User login
Improving compliance with cosmeceutical-prescription combinations
As clinicians who have been in practice for even a relatively short period of time know, patient compliance is an integral aspect of achieving optimal patient outcomes. However, studies show that patient compliance with treatment of many dermatologic disorders, including acne and psoriasis, is often poor.1,2
In 2007, Feldman showed that patients are more likely to use their products in the days before and the days after their dermatologist visit.3 He suggested that more frequent office visits would boost compliance. I have found that this is true and I recommend seeing patients every 4 weeks when implementing a new treatment regimen. I have also found that combining prescription medications with the proper corresponding skin care products helps decrease side effects and speed results when patients apply the products correctly.

To increase the chance of patients using the products correctly, they should be educated about how and when to use the products. I cannot overemphasize the importance of this, as illustrated by the following story of a patient who came in with facial redness and irritation. Upon questioning, I learned that she was using her facial cleanser but was not washing it off and left it on all day. She said, “No one told me to wash it off!” While washing a cleanser off may seem obvious, cultural, gender, ethnic, and geographical differences can lead to misunderstandings.
The problem with patient education is that it takes time. It is best if education is provided by staff, but keeping them trained and up to date is also difficult. Most dermatologists only have 3-5 minutes per patient so streamlining the process of designing a treatment plan and educating the patient and recruiting your staff to help is crucial. Before I discuss how to streamline the process, let’s first look at our goals for patients.
To achieve good patient outcomes, the patient needs to:
- Understand what medications and products to use.
- Understand when and how to use the products.
- Understand the order in which to use the products (step 1, step 2, etc.).
- Purchase the products (from you or elsewhere).
- Tell you if they do not purchase the products, for whatever reason (insurance will not cover, too expensive, could not find them, etc.).
- Use the products consistently.
- Inform you if they do not use the products (too busy, did not have them on a trip, etc.).
- Report any side effects so you can adjust the therapy accordingly.
You can see why it is so difficult to get patients to be compliant. Many factors – such as time, memory, education level, understanding, motivation, cost, convenience, and insurance coverage – can get in the way of these important components. Giving patients a printed regimen with instructions, selling the products in your practice, and providing some sort of interaction to keep patients engaged is key. In my June 2015 Dermatology News column, I discussed why you should consider selling products in your practice. In the future, I will discuss ways to engage your patients, but for now, let’s focus on how to quickly and effectively provide your patients with printed regimens and patient instructions without increasing office visit times.
Streamlining the Process of Generating a Skin Care Regimen That Includes Prescription Medications
Identify patients’ phenotypes
Divide patients into phenotypes based on skin care needs to save yourself time with the recommendation process.
Many doctors do this with a disease-based approach, such as acne, rosacea, eczema, psoriasis, etc. I prefer to classify my patients according to 16 Baumann Skin Types based on four parameters: hydration status, propensity for inflammation; presence or absence of uneven pigmentation; and presence of lifestyle habits, such as sun exposure, that increase an individual’s risk of skin aging.4,5,6 To quickly diagnose the patient as a particular Baumann Skin Type, I use a tablet-based validated questionnaire called the Baumann Skin Type Indicator (BSTI).7 This questionnaire is self-administered by the patient in the waiting room and serves several purposes that facilitate my practice:
- To collect historical and current data.
- To diagnose skin type.
- To ask specifically about skin allergies.
- To learn preferences such as tinted vs. nontinted, or chemical vs. physical sunscreen.
- To inquire about what issues the patient wants to discuss, such as thinning eyelashes, hair loss, dry body skin, toenail fungus, warts, eczema, and other topics that might not come up during the appointment.
- To learn and document habits that affect the skin, such as tanning bed exposure, sun exposure, and smoking.
- To stimulate the patient to think about how daily actions such as sunscreen use and sun exposure affect their skin health.
Whether you choose to use my questionnaire or one of your own, using a validated method that can be initiated by staff in the waiting room saves time in the exam room.
Include prescription medications in the skin care regimen
Often, we think of skin care regimens and prescription medications as two different entities. In actuality, these should be combined.
For example, when treating acne, every item the patient uses plays a role. For example, if they are washing the face with Ivory soap and then applying benzoyl peroxide and a retinoid they will experience dryness and irritation. Then they will buy a moisturizer that might cause acne. (It is very hard for them to know which moisturizers and sunscreens will not worsen acne). By providing them with the exact names of cleansers, moisturizers, and sunscreens to use, they will be better able to tolerate their prescription acne medications.
The same is true with psoriasis, eczema, seborrheic dermatitis, contact dermatitis, and most of the other ailments that dermatologists treat. You must also tell them the order to use them in. For example, I always have patients apply the retinoid over the noncomedogenic moisturizer for the first few weeks to help them adjust to the retinoid. Later, once they have passed the high-risk period of retinoid dermatitis, I move the retinoid to under the moisturizer.
Psoriasis treatment (topical) is another good example. If they are going to use a surfactant-laden soap on their skin, they will impair their barrier and absorb more of the topically applied drug. Conversely, if they use a barrier repair moisturizer, they will absorb less. Telling the patients exactly which body cleansers and moisturizers to use with topical psoriasis medications will help standardize the response. For this reason, giving patients printed regimens is not limited to treatment of acne, rosacea, and photoaging, but rather should be done for patients with all skin issues and phenotypes.
Have informational material for each phenotype at your fingertips
You can have a plan for each patient phenotype that is designed ahead of time. You will save yourself hours of time if you have preprinted instructions sheets made for each of these phenotypes. You can use Touch MD, The Canfield Visia Camera Patient Portal, your EMR, or other systems to organize this material and deliver it to patients.
I personally use the Skin Type Solutions Software System (STSFranchise.com) that I developed and patented to house and export my patient instructions. Using a standardized methodology to provide educational information through video, preprinted sheets, emails, and other methods allows you to educate your patients at their pace and in the media with which they are most comfortable. To have this flexibility, the educational information must be developed prior to the patient visit. Categorizing the education information by phenotype makes this possible.
What the informational material should contain
Educational information should include important information about the phenotype, the do’s and don’ts for the phenotype, an exact skin care regimen containing clear steps that include product names including brand names, prescription medications, the order in which the products should be applied, and clear instructions on how to use the products.
The patient should be informed about what to do if anticipated adverse events occur, such as redness and peeling from retinoids or dryness from benzoyl peroxide. The same is true about injectable biologic medications for psoriasis. The patients need information on where to inject the product, how often, how to clean the skin beforehand, and what to put on the skin after the injections. It is always important with any skin issue for the patient to know when to contact the office. The American Academy of Dermatology and other organizations offer educational brochures for patients, but they cannot be customized. Patients prefer a customized approach to educational material. They don’t want to read information that does not apply to them. I have found that dividing patients into 16 distinct Baumann Skin Types helps target the right information to the corresponding skin phenotypes.
Summary
Patients need education and guidance to be compliant and improve their outcomes. Your staff needs to be a part of the education process, but taking the time to train your staff and educate your patients is always an issue. Developing a standardized methodology will help overcome these hurdles and solve this problem. The methodology should provide directed education and clear communication with written instructions delivered in the media of the patient’s choice. Doing this will yield better compliance and outcomes.
If you have any questions, suggestions or ideas of how to solve these issues, please share them with me at [email protected].
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. JAMA Dermatol. 2015 Jun;151(6):623-6.
2. J Am Acad Dermatol. 2004 Aug;51(2):212-6.
3. J Am Acad Dermatol. 2007 Jul;57(1):81-3.
4. Dermatol Clin. 2008 Jul;26(3):359-73.
5. Baumann L. Cosmetics and skin care in dermatology. In: Wolff K, ed. Fitzpatrick’s Dermatology in General Medicine, 7th ed. New York, NY: McGraw-Hill; 2008:2357-2364.
6. Baumann L. The Baumann skin typing system. In: Farage MA, Miller KW, Maibach HI, eds. Textbook of Aging Skin. Berling, Germany: Springer-Verlag; 2010:929-944.
7. Journal of Cosmetics, Dermatological Sciences and Applications. 2016;6(1):34-40.
As clinicians who have been in practice for even a relatively short period of time know, patient compliance is an integral aspect of achieving optimal patient outcomes. However, studies show that patient compliance with treatment of many dermatologic disorders, including acne and psoriasis, is often poor.1,2
In 2007, Feldman showed that patients are more likely to use their products in the days before and the days after their dermatologist visit.3 He suggested that more frequent office visits would boost compliance. I have found that this is true and I recommend seeing patients every 4 weeks when implementing a new treatment regimen. I have also found that combining prescription medications with the proper corresponding skin care products helps decrease side effects and speed results when patients apply the products correctly.
To increase the chance of patients using the products correctly, they should be educated about how and when to use the products. I cannot overemphasize the importance of this, as illustrated by the following story of a patient who came in with facial redness and irritation. Upon questioning, I learned that she was using her facial cleanser but was not washing it off and left it on all day. She said, “No one told me to wash it off!” While washing a cleanser off may seem obvious, cultural, gender, ethnic, and geographical differences can lead to misunderstandings.
The problem with patient education is that it takes time. It is best if education is provided by staff, but keeping them trained and up to date is also difficult. Most dermatologists only have 3-5 minutes per patient so streamlining the process of designing a treatment plan and educating the patient and recruiting your staff to help is crucial. Before I discuss how to streamline the process, let’s first look at our goals for patients.
To achieve good patient outcomes, the patient needs to:
- Understand what medications and products to use.
- Understand when and how to use the products.
- Understand the order in which to use the products (step 1, step 2, etc.).
- Purchase the products (from you or elsewhere).
- Tell you if they do not purchase the products, for whatever reason (insurance will not cover, too expensive, could not find them, etc.).
- Use the products consistently.
- Inform you if they do not use the products (too busy, did not have them on a trip, etc.).
- Report any side effects so you can adjust the therapy accordingly.
You can see why it is so difficult to get patients to be compliant. Many factors – such as time, memory, education level, understanding, motivation, cost, convenience, and insurance coverage – can get in the way of these important components. Giving patients a printed regimen with instructions, selling the products in your practice, and providing some sort of interaction to keep patients engaged is key. In my June 2015 Dermatology News column, I discussed why you should consider selling products in your practice. In the future, I will discuss ways to engage your patients, but for now, let’s focus on how to quickly and effectively provide your patients with printed regimens and patient instructions without increasing office visit times.
Streamlining the Process of Generating a Skin Care Regimen That Includes Prescription Medications
Identify patients’ phenotypes
Divide patients into phenotypes based on skin care needs to save yourself time with the recommendation process.
Many doctors do this with a disease-based approach, such as acne, rosacea, eczema, psoriasis, etc. I prefer to classify my patients according to 16 Baumann Skin Types based on four parameters: hydration status, propensity for inflammation; presence or absence of uneven pigmentation; and presence of lifestyle habits, such as sun exposure, that increase an individual’s risk of skin aging.4,5,6 To quickly diagnose the patient as a particular Baumann Skin Type, I use a tablet-based validated questionnaire called the Baumann Skin Type Indicator (BSTI).7 This questionnaire is self-administered by the patient in the waiting room and serves several purposes that facilitate my practice:
- To collect historical and current data.
- To diagnose skin type.
- To ask specifically about skin allergies.
- To learn preferences such as tinted vs. nontinted, or chemical vs. physical sunscreen.
- To inquire about what issues the patient wants to discuss, such as thinning eyelashes, hair loss, dry body skin, toenail fungus, warts, eczema, and other topics that might not come up during the appointment.
- To learn and document habits that affect the skin, such as tanning bed exposure, sun exposure, and smoking.
- To stimulate the patient to think about how daily actions such as sunscreen use and sun exposure affect their skin health.
Whether you choose to use my questionnaire or one of your own, using a validated method that can be initiated by staff in the waiting room saves time in the exam room.
Include prescription medications in the skin care regimen
Often, we think of skin care regimens and prescription medications as two different entities. In actuality, these should be combined.
For example, when treating acne, every item the patient uses plays a role. For example, if they are washing the face with Ivory soap and then applying benzoyl peroxide and a retinoid they will experience dryness and irritation. Then they will buy a moisturizer that might cause acne. (It is very hard for them to know which moisturizers and sunscreens will not worsen acne). By providing them with the exact names of cleansers, moisturizers, and sunscreens to use, they will be better able to tolerate their prescription acne medications.
The same is true with psoriasis, eczema, seborrheic dermatitis, contact dermatitis, and most of the other ailments that dermatologists treat. You must also tell them the order to use them in. For example, I always have patients apply the retinoid over the noncomedogenic moisturizer for the first few weeks to help them adjust to the retinoid. Later, once they have passed the high-risk period of retinoid dermatitis, I move the retinoid to under the moisturizer.
Psoriasis treatment (topical) is another good example. If they are going to use a surfactant-laden soap on their skin, they will impair their barrier and absorb more of the topically applied drug. Conversely, if they use a barrier repair moisturizer, they will absorb less. Telling the patients exactly which body cleansers and moisturizers to use with topical psoriasis medications will help standardize the response. For this reason, giving patients printed regimens is not limited to treatment of acne, rosacea, and photoaging, but rather should be done for patients with all skin issues and phenotypes.
Have informational material for each phenotype at your fingertips
You can have a plan for each patient phenotype that is designed ahead of time. You will save yourself hours of time if you have preprinted instructions sheets made for each of these phenotypes. You can use Touch MD, The Canfield Visia Camera Patient Portal, your EMR, or other systems to organize this material and deliver it to patients.
I personally use the Skin Type Solutions Software System (STSFranchise.com) that I developed and patented to house and export my patient instructions. Using a standardized methodology to provide educational information through video, preprinted sheets, emails, and other methods allows you to educate your patients at their pace and in the media with which they are most comfortable. To have this flexibility, the educational information must be developed prior to the patient visit. Categorizing the education information by phenotype makes this possible.
What the informational material should contain
Educational information should include important information about the phenotype, the do’s and don’ts for the phenotype, an exact skin care regimen containing clear steps that include product names including brand names, prescription medications, the order in which the products should be applied, and clear instructions on how to use the products.
The patient should be informed about what to do if anticipated adverse events occur, such as redness and peeling from retinoids or dryness from benzoyl peroxide. The same is true about injectable biologic medications for psoriasis. The patients need information on where to inject the product, how often, how to clean the skin beforehand, and what to put on the skin after the injections. It is always important with any skin issue for the patient to know when to contact the office. The American Academy of Dermatology and other organizations offer educational brochures for patients, but they cannot be customized. Patients prefer a customized approach to educational material. They don’t want to read information that does not apply to them. I have found that dividing patients into 16 distinct Baumann Skin Types helps target the right information to the corresponding skin phenotypes.
Summary
Patients need education and guidance to be compliant and improve their outcomes. Your staff needs to be a part of the education process, but taking the time to train your staff and educate your patients is always an issue. Developing a standardized methodology will help overcome these hurdles and solve this problem. The methodology should provide directed education and clear communication with written instructions delivered in the media of the patient’s choice. Doing this will yield better compliance and outcomes.
If you have any questions, suggestions or ideas of how to solve these issues, please share them with me at [email protected].
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. JAMA Dermatol. 2015 Jun;151(6):623-6.
2. J Am Acad Dermatol. 2004 Aug;51(2):212-6.
3. J Am Acad Dermatol. 2007 Jul;57(1):81-3.
4. Dermatol Clin. 2008 Jul;26(3):359-73.
5. Baumann L. Cosmetics and skin care in dermatology. In: Wolff K, ed. Fitzpatrick’s Dermatology in General Medicine, 7th ed. New York, NY: McGraw-Hill; 2008:2357-2364.
6. Baumann L. The Baumann skin typing system. In: Farage MA, Miller KW, Maibach HI, eds. Textbook of Aging Skin. Berling, Germany: Springer-Verlag; 2010:929-944.
7. Journal of Cosmetics, Dermatological Sciences and Applications. 2016;6(1):34-40.
As clinicians who have been in practice for even a relatively short period of time know, patient compliance is an integral aspect of achieving optimal patient outcomes. However, studies show that patient compliance with treatment of many dermatologic disorders, including acne and psoriasis, is often poor.1,2
In 2007, Feldman showed that patients are more likely to use their products in the days before and the days after their dermatologist visit.3 He suggested that more frequent office visits would boost compliance. I have found that this is true and I recommend seeing patients every 4 weeks when implementing a new treatment regimen. I have also found that combining prescription medications with the proper corresponding skin care products helps decrease side effects and speed results when patients apply the products correctly.
To increase the chance of patients using the products correctly, they should be educated about how and when to use the products. I cannot overemphasize the importance of this, as illustrated by the following story of a patient who came in with facial redness and irritation. Upon questioning, I learned that she was using her facial cleanser but was not washing it off and left it on all day. She said, “No one told me to wash it off!” While washing a cleanser off may seem obvious, cultural, gender, ethnic, and geographical differences can lead to misunderstandings.
The problem with patient education is that it takes time. It is best if education is provided by staff, but keeping them trained and up to date is also difficult. Most dermatologists only have 3-5 minutes per patient so streamlining the process of designing a treatment plan and educating the patient and recruiting your staff to help is crucial. Before I discuss how to streamline the process, let’s first look at our goals for patients.
To achieve good patient outcomes, the patient needs to:
- Understand what medications and products to use.
- Understand when and how to use the products.
- Understand the order in which to use the products (step 1, step 2, etc.).
- Purchase the products (from you or elsewhere).
- Tell you if they do not purchase the products, for whatever reason (insurance will not cover, too expensive, could not find them, etc.).
- Use the products consistently.
- Inform you if they do not use the products (too busy, did not have them on a trip, etc.).
- Report any side effects so you can adjust the therapy accordingly.
You can see why it is so difficult to get patients to be compliant. Many factors – such as time, memory, education level, understanding, motivation, cost, convenience, and insurance coverage – can get in the way of these important components. Giving patients a printed regimen with instructions, selling the products in your practice, and providing some sort of interaction to keep patients engaged is key. In my June 2015 Dermatology News column, I discussed why you should consider selling products in your practice. In the future, I will discuss ways to engage your patients, but for now, let’s focus on how to quickly and effectively provide your patients with printed regimens and patient instructions without increasing office visit times.
Streamlining the Process of Generating a Skin Care Regimen That Includes Prescription Medications
Identify patients’ phenotypes
Divide patients into phenotypes based on skin care needs to save yourself time with the recommendation process.
Many doctors do this with a disease-based approach, such as acne, rosacea, eczema, psoriasis, etc. I prefer to classify my patients according to 16 Baumann Skin Types based on four parameters: hydration status, propensity for inflammation; presence or absence of uneven pigmentation; and presence of lifestyle habits, such as sun exposure, that increase an individual’s risk of skin aging.4,5,6 To quickly diagnose the patient as a particular Baumann Skin Type, I use a tablet-based validated questionnaire called the Baumann Skin Type Indicator (BSTI).7 This questionnaire is self-administered by the patient in the waiting room and serves several purposes that facilitate my practice:
- To collect historical and current data.
- To diagnose skin type.
- To ask specifically about skin allergies.
- To learn preferences such as tinted vs. nontinted, or chemical vs. physical sunscreen.
- To inquire about what issues the patient wants to discuss, such as thinning eyelashes, hair loss, dry body skin, toenail fungus, warts, eczema, and other topics that might not come up during the appointment.
- To learn and document habits that affect the skin, such as tanning bed exposure, sun exposure, and smoking.
- To stimulate the patient to think about how daily actions such as sunscreen use and sun exposure affect their skin health.
Whether you choose to use my questionnaire or one of your own, using a validated method that can be initiated by staff in the waiting room saves time in the exam room.
Include prescription medications in the skin care regimen
Often, we think of skin care regimens and prescription medications as two different entities. In actuality, these should be combined.
For example, when treating acne, every item the patient uses plays a role. For example, if they are washing the face with Ivory soap and then applying benzoyl peroxide and a retinoid they will experience dryness and irritation. Then they will buy a moisturizer that might cause acne. (It is very hard for them to know which moisturizers and sunscreens will not worsen acne). By providing them with the exact names of cleansers, moisturizers, and sunscreens to use, they will be better able to tolerate their prescription acne medications.
