User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Biopsy bests HCRT for lung fibrosis, has risks
Surgical lung biopsy performs well and is relatively safe for evaluating suspected interstitial lung diseases, but may be especially helpful in confirming the diagnosis and directing the treatment of patients with idiopathic pulmonary fibrosis with atypical signs and symptoms, researchers have found.
In patients with immune disorders or severe respiratory dysfunction, or on mechanical ventilation, clinicians should weigh the diagnostic benefits of surgical lung biopsy (SLB) against its potential risks, according to a systematic review and meta-analysis of 23 studies published between 2000 and 2014, comprising 2,148 patients. Dr. Qian Han of the Guangzhou Institute of Respiratory Disease in China led the investigative team. The findings were published in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
The meta-analysis focused on diagnostic yield of biopsy samples and postbiopsy mortality within 90 days of surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.057). The mean age of patients across the studies ranged from 36 to 62 years. The population of the meta-analysis included 1,632 (76%) who had undergone video-assisted thoracic surgery (VATS) and 268 (12.5%) who had open-lung biopsy.
Slightly more than one third (33.5%) of diagnoses involved idiopathic pulmonary fibrosis, followed by nonspecific interstitial pneumonia (12%), hypersensitivity pneumonitis (9.6%), cryptogenic organizing pneumonia (7.5%), sarcoidosis (6.8%), and connective tissue disease related to interstitial lung disease (4%).
The median diagnostic yield across all studies was 95%, ranging from 42% to 100% depending on the study. One study showed a diagnostic yield below 70%. Eight studies showed that the biopsy influenced a change in the treatment plan 42%-90% of the time. In the entire meta-analysis, treatment plans were altered for 59.5% of patients who received a specific diagnosis and in 55.2% of those without a definitive diagnosis.
“These results suggested that an alteration in treatment may not be directed by a definitive histological diagnosis and nonspecific histological results could also be useful in clinical practice,” Dr. Han said.
Eleven of the studies used CT guidance to obtain biopsies without a preference to lobe, but two studies predisposed to the right lobes had diagnostic yields of 84% and 94%. One study avoided the lingual or middle lobe, with a diagnostic yield of 97%, and another focused on the lingular lobe only, with a 100% yield. Two studies showed that biopsy samples from lingual or middle lobes had the same diagnostic yield as did those from other lobes.
With regard to diagnostic performance based on biopsy numbers, one study showed that multiple biopsies may increase the diagnostic yield. Twelve studies obtained one to three samples, and among them eight studies suggested one sample containing both lesion and normal tissue was sufficient to represent pathological changes. One study showed that multiple biopsies may increase diagnostic yield.
Of the 16 studies that provided sufficient data on mortality rates, the pooled 30- and 90-day mortality rates were 2.2% (95% CI 1.0-4.0%) and 3.4% (95% CI 1.8-5.5%), respectively. The composite postoperative mortality rate was 3.6% (95% CI 2.1%-5.5%).
In their discussion, Dr. Han and colleagues addressed the controversy surrounding lingual vs. middle lobe biopsy by noting that high-resolution CT (HRCT) can be valuable in identifying the appropriate biopsy location. While multiple studies supported the effectiveness of only one biopsy as long as it contained both normal and abnormal tissue, the researchers pointed out that future studies evaluating biopsy samples would do well to evaluate biopsy number combined with sample size.
HRCT, while highly specific, may be less sensitive than SLB in the diagnosis of idiopathic pulmonary fibrosis, they found. Two studies the meta-analysis looked at compared the diagnostic yield between SLB and HRCT; SLB finally diagnosed idiopathic pulmonary fibrosis in 75%-91% of suspected cases and in 19%-74% of cases when HRCT did not raise suspicion of the disease. “These findings suggested that HRCT, albeit highly specific, is less sensitive in the diagnosis of IPF, therefore necessitating the utility of SLB in the diagnosis of these HRCT-omitted cases,” Dr. Han said.
On the safety issue, while studies that excluded patients on mechanical ventilation reported lower mortality rates and two studies identified ventilator dependence as an independent risk factor for mortality, the investigators reported that the higher mortality rates were probably the result of a sicker patient population rather than the SLB procedure itself. They wrote that to “indiscreetly refuse” to perform SLB in these patients is “overcautious and inappropriate” given the benefits of SLB in validating diagnoses and influencing treatment plans.
Dr. Han and his colleagues reported having no relevant disclosures.
The role of surgical biopsy in the high-risk population with interstitial lung disease is well suited for surgical review because thoracic surgeons must weigh the risks, including potential mortality, and benefits when discussion options with patients and families, Dr. Katie S. Nason noted in her invited editorial commentary.

|
Dr. Katie S. Nason |
Current guidelines suggest that SLB is no longer essential for diagnosis of idiopathic pulmonary fibrosis and they now consider an HRCT scan showing unusual interstitial pneumonia (UIP) sufficient for diagnosis. “However, in the absence of diagnostic imaging criteria for UIP, specifically honeycombing, surgical lung biopsy with interpretation by an expert pathologist is necessary and should be performed to further define patients with possible UIP,” Dr. Nason wrote. “Comprehensive application of this approach will delineate circumstances in which a surgical biopsy will be more informative than an HRCT scan as well as when a surgical biopsy is not necessary.”
She called for a multi-institutional, international registry to collect and better understand data on the diagnostic yield and mortality after SLB for interstitial lung disease.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
The role of surgical biopsy in the high-risk population with interstitial lung disease is well suited for surgical review because thoracic surgeons must weigh the risks, including potential mortality, and benefits when discussion options with patients and families, Dr. Katie S. Nason noted in her invited editorial commentary.
|
|
Dr. Katie S. Nason |
Current guidelines suggest that SLB is no longer essential for diagnosis of idiopathic pulmonary fibrosis and they now consider an HRCT scan showing unusual interstitial pneumonia (UIP) sufficient for diagnosis. “However, in the absence of diagnostic imaging criteria for UIP, specifically honeycombing, surgical lung biopsy with interpretation by an expert pathologist is necessary and should be performed to further define patients with possible UIP,” Dr. Nason wrote. “Comprehensive application of this approach will delineate circumstances in which a surgical biopsy will be more informative than an HRCT scan as well as when a surgical biopsy is not necessary.”
She called for a multi-institutional, international registry to collect and better understand data on the diagnostic yield and mortality after SLB for interstitial lung disease.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
The role of surgical biopsy in the high-risk population with interstitial lung disease is well suited for surgical review because thoracic surgeons must weigh the risks, including potential mortality, and benefits when discussion options with patients and families, Dr. Katie S. Nason noted in her invited editorial commentary.
|
|
Dr. Katie S. Nason |
Current guidelines suggest that SLB is no longer essential for diagnosis of idiopathic pulmonary fibrosis and they now consider an HRCT scan showing unusual interstitial pneumonia (UIP) sufficient for diagnosis. “However, in the absence of diagnostic imaging criteria for UIP, specifically honeycombing, surgical lung biopsy with interpretation by an expert pathologist is necessary and should be performed to further define patients with possible UIP,” Dr. Nason wrote. “Comprehensive application of this approach will delineate circumstances in which a surgical biopsy will be more informative than an HRCT scan as well as when a surgical biopsy is not necessary.”
She called for a multi-institutional, international registry to collect and better understand data on the diagnostic yield and mortality after SLB for interstitial lung disease.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
Surgical lung biopsy performs well and is relatively safe for evaluating suspected interstitial lung diseases, but may be especially helpful in confirming the diagnosis and directing the treatment of patients with idiopathic pulmonary fibrosis with atypical signs and symptoms, researchers have found.
In patients with immune disorders or severe respiratory dysfunction, or on mechanical ventilation, clinicians should weigh the diagnostic benefits of surgical lung biopsy (SLB) against its potential risks, according to a systematic review and meta-analysis of 23 studies published between 2000 and 2014, comprising 2,148 patients. Dr. Qian Han of the Guangzhou Institute of Respiratory Disease in China led the investigative team. The findings were published in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
The meta-analysis focused on diagnostic yield of biopsy samples and postbiopsy mortality within 90 days of surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.057). The mean age of patients across the studies ranged from 36 to 62 years. The population of the meta-analysis included 1,632 (76%) who had undergone video-assisted thoracic surgery (VATS) and 268 (12.5%) who had open-lung biopsy.
Slightly more than one third (33.5%) of diagnoses involved idiopathic pulmonary fibrosis, followed by nonspecific interstitial pneumonia (12%), hypersensitivity pneumonitis (9.6%), cryptogenic organizing pneumonia (7.5%), sarcoidosis (6.8%), and connective tissue disease related to interstitial lung disease (4%).
The median diagnostic yield across all studies was 95%, ranging from 42% to 100% depending on the study. One study showed a diagnostic yield below 70%. Eight studies showed that the biopsy influenced a change in the treatment plan 42%-90% of the time. In the entire meta-analysis, treatment plans were altered for 59.5% of patients who received a specific diagnosis and in 55.2% of those without a definitive diagnosis.
“These results suggested that an alteration in treatment may not be directed by a definitive histological diagnosis and nonspecific histological results could also be useful in clinical practice,” Dr. Han said.
Eleven of the studies used CT guidance to obtain biopsies without a preference to lobe, but two studies predisposed to the right lobes had diagnostic yields of 84% and 94%. One study avoided the lingual or middle lobe, with a diagnostic yield of 97%, and another focused on the lingular lobe only, with a 100% yield. Two studies showed that biopsy samples from lingual or middle lobes had the same diagnostic yield as did those from other lobes.
With regard to diagnostic performance based on biopsy numbers, one study showed that multiple biopsies may increase the diagnostic yield. Twelve studies obtained one to three samples, and among them eight studies suggested one sample containing both lesion and normal tissue was sufficient to represent pathological changes. One study showed that multiple biopsies may increase diagnostic yield.
Of the 16 studies that provided sufficient data on mortality rates, the pooled 30- and 90-day mortality rates were 2.2% (95% CI 1.0-4.0%) and 3.4% (95% CI 1.8-5.5%), respectively. The composite postoperative mortality rate was 3.6% (95% CI 2.1%-5.5%).
