User login
Cosmetic Corner: Dermatologists Weigh in on Men’s Products
To improve patient care and outcomes, leading dermatologists offered their recommendations on men’s products. Consideration must be given to:
- bareMinerals SPF 30 Natural Sunscreen
Bare Escentuals Beauty, Inc
“I recommend this product to my male patients when they are not wearing a hat. It protects the scalp from UV damage without a heavy greasy finish.”—Shari Lipner, MD, PhD, New York, New York
- Ducray Alopexy 5% For Men
Pierre Fabre Laboratories
“This dermatologist-dispensed product for men addresses chronic hair loss as well as thinning hair. It contains an optimal level of minoxidil 5% in an elegant unscented formulation and is designed to spray on smoothly and evenly.”—Jeannette Graf, MD, Great Neck, New York
- Facial Fuel Energizing Scrub
Kiehl’s
“This product is great for oily skin and enlarged pores. The particles in the product allow one to get a deep-clean feeling.”—Gary Goldenberg, MD, New York, New York
- Physical Matte UV Defense SPF 50
SkinCeuticals
“For men I like to keep things simple. I recommend what I use with the single most important thing being daily sun protection. SkinCeuticals Physical Matte UV Defense SPF 50 is my favorite and I use it after I shave. It goes on smoothly and has a natural tint along with a high SPF.”—Jerome Potozkin, MD, Danville, California
- Ultimate Brushless Shave Cream
Kiehl’s
“I recommend this product for men with frequent irritation from shaving. This cream-based product helps to provide a close shave without as much irritation from other gel-based products. A small amount goes a long way!”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please email your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on men’s products. Consideration must be given to:
- bareMinerals SPF 30 Natural Sunscreen
Bare Escentuals Beauty, Inc
“I recommend this product to my male patients when they are not wearing a hat. It protects the scalp from UV damage without a heavy greasy finish.”—Shari Lipner, MD, PhD, New York, New York
- Ducray Alopexy 5% For Men
Pierre Fabre Laboratories
“This dermatologist-dispensed product for men addresses chronic hair loss as well as thinning hair. It contains an optimal level of minoxidil 5% in an elegant unscented formulation and is designed to spray on smoothly and evenly.”—Jeannette Graf, MD, Great Neck, New York
- Facial Fuel Energizing Scrub
Kiehl’s
“This product is great for oily skin and enlarged pores. The particles in the product allow one to get a deep-clean feeling.”—Gary Goldenberg, MD, New York, New York
- Physical Matte UV Defense SPF 50
SkinCeuticals
“For men I like to keep things simple. I recommend what I use with the single most important thing being daily sun protection. SkinCeuticals Physical Matte UV Defense SPF 50 is my favorite and I use it after I shave. It goes on smoothly and has a natural tint along with a high SPF.”—Jerome Potozkin, MD, Danville, California
- Ultimate Brushless Shave Cream
Kiehl’s
“I recommend this product for men with frequent irritation from shaving. This cream-based product helps to provide a close shave without as much irritation from other gel-based products. A small amount goes a long way!”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please email your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on men’s products. Consideration must be given to:
- bareMinerals SPF 30 Natural Sunscreen
Bare Escentuals Beauty, Inc
“I recommend this product to my male patients when they are not wearing a hat. It protects the scalp from UV damage without a heavy greasy finish.”—Shari Lipner, MD, PhD, New York, New York
- Ducray Alopexy 5% For Men
Pierre Fabre Laboratories
“This dermatologist-dispensed product for men addresses chronic hair loss as well as thinning hair. It contains an optimal level of minoxidil 5% in an elegant unscented formulation and is designed to spray on smoothly and evenly.”—Jeannette Graf, MD, Great Neck, New York
- Facial Fuel Energizing Scrub
Kiehl’s
“This product is great for oily skin and enlarged pores. The particles in the product allow one to get a deep-clean feeling.”—Gary Goldenberg, MD, New York, New York
- Physical Matte UV Defense SPF 50
SkinCeuticals
“For men I like to keep things simple. I recommend what I use with the single most important thing being daily sun protection. SkinCeuticals Physical Matte UV Defense SPF 50 is my favorite and I use it after I shave. It goes on smoothly and has a natural tint along with a high SPF.”—Jerome Potozkin, MD, Danville, California
- Ultimate Brushless Shave Cream
Kiehl’s
“I recommend this product for men with frequent irritation from shaving. This cream-based product helps to provide a close shave without as much irritation from other gel-based products. A small amount goes a long way!”—Anthony M. Rossi, MD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments and cleansing devices will be featured in upcoming editions of Cosmetic Corner. Please email your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Hyaluronic Acid Gel Filler for Nipple Enhancement Following Breast Reconstruction
The most frequently used surgical techniques in nipple-areola complex (NAC) reconstruction involve the use of local tissue flaps and yield the fewest complications, though these techniques can be associated with up to a 75% loss in nipple projection over time.1 In a best-case scenario for both the surgeon and the patient, the NAC is preserved during mastectomy; however, even when the tissues are spared, an eventual loss of nipple projection is expected due to atrophy and contraction of the healing skin.2 Loss of nipple projection is the most common attribute that patients dislike regarding their NAC reconstruction results.Additional efforts made to restore the natural look and feel of the NAC provides undeniable benefit to the patient in the form of improved body image and psychosocial well-being.3
Augmentation with a grafted material can include cartilage or fat (autologous grafts), calcium hydroxylapatite or polymethyl methacrylate (PMMA)(alloplastic grafts), and acellular dermal matrix or biologic collagen (allografts). Among these options, successive treatment with autologous fat has been shown to provide satisfactory projections over time with minimal complications.4 However, an additional consideration associated with graft augmentation is the need for an additional surgical site (autologous grafts) or the possibility that graft material may not be compatible with subsequent breast examination techniques. For example, calcium hydroxylapatite is a radiopaque material that may interfere with the interpretation of radiography and mammography.5
The use of injectable hyaluronic acid (HA) dermal fillers to enhance nipple projection represents a noninvasive procedure with immediate and adjustable results. A variety of dermal fillers that do not interfere with subsequent breast imaging needs have already been successfully used for nipple reconstruction including HA 60% plus acrylic hydrogel 40%, PMMA microspheres in a bovine collagen 3.5% gel, and poly-L-lactic acid.5-7
The results achieved with HA 60% plus acrylic hydrogel 40% were as much as a 2.5-mm mean increase in nipple projection after 12 months for 70 nipples reconstructed using a small wedge from the labia minora.5 In these treatments, an initial injection of 0.1 to 0.3 mL of filler into each nipple along with a 0.2-mL injection at the base of each nipple was made. Further optional treatments at 2 and 4 months after the initial injection were made using up to 0.3 mL additional volume depending on filler reabsorption.5 Results achieved with PMMA microspheres in a bovine collagen 3.5% gel included a 1.6-mm mean increase in nipple projection at 9 months versus baseline for 33 nipples in 23 patients, which involved up to 2 injections at baseline and again at 3 months.6 Treatment with poly-L-lactic acid provided a 2.3-mm mean increase in nipple projection for 12 patients after 1 year of treatment, which involved 0.5-mL injections every 4 weeks over a series of 4 treatments.7
This report describes the technique and cosmetic outcome using an injectable HA gel to postoperatively restore the 3-dimensional contour of the nipple following surgical breast reconstruction. This chemically cross-linked, stabilized HA gel suspended in phosphate-buffered saline at a pH of 7 and a concentration of 20 mg/mL with lidocaine 0.3% is indicated for mid to deep dermal implantation for the correction of moderate to severe facial wrinkles and folds, such as the nasolabial folds.8
Case Report
A 49-year-old woman with a history of breast cancer with a focal, high-grade ductal carcinoma in situ underwent a complete bilateral mastectomy. The sentinel lymph nodes were negative at the time of mastectomy. One year later, the patient elected to have breast and nipple-areola (flap) reconstruction. Following the reconstructive surgery, her nipples had become visibly atrophic and flat, and she was interested in cosmetic enhancement.
After informed consent had been obtained from the patient, a baseline measurement of each nipple was made while the patient was standing. Each nipple was then injected with up to 0.1 to 0.2 mL of HA gel filler using a 30-gauge needle inserted 2-mm deep (bilaterally) into each nipple. The patient tolerated the procedure well with no pain, bleeding, or bruising. Although HA gel filler contains lidocaine 0.3% and tricaine can further be used to ensure patient comfort, the nipple reconstruction surgery left the patient with little sensation in the treatment area. Rubbing alcohol was used to prepare the skin prior to the procedure, and fractionated coconut oil spray with a nonadherent dressing was used postprocedure.
Following the injection, an immediate increase of 1.6 and 1.5 mm in nipple projection in the right and left breasts, respectively, was achieved with HA gel. The nipple projection of the right breast was 1.7 mm before injection (Figure, A) and 3.3 mm immediately postinjection (Figure, C). The nipple projection of the left breast was 1.8 mm before injection (Figure, B) and 3.3 mm immediately postinjection (Figure, D).

Comment
With a single treatment consisting of 0.2 mL or less of filler volume, the HA gel used in this procedure provided an immediate mean increase in nipple projection of 1.5 mm. Although our assessment involved a single patient evaluated at baseline and immediately post-injection of HA filler only, it is reasonable to assume that subsequent reinjections would provide results comparable to other fillers. Although other fillers that are semipermanent (acrylic hydrogel) and nonbiodegradable (PMMA) make them more durable, these properties also make the augmentation less reversible in the case of overfilling. As with all dermal fillers, rare side effects associated with injection of HA gel filler could potentially include injection-site inflammation, extrusion of filler at the needle insertion site, minimal pain or discomfort during or after injections, bruising, swelling, or delayed-type hypersensitivity reaction. Ideally, HA gel is a soft transparent filler that is reversible with hyaluronidase, an advantage not shared by other filler materials.9
Conclusion
Nipple augmentation with HA gel is a simple noninvasive
- Sisti A, Grimaldi L, Tassinari J, et al. Nipple-areola complex reconstruction techniques: a literature review. Eur J Surg Oncol. 2016;42:441-465.
- Murthy V, Chamberlain RS. Defining a place for nipple sparing mastectomy in modern breast care: an evidence based review. Breast J. 2013;19:571-581.
- Jabor MA, Shayani P, Collins DR Jr, et al. Nipple-areola reconstruction: satisfaction and clinical determinants. Plast Reconstr Surg. 2002;110:457-463.
- Kaoutzanis C, Xin M, Ballard TN, et al. Autologous fat grafting after breast reconstruction in postmastectomy patients: complications, biopsy rates, and locoregional cancer recurrence rates. Ann Plast Surg. 2016;76:270-275.
- Panettiere P, Marchetti L, Accorsi D. Filler injection enhances the projection of the reconstructed nipple: an original easy technique. Aesthet Plast Surg. 2005;29:287-294.
- McCarthy CM, Van Laeken N, Lennox P, et al. The efficacy of Artecoll injections for the augmentation of nipple projection in breast reconstruction. Eplasty. 2010;10:E7.
- Dessy LA, Troccola A, Ranno RL, et al. The use of Poly-lactic acid to improve projection of reconstructed nipple. Breast. 2011;20:220-224.
