User login
Could GLP-1 receptor agonists ease knee osteoarthritis pain, slow progression?
Could glucagon-like peptide-1 receptor agonists, such as liraglutide and semaglutide, also be potential disease-modifying treatments for knee osteoarthritis (KOA)?
Weight loss is recommended for patients with KOA, and GLP-1 receptor agonists are approved for weight loss. New early research suggests these drugs might have a disease-modifying effect for KOA.
Three recently published studies investigated this:
- The LOSEIT phase 4, randomized controlled trial of liraglutide vs. placebo in patients with obesity/overweight and KOA.
- A large observational study out of China in patients with KOA and type 2 diabetes.
- A preclinical trial of liraglutide in mouse models of KOA.
The preclinical trial and the observational study report promising results, and the lack of KOA pain relief in patients in the phase 4 trial may be explained by the trial design. Three other trials are in the works.
This news organization invited two researchers and two outside experts to discuss these studies and potential future treatment of KOA with GLP-1 receptor agonists.
The big picture, as seen by two experts
The GLP-1 receptor agonists liraglutide (Victoza) and semaglutide (Ozempic) are approved for type 2 diabetes, and, in higher doses, liraglutide (Saxenda) and semaglutide (Wegovy) are approved for weight loss in patients with obesity (or overweight with comorbidities), and given as weekly injections.

Victoza and Saxenda are expected to come off patent in December 2023, and in 2026, respectively.
Lauren King, MD, PhD, a rheumatologist and clinician scientist who was not involved with the recent investigational studies of GLP-1 receptor agonists for KOA, noted that obesity is the most important, guideline-recommended, modifiable risk factor for KOA.
“In people with overweight and obesity, losing weight can improve knee osteoarthritis symptoms, and some evidence supports that it may also slow joint structural changes,” Dr. King, of the department of medicine at the University of Toronto, said in an interview.
Large trials of GLP-1 receptor agonists in people with overweight and obesity, such as the STEP trials of semaglutide, she noted, “provide evidence that these medications are safe and effective, facilitating clinically relevant and sustained weight loss.”
Further research is needed, she said, to better understand disease-modifying effects of GLP-1 receptor agonists in patients with KOA.
Similarly, W. Timothy Garvey, MD, professor in the department of nutrition sciences at the University of Alabama at Birmingham and director of the UAB Diabetes Research Center, who was not involved with this research, noted that weight loss improves KOA symptoms.
Dr. Garvey was lead investigator in the STEP 5 trial of semaglutide and lead author of the American Association of Clinical Endocrinologists 2016 Obesity Management guidelines.
“The question is whether these GLP-1 receptor agonists have anything to offer over and above weight loss per se, and we don’t know for sure,” he said.
They “do have anti-inflammatory actions,” and “there are GLP-1 receptors in locations where you think GLP-1 receptor agonism may help inflammation in the knee, in joints, and in other tissues,” he noted.
He looks forward to results of the phase 3 trial of semaglutide in patients with KOA, expected this fall.
Three published studies
LOSEIT: RCT of liraglutide for pain and weight control in KOA
Henrik Rindel Gudbergsen, MD, PhD, and colleagues published results of the only randomized controlled trial of a GLP-1 receptor agonist (liraglutide, Saxenda) vs. placebo in patients with overweight/obesity and KOA, the LOSEIT trial.
All patients first entered an 8-week, pre-randomization phase where they had strict caloric restriction (and ate meal replacements) and lost at least 5% of their initial weight. They also had less knee pain at the end of this phase.
Then they were randomly assigned to receive 3 mg liraglutide or placebo daily injections for 1 year.
From randomization until week 52, the liraglutide group had greater mean weight loss than the placebo group (but this was < 5% of their weight). They did not have greater reduction in knee pain than patients in the placebo group.
“Our interpretation was that dieting results in weight loss and diminishes knee pain (which we knew), and that the impact of liraglutide following severe calorie restriction and weight loss and improvement of pain was limited,” Dr. Gudbergsen, a physician and associate professor at The Parker Institute, University of Copenhagen, told this news organization.
“That was the surprise for us as investigators,” he said, “and, I assume, why Novo Nordisk is now pursuing the investigation of semaglutide for KOA, as this is expected to create a larger effect on body weight and knee symptoms.”
The weight loss was about 12.5 kg (27.5 pounds) prior to randomization, and the subsequent weight loss with liraglutide was about 2.8 kg (6 pounds; about 4% of their weight). “Thus, it could seem that the participants’ potential for weight loss as well as symptom reduction was fully exploited in the pre–random assignment dietary intervention period,” according to the researchers.
“It seems highly relevant to use liraglutide or semaglutide for patients impacted by obesity and KOA, as it is in line with guidelines suggesting weight loss for this group,” Dr. Gudbergsen said. “However, whether liraglutide and/or semaglutide, acting via an anti-inflammatory effect, for example, has an added positive impact on cartilage quality remains to be clarified,” he said.
Others who were not involved in this study suggest that the lack of pain-reduction benefit with liraglutide vs. placebo can be explained by the short-term use of liraglutide (1 year), small weight loss (< 5%), and systemic rather than intraarticular injection.
The LOSEIT trial design “is problematic and could not provide a confirmative conclusion,” Hongyi Zhu, MD, PhD, Shanghai Sixth People’s Hospital, China, and colleagues wrote in their observational study. The small weight loss of < 5% in the liraglutide group may explain why the pain relief was not better than with placebo. A longer study duration with significant weight loss/maintenance may be needed, they noted.
Francis Berenbaum, MD, PhD, senior author of a preclinical study of liraglutide, said that in the LOSEIT trial, “daily systemic injections of liraglutide did not ameliorate OA-related pain, probably because of poor access and hence poor local concentrations of liraglutide in the knee joint.”
Dr. Berenbaum is professor of rheumatology at Sorbonne University and director of the department of rheumatology at AP-HP Saint-Antoine Hospital in Paris. He is cofounder and CEO of 4Moving Biotech (a subsidiary of 4P Pharma, an innovator accelerator biotech company), which is testing liraglutide for KOA.
In experiments in mice, systemic injections of liraglutide did not lead to high enough concentration in synovial fluid to show efficacy for pain relief, he told this news organization. “In order to get the direct effect of liraglutide, it should be injected intraarticularly,” he said.
Observational study of patients with diabetes and KOA
Dr. Zhu and colleagues recently published results of the first clinical investigation of long-term effects of GLP-1 receptor agonists on KOA in patients with comorbid type 2 diabetes.
They analyzed data from a subset of patients with KOA and type 2 diabetes from the Shanghai Osteoarthritis Cohort, including 233 patients who received a GLP-1 receptor agonist (semaglutide, liraglutide, or dulaglutide [Trulicity]) for at least 2 years and 1,574 patients who did not receive this therapy.
The patients had a mean weight of 66 kg (145 pounds), a mean body mass index of 27 kg/m2, and a mean A1c of 7.3%.
“According to conventional wisdom, a weight change greater than 5% is considered clinically relevant for KOA,” the researchers wrote. They found that patients had substantial weight loss after GLP-1 receptor agonist therapy.
The primary outcome, the incidence of knee surgery, was lower in the patients who received a GLP-1 receptor agonist than in the other patients (1.7% vs. 5.9%; adjusted P = .014).
Patients who received a GLP-1 receptor agonist also had greater improvements in secondary outcomes than did other patients, including pain subscale scores and cartilage-loss velocity of the medial femorotibial joint in patients with predominantly lateral OA.
“The effects of GLP-1 receptor agonists on arthritic knees were largely mediated by weight loss instead of glycemic control,” Dr. Zhu and colleagues reported.
They concluded that with long-enough treatment, “GLP-1 receptor agonist therapies might be disease-modifying for KOA patients with comorbid [type 2 diabetes mellitus].”
They called for further research to elucidate the effects of GLP-1 receptor agonists on the disease process, joint structure, and patient-reported outcomes of OA.
Dr. Garvey noted that “whether your BMI is 30 or 40, if there are complications, that tells you that degree of adiposity is sufficient to impair health.” So, if a patient in southeast China has a BMI of 27 kg/m2 and has osteoarthritis, he or she could still benefit from weight loss, he said.
Liraglutide and pain-related behavior in mouse models of OA
Dr. Berenbaum and colleagues reported that liraglutide alleviated pain-related behavior in sodium monoiodoacetate mouse models of KOA.
In addition, liraglutide had anti-inflammatory and anticatabolic effects in synovial fluid from the knees of six patients with OA of varying severity.
The researchers analyzed generic liraglutide (from Hybio Pharmaceuticals, Shenzhen, China) and nongeneric liraglutide (from Novo Nordisk, Bagsværd, Denmark).
They found that “when injected intra-articularly, liraglutide blunts the inflammatory process that is present in OA synovial tissue, explaining the acute analgesic effect,” Dr. Berenbaum said.
“Liraglutide could be a game-changer,” he said, “by demonstrating not only an effect on joint structures like synovial tissue and cartilage, but also on symptoms in a short-term period.”
Dr. Garvey said the symptom improvements after intrasynovial infusion of liraglutide in this trial were “impressive.” This study “adds credence to the hypothesis that these GLP-1 receptor agonists could have effects above and beyond weight loss,” he said.
Two trials near completion, one is upcoming
Phase 1 and 2 trials of 4P-004
“We are now in a phase 1 clinical trial [of 4P-004/liraglutide] in patients suffering from knee OA and should start a large phase 2 trial next year,” said Dr. Berenbaum.
The phase 1 LASARE trial, sponsored by 4Moving Biotech, planned to enroll 32 patients with KOA.
The primary outcome is safety and tolerability of single IA administration of 4P-004 at escalating doses in patients with KOA. Secondary outcomes include plasma concentration of liraglutide when administered this way.
Phase 3 trial of semaglutide for KOA
Novo Nordisk is performing a phase 3 study, “Effect of Subcutaneous Semaglutide 2.4 mg Once-weekly Compared to Placebo in Subjects With Obesity and Knee Osteoarthritis,” with an expected enrollment of 407 patients with KOA and estimated trial completion in September.
Eligible patients were aged 18 and older, with BMI > 30 kg/m2 and KOA with Kellgren-Lawrence grades 2 or 3. The co-primary outcomes are change in body weight and change in WOMAC pain score, from baseline to 68 weeks.
The LOSEIT trial was supported by Novo Nordisk and the Cambridge Weight Plan. The observational study in China was supported by the Shanghai Shenkang Hospital Development Centre, the Clinical Research Plan of SHDC, and the National Natural Science Foundation of China. The preclinical trial was supported by 4P Pharma/4Moving Biotech.
Dr. Berenbaum is CEO of 4Moving Biotech and chair of the scientific advisory board of 4P Pharma. He has received personal fees from 4P Pharma as well as numerous other pharmaceutical companies. Dr. Garvey has reported being a consultant to Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Merck, Fractyl Health, and Alnylam Pharmaceuticals, and reported being an investigator for studies sponsored by Novo Nordisk, Eli Lilly, Pfizer, and Epitomee. Dr. Gudbergsen, Dr. King, and Dr. Zhu report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Could glucagon-like peptide-1 receptor agonists, such as liraglutide and semaglutide, also be potential disease-modifying treatments for knee osteoarthritis (KOA)?
Weight loss is recommended for patients with KOA, and GLP-1 receptor agonists are approved for weight loss. New early research suggests these drugs might have a disease-modifying effect for KOA.
Three recently published studies investigated this:
- The LOSEIT phase 4, randomized controlled trial of liraglutide vs. placebo in patients with obesity/overweight and KOA.
- A large observational study out of China in patients with KOA and type 2 diabetes.
- A preclinical trial of liraglutide in mouse models of KOA.
The preclinical trial and the observational study report promising results, and the lack of KOA pain relief in patients in the phase 4 trial may be explained by the trial design. Three other trials are in the works.
This news organization invited two researchers and two outside experts to discuss these studies and potential future treatment of KOA with GLP-1 receptor agonists.
The big picture, as seen by two experts
The GLP-1 receptor agonists liraglutide (Victoza) and semaglutide (Ozempic) are approved for type 2 diabetes, and, in higher doses, liraglutide (Saxenda) and semaglutide (Wegovy) are approved for weight loss in patients with obesity (or overweight with comorbidities), and given as weekly injections.
Victoza and Saxenda are expected to come off patent in December 2023, and in 2026, respectively.
Lauren King, MD, PhD, a rheumatologist and clinician scientist who was not involved with the recent investigational studies of GLP-1 receptor agonists for KOA, noted that obesity is the most important, guideline-recommended, modifiable risk factor for KOA.
“In people with overweight and obesity, losing weight can improve knee osteoarthritis symptoms, and some evidence supports that it may also slow joint structural changes,” Dr. King, of the department of medicine at the University of Toronto, said in an interview.
Large trials of GLP-1 receptor agonists in people with overweight and obesity, such as the STEP trials of semaglutide, she noted, “provide evidence that these medications are safe and effective, facilitating clinically relevant and sustained weight loss.”
Further research is needed, she said, to better understand disease-modifying effects of GLP-1 receptor agonists in patients with KOA.
Similarly, W. Timothy Garvey, MD, professor in the department of nutrition sciences at the University of Alabama at Birmingham and director of the UAB Diabetes Research Center, who was not involved with this research, noted that weight loss improves KOA symptoms.
Dr. Garvey was lead investigator in the STEP 5 trial of semaglutide and lead author of the American Association of Clinical Endocrinologists 2016 Obesity Management guidelines.
“The question is whether these GLP-1 receptor agonists have anything to offer over and above weight loss per se, and we don’t know for sure,” he said.
They “do have anti-inflammatory actions,” and “there are GLP-1 receptors in locations where you think GLP-1 receptor agonism may help inflammation in the knee, in joints, and in other tissues,” he noted.
He looks forward to results of the phase 3 trial of semaglutide in patients with KOA, expected this fall.
Three published studies
LOSEIT: RCT of liraglutide for pain and weight control in KOA
Henrik Rindel Gudbergsen, MD, PhD, and colleagues published results of the only randomized controlled trial of a GLP-1 receptor agonist (liraglutide, Saxenda) vs. placebo in patients with overweight/obesity and KOA, the LOSEIT trial.
All patients first entered an 8-week, pre-randomization phase where they had strict caloric restriction (and ate meal replacements) and lost at least 5% of their initial weight. They also had less knee pain at the end of this phase.
Then they were randomly assigned to receive 3 mg liraglutide or placebo daily injections for 1 year.
From randomization until week 52, the liraglutide group had greater mean weight loss than the placebo group (but this was < 5% of their weight). They did not have greater reduction in knee pain than patients in the placebo group.
“Our interpretation was that dieting results in weight loss and diminishes knee pain (which we knew), and that the impact of liraglutide following severe calorie restriction and weight loss and improvement of pain was limited,” Dr. Gudbergsen, a physician and associate professor at The Parker Institute, University of Copenhagen, told this news organization.
“That was the surprise for us as investigators,” he said, “and, I assume, why Novo Nordisk is now pursuing the investigation of semaglutide for KOA, as this is expected to create a larger effect on body weight and knee symptoms.”
The weight loss was about 12.5 kg (27.5 pounds) prior to randomization, and the subsequent weight loss with liraglutide was about 2.8 kg (6 pounds; about 4% of their weight). “Thus, it could seem that the participants’ potential for weight loss as well as symptom reduction was fully exploited in the pre–random assignment dietary intervention period,” according to the researchers.
“It seems highly relevant to use liraglutide or semaglutide for patients impacted by obesity and KOA, as it is in line with guidelines suggesting weight loss for this group,” Dr. Gudbergsen said. “However, whether liraglutide and/or semaglutide, acting via an anti-inflammatory effect, for example, has an added positive impact on cartilage quality remains to be clarified,” he said.
Others who were not involved in this study suggest that the lack of pain-reduction benefit with liraglutide vs. placebo can be explained by the short-term use of liraglutide (1 year), small weight loss (< 5%), and systemic rather than intraarticular injection.
The LOSEIT trial design “is problematic and could not provide a confirmative conclusion,” Hongyi Zhu, MD, PhD, Shanghai Sixth People’s Hospital, China, and colleagues wrote in their observational study. The small weight loss of < 5% in the liraglutide group may explain why the pain relief was not better than with placebo. A longer study duration with significant weight loss/maintenance may be needed, they noted.
Francis Berenbaum, MD, PhD, senior author of a preclinical study of liraglutide, said that in the LOSEIT trial, “daily systemic injections of liraglutide did not ameliorate OA-related pain, probably because of poor access and hence poor local concentrations of liraglutide in the knee joint.”
Dr. Berenbaum is professor of rheumatology at Sorbonne University and director of the department of rheumatology at AP-HP Saint-Antoine Hospital in Paris. He is cofounder and CEO of 4Moving Biotech (a subsidiary of 4P Pharma, an innovator accelerator biotech company), which is testing liraglutide for KOA.
In experiments in mice, systemic injections of liraglutide did not lead to high enough concentration in synovial fluid to show efficacy for pain relief, he told this news organization. “In order to get the direct effect of liraglutide, it should be injected intraarticularly,” he said.
Observational study of patients with diabetes and KOA
Dr. Zhu and colleagues recently published results of the first clinical investigation of long-term effects of GLP-1 receptor agonists on KOA in patients with comorbid type 2 diabetes.
They analyzed data from a subset of patients with KOA and type 2 diabetes from the Shanghai Osteoarthritis Cohort, including 233 patients who received a GLP-1 receptor agonist (semaglutide, liraglutide, or dulaglutide [Trulicity]) for at least 2 years and 1,574 patients who did not receive this therapy.
The patients had a mean weight of 66 kg (145 pounds), a mean body mass index of 27 kg/m2, and a mean A1c of 7.3%.
“According to conventional wisdom, a weight change greater than 5% is considered clinically relevant for KOA,” the researchers wrote. They found that patients had substantial weight loss after GLP-1 receptor agonist therapy.
The primary outcome, the incidence of knee surgery, was lower in the patients who received a GLP-1 receptor agonist than in the other patients (1.7% vs. 5.9%; adjusted P = .014).
Patients who received a GLP-1 receptor agonist also had greater improvements in secondary outcomes than did other patients, including pain subscale scores and cartilage-loss velocity of the medial femorotibial joint in patients with predominantly lateral OA.
“The effects of GLP-1 receptor agonists on arthritic knees were largely mediated by weight loss instead of glycemic control,” Dr. Zhu and colleagues reported.
They concluded that with long-enough treatment, “GLP-1 receptor agonist therapies might be disease-modifying for KOA patients with comorbid [type 2 diabetes mellitus].”
They called for further research to elucidate the effects of GLP-1 receptor agonists on the disease process, joint structure, and patient-reported outcomes of OA.
Dr. Garvey noted that “whether your BMI is 30 or 40, if there are complications, that tells you that degree of adiposity is sufficient to impair health.” So, if a patient in southeast China has a BMI of 27 kg/m2 and has osteoarthritis, he or she could still benefit from weight loss, he said.
Liraglutide and pain-related behavior in mouse models of OA
Dr. Berenbaum and colleagues reported that liraglutide alleviated pain-related behavior in sodium monoiodoacetate mouse models of KOA.
In addition, liraglutide had anti-inflammatory and anticatabolic effects in synovial fluid from the knees of six patients with OA of varying severity.
The researchers analyzed generic liraglutide (from Hybio Pharmaceuticals, Shenzhen, China) and nongeneric liraglutide (from Novo Nordisk, Bagsværd, Denmark).
They found that “when injected intra-articularly, liraglutide blunts the inflammatory process that is present in OA synovial tissue, explaining the acute analgesic effect,” Dr. Berenbaum said.
“Liraglutide could be a game-changer,” he said, “by demonstrating not only an effect on joint structures like synovial tissue and cartilage, but also on symptoms in a short-term period.”
Dr. Garvey said the symptom improvements after intrasynovial infusion of liraglutide in this trial were “impressive.” This study “adds credence to the hypothesis that these GLP-1 receptor agonists could have effects above and beyond weight loss,” he said.
Two trials near completion, one is upcoming
Phase 1 and 2 trials of 4P-004
“We are now in a phase 1 clinical trial [of 4P-004/liraglutide] in patients suffering from knee OA and should start a large phase 2 trial next year,” said Dr. Berenbaum.
The phase 1 LASARE trial, sponsored by 4Moving Biotech, planned to enroll 32 patients with KOA.
The primary outcome is safety and tolerability of single IA administration of 4P-004 at escalating doses in patients with KOA. Secondary outcomes include plasma concentration of liraglutide when administered this way.
Phase 3 trial of semaglutide for KOA
Novo Nordisk is performing a phase 3 study, “Effect of Subcutaneous Semaglutide 2.4 mg Once-weekly Compared to Placebo in Subjects With Obesity and Knee Osteoarthritis,” with an expected enrollment of 407 patients with KOA and estimated trial completion in September.
Eligible patients were aged 18 and older, with BMI > 30 kg/m2 and KOA with Kellgren-Lawrence grades 2 or 3. The co-primary outcomes are change in body weight and change in WOMAC pain score, from baseline to 68 weeks.
The LOSEIT trial was supported by Novo Nordisk and the Cambridge Weight Plan. The observational study in China was supported by the Shanghai Shenkang Hospital Development Centre, the Clinical Research Plan of SHDC, and the National Natural Science Foundation of China. The preclinical trial was supported by 4P Pharma/4Moving Biotech.
Dr. Berenbaum is CEO of 4Moving Biotech and chair of the scientific advisory board of 4P Pharma. He has received personal fees from 4P Pharma as well as numerous other pharmaceutical companies. Dr. Garvey has reported being a consultant to Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Merck, Fractyl Health, and Alnylam Pharmaceuticals, and reported being an investigator for studies sponsored by Novo Nordisk, Eli Lilly, Pfizer, and Epitomee. Dr. Gudbergsen, Dr. King, and Dr. Zhu report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Could glucagon-like peptide-1 receptor agonists, such as liraglutide and semaglutide, also be potential disease-modifying treatments for knee osteoarthritis (KOA)?
Weight loss is recommended for patients with KOA, and GLP-1 receptor agonists are approved for weight loss. New early research suggests these drugs might have a disease-modifying effect for KOA.
Three recently published studies investigated this:
- The LOSEIT phase 4, randomized controlled trial of liraglutide vs. placebo in patients with obesity/overweight and KOA.
- A large observational study out of China in patients with KOA and type 2 diabetes.
- A preclinical trial of liraglutide in mouse models of KOA.
The preclinical trial and the observational study report promising results, and the lack of KOA pain relief in patients in the phase 4 trial may be explained by the trial design. Three other trials are in the works.
This news organization invited two researchers and two outside experts to discuss these studies and potential future treatment of KOA with GLP-1 receptor agonists.
The big picture, as seen by two experts
The GLP-1 receptor agonists liraglutide (Victoza) and semaglutide (Ozempic) are approved for type 2 diabetes, and, in higher doses, liraglutide (Saxenda) and semaglutide (Wegovy) are approved for weight loss in patients with obesity (or overweight with comorbidities), and given as weekly injections.
Victoza and Saxenda are expected to come off patent in December 2023, and in 2026, respectively.
Lauren King, MD, PhD, a rheumatologist and clinician scientist who was not involved with the recent investigational studies of GLP-1 receptor agonists for KOA, noted that obesity is the most important, guideline-recommended, modifiable risk factor for KOA.
“In people with overweight and obesity, losing weight can improve knee osteoarthritis symptoms, and some evidence supports that it may also slow joint structural changes,” Dr. King, of the department of medicine at the University of Toronto, said in an interview.
Large trials of GLP-1 receptor agonists in people with overweight and obesity, such as the STEP trials of semaglutide, she noted, “provide evidence that these medications are safe and effective, facilitating clinically relevant and sustained weight loss.”
Further research is needed, she said, to better understand disease-modifying effects of GLP-1 receptor agonists in patients with KOA.
Similarly, W. Timothy Garvey, MD, professor in the department of nutrition sciences at the University of Alabama at Birmingham and director of the UAB Diabetes Research Center, who was not involved with this research, noted that weight loss improves KOA symptoms.
Dr. Garvey was lead investigator in the STEP 5 trial of semaglutide and lead author of the American Association of Clinical Endocrinologists 2016 Obesity Management guidelines.
“The question is whether these GLP-1 receptor agonists have anything to offer over and above weight loss per se, and we don’t know for sure,” he said.
They “do have anti-inflammatory actions,” and “there are GLP-1 receptors in locations where you think GLP-1 receptor agonism may help inflammation in the knee, in joints, and in other tissues,” he noted.
He looks forward to results of the phase 3 trial of semaglutide in patients with KOA, expected this fall.
Three published studies
LOSEIT: RCT of liraglutide for pain and weight control in KOA
Henrik Rindel Gudbergsen, MD, PhD, and colleagues published results of the only randomized controlled trial of a GLP-1 receptor agonist (liraglutide, Saxenda) vs. placebo in patients with overweight/obesity and KOA, the LOSEIT trial.
All patients first entered an 8-week, pre-randomization phase where they had strict caloric restriction (and ate meal replacements) and lost at least 5% of their initial weight. They also had less knee pain at the end of this phase.
Then they were randomly assigned to receive 3 mg liraglutide or placebo daily injections for 1 year.
From randomization until week 52, the liraglutide group had greater mean weight loss than the placebo group (but this was < 5% of their weight). They did not have greater reduction in knee pain than patients in the placebo group.
“Our interpretation was that dieting results in weight loss and diminishes knee pain (which we knew), and that the impact of liraglutide following severe calorie restriction and weight loss and improvement of pain was limited,” Dr. Gudbergsen, a physician and associate professor at The Parker Institute, University of Copenhagen, told this news organization.
“That was the surprise for us as investigators,” he said, “and, I assume, why Novo Nordisk is now pursuing the investigation of semaglutide for KOA, as this is expected to create a larger effect on body weight and knee symptoms.”
The weight loss was about 12.5 kg (27.5 pounds) prior to randomization, and the subsequent weight loss with liraglutide was about 2.8 kg (6 pounds; about 4% of their weight). “Thus, it could seem that the participants’ potential for weight loss as well as symptom reduction was fully exploited in the pre–random assignment dietary intervention period,” according to the researchers.
“It seems highly relevant to use liraglutide or semaglutide for patients impacted by obesity and KOA, as it is in line with guidelines suggesting weight loss for this group,” Dr. Gudbergsen said. “However, whether liraglutide and/or semaglutide, acting via an anti-inflammatory effect, for example, has an added positive impact on cartilage quality remains to be clarified,” he said.
Others who were not involved in this study suggest that the lack of pain-reduction benefit with liraglutide vs. placebo can be explained by the short-term use of liraglutide (1 year), small weight loss (< 5%), and systemic rather than intraarticular injection.
The LOSEIT trial design “is problematic and could not provide a confirmative conclusion,” Hongyi Zhu, MD, PhD, Shanghai Sixth People’s Hospital, China, and colleagues wrote in their observational study. The small weight loss of < 5% in the liraglutide group may explain why the pain relief was not better than with placebo. A longer study duration with significant weight loss/maintenance may be needed, they noted.
Francis Berenbaum, MD, PhD, senior author of a preclinical study of liraglutide, said that in the LOSEIT trial, “daily systemic injections of liraglutide did not ameliorate OA-related pain, probably because of poor access and hence poor local concentrations of liraglutide in the knee joint.”
Dr. Berenbaum is professor of rheumatology at Sorbonne University and director of the department of rheumatology at AP-HP Saint-Antoine Hospital in Paris. He is cofounder and CEO of 4Moving Biotech (a subsidiary of 4P Pharma, an innovator accelerator biotech company), which is testing liraglutide for KOA.
In experiments in mice, systemic injections of liraglutide did not lead to high enough concentration in synovial fluid to show efficacy for pain relief, he told this news organization. “In order to get the direct effect of liraglutide, it should be injected intraarticularly,” he said.
Observational study of patients with diabetes and KOA
Dr. Zhu and colleagues recently published results of the first clinical investigation of long-term effects of GLP-1 receptor agonists on KOA in patients with comorbid type 2 diabetes.
They analyzed data from a subset of patients with KOA and type 2 diabetes from the Shanghai Osteoarthritis Cohort, including 233 patients who received a GLP-1 receptor agonist (semaglutide, liraglutide, or dulaglutide [Trulicity]) for at least 2 years and 1,574 patients who did not receive this therapy.
The patients had a mean weight of 66 kg (145 pounds), a mean body mass index of 27 kg/m2, and a mean A1c of 7.3%.
“According to conventional wisdom, a weight change greater than 5% is considered clinically relevant for KOA,” the researchers wrote. They found that patients had substantial weight loss after GLP-1 receptor agonist therapy.
The primary outcome, the incidence of knee surgery, was lower in the patients who received a GLP-1 receptor agonist than in the other patients (1.7% vs. 5.9%; adjusted P = .014).
Patients who received a GLP-1 receptor agonist also had greater improvements in secondary outcomes than did other patients, including pain subscale scores and cartilage-loss velocity of the medial femorotibial joint in patients with predominantly lateral OA.
“The effects of GLP-1 receptor agonists on arthritic knees were largely mediated by weight loss instead of glycemic control,” Dr. Zhu and colleagues reported.
They concluded that with long-enough treatment, “GLP-1 receptor agonist therapies might be disease-modifying for KOA patients with comorbid [type 2 diabetes mellitus].”
They called for further research to elucidate the effects of GLP-1 receptor agonists on the disease process, joint structure, and patient-reported outcomes of OA.
