User login
Factors that change our brains; The APA’s stance on neuroimaging
Factors that change our brains
I greatly enjoyed Dr. Nasrallah’s editorial, “Your patient’s brain is different at every visit” (From the Editor,
In reading this editorial, it is clear that a myriad of factors we consider and address with our patients during each visit underly intricate neurobiologic mechanisms and processes that ever deepen our understanding of the brain. In discussing the changes taking place in our patients, I can’t help but wonder what changes are also occurring in our brains (as Dr. Nasrallah noted). What would be the resulting impact of these changes in our next patient interaction and/or subsequent interaction(s) with the same patient? Looking through the editorial’s bullet points, many (if not all) of the factors contributing to brain changes apply equally and naturally to clinicians as well as patients. In this light, the editorial serves not only as a broad guideline for patient psychoeducation but also as a reminder of wellness and well-being for clinicians.
As a “fresh-out-of-training” psychiatrist, I can definitely work on several of the factors, such as diet and exercise. Trainees and residents can be more susceptible to overlook and befall some of these factors and changes, and may already be basing the clinical advice they give to their patients on these same factors and changes. As a child psychiatrist, I value the importance of modeling healthy behaviors for my patients, and their families and with coworkers or colleagues. In accordance with the impact these factors have on our brains, it’s important to emphasize what we can do to further strengthen rapport and therapeutic value through modeling. I strive to model the desired behaviors, attitudes, and dynamics that are the external, observable manifestation or symptomology of what takes place in my brain. To do so, I understand I need to be mindful in proactively managing the contributing factors, such as those listed in Dr. Nasrallah’s editorial. I imagine patients and their families would easily notice if we are in suboptimal physical and/or mental health that results in us not being prompt, fully engaged, or receptive. I believe that attending to these facets during training falls under the umbrella of professionalism. Being a professional in our field often entails practicing what we preach. So, I’m grateful that what we preach is informed by our field’s exciting research, continued advancements, and expertise that benefits our patients and us professionally and personally.
Philip Yen-Tsun Liu, MD
Child and adolescent psychiatrist
innovaTel Telepsychiatry
San Antonio, Texas
Dr. Nasrallah responds
I would like to thank Dr. Liu for his thoughtful response to my editorial. He seems to be very cognizant of the fact that experiential neuroplasticity and brain tissue remodeling occurs in both the patient and physician. I admire his focus on psychoeducation, wellness, and professionalism. He is right that we as psychiatrists (and nurse practitioners) must be role models for our patients in multiple ways, because it may help enhance clinical outcomes and have a positive impact on their brains.
I would also like to point Dr. Liu to the editorial “The most powerful placebo is not a pill” (From the Editor,
Henry A. Nasrallah, MD
Editor-in-Chief
Sydney W. Souers Endowed Chair
Professor and Chairman
Department of Psychiatry and Behavioral Neuroscience
Saint Louis University School of Medicine
St. Louis, Missouri
The APA’s stance on neuroimaging
Can anyone in the modern world argue that the brain is irrelevant to psychiatry? Yet surprisingly, in September 2018, the American Psychiatric Association (APA) officially declared that neuroimaging of the brain has no clinical value in psychiatry.1
Unfortunately, the APA focused almost exclusively on functional magnetic resonance imaging (fMRI) and neglected an extensive library of studies of single-photon emission computed tomography (SPECT) and positron emission tomography (PET). The APA’s position on neuroimaging is as follows1,2:
- A neuroimaging finding must have a sensitivity and specificity (S/sp) of no less than 80%.
- The psychiatric imaging literature does not support using neuroimaging in psychiatric diagnostics or treatment.
- Neuroimaging has not had a significant impact on the diagnosis and treatment of psychiatric disorders.
The APA set unrealistic standards for biomarkers in a field that lacks pathologic markers of specific disease entities.3 Moreover, numerous widely used tests fall below the APA’s unrealistic S/sp cutoff, including the Hamilton Depression Rating Scale,4 Zung Depression Scale,5 the clock drawing test,6 and even the chest X-ray.3 Curiously, numerous replicated SPECT and PET studies were not included in the APA’s analysis.1-3 For example, in a study of 196 veterans, posttraumatic stress disorder was distinguished from traumatic brain injury with an S/sp of 0.92/0.85.7,8 Also, fluorodeoxyglucose (FDG)-PET has an S/sp of 0.84/0.74 in differentiating patients with Alzheimer’s disease from controls, while perfusion SPECT, using multi-detector cameras, has an S/sp of 0.93/0.84.3,9 Moreover, both FDG-PET and SPECT can differentiate other forms of dementia from Alzheimer’s disease, yielding an additional benefit compared to amyloid imaging alone.2,9 As President of the International Society of Applied Neuroimaging, I suggest neuroimaging should not be feared. Neuroimaging does not replace the diagnostician; rather, it aids him/her in a complex case.
Theodore A. Henderson, MD, PhD
President
Neuro-Luminance Brain Health Centers, Inc.
Denver, Colorado
Director
The Synaptic Space
Vice President
The Neuro-Laser Foundation
President
International Society of Applied Neuroimaging
Centennial, Colorado
Disclosure
The author has no ownership in, and receives no remuneration from, any neuroimaging company.
References
1. First MB, Drevets WC, Carter C, et al. Clinical applications of neuroimaging in psychiatric disorders. Am J Psychiatry. 2018:175:
2. First MB, Drevets WC, Carter C, et al. Data supplement for Clinical applications of neuroimaging in psychiatric disorders. Am J Psychiatry. 2018;175(suppl).
3. Henderson TA. Brain SPECT imaging in neuropsychiatric diagnosis and monitoring. EPatient. http://nmpangea.com/2018/10/09/738/. Published 2018. Accessed May 31, 2019.
4. Bagby RM, Ryder AG, Schuller DR, et al. The Hamilton Depression Rating Scale: has the gold standard become a lead weight? Am J Psychiatry. 2004;161(12):2163-2177.
5. Biggs JT, Wylie LT, Ziegler VE. Validity of the Zung Self-rating Depression Scale. Br J Psychiatry. 1978;132:381-385.
6. Seigerschmidt E, Mösch E, Siemen M, et al. The clock drawing test and questionable dementia: reliability and validity. Int J Geriatr Psychiatry. 2002;17(11):1048-1054.
7. Raji CA, Willeumier K, Taylor D, et al. Functional neuroimaging with default mode network regions distinguishes PTSD from TBI in a military veteran population. Brain Imaging Behav. 2015;9(3):527-534.
8. Amen DG, Raji CA, Willeumier K, et al. Functional neuroimaging distinguishes posttraumatic stress disorder from traumatic brain injury in focused and large community datasets. PLoS One. 2015;10(7):e0129659. doi: 10.1371/journal.pone.0129659.
9. Henderson TA. The diagnosis and evaluation of dementia and mild cognitive impairment with emphasis on SPECT perfusion neuroimaging. CNS Spectr. 2012;17(4):176-206.
Factors that change our brains
I greatly enjoyed Dr. Nasrallah’s editorial, “Your patient’s brain is different at every visit” (From the Editor,
In reading this editorial, it is clear that a myriad of factors we consider and address with our patients during each visit underly intricate neurobiologic mechanisms and processes that ever deepen our understanding of the brain. In discussing the changes taking place in our patients, I can’t help but wonder what changes are also occurring in our brains (as Dr. Nasrallah noted). What would be the resulting impact of these changes in our next patient interaction and/or subsequent interaction(s) with the same patient? Looking through the editorial’s bullet points, many (if not all) of the factors contributing to brain changes apply equally and naturally to clinicians as well as patients. In this light, the editorial serves not only as a broad guideline for patient psychoeducation but also as a reminder of wellness and well-being for clinicians.
As a “fresh-out-of-training” psychiatrist, I can definitely work on several of the factors, such as diet and exercise. Trainees and residents can be more susceptible to overlook and befall some of these factors and changes, and may already be basing the clinical advice they give to their patients on these same factors and changes. As a child psychiatrist, I value the importance of modeling healthy behaviors for my patients, and their families and with coworkers or colleagues. In accordance with the impact these factors have on our brains, it’s important to emphasize what we can do to further strengthen rapport and therapeutic value through modeling. I strive to model the desired behaviors, attitudes, and dynamics that are the external, observable manifestation or symptomology of what takes place in my brain. To do so, I understand I need to be mindful in proactively managing the contributing factors, such as those listed in Dr. Nasrallah’s editorial. I imagine patients and their families would easily notice if we are in suboptimal physical and/or mental health that results in us not being prompt, fully engaged, or receptive. I believe that attending to these facets during training falls under the umbrella of professionalism. Being a professional in our field often entails practicing what we preach. So, I’m grateful that what we preach is informed by our field’s exciting research, continued advancements, and expertise that benefits our patients and us professionally and personally.
Philip Yen-Tsun Liu, MD
Child and adolescent psychiatrist
innovaTel Telepsychiatry
San Antonio, Texas
Dr. Nasrallah responds
I would like to thank Dr. Liu for his thoughtful response to my editorial. He seems to be very cognizant of the fact that experiential neuroplasticity and brain tissue remodeling occurs in both the patient and physician. I admire his focus on psychoeducation, wellness, and professionalism. He is right that we as psychiatrists (and nurse practitioners) must be role models for our patients in multiple ways, because it may help enhance clinical outcomes and have a positive impact on their brains.
I would also like to point Dr. Liu to the editorial “The most powerful placebo is not a pill” (From the Editor,
Henry A. Nasrallah, MD
Editor-in-Chief
Sydney W. Souers Endowed Chair
Professor and Chairman
Department of Psychiatry and Behavioral Neuroscience
Saint Louis University School of Medicine
St. Louis, Missouri
The APA’s stance on neuroimaging
Can anyone in the modern world argue that the brain is irrelevant to psychiatry? Yet surprisingly, in September 2018, the American Psychiatric Association (APA) officially declared that neuroimaging of the brain has no clinical value in psychiatry.1
Unfortunately, the APA focused almost exclusively on functional magnetic resonance imaging (fMRI) and neglected an extensive library of studies of single-photon emission computed tomography (SPECT) and positron emission tomography (PET). The APA’s position on neuroimaging is as follows1,2:
- A neuroimaging finding must have a sensitivity and specificity (S/sp) of no less than 80%.
- The psychiatric imaging literature does not support using neuroimaging in psychiatric diagnostics or treatment.
- Neuroimaging has not had a significant impact on the diagnosis and treatment of psychiatric disorders.
The APA set unrealistic standards for biomarkers in a field that lacks pathologic markers of specific disease entities.3 Moreover, numerous widely used tests fall below the APA’s unrealistic S/sp cutoff, including the Hamilton Depression Rating Scale,4 Zung Depression Scale,5 the clock drawing test,6 and even the chest X-ray.3 Curiously, numerous replicated SPECT and PET studies were not included in the APA’s analysis.1-3 For example, in a study of 196 veterans, posttraumatic stress disorder was distinguished from traumatic brain injury with an S/sp of 0.92/0.85.7,8 Also, fluorodeoxyglucose (FDG)-PET has an S/sp of 0.84/0.74 in differentiating patients with Alzheimer’s disease from controls, while perfusion SPECT, using multi-detector cameras, has an S/sp of 0.93/0.84.3,9 Moreover, both FDG-PET and SPECT can differentiate other forms of dementia from Alzheimer’s disease, yielding an additional benefit compared to amyloid imaging alone.2,9 As President of the International Society of Applied Neuroimaging, I suggest neuroimaging should not be feared. Neuroimaging does not replace the diagnostician; rather, it aids him/her in a complex case.
Theodore A. Henderson, MD, PhD
President
Neuro-Luminance Brain Health Centers, Inc.
Denver, Colorado
Director
The Synaptic Space
Vice President
The Neuro-Laser Foundation
President
International Society of Applied Neuroimaging
Centennial, Colorado
Disclosure
The author has no ownership in, and receives no remuneration from, any neuroimaging company.
References
1. First MB, Drevets WC, Carter C, et al. Clinical applications of neuroimaging in psychiatric disorders. Am J Psychiatry. 2018:175:
2. First MB, Drevets WC, Carter C, et al. Data supplement for Clinical applications of neuroimaging in psychiatric disorders. Am J Psychiatry. 2018;175(suppl).
3. Henderson TA. Brain SPECT imaging in neuropsychiatric diagnosis and monitoring. EPatient. http://nmpangea.com/2018/10/09/738/. Published 2018. Accessed May 31, 2019.
4. Bagby RM, Ryder AG, Schuller DR, et al. The Hamilton Depression Rating Scale: has the gold standard become a lead weight? Am J Psychiatry. 2004;161(12):2163-2177.
5. Biggs JT, Wylie LT, Ziegler VE. Validity of the Zung Self-rating Depression Scale. Br J Psychiatry. 1978;132:381-385.
6. Seigerschmidt E, Mösch E, Siemen M, et al. The clock drawing test and questionable dementia: reliability and validity. Int J Geriatr Psychiatry. 2002;17(11):1048-1054.
7. Raji CA, Willeumier K, Taylor D, et al. Functional neuroimaging with default mode network regions distinguishes PTSD from TBI in a military veteran population. Brain Imaging Behav. 2015;9(3):527-534.
8. Amen DG, Raji CA, Willeumier K, et al. Functional neuroimaging distinguishes posttraumatic stress disorder from traumatic brain injury in focused and large community datasets. PLoS One. 2015;10(7):e0129659. doi: 10.1371/journal.pone.0129659.
9. Henderson TA. The diagnosis and evaluation of dementia and mild cognitive impairment with emphasis on SPECT perfusion neuroimaging. CNS Spectr. 2012;17(4):176-206.
Factors that change our brains
I greatly enjoyed Dr. Nasrallah’s editorial, “Your patient’s brain is different at every visit” (From the Editor,
In reading this editorial, it is clear that a myriad of factors we consider and address with our patients during each visit underly intricate neurobiologic mechanisms and processes that ever deepen our understanding of the brain. In discussing the changes taking place in our patients, I can’t help but wonder what changes are also occurring in our brains (as Dr. Nasrallah noted). What would be the resulting impact of these changes in our next patient interaction and/or subsequent interaction(s) with the same patient? Looking through the editorial’s bullet points, many (if not all) of the factors contributing to brain changes apply equally and naturally to clinicians as well as patients. In this light, the editorial serves not only as a broad guideline for patient psychoeducation but also as a reminder of wellness and well-being for clinicians.
As a “fresh-out-of-training” psychiatrist, I can definitely work on several of the factors, such as diet and exercise. Trainees and residents can be more susceptible to overlook and befall some of these factors and changes, and may already be basing the clinical advice they give to their patients on these same factors and changes. As a child psychiatrist, I value the importance of modeling healthy behaviors for my patients, and their families and with coworkers or colleagues. In accordance with the impact these factors have on our brains, it’s important to emphasize what we can do to further strengthen rapport and therapeutic value through modeling. I strive to model the desired behaviors, attitudes, and dynamics that are the external, observable manifestation or symptomology of what takes place in my brain. To do so, I understand I need to be mindful in proactively managing the contributing factors, such as those listed in Dr. Nasrallah’s editorial. I imagine patients and their families would easily notice if we are in suboptimal physical and/or mental health that results in us not being prompt, fully engaged, or receptive. I believe that attending to these facets during training falls under the umbrella of professionalism. Being a professional in our field often entails practicing what we preach. So, I’m grateful that what we preach is informed by our field’s exciting research, continued advancements, and expertise that benefits our patients and us professionally and personally.
