User login
Research protocol overkill
This is a lot of paper.

It’s not a chart. Or mortgage forms. Or Family and Medical Leave Act paperwork.
It’s a research protocol for a study I’m involved in.
Now, I understand that research needs detailed protocols. It’s serious business, and when it’s happening at multiple sites they all need to know exactly what the plan is, what steps should be followed, who qualifies and who doesn’t, and so on.
But here’s what irritates me: That huge pile showed up at my office about an hour after all of the same documents were delivered to me by email, as PDFs.
Not only that, but someone had paid a messenger service to get them to me promptly. When I asked why I was told “because it’s the protocol that each site have both paper and digital copies.”
I don’t understand this at all. To me, the whole thing seems pretty wasteful on multiple levels. I’m told there are 28 sites for this study, so there’s a minimum stack of 28 times that one involved. Of course, each site probably has three to five copies (at least). Then, if the protocol is amended in a few months ... you get the idea.
To me this seems ridiculously wasteful. That’s a lot of paper and ink and shipping charges. If the whole thing can be sent digitally for a lot less money, why are they requiring both? If they need a signed signature sheet saying I read it, why not just print up that sheet? It’s one page instead of a huge pile. If I can digitally sign a document to refinance my house, why can’t I do it to acknowledge reading the protocol? I’m more likely to read study data on my iPad, anyway.

Not only that, now I have to store that stack in my office for several years, in spite of also having it on my hard drive.
Obviously, this is just a fraction of research costs, but it’s still money wasted.
The environmental issues of trees, water to make paper, the ink cartridges, and fuel to transport documents are all there, too. I could certainly go on.
I guess the overlying problem is that we’re still between two worlds (paper and digital) and, in spite of the marked shift to the latter, many are still insisting we try to live in both. At some point it gets silly. And costly.
I’m sure we won’t become completely paperless in my career, but there are plenty of ways we can eliminate its often-unnecessary overhead. Money is just the most obvious one.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This is a lot of paper.
It’s not a chart. Or mortgage forms. Or Family and Medical Leave Act paperwork.
It’s a research protocol for a study I’m involved in.
Now, I understand that research needs detailed protocols. It’s serious business, and when it’s happening at multiple sites they all need to know exactly what the plan is, what steps should be followed, who qualifies and who doesn’t, and so on.
But here’s what irritates me: That huge pile showed up at my office about an hour after all of the same documents were delivered to me by email, as PDFs.
Not only that, but someone had paid a messenger service to get them to me promptly. When I asked why I was told “because it’s the protocol that each site have both paper and digital copies.”
I don’t understand this at all. To me, the whole thing seems pretty wasteful on multiple levels. I’m told there are 28 sites for this study, so there’s a minimum stack of 28 times that one involved. Of course, each site probably has three to five copies (at least). Then, if the protocol is amended in a few months ... you get the idea.
To me this seems ridiculously wasteful. That’s a lot of paper and ink and shipping charges. If the whole thing can be sent digitally for a lot less money, why are they requiring both? If they need a signed signature sheet saying I read it, why not just print up that sheet? It’s one page instead of a huge pile. If I can digitally sign a document to refinance my house, why can’t I do it to acknowledge reading the protocol? I’m more likely to read study data on my iPad, anyway.
Not only that, now I have to store that stack in my office for several years, in spite of also having it on my hard drive.
Obviously, this is just a fraction of research costs, but it’s still money wasted.
The environmental issues of trees, water to make paper, the ink cartridges, and fuel to transport documents are all there, too. I could certainly go on.
I guess the overlying problem is that we’re still between two worlds (paper and digital) and, in spite of the marked shift to the latter, many are still insisting we try to live in both. At some point it gets silly. And costly.
I’m sure we won’t become completely paperless in my career, but there are plenty of ways we can eliminate its often-unnecessary overhead. Money is just the most obvious one.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This is a lot of paper.
It’s not a chart. Or mortgage forms. Or Family and Medical Leave Act paperwork.
It’s a research protocol for a study I’m involved in.
Now, I understand that research needs detailed protocols. It’s serious business, and when it’s happening at multiple sites they all need to know exactly what the plan is, what steps should be followed, who qualifies and who doesn’t, and so on.
But here’s what irritates me: That huge pile showed up at my office about an hour after all of the same documents were delivered to me by email, as PDFs.
Not only that, but someone had paid a messenger service to get them to me promptly. When I asked why I was told “because it’s the protocol that each site have both paper and digital copies.”
I don’t understand this at all. To me, the whole thing seems pretty wasteful on multiple levels. I’m told there are 28 sites for this study, so there’s a minimum stack of 28 times that one involved. Of course, each site probably has three to five copies (at least). Then, if the protocol is amended in a few months ... you get the idea.
To me this seems ridiculously wasteful. That’s a lot of paper and ink and shipping charges. If the whole thing can be sent digitally for a lot less money, why are they requiring both? If they need a signed signature sheet saying I read it, why not just print up that sheet? It’s one page instead of a huge pile. If I can digitally sign a document to refinance my house, why can’t I do it to acknowledge reading the protocol? I’m more likely to read study data on my iPad, anyway.
Not only that, now I have to store that stack in my office for several years, in spite of also having it on my hard drive.
Obviously, this is just a fraction of research costs, but it’s still money wasted.
The environmental issues of trees, water to make paper, the ink cartridges, and fuel to transport documents are all there, too. I could certainly go on.
I guess the overlying problem is that we’re still between two worlds (paper and digital) and, in spite of the marked shift to the latter, many are still insisting we try to live in both. At some point it gets silly. And costly.
I’m sure we won’t become completely paperless in my career, but there are plenty of ways we can eliminate its often-unnecessary overhead. Money is just the most obvious one.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Are patient portals living up to the hype? Ask your mother-in-law!
While preparing to write this technology column, I received a great deal of insight from the unlikeliest of sources: my mother-in-law.

Now don’t get me wrong – she’s a truly lovely, intelligent, and capable woman. I have sought her advice often on many things and have always been impressed by her wisdom and pragmatism, but I’ve just never thought of asking her for her opinion on medicine or technology, as I considered her knowledge of both subjects to be limited.
This occasion changed my opinion. In fact, I believe that, as health care IT becomes more complex, people like my mother-in-law may be exactly who we should be looking to for answers.
A few weeks ago, my mother-in-law and I were discussing her recent trip to the doctor. When she mentioned some lab tests, I suggested that we log in to her patient portal to view the results. This elicited several questions and a declaration of frustration.
“Which portal?” she asked. “I have so many and can’t keep all of the websites and passwords straight! Why can’t all of my doctors use the same portal, and why do they all have different password requirements?”
As she spoke these words, I was immediately struck with an unfortunate reality of EHRs: We have done a brilliant job creating state-of-the-art digital castles and have filled them with the data needed to revolutionize care and improve population health – but we haven’t given our patients the keys to get inside.
We must ask ourselves if, in trying to construct fortresses of information around our patients, we have lost sight of the individuals in the center. I believe that we can answer this question and improve the benefits of patient portals, but we all must agree to a few simple steps to streamline the experience for everyone.
Make it easy
A study recently published in the Journal of General Internal Medicine surveyed several hospitals on their usage of patient portals. After determining whether or not the institutions had such portals, the authors then investigated to find out what, if any, guidance was provided to patients about how to use them.
Their findings are frustrating, though not surprising. While 89% of hospitals had some form of patient portal, only 65% of those “had links that were easily found, defined as links accessible within two clicks from the home page.”
Furthermore, even in cases where portals were easily found, good instructions on how to use them were missing. Those instructions that did exist centered on rules and restrictions and laying out “terms and conditions” and informing patients on “what not to do,” rather than explaining how to make the most of the experience.
According to the authors, “this focus on curtailing behavior, and the hurdles placed on finding and understanding guidance, suggest that some hospitals may be prioritizing reducing liability over improving the patient experience with portals.”
If we want our patients to use them, portals must be easy to access and intuitive to use. They also must provide value.
Make it meaningful
Patient portals have proliferated exponentially over the last 10 years, thanks to government incentive programs. One such program, known as “meaningful use,” is primarily responsible for this, as it made implementation of a patient portal one of its core requirements.
Sadly, in spite of its oft-reviled name, the meaningful use program never defined patient-friendly standards of usability for patient portals. As a result, current portals just aren’t very good. Patients like my mother-in-law find them to be too numerous, too unfriendly to use, and too limited, so they are not being used to their full potential.
In fact, many institutions may choose not to enable all of the available features in order to limit technical issues and reduce the burden on providers. In the study referenced above, only 63% of portals offered the ability for patients to communicate directly with their physicians, and only 43% offered the ability to refill prescriptions.
When enabled, these functions improve patient engagement and efficiency. Without them, patients are less likely to log on, and physicians are forced to rely on less-efficient telephone calls or traditional letters to communicate results to their patients.
Put the patient, not the portal, at the center
History has all but forgotten the attempts by tech giants such as Google and Microsoft to create personal health records. While these initially seemed like a wonderful concept, they sadly proved to be a total flop. Some patients embraced the idea, but security concerns and the lack of buy-in from EHR vendors significantly limited their uptake.
They may simply have been ahead of their time.
A decade later, wearable technology and telemedicine are ushering in a new era of patient-centric care. Individuals have been embracing a greater share of the responsibility for their own personal health information, yet most EHRs lack the ability to easily incorporate data acquired outside physicians’ offices.
It’s time for EHR vendors to go all in and change that. Instead of enslaving patients to the tyranny of fragmented health records, they should prioritize the creation of a robust, standardized, and portable health record that travels with the patient, not the other way around.
Have any other ideas on how to improve patient engagement? We’d love to hear about them and share them in a future column.
If you want to contribute but don’t have any ideas, we have a suggestion: Ask your mother-in-law. You may be surprised at what you learn!
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Hospital–Jefferson Health. Follow him on twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health.
Reference
Lee JL et al. J Gen Intern Med. 2019 Nov 12. doi: 10.1007/s11606-019-05528-z.
While preparing to write this technology column, I received a great deal of insight from the unlikeliest of sources: my mother-in-law.
Now don’t get me wrong – she’s a truly lovely, intelligent, and capable woman. I have sought her advice often on many things and have always been impressed by her wisdom and pragmatism, but I’ve just never thought of asking her for her opinion on medicine or technology, as I considered her knowledge of both subjects to be limited.
This occasion changed my opinion. In fact, I believe that, as health care IT becomes more complex, people like my mother-in-law may be exactly who we should be looking to for answers.
A few weeks ago, my mother-in-law and I were discussing her recent trip to the doctor. When she mentioned some lab tests, I suggested that we log in to her patient portal to view the results. This elicited several questions and a declaration of frustration.
“Which portal?” she asked. “I have so many and can’t keep all of the websites and passwords straight! Why can’t all of my doctors use the same portal, and why do they all have different password requirements?”
As she spoke these words, I was immediately struck with an unfortunate reality of EHRs: We have done a brilliant job creating state-of-the-art digital castles and have filled them with the data needed to revolutionize care and improve population health – but we haven’t given our patients the keys to get inside.
We must ask ourselves if, in trying to construct fortresses of information around our patients, we have lost sight of the individuals in the center. I believe that we can answer this question and improve the benefits of patient portals, but we all must agree to a few simple steps to streamline the experience for everyone.
Make it easy
A study recently published in the Journal of General Internal Medicine surveyed several hospitals on their usage of patient portals. After determining whether or not the institutions had such portals, the authors then investigated to find out what, if any, guidance was provided to patients about how to use them.
Their findings are frustrating, though not surprising. While 89% of hospitals had some form of patient portal, only 65% of those “had links that were easily found, defined as links accessible within two clicks from the home page.”
Furthermore, even in cases where portals were easily found, good instructions on how to use them were missing. Those instructions that did exist centered on rules and restrictions and laying out “terms and conditions” and informing patients on “what not to do,” rather than explaining how to make the most of the experience.
According to the authors, “this focus on curtailing behavior, and the hurdles placed on finding and understanding guidance, suggest that some hospitals may be prioritizing reducing liability over improving the patient experience with portals.”
If we want our patients to use them, portals must be easy to access and intuitive to use. They also must provide value.
Make it meaningful
Patient portals have proliferated exponentially over the last 10 years, thanks to government incentive programs. One such program, known as “meaningful use,” is primarily responsible for this, as it made implementation of a patient portal one of its core requirements.
Sadly, in spite of its oft-reviled name, the meaningful use program never defined patient-friendly standards of usability for patient portals. As a result, current portals just aren’t very good. Patients like my mother-in-law find them to be too numerous, too unfriendly to use, and too limited, so they are not being used to their full potential.
In fact, many institutions may choose not to enable all of the available features in order to limit technical issues and reduce the burden on providers. In the study referenced above, only 63% of portals offered the ability for patients to communicate directly with their physicians, and only 43% offered the ability to refill prescriptions.
When enabled, these functions improve patient engagement and efficiency. Without them, patients are less likely to log on, and physicians are forced to rely on less-efficient telephone calls or traditional letters to communicate results to their patients.
Put the patient, not the portal, at the center
History has all but forgotten the attempts by tech giants such as Google and Microsoft to create personal health records. While these initially seemed like a wonderful concept, they sadly proved to be a total flop. Some patients embraced the idea, but security concerns and the lack of buy-in from EHR vendors significantly limited their uptake.
They may simply have been ahead of their time.
A decade later, wearable technology and telemedicine are ushering in a new era of patient-centric care. Individuals have been embracing a greater share of the responsibility for their own personal health information, yet most EHRs lack the ability to easily incorporate data acquired outside physicians’ offices.
It’s time for EHR vendors to go all in and change that. Instead of enslaving patients to the tyranny of fragmented health records, they should prioritize the creation of a robust, standardized, and portable health record that travels with the patient, not the other way around.
Have any other ideas on how to improve patient engagement? We’d love to hear about them and share them in a future column.
If you want to contribute but don’t have any ideas, we have a suggestion: Ask your mother-in-law. You may be surprised at what you learn!
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Hospital–Jefferson Health. Follow him on twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health.
Reference
Lee JL et al. J Gen Intern Med. 2019 Nov 12. doi: 10.1007/s11606-019-05528-z.
While preparing to write this technology column, I received a great deal of insight from the unlikeliest of sources: my mother-in-law.
Now don’t get me wrong – she’s a truly lovely, intelligent, and capable woman. I have sought her advice often on many things and have always been impressed by her wisdom and pragmatism, but I’ve just never thought of asking her for her opinion on medicine or technology, as I considered her knowledge of both subjects to be limited.
This occasion changed my opinion. In fact, I believe that, as health care IT becomes more complex, people like my mother-in-law may be exactly who we should be looking to for answers.
A few weeks ago, my mother-in-law and I were discussing her recent trip to the doctor. When she mentioned some lab tests, I suggested that we log in to her patient portal to view the results. This elicited several questions and a declaration of frustration.
“Which portal?” she asked. “I have so many and can’t keep all of the websites and passwords straight! Why can’t all of my doctors use the same portal, and why do they all have different password requirements?”
As she spoke these words, I was immediately struck with an unfortunate reality of EHRs: We have done a brilliant job creating state-of-the-art digital castles and have filled them with the data needed to revolutionize care and improve population health – but we haven’t given our patients the keys to get inside.
We must ask ourselves if, in trying to construct fortresses of information around our patients, we have lost sight of the individuals in the center. I believe that we can answer this question and improve the benefits of patient portals, but we all must agree to a few simple steps to streamline the experience for everyone.
Make it easy
A study recently published in the Journal of General Internal Medicine surveyed several hospitals on their usage of patient portals. After determining whether or not the institutions had such portals, the authors then investigated to find out what, if any, guidance was provided to patients about how to use them.
Their findings are frustrating, though not surprising. While 89% of hospitals had some form of patient portal, only 65% of those “had links that were easily found, defined as links accessible within two clicks from the home page.”
Furthermore, even in cases where portals were easily found, good instructions on how to use them were missing. Those instructions that did exist centered on rules and restrictions and laying out “terms and conditions” and informing patients on “what not to do,” rather than explaining how to make the most of the experience.
According to the authors, “this focus on curtailing behavior, and the hurdles placed on finding and understanding guidance, suggest that some hospitals may be prioritizing reducing liability over improving the patient experience with portals.”
If we want our patients to use them, portals must be easy to access and intuitive to use. They also must provide value.
Make it meaningful
Patient portals have proliferated exponentially over the last 10 years, thanks to government incentive programs. One such program, known as “meaningful use,” is primarily responsible for this, as it made implementation of a patient portal one of its core requirements.
Sadly, in spite of its oft-reviled name, the meaningful use program never defined patient-friendly standards of usability for patient portals. As a result, current portals just aren’t very good. Patients like my mother-in-law find them to be too numerous, too unfriendly to use, and too limited, so they are not being used to their full potential.
In fact, many institutions may choose not to enable all of the available features in order to limit technical issues and reduce the burden on providers. In the study referenced above, only 63% of portals offered the ability for patients to communicate directly with their physicians, and only 43% offered the ability to refill prescriptions.
When enabled, these functions improve patient engagement and efficiency. Without them, patients are less likely to log on, and physicians are forced to rely on less-efficient telephone calls or traditional letters to communicate results to their patients.
Put the patient, not the portal, at the center
History has all but forgotten the attempts by tech giants such as Google and Microsoft to create personal health records. While these initially seemed like a wonderful concept, they sadly proved to be a total flop. Some patients embraced the idea, but security concerns and the lack of buy-in from EHR vendors significantly limited their uptake.
They may simply have been ahead of their time.
A decade later, wearable technology and telemedicine are ushering in a new era of patient-centric care. Individuals have been embracing a greater share of the responsibility for their own personal health information, yet most EHRs lack the ability to easily incorporate data acquired outside physicians’ offices.
It’s time for EHR vendors to go all in and change that. Instead of enslaving patients to the tyranny of fragmented health records, they should prioritize the creation of a robust, standardized, and portable health record that travels with the patient, not the other way around.
Have any other ideas on how to improve patient engagement? We’d love to hear about them and share them in a future column.
If you want to contribute but don’t have any ideas, we have a suggestion: Ask your mother-in-law. You may be surprised at what you learn!
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Hospital–Jefferson Health. Follow him on twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Hospital–Jefferson Health.
Reference
Lee JL et al. J Gen Intern Med. 2019 Nov 12. doi: 10.1007/s11606-019-05528-z.
Nail dystrophy and nail plate thinning
At a follow-up visit, a biopsy of the skin on the fingertips was performed, which showed lichenoid lymphocytic inflammatory infiltrate with associated hyperkeratosis, hypergranulosis, and acanthosis.
No fungal elements were seen. The findings were consistent with lichen planus.

