User login
Vaping among teens increased significantly from 2017 to 2018
according to data from national cross-sectional surveys.
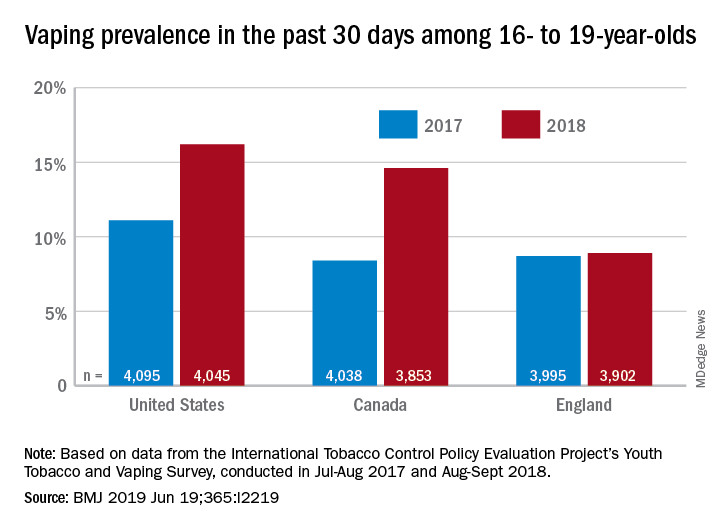
The prevalence of vaping in the past 30 days rose from 11% to 16% in the United States and from 8% to 14.6% in Canada, while use in England showed an nonsignificant increase of 8.7% to 8.9%, David Hammond, PhD, of the University of Waterloo (Canada) and associates said in the BMJ.
Embedded in those U.S. and Canadian increases is the recent evolution of the vaping market brought about by “the growth of JUUL e-cigarettes and similar products [that use] benzoic acid and nicotine salt technology to deliver higher concentrations of nicotine than conventional e-cigarettes,” they explained.
In England, the JUUL system is limited to less than half the nicotine concentration, at 20 mg/mL, compared with more than 50 mg/mL in the United States and Canada, and it was not available at all types of retail outlets at the time of the surveys. That situation changed in March 2019, when the company expanded to convenience stores, the investigators noted.
In the United States, JUUL was the second-most popular product among past–30-day vapers who had a usual brand in 2017, with 9% reporting use. In 2018, JUUL was the most popular brand and use was up to 28%. In Canada, the brand was not among the top five in 2017, but was third in 2018 at 10% in those who reported vaping in the past 30 days. The leading Canadian brand in 2018 was Smok, which released a nicotine-salt version in March of 2018, Dr. Hammond and associates reported.
“Before 2018, there was relatively little evidence of regular vaping among adolescents that might be indicative of nicotine addiction; however, the emergence of JUUL and nicotine salt–based products might signal a change,” they wrote.
The International Tobacco Control Policy Evaluation Project’s Youth Tobacco and Vaping Survey was conducted online in each country in two waves – July to August 2017 and August to September 2018 – with a sample size of approximately 12,000 for each.
The study was funded by the U.S. National Institutes of Health. Dr. Hammond is supported by a Canadian Institutes of Health Research–Public Health Agency of Canada applied public health research chair. The investigators said that they had no other financial disclosures to report, but several have served as paid witnesses in legal challenges against tobacco companies.
SOURCE: Hammond D et al. BMJ 2019 Jun 19. doi: 10.1136/bmj.l2219.
according to data from national cross-sectional surveys.
The prevalence of vaping in the past 30 days rose from 11% to 16% in the United States and from 8% to 14.6% in Canada, while use in England showed an nonsignificant increase of 8.7% to 8.9%, David Hammond, PhD, of the University of Waterloo (Canada) and associates said in the BMJ.
Embedded in those U.S. and Canadian increases is the recent evolution of the vaping market brought about by “the growth of JUUL e-cigarettes and similar products [that use] benzoic acid and nicotine salt technology to deliver higher concentrations of nicotine than conventional e-cigarettes,” they explained.
In England, the JUUL system is limited to less than half the nicotine concentration, at 20 mg/mL, compared with more than 50 mg/mL in the United States and Canada, and it was not available at all types of retail outlets at the time of the surveys. That situation changed in March 2019, when the company expanded to convenience stores, the investigators noted.
In the United States, JUUL was the second-most popular product among past–30-day vapers who had a usual brand in 2017, with 9% reporting use. In 2018, JUUL was the most popular brand and use was up to 28%. In Canada, the brand was not among the top five in 2017, but was third in 2018 at 10% in those who reported vaping in the past 30 days. The leading Canadian brand in 2018 was Smok, which released a nicotine-salt version in March of 2018, Dr. Hammond and associates reported.
“Before 2018, there was relatively little evidence of regular vaping among adolescents that might be indicative of nicotine addiction; however, the emergence of JUUL and nicotine salt–based products might signal a change,” they wrote.
The International Tobacco Control Policy Evaluation Project’s Youth Tobacco and Vaping Survey was conducted online in each country in two waves – July to August 2017 and August to September 2018 – with a sample size of approximately 12,000 for each.
The study was funded by the U.S. National Institutes of Health. Dr. Hammond is supported by a Canadian Institutes of Health Research–Public Health Agency of Canada applied public health research chair. The investigators said that they had no other financial disclosures to report, but several have served as paid witnesses in legal challenges against tobacco companies.
SOURCE: Hammond D et al. BMJ 2019 Jun 19. doi: 10.1136/bmj.l2219.
according to data from national cross-sectional surveys.
The prevalence of vaping in the past 30 days rose from 11% to 16% in the United States and from 8% to 14.6% in Canada, while use in England showed an nonsignificant increase of 8.7% to 8.9%, David Hammond, PhD, of the University of Waterloo (Canada) and associates said in the BMJ.
Embedded in those U.S. and Canadian increases is the recent evolution of the vaping market brought about by “the growth of JUUL e-cigarettes and similar products [that use] benzoic acid and nicotine salt technology to deliver higher concentrations of nicotine than conventional e-cigarettes,” they explained.
In England, the JUUL system is limited to less than half the nicotine concentration, at 20 mg/mL, compared with more than 50 mg/mL in the United States and Canada, and it was not available at all types of retail outlets at the time of the surveys. That situation changed in March 2019, when the company expanded to convenience stores, the investigators noted.
In the United States, JUUL was the second-most popular product among past–30-day vapers who had a usual brand in 2017, with 9% reporting use. In 2018, JUUL was the most popular brand and use was up to 28%. In Canada, the brand was not among the top five in 2017, but was third in 2018 at 10% in those who reported vaping in the past 30 days. The leading Canadian brand in 2018 was Smok, which released a nicotine-salt version in March of 2018, Dr. Hammond and associates reported.
“Before 2018, there was relatively little evidence of regular vaping among adolescents that might be indicative of nicotine addiction; however, the emergence of JUUL and nicotine salt–based products might signal a change,” they wrote.
The International Tobacco Control Policy Evaluation Project’s Youth Tobacco and Vaping Survey was conducted online in each country in two waves – July to August 2017 and August to September 2018 – with a sample size of approximately 12,000 for each.
The study was funded by the U.S. National Institutes of Health. Dr. Hammond is supported by a Canadian Institutes of Health Research–Public Health Agency of Canada applied public health research chair. The investigators said that they had no other financial disclosures to report, but several have served as paid witnesses in legal challenges against tobacco companies.
SOURCE: Hammond D et al. BMJ 2019 Jun 19. doi: 10.1136/bmj.l2219.
FROM THE BMJ
Key clinical point: Recent increases in vaping prevalence among teens “might be indicative of nicotine addiction.”
Major finding: Vaping prevalence increased from 11% to 16% in the United States and from 8% to 14.6% in Canada.
Study details: Two waves of a national, cross-sectional survey that included approximately 12,000 respondents each.
Disclosures: The study was funded by the U.S. National Institutes of Health. Dr. Hammond is supported by a Canadian Institutes of Health Research–Public Health Agency of Canada applied public health research chair. The investigators said that they had no other financial disclosures to report, but several have served as paid witnesses in legal challenges against tobacco companies.
Source: Hammond D et al. BMJ. 2019 Jun 19. doi: 10.1136/bmj.l2219.
Nicotine replacement therapy beats varenicline for smokers with OUD
SAN ANTONIO – People who smoke and have opioid use disorder have a lower likelihood of drug use several months after initiating smoking cessation treatment if they are treated with nicotine replacement therapy rather than varenicline, new research suggests.
“Differences were not due to the pretreatment differences in drug use, which were covaried,” wrote Damaris J. Rohsenow, PhD, and colleagues at Brown University’s Center for Alcohol and Addiction Studies, Providence, R.I. “Results suggest it may be preferable to offer smokers with opioid use disorder [nicotine replacement therapy] rather than varenicline, given their lower adherence and more illicit drug use days during follow-up when given varenicline compared to [nicotine replacement therapy].”
They shared their research poster at the annual meeting of the College on Problems of Drug Dependence.
About 80%-90% of patients with OUD smoke, and those patients have a particularly difficult time with smoking cessation partly because of nonadherence to cessation medications, the authors noted. Smoking increases the risk of relapse from any substance use disorder, and pain – frequently comorbid with smoking – contributes to opioid use, they added.
Though smoking treatment has been shown not to increase drug or alcohol use, varenicline and nicotine replacement therapy have different effects on a4b2 nicotinic acetylcholinergic receptors (nAChRs). The authors noted that nicotine offers greater pain inhibition via full agonist effects across multiple nAChRs, whereas varenicline has only a partial agonist effect on a single nAChR.
“Smokers may receive more rewarding dopamine effects from the full nicotine agonist,” they wrote. The researchers therefore aimed to compare responses to nicotine replacement therapy and varenicline among smokers with and without OUD.
Ninety patients without OUD and 47 patients with it were randomly assigned to receive transdermal nicotine replacement therapy with placebo capsules or varenicline capsules with a placebo patch for 12 weeks with 3- and 6-month follow-ups. At baseline, those with OUD were significantly more likely to be white and slightly younger and have twice as many drug use days than those without the disorder.
Differences also existed between those with and without OUD for comorbid alcohol use disorder (55% vs. 81%), marijuana use disorder (32% vs. 19%) and cocaine use disorder (70% vs. 55%).
Those without OUD had slightly greater medication adherence, but with only borderline significance just among those taking varenicline. Loss to follow-up, meanwhile, was significantly greater for those with OUD in both treatment groups.
Those patients had 16.5 drug use days at 4-6 months’ follow-up, compared with 0.13 days among those with OUD using nicotine replacement therapy (P less than .026). Among those without OUD, nicotine replacement therapy patients had 5 drug use days, and varenicline patients had 2.5 drug use days.
“Given interactions between nicotine and the opioid system and given that [nicotine replacement therapy] binds to more types of nAChRs than varenicline does, it is possible that [nicotine replacement therapy] dampens desire to use opiates compared to varenicline by stimulating more nAChRs,” the authors wrote. “Increasing nicotine dose may be better for smokers with opioid use disorder,” they added, though they noted the small size of the study and the need for replication with larger populations.
The research was funded by the National Institute on Drug Abuse and the Department of Veterans Affairs. The authors reported no disclosures.
SAN ANTONIO – People who smoke and have opioid use disorder have a lower likelihood of drug use several months after initiating smoking cessation treatment if they are treated with nicotine replacement therapy rather than varenicline, new research suggests.
“Differences were not due to the pretreatment differences in drug use, which were covaried,” wrote Damaris J. Rohsenow, PhD, and colleagues at Brown University’s Center for Alcohol and Addiction Studies, Providence, R.I. “Results suggest it may be preferable to offer smokers with opioid use disorder [nicotine replacement therapy] rather than varenicline, given their lower adherence and more illicit drug use days during follow-up when given varenicline compared to [nicotine replacement therapy].”
They shared their research poster at the annual meeting of the College on Problems of Drug Dependence.
About 80%-90% of patients with OUD smoke, and those patients have a particularly difficult time with smoking cessation partly because of nonadherence to cessation medications, the authors noted. Smoking increases the risk of relapse from any substance use disorder, and pain – frequently comorbid with smoking – contributes to opioid use, they added.
Though smoking treatment has been shown not to increase drug or alcohol use, varenicline and nicotine replacement therapy have different effects on a4b2 nicotinic acetylcholinergic receptors (nAChRs). The authors noted that nicotine offers greater pain inhibition via full agonist effects across multiple nAChRs, whereas varenicline has only a partial agonist effect on a single nAChR.
“Smokers may receive more rewarding dopamine effects from the full nicotine agonist,” they wrote. The researchers therefore aimed to compare responses to nicotine replacement therapy and varenicline among smokers with and without OUD.
Ninety patients without OUD and 47 patients with it were randomly assigned to receive transdermal nicotine replacement therapy with placebo capsules or varenicline capsules with a placebo patch for 12 weeks with 3- and 6-month follow-ups. At baseline, those with OUD were significantly more likely to be white and slightly younger and have twice as many drug use days than those without the disorder.
Differences also existed between those with and without OUD for comorbid alcohol use disorder (55% vs. 81%), marijuana use disorder (32% vs. 19%) and cocaine use disorder (70% vs. 55%).
Those without OUD had slightly greater medication adherence, but with only borderline significance just among those taking varenicline. Loss to follow-up, meanwhile, was significantly greater for those with OUD in both treatment groups.
Those patients had 16.5 drug use days at 4-6 months’ follow-up, compared with 0.13 days among those with OUD using nicotine replacement therapy (P less than .026). Among those without OUD, nicotine replacement therapy patients had 5 drug use days, and varenicline patients had 2.5 drug use days.
“Given interactions between nicotine and the opioid system and given that [nicotine replacement therapy] binds to more types of nAChRs than varenicline does, it is possible that [nicotine replacement therapy] dampens desire to use opiates compared to varenicline by stimulating more nAChRs,” the authors wrote. “Increasing nicotine dose may be better for smokers with opioid use disorder,” they added, though they noted the small size of the study and the need for replication with larger populations.
The research was funded by the National Institute on Drug Abuse and the Department of Veterans Affairs. The authors reported no disclosures.
SAN ANTONIO – People who smoke and have opioid use disorder have a lower likelihood of drug use several months after initiating smoking cessation treatment if they are treated with nicotine replacement therapy rather than varenicline, new research suggests.
“Differences were not due to the pretreatment differences in drug use, which were covaried,” wrote Damaris J. Rohsenow, PhD, and colleagues at Brown University’s Center for Alcohol and Addiction Studies, Providence, R.I. “Results suggest it may be preferable to offer smokers with opioid use disorder [nicotine replacement therapy] rather than varenicline, given their lower adherence and more illicit drug use days during follow-up when given varenicline compared to [nicotine replacement therapy].”
They shared their research poster at the annual meeting of the College on Problems of Drug Dependence.