In their discussion, Dr. Han and colleagues addressed the controversy surrounding lingual vs. middle lobe biopsy by noting that high-resolution CT (HRCT) can be valuable in identifying the appropriate biopsy location. While multiple studies supported the effectiveness of only one biopsy as long as it contained both normal and abnormal tissue, the researchers pointed out that future studies evaluating biopsy samples would do well to evaluate biopsy number combined with sample size.
HRCT, while highly specific, may be less sensitive than SLB in the diagnosis of idiopathic pulmonary fibrosis, they found. Two studies the meta-analysis looked at compared the diagnostic yield between SLB and HRCT; SLB finally diagnosed idiopathic pulmonary fibrosis in 75%-91% of suspected cases and in 19%-74% of cases when HRCT did not raise suspicion of the disease. “These findings suggested that HRCT, albeit highly specific, is less sensitive in the diagnosis of IPF, therefore necessitating the utility of SLB in the diagnosis of these HRCT-omitted cases,” Dr. Han said.
On the safety issue, while studies that excluded patients on mechanical ventilation reported lower mortality rates and two studies identified ventilator dependence as an independent risk factor for mortality, the investigators reported that the higher mortality rates were probably the result of a sicker patient population rather than the SLB procedure itself. They wrote that to “indiscreetly refuse” to perform SLB in these patients is “overcautious and inappropriate” given the benefits of SLB in validating diagnoses and influencing treatment plans.
Dr. Han and his colleagues reported having no relevant disclosures.
Surgical lung biopsy performs well and is relatively safe for evaluating suspected interstitial lung diseases, but may be especially helpful in confirming the diagnosis and directing the treatment of patients with idiopathic pulmonary fibrosis with atypical signs and symptoms, researchers have found.
In patients with immune disorders or severe respiratory dysfunction, or on mechanical ventilation, clinicians should weigh the diagnostic benefits of surgical lung biopsy (SLB) against its potential risks, according to a systematic review and meta-analysis of 23 studies published between 2000 and 2014, comprising 2,148 patients. Dr. Qian Han of the Guangzhou Institute of Respiratory Disease in China led the investigative team. The findings were published in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
The meta-analysis focused on diagnostic yield of biopsy samples and postbiopsy mortality within 90 days of surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.057). The mean age of patients across the studies ranged from 36 to 62 years. The population of the meta-analysis included 1,632 (76%) who had undergone video-assisted thoracic surgery (VATS) and 268 (12.5%) who had open-lung biopsy.
Slightly more than one third (33.5%) of diagnoses involved idiopathic pulmonary fibrosis, followed by nonspecific interstitial pneumonia (12%), hypersensitivity pneumonitis (9.6%), cryptogenic organizing pneumonia (7.5%), sarcoidosis (6.8%), and connective tissue disease related to interstitial lung disease (4%).
The median diagnostic yield across all studies was 95%, ranging from 42% to 100% depending on the study. One study showed a diagnostic yield below 70%. Eight studies showed that the biopsy influenced a change in the treatment plan 42%-90% of the time. In the entire meta-analysis, treatment plans were altered for 59.5% of patients who received a specific diagnosis and in 55.2% of those without a definitive diagnosis.
“These results suggested that an alteration in treatment may not be directed by a definitive histological diagnosis and nonspecific histological results could also be useful in clinical practice,” Dr. Han said.
Eleven of the studies used CT guidance to obtain biopsies without a preference to lobe, but two studies predisposed to the right lobes had diagnostic yields of 84% and 94%. One study avoided the lingual or middle lobe, with a diagnostic yield of 97%, and another focused on the lingular lobe only, with a 100% yield. Two studies showed that biopsy samples from lingual or middle lobes had the same diagnostic yield as did those from other lobes.
With regard to diagnostic performance based on biopsy numbers, one study showed that multiple biopsies may increase the diagnostic yield. Twelve studies obtained one to three samples, and among them eight studies suggested one sample containing both lesion and normal tissue was sufficient to represent pathological changes. One study showed that multiple biopsies may increase diagnostic yield.
Of the 16 studies that provided sufficient data on mortality rates, the pooled 30- and 90-day mortality rates were 2.2% (95% CI 1.0-4.0%) and 3.4% (95% CI 1.8-5.5%), respectively. The composite postoperative mortality rate was 3.6% (95% CI 2.1%-5.5%).
In their discussion, Dr. Han and colleagues addressed the controversy surrounding lingual vs. middle lobe biopsy by noting that high-resolution CT (HRCT) can be valuable in identifying the appropriate biopsy location. While multiple studies supported the effectiveness of only one biopsy as long as it contained both normal and abnormal tissue, the researchers pointed out that future studies evaluating biopsy samples would do well to evaluate biopsy number combined with sample size.
HRCT, while highly specific, may be less sensitive than SLB in the diagnosis of idiopathic pulmonary fibrosis, they found. Two studies the meta-analysis looked at compared the diagnostic yield between SLB and HRCT; SLB finally diagnosed idiopathic pulmonary fibrosis in 75%-91% of suspected cases and in 19%-74% of cases when HRCT did not raise suspicion of the disease. “These findings suggested that HRCT, albeit highly specific, is less sensitive in the diagnosis of IPF, therefore necessitating the utility of SLB in the diagnosis of these HRCT-omitted cases,” Dr. Han said.
On the safety issue, while studies that excluded patients on mechanical ventilation reported lower mortality rates and two studies identified ventilator dependence as an independent risk factor for mortality, the investigators reported that the higher mortality rates were probably the result of a sicker patient population rather than the SLB procedure itself. They wrote that to “indiscreetly refuse” to perform SLB in these patients is “overcautious and inappropriate” given the benefits of SLB in validating diagnoses and influencing treatment plans.
Dr. Han and his colleagues reported having no relevant disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgical lung biopsy is helpful to confirm interstitial lung disease in patients with unique signs and symptoms, but the benefit of SLB should be balanced against the risks in patients with more severe disease.
Major finding: In two studies that compared the diagnostic yield between SLB and HRCT; SLB diagnosed idiopathic pulmonary fibrosis in 75%-91% of suspected cases and in 19%-74% of cases when HRCT did not raise suspicion of the disease.
Data source: Meta-analysis of 23 studies published between 2000 and 2014 and involving 2,148 patients.
Disclosures: The National Natural Science Foundation of China Young Investigator Funding supported the work. The investigators reported having no conflicts of interest.

Class of 2015: New drugs projected to earn billions and billions
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
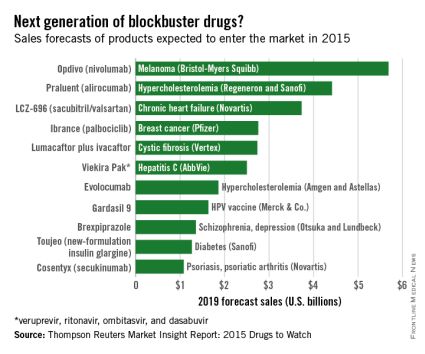
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Of all drugs to be released in 2015, the melanoma drug Opdivo (nivolumab) is expected to have the brightest future, according to a report from Thomson Reuters.
With sales forecast to reach nearly $5.7 billion by 2019, Opdivo is at the head of a large 2015 “blockbuster” drug class. Opdivo is followed by a pair of drugs for the cardiovascular system: Praluent (alirocumab) for hypercholesterolemia with projected sales of $4.4 billion and LCZ-696 (sacubitril and valsartan) for chronic heart failure with projected 2019 sales of $3.7 billion, Thomson Reuters said.
With estimated sales of $2.8 billion, the breast cancer drug Ibrance (palbociclib) is the second oncologic drug making the blockbuster list, with the first noncancer or non-CV drug – lumacaftor plus ivacaftor for cystic fibrosis – rounding out the Top 5 with projected sales of $2.7 billion by 2019.
Next comes Viekira Pak (ombitasvir, paritaprevir, and ritonavir tablets, copackaged with dasabuvir tablets), a hepatitis C virus drug with estimated 2019 sales of $2.5 billion, followed by the hypercholesterolemia/hyperlipidemia drug evolocumab, with projected sales of $1.9 billion. This $2.5 billion disparity between evolocumab and Praluent may be explained by Praluent’s arrival on the market a month sooner, and also because Praluent had a reduced rate of cardiac death, heart attack, and stroke in a phase III trial, a point likely to be relevant to most patients, according to the report.
Overall, 11 drugs are expected to reach $1 billion in sales by 2019, many more than the three blockbusters predicted from the 2014 stock of drugs. However, the two highest-selling new drugs from 2014, Sovaldi (sofosbuvir) and Harvoni (sofosbuvir plus ledipasvir) – both HCV drugs – are each predicted to reach sales of more than $10 billion by 2017, far exceeding anything from 2015, the report said.
The Thomson Reuters Market Insight Report used data collected from 2013 through early February 2015.
Low-risk PE patients can be treated as outpatients
Patients with pulmonary embolism considered as low risk can be treated successfully as outpatients, according to a research letter by Dr. Margaret Fang and her associates.
Of nearly 5,000 patients included in the study, 494 were discharged from emergency departments. The proportion of PE patients discharged increased from 5.6% in 2004 to 11.1% in 2010. Just under 19% of those discharged visited the ED within 30 days, and 7.9% were hospitalized. Eleven patients were diagnosed with hemorrhage within 30 days, and there were two deaths within 90 days.
“Although still representing relatively few patients with PE, the proportion of discharges from ED settings nearly doubled during the 7-year study. Shifting appropriate patients to outpatient treatment may have benefits in terms of improved quality of life, enhanced physical and social functioning, and reduced costs of medical care,” the investigators said.
Find the full study in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2015.0936).
Patients with pulmonary embolism considered as low risk can be treated successfully as outpatients, according to a research letter by Dr. Margaret Fang and her associates.
Of nearly 5,000 patients included in the study, 494 were discharged from emergency departments. The proportion of PE patients discharged increased from 5.6% in 2004 to 11.1% in 2010. Just under 19% of those discharged visited the ED within 30 days, and 7.9% were hospitalized. Eleven patients were diagnosed with hemorrhage within 30 days, and there were two deaths within 90 days.