The patient was started on hydroxychloroquine. It was recommended she start a 6-week course of oral prednisone, but the mother was opposed to systemic treatment because of potential side effects.
She continued topical betamethasone without much change. Topical tacrolimus later was recommended to use on off days of betamethasone, which led to no improvement. Narrow-band UVB also was started with minimal improvement. Unfortunately,
Nail lichen planus (NLP) in children is not a common condition.1 In a recent series from Chiheb et al., NLP was reported in 90 patients, of which 40% were children; a quarter of the patients reported having extracutaneous involvement as well.2 In another childhood LP series,14 % of the children presented with nail disease.3 It can be a severe disease that, if not treated aggressively, may lead to destruction of the nail bed. This condition seems to be more prevalent in boys than girls and more prevalent in African American children.3 Unfortunately, in this patient’s case, the mother was hesitant to use systemic therapy and aggressive treatment was delayed.
Possible but not clear associations with autoimmune conditions such as vitiligo, autoimmune thyroiditis, myasthenia gravis, alopecia areata, thymoma, autoimmune polyendocrinopathy, atopic dermatitis, and lichen nitidus have been described in children with LP.
The clinical characteristics of NLP include nail plate thinning with longitudinal ridging and fissuring, with or without pterygium; trachyonychia; and erythema of the lunula when the nail matrix is involved. When the nail bed is affected, the patient can present with onycholysis with or without subungual hyperkeratosis and violaceous hue of the nail bed.4 NLP can have three different clinical presentations described by Tosti et al., which include typical NLP, 20‐nail dystrophy (trachyonychia), and idiopathic nail atrophy. Idiopathic nail atrophy is described solely in children as an acute and rapid progression that leads to destruction of the nail within months, which appears to be the clinical presentation in our patient.

The differential diagnosis of nail dystrophy in children includes infectious processes such as onychomycosis, especially when children present with onycholysis and subungual hyperkeratosis. Because of this, it is recommended to perform a nail culture or submit a sample of nail clippings for microscopic evaluation to confirm the diagnosis of onychomycosis prior to starting systemic therapy in children. Fingernail involvement without toenail involvement is an unusual presentation of onychomycosis.
Twenty-nail dystrophy – also known as trachyonychia – can be caused by several inflammatory skin conditions such as lichen planus, psoriasis, eczema, pemphigus vulgaris, and alopecia areata. Clinically, there is uniformly monomorphic thinning of the nail plate with longitudinal ridging without splitting or pterygium.1 This is a benign condition and should not cause scarring. About 10% of the cases of 20-nail dystrophy are caused by lichen planus.
Nail psoriasis is characterized by nail pitting, oil spots on the nail plate, leukonychia, subungual hyperkeratosis, and onycholysis, as well as nail crumbling, which were not seen in our patient. Although her initial presentation was of 20-nail dystrophy, which also can be a presentation of nail psoriasis, its rapid evolution with associated nail atrophy and pterygium make it unlikely to be psoriasis in this particular patient.
Patients with pachyonychia congenita – which is a genetic disorder or keratinization caused by mutations on several genes encoding keratin such as K6a, K16, K17, K6b, and possibly K6c – present with nail thickening (pachyonychia) and discoloration of the nails, as well as pincer nails. These patients also present with oral leukokeratosis and focal palmoplantar keratoderma.
The main treatment of lichen planus is potent topical corticosteroids.
For nail disease, topical treatment may not be effective and systemic treatment may be necessary. Systemic corticosteroids have been used in several pediatric series varying from a short course given at a dose of 1- 2 mg/kg per day for 2 weeks to a longer 3-month course followed by tapering.3 There are several protocols of intramuscular triamcinolone at a dose of 0.5 mg/kg in children in once a month injections for about 3 months that have been reported successful with minimal side effects.1 Other medications reported useful in patients with NLP include dapsone and acitretin. Other treatment options include narrow-band UVB and PUVA.3
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at [email protected].
References
1. Arch Dermatol. 2001 Aug;137(8):1027-32.
2. Ann Dermatol Venereol. 2015 Jan;142(1):21-5.
3. Pediatr Dermatol. 2014 Jan-Feb;31(1):59-67.
4. Dermatological diseases, in “Nails: Diagnosis, Therapy, and Surgery,” 3rd ed. (Oxford: Elsevier Saunders, 2005, p. 105).
At a follow-up visit, a biopsy of the skin on the fingertips was performed, which showed lichenoid lymphocytic inflammatory infiltrate with associated hyperkeratosis, hypergranulosis, and acanthosis.
No fungal elements were seen. The findings were consistent with lichen planus.
The patient was started on hydroxychloroquine. It was recommended she start a 6-week course of oral prednisone, but the mother was opposed to systemic treatment because of potential side effects.
She continued topical betamethasone without much change. Topical tacrolimus later was recommended to use on off days of betamethasone, which led to no improvement. Narrow-band UVB also was started with minimal improvement. Unfortunately,
Nail lichen planus (NLP) in children is not a common condition.1 In a recent series from Chiheb et al., NLP was reported in 90 patients, of which 40% were children; a quarter of the patients reported having extracutaneous involvement as well.2 In another childhood LP series,14 % of the children presented with nail disease.3 It can be a severe disease that, if not treated aggressively, may lead to destruction of the nail bed. This condition seems to be more prevalent in boys than girls and more prevalent in African American children.3 Unfortunately, in this patient’s case, the mother was hesitant to use systemic therapy and aggressive treatment was delayed.
Possible but not clear associations with autoimmune conditions such as vitiligo, autoimmune thyroiditis, myasthenia gravis, alopecia areata, thymoma, autoimmune polyendocrinopathy, atopic dermatitis, and lichen nitidus have been described in children with LP.
The clinical characteristics of NLP include nail plate thinning with longitudinal ridging and fissuring, with or without pterygium; trachyonychia; and erythema of the lunula when the nail matrix is involved. When the nail bed is affected, the patient can present with onycholysis with or without subungual hyperkeratosis and violaceous hue of the nail bed.4 NLP can have three different clinical presentations described by Tosti et al., which include typical NLP, 20‐nail dystrophy (trachyonychia), and idiopathic nail atrophy. Idiopathic nail atrophy is described solely in children as an acute and rapid progression that leads to destruction of the nail within months, which appears to be the clinical presentation in our patient.
The differential diagnosis of nail dystrophy in children includes infectious processes such as onychomycosis, especially when children present with onycholysis and subungual hyperkeratosis. Because of this, it is recommended to perform a nail culture or submit a sample of nail clippings for microscopic evaluation to confirm the diagnosis of onychomycosis prior to starting systemic therapy in children. Fingernail involvement without toenail involvement is an unusual presentation of onychomycosis.
Twenty-nail dystrophy – also known as trachyonychia – can be caused by several inflammatory skin conditions such as lichen planus, psoriasis, eczema, pemphigus vulgaris, and alopecia areata. Clinically, there is uniformly monomorphic thinning of the nail plate with longitudinal ridging without splitting or pterygium.1 This is a benign condition and should not cause scarring. About 10% of the cases of 20-nail dystrophy are caused by lichen planus.
Nail psoriasis is characterized by nail pitting, oil spots on the nail plate, leukonychia, subungual hyperkeratosis, and onycholysis, as well as nail crumbling, which were not seen in our patient. Although her initial presentation was of 20-nail dystrophy, which also can be a presentation of nail psoriasis, its rapid evolution with associated nail atrophy and pterygium make it unlikely to be psoriasis in this particular patient.
Patients with pachyonychia congenita – which is a genetic disorder or keratinization caused by mutations on several genes encoding keratin such as K6a, K16, K17, K6b, and possibly K6c – present with nail thickening (pachyonychia) and discoloration of the nails, as well as pincer nails. These patients also present with oral leukokeratosis and focal palmoplantar keratoderma.
The main treatment of lichen planus is potent topical corticosteroids.
For nail disease, topical treatment may not be effective and systemic treatment may be necessary. Systemic corticosteroids have been used in several pediatric series varying from a short course given at a dose of 1- 2 mg/kg per day for 2 weeks to a longer 3-month course followed by tapering.3 There are several protocols of intramuscular triamcinolone at a dose of 0.5 mg/kg in children in once a month injections for about 3 months that have been reported successful with minimal side effects.1 Other medications reported useful in patients with NLP include dapsone and acitretin. Other treatment options include narrow-band UVB and PUVA.3
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at [email protected].
References
1. Arch Dermatol. 2001 Aug;137(8):1027-32.
2. Ann Dermatol Venereol. 2015 Jan;142(1):21-5.
3. Pediatr Dermatol. 2014 Jan-Feb;31(1):59-67.
4. Dermatological diseases, in “Nails: Diagnosis, Therapy, and Surgery,” 3rd ed. (Oxford: Elsevier Saunders, 2005, p. 105).
At a follow-up visit, a biopsy of the skin on the fingertips was performed, which showed lichenoid lymphocytic inflammatory infiltrate with associated hyperkeratosis, hypergranulosis, and acanthosis.
No fungal elements were seen. The findings were consistent with lichen planus.
The patient was started on hydroxychloroquine. It was recommended she start a 6-week course of oral prednisone, but the mother was opposed to systemic treatment because of potential side effects.
She continued topical betamethasone without much change. Topical tacrolimus later was recommended to use on off days of betamethasone, which led to no improvement. Narrow-band UVB also was started with minimal improvement. Unfortunately,
Nail lichen planus (NLP) in children is not a common condition.1 In a recent series from Chiheb et al., NLP was reported in 90 patients, of which 40% were children; a quarter of the patients reported having extracutaneous involvement as well.2 In another childhood LP series,14 % of the children presented with nail disease.3 It can be a severe disease that, if not treated aggressively, may lead to destruction of the nail bed. This condition seems to be more prevalent in boys than girls and more prevalent in African American children.3 Unfortunately, in this patient’s case, the mother was hesitant to use systemic therapy and aggressive treatment was delayed.
Possible but not clear associations with autoimmune conditions such as vitiligo, autoimmune thyroiditis, myasthenia gravis, alopecia areata, thymoma, autoimmune polyendocrinopathy, atopic dermatitis, and lichen nitidus have been described in children with LP.
The clinical characteristics of NLP include nail plate thinning with longitudinal ridging and fissuring, with or without pterygium; trachyonychia; and erythema of the lunula when the nail matrix is involved. When the nail bed is affected, the patient can present with onycholysis with or without subungual hyperkeratosis and violaceous hue of the nail bed.4 NLP can have three different clinical presentations described by Tosti et al., which include typical NLP, 20‐nail dystrophy (trachyonychia), and idiopathic nail atrophy. Idiopathic nail atrophy is described solely in children as an acute and rapid progression that leads to destruction of the nail within months, which appears to be the clinical presentation in our patient.
The differential diagnosis of nail dystrophy in children includes infectious processes such as onychomycosis, especially when children present with onycholysis and subungual hyperkeratosis. Because of this, it is recommended to perform a nail culture or submit a sample of nail clippings for microscopic evaluation to confirm the diagnosis of onychomycosis prior to starting systemic therapy in children. Fingernail involvement without toenail involvement is an unusual presentation of onychomycosis.
Twenty-nail dystrophy – also known as trachyonychia – can be caused by several inflammatory skin conditions such as lichen planus, psoriasis, eczema, pemphigus vulgaris, and alopecia areata. Clinically, there is uniformly monomorphic thinning of the nail plate with longitudinal ridging without splitting or pterygium.1 This is a benign condition and should not cause scarring. About 10% of the cases of 20-nail dystrophy are caused by lichen planus.
Nail psoriasis is characterized by nail pitting, oil spots on the nail plate, leukonychia, subungual hyperkeratosis, and onycholysis, as well as nail crumbling, which were not seen in our patient. Although her initial presentation was of 20-nail dystrophy, which also can be a presentation of nail psoriasis, its rapid evolution with associated nail atrophy and pterygium make it unlikely to be psoriasis in this particular patient.
Patients with pachyonychia congenita – which is a genetic disorder or keratinization caused by mutations on several genes encoding keratin such as K6a, K16, K17, K6b, and possibly K6c – present with nail thickening (pachyonychia) and discoloration of the nails, as well as pincer nails. These patients also present with oral leukokeratosis and focal palmoplantar keratoderma.
The main treatment of lichen planus is potent topical corticosteroids.
For nail disease, topical treatment may not be effective and systemic treatment may be necessary. Systemic corticosteroids have been used in several pediatric series varying from a short course given at a dose of 1- 2 mg/kg per day for 2 weeks to a longer 3-month course followed by tapering.3 There are several protocols of intramuscular triamcinolone at a dose of 0.5 mg/kg in children in once a month injections for about 3 months that have been reported successful with minimal side effects.1 Other medications reported useful in patients with NLP include dapsone and acitretin. Other treatment options include narrow-band UVB and PUVA.3
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. Email her at [email protected].
References
1. Arch Dermatol. 2001 Aug;137(8):1027-32.
2. Ann Dermatol Venereol. 2015 Jan;142(1):21-5.
3. Pediatr Dermatol. 2014 Jan-Feb;31(1):59-67.
4. Dermatological diseases, in “Nails: Diagnosis, Therapy, and Surgery,” 3rd ed. (Oxford: Elsevier Saunders, 2005, p. 105).
An 8-year-old female child comes to our pediatric dermatology clinic for evaluation of onychomycosis on her fingernails. The mother stated the child started developing funny-looking nails 1 year prior to the visit. It started with only two fingernails affected and now has spread to all her fingernails. Her toenails are not involved.

She denied any pain or itching. She initially was treated with topical antifungal medications as well as tea tree oil, apple cider vinegar, and a 6-week course of oral griseofulvin without any improvement. Her nails progressively have gotten much worse. She has no history of atopic dermatitis or any other skin conditions. She denied any joint pain, sun sensitivity, hair loss, or any other symptoms. The mother denied any family history of nail fungus, ringworm, psoriasis, or eczema.
She likes to play basketball and enjoys arts and crafts. She has a cat and a dog; neither of them have any skin problems.
On physical examination, there is nail dystrophy with nail plate thinning and longitudinal fissuring of all fingernails but not of the toenails. She also has hyperpigmented violaceous plaques on the surrounding periungual skin. There are no other skin lesions, and there are no oral or genital lesions. There is no scalp involvement or hair loss. At follow-up several months later, she had complete destruction of the nail plate with scar formation.
A fungal culture was performed, as well as microscopic analysis of the nail with periodic acid fast and giemsa stains, which showed no fungal organisms.
She initially was treated with topical betamethasone twice a day for 6 weeks and then 2 weeks on and 2 weeks off without much change.
The evolution of social media and visual abstracts in hospital medicine
In recent years, social media platforms like Twitter, Facebook, and Instagram have become popular gathering spots for clinicians to connect, engage, and share medical content. Medical journals, which often act as purveyors of this content, have recognized social media’s growing power and influence and have begun looking for ways to better engage their audiences.