The same is true with psoriasis, eczema, seborrheic dermatitis, contact dermatitis, and most of the other ailments that dermatologists treat. You must also tell them the order to use them in. For example, I always have patients apply the retinoid over the noncomedogenic moisturizer for the first few weeks to help them adjust to the retinoid. Later, once they have passed the high-risk period of retinoid dermatitis, I move the retinoid to under the moisturizer.
Psoriasis treatment (topical) is another good example. If they are going to use a surfactant-laden soap on their skin, they will impair their barrier and absorb more of the topically applied drug. Conversely, if they use a barrier repair moisturizer, they will absorb less. Telling the patients exactly which body cleansers and moisturizers to use with topical psoriasis medications will help standardize the response. For this reason, giving patients printed regimens is not limited to treatment of acne, rosacea, and photoaging, but rather should be done for patients with all skin issues and phenotypes.
Have informational material for each phenotype at your fingertips
You can have a plan for each patient phenotype that is designed ahead of time. You will save yourself hours of time if you have preprinted instructions sheets made for each of these phenotypes. You can use Touch MD, The Canfield Visia Camera Patient Portal, your EMR, or other systems to organize this material and deliver it to patients.
I personally use the Skin Type Solutions Software System (STSFranchise.com) that I developed and patented to house and export my patient instructions. Using a standardized methodology to provide educational information through video, preprinted sheets, emails, and other methods allows you to educate your patients at their pace and in the media with which they are most comfortable. To have this flexibility, the educational information must be developed prior to the patient visit. Categorizing the education information by phenotype makes this possible.
What the informational material should contain
Educational information should include important information about the phenotype, the do’s and don’ts for the phenotype, an exact skin care regimen containing clear steps that include product names including brand names, prescription medications, the order in which the products should be applied, and clear instructions on how to use the products.
The patient should be informed about what to do if anticipated adverse events occur, such as redness and peeling from retinoids or dryness from benzoyl peroxide. The same is true about injectable biologic medications for psoriasis. The patients need information on where to inject the product, how often, how to clean the skin beforehand, and what to put on the skin after the injections. It is always important with any skin issue for the patient to know when to contact the office. The American Academy of Dermatology and other organizations offer educational brochures for patients, but they cannot be customized. Patients prefer a customized approach to educational material. They don’t want to read information that does not apply to them. I have found that dividing patients into 16 distinct Baumann Skin Types helps target the right information to the corresponding skin phenotypes.
Summary
Patients need education and guidance to be compliant and improve their outcomes. Your staff needs to be a part of the education process, but taking the time to train your staff and educate your patients is always an issue. Developing a standardized methodology will help overcome these hurdles and solve this problem. The methodology should provide directed education and clear communication with written instructions delivered in the media of the patient’s choice. Doing this will yield better compliance and outcomes.
If you have any questions, suggestions or ideas of how to solve these issues, please share them with me at [email protected].
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. JAMA Dermatol. 2015 Jun;151(6):623-6.
2. J Am Acad Dermatol. 2004 Aug;51(2):212-6.
3. J Am Acad Dermatol. 2007 Jul;57(1):81-3.
4. Dermatol Clin. 2008 Jul;26(3):359-73.
5. Baumann L. Cosmetics and skin care in dermatology. In: Wolff K, ed. Fitzpatrick’s Dermatology in General Medicine, 7th ed. New York, NY: McGraw-Hill; 2008:2357-2364.
6. Baumann L. The Baumann skin typing system. In: Farage MA, Miller KW, Maibach HI, eds. Textbook of Aging Skin. Berling, Germany: Springer-Verlag; 2010:929-944.
7. Journal of Cosmetics, Dermatological Sciences and Applications. 2016;6(1):34-40.

Study reveals crazy quilt of laser laws across the United States
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)

She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)
She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
SAN DIEGO – Laser hair removal isn’t typically in an office cleaner’s job description. So it’s no wonder that Virginia legislators were spooked when they heard from a constituent who was treated by a spa worker who turned out to be a janitor.
Earlier this year, legislators in the Old Dominion passed a bill limiting laser hair removal procedures to a “properly trained” medical doctor, physician assistant, or nurse practitioner – or a “properly trained” person who is supervised by one of these professionals. Therefore, it’s still possible for a “properly trained” person without a degree of any kind to operate a laser in Virginia.
To the north in New Jersey, the rules are much stricter: Only physicians can perform laser procedures. But in New York, it appears that anyone can fire up a laser and go to work on unwanted hair. And in Florida, nonphysicians can perform laser procedures only if they’re physician assistants or nurse practitioners. But they’re only allowed to remove hair with lasers at a clinic that just performs laser hair removal.
Such is the chaotic state of laser law in the United States, a new study finds. The rules, which vary widely from state to state, are often vague and confusing. And, as Virginia’s new law shows, they’re still evolving. (The study is current as of March 2016.)
She and study coauthor Mathew M. Avram, MD, JD, director of the Laser and Cosmetic Center at Massachusetts General, analyzed regulations in the 50 states regarding the operation of lasers. They reported their findings at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. DiGiorgio said that laser operator laws address three issues:
1. Who can operate a laser?
At other clinics across the country, nonphysician employees — such as nurse practitioners and registered nurses – often operate lasers. Whether they can legally actually do so isn’t always obvious.
New Jersey is the only state that requires laser operators to be physicians. At the other extreme, 11 states, including Massachusetts, Colorado, Florida, Missouri, New York, and Pennsylvania, have “no” limits on who can perform laser procedures. (At Massachusetts General Hospital, physicians perform all laser procedures.)
So does that mean anyone can perform a laser procedure? It’s not clear. “The laws are a lot more vague than they should be,” Dr. DiGiorgio said in an interview.
Eighteen states allow people to perform laser procedures as part of the “practice of medicine,” although legislation can be vague on what that means. Those states include Illinois, Michigan, Minnesota, North Carolina, and Texas.
Another 19 states, including California, Ohio, Washington, Wisconsin, and now Virginia, have specific limits on who can perform laser procedures. In California, for example, physician assistants and registered nurses – but not licensed vocational nurses – are allowed to use lasers to remove hair, spider veins, and tattoos. Unlicensed medical assistants, cosmetologists, electrologists, and estheticians are not allowed to perform the procedures
2. Can someone delegate laser procedures to someone else?
In nine states, including Iowa and New Hampshire, there’s no oversight of delegation or nonphysicians can delegate procedures to someone else.
In another nine states, certain procedures can be delegated with no physician oversight, such as laser hair removal in Alaska and ablative procedures (to advanced practice registered nurses only) in Utah.
3. Is supervision required of nonphysicians?
Physicians don’t need to supervise certain laser procedures in 11 states, including Hawaii, Oregon, and Vermont, where they can be performed by a nonphysician with no supervision or under supervision by a non-physician.
In 17 states, supervision isn’t always required or it’s under the discretion of the supervising physician. These states include California, Michigan, Pennsylvania, and Wisconsin.
In 11 states, including Illinois and Massachusetts, only certain procedures require on-site supervision. Six states, including Connecticut and Maryland, require on-site physician supervision for all laser procedures, but Dr. DiGiorgio said the requirements can be vague about what “on site” actually means.
Idaho requires the physician to be on site or immediately available, and South Carolina allows registered nurses to perform laser hair and leg vein removal if a physician is on site and can respond within 5 minutes.
“We don’t know what the ideal regulation is,” Dr. DiGiorgio said. But she believes laser regulations are crucial to safety, especially as fields such as plastic surgery, ophthalmology, and gynecology embrace cosmetic laser procedures.
Information about state-by-state laser operator laws is available on the American Med Spa Association website.
Dr. DiGiorgio reported no relevant disclosures.
AT LASER 2017
Key clinical point:
Major finding: The study found wide variations in who can operate lasers, and in regulations regarding the delegation and supervision of laser treatments in the different states.
Data source: Analysis of regulations in the 50 states regarding the operation of lasers.
Disclosures: Dr. DiGiorgio reported no relevant disclosures
Blepharoplasty Markers: Comparison of Ink Drying Time and Ink Spread
Blepharoplasty, or surgical manipulation of the upper and/or lower eyelids, is a commonly performed cosmetic procedure to improve the appearance and function of the eyelids by repositioning and/or removing excess skin and soft tissue from the eyelids, most often through external incisions that minimize scarring and maximize the aesthetic outcomes of the surgery. Therefore, the placement of the incisions is an important determinant of the surgical outcome, and the preoperative marking of the eyelids to indicate where the incisions should be placed is a crucial part of preparation for the surgery.
Preoperative marking has unique challenges due to the dynamicity of the eyelids and the delicate nature of the surgery. The mark must be narrow to minimize the risk of placing the incision higher or lower than intended. The mark also must dry quickly because the patient may blink and create multiple impressions of the marking on skinfolds in contact with the wet ink. Fast drying of the ink used to create the marks improves the efficiency and clarity of the presurgical planning.
We present data on the performance of the various blepharoplasty markers regarding drying time and ink spread width based on an evaluation of 13 surgical markers.
Methods
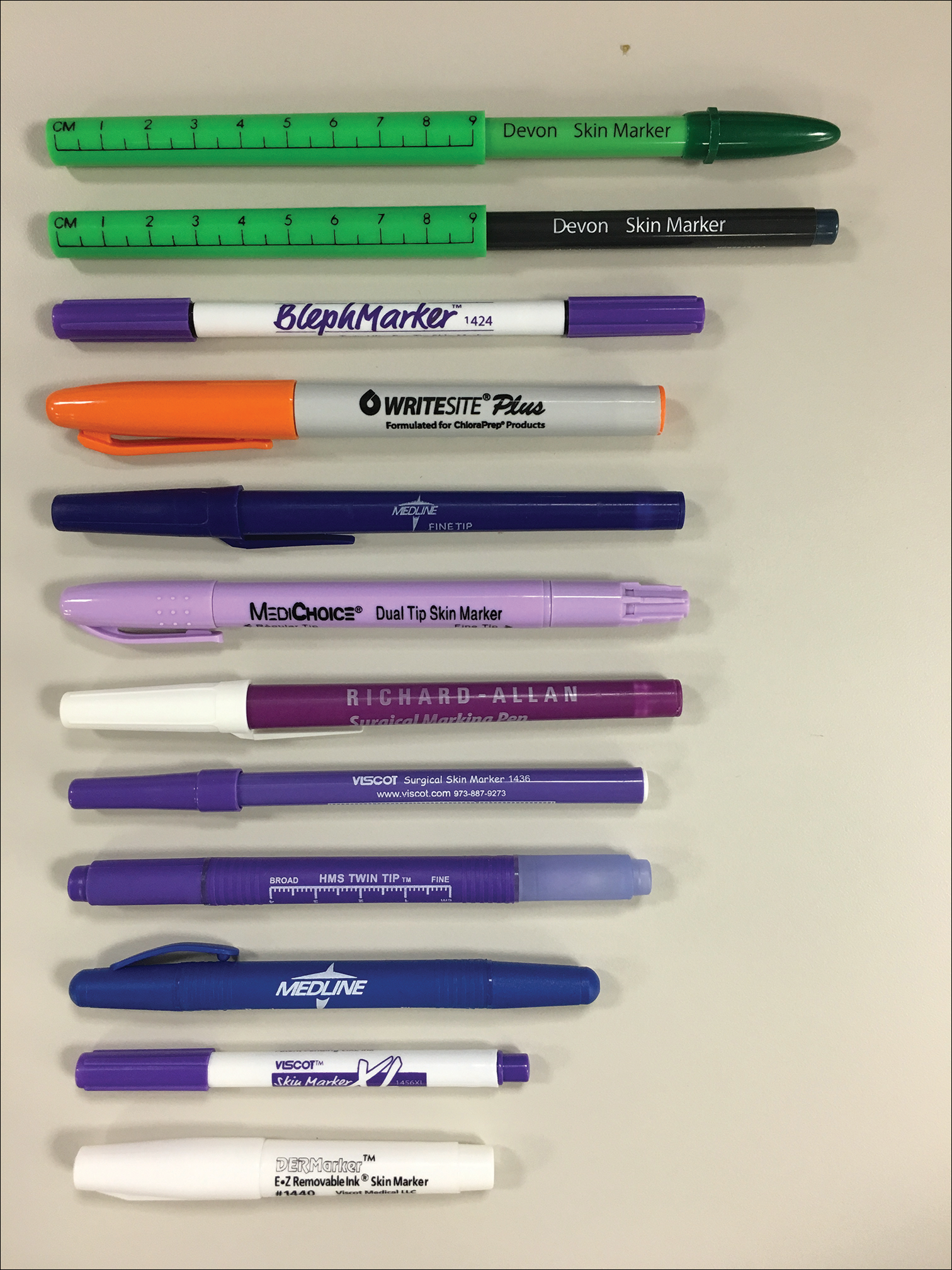
Eleven unique fine tip (FT) markers and 2 standard tip (ST) markers were obtained based on their accessibility at the researchers’ home institution and availability for direct purchase in small quantities from the distributors (Figure 1). Four markers were double tipped with one FT end and one ST end; for these markers, only the FT end was studied. The experiments were conducted on the bilateral upper eyelids and on hairless patches of skin of a single patient in a minor procedure room with surgical lighting and minimal draft of air. The sole experimenter (J.M.K.) conducting the study was not blinded.
The drying time of each marker was measured by marking 1-in lines on a patch of hairless skin that was first cleaned with an alcohol pad, then dried. Drying time for each marking was measured in increments of 5 seconds; at each time point, the markings were wiped with a single-ply, light-duty tissue under the weight of 10 US quarters to ensure that the same weight/pressure was applied when wiping the skin. Smudges observed with the naked eye on either the wipe or the patients’ skin were interpreted as nondry status of the marking. The first time point at which a marking was found to have no visible smudges either on the skin or the wipe was recorded as the drying time of the respective marker.
Ink spread was measured on clean eyelid skin by drawing curved lines along the natural crease as would be done for actual blepharoplasty planning. Each line was allowed to dry for 2 minutes. The greatest perpendicular spread width along the line observed with the naked eye was measured using a digital Vernier caliper with 0.01-mm graduations. Three measurements were obtained per marker and the values averaged to arrive at the final spread width.
Results
Drying time among the 13 total markers (11 FT and 2 ST) ranged from 5 to 70 seconds, with a mean of 20.8 seconds and median of 5 seconds (Table). The drying time for the DERMarker E-Z Removable Ink Mini Skin Marker (Delasco, LLC) with an ST was 5 seconds, while the drying time for the other ST marker, WriteSite Plus Surgical Skin Marker (Aspen Surgical, Inc), was 70 seconds. The FT markers spanned the entire range of drying times. The ink spread width among the markers ranged from 0.53 to 2.27 mm with a median of 0.9 mm and mean of 1.13 mm (Table). The 2 ST markers were found to make some of the widest marks measured, including the WriteSite Plus Surgical Skin Marker, a nonsterile ST marker that created the widest ink marks. The second widest mark was made by an FT marker (Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker [Viscot Medical, LLC]).
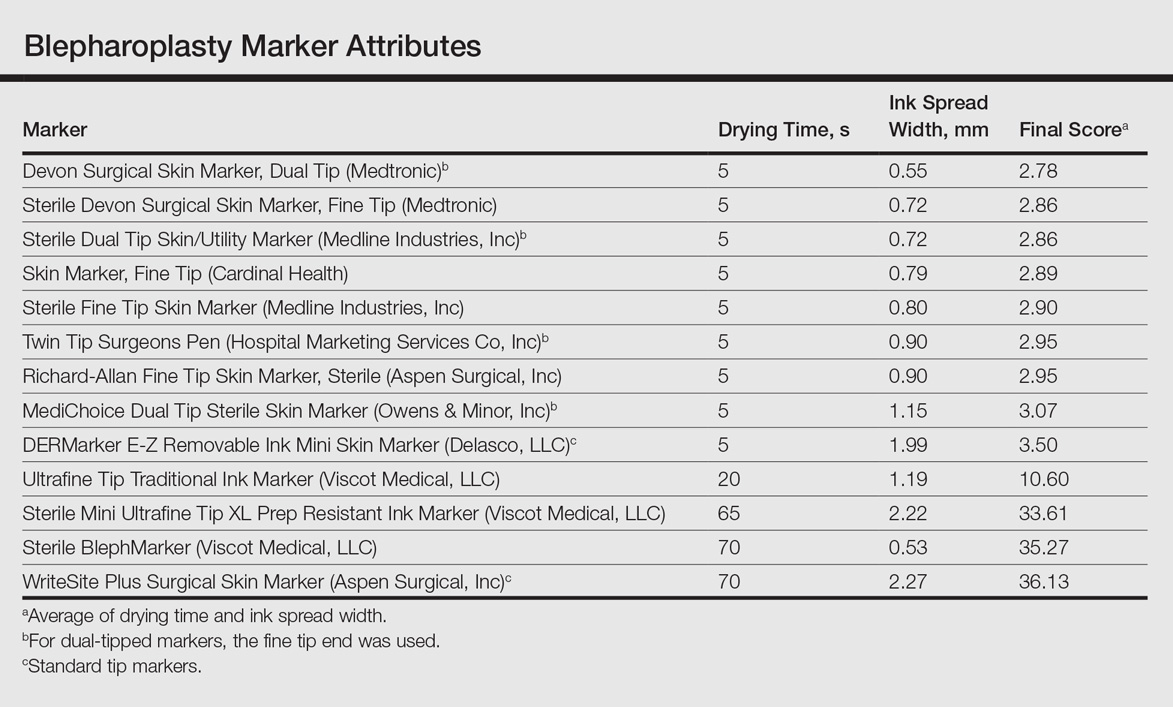
To prioritize short drying time coupled with minimal ink spread width, the values associated with each marker were averaged to arrive at the overall score for each marker. The smaller the overall score, the higher we ranked the marker. The Devon Surgical Skin Marker, Dual Tip (Medtronic) ranked the highest among the 13 markers with a final score of 2.78. Runner-up markers included the Sterile Devon Surgical Skin marker, Fine Tip (Medtronic)(final score, 2.86); the Sterile Dual Tip Skin/Utility Marker (Medline Industries, Inc)(final score, 2.86); and the Skin Marker, Fine Tip (Cardinal Health)(final score, 2.89). The 2 lowest-ranking markers were the WriteSite Plus Surgical Skin Marker, an ST marker (final score, 36.13), followed by the Sterile BlephMarker (Viscot Medical, LLC)(final score, 35.27).
