User login
The Importance of Service Learning in Dermatology Residency: An Actionable Approach to Improve Resident Education and Skin Health Equity
Access to specialty care such as dermatology is a challenge for patients living in underserved communities.1 In 2019, there were 29.6 million individuals without health insurance in the United States—9.2% of the population—up from 28.6 million the prior year.2 Furthermore, Black and Hispanic patients, American Indian and Alaskan Natives, and Native Hawaiian and other Pacific Islanders are more likely to be uninsured than their White counterparts.3 Community service activities such as free skin cancer screenings, partnerships with community practices, and teledermatology consultations through free clinics are instrumental in mitigating health care disparities and improving access to dermatologic care. In this article, we build on existing models from dermatology residency programs across the country to propose actionable methods to expand service-learning opportunities in dermatology residency training and increase health care equity in dermatology.
Why Service Learning?
Service learning is an educational approach that combines learning objectives with community service to provide a comprehensive scholastic experience and meet societal needs.4 In pilot studies of family medicine residents, service-learning initiatives enhanced the standard residency curriculum by promoting clinical practice resourcefulness.5 Dermatology Accreditation Council for Graduate Medical Education requirements mandate that residents demonstrate an awareness of the larger context of health care, including social determinants of health.6 Likewise, dermatology residents must recognize the impact of socioeconomic status on health care utilization, treatment options, and patient adherence. With this understanding, residents can advocate for quality patient care and improve community-based health care systems.6
Service-learning projects can effectively meet the specific health needs of a community. In a service-learning environment, residents will understand a community-based health care approach and work with attending physician role models who exhibit a community service ethic.7 Residents also can gain interprofessional experience through collaborating with a team of social workers, community health workers, care coordinators, pharmacists, nurses, medical students, and attending physicians. Furthermore, residents can practice communicating effectively with patients and families across a range of socioeconomic and cultural backgrounds. Interprofessional, team-based care and interpersonal skill acquisition are both Accreditation Council for Graduate Medical Education requirements for dermatology training.6 Through increased service-learning opportunities, dermatology trainees will learn to recognize and mitigate social determinants of health with a holistic, patient-centered treatment plan.
Free or low-cost medical clinics provide health care to more than 15 million Americans, many of whom identify with marginalized racial and ethnic groups.8 In a dermatology access study, a sample of clinics listed in the National Association of Free and Charitable Clinics database were contacted regarding the availability of dermatologic care; however, more than half of the sites were unresponsive or closed, and the remaining clinics offered limited access to dermatology services.9 The scarcity of free and low-cost dermatologic services likely contributes to adverse skin health outcomes for patients in underserved communities.10 By increasing service learning within dermatology residency training programs, access to dermatologic care will improve for underserved and uninsured populations.
Actionable Methods to Increase Service Learning in Dermatology Residency Training Programs
Utilize Programming Offered Through National Dermatology Associations and Societies
The American Academy of Dermatology (AAD) has developed programming through which faculty, residents, and private practice dermatologists perform community service targeting underserved populations. SPOT me , a skin cancer screening program, is the AAD’s longest-standing public health program through which it provides complimentary screening forms, handouts, and advertisements to facilitate skin cancer screening. AccessDerm is the AAD’s philanthropic teledermatology program that delivers dermatologic care to underserved communities. Camp Discovery and the Shade Structure Grant Program are additional initiatives promoted by the AAD to support volunteer services for communities while learning about dermatology. Residents may apply for AAD grants to subsidize participation in the Native American Health Service Resident Rotation Program, the Skin Care for Developing Countries program, or an international grant.
The Women’s Dermatologic Society hosts 3 primary umbrella community outreach initiatives: Play Safe in the Sun, Coast-2-Coast, and the Transforming Interconnecting Project Program Women’s Shelter Initiative. From uplifting and educating individuals in women’s shelters about skin care, oral hygiene, self-care, nutrition, and social skills to providing complimentary skin cancer screenings, the Women’s Dermatologic Society provides easily accessible tool kits and syllabi to facilitate project composition and completion by its members.
Implement Residency Class Service-Learning Projects
Incoming dermatology residents are regularly encouraged to draft research proposals at the beginning of each academic year. Encouraging residency classes to work collectively on a dermatology service-learning project likely will increase resident camaraderie and project success while minimizing internal competition. In developing a service-learning proposal, residents should engage with community leaders and groups to best understand how to meet the skin health needs of underserved communities. The project should have clear objectives, benchmarks, and full support of the dermatology department. Short-term service-learning projects are completed when set goals are achieved, while sustainable projects continue with each new resident class.
Partner With Existing Community or Federally Funded Clinics
Establishing partnerships with free or federally funded health centers is a reliable way to increase service-learning opportunities in dermatology residency training. Personal malpractice carriers often include free clinic coverage, and most states offer limited liability or immunity for physicians who volunteer their professional services or subsidize malpractice insurance purchases.11 In light of the global coronavirus disease 2019 pandemic, teledermatology options should be explored alongside in-person services. Although logistics may vary based on institutional preference, the following are our recommendations for building community partnerships for dermatology service learning (Figure):
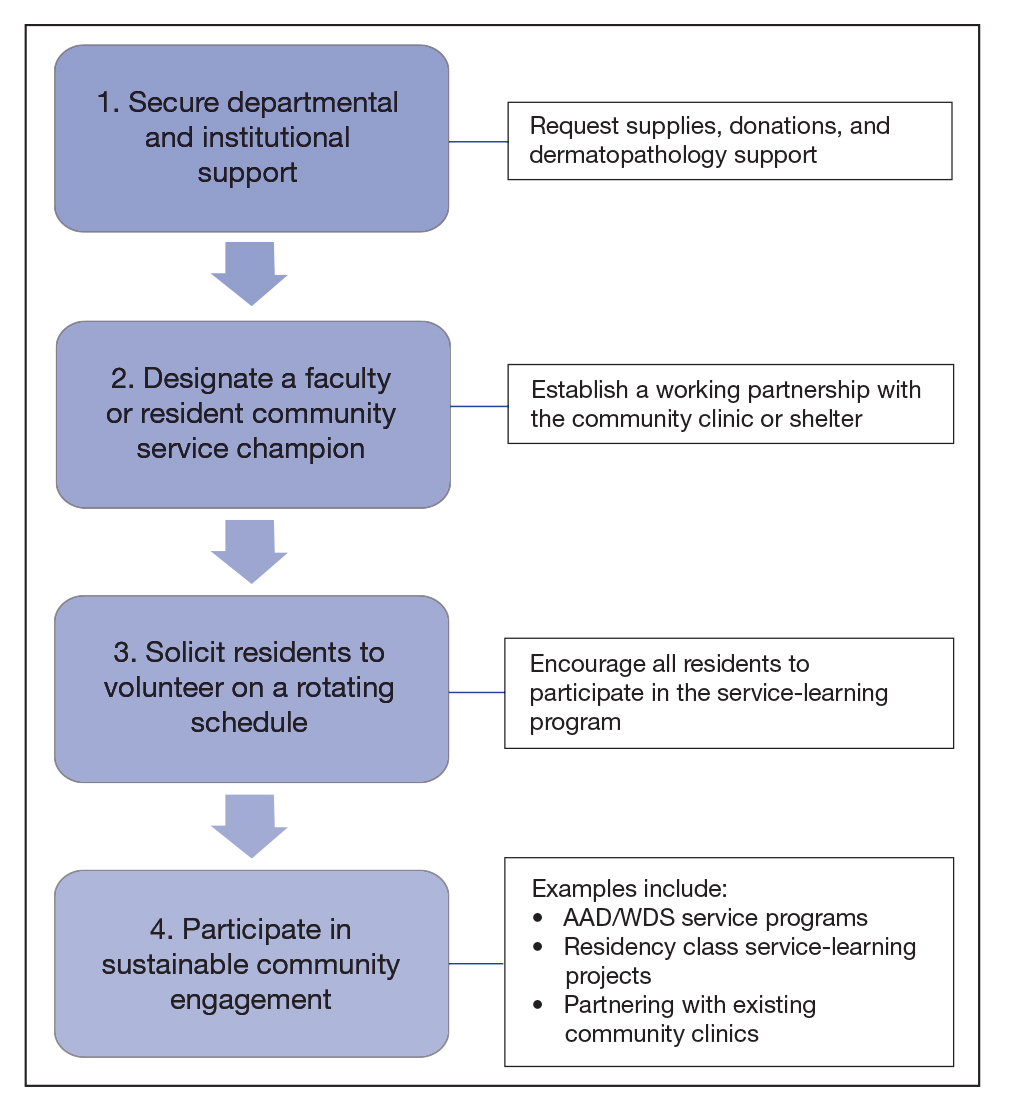
• Secure departmental and institutional support. This includes requesting supplies, donations, and dermatopathology support
• Designate a resident or faculty community service champion to lead clinic correspondence and oversee operative logistics. This individual will establish a working partnership with the community clinic, assess the needs of the patient population, and manage the clinic schedule. The champion also will initiate and maintain open lines of communication with community providers for continuity of care. This partnership with community providers allows for shared resources and mutual learning
• Solicit residents to volunteer on a rotating schedule. Although some residents are fully committed to community service and health care justice, all residents need to participate in the service-learning program
• Participate in sustainable community engagement on a schedule that suits the needs of the community and takes into consideration resident and attending availability
Final Thoughts
Service learning in dermatology residency training is essential to improve access to equitable dermatologic care and train clinically competent dermatologists who have experience practicing in resource-limited settings. Service learning places cultural awareness and an understanding of socioeconomic determinants of health at the forefront.12 Some dermatology residency programs treat a high percentage of medically underserved patients; others have integrated service learning into dermatology rotations, and a few programs offer community engagement–focused residency tracks.13-16 Each dermatology program should evaluate its workforce, resources, and nearby underserved communities to strategically develop a program-specific service-learning program. Service-learning clinics often are the sole means by which patients from underserved communities receive dermatologic care.17 A commitment to service learning in dermatology residency programs will improve skin health equity and improve dermatology residency education.
- Cook NL, Hicks LS, O’Malley J, et al. Access to specialty care and medical services in community health centers. Health Aff (Millwood). 2007;26:1459-1468.
- Broaddus M, Aron-Dine A. Uninsured rate rose again in 2019, further eroding earlier progress. Center on Budget and Policy Priorities website. Published September 15, 2020. Accessed February 9, 2021. https://www.cbpp.org/research/health/uninsured-rate-rose-again-in-2019-further-eroding-earlier-progress
- Artiga S, Orgera K, Damico A. Changes in health coverage by race and ethnicity since the ACA, 2010-2018. Kaiser Family Foundation website. Published March 5, 2020. Accessed February 9, 2021. https://www.kff.org/racial-equity-and-health-policy/issue-brief/changes-in-health-coverage-by-race-and-ethnicity-since-the-aca-2010-2018/
- Martinez MG. H.R.2010 - 103rd Congress (1993-1994): National and Community Service Trust Act of 1993. AmeriCorps website. Accessed November 24, 2020. https://www.congress.gov/bill/103rd-congress/house-bill/2010
- Gefter L, Merrell SB, Rosas LG, et al. Service-based learning for residents: a success for communities and medical education. Fam Med. 2015;47:803-806.
- ACGME Program Requirements for Graduate Medical Education in Dermatology. Accreditation Council for Graduate Medical Education website. Updated July 1, 2020. Accessed February 9, 2021. https://acgme.org/Portals/0/PFAssets/ProgramRequirements/080_Dermatology_2020.pdf?ver=2020-06-29-161626-133
- 7. Blanco G, Vasquez R, Nezafati K, et al. How residency programs can foster practice for the underserved. J Am Acad Dermatol. 2012;67:158-159.
- Darnell JS. Free clinics in the United States: a nationwide survey. Arch Intern Med. 2010;170:946.
- Madray V, Ginjupalli S, Hashmi O, et al. Access to dermatology services at free medical clinics: a nationwide cross-sectional survey. J Am Acad Dermatol. 2019;81:245-246.
- Shi L, Stevens GD. Vulnerability and unmet health care needs: the influence of multiple risk factors. J Gen Intern Med. 2005;20:148-154.
- Benrud L, Darrah J, Johnson A. Liability considerations for physician volunteers in the US. Virtual Mentor. 2010;12:207-212.
- Service-learning plays vital role in understanding social determinants of health. AAMC website. Published September 27, 2016. Accessed February 22, 2021. https://www.aamc.org/news-insights/service-learning-plays-vital-role-understanding-social-determinants-health
- Sheu J, Gonzalez E, Gaeta JM, et al. Boston Health Care for the Homeless Program–Harvard Dermatology collaboration: a service-learning model providing care for an underserved population. J Grad Med Educ. 2014;6:789-790.
- Ojeda VD, Romero L, Ortiz A. A model for sustainable laser tattoo removal services for adult probationers. Int J Prison Health. 2019;15:308-315.
- Diversity & Community Track (Dermatology Diversity and Community Engagement residency position). Penn Medicine Dermatology website. Accessed February 9, 2021. https://dermatology.upenn.edu/residents/diversity-community-track/
- Duke Dermatology Diversity and Community Engagement residency position (1529080A2). Duke Dermatology website. Accessed February 9, 2021. https://dermatology.duke.edu/node/4742
- Buster KJ, Stevens EI, Elmets CA. Dermatologic health disparities. Dermatol Clin. 2012;30:53-59.
Access to specialty care such as dermatology is a challenge for patients living in underserved communities.1 In 2019, there were 29.6 million individuals without health insurance in the United States—9.2% of the population—up from 28.6 million the prior year.2 Furthermore, Black and Hispanic patients, American Indian and Alaskan Natives, and Native Hawaiian and other Pacific Islanders are more likely to be uninsured than their White counterparts.3 Community service activities such as free skin cancer screenings, partnerships with community practices, and teledermatology consultations through free clinics are instrumental in mitigating health care disparities and improving access to dermatologic care. In this article, we build on existing models from dermatology residency programs across the country to propose actionable methods to expand service-learning opportunities in dermatology residency training and increase health care equity in dermatology.
Why Service Learning?
Service learning is an educational approach that combines learning objectives with community service to provide a comprehensive scholastic experience and meet societal needs.4 In pilot studies of family medicine residents, service-learning initiatives enhanced the standard residency curriculum by promoting clinical practice resourcefulness.5 Dermatology Accreditation Council for Graduate Medical Education requirements mandate that residents demonstrate an awareness of the larger context of health care, including social determinants of health.6 Likewise, dermatology residents must recognize the impact of socioeconomic status on health care utilization, treatment options, and patient adherence. With this understanding, residents can advocate for quality patient care and improve community-based health care systems.6
Service-learning projects can effectively meet the specific health needs of a community. In a service-learning environment, residents will understand a community-based health care approach and work with attending physician role models who exhibit a community service ethic.7 Residents also can gain interprofessional experience through collaborating with a team of social workers, community health workers, care coordinators, pharmacists, nurses, medical students, and attending physicians. Furthermore, residents can practice communicating effectively with patients and families across a range of socioeconomic and cultural backgrounds. Interprofessional, team-based care and interpersonal skill acquisition are both Accreditation Council for Graduate Medical Education requirements for dermatology training.6 Through increased service-learning opportunities, dermatology trainees will learn to recognize and mitigate social determinants of health with a holistic, patient-centered treatment plan.
Free or low-cost medical clinics provide health care to more than 15 million Americans, many of whom identify with marginalized racial and ethnic groups.8 In a dermatology access study, a sample of clinics listed in the National Association of Free and Charitable Clinics database were contacted regarding the availability of dermatologic care; however, more than half of the sites were unresponsive or closed, and the remaining clinics offered limited access to dermatology services.9 The scarcity of free and low-cost dermatologic services likely contributes to adverse skin health outcomes for patients in underserved communities.10 By increasing service learning within dermatology residency training programs, access to dermatologic care will improve for underserved and uninsured populations.
Actionable Methods to Increase Service Learning in Dermatology Residency Training Programs
Utilize Programming Offered Through National Dermatology Associations and Societies
The American Academy of Dermatology (AAD) has developed programming through which faculty, residents, and private practice dermatologists perform community service targeting underserved populations. SPOT me , a skin cancer screening program, is the AAD’s longest-standing public health program through which it provides complimentary screening forms, handouts, and advertisements to facilitate skin cancer screening. AccessDerm is the AAD’s philanthropic teledermatology program that delivers dermatologic care to underserved communities. Camp Discovery and the Shade Structure Grant Program are additional initiatives promoted by the AAD to support volunteer services for communities while learning about dermatology. Residents may apply for AAD grants to subsidize participation in the Native American Health Service Resident Rotation Program, the Skin Care for Developing Countries program, or an international grant.
The Women’s Dermatologic Society hosts 3 primary umbrella community outreach initiatives: Play Safe in the Sun, Coast-2-Coast, and the Transforming Interconnecting Project Program Women’s Shelter Initiative. From uplifting and educating individuals in women’s shelters about skin care, oral hygiene, self-care, nutrition, and social skills to providing complimentary skin cancer screenings, the Women’s Dermatologic Society provides easily accessible tool kits and syllabi to facilitate project composition and completion by its members.
Implement Residency Class Service-Learning Projects
Incoming dermatology residents are regularly encouraged to draft research proposals at the beginning of each academic year. Encouraging residency classes to work collectively on a dermatology service-learning project likely will increase resident camaraderie and project success while minimizing internal competition. In developing a service-learning proposal, residents should engage with community leaders and groups to best understand how to meet the skin health needs of underserved communities. The project should have clear objectives, benchmarks, and full support of the dermatology department. Short-term service-learning projects are completed when set goals are achieved, while sustainable projects continue with each new resident class.
Partner With Existing Community or Federally Funded Clinics
Establishing partnerships with free or federally funded health centers is a reliable way to increase service-learning opportunities in dermatology residency training. Personal malpractice carriers often include free clinic coverage, and most states offer limited liability or immunity for physicians who volunteer their professional services or subsidize malpractice insurance purchases.11 In light of the global coronavirus disease 2019 pandemic, teledermatology options should be explored alongside in-person services. Although logistics may vary based on institutional preference, the following are our recommendations for building community partnerships for dermatology service learning (Figure):
• Secure departmental and institutional support. This includes requesting supplies, donations, and dermatopathology support
• Designate a resident or faculty community service champion to lead clinic correspondence and oversee operative logistics. This individual will establish a working partnership with the community clinic, assess the needs of the patient population, and manage the clinic schedule. The champion also will initiate and maintain open lines of communication with community providers for continuity of care. This partnership with community providers allows for shared resources and mutual learning
• Solicit residents to volunteer on a rotating schedule. Although some residents are fully committed to community service and health care justice, all residents need to participate in the service-learning program
• Participate in sustainable community engagement on a schedule that suits the needs of the community and takes into consideration resident and attending availability
Final Thoughts
Service learning in dermatology residency training is essential to improve access to equitable dermatologic care and train clinically competent dermatologists who have experience practicing in resource-limited settings. Service learning places cultural awareness and an understanding of socioeconomic determinants of health at the forefront.12 Some dermatology residency programs treat a high percentage of medically underserved patients; others have integrated service learning into dermatology rotations, and a few programs offer community engagement–focused residency tracks.13-16 Each dermatology program should evaluate its workforce, resources, and nearby underserved communities to strategically develop a program-specific service-learning program. Service-learning clinics often are the sole means by which patients from underserved communities receive dermatologic care.17 A commitment to service learning in dermatology residency programs will improve skin health equity and improve dermatology residency education.
Access to specialty care such as dermatology is a challenge for patients living in underserved communities.1 In 2019, there were 29.6 million individuals without health insurance in the United States—9.2% of the population—up from 28.6 million the prior year.2 Furthermore, Black and Hispanic patients, American Indian and Alaskan Natives, and Native Hawaiian and other Pacific Islanders are more likely to be uninsured than their White counterparts.3 Community service activities such as free skin cancer screenings, partnerships with community practices, and teledermatology consultations through free clinics are instrumental in mitigating health care disparities and improving access to dermatologic care. In this article, we build on existing models from dermatology residency programs across the country to propose actionable methods to expand service-learning opportunities in dermatology residency training and increase health care equity in dermatology.
Why Service Learning?
Service learning is an educational approach that combines learning objectives with community service to provide a comprehensive scholastic experience and meet societal needs.4 In pilot studies of family medicine residents, service-learning initiatives enhanced the standard residency curriculum by promoting clinical practice resourcefulness.5 Dermatology Accreditation Council for Graduate Medical Education requirements mandate that residents demonstrate an awareness of the larger context of health care, including social determinants of health.6 Likewise, dermatology residents must recognize the impact of socioeconomic status on health care utilization, treatment options, and patient adherence. With this understanding, residents can advocate for quality patient care and improve community-based health care systems.6
Service-learning projects can effectively meet the specific health needs of a community. In a service-learning environment, residents will understand a community-based health care approach and work with attending physician role models who exhibit a community service ethic.7 Residents also can gain interprofessional experience through collaborating with a team of social workers, community health workers, care coordinators, pharmacists, nurses, medical students, and attending physicians. Furthermore, residents can practice communicating effectively with patients and families across a range of socioeconomic and cultural backgrounds. Interprofessional, team-based care and interpersonal skill acquisition are both Accreditation Council for Graduate Medical Education requirements for dermatology training.6 Through increased service-learning opportunities, dermatology trainees will learn to recognize and mitigate social determinants of health with a holistic, patient-centered treatment plan.
Free or low-cost medical clinics provide health care to more than 15 million Americans, many of whom identify with marginalized racial and ethnic groups.8 In a dermatology access study, a sample of clinics listed in the National Association of Free and Charitable Clinics database were contacted regarding the availability of dermatologic care; however, more than half of the sites were unresponsive or closed, and the remaining clinics offered limited access to dermatology services.9 The scarcity of free and low-cost dermatologic services likely contributes to adverse skin health outcomes for patients in underserved communities.10 By increasing service learning within dermatology residency training programs, access to dermatologic care will improve for underserved and uninsured populations.