In 2016, the Annals of Surgery was looking to better disseminate the work being published in its pages and looked to Twitter as one way of accomplishing this. At the time, most journals were only posting the title or a brief description of the published manuscript and hoping their Twitter followers would click on the article link. As journal editors were finding, if the audience was not immediately familiar with the topic or able to quickly capture the nuances of the study, there was a good chance the reader would continue to scroll past the post and never view the article.
Recognizing that social media heavily relies on visual material to garner attention, Annals turned to Andrew Ibrahim, MD, an architect turned surgeon, to help them rethink their social media strategy. Using the design training he had previously received in his career as an architect, Dr. Ibrahim created a simple visual tool that could be used to capture the often complicated and nuanced aspects of a research study. He called his creation a “visual abstract.”
But what is a visual abstract? Simply, they are visual representations of the key findings of a published manuscript; or put another way, a “movie trailer” to the full manuscript. While they can take many different forms and designs, they often consist of three key components: (1) a simple, easy to understand title, (2) a primary focus on outcomes, and (3) the use of visual cues or images to help the reader absorb and remember the take home message. This simplified delivery of complex information allows the producer to efficiently share complex findings in a format that allows for rapid visualization and interpretation.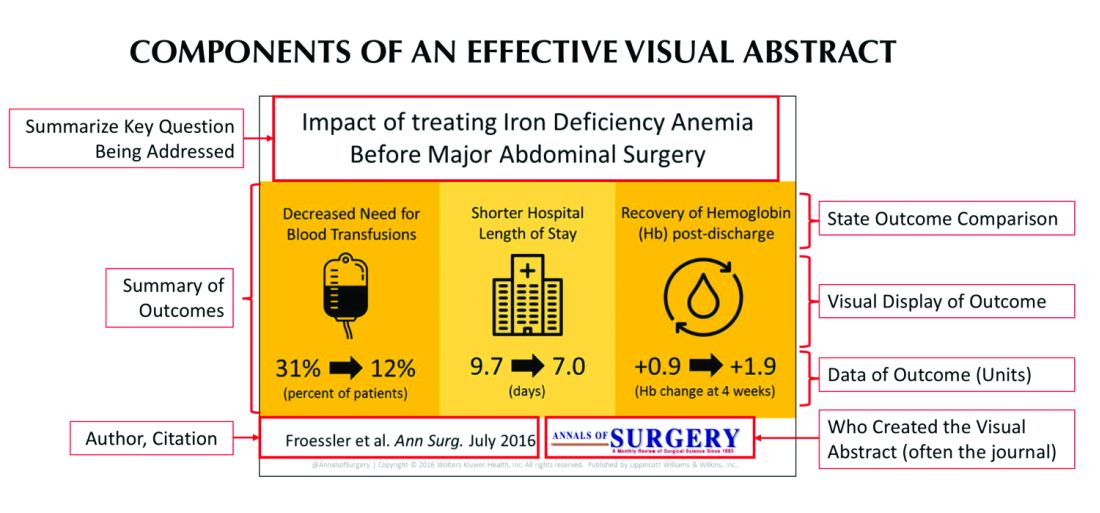
Since its inception, several studies have examined the influence visual abstracts have on disseminating research. One study conducted by Dr. Ibrahim and his colleagues found that articles tweeted with a visual abstract had an almost eightfold increase in the number of Twitter impressions (a measure of social media dissemination) and a threefold increase in article visits, compared with those manuscripts tweeted with the article title only.1 These results reflect what behavioral scientists have long understood: Humans process visual data better than any other type of data.2 For instance, according to research compiled by 3M, the company behind popular sticky notes, visual data is processed 60,000 times faster than text and has been shown to improve learning by 400%.3 Likewise, digital marketers have found that pages with videos and images draw on average 94% more views than their text-only counterparts.4
This knowledge, along with the substantial difference in engagement and dissemination characteristics from Dr. Ibrahim’s study, was far beyond what anyone might have expected and started a trend in medicine that continues to grow today. Medical journals across all practices and disciplines, including several leading journals, such as the New England Journal of Medicine, the Journal of the American Medical Association, and the Journal of Hospital Medicine (JHM), are utilizing this new tool to help disseminate their work in social media.
Visual abstracts have expanded beyond the social media sphere and are now frequently used in Grand Rounds presentations and as teaching tools among medical educators. JHM was one of the first journals to adopt the use of visual abstracts and has since published more than 150 in total. Given the growing popularity and expanded use of visual abstracts, JHM recently began archiving them on the journal’s website to allow clinicians to use the material in their own creative ways.
Visual abstracts are just one piece of the growing enterprise in social media for JHM. Recognizing the growing utilization of social media among physicians, JHM has taken a leading role in the use of online journal clubs. Since 2014, JHM has run a monthly Twitter-based journal club that discusses recently published articles and hospital medicine–based topics, called #JHMChat.5 This forum has allowed hospitalists from across the country, and around the world, to connect, network, and engage around topics important to the field of hospital medicine. The journal frequently reaches beyond hospital medicine borders and partners with other specialties and interest groups to gain perspective and insights into shared topic areas. To date, #JHMChat has one of the most robust online communities and continues to attract new followers each month.
As social media use continues to expand among clinicians, engagement tools like visual abstracts and Twitter chats will certainly continue to grow. Given that more clinicians are scrolling through websites than flipping through journal pages, medical journals like JHM will continually look for novel ways to engage their audiences and create communities among their followers. While a former architect who now practices as a surgeon led the way with visual abstracts, it remains to be seen who will create the next tool used to capture our attention on the ever-evolving sphere of social media.
Dr. Wray is a hospitalist at the University of California, San Francisco, and the San Francisco Veterans Affairs Medical Center. He also serves as a digital media and associate editor for the Journal of Hospital Medicine.
References
1. Ibrahim AM et al. Visual abstracts to disseminate research on social media: A prospective, case-control crossover study. Ann Surg. 2017;266(6):e46.
2. Tufte ER. The Visual Display of Quantitative Information. Second edition. Cheshire, Conn. Graphics Press, 2001. https://search.library.wisc.edu/catalog/999913808702121.
3. Polishing Your Presentation. http://web.archive.org/web/20001014041642/http://www.3m.com:80/meetingnetwork/files/meetingguide_pres.pdf. Accessed May 28, 2017.
4. 7 reasons you need visual content in your marketing strategy. https://medium.com/@nikos_iliopoulos/7-reasons-you-need-visual-content-in-your-marketing-strategy-bc77ca5521ac. Accessed May 28, 2017.
5. Wray CM et al. The adoption of an online journal club to improve research dissemination and social media engagement among hospitalists. J Hosp Med. 2018. doi: 10.12788/jhm.2987.
In recent years, social media platforms like Twitter, Facebook, and Instagram have become popular gathering spots for clinicians to connect, engage, and share medical content. Medical journals, which often act as purveyors of this content, have recognized social media’s growing power and influence and have begun looking for ways to better engage their audiences.
In 2016, the Annals of Surgery was looking to better disseminate the work being published in its pages and looked to Twitter as one way of accomplishing this. At the time, most journals were only posting the title or a brief description of the published manuscript and hoping their Twitter followers would click on the article link. As journal editors were finding, if the audience was not immediately familiar with the topic or able to quickly capture the nuances of the study, there was a good chance the reader would continue to scroll past the post and never view the article.
Recognizing that social media heavily relies on visual material to garner attention, Annals turned to Andrew Ibrahim, MD, an architect turned surgeon, to help them rethink their social media strategy. Using the design training he had previously received in his career as an architect, Dr. Ibrahim created a simple visual tool that could be used to capture the often complicated and nuanced aspects of a research study. He called his creation a “visual abstract.”
But what is a visual abstract? Simply, they are visual representations of the key findings of a published manuscript; or put another way, a “movie trailer” to the full manuscript. While they can take many different forms and designs, they often consist of three key components: (1) a simple, easy to understand title, (2) a primary focus on outcomes, and (3) the use of visual cues or images to help the reader absorb and remember the take home message. This simplified delivery of complex information allows the producer to efficiently share complex findings in a format that allows for rapid visualization and interpretation.
Since its inception, several studies have examined the influence visual abstracts have on disseminating research. One study conducted by Dr. Ibrahim and his colleagues found that articles tweeted with a visual abstract had an almost eightfold increase in the number of Twitter impressions (a measure of social media dissemination) and a threefold increase in article visits, compared with those manuscripts tweeted with the article title only.1 These results reflect what behavioral scientists have long understood: Humans process visual data better than any other type of data.2 For instance, according to research compiled by 3M, the company behind popular sticky notes, visual data is processed 60,000 times faster than text and has been shown to improve learning by 400%.3 Likewise, digital marketers have found that pages with videos and images draw on average 94% more views than their text-only counterparts.4
This knowledge, along with the substantial difference in engagement and dissemination characteristics from Dr. Ibrahim’s study, was far beyond what anyone might have expected and started a trend in medicine that continues to grow today. Medical journals across all practices and disciplines, including several leading journals, such as the New England Journal of Medicine, the Journal of the American Medical Association, and the Journal of Hospital Medicine (JHM), are utilizing this new tool to help disseminate their work in social media.
Visual abstracts have expanded beyond the social media sphere and are now frequently used in Grand Rounds presentations and as teaching tools among medical educators. JHM was one of the first journals to adopt the use of visual abstracts and has since published more than 150 in total. Given the growing popularity and expanded use of visual abstracts, JHM recently began archiving them on the journal’s website to allow clinicians to use the material in their own creative ways.
Visual abstracts are just one piece of the growing enterprise in social media for JHM. Recognizing the growing utilization of social media among physicians, JHM has taken a leading role in the use of online journal clubs. Since 2014, JHM has run a monthly Twitter-based journal club that discusses recently published articles and hospital medicine–based topics, called #JHMChat.5 This forum has allowed hospitalists from across the country, and around the world, to connect, network, and engage around topics important to the field of hospital medicine. The journal frequently reaches beyond hospital medicine borders and partners with other specialties and interest groups to gain perspective and insights into shared topic areas. To date, #JHMChat has one of the most robust online communities and continues to attract new followers each month.
As social media use continues to expand among clinicians, engagement tools like visual abstracts and Twitter chats will certainly continue to grow. Given that more clinicians are scrolling through websites than flipping through journal pages, medical journals like JHM will continually look for novel ways to engage their audiences and create communities among their followers. While a former architect who now practices as a surgeon led the way with visual abstracts, it remains to be seen who will create the next tool used to capture our attention on the ever-evolving sphere of social media.
Dr. Wray is a hospitalist at the University of California, San Francisco, and the San Francisco Veterans Affairs Medical Center. He also serves as a digital media and associate editor for the Journal of Hospital Medicine.
References
1. Ibrahim AM et al. Visual abstracts to disseminate research on social media: A prospective, case-control crossover study. Ann Surg. 2017;266(6):e46.
2. Tufte ER. The Visual Display of Quantitative Information. Second edition. Cheshire, Conn. Graphics Press, 2001. https://search.library.wisc.edu/catalog/999913808702121.
3. Polishing Your Presentation. http://web.archive.org/web/20001014041642/http://www.3m.com:80/meetingnetwork/files/meetingguide_pres.pdf. Accessed May 28, 2017.
4. 7 reasons you need visual content in your marketing strategy. https://medium.com/@nikos_iliopoulos/7-reasons-you-need-visual-content-in-your-marketing-strategy-bc77ca5521ac. Accessed May 28, 2017.
5. Wray CM et al. The adoption of an online journal club to improve research dissemination and social media engagement among hospitalists. J Hosp Med. 2018. doi: 10.12788/jhm.2987.
In recent years, social media platforms like Twitter, Facebook, and Instagram have become popular gathering spots for clinicians to connect, engage, and share medical content. Medical journals, which often act as purveyors of this content, have recognized social media’s growing power and influence and have begun looking for ways to better engage their audiences.
In 2016, the Annals of Surgery was looking to better disseminate the work being published in its pages and looked to Twitter as one way of accomplishing this. At the time, most journals were only posting the title or a brief description of the published manuscript and hoping their Twitter followers would click on the article link. As journal editors were finding, if the audience was not immediately familiar with the topic or able to quickly capture the nuances of the study, there was a good chance the reader would continue to scroll past the post and never view the article.
Recognizing that social media heavily relies on visual material to garner attention, Annals turned to Andrew Ibrahim, MD, an architect turned surgeon, to help them rethink their social media strategy. Using the design training he had previously received in his career as an architect, Dr. Ibrahim created a simple visual tool that could be used to capture the often complicated and nuanced aspects of a research study. He called his creation a “visual abstract.”
But what is a visual abstract? Simply, they are visual representations of the key findings of a published manuscript; or put another way, a “movie trailer” to the full manuscript. While they can take many different forms and designs, they often consist of three key components: (1) a simple, easy to understand title, (2) a primary focus on outcomes, and (3) the use of visual cues or images to help the reader absorb and remember the take home message. This simplified delivery of complex information allows the producer to efficiently share complex findings in a format that allows for rapid visualization and interpretation.
Since its inception, several studies have examined the influence visual abstracts have on disseminating research. One study conducted by Dr. Ibrahim and his colleagues found that articles tweeted with a visual abstract had an almost eightfold increase in the number of Twitter impressions (a measure of social media dissemination) and a threefold increase in article visits, compared with those manuscripts tweeted with the article title only.1 These results reflect what behavioral scientists have long understood: Humans process visual data better than any other type of data.2 For instance, according to research compiled by 3M, the company behind popular sticky notes, visual data is processed 60,000 times faster than text and has been shown to improve learning by 400%.3 Likewise, digital marketers have found that pages with videos and images draw on average 94% more views than their text-only counterparts.4
This knowledge, along with the substantial difference in engagement and dissemination characteristics from Dr. Ibrahim’s study, was far beyond what anyone might have expected and started a trend in medicine that continues to grow today. Medical journals across all practices and disciplines, including several leading journals, such as the New England Journal of Medicine, the Journal of the American Medical Association, and the Journal of Hospital Medicine (JHM), are utilizing this new tool to help disseminate their work in social media.
Visual abstracts have expanded beyond the social media sphere and are now frequently used in Grand Rounds presentations and as teaching tools among medical educators. JHM was one of the first journals to adopt the use of visual abstracts and has since published more than 150 in total. Given the growing popularity and expanded use of visual abstracts, JHM recently began archiving them on the journal’s website to allow clinicians to use the material in their own creative ways.
Visual abstracts are just one piece of the growing enterprise in social media for JHM. Recognizing the growing utilization of social media among physicians, JHM has taken a leading role in the use of online journal clubs. Since 2014, JHM has run a monthly Twitter-based journal club that discusses recently published articles and hospital medicine–based topics, called #JHMChat.5 This forum has allowed hospitalists from across the country, and around the world, to connect, network, and engage around topics important to the field of hospital medicine. The journal frequently reaches beyond hospital medicine borders and partners with other specialties and interest groups to gain perspective and insights into shared topic areas. To date, #JHMChat has one of the most robust online communities and continues to attract new followers each month.
As social media use continues to expand among clinicians, engagement tools like visual abstracts and Twitter chats will certainly continue to grow. Given that more clinicians are scrolling through websites than flipping through journal pages, medical journals like JHM will continually look for novel ways to engage their audiences and create communities among their followers. While a former architect who now practices as a surgeon led the way with visual abstracts, it remains to be seen who will create the next tool used to capture our attention on the ever-evolving sphere of social media.
Dr. Wray is a hospitalist at the University of California, San Francisco, and the San Francisco Veterans Affairs Medical Center. He also serves as a digital media and associate editor for the Journal of Hospital Medicine.
References
1. Ibrahim AM et al. Visual abstracts to disseminate research on social media: A prospective, case-control crossover study. Ann Surg. 2017;266(6):e46.
2. Tufte ER. The Visual Display of Quantitative Information. Second edition. Cheshire, Conn. Graphics Press, 2001. https://search.library.wisc.edu/catalog/999913808702121.
3. Polishing Your Presentation. http://web.archive.org/web/20001014041642/http://www.3m.com:80/meetingnetwork/files/meetingguide_pres.pdf. Accessed May 28, 2017.
4. 7 reasons you need visual content in your marketing strategy. https://medium.com/@nikos_iliopoulos/7-reasons-you-need-visual-content-in-your-marketing-strategy-bc77ca5521ac. Accessed May 28, 2017.
5. Wray CM et al. The adoption of an online journal club to improve research dissemination and social media engagement among hospitalists. J Hosp Med. 2018. doi: 10.12788/jhm.2987.
Play it as it lies: Handling lying by kids
“Not my son!” your patient’s parent rants. “If he lies to me, he will regret it for a long time.” While your first reaction may be to agree that a child lying to a parent crosses a kind of moral line in the sand, lying is a far more nuanced part of parenting worth a deeper understanding.
In order to lie, a child has to develop cognitive and social understanding. Typically developing children look to see what is interesting to others, called “joint attention,” at around 12-18 months. Failure to do this is one of the early signs of autism reflecting atypical social understanding. At around 3.5 years, children may attempt to deceive if they have broken a rule. The study demonstrating this may sound a lot like home: Children are left alone with a tempting toy but told not to touch it. Although they do touch it while the adult is out of sight, they say rather sweetly (and eventually convincingly) that they did not, even though the toy was clearly moved! While boys generally have more behavior problems, girls and children with better verbal skills achieve deceit at an earlier age, some as young as 2 years. At this stage, children become aware that the adult can’t know exactly what they know. If the parent shows high emotion to what they consider a lie, this can be a topic for testing! Children with ADHD often lack the inhibition needed for early mastery of deception, and children with autism later or not at all. They don’t see the social point to lying nor can they fake a facial expression. They have a case of intractable honesty!
The inability to refrain from telling the truth can result in social rejection, for example when a child rats on a peer for a trivial misdeed in class. Even though he is speaking the truth and “following the (teacher’s) rules,” he did not see that the cost of breaking the (peer) social rules was more important. By age 6 years, children typically figure out that what another person thinks may not be true – their belief may be incorrect or a “false belief.” This understanding is called Theory of Mind, missing or delayed in autism. Only 40% of high-functioning children with autism passed false belief testing at ages 6- to 13-years-old, compared with 95% of typical age-matched peers (Physiol Behav. 2010 Jun 1;100[3]:268-76). The percentage of children on the spectrum understanding false beliefs more closely matched that of preschoolers (39%). At a later age and given extra time to think, some children with autism can do better at this kind of perspective taking, but many continue having difficulty understanding thoughts of others, especially social expectations or motivations (such as flirting, status seeking, and making an excuse) even as adults. This can impair social relationships even when desire to fit in and IQ are otherwise high.
On the other hand, ADHD is a common condition in which “lying” comes from saying the first thing that comes to mind even if the child knows otherwise. A wise parent of one of my patients with ADHD told me about her “30 second rule” where she would give her child that extra time and walk away briefly to “be sure that is what you wanted to say,” with praise rather than give a consequence for changing the story to the truth. This is an important concept we pediatricians need to know: Punishing lying in children tends to result in more, not less, lying and more sneakiness. Instead, parents need to be advised to recall the origins of the word discipline as being “to teach.”
When children lie there are four basic scenarios: They may not know the rules, they may know but have something they want more, they may be impulsive, or they may have developed an attitude of seeking to con the adults whom they feel are mean as a way to have some power in the relationship and get back at them. Clearly, we do not want to push children to this fourth resort by harsh reactions to lying. We have seen particular difficulty with harsh reactions to lying in parents from strong, rule-oriented careers such as police officers, military, and ministers. Asking “How would your parent have handled this?” often will reveal reasons for their tough but backfiring stance.
Lying can work to get what one wants and nearly all children try it. As with other new milestones, children practice this “skill,” much to parents’ dismay. Parents generally can tell if children are lying; they see it on their faces, hear the story from siblings, or see evidence of what happened. Lying provides an important opportunity for the adult to stop, take some breaths, touch the child, and empathize: “It is hard to admit a mistake. I know you did not mean to do it. But you are young, and I know that you are good and honest inside, and will get stronger and braver at telling the truth as you get older. Will you promise to try harder?” In some cases a consequence may be appropriate, for example if something was broken. Usually, simply empathizing and focusing on the expectation for improvement will increase the child’s desire to please the parents rather than get back at them. Actual rewards for honesty improve truth telling by 1.5 times if the reward is big enough.
But it is important to recognize that we all make split second tactical decisions about our actions based on how safe we feel in the situation and our knowledge of social rules and costs. Children over time need to learn that it is safe to tell the truth among family members and that they will not be harshly dealt with. It is a subtle task, but important to learn that deception is a tool that can be important used judiciously when required socially (I have a curfew) or in dangerous situations (I did not see the thug), but can undermine relationships and should not be used with your allies (family and friends).