Dr. Garvey noted that “whether your BMI is 30 or 40, if there are complications, that tells you that degree of adiposity is sufficient to impair health.” So, if a patient in southeast China has a BMI of 27 kg/m2 and has osteoarthritis, he or she could still benefit from weight loss, he said.
Liraglutide and pain-related behavior in mouse models of OA
Dr. Berenbaum and colleagues reported that liraglutide alleviated pain-related behavior in sodium monoiodoacetate mouse models of KOA.
In addition, liraglutide had anti-inflammatory and anticatabolic effects in synovial fluid from the knees of six patients with OA of varying severity.
The researchers analyzed generic liraglutide (from Hybio Pharmaceuticals, Shenzhen, China) and nongeneric liraglutide (from Novo Nordisk, Bagsværd, Denmark).
They found that “when injected intra-articularly, liraglutide blunts the inflammatory process that is present in OA synovial tissue, explaining the acute analgesic effect,” Dr. Berenbaum said.
“Liraglutide could be a game-changer,” he said, “by demonstrating not only an effect on joint structures like synovial tissue and cartilage, but also on symptoms in a short-term period.”
Dr. Garvey said the symptom improvements after intrasynovial infusion of liraglutide in this trial were “impressive.” This study “adds credence to the hypothesis that these GLP-1 receptor agonists could have effects above and beyond weight loss,” he said.
Two trials near completion, one is upcoming
Phase 1 and 2 trials of 4P-004
“We are now in a phase 1 clinical trial [of 4P-004/liraglutide] in patients suffering from knee OA and should start a large phase 2 trial next year,” said Dr. Berenbaum.
The phase 1 LASARE trial, sponsored by 4Moving Biotech, planned to enroll 32 patients with KOA.
The primary outcome is safety and tolerability of single IA administration of 4P-004 at escalating doses in patients with KOA. Secondary outcomes include plasma concentration of liraglutide when administered this way.
Phase 3 trial of semaglutide for KOA
Novo Nordisk is performing a phase 3 study, “Effect of Subcutaneous Semaglutide 2.4 mg Once-weekly Compared to Placebo in Subjects With Obesity and Knee Osteoarthritis,” with an expected enrollment of 407 patients with KOA and estimated trial completion in September.
Eligible patients were aged 18 and older, with BMI > 30 kg/m2 and KOA with Kellgren-Lawrence grades 2 or 3. The co-primary outcomes are change in body weight and change in WOMAC pain score, from baseline to 68 weeks.
The LOSEIT trial was supported by Novo Nordisk and the Cambridge Weight Plan. The observational study in China was supported by the Shanghai Shenkang Hospital Development Centre, the Clinical Research Plan of SHDC, and the National Natural Science Foundation of China. The preclinical trial was supported by 4P Pharma/4Moving Biotech.
Dr. Berenbaum is CEO of 4Moving Biotech and chair of the scientific advisory board of 4P Pharma. He has received personal fees from 4P Pharma as well as numerous other pharmaceutical companies. Dr. Garvey has reported being a consultant to Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Merck, Fractyl Health, and Alnylam Pharmaceuticals, and reported being an investigator for studies sponsored by Novo Nordisk, Eli Lilly, Pfizer, and Epitomee. Dr. Gudbergsen, Dr. King, and Dr. Zhu report no relevant financial relationships.
A version of this article appeared on Medscape.com.
Kidnapping and treatment risks come with medical tourism
In March 2023, four “medical tourists” from South Carolina who were seeking health care in Mexico were kidnapped by a drug cartel. Two were killed when they were trapped in a shootout. One of them was scheduled for tummy-tuck surgery, and others were seeking cheaper prescription drugs.
The news reached Bruce Hermann, MD, a plastic surgeon in Denton, Tex., who brought up the incident in a segment of his podcast, “Nip Talk,” in which he talked about the risks of medical tourism. But violence in foreign countries isn’t Dr. Hermann’s primary concern.
“Being the victim of a crime is lower down the risk strata,” Dr. Hermann said in an interview. “A bigger concern is the lack of regulations of doctors and facilities in countries like Mexico.”
Some employers pay for treatment at certain foreign clinics, and Blue Shield of California’s HMO plan, Access Baja, covers care in certain clinics in Mexico’s Baja peninsula. But U.S. health insurance generally does not cover medical tourism.
Despite its popularity, medical tourism is not siphoning off a significant number of patients from U.S. doctors, with the possible exception of plastic surgery. One study found that medical tourism accounts for less than 2% of U.S. spending on noncosmetic health care.
Still, as many as 1.2 million Americans travel to Mexico each year seeking health care at lower costs, particularly dental care, bariatric surgery, and cosmetic procedures.
Physicians such as Dr. Hermann see the results when things go awry. Dr. Hermann said when he takes calls at a nearby level II trauma center, he sees, on average, one patient a month with complications from plastic surgeries performed abroad.
Patients tell Dr. Hermann they often had little preoperative time with the surgeons, and some may not even see their surgeon. They have to fly back home just days after their procedures, so complications that typically arise later are missed, he said.
Who opts for medical tourism?
There are few statistics on the number of medical tourists or the clinical problems they have. Josef Woodman, CEO of Patients Beyond Borders, a medical tourism consultancy in Chapel Hill, N.C., has developed a profile of medical tourism that is based on his close contacts within the industry.
Mr. Woodman said the vast majority of U.S. medical tourists go to Mexico, which accounts for an estimated 1 million to 1.2 million medical visitors a year. He said Costa Rica is another popular destination, followed by other Latin American countries and some in the Far East, the Middle East, and Eastern Europe.
Mr. Woodman estimates that dental treatments make up 65% of all medical tourism. Cosmetic procedures come in a distant second, at 15%. Cosmetic procedures can be expensive and are rarely covered by insurance. They can be performed at half the price abroad, he said.
According to Mr. Woodman, other significant fields for medical tourism are orthopedics, which accounts for 5% of all visits, and bariatrics, with 3%-5%. Hip and knee replacements are expensive, and in the case of bariatrics, U.S. insurers often deny coverage, he said.
People also go abroad for fertility care and organ transplants, and one Jamaica company even offered dialysis vacations for U.S. tourists.
On the other hand, medical tourism does not work well for cancer treatments, because cancer care involves long periods of treatment and cannot be completed in a trip or two, Mr. Woodman said. “The media also plays up major procedures like open heart surgery, but they are in fact very rare,” he added.
What patients are looking for
Medical tourists typically pay 50%-70% of what they would pay in the United States for the same procedure, Mr. Woodman said. Prices are lower because patients pay in cash, foreign wages are lower, and expenses such as malpractice insurance are much lower.
“Many medical tourists don’t have a choice,” Mr. Woodman said. “They cannot afford the U.S. price for the procedure, even if they have health insurance, because they often have a high deductible.” In one study, the majority of medical tourists to Mexico reported an income of $25,000-$50,000 a year.
That same study also found that the average age of medical tourists was just under 65. These older patients often come for a vacation. “A sizable number of medical tourists are looking for surgery plus a vacation, a tummy-tuck and a stay at an all-inclusive resort,” said Steven P. Davison, MD, DDS, a plastic surgeon in Washington, who has written on the phenomenon.
Another large group of medical tourists are immigrants to the United States who want surgery in their country of origin, such as Brazil or Iran, Dr. Davison said, perhaps because they feel more comfortable or have family members who can act as caregivers. He said some go to places that have expertise in a certain procedure.
“For instance, they get their hair transplantation done in Turkey because surgeons there have the expertise and it’s cheaper than in the United States,” Dr. Davison said.
Arranging the trip
Patients often find foreign providers through online brokers who can arrange the flight, hotel, clinic, and physician. Brokers are not unbiased because they are usually paid by the clinic. Mr. Woodman said this arrangement works when the broker can offer a wide variety of options but not when the broker represents just a few clinics.
Mr. Woodman said patients could conceivably make their own arrangements without a broker, and some do so. “All the tools are on the Internet,” he said. “However, many people don’t trust themselves to do this work.”
Even for patients who depend on brokers, Mr. Woodman advises verifying the quality of the clinic and its doctors before signing on. Most countries have online lists of registered doctors, and patients seeking health care can research complaints against a doctor.
There is no insurance that patients can have to guard against the risks of medical tourism, Mr. Woodman said. “When you could get it, it was prohibitively expensive,” he said. “You can get travel insurance, but that just covers peripheral problems, such as flight cancellations, accidental injury, and emergency care. It has nothing to do with problems stemming from planned procedures.
“Some clinics and hospitals serving medical tourists provide warranties on their work,” he added. “However, plastic surgery clinics are less likely to offer warranties, because patients are so frequently dissatisfied.”
How things can go wrong
Mr. Woodman said medical tourists may often receive substandard care when they select a provider who offers unusually large savings, such as 80% off the U.S. price. “Those providers are likely cutting corners to get that kind of savings, and you should stay away from them,” he said.
Even when receiving care at an excellent clinic, patients can get infections if postoperative requirements are not followed, according to Darrick E. Antell, MD, a plastic surgeon in New York, who has treated medical tourists upon their return to the United States.
Typically, patients are told to stay in their rooms for several days after the operation, but friends may push them to go out and have fun, he said. Sometimes patients choose exotic arrangements that place them at risk for infection. As an example, Dr. Antell mentioned a broker who offered a safari in combination with plastic surgery.
Dr. Hermann said tummy tucks are riskier because they involve large incisions, and many such patients are overweight, which impairs healing. “Tummy-tuck patients need a longer recovery, and they often have more discomfort than other plastic surgery,” he said.
When things go wrong, medical tourists have few legal protections. “They usually don’t go to an accredited facility, there is no credentialing of physicians, and their ability to sue is extremely limited,” Dr. Davison said. Patients would have to return to the foreign country and hire a lawyer there, and even then, it is harder to win a case and to receive an award as high as in the United States, he added.
Dealing with follow-ups
An inherent flaw with medical tourism, Dr. Antell said, is that patients typically go back home before postoperative care is fully completed. “They may stay just a few days after surgery, and then fly back home,” he said.
“Patients who have complex operations abroad should stay for 8-10 days to have a proper follow-up,” he said. “But they fly back early, which can also lead to getting pulmonary embolisms on the flight.
“A checkup right after surgery doesn’t uncover many complications, because these tend to occur 7-12 days after surgery,” Dr. Hermann said.
“If they come to me within 3 months after surgery, I charge an upfront fee just to see them, because it takes an hour of my time,” Dr. Davison said. “Then I will take care of acute emergency, such as taking out an infected implant.”
Hermann said many patients wait too long to have their complications treated in the United States. “They may first try calling their doctor in Mexico, who tells them to take some antibiotics or something,” he said. “So when they finally do seek care, the infection is pretty far along.”
What U.S. doctors can do
Patients rarely tell their U.S. doctors that they are planning a trip to a foreign country to undergo medical treatment, even though they have to request a copy of their medical records for the foreign doctor, Mr. Woodman said.
Dr. Hermann said only one of his patients told him she was planning to go aboard for plastic surgery. “She was a young mom, and I tried to talk her out of it,” he said. “I don’t know what happened because she didn’t come back.”
Dr. Hermann said doctors should assume that they won’t be able to change their patients’ minds, and they should try to help their patients make the best of it.
“They should insist on seeing the doctor ahead of time and make sure they get along with them,” he said. “Ask for credentialing of the doctor and the facility, and stay there several weeks post op. But they’re probably not going to do all of this.”
A version of this article first appeared on Medscape.com.
In March 2023, four “medical tourists” from South Carolina who were seeking health care in Mexico were kidnapped by a drug cartel. Two were killed when they were trapped in a shootout. One of them was scheduled for tummy-tuck surgery, and others were seeking cheaper prescription drugs.
The news reached Bruce Hermann, MD, a plastic surgeon in Denton, Tex., who brought up the incident in a segment of his podcast, “Nip Talk,” in which he talked about the risks of medical tourism. But violence in foreign countries isn’t Dr. Hermann’s primary concern.
“Being the victim of a crime is lower down the risk strata,” Dr. Hermann said in an interview. “A bigger concern is the lack of regulations of doctors and facilities in countries like Mexico.”
Some employers pay for treatment at certain foreign clinics, and Blue Shield of California’s HMO plan, Access Baja, covers care in certain clinics in Mexico’s Baja peninsula. But U.S. health insurance generally does not cover medical tourism.
Despite its popularity, medical tourism is not siphoning off a significant number of patients from U.S. doctors, with the possible exception of plastic surgery. One study found that medical tourism accounts for less than 2% of U.S. spending on noncosmetic health care.
Still, as many as 1.2 million Americans travel to Mexico each year seeking health care at lower costs, particularly dental care, bariatric surgery, and cosmetic procedures.
Physicians such as Dr. Hermann see the results when things go awry. Dr. Hermann said when he takes calls at a nearby level II trauma center, he sees, on average, one patient a month with complications from plastic surgeries performed abroad.
Patients tell Dr. Hermann they often had little preoperative time with the surgeons, and some may not even see their surgeon. They have to fly back home just days after their procedures, so complications that typically arise later are missed, he said.
Who opts for medical tourism?
There are few statistics on the number of medical tourists or the clinical problems they have. Josef Woodman, CEO of Patients Beyond Borders, a medical tourism consultancy in Chapel Hill, N.C., has developed a profile of medical tourism that is based on his close contacts within the industry.
Mr. Woodman said the vast majority of U.S. medical tourists go to Mexico, which accounts for an estimated 1 million to 1.2 million medical visitors a year. He said Costa Rica is another popular destination, followed by other Latin American countries and some in the Far East, the Middle East, and Eastern Europe.
Mr. Woodman estimates that dental treatments make up 65% of all medical tourism. Cosmetic procedures come in a distant second, at 15%. Cosmetic procedures can be expensive and are rarely covered by insurance. They can be performed at half the price abroad, he said.
According to Mr. Woodman, other significant fields for medical tourism are orthopedics, which accounts for 5% of all visits, and bariatrics, with 3%-5%. Hip and knee replacements are expensive, and in the case of bariatrics, U.S. insurers often deny coverage, he said.
People also go abroad for fertility care and organ transplants, and one Jamaica company even offered dialysis vacations for U.S. tourists.
On the other hand, medical tourism does not work well for cancer treatments, because cancer care involves long periods of treatment and cannot be completed in a trip or two, Mr. Woodman said. “The media also plays up major procedures like open heart surgery, but they are in fact very rare,” he added.
What patients are looking for
Medical tourists typically pay 50%-70% of what they would pay in the United States for the same procedure, Mr. Woodman said. Prices are lower because patients pay in cash, foreign wages are lower, and expenses such as malpractice insurance are much lower.
“Many medical tourists don’t have a choice,” Mr. Woodman said. “They cannot afford the U.S. price for the procedure, even if they have health insurance, because they often have a high deductible.” In one study, the majority of medical tourists to Mexico reported an income of $25,000-$50,000 a year.
That same study also found that the average age of medical tourists was just under 65. These older patients often come for a vacation. “A sizable number of medical tourists are looking for surgery plus a vacation, a tummy-tuck and a stay at an all-inclusive resort,” said Steven P. Davison, MD, DDS, a plastic surgeon in Washington, who has written on the phenomenon.
Another large group of medical tourists are immigrants to the United States who want surgery in their country of origin, such as Brazil or Iran, Dr. Davison said, perhaps because they feel more comfortable or have family members who can act as caregivers. He said some go to places that have expertise in a certain procedure.
“For instance, they get their hair transplantation done in Turkey because surgeons there have the expertise and it’s cheaper than in the United States,” Dr. Davison said.
Arranging the trip
Patients often find foreign providers through online brokers who can arrange the flight, hotel, clinic, and physician. Brokers are not unbiased because they are usually paid by the clinic. Mr. Woodman said this arrangement works when the broker can offer a wide variety of options but not when the broker represents just a few clinics.
Mr. Woodman said patients could conceivably make their own arrangements without a broker, and some do so. “All the tools are on the Internet,” he said. “However, many people don’t trust themselves to do this work.”
Even for patients who depend on brokers, Mr. Woodman advises verifying the quality of the clinic and its doctors before signing on. Most countries have online lists of registered doctors, and patients seeking health care can research complaints against a doctor.
There is no insurance that patients can have to guard against the risks of medical tourism, Mr. Woodman said. “When you could get it, it was prohibitively expensive,” he said. “You can get travel insurance, but that just covers peripheral problems, such as flight cancellations, accidental injury, and emergency care. It has nothing to do with problems stemming from planned procedures.
“Some clinics and hospitals serving medical tourists provide warranties on their work,” he added. “However, plastic surgery clinics are less likely to offer warranties, because patients are so frequently dissatisfied.”
How things can go wrong
Mr. Woodman said medical tourists may often receive substandard care when they select a provider who offers unusually large savings, such as 80% off the U.S. price. “Those providers are likely cutting corners to get that kind of savings, and you should stay away from them,” he said.
Even when receiving care at an excellent clinic, patients can get infections if postoperative requirements are not followed, according to Darrick E. Antell, MD, a plastic surgeon in New York, who has treated medical tourists upon their return to the United States.
Typically, patients are told to stay in their rooms for several days after the operation, but friends may push them to go out and have fun, he said. Sometimes patients choose exotic arrangements that place them at risk for infection. As an example, Dr. Antell mentioned a broker who offered a safari in combination with plastic surgery.
Dr. Hermann said tummy tucks are riskier because they involve large incisions, and many such patients are overweight, which impairs healing. “Tummy-tuck patients need a longer recovery, and they often have more discomfort than other plastic surgery,” he said.
When things go wrong, medical tourists have few legal protections. “They usually don’t go to an accredited facility, there is no credentialing of physicians, and their ability to sue is extremely limited,” Dr. Davison said. Patients would have to return to the foreign country and hire a lawyer there, and even then, it is harder to win a case and to receive an award as high as in the United States, he added.
Dealing with follow-ups
An inherent flaw with medical tourism, Dr. Antell said, is that patients typically go back home before postoperative care is fully completed. “They may stay just a few days after surgery, and then fly back home,” he said.
“Patients who have complex operations abroad should stay for 8-10 days to have a proper follow-up,” he said. “But they fly back early, which can also lead to getting pulmonary embolisms on the flight.
“A checkup right after surgery doesn’t uncover many complications, because these tend to occur 7-12 days after surgery,” Dr. Hermann said.
“If they come to me within 3 months after surgery, I charge an upfront fee just to see them, because it takes an hour of my time,” Dr. Davison said. “Then I will take care of acute emergency, such as taking out an infected implant.”
Hermann said many patients wait too long to have their complications treated in the United States. “They may first try calling their doctor in Mexico, who tells them to take some antibiotics or something,” he said. “So when they finally do seek care, the infection is pretty far along.”
What U.S. doctors can do
Patients rarely tell their U.S. doctors that they are planning a trip to a foreign country to undergo medical treatment, even though they have to request a copy of their medical records for the foreign doctor, Mr. Woodman said.
Dr. Hermann said only one of his patients told him she was planning to go aboard for plastic surgery. “She was a young mom, and I tried to talk her out of it,” he said. “I don’t know what happened because she didn’t come back.”
Dr. Hermann said doctors should assume that they won’t be able to change their patients’ minds, and they should try to help their patients make the best of it.
“They should insist on seeing the doctor ahead of time and make sure they get along with them,” he said. “Ask for credentialing of the doctor and the facility, and stay there several weeks post op. But they’re probably not going to do all of this.”
A version of this article first appeared on Medscape.com.
In March 2023, four “medical tourists” from South Carolina who were seeking health care in Mexico were kidnapped by a drug cartel. Two were killed when they were trapped in a shootout. One of them was scheduled for tummy-tuck surgery, and others were seeking cheaper prescription drugs.
The news reached Bruce Hermann, MD, a plastic surgeon in Denton, Tex., who brought up the incident in a segment of his podcast, “Nip Talk,” in which he talked about the risks of medical tourism. But violence in foreign countries isn’t Dr. Hermann’s primary concern.
“Being the victim of a crime is lower down the risk strata,” Dr. Hermann said in an interview. “A bigger concern is the lack of regulations of doctors and facilities in countries like Mexico.”
Some employers pay for treatment at certain foreign clinics, and Blue Shield of California’s HMO plan, Access Baja, covers care in certain clinics in Mexico’s Baja peninsula. But U.S. health insurance generally does not cover medical tourism.
Despite its popularity, medical tourism is not siphoning off a significant number of patients from U.S. doctors, with the possible exception of plastic surgery. One study found that medical tourism accounts for less than 2% of U.S. spending on noncosmetic health care.
Still, as many as 1.2 million Americans travel to Mexico each year seeking health care at lower costs, particularly dental care, bariatric surgery, and cosmetic procedures.
Physicians such as Dr. Hermann see the results when things go awry. Dr. Hermann said when he takes calls at a nearby level II trauma center, he sees, on average, one patient a month with complications from plastic surgeries performed abroad.
Patients tell Dr. Hermann they often had little preoperative time with the surgeons, and some may not even see their surgeon. They have to fly back home just days after their procedures, so complications that typically arise later are missed, he said.
Who opts for medical tourism?
There are few statistics on the number of medical tourists or the clinical problems they have. Josef Woodman, CEO of Patients Beyond Borders, a medical tourism consultancy in Chapel Hill, N.C., has developed a profile of medical tourism that is based on his close contacts within the industry.
Mr. Woodman said the vast majority of U.S. medical tourists go to Mexico, which accounts for an estimated 1 million to 1.2 million medical visitors a year. He said Costa Rica is another popular destination, followed by other Latin American countries and some in the Far East, the Middle East, and Eastern Europe.
Mr. Woodman estimates that dental treatments make up 65% of all medical tourism. Cosmetic procedures come in a distant second, at 15%. Cosmetic procedures can be expensive and are rarely covered by insurance. They can be performed at half the price abroad, he said.
According to Mr. Woodman, other significant fields for medical tourism are orthopedics, which accounts for 5% of all visits, and bariatrics, with 3%-5%. Hip and knee replacements are expensive, and in the case of bariatrics, U.S. insurers often deny coverage, he said.
People also go abroad for fertility care and organ transplants, and one Jamaica company even offered dialysis vacations for U.S. tourists.
On the other hand, medical tourism does not work well for cancer treatments, because cancer care involves long periods of treatment and cannot be completed in a trip or two, Mr. Woodman said. “The media also plays up major procedures like open heart surgery, but they are in fact very rare,” he added.
What patients are looking for
Medical tourists typically pay 50%-70% of what they would pay in the United States for the same procedure, Mr. Woodman said. Prices are lower because patients pay in cash, foreign wages are lower, and expenses such as malpractice insurance are much lower.
“Many medical tourists don’t have a choice,” Mr. Woodman said. “They cannot afford the U.S. price for the procedure, even if they have health insurance, because they often have a high deductible.” In one study, the majority of medical tourists to Mexico reported an income of $25,000-$50,000 a year.
That same study also found that the average age of medical tourists was just under 65. These older patients often come for a vacation. “A sizable number of medical tourists are looking for surgery plus a vacation, a tummy-tuck and a stay at an all-inclusive resort,” said Steven P. Davison, MD, DDS, a plastic surgeon in Washington, who has written on the phenomenon.
Another large group of medical tourists are immigrants to the United States who want surgery in their country of origin, such as Brazil or Iran, Dr. Davison said, perhaps because they feel more comfortable or have family members who can act as caregivers. He said some go to places that have expertise in a certain procedure.
“For instance, they get their hair transplantation done in Turkey because surgeons there have the expertise and it’s cheaper than in the United States,” Dr. Davison said.
Arranging the trip
Patients often find foreign providers through online brokers who can arrange the flight, hotel, clinic, and physician. Brokers are not unbiased because they are usually paid by the clinic. Mr. Woodman said this arrangement works when the broker can offer a wide variety of options but not when the broker represents just a few clinics.
Mr. Woodman said patients could conceivably make their own arrangements without a broker, and some do so. “All the tools are on the Internet,” he said. “However, many people don’t trust themselves to do this work.”
Even for patients who depend on brokers, Mr. Woodman advises verifying the quality of the clinic and its doctors before signing on. Most countries have online lists of registered doctors, and patients seeking health care can research complaints against a doctor.
There is no insurance that patients can have to guard against the risks of medical tourism, Mr. Woodman said. “When you could get it, it was prohibitively expensive,” he said. “You can get travel insurance, but that just covers peripheral problems, such as flight cancellations, accidental injury, and emergency care. It has nothing to do with problems stemming from planned procedures.
“Some clinics and hospitals serving medical tourists provide warranties on their work,” he added. “However, plastic surgery clinics are less likely to offer warranties, because patients are so frequently dissatisfied.”
How things can go wrong
Mr. Woodman said medical tourists may often receive substandard care when they select a provider who offers unusually large savings, such as 80% off the U.S. price. “Those providers are likely cutting corners to get that kind of savings, and you should stay away from them,” he said.
Even when receiving care at an excellent clinic, patients can get infections if postoperative requirements are not followed, according to Darrick E. Antell, MD, a plastic surgeon in New York, who has treated medical tourists upon their return to the United States.
Typically, patients are told to stay in their rooms for several days after the operation, but friends may push them to go out and have fun, he said. Sometimes patients choose exotic arrangements that place them at risk for infection. As an example, Dr. Antell mentioned a broker who offered a safari in combination with plastic surgery.
Dr. Hermann said tummy tucks are riskier because they involve large incisions, and many such patients are overweight, which impairs healing. “Tummy-tuck patients need a longer recovery, and they often have more discomfort than other plastic surgery,” he said.
When things go wrong, medical tourists have few legal protections. “They usually don’t go to an accredited facility, there is no credentialing of physicians, and their ability to sue is extremely limited,” Dr. Davison said. Patients would have to return to the foreign country and hire a lawyer there, and even then, it is harder to win a case and to receive an award as high as in the United States, he added.
Dealing with follow-ups
An inherent flaw with medical tourism, Dr. Antell said, is that patients typically go back home before postoperative care is fully completed. “They may stay just a few days after surgery, and then fly back home,” he said.
“Patients who have complex operations abroad should stay for 8-10 days to have a proper follow-up,” he said. “But they fly back early, which can also lead to getting pulmonary embolisms on the flight.
“A checkup right after surgery doesn’t uncover many complications, because these tend to occur 7-12 days after surgery,” Dr. Hermann said.
“If they come to me within 3 months after surgery, I charge an upfront fee just to see them, because it takes an hour of my time,” Dr. Davison said. “Then I will take care of acute emergency, such as taking out an infected implant.”
Hermann said many patients wait too long to have their complications treated in the United States. “They may first try calling their doctor in Mexico, who tells them to take some antibiotics or something,” he said. “So when they finally do seek care, the infection is pretty far along.”
What U.S. doctors can do
Patients rarely tell their U.S. doctors that they are planning a trip to a foreign country to undergo medical treatment, even though they have to request a copy of their medical records for the foreign doctor, Mr. Woodman said.
Dr. Hermann said only one of his patients told him she was planning to go aboard for plastic surgery. “She was a young mom, and I tried to talk her out of it,” he said. “I don’t know what happened because she didn’t come back.”
Dr. Hermann said doctors should assume that they won’t be able to change their patients’ minds, and they should try to help their patients make the best of it.
“They should insist on seeing the doctor ahead of time and make sure they get along with them,” he said. “Ask for credentialing of the doctor and the facility, and stay there several weeks post op. But they’re probably not going to do all of this.”
A version of this article first appeared on Medscape.com.
Chaperones for physical exams? Doctors and patients weigh in
News of physicians accused or convicted of sexually inappropriate behavior toward patients during medical exams has been frequent recently. And patient advocates have brought up the fact that many patients are uncomfortable during sensitive exams.
As a result, more
For some institutions, the movement has been toward mandating chaperones. Chaperones can be present for any examination of what are often referred to as sensitive areas, such as breasts, genitalia, and the perianal area. For example, Yale University Health requires patients to use a medical staff member as a chaperone for all sensitive exams except in emergency situations. UCLA Health, on the other hand, allows any adult or child aged 12 years or older to decline a chaperone if they wish to do so. Michigan Medicine provides a chaperone on request, although a patient can opt out.
Many physicians fully support the concept. “If a patient requests a chaperone I think we all, as practitioners, should honor that request respectfully,” said Shieva Ghofrany, MD, an ob.gyn. practicing in Stamford, Conn., and cofounder of tribecalledv, a women’s health knowledge platform. “It’s a clear sign a patient wants to ensure that they feel safe and comfortable.”
However, using a chaperone can be challenging for many primary care physicians and specialists in terms of logistics. Should a chaperone’s job be purely observational? Or should the chaperone also be a medical professional who assists during the procedure? How, specifically, should a chaperone perform their duty during an exam? Where should the chaperone stand? What about legal and ethical ramifications?
Who should be a chaperone?
The role of a chaperone is sometimes vaguely defined. It’s logical that a chaperone should have sufficient medical knowledge. Could it be a medical student? Should it be a nurse or another doctor? Would a patient representative suffice even if they aren’t a direct-care clinician?
There are no set standards about who can assume the role. However, the American Medical Association recommends that a patient chaperone be an authorized member of a health care team. For many patients, this is vital.
“As a survivor of sexual assault by an ob.gyn. while I was pregnant, I can assure you that the heinous crime committed against me and hundreds of other women would have been prevented had there been another medical professional in the room,” said Laurie Kanyok, founder of a dance company in New York City, whose former doctor was recently convicted of federal sex abuse charges and is scheduled to be sentenced in July 2023. “The chaperone should be a physician assistant, nurse or medical professional. Qualified professionals better understand the nature and protocols of an exam.”
For children and adolescents, allowing a parent to be a chaperone might be a logical and comforting choice. However, a new British study found that it’s not appropriate.
