User login
Happiness in my solo practice
I don’t want to rule the world.

Some doctors do, albeit in a non–Attila-the-Hun sort of way. They want to have offices on every street corner, in every suburb of a given city, sometimes more than one city. Like the Starbucks of medicine.
That’s not me. I’m happy in my little one-office world.
Maybe I just don’t have the ambition, or the business mindset, or whatever it takes to want to do that. I understand it’s all part of wanting to be successful, and obviously those doctors are more driven in that direction than I am. The more offices, the more patients can be seen, and the more money you make.
It’s not quite that simple, though. No one can be in more than one place at the same time, so to see more patients at more places you need more doctors. To pay more doctors requires more money, which in turn requires more patients.
There’s nothing wrong with taking over the world (or at least a suburb) if you like that sort of thing. But to me, more money brings more headaches. More offices to rent, more staff to hire, more people to handle billing, IT, HR, payroll, accounting, contracts, and so on.
You can have it. I’ve taken over all the world I want, in my case a 1,200-square-foot suite on the second floor of a small-to-medium-size medical building. To some that may sound unambitious, but to me, it’s perfect.
I know where my Keurig, Sodastream, and office supplies are. Except for my secretary and her cheerfully rambunctious young daughter, I don’t have to worry about sharing stuff here, or if anyone wants a different carpet color, or what’s going on at a satellite office halfway across town.
If other doctors want to try and take over the world, more power to them, but I’m happy with this. Enough is as good as a feast.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I don’t want to rule the world.
Some doctors do, albeit in a non–Attila-the-Hun sort of way. They want to have offices on every street corner, in every suburb of a given city, sometimes more than one city. Like the Starbucks of medicine.
That’s not me. I’m happy in my little one-office world.
Maybe I just don’t have the ambition, or the business mindset, or whatever it takes to want to do that. I understand it’s all part of wanting to be successful, and obviously those doctors are more driven in that direction than I am. The more offices, the more patients can be seen, and the more money you make.
It’s not quite that simple, though. No one can be in more than one place at the same time, so to see more patients at more places you need more doctors. To pay more doctors requires more money, which in turn requires more patients.
There’s nothing wrong with taking over the world (or at least a suburb) if you like that sort of thing. But to me, more money brings more headaches. More offices to rent, more staff to hire, more people to handle billing, IT, HR, payroll, accounting, contracts, and so on.
You can have it. I’ve taken over all the world I want, in my case a 1,200-square-foot suite on the second floor of a small-to-medium-size medical building. To some that may sound unambitious, but to me, it’s perfect.
I know where my Keurig, Sodastream, and office supplies are. Except for my secretary and her cheerfully rambunctious young daughter, I don’t have to worry about sharing stuff here, or if anyone wants a different carpet color, or what’s going on at a satellite office halfway across town.
If other doctors want to try and take over the world, more power to them, but I’m happy with this. Enough is as good as a feast.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I don’t want to rule the world.
Some doctors do, albeit in a non–Attila-the-Hun sort of way. They want to have offices on every street corner, in every suburb of a given city, sometimes more than one city. Like the Starbucks of medicine.
That’s not me. I’m happy in my little one-office world.
Maybe I just don’t have the ambition, or the business mindset, or whatever it takes to want to do that. I understand it’s all part of wanting to be successful, and obviously those doctors are more driven in that direction than I am. The more offices, the more patients can be seen, and the more money you make.
It’s not quite that simple, though. No one can be in more than one place at the same time, so to see more patients at more places you need more doctors. To pay more doctors requires more money, which in turn requires more patients.
There’s nothing wrong with taking over the world (or at least a suburb) if you like that sort of thing. But to me, more money brings more headaches. More offices to rent, more staff to hire, more people to handle billing, IT, HR, payroll, accounting, contracts, and so on.
You can have it. I’ve taken over all the world I want, in my case a 1,200-square-foot suite on the second floor of a small-to-medium-size medical building. To some that may sound unambitious, but to me, it’s perfect.
I know where my Keurig, Sodastream, and office supplies are. Except for my secretary and her cheerfully rambunctious young daughter, I don’t have to worry about sharing stuff here, or if anyone wants a different carpet color, or what’s going on at a satellite office halfway across town.
If other doctors want to try and take over the world, more power to them, but I’m happy with this. Enough is as good as a feast.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Does this patient have bacterial conjunctivitis?
A 54-year-old pharmacist with a history of gout, hypertension, and conjunctivitis presents for evaluation of pink eye in the summer. The morning before coming into the office, he noticed that his right eye was red and inflamed. He self-treated with saline washes and eye drops, but upon awakening the next day, he found his right eye to be crusted shut with surrounding yellow discharge. He has not had any changes to his vision but endorses a somewhat uncomfortable, “gritty” sensation. He reports no recent cough, nasal congestion, or allergies, and he has not been around any sick contacts. His blood pressure is 102/58 mm Hg, pulse is 76 bpm, and body mass index is 27.3 kg/m2. His eye exam reveals unilateral conjunctival injections but no hyperemia of the conjunctiva adjacent to the cornea. Mucopurulent discharge was neither found on the undersurface of the eyelid nor emerging from the eye. Which of the following is the best treatment for this patient’s condition?
A) Erythromycin 5 mg/gram ophthalmic ointment.
B) Ofloxacin 0.3% ophthalmic drops.
C) Antihistamine drops.
D) Eye lubricant drops.
E) No treatment necessary.
This patient is an adult presenting with presumed conjunctivitis. Because he is presenting in the summer without observed purulent discharge, his condition is unlikely to be bacterial. This patient does not need treatment, although eye lubricant drops could reduce his discomfort.
After ruling out serious eye disease, clinicians need to determine which cases of suspected conjunctivitis are most likely to be bacterial to allow for judicious use of antibiotic eye drops. This is an important undertaking as most patients assume that antibiotics are needed.
How do we know which history and clinical exam findings to lean on when attempting to categorize conjunctivitis as bacterial or not? If a patient reports purulent discharge, doesn’t that mean it is bacterial? Surprisingly, a systematic review published in 2016 by Narayana and McGee found that a patient’s self-report of “purulent drainage” is diagnostically unhelpful, but if a clinician finds it on exam, the likelihood of a bacterial etiology increases.3
Narayana and McGee analyzed three studies that enrolled a total of 281 patients with presumed conjunctivitis who underwent bacterial cultures. They then determined which findings increased the probability of positive bacterial culture. From strongest to weakest, the best indicators of a bacterial cause were found to be: complete redness of the conjunctival membrane obscuring tarsal vessels (the vessels visible on the inside of everted upper or lower eyelids) (likelihood ratio, 4.6), observed purulent discharge (LR, 3.9), matting of both eyes in the morning (LR, 3.6), and presence during winter/spring months (LR, 1.9). On the other hand, failure to observe a red eye at 20 feet (LR, 0.2), absence of morning gluing of either eye (LR, 0.3), and presentation during summer months (LR, 0.4) all decreased the probability of a bacterial cause. This review and different study by Stenson et al. unfortunately have conflicting evidence regarding whether the following findings are diagnostically helpful: qualities of eye discomfort (such as burning or itching), preauricular adenopathy, conjunctival follicles, and conjunctival papillae.3,4 Rietveld and colleagues found that a history of conjunctivitis decreased the likelihood of bacterial conjunctivitis.5

