User login
ACIP issues adult vaccination schedule 2022
by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC).
The Clinical Guideline on the “Recommended Adult Immunization Schedule, United States, 2022” appears online Feb. 17 in Annals of Internal Medicine and in the CDC’s Morbidity and Mortality Weekly Report.
The document features changes to the zoster, pneumococcal, and hepatitis B vaccines. COVID-19 vaccinations are now included in the notes section of the schedule and can be co-administered with other vaccines, according to ACIP.
The 2022 schedule is particularly important because the pandemic has caused many adults to fall behind in routine vaccinations, according to lead author Neil Murthy, MD, MPH, MSJ, of the CDC’s immunization services division, National Center for Immunization and Respiratory Diseases, and colleagues.
“Providers should administer all due and overdue vaccines according to the routine immunization schedule during the same visit,” the group wrote. “In addition, providers should implement strategies to catch up all patients on any overdue vaccines.”
Among other changes appearing in the 2022 recommendations:
- A new step 4 in the form of an appendix lists all the contraindications and precautions for each vaccine.
- The zoster vaccine now is recommended for use in everyone aged 19 years and older who are or will be immunodeficient or immunosuppressed through disease or therapy. The new purple color bar reflects ACIP’s new two-dose series regimen for immunocompromised adults aged 19 to 49.
- The simplified pneumococcal recommendation includes guidance on using the new PCV15 and PCV20 vaccines.
- The hepatitis B recommendation has been made more inclusive, with vaccination recommended for all adults aged 19 to 59. The Special Situations section in the Notes outlines the risk-based recommendations for the hepatitis B vaccine in adults aged 60 and older. The schedule has been harmonized with the 2022 Child and Adolescent Immunization Schedule.
A welcome change
Sandra A. Fryhofer, MD, a member of the ACIP Combined Immunization Work Group, said the new pneumococcal recommendation is a particularly welcome change.
“The old recommendation was complicated and confusing. The new one is much more straightforward,” Dr. Fryhofer, an internist in Atlanta, said in an interview. Now there are only two options: a two-vaccine series of PCV15 (Vaxneuvance), in combination with the already familiar PPSV23 polysaccharide vaccine (Pneumovax 23), and a single dose of the new PCV20, Prevnar 20.
“Some work group members favored a universal age-based recommendation starting at 50 instead of 65,” Fryhofer said. “This would provide more opportunities to vaccinate adults but could lead to waning immunity later in life when risk of disease is higher.”
Although none of the updates is likely to stir controversy, discussion among ACIP members was particularly lively around hepatitis B vaccination, Dr. Fryhofer said. This vaccine has historically been recommended based on risk and has had poor uptake, while age-based vaccine recommendations generally have greater uptake.
“ACIP approved hepatitis B vaccine universally for those up to age 60, but for those 60 and older, the recommendation remains risk-based with a loophole: Anyone 60 and older who wants it can get it,” she told this news organization. “Some of the risk indications for hepatitis B vaccination may be uncomfortable or embarrassing to disclose, especially for older patients. The loophole takes care of that, but patients may have to ask for the vaccine.”
As usual, the graphics have been fine-tuned for greater accuracy and readability. “You can print a color copy to have in the exam room or at your workspace or give it a bookmark and check it online,” Dr. Fryhofer said. “It’s a great resource to have at your fingertips.”
Dr. Fryhofer has made a series of videos explaining ACIP’s approval process, the use of the schedule, and changes to vaccines including influenza. These can be accessed on the American College of Physicians website.
The authors of the recommendations stress that physicians should pay careful attention to the notes section for each vaccine, as these details clarify who needs what vaccine, when, and at what dose.
Co-author Henry Bernstein, DO, reported that he is the editor of Current Opinion in Pediatrics Office Pediatrics Series and received a presentation honorarium from the Florida chapter of the American Academy of Pediatrics. Co-author Kevin Ault, MD, reported having received a grant from the National Cancer Institute, consulting fees from PathoVax, and payments supporting attending meetings and/or travel from the American College of Obstetricians and Gynecologists.
A version of this article first appeared on Medscape.com.
by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC).
The Clinical Guideline on the “Recommended Adult Immunization Schedule, United States, 2022” appears online Feb. 17 in Annals of Internal Medicine and in the CDC’s Morbidity and Mortality Weekly Report.
The document features changes to the zoster, pneumococcal, and hepatitis B vaccines. COVID-19 vaccinations are now included in the notes section of the schedule and can be co-administered with other vaccines, according to ACIP.
The 2022 schedule is particularly important because the pandemic has caused many adults to fall behind in routine vaccinations, according to lead author Neil Murthy, MD, MPH, MSJ, of the CDC’s immunization services division, National Center for Immunization and Respiratory Diseases, and colleagues.
“Providers should administer all due and overdue vaccines according to the routine immunization schedule during the same visit,” the group wrote. “In addition, providers should implement strategies to catch up all patients on any overdue vaccines.”
Among other changes appearing in the 2022 recommendations:
- A new step 4 in the form of an appendix lists all the contraindications and precautions for each vaccine.
- The zoster vaccine now is recommended for use in everyone aged 19 years and older who are or will be immunodeficient or immunosuppressed through disease or therapy. The new purple color bar reflects ACIP’s new two-dose series regimen for immunocompromised adults aged 19 to 49.
- The simplified pneumococcal recommendation includes guidance on using the new PCV15 and PCV20 vaccines.
- The hepatitis B recommendation has been made more inclusive, with vaccination recommended for all adults aged 19 to 59. The Special Situations section in the Notes outlines the risk-based recommendations for the hepatitis B vaccine in adults aged 60 and older. The schedule has been harmonized with the 2022 Child and Adolescent Immunization Schedule.
A welcome change
Sandra A. Fryhofer, MD, a member of the ACIP Combined Immunization Work Group, said the new pneumococcal recommendation is a particularly welcome change.
“The old recommendation was complicated and confusing. The new one is much more straightforward,” Dr. Fryhofer, an internist in Atlanta, said in an interview. Now there are only two options: a two-vaccine series of PCV15 (Vaxneuvance), in combination with the already familiar PPSV23 polysaccharide vaccine (Pneumovax 23), and a single dose of the new PCV20, Prevnar 20.
“Some work group members favored a universal age-based recommendation starting at 50 instead of 65,” Fryhofer said. “This would provide more opportunities to vaccinate adults but could lead to waning immunity later in life when risk of disease is higher.”
Although none of the updates is likely to stir controversy, discussion among ACIP members was particularly lively around hepatitis B vaccination, Dr. Fryhofer said. This vaccine has historically been recommended based on risk and has had poor uptake, while age-based vaccine recommendations generally have greater uptake.
“ACIP approved hepatitis B vaccine universally for those up to age 60, but for those 60 and older, the recommendation remains risk-based with a loophole: Anyone 60 and older who wants it can get it,” she told this news organization. “Some of the risk indications for hepatitis B vaccination may be uncomfortable or embarrassing to disclose, especially for older patients. The loophole takes care of that, but patients may have to ask for the vaccine.”
As usual, the graphics have been fine-tuned for greater accuracy and readability. “You can print a color copy to have in the exam room or at your workspace or give it a bookmark and check it online,” Dr. Fryhofer said. “It’s a great resource to have at your fingertips.”
Dr. Fryhofer has made a series of videos explaining ACIP’s approval process, the use of the schedule, and changes to vaccines including influenza. These can be accessed on the American College of Physicians website.
The authors of the recommendations stress that physicians should pay careful attention to the notes section for each vaccine, as these details clarify who needs what vaccine, when, and at what dose.
Co-author Henry Bernstein, DO, reported that he is the editor of Current Opinion in Pediatrics Office Pediatrics Series and received a presentation honorarium from the Florida chapter of the American Academy of Pediatrics. Co-author Kevin Ault, MD, reported having received a grant from the National Cancer Institute, consulting fees from PathoVax, and payments supporting attending meetings and/or travel from the American College of Obstetricians and Gynecologists.
A version of this article first appeared on Medscape.com.
by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC).
The Clinical Guideline on the “Recommended Adult Immunization Schedule, United States, 2022” appears online Feb. 17 in Annals of Internal Medicine and in the CDC’s Morbidity and Mortality Weekly Report.
The document features changes to the zoster, pneumococcal, and hepatitis B vaccines. COVID-19 vaccinations are now included in the notes section of the schedule and can be co-administered with other vaccines, according to ACIP.
The 2022 schedule is particularly important because the pandemic has caused many adults to fall behind in routine vaccinations, according to lead author Neil Murthy, MD, MPH, MSJ, of the CDC’s immunization services division, National Center for Immunization and Respiratory Diseases, and colleagues.
“Providers should administer all due and overdue vaccines according to the routine immunization schedule during the same visit,” the group wrote. “In addition, providers should implement strategies to catch up all patients on any overdue vaccines.”
Among other changes appearing in the 2022 recommendations:
- A new step 4 in the form of an appendix lists all the contraindications and precautions for each vaccine.
- The zoster vaccine now is recommended for use in everyone aged 19 years and older who are or will be immunodeficient or immunosuppressed through disease or therapy. The new purple color bar reflects ACIP’s new two-dose series regimen for immunocompromised adults aged 19 to 49.
- The simplified pneumococcal recommendation includes guidance on using the new PCV15 and PCV20 vaccines.
- The hepatitis B recommendation has been made more inclusive, with vaccination recommended for all adults aged 19 to 59. The Special Situations section in the Notes outlines the risk-based recommendations for the hepatitis B vaccine in adults aged 60 and older. The schedule has been harmonized with the 2022 Child and Adolescent Immunization Schedule.
A welcome change
Sandra A. Fryhofer, MD, a member of the ACIP Combined Immunization Work Group, said the new pneumococcal recommendation is a particularly welcome change.
“The old recommendation was complicated and confusing. The new one is much more straightforward,” Dr. Fryhofer, an internist in Atlanta, said in an interview. Now there are only two options: a two-vaccine series of PCV15 (Vaxneuvance), in combination with the already familiar PPSV23 polysaccharide vaccine (Pneumovax 23), and a single dose of the new PCV20, Prevnar 20.
“Some work group members favored a universal age-based recommendation starting at 50 instead of 65,” Fryhofer said. “This would provide more opportunities to vaccinate adults but could lead to waning immunity later in life when risk of disease is higher.”
Although none of the updates is likely to stir controversy, discussion among ACIP members was particularly lively around hepatitis B vaccination, Dr. Fryhofer said. This vaccine has historically been recommended based on risk and has had poor uptake, while age-based vaccine recommendations generally have greater uptake.
“ACIP approved hepatitis B vaccine universally for those up to age 60, but for those 60 and older, the recommendation remains risk-based with a loophole: Anyone 60 and older who wants it can get it,” she told this news organization. “Some of the risk indications for hepatitis B vaccination may be uncomfortable or embarrassing to disclose, especially for older patients. The loophole takes care of that, but patients may have to ask for the vaccine.”
As usual, the graphics have been fine-tuned for greater accuracy and readability. “You can print a color copy to have in the exam room or at your workspace or give it a bookmark and check it online,” Dr. Fryhofer said. “It’s a great resource to have at your fingertips.”
Dr. Fryhofer has made a series of videos explaining ACIP’s approval process, the use of the schedule, and changes to vaccines including influenza. These can be accessed on the American College of Physicians website.
The authors of the recommendations stress that physicians should pay careful attention to the notes section for each vaccine, as these details clarify who needs what vaccine, when, and at what dose.
Co-author Henry Bernstein, DO, reported that he is the editor of Current Opinion in Pediatrics Office Pediatrics Series and received a presentation honorarium from the Florida chapter of the American Academy of Pediatrics. Co-author Kevin Ault, MD, reported having received a grant from the National Cancer Institute, consulting fees from PathoVax, and payments supporting attending meetings and/or travel from the American College of Obstetricians and Gynecologists.
A version of this article first appeared on Medscape.com.
Patients are interrupting DMARD use well into the COVID-19 pandemic
The COVID-19 pandemic led to a decrease in the proportion of patients with rheumatic diseases who stopped taking their disease-modifying antirheumatic drugs (DMARDs), but the percentage who interrupted DMARD treatment increased later in the pandemic, according to speakers at the 2022 Rheumatology Winter Clinical Symposium.
“People seem to be less anxious, but they’re interrupting their DMARD therapy more, more recently than in the pits of COVID, if you will,” said Arthur Kavanaugh, MD, professor of medicine at the University of California, San Diego, and director of RWCS.

Dr. Kavanaugh and his copresenter Jack Cush, MD, were discussing the results of a recent study published in Arthritis Care & Research that evaluated 2,424 patients with rheumatic diseases who completed a baseline and at least one follow-up survey issued by patient organizations between March 2020 and May 2021, with a median of five follow-up surveys completed. The patients included in the study were aged a mean of 57 years, 86.6% were women, 90.5% were White, 41.8% had rheumatoid arthritis (RA), 14.8% had antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, and 12.4% had psoriatic arthritis. Overall, 52.6% were on biologics or a Janus kinase (JAK) inhibitor, 30.0% were receiving methotrexate, 21.4% were taking hydroxychloroquine, and 28.6% were receiving low-dose (24.0%) or high-dose (4.6%) glucocorticoids.
