User login
Exercise halves T2D risk in adults with obesity
“Physical exercise combined with diet restriction has been proven to be effective in prevention of diabetes. However, the long-term effect of exercise on prevention of diabetes, and the difference of exercise intensity in prevention of diabetes have not been well studied,” said corresponding author Xiaoying Li, MD, of Zhongshan Hospital, Fudan University, Shanghai, in an interview.
In the research letter published in JAMA Internal Medicine, Dr. Li and colleagues analyzed the results of a study of 220 adults with central obesity and nonalcoholic fatty liver disease, but no incident diabetes, randomized to a 12-month program of vigorous exercise (73 patients), moderate aerobic exercise (73 patients) or no exercise (74 patients).
A total of 208 participants completed the 1-year intervention; of these, 195 and 178 remained to provide data at 2 years and 10 years, respectively. The mean age of the participants was 53.9 years, 32.3% were male, and the mean waist circumference was 96.1 cm at baseline.
The cumulative incidence of type 2 diabetes in the vigorous exercise, moderate exercise, and nonexercise groups was 2.1 per 100 person-years 1.9 per 100 person-years, and 4.1 per 100 person-years, respectively, over the 10-year follow-up period. This translated to a reduction in type 2 diabetes risk of 49% in the vigorous exercise group and 53% in the moderate exercise group compared with the nonexercise group.
In addition, individuals in the vigorous and moderate exercise groups significantly reduced their HbA1c and waist circumference compared with the nonexercisers. Levels of plasma fasting glucose and weight regain were lower in both exercise groups compared with nonexercisers, but these differences were not significant.
The exercise intervention was described in a 2016 study, which was also published in JAMA Internal Medicine. That study’s purpose was to compare the effects of exercise on patients with nonalcoholic fatty liver disease. Participants were coached and supervised for their exercise programs. The program for the vigorous group involved jogging for 150 minutes per week at 65%-80% of maximum heart rate for 6 months and brisk walking 150 minutes per week at 45%-55% of maximum heart rate for another 6 months. The program for the moderate exercise group involved brisk walking 150 minutes per week for 12 months.
Both exercise groups showed a trend towards higher levels of leisure time physical activity after 10 years compared with the nonexercise groups, although the difference was not significant.
The main limitation of the study was that incident prediabetes was not prespecified, which may have led to some confounding, the researchers noted. In addition, the participants were highly supervised for a 12-month program only. However, the results support the long-term value of physical exercise as a method of obesity management and to delay progression to type 2 diabetes in obese individuals, they said. Vigorous and moderate aerobic exercise programs could be implemented for this patient population, they concluded.
“Surprisingly, our findings demonstrated that a 12-month vigorous aerobic exercise or moderate aerobic exercise could significantly reduce the risk of incident diabetes by 50% over the 10-year follow-up,” Dr. Li said in an interview. The results suggest that physical exercise for some period of time can produce a long-term beneficial effect in prevention of type 2 diabetes, he said.
Potential barriers to the routine use of an exercise intervention in patients with obesity include the unwillingness of this population to engage in vigorous exercise, and the potential for musculoskeletal injury, said Dr. Li. In these cases, obese patients should be encouraged to pursue moderate exercise, Dr. Li said.
Looking ahead, more research is needed to examine the potential mechanism behind the effect of exercise on diabetes prevention, said Dr. Li.
Findings fill gap in long-term outcome data
The current study is important because of the long-term follow-up data, said Jill Kanaley, PhD, professor and interim chair of nutrition and exercise physiology at the University of Missouri, in an interview. “We seldom follow up on our training studies, thus it is important to see if there is any long-term impact of these interventions,” she said.
Dr. Kanaley said she was surprised to see the residual benefits of the exercise intervention 10 years later.
“We often wonder how long the impact of the exercise training will stay with someone so that they continue to exercise and watch their weight; this study seems to indicate that there is an educational component that stays with them,” she said.
The main clinical takeaway from the current study was the minimal weight gain over time, Dr. Kanaley said.
Although time may be a barrier to the routine use of an exercise intervention, patients have to realize that they can usually find the time, especially given the multiple benefits, said Dr. Kanaley. “The exercise interventions provide more benefits than just weight control and glucose levels,” she said.
“The 30-60 minutes of exercise does not have to come all at the same time,” Dr. Kanaley noted. “It could be three 15-minute bouts of exercise/physical activity to get their 45 minutes in,” she noted. Exercise does not have to be heavy vigorous exercise, even walking is beneficial, she said. For people who complain of boredom with an exercise routine, Dr. Kanaley encourages mixing it up, with activities such as different exercise classes, running, or walking on a different day of any given week.
Although the current study was conducted in China, the findings may translate to a U.S. population, Dr. Kanaley said in an interview. However, “frequently our Western diet is less healthy than the traditional Chinese diet. This may have provided an immeasurable benefit to these subjects,” although study participants did not make specific adjustments to their diets, she said.
Additional research is needed to confirm the findings, said Dr. Kanaley. “Ideally, the study should be repeated in a population with a Western diet,” she noted.
Next steps for research include maintenance of activity
Evidence on the long-term benefits of exercise programs is limited, said Amanda Paluch, PhD, a physical activity epidemiologist at the University of Massachusetts, Amherst, in an interview.
“Chronic diseases such as diabetes can take years to develop, so understanding these important health outcomes requires years of follow-up. This study followed their study participants for 10 years, which gives us a nice glimpse of the long-term benefits of exercise training on diabetes prevention,” she said.
Data from previous observational studies of individuals’ current activity levels (without an intervention) suggest that adults who are more physically active have a lower risk of diabetes over time, said Dr. Paluch. However, the current study is one of the few with rigorous exercise interventions with extensive follow-up on diabetes risk, and it provides important evidence that a 12-month structured exercise program in inactive adults with obesity can result in meaningful long-term health benefits by lowering the risk of diabetes, she said.
“The individuals in the current study participated in a structured exercise program where their exercise sessions were supervised and coached,” Dr. Paluch noted. “Having a personalized coach may not be within the budget or time constraints for many people,” she said. Her message to clinicians for their patients: “When looking to start an exercise routine, identify an activity you enjoy and find feasible to fit into your existing life and schedule,” she said.
“Although this study was conducted in China, the results are meaningful for the U.S. population, as we would expect the physiological benefit of exercise to be consistent across various populations,” Dr. Paluch said. “However, there are certainly differences across countries at the individual level to the larger community-wide level that may influence a person’s ability to maintain physical activity and prevent diabetes, so replicating similar studies in other countries, including the U.S., would be of value.”
“Additionally, we need more research on how to encourage maintenance of physical activity in the long-term, after the initial exercise program is over,” she said.
“From this current study, we cannot tease out whether diabetes risk is reduced because of the 12-month exercise intervention or the benefit is from maintaining physical activity regularly over the 10 years of follow-up, or a combination of the two,” said Dr. Paluch. Future studies should consider teasing out participants who were only active during the exercise intervention, then ceased being active vs. participants who continued with vigorous activity long-term, she said.
The study was supported by the National Nature Science Foundation, the National Key Research and Development Program of China, and the Shanghai Municipal Science and Technology Major Project. The researchers, Dr. Kanaley, and Dr. Paluch had no financial conflicts to disclose.
“Physical exercise combined with diet restriction has been proven to be effective in prevention of diabetes. However, the long-term effect of exercise on prevention of diabetes, and the difference of exercise intensity in prevention of diabetes have not been well studied,” said corresponding author Xiaoying Li, MD, of Zhongshan Hospital, Fudan University, Shanghai, in an interview.
In the research letter published in JAMA Internal Medicine, Dr. Li and colleagues analyzed the results of a study of 220 adults with central obesity and nonalcoholic fatty liver disease, but no incident diabetes, randomized to a 12-month program of vigorous exercise (73 patients), moderate aerobic exercise (73 patients) or no exercise (74 patients).
A total of 208 participants completed the 1-year intervention; of these, 195 and 178 remained to provide data at 2 years and 10 years, respectively. The mean age of the participants was 53.9 years, 32.3% were male, and the mean waist circumference was 96.1 cm at baseline.
The cumulative incidence of type 2 diabetes in the vigorous exercise, moderate exercise, and nonexercise groups was 2.1 per 100 person-years 1.9 per 100 person-years, and 4.1 per 100 person-years, respectively, over the 10-year follow-up period. This translated to a reduction in type 2 diabetes risk of 49% in the vigorous exercise group and 53% in the moderate exercise group compared with the nonexercise group.
In addition, individuals in the vigorous and moderate exercise groups significantly reduced their HbA1c and waist circumference compared with the nonexercisers. Levels of plasma fasting glucose and weight regain were lower in both exercise groups compared with nonexercisers, but these differences were not significant.
The exercise intervention was described in a 2016 study, which was also published in JAMA Internal Medicine. That study’s purpose was to compare the effects of exercise on patients with nonalcoholic fatty liver disease. Participants were coached and supervised for their exercise programs. The program for the vigorous group involved jogging for 150 minutes per week at 65%-80% of maximum heart rate for 6 months and brisk walking 150 minutes per week at 45%-55% of maximum heart rate for another 6 months. The program for the moderate exercise group involved brisk walking 150 minutes per week for 12 months.
Both exercise groups showed a trend towards higher levels of leisure time physical activity after 10 years compared with the nonexercise groups, although the difference was not significant.
The main limitation of the study was that incident prediabetes was not prespecified, which may have led to some confounding, the researchers noted. In addition, the participants were highly supervised for a 12-month program only. However, the results support the long-term value of physical exercise as a method of obesity management and to delay progression to type 2 diabetes in obese individuals, they said. Vigorous and moderate aerobic exercise programs could be implemented for this patient population, they concluded.
“Surprisingly, our findings demonstrated that a 12-month vigorous aerobic exercise or moderate aerobic exercise could significantly reduce the risk of incident diabetes by 50% over the 10-year follow-up,” Dr. Li said in an interview. The results suggest that physical exercise for some period of time can produce a long-term beneficial effect in prevention of type 2 diabetes, he said.
Potential barriers to the routine use of an exercise intervention in patients with obesity include the unwillingness of this population to engage in vigorous exercise, and the potential for musculoskeletal injury, said Dr. Li. In these cases, obese patients should be encouraged to pursue moderate exercise, Dr. Li said.
Looking ahead, more research is needed to examine the potential mechanism behind the effect of exercise on diabetes prevention, said Dr. Li.
Findings fill gap in long-term outcome data
The current study is important because of the long-term follow-up data, said Jill Kanaley, PhD, professor and interim chair of nutrition and exercise physiology at the University of Missouri, in an interview. “We seldom follow up on our training studies, thus it is important to see if there is any long-term impact of these interventions,” she said.
Dr. Kanaley said she was surprised to see the residual benefits of the exercise intervention 10 years later.
“We often wonder how long the impact of the exercise training will stay with someone so that they continue to exercise and watch their weight; this study seems to indicate that there is an educational component that stays with them,” she said.
The main clinical takeaway from the current study was the minimal weight gain over time, Dr. Kanaley said.
Although time may be a barrier to the routine use of an exercise intervention, patients have to realize that they can usually find the time, especially given the multiple benefits, said Dr. Kanaley. “The exercise interventions provide more benefits than just weight control and glucose levels,” she said.
“The 30-60 minutes of exercise does not have to come all at the same time,” Dr. Kanaley noted. “It could be three 15-minute bouts of exercise/physical activity to get their 45 minutes in,” she noted. Exercise does not have to be heavy vigorous exercise, even walking is beneficial, she said. For people who complain of boredom with an exercise routine, Dr. Kanaley encourages mixing it up, with activities such as different exercise classes, running, or walking on a different day of any given week.
Although the current study was conducted in China, the findings may translate to a U.S. population, Dr. Kanaley said in an interview. However, “frequently our Western diet is less healthy than the traditional Chinese diet. This may have provided an immeasurable benefit to these subjects,” although study participants did not make specific adjustments to their diets, she said.
Additional research is needed to confirm the findings, said Dr. Kanaley. “Ideally, the study should be repeated in a population with a Western diet,” she noted.
Next steps for research include maintenance of activity
Evidence on the long-term benefits of exercise programs is limited, said Amanda Paluch, PhD, a physical activity epidemiologist at the University of Massachusetts, Amherst, in an interview.
“Chronic diseases such as diabetes can take years to develop, so understanding these important health outcomes requires years of follow-up. This study followed their study participants for 10 years, which gives us a nice glimpse of the long-term benefits of exercise training on diabetes prevention,” she said.
Data from previous observational studies of individuals’ current activity levels (without an intervention) suggest that adults who are more physically active have a lower risk of diabetes over time, said Dr. Paluch. However, the current study is one of the few with rigorous exercise interventions with extensive follow-up on diabetes risk, and it provides important evidence that a 12-month structured exercise program in inactive adults with obesity can result in meaningful long-term health benefits by lowering the risk of diabetes, she said.
“The individuals in the current study participated in a structured exercise program where their exercise sessions were supervised and coached,” Dr. Paluch noted. “Having a personalized coach may not be within the budget or time constraints for many people,” she said. Her message to clinicians for their patients: “When looking to start an exercise routine, identify an activity you enjoy and find feasible to fit into your existing life and schedule,” she said.
“Although this study was conducted in China, the results are meaningful for the U.S. population, as we would expect the physiological benefit of exercise to be consistent across various populations,” Dr. Paluch said. “However, there are certainly differences across countries at the individual level to the larger community-wide level that may influence a person’s ability to maintain physical activity and prevent diabetes, so replicating similar studies in other countries, including the U.S., would be of value.”
“Additionally, we need more research on how to encourage maintenance of physical activity in the long-term, after the initial exercise program is over,” she said.
“From this current study, we cannot tease out whether diabetes risk is reduced because of the 12-month exercise intervention or the benefit is from maintaining physical activity regularly over the 10 years of follow-up, or a combination of the two,” said Dr. Paluch. Future studies should consider teasing out participants who were only active during the exercise intervention, then ceased being active vs. participants who continued with vigorous activity long-term, she said.
The study was supported by the National Nature Science Foundation, the National Key Research and Development Program of China, and the Shanghai Municipal Science and Technology Major Project. The researchers, Dr. Kanaley, and Dr. Paluch had no financial conflicts to disclose.
“Physical exercise combined with diet restriction has been proven to be effective in prevention of diabetes. However, the long-term effect of exercise on prevention of diabetes, and the difference of exercise intensity in prevention of diabetes have not been well studied,” said corresponding author Xiaoying Li, MD, of Zhongshan Hospital, Fudan University, Shanghai, in an interview.
In the research letter published in JAMA Internal Medicine, Dr. Li and colleagues analyzed the results of a study of 220 adults with central obesity and nonalcoholic fatty liver disease, but no incident diabetes, randomized to a 12-month program of vigorous exercise (73 patients), moderate aerobic exercise (73 patients) or no exercise (74 patients).
A total of 208 participants completed the 1-year intervention; of these, 195 and 178 remained to provide data at 2 years and 10 years, respectively. The mean age of the participants was 53.9 years, 32.3% were male, and the mean waist circumference was 96.1 cm at baseline.
The cumulative incidence of type 2 diabetes in the vigorous exercise, moderate exercise, and nonexercise groups was 2.1 per 100 person-years 1.9 per 100 person-years, and 4.1 per 100 person-years, respectively, over the 10-year follow-up period. This translated to a reduction in type 2 diabetes risk of 49% in the vigorous exercise group and 53% in the moderate exercise group compared with the nonexercise group.
In addition, individuals in the vigorous and moderate exercise groups significantly reduced their HbA1c and waist circumference compared with the nonexercisers. Levels of plasma fasting glucose and weight regain were lower in both exercise groups compared with nonexercisers, but these differences were not significant.
The exercise intervention was described in a 2016 study, which was also published in JAMA Internal Medicine. That study’s purpose was to compare the effects of exercise on patients with nonalcoholic fatty liver disease. Participants were coached and supervised for their exercise programs. The program for the vigorous group involved jogging for 150 minutes per week at 65%-80% of maximum heart rate for 6 months and brisk walking 150 minutes per week at 45%-55% of maximum heart rate for another 6 months. The program for the moderate exercise group involved brisk walking 150 minutes per week for 12 months.
Both exercise groups showed a trend towards higher levels of leisure time physical activity after 10 years compared with the nonexercise groups, although the difference was not significant.
The main limitation of the study was that incident prediabetes was not prespecified, which may have led to some confounding, the researchers noted. In addition, the participants were highly supervised for a 12-month program only. However, the results support the long-term value of physical exercise as a method of obesity management and to delay progression to type 2 diabetes in obese individuals, they said. Vigorous and moderate aerobic exercise programs could be implemented for this patient population, they concluded.
“Surprisingly, our findings demonstrated that a 12-month vigorous aerobic exercise or moderate aerobic exercise could significantly reduce the risk of incident diabetes by 50% over the 10-year follow-up,” Dr. Li said in an interview. The results suggest that physical exercise for some period of time can produce a long-term beneficial effect in prevention of type 2 diabetes, he said.
Potential barriers to the routine use of an exercise intervention in patients with obesity include the unwillingness of this population to engage in vigorous exercise, and the potential for musculoskeletal injury, said Dr. Li. In these cases, obese patients should be encouraged to pursue moderate exercise, Dr. Li said.
