User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Don’t be scared of red eye, expert says
LAS VEGAS – Few conditions worry parents or school nurses more than when a child develops red eye, but how do you as the treating clinician know when to worry?
“Our challenge is to make the right diagnosis, not to worsen the problem, to figure when to refer, and to make that mother who had to take off from work to bring her child into the office – somehow we have to make her happy,” Dr. David B. Granet said at a pediatric update sponsored by the American Academy of Pediatrics California District 9.

Concomitant pain or photophobia typically means that something other than bacterial conjunctivitis is at play, said Dr. Granet, professor of ophthalmology and pediatrics at the University of California, San Diego. “Is there contact lens use?” he asked. “Is there proptosis or a history of trauma or injury? How long has it been going on? Most bacterial and viral infections will eventually go away. Is there a corneal opacity? Is there cellulitis, loss of vision, or herpes simplex virus?”
If parents call in suspecting that their child’s eye has been contaminated with a chemical, instruct them to irrigate the eye before they head to the emergency department, he advised. “Whoever’s answering the phone in your office ought to be able to separate out what’s worrisome and what’s not,” he said. “Like everything else we do, the history matters.”
For children who present to your office, consider “anything that can go wrong to make the eye red,” he continued, including nasolacrimal duct obstruction, adnexal disease, foreign body/trauma, uveitis, neoplasm, structural change, or conjunctivitis. “Has the vision changed? If so, that’s your vital sign for referral,” he said. “It’s generally a better sign to have both eyes involved with redness than just one. One eye involved means herpes simplex virus, uveitis, or trauma. Both eyes involved usually means infective or allergic conjunctivitis.”
The three most common conditions that cause a red or pink eye are allergic, bacterial, and viral conjunctivitis. Allergic conjunctivitis “is not just itching; that’s the symptom,” Dr. Granet said. “You get redness, swelling of the conjunctiva, lid edema, mucous discharge, and tearing. All of these occur when the patient rubs their eye. The best treatment for allergic conjunctivitis is avoidance of the allergen.”
He also recommended that affected children wash their hair before they go to sleep. “If their hair has been catching allergen all day long and they lie down on their pillow and start to roll [their head around in] it, that can cause a reaction,” he said.
Ketotifen fumarate (Zaditor) is an available over-the-counter treatment option, but olopatadine HCl (Pataday) is the most popular prescription written by pediatricians. “If you give any antihistamine, in low doses you start to prevent the release of histamine,” Dr. Granet said. “As the dose increases, you have a catastrophic event and you start to destruct the mast cell.”
Viral conjunctivitis usually affects older children and presents as a unilateral condition, then affects the fellow eye. It may be associated with pharyngitis and preauricular or submandibular adenopathy. Bacterial conjunctivitis, on the other hand, typically affects preschool-aged children, is often bilateral but can be unilateral, and yields mucopurulent discharge with matting. It is not associated with adenopathy, but it may be associated with otitis media, and it’s highly contagious. Topical antibiotic ointment therapy is indicated for bacterial conjunctivitis “not because this is a deadly disease, but because we want to reduce the chance for spread,” Dr. Granet said. “We know that communicable diseases are responsible for loss of 164 million school days each year. Additionally, there is a significant cost to a family when a parent misses work. Finally, if the diagnosis is in doubt, treatment with an antibiotic geared to work within a few days will help identify masquerade diseases early.”
Because of concerns about antibiotic resistance, fluoroquinolones are often the first choice for treating bacterial conjunctivitis. Dr. Granet led a multicenter comparison of moxifloxacin versus polymyxin B sulfate–trimethoprim ophthalmic solution in the speed of clinical efficacy for the treatment of bacterial conjunctivitis (J. Pediatr. Ophthalmol. Strabismus 2008;45:340-9). The investigators found that after day 2 of treatment, clinical cure was achieved by 81% of kids in the moxifloxacin group, compared with 44% of those in the polymyxin B sulfate–trimethoprim group. In addition, only 2.3% of kids in the moxifloxacin group were nonresponders, compared with 19.5% of those in the polymyxin B sulfate–trimethoprim group.
Common treatments for viral conjunctivitis include hygiene-related approaches like hand washing and not sharing towels and glasses. But these only prevent spread and don’t make the disease go away faster. The infection usually resolves in about 2 weeks.
Dr. Granet disclosed that he is a member of the speakers bureau for Alcon Labs and is a consultant for Diopsys.
On Twitter @dougbrunk
LAS VEGAS – Few conditions worry parents or school nurses more than when a child develops red eye, but how do you as the treating clinician know when to worry?
“Our challenge is to make the right diagnosis, not to worsen the problem, to figure when to refer, and to make that mother who had to take off from work to bring her child into the office – somehow we have to make her happy,” Dr. David B. Granet said at a pediatric update sponsored by the American Academy of Pediatrics California District 9.
Concomitant pain or photophobia typically means that something other than bacterial conjunctivitis is at play, said Dr. Granet, professor of ophthalmology and pediatrics at the University of California, San Diego. “Is there contact lens use?” he asked. “Is there proptosis or a history of trauma or injury? How long has it been going on? Most bacterial and viral infections will eventually go away. Is there a corneal opacity? Is there cellulitis, loss of vision, or herpes simplex virus?”
If parents call in suspecting that their child’s eye has been contaminated with a chemical, instruct them to irrigate the eye before they head to the emergency department, he advised. “Whoever’s answering the phone in your office ought to be able to separate out what’s worrisome and what’s not,” he said. “Like everything else we do, the history matters.”
For children who present to your office, consider “anything that can go wrong to make the eye red,” he continued, including nasolacrimal duct obstruction, adnexal disease, foreign body/trauma, uveitis, neoplasm, structural change, or conjunctivitis. “Has the vision changed? If so, that’s your vital sign for referral,” he said. “It’s generally a better sign to have both eyes involved with redness than just one. One eye involved means herpes simplex virus, uveitis, or trauma. Both eyes involved usually means infective or allergic conjunctivitis.”
The three most common conditions that cause a red or pink eye are allergic, bacterial, and viral conjunctivitis. Allergic conjunctivitis “is not just itching; that’s the symptom,” Dr. Granet said. “You get redness, swelling of the conjunctiva, lid edema, mucous discharge, and tearing. All of these occur when the patient rubs their eye. The best treatment for allergic conjunctivitis is avoidance of the allergen.”
He also recommended that affected children wash their hair before they go to sleep. “If their hair has been catching allergen all day long and they lie down on their pillow and start to roll [their head around in] it, that can cause a reaction,” he said.
Ketotifen fumarate (Zaditor) is an available over-the-counter treatment option, but olopatadine HCl (Pataday) is the most popular prescription written by pediatricians. “If you give any antihistamine, in low doses you start to prevent the release of histamine,” Dr. Granet said. “As the dose increases, you have a catastrophic event and you start to destruct the mast cell.”
Viral conjunctivitis usually affects older children and presents as a unilateral condition, then affects the fellow eye. It may be associated with pharyngitis and preauricular or submandibular adenopathy. Bacterial conjunctivitis, on the other hand, typically affects preschool-aged children, is often bilateral but can be unilateral, and yields mucopurulent discharge with matting. It is not associated with adenopathy, but it may be associated with otitis media, and it’s highly contagious. Topical antibiotic ointment therapy is indicated for bacterial conjunctivitis “not because this is a deadly disease, but because we want to reduce the chance for spread,” Dr. Granet said. “We know that communicable diseases are responsible for loss of 164 million school days each year. Additionally, there is a significant cost to a family when a parent misses work. Finally, if the diagnosis is in doubt, treatment with an antibiotic geared to work within a few days will help identify masquerade diseases early.”
Because of concerns about antibiotic resistance, fluoroquinolones are often the first choice for treating bacterial conjunctivitis. Dr. Granet led a multicenter comparison of moxifloxacin versus polymyxin B sulfate–trimethoprim ophthalmic solution in the speed of clinical efficacy for the treatment of bacterial conjunctivitis (J. Pediatr. Ophthalmol. Strabismus 2008;45:340-9). The investigators found that after day 2 of treatment, clinical cure was achieved by 81% of kids in the moxifloxacin group, compared with 44% of those in the polymyxin B sulfate–trimethoprim group. In addition, only 2.3% of kids in the moxifloxacin group were nonresponders, compared with 19.5% of those in the polymyxin B sulfate–trimethoprim group.
Common treatments for viral conjunctivitis include hygiene-related approaches like hand washing and not sharing towels and glasses. But these only prevent spread and don’t make the disease go away faster. The infection usually resolves in about 2 weeks.
Dr. Granet disclosed that he is a member of the speakers bureau for Alcon Labs and is a consultant for Diopsys.
On Twitter @dougbrunk
LAS VEGAS – Few conditions worry parents or school nurses more than when a child develops red eye, but how do you as the treating clinician know when to worry?
“Our challenge is to make the right diagnosis, not to worsen the problem, to figure when to refer, and to make that mother who had to take off from work to bring her child into the office – somehow we have to make her happy,” Dr. David B. Granet said at a pediatric update sponsored by the American Academy of Pediatrics California District 9.
Concomitant pain or photophobia typically means that something other than bacterial conjunctivitis is at play, said Dr. Granet, professor of ophthalmology and pediatrics at the University of California, San Diego. “Is there contact lens use?” he asked. “Is there proptosis or a history of trauma or injury? How long has it been going on? Most bacterial and viral infections will eventually go away. Is there a corneal opacity? Is there cellulitis, loss of vision, or herpes simplex virus?”
If parents call in suspecting that their child’s eye has been contaminated with a chemical, instruct them to irrigate the eye before they head to the emergency department, he advised. “Whoever’s answering the phone in your office ought to be able to separate out what’s worrisome and what’s not,” he said. “Like everything else we do, the history matters.”
For children who present to your office, consider “anything that can go wrong to make the eye red,” he continued, including nasolacrimal duct obstruction, adnexal disease, foreign body/trauma, uveitis, neoplasm, structural change, or conjunctivitis. “Has the vision changed? If so, that’s your vital sign for referral,” he said. “It’s generally a better sign to have both eyes involved with redness than just one. One eye involved means herpes simplex virus, uveitis, or trauma. Both eyes involved usually means infective or allergic conjunctivitis.”
The three most common conditions that cause a red or pink eye are allergic, bacterial, and viral conjunctivitis. Allergic conjunctivitis “is not just itching; that’s the symptom,” Dr. Granet said. “You get redness, swelling of the conjunctiva, lid edema, mucous discharge, and tearing. All of these occur when the patient rubs their eye. The best treatment for allergic conjunctivitis is avoidance of the allergen.”
He also recommended that affected children wash their hair before they go to sleep. “If their hair has been catching allergen all day long and they lie down on their pillow and start to roll [their head around in] it, that can cause a reaction,” he said.
Ketotifen fumarate (Zaditor) is an available over-the-counter treatment option, but olopatadine HCl (Pataday) is the most popular prescription written by pediatricians. “If you give any antihistamine, in low doses you start to prevent the release of histamine,” Dr. Granet said. “As the dose increases, you have a catastrophic event and you start to destruct the mast cell.”
Viral conjunctivitis usually affects older children and presents as a unilateral condition, then affects the fellow eye. It may be associated with pharyngitis and preauricular or submandibular adenopathy. Bacterial conjunctivitis, on the other hand, typically affects preschool-aged children, is often bilateral but can be unilateral, and yields mucopurulent discharge with matting. It is not associated with adenopathy, but it may be associated with otitis media, and it’s highly contagious. Topical antibiotic ointment therapy is indicated for bacterial conjunctivitis “not because this is a deadly disease, but because we want to reduce the chance for spread,” Dr. Granet said. “We know that communicable diseases are responsible for loss of 164 million school days each year. Additionally, there is a significant cost to a family when a parent misses work. Finally, if the diagnosis is in doubt, treatment with an antibiotic geared to work within a few days will help identify masquerade diseases early.”
Because of concerns about antibiotic resistance, fluoroquinolones are often the first choice for treating bacterial conjunctivitis. Dr. Granet led a multicenter comparison of moxifloxacin versus polymyxin B sulfate–trimethoprim ophthalmic solution in the speed of clinical efficacy for the treatment of bacterial conjunctivitis (J. Pediatr. Ophthalmol. Strabismus 2008;45:340-9). The investigators found that after day 2 of treatment, clinical cure was achieved by 81% of kids in the moxifloxacin group, compared with 44% of those in the polymyxin B sulfate–trimethoprim group. In addition, only 2.3% of kids in the moxifloxacin group were nonresponders, compared with 19.5% of those in the polymyxin B sulfate–trimethoprim group.