Actionable Methods to Increase Service Learning in Dermatology Residency Training Programs
Utilize Programming Offered Through National Dermatology Associations and Societies
The American Academy of Dermatology (AAD) has developed programming through which faculty, residents, and private practice dermatologists perform community service targeting underserved populations. SPOT me , a skin cancer screening program, is the AAD’s longest-standing public health program through which it provides complimentary screening forms, handouts, and advertisements to facilitate skin cancer screening. AccessDerm is the AAD’s philanthropic teledermatology program that delivers dermatologic care to underserved communities. Camp Discovery and the Shade Structure Grant Program are additional initiatives promoted by the AAD to support volunteer services for communities while learning about dermatology. Residents may apply for AAD grants to subsidize participation in the Native American Health Service Resident Rotation Program, the Skin Care for Developing Countries program, or an international grant.
The Women’s Dermatologic Society hosts 3 primary umbrella community outreach initiatives: Play Safe in the Sun, Coast-2-Coast, and the Transforming Interconnecting Project Program Women’s Shelter Initiative. From uplifting and educating individuals in women’s shelters about skin care, oral hygiene, self-care, nutrition, and social skills to providing complimentary skin cancer screenings, the Women’s Dermatologic Society provides easily accessible tool kits and syllabi to facilitate project composition and completion by its members.
Implement Residency Class Service-Learning Projects
Incoming dermatology residents are regularly encouraged to draft research proposals at the beginning of each academic year. Encouraging residency classes to work collectively on a dermatology service-learning project likely will increase resident camaraderie and project success while minimizing internal competition. In developing a service-learning proposal, residents should engage with community leaders and groups to best understand how to meet the skin health needs of underserved communities. The project should have clear objectives, benchmarks, and full support of the dermatology department. Short-term service-learning projects are completed when set goals are achieved, while sustainable projects continue with each new resident class.
Partner With Existing Community or Federally Funded Clinics
Establishing partnerships with free or federally funded health centers is a reliable way to increase service-learning opportunities in dermatology residency training. Personal malpractice carriers often include free clinic coverage, and most states offer limited liability or immunity for physicians who volunteer their professional services or subsidize malpractice insurance purchases.11 In light of the global coronavirus disease 2019 pandemic, teledermatology options should be explored alongside in-person services. Although logistics may vary based on institutional preference, the following are our recommendations for building community partnerships for dermatology service learning (Figure):
• Secure departmental and institutional support. This includes requesting supplies, donations, and dermatopathology support
• Designate a resident or faculty community service champion to lead clinic correspondence and oversee operative logistics. This individual will establish a working partnership with the community clinic, assess the needs of the patient population, and manage the clinic schedule. The champion also will initiate and maintain open lines of communication with community providers for continuity of care. This partnership with community providers allows for shared resources and mutual learning
• Solicit residents to volunteer on a rotating schedule. Although some residents are fully committed to community service and health care justice, all residents need to participate in the service-learning program
• Participate in sustainable community engagement on a schedule that suits the needs of the community and takes into consideration resident and attending availability
Final Thoughts
Service learning in dermatology residency training is essential to improve access to equitable dermatologic care and train clinically competent dermatologists who have experience practicing in resource-limited settings. Service learning places cultural awareness and an understanding of socioeconomic determinants of health at the forefront.12 Some dermatology residency programs treat a high percentage of medically underserved patients; others have integrated service learning into dermatology rotations, and a few programs offer community engagement–focused residency tracks.13-16 Each dermatology program should evaluate its workforce, resources, and nearby underserved communities to strategically develop a program-specific service-learning program. Service-learning clinics often are the sole means by which patients from underserved communities receive dermatologic care.17 A commitment to service learning in dermatology residency programs will improve skin health equity and improve dermatology residency education.
- Cook NL, Hicks LS, O’Malley J, et al. Access to specialty care and medical services in community health centers. Health Aff (Millwood). 2007;26:1459-1468.
- Broaddus M, Aron-Dine A. Uninsured rate rose again in 2019, further eroding earlier progress. Center on Budget and Policy Priorities website. Published September 15, 2020. Accessed February 9, 2021. https://www.cbpp.org/research/health/uninsured-rate-rose-again-in-2019-further-eroding-earlier-progress
- Artiga S, Orgera K, Damico A. Changes in health coverage by race and ethnicity since the ACA, 2010-2018. Kaiser Family Foundation website. Published March 5, 2020. Accessed February 9, 2021. https://www.kff.org/racial-equity-and-health-policy/issue-brief/changes-in-health-coverage-by-race-and-ethnicity-since-the-aca-2010-2018/
- Martinez MG. H.R.2010 - 103rd Congress (1993-1994): National and Community Service Trust Act of 1993. AmeriCorps website. Accessed November 24, 2020. https://www.congress.gov/bill/103rd-congress/house-bill/2010
- Gefter L, Merrell SB, Rosas LG, et al. Service-based learning for residents: a success for communities and medical education. Fam Med. 2015;47:803-806.
- ACGME Program Requirements for Graduate Medical Education in Dermatology. Accreditation Council for Graduate Medical Education website. Updated July 1, 2020. Accessed February 9, 2021. https://acgme.org/Portals/0/PFAssets/ProgramRequirements/080_Dermatology_2020.pdf?ver=2020-06-29-161626-133
- 7. Blanco G, Vasquez R, Nezafati K, et al. How residency programs can foster practice for the underserved. J Am Acad Dermatol. 2012;67:158-159.
- Darnell JS. Free clinics in the United States: a nationwide survey. Arch Intern Med. 2010;170:946.
- Madray V, Ginjupalli S, Hashmi O, et al. Access to dermatology services at free medical clinics: a nationwide cross-sectional survey. J Am Acad Dermatol. 2019;81:245-246.
- Shi L, Stevens GD. Vulnerability and unmet health care needs: the influence of multiple risk factors. J Gen Intern Med. 2005;20:148-154.
- Benrud L, Darrah J, Johnson A. Liability considerations for physician volunteers in the US. Virtual Mentor. 2010;12:207-212.
- Service-learning plays vital role in understanding social determinants of health. AAMC website. Published September 27, 2016. Accessed February 22, 2021. https://www.aamc.org/news-insights/service-learning-plays-vital-role-understanding-social-determinants-health
- Sheu J, Gonzalez E, Gaeta JM, et al. Boston Health Care for the Homeless Program–Harvard Dermatology collaboration: a service-learning model providing care for an underserved population. J Grad Med Educ. 2014;6:789-790.
- Ojeda VD, Romero L, Ortiz A. A model for sustainable laser tattoo removal services for adult probationers. Int J Prison Health. 2019;15:308-315.
- Diversity & Community Track (Dermatology Diversity and Community Engagement residency position). Penn Medicine Dermatology website. Accessed February 9, 2021. https://dermatology.upenn.edu/residents/diversity-community-track/
- Duke Dermatology Diversity and Community Engagement residency position (1529080A2). Duke Dermatology website. Accessed February 9, 2021. https://dermatology.duke.edu/node/4742
- Buster KJ, Stevens EI, Elmets CA. Dermatologic health disparities. Dermatol Clin. 2012;30:53-59.
- Cook NL, Hicks LS, O’Malley J, et al. Access to specialty care and medical services in community health centers. Health Aff (Millwood). 2007;26:1459-1468.
- Broaddus M, Aron-Dine A. Uninsured rate rose again in 2019, further eroding earlier progress. Center on Budget and Policy Priorities website. Published September 15, 2020. Accessed February 9, 2021. https://www.cbpp.org/research/health/uninsured-rate-rose-again-in-2019-further-eroding-earlier-progress
- Artiga S, Orgera K, Damico A. Changes in health coverage by race and ethnicity since the ACA, 2010-2018. Kaiser Family Foundation website. Published March 5, 2020. Accessed February 9, 2021. https://www.kff.org/racial-equity-and-health-policy/issue-brief/changes-in-health-coverage-by-race-and-ethnicity-since-the-aca-2010-2018/
- Martinez MG. H.R.2010 - 103rd Congress (1993-1994): National and Community Service Trust Act of 1993. AmeriCorps website. Accessed November 24, 2020. https://www.congress.gov/bill/103rd-congress/house-bill/2010
- Gefter L, Merrell SB, Rosas LG, et al. Service-based learning for residents: a success for communities and medical education. Fam Med. 2015;47:803-806.
- ACGME Program Requirements for Graduate Medical Education in Dermatology. Accreditation Council for Graduate Medical Education website. Updated July 1, 2020. Accessed February 9, 2021. https://acgme.org/Portals/0/PFAssets/ProgramRequirements/080_Dermatology_2020.pdf?ver=2020-06-29-161626-133
- 7. Blanco G, Vasquez R, Nezafati K, et al. How residency programs can foster practice for the underserved. J Am Acad Dermatol. 2012;67:158-159.
- Darnell JS. Free clinics in the United States: a nationwide survey. Arch Intern Med. 2010;170:946.
- Madray V, Ginjupalli S, Hashmi O, et al. Access to dermatology services at free medical clinics: a nationwide cross-sectional survey. J Am Acad Dermatol. 2019;81:245-246.
- Shi L, Stevens GD. Vulnerability and unmet health care needs: the influence of multiple risk factors. J Gen Intern Med. 2005;20:148-154.
- Benrud L, Darrah J, Johnson A. Liability considerations for physician volunteers in the US. Virtual Mentor. 2010;12:207-212.
- Service-learning plays vital role in understanding social determinants of health. AAMC website. Published September 27, 2016. Accessed February 22, 2021. https://www.aamc.org/news-insights/service-learning-plays-vital-role-understanding-social-determinants-health
- Sheu J, Gonzalez E, Gaeta JM, et al. Boston Health Care for the Homeless Program–Harvard Dermatology collaboration: a service-learning model providing care for an underserved population. J Grad Med Educ. 2014;6:789-790.
- Ojeda VD, Romero L, Ortiz A. A model for sustainable laser tattoo removal services for adult probationers. Int J Prison Health. 2019;15:308-315.
- Diversity & Community Track (Dermatology Diversity and Community Engagement residency position). Penn Medicine Dermatology website. Accessed February 9, 2021. https://dermatology.upenn.edu/residents/diversity-community-track/
- Duke Dermatology Diversity and Community Engagement residency position (1529080A2). Duke Dermatology website. Accessed February 9, 2021. https://dermatology.duke.edu/node/4742
- Buster KJ, Stevens EI, Elmets CA. Dermatologic health disparities. Dermatol Clin. 2012;30:53-59.
Practice Points
- In 2019, nearly 30 million Americans did not have health insurance. Dermatologists in the United States should be cognizant of the challenges faced by underserved patients when accessing dermatologic care.
- Service learning is an educational approach that combines learning objectives with community service to provide a comprehensive learning experience, meet societal needs, and fulfill Accreditation Council for Graduate Medical Education requirements.
- Actionable methods to increase service learning in dermatology residency training include volunteering in community service programs offered by national dermatology organizations, implementing service-learning projects, and partnering with free and federally funded community practices.
- Dermatology residents who participate in service learning will help increase access to equitable dermatologic care and experience practicing in settings with limited resources.
JAMA podcast on racism in medicine faces backlash
Published on Feb. 23, the episode is hosted on JAMA’s learning platform for doctors and is available for continuing medical education credits.
“No physician is racist, so how can there be structural racism in health care? An explanation of the idea by doctors for doctors in this user-friendly podcast,” JAMA wrote in a Twitter post to promote the episode. That tweet has since been deleted.
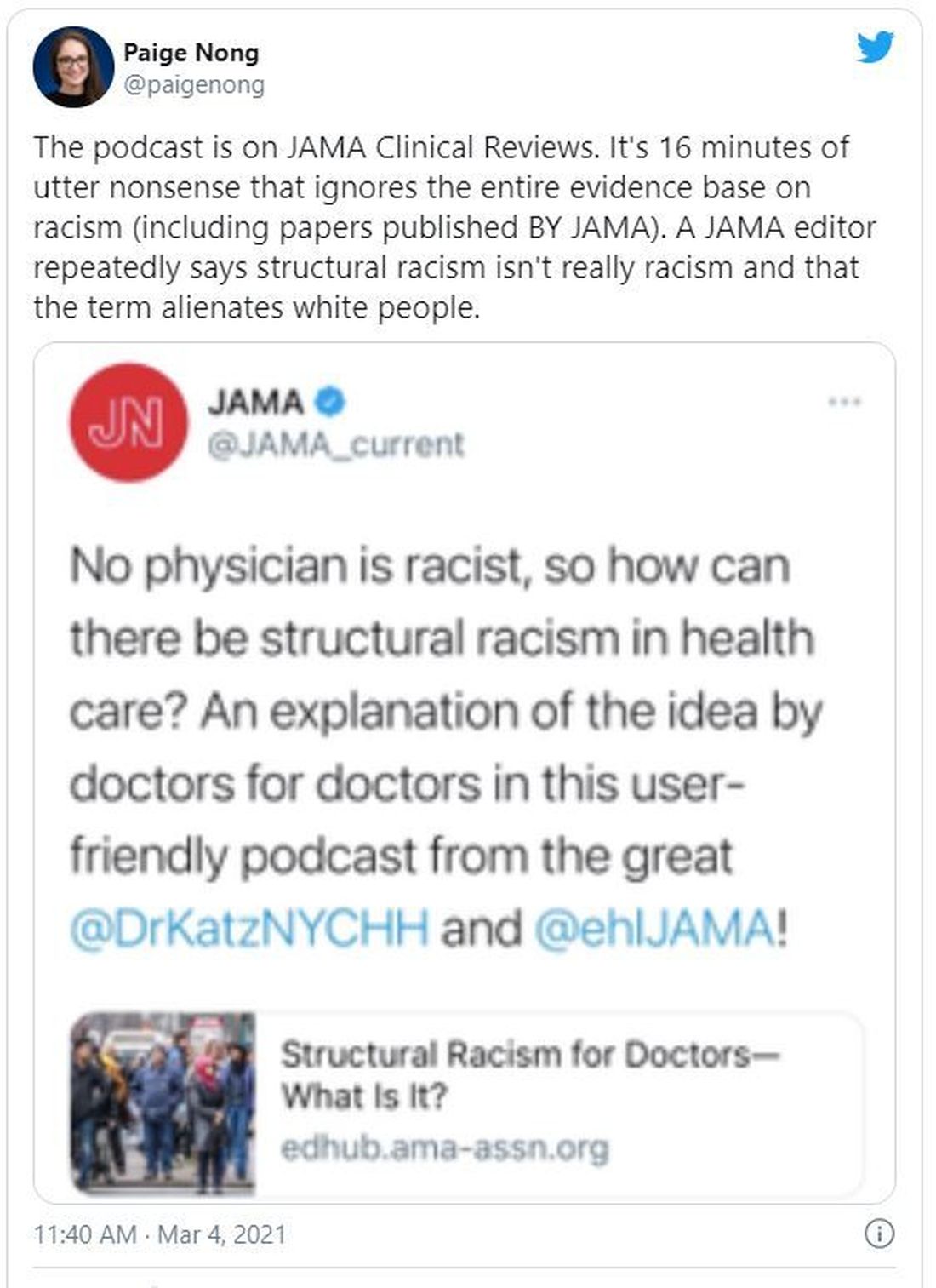
The episode features host Ed Livingston, MD, deputy editor for clinical reviews and education at JAMA, and guest Mitchell Katz, MD, president and CEO for NYC Health + Hospitals and deputy editor for JAMA Internal Medicine. Dr. Livingston approaches the episode as “structural racism for skeptics,” and Dr. Katz tries to explain how structural racism deepens health disparities and what health systems can do about it.
“Many physicians are skeptical of structural racism, the idea that economic, educational, and other societal systems preferentially disadvantage Black Americans and other communities of color,” the episode description says.
In the podcast, Dr. Livingston and Dr. Katz speak about health care disparities and racial inequality. Dr. Livingston, who says he “didn’t understand the concept” going into the episode, suggests that racism was made illegal in the 1960s and that the discussion of “structural racism” should shift away from the term “racism” and focus on socioeconomic status instead.
“What you’re talking about isn’t so much racism ... it isn’t their race, it isn’t their color, it’s their socioeconomic status,” Dr. Livingston says. “Is that a fair statement?”
But Dr. Katz says that “acknowledging structural racism can be helpful to us. Structural racism refers to a system in which policies or practices or how we look at people perpetuates racial inequality.”
Dr. Katz points to the creation of a hospital in San Francisco in the 1880s to treat patients of Chinese ethnicity separately. Outside of health care, he talks about environmental racism between neighborhoods with inequalities in hospitals, schools, and social services.
“All of those things have an impact on that minority person,” Dr. Katz says. “The big thing we can all do is move away from trying to interrogate each other’s opinions and move to a place where we are looking at the policies of our institutions and making sure that they promote equality.”
Dr. Livingston concludes the episode by reemphasizing that “racism” should be taken out of the conversation and it should instead focus on the “structural” aspect of socioeconomics.
“Minorities ... aren’t [in those neighborhoods] because they’re not allowed to buy houses or they can’t get a job because they’re Black or Hispanic. That would be illegal,” Dr. Livingston says. “But disproportionality does exist.”
Efforts to reach Dr. Livingston were unsuccessful. Dr. Katz distanced himself from Dr. Livingston in a statement released on March 4.
“Systemic and interpersonal racism both still exist in our country — they must be rooted out. I do not share the JAMA host’s belief of doing away with the word ‘racism’ will help us be more successful in ending inequities that exists across racial and ethnic lines,” Dr. Katz said. “Further, I believe that we will only produce an equitable society when social and political structures do not continue to produce and perpetuate disparate results based on social race and ethnicity.”
Dr. Katz reiterated that both interpersonal and structural racism continue to exist in the United States, “and it is woefully naive to say that no physician is a racist just because the Civil Rights Act of 1964 forbade it.”
He also recommended JAMA use this controversy “as a learning opportunity for continued dialogue and create another podcast series as an open conversation that invites diverse experts in the field to have an open discussion about structural racism in healthcare.”
The podcast and JAMA’s tweet promoting it were widely criticized on Twitter. In interviews with WebMD, many doctors expressed disbelief that such a respected journal would lend its name to this podcast episode.
B. Bobby Chiong, MD, a radiologist in New York, said although JAMA’s effort to engage with its audience about racism is laudable, it missed the mark.
“I think the backlash comes from how they tried to make a podcast about the subject and somehow made themselves an example of unconscious bias and unfamiliarity with just how embedded in our system is structural racism,” he said.
Perhaps the podcast’s worst offense was its failure to address the painful history of racial bias in this country that still permeates the medical community, says Tamara Saint-Surin, MD, assistant professor at the University of North Carolina at Chapel Hill.
“For physicians in leadership to have the belief that structural racism does not exist in medicine, they don’t really appreciate what affects their patients and what their patients were dealing with,” Dr. Saint-Surin said in an interview. “It was a very harmful podcast and goes to show we still have so much work to do.”
Along with a flawed premise, she says, the podcast was not nearly long enough to address such a nuanced issue. And Dr. Livingston focused on interpersonal racism rather than structural racism, she said, failing to address widespread problems such as higher rates of asthma among Black populations living in areas with poor air quality.
The number of Black doctors remains low and the lack of representation adds to an environment already rife with racism, according to many medical professionals.
Shirlene Obuobi, MD, an internal medicine doctor in Chicago, said JAMA failed to live up to its own standards by publishing material that lacked research and expertise.
“I can’t submit a clinical trial to JAMA without them combing through methods with a fine-tooth comb,” Dr. Obuobi said. “They didn’t uphold the standards they normally apply to anyone else.”
Both the editor of JAMA and the head of the American Medical Association issued statements criticizing the episode and the tweet that promoted it.
JAMA Editor-in-Chief Howard Bauchner, MD, said, “The language of the tweet, and some portions of the podcast, do not reflect my commitment as editorial leader of JAMA and JAMA Network to call out and discuss the adverse effects of injustice, inequity, and racism in society and medicine as JAMA has done for many years.” He said JAMA will schedule a future podcast to address the concerns raised about the recent episode.
AMA CEO James L. Madara, MD, said, “The AMA’s House of Delegates passed policy stating that racism is structural, systemic, cultural, and interpersonal, and we are deeply disturbed – and angered – by a recent JAMA podcast that questioned the existence of structural racism and the affiliated tweet that promoted the podcast and stated ‘no physician is racist, so how can there be structural racism in health care?’ ”
He continued: “JAMA has editorial independence from AMA, but this tweet and podcast are inconsistent with the policies and views of AMA, and I’m concerned about and acknowledge the harms they have caused. Structural racism in health care and our society exists, and it is incumbent on all of us to fix it.”
This article was updated 3/5/21.
A version of this article first appeared on WebMD.com.
Published on Feb. 23, the episode is hosted on JAMA’s learning platform for doctors and is available for continuing medical education credits.
“No physician is racist, so how can there be structural racism in health care? An explanation of the idea by doctors for doctors in this user-friendly podcast,” JAMA wrote in a Twitter post to promote the episode. That tweet has since been deleted.
The episode features host Ed Livingston, MD, deputy editor for clinical reviews and education at JAMA, and guest Mitchell Katz, MD, president and CEO for NYC Health + Hospitals and deputy editor for JAMA Internal Medicine. Dr. Livingston approaches the episode as “structural racism for skeptics,” and Dr. Katz tries to explain how structural racism deepens health disparities and what health systems can do about it.
“Many physicians are skeptical of structural racism, the idea that economic, educational, and other societal systems preferentially disadvantage Black Americans and other communities of color,” the episode description says.
In the podcast, Dr. Livingston and Dr. Katz speak about health care disparities and racial inequality. Dr. Livingston, who says he “didn’t understand the concept” going into the episode, suggests that racism was made illegal in the 1960s and that the discussion of “structural racism” should shift away from the term “racism” and focus on socioeconomic status instead.
“What you’re talking about isn’t so much racism ... it isn’t their race, it isn’t their color, it’s their socioeconomic status,” Dr. Livingston says. “Is that a fair statement?”
But Dr. Katz says that “acknowledging structural racism can be helpful to us. Structural racism refers to a system in which policies or practices or how we look at people perpetuates racial inequality.”