About 80%-90% of patients with OUD smoke, and those patients have a particularly difficult time with smoking cessation partly because of nonadherence to cessation medications, the authors noted. Smoking increases the risk of relapse from any substance use disorder, and pain – frequently comorbid with smoking – contributes to opioid use, they added.
Though smoking treatment has been shown not to increase drug or alcohol use, varenicline and nicotine replacement therapy have different effects on a4b2 nicotinic acetylcholinergic receptors (nAChRs). The authors noted that nicotine offers greater pain inhibition via full agonist effects across multiple nAChRs, whereas varenicline has only a partial agonist effect on a single nAChR.
“Smokers may receive more rewarding dopamine effects from the full nicotine agonist,” they wrote. The researchers therefore aimed to compare responses to nicotine replacement therapy and varenicline among smokers with and without OUD.
Ninety patients without OUD and 47 patients with it were randomly assigned to receive transdermal nicotine replacement therapy with placebo capsules or varenicline capsules with a placebo patch for 12 weeks with 3- and 6-month follow-ups. At baseline, those with OUD were significantly more likely to be white and slightly younger and have twice as many drug use days than those without the disorder.
Differences also existed between those with and without OUD for comorbid alcohol use disorder (55% vs. 81%), marijuana use disorder (32% vs. 19%) and cocaine use disorder (70% vs. 55%).
Those without OUD had slightly greater medication adherence, but with only borderline significance just among those taking varenicline. Loss to follow-up, meanwhile, was significantly greater for those with OUD in both treatment groups.
Those patients had 16.5 drug use days at 4-6 months’ follow-up, compared with 0.13 days among those with OUD using nicotine replacement therapy (P less than .026). Among those without OUD, nicotine replacement therapy patients had 5 drug use days, and varenicline patients had 2.5 drug use days.
“Given interactions between nicotine and the opioid system and given that [nicotine replacement therapy] binds to more types of nAChRs than varenicline does, it is possible that [nicotine replacement therapy] dampens desire to use opiates compared to varenicline by stimulating more nAChRs,” the authors wrote. “Increasing nicotine dose may be better for smokers with opioid use disorder,” they added, though they noted the small size of the study and the need for replication with larger populations.
The research was funded by the National Institute on Drug Abuse and the Department of Veterans Affairs. The authors reported no disclosures.
REPORTING FROM CPDD 2019
Abuse rate of gabapentin, pregabalin far below that of opioids
SAN ANTONIO – Prescription opioid abuse has continued declining since 2011, but opioids remain far more commonly abused than other prescription drugs, including gabapentin and pregabalin, new research shows.
“Both gabapentin and pregabalin are abused but at rates that are 6-56 times less frequent than for opioid analgesics,” wrote Kofi Asomaning, DSci, of Pfizer, and associates at Pfizer and Denver Health’s Rocky Mountain Poison and Drug Center.
“Gabapentin is generally more frequently abused than pregabalin,” they reported in a research poster at the annual meeting of the College on Problems of Drug Dependence.
The researchers analyzed data from the RADARS System Survey of Non-Medical Use of Prescription Drugs Program (NMURx), the RADARS System Treatment Center Programs Combined, and the American Association of Poison Control Centers National Poison Data System (NPDS).
All those use self-reported data. The first is a confidential, anonymous web-based survey used to estimate population-level prevalence, and the second surveys patients with opioid use disorder entering treatment. The NPDS tracks all cases reported to poison control centers nationally.
Analysis of the NMURx data revealed similar lifetime abuse prevalence rates for gabapentin and pregabalin at 0.4%, several magnitudes lower than the 5.3% rate identified with opioids.
Gabapentin, however, had higher rates of abuse in the past month in the Treatment Center Programs Combined. For the third to fourth quarter of 2017, 0.12 per 100,000 population reportedly abused gabapentin, compared with 0.01 per 100,000 for pregabalin. The rate for past-month abuse of opioids was 0.79 per 100,000.
A similar pattern for the same quarter emerged from the NPDS data: Rate of gabapentin abuse was 0.06 per 100,000, rate for pregabalin was 0.01 per 100,000, and rate for opioids was 0.40 per 100,000.
Both pregabalin and opioids were predominantly ingested, though a very small amount of each was inhaled and a similarly small amount of opioids was injected. Data on exposure route for gabapentin were not provided, though it was used more frequently than pregabalin.
The research was funded by Pfizer. The RADARS system is owned by Denver Health and Hospital Authority under the Colorado state government. RADARS receives some funding from pharmaceutical industry subscriptions. Dr. Asomaning and Diane L. Martire, MD, MPH, are Pfizer employees who have financial interests with Pfizer.
SAN ANTONIO – Prescription opioid abuse has continued declining since 2011, but opioids remain far more commonly abused than other prescription drugs, including gabapentin and pregabalin, new research shows.
“Both gabapentin and pregabalin are abused but at rates that are 6-56 times less frequent than for opioid analgesics,” wrote Kofi Asomaning, DSci, of Pfizer, and associates at Pfizer and Denver Health’s Rocky Mountain Poison and Drug Center.
“Gabapentin is generally more frequently abused than pregabalin,” they reported in a research poster at the annual meeting of the College on Problems of Drug Dependence.
The researchers analyzed data from the RADARS System Survey of Non-Medical Use of Prescription Drugs Program (NMURx), the RADARS System Treatment Center Programs Combined, and the American Association of Poison Control Centers National Poison Data System (NPDS).
All those use self-reported data. The first is a confidential, anonymous web-based survey used to estimate population-level prevalence, and the second surveys patients with opioid use disorder entering treatment. The NPDS tracks all cases reported to poison control centers nationally.
Analysis of the NMURx data revealed similar lifetime abuse prevalence rates for gabapentin and pregabalin at 0.4%, several magnitudes lower than the 5.3% rate identified with opioids.
Gabapentin, however, had higher rates of abuse in the past month in the Treatment Center Programs Combined. For the third to fourth quarter of 2017, 0.12 per 100,000 population reportedly abused gabapentin, compared with 0.01 per 100,000 for pregabalin. The rate for past-month abuse of opioids was 0.79 per 100,000.
A similar pattern for the same quarter emerged from the NPDS data: Rate of gabapentin abuse was 0.06 per 100,000, rate for pregabalin was 0.01 per 100,000, and rate for opioids was 0.40 per 100,000.
Both pregabalin and opioids were predominantly ingested, though a very small amount of each was inhaled and a similarly small amount of opioids was injected. Data on exposure route for gabapentin were not provided, though it was used more frequently than pregabalin.
The research was funded by Pfizer. The RADARS system is owned by Denver Health and Hospital Authority under the Colorado state government. RADARS receives some funding from pharmaceutical industry subscriptions. Dr. Asomaning and Diane L. Martire, MD, MPH, are Pfizer employees who have financial interests with Pfizer.
SAN ANTONIO – Prescription opioid abuse has continued declining since 2011, but opioids remain far more commonly abused than other prescription drugs, including gabapentin and pregabalin, new research shows.
“Both gabapentin and pregabalin are abused but at rates that are 6-56 times less frequent than for opioid analgesics,” wrote Kofi Asomaning, DSci, of Pfizer, and associates at Pfizer and Denver Health’s Rocky Mountain Poison and Drug Center.
“Gabapentin is generally more frequently abused than pregabalin,” they reported in a research poster at the annual meeting of the College on Problems of Drug Dependence.
The researchers analyzed data from the RADARS System Survey of Non-Medical Use of Prescription Drugs Program (NMURx), the RADARS System Treatment Center Programs Combined, and the American Association of Poison Control Centers National Poison Data System (NPDS).
All those use self-reported data. The first is a confidential, anonymous web-based survey used to estimate population-level prevalence, and the second surveys patients with opioid use disorder entering treatment. The NPDS tracks all cases reported to poison control centers nationally.
Analysis of the NMURx data revealed similar lifetime abuse prevalence rates for gabapentin and pregabalin at 0.4%, several magnitudes lower than the 5.3% rate identified with opioids.
Gabapentin, however, had higher rates of abuse in the past month in the Treatment Center Programs Combined. For the third to fourth quarter of 2017, 0.12 per 100,000 population reportedly abused gabapentin, compared with 0.01 per 100,000 for pregabalin. The rate for past-month abuse of opioids was 0.79 per 100,000.
A similar pattern for the same quarter emerged from the NPDS data: Rate of gabapentin abuse was 0.06 per 100,000, rate for pregabalin was 0.01 per 100,000, and rate for opioids was 0.40 per 100,000.
Both pregabalin and opioids were predominantly ingested, though a very small amount of each was inhaled and a similarly small amount of opioids was injected. Data on exposure route for gabapentin were not provided, though it was used more frequently than pregabalin.
The research was funded by Pfizer. The RADARS system is owned by Denver Health and Hospital Authority under the Colorado state government. RADARS receives some funding from pharmaceutical industry subscriptions. Dr. Asomaning and Diane L. Martire, MD, MPH, are Pfizer employees who have financial interests with Pfizer.
REPORTING FROM CPDD 2019
Gabapentinoids associated with suicidal behavior, overdose
Young patients might be at increased risk of suicidal behavior, unintentional overdose, injuries, and traffic incidents during treatment periods with gabapentinoids, compared with periods without treatment with those medications, a cohort study of almost 200,000 people shows. Pregabalin is associated with higher hazards of those outcomes than is gabapentin, and the associations are strongest in patients aged 15-24 years, the researchers reported.
“If our findings are triangulated with other forms of evidence, ,” wrote Yasmina Molero, PhD, and associates. “Further restrictions for off-label prescription may need consideration.” The study was published in BMJ.
The use of gabapentinoids has risen in the United States (JAMA Intern Med. 2018;178[2]:292-4), and overdose deaths tied to gabapentin have led some states to explore reclassification of the drug as a controlled substance (Risk Manag Healthc Policy. 2018;11:109-16). In the United Kingdom, gabapentinoids are being reclassified as a class C controlled drug because of concerns about the risk of addiction, overdose, and safety, wrote Dr. Molero of the department of psychiatry at Warneford Hospital at the University of Oxford, England, and associates.
To study associations between gabapentinoids and adverse outcomes related to coordination, mental health, and criminality, Dr. Molero and her associates analyzed data from 191,973 people from the Swedish Prescribed Drug Register who collected prescriptions for pregabalin or gabapentin between 2006 and 2013. The researchers included patients aged 15 years and older in their analyses.
They examined suicidal behavior, unintentional overdoses, head or body injuries, road traffic incidents and offenses, and arrests for violent crime using the Swedish Patient Register and the National Crime Register. In addition, they defined suicidal behavior as emergency hospital visits attributable to self-injurious behavior or suicide attempt, or death by suicide. Unintentional overdoses were defined as emergency hospital visits or death attributable to poisoning by illicit drugs, medications, or biologic substances; accidental poisoning by noxious substances; or acute intoxications and overdoses by alcohol and illicit drugs, excluding intentional self-poisoning, wrote Dr. Molero, who is affiliated with the Karolinska Institute in Stockholm, and her associates.
Of the nearly 192,000 participants who collected prescriptions of gabapentinoids on at least two consecutive occasions, 120,664 received pregabalin, and 85,360 received gabapentin; 14,051 of the participants received both drugs. Fifty-nine percent were women, and most patients were aged 45 or older.
During the study period, 10,026 participants (5.2%) were treated for suicidal behavior or died from suicide, 17,144 participants (8.9%) experienced an unintentional overdose, and 12,070 participants (6.3%) had a road traffic incident or offense. In addition, 70,522 participants (36.7%) had head or body injuries, and 7,984 participants (4.1%) were arrested for a violent crime.
The study used a within-individual design that compared when a person was taking a gabapentinoid with when he or she was not. During treatment periods, participants were at increased risk of suicidal behavior or death from suicide (age-adjusted hazard ratio, 1.26), unintentional overdose (1.24), head or body injuries (1.22), and road traffic incidents or offenses (1.13). Associations with arrests for violent crime were not significant.
Gabapentinoid treatment was associated with increased hazards of suicidal behavior in people young than 55 years, but hazards were reduced or not significant in participants aged 55 years and older. Participants aged 15-24 years had the highest hazards of suicidal behavior (1.67).
In a sensitivity analysis, the researchers examined participants who had a diagnosis of comorbid epilepsy, psychiatric disorders, or musculoskeletal disorders before the start of gabapentinoid treatment. Among patients with comorbid epilepsy, gabapentinoids were not significantly associated with suicidal behavior and were associated with reduced hazards for all other outcomes.
“In comorbid psychiatric disorders, gabapentinoids were associated with lower risk for all outcomes,” the researchers said. Among patients with comorbid musculoskeletal disorders, gabapentinoids were associated with reductions in head or body injuries, traffic incidents, and arrests for violent crime.
Dr. Molero and her associates noted that they lacked information about alcohol and drug use, as well as treatment adherence and the conditions for which gabapentinoids had been prescribed. Furthermore, differences in prescription practices and outcome rates might affect the generalizability of the results to other countries.
The different results for pregabalin and gabapentin “could be due to their different pharmacodynamic and pharmacokinetic profiles; pregabalin has a higher potency, greater bioavailability, and quicker absorption than gabapentin. Pregabalin also has been associated with withdrawal symptoms following rapid discontinuation, which could be related to suicidal behavior,” Dr. Molero and colleagues said. “The reduced hazards in older people could reflect pharmacodynamic differences related to age, less concurrent use of alcohol or drugs, different indications for treatment, or reduced symptom severity of underlying conditions.”
The Wellcome Trust, Swedish Research Council, and Karolinska Institute supported the study. The authors had no disclosures relevant to the study. One author reported grants from Shire and Evolan and has served as a speaker for Shire.
SOURCE: Molero Y et al. BMJ. 2019 Jun 12. doi: 10.1136/bmj.l2147.
The findings by Molero et al. advance clinical knowledge about the drug class of gabapentinoids, wrote Derek K. Tracy, MB BCh. Though the study does not establish causality, it does rely on a solid, large dataset. The study shows the importance of uncoupling pregabalin and gabapentin. Both drugs are indeed gabapentinoids, but their use can lead to different outcomes, depending on the age of patients. For example, pregabalin – not gabapentin – appears tied to higher risks of harm. The demographic group that is most vulnerable is patients aged 15-24, the researchers found. Factors driving those age-related differences in risks tied to the drugs need to be understood.
Dr. Tracy is a consultant psychiatrist at Queen Mary’s Hospital in London. He is a trustee of the charity Mentor and has received honoraria from Janssen for delivering educational talks on novel psychoactive substances. His comments were adapted from an editorial (BMJ. 2019 Jun 12. doi: 10.1136/bmj.14021 ).
The findings by Molero et al. advance clinical knowledge about the drug class of gabapentinoids, wrote Derek K. Tracy, MB BCh. Though the study does not establish causality, it does rely on a solid, large dataset. The study shows the importance of uncoupling pregabalin and gabapentin. Both drugs are indeed gabapentinoids, but their use can lead to different outcomes, depending on the age of patients. For example, pregabalin – not gabapentin – appears tied to higher risks of harm. The demographic group that is most vulnerable is patients aged 15-24, the researchers found. Factors driving those age-related differences in risks tied to the drugs need to be understood.