- Restylane L [package insert]. Fort Worth, TX: Galderma Laboratories, LP; 2016.
- Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
The most frequently used surgical techniques in nipple-areola complex (NAC) reconstruction involve the use of local tissue flaps and yield the fewest complications, though these techniques can be associated with up to a 75% loss in nipple projection over time.1 In a best-case scenario for both the surgeon and the patient, the NAC is preserved during mastectomy; however, even when the tissues are spared, an eventual loss of nipple projection is expected due to atrophy and contraction of the healing skin.2 Loss of nipple projection is the most common attribute that patients dislike regarding their NAC reconstruction results.Additional efforts made to restore the natural look and feel of the NAC provides undeniable benefit to the patient in the form of improved body image and psychosocial well-being.3
Augmentation with a grafted material can include cartilage or fat (autologous grafts), calcium hydroxylapatite or polymethyl methacrylate (PMMA)(alloplastic grafts), and acellular dermal matrix or biologic collagen (allografts). Among these options, successive treatment with autologous fat has been shown to provide satisfactory projections over time with minimal complications.4 However, an additional consideration associated with graft augmentation is the need for an additional surgical site (autologous grafts) or the possibility that graft material may not be compatible with subsequent breast examination techniques. For example, calcium hydroxylapatite is a radiopaque material that may interfere with the interpretation of radiography and mammography.5
The use of injectable hyaluronic acid (HA) dermal fillers to enhance nipple projection represents a noninvasive procedure with immediate and adjustable results. A variety of dermal fillers that do not interfere with subsequent breast imaging needs have already been successfully used for nipple reconstruction including HA 60% plus acrylic hydrogel 40%, PMMA microspheres in a bovine collagen 3.5% gel, and poly-L-lactic acid.5-7
The results achieved with HA 60% plus acrylic hydrogel 40% were as much as a 2.5-mm mean increase in nipple projection after 12 months for 70 nipples reconstructed using a small wedge from the labia minora.5 In these treatments, an initial injection of 0.1 to 0.3 mL of filler into each nipple along with a 0.2-mL injection at the base of each nipple was made. Further optional treatments at 2 and 4 months after the initial injection were made using up to 0.3 mL additional volume depending on filler reabsorption.5 Results achieved with PMMA microspheres in a bovine collagen 3.5% gel included a 1.6-mm mean increase in nipple projection at 9 months versus baseline for 33 nipples in 23 patients, which involved up to 2 injections at baseline and again at 3 months.6 Treatment with poly-L-lactic acid provided a 2.3-mm mean increase in nipple projection for 12 patients after 1 year of treatment, which involved 0.5-mL injections every 4 weeks over a series of 4 treatments.7
This report describes the technique and cosmetic outcome using an injectable HA gel to postoperatively restore the 3-dimensional contour of the nipple following surgical breast reconstruction. This chemically cross-linked, stabilized HA gel suspended in phosphate-buffered saline at a pH of 7 and a concentration of 20 mg/mL with lidocaine 0.3% is indicated for mid to deep dermal implantation for the correction of moderate to severe facial wrinkles and folds, such as the nasolabial folds.8
Case Report
A 49-year-old woman with a history of breast cancer with a focal, high-grade ductal carcinoma in situ underwent a complete bilateral mastectomy. The sentinel lymph nodes were negative at the time of mastectomy. One year later, the patient elected to have breast and nipple-areola (flap) reconstruction. Following the reconstructive surgery, her nipples had become visibly atrophic and flat, and she was interested in cosmetic enhancement.
After informed consent had been obtained from the patient, a baseline measurement of each nipple was made while the patient was standing. Each nipple was then injected with up to 0.1 to 0.2 mL of HA gel filler using a 30-gauge needle inserted 2-mm deep (bilaterally) into each nipple. The patient tolerated the procedure well with no pain, bleeding, or bruising. Although HA gel filler contains lidocaine 0.3% and tricaine can further be used to ensure patient comfort, the nipple reconstruction surgery left the patient with little sensation in the treatment area. Rubbing alcohol was used to prepare the skin prior to the procedure, and fractionated coconut oil spray with a nonadherent dressing was used postprocedure.
Following the injection, an immediate increase of 1.6 and 1.5 mm in nipple projection in the right and left breasts, respectively, was achieved with HA gel. The nipple projection of the right breast was 1.7 mm before injection (Figure, A) and 3.3 mm immediately postinjection (Figure, C). The nipple projection of the left breast was 1.8 mm before injection (Figure, B) and 3.3 mm immediately postinjection (Figure, D).
Comment
With a single treatment consisting of 0.2 mL or less of filler volume, the HA gel used in this procedure provided an immediate mean increase in nipple projection of 1.5 mm. Although our assessment involved a single patient evaluated at baseline and immediately post-injection of HA filler only, it is reasonable to assume that subsequent reinjections would provide results comparable to other fillers. Although other fillers that are semipermanent (acrylic hydrogel) and nonbiodegradable (PMMA) make them more durable, these properties also make the augmentation less reversible in the case of overfilling. As with all dermal fillers, rare side effects associated with injection of HA gel filler could potentially include injection-site inflammation, extrusion of filler at the needle insertion site, minimal pain or discomfort during or after injections, bruising, swelling, or delayed-type hypersensitivity reaction. Ideally, HA gel is a soft transparent filler that is reversible with hyaluronidase, an advantage not shared by other filler materials.9
Conclusion
Nipple augmentation with HA gel is a simple noninvasive
The most frequently used surgical techniques in nipple-areola complex (NAC) reconstruction involve the use of local tissue flaps and yield the fewest complications, though these techniques can be associated with up to a 75% loss in nipple projection over time.1 In a best-case scenario for both the surgeon and the patient, the NAC is preserved during mastectomy; however, even when the tissues are spared, an eventual loss of nipple projection is expected due to atrophy and contraction of the healing skin.2 Loss of nipple projection is the most common attribute that patients dislike regarding their NAC reconstruction results.Additional efforts made to restore the natural look and feel of the NAC provides undeniable benefit to the patient in the form of improved body image and psychosocial well-being.3
Augmentation with a grafted material can include cartilage or fat (autologous grafts), calcium hydroxylapatite or polymethyl methacrylate (PMMA)(alloplastic grafts), and acellular dermal matrix or biologic collagen (allografts). Among these options, successive treatment with autologous fat has been shown to provide satisfactory projections over time with minimal complications.4 However, an additional consideration associated with graft augmentation is the need for an additional surgical site (autologous grafts) or the possibility that graft material may not be compatible with subsequent breast examination techniques. For example, calcium hydroxylapatite is a radiopaque material that may interfere with the interpretation of radiography and mammography.5
The use of injectable hyaluronic acid (HA) dermal fillers to enhance nipple projection represents a noninvasive procedure with immediate and adjustable results. A variety of dermal fillers that do not interfere with subsequent breast imaging needs have already been successfully used for nipple reconstruction including HA 60% plus acrylic hydrogel 40%, PMMA microspheres in a bovine collagen 3.5% gel, and poly-L-lactic acid.5-7
The results achieved with HA 60% plus acrylic hydrogel 40% were as much as a 2.5-mm mean increase in nipple projection after 12 months for 70 nipples reconstructed using a small wedge from the labia minora.5 In these treatments, an initial injection of 0.1 to 0.3 mL of filler into each nipple along with a 0.2-mL injection at the base of each nipple was made. Further optional treatments at 2 and 4 months after the initial injection were made using up to 0.3 mL additional volume depending on filler reabsorption.5 Results achieved with PMMA microspheres in a bovine collagen 3.5% gel included a 1.6-mm mean increase in nipple projection at 9 months versus baseline for 33 nipples in 23 patients, which involved up to 2 injections at baseline and again at 3 months.6 Treatment with poly-L-lactic acid provided a 2.3-mm mean increase in nipple projection for 12 patients after 1 year of treatment, which involved 0.5-mL injections every 4 weeks over a series of 4 treatments.7
This report describes the technique and cosmetic outcome using an injectable HA gel to postoperatively restore the 3-dimensional contour of the nipple following surgical breast reconstruction. This chemically cross-linked, stabilized HA gel suspended in phosphate-buffered saline at a pH of 7 and a concentration of 20 mg/mL with lidocaine 0.3% is indicated for mid to deep dermal implantation for the correction of moderate to severe facial wrinkles and folds, such as the nasolabial folds.8
Case Report
A 49-year-old woman with a history of breast cancer with a focal, high-grade ductal carcinoma in situ underwent a complete bilateral mastectomy. The sentinel lymph nodes were negative at the time of mastectomy. One year later, the patient elected to have breast and nipple-areola (flap) reconstruction. Following the reconstructive surgery, her nipples had become visibly atrophic and flat, and she was interested in cosmetic enhancement.
After informed consent had been obtained from the patient, a baseline measurement of each nipple was made while the patient was standing. Each nipple was then injected with up to 0.1 to 0.2 mL of HA gel filler using a 30-gauge needle inserted 2-mm deep (bilaterally) into each nipple. The patient tolerated the procedure well with no pain, bleeding, or bruising. Although HA gel filler contains lidocaine 0.3% and tricaine can further be used to ensure patient comfort, the nipple reconstruction surgery left the patient with little sensation in the treatment area. Rubbing alcohol was used to prepare the skin prior to the procedure, and fractionated coconut oil spray with a nonadherent dressing was used postprocedure.
Following the injection, an immediate increase of 1.6 and 1.5 mm in nipple projection in the right and left breasts, respectively, was achieved with HA gel. The nipple projection of the right breast was 1.7 mm before injection (Figure, A) and 3.3 mm immediately postinjection (Figure, C). The nipple projection of the left breast was 1.8 mm before injection (Figure, B) and 3.3 mm immediately postinjection (Figure, D).
Comment
With a single treatment consisting of 0.2 mL or less of filler volume, the HA gel used in this procedure provided an immediate mean increase in nipple projection of 1.5 mm. Although our assessment involved a single patient evaluated at baseline and immediately post-injection of HA filler only, it is reasonable to assume that subsequent reinjections would provide results comparable to other fillers. Although other fillers that are semipermanent (acrylic hydrogel) and nonbiodegradable (PMMA) make them more durable, these properties also make the augmentation less reversible in the case of overfilling. As with all dermal fillers, rare side effects associated with injection of HA gel filler could potentially include injection-site inflammation, extrusion of filler at the needle insertion site, minimal pain or discomfort during or after injections, bruising, swelling, or delayed-type hypersensitivity reaction. Ideally, HA gel is a soft transparent filler that is reversible with hyaluronidase, an advantage not shared by other filler materials.9
Conclusion
Nipple augmentation with HA gel is a simple noninvasive
- Sisti A, Grimaldi L, Tassinari J, et al. Nipple-areola complex reconstruction techniques: a literature review. Eur J Surg Oncol. 2016;42:441-465.
- Murthy V, Chamberlain RS. Defining a place for nipple sparing mastectomy in modern breast care: an evidence based review. Breast J. 2013;19:571-581.
- Jabor MA, Shayani P, Collins DR Jr, et al. Nipple-areola reconstruction: satisfaction and clinical determinants. Plast Reconstr Surg. 2002;110:457-463.
