User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Early pneumonia linked with later asthma and COPD
Lower respiratory illness in childhood is associated with later development of asthma and wheezing that can persist into adulthood, and may be a risk factor for adult chronic obstructive pulmonary disease (COPD), a prospective study has found.
Researchers assessed the lung function of 646 children – 338 of whom had experienced lower respiratory illness before age 3 years, and 308 controls – and found those who had early pneumonia had a nearly twofold increase in the risk of asthma and wheeze up to age 26 years.
They also had the most severe subsequent deficits in lung function, while those with early non-pneumonia lower respiratory illness had smaller but still significant impairments in lung function and increased risk of wheezing, according to a paper published online in Pediatrics (2015;135:607-15 [10.1542/peds.2014-3060]).
“Because there is considerable evidence that asthma associated with airflow limitation is a strong risk factor for subsequent chronic obstructive pulmonary disease, the prevention of early-life pneumonia and of the factors that determine low lung function in infancy may contribute significantly to decrease the public health burden of chronic obstructive pulmonary disease,” wrote Dr. Johnny Y.C. Chan of the Kwong Wah Hospital, Hong Kong, and his associates.
The study was funded by the National Institutes of Health, and no conflicts of interest were declared.
Lower respiratory illness in childhood is associated with later development of asthma and wheezing that can persist into adulthood, and may be a risk factor for adult chronic obstructive pulmonary disease (COPD), a prospective study has found.
Researchers assessed the lung function of 646 children – 338 of whom had experienced lower respiratory illness before age 3 years, and 308 controls – and found those who had early pneumonia had a nearly twofold increase in the risk of asthma and wheeze up to age 26 years.
They also had the most severe subsequent deficits in lung function, while those with early non-pneumonia lower respiratory illness had smaller but still significant impairments in lung function and increased risk of wheezing, according to a paper published online in Pediatrics (2015;135:607-15 [10.1542/peds.2014-3060]).
“Because there is considerable evidence that asthma associated with airflow limitation is a strong risk factor for subsequent chronic obstructive pulmonary disease, the prevention of early-life pneumonia and of the factors that determine low lung function in infancy may contribute significantly to decrease the public health burden of chronic obstructive pulmonary disease,” wrote Dr. Johnny Y.C. Chan of the Kwong Wah Hospital, Hong Kong, and his associates.
The study was funded by the National Institutes of Health, and no conflicts of interest were declared.
Lower respiratory illness in childhood is associated with later development of asthma and wheezing that can persist into adulthood, and may be a risk factor for adult chronic obstructive pulmonary disease (COPD), a prospective study has found.
Researchers assessed the lung function of 646 children – 338 of whom had experienced lower respiratory illness before age 3 years, and 308 controls – and found those who had early pneumonia had a nearly twofold increase in the risk of asthma and wheeze up to age 26 years.
They also had the most severe subsequent deficits in lung function, while those with early non-pneumonia lower respiratory illness had smaller but still significant impairments in lung function and increased risk of wheezing, according to a paper published online in Pediatrics (2015;135:607-15 [10.1542/peds.2014-3060]).
“Because there is considerable evidence that asthma associated with airflow limitation is a strong risk factor for subsequent chronic obstructive pulmonary disease, the prevention of early-life pneumonia and of the factors that determine low lung function in infancy may contribute significantly to decrease the public health burden of chronic obstructive pulmonary disease,” wrote Dr. Johnny Y.C. Chan of the Kwong Wah Hospital, Hong Kong, and his associates.
The study was funded by the National Institutes of Health, and no conflicts of interest were declared.
Key clinical point: Lower respiratory illness in childhood is associated with later development of asthma and wheezing that can persist into adulthood.
Major finding: Children who experienced pneumonia before age 3 years had a nearly twofold increase in the risk of asthma and wheeze up to age 26.
Data source: Prospective cohort study in 338 children with early lower respiratory illness and 308 controls.
Disclosures: The study was funded by the National Institutes of Health, and no conflicts of interest were declared.
Avoid voriconazole in transplant patients at risk for skin cancer
SAN FRANCISCO – Voriconazole increased the risk of squamous cell carcinoma by 73% in a review of 455 lung transplant patients at the University of California, San Francisco.
The increase was for any exposure to the drug after transplant (adjusted hazard ratio, 1.73; P = .03). The investigators also found that each additional 30-day exposure at 200 mg of voriconazole twice daily increased the risk of squamous cell carcinoma (SCC) by 3.0% (HR, 1.03; P < .001). The results were adjusted for age at transplant, sex, and race. Overall, SCC risk was highest among white men aged 50 years or older at the time of transplant.

Although voriconazole did protect against posttransplant Aspergillus colonization (aHR, 0.50; P < .001), it did not reduce the risk of invasive aspergillosis. The drug reduced all-cause mortality only among colonized subjects (aHR, 0.34; P = .03), and offered no mortality benefit among those who were not colonized.
There was no difference in all-cause mortality between patients who had any exposure to voriconazole and those who did not, “but we actually found a 2% increased risk of death for each 1 month on the medication. Patients who weren’t colonized were the ones contributing to this increased risk of death,” said lead investigator Matthew Mansh, now a medical student at Stanford (Calif.) University.
There was no increased risk of SCC with alternative antifungals, including inhaled amphotericin and posaconazole. These alternatives should be considered instead of voriconazole in people at higher risk for skin cancer after lung transplants, according to the study, Mr. Mansh noted.
Voriconazole, which is widely used for antifungal prophylaxis after solid organ transplants, has been linked to skin cancer. The reason for the carcinogenic effect is not known; researchers are working to unravel the molecular mechanisms.
“Physicians should be cautious when using voriconazole in the care of transplant recipients. If you see a patient who is developing phototoxicity” with voriconazole, “and if they don’t have evidence of Aspergillus colonization, you may want to limit exposure to high doses of this drug or suggest an alternative,” Mr. Mansh said.
“We have now demonstrated that the alternatives “don’t carry this increased risk of cutaneous SCC,” Mr. Mansh said at the American Academy of Dermatology annual meeting.
The mean age of the study patients at transplant was 52 years, and the majority of patients were white; slightly more than half were men. Most had bilateral lung transplants, with pulmonary fibrosis at the leading indication.
Voriconazole was used in 85% of the patients for an average of 10 months. A quarter of voriconazole patients developed SCC within 5 years of transplant, and 43% within 10 years. Among patients who did not receive the drug, 15% developed SCC within 5 years of transplant, and 28% developed SCC within 10 years of transplant.