Dr. Tracy is a consultant psychiatrist at Queen Mary’s Hospital in London. He is a trustee of the charity Mentor and has received honoraria from Janssen for delivering educational talks on novel psychoactive substances. His comments were adapted from an editorial (BMJ. 2019 Jun 12. doi: 10.1136/bmj.14021 ).
The findings by Molero et al. advance clinical knowledge about the drug class of gabapentinoids, wrote Derek K. Tracy, MB BCh. Though the study does not establish causality, it does rely on a solid, large dataset. The study shows the importance of uncoupling pregabalin and gabapentin. Both drugs are indeed gabapentinoids, but their use can lead to different outcomes, depending on the age of patients. For example, pregabalin – not gabapentin – appears tied to higher risks of harm. The demographic group that is most vulnerable is patients aged 15-24, the researchers found. Factors driving those age-related differences in risks tied to the drugs need to be understood.
Dr. Tracy is a consultant psychiatrist at Queen Mary’s Hospital in London. He is a trustee of the charity Mentor and has received honoraria from Janssen for delivering educational talks on novel psychoactive substances. His comments were adapted from an editorial (BMJ. 2019 Jun 12. doi: 10.1136/bmj.14021 ).
Young patients might be at increased risk of suicidal behavior, unintentional overdose, injuries, and traffic incidents during treatment periods with gabapentinoids, compared with periods without treatment with those medications, a cohort study of almost 200,000 people shows. Pregabalin is associated with higher hazards of those outcomes than is gabapentin, and the associations are strongest in patients aged 15-24 years, the researchers reported.
“If our findings are triangulated with other forms of evidence, ,” wrote Yasmina Molero, PhD, and associates. “Further restrictions for off-label prescription may need consideration.” The study was published in BMJ.
The use of gabapentinoids has risen in the United States (JAMA Intern Med. 2018;178[2]:292-4), and overdose deaths tied to gabapentin have led some states to explore reclassification of the drug as a controlled substance (Risk Manag Healthc Policy. 2018;11:109-16). In the United Kingdom, gabapentinoids are being reclassified as a class C controlled drug because of concerns about the risk of addiction, overdose, and safety, wrote Dr. Molero of the department of psychiatry at Warneford Hospital at the University of Oxford, England, and associates.
To study associations between gabapentinoids and adverse outcomes related to coordination, mental health, and criminality, Dr. Molero and her associates analyzed data from 191,973 people from the Swedish Prescribed Drug Register who collected prescriptions for pregabalin or gabapentin between 2006 and 2013. The researchers included patients aged 15 years and older in their analyses.
They examined suicidal behavior, unintentional overdoses, head or body injuries, road traffic incidents and offenses, and arrests for violent crime using the Swedish Patient Register and the National Crime Register. In addition, they defined suicidal behavior as emergency hospital visits attributable to self-injurious behavior or suicide attempt, or death by suicide. Unintentional overdoses were defined as emergency hospital visits or death attributable to poisoning by illicit drugs, medications, or biologic substances; accidental poisoning by noxious substances; or acute intoxications and overdoses by alcohol and illicit drugs, excluding intentional self-poisoning, wrote Dr. Molero, who is affiliated with the Karolinska Institute in Stockholm, and her associates.
Of the nearly 192,000 participants who collected prescriptions of gabapentinoids on at least two consecutive occasions, 120,664 received pregabalin, and 85,360 received gabapentin; 14,051 of the participants received both drugs. Fifty-nine percent were women, and most patients were aged 45 or older.
During the study period, 10,026 participants (5.2%) were treated for suicidal behavior or died from suicide, 17,144 participants (8.9%) experienced an unintentional overdose, and 12,070 participants (6.3%) had a road traffic incident or offense. In addition, 70,522 participants (36.7%) had head or body injuries, and 7,984 participants (4.1%) were arrested for a violent crime.
The study used a within-individual design that compared when a person was taking a gabapentinoid with when he or she was not. During treatment periods, participants were at increased risk of suicidal behavior or death from suicide (age-adjusted hazard ratio, 1.26), unintentional overdose (1.24), head or body injuries (1.22), and road traffic incidents or offenses (1.13). Associations with arrests for violent crime were not significant.
Gabapentinoid treatment was associated with increased hazards of suicidal behavior in people young than 55 years, but hazards were reduced or not significant in participants aged 55 years and older. Participants aged 15-24 years had the highest hazards of suicidal behavior (1.67).
In a sensitivity analysis, the researchers examined participants who had a diagnosis of comorbid epilepsy, psychiatric disorders, or musculoskeletal disorders before the start of gabapentinoid treatment. Among patients with comorbid epilepsy, gabapentinoids were not significantly associated with suicidal behavior and were associated with reduced hazards for all other outcomes.
“In comorbid psychiatric disorders, gabapentinoids were associated with lower risk for all outcomes,” the researchers said. Among patients with comorbid musculoskeletal disorders, gabapentinoids were associated with reductions in head or body injuries, traffic incidents, and arrests for violent crime.
Dr. Molero and her associates noted that they lacked information about alcohol and drug use, as well as treatment adherence and the conditions for which gabapentinoids had been prescribed. Furthermore, differences in prescription practices and outcome rates might affect the generalizability of the results to other countries.
The different results for pregabalin and gabapentin “could be due to their different pharmacodynamic and pharmacokinetic profiles; pregabalin has a higher potency, greater bioavailability, and quicker absorption than gabapentin. Pregabalin also has been associated with withdrawal symptoms following rapid discontinuation, which could be related to suicidal behavior,” Dr. Molero and colleagues said. “The reduced hazards in older people could reflect pharmacodynamic differences related to age, less concurrent use of alcohol or drugs, different indications for treatment, or reduced symptom severity of underlying conditions.”
The Wellcome Trust, Swedish Research Council, and Karolinska Institute supported the study. The authors had no disclosures relevant to the study. One author reported grants from Shire and Evolan and has served as a speaker for Shire.
SOURCE: Molero Y et al. BMJ. 2019 Jun 12. doi: 10.1136/bmj.l2147.
Young patients might be at increased risk of suicidal behavior, unintentional overdose, injuries, and traffic incidents during treatment periods with gabapentinoids, compared with periods without treatment with those medications, a cohort study of almost 200,000 people shows. Pregabalin is associated with higher hazards of those outcomes than is gabapentin, and the associations are strongest in patients aged 15-24 years, the researchers reported.
“If our findings are triangulated with other forms of evidence, ,” wrote Yasmina Molero, PhD, and associates. “Further restrictions for off-label prescription may need consideration.” The study was published in BMJ.
The use of gabapentinoids has risen in the United States (JAMA Intern Med. 2018;178[2]:292-4), and overdose deaths tied to gabapentin have led some states to explore reclassification of the drug as a controlled substance (Risk Manag Healthc Policy. 2018;11:109-16). In the United Kingdom, gabapentinoids are being reclassified as a class C controlled drug because of concerns about the risk of addiction, overdose, and safety, wrote Dr. Molero of the department of psychiatry at Warneford Hospital at the University of Oxford, England, and associates.
To study associations between gabapentinoids and adverse outcomes related to coordination, mental health, and criminality, Dr. Molero and her associates analyzed data from 191,973 people from the Swedish Prescribed Drug Register who collected prescriptions for pregabalin or gabapentin between 2006 and 2013. The researchers included patients aged 15 years and older in their analyses.
They examined suicidal behavior, unintentional overdoses, head or body injuries, road traffic incidents and offenses, and arrests for violent crime using the Swedish Patient Register and the National Crime Register. In addition, they defined suicidal behavior as emergency hospital visits attributable to self-injurious behavior or suicide attempt, or death by suicide. Unintentional overdoses were defined as emergency hospital visits or death attributable to poisoning by illicit drugs, medications, or biologic substances; accidental poisoning by noxious substances; or acute intoxications and overdoses by alcohol and illicit drugs, excluding intentional self-poisoning, wrote Dr. Molero, who is affiliated with the Karolinska Institute in Stockholm, and her associates.
Of the nearly 192,000 participants who collected prescriptions of gabapentinoids on at least two consecutive occasions, 120,664 received pregabalin, and 85,360 received gabapentin; 14,051 of the participants received both drugs. Fifty-nine percent were women, and most patients were aged 45 or older.
During the study period, 10,026 participants (5.2%) were treated for suicidal behavior or died from suicide, 17,144 participants (8.9%) experienced an unintentional overdose, and 12,070 participants (6.3%) had a road traffic incident or offense. In addition, 70,522 participants (36.7%) had head or body injuries, and 7,984 participants (4.1%) were arrested for a violent crime.
The study used a within-individual design that compared when a person was taking a gabapentinoid with when he or she was not. During treatment periods, participants were at increased risk of suicidal behavior or death from suicide (age-adjusted hazard ratio, 1.26), unintentional overdose (1.24), head or body injuries (1.22), and road traffic incidents or offenses (1.13). Associations with arrests for violent crime were not significant.
Gabapentinoid treatment was associated with increased hazards of suicidal behavior in people young than 55 years, but hazards were reduced or not significant in participants aged 55 years and older. Participants aged 15-24 years had the highest hazards of suicidal behavior (1.67).
In a sensitivity analysis, the researchers examined participants who had a diagnosis of comorbid epilepsy, psychiatric disorders, or musculoskeletal disorders before the start of gabapentinoid treatment. Among patients with comorbid epilepsy, gabapentinoids were not significantly associated with suicidal behavior and were associated with reduced hazards for all other outcomes.
“In comorbid psychiatric disorders, gabapentinoids were associated with lower risk for all outcomes,” the researchers said. Among patients with comorbid musculoskeletal disorders, gabapentinoids were associated with reductions in head or body injuries, traffic incidents, and arrests for violent crime.
Dr. Molero and her associates noted that they lacked information about alcohol and drug use, as well as treatment adherence and the conditions for which gabapentinoids had been prescribed. Furthermore, differences in prescription practices and outcome rates might affect the generalizability of the results to other countries.
The different results for pregabalin and gabapentin “could be due to their different pharmacodynamic and pharmacokinetic profiles; pregabalin has a higher potency, greater bioavailability, and quicker absorption than gabapentin. Pregabalin also has been associated with withdrawal symptoms following rapid discontinuation, which could be related to suicidal behavior,” Dr. Molero and colleagues said. “The reduced hazards in older people could reflect pharmacodynamic differences related to age, less concurrent use of alcohol or drugs, different indications for treatment, or reduced symptom severity of underlying conditions.”
The Wellcome Trust, Swedish Research Council, and Karolinska Institute supported the study. The authors had no disclosures relevant to the study. One author reported grants from Shire and Evolan and has served as a speaker for Shire.
SOURCE: Molero Y et al. BMJ. 2019 Jun 12. doi: 10.1136/bmj.l2147.
FROM BMJ
Key clinical point: Patients might be at increased risk of suicidal behavior, unintentional overdose, head and body injuries, and traffic incidents during periods of treatment with gabapentinoids. Pregabalin is associated with higher hazards of these outcomes than is gabapentin, and the associations are strongest in patients aged 15-24 years.
Major finding: During treatment periods, patients were at increased risk of suicidal behavior or death from suicide (age-adjusted hazard ratio, 1.26), unintentional overdose (1.24), head or body injuries (1.22), and road traffic incidents or offenses (1.13).
Study details: An analysis of data from 191,973 people from the Swedish Prescribed Drug Register, which collected prescriptions for pregabalin or gabapentin between 2006 and 2013.
Disclosures: The Wellcome Trust, Swedish Research Council, and Karolinska Institute supported the study. The authors had no relevant disclosures. One author reported grants from Shire and Evolan, and has served as a speaker for Shire.
Source: Molero Y et al. BMJ. 2019 Jun 12. doi: 10.1136/bmj.l2147.
Cannabis withdrawal syndrome real but underrecognized
SAN FRANCISCO – Marijuana withdrawal syndrome is real, and physicians and patients should recognize the phenomenon and take it seriously as legalization rolls out across the United States, an investigation from Columbia University in New York suggests,

“Most clinicians don’t really believe there is a withdrawal syndrome, but there definitely is. The prevalence we found was 12% among frequent cannabis users,” meaning three or more times a week, said psychiatrist and lead investigator Ofir Livne, MD, who until recently was a research fellow at Columbia but now is affiliated with Tel Aviv University in Israel (Drug Alcohol Depend. 2019 Feb 1;195:170-7).
“Usually what happens is a cannabis user will feel a bit agitated, and they’ll take another joint without even realizing they are just perpetuating the addiction.”
Dr. Livne said the syndrome is seen with other substances but is underrecognized with cannabis. “The word needs to get out more,” he said at the annual meeting of the American Psychiatric Association.
The symptoms can last for several days – or longer.
To get an idea of the extent of the problem, he and his team analyzed data from the National Epidemiologic Survey on Alcohol and Related Conditions-III. The survey collected data on more than 36,000 adults about drug use, associated effects, and other issues in 2012-13.
The investigators focused on the 1,527 people who reported frequent use in the preceding 12 months, and looked to see whether the symptoms they reported when they stopped or cut back would qualify them for cannabis withdrawal syndrome (CWS) in the DSM-5, the first edition of the manual to include the diagnosis.
Overall, 12.1% made the cut. The most common symptoms were nervousness/anxiety (76%), irritability (72%), sleep difficulty (68%), and depressed mood (59%). CWS patients also had lower health-related quality of life scores than peers without CWS.
Physical symptoms associated with CWS included headache, tremors, and sweating, among others. Overall, 70% of people reported some sort of physical discomfort associated with withdrawal.
“We also saw that frequent cannabis users who experience withdrawal are a lot more prone to other psychiatric disorders,” Dr. Livne said, including mood disorders (adjusted odds ratio, 1.9-2.6), anxiety disorders (aOR, 2.4-2.5), and personality disorders (aOR, 1.7-2.2). They more often had a family history of depression (aOR, 2.5).
“This study provides the first nationally representative large-scale report on the DSM-5 cannabis withdrawal syndrome. ... Its shared symptoms with depressive and anxiety disorders call for clinician awareness of CWS and the factors associated with it,” Dr. Livne and his colleagues concluded.
The work was adjusted for social demographics and other confounders, including tobacco withdrawal, which has overlapping symptoms.
It’s possible that in some cases, the survey simply caught a return of the anxiety and other issues that caused people to use in the first place, instead of true withdrawal, but Dr. Livne didn’t think so. “Some of them might have been prone to anxiety, but we controlled for that as much as we could,” he said.
The work was funded by the National Institute on Drug Abuse. Dr. Livne had no disclosures.