Looking ahead, more research is needed to examine the potential mechanism behind the effect of exercise on diabetes prevention, said Dr. Li.
Findings fill gap in long-term outcome data
The current study is important because of the long-term follow-up data, said Jill Kanaley, PhD, professor and interim chair of nutrition and exercise physiology at the University of Missouri, in an interview. “We seldom follow up on our training studies, thus it is important to see if there is any long-term impact of these interventions,” she said.
Dr. Kanaley said she was surprised to see the residual benefits of the exercise intervention 10 years later.
“We often wonder how long the impact of the exercise training will stay with someone so that they continue to exercise and watch their weight; this study seems to indicate that there is an educational component that stays with them,” she said.
The main clinical takeaway from the current study was the minimal weight gain over time, Dr. Kanaley said.
Although time may be a barrier to the routine use of an exercise intervention, patients have to realize that they can usually find the time, especially given the multiple benefits, said Dr. Kanaley. “The exercise interventions provide more benefits than just weight control and glucose levels,” she said.
“The 30-60 minutes of exercise does not have to come all at the same time,” Dr. Kanaley noted. “It could be three 15-minute bouts of exercise/physical activity to get their 45 minutes in,” she noted. Exercise does not have to be heavy vigorous exercise, even walking is beneficial, she said. For people who complain of boredom with an exercise routine, Dr. Kanaley encourages mixing it up, with activities such as different exercise classes, running, or walking on a different day of any given week.
Although the current study was conducted in China, the findings may translate to a U.S. population, Dr. Kanaley said in an interview. However, “frequently our Western diet is less healthy than the traditional Chinese diet. This may have provided an immeasurable benefit to these subjects,” although study participants did not make specific adjustments to their diets, she said.
Additional research is needed to confirm the findings, said Dr. Kanaley. “Ideally, the study should be repeated in a population with a Western diet,” she noted.
Next steps for research include maintenance of activity
Evidence on the long-term benefits of exercise programs is limited, said Amanda Paluch, PhD, a physical activity epidemiologist at the University of Massachusetts, Amherst, in an interview.
“Chronic diseases such as diabetes can take years to develop, so understanding these important health outcomes requires years of follow-up. This study followed their study participants for 10 years, which gives us a nice glimpse of the long-term benefits of exercise training on diabetes prevention,” she said.
Data from previous observational studies of individuals’ current activity levels (without an intervention) suggest that adults who are more physically active have a lower risk of diabetes over time, said Dr. Paluch. However, the current study is one of the few with rigorous exercise interventions with extensive follow-up on diabetes risk, and it provides important evidence that a 12-month structured exercise program in inactive adults with obesity can result in meaningful long-term health benefits by lowering the risk of diabetes, she said.
“The individuals in the current study participated in a structured exercise program where their exercise sessions were supervised and coached,” Dr. Paluch noted. “Having a personalized coach may not be within the budget or time constraints for many people,” she said. Her message to clinicians for their patients: “When looking to start an exercise routine, identify an activity you enjoy and find feasible to fit into your existing life and schedule,” she said.
“Although this study was conducted in China, the results are meaningful for the U.S. population, as we would expect the physiological benefit of exercise to be consistent across various populations,” Dr. Paluch said. “However, there are certainly differences across countries at the individual level to the larger community-wide level that may influence a person’s ability to maintain physical activity and prevent diabetes, so replicating similar studies in other countries, including the U.S., would be of value.”
“Additionally, we need more research on how to encourage maintenance of physical activity in the long-term, after the initial exercise program is over,” she said.
“From this current study, we cannot tease out whether diabetes risk is reduced because of the 12-month exercise intervention or the benefit is from maintaining physical activity regularly over the 10 years of follow-up, or a combination of the two,” said Dr. Paluch. Future studies should consider teasing out participants who were only active during the exercise intervention, then ceased being active vs. participants who continued with vigorous activity long-term, she said.
The study was supported by the National Nature Science Foundation, the National Key Research and Development Program of China, and the Shanghai Municipal Science and Technology Major Project. The researchers, Dr. Kanaley, and Dr. Paluch had no financial conflicts to disclose.
FROM JAMA INTERNAL MEDICINE
Massive rise in drug overdose deaths driven by opioids
The 376% represents the change in age-adjusted overdose deaths per 100,000 population, which went from 6.9 in 2001 to 32.4 in 2021, as the total number of deaths rose from 19,394 to 106,699 (450%) over that time period, the NCHS said in a recent data brief. That total made 2021 the first year ever with more than 100,000 overdose deaths.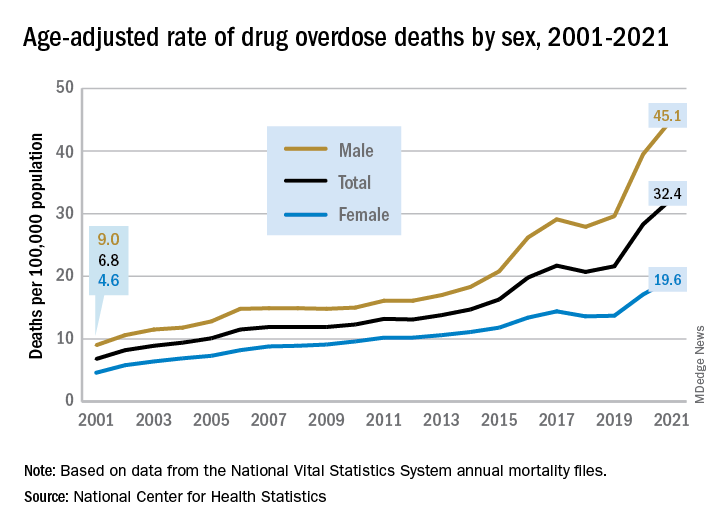
Since the age-adjusted rate stood at 21.6 per 100,000 in 2019, that means 42% of the total increase over 20 years actually occurred in 2020 and 2021. The number of deaths increased by about 36,000 over those 2 years, accounting for 41% of the total annual increase from 2001 to 2021, based on data from the National Vital Statistics System mortality files.
The overdose death rate was significantly higher for males than females for all of the years from 2001 to 2021, with males seeing an increase from 9.0 to 45.1 per 100,000 and females going from 4.6 to 19.6 deaths per 100,000. In the single year from 2020 to 2021, the age-adjusted rate was up by 14% for males and 15% for females, the mortality-file data show.
Analysis by age showed an even larger effect in some groups from 2020 to 2021. Drug overdose deaths jumped 28% among adults aged 65 years and older, more than any other group, and by 21% in those aged 55-64 years, according to the NCHS.
The only age group for which deaths didn’t increase significantly from 2020 to 2021 was 15- to 24-year-olds, whose rate rose by just 3%. The age group with the highest rate in both 2020 and 2021, however, was the 35- to 44-year-olds: 53.9 and 62.0 overdose deaths per 100,000, respectively, for an increase of 15%, the NCHS said in the report.
The drugs now involved in overdose deaths are most often opioids, a change from 2001. That year, opioids were involved in 49% of all overdose deaths, but by 2021 that share had increased to 75%. The trend for opioid-related deaths almost matches that of overall deaths over the 20-year span, and the significantly increasing trend that began for all overdose deaths in 2013 closely follows that of synthetic opioids such as fentanyl and tramadol, the report shows.
Overdose deaths involving cocaine and psychostimulants such as methamphetamine, amphetamine, and methylphenidate also show similar increases. The cocaine-related death rate rose 22% from 2020 to 2021 and is up by 421% since 2012, while the corresponding increases for psychostimulant deaths were 33% and 2,400%, the NCHS said.
The 376% represents the change in age-adjusted overdose deaths per 100,000 population, which went from 6.9 in 2001 to 32.4 in 2021, as the total number of deaths rose from 19,394 to 106,699 (450%) over that time period, the NCHS said in a recent data brief. That total made 2021 the first year ever with more than 100,000 overdose deaths.
Since the age-adjusted rate stood at 21.6 per 100,000 in 2019, that means 42% of the total increase over 20 years actually occurred in 2020 and 2021. The number of deaths increased by about 36,000 over those 2 years, accounting for 41% of the total annual increase from 2001 to 2021, based on data from the National Vital Statistics System mortality files.
The overdose death rate was significantly higher for males than females for all of the years from 2001 to 2021, with males seeing an increase from 9.0 to 45.1 per 100,000 and females going from 4.6 to 19.6 deaths per 100,000. In the single year from 2020 to 2021, the age-adjusted rate was up by 14% for males and 15% for females, the mortality-file data show.
Analysis by age showed an even larger effect in some groups from 2020 to 2021. Drug overdose deaths jumped 28% among adults aged 65 years and older, more than any other group, and by 21% in those aged 55-64 years, according to the NCHS.
The only age group for which deaths didn’t increase significantly from 2020 to 2021 was 15- to 24-year-olds, whose rate rose by just 3%. The age group with the highest rate in both 2020 and 2021, however, was the 35- to 44-year-olds: 53.9 and 62.0 overdose deaths per 100,000, respectively, for an increase of 15%, the NCHS said in the report.
The drugs now involved in overdose deaths are most often opioids, a change from 2001. That year, opioids were involved in 49% of all overdose deaths, but by 2021 that share had increased to 75%. The trend for opioid-related deaths almost matches that of overall deaths over the 20-year span, and the significantly increasing trend that began for all overdose deaths in 2013 closely follows that of synthetic opioids such as fentanyl and tramadol, the report shows.
Overdose deaths involving cocaine and psychostimulants such as methamphetamine, amphetamine, and methylphenidate also show similar increases. The cocaine-related death rate rose 22% from 2020 to 2021 and is up by 421% since 2012, while the corresponding increases for psychostimulant deaths were 33% and 2,400%, the NCHS said.
The 376% represents the change in age-adjusted overdose deaths per 100,000 population, which went from 6.9 in 2001 to 32.4 in 2021, as the total number of deaths rose from 19,394 to 106,699 (450%) over that time period, the NCHS said in a recent data brief. That total made 2021 the first year ever with more than 100,000 overdose deaths.
Since the age-adjusted rate stood at 21.6 per 100,000 in 2019, that means 42% of the total increase over 20 years actually occurred in 2020 and 2021. The number of deaths increased by about 36,000 over those 2 years, accounting for 41% of the total annual increase from 2001 to 2021, based on data from the National Vital Statistics System mortality files.
The overdose death rate was significantly higher for males than females for all of the years from 2001 to 2021, with males seeing an increase from 9.0 to 45.1 per 100,000 and females going from 4.6 to 19.6 deaths per 100,000. In the single year from 2020 to 2021, the age-adjusted rate was up by 14% for males and 15% for females, the mortality-file data show.
Analysis by age showed an even larger effect in some groups from 2020 to 2021. Drug overdose deaths jumped 28% among adults aged 65 years and older, more than any other group, and by 21% in those aged 55-64 years, according to the NCHS.
The only age group for which deaths didn’t increase significantly from 2020 to 2021 was 15- to 24-year-olds, whose rate rose by just 3%. The age group with the highest rate in both 2020 and 2021, however, was the 35- to 44-year-olds: 53.9 and 62.0 overdose deaths per 100,000, respectively, for an increase of 15%, the NCHS said in the report.
The drugs now involved in overdose deaths are most often opioids, a change from 2001. That year, opioids were involved in 49% of all overdose deaths, but by 2021 that share had increased to 75%. The trend for opioid-related deaths almost matches that of overall deaths over the 20-year span, and the significantly increasing trend that began for all overdose deaths in 2013 closely follows that of synthetic opioids such as fentanyl and tramadol, the report shows.
Overdose deaths involving cocaine and psychostimulants such as methamphetamine, amphetamine, and methylphenidate also show similar increases. The cocaine-related death rate rose 22% from 2020 to 2021 and is up by 421% since 2012, while the corresponding increases for psychostimulant deaths were 33% and 2,400%, the NCHS said.
Washington medical board charges doctor with spreading COVID misinformation
Doctors and professional organizations are standing guard, hoping to protect patients from any harm that results from mistruths spread by colleagues.
Case in point: Several physicians and the American Board of Pathology filed complaints with Washington and Idaho medical boards alleging that Ryan Cole, MD, a board-certified pathologist who practices in Boise, Idaho, but who also holds a license in Washington, has spread antivaccine and pro-ivermectin statements on social media. Dr. Cole is one of the founders of America’s Frontline Doctors, a right-wing political organization. Dr. Cole did not respond to a request for comment.
Gary W. Procop, MD, CEO, American Board of Pathology, told this news organization that “as physicians and board-certified pathologists, we have a public trust, and we must be accountable to patients, society, and the profession. Misinformation can cause real harm to patients, which may include death. Misinformation diverts patients away from lifesaving vaccination and other preventive measures, promotes viral transmission, and recommends ineffective therapies that may be toxic instead of evidence-based medical care.”
Cavalcade of complaints
Several doctors also chimed in with formal complaints alleging that Cole is spreading unreliable information, according to a report from KTVB News. For example, a Boise doctor wrote in his complaint that Dr. Cole is “a major purveyor of misinformation” and called it “amazing” that the physician was continuing to publicly support debunked information about COVID-19 more than a year into the pandemic. The doctor also stated, “Cole is a health menace, abusing his status as a physician to mislead the public.”
As a result of such complaints, the Washington medical board has charged Cole with COVID-19–related violations. It is unclear whether or not the Idaho medical board will sanction the doctor. At least 12 medical boards have sanctioned doctors for similar violations since the start of the pandemic.
The statement of charges from the Washington medical board contends that since March 2021, Dr. Cole has made numerous misleading statements regarding the COVID-19 pandemic, vaccines, the use of ivermectin to treat COVID-19, and the effectiveness of masks.
In addition, the statement alleges that Dr. Cole treated several COVID-19 patients via telemedicine. During these sessions, he prescribed ivermectin, an antiparasite drug that has not been found to have any effectiveness in treating, curing, or preventing COVID-19. One of the patients died after receiving this treatment, according to the complaint.
Citing a study published in the New England Journal of Medicine, Dr. Procop pointed out that use of ivermectin, which is not approved by the U.S. Food and Drug Administration to treat COVID-19, is particularly troubling.
“There is a concern whenever an ineffective treatment is prescribed when more effective and scientifically proven therapies are available. Therapeutics have potential side effects, and toxicities have been associated with the use of ivermectin,” Dr. Procop said. “The benefits of therapy should always outweigh the risks of treatment.”
If the Washington medical board finds that Dr. Cole has engaged in unprofessional conduct, possible sanctions include revocation or suspension of his license. Washington state law also provides for a range of other possible sanctions, including restriction or limitation of his practice, requiring that he complete a specific program of remedial education or treatment, monitoring of his practice, censure or reprimand, probation, a fine of up to $5,000 for each violation, or refunding fees that his practice has billed to and collected from patients. Dr. Cole had until January 30 to respond to the medical board’s statement.
“The American Board of Pathology supports the actions of the Washington State Medical Board regarding their inquiries into any physician that holds license in their state who makes false and misleading medical claims, or provides medical care beyond their scope of practice, as indicated by their training,” Dr. Procop said.
Law in limbo
While medical boards are seeking to sanction professionals who spread falsehoods, the pause button has been hit on the California law that allows regulators to punish doctors for spreading false information about COVID-19 vaccinations and treatments.
The law went into effect Jan. 1 but was temporarily halted when U.S. District Judge William B. Shubb of the Eastern District of California granted a preliminary injunction against the law on Jan. 25, according to a report in the Sacramento Bee.
Mr. Shubb said the measure’s definition of “misinformation” was “unconstitutionally vague” under the due process clause of the 14th Amendment. He also criticized the law’s definition of “misinformation” as being “grammatically incoherent.”
A version of this article first appeared on Medscape.com.
Doctors and professional organizations are standing guard, hoping to protect patients from any harm that results from mistruths spread by colleagues.
Case in point: Several physicians and the American Board of Pathology filed complaints with Washington and Idaho medical boards alleging that Ryan Cole, MD, a board-certified pathologist who practices in Boise, Idaho, but who also holds a license in Washington, has spread antivaccine and pro-ivermectin statements on social media. Dr. Cole is one of the founders of America’s Frontline Doctors, a right-wing political organization. Dr. Cole did not respond to a request for comment.
Gary W. Procop, MD, CEO, American Board of Pathology, told this news organization that “as physicians and board-certified pathologists, we have a public trust, and we must be accountable to patients, society, and the profession. Misinformation can cause real harm to patients, which may include death. Misinformation diverts patients away from lifesaving vaccination and other preventive measures, promotes viral transmission, and recommends ineffective therapies that may be toxic instead of evidence-based medical care.”
Cavalcade of complaints
Several doctors also chimed in with formal complaints alleging that Cole is spreading unreliable information, according to a report from KTVB News. For example, a Boise doctor wrote in his complaint that Dr. Cole is “a major purveyor of misinformation” and called it “amazing” that the physician was continuing to publicly support debunked information about COVID-19 more than a year into the pandemic. The doctor also stated, “Cole is a health menace, abusing his status as a physician to mislead the public.”
As a result of such complaints, the Washington medical board has charged Cole with COVID-19–related violations. It is unclear whether or not the Idaho medical board will sanction the doctor. At least 12 medical boards have sanctioned doctors for similar violations since the start of the pandemic.