“The benefit of voriconazole in terms of death was limited to patients with evidence of Aspergillus colonization, and it wasn’t dose dependent. Patients who had a higher cumulative exposure did not get more benefit,” Mr. Mansh said.
Mr. Mansh had no relevant disclosures.

|
Dr. Paul T. Nghiem |
This is a carefully done study with a practical message: voriconazole patients are at a prolonged increased risk for squamous cell carcinoma. If patients develop phototoxicity or are fair-skinned, have sun damage, a history of squamous cell carcinoma or other risk factors, I think it’s highly appropriate to suggest an alternative. The alternatives are not at all associated with phototoxicity or squamous cell carcinoma.
Dr. Paul T. Nghiem moderated the late-breaker presentation in which the study was presented and is a professor of dermatology at the University of Washington, Seattle. Dr. Nghiem had no disclosures related to the study.
|
|
Dr. Paul T. Nghiem |
This is a carefully done study with a practical message: voriconazole patients are at a prolonged increased risk for squamous cell carcinoma. If patients develop phototoxicity or are fair-skinned, have sun damage, a history of squamous cell carcinoma or other risk factors, I think it’s highly appropriate to suggest an alternative. The alternatives are not at all associated with phototoxicity or squamous cell carcinoma.
Dr. Paul T. Nghiem moderated the late-breaker presentation in which the study was presented and is a professor of dermatology at the University of Washington, Seattle. Dr. Nghiem had no disclosures related to the study.
|
|
Dr. Paul T. Nghiem |
This is a carefully done study with a practical message: voriconazole patients are at a prolonged increased risk for squamous cell carcinoma. If patients develop phototoxicity or are fair-skinned, have sun damage, a history of squamous cell carcinoma or other risk factors, I think it’s highly appropriate to suggest an alternative. The alternatives are not at all associated with phototoxicity or squamous cell carcinoma.
Dr. Paul T. Nghiem moderated the late-breaker presentation in which the study was presented and is a professor of dermatology at the University of Washington, Seattle. Dr. Nghiem had no disclosures related to the study.
SAN FRANCISCO – Voriconazole increased the risk of squamous cell carcinoma by 73% in a review of 455 lung transplant patients at the University of California, San Francisco.
The increase was for any exposure to the drug after transplant (adjusted hazard ratio, 1.73; P = .03). The investigators also found that each additional 30-day exposure at 200 mg of voriconazole twice daily increased the risk of squamous cell carcinoma (SCC) by 3.0% (HR, 1.03; P < .001). The results were adjusted for age at transplant, sex, and race. Overall, SCC risk was highest among white men aged 50 years or older at the time of transplant.
Although voriconazole did protect against posttransplant Aspergillus colonization (aHR, 0.50; P < .001), it did not reduce the risk of invasive aspergillosis. The drug reduced all-cause mortality only among colonized subjects (aHR, 0.34; P = .03), and offered no mortality benefit among those who were not colonized.
There was no difference in all-cause mortality between patients who had any exposure to voriconazole and those who did not, “but we actually found a 2% increased risk of death for each 1 month on the medication. Patients who weren’t colonized were the ones contributing to this increased risk of death,” said lead investigator Matthew Mansh, now a medical student at Stanford (Calif.) University.
There was no increased risk of SCC with alternative antifungals, including inhaled amphotericin and posaconazole. These alternatives should be considered instead of voriconazole in people at higher risk for skin cancer after lung transplants, according to the study, Mr. Mansh noted.
Voriconazole, which is widely used for antifungal prophylaxis after solid organ transplants, has been linked to skin cancer. The reason for the carcinogenic effect is not known; researchers are working to unravel the molecular mechanisms.
“Physicians should be cautious when using voriconazole in the care of transplant recipients. If you see a patient who is developing phototoxicity” with voriconazole, “and if they don’t have evidence of Aspergillus colonization, you may want to limit exposure to high doses of this drug or suggest an alternative,” Mr. Mansh said.
“We have now demonstrated that the alternatives “don’t carry this increased risk of cutaneous SCC,” Mr. Mansh said at the American Academy of Dermatology annual meeting.
The mean age of the study patients at transplant was 52 years, and the majority of patients were white; slightly more than half were men. Most had bilateral lung transplants, with pulmonary fibrosis at the leading indication.
Voriconazole was used in 85% of the patients for an average of 10 months. A quarter of voriconazole patients developed SCC within 5 years of transplant, and 43% within 10 years. Among patients who did not receive the drug, 15% developed SCC within 5 years of transplant, and 28% developed SCC within 10 years of transplant.
“The benefit of voriconazole in terms of death was limited to patients with evidence of Aspergillus colonization, and it wasn’t dose dependent. Patients who had a higher cumulative exposure did not get more benefit,” Mr. Mansh said.
Mr. Mansh had no relevant disclosures.
SAN FRANCISCO – Voriconazole increased the risk of squamous cell carcinoma by 73% in a review of 455 lung transplant patients at the University of California, San Francisco.
The increase was for any exposure to the drug after transplant (adjusted hazard ratio, 1.73; P = .03). The investigators also found that each additional 30-day exposure at 200 mg of voriconazole twice daily increased the risk of squamous cell carcinoma (SCC) by 3.0% (HR, 1.03; P < .001). The results were adjusted for age at transplant, sex, and race. Overall, SCC risk was highest among white men aged 50 years or older at the time of transplant.
Although voriconazole did protect against posttransplant Aspergillus colonization (aHR, 0.50; P < .001), it did not reduce the risk of invasive aspergillosis. The drug reduced all-cause mortality only among colonized subjects (aHR, 0.34; P = .03), and offered no mortality benefit among those who were not colonized.
There was no difference in all-cause mortality between patients who had any exposure to voriconazole and those who did not, “but we actually found a 2% increased risk of death for each 1 month on the medication. Patients who weren’t colonized were the ones contributing to this increased risk of death,” said lead investigator Matthew Mansh, now a medical student at Stanford (Calif.) University.
There was no increased risk of SCC with alternative antifungals, including inhaled amphotericin and posaconazole. These alternatives should be considered instead of voriconazole in people at higher risk for skin cancer after lung transplants, according to the study, Mr. Mansh noted.