- Kaoutzanis C, Xin M, Ballard TN, et al. Autologous fat grafting after breast reconstruction in postmastectomy patients: complications, biopsy rates, and locoregional cancer recurrence rates. Ann Plast Surg. 2016;76:270-275.
- Panettiere P, Marchetti L, Accorsi D. Filler injection enhances the projection of the reconstructed nipple: an original easy technique. Aesthet Plast Surg. 2005;29:287-294.
- McCarthy CM, Van Laeken N, Lennox P, et al. The efficacy of Artecoll injections for the augmentation of nipple projection in breast reconstruction. Eplasty. 2010;10:E7.
- Dessy LA, Troccola A, Ranno RL, et al. The use of Poly-lactic acid to improve projection of reconstructed nipple. Breast. 2011;20:220-224.
- Restylane L [package insert]. Fort Worth, TX: Galderma Laboratories, LP; 2016.
- Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
- Sisti A, Grimaldi L, Tassinari J, et al. Nipple-areola complex reconstruction techniques: a literature review. Eur J Surg Oncol. 2016;42:441-465.
- Murthy V, Chamberlain RS. Defining a place for nipple sparing mastectomy in modern breast care: an evidence based review. Breast J. 2013;19:571-581.
- Jabor MA, Shayani P, Collins DR Jr, et al. Nipple-areola reconstruction: satisfaction and clinical determinants. Plast Reconstr Surg. 2002;110:457-463.
- Kaoutzanis C, Xin M, Ballard TN, et al. Autologous fat grafting after breast reconstruction in postmastectomy patients: complications, biopsy rates, and locoregional cancer recurrence rates. Ann Plast Surg. 2016;76:270-275.
- Panettiere P, Marchetti L, Accorsi D. Filler injection enhances the projection of the reconstructed nipple: an original easy technique. Aesthet Plast Surg. 2005;29:287-294.
- McCarthy CM, Van Laeken N, Lennox P, et al. The efficacy of Artecoll injections for the augmentation of nipple projection in breast reconstruction. Eplasty. 2010;10:E7.
- Dessy LA, Troccola A, Ranno RL, et al. The use of Poly-lactic acid to improve projection of reconstructed nipple. Breast. 2011;20:220-224.
- Restylane L [package insert]. Fort Worth, TX: Galderma Laboratories, LP; 2016.
- Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
Practice Points
- The use of injectable hyaluronic acid (HA) gel to restore 3-dimensional contour of the nipple following nipple-areola complex (NAC) reconstruction is a noninvasive procedure that contributes to patient well-being.
- The use of HA gel for NAC augmentation can be performed in an office setting and may eliminate the need for secondary reconstructive surgeries.

Nomadic Mongolian skin care practices
In a large country of only 3 million people (where wild horses outnumber people), with an estimated 2 million who live in the capital and 1 million who live a traditional nomadic lifestyle, traditional skin care and beauty practices can still be found.
In the capital city of Ulaanbaatar, women practice many of the same beauty regimens as those of women in other parts of mainstream Asia, with access to department store beauty counters and shopping malls found in major cities throughout the world. With the influx of movies and media into Mongolia from South Korea in the late 1990s, South Korean beauty regimens and standards have weaved their way into the urban culture. However, in rural Mongolia, where a nomadic way of life still predominates, certain beauty and cultural practices remain intact without the influence of mainstream culture.

Homemade yogurt, a staple in rural Mongolia, is used on the face to help brighten the skin. In rural Mongolia, the yogurt is made and eaten fresh, thus lasts for 1-2 days if not refrigerated. The yogurt comes from cows and goats (rarely from other animals) that graze on open land without pesticides and are not fed hormones and grains. My personal diet doesn’t consist of much dairy, but I can say firsthand that in my opinion, it is delicious there. Yogurt is also applied to the skin to treat acne, but for acne the yogurt is fermented more than usual, so there is more acid to reduce the skin inflammation. (Lactic acid is typically what is found in fermented yogurt.)


Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Resource:
In a large country of only 3 million people (where wild horses outnumber people), with an estimated 2 million who live in the capital and 1 million who live a traditional nomadic lifestyle, traditional skin care and beauty practices can still be found.
In the capital city of Ulaanbaatar, women practice many of the same beauty regimens as those of women in other parts of mainstream Asia, with access to department store beauty counters and shopping malls found in major cities throughout the world. With the influx of movies and media into Mongolia from South Korea in the late 1990s, South Korean beauty regimens and standards have weaved their way into the urban culture. However, in rural Mongolia, where a nomadic way of life still predominates, certain beauty and cultural practices remain intact without the influence of mainstream culture.
Homemade yogurt, a staple in rural Mongolia, is used on the face to help brighten the skin. In rural Mongolia, the yogurt is made and eaten fresh, thus lasts for 1-2 days if not refrigerated. The yogurt comes from cows and goats (rarely from other animals) that graze on open land without pesticides and are not fed hormones and grains. My personal diet doesn’t consist of much dairy, but I can say firsthand that in my opinion, it is delicious there. Yogurt is also applied to the skin to treat acne, but for acne the yogurt is fermented more than usual, so there is more acid to reduce the skin inflammation. (Lactic acid is typically what is found in fermented yogurt.)
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Resource:
In a large country of only 3 million people (where wild horses outnumber people), with an estimated 2 million who live in the capital and 1 million who live a traditional nomadic lifestyle, traditional skin care and beauty practices can still be found.
In the capital city of Ulaanbaatar, women practice many of the same beauty regimens as those of women in other parts of mainstream Asia, with access to department store beauty counters and shopping malls found in major cities throughout the world. With the influx of movies and media into Mongolia from South Korea in the late 1990s, South Korean beauty regimens and standards have weaved their way into the urban culture. However, in rural Mongolia, where a nomadic way of life still predominates, certain beauty and cultural practices remain intact without the influence of mainstream culture.
Homemade yogurt, a staple in rural Mongolia, is used on the face to help brighten the skin. In rural Mongolia, the yogurt is made and eaten fresh, thus lasts for 1-2 days if not refrigerated. The yogurt comes from cows and goats (rarely from other animals) that graze on open land without pesticides and are not fed hormones and grains. My personal diet doesn’t consist of much dairy, but I can say firsthand that in my opinion, it is delicious there. Yogurt is also applied to the skin to treat acne, but for acne the yogurt is fermented more than usual, so there is more acid to reduce the skin inflammation. (Lactic acid is typically what is found in fermented yogurt.)
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Resource:

Isotretinoin patients need not postpone skin surgery
Skin procedures including superficial chemical peels, laser hair removal, minor cutaneous surgery, manual dermabrasion, and fractional ablative and fractional nonablative laser procedures can be performed safely on patients who have recently been or are currently being treated with isotretinoin, according to new recommendations from a consensus panel.
The recommendations were published online in JAMA Dermatology.
Postponing surgical procedures in patients taking isotretinoin because of the potential for keloid formation and delayed wound healing “has persisted despite increasing reports to the contrary,” wrote Leah K. Spring, DO, of Naval Hospital Camp Lejeune, Camp Lejeune, N.C., and her colleagues (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2017.2077).
This protocol is based on 11 patients with delayed healing and keloids, the researchers noted. “In our consensus-based assessment, these initial cases presented a hypothesis to be tested, rather than the foundation for medical dogma on which more than 30 years of clinical practice was built,” they wrote.
To establish the current level of evidence for delaying procedures in isotretinoin patients and to make recommendations, an expert panel reviewed data from 32 publications and more than 1,485 procedures. The literature was divided into five areas: dermabrasion, chemical peels, cutaneous surgery, laser hair removal, and ablative/nonablative laser treatments.
The researchers determined that evidence does not support the safety of mechanical dermabrasion or fully ablative laser surgeries for current or recent isotretinoin users. Manual dermabrasion and microdermabrasion were deemed safe for isotretinoin patients based on the latest evidence, however, as were fractional ablative and fractional nonablative procedures.
In addition, the evidence did not support refraining from chemical peels, laser hair removal, or cutaneous surgery for current and recent isotretinoin patients, although the panel recommended additional prospective, controlled clinical trials in these areas.
In the area of cutaneous surgery, the consensus panel also noted the need for “a rigorous evaluation of the aforementioned specific warning that muscle flap insertion should be delayed until the patient displays normal [creatine phosphokinase (CPK)] levels or, at least, CPK levels below twofold of normal.”
The recommendations can be a resource for discussions with patients about the risks of procedures concurrent with isotretinoin, Dr. Spring and her associates emphasized. “For some patients and some conditions, an informed decision may lead to earlier and potentially more effective interventions.”
Lead author Dr. Spring had no relevant financial conflicts to disclose. Several members of the consensus group disclosed relationships with multiple companies including Allergan, Merz, Leo, Promius, Lumenis, Cynosure, and Valeant.
Skin procedures including superficial chemical peels, laser hair removal, minor cutaneous surgery, manual dermabrasion, and fractional ablative and fractional nonablative laser procedures can be performed safely on patients who have recently been or are currently being treated with isotretinoin, according to new recommendations from a consensus panel.
The recommendations were published online in JAMA Dermatology.
Postponing surgical procedures in patients taking isotretinoin because of the potential for keloid formation and delayed wound healing “has persisted despite increasing reports to the contrary,” wrote Leah K. Spring, DO, of Naval Hospital Camp Lejeune, Camp Lejeune, N.C., and her colleagues (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2017.2077).
This protocol is based on 11 patients with delayed healing and keloids, the researchers noted. “In our consensus-based assessment, these initial cases presented a hypothesis to be tested, rather than the foundation for medical dogma on which more than 30 years of clinical practice was built,” they wrote.
To establish the current level of evidence for delaying procedures in isotretinoin patients and to make recommendations, an expert panel reviewed data from 32 publications and more than 1,485 procedures. The literature was divided into five areas: dermabrasion, chemical peels, cutaneous surgery, laser hair removal, and ablative/nonablative laser treatments.
The researchers determined that evidence does not support the safety of mechanical dermabrasion or fully ablative laser surgeries for current or recent isotretinoin users. Manual dermabrasion and microdermabrasion were deemed safe for isotretinoin patients based on the latest evidence, however, as were fractional ablative and fractional nonablative procedures.
In addition, the evidence did not support refraining from chemical peels, laser hair removal, or cutaneous surgery for current and recent isotretinoin patients, although the panel recommended additional prospective, controlled clinical trials in these areas.
In the area of cutaneous surgery, the consensus panel also noted the need for “a rigorous evaluation of the aforementioned specific warning that muscle flap insertion should be delayed until the patient displays normal [creatine phosphokinase (CPK)] levels or, at least, CPK levels below twofold of normal.”
The recommendations can be a resource for discussions with patients about the risks of procedures concurrent with isotretinoin, Dr. Spring and her associates emphasized. “For some patients and some conditions, an informed decision may lead to earlier and potentially more effective interventions.”
Lead author Dr. Spring had no relevant financial conflicts to disclose. Several members of the consensus group disclosed relationships with multiple companies including Allergan, Merz, Leo, Promius, Lumenis, Cynosure, and Valeant.
Skin procedures including superficial chemical peels, laser hair removal, minor cutaneous surgery, manual dermabrasion, and fractional ablative and fractional nonablative laser procedures can be performed safely on patients who have recently been or are currently being treated with isotretinoin, according to new recommendations from a consensus panel.