Patients’ T-scores on the anxiety short form Patient-Reported Outcomes Measurement Information System (PROMIS) survey significantly decreased from a score of 58.7 in April 2020 to a score of 53.7 in May 2021 (P < .001), but there was a significant decrease in the interruption of DMARD treatment between April and December 2020 (11.2% vs. 7.5%; P < .001). This percentage rose significantly to 14.0% by May 2021 (P < .001). Patients who stopped using DMARDs were significantly associated with predicted incidence of severe flare in the next survey in adjusted models (12.9% vs. 8.0%; odds ratio, 1.71; 95% confidence interval, 1.23-2.36).
The results tell us “that we as a discipline are not doing a good job educating our patients,” said Dr. Cush, a rheumatologist based in Dallas, Tex., and executive editor of RheumNow.com.
“I wish we – and I’m really talking about myself – but myself and my practice were more proactive when COVID happened [in] sending out regular bulletins: ‘Don’t stop your therapy; these are the things you get; get the test that you need to get done,’ ” he said. “We let a lot of things go on autopilot with the patient driving throughout COVID. Even now, it’s happening. And this is a problem, and there are going to be consequences to this.”
Dr. Kavanaugh agreed with Dr. Cush’s assessment, suggesting that the pandemic came up quickly enough that it was difficult to be proactive with the situation.
Patients on JAK inhibitors as new COVID-19 risk group?
Another standout study on COVID-19 from 2021 was an analysis of the COVID-19 Global Rheumatology Alliance physician registry that examined risk of COVID-19 severity for patients with RA taking biologic or targeted synthetic DMARDs (tsDMARDs), which was presented at the 2021 EULAR congress and later published in Annals of the Rheumatic Diseases.
The researchers evaluated 2,869 patients March 2020 and April 2021 who were receiving abatacept (237 patients), rituximab (364 patients), interleukin (IL)-6 inhibitors (317 patients), JAK inhibitors (563 patients), or tumor necrosis factor (TNF) inhibitors such as infliximab, etanercept, adalimumab, certolizumab pegol, and golimumab (1,388 patients) before developing COVID-19. Data about biologics or tsDMARDs were collected as a drug class. Patients in the study were mostly White (69.0%) women (80.8%) with a mean age of 56.7 years who lived in Europe (51.8%) or North America (35.0%). The researchers examined the severity of COVID-19 among all patients studied and calculated odds ratios based on drug class, with the TNF inhibitor group serving as a reference.
“[I]n this case, they said that the baseline use of rituximab was associated with more severity, and you see the severity being hospitalization and ICU and deaths. They found a signal for the JAK inhibitors that is not found in the other studies,” Dr. Kavanaugh said.
Overall, they found 21% of patients in the registry were hospitalized and 5.5% died, with rituximab (OR, 4.15; 95% CI, 3.16-5.44) and JAK inhibitors (OR, 2.06; 95% CI, 1.60-2.65) associated with more severe COVID-19 outcomes. Specifically, rituximab was associated with greater likelihood of hospitalization (OR, 4.53; 95% CI, 3.32-6.18), hospitalization with oxygen/ventilation (OR, 2.87; 95% CI, 2.03-4.06), need for mechanical ventilation (OR, 4.05; 95% CI, 3.08-5.33), and mortality (OR, 4.57; 95% CI, 3.32-9.01), compared with TNF inhibitors. For JAK inhibitors, there was also a greater likelihood of hospitalization (OR, 2.40; 95% CI, 1.78-3.24), hospitalization with oxygen/ventilation (OR, 1.55; 95% CI, 1.04-2.18), need for mechanical ventilation (OR, 2.03; 95% CI, 1.56-2.62), and mortality (OR, 2.04; 95% CI, 1.58-2.65), compared with the TNF inhibitors group. Associations between COVID-19 severity and abatacept or IL-6 inhibitors were not identified.
Commenting on the study in a question-and-answer session, Roy Fleischmann, MD, said the part of the study that identified a signal for JAK inhibitors was “very interesting.” He called attention to a rapid response comment to the study, which questioned if it was the drug class itself that caused the risk for severe disease. “This is very important, because actually, the patients who stop the JAK [inhibitor], that’s what drove the illness. The patients [who] continued the JAK [inhibitor], very few of them had illness,” said Dr. Fleischmann, clinical professor of medicine at the University of Texas Southwestern Medical School and codirector of the Metroplex Clinical Research Center, both in Dallas, Tex.
Confusion among patients during COVID-19
Alvin Wells, MD, PhD, asked the copresenters during the Q&A session whether they had any clinical pearls for the audience on how they manage treatment of patients with rheumatic disease with potential COVID-19 risk. “I think the confusion with our patients and COVID is what the ACR has put out with their guidelines,” said Dr. Wells, director of the department of rheumatology at Advocate Aurora Health in Franklin, Wisc.
Dr. Cush said he has three rules he follows: lower and discontinue steroids, avoid rituximab as a starting treatment and negotiate if patients are already taking it, and don’t stop any therapy.
“I want disease control. I think being under control is what keeps you away from risk of COVID and hospitalization,” Dr. Cush said. “I think being uncontrolled and inflamed, whether it’s our [patients with] inflammatory arthritis or lupus or, worse, vasculitis [or] myositis, those are the ones at high risk of progression from being just infected to being sick and in the hospital.”
Eric Ruderman, MD, professor of rheumatology at Northwestern University, Chicago, posed the question of getting somewhat back to normal during COVID-19 with regard to recently infected patients presenting at infusion centers, whether patients are more likely to continue testing positive, and when patients are cleared to come back. Dr. Ruderman said his center has a 20-day rule for returning after having COVID-19, while Dr. Cush said his center allows patients to come in if they test negative after 7-10 days.
“One of the things we’re struggling with is our infusion center, and one of the questions that keeps coming up is when can people come back after a COVID infection?” he said. “If you’re on a drug at home, that’s up to you and the patient. But in the infusion [center], then you have other people sitting around there.”
Dr. Kavanaugh said there is no current data for how long patients with rheumatic disease shed virus, or how long a positive test can be measured. “You definitely will continue to shed, and you’ll be detectable for a while,” he said.
Dr. Cush and Dr. Kavanaugh reported having financial relationships with numerous pharmaceutical companies.
The COVID-19 pandemic led to a decrease in the proportion of patients with rheumatic diseases who stopped taking their disease-modifying antirheumatic drugs (DMARDs), but the percentage who interrupted DMARD treatment increased later in the pandemic, according to speakers at the 2022 Rheumatology Winter Clinical Symposium.
“People seem to be less anxious, but they’re interrupting their DMARD therapy more, more recently than in the pits of COVID, if you will,” said Arthur Kavanaugh, MD, professor of medicine at the University of California, San Diego, and director of RWCS.
Dr. Kavanaugh and his copresenter Jack Cush, MD, were discussing the results of a recent study published in Arthritis Care & Research that evaluated 2,424 patients with rheumatic diseases who completed a baseline and at least one follow-up survey issued by patient organizations between March 2020 and May 2021, with a median of five follow-up surveys completed. The patients included in the study were aged a mean of 57 years, 86.6% were women, 90.5% were White, 41.8% had rheumatoid arthritis (RA), 14.8% had antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, and 12.4% had psoriatic arthritis. Overall, 52.6% were on biologics or a Janus kinase (JAK) inhibitor, 30.0% were receiving methotrexate, 21.4% were taking hydroxychloroquine, and 28.6% were receiving low-dose (24.0%) or high-dose (4.6%) glucocorticoids.
Patients’ T-scores on the anxiety short form Patient-Reported Outcomes Measurement Information System (PROMIS) survey significantly decreased from a score of 58.7 in April 2020 to a score of 53.7 in May 2021 (P < .001), but there was a significant decrease in the interruption of DMARD treatment between April and December 2020 (11.2% vs. 7.5%; P < .001). This percentage rose significantly to 14.0% by May 2021 (P < .001). Patients who stopped using DMARDs were significantly associated with predicted incidence of severe flare in the next survey in adjusted models (12.9% vs. 8.0%; odds ratio, 1.71; 95% confidence interval, 1.23-2.36).
The results tell us “that we as a discipline are not doing a good job educating our patients,” said Dr. Cush, a rheumatologist based in Dallas, Tex., and executive editor of RheumNow.com.
“I wish we – and I’m really talking about myself – but myself and my practice were more proactive when COVID happened [in] sending out regular bulletins: ‘Don’t stop your therapy; these are the things you get; get the test that you need to get done,’ ” he said. “We let a lot of things go on autopilot with the patient driving throughout COVID. Even now, it’s happening. And this is a problem, and there are going to be consequences to this.”
Dr. Kavanaugh agreed with Dr. Cush’s assessment, suggesting that the pandemic came up quickly enough that it was difficult to be proactive with the situation.
Patients on JAK inhibitors as new COVID-19 risk group?
Another standout study on COVID-19 from 2021 was an analysis of the COVID-19 Global Rheumatology Alliance physician registry that examined risk of COVID-19 severity for patients with RA taking biologic or targeted synthetic DMARDs (tsDMARDs), which was presented at the 2021 EULAR congress and later published in Annals of the Rheumatic Diseases.
The researchers evaluated 2,869 patients March 2020 and April 2021 who were receiving abatacept (237 patients), rituximab (364 patients), interleukin (IL)-6 inhibitors (317 patients), JAK inhibitors (563 patients), or tumor necrosis factor (TNF) inhibitors such as infliximab, etanercept, adalimumab, certolizumab pegol, and golimumab (1,388 patients) before developing COVID-19. Data about biologics or tsDMARDs were collected as a drug class. Patients in the study were mostly White (69.0%) women (80.8%) with a mean age of 56.7 years who lived in Europe (51.8%) or North America (35.0%). The researchers examined the severity of COVID-19 among all patients studied and calculated odds ratios based on drug class, with the TNF inhibitor group serving as a reference.
“[I]n this case, they said that the baseline use of rituximab was associated with more severity, and you see the severity being hospitalization and ICU and deaths. They found a signal for the JAK inhibitors that is not found in the other studies,” Dr. Kavanaugh said.
Overall, they found 21% of patients in the registry were hospitalized and 5.5% died, with rituximab (OR, 4.15; 95% CI, 3.16-5.44) and JAK inhibitors (OR, 2.06; 95% CI, 1.60-2.65) associated with more severe COVID-19 outcomes. Specifically, rituximab was associated with greater likelihood of hospitalization (OR, 4.53; 95% CI, 3.32-6.18), hospitalization with oxygen/ventilation (OR, 2.87; 95% CI, 2.03-4.06), need for mechanical ventilation (OR, 4.05; 95% CI, 3.08-5.33), and mortality (OR, 4.57; 95% CI, 3.32-9.01), compared with TNF inhibitors. For JAK inhibitors, there was also a greater likelihood of hospitalization (OR, 2.40; 95% CI, 1.78-3.24), hospitalization with oxygen/ventilation (OR, 1.55; 95% CI, 1.04-2.18), need for mechanical ventilation (OR, 2.03; 95% CI, 1.56-2.62), and mortality (OR, 2.04; 95% CI, 1.58-2.65), compared with the TNF inhibitors group. Associations between COVID-19 severity and abatacept or IL-6 inhibitors were not identified.
Commenting on the study in a question-and-answer session, Roy Fleischmann, MD, said the part of the study that identified a signal for JAK inhibitors was “very interesting.” He called attention to a rapid response comment to the study, which questioned if it was the drug class itself that caused the risk for severe disease. “This is very important, because actually, the patients who stop the JAK [inhibitor], that’s what drove the illness. The patients [who] continued the JAK [inhibitor], very few of them had illness,” said Dr. Fleischmann, clinical professor of medicine at the University of Texas Southwestern Medical School and codirector of the Metroplex Clinical Research Center, both in Dallas, Tex.
Confusion among patients during COVID-19
Alvin Wells, MD, PhD, asked the copresenters during the Q&A session whether they had any clinical pearls for the audience on how they manage treatment of patients with rheumatic disease with potential COVID-19 risk. “I think the confusion with our patients and COVID is what the ACR has put out with their guidelines,” said Dr. Wells, director of the department of rheumatology at Advocate Aurora Health in Franklin, Wisc.
Dr. Cush said he has three rules he follows: lower and discontinue steroids, avoid rituximab as a starting treatment and negotiate if patients are already taking it, and don’t stop any therapy.
“I want disease control. I think being under control is what keeps you away from risk of COVID and hospitalization,” Dr. Cush said. “I think being uncontrolled and inflamed, whether it’s our [patients with] inflammatory arthritis or lupus or, worse, vasculitis [or] myositis, those are the ones at high risk of progression from being just infected to being sick and in the hospital.”
Eric Ruderman, MD, professor of rheumatology at Northwestern University, Chicago, posed the question of getting somewhat back to normal during COVID-19 with regard to recently infected patients presenting at infusion centers, whether patients are more likely to continue testing positive, and when patients are cleared to come back. Dr. Ruderman said his center has a 20-day rule for returning after having COVID-19, while Dr. Cush said his center allows patients to come in if they test negative after 7-10 days.
“One of the things we’re struggling with is our infusion center, and one of the questions that keeps coming up is when can people come back after a COVID infection?” he said. “If you’re on a drug at home, that’s up to you and the patient. But in the infusion [center], then you have other people sitting around there.”
Dr. Kavanaugh said there is no current data for how long patients with rheumatic disease shed virus, or how long a positive test can be measured. “You definitely will continue to shed, and you’ll be detectable for a while,” he said.
Dr. Cush and Dr. Kavanaugh reported having financial relationships with numerous pharmaceutical companies.