Voriconazole, which is widely used for antifungal prophylaxis after solid organ transplants, has been linked to skin cancer. The reason for the carcinogenic effect is not known; researchers are working to unravel the molecular mechanisms.
“Physicians should be cautious when using voriconazole in the care of transplant recipients. If you see a patient who is developing phototoxicity” with voriconazole, “and if they don’t have evidence of Aspergillus colonization, you may want to limit exposure to high doses of this drug or suggest an alternative,” Mr. Mansh said.
“We have now demonstrated that the alternatives “don’t carry this increased risk of cutaneous SCC,” Mr. Mansh said at the American Academy of Dermatology annual meeting.
The mean age of the study patients at transplant was 52 years, and the majority of patients were white; slightly more than half were men. Most had bilateral lung transplants, with pulmonary fibrosis at the leading indication.
Voriconazole was used in 85% of the patients for an average of 10 months. A quarter of voriconazole patients developed SCC within 5 years of transplant, and 43% within 10 years. Among patients who did not receive the drug, 15% developed SCC within 5 years of transplant, and 28% developed SCC within 10 years of transplant.
“The benefit of voriconazole in terms of death was limited to patients with evidence of Aspergillus colonization, and it wasn’t dose dependent. Patients who had a higher cumulative exposure did not get more benefit,” Mr. Mansh said.
Mr. Mansh had no relevant disclosures.
AT AAD 2015
Key clinical point: Use an alternative antifungal after lung transplant in white men aged 50 years and older.
Major finding: Exposure to voriconazole increased the risk of squamous cell carcinoma by 73% after lung transplant (aHR, 1.73; P = .03); each additional 30‐day exposure at 200 mg twice daily increased the risk by 3.0% (HR 1.03; P < .001).
Data source: Retrospective cohort study of 455 lung transplant patients
Disclosures: The lead investigator had no relevant disclosures.
No increased risk of lung disease with methotrexate
Methotrexate is not associated with an increased risk of pulmonary disease in patients taking it for the treatment of psoriatic arthritis, psoriasis, or inflammatory bowel disease, a meta-analysis has found.
The analysis of results from seven double-blind, randomized, controlled studies, involving a total of 1,640 participants, showed no increased risk of total adverse respiratory events – infectious or noninfectious – or pulmonary deaths in patients taking methotrexate, compared with controls, according to Dr. Richard Conway of the department of rheumatology at Galway (Ireland) University Hospitals and his coauthors.

Methotrexate has previously been implicated as a cause of lung toxicity, and the prevalence of methotrexate-related interstitial lung disease has been reported as high as 11.6% in rheumatoid arthritis, but studies of methotrexate-induced lung disease are confounded by the higher risk of pulmonary infections among patients with rheumatoid arthritis, the authors said (BMJ 2015 [doi:10.1136/bmj.h1269]).
“These findings, coupled with those of a previous study in rheumatoid arthritis, suggest that methotrexate-related lung disease is rare, if it exists at all,” the investigators wrote.
The investigators had no specific source of funding for the study and had no conflicts of interest to declare.
Methotrexate is not associated with an increased risk of pulmonary disease in patients taking it for the treatment of psoriatic arthritis, psoriasis, or inflammatory bowel disease, a meta-analysis has found.
The analysis of results from seven double-blind, randomized, controlled studies, involving a total of 1,640 participants, showed no increased risk of total adverse respiratory events – infectious or noninfectious – or pulmonary deaths in patients taking methotrexate, compared with controls, according to Dr. Richard Conway of the department of rheumatology at Galway (Ireland) University Hospitals and his coauthors.
Methotrexate has previously been implicated as a cause of lung toxicity, and the prevalence of methotrexate-related interstitial lung disease has been reported as high as 11.6% in rheumatoid arthritis, but studies of methotrexate-induced lung disease are confounded by the higher risk of pulmonary infections among patients with rheumatoid arthritis, the authors said (BMJ 2015 [doi:10.1136/bmj.h1269]).
“These findings, coupled with those of a previous study in rheumatoid arthritis, suggest that methotrexate-related lung disease is rare, if it exists at all,” the investigators wrote.
The investigators had no specific source of funding for the study and had no conflicts of interest to declare.
Methotrexate is not associated with an increased risk of pulmonary disease in patients taking it for the treatment of psoriatic arthritis, psoriasis, or inflammatory bowel disease, a meta-analysis has found.
The analysis of results from seven double-blind, randomized, controlled studies, involving a total of 1,640 participants, showed no increased risk of total adverse respiratory events – infectious or noninfectious – or pulmonary deaths in patients taking methotrexate, compared with controls, according to Dr. Richard Conway of the department of rheumatology at Galway (Ireland) University Hospitals and his coauthors.
Methotrexate has previously been implicated as a cause of lung toxicity, and the prevalence of methotrexate-related interstitial lung disease has been reported as high as 11.6% in rheumatoid arthritis, but studies of methotrexate-induced lung disease are confounded by the higher risk of pulmonary infections among patients with rheumatoid arthritis, the authors said (BMJ 2015 [doi:10.1136/bmj.h1269]).
“These findings, coupled with those of a previous study in rheumatoid arthritis, suggest that methotrexate-related lung disease is rare, if it exists at all,” the investigators wrote.
The investigators had no specific source of funding for the study and had no conflicts of interest to declare.
FROM BMJ
Key clinical point: Methotrexate is not associated with an increased risk of pulmonary disease.
Major finding: There was no increased risk of total adverse respiratory events – infectious or noninfectious – or pulmonary deaths in patients taking methotrexate, compared with controls.
Data source: Meta-analysis of seven double-blind, randomized, controlled studies, involving a total of 1,640 participants.
Disclosures: The investigators had no specific source of funding for the study and had no conflicts of interest to declare.

Beta-lactam monotherapy effective for suspected community-acquired pneumonia
Among adults suspected of having community-acquired pneumonia who are hospitalized in non-ICU wards, empirical treatment with beta-lactam monotherapy is noninferior both to beta-lactam plus macrolide combination therapy and to fluoroquinolone monotherapy, according to a report published online April 2 in the New England Journal of Medicine.
Current guidelines recommend the latter two approaches, which has caused a widespread increase in the use of macrolides and fluoroquinolones – and in turn has increased antibiotic resistance.
Moreover, “the evidence in support of these recommendations is limited,” said Dr. Douwe F. Postma of the Julius Center for Health Sciences and Primary Care and the University of Utrecht (the Netherlands), and his associates.