The statement of charges from the Washington medical board contends that since March 2021, Dr. Cole has made numerous misleading statements regarding the COVID-19 pandemic, vaccines, the use of ivermectin to treat COVID-19, and the effectiveness of masks.
In addition, the statement alleges that Dr. Cole treated several COVID-19 patients via telemedicine. During these sessions, he prescribed ivermectin, an antiparasite drug that has not been found to have any effectiveness in treating, curing, or preventing COVID-19. One of the patients died after receiving this treatment, according to the complaint.
Citing a study published in the New England Journal of Medicine, Dr. Procop pointed out that use of ivermectin, which is not approved by the U.S. Food and Drug Administration to treat COVID-19, is particularly troubling.
“There is a concern whenever an ineffective treatment is prescribed when more effective and scientifically proven therapies are available. Therapeutics have potential side effects, and toxicities have been associated with the use of ivermectin,” Dr. Procop said. “The benefits of therapy should always outweigh the risks of treatment.”
If the Washington medical board finds that Dr. Cole has engaged in unprofessional conduct, possible sanctions include revocation or suspension of his license. Washington state law also provides for a range of other possible sanctions, including restriction or limitation of his practice, requiring that he complete a specific program of remedial education or treatment, monitoring of his practice, censure or reprimand, probation, a fine of up to $5,000 for each violation, or refunding fees that his practice has billed to and collected from patients. Dr. Cole had until January 30 to respond to the medical board’s statement.
“The American Board of Pathology supports the actions of the Washington State Medical Board regarding their inquiries into any physician that holds license in their state who makes false and misleading medical claims, or provides medical care beyond their scope of practice, as indicated by their training,” Dr. Procop said.
Law in limbo
While medical boards are seeking to sanction professionals who spread falsehoods, the pause button has been hit on the California law that allows regulators to punish doctors for spreading false information about COVID-19 vaccinations and treatments.
The law went into effect Jan. 1 but was temporarily halted when U.S. District Judge William B. Shubb of the Eastern District of California granted a preliminary injunction against the law on Jan. 25, according to a report in the Sacramento Bee.
Mr. Shubb said the measure’s definition of “misinformation” was “unconstitutionally vague” under the due process clause of the 14th Amendment. He also criticized the law’s definition of “misinformation” as being “grammatically incoherent.”
A version of this article first appeared on Medscape.com.
Doctors and professional organizations are standing guard, hoping to protect patients from any harm that results from mistruths spread by colleagues.
Case in point: Several physicians and the American Board of Pathology filed complaints with Washington and Idaho medical boards alleging that Ryan Cole, MD, a board-certified pathologist who practices in Boise, Idaho, but who also holds a license in Washington, has spread antivaccine and pro-ivermectin statements on social media. Dr. Cole is one of the founders of America’s Frontline Doctors, a right-wing political organization. Dr. Cole did not respond to a request for comment.
Gary W. Procop, MD, CEO, American Board of Pathology, told this news organization that “as physicians and board-certified pathologists, we have a public trust, and we must be accountable to patients, society, and the profession. Misinformation can cause real harm to patients, which may include death. Misinformation diverts patients away from lifesaving vaccination and other preventive measures, promotes viral transmission, and recommends ineffective therapies that may be toxic instead of evidence-based medical care.”
Cavalcade of complaints
Several doctors also chimed in with formal complaints alleging that Cole is spreading unreliable information, according to a report from KTVB News. For example, a Boise doctor wrote in his complaint that Dr. Cole is “a major purveyor of misinformation” and called it “amazing” that the physician was continuing to publicly support debunked information about COVID-19 more than a year into the pandemic. The doctor also stated, “Cole is a health menace, abusing his status as a physician to mislead the public.”
As a result of such complaints, the Washington medical board has charged Cole with COVID-19–related violations. It is unclear whether or not the Idaho medical board will sanction the doctor. At least 12 medical boards have sanctioned doctors for similar violations since the start of the pandemic.
The statement of charges from the Washington medical board contends that since March 2021, Dr. Cole has made numerous misleading statements regarding the COVID-19 pandemic, vaccines, the use of ivermectin to treat COVID-19, and the effectiveness of masks.
In addition, the statement alleges that Dr. Cole treated several COVID-19 patients via telemedicine. During these sessions, he prescribed ivermectin, an antiparasite drug that has not been found to have any effectiveness in treating, curing, or preventing COVID-19. One of the patients died after receiving this treatment, according to the complaint.
Citing a study published in the New England Journal of Medicine, Dr. Procop pointed out that use of ivermectin, which is not approved by the U.S. Food and Drug Administration to treat COVID-19, is particularly troubling.
“There is a concern whenever an ineffective treatment is prescribed when more effective and scientifically proven therapies are available. Therapeutics have potential side effects, and toxicities have been associated with the use of ivermectin,” Dr. Procop said. “The benefits of therapy should always outweigh the risks of treatment.”
If the Washington medical board finds that Dr. Cole has engaged in unprofessional conduct, possible sanctions include revocation or suspension of his license. Washington state law also provides for a range of other possible sanctions, including restriction or limitation of his practice, requiring that he complete a specific program of remedial education or treatment, monitoring of his practice, censure or reprimand, probation, a fine of up to $5,000 for each violation, or refunding fees that his practice has billed to and collected from patients. Dr. Cole had until January 30 to respond to the medical board’s statement.
“The American Board of Pathology supports the actions of the Washington State Medical Board regarding their inquiries into any physician that holds license in their state who makes false and misleading medical claims, or provides medical care beyond their scope of practice, as indicated by their training,” Dr. Procop said.
Law in limbo
While medical boards are seeking to sanction professionals who spread falsehoods, the pause button has been hit on the California law that allows regulators to punish doctors for spreading false information about COVID-19 vaccinations and treatments.
The law went into effect Jan. 1 but was temporarily halted when U.S. District Judge William B. Shubb of the Eastern District of California granted a preliminary injunction against the law on Jan. 25, according to a report in the Sacramento Bee.
Mr. Shubb said the measure’s definition of “misinformation” was “unconstitutionally vague” under the due process clause of the 14th Amendment. He also criticized the law’s definition of “misinformation” as being “grammatically incoherent.”
A version of this article first appeared on Medscape.com.
Difficulty fitting family into career: Female oncologists
In a survey of just over 1,000 female oncologists, 95% said their career plans were at least somewhat associated with the timing of when to start a family.
The most striking finding was that one third of respondents had miscarried and another one third reported difficulty with infertility that required fertility counseling and/or treatment.
One third reported experiencing discrimination during pregnancy, and another third said they experienced discrimination for taking maternity leave, and having more than one child increased the likelihood of this.
The most common negative factor associated with family planning was long work hours and heavy workload (66.6%),
These findings suggest there are systemic changes needed not only in the healthcare setting but in society as a whole around women in the workplace and their choices of childbearing, say the authors.
The study was published online in JAMA Network Open and led by Anna Lee MD, MPH, from the department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston.
In an invited commentary, Mona Saleh, MD, and Stephanie Blank, MD, from the department of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai in New York, suggest that cultural changes are needed that go beyond women in medicine.
“These cultural values are so deeply pervasive (one could also say invasive) that they affect even these most educated and wealthy professional women, such as those who participated in this survey,” the editorialists write.
“[The researchers] advocate for early education on assisted reproductive technology (ART) risks, benefits, and success rates, but this is not getting at the underlying issue: Pregnancy discrimination and unfair distribution of childbearing responsibilities are a reflection of a larger problematic culture rather than an issue specific to women in medicine,” they add.
Survey details
The survey comprised a novel 39-item questionnaire distributed to 1,004 U.S. female oncologists from May 7 to June 30, 2020, via email and social media channels.
Most respondents (84.4%) were married, and 71% were currently working full-time.
About one-third (35%) worked in radiation oncology, another third (34.3%) in medical oncology, 18.4% in surgical oncology, and 9.1% in pediatric oncology.
A total of 768 respondents (76.5%) had children, and of these, 415 (41.3%) first gave birth during postgraduate training and 275 (27.4%) gave birth in years 1-5 as an attending physician.
Of all respondents who had been pregnant, approximately two-thirds (65.7%) had some type of pregnancy complication. About one-third of respondents (31.7%) reported having experienced a miscarriage after a confirmed pregnancy; of those, 61.6% reported one miscarriage, while the remainder had two or more miscarriages (38.4%).
Approximately one-third (31.4%) of respondents reported difficulty with infertility that required fertility counseling and/or treatment.
The questionnaire also asked about assisted reproductive technology, and 164 participants (16.3%) reported the use of fertility medications, and 53 (5.3%) reported cryopreservation of eggs. Nearly 13% reported the use of intrauterine insemination and 13.2% reported the use of in vivo fertilization. Among those who experienced fertility concerns, 36.6% (232 of 634) reported facing financial burdens because of fertility or pregnancy that was in some way associated with their career choice.
When asked on the survey if fertility preservation should be discussed with women during medical school and/or residency, 65.7% of respondents stated that it should.
However, the editorialists suggest that “encouraging formal and directed education regarding the infertility risks specifically toward female physicians (which Lee et al. recommend) could be perceived as a blanket recommendation that it is best for women in medicine to delay childbearing and pursue ART.”
“Medical schools and residency and fellowship training programs should instead focus their energy on creating a framework and culture that normalizes conception during these points in training while also subsidizing and supporting trainees and physicians who prefer to use ART and delay fertility until after training,” they suggest.
The editorialists also emphasized that women may choose to become pregnant at any point during the years that it takes to go from being a medical student to resident/fellow to attending physician, and they should be supported by their workplace on their decisions.
The study was funded by grants from National Institutes of Health/National Cancer Institute Cancer Center.
Dr. Lee and coauthors reported no relevant financial relationships. Dr. Blank reported receiving grants from AstraZeneca, Aravive, Akesobio, GlaxoSmithKline, Merck, and Seattle Genetics outside the submitted work. Dr. Saleh reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a survey of just over 1,000 female oncologists, 95% said their career plans were at least somewhat associated with the timing of when to start a family.
The most striking finding was that one third of respondents had miscarried and another one third reported difficulty with infertility that required fertility counseling and/or treatment.
One third reported experiencing discrimination during pregnancy, and another third said they experienced discrimination for taking maternity leave, and having more than one child increased the likelihood of this.
The most common negative factor associated with family planning was long work hours and heavy workload (66.6%),
These findings suggest there are systemic changes needed not only in the healthcare setting but in society as a whole around women in the workplace and their choices of childbearing, say the authors.
The study was published online in JAMA Network Open and led by Anna Lee MD, MPH, from the department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston.
In an invited commentary, Mona Saleh, MD, and Stephanie Blank, MD, from the department of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai in New York, suggest that cultural changes are needed that go beyond women in medicine.
“These cultural values are so deeply pervasive (one could also say invasive) that they affect even these most educated and wealthy professional women, such as those who participated in this survey,” the editorialists write.
“[The researchers] advocate for early education on assisted reproductive technology (ART) risks, benefits, and success rates, but this is not getting at the underlying issue: Pregnancy discrimination and unfair distribution of childbearing responsibilities are a reflection of a larger problematic culture rather than an issue specific to women in medicine,” they add.
Survey details
The survey comprised a novel 39-item questionnaire distributed to 1,004 U.S. female oncologists from May 7 to June 30, 2020, via email and social media channels.
Most respondents (84.4%) were married, and 71% were currently working full-time.
About one-third (35%) worked in radiation oncology, another third (34.3%) in medical oncology, 18.4% in surgical oncology, and 9.1% in pediatric oncology.
A total of 768 respondents (76.5%) had children, and of these, 415 (41.3%) first gave birth during postgraduate training and 275 (27.4%) gave birth in years 1-5 as an attending physician.
Of all respondents who had been pregnant, approximately two-thirds (65.7%) had some type of pregnancy complication. About one-third of respondents (31.7%) reported having experienced a miscarriage after a confirmed pregnancy; of those, 61.6% reported one miscarriage, while the remainder had two or more miscarriages (38.4%).
Approximately one-third (31.4%) of respondents reported difficulty with infertility that required fertility counseling and/or treatment.
The questionnaire also asked about assisted reproductive technology, and 164 participants (16.3%) reported the use of fertility medications, and 53 (5.3%) reported cryopreservation of eggs. Nearly 13% reported the use of intrauterine insemination and 13.2% reported the use of in vivo fertilization. Among those who experienced fertility concerns, 36.6% (232 of 634) reported facing financial burdens because of fertility or pregnancy that was in some way associated with their career choice.
When asked on the survey if fertility preservation should be discussed with women during medical school and/or residency, 65.7% of respondents stated that it should.
However, the editorialists suggest that “encouraging formal and directed education regarding the infertility risks specifically toward female physicians (which Lee et al. recommend) could be perceived as a blanket recommendation that it is best for women in medicine to delay childbearing and pursue ART.”
“Medical schools and residency and fellowship training programs should instead focus their energy on creating a framework and culture that normalizes conception during these points in training while also subsidizing and supporting trainees and physicians who prefer to use ART and delay fertility until after training,” they suggest.
The editorialists also emphasized that women may choose to become pregnant at any point during the years that it takes to go from being a medical student to resident/fellow to attending physician, and they should be supported by their workplace on their decisions.
The study was funded by grants from National Institutes of Health/National Cancer Institute Cancer Center.
Dr. Lee and coauthors reported no relevant financial relationships. Dr. Blank reported receiving grants from AstraZeneca, Aravive, Akesobio, GlaxoSmithKline, Merck, and Seattle Genetics outside the submitted work. Dr. Saleh reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a survey of just over 1,000 female oncologists, 95% said their career plans were at least somewhat associated with the timing of when to start a family.
The most striking finding was that one third of respondents had miscarried and another one third reported difficulty with infertility that required fertility counseling and/or treatment.
One third reported experiencing discrimination during pregnancy, and another third said they experienced discrimination for taking maternity leave, and having more than one child increased the likelihood of this.
The most common negative factor associated with family planning was long work hours and heavy workload (66.6%),
These findings suggest there are systemic changes needed not only in the healthcare setting but in society as a whole around women in the workplace and their choices of childbearing, say the authors.
The study was published online in JAMA Network Open and led by Anna Lee MD, MPH, from the department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston.
In an invited commentary, Mona Saleh, MD, and Stephanie Blank, MD, from the department of obstetrics, gynecology, and reproductive science at the Icahn School of Medicine at Mount Sinai in New York, suggest that cultural changes are needed that go beyond women in medicine.
“These cultural values are so deeply pervasive (one could also say invasive) that they affect even these most educated and wealthy professional women, such as those who participated in this survey,” the editorialists write.
“[The researchers] advocate for early education on assisted reproductive technology (ART) risks, benefits, and success rates, but this is not getting at the underlying issue: Pregnancy discrimination and unfair distribution of childbearing responsibilities are a reflection of a larger problematic culture rather than an issue specific to women in medicine,” they add.
Survey details
The survey comprised a novel 39-item questionnaire distributed to 1,004 U.S. female oncologists from May 7 to June 30, 2020, via email and social media channels.
Most respondents (84.4%) were married, and 71% were currently working full-time.
About one-third (35%) worked in radiation oncology, another third (34.3%) in medical oncology, 18.4% in surgical oncology, and 9.1% in pediatric oncology.
A total of 768 respondents (76.5%) had children, and of these, 415 (41.3%) first gave birth during postgraduate training and 275 (27.4%) gave birth in years 1-5 as an attending physician.
Of all respondents who had been pregnant, approximately two-thirds (65.7%) had some type of pregnancy complication. About one-third of respondents (31.7%) reported having experienced a miscarriage after a confirmed pregnancy; of those, 61.6% reported one miscarriage, while the remainder had two or more miscarriages (38.4%).
Approximately one-third (31.4%) of respondents reported difficulty with infertility that required fertility counseling and/or treatment.
The questionnaire also asked about assisted reproductive technology, and 164 participants (16.3%) reported the use of fertility medications, and 53 (5.3%) reported cryopreservation of eggs. Nearly 13% reported the use of intrauterine insemination and 13.2% reported the use of in vivo fertilization. Among those who experienced fertility concerns, 36.6% (232 of 634) reported facing financial burdens because of fertility or pregnancy that was in some way associated with their career choice.
When asked on the survey if fertility preservation should be discussed with women during medical school and/or residency, 65.7% of respondents stated that it should.
However, the editorialists suggest that “encouraging formal and directed education regarding the infertility risks specifically toward female physicians (which Lee et al. recommend) could be perceived as a blanket recommendation that it is best for women in medicine to delay childbearing and pursue ART.”
“Medical schools and residency and fellowship training programs should instead focus their energy on creating a framework and culture that normalizes conception during these points in training while also subsidizing and supporting trainees and physicians who prefer to use ART and delay fertility until after training,” they suggest.
The editorialists also emphasized that women may choose to become pregnant at any point during the years that it takes to go from being a medical student to resident/fellow to attending physician, and they should be supported by their workplace on their decisions.
The study was funded by grants from National Institutes of Health/National Cancer Institute Cancer Center.
Dr. Lee and coauthors reported no relevant financial relationships. Dr. Blank reported receiving grants from AstraZeneca, Aravive, Akesobio, GlaxoSmithKline, Merck, and Seattle Genetics outside the submitted work. Dr. Saleh reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Can a nationwide liver paired donation program work?
