.
- Armstrong AW, Kwong MW, Ledo L, et al. Practice models and challenges in teledermatology: a study of collective experiences from teledermatologists. PloS One. 2011;6:e28687.
- Lewis H, Becevic M, Myers D, et al. Dermatology ECHO—an innovative solution to address limited access to dermatology expertise. Rural Remote Health. 2018;18:4415.
- Edison KE, Dyer JA, Whited JD, et al. Practice gaps. the barriers and the promise of teledermatology. JAMA Dermatol. 2012:148:650-651.
To the Editor:
There is an irrefutable trend toward urban dermatology practice in the United States, leading to growing problems with rural access to care. The provision of rural clinical experiences and telehealth in dermatology residency training might increase the likelihood of trainees establishing a rural practice.
In 2017, the American Academy of Dermatology released an updated statement supporting direct patient access to board-certified dermatologists in an effort to reduce morbidity and mortality associated with skin disease.1 Twenty percent of the US population lives in a rural and medically underserved location, yet these areas remain largely underserved, in part because of an irrefutable trend toward urban dermatology practice.2-4 Successful approaches to improving rural access to dermatology care are poorly defined in the literature.
Several variables have been shown to influence a young physician’s decision to establish a clinical practice in geographically isolated areas, including rural upbringing, longitudinal rural clinical experiences during medical training, and family influences.5 Location of residency training is an additional variable that impacts practice location, though migration following dermatology residency is a complex phenomenon. However, training location does not guarantee retention of dermatology graduates in any particular geographic area.6 Practice incentives and stipends might encourage rural dermatology practice, yet these programs are underfunded. Last, telemedicine in dermatology (including teledermatology and teledermoscopy), though not always an ideal substitute for a live visit, can improve access to care in geographically isolated or underserved areas in general.7-9
Focused recruitment of medical students interested in rural dermatology practice to accredited dermatology residency programs aligned with this goal represents another approach to improve geographic diversity in the field of dermatology. Online access to this information would be useful for both applicants and their mentors.
We assessed viewable online curricula related to rural dermatology and telemedicine experiences at all Accreditation Council for Graduate Medical Education (ACGME)–accredited residency programs. Telemedicine experiences at Veterans Health Administration (VHA) health systems also were assessed.
Methods
This study was exempt from review by the institutional review board at the University of Minnesota (Minneapolis, Minnesota)(IRB #STUDY00004915) because no human subjects were involved. Online curricula of all ACGME-accredited dermatology residency programs in the United States and Puerto Rico were reviewed from November to December 2018. The following information was recorded: specialized “rural-track” training; optional elective time in rural settings; teledermatology training; and teledermoscopy training.
Additionally, population density at each program’s primary location was determined using US Census Bureau data and with consideration to communities contained within particular Metropolitan Statistical Areas (MSAs)(eTable). Data were obtained from the VHA system to assess teledermatology services at VHA locations affiliated with residency programs.
Results
Of 154 dermatology residency programs identified in the United States and Puerto Rico, 142 were accredited at the time of data collection. Fifteen (10%) were based in communities of 50,000 individuals or fewer that were not near a large metropolitan area. One program (<1%) offered a specific rural track. Fifty-six programs (39%) cited optional rotations or clinical electives, or both, that could be utilized for a rural experience. Eighteen (12%) offered teledermatology experiences and 1 (<1%) offered teledermoscopy during training. Fifty-three programs (37%) offered a rotation at a VHA hospital that had an active teledermatology service.
Comment
Program websites are a free and easily accessible means of acquiring relevant information. The paucity of readily available data on rural dermatology and teledermatology opportunities is unfortunate and a detriment to dermatology residency applicants interested in rural practice, which may result in a missed opportunity to foster a true passion for rural medicine. A brief comment on a website can be impactful, leading to a postgraduate year 4 dermatology elective rotation at a prospective fellowship training site or a rural dermatology experience.
The paucity of dermatologists working directly in rural areas has led to development of teledermatology initiatives to reach deeply into underserved regions. One of the largest providers of teledermatology is the VHA, which standardized its teledermatology efforts in 2012 and provides remarkable educational opportunities for dermatology residents. However, many residency program and VHA websites provide no information about the participation of dermatology residents in the provision of teledermatology services.
A limitation of this study is that it is based on online published curricula. Dermatology residency programs with excellent rural curricula that are not published online might exist.
Residency program directors with an interest in geographic diversity are encouraged to provide rural and teledermatology opportunities and to update these offerings on their websites, which is a simple modifiable strategy that can impact the rural dermatology care gap by recruiting students interested in filling this role. These efforts should be studied to determine whether this strategy impacts resident selection as well as whether focused rural and telemedicine exposure during training increases the likelihood of establishing a rural dermatology practice in the future.
To the Editor:
There is an irrefutable trend toward urban dermatology practice in the United States, leading to growing problems with rural access to care. The provision of rural clinical experiences and telehealth in dermatology residency training might increase the likelihood of trainees establishing a rural practice.
In 2017, the American Academy of Dermatology released an updated statement supporting direct patient access to board-certified dermatologists in an effort to reduce morbidity and mortality associated with skin disease.1 Twenty percent of the US population lives in a rural and medically underserved location, yet these areas remain largely underserved, in part because of an irrefutable trend toward urban dermatology practice.2-4 Successful approaches to improving rural access to dermatology care are poorly defined in the literature.
Several variables have been shown to influence a young physician’s decision to establish a clinical practice in geographically isolated areas, including rural upbringing, longitudinal rural clinical experiences during medical training, and family influences.5 Location of residency training is an additional variable that impacts practice location, though migration following dermatology residency is a complex phenomenon. However, training location does not guarantee retention of dermatology graduates in any particular geographic area.6 Practice incentives and stipends might encourage rural dermatology practice, yet these programs are underfunded. Last, telemedicine in dermatology (including teledermatology and teledermoscopy), though not always an ideal substitute for a live visit, can improve access to care in geographically isolated or underserved areas in general.7-9
Focused recruitment of medical students interested in rural dermatology practice to accredited dermatology residency programs aligned with this goal represents another approach to improve geographic diversity in the field of dermatology. Online access to this information would be useful for both applicants and their mentors.
We assessed viewable online curricula related to rural dermatology and telemedicine experiences at all Accreditation Council for Graduate Medical Education (ACGME)–accredited residency programs. Telemedicine experiences at Veterans Health Administration (VHA) health systems also were assessed.
Methods
This study was exempt from review by the institutional review board at the University of Minnesota (Minneapolis, Minnesota)(IRB #STUDY00004915) because no human subjects were involved. Online curricula of all ACGME-accredited dermatology residency programs in the United States and Puerto Rico were reviewed from November to December 2018. The following information was recorded: specialized “rural-track” training; optional elective time in rural settings; teledermatology training; and teledermoscopy training.
Additionally, population density at each program’s primary location was determined using US Census Bureau data and with consideration to communities contained within particular Metropolitan Statistical Areas (MSAs)(eTable). Data were obtained from the VHA system to assess teledermatology services at VHA locations affiliated with residency programs.
Results
Of 154 dermatology residency programs identified in the United States and Puerto Rico, 142 were accredited at the time of data collection. Fifteen (10%) were based in communities of 50,000 individuals or fewer that were not near a large metropolitan area. One program (<1%) offered a specific rural track. Fifty-six programs (39%) cited optional rotations or clinical electives, or both, that could be utilized for a rural experience. Eighteen (12%) offered teledermatology experiences and 1 (<1%) offered teledermoscopy during training. Fifty-three programs (37%) offered a rotation at a VHA hospital that had an active teledermatology service.
Comment
Program websites are a free and easily accessible means of acquiring relevant information. The paucity of readily available data on rural dermatology and teledermatology opportunities is unfortunate and a detriment to dermatology residency applicants interested in rural practice, which may result in a missed opportunity to foster a true passion for rural medicine. A brief comment on a website can be impactful, leading to a postgraduate year 4 dermatology elective rotation at a prospective fellowship training site or a rural dermatology experience.
The paucity of dermatologists working directly in rural areas has led to development of teledermatology initiatives to reach deeply into underserved regions. One of the largest providers of teledermatology is the VHA, which standardized its teledermatology efforts in 2012 and provides remarkable educational opportunities for dermatology residents. However, many residency program and VHA websites provide no information about the participation of dermatology residents in the provision of teledermatology services.
A limitation of this study is that it is based on online published curricula. Dermatology residency programs with excellent rural curricula that are not published online might exist.
Residency program directors with an interest in geographic diversity are encouraged to provide rural and teledermatology opportunities and to update these offerings on their websites, which is a simple modifiable strategy that can impact the rural dermatology care gap by recruiting students interested in filling this role. These efforts should be studied to determine whether this strategy impacts resident selection as well as whether focused rural and telemedicine exposure during training increases the likelihood of establishing a rural dermatology practice in the future.
- American Academy of Dermatology. Position statement on access to specialty care and direct access to dermatologic care. Revised May 20, 2017. Accessed December 13, 2020. https://server.aad.org/forms/Policies/Uploads/PS/PS-Access%20to%20Specialty%20Care%20and%20Direct%20Access%20to%20Dermatologic%20Care.pdf
- Dill MJ, Salsberg ES. The Complexities of Physician Supply and Demand: Projections Through 2025. Center for Workforce Studies, Association of American Medical Colleges (AAMC); November 2008. Accessed December 13, 2020. http://innovationlabs.com/pa_future/1/background_docs/AAMC%20Complexities%20of%20physician%20demand,%202008.pdf
- Glazer AM, Rigel DS. Analysis of trends in geographic distribution of US dermatology workforce density. JAMA Dermatol. 2017;153:472-473.
- Yoo JY, Rigel DS. Trends in dermatology: geographic density of US dermatologists. Arch Dermatol. 2010;146:779.
- Feng H, Berk-Krauss J, Feng PW, et al. Comparison of dermatologist density between urban and rural counties in the United States. JAMA Dermatol. 2018;154:1265-1271.
- Landow SM, Oh DH, Weinstock MA. Teledermatology within the Veterans Health Administration, 2002-2014. Telemed J E Health. 2015;21:769-773.
- Armstrong AW, Kwong MW, Ledo L, et al. Practice models and challenges in teledermatology: a study of collective experiences from teledermatologists. PloS One. 2011;6:e28687.
- Lewis H, Becevic M, Myers D, et al. Dermatology ECHO—an innovative solution to address limited access to dermatology expertise. Rural Remote Health. 2018;18:4415.
- Edison KE, Dyer JA, Whited JD, et al. Practice gaps. the barriers and the promise of teledermatology. JAMA Dermatol. 2012:148:650-651.
- American Academy of Dermatology. Position statement on access to specialty care and direct access to dermatologic care. Revised May 20, 2017. Accessed December 13, 2020. https://server.aad.org/forms/Policies/Uploads/PS/PS-Access%20to%20Specialty%20Care%20and%20Direct%20Access%20to%20Dermatologic%20Care.pdf
- Dill MJ, Salsberg ES. The Complexities of Physician Supply and Demand: Projections Through 2025. Center for Workforce Studies, Association of American Medical Colleges (AAMC); November 2008. Accessed December 13, 2020. http://innovationlabs.com/pa_future/1/background_docs/AAMC%20Complexities%20of%20physician%20demand,%202008.pdf
- Glazer AM, Rigel DS. Analysis of trends in geographic distribution of US dermatology workforce density. JAMA Dermatol. 2017;153:472-473.
- Yoo JY, Rigel DS. Trends in dermatology: geographic density of US dermatologists. Arch Dermatol. 2010;146:779.
- Feng H, Berk-Krauss J, Feng PW, et al. Comparison of dermatologist density between urban and rural counties in the United States. JAMA Dermatol. 2018;154:1265-1271.
- Landow SM, Oh DH, Weinstock MA. Teledermatology within the Veterans Health Administration, 2002-2014. Telemed J E Health. 2015;21:769-773.
- Armstrong AW, Kwong MW, Ledo L, et al. Practice models and challenges in teledermatology: a study of collective experiences from teledermatologists. PloS One. 2011;6:e28687.
- Lewis H, Becevic M, Myers D, et al. Dermatology ECHO—an innovative solution to address limited access to dermatology expertise. Rural Remote Health. 2018;18:4415.
- Edison KE, Dyer JA, Whited JD, et al. Practice gaps. the barriers and the promise of teledermatology. JAMA Dermatol. 2012:148:650-651.
Practice Points
- Access to dermatologic care in rural areas is a growing problem.
- Dermatology residency programs can influence medical students and resident dermatologists to provide care in rural and geographically isolated areas.
- Presenting detailed curricula that impact access to care on residency program websites could attract applicants with these career goals.
Racism in medicine: Implicit and explicit
With the shootings of Breonna Taylor, George Floyd, and other Black citizens setting off protests and unrest, race was at the forefront of national conversation in the United States – along with COVID-19 – over the past year.

“We’ve heard things like, ‘We’re in a post-racial society,’ but I think 2020 in particular has emphasized that we’re not,” said Gregory Johnson, MD, SFHM, chief medical officer of hospital medicine at Sound Physicians, a national physician practice. “Racism is very present in our lives, it’s very present in our world, and it is absolutely present in medicine.”
Yes, race is still an issue in the U.S. as we head into 2021, though this may have come as something of a surprise to people who do not live with racism daily.
“If you have a brain, you have bias, and that bias will likely apply to race as well,” Dr. Johnson said. “When we’re talking about institutional racism, the educational system and the media have led us to create presumptions and prejudices that we don’t necessarily recognize off the top because they’ve just been a part of the fabric of who we are as we’ve grown up.”
The term “racism” has extremely negative connotations because there’s character judgment attached to it, but to say someone is racist or racially insensitive does not equate them with being a Klansman, said Dr. Johnson. “I think we as people have to acknowledge that, yes, it’s possible for me to be racist and I might not be 100% aware of it. It’s being open to the possibility – or rather probability – that you are and then taking steps to figure out how you can address that, so you can limit it. And that requires constant self-evaluation and work,” he said.
Racism in the medical environment
Institutional racism is evident before students are even accepted into medical school, said Areeba Kara, MD, SFHM, associate professor of clinical medicine at Indiana University, Indianapolis, and a hospitalist at IU Health Physicians.

Mean MCAT scores are lower for applicants traditionally underrepresented in medicine (UIM) compared to the scores of well-represented groups.1 “Lower scores are associated with lower acceptance rates into medical school,” Dr. Kara said. “These differences reflect unequal educational opportunities rooted in centuries of legal discrimination.”
Racism is apparent in both the hidden medical education curriculum and in lessons implicitly taught to students, said Ndidi Unaka, MD, MEd, associate program director of the pediatric residency training program at Cincinnati Children’s Hospital.
“These lessons inform the way in which we as physicians see our patients, each other, and how we practice,” she said. “We reinforce race-based medicine and shape clinical decision making through flawed guidelines and practices, which exacerbates health inequities. We teach that race – rather than racism – is a risk factor for poor health outcomes. Our students and trainees watch as we assume the worst of our patients from marginalized communities of color.”
Terms describing patients of color, such as “difficult,” “non-compliant,” or “frequent flyer” are thrown around and sometimes, instead of finding out why, “we view these states of being as static, root causes for poor outcomes rather than symptoms of social conditions and obstacles that impact overall health and wellbeing,” Dr. Unaka said.

Leadership opportunities
Though hospital medicine is a growing field, Dr. Kara noted that the 2020 State of Hospital Medicine Report found that only 5.5% of hospital medical group leaders were Black, and just 2.2% were Hispanic/Latino.2 “I think these numbers speak for themselves,” she said.
Dr. Unaka said that the lack of UIM hospitalists and physician leaders creates fewer opportunities for “race-concordant mentorship relationships.” It also forces UIM physicians to shoulder more responsibilities – often obligations that do little to help them move forward in their careers – all in the name of diversity. And when UIM physicians are given leadership opportunities, Dr. Unaka said they are often unsure as to whether their appointments are genuine or just a hollow gesture made for the sake of diversity.
Dr. Johnson pointed out that Black and Latinx populations primarily get their care from hospital-based specialties, yet this is not reflected in the number of UIM practitioners in leadership roles. He said race and ethnicity, as well as gender, need to be factors when individuals are evaluated for leadership opportunities – for the individual’s sake, as well as for the community he or she is serving.
“When we can evaluate for unconscious bias and factor in that diverse groups tend to have better outcomes, whether it’s business or clinical outcomes, it’s one of the opportunities that we collectively have in the specialty to improve what we’re delivering for hospitals and, more importantly, for patients,” he said.
Relationships with colleagues and patients
Racism creeps into interactions and relationships with others as well, whether it’s between clinicians, clinician to patient, or patient to clinician. Sometimes it’s blatant; often it’s subtle.
A common, recurring example Dr. Unaka has experienced in the clinician to clinician relationship is being confused for other Black physicians, making her feel invisible. “The everyday verbal, nonverbal, and environmental slights, snubs, or insults from colleagues are frequent and contribute to feelings of exclusion, isolation, and exhaustion,” she said. Despite this, she is still expected to “address microaggressions and other forms of interpersonal racism and find ways to move through professional spaces in spite of the trauma, fear, and stress associated with my reality and lived experiences.” She said that clinicians who remain silent on the topic of racism participate in the violence and contribute to the disillusionment of UIM physicians.
Dr. Kara said that the discrimination from the health care team is the hardest to deal with. In the clinician to clinician relationship, there is a sense among UIM physicians that they’re being watched more closely and “have to prove themselves at every single turn.” Unfortunately, this comes from the environment, which tends to be adversarial rather than supportive and nurturing, she said.
“There are lots of opportunities for racism or racial insensitivity to crop up from clinician to clinician,” said Dr. Johnson. When he started his career as a physician after his training, Dr. Johnson was informed that his colleagues were watching him because they were not sure about his clinical skills. The fact that he was a former chief resident and board certified in two specialties did not seem to make any difference.