Philip Yen-Tsun Liu, MD
Child and adolescent psychiatrist
innovaTel Telepsychiatry
San Antonio, Texas
Dr. Nasrallah responds
I would like to thank Dr. Liu for his thoughtful response to my editorial. He seems to be very cognizant of the fact that experiential neuroplasticity and brain tissue remodeling occurs in both the patient and physician. I admire his focus on psychoeducation, wellness, and professionalism. He is right that we as psychiatrists (and nurse practitioners) must be role models for our patients in multiple ways, because it may help enhance clinical outcomes and have a positive impact on their brains.
I would also like to point Dr. Liu to the editorial “The most powerful placebo is not a pill” (From the Editor,
Henry A. Nasrallah, MD
Editor-in-Chief
Sydney W. Souers Endowed Chair
Professor and Chairman
Department of Psychiatry and Behavioral Neuroscience
Saint Louis University School of Medicine
St. Louis, Missouri
The APA’s stance on neuroimaging
Can anyone in the modern world argue that the brain is irrelevant to psychiatry? Yet surprisingly, in September 2018, the American Psychiatric Association (APA) officially declared that neuroimaging of the brain has no clinical value in psychiatry.1
Unfortunately, the APA focused almost exclusively on functional magnetic resonance imaging (fMRI) and neglected an extensive library of studies of single-photon emission computed tomography (SPECT) and positron emission tomography (PET). The APA’s position on neuroimaging is as follows1,2:
- A neuroimaging finding must have a sensitivity and specificity (S/sp) of no less than 80%.
- The psychiatric imaging literature does not support using neuroimaging in psychiatric diagnostics or treatment.
- Neuroimaging has not had a significant impact on the diagnosis and treatment of psychiatric disorders.
The APA set unrealistic standards for biomarkers in a field that lacks pathologic markers of specific disease entities.3 Moreover, numerous widely used tests fall below the APA’s unrealistic S/sp cutoff, including the Hamilton Depression Rating Scale,4 Zung Depression Scale,5 the clock drawing test,6 and even the chest X-ray.3 Curiously, numerous replicated SPECT and PET studies were not included in the APA’s analysis.1-3 For example, in a study of 196 veterans, posttraumatic stress disorder was distinguished from traumatic brain injury with an S/sp of 0.92/0.85.7,8 Also, fluorodeoxyglucose (FDG)-PET has an S/sp of 0.84/0.74 in differentiating patients with Alzheimer’s disease from controls, while perfusion SPECT, using multi-detector cameras, has an S/sp of 0.93/0.84.3,9 Moreover, both FDG-PET and SPECT can differentiate other forms of dementia from Alzheimer’s disease, yielding an additional benefit compared to amyloid imaging alone.2,9 As President of the International Society of Applied Neuroimaging, I suggest neuroimaging should not be feared. Neuroimaging does not replace the diagnostician; rather, it aids him/her in a complex case.
Theodore A. Henderson, MD, PhD
President
Neuro-Luminance Brain Health Centers, Inc.
Denver, Colorado
Director
The Synaptic Space
Vice President
The Neuro-Laser Foundation
President
International Society of Applied Neuroimaging
Centennial, Colorado
Disclosure
The author has no ownership in, and receives no remuneration from, any neuroimaging company.
References
1. First MB, Drevets WC, Carter C, et al. Clinical applications of neuroimaging in psychiatric disorders. Am J Psychiatry. 2018:175:
2. First MB, Drevets WC, Carter C, et al. Data supplement for Clinical applications of neuroimaging in psychiatric disorders. Am J Psychiatry. 2018;175(suppl).
3. Henderson TA. Brain SPECT imaging in neuropsychiatric diagnosis and monitoring. EPatient. http://nmpangea.com/2018/10/09/738/. Published 2018. Accessed May 31, 2019.
4. Bagby RM, Ryder AG, Schuller DR, et al. The Hamilton Depression Rating Scale: has the gold standard become a lead weight? Am J Psychiatry. 2004;161(12):2163-2177.
5. Biggs JT, Wylie LT, Ziegler VE. Validity of the Zung Self-rating Depression Scale. Br J Psychiatry. 1978;132:381-385.
6. Seigerschmidt E, Mösch E, Siemen M, et al. The clock drawing test and questionable dementia: reliability and validity. Int J Geriatr Psychiatry. 2002;17(11):1048-1054.
7. Raji CA, Willeumier K, Taylor D, et al. Functional neuroimaging with default mode network regions distinguishes PTSD from TBI in a military veteran population. Brain Imaging Behav. 2015;9(3):527-534.
8. Amen DG, Raji CA, Willeumier K, et al. Functional neuroimaging distinguishes posttraumatic stress disorder from traumatic brain injury in focused and large community datasets. PLoS One. 2015;10(7):e0129659. doi: 10.1371/journal.pone.0129659.
9. Henderson TA. The diagnosis and evaluation of dementia and mild cognitive impairment with emphasis on SPECT perfusion neuroimaging. CNS Spectr. 2012;17(4):176-206.
The 21st Century Cures Act: Tearing down fortresses to put patients first
"A fortress not only protects those inside of it, but it also enslaves them to work.”
– Anthony T. Hincks
As physicians, we spend a great deal of time intending to do our best for the people we serve. We believe fundamentally in the idea that our patients come first, and we toil daily to exercise that belief. We also want our patients to feel they are driving their care as active participants along the journey. Yet time and time again, despite our greatest attempts, those efforts are stymied by the state of modern medicine;

Over the past 10 years, we have done a tremendous job of constructing expensive fortresses around patient information known as electronic health records (EHRs). Billions of dollars have been spent implementing, upgrading, and optimizing. In spite of this, physicians are increasingly frustrated by EHRs (and in many cases, long to return to the days of paper). It isn’t surprising, then, that patients are frustrated as well. We use terms such as “patient-centered care,” but patients feel like they are not in the center at all. Instead, they can find themselves feeling like complete outsiders, at the mercy of the medical juggernaut to make sure they have the appropriate information when they need it. There are several issues that contribute to the frustrations of physicians and patients, but two in particular warrant attention. The first is the diversity of Health IT systems and ongoing issues with EHR interoperability. The second is a provincial attitude surrounding transparency and medical record ownership. We will discuss both of these here, as well as recent legislation designed to advance both concerns.
We have written in previous columns about the many challenges of interoperability. Electronic health records, sold by different vendors, typically won’t “talk” to each other. In spite of years of maturation, issues of compatibility remain. Patient data locked inside of one EHR is not easily accessible by a physician using a different EHR. While efforts have been made to streamline information sharing, there are still many fortresses that cannot be breached.
Bridging the moat
The 21st Century Cures Act, enacted by Congress in December of 2016, seeks to define and require interoperability while addressing many other significant problems in health care. According to the legislation, true interoperability means that health IT should enable the secure exchange of electronic health information with other electronic record systems without special effort on the part of the user; the process should be seamless and shouldn’t be cumbersome for physicians or patients. It also must be fully supported by EHR vendors, but those vendors have been expressing significant concerns with the ways in which the act is being interpreted.
In a recent blog post, the HIMSS Electronic Health Record Association – a consortium of vendors including Epic, Allscripts, eClinicalWorks, as well as several others – expressed “significant concerns regarding timelines, ambiguous language, disincentives for innovation, and definitions related to information blocking.”1 This is not surprising, as the onus for improving interoperability falls squarely on their shoulders, and the work to get there is arduous. Regardless of one’s interpretation, the goal of the Cures act is clear: Arrive at true interoperability in the shortest period of time, while eliminating barriers that prevent patients from accessing their health records. In other words, it asks for the avoidance of “information blocking.”
Breaching the gate
Information blocking, as defined by the Cures Act, is “a practice by a health care provider, health IT developer, health information exchange, or health information network that … is likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information.”2 This practice is explicitly prohibited by the legislation – and is ethically wrong – yet it continues to occur implicitly every day as it has for many years. Even if unintentional and solely because of the growing complexity of our information systems, it makes accessing health information incredibly cumbersome for patients. Even worse, attempts to improve patients’ ability to access their health records have only created additional obstacles.
HIPAA (the Health Insurance Portability and Accountability Act of 1996) was designed to protect patient confidentiality and create security around protected health information. While noble in purpose, many have found it burdensome to work within the parameters set forth in the law. Physicians and patients needing legitimate access to clinical data discover endless release forms and convoluted processes standing in their way. Access to the information eventually comes in the form of reams of printed paper or faxed notes that cannot be easily consumed by or integrated into other systems.
The Meaningful Use initiative, while envisioned to improve data exchange and enhance population health, did little to help. Instead of enabling documentation efficiency and improving patient access, it promoted the proliferation of incompatible EHRs and poorly conceived patient portals. It also created heavy costs for both the federal government and physicians and was largely ineffective at producing systems whose use could be considered meaningful. The federal government paid out as much as $44,000 per physician to incentivize them to purchase medical records, while physicians often spent more than the $44,000 and, in many cases, wound up with EHRs that didn’t work well and had to be replaced.
Authors and supporters of the 21st Century Cures Act are hoping to avoid the shortcomings of prior legislation by attaching financial penalties to health care providers or IT vendors who engage in information blocking. While allowing for exceptions in appropriate cases, the law is clear: Patients deserve complete access to their medical records. While this goes against tradition, it has been proven to result in better outcomes.
Initiatives such as the OpenNotes movement have been pushing the value of full transparency for some time, and their website includes a long list of numerous examples to prove it. Indeed, several studies have demonstrated increased physician and patient satisfaction when both parties have ready access to health information. We believe that we, as physicians, should fully support the idea and lobby our EHR vendors to do the same.
It is time to tear down the impenetrable fortresses of traditional medicine, then work diligently to rebuild them with our patients safely inside.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
References
1. The Electronic Health Record Association blog
"A fortress not only protects those inside of it, but it also enslaves them to work.”
– Anthony T. Hincks
As physicians, we spend a great deal of time intending to do our best for the people we serve. We believe fundamentally in the idea that our patients come first, and we toil daily to exercise that belief. We also want our patients to feel they are driving their care as active participants along the journey. Yet time and time again, despite our greatest attempts, those efforts are stymied by the state of modern medicine;
Over the past 10 years, we have done a tremendous job of constructing expensive fortresses around patient information known as electronic health records (EHRs). Billions of dollars have been spent implementing, upgrading, and optimizing. In spite of this, physicians are increasingly frustrated by EHRs (and in many cases, long to return to the days of paper). It isn’t surprising, then, that patients are frustrated as well. We use terms such as “patient-centered care,” but patients feel like they are not in the center at all. Instead, they can find themselves feeling like complete outsiders, at the mercy of the medical juggernaut to make sure they have the appropriate information when they need it. There are several issues that contribute to the frustrations of physicians and patients, but two in particular warrant attention. The first is the diversity of Health IT systems and ongoing issues with EHR interoperability. The second is a provincial attitude surrounding transparency and medical record ownership. We will discuss both of these here, as well as recent legislation designed to advance both concerns.
We have written in previous columns about the many challenges of interoperability. Electronic health records, sold by different vendors, typically won’t “talk” to each other. In spite of years of maturation, issues of compatibility remain. Patient data locked inside of one EHR is not easily accessible by a physician using a different EHR. While efforts have been made to streamline information sharing, there are still many fortresses that cannot be breached.
Bridging the moat
The 21st Century Cures Act, enacted by Congress in December of 2016, seeks to define and require interoperability while addressing many other significant problems in health care. According to the legislation, true interoperability means that health IT should enable the secure exchange of electronic health information with other electronic record systems without special effort on the part of the user; the process should be seamless and shouldn’t be cumbersome for physicians or patients. It also must be fully supported by EHR vendors, but those vendors have been expressing significant concerns with the ways in which the act is being interpreted.
In a recent blog post, the HIMSS Electronic Health Record Association – a consortium of vendors including Epic, Allscripts, eClinicalWorks, as well as several others – expressed “significant concerns regarding timelines, ambiguous language, disincentives for innovation, and definitions related to information blocking.”1 This is not surprising, as the onus for improving interoperability falls squarely on their shoulders, and the work to get there is arduous. Regardless of one’s interpretation, the goal of the Cures act is clear: Arrive at true interoperability in the shortest period of time, while eliminating barriers that prevent patients from accessing their health records. In other words, it asks for the avoidance of “information blocking.”
Breaching the gate
Information blocking, as defined by the Cures Act, is “a practice by a health care provider, health IT developer, health information exchange, or health information network that … is likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information.”2 This practice is explicitly prohibited by the legislation – and is ethically wrong – yet it continues to occur implicitly every day as it has for many years. Even if unintentional and solely because of the growing complexity of our information systems, it makes accessing health information incredibly cumbersome for patients. Even worse, attempts to improve patients’ ability to access their health records have only created additional obstacles.
HIPAA (the Health Insurance Portability and Accountability Act of 1996) was designed to protect patient confidentiality and create security around protected health information. While noble in purpose, many have found it burdensome to work within the parameters set forth in the law. Physicians and patients needing legitimate access to clinical data discover endless release forms and convoluted processes standing in their way. Access to the information eventually comes in the form of reams of printed paper or faxed notes that cannot be easily consumed by or integrated into other systems.
The Meaningful Use initiative, while envisioned to improve data exchange and enhance population health, did little to help. Instead of enabling documentation efficiency and improving patient access, it promoted the proliferation of incompatible EHRs and poorly conceived patient portals. It also created heavy costs for both the federal government and physicians and was largely ineffective at producing systems whose use could be considered meaningful. The federal government paid out as much as $44,000 per physician to incentivize them to purchase medical records, while physicians often spent more than the $44,000 and, in many cases, wound up with EHRs that didn’t work well and had to be replaced.
Authors and supporters of the 21st Century Cures Act are hoping to avoid the shortcomings of prior legislation by attaching financial penalties to health care providers or IT vendors who engage in information blocking. While allowing for exceptions in appropriate cases, the law is clear: Patients deserve complete access to their medical records. While this goes against tradition, it has been proven to result in better outcomes.
Initiatives such as the OpenNotes movement have been pushing the value of full transparency for some time, and their website includes a long list of numerous examples to prove it. Indeed, several studies have demonstrated increased physician and patient satisfaction when both parties have ready access to health information. We believe that we, as physicians, should fully support the idea and lobby our EHR vendors to do the same.
It is time to tear down the impenetrable fortresses of traditional medicine, then work diligently to rebuild them with our patients safely inside.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
References
1. The Electronic Health Record Association blog
"A fortress not only protects those inside of it, but it also enslaves them to work.”
– Anthony T. Hincks
As physicians, we spend a great deal of time intending to do our best for the people we serve. We believe fundamentally in the idea that our patients come first, and we toil daily to exercise that belief. We also want our patients to feel they are driving their care as active participants along the journey. Yet time and time again, despite our greatest attempts, those efforts are stymied by the state of modern medicine;
Over the past 10 years, we have done a tremendous job of constructing expensive fortresses around patient information known as electronic health records (EHRs). Billions of dollars have been spent implementing, upgrading, and optimizing. In spite of this, physicians are increasingly frustrated by EHRs (and in many cases, long to return to the days of paper). It isn’t surprising, then, that patients are frustrated as well. We use terms such as “patient-centered care,” but patients feel like they are not in the center at all. Instead, they can find themselves feeling like complete outsiders, at the mercy of the medical juggernaut to make sure they have the appropriate information when they need it. There are several issues that contribute to the frustrations of physicians and patients, but two in particular warrant attention. The first is the diversity of Health IT systems and ongoing issues with EHR interoperability. The second is a provincial attitude surrounding transparency and medical record ownership. We will discuss both of these here, as well as recent legislation designed to advance both concerns.