Ultimately, if the former indicators are kept in mind, primary care clinicians should be able to decrease the prescribing of topical antimicrobials to patients with non-bacterial conjunctivitis.
Pearl: The best indicators of a bacterial cause in patients with presumed conjunctivitis are complete redness of the conjunctival membrane obscuring tarsal vessels, observed purulent discharge, and matting of both eyes in the morning. Presentation during the summer months and having a history of conjunctivitis decreases the likelihood of bacterial conjunctivitis.
Ms. Momany is a fourth-year medical student at University of Washington, Seattle. Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington and serves as third-year medical student clerkship director at that university. Contact Dr. Paauw at [email protected].
References
1. Azari AA and Barney NP. JAMA. 2013 Oct 23; 310(16):1721-9.
2. Smith AF and Waycaster C. BMC Ophthalmol. 2009 Nov 25. doi: 10.1186/1471-2415-9-13.
3) Narayana S and McGee S. Am J Med. 2015;128(11):1220-4.e1.
4) Stenson S et al. Arch Ophthalmol. 1982;100(8):1275-7.
5) Rietveld RP et al. BMJ. 2004 Jul 24;329(7459):206-10.
A 54-year-old pharmacist with a history of gout, hypertension, and conjunctivitis presents for evaluation of pink eye in the summer. The morning before coming into the office, he noticed that his right eye was red and inflamed. He self-treated with saline washes and eye drops, but upon awakening the next day, he found his right eye to be crusted shut with surrounding yellow discharge. He has not had any changes to his vision but endorses a somewhat uncomfortable, “gritty” sensation. He reports no recent cough, nasal congestion, or allergies, and he has not been around any sick contacts. His blood pressure is 102/58 mm Hg, pulse is 76 bpm, and body mass index is 27.3 kg/m2. His eye exam reveals unilateral conjunctival injections but no hyperemia of the conjunctiva adjacent to the cornea. Mucopurulent discharge was neither found on the undersurface of the eyelid nor emerging from the eye. Which of the following is the best treatment for this patient’s condition?
A) Erythromycin 5 mg/gram ophthalmic ointment.
B) Ofloxacin 0.3% ophthalmic drops.
C) Antihistamine drops.
D) Eye lubricant drops.
E) No treatment necessary.
This patient is an adult presenting with presumed conjunctivitis. Because he is presenting in the summer without observed purulent discharge, his condition is unlikely to be bacterial. This patient does not need treatment, although eye lubricant drops could reduce his discomfort.
After ruling out serious eye disease, clinicians need to determine which cases of suspected conjunctivitis are most likely to be bacterial to allow for judicious use of antibiotic eye drops. This is an important undertaking as most patients assume that antibiotics are needed.
How do we know which history and clinical exam findings to lean on when attempting to categorize conjunctivitis as bacterial or not? If a patient reports purulent discharge, doesn’t that mean it is bacterial? Surprisingly, a systematic review published in 2016 by Narayana and McGee found that a patient’s self-report of “purulent drainage” is diagnostically unhelpful, but if a clinician finds it on exam, the likelihood of a bacterial etiology increases.3
Narayana and McGee analyzed three studies that enrolled a total of 281 patients with presumed conjunctivitis who underwent bacterial cultures. They then determined which findings increased the probability of positive bacterial culture. From strongest to weakest, the best indicators of a bacterial cause were found to be: complete redness of the conjunctival membrane obscuring tarsal vessels (the vessels visible on the inside of everted upper or lower eyelids) (likelihood ratio, 4.6), observed purulent discharge (LR, 3.9), matting of both eyes in the morning (LR, 3.6), and presence during winter/spring months (LR, 1.9). On the other hand, failure to observe a red eye at 20 feet (LR, 0.2), absence of morning gluing of either eye (LR, 0.3), and presentation during summer months (LR, 0.4) all decreased the probability of a bacterial cause. This review and different study by Stenson et al. unfortunately have conflicting evidence regarding whether the following findings are diagnostically helpful: qualities of eye discomfort (such as burning or itching), preauricular adenopathy, conjunctival follicles, and conjunctival papillae.3,4 Rietveld and colleagues found that a history of conjunctivitis decreased the likelihood of bacterial conjunctivitis.5
Ultimately, if the former indicators are kept in mind, primary care clinicians should be able to decrease the prescribing of topical antimicrobials to patients with non-bacterial conjunctivitis.
Pearl: The best indicators of a bacterial cause in patients with presumed conjunctivitis are complete redness of the conjunctival membrane obscuring tarsal vessels, observed purulent discharge, and matting of both eyes in the morning. Presentation during the summer months and having a history of conjunctivitis decreases the likelihood of bacterial conjunctivitis.
Ms. Momany is a fourth-year medical student at University of Washington, Seattle. Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington and serves as third-year medical student clerkship director at that university. Contact Dr. Paauw at [email protected].
References
1. Azari AA and Barney NP. JAMA. 2013 Oct 23; 310(16):1721-9.
2. Smith AF and Waycaster C. BMC Ophthalmol. 2009 Nov 25. doi: 10.1186/1471-2415-9-13.
3) Narayana S and McGee S. Am J Med. 2015;128(11):1220-4.e1.
4) Stenson S et al. Arch Ophthalmol. 1982;100(8):1275-7.
5) Rietveld RP et al. BMJ. 2004 Jul 24;329(7459):206-10.
A 54-year-old pharmacist with a history of gout, hypertension, and conjunctivitis presents for evaluation of pink eye in the summer. The morning before coming into the office, he noticed that his right eye was red and inflamed. He self-treated with saline washes and eye drops, but upon awakening the next day, he found his right eye to be crusted shut with surrounding yellow discharge. He has not had any changes to his vision but endorses a somewhat uncomfortable, “gritty” sensation. He reports no recent cough, nasal congestion, or allergies, and he has not been around any sick contacts. His blood pressure is 102/58 mm Hg, pulse is 76 bpm, and body mass index is 27.3 kg/m2. His eye exam reveals unilateral conjunctival injections but no hyperemia of the conjunctiva adjacent to the cornea. Mucopurulent discharge was neither found on the undersurface of the eyelid nor emerging from the eye. Which of the following is the best treatment for this patient’s condition?
A) Erythromycin 5 mg/gram ophthalmic ointment.
B) Ofloxacin 0.3% ophthalmic drops.
C) Antihistamine drops.
D) Eye lubricant drops.
E) No treatment necessary.
This patient is an adult presenting with presumed conjunctivitis. Because he is presenting in the summer without observed purulent discharge, his condition is unlikely to be bacterial. This patient does not need treatment, although eye lubricant drops could reduce his discomfort.
After ruling out serious eye disease, clinicians need to determine which cases of suspected conjunctivitis are most likely to be bacterial to allow for judicious use of antibiotic eye drops. This is an important undertaking as most patients assume that antibiotics are needed.
How do we know which history and clinical exam findings to lean on when attempting to categorize conjunctivitis as bacterial or not? If a patient reports purulent discharge, doesn’t that mean it is bacterial? Surprisingly, a systematic review published in 2016 by Narayana and McGee found that a patient’s self-report of “purulent drainage” is diagnostically unhelpful, but if a clinician finds it on exam, the likelihood of a bacterial etiology increases.3
Narayana and McGee analyzed three studies that enrolled a total of 281 patients with presumed conjunctivitis who underwent bacterial cultures. They then determined which findings increased the probability of positive bacterial culture. From strongest to weakest, the best indicators of a bacterial cause were found to be: complete redness of the conjunctival membrane obscuring tarsal vessels (the vessels visible on the inside of everted upper or lower eyelids) (likelihood ratio, 4.6), observed purulent discharge (LR, 3.9), matting of both eyes in the morning (LR, 3.6), and presence during winter/spring months (LR, 1.9). On the other hand, failure to observe a red eye at 20 feet (LR, 0.2), absence of morning gluing of either eye (LR, 0.3), and presentation during summer months (LR, 0.4) all decreased the probability of a bacterial cause. This review and different study by Stenson et al. unfortunately have conflicting evidence regarding whether the following findings are diagnostically helpful: qualities of eye discomfort (such as burning or itching), preauricular adenopathy, conjunctival follicles, and conjunctival papillae.3,4 Rietveld and colleagues found that a history of conjunctivitis decreased the likelihood of bacterial conjunctivitis.5
Ultimately, if the former indicators are kept in mind, primary care clinicians should be able to decrease the prescribing of topical antimicrobials to patients with non-bacterial conjunctivitis.
Pearl: The best indicators of a bacterial cause in patients with presumed conjunctivitis are complete redness of the conjunctival membrane obscuring tarsal vessels, observed purulent discharge, and matting of both eyes in the morning. Presentation during the summer months and having a history of conjunctivitis decreases the likelihood of bacterial conjunctivitis.
Ms. Momany is a fourth-year medical student at University of Washington, Seattle. Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington and serves as third-year medical student clerkship director at that university. Contact Dr. Paauw at [email protected].
References
1. Azari AA and Barney NP. JAMA. 2013 Oct 23; 310(16):1721-9.
2. Smith AF and Waycaster C. BMC Ophthalmol. 2009 Nov 25. doi: 10.1186/1471-2415-9-13.
3) Narayana S and McGee S. Am J Med. 2015;128(11):1220-4.e1.
4) Stenson S et al. Arch Ophthalmol. 1982;100(8):1275-7.
5) Rietveld RP et al. BMJ. 2004 Jul 24;329(7459):206-10.
Financial Education for Health Care Providers
Health care provider (HCP) well-being has become a central topic as health care agencies increasingly recognize that stress leads to turnover and reduced efficacy.1 Financial health of HCPs is one aspect of overall well-being that has received little attention. We all work at the US Department of Veterans Affairs (VA) as psychologists and believe that there is a need to attend to financial literacy within the health care professions, a call that also has been made by physicians.2 For instance, a frequently mentioned aspect of financial literacy involves learning to effectively manage student loan debt. Another less often discussed facet is the need to save money for retirement early in one’s career to reap the benefits of compound interest: This is a particular concern for HCPs who were in graduate/medical school when they would have optimally started saving for retirement. Delaying retirement savings can have significant financial consequences, which can have a negative effect on well-being.
A few years ago, we started teaching advanced psychology trainees about financial well-being and were startled at the students’ lack of knowledge. For example, many students did not understand basic financial concepts, including the difference between a pension and a 401k/403b system of retirement savings—a knowledge gap that the authors speculate persists throughout some professionals’ careers. Research suggests that lack of knowledge in an area feels aversive and may result in procrastination or an inability to move toward a goal.3,4 Yet, postponing saving is problematic as it attenuates the effect of compound interest, thus making it difficult to accrue wealth.5 To address the lack of financial training among psychologists, the authors designed a seminar to provide retirement/financial-planning information to early career psychologists. This information fits the concept of “just in time” education: Disseminating knowledge when it is most likely to be useful, put into practice, and thus retained.6
Methods
In consultation with human resources officials at the VA, a 90-minute seminar was created to educate psychologists about saving for retirement. The seminar was recorded so that psychologists who were not able to attend in-person could view it at a later date. The seminar mainly covered systems of retirement (especially the VAspecific Thrift Savings Plan [TSP]), basic concepts of investing, ways of determining how much to save for retirement, and tax advantages of increased saving. It also provided simple retirement planning rules of thumb, as such heuristics have been shown to lead to greater behavior change than more unsystematic approaches.7 Key points included:
- Psychologists should try to approximately replace their current salary during retirement;
- There is no option to borrow money for retirement; the only sources of income for the retiree are social security, a possible pension, and any money saved;
- Psychologists and many other HCPs were in school during their prime saving years and tend to have lower salaries than that of other professional groups with similar amounts of education, so they should save aggressively earlier in their career;
- Early career psychologists should ensure that money saved for retirement is invested in relatively “aggressive” options, such as stock index funds (vs bond funds); and
- The tax benefits of allocating more income toward retirement savings in a tax-deferred savings plan such as the TSP can make it seem cheaper to invest, which can make it more attractive to immediately increase one’s savings.
As with any other savings plan, there are no guarantees or one-size-fits-all solutions, and finance professionals typically advise diversifying retirement savings (eg, stocks, bonds, real estate), to include both TSP and non-TSP plans in the case of VA employees.
To assess the usefulness of this seminar, the authors conducted a process improvement case study. The institutional review board of the Milwaukee VA Medical Center (VAMC) determined the study to be exempt as it was considered process improvement rather than research. Two assessment measures were created: a 5-item, anonymous measure of attendee satisfaction was administered immediately following the seminar, which assessed the extent to which presenters were engaging, material was presented clearly, presenters effectively used examples and illustrations, presenters effectively used slides/visual aids, and objectives were met (5-point Likert scale from “Needs major improvement” to “Excellent”).
Second, an internally developed anonymous pre- and postseminar survey was administered to assess changes in retirement- related knowledge, attitudes, and behaviors (3 months before the seminar [8 questions] and 2 months after [9 questions]). The survey assessed knowledge of retirement benefits (eg, difference between Roth and traditional retirement savings plans), general investment actions (eg, investing in TSP, investing in the TSP G fund, and investing sufficiently to earn the full employer match), and postseminar actions taken (eg, logging on to tsp.gov, increasing TSP contribution). Participants’ responses were anonymous, so the authors compared average behavior before and after the seminar rather than comparing individuals’ pre- and postseminar comments.
Results
About one-third (n = 28) of the Milwaukee VAMC psychologists attended, viewed, or presented/designed the seminar. Of the 12 participants who attended the seminar in person, all rated the presentation as excellent in each domain, with the exception of 1 participant (good). Anecdotally, participants approached presenters immediately after the presentation and up to 2 years later to indicate that the presentation was a useful retirement planning resource. A total of 27 psychologists completed the preseminar survey. Sixteen psychologists completed the postseminar survey and indicated that they attended/viewed the retirement seminar. Participants’ perceived knowledge of retirement benefits was assessed with response options, including nonexistent, vague, good, and sophisticated.
There was a significant change from preto postseminar, such that psychologists at postseminar felt that they had a better understanding of their retirement benefit options (Mann-Whitney U = 65.5, n1 = 27, n2 = 16, P < .01). The modal response preseminar was “vague” (67%) and postseminar was “good” (88%). There also were changes that were meaningful though not statistically significant: The percentage who had moved their money from the default, low-yield fund increased from 70% at preseminar to 88% at postseminar (Fisher exact test, 1-sided, P = .31). Also, fewer people reported on the postseminar survey that they were not sure whether they were invested in a Roth individual retirement account (IRA) or traditional TSP, indicating a trend toward significantly increased knowledge of their investments (Fisher exact test, 1-sided, P = .076).
Most important at follow-up, several behavior changes were reported. Most people (56%) had logged on to the TSP website to check on their account. A substantial number (26%) increased their contribution amount, and 6% moved money from the default fund. Overall, every respondent at follow-up confirmed having taken at least 1 of the actions assessed by the survey.
Conclusion
Based on the authors’ experience and research into financial education among HCPs, it is recommended that psychologists and other disciplines offer opportunities for retirement education at all levels of training. Financial education is likely to be most helpful if it is tailored toward a specific discipline, workplace, and time frame (eg, early career physicians may need more information about loan repayment and may need to invest in more aggressive retirement funds).8 Although many employers provide access to general financial education from outside companies, information provided by informed members of one’s field may be particularly helpful (eg, our seminar was curated for a psychology audience).
We found that the process of creating such a seminar was not burdensome and was educational for presenters as well as attendees. Further, it need not be intimidating to accumulate information to share; especially for those health care providers who have not made financial well-being a priority, learning and deploying a few targeted strategies can lead to increased peace of mind about retirement savings. Overall, we encourage a focus on financial literacy for all health care professions, including physicians who often may graduate with greater debts. Emphasizing early and aggressive financial literacy as an important aspect of provider well-being may help to produce healthier, wealthier, and overall better health care providers.2
Acknowledgments
This manuscript is partially the result of work supported with resources and the use of facilities at the Clement J. Zablocki VAMC, Milwaukee, Wisconsin. We thank Milwaukee VA retirement specialist, Vicki Heckman, for her invaluable advice in the preparation of these materials and the Psychology Advancement Workgroup at the Milwaukee VAMC for providing the impetus and support for this project.
1. Zhang Y, Feng X. The relationship between job satisfaction, burnout, and turnover intention among physicians from urban state-owned medical institutions in Hubei, China: a cross-sectional study. BMC Health Serv Res. 2011;11(1):235.
2. Chandrakantan A. Why is there no financial literacy 101 for doctors? https://opmed.doximity.com/an-open -call-to-residency-training-programs-and-trainees-to -facilitate-financial-literacy-bb762e585ed8. Published August 21, 2017. Accessed August 22, 2019.
3. Iyengar SS, Huberman G, Jiang W. How much choice is too much: determinants of individual contributions in 401K retirement plans. In: Mitchell OS, Utkus S, eds. Pension Design and Structure: New Lessons From Behavioral Finance. Oxford: Oxford University Press; 2004:83-95.
4. Parker AM, de Bruin WB, Yoong J, Willis R. Inappropriate confidence and retirement planning: four studies with a national sample. J Behav Decis Mak. 2012;25(4):382-389.
5. Lusardi A, Mitchell OS. Baby boomer retirement security: the roles of planning, financial literacy, and housing wealth. J Monet Econ. 2007;54(1):205-224.
6. Chub C. It’s time to teach financial literacy to young doctors. https://www.cnbc.com/2016/12/08/teaching -financial-literacy-to-young-doctors.html. Published December 8, 2016. Accessed August 22, 2019.
7. Binswanger J, Carman KG. How real people make longterm decisions: the case of retirement preparation. J Econ Behav Org. 2012;81(1):39-60.
8. Knoll MA. The role of behavioral economics and behavioral decision making in Americans’ retirement savings decisions. Soc Secur Bull. 2010;70(4):1-23.
Health care provider (HCP) well-being has become a central topic as health care agencies increasingly recognize that stress leads to turnover and reduced efficacy.1 Financial health of HCPs is one aspect of overall well-being that has received little attention. We all work at the US Department of Veterans Affairs (VA) as psychologists and believe that there is a need to attend to financial literacy within the health care professions, a call that also has been made by physicians.2 For instance, a frequently mentioned aspect of financial literacy involves learning to effectively manage student loan debt. Another less often discussed facet is the need to save money for retirement early in one’s career to reap the benefits of compound interest: This is a particular concern for HCPs who were in graduate/medical school when they would have optimally started saving for retirement. Delaying retirement savings can have significant financial consequences, which can have a negative effect on well-being.
A few years ago, we started teaching advanced psychology trainees about financial well-being and were startled at the students’ lack of knowledge. For example, many students did not understand basic financial concepts, including the difference between a pension and a 401k/403b system of retirement savings—a knowledge gap that the authors speculate persists throughout some professionals’ careers. Research suggests that lack of knowledge in an area feels aversive and may result in procrastination or an inability to move toward a goal.3,4 Yet, postponing saving is problematic as it attenuates the effect of compound interest, thus making it difficult to accrue wealth.5 To address the lack of financial training among psychologists, the authors designed a seminar to provide retirement/financial-planning information to early career psychologists. This information fits the concept of “just in time” education: Disseminating knowledge when it is most likely to be useful, put into practice, and thus retained.6
Methods
In consultation with human resources officials at the VA, a 90-minute seminar was created to educate psychologists about saving for retirement. The seminar was recorded so that psychologists who were not able to attend in-person could view it at a later date. The seminar mainly covered systems of retirement (especially the VAspecific Thrift Savings Plan [TSP]), basic concepts of investing, ways of determining how much to save for retirement, and tax advantages of increased saving. It also provided simple retirement planning rules of thumb, as such heuristics have been shown to lead to greater behavior change than more unsystematic approaches.7 Key points included:
- Psychologists should try to approximately replace their current salary during retirement;
- There is no option to borrow money for retirement; the only sources of income for the retiree are social security, a possible pension, and any money saved;
- Psychologists and many other HCPs were in school during their prime saving years and tend to have lower salaries than that of other professional groups with similar amounts of education, so they should save aggressively earlier in their career;
- Early career psychologists should ensure that money saved for retirement is invested in relatively “aggressive” options, such as stock index funds (vs bond funds); and
- The tax benefits of allocating more income toward retirement savings in a tax-deferred savings plan such as the TSP can make it seem cheaper to invest, which can make it more attractive to immediately increase one’s savings.
As with any other savings plan, there are no guarantees or one-size-fits-all solutions, and finance professionals typically advise diversifying retirement savings (eg, stocks, bonds, real estate), to include both TSP and non-TSP plans in the case of VA employees.
To assess the usefulness of this seminar, the authors conducted a process improvement case study. The institutional review board of the Milwaukee VA Medical Center (VAMC) determined the study to be exempt as it was considered process improvement rather than research. Two assessment measures were created: a 5-item, anonymous measure of attendee satisfaction was administered immediately following the seminar, which assessed the extent to which presenters were engaging, material was presented clearly, presenters effectively used examples and illustrations, presenters effectively used slides/visual aids, and objectives were met (5-point Likert scale from “Needs major improvement” to “Excellent”).
Second, an internally developed anonymous pre- and postseminar survey was administered to assess changes in retirement- related knowledge, attitudes, and behaviors (3 months before the seminar [8 questions] and 2 months after [9 questions]). The survey assessed knowledge of retirement benefits (eg, difference between Roth and traditional retirement savings plans), general investment actions (eg, investing in TSP, investing in the TSP G fund, and investing sufficiently to earn the full employer match), and postseminar actions taken (eg, logging on to tsp.gov, increasing TSP contribution). Participants’ responses were anonymous, so the authors compared average behavior before and after the seminar rather than comparing individuals’ pre- and postseminar comments.
Results
About one-third (n = 28) of the Milwaukee VAMC psychologists attended, viewed, or presented/designed the seminar. Of the 12 participants who attended the seminar in person, all rated the presentation as excellent in each domain, with the exception of 1 participant (good). Anecdotally, participants approached presenters immediately after the presentation and up to 2 years later to indicate that the presentation was a useful retirement planning resource. A total of 27 psychologists completed the preseminar survey. Sixteen psychologists completed the postseminar survey and indicated that they attended/viewed the retirement seminar. Participants’ perceived knowledge of retirement benefits was assessed with response options, including nonexistent, vague, good, and sophisticated.
There was a significant change from preto postseminar, such that psychologists at postseminar felt that they had a better understanding of their retirement benefit options (Mann-Whitney U = 65.5, n1 = 27, n2 = 16, P < .01). The modal response preseminar was “vague” (67%) and postseminar was “good” (88%). There also were changes that were meaningful though not statistically significant: The percentage who had moved their money from the default, low-yield fund increased from 70% at preseminar to 88% at postseminar (Fisher exact test, 1-sided, P = .31). Also, fewer people reported on the postseminar survey that they were not sure whether they were invested in a Roth individual retirement account (IRA) or traditional TSP, indicating a trend toward significantly increased knowledge of their investments (Fisher exact test, 1-sided, P = .076).
Most important at follow-up, several behavior changes were reported. Most people (56%) had logged on to the TSP website to check on their account. A substantial number (26%) increased their contribution amount, and 6% moved money from the default fund. Overall, every respondent at follow-up confirmed having taken at least 1 of the actions assessed by the survey.
Conclusion
Based on the authors’ experience and research into financial education among HCPs, it is recommended that psychologists and other disciplines offer opportunities for retirement education at all levels of training. Financial education is likely to be most helpful if it is tailored toward a specific discipline, workplace, and time frame (eg, early career physicians may need more information about loan repayment and may need to invest in more aggressive retirement funds).8 Although many employers provide access to general financial education from outside companies, information provided by informed members of one’s field may be particularly helpful (eg, our seminar was curated for a psychology audience).
We found that the process of creating such a seminar was not burdensome and was educational for presenters as well as attendees. Further, it need not be intimidating to accumulate information to share; especially for those health care providers who have not made financial well-being a priority, learning and deploying a few targeted strategies can lead to increased peace of mind about retirement savings. Overall, we encourage a focus on financial literacy for all health care professions, including physicians who often may graduate with greater debts. Emphasizing early and aggressive financial literacy as an important aspect of provider well-being may help to produce healthier, wealthier, and overall better health care providers.2
Acknowledgments
This manuscript is partially the result of work supported with resources and the use of facilities at the Clement J. Zablocki VAMC, Milwaukee, Wisconsin. We thank Milwaukee VA retirement specialist, Vicki Heckman, for her invaluable advice in the preparation of these materials and the Psychology Advancement Workgroup at the Milwaukee VAMC for providing the impetus and support for this project.
Health care provider (HCP) well-being has become a central topic as health care agencies increasingly recognize that stress leads to turnover and reduced efficacy.1 Financial health of HCPs is one aspect of overall well-being that has received little attention. We all work at the US Department of Veterans Affairs (VA) as psychologists and believe that there is a need to attend to financial literacy within the health care professions, a call that also has been made by physicians.2 For instance, a frequently mentioned aspect of financial literacy involves learning to effectively manage student loan debt. Another less often discussed facet is the need to save money for retirement early in one’s career to reap the benefits of compound interest: This is a particular concern for HCPs who were in graduate/medical school when they would have optimally started saving for retirement. Delaying retirement savings can have significant financial consequences, which can have a negative effect on well-being.
A few years ago, we started teaching advanced psychology trainees about financial well-being and were startled at the students’ lack of knowledge. For example, many students did not understand basic financial concepts, including the difference between a pension and a 401k/403b system of retirement savings—a knowledge gap that the authors speculate persists throughout some professionals’ careers. Research suggests that lack of knowledge in an area feels aversive and may result in procrastination or an inability to move toward a goal.3,4 Yet, postponing saving is problematic as it attenuates the effect of compound interest, thus making it difficult to accrue wealth.5 To address the lack of financial training among psychologists, the authors designed a seminar to provide retirement/financial-planning information to early career psychologists. This information fits the concept of “just in time” education: Disseminating knowledge when it is most likely to be useful, put into practice, and thus retained.6
Methods
In consultation with human resources officials at the VA, a 90-minute seminar was created to educate psychologists about saving for retirement. The seminar was recorded so that psychologists who were not able to attend in-person could view it at a later date. The seminar mainly covered systems of retirement (especially the VAspecific Thrift Savings Plan [TSP]), basic concepts of investing, ways of determining how much to save for retirement, and tax advantages of increased saving. It also provided simple retirement planning rules of thumb, as such heuristics have been shown to lead to greater behavior change than more unsystematic approaches.7 Key points included:
- Psychologists should try to approximately replace their current salary during retirement;
- There is no option to borrow money for retirement; the only sources of income for the retiree are social security, a possible pension, and any money saved;
- Psychologists and many other HCPs were in school during their prime saving years and tend to have lower salaries than that of other professional groups with similar amounts of education, so they should save aggressively earlier in their career;
- Early career psychologists should ensure that money saved for retirement is invested in relatively “aggressive” options, such as stock index funds (vs bond funds); and
- The tax benefits of allocating more income toward retirement savings in a tax-deferred savings plan such as the TSP can make it seem cheaper to invest, which can make it more attractive to immediately increase one’s savings.
As with any other savings plan, there are no guarantees or one-size-fits-all solutions, and finance professionals typically advise diversifying retirement savings (eg, stocks, bonds, real estate), to include both TSP and non-TSP plans in the case of VA employees.
To assess the usefulness of this seminar, the authors conducted a process improvement case study. The institutional review board of the Milwaukee VA Medical Center (VAMC) determined the study to be exempt as it was considered process improvement rather than research. Two assessment measures were created: a 5-item, anonymous measure of attendee satisfaction was administered immediately following the seminar, which assessed the extent to which presenters were engaging, material was presented clearly, presenters effectively used examples and illustrations, presenters effectively used slides/visual aids, and objectives were met (5-point Likert scale from “Needs major improvement” to “Excellent”).
Second, an internally developed anonymous pre- and postseminar survey was administered to assess changes in retirement- related knowledge, attitudes, and behaviors (3 months before the seminar [8 questions] and 2 months after [9 questions]). The survey assessed knowledge of retirement benefits (eg, difference between Roth and traditional retirement savings plans), general investment actions (eg, investing in TSP, investing in the TSP G fund, and investing sufficiently to earn the full employer match), and postseminar actions taken (eg, logging on to tsp.gov, increasing TSP contribution). Participants’ responses were anonymous, so the authors compared average behavior before and after the seminar rather than comparing individuals’ pre- and postseminar comments.
Results
About one-third (n = 28) of the Milwaukee VAMC psychologists attended, viewed, or presented/designed the seminar. Of the 12 participants who attended the seminar in person, all rated the presentation as excellent in each domain, with the exception of 1 participant (good). Anecdotally, participants approached presenters immediately after the presentation and up to 2 years later to indicate that the presentation was a useful retirement planning resource. A total of 27 psychologists completed the preseminar survey. Sixteen psychologists completed the postseminar survey and indicated that they attended/viewed the retirement seminar. Participants’ perceived knowledge of retirement benefits was assessed with response options, including nonexistent, vague, good, and sophisticated.
There was a significant change from preto postseminar, such that psychologists at postseminar felt that they had a better understanding of their retirement benefit options (Mann-Whitney U = 65.5, n1 = 27, n2 = 16, P < .01). The modal response preseminar was “vague” (67%) and postseminar was “good” (88%). There also were changes that were meaningful though not statistically significant: The percentage who had moved their money from the default, low-yield fund increased from 70% at preseminar to 88% at postseminar (Fisher exact test, 1-sided, P = .31). Also, fewer people reported on the postseminar survey that they were not sure whether they were invested in a Roth individual retirement account (IRA) or traditional TSP, indicating a trend toward significantly increased knowledge of their investments (Fisher exact test, 1-sided, P = .076).
Most important at follow-up, several behavior changes were reported. Most people (56%) had logged on to the TSP website to check on their account. A substantial number (26%) increased their contribution amount, and 6% moved money from the default fund. Overall, every respondent at follow-up confirmed having taken at least 1 of the actions assessed by the survey.
Conclusion
Based on the authors’ experience and research into financial education among HCPs, it is recommended that psychologists and other disciplines offer opportunities for retirement education at all levels of training. Financial education is likely to be most helpful if it is tailored toward a specific discipline, workplace, and time frame (eg, early career physicians may need more information about loan repayment and may need to invest in more aggressive retirement funds).8 Although many employers provide access to general financial education from outside companies, information provided by informed members of one’s field may be particularly helpful (eg, our seminar was curated for a psychology audience).
We found that the process of creating such a seminar was not burdensome and was educational for presenters as well as attendees. Further, it need not be intimidating to accumulate information to share; especially for those health care providers who have not made financial well-being a priority, learning and deploying a few targeted strategies can lead to increased peace of mind about retirement savings. Overall, we encourage a focus on financial literacy for all health care professions, including physicians who often may graduate with greater debts. Emphasizing early and aggressive financial literacy as an important aspect of provider well-being may help to produce healthier, wealthier, and overall better health care providers.2
Acknowledgments
This manuscript is partially the result of work supported with resources and the use of facilities at the Clement J. Zablocki VAMC, Milwaukee, Wisconsin. We thank Milwaukee VA retirement specialist, Vicki Heckman, for her invaluable advice in the preparation of these materials and the Psychology Advancement Workgroup at the Milwaukee VAMC for providing the impetus and support for this project.
1. Zhang Y, Feng X. The relationship between job satisfaction, burnout, and turnover intention among physicians from urban state-owned medical institutions in Hubei, China: a cross-sectional study. BMC Health Serv Res. 2011;11(1):235.
2. Chandrakantan A. Why is there no financial literacy 101 for doctors? https://opmed.doximity.com/an-open -call-to-residency-training-programs-and-trainees-to -facilitate-financial-literacy-bb762e585ed8. Published August 21, 2017. Accessed August 22, 2019.
3. Iyengar SS, Huberman G, Jiang W. How much choice is too much: determinants of individual contributions in 401K retirement plans. In: Mitchell OS, Utkus S, eds. Pension Design and Structure: New Lessons From Behavioral Finance. Oxford: Oxford University Press; 2004:83-95.
4. Parker AM, de Bruin WB, Yoong J, Willis R. Inappropriate confidence and retirement planning: four studies with a national sample. J Behav Decis Mak. 2012;25(4):382-389.
5. Lusardi A, Mitchell OS. Baby boomer retirement security: the roles of planning, financial literacy, and housing wealth. J Monet Econ. 2007;54(1):205-224.
6. Chub C. It’s time to teach financial literacy to young doctors. https://www.cnbc.com/2016/12/08/teaching -financial-literacy-to-young-doctors.html. Published December 8, 2016. Accessed August 22, 2019.
7. Binswanger J, Carman KG. How real people make longterm decisions: the case of retirement preparation. J Econ Behav Org. 2012;81(1):39-60.
8. Knoll MA. The role of behavioral economics and behavioral decision making in Americans’ retirement savings decisions. Soc Secur Bull. 2010;70(4):1-23.
1. Zhang Y, Feng X. The relationship between job satisfaction, burnout, and turnover intention among physicians from urban state-owned medical institutions in Hubei, China: a cross-sectional study. BMC Health Serv Res. 2011;11(1):235.
2. Chandrakantan A. Why is there no financial literacy 101 for doctors? https://opmed.doximity.com/an-open -call-to-residency-training-programs-and-trainees-to -facilitate-financial-literacy-bb762e585ed8. Published August 21, 2017. Accessed August 22, 2019.
3. Iyengar SS, Huberman G, Jiang W. How much choice is too much: determinants of individual contributions in 401K retirement plans. In: Mitchell OS, Utkus S, eds. Pension Design and Structure: New Lessons From Behavioral Finance. Oxford: Oxford University Press; 2004:83-95.
4. Parker AM, de Bruin WB, Yoong J, Willis R. Inappropriate confidence and retirement planning: four studies with a national sample. J Behav Decis Mak. 2012;25(4):382-389.
5. Lusardi A, Mitchell OS. Baby boomer retirement security: the roles of planning, financial literacy, and housing wealth. J Monet Econ. 2007;54(1):205-224.
6. Chub C. It’s time to teach financial literacy to young doctors. https://www.cnbc.com/2016/12/08/teaching -financial-literacy-to-young-doctors.html. Published December 8, 2016. Accessed August 22, 2019.
7. Binswanger J, Carman KG. How real people make longterm decisions: the case of retirement preparation. J Econ Behav Org. 2012;81(1):39-60.
8. Knoll MA. The role of behavioral economics and behavioral decision making in Americans’ retirement savings decisions. Soc Secur Bull. 2010;70(4):1-23.
Talking to overweight children
You are seeing a 9-year-old for her annual health maintenance visit. A quick look at her growth chart easily confirms your first impression that she is obese. How are you going to address the weight that you know, and she probably suspects, is going to make her vulnerable to a myriad of health problems as she gets older?
If she has been your patient since she was in preschool, this is certainly not the first time that her growth chart has been concerning. When did you first start discussing her weight with her parents? What words did you use? What strategies have you suggested? What referrals have you made? Maybe you have already given up and decided to not even “go there” at this visit because your experience with overweight patients has been so disappointing.
In her op ed in the New York Times, Dr. Perri Klass reconsiders these kinds of questions as she reviews an article in the journal Childhood Obesity (“Let’s Not Just Dismiss the Weight Watchers Kurbo App,” by Michelle I. Cardel, PhD, MS, RD, and Elsie M. Taveras, MD, MPH, August 2019) written by a nutrition scientist and a pediatrician who are concerned about a new weight loss app for children recently released by Weight Watchers. (The Checkup, “Helping Children Learn to Eat Well,” The New York Times, Aug. 26, 2019). Although the authors of the journal article question some of the science behind the app, their primary concerns are that the app is aimed at children without a way to guarantee parental involvement, and in their opinion the app also places too much emphasis on weight loss.
Their concerns go right to the heart of what troubles me about managing obesity in children. How should I talk to a child about her weight? What words can I choose without shaming? Maybe I shouldn’t be talking to her at all. When a child is 18 months old, we don’t talk to her about her growth chart. Not because she couldn’t understand, but because the solution rests not with her but with her parents.
Does that point come when we have given up on the parents’ ability to create and maintain an environment that discourages obesity? Is that the point when we begin asking the child to unlearn a complex set of behaviors that have been enabled or at least tolerated and poorly modeled at home?
When we begin to talk to a child about his weight do we begin by telling him that he may not have been a contributor to the problem when it began but from now on he needs to be a major player in its management? Of course we don’t share that reality with an 8-year-old, but sometime during his struggle to manage his weight he will connect the dots.

If you are beginning to suspect that I have built my pediatric career around a scaffolding of parent blaming and shaming you are wrong. I know that there are children who have inherited a suite of genes that make them vulnerable to obesity. And I know that too many children grow up in environments in which their parents are powerless to control the family diet for economic reasons. But I am sure that like me you mutter to yourself and your colleagues about the number of patients you are seeing each day whose growth charts are a clear reflection of less than optimal parenting.
Does all of this mean we throw in the towel and stop trying to help overweight children after they turn 6 years old? Of course not. But, it does mean we must redouble our efforts to help parents manage their children’s diets and activity levels in those first critical preschool years.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
You are seeing a 9-year-old for her annual health maintenance visit. A quick look at her growth chart easily confirms your first impression that she is obese. How are you going to address the weight that you know, and she probably suspects, is going to make her vulnerable to a myriad of health problems as she gets older?
If she has been your patient since she was in preschool, this is certainly not the first time that her growth chart has been concerning. When did you first start discussing her weight with her parents? What words did you use? What strategies have you suggested? What referrals have you made? Maybe you have already given up and decided to not even “go there” at this visit because your experience with overweight patients has been so disappointing.
In her op ed in the New York Times, Dr. Perri Klass reconsiders these kinds of questions as she reviews an article in the journal Childhood Obesity (“Let’s Not Just Dismiss the Weight Watchers Kurbo App,” by Michelle I. Cardel, PhD, MS, RD, and Elsie M. Taveras, MD, MPH, August 2019) written by a nutrition scientist and a pediatrician who are concerned about a new weight loss app for children recently released by Weight Watchers. (The Checkup, “Helping Children Learn to Eat Well,” The New York Times, Aug. 26, 2019). Although the authors of the journal article question some of the science behind the app, their primary concerns are that the app is aimed at children without a way to guarantee parental involvement, and in their opinion the app also places too much emphasis on weight loss.
Their concerns go right to the heart of what troubles me about managing obesity in children. How should I talk to a child about her weight? What words can I choose without shaming? Maybe I shouldn’t be talking to her at all. When a child is 18 months old, we don’t talk to her about her growth chart. Not because she couldn’t understand, but because the solution rests not with her but with her parents.
Does that point come when we have given up on the parents’ ability to create and maintain an environment that discourages obesity? Is that the point when we begin asking the child to unlearn a complex set of behaviors that have been enabled or at least tolerated and poorly modeled at home?
When we begin to talk to a child about his weight do we begin by telling him that he may not have been a contributor to the problem when it began but from now on he needs to be a major player in its management? Of course we don’t share that reality with an 8-year-old, but sometime during his struggle to manage his weight he will connect the dots.
If you are beginning to suspect that I have built my pediatric career around a scaffolding of parent blaming and shaming you are wrong. I know that there are children who have inherited a suite of genes that make them vulnerable to obesity. And I know that too many children grow up in environments in which their parents are powerless to control the family diet for economic reasons. But I am sure that like me you mutter to yourself and your colleagues about the number of patients you are seeing each day whose growth charts are a clear reflection of less than optimal parenting.
Does all of this mean we throw in the towel and stop trying to help overweight children after they turn 6 years old? Of course not. But, it does mean we must redouble our efforts to help parents manage their children’s diets and activity levels in those first critical preschool years.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
You are seeing a 9-year-old for her annual health maintenance visit. A quick look at her growth chart easily confirms your first impression that she is obese. How are you going to address the weight that you know, and she probably suspects, is going to make her vulnerable to a myriad of health problems as she gets older?
If she has been your patient since she was in preschool, this is certainly not the first time that her growth chart has been concerning. When did you first start discussing her weight with her parents? What words did you use? What strategies have you suggested? What referrals have you made? Maybe you have already given up and decided to not even “go there” at this visit because your experience with overweight patients has been so disappointing.
In her op ed in the New York Times, Dr. Perri Klass reconsiders these kinds of questions as she reviews an article in the journal Childhood Obesity (“Let’s Not Just Dismiss the Weight Watchers Kurbo App,” by Michelle I. Cardel, PhD, MS, RD, and Elsie M. Taveras, MD, MPH, August 2019) written by a nutrition scientist and a pediatrician who are concerned about a new weight loss app for children recently released by Weight Watchers. (The Checkup, “Helping Children Learn to Eat Well,” The New York Times, Aug. 26, 2019). Although the authors of the journal article question some of the science behind the app, their primary concerns are that the app is aimed at children without a way to guarantee parental involvement, and in their opinion the app also places too much emphasis on weight loss.
Their concerns go right to the heart of what troubles me about managing obesity in children. How should I talk to a child about her weight? What words can I choose without shaming? Maybe I shouldn’t be talking to her at all. When a child is 18 months old, we don’t talk to her about her growth chart. Not because she couldn’t understand, but because the solution rests not with her but with her parents.
Does that point come when we have given up on the parents’ ability to create and maintain an environment that discourages obesity? Is that the point when we begin asking the child to unlearn a complex set of behaviors that have been enabled or at least tolerated and poorly modeled at home?
When we begin to talk to a child about his weight do we begin by telling him that he may not have been a contributor to the problem when it began but from now on he needs to be a major player in its management? Of course we don’t share that reality with an 8-year-old, but sometime during his struggle to manage his weight he will connect the dots.
If you are beginning to suspect that I have built my pediatric career around a scaffolding of parent blaming and shaming you are wrong. I know that there are children who have inherited a suite of genes that make them vulnerable to obesity. And I know that too many children grow up in environments in which their parents are powerless to control the family diet for economic reasons. But I am sure that like me you mutter to yourself and your colleagues about the number of patients you are seeing each day whose growth charts are a clear reflection of less than optimal parenting.
Does all of this mean we throw in the towel and stop trying to help overweight children after they turn 6 years old? Of course not. But, it does mean we must redouble our efforts to help parents manage their children’s diets and activity levels in those first critical preschool years.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Taking vaccines to the next level via mucosal immunity
Vaccines are marvelous, and there are many well documented success stories, including rotavirus (RV) vaccines, where a live vaccine is administered to the gastrointestinal mucosa via oral drops. Antigens presented at the mucosal/epithelial surface not only induce systemic serum IgG – as do injectable vaccines – but also induce secretory IgA (sIgA), which is most helpful in diseases that directly affect the mucosa.