Study authors Rebecca Jane Moon and Justin Huw Davies looked at pubertal staging–related exams and contend that a chaperone should always be impartial, and a parent’s presence could conceivably open up a physician to false charges of misconduct.
The solution: A parent should have the option be present during any physical exam of their child, with a medical professional additionally acting as chaperone. This can also work for any patient who wishes to bring a trusted friend or family member to their medical appointments.
How does a chaperoned exam work?
A research team from the Medical College of Wisconsin and Louisiana State University Health conducted a recent systematic review of patient and clinician perspectives on carrying out a chaperoned urology exam. The review found that the protocol could use improvement. For example, it was reported that over one-quarter of patients didn’t feel comfortable asking for a chaperone if they were not offered one. “Patients should not have to request this,” said Diana Londoño, MD, a board-certified urologist and assistant clinical professor at City of Hope National Medical Center in Duarte, Calif.
The researchers also found that 93% of female patients preferred a chaperone of the same gender, whereas male patients were split on this issue. Key duties of a chaperone should be to ensure privacy, help interpret instructions from doctor to patient, and continually clarify that consent is being requested as a sensitive exam proceeds, the researchers report. Although clinical practice standards for chaperones aren’t uniform, keeping these important points in mind can easily be adopted by any health care provider.
Many doctors do follow their own set guidelines. “Often, we have our medical assistants be our chaperones,” explained Dr. Ghofrany. “Ideally they ‘room’ the patient – take vitals and ask the patient what specific concerns they would like to address. This helps with exam set-up.
“For example, if a patient has a breast concern versus a concern about their genital area, this would change what drapes are used. The medical assistant would then stand near me if they are helping with a Pap smear or cultures, or they may stand by the patient’s head at the bedside and offer support if needed. Some patients want to hold someone’s hand during an uncomfortable exam.”
The issue of positioning is important. A patient may feel very uneasy if it appears that the chaperone is looking at their body from the doctor’s angle, negating the point of reassurance. The key is to explain before an exam exactly how a chaperone is needed during the exam itself and whether the chaperone is a medical assistant or nurse.
“Chaperones usually stand next to me on either side or on the side of the patient facing me, depending on if they are immediately assisting me or helping the patient,” said Dr. Londoño. If a chaperone will be moving back and forth during the exam, that should be conveyed as well. For virtual visits, a chaperone can act as a third party and be present on a split screen, a process Michigan Medicine uses.
It’s also important to inform patients that a chaperone can step in and stop an exam at any point, both at the patient’s request or because of any observation of inappropriate physician behavior. Understanding this can help reluctant patients feel less worry.
When Christian Miller was diagnosed with a sleep disorder, his doctor suggested having a chaperone present during his physical exams. At first, he was apprehensive but then found the experience to be very positive. “Having someone there with me gave me an extra measure of assurance that nothing untoward would happen,” he said. “I found that having a chaperone was reassuring. The chaperone was not intrusive but stood close enough to ensure everything went smoothly and respectfully.”
Do chaperones help protect physicians legally?
Some states mandate that chaperones be present by patient request during sensitive exams, such as Texas and Oregon. For the most part, though, physicians have no legal obligation to offer chaperones, although it could be in their best interest to do so.
Ob.gyn. is one of the most litigated specialties, for example, so these physicians may find chaperones can play a key role in averting lawsuits. According to data from Physicians’ Insurance, having a reliable witness in an exam room can mitigate claims, and doctors should follow a clear practice policy regarding chaperones for all patients to further reduce liability.
Another advantage to having a chaperone present: protection for a doctor against a problematic patient. The risk for assault or aggression during an exam can of course go both ways. It’s important to be able to prove any patient misconduct through a witness, and a chaperone can lessen the prospect of violence in any form. “Having a chaperone in an exam room is about protecting the doctors as well as the patient,” said Ms. Kanyok.
A chaperone can also defuse ethical dilemmas. Consider a patient who refuses to allow a chaperone in an exam, but a chaperone is required by the physician’s health care organization. Asking a patient to state their reasons for wanting privacy with the chaperone present before the actual exam can help document the patient’s wish respectfully as well as protect a physician and organization from any potential liability if the patient refuses the exam altogether or if an exception for the patient is made.
Making a chaperone policy work best
- Have your staff inform patients of a medical chaperone policy at the time an appointment is made. Have fact sheets available for the patient before appointments fully outlining your policy.
- Inform the chaperone fully about the details of the exam and the patient’s case prior to the exam, in accordance with HIPAA.
- The chaperone can introduce themselves to the patient in the waiting room or exam room before you enter the room. The chaperone can go over the policy again verbally and answer any questions the patient may have initially. You can then clarify whether the patient understands your chaperone policy when you come in.
- Document, document, document. Write down who the chaperone was for each exam in patient notes and note the details of any interactions that are significant, such as patient questions or conflicts.
- Practice respect, above all. “A patient’s safety and level of comfort should be prioritized,” said Ms. Kanyok.
A version of this article first appeared on Medscape.com.
News of physicians accused or convicted of sexually inappropriate behavior toward patients during medical exams has been frequent recently. And patient advocates have brought up the fact that many patients are uncomfortable during sensitive exams.
As a result, more
For some institutions, the movement has been toward mandating chaperones. Chaperones can be present for any examination of what are often referred to as sensitive areas, such as breasts, genitalia, and the perianal area. For example, Yale University Health requires patients to use a medical staff member as a chaperone for all sensitive exams except in emergency situations. UCLA Health, on the other hand, allows any adult or child aged 12 years or older to decline a chaperone if they wish to do so. Michigan Medicine provides a chaperone on request, although a patient can opt out.
Many physicians fully support the concept. “If a patient requests a chaperone I think we all, as practitioners, should honor that request respectfully,” said Shieva Ghofrany, MD, an ob.gyn. practicing in Stamford, Conn., and cofounder of tribecalledv, a women’s health knowledge platform. “It’s a clear sign a patient wants to ensure that they feel safe and comfortable.”
However, using a chaperone can be challenging for many primary care physicians and specialists in terms of logistics. Should a chaperone’s job be purely observational? Or should the chaperone also be a medical professional who assists during the procedure? How, specifically, should a chaperone perform their duty during an exam? Where should the chaperone stand? What about legal and ethical ramifications?
Who should be a chaperone?
The role of a chaperone is sometimes vaguely defined. It’s logical that a chaperone should have sufficient medical knowledge. Could it be a medical student? Should it be a nurse or another doctor? Would a patient representative suffice even if they aren’t a direct-care clinician?
There are no set standards about who can assume the role. However, the American Medical Association recommends that a patient chaperone be an authorized member of a health care team. For many patients, this is vital.
“As a survivor of sexual assault by an ob.gyn. while I was pregnant, I can assure you that the heinous crime committed against me and hundreds of other women would have been prevented had there been another medical professional in the room,” said Laurie Kanyok, founder of a dance company in New York City, whose former doctor was recently convicted of federal sex abuse charges and is scheduled to be sentenced in July 2023. “The chaperone should be a physician assistant, nurse or medical professional. Qualified professionals better understand the nature and protocols of an exam.”
For children and adolescents, allowing a parent to be a chaperone might be a logical and comforting choice. However, a new British study found that it’s not appropriate.
Study authors Rebecca Jane Moon and Justin Huw Davies looked at pubertal staging–related exams and contend that a chaperone should always be impartial, and a parent’s presence could conceivably open up a physician to false charges of misconduct.
The solution: A parent should have the option be present during any physical exam of their child, with a medical professional additionally acting as chaperone. This can also work for any patient who wishes to bring a trusted friend or family member to their medical appointments.
How does a chaperoned exam work?
A research team from the Medical College of Wisconsin and Louisiana State University Health conducted a recent systematic review of patient and clinician perspectives on carrying out a chaperoned urology exam. The review found that the protocol could use improvement. For example, it was reported that over one-quarter of patients didn’t feel comfortable asking for a chaperone if they were not offered one. “Patients should not have to request this,” said Diana Londoño, MD, a board-certified urologist and assistant clinical professor at City of Hope National Medical Center in Duarte, Calif.
The researchers also found that 93% of female patients preferred a chaperone of the same gender, whereas male patients were split on this issue. Key duties of a chaperone should be to ensure privacy, help interpret instructions from doctor to patient, and continually clarify that consent is being requested as a sensitive exam proceeds, the researchers report. Although clinical practice standards for chaperones aren’t uniform, keeping these important points in mind can easily be adopted by any health care provider.
Many doctors do follow their own set guidelines. “Often, we have our medical assistants be our chaperones,” explained Dr. Ghofrany. “Ideally they ‘room’ the patient – take vitals and ask the patient what specific concerns they would like to address. This helps with exam set-up.
“For example, if a patient has a breast concern versus a concern about their genital area, this would change what drapes are used. The medical assistant would then stand near me if they are helping with a Pap smear or cultures, or they may stand by the patient’s head at the bedside and offer support if needed. Some patients want to hold someone’s hand during an uncomfortable exam.”
The issue of positioning is important. A patient may feel very uneasy if it appears that the chaperone is looking at their body from the doctor’s angle, negating the point of reassurance. The key is to explain before an exam exactly how a chaperone is needed during the exam itself and whether the chaperone is a medical assistant or nurse.
“Chaperones usually stand next to me on either side or on the side of the patient facing me, depending on if they are immediately assisting me or helping the patient,” said Dr. Londoño. If a chaperone will be moving back and forth during the exam, that should be conveyed as well. For virtual visits, a chaperone can act as a third party and be present on a split screen, a process Michigan Medicine uses.
It’s also important to inform patients that a chaperone can step in and stop an exam at any point, both at the patient’s request or because of any observation of inappropriate physician behavior. Understanding this can help reluctant patients feel less worry.
When Christian Miller was diagnosed with a sleep disorder, his doctor suggested having a chaperone present during his physical exams. At first, he was apprehensive but then found the experience to be very positive. “Having someone there with me gave me an extra measure of assurance that nothing untoward would happen,” he said. “I found that having a chaperone was reassuring. The chaperone was not intrusive but stood close enough to ensure everything went smoothly and respectfully.”
Do chaperones help protect physicians legally?
Some states mandate that chaperones be present by patient request during sensitive exams, such as Texas and Oregon. For the most part, though, physicians have no legal obligation to offer chaperones, although it could be in their best interest to do so.
Ob.gyn. is one of the most litigated specialties, for example, so these physicians may find chaperones can play a key role in averting lawsuits. According to data from Physicians’ Insurance, having a reliable witness in an exam room can mitigate claims, and doctors should follow a clear practice policy regarding chaperones for all patients to further reduce liability.
Another advantage to having a chaperone present: protection for a doctor against a problematic patient. The risk for assault or aggression during an exam can of course go both ways. It’s important to be able to prove any patient misconduct through a witness, and a chaperone can lessen the prospect of violence in any form. “Having a chaperone in an exam room is about protecting the doctors as well as the patient,” said Ms. Kanyok.
A chaperone can also defuse ethical dilemmas. Consider a patient who refuses to allow a chaperone in an exam, but a chaperone is required by the physician’s health care organization. Asking a patient to state their reasons for wanting privacy with the chaperone present before the actual exam can help document the patient’s wish respectfully as well as protect a physician and organization from any potential liability if the patient refuses the exam altogether or if an exception for the patient is made.
Making a chaperone policy work best
- Have your staff inform patients of a medical chaperone policy at the time an appointment is made. Have fact sheets available for the patient before appointments fully outlining your policy.
- Inform the chaperone fully about the details of the exam and the patient’s case prior to the exam, in accordance with HIPAA.
- The chaperone can introduce themselves to the patient in the waiting room or exam room before you enter the room. The chaperone can go over the policy again verbally and answer any questions the patient may have initially. You can then clarify whether the patient understands your chaperone policy when you come in.
- Document, document, document. Write down who the chaperone was for each exam in patient notes and note the details of any interactions that are significant, such as patient questions or conflicts.
- Practice respect, above all. “A patient’s safety and level of comfort should be prioritized,” said Ms. Kanyok.
A version of this article first appeared on Medscape.com.
News of physicians accused or convicted of sexually inappropriate behavior toward patients during medical exams has been frequent recently. And patient advocates have brought up the fact that many patients are uncomfortable during sensitive exams.
As a result, more
For some institutions, the movement has been toward mandating chaperones. Chaperones can be present for any examination of what are often referred to as sensitive areas, such as breasts, genitalia, and the perianal area. For example, Yale University Health requires patients to use a medical staff member as a chaperone for all sensitive exams except in emergency situations. UCLA Health, on the other hand, allows any adult or child aged 12 years or older to decline a chaperone if they wish to do so. Michigan Medicine provides a chaperone on request, although a patient can opt out.
Many physicians fully support the concept. “If a patient requests a chaperone I think we all, as practitioners, should honor that request respectfully,” said Shieva Ghofrany, MD, an ob.gyn. practicing in Stamford, Conn., and cofounder of tribecalledv, a women’s health knowledge platform. “It’s a clear sign a patient wants to ensure that they feel safe and comfortable.”
However, using a chaperone can be challenging for many primary care physicians and specialists in terms of logistics. Should a chaperone’s job be purely observational? Or should the chaperone also be a medical professional who assists during the procedure? How, specifically, should a chaperone perform their duty during an exam? Where should the chaperone stand? What about legal and ethical ramifications?
Who should be a chaperone?
The role of a chaperone is sometimes vaguely defined. It’s logical that a chaperone should have sufficient medical knowledge. Could it be a medical student? Should it be a nurse or another doctor? Would a patient representative suffice even if they aren’t a direct-care clinician?
There are no set standards about who can assume the role. However, the American Medical Association recommends that a patient chaperone be an authorized member of a health care team. For many patients, this is vital.
“As a survivor of sexual assault by an ob.gyn. while I was pregnant, I can assure you that the heinous crime committed against me and hundreds of other women would have been prevented had there been another medical professional in the room,” said Laurie Kanyok, founder of a dance company in New York City, whose former doctor was recently convicted of federal sex abuse charges and is scheduled to be sentenced in July 2023. “The chaperone should be a physician assistant, nurse or medical professional. Qualified professionals better understand the nature and protocols of an exam.”
For children and adolescents, allowing a parent to be a chaperone might be a logical and comforting choice. However, a new British study found that it’s not appropriate.
Study authors Rebecca Jane Moon and Justin Huw Davies looked at pubertal staging–related exams and contend that a chaperone should always be impartial, and a parent’s presence could conceivably open up a physician to false charges of misconduct.
The solution: A parent should have the option be present during any physical exam of their child, with a medical professional additionally acting as chaperone. This can also work for any patient who wishes to bring a trusted friend or family member to their medical appointments.
How does a chaperoned exam work?
A research team from the Medical College of Wisconsin and Louisiana State University Health conducted a recent systematic review of patient and clinician perspectives on carrying out a chaperoned urology exam. The review found that the protocol could use improvement. For example, it was reported that over one-quarter of patients didn’t feel comfortable asking for a chaperone if they were not offered one. “Patients should not have to request this,” said Diana Londoño, MD, a board-certified urologist and assistant clinical professor at City of Hope National Medical Center in Duarte, Calif.
The researchers also found that 93% of female patients preferred a chaperone of the same gender, whereas male patients were split on this issue. Key duties of a chaperone should be to ensure privacy, help interpret instructions from doctor to patient, and continually clarify that consent is being requested as a sensitive exam proceeds, the researchers report. Although clinical practice standards for chaperones aren’t uniform, keeping these important points in mind can easily be adopted by any health care provider.
Many doctors do follow their own set guidelines. “Often, we have our medical assistants be our chaperones,” explained Dr. Ghofrany. “Ideally they ‘room’ the patient – take vitals and ask the patient what specific concerns they would like to address. This helps with exam set-up.
“For example, if a patient has a breast concern versus a concern about their genital area, this would change what drapes are used. The medical assistant would then stand near me if they are helping with a Pap smear or cultures, or they may stand by the patient’s head at the bedside and offer support if needed. Some patients want to hold someone’s hand during an uncomfortable exam.”
The issue of positioning is important. A patient may feel very uneasy if it appears that the chaperone is looking at their body from the doctor’s angle, negating the point of reassurance. The key is to explain before an exam exactly how a chaperone is needed during the exam itself and whether the chaperone is a medical assistant or nurse.
“Chaperones usually stand next to me on either side or on the side of the patient facing me, depending on if they are immediately assisting me or helping the patient,” said Dr. Londoño. If a chaperone will be moving back and forth during the exam, that should be conveyed as well. For virtual visits, a chaperone can act as a third party and be present on a split screen, a process Michigan Medicine uses.
It’s also important to inform patients that a chaperone can step in and stop an exam at any point, both at the patient’s request or because of any observation of inappropriate physician behavior. Understanding this can help reluctant patients feel less worry.
When Christian Miller was diagnosed with a sleep disorder, his doctor suggested having a chaperone present during his physical exams. At first, he was apprehensive but then found the experience to be very positive. “Having someone there with me gave me an extra measure of assurance that nothing untoward would happen,” he said. “I found that having a chaperone was reassuring. The chaperone was not intrusive but stood close enough to ensure everything went smoothly and respectfully.”
Do chaperones help protect physicians legally?
Some states mandate that chaperones be present by patient request during sensitive exams, such as Texas and Oregon. For the most part, though, physicians have no legal obligation to offer chaperones, although it could be in their best interest to do so.
Ob.gyn. is one of the most litigated specialties, for example, so these physicians may find chaperones can play a key role in averting lawsuits. According to data from Physicians’ Insurance, having a reliable witness in an exam room can mitigate claims, and doctors should follow a clear practice policy regarding chaperones for all patients to further reduce liability.
Another advantage to having a chaperone present: protection for a doctor against a problematic patient. The risk for assault or aggression during an exam can of course go both ways. It’s important to be able to prove any patient misconduct through a witness, and a chaperone can lessen the prospect of violence in any form. “Having a chaperone in an exam room is about protecting the doctors as well as the patient,” said Ms. Kanyok.
A chaperone can also defuse ethical dilemmas. Consider a patient who refuses to allow a chaperone in an exam, but a chaperone is required by the physician’s health care organization. Asking a patient to state their reasons for wanting privacy with the chaperone present before the actual exam can help document the patient’s wish respectfully as well as protect a physician and organization from any potential liability if the patient refuses the exam altogether or if an exception for the patient is made.
Making a chaperone policy work best
- Have your staff inform patients of a medical chaperone policy at the time an appointment is made. Have fact sheets available for the patient before appointments fully outlining your policy.
- Inform the chaperone fully about the details of the exam and the patient’s case prior to the exam, in accordance with HIPAA.
- The chaperone can introduce themselves to the patient in the waiting room or exam room before you enter the room. The chaperone can go over the policy again verbally and answer any questions the patient may have initially. You can then clarify whether the patient understands your chaperone policy when you come in.
- Document, document, document. Write down who the chaperone was for each exam in patient notes and note the details of any interactions that are significant, such as patient questions or conflicts.
- Practice respect, above all. “A patient’s safety and level of comfort should be prioritized,” said Ms. Kanyok.
A version of this article first appeared on Medscape.com.
Over-the-counter switches improve access but come with risks
On July 13, the Food and Drug Administration approved the first over-the-counter (OTC) norgestrel birth control pill (Opill). The daily oral contraceptive was approved for prescription use 5 decades ago, providing regulators with a half-century of data to show that the progestin-only drug can be used safely without a prescription.
The drug is the latest in a series of medications that have made the switch from behind the pharmacy counter to retail shelves.
Why switch?
When a drug manufacturer submits a proposal for a switch to OTC, the key question that the FDA considers is patient safety. Some risks can be mitigated by approving OTC drugs at lower doses than what is available as the prescription version.
“There is no drug that doesn’t have risks,” said Almut G. Winterstein, RPh, PhD, a distinguished professor in pharmaceutical outcomes and policy and director of the Center for Drug Evaluation and Safety at the University of Florida, Gainesville. “Risks are mitigated by putting specific constraints around access to those medications.”
Dr. Winterstein, a former chair of the FDA’s Drug Safety and Risk Management Advisory Committee, said that nonprescription drugs are unnecessary in a functional health care system.
Many patients may struggle with accessing health clinicians, so making medications available OTC fills gaps left by not being able to get a prescription, according to Dr. Winterstein.
A 2012 paper funded by the Consumer Healthcare Products Association (CHPA), the organization representing manufacturers and distributors of OTC medications, estimated that one quarter of people who bought OTC drugs would not otherwise seek treatment if these treatments were available only via prescription. The CHPA notes that the number of those who experience allergies who use nonprescription antihistamines and allergy-relief drugs increased by about 10% between 2009 and 2015.
Cholesterol drugs
Approximately 80 million U.S. adults are eligible for cholesterol-lowering medications, particularly statins, but nearly half don’t take them, according to the Centers for Disease Control and Prevention.
Fear of side effects is the most common reason people might avoid taking these drugs. But eliminating the need for a refill may encourage uptake of the statins.
“It’s refill, refill, refill,” said Allen J. Taylor, MD, chairman of cardiology at MedStar Heart and Vascular Institute, in Washington. “We spend a ton of time refilling statins and it’s a headache for patients, too.”
The need to secure regular prescriptions for the drug, “doesn’t put enough trust and faith in pharmacists and doesn’t put enough trust and faith in patients,” Dr. Taylor said.
Moving statins to the front end of a pharmacy might not be the best move given the potential for drug interactions, but a nonprescription behind-the-counter approach could work, according to Dr. Taylor.
“The concerns are modest at most, to where they can be monitored by a pharmacist,” he said. “There’s probably more people that would take a statin if they had that kind of access.”
Many statin manufacturers have attempted to make the prescription-to-OTC switch. In 2005, an FDA advisory panel rejected Merck’s proposal for OTC sales of lovastatin after reviewing a study that found only 55% of OTC purchases would have been medically appropriate.
In 2015, Pfizer pulled its application to make the cholesterol drug atorvastatin available to patients OTC because patients were not using the drug correctly. AstraZeneca is investigating an online platform that would allow patients to self-assess their eligibility for rosuvastatin.
Asthma inhalers
Inhalers are the main rescue therapy for asthma aside from a visit to the ED.
The only inhaler available OTC is epinephrine sold under the brand name Primatene Mist, but this type of medicine device is not recommended as a first-line therapy for acute asthma symptoms, according to the American Medical Association.
“It’s been around for a long time and has stayed over the counter even though newer, safer agents have come onto the market which aren’t available over the counter,” said William B. Feldman, MD, DPhil, MPH, a pulmonologist at Brigham and Women’s Hospital, Boston.
Patients who have a hard time getting to a doctor or patients who lack insurance often face barriers accessing albuterol inhalers and beta agonist–corticosteroid combinations, according to Dr. Feldman. A switch to OTC distribution would widen access.
“What we’re advocating is, if they’re going to have access to Primatene Mist, wouldn’t it be sensible to have access to a safer and more effective therapy?” Dr. Feldman said.
Triptans
Migraines affect an estimated 39 million people in the United States, according to the American Migraine Foundation. Several drugs to treat migraine are available OTC, including nonsteroidal anti-inflammatory drugs, aspirin, and acetaminophen. Triptans, drugs used for the short-term treatment of acute symptoms, are prescription-only in the United States.
But in the United Kingdom, triptans first became available in retail stores in 2006, leading to reduced costs for patients, employers, and the government. One study found that government health expenditures would be reduced by $84 million annually if the OTC switch were made in six European countries.
However, overuse of the drug and potential contraindications have been cited as concerns with OTC access.
For Dr. Winterstein, the decision to switch isn’t just about the freedom to buy a drug; it comes down to weighing potential risks and benefits.
“Drugs are only as good as if they’re used in the context of how they should be used,” Dr. Winterstein said. “It’s not candy.”
A version of this article first appeared on Medscape.com.
On July 13, the Food and Drug Administration approved the first over-the-counter (OTC) norgestrel birth control pill (Opill). The daily oral contraceptive was approved for prescription use 5 decades ago, providing regulators with a half-century of data to show that the progestin-only drug can be used safely without a prescription.
The drug is the latest in a series of medications that have made the switch from behind the pharmacy counter to retail shelves.
Why switch?
When a drug manufacturer submits a proposal for a switch to OTC, the key question that the FDA considers is patient safety. Some risks can be mitigated by approving OTC drugs at lower doses than what is available as the prescription version.
“There is no drug that doesn’t have risks,” said Almut G. Winterstein, RPh, PhD, a distinguished professor in pharmaceutical outcomes and policy and director of the Center for Drug Evaluation and Safety at the University of Florida, Gainesville. “Risks are mitigated by putting specific constraints around access to those medications.”
Dr. Winterstein, a former chair of the FDA’s Drug Safety and Risk Management Advisory Committee, said that nonprescription drugs are unnecessary in a functional health care system.
Many patients may struggle with accessing health clinicians, so making medications available OTC fills gaps left by not being able to get a prescription, according to Dr. Winterstein.
A 2012 paper funded by the Consumer Healthcare Products Association (CHPA), the organization representing manufacturers and distributors of OTC medications, estimated that one quarter of people who bought OTC drugs would not otherwise seek treatment if these treatments were available only via prescription. The CHPA notes that the number of those who experience allergies who use nonprescription antihistamines and allergy-relief drugs increased by about 10% between 2009 and 2015.
Cholesterol drugs
Approximately 80 million U.S. adults are eligible for cholesterol-lowering medications, particularly statins, but nearly half don’t take them, according to the Centers for Disease Control and Prevention.
Fear of side effects is the most common reason people might avoid taking these drugs. But eliminating the need for a refill may encourage uptake of the statins.
“It’s refill, refill, refill,” said Allen J. Taylor, MD, chairman of cardiology at MedStar Heart and Vascular Institute, in Washington. “We spend a ton of time refilling statins and it’s a headache for patients, too.”
The need to secure regular prescriptions for the drug, “doesn’t put enough trust and faith in pharmacists and doesn’t put enough trust and faith in patients,” Dr. Taylor said.
Moving statins to the front end of a pharmacy might not be the best move given the potential for drug interactions, but a nonprescription behind-the-counter approach could work, according to Dr. Taylor.
“The concerns are modest at most, to where they can be monitored by a pharmacist,” he said. “There’s probably more people that would take a statin if they had that kind of access.”
Many statin manufacturers have attempted to make the prescription-to-OTC switch. In 2005, an FDA advisory panel rejected Merck’s proposal for OTC sales of lovastatin after reviewing a study that found only 55% of OTC purchases would have been medically appropriate.
In 2015, Pfizer pulled its application to make the cholesterol drug atorvastatin available to patients OTC because patients were not using the drug correctly. AstraZeneca is investigating an online platform that would allow patients to self-assess their eligibility for rosuvastatin.
Asthma inhalers
Inhalers are the main rescue therapy for asthma aside from a visit to the ED.
The only inhaler available OTC is epinephrine sold under the brand name Primatene Mist, but this type of medicine device is not recommended as a first-line therapy for acute asthma symptoms, according to the American Medical Association.
“It’s been around for a long time and has stayed over the counter even though newer, safer agents have come onto the market which aren’t available over the counter,” said William B. Feldman, MD, DPhil, MPH, a pulmonologist at Brigham and Women’s Hospital, Boston.
Patients who have a hard time getting to a doctor or patients who lack insurance often face barriers accessing albuterol inhalers and beta agonist–corticosteroid combinations, according to Dr. Feldman. A switch to OTC distribution would widen access.
“What we’re advocating is, if they’re going to have access to Primatene Mist, wouldn’t it be sensible to have access to a safer and more effective therapy?” Dr. Feldman said.
Triptans
Migraines affect an estimated 39 million people in the United States, according to the American Migraine Foundation. Several drugs to treat migraine are available OTC, including nonsteroidal anti-inflammatory drugs, aspirin, and acetaminophen. Triptans, drugs used for the short-term treatment of acute symptoms, are prescription-only in the United States.
But in the United Kingdom, triptans first became available in retail stores in 2006, leading to reduced costs for patients, employers, and the government. One study found that government health expenditures would be reduced by $84 million annually if the OTC switch were made in six European countries.
However, overuse of the drug and potential contraindications have been cited as concerns with OTC access.
For Dr. Winterstein, the decision to switch isn’t just about the freedom to buy a drug; it comes down to weighing potential risks and benefits.
“Drugs are only as good as if they’re used in the context of how they should be used,” Dr. Winterstein said. “It’s not candy.”
A version of this article first appeared on Medscape.com.
On July 13, the Food and Drug Administration approved the first over-the-counter (OTC) norgestrel birth control pill (Opill). The daily oral contraceptive was approved for prescription use 5 decades ago, providing regulators with a half-century of data to show that the progestin-only drug can be used safely without a prescription.
The drug is the latest in a series of medications that have made the switch from behind the pharmacy counter to retail shelves.
Why switch?
When a drug manufacturer submits a proposal for a switch to OTC, the key question that the FDA considers is patient safety. Some risks can be mitigated by approving OTC drugs at lower doses than what is available as the prescription version.
“There is no drug that doesn’t have risks,” said Almut G. Winterstein, RPh, PhD, a distinguished professor in pharmaceutical outcomes and policy and director of the Center for Drug Evaluation and Safety at the University of Florida, Gainesville. “Risks are mitigated by putting specific constraints around access to those medications.”
Dr. Winterstein, a former chair of the FDA’s Drug Safety and Risk Management Advisory Committee, said that nonprescription drugs are unnecessary in a functional health care system.
Many patients may struggle with accessing health clinicians, so making medications available OTC fills gaps left by not being able to get a prescription, according to Dr. Winterstein.