To compare outcomes among the three treatment strategies, Dr. Postma and his colleagues conducted the Community-Acquired Pneumonia – Study on the Initial Treatment with Antibiotics of Lower Respiratory Tract Infections (CAP-START) trial in seven Dutch hospitals during a 2.5-year period (N. Engl. J. Med. 2015;372:1312-23).
The cluster-randomized, crossover study called for participating hospitals to rotate using each of the empirical strategies during consecutive 4-month periods for all eligible patients. A total of 656 patients were assigned to receive beta-lactam monotherapy, 739 to receive beta-lactam plus macrolide combination therapy, and 888 to receive fluoroquinolone monotherapy. The median patient age was 70 years.
The primary outcome – all-cause mortality at 90 days after admission – favored beta-lactam monotherapy over the combination therapy by an absolute difference in adjusted risk of death of 1.9 percentage points, and favored beta-lactam monotherapy over fluoroquinolone monotherapy by less than 1 percentage point. That demonstrated the noninferiority of beta-lactam monotherapy, the researchers noted.
Both secondary outcomes – length of hospital stay and treatment-related complications – also were similar among the three study groups, the investigators added.
That noninferiority was confirmed in several further analyses of the data, including a sensitivity analysis restricted only to patients who had radiologically confirmed CAP and another sensitivity analysis that examined 30-day all-cause mortality.
“These findings, together with the slightly longer length of hospital stay with [macrolide monotherapy], reported associations with the development of resistance, and possible increased risk of cardiac events, indicate that the addition of macrolides for empirical treatment of CAP should be reconsidered,” Dr. Postma and his associates said.
The Netherlands Organization for Health Research and Development supported the study. Dr. Postma and his associates reported having no financial disclosures.
Among adults suspected of having community-acquired pneumonia who are hospitalized in non-ICU wards, empirical treatment with beta-lactam monotherapy is noninferior both to beta-lactam plus macrolide combination therapy and to fluoroquinolone monotherapy, according to a report published online April 2 in the New England Journal of Medicine.
Current guidelines recommend the latter two approaches, which has caused a widespread increase in the use of macrolides and fluoroquinolones – and in turn has increased antibiotic resistance.
Moreover, “the evidence in support of these recommendations is limited,” said Dr. Douwe F. Postma of the Julius Center for Health Sciences and Primary Care and the University of Utrecht (the Netherlands), and his associates.
To compare outcomes among the three treatment strategies, Dr. Postma and his colleagues conducted the Community-Acquired Pneumonia – Study on the Initial Treatment with Antibiotics of Lower Respiratory Tract Infections (CAP-START) trial in seven Dutch hospitals during a 2.5-year period (N. Engl. J. Med. 2015;372:1312-23).
The cluster-randomized, crossover study called for participating hospitals to rotate using each of the empirical strategies during consecutive 4-month periods for all eligible patients. A total of 656 patients were assigned to receive beta-lactam monotherapy, 739 to receive beta-lactam plus macrolide combination therapy, and 888 to receive fluoroquinolone monotherapy. The median patient age was 70 years.
The primary outcome – all-cause mortality at 90 days after admission – favored beta-lactam monotherapy over the combination therapy by an absolute difference in adjusted risk of death of 1.9 percentage points, and favored beta-lactam monotherapy over fluoroquinolone monotherapy by less than 1 percentage point. That demonstrated the noninferiority of beta-lactam monotherapy, the researchers noted.
Both secondary outcomes – length of hospital stay and treatment-related complications – also were similar among the three study groups, the investigators added.
That noninferiority was confirmed in several further analyses of the data, including a sensitivity analysis restricted only to patients who had radiologically confirmed CAP and another sensitivity analysis that examined 30-day all-cause mortality.
“These findings, together with the slightly longer length of hospital stay with [macrolide monotherapy], reported associations with the development of resistance, and possible increased risk of cardiac events, indicate that the addition of macrolides for empirical treatment of CAP should be reconsidered,” Dr. Postma and his associates said.
The Netherlands Organization for Health Research and Development supported the study. Dr. Postma and his associates reported having no financial disclosures.
Among adults suspected of having community-acquired pneumonia who are hospitalized in non-ICU wards, empirical treatment with beta-lactam monotherapy is noninferior both to beta-lactam plus macrolide combination therapy and to fluoroquinolone monotherapy, according to a report published online April 2 in the New England Journal of Medicine.
Current guidelines recommend the latter two approaches, which has caused a widespread increase in the use of macrolides and fluoroquinolones – and in turn has increased antibiotic resistance.
Moreover, “the evidence in support of these recommendations is limited,” said Dr. Douwe F. Postma of the Julius Center for Health Sciences and Primary Care and the University of Utrecht (the Netherlands), and his associates.
To compare outcomes among the three treatment strategies, Dr. Postma and his colleagues conducted the Community-Acquired Pneumonia – Study on the Initial Treatment with Antibiotics of Lower Respiratory Tract Infections (CAP-START) trial in seven Dutch hospitals during a 2.5-year period (N. Engl. J. Med. 2015;372:1312-23).
The cluster-randomized, crossover study called for participating hospitals to rotate using each of the empirical strategies during consecutive 4-month periods for all eligible patients. A total of 656 patients were assigned to receive beta-lactam monotherapy, 739 to receive beta-lactam plus macrolide combination therapy, and 888 to receive fluoroquinolone monotherapy. The median patient age was 70 years.
The primary outcome – all-cause mortality at 90 days after admission – favored beta-lactam monotherapy over the combination therapy by an absolute difference in adjusted risk of death of 1.9 percentage points, and favored beta-lactam monotherapy over fluoroquinolone monotherapy by less than 1 percentage point. That demonstrated the noninferiority of beta-lactam monotherapy, the researchers noted.
Both secondary outcomes – length of hospital stay and treatment-related complications – also were similar among the three study groups, the investigators added.
That noninferiority was confirmed in several further analyses of the data, including a sensitivity analysis restricted only to patients who had radiologically confirmed CAP and another sensitivity analysis that examined 30-day all-cause mortality.
“These findings, together with the slightly longer length of hospital stay with [macrolide monotherapy], reported associations with the development of resistance, and possible increased risk of cardiac events, indicate that the addition of macrolides for empirical treatment of CAP should be reconsidered,” Dr. Postma and his associates said.