“Although still representing relatively few patients with PE, the proportion of discharges from ED settings nearly doubled during the 7-year study. Shifting appropriate patients to outpatient treatment may have benefits in terms of improved quality of life, enhanced physical and social functioning, and reduced costs of medical care,” the investigators said.
Find the full study in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2015.0936).
Patients with pulmonary embolism considered as low risk can be treated successfully as outpatients, according to a research letter by Dr. Margaret Fang and her associates.
Of nearly 5,000 patients included in the study, 494 were discharged from emergency departments. The proportion of PE patients discharged increased from 5.6% in 2004 to 11.1% in 2010. Just under 19% of those discharged visited the ED within 30 days, and 7.9% were hospitalized. Eleven patients were diagnosed with hemorrhage within 30 days, and there were two deaths within 90 days.
“Although still representing relatively few patients with PE, the proportion of discharges from ED settings nearly doubled during the 7-year study. Shifting appropriate patients to outpatient treatment may have benefits in terms of improved quality of life, enhanced physical and social functioning, and reduced costs of medical care,” the investigators said.
Find the full study in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2015.0936).
Send kids home 2 hours after food challenge testing
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
HOUSTON – Food-allergic children undergoing a double-blind, placebo-controlled food challenge test can safely be discharged home after 2 hours provided they haven’t experienced a severe immediate reaction in the interim, according to a large retrospective Dutch study.
Late reactions are unpredictable and very seldom severe, Jacquelien Saleh-Langenberg reported at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
She presented a study of 1,142 children who underwent double-blind, placebo-controlled food challenge testing at a tertiary clinic at the University of Groningen in the Netherlands, where she is a combined medical student and Ph.D. candidate. The food-allergic children were challenged with cow’s milk, peanut, cashew, hazelnut, and egg.
A total of 400 children developed late reactions: 20.8% of children reported late reactions only on an active challenge day, 9.6% only on a placebo challenge day, and 4.6% reported reactions on both active and placebo challenge days.
Of particular interest was the finding that 89 subjects developed isolated reactions on an active challenge day and 92 did so on a placebo challenge day.
“Isolated late reactions occurred with comparable frequency after active and placebo challenge and are thus unlikely to be a real phenomenon,” Ms. Saleh-Langenberg concluded.
Late reactions were manifest as gastrointestinal symptoms in 45% of cases and cutaneous symptoms in about one-third, with respiratory symptoms accounting for most of the remainder. Ninety-eight percent of late reactions were rated as mild to moderate, having a score of 1-6 on a 12-point severity scale.
The investigators developed a predictive model for late reactions occurring on an active challenge day. It proved to have little practical value, though. The model, which included age, allergic rhinitis, severity of any immediate reaction, and hazelnut allergy, explained a mere 8% of the variance in the incidence of late reactions.
When late reactions occurred on an active challenge day, they did so a mean of 3.5 hours after testing. When they occurred on a placebo challenge day, they happened a mean of 4 hours after the challenge. The reactions took an average of 2 hours and 1 hour, respectively, to disappear.
Ms. Saleh-Langenberg reported no conflicts of interest with regard to this university-supported study.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: Food-allergic children who don’t experience a severe immediate reaction following double-blind, placebo-controlled food challenges can safely be discharged home 2 hours post-testing.
Major finding: No severe late reactions occurred in a large cohort of children who underwent double-blind, placebo-controlled food challenges with cow’s milk, cashew, peanut, egg, and hazelnut.
Data source: This retrospective study included 1,142 Dutch children who underwent double-blind, placebo-controlled food challenges at a university clinic.
Disclosures: The presenter reported no conflicts of interest with regard to this university-supported study.

Aspirin desensitization making headway in U.S.
HOUSTON – About 63% of allergists and fellows in training perform aspirin desensitization for aspirin-exacerbated respiratory disease, according to a national survey.
That figure is lower than it should be, given the wealth of published evidence that aspirin desensitization is a safe and effective component of the treatment of aspirin-exacerbated respiratory disease (AERD), Dr. Jeremy D. Waldram asserted in presenting the survey findings at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Moreover, the figure likely overcalls the true rate, since participation in the survey was voluntary and fans of aspirin desensitization were probably more inclined to complete the 16-item questionnaire, added Dr. Waldram, a fellow in allergy and immunology at the Scripps Clinic in San Diego.

Was he surprised to find that aspirin desensitization isn’t more widely utilized?
“I think the number that surprised me more was that among the 37.5% of allergists who don’t do aspirin desensitization, almost 30% of them don’t even refer their patients to others who do the procedure. We don’t know why they don’t refer out; it wasn’t a question included in the survey. Perhaps they see patients who are of a less severe phenotype,” he said in an interview.
The 684 survey responses represented a 15% response rate. While 37.5% of respondents indicated they don’t perform aspirin desensitization, 73% of those who reported doing the procedure said they do an average of 1-5 cases annually.
Among allergists who don’t perform aspirin desensitization, safety concerns were the leading reason cited. Indeed, 70% of those who don’t do aspirin desensitization indicated safety risks were the main reason. More than one reason could be given, however, and 30% of allergists cited poor compensation for the procedure as a deterrent, nearly 60% said the logistics of monitoring care were too onerous, and one-third said they didn’t perform aspirin desensitization because they hadn’t been trained to do it.
Of allergists who reported doing aspirin desensitization, 52% perform the procedure in an outpatient setting unattached to a hospital. Another 21% do so in an outpatient clinic that’s physically attached to a hospital.
Within the past 5 years, 9% of respondents said that they’ve had a patient react severely to aspirin desensitization, requiring an unanticipated transfer to a higher level of care. That’s contrary to the experience among allergists at the Scripps Clinic, which is widely credited with pioneering the outpatient approach.
“We essentially do all our aspirin desensitizations for AERD in the outpatient setting. In 1,500 treated patients we’ve never had one that we had to transfer to a higher level of care. We don’t have any special setup. It’s a typical outpatient clinic. We usually don’t start IVs or do anything above and beyond,” Dr. Waldram said.
While 26% of respondents reported they generally recommend aspirin desensitization immediately upon identifying a patient history that supports the diagnosis of AERD, another 54% said they usually recommend the procedure to patients only after they’ve failed to improve on typical medical therapy.
Twenty percent of physicians rated aspirin desensitization as “extremely helpful for the majority of patients,” another 49% said they find it most beneficial as an adjuvant to ongoing medical therapy.
Forty-four percent of allergists who perform aspirin desensitization reported that they learned to do the procedure during fellowship training. Fourteen percent said they learned to the procedure at an annual meeting, and 36% picked it up by reviewing the relevant literature.
Several allergists commented that had Dr. Waldram’s survey been conducted even a couple of years ago the rate of utilization of aspirin desensitization would have been far lower. They interpreted his reported 62.5% rate as a sign of progress. Dr. Waldram said he believes the key to further boosting utilization of aspirin desensitization lies in increasing exposure to the procedure during fellowship training. He noted that internal medicine-trained fellows who responded to the survey had a significantly higher aspirin desensitization utilization rate than those who came to their allergy fellowship with a background in pediatrics.
The hallmarks of AERD are difficult-to-treat nasal polyps, chronic eosinophilic sinusitis, and asthma in a patient with sensitivity to aspirin and other COX-1 inhibitors.
Dr. Waldram reported having no financial conflicts with regard to his study, which was conducted free of commercial support.
HOUSTON – About 63% of allergists and fellows in training perform aspirin desensitization for aspirin-exacerbated respiratory disease, according to a national survey.
That figure is lower than it should be, given the wealth of published evidence that aspirin desensitization is a safe and effective component of the treatment of aspirin-exacerbated respiratory disease (AERD), Dr. Jeremy D. Waldram asserted in presenting the survey findings at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Moreover, the figure likely overcalls the true rate, since participation in the survey was voluntary and fans of aspirin desensitization were probably more inclined to complete the 16-item questionnaire, added Dr. Waldram, a fellow in allergy and immunology at the Scripps Clinic in San Diego.
Was he surprised to find that aspirin desensitization isn’t more widely utilized?
“I think the number that surprised me more was that among the 37.5% of allergists who don’t do aspirin desensitization, almost 30% of them don’t even refer their patients to others who do the procedure. We don’t know why they don’t refer out; it wasn’t a question included in the survey. Perhaps they see patients who are of a less severe phenotype,” he said in an interview.
The 684 survey responses represented a 15% response rate. While 37.5% of respondents indicated they don’t perform aspirin desensitization, 73% of those who reported doing the procedure said they do an average of 1-5 cases annually.
Among allergists who don’t perform aspirin desensitization, safety concerns were the leading reason cited. Indeed, 70% of those who don’t do aspirin desensitization indicated safety risks were the main reason. More than one reason could be given, however, and 30% of allergists cited poor compensation for the procedure as a deterrent, nearly 60% said the logistics of monitoring care were too onerous, and one-third said they didn’t perform aspirin desensitization because they hadn’t been trained to do it.
Of allergists who reported doing aspirin desensitization, 52% perform the procedure in an outpatient setting unattached to a hospital. Another 21% do so in an outpatient clinic that’s physically attached to a hospital.
Within the past 5 years, 9% of respondents said that they’ve had a patient react severely to aspirin desensitization, requiring an unanticipated transfer to a higher level of care. That’s contrary to the experience among allergists at the Scripps Clinic, which is widely credited with pioneering the outpatient approach.
“We essentially do all our aspirin desensitizations for AERD in the outpatient setting. In 1,500 treated patients we’ve never had one that we had to transfer to a higher level of care. We don’t have any special setup. It’s a typical outpatient clinic. We usually don’t start IVs or do anything above and beyond,” Dr. Waldram said.
While 26% of respondents reported they generally recommend aspirin desensitization immediately upon identifying a patient history that supports the diagnosis of AERD, another 54% said they usually recommend the procedure to patients only after they’ve failed to improve on typical medical therapy.
Twenty percent of physicians rated aspirin desensitization as “extremely helpful for the majority of patients,” another 49% said they find it most beneficial as an adjuvant to ongoing medical therapy.