The recommendations were published online in JAMA Dermatology.
Postponing surgical procedures in patients taking isotretinoin because of the potential for keloid formation and delayed wound healing “has persisted despite increasing reports to the contrary,” wrote Leah K. Spring, DO, of Naval Hospital Camp Lejeune, Camp Lejeune, N.C., and her colleagues (JAMA Dermatol. 2017. doi: 10.1001/jamadermatol.2017.2077).
This protocol is based on 11 patients with delayed healing and keloids, the researchers noted. “In our consensus-based assessment, these initial cases presented a hypothesis to be tested, rather than the foundation for medical dogma on which more than 30 years of clinical practice was built,” they wrote.
To establish the current level of evidence for delaying procedures in isotretinoin patients and to make recommendations, an expert panel reviewed data from 32 publications and more than 1,485 procedures. The literature was divided into five areas: dermabrasion, chemical peels, cutaneous surgery, laser hair removal, and ablative/nonablative laser treatments.
The researchers determined that evidence does not support the safety of mechanical dermabrasion or fully ablative laser surgeries for current or recent isotretinoin users. Manual dermabrasion and microdermabrasion were deemed safe for isotretinoin patients based on the latest evidence, however, as were fractional ablative and fractional nonablative procedures.
In addition, the evidence did not support refraining from chemical peels, laser hair removal, or cutaneous surgery for current and recent isotretinoin patients, although the panel recommended additional prospective, controlled clinical trials in these areas.
In the area of cutaneous surgery, the consensus panel also noted the need for “a rigorous evaluation of the aforementioned specific warning that muscle flap insertion should be delayed until the patient displays normal [creatine phosphokinase (CPK)] levels or, at least, CPK levels below twofold of normal.”
The recommendations can be a resource for discussions with patients about the risks of procedures concurrent with isotretinoin, Dr. Spring and her associates emphasized. “For some patients and some conditions, an informed decision may lead to earlier and potentially more effective interventions.”
Lead author Dr. Spring had no relevant financial conflicts to disclose. Several members of the consensus group disclosed relationships with multiple companies including Allergan, Merz, Leo, Promius, Lumenis, Cynosure, and Valeant.
FROM JAMA DERMATOLOGY
Key clinical point:
Major finding: Experts found insufficient evidence to postpone manual dermabrasion, superficial chemical peels, fractional ablative or nonablative laser resurfacing, laser hair removal, or cutaneous surgery in patients taking isotretinoin or those who have taken it within the past 6 to 12 months.
Data source: The data come from 32 clinical publications and a total of 1,485 procedures.
Disclosures: Lead author Dr. Spring had no relevant financial conflicts to disclose. Several members of the consensus group disclosed relationships with multiple companies, including Allergan, Merz, Leo, Promius, Lumenis, Cynosure, and Valeant.
Cosmetic Corner: Dermatologists Weigh in on Redness-Reducing Products
To improve patient care and outcomes, leading dermatologists offered their recommendations on redness-reducing products. Consideration must be given to:
- Avène Antirougeurs FORT Relief Concentrate
Pierre Fabre Dermo-Cosmetique USA
“This formula has medical-grade ruscus extract to support microcirculation and soothe skin reactivity and redness, as well as soothing Avène Thermal Spring Water.” — Jeannette Graf, MD, New York, New York
- Eucerin Redness Relief
Beiersdorf Inc
“Eucerin’s Redness Relief product line has worked well for some of my patients.” — Gary Goldenberg, MD, New York, New York
- Redness Solutions Daily Protective Base Broad Spectrum SPF 15
Clinique Laboratories, LLC
“This oil-free makeup primer has a sheer green tint that camouflages redness while also protecting from UV rays.” — Shari Lipner, MD, PhD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments, cleansing devices, and men’s products will be featured in upcoming editions of Cosmetic Corner. Please email your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on redness-reducing products. Consideration must be given to:
- Avène Antirougeurs FORT Relief Concentrate
Pierre Fabre Dermo-Cosmetique USA
“This formula has medical-grade ruscus extract to support microcirculation and soothe skin reactivity and redness, as well as soothing Avène Thermal Spring Water.” — Jeannette Graf, MD, New York, New York
- Eucerin Redness Relief
Beiersdorf Inc
“Eucerin’s Redness Relief product line has worked well for some of my patients.” — Gary Goldenberg, MD, New York, New York
- Redness Solutions Daily Protective Base Broad Spectrum SPF 15
Clinique Laboratories, LLC
“This oil-free makeup primer has a sheer green tint that camouflages redness while also protecting from UV rays.” — Shari Lipner, MD, PhD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments, cleansing devices, and men’s products will be featured in upcoming editions of Cosmetic Corner. Please email your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on redness-reducing products. Consideration must be given to:
- Avène Antirougeurs FORT Relief Concentrate
Pierre Fabre Dermo-Cosmetique USA
“This formula has medical-grade ruscus extract to support microcirculation and soothe skin reactivity and redness, as well as soothing Avène Thermal Spring Water.” — Jeannette Graf, MD, New York, New York
- Eucerin Redness Relief
Beiersdorf Inc
“Eucerin’s Redness Relief product line has worked well for some of my patients.” — Gary Goldenberg, MD, New York, New York
- Redness Solutions Daily Protective Base Broad Spectrum SPF 15
Clinique Laboratories, LLC
“This oil-free makeup primer has a sheer green tint that camouflages redness while also protecting from UV rays.” — Shari Lipner, MD, PhD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments, cleansing devices, and men’s products will be featured in upcoming editions of Cosmetic Corner. Please email your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Pre- and postprocedure skin care guide for your surgical patients
Whether patients are having a biopsy, surgical excision, or Mohs surgery, the outcome will be improved when the proper skin care is used before and after the procedure. This is a guide that you can use to educate your patients about pre- and postprocedure skin care needs.
Presurgery skin care and supplements
The goal is to speed healing and minimize infection, scarring, and hyperpigmentation. For 2 weeks prior to surgery, recommend products that have been shown to speed wound healing by increasing keratinization and/or collagen production. Ingredients that should be used prior to wounding include retinoids such as tretinoin and retinol. Several studies have convincingly shown that pretreatment with tretinoin speeds wound healing.1,2,3 Kligman and associates evaluated healing after punch biopsy and found the wounds on arms pretreated with tretinoin cream 0.05% to 0.1% were significantly smaller – by 35% to 37% – on days 1 and 4, and were 47% to 50% smaller on days 6, 8, and 11, compared with the untreated arms.4 Most studies suggest a 2- to 4-week tretinoin pretreatment regimen5 because peak epidermal hypertrophy occurs after 7 days of tretinoin application and normalizes after 14 days of continued treatment.6 This approach allows the skin to recover from any retinoid dermatitis prior to surgery. Adapalene should be started 5-6 weeks prior to procedures because it has a longer half-life and requires an earlier initiation period.7
Although wound healing studies have not been conducted in this area, pretreating skin with topical ascorbic acid8 and hydroxyacids9 might help speed wound healing by increasing collagen synthesis.
Ingredients and activities to avoid presurgery
Patients should avoid using ingredients that could promote skin tumor growth. Although there are no studies evaluating the effects of growth factors on promoting the growth of skin cancer, caution is prudent. To reduce bruising, patients should avoid aspirin, ibuprofen, naproxen, St. John’s Wort, vitamin E, omega-3 fatty acids supplements, flax seed oil, ginseng, salmon, and alcohol. Most physicians agree that these should be avoided for 10 days prior to the procedure. Smoking should be avoided 4 weeks prior to the procedure.
Postsurgery skin care and supplements
Oral vitamin C and zinc supplements have been shown to speed wound healing in rats when taken immediately after a procedure.10 Oral Arnica tablets and tinctures are often used prior to and after surgery to reduce bruising and inflammation. There is much anecdotal support for the use of Arnica, but clinical trial evidence substantiating its efficacy to prevent bruising and reduce swelling is scant.

A protein important in wound repair, defensin, is available in a topical formulation. Defensin14 has been shown to activate the leucine-rich repeat-containing G-protein–coupled receptors 5 and 6 (also known as LGR5 and LGR6) stem cells. It speeds wound healing by increasing LGR stem cell migration into wound beds. Wounds should be covered to provide protection from sun exposure until reepithelialization occurs. Which occlusive ointments and wound repair products to use are beyond the scope of this article. Once epithelized, zinc oxide sunscreens can be used. These have been shown to be safe with minimal penetration into the skin.15
Ingredients to avoid post surgery
Topical retinoids should not be used post skin cancer surgery until epithelialization is complete. A study by Hung et al.16 in a porcine model used 0.05% tretinoin cream daily for 10 days prior to partial-thickness skin wounding demonstrated that use of tretinoin 10 days prior to wounding sped reepithelialization while use after the procedure slowed wound healing.
Acidic products will sting wounded skin. For this reason, benzoic acid, hydroxy acids, and ascorbic acid should be avoided until the skin has completely reepithelialized. Products with preservatives and fragrance should be avoided if possible.
Vitamin E derived from oral supplement capsules slowed healing after skin cancer surgery and had a high rate of contact dermatitis.17 Chemical sunscreens are more likely to cause an allergic contact dermatitis and should be avoided for 4 weeks after skin surgery. Organic products with essential oils and botanical ingredients may present a higher risk of contact dermatitis due to allergen exposure.
Conclusion
To ensure the best outcome from surgical treatments, patient education is a must! The more that patients know and understand about the ways in which they can prepare for their procedure and treat their skin after the procedure, the better the outcomes will be. Providers should give this type of information in an easy-to-follow printed instruction sheet because studies show that patients cannot remember most of the oral instructions offered by practitioners.
Encourage your patients to ask questions during their consultation and procedure and to get in touch with your office should they have any concerns when they leave. These steps help improve patient compliance and satisfaction, which will help you maintain a trusting relationship with established patients and attract new ones through word-of-mouth referrals.
Please email me at [email protected] if you have any other pre- and postprocedure skin care advice.
Dr. Leslie S. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Aesthetic Plast Surg. 1995 May-Jun;19(3):243-6.
2. Plast Reconstr Surg. 2011 Mar;127(3):1343-5.
3. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S79-81.
4. Br J Dermatol. 1995 Jan;132(1):46-53.
5. J Am Acad Dermatol. 2004 Dec;51(6):940-6.
6. J Korean Med Sci. 1996 Aug;11(4):335-41.
7. Eur J Dermatol. 2002 Mar-Apr;12(2):145-8.
8. Proc Natl Acad Sci U S A. 1981 May;78(5):2879-82.
9. Exp Dermatol. 2003;12 Suppl 2:57-63.
10. Surg Today. 2004;34(9):747-51.
11. Ophthal Plast Reconstr Surg. 2017 Jan/Feb;33(1):47-52.
12. Wound Repair Regen. 1998 Mar-Apr;6(2):167-77.
13. Dermatol Surg. 1998 Jun;24(6):661-4.
14. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
15. ACS Nano. 2016 Feb 23;10(2):1810-9.
16. Arch Dermatol. 1989 Jan;125(1):65-9.
17. Dermatol Surg. 1999 Apr;25(4):311-5.
Retinoids should be used 2-3 times prior to procedures to speed healing.