The Netherlands Organization for Health Research and Development supported the study. Dr. Postma and his associates reported having no financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Empirical beta-lactam monotherapy is noninferior to recommended treatments for suspected community-acquired pneumonia.
Major finding: The primary outcome – all-cause mortality at 90 days after admission – favored beta-lactam monotherapy over beta-lactam plus macrolide combination therapy and macrolide monotherapy.
Data source: A multicenter, cluster-randomized, crossover trial comparing 90-day outcomes after three different empirical antibiotic therapies in 2,283 adults suspected of having community-acquired pneumonia.
Disclosures: The Netherlands Organization for Health Research and Development supported the study. Dr. Postma and his associates reported having no financial disclosures.
Anxiety tied to fear of falling • fatigue • difficulty concentrating • Dx?
THE CASE
A 21-year-old college student was referred to us by the counseling center at our university for a psychiatric evaluation after 11 psychotherapy sessions over 3 months had failed to reduce her feelings of anxiety and panic.
During our evaluation, the patient described feeling “not quite right” for many months. She had been experiencing mental fogginess, fatigue, and worsening concentration/ memory. Her anxiety, which had been gradually increasing, was the result of being unsure about her gait. She first noticed this while walking down some bleachers; she felt dizzy, was afraid of falling, and couldn’t walk down without assistance. All episodes of “panic” occurred in situations where she experienced disequilibrium, unsteady gait, and fear of falling. She grew fearful of driving or going anywhere without assistance.
The patient had celiac disease that was well controlled with a gluten-free diet. She had no personal or family psychiatric history and no history of substance abuse.
THE DIAGNOSIS
Physical exam and lab studies, including a complete blood count, comprehensive metabolic panel, and thyrotropin and folate levels, were normal. Her homocysteine level was 11.8 μmol/L (reference range, 5.4-11.9 μmol/L) and vitamin B12 level was 292 pg/mL (reference range, 200-1100 pg/mL). Her lab report included a note that read, “Although the reference range for vitamin B12 is 200 to 1100 pg/mL, it has been reported that between 5% and 10% of patients with values between 200 and 400 pg/mL may experience neuropsychiatric and hematologic abnormalities due to occult B12 deficiency; <1% of patients with values >400 pg/mL will have symptoms.”
Based on this vitamin B12 level, the patient’s symptoms, and her borderline high homocysteine level, we diagnosed vitamin B12 deficiency.
DISCUSSION
There are no recommendations by the US Preventive Services Task Force or any other major US medical society for routine vitamin B12 screening.1 In Canada, the Medical Services Commission of the British Columbia Ministry of Health recommends B12 screening for patients who present with macrocytic anemia or unexplained neurologic symptoms (eg, paresthesia, numbness, poor motor coordination, memory lapses, or cognitive or personality changes).2
Vitamin B12 deficiency can be caused by numerous conditions, including those that cause malabsorption (such as gastric bypass). It can also be caused by diseases such as human immunodeficiency virus infection or Crohn’s disease, long-term adherence to a vegetarian or vegan diet, or by any other lack of dietary intake.1 The condition can cause hematologic-related signs and symptoms such as megaloblastic anemia, fatigue, and syncope. It also can have neurologic manifestations, including paresthesia, weakness, motor disturbances (including gait abnormalities), vision loss, and a wide range of cognitive and behavioral changes.1 Anemia is uncommon because since 1998, the US Food and Drug Administration has required fortification of all enriched grain and cereal products with folic acid; thus, vitamin B12 deficiency may proceed without anemia revealing its presence.1
A controversial topic. Vitamin B12 deficiency is a complicated and controversial subject. Specifically, there is uncertainty about the clinical importance of lower serum levels of vitamin B12 (200-400 pg/mL), their impact on well-being, and the need for treatment. In addition to measuring a patient’s serum B12 level, testing a second biomarker (such as homocysteine or methylmalonic acid) can be helpful in establishing a diagnosis of B12 deficiency.1 Levels of each of these are elevated in patients with B12 deficiency.1
Although vitamin B12 deficiency has been well studied in older patients,3 little has been published about the condition in young adults. National Health and Nutrition Examination Survey (NHANES) data from 2000 to 2004 shows that almost 40% of people ages 19 to 30 years have a B12 level <400 pg/mL.1 How many of these individuals are at risk of complications of B12 deficiency is unknown.
B12 supplementation might improve depression, anxiety
B12 supplementation is inexpensive and has no significant adverse effects.1 It can be administered orally, parenterally (intramuscularly or subcutaneously), or intranasally.1 A common oral regimen is 1 mg/d; parental regimens vary widely, but might include a 1-mg injection once a week for 8 weeks, then once a month for life.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety. A Pakistani study randomized 73 patients with depression and “low normal” B12 levels (190-300 pg/mL) to an antidepressant only (equivalent to imipramine 100-250 mg/d or fluoxetine 20-40 mg/d) or an antidepressant plus parenteral B12 (1000 mcg once a week).4 At 3 months follow-up, 100% of the treatment group showed at least a 20% reduction in their Hamilton Depression Rating Scale (HAM-D) score, compared to 69% in the control arm (P<.001).4
A Swedish study analyzed the effects of several B vitamins, including 0.5 mg/d of B12 vs placebo on mood in 65 celiac patients on a gluten-free diet who had borderline/low normal B12 levels (>191 pg/mL).5 Patients who scored low on a measure of psychological well-being at the beginning of the study and who received B12 experienced significant improvements in anxiety and depressed mood compared to those who received placebo.
Our patient
Because neurologic and psychiatric symptoms require assured compliance and urgent treatment, our patient received vitamin B12 parenterally as cyanocobalamin 1 mg/mL. She was given this dosage intramuscularly once a day for 5 days, then once a week for 4 weeks. She will continue to receive it once a month indefinitely.
The patient was advised that if she wished to switch to oral therapy, she could do so after several months of parenteral treatment, as long as she had close follow-up with frequent B12 measurements to assure that she was absorbing oral therapy. Her anxiety and mood symptoms resolved within one month, and her disequilibrium was almost entirely resolved within 3 months of treatment.
THE TAKEAWAY
Although more common in older patients, vitamin B12 deficiency can also affect younger patients. “Low normal” B12 levels (200-400 pg/mL) may affect psychological well-being.