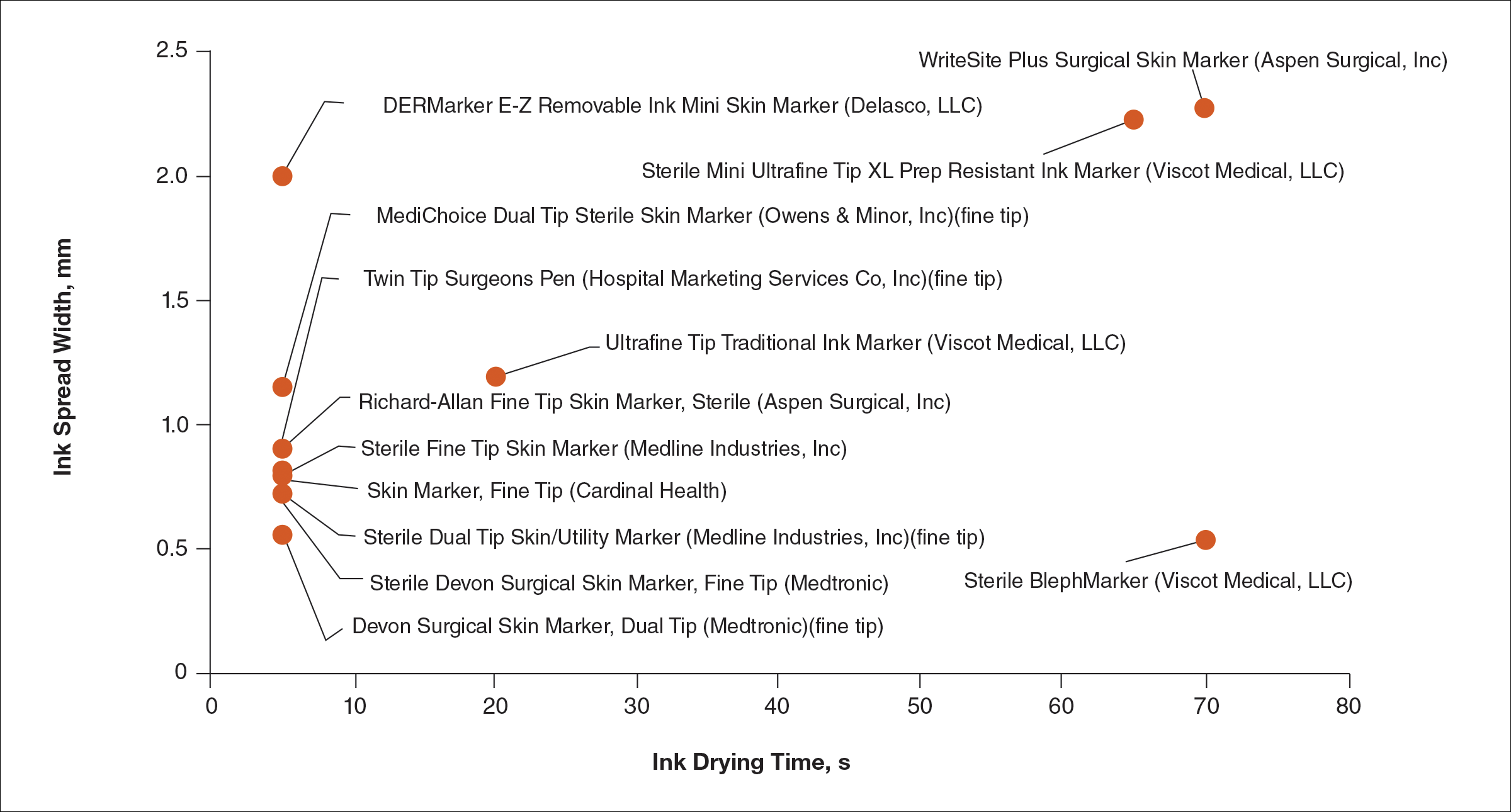
Figure 2 shows the drying time and ink spread width for all 13 markers.
Comment
Blepharoplasty surgeons generally agree that meticulous presurgical planning with marking of the eyelids is critical for successful surgical outcomes.1,2 Fine tip markers have been recommended for this purpose due to the relative precision of the marks, but the prerequisite of these markers is that the marks must have minimal ink spread through skinfolds to allow for precision as well as short drying time to avoid unintentional duplication of the ink on overlapping skin, especially with the likely chance of reflexive blinking by the patient. The associated assumption is that FT markers automatically leave precise marks with minimal drying time. This study systemically compared these 2 qualities for 13 markers, and the results are notable for the unexpected wide range of performance. Although most of the FT markers had ink spread width of less than 1 mm, the Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker was an outlier among FT markers, with ink spread greater than 2 mm, making it too broad and imprecise for practical use. This result indicates that not every FT marker actually makes fine marks. The 2 ST markers in the study—DERMarker E-Z Removable Ink Mini Skin Marker and WriteSite Plus Surgical Skin Marker—left broad marks as anticipated.
The drying time of the markers also ranged from 5 to 70 seconds among both FT and ST markers. Indeed, most of the FT markers were dry at or before 5 seconds of marking, but 2 FT markers—Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker and Sterile BlephMarker—dried at 65 and 70 seconds, respectively. Such a long drying time would be considered impractical for use in blepharoplasty marking and also unexpected of FT markers, which usually are marketed for their precision and efficiency. Notable in the discussion of drying time is that one of the 2 ST markers in the study, the DERMarker E-Z Removable Ink Mini Skin Marker, had the shortest possible drying time of 5 seconds, while the other ST marker, WriteSite Plus Surgical Skin Marker, dried at 70 seconds. This observation coupled with the unexpected results of broad marks and long drying time for some of the FT markers indicates that a surgeon cannot simply assume that a FT marker would provide marks with precision and fast drying time, or that an ST marker would be the opposite.
Future directions for study include the addition of other markers and the extent of resistance to antiseptic routines that can fade the markings.
Conclusion
Among the 13 markers studied, FT markers typically had the shortest drying time and least ink
Acknowledgement
The authors would like to thank Laura B. Hall, MD (New Haven, Connecticut), for her participation as the volunteer in this study.
- Hartstein ME, Massry GG, Holds JB. Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. New York, NY: Springer New York; 2015.
- Gladstone G, Black EH. Oculoplastic Surgery Atlas. New York, NY: Springer New York; 2005.
Blepharoplasty, or surgical manipulation of the upper and/or lower eyelids, is a commonly performed cosmetic procedure to improve the appearance and function of the eyelids by repositioning and/or removing excess skin and soft tissue from the eyelids, most often through external incisions that minimize scarring and maximize the aesthetic outcomes of the surgery. Therefore, the placement of the incisions is an important determinant of the surgical outcome, and the preoperative marking of the eyelids to indicate where the incisions should be placed is a crucial part of preparation for the surgery.
Preoperative marking has unique challenges due to the dynamicity of the eyelids and the delicate nature of the surgery. The mark must be narrow to minimize the risk of placing the incision higher or lower than intended. The mark also must dry quickly because the patient may blink and create multiple impressions of the marking on skinfolds in contact with the wet ink. Fast drying of the ink used to create the marks improves the efficiency and clarity of the presurgical planning.
We present data on the performance of the various blepharoplasty markers regarding drying time and ink spread width based on an evaluation of 13 surgical markers.
Methods
Eleven unique fine tip (FT) markers and 2 standard tip (ST) markers were obtained based on their accessibility at the researchers’ home institution and availability for direct purchase in small quantities from the distributors (Figure 1). Four markers were double tipped with one FT end and one ST end; for these markers, only the FT end was studied. The experiments were conducted on the bilateral upper eyelids and on hairless patches of skin of a single patient in a minor procedure room with surgical lighting and minimal draft of air. The sole experimenter (J.M.K.) conducting the study was not blinded.
The drying time of each marker was measured by marking 1-in lines on a patch of hairless skin that was first cleaned with an alcohol pad, then dried. Drying time for each marking was measured in increments of 5 seconds; at each time point, the markings were wiped with a single-ply, light-duty tissue under the weight of 10 US quarters to ensure that the same weight/pressure was applied when wiping the skin. Smudges observed with the naked eye on either the wipe or the patients’ skin were interpreted as nondry status of the marking. The first time point at which a marking was found to have no visible smudges either on the skin or the wipe was recorded as the drying time of the respective marker.
Ink spread was measured on clean eyelid skin by drawing curved lines along the natural crease as would be done for actual blepharoplasty planning. Each line was allowed to dry for 2 minutes. The greatest perpendicular spread width along the line observed with the naked eye was measured using a digital Vernier caliper with 0.01-mm graduations. Three measurements were obtained per marker and the values averaged to arrive at the final spread width.
Results
Drying time among the 13 total markers (11 FT and 2 ST) ranged from 5 to 70 seconds, with a mean of 20.8 seconds and median of 5 seconds (Table). The drying time for the DERMarker E-Z Removable Ink Mini Skin Marker (Delasco, LLC) with an ST was 5 seconds, while the drying time for the other ST marker, WriteSite Plus Surgical Skin Marker (Aspen Surgical, Inc), was 70 seconds. The FT markers spanned the entire range of drying times. The ink spread width among the markers ranged from 0.53 to 2.27 mm with a median of 0.9 mm and mean of 1.13 mm (Table). The 2 ST markers were found to make some of the widest marks measured, including the WriteSite Plus Surgical Skin Marker, a nonsterile ST marker that created the widest ink marks. The second widest mark was made by an FT marker (Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker [Viscot Medical, LLC]).
To prioritize short drying time coupled with minimal ink spread width, the values associated with each marker were averaged to arrive at the overall score for each marker. The smaller the overall score, the higher we ranked the marker. The Devon Surgical Skin Marker, Dual Tip (Medtronic) ranked the highest among the 13 markers with a final score of 2.78. Runner-up markers included the Sterile Devon Surgical Skin marker, Fine Tip (Medtronic)(final score, 2.86); the Sterile Dual Tip Skin/Utility Marker (Medline Industries, Inc)(final score, 2.86); and the Skin Marker, Fine Tip (Cardinal Health)(final score, 2.89). The 2 lowest-ranking markers were the WriteSite Plus Surgical Skin Marker, an ST marker (final score, 36.13), followed by the Sterile BlephMarker (Viscot Medical, LLC)(final score, 35.27).
Figure 2 shows the drying time and ink spread width for all 13 markers.
Comment
Blepharoplasty surgeons generally agree that meticulous presurgical planning with marking of the eyelids is critical for successful surgical outcomes.1,2 Fine tip markers have been recommended for this purpose due to the relative precision of the marks, but the prerequisite of these markers is that the marks must have minimal ink spread through skinfolds to allow for precision as well as short drying time to avoid unintentional duplication of the ink on overlapping skin, especially with the likely chance of reflexive blinking by the patient. The associated assumption is that FT markers automatically leave precise marks with minimal drying time. This study systemically compared these 2 qualities for 13 markers, and the results are notable for the unexpected wide range of performance. Although most of the FT markers had ink spread width of less than 1 mm, the Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker was an outlier among FT markers, with ink spread greater than 2 mm, making it too broad and imprecise for practical use. This result indicates that not every FT marker actually makes fine marks. The 2 ST markers in the study—DERMarker E-Z Removable Ink Mini Skin Marker and WriteSite Plus Surgical Skin Marker—left broad marks as anticipated.
The drying time of the markers also ranged from 5 to 70 seconds among both FT and ST markers. Indeed, most of the FT markers were dry at or before 5 seconds of marking, but 2 FT markers—Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker and Sterile BlephMarker—dried at 65 and 70 seconds, respectively. Such a long drying time would be considered impractical for use in blepharoplasty marking and also unexpected of FT markers, which usually are marketed for their precision and efficiency. Notable in the discussion of drying time is that one of the 2 ST markers in the study, the DERMarker E-Z Removable Ink Mini Skin Marker, had the shortest possible drying time of 5 seconds, while the other ST marker, WriteSite Plus Surgical Skin Marker, dried at 70 seconds. This observation coupled with the unexpected results of broad marks and long drying time for some of the FT markers indicates that a surgeon cannot simply assume that a FT marker would provide marks with precision and fast drying time, or that an ST marker would be the opposite.
Future directions for study include the addition of other markers and the extent of resistance to antiseptic routines that can fade the markings.
Conclusion
Among the 13 markers studied, FT markers typically had the shortest drying time and least ink
Acknowledgement
The authors would like to thank Laura B. Hall, MD (New Haven, Connecticut), for her participation as the volunteer in this study.
Blepharoplasty, or surgical manipulation of the upper and/or lower eyelids, is a commonly performed cosmetic procedure to improve the appearance and function of the eyelids by repositioning and/or removing excess skin and soft tissue from the eyelids, most often through external incisions that minimize scarring and maximize the aesthetic outcomes of the surgery. Therefore, the placement of the incisions is an important determinant of the surgical outcome, and the preoperative marking of the eyelids to indicate where the incisions should be placed is a crucial part of preparation for the surgery.
Preoperative marking has unique challenges due to the dynamicity of the eyelids and the delicate nature of the surgery. The mark must be narrow to minimize the risk of placing the incision higher or lower than intended. The mark also must dry quickly because the patient may blink and create multiple impressions of the marking on skinfolds in contact with the wet ink. Fast drying of the ink used to create the marks improves the efficiency and clarity of the presurgical planning.
We present data on the performance of the various blepharoplasty markers regarding drying time and ink spread width based on an evaluation of 13 surgical markers.
Methods
Eleven unique fine tip (FT) markers and 2 standard tip (ST) markers were obtained based on their accessibility at the researchers’ home institution and availability for direct purchase in small quantities from the distributors (Figure 1). Four markers were double tipped with one FT end and one ST end; for these markers, only the FT end was studied. The experiments were conducted on the bilateral upper eyelids and on hairless patches of skin of a single patient in a minor procedure room with surgical lighting and minimal draft of air. The sole experimenter (J.M.K.) conducting the study was not blinded.
The drying time of each marker was measured by marking 1-in lines on a patch of hairless skin that was first cleaned with an alcohol pad, then dried. Drying time for each marking was measured in increments of 5 seconds; at each time point, the markings were wiped with a single-ply, light-duty tissue under the weight of 10 US quarters to ensure that the same weight/pressure was applied when wiping the skin. Smudges observed with the naked eye on either the wipe or the patients’ skin were interpreted as nondry status of the marking. The first time point at which a marking was found to have no visible smudges either on the skin or the wipe was recorded as the drying time of the respective marker.
Ink spread was measured on clean eyelid skin by drawing curved lines along the natural crease as would be done for actual blepharoplasty planning. Each line was allowed to dry for 2 minutes. The greatest perpendicular spread width along the line observed with the naked eye was measured using a digital Vernier caliper with 0.01-mm graduations. Three measurements were obtained per marker and the values averaged to arrive at the final spread width.
Results
Drying time among the 13 total markers (11 FT and 2 ST) ranged from 5 to 70 seconds, with a mean of 20.8 seconds and median of 5 seconds (Table). The drying time for the DERMarker E-Z Removable Ink Mini Skin Marker (Delasco, LLC) with an ST was 5 seconds, while the drying time for the other ST marker, WriteSite Plus Surgical Skin Marker (Aspen Surgical, Inc), was 70 seconds. The FT markers spanned the entire range of drying times. The ink spread width among the markers ranged from 0.53 to 2.27 mm with a median of 0.9 mm and mean of 1.13 mm (Table). The 2 ST markers were found to make some of the widest marks measured, including the WriteSite Plus Surgical Skin Marker, a nonsterile ST marker that created the widest ink marks. The second widest mark was made by an FT marker (Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker [Viscot Medical, LLC]).
To prioritize short drying time coupled with minimal ink spread width, the values associated with each marker were averaged to arrive at the overall score for each marker. The smaller the overall score, the higher we ranked the marker. The Devon Surgical Skin Marker, Dual Tip (Medtronic) ranked the highest among the 13 markers with a final score of 2.78. Runner-up markers included the Sterile Devon Surgical Skin marker, Fine Tip (Medtronic)(final score, 2.86); the Sterile Dual Tip Skin/Utility Marker (Medline Industries, Inc)(final score, 2.86); and the Skin Marker, Fine Tip (Cardinal Health)(final score, 2.89). The 2 lowest-ranking markers were the WriteSite Plus Surgical Skin Marker, an ST marker (final score, 36.13), followed by the Sterile BlephMarker (Viscot Medical, LLC)(final score, 35.27).
Figure 2 shows the drying time and ink spread width for all 13 markers.
Comment
Blepharoplasty surgeons generally agree that meticulous presurgical planning with marking of the eyelids is critical for successful surgical outcomes.1,2 Fine tip markers have been recommended for this purpose due to the relative precision of the marks, but the prerequisite of these markers is that the marks must have minimal ink spread through skinfolds to allow for precision as well as short drying time to avoid unintentional duplication of the ink on overlapping skin, especially with the likely chance of reflexive blinking by the patient. The associated assumption is that FT markers automatically leave precise marks with minimal drying time. This study systemically compared these 2 qualities for 13 markers, and the results are notable for the unexpected wide range of performance. Although most of the FT markers had ink spread width of less than 1 mm, the Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker was an outlier among FT markers, with ink spread greater than 2 mm, making it too broad and imprecise for practical use. This result indicates that not every FT marker actually makes fine marks. The 2 ST markers in the study—DERMarker E-Z Removable Ink Mini Skin Marker and WriteSite Plus Surgical Skin Marker—left broad marks as anticipated.
The drying time of the markers also ranged from 5 to 70 seconds among both FT and ST markers. Indeed, most of the FT markers were dry at or before 5 seconds of marking, but 2 FT markers—Sterile Mini Ultrafine Tip XL Prep Resistant Ink Marker and Sterile BlephMarker—dried at 65 and 70 seconds, respectively. Such a long drying time would be considered impractical for use in blepharoplasty marking and also unexpected of FT markers, which usually are marketed for their precision and efficiency. Notable in the discussion of drying time is that one of the 2 ST markers in the study, the DERMarker E-Z Removable Ink Mini Skin Marker, had the shortest possible drying time of 5 seconds, while the other ST marker, WriteSite Plus Surgical Skin Marker, dried at 70 seconds. This observation coupled with the unexpected results of broad marks and long drying time for some of the FT markers indicates that a surgeon cannot simply assume that a FT marker would provide marks with precision and fast drying time, or that an ST marker would be the opposite.
Future directions for study include the addition of other markers and the extent of resistance to antiseptic routines that can fade the markings.
Conclusion
Among the 13 markers studied, FT markers typically had the shortest drying time and least ink
Acknowledgement
The authors would like to thank Laura B. Hall, MD (New Haven, Connecticut), for her participation as the volunteer in this study.
- Hartstein ME, Massry GG, Holds JB. Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. New York, NY: Springer New York; 2015.
- Gladstone G, Black EH. Oculoplastic Surgery Atlas. New York, NY: Springer New York; 2005.
- Hartstein ME, Massry GG, Holds JB. Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. New York, NY: Springer New York; 2015.
- Gladstone G, Black EH. Oculoplastic Surgery Atlas. New York, NY: Springer New York; 2005.
Resident Pearl
Based on the data presented in this study, blepharoplasty surgeons may choose to use the markers shown to have measurably short drying time and minimal ink spread to maximize efficiency of preincisional lid marking.
Nitrous oxide linked to less pain in tattoo removal
SAN DIEGO – The results of a small, single-site study suggest that nitrous oxide (NO) can play a significant role in reducing pain during laser tattoo removal.
“Nitrous oxide is a safe and effective option for patients, particularly those who have large tattoos that can’t be adequately numbed with injections or topical numbing,” the study’s lead author, Jared Mallalieu, DO, said in an interview. “NO has allowed us to treat larger tattoos – full sleeve or large back tattoos – in a single setting, which has made treatment more convenient for patients.”
Patients fared better on pain measures when they received NO, compared with topical and injectable anesthetics, according to Dr. Mallalieu, a cosmetic surgeon at the Laser Center of Maryland, Severna Park. The results were so dramatic that EMLA cream is now rarely used for patients in his clinic, although injectable lidocaine is used on smaller tattoos (smaller than 5 inches by 5 inches), he said.
The use of NO comes with challenges, however, in terms of the extra time and patient monitoring required, he said.
Dr. Mallalieu and his associates reported the results in an e-poster at the annual meeting of the American Society for Laser Medicine and Surgery.
Laser tattoo removal can be an agonizing process. “Patients describe it as being significantly more painful than getting a tattoo,” Dr. Mallalieu said. “The intense pain only lasts during the treatment,” he said, “though many patients will note some discomfort for a few hours after a treatment session.”
Most clinics use a topical cream, such as lidocaine/prilocaine (EMLA) or topical benzocaine/lidocaine/tetracaine (BLT), as an anesthetic for these procedures. “Our center has also used 1% lidocaine with epinephrine in small doses of up to 7 mg/kg,” he said. “The injections are much better than the cream.”
Sometimes the clinic uses a device that blows cold air on the skin, which “helps a little,” he added.
For the study, conducted in 2014, 23 laser tattoo removal patients were surveyed about their pain levels using a 1-10 scale, after undergoing a total of 41 single-location procedures.

The average pain rating during the procedure was 9.1 for those treated only with lidocaine/prilocaine, 5.4 for injections of lidocaine with epinephrine alone, and 6.8 for both lidocaine/prilocaine and lidocaine with epinephrine injections.
The average pain rating for NO alone was 2.6, and was 3.6 for those who received both the injection treatment and lidocaine/prilocaine. Three of 12 NO patients reported anxiety.