A 2012 paper funded by the Consumer Healthcare Products Association (CHPA), the organization representing manufacturers and distributors of OTC medications, estimated that one quarter of people who bought OTC drugs would not otherwise seek treatment if these treatments were available only via prescription. The CHPA notes that the number of those who experience allergies who use nonprescription antihistamines and allergy-relief drugs increased by about 10% between 2009 and 2015.
Cholesterol drugs
Approximately 80 million U.S. adults are eligible for cholesterol-lowering medications, particularly statins, but nearly half don’t take them, according to the Centers for Disease Control and Prevention.
Fear of side effects is the most common reason people might avoid taking these drugs. But eliminating the need for a refill may encourage uptake of the statins.
“It’s refill, refill, refill,” said Allen J. Taylor, MD, chairman of cardiology at MedStar Heart and Vascular Institute, in Washington. “We spend a ton of time refilling statins and it’s a headache for patients, too.”
The need to secure regular prescriptions for the drug, “doesn’t put enough trust and faith in pharmacists and doesn’t put enough trust and faith in patients,” Dr. Taylor said.
Moving statins to the front end of a pharmacy might not be the best move given the potential for drug interactions, but a nonprescription behind-the-counter approach could work, according to Dr. Taylor.
“The concerns are modest at most, to where they can be monitored by a pharmacist,” he said. “There’s probably more people that would take a statin if they had that kind of access.”
Many statin manufacturers have attempted to make the prescription-to-OTC switch. In 2005, an FDA advisory panel rejected Merck’s proposal for OTC sales of lovastatin after reviewing a study that found only 55% of OTC purchases would have been medically appropriate.
In 2015, Pfizer pulled its application to make the cholesterol drug atorvastatin available to patients OTC because patients were not using the drug correctly. AstraZeneca is investigating an online platform that would allow patients to self-assess their eligibility for rosuvastatin.
Asthma inhalers
Inhalers are the main rescue therapy for asthma aside from a visit to the ED.
The only inhaler available OTC is epinephrine sold under the brand name Primatene Mist, but this type of medicine device is not recommended as a first-line therapy for acute asthma symptoms, according to the American Medical Association.
“It’s been around for a long time and has stayed over the counter even though newer, safer agents have come onto the market which aren’t available over the counter,” said William B. Feldman, MD, DPhil, MPH, a pulmonologist at Brigham and Women’s Hospital, Boston.
Patients who have a hard time getting to a doctor or patients who lack insurance often face barriers accessing albuterol inhalers and beta agonist–corticosteroid combinations, according to Dr. Feldman. A switch to OTC distribution would widen access.
“What we’re advocating is, if they’re going to have access to Primatene Mist, wouldn’t it be sensible to have access to a safer and more effective therapy?” Dr. Feldman said.
Triptans
Migraines affect an estimated 39 million people in the United States, according to the American Migraine Foundation. Several drugs to treat migraine are available OTC, including nonsteroidal anti-inflammatory drugs, aspirin, and acetaminophen. Triptans, drugs used for the short-term treatment of acute symptoms, are prescription-only in the United States.
But in the United Kingdom, triptans first became available in retail stores in 2006, leading to reduced costs for patients, employers, and the government. One study found that government health expenditures would be reduced by $84 million annually if the OTC switch were made in six European countries.
However, overuse of the drug and potential contraindications have been cited as concerns with OTC access.
For Dr. Winterstein, the decision to switch isn’t just about the freedom to buy a drug; it comes down to weighing potential risks and benefits.
“Drugs are only as good as if they’re used in the context of how they should be used,” Dr. Winterstein said. “It’s not candy.”
A version of this article first appeared on Medscape.com.
Indian Health Service dermatologist: ‘I saw a real need to be of service’
After completing his dermatology residency at Johns Hopkins Hospital in 2010, Christopher Bengson, MD, MHS, then a Lieutenant Commander in the U.S. Public Health Service, accepted an offer to become a full-time dermatologist at Phoenix Indian Medical Center (PIMC) in Arizona, fulfilling a long desire to provide care for underserved individuals. Thirteen years later, .
As one of the largest hospitals in the IHS system, PIMC provides direct health care services to a population of more than 156,000, including tribal members from The Fort McDowell Yavapai Nation, the Salt River Pima-Maricopa Indian Community, and the San Lucy District of the Tohono O’odham Nation, the Tonto Apache Tribe, the Yavapai-Apache Indian Tribe, and the Yavapai-Prescott Indian Tribe. Dr. Bengson also cares for tribal members who travel to PIMC from as far away as Washington State and Hawaii to receive dermatologic care.
“There is a disproportionate number of Native American patients that come in with severe psoriasis, hidradenitis suppurativa, and dissecting cellulitis of the scalp compared to the general U.S. population, and I’ve been surprised by how many have nonmelanoma skin cancers and autoimmune connective tissue diseases like lupus, as the prevailing sentiment among his patients is that Native people do not get skin cancer,” he said in an interview. “Those who travel great distances are those who come see me for the surgical removal of skin cancers.”
Interesting cases he’s seen in his nearly 13 years on the job include Epstein-Barr virus-induced NK/T-cell lymphoma, anaplastic large cell lymphoma, subcutaneous panniculitis-like T-cell lymphoma, and necrobiotic xanthogranuloma, “tumors that have generally gone to tertiary care facilities for treatment, but we’ve been able to manage here.”
In 2017, Dr. Bengson was appointed as the IHS’s first chief clinical consultant for dermatology, a post that provides him the opportunity to interface with Native people and IHS-affiliated clinicians nationwide regarding skin-related questions and concerns. As the only full-time dermatologist employed by the IHS, he also views his role as providing an opportunity to change the perception that some Native Americans may still hold about federally delivered health care, “where there may be a cultural distrust of government health care in indigenous communities, driven by generational historical traumas that have come out of boarding schools, population relocation to desolate and isolated areas of the country, and contracts that were simply not honored,” he explained.
“While none of these issues are new, what has been great for me is that I’m going on 13 years of being at the same facility, and I’ve treated family members, their kids, and even their grandkids. In some ways the primary barrier of continuity of care – at least at PIMC – has been eliminated by me just being here for a long period of time.”
In Dr. Bengson’s opinion, efforts to improve access to attract more Native Americans to dermatology are laudable, including the American Academy of Dermatology’s Pathways Program, which aims to increase the number of dermatology residents from Black, Latino, and indigenous communities from approximately 100 residents to 250 residents by 2027, or by over 150%, through community-based engagement strategies that begin in high school.
“To have an objective benchmark is encouraging,” he said. However, he encourages dermatology residency program directors to rethink how they recruit Native Americans, many of whom hail from rural areas. “If you’re recruiting primarily from urban settings, you’re very unlikely to include Native Americans as a larger group of minorities,” he said. “When you look at the number of department chairs who are Native American, it’s on the order of 0.1%, [so] it’s no surprise that dermatologists coming out of a residency program don’t want to go to reservations to provide dermatologic care. We pay a lot of lip service to mentorship programs and things like that, but you need a mentor who follows you through the process – and it’s a long process.”
He believes that residency program directors should reconsider the metrics used to select dermatology residents and should consider the degree of adversity that a Native American applicant may have had to overcome to make it to the residency selection committees.
Despite obstacles to attracting young Native Americans to a career in medicine, Dr. Bengson sees encouraging signs ahead. Some of his Native American patients and family members of patients have enrolled in medical school and have asked to rotate with him at PIMC at the premedical and medical student level. “Some have moved on, not necessarily to dermatology, but to other specialties and careers in health care,” he said. “When you have such high rates of obesity, diabetes, hypertension, coronary artery disease, and stroke in Native American communities, nodulocystic acne and other skin conditions that are not threats to life and limb become less of a priority. We need to get more people in the pipeline to deliver medical services even if it may not be in dermatology, as the need for dedicated health care professionals is so great across all disciplines.”
After completing his dermatology residency at Johns Hopkins Hospital in 2010, Christopher Bengson, MD, MHS, then a Lieutenant Commander in the U.S. Public Health Service, accepted an offer to become a full-time dermatologist at Phoenix Indian Medical Center (PIMC) in Arizona, fulfilling a long desire to provide care for underserved individuals. Thirteen years later, .
As one of the largest hospitals in the IHS system, PIMC provides direct health care services to a population of more than 156,000, including tribal members from The Fort McDowell Yavapai Nation, the Salt River Pima-Maricopa Indian Community, and the San Lucy District of the Tohono O’odham Nation, the Tonto Apache Tribe, the Yavapai-Apache Indian Tribe, and the Yavapai-Prescott Indian Tribe. Dr. Bengson also cares for tribal members who travel to PIMC from as far away as Washington State and Hawaii to receive dermatologic care.
“There is a disproportionate number of Native American patients that come in with severe psoriasis, hidradenitis suppurativa, and dissecting cellulitis of the scalp compared to the general U.S. population, and I’ve been surprised by how many have nonmelanoma skin cancers and autoimmune connective tissue diseases like lupus, as the prevailing sentiment among his patients is that Native people do not get skin cancer,” he said in an interview. “Those who travel great distances are those who come see me for the surgical removal of skin cancers.”
Interesting cases he’s seen in his nearly 13 years on the job include Epstein-Barr virus-induced NK/T-cell lymphoma, anaplastic large cell lymphoma, subcutaneous panniculitis-like T-cell lymphoma, and necrobiotic xanthogranuloma, “tumors that have generally gone to tertiary care facilities for treatment, but we’ve been able to manage here.”
In 2017, Dr. Bengson was appointed as the IHS’s first chief clinical consultant for dermatology, a post that provides him the opportunity to interface with Native people and IHS-affiliated clinicians nationwide regarding skin-related questions and concerns. As the only full-time dermatologist employed by the IHS, he also views his role as providing an opportunity to change the perception that some Native Americans may still hold about federally delivered health care, “where there may be a cultural distrust of government health care in indigenous communities, driven by generational historical traumas that have come out of boarding schools, population relocation to desolate and isolated areas of the country, and contracts that were simply not honored,” he explained.
“While none of these issues are new, what has been great for me is that I’m going on 13 years of being at the same facility, and I’ve treated family members, their kids, and even their grandkids. In some ways the primary barrier of continuity of care – at least at PIMC – has been eliminated by me just being here for a long period of time.”
In Dr. Bengson’s opinion, efforts to improve access to attract more Native Americans to dermatology are laudable, including the American Academy of Dermatology’s Pathways Program, which aims to increase the number of dermatology residents from Black, Latino, and indigenous communities from approximately 100 residents to 250 residents by 2027, or by over 150%, through community-based engagement strategies that begin in high school.
“To have an objective benchmark is encouraging,” he said. However, he encourages dermatology residency program directors to rethink how they recruit Native Americans, many of whom hail from rural areas. “If you’re recruiting primarily from urban settings, you’re very unlikely to include Native Americans as a larger group of minorities,” he said. “When you look at the number of department chairs who are Native American, it’s on the order of 0.1%, [so] it’s no surprise that dermatologists coming out of a residency program don’t want to go to reservations to provide dermatologic care. We pay a lot of lip service to mentorship programs and things like that, but you need a mentor who follows you through the process – and it’s a long process.”
He believes that residency program directors should reconsider the metrics used to select dermatology residents and should consider the degree of adversity that a Native American applicant may have had to overcome to make it to the residency selection committees.
Despite obstacles to attracting young Native Americans to a career in medicine, Dr. Bengson sees encouraging signs ahead. Some of his Native American patients and family members of patients have enrolled in medical school and have asked to rotate with him at PIMC at the premedical and medical student level. “Some have moved on, not necessarily to dermatology, but to other specialties and careers in health care,” he said. “When you have such high rates of obesity, diabetes, hypertension, coronary artery disease, and stroke in Native American communities, nodulocystic acne and other skin conditions that are not threats to life and limb become less of a priority. We need to get more people in the pipeline to deliver medical services even if it may not be in dermatology, as the need for dedicated health care professionals is so great across all disciplines.”
After completing his dermatology residency at Johns Hopkins Hospital in 2010, Christopher Bengson, MD, MHS, then a Lieutenant Commander in the U.S. Public Health Service, accepted an offer to become a full-time dermatologist at Phoenix Indian Medical Center (PIMC) in Arizona, fulfilling a long desire to provide care for underserved individuals. Thirteen years later, .
As one of the largest hospitals in the IHS system, PIMC provides direct health care services to a population of more than 156,000, including tribal members from The Fort McDowell Yavapai Nation, the Salt River Pima-Maricopa Indian Community, and the San Lucy District of the Tohono O’odham Nation, the Tonto Apache Tribe, the Yavapai-Apache Indian Tribe, and the Yavapai-Prescott Indian Tribe. Dr. Bengson also cares for tribal members who travel to PIMC from as far away as Washington State and Hawaii to receive dermatologic care.
“There is a disproportionate number of Native American patients that come in with severe psoriasis, hidradenitis suppurativa, and dissecting cellulitis of the scalp compared to the general U.S. population, and I’ve been surprised by how many have nonmelanoma skin cancers and autoimmune connective tissue diseases like lupus, as the prevailing sentiment among his patients is that Native people do not get skin cancer,” he said in an interview. “Those who travel great distances are those who come see me for the surgical removal of skin cancers.”
Interesting cases he’s seen in his nearly 13 years on the job include Epstein-Barr virus-induced NK/T-cell lymphoma, anaplastic large cell lymphoma, subcutaneous panniculitis-like T-cell lymphoma, and necrobiotic xanthogranuloma, “tumors that have generally gone to tertiary care facilities for treatment, but we’ve been able to manage here.”
In 2017, Dr. Bengson was appointed as the IHS’s first chief clinical consultant for dermatology, a post that provides him the opportunity to interface with Native people and IHS-affiliated clinicians nationwide regarding skin-related questions and concerns. As the only full-time dermatologist employed by the IHS, he also views his role as providing an opportunity to change the perception that some Native Americans may still hold about federally delivered health care, “where there may be a cultural distrust of government health care in indigenous communities, driven by generational historical traumas that have come out of boarding schools, population relocation to desolate and isolated areas of the country, and contracts that were simply not honored,” he explained.
“While none of these issues are new, what has been great for me is that I’m going on 13 years of being at the same facility, and I’ve treated family members, their kids, and even their grandkids. In some ways the primary barrier of continuity of care – at least at PIMC – has been eliminated by me just being here for a long period of time.”
In Dr. Bengson’s opinion, efforts to improve access to attract more Native Americans to dermatology are laudable, including the American Academy of Dermatology’s Pathways Program, which aims to increase the number of dermatology residents from Black, Latino, and indigenous communities from approximately 100 residents to 250 residents by 2027, or by over 150%, through community-based engagement strategies that begin in high school.
“To have an objective benchmark is encouraging,” he said. However, he encourages dermatology residency program directors to rethink how they recruit Native Americans, many of whom hail from rural areas. “If you’re recruiting primarily from urban settings, you’re very unlikely to include Native Americans as a larger group of minorities,” he said. “When you look at the number of department chairs who are Native American, it’s on the order of 0.1%, [so] it’s no surprise that dermatologists coming out of a residency program don’t want to go to reservations to provide dermatologic care. We pay a lot of lip service to mentorship programs and things like that, but you need a mentor who follows you through the process – and it’s a long process.”
He believes that residency program directors should reconsider the metrics used to select dermatology residents and should consider the degree of adversity that a Native American applicant may have had to overcome to make it to the residency selection committees.
Despite obstacles to attracting young Native Americans to a career in medicine, Dr. Bengson sees encouraging signs ahead. Some of his Native American patients and family members of patients have enrolled in medical school and have asked to rotate with him at PIMC at the premedical and medical student level. “Some have moved on, not necessarily to dermatology, but to other specialties and careers in health care,” he said. “When you have such high rates of obesity, diabetes, hypertension, coronary artery disease, and stroke in Native American communities, nodulocystic acne and other skin conditions that are not threats to life and limb become less of a priority. We need to get more people in the pipeline to deliver medical services even if it may not be in dermatology, as the need for dedicated health care professionals is so great across all disciplines.”
Dermatologic care in Indian Country marked by unique challenges, opportunities
As a proud member of the Oglala Lakota Nation from the Pine Ridge Indian Reservation in southwestern South Dakota, Drew Hicks grew up with limited access to basic health care, let alone the luxury of scheduling an appointment with a dermatologist or another medical specialist.
The area – once home to the Lakota war leader Crazy Horse – encompasses nearly 47,000 residents scattered over about 2.2 million acres, larger than the size of Rhode Island, with land marked by rolling mixed grass prairie, sandhills, and badlands. Some of the Oglala Lakota people live in substandard housing and lack regular access to food, running water, and refrigeration, not to mention cell phone and Internet service. “It’s sparse,” said Mr. Hicks, the son of Tribal ranchers who now is a 3rd-year medical student at the Mayo Clinic College of Medicine and Science in Rochester, Minn., and has an early interest in pursuing dermatology. “There is a lot of territory and not a lot of health care serving the population.” From the Hicks home, the nearest place to receive health care is a family medicine practice in Martin, S.D. – about a 15-minute drive on gravel roads in the best of conditions, but in poor weather, it can be difficult, he said. “So, there are environmental challenges besides the limited number of health care providers.”

Clinicians in the practice “did have to be the point of care for everything from dermatologic issues to emergency medicine to delivering a baby, because the next-closest medical facility of any magnitude is 2 hours away,” he said.

Challenges of health literacy and limited access to comprehensive health care at Pine Ridge and other American Indian (AI) and Alaska Native (AN) reservations have long-term consequences. “My own mom struggled to control her blood pressure for years and now has chronic kidney disease,” Mr. Hicks said. “It’s not an uncommon story. Diabetes on the reservation is a big issue.” Then there’s his father, who survived two bouts with melanoma that was diagnosed at an advanced stage. “I think about how that has impacted him, and wonder, had we had a dermatologist who serviced our area, would we have caught things sooner?” he said. “I feel there is so much room for impactful health care deliveries to communities like Pine Ridge.” At the same time, he emphasized, “this isn’t poverty porn. We’re a resilient people. Any effort to engage with AIs or ANs should be from a perspective of a learner, having cultural humility, and seeking out community leaders to help lead you.”
According to the 2020 Census, there are 574 federally recognized sovereign tribal nations in the United States and federal- and state-recognized American Indian reservations in 35 states. AI/AN people make up about 2.9% of the total U.S. population, or 9.7 million, and their life expectancy is an average of 4.4 years less, compared with the general population (a mean of 73.7 vs. 78.1 years, respectively). Because of limited access to dermatologic care in these areas, the risk for developing significant skin conditions and diseases that may go undetected for long stretches of time is increased.
“That can mean advanced skin cancers like basal cell carcinomas that have become larger than what you would see in a typical metropolitan population,” said Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, who spent part of her dermatology residency rotating at the Chinle (Ariz.) Service Unit, an Indian Health Service facility, in 2017 and now provides teledermatology and regular in-person dermatology care at that clinic. “The climate there is dry, so you can see bad eczema and dry skin. There’s also a lot of acne and hidradenitis suppurativa. I think the acne and HS is due to the hyperglycemic index diet from the food deserts. Skin disease reflects the climate, the food desert, and the lack of close specialty care.”
Acne scarring common
Some published evidence suggests that acne is more prevalent and severe in AI/AN individuals. In a survey of 158 AI/AN individuals with a mean age of 32 years, 79.1% reported a history of acne, 55.1% reported acne scarring, and 31% reported having active lesions. “Looking back on my experience in high school, I definitely see that in myself and in my peers,” Mr. Hicks said. And, while there are limited published studies about the incidence of melanoma in this population, an analysis from 2006 found that the incidence was 3.1 per 100,000 between 2001 and 2005, which was an increase from 1.6 per 100,000 reported between 1992 and 2000.
There’s a lot to unpack for dermatologists caring for the AI/AN population besides the raw health disparities: a long history of distrust between AI/AN people and the federal government, structural racism, geographic isolation, health literacy challenges, and high rates of poverty and unemployment. And while individuals from federally recognized tribes have a legal right to receive health care provided by the Indian Health Service, a component of the Department of Health & Human Services, the U.S. Government Accountability Office found that in 2017 per capita spending available to the IHS was $4,078, compared with $8,109 for Medicaid, $10,692 for the Veterans Health Administration, and $13,185 for Medicare.

“Everyone deserves healthy skin and good health,” said Dr. Kohn, whose husband is AI and works in AI law. “Knowing that there are pockets of people who lack that access to care really bothers me. I think the American Indians are frequently overlooked. They’re just not even counted for in certain surveys,” she added, noting that categories are usually defined as Black, Hispanic, Asian, or White.
According to Dr. Kohn, who coauthored a chapter titled “Dermatology on American Indian and Alaska Native Reservations,” for the 2021 book “Dermatology in Rural Settings”, 70% of AIs live in urban areas, “so it’s not just people who live on reservations, though the disparity is greatest there.” To help deliver dermatologic care in the rural areas “where you’re on tribal lands, you must partner with the tribes,” she added. “You must get their permission, operate under their laws and regulations and their rules, learn the local customs, learn about the culture, learn the people, and learn their resources before you practice. That’s the only ethical way to practice.” This also means appreciating the fact that some AI/AN individuals may not understand what a dermatologist could do for them. “One of the bigger hurdles to overcome,” she said, is educating the population that dermatologists can cure skin diseases and that there are good medications for treating the diseases.
Shortcomings of teledermatology
Some dermatologists perform teledermatology visits for tribes, often from an office located in a different time zone. “And, they don’t have a sense of what resources are available for the people they’re serving,” Dr. Kohn said. “For example, if they diagnose a potential skin cancer on the face and say, ‘you need a biopsy,’ but the closest dermatologist is 4 hours away, is that really serving the patient? Or, if you tell a patient, ‘I want you to go out and buy Vanicream for your skin,’ but Vanicream costs $17 and the patient can’t even afford to buy food, are you really doing them a service?”
In a survey-based study of 238 AI individuals that is scheduled to be published in late 2023, Dr. Kohn and colleagues asked respondents at two regional powwows in Denver if they would be open to teledermatology – either in their home or in a primary care clinic. Most respondents (70%) lived in urban areas, the rest in rural settings. Nearly half of respondents (42%) “did not want to do teledermatology, even though they couldn’t access in-person dermatology,” Dr. Kohn said. “So, for people who think teledermatology is the answer [to improving access], the respondents to our survey weren’t interested in pursuing that as a solution. I was surprised by that.” When the researchers broke down the responses by age, teenage respondents were even less interested in teledermatology than adults were. “I think there’s something about having someone see you in person, knowing who you are,” she said.
Partnerships with tribes
To foster more sustainable change in the delivery of skin care beyond remote teledermatology and periodic visits from volunteers, some dermatology residencies have established partnerships with tribes, including Massachusetts General Hospital’s teaching partnership with the Rosebud Sioux tribe in Rosebud, S.D., and the University of Utah dermatology department’s resident continuity clinic with Navajo Nation in Montezuma Creek, Utah. In 2016, officials from the Utah Navajo Health System reached out to the University of Utah’s dermatology department to inquire about the potential for creating a teledermatology clinic to serve patients who receive primary care at the Montezuma Creek Community Health Center, located in Southeastern Utah on the northern tip of the Navajo Nation.
Stephanie Klein, MD, associate professor of dermatology at the university, spearheaded the clinic’s launch but soon encountered obstacles that ranged from not being able to visualize the patient’s skin clearly on her computer screen to difficulty making a personal connection with patients despite help from Navajo translators. “It was hard to build a relationship,” she said. A few years later, she drove down to meet with officials of the health system and posed the question: “What is the ideal thing you would want from dermatology?”
Continuity, they told her. “They said that a lot of the services they receive in the form of outreach are rotational, where someone might come in for a day, or a week, or five people may rotate throughout the year,” which did not serve them well, said Dr. Klein, who subsequently collaborated with Utah Navajo Health System clinicians to establish a resident continuity clinic, which launched in January 2021.

The arrangement also serves as a continuity clinic for Dr. Klein as an attending physician. Each month, she and one dermatology resident drive 6.5 hours from Salt Lake City to Montezuma Creek, where they spend 1 or 2 full days seeing about 25 patients referred by the primary care clinicians who work there. About one-quarter of the time they fly, thanks to financial support from a private donor. The flight takes about an hour, then it’s an hour-long drive to the actual clinic. “It’s a commitment,” Dr. Klein said. “A resident can come with me if they commit to the clinic for at least 1 year. This enables us to have continuity of care; it allows us to build relationships with the patients and with the care team there.” As for the prior teledermatology visits she had with residents, “I still do those, but now I do them in between the in-person visits, so I’m not meeting people over telehealth; I’m just following up with them.”

Situated in the high desert among rock formations, the estimated population of Montezuma Creek is just over 320 people. “It’s a beautiful place with otherworldly buttes and mesas, and the Blue Mountains rising up in the distance,” said Lowell Nicholson, MD, a dermatology resident at the University of Utah who is in his second year of a 2-year commitment to the clinic. “But the landscape can be harsh, and it is underserved from an infrastructure perspective,” with large areas with no cell phone service and limited access to running water and refrigeration. “People in general travel quite far to get their medical care and most of the roads are dirt or gravel, so after a big snowstorm or if it’s been raining, they can become impassable.”

Dermatologic conditions they often encounter include vitiligo, photodermatoses, hidradenitis suppurativa, eczema, psoriasis, and severe acne, often with lots of acne-associated scarring. “In general, we tend to see dramatic or advanced presentations of general dermatology diagnoses,” Dr. Nicholson said. “We see a lot of really extensive psoriasis, which can be socially stigmatizing.”
He recalled one middle-aged man who isolated himself from others because his psoriasis became unbearable. The man refused to leave his house, visit family members, or attend tribal meetups. “He tried to see his regular doctor about it and was given topicals, but his disease was just too extensive,” said Dr. Nicholson, who suggested trying a biologic but learned that the man did not have regular access to refrigeration. “That wasn’t going to work, but we started him on an oral medication, apremilast, which has completely cleared his skin,” he said. “He’s doing great. The last time we saw him he was re-engaged with his family, and he told us he was going on dates. We really improved his quality of life.”
Dr. Klein recalled seeing a 6-year-old girl at the clinic with atopic dermatitis so severe that it caused her to miss several days of school. “When she was in school, she was so distracted by the itching – it was so overwhelming,” she said. She was struggling with topical medicines that weren’t effective, but Dr. Klein got her on dupilumab, and during a follow-up visit the girl told her, “This is the first time in my life I can think about things” other than itching.
According to Dr. Nicholson, some patients seen at the Montezuma Creek clinic are on Medicare or carry standard insurance. “Others have a mix, and others are getting all their medications through the Montezuma Creek clinic or through the IHS clinics,” he said. “I have been surprised at the formulary and our ability to get relatively expensive medications for our patients, like biologics and TNF inhibitors. But it takes some creativity to know what is going to work for your patients’ living situation.”
Training more AI/AN dermatologists key
While efforts to increase the culturally respectful and sustainable dermatologic care for AI/AN individuals continue through programs like the continuity clinic at Montezuma Creek, sources interviewed for this story emphasized the importance of training more AI/AN dermatologists. “Of the people who graduate from high school, AIs have the lowest rate of going on to college,” said Dr. Kohn, who serves as a mentor to Mr. Hicks. “Let’s say they get all the way to medical school; it’s about good mentorship and support in what they’re pursuing. We are seeing more AIs in medical school now, something that I personally notice, and I notice it from what Chinle Service Unit tells me. They have received many requests from Native medical students and premed students who want to rotate at Chinle. Native trainees want the experience of being there.”
According to the Association of American Medical Colleges, the number of AI/AN applicants to medical schools increased from 72 in 2020-2021 to 105 in 2021-2022 but dipped slightly to 94 in 2022-2023. Inspired by a passion to serve Pine Ridge or a community like it, Mr. Hicks decided to apply for medical school. While he doesn’t want to “close any doors” on which medical specialty he ultimately chooses to practice, the current front-runner is dermatology, he said, largely because of the influence of Dr. Kohn and two Mayo dermatologists who have become mentors: Molly Lohman, MD, and Hafsa M. Cantwell, MD. “I didn’t see anyone from my background who was a doctor, so having those role models is so important for Native kids to think, ‘I can do this, too,’ and to pursue it,” he said.
As a proud member of the Oglala Lakota Nation from the Pine Ridge Indian Reservation in southwestern South Dakota, Drew Hicks grew up with limited access to basic health care, let alone the luxury of scheduling an appointment with a dermatologist or another medical specialist.
The area – once home to the Lakota war leader Crazy Horse – encompasses nearly 47,000 residents scattered over about 2.2 million acres, larger than the size of Rhode Island, with land marked by rolling mixed grass prairie, sandhills, and badlands. Some of the Oglala Lakota people live in substandard housing and lack regular access to food, running water, and refrigeration, not to mention cell phone and Internet service. “It’s sparse,” said Mr. Hicks, the son of Tribal ranchers who now is a 3rd-year medical student at the Mayo Clinic College of Medicine and Science in Rochester, Minn., and has an early interest in pursuing dermatology. “There is a lot of territory and not a lot of health care serving the population.” From the Hicks home, the nearest place to receive health care is a family medicine practice in Martin, S.D. – about a 15-minute drive on gravel roads in the best of conditions, but in poor weather, it can be difficult, he said. “So, there are environmental challenges besides the limited number of health care providers.”
Clinicians in the practice “did have to be the point of care for everything from dermatologic issues to emergency medicine to delivering a baby, because the next-closest medical facility of any magnitude is 2 hours away,” he said.