For a patient who needs a liver, living donation offers an alternative to staying on a list of more than 10,000 people waiting for a transplant. But what happens when your donor is not a match?
“It’s an exciting time to be caring for patients who need liver transplants,” Benjamin Samstein, MD, chief of liver transplantation at New York–Presbyterian/Weill Cornell Medical Center, New York, said in an interview. He is the principal investigator for the UNOS pilot program. “I do believe it is within our grasp to make sure that nobody dies while waiting for an organ,” he said.
The initiative involves 15 U.S. transplant centers. So far, one recipient-donor pair has enrolled in the program. The pilot program has three main goals: Increase access to living donor transplants; increase access to transplants earlier, when recipients are in better health; and work out how to create and sustain a national program.
What is paired donation?
In 2020, 1,095 people died while waiting for a liver transplant, according to a report from the Organ Procurement and Transplant Network (OPTN) – a public-private partnership that includes more than 250 transplant centers and 50 organ procurement organizations across the country.
Most liver transplants involve deceased donors. One way to improve access to lifesaving transplants is through living donation, by which a healthy individual donates part of his or her liver. Someone can participate in nondirected or “altruistic” donation, in which someone donates a liver to someone they don’t know, or they can donate to a specific individual (usually a blood relative or a spouse).
With living liver donation, someone may receive a liver earlier, before getting sick enough to be given priority on the wait-list for deceased donation. Because the recipients are in better health, they may have an easier time recovering from the surgery, Ruthanne Leishman, who manages paired donation programs at UNOS, said in an interview.
In some cases, an individual will want to donate an organ to a specific person, but testing reveals that the two would not be a good match. Paired donation allows incompatible donors and recipients to find matches with other incompatible pairs. Each donor matches with the other pairs’ recipient, so the organs are essentially swapped or exchanged between the two pairs.
“People who want to donate get excited about the fact that they are not just helping their loved one but they’re also helping somebody else,” Ms. Leishman said.
Paired kidney donation programs have been running since 2002, but paired liver donation is relatively new. Since the first U.S. living-donor liver transplant in 1989, the procedure has become safer and is a viable alternative to deceased liver donation. A growing number of living donor programs are popping up at transplant centers across the country.
Still, living-donor liver donation makes up a small percentage of the liver transplants that are performed every year. In 2022, 603 living-donor liver transplants were performed in the United States, compared to 8,925 liver transplants from deceased donors, according to OPTN data. Dr. Samstein estimates a couple dozen paired liver exchanges may have been performed in the United States over the past few years within individual hospital systems. A goal of this pilot program, along with increasing access to liver transplants, is to see whether paired liver donation works on a national level, Ms. Leishman said.
Challenges to building a national program
There are several notable differences between living donor kidney transplants and living donor liver transplants. For example, living donor liver transplant is a more complicated surgery and poses greater risk to the donor. According to the OPTN 2020 Annual Report, from 2015 to 2019, the rehospitalization rate for living liver donors was twice that of living kidney donors up to 6 weeks after transplant (4.7% vs. 2.4%). One year post transplant, the cumulative rehospitalization rate was 11.0% for living liver donors and 4.8% for living kidney donors.
The risk of dying because of living donation is also higher for liver donors compared to kidney donors. The National Kidney Association states that the odds of dying during kidney donation are about 3 in 100,000, while estimates for risk of death for living liver donors range from 1 in 500 to 1 in 1,000. But some of these estimates are from 10 or more years ago, and outcomes have likely improved, said Whitney Jackson, MD, medical director of living donor liver transplant at UCHealth University of Colorado Hospital, Aurora. Her program is participating in the UNOS pilot.
More recent data from OPTN provides some idea of risk: Of 3,967 liver donors who donated between March 1, 2008, to Sept. 30, 2022, three deaths were reported within 30 days of transplant. However, the causes of death were not specified and therefore may be unrelated to the surgery. By comparison, of 74,555 kidney donors during that date range, 10 deaths were reported at 30 days post surgery.
In addition to a more complex surgery, surgeons also have a smaller time window in which to transplant a liver than than they do to transplant a kidney. A kidney can remain viable in cold storage for 24-36 hours, and it can be transported via commercial airlines cross country. Livers have to be transplanted within 8-12 hours, according to the OPTN website. For living donation, the graft needs to be transplanted within about 4 hours, Dr. Samstein noted; this poses a logistical challenge for a national organ paired donation program.
“We worked around that with the idea that we would move the donor rather than the organ,” he said. The program will require a donor (and a support person) to travel to the recipient’s transplant center where the surgery will be performed. While 3 of the 15 pilot paired donation transplant centers are in New York City, the other programs are scattered across the country, meaning a donor may have to fly to a different city to undergo surgery.
Including the preoperative evaluation, meeting the surgical team, the surgery itself, and follow-up, the donor could stay for about a month. The program offers up to $10,000 of financial assistance for travel expenses (for both the donor and support person), as well as lost wages and dependent care (for the donor only). Health insurance coverage will also be provided by the pilot program, in partnership with the American Foundation for Donation and Transplant.
The program requires that transplant candidates (the recipients) be at least 12 years old, be on the waiting list for deceased liver donation at one of the pilot’s transplant centers, and have a Model for End-Stage Liver Disease (MELD) score of 25 or less. All potential donors must be 18 years or older and must undergo a medical and psychosocial evaluation. Nondirected donors can register with the program, and they will be paired with a candidate on the liver transplant waiting list at the same transplant center.
The 1-year pilot program is set to begin when the program conducts its first match run – an algorithm will help match pairs who are enrolled in the program. About five to seven enrolled pairs would be ideal for the first match run, a UNOS spokesperson said. It is possible that the 1-year pilot program could run without performing any paired transplants, but that’s unlikely if multiple pairs are enrolled in the system, the spokesperson said. At the time of this story’s publication, the one enrolled pair are a mother and daughter who are registered at the UCHealth Transplant Center in Colorado.
Is a national liver paired donor program feasible?
While the UNOS pilot program offers financial assistance for expenses related to liver donation, some transplant surgeons are skeptical about the potential travel component of the pilot program.
The pilot program requires that the donor bring one support person if there is a need to travel for the surgery, but undergoing major abdominal surgery from a transplant team they are not familiar with may be stressful, said Peter Abt, MD, a transplant surgeon at the Hospital of the University of Pennsylvania and the Children’s Hospital of Philadelphia. “That’s a big ask,” he said, “and I’m not sure many potential donors would be up to that.”
John Roberts, MD, a transplant surgeon at the University of California, San Francisco, agreed that the travel component may put additional stress on the donor, but “if it’s the only way for the recipient to get a transplant, then the donor might be motivated,” he added.
Dr. Jackson remains optimistic. “Our experience so far has been that, yes, some people have been hesitant for things like traveling, but a lot of people who seem to be genuinely dedicated to the idea of living donation have been very enthusiastic,” she noted.
Dr. Leishman agreed that the travel aspect appears to one of the greatest barriers to participants entering the program but noted that a goal of the pilot program is to understand better what works - and what doesn’t – when considering a liver paired donation program on a national scale. “[Our] steering committee has put together a really nice framework that they think will work, but they know it’s not perfect. We’re going to have to tweak it along the way,” she said.
More information on the paired liver donation pilot program can be found on the UNOS website.
The sources interviewed for this article reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
This article was updated 2/15/23.
For a patient who needs a liver, living donation offers an alternative to staying on a list of more than 10,000 people waiting for a transplant. But what happens when your donor is not a match?
“It’s an exciting time to be caring for patients who need liver transplants,” Benjamin Samstein, MD, chief of liver transplantation at New York–Presbyterian/Weill Cornell Medical Center, New York, said in an interview. He is the principal investigator for the UNOS pilot program. “I do believe it is within our grasp to make sure that nobody dies while waiting for an organ,” he said.
The initiative involves 15 U.S. transplant centers. So far, one recipient-donor pair has enrolled in the program. The pilot program has three main goals: Increase access to living donor transplants; increase access to transplants earlier, when recipients are in better health; and work out how to create and sustain a national program.
What is paired donation?
In 2020, 1,095 people died while waiting for a liver transplant, according to a report from the Organ Procurement and Transplant Network (OPTN) – a public-private partnership that includes more than 250 transplant centers and 50 organ procurement organizations across the country.
Most liver transplants involve deceased donors. One way to improve access to lifesaving transplants is through living donation, by which a healthy individual donates part of his or her liver. Someone can participate in nondirected or “altruistic” donation, in which someone donates a liver to someone they don’t know, or they can donate to a specific individual (usually a blood relative or a spouse).
With living liver donation, someone may receive a liver earlier, before getting sick enough to be given priority on the wait-list for deceased donation. Because the recipients are in better health, they may have an easier time recovering from the surgery, Ruthanne Leishman, who manages paired donation programs at UNOS, said in an interview.
In some cases, an individual will want to donate an organ to a specific person, but testing reveals that the two would not be a good match. Paired donation allows incompatible donors and recipients to find matches with other incompatible pairs. Each donor matches with the other pairs’ recipient, so the organs are essentially swapped or exchanged between the two pairs.
“People who want to donate get excited about the fact that they are not just helping their loved one but they’re also helping somebody else,” Ms. Leishman said.
Paired kidney donation programs have been running since 2002, but paired liver donation is relatively new. Since the first U.S. living-donor liver transplant in 1989, the procedure has become safer and is a viable alternative to deceased liver donation. A growing number of living donor programs are popping up at transplant centers across the country.
Still, living-donor liver donation makes up a small percentage of the liver transplants that are performed every year. In 2022, 603 living-donor liver transplants were performed in the United States, compared to 8,925 liver transplants from deceased donors, according to OPTN data. Dr. Samstein estimates a couple dozen paired liver exchanges may have been performed in the United States over the past few years within individual hospital systems. A goal of this pilot program, along with increasing access to liver transplants, is to see whether paired liver donation works on a national level, Ms. Leishman said.
Challenges to building a national program
There are several notable differences between living donor kidney transplants and living donor liver transplants. For example, living donor liver transplant is a more complicated surgery and poses greater risk to the donor. According to the OPTN 2020 Annual Report, from 2015 to 2019, the rehospitalization rate for living liver donors was twice that of living kidney donors up to 6 weeks after transplant (4.7% vs. 2.4%). One year post transplant, the cumulative rehospitalization rate was 11.0% for living liver donors and 4.8% for living kidney donors.
The risk of dying because of living donation is also higher for liver donors compared to kidney donors. The National Kidney Association states that the odds of dying during kidney donation are about 3 in 100,000, while estimates for risk of death for living liver donors range from 1 in 500 to 1 in 1,000. But some of these estimates are from 10 or more years ago, and outcomes have likely improved, said Whitney Jackson, MD, medical director of living donor liver transplant at UCHealth University of Colorado Hospital, Aurora. Her program is participating in the UNOS pilot.
More recent data from OPTN provides some idea of risk: Of 3,967 liver donors who donated between March 1, 2008, to Sept. 30, 2022, three deaths were reported within 30 days of transplant. However, the causes of death were not specified and therefore may be unrelated to the surgery. By comparison, of 74,555 kidney donors during that date range, 10 deaths were reported at 30 days post surgery.
In addition to a more complex surgery, surgeons also have a smaller time window in which to transplant a liver than than they do to transplant a kidney. A kidney can remain viable in cold storage for 24-36 hours, and it can be transported via commercial airlines cross country. Livers have to be transplanted within 8-12 hours, according to the OPTN website. For living donation, the graft needs to be transplanted within about 4 hours, Dr. Samstein noted; this poses a logistical challenge for a national organ paired donation program.
“We worked around that with the idea that we would move the donor rather than the organ,” he said. The program will require a donor (and a support person) to travel to the recipient’s transplant center where the surgery will be performed. While 3 of the 15 pilot paired donation transplant centers are in New York City, the other programs are scattered across the country, meaning a donor may have to fly to a different city to undergo surgery.
Including the preoperative evaluation, meeting the surgical team, the surgery itself, and follow-up, the donor could stay for about a month. The program offers up to $10,000 of financial assistance for travel expenses (for both the donor and support person), as well as lost wages and dependent care (for the donor only). Health insurance coverage will also be provided by the pilot program, in partnership with the American Foundation for Donation and Transplant.
The program requires that transplant candidates (the recipients) be at least 12 years old, be on the waiting list for deceased liver donation at one of the pilot’s transplant centers, and have a Model for End-Stage Liver Disease (MELD) score of 25 or less. All potential donors must be 18 years or older and must undergo a medical and psychosocial evaluation. Nondirected donors can register with the program, and they will be paired with a candidate on the liver transplant waiting list at the same transplant center.
The 1-year pilot program is set to begin when the program conducts its first match run – an algorithm will help match pairs who are enrolled in the program. About five to seven enrolled pairs would be ideal for the first match run, a UNOS spokesperson said. It is possible that the 1-year pilot program could run without performing any paired transplants, but that’s unlikely if multiple pairs are enrolled in the system, the spokesperson said. At the time of this story’s publication, the one enrolled pair are a mother and daughter who are registered at the UCHealth Transplant Center in Colorado.
Is a national liver paired donor program feasible?
While the UNOS pilot program offers financial assistance for expenses related to liver donation, some transplant surgeons are skeptical about the potential travel component of the pilot program.
The pilot program requires that the donor bring one support person if there is a need to travel for the surgery, but undergoing major abdominal surgery from a transplant team they are not familiar with may be stressful, said Peter Abt, MD, a transplant surgeon at the Hospital of the University of Pennsylvania and the Children’s Hospital of Philadelphia. “That’s a big ask,” he said, “and I’m not sure many potential donors would be up to that.”
John Roberts, MD, a transplant surgeon at the University of California, San Francisco, agreed that the travel component may put additional stress on the donor, but “if it’s the only way for the recipient to get a transplant, then the donor might be motivated,” he added.
Dr. Jackson remains optimistic. “Our experience so far has been that, yes, some people have been hesitant for things like traveling, but a lot of people who seem to be genuinely dedicated to the idea of living donation have been very enthusiastic,” she noted.
Dr. Leishman agreed that the travel aspect appears to one of the greatest barriers to participants entering the program but noted that a goal of the pilot program is to understand better what works - and what doesn’t – when considering a liver paired donation program on a national scale. “[Our] steering committee has put together a really nice framework that they think will work, but they know it’s not perfect. We’re going to have to tweak it along the way,” she said.
More information on the paired liver donation pilot program can be found on the UNOS website.
The sources interviewed for this article reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
This article was updated 2/15/23.
For a patient who needs a liver, living donation offers an alternative to staying on a list of more than 10,000 people waiting for a transplant. But what happens when your donor is not a match?
“It’s an exciting time to be caring for patients who need liver transplants,” Benjamin Samstein, MD, chief of liver transplantation at New York–Presbyterian/Weill Cornell Medical Center, New York, said in an interview. He is the principal investigator for the UNOS pilot program. “I do believe it is within our grasp to make sure that nobody dies while waiting for an organ,” he said.
The initiative involves 15 U.S. transplant centers. So far, one recipient-donor pair has enrolled in the program. The pilot program has three main goals: Increase access to living donor transplants; increase access to transplants earlier, when recipients are in better health; and work out how to create and sustain a national program.
What is paired donation?
In 2020, 1,095 people died while waiting for a liver transplant, according to a report from the Organ Procurement and Transplant Network (OPTN) – a public-private partnership that includes more than 250 transplant centers and 50 organ procurement organizations across the country.
Most liver transplants involve deceased donors. One way to improve access to lifesaving transplants is through living donation, by which a healthy individual donates part of his or her liver. Someone can participate in nondirected or “altruistic” donation, in which someone donates a liver to someone they don’t know, or they can donate to a specific individual (usually a blood relative or a spouse).
With living liver donation, someone may receive a liver earlier, before getting sick enough to be given priority on the wait-list for deceased donation. Because the recipients are in better health, they may have an easier time recovering from the surgery, Ruthanne Leishman, who manages paired donation programs at UNOS, said in an interview.
In some cases, an individual will want to donate an organ to a specific person, but testing reveals that the two would not be a good match. Paired donation allows incompatible donors and recipients to find matches with other incompatible pairs. Each donor matches with the other pairs’ recipient, so the organs are essentially swapped or exchanged between the two pairs.
“People who want to donate get excited about the fact that they are not just helping their loved one but they’re also helping somebody else,” Ms. Leishman said.
Paired kidney donation programs have been running since 2002, but paired liver donation is relatively new. Since the first U.S. living-donor liver transplant in 1989, the procedure has become safer and is a viable alternative to deceased liver donation. A growing number of living donor programs are popping up at transplant centers across the country.
Still, living-donor liver donation makes up a small percentage of the liver transplants that are performed every year. In 2022, 603 living-donor liver transplants were performed in the United States, compared to 8,925 liver transplants from deceased donors, according to OPTN data. Dr. Samstein estimates a couple dozen paired liver exchanges may have been performed in the United States over the past few years within individual hospital systems. A goal of this pilot program, along with increasing access to liver transplants, is to see whether paired liver donation works on a national level, Ms. Leishman said.