We have written in previous columns about the many challenges of interoperability. Electronic health records, sold by different vendors, typically won’t “talk” to each other. In spite of years of maturation, issues of compatibility remain. Patient data locked inside of one EHR is not easily accessible by a physician using a different EHR. While efforts have been made to streamline information sharing, there are still many fortresses that cannot be breached.
Bridging the moat
The 21st Century Cures Act, enacted by Congress in December of 2016, seeks to define and require interoperability while addressing many other significant problems in health care. According to the legislation, true interoperability means that health IT should enable the secure exchange of electronic health information with other electronic record systems without special effort on the part of the user; the process should be seamless and shouldn’t be cumbersome for physicians or patients. It also must be fully supported by EHR vendors, but those vendors have been expressing significant concerns with the ways in which the act is being interpreted.
In a recent blog post, the HIMSS Electronic Health Record Association – a consortium of vendors including Epic, Allscripts, eClinicalWorks, as well as several others – expressed “significant concerns regarding timelines, ambiguous language, disincentives for innovation, and definitions related to information blocking.”1 This is not surprising, as the onus for improving interoperability falls squarely on their shoulders, and the work to get there is arduous. Regardless of one’s interpretation, the goal of the Cures act is clear: Arrive at true interoperability in the shortest period of time, while eliminating barriers that prevent patients from accessing their health records. In other words, it asks for the avoidance of “information blocking.”
Breaching the gate
Information blocking, as defined by the Cures Act, is “a practice by a health care provider, health IT developer, health information exchange, or health information network that … is likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information.”2 This practice is explicitly prohibited by the legislation – and is ethically wrong – yet it continues to occur implicitly every day as it has for many years. Even if unintentional and solely because of the growing complexity of our information systems, it makes accessing health information incredibly cumbersome for patients. Even worse, attempts to improve patients’ ability to access their health records have only created additional obstacles.
HIPAA (the Health Insurance Portability and Accountability Act of 1996) was designed to protect patient confidentiality and create security around protected health information. While noble in purpose, many have found it burdensome to work within the parameters set forth in the law. Physicians and patients needing legitimate access to clinical data discover endless release forms and convoluted processes standing in their way. Access to the information eventually comes in the form of reams of printed paper or faxed notes that cannot be easily consumed by or integrated into other systems.
The Meaningful Use initiative, while envisioned to improve data exchange and enhance population health, did little to help. Instead of enabling documentation efficiency and improving patient access, it promoted the proliferation of incompatible EHRs and poorly conceived patient portals. It also created heavy costs for both the federal government and physicians and was largely ineffective at producing systems whose use could be considered meaningful. The federal government paid out as much as $44,000 per physician to incentivize them to purchase medical records, while physicians often spent more than the $44,000 and, in many cases, wound up with EHRs that didn’t work well and had to be replaced.
Authors and supporters of the 21st Century Cures Act are hoping to avoid the shortcomings of prior legislation by attaching financial penalties to health care providers or IT vendors who engage in information blocking. While allowing for exceptions in appropriate cases, the law is clear: Patients deserve complete access to their medical records. While this goes against tradition, it has been proven to result in better outcomes.
Initiatives such as the OpenNotes movement have been pushing the value of full transparency for some time, and their website includes a long list of numerous examples to prove it. Indeed, several studies have demonstrated increased physician and patient satisfaction when both parties have ready access to health information. We believe that we, as physicians, should fully support the idea and lobby our EHR vendors to do the same.
It is time to tear down the impenetrable fortresses of traditional medicine, then work diligently to rebuild them with our patients safely inside.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
References
1. The Electronic Health Record Association blog
Scoring below the cut but still depressed: What to do?
Depression is one of the most common mental health conditions in childhood, especially during socially turbulent adolescence when the brain is rapidly changing and parent-child relationships are strained by the teen’s striving for independence and identity. Often parents of teens call me worrying about possible depression, but in the next breath say “but maybe it is just puberty.” Because suicide is one of the most common causes of death among teens and is often associated with depression, we pediatricians have the scary job of sorting out symptoms and making a plan.
The Guidelines for Adolescent Depression in Primary Care (GLAD-PC)1,2 were revised in 2018 to help. This expert consensus document contains specific and practical guidance for all levels of depression. But for mild depression, GLAD-PC now advises pediatricians in Recommendation II to go beyond “watchful waiting.” It states, “After initial diagnosis,
Although a little vague, mild depression is diagnosed when there are “closer to 5” significant symptoms of depression, with “distressing but manageable” severity and only “mildly impaired” functioning. The most commonly used self-report adolescent depression screen, the Patient Health Questionnaire–Modified–9 (PHQ-9), has a recommended cut score of greater than 10, but 5-9 is considered mild depression symptoms. A clinical interview also is always required.
So what is this “active support” being recommended? After making an assessment of symptoms, severity, and impact – and ruling out significant suicide risk – the task is rather familiar to us from other medical conditions. We need to talk clearly and empathetically with the teen (and parents with consent) about depression and its neurological etiology, ask about contributing stress and genetic factors, and describe the typical course with optimism. This discussion is critical to pushing guilt or blame aside to rally family support. Substance use – (including alcohol) both a cause and attempted coping strategy for depression – must be addressed because it adds to risk for suicide or crashes and because it interacts with medicines.
Perhaps the biggest difference between active support for depression versus that for other conditions is that teens are likely reluctant, hopeless, and/or lacking energy to participate in the plan. The plan, therefore, needs to be approached in smaller steps and build on prior teen strengths, goals, or talents to motivate them and create reward to counteract general lethargy. You may know this teen used to play basketball, or sing at church, or love playing with a baby sister – all activities to try to reawaken. Parents can help recall these and are key to setting up opportunities.
GLAD-PC provides a “Self-Care Success!” worksheet of categories for goal setting for active support. These goals include:
- Stay physically active. Specified days/month, minutes/session, and dates and times.
- Engage spirituality and fun activities. Specify times/week, when, and with whom).
- Eat balanced meals. Specify number/day and names of foods.
- Spend time with people who can support you. Specify number/month, minutes/time, with whom, and doing what.
- Spend time relaxing. Specify days/week, minutes/time, and doing what.
- Determine small goals and simple steps. Establish these for a specified problem.
There is now evidence for these you can share with your teen patients and families.
Exercise
Exercise has a moderate effect size of 0.56 on depression, comparable to medications for mild to moderate depression and a useful adjunct to medications. The national Office of Disease Prevention and Health Promotion recommends that 6- to 17-year-olds get 60 minutes/day of moderate exercise or undertake vigorous “out of breath” exercise three times a week to maintain health. A meta-analysis of studies of yoga for people with depressive symptoms (not necessarily diagnosed depression) found reduced symptoms in 14 of 23 studies.
Pleasure
Advising fun has to include acknowledgment that a depressed teen is not motivated to do formerly fun things and may not get as much/any pleasure from it. You need to explain that “doing precedes feeling.” While what is fun is personal, new findings indicate that 2 hours/week “in nature” lowers stress, boosts mental health, and increases sense of well-being.
Nutrition
The MIND diet (Mediterranean-type diet high in leafy vegetables and berries but low in red meat) has evidence for lower odds of depression and psychological distress. Fatty acid supplements, specifically eicosapentaenoic acid at greater than 800 mg/day (930 mg), is better than placebo (P less than .001) for reducing mild depression within as little as 4 weeks. Natural S-Adenosyl-L-methionine (SAMe) has many studies showing benefit, according to National Center for Complementary and Alternative Medicine, a government-run website. NCCAM notes that St. John’s Wort has evidence for effectiveness equal to prescribed antidepressants for mild depression but with dangerous potential side effects, such as worsening of psychotic symptoms in bipolar disorder or schizophrenia, plus potentially life threatening drug interactions. While safe, valerian and probiotics have no evidence for reducing depression.
Social support
Family is usually the most important support for depressed teens even though they may be pushing family away, may refuse to come on outings, or may even refuse to come out of the bedroom. We should encourage parents and siblings to “hang out,” sitting quietly, available to listen rather than probing, cajoling, or nagging as they may have been doing. Parents also provide support by assuring adherence to visits, goals, and medications. Peer support helps a teen feel less alone and may increase social skills, but it can be difficult to sustain because friends may find depression threatening or give up when the teen avoids them and refuses activities. The National Association for Mental Illness has an online support group (www.strengthofus.org), as well as many excellent family resources. Sometimes medical efforts to be nonsectarian result in failure to recognize and remind teens and families of the value of religion, which is free and universally available, as a source of social support.
Relaxation
An evaluation of 15 studies concluded that relaxation techniques reduced depressive symptoms better than no treatment but not as much cognitive-behavior therapy (CBT). Yoga is another source of relaxation training. Mindfulness includes relaxation and specifies working to stay nonjudgmental about thoughts passing through one’s mind, recognizing and “arguing” with negative thinking, which is also part of CBT. Guided relaxation with a person, audiotape, or app (Calm or Headspace, among others) may be better for depressed teens because it inserts a voice to guide thoughts, which could potentially fend off ruminating on sad things.
Setting goals to address problems
In mild depression, compared with more endogenous moderate to severe major depressive disorder, a specific life stressor or relationship issue may be the precipitant. Identifying such factors (never forgetting possible trauma or abuse, which are harder to reveal), empathizing with the pain, and addressing them such as using Problem Solving Treatment for Primary Care (PST-PC) are within primary care skills. PST-PC involves four to six 30-minute sessions over 6-10 weeks during which you can provide perspective, help your patient set realistic goals and solutions to try out for situations that can be changed or coping strategies for emotion-focused unchangeable issues, iteratively check on progress via calls or televisits (the monitoring component), and renew problem-solving efforts as needed.

If mild depression fails to improve over several months or worsens, GLAD-PC describes evidence-based treatments. Even if it remits, your active support and monitoring should continue because depression tends to recur. You may not realize how valuable these seemingly simple active supports are to keeping mild depression in your teen patients at bay.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
References
1. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4081.
2. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4082.
Depression is one of the most common mental health conditions in childhood, especially during socially turbulent adolescence when the brain is rapidly changing and parent-child relationships are strained by the teen’s striving for independence and identity. Often parents of teens call me worrying about possible depression, but in the next breath say “but maybe it is just puberty.” Because suicide is one of the most common causes of death among teens and is often associated with depression, we pediatricians have the scary job of sorting out symptoms and making a plan.
The Guidelines for Adolescent Depression in Primary Care (GLAD-PC)1,2 were revised in 2018 to help. This expert consensus document contains specific and practical guidance for all levels of depression. But for mild depression, GLAD-PC now advises pediatricians in Recommendation II to go beyond “watchful waiting.” It states, “After initial diagnosis,
Although a little vague, mild depression is diagnosed when there are “closer to 5” significant symptoms of depression, with “distressing but manageable” severity and only “mildly impaired” functioning. The most commonly used self-report adolescent depression screen, the Patient Health Questionnaire–Modified–9 (PHQ-9), has a recommended cut score of greater than 10, but 5-9 is considered mild depression symptoms. A clinical interview also is always required.
So what is this “active support” being recommended? After making an assessment of symptoms, severity, and impact – and ruling out significant suicide risk – the task is rather familiar to us from other medical conditions. We need to talk clearly and empathetically with the teen (and parents with consent) about depression and its neurological etiology, ask about contributing stress and genetic factors, and describe the typical course with optimism. This discussion is critical to pushing guilt or blame aside to rally family support. Substance use – (including alcohol) both a cause and attempted coping strategy for depression – must be addressed because it adds to risk for suicide or crashes and because it interacts with medicines.
Perhaps the biggest difference between active support for depression versus that for other conditions is that teens are likely reluctant, hopeless, and/or lacking energy to participate in the plan. The plan, therefore, needs to be approached in smaller steps and build on prior teen strengths, goals, or talents to motivate them and create reward to counteract general lethargy. You may know this teen used to play basketball, or sing at church, or love playing with a baby sister – all activities to try to reawaken. Parents can help recall these and are key to setting up opportunities.
GLAD-PC provides a “Self-Care Success!” worksheet of categories for goal setting for active support. These goals include:
- Stay physically active. Specified days/month, minutes/session, and dates and times.
- Engage spirituality and fun activities. Specify times/week, when, and with whom).
- Eat balanced meals. Specify number/day and names of foods.
- Spend time with people who can support you. Specify number/month, minutes/time, with whom, and doing what.
- Spend time relaxing. Specify days/week, minutes/time, and doing what.
- Determine small goals and simple steps. Establish these for a specified problem.
There is now evidence for these you can share with your teen patients and families.
Exercise
Exercise has a moderate effect size of 0.56 on depression, comparable to medications for mild to moderate depression and a useful adjunct to medications. The national Office of Disease Prevention and Health Promotion recommends that 6- to 17-year-olds get 60 minutes/day of moderate exercise or undertake vigorous “out of breath” exercise three times a week to maintain health. A meta-analysis of studies of yoga for people with depressive symptoms (not necessarily diagnosed depression) found reduced symptoms in 14 of 23 studies.
Pleasure
Advising fun has to include acknowledgment that a depressed teen is not motivated to do formerly fun things and may not get as much/any pleasure from it. You need to explain that “doing precedes feeling.” While what is fun is personal, new findings indicate that 2 hours/week “in nature” lowers stress, boosts mental health, and increases sense of well-being.
Nutrition
The MIND diet (Mediterranean-type diet high in leafy vegetables and berries but low in red meat) has evidence for lower odds of depression and psychological distress. Fatty acid supplements, specifically eicosapentaenoic acid at greater than 800 mg/day (930 mg), is better than placebo (P less than .001) for reducing mild depression within as little as 4 weeks. Natural S-Adenosyl-L-methionine (SAMe) has many studies showing benefit, according to National Center for Complementary and Alternative Medicine, a government-run website. NCCAM notes that St. John’s Wort has evidence for effectiveness equal to prescribed antidepressants for mild depression but with dangerous potential side effects, such as worsening of psychotic symptoms in bipolar disorder or schizophrenia, plus potentially life threatening drug interactions. While safe, valerian and probiotics have no evidence for reducing depression.
Social support
Family is usually the most important support for depressed teens even though they may be pushing family away, may refuse to come on outings, or may even refuse to come out of the bedroom. We should encourage parents and siblings to “hang out,” sitting quietly, available to listen rather than probing, cajoling, or nagging as they may have been doing. Parents also provide support by assuring adherence to visits, goals, and medications. Peer support helps a teen feel less alone and may increase social skills, but it can be difficult to sustain because friends may find depression threatening or give up when the teen avoids them and refuses activities. The National Association for Mental Illness has an online support group (www.strengthofus.org), as well as many excellent family resources. Sometimes medical efforts to be nonsectarian result in failure to recognize and remind teens and families of the value of religion, which is free and universally available, as a source of social support.