Mucosal vs. systemic immunity
Antibody being present on mucosal surfaces (point of initial pathogen contact) has a chance to neutralize the pathogen before it gains a foothold. Pathogen-specific mucosal lymphoid elements (e.g. in Peyer’s patches in the gut) also appear critical for optimal protection.1 The presence of both mucosal immune elements means that infection is severely limited or at times entirely prevented. So virus entering the GI tract causes minimal to no gut lining injury. Hence, there is no or mostly reduced vomiting/diarrhea. A downside of mucosally-administered live vaccines is that preexisting antibody to the vaccine antigens can reduce or block vaccine virus replication in the vaccinee, blunting or preventing protection. Note: Preexisting antibody also affects injectable live vaccines, such as the measles vaccine, similarly.
Classic injectable live or nonlive vaccines provide their most potent protection via systemic cellular responses antibody and/or antibodies in serum and extracellular fluid (ECF) where IgG and IgM are in highest concentrations. So even successful injectable vaccines still allow mucosal infection to start but then intercept further spread and prevent most of the downstream damage (think pertussis) or neutralize an infection-generated toxin (pertussis or tetanus). It usually is only after infection-induced damage occurs that systemic IgG and IgM gain better access to respiratory epithelial surfaces, but still only at a fraction of circulating concentrations. Indeed, pertussis vaccine–induced systemic immunity allows the pathogen to attack and replicate in/on host surface cells, causing toxin release and variable amounts of local mucosal injury/inflammation before vaccine-induced systemic immunity gains adequate access to the pathogen and/or to its toxin which may enter systemic circulation.
Live attenuated influenza vaccine (LAIV) induces mucosal immunity
Another “standard” vaccine that induces mucosal immunity – LAIV – was developed to improve on protection afforded by injectable influenza vaccines (IIVs), but LAIV has had hiccups in the United States. One example is several years of negligible protection against H1N1 disease. As long as LAIV’s vaccine strain had reasonably matched the circulating strains, LAIV worked at least as well as injectable influenza vaccine, and even offered some cross-protection against mildly mismatched strains. But after a number of years of LAIV use, vaccine effectiveness in the United States vs. H1N1 strains appeared to fade due to previously undetected but significant changes in the circulating H1N1 strain. The lesson is that mucosal immunity’s advantages are lost if too much change occurs in the pathogen target for sIgA and mucosally-associated lymphoid tissue cells (MALT)).
Other vaccines likely need to induce mucosal immunity
Protection at the mucosal level will likely be needed for success against norovirus, parainfluenza, respiratory syncytial virus (RSV), Neisseria gonorrhea, and chlamydia. Another helpful aspect of mucosal immunity is that immune cells and sIgA not only reside on the mucosa where the antigen was originally presented, but there is also a reasonable chance that these components will traffic to other mucosal surfaces.2 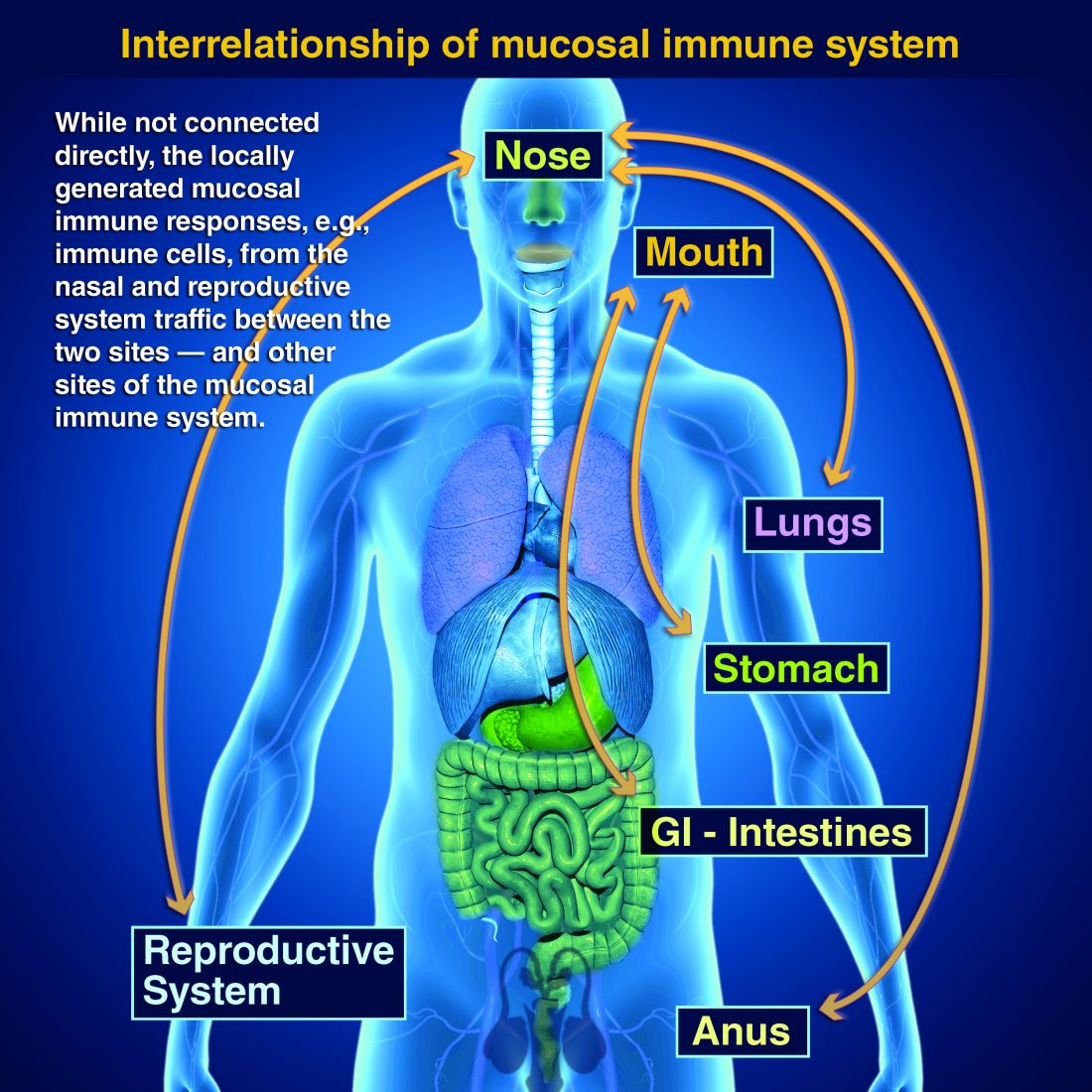
So intranasal vaccine could be expected to protect distant mucosal surfaces (urogenital, GI, and respiratory), leading to vaccine-induced systemic antibody plus mucosal immunity (sIGA and MALT responses) at each site.
Let’s look at a novel “two-site” chlamydia vaccine
Recently a phase 1 chlamydia vaccine that used a novel two-pronged administration site/schedule was successful at inducing both mucosal and systemic immunity in a proof-of-concept study – achieving the best of both worlds.3 This may be a template for vaccines in years to come. British investigators studied 50 healthy women aged 19-45 years in a double-blind, parallel, randomized, placebo-controlled trial that used a recombinant chlamydia protein subunit antigen (CTH522). The vaccine schedule involved three injectable priming doses followed soon thereafter by two intranasal boosting doses. There were three groups:
1. CTH522 adjuvanted with CAF01 liposomes (CTH522:CAF01).
2. CTH522 adjuvanted with aluminum hydroxide (CTH522:AH).
3. Placebo (saline).
The intramuscular (IM) priming schedule was 0, 1, and 4 months. The intranasal vaccine booster doses or placebo were given at 4.5 and 5 months. No related serious adverse reactions occurred. For injectable dosing, the most frequent adverse event was mild local injection-site reactions in all subjects in both vaccine groups vs. in 60% of placebo recipients (P = .053). The adjuvants were the likely cause for local reactions. Intranasal doses had local reactions in 47% of both vaccine groups and 60% of placebo recipients; P = 1.000).
Both vaccines produced systemic IgG seroconversion (including neutralizing antibody) plus small amounts of IgG in the nasal cavity and genital tract in all vaccine recipients; no placebo recipient seroconverted. Interestingly, liposomally-adjuvanted vaccine produced a more rapid systemic IgG response and higher serum titers than the alum-adjuvanted vaccine. Likewise, the IM liposomal vaccine also induced higher but still small mucosal IgG antibody responses (P = .0091). Intranasal IM-induced IgG titers were not boosted by later intranasal vaccine dosing.
Subjects getting liposomal vaccine (but not alum vaccine or placebo) boosters had detectable sIgA titers in both nasal and genital tract secretions. Liposomal vaccine recipients also had fivefold to sixfold higher median titers than alum vaccine recipients after the priming dose, and these higher titers persisted to the end of the study. All liposomal vaccine recipients developed antichlamydial cell-mediated responses vs. 57% alum-adjuvanted vaccine recipients. (P = .01). So both use of two-site dosing and the liposomal adjuvant appeared critical to better responses.

In summary
While this candidate vaccine has hurdles to overcome before coming into routine use, the proof-of-principle that a combination injectable-intranasal vaccine schedule can induce robust systemic and mucosal immunity when given with an appropriate adjuvant is very promising. Adding more vaccines to the schedule then becomes an issue, but that is one of those “good” problems we can deal with later.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital-Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines, receives funding from GlaxoSmithKline for studies on pneumococcal and rotavirus vaccines, and from Pfizer for a study on pneumococcal vaccine on which Dr. Harrison is a sub-investigator. The hospital also receives Centers for Disease Control and Prevention funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus, and also for rotavirus. Email Dr. Harrison at [email protected].
References
1. PLOS Biology. 2012 Sep 1. doi: 10.1371/journal.pbio.1001397.
2. Mucosal Immunity in the Human Female Reproductive Tract in “Mucosal Immunology,” 4th ed., Volume 2 (Cambridge, MA: Academic Press, 2015, pp. 2097-124).
3. Lancet Infect Dis. 2019. doi: 10.1016/S1473-3099(19)30279-8.
Vaccines are marvelous, and there are many well documented success stories, including rotavirus (RV) vaccines, where a live vaccine is administered to the gastrointestinal mucosa via oral drops. Antigens presented at the mucosal/epithelial surface not only induce systemic serum IgG – as do injectable vaccines – but also induce secretory IgA (sIgA), which is most helpful in diseases that directly affect the mucosa.
Mucosal vs. systemic immunity
Antibody being present on mucosal surfaces (point of initial pathogen contact) has a chance to neutralize the pathogen before it gains a foothold. Pathogen-specific mucosal lymphoid elements (e.g. in Peyer’s patches in the gut) also appear critical for optimal protection.1 The presence of both mucosal immune elements means that infection is severely limited or at times entirely prevented. So virus entering the GI tract causes minimal to no gut lining injury. Hence, there is no or mostly reduced vomiting/diarrhea. A downside of mucosally-administered live vaccines is that preexisting antibody to the vaccine antigens can reduce or block vaccine virus replication in the vaccinee, blunting or preventing protection. Note: Preexisting antibody also affects injectable live vaccines, such as the measles vaccine, similarly.
Classic injectable live or nonlive vaccines provide their most potent protection via systemic cellular responses antibody and/or antibodies in serum and extracellular fluid (ECF) where IgG and IgM are in highest concentrations. So even successful injectable vaccines still allow mucosal infection to start but then intercept further spread and prevent most of the downstream damage (think pertussis) or neutralize an infection-generated toxin (pertussis or tetanus). It usually is only after infection-induced damage occurs that systemic IgG and IgM gain better access to respiratory epithelial surfaces, but still only at a fraction of circulating concentrations. Indeed, pertussis vaccine–induced systemic immunity allows the pathogen to attack and replicate in/on host surface cells, causing toxin release and variable amounts of local mucosal injury/inflammation before vaccine-induced systemic immunity gains adequate access to the pathogen and/or to its toxin which may enter systemic circulation.
Live attenuated influenza vaccine (LAIV) induces mucosal immunity
Another “standard” vaccine that induces mucosal immunity – LAIV – was developed to improve on protection afforded by injectable influenza vaccines (IIVs), but LAIV has had hiccups in the United States. One example is several years of negligible protection against H1N1 disease. As long as LAIV’s vaccine strain had reasonably matched the circulating strains, LAIV worked at least as well as injectable influenza vaccine, and even offered some cross-protection against mildly mismatched strains. But after a number of years of LAIV use, vaccine effectiveness in the United States vs. H1N1 strains appeared to fade due to previously undetected but significant changes in the circulating H1N1 strain. The lesson is that mucosal immunity’s advantages are lost if too much change occurs in the pathogen target for sIgA and mucosally-associated lymphoid tissue cells (MALT)).
Other vaccines likely need to induce mucosal immunity
Protection at the mucosal level will likely be needed for success against norovirus, parainfluenza, respiratory syncytial virus (RSV), Neisseria gonorrhea, and chlamydia. Another helpful aspect of mucosal immunity is that immune cells and sIgA not only reside on the mucosa where the antigen was originally presented, but there is also a reasonable chance that these components will traffic to other mucosal surfaces.2
So intranasal vaccine could be expected to protect distant mucosal surfaces (urogenital, GI, and respiratory), leading to vaccine-induced systemic antibody plus mucosal immunity (sIGA and MALT responses) at each site.
Let’s look at a novel “two-site” chlamydia vaccine
Recently a phase 1 chlamydia vaccine that used a novel two-pronged administration site/schedule was successful at inducing both mucosal and systemic immunity in a proof-of-concept study – achieving the best of both worlds.3 This may be a template for vaccines in years to come. British investigators studied 50 healthy women aged 19-45 years in a double-blind, parallel, randomized, placebo-controlled trial that used a recombinant chlamydia protein subunit antigen (CTH522). The vaccine schedule involved three injectable priming doses followed soon thereafter by two intranasal boosting doses. There were three groups:
1. CTH522 adjuvanted with CAF01 liposomes (CTH522:CAF01).
2. CTH522 adjuvanted with aluminum hydroxide (CTH522:AH).
3. Placebo (saline).
The intramuscular (IM) priming schedule was 0, 1, and 4 months. The intranasal vaccine booster doses or placebo were given at 4.5 and 5 months. No related serious adverse reactions occurred. For injectable dosing, the most frequent adverse event was mild local injection-site reactions in all subjects in both vaccine groups vs. in 60% of placebo recipients (P = .053). The adjuvants were the likely cause for local reactions. Intranasal doses had local reactions in 47% of both vaccine groups and 60% of placebo recipients; P = 1.000).
Both vaccines produced systemic IgG seroconversion (including neutralizing antibody) plus small amounts of IgG in the nasal cavity and genital tract in all vaccine recipients; no placebo recipient seroconverted. Interestingly, liposomally-adjuvanted vaccine produced a more rapid systemic IgG response and higher serum titers than the alum-adjuvanted vaccine. Likewise, the IM liposomal vaccine also induced higher but still small mucosal IgG antibody responses (P = .0091). Intranasal IM-induced IgG titers were not boosted by later intranasal vaccine dosing.
Subjects getting liposomal vaccine (but not alum vaccine or placebo) boosters had detectable sIgA titers in both nasal and genital tract secretions. Liposomal vaccine recipients also had fivefold to sixfold higher median titers than alum vaccine recipients after the priming dose, and these higher titers persisted to the end of the study. All liposomal vaccine recipients developed antichlamydial cell-mediated responses vs. 57% alum-adjuvanted vaccine recipients. (P = .01). So both use of two-site dosing and the liposomal adjuvant appeared critical to better responses.
In summary
While this candidate vaccine has hurdles to overcome before coming into routine use, the proof-of-principle that a combination injectable-intranasal vaccine schedule can induce robust systemic and mucosal immunity when given with an appropriate adjuvant is very promising. Adding more vaccines to the schedule then becomes an issue, but that is one of those “good” problems we can deal with later.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital-Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines, receives funding from GlaxoSmithKline for studies on pneumococcal and rotavirus vaccines, and from Pfizer for a study on pneumococcal vaccine on which Dr. Harrison is a sub-investigator. The hospital also receives Centers for Disease Control and Prevention funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus, and also for rotavirus. Email Dr. Harrison at [email protected].
References
1. PLOS Biology. 2012 Sep 1. doi: 10.1371/journal.pbio.1001397.
2. Mucosal Immunity in the Human Female Reproductive Tract in “Mucosal Immunology,” 4th ed., Volume 2 (Cambridge, MA: Academic Press, 2015, pp. 2097-124).
3. Lancet Infect Dis. 2019. doi: 10.1016/S1473-3099(19)30279-8.
Vaccines are marvelous, and there are many well documented success stories, including rotavirus (RV) vaccines, where a live vaccine is administered to the gastrointestinal mucosa via oral drops. Antigens presented at the mucosal/epithelial surface not only induce systemic serum IgG – as do injectable vaccines – but also induce secretory IgA (sIgA), which is most helpful in diseases that directly affect the mucosa.
Mucosal vs. systemic immunity
Antibody being present on mucosal surfaces (point of initial pathogen contact) has a chance to neutralize the pathogen before it gains a foothold. Pathogen-specific mucosal lymphoid elements (e.g. in Peyer’s patches in the gut) also appear critical for optimal protection.1 The presence of both mucosal immune elements means that infection is severely limited or at times entirely prevented. So virus entering the GI tract causes minimal to no gut lining injury. Hence, there is no or mostly reduced vomiting/diarrhea. A downside of mucosally-administered live vaccines is that preexisting antibody to the vaccine antigens can reduce or block vaccine virus replication in the vaccinee, blunting or preventing protection. Note: Preexisting antibody also affects injectable live vaccines, such as the measles vaccine, similarly.
Classic injectable live or nonlive vaccines provide their most potent protection via systemic cellular responses antibody and/or antibodies in serum and extracellular fluid (ECF) where IgG and IgM are in highest concentrations. So even successful injectable vaccines still allow mucosal infection to start but then intercept further spread and prevent most of the downstream damage (think pertussis) or neutralize an infection-generated toxin (pertussis or tetanus). It usually is only after infection-induced damage occurs that systemic IgG and IgM gain better access to respiratory epithelial surfaces, but still only at a fraction of circulating concentrations. Indeed, pertussis vaccine–induced systemic immunity allows the pathogen to attack and replicate in/on host surface cells, causing toxin release and variable amounts of local mucosal injury/inflammation before vaccine-induced systemic immunity gains adequate access to the pathogen and/or to its toxin which may enter systemic circulation.
Live attenuated influenza vaccine (LAIV) induces mucosal immunity
Another “standard” vaccine that induces mucosal immunity – LAIV – was developed to improve on protection afforded by injectable influenza vaccines (IIVs), but LAIV has had hiccups in the United States. One example is several years of negligible protection against H1N1 disease. As long as LAIV’s vaccine strain had reasonably matched the circulating strains, LAIV worked at least as well as injectable influenza vaccine, and even offered some cross-protection against mildly mismatched strains. But after a number of years of LAIV use, vaccine effectiveness in the United States vs. H1N1 strains appeared to fade due to previously undetected but significant changes in the circulating H1N1 strain. The lesson is that mucosal immunity’s advantages are lost if too much change occurs in the pathogen target for sIgA and mucosally-associated lymphoid tissue cells (MALT)).
Other vaccines likely need to induce mucosal immunity
Protection at the mucosal level will likely be needed for success against norovirus, parainfluenza, respiratory syncytial virus (RSV), Neisseria gonorrhea, and chlamydia. Another helpful aspect of mucosal immunity is that immune cells and sIgA not only reside on the mucosa where the antigen was originally presented, but there is also a reasonable chance that these components will traffic to other mucosal surfaces.2
So intranasal vaccine could be expected to protect distant mucosal surfaces (urogenital, GI, and respiratory), leading to vaccine-induced systemic antibody plus mucosal immunity (sIGA and MALT responses) at each site.
Let’s look at a novel “two-site” chlamydia vaccine
Recently a phase 1 chlamydia vaccine that used a novel two-pronged administration site/schedule was successful at inducing both mucosal and systemic immunity in a proof-of-concept study – achieving the best of both worlds.3 This may be a template for vaccines in years to come. British investigators studied 50 healthy women aged 19-45 years in a double-blind, parallel, randomized, placebo-controlled trial that used a recombinant chlamydia protein subunit antigen (CTH522). The vaccine schedule involved three injectable priming doses followed soon thereafter by two intranasal boosting doses. There were three groups:
1. CTH522 adjuvanted with CAF01 liposomes (CTH522:CAF01).
2. CTH522 adjuvanted with aluminum hydroxide (CTH522:AH).
3. Placebo (saline).
The intramuscular (IM) priming schedule was 0, 1, and 4 months. The intranasal vaccine booster doses or placebo were given at 4.5 and 5 months. No related serious adverse reactions occurred. For injectable dosing, the most frequent adverse event was mild local injection-site reactions in all subjects in both vaccine groups vs. in 60% of placebo recipients (P = .053). The adjuvants were the likely cause for local reactions. Intranasal doses had local reactions in 47% of both vaccine groups and 60% of placebo recipients; P = 1.000).
Both vaccines produced systemic IgG seroconversion (including neutralizing antibody) plus small amounts of IgG in the nasal cavity and genital tract in all vaccine recipients; no placebo recipient seroconverted. Interestingly, liposomally-adjuvanted vaccine produced a more rapid systemic IgG response and higher serum titers than the alum-adjuvanted vaccine. Likewise, the IM liposomal vaccine also induced higher but still small mucosal IgG antibody responses (P = .0091). Intranasal IM-induced IgG titers were not boosted by later intranasal vaccine dosing.
Subjects getting liposomal vaccine (but not alum vaccine or placebo) boosters had detectable sIgA titers in both nasal and genital tract secretions. Liposomal vaccine recipients also had fivefold to sixfold higher median titers than alum vaccine recipients after the priming dose, and these higher titers persisted to the end of the study. All liposomal vaccine recipients developed antichlamydial cell-mediated responses vs. 57% alum-adjuvanted vaccine recipients. (P = .01). So both use of two-site dosing and the liposomal adjuvant appeared critical to better responses.
In summary
While this candidate vaccine has hurdles to overcome before coming into routine use, the proof-of-principle that a combination injectable-intranasal vaccine schedule can induce robust systemic and mucosal immunity when given with an appropriate adjuvant is very promising. Adding more vaccines to the schedule then becomes an issue, but that is one of those “good” problems we can deal with later.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospital-Kansas City, Mo. Children’s Mercy Hospital receives grant funding to study two candidate RSV vaccines, receives funding from GlaxoSmithKline for studies on pneumococcal and rotavirus vaccines, and from Pfizer for a study on pneumococcal vaccine on which Dr. Harrison is a sub-investigator. The hospital also receives Centers for Disease Control and Prevention funding under the New Vaccine Surveillance Network for multicenter surveillance of acute respiratory infections, including influenza, RSV, and parainfluenza virus, and also for rotavirus. Email Dr. Harrison at [email protected].
References
1. PLOS Biology. 2012 Sep 1. doi: 10.1371/journal.pbio.1001397.
2. Mucosal Immunity in the Human Female Reproductive Tract in “Mucosal Immunology,” 4th ed., Volume 2 (Cambridge, MA: Academic Press, 2015, pp. 2097-124).
3. Lancet Infect Dis. 2019. doi: 10.1016/S1473-3099(19)30279-8.
My patient tells me that they are transgender – now what?
I am privileged to work in a university hospital system where I have access to colleagues with expertise in LGBT health; however, medical providers in the community may not enjoy such resources. Many transgender and gender-diverse (TGD) youth now are seeking help from their community primary care providers to affirm their gender identity, but many community primary care providers do not have the luxury of referring these patients to an expert in gender-affirming care when their TGD patients express the desire to affirm their gender through medical and surgical means. This is even more difficult if the nearest referral center is hundreds of miles away. Nevertheless,

If a TGD youth discloses their gender identity to you, it is critical that you make the patient feel safe and supported. Showing support is important in maintaining rapport between you and the patient. Furthermore, you may be one of the very few adults in the child’s life whom they can trust.
First of all, thank them. For many TGD patients, disclosing their gender identity to a health care provider can be a herculean task. They may have spent many hours trying to find the right words to say to disclose an important aspect of themselves to you. They also probably spent a fair amount of time worrying about whether or not you would react positively to this disclosure. This fear is reasonable. About one-fifth of transgender people have reported being kicked out of a medical practice because of their disclosure of their gender identity.1
Secondly, assure the TGD patient that your treatment would be no different from the care provided for other patients. Discrimination from a health care provider has frequently been reported by TGD patients1 and is expected from this population.2 By emphasizing this, you have signaled to them that you are committed to treating them with dignity and respect. Furthermore, signal your commitment to this treatment by making the clinic a safe and welcoming place for LGBT youth. Several resources exist that can help with this. The American Medical Association provides a good example on how to draft a nondiscrimination statement that can be posted in waiting areas;3 the Fenway Institute has a good example of an intake form that is LGBT friendly.4
In addition, a good way to help affirm their gender identity is to tell them that being transgender or gender-diverse is normal and healthy. Many times, TGD youth will hear narratives that gender diversity is pathological or aberrant; however, hearing that they are healthy and normal, especially from a health care provider, can make a powerful impact on feeling supported and affirmed.
Furthermore, inform your TGD youth of their right to confidentiality. Many TGD youth may not be out to their parents, and you may be the first person to whom they disclosed their gender identity. This is especially helpful if you describe their right to and the limits of confidentiality (e.g., suicidality) at the beginning of the visit. Assurance of confidentiality is a vital reason adolescents and young adults seek health care from a medical provider,5 and the same can be said of TGD youth; however, keep in mind that if they do desire to transition using cross-sex hormones or surgery, parental permission is required.
If they are not out to their parents and they are planning to come out to their parents, offer to be there when they do. Having someone to support the child – someone who is a medical provider – can add to the sense of legitimacy that what the child is experiencing is normal and healthy. Providing guidance on how parents can support their TGD child is essential for successful affirmation, and some suggestions can be found in an LGBT Youth Consult column I wrote titled, “Guidance for parents of LGBT youth.”
If you practice in a location where the nearest expert in gender-affirming care can be hundreds of miles away, educate yourself on gender-affirming care. Several guidelines are available. The World Professional Society for Transgender Standards of Care (SOC) focuses on the mental health aspects of gender-affirming care. The SOC recommends, but no longer requires, letters from a mental health therapist to start gender-affirming medical treatments and does allow for a discussion between you and the patient on the risks, benefits, alternatives, unknowns, limitations of treatment, and risks of not treating (i.e., obtaining informed consent) as the threshold for hormone therapy.6 This approach, known as the “informed consent model,” can be helpful in expanding health care access for TGD youth. Furthermore, there’s the Endocrine Society Clinical Practice Guidelines7 and the University of California, San Francisco, Guidelines,8 which focus on the medical aspects of gender-affirming care, such as when to start pubertal blockers and dosing for cross-sex hormones. Finally, there are resources that allow providers to consult an expert remotely for more complicated cases. Transline is a transgender medical consultation service staffed by medical providers with expertise in gender-affirming care. Providers can learn more about this valuable service on the website: http://project-health.org/transline/.