The COVID-19 pandemic led to a decrease in the proportion of patients with rheumatic diseases who stopped taking their disease-modifying antirheumatic drugs (DMARDs), but the percentage who interrupted DMARD treatment increased later in the pandemic, according to speakers at the 2022 Rheumatology Winter Clinical Symposium.
“People seem to be less anxious, but they’re interrupting their DMARD therapy more, more recently than in the pits of COVID, if you will,” said Arthur Kavanaugh, MD, professor of medicine at the University of California, San Diego, and director of RWCS.
Dr. Kavanaugh and his copresenter Jack Cush, MD, were discussing the results of a recent study published in Arthritis Care & Research that evaluated 2,424 patients with rheumatic diseases who completed a baseline and at least one follow-up survey issued by patient organizations between March 2020 and May 2021, with a median of five follow-up surveys completed. The patients included in the study were aged a mean of 57 years, 86.6% were women, 90.5% were White, 41.8% had rheumatoid arthritis (RA), 14.8% had antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis, and 12.4% had psoriatic arthritis. Overall, 52.6% were on biologics or a Janus kinase (JAK) inhibitor, 30.0% were receiving methotrexate, 21.4% were taking hydroxychloroquine, and 28.6% were receiving low-dose (24.0%) or high-dose (4.6%) glucocorticoids.
Patients’ T-scores on the anxiety short form Patient-Reported Outcomes Measurement Information System (PROMIS) survey significantly decreased from a score of 58.7 in April 2020 to a score of 53.7 in May 2021 (P < .001), but there was a significant decrease in the interruption of DMARD treatment between April and December 2020 (11.2% vs. 7.5%; P < .001). This percentage rose significantly to 14.0% by May 2021 (P < .001). Patients who stopped using DMARDs were significantly associated with predicted incidence of severe flare in the next survey in adjusted models (12.9% vs. 8.0%; odds ratio, 1.71; 95% confidence interval, 1.23-2.36).
The results tell us “that we as a discipline are not doing a good job educating our patients,” said Dr. Cush, a rheumatologist based in Dallas, Tex., and executive editor of RheumNow.com.
“I wish we – and I’m really talking about myself – but myself and my practice were more proactive when COVID happened [in] sending out regular bulletins: ‘Don’t stop your therapy; these are the things you get; get the test that you need to get done,’ ” he said. “We let a lot of things go on autopilot with the patient driving throughout COVID. Even now, it’s happening. And this is a problem, and there are going to be consequences to this.”
Dr. Kavanaugh agreed with Dr. Cush’s assessment, suggesting that the pandemic came up quickly enough that it was difficult to be proactive with the situation.
Patients on JAK inhibitors as new COVID-19 risk group?
Another standout study on COVID-19 from 2021 was an analysis of the COVID-19 Global Rheumatology Alliance physician registry that examined risk of COVID-19 severity for patients with RA taking biologic or targeted synthetic DMARDs (tsDMARDs), which was presented at the 2021 EULAR congress and later published in Annals of the Rheumatic Diseases.
The researchers evaluated 2,869 patients March 2020 and April 2021 who were receiving abatacept (237 patients), rituximab (364 patients), interleukin (IL)-6 inhibitors (317 patients), JAK inhibitors (563 patients), or tumor necrosis factor (TNF) inhibitors such as infliximab, etanercept, adalimumab, certolizumab pegol, and golimumab (1,388 patients) before developing COVID-19. Data about biologics or tsDMARDs were collected as a drug class. Patients in the study were mostly White (69.0%) women (80.8%) with a mean age of 56.7 years who lived in Europe (51.8%) or North America (35.0%). The researchers examined the severity of COVID-19 among all patients studied and calculated odds ratios based on drug class, with the TNF inhibitor group serving as a reference.
“[I]n this case, they said that the baseline use of rituximab was associated with more severity, and you see the severity being hospitalization and ICU and deaths. They found a signal for the JAK inhibitors that is not found in the other studies,” Dr. Kavanaugh said.
Overall, they found 21% of patients in the registry were hospitalized and 5.5% died, with rituximab (OR, 4.15; 95% CI, 3.16-5.44) and JAK inhibitors (OR, 2.06; 95% CI, 1.60-2.65) associated with more severe COVID-19 outcomes. Specifically, rituximab was associated with greater likelihood of hospitalization (OR, 4.53; 95% CI, 3.32-6.18), hospitalization with oxygen/ventilation (OR, 2.87; 95% CI, 2.03-4.06), need for mechanical ventilation (OR, 4.05; 95% CI, 3.08-5.33), and mortality (OR, 4.57; 95% CI, 3.32-9.01), compared with TNF inhibitors. For JAK inhibitors, there was also a greater likelihood of hospitalization (OR, 2.40; 95% CI, 1.78-3.24), hospitalization with oxygen/ventilation (OR, 1.55; 95% CI, 1.04-2.18), need for mechanical ventilation (OR, 2.03; 95% CI, 1.56-2.62), and mortality (OR, 2.04; 95% CI, 1.58-2.65), compared with the TNF inhibitors group. Associations between COVID-19 severity and abatacept or IL-6 inhibitors were not identified.
Commenting on the study in a question-and-answer session, Roy Fleischmann, MD, said the part of the study that identified a signal for JAK inhibitors was “very interesting.” He called attention to a rapid response comment to the study, which questioned if it was the drug class itself that caused the risk for severe disease. “This is very important, because actually, the patients who stop the JAK [inhibitor], that’s what drove the illness. The patients [who] continued the JAK [inhibitor], very few of them had illness,” said Dr. Fleischmann, clinical professor of medicine at the University of Texas Southwestern Medical School and codirector of the Metroplex Clinical Research Center, both in Dallas, Tex.
Confusion among patients during COVID-19
Alvin Wells, MD, PhD, asked the copresenters during the Q&A session whether they had any clinical pearls for the audience on how they manage treatment of patients with rheumatic disease with potential COVID-19 risk. “I think the confusion with our patients and COVID is what the ACR has put out with their guidelines,” said Dr. Wells, director of the department of rheumatology at Advocate Aurora Health in Franklin, Wisc.
Dr. Cush said he has three rules he follows: lower and discontinue steroids, avoid rituximab as a starting treatment and negotiate if patients are already taking it, and don’t stop any therapy.
“I want disease control. I think being under control is what keeps you away from risk of COVID and hospitalization,” Dr. Cush said. “I think being uncontrolled and inflamed, whether it’s our [patients with] inflammatory arthritis or lupus or, worse, vasculitis [or] myositis, those are the ones at high risk of progression from being just infected to being sick and in the hospital.”
Eric Ruderman, MD, professor of rheumatology at Northwestern University, Chicago, posed the question of getting somewhat back to normal during COVID-19 with regard to recently infected patients presenting at infusion centers, whether patients are more likely to continue testing positive, and when patients are cleared to come back. Dr. Ruderman said his center has a 20-day rule for returning after having COVID-19, while Dr. Cush said his center allows patients to come in if they test negative after 7-10 days.
“One of the things we’re struggling with is our infusion center, and one of the questions that keeps coming up is when can people come back after a COVID infection?” he said. “If you’re on a drug at home, that’s up to you and the patient. But in the infusion [center], then you have other people sitting around there.”
Dr. Kavanaugh said there is no current data for how long patients with rheumatic disease shed virus, or how long a positive test can be measured. “You definitely will continue to shed, and you’ll be detectable for a while,” he said.
Dr. Cush and Dr. Kavanaugh reported having financial relationships with numerous pharmaceutical companies.
FROM RWCS 2022
Thirty-seven percent of COVID-19 patients lose sense of taste, study says
, according to a new study.
Many COVID-19 patients report losing their sense of taste as well as their sense of smell, but scientists have been skeptical because the two senses are closely related and it was relatively rare for people to lose their taste sense before the COVID pandemic, says the Monell Chemical Senses Center, a nonprofit research institute in Philadelphia.
But a new Monell Center analysis found that 37% – or about four in every 10 -- of COVID-19 patients actually did lose their sense of taste and that “reports of taste loss are in fact genuine and distinguishable from smell loss.”
Taste dysfunction can be total taste loss, partial taste loss, and taste distortion. It’s an “underrated” symptom that could help doctors better treat COVID patients, the Monell Center said in a news release.
“It is time to turn to the tongue” to learn why taste is affected and to start on how to reverse or repair the loss, said Mackenzie Hannum, PhD, an author of the report and a postdoctoral fellow in the lab of Danielle Reed, PhD.
Researchers looked at data regarding 138,785 COVID patients from 241 studies that assessed taste loss and were published between May 15, 2020, and June 1, 2021. Of those patients, 32,918 said they had some form of taste loss. Further, female patients were more likely than males to lose their sense of taste, and people 36-50 years old had the highest rate of taste loss.
The information came from self-reports and direct reports.
“Self-reports are more subjective and can be in the form of questionnaires, interviews, health records, for example,” Dr. Hannum said. “On the other hand, direct measures of taste are more objective. They are conducted using testing kits that contain various sweet, salty, and sometimes bitter and sour solutions given to participants via drops, strips, or sprays.”
Though self-reports were subjective, they proved just as good as direct reports at detecting taste loss, the study said.
“Here self-reports are backed up by direct measures, proving that loss of taste is a real, distinct symptom of COVID-19 that is not to be confused with smell loss,” said study co-author Vicente Ramirez, a visiting scientist at Monell and a doctoral student at the University of California, Merced.
A version of this article first appeared on WebMD.com.
, according to a new study.
Many COVID-19 patients report losing their sense of taste as well as their sense of smell, but scientists have been skeptical because the two senses are closely related and it was relatively rare for people to lose their taste sense before the COVID pandemic, says the Monell Chemical Senses Center, a nonprofit research institute in Philadelphia.
But a new Monell Center analysis found that 37% – or about four in every 10 -- of COVID-19 patients actually did lose their sense of taste and that “reports of taste loss are in fact genuine and distinguishable from smell loss.”
Taste dysfunction can be total taste loss, partial taste loss, and taste distortion. It’s an “underrated” symptom that could help doctors better treat COVID patients, the Monell Center said in a news release.
“It is time to turn to the tongue” to learn why taste is affected and to start on how to reverse or repair the loss, said Mackenzie Hannum, PhD, an author of the report and a postdoctoral fellow in the lab of Danielle Reed, PhD.
Researchers looked at data regarding 138,785 COVID patients from 241 studies that assessed taste loss and were published between May 15, 2020, and June 1, 2021. Of those patients, 32,918 said they had some form of taste loss. Further, female patients were more likely than males to lose their sense of taste, and people 36-50 years old had the highest rate of taste loss.
The information came from self-reports and direct reports.
“Self-reports are more subjective and can be in the form of questionnaires, interviews, health records, for example,” Dr. Hannum said. “On the other hand, direct measures of taste are more objective. They are conducted using testing kits that contain various sweet, salty, and sometimes bitter and sour solutions given to participants via drops, strips, or sprays.”
Though self-reports were subjective, they proved just as good as direct reports at detecting taste loss, the study said.
“Here self-reports are backed up by direct measures, proving that loss of taste is a real, distinct symptom of COVID-19 that is not to be confused with smell loss,” said study co-author Vicente Ramirez, a visiting scientist at Monell and a doctoral student at the University of California, Merced.
A version of this article first appeared on WebMD.com.
, according to a new study.
Many COVID-19 patients report losing their sense of taste as well as their sense of smell, but scientists have been skeptical because the two senses are closely related and it was relatively rare for people to lose their taste sense before the COVID pandemic, says the Monell Chemical Senses Center, a nonprofit research institute in Philadelphia.
But a new Monell Center analysis found that 37% – or about four in every 10 -- of COVID-19 patients actually did lose their sense of taste and that “reports of taste loss are in fact genuine and distinguishable from smell loss.”
Taste dysfunction can be total taste loss, partial taste loss, and taste distortion. It’s an “underrated” symptom that could help doctors better treat COVID patients, the Monell Center said in a news release.
“It is time to turn to the tongue” to learn why taste is affected and to start on how to reverse or repair the loss, said Mackenzie Hannum, PhD, an author of the report and a postdoctoral fellow in the lab of Danielle Reed, PhD.
Researchers looked at data regarding 138,785 COVID patients from 241 studies that assessed taste loss and were published between May 15, 2020, and June 1, 2021. Of those patients, 32,918 said they had some form of taste loss. Further, female patients were more likely than males to lose their sense of taste, and people 36-50 years old had the highest rate of taste loss.
The information came from self-reports and direct reports.
“Self-reports are more subjective and can be in the form of questionnaires, interviews, health records, for example,” Dr. Hannum said. “On the other hand, direct measures of taste are more objective. They are conducted using testing kits that contain various sweet, salty, and sometimes bitter and sour solutions given to participants via drops, strips, or sprays.”
Though self-reports were subjective, they proved just as good as direct reports at detecting taste loss, the study said.
“Here self-reports are backed up by direct measures, proving that loss of taste is a real, distinct symptom of COVID-19 that is not to be confused with smell loss,” said study co-author Vicente Ramirez, a visiting scientist at Monell and a doctoral student at the University of California, Merced.
A version of this article first appeared on WebMD.com.
FROM CHEMICAL SENSES
Babies better protected from COVID if mother vaccinated during pregnancy: study
In a first of its kind study, researchers found women who received two mRNA COVID vaccine doses during pregnancy were 61% less likely to have a baby hospitalized for COVID-19 during the first 6 months of life.