Relaxation
An evaluation of 15 studies concluded that relaxation techniques reduced depressive symptoms better than no treatment but not as much cognitive-behavior therapy (CBT). Yoga is another source of relaxation training. Mindfulness includes relaxation and specifies working to stay nonjudgmental about thoughts passing through one’s mind, recognizing and “arguing” with negative thinking, which is also part of CBT. Guided relaxation with a person, audiotape, or app (Calm or Headspace, among others) may be better for depressed teens because it inserts a voice to guide thoughts, which could potentially fend off ruminating on sad things.
Setting goals to address problems
In mild depression, compared with more endogenous moderate to severe major depressive disorder, a specific life stressor or relationship issue may be the precipitant. Identifying such factors (never forgetting possible trauma or abuse, which are harder to reveal), empathizing with the pain, and addressing them such as using Problem Solving Treatment for Primary Care (PST-PC) are within primary care skills. PST-PC involves four to six 30-minute sessions over 6-10 weeks during which you can provide perspective, help your patient set realistic goals and solutions to try out for situations that can be changed or coping strategies for emotion-focused unchangeable issues, iteratively check on progress via calls or televisits (the monitoring component), and renew problem-solving efforts as needed.
If mild depression fails to improve over several months or worsens, GLAD-PC describes evidence-based treatments. Even if it remits, your active support and monitoring should continue because depression tends to recur. You may not realize how valuable these seemingly simple active supports are to keeping mild depression in your teen patients at bay.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
References
1. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4081.
2. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4082.
Depression is one of the most common mental health conditions in childhood, especially during socially turbulent adolescence when the brain is rapidly changing and parent-child relationships are strained by the teen’s striving for independence and identity. Often parents of teens call me worrying about possible depression, but in the next breath say “but maybe it is just puberty.” Because suicide is one of the most common causes of death among teens and is often associated with depression, we pediatricians have the scary job of sorting out symptoms and making a plan.
The Guidelines for Adolescent Depression in Primary Care (GLAD-PC)1,2 were revised in 2018 to help. This expert consensus document contains specific and practical guidance for all levels of depression. But for mild depression, GLAD-PC now advises pediatricians in Recommendation II to go beyond “watchful waiting.” It states, “After initial diagnosis,
Although a little vague, mild depression is diagnosed when there are “closer to 5” significant symptoms of depression, with “distressing but manageable” severity and only “mildly impaired” functioning. The most commonly used self-report adolescent depression screen, the Patient Health Questionnaire–Modified–9 (PHQ-9), has a recommended cut score of greater than 10, but 5-9 is considered mild depression symptoms. A clinical interview also is always required.
So what is this “active support” being recommended? After making an assessment of symptoms, severity, and impact – and ruling out significant suicide risk – the task is rather familiar to us from other medical conditions. We need to talk clearly and empathetically with the teen (and parents with consent) about depression and its neurological etiology, ask about contributing stress and genetic factors, and describe the typical course with optimism. This discussion is critical to pushing guilt or blame aside to rally family support. Substance use – (including alcohol) both a cause and attempted coping strategy for depression – must be addressed because it adds to risk for suicide or crashes and because it interacts with medicines.
Perhaps the biggest difference between active support for depression versus that for other conditions is that teens are likely reluctant, hopeless, and/or lacking energy to participate in the plan. The plan, therefore, needs to be approached in smaller steps and build on prior teen strengths, goals, or talents to motivate them and create reward to counteract general lethargy. You may know this teen used to play basketball, or sing at church, or love playing with a baby sister – all activities to try to reawaken. Parents can help recall these and are key to setting up opportunities.
GLAD-PC provides a “Self-Care Success!” worksheet of categories for goal setting for active support. These goals include:
- Stay physically active. Specified days/month, minutes/session, and dates and times.
- Engage spirituality and fun activities. Specify times/week, when, and with whom).
- Eat balanced meals. Specify number/day and names of foods.
- Spend time with people who can support you. Specify number/month, minutes/time, with whom, and doing what.
- Spend time relaxing. Specify days/week, minutes/time, and doing what.
- Determine small goals and simple steps. Establish these for a specified problem.
There is now evidence for these you can share with your teen patients and families.
Exercise
Exercise has a moderate effect size of 0.56 on depression, comparable to medications for mild to moderate depression and a useful adjunct to medications. The national Office of Disease Prevention and Health Promotion recommends that 6- to 17-year-olds get 60 minutes/day of moderate exercise or undertake vigorous “out of breath” exercise three times a week to maintain health. A meta-analysis of studies of yoga for people with depressive symptoms (not necessarily diagnosed depression) found reduced symptoms in 14 of 23 studies.
Pleasure
Advising fun has to include acknowledgment that a depressed teen is not motivated to do formerly fun things and may not get as much/any pleasure from it. You need to explain that “doing precedes feeling.” While what is fun is personal, new findings indicate that 2 hours/week “in nature” lowers stress, boosts mental health, and increases sense of well-being.
Nutrition
The MIND diet (Mediterranean-type diet high in leafy vegetables and berries but low in red meat) has evidence for lower odds of depression and psychological distress. Fatty acid supplements, specifically eicosapentaenoic acid at greater than 800 mg/day (930 mg), is better than placebo (P less than .001) for reducing mild depression within as little as 4 weeks. Natural S-Adenosyl-L-methionine (SAMe) has many studies showing benefit, according to National Center for Complementary and Alternative Medicine, a government-run website. NCCAM notes that St. John’s Wort has evidence for effectiveness equal to prescribed antidepressants for mild depression but with dangerous potential side effects, such as worsening of psychotic symptoms in bipolar disorder or schizophrenia, plus potentially life threatening drug interactions. While safe, valerian and probiotics have no evidence for reducing depression.
Social support
Family is usually the most important support for depressed teens even though they may be pushing family away, may refuse to come on outings, or may even refuse to come out of the bedroom. We should encourage parents and siblings to “hang out,” sitting quietly, available to listen rather than probing, cajoling, or nagging as they may have been doing. Parents also provide support by assuring adherence to visits, goals, and medications. Peer support helps a teen feel less alone and may increase social skills, but it can be difficult to sustain because friends may find depression threatening or give up when the teen avoids them and refuses activities. The National Association for Mental Illness has an online support group (www.strengthofus.org), as well as many excellent family resources. Sometimes medical efforts to be nonsectarian result in failure to recognize and remind teens and families of the value of religion, which is free and universally available, as a source of social support.
Relaxation
An evaluation of 15 studies concluded that relaxation techniques reduced depressive symptoms better than no treatment but not as much cognitive-behavior therapy (CBT). Yoga is another source of relaxation training. Mindfulness includes relaxation and specifies working to stay nonjudgmental about thoughts passing through one’s mind, recognizing and “arguing” with negative thinking, which is also part of CBT. Guided relaxation with a person, audiotape, or app (Calm or Headspace, among others) may be better for depressed teens because it inserts a voice to guide thoughts, which could potentially fend off ruminating on sad things.
Setting goals to address problems
In mild depression, compared with more endogenous moderate to severe major depressive disorder, a specific life stressor or relationship issue may be the precipitant. Identifying such factors (never forgetting possible trauma or abuse, which are harder to reveal), empathizing with the pain, and addressing them such as using Problem Solving Treatment for Primary Care (PST-PC) are within primary care skills. PST-PC involves four to six 30-minute sessions over 6-10 weeks during which you can provide perspective, help your patient set realistic goals and solutions to try out for situations that can be changed or coping strategies for emotion-focused unchangeable issues, iteratively check on progress via calls or televisits (the monitoring component), and renew problem-solving efforts as needed.
If mild depression fails to improve over several months or worsens, GLAD-PC describes evidence-based treatments. Even if it remits, your active support and monitoring should continue because depression tends to recur. You may not realize how valuable these seemingly simple active supports are to keeping mild depression in your teen patients at bay.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
References
1. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4081.
2. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4082.
The right of conscientious objection
This particularly is true for those who consider medicine a vocation, or a calling, rather than just a job.

On May 2, 2019, the Department of Health and Human Services made public a 440-page document known as the Final Conscience Rule.1 It isn’t quite final. And the state of California already is suing to stop it.2 But the document represents the culmination of years of legal wrangling over whether physicians are allowed to have consciences or whether they must function as automatons providing any legally permitted care that a patient might demand. This comprehensive document provides a history of the issues, but was written in dense legalese, as if it expected to be answering challenges in court.
The short answer in the United States is that religious liberty continues to triumph over editorials in the New England Journal of Medicine. Consciences are allowed. The Final Conscience Rule begins with “The United States has a long history of providing protections in health care for individuals and entities on the basis of religious beliefs or moral convictions.” That history includes the Religious Freedom and Restoration Act of 1993.3 RFRA was introduced into the Senate by Sen. Ted Kennedy (D-Mass.), a bastion of liberal health care policies, and passed by a 97-3 vote. It was introduced into the House by then-Rep. Chuck Schumer (D-N.Y.) and passed by a unanimous voice vote. RFRA is not the invention of Republican fundamentalists.
For my colleagues in Canada, the Ontario Court of Appeals (ONCA, the highest provincial court) decided on May 15, 2019, that the opposite situation is the law in Canada. A recent Ontario law concerning medical assistance in dying (also known as physician-assisted suicide) requires Ontario physicians to either provide the assistance when requested or to make an effective referral, defined as “a referral made in good faith, to a non-objecting, available, and accessible physician, other health-care professional, or agency.” Some Canadian physicians objected to this requirement as a violation of their consciences and their Hippocratic Oaths. They lost. The ONCA decision is 74 readable, double-spaced pages and spells out the ethics and legal principles. In summary, the ONCA said the policies on requiring an effective referral “strike a reasonable balance between patients’ interests and physicians’ Charter-protected religious freedom. In short, they are reasonable limits prescribed by law that are demonstrably justified in a free and democratic society.”4
The California physician-assisted dying law, known as the End of Life Option Act, which became effective in 2016, has policies which are very different from the Ontario policies. The California law has clear protections for the consciences of physicians. The law empowers them to avoid being compelled or coerced into cooperating with these deaths. “Participation in activities authorized pursuant to this part shall be voluntary. … A person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.”5 If it seems strange that California would strongly protect conscience with its own statute but challenge the new federal regulations, welcome to tribal politics.

The point is that the role of physicians in abortion, physician aid in dying, and other controversial practices is not going to be decided by philosophical discussions about the ideal scope and purpose of medicine. Compromises are involved that reflect the values of society. Canada is more anticlerical than the United States, and Ontario chose a different path. French culture is even more extreme. Recently, mayors in two towns in France told their elementary schools to stop offering alternative entrées on days when pork was served for hot lunches. Secular schools were not to provide accommodation for students (Muslim and Jewish) who religiously objected to pork. Since the French Revolution, the emphasis is on assimilation and laïcité (France’s principle of secularism in public affairs). The cathedral Notre-Dame de Paris – recently damaged by fire – is owned by the state, not the Catholic Church. The United States has a different history and culture. It has supported religious liberty and reasonable accommodations. That is the loving thing to do. But as a reminder, the Peace of Westphalia in 1648, which ended European religious wars between Protestants and Catholics, was not a result of enlightened thinking and agapeic love. The fighting parties looked in the abyss of mutual annihilation and opted for coexistence instead.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
References
1. Department of Health and Human Services, “HHS Announces Final Conscience Rule Protecting Health Care Entities and Individuals,” May 2, 2019.
2. “California sues Trump administration over ‘conscience rule’ that could limit abortions,” Los Angeles Times, May 21, 2019.
3. Wikipedia, “Religious Freedom Restoration Act of 1993”
4. Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393.
5. California Assembly Bill No. 15, End of Life Option Act.
The article was updated on June 21, 2019.
This particularly is true for those who consider medicine a vocation, or a calling, rather than just a job.
On May 2, 2019, the Department of Health and Human Services made public a 440-page document known as the Final Conscience Rule.1 It isn’t quite final. And the state of California already is suing to stop it.2 But the document represents the culmination of years of legal wrangling over whether physicians are allowed to have consciences or whether they must function as automatons providing any legally permitted care that a patient might demand. This comprehensive document provides a history of the issues, but was written in dense legalese, as if it expected to be answering challenges in court.
The short answer in the United States is that religious liberty continues to triumph over editorials in the New England Journal of Medicine. Consciences are allowed. The Final Conscience Rule begins with “The United States has a long history of providing protections in health care for individuals and entities on the basis of religious beliefs or moral convictions.” That history includes the Religious Freedom and Restoration Act of 1993.3 RFRA was introduced into the Senate by Sen. Ted Kennedy (D-Mass.), a bastion of liberal health care policies, and passed by a 97-3 vote. It was introduced into the House by then-Rep. Chuck Schumer (D-N.Y.) and passed by a unanimous voice vote. RFRA is not the invention of Republican fundamentalists.
For my colleagues in Canada, the Ontario Court of Appeals (ONCA, the highest provincial court) decided on May 15, 2019, that the opposite situation is the law in Canada. A recent Ontario law concerning medical assistance in dying (also known as physician-assisted suicide) requires Ontario physicians to either provide the assistance when requested or to make an effective referral, defined as “a referral made in good faith, to a non-objecting, available, and accessible physician, other health-care professional, or agency.” Some Canadian physicians objected to this requirement as a violation of their consciences and their Hippocratic Oaths. They lost. The ONCA decision is 74 readable, double-spaced pages and spells out the ethics and legal principles. In summary, the ONCA said the policies on requiring an effective referral “strike a reasonable balance between patients’ interests and physicians’ Charter-protected religious freedom. In short, they are reasonable limits prescribed by law that are demonstrably justified in a free and democratic society.”4
The California physician-assisted dying law, known as the End of Life Option Act, which became effective in 2016, has policies which are very different from the Ontario policies. The California law has clear protections for the consciences of physicians. The law empowers them to avoid being compelled or coerced into cooperating with these deaths. “Participation in activities authorized pursuant to this part shall be voluntary. … A person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.”5 If it seems strange that California would strongly protect conscience with its own statute but challenge the new federal regulations, welcome to tribal politics.
The point is that the role of physicians in abortion, physician aid in dying, and other controversial practices is not going to be decided by philosophical discussions about the ideal scope and purpose of medicine. Compromises are involved that reflect the values of society. Canada is more anticlerical than the United States, and Ontario chose a different path. French culture is even more extreme. Recently, mayors in two towns in France told their elementary schools to stop offering alternative entrées on days when pork was served for hot lunches. Secular schools were not to provide accommodation for students (Muslim and Jewish) who religiously objected to pork. Since the French Revolution, the emphasis is on assimilation and laïcité (France’s principle of secularism in public affairs). The cathedral Notre-Dame de Paris – recently damaged by fire – is owned by the state, not the Catholic Church. The United States has a different history and culture. It has supported religious liberty and reasonable accommodations. That is the loving thing to do. But as a reminder, the Peace of Westphalia in 1648, which ended European religious wars between Protestants and Catholics, was not a result of enlightened thinking and agapeic love. The fighting parties looked in the abyss of mutual annihilation and opted for coexistence instead.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
References
1. Department of Health and Human Services, “HHS Announces Final Conscience Rule Protecting Health Care Entities and Individuals,” May 2, 2019.
2. “California sues Trump administration over ‘conscience rule’ that could limit abortions,” Los Angeles Times, May 21, 2019.
3. Wikipedia, “Religious Freedom Restoration Act of 1993”
4. Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393.