Common treatments for viral conjunctivitis include hygiene-related approaches like hand washing and not sharing towels and glasses. But these only prevent spread and don’t make the disease go away faster. The infection usually resolves in about 2 weeks.
Dr. Granet disclosed that he is a member of the speakers bureau for Alcon Labs and is a consultant for Diopsys.
On Twitter @dougbrunk
EXPERT ANALYSIS AT PEDIATRIC UPDATE

Pulmonary edema is common after convulsive seizures
SEATTLE – Nearly a third of patients who experience a generalized convulsive seizure develop pulmonary edema, suggests a small cohort study reported at the annual meeting of the American Epilepsy Society. The longer the seizure lasts, the higher the probability of this complication.
“There are a few theories about how pulmonary edema can develop” in this context, noted first author Dr. Jeffrey Kennedy of the UC Davis Health System in Sacramento, Calif. Neurogenic mechanisms, hypoxemia, and prolonged negative intrathoracic pressure have all been implicated.
As far as the clinical implications, “postictal pulmonary edema may play a role in the mechanisms of SUDEP (sudden unexpected death in epilepsy),” he proposed at the annual meeting of the American Epilepsy Society.
Session attendee Dr. Kevin Chapman of the child neurology section in the department of pediatrics at Children’s Hospital Colorado, Aurora, asked, “If you identify somebody who has pulmonary edema, what do you do with them?”
“We have been following the patients who are clinically stable,” Dr. Kennedy replied. “We had a patient we identified with Takotsubo cardiomyopathy, which triggered some additional patient care from our cardiology department.”
“I think it just identifies patients who are at higher risk” for poor outcomes, he speculated. “In the EMU [epilepsy monitoring unit], when it comes to letting patients have more seizures, it does make us conservative as far as restarting medications and maybe trying to start giving them some benzodiazepines to try to shut things down.”
Another attendee commented, “Some of my patients’ relatives are very alarmed when the patient suffers severe cyanosis after a seizure. The first thing that our emergency staff will do when they arrive will be to clasp an oxygen mask over them. So our patients ask us, ‘Please, will we provide them with oxygen?’ I have a sneaking suspicion from your data that they may be justified in that. What would you advise?”
Another study done by the UC Davis group looked at a variety of peri-ictal interventions and found simple nursing practices worked about as well as oxygen, according to Dr. Kennedy (Epilepsia 2013;54:377-82). “It seems like just doing something – stimulating the patient, turning them on their side – is enough, rather than just administering oxygen.”
In an interview, session comoderator Dr. Amy Crepeau, a neurologist at the Mayo Clinic Arizona in Phoenix, said the observed incidence of pulmonary edema raises important questions: “Is this something we need to be more conscientious about and really intervene more closely? Should we be shortening the duration of time before we stop seizures and not letting them go as long? It seems as though they have done that at UC Davis – kind of limited the number of seizures that they allow patients to have in the epilepsy monitoring unit.”

“This study comes back to this issue of who’s at risk for SUDEP, what are the causes for SUDEP, and what are the interventions we can use to try to prevent that or lessen the risk for it,” she added. “We are looking forward to seeing whether these patients have any increased risk of SUDEP that associates with the pulmonary edema.”
Dr. Kennedy and colleagues studied 24 consecutive adult patients, mean age 32, who experienced generalized convulsive seizures while undergoing monitoring in the UC Davis EMU, where all patients with such seizures receive a chest x-ray soon afterward as a safety measure.
Overall, 29% of the patients were found to have pulmonary edema, with or without focal infiltrates, on their chest x-ray, and another 17% were found to have focal infiltrates only.
The mean time elapsed between the seizure and the chest x-ray acquisition was 225 minutes in the patients with abnormal findings and 196 minutes in the patients with normal findings, a nonsignificant difference, reported Dr. Kennedy, who disclosed that he had no relevant conflicts of interest.
The seizure duration was more than twice as long among patients with chest x-ray abnormalities as among counterparts without these abnormalities (250 vs. 101 seconds; P = .002), and the probability of abnormalities increased with seizure duration.
The groups with and without chest x-rays abnormalities did not differ significantly with respect to a variety of demographic and cardiorespiratory and other clinical factors, however.
SEATTLE – Nearly a third of patients who experience a generalized convulsive seizure develop pulmonary edema, suggests a small cohort study reported at the annual meeting of the American Epilepsy Society. The longer the seizure lasts, the higher the probability of this complication.
“There are a few theories about how pulmonary edema can develop” in this context, noted first author Dr. Jeffrey Kennedy of the UC Davis Health System in Sacramento, Calif. Neurogenic mechanisms, hypoxemia, and prolonged negative intrathoracic pressure have all been implicated.
As far as the clinical implications, “postictal pulmonary edema may play a role in the mechanisms of SUDEP (sudden unexpected death in epilepsy),” he proposed at the annual meeting of the American Epilepsy Society.
Session attendee Dr. Kevin Chapman of the child neurology section in the department of pediatrics at Children’s Hospital Colorado, Aurora, asked, “If you identify somebody who has pulmonary edema, what do you do with them?”
“We have been following the patients who are clinically stable,” Dr. Kennedy replied. “We had a patient we identified with Takotsubo cardiomyopathy, which triggered some additional patient care from our cardiology department.”
“I think it just identifies patients who are at higher risk” for poor outcomes, he speculated. “In the EMU [epilepsy monitoring unit], when it comes to letting patients have more seizures, it does make us conservative as far as restarting medications and maybe trying to start giving them some benzodiazepines to try to shut things down.”
Another attendee commented, “Some of my patients’ relatives are very alarmed when the patient suffers severe cyanosis after a seizure. The first thing that our emergency staff will do when they arrive will be to clasp an oxygen mask over them. So our patients ask us, ‘Please, will we provide them with oxygen?’ I have a sneaking suspicion from your data that they may be justified in that. What would you advise?”
Another study done by the UC Davis group looked at a variety of peri-ictal interventions and found simple nursing practices worked about as well as oxygen, according to Dr. Kennedy (Epilepsia 2013;54:377-82). “It seems like just doing something – stimulating the patient, turning them on their side – is enough, rather than just administering oxygen.”
In an interview, session comoderator Dr. Amy Crepeau, a neurologist at the Mayo Clinic Arizona in Phoenix, said the observed incidence of pulmonary edema raises important questions: “Is this something we need to be more conscientious about and really intervene more closely? Should we be shortening the duration of time before we stop seizures and not letting them go as long? It seems as though they have done that at UC Davis – kind of limited the number of seizures that they allow patients to have in the epilepsy monitoring unit.”
“This study comes back to this issue of who’s at risk for SUDEP, what are the causes for SUDEP, and what are the interventions we can use to try to prevent that or lessen the risk for it,” she added. “We are looking forward to seeing whether these patients have any increased risk of SUDEP that associates with the pulmonary edema.”
Dr. Kennedy and colleagues studied 24 consecutive adult patients, mean age 32, who experienced generalized convulsive seizures while undergoing monitoring in the UC Davis EMU, where all patients with such seizures receive a chest x-ray soon afterward as a safety measure.
Overall, 29% of the patients were found to have pulmonary edema, with or without focal infiltrates, on their chest x-ray, and another 17% were found to have focal infiltrates only.
The mean time elapsed between the seizure and the chest x-ray acquisition was 225 minutes in the patients with abnormal findings and 196 minutes in the patients with normal findings, a nonsignificant difference, reported Dr. Kennedy, who disclosed that he had no relevant conflicts of interest.
The seizure duration was more than twice as long among patients with chest x-ray abnormalities as among counterparts without these abnormalities (250 vs. 101 seconds; P = .002), and the probability of abnormalities increased with seizure duration.
The groups with and without chest x-rays abnormalities did not differ significantly with respect to a variety of demographic and cardiorespiratory and other clinical factors, however.
SEATTLE – Nearly a third of patients who experience a generalized convulsive seizure develop pulmonary edema, suggests a small cohort study reported at the annual meeting of the American Epilepsy Society. The longer the seizure lasts, the higher the probability of this complication.
“There are a few theories about how pulmonary edema can develop” in this context, noted first author Dr. Jeffrey Kennedy of the UC Davis Health System in Sacramento, Calif. Neurogenic mechanisms, hypoxemia, and prolonged negative intrathoracic pressure have all been implicated.
As far as the clinical implications, “postictal pulmonary edema may play a role in the mechanisms of SUDEP (sudden unexpected death in epilepsy),” he proposed at the annual meeting of the American Epilepsy Society.
Session attendee Dr. Kevin Chapman of the child neurology section in the department of pediatrics at Children’s Hospital Colorado, Aurora, asked, “If you identify somebody who has pulmonary edema, what do you do with them?”
“We have been following the patients who are clinically stable,” Dr. Kennedy replied. “We had a patient we identified with Takotsubo cardiomyopathy, which triggered some additional patient care from our cardiology department.”
“I think it just identifies patients who are at higher risk” for poor outcomes, he speculated. “In the EMU [epilepsy monitoring unit], when it comes to letting patients have more seizures, it does make us conservative as far as restarting medications and maybe trying to start giving them some benzodiazepines to try to shut things down.”
Another attendee commented, “Some of my patients’ relatives are very alarmed when the patient suffers severe cyanosis after a seizure. The first thing that our emergency staff will do when they arrive will be to clasp an oxygen mask over them. So our patients ask us, ‘Please, will we provide them with oxygen?’ I have a sneaking suspicion from your data that they may be justified in that. What would you advise?”
Another study done by the UC Davis group looked at a variety of peri-ictal interventions and found simple nursing practices worked about as well as oxygen, according to Dr. Kennedy (Epilepsia 2013;54:377-82). “It seems like just doing something – stimulating the patient, turning them on their side – is enough, rather than just administering oxygen.”
In an interview, session comoderator Dr. Amy Crepeau, a neurologist at the Mayo Clinic Arizona in Phoenix, said the observed incidence of pulmonary edema raises important questions: “Is this something we need to be more conscientious about and really intervene more closely? Should we be shortening the duration of time before we stop seizures and not letting them go as long? It seems as though they have done that at UC Davis – kind of limited the number of seizures that they allow patients to have in the epilepsy monitoring unit.”
“This study comes back to this issue of who’s at risk for SUDEP, what are the causes for SUDEP, and what are the interventions we can use to try to prevent that or lessen the risk for it,” she added. “We are looking forward to seeing whether these patients have any increased risk of SUDEP that associates with the pulmonary edema.”
Dr. Kennedy and colleagues studied 24 consecutive adult patients, mean age 32, who experienced generalized convulsive seizures while undergoing monitoring in the UC Davis EMU, where all patients with such seizures receive a chest x-ray soon afterward as a safety measure.
Overall, 29% of the patients were found to have pulmonary edema, with or without focal infiltrates, on their chest x-ray, and another 17% were found to have focal infiltrates only.
The mean time elapsed between the seizure and the chest x-ray acquisition was 225 minutes in the patients with abnormal findings and 196 minutes in the patients with normal findings, a nonsignificant difference, reported Dr. Kennedy, who disclosed that he had no relevant conflicts of interest.
The seizure duration was more than twice as long among patients with chest x-ray abnormalities as among counterparts without these abnormalities (250 vs. 101 seconds; P = .002), and the probability of abnormalities increased with seizure duration.
The groups with and without chest x-rays abnormalities did not differ significantly with respect to a variety of demographic and cardiorespiratory and other clinical factors, however.
AT AES 2014
Key clinical point: Postictal pulmonary edema is common in patients having convulsive seizures.
Major finding: Overall, 29% of patients had postictal pulmonary edema on a chest x-ray.
Data source: A cohort study of 24 consecutive adult patients who had generalized convulsive seizures while being monitored.
Disclosures: Dr. Kennedy disclosed that he has no relevant conflicts of interest.

Study ignites concern that e-cigarettes may ‘renormalize’ smoking
A large portion of young people using e-cigarettes are also smoking tobacco cigarettes, a cross-sectional study from Hawaii showed, raising concerns that the rise in the popularity of “vaping” may be renormalizing cigarette smoking.
Electronic cigarettes are a rising phenomenon in the United States, with projected sales in 2013 reaching $11.7 billion, Thomas A. Willis, Ph.D., and his associates at the University of Hawaii in Honolulu wrote in Pediatrics (2014 Feb. 15 [doi:10.1542/peds.2014-0760]).
There are two schools of thought on the use of e-cigarettes in adolescents, Dr. Willis and his colleagues wrote. One suggests that youth who try e-cigarettes are motivated by health values and concerns, making it unlikely that they also would try cigarettes or other substances.
However, the contrasting model argues that e-cigarettes appeal to young people wishing to rebel against conventional values, making it likely that they also would try tobacco and alcohol. “Although both formulations are plausible, there is little empirical evidence to support or reject either theory at this time,” the study authors wrote.