Working in a major medical center is not necessary in providing gender-affirming care to TGD youth. Being respectful, supportive, and having the willingness to learn are the minimal requirements. Resources are available to help guide you on the more technical aspects of gender-affirming care. Maintaining a supportive environment and using these resources will help you expand health care access for this population.
Dr. Montano is an assistant professor of pediatrics at the University of Pittsburgh and an adolescent medicine physician at Children’s Hospital of Pittsburgh of UPMC. Email him at [email protected].
References
1. Injustice at every turn: A report of the national transgender discrimination survey (National Center for Transgender Equality and National Gay and Lesbian Task Force, 2011).
2. Psychol Bull. 2003 Sep;129(5):674-97.
3. “Creating an LGBTQ-friendly practice,” American Medical Association.
4. Fenway Health Client Registration Form.
5. JAMA. 1993 Mar 17;269(11):1404-7.
6. Int J Transgenderism 2012;13:165-232.
7. J Clin Endocrinol Metab. 2017 Nov 1;102(11):3869-903.
8. “Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People,” 2nd edition (San Francisco, CA: University of California, San Francisco, June 17, 2016).
I am privileged to work in a university hospital system where I have access to colleagues with expertise in LGBT health; however, medical providers in the community may not enjoy such resources. Many transgender and gender-diverse (TGD) youth now are seeking help from their community primary care providers to affirm their gender identity, but many community primary care providers do not have the luxury of referring these patients to an expert in gender-affirming care when their TGD patients express the desire to affirm their gender through medical and surgical means. This is even more difficult if the nearest referral center is hundreds of miles away. Nevertheless,
If a TGD youth discloses their gender identity to you, it is critical that you make the patient feel safe and supported. Showing support is important in maintaining rapport between you and the patient. Furthermore, you may be one of the very few adults in the child’s life whom they can trust.
First of all, thank them. For many TGD patients, disclosing their gender identity to a health care provider can be a herculean task. They may have spent many hours trying to find the right words to say to disclose an important aspect of themselves to you. They also probably spent a fair amount of time worrying about whether or not you would react positively to this disclosure. This fear is reasonable. About one-fifth of transgender people have reported being kicked out of a medical practice because of their disclosure of their gender identity.1
Secondly, assure the TGD patient that your treatment would be no different from the care provided for other patients. Discrimination from a health care provider has frequently been reported by TGD patients1 and is expected from this population.2 By emphasizing this, you have signaled to them that you are committed to treating them with dignity and respect. Furthermore, signal your commitment to this treatment by making the clinic a safe and welcoming place for LGBT youth. Several resources exist that can help with this. The American Medical Association provides a good example on how to draft a nondiscrimination statement that can be posted in waiting areas;3 the Fenway Institute has a good example of an intake form that is LGBT friendly.4
In addition, a good way to help affirm their gender identity is to tell them that being transgender or gender-diverse is normal and healthy. Many times, TGD youth will hear narratives that gender diversity is pathological or aberrant; however, hearing that they are healthy and normal, especially from a health care provider, can make a powerful impact on feeling supported and affirmed.
Furthermore, inform your TGD youth of their right to confidentiality. Many TGD youth may not be out to their parents, and you may be the first person to whom they disclosed their gender identity. This is especially helpful if you describe their right to and the limits of confidentiality (e.g., suicidality) at the beginning of the visit. Assurance of confidentiality is a vital reason adolescents and young adults seek health care from a medical provider,5 and the same can be said of TGD youth; however, keep in mind that if they do desire to transition using cross-sex hormones or surgery, parental permission is required.
If they are not out to their parents and they are planning to come out to their parents, offer to be there when they do. Having someone to support the child – someone who is a medical provider – can add to the sense of legitimacy that what the child is experiencing is normal and healthy. Providing guidance on how parents can support their TGD child is essential for successful affirmation, and some suggestions can be found in an LGBT Youth Consult column I wrote titled, “Guidance for parents of LGBT youth.”
If you practice in a location where the nearest expert in gender-affirming care can be hundreds of miles away, educate yourself on gender-affirming care. Several guidelines are available. The World Professional Society for Transgender Standards of Care (SOC) focuses on the mental health aspects of gender-affirming care. The SOC recommends, but no longer requires, letters from a mental health therapist to start gender-affirming medical treatments and does allow for a discussion between you and the patient on the risks, benefits, alternatives, unknowns, limitations of treatment, and risks of not treating (i.e., obtaining informed consent) as the threshold for hormone therapy.6 This approach, known as the “informed consent model,” can be helpful in expanding health care access for TGD youth. Furthermore, there’s the Endocrine Society Clinical Practice Guidelines7 and the University of California, San Francisco, Guidelines,8 which focus on the medical aspects of gender-affirming care, such as when to start pubertal blockers and dosing for cross-sex hormones. Finally, there are resources that allow providers to consult an expert remotely for more complicated cases. Transline is a transgender medical consultation service staffed by medical providers with expertise in gender-affirming care. Providers can learn more about this valuable service on the website: http://project-health.org/transline/.
Working in a major medical center is not necessary in providing gender-affirming care to TGD youth. Being respectful, supportive, and having the willingness to learn are the minimal requirements. Resources are available to help guide you on the more technical aspects of gender-affirming care. Maintaining a supportive environment and using these resources will help you expand health care access for this population.
Dr. Montano is an assistant professor of pediatrics at the University of Pittsburgh and an adolescent medicine physician at Children’s Hospital of Pittsburgh of UPMC. Email him at [email protected].
References
1. Injustice at every turn: A report of the national transgender discrimination survey (National Center for Transgender Equality and National Gay and Lesbian Task Force, 2011).
2. Psychol Bull. 2003 Sep;129(5):674-97.
3. “Creating an LGBTQ-friendly practice,” American Medical Association.
4. Fenway Health Client Registration Form.
5. JAMA. 1993 Mar 17;269(11):1404-7.
6. Int J Transgenderism 2012;13:165-232.
7. J Clin Endocrinol Metab. 2017 Nov 1;102(11):3869-903.
8. “Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People,” 2nd edition (San Francisco, CA: University of California, San Francisco, June 17, 2016).
I am privileged to work in a university hospital system where I have access to colleagues with expertise in LGBT health; however, medical providers in the community may not enjoy such resources. Many transgender and gender-diverse (TGD) youth now are seeking help from their community primary care providers to affirm their gender identity, but many community primary care providers do not have the luxury of referring these patients to an expert in gender-affirming care when their TGD patients express the desire to affirm their gender through medical and surgical means. This is even more difficult if the nearest referral center is hundreds of miles away. Nevertheless,
If a TGD youth discloses their gender identity to you, it is critical that you make the patient feel safe and supported. Showing support is important in maintaining rapport between you and the patient. Furthermore, you may be one of the very few adults in the child’s life whom they can trust.
First of all, thank them. For many TGD patients, disclosing their gender identity to a health care provider can be a herculean task. They may have spent many hours trying to find the right words to say to disclose an important aspect of themselves to you. They also probably spent a fair amount of time worrying about whether or not you would react positively to this disclosure. This fear is reasonable. About one-fifth of transgender people have reported being kicked out of a medical practice because of their disclosure of their gender identity.1
Secondly, assure the TGD patient that your treatment would be no different from the care provided for other patients. Discrimination from a health care provider has frequently been reported by TGD patients1 and is expected from this population.2 By emphasizing this, you have signaled to them that you are committed to treating them with dignity and respect. Furthermore, signal your commitment to this treatment by making the clinic a safe and welcoming place for LGBT youth. Several resources exist that can help with this. The American Medical Association provides a good example on how to draft a nondiscrimination statement that can be posted in waiting areas;3 the Fenway Institute has a good example of an intake form that is LGBT friendly.4
In addition, a good way to help affirm their gender identity is to tell them that being transgender or gender-diverse is normal and healthy. Many times, TGD youth will hear narratives that gender diversity is pathological or aberrant; however, hearing that they are healthy and normal, especially from a health care provider, can make a powerful impact on feeling supported and affirmed.
Furthermore, inform your TGD youth of their right to confidentiality. Many TGD youth may not be out to their parents, and you may be the first person to whom they disclosed their gender identity. This is especially helpful if you describe their right to and the limits of confidentiality (e.g., suicidality) at the beginning of the visit. Assurance of confidentiality is a vital reason adolescents and young adults seek health care from a medical provider,5 and the same can be said of TGD youth; however, keep in mind that if they do desire to transition using cross-sex hormones or surgery, parental permission is required.
If they are not out to their parents and they are planning to come out to their parents, offer to be there when they do. Having someone to support the child – someone who is a medical provider – can add to the sense of legitimacy that what the child is experiencing is normal and healthy. Providing guidance on how parents can support their TGD child is essential for successful affirmation, and some suggestions can be found in an LGBT Youth Consult column I wrote titled, “Guidance for parents of LGBT youth.”
If you practice in a location where the nearest expert in gender-affirming care can be hundreds of miles away, educate yourself on gender-affirming care. Several guidelines are available. The World Professional Society for Transgender Standards of Care (SOC) focuses on the mental health aspects of gender-affirming care. The SOC recommends, but no longer requires, letters from a mental health therapist to start gender-affirming medical treatments and does allow for a discussion between you and the patient on the risks, benefits, alternatives, unknowns, limitations of treatment, and risks of not treating (i.e., obtaining informed consent) as the threshold for hormone therapy.6 This approach, known as the “informed consent model,” can be helpful in expanding health care access for TGD youth. Furthermore, there’s the Endocrine Society Clinical Practice Guidelines7 and the University of California, San Francisco, Guidelines,8 which focus on the medical aspects of gender-affirming care, such as when to start pubertal blockers and dosing for cross-sex hormones. Finally, there are resources that allow providers to consult an expert remotely for more complicated cases. Transline is a transgender medical consultation service staffed by medical providers with expertise in gender-affirming care. Providers can learn more about this valuable service on the website: http://project-health.org/transline/.
Working in a major medical center is not necessary in providing gender-affirming care to TGD youth. Being respectful, supportive, and having the willingness to learn are the minimal requirements. Resources are available to help guide you on the more technical aspects of gender-affirming care. Maintaining a supportive environment and using these resources will help you expand health care access for this population.
Dr. Montano is an assistant professor of pediatrics at the University of Pittsburgh and an adolescent medicine physician at Children’s Hospital of Pittsburgh of UPMC. Email him at [email protected].
References
1. Injustice at every turn: A report of the national transgender discrimination survey (National Center for Transgender Equality and National Gay and Lesbian Task Force, 2011).
2. Psychol Bull. 2003 Sep;129(5):674-97.
3. “Creating an LGBTQ-friendly practice,” American Medical Association.
4. Fenway Health Client Registration Form.
5. JAMA. 1993 Mar 17;269(11):1404-7.
6. Int J Transgenderism 2012;13:165-232.
7. J Clin Endocrinol Metab. 2017 Nov 1;102(11):3869-903.
8. “Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People,” 2nd edition (San Francisco, CA: University of California, San Francisco, June 17, 2016).

Pneumonia with tender, dry, crusted lips
Mycoplasma pneumoniae infection commonly manifests as an upper or lower respiratory tract infection with associated fever, dyspnea, cough, and coryza. However, patients can present with extrapulmonary complications with dermatologic findings including mucocutaneous eruptions. M. pneumoniae–associated mucocutaneous disease has prominent mucositis and typically sparse cutaneous involvement. The mucositis usually involves the lips and oral mucosa, eye conjunctivae, and nasal mucosa and can involve urogenital lesions. It predominantly is observed in children and adolescents. This condition is essentially a subtype of Stevens-Johnson syndrome, with a specific infection-associated etiology, and has been called “Mycoplasma pneumoniae–induced rash and mucositis,” shortened to “MIRM.”

Severe reactive mucocutaneous eruptions include erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN). While there has been semantic confusion over the years, there are some distinctive characteristics.
EM is characterized by typical three-ringed target papules that are predominantly acral in location and often without mucosal involvement. The lesions are “multiforme” in that they can appear polymorphous and evolve during an episode, with erythematous macules progressing to edematous papules, sometimes with a halo of pallor and concentric “target-like” appearance. Lesions of EM are fixed, meaning individual lesions last 7-10 days, unlike urticarial lesions that last hours. EM classically is associated with herpes simplex virus infections which usually precede its development.
SJS and TEN display atypical macules and papules which develop into erythematous vesicles, bullae, and potentially extensive desquamation, usually presenting with fever and systemic symptoms, with multiple mucosal sites involved. SJS usually is defined by having bullae restricted to less than 10% of body surface area (BSA), TEN as greater than 30% BSA, and “overlap SJS-TEN” as 20%-30% skin detachment.1 SJS and TEN commonly are induced by medications and on a spectrum of drug hypersensitivity–induced epidermal necrolysis.
MIRM has been highlighted as a distinct, common condition, usually mucous-membrane predominant with involvement of two or more mucosal sites, less than 10% total BSA, the presence of few vesiculobullous lesions or scattered atypical targets with or without targetoid lesions (without rash is called MIRM sine rash), and clinical and laboratory evidence of atypical pneumonia.2 Other infections can cause similar eruptions (for example, Chlamydia pneumoniae), and a recent proposal by the Pediatric Dermatology Research Alliance has suggested the term “Reactive Infectious Mucocutaneous Eruption” (RIME) to include MIRM and other infection-induced reactions.
Laboratory diagnosis of M. pneumoniae is via serology or polymerase chain reaction. Antibody titers begin to rise approximately 7-9 days after infection and peak at 3-4 weeks. Enzyme immunoassay is more sensitive in detecting acute infection than culture and has sensitivity comparable to the polymerase chain reaction if there has been sufficient time to develop an antibody response.

The differential diagnosis between RIME/MIRM, SJS, and TEN may be difficult to distinguish in the first few days of presentation, and consideration of infections and possible medication causes is important. DRESS syndrome (drug reaction with eosinophilia and systemic symptoms) also is in the differential diagnosis. DRESS usually has a long latency (2-8 weeks) between drug exposure and disease onset.
Treatment of RIME/MIRM is supportive care and treatment of any underlying infection. Steroids and intravenous immune globulin (IVIG) have been used to treat reactive mucositis, as well as cyclosporine and biologic agents (such as etanercept), in an attempt to minimize the extent and duration of mucous membrane vesiculation and denudation. While these drugs may help shorten the duration of the disease course, controlled trials are lacking and there is little comparative literature on efficacy or safety of these agents.
Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Dr. Bhatti is a research fellow in pediatric dermatology at Rady Children’s Hospital and the University of California, San Diego. They said they have no financial disclosures. Email Dr. Eichenfield and Dr. Bhatti at [email protected].
References
1. Arch Dermatol. 1993 Jan;129(1):92-6.
2. J Am Acad Dermatol. 2015 Feb;72(2):239-45.
Mycoplasma pneumoniae infection commonly manifests as an upper or lower respiratory tract infection with associated fever, dyspnea, cough, and coryza. However, patients can present with extrapulmonary complications with dermatologic findings including mucocutaneous eruptions. M. pneumoniae–associated mucocutaneous disease has prominent mucositis and typically sparse cutaneous involvement. The mucositis usually involves the lips and oral mucosa, eye conjunctivae, and nasal mucosa and can involve urogenital lesions. It predominantly is observed in children and adolescents. This condition is essentially a subtype of Stevens-Johnson syndrome, with a specific infection-associated etiology, and has been called “Mycoplasma pneumoniae–induced rash and mucositis,” shortened to “MIRM.”
Severe reactive mucocutaneous eruptions include erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN). While there has been semantic confusion over the years, there are some distinctive characteristics.
EM is characterized by typical three-ringed target papules that are predominantly acral in location and often without mucosal involvement. The lesions are “multiforme” in that they can appear polymorphous and evolve during an episode, with erythematous macules progressing to edematous papules, sometimes with a halo of pallor and concentric “target-like” appearance. Lesions of EM are fixed, meaning individual lesions last 7-10 days, unlike urticarial lesions that last hours. EM classically is associated with herpes simplex virus infections which usually precede its development.
SJS and TEN display atypical macules and papules which develop into erythematous vesicles, bullae, and potentially extensive desquamation, usually presenting with fever and systemic symptoms, with multiple mucosal sites involved. SJS usually is defined by having bullae restricted to less than 10% of body surface area (BSA), TEN as greater than 30% BSA, and “overlap SJS-TEN” as 20%-30% skin detachment.1 SJS and TEN commonly are induced by medications and on a spectrum of drug hypersensitivity–induced epidermal necrolysis.
MIRM has been highlighted as a distinct, common condition, usually mucous-membrane predominant with involvement of two or more mucosal sites, less than 10% total BSA, the presence of few vesiculobullous lesions or scattered atypical targets with or without targetoid lesions (without rash is called MIRM sine rash), and clinical and laboratory evidence of atypical pneumonia.2 Other infections can cause similar eruptions (for example, Chlamydia pneumoniae), and a recent proposal by the Pediatric Dermatology Research Alliance has suggested the term “Reactive Infectious Mucocutaneous Eruption” (RIME) to include MIRM and other infection-induced reactions.
Laboratory diagnosis of M. pneumoniae is via serology or polymerase chain reaction. Antibody titers begin to rise approximately 7-9 days after infection and peak at 3-4 weeks. Enzyme immunoassay is more sensitive in detecting acute infection than culture and has sensitivity comparable to the polymerase chain reaction if there has been sufficient time to develop an antibody response.
The differential diagnosis between RIME/MIRM, SJS, and TEN may be difficult to distinguish in the first few days of presentation, and consideration of infections and possible medication causes is important. DRESS syndrome (drug reaction with eosinophilia and systemic symptoms) also is in the differential diagnosis. DRESS usually has a long latency (2-8 weeks) between drug exposure and disease onset.
Treatment of RIME/MIRM is supportive care and treatment of any underlying infection. Steroids and intravenous immune globulin (IVIG) have been used to treat reactive mucositis, as well as cyclosporine and biologic agents (such as etanercept), in an attempt to minimize the extent and duration of mucous membrane vesiculation and denudation. While these drugs may help shorten the duration of the disease course, controlled trials are lacking and there is little comparative literature on efficacy or safety of these agents.
Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Dr. Bhatti is a research fellow in pediatric dermatology at Rady Children’s Hospital and the University of California, San Diego. They said they have no financial disclosures. Email Dr. Eichenfield and Dr. Bhatti at [email protected].
References
1. Arch Dermatol. 1993 Jan;129(1):92-6.
2. J Am Acad Dermatol. 2015 Feb;72(2):239-45.
Mycoplasma pneumoniae infection commonly manifests as an upper or lower respiratory tract infection with associated fever, dyspnea, cough, and coryza. However, patients can present with extrapulmonary complications with dermatologic findings including mucocutaneous eruptions. M. pneumoniae–associated mucocutaneous disease has prominent mucositis and typically sparse cutaneous involvement. The mucositis usually involves the lips and oral mucosa, eye conjunctivae, and nasal mucosa and can involve urogenital lesions. It predominantly is observed in children and adolescents. This condition is essentially a subtype of Stevens-Johnson syndrome, with a specific infection-associated etiology, and has been called “Mycoplasma pneumoniae–induced rash and mucositis,” shortened to “MIRM.”
Severe reactive mucocutaneous eruptions include erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN). While there has been semantic confusion over the years, there are some distinctive characteristics.
EM is characterized by typical three-ringed target papules that are predominantly acral in location and often without mucosal involvement. The lesions are “multiforme” in that they can appear polymorphous and evolve during an episode, with erythematous macules progressing to edematous papules, sometimes with a halo of pallor and concentric “target-like” appearance. Lesions of EM are fixed, meaning individual lesions last 7-10 days, unlike urticarial lesions that last hours. EM classically is associated with herpes simplex virus infections which usually precede its development.
SJS and TEN display atypical macules and papules which develop into erythematous vesicles, bullae, and potentially extensive desquamation, usually presenting with fever and systemic symptoms, with multiple mucosal sites involved. SJS usually is defined by having bullae restricted to less than 10% of body surface area (BSA), TEN as greater than 30% BSA, and “overlap SJS-TEN” as 20%-30% skin detachment.1 SJS and TEN commonly are induced by medications and on a spectrum of drug hypersensitivity–induced epidermal necrolysis.
MIRM has been highlighted as a distinct, common condition, usually mucous-membrane predominant with involvement of two or more mucosal sites, less than 10% total BSA, the presence of few vesiculobullous lesions or scattered atypical targets with or without targetoid lesions (without rash is called MIRM sine rash), and clinical and laboratory evidence of atypical pneumonia.2 Other infections can cause similar eruptions (for example, Chlamydia pneumoniae), and a recent proposal by the Pediatric Dermatology Research Alliance has suggested the term “Reactive Infectious Mucocutaneous Eruption” (RIME) to include MIRM and other infection-induced reactions.
Laboratory diagnosis of M. pneumoniae is via serology or polymerase chain reaction. Antibody titers begin to rise approximately 7-9 days after infection and peak at 3-4 weeks. Enzyme immunoassay is more sensitive in detecting acute infection than culture and has sensitivity comparable to the polymerase chain reaction if there has been sufficient time to develop an antibody response.
The differential diagnosis between RIME/MIRM, SJS, and TEN may be difficult to distinguish in the first few days of presentation, and consideration of infections and possible medication causes is important. DRESS syndrome (drug reaction with eosinophilia and systemic symptoms) also is in the differential diagnosis. DRESS usually has a long latency (2-8 weeks) between drug exposure and disease onset.
Treatment of RIME/MIRM is supportive care and treatment of any underlying infection. Steroids and intravenous immune globulin (IVIG) have been used to treat reactive mucositis, as well as cyclosporine and biologic agents (such as etanercept), in an attempt to minimize the extent and duration of mucous membrane vesiculation and denudation. While these drugs may help shorten the duration of the disease course, controlled trials are lacking and there is little comparative literature on efficacy or safety of these agents.
Dr. Eichenfield is chief of pediatric and adolescent dermatology at Rady Children’s Hospital–San Diego. He is vice chair of the department of dermatology and professor of dermatology and pediatrics at the University of California, San Diego. Dr. Bhatti is a research fellow in pediatric dermatology at Rady Children’s Hospital and the University of California, San Diego. They said they have no financial disclosures. Email Dr. Eichenfield and Dr. Bhatti at [email protected].
References
1. Arch Dermatol. 1993 Jan;129(1):92-6.
2. J Am Acad Dermatol. 2015 Feb;72(2):239-45.