Dr. Katz points to the creation of a hospital in San Francisco in the 1880s to treat patients of Chinese ethnicity separately. Outside of health care, he talks about environmental racism between neighborhoods with inequalities in hospitals, schools, and social services.
“All of those things have an impact on that minority person,” Dr. Katz says. “The big thing we can all do is move away from trying to interrogate each other’s opinions and move to a place where we are looking at the policies of our institutions and making sure that they promote equality.”
Dr. Livingston concludes the episode by reemphasizing that “racism” should be taken out of the conversation and it should instead focus on the “structural” aspect of socioeconomics.
“Minorities ... aren’t [in those neighborhoods] because they’re not allowed to buy houses or they can’t get a job because they’re Black or Hispanic. That would be illegal,” Dr. Livingston says. “But disproportionality does exist.”
Efforts to reach Dr. Livingston were unsuccessful. Dr. Katz distanced himself from Dr. Livingston in a statement released on March 4.
“Systemic and interpersonal racism both still exist in our country — they must be rooted out. I do not share the JAMA host’s belief of doing away with the word ‘racism’ will help us be more successful in ending inequities that exists across racial and ethnic lines,” Dr. Katz said. “Further, I believe that we will only produce an equitable society when social and political structures do not continue to produce and perpetuate disparate results based on social race and ethnicity.”
Dr. Katz reiterated that both interpersonal and structural racism continue to exist in the United States, “and it is woefully naive to say that no physician is a racist just because the Civil Rights Act of 1964 forbade it.”
He also recommended JAMA use this controversy “as a learning opportunity for continued dialogue and create another podcast series as an open conversation that invites diverse experts in the field to have an open discussion about structural racism in healthcare.”
The podcast and JAMA’s tweet promoting it were widely criticized on Twitter. In interviews with WebMD, many doctors expressed disbelief that such a respected journal would lend its name to this podcast episode.
B. Bobby Chiong, MD, a radiologist in New York, said although JAMA’s effort to engage with its audience about racism is laudable, it missed the mark.
“I think the backlash comes from how they tried to make a podcast about the subject and somehow made themselves an example of unconscious bias and unfamiliarity with just how embedded in our system is structural racism,” he said.
Perhaps the podcast’s worst offense was its failure to address the painful history of racial bias in this country that still permeates the medical community, says Tamara Saint-Surin, MD, assistant professor at the University of North Carolina at Chapel Hill.
“For physicians in leadership to have the belief that structural racism does not exist in medicine, they don’t really appreciate what affects their patients and what their patients were dealing with,” Dr. Saint-Surin said in an interview. “It was a very harmful podcast and goes to show we still have so much work to do.”
Along with a flawed premise, she says, the podcast was not nearly long enough to address such a nuanced issue. And Dr. Livingston focused on interpersonal racism rather than structural racism, she said, failing to address widespread problems such as higher rates of asthma among Black populations living in areas with poor air quality.
The number of Black doctors remains low and the lack of representation adds to an environment already rife with racism, according to many medical professionals.
Shirlene Obuobi, MD, an internal medicine doctor in Chicago, said JAMA failed to live up to its own standards by publishing material that lacked research and expertise.
“I can’t submit a clinical trial to JAMA without them combing through methods with a fine-tooth comb,” Dr. Obuobi said. “They didn’t uphold the standards they normally apply to anyone else.”
Both the editor of JAMA and the head of the American Medical Association issued statements criticizing the episode and the tweet that promoted it.
JAMA Editor-in-Chief Howard Bauchner, MD, said, “The language of the tweet, and some portions of the podcast, do not reflect my commitment as editorial leader of JAMA and JAMA Network to call out and discuss the adverse effects of injustice, inequity, and racism in society and medicine as JAMA has done for many years.” He said JAMA will schedule a future podcast to address the concerns raised about the recent episode.
AMA CEO James L. Madara, MD, said, “The AMA’s House of Delegates passed policy stating that racism is structural, systemic, cultural, and interpersonal, and we are deeply disturbed – and angered – by a recent JAMA podcast that questioned the existence of structural racism and the affiliated tweet that promoted the podcast and stated ‘no physician is racist, so how can there be structural racism in health care?’ ”
He continued: “JAMA has editorial independence from AMA, but this tweet and podcast are inconsistent with the policies and views of AMA, and I’m concerned about and acknowledge the harms they have caused. Structural racism in health care and our society exists, and it is incumbent on all of us to fix it.”
This article was updated 3/5/21.
A version of this article first appeared on WebMD.com.
Published on Feb. 23, the episode is hosted on JAMA’s learning platform for doctors and is available for continuing medical education credits.
“No physician is racist, so how can there be structural racism in health care? An explanation of the idea by doctors for doctors in this user-friendly podcast,” JAMA wrote in a Twitter post to promote the episode. That tweet has since been deleted.
The episode features host Ed Livingston, MD, deputy editor for clinical reviews and education at JAMA, and guest Mitchell Katz, MD, president and CEO for NYC Health + Hospitals and deputy editor for JAMA Internal Medicine. Dr. Livingston approaches the episode as “structural racism for skeptics,” and Dr. Katz tries to explain how structural racism deepens health disparities and what health systems can do about it.
“Many physicians are skeptical of structural racism, the idea that economic, educational, and other societal systems preferentially disadvantage Black Americans and other communities of color,” the episode description says.
In the podcast, Dr. Livingston and Dr. Katz speak about health care disparities and racial inequality. Dr. Livingston, who says he “didn’t understand the concept” going into the episode, suggests that racism was made illegal in the 1960s and that the discussion of “structural racism” should shift away from the term “racism” and focus on socioeconomic status instead.
“What you’re talking about isn’t so much racism ... it isn’t their race, it isn’t their color, it’s their socioeconomic status,” Dr. Livingston says. “Is that a fair statement?”
But Dr. Katz says that “acknowledging structural racism can be helpful to us. Structural racism refers to a system in which policies or practices or how we look at people perpetuates racial inequality.”
Dr. Katz points to the creation of a hospital in San Francisco in the 1880s to treat patients of Chinese ethnicity separately. Outside of health care, he talks about environmental racism between neighborhoods with inequalities in hospitals, schools, and social services.
“All of those things have an impact on that minority person,” Dr. Katz says. “The big thing we can all do is move away from trying to interrogate each other’s opinions and move to a place where we are looking at the policies of our institutions and making sure that they promote equality.”
Dr. Livingston concludes the episode by reemphasizing that “racism” should be taken out of the conversation and it should instead focus on the “structural” aspect of socioeconomics.
“Minorities ... aren’t [in those neighborhoods] because they’re not allowed to buy houses or they can’t get a job because they’re Black or Hispanic. That would be illegal,” Dr. Livingston says. “But disproportionality does exist.”
Efforts to reach Dr. Livingston were unsuccessful. Dr. Katz distanced himself from Dr. Livingston in a statement released on March 4.
“Systemic and interpersonal racism both still exist in our country — they must be rooted out. I do not share the JAMA host’s belief of doing away with the word ‘racism’ will help us be more successful in ending inequities that exists across racial and ethnic lines,” Dr. Katz said. “Further, I believe that we will only produce an equitable society when social and political structures do not continue to produce and perpetuate disparate results based on social race and ethnicity.”
Dr. Katz reiterated that both interpersonal and structural racism continue to exist in the United States, “and it is woefully naive to say that no physician is a racist just because the Civil Rights Act of 1964 forbade it.”
He also recommended JAMA use this controversy “as a learning opportunity for continued dialogue and create another podcast series as an open conversation that invites diverse experts in the field to have an open discussion about structural racism in healthcare.”
The podcast and JAMA’s tweet promoting it were widely criticized on Twitter. In interviews with WebMD, many doctors expressed disbelief that such a respected journal would lend its name to this podcast episode.
B. Bobby Chiong, MD, a radiologist in New York, said although JAMA’s effort to engage with its audience about racism is laudable, it missed the mark.
“I think the backlash comes from how they tried to make a podcast about the subject and somehow made themselves an example of unconscious bias and unfamiliarity with just how embedded in our system is structural racism,” he said.
Perhaps the podcast’s worst offense was its failure to address the painful history of racial bias in this country that still permeates the medical community, says Tamara Saint-Surin, MD, assistant professor at the University of North Carolina at Chapel Hill.
“For physicians in leadership to have the belief that structural racism does not exist in medicine, they don’t really appreciate what affects their patients and what their patients were dealing with,” Dr. Saint-Surin said in an interview. “It was a very harmful podcast and goes to show we still have so much work to do.”
Along with a flawed premise, she says, the podcast was not nearly long enough to address such a nuanced issue. And Dr. Livingston focused on interpersonal racism rather than structural racism, she said, failing to address widespread problems such as higher rates of asthma among Black populations living in areas with poor air quality.
The number of Black doctors remains low and the lack of representation adds to an environment already rife with racism, according to many medical professionals.
Shirlene Obuobi, MD, an internal medicine doctor in Chicago, said JAMA failed to live up to its own standards by publishing material that lacked research and expertise.
“I can’t submit a clinical trial to JAMA without them combing through methods with a fine-tooth comb,” Dr. Obuobi said. “They didn’t uphold the standards they normally apply to anyone else.”
Both the editor of JAMA and the head of the American Medical Association issued statements criticizing the episode and the tweet that promoted it.
JAMA Editor-in-Chief Howard Bauchner, MD, said, “The language of the tweet, and some portions of the podcast, do not reflect my commitment as editorial leader of JAMA and JAMA Network to call out and discuss the adverse effects of injustice, inequity, and racism in society and medicine as JAMA has done for many years.” He said JAMA will schedule a future podcast to address the concerns raised about the recent episode.
AMA CEO James L. Madara, MD, said, “The AMA’s House of Delegates passed policy stating that racism is structural, systemic, cultural, and interpersonal, and we are deeply disturbed – and angered – by a recent JAMA podcast that questioned the existence of structural racism and the affiliated tweet that promoted the podcast and stated ‘no physician is racist, so how can there be structural racism in health care?’ ”
He continued: “JAMA has editorial independence from AMA, but this tweet and podcast are inconsistent with the policies and views of AMA, and I’m concerned about and acknowledge the harms they have caused. Structural racism in health care and our society exists, and it is incumbent on all of us to fix it.”
This article was updated 3/5/21.
A version of this article first appeared on WebMD.com.
Addressing structural racism: An update from the APA
The coronavirus disease 2019 pandemic, which as of mid-February 2021 had caused more than 486,000 deaths in the United States, has changed our lives forever. Elders and Black, Indigenous, and People of Color (BIPOC) have been overrepresented among those lost. That, when juxtaposed with the civil unrest that followed the brutal killing of George Floyd, an unarmed Black man, by a White law enforcement officer on May 25, 2020, have compelled us to talk about US race relations in unprecedented ways. These and other traumas disproportionately affect the quality of life and health of minority and underserved individuals. The international outcry about racism, serial trauma, and health disparities left the medical profession well positioned to promulgate changes that are conducive to achieving health equity.
Race is a social construct
In November 2020, the American Medical Association (AMA) Board of Trustees made several public acknowledgments about race.1 First, race is a social, nonbiological classification that is different from biology, ethnicity, or genetic ancestry.1 Next, race contributes to health disparities and poor health outcomes for minorities and members of underserved communities.1 Also, racism, which includes disproportionate police brutality against Black and Indigenous people, is a driver of health inequity for them and people in marginalized communities.1
The AMA also commented on how serial trauma and racism can affect one’s health. The AMA acknowledged that exposure to serial trauma throughout one’s life can have a cumulative effect that is “associated with chronic stress, higher rates of comorbidities and lower life expectancy” and results in increased health care costs and decreased quality of life for those who are affected.1 Also, the AMA proclaimed that racism is a threat to public health and pledged to dismantle discriminatory practices and policies in health care, including medical education and research.2
Diversity and inclusion in psychiatry
While the AMA has been striving to reduce bias in health care systems, psychiatry has been forging its path. In March 2015, the American Psychiatric Association’s (APA) Board of Trustees approved the APA’s Strategic Initiative, which has 4 goals: 1) advancing the integration of psychiatry in health care; 2) supporting research; 3) supporting education; and 4) promoting diversity and inclusion in psychiatry.3 The latter goal includes advocating for antiracist policies that promote cultural competence and health equity in education, research and psychiatric care; increased recruitment and retention of psychiatrists from groups that historically have been underrepresented in medicine and medical leadership; and ensuring representation of these groups in APA governance at all levels.3
The APA’s antiracism agenda
In March 2020, outgoing APA President Bruce Schwartz concurred with Board members that diversity and inclusion in the APA warranted a closer review. On May 5, 2020, APA President Jeff Geller committed to authorizing a systematic study of diversity and inclusion in various branches of the APA, including councils and governance. By the end of May, with civil unrest in full swing in the United States, President Geller decided to expand the APA’s diversity agenda.
President Geller appointed the APA Presidential Task Force to Address Structural Racism Throughout Psychiatry (SR Task Force), which had its virtual inaugural meeting on June 27, 2020.4 The SR Task Force exists to focus on structural racism (aka institutional racism) in organized psychiatry, psychiatric patients, and those who provide psychiatric services to patients. The charge, which is subject to revision, if warranted, is clear: provide resources and education on the history of structural racism in the APA and psychiatry, explain how structural racism impacts psychiatric patients and the profession, craft actionable recommendations to dismantle structural racism in the APA and psychiatry, report those findings to the APA’s Board of Trustees, and implement a quality assurance protocol to ensure that the Task Force’s work is consistent with its charge. President Geller decided to have the Task Force focus on anti-Black racism in its inaugural year and believes that the outcome will benefit all psychiatrists, other mental health professionals, and patients who identify as members of minority and underserved groups in the United States and the profession of psychiatry.5
Presidential Task Forces in APA
Presidential Task Forces report directly to the Board of Trustees, which expedites the review of progress reports and deliberation on and, when favorable, implementation of recommendations. Also, Presidential Task Forces are afforded additional APA resources. For example, the SR Task Force has 16 APA staff members who have been appointed or volunteered to assist the Task Force in some way. Many APA staff have graduate degrees in law, education, and other subjects. The skill sets, networks, institutional memory, and commitment that they bring to the project are conducive to advancing the SR Task Force’s agenda at a brisk pace.
Continue to: The APA President...
The APA President decides whom to appoint to each Task Force. President Geller propitiously appointed subject matter experts and members of the Board of Trustees to serve on the SR Task Force. Subject matter experts contribute historical and contemporary content about racism, including anti-Black racism, to the discussion. The data are used to craft research questions that may yield pertinent data. (Note that not all subject matter experts are Black, nor are all Board members White.) APA staff support the Task Force by sharing their expertise, compiling data, coordinating meetings, collaborating on program development, disseminating the work product to APA members and the media, and other important tasks.
The SR Task Force’s work
The SR Task Force strives for transparency in a process that is informed by APA members. The group immediately set up a web hub that is used to communicate with APA members.5 Individual members also use social media to alert members to SR Task Force activities and events. Member input has been solicited by posting several brief surveys on the SR Task Force web hub. Topics have included the effect of structural racism on patient care, psychiatric practice, and organized psychiatry, including the APA. The responses, which collectively totaled >1,600, were reviewed and used to inform Task Force priorities while working within the scope of the charge.5
Based on member feedback, the first large project of the SR Task Force has been to examine structural racism in the APA. The SR Task Force formed workgroups to study data pertaining to diversity and inclusion in the APA Assembly, governance (the Board of Trustees), Councils and Committees, and Scientific Program Committee. As APA Publishing and the DSM Steering Committee have internal processes to address structural racism, the SR Task Force did not convene workgroups to study this. However, the SR Task Force will be meeting with leaders of those groups to learn about their protocols and will request that information be made available to APA members.
The SR Task Force reviews and interprets data that are compiled by each workgroup, deliberates on its significance, and when appropriate, drafts achievable recommendations to improve diversity and inclusion in the APA. This is where Trustee involvement is invaluable to the SR Task Force, because the report and recommendations will be presented to the Board of Trustees.
There is no guarantee that the recommendations contained in a report that is accepted by the Board of Trustees will be implemented unless they are approved. It is imperative, therefore, that SR Task Force recommendations to the Board take into consideration Board structure, processes, goals, efficiency, history, and other matters. The learning curve can be steep, especially when the first major report was due 3 months after the SR Task Force was appointed. Clarity and efficiency are key in report preparation. For example, during the Winter 2020 Board of Trustees meeting, the SR Task Force presented its report, answered questions, and offered 7 action items to the Board for deliberation and voting. The endeavor, which was completed in 20 minutes, resulted in the Board supporting 6 of the recommendations and deferring the deliberation of the seventh recommendation to the spring Board meeting, due to logistical concerns.
Continue to: Thus far, the SR Task Force Workgroups...
Thus far, the SR Task Force Workgroups on the Assembly and Governance have presented their reports. 5 The SR Task Force reports on the Scientific Program Committee and Councils and Committees are scheduled to be presented to the Board during the Spring 2021 meeting.
The SR Task Force has been fulfilling the commitment to provide relevant educational materials to members in several ways. There have been 4 virtual Structural Racism Town Hall meetings that featured subject matter experts. The first Town Hall session addressed the initial steps towards dismantling structural racism and included President Geller’s announcement about appointing a SR Task Force. The next Town Hall meeting addressed structural racism in medicine and psychiatry, its effect on children and individuals who identify as transgender, and its intersectionality (the cumulative effect of discrimination on a person who belongs to 2 non-dominant groups.) The panel in the third Town Hall meeting reviewed the impact of structural racism, including intersectionality, on transgenerational trauma in several minority groups. The meeting ended with an update of Task Force activities. The February 2021 Town Hall meeting focused on how structural racism affects recruitment and retention of minority psychiatry residents, and how this can undermine efforts to grow a diverse workforce. Recordings of these and other events can be accessed on the SR Task Force web hub.5 The SR Task Force members plan to present a review of the year’s work during the next Town Hall meeting, which is scheduled to occur on Saturday, May 1, 2021, during the APA’s Annual Meeting.
The SR Task Force web hub contains other resources, including APA position statements, press releases, and news articles, and a glossary of relevant terms. It also includes internet links to President Geller’s 9-part series on the history of Structural Racism in the APA. There are CME and other webinars, a curated list of references, videos, podcasts, and other media.4
The SR Task Force believes that much of the antiracism work needs to occur beyond APA headquarters. Consequently, President Geller challenged all APA Councils to work on an antiracism project to support the APA’s antiracism agenda. APA committees and caucuses have been encouraged to do the same. The SR Task Force has asked APA District Branches and Allied Organizations to share information about what they are doing to educate members about structural racism and what they are doing for input regarding their antiracist activities. Additionally, Task Force members have been speaking with these and other groups to inform them about the APA’s antiracism work.
APA’s Board of Trustees actions
It would be inappropriate for the APA to task groups with focusing on antiracism unless the organization was doing its part. In July 2020, the Board of Trustees had a 2-hour round table discussion during which each member spoke about the problem and how the APA should address it. Next, President Geller appointed a Board Workgroup to clarify the definitions of “minority” and “underrepresented.” Although the APA Assembly has defined the terms, the APA has not. Additionally, the APA Board of Trustees retained a consultant to assess all aspects of how it functions as a Board. The Board’s management of matters pertaining to diversity and inclusion was part of the examination. The recommendations are being reviewed and the Board will undergo diversity training.
Continue to: President Geller's study...
President Geller’s study of racism in the APA, which involved a review of past APA presidential addresses, brought to light a long-term pattern of racism in the organization.5 On January 18, 2021, Martin Luther King, Jr. Day, the APA acknowledged and apologized to psychiatrists, patients, and the public for its history of engaging in and passively condoning racist behavior.6 The APA has committed to being better informed about diversity and inclusion at every level. Lastly, hired consultants with expertise in diversity and inclusion are working with APA staff at every level so that the environment can be a welcoming and comfortable workspace for recruiting and retaining a diverse workforce.
Although it may seem that the APA has engaged in many antiracist activities in a brief period, there is much more to accomplish. The Task Force hopes that the work will speak for itself and will be sustained over time. It’s long overdue.
1. American Medical Association. New AMA policies recognize race as a social, not biological, construct. Published November 16, 2020. Accessed February 1, 2021. https://www.ama-assn.org/press-center/press-releases/new-ama-policies-recognize-race-social-not-biological-construct
2. American Medical Association. New AMA policy recognizes racism as a public health threat. Published November 16, 2020. Accessed February 1, 2021. https://www.ama-assn.org/press-center/press-releases/new-ama-policy-recognizes-racism-public-health-threat
3. American Psychiatric Association. Board-approved recommendation on strategic planning. Published March 2015. Accessed February 1, 2021. https://www.psychiatry.org/about-apa/read-apa-organization-documents-and-policies/strategic-plan
4. Geller J. Structural racism in American psychiatry and APA. Parts 1-9. Published July-November 2020. Accessed February 8, 2021. https://psychnews.psychiatryonline.org/topic/news-president?sortBy=Ppub
5. American Psychiatric Association. Structural Racism Task Force. Accessed February 8, 2021. https://www.psychiatry.org/psychiatrists/structural-racism-task-force
6. American Psychiatric Association. APA’s apology to black, indigenous and people of color for its support of structural racism in psychiatry. Published January 18, 2021. Accessed February 8, 2021. https://www.psychiatry.org/newsroom/apa-apology-for-its-support-of-structural-racism-in-psychiatry
The coronavirus disease 2019 pandemic, which as of mid-February 2021 had caused more than 486,000 deaths in the United States, has changed our lives forever. Elders and Black, Indigenous, and People of Color (BIPOC) have been overrepresented among those lost. That, when juxtaposed with the civil unrest that followed the brutal killing of George Floyd, an unarmed Black man, by a White law enforcement officer on May 25, 2020, have compelled us to talk about US race relations in unprecedented ways. These and other traumas disproportionately affect the quality of life and health of minority and underserved individuals. The international outcry about racism, serial trauma, and health disparities left the medical profession well positioned to promulgate changes that are conducive to achieving health equity.