Another benefit is that patients can drive after receiving NO, unlike other anesthetics, which leave patients sedated, he said. “Levels of NO are titrated to keep the patient sedated, but breathing on their own,” and patients can be easily woken up within moments of stopping the NO.
However, the use of NO requires more time to set up and more monitoring, he added. The average treatment time for procedures with NO was 27 minutes compared with 4 minutes for the other procedure, and “the patient is put on a monitor that measures pulse rate and oxygenation levels,” which not only takes more time, but requires additional staff to watch the patient. “Also, it takes about 3-5 minutes to slowly the titrate the NO to a perfect level.”
The study points out that physicians at the clinic are the only ones who perform the procedures that use NO, but at many clinics, nonphysicians perform tattoo removals.
As for cost, “NO and oxygen tanks are rather inexpensive to purchase and maintain, and there are various small units which serve to titrate the gas,” Dr. Mallalieu said. “We do charge our patients a small fee because of the added personnel and time cost associated with the procedure. As tattoo removal is considered a cosmetic procedure, insurance doesn’t come into play.”
Training to administer NO brings up the issue of what is allowed in the state, he said. Physicians can give sedation to patients, “but some states may limit the degree to which a patient can be sedated in an office. If the physician has a certified operating room, this is not a problem,” he added. “Because dentists commonly use NO, we followed the American Dental Association guidelines ... As we employ an anesthesiologist, we were quite familiar with it. That said, the administration of NO is not complex and [is] easily mastered.”
Dr. Mallalieu reported no relevant disclosures.
SAN DIEGO – The results of a small, single-site study suggest that nitrous oxide (NO) can play a significant role in reducing pain during laser tattoo removal.
“Nitrous oxide is a safe and effective option for patients, particularly those who have large tattoos that can’t be adequately numbed with injections or topical numbing,” the study’s lead author, Jared Mallalieu, DO, said in an interview. “NO has allowed us to treat larger tattoos – full sleeve or large back tattoos – in a single setting, which has made treatment more convenient for patients.”
Patients fared better on pain measures when they received NO, compared with topical and injectable anesthetics, according to Dr. Mallalieu, a cosmetic surgeon at the Laser Center of Maryland, Severna Park. The results were so dramatic that EMLA cream is now rarely used for patients in his clinic, although injectable lidocaine is used on smaller tattoos (smaller than 5 inches by 5 inches), he said.
The use of NO comes with challenges, however, in terms of the extra time and patient monitoring required, he said.
Dr. Mallalieu and his associates reported the results in an e-poster at the annual meeting of the American Society for Laser Medicine and Surgery.
Laser tattoo removal can be an agonizing process. “Patients describe it as being significantly more painful than getting a tattoo,” Dr. Mallalieu said. “The intense pain only lasts during the treatment,” he said, “though many patients will note some discomfort for a few hours after a treatment session.”
Most clinics use a topical cream, such as lidocaine/prilocaine (EMLA) or topical benzocaine/lidocaine/tetracaine (BLT), as an anesthetic for these procedures. “Our center has also used 1% lidocaine with epinephrine in small doses of up to 7 mg/kg,” he said. “The injections are much better than the cream.”
Sometimes the clinic uses a device that blows cold air on the skin, which “helps a little,” he added.
For the study, conducted in 2014, 23 laser tattoo removal patients were surveyed about their pain levels using a 1-10 scale, after undergoing a total of 41 single-location procedures.
The average pain rating during the procedure was 9.1 for those treated only with lidocaine/prilocaine, 5.4 for injections of lidocaine with epinephrine alone, and 6.8 for both lidocaine/prilocaine and lidocaine with epinephrine injections.
The average pain rating for NO alone was 2.6, and was 3.6 for those who received both the injection treatment and lidocaine/prilocaine. Three of 12 NO patients reported anxiety.
Another benefit is that patients can drive after receiving NO, unlike other anesthetics, which leave patients sedated, he said. “Levels of NO are titrated to keep the patient sedated, but breathing on their own,” and patients can be easily woken up within moments of stopping the NO.
However, the use of NO requires more time to set up and more monitoring, he added. The average treatment time for procedures with NO was 27 minutes compared with 4 minutes for the other procedure, and “the patient is put on a monitor that measures pulse rate and oxygenation levels,” which not only takes more time, but requires additional staff to watch the patient. “Also, it takes about 3-5 minutes to slowly the titrate the NO to a perfect level.”
The study points out that physicians at the clinic are the only ones who perform the procedures that use NO, but at many clinics, nonphysicians perform tattoo removals.
As for cost, “NO and oxygen tanks are rather inexpensive to purchase and maintain, and there are various small units which serve to titrate the gas,” Dr. Mallalieu said. “We do charge our patients a small fee because of the added personnel and time cost associated with the procedure. As tattoo removal is considered a cosmetic procedure, insurance doesn’t come into play.”
Training to administer NO brings up the issue of what is allowed in the state, he said. Physicians can give sedation to patients, “but some states may limit the degree to which a patient can be sedated in an office. If the physician has a certified operating room, this is not a problem,” he added. “Because dentists commonly use NO, we followed the American Dental Association guidelines ... As we employ an anesthesiologist, we were quite familiar with it. That said, the administration of NO is not complex and [is] easily mastered.”
Dr. Mallalieu reported no relevant disclosures.
SAN DIEGO – The results of a small, single-site study suggest that nitrous oxide (NO) can play a significant role in reducing pain during laser tattoo removal.
“Nitrous oxide is a safe and effective option for patients, particularly those who have large tattoos that can’t be adequately numbed with injections or topical numbing,” the study’s lead author, Jared Mallalieu, DO, said in an interview. “NO has allowed us to treat larger tattoos – full sleeve or large back tattoos – in a single setting, which has made treatment more convenient for patients.”
Patients fared better on pain measures when they received NO, compared with topical and injectable anesthetics, according to Dr. Mallalieu, a cosmetic surgeon at the Laser Center of Maryland, Severna Park. The results were so dramatic that EMLA cream is now rarely used for patients in his clinic, although injectable lidocaine is used on smaller tattoos (smaller than 5 inches by 5 inches), he said.
The use of NO comes with challenges, however, in terms of the extra time and patient monitoring required, he said.
Dr. Mallalieu and his associates reported the results in an e-poster at the annual meeting of the American Society for Laser Medicine and Surgery.
Laser tattoo removal can be an agonizing process. “Patients describe it as being significantly more painful than getting a tattoo,” Dr. Mallalieu said. “The intense pain only lasts during the treatment,” he said, “though many patients will note some discomfort for a few hours after a treatment session.”
Most clinics use a topical cream, such as lidocaine/prilocaine (EMLA) or topical benzocaine/lidocaine/tetracaine (BLT), as an anesthetic for these procedures. “Our center has also used 1% lidocaine with epinephrine in small doses of up to 7 mg/kg,” he said. “The injections are much better than the cream.”
Sometimes the clinic uses a device that blows cold air on the skin, which “helps a little,” he added.
For the study, conducted in 2014, 23 laser tattoo removal patients were surveyed about their pain levels using a 1-10 scale, after undergoing a total of 41 single-location procedures.
The average pain rating during the procedure was 9.1 for those treated only with lidocaine/prilocaine, 5.4 for injections of lidocaine with epinephrine alone, and 6.8 for both lidocaine/prilocaine and lidocaine with epinephrine injections.
The average pain rating for NO alone was 2.6, and was 3.6 for those who received both the injection treatment and lidocaine/prilocaine. Three of 12 NO patients reported anxiety.
Another benefit is that patients can drive after receiving NO, unlike other anesthetics, which leave patients sedated, he said. “Levels of NO are titrated to keep the patient sedated, but breathing on their own,” and patients can be easily woken up within moments of stopping the NO.
However, the use of NO requires more time to set up and more monitoring, he added. The average treatment time for procedures with NO was 27 minutes compared with 4 minutes for the other procedure, and “the patient is put on a monitor that measures pulse rate and oxygenation levels,” which not only takes more time, but requires additional staff to watch the patient. “Also, it takes about 3-5 minutes to slowly the titrate the NO to a perfect level.”
The study points out that physicians at the clinic are the only ones who perform the procedures that use NO, but at many clinics, nonphysicians perform tattoo removals.
As for cost, “NO and oxygen tanks are rather inexpensive to purchase and maintain, and there are various small units which serve to titrate the gas,” Dr. Mallalieu said. “We do charge our patients a small fee because of the added personnel and time cost associated with the procedure. As tattoo removal is considered a cosmetic procedure, insurance doesn’t come into play.”
Training to administer NO brings up the issue of what is allowed in the state, he said. Physicians can give sedation to patients, “but some states may limit the degree to which a patient can be sedated in an office. If the physician has a certified operating room, this is not a problem,” he added. “Because dentists commonly use NO, we followed the American Dental Association guidelines ... As we employ an anesthesiologist, we were quite familiar with it. That said, the administration of NO is not complex and [is] easily mastered.”
Dr. Mallalieu reported no relevant disclosures.
Twitter Q&A Transcript April 18, 2017
On April 18, 2017, Gary Goldenberg, MD, took over the @CutisJournal Twitter account for 1 hour to answer reader questions about updates in cosmetic dermatology. Below is a transcript of the Twitter Q&A session (#AskCutisJournal).

@carriekovarik
What can help #hyperpigmentation from prior #HIV related #prurigo in darker pts since this is a stigma of disease? #AskCutisJournal
@carriekovarik Aside from lightening agents & moisturizers, success with #microneedling. Go low & slow 2 prevent more hyperpigmentation.
RELATED ARTICLE:
Microneedling Therapy With and Without Platelet-Rich Plasma
@NailDoc12
What's new for treatment of melasma?
@NailDoc12 I recommend combo of prevention, sunscreen & lightening cream w/ microneedling w/ PRP or ktp laser such as #Cutera #ExcelV.
RELATED ARTICLE:
Dermatologists Weigh in on Skin-Lightening Agents
@NailDoc12
Is there good evidence for use of PRP for skin aging?
@NailDoc12 Pts swear by #PRP. Use after fillers/Botox & microneedling or laser. Pts say it improves skin quality, gives it a "glow" (1/2)
@NailDoc12 Growth factors in PRP improve tissue vascularity & help cells regenerate & normalize. Helps w/wound healing post procedure (2/2)
RELATED VIDEO:
Microneedling With Platelet-Rich Plasma
@anthonymrossi
@CutisJournal #AskCutisJournal What is your approach to global facial rejuvenation? Do you like to start with injectables or laser?
@anthonymrossi Total rejuvenation is just that. I rec combo tx 2 improve skin quality (laser and/or microneedling with PRP) (1/2)
@anthonymrossi Plus wrinkle relaxers for dynamic wrinkles, & fillers to address volume loss and deep wrinkles & lines (2/2)
RELATED VIDEO:
Facial Rejuvenation With Fractional Laser Resurfacing
@SkindocDLCC
@CutisJournal #AskCutisJournal Whats your favorite filler for cheek lifting?
@SkindocDLCC Filler naive pts: #RestylaneLyft or #JuvedermVoluma. Experienced pts: #Radiesse or #Bellafill
@SkindocDLCC
@CutisJournal @Goldenberg_Derm What filler do you like for a sharper jawline? #AskCutisJournal
@SkindocDLCC I prefer long-lasting fillers, such as #Radiesse or #Bellafill. This is true for both male & female pts
RELATED ARTICLE:
Efficacy and Safety of New Dermal Fillers
@SkindocDLCC
@CutisJournal @Goldenberg_Derm How do you get a smooth forehead with neurotoxin without a heavy brow? #AskCutisJournal
@SkindocDLCC Precise placement of product is important. Some pts may require more product to completely smooth out forehead (1/2)
@SkindocDLCC Those pts may need a combo tx with laser such as #CO2 or #microneedling with #PRP (2/2)
@SkindocDLCC
@CutisJournal @Goldenberg_Derm How do you combine PRP and fillers? #AskCutisJournal
@SkindocDLCC I regularly use #PRP with fillers 2 enhance the effect (1/3)
@SkindocDLCC PRP helps stimulate collagen & increase vascularity needed for collagen production (2/3)
@SkindocDLCC I use a mesotherapy needle to inject #PRP after injecting filler and/or neurotoxins (3/3)
@MilitelloDerm
@CutisJournal @Goldenberg_Derm What is your favorite filler for tear troughs?
@MilitelloDerm I prefer Restylane or Juvederm Ultra. These fillers give the best volume effect & last longer than other options in my hands
RELATED ARTICLE:
Periocular Fillers and Related Anatomy

On April 18, 2017, Gary Goldenberg, MD, took over the @CutisJournal Twitter account for 1 hour to answer reader questions about updates in cosmetic dermatology. Below is a transcript of the Twitter Q&A session (#AskCutisJournal).
@carriekovarik
What can help #hyperpigmentation from prior #HIV related #prurigo in darker pts since this is a stigma of disease? #AskCutisJournal
@carriekovarik Aside from lightening agents & moisturizers, success with #microneedling. Go low & slow 2 prevent more hyperpigmentation.
RELATED ARTICLE:
Microneedling Therapy With and Without Platelet-Rich Plasma
@NailDoc12
What's new for treatment of melasma?
@NailDoc12 I recommend combo of prevention, sunscreen & lightening cream w/ microneedling w/ PRP or ktp laser such as #Cutera #ExcelV.
RELATED ARTICLE:
Dermatologists Weigh in on Skin-Lightening Agents
@NailDoc12
Is there good evidence for use of PRP for skin aging?
@NailDoc12 Pts swear by #PRP. Use after fillers/Botox & microneedling or laser. Pts say it improves skin quality, gives it a "glow" (1/2)
@NailDoc12 Growth factors in PRP improve tissue vascularity & help cells regenerate & normalize. Helps w/wound healing post procedure (2/2)
RELATED VIDEO:
Microneedling With Platelet-Rich Plasma
@anthonymrossi
@CutisJournal #AskCutisJournal What is your approach to global facial rejuvenation? Do you like to start with injectables or laser?
@anthonymrossi Total rejuvenation is just that. I rec combo tx 2 improve skin quality (laser and/or microneedling with PRP) (1/2)
@anthonymrossi Plus wrinkle relaxers for dynamic wrinkles, & fillers to address volume loss and deep wrinkles & lines (2/2)
RELATED VIDEO:
Facial Rejuvenation With Fractional Laser Resurfacing
@SkindocDLCC
@CutisJournal #AskCutisJournal Whats your favorite filler for cheek lifting?
@SkindocDLCC Filler naive pts: #RestylaneLyft or #JuvedermVoluma. Experienced pts: #Radiesse or #Bellafill
@SkindocDLCC
@CutisJournal @Goldenberg_Derm What filler do you like for a sharper jawline? #AskCutisJournal
@SkindocDLCC I prefer long-lasting fillers, such as #Radiesse or #Bellafill. This is true for both male & female pts
RELATED ARTICLE:
Efficacy and Safety of New Dermal Fillers
@SkindocDLCC
@CutisJournal @Goldenberg_Derm How do you get a smooth forehead with neurotoxin without a heavy brow? #AskCutisJournal
@SkindocDLCC Precise placement of product is important. Some pts may require more product to completely smooth out forehead (1/2)
@SkindocDLCC Those pts may need a combo tx with laser such as #CO2 or #microneedling with #PRP (2/2)
@SkindocDLCC
@CutisJournal @Goldenberg_Derm How do you combine PRP and fillers? #AskCutisJournal
@SkindocDLCC I regularly use #PRP with fillers 2 enhance the effect (1/3)
@SkindocDLCC PRP helps stimulate collagen & increase vascularity needed for collagen production (2/3)
@SkindocDLCC I use a mesotherapy needle to inject #PRP after injecting filler and/or neurotoxins (3/3)
@MilitelloDerm
@CutisJournal @Goldenberg_Derm What is your favorite filler for tear troughs?
@MilitelloDerm I prefer Restylane or Juvederm Ultra. These fillers give the best volume effect & last longer than other options in my hands
RELATED ARTICLE:
Periocular Fillers and Related Anatomy
On April 18, 2017, Gary Goldenberg, MD, took over the @CutisJournal Twitter account for 1 hour to answer reader questions about updates in cosmetic dermatology. Below is a transcript of the Twitter Q&A session (#AskCutisJournal).
@carriekovarik
What can help #hyperpigmentation from prior #HIV related #prurigo in darker pts since this is a stigma of disease? #AskCutisJournal
@carriekovarik Aside from lightening agents & moisturizers, success with #microneedling. Go low & slow 2 prevent more hyperpigmentation.
RELATED ARTICLE:
Microneedling Therapy With and Without Platelet-Rich Plasma
@NailDoc12
What's new for treatment of melasma?
@NailDoc12 I recommend combo of prevention, sunscreen & lightening cream w/ microneedling w/ PRP or ktp laser such as #Cutera #ExcelV.
RELATED ARTICLE:
Dermatologists Weigh in on Skin-Lightening Agents
@NailDoc12
Is there good evidence for use of PRP for skin aging?
@NailDoc12 Pts swear by #PRP. Use after fillers/Botox & microneedling or laser. Pts say it improves skin quality, gives it a "glow" (1/2)
@NailDoc12 Growth factors in PRP improve tissue vascularity & help cells regenerate & normalize. Helps w/wound healing post procedure (2/2)
RELATED VIDEO:
Microneedling With Platelet-Rich Plasma
@anthonymrossi
@CutisJournal #AskCutisJournal What is your approach to global facial rejuvenation? Do you like to start with injectables or laser?
@anthonymrossi Total rejuvenation is just that. I rec combo tx 2 improve skin quality (laser and/or microneedling with PRP) (1/2)
@anthonymrossi Plus wrinkle relaxers for dynamic wrinkles, & fillers to address volume loss and deep wrinkles & lines (2/2)
RELATED VIDEO:
Facial Rejuvenation With Fractional Laser Resurfacing
@SkindocDLCC
@CutisJournal #AskCutisJournal Whats your favorite filler for cheek lifting?
@SkindocDLCC Filler naive pts: #RestylaneLyft or #JuvedermVoluma. Experienced pts: #Radiesse or #Bellafill
@SkindocDLCC
@CutisJournal @Goldenberg_Derm What filler do you like for a sharper jawline? #AskCutisJournal
@SkindocDLCC I prefer long-lasting fillers, such as #Radiesse or #Bellafill. This is true for both male & female pts
RELATED ARTICLE:
Efficacy and Safety of New Dermal Fillers
@SkindocDLCC
@CutisJournal @Goldenberg_Derm How do you get a smooth forehead with neurotoxin without a heavy brow? #AskCutisJournal
@SkindocDLCC Precise placement of product is important. Some pts may require more product to completely smooth out forehead (1/2)
@SkindocDLCC Those pts may need a combo tx with laser such as #CO2 or #microneedling with #PRP (2/2)
@SkindocDLCC
@CutisJournal @Goldenberg_Derm How do you combine PRP and fillers? #AskCutisJournal
@SkindocDLCC I regularly use #PRP with fillers 2 enhance the effect (1/3)
@SkindocDLCC PRP helps stimulate collagen & increase vascularity needed for collagen production (2/3)
@SkindocDLCC I use a mesotherapy needle to inject #PRP after injecting filler and/or neurotoxins (3/3)
@MilitelloDerm
@CutisJournal @Goldenberg_Derm What is your favorite filler for tear troughs?
@MilitelloDerm I prefer Restylane or Juvederm Ultra. These fillers give the best volume effect & last longer than other options in my hands
RELATED ARTICLE:
Periocular Fillers and Related Anatomy
Know your new hyaluronic acid–based fillers
WAILEA, HAWAII – American dermatologists are now gaining access to a lot of new hyaluronic acid-based fillers, designed to address limitations in the older, tried-and-true product lines, according to Nowell Solish, MD.
These products have been available in Canada for years. Dr. Solish, a dermatologist at the University of Toronto, shared insights regarding their optimal use, based on his extensive experience with them.

Allergan’s earlier Juvéderm Ultra range of dermal fillers is based on Hylacross, which utilizes crosslinked high–molecular weight HA.