SAN FRANCISCO – Marijuana withdrawal syndrome is real, and physicians and patients should recognize the phenomenon and take it seriously as legalization rolls out across the United States, an investigation from Columbia University in New York suggests,
“Most clinicians don’t really believe there is a withdrawal syndrome, but there definitely is. The prevalence we found was 12% among frequent cannabis users,” meaning three or more times a week, said psychiatrist and lead investigator Ofir Livne, MD, who until recently was a research fellow at Columbia but now is affiliated with Tel Aviv University in Israel (Drug Alcohol Depend. 2019 Feb 1;195:170-7).
“Usually what happens is a cannabis user will feel a bit agitated, and they’ll take another joint without even realizing they are just perpetuating the addiction.”
Dr. Livne said the syndrome is seen with other substances but is underrecognized with cannabis. “The word needs to get out more,” he said at the annual meeting of the American Psychiatric Association.
The symptoms can last for several days – or longer.
To get an idea of the extent of the problem, he and his team analyzed data from the National Epidemiologic Survey on Alcohol and Related Conditions-III. The survey collected data on more than 36,000 adults about drug use, associated effects, and other issues in 2012-13.
The investigators focused on the 1,527 people who reported frequent use in the preceding 12 months, and looked to see whether the symptoms they reported when they stopped or cut back would qualify them for cannabis withdrawal syndrome (CWS) in the DSM-5, the first edition of the manual to include the diagnosis.
Overall, 12.1% made the cut. The most common symptoms were nervousness/anxiety (76%), irritability (72%), sleep difficulty (68%), and depressed mood (59%). CWS patients also had lower health-related quality of life scores than peers without CWS.
Physical symptoms associated with CWS included headache, tremors, and sweating, among others. Overall, 70% of people reported some sort of physical discomfort associated with withdrawal.
“We also saw that frequent cannabis users who experience withdrawal are a lot more prone to other psychiatric disorders,” Dr. Livne said, including mood disorders (adjusted odds ratio, 1.9-2.6), anxiety disorders (aOR, 2.4-2.5), and personality disorders (aOR, 1.7-2.2). They more often had a family history of depression (aOR, 2.5).
“This study provides the first nationally representative large-scale report on the DSM-5 cannabis withdrawal syndrome. ... Its shared symptoms with depressive and anxiety disorders call for clinician awareness of CWS and the factors associated with it,” Dr. Livne and his colleagues concluded.
The work was adjusted for social demographics and other confounders, including tobacco withdrawal, which has overlapping symptoms.
It’s possible that in some cases, the survey simply caught a return of the anxiety and other issues that caused people to use in the first place, instead of true withdrawal, but Dr. Livne didn’t think so. “Some of them might have been prone to anxiety, but we controlled for that as much as we could,” he said.
The work was funded by the National Institute on Drug Abuse. Dr. Livne had no disclosures.
SAN FRANCISCO – Marijuana withdrawal syndrome is real, and physicians and patients should recognize the phenomenon and take it seriously as legalization rolls out across the United States, an investigation from Columbia University in New York suggests,
“Most clinicians don’t really believe there is a withdrawal syndrome, but there definitely is. The prevalence we found was 12% among frequent cannabis users,” meaning three or more times a week, said psychiatrist and lead investigator Ofir Livne, MD, who until recently was a research fellow at Columbia but now is affiliated with Tel Aviv University in Israel (Drug Alcohol Depend. 2019 Feb 1;195:170-7).
“Usually what happens is a cannabis user will feel a bit agitated, and they’ll take another joint without even realizing they are just perpetuating the addiction.”
Dr. Livne said the syndrome is seen with other substances but is underrecognized with cannabis. “The word needs to get out more,” he said at the annual meeting of the American Psychiatric Association.
The symptoms can last for several days – or longer.
To get an idea of the extent of the problem, he and his team analyzed data from the National Epidemiologic Survey on Alcohol and Related Conditions-III. The survey collected data on more than 36,000 adults about drug use, associated effects, and other issues in 2012-13.
The investigators focused on the 1,527 people who reported frequent use in the preceding 12 months, and looked to see whether the symptoms they reported when they stopped or cut back would qualify them for cannabis withdrawal syndrome (CWS) in the DSM-5, the first edition of the manual to include the diagnosis.
Overall, 12.1% made the cut. The most common symptoms were nervousness/anxiety (76%), irritability (72%), sleep difficulty (68%), and depressed mood (59%). CWS patients also had lower health-related quality of life scores than peers without CWS.
Physical symptoms associated with CWS included headache, tremors, and sweating, among others. Overall, 70% of people reported some sort of physical discomfort associated with withdrawal.
“We also saw that frequent cannabis users who experience withdrawal are a lot more prone to other psychiatric disorders,” Dr. Livne said, including mood disorders (adjusted odds ratio, 1.9-2.6), anxiety disorders (aOR, 2.4-2.5), and personality disorders (aOR, 1.7-2.2). They more often had a family history of depression (aOR, 2.5).
“This study provides the first nationally representative large-scale report on the DSM-5 cannabis withdrawal syndrome. ... Its shared symptoms with depressive and anxiety disorders call for clinician awareness of CWS and the factors associated with it,” Dr. Livne and his colleagues concluded.
The work was adjusted for social demographics and other confounders, including tobacco withdrawal, which has overlapping symptoms.
It’s possible that in some cases, the survey simply caught a return of the anxiety and other issues that caused people to use in the first place, instead of true withdrawal, but Dr. Livne didn’t think so. “Some of them might have been prone to anxiety, but we controlled for that as much as we could,” he said.
The work was funded by the National Institute on Drug Abuse. Dr. Livne had no disclosures.
REPORTING FROM APA 2019

Deaths from drugs, alcohol, and suicide increase among millennials
The number of Americans who die each year from alcohol, drugs, or suicide increased to an all-time high in 2017, and the increase was especially pronounced among young adults, according a June 13 report from two public health policy and advocacy organizations. A separate report found that rates of these “deaths of despair” vary widely by state.
The report by Trust for America’s Health and Well Being Trust examined Centers for Disease Control and Prevention (CDC) data with a focus on adults aged 18-34 years. Between 2007 and 2017, alcohol-induced deaths increased by 69%, drug-related deaths by 108%, and suicide by 35% in this age group. These deaths increased in other age groups, too, but often to a lesser extent.
In 1999, there were 7 drug deaths per 100,000 people across age groups, which increased to 22.7 drug deaths per 100,000 people in 2017. Among adults aged 18-34, however, the rate was nearly 31 drug overdose deaths per 100,000 people. Opioid overdoses are largely responsible for the increase in drug-related deaths, and synthetic opioid death rates increased by 6,000% between 1999 and 2017, the report said.
... including the opioid crisis, the skyrocketing costs of education and housing, and entering the job market during the great recession,” according to the report, which was funded with grants from Well Being Trust and the Robert Wood Johnson Foundation.
Screening, treatment, and addressing risk and protective factors are among the measures that the groups recommend to reduce “deaths of despair.”
On June 12, the Commonwealth Fund released a report that examines how drug, alcohol, and suicide death rates across age groups may vary widely by state.
“In Pennsylvania, Maryland, and Ohio, mortality rates from drug overdoses were at least five times higher than rates for alcohol-related deaths and about three times higher than suicide rates,” according to the Commonwealth Fund analysis. “In other states, deaths from suicide and alcohol dominate. In 2017, Montana, Nebraska, the Dakotas, Oregon, and Wyoming saw higher rates of death from suicide and alcohol than from drugs.”
Substance use disorders and suicide might be related, and researchers have suggested that many overdoses may be suicide attempts.
“We assumed that overdoses were accidental ... only to find that many users were actively suicidal, others were playing a version of Russian roulette, and others had passive suicidal ideation,” said Mark S. Gold, MD, adjunct professor of psychiatry at Washington University in St. Louis, in an interview. Opioid use disorders often are treated as “simply opioid deficiency syndromes,” and physicians may miss when patients have physical, sexual, or emotional trauma, anxiety disorders, or major depression, he said.
The number of Americans who die each year from alcohol, drugs, or suicide increased to an all-time high in 2017, and the increase was especially pronounced among young adults, according a June 13 report from two public health policy and advocacy organizations. A separate report found that rates of these “deaths of despair” vary widely by state.
The report by Trust for America’s Health and Well Being Trust examined Centers for Disease Control and Prevention (CDC) data with a focus on adults aged 18-34 years. Between 2007 and 2017, alcohol-induced deaths increased by 69%, drug-related deaths by 108%, and suicide by 35% in this age group. These deaths increased in other age groups, too, but often to a lesser extent.
In 1999, there were 7 drug deaths per 100,000 people across age groups, which increased to 22.7 drug deaths per 100,000 people in 2017. Among adults aged 18-34, however, the rate was nearly 31 drug overdose deaths per 100,000 people. Opioid overdoses are largely responsible for the increase in drug-related deaths, and synthetic opioid death rates increased by 6,000% between 1999 and 2017, the report said.
... including the opioid crisis, the skyrocketing costs of education and housing, and entering the job market during the great recession,” according to the report, which was funded with grants from Well Being Trust and the Robert Wood Johnson Foundation.
Screening, treatment, and addressing risk and protective factors are among the measures that the groups recommend to reduce “deaths of despair.”
On June 12, the Commonwealth Fund released a report that examines how drug, alcohol, and suicide death rates across age groups may vary widely by state.
“In Pennsylvania, Maryland, and Ohio, mortality rates from drug overdoses were at least five times higher than rates for alcohol-related deaths and about three times higher than suicide rates,” according to the Commonwealth Fund analysis. “In other states, deaths from suicide and alcohol dominate. In 2017, Montana, Nebraska, the Dakotas, Oregon, and Wyoming saw higher rates of death from suicide and alcohol than from drugs.”
Substance use disorders and suicide might be related, and researchers have suggested that many overdoses may be suicide attempts.
“We assumed that overdoses were accidental ... only to find that many users were actively suicidal, others were playing a version of Russian roulette, and others had passive suicidal ideation,” said Mark S. Gold, MD, adjunct professor of psychiatry at Washington University in St. Louis, in an interview. Opioid use disorders often are treated as “simply opioid deficiency syndromes,” and physicians may miss when patients have physical, sexual, or emotional trauma, anxiety disorders, or major depression, he said.
The number of Americans who die each year from alcohol, drugs, or suicide increased to an all-time high in 2017, and the increase was especially pronounced among young adults, according a June 13 report from two public health policy and advocacy organizations. A separate report found that rates of these “deaths of despair” vary widely by state.
The report by Trust for America’s Health and Well Being Trust examined Centers for Disease Control and Prevention (CDC) data with a focus on adults aged 18-34 years. Between 2007 and 2017, alcohol-induced deaths increased by 69%, drug-related deaths by 108%, and suicide by 35% in this age group. These deaths increased in other age groups, too, but often to a lesser extent.
In 1999, there were 7 drug deaths per 100,000 people across age groups, which increased to 22.7 drug deaths per 100,000 people in 2017. Among adults aged 18-34, however, the rate was nearly 31 drug overdose deaths per 100,000 people. Opioid overdoses are largely responsible for the increase in drug-related deaths, and synthetic opioid death rates increased by 6,000% between 1999 and 2017, the report said.
... including the opioid crisis, the skyrocketing costs of education and housing, and entering the job market during the great recession,” according to the report, which was funded with grants from Well Being Trust and the Robert Wood Johnson Foundation.
Screening, treatment, and addressing risk and protective factors are among the measures that the groups recommend to reduce “deaths of despair.”
On June 12, the Commonwealth Fund released a report that examines how drug, alcohol, and suicide death rates across age groups may vary widely by state.
“In Pennsylvania, Maryland, and Ohio, mortality rates from drug overdoses were at least five times higher than rates for alcohol-related deaths and about three times higher than suicide rates,” according to the Commonwealth Fund analysis. “In other states, deaths from suicide and alcohol dominate. In 2017, Montana, Nebraska, the Dakotas, Oregon, and Wyoming saw higher rates of death from suicide and alcohol than from drugs.”
Substance use disorders and suicide might be related, and researchers have suggested that many overdoses may be suicide attempts.
“We assumed that overdoses were accidental ... only to find that many users were actively suicidal, others were playing a version of Russian roulette, and others had passive suicidal ideation,” said Mark S. Gold, MD, adjunct professor of psychiatry at Washington University in St. Louis, in an interview. Opioid use disorders often are treated as “simply opioid deficiency syndromes,” and physicians may miss when patients have physical, sexual, or emotional trauma, anxiety disorders, or major depression, he said.
Psilocybin promising for alcohol use disorder
SAN FRANCISCO – Patients with alcohol use disorder reported a substantial decrease in drinking days, drinks per drinking day, and cravings in an ongoing trial of psilocybin at New York University.

“If this keeps going the way it looks like it’s going, I think it will lead to a large phase 3 trial that could be part of getting psilocybin rescheduled” from a schedule I drug, said NYU psychiatrist and lead investigator Kelley O’Donnell, MD, PhD.
The work builds on positive results from the 1950s and 1960s of LSD for alcoholism, before LSD research was largely abandoned. Researchers such as Dr. O’Donnell are revisiting the approach, but with psilocybin because, among other reasons, it has less stigma and a shorter duration that allows for outpatient use (J Psychopharmacol. 2012 Jul;26[7]:994-1002). The Drug Enforcement Administration currently classifies psilocybin, the psychoactive ingredient in hallucinogenic, or “magic” mushrooms, as schedule I. The results found by Dr. O’Donnell’s team and other factors, such as the low risk of abuse tied to the use of psilocybin, are leading some researchers to suggest that the drug should be reclassified to “no more restrictively than schedule IV” (Neuropsychopharm. 2018 Nov;142:143-66).
Dr. O’Donnell’s presentation was part of a recurring theme at the annual meeting of the American Psychiatric Association – the transformation of what were once considered street drugs into therapeutic tools. Favorable results also were reported for 3,4-Methylenedioxymethamphetamine (MDMA), commonly known as ecstasy, for posttraumatic stress disorder; ketamine for depression and suicidality; and marijuana for pain and other problems.
Concerning psilocybin for alcohol use disorder (AUD), Dr. O’Donnell said: “Some people have really profound psychological experiences that shift the way they think about themselves and the way alcohol is affecting their relationships. Therapy can work with that shift in meaning [to create] lasting change.”
Many people “say that they get exactly what they needed.” Sometimes, patients revisit a past trauma but with a greater openness and flexibility – and a growing sense of peace. “They access affective states they just don’t have access to normally,” she said.
In another case, a woman hallucinated that she was sitting on a throne ascending through the universe, surrounded by the faces and voices of people she knew telling her she is a valuable and worthwhile person, and could take her place within the center of her universe without the sense of defectiveness and shame that often triggered her drinking. Happy little beer bottles told her: “We don’t need to be the enemy. We don’t need to be a part of your life,” Dr. O’Donnell said.
She and her team are pitting psilocybin against diphenhydramine as a control in the NYU AUD trial.