In addition, two doses of the Pfizer/BioNTech or Moderna COVID vaccine later in a pregnancy were linked to an even higher level of protection, 80%, compared with 32% when given before 20 weeks’ gestation.
This finding suggests a greater transfer of maternal antibodies closer to birth, but more research is needed, cautioned senior study author Manish Patel, MD, during a Tuesday media telebriefing held by the Centers for Disease Control and Prevention.
Unanswered questions include how the babies got infected or if there is any protection afforded to babies for women vaccinated before pregnancy.
“We cannot be sure about the source of the infection,” said Dr. Patel, a medical epidemiologist with the CDC COVID-19 Emergency Response Team.
Dana Meaney-Delman, MD, MPH, agreed, but added that “perinatal transmission of the virus is very rare” with SARS-CoV-2. She is a practicing obstetrician and gynecologist and chief of the CDC Infant Outcomes Monitoring Research and Prevention Branch.
The study numbers were too small to show if a booster shot during pregnancy or breastfeeding could provide even greater protection for babies, Dr. Patel said.
The early release study was published online Feb. 15 in the CDC’s Morbidity and Mortality Weekly Report (MMWR).
Many previous studies looking at COVID-19 immunization during pregnancy focused on maternal health and “have clearly shown that receiving an mRNA COVID-19 vaccine during pregnancy reduces the risk for severe illness,” Dr. Meaney-Delman said.
Some dual protection suggested
Now there is evidence for a potential benefit to babies as well when a pregnant woman gets vaccinated. The study “provides real-world evidence that getting COVID-19 vaccination during pregnancy might help protect infants less than 6 months [of age],” Dr. Meaney-Delman said.
“These findings continue to emphasize the importance of COVID-19 vaccination during pregnancy to protect people who are pregnant and also to protect their babies,” she said.
Dr. Patel and colleagues studied 379 infants younger than 6 months hospitalized between July 1, 2021 and Jan. 17 of this year. Delta and then the Omicron variant predominated during this time.
The infants were admitted to one of 20 children’s hospitals in 17 states. The researchers compared 176 infants admitted with a positive COVID-19 PCR test to another 203 infants with a negative PCR test who served as controls.
Half as many mothers of infants admitted with COVID-19 were vaccinated during pregnancy, 16%, versus 32% of mothers of the control infants.
Vaccination with two doses of mRNA vaccine during pregnancy was 61% effective (95% confidence interval, 31%-78%) at preventing hospitalization among these infants. Because the study was epidemiological, the lower risk was an association, not a cause-and-effect finding, Dr. Patel said.
Babies admitted to the hospital positive for COVID-19 were more likely to be non-Hispanic Black, 18%, versus 9% of control group babies; and more likely to be Hispanic, 34% versus 28%, respectively.
A total 24% of infants with COVID-19 were admitted to the ICU, including the baby of an unvaccinated mother who required extracorporeal membrane oxygenation (ECMO). Another baby of an unvaccinated mother was the only infant death during the study.
Maternal vaccination trends
A reporter pointed out that COVID-19 vaccination rates tend to be low among pregnant women. “So there is some exciting news,” Dr. Meaney-Delman said, referring to a steady increase in the percentages of pregnant women in the U.S. choosing to get vaccinated, according to the CDC Data Tracker website.
“The numbers are encouraging, [but] they’re not quite where we need them to be, and they do differ by race and ethnicity,” she added.
A version of this article first appeared on Medscape.com.
In a first of its kind study, researchers found women who received two mRNA COVID vaccine doses during pregnancy were 61% less likely to have a baby hospitalized for COVID-19 during the first 6 months of life.
In addition, two doses of the Pfizer/BioNTech or Moderna COVID vaccine later in a pregnancy were linked to an even higher level of protection, 80%, compared with 32% when given before 20 weeks’ gestation.
This finding suggests a greater transfer of maternal antibodies closer to birth, but more research is needed, cautioned senior study author Manish Patel, MD, during a Tuesday media telebriefing held by the Centers for Disease Control and Prevention.
Unanswered questions include how the babies got infected or if there is any protection afforded to babies for women vaccinated before pregnancy.
“We cannot be sure about the source of the infection,” said Dr. Patel, a medical epidemiologist with the CDC COVID-19 Emergency Response Team.
Dana Meaney-Delman, MD, MPH, agreed, but added that “perinatal transmission of the virus is very rare” with SARS-CoV-2. She is a practicing obstetrician and gynecologist and chief of the CDC Infant Outcomes Monitoring Research and Prevention Branch.
The study numbers were too small to show if a booster shot during pregnancy or breastfeeding could provide even greater protection for babies, Dr. Patel said.
The early release study was published online Feb. 15 in the CDC’s Morbidity and Mortality Weekly Report (MMWR).
Many previous studies looking at COVID-19 immunization during pregnancy focused on maternal health and “have clearly shown that receiving an mRNA COVID-19 vaccine during pregnancy reduces the risk for severe illness,” Dr. Meaney-Delman said.
Some dual protection suggested
Now there is evidence for a potential benefit to babies as well when a pregnant woman gets vaccinated. The study “provides real-world evidence that getting COVID-19 vaccination during pregnancy might help protect infants less than 6 months [of age],” Dr. Meaney-Delman said.
“These findings continue to emphasize the importance of COVID-19 vaccination during pregnancy to protect people who are pregnant and also to protect their babies,” she said.
Dr. Patel and colleagues studied 379 infants younger than 6 months hospitalized between July 1, 2021 and Jan. 17 of this year. Delta and then the Omicron variant predominated during this time.
The infants were admitted to one of 20 children’s hospitals in 17 states. The researchers compared 176 infants admitted with a positive COVID-19 PCR test to another 203 infants with a negative PCR test who served as controls.
Half as many mothers of infants admitted with COVID-19 were vaccinated during pregnancy, 16%, versus 32% of mothers of the control infants.
Vaccination with two doses of mRNA vaccine during pregnancy was 61% effective (95% confidence interval, 31%-78%) at preventing hospitalization among these infants. Because the study was epidemiological, the lower risk was an association, not a cause-and-effect finding, Dr. Patel said.
Babies admitted to the hospital positive for COVID-19 were more likely to be non-Hispanic Black, 18%, versus 9% of control group babies; and more likely to be Hispanic, 34% versus 28%, respectively.
A total 24% of infants with COVID-19 were admitted to the ICU, including the baby of an unvaccinated mother who required extracorporeal membrane oxygenation (ECMO). Another baby of an unvaccinated mother was the only infant death during the study.
Maternal vaccination trends
A reporter pointed out that COVID-19 vaccination rates tend to be low among pregnant women. “So there is some exciting news,” Dr. Meaney-Delman said, referring to a steady increase in the percentages of pregnant women in the U.S. choosing to get vaccinated, according to the CDC Data Tracker website.
“The numbers are encouraging, [but] they’re not quite where we need them to be, and they do differ by race and ethnicity,” she added.
A version of this article first appeared on Medscape.com.
In a first of its kind study, researchers found women who received two mRNA COVID vaccine doses during pregnancy were 61% less likely to have a baby hospitalized for COVID-19 during the first 6 months of life.
In addition, two doses of the Pfizer/BioNTech or Moderna COVID vaccine later in a pregnancy were linked to an even higher level of protection, 80%, compared with 32% when given before 20 weeks’ gestation.
This finding suggests a greater transfer of maternal antibodies closer to birth, but more research is needed, cautioned senior study author Manish Patel, MD, during a Tuesday media telebriefing held by the Centers for Disease Control and Prevention.
Unanswered questions include how the babies got infected or if there is any protection afforded to babies for women vaccinated before pregnancy.
“We cannot be sure about the source of the infection,” said Dr. Patel, a medical epidemiologist with the CDC COVID-19 Emergency Response Team.
Dana Meaney-Delman, MD, MPH, agreed, but added that “perinatal transmission of the virus is very rare” with SARS-CoV-2. She is a practicing obstetrician and gynecologist and chief of the CDC Infant Outcomes Monitoring Research and Prevention Branch.
The study numbers were too small to show if a booster shot during pregnancy or breastfeeding could provide even greater protection for babies, Dr. Patel said.
The early release study was published online Feb. 15 in the CDC’s Morbidity and Mortality Weekly Report (MMWR).
Many previous studies looking at COVID-19 immunization during pregnancy focused on maternal health and “have clearly shown that receiving an mRNA COVID-19 vaccine during pregnancy reduces the risk for severe illness,” Dr. Meaney-Delman said.
Some dual protection suggested
Now there is evidence for a potential benefit to babies as well when a pregnant woman gets vaccinated. The study “provides real-world evidence that getting COVID-19 vaccination during pregnancy might help protect infants less than 6 months [of age],” Dr. Meaney-Delman said.
“These findings continue to emphasize the importance of COVID-19 vaccination during pregnancy to protect people who are pregnant and also to protect their babies,” she said.
Dr. Patel and colleagues studied 379 infants younger than 6 months hospitalized between July 1, 2021 and Jan. 17 of this year. Delta and then the Omicron variant predominated during this time.
The infants were admitted to one of 20 children’s hospitals in 17 states. The researchers compared 176 infants admitted with a positive COVID-19 PCR test to another 203 infants with a negative PCR test who served as controls.
Half as many mothers of infants admitted with COVID-19 were vaccinated during pregnancy, 16%, versus 32% of mothers of the control infants.
Vaccination with two doses of mRNA vaccine during pregnancy was 61% effective (95% confidence interval, 31%-78%) at preventing hospitalization among these infants. Because the study was epidemiological, the lower risk was an association, not a cause-and-effect finding, Dr. Patel said.
Babies admitted to the hospital positive for COVID-19 were more likely to be non-Hispanic Black, 18%, versus 9% of control group babies; and more likely to be Hispanic, 34% versus 28%, respectively.
A total 24% of infants with COVID-19 were admitted to the ICU, including the baby of an unvaccinated mother who required extracorporeal membrane oxygenation (ECMO). Another baby of an unvaccinated mother was the only infant death during the study.
Maternal vaccination trends
A reporter pointed out that COVID-19 vaccination rates tend to be low among pregnant women. “So there is some exciting news,” Dr. Meaney-Delman said, referring to a steady increase in the percentages of pregnant women in the U.S. choosing to get vaccinated, according to the CDC Data Tracker website.
“The numbers are encouraging, [but] they’re not quite where we need them to be, and they do differ by race and ethnicity,” she added.
A version of this article first appeared on Medscape.com.
CDC preparing to update mask guidance
, CDC Director Rochelle P. Walensky, MD, said on Feb. 16.
“As we consider future metrics, which will be updated soon, we recognize the importance of not just cases … but critically, medically severe disease that leads to hospitalizations,” Dr. Walensky said at a White House news briefing. “We must consider hospital capacity as an additional important barometer.”![]()
She later added, “We are looking at an overview of much of our guidance, and masking in all settings will be a part of that.”
Coronavirus cases continue to drop nationwide. This week’s 7-day daily average of cases is 147,000, a decrease of 40%. Hospitalizations have dropped 28% to 9,500, and daily deaths are 2,200, a decrease of 9%.
“Omicron cases are declining, and we are all cautiously optimistic about the trajectory we’re on,” Dr. Walensky said. “Things are moving in the right direction, but we want to remain vigilant to do all we can so this trajectory continues.”
Dr. Walensky said public masking remains especially important if someone is symptomatic or not feeling well, or if there has been a COVID-19 exposure. Those who are within 10 days of being diagnosed with the virus should also remain masked in public.
“We all share the same goal: to get to a point where COVID-19 is no longer disrupting our daily lives. A time when it won’t be a constant crisis,” Dr. Walensky said. “Moving from this pandemic will be a process led by science and epidemiological trends, and one that relies on the powerful tools we already have.”
A version of this article first appeared on WebMD.com.
, CDC Director Rochelle P. Walensky, MD, said on Feb. 16.
“As we consider future metrics, which will be updated soon, we recognize the importance of not just cases … but critically, medically severe disease that leads to hospitalizations,” Dr. Walensky said at a White House news briefing. “We must consider hospital capacity as an additional important barometer.”![]()
She later added, “We are looking at an overview of much of our guidance, and masking in all settings will be a part of that.”
Coronavirus cases continue to drop nationwide. This week’s 7-day daily average of cases is 147,000, a decrease of 40%. Hospitalizations have dropped 28% to 9,500, and daily deaths are 2,200, a decrease of 9%.
“Omicron cases are declining, and we are all cautiously optimistic about the trajectory we’re on,” Dr. Walensky said. “Things are moving in the right direction, but we want to remain vigilant to do all we can so this trajectory continues.”
Dr. Walensky said public masking remains especially important if someone is symptomatic or not feeling well, or if there has been a COVID-19 exposure. Those who are within 10 days of being diagnosed with the virus should also remain masked in public.
“We all share the same goal: to get to a point where COVID-19 is no longer disrupting our daily lives. A time when it won’t be a constant crisis,” Dr. Walensky said. “Moving from this pandemic will be a process led by science and epidemiological trends, and one that relies on the powerful tools we already have.”
A version of this article first appeared on WebMD.com.
, CDC Director Rochelle P. Walensky, MD, said on Feb. 16.
“As we consider future metrics, which will be updated soon, we recognize the importance of not just cases … but critically, medically severe disease that leads to hospitalizations,” Dr. Walensky said at a White House news briefing. “We must consider hospital capacity as an additional important barometer.”![]()
She later added, “We are looking at an overview of much of our guidance, and masking in all settings will be a part of that.”