Forty-four percent of allergists who perform aspirin desensitization reported that they learned to do the procedure during fellowship training. Fourteen percent said they learned to the procedure at an annual meeting, and 36% picked it up by reviewing the relevant literature.
Several allergists commented that had Dr. Waldram’s survey been conducted even a couple of years ago the rate of utilization of aspirin desensitization would have been far lower. They interpreted his reported 62.5% rate as a sign of progress. Dr. Waldram said he believes the key to further boosting utilization of aspirin desensitization lies in increasing exposure to the procedure during fellowship training. He noted that internal medicine-trained fellows who responded to the survey had a significantly higher aspirin desensitization utilization rate than those who came to their allergy fellowship with a background in pediatrics.
The hallmarks of AERD are difficult-to-treat nasal polyps, chronic eosinophilic sinusitis, and asthma in a patient with sensitivity to aspirin and other COX-1 inhibitors.
Dr. Waldram reported having no financial conflicts with regard to his study, which was conducted free of commercial support.
HOUSTON – About 63% of allergists and fellows in training perform aspirin desensitization for aspirin-exacerbated respiratory disease, according to a national survey.
That figure is lower than it should be, given the wealth of published evidence that aspirin desensitization is a safe and effective component of the treatment of aspirin-exacerbated respiratory disease (AERD), Dr. Jeremy D. Waldram asserted in presenting the survey findings at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Moreover, the figure likely overcalls the true rate, since participation in the survey was voluntary and fans of aspirin desensitization were probably more inclined to complete the 16-item questionnaire, added Dr. Waldram, a fellow in allergy and immunology at the Scripps Clinic in San Diego.
Was he surprised to find that aspirin desensitization isn’t more widely utilized?
“I think the number that surprised me more was that among the 37.5% of allergists who don’t do aspirin desensitization, almost 30% of them don’t even refer their patients to others who do the procedure. We don’t know why they don’t refer out; it wasn’t a question included in the survey. Perhaps they see patients who are of a less severe phenotype,” he said in an interview.
The 684 survey responses represented a 15% response rate. While 37.5% of respondents indicated they don’t perform aspirin desensitization, 73% of those who reported doing the procedure said they do an average of 1-5 cases annually.
Among allergists who don’t perform aspirin desensitization, safety concerns were the leading reason cited. Indeed, 70% of those who don’t do aspirin desensitization indicated safety risks were the main reason. More than one reason could be given, however, and 30% of allergists cited poor compensation for the procedure as a deterrent, nearly 60% said the logistics of monitoring care were too onerous, and one-third said they didn’t perform aspirin desensitization because they hadn’t been trained to do it.
Of allergists who reported doing aspirin desensitization, 52% perform the procedure in an outpatient setting unattached to a hospital. Another 21% do so in an outpatient clinic that’s physically attached to a hospital.
Within the past 5 years, 9% of respondents said that they’ve had a patient react severely to aspirin desensitization, requiring an unanticipated transfer to a higher level of care. That’s contrary to the experience among allergists at the Scripps Clinic, which is widely credited with pioneering the outpatient approach.
“We essentially do all our aspirin desensitizations for AERD in the outpatient setting. In 1,500 treated patients we’ve never had one that we had to transfer to a higher level of care. We don’t have any special setup. It’s a typical outpatient clinic. We usually don’t start IVs or do anything above and beyond,” Dr. Waldram said.
While 26% of respondents reported they generally recommend aspirin desensitization immediately upon identifying a patient history that supports the diagnosis of AERD, another 54% said they usually recommend the procedure to patients only after they’ve failed to improve on typical medical therapy.
Twenty percent of physicians rated aspirin desensitization as “extremely helpful for the majority of patients,” another 49% said they find it most beneficial as an adjuvant to ongoing medical therapy.
Forty-four percent of allergists who perform aspirin desensitization reported that they learned to do the procedure during fellowship training. Fourteen percent said they learned to the procedure at an annual meeting, and 36% picked it up by reviewing the relevant literature.
Several allergists commented that had Dr. Waldram’s survey been conducted even a couple of years ago the rate of utilization of aspirin desensitization would have been far lower. They interpreted his reported 62.5% rate as a sign of progress. Dr. Waldram said he believes the key to further boosting utilization of aspirin desensitization lies in increasing exposure to the procedure during fellowship training. He noted that internal medicine-trained fellows who responded to the survey had a significantly higher aspirin desensitization utilization rate than those who came to their allergy fellowship with a background in pediatrics.
The hallmarks of AERD are difficult-to-treat nasal polyps, chronic eosinophilic sinusitis, and asthma in a patient with sensitivity to aspirin and other COX-1 inhibitors.
Dr. Waldram reported having no financial conflicts with regard to his study, which was conducted free of commercial support.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: Aspirin desensitization for patients with aspirin-exacerbated respiratory disease is catching on among U.S. allergists.
Major finding: Roughly 63% of allergists and allergy fellows who responded to a national survey indicated they perform aspirin desensitization for aspirin-exacerbated respiratory disease.
Data source: This was a 16-question survey of aspirin desensitization practices among U.S. allergists and allergy fellows. The national survey drew 684 responses.
Disclosures: The presenter reported having no financial conflicts with regard to his study, which was funded without commercial support.
Chronic illness more common in 9/11 first responders
Emergency medical workers who worked on-site immediately after the 9/11 attacks in New York are at significantly higher risk of chronic illness than employees who did not work there, according to Jennifer Yip and her associates.
Incidence of both gastroesophageal reflux disease and obstructive airways disease was 12%, with rhinosinusitis incidence at 11%. On-site EMS workers had depression rates of 17% and posttraumatic stress disorder rates of 7%. On-site EMS workers were four times more likely to have GERD or rhinosinusitis, seven times more likely to have PTSD, and twice as likely to have depression as a similar group of workers who were not at the World Trade Center.
The study findings demonstrate “that the burden of disease over the 12-year study period was substantial, highlighting the need for continued monitoring and treatment of EMS workers,” the investigators concluded.Find the full study in Occupational and Environmental Medicine (doi:10.1136/oemed-2014-102601).
Emergency medical workers who worked on-site immediately after the 9/11 attacks in New York are at significantly higher risk of chronic illness than employees who did not work there, according to Jennifer Yip and her associates.
Incidence of both gastroesophageal reflux disease and obstructive airways disease was 12%, with rhinosinusitis incidence at 11%. On-site EMS workers had depression rates of 17% and posttraumatic stress disorder rates of 7%. On-site EMS workers were four times more likely to have GERD or rhinosinusitis, seven times more likely to have PTSD, and twice as likely to have depression as a similar group of workers who were not at the World Trade Center.
The study findings demonstrate “that the burden of disease over the 12-year study period was substantial, highlighting the need for continued monitoring and treatment of EMS workers,” the investigators concluded.Find the full study in Occupational and Environmental Medicine (doi:10.1136/oemed-2014-102601).
Emergency medical workers who worked on-site immediately after the 9/11 attacks in New York are at significantly higher risk of chronic illness than employees who did not work there, according to Jennifer Yip and her associates.
Incidence of both gastroesophageal reflux disease and obstructive airways disease was 12%, with rhinosinusitis incidence at 11%. On-site EMS workers had depression rates of 17% and posttraumatic stress disorder rates of 7%. On-site EMS workers were four times more likely to have GERD or rhinosinusitis, seven times more likely to have PTSD, and twice as likely to have depression as a similar group of workers who were not at the World Trade Center.
The study findings demonstrate “that the burden of disease over the 12-year study period was substantial, highlighting the need for continued monitoring and treatment of EMS workers,” the investigators concluded.Find the full study in Occupational and Environmental Medicine (doi:10.1136/oemed-2014-102601).
Respiratory Disorders Most Common Cause of Childhood Hospitalization
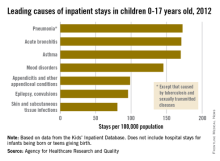
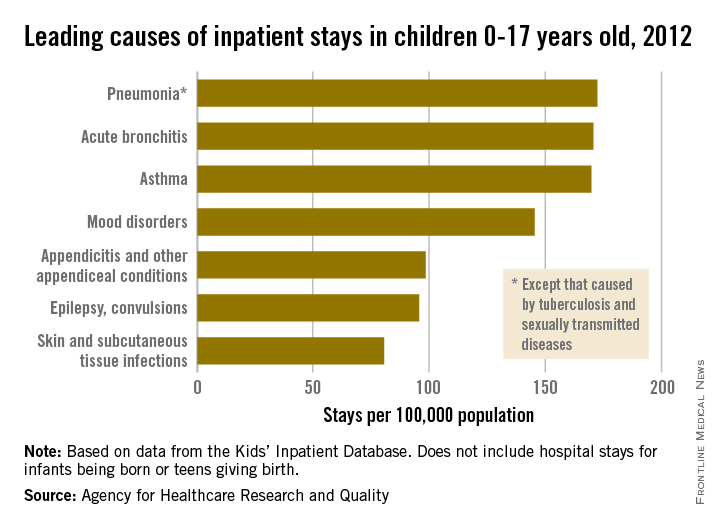
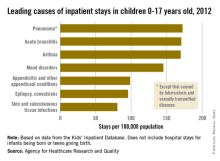
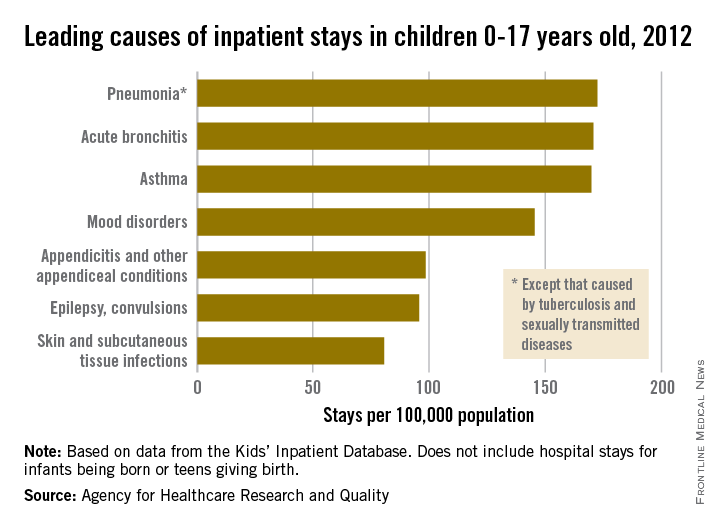
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
Respiratory disorders most common cause of childhood hospitalization
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
The three most common causes of nonneonatal and nonmaternal hospitalization in 2012 for children under 18 years were all respiratory disorders, according to a report from the Agency for Healthcare Research and Quality.