People are randomized, then undergo therapy focused equally on their alcohol use and preparing them for the drug experience. At week 4, they take their study medication – either 25 mg per 70 kg psilocybin or 50 mg diphenhydramine – in a relaxed living room–like setting, with classical or world music in the background. The study team avoids music with words in English. Two therapists, usually a man and a woman, are there as guides. The experience lasts a few hours; patients are debriefed afterward.
Patients undergo another round of counseling to understand the meaning of the experience, followed by a second dose, either 40 mg per 70 kg psilocybin or 100 mg diphenhydramine, at week 8. Patients are debriefed again and undergo a third month of counseling.
The results have not yet been unblinded, but Dr. O’Donnell and her team did find that, among their first 56 subjects, more intense mystical experiences, as gauged by the self-reported Mystical Experience Questionnaire (MEQ), correlated with greater treatment success.
Patients fill out the MEQ 8 hours after their dose, rating dimensions such as ego dissolution, oceanic boundlessness, joy, compassion, and openness. The maximum score is 1, the lowest 0, meaning no mystical effects. The median score among the 56 subjects was 0.26. The 30 or so patients who scored at or above that mark after their first medication session – as a group, their mean first MEQ score was 0.65 – reported a smaller percentage of drinking days at week 12 than those who scored below 0.26 (19% vs. 40%; P less than .05), with fewer drinks per drinking day (2.63 vs. 7.01; P less than .01); and lower craving (8.43 vs. 13.86 points on 30-point Penn Alcohol Craving Scale, P less than .01).
The groups were evenly matched at baseline. Both reported drinking an average of 3 out of 4 days, with an mean of 7.5 drinks per drinking day and a craving score of about 18. No differences were found in anxiety and depression scores, which were minimal in both groups.
More than half the subjects were men; the mean age was 46; and subjects were fairly well educated, reporting an average of 17 school years.
Dr. O’Donnell said she’s seen a range of experiences on psilocybin, but that bad trips are rare. Benzodiazepines are kept on hand, however, to help people who get too anxious, and an atypical antipsychotic is on hand to reverse hallucinatory effects.
Her team hopes to enroll 100 subjects and plans for follow-up past 12 weeks. Both Denver and Oakland, Calif., recently decriminalized psilocybin.
The work is being funded by the Heffter Research Institute. Dr. O’Donnell had no disclosures.
SAN FRANCISCO – Patients with alcohol use disorder reported a substantial decrease in drinking days, drinks per drinking day, and cravings in an ongoing trial of psilocybin at New York University.
“If this keeps going the way it looks like it’s going, I think it will lead to a large phase 3 trial that could be part of getting psilocybin rescheduled” from a schedule I drug, said NYU psychiatrist and lead investigator Kelley O’Donnell, MD, PhD.
The work builds on positive results from the 1950s and 1960s of LSD for alcoholism, before LSD research was largely abandoned. Researchers such as Dr. O’Donnell are revisiting the approach, but with psilocybin because, among other reasons, it has less stigma and a shorter duration that allows for outpatient use (J Psychopharmacol. 2012 Jul;26[7]:994-1002). The Drug Enforcement Administration currently classifies psilocybin, the psychoactive ingredient in hallucinogenic, or “magic” mushrooms, as schedule I. The results found by Dr. O’Donnell’s team and other factors, such as the low risk of abuse tied to the use of psilocybin, are leading some researchers to suggest that the drug should be reclassified to “no more restrictively than schedule IV” (Neuropsychopharm. 2018 Nov;142:143-66).
Dr. O’Donnell’s presentation was part of a recurring theme at the annual meeting of the American Psychiatric Association – the transformation of what were once considered street drugs into therapeutic tools. Favorable results also were reported for 3,4-Methylenedioxymethamphetamine (MDMA), commonly known as ecstasy, for posttraumatic stress disorder; ketamine for depression and suicidality; and marijuana for pain and other problems.
Concerning psilocybin for alcohol use disorder (AUD), Dr. O’Donnell said: “Some people have really profound psychological experiences that shift the way they think about themselves and the way alcohol is affecting their relationships. Therapy can work with that shift in meaning [to create] lasting change.”
Many people “say that they get exactly what they needed.” Sometimes, patients revisit a past trauma but with a greater openness and flexibility – and a growing sense of peace. “They access affective states they just don’t have access to normally,” she said.
In another case, a woman hallucinated that she was sitting on a throne ascending through the universe, surrounded by the faces and voices of people she knew telling her she is a valuable and worthwhile person, and could take her place within the center of her universe without the sense of defectiveness and shame that often triggered her drinking. Happy little beer bottles told her: “We don’t need to be the enemy. We don’t need to be a part of your life,” Dr. O’Donnell said.
She and her team are pitting psilocybin against diphenhydramine as a control in the NYU AUD trial.
People are randomized, then undergo therapy focused equally on their alcohol use and preparing them for the drug experience. At week 4, they take their study medication – either 25 mg per 70 kg psilocybin or 50 mg diphenhydramine – in a relaxed living room–like setting, with classical or world music in the background. The study team avoids music with words in English. Two therapists, usually a man and a woman, are there as guides. The experience lasts a few hours; patients are debriefed afterward.
Patients undergo another round of counseling to understand the meaning of the experience, followed by a second dose, either 40 mg per 70 kg psilocybin or 100 mg diphenhydramine, at week 8. Patients are debriefed again and undergo a third month of counseling.
The results have not yet been unblinded, but Dr. O’Donnell and her team did find that, among their first 56 subjects, more intense mystical experiences, as gauged by the self-reported Mystical Experience Questionnaire (MEQ), correlated with greater treatment success.
Patients fill out the MEQ 8 hours after their dose, rating dimensions such as ego dissolution, oceanic boundlessness, joy, compassion, and openness. The maximum score is 1, the lowest 0, meaning no mystical effects. The median score among the 56 subjects was 0.26. The 30 or so patients who scored at or above that mark after their first medication session – as a group, their mean first MEQ score was 0.65 – reported a smaller percentage of drinking days at week 12 than those who scored below 0.26 (19% vs. 40%; P less than .05), with fewer drinks per drinking day (2.63 vs. 7.01; P less than .01); and lower craving (8.43 vs. 13.86 points on 30-point Penn Alcohol Craving Scale, P less than .01).
The groups were evenly matched at baseline. Both reported drinking an average of 3 out of 4 days, with an mean of 7.5 drinks per drinking day and a craving score of about 18. No differences were found in anxiety and depression scores, which were minimal in both groups.
More than half the subjects were men; the mean age was 46; and subjects were fairly well educated, reporting an average of 17 school years.
Dr. O’Donnell said she’s seen a range of experiences on psilocybin, but that bad trips are rare. Benzodiazepines are kept on hand, however, to help people who get too anxious, and an atypical antipsychotic is on hand to reverse hallucinatory effects.
Her team hopes to enroll 100 subjects and plans for follow-up past 12 weeks. Both Denver and Oakland, Calif., recently decriminalized psilocybin.
The work is being funded by the Heffter Research Institute. Dr. O’Donnell had no disclosures.
SAN FRANCISCO – Patients with alcohol use disorder reported a substantial decrease in drinking days, drinks per drinking day, and cravings in an ongoing trial of psilocybin at New York University.
“If this keeps going the way it looks like it’s going, I think it will lead to a large phase 3 trial that could be part of getting psilocybin rescheduled” from a schedule I drug, said NYU psychiatrist and lead investigator Kelley O’Donnell, MD, PhD.
The work builds on positive results from the 1950s and 1960s of LSD for alcoholism, before LSD research was largely abandoned. Researchers such as Dr. O’Donnell are revisiting the approach, but with psilocybin because, among other reasons, it has less stigma and a shorter duration that allows for outpatient use (J Psychopharmacol. 2012 Jul;26[7]:994-1002). The Drug Enforcement Administration currently classifies psilocybin, the psychoactive ingredient in hallucinogenic, or “magic” mushrooms, as schedule I. The results found by Dr. O’Donnell’s team and other factors, such as the low risk of abuse tied to the use of psilocybin, are leading some researchers to suggest that the drug should be reclassified to “no more restrictively than schedule IV” (Neuropsychopharm. 2018 Nov;142:143-66).
Dr. O’Donnell’s presentation was part of a recurring theme at the annual meeting of the American Psychiatric Association – the transformation of what were once considered street drugs into therapeutic tools. Favorable results also were reported for 3,4-Methylenedioxymethamphetamine (MDMA), commonly known as ecstasy, for posttraumatic stress disorder; ketamine for depression and suicidality; and marijuana for pain and other problems.
Concerning psilocybin for alcohol use disorder (AUD), Dr. O’Donnell said: “Some people have really profound psychological experiences that shift the way they think about themselves and the way alcohol is affecting their relationships. Therapy can work with that shift in meaning [to create] lasting change.”
Many people “say that they get exactly what they needed.” Sometimes, patients revisit a past trauma but with a greater openness and flexibility – and a growing sense of peace. “They access affective states they just don’t have access to normally,” she said.
In another case, a woman hallucinated that she was sitting on a throne ascending through the universe, surrounded by the faces and voices of people she knew telling her she is a valuable and worthwhile person, and could take her place within the center of her universe without the sense of defectiveness and shame that often triggered her drinking. Happy little beer bottles told her: “We don’t need to be the enemy. We don’t need to be a part of your life,” Dr. O’Donnell said.
She and her team are pitting psilocybin against diphenhydramine as a control in the NYU AUD trial.
People are randomized, then undergo therapy focused equally on their alcohol use and preparing them for the drug experience. At week 4, they take their study medication – either 25 mg per 70 kg psilocybin or 50 mg diphenhydramine – in a relaxed living room–like setting, with classical or world music in the background. The study team avoids music with words in English. Two therapists, usually a man and a woman, are there as guides. The experience lasts a few hours; patients are debriefed afterward.
Patients undergo another round of counseling to understand the meaning of the experience, followed by a second dose, either 40 mg per 70 kg psilocybin or 100 mg diphenhydramine, at week 8. Patients are debriefed again and undergo a third month of counseling.
The results have not yet been unblinded, but Dr. O’Donnell and her team did find that, among their first 56 subjects, more intense mystical experiences, as gauged by the self-reported Mystical Experience Questionnaire (MEQ), correlated with greater treatment success.
Patients fill out the MEQ 8 hours after their dose, rating dimensions such as ego dissolution, oceanic boundlessness, joy, compassion, and openness. The maximum score is 1, the lowest 0, meaning no mystical effects. The median score among the 56 subjects was 0.26. The 30 or so patients who scored at or above that mark after their first medication session – as a group, their mean first MEQ score was 0.65 – reported a smaller percentage of drinking days at week 12 than those who scored below 0.26 (19% vs. 40%; P less than .05), with fewer drinks per drinking day (2.63 vs. 7.01; P less than .01); and lower craving (8.43 vs. 13.86 points on 30-point Penn Alcohol Craving Scale, P less than .01).
The groups were evenly matched at baseline. Both reported drinking an average of 3 out of 4 days, with an mean of 7.5 drinks per drinking day and a craving score of about 18. No differences were found in anxiety and depression scores, which were minimal in both groups.
More than half the subjects were men; the mean age was 46; and subjects were fairly well educated, reporting an average of 17 school years.
Dr. O’Donnell said she’s seen a range of experiences on psilocybin, but that bad trips are rare. Benzodiazepines are kept on hand, however, to help people who get too anxious, and an atypical antipsychotic is on hand to reverse hallucinatory effects.
Her team hopes to enroll 100 subjects and plans for follow-up past 12 weeks. Both Denver and Oakland, Calif., recently decriminalized psilocybin.
The work is being funded by the Heffter Research Institute. Dr. O’Donnell had no disclosures.
REPORTING FROM APA 2019
Would you be able to recognize the signs and symptoms of this particular drug overdose?
CASE 1
Two days after reviving her boyfriend with naloxone, a woman and her 30-year-old boyfriend presented to our family medicine clinic. They explained that he had injected heroin and shortly thereafter he stopped breathing and his lips turned blue. The patient’s girlfriend did not call emergency medical services (EMS) at the time because she was afraid of getting arrested due to past incarceration for possession of illegal drugs. Instead, she revived him with naloxone that she found in his bag.
Both the patient and his girlfriend were scared and surprised by his “terrible reaction,” as he had previously purchased heroin from the same dealer and used the same dose without similar effects. However, the patient did note that the drug he purchased this time had a bright white tinge, when normally the drug was light yellow.
On physical examination, the patient’s heart rate and blood pressure were normal. There were needle track marks on both forearms, elbows, and upper arms. A laboratory workup obtained during this visit revealed anemia and a normal basic metabolic panel. A hepatitis C virus antibody test was positive, and a hepatic function panel revealed elevated transaminase levels. Urine toxicology was positive for opioids and negative for other substances.
CASE 2
A 58-year-old man with a history of chronic hepatitis C, polysubstance abuse, and schizophrenia was transported to the emergency department by EMS after his family found him unresponsive in his bedroom. The patient had agonal breathing when EMS arrived, so they administered naloxone (4 mg intranasal and 4 mg intravenous). His breathing improved, but his mental status did not. He was still obtunded upon arrival in the emergency department and vomited 4 tan-colored patches. The patient was tachycardic (heart rate, 108 beats/min), hypertensive (blood pressure, 189/95 mm Hg), and had rapid shallow breathing (respiratory rate, 38 breaths/min). He was intubated for airway protection, at which time 2 more tan-colored patches were removed from his pharynx.
Laboratory evaluation revealed an acute kidney injury with a high anion metabolic acidosis. A hepatic function panel showed elevated transaminase levels. Plasma acetaminophen and salicylate levels were normal. A computed tomography head scan was normal. Urine toxicology was negative for opioids but was positive for cocaine and benzodiazepines.
THE DIAGNOSIS
Opioid overdose caused the acute respiratory depression in both cases. In Case 1, the patient unknowingly overdosed on heroin laced with fentanyl, known as China White, which likely caused the drug’s bright white tinge. In Case 2, the patient’s overdose was the result of oral ingestion of fentanyl patches. (Limited urine toxicology was negative for opiates because fentanyl is a fully synthetic opioid that shows up only with a specific or extended assay. More on this in a bit.)
DISCUSSION
The fatal drug overdose epidemic in the United States is growing. From 2000 to 2014, the mortality rate from drug overdose increased by 137%, including a 200% increase in the rate of overdose deaths related to opioids (ie, pain medications, heroin).1 Between 2013 and 2014, the age-adjusted mortality rate related to methadone, a synthetic opioid, remained unchanged; however, age-adjusted mortality rates related to natural and semisynthetic opioid pain medications, heroin, and synthetic opioids other than methadone (eg, fentanyl) increased by 9%, 26%, and 80%, respectively. In 2014, a sharp increase in overdose deaths related to synthetic opioids other than methadone coincided with law enforcement reports of increased availability of illegal fentanyl; however, the toxicology panel used by coroners and medical examiners at that time could not distinguish between illegal and prescription fentanyl.1
Continue to: Among 70,237 drug overdose deaths...