Narrative Medicine: A Re-emerging Philosophy of Patient Care
Narrative medicine (NM) centers on understanding patients’ lives, caring for the caregivers (including the clinicians), and giving voice to the suffering.1 It is an antidote for medical “progress,” which often stresses technology and pharmacologic interventions, leaving the patient out of his/her own medical story—with negative consequences.
This missing patient narrative goes beyond the template information solicited and recorded in the history of present illness (HPI) and review of systems (ROS). It is well expressed by Francis W. Peabody, MD, (1881-1927) in a published lecture for Harvard Medical School students: “One of the essential qualities of the clinician is an interest in humanity, for the secret of the care of the patient is in caring for the patient.”2
This article serves as an introduction to NM, its evolution, and its power to improve medical diagnoses and reduce clinician burnout. While its roots are in palliative and chronic care, NM has a place in the day-to-day care of patients in acute settings as well.
VIGNETTE
It’s been a busy day in clinic; the clock ticks toward closing. Scanning the monitor, you permit a brief moment of relief as you spy the perfect end-of-shift, quickie patient case: “Sore throat x 2 days,” with a rapid strep test under way. You quickly check lab coat pockets for examination tools and hasten down the hall noting age 22, white female, self-pay. Vitals reveal a low-grade fever. Maybe this sore throat will be bacterial; all the easier as there will be no need to do the “antibiotics don’t work for viruses” sermon.
You knock briefly, enter the exam room, place the laptop on the counter, and immediately recognize the patient from multiple visits over the past 2 years, mostly for gynecologic issues. You recall treating her for gonorrhea and discussing her worry about HIV. She told you that she’s a graduate student, although she is overdressed for a week night, wearing a silk blouse, short skirt, and high heels. She offers a winning smile and tells you with her pleasant accent that she is running late for an appointment.
The patient describes her symptoms: unrelenting sore throat for 2 days and pain with swallowing. She complains of feeling feverish and fatigued, with no appetite and “swollen glands.” She denies cough and runny nose; she looks and sounds exhausted. She denies smoking and excessive alcohol intake. You vaguely hone in on the accent, thinking it might be South African. Her HPI and ROS completed, you record her physical findings of pharyngeal erythema, no exudates, and moderate anterior lymphadenopathy.
You have a nagging thought about her “story.” As an urgent care clinician, you know you are likely her only health care provider and you feel some connection. It is late, and the patient is in a rush, so you promise yourself to delve deeper the next time she presents.
Continue to: You confirm the negative strep test results...
You confirm the negative strep test results and deliver the well-rehearsed sermon. She appears surprised, asking if you are sure. You suggest that she schedule a full physical in the near future. She hops off the table, heels clicking on the tile floor, as you complete your note. You do not suspect she is off to meet her scheduled man of the evening as assigned by her escort service.
Before you clock out, you check the extended patient appointment schedule and do not see her name. You vow to call her the next day and discover that she has no listed phone number. An uncomfortable feeling settles in: Are you missing something?
IN URGENT CARE
NM is an interactive patient approach more often applied to seriously ill or chronic disease patients, for whom it meaningfully supports a patient’s existence as central to the diagnostic testing and treatment of health care concerns. One can professionally debate that NM has no place in urgent care; however, this is where many patients’ acute and chronic conditions are discovered. It is where elevated blood glucose becomes type 2 diabetes and abnormal complete blood counts become blood cancer. With deeper application of NM’s principles, our simple-appearing acute pharyngitis case might have received a different workup.
NM practitioners subscribe to careful listening. Rita Charon, MD, a leading proponent of NM, describes this approach to patient care as a “rigorous intellectual and clinical discipline to fortify health care with its capacity to skillfully receive the accounts persons give of themselves—to recognize, absorb, interpret, and be moved to action by the stories of others.”3 It is a patient care revival that helps clinicians recognize and shield themselves from the powerful stampede of technology, templated patient interviews, digital documentation, and diminution of clinician and patient bonding.
The clinician in this patient encounter has functionally intact radar, sensing something awry, but communication falls short. NM’s strength is to bond the clinician to the patient, enhancing subtle, and at times pivotal, information exchange. It generates patient trust even in brief encounters, fostering improved clinical decision-making. A stronger NM focus might have encouraged this clinician to investigate more deeply the patient’s fancy clothing and surprised response to the negative strep test results by posing a simple query, such as ”What do you think might be going on?”
Continue to: MEDICAL ERROR
MEDICAL ERROR
Pharyngitis is common, making it prime territory for medical error—even for experienced clinicians—because of 3 human tendencies that NM recognizes and seeks to avoid.4 These human tendencies, insightfully delineated decades ago by experimental psychologists Amos Tversky and Daniel Kahneman, authors of Anchoring, Availability and Attribution, appear most commonly under uncertain conditions and time pressures, such as in urgent care. How does this patient encounter reflect these tendencies?5
Anchoring refers to the tendency to grasp the first symptom, physical finding, or laboratory abnormality, and hold onto it tightly.5 Such initial diagnostic impressions/information may prove true; however, other unconsidered diagnoses may include the correct one. In this encounter, the clinician entered the exam room with an early fixed diagnosis and applied the rapid strep results to diagnose viral pharyngitis. Other, conflicting hints were fleetingly noted and not addressed.
Availability refers to the tendency to assume that a quickly recalled experience explains a novel situation.5 Clinicians regularly diagnose viral pharyngitis, leading to familiarity and availability. This is contrary to NM’s view of every patient having a unique and noteworthy story.
Attribution refers to the tendency to invoke stereotypical images and assign symptoms and findings to the stereotype, which is often negative (eg, hypochondriac, drinker).5
In this encounter, the clinician would have benefited from considering other categories of diagnoses that could occur in this patient, expanding the differential diagnosis list, by soliciting a deeper patient story, fostering trust, and following clinical intuition. Had this bond been cultivated over prior visits, even in an urgent care setting, the graduate student ruse would have been discovered and the patient’s true occupation—female sex worker—revealed. The clinician would have modified the laboratory testing, discovering human herpesvirus type 8 (HHV-8) as the pharyngitis etiology, which is disproportionately linked to HIV co-infection and increases the risk for Kaposi sarcoma (KS) 20,000-fold. The prevalence of HHV-8 is 17% in the United States and is much higher (50%) in South Africa, the origin of the patient’s accent.6 Deeper patient relationships enable uncomfortable history-taking questions, with improved reliability. This missed diagnosis has wide-ranging negative consequences for the patient and her escort encounters.6
Continue to: THE FLEXNER REPORT
THE FLEXNER REPORT: NARRATIVE MEDICINE'S EXCISION
It is clear that the scientific revolution prompted the removal of NM from clinical practice. The 1910 Flexner Report, funded by the Carnegie Foundation for the Advancement of Teaching Science and authored by research scholar and physician Abraham Flexner, analyzed the functioning of 155 US and Canadian medical schools.7 His report supported the socially desirable goal of reforming medical education by exposing mediocre quality, unsavory profit motives, inadequate facilities, and nonscientific approaches, and publishing a list of those falling below the gold standard (which was the German medical education system). Harvard and Johns Hopkins received a gold seal, many other medical schools closed, and several responded to the challenge and excelled.8
Medical school curricula transitioned to exclusively theoretical and scientific teaching, objectifying values and rewarding research and efficiency. The subjective patient story was surgically excised and replaced with objective science. Not all change is good, however, and years later, Flexner reflected that scientific medicine was “sadly deficient in cultural and philosophic background.”8 His report also dramatically suppressed the use of complementary and alternative medicine and psychiatry, another medical boomerang.9 Scientific rigor is desirable—but not to the exclusion of the central patient role and other potential health care modalities.
THE PROBLEM-ORIENTED MEDICAL RECORD AND EHR
Decades after Flexner’s report on medical education curricula, another reformer, Lawrence Weed, MD, trained his eye on medical documentation’s organization and structure. He published a seminal article, “Medical Records that Guide and Teach” in the New England Journal of Medicine.10 Truly a pioneer, he demonstrated how typical medical record case documentation circa 1967 could be more efficient and espoused the problem-oriented medical record. He conceptualized designs for reorganizing medical records, prophetically promoted use of “paramedical” personnel, and encouraged computer integration.10
Coinciding with the birth of the PA profession and the recent inception of the NP profession, Weed endorsed the use of trained interviewers who would apply a “branching” question algorithm with associated computer data entry designed to protect expensive physician time. The patient story would be a jigsaw puzzle, as physicians could fill in missing information.10
Weed’s goals had merit by stressing structure for the disorganized, then-handwritten medical record, benefitting the growth of team-based patient care. However, efficiency and precision continued to marginalize a key component of the patient’s illness narrative in favor of speed, objectivity, and achievable billing essentials.11 His recommendations have eradicated the free-text box, replacing it with a selection of pull-down choices or prewritten templates. With a series of clicks, the subjective patient’s own narrative is sterilized, removing valuable details from the team’s view.11 The “s” of the Subjective Objective Assessment and Plan note is washed away (Table 1).

Continue to: Weed's clinical documentation...
Weed’s clinical documentation efficiency system caught fire. However, similar to Flexner’s later second thoughts, Weed also cast doubt on the full effect of his recommendations. In a 2009 interview conducted by a former medical student of his, Weed revealed views that more closely resemble our current competency-based medical education and stress the value of interpersonal skills in patient care12:
- Computerization of the medical record—with its vast amount of information and physician-processing capacity—“inevitably” leads to dangerous cognitive shortcuts. Medical education seeks to instill “medical knowledge and clinical judgment,” giving students “misplaced faith in the completeness and accuracy of their own intellects and is the antithesis of a truly scientific education.”12
- Medical student recruitment and instruction have long emphasized memory and regurgitation of facts, while students should be selected for their hands-on and interpersonal skills. Medical school should be “teaching a core of behavior instead of a core of knowledge.”12 These are areas in which NM helps.
FLEXNER, WEED, AND NOW, CHARON
Medicine’s history is blemished by errors, some significant. Flexner neatly compartmentalized medical education, Weed digitized the clinician/patient interaction, and Charon revitalizes the reason clinicians chose a health care profession. Charon—as a practicing internist, as well as a professor in the Department of Medicine and Executive Director of the Program in Narrative Medicine at Columbia University’s Vagelos College of Physicians and Surgeons in New York City—is fully qualified to speak to the importance of NM in medical education and medical practice. Her 2006 book reminds us that sore throats are not always simple, boring, and routine; each one is as unique as the person housing that particular pharynx.13
How does NM drive clinicians to be better, countering cognitive errors while incorporating the patient’s cultural and philosophic background? According to Charon, the NM concept results from conversation among scholars and clinicians teaching and practicing at Columbia University in early 2000, fueled by decades of insight from literature, medical (health care) humanities, ethics, health care communication, and primary care medicine.3 NM supports patient-centric teaching and care, reminding us that it combines the historical doctor-at-bedside, who exhibited careful, empathetic questioning and listening, with the benefits of modern medical science.
Charon describes 3 main clinician-to-patient interactions, allowing us to regain some of what we have lost: attention, representation, and affiliation (Table 2). In addition to medical error reduction, these 3 interactive behaviors counter the aforementioned 3As (anchoring, availability, and attribution) of cognitive error.5Attention initiates the clinician’s heightened and committed listening to the patient.3 In our patient encounter, essential information is undisclosed, leading to a missed diagnosis and an incomplete representation in the written note. The clinician, due to insufficient attention, missed important clues such as the patient’s dress, accent, and profession, which limited the representation. This almost seems nonsensical; who would care about a patient’s dress or accent and, of practical concern today, where would one record it? And could another urgent care clinician or specialist find these notes? How might a more serious future medical outcome be averted? Affiliation results in a connection of careful listening and full documentation as the clinician becomes invested in the whole patient, not just the sore throat.3