Coronavirus cases continue to drop nationwide. This week’s 7-day daily average of cases is 147,000, a decrease of 40%. Hospitalizations have dropped 28% to 9,500, and daily deaths are 2,200, a decrease of 9%.
“Omicron cases are declining, and we are all cautiously optimistic about the trajectory we’re on,” Dr. Walensky said. “Things are moving in the right direction, but we want to remain vigilant to do all we can so this trajectory continues.”
Dr. Walensky said public masking remains especially important if someone is symptomatic or not feeling well, or if there has been a COVID-19 exposure. Those who are within 10 days of being diagnosed with the virus should also remain masked in public.
“We all share the same goal: to get to a point where COVID-19 is no longer disrupting our daily lives. A time when it won’t be a constant crisis,” Dr. Walensky said. “Moving from this pandemic will be a process led by science and epidemiological trends, and one that relies on the powerful tools we already have.”
A version of this article first appeared on WebMD.com.
Stroke risk is highest right after COVID infection
, new research shows.
The study among Medicare beneficiaries with COVID-19 also showed that stroke risk is higher for relatively young older adults, those aged 65 to 74 years, and those without a history of stroke.
The study highlights the impact COVID-19 has on the cardiovascular system, said study author Quanhe Yang, PhD, senior scientist, Division for Heart Disease and Stroke Prevention, Centers for Disease Control and Prevention, Atlanta.
“Clinicians and patients should understand that stroke might be one of the very important clinical consequences of COVID-19.”
The study was presented during the hybrid International Stroke Conference held in New Orleans and online. The meeting was presented by the American Stroke Association, a division of the American Heart Association.
Stroke is the fifth leading cause of death in the U.S. As an increasing number of people become infected with COVID-19, “it’s important to determine if there’s a relationship between COVID and the risk of stroke,” said Dr. Yang.
Findings from prior research examining the link between stroke and COVID-19 have been inconsistent, he noted. Some studies found an association while others did not, and in still others, the association was not as strong as expected.
Many factors may contribute to these inconsistent findings, said Dr. Yang, including differences in study design, inclusion criteria, comparison groups, sample sizes, and countries where the research was carried out. Dr. Yang pointed out that many of these studies were done in the early stages of the pandemic or didn’t include older adults, the population most at risk for stroke.
The current study included 19,553 Medicare beneficiaries aged 65 years and older diagnosed with COVID-19 and hospitalized with acute ischemic stroke. The median age at diagnosis of COVID-19 was 80.5 years, 57.5% were women, and more than 75% were non-Hispanic Whites.
To ensure the stroke occurred after a COVID infection, researchers used a self-controlled case series study design, a “within person” comparison between the risk period and the control period.
They divided the study period (Jan. 1, 2019 to Feb. 28, 2021) into the exposure or stroke risk periods after the COVID diagnosis (0-3 days; 4-7 days; 8-15 days; and 15-28 days) and control periods.
Strokes that occurred 7 days before or 28 days after a COVID diagnosis served as a control period. “Any stroke that occurred outside the risk window is in the control period,” explained Dr. Yang.
He added that the control period provides a baseline. “Without COVID-19, this is what I would expect” in terms of the number of strokes.
To estimate the incidence rate ratio (IRR), investigators compared the incidence of acute ischemic stroke in the various risk periods with control periods.
The IRR was 10.97 (95% confidence interval, 10.30-11.68) at 0-3 days. The risk then quickly declined but stayed higher than the control period. The IRRs were: 1.59 (95% CI, 1.35-1.87) at 4-7 days; 1.23 (95% CI, 1.07-1.41) at 8-14 days; and 1.06 (95% CI, 0.95-1.18) at 15-28 days.
The temporary increase in stroke risk early after an infection isn’t novel; the pattern has been observed with influenza, respiratory infections, and shingles, said Dr. Yang. “But COVID-19 appears to be particularly risky.”
Although the mechanism driving the early increased stroke risk isn’t fully understood, it’s likely tied to an “exaggerated inflammatory response,” said Dr. Yang. This can trigger the cascade of events setting the stage for a stroke – a hypercoagulation state leading to the formation of blood clots that then block arteries to the brain, he said.
It’s also possible the infection directly affects endothelial cells, leading to rupture of plaque, again blocking arteries and raising stroke risks, added Dr. Yang.
The association was stronger among younger beneficiaries, aged 65 to 74 years, compared with those 85 years and older, a finding Dr. Yang said was somewhat surprising. But he noted other studies have found stroke patients with COVID are younger than stroke patients without COVID – by some 5 to 6 years.
“If COVID-19 disproportionately affects younger patients, that may explain the stronger association,” said Dr. Yang. “Stroke risk increases tremendously with age, so if you’re a younger age, your baseline stroke risk is lower.”
The association was also stronger among beneficiaries without a history of stroke. Again, this could be related to the stronger association among younger patients who are less likely to have suffered a stroke. The association was largely consistent across sex and race/ethnicities.
Dr. Yang stressed that the findings need to be confirmed with further studies.
The study was carried out before widespread use of vaccinations in the U.S. Once those data are available, Dr. Yang and his colleagues plan to determine if vaccinations modify the association between COVID-19 and stroke risk.
The new results contribute to the mounting evidence that a COVID-19 infection “can actually affect multiple human organs structurally or functionally in addition to the impact on [the] respiratory system,” said Dr. Yang.
Some dates of COVID-19 diagnoses may be incorrect due to limited test availability, particularly early in the pandemic. Another limitation of the study was possible misclassification from the use of Medicare real-time preliminary claims.
In a provided statement, Louise D. McCullough, MD, PhD, chair of the ISC 2022 and professor and chair of neurology, McGovern Medical School, University of Texas Health Science Center at Houston, noted that the study focused on older adults because it was examining Medicare beneficiaries.
“But everyone is likely at risk for stroke after COVID,” she said. “Any infection is linked to stroke risk, probably because any infection will cause inflammation, and inflammation can cause clots or thrombus, which is the cause of stroke.”
There was no outside funding for the study. No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
, new research shows.
The study among Medicare beneficiaries with COVID-19 also showed that stroke risk is higher for relatively young older adults, those aged 65 to 74 years, and those without a history of stroke.
The study highlights the impact COVID-19 has on the cardiovascular system, said study author Quanhe Yang, PhD, senior scientist, Division for Heart Disease and Stroke Prevention, Centers for Disease Control and Prevention, Atlanta.
“Clinicians and patients should understand that stroke might be one of the very important clinical consequences of COVID-19.”
The study was presented during the hybrid International Stroke Conference held in New Orleans and online. The meeting was presented by the American Stroke Association, a division of the American Heart Association.
Stroke is the fifth leading cause of death in the U.S. As an increasing number of people become infected with COVID-19, “it’s important to determine if there’s a relationship between COVID and the risk of stroke,” said Dr. Yang.
Findings from prior research examining the link between stroke and COVID-19 have been inconsistent, he noted. Some studies found an association while others did not, and in still others, the association was not as strong as expected.
Many factors may contribute to these inconsistent findings, said Dr. Yang, including differences in study design, inclusion criteria, comparison groups, sample sizes, and countries where the research was carried out. Dr. Yang pointed out that many of these studies were done in the early stages of the pandemic or didn’t include older adults, the population most at risk for stroke.
The current study included 19,553 Medicare beneficiaries aged 65 years and older diagnosed with COVID-19 and hospitalized with acute ischemic stroke. The median age at diagnosis of COVID-19 was 80.5 years, 57.5% were women, and more than 75% were non-Hispanic Whites.
To ensure the stroke occurred after a COVID infection, researchers used a self-controlled case series study design, a “within person” comparison between the risk period and the control period.
They divided the study period (Jan. 1, 2019 to Feb. 28, 2021) into the exposure or stroke risk periods after the COVID diagnosis (0-3 days; 4-7 days; 8-15 days; and 15-28 days) and control periods.
Strokes that occurred 7 days before or 28 days after a COVID diagnosis served as a control period. “Any stroke that occurred outside the risk window is in the control period,” explained Dr. Yang.
He added that the control period provides a baseline. “Without COVID-19, this is what I would expect” in terms of the number of strokes.
To estimate the incidence rate ratio (IRR), investigators compared the incidence of acute ischemic stroke in the various risk periods with control periods.
The IRR was 10.97 (95% confidence interval, 10.30-11.68) at 0-3 days. The risk then quickly declined but stayed higher than the control period. The IRRs were: 1.59 (95% CI, 1.35-1.87) at 4-7 days; 1.23 (95% CI, 1.07-1.41) at 8-14 days; and 1.06 (95% CI, 0.95-1.18) at 15-28 days.
The temporary increase in stroke risk early after an infection isn’t novel; the pattern has been observed with influenza, respiratory infections, and shingles, said Dr. Yang. “But COVID-19 appears to be particularly risky.”
Although the mechanism driving the early increased stroke risk isn’t fully understood, it’s likely tied to an “exaggerated inflammatory response,” said Dr. Yang. This can trigger the cascade of events setting the stage for a stroke – a hypercoagulation state leading to the formation of blood clots that then block arteries to the brain, he said.
It’s also possible the infection directly affects endothelial cells, leading to rupture of plaque, again blocking arteries and raising stroke risks, added Dr. Yang.
The association was stronger among younger beneficiaries, aged 65 to 74 years, compared with those 85 years and older, a finding Dr. Yang said was somewhat surprising. But he noted other studies have found stroke patients with COVID are younger than stroke patients without COVID – by some 5 to 6 years.
“If COVID-19 disproportionately affects younger patients, that may explain the stronger association,” said Dr. Yang. “Stroke risk increases tremendously with age, so if you’re a younger age, your baseline stroke risk is lower.”
The association was also stronger among beneficiaries without a history of stroke. Again, this could be related to the stronger association among younger patients who are less likely to have suffered a stroke. The association was largely consistent across sex and race/ethnicities.
Dr. Yang stressed that the findings need to be confirmed with further studies.
The study was carried out before widespread use of vaccinations in the U.S. Once those data are available, Dr. Yang and his colleagues plan to determine if vaccinations modify the association between COVID-19 and stroke risk.
The new results contribute to the mounting evidence that a COVID-19 infection “can actually affect multiple human organs structurally or functionally in addition to the impact on [the] respiratory system,” said Dr. Yang.
Some dates of COVID-19 diagnoses may be incorrect due to limited test availability, particularly early in the pandemic. Another limitation of the study was possible misclassification from the use of Medicare real-time preliminary claims.
In a provided statement, Louise D. McCullough, MD, PhD, chair of the ISC 2022 and professor and chair of neurology, McGovern Medical School, University of Texas Health Science Center at Houston, noted that the study focused on older adults because it was examining Medicare beneficiaries.
“But everyone is likely at risk for stroke after COVID,” she said. “Any infection is linked to stroke risk, probably because any infection will cause inflammation, and inflammation can cause clots or thrombus, which is the cause of stroke.”
There was no outside funding for the study. No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
, new research shows.
The study among Medicare beneficiaries with COVID-19 also showed that stroke risk is higher for relatively young older adults, those aged 65 to 74 years, and those without a history of stroke.
The study highlights the impact COVID-19 has on the cardiovascular system, said study author Quanhe Yang, PhD, senior scientist, Division for Heart Disease and Stroke Prevention, Centers for Disease Control and Prevention, Atlanta.
“Clinicians and patients should understand that stroke might be one of the very important clinical consequences of COVID-19.”
The study was presented during the hybrid International Stroke Conference held in New Orleans and online. The meeting was presented by the American Stroke Association, a division of the American Heart Association.
Stroke is the fifth leading cause of death in the U.S. As an increasing number of people become infected with COVID-19, “it’s important to determine if there’s a relationship between COVID and the risk of stroke,” said Dr. Yang.
Findings from prior research examining the link between stroke and COVID-19 have been inconsistent, he noted. Some studies found an association while others did not, and in still others, the association was not as strong as expected.
Many factors may contribute to these inconsistent findings, said Dr. Yang, including differences in study design, inclusion criteria, comparison groups, sample sizes, and countries where the research was carried out. Dr. Yang pointed out that many of these studies were done in the early stages of the pandemic or didn’t include older adults, the population most at risk for stroke.
The current study included 19,553 Medicare beneficiaries aged 65 years and older diagnosed with COVID-19 and hospitalized with acute ischemic stroke. The median age at diagnosis of COVID-19 was 80.5 years, 57.5% were women, and more than 75% were non-Hispanic Whites.
To ensure the stroke occurred after a COVID infection, researchers used a self-controlled case series study design, a “within person” comparison between the risk period and the control period.
They divided the study period (Jan. 1, 2019 to Feb. 28, 2021) into the exposure or stroke risk periods after the COVID diagnosis (0-3 days; 4-7 days; 8-15 days; and 15-28 days) and control periods.
Strokes that occurred 7 days before or 28 days after a COVID diagnosis served as a control period. “Any stroke that occurred outside the risk window is in the control period,” explained Dr. Yang.
He added that the control period provides a baseline. “Without COVID-19, this is what I would expect” in terms of the number of strokes.
To estimate the incidence rate ratio (IRR), investigators compared the incidence of acute ischemic stroke in the various risk periods with control periods.