5. California Assembly Bill No. 15, End of Life Option Act.
The article was updated on June 21, 2019.
This particularly is true for those who consider medicine a vocation, or a calling, rather than just a job.
On May 2, 2019, the Department of Health and Human Services made public a 440-page document known as the Final Conscience Rule.1 It isn’t quite final. And the state of California already is suing to stop it.2 But the document represents the culmination of years of legal wrangling over whether physicians are allowed to have consciences or whether they must function as automatons providing any legally permitted care that a patient might demand. This comprehensive document provides a history of the issues, but was written in dense legalese, as if it expected to be answering challenges in court.
The short answer in the United States is that religious liberty continues to triumph over editorials in the New England Journal of Medicine. Consciences are allowed. The Final Conscience Rule begins with “The United States has a long history of providing protections in health care for individuals and entities on the basis of religious beliefs or moral convictions.” That history includes the Religious Freedom and Restoration Act of 1993.3 RFRA was introduced into the Senate by Sen. Ted Kennedy (D-Mass.), a bastion of liberal health care policies, and passed by a 97-3 vote. It was introduced into the House by then-Rep. Chuck Schumer (D-N.Y.) and passed by a unanimous voice vote. RFRA is not the invention of Republican fundamentalists.
For my colleagues in Canada, the Ontario Court of Appeals (ONCA, the highest provincial court) decided on May 15, 2019, that the opposite situation is the law in Canada. A recent Ontario law concerning medical assistance in dying (also known as physician-assisted suicide) requires Ontario physicians to either provide the assistance when requested or to make an effective referral, defined as “a referral made in good faith, to a non-objecting, available, and accessible physician, other health-care professional, or agency.” Some Canadian physicians objected to this requirement as a violation of their consciences and their Hippocratic Oaths. They lost. The ONCA decision is 74 readable, double-spaced pages and spells out the ethics and legal principles. In summary, the ONCA said the policies on requiring an effective referral “strike a reasonable balance between patients’ interests and physicians’ Charter-protected religious freedom. In short, they are reasonable limits prescribed by law that are demonstrably justified in a free and democratic society.”4
The California physician-assisted dying law, known as the End of Life Option Act, which became effective in 2016, has policies which are very different from the Ontario policies. The California law has clear protections for the consciences of physicians. The law empowers them to avoid being compelled or coerced into cooperating with these deaths. “Participation in activities authorized pursuant to this part shall be voluntary. … A person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.”5 If it seems strange that California would strongly protect conscience with its own statute but challenge the new federal regulations, welcome to tribal politics.
The point is that the role of physicians in abortion, physician aid in dying, and other controversial practices is not going to be decided by philosophical discussions about the ideal scope and purpose of medicine. Compromises are involved that reflect the values of society. Canada is more anticlerical than the United States, and Ontario chose a different path. French culture is even more extreme. Recently, mayors in two towns in France told their elementary schools to stop offering alternative entrées on days when pork was served for hot lunches. Secular schools were not to provide accommodation for students (Muslim and Jewish) who religiously objected to pork. Since the French Revolution, the emphasis is on assimilation and laïcité (France’s principle of secularism in public affairs). The cathedral Notre-Dame de Paris – recently damaged by fire – is owned by the state, not the Catholic Church. The United States has a different history and culture. It has supported religious liberty and reasonable accommodations. That is the loving thing to do. But as a reminder, the Peace of Westphalia in 1648, which ended European religious wars between Protestants and Catholics, was not a result of enlightened thinking and agapeic love. The fighting parties looked in the abyss of mutual annihilation and opted for coexistence instead.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
References
1. Department of Health and Human Services, “HHS Announces Final Conscience Rule Protecting Health Care Entities and Individuals,” May 2, 2019.
2. “California sues Trump administration over ‘conscience rule’ that could limit abortions,” Los Angeles Times, May 21, 2019.
3. Wikipedia, “Religious Freedom Restoration Act of 1993”
4. Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393.
5. California Assembly Bill No. 15, End of Life Option Act.
The article was updated on June 21, 2019.
A healthy 8-year-old boy presents with several skin-colored, round 1-3 mm papules on the nose, forehead, and cheeks
A shave biopsy of one of the lesions was performed that showed a proliferation of nests of basaloid cells on the dermis with palisading and rare vacuolated clear cell change. A rare ductal structure with luminal proteinaceous contents was noted. The findings were consistent with a trichoepithelioma.

Trichoepitheliomas are rare, benign, adnexal skin tumors that can start in early childhood or during puberty. The lesions are most commonly seen in girls as skin color papules on the face, and sometimes on the trunk and the neck. Trichoepitheliomas can appear as a benign single lesion nonfamilial form or as a familial form with multiple lesions.1 Brooke-Spiegler syndrome (BSS) is a rare autosomal dominant condition where affected individuals have multiple trichoepitheliomas, cylindromas, and spiradenomas. Depending on the predominant type of lesion, phenotypic variants include multiple familial trichoepithelioma type 1 and familial cylindromatosis.2 BSS is caused by mutations within CYLD, a tumor-suppressor gene located on chromosome 16q12-q13.3 Our patient presented only with trichoepitheliomas with no other lesions on the scalp, neck, or torso.
Multiple trichoepitheliomas also can be seen in other syndromes including Rombo syndrome, which is characterized by basal cell carcinomas, milia, hypotrichosis, distal vasodilation, and atrophoderma vermiculata; none seen in our patient. Bazex-Dupré-Christol syndrome is an X-linked dominant condition in which affected individuals can present with multiple trichoepitheliomas, as well as milia, hypotrichosis, follicular atrophoderma, and basal cell carcinomas.
The differential diagnosis of skin color papules on the central face on a child should include acne, flat warts, and angiofibromas seen in tuberous sclerosis. Our patient’s lesions were monomorphous, and there were no comedones, pustules, or inflammatory papules characteristic of acne.
He had warts on his hands which could make it suspicious for the face lesions to be verrucous in nature. Flat warts also present as skin color papules, but characteristically are flat, not round and shiny as our patient’s lesions were. Angiofibromas, as seen in individuals with tuberous sclerosis, also can start at an early age in the same location as trichoepitheliomas in BSS, but clinically the lesions are pinker and redder rather than the skin-color, round shape papules characteristic of trichoepitheliomas. Patients may have other findings suggestive of tuberous sclerosis including confetti hypopigmentation, ash leaf spots, shagreen patch, and a history of seizures or developmental delay – none of which were present in our patient. Children with basal cell nevus syndrome can present with skin color to shiny telangiectatic papules (basal cell carcinomas) that can be single or multiple on the face, chest, and back. The lesions usually are not seen in clusters around the nose and central face as seen in patients with BSS. Patients with basal cell nevus syndrome can develop jaw bone cysts, brain tumors (medulloblastoma), and fibromas on the heart or ovaries, palmar pits and be macrocephalic.4
Trichoepitheliomas usually are treated surgically but other nonsurgical removing techniques include laser resurfacing, curettage, and electrocautery.5 Malignant transformation can occur in 5%-10% of the individuals and should be managed by a multidisciplinary team. Topical treatment with sirolimus previously has been reported to be effective in young patients.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email Dr. Matiz at [email protected].
References
1. Acta Dermatovenerol Croat. 2018 Jun;26(2):162-5.
2. Eur J Med Genet. 2015;58(5):271-8.
3. Am J Dermatopathol. 2014;36(11):868-74.
4. Int J Dermatol. 2016 Apr;55(4):367-75.
5. Int J Dermatol. 2007;46(6):583-6.
6. Dermatol Ther. 2017 Mar. doi: 10.1111/dth.12458.
A shave biopsy of one of the lesions was performed that showed a proliferation of nests of basaloid cells on the dermis with palisading and rare vacuolated clear cell change. A rare ductal structure with luminal proteinaceous contents was noted. The findings were consistent with a trichoepithelioma.
Trichoepitheliomas are rare, benign, adnexal skin tumors that can start in early childhood or during puberty. The lesions are most commonly seen in girls as skin color papules on the face, and sometimes on the trunk and the neck. Trichoepitheliomas can appear as a benign single lesion nonfamilial form or as a familial form with multiple lesions.1 Brooke-Spiegler syndrome (BSS) is a rare autosomal dominant condition where affected individuals have multiple trichoepitheliomas, cylindromas, and spiradenomas. Depending on the predominant type of lesion, phenotypic variants include multiple familial trichoepithelioma type 1 and familial cylindromatosis.2 BSS is caused by mutations within CYLD, a tumor-suppressor gene located on chromosome 16q12-q13.3 Our patient presented only with trichoepitheliomas with no other lesions on the scalp, neck, or torso.
Multiple trichoepitheliomas also can be seen in other syndromes including Rombo syndrome, which is characterized by basal cell carcinomas, milia, hypotrichosis, distal vasodilation, and atrophoderma vermiculata; none seen in our patient. Bazex-Dupré-Christol syndrome is an X-linked dominant condition in which affected individuals can present with multiple trichoepitheliomas, as well as milia, hypotrichosis, follicular atrophoderma, and basal cell carcinomas.
The differential diagnosis of skin color papules on the central face on a child should include acne, flat warts, and angiofibromas seen in tuberous sclerosis. Our patient’s lesions were monomorphous, and there were no comedones, pustules, or inflammatory papules characteristic of acne.
He had warts on his hands which could make it suspicious for the face lesions to be verrucous in nature. Flat warts also present as skin color papules, but characteristically are flat, not round and shiny as our patient’s lesions were. Angiofibromas, as seen in individuals with tuberous sclerosis, also can start at an early age in the same location as trichoepitheliomas in BSS, but clinically the lesions are pinker and redder rather than the skin-color, round shape papules characteristic of trichoepitheliomas. Patients may have other findings suggestive of tuberous sclerosis including confetti hypopigmentation, ash leaf spots, shagreen patch, and a history of seizures or developmental delay – none of which were present in our patient. Children with basal cell nevus syndrome can present with skin color to shiny telangiectatic papules (basal cell carcinomas) that can be single or multiple on the face, chest, and back. The lesions usually are not seen in clusters around the nose and central face as seen in patients with BSS. Patients with basal cell nevus syndrome can develop jaw bone cysts, brain tumors (medulloblastoma), and fibromas on the heart or ovaries, palmar pits and be macrocephalic.4
Trichoepitheliomas usually are treated surgically but other nonsurgical removing techniques include laser resurfacing, curettage, and electrocautery.5 Malignant transformation can occur in 5%-10% of the individuals and should be managed by a multidisciplinary team. Topical treatment with sirolimus previously has been reported to be effective in young patients.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email Dr. Matiz at [email protected].
References
1. Acta Dermatovenerol Croat. 2018 Jun;26(2):162-5.
2. Eur J Med Genet. 2015;58(5):271-8.
3. Am J Dermatopathol. 2014;36(11):868-74.
4. Int J Dermatol. 2016 Apr;55(4):367-75.
5. Int J Dermatol. 2007;46(6):583-6.
6. Dermatol Ther. 2017 Mar. doi: 10.1111/dth.12458.
A shave biopsy of one of the lesions was performed that showed a proliferation of nests of basaloid cells on the dermis with palisading and rare vacuolated clear cell change. A rare ductal structure with luminal proteinaceous contents was noted. The findings were consistent with a trichoepithelioma.
Trichoepitheliomas are rare, benign, adnexal skin tumors that can start in early childhood or during puberty. The lesions are most commonly seen in girls as skin color papules on the face, and sometimes on the trunk and the neck. Trichoepitheliomas can appear as a benign single lesion nonfamilial form or as a familial form with multiple lesions.1 Brooke-Spiegler syndrome (BSS) is a rare autosomal dominant condition where affected individuals have multiple trichoepitheliomas, cylindromas, and spiradenomas. Depending on the predominant type of lesion, phenotypic variants include multiple familial trichoepithelioma type 1 and familial cylindromatosis.2 BSS is caused by mutations within CYLD, a tumor-suppressor gene located on chromosome 16q12-q13.3 Our patient presented only with trichoepitheliomas with no other lesions on the scalp, neck, or torso.
Multiple trichoepitheliomas also can be seen in other syndromes including Rombo syndrome, which is characterized by basal cell carcinomas, milia, hypotrichosis, distal vasodilation, and atrophoderma vermiculata; none seen in our patient. Bazex-Dupré-Christol syndrome is an X-linked dominant condition in which affected individuals can present with multiple trichoepitheliomas, as well as milia, hypotrichosis, follicular atrophoderma, and basal cell carcinomas.
The differential diagnosis of skin color papules on the central face on a child should include acne, flat warts, and angiofibromas seen in tuberous sclerosis. Our patient’s lesions were monomorphous, and there were no comedones, pustules, or inflammatory papules characteristic of acne.
He had warts on his hands which could make it suspicious for the face lesions to be verrucous in nature. Flat warts also present as skin color papules, but characteristically are flat, not round and shiny as our patient’s lesions were. Angiofibromas, as seen in individuals with tuberous sclerosis, also can start at an early age in the same location as trichoepitheliomas in BSS, but clinically the lesions are pinker and redder rather than the skin-color, round shape papules characteristic of trichoepitheliomas. Patients may have other findings suggestive of tuberous sclerosis including confetti hypopigmentation, ash leaf spots, shagreen patch, and a history of seizures or developmental delay – none of which were present in our patient. Children with basal cell nevus syndrome can present with skin color to shiny telangiectatic papules (basal cell carcinomas) that can be single or multiple on the face, chest, and back. The lesions usually are not seen in clusters around the nose and central face as seen in patients with BSS. Patients with basal cell nevus syndrome can develop jaw bone cysts, brain tumors (medulloblastoma), and fibromas on the heart or ovaries, palmar pits and be macrocephalic.4
Trichoepitheliomas usually are treated surgically but other nonsurgical removing techniques include laser resurfacing, curettage, and electrocautery.5 Malignant transformation can occur in 5%-10% of the individuals and should be managed by a multidisciplinary team. Topical treatment with sirolimus previously has been reported to be effective in young patients.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email Dr. Matiz at [email protected].
References
1. Acta Dermatovenerol Croat. 2018 Jun;26(2):162-5.
2. Eur J Med Genet. 2015;58(5):271-8.
3. Am J Dermatopathol. 2014;36(11):868-74.
4. Int J Dermatol. 2016 Apr;55(4):367-75.
5. Int J Dermatol. 2007;46(6):583-6.
6. Dermatol Ther. 2017 Mar. doi: 10.1111/dth.12458.
A white 8-year-old boy comes to our pediatric dermatology clinic with his mother for evaluation of acne. The lesions started about a year ago on his nose and now have spread to his cheeks. The bumps are not symptomatic. He has been applying over the counter salicylic acid and benzoyl peroxide gels with no help. The mother reports he has been growing well, denies any growth spurt, no axillary or genital hair or body odor noted.

None of the family members have a history of acne. The mother cannot recall any family members with similar lesions on the face. He has had some warts on his fingers for years and has been treated with over the counter salicylic acid. There is no family history of skin cancer.
On physical exam, he is a healthy young boy with several skin color, round papules 1-3 mm on the nose, forehead, and cheeks. There are no lesions on the scalp. He has abundant brown hair. He has few verrucous papules on the fingers. Axillary and genital hair is not noted. There is no body odor and he is Tanner stage I.