Conducting a school-based survey of 1,941 high school students living in Oahu, Hawaii, who were on average 14.6 years old, the researchers sought to determine what risk factors and conversely,which protective factors lead to a higher or lower likelihood of substance use. They found that 17% of respondents used e-cigarettes only, 12% used e-cigarettes and tobacco cigarettes (dual users), 3% used cigarettes only, and 68% were nonusers. The use of e-cigarettes in the student population was higher than seen in other data, although the authors noted that young people in Hawaii are particularly exposed to aggressive marketing.
According to the authors, some support for both schools of thought can be found in their data.
For example, people who used e-cigarettes only did not score high on rebelliousness and sensation seeking, compared with dual users. This finding supports the first model by showing that people who fall into this group are less prone to deviance, the investigators said. However, consistent with the model, dual users scored higher across several risk factors and lower on protective factors, compared with the other groups. “Dual users clearly represent people who are prone to problem behavior,” they wrote. “The fact that e-cigarette–only users were intermediate in risk status [between nonusers and dual users] raises the possibility that e-cigarettes are recruiting medium-risk adolescents who otherwise would be less susceptible to tobacco product use.”
Dr. Willis and his colleagues cited two limitations: The study was cross-sectional, and it was conducted in a single geographic area. “However, our findings on the association of e-cigarette use with current smoking status are consistent with those of other studies ... and our results on demographics are consistent with these and other studies,” the investigators wrote.
Attention should be given to the prominence of e-cigarette advertising and the perceived attractiveness of e-cigarettes, they added.
The study was funded by a grant from the National Cancer Institute. The authors said they had no relevant financial conflicts to disclose.
A large portion of young people using e-cigarettes are also smoking tobacco cigarettes, a cross-sectional study from Hawaii showed, raising concerns that the rise in the popularity of “vaping” may be renormalizing cigarette smoking.
Electronic cigarettes are a rising phenomenon in the United States, with projected sales in 2013 reaching $11.7 billion, Thomas A. Willis, Ph.D., and his associates at the University of Hawaii in Honolulu wrote in Pediatrics (2014 Feb. 15 [doi:10.1542/peds.2014-0760]).
There are two schools of thought on the use of e-cigarettes in adolescents, Dr. Willis and his colleagues wrote. One suggests that youth who try e-cigarettes are motivated by health values and concerns, making it unlikely that they also would try cigarettes or other substances.
However, the contrasting model argues that e-cigarettes appeal to young people wishing to rebel against conventional values, making it likely that they also would try tobacco and alcohol. “Although both formulations are plausible, there is little empirical evidence to support or reject either theory at this time,” the study authors wrote.
Conducting a school-based survey of 1,941 high school students living in Oahu, Hawaii, who were on average 14.6 years old, the researchers sought to determine what risk factors and conversely,which protective factors lead to a higher or lower likelihood of substance use. They found that 17% of respondents used e-cigarettes only, 12% used e-cigarettes and tobacco cigarettes (dual users), 3% used cigarettes only, and 68% were nonusers. The use of e-cigarettes in the student population was higher than seen in other data, although the authors noted that young people in Hawaii are particularly exposed to aggressive marketing.
According to the authors, some support for both schools of thought can be found in their data.
For example, people who used e-cigarettes only did not score high on rebelliousness and sensation seeking, compared with dual users. This finding supports the first model by showing that people who fall into this group are less prone to deviance, the investigators said. However, consistent with the model, dual users scored higher across several risk factors and lower on protective factors, compared with the other groups. “Dual users clearly represent people who are prone to problem behavior,” they wrote. “The fact that e-cigarette–only users were intermediate in risk status [between nonusers and dual users] raises the possibility that e-cigarettes are recruiting medium-risk adolescents who otherwise would be less susceptible to tobacco product use.”
Dr. Willis and his colleagues cited two limitations: The study was cross-sectional, and it was conducted in a single geographic area. “However, our findings on the association of e-cigarette use with current smoking status are consistent with those of other studies ... and our results on demographics are consistent with these and other studies,” the investigators wrote.
Attention should be given to the prominence of e-cigarette advertising and the perceived attractiveness of e-cigarettes, they added.
The study was funded by a grant from the National Cancer Institute. The authors said they had no relevant financial conflicts to disclose.
A large portion of young people using e-cigarettes are also smoking tobacco cigarettes, a cross-sectional study from Hawaii showed, raising concerns that the rise in the popularity of “vaping” may be renormalizing cigarette smoking.
Electronic cigarettes are a rising phenomenon in the United States, with projected sales in 2013 reaching $11.7 billion, Thomas A. Willis, Ph.D., and his associates at the University of Hawaii in Honolulu wrote in Pediatrics (2014 Feb. 15 [doi:10.1542/peds.2014-0760]).
There are two schools of thought on the use of e-cigarettes in adolescents, Dr. Willis and his colleagues wrote. One suggests that youth who try e-cigarettes are motivated by health values and concerns, making it unlikely that they also would try cigarettes or other substances.
However, the contrasting model argues that e-cigarettes appeal to young people wishing to rebel against conventional values, making it likely that they also would try tobacco and alcohol. “Although both formulations are plausible, there is little empirical evidence to support or reject either theory at this time,” the study authors wrote.
Conducting a school-based survey of 1,941 high school students living in Oahu, Hawaii, who were on average 14.6 years old, the researchers sought to determine what risk factors and conversely,which protective factors lead to a higher or lower likelihood of substance use. They found that 17% of respondents used e-cigarettes only, 12% used e-cigarettes and tobacco cigarettes (dual users), 3% used cigarettes only, and 68% were nonusers. The use of e-cigarettes in the student population was higher than seen in other data, although the authors noted that young people in Hawaii are particularly exposed to aggressive marketing.
According to the authors, some support for both schools of thought can be found in their data.
For example, people who used e-cigarettes only did not score high on rebelliousness and sensation seeking, compared with dual users. This finding supports the first model by showing that people who fall into this group are less prone to deviance, the investigators said. However, consistent with the model, dual users scored higher across several risk factors and lower on protective factors, compared with the other groups. “Dual users clearly represent people who are prone to problem behavior,” they wrote. “The fact that e-cigarette–only users were intermediate in risk status [between nonusers and dual users] raises the possibility that e-cigarettes are recruiting medium-risk adolescents who otherwise would be less susceptible to tobacco product use.”
Dr. Willis and his colleagues cited two limitations: The study was cross-sectional, and it was conducted in a single geographic area. “However, our findings on the association of e-cigarette use with current smoking status are consistent with those of other studies ... and our results on demographics are consistent with these and other studies,” the investigators wrote.
Attention should be given to the prominence of e-cigarette advertising and the perceived attractiveness of e-cigarettes, they added.
The study was funded by a grant from the National Cancer Institute. The authors said they had no relevant financial conflicts to disclose.
FROM PEDIATRICS
Key clinical point: A high percentage of youth using e-cigarettes also are using tobacco, which suggests that e-cigarettes may be “renormalizing” smoking and recruiting adolescents who would have been less susceptible to tobacco use.
Major finding: Seventeen percent of respondents used e-cigarettes only, and this group was deemed to be at “intermediate” risk of substance abuse, compared with dual users and nonusers.
Data source: A cross-sectional survey of 1,941 adolescents who were on average 14.6 years old and from several schools in Oahu, Hawaii.
Disclosures: The study was funded by a grant from the National Cancer Institute. The authors said they had no relevant financial conflicts to disclose.
Kidney function declines faster with high sleep apnea risk
PHILADELPHIA – Patients with type 2 diabetes, chronic kidney disease, and a high risk of obstructive sleep apnea have more rapid loss of kidney function than do similar patients with a low risk of sleep apnea, findings from a retrospective cohort study suggest.
Of 56 patients with diabetic nephropathy who underwent screening for obstructive sleep apnea, 34 (61%) were at high risk. Compared with 22 patients with a low risk score, the high-risk patients had a significantly greater loss of estimated glomerular filtration rate over time (median loss of -3.4 vs. 1.5 ml/min/1.73 m2 per year for the high- vs. low-risk patients, respectively), Dr. Roberto Pisoni reported in a poster at the annual meeting of the American Society of Nephrology.
This finding was despite comparable blood pressure for the high- and low-risk groups (systolic: 141.7 and 143.7 mm Hg; diastolic: 72.0 and 72.4 mm Hg, respectively), proteinuria upon admission to a chronic kidney disease clinic (urinary protein/creatinine ratio, 1.9 and 1.6 g/g, respectively), and time spent in clinic (1.9 vs. 2.1 years, respectively), said Dr. Pisoni of the Medical University of South Carolina, Charleston.
Patients in the high- and low-risk groups also had similar baseline gender, body mass index, use of renin-angiotensin-aldosterone system blockers, eGFR, and co-morbidities, he noted.
Data used for this study were from the University of Alabama at Birmingham Chronic Kidney Disease Database. Patients had completed the Berlin questionnaire to assess for sleep apnea during a 9-month study period.
Obstructive sleep apnea is common in patients with type 2 diabetes and is also associated with glomerular hyperfiltration and proteinuria in patients with normal renal function, which raised the question of whether it might be related to chronic kidney disease progression, Dr. Pisoni explained. He noted that the association between obstructive sleep apnea and diabetic nephropathy has not been fully investigated.
The study demonstrated that the “simple approach” of assessing obstructive sleep apnea risk identifies patients who are also at increased risk of CKD progression, he said, adding that the findings require replication in a prospective cohort.
Dr. Pisoni reported having no disclosures.
PHILADELPHIA – Patients with type 2 diabetes, chronic kidney disease, and a high risk of obstructive sleep apnea have more rapid loss of kidney function than do similar patients with a low risk of sleep apnea, findings from a retrospective cohort study suggest.
Of 56 patients with diabetic nephropathy who underwent screening for obstructive sleep apnea, 34 (61%) were at high risk. Compared with 22 patients with a low risk score, the high-risk patients had a significantly greater loss of estimated glomerular filtration rate over time (median loss of -3.4 vs. 1.5 ml/min/1.73 m2 per year for the high- vs. low-risk patients, respectively), Dr. Roberto Pisoni reported in a poster at the annual meeting of the American Society of Nephrology.
This finding was despite comparable blood pressure for the high- and low-risk groups (systolic: 141.7 and 143.7 mm Hg; diastolic: 72.0 and 72.4 mm Hg, respectively), proteinuria upon admission to a chronic kidney disease clinic (urinary protein/creatinine ratio, 1.9 and 1.6 g/g, respectively), and time spent in clinic (1.9 vs. 2.1 years, respectively), said Dr. Pisoni of the Medical University of South Carolina, Charleston.
Patients in the high- and low-risk groups also had similar baseline gender, body mass index, use of renin-angiotensin-aldosterone system blockers, eGFR, and co-morbidities, he noted.
Data used for this study were from the University of Alabama at Birmingham Chronic Kidney Disease Database. Patients had completed the Berlin questionnaire to assess for sleep apnea during a 9-month study period.
Obstructive sleep apnea is common in patients with type 2 diabetes and is also associated with glomerular hyperfiltration and proteinuria in patients with normal renal function, which raised the question of whether it might be related to chronic kidney disease progression, Dr. Pisoni explained. He noted that the association between obstructive sleep apnea and diabetic nephropathy has not been fully investigated.
The study demonstrated that the “simple approach” of assessing obstructive sleep apnea risk identifies patients who are also at increased risk of CKD progression, he said, adding that the findings require replication in a prospective cohort.
Dr. Pisoni reported having no disclosures.
PHILADELPHIA – Patients with type 2 diabetes, chronic kidney disease, and a high risk of obstructive sleep apnea have more rapid loss of kidney function than do similar patients with a low risk of sleep apnea, findings from a retrospective cohort study suggest.
Of 56 patients with diabetic nephropathy who underwent screening for obstructive sleep apnea, 34 (61%) were at high risk. Compared with 22 patients with a low risk score, the high-risk patients had a significantly greater loss of estimated glomerular filtration rate over time (median loss of -3.4 vs. 1.5 ml/min/1.73 m2 per year for the high- vs. low-risk patients, respectively), Dr. Roberto Pisoni reported in a poster at the annual meeting of the American Society of Nephrology.
This finding was despite comparable blood pressure for the high- and low-risk groups (systolic: 141.7 and 143.7 mm Hg; diastolic: 72.0 and 72.4 mm Hg, respectively), proteinuria upon admission to a chronic kidney disease clinic (urinary protein/creatinine ratio, 1.9 and 1.6 g/g, respectively), and time spent in clinic (1.9 vs. 2.1 years, respectively), said Dr. Pisoni of the Medical University of South Carolina, Charleston.