Challenges of health literacy and limited access to comprehensive health care at Pine Ridge and other American Indian (AI) and Alaska Native (AN) reservations have long-term consequences. “My own mom struggled to control her blood pressure for years and now has chronic kidney disease,” Mr. Hicks said. “It’s not an uncommon story. Diabetes on the reservation is a big issue.” Then there’s his father, who survived two bouts with melanoma that was diagnosed at an advanced stage. “I think about how that has impacted him, and wonder, had we had a dermatologist who serviced our area, would we have caught things sooner?” he said. “I feel there is so much room for impactful health care deliveries to communities like Pine Ridge.” At the same time, he emphasized, “this isn’t poverty porn. We’re a resilient people. Any effort to engage with AIs or ANs should be from a perspective of a learner, having cultural humility, and seeking out community leaders to help lead you.”
According to the 2020 Census, there are 574 federally recognized sovereign tribal nations in the United States and federal- and state-recognized American Indian reservations in 35 states. AI/AN people make up about 2.9% of the total U.S. population, or 9.7 million, and their life expectancy is an average of 4.4 years less, compared with the general population (a mean of 73.7 vs. 78.1 years, respectively). Because of limited access to dermatologic care in these areas, the risk for developing significant skin conditions and diseases that may go undetected for long stretches of time is increased.
“That can mean advanced skin cancers like basal cell carcinomas that have become larger than what you would see in a typical metropolitan population,” said Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, who spent part of her dermatology residency rotating at the Chinle (Ariz.) Service Unit, an Indian Health Service facility, in 2017 and now provides teledermatology and regular in-person dermatology care at that clinic. “The climate there is dry, so you can see bad eczema and dry skin. There’s also a lot of acne and hidradenitis suppurativa. I think the acne and HS is due to the hyperglycemic index diet from the food deserts. Skin disease reflects the climate, the food desert, and the lack of close specialty care.”
Acne scarring common
Some published evidence suggests that acne is more prevalent and severe in AI/AN individuals. In a survey of 158 AI/AN individuals with a mean age of 32 years, 79.1% reported a history of acne, 55.1% reported acne scarring, and 31% reported having active lesions. “Looking back on my experience in high school, I definitely see that in myself and in my peers,” Mr. Hicks said. And, while there are limited published studies about the incidence of melanoma in this population, an analysis from 2006 found that the incidence was 3.1 per 100,000 between 2001 and 2005, which was an increase from 1.6 per 100,000 reported between 1992 and 2000.
There’s a lot to unpack for dermatologists caring for the AI/AN population besides the raw health disparities: a long history of distrust between AI/AN people and the federal government, structural racism, geographic isolation, health literacy challenges, and high rates of poverty and unemployment. And while individuals from federally recognized tribes have a legal right to receive health care provided by the Indian Health Service, a component of the Department of Health & Human Services, the U.S. Government Accountability Office found that in 2017 per capita spending available to the IHS was $4,078, compared with $8,109 for Medicaid, $10,692 for the Veterans Health Administration, and $13,185 for Medicare.
“Everyone deserves healthy skin and good health,” said Dr. Kohn, whose husband is AI and works in AI law. “Knowing that there are pockets of people who lack that access to care really bothers me. I think the American Indians are frequently overlooked. They’re just not even counted for in certain surveys,” she added, noting that categories are usually defined as Black, Hispanic, Asian, or White.
According to Dr. Kohn, who coauthored a chapter titled “Dermatology on American Indian and Alaska Native Reservations,” for the 2021 book “Dermatology in Rural Settings”, 70% of AIs live in urban areas, “so it’s not just people who live on reservations, though the disparity is greatest there.” To help deliver dermatologic care in the rural areas “where you’re on tribal lands, you must partner with the tribes,” she added. “You must get their permission, operate under their laws and regulations and their rules, learn the local customs, learn about the culture, learn the people, and learn their resources before you practice. That’s the only ethical way to practice.” This also means appreciating the fact that some AI/AN individuals may not understand what a dermatologist could do for them. “One of the bigger hurdles to overcome,” she said, is educating the population that dermatologists can cure skin diseases and that there are good medications for treating the diseases.
Shortcomings of teledermatology
Some dermatologists perform teledermatology visits for tribes, often from an office located in a different time zone. “And, they don’t have a sense of what resources are available for the people they’re serving,” Dr. Kohn said. “For example, if they diagnose a potential skin cancer on the face and say, ‘you need a biopsy,’ but the closest dermatologist is 4 hours away, is that really serving the patient? Or, if you tell a patient, ‘I want you to go out and buy Vanicream for your skin,’ but Vanicream costs $17 and the patient can’t even afford to buy food, are you really doing them a service?”
In a survey-based study of 238 AI individuals that is scheduled to be published in late 2023, Dr. Kohn and colleagues asked respondents at two regional powwows in Denver if they would be open to teledermatology – either in their home or in a primary care clinic. Most respondents (70%) lived in urban areas, the rest in rural settings. Nearly half of respondents (42%) “did not want to do teledermatology, even though they couldn’t access in-person dermatology,” Dr. Kohn said. “So, for people who think teledermatology is the answer [to improving access], the respondents to our survey weren’t interested in pursuing that as a solution. I was surprised by that.” When the researchers broke down the responses by age, teenage respondents were even less interested in teledermatology than adults were. “I think there’s something about having someone see you in person, knowing who you are,” she said.
Partnerships with tribes
To foster more sustainable change in the delivery of skin care beyond remote teledermatology and periodic visits from volunteers, some dermatology residencies have established partnerships with tribes, including Massachusetts General Hospital’s teaching partnership with the Rosebud Sioux tribe in Rosebud, S.D., and the University of Utah dermatology department’s resident continuity clinic with Navajo Nation in Montezuma Creek, Utah. In 2016, officials from the Utah Navajo Health System reached out to the University of Utah’s dermatology department to inquire about the potential for creating a teledermatology clinic to serve patients who receive primary care at the Montezuma Creek Community Health Center, located in Southeastern Utah on the northern tip of the Navajo Nation.
Stephanie Klein, MD, associate professor of dermatology at the university, spearheaded the clinic’s launch but soon encountered obstacles that ranged from not being able to visualize the patient’s skin clearly on her computer screen to difficulty making a personal connection with patients despite help from Navajo translators. “It was hard to build a relationship,” she said. A few years later, she drove down to meet with officials of the health system and posed the question: “What is the ideal thing you would want from dermatology?”
Continuity, they told her. “They said that a lot of the services they receive in the form of outreach are rotational, where someone might come in for a day, or a week, or five people may rotate throughout the year,” which did not serve them well, said Dr. Klein, who subsequently collaborated with Utah Navajo Health System clinicians to establish a resident continuity clinic, which launched in January 2021.
The arrangement also serves as a continuity clinic for Dr. Klein as an attending physician. Each month, she and one dermatology resident drive 6.5 hours from Salt Lake City to Montezuma Creek, where they spend 1 or 2 full days seeing about 25 patients referred by the primary care clinicians who work there. About one-quarter of the time they fly, thanks to financial support from a private donor. The flight takes about an hour, then it’s an hour-long drive to the actual clinic. “It’s a commitment,” Dr. Klein said. “A resident can come with me if they commit to the clinic for at least 1 year. This enables us to have continuity of care; it allows us to build relationships with the patients and with the care team there.” As for the prior teledermatology visits she had with residents, “I still do those, but now I do them in between the in-person visits, so I’m not meeting people over telehealth; I’m just following up with them.”
Situated in the high desert among rock formations, the estimated population of Montezuma Creek is just over 320 people. “It’s a beautiful place with otherworldly buttes and mesas, and the Blue Mountains rising up in the distance,” said Lowell Nicholson, MD, a dermatology resident at the University of Utah who is in his second year of a 2-year commitment to the clinic. “But the landscape can be harsh, and it is underserved from an infrastructure perspective,” with large areas with no cell phone service and limited access to running water and refrigeration. “People in general travel quite far to get their medical care and most of the roads are dirt or gravel, so after a big snowstorm or if it’s been raining, they can become impassable.”
Dermatologic conditions they often encounter include vitiligo, photodermatoses, hidradenitis suppurativa, eczema, psoriasis, and severe acne, often with lots of acne-associated scarring. “In general, we tend to see dramatic or advanced presentations of general dermatology diagnoses,” Dr. Nicholson said. “We see a lot of really extensive psoriasis, which can be socially stigmatizing.”
He recalled one middle-aged man who isolated himself from others because his psoriasis became unbearable. The man refused to leave his house, visit family members, or attend tribal meetups. “He tried to see his regular doctor about it and was given topicals, but his disease was just too extensive,” said Dr. Nicholson, who suggested trying a biologic but learned that the man did not have regular access to refrigeration. “That wasn’t going to work, but we started him on an oral medication, apremilast, which has completely cleared his skin,” he said. “He’s doing great. The last time we saw him he was re-engaged with his family, and he told us he was going on dates. We really improved his quality of life.”
Dr. Klein recalled seeing a 6-year-old girl at the clinic with atopic dermatitis so severe that it caused her to miss several days of school. “When she was in school, she was so distracted by the itching – it was so overwhelming,” she said. She was struggling with topical medicines that weren’t effective, but Dr. Klein got her on dupilumab, and during a follow-up visit the girl told her, “This is the first time in my life I can think about things” other than itching.
According to Dr. Nicholson, some patients seen at the Montezuma Creek clinic are on Medicare or carry standard insurance. “Others have a mix, and others are getting all their medications through the Montezuma Creek clinic or through the IHS clinics,” he said. “I have been surprised at the formulary and our ability to get relatively expensive medications for our patients, like biologics and TNF inhibitors. But it takes some creativity to know what is going to work for your patients’ living situation.”
Training more AI/AN dermatologists key
While efforts to increase the culturally respectful and sustainable dermatologic care for AI/AN individuals continue through programs like the continuity clinic at Montezuma Creek, sources interviewed for this story emphasized the importance of training more AI/AN dermatologists. “Of the people who graduate from high school, AIs have the lowest rate of going on to college,” said Dr. Kohn, who serves as a mentor to Mr. Hicks. “Let’s say they get all the way to medical school; it’s about good mentorship and support in what they’re pursuing. We are seeing more AIs in medical school now, something that I personally notice, and I notice it from what Chinle Service Unit tells me. They have received many requests from Native medical students and premed students who want to rotate at Chinle. Native trainees want the experience of being there.”
According to the Association of American Medical Colleges, the number of AI/AN applicants to medical schools increased from 72 in 2020-2021 to 105 in 2021-2022 but dipped slightly to 94 in 2022-2023. Inspired by a passion to serve Pine Ridge or a community like it, Mr. Hicks decided to apply for medical school. While he doesn’t want to “close any doors” on which medical specialty he ultimately chooses to practice, the current front-runner is dermatology, he said, largely because of the influence of Dr. Kohn and two Mayo dermatologists who have become mentors: Molly Lohman, MD, and Hafsa M. Cantwell, MD. “I didn’t see anyone from my background who was a doctor, so having those role models is so important for Native kids to think, ‘I can do this, too,’ and to pursue it,” he said.
As a proud member of the Oglala Lakota Nation from the Pine Ridge Indian Reservation in southwestern South Dakota, Drew Hicks grew up with limited access to basic health care, let alone the luxury of scheduling an appointment with a dermatologist or another medical specialist.
The area – once home to the Lakota war leader Crazy Horse – encompasses nearly 47,000 residents scattered over about 2.2 million acres, larger than the size of Rhode Island, with land marked by rolling mixed grass prairie, sandhills, and badlands. Some of the Oglala Lakota people live in substandard housing and lack regular access to food, running water, and refrigeration, not to mention cell phone and Internet service. “It’s sparse,” said Mr. Hicks, the son of Tribal ranchers who now is a 3rd-year medical student at the Mayo Clinic College of Medicine and Science in Rochester, Minn., and has an early interest in pursuing dermatology. “There is a lot of territory and not a lot of health care serving the population.” From the Hicks home, the nearest place to receive health care is a family medicine practice in Martin, S.D. – about a 15-minute drive on gravel roads in the best of conditions, but in poor weather, it can be difficult, he said. “So, there are environmental challenges besides the limited number of health care providers.”
Clinicians in the practice “did have to be the point of care for everything from dermatologic issues to emergency medicine to delivering a baby, because the next-closest medical facility of any magnitude is 2 hours away,” he said.
Challenges of health literacy and limited access to comprehensive health care at Pine Ridge and other American Indian (AI) and Alaska Native (AN) reservations have long-term consequences. “My own mom struggled to control her blood pressure for years and now has chronic kidney disease,” Mr. Hicks said. “It’s not an uncommon story. Diabetes on the reservation is a big issue.” Then there’s his father, who survived two bouts with melanoma that was diagnosed at an advanced stage. “I think about how that has impacted him, and wonder, had we had a dermatologist who serviced our area, would we have caught things sooner?” he said. “I feel there is so much room for impactful health care deliveries to communities like Pine Ridge.” At the same time, he emphasized, “this isn’t poverty porn. We’re a resilient people. Any effort to engage with AIs or ANs should be from a perspective of a learner, having cultural humility, and seeking out community leaders to help lead you.”
According to the 2020 Census, there are 574 federally recognized sovereign tribal nations in the United States and federal- and state-recognized American Indian reservations in 35 states. AI/AN people make up about 2.9% of the total U.S. population, or 9.7 million, and their life expectancy is an average of 4.4 years less, compared with the general population (a mean of 73.7 vs. 78.1 years, respectively). Because of limited access to dermatologic care in these areas, the risk for developing significant skin conditions and diseases that may go undetected for long stretches of time is increased.
“That can mean advanced skin cancers like basal cell carcinomas that have become larger than what you would see in a typical metropolitan population,” said Lucinda Kohn, MD, assistant professor of dermatology in the Centers for American Indian and Alaska Native Health at the University of Colorado at Denver, Aurora, who spent part of her dermatology residency rotating at the Chinle (Ariz.) Service Unit, an Indian Health Service facility, in 2017 and now provides teledermatology and regular in-person dermatology care at that clinic. “The climate there is dry, so you can see bad eczema and dry skin. There’s also a lot of acne and hidradenitis suppurativa. I think the acne and HS is due to the hyperglycemic index diet from the food deserts. Skin disease reflects the climate, the food desert, and the lack of close specialty care.”
Acne scarring common
Some published evidence suggests that acne is more prevalent and severe in AI/AN individuals. In a survey of 158 AI/AN individuals with a mean age of 32 years, 79.1% reported a history of acne, 55.1% reported acne scarring, and 31% reported having active lesions. “Looking back on my experience in high school, I definitely see that in myself and in my peers,” Mr. Hicks said. And, while there are limited published studies about the incidence of melanoma in this population, an analysis from 2006 found that the incidence was 3.1 per 100,000 between 2001 and 2005, which was an increase from 1.6 per 100,000 reported between 1992 and 2000.
There’s a lot to unpack for dermatologists caring for the AI/AN population besides the raw health disparities: a long history of distrust between AI/AN people and the federal government, structural racism, geographic isolation, health literacy challenges, and high rates of poverty and unemployment. And while individuals from federally recognized tribes have a legal right to receive health care provided by the Indian Health Service, a component of the Department of Health & Human Services, the U.S. Government Accountability Office found that in 2017 per capita spending available to the IHS was $4,078, compared with $8,109 for Medicaid, $10,692 for the Veterans Health Administration, and $13,185 for Medicare.
“Everyone deserves healthy skin and good health,” said Dr. Kohn, whose husband is AI and works in AI law. “Knowing that there are pockets of people who lack that access to care really bothers me. I think the American Indians are frequently overlooked. They’re just not even counted for in certain surveys,” she added, noting that categories are usually defined as Black, Hispanic, Asian, or White.
According to Dr. Kohn, who coauthored a chapter titled “Dermatology on American Indian and Alaska Native Reservations,” for the 2021 book “Dermatology in Rural Settings”, 70% of AIs live in urban areas, “so it’s not just people who live on reservations, though the disparity is greatest there.” To help deliver dermatologic care in the rural areas “where you’re on tribal lands, you must partner with the tribes,” she added. “You must get their permission, operate under their laws and regulations and their rules, learn the local customs, learn about the culture, learn the people, and learn their resources before you practice. That’s the only ethical way to practice.” This also means appreciating the fact that some AI/AN individuals may not understand what a dermatologist could do for them. “One of the bigger hurdles to overcome,” she said, is educating the population that dermatologists can cure skin diseases and that there are good medications for treating the diseases.
Shortcomings of teledermatology
Some dermatologists perform teledermatology visits for tribes, often from an office located in a different time zone. “And, they don’t have a sense of what resources are available for the people they’re serving,” Dr. Kohn said. “For example, if they diagnose a potential skin cancer on the face and say, ‘you need a biopsy,’ but the closest dermatologist is 4 hours away, is that really serving the patient? Or, if you tell a patient, ‘I want you to go out and buy Vanicream for your skin,’ but Vanicream costs $17 and the patient can’t even afford to buy food, are you really doing them a service?”
In a survey-based study of 238 AI individuals that is scheduled to be published in late 2023, Dr. Kohn and colleagues asked respondents at two regional powwows in Denver if they would be open to teledermatology – either in their home or in a primary care clinic. Most respondents (70%) lived in urban areas, the rest in rural settings. Nearly half of respondents (42%) “did not want to do teledermatology, even though they couldn’t access in-person dermatology,” Dr. Kohn said. “So, for people who think teledermatology is the answer [to improving access], the respondents to our survey weren’t interested in pursuing that as a solution. I was surprised by that.” When the researchers broke down the responses by age, teenage respondents were even less interested in teledermatology than adults were. “I think there’s something about having someone see you in person, knowing who you are,” she said.
Partnerships with tribes
To foster more sustainable change in the delivery of skin care beyond remote teledermatology and periodic visits from volunteers, some dermatology residencies have established partnerships with tribes, including Massachusetts General Hospital’s teaching partnership with the Rosebud Sioux tribe in Rosebud, S.D., and the University of Utah dermatology department’s resident continuity clinic with Navajo Nation in Montezuma Creek, Utah. In 2016, officials from the Utah Navajo Health System reached out to the University of Utah’s dermatology department to inquire about the potential for creating a teledermatology clinic to serve patients who receive primary care at the Montezuma Creek Community Health Center, located in Southeastern Utah on the northern tip of the Navajo Nation.
Stephanie Klein, MD, associate professor of dermatology at the university, spearheaded the clinic’s launch but soon encountered obstacles that ranged from not being able to visualize the patient’s skin clearly on her computer screen to difficulty making a personal connection with patients despite help from Navajo translators. “It was hard to build a relationship,” she said. A few years later, she drove down to meet with officials of the health system and posed the question: “What is the ideal thing you would want from dermatology?”
Continuity, they told her. “They said that a lot of the services they receive in the form of outreach are rotational, where someone might come in for a day, or a week, or five people may rotate throughout the year,” which did not serve them well, said Dr. Klein, who subsequently collaborated with Utah Navajo Health System clinicians to establish a resident continuity clinic, which launched in January 2021.
The arrangement also serves as a continuity clinic for Dr. Klein as an attending physician. Each month, she and one dermatology resident drive 6.5 hours from Salt Lake City to Montezuma Creek, where they spend 1 or 2 full days seeing about 25 patients referred by the primary care clinicians who work there. About one-quarter of the time they fly, thanks to financial support from a private donor. The flight takes about an hour, then it’s an hour-long drive to the actual clinic. “It’s a commitment,” Dr. Klein said. “A resident can come with me if they commit to the clinic for at least 1 year. This enables us to have continuity of care; it allows us to build relationships with the patients and with the care team there.” As for the prior teledermatology visits she had with residents, “I still do those, but now I do them in between the in-person visits, so I’m not meeting people over telehealth; I’m just following up with them.”
Situated in the high desert among rock formations, the estimated population of Montezuma Creek is just over 320 people. “It’s a beautiful place with otherworldly buttes and mesas, and the Blue Mountains rising up in the distance,” said Lowell Nicholson, MD, a dermatology resident at the University of Utah who is in his second year of a 2-year commitment to the clinic. “But the landscape can be harsh, and it is underserved from an infrastructure perspective,” with large areas with no cell phone service and limited access to running water and refrigeration. “People in general travel quite far to get their medical care and most of the roads are dirt or gravel, so after a big snowstorm or if it’s been raining, they can become impassable.”
Dermatologic conditions they often encounter include vitiligo, photodermatoses, hidradenitis suppurativa, eczema, psoriasis, and severe acne, often with lots of acne-associated scarring. “In general, we tend to see dramatic or advanced presentations of general dermatology diagnoses,” Dr. Nicholson said. “We see a lot of really extensive psoriasis, which can be socially stigmatizing.”
He recalled one middle-aged man who isolated himself from others because his psoriasis became unbearable. The man refused to leave his house, visit family members, or attend tribal meetups. “He tried to see his regular doctor about it and was given topicals, but his disease was just too extensive,” said Dr. Nicholson, who suggested trying a biologic but learned that the man did not have regular access to refrigeration. “That wasn’t going to work, but we started him on an oral medication, apremilast, which has completely cleared his skin,” he said. “He’s doing great. The last time we saw him he was re-engaged with his family, and he told us he was going on dates. We really improved his quality of life.”
Dr. Klein recalled seeing a 6-year-old girl at the clinic with atopic dermatitis so severe that it caused her to miss several days of school. “When she was in school, she was so distracted by the itching – it was so overwhelming,” she said. She was struggling with topical medicines that weren’t effective, but Dr. Klein got her on dupilumab, and during a follow-up visit the girl told her, “This is the first time in my life I can think about things” other than itching.
According to Dr. Nicholson, some patients seen at the Montezuma Creek clinic are on Medicare or carry standard insurance. “Others have a mix, and others are getting all their medications through the Montezuma Creek clinic or through the IHS clinics,” he said. “I have been surprised at the formulary and our ability to get relatively expensive medications for our patients, like biologics and TNF inhibitors. But it takes some creativity to know what is going to work for your patients’ living situation.”
Training more AI/AN dermatologists key
While efforts to increase the culturally respectful and sustainable dermatologic care for AI/AN individuals continue through programs like the continuity clinic at Montezuma Creek, sources interviewed for this story emphasized the importance of training more AI/AN dermatologists. “Of the people who graduate from high school, AIs have the lowest rate of going on to college,” said Dr. Kohn, who serves as a mentor to Mr. Hicks. “Let’s say they get all the way to medical school; it’s about good mentorship and support in what they’re pursuing. We are seeing more AIs in medical school now, something that I personally notice, and I notice it from what Chinle Service Unit tells me. They have received many requests from Native medical students and premed students who want to rotate at Chinle. Native trainees want the experience of being there.”
According to the Association of American Medical Colleges, the number of AI/AN applicants to medical schools increased from 72 in 2020-2021 to 105 in 2021-2022 but dipped slightly to 94 in 2022-2023. Inspired by a passion to serve Pine Ridge or a community like it, Mr. Hicks decided to apply for medical school. While he doesn’t want to “close any doors” on which medical specialty he ultimately chooses to practice, the current front-runner is dermatology, he said, largely because of the influence of Dr. Kohn and two Mayo dermatologists who have become mentors: Molly Lohman, MD, and Hafsa M. Cantwell, MD. “I didn’t see anyone from my background who was a doctor, so having those role models is so important for Native kids to think, ‘I can do this, too,’ and to pursue it,” he said.
U.S. mammogram update sparks concern, reignites debates
, while also renewing debates about the timing of these tests and the screening approaches used.
The U.S. Preventive Services Task Force is currently finalizing an update to its recommendations on breast cancer screening. In May, the task force released a proposed update that dropped the initial age for routine mammogram screening from 50 to 40.
The task force intends to give a “B” rating to this recommendation, which covers screening every other year up to age 74 for women deemed average risk for breast cancer.
The task force’s rating carries clout, A. Mark Fendrick, MD, director of the Value-Based Insurance Design at the University of Michigan, Ann Arbor, said in an interview.
For one, the Affordable Care Act requires that private insurers cover services that get top A or B marks from USPSTF without charging copays.
However, Dr. Fendrick noted, such coverage does not necessarily apply to follow-up testing when a routine mammogram comes back with a positive finding. The expense of follow-up testing may deter some women from seeking follow-up diagnostic imaging or biopsies after an abnormal result on a screening mammogram.
A recent analysis in JAMA Network Open found that women facing higher anticipated out-of-pocket costs for breast cancer diagnostic tests, based on their health insurance plan, were less likely to get that follow-up screening. For instance, the use of breast MRI decreased by nearly 24% between patients undergoing subsequent diagnostic testing in plans with the lowest out-of-pocket costs vs. those with the highest.
“The study’s central finding that some women who have an abnormal result on a mammogram may not get appropriate follow-up because of cost is worrisome,” said Dr. Fendrick and Ilana B. Richman, MD, MHS, in an accompanying commentary to the JAMA analysis. “On an individual level, high out-of-pocket costs may directly contribute to worse health outcomes or require individuals to use scarce financial resources that may otherwise be used for critical items such as food or rent.”
For patients to fully benefit from early detection, the USPSTF would also need to make clear that follow-up diagnostic mammograms are covered, Dr. Fendrick said.
The ongoing debates
Concerns over the costs of potential follow-up tests are not the only issues experts have highlighted since USPSTF released its updated draft guidance on screening mammography.
The task force’s proposed update has also reignited questions and uncertainties surrounding when to screen, how often, and what types are best.
When it comes to frequency, the major organizations that provide screening guidance don’t see eye to eye. The USPSTF recommends breast cancer screening every other year, while the American College of Radiology recommends screening every year because that approach leads to saves “the most lives.”
At this time, the American College of Obstetricians and Gynecologists guidance currently teeters in the middle, suggesting either annual or biennial screening and highlighting the pros and cons of either approach. According to ACOG, “annual screening intervals appear to result in the least number of breast cancer deaths, particularly in younger women, but at the cost of additional callbacks and biopsies.”
When to begin screening represents another point of contention. While some experts, such as ACOG, agree with the task force’s decision to lower the screening start age to 40, others point to the need for greater nuance on setting the appropriate screening age. The main issue: the task force’s draft sets a uniform age to begin screening, but the risk for breast cancer and breast cancer mortality is not uniform across different racial and ethnic groups.
A recent study published in JAMA Network Open found that, among women aged 40-49, breast cancer mortality was highest among Black women (27 deaths per 100,000 person-years) followed by White women (15 deaths per 100,000 person-years). Based on a recommended screening age of 50, the authors suggested that Black women should start screening at age 42, whereas White women could start at 51.
“These findings suggest that health policy makers and clinicians could consider an alternative, race and ethnicity–adapted approach in which Black female patients start screening earlier,” writes Tianhui Chen, PhD, of China’s Zhejiang Cancer Hospital and coauthor of the study.
Weighing in on the guidance, the nonprofit National Center for Health Research urged the task force to consider suggesting different screening schedules based on race and ethnicity data. That would mean the recommendation to start at age 40 should only apply to Black women and other groups with higher-than-average risk for breast cancer at a younger age.
“Women are capable of understanding why the age to start mammography screening may be different for women with different risk factors,” the National Center for Health Research wrote in a comment to USPSTF, provided to this news organization by request. “What is confusing is when some physician groups recommend annual mammograms for all women starting at age 40, even though the data do not support that recommendation.”
While the ACR agreed with the task force’s recommendation to lower the screening age, the organization suggested starting risk assessments based on racial variations in breast cancer incidence and death even earlier. Specifically, the ACR recommended that high-risk groups, such as Black women, get risk assessments by age 25 to determine whether mammography before age 40 is needed.
Screening options for women with dense breasts may be some of the most challenging to weigh. Having dense breasts increases an individual’s risk for breast cancer, and mammography alone is not as effective at identifying breast cancer among these women. However, the evidence on the benefits vs. harms of additional screening beyond mammography remains mixed.
As a result, the task force decided to maintain its “I” grade on additional screening beyond mammography for these women – a grade that indicates insufficient evidence to determine the benefits and harms for a service.
The task force largely based its decision on the findings of two key reports. One report from the Cancer Intervention and Surveillance Modeling Network, which modeled potential outcomes of different screening strategies, indicated that extra screening might reduce breast cancer mortality in those with dense breasts, but at a cost of more false-positive reports.
The second report, a review from the Kaiser Permanente Evidence-based Practice Center, reaffirmed the benefits of routine mammography for reducing deaths from breast cancer, but found no solid evidence that different strategies – including supplemental screening in women with denser breasts – lowered breast cancer mortality or the risk of progression to advanced cancer. Further studies may show which approaches work best to reduce breast cancer deaths, the report said.
In this instance, ACOG agreed with USPSTF: “Based on the lack of data, ACOG does not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
Women with dense breasts should still be encouraged to receive regular screening mammography, even if the results they get may not be as accurate as those for women with less dense breasts, said Diana L. Miglioretti, PhD, of the University of California, Davis, who worked on a report for the USPSTF guidelines.
What’s next?
Despite ongoing debate and uncertainties surrounding some breast screening guidance, support for ending copay requirements for follow-up tests after a positive mammogram finding is widespread.
According to Dr. Fendrick, the USPSTF should expand coverage of follow-up testing after a positive mammogram to ensure people receive routine screening and any necessary diagnostic tests, as it did with colon cancer.
Before 2021, patients could face high costs for a colonoscopy following a positive stool-based Cologuard test. But in 2021, the USPSTF said that positive results on stool-based tests would require follow-up with colonoscopy, defining this follow-up as part of the screening benefit. In 2022, Medicare followed by setting a policy that ended the copay for these follow-up colonoscopies.