PREPROFESSIONAL AND PROFESSIONAL EDUCATION
Preprofessional humanities education may result in stronger NM conceptualization. The Association of American Medical Colleges (AAMC) recognizes the value of arts and humanities in medical education in developing qualities of professionalism, communication skills, and emotional intelligence in physicians. The AAMC Curriculum Inventory and Reports (2015-2016) shows that 119 medical schools require humanities education, including
- Visual arts to improve observational skills
- History education to frame modern-day Ebola outbreaks (eg, using the framework of the Black Death),
- Literature and poetry to enhance insight into different ways of living and thinking, fostering critical thinking.14
Continue to: NM has been offered in...
NM has been offered in medical schools with positive outcomes. Published results of a 2010 qualitative study of 130 Columbia University medical students who completed a required intensive half-semester of NM seminars testify to its salience.15 Students articulated NM’s importance to critical thinking and reflection, through improved attention and affiliation with their patients, improved ability to examine assumptions and develop new skills, and improved clarity of communication.15
A small number of PA programs, far fewer than medical schools, are incorporating NM coursework, through application of literature, visual media, creative writing, and other approaches based on the humanities.16 The nursing profession, which prefers the term narrative health care to narrative medicine, endorses its inclusion in nursing education. A 2018 article in Nursing Education Perspectives supports the study of humanities to complement technical competencies such as the ability to “absorb, analyze, and interpret complex artifacts” and to “participate effectively in deliberative conversations.”17
THE PRACTICING CLINICIAN: MENTAL HEALTH AND NARRATIVE MEDICINE
The value of NM extends beyond the patient to embrace caregivers as well; this is important, in light of increased attention to mental health status among clinicians. Although the term used most frequently is physician burnout, data indicate that patient management by MDs, NPs, and PAs is becoming indistinguishable—and thus risk for associated negative mental health consequences may be shared
The National Academy of Medicine is also addressing the issues of clinician well-being (see https://nam.edu/initiatives/clinician-resilience-and-well-being/). Former US Surgeon General Vivek Murthy, MD, has spoken about the epidemic of loneliness that affects clinicians. This can result from playing the physician role, lack of family support, and increased dependency on technology—yet, on a basic level, lack of interpersonal communication and connection are at the core.21 Communication between clinicians can lead to greater social cohesion and compassion, and effective uninterrupted listening and expression of their feelings helps. This begs the question: If physicians need to communicate better and practice active listening among themselves, how does this translate to the physician-to-patient bond?
THE CLINICIANS' PERSONAL BALM
Caruso Brown and Garden describe how the illness experiences of physicians, through their own reflective writing, create an empathy bridge between the professional healer and a sick patient, allowing them to be better and healthier clinicians.22 Recent best-selling physician narratives such as those by Atul Gawande,23 Siddhartha Mukherjee,24 and Paul Kalanithi25 support the similarities between the sick physician and the sick patient. Illness narratives written by physicians-turned-patients are not dissimilar to illness narratives written by patients. Reflective writing by clinicians fosters a deeper understanding not only of how patients feel, but also of the relationship they desire and deserve.22
Continue to: Writing a novel...
Writing a novel is beyond the time and ability of many clinicians. However, they can closely read literature (another NM tool), discuss books and other types of writing, participate in a book club, establish a hospital or office support group, and find a buddy or trustworthy confidant with whom to decompress and vent.3 Active journal clubs can alternate clinical guidelines with literature to expand their perspectives. An international voice, Maria Giulia Marini, Research and Health Director of the Fondazione ISTUD in Milan, Italy, and European proponent of NM, offers similar suggestions, indicating that making nonmedical works parts of a clinician’s life encourages empathy and promotes understanding between clinician and patient, as well as a holistic management approach, encourages personal and collegial reflection (eg, sharing tough experiences), sets a patient-centered agenda, and challenges the norm.26
NARRATIVE MEDICINE'S FUTURE ROLE
The field of medical humanities has experienced growth through publications, national and international conferences, and formal discussion between executives of the AAMC and the National Endowment for the Humanities to design and incorporate joint programs teaching humanities in medical schools.27 As of March 2019, there were 85 established baccalaureate health humanities programs in the US, with additional programs in development.28
Clinicians and professional organizations cannot help but see the suffering of patients, with its concomitant provider burden. The urgent care patient encounter in our example met the standard of care of the typical interaction that achieves billing protocols; the HPI, ROS, and physical exam would not raise an eyebrow. Yet, an NM approach provides more. Asking the atypical questions about accents, out-of-the-ordinary dress and behavior, and wondering about the mentioned late-night appointment attends to NM’s focused active listening, with resultant quality documentation and a whole patient encounter, even in an acute care case.
Don’t be afraid. Consider that as in novels and movies, strange things happen. The iconic book The House of God reminds clinicians that, upon hearing hoof beats, we should first think of horses—however, sometimes a zebra is correct.29 When an urgent care clinician interprets the hoof beats, a zebra may be in the differential diagnosis; in the case presented, the patient might fortunately be spared a future KS diagnosis. And the clinician may avoid personal anguish at what could have been a better outcome. NM can help clinicians remember that sore throats are as unique as people.
1. Krisberg K. Narrative medicine: Every patient has a story. AAMC News. March 28, 2018. https://news.aamc.org/medical-education/article/narrative-medicine-every-patient-has-story. Accessed October 10, 2018.
2. Peabody FW. The care of the patient. JAMA. 1927;80(12):877-882.
3. Charon R, DasGupta S, Hermann N, et al. The Principles and Practice of Narrative Medicine. New York, NY: Oxford University Press; 2017:1, 3.
4. Murphy JG , Stee LA, McAvoy MT, Oshiro J. Journal reporting of medical errors: the wisdom of Solomon, the bravery of Achilles, and the foolishness of Pan. Chest. 2007;131(3):890-896.
5. Groopman J, Hartzband P. Mindful medicine: Critical thinking leads to right diagnosis. ACP Internist. January 2008. https://acpinternist.org/archives/2008/01/groopman.htm. Accessed May 11, 2018.
6. Nzivo MM, Lwembe RM, Odari EO, Budambula NLM. Human herpes virus type 8 among female-sex workers. J Hum Virol Retrovirol 2017;5(6):00176.
7. Flexner A. Medical education in the United States and Canada—a report to the Carnegie Foundation for the Advancement of Teaching. Bulletin No. 4. Boston, MA: DB Updike, Merrymount Press; 1910.
8. Cooke M, Irby DM, Sullivan W, Ludmerer KM. American medical education 100 years after the Flexner Report. N Engl J Med. 2006;355(13):1339-1344.
9. Stahnisch FW, Verhoef M. The Flexner Report of 1910 and its impact on complementary and alternative medicine and psychiatry in North America in the 20th Century. Evid Based Complement Alternat Med. 2012;2012:647896.
10. Weed LL. Medical records that guide and teach. NEJM. 1968;278(12):652-657.
11. Ommaya AK, Cipriano PF, Hoyt DB, et al. Care-centered clinical documentation in the digital environment: solutions to alleviate burnout. NAM.edu/Perspectives. January 29, 2018. Accessed June 19, 2018.
12. Jacobs L. Interview with Lawrence Weed, MD - The father of the problem-oriented medical record looks ahead. The Permanente Journal. Summer 2009;13(3):84-89. https://doi.org/10.7812/TPP/09-068. Accessed August 2, 2019.
13. Charon R. Narrative Medicine: Honoring the Stories of Illness. New York, NY: Oxford University Press; 2006.
14. Mann S. Focusing on arts, humanities to develop well-rounded physicians. AAMC News. August 15, 2017. https://news.aamc.org/medical-education/article/focusing-arts-humanities-well-rounded-physicians/. Accessed Oct 10, 2018.
15. Miller E, Balmer D, Hermann N, et al. Sounding narrative medicine: studying students’ professional identity development at Columbia University College of Physicians and Surgeons. Acad Med. 2014;89(2):335-342.
16. Grant JP, Gregory T. The Sacred Seven elective: integrating the health humanities into physician assistant education. J Physician Assist Educ. 2017;28(4):220-222.
17. Lim F, Marsaglia MJ. Nursing humanities: teaching for a sense of salience. Nurs Educ Perspect. 2018;39(2):121-122.
18. Hooker RS. PAs, NPs, PAs, physicians and regression to the mean. JAAPA. 2018;31(7):13-14.
19. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;338:2272-2281.
20. Kearney MK, Weininger RB, Vachon ML, et al. Self-care of physicians caring for patients at the end of life: “Being connected … a key to my survival.” JAMA. 2009;301(11):1155–1164, E1.
21. Firth S. Former Surgeon General talks love, loneliness, and burnout: NAM panel addresses growing crisis in medicine. Medpage Today. May 4, 2018. www.medpagetoday.com/publichealthpolicy/generalprofessionalissues/72720. Accessed June 15, 2018.
22. Caruso Brown AE, Garden R. Images of healing and learning: from silence into language: Questioning the power of physician illness narratives. AMA J Ethics. 2017;19(5):501-507.
23. Gawande A. Being Mortal: Medicine and What Matters in the End. 1st ed. New York, NY: Metropolitan Books; 2014.
24. Mukherjee S. The Emperor of All Maladies: A Biography of Cancer. New York, NY: Simon & Schuster; 2010.
25. Kalanithi P. When Breath Becomes Air. New York, NY: Penguin Random House; 2016.
26. Marini MG. Narrative Medicine: Bridging the Gap Between Evidence-Based Care and Medical Humanities. Cham, Switzerland: Springer International Publishing; 2016.
27. Charon R. To see the suffering. Acad Med. 2017;92(12):1668-1670.
28. Lamb EG, Berry SL, Jones T. Health Humanities Baccalaureate Programs in the United States. Hiram, OH: Center for Literature and Medicine, Hiram College; March 2019.
29. Shem S. The House of God. New York, NY: Berkley Random House; 1978.
Narrative medicine (NM) centers on understanding patients’ lives, caring for the caregivers (including the clinicians), and giving voice to the suffering.1 It is an antidote for medical “progress,” which often stresses technology and pharmacologic interventions, leaving the patient out of his/her own medical story—with negative consequences.
This missing patient narrative goes beyond the template information solicited and recorded in the history of present illness (HPI) and review of systems (ROS). It is well expressed by Francis W. Peabody, MD, (1881-1927) in a published lecture for Harvard Medical School students: “One of the essential qualities of the clinician is an interest in humanity, for the secret of the care of the patient is in caring for the patient.”2
This article serves as an introduction to NM, its evolution, and its power to improve medical diagnoses and reduce clinician burnout. While its roots are in palliative and chronic care, NM has a place in the day-to-day care of patients in acute settings as well.
VIGNETTE
It’s been a busy day in clinic; the clock ticks toward closing. Scanning the monitor, you permit a brief moment of relief as you spy the perfect end-of-shift, quickie patient case: “Sore throat x 2 days,” with a rapid strep test under way. You quickly check lab coat pockets for examination tools and hasten down the hall noting age 22, white female, self-pay. Vitals reveal a low-grade fever. Maybe this sore throat will be bacterial; all the easier as there will be no need to do the “antibiotics don’t work for viruses” sermon.
You knock briefly, enter the exam room, place the laptop on the counter, and immediately recognize the patient from multiple visits over the past 2 years, mostly for gynecologic issues. You recall treating her for gonorrhea and discussing her worry about HIV. She told you that she’s a graduate student, although she is overdressed for a week night, wearing a silk blouse, short skirt, and high heels. She offers a winning smile and tells you with her pleasant accent that she is running late for an appointment.
The patient describes her symptoms: unrelenting sore throat for 2 days and pain with swallowing. She complains of feeling feverish and fatigued, with no appetite and “swollen glands.” She denies cough and runny nose; she looks and sounds exhausted. She denies smoking and excessive alcohol intake. You vaguely hone in on the accent, thinking it might be South African. Her HPI and ROS completed, you record her physical findings of pharyngeal erythema, no exudates, and moderate anterior lymphadenopathy.
You have a nagging thought about her “story.” As an urgent care clinician, you know you are likely her only health care provider and you feel some connection. It is late, and the patient is in a rush, so you promise yourself to delve deeper the next time she presents.
Continue to: You confirm the negative strep test results...
You confirm the negative strep test results and deliver the well-rehearsed sermon. She appears surprised, asking if you are sure. You suggest that she schedule a full physical in the near future. She hops off the table, heels clicking on the tile floor, as you complete your note. You do not suspect she is off to meet her scheduled man of the evening as assigned by her escort service.
Before you clock out, you check the extended patient appointment schedule and do not see her name. You vow to call her the next day and discover that she has no listed phone number. An uncomfortable feeling settles in: Are you missing something?
IN URGENT CARE
NM is an interactive patient approach more often applied to seriously ill or chronic disease patients, for whom it meaningfully supports a patient’s existence as central to the diagnostic testing and treatment of health care concerns. One can professionally debate that NM has no place in urgent care; however, this is where many patients’ acute and chronic conditions are discovered. It is where elevated blood glucose becomes type 2 diabetes and abnormal complete blood counts become blood cancer. With deeper application of NM’s principles, our simple-appearing acute pharyngitis case might have received a different workup.
NM practitioners subscribe to careful listening. Rita Charon, MD, a leading proponent of NM, describes this approach to patient care as a “rigorous intellectual and clinical discipline to fortify health care with its capacity to skillfully receive the accounts persons give of themselves—to recognize, absorb, interpret, and be moved to action by the stories of others.”3 It is a patient care revival that helps clinicians recognize and shield themselves from the powerful stampede of technology, templated patient interviews, digital documentation, and diminution of clinician and patient bonding.
The clinician in this patient encounter has functionally intact radar, sensing something awry, but communication falls short. NM’s strength is to bond the clinician to the patient, enhancing subtle, and at times pivotal, information exchange. It generates patient trust even in brief encounters, fostering improved clinical decision-making. A stronger NM focus might have encouraged this clinician to investigate more deeply the patient’s fancy clothing and surprised response to the negative strep test results by posing a simple query, such as ”What do you think might be going on?”
Continue to: MEDICAL ERROR
MEDICAL ERROR
Pharyngitis is common, making it prime territory for medical error—even for experienced clinicians—because of 3 human tendencies that NM recognizes and seeks to avoid.4 These human tendencies, insightfully delineated decades ago by experimental psychologists Amos Tversky and Daniel Kahneman, authors of Anchoring, Availability and Attribution, appear most commonly under uncertain conditions and time pressures, such as in urgent care. How does this patient encounter reflect these tendencies?5
Anchoring refers to the tendency to grasp the first symptom, physical finding, or laboratory abnormality, and hold onto it tightly.5 Such initial diagnostic impressions/information may prove true; however, other unconsidered diagnoses may include the correct one. In this encounter, the clinician entered the exam room with an early fixed diagnosis and applied the rapid strep results to diagnose viral pharyngitis. Other, conflicting hints were fleetingly noted and not addressed.
Availability refers to the tendency to assume that a quickly recalled experience explains a novel situation.5 Clinicians regularly diagnose viral pharyngitis, leading to familiarity and availability. This is contrary to NM’s view of every patient having a unique and noteworthy story.
Attribution refers to the tendency to invoke stereotypical images and assign symptoms and findings to the stereotype, which is often negative (eg, hypochondriac, drinker).5
In this encounter, the clinician would have benefited from considering other categories of diagnoses that could occur in this patient, expanding the differential diagnosis list, by soliciting a deeper patient story, fostering trust, and following clinical intuition. Had this bond been cultivated over prior visits, even in an urgent care setting, the graduate student ruse would have been discovered and the patient’s true occupation—female sex worker—revealed. The clinician would have modified the laboratory testing, discovering human herpesvirus type 8 (HHV-8) as the pharyngitis etiology, which is disproportionately linked to HIV co-infection and increases the risk for Kaposi sarcoma (KS) 20,000-fold. The prevalence of HHV-8 is 17% in the United States and is much higher (50%) in South Africa, the origin of the patient’s accent.6 Deeper patient relationships enable uncomfortable history-taking questions, with improved reliability. This missed diagnosis has wide-ranging negative consequences for the patient and her escort encounters.6
Continue to: THE FLEXNER REPORT
THE FLEXNER REPORT: NARRATIVE MEDICINE'S EXCISION
It is clear that the scientific revolution prompted the removal of NM from clinical practice. The 1910 Flexner Report, funded by the Carnegie Foundation for the Advancement of Teaching Science and authored by research scholar and physician Abraham Flexner, analyzed the functioning of 155 US and Canadian medical schools.7 His report supported the socially desirable goal of reforming medical education by exposing mediocre quality, unsavory profit motives, inadequate facilities, and nonscientific approaches, and publishing a list of those falling below the gold standard (which was the German medical education system). Harvard and Johns Hopkins received a gold seal, many other medical schools closed, and several responded to the challenge and excelled.8
Medical school curricula transitioned to exclusively theoretical and scientific teaching, objectifying values and rewarding research and efficiency. The subjective patient story was surgically excised and replaced with objective science. Not all change is good, however, and years later, Flexner reflected that scientific medicine was “sadly deficient in cultural and philosophic background.”8 His report also dramatically suppressed the use of complementary and alternative medicine and psychiatry, another medical boomerang.9 Scientific rigor is desirable—but not to the exclusion of the central patient role and other potential health care modalities.
THE PROBLEM-ORIENTED MEDICAL RECORD AND EHR
Decades after Flexner’s report on medical education curricula, another reformer, Lawrence Weed, MD, trained his eye on medical documentation’s organization and structure. He published a seminal article, “Medical Records that Guide and Teach” in the New England Journal of Medicine.10 Truly a pioneer, he demonstrated how typical medical record case documentation circa 1967 could be more efficient and espoused the problem-oriented medical record. He conceptualized designs for reorganizing medical records, prophetically promoted use of “paramedical” personnel, and encouraged computer integration.10
Coinciding with the birth of the PA profession and the recent inception of the NP profession, Weed endorsed the use of trained interviewers who would apply a “branching” question algorithm with associated computer data entry designed to protect expensive physician time. The patient story would be a jigsaw puzzle, as physicians could fill in missing information.10
Weed’s goals had merit by stressing structure for the disorganized, then-handwritten medical record, benefitting the growth of team-based patient care. However, efficiency and precision continued to marginalize a key component of the patient’s illness narrative in favor of speed, objectivity, and achievable billing essentials.11 His recommendations have eradicated the free-text box, replacing it with a selection of pull-down choices or prewritten templates. With a series of clicks, the subjective patient’s own narrative is sterilized, removing valuable details from the team’s view.11 The “s” of the Subjective Objective Assessment and Plan note is washed away (Table 1).
Continue to: Weed's clinical documentation...
Weed’s clinical documentation efficiency system caught fire. However, similar to Flexner’s later second thoughts, Weed also cast doubt on the full effect of his recommendations. In a 2009 interview conducted by a former medical student of his, Weed revealed views that more closely resemble our current competency-based medical education and stress the value of interpersonal skills in patient care12:
- Computerization of the medical record—with its vast amount of information and physician-processing capacity—“inevitably” leads to dangerous cognitive shortcuts. Medical education seeks to instill “medical knowledge and clinical judgment,” giving students “misplaced faith in the completeness and accuracy of their own intellects and is the antithesis of a truly scientific education.”12
- Medical student recruitment and instruction have long emphasized memory and regurgitation of facts, while students should be selected for their hands-on and interpersonal skills. Medical school should be “teaching a core of behavior instead of a core of knowledge.”12 These are areas in which NM helps.
FLEXNER, WEED, AND NOW, CHARON
Medicine’s history is blemished by errors, some significant. Flexner neatly compartmentalized medical education, Weed digitized the clinician/patient interaction, and Charon revitalizes the reason clinicians chose a health care profession. Charon—as a practicing internist, as well as a professor in the Department of Medicine and Executive Director of the Program in Narrative Medicine at Columbia University’s Vagelos College of Physicians and Surgeons in New York City—is fully qualified to speak to the importance of NM in medical education and medical practice. Her 2006 book reminds us that sore throats are not always simple, boring, and routine; each one is as unique as the person housing that particular pharynx.13
How does NM drive clinicians to be better, countering cognitive errors while incorporating the patient’s cultural and philosophic background? According to Charon, the NM concept results from conversation among scholars and clinicians teaching and practicing at Columbia University in early 2000, fueled by decades of insight from literature, medical (health care) humanities, ethics, health care communication, and primary care medicine.3 NM supports patient-centric teaching and care, reminding us that it combines the historical doctor-at-bedside, who exhibited careful, empathetic questioning and listening, with the benefits of modern medical science.
Charon describes 3 main clinician-to-patient interactions, allowing us to regain some of what we have lost: attention, representation, and affiliation (Table 2). In addition to medical error reduction, these 3 interactive behaviors counter the aforementioned 3As (anchoring, availability, and attribution) of cognitive error.5Attention initiates the clinician’s heightened and committed listening to the patient.3 In our patient encounter, essential information is undisclosed, leading to a missed diagnosis and an incomplete representation in the written note. The clinician, due to insufficient attention, missed important clues such as the patient’s dress, accent, and profession, which limited the representation. This almost seems nonsensical; who would care about a patient’s dress or accent and, of practical concern today, where would one record it? And could another urgent care clinician or specialist find these notes? How might a more serious future medical outcome be averted? Affiliation results in a connection of careful listening and full documentation as the clinician becomes invested in the whole patient, not just the sore throat.3
PREPROFESSIONAL AND PROFESSIONAL EDUCATION
Preprofessional humanities education may result in stronger NM conceptualization. The Association of American Medical Colleges (AAMC) recognizes the value of arts and humanities in medical education in developing qualities of professionalism, communication skills, and emotional intelligence in physicians. The AAMC Curriculum Inventory and Reports (2015-2016) shows that 119 medical schools require humanities education, including
- Visual arts to improve observational skills
- History education to frame modern-day Ebola outbreaks (eg, using the framework of the Black Death),
- Literature and poetry to enhance insight into different ways of living and thinking, fostering critical thinking.14
Continue to: NM has been offered in...
NM has been offered in medical schools with positive outcomes. Published results of a 2010 qualitative study of 130 Columbia University medical students who completed a required intensive half-semester of NM seminars testify to its salience.15 Students articulated NM’s importance to critical thinking and reflection, through improved attention and affiliation with their patients, improved ability to examine assumptions and develop new skills, and improved clarity of communication.15
A small number of PA programs, far fewer than medical schools, are incorporating NM coursework, through application of literature, visual media, creative writing, and other approaches based on the humanities.16 The nursing profession, which prefers the term narrative health care to narrative medicine, endorses its inclusion in nursing education. A 2018 article in Nursing Education Perspectives supports the study of humanities to complement technical competencies such as the ability to “absorb, analyze, and interpret complex artifacts” and to “participate effectively in deliberative conversations.”17
THE PRACTICING CLINICIAN: MENTAL HEALTH AND NARRATIVE MEDICINE
The value of NM extends beyond the patient to embrace caregivers as well; this is important, in light of increased attention to mental health status among clinicians. Although the term used most frequently is physician burnout, data indicate that patient management by MDs, NPs, and PAs is becoming indistinguishable—and thus risk for associated negative mental health consequences may be shared
The National Academy of Medicine is also addressing the issues of clinician well-being (see https://nam.edu/initiatives/clinician-resilience-and-well-being/). Former US Surgeon General Vivek Murthy, MD, has spoken about the epidemic of loneliness that affects clinicians. This can result from playing the physician role, lack of family support, and increased dependency on technology—yet, on a basic level, lack of interpersonal communication and connection are at the core.21 Communication between clinicians can lead to greater social cohesion and compassion, and effective uninterrupted listening and expression of their feelings helps. This begs the question: If physicians need to communicate better and practice active listening among themselves, how does this translate to the physician-to-patient bond?
THE CLINICIANS' PERSONAL BALM
Caruso Brown and Garden describe how the illness experiences of physicians, through their own reflective writing, create an empathy bridge between the professional healer and a sick patient, allowing them to be better and healthier clinicians.22 Recent best-selling physician narratives such as those by Atul Gawande,23 Siddhartha Mukherjee,24 and Paul Kalanithi25 support the similarities between the sick physician and the sick patient. Illness narratives written by physicians-turned-patients are not dissimilar to illness narratives written by patients. Reflective writing by clinicians fosters a deeper understanding not only of how patients feel, but also of the relationship they desire and deserve.22
Continue to: Writing a novel...
Writing a novel is beyond the time and ability of many clinicians. However, they can closely read literature (another NM tool), discuss books and other types of writing, participate in a book club, establish a hospital or office support group, and find a buddy or trustworthy confidant with whom to decompress and vent.3 Active journal clubs can alternate clinical guidelines with literature to expand their perspectives. An international voice, Maria Giulia Marini, Research and Health Director of the Fondazione ISTUD in Milan, Italy, and European proponent of NM, offers similar suggestions, indicating that making nonmedical works parts of a clinician’s life encourages empathy and promotes understanding between clinician and patient, as well as a holistic management approach, encourages personal and collegial reflection (eg, sharing tough experiences), sets a patient-centered agenda, and challenges the norm.26
NARRATIVE MEDICINE'S FUTURE ROLE
The field of medical humanities has experienced growth through publications, national and international conferences, and formal discussion between executives of the AAMC and the National Endowment for the Humanities to design and incorporate joint programs teaching humanities in medical schools.27 As of March 2019, there were 85 established baccalaureate health humanities programs in the US, with additional programs in development.28