Race is a social construct
In November 2020, the American Medical Association (AMA) Board of Trustees made several public acknowledgments about race.1 First, race is a social, nonbiological classification that is different from biology, ethnicity, or genetic ancestry.1 Next, race contributes to health disparities and poor health outcomes for minorities and members of underserved communities.1 Also, racism, which includes disproportionate police brutality against Black and Indigenous people, is a driver of health inequity for them and people in marginalized communities.1
The AMA also commented on how serial trauma and racism can affect one’s health. The AMA acknowledged that exposure to serial trauma throughout one’s life can have a cumulative effect that is “associated with chronic stress, higher rates of comorbidities and lower life expectancy” and results in increased health care costs and decreased quality of life for those who are affected.1 Also, the AMA proclaimed that racism is a threat to public health and pledged to dismantle discriminatory practices and policies in health care, including medical education and research.2
Diversity and inclusion in psychiatry
While the AMA has been striving to reduce bias in health care systems, psychiatry has been forging its path. In March 2015, the American Psychiatric Association’s (APA) Board of Trustees approved the APA’s Strategic Initiative, which has 4 goals: 1) advancing the integration of psychiatry in health care; 2) supporting research; 3) supporting education; and 4) promoting diversity and inclusion in psychiatry.3 The latter goal includes advocating for antiracist policies that promote cultural competence and health equity in education, research and psychiatric care; increased recruitment and retention of psychiatrists from groups that historically have been underrepresented in medicine and medical leadership; and ensuring representation of these groups in APA governance at all levels.3
The APA’s antiracism agenda
In March 2020, outgoing APA President Bruce Schwartz concurred with Board members that diversity and inclusion in the APA warranted a closer review. On May 5, 2020, APA President Jeff Geller committed to authorizing a systematic study of diversity and inclusion in various branches of the APA, including councils and governance. By the end of May, with civil unrest in full swing in the United States, President Geller decided to expand the APA’s diversity agenda.
President Geller appointed the APA Presidential Task Force to Address Structural Racism Throughout Psychiatry (SR Task Force), which had its virtual inaugural meeting on June 27, 2020.4 The SR Task Force exists to focus on structural racism (aka institutional racism) in organized psychiatry, psychiatric patients, and those who provide psychiatric services to patients. The charge, which is subject to revision, if warranted, is clear: provide resources and education on the history of structural racism in the APA and psychiatry, explain how structural racism impacts psychiatric patients and the profession, craft actionable recommendations to dismantle structural racism in the APA and psychiatry, report those findings to the APA’s Board of Trustees, and implement a quality assurance protocol to ensure that the Task Force’s work is consistent with its charge. President Geller decided to have the Task Force focus on anti-Black racism in its inaugural year and believes that the outcome will benefit all psychiatrists, other mental health professionals, and patients who identify as members of minority and underserved groups in the United States and the profession of psychiatry.5
Presidential Task Forces in APA
Presidential Task Forces report directly to the Board of Trustees, which expedites the review of progress reports and deliberation on and, when favorable, implementation of recommendations. Also, Presidential Task Forces are afforded additional APA resources. For example, the SR Task Force has 16 APA staff members who have been appointed or volunteered to assist the Task Force in some way. Many APA staff have graduate degrees in law, education, and other subjects. The skill sets, networks, institutional memory, and commitment that they bring to the project are conducive to advancing the SR Task Force’s agenda at a brisk pace.
Continue to: The APA President...
The APA President decides whom to appoint to each Task Force. President Geller propitiously appointed subject matter experts and members of the Board of Trustees to serve on the SR Task Force. Subject matter experts contribute historical and contemporary content about racism, including anti-Black racism, to the discussion. The data are used to craft research questions that may yield pertinent data. (Note that not all subject matter experts are Black, nor are all Board members White.) APA staff support the Task Force by sharing their expertise, compiling data, coordinating meetings, collaborating on program development, disseminating the work product to APA members and the media, and other important tasks.
The SR Task Force’s work
The SR Task Force strives for transparency in a process that is informed by APA members. The group immediately set up a web hub that is used to communicate with APA members.5 Individual members also use social media to alert members to SR Task Force activities and events. Member input has been solicited by posting several brief surveys on the SR Task Force web hub. Topics have included the effect of structural racism on patient care, psychiatric practice, and organized psychiatry, including the APA. The responses, which collectively totaled >1,600, were reviewed and used to inform Task Force priorities while working within the scope of the charge.5
Based on member feedback, the first large project of the SR Task Force has been to examine structural racism in the APA. The SR Task Force formed workgroups to study data pertaining to diversity and inclusion in the APA Assembly, governance (the Board of Trustees), Councils and Committees, and Scientific Program Committee. As APA Publishing and the DSM Steering Committee have internal processes to address structural racism, the SR Task Force did not convene workgroups to study this. However, the SR Task Force will be meeting with leaders of those groups to learn about their protocols and will request that information be made available to APA members.
The SR Task Force reviews and interprets data that are compiled by each workgroup, deliberates on its significance, and when appropriate, drafts achievable recommendations to improve diversity and inclusion in the APA. This is where Trustee involvement is invaluable to the SR Task Force, because the report and recommendations will be presented to the Board of Trustees.
There is no guarantee that the recommendations contained in a report that is accepted by the Board of Trustees will be implemented unless they are approved. It is imperative, therefore, that SR Task Force recommendations to the Board take into consideration Board structure, processes, goals, efficiency, history, and other matters. The learning curve can be steep, especially when the first major report was due 3 months after the SR Task Force was appointed. Clarity and efficiency are key in report preparation. For example, during the Winter 2020 Board of Trustees meeting, the SR Task Force presented its report, answered questions, and offered 7 action items to the Board for deliberation and voting. The endeavor, which was completed in 20 minutes, resulted in the Board supporting 6 of the recommendations and deferring the deliberation of the seventh recommendation to the spring Board meeting, due to logistical concerns.
Continue to: Thus far, the SR Task Force Workgroups...
Thus far, the SR Task Force Workgroups on the Assembly and Governance have presented their reports. 5 The SR Task Force reports on the Scientific Program Committee and Councils and Committees are scheduled to be presented to the Board during the Spring 2021 meeting.
The SR Task Force has been fulfilling the commitment to provide relevant educational materials to members in several ways. There have been 4 virtual Structural Racism Town Hall meetings that featured subject matter experts. The first Town Hall session addressed the initial steps towards dismantling structural racism and included President Geller’s announcement about appointing a SR Task Force. The next Town Hall meeting addressed structural racism in medicine and psychiatry, its effect on children and individuals who identify as transgender, and its intersectionality (the cumulative effect of discrimination on a person who belongs to 2 non-dominant groups.) The panel in the third Town Hall meeting reviewed the impact of structural racism, including intersectionality, on transgenerational trauma in several minority groups. The meeting ended with an update of Task Force activities. The February 2021 Town Hall meeting focused on how structural racism affects recruitment and retention of minority psychiatry residents, and how this can undermine efforts to grow a diverse workforce. Recordings of these and other events can be accessed on the SR Task Force web hub.5 The SR Task Force members plan to present a review of the year’s work during the next Town Hall meeting, which is scheduled to occur on Saturday, May 1, 2021, during the APA’s Annual Meeting.
The SR Task Force web hub contains other resources, including APA position statements, press releases, and news articles, and a glossary of relevant terms. It also includes internet links to President Geller’s 9-part series on the history of Structural Racism in the APA. There are CME and other webinars, a curated list of references, videos, podcasts, and other media.4
The SR Task Force believes that much of the antiracism work needs to occur beyond APA headquarters. Consequently, President Geller challenged all APA Councils to work on an antiracism project to support the APA’s antiracism agenda. APA committees and caucuses have been encouraged to do the same. The SR Task Force has asked APA District Branches and Allied Organizations to share information about what they are doing to educate members about structural racism and what they are doing for input regarding their antiracist activities. Additionally, Task Force members have been speaking with these and other groups to inform them about the APA’s antiracism work.
APA’s Board of Trustees actions
It would be inappropriate for the APA to task groups with focusing on antiracism unless the organization was doing its part. In July 2020, the Board of Trustees had a 2-hour round table discussion during which each member spoke about the problem and how the APA should address it. Next, President Geller appointed a Board Workgroup to clarify the definitions of “minority” and “underrepresented.” Although the APA Assembly has defined the terms, the APA has not. Additionally, the APA Board of Trustees retained a consultant to assess all aspects of how it functions as a Board. The Board’s management of matters pertaining to diversity and inclusion was part of the examination. The recommendations are being reviewed and the Board will undergo diversity training.
Continue to: President Geller's study...
President Geller’s study of racism in the APA, which involved a review of past APA presidential addresses, brought to light a long-term pattern of racism in the organization.5 On January 18, 2021, Martin Luther King, Jr. Day, the APA acknowledged and apologized to psychiatrists, patients, and the public for its history of engaging in and passively condoning racist behavior.6 The APA has committed to being better informed about diversity and inclusion at every level. Lastly, hired consultants with expertise in diversity and inclusion are working with APA staff at every level so that the environment can be a welcoming and comfortable workspace for recruiting and retaining a diverse workforce.
Although it may seem that the APA has engaged in many antiracist activities in a brief period, there is much more to accomplish. The Task Force hopes that the work will speak for itself and will be sustained over time. It’s long overdue.
The coronavirus disease 2019 pandemic, which as of mid-February 2021 had caused more than 486,000 deaths in the United States, has changed our lives forever. Elders and Black, Indigenous, and People of Color (BIPOC) have been overrepresented among those lost. That, when juxtaposed with the civil unrest that followed the brutal killing of George Floyd, an unarmed Black man, by a White law enforcement officer on May 25, 2020, have compelled us to talk about US race relations in unprecedented ways. These and other traumas disproportionately affect the quality of life and health of minority and underserved individuals. The international outcry about racism, serial trauma, and health disparities left the medical profession well positioned to promulgate changes that are conducive to achieving health equity.
Race is a social construct
In November 2020, the American Medical Association (AMA) Board of Trustees made several public acknowledgments about race.1 First, race is a social, nonbiological classification that is different from biology, ethnicity, or genetic ancestry.1 Next, race contributes to health disparities and poor health outcomes for minorities and members of underserved communities.1 Also, racism, which includes disproportionate police brutality against Black and Indigenous people, is a driver of health inequity for them and people in marginalized communities.1
The AMA also commented on how serial trauma and racism can affect one’s health. The AMA acknowledged that exposure to serial trauma throughout one’s life can have a cumulative effect that is “associated with chronic stress, higher rates of comorbidities and lower life expectancy” and results in increased health care costs and decreased quality of life for those who are affected.1 Also, the AMA proclaimed that racism is a threat to public health and pledged to dismantle discriminatory practices and policies in health care, including medical education and research.2
Diversity and inclusion in psychiatry
While the AMA has been striving to reduce bias in health care systems, psychiatry has been forging its path. In March 2015, the American Psychiatric Association’s (APA) Board of Trustees approved the APA’s Strategic Initiative, which has 4 goals: 1) advancing the integration of psychiatry in health care; 2) supporting research; 3) supporting education; and 4) promoting diversity and inclusion in psychiatry.3 The latter goal includes advocating for antiracist policies that promote cultural competence and health equity in education, research and psychiatric care; increased recruitment and retention of psychiatrists from groups that historically have been underrepresented in medicine and medical leadership; and ensuring representation of these groups in APA governance at all levels.3
The APA’s antiracism agenda
In March 2020, outgoing APA President Bruce Schwartz concurred with Board members that diversity and inclusion in the APA warranted a closer review. On May 5, 2020, APA President Jeff Geller committed to authorizing a systematic study of diversity and inclusion in various branches of the APA, including councils and governance. By the end of May, with civil unrest in full swing in the United States, President Geller decided to expand the APA’s diversity agenda.
President Geller appointed the APA Presidential Task Force to Address Structural Racism Throughout Psychiatry (SR Task Force), which had its virtual inaugural meeting on June 27, 2020.4 The SR Task Force exists to focus on structural racism (aka institutional racism) in organized psychiatry, psychiatric patients, and those who provide psychiatric services to patients. The charge, which is subject to revision, if warranted, is clear: provide resources and education on the history of structural racism in the APA and psychiatry, explain how structural racism impacts psychiatric patients and the profession, craft actionable recommendations to dismantle structural racism in the APA and psychiatry, report those findings to the APA’s Board of Trustees, and implement a quality assurance protocol to ensure that the Task Force’s work is consistent with its charge. President Geller decided to have the Task Force focus on anti-Black racism in its inaugural year and believes that the outcome will benefit all psychiatrists, other mental health professionals, and patients who identify as members of minority and underserved groups in the United States and the profession of psychiatry.5
Presidential Task Forces in APA
Presidential Task Forces report directly to the Board of Trustees, which expedites the review of progress reports and deliberation on and, when favorable, implementation of recommendations. Also, Presidential Task Forces are afforded additional APA resources. For example, the SR Task Force has 16 APA staff members who have been appointed or volunteered to assist the Task Force in some way. Many APA staff have graduate degrees in law, education, and other subjects. The skill sets, networks, institutional memory, and commitment that they bring to the project are conducive to advancing the SR Task Force’s agenda at a brisk pace.
Continue to: The APA President...
The APA President decides whom to appoint to each Task Force. President Geller propitiously appointed subject matter experts and members of the Board of Trustees to serve on the SR Task Force. Subject matter experts contribute historical and contemporary content about racism, including anti-Black racism, to the discussion. The data are used to craft research questions that may yield pertinent data. (Note that not all subject matter experts are Black, nor are all Board members White.) APA staff support the Task Force by sharing their expertise, compiling data, coordinating meetings, collaborating on program development, disseminating the work product to APA members and the media, and other important tasks.
The SR Task Force’s work
The SR Task Force strives for transparency in a process that is informed by APA members. The group immediately set up a web hub that is used to communicate with APA members.5 Individual members also use social media to alert members to SR Task Force activities and events. Member input has been solicited by posting several brief surveys on the SR Task Force web hub. Topics have included the effect of structural racism on patient care, psychiatric practice, and organized psychiatry, including the APA. The responses, which collectively totaled >1,600, were reviewed and used to inform Task Force priorities while working within the scope of the charge.5
Based on member feedback, the first large project of the SR Task Force has been to examine structural racism in the APA. The SR Task Force formed workgroups to study data pertaining to diversity and inclusion in the APA Assembly, governance (the Board of Trustees), Councils and Committees, and Scientific Program Committee. As APA Publishing and the DSM Steering Committee have internal processes to address structural racism, the SR Task Force did not convene workgroups to study this. However, the SR Task Force will be meeting with leaders of those groups to learn about their protocols and will request that information be made available to APA members.
The SR Task Force reviews and interprets data that are compiled by each workgroup, deliberates on its significance, and when appropriate, drafts achievable recommendations to improve diversity and inclusion in the APA. This is where Trustee involvement is invaluable to the SR Task Force, because the report and recommendations will be presented to the Board of Trustees.
There is no guarantee that the recommendations contained in a report that is accepted by the Board of Trustees will be implemented unless they are approved. It is imperative, therefore, that SR Task Force recommendations to the Board take into consideration Board structure, processes, goals, efficiency, history, and other matters. The learning curve can be steep, especially when the first major report was due 3 months after the SR Task Force was appointed. Clarity and efficiency are key in report preparation. For example, during the Winter 2020 Board of Trustees meeting, the SR Task Force presented its report, answered questions, and offered 7 action items to the Board for deliberation and voting. The endeavor, which was completed in 20 minutes, resulted in the Board supporting 6 of the recommendations and deferring the deliberation of the seventh recommendation to the spring Board meeting, due to logistical concerns.
Continue to: Thus far, the SR Task Force Workgroups...
Thus far, the SR Task Force Workgroups on the Assembly and Governance have presented their reports. 5 The SR Task Force reports on the Scientific Program Committee and Councils and Committees are scheduled to be presented to the Board during the Spring 2021 meeting.
The SR Task Force has been fulfilling the commitment to provide relevant educational materials to members in several ways. There have been 4 virtual Structural Racism Town Hall meetings that featured subject matter experts. The first Town Hall session addressed the initial steps towards dismantling structural racism and included President Geller’s announcement about appointing a SR Task Force. The next Town Hall meeting addressed structural racism in medicine and psychiatry, its effect on children and individuals who identify as transgender, and its intersectionality (the cumulative effect of discrimination on a person who belongs to 2 non-dominant groups.) The panel in the third Town Hall meeting reviewed the impact of structural racism, including intersectionality, on transgenerational trauma in several minority groups. The meeting ended with an update of Task Force activities. The February 2021 Town Hall meeting focused on how structural racism affects recruitment and retention of minority psychiatry residents, and how this can undermine efforts to grow a diverse workforce. Recordings of these and other events can be accessed on the SR Task Force web hub.5 The SR Task Force members plan to present a review of the year’s work during the next Town Hall meeting, which is scheduled to occur on Saturday, May 1, 2021, during the APA’s Annual Meeting.
The SR Task Force web hub contains other resources, including APA position statements, press releases, and news articles, and a glossary of relevant terms. It also includes internet links to President Geller’s 9-part series on the history of Structural Racism in the APA. There are CME and other webinars, a curated list of references, videos, podcasts, and other media.4
The SR Task Force believes that much of the antiracism work needs to occur beyond APA headquarters. Consequently, President Geller challenged all APA Councils to work on an antiracism project to support the APA’s antiracism agenda. APA committees and caucuses have been encouraged to do the same. The SR Task Force has asked APA District Branches and Allied Organizations to share information about what they are doing to educate members about structural racism and what they are doing for input regarding their antiracist activities. Additionally, Task Force members have been speaking with these and other groups to inform them about the APA’s antiracism work.
APA’s Board of Trustees actions
It would be inappropriate for the APA to task groups with focusing on antiracism unless the organization was doing its part. In July 2020, the Board of Trustees had a 2-hour round table discussion during which each member spoke about the problem and how the APA should address it. Next, President Geller appointed a Board Workgroup to clarify the definitions of “minority” and “underrepresented.” Although the APA Assembly has defined the terms, the APA has not. Additionally, the APA Board of Trustees retained a consultant to assess all aspects of how it functions as a Board. The Board’s management of matters pertaining to diversity and inclusion was part of the examination. The recommendations are being reviewed and the Board will undergo diversity training.
Continue to: President Geller's study...
President Geller’s study of racism in the APA, which involved a review of past APA presidential addresses, brought to light a long-term pattern of racism in the organization.5 On January 18, 2021, Martin Luther King, Jr. Day, the APA acknowledged and apologized to psychiatrists, patients, and the public for its history of engaging in and passively condoning racist behavior.6 The APA has committed to being better informed about diversity and inclusion at every level. Lastly, hired consultants with expertise in diversity and inclusion are working with APA staff at every level so that the environment can be a welcoming and comfortable workspace for recruiting and retaining a diverse workforce.
Although it may seem that the APA has engaged in many antiracist activities in a brief period, there is much more to accomplish. The Task Force hopes that the work will speak for itself and will be sustained over time. It’s long overdue.
1. American Medical Association. New AMA policies recognize race as a social, not biological, construct. Published November 16, 2020. Accessed February 1, 2021. https://www.ama-assn.org/press-center/press-releases/new-ama-policies-recognize-race-social-not-biological-construct
2. American Medical Association. New AMA policy recognizes racism as a public health threat. Published November 16, 2020. Accessed February 1, 2021. https://www.ama-assn.org/press-center/press-releases/new-ama-policy-recognizes-racism-public-health-threat
3. American Psychiatric Association. Board-approved recommendation on strategic planning. Published March 2015. Accessed February 1, 2021. https://www.psychiatry.org/about-apa/read-apa-organization-documents-and-policies/strategic-plan
4. Geller J. Structural racism in American psychiatry and APA. Parts 1-9. Published July-November 2020. Accessed February 8, 2021. https://psychnews.psychiatryonline.org/topic/news-president?sortBy=Ppub
5. American Psychiatric Association. Structural Racism Task Force. Accessed February 8, 2021. https://www.psychiatry.org/psychiatrists/structural-racism-task-force
6. American Psychiatric Association. APA’s apology to black, indigenous and people of color for its support of structural racism in psychiatry. Published January 18, 2021. Accessed February 8, 2021. https://www.psychiatry.org/newsroom/apa-apology-for-its-support-of-structural-racism-in-psychiatry
1. American Medical Association. New AMA policies recognize race as a social, not biological, construct. Published November 16, 2020. Accessed February 1, 2021. https://www.ama-assn.org/press-center/press-releases/new-ama-policies-recognize-race-social-not-biological-construct
2. American Medical Association. New AMA policy recognizes racism as a public health threat. Published November 16, 2020. Accessed February 1, 2021. https://www.ama-assn.org/press-center/press-releases/new-ama-policy-recognizes-racism-public-health-threat
3. American Psychiatric Association. Board-approved recommendation on strategic planning. Published March 2015. Accessed February 1, 2021. https://www.psychiatry.org/about-apa/read-apa-organization-documents-and-policies/strategic-plan
4. Geller J. Structural racism in American psychiatry and APA. Parts 1-9. Published July-November 2020. Accessed February 8, 2021. https://psychnews.psychiatryonline.org/topic/news-president?sortBy=Ppub
5. American Psychiatric Association. Structural Racism Task Force. Accessed February 8, 2021. https://www.psychiatry.org/psychiatrists/structural-racism-task-force
6. American Psychiatric Association. APA’s apology to black, indigenous and people of color for its support of structural racism in psychiatry. Published January 18, 2021. Accessed February 8, 2021. https://www.psychiatry.org/newsroom/apa-apology-for-its-support-of-structural-racism-in-psychiatry

Eruptive Annular Papules on the Trunk of an Organ Transplant Recipient
The Diagnosis: Epidermodysplasia Verruciformis
Histopathologic examination of our patient's biopsy specimen revealed mild acanthosis with prominent hypergranulosis and enlarged keratinocytes with blue-gray cytoplasm (Figure). A diagnosis of acquired epidermodysplasia verruciformis (EV) was rendered. The patient was treated with photodynamic therapy utilizing 5-aminolevulinic acid.