Patients in the high- and low-risk groups also had similar baseline gender, body mass index, use of renin-angiotensin-aldosterone system blockers, eGFR, and co-morbidities, he noted.
Data used for this study were from the University of Alabama at Birmingham Chronic Kidney Disease Database. Patients had completed the Berlin questionnaire to assess for sleep apnea during a 9-month study period.
Obstructive sleep apnea is common in patients with type 2 diabetes and is also associated with glomerular hyperfiltration and proteinuria in patients with normal renal function, which raised the question of whether it might be related to chronic kidney disease progression, Dr. Pisoni explained. He noted that the association between obstructive sleep apnea and diabetic nephropathy has not been fully investigated.
The study demonstrated that the “simple approach” of assessing obstructive sleep apnea risk identifies patients who are also at increased risk of CKD progression, he said, adding that the findings require replication in a prospective cohort.
Dr. Pisoni reported having no disclosures.
Key clinical point: Screening for OSA risk might help identify patients at higher risk for CKD progression.
Major finding: Median loss of eGFR was -3.4 vs. 1.5 ml/min/1.73 m2 per year in patients at high vs. low risk for OSA.
Data source: A retrospective cohort study involving 56 patients.
Disclosures: Dr. Pisoni reported having no disclosures.
Antibiotic prescribing leaves room for improvement
Despite all efforts to curtail the use of antibiotics, an average of 27.3% of children used an antibiotic each year from 2004 to 2010, according to a study from the Agency for Healthcare Research and Quality.
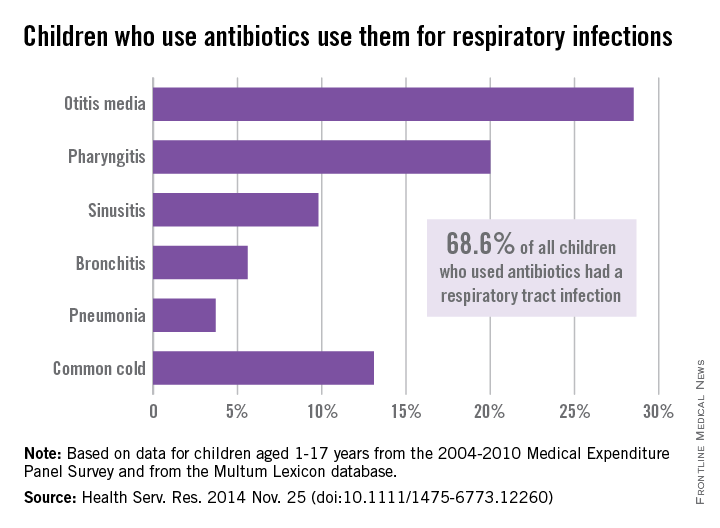
The most popular indication for antibiotic use – comprising an average of 68.6% annually of all children aged 1-17 years who used an antibiotic – was common respiratory tract infection (RTI), reported Eric M. Sarpong, Ph.D., and G. Edward Miller, Ph.D., who are both with the AHRQ in Rockville, Md.
Among the various RTIs, children who got an antibiotic were most likely to have otitis media (28.5%), followed by pharyngitis (20%). “Furthermore, significant proportions of children used antibiotics to treat three conditions – bronchitis (5.6%), sinusitis (9.8%), and the common cold (13.1%) – for which antibiotics are rarely, or never, indicated,” the investigators wrote (Health Serv. Res. 2014 Nov. 25 [doi:10.1111/1475-6773.12260]).
After controlling for a range of factors, including race/ethnicity, age, insurance status, and location, the findings suggest that “an opportunity, as well as a need, exists for further improvement in the judicious and appropriate prescribing of antibiotics for children,” Dr. Sarpong and Dr. Miller noted.
The analysis used data from the Medical Expenditure Panel Survey Household Component, which was linked to the Multum Lexicon database to assess acquisition of antibiotics.
The investigators said that they had no conflicts of interest regarding the study.

Despite all efforts to curtail the use of antibiotics, an average of 27.3% of children used an antibiotic each year from 2004 to 2010, according to a study from the Agency for Healthcare Research and Quality.
The most popular indication for antibiotic use – comprising an average of 68.6% annually of all children aged 1-17 years who used an antibiotic – was common respiratory tract infection (RTI), reported Eric M. Sarpong, Ph.D., and G. Edward Miller, Ph.D., who are both with the AHRQ in Rockville, Md.
Among the various RTIs, children who got an antibiotic were most likely to have otitis media (28.5%), followed by pharyngitis (20%). “Furthermore, significant proportions of children used antibiotics to treat three conditions – bronchitis (5.6%), sinusitis (9.8%), and the common cold (13.1%) – for which antibiotics are rarely, or never, indicated,” the investigators wrote (Health Serv. Res. 2014 Nov. 25 [doi:10.1111/1475-6773.12260]).
After controlling for a range of factors, including race/ethnicity, age, insurance status, and location, the findings suggest that “an opportunity, as well as a need, exists for further improvement in the judicious and appropriate prescribing of antibiotics for children,” Dr. Sarpong and Dr. Miller noted.
The analysis used data from the Medical Expenditure Panel Survey Household Component, which was linked to the Multum Lexicon database to assess acquisition of antibiotics.
The investigators said that they had no conflicts of interest regarding the study.
Despite all efforts to curtail the use of antibiotics, an average of 27.3% of children used an antibiotic each year from 2004 to 2010, according to a study from the Agency for Healthcare Research and Quality.
The most popular indication for antibiotic use – comprising an average of 68.6% annually of all children aged 1-17 years who used an antibiotic – was common respiratory tract infection (RTI), reported Eric M. Sarpong, Ph.D., and G. Edward Miller, Ph.D., who are both with the AHRQ in Rockville, Md.
Among the various RTIs, children who got an antibiotic were most likely to have otitis media (28.5%), followed by pharyngitis (20%). “Furthermore, significant proportions of children used antibiotics to treat three conditions – bronchitis (5.6%), sinusitis (9.8%), and the common cold (13.1%) – for which antibiotics are rarely, or never, indicated,” the investigators wrote (Health Serv. Res. 2014 Nov. 25 [doi:10.1111/1475-6773.12260]).
After controlling for a range of factors, including race/ethnicity, age, insurance status, and location, the findings suggest that “an opportunity, as well as a need, exists for further improvement in the judicious and appropriate prescribing of antibiotics for children,” Dr. Sarpong and Dr. Miller noted.
The analysis used data from the Medical Expenditure Panel Survey Household Component, which was linked to the Multum Lexicon database to assess acquisition of antibiotics.
The investigators said that they had no conflicts of interest regarding the study.
FROM HEALTH SERVICES RESEARCH
LAMA/LABA may enable withdrawal of inhaled corticosteroids in COPD
AUSTIN, TEX. – Inhaled corticosteroids can be successfully withdrawn without increasing the risk of exacerbations in patients who have chronic obstructive pulmonary disease and are receiving dual bronchodilator therapy with a long-acting muscarinic antagonist (LAMA) and a long-acting beta2-agonist (LABA), according to findings from the WISDOM study.
However, inhaled corticosteroid (ICS) withdrawal should be conducted with caution, as a small but statistically significantly greater decrease in lung function occurred in patients who withdrew completely, compared with those who did not during the 12-month, double-blind, parallel-group study, Dr. Helgo Magnussen reported at the annual meeting of the American College of Chest Physicians.
“In patients with severe but stable COPD who are receiving combination therapy with tiotropium, salmeterol and ICS, a stepwise withdrawal of ICS was noninferior to continuation of ICS with respect to the risk of moderate or severe exacerbations. Despite this, if you do [withdraw ICS] – and we believe you can try to withdraw ICS – please observe the symptoms and lung function, because we found this signal [for decreased lung function],” he said.
Study subjects were 2,485 adults over age 40 years with severe or very severe COPD and a history of exacerbations. All patients received triple therapy with the LAMA tiotropium at 18 mcg four times daily, the LABA salmeterol at 50 mcg twice daily, and the ICS fluticasone at 500 mcg twice daily for a 6-week run-in period.
The patients were randomized to continue the triple therapy or to undergo ICS withdrawal over 12 weeks, with a dose reduction every 6 weeks.
ICS withdrawal met the prespecified noninferiority criterion of 1.20 for the upper limit of the 95% confidence interval, compared with continued ICS with respect to moderate or severe COPD exacerbation (hazard ratio, 1.06), but the adjusted mean reduction from baseline in the trough forced expiratory volume in 1 second (FEV1) at week 18 was 38 mL greater in the ICS withdrawal group, said Dr. Magnussen of the Pulmonary Research Institute at Lung Clinic Grosshansdorf (Germany), Airway Research Center North.
A similar between-group difference of 43 mL was seen at week 52, he said, noting that this did not differ significantly from the difference seen at week 18, demonstrating that there is no further decline in lung function after complete ICS withdrawal at week 18.
Also, the decline in lung function – even at the peak decrease in function at week 18, was not associated with an increase in dyspnea; the difference in change from baseline in the modified Medical Research Council (mMRC) dyspnea scale was nonsignificant for ICS withdrawal, compared with ICS continuation at week 18 or week 52. The change from baseline in the St. George’s Respiratory Questionnaire (SGRQ) total score was 0.55 with ICS withdrawal, compared with –0.42 with ICS at week 27, and 1.15, compared with –0.07 for withdrawal vs. continuation, respectively, at week 52. This difference, though statistically significant, was not considered clinically relevant, Dr. Magnussen said.
ICS treatment is recommended along with long-acting bronchodilators in patients with frequent exacerbations of severe COPD, but the benefits of ICS use in addition to dual bronchodilator therapy have not been fully elucidated, he said.
The findings of the WISDOM study (N. Engl. J. Med. 2014;371:1285-94), suggest that ICS discontinuation is possible.This study was funded by Boehringer Ingelheim. Dr. Magnussen reported receiving consultant fees and/or serving on a speakers bureau or advisory committee for Almirall, Boehringer Ingelheim, Chiesi, Berli-Chemi, and Novartis. His employer, the Pulmonary Research Institute, received payments for conducting the study.
AUSTIN, TEX. – Inhaled corticosteroids can be successfully withdrawn without increasing the risk of exacerbations in patients who have chronic obstructive pulmonary disease and are receiving dual bronchodilator therapy with a long-acting muscarinic antagonist (LAMA) and a long-acting beta2-agonist (LABA), according to findings from the WISDOM study.
However, inhaled corticosteroid (ICS) withdrawal should be conducted with caution, as a small but statistically significantly greater decrease in lung function occurred in patients who withdrew completely, compared with those who did not during the 12-month, double-blind, parallel-group study, Dr. Helgo Magnussen reported at the annual meeting of the American College of Chest Physicians.
“In patients with severe but stable COPD who are receiving combination therapy with tiotropium, salmeterol and ICS, a stepwise withdrawal of ICS was noninferior to continuation of ICS with respect to the risk of moderate or severe exacerbations. Despite this, if you do [withdraw ICS] – and we believe you can try to withdraw ICS – please observe the symptoms and lung function, because we found this signal [for decreased lung function],” he said.
Study subjects were 2,485 adults over age 40 years with severe or very severe COPD and a history of exacerbations. All patients received triple therapy with the LAMA tiotropium at 18 mcg four times daily, the LABA salmeterol at 50 mcg twice daily, and the ICS fluticasone at 500 mcg twice daily for a 6-week run-in period.
The patients were randomized to continue the triple therapy or to undergo ICS withdrawal over 12 weeks, with a dose reduction every 6 weeks.
ICS withdrawal met the prespecified noninferiority criterion of 1.20 for the upper limit of the 95% confidence interval, compared with continued ICS with respect to moderate or severe COPD exacerbation (hazard ratio, 1.06), but the adjusted mean reduction from baseline in the trough forced expiratory volume in 1 second (FEV1) at week 18 was 38 mL greater in the ICS withdrawal group, said Dr. Magnussen of the Pulmonary Research Institute at Lung Clinic Grosshansdorf (Germany), Airway Research Center North.
A similar between-group difference of 43 mL was seen at week 52, he said, noting that this did not differ significantly from the difference seen at week 18, demonstrating that there is no further decline in lung function after complete ICS withdrawal at week 18.
Also, the decline in lung function – even at the peak decrease in function at week 18, was not associated with an increase in dyspnea; the difference in change from baseline in the modified Medical Research Council (mMRC) dyspnea scale was nonsignificant for ICS withdrawal, compared with ICS continuation at week 18 or week 52. The change from baseline in the St. George’s Respiratory Questionnaire (SGRQ) total score was 0.55 with ICS withdrawal, compared with –0.42 with ICS at week 27, and 1.15, compared with –0.07 for withdrawal vs. continuation, respectively, at week 52. This difference, though statistically significant, was not considered clinically relevant, Dr. Magnussen said.