Consider testing serum B12 and a second biomarker—such as homocysteine or methylmalonic acid, if indicated—in patients who present with depressed mood, anxiety, cognitive symptoms, and/or fatigue. Vitamin B12 supplementation can be administered orally and has no major adverse effects.
1. Centers for Disease Control and Prevention. Why vitamin B12 deficiency should be on your radar screen. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/b12/. Accessed February 26, 2015.
2. Guidelines and Protocols Advisory Committee, Medical Services Commission, British Columbia Ministry of Health. Cobalamin (vitamin B12) Deficiency - Investigation & Management. British Columbia Ministry of Health Web site. Available at: http://www.bcguidelines.ca/guideline_cobalamin.html. Accessed March 13, 2015.
3. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly outpatients. J Am Geriatr Soc. 1992;40:1197-1204.
4. Syed EU, Wasay M, Awan S. Vitamin B12 supplementation in treating major depressive disorder: a randomized controlled trial. Open Neurol J. 2013;7:44-48
5. Hallert C, Svensson M, Tholstrup J, et al. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Ailment Pharmacol Ther. 2009;29:811-816.
THE CASE
A 21-year-old college student was referred to us by the counseling center at our university for a psychiatric evaluation after 11 psychotherapy sessions over 3 months had failed to reduce her feelings of anxiety and panic.
During our evaluation, the patient described feeling “not quite right” for many months. She had been experiencing mental fogginess, fatigue, and worsening concentration/ memory. Her anxiety, which had been gradually increasing, was the result of being unsure about her gait. She first noticed this while walking down some bleachers; she felt dizzy, was afraid of falling, and couldn’t walk down without assistance. All episodes of “panic” occurred in situations where she experienced disequilibrium, unsteady gait, and fear of falling. She grew fearful of driving or going anywhere without assistance.
The patient had celiac disease that was well controlled with a gluten-free diet. She had no personal or family psychiatric history and no history of substance abuse.
THE DIAGNOSIS
Physical exam and lab studies, including a complete blood count, comprehensive metabolic panel, and thyrotropin and folate levels, were normal. Her homocysteine level was 11.8 μmol/L (reference range, 5.4-11.9 μmol/L) and vitamin B12 level was 292 pg/mL (reference range, 200-1100 pg/mL). Her lab report included a note that read, “Although the reference range for vitamin B12 is 200 to 1100 pg/mL, it has been reported that between 5% and 10% of patients with values between 200 and 400 pg/mL may experience neuropsychiatric and hematologic abnormalities due to occult B12 deficiency; <1% of patients with values >400 pg/mL will have symptoms.”
Based on this vitamin B12 level, the patient’s symptoms, and her borderline high homocysteine level, we diagnosed vitamin B12 deficiency.
DISCUSSION
There are no recommendations by the US Preventive Services Task Force or any other major US medical society for routine vitamin B12 screening.1 In Canada, the Medical Services Commission of the British Columbia Ministry of Health recommends B12 screening for patients who present with macrocytic anemia or unexplained neurologic symptoms (eg, paresthesia, numbness, poor motor coordination, memory lapses, or cognitive or personality changes).2
Vitamin B12 deficiency can be caused by numerous conditions, including those that cause malabsorption (such as gastric bypass). It can also be caused by diseases such as human immunodeficiency virus infection or Crohn’s disease, long-term adherence to a vegetarian or vegan diet, or by any other lack of dietary intake.1 The condition can cause hematologic-related signs and symptoms such as megaloblastic anemia, fatigue, and syncope. It also can have neurologic manifestations, including paresthesia, weakness, motor disturbances (including gait abnormalities), vision loss, and a wide range of cognitive and behavioral changes.1 Anemia is uncommon because since 1998, the US Food and Drug Administration has required fortification of all enriched grain and cereal products with folic acid; thus, vitamin B12 deficiency may proceed without anemia revealing its presence.1
A controversial topic. Vitamin B12 deficiency is a complicated and controversial subject. Specifically, there is uncertainty about the clinical importance of lower serum levels of vitamin B12 (200-400 pg/mL), their impact on well-being, and the need for treatment. In addition to measuring a patient’s serum B12 level, testing a second biomarker (such as homocysteine or methylmalonic acid) can be helpful in establishing a diagnosis of B12 deficiency.1 Levels of each of these are elevated in patients with B12 deficiency.1
Although vitamin B12 deficiency has been well studied in older patients,3 little has been published about the condition in young adults. National Health and Nutrition Examination Survey (NHANES) data from 2000 to 2004 shows that almost 40% of people ages 19 to 30 years have a B12 level <400 pg/mL.1 How many of these individuals are at risk of complications of B12 deficiency is unknown.
B12 supplementation might improve depression, anxiety
B12 supplementation is inexpensive and has no significant adverse effects.1 It can be administered orally, parenterally (intramuscularly or subcutaneously), or intranasally.1 A common oral regimen is 1 mg/d; parental regimens vary widely, but might include a 1-mg injection once a week for 8 weeks, then once a month for life.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety. A Pakistani study randomized 73 patients with depression and “low normal” B12 levels (190-300 pg/mL) to an antidepressant only (equivalent to imipramine 100-250 mg/d or fluoxetine 20-40 mg/d) or an antidepressant plus parenteral B12 (1000 mcg once a week).4 At 3 months follow-up, 100% of the treatment group showed at least a 20% reduction in their Hamilton Depression Rating Scale (HAM-D) score, compared to 69% in the control arm (P<.001).4
A Swedish study analyzed the effects of several B vitamins, including 0.5 mg/d of B12 vs placebo on mood in 65 celiac patients on a gluten-free diet who had borderline/low normal B12 levels (>191 pg/mL).5 Patients who scored low on a measure of psychological well-being at the beginning of the study and who received B12 experienced significant improvements in anxiety and depressed mood compared to those who received placebo.
Our patient
Because neurologic and psychiatric symptoms require assured compliance and urgent treatment, our patient received vitamin B12 parenterally as cyanocobalamin 1 mg/mL. She was given this dosage intramuscularly once a day for 5 days, then once a week for 4 weeks. She will continue to receive it once a month indefinitely.
The patient was advised that if she wished to switch to oral therapy, she could do so after several months of parenteral treatment, as long as she had close follow-up with frequent B12 measurements to assure that she was absorbing oral therapy. Her anxiety and mood symptoms resolved within one month, and her disequilibrium was almost entirely resolved within 3 months of treatment.