Pneumonia was the most common cause of hospitalization in children, with stays occurring at a rate of 169/100,000 population. There was very little difference in the rate between pneumonia and the next two most common diagnoses, acute bronchitis and asthma, which occurred at a rate of 168/100,000 and 167/100,000, respectively.
Mood disorders were the most common nonrespiratory and nonmaternal hospitalization diagnosis, with a hospital admission incidence of 144/100,000 population. This was followed by appendicitis (97/100,000), epilepsy and convulsions (95/100,000), and skin and subcutaneous tissue infections (80/100,000). The overall rate of hospitalization in children under age 18 years for nonneonatal and nonmaternal diagnoses was just over 2,500/100,000.
The incidence of six of the seven most common causes of hospitalization, and all but 1 of the 24 reported diagnostic categories, either decreased or remained steady from 2000 to 2012. Only skin and subcutaneous tissue conditions saw a significant increase in that time period. “Understanding the reasons why children are hospitalized and examining trends over time is critical to inform clinical practice and health policy,” the researchers commented.
The AHRQ report used data collected by the Healthcare Cost and Utilization Project Kids’ Inpatient Database.
Bronchial thermoplasty gains momentum for severe asthma
HOUSTON – Bronchial thermoplasty has emerged as an important treatment option for patients with severe asthma at specialized centers, Dr. Mario Castro observed at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The most recent international European Respiratory Society/American Thoracic Society practice guidelines on severe asthma recommend that bronchial thermoplasty for severe persistent asthma be utilized only in the setting of a clinical study or independent registry. The guidelines cited “very low confidence” in the available estimates of the novel treatment’s longer-term benefits and harms, as well as the lack of data regarding the phenotypes of asthma patients most likely to benefit (Eur. Respir. J. 2014 Feb;43:343-73).

Dr. Castro, a member of the task force that developed the ERS/ATS guidelines, said the group’s cautious stance was appropriate given the evidence available at the time of deliberations. However, at the AAAAI meeting, he highlighted more recent study results that address many of the task force’s concerns and that he said might lead to a more enthusiastic recommendation for bronchial thermoplasty in future guidelines.
One key piece of evidence unavailable to the task force comes from results reported in the 5-year prospective follow-up of 162 bronchial thermoplasty-treated patients in the international Asthma Intervention Research 2 (AIR2) trial.
“It’s quite striking that the exacerbation rate did not start to creep back up over time in this severe asthma population. We believe this study shows for the first time that this therapy may actually be a disease modifier, and that you can do this procedure in an identified population and the benefits of this one-time treatment are sustained over at least a 5-year time period,” said Dr. Castro, an AIR2 investigator and professor of pulmonary and critical care medicine and pediatrics at Washington University in St. Louis.
Compared with the baseline established during the year prior to bronchial thermoplasty, at 5 years post procedure, there was a 44% decrease in the percentage of AIR2 participants with severe exacerbations requiring oral corticosteroids, and a 48% reduction in the severe exacerbation event rate. Moreover, there was a 78% reduction in the percentage of patients with an emergency department visit for asthma and an 88% drop in the ED visit event rate (J. Allergy Clin. Immunol. 2013;132:1295-302).
With regard to safety, annual high-resolution CT scans showed no structural abnormalities from baseline to 5 years post-bronchial thermoplasty that could be attributed to the procedure. Prebronchodilator forced expiratory volume in 1 second (FEV1) values remained steady between years 1 and 5 post procedure despite an 18% decrease in the average daily dose of inhaled corticosteroids.
In a separate study, Dr. Castro and coinvestigators at Washington University identified a number of predictors of who will get the best responses to bronchial thermoplasty. This was a small study involving 42 patients with severe persistent asthma as reflected in their baseline mean inhaled corticosteroid dose of 2,185 mcg/day. Eighty percent of patients required bursts of oral corticosteroids during the year prior to the procedure. Their average baseline Asthma Quality of Life Questionnaire (AQLQ) score was 3.42. The baseline FEV1 postbronchodilator averaged 70%, with a range of 44%-121%.
Predictors of a clinically meaningful improvement in quality of life as defined by at least a 0.5-point improvement in AQLQ score 1 year post procedure included a shorter duration of asthma – 19 years, as compared with an average of 45 years in nonresponders – and a greater number of severe exacerbations during the year prior to bronchial thermoplasty.
Using another important yardstick of clinical improvement – at least a 240 mcg/day dose reduction in inhaled corticosteroids or a 2.5 mg/day decrease in oral corticosteroids at 1 year post procedure – significant predictors of benefit included older age (55 vs. 43 years), a lower baseline AQLQ score (2.4 vs. 4.0), and greater need for oral corticosteroids.
In addition, several quantitative metrics obtained through multidetector CT scans of the chest showed promise as predictors of a corticosteroid dose reduction. Responders showed less baseline air trapping, with an average of 6.1% of the lung having a density below –850 Hounsfield units, compared with 12.1% in nonresponders. Responders also had less baseline emphysema-like lung, with 3.2% of the lung having a density below –950 Hounsfield units at total lung capacity, compared with 5.8% in nonresponders, according to Dr. Castro.
This as-yet unpublished study was funded by the National Institutes of Health. AIR2 was sponsored by Boston Scientific. Dr. Castro reported research grants from the NIH, the American Lung Association, Boston Scientific, and other companies.
An estimated 5% of asthma patients are categorized as having severe disease. Bronchial thermoplasty has been approved by the FDA for the treatment of severe asthma since 2010. The outpatient procedure entails delivery of radiofrequency energy to the lungs in three sessions spaced several weeks apart.
HOUSTON – Bronchial thermoplasty has emerged as an important treatment option for patients with severe asthma at specialized centers, Dr. Mario Castro observed at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The most recent international European Respiratory Society/American Thoracic Society practice guidelines on severe asthma recommend that bronchial thermoplasty for severe persistent asthma be utilized only in the setting of a clinical study or independent registry. The guidelines cited “very low confidence” in the available estimates of the novel treatment’s longer-term benefits and harms, as well as the lack of data regarding the phenotypes of asthma patients most likely to benefit (Eur. Respir. J. 2014 Feb;43:343-73).
Dr. Castro, a member of the task force that developed the ERS/ATS guidelines, said the group’s cautious stance was appropriate given the evidence available at the time of deliberations. However, at the AAAAI meeting, he highlighted more recent study results that address many of the task force’s concerns and that he said might lead to a more enthusiastic recommendation for bronchial thermoplasty in future guidelines.
One key piece of evidence unavailable to the task force comes from results reported in the 5-year prospective follow-up of 162 bronchial thermoplasty-treated patients in the international Asthma Intervention Research 2 (AIR2) trial.
“It’s quite striking that the exacerbation rate did not start to creep back up over time in this severe asthma population. We believe this study shows for the first time that this therapy may actually be a disease modifier, and that you can do this procedure in an identified population and the benefits of this one-time treatment are sustained over at least a 5-year time period,” said Dr. Castro, an AIR2 investigator and professor of pulmonary and critical care medicine and pediatrics at Washington University in St. Louis.
Compared with the baseline established during the year prior to bronchial thermoplasty, at 5 years post procedure, there was a 44% decrease in the percentage of AIR2 participants with severe exacerbations requiring oral corticosteroids, and a 48% reduction in the severe exacerbation event rate. Moreover, there was a 78% reduction in the percentage of patients with an emergency department visit for asthma and an 88% drop in the ED visit event rate (J. Allergy Clin. Immunol. 2013;132:1295-302).
With regard to safety, annual high-resolution CT scans showed no structural abnormalities from baseline to 5 years post-bronchial thermoplasty that could be attributed to the procedure. Prebronchodilator forced expiratory volume in 1 second (FEV1) values remained steady between years 1 and 5 post procedure despite an 18% decrease in the average daily dose of inhaled corticosteroids.
In a separate study, Dr. Castro and coinvestigators at Washington University identified a number of predictors of who will get the best responses to bronchial thermoplasty. This was a small study involving 42 patients with severe persistent asthma as reflected in their baseline mean inhaled corticosteroid dose of 2,185 mcg/day. Eighty percent of patients required bursts of oral corticosteroids during the year prior to the procedure. Their average baseline Asthma Quality of Life Questionnaire (AQLQ) score was 3.42. The baseline FEV1 postbronchodilator averaged 70%, with a range of 44%-121%.
Predictors of a clinically meaningful improvement in quality of life as defined by at least a 0.5-point improvement in AQLQ score 1 year post procedure included a shorter duration of asthma – 19 years, as compared with an average of 45 years in nonresponders – and a greater number of severe exacerbations during the year prior to bronchial thermoplasty.
Using another important yardstick of clinical improvement – at least a 240 mcg/day dose reduction in inhaled corticosteroids or a 2.5 mg/day decrease in oral corticosteroids at 1 year post procedure – significant predictors of benefit included older age (55 vs. 43 years), a lower baseline AQLQ score (2.4 vs. 4.0), and greater need for oral corticosteroids.
In addition, several quantitative metrics obtained through multidetector CT scans of the chest showed promise as predictors of a corticosteroid dose reduction. Responders showed less baseline air trapping, with an average of 6.1% of the lung having a density below –850 Hounsfield units, compared with 12.1% in nonresponders. Responders also had less baseline emphysema-like lung, with 3.2% of the lung having a density below –950 Hounsfield units at total lung capacity, compared with 5.8% in nonresponders, according to Dr. Castro.