Patients refusing care from UIM physicians or expressing disapproval – both verbal and nonverbal – of such care, happens all too often. “It’s easier for me to excuse patients and their families as we often meet them on their worst days,” said Dr. Kara. Still, “understanding my oath to care for people and do no harm, but at the same time, recognizing that this is an individual that is rejecting my care without having any idea of who I am as a physician is frustrating,” Dr. Johnson acknowledged.
Then there’s the complex clinician to patient relationship, which research clearly shows contributes to health disparities.3 For one thing, the physician workforce does not reflect the patient population, Dr. Unaka said. “We cannot ignore the lack of race concordance between patients and clinicians, nor can the continued misplacement of blame for medical mistrust be at the feet of our patients,” she said.
Dr. Unaka feels that clinicians need to accept both that health inequities exist and that frontline physicians themselves contribute to the inequities. “Our diagnostic and therapeutic decisions are not immune to bias and are influenced by our deeply held beliefs about specific populations,” she said. “And the health care system that our patients navigate is no different than other systems, settings, and environments that are marred by racism in all its forms.”
Systemic racism greatly impacts patient care, said Dr. Kara. She pointed to several examples: Research showing that race concordance between patients and providers in an emergency department setting led to better pain control with fewer analgesics.4 The high maternal and infant mortality rates amongst Black women and children.5 Evidence of poorer outcomes in sepsis patients with limited English proficiency.6 “There are plenty more,” she said. “We need to be asking ourselves what we are going to do about it.”
Moving forward
That racial biases are steeped so thoroughly into our culture and consciousness means that moving beyond them is a continual, purposeful work in progress. But it is work that is critical for everyone, and certainly necessary for those who care for their fellow human beings when they are in a vulnerable state.
Health care systems need to move toward equity – giving everyone what they need to thrive – rather than focusing on equality – giving everyone the same thing, said Jenny Baenziger, MD, assistant professor of clinical medicine and pediatrics at Indiana University, Indianapolis, and associate director of education at IU Center for Global Health. “We know that minoritized patients are going to need more attention, more advocacy, more sensitivity, and more creative solutions in order to help them achieve health in a world that is often stacked against them,” she said.

“The unique needs of each patient, family unit, and/or population must be taken into consideration,” said Dr. Unaka. She said hospitalists need to embrace creative approaches that can better serve the specific needs of patients. Equitable practices should be the default, which means data transparency, thoroughly dissecting hospital processes to find existing inequities, giving stakeholders – especially patients and families of color – a voice, and tearing down oppressive systems that contribute to poor health outcomes and oppression, she said.
“It’s time for us to talk about racism openly,” said Dr. Kara. “Believe your colleagues when they share their fears and treat each other with respect. We should be actively learning about and celebrating our diversity.” She encourages finding out what your institution is doing on this front and getting involved.
Dr. Johnson believes that first and foremost, hospitalists need to be exposed to the data on health care disparities. “The next step is asking what we as hospitalists, or any other specialty, can do to intervene and improve in those areas,” he said. Focusing on unconscious bias training is important, he said, so clinicians can see what biases they might be bringing into the hospital and to the bedside. Maintaining a diverse workforce and bringing UIM physicians into leadership roles to encourage diversity of ideas and approaches are also critical to promoting equity, he said.
“You cannot fix what you cannot face,” said Dr. Unaka. Education on how racism impacts patients and colleagues is essential, she believes, as is advocacy for changing inequitable health system policies. She recommends expanding social and professional circles. “Diverse social groups allow us to consider the perspectives of others; diverse professional groups allow us to ask better research questions and practice better medicine.”
Start by developing the ability to question personal assumptions and pinpoint implicit biases, suggested Dr. Baenziger. “Asking for feedback can be scary and difficult, but we should take a deep breath and do it anyway,” she said. “Simply ask your team, ‘I’ve been thinking a lot about racial equity and disparities. How can I do better at my interactions with people of color? What are my blind spots?’” Dr. Baenziger said that “to help us remember how beautifully complicated and diverse people are,” all health care professionals need to watch Nigerian novelist Chimamanda Ngozi Adichie’s TED talk “The Danger of a Single Story.”
Dr. Baenziger also stressed the importance of conversations about “places where race is built into our clinical assessments, like eGFR,” as well as being aware that many of the research studies that are used to support everyday clinical decisions didn’t include people of color. She also encouraged clinicians to consider how and when they include race in their notes.7 “Is it really helpful to make sure people know right away that you are treating a ‘46-year-old Hispanic male’ or can the fact that he is Hispanic be saved for the social history section with other important details of his life such as being a father, veteran, and mechanic?” she asked.
“Racism is real and very much a part of our history. We can no longer be in denial regarding the racism that exists in medicine and the impact it has on our patients,” Dr. Unaka said. “As a profession, we cannot hide behind our espoused core values. We must live up to them.”
References
1. Lucey CR, Saguil, A. The Consequences of Structural Racism on MCAT Scores and Medical School Admissions: The Past Is Prologue. Acad Med. 2020 Mar;95(3):351-356. doi: 10.1097/ACM.0000000000002939.
2. Flores L. Increasing racial diversity in hospital medicine’s leadership ranks. The Hospitalist. 2020 Oct 21.
3. Smedley BD, et al, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Institute of Medicine Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Washington: National Academies Press; 2003.
4. Heins A, et al. Physician Race/Ethnicity Predicts Successful Emergency Department Analgesia. J Pain. 2010 July;11(7):692-697. doi: 10.1016/j.jpain.2009.10.017.
5. U.S. Department of Health and Human Serves, Office of Minority Health. Infant Mortality and African Americans. 2019 Nov 8. minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=23.
6. Jacobs ZG, et al. The Association between Limited English Proficiency and Sepsis Mortality. J Hosp Med. 2020;3;140-146. Published Online First 2019 Nov 20. doi:10.12788/jhm.3334.
7. Finucane TE. Mention of a Patient’s “Race” in Clinical Presentations. Virtual Mentor. 2014;16(6):423-427. doi: 10.1001/virtualmentor.2014.16.6.ecas1-1406.
With the shootings of Breonna Taylor, George Floyd, and other Black citizens setting off protests and unrest, race was at the forefront of national conversation in the United States – along with COVID-19 – over the past year.
“We’ve heard things like, ‘We’re in a post-racial society,’ but I think 2020 in particular has emphasized that we’re not,” said Gregory Johnson, MD, SFHM, chief medical officer of hospital medicine at Sound Physicians, a national physician practice. “Racism is very present in our lives, it’s very present in our world, and it is absolutely present in medicine.”
Yes, race is still an issue in the U.S. as we head into 2021, though this may have come as something of a surprise to people who do not live with racism daily.
“If you have a brain, you have bias, and that bias will likely apply to race as well,” Dr. Johnson said. “When we’re talking about institutional racism, the educational system and the media have led us to create presumptions and prejudices that we don’t necessarily recognize off the top because they’ve just been a part of the fabric of who we are as we’ve grown up.”
The term “racism” has extremely negative connotations because there’s character judgment attached to it, but to say someone is racist or racially insensitive does not equate them with being a Klansman, said Dr. Johnson. “I think we as people have to acknowledge that, yes, it’s possible for me to be racist and I might not be 100% aware of it. It’s being open to the possibility – or rather probability – that you are and then taking steps to figure out how you can address that, so you can limit it. And that requires constant self-evaluation and work,” he said.
Racism in the medical environment
Institutional racism is evident before students are even accepted into medical school, said Areeba Kara, MD, SFHM, associate professor of clinical medicine at Indiana University, Indianapolis, and a hospitalist at IU Health Physicians.
Mean MCAT scores are lower for applicants traditionally underrepresented in medicine (UIM) compared to the scores of well-represented groups.1 “Lower scores are associated with lower acceptance rates into medical school,” Dr. Kara said. “These differences reflect unequal educational opportunities rooted in centuries of legal discrimination.”
Racism is apparent in both the hidden medical education curriculum and in lessons implicitly taught to students, said Ndidi Unaka, MD, MEd, associate program director of the pediatric residency training program at Cincinnati Children’s Hospital.
“These lessons inform the way in which we as physicians see our patients, each other, and how we practice,” she said. “We reinforce race-based medicine and shape clinical decision making through flawed guidelines and practices, which exacerbates health inequities. We teach that race – rather than racism – is a risk factor for poor health outcomes. Our students and trainees watch as we assume the worst of our patients from marginalized communities of color.”
Terms describing patients of color, such as “difficult,” “non-compliant,” or “frequent flyer” are thrown around and sometimes, instead of finding out why, “we view these states of being as static, root causes for poor outcomes rather than symptoms of social conditions and obstacles that impact overall health and wellbeing,” Dr. Unaka said.
Leadership opportunities
Though hospital medicine is a growing field, Dr. Kara noted that the 2020 State of Hospital Medicine Report found that only 5.5% of hospital medical group leaders were Black, and just 2.2% were Hispanic/Latino.2 “I think these numbers speak for themselves,” she said.
Dr. Unaka said that the lack of UIM hospitalists and physician leaders creates fewer opportunities for “race-concordant mentorship relationships.” It also forces UIM physicians to shoulder more responsibilities – often obligations that do little to help them move forward in their careers – all in the name of diversity. And when UIM physicians are given leadership opportunities, Dr. Unaka said they are often unsure as to whether their appointments are genuine or just a hollow gesture made for the sake of diversity.
Dr. Johnson pointed out that Black and Latinx populations primarily get their care from hospital-based specialties, yet this is not reflected in the number of UIM practitioners in leadership roles. He said race and ethnicity, as well as gender, need to be factors when individuals are evaluated for leadership opportunities – for the individual’s sake, as well as for the community he or she is serving.
“When we can evaluate for unconscious bias and factor in that diverse groups tend to have better outcomes, whether it’s business or clinical outcomes, it’s one of the opportunities that we collectively have in the specialty to improve what we’re delivering for hospitals and, more importantly, for patients,” he said.
Relationships with colleagues and patients
Racism creeps into interactions and relationships with others as well, whether it’s between clinicians, clinician to patient, or patient to clinician. Sometimes it’s blatant; often it’s subtle.
A common, recurring example Dr. Unaka has experienced in the clinician to clinician relationship is being confused for other Black physicians, making her feel invisible. “The everyday verbal, nonverbal, and environmental slights, snubs, or insults from colleagues are frequent and contribute to feelings of exclusion, isolation, and exhaustion,” she said. Despite this, she is still expected to “address microaggressions and other forms of interpersonal racism and find ways to move through professional spaces in spite of the trauma, fear, and stress associated with my reality and lived experiences.” She said that clinicians who remain silent on the topic of racism participate in the violence and contribute to the disillusionment of UIM physicians.
Dr. Kara said that the discrimination from the health care team is the hardest to deal with. In the clinician to clinician relationship, there is a sense among UIM physicians that they’re being watched more closely and “have to prove themselves at every single turn.” Unfortunately, this comes from the environment, which tends to be adversarial rather than supportive and nurturing, she said.
“There are lots of opportunities for racism or racial insensitivity to crop up from clinician to clinician,” said Dr. Johnson. When he started his career as a physician after his training, Dr. Johnson was informed that his colleagues were watching him because they were not sure about his clinical skills. The fact that he was a former chief resident and board certified in two specialties did not seem to make any difference.
Patients refusing care from UIM physicians or expressing disapproval – both verbal and nonverbal – of such care, happens all too often. “It’s easier for me to excuse patients and their families as we often meet them on their worst days,” said Dr. Kara. Still, “understanding my oath to care for people and do no harm, but at the same time, recognizing that this is an individual that is rejecting my care without having any idea of who I am as a physician is frustrating,” Dr. Johnson acknowledged.
Then there’s the complex clinician to patient relationship, which research clearly shows contributes to health disparities.3 For one thing, the physician workforce does not reflect the patient population, Dr. Unaka said. “We cannot ignore the lack of race concordance between patients and clinicians, nor can the continued misplacement of blame for medical mistrust be at the feet of our patients,” she said.
Dr. Unaka feels that clinicians need to accept both that health inequities exist and that frontline physicians themselves contribute to the inequities. “Our diagnostic and therapeutic decisions are not immune to bias and are influenced by our deeply held beliefs about specific populations,” she said. “And the health care system that our patients navigate is no different than other systems, settings, and environments that are marred by racism in all its forms.”
Systemic racism greatly impacts patient care, said Dr. Kara. She pointed to several examples: Research showing that race concordance between patients and providers in an emergency department setting led to better pain control with fewer analgesics.4 The high maternal and infant mortality rates amongst Black women and children.5 Evidence of poorer outcomes in sepsis patients with limited English proficiency.6 “There are plenty more,” she said. “We need to be asking ourselves what we are going to do about it.”
Moving forward
That racial biases are steeped so thoroughly into our culture and consciousness means that moving beyond them is a continual, purposeful work in progress. But it is work that is critical for everyone, and certainly necessary for those who care for their fellow human beings when they are in a vulnerable state.
Health care systems need to move toward equity – giving everyone what they need to thrive – rather than focusing on equality – giving everyone the same thing, said Jenny Baenziger, MD, assistant professor of clinical medicine and pediatrics at Indiana University, Indianapolis, and associate director of education at IU Center for Global Health. “We know that minoritized patients are going to need more attention, more advocacy, more sensitivity, and more creative solutions in order to help them achieve health in a world that is often stacked against them,” she said.
“The unique needs of each patient, family unit, and/or population must be taken into consideration,” said Dr. Unaka. She said hospitalists need to embrace creative approaches that can better serve the specific needs of patients. Equitable practices should be the default, which means data transparency, thoroughly dissecting hospital processes to find existing inequities, giving stakeholders – especially patients and families of color – a voice, and tearing down oppressive systems that contribute to poor health outcomes and oppression, she said.
“It’s time for us to talk about racism openly,” said Dr. Kara. “Believe your colleagues when they share their fears and treat each other with respect. We should be actively learning about and celebrating our diversity.” She encourages finding out what your institution is doing on this front and getting involved.
Dr. Johnson believes that first and foremost, hospitalists need to be exposed to the data on health care disparities. “The next step is asking what we as hospitalists, or any other specialty, can do to intervene and improve in those areas,” he said. Focusing on unconscious bias training is important, he said, so clinicians can see what biases they might be bringing into the hospital and to the bedside. Maintaining a diverse workforce and bringing UIM physicians into leadership roles to encourage diversity of ideas and approaches are also critical to promoting equity, he said.
“You cannot fix what you cannot face,” said Dr. Unaka. Education on how racism impacts patients and colleagues is essential, she believes, as is advocacy for changing inequitable health system policies. She recommends expanding social and professional circles. “Diverse social groups allow us to consider the perspectives of others; diverse professional groups allow us to ask better research questions and practice better medicine.”
Start by developing the ability to question personal assumptions and pinpoint implicit biases, suggested Dr. Baenziger. “Asking for feedback can be scary and difficult, but we should take a deep breath and do it anyway,” she said. “Simply ask your team, ‘I’ve been thinking a lot about racial equity and disparities. How can I do better at my interactions with people of color? What are my blind spots?’” Dr. Baenziger said that “to help us remember how beautifully complicated and diverse people are,” all health care professionals need to watch Nigerian novelist Chimamanda Ngozi Adichie’s TED talk “The Danger of a Single Story.”
Dr. Baenziger also stressed the importance of conversations about “places where race is built into our clinical assessments, like eGFR,” as well as being aware that many of the research studies that are used to support everyday clinical decisions didn’t include people of color. She also encouraged clinicians to consider how and when they include race in their notes.7 “Is it really helpful to make sure people know right away that you are treating a ‘46-year-old Hispanic male’ or can the fact that he is Hispanic be saved for the social history section with other important details of his life such as being a father, veteran, and mechanic?” she asked.
“Racism is real and very much a part of our history. We can no longer be in denial regarding the racism that exists in medicine and the impact it has on our patients,” Dr. Unaka said. “As a profession, we cannot hide behind our espoused core values. We must live up to them.”
References
1. Lucey CR, Saguil, A. The Consequences of Structural Racism on MCAT Scores and Medical School Admissions: The Past Is Prologue. Acad Med. 2020 Mar;95(3):351-356. doi: 10.1097/ACM.0000000000002939.
2. Flores L. Increasing racial diversity in hospital medicine’s leadership ranks. The Hospitalist. 2020 Oct 21.
3. Smedley BD, et al, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Institute of Medicine Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Washington: National Academies Press; 2003.
4. Heins A, et al. Physician Race/Ethnicity Predicts Successful Emergency Department Analgesia. J Pain. 2010 July;11(7):692-697. doi: 10.1016/j.jpain.2009.10.017.
5. U.S. Department of Health and Human Serves, Office of Minority Health. Infant Mortality and African Americans. 2019 Nov 8. minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=23.
6. Jacobs ZG, et al. The Association between Limited English Proficiency and Sepsis Mortality. J Hosp Med. 2020;3;140-146. Published Online First 2019 Nov 20. doi:10.12788/jhm.3334.
7. Finucane TE. Mention of a Patient’s “Race” in Clinical Presentations. Virtual Mentor. 2014;16(6):423-427. doi: 10.1001/virtualmentor.2014.16.6.ecas1-1406.
With the shootings of Breonna Taylor, George Floyd, and other Black citizens setting off protests and unrest, race was at the forefront of national conversation in the United States – along with COVID-19 – over the past year.
“We’ve heard things like, ‘We’re in a post-racial society,’ but I think 2020 in particular has emphasized that we’re not,” said Gregory Johnson, MD, SFHM, chief medical officer of hospital medicine at Sound Physicians, a national physician practice. “Racism is very present in our lives, it’s very present in our world, and it is absolutely present in medicine.”
Yes, race is still an issue in the U.S. as we head into 2021, though this may have come as something of a surprise to people who do not live with racism daily.