“These products have been around a long time and have lots of benefits, but there were definitely some things missing in the product line,” he explained. “We wanted more control of gel swelling – that is, how much water the hyaluronic acid takes up.”
The Vycross technology employs a proprietary mix of low– and high–molecular weight HA, which results in a highly crosslinked gel that’s moldable immediately after injection, displays minimal gel swelling, and is designed to last longer than earlier-generation fillers.
The main difference between the three products lies in their HA concentrations: Juvéderm Voluma XC has the highest concentration of HA and Juvéderm Volbella XC the lowest, with Volift in between.
The company claims that outcomes with Volbella and Volift last up to 12 months, while Voluma outcomes lasts for up to 24 months. Dr. Solish suggested that his American colleagues take that with a grain of salt.
“I would say I always underpromise and overdeliver with my patients,” he noted. “I think you can probably detect Voluma at 2 years, but, the question is, how good is the effect? How happy is the patient? I think 2 years is a little bit of a stretch. I think it lasts for about 9 months to a year before reinjection.”
Voluma has been available in the United States for several years, while Dr. Solish has been using it far longer. His impression is that Voluma is great for creating volume, especially in the cheeks, midface, and submalar area. He finds that he gets his best results by implanting the product in a series of small, 0.2-mL, tent-like boluses. The reinjection volume is typically substantially less than that employed in initial treatment.
Volbella received approval from the FDA in autumn 2016 for perioral injection and is just now reaching the U.S. marketplace.
“In my humble opinion, I don’t think Volbella is really good for volume,” he explained. “I think it’s great for what I call lip hydration, to give that lip a lipstick look. Where I find that I use this product the most is for the perioral rhytids – the vertical lip lines people sometimes call smokers’ lines. I implant it in the lip mucosa to straighten out the folds.”
Dr. Solish cautioned that Volbella is a fast-flowing product.
“The thing you have to be careful about with Volbella is it has a very low extrusion force,” he noted. “That means it’s very easy to unload the syringe and get too much product out. And there’s no question that there’s a direct correlation between speed of injection and adverse events, mainly edema. So, just remember to slow your hand down, or off-label to add a 31- or even 32-gauge needle to the syringe.”
Volift is not yet approved in the United States, but it’s coming. Dr. Solish called it “a good workhorse product” for mild-to-moderate lines around the face.
“Sales will be much higher than for Volbella, because Volift is great for the in-between things,” the dermatologist continued. “You have Voluma for volume on the midface and cheeks, but Volift is great for nasolabial folds and, especially, for marionette lines and smile lines, where you don’t want a lot of bulk.”
The main adverse event encountered with any of the three products is delayed-onset development of nonpainful inflammatory nodules arising 3-6 months post injection. In one Canadian study, the incidence was less than 0.5% (Dermatol Surg. 2015 Sep;41[9]:1060-7).
Dr. Solish recommended treating the nodules with weekly or biweekly intralesional injections of hyaluronidase, followed by intralesional injections of 0.1 mL/cm2 of triamcinolone (Kenalog) at 2.5 mg/mL to 5.0 mg/mL.
Turning to Galderma’s NASHA technology, Dr. Solish explained that it relies on naturally occurring entanglement of HA chains to create gel particles formulated at 20 mg/dL. By varying the gel particle size and the amount of crosslinking, the company has created a series of products with different properties.
Restylane Refyne features smaller-size particles and less crosslinking, which makes for a softer gel. It’s an excellent option for marionette lines, mild nasolabial folds, and small perioral lines, and “it’s my absolute go-to for tear troughs,” Dr. Solish said.
In contrast, Restylane Defyne has bigger gel particles and more extensive HA crosslinking. It is firmer than Refyne and is best suited for achieving lift and volume. He implants it in the cheeks, forehead, temples, and deeper nasolabial folds.
In addition to these two products, which are new to the United States, Galderma has rebranded Perlane as Restylane Lyft, approved for midfacial augmentation. Another product, Restylane Silk, is similar to Volbella in that it is fast-flowing and not a big volumizer. Dr. Solish called it “lipstick in a syringe,” best suited for improving definition of the lips and for addressing perioral fine lines.
Dr. Solish reported serving as an investigator and/or consultant for Allergan, Galderma, Indeed, Merz, Revance Therapeutics, and Valeant. The SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – American dermatologists are now gaining access to a lot of new hyaluronic acid-based fillers, designed to address limitations in the older, tried-and-true product lines, according to Nowell Solish, MD.
These products have been available in Canada for years. Dr. Solish, a dermatologist at the University of Toronto, shared insights regarding their optimal use, based on his extensive experience with them.
Allergan’s earlier Juvéderm Ultra range of dermal fillers is based on Hylacross, which utilizes crosslinked high–molecular weight HA.
“These products have been around a long time and have lots of benefits, but there were definitely some things missing in the product line,” he explained. “We wanted more control of gel swelling – that is, how much water the hyaluronic acid takes up.”
The Vycross technology employs a proprietary mix of low– and high–molecular weight HA, which results in a highly crosslinked gel that’s moldable immediately after injection, displays minimal gel swelling, and is designed to last longer than earlier-generation fillers.
The main difference between the three products lies in their HA concentrations: Juvéderm Voluma XC has the highest concentration of HA and Juvéderm Volbella XC the lowest, with Volift in between.
The company claims that outcomes with Volbella and Volift last up to 12 months, while Voluma outcomes lasts for up to 24 months. Dr. Solish suggested that his American colleagues take that with a grain of salt.
“I would say I always underpromise and overdeliver with my patients,” he noted. “I think you can probably detect Voluma at 2 years, but, the question is, how good is the effect? How happy is the patient? I think 2 years is a little bit of a stretch. I think it lasts for about 9 months to a year before reinjection.”
Voluma has been available in the United States for several years, while Dr. Solish has been using it far longer. His impression is that Voluma is great for creating volume, especially in the cheeks, midface, and submalar area. He finds that he gets his best results by implanting the product in a series of small, 0.2-mL, tent-like boluses. The reinjection volume is typically substantially less than that employed in initial treatment.
Volbella received approval from the FDA in autumn 2016 for perioral injection and is just now reaching the U.S. marketplace.
“In my humble opinion, I don’t think Volbella is really good for volume,” he explained. “I think it’s great for what I call lip hydration, to give that lip a lipstick look. Where I find that I use this product the most is for the perioral rhytids – the vertical lip lines people sometimes call smokers’ lines. I implant it in the lip mucosa to straighten out the folds.”
Dr. Solish cautioned that Volbella is a fast-flowing product.
“The thing you have to be careful about with Volbella is it has a very low extrusion force,” he noted. “That means it’s very easy to unload the syringe and get too much product out. And there’s no question that there’s a direct correlation between speed of injection and adverse events, mainly edema. So, just remember to slow your hand down, or off-label to add a 31- or even 32-gauge needle to the syringe.”
Volift is not yet approved in the United States, but it’s coming. Dr. Solish called it “a good workhorse product” for mild-to-moderate lines around the face.
“Sales will be much higher than for Volbella, because Volift is great for the in-between things,” the dermatologist continued. “You have Voluma for volume on the midface and cheeks, but Volift is great for nasolabial folds and, especially, for marionette lines and smile lines, where you don’t want a lot of bulk.”
The main adverse event encountered with any of the three products is delayed-onset development of nonpainful inflammatory nodules arising 3-6 months post injection. In one Canadian study, the incidence was less than 0.5% (Dermatol Surg. 2015 Sep;41[9]:1060-7).
Dr. Solish recommended treating the nodules with weekly or biweekly intralesional injections of hyaluronidase, followed by intralesional injections of 0.1 mL/cm2 of triamcinolone (Kenalog) at 2.5 mg/mL to 5.0 mg/mL.
Turning to Galderma’s NASHA technology, Dr. Solish explained that it relies on naturally occurring entanglement of HA chains to create gel particles formulated at 20 mg/dL. By varying the gel particle size and the amount of crosslinking, the company has created a series of products with different properties.
Restylane Refyne features smaller-size particles and less crosslinking, which makes for a softer gel. It’s an excellent option for marionette lines, mild nasolabial folds, and small perioral lines, and “it’s my absolute go-to for tear troughs,” Dr. Solish said.
In contrast, Restylane Defyne has bigger gel particles and more extensive HA crosslinking. It is firmer than Refyne and is best suited for achieving lift and volume. He implants it in the cheeks, forehead, temples, and deeper nasolabial folds.
In addition to these two products, which are new to the United States, Galderma has rebranded Perlane as Restylane Lyft, approved for midfacial augmentation. Another product, Restylane Silk, is similar to Volbella in that it is fast-flowing and not a big volumizer. Dr. Solish called it “lipstick in a syringe,” best suited for improving definition of the lips and for addressing perioral fine lines.
Dr. Solish reported serving as an investigator and/or consultant for Allergan, Galderma, Indeed, Merz, Revance Therapeutics, and Valeant. The SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – American dermatologists are now gaining access to a lot of new hyaluronic acid-based fillers, designed to address limitations in the older, tried-and-true product lines, according to Nowell Solish, MD.
These products have been available in Canada for years. Dr. Solish, a dermatologist at the University of Toronto, shared insights regarding their optimal use, based on his extensive experience with them.
Allergan’s earlier Juvéderm Ultra range of dermal fillers is based on Hylacross, which utilizes crosslinked high–molecular weight HA.
“These products have been around a long time and have lots of benefits, but there were definitely some things missing in the product line,” he explained. “We wanted more control of gel swelling – that is, how much water the hyaluronic acid takes up.”
The Vycross technology employs a proprietary mix of low– and high–molecular weight HA, which results in a highly crosslinked gel that’s moldable immediately after injection, displays minimal gel swelling, and is designed to last longer than earlier-generation fillers.
The main difference between the three products lies in their HA concentrations: Juvéderm Voluma XC has the highest concentration of HA and Juvéderm Volbella XC the lowest, with Volift in between.
The company claims that outcomes with Volbella and Volift last up to 12 months, while Voluma outcomes lasts for up to 24 months. Dr. Solish suggested that his American colleagues take that with a grain of salt.
“I would say I always underpromise and overdeliver with my patients,” he noted. “I think you can probably detect Voluma at 2 years, but, the question is, how good is the effect? How happy is the patient? I think 2 years is a little bit of a stretch. I think it lasts for about 9 months to a year before reinjection.”
Voluma has been available in the United States for several years, while Dr. Solish has been using it far longer. His impression is that Voluma is great for creating volume, especially in the cheeks, midface, and submalar area. He finds that he gets his best results by implanting the product in a series of small, 0.2-mL, tent-like boluses. The reinjection volume is typically substantially less than that employed in initial treatment.
Volbella received approval from the FDA in autumn 2016 for perioral injection and is just now reaching the U.S. marketplace.
“In my humble opinion, I don’t think Volbella is really good for volume,” he explained. “I think it’s great for what I call lip hydration, to give that lip a lipstick look. Where I find that I use this product the most is for the perioral rhytids – the vertical lip lines people sometimes call smokers’ lines. I implant it in the lip mucosa to straighten out the folds.”
Dr. Solish cautioned that Volbella is a fast-flowing product.
“The thing you have to be careful about with Volbella is it has a very low extrusion force,” he noted. “That means it’s very easy to unload the syringe and get too much product out. And there’s no question that there’s a direct correlation between speed of injection and adverse events, mainly edema. So, just remember to slow your hand down, or off-label to add a 31- or even 32-gauge needle to the syringe.”
Volift is not yet approved in the United States, but it’s coming. Dr. Solish called it “a good workhorse product” for mild-to-moderate lines around the face.
“Sales will be much higher than for Volbella, because Volift is great for the in-between things,” the dermatologist continued. “You have Voluma for volume on the midface and cheeks, but Volift is great for nasolabial folds and, especially, for marionette lines and smile lines, where you don’t want a lot of bulk.”
The main adverse event encountered with any of the three products is delayed-onset development of nonpainful inflammatory nodules arising 3-6 months post injection. In one Canadian study, the incidence was less than 0.5% (Dermatol Surg. 2015 Sep;41[9]:1060-7).
Dr. Solish recommended treating the nodules with weekly or biweekly intralesional injections of hyaluronidase, followed by intralesional injections of 0.1 mL/cm2 of triamcinolone (Kenalog) at 2.5 mg/mL to 5.0 mg/mL.
Turning to Galderma’s NASHA technology, Dr. Solish explained that it relies on naturally occurring entanglement of HA chains to create gel particles formulated at 20 mg/dL. By varying the gel particle size and the amount of crosslinking, the company has created a series of products with different properties.
Restylane Refyne features smaller-size particles and less crosslinking, which makes for a softer gel. It’s an excellent option for marionette lines, mild nasolabial folds, and small perioral lines, and “it’s my absolute go-to for tear troughs,” Dr. Solish said.
In contrast, Restylane Defyne has bigger gel particles and more extensive HA crosslinking. It is firmer than Refyne and is best suited for achieving lift and volume. He implants it in the cheeks, forehead, temples, and deeper nasolabial folds.
In addition to these two products, which are new to the United States, Galderma has rebranded Perlane as Restylane Lyft, approved for midfacial augmentation. Another product, Restylane Silk, is similar to Volbella in that it is fast-flowing and not a big volumizer. Dr. Solish called it “lipstick in a syringe,” best suited for improving definition of the lips and for addressing perioral fine lines.
Dr. Solish reported serving as an investigator and/or consultant for Allergan, Galderma, Indeed, Merz, Revance Therapeutics, and Valeant. The SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR
Hard water versus your skin
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.

Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.

Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.
Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.
Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.
Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.
Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Perfluorodecalin-spiked patch improves tattoo removal results
Laser tattoo removal with use of a perfluorodecalin (PFD)-infused patch allowed significantly more passes during a 5-minute treatment session, in a randomized trial of 30 adults.
In the study, published online in Lasers in Surgery and Medicine, an average of 3.7 laser treatment passes (range 2-4) were used when the laser was combined with a PFD-infused patch during a 5-minute session, compared with an average of 1.4 passes (range 1-3) with the laser alone (P less than .0001).
“Laser-assisted tattoo removal is generally regarded as safe and effective, but the procedure is subject to several important limitations,” wrote Brian S. Biesman, MD, and Cara Costner, RN, FNP, who practice in Nashville, Tenn. These limitations include the need to wait for epidermal whitening to dissipate between laser passes, but “one strategy for improving the efficiency of laser-assisted tattoo removal involves the topical use of an optical clearing agent to reduce the epidermal whitening effect,” they explained.

“Topical use of PFD reduces optical scattering at the skin surface, which helps to improve energy delivery to the tattoo ink in deeper layers of the skin and may reduce the potential of epidermal injury and treatment-related AEs,” they added (Lasers Surg Med. 2017 March 20. doi: 10.1002/lsm.22659).
They enrolled 16 women and 14 men seeking tattoo removal in the randomized, split-area study. The mean age of the subjects was 37 years; most were Fitzpatrick skin type II or III. One side of each tattoo was treated with the 755-nm Q-Switched Alexandrite nanosecond laser alone, and the other half was treated with the same laser through the PFD patch.
Patients’ reports of pain based on the Visual Analog Scale were approximately one point lower on the areas treated with the laser and the patch compared with the laser alone. Compared with the laser-only areas, a lower proportion of the areas treated with the patch were affected by edema (36.7% vs. 63.3%) or erythema (33.3% vs. 70%). None of the patients had hypopigmentation or hyperpigmentation. “All AEs [adverse events] were transient and had resolved by the 1-month follow-up visit,” at which time all 30 patients said they preferred to continue their tattoo removal using the PFD patch, the investigators wrote.
The findings were limited by several factors, including the use of a single laser and the predominance of black or dark blue tattoos, as well as the lack of patients with darker skin types. However, “incorporation of the PFD patch into laser tattoo removal procedures may afford multiple benefits to the patient and provider, including increased efficiency, improved patient safety, fewer AEs associated with epidermal injury, and protection of the patient and provider from tissue splatter and laser plume,” the authors concluded.
Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Laser tattoo removal with use of a perfluorodecalin (PFD)-infused patch allowed significantly more passes during a 5-minute treatment session, in a randomized trial of 30 adults.
In the study, published online in Lasers in Surgery and Medicine, an average of 3.7 laser treatment passes (range 2-4) were used when the laser was combined with a PFD-infused patch during a 5-minute session, compared with an average of 1.4 passes (range 1-3) with the laser alone (P less than .0001).
“Laser-assisted tattoo removal is generally regarded as safe and effective, but the procedure is subject to several important limitations,” wrote Brian S. Biesman, MD, and Cara Costner, RN, FNP, who practice in Nashville, Tenn. These limitations include the need to wait for epidermal whitening to dissipate between laser passes, but “one strategy for improving the efficiency of laser-assisted tattoo removal involves the topical use of an optical clearing agent to reduce the epidermal whitening effect,” they explained.
“Topical use of PFD reduces optical scattering at the skin surface, which helps to improve energy delivery to the tattoo ink in deeper layers of the skin and may reduce the potential of epidermal injury and treatment-related AEs,” they added (Lasers Surg Med. 2017 March 20. doi: 10.1002/lsm.22659).
They enrolled 16 women and 14 men seeking tattoo removal in the randomized, split-area study. The mean age of the subjects was 37 years; most were Fitzpatrick skin type II or III. One side of each tattoo was treated with the 755-nm Q-Switched Alexandrite nanosecond laser alone, and the other half was treated with the same laser through the PFD patch.
Patients’ reports of pain based on the Visual Analog Scale were approximately one point lower on the areas treated with the laser and the patch compared with the laser alone. Compared with the laser-only areas, a lower proportion of the areas treated with the patch were affected by edema (36.7% vs. 63.3%) or erythema (33.3% vs. 70%). None of the patients had hypopigmentation or hyperpigmentation. “All AEs [adverse events] were transient and had resolved by the 1-month follow-up visit,” at which time all 30 patients said they preferred to continue their tattoo removal using the PFD patch, the investigators wrote.
The findings were limited by several factors, including the use of a single laser and the predominance of black or dark blue tattoos, as well as the lack of patients with darker skin types. However, “incorporation of the PFD patch into laser tattoo removal procedures may afford multiple benefits to the patient and provider, including increased efficiency, improved patient safety, fewer AEs associated with epidermal injury, and protection of the patient and provider from tissue splatter and laser plume,” the authors concluded.
Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Laser tattoo removal with use of a perfluorodecalin (PFD)-infused patch allowed significantly more passes during a 5-minute treatment session, in a randomized trial of 30 adults.
In the study, published online in Lasers in Surgery and Medicine, an average of 3.7 laser treatment passes (range 2-4) were used when the laser was combined with a PFD-infused patch during a 5-minute session, compared with an average of 1.4 passes (range 1-3) with the laser alone (P less than .0001).
“Laser-assisted tattoo removal is generally regarded as safe and effective, but the procedure is subject to several important limitations,” wrote Brian S. Biesman, MD, and Cara Costner, RN, FNP, who practice in Nashville, Tenn. These limitations include the need to wait for epidermal whitening to dissipate between laser passes, but “one strategy for improving the efficiency of laser-assisted tattoo removal involves the topical use of an optical clearing agent to reduce the epidermal whitening effect,” they explained.
“Topical use of PFD reduces optical scattering at the skin surface, which helps to improve energy delivery to the tattoo ink in deeper layers of the skin and may reduce the potential of epidermal injury and treatment-related AEs,” they added (Lasers Surg Med. 2017 March 20. doi: 10.1002/lsm.22659).
They enrolled 16 women and 14 men seeking tattoo removal in the randomized, split-area study. The mean age of the subjects was 37 years; most were Fitzpatrick skin type II or III. One side of each tattoo was treated with the 755-nm Q-Switched Alexandrite nanosecond laser alone, and the other half was treated with the same laser through the PFD patch.
Patients’ reports of pain based on the Visual Analog Scale were approximately one point lower on the areas treated with the laser and the patch compared with the laser alone. Compared with the laser-only areas, a lower proportion of the areas treated with the patch were affected by edema (36.7% vs. 63.3%) or erythema (33.3% vs. 70%). None of the patients had hypopigmentation or hyperpigmentation. “All AEs [adverse events] were transient and had resolved by the 1-month follow-up visit,” at which time all 30 patients said they preferred to continue their tattoo removal using the PFD patch, the investigators wrote.