Challenges to building a national program
There are several notable differences between living donor kidney transplants and living donor liver transplants. For example, living donor liver transplant is a more complicated surgery and poses greater risk to the donor. According to the OPTN 2020 Annual Report, from 2015 to 2019, the rehospitalization rate for living liver donors was twice that of living kidney donors up to 6 weeks after transplant (4.7% vs. 2.4%). One year post transplant, the cumulative rehospitalization rate was 11.0% for living liver donors and 4.8% for living kidney donors.
The risk of dying because of living donation is also higher for liver donors compared to kidney donors. The National Kidney Association states that the odds of dying during kidney donation are about 3 in 100,000, while estimates for risk of death for living liver donors range from 1 in 500 to 1 in 1,000. But some of these estimates are from 10 or more years ago, and outcomes have likely improved, said Whitney Jackson, MD, medical director of living donor liver transplant at UCHealth University of Colorado Hospital, Aurora. Her program is participating in the UNOS pilot.
More recent data from OPTN provides some idea of risk: Of 3,967 liver donors who donated between March 1, 2008, to Sept. 30, 2022, three deaths were reported within 30 days of transplant. However, the causes of death were not specified and therefore may be unrelated to the surgery. By comparison, of 74,555 kidney donors during that date range, 10 deaths were reported at 30 days post surgery.
In addition to a more complex surgery, surgeons also have a smaller time window in which to transplant a liver than than they do to transplant a kidney. A kidney can remain viable in cold storage for 24-36 hours, and it can be transported via commercial airlines cross country. Livers have to be transplanted within 8-12 hours, according to the OPTN website. For living donation, the graft needs to be transplanted within about 4 hours, Dr. Samstein noted; this poses a logistical challenge for a national organ paired donation program.
“We worked around that with the idea that we would move the donor rather than the organ,” he said. The program will require a donor (and a support person) to travel to the recipient’s transplant center where the surgery will be performed. While 3 of the 15 pilot paired donation transplant centers are in New York City, the other programs are scattered across the country, meaning a donor may have to fly to a different city to undergo surgery.
Including the preoperative evaluation, meeting the surgical team, the surgery itself, and follow-up, the donor could stay for about a month. The program offers up to $10,000 of financial assistance for travel expenses (for both the donor and support person), as well as lost wages and dependent care (for the donor only). Health insurance coverage will also be provided by the pilot program, in partnership with the American Foundation for Donation and Transplant.
The program requires that transplant candidates (the recipients) be at least 12 years old, be on the waiting list for deceased liver donation at one of the pilot’s transplant centers, and have a Model for End-Stage Liver Disease (MELD) score of 25 or less. All potential donors must be 18 years or older and must undergo a medical and psychosocial evaluation. Nondirected donors can register with the program, and they will be paired with a candidate on the liver transplant waiting list at the same transplant center.
The 1-year pilot program is set to begin when the program conducts its first match run – an algorithm will help match pairs who are enrolled in the program. About five to seven enrolled pairs would be ideal for the first match run, a UNOS spokesperson said. It is possible that the 1-year pilot program could run without performing any paired transplants, but that’s unlikely if multiple pairs are enrolled in the system, the spokesperson said. At the time of this story’s publication, the one enrolled pair are a mother and daughter who are registered at the UCHealth Transplant Center in Colorado.
Is a national liver paired donor program feasible?
While the UNOS pilot program offers financial assistance for expenses related to liver donation, some transplant surgeons are skeptical about the potential travel component of the pilot program.
The pilot program requires that the donor bring one support person if there is a need to travel for the surgery, but undergoing major abdominal surgery from a transplant team they are not familiar with may be stressful, said Peter Abt, MD, a transplant surgeon at the Hospital of the University of Pennsylvania and the Children’s Hospital of Philadelphia. “That’s a big ask,” he said, “and I’m not sure many potential donors would be up to that.”
John Roberts, MD, a transplant surgeon at the University of California, San Francisco, agreed that the travel component may put additional stress on the donor, but “if it’s the only way for the recipient to get a transplant, then the donor might be motivated,” he added.
Dr. Jackson remains optimistic. “Our experience so far has been that, yes, some people have been hesitant for things like traveling, but a lot of people who seem to be genuinely dedicated to the idea of living donation have been very enthusiastic,” she noted.
Dr. Leishman agreed that the travel aspect appears to one of the greatest barriers to participants entering the program but noted that a goal of the pilot program is to understand better what works - and what doesn’t – when considering a liver paired donation program on a national scale. “[Our] steering committee has put together a really nice framework that they think will work, but they know it’s not perfect. We’re going to have to tweak it along the way,” she said.
More information on the paired liver donation pilot program can be found on the UNOS website.
The sources interviewed for this article reported no financial conflicts of interest.
A version of this article first appeared on Medscape.com.
This article was updated 2/15/23.
Citing workplace violence, one-fourth of critical care workers are ready to quit
A surgeon in Tulsa shot by a disgruntled patient. A doctor in India beaten by a group of bereaved family members. A general practitioner in the United Kingdom threatened with stabbing. A new study identifies this trend and finds that 25% of health care workers polled were willing to quit because of such violence.
“That was pretty appalling,” Rahul Kashyap, MD, MBA, MBBS, recalls. Dr. Kashyap is one of the leaders of the Violence Study of Healthcare Workers and Systems (ViSHWaS), which polled an international sample of physicians, nurses, and hospital staff. This study has worrying implications, Dr. Kashyap says. In a time when hospital staff are reporting burnout in record numbers, further deterrents may be the last thing our health care system needs. But Dr. Kashyap hopes that bringing awareness to these trends may allow physicians, policymakers, and the public to mobilize and intervene before it’s too late.
Previous studies have revealed similar trends. The rate of workplace violence directed at U.S. health care workers is five times that of workers in any other industry, according to the Bureau of Labor Statistics. The same study found that attacks had increased 63% from 2011 to 2018. Other polls that focus on the pandemic show that nearly half of U.S. nurses believe that violence increased since the world shut down. Well before the pandemic, however, a study from the Indian Medical Association found that 75% of doctors experienced workplace violence.
With this history in mind, perhaps it’s not surprising that the idea for the study came from the authors’ personal experiences. They had seen coworkers go through attacks, or they had endured attacks themselves, Dr. Kashyap says. But they couldn’t find any global data to back up these experiences. So Dr. Kashyap and his colleagues formed a web of volunteers dedicated to creating a cross-sectional study.
They got in touch with researchers from countries across Asia, the Middle East, South America, North America, and Africa. The initial group agreed to reach out to their contacts, casting a wide net. Researchers used WhatsApp, LinkedIn, and text messages to distribute the survey. Health care workers in each country completed the brief questionnaire, recalling their prepandemic world and evaluating their current one.
Within 2 months, they had reached health care workers in more than 100 countries. They concluded the study when they received about 5,000 results, according to Dr. Kashyap, and then began the process of stratifying the data. For this report, they focused on critical care, emergency medicine, and anesthesiology, which resulted in 598 responses from 69 countries. Of these, India and the United States had the highest number of participants.
In all, 73% of participants reported facing physical or verbal violence while in the hospital; 48% said they felt less motivated to work because of that violence; 39% of respondents believed that the amount of violence they experienced was the same as before the COVID-19 pandemic; and 36% of respondents believed that violence had increased. Even though they were trained on guidelines from the Occupational Safety and Health Administration, 20% of participants felt unprepared to face violence.
Although the study didn’t analyze the reasons workers felt this way, Dr. Kashyap speculates that it could be related to the medical distrust that grew during the pandemic or the stress patients and health care professionals experienced during its peak.
Regardless, the researchers say their study is a starting point. Now that the trend has been highlighted, it may be acted on.
Moving forward, Dr. Kashyap believes that controlling for different variables could determine whether factors like gender or shift time put a worker at higher risk for violence. He hopes it’s possible to interrupt these patterns and reestablish trust in the hospital environment. “It’s aspirational, but you’re hoping that through studies like ViSHWaS, which means trust in Hindi ... [we could restore] the trust and confidence among health care providers for the patients and family members.”
A version of this article first appeared on Medscape.com.
A surgeon in Tulsa shot by a disgruntled patient. A doctor in India beaten by a group of bereaved family members. A general practitioner in the United Kingdom threatened with stabbing. A new study identifies this trend and finds that 25% of health care workers polled were willing to quit because of such violence.
“That was pretty appalling,” Rahul Kashyap, MD, MBA, MBBS, recalls. Dr. Kashyap is one of the leaders of the Violence Study of Healthcare Workers and Systems (ViSHWaS), which polled an international sample of physicians, nurses, and hospital staff. This study has worrying implications, Dr. Kashyap says. In a time when hospital staff are reporting burnout in record numbers, further deterrents may be the last thing our health care system needs. But Dr. Kashyap hopes that bringing awareness to these trends may allow physicians, policymakers, and the public to mobilize and intervene before it’s too late.
Previous studies have revealed similar trends. The rate of workplace violence directed at U.S. health care workers is five times that of workers in any other industry, according to the Bureau of Labor Statistics. The same study found that attacks had increased 63% from 2011 to 2018. Other polls that focus on the pandemic show that nearly half of U.S. nurses believe that violence increased since the world shut down. Well before the pandemic, however, a study from the Indian Medical Association found that 75% of doctors experienced workplace violence.
With this history in mind, perhaps it’s not surprising that the idea for the study came from the authors’ personal experiences. They had seen coworkers go through attacks, or they had endured attacks themselves, Dr. Kashyap says. But they couldn’t find any global data to back up these experiences. So Dr. Kashyap and his colleagues formed a web of volunteers dedicated to creating a cross-sectional study.
They got in touch with researchers from countries across Asia, the Middle East, South America, North America, and Africa. The initial group agreed to reach out to their contacts, casting a wide net. Researchers used WhatsApp, LinkedIn, and text messages to distribute the survey. Health care workers in each country completed the brief questionnaire, recalling their prepandemic world and evaluating their current one.
Within 2 months, they had reached health care workers in more than 100 countries. They concluded the study when they received about 5,000 results, according to Dr. Kashyap, and then began the process of stratifying the data. For this report, they focused on critical care, emergency medicine, and anesthesiology, which resulted in 598 responses from 69 countries. Of these, India and the United States had the highest number of participants.
In all, 73% of participants reported facing physical or verbal violence while in the hospital; 48% said they felt less motivated to work because of that violence; 39% of respondents believed that the amount of violence they experienced was the same as before the COVID-19 pandemic; and 36% of respondents believed that violence had increased. Even though they were trained on guidelines from the Occupational Safety and Health Administration, 20% of participants felt unprepared to face violence.
Although the study didn’t analyze the reasons workers felt this way, Dr. Kashyap speculates that it could be related to the medical distrust that grew during the pandemic or the stress patients and health care professionals experienced during its peak.
Regardless, the researchers say their study is a starting point. Now that the trend has been highlighted, it may be acted on.
Moving forward, Dr. Kashyap believes that controlling for different variables could determine whether factors like gender or shift time put a worker at higher risk for violence. He hopes it’s possible to interrupt these patterns and reestablish trust in the hospital environment. “It’s aspirational, but you’re hoping that through studies like ViSHWaS, which means trust in Hindi ... [we could restore] the trust and confidence among health care providers for the patients and family members.”
A version of this article first appeared on Medscape.com.
A surgeon in Tulsa shot by a disgruntled patient. A doctor in India beaten by a group of bereaved family members. A general practitioner in the United Kingdom threatened with stabbing. A new study identifies this trend and finds that 25% of health care workers polled were willing to quit because of such violence.
“That was pretty appalling,” Rahul Kashyap, MD, MBA, MBBS, recalls. Dr. Kashyap is one of the leaders of the Violence Study of Healthcare Workers and Systems (ViSHWaS), which polled an international sample of physicians, nurses, and hospital staff. This study has worrying implications, Dr. Kashyap says. In a time when hospital staff are reporting burnout in record numbers, further deterrents may be the last thing our health care system needs. But Dr. Kashyap hopes that bringing awareness to these trends may allow physicians, policymakers, and the public to mobilize and intervene before it’s too late.
Previous studies have revealed similar trends. The rate of workplace violence directed at U.S. health care workers is five times that of workers in any other industry, according to the Bureau of Labor Statistics. The same study found that attacks had increased 63% from 2011 to 2018. Other polls that focus on the pandemic show that nearly half of U.S. nurses believe that violence increased since the world shut down. Well before the pandemic, however, a study from the Indian Medical Association found that 75% of doctors experienced workplace violence.
With this history in mind, perhaps it’s not surprising that the idea for the study came from the authors’ personal experiences. They had seen coworkers go through attacks, or they had endured attacks themselves, Dr. Kashyap says. But they couldn’t find any global data to back up these experiences. So Dr. Kashyap and his colleagues formed a web of volunteers dedicated to creating a cross-sectional study.
They got in touch with researchers from countries across Asia, the Middle East, South America, North America, and Africa. The initial group agreed to reach out to their contacts, casting a wide net. Researchers used WhatsApp, LinkedIn, and text messages to distribute the survey. Health care workers in each country completed the brief questionnaire, recalling their prepandemic world and evaluating their current one.
Within 2 months, they had reached health care workers in more than 100 countries. They concluded the study when they received about 5,000 results, according to Dr. Kashyap, and then began the process of stratifying the data. For this report, they focused on critical care, emergency medicine, and anesthesiology, which resulted in 598 responses from 69 countries. Of these, India and the United States had the highest number of participants.
In all, 73% of participants reported facing physical or verbal violence while in the hospital; 48% said they felt less motivated to work because of that violence; 39% of respondents believed that the amount of violence they experienced was the same as before the COVID-19 pandemic; and 36% of respondents believed that violence had increased. Even though they were trained on guidelines from the Occupational Safety and Health Administration, 20% of participants felt unprepared to face violence.
Although the study didn’t analyze the reasons workers felt this way, Dr. Kashyap speculates that it could be related to the medical distrust that grew during the pandemic or the stress patients and health care professionals experienced during its peak.
Regardless, the researchers say their study is a starting point. Now that the trend has been highlighted, it may be acted on.
Moving forward, Dr. Kashyap believes that controlling for different variables could determine whether factors like gender or shift time put a worker at higher risk for violence. He hopes it’s possible to interrupt these patterns and reestablish trust in the hospital environment. “It’s aspirational, but you’re hoping that through studies like ViSHWaS, which means trust in Hindi ... [we could restore] the trust and confidence among health care providers for the patients and family members.”
A version of this article first appeared on Medscape.com.
Feds charge 25 nursing school execs, staff in fake diploma scheme
The U.S. Department of Justice recently announced charges against 25 owners, operators, and employees of three Florida nursing schools in a fraud scheme in which they sold as many as 7,600 fake nursing degrees.
The purchasers in the diploma scheme paid $10,000 to $15,000 for degrees and transcripts and some 2,800 of the buyers passed the national nursing licensing exam to become registered nurses (RNs) and licensed practice nurses/vocational nurses (LPN/VNs) around the country, according to The New York Times.
Many of the degree recipients went on to work at hospitals, nursing homes, and Veterans Affairs medical centers, according to the U.S. Attorney’s Office for the Southern District of Florida.
Several national nursing organizations cooperated with the investigation, and the Delaware Division of Professional Regulation already annulled 26 licenses, according to the Delaware Nurses Association. Fake licenses were issued in five states, according to federal reports.
“We are deeply unsettled by this egregious act,” DNA President Stephanie McClellan, MSN, RN, CMSRN, said in the group’s press statement. “We want all Delaware nurses to be aware of this active issue and to speak up if there is a concern regarding capacity to practice safely by a colleague/peer,” she said.
The Oregon State Board of Nursing is also investigating at least a dozen nurses who may have paid for their degrees, according to a Portland CBS affiliate.
The National Council of State Boards of Nursing said in a statement that it had helped authorities identify and monitor the individuals who allegedly provided the false degrees.
Nursing community reacts
News of the fraud scheme spread through the nursing community, including social media. “The recent report on falsified nursing school degrees is both heartbreaking and serves as an eye-opener,” tweeted Usha Menon, PhD, RN, FAAN, dean and health professor of the University of South Florida Health College of Nursing. “There was enough of a need that prompted these bad actors to develop a scheme that could’ve endangered dozens of lives.”
Jennifer Mensik Kennedy, PhD, MBA, RN, the new president of the American Nurses Association, also weighed in. “The accusation that personnel at once-accredited nursing schools allegedly participated in this scheme is simply deplorable. These unlawful and unethical acts disparage the reputation of actual nurses everywhere who have rightfully earned [their titles] through their education, hard work, dedication, and time.”
The false degrees and transcripts were issued by three once-accredited and now-shuttered nursing schools in South Florida: Palm Beach School of Nursing, Sacred Heart International Institute, and Sienna College.
The alleged co-conspirators reportedly made $114 million from the scheme, which dates back to 2016, according to several news reports. Each defendant faces up to 20 years in prison.
Most LPN programs charge $10,000 to $15,000 to complete a program, Robert Rosseter, a spokesperson for the American Association of Colleges of Nursing (AACN), told this news organization.
None were AACN members, and none were accredited by the Commission on Collegiate Nursing Education, which is AACN’s autonomous accrediting agency, Mr. Rosseter said. AACN membership is voluntary and is open to schools offering baccalaureate or higher degrees, he explained.