This as-yet unpublished study was funded by the National Institutes of Health. AIR2 was sponsored by Boston Scientific. Dr. Castro reported research grants from the NIH, the American Lung Association, Boston Scientific, and other companies.
An estimated 5% of asthma patients are categorized as having severe disease. Bronchial thermoplasty has been approved by the FDA for the treatment of severe asthma since 2010. The outpatient procedure entails delivery of radiofrequency energy to the lungs in three sessions spaced several weeks apart.
HOUSTON – Bronchial thermoplasty has emerged as an important treatment option for patients with severe asthma at specialized centers, Dr. Mario Castro observed at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The most recent international European Respiratory Society/American Thoracic Society practice guidelines on severe asthma recommend that bronchial thermoplasty for severe persistent asthma be utilized only in the setting of a clinical study or independent registry. The guidelines cited “very low confidence” in the available estimates of the novel treatment’s longer-term benefits and harms, as well as the lack of data regarding the phenotypes of asthma patients most likely to benefit (Eur. Respir. J. 2014 Feb;43:343-73).
Dr. Castro, a member of the task force that developed the ERS/ATS guidelines, said the group’s cautious stance was appropriate given the evidence available at the time of deliberations. However, at the AAAAI meeting, he highlighted more recent study results that address many of the task force’s concerns and that he said might lead to a more enthusiastic recommendation for bronchial thermoplasty in future guidelines.
One key piece of evidence unavailable to the task force comes from results reported in the 5-year prospective follow-up of 162 bronchial thermoplasty-treated patients in the international Asthma Intervention Research 2 (AIR2) trial.
“It’s quite striking that the exacerbation rate did not start to creep back up over time in this severe asthma population. We believe this study shows for the first time that this therapy may actually be a disease modifier, and that you can do this procedure in an identified population and the benefits of this one-time treatment are sustained over at least a 5-year time period,” said Dr. Castro, an AIR2 investigator and professor of pulmonary and critical care medicine and pediatrics at Washington University in St. Louis.
Compared with the baseline established during the year prior to bronchial thermoplasty, at 5 years post procedure, there was a 44% decrease in the percentage of AIR2 participants with severe exacerbations requiring oral corticosteroids, and a 48% reduction in the severe exacerbation event rate. Moreover, there was a 78% reduction in the percentage of patients with an emergency department visit for asthma and an 88% drop in the ED visit event rate (J. Allergy Clin. Immunol. 2013;132:1295-302).
With regard to safety, annual high-resolution CT scans showed no structural abnormalities from baseline to 5 years post-bronchial thermoplasty that could be attributed to the procedure. Prebronchodilator forced expiratory volume in 1 second (FEV1) values remained steady between years 1 and 5 post procedure despite an 18% decrease in the average daily dose of inhaled corticosteroids.
In a separate study, Dr. Castro and coinvestigators at Washington University identified a number of predictors of who will get the best responses to bronchial thermoplasty. This was a small study involving 42 patients with severe persistent asthma as reflected in their baseline mean inhaled corticosteroid dose of 2,185 mcg/day. Eighty percent of patients required bursts of oral corticosteroids during the year prior to the procedure. Their average baseline Asthma Quality of Life Questionnaire (AQLQ) score was 3.42. The baseline FEV1 postbronchodilator averaged 70%, with a range of 44%-121%.
Predictors of a clinically meaningful improvement in quality of life as defined by at least a 0.5-point improvement in AQLQ score 1 year post procedure included a shorter duration of asthma – 19 years, as compared with an average of 45 years in nonresponders – and a greater number of severe exacerbations during the year prior to bronchial thermoplasty.
Using another important yardstick of clinical improvement – at least a 240 mcg/day dose reduction in inhaled corticosteroids or a 2.5 mg/day decrease in oral corticosteroids at 1 year post procedure – significant predictors of benefit included older age (55 vs. 43 years), a lower baseline AQLQ score (2.4 vs. 4.0), and greater need for oral corticosteroids.
In addition, several quantitative metrics obtained through multidetector CT scans of the chest showed promise as predictors of a corticosteroid dose reduction. Responders showed less baseline air trapping, with an average of 6.1% of the lung having a density below –850 Hounsfield units, compared with 12.1% in nonresponders. Responders also had less baseline emphysema-like lung, with 3.2% of the lung having a density below –950 Hounsfield units at total lung capacity, compared with 5.8% in nonresponders, according to Dr. Castro.
This as-yet unpublished study was funded by the National Institutes of Health. AIR2 was sponsored by Boston Scientific. Dr. Castro reported research grants from the NIH, the American Lung Association, Boston Scientific, and other companies.
An estimated 5% of asthma patients are categorized as having severe disease. Bronchial thermoplasty has been approved by the FDA for the treatment of severe asthma since 2010. The outpatient procedure entails delivery of radiofrequency energy to the lungs in three sessions spaced several weeks apart.
EXPERT ANALYSIS FROM THE 2015 AAAAI ANNUAL MEETING

‘Mossy Oak sign’ suggests delayed anaphylaxis to red meat
HOUSTON– In central Virginia, where IgE-mediated delayed allergic reactions to red meat have become the most common cause of anaphylaxis in adults, physicians have taken to looking for what they call the ‘Mossy Oak sign.’
“If a patient shows up in a blaze-orange cap and hunter’s camouflage fatigues, an allergy fellow will tell me, ‘There’s a positive Mossy Oak sign in room 2,’ and I know that probably means the patient has delayed anaphylaxis to alpha-gal,” Dr. Scott P. Commins said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.

Alpha-gal is short for galactose-alpha-1,3,-galactose, an oligosaccharide present on thyroglobulin and other tissues in nonprimate mammals. It’s not normally present in humans, but when a lone star tick (Amblyomma americanum) that has fed on a nonprimate mammal bites a human, the alpha-gal is transferred, eliciting serum IgE antibodies.
Mossy Oak is a popular brand of hunter’s camouflage clothing. A positive Mossy Oak sign is useful in clinical practice because a patient who presents to a medical clinic dressed in hunting regalia is someone who spends a lot of time outdoors in the woods and fields where ticks lurk. He’s also typically someone who enjoys eating red meat. And whether it’s venison, beef, pork, lamb, goat, or bison, it contains alpha-gal. The result, in a patient who’s been primed via tick bite, can be a life-threatening anaphylactic or urticarial reaction arising 3-6 hours later, explained Dr. Commins, an allergist at the University of Virginia, Charlottesville.
He and his coinvestigators have played a central role in the still-unfolding story of this novel disease involving late-onset anaphylaxis to mammalian meat. Dr. Commins was the lead author of the paper that first described the syndrome (J. Allergy Clin. Immunol. 2009;123:426-33), as well as a subsequent paper that established the lone star tick as the culprit, making this syndrome the first known example of a response to an ectoparasite giving rise to a serious form of food allergy (J. Allergy Clin. Immunol. 2011;127:1286-93). More recently, the investigators have shown that alpha-gal-specific IgE does not cause or worsen asthma (Am. J. Respir. Crit. Care Med. 2012;185:723-30).
In a wide-ranging talk, Dr. Commins addressed the diagnosis and management of delayed anaphylaxis to red meat. He also touched upon some provocative emerging issues, including the possible risks posed by placing a porcine heart valve or bioprosthetic ligament in a patient with serum IgE antibodies to alpha-gal.

The investigators stumbled upon the phenomenon of tick-transmitted delayed anaphylaxis to red meat while they were trying to unravel the explanation for the markedly regional occurrence of IgE-mediated hypersensitivity reactions to the chimeric monoclonal antibody cetuximab (Erbitux) previously reported in the oncology literature (J. Clin. Oncol. 2007;25:3644-8). Dr. Commins and his colleagues realized that the same southeastern and south-central states where reactions to the initial infusion of cetuximab were concentrated were the states where the lone star tick abounds.
Incidentally, scientists at the Centers for Disease Control and Prevention follow the lone star tick closely because it is the primary vector for ehrlichiosis. CDC researchers say the tick’s range is steadily expanding and now includes 28 states, with New York’s Long Island a hot spot.
There is no public health requirement to report serum IgE-mediated delayed reactions to red meat, so the exact number of affected patients is unknown. But it’s clear that many thousands of individuals are affected, and estimates are being revised upward as the novel syndrome becomes more widely known. The disorder is common in Europe and Australia as well.
Classically, IgE-mediated anaphylactic reactions occur within 5-30 minutes after exposure to the offending agent. Thus, the 3- to 6-hour delay in symptom onset in patients with a reaction to the alpha-gal in red meat is remarkable; the explanation for the time lag remains unclear.
Dr. Commins and others have shown that individuals with serum IgE antibodies to alpha-gal also typically have serum IgE antibodies to cat, dog, beef, and pork, but not to egg, peanut, chicken, fish, or house dust mite.
Diagnosis of IgE-mediated urticarial or anaphylactic reactions to mammalian meat is made on the basis of the presence of serum IgE antibodies to alpha-gal. Dr. Commins recommended considering the diagnosis and ordering the blood test in the setting of new-onset anaphylaxis in a patient who enjoys hunting or other outdoor activities in a state where the lone star tick is found, particularly if the symptoms occur at night, hours after a big meat-heavy meal. A history of recent or persistent tick bites is an obvious clue.
“Also, it’s striking how many patients develop palmar erythema and itching during an episode. Not all report it, but when they do it’s usually a pretty good giveaway that they might have IgE to alpha-gal,” according to the allergist.
He added that it’s entirely reasonable to order a screening test for IgE to alpha-gal in patients in lone star tick–abiding states whose anaphylactic reactions seem to occur randomly without an apparent trigger.
Dr. Commins and his coinvestigators have assembled a database of roughly 500 of their patients with IgE to alpha-gal, about half of whom have a history of atopy. The investigators have found that an individual’s atopic status has no bearing on IgE antibody titer or the severity of the delayed reactions. Moreover, neither the alpha-gal IgE antibody level, the ratio of alpha-gal-specific IgE to total IgE, nor IgG antibodies correlate with reaction severity, he continued.