“If you have a brain, you have bias, and that bias will likely apply to race as well,” Dr. Johnson said. “When we’re talking about institutional racism, the educational system and the media have led us to create presumptions and prejudices that we don’t necessarily recognize off the top because they’ve just been a part of the fabric of who we are as we’ve grown up.”
The term “racism” has extremely negative connotations because there’s character judgment attached to it, but to say someone is racist or racially insensitive does not equate them with being a Klansman, said Dr. Johnson. “I think we as people have to acknowledge that, yes, it’s possible for me to be racist and I might not be 100% aware of it. It’s being open to the possibility – or rather probability – that you are and then taking steps to figure out how you can address that, so you can limit it. And that requires constant self-evaluation and work,” he said.
Racism in the medical environment
Institutional racism is evident before students are even accepted into medical school, said Areeba Kara, MD, SFHM, associate professor of clinical medicine at Indiana University, Indianapolis, and a hospitalist at IU Health Physicians.
Mean MCAT scores are lower for applicants traditionally underrepresented in medicine (UIM) compared to the scores of well-represented groups.1 “Lower scores are associated with lower acceptance rates into medical school,” Dr. Kara said. “These differences reflect unequal educational opportunities rooted in centuries of legal discrimination.”
Racism is apparent in both the hidden medical education curriculum and in lessons implicitly taught to students, said Ndidi Unaka, MD, MEd, associate program director of the pediatric residency training program at Cincinnati Children’s Hospital.
“These lessons inform the way in which we as physicians see our patients, each other, and how we practice,” she said. “We reinforce race-based medicine and shape clinical decision making through flawed guidelines and practices, which exacerbates health inequities. We teach that race – rather than racism – is a risk factor for poor health outcomes. Our students and trainees watch as we assume the worst of our patients from marginalized communities of color.”
Terms describing patients of color, such as “difficult,” “non-compliant,” or “frequent flyer” are thrown around and sometimes, instead of finding out why, “we view these states of being as static, root causes for poor outcomes rather than symptoms of social conditions and obstacles that impact overall health and wellbeing,” Dr. Unaka said.
Leadership opportunities
Though hospital medicine is a growing field, Dr. Kara noted that the 2020 State of Hospital Medicine Report found that only 5.5% of hospital medical group leaders were Black, and just 2.2% were Hispanic/Latino.2 “I think these numbers speak for themselves,” she said.
Dr. Unaka said that the lack of UIM hospitalists and physician leaders creates fewer opportunities for “race-concordant mentorship relationships.” It also forces UIM physicians to shoulder more responsibilities – often obligations that do little to help them move forward in their careers – all in the name of diversity. And when UIM physicians are given leadership opportunities, Dr. Unaka said they are often unsure as to whether their appointments are genuine or just a hollow gesture made for the sake of diversity.
Dr. Johnson pointed out that Black and Latinx populations primarily get their care from hospital-based specialties, yet this is not reflected in the number of UIM practitioners in leadership roles. He said race and ethnicity, as well as gender, need to be factors when individuals are evaluated for leadership opportunities – for the individual’s sake, as well as for the community he or she is serving.
“When we can evaluate for unconscious bias and factor in that diverse groups tend to have better outcomes, whether it’s business or clinical outcomes, it’s one of the opportunities that we collectively have in the specialty to improve what we’re delivering for hospitals and, more importantly, for patients,” he said.
Relationships with colleagues and patients
Racism creeps into interactions and relationships with others as well, whether it’s between clinicians, clinician to patient, or patient to clinician. Sometimes it’s blatant; often it’s subtle.
A common, recurring example Dr. Unaka has experienced in the clinician to clinician relationship is being confused for other Black physicians, making her feel invisible. “The everyday verbal, nonverbal, and environmental slights, snubs, or insults from colleagues are frequent and contribute to feelings of exclusion, isolation, and exhaustion,” she said. Despite this, she is still expected to “address microaggressions and other forms of interpersonal racism and find ways to move through professional spaces in spite of the trauma, fear, and stress associated with my reality and lived experiences.” She said that clinicians who remain silent on the topic of racism participate in the violence and contribute to the disillusionment of UIM physicians.
Dr. Kara said that the discrimination from the health care team is the hardest to deal with. In the clinician to clinician relationship, there is a sense among UIM physicians that they’re being watched more closely and “have to prove themselves at every single turn.” Unfortunately, this comes from the environment, which tends to be adversarial rather than supportive and nurturing, she said.
“There are lots of opportunities for racism or racial insensitivity to crop up from clinician to clinician,” said Dr. Johnson. When he started his career as a physician after his training, Dr. Johnson was informed that his colleagues were watching him because they were not sure about his clinical skills. The fact that he was a former chief resident and board certified in two specialties did not seem to make any difference.
Patients refusing care from UIM physicians or expressing disapproval – both verbal and nonverbal – of such care, happens all too often. “It’s easier for me to excuse patients and their families as we often meet them on their worst days,” said Dr. Kara. Still, “understanding my oath to care for people and do no harm, but at the same time, recognizing that this is an individual that is rejecting my care without having any idea of who I am as a physician is frustrating,” Dr. Johnson acknowledged.
Then there’s the complex clinician to patient relationship, which research clearly shows contributes to health disparities.3 For one thing, the physician workforce does not reflect the patient population, Dr. Unaka said. “We cannot ignore the lack of race concordance between patients and clinicians, nor can the continued misplacement of blame for medical mistrust be at the feet of our patients,” she said.
Dr. Unaka feels that clinicians need to accept both that health inequities exist and that frontline physicians themselves contribute to the inequities. “Our diagnostic and therapeutic decisions are not immune to bias and are influenced by our deeply held beliefs about specific populations,” she said. “And the health care system that our patients navigate is no different than other systems, settings, and environments that are marred by racism in all its forms.”
Systemic racism greatly impacts patient care, said Dr. Kara. She pointed to several examples: Research showing that race concordance between patients and providers in an emergency department setting led to better pain control with fewer analgesics.4 The high maternal and infant mortality rates amongst Black women and children.5 Evidence of poorer outcomes in sepsis patients with limited English proficiency.6 “There are plenty more,” she said. “We need to be asking ourselves what we are going to do about it.”
Moving forward
That racial biases are steeped so thoroughly into our culture and consciousness means that moving beyond them is a continual, purposeful work in progress. But it is work that is critical for everyone, and certainly necessary for those who care for their fellow human beings when they are in a vulnerable state.
Health care systems need to move toward equity – giving everyone what they need to thrive – rather than focusing on equality – giving everyone the same thing, said Jenny Baenziger, MD, assistant professor of clinical medicine and pediatrics at Indiana University, Indianapolis, and associate director of education at IU Center for Global Health. “We know that minoritized patients are going to need more attention, more advocacy, more sensitivity, and more creative solutions in order to help them achieve health in a world that is often stacked against them,” she said.
“The unique needs of each patient, family unit, and/or population must be taken into consideration,” said Dr. Unaka. She said hospitalists need to embrace creative approaches that can better serve the specific needs of patients. Equitable practices should be the default, which means data transparency, thoroughly dissecting hospital processes to find existing inequities, giving stakeholders – especially patients and families of color – a voice, and tearing down oppressive systems that contribute to poor health outcomes and oppression, she said.
“It’s time for us to talk about racism openly,” said Dr. Kara. “Believe your colleagues when they share their fears and treat each other with respect. We should be actively learning about and celebrating our diversity.” She encourages finding out what your institution is doing on this front and getting involved.
Dr. Johnson believes that first and foremost, hospitalists need to be exposed to the data on health care disparities. “The next step is asking what we as hospitalists, or any other specialty, can do to intervene and improve in those areas,” he said. Focusing on unconscious bias training is important, he said, so clinicians can see what biases they might be bringing into the hospital and to the bedside. Maintaining a diverse workforce and bringing UIM physicians into leadership roles to encourage diversity of ideas and approaches are also critical to promoting equity, he said.
“You cannot fix what you cannot face,” said Dr. Unaka. Education on how racism impacts patients and colleagues is essential, she believes, as is advocacy for changing inequitable health system policies. She recommends expanding social and professional circles. “Diverse social groups allow us to consider the perspectives of others; diverse professional groups allow us to ask better research questions and practice better medicine.”
Start by developing the ability to question personal assumptions and pinpoint implicit biases, suggested Dr. Baenziger. “Asking for feedback can be scary and difficult, but we should take a deep breath and do it anyway,” she said. “Simply ask your team, ‘I’ve been thinking a lot about racial equity and disparities. How can I do better at my interactions with people of color? What are my blind spots?’” Dr. Baenziger said that “to help us remember how beautifully complicated and diverse people are,” all health care professionals need to watch Nigerian novelist Chimamanda Ngozi Adichie’s TED talk “The Danger of a Single Story.”
Dr. Baenziger also stressed the importance of conversations about “places where race is built into our clinical assessments, like eGFR,” as well as being aware that many of the research studies that are used to support everyday clinical decisions didn’t include people of color. She also encouraged clinicians to consider how and when they include race in their notes.7 “Is it really helpful to make sure people know right away that you are treating a ‘46-year-old Hispanic male’ or can the fact that he is Hispanic be saved for the social history section with other important details of his life such as being a father, veteran, and mechanic?” she asked.
“Racism is real and very much a part of our history. We can no longer be in denial regarding the racism that exists in medicine and the impact it has on our patients,” Dr. Unaka said. “As a profession, we cannot hide behind our espoused core values. We must live up to them.”
References
1. Lucey CR, Saguil, A. The Consequences of Structural Racism on MCAT Scores and Medical School Admissions: The Past Is Prologue. Acad Med. 2020 Mar;95(3):351-356. doi: 10.1097/ACM.0000000000002939.
2. Flores L. Increasing racial diversity in hospital medicine’s leadership ranks. The Hospitalist. 2020 Oct 21.
3. Smedley BD, et al, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Institute of Medicine Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Washington: National Academies Press; 2003.
4. Heins A, et al. Physician Race/Ethnicity Predicts Successful Emergency Department Analgesia. J Pain. 2010 July;11(7):692-697. doi: 10.1016/j.jpain.2009.10.017.
5. U.S. Department of Health and Human Serves, Office of Minority Health. Infant Mortality and African Americans. 2019 Nov 8. minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=23.
6. Jacobs ZG, et al. The Association between Limited English Proficiency and Sepsis Mortality. J Hosp Med. 2020;3;140-146. Published Online First 2019 Nov 20. doi:10.12788/jhm.3334.
7. Finucane TE. Mention of a Patient’s “Race” in Clinical Presentations. Virtual Mentor. 2014;16(6):423-427. doi: 10.1001/virtualmentor.2014.16.6.ecas1-1406.
Disparities in child abuse evaluation arise from implicit bias
according to research discussed by Tiffani J. Johnson, MD, an assistant professor of emergency medicine at the University of California, Davis.

“These disparities in child abuse evaluation and reporting are bidirectional,” she said. “We also recognize that abuse is more likely to be unrecognized in White children.”
Dr. Johnson presented data on the health disparities in child abuse reporting in a session at the annual meeting of the American Academy of Pediatrics, held virtually this year. Health care disparities, as defined by the National Academy of Sciences, refers to differences in the quality of care between minority and nonminority populations that are not caused by clinical appropriateness, access, need, or patient preference, she explained. Instead, they result from discrimination, bias, stereotyping, and uncertainty.
Disparities lead to harm in all children
For example, a 2018 systematic review found that Black and other non-White children were significantly more likely than White children to be evaluated with a skeletal survey. In one of the studies included, at a large urban academic center, Black and Latinx children with accidental fractures were 8.75 times more likely to undergo a skeletal survey than White children and 4.3 times more likely to be reported to child protective services.
“And let me emphasize that these are children who were ultimately found to have accidental fractures,” Dr. Johnson said.
Meanwhile, in an analysis of known cases of head trauma, researchers found that abuse was missed in 37% of White children, compared with 19% of non-White children.
“These only represent the tip of the iceberg as a true number of cases of abuse may never really be detected because some cases are still unknown,” Dr. Johnson told attendees. And the harm of these disparities runs in both directions.
“Failing to diagnose abuse in White children clearly puts them at increased risk for return visits and return evaluations for repeated abuse by the perpetrators,” she said. But harm also can result from overreporting and investigation, including psychological trauma and a waste of limited resources. Overinvestigation also can erode family-physician relationships and perpetuate distrust of medical care in communities of color.
Yet at the same time, it’s clear that Black children, adolescents, and young adults are not protected from harm in society more generally, when at home, where they learn, or where they play, Dr. Johnson said, referencing the deaths of Breonna Taylor and Tamir Rice as examples.
“And now we’re seeing increased evidence that children are not protected in the health care center when we think about the many disparities that have been identified in the care and outcomes of children, including the disproportionality in terms of child abuse evaluation and referrals,” Dr. Johnson said.
Racism is a root cause of that harm to Black children, she said, as the systemic structure of opportunities unfairly disadvantages some individuals and communities while unfairly advantaging others, thereby “sapping the strength of the whole society through the waste of human resources.”
Tonya Chaffee, MD, MPH, a clinical professor of health sciences at the University of California, San Francisco, who attended the session, said she particularly appreciated “seeing data on which racial/ethnic populations have child abuse reports made and the disparities that exist that are similar to what we are noticing in our own institution.”
Role of individual-level implicit bias and racism
While institutional and structural racism play a substantial role in health care disparities, Dr. Johnson focused primarily on the impact of personal racism when it comes to child abuse evaluations, through overt discrimination, explicit bias, implicit bias, and stigmatization. The most challenging of these to identify and acknowledge is often implicit bias, a tendency to believe, even unconsciously, that some people or ideas are better than others, which results in unfair treatment.
For example, a 2016 study found that half of medical students and residents held at least one biological belief about differences between Black and White individuals that was actually false, such as Black people having more pain tolerance or stronger bones than White people, which then affected treatment recommendations.
“Implicit bias refers to our attitudes that lie below the surface, but they can still influence our behaviors,” Dr. Johnson explained. She encouraged providers to take the implicit bias test online to learn about their own unrecognized implicit biases. These biases have a hand in influencing decisions particularly in fast-paced environments where cognitive load is high – such as EDs, where many child abuse evaluations occur.
For example, in one study Dr. Johnson led, the researchers measured implicit bias in participants before and after an ED shift to assess how cognitive load affected bias. They found that participants who care for more than 10 patients, the average score for implicit bias increased.
Similarly, “when the ED was more overcrowded, there was also increased bias at the end of the shift, compared to the beginning of the shift,” Dr. Johnson said. She asked clinicians to take into consideration that at the start of the shift, they may feel well rested and freshly caffeinated, able to suppress or overcome the biases that they know they have.
“But our biases [are] more likely to come into play with every subsequent decision that we make throughout the day when we’re engaged in clinical encounters,” such as who does and does not receive a skeletal survey or get referred to child protective services, she said.
In another study where she hypothesized that resident physicians would have less bias on the child race implicit bias test than on the adult race one, Dr. Johnson reported that 85% of 91 residents working in an ED had an implicit pro-White/anti-Black bias in the test on adult race, but an even higher bias score – 91% – with child race.
Research has found that even children’s names can conjure implicit bias when it comes to stereotypically “White-sounding” names versus stereotypically “Black-sounding names.”
The implicit bias among clinicians extends beyond care of different children. Research has also identified association between higher implicit bias scores and less interpersonal treatment, less supportive communication, less patient-centered communication, poorer patient ratings of satisfaction, and greater patient-reported difficulty with following recommendations, Dr. Johnson said.
“I want you to think about that because I know that when we’re engaging with parents and making decisions about whether or not we’re going to do a skeletal survey or report someone for it, there is a lot of subjectivity that comes into play with how you’re interacting with families,” Dr. Johnson said. Those verbal and nonverbal cues may be triggering to parents, which then affects your interaction with them. Further, research shows that these biases may impact treatment decisions as well.
Personal-mediated racism also shows up in the use of stigmatizing language, Dr. Johnson said.
“When providers read stigmatizing language in the patient’s medical records, it was associated with them having more negative attitudes about that patient,” which then influenced their clinical decision-making, she said. “So when providers got primed with stigmatizing language, they subsequently had less aggressive pain management for those patients.”
Clinical implications for patient care
Dr. Johnson encouraged attendees to be careful about the language and tone they use in communicating with other health care providers and during documentation in medical records. Disparities in child abuse evaluation and reporting tend to be greater in EDs with more subjective conditions, whereas disparities are lower in departments with more established protocols.
She recommended several changes to practice that can reduce the impact of implicit bias. Universal screening for child abuse can increase how many injuries are found, but usually at the cost of increased resources and radiation. Another option is use of validated clinical decision support rules to identify who is at high or low risk for maltreatment, something Dr. Johnson is working on in her research.
But it’s also important for individual providers to confront their personal biases. Evidence-based strategies for reducing bias include perspective taking, focusing on common identities with patients, using counter-stereotypical imaging, seeking increased opportunity for cross-cultural contact, and mindfulness meditation.
“When you interact with people of different backgrounds, it helps to reduce the impact of stereotypes in society about those individuals,” Dr. Johnson told attendees. It’s also important to recognize how diversity in your clinical team can reduce bias.
“We need to work with our institutions to confront racial biases in child abuse reporting and develop quality improvement projects to ensure reporting is done objectively,” Dr. Chaffee said in an interview after attending the session. “This will require training and likely policy changes, including how reports are made to child welfare and/or the police moving forward.”
according to research discussed by Tiffani J. Johnson, MD, an assistant professor of emergency medicine at the University of California, Davis.
“These disparities in child abuse evaluation and reporting are bidirectional,” she said. “We also recognize that abuse is more likely to be unrecognized in White children.”
Dr. Johnson presented data on the health disparities in child abuse reporting in a session at the annual meeting of the American Academy of Pediatrics, held virtually this year. Health care disparities, as defined by the National Academy of Sciences, refers to differences in the quality of care between minority and nonminority populations that are not caused by clinical appropriateness, access, need, or patient preference, she explained. Instead, they result from discrimination, bias, stereotyping, and uncertainty.