“What is disturbing about this investigation is that there are over 7,600 people around the country with fraudulent nursing credentials who are potentially in critical health care roles treating patients,” Chad Yarbrough, acting special agent in charge for the FBI in Miami, said in the federal justice department release.
‘Operation Nightingale’ based on tip
The federal action, dubbed “Operation Nightingale” after the nursing pioneer Florence Nightingale, began in 2019. It was based on a tip related to a case in Maryland, according to Nurse.org.
That case ensnared Palm Beach School of Nursing owner Johanah Napoleon, who reportedly was selling fake degrees for $6,000 to $18,000 each to two individuals in Maryland and Virginia. Ms. Napoleon was charged in 2021 and eventually pled guilty. The Florida Board of Nursing shut down the Palm Beach school in 2017 owing to its students’ low passing rate on the national licensing exam.
Two participants in the bigger scheme who had also worked with Ms. Napoleon – Geralda Adrien and Woosvelt Predestin – were indicted in 2021. Ms. Adrien owned private education companies for people who at aspired to be nurses, and Mr. Predestin was an employee. They were sentenced to 27 months in prison last year and helped the federal officials build the larger case.
The 25 individuals who were charged Jan. 25 operated in Delaware, New York, New Jersey, Texas, and Florida.
Schemes lured immigrants
In the scheme involving Siena College, some of the individuals acted as recruiters to direct nurses who were looking for employment to the school, where they allegedly would then pay for an RN or LPN/VN degree. The recipients of the false documents then used them to obtain jobs, including at a hospital in Georgia and a Veterans Affairs medical center in Maryland, according to one indictment. The president of Siena and her co-conspirators sold more than 2,000 fake diplomas, according to charging documents.
At the Palm Beach College of Nursing, individuals at various nursing prep and education programs allegedly helped others obtain fake degrees and transcripts, which were then used to pass RN and LPN/VN licensing exams in states that included Massachusetts, New Jersey, New York, and Ohio, according to the indictment.
Some individuals then secured employment with a nursing home in Ohio, a home health agency for pediatric patients in Massachusetts, and skilled nursing facilities in New York and New Jersey.
Prosecutors allege that the president of Sacred Heart International Institute and two other co-conspirators sold 588 fake diplomas.
The FBI said that some of the aspiring nurses who were talked into buying the degrees were LPNs who wanted to become RNs and that most of those lured into the scheme were from South Florida’s Haitian American immigrant community, Nurse.org reported.
A version of this article first appeared on Medscape.com.
The U.S. Department of Justice recently announced charges against 25 owners, operators, and employees of three Florida nursing schools in a fraud scheme in which they sold as many as 7,600 fake nursing degrees.
The purchasers in the diploma scheme paid $10,000 to $15,000 for degrees and transcripts and some 2,800 of the buyers passed the national nursing licensing exam to become registered nurses (RNs) and licensed practice nurses/vocational nurses (LPN/VNs) around the country, according to The New York Times.
Many of the degree recipients went on to work at hospitals, nursing homes, and Veterans Affairs medical centers, according to the U.S. Attorney’s Office for the Southern District of Florida.
Several national nursing organizations cooperated with the investigation, and the Delaware Division of Professional Regulation already annulled 26 licenses, according to the Delaware Nurses Association. Fake licenses were issued in five states, according to federal reports.
“We are deeply unsettled by this egregious act,” DNA President Stephanie McClellan, MSN, RN, CMSRN, said in the group’s press statement. “We want all Delaware nurses to be aware of this active issue and to speak up if there is a concern regarding capacity to practice safely by a colleague/peer,” she said.
The Oregon State Board of Nursing is also investigating at least a dozen nurses who may have paid for their degrees, according to a Portland CBS affiliate.
The National Council of State Boards of Nursing said in a statement that it had helped authorities identify and monitor the individuals who allegedly provided the false degrees.
Nursing community reacts
News of the fraud scheme spread through the nursing community, including social media. “The recent report on falsified nursing school degrees is both heartbreaking and serves as an eye-opener,” tweeted Usha Menon, PhD, RN, FAAN, dean and health professor of the University of South Florida Health College of Nursing. “There was enough of a need that prompted these bad actors to develop a scheme that could’ve endangered dozens of lives.”
Jennifer Mensik Kennedy, PhD, MBA, RN, the new president of the American Nurses Association, also weighed in. “The accusation that personnel at once-accredited nursing schools allegedly participated in this scheme is simply deplorable. These unlawful and unethical acts disparage the reputation of actual nurses everywhere who have rightfully earned [their titles] through their education, hard work, dedication, and time.”
The false degrees and transcripts were issued by three once-accredited and now-shuttered nursing schools in South Florida: Palm Beach School of Nursing, Sacred Heart International Institute, and Sienna College.
The alleged co-conspirators reportedly made $114 million from the scheme, which dates back to 2016, according to several news reports. Each defendant faces up to 20 years in prison.
Most LPN programs charge $10,000 to $15,000 to complete a program, Robert Rosseter, a spokesperson for the American Association of Colleges of Nursing (AACN), told this news organization.
None were AACN members, and none were accredited by the Commission on Collegiate Nursing Education, which is AACN’s autonomous accrediting agency, Mr. Rosseter said. AACN membership is voluntary and is open to schools offering baccalaureate or higher degrees, he explained.
“What is disturbing about this investigation is that there are over 7,600 people around the country with fraudulent nursing credentials who are potentially in critical health care roles treating patients,” Chad Yarbrough, acting special agent in charge for the FBI in Miami, said in the federal justice department release.
‘Operation Nightingale’ based on tip
The federal action, dubbed “Operation Nightingale” after the nursing pioneer Florence Nightingale, began in 2019. It was based on a tip related to a case in Maryland, according to Nurse.org.
That case ensnared Palm Beach School of Nursing owner Johanah Napoleon, who reportedly was selling fake degrees for $6,000 to $18,000 each to two individuals in Maryland and Virginia. Ms. Napoleon was charged in 2021 and eventually pled guilty. The Florida Board of Nursing shut down the Palm Beach school in 2017 owing to its students’ low passing rate on the national licensing exam.
Two participants in the bigger scheme who had also worked with Ms. Napoleon – Geralda Adrien and Woosvelt Predestin – were indicted in 2021. Ms. Adrien owned private education companies for people who at aspired to be nurses, and Mr. Predestin was an employee. They were sentenced to 27 months in prison last year and helped the federal officials build the larger case.
The 25 individuals who were charged Jan. 25 operated in Delaware, New York, New Jersey, Texas, and Florida.
Schemes lured immigrants
In the scheme involving Siena College, some of the individuals acted as recruiters to direct nurses who were looking for employment to the school, where they allegedly would then pay for an RN or LPN/VN degree. The recipients of the false documents then used them to obtain jobs, including at a hospital in Georgia and a Veterans Affairs medical center in Maryland, according to one indictment. The president of Siena and her co-conspirators sold more than 2,000 fake diplomas, according to charging documents.
At the Palm Beach College of Nursing, individuals at various nursing prep and education programs allegedly helped others obtain fake degrees and transcripts, which were then used to pass RN and LPN/VN licensing exams in states that included Massachusetts, New Jersey, New York, and Ohio, according to the indictment.
Some individuals then secured employment with a nursing home in Ohio, a home health agency for pediatric patients in Massachusetts, and skilled nursing facilities in New York and New Jersey.
Prosecutors allege that the president of Sacred Heart International Institute and two other co-conspirators sold 588 fake diplomas.
The FBI said that some of the aspiring nurses who were talked into buying the degrees were LPNs who wanted to become RNs and that most of those lured into the scheme were from South Florida’s Haitian American immigrant community, Nurse.org reported.
A version of this article first appeared on Medscape.com.
The U.S. Department of Justice recently announced charges against 25 owners, operators, and employees of three Florida nursing schools in a fraud scheme in which they sold as many as 7,600 fake nursing degrees.
The purchasers in the diploma scheme paid $10,000 to $15,000 for degrees and transcripts and some 2,800 of the buyers passed the national nursing licensing exam to become registered nurses (RNs) and licensed practice nurses/vocational nurses (LPN/VNs) around the country, according to The New York Times.
Many of the degree recipients went on to work at hospitals, nursing homes, and Veterans Affairs medical centers, according to the U.S. Attorney’s Office for the Southern District of Florida.
Several national nursing organizations cooperated with the investigation, and the Delaware Division of Professional Regulation already annulled 26 licenses, according to the Delaware Nurses Association. Fake licenses were issued in five states, according to federal reports.
“We are deeply unsettled by this egregious act,” DNA President Stephanie McClellan, MSN, RN, CMSRN, said in the group’s press statement. “We want all Delaware nurses to be aware of this active issue and to speak up if there is a concern regarding capacity to practice safely by a colleague/peer,” she said.
The Oregon State Board of Nursing is also investigating at least a dozen nurses who may have paid for their degrees, according to a Portland CBS affiliate.
The National Council of State Boards of Nursing said in a statement that it had helped authorities identify and monitor the individuals who allegedly provided the false degrees.
Nursing community reacts
News of the fraud scheme spread through the nursing community, including social media. “The recent report on falsified nursing school degrees is both heartbreaking and serves as an eye-opener,” tweeted Usha Menon, PhD, RN, FAAN, dean and health professor of the University of South Florida Health College of Nursing. “There was enough of a need that prompted these bad actors to develop a scheme that could’ve endangered dozens of lives.”
Jennifer Mensik Kennedy, PhD, MBA, RN, the new president of the American Nurses Association, also weighed in. “The accusation that personnel at once-accredited nursing schools allegedly participated in this scheme is simply deplorable. These unlawful and unethical acts disparage the reputation of actual nurses everywhere who have rightfully earned [their titles] through their education, hard work, dedication, and time.”
The false degrees and transcripts were issued by three once-accredited and now-shuttered nursing schools in South Florida: Palm Beach School of Nursing, Sacred Heart International Institute, and Sienna College.
The alleged co-conspirators reportedly made $114 million from the scheme, which dates back to 2016, according to several news reports. Each defendant faces up to 20 years in prison.
Most LPN programs charge $10,000 to $15,000 to complete a program, Robert Rosseter, a spokesperson for the American Association of Colleges of Nursing (AACN), told this news organization.
None were AACN members, and none were accredited by the Commission on Collegiate Nursing Education, which is AACN’s autonomous accrediting agency, Mr. Rosseter said. AACN membership is voluntary and is open to schools offering baccalaureate or higher degrees, he explained.
“What is disturbing about this investigation is that there are over 7,600 people around the country with fraudulent nursing credentials who are potentially in critical health care roles treating patients,” Chad Yarbrough, acting special agent in charge for the FBI in Miami, said in the federal justice department release.
‘Operation Nightingale’ based on tip
The federal action, dubbed “Operation Nightingale” after the nursing pioneer Florence Nightingale, began in 2019. It was based on a tip related to a case in Maryland, according to Nurse.org.
That case ensnared Palm Beach School of Nursing owner Johanah Napoleon, who reportedly was selling fake degrees for $6,000 to $18,000 each to two individuals in Maryland and Virginia. Ms. Napoleon was charged in 2021 and eventually pled guilty. The Florida Board of Nursing shut down the Palm Beach school in 2017 owing to its students’ low passing rate on the national licensing exam.
Two participants in the bigger scheme who had also worked with Ms. Napoleon – Geralda Adrien and Woosvelt Predestin – were indicted in 2021. Ms. Adrien owned private education companies for people who at aspired to be nurses, and Mr. Predestin was an employee. They were sentenced to 27 months in prison last year and helped the federal officials build the larger case.
The 25 individuals who were charged Jan. 25 operated in Delaware, New York, New Jersey, Texas, and Florida.
Schemes lured immigrants
In the scheme involving Siena College, some of the individuals acted as recruiters to direct nurses who were looking for employment to the school, where they allegedly would then pay for an RN or LPN/VN degree. The recipients of the false documents then used them to obtain jobs, including at a hospital in Georgia and a Veterans Affairs medical center in Maryland, according to one indictment. The president of Siena and her co-conspirators sold more than 2,000 fake diplomas, according to charging documents.
At the Palm Beach College of Nursing, individuals at various nursing prep and education programs allegedly helped others obtain fake degrees and transcripts, which were then used to pass RN and LPN/VN licensing exams in states that included Massachusetts, New Jersey, New York, and Ohio, according to the indictment.
Some individuals then secured employment with a nursing home in Ohio, a home health agency for pediatric patients in Massachusetts, and skilled nursing facilities in New York and New Jersey.
Prosecutors allege that the president of Sacred Heart International Institute and two other co-conspirators sold 588 fake diplomas.
The FBI said that some of the aspiring nurses who were talked into buying the degrees were LPNs who wanted to become RNs and that most of those lured into the scheme were from South Florida’s Haitian American immigrant community, Nurse.org reported.
A version of this article first appeared on Medscape.com.
Biden to end COVID emergencies in May
Doing so will have many effects, including the end of free vaccines and health services to fight the pandemic. The public health emergency has been renewed every 90 days since it was declared by the Trump administration in January 2020.
The declaration allowed major changes throughout the health care system to deal with the pandemic, including the free distribution of vaccines, testing, and treatments. In addition, telehealth services were expanded, and Medicaid and the Children’s Health Insurance Program were extended to millions more Americans.
Biden said the COVID-19 national emergency is set to expire March 1 while the declared public health emergency would currently expire on April 11. The president said both will be extended to end May 11.
There were nearly 300,000 newly reported COVID-19 cases in the United States for the week ending Jan. 25, according to CDC data, as well as more than 3,750 deaths.
A version of this article first appeared on WebMD.com.
Doing so will have many effects, including the end of free vaccines and health services to fight the pandemic. The public health emergency has been renewed every 90 days since it was declared by the Trump administration in January 2020.
The declaration allowed major changes throughout the health care system to deal with the pandemic, including the free distribution of vaccines, testing, and treatments. In addition, telehealth services were expanded, and Medicaid and the Children’s Health Insurance Program were extended to millions more Americans.
Biden said the COVID-19 national emergency is set to expire March 1 while the declared public health emergency would currently expire on April 11. The president said both will be extended to end May 11.
There were nearly 300,000 newly reported COVID-19 cases in the United States for the week ending Jan. 25, according to CDC data, as well as more than 3,750 deaths.
A version of this article first appeared on WebMD.com.
Doing so will have many effects, including the end of free vaccines and health services to fight the pandemic. The public health emergency has been renewed every 90 days since it was declared by the Trump administration in January 2020.
The declaration allowed major changes throughout the health care system to deal with the pandemic, including the free distribution of vaccines, testing, and treatments. In addition, telehealth services were expanded, and Medicaid and the Children’s Health Insurance Program were extended to millions more Americans.
Biden said the COVID-19 national emergency is set to expire March 1 while the declared public health emergency would currently expire on April 11. The president said both will be extended to end May 11.
There were nearly 300,000 newly reported COVID-19 cases in the United States for the week ending Jan. 25, according to CDC data, as well as more than 3,750 deaths.
A version of this article first appeared on WebMD.com.
Female doctors have higher infertility rates and riskier pregnancies: What can be done?
In 2021, Eugene Kim, MD, division director of pediatric surgery and vice chair in the department of surgery at Cedars-Sinai Medical Center, Los Angeles, gave his presidential address to the Association for Academic Surgery.
“Presidents tend to give a message of hope or inspiration; I probably took it in a different way,” he said.
Dr. Kim told the story of one of his clinical partners, Eveline Shue, who, after five rounds of in vitro fertilization (IVF), became pregnant with twins. A high-achiever in her field, Ms. Shue continued working the grueling hours required by her job throughout pregnancy until she noticed concerning symptoms – musculoskeletal issues, extreme swelling, and more. She and her group decided that she should step back from work in her third trimester. A few days later, Ms. Shue suffered a stroke. She was rushed to the hospital where her babies were delivered by emergency C-section. Ms. Shue underwent brain surgery but later recovered and is still practicing in Southern California.
“I remember being at her bedside thinking, ‘How could we have let this happen? How could we have prevented this?’ ”
Dr. Kim’s speech kicked off a firestorm of awareness about pregnancy complications among physicians. “I got scores of emails from women around the country, surgeons in particular, who felt like their issues had been seen. The conversation was long overdue,” he said.
Family planning issues, pregnancy complications, infertility, and pregnancy loss are common, pervasive, and often silent issues in medicine. In July 2021, Dr. Kim and a group of other researchers published a study in JAMA Surgery. It revealed staggering truths: When compared to non-surgeons, female surgeons were more likely to delay pregnancy, use assisted reproductive technology such as IVF, have non-elective C-sections, and suffer pregnancy loss. In the study, 42% of surgeons had experienced pregnancy loss – more than double the rate of the general population. Almost half had serious pregnancy complications.
Research has found that female physicians in general have a significantly greater incidence of miscarriage, infertility, and pregnancy complications than the general population. According to a 2016 survey in the Journal of Women’s Health, the infertility rate for physicians is nearly 1 in 4, about double the rate of the general public.
The barriers to starting a family
Physicians face significant professional barriers that impact family planning. Demanding jobs with exhausting and often unpredictable hours contribute to a culture that, traditionally, has been far from family friendly. As a result, many physicians start families later. “For a pediatric surgeon, you finish training at age 35 – minimum,” says Dr. Kim. “Simply being a surgeon makes you a high-risk pregnancy candidate just because of the career.”