For breast screening, there are efforts underway in Congress to end copays for breast screening. In May, Rep. Rosa DeLauro (D-Conn.) introduced a bill, the Find It Early Act, that would require both private and government insurers to cover the out-of-pocket costs for many women receiving screening with ultrasound and MRI.
When the USPSTF finalizes its breast screening guidelines, the recommendations will be woven into discussions between primary care physicians and patients about breast cancer screening.
As guidelines and evidence evolve, “we’re learning to adjust” and communicate these changes to patients, said Tochi Iroku-Malize, MD, president of the American Academy of Family Physicians.
However, gaps in the guidance will leave some open-ended questions about optimal screening practices and how much screening may cost.
Given that, Dr. Iroku-Malize takes many factors into account when discussing screening options with her patients. Based on the new information and the patient’s information, she said she will tell her patients, “We’re going to adjust our guidance as to what you need.”
A version of this article first appeared on Medscape.com.
, while also renewing debates about the timing of these tests and the screening approaches used.
The U.S. Preventive Services Task Force is currently finalizing an update to its recommendations on breast cancer screening. In May, the task force released a proposed update that dropped the initial age for routine mammogram screening from 50 to 40.
The task force intends to give a “B” rating to this recommendation, which covers screening every other year up to age 74 for women deemed average risk for breast cancer.
The task force’s rating carries clout, A. Mark Fendrick, MD, director of the Value-Based Insurance Design at the University of Michigan, Ann Arbor, said in an interview.
For one, the Affordable Care Act requires that private insurers cover services that get top A or B marks from USPSTF without charging copays.
However, Dr. Fendrick noted, such coverage does not necessarily apply to follow-up testing when a routine mammogram comes back with a positive finding. The expense of follow-up testing may deter some women from seeking follow-up diagnostic imaging or biopsies after an abnormal result on a screening mammogram.
A recent analysis in JAMA Network Open found that women facing higher anticipated out-of-pocket costs for breast cancer diagnostic tests, based on their health insurance plan, were less likely to get that follow-up screening. For instance, the use of breast MRI decreased by nearly 24% between patients undergoing subsequent diagnostic testing in plans with the lowest out-of-pocket costs vs. those with the highest.
“The study’s central finding that some women who have an abnormal result on a mammogram may not get appropriate follow-up because of cost is worrisome,” said Dr. Fendrick and Ilana B. Richman, MD, MHS, in an accompanying commentary to the JAMA analysis. “On an individual level, high out-of-pocket costs may directly contribute to worse health outcomes or require individuals to use scarce financial resources that may otherwise be used for critical items such as food or rent.”
For patients to fully benefit from early detection, the USPSTF would also need to make clear that follow-up diagnostic mammograms are covered, Dr. Fendrick said.
The ongoing debates
Concerns over the costs of potential follow-up tests are not the only issues experts have highlighted since USPSTF released its updated draft guidance on screening mammography.
The task force’s proposed update has also reignited questions and uncertainties surrounding when to screen, how often, and what types are best.
When it comes to frequency, the major organizations that provide screening guidance don’t see eye to eye. The USPSTF recommends breast cancer screening every other year, while the American College of Radiology recommends screening every year because that approach leads to saves “the most lives.”
At this time, the American College of Obstetricians and Gynecologists guidance currently teeters in the middle, suggesting either annual or biennial screening and highlighting the pros and cons of either approach. According to ACOG, “annual screening intervals appear to result in the least number of breast cancer deaths, particularly in younger women, but at the cost of additional callbacks and biopsies.”
When to begin screening represents another point of contention. While some experts, such as ACOG, agree with the task force’s decision to lower the screening start age to 40, others point to the need for greater nuance on setting the appropriate screening age. The main issue: the task force’s draft sets a uniform age to begin screening, but the risk for breast cancer and breast cancer mortality is not uniform across different racial and ethnic groups.
A recent study published in JAMA Network Open found that, among women aged 40-49, breast cancer mortality was highest among Black women (27 deaths per 100,000 person-years) followed by White women (15 deaths per 100,000 person-years). Based on a recommended screening age of 50, the authors suggested that Black women should start screening at age 42, whereas White women could start at 51.
“These findings suggest that health policy makers and clinicians could consider an alternative, race and ethnicity–adapted approach in which Black female patients start screening earlier,” writes Tianhui Chen, PhD, of China’s Zhejiang Cancer Hospital and coauthor of the study.
Weighing in on the guidance, the nonprofit National Center for Health Research urged the task force to consider suggesting different screening schedules based on race and ethnicity data. That would mean the recommendation to start at age 40 should only apply to Black women and other groups with higher-than-average risk for breast cancer at a younger age.
“Women are capable of understanding why the age to start mammography screening may be different for women with different risk factors,” the National Center for Health Research wrote in a comment to USPSTF, provided to this news organization by request. “What is confusing is when some physician groups recommend annual mammograms for all women starting at age 40, even though the data do not support that recommendation.”
While the ACR agreed with the task force’s recommendation to lower the screening age, the organization suggested starting risk assessments based on racial variations in breast cancer incidence and death even earlier. Specifically, the ACR recommended that high-risk groups, such as Black women, get risk assessments by age 25 to determine whether mammography before age 40 is needed.
Screening options for women with dense breasts may be some of the most challenging to weigh. Having dense breasts increases an individual’s risk for breast cancer, and mammography alone is not as effective at identifying breast cancer among these women. However, the evidence on the benefits vs. harms of additional screening beyond mammography remains mixed.
As a result, the task force decided to maintain its “I” grade on additional screening beyond mammography for these women – a grade that indicates insufficient evidence to determine the benefits and harms for a service.
The task force largely based its decision on the findings of two key reports. One report from the Cancer Intervention and Surveillance Modeling Network, which modeled potential outcomes of different screening strategies, indicated that extra screening might reduce breast cancer mortality in those with dense breasts, but at a cost of more false-positive reports.
The second report, a review from the Kaiser Permanente Evidence-based Practice Center, reaffirmed the benefits of routine mammography for reducing deaths from breast cancer, but found no solid evidence that different strategies – including supplemental screening in women with denser breasts – lowered breast cancer mortality or the risk of progression to advanced cancer. Further studies may show which approaches work best to reduce breast cancer deaths, the report said.
In this instance, ACOG agreed with USPSTF: “Based on the lack of data, ACOG does not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
Women with dense breasts should still be encouraged to receive regular screening mammography, even if the results they get may not be as accurate as those for women with less dense breasts, said Diana L. Miglioretti, PhD, of the University of California, Davis, who worked on a report for the USPSTF guidelines.
What’s next?
Despite ongoing debate and uncertainties surrounding some breast screening guidance, support for ending copay requirements for follow-up tests after a positive mammogram finding is widespread.
According to Dr. Fendrick, the USPSTF should expand coverage of follow-up testing after a positive mammogram to ensure people receive routine screening and any necessary diagnostic tests, as it did with colon cancer.
Before 2021, patients could face high costs for a colonoscopy following a positive stool-based Cologuard test. But in 2021, the USPSTF said that positive results on stool-based tests would require follow-up with colonoscopy, defining this follow-up as part of the screening benefit. In 2022, Medicare followed by setting a policy that ended the copay for these follow-up colonoscopies.
For breast screening, there are efforts underway in Congress to end copays for breast screening. In May, Rep. Rosa DeLauro (D-Conn.) introduced a bill, the Find It Early Act, that would require both private and government insurers to cover the out-of-pocket costs for many women receiving screening with ultrasound and MRI.
When the USPSTF finalizes its breast screening guidelines, the recommendations will be woven into discussions between primary care physicians and patients about breast cancer screening.
As guidelines and evidence evolve, “we’re learning to adjust” and communicate these changes to patients, said Tochi Iroku-Malize, MD, president of the American Academy of Family Physicians.
However, gaps in the guidance will leave some open-ended questions about optimal screening practices and how much screening may cost.
Given that, Dr. Iroku-Malize takes many factors into account when discussing screening options with her patients. Based on the new information and the patient’s information, she said she will tell her patients, “We’re going to adjust our guidance as to what you need.”
A version of this article first appeared on Medscape.com.
, while also renewing debates about the timing of these tests and the screening approaches used.
The U.S. Preventive Services Task Force is currently finalizing an update to its recommendations on breast cancer screening. In May, the task force released a proposed update that dropped the initial age for routine mammogram screening from 50 to 40.
The task force intends to give a “B” rating to this recommendation, which covers screening every other year up to age 74 for women deemed average risk for breast cancer.
The task force’s rating carries clout, A. Mark Fendrick, MD, director of the Value-Based Insurance Design at the University of Michigan, Ann Arbor, said in an interview.
For one, the Affordable Care Act requires that private insurers cover services that get top A or B marks from USPSTF without charging copays.
However, Dr. Fendrick noted, such coverage does not necessarily apply to follow-up testing when a routine mammogram comes back with a positive finding. The expense of follow-up testing may deter some women from seeking follow-up diagnostic imaging or biopsies after an abnormal result on a screening mammogram.
A recent analysis in JAMA Network Open found that women facing higher anticipated out-of-pocket costs for breast cancer diagnostic tests, based on their health insurance plan, were less likely to get that follow-up screening. For instance, the use of breast MRI decreased by nearly 24% between patients undergoing subsequent diagnostic testing in plans with the lowest out-of-pocket costs vs. those with the highest.
“The study’s central finding that some women who have an abnormal result on a mammogram may not get appropriate follow-up because of cost is worrisome,” said Dr. Fendrick and Ilana B. Richman, MD, MHS, in an accompanying commentary to the JAMA analysis. “On an individual level, high out-of-pocket costs may directly contribute to worse health outcomes or require individuals to use scarce financial resources that may otherwise be used for critical items such as food or rent.”
For patients to fully benefit from early detection, the USPSTF would also need to make clear that follow-up diagnostic mammograms are covered, Dr. Fendrick said.
The ongoing debates
Concerns over the costs of potential follow-up tests are not the only issues experts have highlighted since USPSTF released its updated draft guidance on screening mammography.
The task force’s proposed update has also reignited questions and uncertainties surrounding when to screen, how often, and what types are best.
When it comes to frequency, the major organizations that provide screening guidance don’t see eye to eye. The USPSTF recommends breast cancer screening every other year, while the American College of Radiology recommends screening every year because that approach leads to saves “the most lives.”
At this time, the American College of Obstetricians and Gynecologists guidance currently teeters in the middle, suggesting either annual or biennial screening and highlighting the pros and cons of either approach. According to ACOG, “annual screening intervals appear to result in the least number of breast cancer deaths, particularly in younger women, but at the cost of additional callbacks and biopsies.”
When to begin screening represents another point of contention. While some experts, such as ACOG, agree with the task force’s decision to lower the screening start age to 40, others point to the need for greater nuance on setting the appropriate screening age. The main issue: the task force’s draft sets a uniform age to begin screening, but the risk for breast cancer and breast cancer mortality is not uniform across different racial and ethnic groups.
A recent study published in JAMA Network Open found that, among women aged 40-49, breast cancer mortality was highest among Black women (27 deaths per 100,000 person-years) followed by White women (15 deaths per 100,000 person-years). Based on a recommended screening age of 50, the authors suggested that Black women should start screening at age 42, whereas White women could start at 51.
“These findings suggest that health policy makers and clinicians could consider an alternative, race and ethnicity–adapted approach in which Black female patients start screening earlier,” writes Tianhui Chen, PhD, of China’s Zhejiang Cancer Hospital and coauthor of the study.
Weighing in on the guidance, the nonprofit National Center for Health Research urged the task force to consider suggesting different screening schedules based on race and ethnicity data. That would mean the recommendation to start at age 40 should only apply to Black women and other groups with higher-than-average risk for breast cancer at a younger age.
“Women are capable of understanding why the age to start mammography screening may be different for women with different risk factors,” the National Center for Health Research wrote in a comment to USPSTF, provided to this news organization by request. “What is confusing is when some physician groups recommend annual mammograms for all women starting at age 40, even though the data do not support that recommendation.”
While the ACR agreed with the task force’s recommendation to lower the screening age, the organization suggested starting risk assessments based on racial variations in breast cancer incidence and death even earlier. Specifically, the ACR recommended that high-risk groups, such as Black women, get risk assessments by age 25 to determine whether mammography before age 40 is needed.
Screening options for women with dense breasts may be some of the most challenging to weigh. Having dense breasts increases an individual’s risk for breast cancer, and mammography alone is not as effective at identifying breast cancer among these women. However, the evidence on the benefits vs. harms of additional screening beyond mammography remains mixed.
As a result, the task force decided to maintain its “I” grade on additional screening beyond mammography for these women – a grade that indicates insufficient evidence to determine the benefits and harms for a service.
The task force largely based its decision on the findings of two key reports. One report from the Cancer Intervention and Surveillance Modeling Network, which modeled potential outcomes of different screening strategies, indicated that extra screening might reduce breast cancer mortality in those with dense breasts, but at a cost of more false-positive reports.
The second report, a review from the Kaiser Permanente Evidence-based Practice Center, reaffirmed the benefits of routine mammography for reducing deaths from breast cancer, but found no solid evidence that different strategies – including supplemental screening in women with denser breasts – lowered breast cancer mortality or the risk of progression to advanced cancer. Further studies may show which approaches work best to reduce breast cancer deaths, the report said.
In this instance, ACOG agreed with USPSTF: “Based on the lack of data, ACOG does not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
Women with dense breasts should still be encouraged to receive regular screening mammography, even if the results they get may not be as accurate as those for women with less dense breasts, said Diana L. Miglioretti, PhD, of the University of California, Davis, who worked on a report for the USPSTF guidelines.
What’s next?
Despite ongoing debate and uncertainties surrounding some breast screening guidance, support for ending copay requirements for follow-up tests after a positive mammogram finding is widespread.
According to Dr. Fendrick, the USPSTF should expand coverage of follow-up testing after a positive mammogram to ensure people receive routine screening and any necessary diagnostic tests, as it did with colon cancer.
Before 2021, patients could face high costs for a colonoscopy following a positive stool-based Cologuard test. But in 2021, the USPSTF said that positive results on stool-based tests would require follow-up with colonoscopy, defining this follow-up as part of the screening benefit. In 2022, Medicare followed by setting a policy that ended the copay for these follow-up colonoscopies.
For breast screening, there are efforts underway in Congress to end copays for breast screening. In May, Rep. Rosa DeLauro (D-Conn.) introduced a bill, the Find It Early Act, that would require both private and government insurers to cover the out-of-pocket costs for many women receiving screening with ultrasound and MRI.
When the USPSTF finalizes its breast screening guidelines, the recommendations will be woven into discussions between primary care physicians and patients about breast cancer screening.
As guidelines and evidence evolve, “we’re learning to adjust” and communicate these changes to patients, said Tochi Iroku-Malize, MD, president of the American Academy of Family Physicians.
However, gaps in the guidance will leave some open-ended questions about optimal screening practices and how much screening may cost.
Given that, Dr. Iroku-Malize takes many factors into account when discussing screening options with her patients. Based on the new information and the patient’s information, she said she will tell her patients, “We’re going to adjust our guidance as to what you need.”
A version of this article first appeared on Medscape.com.
Humira biosimilars: Five things to know
The best-selling drug Humira (adalimumab) now faces competition in the United States after a 20-year monopoly. The first adalimumab biosimilar, Amjevita, launched in the United States on January 31, and in July, seven additional biosimilars became available. These drugs have the potential to lower prescription drug prices, but when and by how much remains to be seen.
Here’s what you need to know about adalimumab biosimilars.
What Humira biosimilars are now available?
Eight different biosimilars have launched in 2023 with discounts as large at 85% from Humira’s list price of $6,922. A few companies also offer two price points.
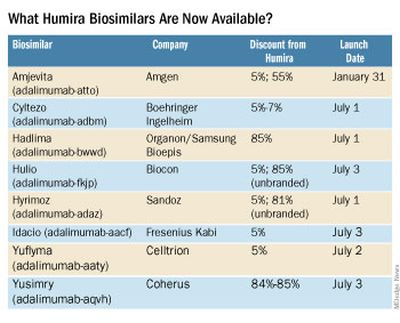
Three of these biosimilars – Hadlima, Hyrimoz, and Yuflyma – are available in high concentration formulations. This high concentration formulation makes up 85% of Humira prescriptions, according to a report from Goodroot, a collection of companies focused on lowering health care costs.
Cyltezo is currently the only adalimumab biosimilar with an interchangeability designation, meaning that a pharmacist can substitute the biosimilar for an equivalent Humira prescription without the intervention of a clinician. A total of 47 states allow for these substitutions without prior approval from a clinician, according to Goodroot, and the clinician must be notified of the switch within a certain time frame. A total of 40 states require that patients be notified of the switch before substitution.
However, it’s not clear if this interchangeability designation will prove an advantage for Cyltezo, as it is interchangeable with the lower concentration version of Humira that makes up just 15% of prescriptions.
Most of the companies behind these biosimilars are pursuing interchangeability designations for their drugs, except for Fresenius Kabi (Idacio) and Coherus (Yusimry).
A ninth biosimilar, Pfizer’s adalimumab-afzb (Abrilada), is not yet on the market and is currently awaiting an approval decision from the Food and Drug Administration to add an interchangeability designation to its prior approval for a low-concentration formulation.
Why are they priced differently?
The two price points offer different deals to payers. Pharmacy benefit managers make confidential agreements with drug manufacturers to get a discount – called a rebate – to get the drug on the PBM’s formulary. The PBM keeps a portion of that rebate, and the rest is passed on to the insurance company and patients. Biosimilars at a higher price point will likely offer larger rebates. Biosimilars offered at lower price points incorporate this discount up front in their list pricing and likely will not offer large rebates.
Will biosimilars be covered by payers?
Currently, biosimilars are being offered on formularies at parity with Humira, meaning they are on the same tier. The PBM companies OptumRx and Cigna Group’s Express Scripts will offer Amjevita (at both price points), Cyltezo, and Hyrimoz (at both price points).
“This decision allows our clients flexibility to provide access to the lower list price, so members in high-deductible plans and benefit designs with coinsurance can experience lower out-of-pocket costs,” said OptumRx spokesperson Isaac Sorensen in an email.
Mark Cuban Cost Plus Drug Company, which uses a direct-to-consumer model, will offer Yusimry for $567.27 on its website. SmithRx, a PBM based in San Francisco, announced it would partner with Cost Plus Drugs to offer Yusimry, adding that SmithRx members can use their insurance benefits to further reduce out-of-pocket costs. RxPreferred, another PBM, will also offer Yusimry through its partnership with Cuban’s company.
The news website Formulary Watch previously reported that CVS Caremark, another of the biggest PBMs, will be offering Amjevita, but as a nonpreferred brand, while Humira remains the preferred brand. CVS Caremark did not respond to a request for comment.
Will patients pay less?
Biosimilars have been touted as a potential solution to lower spending on biologic drugs, but it’s unknown if patients will ultimately benefit with lower out-of-pocket costs. It’s “impossible to predict” if the discount that third-party payers pay will be passed on to consumers, said Mark Fendrick, MD, who directs the University of Michigan Center for Value-based Insurance Design in Ann Arbor.

Generally, a consumer’s copay is a percentage of a drug’s list price, so it stands to reason that a low drug price would result in lower out-of-pocket payments. While this is mostly true, Humira has a successful copay assistance program to lower prescription costs for consumers. According to a 2022 IQVIA report, 82% of commercial prescriptions cost patients less than $10 for Humira because of this program.
To appeal to patients, biosimilar companies will need to offer similar savings, Dr. Fendrick added. “There will be some discontent if patients are actually asked to pay more out-of-pocket for a less expensive drug,” he said.
All eight companies behind these biosimilars are offering or will be launching copay saving programs, many which advertise copays as low as $0 per month for eligible patients.
How will Humira respond?
Marta Wosińska, PhD, a health care economist at the Brookings Institute, Washington, predicts payers will use these lower biosimilar prices to negotiate better deals with AbbVie, Humira’s manufacturer. “We have a lot of players coming into [the market] right now, so the competition is really fierce,” she said. In response, AbbVie will need to increase rebates on Humira and/or lower its price to compete with these biosimilars.
“The ball is in AbbVie’s court,” she said. “If [the company] is not willing to drop price sufficiently, then payers will start switching to biosimilars.”
Dr. Fendrick reported past financial relationships and consulting arrangements with AbbVie, Amgen, Arnold Ventures, Bayer, CareFirst, BlueCross BlueShield, and many other companies. Dr. Wosińska has received funding from Arnold Ventures and serves as an expert witness on antitrust cases involving generic medication.
A version of this article first appeared on Medscape.com.
The best-selling drug Humira (adalimumab) now faces competition in the United States after a 20-year monopoly. The first adalimumab biosimilar, Amjevita, launched in the United States on January 31, and in July, seven additional biosimilars became available. These drugs have the potential to lower prescription drug prices, but when and by how much remains to be seen.
Here’s what you need to know about adalimumab biosimilars.
What Humira biosimilars are now available?
Eight different biosimilars have launched in 2023 with discounts as large at 85% from Humira’s list price of $6,922. A few companies also offer two price points.
Three of these biosimilars – Hadlima, Hyrimoz, and Yuflyma – are available in high concentration formulations. This high concentration formulation makes up 85% of Humira prescriptions, according to a report from Goodroot, a collection of companies focused on lowering health care costs.
Cyltezo is currently the only adalimumab biosimilar with an interchangeability designation, meaning that a pharmacist can substitute the biosimilar for an equivalent Humira prescription without the intervention of a clinician. A total of 47 states allow for these substitutions without prior approval from a clinician, according to Goodroot, and the clinician must be notified of the switch within a certain time frame. A total of 40 states require that patients be notified of the switch before substitution.
However, it’s not clear if this interchangeability designation will prove an advantage for Cyltezo, as it is interchangeable with the lower concentration version of Humira that makes up just 15% of prescriptions.
Most of the companies behind these biosimilars are pursuing interchangeability designations for their drugs, except for Fresenius Kabi (Idacio) and Coherus (Yusimry).
A ninth biosimilar, Pfizer’s adalimumab-afzb (Abrilada), is not yet on the market and is currently awaiting an approval decision from the Food and Drug Administration to add an interchangeability designation to its prior approval for a low-concentration formulation.
Why are they priced differently?
The two price points offer different deals to payers. Pharmacy benefit managers make confidential agreements with drug manufacturers to get a discount – called a rebate – to get the drug on the PBM’s formulary. The PBM keeps a portion of that rebate, and the rest is passed on to the insurance company and patients. Biosimilars at a higher price point will likely offer larger rebates. Biosimilars offered at lower price points incorporate this discount up front in their list pricing and likely will not offer large rebates.
Will biosimilars be covered by payers?
Currently, biosimilars are being offered on formularies at parity with Humira, meaning they are on the same tier. The PBM companies OptumRx and Cigna Group’s Express Scripts will offer Amjevita (at both price points), Cyltezo, and Hyrimoz (at both price points).
“This decision allows our clients flexibility to provide access to the lower list price, so members in high-deductible plans and benefit designs with coinsurance can experience lower out-of-pocket costs,” said OptumRx spokesperson Isaac Sorensen in an email.
Mark Cuban Cost Plus Drug Company, which uses a direct-to-consumer model, will offer Yusimry for $567.27 on its website. SmithRx, a PBM based in San Francisco, announced it would partner with Cost Plus Drugs to offer Yusimry, adding that SmithRx members can use their insurance benefits to further reduce out-of-pocket costs. RxPreferred, another PBM, will also offer Yusimry through its partnership with Cuban’s company.
The news website Formulary Watch previously reported that CVS Caremark, another of the biggest PBMs, will be offering Amjevita, but as a nonpreferred brand, while Humira remains the preferred brand. CVS Caremark did not respond to a request for comment.
Will patients pay less?
Biosimilars have been touted as a potential solution to lower spending on biologic drugs, but it’s unknown if patients will ultimately benefit with lower out-of-pocket costs. It’s “impossible to predict” if the discount that third-party payers pay will be passed on to consumers, said Mark Fendrick, MD, who directs the University of Michigan Center for Value-based Insurance Design in Ann Arbor.
Generally, a consumer’s copay is a percentage of a drug’s list price, so it stands to reason that a low drug price would result in lower out-of-pocket payments. While this is mostly true, Humira has a successful copay assistance program to lower prescription costs for consumers. According to a 2022 IQVIA report, 82% of commercial prescriptions cost patients less than $10 for Humira because of this program.
To appeal to patients, biosimilar companies will need to offer similar savings, Dr. Fendrick added. “There will be some discontent if patients are actually asked to pay more out-of-pocket for a less expensive drug,” he said.
All eight companies behind these biosimilars are offering or will be launching copay saving programs, many which advertise copays as low as $0 per month for eligible patients.
How will Humira respond?
Marta Wosińska, PhD, a health care economist at the Brookings Institute, Washington, predicts payers will use these lower biosimilar prices to negotiate better deals with AbbVie, Humira’s manufacturer. “We have a lot of players coming into [the market] right now, so the competition is really fierce,” she said. In response, AbbVie will need to increase rebates on Humira and/or lower its price to compete with these biosimilars.
“The ball is in AbbVie’s court,” she said. “If [the company] is not willing to drop price sufficiently, then payers will start switching to biosimilars.”
Dr. Fendrick reported past financial relationships and consulting arrangements with AbbVie, Amgen, Arnold Ventures, Bayer, CareFirst, BlueCross BlueShield, and many other companies. Dr. Wosińska has received funding from Arnold Ventures and serves as an expert witness on antitrust cases involving generic medication.
A version of this article first appeared on Medscape.com.
The best-selling drug Humira (adalimumab) now faces competition in the United States after a 20-year monopoly. The first adalimumab biosimilar, Amjevita, launched in the United States on January 31, and in July, seven additional biosimilars became available. These drugs have the potential to lower prescription drug prices, but when and by how much remains to be seen.
Here’s what you need to know about adalimumab biosimilars.
What Humira biosimilars are now available?
Eight different biosimilars have launched in 2023 with discounts as large at 85% from Humira’s list price of $6,922. A few companies also offer two price points.
Three of these biosimilars – Hadlima, Hyrimoz, and Yuflyma – are available in high concentration formulations. This high concentration formulation makes up 85% of Humira prescriptions, according to a report from Goodroot, a collection of companies focused on lowering health care costs.
Cyltezo is currently the only adalimumab biosimilar with an interchangeability designation, meaning that a pharmacist can substitute the biosimilar for an equivalent Humira prescription without the intervention of a clinician. A total of 47 states allow for these substitutions without prior approval from a clinician, according to Goodroot, and the clinician must be notified of the switch within a certain time frame. A total of 40 states require that patients be notified of the switch before substitution.
However, it’s not clear if this interchangeability designation will prove an advantage for Cyltezo, as it is interchangeable with the lower concentration version of Humira that makes up just 15% of prescriptions.
Most of the companies behind these biosimilars are pursuing interchangeability designations for their drugs, except for Fresenius Kabi (Idacio) and Coherus (Yusimry).
A ninth biosimilar, Pfizer’s adalimumab-afzb (Abrilada), is not yet on the market and is currently awaiting an approval decision from the Food and Drug Administration to add an interchangeability designation to its prior approval for a low-concentration formulation.
Why are they priced differently?
The two price points offer different deals to payers. Pharmacy benefit managers make confidential agreements with drug manufacturers to get a discount – called a rebate – to get the drug on the PBM’s formulary. The PBM keeps a portion of that rebate, and the rest is passed on to the insurance company and patients. Biosimilars at a higher price point will likely offer larger rebates. Biosimilars offered at lower price points incorporate this discount up front in their list pricing and likely will not offer large rebates.
Will biosimilars be covered by payers?
Currently, biosimilars are being offered on formularies at parity with Humira, meaning they are on the same tier. The PBM companies OptumRx and Cigna Group’s Express Scripts will offer Amjevita (at both price points), Cyltezo, and Hyrimoz (at both price points).
“This decision allows our clients flexibility to provide access to the lower list price, so members in high-deductible plans and benefit designs with coinsurance can experience lower out-of-pocket costs,” said OptumRx spokesperson Isaac Sorensen in an email.
Mark Cuban Cost Plus Drug Company, which uses a direct-to-consumer model, will offer Yusimry for $567.27 on its website. SmithRx, a PBM based in San Francisco, announced it would partner with Cost Plus Drugs to offer Yusimry, adding that SmithRx members can use their insurance benefits to further reduce out-of-pocket costs. RxPreferred, another PBM, will also offer Yusimry through its partnership with Cuban’s company.
The news website Formulary Watch previously reported that CVS Caremark, another of the biggest PBMs, will be offering Amjevita, but as a nonpreferred brand, while Humira remains the preferred brand. CVS Caremark did not respond to a request for comment.
Will patients pay less?
Biosimilars have been touted as a potential solution to lower spending on biologic drugs, but it’s unknown if patients will ultimately benefit with lower out-of-pocket costs. It’s “impossible to predict” if the discount that third-party payers pay will be passed on to consumers, said Mark Fendrick, MD, who directs the University of Michigan Center for Value-based Insurance Design in Ann Arbor.
Generally, a consumer’s copay is a percentage of a drug’s list price, so it stands to reason that a low drug price would result in lower out-of-pocket payments. While this is mostly true, Humira has a successful copay assistance program to lower prescription costs for consumers. According to a 2022 IQVIA report, 82% of commercial prescriptions cost patients less than $10 for Humira because of this program.
To appeal to patients, biosimilar companies will need to offer similar savings, Dr. Fendrick added. “There will be some discontent if patients are actually asked to pay more out-of-pocket for a less expensive drug,” he said.
All eight companies behind these biosimilars are offering or will be launching copay saving programs, many which advertise copays as low as $0 per month for eligible patients.