Disparities lead to harm in all children
For example, a 2018 systematic review found that Black and other non-White children were significantly more likely than White children to be evaluated with a skeletal survey. In one of the studies included, at a large urban academic center, Black and Latinx children with accidental fractures were 8.75 times more likely to undergo a skeletal survey than White children and 4.3 times more likely to be reported to child protective services.
“And let me emphasize that these are children who were ultimately found to have accidental fractures,” Dr. Johnson said.
Meanwhile, in an analysis of known cases of head trauma, researchers found that abuse was missed in 37% of White children, compared with 19% of non-White children.
“These only represent the tip of the iceberg as a true number of cases of abuse may never really be detected because some cases are still unknown,” Dr. Johnson told attendees. And the harm of these disparities runs in both directions.
“Failing to diagnose abuse in White children clearly puts them at increased risk for return visits and return evaluations for repeated abuse by the perpetrators,” she said. But harm also can result from overreporting and investigation, including psychological trauma and a waste of limited resources. Overinvestigation also can erode family-physician relationships and perpetuate distrust of medical care in communities of color.
Yet at the same time, it’s clear that Black children, adolescents, and young adults are not protected from harm in society more generally, when at home, where they learn, or where they play, Dr. Johnson said, referencing the deaths of Breonna Taylor and Tamir Rice as examples.
“And now we’re seeing increased evidence that children are not protected in the health care center when we think about the many disparities that have been identified in the care and outcomes of children, including the disproportionality in terms of child abuse evaluation and referrals,” Dr. Johnson said.
Racism is a root cause of that harm to Black children, she said, as the systemic structure of opportunities unfairly disadvantages some individuals and communities while unfairly advantaging others, thereby “sapping the strength of the whole society through the waste of human resources.”
Tonya Chaffee, MD, MPH, a clinical professor of health sciences at the University of California, San Francisco, who attended the session, said she particularly appreciated “seeing data on which racial/ethnic populations have child abuse reports made and the disparities that exist that are similar to what we are noticing in our own institution.”
Role of individual-level implicit bias and racism
While institutional and structural racism play a substantial role in health care disparities, Dr. Johnson focused primarily on the impact of personal racism when it comes to child abuse evaluations, through overt discrimination, explicit bias, implicit bias, and stigmatization. The most challenging of these to identify and acknowledge is often implicit bias, a tendency to believe, even unconsciously, that some people or ideas are better than others, which results in unfair treatment.
For example, a 2016 study found that half of medical students and residents held at least one biological belief about differences between Black and White individuals that was actually false, such as Black people having more pain tolerance or stronger bones than White people, which then affected treatment recommendations.
“Implicit bias refers to our attitudes that lie below the surface, but they can still influence our behaviors,” Dr. Johnson explained. She encouraged providers to take the implicit bias test online to learn about their own unrecognized implicit biases. These biases have a hand in influencing decisions particularly in fast-paced environments where cognitive load is high – such as EDs, where many child abuse evaluations occur.
For example, in one study Dr. Johnson led, the researchers measured implicit bias in participants before and after an ED shift to assess how cognitive load affected bias. They found that participants who care for more than 10 patients, the average score for implicit bias increased.
Similarly, “when the ED was more overcrowded, there was also increased bias at the end of the shift, compared to the beginning of the shift,” Dr. Johnson said. She asked clinicians to take into consideration that at the start of the shift, they may feel well rested and freshly caffeinated, able to suppress or overcome the biases that they know they have.
“But our biases [are] more likely to come into play with every subsequent decision that we make throughout the day when we’re engaged in clinical encounters,” such as who does and does not receive a skeletal survey or get referred to child protective services, she said.
In another study where she hypothesized that resident physicians would have less bias on the child race implicit bias test than on the adult race one, Dr. Johnson reported that 85% of 91 residents working in an ED had an implicit pro-White/anti-Black bias in the test on adult race, but an even higher bias score – 91% – with child race.
Research has found that even children’s names can conjure implicit bias when it comes to stereotypically “White-sounding” names versus stereotypically “Black-sounding names.”
The implicit bias among clinicians extends beyond care of different children. Research has also identified association between higher implicit bias scores and less interpersonal treatment, less supportive communication, less patient-centered communication, poorer patient ratings of satisfaction, and greater patient-reported difficulty with following recommendations, Dr. Johnson said.
“I want you to think about that because I know that when we’re engaging with parents and making decisions about whether or not we’re going to do a skeletal survey or report someone for it, there is a lot of subjectivity that comes into play with how you’re interacting with families,” Dr. Johnson said. Those verbal and nonverbal cues may be triggering to parents, which then affects your interaction with them. Further, research shows that these biases may impact treatment decisions as well.
Personal-mediated racism also shows up in the use of stigmatizing language, Dr. Johnson said.
“When providers read stigmatizing language in the patient’s medical records, it was associated with them having more negative attitudes about that patient,” which then influenced their clinical decision-making, she said. “So when providers got primed with stigmatizing language, they subsequently had less aggressive pain management for those patients.”
Clinical implications for patient care
Dr. Johnson encouraged attendees to be careful about the language and tone they use in communicating with other health care providers and during documentation in medical records. Disparities in child abuse evaluation and reporting tend to be greater in EDs with more subjective conditions, whereas disparities are lower in departments with more established protocols.
She recommended several changes to practice that can reduce the impact of implicit bias. Universal screening for child abuse can increase how many injuries are found, but usually at the cost of increased resources and radiation. Another option is use of validated clinical decision support rules to identify who is at high or low risk for maltreatment, something Dr. Johnson is working on in her research.
But it’s also important for individual providers to confront their personal biases. Evidence-based strategies for reducing bias include perspective taking, focusing on common identities with patients, using counter-stereotypical imaging, seeking increased opportunity for cross-cultural contact, and mindfulness meditation.
“When you interact with people of different backgrounds, it helps to reduce the impact of stereotypes in society about those individuals,” Dr. Johnson told attendees. It’s also important to recognize how diversity in your clinical team can reduce bias.
“We need to work with our institutions to confront racial biases in child abuse reporting and develop quality improvement projects to ensure reporting is done objectively,” Dr. Chaffee said in an interview after attending the session. “This will require training and likely policy changes, including how reports are made to child welfare and/or the police moving forward.”
according to research discussed by Tiffani J. Johnson, MD, an assistant professor of emergency medicine at the University of California, Davis.
“These disparities in child abuse evaluation and reporting are bidirectional,” she said. “We also recognize that abuse is more likely to be unrecognized in White children.”
Dr. Johnson presented data on the health disparities in child abuse reporting in a session at the annual meeting of the American Academy of Pediatrics, held virtually this year. Health care disparities, as defined by the National Academy of Sciences, refers to differences in the quality of care between minority and nonminority populations that are not caused by clinical appropriateness, access, need, or patient preference, she explained. Instead, they result from discrimination, bias, stereotyping, and uncertainty.
Disparities lead to harm in all children
For example, a 2018 systematic review found that Black and other non-White children were significantly more likely than White children to be evaluated with a skeletal survey. In one of the studies included, at a large urban academic center, Black and Latinx children with accidental fractures were 8.75 times more likely to undergo a skeletal survey than White children and 4.3 times more likely to be reported to child protective services.
“And let me emphasize that these are children who were ultimately found to have accidental fractures,” Dr. Johnson said.
Meanwhile, in an analysis of known cases of head trauma, researchers found that abuse was missed in 37% of White children, compared with 19% of non-White children.
“These only represent the tip of the iceberg as a true number of cases of abuse may never really be detected because some cases are still unknown,” Dr. Johnson told attendees. And the harm of these disparities runs in both directions.
“Failing to diagnose abuse in White children clearly puts them at increased risk for return visits and return evaluations for repeated abuse by the perpetrators,” she said. But harm also can result from overreporting and investigation, including psychological trauma and a waste of limited resources. Overinvestigation also can erode family-physician relationships and perpetuate distrust of medical care in communities of color.
Yet at the same time, it’s clear that Black children, adolescents, and young adults are not protected from harm in society more generally, when at home, where they learn, or where they play, Dr. Johnson said, referencing the deaths of Breonna Taylor and Tamir Rice as examples.
“And now we’re seeing increased evidence that children are not protected in the health care center when we think about the many disparities that have been identified in the care and outcomes of children, including the disproportionality in terms of child abuse evaluation and referrals,” Dr. Johnson said.
Racism is a root cause of that harm to Black children, she said, as the systemic structure of opportunities unfairly disadvantages some individuals and communities while unfairly advantaging others, thereby “sapping the strength of the whole society through the waste of human resources.”
Tonya Chaffee, MD, MPH, a clinical professor of health sciences at the University of California, San Francisco, who attended the session, said she particularly appreciated “seeing data on which racial/ethnic populations have child abuse reports made and the disparities that exist that are similar to what we are noticing in our own institution.”
Role of individual-level implicit bias and racism
While institutional and structural racism play a substantial role in health care disparities, Dr. Johnson focused primarily on the impact of personal racism when it comes to child abuse evaluations, through overt discrimination, explicit bias, implicit bias, and stigmatization. The most challenging of these to identify and acknowledge is often implicit bias, a tendency to believe, even unconsciously, that some people or ideas are better than others, which results in unfair treatment.
For example, a 2016 study found that half of medical students and residents held at least one biological belief about differences between Black and White individuals that was actually false, such as Black people having more pain tolerance or stronger bones than White people, which then affected treatment recommendations.
“Implicit bias refers to our attitudes that lie below the surface, but they can still influence our behaviors,” Dr. Johnson explained. She encouraged providers to take the implicit bias test online to learn about their own unrecognized implicit biases. These biases have a hand in influencing decisions particularly in fast-paced environments where cognitive load is high – such as EDs, where many child abuse evaluations occur.
For example, in one study Dr. Johnson led, the researchers measured implicit bias in participants before and after an ED shift to assess how cognitive load affected bias. They found that participants who care for more than 10 patients, the average score for implicit bias increased.
Similarly, “when the ED was more overcrowded, there was also increased bias at the end of the shift, compared to the beginning of the shift,” Dr. Johnson said. She asked clinicians to take into consideration that at the start of the shift, they may feel well rested and freshly caffeinated, able to suppress or overcome the biases that they know they have.
“But our biases [are] more likely to come into play with every subsequent decision that we make throughout the day when we’re engaged in clinical encounters,” such as who does and does not receive a skeletal survey or get referred to child protective services, she said.
In another study where she hypothesized that resident physicians would have less bias on the child race implicit bias test than on the adult race one, Dr. Johnson reported that 85% of 91 residents working in an ED had an implicit pro-White/anti-Black bias in the test on adult race, but an even higher bias score – 91% – with child race.
Research has found that even children’s names can conjure implicit bias when it comes to stereotypically “White-sounding” names versus stereotypically “Black-sounding names.”
The implicit bias among clinicians extends beyond care of different children. Research has also identified association between higher implicit bias scores and less interpersonal treatment, less supportive communication, less patient-centered communication, poorer patient ratings of satisfaction, and greater patient-reported difficulty with following recommendations, Dr. Johnson said.
“I want you to think about that because I know that when we’re engaging with parents and making decisions about whether or not we’re going to do a skeletal survey or report someone for it, there is a lot of subjectivity that comes into play with how you’re interacting with families,” Dr. Johnson said. Those verbal and nonverbal cues may be triggering to parents, which then affects your interaction with them. Further, research shows that these biases may impact treatment decisions as well.
Personal-mediated racism also shows up in the use of stigmatizing language, Dr. Johnson said.
“When providers read stigmatizing language in the patient’s medical records, it was associated with them having more negative attitudes about that patient,” which then influenced their clinical decision-making, she said. “So when providers got primed with stigmatizing language, they subsequently had less aggressive pain management for those patients.”
Clinical implications for patient care
Dr. Johnson encouraged attendees to be careful about the language and tone they use in communicating with other health care providers and during documentation in medical records. Disparities in child abuse evaluation and reporting tend to be greater in EDs with more subjective conditions, whereas disparities are lower in departments with more established protocols.
She recommended several changes to practice that can reduce the impact of implicit bias. Universal screening for child abuse can increase how many injuries are found, but usually at the cost of increased resources and radiation. Another option is use of validated clinical decision support rules to identify who is at high or low risk for maltreatment, something Dr. Johnson is working on in her research.
But it’s also important for individual providers to confront their personal biases. Evidence-based strategies for reducing bias include perspective taking, focusing on common identities with patients, using counter-stereotypical imaging, seeking increased opportunity for cross-cultural contact, and mindfulness meditation.
“When you interact with people of different backgrounds, it helps to reduce the impact of stereotypes in society about those individuals,” Dr. Johnson told attendees. It’s also important to recognize how diversity in your clinical team can reduce bias.
“We need to work with our institutions to confront racial biases in child abuse reporting and develop quality improvement projects to ensure reporting is done objectively,” Dr. Chaffee said in an interview after attending the session. “This will require training and likely policy changes, including how reports are made to child welfare and/or the police moving forward.”
FROM AAP 2020
Study shows no link between race and mortality in clear cell RCC
The issue of race and survival in patients with clear cell renal cell carcinoma (ccRCC) has been debated in the literature.
Some studies have shown worse survival for Black patients, while others have suggested that Black race is instead a stand-in for social determinants, including access to care.
New research suggests that Black race is not correlated with increased mortality from ccRCC. These results were published in Urology.
“Despite well documented racial biases and race-specific outcomes in the health care landscape, our study found race was not associated with 5-year cause-specific survival from ccRCC,” wrote investigator Dhaval Jivanji, a medical student at Florida International University, Miami, and colleagues.
In their retrospective study, the investigators examined 5-year survival in ccRCC patients, comparing results across races. The team used data from the Surveillance Epidemiology, and End Results (SEER) database, which collects cancer data from 13 states using population-based cancer registries. They extracted data on demographics, prevalence, and mortality, in relation to ccRCC.
A total of 8,421 subjects with ccRCC were included in the analysis, which covered the years 2007-2015. The primary outcome was 5-year survival, defined as cause-specific mortality up to the first 60 months from time of cancer diagnosis.
In addition to race, variables included in the statistical model were age (18-50, 51-60, 61-70,71-80, >80), sex (male/female), SEER Summary tumor staging (localized, regionalized, distant), insurance status (uninsured, insured, insured not specific, Medicaid), and marital status (single, married/partner, separated/divorced/widowed).
Demographic determinism
In the adjusted analysis, the researchers found no association between race and 5-year cause-specific survival in patients with ccRCC.
The hazard ratios for death were 0.96 for Black patients, 1.01 for American Indian/Alaska Native patients, and 0.99 for Asian/Pacific Islander patients, with White patients as the comparator.
In terms of the other covariates studied, the researchers found that older age (>50 years) and the presence of regional or distant tumors were associated with an increased hazard of death, while female sex and having insurance were associated with a decreased hazard of death.
“Our study found that age, tumor stage, and insurance status are significantly associated with 5-year cause-specific survival. Future studies will benefit from complete assessment of other demographic factors, including income, medical comorbidities, and access to care. These are negative predictors, and [their] potential impact on overall survival should be considered by the clinician in treatment and management plans for RCC patients,” the researchers concluded.
In an editorial commentary published within the main article, Paul Russo, MD, of Weill Cornell Medicine, New York, stated: “Investigations such as this utilizing the SEER registries provide a 30,000-foot demographic view of some disease elements but lack important granularity, such as tumor size and grade, family income, critical medical comorbidities, and patient access to hospitals with surgical and medical oncologic expertise.”
Dr. Russo said it is well known that disparate access to diagnosis, surgical intervention, and expert treatment have an impact on survival.
He went on to ask: “Could African Americans have had superior outcomes if the data was controlled for these important variables? As urologic surgeons, we must join the greater medical community in understanding the root causes leading to structural racial and economic disparities, inequities in access to care, and the profound negative impact these disparities have on health outcomes in general and cancer outcomes specifically.”
The authors did not disclose funding or conflicts of interest.
SOURCE: Jivanji D et al. Urology. 2020. doi: 10.1016/j.urology.2020.10.055.
The issue of race and survival in patients with clear cell renal cell carcinoma (ccRCC) has been debated in the literature.
Some studies have shown worse survival for Black patients, while others have suggested that Black race is instead a stand-in for social determinants, including access to care.
New research suggests that Black race is not correlated with increased mortality from ccRCC. These results were published in Urology.
“Despite well documented racial biases and race-specific outcomes in the health care landscape, our study found race was not associated with 5-year cause-specific survival from ccRCC,” wrote investigator Dhaval Jivanji, a medical student at Florida International University, Miami, and colleagues.
In their retrospective study, the investigators examined 5-year survival in ccRCC patients, comparing results across races. The team used data from the Surveillance Epidemiology, and End Results (SEER) database, which collects cancer data from 13 states using population-based cancer registries. They extracted data on demographics, prevalence, and mortality, in relation to ccRCC.
A total of 8,421 subjects with ccRCC were included in the analysis, which covered the years 2007-2015. The primary outcome was 5-year survival, defined as cause-specific mortality up to the first 60 months from time of cancer diagnosis.
In addition to race, variables included in the statistical model were age (18-50, 51-60, 61-70,71-80, >80), sex (male/female), SEER Summary tumor staging (localized, regionalized, distant), insurance status (uninsured, insured, insured not specific, Medicaid), and marital status (single, married/partner, separated/divorced/widowed).
Demographic determinism
In the adjusted analysis, the researchers found no association between race and 5-year cause-specific survival in patients with ccRCC.
The hazard ratios for death were 0.96 for Black patients, 1.01 for American Indian/Alaska Native patients, and 0.99 for Asian/Pacific Islander patients, with White patients as the comparator.
In terms of the other covariates studied, the researchers found that older age (>50 years) and the presence of regional or distant tumors were associated with an increased hazard of death, while female sex and having insurance were associated with a decreased hazard of death.