In 2020, Ariela L. Marshall, MD, an associate professor of clinical medicine at the University of Pennsylvania’s Perelman school of medicine, co-authored a commentary article in Academic Medicine titled “Physician Fertility: A Call to Action” which was based on her own experiences with infertility. Dr. Marshall was 34 when she and her husband decided to start a family, and she says her infertility diagnosis “came as a shock.”
“I never stopped to think about the consequences of a career path where I’m not going to be established until my 30s,” Dr. Marshall says. “I never thought about how long hours, overnight shifts, or working all the time could impact my fertility.”
It would take four cycles of IVF egg retrieval to create embryos and one failed implantation before Dr. Marshall became pregnant with her son.
When it comes to the timing of pregnancy, medical culture also plays a role. “There’s a lot of messaging around when it’s appropriate to carry a baby – and it’s not until after training is done,” says Arghavan Salles, MD, PhD, a clinical associate professor and special advisor for DEI programs at Stanford (Calif.) University’s department of medicine.
There are always exceptions. Some institutions are more flexible than others about pregnancy during residency. But Dr. Salles notes that this attitude is “not universal,” partly because of the lack of a comprehensive approach to pregnancy or parenthood in the United States. “There’s no federal paid parental leave in this country,” reminds Dr. Salles. “That signals that we don’t value parenting.”
The trickle-down effect of this in medicine is more like a waterfall. Some physicians complain when other physicians are out on leave. There’s an additional burden of work when people take time away, and there are often no support structures in place for backup or fill-in care. Dr. Salles said doctors often tell her that they were responsible for finding coverage for any time off during pregnancy or after becoming a parent. A paper of hers published in JAMA Surgery found that, for physicians, a fear of burdening others was a major barrier to getting pregnant during residency in the first place.
The physical consequences
Although research supports the benefits of physical activity throughout pregnancy, a job such as surgery that requires being on your feet for long periods of time “is not the same as exercise,” explains Erika Lu Rangel, MD, a gastrointestinal surgeon at Brigham and Women’s Hospital, Boston, and Dr. Kim’s lead author on the JAMA Surgery article.
Surgeons operating for more than 12 hours a week are at higher risk for pregnancy complications, the study found. Dr. Rangel also cites data suggesting that night shifts or swing shifts (the hours between day and night) put women at higher risk for pregnancy complications.
Equally alarming: Medical trainees appear to have “almost as high a rate of pregnancy complications as surgeons who have already completed their training,” said Dr. Rangel. It is a concerning finding since, as a younger cohort, they should have lower complication rates based on their age. But doctors in training may be on their feet even more than surgeons during long shifts.
Like Dr. Salles, Dr. Rangel sees these issues as part of a pervasive culture of “presenteeism” in medicine, and she points out that many surgeons don’t even take time off to grieve pregnancy loss or physically recover from it. “We work even when we’re sick and even when it’s not good for our health,” she said. “I think that’s an unhealthy behavior that we cultivate from the time that we’re trainees, and we carry it on through when we’re in practice.”
Penn Medicine’s Dr. Marshall remembers that her own maternity leave was “not an easy process to navigate.” From her hospital room on a magnesium drip for preeclampsia, she still attended Zoom meetings with her colleagues. “Nobody says, ‘Oh, you have to do this,’ ” Dr. Marshall explains, “but you wind up feeling guilty if you’re not there at all moments for everyone. That’s also something that needs to change.”
Dr. Rangel was pregnant with her oldest son as a fourth-year surgery resident. The day she gave birth to him she remembers waking up with a flu-like illness and a fever. She went to work anyway, because “you don’t call in sick as a resident.” She was barely able to complete her rounds and then had to lie down between cases. A co-resident found her and took her to labor and delivery. She had gone into premature labor at 37 weeks, and her son went into the NICU with complications.
“I remember feeling this enormous guilt,” says Dr. Rangel. “I’d been a mom for just a few minutes, and I felt like I had already failed him because I had prioritized what the residency thought of me above what I knew was necessary for his health.”
Hope for the future
Disturbed by the status quo, many physicians are pushing for change. “I think there’s a really important and positive conversation going on in the medical community right now about ways that we need to support new parent physicians,” said Dr. Rangel.
Parental leave is a key part of that support. Last year, The American Board of Medical Specialties enacted a mandate that all specialty boards 2 years or more in duration must provide at least 6 weeks of parental and caregiver leave. In 2023, the Accreditation Council for Graduate Medical Education (ACGME) required that all training programs match that policy. “This sends a message to policymakers and leaders in American medicine that this is a priority,” said Dr. Rangel.
In January 2022, a group from the University of Michigan also published an article in the Annals of Surgery called “Safe and Supported Pregnancy: A Call to Action for Surgery Chairs and Program Directors”. The essay urged leading groups such as the ACGME and the American Board of Surgery to “directly address the health and safety of pregnant trainees” and specifically, to “allow for further flexibility during training for pregnancy and peripartum periods,” calling these “fundamental necessities for cultural progress.”
Others have recommended allowing pregnant trainees more flexibility in their schedules or front-loading certain parts of the training that may be more difficult as a pregnancy progresses. Insurance coverage for fertility preservation and reproductive endocrinology services, and support for reentry (including lactation and childcare) are also issues that must be addressed, says Dr. Salles.
A new paper of Dr. Rangel’s, published in JAMA Surgery, suggests that things like mentorship for residents from faculty can also be important pieces of the puzzle.
Education about reproductive health must start earlier, too – as early as medical school. Research suggests only 8% of physicians receive education on the risks of delaying pregnancy. Those who do are significantly less likely to experience pregnancy loss or seek infertility treatment.
Dr. Salles recalls sitting in a classroom learning about advanced maternal age at a time when age 35 seemed unimaginably distant. “It was never taught – at least to my recollection – in a way that was like, ‘this could be your future,’ ” Dr. Salles says.” It was more like this abstract patient who might have advanced maternal age and what the consequences would be. Maybe some of my colleagues put two and two together, but I definitely didn’t.”
Dr. Marshall is the curriculum chair for the IGNITEMed Initiative, which aims to educate medical students about issues not discussed in traditional medical school curricula. Dr. Marshall and her colleague Julia Files, MD, talk with IGNITEMed students about reproductive life planning.
“Raising awareness is a very big thing. That’s not just true for medical students but for professionals at every level of medicine,” Dr. Marshall said. “Residency and fellowship training program directors, department chairs, and hospital CEOs all need to understand that these issues are very common in the people they oversee – and that they are medical issues, like any other medical issue, where people need time off and support.”
A version of this article first appeared on Medscape.com.
In 2021, Eugene Kim, MD, division director of pediatric surgery and vice chair in the department of surgery at Cedars-Sinai Medical Center, Los Angeles, gave his presidential address to the Association for Academic Surgery.
“Presidents tend to give a message of hope or inspiration; I probably took it in a different way,” he said.
Dr. Kim told the story of one of his clinical partners, Eveline Shue, who, after five rounds of in vitro fertilization (IVF), became pregnant with twins. A high-achiever in her field, Ms. Shue continued working the grueling hours required by her job throughout pregnancy until she noticed concerning symptoms – musculoskeletal issues, extreme swelling, and more. She and her group decided that she should step back from work in her third trimester. A few days later, Ms. Shue suffered a stroke. She was rushed to the hospital where her babies were delivered by emergency C-section. Ms. Shue underwent brain surgery but later recovered and is still practicing in Southern California.
“I remember being at her bedside thinking, ‘How could we have let this happen? How could we have prevented this?’ ”
Dr. Kim’s speech kicked off a firestorm of awareness about pregnancy complications among physicians. “I got scores of emails from women around the country, surgeons in particular, who felt like their issues had been seen. The conversation was long overdue,” he said.
Family planning issues, pregnancy complications, infertility, and pregnancy loss are common, pervasive, and often silent issues in medicine. In July 2021, Dr. Kim and a group of other researchers published a study in JAMA Surgery. It revealed staggering truths: When compared to non-surgeons, female surgeons were more likely to delay pregnancy, use assisted reproductive technology such as IVF, have non-elective C-sections, and suffer pregnancy loss. In the study, 42% of surgeons had experienced pregnancy loss – more than double the rate of the general population. Almost half had serious pregnancy complications.
Research has found that female physicians in general have a significantly greater incidence of miscarriage, infertility, and pregnancy complications than the general population. According to a 2016 survey in the Journal of Women’s Health, the infertility rate for physicians is nearly 1 in 4, about double the rate of the general public.
The barriers to starting a family
Physicians face significant professional barriers that impact family planning. Demanding jobs with exhausting and often unpredictable hours contribute to a culture that, traditionally, has been far from family friendly. As a result, many physicians start families later. “For a pediatric surgeon, you finish training at age 35 – minimum,” says Dr. Kim. “Simply being a surgeon makes you a high-risk pregnancy candidate just because of the career.”
In 2020, Ariela L. Marshall, MD, an associate professor of clinical medicine at the University of Pennsylvania’s Perelman school of medicine, co-authored a commentary article in Academic Medicine titled “Physician Fertility: A Call to Action” which was based on her own experiences with infertility. Dr. Marshall was 34 when she and her husband decided to start a family, and she says her infertility diagnosis “came as a shock.”
“I never stopped to think about the consequences of a career path where I’m not going to be established until my 30s,” Dr. Marshall says. “I never thought about how long hours, overnight shifts, or working all the time could impact my fertility.”
It would take four cycles of IVF egg retrieval to create embryos and one failed implantation before Dr. Marshall became pregnant with her son.
When it comes to the timing of pregnancy, medical culture also plays a role. “There’s a lot of messaging around when it’s appropriate to carry a baby – and it’s not until after training is done,” says Arghavan Salles, MD, PhD, a clinical associate professor and special advisor for DEI programs at Stanford (Calif.) University’s department of medicine.
There are always exceptions. Some institutions are more flexible than others about pregnancy during residency. But Dr. Salles notes that this attitude is “not universal,” partly because of the lack of a comprehensive approach to pregnancy or parenthood in the United States. “There’s no federal paid parental leave in this country,” reminds Dr. Salles. “That signals that we don’t value parenting.”
The trickle-down effect of this in medicine is more like a waterfall. Some physicians complain when other physicians are out on leave. There’s an additional burden of work when people take time away, and there are often no support structures in place for backup or fill-in care. Dr. Salles said doctors often tell her that they were responsible for finding coverage for any time off during pregnancy or after becoming a parent. A paper of hers published in JAMA Surgery found that, for physicians, a fear of burdening others was a major barrier to getting pregnant during residency in the first place.
The physical consequences
Although research supports the benefits of physical activity throughout pregnancy, a job such as surgery that requires being on your feet for long periods of time “is not the same as exercise,” explains Erika Lu Rangel, MD, a gastrointestinal surgeon at Brigham and Women’s Hospital, Boston, and Dr. Kim’s lead author on the JAMA Surgery article.
Surgeons operating for more than 12 hours a week are at higher risk for pregnancy complications, the study found. Dr. Rangel also cites data suggesting that night shifts or swing shifts (the hours between day and night) put women at higher risk for pregnancy complications.
Equally alarming: Medical trainees appear to have “almost as high a rate of pregnancy complications as surgeons who have already completed their training,” said Dr. Rangel. It is a concerning finding since, as a younger cohort, they should have lower complication rates based on their age. But doctors in training may be on their feet even more than surgeons during long shifts.
Like Dr. Salles, Dr. Rangel sees these issues as part of a pervasive culture of “presenteeism” in medicine, and she points out that many surgeons don’t even take time off to grieve pregnancy loss or physically recover from it. “We work even when we’re sick and even when it’s not good for our health,” she said. “I think that’s an unhealthy behavior that we cultivate from the time that we’re trainees, and we carry it on through when we’re in practice.”
Penn Medicine’s Dr. Marshall remembers that her own maternity leave was “not an easy process to navigate.” From her hospital room on a magnesium drip for preeclampsia, she still attended Zoom meetings with her colleagues. “Nobody says, ‘Oh, you have to do this,’ ” Dr. Marshall explains, “but you wind up feeling guilty if you’re not there at all moments for everyone. That’s also something that needs to change.”
Dr. Rangel was pregnant with her oldest son as a fourth-year surgery resident. The day she gave birth to him she remembers waking up with a flu-like illness and a fever. She went to work anyway, because “you don’t call in sick as a resident.” She was barely able to complete her rounds and then had to lie down between cases. A co-resident found her and took her to labor and delivery. She had gone into premature labor at 37 weeks, and her son went into the NICU with complications.
“I remember feeling this enormous guilt,” says Dr. Rangel. “I’d been a mom for just a few minutes, and I felt like I had already failed him because I had prioritized what the residency thought of me above what I knew was necessary for his health.”
Hope for the future
Disturbed by the status quo, many physicians are pushing for change. “I think there’s a really important and positive conversation going on in the medical community right now about ways that we need to support new parent physicians,” said Dr. Rangel.
Parental leave is a key part of that support. Last year, The American Board of Medical Specialties enacted a mandate that all specialty boards 2 years or more in duration must provide at least 6 weeks of parental and caregiver leave. In 2023, the Accreditation Council for Graduate Medical Education (ACGME) required that all training programs match that policy. “This sends a message to policymakers and leaders in American medicine that this is a priority,” said Dr. Rangel.
In January 2022, a group from the University of Michigan also published an article in the Annals of Surgery called “Safe and Supported Pregnancy: A Call to Action for Surgery Chairs and Program Directors”. The essay urged leading groups such as the ACGME and the American Board of Surgery to “directly address the health and safety of pregnant trainees” and specifically, to “allow for further flexibility during training for pregnancy and peripartum periods,” calling these “fundamental necessities for cultural progress.”
Others have recommended allowing pregnant trainees more flexibility in their schedules or front-loading certain parts of the training that may be more difficult as a pregnancy progresses. Insurance coverage for fertility preservation and reproductive endocrinology services, and support for reentry (including lactation and childcare) are also issues that must be addressed, says Dr. Salles.
A new paper of Dr. Rangel’s, published in JAMA Surgery, suggests that things like mentorship for residents from faculty can also be important pieces of the puzzle.
Education about reproductive health must start earlier, too – as early as medical school. Research suggests only 8% of physicians receive education on the risks of delaying pregnancy. Those who do are significantly less likely to experience pregnancy loss or seek infertility treatment.
Dr. Salles recalls sitting in a classroom learning about advanced maternal age at a time when age 35 seemed unimaginably distant. “It was never taught – at least to my recollection – in a way that was like, ‘this could be your future,’ ” Dr. Salles says.” It was more like this abstract patient who might have advanced maternal age and what the consequences would be. Maybe some of my colleagues put two and two together, but I definitely didn’t.”
Dr. Marshall is the curriculum chair for the IGNITEMed Initiative, which aims to educate medical students about issues not discussed in traditional medical school curricula. Dr. Marshall and her colleague Julia Files, MD, talk with IGNITEMed students about reproductive life planning.
“Raising awareness is a very big thing. That’s not just true for medical students but for professionals at every level of medicine,” Dr. Marshall said. “Residency and fellowship training program directors, department chairs, and hospital CEOs all need to understand that these issues are very common in the people they oversee – and that they are medical issues, like any other medical issue, where people need time off and support.”
A version of this article first appeared on Medscape.com.
In 2021, Eugene Kim, MD, division director of pediatric surgery and vice chair in the department of surgery at Cedars-Sinai Medical Center, Los Angeles, gave his presidential address to the Association for Academic Surgery.
“Presidents tend to give a message of hope or inspiration; I probably took it in a different way,” he said.
Dr. Kim told the story of one of his clinical partners, Eveline Shue, who, after five rounds of in vitro fertilization (IVF), became pregnant with twins. A high-achiever in her field, Ms. Shue continued working the grueling hours required by her job throughout pregnancy until she noticed concerning symptoms – musculoskeletal issues, extreme swelling, and more. She and her group decided that she should step back from work in her third trimester. A few days later, Ms. Shue suffered a stroke. She was rushed to the hospital where her babies were delivered by emergency C-section. Ms. Shue underwent brain surgery but later recovered and is still practicing in Southern California.
“I remember being at her bedside thinking, ‘How could we have let this happen? How could we have prevented this?’ ”
Dr. Kim’s speech kicked off a firestorm of awareness about pregnancy complications among physicians. “I got scores of emails from women around the country, surgeons in particular, who felt like their issues had been seen. The conversation was long overdue,” he said.
Family planning issues, pregnancy complications, infertility, and pregnancy loss are common, pervasive, and often silent issues in medicine. In July 2021, Dr. Kim and a group of other researchers published a study in JAMA Surgery. It revealed staggering truths: When compared to non-surgeons, female surgeons were more likely to delay pregnancy, use assisted reproductive technology such as IVF, have non-elective C-sections, and suffer pregnancy loss. In the study, 42% of surgeons had experienced pregnancy loss – more than double the rate of the general population. Almost half had serious pregnancy complications.
Research has found that female physicians in general have a significantly greater incidence of miscarriage, infertility, and pregnancy complications than the general population. According to a 2016 survey in the Journal of Women’s Health, the infertility rate for physicians is nearly 1 in 4, about double the rate of the general public.