THE TAKEAWAY
Although more common in older patients, vitamin B12 deficiency can also affect younger patients. “Low normal” B12 levels (200-400 pg/mL) may affect psychological well-being.
Consider testing serum B12 and a second biomarker—such as homocysteine or methylmalonic acid, if indicated—in patients who present with depressed mood, anxiety, cognitive symptoms, and/or fatigue. Vitamin B12 supplementation can be administered orally and has no major adverse effects.
THE CASE
A 21-year-old college student was referred to us by the counseling center at our university for a psychiatric evaluation after 11 psychotherapy sessions over 3 months had failed to reduce her feelings of anxiety and panic.
During our evaluation, the patient described feeling “not quite right” for many months. She had been experiencing mental fogginess, fatigue, and worsening concentration/ memory. Her anxiety, which had been gradually increasing, was the result of being unsure about her gait. She first noticed this while walking down some bleachers; she felt dizzy, was afraid of falling, and couldn’t walk down without assistance. All episodes of “panic” occurred in situations where she experienced disequilibrium, unsteady gait, and fear of falling. She grew fearful of driving or going anywhere without assistance.
The patient had celiac disease that was well controlled with a gluten-free diet. She had no personal or family psychiatric history and no history of substance abuse.
THE DIAGNOSIS
Physical exam and lab studies, including a complete blood count, comprehensive metabolic panel, and thyrotropin and folate levels, were normal. Her homocysteine level was 11.8 μmol/L (reference range, 5.4-11.9 μmol/L) and vitamin B12 level was 292 pg/mL (reference range, 200-1100 pg/mL). Her lab report included a note that read, “Although the reference range for vitamin B12 is 200 to 1100 pg/mL, it has been reported that between 5% and 10% of patients with values between 200 and 400 pg/mL may experience neuropsychiatric and hematologic abnormalities due to occult B12 deficiency; <1% of patients with values >400 pg/mL will have symptoms.”
Based on this vitamin B12 level, the patient’s symptoms, and her borderline high homocysteine level, we diagnosed vitamin B12 deficiency.
DISCUSSION
There are no recommendations by the US Preventive Services Task Force or any other major US medical society for routine vitamin B12 screening.1 In Canada, the Medical Services Commission of the British Columbia Ministry of Health recommends B12 screening for patients who present with macrocytic anemia or unexplained neurologic symptoms (eg, paresthesia, numbness, poor motor coordination, memory lapses, or cognitive or personality changes).2
Vitamin B12 deficiency can be caused by numerous conditions, including those that cause malabsorption (such as gastric bypass). It can also be caused by diseases such as human immunodeficiency virus infection or Crohn’s disease, long-term adherence to a vegetarian or vegan diet, or by any other lack of dietary intake.1 The condition can cause hematologic-related signs and symptoms such as megaloblastic anemia, fatigue, and syncope. It also can have neurologic manifestations, including paresthesia, weakness, motor disturbances (including gait abnormalities), vision loss, and a wide range of cognitive and behavioral changes.1 Anemia is uncommon because since 1998, the US Food and Drug Administration has required fortification of all enriched grain and cereal products with folic acid; thus, vitamin B12 deficiency may proceed without anemia revealing its presence.1
A controversial topic. Vitamin B12 deficiency is a complicated and controversial subject. Specifically, there is uncertainty about the clinical importance of lower serum levels of vitamin B12 (200-400 pg/mL), their impact on well-being, and the need for treatment. In addition to measuring a patient’s serum B12 level, testing a second biomarker (such as homocysteine or methylmalonic acid) can be helpful in establishing a diagnosis of B12 deficiency.1 Levels of each of these are elevated in patients with B12 deficiency.1
Although vitamin B12 deficiency has been well studied in older patients,3 little has been published about the condition in young adults. National Health and Nutrition Examination Survey (NHANES) data from 2000 to 2004 shows that almost 40% of people ages 19 to 30 years have a B12 level <400 pg/mL.1 How many of these individuals are at risk of complications of B12 deficiency is unknown.
B12 supplementation might improve depression, anxiety
B12 supplementation is inexpensive and has no significant adverse effects.1 It can be administered orally, parenterally (intramuscularly or subcutaneously), or intranasally.1 A common oral regimen is 1 mg/d; parental regimens vary widely, but might include a 1-mg injection once a week for 8 weeks, then once a month for life.1
Some evidence suggests B12 supplementation may improve symptoms of depression and anxiety. A Pakistani study randomized 73 patients with depression and “low normal” B12 levels (190-300 pg/mL) to an antidepressant only (equivalent to imipramine 100-250 mg/d or fluoxetine 20-40 mg/d) or an antidepressant plus parenteral B12 (1000 mcg once a week).4 At 3 months follow-up, 100% of the treatment group showed at least a 20% reduction in their Hamilton Depression Rating Scale (HAM-D) score, compared to 69% in the control arm (P<.001).4
A Swedish study analyzed the effects of several B vitamins, including 0.5 mg/d of B12 vs placebo on mood in 65 celiac patients on a gluten-free diet who had borderline/low normal B12 levels (>191 pg/mL).5 Patients who scored low on a measure of psychological well-being at the beginning of the study and who received B12 experienced significant improvements in anxiety and depressed mood compared to those who received placebo.
Our patient
Because neurologic and psychiatric symptoms require assured compliance and urgent treatment, our patient received vitamin B12 parenterally as cyanocobalamin 1 mg/mL. She was given this dosage intramuscularly once a day for 5 days, then once a week for 4 weeks. She will continue to receive it once a month indefinitely.
The patient was advised that if she wished to switch to oral therapy, she could do so after several months of parenteral treatment, as long as she had close follow-up with frequent B12 measurements to assure that she was absorbing oral therapy. Her anxiety and mood symptoms resolved within one month, and her disequilibrium was almost entirely resolved within 3 months of treatment.
THE TAKEAWAY
Although more common in older patients, vitamin B12 deficiency can also affect younger patients. “Low normal” B12 levels (200-400 pg/mL) may affect psychological well-being.
Consider testing serum B12 and a second biomarker—such as homocysteine or methylmalonic acid, if indicated—in patients who present with depressed mood, anxiety, cognitive symptoms, and/or fatigue. Vitamin B12 supplementation can be administered orally and has no major adverse effects.
1. Centers for Disease Control and Prevention. Why vitamin B12 deficiency should be on your radar screen. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/b12/. Accessed February 26, 2015.