Among 70,237 drug overdose deaths in the United States in 2017, 47,600 (67.8%) involved an opioid. From 2013 to 2017, drug overdose death rates increased in 35 of 50 states and the District of Columbia, and significant increases in death rates involving synthetic opioids occurred in 15 out of 20 states, likely driven by illicitly manufactured fentanyl.2
Fentanyl-laced heroin: More common, but not new
In October 1991, 3-methylfentanyl was identified in 16 fatal drug overdoses in Allegheny County, Pennsylvania, contributing to a 4-fold increase in overdose deaths compared to the previous year. Fentanyl mixed with heroin and other drugs is commonly found in the Midwest, Northeast, and Southern regions of the United States; in 2014, more than 80% of fentanyl confiscations occurred in 10 states within these regions, with the highest incidence occurring in Ohio.3
When combined with fentanyl, heroin becomes 50 to 100 times more potent, resulting in a subjective high with exaggerated central nervous system depression manifesting as lethargy, miosis, and respiratory depression.4 Most drug users are unaware and unable to identify when heroin is laced with fentanyl, which may contribute to the rise in deaths from unintentional drug overdose.1,5,6
Oral abuse of fentanyl patches can be fatal
Outcomes from oral abuse of fentanyl patches have ranged from transient overdose symptoms, such as lethargy and respiratory depression, to death.7-9 When administered in a medical setting, transbuccal fentanyl has a bioavailability of 50% to 65% across the buccal membrane. Nearly 20% of the drug escapes hepatic first pass metabolism when fentanyl patches are ingested orally and enters the systemic circulation, resulting in severe overdose and potentially death. Prolonged chewing and sucking on fentanyl patches increases the contact time with the buccal membrane, resulting in increased systemic absorption compared to oral ingestion without chewing/sucking.7-9
Urine toxicology screening detects compounds based on a chemical assay for drugs—generally codeine, morphine, and their metabolites. Because fentanyl is a fully synthetic opioid, its structure is not
Continue to: Survival of fentanyl overdose depends on naloxone availability
Survival of fentanyl overdose depends on naloxone availability
Naloxone is a safe and effective antidote to an opioid overdose. It comes in 3 preparations, including intramuscular and subcutaneous injections and an intranasal spray.12 Concerns that naloxone will harm patients with opioid dependence are unfounded. Naloxone can induce symptoms of opioid withdrawal, such as yawning, lacrimation, piloerection, diaphoresis, myalgia, vomiting, and diarrhea. While these withdrawal symptoms are unpleasant, they are not life threatening.12 Due to its high potency, large doses of naloxone (ie, 4–16 mg) are required to reverse the effects of a fentanyl overdose.13 Intranasal naloxone hydrochloride 4 mg delivered in a single spray is preferred due to the ease of administration. Repeat doses may be necessary if respiratory depression continues or recurs prior to the arrival of emergency medical services. Increasing the availability of naloxone to first responders has the potential to save many lives.6
THE TAKEAWAY
Fentanyl is a major contributor to the growing drug overdose crisis in the United States. When laced with heroin or consumed orally in the form of transdermal patches, fentanyl becomes more potent and is increasingly fatal. It’s crucial that primary care physicians be able to identify and educate at-risk patients about the fatal consequences of fentanyl overdose and coordinate care to help get them into an appropriate rehabilitation program.
In order to quickly recognize the signs of fentanyl-related overdose, it’s important to be alert for this possibility. At the bedside, the most easily recognized abnormality associated with fentanyl or other opioid overdose is a decline in respiratory rate culminating in apnea.10 A respiratory rate of 12 breaths/min or less in a patient who is not in physiologic sleep strongly suggests acute opioid intoxication, particularly when accompanied by miosis or stupor. Other signs include bradycardia, hypotension, and seizures from anoxia.10
Apart from the severity of symptoms, it is hard to clinically distinguish fentanyl overdose from other opiate overdose incidents. Given the degree to which illegal opiates are contaminated with fentanyl in the United States,3 it is appropriate to screen for fentanyl with extended panel urine toxicology testing in patients with suspected opioid overdose.
CORRESPONDENCE
Jaividhya Dasarathy, MD, 2500 MetroHealth Medical Center, Cleveland, OH 44109; [email protected]
1. Rudd RA, Aleshire N, Zibbell JE, et al. Increases in drug and opioid overdose deaths—United States, 2000–2014. MMWR Morb Mortal Wkly Rep. 2016;64:1378-1382.
2. Scholl L, Seth P, Kariisa M, et al. Drug and opioid-involved overdose deaths—United States, 2013–2017. MMWR Morb Mortal Wkly Rep. 2019;67:1419-1427.
3. Hibbs J, Perper J, Winek CL. An outbreak of designer drug-related deaths in Pennsylvania. JAMA. 1991;265:1011-1013.
4. Increases in fentanyl drug confiscations and fentanyl-related overdose fatalities. Centers for Disease Control and Prevention Web site. https://emergency.cdc.gov/han/han00384.asp. Published October 26, 2015. Accessed May 3, 2019.
5. Fentanyl. Centers for Disease Control and Prevention Web site. https://www.cdc.gov/drugoverdose/opioids/fentanyl.html. Updated December 19, 2018. Accessed May 3, 2019.
6. Peterson AB, Gladden RM, Delcher C, et al. Increases in fentanyl-related overdose deaths—Florida and Ohio, 2013–2015. MMWR Morb Mortal Wkly Rep. 2016;65:844-849.
7. Streisand JB, Varvel JR, Stanski DR, et al. Absorption and bioavailability of oral transmucosal fentanyl citrate. Anesthesiology. 1991;75:223-229.
8. Kharasch ED, Whittington D, Hoffer C. Influence of hepatic and intestinal cytochrome P4503A activity on the acute disposition and effects of oral transmucosal fentanyl citrate. Anesthesiology. 2004;101:729-737.
9. Woodall KL, Martin TL, McLellan BA. Oral abuse of fentanyl patches (Duragesic): seven case reports. J Forensic Sci. 2008;53:222-225.
10. Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83:66-76.
11. Appropriate Use of Drug Testing in Clinical Addiction Medicine. American Society of Addiction Medicine Web site. https://www.asam.org/docs/default-source/quality-science/appropriate_use_of_drug_testing_in_clinical-1-(7).pdf?sfvrsn=2. Published April 5, 2017. Accessed May 30, 2019.
12. Boyer EW. Management of opioid analgesic overdose. N Engl J Med. 2012;367:146-155.
13. Drugs@FDA: FDA approved drug products. US Food and Drug Administration Web site. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=208411. Accessed May 22, 2019.
CASE 1
Two days after reviving her boyfriend with naloxone, a woman and her 30-year-old boyfriend presented to our family medicine clinic. They explained that he had injected heroin and shortly thereafter he stopped breathing and his lips turned blue. The patient’s girlfriend did not call emergency medical services (EMS) at the time because she was afraid of getting arrested due to past incarceration for possession of illegal drugs. Instead, she revived him with naloxone that she found in his bag.
Both the patient and his girlfriend were scared and surprised by his “terrible reaction,” as he had previously purchased heroin from the same dealer and used the same dose without similar effects. However, the patient did note that the drug he purchased this time had a bright white tinge, when normally the drug was light yellow.
On physical examination, the patient’s heart rate and blood pressure were normal. There were needle track marks on both forearms, elbows, and upper arms. A laboratory workup obtained during this visit revealed anemia and a normal basic metabolic panel. A hepatitis C virus antibody test was positive, and a hepatic function panel revealed elevated transaminase levels. Urine toxicology was positive for opioids and negative for other substances.
CASE 2
A 58-year-old man with a history of chronic hepatitis C, polysubstance abuse, and schizophrenia was transported to the emergency department by EMS after his family found him unresponsive in his bedroom. The patient had agonal breathing when EMS arrived, so they administered naloxone (4 mg intranasal and 4 mg intravenous). His breathing improved, but his mental status did not. He was still obtunded upon arrival in the emergency department and vomited 4 tan-colored patches. The patient was tachycardic (heart rate, 108 beats/min), hypertensive (blood pressure, 189/95 mm Hg), and had rapid shallow breathing (respiratory rate, 38 breaths/min). He was intubated for airway protection, at which time 2 more tan-colored patches were removed from his pharynx.
Laboratory evaluation revealed an acute kidney injury with a high anion metabolic acidosis. A hepatic function panel showed elevated transaminase levels. Plasma acetaminophen and salicylate levels were normal. A computed tomography head scan was normal. Urine toxicology was negative for opioids but was positive for cocaine and benzodiazepines.
THE DIAGNOSIS
Opioid overdose caused the acute respiratory depression in both cases. In Case 1, the patient unknowingly overdosed on heroin laced with fentanyl, known as China White, which likely caused the drug’s bright white tinge. In Case 2, the patient’s overdose was the result of oral ingestion of fentanyl patches. (Limited urine toxicology was negative for opiates because fentanyl is a fully synthetic opioid that shows up only with a specific or extended assay. More on this in a bit.)
DISCUSSION
The fatal drug overdose epidemic in the United States is growing. From 2000 to 2014, the mortality rate from drug overdose increased by 137%, including a 200% increase in the rate of overdose deaths related to opioids (ie, pain medications, heroin).1 Between 2013 and 2014, the age-adjusted mortality rate related to methadone, a synthetic opioid, remained unchanged; however, age-adjusted mortality rates related to natural and semisynthetic opioid pain medications, heroin, and synthetic opioids other than methadone (eg, fentanyl) increased by 9%, 26%, and 80%, respectively. In 2014, a sharp increase in overdose deaths related to synthetic opioids other than methadone coincided with law enforcement reports of increased availability of illegal fentanyl; however, the toxicology panel used by coroners and medical examiners at that time could not distinguish between illegal and prescription fentanyl.1
Continue to: Among 70,237 drug overdose deaths...
Among 70,237 drug overdose deaths in the United States in 2017, 47,600 (67.8%) involved an opioid. From 2013 to 2017, drug overdose death rates increased in 35 of 50 states and the District of Columbia, and significant increases in death rates involving synthetic opioids occurred in 15 out of 20 states, likely driven by illicitly manufactured fentanyl.2
Fentanyl-laced heroin: More common, but not new
In October 1991, 3-methylfentanyl was identified in 16 fatal drug overdoses in Allegheny County, Pennsylvania, contributing to a 4-fold increase in overdose deaths compared to the previous year. Fentanyl mixed with heroin and other drugs is commonly found in the Midwest, Northeast, and Southern regions of the United States; in 2014, more than 80% of fentanyl confiscations occurred in 10 states within these regions, with the highest incidence occurring in Ohio.3
When combined with fentanyl, heroin becomes 50 to 100 times more potent, resulting in a subjective high with exaggerated central nervous system depression manifesting as lethargy, miosis, and respiratory depression.4 Most drug users are unaware and unable to identify when heroin is laced with fentanyl, which may contribute to the rise in deaths from unintentional drug overdose.1,5,6
Oral abuse of fentanyl patches can be fatal
Outcomes from oral abuse of fentanyl patches have ranged from transient overdose symptoms, such as lethargy and respiratory depression, to death.7-9 When administered in a medical setting, transbuccal fentanyl has a bioavailability of 50% to 65% across the buccal membrane. Nearly 20% of the drug escapes hepatic first pass metabolism when fentanyl patches are ingested orally and enters the systemic circulation, resulting in severe overdose and potentially death. Prolonged chewing and sucking on fentanyl patches increases the contact time with the buccal membrane, resulting in increased systemic absorption compared to oral ingestion without chewing/sucking.7-9
Urine toxicology screening detects compounds based on a chemical assay for drugs—generally codeine, morphine, and their metabolites. Because fentanyl is a fully synthetic opioid, its structure is not
Continue to: Survival of fentanyl overdose depends on naloxone availability
Survival of fentanyl overdose depends on naloxone availability
Naloxone is a safe and effective antidote to an opioid overdose. It comes in 3 preparations, including intramuscular and subcutaneous injections and an intranasal spray.12 Concerns that naloxone will harm patients with opioid dependence are unfounded. Naloxone can induce symptoms of opioid withdrawal, such as yawning, lacrimation, piloerection, diaphoresis, myalgia, vomiting, and diarrhea. While these withdrawal symptoms are unpleasant, they are not life threatening.12 Due to its high potency, large doses of naloxone (ie, 4–16 mg) are required to reverse the effects of a fentanyl overdose.13 Intranasal naloxone hydrochloride 4 mg delivered in a single spray is preferred due to the ease of administration. Repeat doses may be necessary if respiratory depression continues or recurs prior to the arrival of emergency medical services. Increasing the availability of naloxone to first responders has the potential to save many lives.6
THE TAKEAWAY
Fentanyl is a major contributor to the growing drug overdose crisis in the United States. When laced with heroin or consumed orally in the form of transdermal patches, fentanyl becomes more potent and is increasingly fatal. It’s crucial that primary care physicians be able to identify and educate at-risk patients about the fatal consequences of fentanyl overdose and coordinate care to help get them into an appropriate rehabilitation program.
In order to quickly recognize the signs of fentanyl-related overdose, it’s important to be alert for this possibility. At the bedside, the most easily recognized abnormality associated with fentanyl or other opioid overdose is a decline in respiratory rate culminating in apnea.10 A respiratory rate of 12 breaths/min or less in a patient who is not in physiologic sleep strongly suggests acute opioid intoxication, particularly when accompanied by miosis or stupor. Other signs include bradycardia, hypotension, and seizures from anoxia.10
Apart from the severity of symptoms, it is hard to clinically distinguish fentanyl overdose from other opiate overdose incidents. Given the degree to which illegal opiates are contaminated with fentanyl in the United States,3 it is appropriate to screen for fentanyl with extended panel urine toxicology testing in patients with suspected opioid overdose.
CORRESPONDENCE
Jaividhya Dasarathy, MD, 2500 MetroHealth Medical Center, Cleveland, OH 44109; [email protected]
CASE 1
Two days after reviving her boyfriend with naloxone, a woman and her 30-year-old boyfriend presented to our family medicine clinic. They explained that he had injected heroin and shortly thereafter he stopped breathing and his lips turned blue. The patient’s girlfriend did not call emergency medical services (EMS) at the time because she was afraid of getting arrested due to past incarceration for possession of illegal drugs. Instead, she revived him with naloxone that she found in his bag.
Both the patient and his girlfriend were scared and surprised by his “terrible reaction,” as he had previously purchased heroin from the same dealer and used the same dose without similar effects. However, the patient did note that the drug he purchased this time had a bright white tinge, when normally the drug was light yellow.
On physical examination, the patient’s heart rate and blood pressure were normal. There were needle track marks on both forearms, elbows, and upper arms. A laboratory workup obtained during this visit revealed anemia and a normal basic metabolic panel. A hepatitis C virus antibody test was positive, and a hepatic function panel revealed elevated transaminase levels. Urine toxicology was positive for opioids and negative for other substances.