Retinoids should not be used after the procedure until reepithelization has occurred.
Vitamin C and zinc supplements taken post procedure might speed wound healing.
Retinoids should be used 2-3 times prior to procedures to speed healing.
Retinoids should not be used after the procedure until reepithelization has occurred.
Vitamin C and zinc supplements taken post procedure might speed wound healing.
Retinoids should be used 2-3 times prior to procedures to speed healing.
Retinoids should not be used after the procedure until reepithelization has occurred.
Vitamin C and zinc supplements taken post procedure might speed wound healing.
Whether patients are having a biopsy, surgical excision, or Mohs surgery, the outcome will be improved when the proper skin care is used before and after the procedure. This is a guide that you can use to educate your patients about pre- and postprocedure skin care needs.
Presurgery skin care and supplements
The goal is to speed healing and minimize infection, scarring, and hyperpigmentation. For 2 weeks prior to surgery, recommend products that have been shown to speed wound healing by increasing keratinization and/or collagen production. Ingredients that should be used prior to wounding include retinoids such as tretinoin and retinol. Several studies have convincingly shown that pretreatment with tretinoin speeds wound healing.1,2,3 Kligman and associates evaluated healing after punch biopsy and found the wounds on arms pretreated with tretinoin cream 0.05% to 0.1% were significantly smaller – by 35% to 37% – on days 1 and 4, and were 47% to 50% smaller on days 6, 8, and 11, compared with the untreated arms.4 Most studies suggest a 2- to 4-week tretinoin pretreatment regimen5 because peak epidermal hypertrophy occurs after 7 days of tretinoin application and normalizes after 14 days of continued treatment.6 This approach allows the skin to recover from any retinoid dermatitis prior to surgery. Adapalene should be started 5-6 weeks prior to procedures because it has a longer half-life and requires an earlier initiation period.7
Although wound healing studies have not been conducted in this area, pretreating skin with topical ascorbic acid8 and hydroxyacids9 might help speed wound healing by increasing collagen synthesis.
Ingredients and activities to avoid presurgery
Patients should avoid using ingredients that could promote skin tumor growth. Although there are no studies evaluating the effects of growth factors on promoting the growth of skin cancer, caution is prudent. To reduce bruising, patients should avoid aspirin, ibuprofen, naproxen, St. John’s Wort, vitamin E, omega-3 fatty acids supplements, flax seed oil, ginseng, salmon, and alcohol. Most physicians agree that these should be avoided for 10 days prior to the procedure. Smoking should be avoided 4 weeks prior to the procedure.
Postsurgery skin care and supplements
Oral vitamin C and zinc supplements have been shown to speed wound healing in rats when taken immediately after a procedure.10 Oral Arnica tablets and tinctures are often used prior to and after surgery to reduce bruising and inflammation. There is much anecdotal support for the use of Arnica, but clinical trial evidence substantiating its efficacy to prevent bruising and reduce swelling is scant.
A protein important in wound repair, defensin, is available in a topical formulation. Defensin14 has been shown to activate the leucine-rich repeat-containing G-protein–coupled receptors 5 and 6 (also known as LGR5 and LGR6) stem cells. It speeds wound healing by increasing LGR stem cell migration into wound beds. Wounds should be covered to provide protection from sun exposure until reepithelialization occurs. Which occlusive ointments and wound repair products to use are beyond the scope of this article. Once epithelized, zinc oxide sunscreens can be used. These have been shown to be safe with minimal penetration into the skin.15
Ingredients to avoid post surgery
Topical retinoids should not be used post skin cancer surgery until epithelialization is complete. A study by Hung et al.16 in a porcine model used 0.05% tretinoin cream daily for 10 days prior to partial-thickness skin wounding demonstrated that use of tretinoin 10 days prior to wounding sped reepithelialization while use after the procedure slowed wound healing.
Acidic products will sting wounded skin. For this reason, benzoic acid, hydroxy acids, and ascorbic acid should be avoided until the skin has completely reepithelialized. Products with preservatives and fragrance should be avoided if possible.
Vitamin E derived from oral supplement capsules slowed healing after skin cancer surgery and had a high rate of contact dermatitis.17 Chemical sunscreens are more likely to cause an allergic contact dermatitis and should be avoided for 4 weeks after skin surgery. Organic products with essential oils and botanical ingredients may present a higher risk of contact dermatitis due to allergen exposure.
Conclusion
To ensure the best outcome from surgical treatments, patient education is a must! The more that patients know and understand about the ways in which they can prepare for their procedure and treat their skin after the procedure, the better the outcomes will be. Providers should give this type of information in an easy-to-follow printed instruction sheet because studies show that patients cannot remember most of the oral instructions offered by practitioners.
Encourage your patients to ask questions during their consultation and procedure and to get in touch with your office should they have any concerns when they leave. These steps help improve patient compliance and satisfaction, which will help you maintain a trusting relationship with established patients and attract new ones through word-of-mouth referrals.
Please email me at [email protected] if you have any other pre- and postprocedure skin care advice.
Dr. Leslie S. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Aesthetic Plast Surg. 1995 May-Jun;19(3):243-6.
2. Plast Reconstr Surg. 2011 Mar;127(3):1343-5.
3. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S79-81.
4. Br J Dermatol. 1995 Jan;132(1):46-53.
5. J Am Acad Dermatol. 2004 Dec;51(6):940-6.
6. J Korean Med Sci. 1996 Aug;11(4):335-41.
7. Eur J Dermatol. 2002 Mar-Apr;12(2):145-8.
8. Proc Natl Acad Sci U S A. 1981 May;78(5):2879-82.
9. Exp Dermatol. 2003;12 Suppl 2:57-63.
10. Surg Today. 2004;34(9):747-51.
11. Ophthal Plast Reconstr Surg. 2017 Jan/Feb;33(1):47-52.
12. Wound Repair Regen. 1998 Mar-Apr;6(2):167-77.
13. Dermatol Surg. 1998 Jun;24(6):661-4.
14. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
15. ACS Nano. 2016 Feb 23;10(2):1810-9.
16. Arch Dermatol. 1989 Jan;125(1):65-9.
17. Dermatol Surg. 1999 Apr;25(4):311-5.
Whether patients are having a biopsy, surgical excision, or Mohs surgery, the outcome will be improved when the proper skin care is used before and after the procedure. This is a guide that you can use to educate your patients about pre- and postprocedure skin care needs.
Presurgery skin care and supplements
The goal is to speed healing and minimize infection, scarring, and hyperpigmentation. For 2 weeks prior to surgery, recommend products that have been shown to speed wound healing by increasing keratinization and/or collagen production. Ingredients that should be used prior to wounding include retinoids such as tretinoin and retinol. Several studies have convincingly shown that pretreatment with tretinoin speeds wound healing.1,2,3 Kligman and associates evaluated healing after punch biopsy and found the wounds on arms pretreated with tretinoin cream 0.05% to 0.1% were significantly smaller – by 35% to 37% – on days 1 and 4, and were 47% to 50% smaller on days 6, 8, and 11, compared with the untreated arms.4 Most studies suggest a 2- to 4-week tretinoin pretreatment regimen5 because peak epidermal hypertrophy occurs after 7 days of tretinoin application and normalizes after 14 days of continued treatment.6 This approach allows the skin to recover from any retinoid dermatitis prior to surgery. Adapalene should be started 5-6 weeks prior to procedures because it has a longer half-life and requires an earlier initiation period.7
Although wound healing studies have not been conducted in this area, pretreating skin with topical ascorbic acid8 and hydroxyacids9 might help speed wound healing by increasing collagen synthesis.
Ingredients and activities to avoid presurgery
Patients should avoid using ingredients that could promote skin tumor growth. Although there are no studies evaluating the effects of growth factors on promoting the growth of skin cancer, caution is prudent. To reduce bruising, patients should avoid aspirin, ibuprofen, naproxen, St. John’s Wort, vitamin E, omega-3 fatty acids supplements, flax seed oil, ginseng, salmon, and alcohol. Most physicians agree that these should be avoided for 10 days prior to the procedure. Smoking should be avoided 4 weeks prior to the procedure.
Postsurgery skin care and supplements
Oral vitamin C and zinc supplements have been shown to speed wound healing in rats when taken immediately after a procedure.10 Oral Arnica tablets and tinctures are often used prior to and after surgery to reduce bruising and inflammation. There is much anecdotal support for the use of Arnica, but clinical trial evidence substantiating its efficacy to prevent bruising and reduce swelling is scant.
A protein important in wound repair, defensin, is available in a topical formulation. Defensin14 has been shown to activate the leucine-rich repeat-containing G-protein–coupled receptors 5 and 6 (also known as LGR5 and LGR6) stem cells. It speeds wound healing by increasing LGR stem cell migration into wound beds. Wounds should be covered to provide protection from sun exposure until reepithelialization occurs. Which occlusive ointments and wound repair products to use are beyond the scope of this article. Once epithelized, zinc oxide sunscreens can be used. These have been shown to be safe with minimal penetration into the skin.15
Ingredients to avoid post surgery
Topical retinoids should not be used post skin cancer surgery until epithelialization is complete. A study by Hung et al.16 in a porcine model used 0.05% tretinoin cream daily for 10 days prior to partial-thickness skin wounding demonstrated that use of tretinoin 10 days prior to wounding sped reepithelialization while use after the procedure slowed wound healing.
Acidic products will sting wounded skin. For this reason, benzoic acid, hydroxy acids, and ascorbic acid should be avoided until the skin has completely reepithelialized. Products with preservatives and fragrance should be avoided if possible.
Vitamin E derived from oral supplement capsules slowed healing after skin cancer surgery and had a high rate of contact dermatitis.17 Chemical sunscreens are more likely to cause an allergic contact dermatitis and should be avoided for 4 weeks after skin surgery. Organic products with essential oils and botanical ingredients may present a higher risk of contact dermatitis due to allergen exposure.
Conclusion
To ensure the best outcome from surgical treatments, patient education is a must! The more that patients know and understand about the ways in which they can prepare for their procedure and treat their skin after the procedure, the better the outcomes will be. Providers should give this type of information in an easy-to-follow printed instruction sheet because studies show that patients cannot remember most of the oral instructions offered by practitioners.
Encourage your patients to ask questions during their consultation and procedure and to get in touch with your office should they have any concerns when they leave. These steps help improve patient compliance and satisfaction, which will help you maintain a trusting relationship with established patients and attract new ones through word-of-mouth referrals.
Please email me at [email protected] if you have any other pre- and postprocedure skin care advice.
Dr. Leslie S. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and “Cosmeceuticals and Cosmetic Ingredients,” (New York: McGraw-Hill, 2014), and a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Aesthetic Plast Surg. 1995 May-Jun;19(3):243-6.
2. Plast Reconstr Surg. 2011 Mar;127(3):1343-5.
3. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S79-81.