Clinicians and professional organizations cannot help but see the suffering of patients, with its concomitant provider burden. The urgent care patient encounter in our example met the standard of care of the typical interaction that achieves billing protocols; the HPI, ROS, and physical exam would not raise an eyebrow. Yet, an NM approach provides more. Asking the atypical questions about accents, out-of-the-ordinary dress and behavior, and wondering about the mentioned late-night appointment attends to NM’s focused active listening, with resultant quality documentation and a whole patient encounter, even in an acute care case.
Don’t be afraid. Consider that as in novels and movies, strange things happen. The iconic book The House of God reminds clinicians that, upon hearing hoof beats, we should first think of horses—however, sometimes a zebra is correct.29 When an urgent care clinician interprets the hoof beats, a zebra may be in the differential diagnosis; in the case presented, the patient might fortunately be spared a future KS diagnosis. And the clinician may avoid personal anguish at what could have been a better outcome. NM can help clinicians remember that sore throats are as unique as people.
Narrative medicine (NM) centers on understanding patients’ lives, caring for the caregivers (including the clinicians), and giving voice to the suffering.1 It is an antidote for medical “progress,” which often stresses technology and pharmacologic interventions, leaving the patient out of his/her own medical story—with negative consequences.
This missing patient narrative goes beyond the template information solicited and recorded in the history of present illness (HPI) and review of systems (ROS). It is well expressed by Francis W. Peabody, MD, (1881-1927) in a published lecture for Harvard Medical School students: “One of the essential qualities of the clinician is an interest in humanity, for the secret of the care of the patient is in caring for the patient.”2
This article serves as an introduction to NM, its evolution, and its power to improve medical diagnoses and reduce clinician burnout. While its roots are in palliative and chronic care, NM has a place in the day-to-day care of patients in acute settings as well.
VIGNETTE
It’s been a busy day in clinic; the clock ticks toward closing. Scanning the monitor, you permit a brief moment of relief as you spy the perfect end-of-shift, quickie patient case: “Sore throat x 2 days,” with a rapid strep test under way. You quickly check lab coat pockets for examination tools and hasten down the hall noting age 22, white female, self-pay. Vitals reveal a low-grade fever. Maybe this sore throat will be bacterial; all the easier as there will be no need to do the “antibiotics don’t work for viruses” sermon.
You knock briefly, enter the exam room, place the laptop on the counter, and immediately recognize the patient from multiple visits over the past 2 years, mostly for gynecologic issues. You recall treating her for gonorrhea and discussing her worry about HIV. She told you that she’s a graduate student, although she is overdressed for a week night, wearing a silk blouse, short skirt, and high heels. She offers a winning smile and tells you with her pleasant accent that she is running late for an appointment.
The patient describes her symptoms: unrelenting sore throat for 2 days and pain with swallowing. She complains of feeling feverish and fatigued, with no appetite and “swollen glands.” She denies cough and runny nose; she looks and sounds exhausted. She denies smoking and excessive alcohol intake. You vaguely hone in on the accent, thinking it might be South African. Her HPI and ROS completed, you record her physical findings of pharyngeal erythema, no exudates, and moderate anterior lymphadenopathy.
You have a nagging thought about her “story.” As an urgent care clinician, you know you are likely her only health care provider and you feel some connection. It is late, and the patient is in a rush, so you promise yourself to delve deeper the next time she presents.
Continue to: You confirm the negative strep test results...
You confirm the negative strep test results and deliver the well-rehearsed sermon. She appears surprised, asking if you are sure. You suggest that she schedule a full physical in the near future. She hops off the table, heels clicking on the tile floor, as you complete your note. You do not suspect she is off to meet her scheduled man of the evening as assigned by her escort service.
Before you clock out, you check the extended patient appointment schedule and do not see her name. You vow to call her the next day and discover that she has no listed phone number. An uncomfortable feeling settles in: Are you missing something?
IN URGENT CARE
NM is an interactive patient approach more often applied to seriously ill or chronic disease patients, for whom it meaningfully supports a patient’s existence as central to the diagnostic testing and treatment of health care concerns. One can professionally debate that NM has no place in urgent care; however, this is where many patients’ acute and chronic conditions are discovered. It is where elevated blood glucose becomes type 2 diabetes and abnormal complete blood counts become blood cancer. With deeper application of NM’s principles, our simple-appearing acute pharyngitis case might have received a different workup.
NM practitioners subscribe to careful listening. Rita Charon, MD, a leading proponent of NM, describes this approach to patient care as a “rigorous intellectual and clinical discipline to fortify health care with its capacity to skillfully receive the accounts persons give of themselves—to recognize, absorb, interpret, and be moved to action by the stories of others.”3 It is a patient care revival that helps clinicians recognize and shield themselves from the powerful stampede of technology, templated patient interviews, digital documentation, and diminution of clinician and patient bonding.
The clinician in this patient encounter has functionally intact radar, sensing something awry, but communication falls short. NM’s strength is to bond the clinician to the patient, enhancing subtle, and at times pivotal, information exchange. It generates patient trust even in brief encounters, fostering improved clinical decision-making. A stronger NM focus might have encouraged this clinician to investigate more deeply the patient’s fancy clothing and surprised response to the negative strep test results by posing a simple query, such as ”What do you think might be going on?”
Continue to: MEDICAL ERROR
MEDICAL ERROR
Pharyngitis is common, making it prime territory for medical error—even for experienced clinicians—because of 3 human tendencies that NM recognizes and seeks to avoid.4 These human tendencies, insightfully delineated decades ago by experimental psychologists Amos Tversky and Daniel Kahneman, authors of Anchoring, Availability and Attribution, appear most commonly under uncertain conditions and time pressures, such as in urgent care. How does this patient encounter reflect these tendencies?5
Anchoring refers to the tendency to grasp the first symptom, physical finding, or laboratory abnormality, and hold onto it tightly.5 Such initial diagnostic impressions/information may prove true; however, other unconsidered diagnoses may include the correct one. In this encounter, the clinician entered the exam room with an early fixed diagnosis and applied the rapid strep results to diagnose viral pharyngitis. Other, conflicting hints were fleetingly noted and not addressed.
Availability refers to the tendency to assume that a quickly recalled experience explains a novel situation.5 Clinicians regularly diagnose viral pharyngitis, leading to familiarity and availability. This is contrary to NM’s view of every patient having a unique and noteworthy story.
Attribution refers to the tendency to invoke stereotypical images and assign symptoms and findings to the stereotype, which is often negative (eg, hypochondriac, drinker).5
In this encounter, the clinician would have benefited from considering other categories of diagnoses that could occur in this patient, expanding the differential diagnosis list, by soliciting a deeper patient story, fostering trust, and following clinical intuition. Had this bond been cultivated over prior visits, even in an urgent care setting, the graduate student ruse would have been discovered and the patient’s true occupation—female sex worker—revealed. The clinician would have modified the laboratory testing, discovering human herpesvirus type 8 (HHV-8) as the pharyngitis etiology, which is disproportionately linked to HIV co-infection and increases the risk for Kaposi sarcoma (KS) 20,000-fold. The prevalence of HHV-8 is 17% in the United States and is much higher (50%) in South Africa, the origin of the patient’s accent.6 Deeper patient relationships enable uncomfortable history-taking questions, with improved reliability. This missed diagnosis has wide-ranging negative consequences for the patient and her escort encounters.6
Continue to: THE FLEXNER REPORT
THE FLEXNER REPORT: NARRATIVE MEDICINE'S EXCISION
It is clear that the scientific revolution prompted the removal of NM from clinical practice. The 1910 Flexner Report, funded by the Carnegie Foundation for the Advancement of Teaching Science and authored by research scholar and physician Abraham Flexner, analyzed the functioning of 155 US and Canadian medical schools.7 His report supported the socially desirable goal of reforming medical education by exposing mediocre quality, unsavory profit motives, inadequate facilities, and nonscientific approaches, and publishing a list of those falling below the gold standard (which was the German medical education system). Harvard and Johns Hopkins received a gold seal, many other medical schools closed, and several responded to the challenge and excelled.8
Medical school curricula transitioned to exclusively theoretical and scientific teaching, objectifying values and rewarding research and efficiency. The subjective patient story was surgically excised and replaced with objective science. Not all change is good, however, and years later, Flexner reflected that scientific medicine was “sadly deficient in cultural and philosophic background.”8 His report also dramatically suppressed the use of complementary and alternative medicine and psychiatry, another medical boomerang.9 Scientific rigor is desirable—but not to the exclusion of the central patient role and other potential health care modalities.
THE PROBLEM-ORIENTED MEDICAL RECORD AND EHR
Decades after Flexner’s report on medical education curricula, another reformer, Lawrence Weed, MD, trained his eye on medical documentation’s organization and structure. He published a seminal article, “Medical Records that Guide and Teach” in the New England Journal of Medicine.10 Truly a pioneer, he demonstrated how typical medical record case documentation circa 1967 could be more efficient and espoused the problem-oriented medical record. He conceptualized designs for reorganizing medical records, prophetically promoted use of “paramedical” personnel, and encouraged computer integration.10
Coinciding with the birth of the PA profession and the recent inception of the NP profession, Weed endorsed the use of trained interviewers who would apply a “branching” question algorithm with associated computer data entry designed to protect expensive physician time. The patient story would be a jigsaw puzzle, as physicians could fill in missing information.10
Weed’s goals had merit by stressing structure for the disorganized, then-handwritten medical record, benefitting the growth of team-based patient care. However, efficiency and precision continued to marginalize a key component of the patient’s illness narrative in favor of speed, objectivity, and achievable billing essentials.11 His recommendations have eradicated the free-text box, replacing it with a selection of pull-down choices or prewritten templates. With a series of clicks, the subjective patient’s own narrative is sterilized, removing valuable details from the team’s view.11 The “s” of the Subjective Objective Assessment and Plan note is washed away (Table 1).
Continue to: Weed's clinical documentation...
Weed’s clinical documentation efficiency system caught fire. However, similar to Flexner’s later second thoughts, Weed also cast doubt on the full effect of his recommendations. In a 2009 interview conducted by a former medical student of his, Weed revealed views that more closely resemble our current competency-based medical education and stress the value of interpersonal skills in patient care12:
- Computerization of the medical record—with its vast amount of information and physician-processing capacity—“inevitably” leads to dangerous cognitive shortcuts. Medical education seeks to instill “medical knowledge and clinical judgment,” giving students “misplaced faith in the completeness and accuracy of their own intellects and is the antithesis of a truly scientific education.”12
- Medical student recruitment and instruction have long emphasized memory and regurgitation of facts, while students should be selected for their hands-on and interpersonal skills. Medical school should be “teaching a core of behavior instead of a core of knowledge.”12 These are areas in which NM helps.
FLEXNER, WEED, AND NOW, CHARON
Medicine’s history is blemished by errors, some significant. Flexner neatly compartmentalized medical education, Weed digitized the clinician/patient interaction, and Charon revitalizes the reason clinicians chose a health care profession. Charon—as a practicing internist, as well as a professor in the Department of Medicine and Executive Director of the Program in Narrative Medicine at Columbia University’s Vagelos College of Physicians and Surgeons in New York City—is fully qualified to speak to the importance of NM in medical education and medical practice. Her 2006 book reminds us that sore throats are not always simple, boring, and routine; each one is as unique as the person housing that particular pharynx.13
How does NM drive clinicians to be better, countering cognitive errors while incorporating the patient’s cultural and philosophic background? According to Charon, the NM concept results from conversation among scholars and clinicians teaching and practicing at Columbia University in early 2000, fueled by decades of insight from literature, medical (health care) humanities, ethics, health care communication, and primary care medicine.3 NM supports patient-centric teaching and care, reminding us that it combines the historical doctor-at-bedside, who exhibited careful, empathetic questioning and listening, with the benefits of modern medical science.
Charon describes 3 main clinician-to-patient interactions, allowing us to regain some of what we have lost: attention, representation, and affiliation (Table 2). In addition to medical error reduction, these 3 interactive behaviors counter the aforementioned 3As (anchoring, availability, and attribution) of cognitive error.5Attention initiates the clinician’s heightened and committed listening to the patient.3 In our patient encounter, essential information is undisclosed, leading to a missed diagnosis and an incomplete representation in the written note. The clinician, due to insufficient attention, missed important clues such as the patient’s dress, accent, and profession, which limited the representation. This almost seems nonsensical; who would care about a patient’s dress or accent and, of practical concern today, where would one record it? And could another urgent care clinician or specialist find these notes? How might a more serious future medical outcome be averted? Affiliation results in a connection of careful listening and full documentation as the clinician becomes invested in the whole patient, not just the sore throat.3
PREPROFESSIONAL AND PROFESSIONAL EDUCATION
Preprofessional humanities education may result in stronger NM conceptualization. The Association of American Medical Colleges (AAMC) recognizes the value of arts and humanities in medical education in developing qualities of professionalism, communication skills, and emotional intelligence in physicians. The AAMC Curriculum Inventory and Reports (2015-2016) shows that 119 medical schools require humanities education, including
- Visual arts to improve observational skills
- History education to frame modern-day Ebola outbreaks (eg, using the framework of the Black Death),
- Literature and poetry to enhance insight into different ways of living and thinking, fostering critical thinking.14
Continue to: NM has been offered in...
NM has been offered in medical schools with positive outcomes. Published results of a 2010 qualitative study of 130 Columbia University medical students who completed a required intensive half-semester of NM seminars testify to its salience.15 Students articulated NM’s importance to critical thinking and reflection, through improved attention and affiliation with their patients, improved ability to examine assumptions and develop new skills, and improved clarity of communication.15
A small number of PA programs, far fewer than medical schools, are incorporating NM coursework, through application of literature, visual media, creative writing, and other approaches based on the humanities.16 The nursing profession, which prefers the term narrative health care to narrative medicine, endorses its inclusion in nursing education. A 2018 article in Nursing Education Perspectives supports the study of humanities to complement technical competencies such as the ability to “absorb, analyze, and interpret complex artifacts” and to “participate effectively in deliberative conversations.”17
THE PRACTICING CLINICIAN: MENTAL HEALTH AND NARRATIVE MEDICINE
The value of NM extends beyond the patient to embrace caregivers as well; this is important, in light of increased attention to mental health status among clinicians. Although the term used most frequently is physician burnout, data indicate that patient management by MDs, NPs, and PAs is becoming indistinguishable—and thus risk for associated negative mental health consequences may be shared
The National Academy of Medicine is also addressing the issues of clinician well-being (see https://nam.edu/initiatives/clinician-resilience-and-well-being/). Former US Surgeon General Vivek Murthy, MD, has spoken about the epidemic of loneliness that affects clinicians. This can result from playing the physician role, lack of family support, and increased dependency on technology—yet, on a basic level, lack of interpersonal communication and connection are at the core.21 Communication between clinicians can lead to greater social cohesion and compassion, and effective uninterrupted listening and expression of their feelings helps. This begs the question: If physicians need to communicate better and practice active listening among themselves, how does this translate to the physician-to-patient bond?
THE CLINICIANS' PERSONAL BALM
Caruso Brown and Garden describe how the illness experiences of physicians, through their own reflective writing, create an empathy bridge between the professional healer and a sick patient, allowing them to be better and healthier clinicians.22 Recent best-selling physician narratives such as those by Atul Gawande,23 Siddhartha Mukherjee,24 and Paul Kalanithi25 support the similarities between the sick physician and the sick patient. Illness narratives written by physicians-turned-patients are not dissimilar to illness narratives written by patients. Reflective writing by clinicians fosters a deeper understanding not only of how patients feel, but also of the relationship they desire and deserve.22
Continue to: Writing a novel...
Writing a novel is beyond the time and ability of many clinicians. However, they can closely read literature (another NM tool), discuss books and other types of writing, participate in a book club, establish a hospital or office support group, and find a buddy or trustworthy confidant with whom to decompress and vent.3 Active journal clubs can alternate clinical guidelines with literature to expand their perspectives. An international voice, Maria Giulia Marini, Research and Health Director of the Fondazione ISTUD in Milan, Italy, and European proponent of NM, offers similar suggestions, indicating that making nonmedical works parts of a clinician’s life encourages empathy and promotes understanding between clinician and patient, as well as a holistic management approach, encourages personal and collegial reflection (eg, sharing tough experiences), sets a patient-centered agenda, and challenges the norm.26
NARRATIVE MEDICINE'S FUTURE ROLE
The field of medical humanities has experienced growth through publications, national and international conferences, and formal discussion between executives of the AAMC and the National Endowment for the Humanities to design and incorporate joint programs teaching humanities in medical schools.27 As of March 2019, there were 85 established baccalaureate health humanities programs in the US, with additional programs in development.28
Clinicians and professional organizations cannot help but see the suffering of patients, with its concomitant provider burden. The urgent care patient encounter in our example met the standard of care of the typical interaction that achieves billing protocols; the HPI, ROS, and physical exam would not raise an eyebrow. Yet, an NM approach provides more. Asking the atypical questions about accents, out-of-the-ordinary dress and behavior, and wondering about the mentioned late-night appointment attends to NM’s focused active listening, with resultant quality documentation and a whole patient encounter, even in an acute care case.
Don’t be afraid. Consider that as in novels and movies, strange things happen. The iconic book The House of God reminds clinicians that, upon hearing hoof beats, we should first think of horses—however, sometimes a zebra is correct.29 When an urgent care clinician interprets the hoof beats, a zebra may be in the differential diagnosis; in the case presented, the patient might fortunately be spared a future KS diagnosis. And the clinician may avoid personal anguish at what could have been a better outcome. NM can help clinicians remember that sore throats are as unique as people.
1. Krisberg K. Narrative medicine: Every patient has a story. AAMC News. March 28, 2018. https://news.aamc.org/medical-education/article/narrative-medicine-every-patient-has-story. Accessed October 10, 2018.
2. Peabody FW. The care of the patient. JAMA. 1927;80(12):877-882.
3. Charon R, DasGupta S, Hermann N, et al. The Principles and Practice of Narrative Medicine. New York, NY: Oxford University Press; 2017:1, 3.
4. Murphy JG , Stee LA, McAvoy MT, Oshiro J. Journal reporting of medical errors: the wisdom of Solomon, the bravery of Achilles, and the foolishness of Pan. Chest. 2007;131(3):890-896.
5. Groopman J, Hartzband P. Mindful medicine: Critical thinking leads to right diagnosis. ACP Internist. January 2008. https://acpinternist.org/archives/2008/01/groopman.htm. Accessed May 11, 2018.
6. Nzivo MM, Lwembe RM, Odari EO, Budambula NLM. Human herpes virus type 8 among female-sex workers. J Hum Virol Retrovirol 2017;5(6):00176.
7. Flexner A. Medical education in the United States and Canada—a report to the Carnegie Foundation for the Advancement of Teaching. Bulletin No. 4. Boston, MA: DB Updike, Merrymount Press; 1910.
8. Cooke M, Irby DM, Sullivan W, Ludmerer KM. American medical education 100 years after the Flexner Report. N Engl J Med. 2006;355(13):1339-1344.
9. Stahnisch FW, Verhoef M. The Flexner Report of 1910 and its impact on complementary and alternative medicine and psychiatry in North America in the 20th Century. Evid Based Complement Alternat Med. 2012;2012:647896.
10. Weed LL. Medical records that guide and teach. NEJM. 1968;278(12):652-657.
11. Ommaya AK, Cipriano PF, Hoyt DB, et al. Care-centered clinical documentation in the digital environment: solutions to alleviate burnout. NAM.edu/Perspectives. January 29, 2018. Accessed June 19, 2018.
12. Jacobs L. Interview with Lawrence Weed, MD - The father of the problem-oriented medical record looks ahead. The Permanente Journal. Summer 2009;13(3):84-89. https://doi.org/10.7812/TPP/09-068. Accessed August 2, 2019.
13. Charon R. Narrative Medicine: Honoring the Stories of Illness. New York, NY: Oxford University Press; 2006.
14. Mann S. Focusing on arts, humanities to develop well-rounded physicians. AAMC News. August 15, 2017. https://news.aamc.org/medical-education/article/focusing-arts-humanities-well-rounded-physicians/. Accessed Oct 10, 2018.
15. Miller E, Balmer D, Hermann N, et al. Sounding narrative medicine: studying students’ professional identity development at Columbia University College of Physicians and Surgeons. Acad Med. 2014;89(2):335-342.
16. Grant JP, Gregory T. The Sacred Seven elective: integrating the health humanities into physician assistant education. J Physician Assist Educ. 2017;28(4):220-222.
17. Lim F, Marsaglia MJ. Nursing humanities: teaching for a sense of salience. Nurs Educ Perspect. 2018;39(2):121-122.
18. Hooker RS. PAs, NPs, PAs, physicians and regression to the mean. JAAPA. 2018;31(7):13-14.
19. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;338:2272-2281.
20. Kearney MK, Weininger RB, Vachon ML, et al. Self-care of physicians caring for patients at the end of life: “Being connected … a key to my survival.” JAMA. 2009;301(11):1155–1164, E1.
21. Firth S. Former Surgeon General talks love, loneliness, and burnout: NAM panel addresses growing crisis in medicine. Medpage Today. May 4, 2018. www.medpagetoday.com/publichealthpolicy/generalprofessionalissues/72720. Accessed June 15, 2018.
22. Caruso Brown AE, Garden R. Images of healing and learning: from silence into language: Questioning the power of physician illness narratives. AMA J Ethics. 2017;19(5):501-507.
23. Gawande A. Being Mortal: Medicine and What Matters in the End. 1st ed. New York, NY: Metropolitan Books; 2014.
24. Mukherjee S. The Emperor of All Maladies: A Biography of Cancer. New York, NY: Simon & Schuster; 2010.
25. Kalanithi P. When Breath Becomes Air. New York, NY: Penguin Random House; 2016.
26. Marini MG. Narrative Medicine: Bridging the Gap Between Evidence-Based Care and Medical Humanities. Cham, Switzerland: Springer International Publishing; 2016.
27. Charon R. To see the suffering. Acad Med. 2017;92(12):1668-1670.
28. Lamb EG, Berry SL, Jones T. Health Humanities Baccalaureate Programs in the United States. Hiram, OH: Center for Literature and Medicine, Hiram College; March 2019.
29. Shem S. The House of God. New York, NY: Berkley Random House; 1978.
1. Krisberg K. Narrative medicine: Every patient has a story. AAMC News. March 28, 2018. https://news.aamc.org/medical-education/article/narrative-medicine-every-patient-has-story. Accessed October 10, 2018.
2. Peabody FW. The care of the patient. JAMA. 1927;80(12):877-882.
3. Charon R, DasGupta S, Hermann N, et al. The Principles and Practice of Narrative Medicine. New York, NY: Oxford University Press; 2017:1, 3.
4. Murphy JG , Stee LA, McAvoy MT, Oshiro J. Journal reporting of medical errors: the wisdom of Solomon, the bravery of Achilles, and the foolishness of Pan. Chest. 2007;131(3):890-896.
5. Groopman J, Hartzband P. Mindful medicine: Critical thinking leads to right diagnosis. ACP Internist. January 2008. https://acpinternist.org/archives/2008/01/groopman.htm. Accessed May 11, 2018.
6. Nzivo MM, Lwembe RM, Odari EO, Budambula NLM. Human herpes virus type 8 among female-sex workers. J Hum Virol Retrovirol 2017;5(6):00176.
7. Flexner A. Medical education in the United States and Canada—a report to the Carnegie Foundation for the Advancement of Teaching. Bulletin No. 4. Boston, MA: DB Updike, Merrymount Press; 1910.
8. Cooke M, Irby DM, Sullivan W, Ludmerer KM. American medical education 100 years after the Flexner Report. N Engl J Med. 2006;355(13):1339-1344.
9. Stahnisch FW, Verhoef M. The Flexner Report of 1910 and its impact on complementary and alternative medicine and psychiatry in North America in the 20th Century. Evid Based Complement Alternat Med. 2012;2012:647896.
10. Weed LL. Medical records that guide and teach. NEJM. 1968;278(12):652-657.
11. Ommaya AK, Cipriano PF, Hoyt DB, et al. Care-centered clinical documentation in the digital environment: solutions to alleviate burnout. NAM.edu/Perspectives. January 29, 2018. Accessed June 19, 2018.
12. Jacobs L. Interview with Lawrence Weed, MD - The father of the problem-oriented medical record looks ahead. The Permanente Journal. Summer 2009;13(3):84-89. https://doi.org/10.7812/TPP/09-068. Accessed August 2, 2019.
13. Charon R. Narrative Medicine: Honoring the Stories of Illness. New York, NY: Oxford University Press; 2006.
14. Mann S. Focusing on arts, humanities to develop well-rounded physicians. AAMC News. August 15, 2017. https://news.aamc.org/medical-education/article/focusing-arts-humanities-well-rounded-physicians/. Accessed Oct 10, 2018.
15. Miller E, Balmer D, Hermann N, et al. Sounding narrative medicine: studying students’ professional identity development at Columbia University College of Physicians and Surgeons. Acad Med. 2014;89(2):335-342.
16. Grant JP, Gregory T. The Sacred Seven elective: integrating the health humanities into physician assistant education. J Physician Assist Educ. 2017;28(4):220-222.
17. Lim F, Marsaglia MJ. Nursing humanities: teaching for a sense of salience. Nurs Educ Perspect. 2018;39(2):121-122.
18. Hooker RS. PAs, NPs, PAs, physicians and regression to the mean. JAAPA. 2018;31(7):13-14.
19. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;338:2272-2281.
20. Kearney MK, Weininger RB, Vachon ML, et al. Self-care of physicians caring for patients at the end of life: “Being connected … a key to my survival.” JAMA. 2009;301(11):1155–1164, E1.
21. Firth S. Former Surgeon General talks love, loneliness, and burnout: NAM panel addresses growing crisis in medicine. Medpage Today. May 4, 2018. www.medpagetoday.com/publichealthpolicy/generalprofessionalissues/72720. Accessed June 15, 2018.
22. Caruso Brown AE, Garden R. Images of healing and learning: from silence into language: Questioning the power of physician illness narratives. AMA J Ethics. 2017;19(5):501-507.
23. Gawande A. Being Mortal: Medicine and What Matters in the End. 1st ed. New York, NY: Metropolitan Books; 2014.
24. Mukherjee S. The Emperor of All Maladies: A Biography of Cancer. New York, NY: Simon & Schuster; 2010.
25. Kalanithi P. When Breath Becomes Air. New York, NY: Penguin Random House; 2016.
26. Marini MG. Narrative Medicine: Bridging the Gap Between Evidence-Based Care and Medical Humanities. Cham, Switzerland: Springer International Publishing; 2016.
27. Charon R. To see the suffering. Acad Med. 2017;92(12):1668-1670.
28. Lamb EG, Berry SL, Jones T. Health Humanities Baccalaureate Programs in the United States. Hiram, OH: Center for Literature and Medicine, Hiram College; March 2019.
29. Shem S. The House of God. New York, NY: Berkley Random House; 1978.