Epidermodysplasia verruciformis is characterized by susceptibility to human papillomavirus (HPV) infections via a defect in cellular immunity. Epidermodysplasia verruciformis was first described as an autosomal-recessive genodermatosis, but it can be acquired in immunosuppressed states with an atypical clinical appearance.1 There are few case reports in skin of color. Acquired EV appears in patients with acquired immunodeficiencies that are susceptible to EV-causing HPVs via a similar mechanism found in inherited EV.2 The most common HPV serotypes involved in EV are HPV-5 and HPV-8. The duration of immunosuppression has been found to be positively correlated with the risk for EV development, with the majority of patients developing lesions after 5 years of immunosuppression.3 There is an approximately 60% risk of malignant transformation of EV lesions into nonmelanoma skin cancer.2 This risk is believed to be lower in patients with darker skin.4
Preventative measures including sun protection and annual surveillance are crucial in EV patients given the high rate of malignant transformation in sun-exposed lesions.5 Treatment options for EV are anecdotal and have variable results, ranging from topicals including 5-fluorouracil and imiquimod to systemic medications including acitretin and interferon.3 Photodynamic therapy can be used for extensive EV. Surgical modalities and other destructive methods also have been tried.6
Epidermodysplasia verruciformis often can be confused with similar dermatoses. Porokeratosis appears as annular pink papules with waferlike peripheral scales. Tinea versicolor is a dermatophyte infection caused by Malassezia furfur and presents as multiple dyspigmented, finely scaling, thin papules and plaques. Subacute cutaneous lupus erythematosus presents as pink, scaly, annular or psoriasiform papules and plaques most commonly on the trunk. Discoid lupus erythematosus presents as pink, hypopigmented or depigmented, atrophic plaques with a peripheral rim of erythema that indicates activity. Secondary syphilis, commonly denoted as the "great mimicker," presents as psoriasiform papules and plaques among other variable morphologies.
- Sa NB, Guerini MB, Barbato MT, et al. Epidermodysplasia verruciformis: clinical presentation with varied forms of lesions. An Bras Dermatol. 2011;86(4 suppl 1):S57-S60.
- Rogers HD, Macgregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:315-320.
- Henley JK, Hossler EW. Acquired epidermodysplasia verruciformis occurring in a renal transplant recipient. Cutis. 2017;99:E9-E12.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Fox SH, Elston DM. Epidermodysplasia verruciformis and the risk for malignancy. Cutis. 2016;98:E10-E12.
- Shruti S, Siraj F, Singh A, et al. Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26:59-61.
The Diagnosis: Epidermodysplasia Verruciformis
Histopathologic examination of our patient's biopsy specimen revealed mild acanthosis with prominent hypergranulosis and enlarged keratinocytes with blue-gray cytoplasm (Figure). A diagnosis of acquired epidermodysplasia verruciformis (EV) was rendered. The patient was treated with photodynamic therapy utilizing 5-aminolevulinic acid.
Epidermodysplasia verruciformis is characterized by susceptibility to human papillomavirus (HPV) infections via a defect in cellular immunity. Epidermodysplasia verruciformis was first described as an autosomal-recessive genodermatosis, but it can be acquired in immunosuppressed states with an atypical clinical appearance.1 There are few case reports in skin of color. Acquired EV appears in patients with acquired immunodeficiencies that are susceptible to EV-causing HPVs via a similar mechanism found in inherited EV.2 The most common HPV serotypes involved in EV are HPV-5 and HPV-8. The duration of immunosuppression has been found to be positively correlated with the risk for EV development, with the majority of patients developing lesions after 5 years of immunosuppression.3 There is an approximately 60% risk of malignant transformation of EV lesions into nonmelanoma skin cancer.2 This risk is believed to be lower in patients with darker skin.4
Preventative measures including sun protection and annual surveillance are crucial in EV patients given the high rate of malignant transformation in sun-exposed lesions.5 Treatment options for EV are anecdotal and have variable results, ranging from topicals including 5-fluorouracil and imiquimod to systemic medications including acitretin and interferon.3 Photodynamic therapy can be used for extensive EV. Surgical modalities and other destructive methods also have been tried.6
Epidermodysplasia verruciformis often can be confused with similar dermatoses. Porokeratosis appears as annular pink papules with waferlike peripheral scales. Tinea versicolor is a dermatophyte infection caused by Malassezia furfur and presents as multiple dyspigmented, finely scaling, thin papules and plaques. Subacute cutaneous lupus erythematosus presents as pink, scaly, annular or psoriasiform papules and plaques most commonly on the trunk. Discoid lupus erythematosus presents as pink, hypopigmented or depigmented, atrophic plaques with a peripheral rim of erythema that indicates activity. Secondary syphilis, commonly denoted as the "great mimicker," presents as psoriasiform papules and plaques among other variable morphologies.
The Diagnosis: Epidermodysplasia Verruciformis
Histopathologic examination of our patient's biopsy specimen revealed mild acanthosis with prominent hypergranulosis and enlarged keratinocytes with blue-gray cytoplasm (Figure). A diagnosis of acquired epidermodysplasia verruciformis (EV) was rendered. The patient was treated with photodynamic therapy utilizing 5-aminolevulinic acid.
Epidermodysplasia verruciformis is characterized by susceptibility to human papillomavirus (HPV) infections via a defect in cellular immunity. Epidermodysplasia verruciformis was first described as an autosomal-recessive genodermatosis, but it can be acquired in immunosuppressed states with an atypical clinical appearance.1 There are few case reports in skin of color. Acquired EV appears in patients with acquired immunodeficiencies that are susceptible to EV-causing HPVs via a similar mechanism found in inherited EV.2 The most common HPV serotypes involved in EV are HPV-5 and HPV-8. The duration of immunosuppression has been found to be positively correlated with the risk for EV development, with the majority of patients developing lesions after 5 years of immunosuppression.3 There is an approximately 60% risk of malignant transformation of EV lesions into nonmelanoma skin cancer.2 This risk is believed to be lower in patients with darker skin.4
Preventative measures including sun protection and annual surveillance are crucial in EV patients given the high rate of malignant transformation in sun-exposed lesions.5 Treatment options for EV are anecdotal and have variable results, ranging from topicals including 5-fluorouracil and imiquimod to systemic medications including acitretin and interferon.3 Photodynamic therapy can be used for extensive EV. Surgical modalities and other destructive methods also have been tried.6
Epidermodysplasia verruciformis often can be confused with similar dermatoses. Porokeratosis appears as annular pink papules with waferlike peripheral scales. Tinea versicolor is a dermatophyte infection caused by Malassezia furfur and presents as multiple dyspigmented, finely scaling, thin papules and plaques. Subacute cutaneous lupus erythematosus presents as pink, scaly, annular or psoriasiform papules and plaques most commonly on the trunk. Discoid lupus erythematosus presents as pink, hypopigmented or depigmented, atrophic plaques with a peripheral rim of erythema that indicates activity. Secondary syphilis, commonly denoted as the "great mimicker," presents as psoriasiform papules and plaques among other variable morphologies.
- Sa NB, Guerini MB, Barbato MT, et al. Epidermodysplasia verruciformis: clinical presentation with varied forms of lesions. An Bras Dermatol. 2011;86(4 suppl 1):S57-S60.
- Rogers HD, Macgregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:315-320.
- Henley JK, Hossler EW. Acquired epidermodysplasia verruciformis occurring in a renal transplant recipient. Cutis. 2017;99:E9-E12.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Fox SH, Elston DM. Epidermodysplasia verruciformis and the risk for malignancy. Cutis. 2016;98:E10-E12.
- Shruti S, Siraj F, Singh A, et al. Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26:59-61.
- Sa NB, Guerini MB, Barbato MT, et al. Epidermodysplasia verruciformis: clinical presentation with varied forms of lesions. An Bras Dermatol. 2011;86(4 suppl 1):S57-S60.
- Rogers HD, Macgregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:315-320.
- Henley JK, Hossler EW. Acquired epidermodysplasia verruciformis occurring in a renal transplant recipient. Cutis. 2017;99:E9-E12.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Fox SH, Elston DM. Epidermodysplasia verruciformis and the risk for malignancy. Cutis. 2016;98:E10-E12.
- Shruti S, Siraj F, Singh A, et al. Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26:59-61.
A 50-year-old Black woman with systemic lupus erythematosus and a renal transplant 15 years prior due to lupus nephritis presented with a nonpruritic rash on the abdomen of 1 year’s duration. Her immunosuppressive regimen consisted of tacrolimus, azathioprine, and prednisone. Physical examination revealed numerous monomorphic, annular, hyperpigmented, and thin papules with central clearing present on the abdomen extending to the flanks and groin. The patient denied any family history of similar lesions. A 4-mm punch biopsy of an abdominal lesion was performed.
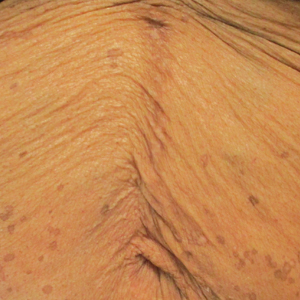
Improving Dermatologic Care for South Asian Patients: Understanding Religious and Cultural Practices
Traditional garments are particularly important in both Sikhism and Islam. Sikhs began wearing symbolic garments in the 16th century as markers of their identity during periods of religious persecution. Today, many Sikhs continue to maintain this tradition of wearing the Five Ks—kesh (uncut hair, often tied in a turban), kanga (wooden hair comb), kirpan (symbolic dagger), kachha (cotton underwear), and kara (steel bracelet).2 Similarly, Islamic traditions also provide guidance for clothing. Many Muslim women wear the hijab (headscarf), a garment that originated as protective headgear for nomadic desert cultures and has come to symbolize modest dress. Traditionally, the hijab is worn in the presence of all men who are not immediate relatives, although patients may make exceptions for medical care. Some Muslim men also may cover their heads with a skullcap and/or maintain long beards (occasionally dyed with henna pigment) as a way of keeping continuity with the tradition of the Prophet Muhammad and his companions.3
Certain styles of headwear can cause high tension on hair follicles and have been associated with traction alopecia.4 Persistent use of the same turban, hijab, or comb also may lead to seborrheic dermatitis or fungal scalp infections. Dermatologists should advise patients about these potential challenges and suggest modifications in accordance with the patient’s religious beliefs; for example, providers can suggest removing headwear at night, using prophylactic antifungal shampoos, and/or tying the hair in a ponytail or loosening the headgear to reduce traction.
Although Hinduism does not have a unifying garment or hair tradition in the vein of Sikhism or Islam, all 3 religions share a strong emphasis on bodily modesty, which may affect dermatologic examinations. Patients from all 3 religions may seek to expose as little skin as possible during a physical examination, and many patients may be uncomfortable with a physician of the opposite gender. Dermatologists may find the following practices to be helpful5:
• Talk through each aspect of the skin examination while it is being performed and expose the least amount of skin necessary during the process
• Offer the patient a chaperone or a same-gender provider, if possible
• Empower patients to assist in adjusting garments themselves to help the physician visualize all parts of the skin
Some Sikhs also may have specific concerns regarding cutting their hair. One aspect of kesh is that every hair is sacred, and thus, many Sikhs refrain from removing hair on any part of the body. As such, providers should carefully obtain the patient’s informed consent before performing any procedure or physical examination maneuvers (eg, hair pull test) that may result in loss of hair.2
Physicians of all disciplines can help address these challenges through increased outreach and cultural awareness; for example, dermatologists can create skin care pamphlets translated into various South Asian languages and distribute them at houses of worship or other community centers. This may help patients identify their skin needs and seek appropriate care. The onus must be on physicians to make these patients feel comfortable seeking care by creating nonjudgmental, culturally knowledgeable clinical environments. When asking about social history, the physician might consider asking an open-ended question such as, “What role does religion/spirituality play in your life?” They can then proceed to ask specific questions about practices that might affect the patient’s care.5
Given the current coronavirus disease 2019 pandemic, South Asian patients may be even further discouraged from seeking dermatologic care. By understanding religious traditions and taking steps to address biases, dermatologists can help mitigate health care disparities and provide culturally competent care to South Asian patients.
- Nadimpalli SB, Cleland CM, Hutchinson MK, et al. The association between discrimination and the health of Sikh Asian Indians. Health Psychol. 2016;35:351-355.
- The five Ks. BBC website. Updated September 29, 2009. Accessed February 4, 2021. https://www.bbc.co.uk/religion/religions/sikhism/customs/fiveks.shtml
- Islam. BBC website. Accessed February 2, 2021. https://www.bbc.co.uk/religion/religions/islam/
- James J, Saladi RN, Fox JL. Traction alopecia in Sikh male patients. J Am Board Fam Med. 2007;20:497-498.
- Hussain A. Recommendations for culturally competent dermatology care of Muslim patients. J Am Acad Dermatol. 2017;77:388-389.
Traditional garments are particularly important in both Sikhism and Islam. Sikhs began wearing symbolic garments in the 16th century as markers of their identity during periods of religious persecution. Today, many Sikhs continue to maintain this tradition of wearing the Five Ks—kesh (uncut hair, often tied in a turban), kanga (wooden hair comb), kirpan (symbolic dagger), kachha (cotton underwear), and kara (steel bracelet).2 Similarly, Islamic traditions also provide guidance for clothing. Many Muslim women wear the hijab (headscarf), a garment that originated as protective headgear for nomadic desert cultures and has come to symbolize modest dress. Traditionally, the hijab is worn in the presence of all men who are not immediate relatives, although patients may make exceptions for medical care. Some Muslim men also may cover their heads with a skullcap and/or maintain long beards (occasionally dyed with henna pigment) as a way of keeping continuity with the tradition of the Prophet Muhammad and his companions.3
Certain styles of headwear can cause high tension on hair follicles and have been associated with traction alopecia.4 Persistent use of the same turban, hijab, or comb also may lead to seborrheic dermatitis or fungal scalp infections. Dermatologists should advise patients about these potential challenges and suggest modifications in accordance with the patient’s religious beliefs; for example, providers can suggest removing headwear at night, using prophylactic antifungal shampoos, and/or tying the hair in a ponytail or loosening the headgear to reduce traction.
Although Hinduism does not have a unifying garment or hair tradition in the vein of Sikhism or Islam, all 3 religions share a strong emphasis on bodily modesty, which may affect dermatologic examinations. Patients from all 3 religions may seek to expose as little skin as possible during a physical examination, and many patients may be uncomfortable with a physician of the opposite gender. Dermatologists may find the following practices to be helpful5:
• Talk through each aspect of the skin examination while it is being performed and expose the least amount of skin necessary during the process
• Offer the patient a chaperone or a same-gender provider, if possible
• Empower patients to assist in adjusting garments themselves to help the physician visualize all parts of the skin
Some Sikhs also may have specific concerns regarding cutting their hair. One aspect of kesh is that every hair is sacred, and thus, many Sikhs refrain from removing hair on any part of the body. As such, providers should carefully obtain the patient’s informed consent before performing any procedure or physical examination maneuvers (eg, hair pull test) that may result in loss of hair.2
Physicians of all disciplines can help address these challenges through increased outreach and cultural awareness; for example, dermatologists can create skin care pamphlets translated into various South Asian languages and distribute them at houses of worship or other community centers. This may help patients identify their skin needs and seek appropriate care. The onus must be on physicians to make these patients feel comfortable seeking care by creating nonjudgmental, culturally knowledgeable clinical environments. When asking about social history, the physician might consider asking an open-ended question such as, “What role does religion/spirituality play in your life?” They can then proceed to ask specific questions about practices that might affect the patient’s care.5
Given the current coronavirus disease 2019 pandemic, South Asian patients may be even further discouraged from seeking dermatologic care. By understanding religious traditions and taking steps to address biases, dermatologists can help mitigate health care disparities and provide culturally competent care to South Asian patients.
Traditional garments are particularly important in both Sikhism and Islam. Sikhs began wearing symbolic garments in the 16th century as markers of their identity during periods of religious persecution. Today, many Sikhs continue to maintain this tradition of wearing the Five Ks—kesh (uncut hair, often tied in a turban), kanga (wooden hair comb), kirpan (symbolic dagger), kachha (cotton underwear), and kara (steel bracelet).2 Similarly, Islamic traditions also provide guidance for clothing. Many Muslim women wear the hijab (headscarf), a garment that originated as protective headgear for nomadic desert cultures and has come to symbolize modest dress. Traditionally, the hijab is worn in the presence of all men who are not immediate relatives, although patients may make exceptions for medical care. Some Muslim men also may cover their heads with a skullcap and/or maintain long beards (occasionally dyed with henna pigment) as a way of keeping continuity with the tradition of the Prophet Muhammad and his companions.3
Certain styles of headwear can cause high tension on hair follicles and have been associated with traction alopecia.4 Persistent use of the same turban, hijab, or comb also may lead to seborrheic dermatitis or fungal scalp infections. Dermatologists should advise patients about these potential challenges and suggest modifications in accordance with the patient’s religious beliefs; for example, providers can suggest removing headwear at night, using prophylactic antifungal shampoos, and/or tying the hair in a ponytail or loosening the headgear to reduce traction.
Although Hinduism does not have a unifying garment or hair tradition in the vein of Sikhism or Islam, all 3 religions share a strong emphasis on bodily modesty, which may affect dermatologic examinations. Patients from all 3 religions may seek to expose as little skin as possible during a physical examination, and many patients may be uncomfortable with a physician of the opposite gender. Dermatologists may find the following practices to be helpful5:
• Talk through each aspect of the skin examination while it is being performed and expose the least amount of skin necessary during the process
• Offer the patient a chaperone or a same-gender provider, if possible
• Empower patients to assist in adjusting garments themselves to help the physician visualize all parts of the skin
Some Sikhs also may have specific concerns regarding cutting their hair. One aspect of kesh is that every hair is sacred, and thus, many Sikhs refrain from removing hair on any part of the body. As such, providers should carefully obtain the patient’s informed consent before performing any procedure or physical examination maneuvers (eg, hair pull test) that may result in loss of hair.2
Physicians of all disciplines can help address these challenges through increased outreach and cultural awareness; for example, dermatologists can create skin care pamphlets translated into various South Asian languages and distribute them at houses of worship or other community centers. This may help patients identify their skin needs and seek appropriate care. The onus must be on physicians to make these patients feel comfortable seeking care by creating nonjudgmental, culturally knowledgeable clinical environments. When asking about social history, the physician might consider asking an open-ended question such as, “What role does religion/spirituality play in your life?” They can then proceed to ask specific questions about practices that might affect the patient’s care.5
Given the current coronavirus disease 2019 pandemic, South Asian patients may be even further discouraged from seeking dermatologic care. By understanding religious traditions and taking steps to address biases, dermatologists can help mitigate health care disparities and provide culturally competent care to South Asian patients.
- Nadimpalli SB, Cleland CM, Hutchinson MK, et al. The association between discrimination and the health of Sikh Asian Indians. Health Psychol. 2016;35:351-355.
- The five Ks. BBC website. Updated September 29, 2009. Accessed February 4, 2021. https://www.bbc.co.uk/religion/religions/sikhism/customs/fiveks.shtml
- Islam. BBC website. Accessed February 2, 2021. https://www.bbc.co.uk/religion/religions/islam/
- James J, Saladi RN, Fox JL. Traction alopecia in Sikh male patients. J Am Board Fam Med. 2007;20:497-498.
- Hussain A. Recommendations for culturally competent dermatology care of Muslim patients. J Am Acad Dermatol. 2017;77:388-389.
- Nadimpalli SB, Cleland CM, Hutchinson MK, et al. The association between discrimination and the health of Sikh Asian Indians. Health Psychol. 2016;35:351-355.
- The five Ks. BBC website. Updated September 29, 2009. Accessed February 4, 2021. https://www.bbc.co.uk/religion/religions/sikhism/customs/fiveks.shtml
- Islam. BBC website. Accessed February 2, 2021. https://www.bbc.co.uk/religion/religions/islam/
- James J, Saladi RN, Fox JL. Traction alopecia in Sikh male patients. J Am Board Fam Med. 2007;20:497-498.
- Hussain A. Recommendations for culturally competent dermatology care of Muslim patients. J Am Acad Dermatol. 2017;77:388-389.
Practice Points
- Providers should familiarize themselves with traditional garments of Sikhism and Islam, including head coverings and other symbolic items.
- Inform patients about health-conscious methods of wearing traditional headwear, such as removing certain headwear at night and tying hair in methods to avoid causing traction alopecia.
- Talk through each aspect of the skin examination while it is being performed and expose the least amount of skin necessary during the process. Offer the patient a chaperone or a same-gender provider, if possible.
- Empower patients to assist in adjusting garments themselves to help the physician visualize all parts of the skin.
Racial/ethnic disparities in cesarean rates increase with greater maternal education
While the likelihood of a cesarean delivery usually drops as maternal education level increases, the disparities seen in cesarean rates between White and Black or Hispanic women actually increase with more maternal education, according to findings from a new study presented at the Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Typically, higher maternal education is associated with a lower likelihood of cesarean delivery, but this protective effect is much smaller for Black women and nonexistent for Hispanic women, leading to bigger gaps between these groups and White women, found Yael Eliner, MD, an ob.gyn. residency applicant at Boston University who conducted this research with her colleagues in the ob.gyn. department at Lenox Hill Hospital, New York, and Hofstra University, Hempstead, N.Y..
Researchers have previously identified racial and ethnic disparities in a wide range of maternal outcomes, including mortality, overall morbidity, preterm birth, low birth weight, fetal growth restriction, hypertensive disorders of pregnancy, diabetes, and cesarean deliveries. But the researchers wanted to know if the usual protective effects seen for cesarean deliveries existed in the racial and ethnic groups with these disparities. Past studies have already found that the protective effect of maternal education is greater for White women than Black women with infant mortality and overall self-rated health.
The researchers conducted a retrospective analysis of all low-risk nulliparous, term, singleton, vertex live births to U.S. residents from 2016 to 2019 by using the natality database of the Centers for Disease Control and Prevention. They looked only at women who were non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, and Hispanic women. They excluded women with pregestational and gestational diabetes, chronic hypertension, and hypertensive disorders of pregnancy.