ICS treatment is recommended along with long-acting bronchodilators in patients with frequent exacerbations of severe COPD, but the benefits of ICS use in addition to dual bronchodilator therapy have not been fully elucidated, he said.
The findings of the WISDOM study (N. Engl. J. Med. 2014;371:1285-94), suggest that ICS discontinuation is possible.This study was funded by Boehringer Ingelheim. Dr. Magnussen reported receiving consultant fees and/or serving on a speakers bureau or advisory committee for Almirall, Boehringer Ingelheim, Chiesi, Berli-Chemi, and Novartis. His employer, the Pulmonary Research Institute, received payments for conducting the study.
AUSTIN, TEX. – Inhaled corticosteroids can be successfully withdrawn without increasing the risk of exacerbations in patients who have chronic obstructive pulmonary disease and are receiving dual bronchodilator therapy with a long-acting muscarinic antagonist (LAMA) and a long-acting beta2-agonist (LABA), according to findings from the WISDOM study.
However, inhaled corticosteroid (ICS) withdrawal should be conducted with caution, as a small but statistically significantly greater decrease in lung function occurred in patients who withdrew completely, compared with those who did not during the 12-month, double-blind, parallel-group study, Dr. Helgo Magnussen reported at the annual meeting of the American College of Chest Physicians.
“In patients with severe but stable COPD who are receiving combination therapy with tiotropium, salmeterol and ICS, a stepwise withdrawal of ICS was noninferior to continuation of ICS with respect to the risk of moderate or severe exacerbations. Despite this, if you do [withdraw ICS] – and we believe you can try to withdraw ICS – please observe the symptoms and lung function, because we found this signal [for decreased lung function],” he said.
Study subjects were 2,485 adults over age 40 years with severe or very severe COPD and a history of exacerbations. All patients received triple therapy with the LAMA tiotropium at 18 mcg four times daily, the LABA salmeterol at 50 mcg twice daily, and the ICS fluticasone at 500 mcg twice daily for a 6-week run-in period.
The patients were randomized to continue the triple therapy or to undergo ICS withdrawal over 12 weeks, with a dose reduction every 6 weeks.
ICS withdrawal met the prespecified noninferiority criterion of 1.20 for the upper limit of the 95% confidence interval, compared with continued ICS with respect to moderate or severe COPD exacerbation (hazard ratio, 1.06), but the adjusted mean reduction from baseline in the trough forced expiratory volume in 1 second (FEV1) at week 18 was 38 mL greater in the ICS withdrawal group, said Dr. Magnussen of the Pulmonary Research Institute at Lung Clinic Grosshansdorf (Germany), Airway Research Center North.
A similar between-group difference of 43 mL was seen at week 52, he said, noting that this did not differ significantly from the difference seen at week 18, demonstrating that there is no further decline in lung function after complete ICS withdrawal at week 18.
Also, the decline in lung function – even at the peak decrease in function at week 18, was not associated with an increase in dyspnea; the difference in change from baseline in the modified Medical Research Council (mMRC) dyspnea scale was nonsignificant for ICS withdrawal, compared with ICS continuation at week 18 or week 52. The change from baseline in the St. George’s Respiratory Questionnaire (SGRQ) total score was 0.55 with ICS withdrawal, compared with –0.42 with ICS at week 27, and 1.15, compared with –0.07 for withdrawal vs. continuation, respectively, at week 52. This difference, though statistically significant, was not considered clinically relevant, Dr. Magnussen said.
ICS treatment is recommended along with long-acting bronchodilators in patients with frequent exacerbations of severe COPD, but the benefits of ICS use in addition to dual bronchodilator therapy have not been fully elucidated, he said.
The findings of the WISDOM study (N. Engl. J. Med. 2014;371:1285-94), suggest that ICS discontinuation is possible.This study was funded by Boehringer Ingelheim. Dr. Magnussen reported receiving consultant fees and/or serving on a speakers bureau or advisory committee for Almirall, Boehringer Ingelheim, Chiesi, Berli-Chemi, and Novartis. His employer, the Pulmonary Research Institute, received payments for conducting the study.
Key clinical point: Dual bronchotherapy might allow some COPD patients to stop using inhaled corticosteroids.
Major finding: There was no difference with respect to COPD exacerbations (HR, 1.06) in LAMA/LABA users who discontinued and those who remained on inhaled corticosteroids.
Data source: The WISDOM study of 2,485 adults with COPD.
Disclosures: This study was funded by Boehringer Ingelheim. Dr. Magnussen reported receiving consultant fees and/or serving on a speakers bureau or advisory committee for Almirall, Boehringer Ingelheim, Chiesi, Berli-Chemi, and Novartis. His employer, the Pulmonary Research Institute, received payments for the conduct of this study.
RAPID: Baseline characteristics may affect response to A1-PI therapy
AUSTIN, TEX. – Higher baseline alpha-1 proteinase inhibitor level, higher body mass index, and female gender may be associated with improved response to alpha-1 proteinase inhibitor augmentation therapy, according to an analysis of data from RAPID.
Better responses to therapy in the trial, as compared with placebo and as measured by mean computed tomography-assessed rate of change in adjusted P15 lung density at total lung capacity, occurred among the 79 female subjects (1.45 g/L per year), and among the 60, 58, and 59 patients with high functional, antigenic, or intermediate functional alpha-1 proteinase inhibitor (A1-PI) levels, respectively (1.08, 1.23, and 1.38 g/L per year), Dr. James Stocks reported at the annual meeting of the American College of Chest Physicians.
The differences in the rate of change with treatment vs. placebo in these subgroups were statistically significant, said Dr. Stocks of the University of Texas Health Science Center at Tyler.
Greater differences in favor of A1-PI – with a trend toward statistical significance – were also seen in the 21 patients with a body mass index of 30 kg/m2 or greater (2.21 g/L per year), the 86 patients under age 54 years (0.96 g/L year), the 87 patients with a carbon monoxide diffusion capacity at or below the median at baseline (0.90 g/L per year), the 8 patients with lower exercise capacity, defined by 400 m or less walked (0.99 g/L per year), and the 88 patients with St. George’s Respiratory Questionnaire symptoms scores at or below the median at baseline (0.93 g/L per year), he said.
RAPID (Randomized, Placebo-Controlled Trial in Alpha-1 Proteinase Inhibitor Deficiency) – the single largest clinical trial of A1-PI augmentation therapy – included 180 A1-PI–deficient patients and demonstrated that weekly intravenous A1-PI therapy at a dose of 60 g/kg per week for 2 years slows progression of emphysema. The annual rate of decline in CT-measured lung density was 34%, compared with placebo. Those findings were reported in May 2013.
According to the current analysis, A1-PI augmentation appears to be efficacious across a wide range of subgroups, Dr. Stocks said. Those with higher BMI may have experienced greater benefit because of receiving a greater amount of A1-PI as a result of weight-based dosing. Younger patients may have experienced greater benefit because of being in the earlier stages of disease, with less emphysematous lung damage and lung density loss.
“It is important to note that were no multiplicity adjustments made in the analysis, and no tests for interaction within a subgroup were significant, so no subgroup could be said to be particularly favored as being suitable for treatment with A1-PI,” he said. It does appear, however, that earlier treatment may help to reduce overall progression of emphysema in affected patients, and that baseline factors such as higher baseline A1-PI, BMI, and gender may impact treatment benefit, he said.
This study was funded by CSL Behring. Dr. Stocks reported receiving funds as an investigator for the commercially sponsored clinical trial.
AUSTIN, TEX. – Higher baseline alpha-1 proteinase inhibitor level, higher body mass index, and female gender may be associated with improved response to alpha-1 proteinase inhibitor augmentation therapy, according to an analysis of data from RAPID.
Better responses to therapy in the trial, as compared with placebo and as measured by mean computed tomography-assessed rate of change in adjusted P15 lung density at total lung capacity, occurred among the 79 female subjects (1.45 g/L per year), and among the 60, 58, and 59 patients with high functional, antigenic, or intermediate functional alpha-1 proteinase inhibitor (A1-PI) levels, respectively (1.08, 1.23, and 1.38 g/L per year), Dr. James Stocks reported at the annual meeting of the American College of Chest Physicians.
The differences in the rate of change with treatment vs. placebo in these subgroups were statistically significant, said Dr. Stocks of the University of Texas Health Science Center at Tyler.
Greater differences in favor of A1-PI – with a trend toward statistical significance – were also seen in the 21 patients with a body mass index of 30 kg/m2 or greater (2.21 g/L per year), the 86 patients under age 54 years (0.96 g/L year), the 87 patients with a carbon monoxide diffusion capacity at or below the median at baseline (0.90 g/L per year), the 8 patients with lower exercise capacity, defined by 400 m or less walked (0.99 g/L per year), and the 88 patients with St. George’s Respiratory Questionnaire symptoms scores at or below the median at baseline (0.93 g/L per year), he said.
RAPID (Randomized, Placebo-Controlled Trial in Alpha-1 Proteinase Inhibitor Deficiency) – the single largest clinical trial of A1-PI augmentation therapy – included 180 A1-PI–deficient patients and demonstrated that weekly intravenous A1-PI therapy at a dose of 60 g/kg per week for 2 years slows progression of emphysema. The annual rate of decline in CT-measured lung density was 34%, compared with placebo. Those findings were reported in May 2013.
According to the current analysis, A1-PI augmentation appears to be efficacious across a wide range of subgroups, Dr. Stocks said. Those with higher BMI may have experienced greater benefit because of receiving a greater amount of A1-PI as a result of weight-based dosing. Younger patients may have experienced greater benefit because of being in the earlier stages of disease, with less emphysematous lung damage and lung density loss.
“It is important to note that were no multiplicity adjustments made in the analysis, and no tests for interaction within a subgroup were significant, so no subgroup could be said to be particularly favored as being suitable for treatment with A1-PI,” he said. It does appear, however, that earlier treatment may help to reduce overall progression of emphysema in affected patients, and that baseline factors such as higher baseline A1-PI, BMI, and gender may impact treatment benefit, he said.
This study was funded by CSL Behring. Dr. Stocks reported receiving funds as an investigator for the commercially sponsored clinical trial.
AUSTIN, TEX. – Higher baseline alpha-1 proteinase inhibitor level, higher body mass index, and female gender may be associated with improved response to alpha-1 proteinase inhibitor augmentation therapy, according to an analysis of data from RAPID.
Better responses to therapy in the trial, as compared with placebo and as measured by mean computed tomography-assessed rate of change in adjusted P15 lung density at total lung capacity, occurred among the 79 female subjects (1.45 g/L per year), and among the 60, 58, and 59 patients with high functional, antigenic, or intermediate functional alpha-1 proteinase inhibitor (A1-PI) levels, respectively (1.08, 1.23, and 1.38 g/L per year), Dr. James Stocks reported at the annual meeting of the American College of Chest Physicians.
The differences in the rate of change with treatment vs. placebo in these subgroups were statistically significant, said Dr. Stocks of the University of Texas Health Science Center at Tyler.
Greater differences in favor of A1-PI – with a trend toward statistical significance – were also seen in the 21 patients with a body mass index of 30 kg/m2 or greater (2.21 g/L per year), the 86 patients under age 54 years (0.96 g/L year), the 87 patients with a carbon monoxide diffusion capacity at or below the median at baseline (0.90 g/L per year), the 8 patients with lower exercise capacity, defined by 400 m or less walked (0.99 g/L per year), and the 88 patients with St. George’s Respiratory Questionnaire symptoms scores at or below the median at baseline (0.93 g/L per year), he said.
RAPID (Randomized, Placebo-Controlled Trial in Alpha-1 Proteinase Inhibitor Deficiency) – the single largest clinical trial of A1-PI augmentation therapy – included 180 A1-PI–deficient patients and demonstrated that weekly intravenous A1-PI therapy at a dose of 60 g/kg per week for 2 years slows progression of emphysema. The annual rate of decline in CT-measured lung density was 34%, compared with placebo. Those findings were reported in May 2013.
According to the current analysis, A1-PI augmentation appears to be efficacious across a wide range of subgroups, Dr. Stocks said. Those with higher BMI may have experienced greater benefit because of receiving a greater amount of A1-PI as a result of weight-based dosing. Younger patients may have experienced greater benefit because of being in the earlier stages of disease, with less emphysematous lung damage and lung density loss.