Long-term survival in stage IV NSCLC
In this edition of “How I will treat my next patient,” I highlight two studies addressing long-term survival for patients with stage IV non–small cell lung cancer (NSCLC). One summarizes survival of patients who received nivolumab therapy in the second- or later-line setting. The other is a retrospective database query regarding whether local consolidation (LC) improves survival after systemic treatment of patients with oligometastatic NSCLC.

Nivolumab therapy
Scott J. Antonia, MD, PhD, and colleagues sought to determine the frequency of long-term survival among advanced NSCLC patients who received nivolumab in the second-line or later settings (Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045[19]30407-3). They aggregated the results of four trials. Checkmate 017 and 057 were phase 3 comparisons of nivolumab with docetaxel for nonsquamous and squamous NSCLC, respectively – with crossover from docetaxel to nivolumab permitted. Checkmate 003 was a dose-escalation trial and Checkmate 063 was a phase 2 study of nivolumab in advanced, refractory squamous NSCLC. A minimum follow-up of 4 years was required.
In total, 664 patients participated in the four trials, more than 85% of whom received the fairly standard dose of 3 mg/kg every 2 weeks. In a very data-dense analysis, among all patients who received nivolumab, the 4-year overall survival was 14% (95% confidence interval, 11%-17%). Four-year overall survival was higher (19%; 95% CI, 15%-24%) in patients with at least 1% programmed death-ligand 1 (PD-L1) expression. There was no difference by histology (squamous vs. nonsquamous). Patients with Eastern Cooperative Oncology Group (ECOG) Performance Status of 0, PD-L1 greater than 10%, and absence of liver metastases were more likely to achieve 4-year overall survival.
Although progression-free survival was low (8%, overall; 19% for patients achieving complete remission or partial remission), depth of response correlated with the 4-year overall survival rate. Those patients in complete or partial remission at 6 months had an overall survival at 4 years of 56%. Stable disease at 6 months showed an overall survival at 4 years of 19%, which was superior to the results for patients with partial disease as best response (4%).
There were two treatment-related deaths with nivolumab, with no unexpected safety signals. Despite allowing continuous treatment in three of the four studies, most potentially immune-related toxic events occurred in the first 2-3 years of therapy. In the two randomized studies (017 and 057), 4-year overall survival was higher with nivolumab (14%) than with docetaxel (5%), with no overlap in the 95% confidence intervals.
What this means in practice
British prime minister, Benjamin Disraeli (and, later, Mark Twain) said, “There are three kinds of lies: lies, damned lies, and statistics.” There are no lies in Dr. Antonia’s paper, but there are plenty of statistics – which oncologists love. The reported data enable us to put some boundaries on the figures we quote when patients ask us, “How well could I do with this treatment?” Dr. Antonia’s paper significantly assists with these very practical discussions. For patients who want more detail, the boundaries can be further refined. Dr. Antonia and colleagues have given us clinical (depth of response, performance status, sites of metastasis) and molecular (proportion of cells with PD-L1) refinements to personalize our consultations with patients.
Unfortunately, the data do not allow us to predict who should not receive an immune checkpoint inhibitor and, instead, receive late-line chemotherapy or early hospice referral. The data summarize well-executed clinical trials, but it is well known that (as reported at the Quality Care Symposium 2019) NSCLC patients participating in clinical trials have significantly improved survival rates – perhaps as much as two times – compared with those not enrolled in trials. These realities, however, should not obscure the fact that immune checkpoint inhibitors are a major advance for metastatic NSCLC patients, including those who have progressed after prior treatment. They offer hope for cancer-free or cancer-controlled survival that would have properly been placed in the category of “a miracle” just a few years ago.
Local consolidation
Johannes Uhlig, MD, and colleagues analyzed 6 years of National Cancer Database records, identifying 34,887 stage IV NSCLC patients who had fewer than two distant metastatic lesions in the liver, lung, brain, or bone (JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702). Treatment groups were divided into patients who received systemic therapy alone (70.3% of the total patients), had surgical resection of the primary site plus systemic therapy (2.4%), or received external beam radiation therapy or thermal ablation (EBRT/TA) of the primary site plus systemic therapy (27.3%). Multivariable Cox proportional hazards models, incorporating a number of clinical variables, were used to compare overall survival between the three groups at a median follow-up of approximately 39 months.
They found that patients treated with surgical consolidation had a 41% lower mortality, in comparison with systemic therapy alone. EBRT/TA was also associated with lower mortality (by 5%), in comparison with systemic therapy alone, but the benefit was more nuanced. For instance, patients with squamous cell histology with low tumor bulk, low nodal burden, and fewer distant sites of disease benefited, but patients with adenocarcinoma and bulkier disease or more than two distant sites did not benefit.
The discussion emphasized all of the caveats that would be appropriate for a retrospective, telescopic record review – patient selection factors; lack of detail about systemic therapy; small numbers of patients in various subsets; exclusion of patients who had consolidative treatment of metastatic sites; and the potential for unbalanced allocation of patients with various actionable, prognostically relevant mutations. Further research, including ongoing trials such as NRG-LU002, was encouraged.
How these results influence clinical practice
Ralph R. Weichselbaum, MD, in his Karnofsky lecture at the 2018 annual meeting of the American Society of Clinical Oncology highlighted the hypothesis that metastatic tumors are enriched differentially for oligometastatic or polymetastatic miRNAs and that these miRNAs could influence future clinical behavior (J Clin Oncol. 2018;36[32]:3240-50). This work, coupled with clinical features (number of sites of disease, pace of progression) could elucidate which oligometastatic NSCLC patients might benefit from aggressive local treatment and achieve long-term, disease-free survival.
As previously reported, Daniel R. Gomez, MD, and colleagues found improved median progression-free survival (14.2 vs. 4.4 months; P = .022) and overall survival (41.2 vs. 17.0 months; P = .017) among patients with oligometastatic NSCLC who were randomized to local consolidation versus standard maintenance therapy/observation (J Clin Oncol. 8 May 2019. doi: 10. 1200/JCO.19.00201). Joshua M. Bauml and colleagues reported impressive results for systemically treated stage IV NSCLC patients who received local consolidation and checkpoint inhibitors for “oligo-remnant disease” (JAMA Oncol. 2019 Jul 11. doi: 10.1001/jamaoncol.2019.1449).
At the present time, clinical practice should remain governed by the general tendency to discourage aggressive local treatment except in highly selected cases with poorly resolved or impending life-altering symptoms. The publication by Dr. Uhlig and colleagues and the previously reported phase 2 trials, support phase 3 randomized trials of local treatment of isolated sites in oligometastatic NSCLC patients, particularly in an era of immune-based systemic treatment that offers finite potential for long-term survival.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I highlight two studies addressing long-term survival for patients with stage IV non–small cell lung cancer (NSCLC). One summarizes survival of patients who received nivolumab therapy in the second- or later-line setting. The other is a retrospective database query regarding whether local consolidation (LC) improves survival after systemic treatment of patients with oligometastatic NSCLC.
Nivolumab therapy
Scott J. Antonia, MD, PhD, and colleagues sought to determine the frequency of long-term survival among advanced NSCLC patients who received nivolumab in the second-line or later settings (Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045[19]30407-3). They aggregated the results of four trials. Checkmate 017 and 057 were phase 3 comparisons of nivolumab with docetaxel for nonsquamous and squamous NSCLC, respectively – with crossover from docetaxel to nivolumab permitted. Checkmate 003 was a dose-escalation trial and Checkmate 063 was a phase 2 study of nivolumab in advanced, refractory squamous NSCLC. A minimum follow-up of 4 years was required.
In total, 664 patients participated in the four trials, more than 85% of whom received the fairly standard dose of 3 mg/kg every 2 weeks. In a very data-dense analysis, among all patients who received nivolumab, the 4-year overall survival was 14% (95% confidence interval, 11%-17%). Four-year overall survival was higher (19%; 95% CI, 15%-24%) in patients with at least 1% programmed death-ligand 1 (PD-L1) expression. There was no difference by histology (squamous vs. nonsquamous). Patients with Eastern Cooperative Oncology Group (ECOG) Performance Status of 0, PD-L1 greater than 10%, and absence of liver metastases were more likely to achieve 4-year overall survival.
Although progression-free survival was low (8%, overall; 19% for patients achieving complete remission or partial remission), depth of response correlated with the 4-year overall survival rate. Those patients in complete or partial remission at 6 months had an overall survival at 4 years of 56%. Stable disease at 6 months showed an overall survival at 4 years of 19%, which was superior to the results for patients with partial disease as best response (4%).
There were two treatment-related deaths with nivolumab, with no unexpected safety signals. Despite allowing continuous treatment in three of the four studies, most potentially immune-related toxic events occurred in the first 2-3 years of therapy. In the two randomized studies (017 and 057), 4-year overall survival was higher with nivolumab (14%) than with docetaxel (5%), with no overlap in the 95% confidence intervals.
What this means in practice
British prime minister, Benjamin Disraeli (and, later, Mark Twain) said, “There are three kinds of lies: lies, damned lies, and statistics.” There are no lies in Dr. Antonia’s paper, but there are plenty of statistics – which oncologists love. The reported data enable us to put some boundaries on the figures we quote when patients ask us, “How well could I do with this treatment?” Dr. Antonia’s paper significantly assists with these very practical discussions. For patients who want more detail, the boundaries can be further refined. Dr. Antonia and colleagues have given us clinical (depth of response, performance status, sites of metastasis) and molecular (proportion of cells with PD-L1) refinements to personalize our consultations with patients.
Unfortunately, the data do not allow us to predict who should not receive an immune checkpoint inhibitor and, instead, receive late-line chemotherapy or early hospice referral. The data summarize well-executed clinical trials, but it is well known that (as reported at the Quality Care Symposium 2019) NSCLC patients participating in clinical trials have significantly improved survival rates – perhaps as much as two times – compared with those not enrolled in trials. These realities, however, should not obscure the fact that immune checkpoint inhibitors are a major advance for metastatic NSCLC patients, including those who have progressed after prior treatment. They offer hope for cancer-free or cancer-controlled survival that would have properly been placed in the category of “a miracle” just a few years ago.
Local consolidation
Johannes Uhlig, MD, and colleagues analyzed 6 years of National Cancer Database records, identifying 34,887 stage IV NSCLC patients who had fewer than two distant metastatic lesions in the liver, lung, brain, or bone (JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702). Treatment groups were divided into patients who received systemic therapy alone (70.3% of the total patients), had surgical resection of the primary site plus systemic therapy (2.4%), or received external beam radiation therapy or thermal ablation (EBRT/TA) of the primary site plus systemic therapy (27.3%). Multivariable Cox proportional hazards models, incorporating a number of clinical variables, were used to compare overall survival between the three groups at a median follow-up of approximately 39 months.
They found that patients treated with surgical consolidation had a 41% lower mortality, in comparison with systemic therapy alone. EBRT/TA was also associated with lower mortality (by 5%), in comparison with systemic therapy alone, but the benefit was more nuanced. For instance, patients with squamous cell histology with low tumor bulk, low nodal burden, and fewer distant sites of disease benefited, but patients with adenocarcinoma and bulkier disease or more than two distant sites did not benefit.
The discussion emphasized all of the caveats that would be appropriate for a retrospective, telescopic record review – patient selection factors; lack of detail about systemic therapy; small numbers of patients in various subsets; exclusion of patients who had consolidative treatment of metastatic sites; and the potential for unbalanced allocation of patients with various actionable, prognostically relevant mutations. Further research, including ongoing trials such as NRG-LU002, was encouraged.
How these results influence clinical practice
Ralph R. Weichselbaum, MD, in his Karnofsky lecture at the 2018 annual meeting of the American Society of Clinical Oncology highlighted the hypothesis that metastatic tumors are enriched differentially for oligometastatic or polymetastatic miRNAs and that these miRNAs could influence future clinical behavior (J Clin Oncol. 2018;36[32]:3240-50). This work, coupled with clinical features (number of sites of disease, pace of progression) could elucidate which oligometastatic NSCLC patients might benefit from aggressive local treatment and achieve long-term, disease-free survival.
As previously reported, Daniel R. Gomez, MD, and colleagues found improved median progression-free survival (14.2 vs. 4.4 months; P = .022) and overall survival (41.2 vs. 17.0 months; P = .017) among patients with oligometastatic NSCLC who were randomized to local consolidation versus standard maintenance therapy/observation (J Clin Oncol. 8 May 2019. doi: 10. 1200/JCO.19.00201). Joshua M. Bauml and colleagues reported impressive results for systemically treated stage IV NSCLC patients who received local consolidation and checkpoint inhibitors for “oligo-remnant disease” (JAMA Oncol. 2019 Jul 11. doi: 10.1001/jamaoncol.2019.1449).
At the present time, clinical practice should remain governed by the general tendency to discourage aggressive local treatment except in highly selected cases with poorly resolved or impending life-altering symptoms. The publication by Dr. Uhlig and colleagues and the previously reported phase 2 trials, support phase 3 randomized trials of local treatment of isolated sites in oligometastatic NSCLC patients, particularly in an era of immune-based systemic treatment that offers finite potential for long-term survival.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I highlight two studies addressing long-term survival for patients with stage IV non–small cell lung cancer (NSCLC). One summarizes survival of patients who received nivolumab therapy in the second- or later-line setting. The other is a retrospective database query regarding whether local consolidation (LC) improves survival after systemic treatment of patients with oligometastatic NSCLC.
Nivolumab therapy
Scott J. Antonia, MD, PhD, and colleagues sought to determine the frequency of long-term survival among advanced NSCLC patients who received nivolumab in the second-line or later settings (Lancet Oncol. 2019 Aug 14. doi: 10.1016/S1470-2045[19]30407-3). They aggregated the results of four trials. Checkmate 017 and 057 were phase 3 comparisons of nivolumab with docetaxel for nonsquamous and squamous NSCLC, respectively – with crossover from docetaxel to nivolumab permitted. Checkmate 003 was a dose-escalation trial and Checkmate 063 was a phase 2 study of nivolumab in advanced, refractory squamous NSCLC. A minimum follow-up of 4 years was required.
In total, 664 patients participated in the four trials, more than 85% of whom received the fairly standard dose of 3 mg/kg every 2 weeks. In a very data-dense analysis, among all patients who received nivolumab, the 4-year overall survival was 14% (95% confidence interval, 11%-17%). Four-year overall survival was higher (19%; 95% CI, 15%-24%) in patients with at least 1% programmed death-ligand 1 (PD-L1) expression. There was no difference by histology (squamous vs. nonsquamous). Patients with Eastern Cooperative Oncology Group (ECOG) Performance Status of 0, PD-L1 greater than 10%, and absence of liver metastases were more likely to achieve 4-year overall survival.
Although progression-free survival was low (8%, overall; 19% for patients achieving complete remission or partial remission), depth of response correlated with the 4-year overall survival rate. Those patients in complete or partial remission at 6 months had an overall survival at 4 years of 56%. Stable disease at 6 months showed an overall survival at 4 years of 19%, which was superior to the results for patients with partial disease as best response (4%).
There were two treatment-related deaths with nivolumab, with no unexpected safety signals. Despite allowing continuous treatment in three of the four studies, most potentially immune-related toxic events occurred in the first 2-3 years of therapy. In the two randomized studies (017 and 057), 4-year overall survival was higher with nivolumab (14%) than with docetaxel (5%), with no overlap in the 95% confidence intervals.
What this means in practice
British prime minister, Benjamin Disraeli (and, later, Mark Twain) said, “There are three kinds of lies: lies, damned lies, and statistics.” There are no lies in Dr. Antonia’s paper, but there are plenty of statistics – which oncologists love. The reported data enable us to put some boundaries on the figures we quote when patients ask us, “How well could I do with this treatment?” Dr. Antonia’s paper significantly assists with these very practical discussions. For patients who want more detail, the boundaries can be further refined. Dr. Antonia and colleagues have given us clinical (depth of response, performance status, sites of metastasis) and molecular (proportion of cells with PD-L1) refinements to personalize our consultations with patients.
Unfortunately, the data do not allow us to predict who should not receive an immune checkpoint inhibitor and, instead, receive late-line chemotherapy or early hospice referral. The data summarize well-executed clinical trials, but it is well known that (as reported at the Quality Care Symposium 2019) NSCLC patients participating in clinical trials have significantly improved survival rates – perhaps as much as two times – compared with those not enrolled in trials. These realities, however, should not obscure the fact that immune checkpoint inhibitors are a major advance for metastatic NSCLC patients, including those who have progressed after prior treatment. They offer hope for cancer-free or cancer-controlled survival that would have properly been placed in the category of “a miracle” just a few years ago.
Local consolidation
Johannes Uhlig, MD, and colleagues analyzed 6 years of National Cancer Database records, identifying 34,887 stage IV NSCLC patients who had fewer than two distant metastatic lesions in the liver, lung, brain, or bone (JAMA Netw Open. 2019 Aug 21. doi: 10.1001/jamanetworkopen.2019.9702). Treatment groups were divided into patients who received systemic therapy alone (70.3% of the total patients), had surgical resection of the primary site plus systemic therapy (2.4%), or received external beam radiation therapy or thermal ablation (EBRT/TA) of the primary site plus systemic therapy (27.3%). Multivariable Cox proportional hazards models, incorporating a number of clinical variables, were used to compare overall survival between the three groups at a median follow-up of approximately 39 months.
They found that patients treated with surgical consolidation had a 41% lower mortality, in comparison with systemic therapy alone. EBRT/TA was also associated with lower mortality (by 5%), in comparison with systemic therapy alone, but the benefit was more nuanced. For instance, patients with squamous cell histology with low tumor bulk, low nodal burden, and fewer distant sites of disease benefited, but patients with adenocarcinoma and bulkier disease or more than two distant sites did not benefit.
The discussion emphasized all of the caveats that would be appropriate for a retrospective, telescopic record review – patient selection factors; lack of detail about systemic therapy; small numbers of patients in various subsets; exclusion of patients who had consolidative treatment of metastatic sites; and the potential for unbalanced allocation of patients with various actionable, prognostically relevant mutations. Further research, including ongoing trials such as NRG-LU002, was encouraged.
How these results influence clinical practice
Ralph R. Weichselbaum, MD, in his Karnofsky lecture at the 2018 annual meeting of the American Society of Clinical Oncology highlighted the hypothesis that metastatic tumors are enriched differentially for oligometastatic or polymetastatic miRNAs and that these miRNAs could influence future clinical behavior (J Clin Oncol. 2018;36[32]:3240-50). This work, coupled with clinical features (number of sites of disease, pace of progression) could elucidate which oligometastatic NSCLC patients might benefit from aggressive local treatment and achieve long-term, disease-free survival.
As previously reported, Daniel R. Gomez, MD, and colleagues found improved median progression-free survival (14.2 vs. 4.4 months; P = .022) and overall survival (41.2 vs. 17.0 months; P = .017) among patients with oligometastatic NSCLC who were randomized to local consolidation versus standard maintenance therapy/observation (J Clin Oncol. 8 May 2019. doi: 10. 1200/JCO.19.00201). Joshua M. Bauml and colleagues reported impressive results for systemically treated stage IV NSCLC patients who received local consolidation and checkpoint inhibitors for “oligo-remnant disease” (JAMA Oncol. 2019 Jul 11. doi: 10.1001/jamaoncol.2019.1449).
At the present time, clinical practice should remain governed by the general tendency to discourage aggressive local treatment except in highly selected cases with poorly resolved or impending life-altering symptoms. The publication by Dr. Uhlig and colleagues and the previously reported phase 2 trials, support phase 3 randomized trials of local treatment of isolated sites in oligometastatic NSCLC patients, particularly in an era of immune-based systemic treatment that offers finite potential for long-term survival.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
Encourage participation in team sports
Participation in sports, competitive team sports in particular, is very good for the physical well-being and emotional development of children and adolescents. Specifically, there is growing evidence that sports promote healthy development socially and emotionally, protecting against drug use, poor body image, and against psychiatric illness in youth.

Sustaining academic productivity and team sports is demanding. By the middle of autumn, the amount of homework can begin to wear on teenagers, and the burden of getting them to practices and games can wear on parents. It can be very tempting for youth and their parents to drop team sports in high school, and turn their time and effort more completely to the serious work of school. But advocating for your patients and their parents to protect the time for team sports participation will pay dividends in the health and well-being of your patients and may even support rather than detract from academic performance.
The benefits of regular exercise for physical health are well established. Most teenagers do not get the recommended 60 minutes daily of moderate to vigorous physical activity. Participating in a team sport enforces this level of activity, in ways that parents typically don’t have to enforce. This level of physical activity typically promotes healthy eating and a healthy weight. Daily exercise promotes adequate, restful sleep, one of the most critical (and usually compromised) components of adolescent health. These exercise habits are easier to maintain into adulthood – when they protect against cardiovascular and inflammatory diseases – if they have been established early.

Beyond physical health, participation in team sports has been shown to promote good mental health and protect against psychiatric illnesses. They generally are less likely to use drugs and more likely to have a healthy body image than are their nonathlete peers. It is worth noting that the mental health benefits of team sports are even more robust than the benefits of solitary exercise in teenagers,1 possibly because of the social connections to peers and adults that grow out of them.
In the Monitoring the Future surveys (biannual national surveys of high school student health and behaviors funded by the National Institutes of Health) from 2010 to 2015, teenagers who participated in team sports were more likely to describe higher self-esteem and lower levels of loneliness. It is important to note that it has been difficult to establish the causal direction of the association between team sports and mental health in youth. We need more prospective randomized controlled trials to assert that the benefit is not simply an artifact of healthier youth choosing to participate in sports, but actually an active consequence of that choice. For now, though, we can say with confidence that physical activity promotes good mental health in youth and may protect against mental illness.

While student athletes benefit from the opportunity to develop deep social connections – ones forged in the intense setting of competition, collaboration, and sustained teamwork – they also benefit from strong mentorship connections with adults, including coaches, trainers, and even the parents of teammates who participate in all of the efforts that go into team sports in youth. While it might seem that all of the mental and physical benefits must be offset by lower academic performance, it turns out that is not the case. It is well established that regular exercise promotes healthy cognitive function, including processing speed, working memory, and even creativity. According to data from the Monitoring the Future survey, adolescents who participated in team sports were more likely to have As and to plan on attending a 4-year college than were their nonathlete peers.
Beyond the physiologic and social benefits of exercise, team sports provide adolescents with a powerful opportunity to get comfortable with failure. Even the best athletes cannot win all the time, and sports are unique in building failure into the work. Practice is almost entirely about failure, gradually getting better at something that is difficult. While everyone aims to win, they also prepare to struggle and lose. Athletes must learn how to persevere through a match that they are losing, and then pick themselves up and prepare again for the next match. When young people get comfortable with facing and managing challenges, managing setbacks and failure, they are ready to face the larger challenges, setbacks, and failures of adult life.
Team sports enable young people to learn what they are actually capable of managing – they build resilience. This promotion of resilience is illustrated in recent research that demonstrated that team sports may be especially protective for young people who have experienced trauma (adverse childhood experiences, or “ACEs”). Researchers at the University of California, Los Angeles, followed teenagers with and without high ACE scores into their mid 20s. They found that those with high ACE scores who participated in team sports as adolescents were 24% less likely to have depression and 30% less likely to have anxiety diagnoses as adults, compared with their peers who did not participate in team sports.2
Of course, the details matter in team sports. If your patients are participating and they or their parents are worried about spending so much time on something other than homework, talk to them about all of these exceptional benefits of team sports. But the culture of the team matters also. Some teams may be focused on winning at all costs, or have a practice culture that is humiliating or bullying. Some teams may have a culture of partying after games, with binge drinking and drug use. Ask your patients about whether they feel they are respected members of the team, and if effort and sportsmanship are valued as well as performance. Do they trust their coaches? Do they believe their coaches know and care about them? If your patients are not participating in a team sport, encourage them to find one (or more) that engage their interests. The benefits of track and field, crew, and tennis can be just as robust as the benefits of football or soccer. Speak with your patients and their parents about the payoff for their physical, mental, and developmental health the time and effort they are putting into a team sport can provide.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
References
1. Int J Nutr Phys Act. 2013 Aug 15. doi: 10.1186/1479-5868-10-98.
2. JAMA Pediatr. 2019 Jul 1;173(7):681-8.
Participation in sports, competitive team sports in particular, is very good for the physical well-being and emotional development of children and adolescents. Specifically, there is growing evidence that sports promote healthy development socially and emotionally, protecting against drug use, poor body image, and against psychiatric illness in youth.
Sustaining academic productivity and team sports is demanding. By the middle of autumn, the amount of homework can begin to wear on teenagers, and the burden of getting them to practices and games can wear on parents. It can be very tempting for youth and their parents to drop team sports in high school, and turn their time and effort more completely to the serious work of school. But advocating for your patients and their parents to protect the time for team sports participation will pay dividends in the health and well-being of your patients and may even support rather than detract from academic performance.
The benefits of regular exercise for physical health are well established. Most teenagers do not get the recommended 60 minutes daily of moderate to vigorous physical activity. Participating in a team sport enforces this level of activity, in ways that parents typically don’t have to enforce. This level of physical activity typically promotes healthy eating and a healthy weight. Daily exercise promotes adequate, restful sleep, one of the most critical (and usually compromised) components of adolescent health. These exercise habits are easier to maintain into adulthood – when they protect against cardiovascular and inflammatory diseases – if they have been established early.
Beyond physical health, participation in team sports has been shown to promote good mental health and protect against psychiatric illnesses. They generally are less likely to use drugs and more likely to have a healthy body image than are their nonathlete peers. It is worth noting that the mental health benefits of team sports are even more robust than the benefits of solitary exercise in teenagers,1 possibly because of the social connections to peers and adults that grow out of them.
In the Monitoring the Future surveys (biannual national surveys of high school student health and behaviors funded by the National Institutes of Health) from 2010 to 2015, teenagers who participated in team sports were more likely to describe higher self-esteem and lower levels of loneliness. It is important to note that it has been difficult to establish the causal direction of the association between team sports and mental health in youth. We need more prospective randomized controlled trials to assert that the benefit is not simply an artifact of healthier youth choosing to participate in sports, but actually an active consequence of that choice. For now, though, we can say with confidence that physical activity promotes good mental health in youth and may protect against mental illness.
While student athletes benefit from the opportunity to develop deep social connections – ones forged in the intense setting of competition, collaboration, and sustained teamwork – they also benefit from strong mentorship connections with adults, including coaches, trainers, and even the parents of teammates who participate in all of the efforts that go into team sports in youth. While it might seem that all of the mental and physical benefits must be offset by lower academic performance, it turns out that is not the case. It is well established that regular exercise promotes healthy cognitive function, including processing speed, working memory, and even creativity. According to data from the Monitoring the Future survey, adolescents who participated in team sports were more likely to have As and to plan on attending a 4-year college than were their nonathlete peers.
Beyond the physiologic and social benefits of exercise, team sports provide adolescents with a powerful opportunity to get comfortable with failure. Even the best athletes cannot win all the time, and sports are unique in building failure into the work. Practice is almost entirely about failure, gradually getting better at something that is difficult. While everyone aims to win, they also prepare to struggle and lose. Athletes must learn how to persevere through a match that they are losing, and then pick themselves up and prepare again for the next match. When young people get comfortable with facing and managing challenges, managing setbacks and failure, they are ready to face the larger challenges, setbacks, and failures of adult life.
Team sports enable young people to learn what they are actually capable of managing – they build resilience. This promotion of resilience is illustrated in recent research that demonstrated that team sports may be especially protective for young people who have experienced trauma (adverse childhood experiences, or “ACEs”). Researchers at the University of California, Los Angeles, followed teenagers with and without high ACE scores into their mid 20s. They found that those with high ACE scores who participated in team sports as adolescents were 24% less likely to have depression and 30% less likely to have anxiety diagnoses as adults, compared with their peers who did not participate in team sports.2
Of course, the details matter in team sports. If your patients are participating and they or their parents are worried about spending so much time on something other than homework, talk to them about all of these exceptional benefits of team sports. But the culture of the team matters also. Some teams may be focused on winning at all costs, or have a practice culture that is humiliating or bullying. Some teams may have a culture of partying after games, with binge drinking and drug use. Ask your patients about whether they feel they are respected members of the team, and if effort and sportsmanship are valued as well as performance. Do they trust their coaches? Do they believe their coaches know and care about them? If your patients are not participating in a team sport, encourage them to find one (or more) that engage their interests. The benefits of track and field, crew, and tennis can be just as robust as the benefits of football or soccer. Speak with your patients and their parents about the payoff for their physical, mental, and developmental health the time and effort they are putting into a team sport can provide.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
References
1. Int J Nutr Phys Act. 2013 Aug 15. doi: 10.1186/1479-5868-10-98.
2. JAMA Pediatr. 2019 Jul 1;173(7):681-8.
Participation in sports, competitive team sports in particular, is very good for the physical well-being and emotional development of children and adolescents. Specifically, there is growing evidence that sports promote healthy development socially and emotionally, protecting against drug use, poor body image, and against psychiatric illness in youth.
Sustaining academic productivity and team sports is demanding. By the middle of autumn, the amount of homework can begin to wear on teenagers, and the burden of getting them to practices and games can wear on parents. It can be very tempting for youth and their parents to drop team sports in high school, and turn their time and effort more completely to the serious work of school. But advocating for your patients and their parents to protect the time for team sports participation will pay dividends in the health and well-being of your patients and may even support rather than detract from academic performance.
The benefits of regular exercise for physical health are well established. Most teenagers do not get the recommended 60 minutes daily of moderate to vigorous physical activity. Participating in a team sport enforces this level of activity, in ways that parents typically don’t have to enforce. This level of physical activity typically promotes healthy eating and a healthy weight. Daily exercise promotes adequate, restful sleep, one of the most critical (and usually compromised) components of adolescent health. These exercise habits are easier to maintain into adulthood – when they protect against cardiovascular and inflammatory diseases – if they have been established early.
Beyond physical health, participation in team sports has been shown to promote good mental health and protect against psychiatric illnesses. They generally are less likely to use drugs and more likely to have a healthy body image than are their nonathlete peers. It is worth noting that the mental health benefits of team sports are even more robust than the benefits of solitary exercise in teenagers,1 possibly because of the social connections to peers and adults that grow out of them.
In the Monitoring the Future surveys (biannual national surveys of high school student health and behaviors funded by the National Institutes of Health) from 2010 to 2015, teenagers who participated in team sports were more likely to describe higher self-esteem and lower levels of loneliness. It is important to note that it has been difficult to establish the causal direction of the association between team sports and mental health in youth. We need more prospective randomized controlled trials to assert that the benefit is not simply an artifact of healthier youth choosing to participate in sports, but actually an active consequence of that choice. For now, though, we can say with confidence that physical activity promotes good mental health in youth and may protect against mental illness.
While student athletes benefit from the opportunity to develop deep social connections – ones forged in the intense setting of competition, collaboration, and sustained teamwork – they also benefit from strong mentorship connections with adults, including coaches, trainers, and even the parents of teammates who participate in all of the efforts that go into team sports in youth. While it might seem that all of the mental and physical benefits must be offset by lower academic performance, it turns out that is not the case. It is well established that regular exercise promotes healthy cognitive function, including processing speed, working memory, and even creativity. According to data from the Monitoring the Future survey, adolescents who participated in team sports were more likely to have As and to plan on attending a 4-year college than were their nonathlete peers.
Beyond the physiologic and social benefits of exercise, team sports provide adolescents with a powerful opportunity to get comfortable with failure. Even the best athletes cannot win all the time, and sports are unique in building failure into the work. Practice is almost entirely about failure, gradually getting better at something that is difficult. While everyone aims to win, they also prepare to struggle and lose. Athletes must learn how to persevere through a match that they are losing, and then pick themselves up and prepare again for the next match. When young people get comfortable with facing and managing challenges, managing setbacks and failure, they are ready to face the larger challenges, setbacks, and failures of adult life.
Team sports enable young people to learn what they are actually capable of managing – they build resilience. This promotion of resilience is illustrated in recent research that demonstrated that team sports may be especially protective for young people who have experienced trauma (adverse childhood experiences, or “ACEs”). Researchers at the University of California, Los Angeles, followed teenagers with and without high ACE scores into their mid 20s. They found that those with high ACE scores who participated in team sports as adolescents were 24% less likely to have depression and 30% less likely to have anxiety diagnoses as adults, compared with their peers who did not participate in team sports.2
Of course, the details matter in team sports. If your patients are participating and they or their parents are worried about spending so much time on something other than homework, talk to them about all of these exceptional benefits of team sports. But the culture of the team matters also. Some teams may be focused on winning at all costs, or have a practice culture that is humiliating or bullying. Some teams may have a culture of partying after games, with binge drinking and drug use. Ask your patients about whether they feel they are respected members of the team, and if effort and sportsmanship are valued as well as performance. Do they trust their coaches? Do they believe their coaches know and care about them? If your patients are not participating in a team sport, encourage them to find one (or more) that engage their interests. The benefits of track and field, crew, and tennis can be just as robust as the benefits of football or soccer. Speak with your patients and their parents about the payoff for their physical, mental, and developmental health the time and effort they are putting into a team sport can provide.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at [email protected].
References
1. Int J Nutr Phys Act. 2013 Aug 15. doi: 10.1186/1479-5868-10-98.
2. JAMA Pediatr. 2019 Jul 1;173(7):681-8.