Maternal education levels were stratified into those without a high school diploma, high school graduates (including those with some college credit), college graduates, and those with advanced degrees. The total population included 2,969,207 mothers with a 23.4% cesarean delivery rate.
Before considering education or other potential confounders, the cesarean delivery rate was 27.4% in Black women and 25.6% in Asian women, compared with 22.4% in White women and 23% in Hispanic women (P < .001).
Among those with less than a high school education, Black (20.9%), Asian (23.1%), and Hispanic (17.9% cesarean delivery prevalence was greater than that among White women (17.2%) (P < .001). The same was true among those with a high school education (with or without some college): 22% of White women in this group had cesarean deliveries compared with 26.3% of Black women, 26.3% of Asian women, and 22.5% of Hispanic women (P < .001).
At higher levels of education, the disparities not only persisted but actually increased.
The prevalence of cesarean deliveries was 23% in White college graduates, compared with 32.5% of Black college graduates, 26.3% of Asian college graduates, and 27.7% of Hispanic college graduates (P < .001). Similarly, in those with an advanced degree, the prevalence of cesarean deliveries in their population set was 23.6% of Whites, 36.3% of Blacks, 26.1% of Asians, and 30.1% of Hispanics (P < .001).
After adjusting for maternal education as well as age, prepregnancy body mass index, weight gain during pregnancy, insurance type, and neonatal birth weight, the researchers still found substantial disparities in cesarean delivery rates. Black women had 1.54 times greater odds of cesarean delivery than White women (P < .001). Similarly, the odds were 1.45 times greater for Asian women and 1.24 times greater for Hispanic women (P < .001).
Controlling for race, ethnicity, and the other confounders, women with less than a high school education or a high school diploma had similar likelihoods of cesarean delivery. The likelihood of a cesarean delivery was slightly reduced for women with a college degree (odds ratio, 0.93) or advanced degree (OR, 0.88). But this protective effect did not dampen racial/ethnic disparities. In fact, even greater disparities were seen at higher levels of education.
“At each level of education, all the racial/ethnic groups had significantly higher odds of a cesarean delivery than White women,” Dr. Eliner said. “Additionally, the racial/ethnic disparity in cesarean delivery rates increased with increasing level of education, and we specifically see a meaningful jump in the odds ratio at the college graduate level.”
She pointed out that the OR for cesarean delivery in Black women was 1.4 times greater than White women in the group with less than a high school education and 1.44 times greater in those with high school diplomas. Then it jumped to 1.69 in the college graduates group and 1.7 in the advanced degree group.
Higher maternal education was associated with a lower likelihood of cesarean delivery in White women and Asian women. White women with advanced degrees were 17% less likely to have a cesarean than White women with less than a high school education, and the respective reduction in risk was 19% for Asian women.
In Black women, however, education has a much smaller protective effect: An advanced degree reduced the odds of a cesarean delivery by only 7% and no significant difference showed up between high school graduates and college graduates, Dr. Eliner reported.
In Hispanic women, no protective effect showed up, and the odds of a cesarean delivery actually increased slightly in high school and college graduates above those with less than a high school education.
Dr. Eliner discussed a couple possible reasons for a less protective effect from maternal education in Black and Hispanic groups, including higher levels of chronic stress found in past research among racial/ethnic minorities with higher levels of education.
“The impact of racism as a chronic stressor and its association with adverse obstetric and prenatal outcomes is an emerging theme in health disparity research and is yet to be fully understood,” Dr. Eliner said in an interview. “Nonetheless, there is some evidence suggesting that racial/ethnic minorities with higher levels of education suffer from higher levels of stress.”
Implicit and explicit interpersonal bias and institutional racism may also play a role in the disparities, she said, and these factors may disproportionately affect the quality of care for more educated women. She also suggested that White women may be more comfortable advocating for their care.
“While less educated women from all racial/ethnic groups may lack the self-advocacy skills to discuss their labor course, educated White women may be more confident than women from educated minority groups,” Dr. Eliner told attendees. “They may therefore be better equipped to discuss the need for a cesarean delivery with their provider.”
Dr. Eliner elaborated on this: “Given the historical and current disparities of the health care system, women in racial/ethnic minorities may potentially be guarded in their interaction with medical professionals, with a reduced trust in the health care system, and may thus not feel empowered to advocate for themselves in this setting,” she said.

Allison Bryant Mantha, MD, MPH, vice chair for quality, equity, and safety in the ob.gyn. department at Massachusetts General Hospital, Boston, suggested that bias and racism may play a role in this self-advocacy as well.
“I’m wondering if it might not be equally plausible that the advocacy might be met differently by who’s delivering the message,” Dr. Bryant Mantha said. “I think from the story of Dr. Susan Moore and patients who advocate for themselves, I think that we know there is probably some differential by who’s delivering the message.”
Finally, even though education is usually highly correlated with income and frequently used as a proxy for it, but the effect of education on income varies by race/ethnicity.
Since education alone is not sufficient to reduce these disparities, potential interventions should focus on increasing awareness of the disparities and the role of implicit bias, improving patients’ trust in the medical system, and training more doctors from underrepresented groups, Dr. Eliner said.
“I was also wondering about the overall patient choice,” said Sarahn M. Wheeler, MD, an assistant professor of ob.gyn. at Duke University Medical Center in Durham, N.C., who comoderated the session with Dr. Bryant Mantha. “Did we have any understanding of differences in patient values systems that might go into some of these differences in findings as well? There are lots of interesting concepts to explore and that this abstract brings up.”
Dr. Eliner, Dr. Wheeler, and Dr. Bryant Mantha had no disclosures.
While the likelihood of a cesarean delivery usually drops as maternal education level increases, the disparities seen in cesarean rates between White and Black or Hispanic women actually increase with more maternal education, according to findings from a new study presented at the Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Typically, higher maternal education is associated with a lower likelihood of cesarean delivery, but this protective effect is much smaller for Black women and nonexistent for Hispanic women, leading to bigger gaps between these groups and White women, found Yael Eliner, MD, an ob.gyn. residency applicant at Boston University who conducted this research with her colleagues in the ob.gyn. department at Lenox Hill Hospital, New York, and Hofstra University, Hempstead, N.Y..
Researchers have previously identified racial and ethnic disparities in a wide range of maternal outcomes, including mortality, overall morbidity, preterm birth, low birth weight, fetal growth restriction, hypertensive disorders of pregnancy, diabetes, and cesarean deliveries. But the researchers wanted to know if the usual protective effects seen for cesarean deliveries existed in the racial and ethnic groups with these disparities. Past studies have already found that the protective effect of maternal education is greater for White women than Black women with infant mortality and overall self-rated health.
The researchers conducted a retrospective analysis of all low-risk nulliparous, term, singleton, vertex live births to U.S. residents from 2016 to 2019 by using the natality database of the Centers for Disease Control and Prevention. They looked only at women who were non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, and Hispanic women. They excluded women with pregestational and gestational diabetes, chronic hypertension, and hypertensive disorders of pregnancy.
Maternal education levels were stratified into those without a high school diploma, high school graduates (including those with some college credit), college graduates, and those with advanced degrees. The total population included 2,969,207 mothers with a 23.4% cesarean delivery rate.
Before considering education or other potential confounders, the cesarean delivery rate was 27.4% in Black women and 25.6% in Asian women, compared with 22.4% in White women and 23% in Hispanic women (P < .001).
Among those with less than a high school education, Black (20.9%), Asian (23.1%), and Hispanic (17.9% cesarean delivery prevalence was greater than that among White women (17.2%) (P < .001). The same was true among those with a high school education (with or without some college): 22% of White women in this group had cesarean deliveries compared with 26.3% of Black women, 26.3% of Asian women, and 22.5% of Hispanic women (P < .001).
At higher levels of education, the disparities not only persisted but actually increased.
The prevalence of cesarean deliveries was 23% in White college graduates, compared with 32.5% of Black college graduates, 26.3% of Asian college graduates, and 27.7% of Hispanic college graduates (P < .001). Similarly, in those with an advanced degree, the prevalence of cesarean deliveries in their population set was 23.6% of Whites, 36.3% of Blacks, 26.1% of Asians, and 30.1% of Hispanics (P < .001).
After adjusting for maternal education as well as age, prepregnancy body mass index, weight gain during pregnancy, insurance type, and neonatal birth weight, the researchers still found substantial disparities in cesarean delivery rates. Black women had 1.54 times greater odds of cesarean delivery than White women (P < .001). Similarly, the odds were 1.45 times greater for Asian women and 1.24 times greater for Hispanic women (P < .001).
Controlling for race, ethnicity, and the other confounders, women with less than a high school education or a high school diploma had similar likelihoods of cesarean delivery. The likelihood of a cesarean delivery was slightly reduced for women with a college degree (odds ratio, 0.93) or advanced degree (OR, 0.88). But this protective effect did not dampen racial/ethnic disparities. In fact, even greater disparities were seen at higher levels of education.
“At each level of education, all the racial/ethnic groups had significantly higher odds of a cesarean delivery than White women,” Dr. Eliner said. “Additionally, the racial/ethnic disparity in cesarean delivery rates increased with increasing level of education, and we specifically see a meaningful jump in the odds ratio at the college graduate level.”
She pointed out that the OR for cesarean delivery in Black women was 1.4 times greater than White women in the group with less than a high school education and 1.44 times greater in those with high school diplomas. Then it jumped to 1.69 in the college graduates group and 1.7 in the advanced degree group.
Higher maternal education was associated with a lower likelihood of cesarean delivery in White women and Asian women. White women with advanced degrees were 17% less likely to have a cesarean than White women with less than a high school education, and the respective reduction in risk was 19% for Asian women.
In Black women, however, education has a much smaller protective effect: An advanced degree reduced the odds of a cesarean delivery by only 7% and no significant difference showed up between high school graduates and college graduates, Dr. Eliner reported.
In Hispanic women, no protective effect showed up, and the odds of a cesarean delivery actually increased slightly in high school and college graduates above those with less than a high school education.
Dr. Eliner discussed a couple possible reasons for a less protective effect from maternal education in Black and Hispanic groups, including higher levels of chronic stress found in past research among racial/ethnic minorities with higher levels of education.
“The impact of racism as a chronic stressor and its association with adverse obstetric and prenatal outcomes is an emerging theme in health disparity research and is yet to be fully understood,” Dr. Eliner said in an interview. “Nonetheless, there is some evidence suggesting that racial/ethnic minorities with higher levels of education suffer from higher levels of stress.”
Implicit and explicit interpersonal bias and institutional racism may also play a role in the disparities, she said, and these factors may disproportionately affect the quality of care for more educated women. She also suggested that White women may be more comfortable advocating for their care.
“While less educated women from all racial/ethnic groups may lack the self-advocacy skills to discuss their labor course, educated White women may be more confident than women from educated minority groups,” Dr. Eliner told attendees. “They may therefore be better equipped to discuss the need for a cesarean delivery with their provider.”
Dr. Eliner elaborated on this: “Given the historical and current disparities of the health care system, women in racial/ethnic minorities may potentially be guarded in their interaction with medical professionals, with a reduced trust in the health care system, and may thus not feel empowered to advocate for themselves in this setting,” she said.
Allison Bryant Mantha, MD, MPH, vice chair for quality, equity, and safety in the ob.gyn. department at Massachusetts General Hospital, Boston, suggested that bias and racism may play a role in this self-advocacy as well.
“I’m wondering if it might not be equally plausible that the advocacy might be met differently by who’s delivering the message,” Dr. Bryant Mantha said. “I think from the story of Dr. Susan Moore and patients who advocate for themselves, I think that we know there is probably some differential by who’s delivering the message.”
Finally, even though education is usually highly correlated with income and frequently used as a proxy for it, but the effect of education on income varies by race/ethnicity.
Since education alone is not sufficient to reduce these disparities, potential interventions should focus on increasing awareness of the disparities and the role of implicit bias, improving patients’ trust in the medical system, and training more doctors from underrepresented groups, Dr. Eliner said.
“I was also wondering about the overall patient choice,” said Sarahn M. Wheeler, MD, an assistant professor of ob.gyn. at Duke University Medical Center in Durham, N.C., who comoderated the session with Dr. Bryant Mantha. “Did we have any understanding of differences in patient values systems that might go into some of these differences in findings as well? There are lots of interesting concepts to explore and that this abstract brings up.”
Dr. Eliner, Dr. Wheeler, and Dr. Bryant Mantha had no disclosures.
While the likelihood of a cesarean delivery usually drops as maternal education level increases, the disparities seen in cesarean rates between White and Black or Hispanic women actually increase with more maternal education, according to findings from a new study presented at the Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Typically, higher maternal education is associated with a lower likelihood of cesarean delivery, but this protective effect is much smaller for Black women and nonexistent for Hispanic women, leading to bigger gaps between these groups and White women, found Yael Eliner, MD, an ob.gyn. residency applicant at Boston University who conducted this research with her colleagues in the ob.gyn. department at Lenox Hill Hospital, New York, and Hofstra University, Hempstead, N.Y..
Researchers have previously identified racial and ethnic disparities in a wide range of maternal outcomes, including mortality, overall morbidity, preterm birth, low birth weight, fetal growth restriction, hypertensive disorders of pregnancy, diabetes, and cesarean deliveries. But the researchers wanted to know if the usual protective effects seen for cesarean deliveries existed in the racial and ethnic groups with these disparities. Past studies have already found that the protective effect of maternal education is greater for White women than Black women with infant mortality and overall self-rated health.
The researchers conducted a retrospective analysis of all low-risk nulliparous, term, singleton, vertex live births to U.S. residents from 2016 to 2019 by using the natality database of the Centers for Disease Control and Prevention. They looked only at women who were non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, and Hispanic women. They excluded women with pregestational and gestational diabetes, chronic hypertension, and hypertensive disorders of pregnancy.
Maternal education levels were stratified into those without a high school diploma, high school graduates (including those with some college credit), college graduates, and those with advanced degrees. The total population included 2,969,207 mothers with a 23.4% cesarean delivery rate.
Before considering education or other potential confounders, the cesarean delivery rate was 27.4% in Black women and 25.6% in Asian women, compared with 22.4% in White women and 23% in Hispanic women (P < .001).
Among those with less than a high school education, Black (20.9%), Asian (23.1%), and Hispanic (17.9% cesarean delivery prevalence was greater than that among White women (17.2%) (P < .001). The same was true among those with a high school education (with or without some college): 22% of White women in this group had cesarean deliveries compared with 26.3% of Black women, 26.3% of Asian women, and 22.5% of Hispanic women (P < .001).
At higher levels of education, the disparities not only persisted but actually increased.
The prevalence of cesarean deliveries was 23% in White college graduates, compared with 32.5% of Black college graduates, 26.3% of Asian college graduates, and 27.7% of Hispanic college graduates (P < .001). Similarly, in those with an advanced degree, the prevalence of cesarean deliveries in their population set was 23.6% of Whites, 36.3% of Blacks, 26.1% of Asians, and 30.1% of Hispanics (P < .001).
After adjusting for maternal education as well as age, prepregnancy body mass index, weight gain during pregnancy, insurance type, and neonatal birth weight, the researchers still found substantial disparities in cesarean delivery rates. Black women had 1.54 times greater odds of cesarean delivery than White women (P < .001). Similarly, the odds were 1.45 times greater for Asian women and 1.24 times greater for Hispanic women (P < .001).
Controlling for race, ethnicity, and the other confounders, women with less than a high school education or a high school diploma had similar likelihoods of cesarean delivery. The likelihood of a cesarean delivery was slightly reduced for women with a college degree (odds ratio, 0.93) or advanced degree (OR, 0.88). But this protective effect did not dampen racial/ethnic disparities. In fact, even greater disparities were seen at higher levels of education.
“At each level of education, all the racial/ethnic groups had significantly higher odds of a cesarean delivery than White women,” Dr. Eliner said. “Additionally, the racial/ethnic disparity in cesarean delivery rates increased with increasing level of education, and we specifically see a meaningful jump in the odds ratio at the college graduate level.”
She pointed out that the OR for cesarean delivery in Black women was 1.4 times greater than White women in the group with less than a high school education and 1.44 times greater in those with high school diplomas. Then it jumped to 1.69 in the college graduates group and 1.7 in the advanced degree group.
Higher maternal education was associated with a lower likelihood of cesarean delivery in White women and Asian women. White women with advanced degrees were 17% less likely to have a cesarean than White women with less than a high school education, and the respective reduction in risk was 19% for Asian women.
In Black women, however, education has a much smaller protective effect: An advanced degree reduced the odds of a cesarean delivery by only 7% and no significant difference showed up between high school graduates and college graduates, Dr. Eliner reported.
In Hispanic women, no protective effect showed up, and the odds of a cesarean delivery actually increased slightly in high school and college graduates above those with less than a high school education.
Dr. Eliner discussed a couple possible reasons for a less protective effect from maternal education in Black and Hispanic groups, including higher levels of chronic stress found in past research among racial/ethnic minorities with higher levels of education.
“The impact of racism as a chronic stressor and its association with adverse obstetric and prenatal outcomes is an emerging theme in health disparity research and is yet to be fully understood,” Dr. Eliner said in an interview. “Nonetheless, there is some evidence suggesting that racial/ethnic minorities with higher levels of education suffer from higher levels of stress.”
Implicit and explicit interpersonal bias and institutional racism may also play a role in the disparities, she said, and these factors may disproportionately affect the quality of care for more educated women. She also suggested that White women may be more comfortable advocating for their care.
“While less educated women from all racial/ethnic groups may lack the self-advocacy skills to discuss their labor course, educated White women may be more confident than women from educated minority groups,” Dr. Eliner told attendees. “They may therefore be better equipped to discuss the need for a cesarean delivery with their provider.”
Dr. Eliner elaborated on this: “Given the historical and current disparities of the health care system, women in racial/ethnic minorities may potentially be guarded in their interaction with medical professionals, with a reduced trust in the health care system, and may thus not feel empowered to advocate for themselves in this setting,” she said.
Allison Bryant Mantha, MD, MPH, vice chair for quality, equity, and safety in the ob.gyn. department at Massachusetts General Hospital, Boston, suggested that bias and racism may play a role in this self-advocacy as well.
“I’m wondering if it might not be equally plausible that the advocacy might be met differently by who’s delivering the message,” Dr. Bryant Mantha said. “I think from the story of Dr. Susan Moore and patients who advocate for themselves, I think that we know there is probably some differential by who’s delivering the message.”
Finally, even though education is usually highly correlated with income and frequently used as a proxy for it, but the effect of education on income varies by race/ethnicity.
Since education alone is not sufficient to reduce these disparities, potential interventions should focus on increasing awareness of the disparities and the role of implicit bias, improving patients’ trust in the medical system, and training more doctors from underrepresented groups, Dr. Eliner said.
“I was also wondering about the overall patient choice,” said Sarahn M. Wheeler, MD, an assistant professor of ob.gyn. at Duke University Medical Center in Durham, N.C., who comoderated the session with Dr. Bryant Mantha. “Did we have any understanding of differences in patient values systems that might go into some of these differences in findings as well? There are lots of interesting concepts to explore and that this abstract brings up.”
Dr. Eliner, Dr. Wheeler, and Dr. Bryant Mantha had no disclosures.
FROM THE PREGNANCY MEETING
Family medicine has grown; its composition has evolved
and the men and women who practice it are no exception.
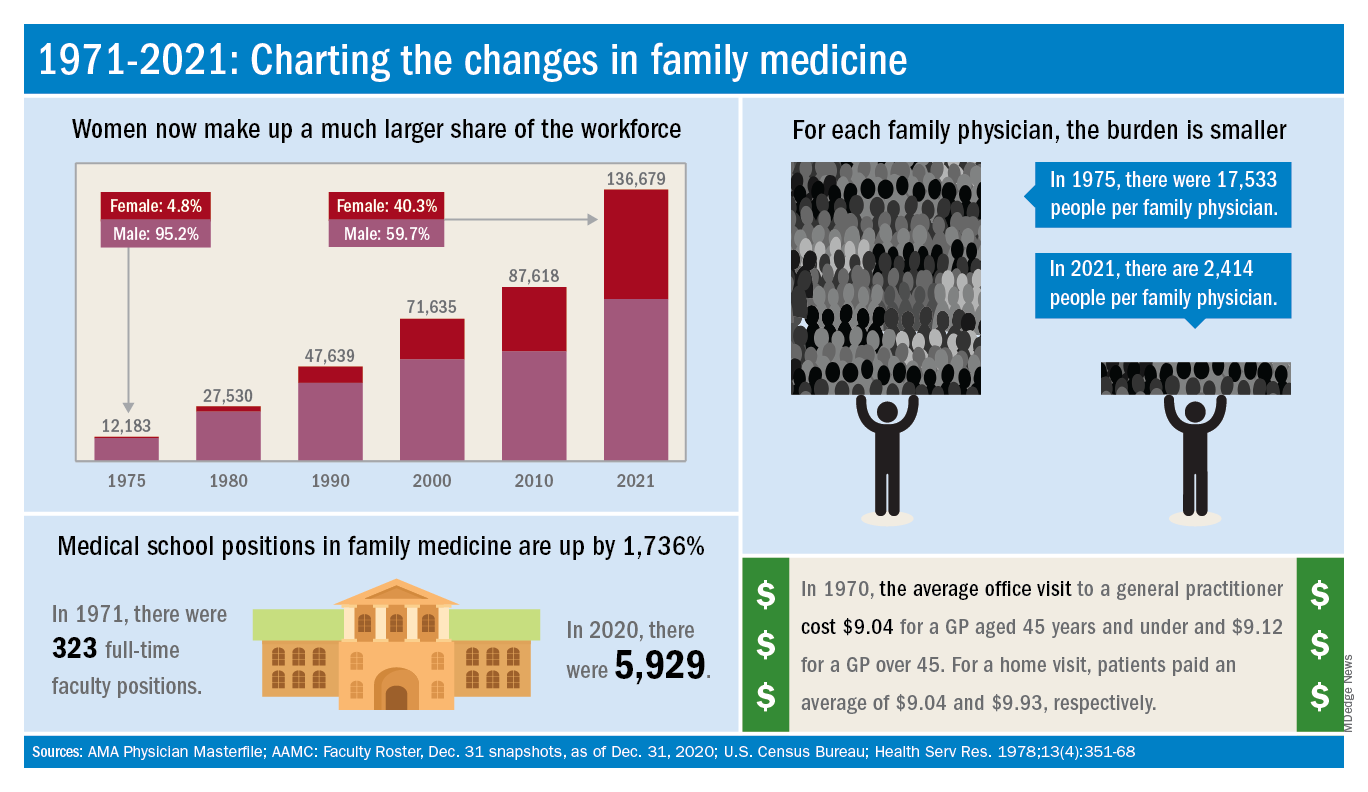
The family medicine workforce of 2021 is not the workforce of 1971. Not even close. Although we would like to give a huge shout-out to anyone who can claim to be a member of both.