4. Br J Dermatol. 1995 Jan;132(1):46-53.
5. J Am Acad Dermatol. 2004 Dec;51(6):940-6.
6. J Korean Med Sci. 1996 Aug;11(4):335-41.
7. Eur J Dermatol. 2002 Mar-Apr;12(2):145-8.
8. Proc Natl Acad Sci U S A. 1981 May;78(5):2879-82.
9. Exp Dermatol. 2003;12 Suppl 2:57-63.
10. Surg Today. 2004;34(9):747-51.
11. Ophthal Plast Reconstr Surg. 2017 Jan/Feb;33(1):47-52.
12. Wound Repair Regen. 1998 Mar-Apr;6(2):167-77.
13. Dermatol Surg. 1998 Jun;24(6):661-4.
14. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
15. ACS Nano. 2016 Feb 23;10(2):1810-9.
16. Arch Dermatol. 1989 Jan;125(1):65-9.
17. Dermatol Surg. 1999 Apr;25(4):311-5.

Histological changes noted, with topical application of cosmetic product, in small study
Histological changes were observed in skin treated with a product developed to target changes in the extracellular matrix associated with aging, in a study of six patients in their 60s.
The results were presented in a poster at the Summit in Aesthetic Medicine held by Global Academy for Medical Education.
The product, which contains tripeptide and hexapeptide ingredients, was applied to the forearms and preauricular regions of the participants, which were biopsied 3-8 weeks later. Compared with biopsies at baseline, the investigators found evidence of changes in the extracellular matrix, with “changes in collagen and elastin ... with mature old collagen replaced by freshened new collagen,” as well as “upregulated and redistributed elastin,” and “thickened epidermis with healthy cuboidal basal cells” that replaced flattened cells in the dermoepidermal junction, according to the poster
The study was limited by the small sample of patients, the authors noted. This study was sponsored by Alastin Skincare, the product’s manufacturer. The lead author, Antoanella Calame, MD, chief of dermatology at Scripps Memorial Hospital, La Jolla, California, disclosed consulting fees from Alastin. The other author, Alan Widgerow, MD, professor of plastic surgery at University of California, Irvine, is the chief medical officer of Alastin.
Global Academy and this news organization are owned the same company.
[email protected]
On Twitter @eaztweets
Histological changes were observed in skin treated with a product developed to target changes in the extracellular matrix associated with aging, in a study of six patients in their 60s.
The results were presented in a poster at the Summit in Aesthetic Medicine held by Global Academy for Medical Education.
The product, which contains tripeptide and hexapeptide ingredients, was applied to the forearms and preauricular regions of the participants, which were biopsied 3-8 weeks later. Compared with biopsies at baseline, the investigators found evidence of changes in the extracellular matrix, with “changes in collagen and elastin ... with mature old collagen replaced by freshened new collagen,” as well as “upregulated and redistributed elastin,” and “thickened epidermis with healthy cuboidal basal cells” that replaced flattened cells in the dermoepidermal junction, according to the poster
The study was limited by the small sample of patients, the authors noted. This study was sponsored by Alastin Skincare, the product’s manufacturer. The lead author, Antoanella Calame, MD, chief of dermatology at Scripps Memorial Hospital, La Jolla, California, disclosed consulting fees from Alastin. The other author, Alan Widgerow, MD, professor of plastic surgery at University of California, Irvine, is the chief medical officer of Alastin.
Global Academy and this news organization are owned the same company.
[email protected]
On Twitter @eaztweets
Histological changes were observed in skin treated with a product developed to target changes in the extracellular matrix associated with aging, in a study of six patients in their 60s.
The results were presented in a poster at the Summit in Aesthetic Medicine held by Global Academy for Medical Education.
The product, which contains tripeptide and hexapeptide ingredients, was applied to the forearms and preauricular regions of the participants, which were biopsied 3-8 weeks later. Compared with biopsies at baseline, the investigators found evidence of changes in the extracellular matrix, with “changes in collagen and elastin ... with mature old collagen replaced by freshened new collagen,” as well as “upregulated and redistributed elastin,” and “thickened epidermis with healthy cuboidal basal cells” that replaced flattened cells in the dermoepidermal junction, according to the poster
The study was limited by the small sample of patients, the authors noted. This study was sponsored by Alastin Skincare, the product’s manufacturer. The lead author, Antoanella Calame, MD, chief of dermatology at Scripps Memorial Hospital, La Jolla, California, disclosed consulting fees from Alastin. The other author, Alan Widgerow, MD, professor of plastic surgery at University of California, Irvine, is the chief medical officer of Alastin.
Global Academy and this news organization are owned the same company.
[email protected]
On Twitter @eaztweets
Benefits of topical product evaluated in patients undergoing laser treatment
The use of a combination product applied to treated areas before and after laser treatment of the face or decollete appeared to improve healing, compared with standard care, in a split-face study of 10 patients undergoing fractional CO2 laser treatment of the face and decollete.
The results were presented in a poster at the Summit in Aesthetic Medicine held by Global Academy for Medical Education. The product, manufactured by Alastin Skincare, is a topical formulation designed for use before and after laser therapy.
Before and after treatment, patients in the trial were given the topical treatment on one side of their faces or decollete and a standard treatment on the other, according to the poster.
Based on the blinded investigator ratings, the sides treated with the new product scored higher on day 4 for lentigines (P = .009), texture (P = .043), and Global Skin Quality (P = .051), according to Deanne Robinson, MD, director of the body sculpting center at the Connecticut Dermatology Group and the author of the study.
In addition, patients said they were more satisfied with the side treated with the product in terms of looking better and feeling better on that side (P = .05).
Dr. Robinson reported no financial conflicts. Global Academy and this news organization are owned the same company.
[email protected]
On Twitter @eaztweets
The use of a combination product applied to treated areas before and after laser treatment of the face or decollete appeared to improve healing, compared with standard care, in a split-face study of 10 patients undergoing fractional CO2 laser treatment of the face and decollete.
The results were presented in a poster at the Summit in Aesthetic Medicine held by Global Academy for Medical Education. The product, manufactured by Alastin Skincare, is a topical formulation designed for use before and after laser therapy.
Before and after treatment, patients in the trial were given the topical treatment on one side of their faces or decollete and a standard treatment on the other, according to the poster.
Based on the blinded investigator ratings, the sides treated with the new product scored higher on day 4 for lentigines (P = .009), texture (P = .043), and Global Skin Quality (P = .051), according to Deanne Robinson, MD, director of the body sculpting center at the Connecticut Dermatology Group and the author of the study.
In addition, patients said they were more satisfied with the side treated with the product in terms of looking better and feeling better on that side (P = .05).
Dr. Robinson reported no financial conflicts. Global Academy and this news organization are owned the same company.
[email protected]
On Twitter @eaztweets
The use of a combination product applied to treated areas before and after laser treatment of the face or decollete appeared to improve healing, compared with standard care, in a split-face study of 10 patients undergoing fractional CO2 laser treatment of the face and decollete.
The results were presented in a poster at the Summit in Aesthetic Medicine held by Global Academy for Medical Education. The product, manufactured by Alastin Skincare, is a topical formulation designed for use before and after laser therapy.
Before and after treatment, patients in the trial were given the topical treatment on one side of their faces or decollete and a standard treatment on the other, according to the poster.
Based on the blinded investigator ratings, the sides treated with the new product scored higher on day 4 for lentigines (P = .009), texture (P = .043), and Global Skin Quality (P = .051), according to Deanne Robinson, MD, director of the body sculpting center at the Connecticut Dermatology Group and the author of the study.
In addition, patients said they were more satisfied with the side treated with the product in terms of looking better and feeling better on that side (P = .05).
Dr. Robinson reported no financial conflicts. Global Academy and this news organization are owned the same company.
[email protected]
On Twitter @eaztweets
The hype behind facial oils
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
The therapeutic benefits of plant oils have been documented for hundreds of years. The properties of medicinal and aromatic plants have been explored for their essential oils. Essential oils are synthesized and used in a multibillion dollar global market for their curative properties, which include antimicrobial, antioxidant, anti-inflammatory, chemoprotective, antiproliferative, antiatherogenic, and antidiabetic properties. More than 80% of the global population depends on traditional plant-based medicine for treating health problems. There are currently over 3,000 known essential oils, among which 300 are commercially available for food, pharmaceutical, cosmetic, sanitary, and perfume industries. The extraction of these oils and their use in cosmeceuticals has increased in the last decade, as minor ingredients in creams and skin cleansing preparations.
However, these oils are now being marketed for direct application on the skin. What’s the hype about facial oils and why are there hundreds currently on the market?
Choosing the right oil, however, is not easy. Most consumers shy away from pure oils because they fear breakouts or increased “oiliness” of their skin. Understanding the properties of the oils can help determine which oils will benefit specific skin types. Argan oil and sunflower oil, for example, are rich in essential fatty acids and vitamin E, which hydrate the skin and have antiaging properties. Tea tree oil has antibacterial and anti-inflammatory qualities which are great for acne-prone skin. Oils such as these are particularly effective if acne medications are used. Acne medications can strip the natural barrier of the skin and without proper hydration excess sebum is produced and can cause clogging of pores.
Essential oils have antiaging properties as well. A study of sixty postmenopausal women who received oral or topical argan oil had significantly improved elasticity of the skin after 60 days, compared with the consumption of olive oil, which produced no improvement of skin elasticity. Sunflower oil has been used in skin preparations for its rich antioxidant properties, which decrease free radical damage from UV radiation.
The use of oils is multidimensional. Oils are highly effective for removing makeup and are the best source for cleansing of dry, dehydrated, or sensitive skin. Similarly, oils applied to the hair can help restore the natural oils of the hair, which are often stripped from overwashing and from chemical hair treatments. Facial oils also help improve skin hydration and restore the natural barrier of the skin. In addition, facial oils can be used in place of moisturizers or under a moisturizer to help prevent transepidermal water loss in dehydrated or atopic skin.
But these oils have a downside. Fragrant plant-based oils can cause skin irritation, photosensitivity, and potentially, allergic reactions. Consumers with plant-based allergies or sensitive skin should therefore steer clear of fragrant oils and test every oil on their inner forearm prior to applying them on the face.
I am a believer in these products. Oils have come a long way in cosmetic products and their manufacturing process has been improved over the last decade, making them easy to use, noncomedogenic, and nongreasy. They are an essential part of skin care for anyone with inflamed, dry, or irritated skin. More cosmetically elegant than their predecessors, when used correctly, oils are among the best products in the cosmeceutical market today.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
References
J Pharm Pharmacol. 2010 Dec;62(12):1669-75.
Inflamm Allergy Drug Targets. 2014;13(3):168-76.
Issue Biol. Sci. Pharm. Res. 2(1):001-007.
Evid Based Complement Alternat Med. 2017;2017:4517971.
Clin Interv Aging. 2015; 10: 339-49.
Evid Based Complement Alternat Med. 2013;2013:827248.
Dermatoendocrinol. 2012 Jul 1;4(3):298-307.
http://www.circulating-oils-library.com/en/start.