But parenting involves lying also, which can be a model for the child. Sarcasm is a peculiar form of problematic adult lying. The adults say the opposite or an exaggeration of what they really mean, usually with a smirk or other nonverbal cue to their intent. This is confusing, if not infuriating, to immature children or those who do not understand this twisted communication. It is best to avoid sarcasm with children, or at least be sure to explain it so the children gain understanding over time.
Parents need to “lie” to their children to some extent to reassure and allow for development of confidence. What adult hasn’t said “It’s going to be all right” about a looming storm, car crash, or illness, when actually there is uncertainty. Children count on adults to keep them safe emotionally and physically from things they can’t yet handle. To move forward developmentally, children need adults to be brave leaders, even when the adults don’t feel confident. Some parents think their children must know the “truth” in every instance. Those children are often painfully anxious and overwhelmed.
There is plenty of time for more facts later when the child has the thinking and emotional power to handle the truth.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
“Not my son!” your patient’s parent rants. “If he lies to me, he will regret it for a long time.” While your first reaction may be to agree that a child lying to a parent crosses a kind of moral line in the sand, lying is a far more nuanced part of parenting worth a deeper understanding.
In order to lie, a child has to develop cognitive and social understanding. Typically developing children look to see what is interesting to others, called “joint attention,” at around 12-18 months. Failure to do this is one of the early signs of autism reflecting atypical social understanding. At around 3.5 years, children may attempt to deceive if they have broken a rule. The study demonstrating this may sound a lot like home: Children are left alone with a tempting toy but told not to touch it. Although they do touch it while the adult is out of sight, they say rather sweetly (and eventually convincingly) that they did not, even though the toy was clearly moved! While boys generally have more behavior problems, girls and children with better verbal skills achieve deceit at an earlier age, some as young as 2 years. At this stage, children become aware that the adult can’t know exactly what they know. If the parent shows high emotion to what they consider a lie, this can be a topic for testing! Children with ADHD often lack the inhibition needed for early mastery of deception, and children with autism later or not at all. They don’t see the social point to lying nor can they fake a facial expression. They have a case of intractable honesty!
The inability to refrain from telling the truth can result in social rejection, for example when a child rats on a peer for a trivial misdeed in class. Even though he is speaking the truth and “following the (teacher’s) rules,” he did not see that the cost of breaking the (peer) social rules was more important. By age 6 years, children typically figure out that what another person thinks may not be true – their belief may be incorrect or a “false belief.” This understanding is called Theory of Mind, missing or delayed in autism. Only 40% of high-functioning children with autism passed false belief testing at ages 6- to 13-years-old, compared with 95% of typical age-matched peers (Physiol Behav. 2010 Jun 1;100[3]:268-76). The percentage of children on the spectrum understanding false beliefs more closely matched that of preschoolers (39%). At a later age and given extra time to think, some children with autism can do better at this kind of perspective taking, but many continue having difficulty understanding thoughts of others, especially social expectations or motivations (such as flirting, status seeking, and making an excuse) even as adults. This can impair social relationships even when desire to fit in and IQ are otherwise high.
On the other hand, ADHD is a common condition in which “lying” comes from saying the first thing that comes to mind even if the child knows otherwise. A wise parent of one of my patients with ADHD told me about her “30 second rule” where she would give her child that extra time and walk away briefly to “be sure that is what you wanted to say,” with praise rather than give a consequence for changing the story to the truth. This is an important concept we pediatricians need to know: Punishing lying in children tends to result in more, not less, lying and more sneakiness. Instead, parents need to be advised to recall the origins of the word discipline as being “to teach.”
When children lie there are four basic scenarios: They may not know the rules, they may know but have something they want more, they may be impulsive, or they may have developed an attitude of seeking to con the adults whom they feel are mean as a way to have some power in the relationship and get back at them. Clearly, we do not want to push children to this fourth resort by harsh reactions to lying. We have seen particular difficulty with harsh reactions to lying in parents from strong, rule-oriented careers such as police officers, military, and ministers. Asking “How would your parent have handled this?” often will reveal reasons for their tough but backfiring stance.
Lying can work to get what one wants and nearly all children try it. As with other new milestones, children practice this “skill,” much to parents’ dismay. Parents generally can tell if children are lying; they see it on their faces, hear the story from siblings, or see evidence of what happened. Lying provides an important opportunity for the adult to stop, take some breaths, touch the child, and empathize: “It is hard to admit a mistake. I know you did not mean to do it. But you are young, and I know that you are good and honest inside, and will get stronger and braver at telling the truth as you get older. Will you promise to try harder?” In some cases a consequence may be appropriate, for example if something was broken. Usually, simply empathizing and focusing on the expectation for improvement will increase the child’s desire to please the parents rather than get back at them. Actual rewards for honesty improve truth telling by 1.5 times if the reward is big enough.
But it is important to recognize that we all make split second tactical decisions about our actions based on how safe we feel in the situation and our knowledge of social rules and costs. Children over time need to learn that it is safe to tell the truth among family members and that they will not be harshly dealt with. It is a subtle task, but important to learn that deception is a tool that can be important used judiciously when required socially (I have a curfew) or in dangerous situations (I did not see the thug), but can undermine relationships and should not be used with your allies (family and friends).
But parenting involves lying also, which can be a model for the child. Sarcasm is a peculiar form of problematic adult lying. The adults say the opposite or an exaggeration of what they really mean, usually with a smirk or other nonverbal cue to their intent. This is confusing, if not infuriating, to immature children or those who do not understand this twisted communication. It is best to avoid sarcasm with children, or at least be sure to explain it so the children gain understanding over time.
Parents need to “lie” to their children to some extent to reassure and allow for development of confidence. What adult hasn’t said “It’s going to be all right” about a looming storm, car crash, or illness, when actually there is uncertainty. Children count on adults to keep them safe emotionally and physically from things they can’t yet handle. To move forward developmentally, children need adults to be brave leaders, even when the adults don’t feel confident. Some parents think their children must know the “truth” in every instance. Those children are often painfully anxious and overwhelmed.
There is plenty of time for more facts later when the child has the thinking and emotional power to handle the truth.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].
“Not my son!” your patient’s parent rants. “If he lies to me, he will regret it for a long time.” While your first reaction may be to agree that a child lying to a parent crosses a kind of moral line in the sand, lying is a far more nuanced part of parenting worth a deeper understanding.
In order to lie, a child has to develop cognitive and social understanding. Typically developing children look to see what is interesting to others, called “joint attention,” at around 12-18 months. Failure to do this is one of the early signs of autism reflecting atypical social understanding. At around 3.5 years, children may attempt to deceive if they have broken a rule. The study demonstrating this may sound a lot like home: Children are left alone with a tempting toy but told not to touch it. Although they do touch it while the adult is out of sight, they say rather sweetly (and eventually convincingly) that they did not, even though the toy was clearly moved! While boys generally have more behavior problems, girls and children with better verbal skills achieve deceit at an earlier age, some as young as 2 years. At this stage, children become aware that the adult can’t know exactly what they know. If the parent shows high emotion to what they consider a lie, this can be a topic for testing! Children with ADHD often lack the inhibition needed for early mastery of deception, and children with autism later or not at all. They don’t see the social point to lying nor can they fake a facial expression. They have a case of intractable honesty!
The inability to refrain from telling the truth can result in social rejection, for example when a child rats on a peer for a trivial misdeed in class. Even though he is speaking the truth and “following the (teacher’s) rules,” he did not see that the cost of breaking the (peer) social rules was more important. By age 6 years, children typically figure out that what another person thinks may not be true – their belief may be incorrect or a “false belief.” This understanding is called Theory of Mind, missing or delayed in autism. Only 40% of high-functioning children with autism passed false belief testing at ages 6- to 13-years-old, compared with 95% of typical age-matched peers (Physiol Behav. 2010 Jun 1;100[3]:268-76). The percentage of children on the spectrum understanding false beliefs more closely matched that of preschoolers (39%). At a later age and given extra time to think, some children with autism can do better at this kind of perspective taking, but many continue having difficulty understanding thoughts of others, especially social expectations or motivations (such as flirting, status seeking, and making an excuse) even as adults. This can impair social relationships even when desire to fit in and IQ are otherwise high.
On the other hand, ADHD is a common condition in which “lying” comes from saying the first thing that comes to mind even if the child knows otherwise. A wise parent of one of my patients with ADHD told me about her “30 second rule” where she would give her child that extra time and walk away briefly to “be sure that is what you wanted to say,” with praise rather than give a consequence for changing the story to the truth. This is an important concept we pediatricians need to know: Punishing lying in children tends to result in more, not less, lying and more sneakiness. Instead, parents need to be advised to recall the origins of the word discipline as being “to teach.”
When children lie there are four basic scenarios: They may not know the rules, they may know but have something they want more, they may be impulsive, or they may have developed an attitude of seeking to con the adults whom they feel are mean as a way to have some power in the relationship and get back at them. Clearly, we do not want to push children to this fourth resort by harsh reactions to lying. We have seen particular difficulty with harsh reactions to lying in parents from strong, rule-oriented careers such as police officers, military, and ministers. Asking “How would your parent have handled this?” often will reveal reasons for their tough but backfiring stance.
Lying can work to get what one wants and nearly all children try it. As with other new milestones, children practice this “skill,” much to parents’ dismay. Parents generally can tell if children are lying; they see it on their faces, hear the story from siblings, or see evidence of what happened. Lying provides an important opportunity for the adult to stop, take some breaths, touch the child, and empathize: “It is hard to admit a mistake. I know you did not mean to do it. But you are young, and I know that you are good and honest inside, and will get stronger and braver at telling the truth as you get older. Will you promise to try harder?” In some cases a consequence may be appropriate, for example if something was broken. Usually, simply empathizing and focusing on the expectation for improvement will increase the child’s desire to please the parents rather than get back at them. Actual rewards for honesty improve truth telling by 1.5 times if the reward is big enough.
But it is important to recognize that we all make split second tactical decisions about our actions based on how safe we feel in the situation and our knowledge of social rules and costs. Children over time need to learn that it is safe to tell the truth among family members and that they will not be harshly dealt with. It is a subtle task, but important to learn that deception is a tool that can be important used judiciously when required socially (I have a curfew) or in dangerous situations (I did not see the thug), but can undermine relationships and should not be used with your allies (family and friends).
But parenting involves lying also, which can be a model for the child. Sarcasm is a peculiar form of problematic adult lying. The adults say the opposite or an exaggeration of what they really mean, usually with a smirk or other nonverbal cue to their intent. This is confusing, if not infuriating, to immature children or those who do not understand this twisted communication. It is best to avoid sarcasm with children, or at least be sure to explain it so the children gain understanding over time.
Parents need to “lie” to their children to some extent to reassure and allow for development of confidence. What adult hasn’t said “It’s going to be all right” about a looming storm, car crash, or illness, when actually there is uncertainty. Children count on adults to keep them safe emotionally and physically from things they can’t yet handle. To move forward developmentally, children need adults to be brave leaders, even when the adults don’t feel confident. Some parents think their children must know the “truth” in every instance. Those children are often painfully anxious and overwhelmed.
There is plenty of time for more facts later when the child has the thinking and emotional power to handle the truth.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at [email protected].

Vascular occlusion management
The time course and proper management of vascular occlusion attributable to interarterial hyaluronic acid fillers is critical. Albeit a rare complication, off-label uses of HA fillers, lack of proper training of injectors, and lack of clear appropriate guidelines in the management of these complications are some of the causes of delayed treatment and necrotic complications.
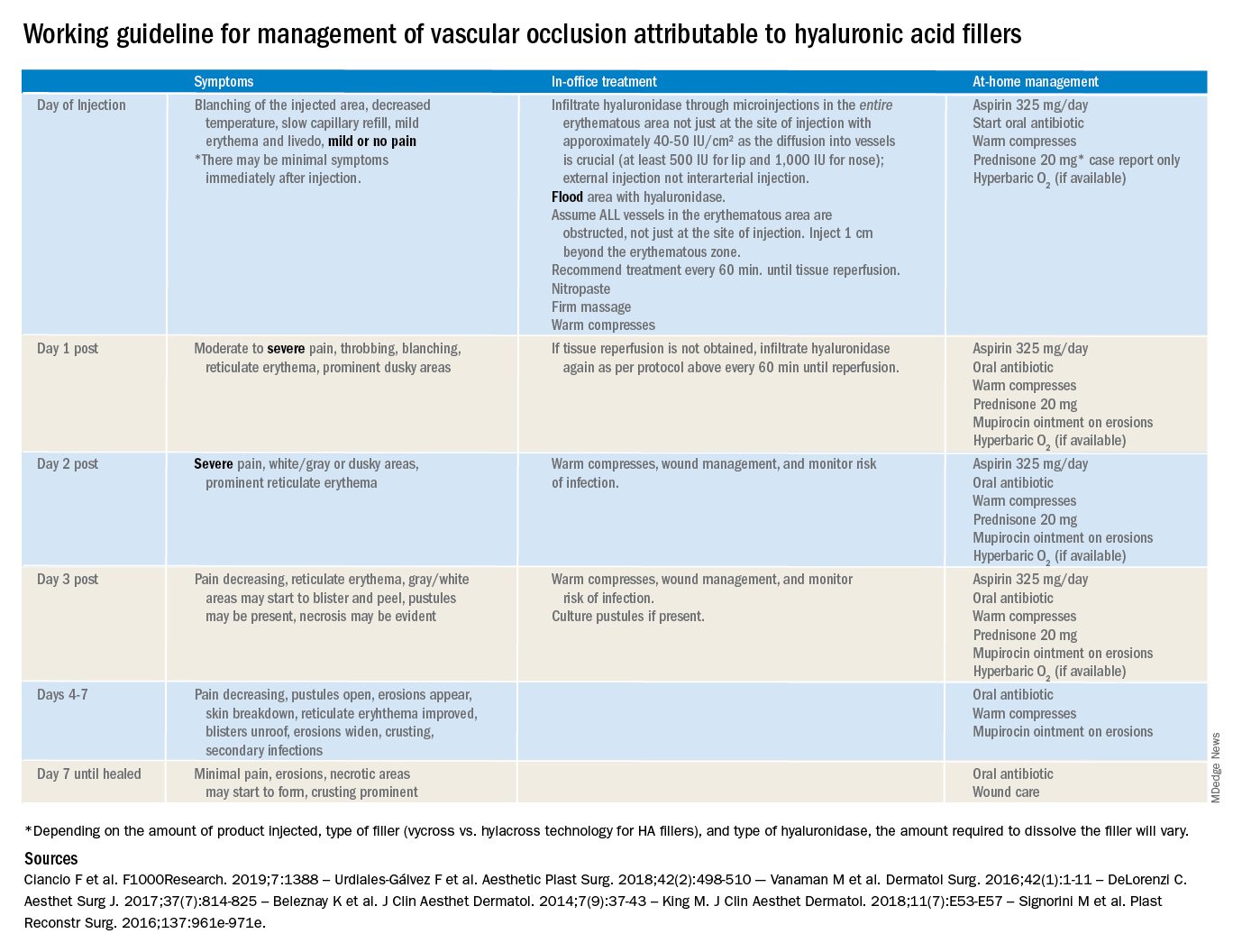
There are currently no definitive guidelines for the management of filler-associated cutaneous necrosis as experience with its treatment continues to evolve and be reported. In an attempt to consolidate the published data, as well as to give somewhat of a clear guideline of expectations, a time course and treatment guide has been outlined. The following is a working guideline for management of vascular occlusion attributable to HA fillers based on reports in the literature. This is not a consensus statement, rather it is a consolidation of the anecdotal reports and case studies outlined to help practitioners. It is also not inclusive of all the presentations of vascular occlusion. There are delayed cases of vascular occlusion beginning several days after injection, as well as alternative treatment options that may be considered.
These guidelines also are not for the devastating complication of blindness because of vascular occlusion secondary to fillers. Blindness is beyond the scope of the current article; however, we believe all experienced injectors should have emergency preparations in place and a relationship with an ophthalmologist or other trained surgeons experienced in performing retrobulbar hyaluronidase injections who can be reached in the event of a suspected occlusion. Any symptoms of eye pain, headache, or visual changes need to be immediately treated. Vascular occlusion is an emergency and timing is critical to prevent permanent blindness and facial deformities.