The findings were limited by several factors, including the use of a single laser and the predominance of black or dark blue tattoos, as well as the lack of patients with darker skin types. However, “incorporation of the PFD patch into laser tattoo removal procedures may afford multiple benefits to the patient and provider, including increased efficiency, improved patient safety, fewer AEs associated with epidermal injury, and protection of the patient and provider from tissue splatter and laser plume,” the authors concluded.
Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Key clinical point: Addition of a perfluorodecalin-infused patch to a laser treatment protocol allowed significantly more laser passes with no difference in adverse events.
Major finding: More laser treatment passes for tattoo removal were possible when the laser was combined with a perfluorodecalin patch vs. laser alone (an average of 3.7 vs. 1.4 passes in a 5-minute session, a significant difference).
Data source: A prospective, randomized study of 30 adults seeking removal of tattoos.
Disclosures: Dr. Biesman disclosed grant support, honoraria, or consulting fees from Allergan, Cutera, Cytrellis, Evolus Galderma, Intraderm, Merz, ON Light Sciences, Revance, Sienna, Suneva, Syneron-Candela, Valeant, and Zeltiq. The study was sponsored by ON Light Sciences.
Cosmetic Corner: Dermatologists Weigh in on Products for Hyperhidrosis
To improve patient care and outcomes, leading dermatologists offered their recommendations on hyperhidrosis products. Consideration must be given to:
- Certain Dri Prescription Strength Clinical Roll-On
Clarion Brands Inc
“This over-the-counter antiperspirant has 12% aluminum chloride, making it very effective in treating hyperhidrosis.”—Shari Lipner, MD, PhD, New York, New York
Recommended by Gary Goldenberg, MD, New York, New York
- miraDry
Miramar Labs, Inc
“miraDry offers a noninvasive reduction of sweating of more than 70% after the first treatment in the underarm area.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- SweatBlock Clinical Strength Antiperspirant Towelettes
SweatBlock
“Each of the towelettes contains 14% aluminum chloride, can be applied to any part of the body, and can last up to 7 days.”—Jeannette Graf, MD, New York, New York
Cutis invites readers to send us their recommendations. Products for athlete’s foot, redness reduction, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on hyperhidrosis products. Consideration must be given to:
- Certain Dri Prescription Strength Clinical Roll-On
Clarion Brands Inc
“This over-the-counter antiperspirant has 12% aluminum chloride, making it very effective in treating hyperhidrosis.”—Shari Lipner, MD, PhD, New York, New York
Recommended by Gary Goldenberg, MD, New York, New York
- miraDry
Miramar Labs, Inc
“miraDry offers a noninvasive reduction of sweating of more than 70% after the first treatment in the underarm area.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- SweatBlock Clinical Strength Antiperspirant Towelettes
SweatBlock
“Each of the towelettes contains 14% aluminum chloride, can be applied to any part of the body, and can last up to 7 days.”—Jeannette Graf, MD, New York, New York
Cutis invites readers to send us their recommendations. Products for athlete’s foot, redness reduction, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on hyperhidrosis products. Consideration must be given to:
- Certain Dri Prescription Strength Clinical Roll-On
Clarion Brands Inc
“This over-the-counter antiperspirant has 12% aluminum chloride, making it very effective in treating hyperhidrosis.”—Shari Lipner, MD, PhD, New York, New York
Recommended by Gary Goldenberg, MD, New York, New York
- miraDry
Miramar Labs, Inc
“miraDry offers a noninvasive reduction of sweating of more than 70% after the first treatment in the underarm area.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- SweatBlock Clinical Strength Antiperspirant Towelettes
SweatBlock
“Each of the towelettes contains 14% aluminum chloride, can be applied to any part of the body, and can last up to 7 days.”—Jeannette Graf, MD, New York, New York
Cutis invites readers to send us their recommendations. Products for athlete’s foot, redness reduction, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]

Electronic Collaboration in Dermatology Resident Training Through Social Networking
More than 1.8 billion individuals utilize social media, a number that continues to grow as the social media market expands.1 Social media enables individuals, groups, and organizations to efficiently disperse and access information2-4 and also provides a structure that encourages collaboration between patients, staff, and physicians that cannot be achieved by other communication modalities.4-6 Expert opinions and related educational materials can be shared globally, improving collaboration between dermatologists.6 A structured social networking site for sharing training materials, research, and ideas can help bring the national dermatology community together in a new way.
Other professions have employed social networking tools to accomplish similar goals of organizing training resources; radiology has an electronic database that allows sharing of training materials and incorporates social networking capabilities.7 Their Web software provides functionality for individual file uploading and supports collaboration and sharing, all while maintaining the security of uploaded information. General surgery has already addressed similar concerns via a task force that incorporates all the essential organizations in surgical education.8 Increased satisfaction and academic abilities have been demonstrated with their collaborative curriculum.9 Gastroenterologists also utilize electronic resources; one study showed that using videos to educate patients prior to colonoscopies was superior to face-to-face education.10 In addition, video education may free up time for office staff to accomplish other tasks.
As a specialty, dermatology has not been a leader in the implementation of social networking for collaboration and training purposes. Every dermatologist is an educator. To maintain a successful practice, dermatologists must keep up-to-date on their own clinical knowledge, provide training to their staff, and educate their patients. Although there are numerous educational resources available to dermatologists, an informal survey of 30 dermatology faculty members revealed a practice gap in awareness and utilization of these expanding electronic resources.11
To better understand the needs of the specialty as a whole, we chose to focus on one aspect of dermatology education: resident training. The goal of our study was to survey dermatology residents and faculty to gain a better understanding of how they currently provide education and what online resources and social networking sites they currently use or would be willing to use. The study included 3 central hypotheses: First, residents would be less satisfied with their current curriculum and residents would report greater contributions to the curriculum relative to faculty. Second, both residents and faculty of smaller programs would be more interested in collaborative educational resources relative to larger programs. Lastly, residents would be more willing than faculty to participate in social networking for educational purposes.
Methods
This study was granted institutional review board exemption. Two surveys were developed by the authors to assess the current structure and satisfaction of dermatology residency curriculum and the willingness to participate in social networking to use and share educational materials. The surveys were evaluated for relevance by the survey evaluation team of the Association of Professors of Dermatology (APD). The instrument was not pilot tested.
The surveys were electronically distributed using an online service to dermatology faculty via the APD listserve, which comprised the entirety of the APD membership in 2014. The resident survey was distributed to the dermatology residents via the American Society for Dermatologic Surgery listserve, which included all residents in training (2013-2014 academic year). Second and third invitations to complete the surveys were distributed 3 and 5 weeks later, respectively.
Resident and faculty responses were compared. Additionally, responses were stratified for large (>9 residents) and small programs (≤9 residents) for comparison. Descriptive statistics including means and medians for continuous variables and frequency tables for categorical variables were generated using research and spreadsheet software.
Results
There were 137 survey respondents; 52 of 426 (12.2%) dermatology faculty and 85 of 1539 (5.5%) dermatology residents responded to the survey. Small programs accounted for 24% of total survey responses and 76% were from large programs.
Current Curriculum
The majority of dermatology faculty (44%) and residents (35%) identified 1 to 2 faculty members as contributing to the creation and organization of their respective curricula; however, a notable percentage of residents (9%) reported that no faculty contributed to the organization of the curriculum. Residents noted that senior residents carry twice the responsibility for structuring the curriculum compared to faculty (61% vs 32% of the workload), but faculty described an even split between senior residents and faculty (47% vs 49% of the workload). Faculty believed their residents spend a similar amount of time in resident- and faculty-led instruction (38% vs 35% of their time); however, the majority of residents reported spending too little time in faculty-led instruction (53%). When residents ranked their preference for learning modes, faculty-led and self-study learning were ranked first and second by 48% and 45% of residents, respectively. Resident-led instruction was ranked last by 66% of residents. Likewise, a majority of residents (53%) described their amount of time in faculty-led instruction as too little.
When asked what subjects in dermatology were lacking at their programs, residents reported clinical trials (47%), skin of color (46%), cosmetic dermatology (34%), and aggressive skin cancer/multidisciplinary tumor board (32%). Although 11% of residents reported lacking inpatient dermatology in their curriculum, 0% of faculty reported the same. A notable percentage of faculty reported nothing was lacking compared to residents (25% vs 7%). Despite these different views between residents and faculty on their contributions to and structure of their curriculums, both faculty and residents claimed overall satisfaction (satisfied or very satisfied) with their program’s ability to optimally cover the field of dermatology in 3 years (100% and 91%, respectively).
Large Versus Small Residency Programs
When stratifying the resident responses for small versus large programs, both program sizes reported more time in resident-led instruction than faculty-led instruction. Likewise, residents in both program sizes equally preferred self-study or faculty-led instruction to resident-led instruction. Residents at small programs more often reported lacking instruction in rheumatology, immunobullous diseases, and basic science/skin biology compared to large-program residents. Compared to large-program faculty, small-program faculty reported lacking instruction in cosmetic dermatology.
Faculty at small programs reported spending too little time preparing for their faculty-led instruction compared to faculty at large programs (44% vs 12%). All (100%) of the faculty at small programs were likely to seek out study materials shared by top educators, while 77% of faculty at large programs were likely to do the same. When asked if faculty would translate what their program does well into an electronic format for sharing, 30% of large-program faculty were likely to do so compared to 11% of small-program faculty (Figure 1).
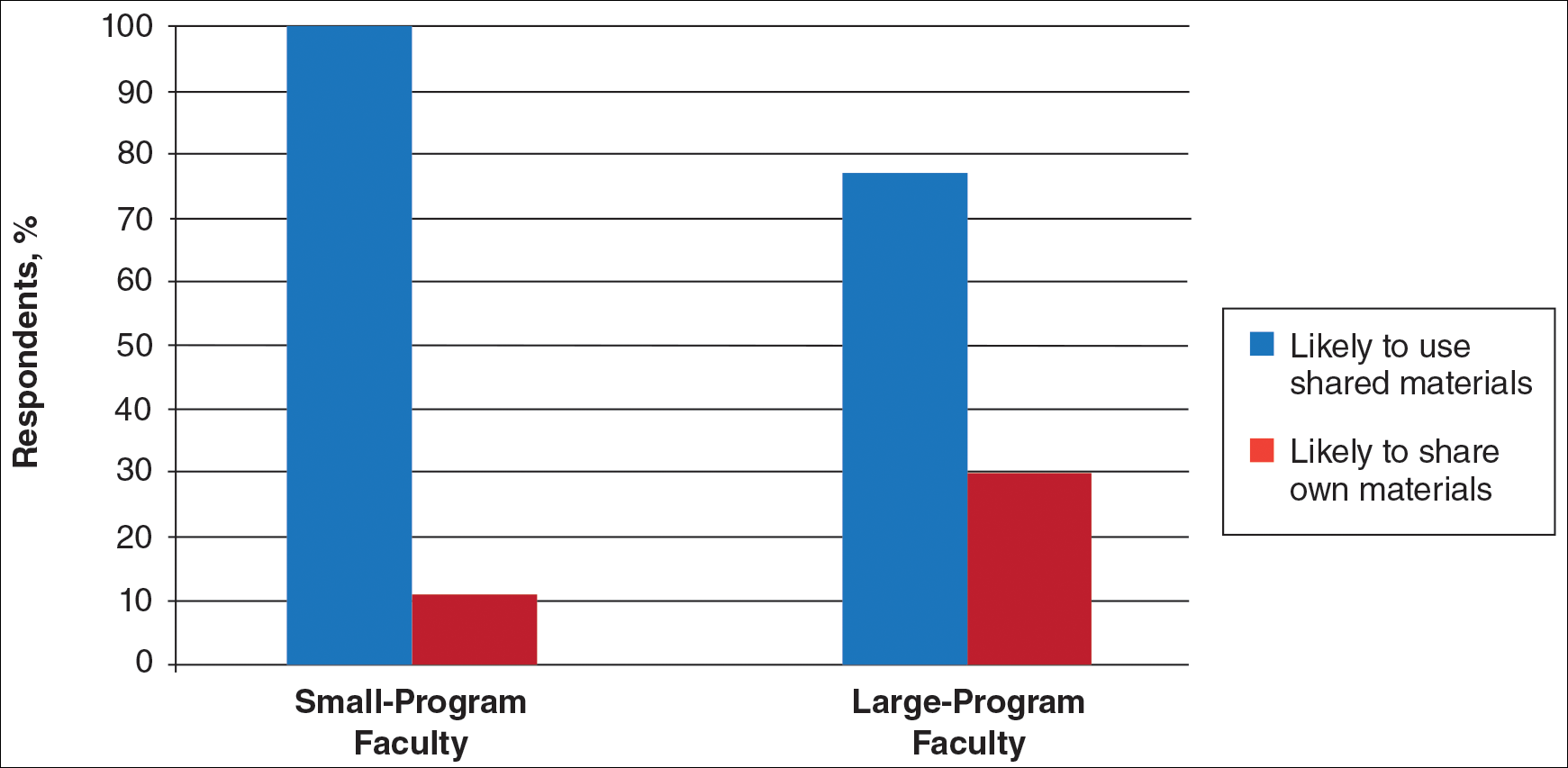
Use of Online Educational Materials and Interest in Collaboration
A majority of faculty and residents stated that they use online educational materials as supplements to traditional classroom lecture and print materials (81% vs 86%); however, almost twice as many residents stated that online educational materials were essential to their current study routines compared to faculty (39% vs 21%).
The majority of faculty (92%) and residents (84%) were either interested or very interested in a collaborative online curriculum. Both residents (85%) and faculty (81%) stated they would be likely to seek out online educational materials shared by top educators. Although both residents and faculty reported many aspects of their curriculums they thought could be beneficial to other dermatology programs (Table 1), only 27% of faculty and 19% of residents were likely to translate those strengths into a shareable electronic format. Several reasons were reported for not contributing to an online curriculum, with lack of time being the most common reason (Table 2).
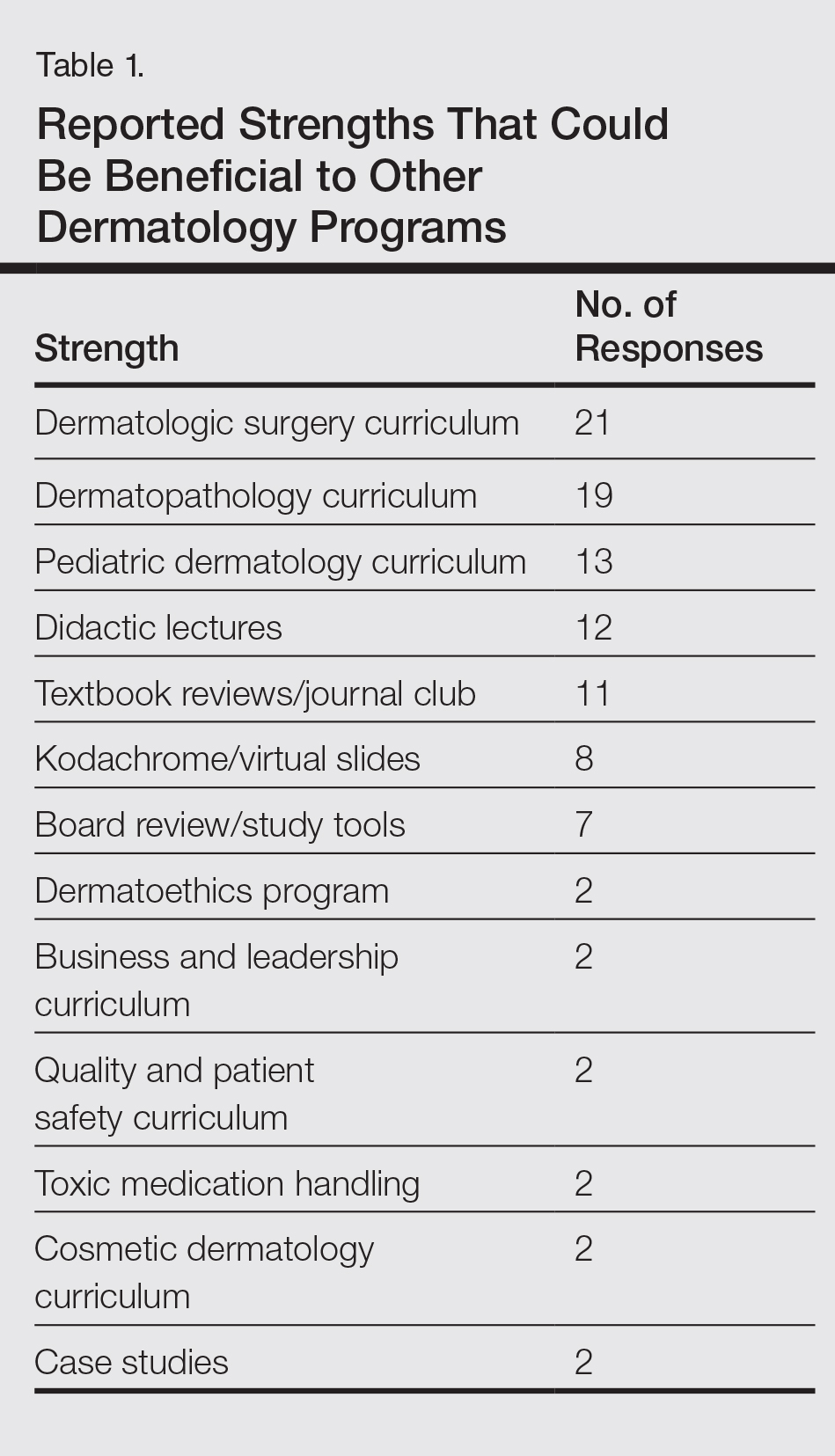
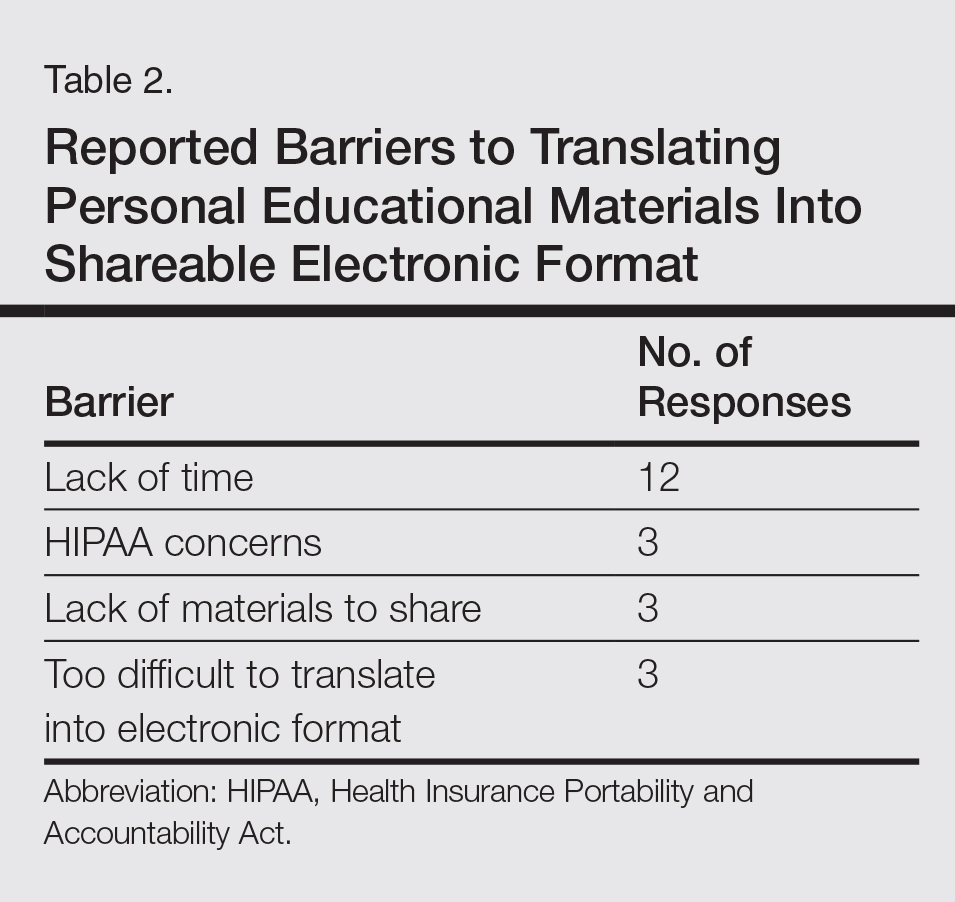
Eighty percent of residents and 88% of faculty reported they were either interested or very interested in being more connected/interactive with their dermatology peers nationally (Figure 2). Likewise, 94% of residents and 87% of faculty agreed that the dermatology community could benefit from a social networking site for educational collaboration. Four times as many residents versus faculty currently use social networking sites (eg, Facebook, LinkedIn, Google Groups) as a primary mode of communication with distant professional peers. The majority of residents (52%) reported they would be likely to participate in a professional social networking site, while the majority of faculty (50%) stated they were neutral on their likelihood of participating. Both residents and faculty reported lack of time as a common reason for being unlikely to utilize a professional social networking site. Other barriers to participation are listed in Table 3.