“Our study found that age, tumor stage, and insurance status are significantly associated with 5-year cause-specific survival. Future studies will benefit from complete assessment of other demographic factors, including income, medical comorbidities, and access to care. These are negative predictors, and [their] potential impact on overall survival should be considered by the clinician in treatment and management plans for RCC patients,” the researchers concluded.
In an editorial commentary published within the main article, Paul Russo, MD, of Weill Cornell Medicine, New York, stated: “Investigations such as this utilizing the SEER registries provide a 30,000-foot demographic view of some disease elements but lack important granularity, such as tumor size and grade, family income, critical medical comorbidities, and patient access to hospitals with surgical and medical oncologic expertise.”
Dr. Russo said it is well known that disparate access to diagnosis, surgical intervention, and expert treatment have an impact on survival.
He went on to ask: “Could African Americans have had superior outcomes if the data was controlled for these important variables? As urologic surgeons, we must join the greater medical community in understanding the root causes leading to structural racial and economic disparities, inequities in access to care, and the profound negative impact these disparities have on health outcomes in general and cancer outcomes specifically.”
The authors did not disclose funding or conflicts of interest.
SOURCE: Jivanji D et al. Urology. 2020. doi: 10.1016/j.urology.2020.10.055.
The issue of race and survival in patients with clear cell renal cell carcinoma (ccRCC) has been debated in the literature.
Some studies have shown worse survival for Black patients, while others have suggested that Black race is instead a stand-in for social determinants, including access to care.
New research suggests that Black race is not correlated with increased mortality from ccRCC. These results were published in Urology.
“Despite well documented racial biases and race-specific outcomes in the health care landscape, our study found race was not associated with 5-year cause-specific survival from ccRCC,” wrote investigator Dhaval Jivanji, a medical student at Florida International University, Miami, and colleagues.
In their retrospective study, the investigators examined 5-year survival in ccRCC patients, comparing results across races. The team used data from the Surveillance Epidemiology, and End Results (SEER) database, which collects cancer data from 13 states using population-based cancer registries. They extracted data on demographics, prevalence, and mortality, in relation to ccRCC.
A total of 8,421 subjects with ccRCC were included in the analysis, which covered the years 2007-2015. The primary outcome was 5-year survival, defined as cause-specific mortality up to the first 60 months from time of cancer diagnosis.
In addition to race, variables included in the statistical model were age (18-50, 51-60, 61-70,71-80, >80), sex (male/female), SEER Summary tumor staging (localized, regionalized, distant), insurance status (uninsured, insured, insured not specific, Medicaid), and marital status (single, married/partner, separated/divorced/widowed).
Demographic determinism
In the adjusted analysis, the researchers found no association between race and 5-year cause-specific survival in patients with ccRCC.
The hazard ratios for death were 0.96 for Black patients, 1.01 for American Indian/Alaska Native patients, and 0.99 for Asian/Pacific Islander patients, with White patients as the comparator.
In terms of the other covariates studied, the researchers found that older age (>50 years) and the presence of regional or distant tumors were associated with an increased hazard of death, while female sex and having insurance were associated with a decreased hazard of death.
“Our study found that age, tumor stage, and insurance status are significantly associated with 5-year cause-specific survival. Future studies will benefit from complete assessment of other demographic factors, including income, medical comorbidities, and access to care. These are negative predictors, and [their] potential impact on overall survival should be considered by the clinician in treatment and management plans for RCC patients,” the researchers concluded.
In an editorial commentary published within the main article, Paul Russo, MD, of Weill Cornell Medicine, New York, stated: “Investigations such as this utilizing the SEER registries provide a 30,000-foot demographic view of some disease elements but lack important granularity, such as tumor size and grade, family income, critical medical comorbidities, and patient access to hospitals with surgical and medical oncologic expertise.”
Dr. Russo said it is well known that disparate access to diagnosis, surgical intervention, and expert treatment have an impact on survival.
He went on to ask: “Could African Americans have had superior outcomes if the data was controlled for these important variables? As urologic surgeons, we must join the greater medical community in understanding the root causes leading to structural racial and economic disparities, inequities in access to care, and the profound negative impact these disparities have on health outcomes in general and cancer outcomes specifically.”
The authors did not disclose funding or conflicts of interest.
SOURCE: Jivanji D et al. Urology. 2020. doi: 10.1016/j.urology.2020.10.055.
FROM UROLOGY
Breast cancer survival disparities: Need to address obesity
The poorer survival rates in Black women compared with White women with breast cancer could be explained to some extent by the finding of much higher rates of obesity, obesity-related comorbidities, and overall comorbidities in Black women, say researchers reporting a retrospective chart review from their clinic.
Kirsten A. Nyrop, PhD, deputy director for research for the Geriatric Oncology Program at the University of North Carolina, Chapel Hill, and colleagues analyzed medical charts for 144 Black women and 404 White women with early breast cancer.
Obesity rates were nearly double among Black women, at 62% vs 32%.
In addition, significantly more Black women had two or more total comorbidities (62% vs 47%), two or more obesity-related comorbidities (33% vs 10%), hypertension (60% vs 32%), type 2 diabetes (23% vs 6%), and hypercholesterolemia or hyperlipidemia (28% vs 18%).
These racial disparities persisted after adjustment for age and body mass index, both independent predictors of chronic diseases.
The difference in obesity and comorbidity did not translate to differences in treatment decisions such as surgery type, chemotherapy regimen, radiation, or endocrine treatment, the researchers note.
The findings were published online December 7 in the journal Cancer.
They underscore the likely role of obesity and related complications in the racial disparities seen in breast cancer survival outcomes, the authors conclude.
Experts writing in an accompanying editorial agree, while emphasizing the well documented differences in survival.
Compared with White women with breast cancer, Black women with breast cancer have a 42% higher mortality rate and a greater likelihood of dying from breast cancer regardless of their age at diagnosis, note Caitlin E. Taylor, MD, and Jane Lowe Meisel, MD, of Emory University, Atlanta, Georgia.
“Although it is clear that the causes of such disparities are complex and multifactorial, questions remain regarding to what extent patient comorbidities, and specifically obesity, may be playing a role,” they write.
The obesity- and comorbidity-related disparities identified by Nyrop et al “undoubtedly contribute to the overall disparities noted in breast cancer outcomes among Black women,” they add.
Takeaway messages
Nyrop and colleagues say their findings have two important takeaway messages:
1) It is important to manage comorbidities in women with newly diagnosed early breast cancer to reduce the risk of mortality from competing causes, and
2) Excess weight at diagnosis and weight gain after primary treatment increase the risk of obesity-related disease that can affect survival, and patients should be educated about the association.
Such conversations should be “patient-centered and culturally appropriate,” they note.
In their editorial, Taylor and Meisel agree with the authors’ conclusions. “Given the higher prevalence of obesity and related comorbidities among Black patients, addressing these issues must become an integral part of early breast cancer management to prolong overall survival and continue improving outcomes for these women.”
In fact, addressing comorbidities early in breast cancer management is important for patients of all racial and ethnic backgrounds, the editorialists add, concluding that the role of obesity as “a critical player underlying breast cancer mortality” is increasingly clear, and that its management is crucial for improved outcomes and quality of life.
This study was supported by the Breast Cancer Research Foundation, the National Cancer Institute’s Breast Cancer Specialized Program of Research Excellence, and the University of North Carolina Lineberger Comprehensive Cancer Center/University Cancer Research Fund. The study authors have disclosed no relevant financial relationships. Meisel has received research support from Pfizer, Eli Lilly, and Seattle Genetics and has served as a paid advisor for Pfizer, PUMA, Novartis, and Clovis Oncology. Taylor has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The poorer survival rates in Black women compared with White women with breast cancer could be explained to some extent by the finding of much higher rates of obesity, obesity-related comorbidities, and overall comorbidities in Black women, say researchers reporting a retrospective chart review from their clinic.
Kirsten A. Nyrop, PhD, deputy director for research for the Geriatric Oncology Program at the University of North Carolina, Chapel Hill, and colleagues analyzed medical charts for 144 Black women and 404 White women with early breast cancer.
Obesity rates were nearly double among Black women, at 62% vs 32%.
In addition, significantly more Black women had two or more total comorbidities (62% vs 47%), two or more obesity-related comorbidities (33% vs 10%), hypertension (60% vs 32%), type 2 diabetes (23% vs 6%), and hypercholesterolemia or hyperlipidemia (28% vs 18%).
These racial disparities persisted after adjustment for age and body mass index, both independent predictors of chronic diseases.
The difference in obesity and comorbidity did not translate to differences in treatment decisions such as surgery type, chemotherapy regimen, radiation, or endocrine treatment, the researchers note.
The findings were published online December 7 in the journal Cancer.
They underscore the likely role of obesity and related complications in the racial disparities seen in breast cancer survival outcomes, the authors conclude.
Experts writing in an accompanying editorial agree, while emphasizing the well documented differences in survival.
Compared with White women with breast cancer, Black women with breast cancer have a 42% higher mortality rate and a greater likelihood of dying from breast cancer regardless of their age at diagnosis, note Caitlin E. Taylor, MD, and Jane Lowe Meisel, MD, of Emory University, Atlanta, Georgia.
“Although it is clear that the causes of such disparities are complex and multifactorial, questions remain regarding to what extent patient comorbidities, and specifically obesity, may be playing a role,” they write.
The obesity- and comorbidity-related disparities identified by Nyrop et al “undoubtedly contribute to the overall disparities noted in breast cancer outcomes among Black women,” they add.
Takeaway messages
Nyrop and colleagues say their findings have two important takeaway messages:
1) It is important to manage comorbidities in women with newly diagnosed early breast cancer to reduce the risk of mortality from competing causes, and
2) Excess weight at diagnosis and weight gain after primary treatment increase the risk of obesity-related disease that can affect survival, and patients should be educated about the association.
Such conversations should be “patient-centered and culturally appropriate,” they note.
In their editorial, Taylor and Meisel agree with the authors’ conclusions. “Given the higher prevalence of obesity and related comorbidities among Black patients, addressing these issues must become an integral part of early breast cancer management to prolong overall survival and continue improving outcomes for these women.”
In fact, addressing comorbidities early in breast cancer management is important for patients of all racial and ethnic backgrounds, the editorialists add, concluding that the role of obesity as “a critical player underlying breast cancer mortality” is increasingly clear, and that its management is crucial for improved outcomes and quality of life.
This study was supported by the Breast Cancer Research Foundation, the National Cancer Institute’s Breast Cancer Specialized Program of Research Excellence, and the University of North Carolina Lineberger Comprehensive Cancer Center/University Cancer Research Fund. The study authors have disclosed no relevant financial relationships. Meisel has received research support from Pfizer, Eli Lilly, and Seattle Genetics and has served as a paid advisor for Pfizer, PUMA, Novartis, and Clovis Oncology. Taylor has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The poorer survival rates in Black women compared with White women with breast cancer could be explained to some extent by the finding of much higher rates of obesity, obesity-related comorbidities, and overall comorbidities in Black women, say researchers reporting a retrospective chart review from their clinic.
Kirsten A. Nyrop, PhD, deputy director for research for the Geriatric Oncology Program at the University of North Carolina, Chapel Hill, and colleagues analyzed medical charts for 144 Black women and 404 White women with early breast cancer.
Obesity rates were nearly double among Black women, at 62% vs 32%.
In addition, significantly more Black women had two or more total comorbidities (62% vs 47%), two or more obesity-related comorbidities (33% vs 10%), hypertension (60% vs 32%), type 2 diabetes (23% vs 6%), and hypercholesterolemia or hyperlipidemia (28% vs 18%).
These racial disparities persisted after adjustment for age and body mass index, both independent predictors of chronic diseases.
The difference in obesity and comorbidity did not translate to differences in treatment decisions such as surgery type, chemotherapy regimen, radiation, or endocrine treatment, the researchers note.
The findings were published online December 7 in the journal Cancer.
They underscore the likely role of obesity and related complications in the racial disparities seen in breast cancer survival outcomes, the authors conclude.
Experts writing in an accompanying editorial agree, while emphasizing the well documented differences in survival.
Compared with White women with breast cancer, Black women with breast cancer have a 42% higher mortality rate and a greater likelihood of dying from breast cancer regardless of their age at diagnosis, note Caitlin E. Taylor, MD, and Jane Lowe Meisel, MD, of Emory University, Atlanta, Georgia.
“Although it is clear that the causes of such disparities are complex and multifactorial, questions remain regarding to what extent patient comorbidities, and specifically obesity, may be playing a role,” they write.
The obesity- and comorbidity-related disparities identified by Nyrop et al “undoubtedly contribute to the overall disparities noted in breast cancer outcomes among Black women,” they add.
Takeaway messages
Nyrop and colleagues say their findings have two important takeaway messages:
1) It is important to manage comorbidities in women with newly diagnosed early breast cancer to reduce the risk of mortality from competing causes, and
2) Excess weight at diagnosis and weight gain after primary treatment increase the risk of obesity-related disease that can affect survival, and patients should be educated about the association.
Such conversations should be “patient-centered and culturally appropriate,” they note.
In their editorial, Taylor and Meisel agree with the authors’ conclusions. “Given the higher prevalence of obesity and related comorbidities among Black patients, addressing these issues must become an integral part of early breast cancer management to prolong overall survival and continue improving outcomes for these women.”
In fact, addressing comorbidities early in breast cancer management is important for patients of all racial and ethnic backgrounds, the editorialists add, concluding that the role of obesity as “a critical player underlying breast cancer mortality” is increasingly clear, and that its management is crucial for improved outcomes and quality of life.
This study was supported by the Breast Cancer Research Foundation, the National Cancer Institute’s Breast Cancer Specialized Program of Research Excellence, and the University of North Carolina Lineberger Comprehensive Cancer Center/University Cancer Research Fund. The study authors have disclosed no relevant financial relationships. Meisel has received research support from Pfizer, Eli Lilly, and Seattle Genetics and has served as a paid advisor for Pfizer, PUMA, Novartis, and Clovis Oncology. Taylor has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Advocate for legislation to improve, protect LGBTQ lives
In January in many states, the start of a new year also means the start of a new legislative session. For LGBTQ youth and their families, these sessions can create a significant amount of anxiety, as legislators in several states introduce legislation to curtail the rights of this population. In some cases, legislators have attempted to criminalize the provision of gender-affirming medical care to the trans and gender-diverse adolescents that many of us provide care to on a daily basis. As pediatricians,
2020 started on a positive note for LGBTQ children and adolescents, with Virginia becoming the 20th state to ban conversion therapy for minors. Legislation was introduced in several other states to prohibit this practice, including Kentucky, Missouri, and Ohio, and but they ultimately died in committee or were never referred. While there is not yet a nationwide ban on conversion therapy, legislation was introduced in the last three U.S. Congress sessions to ban this harmful practice. In June 2020, the Supreme Court decision in Bostock vs. Clayton County stated that employers could not fire an employee solely because of that person’s sexual orientation and/or gender identity.
However, 19 separate bills were introduced in 2020 alone in states across the United States that would prohibit gender-affirming care for adolescents under age 18.1 Many of these bills also would make the provision of gender-affirming medical care codified as felony child abuse, with loss of licensure, fines and/or jail time a possibility for physicians who prescribe hormones or puberty blockers for gender-affirming care to minors. Fortunately, these bills either died in committee or never had a hearing. However, legislation has been prefiled in several states for their 2021 session to again attempt to prohibit minors from obtaining gender-affirming medical care and/or criminalizing the provision of this care by physicians. Other bills were filed or have been prefiled again to allow various medical and mental health providers to refuse to treat LGBTQ patients because of their personal religious beliefs and/or forcing these same providers to tell a parent if a minor reveals to that provider that they are LGBTQ.
Even if this legislation does not pass or get a hearing, the fact that the bills were introduced can have a profound impact on LGBTQ patients and their families. After a bill was introduced in Texas in their 2017 legislative session that would require trans and gender-diverse (TGD) people to use the bathroom based on their sex assigned at birth, the Trevor Project reported that it had an increase of 34% in crisis calls from trans youth who were in distress.2 This was similar, but slightly less, than was reported by the Trevor Project in September 2015 when in the run-up to a vote on Houston’s Equal Rights Ordinance, advertising was run equating trans women as predators who could be lying in wait in bathrooms. On the converse, when LGBTQ youth feel supported in the media, courts, and legislatures, this can have a positive impact on their mental health. A 2017 study found that, in states who enacted same-sex marriage laws prior to the 2015 Supreme Court decision in Obergefell, compared with those who did not, there was a 7% relative reduction in the proportion of high school students who attempted suicide.3
The American Academy of Pediatrics published its policy statement in September 2018 outlining suggestions for pediatricians to provide support to TGD youth.4 In this position statement, recommendation No. 7 states “that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence.” Therefore, it is incumbent upon us to use our voices to support our LGBTQ youth. In 2020, several pediatricians from the South Dakota chapter of the AAP provided testimony – and organized public rallies – against legislation in that state which would have made gender-affirming care to minors under age 16 punishable by a fine and/or up to 10 years in prison.5

So what can you do? First, get to know your local and state legislators. While it was difficult to meet them in person for much of 2020, you can always call their district and/or Capitol offices, email them, or fill out their constituent contact form typically found on their website. Let them know that you oppose bills which introduce discrimination against your LGBTQ patients or threaten to criminalize the care that you provide to these patients.
Second, work with your state medical association or state AAP chapter to encourage them to oppose these harmful laws and support laws that improve the lives of LGBTQ patients. Third, you can write op-eds to your local newspaper, expressing your support for your patients and outlining the detrimental effects that anti-LGBTQ laws have on your patients. Lastly, you can be active on Twitter, Facebook, or other social media platforms sharing stories of how harmful or helpful certain pieces of legislation can be for your patients.