Completeness of Facial Self-application of Sunscreen in Cosmetic Surgery Patients
UV radiation from sun exposure is a risk factor for most types of skin cancer.1 Despite comprising only 1% of the body's surface area, the periocular region is the location of approximately 5% to 10% of skin cancers described in one US study.2 The efficacy of sunscreen in preventing skin cancer is widely accepted, and the American Academy of Dermatology recommends application of broad-spectrum UVA/UVB sunscreen with a sun protection factor of 30 or higher to help prevent skin cancer.3-5
RELATED ARTICLE: Sun Protection for Infants: Parent Behaviors and Beliefs
Reducing the risk of skin cancer from sun exposure relies on many factors, including completeness of application. A number of studies have demonstrated incomplete sunscreen application on the hairline, ears, neck, and dorsal feet.6-8 The purpose of this study was to assess the completeness of facial sunscreen self-application in oculofacial surgery patients using UV photography.
Methods
This single-site, cross-sectional, qualitative study assessed the completeness of facial sunscreen self-application among patients from a single surgeon's (J.A.W.) cosmetic and tertiary-care oculofacial surgery practice at the Duke Eye Center (Durham, North Carolina) between March 2016 and May 2016. Approval from the Duke University institutional review board was obtained, and the research adhered to the tenets of the Declaration of Helsinki and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients, and patients could elect to provide specific written consent for publication of photographs in scientific presentations and publications. Patients younger than 18 years of age; those with known sensitivity to sunscreen or its ingredients; and those with an active lesion, rash, or open wound were excluded from the study.
After obtaining informed consent, patients were photographed using a camera with a UV lens in natural outdoor lighting, first without sunscreen and again after self-application of a sunscreen of their choosing using their routine application technique. Completeness of sunscreen application was graded independently by 3 oculofacial surgeons (N.A.L., J.L., J.A.W.) as complete, partial, none, or cannot determine for 15 facial regions. The majority response was used for analysis.
Results
Forty-four patients were enrolled in the study. Six patients were disqualified due to use of mineral-based formulations (zinc oxide and/or titanium dioxide), as these sunscreens could not be visualized using UV photography. The age range of the remaining 38 patients was 28 to 74 years; 26% (10/38) were men and 74% (28/38) were women.
Complete sunscreen application was most frequently performed on the cheeks (97% [37/38]), chin (95% [36/38]), forehead (92% [35/38]), and temples (92% [35/38]). Complete absence of sunscreen coverage was most common on the lower eyelid margin (84% [32/38]), upper eyelid margin (82% [31/38]), medial canthus (71% 27/38]), and upper eyelid (66% [25/38])(Table)(Figure).
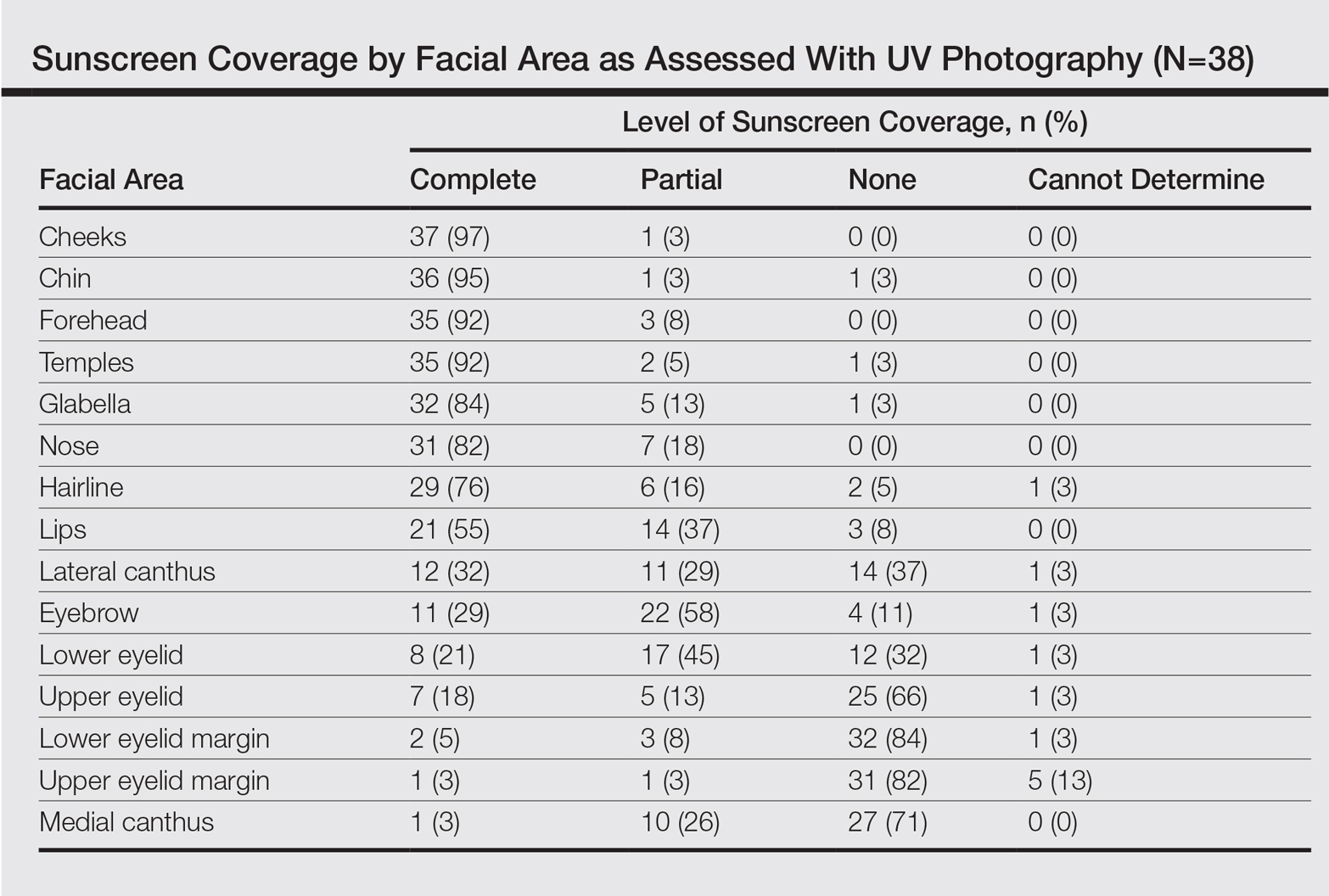
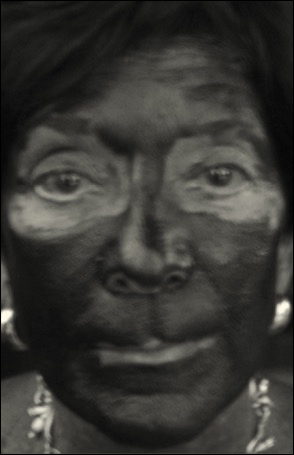
Comment
UV radiation-related skin cancers frequently occur in the periocular area, presumably because it is a frequent site of UV exposure. Clothing, sunglasses, and hats can be used to aid in protection from UV radiation, but these products are only regulated by the US Food and Drug Administration if the product claims to prevent skin cancer. Sunscreen is a proven method of protection from UV radiation and the prevention of skin cancer but must be properly applied for it to be effective.1,2,5,6 Incomplete sunscreen application has been demonstrated in numerous studies. Lademann et al7 studied sunscreen application among 60 beachgoers in Germany and found they typically missed the hairline, ears, and dorsal feet. In a study of 10 women with photosensitivity in England who were asked to apply sunscreen in their routine manner, Azurdia et al6 found the posterior neck, lateral neck, temples, and ears, respectively, were the most frequently missed sites. Yang et al8 assessed sunscreen application in 39 dermatologists and 41 photosensitive patients in China and found the neck, ears, dorsal hands, hairline, temples, and perioral region, respectively, were most commonly left unprotected.
Our study investigated detailed facial self-application of sunscreen and found excellent coverage of the larger facial units such as the forehead, cheeks, chin, and temples. The brow, medial canthus, lateral canthus, and upper and lower eyelids and eyelid margins were infrequently protected with sunscreen during routine application. Our opinion is that patients are unaware that eyelid sunscreen application is important. They may be afraid that the products will sting or cause damage if they get in the eyes. Although some products do sting if they get into the eyes, there is no evidence that sunscreens cause injury to the eyes. The US Food and Drug Administration does not have clear guidelines about applying sunscreens in the periocular area, but in general, mineral blocks are recommended because they have less chance of irritation. Several companies make such products that are designed to be applied to the eyelids.
Limitations of our study included a small sample size and a majority female demographic, which may have affected the results, as women generally are more familiar with the application of lotions to the face. Additionally, the patients were recruited from a tertiary-care clinic and may have had periocular malignancy or may have previously received counseling on the importance of sunscreen use.
Conclusion
Cancer reconstruction of the periocular area is challenging, and even in the best of hands, a patient's quality of life may be negatively affected by postreconstructive appearance or suboptimal function, resulting in ocular exposure. The authors recommend counseling patients on the importance of good sun protection habits, including daily application of sunscreen to the face and periocular region to prevent malignancy in these delicate areas.
- Olsen CM, Wilson LF, Green AC, et al. Cancers inAustralia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471-476.
- Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746-750.
- van de Pols JC, Williams GM, Pandeye N, et al. Prolonged prevention of squamous cell carcinoma of the skin by regular sunscreen use. Cancer Epidemiol Biomarkers Preven. 2006;15:2546-2548.
- Skin Cancer Foundation. Basal cell carcinoma prevention guidelines. http://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-prevention-guidelines. Accessed May 24, 2017.
- American Academy of Dermatology. Basal cell carcinoma: tips for managing. https://www.aad.org/public/diseases/skin-cancer/basal-cell-carcinoma#tips. Accessed May 24, 2017.
- Azurdia RM, Pagliaro JA, Diffey BL, et al. Sunscreen application by photosensitive patients is inadequate for protection. Br J Dermatol. 1999;140:255-258.
- Lademann J, Schanzer S, Richter H, et al. Sunscreen application at the beach. J Cosmet Dermatol. 2004;3:62-68.
- Yang HP, Chen K, Chang BZ, et al. A study of the way in which dermatologists and photosensitive patients apply sunscreen in China. Photodermatol Photoimmunol Photomed. 2009;25:245-249.
UV radiation from sun exposure is a risk factor for most types of skin cancer.1 Despite comprising only 1% of the body's surface area, the periocular region is the location of approximately 5% to 10% of skin cancers described in one US study.2 The efficacy of sunscreen in preventing skin cancer is widely accepted, and the American Academy of Dermatology recommends application of broad-spectrum UVA/UVB sunscreen with a sun protection factor of 30 or higher to help prevent skin cancer.3-5
RELATED ARTICLE: Sun Protection for Infants: Parent Behaviors and Beliefs
Reducing the risk of skin cancer from sun exposure relies on many factors, including completeness of application. A number of studies have demonstrated incomplete sunscreen application on the hairline, ears, neck, and dorsal feet.6-8 The purpose of this study was to assess the completeness of facial sunscreen self-application in oculofacial surgery patients using UV photography.
Methods
This single-site, cross-sectional, qualitative study assessed the completeness of facial sunscreen self-application among patients from a single surgeon's (J.A.W.) cosmetic and tertiary-care oculofacial surgery practice at the Duke Eye Center (Durham, North Carolina) between March 2016 and May 2016. Approval from the Duke University institutional review board was obtained, and the research adhered to the tenets of the Declaration of Helsinki and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients, and patients could elect to provide specific written consent for publication of photographs in scientific presentations and publications. Patients younger than 18 years of age; those with known sensitivity to sunscreen or its ingredients; and those with an active lesion, rash, or open wound were excluded from the study.