How will Humira respond?
Marta Wosińska, PhD, a health care economist at the Brookings Institute, Washington, predicts payers will use these lower biosimilar prices to negotiate better deals with AbbVie, Humira’s manufacturer. “We have a lot of players coming into [the market] right now, so the competition is really fierce,” she said. In response, AbbVie will need to increase rebates on Humira and/or lower its price to compete with these biosimilars.
“The ball is in AbbVie’s court,” she said. “If [the company] is not willing to drop price sufficiently, then payers will start switching to biosimilars.”
Dr. Fendrick reported past financial relationships and consulting arrangements with AbbVie, Amgen, Arnold Ventures, Bayer, CareFirst, BlueCross BlueShield, and many other companies. Dr. Wosińska has received funding from Arnold Ventures and serves as an expert witness on antitrust cases involving generic medication.
A version of this article first appeared on Medscape.com.
In new era of gene therapy, PCPs are ‘boots on the ground’
In Colorado and Wyoming, nearly every baby born since 2020 is tested for signs of a mutation in the SMN1 gene, an indicator of spinal muscular atrophy (SMA). And in 4 years, genetic counselor Melissa Gibbons has seen 24 positive results. She has prepped 24 different pediatricians and family doctors to deliver the news: A seemingly perfect newborn likely has a lethal genetic disease.
Most of these clinicians had never cared for a child with SMA before, nor did they know that lifesaving gene therapy for the condition now exists. Still, the physicians were foundational to getting babies emergency treatment and monitoring the child’s safety after the fact.
“They are boots on the ground for this kind of [work],” Ms. Gibbons, who is the newborn screen coordinator for SMA in both states, told this news organization. “I’m not even sure they realize it.” As of today, the U.S. Food and Drug Administration has approved 16 gene therapies for the treatment of rare and debilitating diseases once considered lethal, such as SMA and cerebral adrenoleukodystrophy.
The newest addition to the list of approvals is Elevidys, Sarepta’s gene therapy for Duchenne muscular dystrophy (DMD). These conditions can now be mitigated, abated for years at a time, and even cured using treatments that tweak a patient’s DNA or RNA.
Hundreds of treatments are under development using the same mechanism. Viruses, liposomes, and other vectors of all kinds are being used to usher new genes into cells, correcting faulty copies or equipping a cell to fight disease. Cells gain the ability to make lifesaving proteins – proteins that heal wounds, restore muscle function, and fight cancer.
Within the decade, a significant fraction of the pediatric population will have gone through gene therapy, experts told this news organization. And primary care stands to be a linchpin in the scale-up of this kind of precision genetic medicine. Pediatricians and general practitioners will be central to finding and monitoring the patients that need these treatments. But the time and support doctors will need to fill that role remain scarce.
“This is a world we are creating right now, quite literally,” said Stanley Nelson, MD, director of the center for Duchenne muscular dystrophy at the University of California, Los Angeles. These cases – some before gene therapy and some after – will show up in primary care offices before the textbook is written.
Unknown side effects, new diseases
Even now, gene therapy is sequestered away in large academic medical research centers. The diagnosis, decision-making, and aftercare are handled by subspecialists working on clinical trials. While the research is ongoing, trial sponsors are keeping a close eye on enrolled patients. But that’s only until these drugs get market approval, Phil Beales, MD, chief medical officer at Congenica, a digital health company specializing in genome analysis support, said. Afterward, “the trialists will no longer have a role in looking after those patients.”
At that point, the role of primary care clinicians will be critically important. Although they probably will not manage gene-therapy patients on their own – comanaging them instead with subspecialists – they will be involved in the ordering and monitoring of safety labs and other tests.
General practitioners “need to know side effects because they are going to deal with side effects when someone calls them in the middle of the night,” said Dr. Beales, who also is chief executive officer of Axovia Therapeutics, a biotech company developing gene therapies.
Some of the side effects that come with gene therapy are established. Adeno-associated virus (AAV) or AAV-mediated gene therapies carry an increased risk for damage to the heart and liver, Dr. Nelson said. Other side effects are less well known and could be specific to the treatment and the tissue it targets. Primary care will be critical in detecting these unexpected side effects and expediting visits with subspecialists, he said.
In rural Wyoming, pediatricians and family doctors are especially important, Ms. Gibbons said. In the 30-90 days after gene therapy, patients need a lot of follow-up for safety reasons.
But aftercare for gene therapy will be more than just monitoring and managing side effects. The diseases themselves will change. Patients will be living with conditions that once were lethal.
In some cases, gene therapy may largely eliminate the disease. The data suggest that thalassemia, for example, can be largely cured for decades with one infusion of a patient’s genetically modified hematopoietic stem cells made using bluebird bio’s Zynteglo, according to Christy Duncan, MD, medical director of clinical research at the gene therapy program at Boston Children’s Hospital.
But other gene therapies, like the one for DMD, will offer a “spectrum of benefits,” Dr. Nelson said. They will be lifesaving, but the signs of the disease will linger. Clinicians will be learning alongside specialists what the new disease state for DMD and other rare diseases looks like after gene therapy.
“As we get hundreds of such therapies, [post–gene therapy] will amount to a substantial part of the pediatric population,” Dr. Nelson said.
Finding patients
Many of these rare diseases that plague young patients are unmistakable. Children with moderate or severe dystrophic epidermolysis bullosa, for instance, carry a mutation that prevents them from making type VII collagen. The babies suffer wounds and excessive bleeding and tend to receive a quick diagnosis within the first 6 months of life, according to Andy Orth, chief commercial officer at Krystal Bio, manufacturer of a new wound-healing gene therapy, Vyjuvek, for the disorder.
Other rare neurologic or muscular diseases can go undiagnosed for years. Until recently, drug companies and researchers have had little motivation to speed up the timeline because early diagnosis of a disease like DMD would not change the outcome, Dr. Nelson said.
But with gene therapy, prognoses are changing. And finding diseases early could soon mean preserving muscular function or preventing neurologic damage, Dr. Duncan said.
Newborn sequencing “is not standard of care yet, but it’s certainly coming,” Josh Peterson, MD, MPH, director of the center for precision medicine at Vanderbilt University Medical Center, in Nashville, Tenn., told this news organization.
A recent survey of 238 specialists in rare diseases found that roughly 90% believe whole-genome sequencing should be available to all newborns. And 80% of those experts endorse 42 genes as disease predictors. Screening for rare diseases at birth could reveal a host of conditions in the first week of life and expedite treatment. But this strategy will often rely on primary care and pediatricians interpreting the results.
Most pediatricians think sequencing is a great idea, but they do not feel comfortable doing it themselves, Dr. Peterson said. The good news, he said, is that manufacturers have made screening tests straightforward. Some drug companies even offer free screenings for gene therapy candidates.
Dr. Peterson predicts pediatricians will need to be equipped to deliver negative results on their own, which will be the case for around 97%-99% of patients. They also will need to be clear on whether a negative result is definitive or if more testing is warranted.
Positive results are more nuanced. Genetic counseling is the ideal resource when delivering this kind of news to patients, but counselors are a scarce resource nationally – and particularly in rural areas, Dr. Nelson said. Physicians likely will have to rely on their own counseling training to some degree.
“I feel very strongly that genetic counselors are in short supply,” Ms. Gibbons in Colorado said. Patients need a friendly resource who can talk them through the disease and how it works. And that discussion is not a one-off, she said.
The number of board-certified genetic counselors in the United States has doubled to more than 6,000 in the past 10 years – a pace that is expected to continue, according to the National Society of Genetic Counselors. “However, the geographical distribution of genetic counselors is most concentrated in urban centers.”
Equally important to the counseling experience, according to Dr. Duncan at Boston Children’s, is a primary care physician’s network of connections. The best newborn screening rollouts across the country have succeeded because clinicians knew where to send people next and how to get families the help they needed, she said.
But she also cautioned that this learning curve will soon be overwhelming. As gene therapy expands, it may be difficult for primary care doctors to keep up with the science, treatment studies, and commercially available therapies. “It’s asking too much,” Dr. Duncan said.
The structure of primary care already stretches practitioners thin and will “affect how well precision medicine can be adopted and disseminated,” Dr. Peterson said. “I think that is a key issue.”
Artificial intelligence may offer a partial solution. Some genetic counseling models already exist, but their utility for clinicians so far is limited, Dr. Beales said. But he said he expects these tools to improve rapidly to help clinicians and patients. On the patient’s end, they may be able to answer questions and supplement basic genetic counseling. On the physician’s end, algorithms could help triage patients and help move them along to the next steps in the care pathway for these rare diseases.
The whole patient
Primary care physicians will not be expected to be experts in gene therapy or solely in charge of patient safety. They will have support from industry and subspecialists leading the development of these treatments, experts agreed.
But generalists should expect to be drawn into multidisciplinary care teams, be the sounding boards for patients making decisions about gene therapy, help arrange insurance coverage, and be the recipients of late-night phone calls about side effects.
All that, while never losing sight of the child’s holistic health. In children so sick, specialists, subspecialists, and even parents tend to focus only on the rare disease. The team can “get distracted from good normal routine care,” Dr. Nelson said. But these children aren’t exempt from check-ups, vaccine regimens, or the other diseases of childhood.
“In a world where we mitigate that core disease,” he said, “we need a partner in the general pediatrics community” investing in their long-term health.
A version of this article first appeared on Medscape.com.
In Colorado and Wyoming, nearly every baby born since 2020 is tested for signs of a mutation in the SMN1 gene, an indicator of spinal muscular atrophy (SMA). And in 4 years, genetic counselor Melissa Gibbons has seen 24 positive results. She has prepped 24 different pediatricians and family doctors to deliver the news: A seemingly perfect newborn likely has a lethal genetic disease.
Most of these clinicians had never cared for a child with SMA before, nor did they know that lifesaving gene therapy for the condition now exists. Still, the physicians were foundational to getting babies emergency treatment and monitoring the child’s safety after the fact.
“They are boots on the ground for this kind of [work],” Ms. Gibbons, who is the newborn screen coordinator for SMA in both states, told this news organization. “I’m not even sure they realize it.” As of today, the U.S. Food and Drug Administration has approved 16 gene therapies for the treatment of rare and debilitating diseases once considered lethal, such as SMA and cerebral adrenoleukodystrophy.
The newest addition to the list of approvals is Elevidys, Sarepta’s gene therapy for Duchenne muscular dystrophy (DMD). These conditions can now be mitigated, abated for years at a time, and even cured using treatments that tweak a patient’s DNA or RNA.
Hundreds of treatments are under development using the same mechanism. Viruses, liposomes, and other vectors of all kinds are being used to usher new genes into cells, correcting faulty copies or equipping a cell to fight disease. Cells gain the ability to make lifesaving proteins – proteins that heal wounds, restore muscle function, and fight cancer.
Within the decade, a significant fraction of the pediatric population will have gone through gene therapy, experts told this news organization. And primary care stands to be a linchpin in the scale-up of this kind of precision genetic medicine. Pediatricians and general practitioners will be central to finding and monitoring the patients that need these treatments. But the time and support doctors will need to fill that role remain scarce.
“This is a world we are creating right now, quite literally,” said Stanley Nelson, MD, director of the center for Duchenne muscular dystrophy at the University of California, Los Angeles. These cases – some before gene therapy and some after – will show up in primary care offices before the textbook is written.
Unknown side effects, new diseases
Even now, gene therapy is sequestered away in large academic medical research centers. The diagnosis, decision-making, and aftercare are handled by subspecialists working on clinical trials. While the research is ongoing, trial sponsors are keeping a close eye on enrolled patients. But that’s only until these drugs get market approval, Phil Beales, MD, chief medical officer at Congenica, a digital health company specializing in genome analysis support, said. Afterward, “the trialists will no longer have a role in looking after those patients.”
At that point, the role of primary care clinicians will be critically important. Although they probably will not manage gene-therapy patients on their own – comanaging them instead with subspecialists – they will be involved in the ordering and monitoring of safety labs and other tests.
General practitioners “need to know side effects because they are going to deal with side effects when someone calls them in the middle of the night,” said Dr. Beales, who also is chief executive officer of Axovia Therapeutics, a biotech company developing gene therapies.
Some of the side effects that come with gene therapy are established. Adeno-associated virus (AAV) or AAV-mediated gene therapies carry an increased risk for damage to the heart and liver, Dr. Nelson said. Other side effects are less well known and could be specific to the treatment and the tissue it targets. Primary care will be critical in detecting these unexpected side effects and expediting visits with subspecialists, he said.
In rural Wyoming, pediatricians and family doctors are especially important, Ms. Gibbons said. In the 30-90 days after gene therapy, patients need a lot of follow-up for safety reasons.
But aftercare for gene therapy will be more than just monitoring and managing side effects. The diseases themselves will change. Patients will be living with conditions that once were lethal.
In some cases, gene therapy may largely eliminate the disease. The data suggest that thalassemia, for example, can be largely cured for decades with one infusion of a patient’s genetically modified hematopoietic stem cells made using bluebird bio’s Zynteglo, according to Christy Duncan, MD, medical director of clinical research at the gene therapy program at Boston Children’s Hospital.
But other gene therapies, like the one for DMD, will offer a “spectrum of benefits,” Dr. Nelson said. They will be lifesaving, but the signs of the disease will linger. Clinicians will be learning alongside specialists what the new disease state for DMD and other rare diseases looks like after gene therapy.
“As we get hundreds of such therapies, [post–gene therapy] will amount to a substantial part of the pediatric population,” Dr. Nelson said.
Finding patients
Many of these rare diseases that plague young patients are unmistakable. Children with moderate or severe dystrophic epidermolysis bullosa, for instance, carry a mutation that prevents them from making type VII collagen. The babies suffer wounds and excessive bleeding and tend to receive a quick diagnosis within the first 6 months of life, according to Andy Orth, chief commercial officer at Krystal Bio, manufacturer of a new wound-healing gene therapy, Vyjuvek, for the disorder.
Other rare neurologic or muscular diseases can go undiagnosed for years. Until recently, drug companies and researchers have had little motivation to speed up the timeline because early diagnosis of a disease like DMD would not change the outcome, Dr. Nelson said.
But with gene therapy, prognoses are changing. And finding diseases early could soon mean preserving muscular function or preventing neurologic damage, Dr. Duncan said.
Newborn sequencing “is not standard of care yet, but it’s certainly coming,” Josh Peterson, MD, MPH, director of the center for precision medicine at Vanderbilt University Medical Center, in Nashville, Tenn., told this news organization.
A recent survey of 238 specialists in rare diseases found that roughly 90% believe whole-genome sequencing should be available to all newborns. And 80% of those experts endorse 42 genes as disease predictors. Screening for rare diseases at birth could reveal a host of conditions in the first week of life and expedite treatment. But this strategy will often rely on primary care and pediatricians interpreting the results.
Most pediatricians think sequencing is a great idea, but they do not feel comfortable doing it themselves, Dr. Peterson said. The good news, he said, is that manufacturers have made screening tests straightforward. Some drug companies even offer free screenings for gene therapy candidates.
Dr. Peterson predicts pediatricians will need to be equipped to deliver negative results on their own, which will be the case for around 97%-99% of patients. They also will need to be clear on whether a negative result is definitive or if more testing is warranted.
Positive results are more nuanced. Genetic counseling is the ideal resource when delivering this kind of news to patients, but counselors are a scarce resource nationally – and particularly in rural areas, Dr. Nelson said. Physicians likely will have to rely on their own counseling training to some degree.
“I feel very strongly that genetic counselors are in short supply,” Ms. Gibbons in Colorado said. Patients need a friendly resource who can talk them through the disease and how it works. And that discussion is not a one-off, she said.
The number of board-certified genetic counselors in the United States has doubled to more than 6,000 in the past 10 years – a pace that is expected to continue, according to the National Society of Genetic Counselors. “However, the geographical distribution of genetic counselors is most concentrated in urban centers.”
Equally important to the counseling experience, according to Dr. Duncan at Boston Children’s, is a primary care physician’s network of connections. The best newborn screening rollouts across the country have succeeded because clinicians knew where to send people next and how to get families the help they needed, she said.
But she also cautioned that this learning curve will soon be overwhelming. As gene therapy expands, it may be difficult for primary care doctors to keep up with the science, treatment studies, and commercially available therapies. “It’s asking too much,” Dr. Duncan said.
The structure of primary care already stretches practitioners thin and will “affect how well precision medicine can be adopted and disseminated,” Dr. Peterson said. “I think that is a key issue.”
Artificial intelligence may offer a partial solution. Some genetic counseling models already exist, but their utility for clinicians so far is limited, Dr. Beales said. But he said he expects these tools to improve rapidly to help clinicians and patients. On the patient’s end, they may be able to answer questions and supplement basic genetic counseling. On the physician’s end, algorithms could help triage patients and help move them along to the next steps in the care pathway for these rare diseases.
The whole patient
Primary care physicians will not be expected to be experts in gene therapy or solely in charge of patient safety. They will have support from industry and subspecialists leading the development of these treatments, experts agreed.
But generalists should expect to be drawn into multidisciplinary care teams, be the sounding boards for patients making decisions about gene therapy, help arrange insurance coverage, and be the recipients of late-night phone calls about side effects.
All that, while never losing sight of the child’s holistic health. In children so sick, specialists, subspecialists, and even parents tend to focus only on the rare disease. The team can “get distracted from good normal routine care,” Dr. Nelson said. But these children aren’t exempt from check-ups, vaccine regimens, or the other diseases of childhood.
“In a world where we mitigate that core disease,” he said, “we need a partner in the general pediatrics community” investing in their long-term health.
A version of this article first appeared on Medscape.com.
In Colorado and Wyoming, nearly every baby born since 2020 is tested for signs of a mutation in the SMN1 gene, an indicator of spinal muscular atrophy (SMA). And in 4 years, genetic counselor Melissa Gibbons has seen 24 positive results. She has prepped 24 different pediatricians and family doctors to deliver the news: A seemingly perfect newborn likely has a lethal genetic disease.
Most of these clinicians had never cared for a child with SMA before, nor did they know that lifesaving gene therapy for the condition now exists. Still, the physicians were foundational to getting babies emergency treatment and monitoring the child’s safety after the fact.
“They are boots on the ground for this kind of [work],” Ms. Gibbons, who is the newborn screen coordinator for SMA in both states, told this news organization. “I’m not even sure they realize it.” As of today, the U.S. Food and Drug Administration has approved 16 gene therapies for the treatment of rare and debilitating diseases once considered lethal, such as SMA and cerebral adrenoleukodystrophy.
The newest addition to the list of approvals is Elevidys, Sarepta’s gene therapy for Duchenne muscular dystrophy (DMD). These conditions can now be mitigated, abated for years at a time, and even cured using treatments that tweak a patient’s DNA or RNA.
Hundreds of treatments are under development using the same mechanism. Viruses, liposomes, and other vectors of all kinds are being used to usher new genes into cells, correcting faulty copies or equipping a cell to fight disease. Cells gain the ability to make lifesaving proteins – proteins that heal wounds, restore muscle function, and fight cancer.
Within the decade, a significant fraction of the pediatric population will have gone through gene therapy, experts told this news organization. And primary care stands to be a linchpin in the scale-up of this kind of precision genetic medicine. Pediatricians and general practitioners will be central to finding and monitoring the patients that need these treatments. But the time and support doctors will need to fill that role remain scarce.
“This is a world we are creating right now, quite literally,” said Stanley Nelson, MD, director of the center for Duchenne muscular dystrophy at the University of California, Los Angeles. These cases – some before gene therapy and some after – will show up in primary care offices before the textbook is written.
Unknown side effects, new diseases
Even now, gene therapy is sequestered away in large academic medical research centers. The diagnosis, decision-making, and aftercare are handled by subspecialists working on clinical trials. While the research is ongoing, trial sponsors are keeping a close eye on enrolled patients. But that’s only until these drugs get market approval, Phil Beales, MD, chief medical officer at Congenica, a digital health company specializing in genome analysis support, said. Afterward, “the trialists will no longer have a role in looking after those patients.”
At that point, the role of primary care clinicians will be critically important. Although they probably will not manage gene-therapy patients on their own – comanaging them instead with subspecialists – they will be involved in the ordering and monitoring of safety labs and other tests.
General practitioners “need to know side effects because they are going to deal with side effects when someone calls them in the middle of the night,” said Dr. Beales, who also is chief executive officer of Axovia Therapeutics, a biotech company developing gene therapies.
Some of the side effects that come with gene therapy are established. Adeno-associated virus (AAV) or AAV-mediated gene therapies carry an increased risk for damage to the heart and liver, Dr. Nelson said. Other side effects are less well known and could be specific to the treatment and the tissue it targets. Primary care will be critical in detecting these unexpected side effects and expediting visits with subspecialists, he said.
In rural Wyoming, pediatricians and family doctors are especially important, Ms. Gibbons said. In the 30-90 days after gene therapy, patients need a lot of follow-up for safety reasons.
But aftercare for gene therapy will be more than just monitoring and managing side effects. The diseases themselves will change. Patients will be living with conditions that once were lethal.
In some cases, gene therapy may largely eliminate the disease. The data suggest that thalassemia, for example, can be largely cured for decades with one infusion of a patient’s genetically modified hematopoietic stem cells made using bluebird bio’s Zynteglo, according to Christy Duncan, MD, medical director of clinical research at the gene therapy program at Boston Children’s Hospital.
But other gene therapies, like the one for DMD, will offer a “spectrum of benefits,” Dr. Nelson said. They will be lifesaving, but the signs of the disease will linger. Clinicians will be learning alongside specialists what the new disease state for DMD and other rare diseases looks like after gene therapy.
“As we get hundreds of such therapies, [post–gene therapy] will amount to a substantial part of the pediatric population,” Dr. Nelson said.
Finding patients
Many of these rare diseases that plague young patients are unmistakable. Children with moderate or severe dystrophic epidermolysis bullosa, for instance, carry a mutation that prevents them from making type VII collagen. The babies suffer wounds and excessive bleeding and tend to receive a quick diagnosis within the first 6 months of life, according to Andy Orth, chief commercial officer at Krystal Bio, manufacturer of a new wound-healing gene therapy, Vyjuvek, for the disorder.
Other rare neurologic or muscular diseases can go undiagnosed for years. Until recently, drug companies and researchers have had little motivation to speed up the timeline because early diagnosis of a disease like DMD would not change the outcome, Dr. Nelson said.
But with gene therapy, prognoses are changing. And finding diseases early could soon mean preserving muscular function or preventing neurologic damage, Dr. Duncan said.
Newborn sequencing “is not standard of care yet, but it’s certainly coming,” Josh Peterson, MD, MPH, director of the center for precision medicine at Vanderbilt University Medical Center, in Nashville, Tenn., told this news organization.
A recent survey of 238 specialists in rare diseases found that roughly 90% believe whole-genome sequencing should be available to all newborns. And 80% of those experts endorse 42 genes as disease predictors. Screening for rare diseases at birth could reveal a host of conditions in the first week of life and expedite treatment. But this strategy will often rely on primary care and pediatricians interpreting the results.
Most pediatricians think sequencing is a great idea, but they do not feel comfortable doing it themselves, Dr. Peterson said. The good news, he said, is that manufacturers have made screening tests straightforward. Some drug companies even offer free screenings for gene therapy candidates.
Dr. Peterson predicts pediatricians will need to be equipped to deliver negative results on their own, which will be the case for around 97%-99% of patients. They also will need to be clear on whether a negative result is definitive or if more testing is warranted.
Positive results are more nuanced. Genetic counseling is the ideal resource when delivering this kind of news to patients, but counselors are a scarce resource nationally – and particularly in rural areas, Dr. Nelson said. Physicians likely will have to rely on their own counseling training to some degree.
“I feel very strongly that genetic counselors are in short supply,” Ms. Gibbons in Colorado said. Patients need a friendly resource who can talk them through the disease and how it works. And that discussion is not a one-off, she said.
The number of board-certified genetic counselors in the United States has doubled to more than 6,000 in the past 10 years – a pace that is expected to continue, according to the National Society of Genetic Counselors. “However, the geographical distribution of genetic counselors is most concentrated in urban centers.”
Equally important to the counseling experience, according to Dr. Duncan at Boston Children’s, is a primary care physician’s network of connections. The best newborn screening rollouts across the country have succeeded because clinicians knew where to send people next and how to get families the help they needed, she said.
But she also cautioned that this learning curve will soon be overwhelming. As gene therapy expands, it may be difficult for primary care doctors to keep up with the science, treatment studies, and commercially available therapies. “It’s asking too much,” Dr. Duncan said.
The structure of primary care already stretches practitioners thin and will “affect how well precision medicine can be adopted and disseminated,” Dr. Peterson said. “I think that is a key issue.”
Artificial intelligence may offer a partial solution. Some genetic counseling models already exist, but their utility for clinicians so far is limited, Dr. Beales said. But he said he expects these tools to improve rapidly to help clinicians and patients. On the patient’s end, they may be able to answer questions and supplement basic genetic counseling. On the physician’s end, algorithms could help triage patients and help move them along to the next steps in the care pathway for these rare diseases.
The whole patient
Primary care physicians will not be expected to be experts in gene therapy or solely in charge of patient safety. They will have support from industry and subspecialists leading the development of these treatments, experts agreed.
But generalists should expect to be drawn into multidisciplinary care teams, be the sounding boards for patients making decisions about gene therapy, help arrange insurance coverage, and be the recipients of late-night phone calls about side effects.
All that, while never losing sight of the child’s holistic health. In children so sick, specialists, subspecialists, and even parents tend to focus only on the rare disease. The team can “get distracted from good normal routine care,” Dr. Nelson said. But these children aren’t exempt from check-ups, vaccine regimens, or the other diseases of childhood.
“In a world where we mitigate that core disease,” he said, “we need a partner in the general pediatrics community” investing in their long-term health.
A version of this article first appeared on Medscape.com.
When did medicine become a battleground for everything?
Like hundreds of other medical experts, Leana Wen, MD, an emergency physician and former Baltimore health commissioner, was an early and avid supporter of COVID vaccines and their ability to prevent severe disease, hospitalization, and death from SARS-CoV-2 infections.
When 51-year-old Scott Eli Harris, of Aubrey, Tex., heard of Dr. Wen’s stance in July 2021, the self-described “fifth-generation U.S. Army veteran and a sniper” sent Dr. Wen an electronic invective laden with racist language and very specific threats to shoot her.
Mr. Harris pled guilty to transmitting threats via interstate commerce last February and began serving 6 months in federal prison in the fall of 2022, but his threats wouldn’t be the last for Dr. Wen. Just 2 days after Mr. Harris was sentenced, charges were unsealed against another man in Massachusetts, who threatened that Dr. Wen would “end up in pieces” if she continued “pushing” her thoughts publicly.’
Dr. Wen has plenty of company. In an August 2022 survey of emergency doctors conducted by the American College of Emergency Physicians, 85% of respondents said violence against them is increasing. One in four doctors said they’re being assaulted by patients and their family and friends multiple times a week, compared with just 8% of doctors who said as much in 2018. About 64% of emergency physicians reported receiving verbal assaults and threats of violence; 40% reported being hit or slapped, and 26% were kicked.
This uptick of violence and threats against physicians didn’t come out of nowhere; violence against health care workers has been gradually increasing over the past decade. Health care providers can attest to the hostility that particular topics have sparked for years: vaccines in pediatrics, abortion in ob.gyn., and gender-affirming care in endocrinology.
But the pandemic fueled the fire. The proliferation of misinformation (often via social media) and the politicization of public health and medicine are at the center of the problem.
‘The people attacking are themselves victims’
The misinformation problem first came to a head in one area of public health: vaccines. The pandemic accelerated antagonism in medicine – thanks, in part, to decades of antivaccine activism.
The antivaccine movement, which has ebbed and flowed in the United States and across the globe since the first vaccine, experienced a new wave in the early 2000s with the combination of concerns about thimerosal in vaccines and a now disproven link between autism and the MMR vaccine. But that movement grew. It picked up steam when activists gained political clout after a 2014 measles outbreak at Disneyland led California schools to tighten up policies regarding vaccinations for kids who enrolled. These stronger public school vaccination laws ran up against religious freedom arguments from antivaccine advocates.
Use of social media continues to grow, and with it, the spread of misinformation. A recent study found that Facebook “users’ social media habits doubled, and in some cases, tripled the amount of fake news they shared.”
In the face of growing confusion, health care providers and public health experts have often struggled to treat their patients – and communicate to the public – without appearing political.

“The people that are doing the attacking are in some ways themselves victims,” said Peter Hotez, MD, PhD, dean of the National School of Tropical Medicine at Baylor College of Medicine, Houston. “They’re victims of the antiscience, antihealth ecosystem coming out of Fox News, the House Freedom Caucus, the CPAC conference, coming out of contrarian intellectuals.”
Many of Dr. Hotez’s colleagues don’t want to talk about the political right as an enabler of scientific disinformation, he said, but that doesn’t change what the evidence shows. The vast majority of state and national bills opposing vaccination, gender-affirming care, comprehensive reproductive care, and other evidence-based medical care often come from Republican legislators.
When politics and health care collide
“We’re in an incredible status quo,” said William Schaffner, MD, the previous director of the Infectious Diseases Society of America and a professor of infectious diseases and preventive medicine at Vanderbilt University, Nashville, Tenn. “You can’t get away from the politics, because you have [political] candidates espousing certain concepts that are antithetical to good public health.”