Sarcoma—rare, but not insignificant
This year, progress in treating rare cancers has been named the advance of the year by the American Society of Clinical Oncology (ASCO). Advancements in treating desmoid tumors, a subtype of sarcoma, was highlighted as one of the prominent breakthroughs for a rare cancer. While sarcoma is statistically rare, the impact of the disease is great, particularly on patients and families. ASCO’s recognition of rare cancer advancements demonstrates what the sarcoma community has long known: that “rare” shouldn’t mean unimportant or overlooked. In fact, the contributions of families, patients, caregivers, clinicians, researchers, foundations, organizations, and agencies in bringing sarcoma to the forefront and giving it prominence—spending time, effort, and energy in finding effective treatments—is of utmost importance, despite the disease’s rarity.
The Sarcoma Foundation of America (SFA) is leading the race to cure sarcoma, and it is doing so through research, advocacy, and education. Since its founding in 2001, donors to the foundation have funded over $9 million in research, with almost $2 million to be invested in research projects this year alone. The SFA supports research focused on discovering and developing new and effective therapies to treat and eradicate sarcoma—often highrisk, high-reward projects that would not likely be funded by the government or commercial interests. Driving the research agenda are members of its Medical Advisory Board—some of the brightest scientific minds in the world today, several of whom also serve on the Editorial Advisory Board of this, the SFA’s official journal. We are thankful for their dedication. Together, their efforts will continue to make a difference in the lives of those impacted by sarcoma.
The Sarcoma Foundation of America
CureSarcoma.org
This year, progress in treating rare cancers has been named the advance of the year by the American Society of Clinical Oncology (ASCO). Advancements in treating desmoid tumors, a subtype of sarcoma, was highlighted as one of the prominent breakthroughs for a rare cancer. While sarcoma is statistically rare, the impact of the disease is great, particularly on patients and families. ASCO’s recognition of rare cancer advancements demonstrates what the sarcoma community has long known: that “rare” shouldn’t mean unimportant or overlooked. In fact, the contributions of families, patients, caregivers, clinicians, researchers, foundations, organizations, and agencies in bringing sarcoma to the forefront and giving it prominence—spending time, effort, and energy in finding effective treatments—is of utmost importance, despite the disease’s rarity.
The Sarcoma Foundation of America (SFA) is leading the race to cure sarcoma, and it is doing so through research, advocacy, and education. Since its founding in 2001, donors to the foundation have funded over $9 million in research, with almost $2 million to be invested in research projects this year alone. The SFA supports research focused on discovering and developing new and effective therapies to treat and eradicate sarcoma—often highrisk, high-reward projects that would not likely be funded by the government or commercial interests. Driving the research agenda are members of its Medical Advisory Board—some of the brightest scientific minds in the world today, several of whom also serve on the Editorial Advisory Board of this, the SFA’s official journal. We are thankful for their dedication. Together, their efforts will continue to make a difference in the lives of those impacted by sarcoma.
The Sarcoma Foundation of America
CureSarcoma.org
This year, progress in treating rare cancers has been named the advance of the year by the American Society of Clinical Oncology (ASCO). Advancements in treating desmoid tumors, a subtype of sarcoma, was highlighted as one of the prominent breakthroughs for a rare cancer. While sarcoma is statistically rare, the impact of the disease is great, particularly on patients and families. ASCO’s recognition of rare cancer advancements demonstrates what the sarcoma community has long known: that “rare” shouldn’t mean unimportant or overlooked. In fact, the contributions of families, patients, caregivers, clinicians, researchers, foundations, organizations, and agencies in bringing sarcoma to the forefront and giving it prominence—spending time, effort, and energy in finding effective treatments—is of utmost importance, despite the disease’s rarity.
The Sarcoma Foundation of America (SFA) is leading the race to cure sarcoma, and it is doing so through research, advocacy, and education. Since its founding in 2001, donors to the foundation have funded over $9 million in research, with almost $2 million to be invested in research projects this year alone. The SFA supports research focused on discovering and developing new and effective therapies to treat and eradicate sarcoma—often highrisk, high-reward projects that would not likely be funded by the government or commercial interests. Driving the research agenda are members of its Medical Advisory Board—some of the brightest scientific minds in the world today, several of whom also serve on the Editorial Advisory Board of this, the SFA’s official journal. We are thankful for their dedication. Together, their efforts will continue to make a difference in the lives of those impacted by sarcoma.
The Sarcoma Foundation of America
CureSarcoma.org
Sexual harassment: Prevention and defense
Unless you have been vacationing on some distant astral plane, you are well aware that sexual misconduct and harassment have dominated news coverage and social media forums over the past year or more. It has ended the careers of a number of formerly respectable celebrities, and the #MeToo movement has empowered many additional harassment victims to come forward with their stories.

Medical offices are far from immune from harassment, of course, and the problem is not limited to staff interactions. According to a Medscape poll, 27% of physicians have been targets of inappropriate behavior in a professional setting. In another poll, 47% of physicians and 71% of nurses reported being harassed (by stalking, persistent attempts at communication, or inappropriate social media contact) by a patient.
The reality is that , have an ethical and legal responsibility to provide a safe and respectful work environment for everyone involved.
The first step in meeting that responsibility is to develop a written policy, if you don’t already have one, starting with a clear definition of sexual harassment. The Equal Employment Opportunity Commission (EEOC) has a good summary on its website of what does and does not constitute harassment, and under what conditions employers may be liable. Once the problem has been defined, a good written policy will provide specific methods for reporting transgressions, along with outlines of investigative and corrective measures to be taken in response. Templates for such documents are available on many websites, if you don’t want to start from scratch.
The next step, once a written policy is in place (and vetted by your attorney), is training for your staff. In particular, you should ensure that those in supervisory roles understand their specific responsibilities, and that everyone knows how to report an incident.
Harassment prevention training is already mandated by law in some states, including New York, California (if you have five or more employees), Maine, Delaware, and Connecticut. Other states, such as Colorado, Florida, Massachusetts, Michigan, Oklahoma, Rhode Island, Tennessee, Utah, and Vermont, have laws that “encourage” employers to provide such training. Other legislation is pending; check for new laws in your state on a regular basis.
Federal EEOC guidelines suggest that all employers “conduct and reinforce” harassment prevention training, whether laws in your particular state require it or not. On a practical level, recent court decisions suggest that offices that do not train their employees may find it difficult to mount an effective defense of a harassment lawsuit, even when they have a written policy in place. They may also be more vulnerable to punitive damage awards.
OSHA and various private companies offer a variety of downloadable training videos at reasonable cost. (As always, I have no financial interest in any product or service mentioned here.)
Misconduct among office staff is a straightforward, zero-tolerance issue. Harassment by patients is more complex, and dealing with it often requires some creativity. No one in your office, however, should think it is something they must accept because it comes from a patient. Any physician or staffer should be empowered to speak up if anyone else’s behavior, including a patient’s, makes them uncomfortable. Even when there is a medical explanation – such as psychiatric or cognitive impairment – it is important (and in some states, mandatory) to call out the behavior and report the incident.
Once reported, it should be documented, so that colleagues and other providers will be aware of the problem, and to protect yourself should the patient ever make false accusations against your practice. At subsequent appointments, take common-sense precautions. Chaperones are always a good idea, but especially so in these situations.
With repeat offenders, everyone has their own barometer of what they can and cannot tolerate. My personal threshold is low; I give one polite warning, explaining that we must provide a respectful and welcoming environment for everyone in the office, and any unacceptable behavior in the future will be grounds for dismissal from my practice. Most get the message; those who don’t are dismissed, politely.

The central point is to prevent harassment whenever possible, and to take every complaint seriously and address it promptly. An effective misconduct policy goes beyond simply avoiding legal liability. Patients and staffers alike should be secure in the knowledge that inappropriate verbal or physical interactions are not acceptable in your office under any circumstances, and will not be ignored or tolerated.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected] .
Unless you have been vacationing on some distant astral plane, you are well aware that sexual misconduct and harassment have dominated news coverage and social media forums over the past year or more. It has ended the careers of a number of formerly respectable celebrities, and the #MeToo movement has empowered many additional harassment victims to come forward with their stories.
Medical offices are far from immune from harassment, of course, and the problem is not limited to staff interactions. According to a Medscape poll, 27% of physicians have been targets of inappropriate behavior in a professional setting. In another poll, 47% of physicians and 71% of nurses reported being harassed (by stalking, persistent attempts at communication, or inappropriate social media contact) by a patient.
The reality is that , have an ethical and legal responsibility to provide a safe and respectful work environment for everyone involved.
The first step in meeting that responsibility is to develop a written policy, if you don’t already have one, starting with a clear definition of sexual harassment. The Equal Employment Opportunity Commission (EEOC) has a good summary on its website of what does and does not constitute harassment, and under what conditions employers may be liable. Once the problem has been defined, a good written policy will provide specific methods for reporting transgressions, along with outlines of investigative and corrective measures to be taken in response. Templates for such documents are available on many websites, if you don’t want to start from scratch.
The next step, once a written policy is in place (and vetted by your attorney), is training for your staff. In particular, you should ensure that those in supervisory roles understand their specific responsibilities, and that everyone knows how to report an incident.
Harassment prevention training is already mandated by law in some states, including New York, California (if you have five or more employees), Maine, Delaware, and Connecticut. Other states, such as Colorado, Florida, Massachusetts, Michigan, Oklahoma, Rhode Island, Tennessee, Utah, and Vermont, have laws that “encourage” employers to provide such training. Other legislation is pending; check for new laws in your state on a regular basis.
Federal EEOC guidelines suggest that all employers “conduct and reinforce” harassment prevention training, whether laws in your particular state require it or not. On a practical level, recent court decisions suggest that offices that do not train their employees may find it difficult to mount an effective defense of a harassment lawsuit, even when they have a written policy in place. They may also be more vulnerable to punitive damage awards.
OSHA and various private companies offer a variety of downloadable training videos at reasonable cost. (As always, I have no financial interest in any product or service mentioned here.)
Misconduct among office staff is a straightforward, zero-tolerance issue. Harassment by patients is more complex, and dealing with it often requires some creativity. No one in your office, however, should think it is something they must accept because it comes from a patient. Any physician or staffer should be empowered to speak up if anyone else’s behavior, including a patient’s, makes them uncomfortable. Even when there is a medical explanation – such as psychiatric or cognitive impairment – it is important (and in some states, mandatory) to call out the behavior and report the incident.
Once reported, it should be documented, so that colleagues and other providers will be aware of the problem, and to protect yourself should the patient ever make false accusations against your practice. At subsequent appointments, take common-sense precautions. Chaperones are always a good idea, but especially so in these situations.
With repeat offenders, everyone has their own barometer of what they can and cannot tolerate. My personal threshold is low; I give one polite warning, explaining that we must provide a respectful and welcoming environment for everyone in the office, and any unacceptable behavior in the future will be grounds for dismissal from my practice. Most get the message; those who don’t are dismissed, politely.
The central point is to prevent harassment whenever possible, and to take every complaint seriously and address it promptly. An effective misconduct policy goes beyond simply avoiding legal liability. Patients and staffers alike should be secure in the knowledge that inappropriate verbal or physical interactions are not acceptable in your office under any circumstances, and will not be ignored or tolerated.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected] .
Unless you have been vacationing on some distant astral plane, you are well aware that sexual misconduct and harassment have dominated news coverage and social media forums over the past year or more. It has ended the careers of a number of formerly respectable celebrities, and the #MeToo movement has empowered many additional harassment victims to come forward with their stories.
Medical offices are far from immune from harassment, of course, and the problem is not limited to staff interactions. According to a Medscape poll, 27% of physicians have been targets of inappropriate behavior in a professional setting. In another poll, 47% of physicians and 71% of nurses reported being harassed (by stalking, persistent attempts at communication, or inappropriate social media contact) by a patient.
The reality is that , have an ethical and legal responsibility to provide a safe and respectful work environment for everyone involved.
The first step in meeting that responsibility is to develop a written policy, if you don’t already have one, starting with a clear definition of sexual harassment. The Equal Employment Opportunity Commission (EEOC) has a good summary on its website of what does and does not constitute harassment, and under what conditions employers may be liable. Once the problem has been defined, a good written policy will provide specific methods for reporting transgressions, along with outlines of investigative and corrective measures to be taken in response. Templates for such documents are available on many websites, if you don’t want to start from scratch.
The next step, once a written policy is in place (and vetted by your attorney), is training for your staff. In particular, you should ensure that those in supervisory roles understand their specific responsibilities, and that everyone knows how to report an incident.
Harassment prevention training is already mandated by law in some states, including New York, California (if you have five or more employees), Maine, Delaware, and Connecticut. Other states, such as Colorado, Florida, Massachusetts, Michigan, Oklahoma, Rhode Island, Tennessee, Utah, and Vermont, have laws that “encourage” employers to provide such training. Other legislation is pending; check for new laws in your state on a regular basis.
Federal EEOC guidelines suggest that all employers “conduct and reinforce” harassment prevention training, whether laws in your particular state require it or not. On a practical level, recent court decisions suggest that offices that do not train their employees may find it difficult to mount an effective defense of a harassment lawsuit, even when they have a written policy in place. They may also be more vulnerable to punitive damage awards.
OSHA and various private companies offer a variety of downloadable training videos at reasonable cost. (As always, I have no financial interest in any product or service mentioned here.)
Misconduct among office staff is a straightforward, zero-tolerance issue. Harassment by patients is more complex, and dealing with it often requires some creativity. No one in your office, however, should think it is something they must accept because it comes from a patient. Any physician or staffer should be empowered to speak up if anyone else’s behavior, including a patient’s, makes them uncomfortable. Even when there is a medical explanation – such as psychiatric or cognitive impairment – it is important (and in some states, mandatory) to call out the behavior and report the incident.
Once reported, it should be documented, so that colleagues and other providers will be aware of the problem, and to protect yourself should the patient ever make false accusations against your practice. At subsequent appointments, take common-sense precautions. Chaperones are always a good idea, but especially so in these situations.
With repeat offenders, everyone has their own barometer of what they can and cannot tolerate. My personal threshold is low; I give one polite warning, explaining that we must provide a respectful and welcoming environment for everyone in the office, and any unacceptable behavior in the future will be grounds for dismissal from my practice. Most get the message; those who don’t are dismissed, politely.
The central point is to prevent harassment whenever possible, and to take every complaint seriously and address it promptly. An effective misconduct policy goes beyond simply avoiding legal liability. Patients and staffers alike should be secure in the knowledge that inappropriate verbal or physical interactions are not acceptable in your office under any circumstances, and will not be ignored or tolerated.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected] .

Get patients vaccinated: Avoid unwelcome international travel souvenirs
Summer officially began June 21, 2019, but many of your patients already may have departed or will soon be headed to international destinations. Reasons for travel are as variable as their destinations and include but are not limited to family vacations, mission trips, study abroad, parental job relocation, and visiting friends and relatives. The majority of the trips are planned at least 3 months in advance; however, for many travelers and their parents, they suddenly get an aha moment and realize there is/are specific vaccines required to obtain a visa or entry to their final destination. Unfortunately, too much emphasis is focused on required vaccines. The well-informed traveler knows that they may be exposed to multiple diseases and many are vaccine preventable.