As with all filler injections, risks and complications can happen, and we cannot stress enough the appropriate level of training, as well as expert understanding of anatomy and injection technique, in minimizing potential risks. We encourage regulations and a required level of training to perform these procedures.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
The time course and proper management of vascular occlusion attributable to interarterial hyaluronic acid fillers is critical. Albeit a rare complication, off-label uses of HA fillers, lack of proper training of injectors, and lack of clear appropriate guidelines in the management of these complications are some of the causes of delayed treatment and necrotic complications.
There are currently no definitive guidelines for the management of filler-associated cutaneous necrosis as experience with its treatment continues to evolve and be reported. In an attempt to consolidate the published data, as well as to give somewhat of a clear guideline of expectations, a time course and treatment guide has been outlined. The following is a working guideline for management of vascular occlusion attributable to HA fillers based on reports in the literature. This is not a consensus statement, rather it is a consolidation of the anecdotal reports and case studies outlined to help practitioners. It is also not inclusive of all the presentations of vascular occlusion. There are delayed cases of vascular occlusion beginning several days after injection, as well as alternative treatment options that may be considered.
These guidelines also are not for the devastating complication of blindness because of vascular occlusion secondary to fillers. Blindness is beyond the scope of the current article; however, we believe all experienced injectors should have emergency preparations in place and a relationship with an ophthalmologist or other trained surgeons experienced in performing retrobulbar hyaluronidase injections who can be reached in the event of a suspected occlusion. Any symptoms of eye pain, headache, or visual changes need to be immediately treated. Vascular occlusion is an emergency and timing is critical to prevent permanent blindness and facial deformities.
As with all filler injections, risks and complications can happen, and we cannot stress enough the appropriate level of training, as well as expert understanding of anatomy and injection technique, in minimizing potential risks. We encourage regulations and a required level of training to perform these procedures.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
The time course and proper management of vascular occlusion attributable to interarterial hyaluronic acid fillers is critical. Albeit a rare complication, off-label uses of HA fillers, lack of proper training of injectors, and lack of clear appropriate guidelines in the management of these complications are some of the causes of delayed treatment and necrotic complications.
There are currently no definitive guidelines for the management of filler-associated cutaneous necrosis as experience with its treatment continues to evolve and be reported. In an attempt to consolidate the published data, as well as to give somewhat of a clear guideline of expectations, a time course and treatment guide has been outlined. The following is a working guideline for management of vascular occlusion attributable to HA fillers based on reports in the literature. This is not a consensus statement, rather it is a consolidation of the anecdotal reports and case studies outlined to help practitioners. It is also not inclusive of all the presentations of vascular occlusion. There are delayed cases of vascular occlusion beginning several days after injection, as well as alternative treatment options that may be considered.
These guidelines also are not for the devastating complication of blindness because of vascular occlusion secondary to fillers. Blindness is beyond the scope of the current article; however, we believe all experienced injectors should have emergency preparations in place and a relationship with an ophthalmologist or other trained surgeons experienced in performing retrobulbar hyaluronidase injections who can be reached in the event of a suspected occlusion. Any symptoms of eye pain, headache, or visual changes need to be immediately treated. Vascular occlusion is an emergency and timing is critical to prevent permanent blindness and facial deformities.
As with all filler injections, risks and complications can happen, and we cannot stress enough the appropriate level of training, as well as expert understanding of anatomy and injection technique, in minimizing potential risks. We encourage regulations and a required level of training to perform these procedures.
Dr. Wesley and Dr. Talakoub are cocontributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They had no relevant disclosures.
My inspiration
Kobe Bryant knew me. Not personally, of course. I never received an autograph or shook his hand. But once in a while if I was up early enough, I’d run into Kobe at the gym in Newport Beach where he and I both worked out. As he did for all his fans at the gym, he’d make eye contact with me and nod hello. He was always focused on his workout – working with a trainer, never with headphones on. In person, he appeared enormous. Unlike most retired professional athletes, he still was in great shape. No doubt he could have suited up in purple and gold, and played against the Clippers that night if needed.

Being from New England, I never was a Laker fan. But I thought, if Kobe can head to the gym after midnight and take a 1,000 shots to prepare for a game, then I could set my alarm for 4 a.m. and take a few dozen more questions from my First Aid books. Head down, “Kryptonite” cranked on my iPod, I wasn’t going to let anyone in that test room outwork me. Neither did he. I put in the time and, like Kobe in the 2002 conference finals against Sacramento, I crushed it.*
When we moved to California, I followed Kobe and the Lakers until he retired. To be clear, I didn’t aspire to be like him, firstly because I’m slightly shorter than Michael Bloomberg, but also because although accomplished, Kobe made some poor choices at times. Indeed, it seems he might have been kinder and more considerate when he was at the top. But in his retirement he looked to be toiling to make reparations, refocusing his prodigious energy and talent for the benefit of others rather than for just for scoring 81 points. His Rolls Royce was there before mine at the gym, and I was there early. He was still getting up early and now preparing to be a great venture capitalist, podcaster, author, and father to his girls.

Watching him carry kettle bells across the floor one morning, I wondered, do people like Kobe Bryant look to others for inspiration? Or are they are born with an endless supply of it? For me, I seemed to push harder and faster when watching idols pass by. Whether it was Kobe or Clayton Christensen (author of “The Innovator’s Dilemma”), Joe Jorizzo, or Barack Obama, I found I could do just a bit more if I had them in mind.
On game days, Kobe spoke of arriving at the arena early, long before anyone. He would use the silent, solo time to reflect on what he needed to do perform that night. I tried this last week, arriving at our clinic early, before any patients or staff. I turned the lights on and took a few minutes to think about what we needed to accomplish that day. I previewed patients on my schedule, searched Up to Date for the latest recommendations on a difficult case. I didn’t know Kobe, but I felt like I did.
When I received the text that Kobe Bryant had died, I was actually working on this column. So I decided to change the topic to write about people who inspire me, ironically inspired by him again. May he rest in peace.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
*This article was updated 2/19/2020.
Kobe Bryant knew me. Not personally, of course. I never received an autograph or shook his hand. But once in a while if I was up early enough, I’d run into Kobe at the gym in Newport Beach where he and I both worked out. As he did for all his fans at the gym, he’d make eye contact with me and nod hello. He was always focused on his workout – working with a trainer, never with headphones on. In person, he appeared enormous. Unlike most retired professional athletes, he still was in great shape. No doubt he could have suited up in purple and gold, and played against the Clippers that night if needed.
Being from New England, I never was a Laker fan. But I thought, if Kobe can head to the gym after midnight and take a 1,000 shots to prepare for a game, then I could set my alarm for 4 a.m. and take a few dozen more questions from my First Aid books. Head down, “Kryptonite” cranked on my iPod, I wasn’t going to let anyone in that test room outwork me. Neither did he. I put in the time and, like Kobe in the 2002 conference finals against Sacramento, I crushed it.*
When we moved to California, I followed Kobe and the Lakers until he retired. To be clear, I didn’t aspire to be like him, firstly because I’m slightly shorter than Michael Bloomberg, but also because although accomplished, Kobe made some poor choices at times. Indeed, it seems he might have been kinder and more considerate when he was at the top. But in his retirement he looked to be toiling to make reparations, refocusing his prodigious energy and talent for the benefit of others rather than for just for scoring 81 points. His Rolls Royce was there before mine at the gym, and I was there early. He was still getting up early and now preparing to be a great venture capitalist, podcaster, author, and father to his girls.
Watching him carry kettle bells across the floor one morning, I wondered, do people like Kobe Bryant look to others for inspiration? Or are they are born with an endless supply of it? For me, I seemed to push harder and faster when watching idols pass by. Whether it was Kobe or Clayton Christensen (author of “The Innovator’s Dilemma”), Joe Jorizzo, or Barack Obama, I found I could do just a bit more if I had them in mind.
On game days, Kobe spoke of arriving at the arena early, long before anyone. He would use the silent, solo time to reflect on what he needed to do perform that night. I tried this last week, arriving at our clinic early, before any patients or staff. I turned the lights on and took a few minutes to think about what we needed to accomplish that day. I previewed patients on my schedule, searched Up to Date for the latest recommendations on a difficult case. I didn’t know Kobe, but I felt like I did.
When I received the text that Kobe Bryant had died, I was actually working on this column. So I decided to change the topic to write about people who inspire me, ironically inspired by him again. May he rest in peace.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
*This article was updated 2/19/2020.
Kobe Bryant knew me. Not personally, of course. I never received an autograph or shook his hand. But once in a while if I was up early enough, I’d run into Kobe at the gym in Newport Beach where he and I both worked out. As he did for all his fans at the gym, he’d make eye contact with me and nod hello. He was always focused on his workout – working with a trainer, never with headphones on. In person, he appeared enormous. Unlike most retired professional athletes, he still was in great shape. No doubt he could have suited up in purple and gold, and played against the Clippers that night if needed.
Being from New England, I never was a Laker fan. But I thought, if Kobe can head to the gym after midnight and take a 1,000 shots to prepare for a game, then I could set my alarm for 4 a.m. and take a few dozen more questions from my First Aid books. Head down, “Kryptonite” cranked on my iPod, I wasn’t going to let anyone in that test room outwork me. Neither did he. I put in the time and, like Kobe in the 2002 conference finals against Sacramento, I crushed it.*
When we moved to California, I followed Kobe and the Lakers until he retired. To be clear, I didn’t aspire to be like him, firstly because I’m slightly shorter than Michael Bloomberg, but also because although accomplished, Kobe made some poor choices at times. Indeed, it seems he might have been kinder and more considerate when he was at the top. But in his retirement he looked to be toiling to make reparations, refocusing his prodigious energy and talent for the benefit of others rather than for just for scoring 81 points. His Rolls Royce was there before mine at the gym, and I was there early. He was still getting up early and now preparing to be a great venture capitalist, podcaster, author, and father to his girls.
Watching him carry kettle bells across the floor one morning, I wondered, do people like Kobe Bryant look to others for inspiration? Or are they are born with an endless supply of it? For me, I seemed to push harder and faster when watching idols pass by. Whether it was Kobe or Clayton Christensen (author of “The Innovator’s Dilemma”), Joe Jorizzo, or Barack Obama, I found I could do just a bit more if I had them in mind.
On game days, Kobe spoke of arriving at the arena early, long before anyone. He would use the silent, solo time to reflect on what he needed to do perform that night. I tried this last week, arriving at our clinic early, before any patients or staff. I turned the lights on and took a few minutes to think about what we needed to accomplish that day. I previewed patients on my schedule, searched Up to Date for the latest recommendations on a difficult case. I didn’t know Kobe, but I felt like I did.
When I received the text that Kobe Bryant had died, I was actually working on this column. So I decided to change the topic to write about people who inspire me, ironically inspired by him again. May he rest in peace.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
*This article was updated 2/19/2020.
Psychopharmacology for aggression? Our field’s ‘nonconsensus’ and the risks
A 13-year-old boy with ADHD, combined type, presents to his family physician with his parents. His parents called for an appointment outside of his routine follow-up care to discuss what they should do to address their son’s new “aggressive behaviors.” He will throw objects when angry, yell, and slam doors at home when he is told to turn off video games. He used to play soccer but doesn’t anymore. He has maintained very good grades and friends. There is not a concern for substance abuse at this time.He speaks in curt sentences during the appointment, and he has his arms crossed or is looking out of the window the entire time.
His parents share in front on him that he has always been a “difficult child” (their words), but they now are struggling to adjust to his aggressive tendencies as he ages. He is growing bigger and angrier. He will not attend therapy and will not see a consultation psychiatrist in the office. A variety of stimulant trials including Ritalin and amphetamine preparations to manage impulsivity in ADHD were ineffective to curb his aggression, and he doesn’t want to take any medication.
They ask, what do we do? They are not worried for their safety but living like this is eroding their quality of life as a family, and the dynamic seems destined to get worse before it gets better.
They wonder, is there a next medication step to manage his aggression?
A family physician presented the above situation to me in my role as a child and adolescent psychiatrist in the medical home. It led us to a fruitful discussion of aggression and what can be done to help families who are all too often in situations like the above, then in your office looking for immediate solutions. The questions are, what can be done with an aggressive child, even and especially without the child’s buy-in to work on that as a problem?
Psychoeducation can go a long way in helping families rethink aggression as a symptom of something deeper, either in the environment or a diagnosis, although we all can empathize with the desire to reconcile the above behavior immediately.
Characterize the aggression
First, it can be helpful to identify a child’s aggression type. There are two types of aggression, reactive and proactive. We most often see reactive aggression in our clinics, which is aggression as a defensive and impulsive response to something in the environment (often limit-setting, as above). Proactive aggression is premeditated and may appear as aggression for aggression’s sake without the emotional drive behind it.
Secondly, it also can be helpful to know that externalizing and internalizing symptoms can represent different sides of the same coin, with the proverbial “coin” as “emotion” and the associated behaviors (throwing objects, in the above example) as the “signs” that there is a complex difficulty in managing painful emotions. Some children (and adults too!) tend to “externalize” strong emotions as aggression or irritability with others, while others “internalize” them by retreating with internal suffering such as “anxiety and depression.” These styles also can be similar among children and their parents.
With those two points in mind, it’s important to consider the diagnosis, which would guide treatment. It’s generally agreed upon that “reactive aggression” is more likely to be related to underlying untreated ADHD, or a depressive or anxiety disorder. This is much more amenable to treatment than aggression related to oppositional defiant disorder or conduct disorder, which are more defined by proactive forms of aggression.
You can pick up on family dynamics that may inadvertently reinforce the same behaviors they so wish to change. In the above example, the parents have clearly identified their son as “the problem.” You can imagine the difficulty of going to school and being a “problem,” and then coming home and feeling the same way. This negative perception can erode a child’s self-esteem over time, which may appear as disengagement or simply not caring in an appointment. It may become harder and harder to engage the child in psychotherapy or even in taking a medication as their only means of resistance to that painful notion about oneself as the “problem.”
It can be useful to begin appointments with “what is going well?” (in the example above, he “has friends and is maintaining grades”) and “what do you like most about your child?” As we all know, positive reinforcement is more powerful than its counterpart. Also problems in a family often are complex, and may involve many family members needing to change to meet their goals, not just the child.
Why you should try behavioral interventions first
Behavioral interventions are the first step always. Parents can do behavioral interventions and change their parenting and family environment through their own behavioral changes – commonly called parent management training. They can assess antecedents of aggression and their own responses, which may contribute or perpetuate a cycle of the aggression – such as giving attention or giving in to fewer limitations to avoid a fight. This small but important point can help protect against a feeling of helplessness that a child will not engage in therapy or skills-building.
In answering the clinician’s question about what to do next, I often feel like the question embedded in this is “what medication is next?” There is a felt pressure to do something “right now” conveyed to a clinician. This drives the impulse to prescribe something immediately – and likely more risky and with less of an evidence base – even before trying the known psychotherapy interventions that have the most evidence to change aggressive tendencies.
In looking deeper into this consultation case, I also found more “food for thought” for one’s thinking about aggression and psychopharmacology in cases like the above: Aggression isn’t an uncomplicated symptom that one can address immediately, and therefore we cannot rely on symptom-specific management to eradicate it. This is similar to prescribing Tylenol to manage a general ache or pain; if the pain persists, we want to know the “whys” of the pain persisting.
Thankfully, there are ways that a parent can better understand behaviors with this philosophy in mind. Applied Behavioral Analysis1 offers some helpful ideas, not only for children with autism spectrum disorder, but that can be applied to one’s understanding of other’s behavior in general. ABA pays attention to antecedents, perpetuating factors, and consequences as well as their interplay in understanding behaviors. You can encourage a family – rather than wanting to “get rid of a problem behavior” – to try to understand it and come up, with help from a psychotherapist or other professional, with a deeper evaluation of the behavior and a specific, collaborative plan.
Most experts see that ADHD, anxiety disorders, depressive disorders, and unrecognized learning disabilities, in sum, are more common underpinnings than not with aggressive children. This also can be confounded by an environment with parents who have those diagnoses untreated as well. Aggression should raise a red flag in our clinics to consider the above even if a family or child simply says aggression is the one issue, and it’s only the child with the issue.
While there have been attempts to find a “spot treatment” for aggression in a medication, medications not only fail to address the underlying issues many times, but have little evidence that support them and may do more harm long term than good.2
Kids need outlets for “normal aggressive drives.” And puberty, as in the case above, is a time of intense emotions of all varieties. In the example above, you may notice that the child is no longer playing soccer, which was likely serving some protective function in many ways for him and as a positive outlet for aggression. In the same way, you may see that kids who are more sedentary or idle (playing unrestricted video games now instead of sports, ) would benefit from revisiting outlets or finding new ones as a family.
Consider medications if the underlying diagnosis merits it
We generally seek to find and treat the underlying diagnosis, if it exists, in the following ways.
If a child has ADHD, as in the case above, you can trial a stimulant or an alpha-adrenergic agent to target impulsivity if that is suspected as the driver of aggression. This may include guanfacine (long-acting Intuniv at night, but I would choose lower dosing such as 0.5 mg to 1 mg at bedtime) to manage ADHD. However, the evidence base that management of ADHD improves aggressive behaviors at all or on their own, is scant. In addition, these medications can represent more harm than good as well, although they are perceived as more innocuous than their antipsychotic counterparts. For example, some patients can begin to have bed-wetting accidents in the evening or become sleepy in classes, which can further erode their sense of self-confidence even if this is clearly attributable to a medication side effect and resolves once the agent is reduced or removed.
In the same way to reorient to diagnosis with children with aggression, you can consider an SSRI for an anxiety disorder or irritable depression. But know that it’s a rare thing for children to say specifically that they are struggling with their emotions, whether they are angry, sad, or nervous and that a deeper dive into this may be warranted. Data by Connor DF et al.3 may indicate anxiety disorders should be highest on one’s differential diagnosis in aggression, followed by consideration for ADHD, which may be a different assumption than one would expect.
Mood stabilizers –lamotrigine (Lamictal), divalproex sodium (Depakote), and lithium – and antipsychotics – aripiprazole (Abilify) and risperidone (Risperdal) – are risky medications and the use of them contradicts the first point, agreed upon by most experts, that diagnosis should drive treatment. One is hardly ever treating a young child for psychosis or bipolar disorder in these circumstances of episodic, reactive aggression. Antipsychotics also carry the notorious risks of metabolic syndrome, among other risks to overall health, which becomes an additive risk over time and potentially into adulthood. I once heard in my child adolescent psychiatry training the haunting phase, “yes, they can ‘work’ quickly but they can work ‘almost too well,’ ” meaning they can sedate or tranquilize an aggressive child when the real goal should be to understand, diagnose, and intervene in ways that see the “big picture” of aggression.
Benzodiazepines generally are avoided in children due to disinhibition and often not even considered, in these circumstances, as they are in adults to manage agitation or aggression, due to this fact.
In many instances in working with families, our role in primary care can be one of illuminating children’s behaviors not just as symptoms to treat, but to understand deeply. This is as true for aggression as it is for anxiety.