Dr. Cooper is assistant professor of pediatrics at the University of Texas, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Email Dr. Cooper at [email protected].
References
1. “Leglislation affecting LGBT rights across country.” www.aclu.org.
2. “Bathroom Bills Fuel Spike In Calls From Trans Youth To Suicide Hotline.” www.outsmartmagazine.com. 2017 Aug.
3. JAMA Pediatr. 2017 Apr 1. doi: 10.1001/jamapediatrics.2016.4529.
4. Pediatrics. 2018 Oct. doi: 10.1542/peds.2018-2162.
5. Wyckoff AS. “State bills seek to place limits on transgender care, ‘punish’ physicians.” AAP News. 2020 Feb 18.
In January in many states, the start of a new year also means the start of a new legislative session. For LGBTQ youth and their families, these sessions can create a significant amount of anxiety, as legislators in several states introduce legislation to curtail the rights of this population. In some cases, legislators have attempted to criminalize the provision of gender-affirming medical care to the trans and gender-diverse adolescents that many of us provide care to on a daily basis. As pediatricians,
2020 started on a positive note for LGBTQ children and adolescents, with Virginia becoming the 20th state to ban conversion therapy for minors. Legislation was introduced in several other states to prohibit this practice, including Kentucky, Missouri, and Ohio, and but they ultimately died in committee or were never referred. While there is not yet a nationwide ban on conversion therapy, legislation was introduced in the last three U.S. Congress sessions to ban this harmful practice. In June 2020, the Supreme Court decision in Bostock vs. Clayton County stated that employers could not fire an employee solely because of that person’s sexual orientation and/or gender identity.
However, 19 separate bills were introduced in 2020 alone in states across the United States that would prohibit gender-affirming care for adolescents under age 18.1 Many of these bills also would make the provision of gender-affirming medical care codified as felony child abuse, with loss of licensure, fines and/or jail time a possibility for physicians who prescribe hormones or puberty blockers for gender-affirming care to minors. Fortunately, these bills either died in committee or never had a hearing. However, legislation has been prefiled in several states for their 2021 session to again attempt to prohibit minors from obtaining gender-affirming medical care and/or criminalizing the provision of this care by physicians. Other bills were filed or have been prefiled again to allow various medical and mental health providers to refuse to treat LGBTQ patients because of their personal religious beliefs and/or forcing these same providers to tell a parent if a minor reveals to that provider that they are LGBTQ.
Even if this legislation does not pass or get a hearing, the fact that the bills were introduced can have a profound impact on LGBTQ patients and their families. After a bill was introduced in Texas in their 2017 legislative session that would require trans and gender-diverse (TGD) people to use the bathroom based on their sex assigned at birth, the Trevor Project reported that it had an increase of 34% in crisis calls from trans youth who were in distress.2 This was similar, but slightly less, than was reported by the Trevor Project in September 2015 when in the run-up to a vote on Houston’s Equal Rights Ordinance, advertising was run equating trans women as predators who could be lying in wait in bathrooms. On the converse, when LGBTQ youth feel supported in the media, courts, and legislatures, this can have a positive impact on their mental health. A 2017 study found that, in states who enacted same-sex marriage laws prior to the 2015 Supreme Court decision in Obergefell, compared with those who did not, there was a 7% relative reduction in the proportion of high school students who attempted suicide.3
The American Academy of Pediatrics published its policy statement in September 2018 outlining suggestions for pediatricians to provide support to TGD youth.4 In this position statement, recommendation No. 7 states “that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence.” Therefore, it is incumbent upon us to use our voices to support our LGBTQ youth. In 2020, several pediatricians from the South Dakota chapter of the AAP provided testimony – and organized public rallies – against legislation in that state which would have made gender-affirming care to minors under age 16 punishable by a fine and/or up to 10 years in prison.5
So what can you do? First, get to know your local and state legislators. While it was difficult to meet them in person for much of 2020, you can always call their district and/or Capitol offices, email them, or fill out their constituent contact form typically found on their website. Let them know that you oppose bills which introduce discrimination against your LGBTQ patients or threaten to criminalize the care that you provide to these patients.
Second, work with your state medical association or state AAP chapter to encourage them to oppose these harmful laws and support laws that improve the lives of LGBTQ patients. Third, you can write op-eds to your local newspaper, expressing your support for your patients and outlining the detrimental effects that anti-LGBTQ laws have on your patients. Lastly, you can be active on Twitter, Facebook, or other social media platforms sharing stories of how harmful or helpful certain pieces of legislation can be for your patients.
Dr. Cooper is assistant professor of pediatrics at the University of Texas, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Email Dr. Cooper at [email protected].
References
1. “Leglislation affecting LGBT rights across country.” www.aclu.org.
2. “Bathroom Bills Fuel Spike In Calls From Trans Youth To Suicide Hotline.” www.outsmartmagazine.com. 2017 Aug.
3. JAMA Pediatr. 2017 Apr 1. doi: 10.1001/jamapediatrics.2016.4529.
4. Pediatrics. 2018 Oct. doi: 10.1542/peds.2018-2162.
5. Wyckoff AS. “State bills seek to place limits on transgender care, ‘punish’ physicians.” AAP News. 2020 Feb 18.
In January in many states, the start of a new year also means the start of a new legislative session. For LGBTQ youth and their families, these sessions can create a significant amount of anxiety, as legislators in several states introduce legislation to curtail the rights of this population. In some cases, legislators have attempted to criminalize the provision of gender-affirming medical care to the trans and gender-diverse adolescents that many of us provide care to on a daily basis. As pediatricians,
2020 started on a positive note for LGBTQ children and adolescents, with Virginia becoming the 20th state to ban conversion therapy for minors. Legislation was introduced in several other states to prohibit this practice, including Kentucky, Missouri, and Ohio, and but they ultimately died in committee or were never referred. While there is not yet a nationwide ban on conversion therapy, legislation was introduced in the last three U.S. Congress sessions to ban this harmful practice. In June 2020, the Supreme Court decision in Bostock vs. Clayton County stated that employers could not fire an employee solely because of that person’s sexual orientation and/or gender identity.
However, 19 separate bills were introduced in 2020 alone in states across the United States that would prohibit gender-affirming care for adolescents under age 18.1 Many of these bills also would make the provision of gender-affirming medical care codified as felony child abuse, with loss of licensure, fines and/or jail time a possibility for physicians who prescribe hormones or puberty blockers for gender-affirming care to minors. Fortunately, these bills either died in committee or never had a hearing. However, legislation has been prefiled in several states for their 2021 session to again attempt to prohibit minors from obtaining gender-affirming medical care and/or criminalizing the provision of this care by physicians. Other bills were filed or have been prefiled again to allow various medical and mental health providers to refuse to treat LGBTQ patients because of their personal religious beliefs and/or forcing these same providers to tell a parent if a minor reveals to that provider that they are LGBTQ.
Even if this legislation does not pass or get a hearing, the fact that the bills were introduced can have a profound impact on LGBTQ patients and their families. After a bill was introduced in Texas in their 2017 legislative session that would require trans and gender-diverse (TGD) people to use the bathroom based on their sex assigned at birth, the Trevor Project reported that it had an increase of 34% in crisis calls from trans youth who were in distress.2 This was similar, but slightly less, than was reported by the Trevor Project in September 2015 when in the run-up to a vote on Houston’s Equal Rights Ordinance, advertising was run equating trans women as predators who could be lying in wait in bathrooms. On the converse, when LGBTQ youth feel supported in the media, courts, and legislatures, this can have a positive impact on their mental health. A 2017 study found that, in states who enacted same-sex marriage laws prior to the 2015 Supreme Court decision in Obergefell, compared with those who did not, there was a 7% relative reduction in the proportion of high school students who attempted suicide.3
The American Academy of Pediatrics published its policy statement in September 2018 outlining suggestions for pediatricians to provide support to TGD youth.4 In this position statement, recommendation No. 7 states “that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence.” Therefore, it is incumbent upon us to use our voices to support our LGBTQ youth. In 2020, several pediatricians from the South Dakota chapter of the AAP provided testimony – and organized public rallies – against legislation in that state which would have made gender-affirming care to minors under age 16 punishable by a fine and/or up to 10 years in prison.5
So what can you do? First, get to know your local and state legislators. While it was difficult to meet them in person for much of 2020, you can always call their district and/or Capitol offices, email them, or fill out their constituent contact form typically found on their website. Let them know that you oppose bills which introduce discrimination against your LGBTQ patients or threaten to criminalize the care that you provide to these patients.
Second, work with your state medical association or state AAP chapter to encourage them to oppose these harmful laws and support laws that improve the lives of LGBTQ patients. Third, you can write op-eds to your local newspaper, expressing your support for your patients and outlining the detrimental effects that anti-LGBTQ laws have on your patients. Lastly, you can be active on Twitter, Facebook, or other social media platforms sharing stories of how harmful or helpful certain pieces of legislation can be for your patients.
Dr. Cooper is assistant professor of pediatrics at the University of Texas, Dallas, and an adolescent medicine specialist at Children’s Medical Center Dallas. He has no relevant financial disclosures. Email Dr. Cooper at [email protected].
References
1. “Leglislation affecting LGBT rights across country.” www.aclu.org.
2. “Bathroom Bills Fuel Spike In Calls From Trans Youth To Suicide Hotline.” www.outsmartmagazine.com. 2017 Aug.
3. JAMA Pediatr. 2017 Apr 1. doi: 10.1001/jamapediatrics.2016.4529.
4. Pediatrics. 2018 Oct. doi: 10.1542/peds.2018-2162.
5. Wyckoff AS. “State bills seek to place limits on transgender care, ‘punish’ physicians.” AAP News. 2020 Feb 18.

Black race linked to poorer survival in AML
Black race is the most important risk factor for patients with acute myeloid leukemia (AML) and is associated with poor survival, according to new findings.
Among patients with AML younger than 60 years, the rate of overall 3-year survival was significantly less among Black patients than White patients (34% vs. 43%). The risk for death was 27% higher for Black patients compared with White patients.
“Our study demonstrates the delicate interplay between a variety of factors that influence survival disparities, particularly for younger Black AML patients,” said first author Bhavana Bhatnagar, DO, of the Ohio State University’s Comprehensive Cancer Center, Columbus. “We were able to confirm the impact of socioeconomic factors while also demonstrating that being Black is, in and of itself, an independent poor prognostic variable for survival.”
She noted that the persistently poor outcomes of young Black patients that were seen despite similar treatments in clinical trials strongly suggest that additional factors have a bearing on their survival.
The findings of the study were presented during the plenary session of the annual meeting of the American Society of Hematology, which was held online this year. The study was simultaneously published in Cancer Discovery.
Racial disparities in cancer outcomes remain a challenge. The term “health disparities” describes the differences of health outcomes among different groups, said Chancellor Donald, MD, of Tulane University, New Orleans, who introduced the article at the meeting. “Racial health disparities usually result from an unequal distribution of power and resources, not genetics.
“The examination of health disparities is certainly a worthwhile endeavor,” he continued. “For generations, differences in key health outcomes have negatively impacted the quality of life and shortened the life span of countless individuals. As scientists, clinicians, and invested members of our shared society, we are obligated to obtain a profound understanding of the mechanisms and impact of this morbid reality.”
Black race a risk factor
For their study, Dr. Bhatnagar and colleagues conducted a nationwide population analysis using data from the Surveillance Epidemiology End Results (SEER) Program of the National Cancer Institute to identify 11,190 adults aged 18-60 years who were diagnosed with AML between 1986 and 2015.
To characterize molecular features, they conducted targeted sequencing of 81 genes in 1,339 patients with AML who were treated on frontline Cancer and Leukemia Group B/Alliance for Clinical Trials in Oncology (Alliance) protocols based on standard-intensity cytarabine/anthracycline induction followed by consolidation between 1986 and 2016. None of these patients received an allogeneic stem cell transplant when they achieved complete remission.
Although overall survival has improved during the past 3 decades, survival disparities between Black and White patients has widened over time (P < .001). The authors found a nonstatistically significant difference in survival between 1986 and 1995 (White patients, n = 1,365; Black patients, n = 160; P = .19). However, the difference was significant between 1996 and 2005 (White patients, n = 2,994; Black patients, n = 480; P = .004). “And it became even more noticeable in the most recent decade,” said Dr. Bhatnagar. “Furthermore, younger Black AML patients were found to have worse survival compared with younger White AML patients.”
Results from the second analysis of patients treated on Alliance protocols did not show any significant differences in early death rates (10% vs. 46%; P = .02) and complete remission rates (71% vs. 71%; P = 1.00). “While relapse rates were slightly higher in Black compared to White patients, this difference did not reach statistical significance,” said Dr. Bhatnagar. “There was also no significant difference in the number of cycles of consolidation chemotherapy administered to these patients.”
However, both disease-free and overall survival were significantly worse for Black patients, suggesting that factors other than treatment selection were likely at play in influencing the survival disparity. The median disease-free survival for Black patients was 0.8 years, vs. 1.4 years for White patients (P = .02). Overall survival was 1.2 years vs. 1.8 years (P = .02).
Relapse rates were slightly higher in Black patients than in White patients, at 71% vs. 59%, but this difference did not reach statistical significance (P = .14).
Differences in biomarkers
With regard to underlying molecular differences between Black and White patients, the investigators found that the most common mutations were in NPM1, FLT3-ITD, and DNM3TA. Mutations were detected in more than 20% of Black patients. Other commonly mutated genes were IDH2, NRAS, TET2, IDH1, and TP53, which were mutated in more than 10% of patients. “All of these genes are established commonly mutated genes in AML,” said Bhatnagar.
On univariable and multivariable outcome analyses, which were used to identify clinical or molecular features that had a bearing on outcome, FLT3-ITD and IDH2 mutations were the only mutations associated with a higher risk for death among Black patients.
“This is actually a very important finding, as both FLT3 and IDH2 are now targetable with small-molecule inhibitors,” said Dr. Bhatnagar. “In addition, it is also worth noting that other gene mutations that have known prognostic significance in AML, such as NPM1, as well as RUNX1 and TP53, did not remain in the final statistical model.
“Importantly, our study provides powerful evidence that suggests differences in underlying disease biology between young Black and White AML patients, as evidenced by differences in the frequencies of recurrent gene mutations, “ she said.
Understudied disparities
Although the study showed that Black patients had worse outcomes, “surprisingly, the authors found these outcomes hold even when the patients are participating in clinical trials,” noted Elisa Weiss, PhD, senior vice president of education, services, and health research for the Leukemia and Lymphoma Society.
“The study makes clear that the medical and science community need to do more to better understand the social, economic, environmental, and biological causes of these disparities,” she said in an interview. “In fact, the findings suggest that there are myriad complex and understudied causes of the identified disparities, and they are likely to lie at the intersection of all levels of the social ecology that impact an individual’s ability to access timely and unbiased care, maintain their mental and physical health, and receive needed social support and resources.”
She noted that the Leukemia and Lymphoma Society has an Equity in Access research program that aims to “advance study of underlying causes of inequitable access to care and identify policies, strategies, and interventions that have the potential to reduce inequities and increase access to health care, services, and programs for blood cancer patients and survivors.”
The research was supported in part by the National Cancer Institute of the National Institutes of Health, other institutions, and through several scholar awards. Dr. Bhatnagar has received advisory board honoraria from Novartis, Kite Pharma, Celgene, Astellas, and Cell Therapeutics. Dr. Weiss has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Black race is the most important risk factor for patients with acute myeloid leukemia (AML) and is associated with poor survival, according to new findings.
Among patients with AML younger than 60 years, the rate of overall 3-year survival was significantly less among Black patients than White patients (34% vs. 43%). The risk for death was 27% higher for Black patients compared with White patients.
“Our study demonstrates the delicate interplay between a variety of factors that influence survival disparities, particularly for younger Black AML patients,” said first author Bhavana Bhatnagar, DO, of the Ohio State University’s Comprehensive Cancer Center, Columbus. “We were able to confirm the impact of socioeconomic factors while also demonstrating that being Black is, in and of itself, an independent poor prognostic variable for survival.”
She noted that the persistently poor outcomes of young Black patients that were seen despite similar treatments in clinical trials strongly suggest that additional factors have a bearing on their survival.
The findings of the study were presented during the plenary session of the annual meeting of the American Society of Hematology, which was held online this year. The study was simultaneously published in Cancer Discovery.
Racial disparities in cancer outcomes remain a challenge. The term “health disparities” describes the differences of health outcomes among different groups, said Chancellor Donald, MD, of Tulane University, New Orleans, who introduced the article at the meeting. “Racial health disparities usually result from an unequal distribution of power and resources, not genetics.
“The examination of health disparities is certainly a worthwhile endeavor,” he continued. “For generations, differences in key health outcomes have negatively impacted the quality of life and shortened the life span of countless individuals. As scientists, clinicians, and invested members of our shared society, we are obligated to obtain a profound understanding of the mechanisms and impact of this morbid reality.”
Black race a risk factor
For their study, Dr. Bhatnagar and colleagues conducted a nationwide population analysis using data from the Surveillance Epidemiology End Results (SEER) Program of the National Cancer Institute to identify 11,190 adults aged 18-60 years who were diagnosed with AML between 1986 and 2015.
To characterize molecular features, they conducted targeted sequencing of 81 genes in 1,339 patients with AML who were treated on frontline Cancer and Leukemia Group B/Alliance for Clinical Trials in Oncology (Alliance) protocols based on standard-intensity cytarabine/anthracycline induction followed by consolidation between 1986 and 2016. None of these patients received an allogeneic stem cell transplant when they achieved complete remission.
Although overall survival has improved during the past 3 decades, survival disparities between Black and White patients has widened over time (P < .001). The authors found a nonstatistically significant difference in survival between 1986 and 1995 (White patients, n = 1,365; Black patients, n = 160; P = .19). However, the difference was significant between 1996 and 2005 (White patients, n = 2,994; Black patients, n = 480; P = .004). “And it became even more noticeable in the most recent decade,” said Dr. Bhatnagar. “Furthermore, younger Black AML patients were found to have worse survival compared with younger White AML patients.”