The IRR was 10.97 (95% confidence interval, 10.30-11.68) at 0-3 days. The risk then quickly declined but stayed higher than the control period. The IRRs were: 1.59 (95% CI, 1.35-1.87) at 4-7 days; 1.23 (95% CI, 1.07-1.41) at 8-14 days; and 1.06 (95% CI, 0.95-1.18) at 15-28 days.
The temporary increase in stroke risk early after an infection isn’t novel; the pattern has been observed with influenza, respiratory infections, and shingles, said Dr. Yang. “But COVID-19 appears to be particularly risky.”
Although the mechanism driving the early increased stroke risk isn’t fully understood, it’s likely tied to an “exaggerated inflammatory response,” said Dr. Yang. This can trigger the cascade of events setting the stage for a stroke – a hypercoagulation state leading to the formation of blood clots that then block arteries to the brain, he said.
It’s also possible the infection directly affects endothelial cells, leading to rupture of plaque, again blocking arteries and raising stroke risks, added Dr. Yang.
The association was stronger among younger beneficiaries, aged 65 to 74 years, compared with those 85 years and older, a finding Dr. Yang said was somewhat surprising. But he noted other studies have found stroke patients with COVID are younger than stroke patients without COVID – by some 5 to 6 years.
“If COVID-19 disproportionately affects younger patients, that may explain the stronger association,” said Dr. Yang. “Stroke risk increases tremendously with age, so if you’re a younger age, your baseline stroke risk is lower.”
The association was also stronger among beneficiaries without a history of stroke. Again, this could be related to the stronger association among younger patients who are less likely to have suffered a stroke. The association was largely consistent across sex and race/ethnicities.
Dr. Yang stressed that the findings need to be confirmed with further studies.
The study was carried out before widespread use of vaccinations in the U.S. Once those data are available, Dr. Yang and his colleagues plan to determine if vaccinations modify the association between COVID-19 and stroke risk.
The new results contribute to the mounting evidence that a COVID-19 infection “can actually affect multiple human organs structurally or functionally in addition to the impact on [the] respiratory system,” said Dr. Yang.
Some dates of COVID-19 diagnoses may be incorrect due to limited test availability, particularly early in the pandemic. Another limitation of the study was possible misclassification from the use of Medicare real-time preliminary claims.
In a provided statement, Louise D. McCullough, MD, PhD, chair of the ISC 2022 and professor and chair of neurology, McGovern Medical School, University of Texas Health Science Center at Houston, noted that the study focused on older adults because it was examining Medicare beneficiaries.
“But everyone is likely at risk for stroke after COVID,” she said. “Any infection is linked to stroke risk, probably because any infection will cause inflammation, and inflammation can cause clots or thrombus, which is the cause of stroke.”
There was no outside funding for the study. No relevant conflicts of interest were disclosed.
A version of this article first appeared on Medscape.com.
FROM ISC 2022
Medical boards pressured to let it slide when doctors spread COVID misinformation
Tennessee’s Board of Medical Examiners unanimously adopted in September 2021 a statement that said doctors spreading COVID misinformation – such as suggesting that vaccines contain microchips – could jeopardize their license to practice.
“I’m very glad that we’re taking this step,” Dr. Stephen Loyd, MD, the panel’s vice president, said at the time. “If you’re spreading this willful misinformation, for me it’s going to be really hard to do anything other than put you on probation or take your license for a year. There has to be a message sent for this. It’s not okay.”
The board’s statement was posted on a government website.
The growing tension in Tennessee between conservative lawmakers and the state’s medical board may be the most prominent example in the country. But the Federation of State Medical Boards, which created the language adopted by at least 15 state boards, is tracking legislation introduced by Republicans in at least 14 states that would restrict a medical board’s authority to discipline doctors for their advice on COVID.
Humayun Chaudhry, DO, the federation’s CEO, called it “an unwelcome trend.” The nonprofit association, based in Euless, Tex., said the statement is merely a COVID-specific restatement of an existing rule: that doctors who engage in behavior that puts patients at risk could face disciplinary action.
Although doctors have leeway to decide which treatments to provide, the medical boards that oversee them have broad authority over licensing. Often, doctors are investigated for violating guidelines on prescribing high-powered drugs. But physicians are sometimes punished for other “unprofessional conduct.” In 2013, Tennessee’s board fined U.S. Rep. Scott DesJarlais for separately having sexual relations with two female patients more than a decade earlier.
Still, stopping doctors from sharing unsound medical advice has proved challenging. Even defining misinformation has been difficult. And during the pandemic, resistance from some state legislatures is complicating the effort.
A relatively small group of physicians peddle COVID misinformation, but many of them associate with America’s Frontline Doctors. Its founder, Simone Gold, MD, has claimed patients are dying from COVID treatments, not the virus itself. Sherri Tenpenny, DO, said in a legislative hearing in Ohio that the COVID vaccine could magnetize patients. Stella Immanuel, MD, has pushed hydroxychloroquine as a COVID cure in Texas, although clinical trials showed that it had no benefit. None of them agreed to requests for comment.
The Texas Medical Board fined Dr. Immanuel $500 for not informing a patient of the risks associated with using hydroxychloroquine as an off-label COVID treatment.
In Tennessee, state lawmakers called a special legislative session in October to address COVID restrictions, and Republican Gov. Bill Lee signed a sweeping package of bills that push back against pandemic rules. One included language directed at the medical board’s recent COVID policy statement, making it more difficult for the panel to investigate complaints about physicians’ advice on COVID vaccines or treatments.
In November, Republican state Rep. John Ragan sent the medical board a letter demanding that the statement be deleted from the state’s website. Rep. Ragan leads a legislative panel that had raised the prospect of defunding the state’s health department over its promotion of COVID vaccines to teens.
Among his demands, Rep. Ragan listed 20 questions he wanted the medical board to answer in writing, including why the misinformation “policy” was proposed nearly two years into the pandemic, which scholars would determine what constitutes misinformation, and how was the “policy” not an infringement on the doctor-patient relationship.
“If you fail to act promptly, your organization will be required to appear before the Joint Government Operations Committee to explain your inaction,” Rep. Ragan wrote in the letter, obtained by Kaiser Health News and Nashville Public Radio.
In response to a request for comment, Rep. Ragan said that “any executive agency, including Board of Medical Examiners, that refuses to follow the law is subject to dissolution.”
He set a deadline of Dec. 7.
In Florida, a Republican-sponsored bill making its way through the state legislature proposes to ban medical boards from revoking or threatening to revoke doctors’ licenses for what they say unless “direct physical harm” of a patient occurred. If the publicized complaint can’t be proved, the board could owe a doctor up to $1.5 million in damages.
Although Florida’s medical board has not adopted the Federation of State Medical Boards’ COVID misinformation statement, the panel has considered misinformation complaints against physicians, including the state’s surgeon general, Joseph Ladapo, MD, PhD.
Dr. Chaudhry said he’s surprised just how many COVID-related complaints are being filed across the country. Often, boards do not publicize investigations before a violation of ethics or standards is confirmed. But in response to a survey by the federation in late 2021, two-thirds of state boards reported an increase in misinformation complaints. And the federation said 12 boards had taken action against a licensed physician.
“At the end of the day, if a physician who is licensed engages in activity that causes harm, the state medical boards are the ones that historically have been set up to look into the situation and make a judgment about what happened or didn’t happen,” Dr. Chaudhry said. “And if you start to chip away at that, it becomes a slippery slope.”
The Georgia Composite Medical Board adopted a version of the federation’s misinformation guidance in early November and has been receiving 10-20 complaints each month, said Debi Dalton, MD, the chairperson. Two months in, no one had been sanctioned.
Dr. Dalton said that even putting out a misinformation policy leaves some “gray” area. Generally, physicians are expected to follow the “consensus,” rather than “the newest information that pops up on social media,” she said.
“We expect physicians to think ethically, professionally, and with the safety of patients in mind,” Dr. Dalton said.
A few physician groups are resisting attempts to root out misinformation, including the Association of American Physicians and Surgeons, known for its stands against government regulation.
Some medical boards have opted against taking a public stand against misinformation.
The Alabama Board of Medical Examiners discussed signing on to the federation’s statement, according to the minutes from an October meeting. But after debating the potential legal ramifications in a private executive session, the board opted not to act.
In Tennessee, the Board of Medical Examiners met on the day Rep. Ragan had set as the deadline and voted to remove the misinformation statement from its website to avoid being called into a legislative hearing. But then, in late January, the board decided to stick with the policy – although it did not republish the statement online immediately – and more specifically defined misinformation, calling it “content that is false, inaccurate or misleading, even if spread unintentionally.”
Board members acknowledged they would likely get more pushback from lawmakers but said they wanted to protect their profession from interference.
“Doctors who are putting forth good evidence-based medicine deserve the protection of this board so they can actually say: ‘Hey, I’m in line with this guideline, and this is a source of truth,’” said Melanie Blake, MD, the board’s president. “We should be a source of truth.”
The medical board was looking into nearly 30 open complaints related to COVID when its misinformation statement came down from its website. As of early February, no Tennessee physician had faced disciplinary action.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. This story is part of a partnership that includes Nashville Public Radio, NPR, and KHN.
Tennessee’s Board of Medical Examiners unanimously adopted in September 2021 a statement that said doctors spreading COVID misinformation – such as suggesting that vaccines contain microchips – could jeopardize their license to practice.
“I’m very glad that we’re taking this step,” Dr. Stephen Loyd, MD, the panel’s vice president, said at the time. “If you’re spreading this willful misinformation, for me it’s going to be really hard to do anything other than put you on probation or take your license for a year. There has to be a message sent for this. It’s not okay.”
The board’s statement was posted on a government website.
The growing tension in Tennessee between conservative lawmakers and the state’s medical board may be the most prominent example in the country. But the Federation of State Medical Boards, which created the language adopted by at least 15 state boards, is tracking legislation introduced by Republicans in at least 14 states that would restrict a medical board’s authority to discipline doctors for their advice on COVID.
Humayun Chaudhry, DO, the federation’s CEO, called it “an unwelcome trend.” The nonprofit association, based in Euless, Tex., said the statement is merely a COVID-specific restatement of an existing rule: that doctors who engage in behavior that puts patients at risk could face disciplinary action.
Although doctors have leeway to decide which treatments to provide, the medical boards that oversee them have broad authority over licensing. Often, doctors are investigated for violating guidelines on prescribing high-powered drugs. But physicians are sometimes punished for other “unprofessional conduct.” In 2013, Tennessee’s board fined U.S. Rep. Scott DesJarlais for separately having sexual relations with two female patients more than a decade earlier.
Still, stopping doctors from sharing unsound medical advice has proved challenging. Even defining misinformation has been difficult. And during the pandemic, resistance from some state legislatures is complicating the effort.
A relatively small group of physicians peddle COVID misinformation, but many of them associate with America’s Frontline Doctors. Its founder, Simone Gold, MD, has claimed patients are dying from COVID treatments, not the virus itself. Sherri Tenpenny, DO, said in a legislative hearing in Ohio that the COVID vaccine could magnetize patients. Stella Immanuel, MD, has pushed hydroxychloroquine as a COVID cure in Texas, although clinical trials showed that it had no benefit. None of them agreed to requests for comment.
The Texas Medical Board fined Dr. Immanuel $500 for not informing a patient of the risks associated with using hydroxychloroquine as an off-label COVID treatment.
In Tennessee, state lawmakers called a special legislative session in October to address COVID restrictions, and Republican Gov. Bill Lee signed a sweeping package of bills that push back against pandemic rules. One included language directed at the medical board’s recent COVID policy statement, making it more difficult for the panel to investigate complaints about physicians’ advice on COVID vaccines or treatments.
In November, Republican state Rep. John Ragan sent the medical board a letter demanding that the statement be deleted from the state’s website. Rep. Ragan leads a legislative panel that had raised the prospect of defunding the state’s health department over its promotion of COVID vaccines to teens.
Among his demands, Rep. Ragan listed 20 questions he wanted the medical board to answer in writing, including why the misinformation “policy” was proposed nearly two years into the pandemic, which scholars would determine what constitutes misinformation, and how was the “policy” not an infringement on the doctor-patient relationship.
“If you fail to act promptly, your organization will be required to appear before the Joint Government Operations Committee to explain your inaction,” Rep. Ragan wrote in the letter, obtained by Kaiser Health News and Nashville Public Radio.
In response to a request for comment, Rep. Ragan said that “any executive agency, including Board of Medical Examiners, that refuses to follow the law is subject to dissolution.”
He set a deadline of Dec. 7.
In Florida, a Republican-sponsored bill making its way through the state legislature proposes to ban medical boards from revoking or threatening to revoke doctors’ licenses for what they say unless “direct physical harm” of a patient occurred. If the publicized complaint can’t be proved, the board could owe a doctor up to $1.5 million in damages.
Although Florida’s medical board has not adopted the Federation of State Medical Boards’ COVID misinformation statement, the panel has considered misinformation complaints against physicians, including the state’s surgeon general, Joseph Ladapo, MD, PhD.
Dr. Chaudhry said he’s surprised just how many COVID-related complaints are being filed across the country. Often, boards do not publicize investigations before a violation of ethics or standards is confirmed. But in response to a survey by the federation in late 2021, two-thirds of state boards reported an increase in misinformation complaints. And the federation said 12 boards had taken action against a licensed physician.
“At the end of the day, if a physician who is licensed engages in activity that causes harm, the state medical boards are the ones that historically have been set up to look into the situation and make a judgment about what happened or didn’t happen,” Dr. Chaudhry said. “And if you start to chip away at that, it becomes a slippery slope.”