In March 2023, Florida Gov. Ron DeSantis’s surgeon general, Joseph Ladapo, MD, PhD, warned that COVID vaccines are harmful to young men, prompting rebukes from federal health authorities. It later came out that Dr. Ladapo had changed some of the results of the study before issuing his warning. But long before 2023, there emerged an increasing gap in COVID deaths between red states and blue states, mirroring the vaccination rates in those states. The redder the state, the higher the death toll.
It’s not just Republican Party culture warriors; medical misinformation is also finding increasing purchase on the far left. Robert F. Kennedy Jr. and Marianne Williamson, both of whom have launched long-shot challenges to President Biden for the 2024 Democratic nomination, had promoted antivaccine ideas long before the COVID pandemic. Mr. Kennedy continues to spread misinformation.
In June 2023, Joe Rogan hosted Mr. Kennedy, on his podcast. During the episode, Mr. Rogan listened uncritically as Mr. Kennedy told his millions of listeners that vaccines cause autism and that 5G causes cancer, among other fringe, often-debunked theories.
Dr. Hotez, a prominent misinformation debunker who was also part of a team that designed a low-cost COVID-19 vaccine, wrote on Twitter that the episode was “just awful.”
The backlash began almost immediately. Mr. Rogan, who has over 11 million followers on Twitter, responded with a public challenge for Dr. Hotez to debate Mr. Kennedy on Mr. Rogan’s show, with a reward of $100,000 to the charity of Dr. Hotez’s choice. More offers streamed in, including from Elon Musk, who tweeted that Dr. Hotez was “afraid of a public debate, because he knows he’s wrong.” More supporters of Mr. Kennedy and Mr. Rogan piled on.
Vaccine skeptics even showed up at Dr. Hotez’s house, filming him as he was returning from buying a Father’s Day cake and taunting him to debate Mr. Kennedy.
A turn in the pandemic
For a precious few weeks at the start of the pandemic, it felt as though the country was all in this together. There were arguments against closing schools and shutting down businesses, but for the most part, the nation had about 4 solid weeks of solidarity.
As masking mandates changed and the public health establishment lost the confidence of Americans, the veneer of solidarity began to chip away.
“Things were changing so rapidly during the pandemic that it was very hard for staff and patients to understand the changing guidelines, whether it was visitor constraints or masking,” said Carrie Nelson, the chief medical officer at the telehealth company AmWell, who worked as a supervisor at a large health care system in the Midwest until 2021.
In the midst of the public health crisis, former President Trump was downplaying the severity of the disease and was silencing officials from the Centers for Disease Control and Prevention, such as Nancy Messonier, who warned from the very beginning of the pandemic’s potential.
When the vaccines came out, the latent antivaccine movement flared up once again. And this time – unlike in decades past – the debate over vaccines had become partisan.
“Before the pandemic,” said Christopher Thomas, an emergency physician on the West Coast who requested that a pseudonym be used because of personal threats he has received, “patients wouldn’t really challenge me or throw out weird questions.” It’s not that he never encountered pushback, but the stakes felt lower, and people largely deferred to his medical expertise. “If we got a parent who had not vaccinated their child, I would totally engage back then,” Dr. Thomas said.
But the pandemic – and America’s response to it – changed the conversation. “The rhetoric ... switched from downplaying the virus to demonizing the vaccines,” Dr. Thomas said.
The toll on health care professionals
By the time vaccines were available, the public had begun to conflate doctors with public health experts, since both were “pushing” the vaccine.
“Most people probably don’t really know the difference between clinical medicine and public health,” said Richard Pan, MD, MPH, a pediatrician and California legislator who sponsored two bills – now laws – that strengthened state childhood vaccination requirements.
At first, it was clearly public health officials, such as Anthony Fauci, MD, who were the face of measures to mitigate the virus. But as doctors became the enforcers of those measures, the line between physicians and public health officials blurred.
A lot of the anger then shifted toward doctors, nurses, and other health care professionals, Dr. Pan said, “because we were, of course, the ones who would be administering the vaccines. They don’t really think of their doctor as a government person until your doctor is carrying a [government] message.”
Given the pressures and struggles of the past few years, it’s no surprise that burnout among health care professionals is high. According to an April 2023 study by the National Council of State Boards of Nursing and the National Forum of State Nursing Workforce Centers, an estimated 800,000 nurses expect to leave the profession by 2027, driven first and foremost by “stress and burnout.”
All of these departures in medicine’s “great resignation” have left hospitals and health care organizations even more short staffed, thereby increasing even more the pressure and burnout on those left.
The pandemic had already badly exacerbated the already widespread problem of burnout in the medical field, which Ms. Nelson said has contributed to the tension.
“The burnout problem that we have in health care is not a good basis for the development of a good therapeutic relationship,” Ms. Nelson said. “Burnout is fraught with apathy and desensitization to human emotions. It takes away the empathy that we once had for people that we see.”
What comes next?
Almost exactly 3 years after the world learned about SARS-CoV-2, Biden declared an end to the coronavirus public health emergency in April 2023. Yet, Americans continue to die from COVID, and the anger that bloomed and spread has not abated.
“I think we’re in a new steady state of violence in health care settings,” Ms. Nelson said. “It’s not gone down, because people are still very distressed.” That’s evident from the high prevalence of mental health conditions, the financial strain of first the pandemic and then inflation, and the overall traumatic impact the pandemic had on people, whether they recognize it or not.
The first step to solving any problem is, as the saying goes, to admit that there is a problem.
“I think people need to start stepping out of their comfort bubbles and start to look at things that make them uncomfortable,” Dr. Thomas said, but he doesn’t see that happening any time soon. “I’ve been very let down by physicians and embarrassed by the American physician organizations.”
The medical board in his state, he said, has stood by as some doctors continue misrepresenting medical evidence. “That’s been really, really hard on me. I didn’t think that the medical boards would go so far as to look the other way for something that was this tremendously bad.”
There are others who can take the lead – if they’re willing.
“There are some things the medical societies and academic health centers can do,” Dr. Hotez said, “starting with building up a culture of physicians and health care providers feeling comfortable in the public domain.” He said the messaging when he was getting his degrees was not to engage the public and not to talk to journalists because that was “self-promotion” or “grandstanding.” But the world is different now. Health care professionals need training in public engagement and communication, he said, and the culture needs to change so that health care providers feel comfortable speaking out without feeling “the sword of Damocles over their heads” every time they talk to a reporter, Dr. Hotez said.
There may be no silver bullet to solve the big-picture trust problem in medicine and public health. No TV appearance or quote in an article can solve it. But on an individual level — through careful relationship building with patients – doctors can strengthen that trust.
Telehealth may help with that, but there’s a fine balance there, Ms. Nelson cautioned. On the one hand, with the doctor and the patient each in their own private spaces, where they feel safe and comfortable, the overall experience can be more therapeutic and less stressful. At the same time, telehealth can pile on change-management tasks that can exacerbate burnout, “so it’s a delicate thing we have to approach.”
One very thin silver lining that could emerge from the way in which patients have begun to try to take charge of their care.
“They should fully understand the reasoning behind the recommendations that physicians are making,” Ms. Nelson said. “I’d like to see us get to a happy medium where it’s a partnership. We can’t go back to the old school where the doctor knows best and you don’t ever question him.
“What we need is the partnership, and I would love to see that as the silver lining, but the anger has got to settle down in order for that kind of productive thing to happen.”
As for the big picture? There’s a limit to what even society’s “miracle workers” can do. “The biggest priority right now for the health system is to protect their staff whatever way they can and do some training in deescalation,” Ms. Nelson said. “But I don’t think health care can solve the societal issues that seem to be creating this.”
A version of this article first appeared on Medscape.com.
Like hundreds of other medical experts, Leana Wen, MD, an emergency physician and former Baltimore health commissioner, was an early and avid supporter of COVID vaccines and their ability to prevent severe disease, hospitalization, and death from SARS-CoV-2 infections.
When 51-year-old Scott Eli Harris, of Aubrey, Tex., heard of Dr. Wen’s stance in July 2021, the self-described “fifth-generation U.S. Army veteran and a sniper” sent Dr. Wen an electronic invective laden with racist language and very specific threats to shoot her.
Mr. Harris pled guilty to transmitting threats via interstate commerce last February and began serving 6 months in federal prison in the fall of 2022, but his threats wouldn’t be the last for Dr. Wen. Just 2 days after Mr. Harris was sentenced, charges were unsealed against another man in Massachusetts, who threatened that Dr. Wen would “end up in pieces” if she continued “pushing” her thoughts publicly.’
Dr. Wen has plenty of company. In an August 2022 survey of emergency doctors conducted by the American College of Emergency Physicians, 85% of respondents said violence against them is increasing. One in four doctors said they’re being assaulted by patients and their family and friends multiple times a week, compared with just 8% of doctors who said as much in 2018. About 64% of emergency physicians reported receiving verbal assaults and threats of violence; 40% reported being hit or slapped, and 26% were kicked.
This uptick of violence and threats against physicians didn’t come out of nowhere; violence against health care workers has been gradually increasing over the past decade. Health care providers can attest to the hostility that particular topics have sparked for years: vaccines in pediatrics, abortion in ob.gyn., and gender-affirming care in endocrinology.
But the pandemic fueled the fire. The proliferation of misinformation (often via social media) and the politicization of public health and medicine are at the center of the problem.
‘The people attacking are themselves victims’
The misinformation problem first came to a head in one area of public health: vaccines. The pandemic accelerated antagonism in medicine – thanks, in part, to decades of antivaccine activism.
The antivaccine movement, which has ebbed and flowed in the United States and across the globe since the first vaccine, experienced a new wave in the early 2000s with the combination of concerns about thimerosal in vaccines and a now disproven link between autism and the MMR vaccine. But that movement grew. It picked up steam when activists gained political clout after a 2014 measles outbreak at Disneyland led California schools to tighten up policies regarding vaccinations for kids who enrolled. These stronger public school vaccination laws ran up against religious freedom arguments from antivaccine advocates.
Use of social media continues to grow, and with it, the spread of misinformation. A recent study found that Facebook “users’ social media habits doubled, and in some cases, tripled the amount of fake news they shared.”
In the face of growing confusion, health care providers and public health experts have often struggled to treat their patients – and communicate to the public – without appearing political.
“The people that are doing the attacking are in some ways themselves victims,” said Peter Hotez, MD, PhD, dean of the National School of Tropical Medicine at Baylor College of Medicine, Houston. “They’re victims of the antiscience, antihealth ecosystem coming out of Fox News, the House Freedom Caucus, the CPAC conference, coming out of contrarian intellectuals.”
Many of Dr. Hotez’s colleagues don’t want to talk about the political right as an enabler of scientific disinformation, he said, but that doesn’t change what the evidence shows. The vast majority of state and national bills opposing vaccination, gender-affirming care, comprehensive reproductive care, and other evidence-based medical care often come from Republican legislators.
When politics and health care collide
“We’re in an incredible status quo,” said William Schaffner, MD, the previous director of the Infectious Diseases Society of America and a professor of infectious diseases and preventive medicine at Vanderbilt University, Nashville, Tenn. “You can’t get away from the politics, because you have [political] candidates espousing certain concepts that are antithetical to good public health.”
In March 2023, Florida Gov. Ron DeSantis’s surgeon general, Joseph Ladapo, MD, PhD, warned that COVID vaccines are harmful to young men, prompting rebukes from federal health authorities. It later came out that Dr. Ladapo had changed some of the results of the study before issuing his warning. But long before 2023, there emerged an increasing gap in COVID deaths between red states and blue states, mirroring the vaccination rates in those states. The redder the state, the higher the death toll.
It’s not just Republican Party culture warriors; medical misinformation is also finding increasing purchase on the far left. Robert F. Kennedy Jr. and Marianne Williamson, both of whom have launched long-shot challenges to President Biden for the 2024 Democratic nomination, had promoted antivaccine ideas long before the COVID pandemic. Mr. Kennedy continues to spread misinformation.
In June 2023, Joe Rogan hosted Mr. Kennedy, on his podcast. During the episode, Mr. Rogan listened uncritically as Mr. Kennedy told his millions of listeners that vaccines cause autism and that 5G causes cancer, among other fringe, often-debunked theories.
Dr. Hotez, a prominent misinformation debunker who was also part of a team that designed a low-cost COVID-19 vaccine, wrote on Twitter that the episode was “just awful.”
The backlash began almost immediately. Mr. Rogan, who has over 11 million followers on Twitter, responded with a public challenge for Dr. Hotez to debate Mr. Kennedy on Mr. Rogan’s show, with a reward of $100,000 to the charity of Dr. Hotez’s choice. More offers streamed in, including from Elon Musk, who tweeted that Dr. Hotez was “afraid of a public debate, because he knows he’s wrong.” More supporters of Mr. Kennedy and Mr. Rogan piled on.
Vaccine skeptics even showed up at Dr. Hotez’s house, filming him as he was returning from buying a Father’s Day cake and taunting him to debate Mr. Kennedy.
A turn in the pandemic
For a precious few weeks at the start of the pandemic, it felt as though the country was all in this together. There were arguments against closing schools and shutting down businesses, but for the most part, the nation had about 4 solid weeks of solidarity.
As masking mandates changed and the public health establishment lost the confidence of Americans, the veneer of solidarity began to chip away.
“Things were changing so rapidly during the pandemic that it was very hard for staff and patients to understand the changing guidelines, whether it was visitor constraints or masking,” said Carrie Nelson, the chief medical officer at the telehealth company AmWell, who worked as a supervisor at a large health care system in the Midwest until 2021.
In the midst of the public health crisis, former President Trump was downplaying the severity of the disease and was silencing officials from the Centers for Disease Control and Prevention, such as Nancy Messonier, who warned from the very beginning of the pandemic’s potential.
When the vaccines came out, the latent antivaccine movement flared up once again. And this time – unlike in decades past – the debate over vaccines had become partisan.
“Before the pandemic,” said Christopher Thomas, an emergency physician on the West Coast who requested that a pseudonym be used because of personal threats he has received, “patients wouldn’t really challenge me or throw out weird questions.” It’s not that he never encountered pushback, but the stakes felt lower, and people largely deferred to his medical expertise. “If we got a parent who had not vaccinated their child, I would totally engage back then,” Dr. Thomas said.
But the pandemic – and America’s response to it – changed the conversation. “The rhetoric ... switched from downplaying the virus to demonizing the vaccines,” Dr. Thomas said.
The toll on health care professionals
By the time vaccines were available, the public had begun to conflate doctors with public health experts, since both were “pushing” the vaccine.
“Most people probably don’t really know the difference between clinical medicine and public health,” said Richard Pan, MD, MPH, a pediatrician and California legislator who sponsored two bills – now laws – that strengthened state childhood vaccination requirements.
At first, it was clearly public health officials, such as Anthony Fauci, MD, who were the face of measures to mitigate the virus. But as doctors became the enforcers of those measures, the line between physicians and public health officials blurred.
A lot of the anger then shifted toward doctors, nurses, and other health care professionals, Dr. Pan said, “because we were, of course, the ones who would be administering the vaccines. They don’t really think of their doctor as a government person until your doctor is carrying a [government] message.”
Given the pressures and struggles of the past few years, it’s no surprise that burnout among health care professionals is high. According to an April 2023 study by the National Council of State Boards of Nursing and the National Forum of State Nursing Workforce Centers, an estimated 800,000 nurses expect to leave the profession by 2027, driven first and foremost by “stress and burnout.”
All of these departures in medicine’s “great resignation” have left hospitals and health care organizations even more short staffed, thereby increasing even more the pressure and burnout on those left.
The pandemic had already badly exacerbated the already widespread problem of burnout in the medical field, which Ms. Nelson said has contributed to the tension.
“The burnout problem that we have in health care is not a good basis for the development of a good therapeutic relationship,” Ms. Nelson said. “Burnout is fraught with apathy and desensitization to human emotions. It takes away the empathy that we once had for people that we see.”
What comes next?
Almost exactly 3 years after the world learned about SARS-CoV-2, Biden declared an end to the coronavirus public health emergency in April 2023. Yet, Americans continue to die from COVID, and the anger that bloomed and spread has not abated.
“I think we’re in a new steady state of violence in health care settings,” Ms. Nelson said. “It’s not gone down, because people are still very distressed.” That’s evident from the high prevalence of mental health conditions, the financial strain of first the pandemic and then inflation, and the overall traumatic impact the pandemic had on people, whether they recognize it or not.
The first step to solving any problem is, as the saying goes, to admit that there is a problem.
“I think people need to start stepping out of their comfort bubbles and start to look at things that make them uncomfortable,” Dr. Thomas said, but he doesn’t see that happening any time soon. “I’ve been very let down by physicians and embarrassed by the American physician organizations.”
The medical board in his state, he said, has stood by as some doctors continue misrepresenting medical evidence. “That’s been really, really hard on me. I didn’t think that the medical boards would go so far as to look the other way for something that was this tremendously bad.”
There are others who can take the lead – if they’re willing.
“There are some things the medical societies and academic health centers can do,” Dr. Hotez said, “starting with building up a culture of physicians and health care providers feeling comfortable in the public domain.” He said the messaging when he was getting his degrees was not to engage the public and not to talk to journalists because that was “self-promotion” or “grandstanding.” But the world is different now. Health care professionals need training in public engagement and communication, he said, and the culture needs to change so that health care providers feel comfortable speaking out without feeling “the sword of Damocles over their heads” every time they talk to a reporter, Dr. Hotez said.
There may be no silver bullet to solve the big-picture trust problem in medicine and public health. No TV appearance or quote in an article can solve it. But on an individual level — through careful relationship building with patients – doctors can strengthen that trust.
Telehealth may help with that, but there’s a fine balance there, Ms. Nelson cautioned. On the one hand, with the doctor and the patient each in their own private spaces, where they feel safe and comfortable, the overall experience can be more therapeutic and less stressful. At the same time, telehealth can pile on change-management tasks that can exacerbate burnout, “so it’s a delicate thing we have to approach.”
One very thin silver lining that could emerge from the way in which patients have begun to try to take charge of their care.
“They should fully understand the reasoning behind the recommendations that physicians are making,” Ms. Nelson said. “I’d like to see us get to a happy medium where it’s a partnership. We can’t go back to the old school where the doctor knows best and you don’t ever question him.
“What we need is the partnership, and I would love to see that as the silver lining, but the anger has got to settle down in order for that kind of productive thing to happen.”
As for the big picture? There’s a limit to what even society’s “miracle workers” can do. “The biggest priority right now for the health system is to protect their staff whatever way they can and do some training in deescalation,” Ms. Nelson said. “But I don’t think health care can solve the societal issues that seem to be creating this.”
A version of this article first appeared on Medscape.com.
Like hundreds of other medical experts, Leana Wen, MD, an emergency physician and former Baltimore health commissioner, was an early and avid supporter of COVID vaccines and their ability to prevent severe disease, hospitalization, and death from SARS-CoV-2 infections.
When 51-year-old Scott Eli Harris, of Aubrey, Tex., heard of Dr. Wen’s stance in July 2021, the self-described “fifth-generation U.S. Army veteran and a sniper” sent Dr. Wen an electronic invective laden with racist language and very specific threats to shoot her.
Mr. Harris pled guilty to transmitting threats via interstate commerce last February and began serving 6 months in federal prison in the fall of 2022, but his threats wouldn’t be the last for Dr. Wen. Just 2 days after Mr. Harris was sentenced, charges were unsealed against another man in Massachusetts, who threatened that Dr. Wen would “end up in pieces” if she continued “pushing” her thoughts publicly.’
Dr. Wen has plenty of company. In an August 2022 survey of emergency doctors conducted by the American College of Emergency Physicians, 85% of respondents said violence against them is increasing. One in four doctors said they’re being assaulted by patients and their family and friends multiple times a week, compared with just 8% of doctors who said as much in 2018. About 64% of emergency physicians reported receiving verbal assaults and threats of violence; 40% reported being hit or slapped, and 26% were kicked.
This uptick of violence and threats against physicians didn’t come out of nowhere; violence against health care workers has been gradually increasing over the past decade. Health care providers can attest to the hostility that particular topics have sparked for years: vaccines in pediatrics, abortion in ob.gyn., and gender-affirming care in endocrinology.
But the pandemic fueled the fire. The proliferation of misinformation (often via social media) and the politicization of public health and medicine are at the center of the problem.
‘The people attacking are themselves victims’
The misinformation problem first came to a head in one area of public health: vaccines. The pandemic accelerated antagonism in medicine – thanks, in part, to decades of antivaccine activism.
The antivaccine movement, which has ebbed and flowed in the United States and across the globe since the first vaccine, experienced a new wave in the early 2000s with the combination of concerns about thimerosal in vaccines and a now disproven link between autism and the MMR vaccine. But that movement grew. It picked up steam when activists gained political clout after a 2014 measles outbreak at Disneyland led California schools to tighten up policies regarding vaccinations for kids who enrolled. These stronger public school vaccination laws ran up against religious freedom arguments from antivaccine advocates.
Use of social media continues to grow, and with it, the spread of misinformation. A recent study found that Facebook “users’ social media habits doubled, and in some cases, tripled the amount of fake news they shared.”
In the face of growing confusion, health care providers and public health experts have often struggled to treat their patients – and communicate to the public – without appearing political.
“The people that are doing the attacking are in some ways themselves victims,” said Peter Hotez, MD, PhD, dean of the National School of Tropical Medicine at Baylor College of Medicine, Houston. “They’re victims of the antiscience, antihealth ecosystem coming out of Fox News, the House Freedom Caucus, the CPAC conference, coming out of contrarian intellectuals.”
Many of Dr. Hotez’s colleagues don’t want to talk about the political right as an enabler of scientific disinformation, he said, but that doesn’t change what the evidence shows. The vast majority of state and national bills opposing vaccination, gender-affirming care, comprehensive reproductive care, and other evidence-based medical care often come from Republican legislators.
When politics and health care collide
“We’re in an incredible status quo,” said William Schaffner, MD, the previous director of the Infectious Diseases Society of America and a professor of infectious diseases and preventive medicine at Vanderbilt University, Nashville, Tenn. “You can’t get away from the politics, because you have [political] candidates espousing certain concepts that are antithetical to good public health.”
In March 2023, Florida Gov. Ron DeSantis’s surgeon general, Joseph Ladapo, MD, PhD, warned that COVID vaccines are harmful to young men, prompting rebukes from federal health authorities. It later came out that Dr. Ladapo had changed some of the results of the study before issuing his warning. But long before 2023, there emerged an increasing gap in COVID deaths between red states and blue states, mirroring the vaccination rates in those states. The redder the state, the higher the death toll.
It’s not just Republican Party culture warriors; medical misinformation is also finding increasing purchase on the far left. Robert F. Kennedy Jr. and Marianne Williamson, both of whom have launched long-shot challenges to President Biden for the 2024 Democratic nomination, had promoted antivaccine ideas long before the COVID pandemic. Mr. Kennedy continues to spread misinformation.
In June 2023, Joe Rogan hosted Mr. Kennedy, on his podcast. During the episode, Mr. Rogan listened uncritically as Mr. Kennedy told his millions of listeners that vaccines cause autism and that 5G causes cancer, among other fringe, often-debunked theories.
Dr. Hotez, a prominent misinformation debunker who was also part of a team that designed a low-cost COVID-19 vaccine, wrote on Twitter that the episode was “just awful.”
The backlash began almost immediately. Mr. Rogan, who has over 11 million followers on Twitter, responded with a public challenge for Dr. Hotez to debate Mr. Kennedy on Mr. Rogan’s show, with a reward of $100,000 to the charity of Dr. Hotez’s choice. More offers streamed in, including from Elon Musk, who tweeted that Dr. Hotez was “afraid of a public debate, because he knows he’s wrong.” More supporters of Mr. Kennedy and Mr. Rogan piled on.
Vaccine skeptics even showed up at Dr. Hotez’s house, filming him as he was returning from buying a Father’s Day cake and taunting him to debate Mr. Kennedy.
A turn in the pandemic
For a precious few weeks at the start of the pandemic, it felt as though the country was all in this together. There were arguments against closing schools and shutting down businesses, but for the most part, the nation had about 4 solid weeks of solidarity.
As masking mandates changed and the public health establishment lost the confidence of Americans, the veneer of solidarity began to chip away.
“Things were changing so rapidly during the pandemic that it was very hard for staff and patients to understand the changing guidelines, whether it was visitor constraints or masking,” said Carrie Nelson, the chief medical officer at the telehealth company AmWell, who worked as a supervisor at a large health care system in the Midwest until 2021.
In the midst of the public health crisis, former President Trump was downplaying the severity of the disease and was silencing officials from the Centers for Disease Control and Prevention, such as Nancy Messonier, who warned from the very beginning of the pandemic’s potential.
When the vaccines came out, the latent antivaccine movement flared up once again. And this time – unlike in decades past – the debate over vaccines had become partisan.
“Before the pandemic,” said Christopher Thomas, an emergency physician on the West Coast who requested that a pseudonym be used because of personal threats he has received, “patients wouldn’t really challenge me or throw out weird questions.” It’s not that he never encountered pushback, but the stakes felt lower, and people largely deferred to his medical expertise. “If we got a parent who had not vaccinated their child, I would totally engage back then,” Dr. Thomas said.
But the pandemic – and America’s response to it – changed the conversation. “The rhetoric ... switched from downplaying the virus to demonizing the vaccines,” Dr. Thomas said.
The toll on health care professionals
By the time vaccines were available, the public had begun to conflate doctors with public health experts, since both were “pushing” the vaccine.
“Most people probably don’t really know the difference between clinical medicine and public health,” said Richard Pan, MD, MPH, a pediatrician and California legislator who sponsored two bills – now laws – that strengthened state childhood vaccination requirements.
At first, it was clearly public health officials, such as Anthony Fauci, MD, who were the face of measures to mitigate the virus. But as doctors became the enforcers of those measures, the line between physicians and public health officials blurred.
A lot of the anger then shifted toward doctors, nurses, and other health care professionals, Dr. Pan said, “because we were, of course, the ones who would be administering the vaccines. They don’t really think of their doctor as a government person until your doctor is carrying a [government] message.”
Given the pressures and struggles of the past few years, it’s no surprise that burnout among health care professionals is high. According to an April 2023 study by the National Council of State Boards of Nursing and the National Forum of State Nursing Workforce Centers, an estimated 800,000 nurses expect to leave the profession by 2027, driven first and foremost by “stress and burnout.”
All of these departures in medicine’s “great resignation” have left hospitals and health care organizations even more short staffed, thereby increasing even more the pressure and burnout on those left.
The pandemic had already badly exacerbated the already widespread problem of burnout in the medical field, which Ms. Nelson said has contributed to the tension.
“The burnout problem that we have in health care is not a good basis for the development of a good therapeutic relationship,” Ms. Nelson said. “Burnout is fraught with apathy and desensitization to human emotions. It takes away the empathy that we once had for people that we see.”
What comes next?
Almost exactly 3 years after the world learned about SARS-CoV-2, Biden declared an end to the coronavirus public health emergency in April 2023. Yet, Americans continue to die from COVID, and the anger that bloomed and spread has not abated.
“I think we’re in a new steady state of violence in health care settings,” Ms. Nelson said. “It’s not gone down, because people are still very distressed.” That’s evident from the high prevalence of mental health conditions, the financial strain of first the pandemic and then inflation, and the overall traumatic impact the pandemic had on people, whether they recognize it or not.
The first step to solving any problem is, as the saying goes, to admit that there is a problem.
“I think people need to start stepping out of their comfort bubbles and start to look at things that make them uncomfortable,” Dr. Thomas said, but he doesn’t see that happening any time soon. “I’ve been very let down by physicians and embarrassed by the American physician organizations.”
The medical board in his state, he said, has stood by as some doctors continue misrepresenting medical evidence. “That’s been really, really hard on me. I didn’t think that the medical boards would go so far as to look the other way for something that was this tremendously bad.”
There are others who can take the lead – if they’re willing.
“There are some things the medical societies and academic health centers can do,” Dr. Hotez said, “starting with building up a culture of physicians and health care providers feeling comfortable in the public domain.” He said the messaging when he was getting his degrees was not to engage the public and not to talk to journalists because that was “self-promotion” or “grandstanding.” But the world is different now. Health care professionals need training in public engagement and communication, he said, and the culture needs to change so that health care providers feel comfortable speaking out without feeling “the sword of Damocles over their heads” every time they talk to a reporter, Dr. Hotez said.
There may be no silver bullet to solve the big-picture trust problem in medicine and public health. No TV appearance or quote in an article can solve it. But on an individual level — through careful relationship building with patients – doctors can strengthen that trust.
Telehealth may help with that, but there’s a fine balance there, Ms. Nelson cautioned. On the one hand, with the doctor and the patient each in their own private spaces, where they feel safe and comfortable, the overall experience can be more therapeutic and less stressful. At the same time, telehealth can pile on change-management tasks that can exacerbate burnout, “so it’s a delicate thing we have to approach.”
One very thin silver lining that could emerge from the way in which patients have begun to try to take charge of their care.
“They should fully understand the reasoning behind the recommendations that physicians are making,” Ms. Nelson said. “I’d like to see us get to a happy medium where it’s a partnership. We can’t go back to the old school where the doctor knows best and you don’t ever question him.
“What we need is the partnership, and I would love to see that as the silver lining, but the anger has got to settle down in order for that kind of productive thing to happen.”
As for the big picture? There’s a limit to what even society’s “miracle workers” can do. “The biggest priority right now for the health system is to protect their staff whatever way they can and do some training in deescalation,” Ms. Nelson said. “But I don’t think health care can solve the societal issues that seem to be creating this.”
A version of this article first appeared on Medscape.com.