Results from the second analysis of patients treated on Alliance protocols did not show any significant differences in early death rates (10% vs. 46%; P = .02) and complete remission rates (71% vs. 71%; P = 1.00). “While relapse rates were slightly higher in Black compared to White patients, this difference did not reach statistical significance,” said Dr. Bhatnagar. “There was also no significant difference in the number of cycles of consolidation chemotherapy administered to these patients.”
However, both disease-free and overall survival were significantly worse for Black patients, suggesting that factors other than treatment selection were likely at play in influencing the survival disparity. The median disease-free survival for Black patients was 0.8 years, vs. 1.4 years for White patients (P = .02). Overall survival was 1.2 years vs. 1.8 years (P = .02).
Relapse rates were slightly higher in Black patients than in White patients, at 71% vs. 59%, but this difference did not reach statistical significance (P = .14).
Differences in biomarkers
With regard to underlying molecular differences between Black and White patients, the investigators found that the most common mutations were in NPM1, FLT3-ITD, and DNM3TA. Mutations were detected in more than 20% of Black patients. Other commonly mutated genes were IDH2, NRAS, TET2, IDH1, and TP53, which were mutated in more than 10% of patients. “All of these genes are established commonly mutated genes in AML,” said Bhatnagar.
On univariable and multivariable outcome analyses, which were used to identify clinical or molecular features that had a bearing on outcome, FLT3-ITD and IDH2 mutations were the only mutations associated with a higher risk for death among Black patients.
“This is actually a very important finding, as both FLT3 and IDH2 are now targetable with small-molecule inhibitors,” said Dr. Bhatnagar. “In addition, it is also worth noting that other gene mutations that have known prognostic significance in AML, such as NPM1, as well as RUNX1 and TP53, did not remain in the final statistical model.
“Importantly, our study provides powerful evidence that suggests differences in underlying disease biology between young Black and White AML patients, as evidenced by differences in the frequencies of recurrent gene mutations, “ she said.
Understudied disparities
Although the study showed that Black patients had worse outcomes, “surprisingly, the authors found these outcomes hold even when the patients are participating in clinical trials,” noted Elisa Weiss, PhD, senior vice president of education, services, and health research for the Leukemia and Lymphoma Society.
“The study makes clear that the medical and science community need to do more to better understand the social, economic, environmental, and biological causes of these disparities,” she said in an interview. “In fact, the findings suggest that there are myriad complex and understudied causes of the identified disparities, and they are likely to lie at the intersection of all levels of the social ecology that impact an individual’s ability to access timely and unbiased care, maintain their mental and physical health, and receive needed social support and resources.”
She noted that the Leukemia and Lymphoma Society has an Equity in Access research program that aims to “advance study of underlying causes of inequitable access to care and identify policies, strategies, and interventions that have the potential to reduce inequities and increase access to health care, services, and programs for blood cancer patients and survivors.”
The research was supported in part by the National Cancer Institute of the National Institutes of Health, other institutions, and through several scholar awards. Dr. Bhatnagar has received advisory board honoraria from Novartis, Kite Pharma, Celgene, Astellas, and Cell Therapeutics. Dr. Weiss has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Black race is the most important risk factor for patients with acute myeloid leukemia (AML) and is associated with poor survival, according to new findings.
Among patients with AML younger than 60 years, the rate of overall 3-year survival was significantly less among Black patients than White patients (34% vs. 43%). The risk for death was 27% higher for Black patients compared with White patients.
“Our study demonstrates the delicate interplay between a variety of factors that influence survival disparities, particularly for younger Black AML patients,” said first author Bhavana Bhatnagar, DO, of the Ohio State University’s Comprehensive Cancer Center, Columbus. “We were able to confirm the impact of socioeconomic factors while also demonstrating that being Black is, in and of itself, an independent poor prognostic variable for survival.”
She noted that the persistently poor outcomes of young Black patients that were seen despite similar treatments in clinical trials strongly suggest that additional factors have a bearing on their survival.
The findings of the study were presented during the plenary session of the annual meeting of the American Society of Hematology, which was held online this year. The study was simultaneously published in Cancer Discovery.
Racial disparities in cancer outcomes remain a challenge. The term “health disparities” describes the differences of health outcomes among different groups, said Chancellor Donald, MD, of Tulane University, New Orleans, who introduced the article at the meeting. “Racial health disparities usually result from an unequal distribution of power and resources, not genetics.
“The examination of health disparities is certainly a worthwhile endeavor,” he continued. “For generations, differences in key health outcomes have negatively impacted the quality of life and shortened the life span of countless individuals. As scientists, clinicians, and invested members of our shared society, we are obligated to obtain a profound understanding of the mechanisms and impact of this morbid reality.”
Black race a risk factor
For their study, Dr. Bhatnagar and colleagues conducted a nationwide population analysis using data from the Surveillance Epidemiology End Results (SEER) Program of the National Cancer Institute to identify 11,190 adults aged 18-60 years who were diagnosed with AML between 1986 and 2015.
To characterize molecular features, they conducted targeted sequencing of 81 genes in 1,339 patients with AML who were treated on frontline Cancer and Leukemia Group B/Alliance for Clinical Trials in Oncology (Alliance) protocols based on standard-intensity cytarabine/anthracycline induction followed by consolidation between 1986 and 2016. None of these patients received an allogeneic stem cell transplant when they achieved complete remission.
Although overall survival has improved during the past 3 decades, survival disparities between Black and White patients has widened over time (P < .001). The authors found a nonstatistically significant difference in survival between 1986 and 1995 (White patients, n = 1,365; Black patients, n = 160; P = .19). However, the difference was significant between 1996 and 2005 (White patients, n = 2,994; Black patients, n = 480; P = .004). “And it became even more noticeable in the most recent decade,” said Dr. Bhatnagar. “Furthermore, younger Black AML patients were found to have worse survival compared with younger White AML patients.”
Results from the second analysis of patients treated on Alliance protocols did not show any significant differences in early death rates (10% vs. 46%; P = .02) and complete remission rates (71% vs. 71%; P = 1.00). “While relapse rates were slightly higher in Black compared to White patients, this difference did not reach statistical significance,” said Dr. Bhatnagar. “There was also no significant difference in the number of cycles of consolidation chemotherapy administered to these patients.”
However, both disease-free and overall survival were significantly worse for Black patients, suggesting that factors other than treatment selection were likely at play in influencing the survival disparity. The median disease-free survival for Black patients was 0.8 years, vs. 1.4 years for White patients (P = .02). Overall survival was 1.2 years vs. 1.8 years (P = .02).
Relapse rates were slightly higher in Black patients than in White patients, at 71% vs. 59%, but this difference did not reach statistical significance (P = .14).
Differences in biomarkers
With regard to underlying molecular differences between Black and White patients, the investigators found that the most common mutations were in NPM1, FLT3-ITD, and DNM3TA. Mutations were detected in more than 20% of Black patients. Other commonly mutated genes were IDH2, NRAS, TET2, IDH1, and TP53, which were mutated in more than 10% of patients. “All of these genes are established commonly mutated genes in AML,” said Bhatnagar.
On univariable and multivariable outcome analyses, which were used to identify clinical or molecular features that had a bearing on outcome, FLT3-ITD and IDH2 mutations were the only mutations associated with a higher risk for death among Black patients.
“This is actually a very important finding, as both FLT3 and IDH2 are now targetable with small-molecule inhibitors,” said Dr. Bhatnagar. “In addition, it is also worth noting that other gene mutations that have known prognostic significance in AML, such as NPM1, as well as RUNX1 and TP53, did not remain in the final statistical model.
“Importantly, our study provides powerful evidence that suggests differences in underlying disease biology between young Black and White AML patients, as evidenced by differences in the frequencies of recurrent gene mutations, “ she said.
Understudied disparities
Although the study showed that Black patients had worse outcomes, “surprisingly, the authors found these outcomes hold even when the patients are participating in clinical trials,” noted Elisa Weiss, PhD, senior vice president of education, services, and health research for the Leukemia and Lymphoma Society.
“The study makes clear that the medical and science community need to do more to better understand the social, economic, environmental, and biological causes of these disparities,” she said in an interview. “In fact, the findings suggest that there are myriad complex and understudied causes of the identified disparities, and they are likely to lie at the intersection of all levels of the social ecology that impact an individual’s ability to access timely and unbiased care, maintain their mental and physical health, and receive needed social support and resources.”
She noted that the Leukemia and Lymphoma Society has an Equity in Access research program that aims to “advance study of underlying causes of inequitable access to care and identify policies, strategies, and interventions that have the potential to reduce inequities and increase access to health care, services, and programs for blood cancer patients and survivors.”
The research was supported in part by the National Cancer Institute of the National Institutes of Health, other institutions, and through several scholar awards. Dr. Bhatnagar has received advisory board honoraria from Novartis, Kite Pharma, Celgene, Astellas, and Cell Therapeutics. Dr. Weiss has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Herpes Zoster May Be a Marker for COVID-19 Infection During Pregnancy
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the most recently identified member of the zoonotic pathogens of coronaviruses. It caused an outbreak of pneumonia in December 2019 in Wuhan, China.1 Among all related acute respiratory syndromes (SARS-CoV, Middle East respiratory syndrome coronavirus), SARS-CoV-2 remains to be the most infectious, has the highest potential for human transmission, and can eventually result in acute respiratory distress syndrome.2,3
Only 15% of coronavirus disease 2019 (COVID-19) cases progress to pneumonia, and approximately 5% of these cases develop acute respiratory distress syndrome, septic shock, and/or multiple organ failure. The majority of cases only exhibit mild to moderate symptoms.4,5 A wide array of skin manifestations in COVID-19 infection have been reported, including maculopapular eruptions, morbilliform rashes, urticaria, chickenpoxlike lesions, livedo reticularis, COVID toes, erythema multiforme, pityriasis rosea, and several other patterns.6 We report a case of herpes zoster (HZ) complication in a COVID-19–positive woman who was 27 weeks pregnant.
Case Report
A 36-year-old woman who was 27 weeks pregnant was referred by her obstetrician to the dermatology clinic. She presented with a low-grade fever and a vesicular painful rash. Physical examination revealed painful, itchy, dysesthetic papules and vesicles on the left side of the forehead along with mild edema of the left upper eyelid but no watering of the eye or photophobia. She reported episodes of fever (temperature, 38.9°C), fatigue, and myalgia over the last week. She had bouts of dyspnea and tachycardia that she thought were related to being in the late second trimester of pregnancy. The area surrounding the vesicular eruption was tender to touch. No dry cough or any gastrointestinal or urinary tract symptoms were noted. She reported a burning sensation when splashing water on the face or when exposed to air currents. One week following the initial symptoms, she experienced a painful vesicular rash along the upper left forehead (Figure) associated with eyelid edema. Oral and ocular mucosae were free of any presentations. She had no relevant history and had not experienced any complications during pregnancy. A diagnosis of HZ was made, and she was prescribed valacyclovir 1 g 3 times daily for 7 days, acetaminophen for the fever, and calamine lotion. We recommended COVID-19 testing based on her symptoms. A chest radiograph and a positive nasopharyngeal smear were consistent with COVID-19 infection. She reported via telephone follow-up 1 week after presentation that her skin condition had improved following the treatment course and that the vesicles eventually dried, leaving a crusting appearance after 5 to 7 days. Regarding her SARS-CoV-2 condition, her oxygen saturation was 95% at presentation; she self-quarantined at home; and she was treated with oseltamivir 75 mg orally every 12 hours for 5 days, azithromycin 500 mg orally daily, acetaminophen, and vitamin C. Electronic fetal heart rate monitoring and ultrasound examinations were performed to assess the condition of the fetus and were reported normal. At the time of writing this article, she was 32 weeks pregnant and tested negative to 2 consecutive nasopharyngeal swabs for COVID-19 and was in good general condition. She continued her pregnancy according to her obstetrician’s recommendations.

Comment
The incubation time of COVID-19 can be up to 14 days. Fever, dry cough, fatigue, and diarrhea have been speculated to be clinical symptoms; however, many cases may be asymptomatic. Aside from a medical or travel history at risk for COVID-19, diagnosis can be confirmed by detection of viral RNA by reverse transcriptase–polymerase chain reaction for nasopharyngeal swabs or bronchoalveolar fluid. Patients who are immunocompromised, older, or male or who have a history of cardiovascular conditions or debilitating chronic conditions are at an increased risk for severe disease and poor outcome compared to younger healthy individuals.7
The vesicular rash of COVID-19 has been reported to have different forms of presentation. A diffuse widespread pattern resembling hand-foot-and-mouth disease and a localized monomorphic pattern resembling chickenpox but with predilection to the trunk has been described.8
Physiologic changes in the immune and cardiopulmonary systems during pregnancy (eg, diaphragm elevation, increased oxygen consumption, edema of the respiratory tract mucosae) make pregnant women intolerant to hypoxia. The mortality rate of the 1918 influenza pandemic was 2.6% in the overall population but 37% among pregnant women.9 In 2009, pregnant women were reported to be at an increased risk for complications from the H1N1 influenza virus pandemic, with a higher estimated rate of hospital admission than the general population.10 In 2003, approximately 50% of pregnant women who received a diagnosis of SARS-CoV were admitted to the intensive care unit, approximately 33% of pregnant women with SARS-CoV required mechanical ventilation, and the mortality rate was as high as 25% for these women.11 To date, data on the effects of COVID-19 in pregnancy are limited to small case series.12-15
It was confirmed that COVID-19 infection is accompanied by a reduction in lymphocytes, monocytes, and eosinophils, along with a notable reduction of CD4/CD8 T cells, B cells, and natural killer cells. It was further revealed that nonsurvivor COVID-19 patients continued to show a decrease in lymphocyte counts along the course of their disease until death.16-18
Different mechanisms for lymphocyte depletion and deficiency were speculated among COVID-19 patients and include direct lymphocyte death through coronavirus angiotensin-converting enzyme 2–lymphocyte-expressed receptors; direct damage to lymphatic organs, such as the thymus and spleen, but this theory needs to be further investigated; direct lymphocyte apoptosis mediated by tumor necrosis factor α, IL-6, and other proinflammatory cytokines; and direct inhibition of lymphocytes by metabolic upset, such as acidosis.19,20
These causes may precipitate lymphopenia and impaired antiviral responses.21 It also has been postulated that the functional damage of CD4+ T cells may predispose patients with COVID-19 to severe disease.22 Such immune changes can render a patient more susceptible to developing shingles by reactivating varicella-zoster virus, which could be a sign of undiagnosed COVID-19 infection in younger age groups.
Two earlier reports discussed HZ among COVID-19–diagnosed patients. Shors23 presented a case of a patient who developed varicella-zoster virus reactivation of the V2 dermatome during the course of COVID-19 infection. In addition, the patient developed severe acute herpetic neuralgia despite the early initiation of antiviral therapy.23 Elsaie et al24 described 2 cases of patients during the pandemic who first presented with HZ before later being diagnosed with COVID-19 infection.
New information and cutaneous manifestations possibly related to COVID-19 are emerging every day. We report a pregnant female presenting with HZ during the course of COVID-19 infection, which suggests that the clinical presentation of HZ at the time of the current pandemic, especially if associated with other signs of COVID-19 infection, should be carefully monitored and reported for further assessment.
Acknowledgment
The authors would like to thank all the health care workers who have been fighting COVID-19 in Egypt and worldwide.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207.
- Zhang YZ, Holes EC. A genomic perspective on the origin and emergence of sars-cov-2. Cell. 2020;181:223-227.
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38:1‐9.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan0, China. Lancet. 2020;395:497-506.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-422.
- Wollina U, Karadag˘ AS, Rowland-Payne C, et al. Cutaneous signs in COVID-19 patients: a review. Dermatol Ther. 2020;33:e13549.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577‐582.
- Fernandez-Nieto D, Ortega-Quijano D, Jimenez-Cauhe J, et al. Clinical and histological characterization of vesicular COVID-19 rashes: a prospective study in a tertiary care hospital. Clin Exp Dermatol. 2020;45:872-875.
- Gottfredsson M. The Spanish flu in Iceland 1918. Lessons in medicine and history [in Icelandic]. Laeknabladid. 2008;94:737-745.
- Jamieson D, Honein M, Rasmussen S, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451-458.
- Ksiazek TG, Erdman D, Goldsmith CS. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953-1966.
- Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809‐815.
- Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCov pneumonia. Transl Pediatr. 2020;9:51-60.
- Liu Y, Chen H, Tang K, et al. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy [published online March 4, 2020]. J Infect. doi:10.1016/j.jinf.2020.02.028.
- Zhang L, Jiang Y, Wei M, et al. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province [in Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2020;55:166-171.
- Henry BM, de Oliveira MHS, Benoit S, et al. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58:1021-1028.
- Cai Q, Huang D, Ou P, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. 2020;75:1742-1752.
- Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-884.
- Kumar A, Anil A, Sharma P, et al. Clinical features of COVID-19 and factors associated with severe clinical course: a systematic review and meta-analysis [preprint]. SSRN. doi:10.2139/ssrn.3566166.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12. https://doi.org/10.1038/s41368-020-0074-x.
- Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395:1517-1520.
- Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020;17:533-535.
- Shors AR. Herpes zoster and severe acute herpetic neuralgia as a complication of COVID-19 infection. JAAD Case Rep. 2020;6:656-657.