After obtaining informed consent, patients were photographed using a camera with a UV lens in natural outdoor lighting, first without sunscreen and again after self-application of a sunscreen of their choosing using their routine application technique. Completeness of sunscreen application was graded independently by 3 oculofacial surgeons (N.A.L., J.L., J.A.W.) as complete, partial, none, or cannot determine for 15 facial regions. The majority response was used for analysis.
Results
Forty-four patients were enrolled in the study. Six patients were disqualified due to use of mineral-based formulations (zinc oxide and/or titanium dioxide), as these sunscreens could not be visualized using UV photography. The age range of the remaining 38 patients was 28 to 74 years; 26% (10/38) were men and 74% (28/38) were women.
Complete sunscreen application was most frequently performed on the cheeks (97% [37/38]), chin (95% [36/38]), forehead (92% [35/38]), and temples (92% [35/38]). Complete absence of sunscreen coverage was most common on the lower eyelid margin (84% [32/38]), upper eyelid margin (82% [31/38]), medial canthus (71% 27/38]), and upper eyelid (66% [25/38])(Table)(Figure).
Comment
UV radiation-related skin cancers frequently occur in the periocular area, presumably because it is a frequent site of UV exposure. Clothing, sunglasses, and hats can be used to aid in protection from UV radiation, but these products are only regulated by the US Food and Drug Administration if the product claims to prevent skin cancer. Sunscreen is a proven method of protection from UV radiation and the prevention of skin cancer but must be properly applied for it to be effective.1,2,5,6 Incomplete sunscreen application has been demonstrated in numerous studies. Lademann et al7 studied sunscreen application among 60 beachgoers in Germany and found they typically missed the hairline, ears, and dorsal feet. In a study of 10 women with photosensitivity in England who were asked to apply sunscreen in their routine manner, Azurdia et al6 found the posterior neck, lateral neck, temples, and ears, respectively, were the most frequently missed sites. Yang et al8 assessed sunscreen application in 39 dermatologists and 41 photosensitive patients in China and found the neck, ears, dorsal hands, hairline, temples, and perioral region, respectively, were most commonly left unprotected.
Our study investigated detailed facial self-application of sunscreen and found excellent coverage of the larger facial units such as the forehead, cheeks, chin, and temples. The brow, medial canthus, lateral canthus, and upper and lower eyelids and eyelid margins were infrequently protected with sunscreen during routine application. Our opinion is that patients are unaware that eyelid sunscreen application is important. They may be afraid that the products will sting or cause damage if they get in the eyes. Although some products do sting if they get into the eyes, there is no evidence that sunscreens cause injury to the eyes. The US Food and Drug Administration does not have clear guidelines about applying sunscreens in the periocular area, but in general, mineral blocks are recommended because they have less chance of irritation. Several companies make such products that are designed to be applied to the eyelids.
Limitations of our study included a small sample size and a majority female demographic, which may have affected the results, as women generally are more familiar with the application of lotions to the face. Additionally, the patients were recruited from a tertiary-care clinic and may have had periocular malignancy or may have previously received counseling on the importance of sunscreen use.
Conclusion
Cancer reconstruction of the periocular area is challenging, and even in the best of hands, a patient's quality of life may be negatively affected by postreconstructive appearance or suboptimal function, resulting in ocular exposure. The authors recommend counseling patients on the importance of good sun protection habits, including daily application of sunscreen to the face and periocular region to prevent malignancy in these delicate areas.
UV radiation from sun exposure is a risk factor for most types of skin cancer.1 Despite comprising only 1% of the body's surface area, the periocular region is the location of approximately 5% to 10% of skin cancers described in one US study.2 The efficacy of sunscreen in preventing skin cancer is widely accepted, and the American Academy of Dermatology recommends application of broad-spectrum UVA/UVB sunscreen with a sun protection factor of 30 or higher to help prevent skin cancer.3-5
RELATED ARTICLE: Sun Protection for Infants: Parent Behaviors and Beliefs
Reducing the risk of skin cancer from sun exposure relies on many factors, including completeness of application. A number of studies have demonstrated incomplete sunscreen application on the hairline, ears, neck, and dorsal feet.6-8 The purpose of this study was to assess the completeness of facial sunscreen self-application in oculofacial surgery patients using UV photography.
Methods
This single-site, cross-sectional, qualitative study assessed the completeness of facial sunscreen self-application among patients from a single surgeon's (J.A.W.) cosmetic and tertiary-care oculofacial surgery practice at the Duke Eye Center (Durham, North Carolina) between March 2016 and May 2016. Approval from the Duke University institutional review board was obtained, and the research adhered to the tenets of the Declaration of Helsinki and complied with the Health Insurance Portability and Accountability Act. Informed consent was obtained from all patients, and patients could elect to provide specific written consent for publication of photographs in scientific presentations and publications. Patients younger than 18 years of age; those with known sensitivity to sunscreen or its ingredients; and those with an active lesion, rash, or open wound were excluded from the study.
After obtaining informed consent, patients were photographed using a camera with a UV lens in natural outdoor lighting, first without sunscreen and again after self-application of a sunscreen of their choosing using their routine application technique. Completeness of sunscreen application was graded independently by 3 oculofacial surgeons (N.A.L., J.L., J.A.W.) as complete, partial, none, or cannot determine for 15 facial regions. The majority response was used for analysis.
Results
Forty-four patients were enrolled in the study. Six patients were disqualified due to use of mineral-based formulations (zinc oxide and/or titanium dioxide), as these sunscreens could not be visualized using UV photography. The age range of the remaining 38 patients was 28 to 74 years; 26% (10/38) were men and 74% (28/38) were women.
Complete sunscreen application was most frequently performed on the cheeks (97% [37/38]), chin (95% [36/38]), forehead (92% [35/38]), and temples (92% [35/38]). Complete absence of sunscreen coverage was most common on the lower eyelid margin (84% [32/38]), upper eyelid margin (82% [31/38]), medial canthus (71% 27/38]), and upper eyelid (66% [25/38])(Table)(Figure).
Comment
UV radiation-related skin cancers frequently occur in the periocular area, presumably because it is a frequent site of UV exposure. Clothing, sunglasses, and hats can be used to aid in protection from UV radiation, but these products are only regulated by the US Food and Drug Administration if the product claims to prevent skin cancer. Sunscreen is a proven method of protection from UV radiation and the prevention of skin cancer but must be properly applied for it to be effective.1,2,5,6 Incomplete sunscreen application has been demonstrated in numerous studies. Lademann et al7 studied sunscreen application among 60 beachgoers in Germany and found they typically missed the hairline, ears, and dorsal feet. In a study of 10 women with photosensitivity in England who were asked to apply sunscreen in their routine manner, Azurdia et al6 found the posterior neck, lateral neck, temples, and ears, respectively, were the most frequently missed sites. Yang et al8 assessed sunscreen application in 39 dermatologists and 41 photosensitive patients in China and found the neck, ears, dorsal hands, hairline, temples, and perioral region, respectively, were most commonly left unprotected.
Our study investigated detailed facial self-application of sunscreen and found excellent coverage of the larger facial units such as the forehead, cheeks, chin, and temples. The brow, medial canthus, lateral canthus, and upper and lower eyelids and eyelid margins were infrequently protected with sunscreen during routine application. Our opinion is that patients are unaware that eyelid sunscreen application is important. They may be afraid that the products will sting or cause damage if they get in the eyes. Although some products do sting if they get into the eyes, there is no evidence that sunscreens cause injury to the eyes. The US Food and Drug Administration does not have clear guidelines about applying sunscreens in the periocular area, but in general, mineral blocks are recommended because they have less chance of irritation. Several companies make such products that are designed to be applied to the eyelids.
Limitations of our study included a small sample size and a majority female demographic, which may have affected the results, as women generally are more familiar with the application of lotions to the face. Additionally, the patients were recruited from a tertiary-care clinic and may have had periocular malignancy or may have previously received counseling on the importance of sunscreen use.
Conclusion
Cancer reconstruction of the periocular area is challenging, and even in the best of hands, a patient's quality of life may be negatively affected by postreconstructive appearance or suboptimal function, resulting in ocular exposure. The authors recommend counseling patients on the importance of good sun protection habits, including daily application of sunscreen to the face and periocular region to prevent malignancy in these delicate areas.
- Olsen CM, Wilson LF, Green AC, et al. Cancers inAustralia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471-476.
- Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746-750.
- van de Pols JC, Williams GM, Pandeye N, et al. Prolonged prevention of squamous cell carcinoma of the skin by regular sunscreen use. Cancer Epidemiol Biomarkers Preven. 2006;15:2546-2548.
- Skin Cancer Foundation. Basal cell carcinoma prevention guidelines. http://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-prevention-guidelines. Accessed May 24, 2017.
- American Academy of Dermatology. Basal cell carcinoma: tips for managing. https://www.aad.org/public/diseases/skin-cancer/basal-cell-carcinoma#tips. Accessed May 24, 2017.
- Azurdia RM, Pagliaro JA, Diffey BL, et al. Sunscreen application by photosensitive patients is inadequate for protection. Br J Dermatol. 1999;140:255-258.
- Lademann J, Schanzer S, Richter H, et al. Sunscreen application at the beach. J Cosmet Dermatol. 2004;3:62-68.
- Yang HP, Chen K, Chang BZ, et al. A study of the way in which dermatologists and photosensitive patients apply sunscreen in China. Photodermatol Photoimmunol Photomed. 2009;25:245-249.
- Olsen CM, Wilson LF, Green AC, et al. Cancers inAustralia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health. 2015;39:471-476.
- Cook BE Jr, Bartley GB. Epidemiologic characteristics and clinical course of patients with malignant eyelid tumors in an incidence cohort in an incidence cohort in Olmsted County, Minnesota. Ophthalmology. 1999;106:746-750.
- van de Pols JC, Williams GM, Pandeye N, et al. Prolonged prevention of squamous cell carcinoma of the skin by regular sunscreen use. Cancer Epidemiol Biomarkers Preven. 2006;15:2546-2548.
- Skin Cancer Foundation. Basal cell carcinoma prevention guidelines. http://www.skincancer.org/skin-cancer-information/basal-cell-carcinoma/bcc-prevention-guidelines. Accessed May 24, 2017.
- American Academy of Dermatology. Basal cell carcinoma: tips for managing. https://www.aad.org/public/diseases/skin-cancer/basal-cell-carcinoma#tips. Accessed May 24, 2017.
- Azurdia RM, Pagliaro JA, Diffey BL, et al. Sunscreen application by photosensitive patients is inadequate for protection. Br J Dermatol. 1999;140:255-258.
- Lademann J, Schanzer S, Richter H, et al. Sunscreen application at the beach. J Cosmet Dermatol. 2004;3:62-68.
- Yang HP, Chen K, Chang BZ, et al. A study of the way in which dermatologists and photosensitive patients apply sunscreen in China. Photodermatol Photoimmunol Photomed. 2009;25:245-249.
Resident Pearl
- Patients may benefit from their physician taking a moment to describe the importance of applying sunscreen to the eyelids while applying it to the rest of the face.