The accompanying table lists vaccines traditionally considered to be travel vaccines. Several require multiple doses administered over 21-28 days to provide protection. Others such as cholera and yellow fever must be completed at least 10 days prior to departure to be effective. Typhoid has two formulations: The oral and injectable typhoid vaccines should be completed 1 and 2 weeks, respectively, prior to travel. Several vaccines have age limitations. Routine immunization of all infants against hepatitis A was recommended in 2006. Depending on your region, there may be adolescents who have not been immunized. Fortunately, hepatitis A vaccine works immediately.
One of the challenges you face is identifying someone in your area that provides travel medicine advice and immunizations to children and adolescents. Most children and teens travel with their parents, but today many adolescents travel independently with organized groups. Most of the vaccines listed are not routinely administered at your office, yet you most likely will be the first call a parent makes seeking travel advice.
Let me tell you about a few vaccines in particular.
Japanese encephalitis
This is most common cause of encephalitis in Asia and parts of the western Pacific. Risk generally is limited to rural agricultural areas where the causative virus is transmitted by a mosquito. Fatality rates are 20%-30%. Among survivors, 30%-50% have significant neurologic, cognitive, and psychiatric sequelae. Candidates for this vaccine are long-term travelers and short-term travelers with extensive outdoor rural activities.
Meningococcal conjugate vaccines (MCV4)
All travelers to the Hajj Pilgrimage (Aug. 9-14, 2019) and/or Umrah must show proof of immunization. Vaccine must be received at least 10 days prior to and no greater than 5 years prior to arrival to Saudi Arabia. Conjugate vaccine must clearly be documented for validity of 5 years. For all health entry requirements, go to www.moh.gov.sa/en/hajj/pages/healthregulations.aspx.
Measles
The Advisory Committee on Immunization Practices recommends all infants 6-11 months old receive one dose of MMR prior to international travel regardless of the destination. This should be followed by two additional countable doses. All persons at least 12 months of age and born after 1956 should receive two doses of MMR at least 28 days apart prior to international travel.
Rabies
Rabies is a viral disease endemic in more than 150 countries with approximately 60,000 fatal cases worldwide each year. Asia and Africa are the areas with the highest risk of exposure, and dogs are the principal hosts. Human rabies is almost always fatal once symptoms develop. Preexposure vaccine is recommended for persons with prolonged and/or remote travel to countries where rabies immunoglobulin is unavailable and the occurrence of animal rabies is high. Post exposure vaccination on days 0 and 3 still would be required.*
Typhoid
A bacterial infection caused by Salmonella enterica serotype Typhi and Paratyphi manifests with fever, headache, abdominal pain, diarrhea, or constipation. When bacteremia occurs, it usually is referred to as enteric fever. It is acquired by consumption of food/water contaminated with human feces. Highest risk areas include Africa, Southern Asia, and Southeast Asia
Yellow fever
Risk is limited to sub-Saharan Africa and the tropical areas of South America. It is transmitted by the bite of an infected mosquito. The vaccine is required for entry into at least 16 countries. In a country where yellow fever is present, persons transiting through for more than 12 hours to reach their final destination may actually cause a change in the entry requirements for the destination country. For example, travel from the United States to Tanzania requires no yellow fever vaccine while travel from the United States to Nairobi (more than 12 hours) to Tanzania requires yellow fever vaccine for entry into Tanzania. Travel sequence and duration is extremely important. Check the Centers for Disease Control and Prevention yellow fever site and/or the consulate for the most up-to-date yellow fever vaccine requirements.

YF-Vax (yellow fever vaccine) produced by Sanofi Pasteur in the United States currently is unavailable. The company is building a new facility, and vaccine will not be available for the remainder of 2019. To assure vaccine for U.S. travelers, Stamaril, a yellow fever vaccine produced by Sanofi Pasteur in France has been made available at more than 250 sites nationwide. Because Stamaril is offered at a limited number of locations, persons in need of vaccine should not delay seeking it. Because of increased demand related to summer travel, travelers in some areas have reported delays of several weeks in scheduling an appointment. To locate a Stamaril site in your area, go to wwwnc.cdc.gov/travel/page/search-for-stamaril-clinics.
There are several other diseases transmitted by mosquitoes and ticks including malaria, dengue, Zika and rickettsial diseases. Vigilant use of mosquito repellents is a must. Prophylactic medication is available for only malaria and should be initiated prior to exposure. Frequency and duration depends on the medication selected.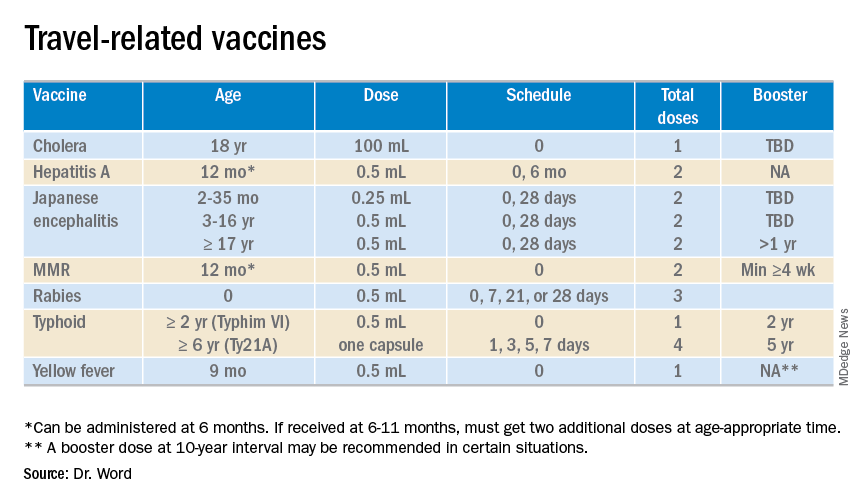
So how do you assist your patients?
Once you’ve identified a travel medicine facility in your area, encourage them to seek pretravel advice 4-6 weeks prior to international travel and make sure their routine immunizations are up to date. Generally, this is not an issue. One challenge is the early administration of MMR. While most practitioners know that early administration for international travel has been recommended for years, many office staff are accustomed to administration at only the 12 month and 4 year visit. When parents call requesting immunization, they often are informed that is it unnecessary and the appointment denied. This is a challenge, especially when coordination of administration of another live vaccine, such as yellow fever, is planned. Familiarizing all members of the health care team with current vaccine recommendations is critical.
For country-specific information, up-to-date travel alerts, and to locate a travel medicine clinic, visit www.cdc.gov/travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Email her at [email protected].
*This article was updated 6/18/2019.
Summer officially began June 21, 2019, but many of your patients already may have departed or will soon be headed to international destinations. Reasons for travel are as variable as their destinations and include but are not limited to family vacations, mission trips, study abroad, parental job relocation, and visiting friends and relatives. The majority of the trips are planned at least 3 months in advance; however, for many travelers and their parents, they suddenly get an aha moment and realize there is/are specific vaccines required to obtain a visa or entry to their final destination. Unfortunately, too much emphasis is focused on required vaccines. The well-informed traveler knows that they may be exposed to multiple diseases and many are vaccine preventable.
The accompanying table lists vaccines traditionally considered to be travel vaccines. Several require multiple doses administered over 21-28 days to provide protection. Others such as cholera and yellow fever must be completed at least 10 days prior to departure to be effective. Typhoid has two formulations: The oral and injectable typhoid vaccines should be completed 1 and 2 weeks, respectively, prior to travel. Several vaccines have age limitations. Routine immunization of all infants against hepatitis A was recommended in 2006. Depending on your region, there may be adolescents who have not been immunized. Fortunately, hepatitis A vaccine works immediately.
One of the challenges you face is identifying someone in your area that provides travel medicine advice and immunizations to children and adolescents. Most children and teens travel with their parents, but today many adolescents travel independently with organized groups. Most of the vaccines listed are not routinely administered at your office, yet you most likely will be the first call a parent makes seeking travel advice.
Let me tell you about a few vaccines in particular.
Japanese encephalitis
This is most common cause of encephalitis in Asia and parts of the western Pacific. Risk generally is limited to rural agricultural areas where the causative virus is transmitted by a mosquito. Fatality rates are 20%-30%. Among survivors, 30%-50% have significant neurologic, cognitive, and psychiatric sequelae. Candidates for this vaccine are long-term travelers and short-term travelers with extensive outdoor rural activities.
Meningococcal conjugate vaccines (MCV4)
All travelers to the Hajj Pilgrimage (Aug. 9-14, 2019) and/or Umrah must show proof of immunization. Vaccine must be received at least 10 days prior to and no greater than 5 years prior to arrival to Saudi Arabia. Conjugate vaccine must clearly be documented for validity of 5 years. For all health entry requirements, go to www.moh.gov.sa/en/hajj/pages/healthregulations.aspx.
Measles
The Advisory Committee on Immunization Practices recommends all infants 6-11 months old receive one dose of MMR prior to international travel regardless of the destination. This should be followed by two additional countable doses. All persons at least 12 months of age and born after 1956 should receive two doses of MMR at least 28 days apart prior to international travel.
Rabies
Rabies is a viral disease endemic in more than 150 countries with approximately 60,000 fatal cases worldwide each year. Asia and Africa are the areas with the highest risk of exposure, and dogs are the principal hosts. Human rabies is almost always fatal once symptoms develop. Preexposure vaccine is recommended for persons with prolonged and/or remote travel to countries where rabies immunoglobulin is unavailable and the occurrence of animal rabies is high. Post exposure vaccination on days 0 and 3 still would be required.*
Typhoid
A bacterial infection caused by Salmonella enterica serotype Typhi and Paratyphi manifests with fever, headache, abdominal pain, diarrhea, or constipation. When bacteremia occurs, it usually is referred to as enteric fever. It is acquired by consumption of food/water contaminated with human feces. Highest risk areas include Africa, Southern Asia, and Southeast Asia
Yellow fever
Risk is limited to sub-Saharan Africa and the tropical areas of South America. It is transmitted by the bite of an infected mosquito. The vaccine is required for entry into at least 16 countries. In a country where yellow fever is present, persons transiting through for more than 12 hours to reach their final destination may actually cause a change in the entry requirements for the destination country. For example, travel from the United States to Tanzania requires no yellow fever vaccine while travel from the United States to Nairobi (more than 12 hours) to Tanzania requires yellow fever vaccine for entry into Tanzania. Travel sequence and duration is extremely important. Check the Centers for Disease Control and Prevention yellow fever site and/or the consulate for the most up-to-date yellow fever vaccine requirements.
YF-Vax (yellow fever vaccine) produced by Sanofi Pasteur in the United States currently is unavailable. The company is building a new facility, and vaccine will not be available for the remainder of 2019. To assure vaccine for U.S. travelers, Stamaril, a yellow fever vaccine produced by Sanofi Pasteur in France has been made available at more than 250 sites nationwide. Because Stamaril is offered at a limited number of locations, persons in need of vaccine should not delay seeking it. Because of increased demand related to summer travel, travelers in some areas have reported delays of several weeks in scheduling an appointment. To locate a Stamaril site in your area, go to wwwnc.cdc.gov/travel/page/search-for-stamaril-clinics.
There are several other diseases transmitted by mosquitoes and ticks including malaria, dengue, Zika and rickettsial diseases. Vigilant use of mosquito repellents is a must. Prophylactic medication is available for only malaria and should be initiated prior to exposure. Frequency and duration depends on the medication selected.
So how do you assist your patients?
Once you’ve identified a travel medicine facility in your area, encourage them to seek pretravel advice 4-6 weeks prior to international travel and make sure their routine immunizations are up to date. Generally, this is not an issue. One challenge is the early administration of MMR. While most practitioners know that early administration for international travel has been recommended for years, many office staff are accustomed to administration at only the 12 month and 4 year visit. When parents call requesting immunization, they often are informed that is it unnecessary and the appointment denied. This is a challenge, especially when coordination of administration of another live vaccine, such as yellow fever, is planned. Familiarizing all members of the health care team with current vaccine recommendations is critical.
For country-specific information, up-to-date travel alerts, and to locate a travel medicine clinic, visit www.cdc.gov/travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Email her at [email protected].
*This article was updated 6/18/2019.
Summer officially began June 21, 2019, but many of your patients already may have departed or will soon be headed to international destinations. Reasons for travel are as variable as their destinations and include but are not limited to family vacations, mission trips, study abroad, parental job relocation, and visiting friends and relatives. The majority of the trips are planned at least 3 months in advance; however, for many travelers and their parents, they suddenly get an aha moment and realize there is/are specific vaccines required to obtain a visa or entry to their final destination. Unfortunately, too much emphasis is focused on required vaccines. The well-informed traveler knows that they may be exposed to multiple diseases and many are vaccine preventable.
The accompanying table lists vaccines traditionally considered to be travel vaccines. Several require multiple doses administered over 21-28 days to provide protection. Others such as cholera and yellow fever must be completed at least 10 days prior to departure to be effective. Typhoid has two formulations: The oral and injectable typhoid vaccines should be completed 1 and 2 weeks, respectively, prior to travel. Several vaccines have age limitations. Routine immunization of all infants against hepatitis A was recommended in 2006. Depending on your region, there may be adolescents who have not been immunized. Fortunately, hepatitis A vaccine works immediately.
One of the challenges you face is identifying someone in your area that provides travel medicine advice and immunizations to children and adolescents. Most children and teens travel with their parents, but today many adolescents travel independently with organized groups. Most of the vaccines listed are not routinely administered at your office, yet you most likely will be the first call a parent makes seeking travel advice.
Let me tell you about a few vaccines in particular.
Japanese encephalitis
This is most common cause of encephalitis in Asia and parts of the western Pacific. Risk generally is limited to rural agricultural areas where the causative virus is transmitted by a mosquito. Fatality rates are 20%-30%. Among survivors, 30%-50% have significant neurologic, cognitive, and psychiatric sequelae. Candidates for this vaccine are long-term travelers and short-term travelers with extensive outdoor rural activities.
Meningococcal conjugate vaccines (MCV4)
All travelers to the Hajj Pilgrimage (Aug. 9-14, 2019) and/or Umrah must show proof of immunization. Vaccine must be received at least 10 days prior to and no greater than 5 years prior to arrival to Saudi Arabia. Conjugate vaccine must clearly be documented for validity of 5 years. For all health entry requirements, go to www.moh.gov.sa/en/hajj/pages/healthregulations.aspx.
Measles
The Advisory Committee on Immunization Practices recommends all infants 6-11 months old receive one dose of MMR prior to international travel regardless of the destination. This should be followed by two additional countable doses. All persons at least 12 months of age and born after 1956 should receive two doses of MMR at least 28 days apart prior to international travel.
Rabies
Rabies is a viral disease endemic in more than 150 countries with approximately 60,000 fatal cases worldwide each year. Asia and Africa are the areas with the highest risk of exposure, and dogs are the principal hosts. Human rabies is almost always fatal once symptoms develop. Preexposure vaccine is recommended for persons with prolonged and/or remote travel to countries where rabies immunoglobulin is unavailable and the occurrence of animal rabies is high. Post exposure vaccination on days 0 and 3 still would be required.*
Typhoid
A bacterial infection caused by Salmonella enterica serotype Typhi and Paratyphi manifests with fever, headache, abdominal pain, diarrhea, or constipation. When bacteremia occurs, it usually is referred to as enteric fever. It is acquired by consumption of food/water contaminated with human feces. Highest risk areas include Africa, Southern Asia, and Southeast Asia
Yellow fever
Risk is limited to sub-Saharan Africa and the tropical areas of South America. It is transmitted by the bite of an infected mosquito. The vaccine is required for entry into at least 16 countries. In a country where yellow fever is present, persons transiting through for more than 12 hours to reach their final destination may actually cause a change in the entry requirements for the destination country. For example, travel from the United States to Tanzania requires no yellow fever vaccine while travel from the United States to Nairobi (more than 12 hours) to Tanzania requires yellow fever vaccine for entry into Tanzania. Travel sequence and duration is extremely important. Check the Centers for Disease Control and Prevention yellow fever site and/or the consulate for the most up-to-date yellow fever vaccine requirements.