Today’s FP workforce is, first of all, much larger than it was in 1971, although we can’t actually prove it because the American Medical Association’s data for that year are “only available in books that are locked away at the empty AMA headquarters,” according to a member of the AMA media relations staff who is, like so many people these days, working at home because of the pandemic.
The face of family medicine in 1975 vs. today
Today’s workforce is much larger than it was in 1975, when there were just over 12,000 family physicians in the United States. As of January 2021, the total was approaching 137,000, including all “physicians and residents in patient care, research, administration, teaching, retired, inactive, etc.,” the AMA explained.
Family physicians as a group are much more diverse than they were in 1975. That year, 8.3% of FPs were international medical graduates (IMGs). By 2010, IMGs made up almost 23% of the workforce, and in the 2020 resident match, 37% of the 4,662 available family medicine slots were filled by IMGs.
Women have made even greater inroads into the family physician ranks over the last 5 decades. In 1975, less than 5% of all FPs were females, but by 2021 the proportion of females in the specialty was just over 40%.
In the first 5 years of the family practice era, 1969-1973, only 12 women and 31 IMGs graduated from FP residency programs, those numbers representing 3.2% and 8.3%, respectively, of the total of 372, according to a 1996 study in JAMA. By 1990-1993, women made up 33% and IMGs 14% of the 9,400 graduates.
Another group that increased its presence in family medicine is doctors of osteopathy, who went from zero residency graduates in 1969-1973 to over 1,100 (11.8%) in 1990-1993, the JAMA report noted. By 2020, almost 1,400 osteopathic physicians entered family medicine residencies, filling 30% of all slots available, according to the National Resident Matching Program.
The medical schools producing all these new residents have raised their games since 1971: the number of full-time faculty in family medicine departments rose from 323 to 5,929 in 2020, based on data from the Association of American Medical Colleges (Faculty Roster, Dec. 31 snapshots, as of Dec. 31, 2020).
A shortage or a surplus of FPs?
It has been suggested, however, that all is not well in primary care land. A study conducted by the American Academy of Family Physicians in 2016 – a year after 2,463 graduates of MD- and DO-granting medical schools entered family medicine residencies – concluded “that the current medical school system is failing, collectively, to produce the primary care workforce that is needed to achieve optimal health.”
Warnings about physician shortages are nothing new, but how about the other side of the coin? The Jan. 15, 1981, issue of Family Practice News covered a somewhat controversial report from the Graduate Medical Education National Advisory Committee, which projected a surplus of 3,000 FPs, and as many as 70,000 physicians overall, by the year 1990.
Just a few months later, in the June 15, 1981, issue of FPN, an AAFP officer predicted that “the flood of new physicians in the next decade may affect family practice more than any other specialty.”
Mostly, though, the issue is shortages. In 2002, a status report on family practice from the Robert Graham Center acknowledged that “many centers of academic medicine continue to resist the development of family practice and primary care. ... Family medicine remains a true counterculture in these environments, and students may continue to face significant discouragement in response to interest they may express in becoming a family physician.”
and the men and women who practice it are no exception.
The family medicine workforce of 2021 is not the workforce of 1971. Not even close. Although we would like to give a huge shout-out to anyone who can claim to be a member of both.
Today’s FP workforce is, first of all, much larger than it was in 1971, although we can’t actually prove it because the American Medical Association’s data for that year are “only available in books that are locked away at the empty AMA headquarters,” according to a member of the AMA media relations staff who is, like so many people these days, working at home because of the pandemic.
The face of family medicine in 1975 vs. today
Today’s workforce is much larger than it was in 1975, when there were just over 12,000 family physicians in the United States. As of January 2021, the total was approaching 137,000, including all “physicians and residents in patient care, research, administration, teaching, retired, inactive, etc.,” the AMA explained.
Family physicians as a group are much more diverse than they were in 1975. That year, 8.3% of FPs were international medical graduates (IMGs). By 2010, IMGs made up almost 23% of the workforce, and in the 2020 resident match, 37% of the 4,662 available family medicine slots were filled by IMGs.
Women have made even greater inroads into the family physician ranks over the last 5 decades. In 1975, less than 5% of all FPs were females, but by 2021 the proportion of females in the specialty was just over 40%.
In the first 5 years of the family practice era, 1969-1973, only 12 women and 31 IMGs graduated from FP residency programs, those numbers representing 3.2% and 8.3%, respectively, of the total of 372, according to a 1996 study in JAMA. By 1990-1993, women made up 33% and IMGs 14% of the 9,400 graduates.
Another group that increased its presence in family medicine is doctors of osteopathy, who went from zero residency graduates in 1969-1973 to over 1,100 (11.8%) in 1990-1993, the JAMA report noted. By 2020, almost 1,400 osteopathic physicians entered family medicine residencies, filling 30% of all slots available, according to the National Resident Matching Program.
The medical schools producing all these new residents have raised their games since 1971: the number of full-time faculty in family medicine departments rose from 323 to 5,929 in 2020, based on data from the Association of American Medical Colleges (Faculty Roster, Dec. 31 snapshots, as of Dec. 31, 2020).
A shortage or a surplus of FPs?
It has been suggested, however, that all is not well in primary care land. A study conducted by the American Academy of Family Physicians in 2016 – a year after 2,463 graduates of MD- and DO-granting medical schools entered family medicine residencies – concluded “that the current medical school system is failing, collectively, to produce the primary care workforce that is needed to achieve optimal health.”
Warnings about physician shortages are nothing new, but how about the other side of the coin? The Jan. 15, 1981, issue of Family Practice News covered a somewhat controversial report from the Graduate Medical Education National Advisory Committee, which projected a surplus of 3,000 FPs, and as many as 70,000 physicians overall, by the year 1990.
Just a few months later, in the June 15, 1981, issue of FPN, an AAFP officer predicted that “the flood of new physicians in the next decade may affect family practice more than any other specialty.”
Mostly, though, the issue is shortages. In 2002, a status report on family practice from the Robert Graham Center acknowledged that “many centers of academic medicine continue to resist the development of family practice and primary care. ... Family medicine remains a true counterculture in these environments, and students may continue to face significant discouragement in response to interest they may express in becoming a family physician.”
and the men and women who practice it are no exception.
The family medicine workforce of 2021 is not the workforce of 1971. Not even close. Although we would like to give a huge shout-out to anyone who can claim to be a member of both.
Today’s FP workforce is, first of all, much larger than it was in 1971, although we can’t actually prove it because the American Medical Association’s data for that year are “only available in books that are locked away at the empty AMA headquarters,” according to a member of the AMA media relations staff who is, like so many people these days, working at home because of the pandemic.
The face of family medicine in 1975 vs. today
Today’s workforce is much larger than it was in 1975, when there were just over 12,000 family physicians in the United States. As of January 2021, the total was approaching 137,000, including all “physicians and residents in patient care, research, administration, teaching, retired, inactive, etc.,” the AMA explained.
Family physicians as a group are much more diverse than they were in 1975. That year, 8.3% of FPs were international medical graduates (IMGs). By 2010, IMGs made up almost 23% of the workforce, and in the 2020 resident match, 37% of the 4,662 available family medicine slots were filled by IMGs.
Women have made even greater inroads into the family physician ranks over the last 5 decades. In 1975, less than 5% of all FPs were females, but by 2021 the proportion of females in the specialty was just over 40%.
In the first 5 years of the family practice era, 1969-1973, only 12 women and 31 IMGs graduated from FP residency programs, those numbers representing 3.2% and 8.3%, respectively, of the total of 372, according to a 1996 study in JAMA. By 1990-1993, women made up 33% and IMGs 14% of the 9,400 graduates.
Another group that increased its presence in family medicine is doctors of osteopathy, who went from zero residency graduates in 1969-1973 to over 1,100 (11.8%) in 1990-1993, the JAMA report noted. By 2020, almost 1,400 osteopathic physicians entered family medicine residencies, filling 30% of all slots available, according to the National Resident Matching Program.
The medical schools producing all these new residents have raised their games since 1971: the number of full-time faculty in family medicine departments rose from 323 to 5,929 in 2020, based on data from the Association of American Medical Colleges (Faculty Roster, Dec. 31 snapshots, as of Dec. 31, 2020).
A shortage or a surplus of FPs?
It has been suggested, however, that all is not well in primary care land. A study conducted by the American Academy of Family Physicians in 2016 – a year after 2,463 graduates of MD- and DO-granting medical schools entered family medicine residencies – concluded “that the current medical school system is failing, collectively, to produce the primary care workforce that is needed to achieve optimal health.”
Warnings about physician shortages are nothing new, but how about the other side of the coin? The Jan. 15, 1981, issue of Family Practice News covered a somewhat controversial report from the Graduate Medical Education National Advisory Committee, which projected a surplus of 3,000 FPs, and as many as 70,000 physicians overall, by the year 1990.
Just a few months later, in the June 15, 1981, issue of FPN, an AAFP officer predicted that “the flood of new physicians in the next decade may affect family practice more than any other specialty.”
Mostly, though, the issue is shortages. In 2002, a status report on family practice from the Robert Graham Center acknowledged that “many centers of academic medicine continue to resist the development of family practice and primary care. ... Family medicine remains a true counterculture in these environments, and students may continue to face significant discouragement in response to interest they may express in becoming a family physician.”
Cardiovascular trials lose more women than men
A new analysis of 11 phase 3/4 cardiovascular clinical trials conducted by the Thrombolysis in Myocardial Infarction (TIMI) group shows that women are more likely than men to discontinue study medications, and to withdraw from trials. The differences could not be explained by different frequencies of reporting adverse events, or by baseline differences.

The findings are significant, since cardiovascular drugs are routinely prescribed to women based on clinical trials that are populated largely by men, according to lead study author Emily Lau, MD, who is an advanced cardiology fellow at Massachusetts General Hospital, Boston. “It highlights an important disparity in clinical research in cardiology, because if women are already not represented well in clinical trials, and if once in clinical trials they don’t complete the study, it’s very hard to extrapolate the clinical trial findings to our female population in an accurate way,” Dr. Lau said in an interview. She also noted that sex-specific and reproductive factors are increasingly recognized as being important in the development and progression of cardiovascular disease.
The study was published in the journal Circulation.
The study refutes previously advanced explanations for higher withdrawal among women, including sex difference and comorbidities, according to an accompanying editorial by Sofia Sederholm Lawesson, MD, PhD, Eva Swahn, MD, PhD, and Joakim Alfredsson, MD, PhD, of Linköping University, Sweden. They also pointed out that the study found a larger between-sex difference in failure to adhere to study drug in North America (odds ratio, 1.35; 95% confidence interval, 1.30-1.41), but a more moderate difference among participants in Europe/Middle East/Africa (OR, 1.13; 95% CI, 1.09-1.17) and Asia/Pacific (OR, 1.13; 95% CI, 1.03-1.23) regions. And there were no sex differences at all among South/Central American populations.
They noted that high rates of nonadherence increase the chances of a false negative finding and overestimation of drug safety. “We know the associations between nonadherence and clinical outcomes. The next step should be to better understand the underlying reasons for, as well as consistent reporting of, nonadherence, and discontinuation in RCTs,” the editorial authors wrote.
Dr. Lau suggested a simple method to better understand reasons for withdrawal: Addition of questions to the case report form that asks about reasons for drug discontinuation or study withdrawal. “Was it an adverse event? Was it because I’m a mother of three and I can’t get to the clinical trial site after work and also pick up my kids? Are there societal barriers for women, or was it the experience of the clinical trial that was maybe less favorable for women compared to men? Or maybe there are medical reasons we simply don’t know. Something as simple as asking those questions can help us better understand the barriers to female retention,” said Dr. Lau.
The analysis included data from 135,879 men (72%) and 51,812 women (28%) enrolled in the trials. After adjustment for baseline differences, women were more likely than were men to permanently discontinue study drug (adjusted odds ratio [aOR], 1.22: P < .001), which did not vary by study duration. The finding was consistent regardless of the type of drug studied, as well as across placebo and active study arms.
Women also were more likely to prematurely discontinue study drug (trial-adjusted OR, 1.18; P < .001). The rate of drug discontinuation due to adverse event was identical in both men and women, at 36%.
Women were more likely to withdraw consent than were men in a meta-analysis and when individual patient-level results were pooled (aOR, 1.26; P < .001 for both).
Dr. Lau received funding from the National Institutes of Health and has no relevant financial disclosures. The editorial authors had various disclosures, including lecture fees from Bayer, Pfizer, and Boehringer Ingelheim, and they served on advisory boards for AstraZeneca and MSD.
A new analysis of 11 phase 3/4 cardiovascular clinical trials conducted by the Thrombolysis in Myocardial Infarction (TIMI) group shows that women are more likely than men to discontinue study medications, and to withdraw from trials. The differences could not be explained by different frequencies of reporting adverse events, or by baseline differences.
The findings are significant, since cardiovascular drugs are routinely prescribed to women based on clinical trials that are populated largely by men, according to lead study author Emily Lau, MD, who is an advanced cardiology fellow at Massachusetts General Hospital, Boston. “It highlights an important disparity in clinical research in cardiology, because if women are already not represented well in clinical trials, and if once in clinical trials they don’t complete the study, it’s very hard to extrapolate the clinical trial findings to our female population in an accurate way,” Dr. Lau said in an interview. She also noted that sex-specific and reproductive factors are increasingly recognized as being important in the development and progression of cardiovascular disease.
The study was published in the journal Circulation.
The study refutes previously advanced explanations for higher withdrawal among women, including sex difference and comorbidities, according to an accompanying editorial by Sofia Sederholm Lawesson, MD, PhD, Eva Swahn, MD, PhD, and Joakim Alfredsson, MD, PhD, of Linköping University, Sweden. They also pointed out that the study found a larger between-sex difference in failure to adhere to study drug in North America (odds ratio, 1.35; 95% confidence interval, 1.30-1.41), but a more moderate difference among participants in Europe/Middle East/Africa (OR, 1.13; 95% CI, 1.09-1.17) and Asia/Pacific (OR, 1.13; 95% CI, 1.03-1.23) regions. And there were no sex differences at all among South/Central American populations.
They noted that high rates of nonadherence increase the chances of a false negative finding and overestimation of drug safety. “We know the associations between nonadherence and clinical outcomes. The next step should be to better understand the underlying reasons for, as well as consistent reporting of, nonadherence, and discontinuation in RCTs,” the editorial authors wrote.
Dr. Lau suggested a simple method to better understand reasons for withdrawal: Addition of questions to the case report form that asks about reasons for drug discontinuation or study withdrawal. “Was it an adverse event? Was it because I’m a mother of three and I can’t get to the clinical trial site after work and also pick up my kids? Are there societal barriers for women, or was it the experience of the clinical trial that was maybe less favorable for women compared to men? Or maybe there are medical reasons we simply don’t know. Something as simple as asking those questions can help us better understand the barriers to female retention,” said Dr. Lau.
The analysis included data from 135,879 men (72%) and 51,812 women (28%) enrolled in the trials. After adjustment for baseline differences, women were more likely than were men to permanently discontinue study drug (adjusted odds ratio [aOR], 1.22: P < .001), which did not vary by study duration. The finding was consistent regardless of the type of drug studied, as well as across placebo and active study arms.
Women also were more likely to prematurely discontinue study drug (trial-adjusted OR, 1.18; P < .001). The rate of drug discontinuation due to adverse event was identical in both men and women, at 36%.
Women were more likely to withdraw consent than were men in a meta-analysis and when individual patient-level results were pooled (aOR, 1.26; P < .001 for both).
Dr. Lau received funding from the National Institutes of Health and has no relevant financial disclosures. The editorial authors had various disclosures, including lecture fees from Bayer, Pfizer, and Boehringer Ingelheim, and they served on advisory boards for AstraZeneca and MSD.
A new analysis of 11 phase 3/4 cardiovascular clinical trials conducted by the Thrombolysis in Myocardial Infarction (TIMI) group shows that women are more likely than men to discontinue study medications, and to withdraw from trials. The differences could not be explained by different frequencies of reporting adverse events, or by baseline differences.
The findings are significant, since cardiovascular drugs are routinely prescribed to women based on clinical trials that are populated largely by men, according to lead study author Emily Lau, MD, who is an advanced cardiology fellow at Massachusetts General Hospital, Boston. “It highlights an important disparity in clinical research in cardiology, because if women are already not represented well in clinical trials, and if once in clinical trials they don’t complete the study, it’s very hard to extrapolate the clinical trial findings to our female population in an accurate way,” Dr. Lau said in an interview. She also noted that sex-specific and reproductive factors are increasingly recognized as being important in the development and progression of cardiovascular disease.
The study was published in the journal Circulation.
The study refutes previously advanced explanations for higher withdrawal among women, including sex difference and comorbidities, according to an accompanying editorial by Sofia Sederholm Lawesson, MD, PhD, Eva Swahn, MD, PhD, and Joakim Alfredsson, MD, PhD, of Linköping University, Sweden. They also pointed out that the study found a larger between-sex difference in failure to adhere to study drug in North America (odds ratio, 1.35; 95% confidence interval, 1.30-1.41), but a more moderate difference among participants in Europe/Middle East/Africa (OR, 1.13; 95% CI, 1.09-1.17) and Asia/Pacific (OR, 1.13; 95% CI, 1.03-1.23) regions. And there were no sex differences at all among South/Central American populations.
They noted that high rates of nonadherence increase the chances of a false negative finding and overestimation of drug safety. “We know the associations between nonadherence and clinical outcomes. The next step should be to better understand the underlying reasons for, as well as consistent reporting of, nonadherence, and discontinuation in RCTs,” the editorial authors wrote.
Dr. Lau suggested a simple method to better understand reasons for withdrawal: Addition of questions to the case report form that asks about reasons for drug discontinuation or study withdrawal. “Was it an adverse event? Was it because I’m a mother of three and I can’t get to the clinical trial site after work and also pick up my kids? Are there societal barriers for women, or was it the experience of the clinical trial that was maybe less favorable for women compared to men? Or maybe there are medical reasons we simply don’t know. Something as simple as asking those questions can help us better understand the barriers to female retention,” said Dr. Lau.
The analysis included data from 135,879 men (72%) and 51,812 women (28%) enrolled in the trials. After adjustment for baseline differences, women were more likely than were men to permanently discontinue study drug (adjusted odds ratio [aOR], 1.22: P < .001), which did not vary by study duration. The finding was consistent regardless of the type of drug studied, as well as across placebo and active study arms.
Women also were more likely to prematurely discontinue study drug (trial-adjusted OR, 1.18; P < .001). The rate of drug discontinuation due to adverse event was identical in both men and women, at 36%.
Women were more likely to withdraw consent than were men in a meta-analysis and when individual patient-level results were pooled (aOR, 1.26; P < .001 for both).
Dr. Lau received funding from the National Institutes of Health and has no relevant financial disclosures. The editorial authors had various disclosures, including lecture fees from Bayer, Pfizer, and Boehringer Ingelheim, and they served on advisory boards for AstraZeneca and MSD.
FROM CIRCULATION
Seen or viewed: A black hematologist’s perspective
After a long day in hematology clinic, I skimmed the inpatient list to see if any of my patients had been admitted. Seeing Ms. Short’s name (changed for privacy), a delightful African American woman I met during my early days of fellowship, had me making the trek to the hospital. She was living with multiple myeloma complicated by extramedullary manifestations that had significantly impacted her quality of life.

During our first encounter, she showed me a growing left subscapular mass the size of an orange that was erythematous, hot, painful, and irritated. As an enthusiastic first-year fellow, I wanted to be aggressive in addressing her concerns in response to her obvious distress about this mass. Ultimately, she left clinic with antibiotics and an appointment with radiation oncology to see if they could use radiation to shrink the subscapular mass.
When I went back in to discuss the plan with her, she grabbed my hand, looked me in my eyes and said: “Thank you, I’ve been mentioning this for a while and you’re the first person to get something done about it.” In that moment I knew that she felt seen.
By the time I made it over to the hospital, she was getting settled in her room to start another cycle of cytoreductive chemotherapy.
“I told them I had a Black doctor!” she exclaimed as I walked into her hospital room. “I was looking for you today in clinic ... I kept telling them I had a Black doctor, but the nurses kept telling me no, that there were only Black nurse practitioners.” She had repeatedly told the staff that I, her “Black doctor,” did indeed exist, and she went on to describe me as “you know, the [heavy-chested] and short Black doctor I saw early this fall.” To this day, her description still makes me chuckle.
Though I laughed at her description, it hurt that I had worked in a clinic for 6 months yet was invisible. Initially disappointed, I left Ms. Short’s room with a smile on my face, energized and encouraged.
My time with Ms. Short prompted me to ruminate on my experience as a Black physician. To put it in perspective, 5% of all physicians are Black, 2% are Black women, and 2.3% are oncologists, even though African Americans make up 13% of the general U.S. population. I reside in a space where I am simultaneously scrutinized because I am one of the few (or the only) Black physicians in the building, and yet I am invisible because my colleagues and coworkers routinely ignore my presence.