“It is important to note that were no multiplicity adjustments made in the analysis, and no tests for interaction within a subgroup were significant, so no subgroup could be said to be particularly favored as being suitable for treatment with A1-PI,” he said. It does appear, however, that earlier treatment may help to reduce overall progression of emphysema in affected patients, and that baseline factors such as higher baseline A1-PI, BMI, and gender may impact treatment benefit, he said.
This study was funded by CSL Behring. Dr. Stocks reported receiving funds as an investigator for the commercially sponsored clinical trial.
Key clinical point: A1-PI augmentation is effective across a wide range of subgroups with A1-PI deficiency.
Major finding: The decreased rate of change in adjusted P15 lung density vs. placebo in those with high functional, antigenic, or intermediate functional A1-PI levels who were treated with A1-PI augmentation was 1.08 g/L per year, 1.23 g/L per year, and 1.38 g/L year, respectively.
Data source: An analysis of data from the 180-patient RAPID study.
Disclosures: This study was funded by CSL Behring. Dr. Stocks reported receiving funds as an investigator for the commercially sponsored clinical trial.
Early sleep abnormalities linked to later obesity
Sleep-disordered breathing and short sleep duration in early childhood are strongly and independently associated with obesity at ages 7, 10, and 15 years, according to a report published online Dec. 11 in the Journal of Pediatrics.
These findings underscore the importance of identifying and treating sleep-disordered breathing and insufficient sleep as early as possible to reduce later obesity, said Karen Bonuck, Ph.D., of the department of family medicine and social medicine, Albert Einstein College of Medicine, Bronx, N.Y., and her associates.

To examine the relationships between sleep abnormalities and obesity in the pediatric population, the investigators analyzed data from a large longitudinal cohort study of children born during 1991-1992 in southwest England. Participating mothers reported on their children’s sleep duration and on the presence and severity of sleep-disordered breathing, which was defined as snoring, observed episodes of apnea, and mouth-breathing during sleep. These were assessed at ages 18 months, 2.5 years, 4.75 years, 5.75 years, and 6.75 years. The children’s body mass index was calculated from height and weight measurements taken at ages 7, 10, and 15 years.
In this analysis of 1,844 of the participating children, those with the most severe sleep-disordered breathing at age 2.5 years were twice as likely as were asymptomatic children to be obese in later childhood. Similarly, children with short sleep duration at ages 5-6 years (less than 10 hours per night) were twice as likely to be obese at age 15 as were those with the longest sleep duration. These negative effects were independent of each other and of comparable magnitude, Dr. Bonuck and her associates said (J. Pediatr. 2014 Dec. 11 [doi:10.1016/j.jpeds.2014.11.001]).
“Our findings affirm the concept of healthy sleep ... as a foundation for healthy weight throughout childhood and into adulthood,” they added.
This study was supported by the U.S. National Heart, Lung, and Blood Institute, the U.K. Medical Research Council, and the University of Bristol (England) Dr. Bonuck and her associates reported having no financial disclosures.
Sleep-disordered breathing and short sleep duration in early childhood are strongly and independently associated with obesity at ages 7, 10, and 15 years, according to a report published online Dec. 11 in the Journal of Pediatrics.
These findings underscore the importance of identifying and treating sleep-disordered breathing and insufficient sleep as early as possible to reduce later obesity, said Karen Bonuck, Ph.D., of the department of family medicine and social medicine, Albert Einstein College of Medicine, Bronx, N.Y., and her associates.
To examine the relationships between sleep abnormalities and obesity in the pediatric population, the investigators analyzed data from a large longitudinal cohort study of children born during 1991-1992 in southwest England. Participating mothers reported on their children’s sleep duration and on the presence and severity of sleep-disordered breathing, which was defined as snoring, observed episodes of apnea, and mouth-breathing during sleep. These were assessed at ages 18 months, 2.5 years, 4.75 years, 5.75 years, and 6.75 years. The children’s body mass index was calculated from height and weight measurements taken at ages 7, 10, and 15 years.
In this analysis of 1,844 of the participating children, those with the most severe sleep-disordered breathing at age 2.5 years were twice as likely as were asymptomatic children to be obese in later childhood. Similarly, children with short sleep duration at ages 5-6 years (less than 10 hours per night) were twice as likely to be obese at age 15 as were those with the longest sleep duration. These negative effects were independent of each other and of comparable magnitude, Dr. Bonuck and her associates said (J. Pediatr. 2014 Dec. 11 [doi:10.1016/j.jpeds.2014.11.001]).
“Our findings affirm the concept of healthy sleep ... as a foundation for healthy weight throughout childhood and into adulthood,” they added.
This study was supported by the U.S. National Heart, Lung, and Blood Institute, the U.K. Medical Research Council, and the University of Bristol (England) Dr. Bonuck and her associates reported having no financial disclosures.
Sleep-disordered breathing and short sleep duration in early childhood are strongly and independently associated with obesity at ages 7, 10, and 15 years, according to a report published online Dec. 11 in the Journal of Pediatrics.
These findings underscore the importance of identifying and treating sleep-disordered breathing and insufficient sleep as early as possible to reduce later obesity, said Karen Bonuck, Ph.D., of the department of family medicine and social medicine, Albert Einstein College of Medicine, Bronx, N.Y., and her associates.
To examine the relationships between sleep abnormalities and obesity in the pediatric population, the investigators analyzed data from a large longitudinal cohort study of children born during 1991-1992 in southwest England. Participating mothers reported on their children’s sleep duration and on the presence and severity of sleep-disordered breathing, which was defined as snoring, observed episodes of apnea, and mouth-breathing during sleep. These were assessed at ages 18 months, 2.5 years, 4.75 years, 5.75 years, and 6.75 years. The children’s body mass index was calculated from height and weight measurements taken at ages 7, 10, and 15 years.
In this analysis of 1,844 of the participating children, those with the most severe sleep-disordered breathing at age 2.5 years were twice as likely as were asymptomatic children to be obese in later childhood. Similarly, children with short sleep duration at ages 5-6 years (less than 10 hours per night) were twice as likely to be obese at age 15 as were those with the longest sleep duration. These negative effects were independent of each other and of comparable magnitude, Dr. Bonuck and her associates said (J. Pediatr. 2014 Dec. 11 [doi:10.1016/j.jpeds.2014.11.001]).
“Our findings affirm the concept of healthy sleep ... as a foundation for healthy weight throughout childhood and into adulthood,” they added.
This study was supported by the U.S. National Heart, Lung, and Blood Institute, the U.K. Medical Research Council, and the University of Bristol (England) Dr. Bonuck and her associates reported having no financial disclosures.
Key clinical point: Sleep-disordered breathing and short sleep duration in early childhood are strongly and independently associated with obesity at ages 7, 10, and 15 years.
Major finding: Among 1,844 children, those who had the most severe sleep-disordered breathing at age 2.5 years were twice as likely as were asymptomatic children to be obese in later childhood.
Data source: A secondary analysis of data from a longitudinal cohort study in England of children followed from birth to age 15 years.
Disclosures: This study was supported by the U.S. National Heart, Lung, and Blood Institute, the U.K. Medical Research Council, and the University of Bristol (England) Dr. Bonuck and her associates reported having no financial disclosures.

Predictions for 2015
Last year, there were five predictions made that appeared to be on the money – but there is more to the story!
1. The approach to diagnosis and treatment of influenza was essential knowledge for clinicians. Last year, we started seeing influenza activity early – with disease confirmed in mid-November, peaking during the week ending December 28, 2013 and trending downward in early January 2014. Hospitalizations were most common in young and middle aged adults and the 2009 H1N1 virus predominated.

This year, again we are seeing influenza early – with nearly all states reporting at least sporadic and local activity, and several states (Alaska, Florida, Louisiana, Massachusetts, and Texas) reporting regional activity as of the week ending November 24, 2014. At my institution, we’ve already tested over 500 children and over 100 were positive – influenza A (H3N2) strains are predominating. That may be important for the two reasons you’ll read below.
2. Invasive staphylococcal disease caused by methicillin-susceptible Staphylococcus aureus (MSSA) was more common than methicillin-resistant Staphylococcus aureus (MRSA), as the national burden of MRSA disease decreased (JAMA 2014;311:1438-9). The rates of clindamycin resistance continue to be pretty steady at approximately 15%-18%, but higher for MSSA than for MRSA – a point that is important to consider when empirically treating suspected invasive staphylococcal infection.
3. Multidrug resistant uropathogens took an increasingly prominent role in 2014, requiring careful approach to diagnosis (every child treated for urinary tract infection should have an appropriately obtained urine culture with an identified pathogen) and treatment (the drug used should be based on antibiotic susceptibility testing results). Particularly concerning is the emergence of carbapenem-resistant Enterobacteriaceae, which cause infection more commonly in hospitalized patients, those with indwelling devices, and those who have received long courses of antibiotics.
4. It was an outbreak year for parechovirus (HPeV), a viral pathogen causing meningitis in very young infants. Such infants present with signs and symptoms of meningitis but rarely show CSF pleocytosis. Diagnosis relies on the detection of the virus by polymerase chain reaction testing in CSF – a test which is not routinely available in many laboratories. At my institution this season, we saw nearly as many cases of parechovirus meningitis (n = 43) as we saw cases of enterovirus meningitis (n = 63). The parechovirus virus we detected was HPeV type 3, which can cause particularly severe disease in neonates.
5. Data confirmed that making human papillomavirus (HPV) vaccine a standard recommendation increased vaccine uptake and coverage. In February of 2014, a “Dear Colleague” letter that was endorsed by six leading medical organizations encouraged providers to promote HPV vaccination by giving a strong recommendation, citing data based on research conducted by the Centers for Disease Control and Prevention. We still have a long way to go as HPV vaccine coverage for teens remains at 35% for the three-dose series while meningococcal and Tdap vaccine (both vaccines that generally receive a standard recommendation by physicians) coverage is at nearly 90%.
So for 2015, I’ll start the discussion by saying there are five major developments I did not see coming for this past year, but that will remain relevant for the year 2015!
1. In June of 2014, live attenuated influenza vaccine (LAIV) was announced by the Advisory Committee on Immunization Practices to be the preferred vaccine in children aged 2-8 years. The American Academy of Pediatrics followed with a recommendation that either inactivated influenza vaccine (IIV) or LAIV be used for children, including children aged 2-8 years – the key being to give the vaccine as soon as one had it available. What was not known then and I did not predict was that newer data would confirm that in children aged 2-8 years who received LAIV last year when 2009 H1N1 strains predominated, there was essentially no coverage against 2009 H1N1 virus. This was in contrast to data from the prior 2 years and is as yet unexplained. The AAP continues to recommend that either vaccine be given and all children be immunized. That may be especially important this year as the influenza season started early. Disease will likely have been widespread by Christmas in many parts of the United States, and it looks like influenza A H3N2 strains will be most commonly noted. So the good news for young children who received LAIV is that 2009 H1N1 strains so far have not been seen this year. The bad news is that there are two H3N2 strains circulating, and potentially only one will be covered by the 2014-2015 seasonal vaccine. Staffing your office and hospital for a likely high census respiratory viral season is going to be essential.
2. The largest U.S. outbreak ever of enterovirus (EV) D-68 respiratory infection occurred between August and October of 2014. This virus – which had been identified in 1962 but was rarely described over the next 36 years except in small clusters of disease – was reported in nearly every state and characterized by unusually severe respiratory tract infection. Many, but not all children, had a history of asthma or prior wheezing, and the clinical presentation was that of severe bronchospasm that was generally resistant to standard bronchodilator therapy. The spectrum of infection likely ranged from mild upper respiratory infection to severe bronchospasm with respiratory failure, and the burden of disease resulting in hospitalization was substantial at many children’s hospitals. The big question now is what will enterovirus season 2015 bring us? The good news here is that we now have a test to rapidly diagnose EV D-68, which will allow us to more clearly understand the burden of disease – and potentially to define antiviral treatment (none of the current antivirals is effective) and prevention (there is no vaccine against EV D-68).
3. The etiology of the neurologic illness, which appeared to mimic polio and presented during the same time frame during which EV D-68 was circulating, is as yet unknown. As of Nov. 26, 2014, the CDC has received reports of 90 children in 32 states who meet a case definition consistent with acute flaccid myelitis. While certain viruses – including West Nile virus, herpes virus, adenovirus, and certain enterovirus types (for example, enterovirus 71, and the classic being polio) – may cause acute flaccid paralysis and can be confirmed by detecting the virus in cerebrospinal fluid and stool, to date virus testing for all viruses, including EV D-68, has been negative in all of the patients reported. Hopefully, 2015 will be the year that will allow us to more clearly understand this neurologic illness – and this is important because so far most children have shown minimal recovery of function.