- Elsaie ML, Youssef EA, Nada HA. Herpes zoster might be an indicator for latent COVID 19 infection [published online May 23, 2020]. Dermatol Ther. doi:10.1111/dth.13666.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the most recently identified member of the zoonotic pathogens of coronaviruses. It caused an outbreak of pneumonia in December 2019 in Wuhan, China.1 Among all related acute respiratory syndromes (SARS-CoV, Middle East respiratory syndrome coronavirus), SARS-CoV-2 remains to be the most infectious, has the highest potential for human transmission, and can eventually result in acute respiratory distress syndrome.2,3
Only 15% of coronavirus disease 2019 (COVID-19) cases progress to pneumonia, and approximately 5% of these cases develop acute respiratory distress syndrome, septic shock, and/or multiple organ failure. The majority of cases only exhibit mild to moderate symptoms.4,5 A wide array of skin manifestations in COVID-19 infection have been reported, including maculopapular eruptions, morbilliform rashes, urticaria, chickenpoxlike lesions, livedo reticularis, COVID toes, erythema multiforme, pityriasis rosea, and several other patterns.6 We report a case of herpes zoster (HZ) complication in a COVID-19–positive woman who was 27 weeks pregnant.
Case Report
A 36-year-old woman who was 27 weeks pregnant was referred by her obstetrician to the dermatology clinic. She presented with a low-grade fever and a vesicular painful rash. Physical examination revealed painful, itchy, dysesthetic papules and vesicles on the left side of the forehead along with mild edema of the left upper eyelid but no watering of the eye or photophobia. She reported episodes of fever (temperature, 38.9°C), fatigue, and myalgia over the last week. She had bouts of dyspnea and tachycardia that she thought were related to being in the late second trimester of pregnancy. The area surrounding the vesicular eruption was tender to touch. No dry cough or any gastrointestinal or urinary tract symptoms were noted. She reported a burning sensation when splashing water on the face or when exposed to air currents. One week following the initial symptoms, she experienced a painful vesicular rash along the upper left forehead (Figure) associated with eyelid edema. Oral and ocular mucosae were free of any presentations. She had no relevant history and had not experienced any complications during pregnancy. A diagnosis of HZ was made, and she was prescribed valacyclovir 1 g 3 times daily for 7 days, acetaminophen for the fever, and calamine lotion. We recommended COVID-19 testing based on her symptoms. A chest radiograph and a positive nasopharyngeal smear were consistent with COVID-19 infection. She reported via telephone follow-up 1 week after presentation that her skin condition had improved following the treatment course and that the vesicles eventually dried, leaving a crusting appearance after 5 to 7 days. Regarding her SARS-CoV-2 condition, her oxygen saturation was 95% at presentation; she self-quarantined at home; and she was treated with oseltamivir 75 mg orally every 12 hours for 5 days, azithromycin 500 mg orally daily, acetaminophen, and vitamin C. Electronic fetal heart rate monitoring and ultrasound examinations were performed to assess the condition of the fetus and were reported normal. At the time of writing this article, she was 32 weeks pregnant and tested negative to 2 consecutive nasopharyngeal swabs for COVID-19 and was in good general condition. She continued her pregnancy according to her obstetrician’s recommendations.
Comment
The incubation time of COVID-19 can be up to 14 days. Fever, dry cough, fatigue, and diarrhea have been speculated to be clinical symptoms; however, many cases may be asymptomatic. Aside from a medical or travel history at risk for COVID-19, diagnosis can be confirmed by detection of viral RNA by reverse transcriptase–polymerase chain reaction for nasopharyngeal swabs or bronchoalveolar fluid. Patients who are immunocompromised, older, or male or who have a history of cardiovascular conditions or debilitating chronic conditions are at an increased risk for severe disease and poor outcome compared to younger healthy individuals.7
The vesicular rash of COVID-19 has been reported to have different forms of presentation. A diffuse widespread pattern resembling hand-foot-and-mouth disease and a localized monomorphic pattern resembling chickenpox but with predilection to the trunk has been described.8
Physiologic changes in the immune and cardiopulmonary systems during pregnancy (eg, diaphragm elevation, increased oxygen consumption, edema of the respiratory tract mucosae) make pregnant women intolerant to hypoxia. The mortality rate of the 1918 influenza pandemic was 2.6% in the overall population but 37% among pregnant women.9 In 2009, pregnant women were reported to be at an increased risk for complications from the H1N1 influenza virus pandemic, with a higher estimated rate of hospital admission than the general population.10 In 2003, approximately 50% of pregnant women who received a diagnosis of SARS-CoV were admitted to the intensive care unit, approximately 33% of pregnant women with SARS-CoV required mechanical ventilation, and the mortality rate was as high as 25% for these women.11 To date, data on the effects of COVID-19 in pregnancy are limited to small case series.12-15
It was confirmed that COVID-19 infection is accompanied by a reduction in lymphocytes, monocytes, and eosinophils, along with a notable reduction of CD4/CD8 T cells, B cells, and natural killer cells. It was further revealed that nonsurvivor COVID-19 patients continued to show a decrease in lymphocyte counts along the course of their disease until death.16-18
Different mechanisms for lymphocyte depletion and deficiency were speculated among COVID-19 patients and include direct lymphocyte death through coronavirus angiotensin-converting enzyme 2–lymphocyte-expressed receptors; direct damage to lymphatic organs, such as the thymus and spleen, but this theory needs to be further investigated; direct lymphocyte apoptosis mediated by tumor necrosis factor α, IL-6, and other proinflammatory cytokines; and direct inhibition of lymphocytes by metabolic upset, such as acidosis.19,20
These causes may precipitate lymphopenia and impaired antiviral responses.21 It also has been postulated that the functional damage of CD4+ T cells may predispose patients with COVID-19 to severe disease.22 Such immune changes can render a patient more susceptible to developing shingles by reactivating varicella-zoster virus, which could be a sign of undiagnosed COVID-19 infection in younger age groups.
Two earlier reports discussed HZ among COVID-19–diagnosed patients. Shors23 presented a case of a patient who developed varicella-zoster virus reactivation of the V2 dermatome during the course of COVID-19 infection. In addition, the patient developed severe acute herpetic neuralgia despite the early initiation of antiviral therapy.23 Elsaie et al24 described 2 cases of patients during the pandemic who first presented with HZ before later being diagnosed with COVID-19 infection.
New information and cutaneous manifestations possibly related to COVID-19 are emerging every day. We report a pregnant female presenting with HZ during the course of COVID-19 infection, which suggests that the clinical presentation of HZ at the time of the current pandemic, especially if associated with other signs of COVID-19 infection, should be carefully monitored and reported for further assessment.
Acknowledgment
The authors would like to thank all the health care workers who have been fighting COVID-19 in Egypt and worldwide.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the most recently identified member of the zoonotic pathogens of coronaviruses. It caused an outbreak of pneumonia in December 2019 in Wuhan, China.1 Among all related acute respiratory syndromes (SARS-CoV, Middle East respiratory syndrome coronavirus), SARS-CoV-2 remains to be the most infectious, has the highest potential for human transmission, and can eventually result in acute respiratory distress syndrome.2,3
Only 15% of coronavirus disease 2019 (COVID-19) cases progress to pneumonia, and approximately 5% of these cases develop acute respiratory distress syndrome, septic shock, and/or multiple organ failure. The majority of cases only exhibit mild to moderate symptoms.4,5 A wide array of skin manifestations in COVID-19 infection have been reported, including maculopapular eruptions, morbilliform rashes, urticaria, chickenpoxlike lesions, livedo reticularis, COVID toes, erythema multiforme, pityriasis rosea, and several other patterns.6 We report a case of herpes zoster (HZ) complication in a COVID-19–positive woman who was 27 weeks pregnant.
Case Report
A 36-year-old woman who was 27 weeks pregnant was referred by her obstetrician to the dermatology clinic. She presented with a low-grade fever and a vesicular painful rash. Physical examination revealed painful, itchy, dysesthetic papules and vesicles on the left side of the forehead along with mild edema of the left upper eyelid but no watering of the eye or photophobia. She reported episodes of fever (temperature, 38.9°C), fatigue, and myalgia over the last week. She had bouts of dyspnea and tachycardia that she thought were related to being in the late second trimester of pregnancy. The area surrounding the vesicular eruption was tender to touch. No dry cough or any gastrointestinal or urinary tract symptoms were noted. She reported a burning sensation when splashing water on the face or when exposed to air currents. One week following the initial symptoms, she experienced a painful vesicular rash along the upper left forehead (Figure) associated with eyelid edema. Oral and ocular mucosae were free of any presentations. She had no relevant history and had not experienced any complications during pregnancy. A diagnosis of HZ was made, and she was prescribed valacyclovir 1 g 3 times daily for 7 days, acetaminophen for the fever, and calamine lotion. We recommended COVID-19 testing based on her symptoms. A chest radiograph and a positive nasopharyngeal smear were consistent with COVID-19 infection. She reported via telephone follow-up 1 week after presentation that her skin condition had improved following the treatment course and that the vesicles eventually dried, leaving a crusting appearance after 5 to 7 days. Regarding her SARS-CoV-2 condition, her oxygen saturation was 95% at presentation; she self-quarantined at home; and she was treated with oseltamivir 75 mg orally every 12 hours for 5 days, azithromycin 500 mg orally daily, acetaminophen, and vitamin C. Electronic fetal heart rate monitoring and ultrasound examinations were performed to assess the condition of the fetus and were reported normal. At the time of writing this article, she was 32 weeks pregnant and tested negative to 2 consecutive nasopharyngeal swabs for COVID-19 and was in good general condition. She continued her pregnancy according to her obstetrician’s recommendations.
Comment
The incubation time of COVID-19 can be up to 14 days. Fever, dry cough, fatigue, and diarrhea have been speculated to be clinical symptoms; however, many cases may be asymptomatic. Aside from a medical or travel history at risk for COVID-19, diagnosis can be confirmed by detection of viral RNA by reverse transcriptase–polymerase chain reaction for nasopharyngeal swabs or bronchoalveolar fluid. Patients who are immunocompromised, older, or male or who have a history of cardiovascular conditions or debilitating chronic conditions are at an increased risk for severe disease and poor outcome compared to younger healthy individuals.7
The vesicular rash of COVID-19 has been reported to have different forms of presentation. A diffuse widespread pattern resembling hand-foot-and-mouth disease and a localized monomorphic pattern resembling chickenpox but with predilection to the trunk has been described.8
Physiologic changes in the immune and cardiopulmonary systems during pregnancy (eg, diaphragm elevation, increased oxygen consumption, edema of the respiratory tract mucosae) make pregnant women intolerant to hypoxia. The mortality rate of the 1918 influenza pandemic was 2.6% in the overall population but 37% among pregnant women.9 In 2009, pregnant women were reported to be at an increased risk for complications from the H1N1 influenza virus pandemic, with a higher estimated rate of hospital admission than the general population.10 In 2003, approximately 50% of pregnant women who received a diagnosis of SARS-CoV were admitted to the intensive care unit, approximately 33% of pregnant women with SARS-CoV required mechanical ventilation, and the mortality rate was as high as 25% for these women.11 To date, data on the effects of COVID-19 in pregnancy are limited to small case series.12-15
It was confirmed that COVID-19 infection is accompanied by a reduction in lymphocytes, monocytes, and eosinophils, along with a notable reduction of CD4/CD8 T cells, B cells, and natural killer cells. It was further revealed that nonsurvivor COVID-19 patients continued to show a decrease in lymphocyte counts along the course of their disease until death.16-18
Different mechanisms for lymphocyte depletion and deficiency were speculated among COVID-19 patients and include direct lymphocyte death through coronavirus angiotensin-converting enzyme 2–lymphocyte-expressed receptors; direct damage to lymphatic organs, such as the thymus and spleen, but this theory needs to be further investigated; direct lymphocyte apoptosis mediated by tumor necrosis factor α, IL-6, and other proinflammatory cytokines; and direct inhibition of lymphocytes by metabolic upset, such as acidosis.19,20
These causes may precipitate lymphopenia and impaired antiviral responses.21 It also has been postulated that the functional damage of CD4+ T cells may predispose patients with COVID-19 to severe disease.22 Such immune changes can render a patient more susceptible to developing shingles by reactivating varicella-zoster virus, which could be a sign of undiagnosed COVID-19 infection in younger age groups.
Two earlier reports discussed HZ among COVID-19–diagnosed patients. Shors23 presented a case of a patient who developed varicella-zoster virus reactivation of the V2 dermatome during the course of COVID-19 infection. In addition, the patient developed severe acute herpetic neuralgia despite the early initiation of antiviral therapy.23 Elsaie et al24 described 2 cases of patients during the pandemic who first presented with HZ before later being diagnosed with COVID-19 infection.
New information and cutaneous manifestations possibly related to COVID-19 are emerging every day. We report a pregnant female presenting with HZ during the course of COVID-19 infection, which suggests that the clinical presentation of HZ at the time of the current pandemic, especially if associated with other signs of COVID-19 infection, should be carefully monitored and reported for further assessment.
Acknowledgment
The authors would like to thank all the health care workers who have been fighting COVID-19 in Egypt and worldwide.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207.
- Zhang YZ, Holes EC. A genomic perspective on the origin and emergence of sars-cov-2. Cell. 2020;181:223-227.
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38:1‐9.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan0, China. Lancet. 2020;395:497-506.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-422.
- Wollina U, Karadag˘ AS, Rowland-Payne C, et al. Cutaneous signs in COVID-19 patients: a review. Dermatol Ther. 2020;33:e13549.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577‐582.
- Fernandez-Nieto D, Ortega-Quijano D, Jimenez-Cauhe J, et al. Clinical and histological characterization of vesicular COVID-19 rashes: a prospective study in a tertiary care hospital. Clin Exp Dermatol. 2020;45:872-875.
- Gottfredsson M. The Spanish flu in Iceland 1918. Lessons in medicine and history [in Icelandic]. Laeknabladid. 2008;94:737-745.
- Jamieson D, Honein M, Rasmussen S, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451-458.
- Ksiazek TG, Erdman D, Goldsmith CS. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953-1966.
- Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809‐815.
- Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCov pneumonia. Transl Pediatr. 2020;9:51-60.
- Liu Y, Chen H, Tang K, et al. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy [published online March 4, 2020]. J Infect. doi:10.1016/j.jinf.2020.02.028.
- Zhang L, Jiang Y, Wei M, et al. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province [in Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2020;55:166-171.
- Henry BM, de Oliveira MHS, Benoit S, et al. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58:1021-1028.
- Cai Q, Huang D, Ou P, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. 2020;75:1742-1752.
- Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-884.
- Kumar A, Anil A, Sharma P, et al. Clinical features of COVID-19 and factors associated with severe clinical course: a systematic review and meta-analysis [preprint]. SSRN. doi:10.2139/ssrn.3566166.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12. https://doi.org/10.1038/s41368-020-0074-x.
- Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395:1517-1520.
- Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020;17:533-535.
- Shors AR. Herpes zoster and severe acute herpetic neuralgia as a complication of COVID-19 infection. JAAD Case Rep. 2020;6:656-657.
- Elsaie ML, Youssef EA, Nada HA. Herpes zoster might be an indicator for latent COVID 19 infection [published online May 23, 2020]. Dermatol Ther. doi:10.1111/dth.13666.
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207.
- Zhang YZ, Holes EC. A genomic perspective on the origin and emergence of sars-cov-2. Cell. 2020;181:223-227.
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020;38:1‐9.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan0, China. Lancet. 2020;395:497-506.
- Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420-422.
- Wollina U, Karadag˘ AS, Rowland-Payne C, et al. Cutaneous signs in COVID-19 patients: a review. Dermatol Ther. 2020;33:e13549.
- Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577‐582.
- Fernandez-Nieto D, Ortega-Quijano D, Jimenez-Cauhe J, et al. Clinical and histological characterization of vesicular COVID-19 rashes: a prospective study in a tertiary care hospital. Clin Exp Dermatol. 2020;45:872-875.
- Gottfredsson M. The Spanish flu in Iceland 1918. Lessons in medicine and history [in Icelandic]. Laeknabladid. 2008;94:737-745.
- Jamieson D, Honein M, Rasmussen S, et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451-458.
- Ksiazek TG, Erdman D, Goldsmith CS. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953-1966.
- Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395:809‐815.
- Zhu H, Wang L, Fang C, et al. Clinical analysis of 10 neonates born to mothers with 2019-nCov pneumonia. Transl Pediatr. 2020;9:51-60.
- Liu Y, Chen H, Tang K, et al. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy [published online March 4, 2020]. J Infect. doi:10.1016/j.jinf.2020.02.028.
- Zhang L, Jiang Y, Wei M, et al. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province [in Chinese]. Zhonghua Fu Chan Ke Za Zhi. 2020;55:166-171.
- Henry BM, de Oliveira MHS, Benoit S, et al. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58:1021-1028.
- Cai Q, Huang D, Ou P, et al. COVID-19 in a designated infectious diseases hospital outside Hubei Province, China. Allergy. 2020;75:1742-1752.
- Ruan Q, Yang K, Wang W, et al. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020;46:846-884.
- Kumar A, Anil A, Sharma P, et al. Clinical features of COVID-19 and factors associated with severe clinical course: a systematic review and meta-analysis [preprint]. SSRN. doi:10.2139/ssrn.3566166.
- Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12. https://doi.org/10.1038/s41368-020-0074-x.
- Li H, Liu L, Zhang D, et al. SARS-CoV-2 and viral sepsis: observations and hypotheses. Lancet. 2020;395:1517-1520.
- Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol. 2020;17:533-535.
- Shors AR. Herpes zoster and severe acute herpetic neuralgia as a complication of COVID-19 infection. JAAD Case Rep. 2020;6:656-657.
- Elsaie ML, Youssef EA, Nada HA. Herpes zoster might be an indicator for latent COVID 19 infection [published online May 23, 2020]. Dermatol Ther. doi:10.1111/dth.13666.
Practice Points
- The vesicular rash of coronavirus disease 2019 (COVID-19) has been reported to have different forms of presentation.
- Pregnant women appear to be at increased risk for complications from COVID-19 infection.
- The clinical presentation of herpes zoster should be carefully monitored and reported for further assessment, especially if associated with other signs of COVID-19 infection.