CASE 2
A 58-year-old man with a history of chronic hepatitis C, polysubstance abuse, and schizophrenia was transported to the emergency department by EMS after his family found him unresponsive in his bedroom. The patient had agonal breathing when EMS arrived, so they administered naloxone (4 mg intranasal and 4 mg intravenous). His breathing improved, but his mental status did not. He was still obtunded upon arrival in the emergency department and vomited 4 tan-colored patches. The patient was tachycardic (heart rate, 108 beats/min), hypertensive (blood pressure, 189/95 mm Hg), and had rapid shallow breathing (respiratory rate, 38 breaths/min). He was intubated for airway protection, at which time 2 more tan-colored patches were removed from his pharynx.
Laboratory evaluation revealed an acute kidney injury with a high anion metabolic acidosis. A hepatic function panel showed elevated transaminase levels. Plasma acetaminophen and salicylate levels were normal. A computed tomography head scan was normal. Urine toxicology was negative for opioids but was positive for cocaine and benzodiazepines.
THE DIAGNOSIS
Opioid overdose caused the acute respiratory depression in both cases. In Case 1, the patient unknowingly overdosed on heroin laced with fentanyl, known as China White, which likely caused the drug’s bright white tinge. In Case 2, the patient’s overdose was the result of oral ingestion of fentanyl patches. (Limited urine toxicology was negative for opiates because fentanyl is a fully synthetic opioid that shows up only with a specific or extended assay. More on this in a bit.)
DISCUSSION
The fatal drug overdose epidemic in the United States is growing. From 2000 to 2014, the mortality rate from drug overdose increased by 137%, including a 200% increase in the rate of overdose deaths related to opioids (ie, pain medications, heroin).1 Between 2013 and 2014, the age-adjusted mortality rate related to methadone, a synthetic opioid, remained unchanged; however, age-adjusted mortality rates related to natural and semisynthetic opioid pain medications, heroin, and synthetic opioids other than methadone (eg, fentanyl) increased by 9%, 26%, and 80%, respectively. In 2014, a sharp increase in overdose deaths related to synthetic opioids other than methadone coincided with law enforcement reports of increased availability of illegal fentanyl; however, the toxicology panel used by coroners and medical examiners at that time could not distinguish between illegal and prescription fentanyl.1
Continue to: Among 70,237 drug overdose deaths...
Among 70,237 drug overdose deaths in the United States in 2017, 47,600 (67.8%) involved an opioid. From 2013 to 2017, drug overdose death rates increased in 35 of 50 states and the District of Columbia, and significant increases in death rates involving synthetic opioids occurred in 15 out of 20 states, likely driven by illicitly manufactured fentanyl.2
Fentanyl-laced heroin: More common, but not new
In October 1991, 3-methylfentanyl was identified in 16 fatal drug overdoses in Allegheny County, Pennsylvania, contributing to a 4-fold increase in overdose deaths compared to the previous year. Fentanyl mixed with heroin and other drugs is commonly found in the Midwest, Northeast, and Southern regions of the United States; in 2014, more than 80% of fentanyl confiscations occurred in 10 states within these regions, with the highest incidence occurring in Ohio.3
When combined with fentanyl, heroin becomes 50 to 100 times more potent, resulting in a subjective high with exaggerated central nervous system depression manifesting as lethargy, miosis, and respiratory depression.4 Most drug users are unaware and unable to identify when heroin is laced with fentanyl, which may contribute to the rise in deaths from unintentional drug overdose.1,5,6
Oral abuse of fentanyl patches can be fatal
Outcomes from oral abuse of fentanyl patches have ranged from transient overdose symptoms, such as lethargy and respiratory depression, to death.7-9 When administered in a medical setting, transbuccal fentanyl has a bioavailability of 50% to 65% across the buccal membrane. Nearly 20% of the drug escapes hepatic first pass metabolism when fentanyl patches are ingested orally and enters the systemic circulation, resulting in severe overdose and potentially death. Prolonged chewing and sucking on fentanyl patches increases the contact time with the buccal membrane, resulting in increased systemic absorption compared to oral ingestion without chewing/sucking.7-9
Urine toxicology screening detects compounds based on a chemical assay for drugs—generally codeine, morphine, and their metabolites. Because fentanyl is a fully synthetic opioid, its structure is not
Continue to: Survival of fentanyl overdose depends on naloxone availability
Survival of fentanyl overdose depends on naloxone availability
Naloxone is a safe and effective antidote to an opioid overdose. It comes in 3 preparations, including intramuscular and subcutaneous injections and an intranasal spray.12 Concerns that naloxone will harm patients with opioid dependence are unfounded. Naloxone can induce symptoms of opioid withdrawal, such as yawning, lacrimation, piloerection, diaphoresis, myalgia, vomiting, and diarrhea. While these withdrawal symptoms are unpleasant, they are not life threatening.12 Due to its high potency, large doses of naloxone (ie, 4–16 mg) are required to reverse the effects of a fentanyl overdose.13 Intranasal naloxone hydrochloride 4 mg delivered in a single spray is preferred due to the ease of administration. Repeat doses may be necessary if respiratory depression continues or recurs prior to the arrival of emergency medical services. Increasing the availability of naloxone to first responders has the potential to save many lives.6
THE TAKEAWAY
Fentanyl is a major contributor to the growing drug overdose crisis in the United States. When laced with heroin or consumed orally in the form of transdermal patches, fentanyl becomes more potent and is increasingly fatal. It’s crucial that primary care physicians be able to identify and educate at-risk patients about the fatal consequences of fentanyl overdose and coordinate care to help get them into an appropriate rehabilitation program.
In order to quickly recognize the signs of fentanyl-related overdose, it’s important to be alert for this possibility. At the bedside, the most easily recognized abnormality associated with fentanyl or other opioid overdose is a decline in respiratory rate culminating in apnea.10 A respiratory rate of 12 breaths/min or less in a patient who is not in physiologic sleep strongly suggests acute opioid intoxication, particularly when accompanied by miosis or stupor. Other signs include bradycardia, hypotension, and seizures from anoxia.10
Apart from the severity of symptoms, it is hard to clinically distinguish fentanyl overdose from other opiate overdose incidents. Given the degree to which illegal opiates are contaminated with fentanyl in the United States,3 it is appropriate to screen for fentanyl with extended panel urine toxicology testing in patients with suspected opioid overdose.
CORRESPONDENCE
Jaividhya Dasarathy, MD, 2500 MetroHealth Medical Center, Cleveland, OH 44109; [email protected]
1. Rudd RA, Aleshire N, Zibbell JE, et al. Increases in drug and opioid overdose deaths—United States, 2000–2014. MMWR Morb Mortal Wkly Rep. 2016;64:1378-1382.
2. Scholl L, Seth P, Kariisa M, et al. Drug and opioid-involved overdose deaths—United States, 2013–2017. MMWR Morb Mortal Wkly Rep. 2019;67:1419-1427.
3. Hibbs J, Perper J, Winek CL. An outbreak of designer drug-related deaths in Pennsylvania. JAMA. 1991;265:1011-1013.
4. Increases in fentanyl drug confiscations and fentanyl-related overdose fatalities. Centers for Disease Control and Prevention Web site. https://emergency.cdc.gov/han/han00384.asp. Published October 26, 2015. Accessed May 3, 2019.
5. Fentanyl. Centers for Disease Control and Prevention Web site. https://www.cdc.gov/drugoverdose/opioids/fentanyl.html. Updated December 19, 2018. Accessed May 3, 2019.
6. Peterson AB, Gladden RM, Delcher C, et al. Increases in fentanyl-related overdose deaths—Florida and Ohio, 2013–2015. MMWR Morb Mortal Wkly Rep. 2016;65:844-849.
7. Streisand JB, Varvel JR, Stanski DR, et al. Absorption and bioavailability of oral transmucosal fentanyl citrate. Anesthesiology. 1991;75:223-229.
8. Kharasch ED, Whittington D, Hoffer C. Influence of hepatic and intestinal cytochrome P4503A activity on the acute disposition and effects of oral transmucosal fentanyl citrate. Anesthesiology. 2004;101:729-737.
9. Woodall KL, Martin TL, McLellan BA. Oral abuse of fentanyl patches (Duragesic): seven case reports. J Forensic Sci. 2008;53:222-225.
10. Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83:66-76.
11. Appropriate Use of Drug Testing in Clinical Addiction Medicine. American Society of Addiction Medicine Web site. https://www.asam.org/docs/default-source/quality-science/appropriate_use_of_drug_testing_in_clinical-1-(7).pdf?sfvrsn=2. Published April 5, 2017. Accessed May 30, 2019.
12. Boyer EW. Management of opioid analgesic overdose. N Engl J Med. 2012;367:146-155.
13. Drugs@FDA: FDA approved drug products. US Food and Drug Administration Web site. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=208411. Accessed May 22, 2019.
1. Rudd RA, Aleshire N, Zibbell JE, et al. Increases in drug and opioid overdose deaths—United States, 2000–2014. MMWR Morb Mortal Wkly Rep. 2016;64:1378-1382.
2. Scholl L, Seth P, Kariisa M, et al. Drug and opioid-involved overdose deaths—United States, 2013–2017. MMWR Morb Mortal Wkly Rep. 2019;67:1419-1427.
3. Hibbs J, Perper J, Winek CL. An outbreak of designer drug-related deaths in Pennsylvania. JAMA. 1991;265:1011-1013.
4. Increases in fentanyl drug confiscations and fentanyl-related overdose fatalities. Centers for Disease Control and Prevention Web site. https://emergency.cdc.gov/han/han00384.asp. Published October 26, 2015. Accessed May 3, 2019.
5. Fentanyl. Centers for Disease Control and Prevention Web site. https://www.cdc.gov/drugoverdose/opioids/fentanyl.html. Updated December 19, 2018. Accessed May 3, 2019.
6. Peterson AB, Gladden RM, Delcher C, et al. Increases in fentanyl-related overdose deaths—Florida and Ohio, 2013–2015. MMWR Morb Mortal Wkly Rep. 2016;65:844-849.
7. Streisand JB, Varvel JR, Stanski DR, et al. Absorption and bioavailability of oral transmucosal fentanyl citrate. Anesthesiology. 1991;75:223-229.
8. Kharasch ED, Whittington D, Hoffer C. Influence of hepatic and intestinal cytochrome P4503A activity on the acute disposition and effects of oral transmucosal fentanyl citrate. Anesthesiology. 2004;101:729-737.
9. Woodall KL, Martin TL, McLellan BA. Oral abuse of fentanyl patches (Duragesic): seven case reports. J Forensic Sci. 2008;53:222-225.
10. Moeller KE, Lee KC, Kissack JC. Urine drug screening: practical guide for clinicians. Mayo Clin Proc. 2008;83:66-76.
11. Appropriate Use of Drug Testing in Clinical Addiction Medicine. American Society of Addiction Medicine Web site. https://www.asam.org/docs/default-source/quality-science/appropriate_use_of_drug_testing_in_clinical-1-(7).pdf?sfvrsn=2. Published April 5, 2017. Accessed May 30, 2019.
12. Boyer EW. Management of opioid analgesic overdose. N Engl J Med. 2012;367:146-155.
13. Drugs@FDA: FDA approved drug products. US Food and Drug Administration Web site. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=208411. Accessed May 22, 2019.

Opioid prescriptions declined 33% over 5 years
Fewer opioid retail prescriptions are being filled, according to a new report issued by the American Medical Association Opioid Task Force.
Opioid prescribing declined by 33% over a 5-year period based on the total number of opioid retail prescriptions filled. Total prescriptions declined from 251.8 million in 2013 to 168.8 million in 2018, according to the report.
The numbers come as the most recent data from the Centers for Disease Control and Prevention show a leveling of deaths involving prescription opioids. The CDC data were most recently updated in January 2019 and cover the period 1999-2017.
A closer look shows that deaths involving prescription opioids, but not other synthetic narcotics, peaked in 2011 and have generally declined since then. Deaths involving other synthetic narcotics, however, have been rising, offsetting the reduction and keeping the total number of deaths involving opioids relatively stable between 2016 and 2017.
Other data released by the AMA Opioid Task Force show that physicians are increasing their use of state-level prescription drug monitoring programs (PDMPs).
In 2017, there were 1.5 million physicians registered to use state PDMPs. That number rose to 1.97 million in 2019. And the physicians are using PDMPs. In 2018, physicians made 460 million PDMP queries, up 56% from 2017 and up 651% from 2014.
More education about opioid prescribing is being sought, with 700,000 physicians completing CME training and accessing other training related to opioid prescribing, pain management, screening for substance use disorders, and other related topics.
While the report does show positive trends, the task force is calling for more action, including more access to naloxone and better access to mental health treatment.
The report notes that more than 66,000 physicians and other health professionals have a federal waiver to prescribe buprenorphine, up more than 28,000 since 2016.
A number of policy recommendations are made in the report, including removing inappropriate administrative burdens or barriers that delay access to medications used in medication-assisted treatment (MAT); removing barriers to comprehensive pain care and rehabilitation programs, and reforming the civil and criminal justice system to help ensure access to high-quality, evidence-based care for opioid use disorder.
“We are at a crossroads in our nation’s efforts to end the opioid epidemic,” AMA Opioid Task Force Chair Patrice A. Harris, MD, stated in the report. “It is time to end delays and barriers to medication-assisted treatment – evidence based care proven to save lives; time for payers, [pharmacy benefit managers] and pharmacy chains to reevaluate and revise policies that restrict opioid therapy to patients based on arbitrary thresholds; and time to commit to helping all patients access evidence-based care for pain and substance use disorders.”
Dr. Harris continued: “Physicians must continue to demonstrate leadership, but unless these actions occur, the progress we are making will not stop patients from dying.”
Fewer opioid retail prescriptions are being filled, according to a new report issued by the American Medical Association Opioid Task Force.
Opioid prescribing declined by 33% over a 5-year period based on the total number of opioid retail prescriptions filled. Total prescriptions declined from 251.8 million in 2013 to 168.8 million in 2018, according to the report.
The numbers come as the most recent data from the Centers for Disease Control and Prevention show a leveling of deaths involving prescription opioids. The CDC data were most recently updated in January 2019 and cover the period 1999-2017.
A closer look shows that deaths involving prescription opioids, but not other synthetic narcotics, peaked in 2011 and have generally declined since then. Deaths involving other synthetic narcotics, however, have been rising, offsetting the reduction and keeping the total number of deaths involving opioids relatively stable between 2016 and 2017.
Other data released by the AMA Opioid Task Force show that physicians are increasing their use of state-level prescription drug monitoring programs (PDMPs).
In 2017, there were 1.5 million physicians registered to use state PDMPs. That number rose to 1.97 million in 2019. And the physicians are using PDMPs. In 2018, physicians made 460 million PDMP queries, up 56% from 2017 and up 651% from 2014.