Based upon their study of 45 affected children, Dr. Commins and coworkers concluded that the clinical presentation and serum IgE pattern are the same as in adults (Pediatrics 2013 May [doi:10.1542/peds.2012-2585]). Since that publication, however, the investigators have realized there is a subgroup of affected teenagers who present with GI symptoms, he added.
Turning to disease management, Dr. Commins said he advocates an avoidance diet that eliminates mammalian meats, rich desserts, and super-premium ice cream.
“I also counsel patients to avoid broths, gravies, and anything that might be a mystery sauce,” he said. “You’d be surprised at how many people with alpha-gal order chicken at a Mexican restaurant thinking that they’re doing the right thing and end up reacting. I don’t know exactly why it happens, so I just say ‘avoid mystery sauces.’ Dairy and cheese are actually fairly well tolerated, although soft cheeses, like brie, can cause a reaction.”
Reactions are inconsistent, and symptoms can vary from episode to episode. Cofactors are a concern, with exercise and alcohol tending to make patients more sensitive to an alpha-gal exposure. The degree of risk posed by vaccines containing gelatin constitutes an emerging and unresolved issue.
“We’ve heard of several reactions to the shingles vaccine because of the gelatin, and the MMR vaccine is also on the radar,” Dr. Commins said.
Implantation of porcine bioprosthetic heart valves in patients with serum IgE antibodies to alpha-gal has been associated with reports of early valve failure; all bioprosthetic valves contain alpha-gal unless they’ve been decellularized. In addition, Dr. Commins is familiar with a case at another university in which three separate attempts to place a bioprosthetic ligament during repeated arthroscopic knee surgeries failed in a patient who had a “screamingly high” level of IgE to alpha-gal.
“I think this bioprosthesis issue is yet to be resolved,” he added.
One audience member, a Texas allergist, said she has a lot of trouble convincing her patients who are avid hunters to give up eating red meats. Dr. Commins said he faces the same issue.
“There is a recalcitrant group that just wants to eat a side of beef every day. I tell them if you’re not going to be on an avoidance diet, at least avoid the fattier cuts and don’t eat tremendous amounts. We believe that the antigen is possibly a glycolipid. Those cuts of meat that are high in fat are the ones patients tell us over and over again give them the worst reactions,” he said.
“The inconsistency of the allergic reactions keeps some patients from taking this disease seriously,” the allergist added. “What eventually happens for some patients is they end up having a really bad reaction. And then that convinces them.”
He monitors affected patients’ alpha-gal IgE levels over time. If and when the IgE becomes negative, he recommends a food challenge test. The patient comes in at 8 a.m., eats three pork sausage patties, and spends the day under observation at the clinic, walking the stairs periodically since exercise is a cofactor. If the challenge goes off without a hitch, the patient is free to go home at 4 or 5 p.m. In the past, that was the patient’s ticket to clearance to safely eat a big meat meal with alcohol, but Dr. Commins has pulled back of late from that recommendation.
“We believe that additional tick bites can make the allergy come back. So if someone passes a challenge in October and then the following spring gets more tick bites, you may have set them up to have a reaction because you’ve told them they can eat meat again. So the utility of a negative food challenge is unclear unless you’re pretty confident a patient is not going to have more tick bites,” he explained.
Dr. Commins reported receiving research grants from the National Institutes of Health to conduct his studies on delayed anaphylactic reactions to red meat. He serves on speakers bureaus for Genentech and Teva.
HOUSTON– In central Virginia, where IgE-mediated delayed allergic reactions to red meat have become the most common cause of anaphylaxis in adults, physicians have taken to looking for what they call the ‘Mossy Oak sign.’
“If a patient shows up in a blaze-orange cap and hunter’s camouflage fatigues, an allergy fellow will tell me, ‘There’s a positive Mossy Oak sign in room 2,’ and I know that probably means the patient has delayed anaphylaxis to alpha-gal,” Dr. Scott P. Commins said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Alpha-gal is short for galactose-alpha-1,3,-galactose, an oligosaccharide present on thyroglobulin and other tissues in nonprimate mammals. It’s not normally present in humans, but when a lone star tick (Amblyomma americanum) that has fed on a nonprimate mammal bites a human, the alpha-gal is transferred, eliciting serum IgE antibodies.
Mossy Oak is a popular brand of hunter’s camouflage clothing. A positive Mossy Oak sign is useful in clinical practice because a patient who presents to a medical clinic dressed in hunting regalia is someone who spends a lot of time outdoors in the woods and fields where ticks lurk. He’s also typically someone who enjoys eating red meat. And whether it’s venison, beef, pork, lamb, goat, or bison, it contains alpha-gal. The result, in a patient who’s been primed via tick bite, can be a life-threatening anaphylactic or urticarial reaction arising 3-6 hours later, explained Dr. Commins, an allergist at the University of Virginia, Charlottesville.
He and his coinvestigators have played a central role in the still-unfolding story of this novel disease involving late-onset anaphylaxis to mammalian meat. Dr. Commins was the lead author of the paper that first described the syndrome (J. Allergy Clin. Immunol. 2009;123:426-33), as well as a subsequent paper that established the lone star tick as the culprit, making this syndrome the first known example of a response to an ectoparasite giving rise to a serious form of food allergy (J. Allergy Clin. Immunol. 2011;127:1286-93). More recently, the investigators have shown that alpha-gal-specific IgE does not cause or worsen asthma (Am. J. Respir. Crit. Care Med. 2012;185:723-30).
In a wide-ranging talk, Dr. Commins addressed the diagnosis and management of delayed anaphylaxis to red meat. He also touched upon some provocative emerging issues, including the possible risks posed by placing a porcine heart valve or bioprosthetic ligament in a patient with serum IgE antibodies to alpha-gal.
The investigators stumbled upon the phenomenon of tick-transmitted delayed anaphylaxis to red meat while they were trying to unravel the explanation for the markedly regional occurrence of IgE-mediated hypersensitivity reactions to the chimeric monoclonal antibody cetuximab (Erbitux) previously reported in the oncology literature (J. Clin. Oncol. 2007;25:3644-8). Dr. Commins and his colleagues realized that the same southeastern and south-central states where reactions to the initial infusion of cetuximab were concentrated were the states where the lone star tick abounds.
Incidentally, scientists at the Centers for Disease Control and Prevention follow the lone star tick closely because it is the primary vector for ehrlichiosis. CDC researchers say the tick’s range is steadily expanding and now includes 28 states, with New York’s Long Island a hot spot.
There is no public health requirement to report serum IgE-mediated delayed reactions to red meat, so the exact number of affected patients is unknown. But it’s clear that many thousands of individuals are affected, and estimates are being revised upward as the novel syndrome becomes more widely known. The disorder is common in Europe and Australia as well.
Classically, IgE-mediated anaphylactic reactions occur within 5-30 minutes after exposure to the offending agent. Thus, the 3- to 6-hour delay in symptom onset in patients with a reaction to the alpha-gal in red meat is remarkable; the explanation for the time lag remains unclear.
Dr. Commins and others have shown that individuals with serum IgE antibodies to alpha-gal also typically have serum IgE antibodies to cat, dog, beef, and pork, but not to egg, peanut, chicken, fish, or house dust mite.
Diagnosis of IgE-mediated urticarial or anaphylactic reactions to mammalian meat is made on the basis of the presence of serum IgE antibodies to alpha-gal. Dr. Commins recommended considering the diagnosis and ordering the blood test in the setting of new-onset anaphylaxis in a patient who enjoys hunting or other outdoor activities in a state where the lone star tick is found, particularly if the symptoms occur at night, hours after a big meat-heavy meal. A history of recent or persistent tick bites is an obvious clue.
“Also, it’s striking how many patients develop palmar erythema and itching during an episode. Not all report it, but when they do it’s usually a pretty good giveaway that they might have IgE to alpha-gal,” according to the allergist.
He added that it’s entirely reasonable to order a screening test for IgE to alpha-gal in patients in lone star tick–abiding states whose anaphylactic reactions seem to occur randomly without an apparent trigger.
Dr. Commins and his coinvestigators have assembled a database of roughly 500 of their patients with IgE to alpha-gal, about half of whom have a history of atopy. The investigators have found that an individual’s atopic status has no bearing on IgE antibody titer or the severity of the delayed reactions. Moreover, neither the alpha-gal IgE antibody level, the ratio of alpha-gal-specific IgE to total IgE, nor IgG antibodies correlate with reaction severity, he continued.
Based upon their study of 45 affected children, Dr. Commins and coworkers concluded that the clinical presentation and serum IgE pattern are the same as in adults (Pediatrics 2013 May [doi:10.1542/peds.2012-2585]). Since that publication, however, the investigators have realized there is a subgroup of affected teenagers who present with GI symptoms, he added.
Turning to disease management, Dr. Commins said he advocates an avoidance diet that eliminates mammalian meats, rich desserts, and super-premium ice cream.
“I also counsel patients to avoid broths, gravies, and anything that might be a mystery sauce,” he said. “You’d be surprised at how many people with alpha-gal order chicken at a Mexican restaurant thinking that they’re doing the right thing and end up reacting. I don’t know exactly why it happens, so I just say ‘avoid mystery sauces.’ Dairy and cheese are actually fairly well tolerated, although soft cheeses, like brie, can cause a reaction.”
Reactions are inconsistent, and symptoms can vary from episode to episode. Cofactors are a concern, with exercise and alcohol tending to make patients more sensitive to an alpha-gal exposure. The degree of risk posed by vaccines containing gelatin constitutes an emerging and unresolved issue.
“We’ve heard of several reactions to the shingles vaccine because of the gelatin, and the MMR vaccine is also on the radar,” Dr. Commins said.
Implantation of porcine bioprosthetic heart valves in patients with serum IgE antibodies to alpha-gal has been associated with reports of early valve failure; all bioprosthetic valves contain alpha-gal unless they’ve been decellularized. In addition, Dr. Commins is familiar with a case at another university in which three separate attempts to place a bioprosthetic ligament during repeated arthroscopic knee surgeries failed in a patient who had a “screamingly high” level of IgE to alpha-gal.
“I think this bioprosthesis issue is yet to be resolved,” he added.