4. If you see a child (or adult) who recently traveled to the Caribbean and returns with fever, rash, and joint pain, especially with severe pain of the hands and feet, think chikungunya virus infection. As of the end of October 2014, local transmission had been identified in 37 countries or territories in the Caribbean (including Puerto Rico and the U.S. Virgin Islands), with a total of 780,206 suspected cases and over 15,000 confirmed cases reported from these areas. Consider this in contrast to the numbers from 2006 through 2011, when 117 cases of chikungunya fever were reported in returning travelers. As of Dec. 2, a total of 1,911 chikungunya virus disease cases have been reported to ArboNET from U.S. states. The mosquito that transmits chikungunya virus can bite in day and night, and prevention relies on appropriate use of mosquito repellents. Physicians should be prepared to discuss the risks of this virus with travelers who plan a trip to the Caribbean, especially those at high risk, including those with underlying medical conditions, preexisting arthritis diagnoses, and pregnant women (because of the potential risk to newborns whose mothers develop intrapartum infection).
5. And lastly, Ebola. While there were reports that Ebola virus disease had emerged in West Africa as early as December of 2013, the scope of the outbreak and extent of loss of human life has been unbelievably huge. Dr. Carrie Byington, who is the current chair of the AAP Committee on Infectious Diseases, wrote an article in AAP News in October 2014 describing the needs of children who have been impacted by Ebola virus disease (EVD). She noted that UNICEF estimated there were at that time, over 4,000 Ebola orphans in the countries most affected by EVD, including Sierra Leone, Liberia, and Guinea, and that these countries urgently needed medical infrastructure for treatment and prevention of this disease. It appears that at least two Ebola vaccines will be deployed in West Africa in 2015, and it is not a moment too soon. While cases in Liberia seemed to be decreasing, it looks like Sierra Leone cases continue to mount.
Dr. Jackson is chief of pediatric infectious diseases at Children’s Mercy Hospital, Kansas City, Mo., and professor of pediatrics at the University of Missouri–Kansas City. Dr. Jackson was a member of the AAP Committee on Infectious Diseases who wrote the AAP clinical report entitled “Guidance on Management of Asymptomatic Neonates Born to Women With Active Genital Herpes Lesions,” but said she had no other conflicts of interest to disclose. E-mail her at [email protected].
Last year, there were five predictions made that appeared to be on the money – but there is more to the story!
1. The approach to diagnosis and treatment of influenza was essential knowledge for clinicians. Last year, we started seeing influenza activity early – with disease confirmed in mid-November, peaking during the week ending December 28, 2013 and trending downward in early January 2014. Hospitalizations were most common in young and middle aged adults and the 2009 H1N1 virus predominated.
This year, again we are seeing influenza early – with nearly all states reporting at least sporadic and local activity, and several states (Alaska, Florida, Louisiana, Massachusetts, and Texas) reporting regional activity as of the week ending November 24, 2014. At my institution, we’ve already tested over 500 children and over 100 were positive – influenza A (H3N2) strains are predominating. That may be important for the two reasons you’ll read below.
2. Invasive staphylococcal disease caused by methicillin-susceptible Staphylococcus aureus (MSSA) was more common than methicillin-resistant Staphylococcus aureus (MRSA), as the national burden of MRSA disease decreased (JAMA 2014;311:1438-9). The rates of clindamycin resistance continue to be pretty steady at approximately 15%-18%, but higher for MSSA than for MRSA – a point that is important to consider when empirically treating suspected invasive staphylococcal infection.
3. Multidrug resistant uropathogens took an increasingly prominent role in 2014, requiring careful approach to diagnosis (every child treated for urinary tract infection should have an appropriately obtained urine culture with an identified pathogen) and treatment (the drug used should be based on antibiotic susceptibility testing results). Particularly concerning is the emergence of carbapenem-resistant Enterobacteriaceae, which cause infection more commonly in hospitalized patients, those with indwelling devices, and those who have received long courses of antibiotics.
4. It was an outbreak year for parechovirus (HPeV), a viral pathogen causing meningitis in very young infants. Such infants present with signs and symptoms of meningitis but rarely show CSF pleocytosis. Diagnosis relies on the detection of the virus by polymerase chain reaction testing in CSF – a test which is not routinely available in many laboratories. At my institution this season, we saw nearly as many cases of parechovirus meningitis (n = 43) as we saw cases of enterovirus meningitis (n = 63). The parechovirus virus we detected was HPeV type 3, which can cause particularly severe disease in neonates.
5. Data confirmed that making human papillomavirus (HPV) vaccine a standard recommendation increased vaccine uptake and coverage. In February of 2014, a “Dear Colleague” letter that was endorsed by six leading medical organizations encouraged providers to promote HPV vaccination by giving a strong recommendation, citing data based on research conducted by the Centers for Disease Control and Prevention. We still have a long way to go as HPV vaccine coverage for teens remains at 35% for the three-dose series while meningococcal and Tdap vaccine (both vaccines that generally receive a standard recommendation by physicians) coverage is at nearly 90%.
So for 2015, I’ll start the discussion by saying there are five major developments I did not see coming for this past year, but that will remain relevant for the year 2015!
1. In June of 2014, live attenuated influenza vaccine (LAIV) was announced by the Advisory Committee on Immunization Practices to be the preferred vaccine in children aged 2-8 years. The American Academy of Pediatrics followed with a recommendation that either inactivated influenza vaccine (IIV) or LAIV be used for children, including children aged 2-8 years – the key being to give the vaccine as soon as one had it available. What was not known then and I did not predict was that newer data would confirm that in children aged 2-8 years who received LAIV last year when 2009 H1N1 strains predominated, there was essentially no coverage against 2009 H1N1 virus. This was in contrast to data from the prior 2 years and is as yet unexplained. The AAP continues to recommend that either vaccine be given and all children be immunized. That may be especially important this year as the influenza season started early. Disease will likely have been widespread by Christmas in many parts of the United States, and it looks like influenza A H3N2 strains will be most commonly noted. So the good news for young children who received LAIV is that 2009 H1N1 strains so far have not been seen this year. The bad news is that there are two H3N2 strains circulating, and potentially only one will be covered by the 2014-2015 seasonal vaccine. Staffing your office and hospital for a likely high census respiratory viral season is going to be essential.
2. The largest U.S. outbreak ever of enterovirus (EV) D-68 respiratory infection occurred between August and October of 2014. This virus – which had been identified in 1962 but was rarely described over the next 36 years except in small clusters of disease – was reported in nearly every state and characterized by unusually severe respiratory tract infection. Many, but not all children, had a history of asthma or prior wheezing, and the clinical presentation was that of severe bronchospasm that was generally resistant to standard bronchodilator therapy. The spectrum of infection likely ranged from mild upper respiratory infection to severe bronchospasm with respiratory failure, and the burden of disease resulting in hospitalization was substantial at many children’s hospitals. The big question now is what will enterovirus season 2015 bring us? The good news here is that we now have a test to rapidly diagnose EV D-68, which will allow us to more clearly understand the burden of disease – and potentially to define antiviral treatment (none of the current antivirals is effective) and prevention (there is no vaccine against EV D-68).
3. The etiology of the neurologic illness, which appeared to mimic polio and presented during the same time frame during which EV D-68 was circulating, is as yet unknown. As of Nov. 26, 2014, the CDC has received reports of 90 children in 32 states who meet a case definition consistent with acute flaccid myelitis. While certain viruses – including West Nile virus, herpes virus, adenovirus, and certain enterovirus types (for example, enterovirus 71, and the classic being polio) – may cause acute flaccid paralysis and can be confirmed by detecting the virus in cerebrospinal fluid and stool, to date virus testing for all viruses, including EV D-68, has been negative in all of the patients reported. Hopefully, 2015 will be the year that will allow us to more clearly understand this neurologic illness – and this is important because so far most children have shown minimal recovery of function.
4. If you see a child (or adult) who recently traveled to the Caribbean and returns with fever, rash, and joint pain, especially with severe pain of the hands and feet, think chikungunya virus infection. As of the end of October 2014, local transmission had been identified in 37 countries or territories in the Caribbean (including Puerto Rico and the U.S. Virgin Islands), with a total of 780,206 suspected cases and over 15,000 confirmed cases reported from these areas. Consider this in contrast to the numbers from 2006 through 2011, when 117 cases of chikungunya fever were reported in returning travelers. As of Dec. 2, a total of 1,911 chikungunya virus disease cases have been reported to ArboNET from U.S. states. The mosquito that transmits chikungunya virus can bite in day and night, and prevention relies on appropriate use of mosquito repellents. Physicians should be prepared to discuss the risks of this virus with travelers who plan a trip to the Caribbean, especially those at high risk, including those with underlying medical conditions, preexisting arthritis diagnoses, and pregnant women (because of the potential risk to newborns whose mothers develop intrapartum infection).
5. And lastly, Ebola. While there were reports that Ebola virus disease had emerged in West Africa as early as December of 2013, the scope of the outbreak and extent of loss of human life has been unbelievably huge. Dr. Carrie Byington, who is the current chair of the AAP Committee on Infectious Diseases, wrote an article in AAP News in October 2014 describing the needs of children who have been impacted by Ebola virus disease (EVD). She noted that UNICEF estimated there were at that time, over 4,000 Ebola orphans in the countries most affected by EVD, including Sierra Leone, Liberia, and Guinea, and that these countries urgently needed medical infrastructure for treatment and prevention of this disease. It appears that at least two Ebola vaccines will be deployed in West Africa in 2015, and it is not a moment too soon. While cases in Liberia seemed to be decreasing, it looks like Sierra Leone cases continue to mount.
Dr. Jackson is chief of pediatric infectious diseases at Children’s Mercy Hospital, Kansas City, Mo., and professor of pediatrics at the University of Missouri–Kansas City. Dr. Jackson was a member of the AAP Committee on Infectious Diseases who wrote the AAP clinical report entitled “Guidance on Management of Asymptomatic Neonates Born to Women With Active Genital Herpes Lesions,” but said she had no other conflicts of interest to disclose. E-mail her at [email protected].
Last year, there were five predictions made that appeared to be on the money – but there is more to the story!
1. The approach to diagnosis and treatment of influenza was essential knowledge for clinicians. Last year, we started seeing influenza activity early – with disease confirmed in mid-November, peaking during the week ending December 28, 2013 and trending downward in early January 2014. Hospitalizations were most common in young and middle aged adults and the 2009 H1N1 virus predominated.
This year, again we are seeing influenza early – with nearly all states reporting at least sporadic and local activity, and several states (Alaska, Florida, Louisiana, Massachusetts, and Texas) reporting regional activity as of the week ending November 24, 2014. At my institution, we’ve already tested over 500 children and over 100 were positive – influenza A (H3N2) strains are predominating. That may be important for the two reasons you’ll read below.
2. Invasive staphylococcal disease caused by methicillin-susceptible Staphylococcus aureus (MSSA) was more common than methicillin-resistant Staphylococcus aureus (MRSA), as the national burden of MRSA disease decreased (JAMA 2014;311:1438-9). The rates of clindamycin resistance continue to be pretty steady at approximately 15%-18%, but higher for MSSA than for MRSA – a point that is important to consider when empirically treating suspected invasive staphylococcal infection.
3. Multidrug resistant uropathogens took an increasingly prominent role in 2014, requiring careful approach to diagnosis (every child treated for urinary tract infection should have an appropriately obtained urine culture with an identified pathogen) and treatment (the drug used should be based on antibiotic susceptibility testing results). Particularly concerning is the emergence of carbapenem-resistant Enterobacteriaceae, which cause infection more commonly in hospitalized patients, those with indwelling devices, and those who have received long courses of antibiotics.
4. It was an outbreak year for parechovirus (HPeV), a viral pathogen causing meningitis in very young infants. Such infants present with signs and symptoms of meningitis but rarely show CSF pleocytosis. Diagnosis relies on the detection of the virus by polymerase chain reaction testing in CSF – a test which is not routinely available in many laboratories. At my institution this season, we saw nearly as many cases of parechovirus meningitis (n = 43) as we saw cases of enterovirus meningitis (n = 63). The parechovirus virus we detected was HPeV type 3, which can cause particularly severe disease in neonates.
5. Data confirmed that making human papillomavirus (HPV) vaccine a standard recommendation increased vaccine uptake and coverage. In February of 2014, a “Dear Colleague” letter that was endorsed by six leading medical organizations encouraged providers to promote HPV vaccination by giving a strong recommendation, citing data based on research conducted by the Centers for Disease Control and Prevention. We still have a long way to go as HPV vaccine coverage for teens remains at 35% for the three-dose series while meningococcal and Tdap vaccine (both vaccines that generally receive a standard recommendation by physicians) coverage is at nearly 90%.