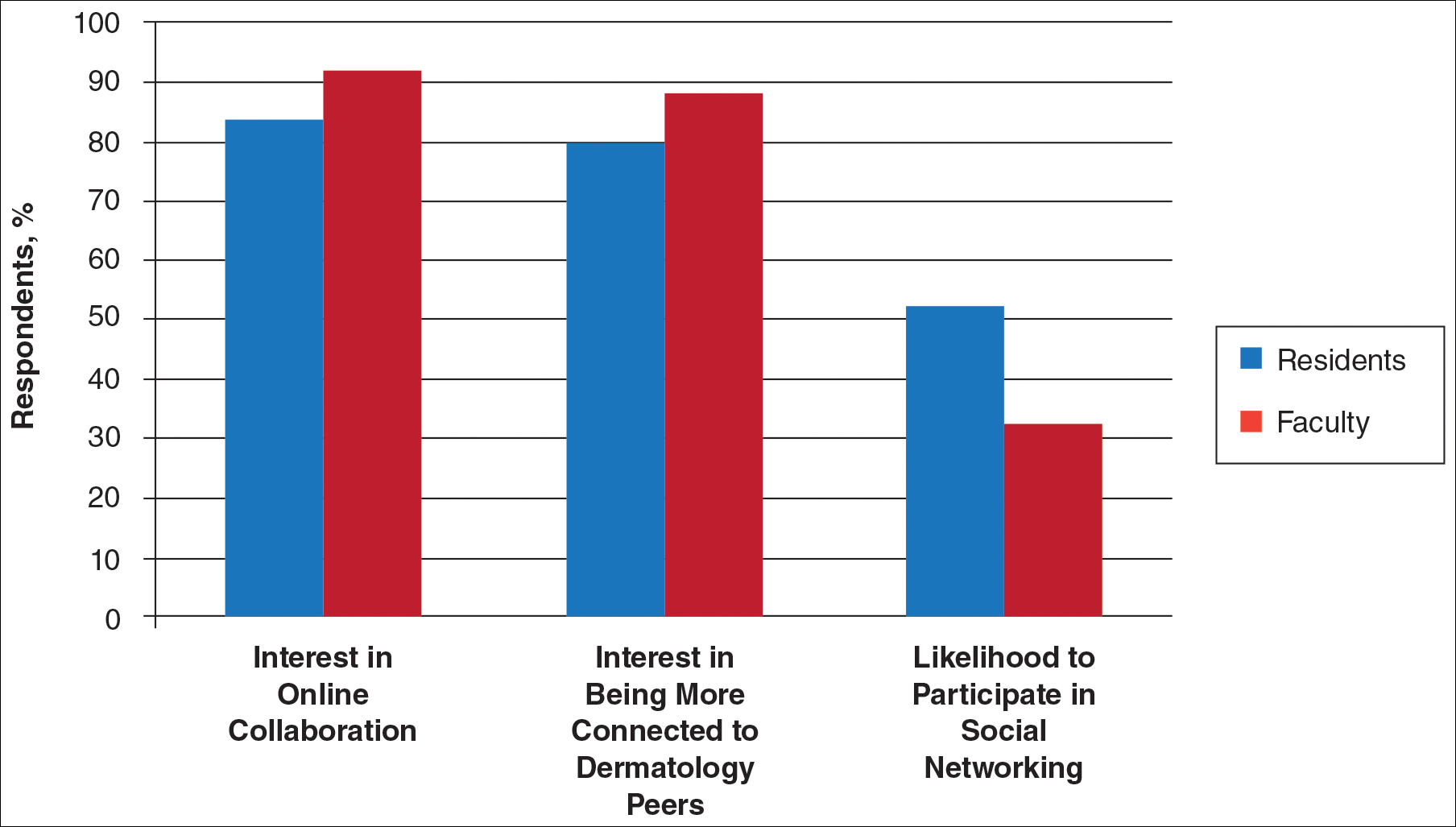
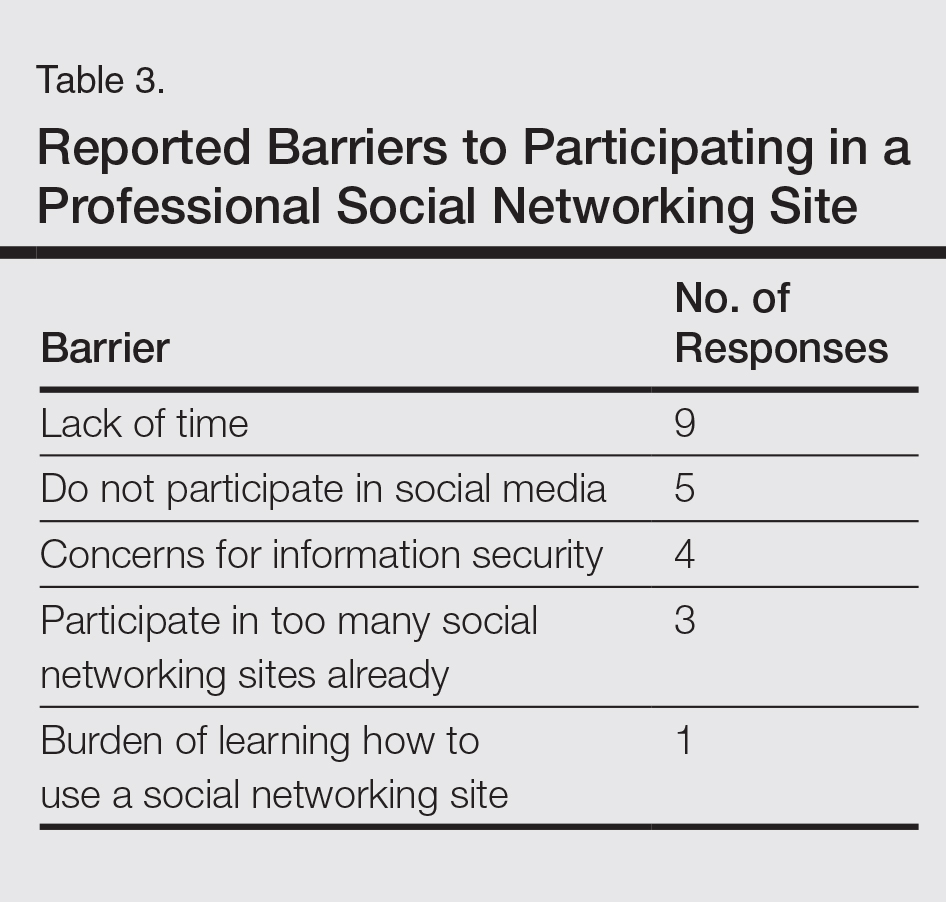
Comment
This study showed how dermatology faculty and residents currently provide training and what online resources and social networking sites they currently use or would be willing to use. The generalizability of the conclusions is limited by the low response rate for the surveys. The results demonstrated the different views between faculty and residents and between large and small residency programs on various topics. This microcosm of dermatology training can likely be applied to other training scenarios in dermatology, including patient education; training of nurses, physician extenders, and office staff; continuing medical education for physicians; and peer-to-peer collaboration.
Hypothesis 1: Partially Proven
We hypothesized that residents would report less satisfaction with their current curriculum and would report greater resident contributions to the curriculum relative to faculty. Overall, residents and faculty reported satisfaction with their curriculums to provide up-to-date information and breadth in the field of dermatology. Despite their overall satisfaction, more residents reported lacking instruction in several dermatology subtopics compared to faculty. Additionally, residents believed they spend twice as much time structuring their curriculum compared to faculty, with some residents reporting no faculty involvement. Although residents preferred faculty-led instruction, a majority of residents reported they do not have enough faculty-led didactics. The preference for faculty-led training is likely due to the expertise of faculty compared to residents.
Hypothesis 2: Partially Proven
We also hypothesized that both residents and faculty of smaller programs would be more interested in collaborative educational resources relative to larger programs. Although there was no difference in interest between residents at small versus large programs, there was a difference between faculty at small versus large programs. Small-program faculty were more interested in using shared materials than larger programs, while large-program faculty were more likely to share their educational materials. Small-program faculty reported spending too little time preparing their lectures, which is possibly due to a lack of time for preparation. Additionally, residents and faculty at smaller programs report their curriculum was lacking specific dermatology topics compared to large programs. These disparities between program sizes indicate a need for a social networking site for training collaboration in dermatology. Large programs have the ability to share what they do well, which small programs are eager to utilize.
Hypothesis 3: Not Proven
We hypothesized that residents would be more willing than faculty to participate in social networking for educational purposes. The majority of faculty and residents were interested in participating in a collaborative online curriculum and using the shared materials from top educators; however, even though such large majorities favored collaboration and sharing, only 27% of faculty and 19% of residents were likely to translate their own materials into a shareable format. Although lack of time was the most common reason for not sharing materials, electronic methods may have the potential to ultimately save time and remove the burden of content creation. The time it would take to translate selected personal training materials into a shareable form would be made up for by the time saved using another educators’ materials. Updating and customizing shared online educational materials can be much quicker and easier than educators creating materials on their own. Dermatologists would be more efficient facilitators of training via high-quality shared materials while decreasing the time burden associated with resident education.5 Another concern for not sharing or participating in a social networking site was skepticism of information security on such a network. The poor organization and information overload of online resources can compound the already existing time constraints on dermatologists, which may limit their ability to utilize such valuable resources. In addition, quality of online resources is not always guaranteed, and determining the sources that are high quality is sometimes a difficult task.6 For online materials to remain useful, there should be a peer-review process to evaluate quality and assess satisfaction.5
Solution: Create a Dermatology Task Force
A dermatology task force could facilitate the resolution of these challenges of online materials. In addition, a task force could cover the administrative support needed to ensure security and provide maintenance on social networks.
The main limitation to implementing a social network is the presence of the administrative infrastructure to jumpstart its creation. A task force incorporating the essential stakeholders in dermatology training is the first step. With inclusive representation from all of the smaller professional dermatology societies, the American Academy of Dermatology is optimally positioned to create this task force. With existing information technologies, a task force could address the concerns revealed in our survey as well as any future concerns that may arise.
The goal is a single social network for dermatologists that has the capability of improving communication and collaboration between professional peers regardless of their practice setting. Such a network is ideal for the practicing dermatologist for the purposes of staff training, patient education, and obtaining continuing medical education credit. Additionally, peer group collaboration would facilitate the understanding and completion of the evolving requirements for Maintenance of Certification from the American Board of Dermatology. The availability of quality shared materials would save time and increase efficiency of an entire dermatology practice. Materials that aid in patient education would allow office staff to dedicate their time to other tasks, thereby increasing productivity. Shared training materials would decrease the burden of staff education, providing more time for advanced hands-on training. This method of collaborative effort is capable of advancing the field of dermatology as a whole. It can overcome geographical and institutional barriers to connect dermatologists with similar interests worldwide; disseminate advances in diagnosis and treatment; and improve the quality of dermatology training of dermatologists, staff, and patients.
- Statistics and facts about social networks. Statista website. http://www.statista.com/topics/1164/social-networks/. Accessed March 22, 2017.
- Baker RC, Klein M, Samaan Z, et al. Effectiveness of an online pediatric primary care curriculum. Acad Pediatr. 2010;10:131-137.
- Dolev JC, O’Sullivan P, Berger T. The eDerm online curriculum: a randomized study of effective skin cancer teaching to medical students. J Am Acad Dermatol. 2011;65:e165-e171.
- Amir M, Sampson BP, Endly D, et al. Social networking sites: emerging and essential tools for communication in dermatology. JAMA Dermatol. 2014;150:56-60.
- Ruiz JG, Mintzer MJ, Leipzig RM. The impact of e-learning in medical education. Acad Med. 2006;81:207-212.
- Hanson AH, Krause LK, Simmons RN, et al. Dermatology education and the internet: traditional and cutting-edge resources. J Am Acad Dermatol. 2011;65:836-842.
- Rowe SP, Siddiqui A, Bonekamp D. The key image and case log application: new radiology software for teaching file creation and case logging that incorporates elements of a social network. Acad Radiol. 2014;21:916-930.
- Bell RH. Surgical council on resident education: a new organization devoted to graduate surgical education. J Am Coll Surg. 2007;204:341-346.
- Kirton OC, Reilly P, Staff I, et al. Development and implementation of an interactive, objective, and simulation-based curriculum for general surgery residents. J Surg Educ. 2012;69:718-723.
- Prakash S, Verma S, McGowan J, et al. Improving the quality of colonoscopy bowel preparation using an educational video. Can J Gastroenterol. 2013;27:696-700.
- Carroll BT. eTools for teaching dermatologic surgery. Paper presented at the Association of Professors of Dermatology 2014 Annual Meeting; September 12-13, 2014; Chicago, IL.
More than 1.8 billion individuals utilize social media, a number that continues to grow as the social media market expands.1 Social media enables individuals, groups, and organizations to efficiently disperse and access information2-4 and also provides a structure that encourages collaboration between patients, staff, and physicians that cannot be achieved by other communication modalities.4-6 Expert opinions and related educational materials can be shared globally, improving collaboration between dermatologists.6 A structured social networking site for sharing training materials, research, and ideas can help bring the national dermatology community together in a new way.
Other professions have employed social networking tools to accomplish similar goals of organizing training resources; radiology has an electronic database that allows sharing of training materials and incorporates social networking capabilities.7 Their Web software provides functionality for individual file uploading and supports collaboration and sharing, all while maintaining the security of uploaded information. General surgery has already addressed similar concerns via a task force that incorporates all the essential organizations in surgical education.8 Increased satisfaction and academic abilities have been demonstrated with their collaborative curriculum.9 Gastroenterologists also utilize electronic resources; one study showed that using videos to educate patients prior to colonoscopies was superior to face-to-face education.10 In addition, video education may free up time for office staff to accomplish other tasks.
As a specialty, dermatology has not been a leader in the implementation of social networking for collaboration and training purposes. Every dermatologist is an educator. To maintain a successful practice, dermatologists must keep up-to-date on their own clinical knowledge, provide training to their staff, and educate their patients. Although there are numerous educational resources available to dermatologists, an informal survey of 30 dermatology faculty members revealed a practice gap in awareness and utilization of these expanding electronic resources.11
To better understand the needs of the specialty as a whole, we chose to focus on one aspect of dermatology education: resident training. The goal of our study was to survey dermatology residents and faculty to gain a better understanding of how they currently provide education and what online resources and social networking sites they currently use or would be willing to use. The study included 3 central hypotheses: First, residents would be less satisfied with their current curriculum and residents would report greater contributions to the curriculum relative to faculty. Second, both residents and faculty of smaller programs would be more interested in collaborative educational resources relative to larger programs. Lastly, residents would be more willing than faculty to participate in social networking for educational purposes.
Methods
This study was granted institutional review board exemption. Two surveys were developed by the authors to assess the current structure and satisfaction of dermatology residency curriculum and the willingness to participate in social networking to use and share educational materials. The surveys were evaluated for relevance by the survey evaluation team of the Association of Professors of Dermatology (APD). The instrument was not pilot tested.
The surveys were electronically distributed using an online service to dermatology faculty via the APD listserve, which comprised the entirety of the APD membership in 2014. The resident survey was distributed to the dermatology residents via the American Society for Dermatologic Surgery listserve, which included all residents in training (2013-2014 academic year). Second and third invitations to complete the surveys were distributed 3 and 5 weeks later, respectively.
Resident and faculty responses were compared. Additionally, responses were stratified for large (>9 residents) and small programs (≤9 residents) for comparison. Descriptive statistics including means and medians for continuous variables and frequency tables for categorical variables were generated using research and spreadsheet software.
Results
There were 137 survey respondents; 52 of 426 (12.2%) dermatology faculty and 85 of 1539 (5.5%) dermatology residents responded to the survey. Small programs accounted for 24% of total survey responses and 76% were from large programs.
Current Curriculum
The majority of dermatology faculty (44%) and residents (35%) identified 1 to 2 faculty members as contributing to the creation and organization of their respective curricula; however, a notable percentage of residents (9%) reported that no faculty contributed to the organization of the curriculum. Residents noted that senior residents carry twice the responsibility for structuring the curriculum compared to faculty (61% vs 32% of the workload), but faculty described an even split between senior residents and faculty (47% vs 49% of the workload). Faculty believed their residents spend a similar amount of time in resident- and faculty-led instruction (38% vs 35% of their time); however, the majority of residents reported spending too little time in faculty-led instruction (53%). When residents ranked their preference for learning modes, faculty-led and self-study learning were ranked first and second by 48% and 45% of residents, respectively. Resident-led instruction was ranked last by 66% of residents. Likewise, a majority of residents (53%) described their amount of time in faculty-led instruction as too little.
When asked what subjects in dermatology were lacking at their programs, residents reported clinical trials (47%), skin of color (46%), cosmetic dermatology (34%), and aggressive skin cancer/multidisciplinary tumor board (32%). Although 11% of residents reported lacking inpatient dermatology in their curriculum, 0% of faculty reported the same. A notable percentage of faculty reported nothing was lacking compared to residents (25% vs 7%). Despite these different views between residents and faculty on their contributions to and structure of their curriculums, both faculty and residents claimed overall satisfaction (satisfied or very satisfied) with their program’s ability to optimally cover the field of dermatology in 3 years (100% and 91%, respectively).
Large Versus Small Residency Programs
When stratifying the resident responses for small versus large programs, both program sizes reported more time in resident-led instruction than faculty-led instruction. Likewise, residents in both program sizes equally preferred self-study or faculty-led instruction to resident-led instruction. Residents at small programs more often reported lacking instruction in rheumatology, immunobullous diseases, and basic science/skin biology compared to large-program residents. Compared to large-program faculty, small-program faculty reported lacking instruction in cosmetic dermatology.
Faculty at small programs reported spending too little time preparing for their faculty-led instruction compared to faculty at large programs (44% vs 12%). All (100%) of the faculty at small programs were likely to seek out study materials shared by top educators, while 77% of faculty at large programs were likely to do the same. When asked if faculty would translate what their program does well into an electronic format for sharing, 30% of large-program faculty were likely to do so compared to 11% of small-program faculty (Figure 1).
Use of Online Educational Materials and Interest in Collaboration
A majority of faculty and residents stated that they use online educational materials as supplements to traditional classroom lecture and print materials (81% vs 86%); however, almost twice as many residents stated that online educational materials were essential to their current study routines compared to faculty (39% vs 21%).
The majority of faculty (92%) and residents (84%) were either interested or very interested in a collaborative online curriculum. Both residents (85%) and faculty (81%) stated they would be likely to seek out online educational materials shared by top educators. Although both residents and faculty reported many aspects of their curriculums they thought could be beneficial to other dermatology programs (Table 1), only 27% of faculty and 19% of residents were likely to translate those strengths into a shareable electronic format. Several reasons were reported for not contributing to an online curriculum, with lack of time being the most common reason (Table 2).