YF-Vax (yellow fever vaccine) produced by Sanofi Pasteur in the United States currently is unavailable. The company is building a new facility, and vaccine will not be available for the remainder of 2019. To assure vaccine for U.S. travelers, Stamaril, a yellow fever vaccine produced by Sanofi Pasteur in France has been made available at more than 250 sites nationwide. Because Stamaril is offered at a limited number of locations, persons in need of vaccine should not delay seeking it. Because of increased demand related to summer travel, travelers in some areas have reported delays of several weeks in scheduling an appointment. To locate a Stamaril site in your area, go to wwwnc.cdc.gov/travel/page/search-for-stamaril-clinics.
There are several other diseases transmitted by mosquitoes and ticks including malaria, dengue, Zika and rickettsial diseases. Vigilant use of mosquito repellents is a must. Prophylactic medication is available for only malaria and should be initiated prior to exposure. Frequency and duration depends on the medication selected.
So how do you assist your patients?
Once you’ve identified a travel medicine facility in your area, encourage them to seek pretravel advice 4-6 weeks prior to international travel and make sure their routine immunizations are up to date. Generally, this is not an issue. One challenge is the early administration of MMR. While most practitioners know that early administration for international travel has been recommended for years, many office staff are accustomed to administration at only the 12 month and 4 year visit. When parents call requesting immunization, they often are informed that is it unnecessary and the appointment denied. This is a challenge, especially when coordination of administration of another live vaccine, such as yellow fever, is planned. Familiarizing all members of the health care team with current vaccine recommendations is critical.
For country-specific information, up-to-date travel alerts, and to locate a travel medicine clinic, visit www.cdc.gov/travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Email her at [email protected].
*This article was updated 6/18/2019.
NSCLC: Local consolidative therapy in oligometastatic disease and immunotherapy in EGFR mutations
In this edition of “How I will treat my next patient,” I take a look at two recent trials in non–small cell lung cancer (NSCLC). One summarizes a late analysis of a previously published randomized trial in stage IV NSCLC with three or fewer sites of metastasis – oligometastatic disease. The other reviews deidentified patient data to discern whether immune-targeted treatment might be valuable in particular subsets of NSCLC patients with EGFR mutations.

Local consolidative therapy
Daniel R. Gomez, MD, and colleagues published an updated analysis of progression-free survival (PFS) and an initial analysis of overall survival (OS) data in a randomized phase 2 trial in oligometastatic NSCLC. As originally published, patients were randomized to local consolidative treatment (LCT) versus standard maintenance therapy or observation (MT/O). Patients were required to have responding or stable disease after first-line systemic therapy prior to randomization.
Among the 49 patients who received LCT, there was a clear benefit of LCT (PFS of 14.2 months vs. 4.4 months for MT/O; P = .022; and median OS 41.2 months vs. 17.0 months; P = .017). The OS benefit was seen despite allowing crossover to LCT for patients who demonstrated disease progression in the MT/O arm.
What this means in practice
These data are exciting and move clinical research forward – if not, at this time, clinical practice. They support the ongoing clinical trials in NSCLC (NRG LU002) and breast cancer (NRG BR002) investigating the role of LCT in the oligometastatic setting.
For patients who are not candidates for (or choose not to participate in) these important phase 2R/3 trials, I believe that LCT should be discussed with all of the caveats that the authors appropriately mention, from the small number of patients because of the premature closure of the trial, to heterogeneous systemic regimens, to the lack of clarity on whether newer systemic therapies are better.
Immune checkpoint blockade
Historically, EGFR-mutated NSCLCs have not derived comparable benefit to EGFR-wild type (WT) tumors from checkpoint inhibitors. For that reason, in EGFR-mutated tumors, guidelines from the National Comprehensive Cancer Network (NCCN) suggest immune-targeted treatment should be used only on clinical trials or after receipt of EGFR-targeted tyrosine kinase inhibitors and cytotoxic chemotherapy. Several recent studies (IMpower and ATLANTIC), however, have suggested that selected EGFR-mutated patients can benefit from immune-targeted treatment.
Katherine Hastings, PhD, of Yale University, New Haven, Conn., and associates found, in a multi-institution clinical-molecular data review, that among the 44 of 171 EGFR-mutated tumors with L858R mutations, benefit from checkpoint inhibitors was comparable to WT tumors with regard to overall response rate and OS, but not PFS. Additionally, tumors with the EGFR T790M mutation demonstrated similar benefit from checkpoint inhibitors as in WT tumors, L858R-mutated tumors (but not exon 19 deleted tumors) had high tumor mutation burden, and PD-L1 expression did not influence outcome from immunotherapy.
What this means in practice
I agree with the modesty of the authors’ conclusion that these findings should not change clinical practice but rather should encourage further research into which patients with EGFR-mutant disease might benefit from immune-targeted therapy. For now, outside of a clinical trial, in EGFR-mutated patients, I will follow NCCN guidelines, using immune-targeted therapy off-study only with attentiveness to the particular immunotherapy regimens that have shown promise in the literature – and later, not earlier.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I take a look at two recent trials in non–small cell lung cancer (NSCLC). One summarizes a late analysis of a previously published randomized trial in stage IV NSCLC with three or fewer sites of metastasis – oligometastatic disease. The other reviews deidentified patient data to discern whether immune-targeted treatment might be valuable in particular subsets of NSCLC patients with EGFR mutations.
Local consolidative therapy
Daniel R. Gomez, MD, and colleagues published an updated analysis of progression-free survival (PFS) and an initial analysis of overall survival (OS) data in a randomized phase 2 trial in oligometastatic NSCLC. As originally published, patients were randomized to local consolidative treatment (LCT) versus standard maintenance therapy or observation (MT/O). Patients were required to have responding or stable disease after first-line systemic therapy prior to randomization.
Among the 49 patients who received LCT, there was a clear benefit of LCT (PFS of 14.2 months vs. 4.4 months for MT/O; P = .022; and median OS 41.2 months vs. 17.0 months; P = .017). The OS benefit was seen despite allowing crossover to LCT for patients who demonstrated disease progression in the MT/O arm.
What this means in practice
These data are exciting and move clinical research forward – if not, at this time, clinical practice. They support the ongoing clinical trials in NSCLC (NRG LU002) and breast cancer (NRG BR002) investigating the role of LCT in the oligometastatic setting.
For patients who are not candidates for (or choose not to participate in) these important phase 2R/3 trials, I believe that LCT should be discussed with all of the caveats that the authors appropriately mention, from the small number of patients because of the premature closure of the trial, to heterogeneous systemic regimens, to the lack of clarity on whether newer systemic therapies are better.
Immune checkpoint blockade
Historically, EGFR-mutated NSCLCs have not derived comparable benefit to EGFR-wild type (WT) tumors from checkpoint inhibitors. For that reason, in EGFR-mutated tumors, guidelines from the National Comprehensive Cancer Network (NCCN) suggest immune-targeted treatment should be used only on clinical trials or after receipt of EGFR-targeted tyrosine kinase inhibitors and cytotoxic chemotherapy. Several recent studies (IMpower and ATLANTIC), however, have suggested that selected EGFR-mutated patients can benefit from immune-targeted treatment.
Katherine Hastings, PhD, of Yale University, New Haven, Conn., and associates found, in a multi-institution clinical-molecular data review, that among the 44 of 171 EGFR-mutated tumors with L858R mutations, benefit from checkpoint inhibitors was comparable to WT tumors with regard to overall response rate and OS, but not PFS. Additionally, tumors with the EGFR T790M mutation demonstrated similar benefit from checkpoint inhibitors as in WT tumors, L858R-mutated tumors (but not exon 19 deleted tumors) had high tumor mutation burden, and PD-L1 expression did not influence outcome from immunotherapy.
What this means in practice
I agree with the modesty of the authors’ conclusion that these findings should not change clinical practice but rather should encourage further research into which patients with EGFR-mutant disease might benefit from immune-targeted therapy. For now, outside of a clinical trial, in EGFR-mutated patients, I will follow NCCN guidelines, using immune-targeted therapy off-study only with attentiveness to the particular immunotherapy regimens that have shown promise in the literature – and later, not earlier.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I take a look at two recent trials in non–small cell lung cancer (NSCLC). One summarizes a late analysis of a previously published randomized trial in stage IV NSCLC with three or fewer sites of metastasis – oligometastatic disease. The other reviews deidentified patient data to discern whether immune-targeted treatment might be valuable in particular subsets of NSCLC patients with EGFR mutations.
Local consolidative therapy
Daniel R. Gomez, MD, and colleagues published an updated analysis of progression-free survival (PFS) and an initial analysis of overall survival (OS) data in a randomized phase 2 trial in oligometastatic NSCLC. As originally published, patients were randomized to local consolidative treatment (LCT) versus standard maintenance therapy or observation (MT/O). Patients were required to have responding or stable disease after first-line systemic therapy prior to randomization.
Among the 49 patients who received LCT, there was a clear benefit of LCT (PFS of 14.2 months vs. 4.4 months for MT/O; P = .022; and median OS 41.2 months vs. 17.0 months; P = .017). The OS benefit was seen despite allowing crossover to LCT for patients who demonstrated disease progression in the MT/O arm.
What this means in practice
These data are exciting and move clinical research forward – if not, at this time, clinical practice. They support the ongoing clinical trials in NSCLC (NRG LU002) and breast cancer (NRG BR002) investigating the role of LCT in the oligometastatic setting.
For patients who are not candidates for (or choose not to participate in) these important phase 2R/3 trials, I believe that LCT should be discussed with all of the caveats that the authors appropriately mention, from the small number of patients because of the premature closure of the trial, to heterogeneous systemic regimens, to the lack of clarity on whether newer systemic therapies are better.
Immune checkpoint blockade
Historically, EGFR-mutated NSCLCs have not derived comparable benefit to EGFR-wild type (WT) tumors from checkpoint inhibitors. For that reason, in EGFR-mutated tumors, guidelines from the National Comprehensive Cancer Network (NCCN) suggest immune-targeted treatment should be used only on clinical trials or after receipt of EGFR-targeted tyrosine kinase inhibitors and cytotoxic chemotherapy. Several recent studies (IMpower and ATLANTIC), however, have suggested that selected EGFR-mutated patients can benefit from immune-targeted treatment.
Katherine Hastings, PhD, of Yale University, New Haven, Conn., and associates found, in a multi-institution clinical-molecular data review, that among the 44 of 171 EGFR-mutated tumors with L858R mutations, benefit from checkpoint inhibitors was comparable to WT tumors with regard to overall response rate and OS, but not PFS. Additionally, tumors with the EGFR T790M mutation demonstrated similar benefit from checkpoint inhibitors as in WT tumors, L858R-mutated tumors (but not exon 19 deleted tumors) had high tumor mutation burden, and PD-L1 expression did not influence outcome from immunotherapy.
What this means in practice
I agree with the modesty of the authors’ conclusion that these findings should not change clinical practice but rather should encourage further research into which patients with EGFR-mutant disease might benefit from immune-targeted therapy. For now, outside of a clinical trial, in EGFR-mutated patients, I will follow NCCN guidelines, using immune-targeted therapy off-study only with attentiveness to the particular immunotherapy regimens that have shown promise in the literature – and later, not earlier.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Learning to live with a slow week at the office
It was a slow week at my office. For whatever reason, almost no one called for an appointment. Roughly 80% of my office slots were empty.
As a result, I began to worry.
You’d think that after 20 years in practice I wouldn’t, but I still do. I wonder if someone has actually read my Yelp reviews (most of which aren’t particularly good), or that I’ve done something to upset my referral base, or that some scandal about me broke in the local news that I’m entirely unaware of.
![]()
Of course, the reality is that business comes and goes in waves. It was also the week after local schools closed for summer, and people were fleeing for summer vacation. In Phoenix, the older population leaves town as it heats up, and our winter visitors from elsewhere went home last month. And, like any business, things go in cycles that often don’t have a rational explanation.

I reassure myself that plenty of weeks are crazy. Patients crammed into every nook and cranny of the schedule, more people needing to be worked in, a huge pile of test results to be reviewed and make decisions on, and a lot of phone calls to be returned.
Then I’ll wish for a quieter week. I’ve given up on finding a happy medium – it doesn’t seem to happen.
So I try to live with the quiet. Close up and go home a little early if there’s no one to see. Catch up on my sleep and reading. Do some online surveys for extra dollars. Throw away expired stuff in my drug sample cabinet.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
It was a slow week at my office. For whatever reason, almost no one called for an appointment. Roughly 80% of my office slots were empty.
As a result, I began to worry.
You’d think that after 20 years in practice I wouldn’t, but I still do. I wonder if someone has actually read my Yelp reviews (most of which aren’t particularly good), or that I’ve done something to upset my referral base, or that some scandal about me broke in the local news that I’m entirely unaware of.
![]()
Of course, the reality is that business comes and goes in waves. It was also the week after local schools closed for summer, and people were fleeing for summer vacation. In Phoenix, the older population leaves town as it heats up, and our winter visitors from elsewhere went home last month. And, like any business, things go in cycles that often don’t have a rational explanation.
I reassure myself that plenty of weeks are crazy. Patients crammed into every nook and cranny of the schedule, more people needing to be worked in, a huge pile of test results to be reviewed and make decisions on, and a lot of phone calls to be returned.
Then I’ll wish for a quieter week. I’ve given up on finding a happy medium – it doesn’t seem to happen.
So I try to live with the quiet. Close up and go home a little early if there’s no one to see. Catch up on my sleep and reading. Do some online surveys for extra dollars. Throw away expired stuff in my drug sample cabinet.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
It was a slow week at my office. For whatever reason, almost no one called for an appointment. Roughly 80% of my office slots were empty.
As a result, I began to worry.
You’d think that after 20 years in practice I wouldn’t, but I still do. I wonder if someone has actually read my Yelp reviews (most of which aren’t particularly good), or that I’ve done something to upset my referral base, or that some scandal about me broke in the local news that I’m entirely unaware of.
![]()
Of course, the reality is that business comes and goes in waves. It was also the week after local schools closed for summer, and people were fleeing for summer vacation. In Phoenix, the older population leaves town as it heats up, and our winter visitors from elsewhere went home last month. And, like any business, things go in cycles that often don’t have a rational explanation.
I reassure myself that plenty of weeks are crazy. Patients crammed into every nook and cranny of the schedule, more people needing to be worked in, a huge pile of test results to be reviewed and make decisions on, and a lot of phone calls to be returned.
Then I’ll wish for a quieter week. I’ve given up on finding a happy medium – it doesn’t seem to happen.
So I try to live with the quiet. Close up and go home a little early if there’s no one to see. Catch up on my sleep and reading. Do some online surveys for extra dollars. Throw away expired stuff in my drug sample cabinet.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.