So for 2015, I’ll start the discussion by saying there are five major developments I did not see coming for this past year, but that will remain relevant for the year 2015!
1. In June of 2014, live attenuated influenza vaccine (LAIV) was announced by the Advisory Committee on Immunization Practices to be the preferred vaccine in children aged 2-8 years. The American Academy of Pediatrics followed with a recommendation that either inactivated influenza vaccine (IIV) or LAIV be used for children, including children aged 2-8 years – the key being to give the vaccine as soon as one had it available. What was not known then and I did not predict was that newer data would confirm that in children aged 2-8 years who received LAIV last year when 2009 H1N1 strains predominated, there was essentially no coverage against 2009 H1N1 virus. This was in contrast to data from the prior 2 years and is as yet unexplained. The AAP continues to recommend that either vaccine be given and all children be immunized. That may be especially important this year as the influenza season started early. Disease will likely have been widespread by Christmas in many parts of the United States, and it looks like influenza A H3N2 strains will be most commonly noted. So the good news for young children who received LAIV is that 2009 H1N1 strains so far have not been seen this year. The bad news is that there are two H3N2 strains circulating, and potentially only one will be covered by the 2014-2015 seasonal vaccine. Staffing your office and hospital for a likely high census respiratory viral season is going to be essential.
2. The largest U.S. outbreak ever of enterovirus (EV) D-68 respiratory infection occurred between August and October of 2014. This virus – which had been identified in 1962 but was rarely described over the next 36 years except in small clusters of disease – was reported in nearly every state and characterized by unusually severe respiratory tract infection. Many, but not all children, had a history of asthma or prior wheezing, and the clinical presentation was that of severe bronchospasm that was generally resistant to standard bronchodilator therapy. The spectrum of infection likely ranged from mild upper respiratory infection to severe bronchospasm with respiratory failure, and the burden of disease resulting in hospitalization was substantial at many children’s hospitals. The big question now is what will enterovirus season 2015 bring us? The good news here is that we now have a test to rapidly diagnose EV D-68, which will allow us to more clearly understand the burden of disease – and potentially to define antiviral treatment (none of the current antivirals is effective) and prevention (there is no vaccine against EV D-68).
3. The etiology of the neurologic illness, which appeared to mimic polio and presented during the same time frame during which EV D-68 was circulating, is as yet unknown. As of Nov. 26, 2014, the CDC has received reports of 90 children in 32 states who meet a case definition consistent with acute flaccid myelitis. While certain viruses – including West Nile virus, herpes virus, adenovirus, and certain enterovirus types (for example, enterovirus 71, and the classic being polio) – may cause acute flaccid paralysis and can be confirmed by detecting the virus in cerebrospinal fluid and stool, to date virus testing for all viruses, including EV D-68, has been negative in all of the patients reported. Hopefully, 2015 will be the year that will allow us to more clearly understand this neurologic illness – and this is important because so far most children have shown minimal recovery of function.
4. If you see a child (or adult) who recently traveled to the Caribbean and returns with fever, rash, and joint pain, especially with severe pain of the hands and feet, think chikungunya virus infection. As of the end of October 2014, local transmission had been identified in 37 countries or territories in the Caribbean (including Puerto Rico and the U.S. Virgin Islands), with a total of 780,206 suspected cases and over 15,000 confirmed cases reported from these areas. Consider this in contrast to the numbers from 2006 through 2011, when 117 cases of chikungunya fever were reported in returning travelers. As of Dec. 2, a total of 1,911 chikungunya virus disease cases have been reported to ArboNET from U.S. states. The mosquito that transmits chikungunya virus can bite in day and night, and prevention relies on appropriate use of mosquito repellents. Physicians should be prepared to discuss the risks of this virus with travelers who plan a trip to the Caribbean, especially those at high risk, including those with underlying medical conditions, preexisting arthritis diagnoses, and pregnant women (because of the potential risk to newborns whose mothers develop intrapartum infection).
5. And lastly, Ebola. While there were reports that Ebola virus disease had emerged in West Africa as early as December of 2013, the scope of the outbreak and extent of loss of human life has been unbelievably huge. Dr. Carrie Byington, who is the current chair of the AAP Committee on Infectious Diseases, wrote an article in AAP News in October 2014 describing the needs of children who have been impacted by Ebola virus disease (EVD). She noted that UNICEF estimated there were at that time, over 4,000 Ebola orphans in the countries most affected by EVD, including Sierra Leone, Liberia, and Guinea, and that these countries urgently needed medical infrastructure for treatment and prevention of this disease. It appears that at least two Ebola vaccines will be deployed in West Africa in 2015, and it is not a moment too soon. While cases in Liberia seemed to be decreasing, it looks like Sierra Leone cases continue to mount.
Dr. Jackson is chief of pediatric infectious diseases at Children’s Mercy Hospital, Kansas City, Mo., and professor of pediatrics at the University of Missouri–Kansas City. Dr. Jackson was a member of the AAP Committee on Infectious Diseases who wrote the AAP clinical report entitled “Guidance on Management of Asymptomatic Neonates Born to Women With Active Genital Herpes Lesions,” but said she had no other conflicts of interest to disclose. E-mail her at [email protected].

Hookah, snus users more likely to start smoking
Smoking water pipe tobacco, or hookahs, more than doubles the odds that a non–cigarette smoker will begin smoking within 2 years, according to a recent study. Using snus increases the risk of starting smoking by more than sixfold.
“Our study demonstrates that [water pipe tobacco] and snus use among non–cigarette smoking adolescents and young adults were longitudinally associated with subsequent cigarette smoking,” Samir S. Soneji, Ph.D., of Dartmouth University, Lebanon, N.H., and his associates reported online [JAMA Pediatr. 2014 Dec. 8 [doi:10.1001/jamapediatrics.2014.2697]).
“Yet, water pipe tobacco remains largely unregulated by the [Food and Drug Administration], and snus is less regulated than other smokeless tobacco,” Dr. Soneji and colleagues wrote. “The success of FDA tobacco regulatory control policies will depend, in part, on their ability to reduce the use of alternative tobacco products that may lead to subsequent cigarette smoking.”

The researchers interviewed 2,541 respondents between October 2010 and June 2011 and then gathered follow-up data 2 years later from 1,596 respondents. Of the original sample, 39% had never tried smoking cigarettes, and 15% were current smokers. Two thirds of follow-up respondents (1,048 of 1,596) were non–cigarette smokers at baseline: 20 of these individuals had used snus, and 71 had smoked water pipe tobacco.
At follow-up, among those who did not smoke cigarettes at baseline, 39% of hookah users had begun smoking, compared with 20% of those who had not used water pipes. Similarly, among baseline nonsmokers, 55% of snus users had begun smoking at follow-up, compared with 21% of those who did not use snus.
After accounting for sociodemographic and behavioral risk factors, those who used hookahs at baseline, compared with non–hookah users, were 2.6 times more likely to start smoking 2 years later; snus users were 3.7 times more likely than non–snus users. Similarly, hookah users were 2.5 times more likely to be current smokers and 2.6 times more likely to be higher-intensity cigarette smokers at follow-up. Snus users were 6.2 times more likely to be current smokers and 4.5 times more likely to be higher-intensity cigarette smokers.
The sociodemographic factors controlled for included age, sex, race/ethnicity, region, urbanicity, and socioeconomic status as based on maternal educational level and annual household income. Behavioral risk factors considered included smoking status of friends and parents, and respondents’ answers to questions about risk taking, sensation seeking, and binge drinking.
The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
Smoking water pipe tobacco, or hookahs, more than doubles the odds that a non–cigarette smoker will begin smoking within 2 years, according to a recent study. Using snus increases the risk of starting smoking by more than sixfold.
“Our study demonstrates that [water pipe tobacco] and snus use among non–cigarette smoking adolescents and young adults were longitudinally associated with subsequent cigarette smoking,” Samir S. Soneji, Ph.D., of Dartmouth University, Lebanon, N.H., and his associates reported online [JAMA Pediatr. 2014 Dec. 8 [doi:10.1001/jamapediatrics.2014.2697]).
“Yet, water pipe tobacco remains largely unregulated by the [Food and Drug Administration], and snus is less regulated than other smokeless tobacco,” Dr. Soneji and colleagues wrote. “The success of FDA tobacco regulatory control policies will depend, in part, on their ability to reduce the use of alternative tobacco products that may lead to subsequent cigarette smoking.”
The researchers interviewed 2,541 respondents between October 2010 and June 2011 and then gathered follow-up data 2 years later from 1,596 respondents. Of the original sample, 39% had never tried smoking cigarettes, and 15% were current smokers. Two thirds of follow-up respondents (1,048 of 1,596) were non–cigarette smokers at baseline: 20 of these individuals had used snus, and 71 had smoked water pipe tobacco.
At follow-up, among those who did not smoke cigarettes at baseline, 39% of hookah users had begun smoking, compared with 20% of those who had not used water pipes. Similarly, among baseline nonsmokers, 55% of snus users had begun smoking at follow-up, compared with 21% of those who did not use snus.
After accounting for sociodemographic and behavioral risk factors, those who used hookahs at baseline, compared with non–hookah users, were 2.6 times more likely to start smoking 2 years later; snus users were 3.7 times more likely than non–snus users. Similarly, hookah users were 2.5 times more likely to be current smokers and 2.6 times more likely to be higher-intensity cigarette smokers at follow-up. Snus users were 6.2 times more likely to be current smokers and 4.5 times more likely to be higher-intensity cigarette smokers.
The sociodemographic factors controlled for included age, sex, race/ethnicity, region, urbanicity, and socioeconomic status as based on maternal educational level and annual household income. Behavioral risk factors considered included smoking status of friends and parents, and respondents’ answers to questions about risk taking, sensation seeking, and binge drinking.
The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
Smoking water pipe tobacco, or hookahs, more than doubles the odds that a non–cigarette smoker will begin smoking within 2 years, according to a recent study. Using snus increases the risk of starting smoking by more than sixfold.
“Our study demonstrates that [water pipe tobacco] and snus use among non–cigarette smoking adolescents and young adults were longitudinally associated with subsequent cigarette smoking,” Samir S. Soneji, Ph.D., of Dartmouth University, Lebanon, N.H., and his associates reported online [JAMA Pediatr. 2014 Dec. 8 [doi:10.1001/jamapediatrics.2014.2697]).
“Yet, water pipe tobacco remains largely unregulated by the [Food and Drug Administration], and snus is less regulated than other smokeless tobacco,” Dr. Soneji and colleagues wrote. “The success of FDA tobacco regulatory control policies will depend, in part, on their ability to reduce the use of alternative tobacco products that may lead to subsequent cigarette smoking.”
The researchers interviewed 2,541 respondents between October 2010 and June 2011 and then gathered follow-up data 2 years later from 1,596 respondents. Of the original sample, 39% had never tried smoking cigarettes, and 15% were current smokers. Two thirds of follow-up respondents (1,048 of 1,596) were non–cigarette smokers at baseline: 20 of these individuals had used snus, and 71 had smoked water pipe tobacco.
At follow-up, among those who did not smoke cigarettes at baseline, 39% of hookah users had begun smoking, compared with 20% of those who had not used water pipes. Similarly, among baseline nonsmokers, 55% of snus users had begun smoking at follow-up, compared with 21% of those who did not use snus.
After accounting for sociodemographic and behavioral risk factors, those who used hookahs at baseline, compared with non–hookah users, were 2.6 times more likely to start smoking 2 years later; snus users were 3.7 times more likely than non–snus users. Similarly, hookah users were 2.5 times more likely to be current smokers and 2.6 times more likely to be higher-intensity cigarette smokers at follow-up. Snus users were 6.2 times more likely to be current smokers and 4.5 times more likely to be higher-intensity cigarette smokers.
The sociodemographic factors controlled for included age, sex, race/ethnicity, region, urbanicity, and socioeconomic status as based on maternal educational level and annual household income. Behavioral risk factors considered included smoking status of friends and parents, and respondents’ answers to questions about risk taking, sensation seeking, and binge drinking.
The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
FROM JAMA PEDIATRICS
Key clinical point: “The increasing use of novel alternative tobacco products introduces new harms to adolescents and young adults.”
Major finding: Hookah users were 2.6 times more likely to start smoking cigarettes and be high-intensity cigarette smokers; snus users were 6.2 times more likely to start smoking and 4.5 times more likely to be high-intensity smokers.
Data source: The findings are based on a prospective longitudinal study of 1,596 individuals aged 15 to 23 between October 2010 and March 2013.
Disclosures: The research was funded by the National Cancer Institute and the National Center for Advancing Translational Sciences. The authors reported no disclosures.