More education about opioid prescribing is being sought, with 700,000 physicians completing CME training and accessing other training related to opioid prescribing, pain management, screening for substance use disorders, and other related topics.
While the report does show positive trends, the task force is calling for more action, including more access to naloxone and better access to mental health treatment.
The report notes that more than 66,000 physicians and other health professionals have a federal waiver to prescribe buprenorphine, up more than 28,000 since 2016.
A number of policy recommendations are made in the report, including removing inappropriate administrative burdens or barriers that delay access to medications used in medication-assisted treatment (MAT); removing barriers to comprehensive pain care and rehabilitation programs, and reforming the civil and criminal justice system to help ensure access to high-quality, evidence-based care for opioid use disorder.
“We are at a crossroads in our nation’s efforts to end the opioid epidemic,” AMA Opioid Task Force Chair Patrice A. Harris, MD, stated in the report. “It is time to end delays and barriers to medication-assisted treatment – evidence based care proven to save lives; time for payers, [pharmacy benefit managers] and pharmacy chains to reevaluate and revise policies that restrict opioid therapy to patients based on arbitrary thresholds; and time to commit to helping all patients access evidence-based care for pain and substance use disorders.”
Dr. Harris continued: “Physicians must continue to demonstrate leadership, but unless these actions occur, the progress we are making will not stop patients from dying.”
Fewer opioid retail prescriptions are being filled, according to a new report issued by the American Medical Association Opioid Task Force.
Opioid prescribing declined by 33% over a 5-year period based on the total number of opioid retail prescriptions filled. Total prescriptions declined from 251.8 million in 2013 to 168.8 million in 2018, according to the report.
The numbers come as the most recent data from the Centers for Disease Control and Prevention show a leveling of deaths involving prescription opioids. The CDC data were most recently updated in January 2019 and cover the period 1999-2017.
A closer look shows that deaths involving prescription opioids, but not other synthetic narcotics, peaked in 2011 and have generally declined since then. Deaths involving other synthetic narcotics, however, have been rising, offsetting the reduction and keeping the total number of deaths involving opioids relatively stable between 2016 and 2017.
Other data released by the AMA Opioid Task Force show that physicians are increasing their use of state-level prescription drug monitoring programs (PDMPs).
In 2017, there were 1.5 million physicians registered to use state PDMPs. That number rose to 1.97 million in 2019. And the physicians are using PDMPs. In 2018, physicians made 460 million PDMP queries, up 56% from 2017 and up 651% from 2014.
More education about opioid prescribing is being sought, with 700,000 physicians completing CME training and accessing other training related to opioid prescribing, pain management, screening for substance use disorders, and other related topics.
While the report does show positive trends, the task force is calling for more action, including more access to naloxone and better access to mental health treatment.
The report notes that more than 66,000 physicians and other health professionals have a federal waiver to prescribe buprenorphine, up more than 28,000 since 2016.
A number of policy recommendations are made in the report, including removing inappropriate administrative burdens or barriers that delay access to medications used in medication-assisted treatment (MAT); removing barriers to comprehensive pain care and rehabilitation programs, and reforming the civil and criminal justice system to help ensure access to high-quality, evidence-based care for opioid use disorder.
“We are at a crossroads in our nation’s efforts to end the opioid epidemic,” AMA Opioid Task Force Chair Patrice A. Harris, MD, stated in the report. “It is time to end delays and barriers to medication-assisted treatment – evidence based care proven to save lives; time for payers, [pharmacy benefit managers] and pharmacy chains to reevaluate and revise policies that restrict opioid therapy to patients based on arbitrary thresholds; and time to commit to helping all patients access evidence-based care for pain and substance use disorders.”
Dr. Harris continued: “Physicians must continue to demonstrate leadership, but unless these actions occur, the progress we are making will not stop patients from dying.”
Pediatricians report low knowledge, comfort discussing e-cigarettes
BALTIMORE – according to a recent study.

“Providers are aware of the increased prevalence, harms [of e-cigs] and [the] positive impact of counseling teens about e-cigs,” said Allison Heinly, MD, of Hasbro Children’s Hospital in Providence, R.I., and her colleagues. But, “providers are less likely to ask, advise, or assist parents [and teens] regarding e-cig use, compared to tobacco, and are less comfortable doing so.” The researchers presented their findings at the Pediatric Academic Societies annual meeting.
A variety of concerns exist regarding ingredients in e-cigarettes, Dr. Heinly noted, including nicotine, volatile organic compounds, carcinogenic chemicals, flavorings, and ultra-fine particles.
Dr. Heinly and her associates aimed to assess pediatricians’ knowledge, attitudes, and behaviors toward both teens’ and parents’ use of e-cigarettes, as well as the barrier pediatricians perceived when it came to screening and counseling those who use e-cigarettes.
Among 69 providers at a large Northeastern urban academic primary care clinic who received surveys, 62 responded, primarily residents (84%). The respondents included 44 pediatric residents, eight triple-board residents, and 10 attending physicians.
The researchers collapsed “most of the time”/“always” and “some of the time”/“never” responses into two categories.
Most of the respondents (82%) knew e-cigarettes are the most common tobacco product that youth use, and nearly all (97%) believed e-cigarettes were addictive and harmful to users’ health. In addition, most (79%) believed using e-cigarettes could be a pathway toward students beginning to use other drugs.
Even though respondents believed counseling teens about use of tobacco or e-cigarettes can reduce the likelihood that they will start using them, providers were much less likely to discuss e-cigarettes than tobacco with teens.
Nearly all the doctors (97%) reported asking teens about their use of tobacco, but only about half (52%) asked about e-cigarette use (P less than .001). And only about one in five doctors (21%) reported counseling teens about using e-cigarettes, compared with 47% of those who advised teens regarding tobacco use (P = .002).
Over a third of responding physicians (37%) reported helping adolescent patients quit using tobacco, but just 7% reported doing so with e-cigarettes (P less than .001).
Doctors overwhelmingly reported feeling comfortable talking about tobacco with teens (98%), but fewer felt comfortable discussing e-cigarettes (77%; P less than .001). Respondents similarly were less comfortable discussing e-cigarettes (55%) than tobacco (87%) with parents (P less than .001).
Very few pediatricians asked parents about their use of e-cigarettes (5%) or advised them about e-cigarettes’ harms (7%), and even fewer reported helping parents quit using them (2%). By contrast, more than half of pediatricians (60%) asked parents about smoking or advised them about tobacco use harms (52%), and nearly one-third (31%) reported helping parents quit smoking (P less than .001 for all comparisons).
The biggest barrier to discussing e-cigarettes with families was, as with discussing tobacco, not having enough time. But about twice as many respondents cited insufficient knowledge as a barrier for e-cigarettes as for tobacco (P = .003). A small percentage of respondents (less than 20%) also reported feeling unsure about the harm of e-cigarettes (P = .001).
Lack of training was a significant barrier to physicians’ discussion of e-cigarettes as well. Many more physicians reported receiving training in medical school on tobacco and traditional cigarettes (78%) than on e-cigarettes (13%), possibly because of how recently e-cigarettes have become widely available (P less than .001).
More physicians reported receiving training related to e-cigarettes during residency (36%), but it still fell well short of how many reported other tobacco and smoking training during residency (61%; P = .001).
The findings “emphasize the importance of increasing training about e-cig counseling,” Dr. Heinly and her associates concluded.
The researchers noted no external funding or disclosures.
BALTIMORE – according to a recent study.
“Providers are aware of the increased prevalence, harms [of e-cigs] and [the] positive impact of counseling teens about e-cigs,” said Allison Heinly, MD, of Hasbro Children’s Hospital in Providence, R.I., and her colleagues. But, “providers are less likely to ask, advise, or assist parents [and teens] regarding e-cig use, compared to tobacco, and are less comfortable doing so.” The researchers presented their findings at the Pediatric Academic Societies annual meeting.
A variety of concerns exist regarding ingredients in e-cigarettes, Dr. Heinly noted, including nicotine, volatile organic compounds, carcinogenic chemicals, flavorings, and ultra-fine particles.
Dr. Heinly and her associates aimed to assess pediatricians’ knowledge, attitudes, and behaviors toward both teens’ and parents’ use of e-cigarettes, as well as the barrier pediatricians perceived when it came to screening and counseling those who use e-cigarettes.
Among 69 providers at a large Northeastern urban academic primary care clinic who received surveys, 62 responded, primarily residents (84%). The respondents included 44 pediatric residents, eight triple-board residents, and 10 attending physicians.
The researchers collapsed “most of the time”/“always” and “some of the time”/“never” responses into two categories.
Most of the respondents (82%) knew e-cigarettes are the most common tobacco product that youth use, and nearly all (97%) believed e-cigarettes were addictive and harmful to users’ health. In addition, most (79%) believed using e-cigarettes could be a pathway toward students beginning to use other drugs.
Even though respondents believed counseling teens about use of tobacco or e-cigarettes can reduce the likelihood that they will start using them, providers were much less likely to discuss e-cigarettes than tobacco with teens.
Nearly all the doctors (97%) reported asking teens about their use of tobacco, but only about half (52%) asked about e-cigarette use (P less than .001). And only about one in five doctors (21%) reported counseling teens about using e-cigarettes, compared with 47% of those who advised teens regarding tobacco use (P = .002).
Over a third of responding physicians (37%) reported helping adolescent patients quit using tobacco, but just 7% reported doing so with e-cigarettes (P less than .001).
Doctors overwhelmingly reported feeling comfortable talking about tobacco with teens (98%), but fewer felt comfortable discussing e-cigarettes (77%; P less than .001). Respondents similarly were less comfortable discussing e-cigarettes (55%) than tobacco (87%) with parents (P less than .001).
Very few pediatricians asked parents about their use of e-cigarettes (5%) or advised them about e-cigarettes’ harms (7%), and even fewer reported helping parents quit using them (2%). By contrast, more than half of pediatricians (60%) asked parents about smoking or advised them about tobacco use harms (52%), and nearly one-third (31%) reported helping parents quit smoking (P less than .001 for all comparisons).
The biggest barrier to discussing e-cigarettes with families was, as with discussing tobacco, not having enough time. But about twice as many respondents cited insufficient knowledge as a barrier for e-cigarettes as for tobacco (P = .003). A small percentage of respondents (less than 20%) also reported feeling unsure about the harm of e-cigarettes (P = .001).
Lack of training was a significant barrier to physicians’ discussion of e-cigarettes as well. Many more physicians reported receiving training in medical school on tobacco and traditional cigarettes (78%) than on e-cigarettes (13%), possibly because of how recently e-cigarettes have become widely available (P less than .001).
More physicians reported receiving training related to e-cigarettes during residency (36%), but it still fell well short of how many reported other tobacco and smoking training during residency (61%; P = .001).
The findings “emphasize the importance of increasing training about e-cig counseling,” Dr. Heinly and her associates concluded.
The researchers noted no external funding or disclosures.
BALTIMORE – according to a recent study.
“Providers are aware of the increased prevalence, harms [of e-cigs] and [the] positive impact of counseling teens about e-cigs,” said Allison Heinly, MD, of Hasbro Children’s Hospital in Providence, R.I., and her colleagues. But, “providers are less likely to ask, advise, or assist parents [and teens] regarding e-cig use, compared to tobacco, and are less comfortable doing so.” The researchers presented their findings at the Pediatric Academic Societies annual meeting.
A variety of concerns exist regarding ingredients in e-cigarettes, Dr. Heinly noted, including nicotine, volatile organic compounds, carcinogenic chemicals, flavorings, and ultra-fine particles.
Dr. Heinly and her associates aimed to assess pediatricians’ knowledge, attitudes, and behaviors toward both teens’ and parents’ use of e-cigarettes, as well as the barrier pediatricians perceived when it came to screening and counseling those who use e-cigarettes.
Among 69 providers at a large Northeastern urban academic primary care clinic who received surveys, 62 responded, primarily residents (84%). The respondents included 44 pediatric residents, eight triple-board residents, and 10 attending physicians.
The researchers collapsed “most of the time”/“always” and “some of the time”/“never” responses into two categories.
Most of the respondents (82%) knew e-cigarettes are the most common tobacco product that youth use, and nearly all (97%) believed e-cigarettes were addictive and harmful to users’ health. In addition, most (79%) believed using e-cigarettes could be a pathway toward students beginning to use other drugs.
Even though respondents believed counseling teens about use of tobacco or e-cigarettes can reduce the likelihood that they will start using them, providers were much less likely to discuss e-cigarettes than tobacco with teens.
Nearly all the doctors (97%) reported asking teens about their use of tobacco, but only about half (52%) asked about e-cigarette use (P less than .001). And only about one in five doctors (21%) reported counseling teens about using e-cigarettes, compared with 47% of those who advised teens regarding tobacco use (P = .002).
Over a third of responding physicians (37%) reported helping adolescent patients quit using tobacco, but just 7% reported doing so with e-cigarettes (P less than .001).
Doctors overwhelmingly reported feeling comfortable talking about tobacco with teens (98%), but fewer felt comfortable discussing e-cigarettes (77%; P less than .001). Respondents similarly were less comfortable discussing e-cigarettes (55%) than tobacco (87%) with parents (P less than .001).
Very few pediatricians asked parents about their use of e-cigarettes (5%) or advised them about e-cigarettes’ harms (7%), and even fewer reported helping parents quit using them (2%). By contrast, more than half of pediatricians (60%) asked parents about smoking or advised them about tobacco use harms (52%), and nearly one-third (31%) reported helping parents quit smoking (P less than .001 for all comparisons).
The biggest barrier to discussing e-cigarettes with families was, as with discussing tobacco, not having enough time. But about twice as many respondents cited insufficient knowledge as a barrier for e-cigarettes as for tobacco (P = .003). A small percentage of respondents (less than 20%) also reported feeling unsure about the harm of e-cigarettes (P = .001).
Lack of training was a significant barrier to physicians’ discussion of e-cigarettes as well. Many more physicians reported receiving training in medical school on tobacco and traditional cigarettes (78%) than on e-cigarettes (13%), possibly because of how recently e-cigarettes have become widely available (P less than .001).
More physicians reported receiving training related to e-cigarettes during residency (36%), but it still fell well short of how many reported other tobacco and smoking training during residency (61%; P = .001).
The findings “emphasize the importance of increasing training about e-cig counseling,” Dr. Heinly and her associates concluded.
The researchers noted no external funding or disclosures.
REPORTING FROM PAS 2019
Key clinical point: Physicians report less training and less comfort when discussing e-cigarettes with teens and parents than when discussing tobacco products.
Major finding: 7% of physicians reported helping adolescent patients quit using e-cigarettes, compared with 37% helping with quitting tobacco use (P less than .001).
Study details: The findings are based on a cross-sectional survey of 62 pediatric residents and attendings at a large urban academic primary care clinic in the Northeast.
Disclosures: The researchers noted no external funding or disclosures.