The Georgia Composite Medical Board adopted a version of the federation’s misinformation guidance in early November and has been receiving 10-20 complaints each month, said Debi Dalton, MD, the chairperson. Two months in, no one had been sanctioned.
Dr. Dalton said that even putting out a misinformation policy leaves some “gray” area. Generally, physicians are expected to follow the “consensus,” rather than “the newest information that pops up on social media,” she said.
“We expect physicians to think ethically, professionally, and with the safety of patients in mind,” Dr. Dalton said.
A few physician groups are resisting attempts to root out misinformation, including the Association of American Physicians and Surgeons, known for its stands against government regulation.
Some medical boards have opted against taking a public stand against misinformation.
The Alabama Board of Medical Examiners discussed signing on to the federation’s statement, according to the minutes from an October meeting. But after debating the potential legal ramifications in a private executive session, the board opted not to act.
In Tennessee, the Board of Medical Examiners met on the day Rep. Ragan had set as the deadline and voted to remove the misinformation statement from its website to avoid being called into a legislative hearing. But then, in late January, the board decided to stick with the policy – although it did not republish the statement online immediately – and more specifically defined misinformation, calling it “content that is false, inaccurate or misleading, even if spread unintentionally.”
Board members acknowledged they would likely get more pushback from lawmakers but said they wanted to protect their profession from interference.
“Doctors who are putting forth good evidence-based medicine deserve the protection of this board so they can actually say: ‘Hey, I’m in line with this guideline, and this is a source of truth,’” said Melanie Blake, MD, the board’s president. “We should be a source of truth.”
The medical board was looking into nearly 30 open complaints related to COVID when its misinformation statement came down from its website. As of early February, no Tennessee physician had faced disciplinary action.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. This story is part of a partnership that includes Nashville Public Radio, NPR, and KHN.
Tennessee’s Board of Medical Examiners unanimously adopted in September 2021 a statement that said doctors spreading COVID misinformation – such as suggesting that vaccines contain microchips – could jeopardize their license to practice.
“I’m very glad that we’re taking this step,” Dr. Stephen Loyd, MD, the panel’s vice president, said at the time. “If you’re spreading this willful misinformation, for me it’s going to be really hard to do anything other than put you on probation or take your license for a year. There has to be a message sent for this. It’s not okay.”
The board’s statement was posted on a government website.
The growing tension in Tennessee between conservative lawmakers and the state’s medical board may be the most prominent example in the country. But the Federation of State Medical Boards, which created the language adopted by at least 15 state boards, is tracking legislation introduced by Republicans in at least 14 states that would restrict a medical board’s authority to discipline doctors for their advice on COVID.
Humayun Chaudhry, DO, the federation’s CEO, called it “an unwelcome trend.” The nonprofit association, based in Euless, Tex., said the statement is merely a COVID-specific restatement of an existing rule: that doctors who engage in behavior that puts patients at risk could face disciplinary action.
Although doctors have leeway to decide which treatments to provide, the medical boards that oversee them have broad authority over licensing. Often, doctors are investigated for violating guidelines on prescribing high-powered drugs. But physicians are sometimes punished for other “unprofessional conduct.” In 2013, Tennessee’s board fined U.S. Rep. Scott DesJarlais for separately having sexual relations with two female patients more than a decade earlier.
Still, stopping doctors from sharing unsound medical advice has proved challenging. Even defining misinformation has been difficult. And during the pandemic, resistance from some state legislatures is complicating the effort.
A relatively small group of physicians peddle COVID misinformation, but many of them associate with America’s Frontline Doctors. Its founder, Simone Gold, MD, has claimed patients are dying from COVID treatments, not the virus itself. Sherri Tenpenny, DO, said in a legislative hearing in Ohio that the COVID vaccine could magnetize patients. Stella Immanuel, MD, has pushed hydroxychloroquine as a COVID cure in Texas, although clinical trials showed that it had no benefit. None of them agreed to requests for comment.
The Texas Medical Board fined Dr. Immanuel $500 for not informing a patient of the risks associated with using hydroxychloroquine as an off-label COVID treatment.
In Tennessee, state lawmakers called a special legislative session in October to address COVID restrictions, and Republican Gov. Bill Lee signed a sweeping package of bills that push back against pandemic rules. One included language directed at the medical board’s recent COVID policy statement, making it more difficult for the panel to investigate complaints about physicians’ advice on COVID vaccines or treatments.
In November, Republican state Rep. John Ragan sent the medical board a letter demanding that the statement be deleted from the state’s website. Rep. Ragan leads a legislative panel that had raised the prospect of defunding the state’s health department over its promotion of COVID vaccines to teens.
Among his demands, Rep. Ragan listed 20 questions he wanted the medical board to answer in writing, including why the misinformation “policy” was proposed nearly two years into the pandemic, which scholars would determine what constitutes misinformation, and how was the “policy” not an infringement on the doctor-patient relationship.
“If you fail to act promptly, your organization will be required to appear before the Joint Government Operations Committee to explain your inaction,” Rep. Ragan wrote in the letter, obtained by Kaiser Health News and Nashville Public Radio.
In response to a request for comment, Rep. Ragan said that “any executive agency, including Board of Medical Examiners, that refuses to follow the law is subject to dissolution.”
He set a deadline of Dec. 7.
In Florida, a Republican-sponsored bill making its way through the state legislature proposes to ban medical boards from revoking or threatening to revoke doctors’ licenses for what they say unless “direct physical harm” of a patient occurred. If the publicized complaint can’t be proved, the board could owe a doctor up to $1.5 million in damages.
Although Florida’s medical board has not adopted the Federation of State Medical Boards’ COVID misinformation statement, the panel has considered misinformation complaints against physicians, including the state’s surgeon general, Joseph Ladapo, MD, PhD.
Dr. Chaudhry said he’s surprised just how many COVID-related complaints are being filed across the country. Often, boards do not publicize investigations before a violation of ethics or standards is confirmed. But in response to a survey by the federation in late 2021, two-thirds of state boards reported an increase in misinformation complaints. And the federation said 12 boards had taken action against a licensed physician.
“At the end of the day, if a physician who is licensed engages in activity that causes harm, the state medical boards are the ones that historically have been set up to look into the situation and make a judgment about what happened or didn’t happen,” Dr. Chaudhry said. “And if you start to chip away at that, it becomes a slippery slope.”
The Georgia Composite Medical Board adopted a version of the federation’s misinformation guidance in early November and has been receiving 10-20 complaints each month, said Debi Dalton, MD, the chairperson. Two months in, no one had been sanctioned.
Dr. Dalton said that even putting out a misinformation policy leaves some “gray” area. Generally, physicians are expected to follow the “consensus,” rather than “the newest information that pops up on social media,” she said.
“We expect physicians to think ethically, professionally, and with the safety of patients in mind,” Dr. Dalton said.
A few physician groups are resisting attempts to root out misinformation, including the Association of American Physicians and Surgeons, known for its stands against government regulation.
Some medical boards have opted against taking a public stand against misinformation.
The Alabama Board of Medical Examiners discussed signing on to the federation’s statement, according to the minutes from an October meeting. But after debating the potential legal ramifications in a private executive session, the board opted not to act.
In Tennessee, the Board of Medical Examiners met on the day Rep. Ragan had set as the deadline and voted to remove the misinformation statement from its website to avoid being called into a legislative hearing. But then, in late January, the board decided to stick with the policy – although it did not republish the statement online immediately – and more specifically defined misinformation, calling it “content that is false, inaccurate or misleading, even if spread unintentionally.”
Board members acknowledged they would likely get more pushback from lawmakers but said they wanted to protect their profession from interference.
“Doctors who are putting forth good evidence-based medicine deserve the protection of this board so they can actually say: ‘Hey, I’m in line with this guideline, and this is a source of truth,’” said Melanie Blake, MD, the board’s president. “We should be a source of truth.”
The medical board was looking into nearly 30 open complaints related to COVID when its misinformation statement came down from its website. As of early February, no Tennessee physician had faced disciplinary action.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation. This story is part of a partnership that includes Nashville Public Radio, NPR, and KHN.
New study shows natural immunity to COVID has enduring strength
It’s a matter of quality, not quantity. That’s the gist of a new Israeli study that shows that unvaccinated people with a prior SARS-CoV-2 infection create antibodies that are more effective in the long run compared with others who were vaccinated but never infected.
“While the quantity of antibodies decreases with time in both COVID-19 recovered patients and vaccinated individuals, ” lead author Carmit Cohen, PhD, said in an interview.
This difference could explain why previously infected patients appear to be better protected against a new infection than those who have only been vaccinated, according to a news release attached to the research.
One key caveat: This research does not include people from the later part of the pandemic.
This means there is a catch in terms of timing, William Schaffner, MD, Vanderbilt University School of Medicine, Nashville, Tenn., said when asked to comment on the study: “The study involved only the early COVID strains – it has no information on either the Delta or Omicron variants. Thus, the results primarily are of scientific or historical interest but are not immediately relevant to the current situation.”
The findings come from an early release of a study to be presented at the European Congress of Clinical Microbiology & Infectious Diseases in April.
An unexpected finding of the study showed that obese people had better protection – a higher and more sustained immune response – compared with overweight and normal-weight individuals.
“The results in the obese group were indeed unexpected and need further research to confirm or dispute,” Dr. Schaffner said. “Obesity does predispose to more severe disease.”
A focus on earlier strains
Dr. Cohen – a senior research assistant in infectious disease prevention at the Sheba Medical Center in Ramat Gan, Israel – and her colleagues recruited participants between March 25, 2020 and Nov. 25, 2020 and completed analysis in April 2021. This means they assessed people with a history of infection from the original, the Alpha, and some Beta strains of SARS-CoV-2.
Dr. Cohen indicated that the next phase of their research will examine innate and acquired immune responses to the more recent Delta and Omicron variants.
The investigators analyzed the antibody-induced immune response up to 1 year in 130 COVID-19 recovered but unvaccinated individuals versus up to 8 months among 402 others matched by age and body mass index (BMI) and without previous infection who received two doses of the Pfizer vaccine.
The numbers of antibodies a month after vaccination were higher than those in the COVID-19 recovered patients. However, these numbers also declined more steeply in the vaccinated group, they note.
To assess the antibody performance, the investigators used the avidity index. This assay measures antibody function based on the strength of the interactions between the antibody and the viral antigen.
They found that the avidity index was higher in vaccinated individuals than in recovered patients initially but changes over time. At up to 6 months, the index did not significantly change in vaccinated individuals, whereas it gradually increased in recovered patients. This increase would potentially protect them from reinfection, the authors note.
These findings stand in stark contrast to an Oct. 29, 2021, Centers for Disease Control and Prevention study that found that COVID-19 vaccines provided five times the protection of natural immunity.
Those results, published in the organization’s Morbidity and Mortality Weekly Report, suggest that vaccination helps people mount a higher, stronger, and more consistent level of immunity against COVID-19 hospitalization than infection alone for at least 6 months.
Protection linked to obesity
Another finding that ran against the scientific grain was the data about obesity.
There was a higher and more persistent antibody performance among people with a BMI of 30 kg/m2.
This could relate to greater disease severity and/or a more pronounced initial response to infection among the obese group.
“Our hypothesis is that patients with obesity begin with a more pronounced response – reflected also by the disease manifestation – and the trend of decline is similar, therefore the kinetics of immune response remain higher throughout the study,” Dr. Cohen said.
“The results in the obese group were indeed unexpected and need further research to confirm or dispute,” said Dr. Schaffner, who is also the current medical director of the National Foundation for Infectious Diseases. “Obesity does predispose to more severe disease.”
Before the boosters
Along with using participants from only the earlier part of the pandemic, another limitation of the study was that the vaccinated group had only two doses of vaccine; boosters were not given during the time of the study, Dr. Schaffner said.
“Again, not the current situation.”
“That said, the strength and duration of natural immunity provided by the early variants was solid for up to a year, confirming previous reports,” he said.
A version of this article first appeared on Medscape.com.
It’s a matter of quality, not quantity. That’s the gist of a new Israeli study that shows that unvaccinated people with a prior SARS-CoV-2 infection create antibodies that are more effective in the long run compared with others who were vaccinated but never infected.
“While the quantity of antibodies decreases with time in both COVID-19 recovered patients and vaccinated individuals, ” lead author Carmit Cohen, PhD, said in an interview.
This difference could explain why previously infected patients appear to be better protected against a new infection than those who have only been vaccinated, according to a news release attached to the research.
One key caveat: This research does not include people from the later part of the pandemic.
This means there is a catch in terms of timing, William Schaffner, MD, Vanderbilt University School of Medicine, Nashville, Tenn., said when asked to comment on the study: “The study involved only the early COVID strains – it has no information on either the Delta or Omicron variants. Thus, the results primarily are of scientific or historical interest but are not immediately relevant to the current situation.”
The findings come from an early release of a study to be presented at the European Congress of Clinical Microbiology & Infectious Diseases in April.
An unexpected finding of the study showed that obese people had better protection – a higher and more sustained immune response – compared with overweight and normal-weight individuals.
“The results in the obese group were indeed unexpected and need further research to confirm or dispute,” Dr. Schaffner said. “Obesity does predispose to more severe disease.”
A focus on earlier strains
Dr. Cohen – a senior research assistant in infectious disease prevention at the Sheba Medical Center in Ramat Gan, Israel – and her colleagues recruited participants between March 25, 2020 and Nov. 25, 2020 and completed analysis in April 2021. This means they assessed people with a history of infection from the original, the Alpha, and some Beta strains of SARS-CoV-2.