Eighty percent of residents and 88% of faculty reported they were either interested or very interested in being more connected/interactive with their dermatology peers nationally (Figure 2). Likewise, 94% of residents and 87% of faculty agreed that the dermatology community could benefit from a social networking site for educational collaboration. Four times as many residents versus faculty currently use social networking sites (eg, Facebook, LinkedIn, Google Groups) as a primary mode of communication with distant professional peers. The majority of residents (52%) reported they would be likely to participate in a professional social networking site, while the majority of faculty (50%) stated they were neutral on their likelihood of participating. Both residents and faculty reported lack of time as a common reason for being unlikely to utilize a professional social networking site. Other barriers to participation are listed in Table 3.
Comment
This study showed how dermatology faculty and residents currently provide training and what online resources and social networking sites they currently use or would be willing to use. The generalizability of the conclusions is limited by the low response rate for the surveys. The results demonstrated the different views between faculty and residents and between large and small residency programs on various topics. This microcosm of dermatology training can likely be applied to other training scenarios in dermatology, including patient education; training of nurses, physician extenders, and office staff; continuing medical education for physicians; and peer-to-peer collaboration.
Hypothesis 1: Partially Proven
We hypothesized that residents would report less satisfaction with their current curriculum and would report greater resident contributions to the curriculum relative to faculty. Overall, residents and faculty reported satisfaction with their curriculums to provide up-to-date information and breadth in the field of dermatology. Despite their overall satisfaction, more residents reported lacking instruction in several dermatology subtopics compared to faculty. Additionally, residents believed they spend twice as much time structuring their curriculum compared to faculty, with some residents reporting no faculty involvement. Although residents preferred faculty-led instruction, a majority of residents reported they do not have enough faculty-led didactics. The preference for faculty-led training is likely due to the expertise of faculty compared to residents.
Hypothesis 2: Partially Proven
We also hypothesized that both residents and faculty of smaller programs would be more interested in collaborative educational resources relative to larger programs. Although there was no difference in interest between residents at small versus large programs, there was a difference between faculty at small versus large programs. Small-program faculty were more interested in using shared materials than larger programs, while large-program faculty were more likely to share their educational materials. Small-program faculty reported spending too little time preparing their lectures, which is possibly due to a lack of time for preparation. Additionally, residents and faculty at smaller programs report their curriculum was lacking specific dermatology topics compared to large programs. These disparities between program sizes indicate a need for a social networking site for training collaboration in dermatology. Large programs have the ability to share what they do well, which small programs are eager to utilize.
Hypothesis 3: Not Proven
We hypothesized that residents would be more willing than faculty to participate in social networking for educational purposes. The majority of faculty and residents were interested in participating in a collaborative online curriculum and using the shared materials from top educators; however, even though such large majorities favored collaboration and sharing, only 27% of faculty and 19% of residents were likely to translate their own materials into a shareable format. Although lack of time was the most common reason for not sharing materials, electronic methods may have the potential to ultimately save time and remove the burden of content creation. The time it would take to translate selected personal training materials into a shareable form would be made up for by the time saved using another educators’ materials. Updating and customizing shared online educational materials can be much quicker and easier than educators creating materials on their own. Dermatologists would be more efficient facilitators of training via high-quality shared materials while decreasing the time burden associated with resident education.5 Another concern for not sharing or participating in a social networking site was skepticism of information security on such a network. The poor organization and information overload of online resources can compound the already existing time constraints on dermatologists, which may limit their ability to utilize such valuable resources. In addition, quality of online resources is not always guaranteed, and determining the sources that are high quality is sometimes a difficult task.6 For online materials to remain useful, there should be a peer-review process to evaluate quality and assess satisfaction.5
Solution: Create a Dermatology Task Force
A dermatology task force could facilitate the resolution of these challenges of online materials. In addition, a task force could cover the administrative support needed to ensure security and provide maintenance on social networks.
The main limitation to implementing a social network is the presence of the administrative infrastructure to jumpstart its creation. A task force incorporating the essential stakeholders in dermatology training is the first step. With inclusive representation from all of the smaller professional dermatology societies, the American Academy of Dermatology is optimally positioned to create this task force. With existing information technologies, a task force could address the concerns revealed in our survey as well as any future concerns that may arise.
The goal is a single social network for dermatologists that has the capability of improving communication and collaboration between professional peers regardless of their practice setting. Such a network is ideal for the practicing dermatologist for the purposes of staff training, patient education, and obtaining continuing medical education credit. Additionally, peer group collaboration would facilitate the understanding and completion of the evolving requirements for Maintenance of Certification from the American Board of Dermatology. The availability of quality shared materials would save time and increase efficiency of an entire dermatology practice. Materials that aid in patient education would allow office staff to dedicate their time to other tasks, thereby increasing productivity. Shared training materials would decrease the burden of staff education, providing more time for advanced hands-on training. This method of collaborative effort is capable of advancing the field of dermatology as a whole. It can overcome geographical and institutional barriers to connect dermatologists with similar interests worldwide; disseminate advances in diagnosis and treatment; and improve the quality of dermatology training of dermatologists, staff, and patients.
More than 1.8 billion individuals utilize social media, a number that continues to grow as the social media market expands.1 Social media enables individuals, groups, and organizations to efficiently disperse and access information2-4 and also provides a structure that encourages collaboration between patients, staff, and physicians that cannot be achieved by other communication modalities.4-6 Expert opinions and related educational materials can be shared globally, improving collaboration between dermatologists.6 A structured social networking site for sharing training materials, research, and ideas can help bring the national dermatology community together in a new way.
Other professions have employed social networking tools to accomplish similar goals of organizing training resources; radiology has an electronic database that allows sharing of training materials and incorporates social networking capabilities.7 Their Web software provides functionality for individual file uploading and supports collaboration and sharing, all while maintaining the security of uploaded information. General surgery has already addressed similar concerns via a task force that incorporates all the essential organizations in surgical education.8 Increased satisfaction and academic abilities have been demonstrated with their collaborative curriculum.9 Gastroenterologists also utilize electronic resources; one study showed that using videos to educate patients prior to colonoscopies was superior to face-to-face education.10 In addition, video education may free up time for office staff to accomplish other tasks.
As a specialty, dermatology has not been a leader in the implementation of social networking for collaboration and training purposes. Every dermatologist is an educator. To maintain a successful practice, dermatologists must keep up-to-date on their own clinical knowledge, provide training to their staff, and educate their patients. Although there are numerous educational resources available to dermatologists, an informal survey of 30 dermatology faculty members revealed a practice gap in awareness and utilization of these expanding electronic resources.11
To better understand the needs of the specialty as a whole, we chose to focus on one aspect of dermatology education: resident training. The goal of our study was to survey dermatology residents and faculty to gain a better understanding of how they currently provide education and what online resources and social networking sites they currently use or would be willing to use. The study included 3 central hypotheses: First, residents would be less satisfied with their current curriculum and residents would report greater contributions to the curriculum relative to faculty. Second, both residents and faculty of smaller programs would be more interested in collaborative educational resources relative to larger programs. Lastly, residents would be more willing than faculty to participate in social networking for educational purposes.
Methods
This study was granted institutional review board exemption. Two surveys were developed by the authors to assess the current structure and satisfaction of dermatology residency curriculum and the willingness to participate in social networking to use and share educational materials. The surveys were evaluated for relevance by the survey evaluation team of the Association of Professors of Dermatology (APD). The instrument was not pilot tested.
The surveys were electronically distributed using an online service to dermatology faculty via the APD listserve, which comprised the entirety of the APD membership in 2014. The resident survey was distributed to the dermatology residents via the American Society for Dermatologic Surgery listserve, which included all residents in training (2013-2014 academic year). Second and third invitations to complete the surveys were distributed 3 and 5 weeks later, respectively.
Resident and faculty responses were compared. Additionally, responses were stratified for large (>9 residents) and small programs (≤9 residents) for comparison. Descriptive statistics including means and medians for continuous variables and frequency tables for categorical variables were generated using research and spreadsheet software.
Results
There were 137 survey respondents; 52 of 426 (12.2%) dermatology faculty and 85 of 1539 (5.5%) dermatology residents responded to the survey. Small programs accounted for 24% of total survey responses and 76% were from large programs.
Current Curriculum
The majority of dermatology faculty (44%) and residents (35%) identified 1 to 2 faculty members as contributing to the creation and organization of their respective curricula; however, a notable percentage of residents (9%) reported that no faculty contributed to the organization of the curriculum. Residents noted that senior residents carry twice the responsibility for structuring the curriculum compared to faculty (61% vs 32% of the workload), but faculty described an even split between senior residents and faculty (47% vs 49% of the workload). Faculty believed their residents spend a similar amount of time in resident- and faculty-led instruction (38% vs 35% of their time); however, the majority of residents reported spending too little time in faculty-led instruction (53%). When residents ranked their preference for learning modes, faculty-led and self-study learning were ranked first and second by 48% and 45% of residents, respectively. Resident-led instruction was ranked last by 66% of residents. Likewise, a majority of residents (53%) described their amount of time in faculty-led instruction as too little.
When asked what subjects in dermatology were lacking at their programs, residents reported clinical trials (47%), skin of color (46%), cosmetic dermatology (34%), and aggressive skin cancer/multidisciplinary tumor board (32%). Although 11% of residents reported lacking inpatient dermatology in their curriculum, 0% of faculty reported the same. A notable percentage of faculty reported nothing was lacking compared to residents (25% vs 7%). Despite these different views between residents and faculty on their contributions to and structure of their curriculums, both faculty and residents claimed overall satisfaction (satisfied or very satisfied) with their program’s ability to optimally cover the field of dermatology in 3 years (100% and 91%, respectively).
Large Versus Small Residency Programs
When stratifying the resident responses for small versus large programs, both program sizes reported more time in resident-led instruction than faculty-led instruction. Likewise, residents in both program sizes equally preferred self-study or faculty-led instruction to resident-led instruction. Residents at small programs more often reported lacking instruction in rheumatology, immunobullous diseases, and basic science/skin biology compared to large-program residents. Compared to large-program faculty, small-program faculty reported lacking instruction in cosmetic dermatology.
Faculty at small programs reported spending too little time preparing for their faculty-led instruction compared to faculty at large programs (44% vs 12%). All (100%) of the faculty at small programs were likely to seek out study materials shared by top educators, while 77% of faculty at large programs were likely to do the same. When asked if faculty would translate what their program does well into an electronic format for sharing, 30% of large-program faculty were likely to do so compared to 11% of small-program faculty (Figure 1).
Use of Online Educational Materials and Interest in Collaboration
A majority of faculty and residents stated that they use online educational materials as supplements to traditional classroom lecture and print materials (81% vs 86%); however, almost twice as many residents stated that online educational materials were essential to their current study routines compared to faculty (39% vs 21%).
The majority of faculty (92%) and residents (84%) were either interested or very interested in a collaborative online curriculum. Both residents (85%) and faculty (81%) stated they would be likely to seek out online educational materials shared by top educators. Although both residents and faculty reported many aspects of their curriculums they thought could be beneficial to other dermatology programs (Table 1), only 27% of faculty and 19% of residents were likely to translate those strengths into a shareable electronic format. Several reasons were reported for not contributing to an online curriculum, with lack of time being the most common reason (Table 2).
Eighty percent of residents and 88% of faculty reported they were either interested or very interested in being more connected/interactive with their dermatology peers nationally (Figure 2). Likewise, 94% of residents and 87% of faculty agreed that the dermatology community could benefit from a social networking site for educational collaboration. Four times as many residents versus faculty currently use social networking sites (eg, Facebook, LinkedIn, Google Groups) as a primary mode of communication with distant professional peers. The majority of residents (52%) reported they would be likely to participate in a professional social networking site, while the majority of faculty (50%) stated they were neutral on their likelihood of participating. Both residents and faculty reported lack of time as a common reason for being unlikely to utilize a professional social networking site. Other barriers to participation are listed in Table 3.
Comment
This study showed how dermatology faculty and residents currently provide training and what online resources and social networking sites they currently use or would be willing to use. The generalizability of the conclusions is limited by the low response rate for the surveys. The results demonstrated the different views between faculty and residents and between large and small residency programs on various topics. This microcosm of dermatology training can likely be applied to other training scenarios in dermatology, including patient education; training of nurses, physician extenders, and office staff; continuing medical education for physicians; and peer-to-peer collaboration.
Hypothesis 1: Partially Proven
We hypothesized that residents would report less satisfaction with their current curriculum and would report greater resident contributions to the curriculum relative to faculty. Overall, residents and faculty reported satisfaction with their curriculums to provide up-to-date information and breadth in the field of dermatology. Despite their overall satisfaction, more residents reported lacking instruction in several dermatology subtopics compared to faculty. Additionally, residents believed they spend twice as much time structuring their curriculum compared to faculty, with some residents reporting no faculty involvement. Although residents preferred faculty-led instruction, a majority of residents reported they do not have enough faculty-led didactics. The preference for faculty-led training is likely due to the expertise of faculty compared to residents.
Hypothesis 2: Partially Proven
We also hypothesized that both residents and faculty of smaller programs would be more interested in collaborative educational resources relative to larger programs. Although there was no difference in interest between residents at small versus large programs, there was a difference between faculty at small versus large programs. Small-program faculty were more interested in using shared materials than larger programs, while large-program faculty were more likely to share their educational materials. Small-program faculty reported spending too little time preparing their lectures, which is possibly due to a lack of time for preparation. Additionally, residents and faculty at smaller programs report their curriculum was lacking specific dermatology topics compared to large programs. These disparities between program sizes indicate a need for a social networking site for training collaboration in dermatology. Large programs have the ability to share what they do well, which small programs are eager to utilize.
Hypothesis 3: Not Proven
We hypothesized that residents would be more willing than faculty to participate in social networking for educational purposes. The majority of faculty and residents were interested in participating in a collaborative online curriculum and using the shared materials from top educators; however, even though such large majorities favored collaboration and sharing, only 27% of faculty and 19% of residents were likely to translate their own materials into a shareable format. Although lack of time was the most common reason for not sharing materials, electronic methods may have the potential to ultimately save time and remove the burden of content creation. The time it would take to translate selected personal training materials into a shareable form would be made up for by the time saved using another educators’ materials. Updating and customizing shared online educational materials can be much quicker and easier than educators creating materials on their own. Dermatologists would be more efficient facilitators of training via high-quality shared materials while decreasing the time burden associated with resident education.5 Another concern for not sharing or participating in a social networking site was skepticism of information security on such a network. The poor organization and information overload of online resources can compound the already existing time constraints on dermatologists, which may limit their ability to utilize such valuable resources. In addition, quality of online resources is not always guaranteed, and determining the sources that are high quality is sometimes a difficult task.6 For online materials to remain useful, there should be a peer-review process to evaluate quality and assess satisfaction.5
Solution: Create a Dermatology Task Force
A dermatology task force could facilitate the resolution of these challenges of online materials. In addition, a task force could cover the administrative support needed to ensure security and provide maintenance on social networks.
The main limitation to implementing a social network is the presence of the administrative infrastructure to jumpstart its creation. A task force incorporating the essential stakeholders in dermatology training is the first step. With inclusive representation from all of the smaller professional dermatology societies, the American Academy of Dermatology is optimally positioned to create this task force. With existing information technologies, a task force could address the concerns revealed in our survey as well as any future concerns that may arise.
The goal is a single social network for dermatologists that has the capability of improving communication and collaboration between professional peers regardless of their practice setting. Such a network is ideal for the practicing dermatologist for the purposes of staff training, patient education, and obtaining continuing medical education credit. Additionally, peer group collaboration would facilitate the understanding and completion of the evolving requirements for Maintenance of Certification from the American Board of Dermatology. The availability of quality shared materials would save time and increase efficiency of an entire dermatology practice. Materials that aid in patient education would allow office staff to dedicate their time to other tasks, thereby increasing productivity. Shared training materials would decrease the burden of staff education, providing more time for advanced hands-on training. This method of collaborative effort is capable of advancing the field of dermatology as a whole. It can overcome geographical and institutional barriers to connect dermatologists with similar interests worldwide; disseminate advances in diagnosis and treatment; and improve the quality of dermatology training of dermatologists, staff, and patients.
- Statistics and facts about social networks. Statista website. http://www.statista.com/topics/1164/social-networks/. Accessed March 22, 2017.
- Baker RC, Klein M, Samaan Z, et al. Effectiveness of an online pediatric primary care curriculum. Acad Pediatr. 2010;10:131-137.
- Dolev JC, O’Sullivan P, Berger T. The eDerm online curriculum: a randomized study of effective skin cancer teaching to medical students. J Am Acad Dermatol. 2011;65:e165-e171.
- Amir M, Sampson BP, Endly D, et al. Social networking sites: emerging and essential tools for communication in dermatology. JAMA Dermatol. 2014;150:56-60.
- Ruiz JG, Mintzer MJ, Leipzig RM. The impact of e-learning in medical education. Acad Med. 2006;81:207-212.
- Hanson AH, Krause LK, Simmons RN, et al. Dermatology education and the internet: traditional and cutting-edge resources. J Am Acad Dermatol. 2011;65:836-842.
- Rowe SP, Siddiqui A, Bonekamp D. The key image and case log application: new radiology software for teaching file creation and case logging that incorporates elements of a social network. Acad Radiol. 2014;21:916-930.
- Bell RH. Surgical council on resident education: a new organization devoted to graduate surgical education. J Am Coll Surg. 2007;204:341-346.
- Kirton OC, Reilly P, Staff I, et al. Development and implementation of an interactive, objective, and simulation-based curriculum for general surgery residents. J Surg Educ. 2012;69:718-723.
- Prakash S, Verma S, McGowan J, et al. Improving the quality of colonoscopy bowel preparation using an educational video. Can J Gastroenterol. 2013;27:696-700.
- Carroll BT. eTools for teaching dermatologic surgery. Paper presented at the Association of Professors of Dermatology 2014 Annual Meeting; September 12-13, 2014; Chicago, IL.
- Statistics and facts about social networks. Statista website. http://www.statista.com/topics/1164/social-networks/. Accessed March 22, 2017.
- Baker RC, Klein M, Samaan Z, et al. Effectiveness of an online pediatric primary care curriculum. Acad Pediatr. 2010;10:131-137.
- Dolev JC, O’Sullivan P, Berger T. The eDerm online curriculum: a randomized study of effective skin cancer teaching to medical students. J Am Acad Dermatol. 2011;65:e165-e171.
- Amir M, Sampson BP, Endly D, et al. Social networking sites: emerging and essential tools for communication in dermatology. JAMA Dermatol. 2014;150:56-60.
- Ruiz JG, Mintzer MJ, Leipzig RM. The impact of e-learning in medical education. Acad Med. 2006;81:207-212.
- Hanson AH, Krause LK, Simmons RN, et al. Dermatology education and the internet: traditional and cutting-edge resources. J Am Acad Dermatol. 2011;65:836-842.
- Rowe SP, Siddiqui A, Bonekamp D. The key image and case log application: new radiology software for teaching file creation and case logging that incorporates elements of a social network. Acad Radiol. 2014;21:916-930.
- Bell RH. Surgical council on resident education: a new organization devoted to graduate surgical education. J Am Coll Surg. 2007;204:341-346.
- Kirton OC, Reilly P, Staff I, et al. Development and implementation of an interactive, objective, and simulation-based curriculum for general surgery residents. J Surg Educ. 2012;69:718-723.
- Prakash S, Verma S, McGowan J, et al. Improving the quality of colonoscopy bowel preparation using an educational video. Can J Gastroenterol. 2013;27:696-700.
- Carroll BT. eTools for teaching dermatologic surgery. Paper presented at the Association of Professors of Dermatology 2014 Annual Meeting; September 12-13, 2014; Chicago, IL.
Practice Points
- Educational collaboration between residency programs via social media can result in more well-rounded dermatologists, which will enhance patient care.
- Social media can connect dermatologists nationwide to improve patient care via collaboration.