Finally, I am reminded of the common question I receive from adult patients in primary care who ask me if anyone has yet made a medication to lose weight that’s safe and effective. Then the counseling commences on our fantasies, from our patients and ourselves, about what medications can do for us and our risks therein.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington. Email her at [email protected].
References
1. ABA in the Treatment of Aggressive Behavior Disorder and Lack of Impulse Control.
2. Managing Aggression in Children: A Practical Approach, The Carlat Child Psychiatry Report, May 2010, The Explosive Child.
3. Child Psychiatry Hum Dev. 2006 May;37[1]:1-14.
A 13-year-old boy with ADHD, combined type, presents to his family physician with his parents. His parents called for an appointment outside of his routine follow-up care to discuss what they should do to address their son’s new “aggressive behaviors.” He will throw objects when angry, yell, and slam doors at home when he is told to turn off video games. He used to play soccer but doesn’t anymore. He has maintained very good grades and friends. There is not a concern for substance abuse at this time.He speaks in curt sentences during the appointment, and he has his arms crossed or is looking out of the window the entire time.
His parents share in front on him that he has always been a “difficult child” (their words), but they now are struggling to adjust to his aggressive tendencies as he ages. He is growing bigger and angrier. He will not attend therapy and will not see a consultation psychiatrist in the office. A variety of stimulant trials including Ritalin and amphetamine preparations to manage impulsivity in ADHD were ineffective to curb his aggression, and he doesn’t want to take any medication.
They ask, what do we do? They are not worried for their safety but living like this is eroding their quality of life as a family, and the dynamic seems destined to get worse before it gets better.
They wonder, is there a next medication step to manage his aggression?
A family physician presented the above situation to me in my role as a child and adolescent psychiatrist in the medical home. It led us to a fruitful discussion of aggression and what can be done to help families who are all too often in situations like the above, then in your office looking for immediate solutions. The questions are, what can be done with an aggressive child, even and especially without the child’s buy-in to work on that as a problem?
Psychoeducation can go a long way in helping families rethink aggression as a symptom of something deeper, either in the environment or a diagnosis, although we all can empathize with the desire to reconcile the above behavior immediately.
Characterize the aggression
First, it can be helpful to identify a child’s aggression type. There are two types of aggression, reactive and proactive. We most often see reactive aggression in our clinics, which is aggression as a defensive and impulsive response to something in the environment (often limit-setting, as above). Proactive aggression is premeditated and may appear as aggression for aggression’s sake without the emotional drive behind it.
Secondly, it also can be helpful to know that externalizing and internalizing symptoms can represent different sides of the same coin, with the proverbial “coin” as “emotion” and the associated behaviors (throwing objects, in the above example) as the “signs” that there is a complex difficulty in managing painful emotions. Some children (and adults too!) tend to “externalize” strong emotions as aggression or irritability with others, while others “internalize” them by retreating with internal suffering such as “anxiety and depression.” These styles also can be similar among children and their parents.
With those two points in mind, it’s important to consider the diagnosis, which would guide treatment. It’s generally agreed upon that “reactive aggression” is more likely to be related to underlying untreated ADHD, or a depressive or anxiety disorder. This is much more amenable to treatment than aggression related to oppositional defiant disorder or conduct disorder, which are more defined by proactive forms of aggression.
You can pick up on family dynamics that may inadvertently reinforce the same behaviors they so wish to change. In the above example, the parents have clearly identified their son as “the problem.” You can imagine the difficulty of going to school and being a “problem,” and then coming home and feeling the same way. This negative perception can erode a child’s self-esteem over time, which may appear as disengagement or simply not caring in an appointment. It may become harder and harder to engage the child in psychotherapy or even in taking a medication as their only means of resistance to that painful notion about oneself as the “problem.”
It can be useful to begin appointments with “what is going well?” (in the example above, he “has friends and is maintaining grades”) and “what do you like most about your child?” As we all know, positive reinforcement is more powerful than its counterpart. Also problems in a family often are complex, and may involve many family members needing to change to meet their goals, not just the child.
Why you should try behavioral interventions first
Behavioral interventions are the first step always. Parents can do behavioral interventions and change their parenting and family environment through their own behavioral changes – commonly called parent management training. They can assess antecedents of aggression and their own responses, which may contribute or perpetuate a cycle of the aggression – such as giving attention or giving in to fewer limitations to avoid a fight. This small but important point can help protect against a feeling of helplessness that a child will not engage in therapy or skills-building.
In answering the clinician’s question about what to do next, I often feel like the question embedded in this is “what medication is next?” There is a felt pressure to do something “right now” conveyed to a clinician. This drives the impulse to prescribe something immediately – and likely more risky and with less of an evidence base – even before trying the known psychotherapy interventions that have the most evidence to change aggressive tendencies.
In looking deeper into this consultation case, I also found more “food for thought” for one’s thinking about aggression and psychopharmacology in cases like the above: Aggression isn’t an uncomplicated symptom that one can address immediately, and therefore we cannot rely on symptom-specific management to eradicate it. This is similar to prescribing Tylenol to manage a general ache or pain; if the pain persists, we want to know the “whys” of the pain persisting.
Thankfully, there are ways that a parent can better understand behaviors with this philosophy in mind. Applied Behavioral Analysis1 offers some helpful ideas, not only for children with autism spectrum disorder, but that can be applied to one’s understanding of other’s behavior in general. ABA pays attention to antecedents, perpetuating factors, and consequences as well as their interplay in understanding behaviors. You can encourage a family – rather than wanting to “get rid of a problem behavior” – to try to understand it and come up, with help from a psychotherapist or other professional, with a deeper evaluation of the behavior and a specific, collaborative plan.
Most experts see that ADHD, anxiety disorders, depressive disorders, and unrecognized learning disabilities, in sum, are more common underpinnings than not with aggressive children. This also can be confounded by an environment with parents who have those diagnoses untreated as well. Aggression should raise a red flag in our clinics to consider the above even if a family or child simply says aggression is the one issue, and it’s only the child with the issue.
While there have been attempts to find a “spot treatment” for aggression in a medication, medications not only fail to address the underlying issues many times, but have little evidence that support them and may do more harm long term than good.2
Kids need outlets for “normal aggressive drives.” And puberty, as in the case above, is a time of intense emotions of all varieties. In the example above, you may notice that the child is no longer playing soccer, which was likely serving some protective function in many ways for him and as a positive outlet for aggression. In the same way, you may see that kids who are more sedentary or idle (playing unrestricted video games now instead of sports, ) would benefit from revisiting outlets or finding new ones as a family.
Consider medications if the underlying diagnosis merits it
We generally seek to find and treat the underlying diagnosis, if it exists, in the following ways.
If a child has ADHD, as in the case above, you can trial a stimulant or an alpha-adrenergic agent to target impulsivity if that is suspected as the driver of aggression. This may include guanfacine (long-acting Intuniv at night, but I would choose lower dosing such as 0.5 mg to 1 mg at bedtime) to manage ADHD. However, the evidence base that management of ADHD improves aggressive behaviors at all or on their own, is scant. In addition, these medications can represent more harm than good as well, although they are perceived as more innocuous than their antipsychotic counterparts. For example, some patients can begin to have bed-wetting accidents in the evening or become sleepy in classes, which can further erode their sense of self-confidence even if this is clearly attributable to a medication side effect and resolves once the agent is reduced or removed.
In the same way to reorient to diagnosis with children with aggression, you can consider an SSRI for an anxiety disorder or irritable depression. But know that it’s a rare thing for children to say specifically that they are struggling with their emotions, whether they are angry, sad, or nervous and that a deeper dive into this may be warranted. Data by Connor DF et al.3 may indicate anxiety disorders should be highest on one’s differential diagnosis in aggression, followed by consideration for ADHD, which may be a different assumption than one would expect.
Mood stabilizers –lamotrigine (Lamictal), divalproex sodium (Depakote), and lithium – and antipsychotics – aripiprazole (Abilify) and risperidone (Risperdal) – are risky medications and the use of them contradicts the first point, agreed upon by most experts, that diagnosis should drive treatment. One is hardly ever treating a young child for psychosis or bipolar disorder in these circumstances of episodic, reactive aggression. Antipsychotics also carry the notorious risks of metabolic syndrome, among other risks to overall health, which becomes an additive risk over time and potentially into adulthood. I once heard in my child adolescent psychiatry training the haunting phase, “yes, they can ‘work’ quickly but they can work ‘almost too well,’ ” meaning they can sedate or tranquilize an aggressive child when the real goal should be to understand, diagnose, and intervene in ways that see the “big picture” of aggression.
Benzodiazepines generally are avoided in children due to disinhibition and often not even considered, in these circumstances, as they are in adults to manage agitation or aggression, due to this fact.
In many instances in working with families, our role in primary care can be one of illuminating children’s behaviors not just as symptoms to treat, but to understand deeply. This is as true for aggression as it is for anxiety.
Finally, I am reminded of the common question I receive from adult patients in primary care who ask me if anyone has yet made a medication to lose weight that’s safe and effective. Then the counseling commences on our fantasies, from our patients and ourselves, about what medications can do for us and our risks therein.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington. Email her at [email protected].
References
1. ABA in the Treatment of Aggressive Behavior Disorder and Lack of Impulse Control.
2. Managing Aggression in Children: A Practical Approach, The Carlat Child Psychiatry Report, May 2010, The Explosive Child.
3. Child Psychiatry Hum Dev. 2006 May;37[1]:1-14.
A 13-year-old boy with ADHD, combined type, presents to his family physician with his parents. His parents called for an appointment outside of his routine follow-up care to discuss what they should do to address their son’s new “aggressive behaviors.” He will throw objects when angry, yell, and slam doors at home when he is told to turn off video games. He used to play soccer but doesn’t anymore. He has maintained very good grades and friends. There is not a concern for substance abuse at this time.He speaks in curt sentences during the appointment, and he has his arms crossed or is looking out of the window the entire time.
His parents share in front on him that he has always been a “difficult child” (their words), but they now are struggling to adjust to his aggressive tendencies as he ages. He is growing bigger and angrier. He will not attend therapy and will not see a consultation psychiatrist in the office. A variety of stimulant trials including Ritalin and amphetamine preparations to manage impulsivity in ADHD were ineffective to curb his aggression, and he doesn’t want to take any medication.
They ask, what do we do? They are not worried for their safety but living like this is eroding their quality of life as a family, and the dynamic seems destined to get worse before it gets better.
They wonder, is there a next medication step to manage his aggression?
A family physician presented the above situation to me in my role as a child and adolescent psychiatrist in the medical home. It led us to a fruitful discussion of aggression and what can be done to help families who are all too often in situations like the above, then in your office looking for immediate solutions. The questions are, what can be done with an aggressive child, even and especially without the child’s buy-in to work on that as a problem?
Psychoeducation can go a long way in helping families rethink aggression as a symptom of something deeper, either in the environment or a diagnosis, although we all can empathize with the desire to reconcile the above behavior immediately.
Characterize the aggression
First, it can be helpful to identify a child’s aggression type. There are two types of aggression, reactive and proactive. We most often see reactive aggression in our clinics, which is aggression as a defensive and impulsive response to something in the environment (often limit-setting, as above). Proactive aggression is premeditated and may appear as aggression for aggression’s sake without the emotional drive behind it.
Secondly, it also can be helpful to know that externalizing and internalizing symptoms can represent different sides of the same coin, with the proverbial “coin” as “emotion” and the associated behaviors (throwing objects, in the above example) as the “signs” that there is a complex difficulty in managing painful emotions. Some children (and adults too!) tend to “externalize” strong emotions as aggression or irritability with others, while others “internalize” them by retreating with internal suffering such as “anxiety and depression.” These styles also can be similar among children and their parents.
With those two points in mind, it’s important to consider the diagnosis, which would guide treatment. It’s generally agreed upon that “reactive aggression” is more likely to be related to underlying untreated ADHD, or a depressive or anxiety disorder. This is much more amenable to treatment than aggression related to oppositional defiant disorder or conduct disorder, which are more defined by proactive forms of aggression.
You can pick up on family dynamics that may inadvertently reinforce the same behaviors they so wish to change. In the above example, the parents have clearly identified their son as “the problem.” You can imagine the difficulty of going to school and being a “problem,” and then coming home and feeling the same way. This negative perception can erode a child’s self-esteem over time, which may appear as disengagement or simply not caring in an appointment. It may become harder and harder to engage the child in psychotherapy or even in taking a medication as their only means of resistance to that painful notion about oneself as the “problem.”
It can be useful to begin appointments with “what is going well?” (in the example above, he “has friends and is maintaining grades”) and “what do you like most about your child?” As we all know, positive reinforcement is more powerful than its counterpart. Also problems in a family often are complex, and may involve many family members needing to change to meet their goals, not just the child.
Why you should try behavioral interventions first
Behavioral interventions are the first step always. Parents can do behavioral interventions and change their parenting and family environment through their own behavioral changes – commonly called parent management training. They can assess antecedents of aggression and their own responses, which may contribute or perpetuate a cycle of the aggression – such as giving attention or giving in to fewer limitations to avoid a fight. This small but important point can help protect against a feeling of helplessness that a child will not engage in therapy or skills-building.
In answering the clinician’s question about what to do next, I often feel like the question embedded in this is “what medication is next?” There is a felt pressure to do something “right now” conveyed to a clinician. This drives the impulse to prescribe something immediately – and likely more risky and with less of an evidence base – even before trying the known psychotherapy interventions that have the most evidence to change aggressive tendencies.
In looking deeper into this consultation case, I also found more “food for thought” for one’s thinking about aggression and psychopharmacology in cases like the above: Aggression isn’t an uncomplicated symptom that one can address immediately, and therefore we cannot rely on symptom-specific management to eradicate it. This is similar to prescribing Tylenol to manage a general ache or pain; if the pain persists, we want to know the “whys” of the pain persisting.
Thankfully, there are ways that a parent can better understand behaviors with this philosophy in mind. Applied Behavioral Analysis1 offers some helpful ideas, not only for children with autism spectrum disorder, but that can be applied to one’s understanding of other’s behavior in general. ABA pays attention to antecedents, perpetuating factors, and consequences as well as their interplay in understanding behaviors. You can encourage a family – rather than wanting to “get rid of a problem behavior” – to try to understand it and come up, with help from a psychotherapist or other professional, with a deeper evaluation of the behavior and a specific, collaborative plan.
Most experts see that ADHD, anxiety disorders, depressive disorders, and unrecognized learning disabilities, in sum, are more common underpinnings than not with aggressive children. This also can be confounded by an environment with parents who have those diagnoses untreated as well. Aggression should raise a red flag in our clinics to consider the above even if a family or child simply says aggression is the one issue, and it’s only the child with the issue.
While there have been attempts to find a “spot treatment” for aggression in a medication, medications not only fail to address the underlying issues many times, but have little evidence that support them and may do more harm long term than good.2
Kids need outlets for “normal aggressive drives.” And puberty, as in the case above, is a time of intense emotions of all varieties. In the example above, you may notice that the child is no longer playing soccer, which was likely serving some protective function in many ways for him and as a positive outlet for aggression. In the same way, you may see that kids who are more sedentary or idle (playing unrestricted video games now instead of sports, ) would benefit from revisiting outlets or finding new ones as a family.
Consider medications if the underlying diagnosis merits it
We generally seek to find and treat the underlying diagnosis, if it exists, in the following ways.
If a child has ADHD, as in the case above, you can trial a stimulant or an alpha-adrenergic agent to target impulsivity if that is suspected as the driver of aggression. This may include guanfacine (long-acting Intuniv at night, but I would choose lower dosing such as 0.5 mg to 1 mg at bedtime) to manage ADHD. However, the evidence base that management of ADHD improves aggressive behaviors at all or on their own, is scant. In addition, these medications can represent more harm than good as well, although they are perceived as more innocuous than their antipsychotic counterparts. For example, some patients can begin to have bed-wetting accidents in the evening or become sleepy in classes, which can further erode their sense of self-confidence even if this is clearly attributable to a medication side effect and resolves once the agent is reduced or removed.
In the same way to reorient to diagnosis with children with aggression, you can consider an SSRI for an anxiety disorder or irritable depression. But know that it’s a rare thing for children to say specifically that they are struggling with their emotions, whether they are angry, sad, or nervous and that a deeper dive into this may be warranted. Data by Connor DF et al.3 may indicate anxiety disorders should be highest on one’s differential diagnosis in aggression, followed by consideration for ADHD, which may be a different assumption than one would expect.
Mood stabilizers –lamotrigine (Lamictal), divalproex sodium (Depakote), and lithium – and antipsychotics – aripiprazole (Abilify) and risperidone (Risperdal) – are risky medications and the use of them contradicts the first point, agreed upon by most experts, that diagnosis should drive treatment. One is hardly ever treating a young child for psychosis or bipolar disorder in these circumstances of episodic, reactive aggression. Antipsychotics also carry the notorious risks of metabolic syndrome, among other risks to overall health, which becomes an additive risk over time and potentially into adulthood. I once heard in my child adolescent psychiatry training the haunting phase, “yes, they can ‘work’ quickly but they can work ‘almost too well,’ ” meaning they can sedate or tranquilize an aggressive child when the real goal should be to understand, diagnose, and intervene in ways that see the “big picture” of aggression.
Benzodiazepines generally are avoided in children due to disinhibition and often not even considered, in these circumstances, as they are in adults to manage agitation or aggression, due to this fact.
In many instances in working with families, our role in primary care can be one of illuminating children’s behaviors not just as symptoms to treat, but to understand deeply. This is as true for aggression as it is for anxiety.
Finally, I am reminded of the common question I receive from adult patients in primary care who ask me if anyone has yet made a medication to lose weight that’s safe and effective. Then the counseling commences on our fantasies, from our patients and ourselves, about what medications can do for us and our risks therein.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington. Email her at [email protected].
References
1. ABA in the Treatment of Aggressive Behavior Disorder and Lack of Impulse Control.
2. Managing Aggression in Children: A Practical Approach, The Carlat Child Psychiatry Report, May 2010, The Explosive Child.
3. Child Psychiatry Hum Dev. 2006 May;37[1]:1-14.
An epidemic of fear and misinformation
As I write this, the 2019 novel coronavirus* continues to spread, exceeding 59,000 cases and 1,300 deaths worldwide. With it spreads fear. In the modern world of social media, misinformation spreads even faster than disease.