Dr. Cohen indicated that the next phase of their research will examine innate and acquired immune responses to the more recent Delta and Omicron variants.
The investigators analyzed the antibody-induced immune response up to 1 year in 130 COVID-19 recovered but unvaccinated individuals versus up to 8 months among 402 others matched by age and body mass index (BMI) and without previous infection who received two doses of the Pfizer vaccine.
The numbers of antibodies a month after vaccination were higher than those in the COVID-19 recovered patients. However, these numbers also declined more steeply in the vaccinated group, they note.
To assess the antibody performance, the investigators used the avidity index. This assay measures antibody function based on the strength of the interactions between the antibody and the viral antigen.
They found that the avidity index was higher in vaccinated individuals than in recovered patients initially but changes over time. At up to 6 months, the index did not significantly change in vaccinated individuals, whereas it gradually increased in recovered patients. This increase would potentially protect them from reinfection, the authors note.
These findings stand in stark contrast to an Oct. 29, 2021, Centers for Disease Control and Prevention study that found that COVID-19 vaccines provided five times the protection of natural immunity.
Those results, published in the organization’s Morbidity and Mortality Weekly Report, suggest that vaccination helps people mount a higher, stronger, and more consistent level of immunity against COVID-19 hospitalization than infection alone for at least 6 months.
Protection linked to obesity
Another finding that ran against the scientific grain was the data about obesity.
There was a higher and more persistent antibody performance among people with a BMI of 30 kg/m2.
This could relate to greater disease severity and/or a more pronounced initial response to infection among the obese group.
“Our hypothesis is that patients with obesity begin with a more pronounced response – reflected also by the disease manifestation – and the trend of decline is similar, therefore the kinetics of immune response remain higher throughout the study,” Dr. Cohen said.
“The results in the obese group were indeed unexpected and need further research to confirm or dispute,” said Dr. Schaffner, who is also the current medical director of the National Foundation for Infectious Diseases. “Obesity does predispose to more severe disease.”
Before the boosters
Along with using participants from only the earlier part of the pandemic, another limitation of the study was that the vaccinated group had only two doses of vaccine; boosters were not given during the time of the study, Dr. Schaffner said.
“Again, not the current situation.”
“That said, the strength and duration of natural immunity provided by the early variants was solid for up to a year, confirming previous reports,” he said.
A version of this article first appeared on Medscape.com.
It’s a matter of quality, not quantity. That’s the gist of a new Israeli study that shows that unvaccinated people with a prior SARS-CoV-2 infection create antibodies that are more effective in the long run compared with others who were vaccinated but never infected.
“While the quantity of antibodies decreases with time in both COVID-19 recovered patients and vaccinated individuals, ” lead author Carmit Cohen, PhD, said in an interview.
This difference could explain why previously infected patients appear to be better protected against a new infection than those who have only been vaccinated, according to a news release attached to the research.
One key caveat: This research does not include people from the later part of the pandemic.
This means there is a catch in terms of timing, William Schaffner, MD, Vanderbilt University School of Medicine, Nashville, Tenn., said when asked to comment on the study: “The study involved only the early COVID strains – it has no information on either the Delta or Omicron variants. Thus, the results primarily are of scientific or historical interest but are not immediately relevant to the current situation.”
The findings come from an early release of a study to be presented at the European Congress of Clinical Microbiology & Infectious Diseases in April.
An unexpected finding of the study showed that obese people had better protection – a higher and more sustained immune response – compared with overweight and normal-weight individuals.
“The results in the obese group were indeed unexpected and need further research to confirm or dispute,” Dr. Schaffner said. “Obesity does predispose to more severe disease.”
A focus on earlier strains
Dr. Cohen – a senior research assistant in infectious disease prevention at the Sheba Medical Center in Ramat Gan, Israel – and her colleagues recruited participants between March 25, 2020 and Nov. 25, 2020 and completed analysis in April 2021. This means they assessed people with a history of infection from the original, the Alpha, and some Beta strains of SARS-CoV-2.
Dr. Cohen indicated that the next phase of their research will examine innate and acquired immune responses to the more recent Delta and Omicron variants.
The investigators analyzed the antibody-induced immune response up to 1 year in 130 COVID-19 recovered but unvaccinated individuals versus up to 8 months among 402 others matched by age and body mass index (BMI) and without previous infection who received two doses of the Pfizer vaccine.
The numbers of antibodies a month after vaccination were higher than those in the COVID-19 recovered patients. However, these numbers also declined more steeply in the vaccinated group, they note.
To assess the antibody performance, the investigators used the avidity index. This assay measures antibody function based on the strength of the interactions between the antibody and the viral antigen.
They found that the avidity index was higher in vaccinated individuals than in recovered patients initially but changes over time. At up to 6 months, the index did not significantly change in vaccinated individuals, whereas it gradually increased in recovered patients. This increase would potentially protect them from reinfection, the authors note.
These findings stand in stark contrast to an Oct. 29, 2021, Centers for Disease Control and Prevention study that found that COVID-19 vaccines provided five times the protection of natural immunity.
Those results, published in the organization’s Morbidity and Mortality Weekly Report, suggest that vaccination helps people mount a higher, stronger, and more consistent level of immunity against COVID-19 hospitalization than infection alone for at least 6 months.
Protection linked to obesity
Another finding that ran against the scientific grain was the data about obesity.
There was a higher and more persistent antibody performance among people with a BMI of 30 kg/m2.
This could relate to greater disease severity and/or a more pronounced initial response to infection among the obese group.
“Our hypothesis is that patients with obesity begin with a more pronounced response – reflected also by the disease manifestation – and the trend of decline is similar, therefore the kinetics of immune response remain higher throughout the study,” Dr. Cohen said.
“The results in the obese group were indeed unexpected and need further research to confirm or dispute,” said Dr. Schaffner, who is also the current medical director of the National Foundation for Infectious Diseases. “Obesity does predispose to more severe disease.”
Before the boosters
Along with using participants from only the earlier part of the pandemic, another limitation of the study was that the vaccinated group had only two doses of vaccine; boosters were not given during the time of the study, Dr. Schaffner said.
“Again, not the current situation.”
“That said, the strength and duration of natural immunity provided by the early variants was solid for up to a year, confirming previous reports,” he said.
A version of this article first appeared on Medscape.com.
Children and COVID: Weekly cases down by more than half
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.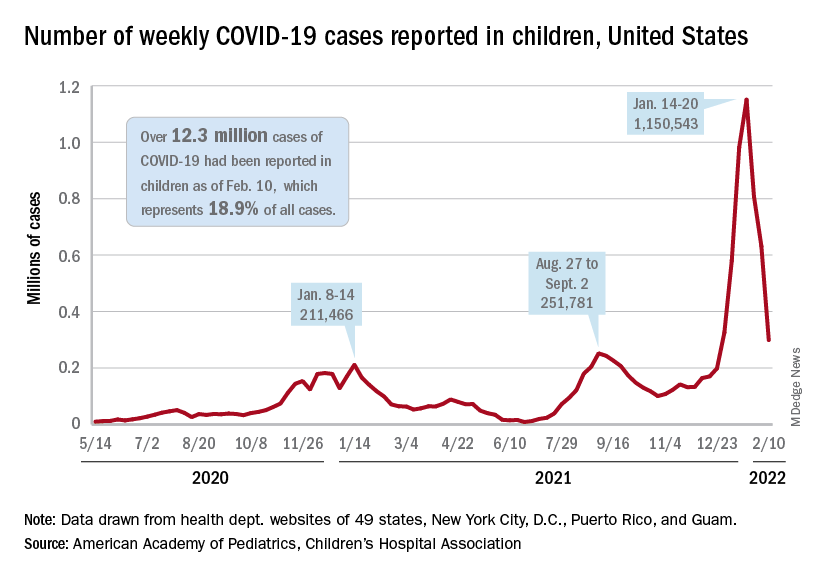
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
A third consecutive week of declines in new COVID-19 cases among children has brought the weekly count down by 74% since the Omicron surge peaked in mid-January, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
and by 74% from the peak of 1.15 million cases recorded for the week of Jan. 14-20, the AAP and CHA said in their weekly COVID report. They also noted that the weekly tally was still higher than anything seen during the Delta surge.
The total number of pediatric cases was over 12.3 million as of Feb. 10, with children representing 18.9% of cases in all ages, according to the AAP/CHA report. The Centers for Disease Control and Prevention puts the two measures at 10.4 million and 17.3% on its COVID Data Tracker, based on availability of age data for 59.6 million total cases as of Feb. 14. The CDC also reported that 1,282 children have died from COVID-19 so far, which is about 0.17% of all deaths with age data available.
The AAP and CHA have been collecting data from state and territorial health departments, which have not always been consistently available over the course of the pandemic. Also, the CDC defines children as those under age 18 years, but that upper boundary varies from 14 to 20 among the states.
The decline of the Omicron variant also can be seen in new admissions of children with confirmed COVID-19, which continued to drop. The 7-day average of 435 admissions per day for the week of Feb. 6-12 was less than half of the peak seen in mid-January, when it reached 914 per day. The daily admission rate on Feb. 12 was 0.60 per 100,000 children aged 0-17 years – again, less than half the peak rate of 1.25 reported on Jan. 16, CDC data show.
The fading threat of Omicron also seems to be reflected in recent vaccination trends. Both initial doses and completions declined for the fourth consecutive week (Feb. 3-9) among children aged 5-11 years, while initiations held steady for 12- to 17-year-olds but completions declined for the third straight week, the AAP said in its separate vaccination report, which is based on data from the CDC.
As of Feb. 14, almost 32% of children aged 5-11 – that’s almost 9.2 million individuals – had received at least one dose of the COVID-19 vaccine and just over 24% (6.9 million) were fully vaccinated, the CDC reported. For children aged 12-17, the corresponding figures are 67% (16.9 million) and 57% (14.4 million). Newly available data from the CDC also indicate that 19.5% (2.8 million) of children aged 12-17 have received a booster dose.
Long COVID symptoms linked to effects on vagus nerve
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.
Several long COVID symptoms could be linked to the effects of the coronavirus on a vital central nerve, according to new research being released in the spring.
The vagus nerve, which runs from the brain into the body, connects to the heart, lungs, intestines, and several muscles involved with swallowing. It plays a role in several body functions that control heart rate, speech, the gag reflex, sweating, and digestion.
Those with long COVID and vagus nerve problems could face long-term issues with their voice, a hard time swallowing, dizziness, a high heart rate, low blood pressure, and diarrhea, the study authors found.
Their findings will be presented at the 2022 European Congress of Clinical Microbiology and Infectious Diseases in late April.
“Most long COVID subjects with vagus nerve dysfunction symptoms had a range of significant, clinically relevant, structural and/or functional alterations in their vagus nerve, including nerve thickening, trouble swallowing, and symptoms of impaired breathing,” the study authors wrote. “Our findings so far thus point at vagus nerve dysfunction as a central pathophysiological feature of long COVID.”
Researchers from the University Hospital Germans Trias i Pujol in Barcelona performed a study to look at vagus nerve functioning in long COVID patients. Among 348 patients, about 66% had at least one symptom that suggested vagus nerve dysfunction. The researchers did a broad evaluation with imaging and functional tests for 22 patients in the university’s Long COVID Clinic from March to June 2021.
Of the 22 patients, 20 were women, and the median age was 44. The most frequent symptoms related to vagus nerve dysfunction were diarrhea (73%), high heart rates (59%), dizziness (45%), swallowing problems (45%), voice problems (45%), and low blood pressure (14%).
Almost all (19 of 22 patients) had three or more symptoms related to vagus nerve dysfunction. The average length of symptoms was 14 months.
Of 22 patients, 6 had a change in the vagus nerve in the neck, which the researchers observed by ultrasound. They had a thickening of the vagus nerve and increased “echogenicity,” which suggests inflammation.
What’s more, 10 of 22 patients had flattened “diaphragmatic curves” during a thoracic ultrasound, which means the diaphragm doesn’t move as well as it should during breathing, and abnormal breathing. In another assessment, 10 of 16 patients had lower maximum inspiration pressures, suggesting a weakness in breathing muscles.
Eating and digestion were also impaired in some patients, with 13 reporting trouble with swallowing. During a gastric and bowel function assessment, eight patients couldn’t move food from the esophagus to the stomach as well as they should, while nine patients had acid reflux. Three patients had a hiatal hernia, which happens when the upper part of the stomach bulges through the diaphragm into the chest cavity.
The voices of some patients changed as well. Eight patients had an abnormal voice handicap index 30 test, which is a standard way to measure voice function. Among those, seven patients had dysphonia, or persistent voice problems.
The study is ongoing, and the research team is continuing to recruit patients to study the links between long COVID and the vagus nerve. The full paper isn’t yet available, and the research hasn’t yet been peer reviewed.
“The study appears to add to a growing collection of data suggesting at least some of the symptoms of long COVID is mediated through a direct impact on the nervous system,” David Strain, MD, a clinical senior lecturer at the University of Exeter (England), told the Science Media Centre.
“Establishing vagal nerve damage is useful information, as there are recognized, albeit not perfect, treatments for other causes of vagal nerve dysfunction that may be extrapolated to be beneficial for people with this type of long COVID,” he said.
A version of this article first appeared on WebMD.com.