One audience member, a Texas allergist, said she has a lot of trouble convincing her patients who are avid hunters to give up eating red meats. Dr. Commins said he faces the same issue.
“There is a recalcitrant group that just wants to eat a side of beef every day. I tell them if you’re not going to be on an avoidance diet, at least avoid the fattier cuts and don’t eat tremendous amounts. We believe that the antigen is possibly a glycolipid. Those cuts of meat that are high in fat are the ones patients tell us over and over again give them the worst reactions,” he said.
“The inconsistency of the allergic reactions keeps some patients from taking this disease seriously,” the allergist added. “What eventually happens for some patients is they end up having a really bad reaction. And then that convinces them.”
He monitors affected patients’ alpha-gal IgE levels over time. If and when the IgE becomes negative, he recommends a food challenge test. The patient comes in at 8 a.m., eats three pork sausage patties, and spends the day under observation at the clinic, walking the stairs periodically since exercise is a cofactor. If the challenge goes off without a hitch, the patient is free to go home at 4 or 5 p.m. In the past, that was the patient’s ticket to clearance to safely eat a big meat meal with alcohol, but Dr. Commins has pulled back of late from that recommendation.
“We believe that additional tick bites can make the allergy come back. So if someone passes a challenge in October and then the following spring gets more tick bites, you may have set them up to have a reaction because you’ve told them they can eat meat again. So the utility of a negative food challenge is unclear unless you’re pretty confident a patient is not going to have more tick bites,” he explained.
Dr. Commins reported receiving research grants from the National Institutes of Health to conduct his studies on delayed anaphylactic reactions to red meat. He serves on speakers bureaus for Genentech and Teva.
HOUSTON– In central Virginia, where IgE-mediated delayed allergic reactions to red meat have become the most common cause of anaphylaxis in adults, physicians have taken to looking for what they call the ‘Mossy Oak sign.’
“If a patient shows up in a blaze-orange cap and hunter’s camouflage fatigues, an allergy fellow will tell me, ‘There’s a positive Mossy Oak sign in room 2,’ and I know that probably means the patient has delayed anaphylaxis to alpha-gal,” Dr. Scott P. Commins said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
Alpha-gal is short for galactose-alpha-1,3,-galactose, an oligosaccharide present on thyroglobulin and other tissues in nonprimate mammals. It’s not normally present in humans, but when a lone star tick (Amblyomma americanum) that has fed on a nonprimate mammal bites a human, the alpha-gal is transferred, eliciting serum IgE antibodies.
Mossy Oak is a popular brand of hunter’s camouflage clothing. A positive Mossy Oak sign is useful in clinical practice because a patient who presents to a medical clinic dressed in hunting regalia is someone who spends a lot of time outdoors in the woods and fields where ticks lurk. He’s also typically someone who enjoys eating red meat. And whether it’s venison, beef, pork, lamb, goat, or bison, it contains alpha-gal. The result, in a patient who’s been primed via tick bite, can be a life-threatening anaphylactic or urticarial reaction arising 3-6 hours later, explained Dr. Commins, an allergist at the University of Virginia, Charlottesville.
He and his coinvestigators have played a central role in the still-unfolding story of this novel disease involving late-onset anaphylaxis to mammalian meat. Dr. Commins was the lead author of the paper that first described the syndrome (J. Allergy Clin. Immunol. 2009;123:426-33), as well as a subsequent paper that established the lone star tick as the culprit, making this syndrome the first known example of a response to an ectoparasite giving rise to a serious form of food allergy (J. Allergy Clin. Immunol. 2011;127:1286-93). More recently, the investigators have shown that alpha-gal-specific IgE does not cause or worsen asthma (Am. J. Respir. Crit. Care Med. 2012;185:723-30).
In a wide-ranging talk, Dr. Commins addressed the diagnosis and management of delayed anaphylaxis to red meat. He also touched upon some provocative emerging issues, including the possible risks posed by placing a porcine heart valve or bioprosthetic ligament in a patient with serum IgE antibodies to alpha-gal.
The investigators stumbled upon the phenomenon of tick-transmitted delayed anaphylaxis to red meat while they were trying to unravel the explanation for the markedly regional occurrence of IgE-mediated hypersensitivity reactions to the chimeric monoclonal antibody cetuximab (Erbitux) previously reported in the oncology literature (J. Clin. Oncol. 2007;25:3644-8). Dr. Commins and his colleagues realized that the same southeastern and south-central states where reactions to the initial infusion of cetuximab were concentrated were the states where the lone star tick abounds.
Incidentally, scientists at the Centers for Disease Control and Prevention follow the lone star tick closely because it is the primary vector for ehrlichiosis. CDC researchers say the tick’s range is steadily expanding and now includes 28 states, with New York’s Long Island a hot spot.
There is no public health requirement to report serum IgE-mediated delayed reactions to red meat, so the exact number of affected patients is unknown. But it’s clear that many thousands of individuals are affected, and estimates are being revised upward as the novel syndrome becomes more widely known. The disorder is common in Europe and Australia as well.
Classically, IgE-mediated anaphylactic reactions occur within 5-30 minutes after exposure to the offending agent. Thus, the 3- to 6-hour delay in symptom onset in patients with a reaction to the alpha-gal in red meat is remarkable; the explanation for the time lag remains unclear.
Dr. Commins and others have shown that individuals with serum IgE antibodies to alpha-gal also typically have serum IgE antibodies to cat, dog, beef, and pork, but not to egg, peanut, chicken, fish, or house dust mite.
Diagnosis of IgE-mediated urticarial or anaphylactic reactions to mammalian meat is made on the basis of the presence of serum IgE antibodies to alpha-gal. Dr. Commins recommended considering the diagnosis and ordering the blood test in the setting of new-onset anaphylaxis in a patient who enjoys hunting or other outdoor activities in a state where the lone star tick is found, particularly if the symptoms occur at night, hours after a big meat-heavy meal. A history of recent or persistent tick bites is an obvious clue.
“Also, it’s striking how many patients develop palmar erythema and itching during an episode. Not all report it, but when they do it’s usually a pretty good giveaway that they might have IgE to alpha-gal,” according to the allergist.
He added that it’s entirely reasonable to order a screening test for IgE to alpha-gal in patients in lone star tick–abiding states whose anaphylactic reactions seem to occur randomly without an apparent trigger.
Dr. Commins and his coinvestigators have assembled a database of roughly 500 of their patients with IgE to alpha-gal, about half of whom have a history of atopy. The investigators have found that an individual’s atopic status has no bearing on IgE antibody titer or the severity of the delayed reactions. Moreover, neither the alpha-gal IgE antibody level, the ratio of alpha-gal-specific IgE to total IgE, nor IgG antibodies correlate with reaction severity, he continued.
Based upon their study of 45 affected children, Dr. Commins and coworkers concluded that the clinical presentation and serum IgE pattern are the same as in adults (Pediatrics 2013 May [doi:10.1542/peds.2012-2585]). Since that publication, however, the investigators have realized there is a subgroup of affected teenagers who present with GI symptoms, he added.
Turning to disease management, Dr. Commins said he advocates an avoidance diet that eliminates mammalian meats, rich desserts, and super-premium ice cream.
“I also counsel patients to avoid broths, gravies, and anything that might be a mystery sauce,” he said. “You’d be surprised at how many people with alpha-gal order chicken at a Mexican restaurant thinking that they’re doing the right thing and end up reacting. I don’t know exactly why it happens, so I just say ‘avoid mystery sauces.’ Dairy and cheese are actually fairly well tolerated, although soft cheeses, like brie, can cause a reaction.”
Reactions are inconsistent, and symptoms can vary from episode to episode. Cofactors are a concern, with exercise and alcohol tending to make patients more sensitive to an alpha-gal exposure. The degree of risk posed by vaccines containing gelatin constitutes an emerging and unresolved issue.
“We’ve heard of several reactions to the shingles vaccine because of the gelatin, and the MMR vaccine is also on the radar,” Dr. Commins said.
Implantation of porcine bioprosthetic heart valves in patients with serum IgE antibodies to alpha-gal has been associated with reports of early valve failure; all bioprosthetic valves contain alpha-gal unless they’ve been decellularized. In addition, Dr. Commins is familiar with a case at another university in which three separate attempts to place a bioprosthetic ligament during repeated arthroscopic knee surgeries failed in a patient who had a “screamingly high” level of IgE to alpha-gal.
“I think this bioprosthesis issue is yet to be resolved,” he added.
One audience member, a Texas allergist, said she has a lot of trouble convincing her patients who are avid hunters to give up eating red meats. Dr. Commins said he faces the same issue.
“There is a recalcitrant group that just wants to eat a side of beef every day. I tell them if you’re not going to be on an avoidance diet, at least avoid the fattier cuts and don’t eat tremendous amounts. We believe that the antigen is possibly a glycolipid. Those cuts of meat that are high in fat are the ones patients tell us over and over again give them the worst reactions,” he said.
“The inconsistency of the allergic reactions keeps some patients from taking this disease seriously,” the allergist added. “What eventually happens for some patients is they end up having a really bad reaction. And then that convinces them.”
He monitors affected patients’ alpha-gal IgE levels over time. If and when the IgE becomes negative, he recommends a food challenge test. The patient comes in at 8 a.m., eats three pork sausage patties, and spends the day under observation at the clinic, walking the stairs periodically since exercise is a cofactor. If the challenge goes off without a hitch, the patient is free to go home at 4 or 5 p.m. In the past, that was the patient’s ticket to clearance to safely eat a big meat meal with alcohol, but Dr. Commins has pulled back of late from that recommendation.
“We believe that additional tick bites can make the allergy come back. So if someone passes a challenge in October and then the following spring gets more tick bites, you may have set them up to have a reaction because you’ve told them they can eat meat again. So the utility of a negative food challenge is unclear unless you’re pretty confident a patient is not going to have more tick bites,” he explained.
Dr. Commins reported receiving research grants from the National Institutes of Health to conduct his studies on delayed anaphylactic reactions to red meat. He serves on speakers bureaus for Genentech and Teva.
EXPERT ANALYSIS FROM THE 2015 AAAAI ANNUAL MEETING