The news about a novel and deadly illness crowds out more substantial worries. Humans are not particularly good at assessing risk or responding rationally and consistently to it. Risk is hard to fully define. If you look up “risk” in Merriam Webster’s online dictionary, you get the simple definition of “possibility of loss or injury; peril.” If you look up risk in Wikipedia, you get 12 pages of explanation and 8 more pages of links and references.
People handle risk differently. Some people are more risk adverse than others. Some get a pleasurable thrill from risk, whether a slot machine or a parachute jump. Most people really don’t comprehend small probabilities, with tens of billions of dollars spent annually on U.S. lotteries.
Because 98% of people who get COVID-19 are recovering, this is not an extinction-level event or the zombie apocalypse. It is a major health hazard, and one where morbidity and mortality might be assuaged by an early and effective public health response, including the population’s adoption of good habits such as hand washing, cough etiquette, and staying home when ill.
Three key factors may help reduce the fear factor.
One key factor is accurate communication of health information to the public. This has been severely harmed in the last few years by the promotion of gossip on social media, such as Facebook, within newsfeeds without any vetting, along with a smaller component of deliberate misinformation from untraceable sources. Compare this situation with the decision in May 1988 when Surgeon General C. Everett Koop chose to snail mail a brochure on AIDS to every household in America. It was unprecedented. One element of this communication is the public’s belief that government and health care officials will responsibly and timely convey the information. There are accusations that the Chinese government initially impeded early warnings about COVID-19. Dr. Koop, to his great credit and lifesaving leadership, overcame queasiness within the Reagan administration about issues of morality and taste in discussing some of the HIV information. Alas, no similar leadership occurred in the decade of the 2010s when deaths from the opioid epidemic in the United States skyrocketed to claim more lives annually than car accidents or suicide.