The barriers to starting a family
Physicians face significant professional barriers that impact family planning. Demanding jobs with exhausting and often unpredictable hours contribute to a culture that, traditionally, has been far from family friendly. As a result, many physicians start families later. “For a pediatric surgeon, you finish training at age 35 – minimum,” says Dr. Kim. “Simply being a surgeon makes you a high-risk pregnancy candidate just because of the career.”
In 2020, Ariela L. Marshall, MD, an associate professor of clinical medicine at the University of Pennsylvania’s Perelman school of medicine, co-authored a commentary article in Academic Medicine titled “Physician Fertility: A Call to Action” which was based on her own experiences with infertility. Dr. Marshall was 34 when she and her husband decided to start a family, and she says her infertility diagnosis “came as a shock.”
“I never stopped to think about the consequences of a career path where I’m not going to be established until my 30s,” Dr. Marshall says. “I never thought about how long hours, overnight shifts, or working all the time could impact my fertility.”
It would take four cycles of IVF egg retrieval to create embryos and one failed implantation before Dr. Marshall became pregnant with her son.
When it comes to the timing of pregnancy, medical culture also plays a role. “There’s a lot of messaging around when it’s appropriate to carry a baby – and it’s not until after training is done,” says Arghavan Salles, MD, PhD, a clinical associate professor and special advisor for DEI programs at Stanford (Calif.) University’s department of medicine.
There are always exceptions. Some institutions are more flexible than others about pregnancy during residency. But Dr. Salles notes that this attitude is “not universal,” partly because of the lack of a comprehensive approach to pregnancy or parenthood in the United States. “There’s no federal paid parental leave in this country,” reminds Dr. Salles. “That signals that we don’t value parenting.”
The trickle-down effect of this in medicine is more like a waterfall. Some physicians complain when other physicians are out on leave. There’s an additional burden of work when people take time away, and there are often no support structures in place for backup or fill-in care. Dr. Salles said doctors often tell her that they were responsible for finding coverage for any time off during pregnancy or after becoming a parent. A paper of hers published in JAMA Surgery found that, for physicians, a fear of burdening others was a major barrier to getting pregnant during residency in the first place.
The physical consequences
Although research supports the benefits of physical activity throughout pregnancy, a job such as surgery that requires being on your feet for long periods of time “is not the same as exercise,” explains Erika Lu Rangel, MD, a gastrointestinal surgeon at Brigham and Women’s Hospital, Boston, and Dr. Kim’s lead author on the JAMA Surgery article.
Surgeons operating for more than 12 hours a week are at higher risk for pregnancy complications, the study found. Dr. Rangel also cites data suggesting that night shifts or swing shifts (the hours between day and night) put women at higher risk for pregnancy complications.
Equally alarming: Medical trainees appear to have “almost as high a rate of pregnancy complications as surgeons who have already completed their training,” said Dr. Rangel. It is a concerning finding since, as a younger cohort, they should have lower complication rates based on their age. But doctors in training may be on their feet even more than surgeons during long shifts.
Like Dr. Salles, Dr. Rangel sees these issues as part of a pervasive culture of “presenteeism” in medicine, and she points out that many surgeons don’t even take time off to grieve pregnancy loss or physically recover from it. “We work even when we’re sick and even when it’s not good for our health,” she said. “I think that’s an unhealthy behavior that we cultivate from the time that we’re trainees, and we carry it on through when we’re in practice.”
Penn Medicine’s Dr. Marshall remembers that her own maternity leave was “not an easy process to navigate.” From her hospital room on a magnesium drip for preeclampsia, she still attended Zoom meetings with her colleagues. “Nobody says, ‘Oh, you have to do this,’ ” Dr. Marshall explains, “but you wind up feeling guilty if you’re not there at all moments for everyone. That’s also something that needs to change.”
Dr. Rangel was pregnant with her oldest son as a fourth-year surgery resident. The day she gave birth to him she remembers waking up with a flu-like illness and a fever. She went to work anyway, because “you don’t call in sick as a resident.” She was barely able to complete her rounds and then had to lie down between cases. A co-resident found her and took her to labor and delivery. She had gone into premature labor at 37 weeks, and her son went into the NICU with complications.
“I remember feeling this enormous guilt,” says Dr. Rangel. “I’d been a mom for just a few minutes, and I felt like I had already failed him because I had prioritized what the residency thought of me above what I knew was necessary for his health.”
Hope for the future
Disturbed by the status quo, many physicians are pushing for change. “I think there’s a really important and positive conversation going on in the medical community right now about ways that we need to support new parent physicians,” said Dr. Rangel.
Parental leave is a key part of that support. Last year, The American Board of Medical Specialties enacted a mandate that all specialty boards 2 years or more in duration must provide at least 6 weeks of parental and caregiver leave. In 2023, the Accreditation Council for Graduate Medical Education (ACGME) required that all training programs match that policy. “This sends a message to policymakers and leaders in American medicine that this is a priority,” said Dr. Rangel.
In January 2022, a group from the University of Michigan also published an article in the Annals of Surgery called “Safe and Supported Pregnancy: A Call to Action for Surgery Chairs and Program Directors”. The essay urged leading groups such as the ACGME and the American Board of Surgery to “directly address the health and safety of pregnant trainees” and specifically, to “allow for further flexibility during training for pregnancy and peripartum periods,” calling these “fundamental necessities for cultural progress.”
Others have recommended allowing pregnant trainees more flexibility in their schedules or front-loading certain parts of the training that may be more difficult as a pregnancy progresses. Insurance coverage for fertility preservation and reproductive endocrinology services, and support for reentry (including lactation and childcare) are also issues that must be addressed, says Dr. Salles.
A new paper of Dr. Rangel’s, published in JAMA Surgery, suggests that things like mentorship for residents from faculty can also be important pieces of the puzzle.
Education about reproductive health must start earlier, too – as early as medical school. Research suggests only 8% of physicians receive education on the risks of delaying pregnancy. Those who do are significantly less likely to experience pregnancy loss or seek infertility treatment.
Dr. Salles recalls sitting in a classroom learning about advanced maternal age at a time when age 35 seemed unimaginably distant. “It was never taught – at least to my recollection – in a way that was like, ‘this could be your future,’ ” Dr. Salles says.” It was more like this abstract patient who might have advanced maternal age and what the consequences would be. Maybe some of my colleagues put two and two together, but I definitely didn’t.”
Dr. Marshall is the curriculum chair for the IGNITEMed Initiative, which aims to educate medical students about issues not discussed in traditional medical school curricula. Dr. Marshall and her colleague Julia Files, MD, talk with IGNITEMed students about reproductive life planning.
“Raising awareness is a very big thing. That’s not just true for medical students but for professionals at every level of medicine,” Dr. Marshall said. “Residency and fellowship training program directors, department chairs, and hospital CEOs all need to understand that these issues are very common in the people they oversee – and that they are medical issues, like any other medical issue, where people need time off and support.”
A version of this article first appeared on Medscape.com.
Long COVID affecting more than one-third of college students, faculty
With a median age of 23 years, the study is unique for evaluating mostly healthy, young adults and for its rare look at long COVID in a university community.
The more symptoms during a bout with COVID, the greater the risk for long COVID, the researchers found. That lines up with previous studies. Also, the more vaccinations and booster shots against SARS-CoV-2, the virus that causes COVID, the lower the long COVID risk.
Women were more likely than men to be affected. Current or prior smoking, seeking medical care for COVID, and receiving antibody treatment also were linked to higher chances for developing long COVID.
Lead author Megan Landry, DrPH, MPH, and colleagues were already assessing students, staff, and faculty at George Washington University, Washington, who tested positive for COVID. Then they started seeing symptoms that lasted 28 days or more after their 10-day isolation period.
“We were starting to recognize that individuals ... were still having symptoms longer than the typical isolation period,” said Dr. Landry. So they developed a questionnaire to figure out the how long these symptoms last and how many people are affected by them.
The list of potential symptoms was long and included trouble thinking, fatigue, loss of smell or taste, shortness of breath, and more.
The study was published online in Emerging Infectious Diseases. Results are based on records and responses from 1,388 students, faculty, and staff from July 2021 to March 2022.
People had a median of four long COVID symptoms, about 63% were women, and 56% were non-Hispanic White. About three-quarters were students and the remainder were faculty and staff.
The finding that 36% of people with a history of COVID reported long COVID symptoms did not surprise Dr. Landry.
“Based on the literature that’s currently out there, it ranges from a 10% to an 80% prevalence of long COVID,” she said. “We kind of figured that we would fall somewhere in there.”
In contrast, that figure seemed high to Eric Topol, MD.
“That’s really high,” said Dr. Topol, founder and director of the Scripps Research Translational Institute in La Jolla, Calif. He added most studies estimate that about 10% of people with a history of acute infection develop long COVID.
Even at 10%, which could be an underestimate, that’s a lot of affected people globally.
“At least 65 million individuals around the world have long COVID, based on a conservative estimated incidence of 10% of infected people and more than 651 million documented COVID-19 cases worldwide; the number is likely much higher due to many undocumented cases,” Dr. Topol and colleagues wrote in a long COVID review article published in Nature Reviews Microbiology.
About 30% of study participants were fully vaccinated with an initial vaccine series, 42% had received a booster dose, and 29% were not fully vaccinated at the time of their first positive test for COVID. Those who were not fully vaccinated were significantly more likely to report symptoms of long COVID.
“I know a lot of people wish they could put COVID on the back burner or brush it under the rug, but COVID is still a real thing. We need to continue supporting vaccines and boosters and make sure people are up to date. Not only for COVID, but for flu as well,” Dr. Topol said
Research continues
“Long COVID is still evolving and we continue to learn more about it every day,” Landry said. “It’s just so new and there are still a lot of unknowns. That’s why it’s important to get this information out.”
People with long COVID often have a hard time with occupational, educational, social, or personal activities, compared with before COVID, with effects that can last for more than 6 months, the authors noted.
“I think across the board, universities in general need to consider the possibility of folks on their campuses are having symptoms of long COVID,” Dr. Landry said.
Moving forward, Dr. Landry and colleagues would like to continue investigating long COVID. For example, in the current study, they did not ask about severity of symptoms or how the symptoms affected daily functioning.
“I would like to continue this and dive deeper into how disruptive their symptoms of long COVID are to their everyday studying, teaching, or their activities to keeping a university running,” Dr. Landry said.
A version of this article originally appeared on WebMD.com.
With a median age of 23 years, the study is unique for evaluating mostly healthy, young adults and for its rare look at long COVID in a university community.
The more symptoms during a bout with COVID, the greater the risk for long COVID, the researchers found. That lines up with previous studies. Also, the more vaccinations and booster shots against SARS-CoV-2, the virus that causes COVID, the lower the long COVID risk.
Women were more likely than men to be affected. Current or prior smoking, seeking medical care for COVID, and receiving antibody treatment also were linked to higher chances for developing long COVID.
Lead author Megan Landry, DrPH, MPH, and colleagues were already assessing students, staff, and faculty at George Washington University, Washington, who tested positive for COVID. Then they started seeing symptoms that lasted 28 days or more after their 10-day isolation period.
“We were starting to recognize that individuals ... were still having symptoms longer than the typical isolation period,” said Dr. Landry. So they developed a questionnaire to figure out the how long these symptoms last and how many people are affected by them.
The list of potential symptoms was long and included trouble thinking, fatigue, loss of smell or taste, shortness of breath, and more.
The study was published online in Emerging Infectious Diseases. Results are based on records and responses from 1,388 students, faculty, and staff from July 2021 to March 2022.
People had a median of four long COVID symptoms, about 63% were women, and 56% were non-Hispanic White. About three-quarters were students and the remainder were faculty and staff.
The finding that 36% of people with a history of COVID reported long COVID symptoms did not surprise Dr. Landry.
“Based on the literature that’s currently out there, it ranges from a 10% to an 80% prevalence of long COVID,” she said. “We kind of figured that we would fall somewhere in there.”
In contrast, that figure seemed high to Eric Topol, MD.
“That’s really high,” said Dr. Topol, founder and director of the Scripps Research Translational Institute in La Jolla, Calif. He added most studies estimate that about 10% of people with a history of acute infection develop long COVID.
Even at 10%, which could be an underestimate, that’s a lot of affected people globally.
“At least 65 million individuals around the world have long COVID, based on a conservative estimated incidence of 10% of infected people and more than 651 million documented COVID-19 cases worldwide; the number is likely much higher due to many undocumented cases,” Dr. Topol and colleagues wrote in a long COVID review article published in Nature Reviews Microbiology.
About 30% of study participants were fully vaccinated with an initial vaccine series, 42% had received a booster dose, and 29% were not fully vaccinated at the time of their first positive test for COVID. Those who were not fully vaccinated were significantly more likely to report symptoms of long COVID.
“I know a lot of people wish they could put COVID on the back burner or brush it under the rug, but COVID is still a real thing. We need to continue supporting vaccines and boosters and make sure people are up to date. Not only for COVID, but for flu as well,” Dr. Topol said
Research continues
“Long COVID is still evolving and we continue to learn more about it every day,” Landry said. “It’s just so new and there are still a lot of unknowns. That’s why it’s important to get this information out.”
People with long COVID often have a hard time with occupational, educational, social, or personal activities, compared with before COVID, with effects that can last for more than 6 months, the authors noted.
“I think across the board, universities in general need to consider the possibility of folks on their campuses are having symptoms of long COVID,” Dr. Landry said.
Moving forward, Dr. Landry and colleagues would like to continue investigating long COVID. For example, in the current study, they did not ask about severity of symptoms or how the symptoms affected daily functioning.
“I would like to continue this and dive deeper into how disruptive their symptoms of long COVID are to their everyday studying, teaching, or their activities to keeping a university running,” Dr. Landry said.
A version of this article originally appeared on WebMD.com.
With a median age of 23 years, the study is unique for evaluating mostly healthy, young adults and for its rare look at long COVID in a university community.
The more symptoms during a bout with COVID, the greater the risk for long COVID, the researchers found. That lines up with previous studies. Also, the more vaccinations and booster shots against SARS-CoV-2, the virus that causes COVID, the lower the long COVID risk.
Women were more likely than men to be affected. Current or prior smoking, seeking medical care for COVID, and receiving antibody treatment also were linked to higher chances for developing long COVID.
Lead author Megan Landry, DrPH, MPH, and colleagues were already assessing students, staff, and faculty at George Washington University, Washington, who tested positive for COVID. Then they started seeing symptoms that lasted 28 days or more after their 10-day isolation period.
“We were starting to recognize that individuals ... were still having symptoms longer than the typical isolation period,” said Dr. Landry. So they developed a questionnaire to figure out the how long these symptoms last and how many people are affected by them.
The list of potential symptoms was long and included trouble thinking, fatigue, loss of smell or taste, shortness of breath, and more.
The study was published online in Emerging Infectious Diseases. Results are based on records and responses from 1,388 students, faculty, and staff from July 2021 to March 2022.
People had a median of four long COVID symptoms, about 63% were women, and 56% were non-Hispanic White. About three-quarters were students and the remainder were faculty and staff.
The finding that 36% of people with a history of COVID reported long COVID symptoms did not surprise Dr. Landry.
“Based on the literature that’s currently out there, it ranges from a 10% to an 80% prevalence of long COVID,” she said. “We kind of figured that we would fall somewhere in there.”
In contrast, that figure seemed high to Eric Topol, MD.
“That’s really high,” said Dr. Topol, founder and director of the Scripps Research Translational Institute in La Jolla, Calif. He added most studies estimate that about 10% of people with a history of acute infection develop long COVID.
Even at 10%, which could be an underestimate, that’s a lot of affected people globally.
“At least 65 million individuals around the world have long COVID, based on a conservative estimated incidence of 10% of infected people and more than 651 million documented COVID-19 cases worldwide; the number is likely much higher due to many undocumented cases,” Dr. Topol and colleagues wrote in a long COVID review article published in Nature Reviews Microbiology.
About 30% of study participants were fully vaccinated with an initial vaccine series, 42% had received a booster dose, and 29% were not fully vaccinated at the time of their first positive test for COVID. Those who were not fully vaccinated were significantly more likely to report symptoms of long COVID.
“I know a lot of people wish they could put COVID on the back burner or brush it under the rug, but COVID is still a real thing. We need to continue supporting vaccines and boosters and make sure people are up to date. Not only for COVID, but for flu as well,” Dr. Topol said
Research continues
“Long COVID is still evolving and we continue to learn more about it every day,” Landry said. “It’s just so new and there are still a lot of unknowns. That’s why it’s important to get this information out.”
People with long COVID often have a hard time with occupational, educational, social, or personal activities, compared with before COVID, with effects that can last for more than 6 months, the authors noted.
“I think across the board, universities in general need to consider the possibility of folks on their campuses are having symptoms of long COVID,” Dr. Landry said.
Moving forward, Dr. Landry and colleagues would like to continue investigating long COVID. For example, in the current study, they did not ask about severity of symptoms or how the symptoms affected daily functioning.
“I would like to continue this and dive deeper into how disruptive their symptoms of long COVID are to their everyday studying, teaching, or their activities to keeping a university running,” Dr. Landry said.
A version of this article originally appeared on WebMD.com.
FROM EMERGING INFECTIOUS DISEASES