Black physicians, let alone hematologists, are so rare that nurses often cannot fathom that a Black woman could be more than a nurse practitioner. Sadly, this is the tip of the iceberg of some of the negative experiences I, and other Black doctors, have had.
How I present myself must be carefully curated to make progress in my career. My peers and superiors seem to hear me better when my hair is straight and not in its naturally curly state. My introversion has been interpreted as being standoffish or disinterested. Any tone other than happy is interpreted as “aggressive” or “angry”. Talking “too much” to Black support staff was reported to my program, as it was viewed as suspicious, disruptive, and “appearances matter”.
I am also expected to be nurturing in ways that White physicians are not required to be. In my presence, White physicians have denigrated an entire patient population that is disproportionately Black by calling them “sicklers.” If there is an interpersonal conflict, I must think about the long-term consequences of voicing my perspective. My non-Black colleagues do not have to think about these things.
Imagine dealing with this at work, then on your commute home being worried about the reality that you may be pulled over and become the next name on the ever-growing list of Black women and men murdered at the hands of police. The cognitive and emotional impact of being invisible is immense and cumulative over the years.
My Blackness creates a bias of inferiority that cannot be overcome by respectability, compliance, professionalism, training, and expertise. This is glaringly apparent on both sides of the physician-patient relationship. Black patients’ concerns are routinely overlooked and dismissed, as seen with Ms. Short, and are reflected in the Black maternal death rate, pain control in Black versus White patients, and personal experience as a patient and an advocate for my family members.
Patients have looked me in the face and said, “all lives matter,” displaying their refusal to recognize that systematic racism and inequality exist. These facts and experiences are the antithesis of “primum non nocere.”
Sadly, my and Ms. Short’s experiences are not singular ones, and racial bias in medicine is a diagnosed, but untreated cancer. Like the malignancies I treat, ignoring the problem has not made it go away; therefore, it continues to fester and spread, causing more destruction. It is of great importance and concern that all physicians recognize, reflect, and correct their implicit biases not only toward their patients, but also colleagues and trainees.
It seems that health care professionals can talk the talk, as many statements have been made against racism and implicit bias in medicine, but can we take true and meaningful action to begin the journey to equity and justice?
I would like to thank Adrienne Glover, MD, MaKenzie Hodge, MD, Maranatha McLean, MD, and Darion Showell, MD, for our stimulating conversations that helped me put pen to paper. I’d also like to thank my family for being my editors.
Daphanie D. Taylor, MD, is a hematology/oncology fellow PGY-6 at Levine Cancer Institute, Charlotte, N.C.
References and further reading
Roy L. “‘It’s My Calling To Change The Statistics’: Why We Need More Black Female Physicians.” Forbes Magazine, 27 Feb. 2020.
“Diversity in Medicine: Facts and Figures 2019.” Association of American Medical Colleges, 2019.
“Facts & Figures: Diversity in Oncology.” American Society of Clinical Oncology. 2020 Jan 16.
After a long day in hematology clinic, I skimmed the inpatient list to see if any of my patients had been admitted. Seeing Ms. Short’s name (changed for privacy), a delightful African American woman I met during my early days of fellowship, had me making the trek to the hospital. She was living with multiple myeloma complicated by extramedullary manifestations that had significantly impacted her quality of life.
During our first encounter, she showed me a growing left subscapular mass the size of an orange that was erythematous, hot, painful, and irritated. As an enthusiastic first-year fellow, I wanted to be aggressive in addressing her concerns in response to her obvious distress about this mass. Ultimately, she left clinic with antibiotics and an appointment with radiation oncology to see if they could use radiation to shrink the subscapular mass.
When I went back in to discuss the plan with her, she grabbed my hand, looked me in my eyes and said: “Thank you, I’ve been mentioning this for a while and you’re the first person to get something done about it.” In that moment I knew that she felt seen.
By the time I made it over to the hospital, she was getting settled in her room to start another cycle of cytoreductive chemotherapy.
“I told them I had a Black doctor!” she exclaimed as I walked into her hospital room. “I was looking for you today in clinic ... I kept telling them I had a Black doctor, but the nurses kept telling me no, that there were only Black nurse practitioners.” She had repeatedly told the staff that I, her “Black doctor,” did indeed exist, and she went on to describe me as “you know, the [heavy-chested] and short Black doctor I saw early this fall.” To this day, her description still makes me chuckle.
Though I laughed at her description, it hurt that I had worked in a clinic for 6 months yet was invisible. Initially disappointed, I left Ms. Short’s room with a smile on my face, energized and encouraged.
My time with Ms. Short prompted me to ruminate on my experience as a Black physician. To put it in perspective, 5% of all physicians are Black, 2% are Black women, and 2.3% are oncologists, even though African Americans make up 13% of the general U.S. population. I reside in a space where I am simultaneously scrutinized because I am one of the few (or the only) Black physicians in the building, and yet I am invisible because my colleagues and coworkers routinely ignore my presence.
Black physicians, let alone hematologists, are so rare that nurses often cannot fathom that a Black woman could be more than a nurse practitioner. Sadly, this is the tip of the iceberg of some of the negative experiences I, and other Black doctors, have had.
How I present myself must be carefully curated to make progress in my career. My peers and superiors seem to hear me better when my hair is straight and not in its naturally curly state. My introversion has been interpreted as being standoffish or disinterested. Any tone other than happy is interpreted as “aggressive” or “angry”. Talking “too much” to Black support staff was reported to my program, as it was viewed as suspicious, disruptive, and “appearances matter”.
I am also expected to be nurturing in ways that White physicians are not required to be. In my presence, White physicians have denigrated an entire patient population that is disproportionately Black by calling them “sicklers.” If there is an interpersonal conflict, I must think about the long-term consequences of voicing my perspective. My non-Black colleagues do not have to think about these things.
Imagine dealing with this at work, then on your commute home being worried about the reality that you may be pulled over and become the next name on the ever-growing list of Black women and men murdered at the hands of police. The cognitive and emotional impact of being invisible is immense and cumulative over the years.
My Blackness creates a bias of inferiority that cannot be overcome by respectability, compliance, professionalism, training, and expertise. This is glaringly apparent on both sides of the physician-patient relationship. Black patients’ concerns are routinely overlooked and dismissed, as seen with Ms. Short, and are reflected in the Black maternal death rate, pain control in Black versus White patients, and personal experience as a patient and an advocate for my family members.
Patients have looked me in the face and said, “all lives matter,” displaying their refusal to recognize that systematic racism and inequality exist. These facts and experiences are the antithesis of “primum non nocere.”
Sadly, my and Ms. Short’s experiences are not singular ones, and racial bias in medicine is a diagnosed, but untreated cancer. Like the malignancies I treat, ignoring the problem has not made it go away; therefore, it continues to fester and spread, causing more destruction. It is of great importance and concern that all physicians recognize, reflect, and correct their implicit biases not only toward their patients, but also colleagues and trainees.
It seems that health care professionals can talk the talk, as many statements have been made against racism and implicit bias in medicine, but can we take true and meaningful action to begin the journey to equity and justice?
I would like to thank Adrienne Glover, MD, MaKenzie Hodge, MD, Maranatha McLean, MD, and Darion Showell, MD, for our stimulating conversations that helped me put pen to paper. I’d also like to thank my family for being my editors.
Daphanie D. Taylor, MD, is a hematology/oncology fellow PGY-6 at Levine Cancer Institute, Charlotte, N.C.
References and further reading
Roy L. “‘It’s My Calling To Change The Statistics’: Why We Need More Black Female Physicians.” Forbes Magazine, 27 Feb. 2020.
“Diversity in Medicine: Facts and Figures 2019.” Association of American Medical Colleges, 2019.
“Facts & Figures: Diversity in Oncology.” American Society of Clinical Oncology. 2020 Jan 16.
After a long day in hematology clinic, I skimmed the inpatient list to see if any of my patients had been admitted. Seeing Ms. Short’s name (changed for privacy), a delightful African American woman I met during my early days of fellowship, had me making the trek to the hospital. She was living with multiple myeloma complicated by extramedullary manifestations that had significantly impacted her quality of life.
During our first encounter, she showed me a growing left subscapular mass the size of an orange that was erythematous, hot, painful, and irritated. As an enthusiastic first-year fellow, I wanted to be aggressive in addressing her concerns in response to her obvious distress about this mass. Ultimately, she left clinic with antibiotics and an appointment with radiation oncology to see if they could use radiation to shrink the subscapular mass.
When I went back in to discuss the plan with her, she grabbed my hand, looked me in my eyes and said: “Thank you, I’ve been mentioning this for a while and you’re the first person to get something done about it.” In that moment I knew that she felt seen.
By the time I made it over to the hospital, she was getting settled in her room to start another cycle of cytoreductive chemotherapy.
“I told them I had a Black doctor!” she exclaimed as I walked into her hospital room. “I was looking for you today in clinic ... I kept telling them I had a Black doctor, but the nurses kept telling me no, that there were only Black nurse practitioners.” She had repeatedly told the staff that I, her “Black doctor,” did indeed exist, and she went on to describe me as “you know, the [heavy-chested] and short Black doctor I saw early this fall.” To this day, her description still makes me chuckle.
Though I laughed at her description, it hurt that I had worked in a clinic for 6 months yet was invisible. Initially disappointed, I left Ms. Short’s room with a smile on my face, energized and encouraged.
My time with Ms. Short prompted me to ruminate on my experience as a Black physician. To put it in perspective, 5% of all physicians are Black, 2% are Black women, and 2.3% are oncologists, even though African Americans make up 13% of the general U.S. population. I reside in a space where I am simultaneously scrutinized because I am one of the few (or the only) Black physicians in the building, and yet I am invisible because my colleagues and coworkers routinely ignore my presence.
Black physicians, let alone hematologists, are so rare that nurses often cannot fathom that a Black woman could be more than a nurse practitioner. Sadly, this is the tip of the iceberg of some of the negative experiences I, and other Black doctors, have had.
How I present myself must be carefully curated to make progress in my career. My peers and superiors seem to hear me better when my hair is straight and not in its naturally curly state. My introversion has been interpreted as being standoffish or disinterested. Any tone other than happy is interpreted as “aggressive” or “angry”. Talking “too much” to Black support staff was reported to my program, as it was viewed as suspicious, disruptive, and “appearances matter”.
I am also expected to be nurturing in ways that White physicians are not required to be. In my presence, White physicians have denigrated an entire patient population that is disproportionately Black by calling them “sicklers.” If there is an interpersonal conflict, I must think about the long-term consequences of voicing my perspective. My non-Black colleagues do not have to think about these things.
Imagine dealing with this at work, then on your commute home being worried about the reality that you may be pulled over and become the next name on the ever-growing list of Black women and men murdered at the hands of police. The cognitive and emotional impact of being invisible is immense and cumulative over the years.
My Blackness creates a bias of inferiority that cannot be overcome by respectability, compliance, professionalism, training, and expertise. This is glaringly apparent on both sides of the physician-patient relationship. Black patients’ concerns are routinely overlooked and dismissed, as seen with Ms. Short, and are reflected in the Black maternal death rate, pain control in Black versus White patients, and personal experience as a patient and an advocate for my family members.
Patients have looked me in the face and said, “all lives matter,” displaying their refusal to recognize that systematic racism and inequality exist. These facts and experiences are the antithesis of “primum non nocere.”
Sadly, my and Ms. Short’s experiences are not singular ones, and racial bias in medicine is a diagnosed, but untreated cancer. Like the malignancies I treat, ignoring the problem has not made it go away; therefore, it continues to fester and spread, causing more destruction. It is of great importance and concern that all physicians recognize, reflect, and correct their implicit biases not only toward their patients, but also colleagues and trainees.
It seems that health care professionals can talk the talk, as many statements have been made against racism and implicit bias in medicine, but can we take true and meaningful action to begin the journey to equity and justice?
I would like to thank Adrienne Glover, MD, MaKenzie Hodge, MD, Maranatha McLean, MD, and Darion Showell, MD, for our stimulating conversations that helped me put pen to paper. I’d also like to thank my family for being my editors.
Daphanie D. Taylor, MD, is a hematology/oncology fellow PGY-6 at Levine Cancer Institute, Charlotte, N.C.
References and further reading
Roy L. “‘It’s My Calling To Change The Statistics’: Why We Need More Black Female Physicians.” Forbes Magazine, 27 Feb. 2020.
“Diversity in Medicine: Facts and Figures 2019.” Association of American Medical Colleges, 2019.
“Facts & Figures: Diversity in Oncology.” American Society of Clinical Oncology. 2020 Jan 16.
AAD announces diversity initiatives
not only within the academy itself, but also in the profession of dermatology overall.

“Last year’s events surrounding social justice issues and the disproportionate impact of COVID-19 on minority communities underscored an urgent need for the academy to outline a strategy to address gaps in diversity, equity, and inclusion across the academy’s programs, provide better access to dermatologic care, and expand the pipeline for prospective dermatologists,” according to an AAD statement introducing the plan.
“The AAD has long recognized the importance of fostering diversity in the dermatology specialty and increasing dermatologic services to underserved populations as a key strategic goal,” Kanya Ferguson, MD, chair of the AAD’s diversity committee, said in an interview.
“The importance and urgency of furthering these goals have been underscored by the social justice events of 2020 and the disproportionate impact that COVID-19 has had, specifically on Black and Latino communities,” added Dr. Ferguson, of the department of dermatology, at the University of Iowa, Iowa City. “The 3-year plan comprehensively expands current diversity, equity, and inclusion initiatives in an effort to accelerate the Academy’s progress toward its strategic goals.”
“Numerous barriers persist that contribute to the narrowing pipeline in medicine and ultimately in dermatology,” Dr. Ferguson noted. “The AAD’s diversity, equity, and inclusion initiatives, toolkits, and resources aim to address some of these barriers through early exposure, pipeline programming, and mentorship.”
As for the next steps, “the diversity committee will be working hard over the next few years to coordinate the integration and adoption of initiatives throughout the Academy’s activities,” she added. “This work will take a significant amount of collaboration and the committee is excited to move this forward in a meaningful and sustainable way.”
The AAD’s diversity committee headed the development of the plan, unanimously approved by the AAD’s board of directors, which outlines four key goals for the next 3 years, presented in the Diversity in Dermatology plan as follows:
“Promote and facilitate diversity, equity, and inclusion within the AAD.” Steps toward this goal include facilitating diverse representation on AAD committees, councils, and task forces, increasing representation of skin of color session speakers and lecture topics at Academy meetings, and ensuring equity in the selection process for awards including the Leadership Forum, Academic Dermatology Leadership Program, Advanced Leadership Forum, Journal of the AAD Editorial Mentorship Program, and other leadership activities.
- “Ensure dermatologic education and research encompasses health disparities and skin of color, and advocate for Black and Latino patient representation in research.” Steps toward this goal include increasing use of images reflecting the full spectrum of skin types, ensuring that skin of color populations receive information about dermatologic diseases, and supporting underrepresented minority (URM) dermatology physician scientists in leadership and professional development.
- “Expand Academy’s Advocacy Priorities to prioritize addressing health inequities.” Steps toward this goal include prioritizing issues that affect minority and marginalized populations, establishing relationships with relevant congressional leadership, and advocating for patient support groups for diseases that disproportionately impact skin of color patients.
- “Increase the number of practicing dermatologists who are underrepresented minorities and provide leadership and professional development programming.” Steps toward this goal include expanding the AAD mentorship program to include physician scientists, expanding diversity champion programs, expanding outreach to URM college students in STEM majors, and launching an AAD Summer Diversity & Inclusion camp for younger students to promote interest in a medical career.
The AAD diversity committee also has assembled a toolkit of resources designed to help its members learn how to talk about race, be an effective ally, and achieve cultural competency. Additional updated resources include guidelines on mentorship and outreach.
not only within the academy itself, but also in the profession of dermatology overall.
“Last year’s events surrounding social justice issues and the disproportionate impact of COVID-19 on minority communities underscored an urgent need for the academy to outline a strategy to address gaps in diversity, equity, and inclusion across the academy’s programs, provide better access to dermatologic care, and expand the pipeline for prospective dermatologists,” according to an AAD statement introducing the plan.
“The AAD has long recognized the importance of fostering diversity in the dermatology specialty and increasing dermatologic services to underserved populations as a key strategic goal,” Kanya Ferguson, MD, chair of the AAD’s diversity committee, said in an interview.
“The importance and urgency of furthering these goals have been underscored by the social justice events of 2020 and the disproportionate impact that COVID-19 has had, specifically on Black and Latino communities,” added Dr. Ferguson, of the department of dermatology, at the University of Iowa, Iowa City. “The 3-year plan comprehensively expands current diversity, equity, and inclusion initiatives in an effort to accelerate the Academy’s progress toward its strategic goals.”
“Numerous barriers persist that contribute to the narrowing pipeline in medicine and ultimately in dermatology,” Dr. Ferguson noted. “The AAD’s diversity, equity, and inclusion initiatives, toolkits, and resources aim to address some of these barriers through early exposure, pipeline programming, and mentorship.”
As for the next steps, “the diversity committee will be working hard over the next few years to coordinate the integration and adoption of initiatives throughout the Academy’s activities,” she added. “This work will take a significant amount of collaboration and the committee is excited to move this forward in a meaningful and sustainable way.”
The AAD’s diversity committee headed the development of the plan, unanimously approved by the AAD’s board of directors, which outlines four key goals for the next 3 years, presented in the Diversity in Dermatology plan as follows:
“Promote and facilitate diversity, equity, and inclusion within the AAD.” Steps toward this goal include facilitating diverse representation on AAD committees, councils, and task forces, increasing representation of skin of color session speakers and lecture topics at Academy meetings, and ensuring equity in the selection process for awards including the Leadership Forum, Academic Dermatology Leadership Program, Advanced Leadership Forum, Journal of the AAD Editorial Mentorship Program, and other leadership activities.
- “Ensure dermatologic education and research encompasses health disparities and skin of color, and advocate for Black and Latino patient representation in research.” Steps toward this goal include increasing use of images reflecting the full spectrum of skin types, ensuring that skin of color populations receive information about dermatologic diseases, and supporting underrepresented minority (URM) dermatology physician scientists in leadership and professional development.
- “Expand Academy’s Advocacy Priorities to prioritize addressing health inequities.” Steps toward this goal include prioritizing issues that affect minority and marginalized populations, establishing relationships with relevant congressional leadership, and advocating for patient support groups for diseases that disproportionately impact skin of color patients.
- “Increase the number of practicing dermatologists who are underrepresented minorities and provide leadership and professional development programming.” Steps toward this goal include expanding the AAD mentorship program to include physician scientists, expanding diversity champion programs, expanding outreach to URM college students in STEM majors, and launching an AAD Summer Diversity & Inclusion camp for younger students to promote interest in a medical career.
The AAD diversity committee also has assembled a toolkit of resources designed to help its members learn how to talk about race, be an effective ally, and achieve cultural competency. Additional updated resources include guidelines on mentorship and outreach.
not only within the academy itself, but also in the profession of dermatology overall.
“Last year’s events surrounding social justice issues and the disproportionate impact of COVID-19 on minority communities underscored an urgent need for the academy to outline a strategy to address gaps in diversity, equity, and inclusion across the academy’s programs, provide better access to dermatologic care, and expand the pipeline for prospective dermatologists,” according to an AAD statement introducing the plan.
“The AAD has long recognized the importance of fostering diversity in the dermatology specialty and increasing dermatologic services to underserved populations as a key strategic goal,” Kanya Ferguson, MD, chair of the AAD’s diversity committee, said in an interview.
“The importance and urgency of furthering these goals have been underscored by the social justice events of 2020 and the disproportionate impact that COVID-19 has had, specifically on Black and Latino communities,” added Dr. Ferguson, of the department of dermatology, at the University of Iowa, Iowa City. “The 3-year plan comprehensively expands current diversity, equity, and inclusion initiatives in an effort to accelerate the Academy’s progress toward its strategic goals.”
“Numerous barriers persist that contribute to the narrowing pipeline in medicine and ultimately in dermatology,” Dr. Ferguson noted. “The AAD’s diversity, equity, and inclusion initiatives, toolkits, and resources aim to address some of these barriers through early exposure, pipeline programming, and mentorship.”
As for the next steps, “the diversity committee will be working hard over the next few years to coordinate the integration and adoption of initiatives throughout the Academy’s activities,” she added. “This work will take a significant amount of collaboration and the committee is excited to move this forward in a meaningful and sustainable way.”
The AAD’s diversity committee headed the development of the plan, unanimously approved by the AAD’s board of directors, which outlines four key goals for the next 3 years, presented in the Diversity in Dermatology plan as follows:
“Promote and facilitate diversity, equity, and inclusion within the AAD.” Steps toward this goal include facilitating diverse representation on AAD committees, councils, and task forces, increasing representation of skin of color session speakers and lecture topics at Academy meetings, and ensuring equity in the selection process for awards including the Leadership Forum, Academic Dermatology Leadership Program, Advanced Leadership Forum, Journal of the AAD Editorial Mentorship Program, and other leadership activities.
- “Ensure dermatologic education and research encompasses health disparities and skin of color, and advocate for Black and Latino patient representation in research.” Steps toward this goal include increasing use of images reflecting the full spectrum of skin types, ensuring that skin of color populations receive information about dermatologic diseases, and supporting underrepresented minority (URM) dermatology physician scientists in leadership and professional development.
- “Expand Academy’s Advocacy Priorities to prioritize addressing health inequities.” Steps toward this goal include prioritizing issues that affect minority and marginalized populations, establishing relationships with relevant congressional leadership, and advocating for patient support groups for diseases that disproportionately impact skin of color patients.
- “Increase the number of practicing dermatologists who are underrepresented minorities and provide leadership and professional development programming.” Steps toward this goal include expanding the AAD mentorship program to include physician scientists, expanding diversity champion programs, expanding outreach to URM college students in STEM majors, and launching an AAD Summer Diversity & Inclusion camp for younger students to promote interest in a medical career.
The AAD diversity committee also has assembled a toolkit of resources designed to help its members learn how to talk about race, be an effective ally, and achieve cultural competency. Additional updated resources include guidelines on mentorship and outreach.