A second factor is the credibility of the scientists. Antivaxxers, climate change deniers, and mercenary scientists have severely damaged that credibility of science, compared with the trust in scientists 50 years ago during the Apollo moon shot.
A third factor is perspective. Poor journalism and clickbait can focus excessively on the rare events as news. Airline crashes make the front page while fatal car accidents, claiming a hundred times more lives annually, don’t even merit a story in local media. Someone wins the lottery weekly but few pay attention to those suffering from gambling debts.
Influenza is killing many times more people than the 2019 novel coronavirus, but the news is focused on cruise ships. In the United States, influenza annually will strike tens of millions, with about 10 per 1,000 hospitalized and 0.5 per 1,000 dying. The novel coronavirus is more lethal. SARS (a coronavirus epidemic in 2003) had 8,000 cases with a mortality rate of 96 per 1,000 while the novel 2019 strain so far is killing about 20 per 1,000. That value may be an overestimate, because there may be a significant fraction of COVID-19 patients with symptoms mild enough that they do not seek medical care and do not get tested and counted.
For perspective, in 1952 the United States reported 50,000 cases of polio (meningitis or paralytic) annually with 3,000 deaths. As many as 95% of cases of poliovirus infection have no or mild symptoms and would not have been reported, so the case fatality rate estimate is skewed. In the 1950s, the United States averaged about 500,000 cases of measles per year, with about 500 deaths annually for a case fatality rate of about 1 per 1,000 in a population that was well nourished with good medical care. In malnourished children without access to modern health care, the case fatality rate can be as high as 100 per 1,000, which is why globally measles killed 142,000 people in 2018, a substantial improvement from 536,000 deaths globally in 2000, but still a leading killer of children worldwide. Vaccines had reduced the annual death toll of polio and measles in the U.S. to zero.
In comparison, in this country the annual incidences are about 70,000 overdose deaths, 50,000 suicides, and 40,000 traffic deaths.
Reassurance is the most common product sold by pediatricians. We look for low-probability, high-impact bad things. Usually we don’t find them and can reassure parents that the child will be okay. Sometimes we spot a higher-risk situation and intervene. My job is to worry professionally so that parents can worry less.
COVID-19 worries me, but irrational people worry me more. The real enemies are fear, disinformation, discrimination, and economic warfare.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
*This article was updated 2/21/2020.
As I write this, the 2019 novel coronavirus* continues to spread, exceeding 59,000 cases and 1,300 deaths worldwide. With it spreads fear. In the modern world of social media, misinformation spreads even faster than disease.
The news about a novel and deadly illness crowds out more substantial worries. Humans are not particularly good at assessing risk or responding rationally and consistently to it. Risk is hard to fully define. If you look up “risk” in Merriam Webster’s online dictionary, you get the simple definition of “possibility of loss or injury; peril.” If you look up risk in Wikipedia, you get 12 pages of explanation and 8 more pages of links and references.
People handle risk differently. Some people are more risk adverse than others. Some get a pleasurable thrill from risk, whether a slot machine or a parachute jump. Most people really don’t comprehend small probabilities, with tens of billions of dollars spent annually on U.S. lotteries.
Because 98% of people who get COVID-19 are recovering, this is not an extinction-level event or the zombie apocalypse. It is a major health hazard, and one where morbidity and mortality might be assuaged by an early and effective public health response, including the population’s adoption of good habits such as hand washing, cough etiquette, and staying home when ill.
Three key factors may help reduce the fear factor.
One key factor is accurate communication of health information to the public. This has been severely harmed in the last few years by the promotion of gossip on social media, such as Facebook, within newsfeeds without any vetting, along with a smaller component of deliberate misinformation from untraceable sources. Compare this situation with the decision in May 1988 when Surgeon General C. Everett Koop chose to snail mail a brochure on AIDS to every household in America. It was unprecedented. One element of this communication is the public’s belief that government and health care officials will responsibly and timely convey the information. There are accusations that the Chinese government initially impeded early warnings about COVID-19. Dr. Koop, to his great credit and lifesaving leadership, overcame queasiness within the Reagan administration about issues of morality and taste in discussing some of the HIV information. Alas, no similar leadership occurred in the decade of the 2010s when deaths from the opioid epidemic in the United States skyrocketed to claim more lives annually than car accidents or suicide.
A second factor is the credibility of the scientists. Antivaxxers, climate change deniers, and mercenary scientists have severely damaged that credibility of science, compared with the trust in scientists 50 years ago during the Apollo moon shot.
A third factor is perspective. Poor journalism and clickbait can focus excessively on the rare events as news. Airline crashes make the front page while fatal car accidents, claiming a hundred times more lives annually, don’t even merit a story in local media. Someone wins the lottery weekly but few pay attention to those suffering from gambling debts.
Influenza is killing many times more people than the 2019 novel coronavirus, but the news is focused on cruise ships. In the United States, influenza annually will strike tens of millions, with about 10 per 1,000 hospitalized and 0.5 per 1,000 dying. The novel coronavirus is more lethal. SARS (a coronavirus epidemic in 2003) had 8,000 cases with a mortality rate of 96 per 1,000 while the novel 2019 strain so far is killing about 20 per 1,000. That value may be an overestimate, because there may be a significant fraction of COVID-19 patients with symptoms mild enough that they do not seek medical care and do not get tested and counted.
For perspective, in 1952 the United States reported 50,000 cases of polio (meningitis or paralytic) annually with 3,000 deaths. As many as 95% of cases of poliovirus infection have no or mild symptoms and would not have been reported, so the case fatality rate estimate is skewed. In the 1950s, the United States averaged about 500,000 cases of measles per year, with about 500 deaths annually for a case fatality rate of about 1 per 1,000 in a population that was well nourished with good medical care. In malnourished children without access to modern health care, the case fatality rate can be as high as 100 per 1,000, which is why globally measles killed 142,000 people in 2018, a substantial improvement from 536,000 deaths globally in 2000, but still a leading killer of children worldwide. Vaccines had reduced the annual death toll of polio and measles in the U.S. to zero.
In comparison, in this country the annual incidences are about 70,000 overdose deaths, 50,000 suicides, and 40,000 traffic deaths.
Reassurance is the most common product sold by pediatricians. We look for low-probability, high-impact bad things. Usually we don’t find them and can reassure parents that the child will be okay. Sometimes we spot a higher-risk situation and intervene. My job is to worry professionally so that parents can worry less.
COVID-19 worries me, but irrational people worry me more. The real enemies are fear, disinformation, discrimination, and economic warfare.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
*This article was updated 2/21/2020.
As I write this, the 2019 novel coronavirus* continues to spread, exceeding 59,000 cases and 1,300 deaths worldwide. With it spreads fear. In the modern world of social media, misinformation spreads even faster than disease.
The news about a novel and deadly illness crowds out more substantial worries. Humans are not particularly good at assessing risk or responding rationally and consistently to it. Risk is hard to fully define. If you look up “risk” in Merriam Webster’s online dictionary, you get the simple definition of “possibility of loss or injury; peril.” If you look up risk in Wikipedia, you get 12 pages of explanation and 8 more pages of links and references.
People handle risk differently. Some people are more risk adverse than others. Some get a pleasurable thrill from risk, whether a slot machine or a parachute jump. Most people really don’t comprehend small probabilities, with tens of billions of dollars spent annually on U.S. lotteries.
Because 98% of people who get COVID-19 are recovering, this is not an extinction-level event or the zombie apocalypse. It is a major health hazard, and one where morbidity and mortality might be assuaged by an early and effective public health response, including the population’s adoption of good habits such as hand washing, cough etiquette, and staying home when ill.
Three key factors may help reduce the fear factor.
One key factor is accurate communication of health information to the public. This has been severely harmed in the last few years by the promotion of gossip on social media, such as Facebook, within newsfeeds without any vetting, along with a smaller component of deliberate misinformation from untraceable sources. Compare this situation with the decision in May 1988 when Surgeon General C. Everett Koop chose to snail mail a brochure on AIDS to every household in America. It was unprecedented. One element of this communication is the public’s belief that government and health care officials will responsibly and timely convey the information. There are accusations that the Chinese government initially impeded early warnings about COVID-19. Dr. Koop, to his great credit and lifesaving leadership, overcame queasiness within the Reagan administration about issues of morality and taste in discussing some of the HIV information. Alas, no similar leadership occurred in the decade of the 2010s when deaths from the opioid epidemic in the United States skyrocketed to claim more lives annually than car accidents or suicide.
A second factor is the credibility of the scientists. Antivaxxers, climate change deniers, and mercenary scientists have severely damaged that credibility of science, compared with the trust in scientists 50 years ago during the Apollo moon shot.
A third factor is perspective. Poor journalism and clickbait can focus excessively on the rare events as news. Airline crashes make the front page while fatal car accidents, claiming a hundred times more lives annually, don’t even merit a story in local media. Someone wins the lottery weekly but few pay attention to those suffering from gambling debts.
Influenza is killing many times more people than the 2019 novel coronavirus, but the news is focused on cruise ships. In the United States, influenza annually will strike tens of millions, with about 10 per 1,000 hospitalized and 0.5 per 1,000 dying. The novel coronavirus is more lethal. SARS (a coronavirus epidemic in 2003) had 8,000 cases with a mortality rate of 96 per 1,000 while the novel 2019 strain so far is killing about 20 per 1,000. That value may be an overestimate, because there may be a significant fraction of COVID-19 patients with symptoms mild enough that they do not seek medical care and do not get tested and counted.
For perspective, in 1952 the United States reported 50,000 cases of polio (meningitis or paralytic) annually with 3,000 deaths. As many as 95% of cases of poliovirus infection have no or mild symptoms and would not have been reported, so the case fatality rate estimate is skewed. In the 1950s, the United States averaged about 500,000 cases of measles per year, with about 500 deaths annually for a case fatality rate of about 1 per 1,000 in a population that was well nourished with good medical care. In malnourished children without access to modern health care, the case fatality rate can be as high as 100 per 1,000, which is why globally measles killed 142,000 people in 2018, a substantial improvement from 536,000 deaths globally in 2000, but still a leading killer of children worldwide. Vaccines had reduced the annual death toll of polio and measles in the U.S. to zero.
In comparison, in this country the annual incidences are about 70,000 overdose deaths, 50,000 suicides, and 40,000 traffic deaths.
Reassurance is the most common product sold by pediatricians. We look for low-probability, high-impact bad things. Usually we don’t find them and can reassure parents that the child will be okay. Sometimes we spot a higher-risk situation and intervene. My job is to worry professionally so that parents can worry less.
COVID-19 worries me, but irrational people worry me more. The real enemies are fear, disinformation, discrimination, and economic warfare.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at [email protected].
*This article was updated 2/21/2020.
An unusual ‘retirement’ option
Whether “retirement” is withdrawing from one’s occupation or from an active working life, it is of utmost importance to not let one’s mind degenerate. Some individuals move on to gathering new intellectual skills by attending new educational courses or meetings, some travel, some become semiprofessional golfers or fishermen, and some find other forms of personal extension. I now serve to develop cost-saving medical programs for county jails in the state of Texas while attempting to improve the overall quality of inmate care.
Initially I was a pediatrician in Houston with special training in allergy and immunology, but because of a medical problem I was forced to abandon my first love – primary pediatrics. My move to a small town at the age of 40 required me to reevaluate my professional life, and I opted to provide care only in my allergy and immunology specialty.
However, living in a small town is different from life in a metropolis, and it was not uncommon for doctors to be asked to assist the community. A number of years ago, our county judge asked if I would help evaluate why our county jail was spending so much money. After several attempts to refuse, I eventually did evaluate the program there, and was flabbergasted by how much money was being wasted. I made some rather simple suggestions as how to correct the problem, but when no primary care doctor stepped forward to implement the changes and run the jail medical program, I became its medical director. When we saved $120,000 the first year, even I was astounded.
While I continued to run my private practice, I did accept other small community’s offers to look into their county jails’ programs. I found that their problems in cost control and quality of health care mirrored those I found in the first jail, and they were easily solvable if the county judge and the local sheriff wanted solutions. I also found that politics makes strange bedfellows, as the saying goes, and often the obvious changes were met with obstruction in one form or another. Nonetheless, I found that I could serve these communities in addition to my individual patients. When it was time for retirement, I continued to have a real desire to make the towns around which I lived and my own community more livable. So
In most things, I found that the same business philosophy and personal medical approach I learned in my pediatrics training and as a private practitioner applied to the jail system. Let me mention some specifics. Using generic medicines was less expensive than using brand names. The diagnoses which patients claimed when they entered jail might or might not be correct, so reevaluating the diagnosis and treatment was appropriate as soon as possible. Hospital and ED visits should be limited to patients’ medically requiring them rather than using the ED as a screening tool.
But I did come to understand that medical care in the county jail is different from medical care outside an incarcerated facility in that sometimes the prisoners had their own reasons for seeking medical care. This was complicated by the fact that often there were critically ill patients presenting to county jails. So carefully established criteria and protocols were an absolute necessity to save lives.
Let me expand on the topic of seeking medical care by the inmate-patients. A relatively small number of these individuals required immediate emergency treatment, without which they could not do well: The diabetic who was not taking his insulin, the out-of-control paranoid schizophrenic who decided he was cured and therefore was unattended, the alcoholic or drug addict who would develop delirium tremens if medications were stopped abruptly. These people had to be identified as quickly as possible and correctly treated. Confounding the problem was the fact that many, and I repeat many, individuals try to use the medical route to manipulate their incarceration environment. I called this the B problem: beds, blankets, barter, buzz, better food, and be out of here. They might claim an illness existed, and often they might believe it did.
A related situation might exist when individuals would demand psychiatric and pain medications, often in large quantities, when they in fact had not taken them for some time in the outside world. Often these patients were addicts, and of course this could create an entire other relationship with the medical team. A third example would be the claim of hypoglycemia so that the prisoner would receive more frequent meals.
One might think that as a pediatrician I was ill prepared to treat adults, and in fact, there was much review of the general medical care needed when I began this program. However, the internists and family physicians in town were glad to assist me whenever I encountered a difficult patient. When hospitalizations were required, the inpatient always was covered by one of the internists on hospital staff. Quite frankly, the doctors seemed pleased to not be dealing with this group of individuals as much as they had in the past.
On a slightly different note, skills honed during my pediatric career were extremely valuable. Children, particularly young children, do not verbally communicate with their parents or their doctor particularly well, so pediatricians are well trained in the skill of observation. The patient who claims a guard hurt his shoulder so badly during an altercation that he cannot move it is found out when he easily whips his arms over his head when asked to remove his shirt. It is not uncommon for an individual to demand antidepressant medications from the medical staff, but when evaluated more thoroughly and for a longer period of time, the patient ends up laughing, even denying any suicidal ideation or any other sign of depression. One also deals with a lot of adolescent behavior from the inmates, such as the individuals who say that unless they don’t get their way (more food) they are not going to take their medications and thus get sicker. That’s Adolescent Medicine 101.
Some of the modalities I utilized in modifying the jail programs will be familiar to every practicing pediatrician. I educate; I teach; I train. Parents of my asthmatic patients had to know what medications to keep handy and when to use them. It is pretty easy to see how that relates to jail medicine. Many patients come into jail with inhalers and with a diagnosis of asthma. Some have the condition, and some do not. By training jail and medical staff how to observe breathing patterns and by performing pulse oximetry, we eliminated a large number of unnecessary ED visits, and we often made the diagnosis of hyperventilation syndrome rather than misdiagnosed asthma.
Jail medicine is a large part of the cost of housing inmates. I did consultation work for a large urban jail, and we saved over $7 million in 1 year. In a medium-sized jail, the cost-savings after a 4-month consultation was over $300,000. This is a lot of money to me, and I suspect is to you, too. Just as in our general communities, we have enough resources to provide medical care and to provide a high level of care for all. However, we cannot waste money by providing inappropriate care or overtesting or overtreating. The medical care must be what treats the disease the patient actually has ... nothing more and nothing less!
If it sounds as if I am cynical about inmate patients, that is not true. However, I am realistic that no one wishes to be in jail. I realize that the medical route is just one that prisoners can and do use to modify their situation. I understand that the medical staff within a jail needs constant education and supervision at first, and with time they become more astute – just like a physician in this arena – at distinguishing the very serious from the mildly serious from malingering. In spite of this, we doctors also can be fooled. However, through constant vigilance and constant education we can get better.
Jail medicine is not for everyone in retirement. Heck, it is not for everyone ever. I found it interesting because it required me to match my diagnostic skills against the diseases and the psychodynamics of individuals who often – not always – made that diagnosis more difficult. Diagnosing illness and curing it – isn’t this why we all went into medicine?
Dr. Yoffe is a retired pediatrician specializing in allergy and immunology who resides in Brenham, Tex. Email him at [email protected].
This article was updated 2/13/2020.
Whether “retirement” is withdrawing from one’s occupation or from an active working life, it is of utmost importance to not let one’s mind degenerate. Some individuals move on to gathering new intellectual skills by attending new educational courses or meetings, some travel, some become semiprofessional golfers or fishermen, and some find other forms of personal extension. I now serve to develop cost-saving medical programs for county jails in the state of Texas while attempting to improve the overall quality of inmate care.
Initially I was a pediatrician in Houston with special training in allergy and immunology, but because of a medical problem I was forced to abandon my first love – primary pediatrics. My move to a small town at the age of 40 required me to reevaluate my professional life, and I opted to provide care only in my allergy and immunology specialty.
However, living in a small town is different from life in a metropolis, and it was not uncommon for doctors to be asked to assist the community. A number of years ago, our county judge asked if I would help evaluate why our county jail was spending so much money. After several attempts to refuse, I eventually did evaluate the program there, and was flabbergasted by how much money was being wasted. I made some rather simple suggestions as how to correct the problem, but when no primary care doctor stepped forward to implement the changes and run the jail medical program, I became its medical director. When we saved $120,000 the first year, even I was astounded.
While I continued to run my private practice, I did accept other small community’s offers to look into their county jails’ programs. I found that their problems in cost control and quality of health care mirrored those I found in the first jail, and they were easily solvable if the county judge and the local sheriff wanted solutions. I also found that politics makes strange bedfellows, as the saying goes, and often the obvious changes were met with obstruction in one form or another. Nonetheless, I found that I could serve these communities in addition to my individual patients. When it was time for retirement, I continued to have a real desire to make the towns around which I lived and my own community more livable. So
In most things, I found that the same business philosophy and personal medical approach I learned in my pediatrics training and as a private practitioner applied to the jail system. Let me mention some specifics. Using generic medicines was less expensive than using brand names. The diagnoses which patients claimed when they entered jail might or might not be correct, so reevaluating the diagnosis and treatment was appropriate as soon as possible. Hospital and ED visits should be limited to patients’ medically requiring them rather than using the ED as a screening tool.
But I did come to understand that medical care in the county jail is different from medical care outside an incarcerated facility in that sometimes the prisoners had their own reasons for seeking medical care. This was complicated by the fact that often there were critically ill patients presenting to county jails. So carefully established criteria and protocols were an absolute necessity to save lives.
Let me expand on the topic of seeking medical care by the inmate-patients. A relatively small number of these individuals required immediate emergency treatment, without which they could not do well: The diabetic who was not taking his insulin, the out-of-control paranoid schizophrenic who decided he was cured and therefore was unattended, the alcoholic or drug addict who would develop delirium tremens if medications were stopped abruptly. These people had to be identified as quickly as possible and correctly treated. Confounding the problem was the fact that many, and I repeat many, individuals try to use the medical route to manipulate their incarceration environment. I called this the B problem: beds, blankets, barter, buzz, better food, and be out of here. They might claim an illness existed, and often they might believe it did.
A related situation might exist when individuals would demand psychiatric and pain medications, often in large quantities, when they in fact had not taken them for some time in the outside world. Often these patients were addicts, and of course this could create an entire other relationship with the medical team. A third example would be the claim of hypoglycemia so that the prisoner would receive more frequent meals.
One might think that as a pediatrician I was ill prepared to treat adults, and in fact, there was much review of the general medical care needed when I began this program. However, the internists and family physicians in town were glad to assist me whenever I encountered a difficult patient. When hospitalizations were required, the inpatient always was covered by one of the internists on hospital staff. Quite frankly, the doctors seemed pleased to not be dealing with this group of individuals as much as they had in the past.
On a slightly different note, skills honed during my pediatric career were extremely valuable. Children, particularly young children, do not verbally communicate with their parents or their doctor particularly well, so pediatricians are well trained in the skill of observation. The patient who claims a guard hurt his shoulder so badly during an altercation that he cannot move it is found out when he easily whips his arms over his head when asked to remove his shirt. It is not uncommon for an individual to demand antidepressant medications from the medical staff, but when evaluated more thoroughly and for a longer period of time, the patient ends up laughing, even denying any suicidal ideation or any other sign of depression. One also deals with a lot of adolescent behavior from the inmates, such as the individuals who say that unless they don’t get their way (more food) they are not going to take their medications and thus get sicker. That’s Adolescent Medicine 101.
Some of the modalities I utilized in modifying the jail programs will be familiar to every practicing pediatrician. I educate; I teach; I train. Parents of my asthmatic patients had to know what medications to keep handy and when to use them. It is pretty easy to see how that relates to jail medicine. Many patients come into jail with inhalers and with a diagnosis of asthma. Some have the condition, and some do not. By training jail and medical staff how to observe breathing patterns and by performing pulse oximetry, we eliminated a large number of unnecessary ED visits, and we often made the diagnosis of hyperventilation syndrome rather than misdiagnosed asthma.
Jail medicine is a large part of the cost of housing inmates. I did consultation work for a large urban jail, and we saved over $7 million in 1 year. In a medium-sized jail, the cost-savings after a 4-month consultation was over $300,000. This is a lot of money to me, and I suspect is to you, too. Just as in our general communities, we have enough resources to provide medical care and to provide a high level of care for all. However, we cannot waste money by providing inappropriate care or overtesting or overtreating. The medical care must be what treats the disease the patient actually has ... nothing more and nothing less!
If it sounds as if I am cynical about inmate patients, that is not true. However, I am realistic that no one wishes to be in jail. I realize that the medical route is just one that prisoners can and do use to modify their situation. I understand that the medical staff within a jail needs constant education and supervision at first, and with time they become more astute – just like a physician in this arena – at distinguishing the very serious from the mildly serious from malingering. In spite of this, we doctors also can be fooled. However, through constant vigilance and constant education we can get better.
Jail medicine is not for everyone in retirement. Heck, it is not for everyone ever. I found it interesting because it required me to match my diagnostic skills against the diseases and the psychodynamics of individuals who often – not always – made that diagnosis more difficult. Diagnosing illness and curing it – isn’t this why we all went into medicine?
Dr. Yoffe is a retired pediatrician specializing in allergy and immunology who resides in Brenham, Tex. Email him at [email protected].
This article was updated 2/13/2020.
Whether “retirement” is withdrawing from one’s occupation or from an active working life, it is of utmost importance to not let one’s mind degenerate. Some individuals move on to gathering new intellectual skills by attending new educational courses or meetings, some travel, some become semiprofessional golfers or fishermen, and some find other forms of personal extension. I now serve to develop cost-saving medical programs for county jails in the state of Texas while attempting to improve the overall quality of inmate care.
Initially I was a pediatrician in Houston with special training in allergy and immunology, but because of a medical problem I was forced to abandon my first love – primary pediatrics. My move to a small town at the age of 40 required me to reevaluate my professional life, and I opted to provide care only in my allergy and immunology specialty.
However, living in a small town is different from life in a metropolis, and it was not uncommon for doctors to be asked to assist the community. A number of years ago, our county judge asked if I would help evaluate why our county jail was spending so much money. After several attempts to refuse, I eventually did evaluate the program there, and was flabbergasted by how much money was being wasted. I made some rather simple suggestions as how to correct the problem, but when no primary care doctor stepped forward to implement the changes and run the jail medical program, I became its medical director. When we saved $120,000 the first year, even I was astounded.
While I continued to run my private practice, I did accept other small community’s offers to look into their county jails’ programs. I found that their problems in cost control and quality of health care mirrored those I found in the first jail, and they were easily solvable if the county judge and the local sheriff wanted solutions. I also found that politics makes strange bedfellows, as the saying goes, and often the obvious changes were met with obstruction in one form or another. Nonetheless, I found that I could serve these communities in addition to my individual patients. When it was time for retirement, I continued to have a real desire to make the towns around which I lived and my own community more livable. So
In most things, I found that the same business philosophy and personal medical approach I learned in my pediatrics training and as a private practitioner applied to the jail system. Let me mention some specifics. Using generic medicines was less expensive than using brand names. The diagnoses which patients claimed when they entered jail might or might not be correct, so reevaluating the diagnosis and treatment was appropriate as soon as possible. Hospital and ED visits should be limited to patients’ medically requiring them rather than using the ED as a screening tool.
But I did come to understand that medical care in the county jail is different from medical care outside an incarcerated facility in that sometimes the prisoners had their own reasons for seeking medical care. This was complicated by the fact that often there were critically ill patients presenting to county jails. So carefully established criteria and protocols were an absolute necessity to save lives.
Let me expand on the topic of seeking medical care by the inmate-patients. A relatively small number of these individuals required immediate emergency treatment, without which they could not do well: The diabetic who was not taking his insulin, the out-of-control paranoid schizophrenic who decided he was cured and therefore was unattended, the alcoholic or drug addict who would develop delirium tremens if medications were stopped abruptly. These people had to be identified as quickly as possible and correctly treated. Confounding the problem was the fact that many, and I repeat many, individuals try to use the medical route to manipulate their incarceration environment. I called this the B problem: beds, blankets, barter, buzz, better food, and be out of here. They might claim an illness existed, and often they might believe it did.
A related situation might exist when individuals would demand psychiatric and pain medications, often in large quantities, when they in fact had not taken them for some time in the outside world. Often these patients were addicts, and of course this could create an entire other relationship with the medical team. A third example would be the claim of hypoglycemia so that the prisoner would receive more frequent meals.
One might think that as a pediatrician I was ill prepared to treat adults, and in fact, there was much review of the general medical care needed when I began this program. However, the internists and family physicians in town were glad to assist me whenever I encountered a difficult patient. When hospitalizations were required, the inpatient always was covered by one of the internists on hospital staff. Quite frankly, the doctors seemed pleased to not be dealing with this group of individuals as much as they had in the past.
On a slightly different note, skills honed during my pediatric career were extremely valuable. Children, particularly young children, do not verbally communicate with their parents or their doctor particularly well, so pediatricians are well trained in the skill of observation. The patient who claims a guard hurt his shoulder so badly during an altercation that he cannot move it is found out when he easily whips his arms over his head when asked to remove his shirt. It is not uncommon for an individual to demand antidepressant medications from the medical staff, but when evaluated more thoroughly and for a longer period of time, the patient ends up laughing, even denying any suicidal ideation or any other sign of depression. One also deals with a lot of adolescent behavior from the inmates, such as the individuals who say that unless they don’t get their way (more food) they are not going to take their medications and thus get sicker. That’s Adolescent Medicine 101.
Some of the modalities I utilized in modifying the jail programs will be familiar to every practicing pediatrician. I educate; I teach; I train. Parents of my asthmatic patients had to know what medications to keep handy and when to use them. It is pretty easy to see how that relates to jail medicine. Many patients come into jail with inhalers and with a diagnosis of asthma. Some have the condition, and some do not. By training jail and medical staff how to observe breathing patterns and by performing pulse oximetry, we eliminated a large number of unnecessary ED visits, and we often made the diagnosis of hyperventilation syndrome rather than misdiagnosed asthma.
Jail medicine is a large part of the cost of housing inmates. I did consultation work for a large urban jail, and we saved over $7 million in 1 year. In a medium-sized jail, the cost-savings after a 4-month consultation was over $300,000. This is a lot of money to me, and I suspect is to you, too. Just as in our general communities, we have enough resources to provide medical care and to provide a high level of care for all. However, we cannot waste money by providing inappropriate care or overtesting or overtreating. The medical care must be what treats the disease the patient actually has ... nothing more and nothing less!
If it sounds as if I am cynical about inmate patients, that is not true. However, I am realistic that no one wishes to be in jail. I realize that the medical route is just one that prisoners can and do use to modify their situation. I understand that the medical staff within a jail needs constant education and supervision at first, and with time they become more astute – just like a physician in this arena – at distinguishing the very serious from the mildly serious from malingering. In spite of this, we doctors also can be fooled. However, through constant vigilance and constant education we can get better.
Jail medicine is not for everyone in retirement. Heck, it is not for everyone ever. I found it interesting because it required me to match my diagnostic skills against the diseases and the psychodynamics of individuals who often – not always – made that diagnosis more difficult. Diagnosing illness and curing it – isn’t this why we all went into medicine?
Dr. Yoffe is a retired pediatrician specializing in allergy and immunology who resides in Brenham, Tex. Email him at [email protected].
This article was updated 2/13/2020.