2. Guidelines and Protocols Advisory Committee, Medical Services Commission, British Columbia Ministry of Health. Cobalamin (vitamin B12) Deficiency - Investigation & Management. British Columbia Ministry of Health Web site. Available at: http://www.bcguidelines.ca/guideline_cobalamin.html. Accessed March 13, 2015.
3. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly outpatients. J Am Geriatr Soc. 1992;40:1197-1204.
4. Syed EU, Wasay M, Awan S. Vitamin B12 supplementation in treating major depressive disorder: a randomized controlled trial. Open Neurol J. 2013;7:44-48
5. Hallert C, Svensson M, Tholstrup J, et al. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Ailment Pharmacol Ther. 2009;29:811-816.
1. Centers for Disease Control and Prevention. Why vitamin B12 deficiency should be on your radar screen. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/b12/. Accessed February 26, 2015.
2. Guidelines and Protocols Advisory Committee, Medical Services Commission, British Columbia Ministry of Health. Cobalamin (vitamin B12) Deficiency - Investigation & Management. British Columbia Ministry of Health Web site. Available at: http://www.bcguidelines.ca/guideline_cobalamin.html. Accessed March 13, 2015.
3. Pennypacker LC, Allen RH, Kelly JP, et al. High prevalence of cobalamin deficiency in elderly outpatients. J Am Geriatr Soc. 1992;40:1197-1204.
4. Syed EU, Wasay M, Awan S. Vitamin B12 supplementation in treating major depressive disorder: a randomized controlled trial. Open Neurol J. 2013;7:44-48
5. Hallert C, Svensson M, Tholstrup J, et al. Clinical trial: B vitamins improve health in patients with coeliac disease living on a gluten-free diet. Ailment Pharmacol Ther. 2009;29:811-816.
Headache • fatigue • blurred vision • Dx?
THE CASE
One month after moving into her mother’s apartment, a 27-year-old woman sought care at our clinic for fatigue, headache, blurred vision, nausea, and morning vomiting. She had weakness and difficulty sleeping, but denied any fever, rashes, neck stiffness, recent travel, trauma, or tobacco or illicit drug use. She did, however, have a 6-year history of migraines. Her physical exam was normal. She was sent home with a prescription for tramadol 50 mg bid for her headaches.
The patient subsequently went to the emergency department 3 times for the same complaints; none of the treatments she received there (mostly acetaminophen with codeine) relieved her symptoms. Three weeks later she returned to our clinic. She was distressed that the symptoms hadn’t gone away, and noted that her family was now experiencing similar symptoms.
Her temperature was 98.1°F (36.7°C), blood pressure was 131/88 mm Hg, pulse was 85 beats/min, and respiratory rate was 18 breaths/min. Physical and neurologic exams were normal.
THE DIAGNOSIS
Although most of the patient’s lab test results were within normal ranges, her carboxyhemoglobin (COHb) level was 4.2%. COHb levels of >2% to 3% in nonsmokers or >9% to 10% in smokers suggest carbon monoxide (CO) poisoning.1,2 Based on this finding and our patient’s symptoms, we diagnosed unintentional CO poisoning. We recommended that she and her mother vacate the apartment and have it inspected.
DISCUSSION
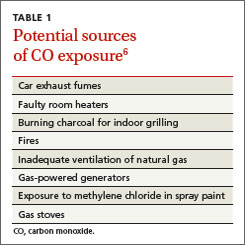
CO is the leading cause of poisoning mortality in the United States, and causes half of all fatal poisonings worldwide.1,3,4 It is a colorless, odorless, and tasteless gas that is produced by the incomplete combustion of carbon-based products, such as coal or gas.5,6 Exposure can occur from car exhaust fumes, faulty room heaters, and other sources (TABLE 1).6 The incidence of CO poisoning is higher during the winter months and after natural disasters. Individuals who have a lowered oxygen capacity, such as older adults, pregnant women (and their fetuses), infants, and patients with anemia, cardiovascular disease, or cerebrovascular disease, are more susceptible to CO poisoning.5,6
COHb, a stable complex of CO that forms in red blood cells when CO is inhaled, impairs oxygen delivery and peripheral utilization, resulting in cellular hypoxia.1 Signs and symptoms of CO poisoning are nonspecific and require a high degree of clinical suspicion for early diagnosis and treatment. Although cherry-red lips, peripheral cyanosis, and retinal hemorrhages are often described as “classic” symptoms of CO poisoning, these are rarely seen.6 The most common symptoms are actually headache (90%), dizziness (82%), and weakness (53%).7 Other symptoms include nausea, vomiting, confusion, visual disturbances, loss of consciousness, angina, seizure, and fatigue.6,7 Symptoms of chronic CO poisoning may differ from those of acute poisoning and can include chronic fatigue, neuropathy, and memory deficit.8
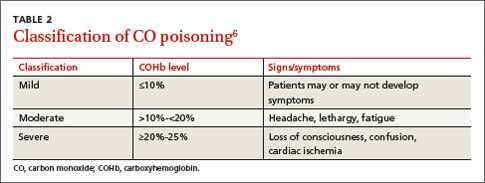
The differential diagnosis for CO poisoning includes flu-like syndrome/influenza/other viral illnesses, migraine or tension headaches, depression, transient ischemic attack, encephalitis, coronary artery disease, gastroenteritis or food poisoning, seizures, and dysrhythmias.1,4 Lab testing for COHb can help narrow the diagnosis. CO poisoning can be classified as mild, moderate, or severe based on COHb levels and the patient’s signs and symptoms (TABLE 2).6 However, COHb level is a poor predictor of clinical presentation and should not be used to dictate management.2,7
Oxygen therapy is the recommended treatment
Early treatment with supplemental oxygen is recommended to reduce the length of time red blood cells are exposed to CO.1 A COHb level >25% is the criterion for hyperbaric oxygen therapy.1,3 Patients should receive treatment until their symptoms become less intense.
Delayed neuropsychiatric sequelae (DNS) can occur in up to one-third of patients with acute CO poisoning more than a month after apparent recovery.1,6,9 DNS symptoms include cognitive changes, emotional lability, visual disturbances, disorientation, depression, dementia, psychotic behavior, parkinsonism, amnesia, and incontinence.1,6,9 Approximately 50% to 75% of patients with DNS recover spontaneously within a year with symptomatic treatment.1,6,9
Our patient
After recommending that our patient (and her mother) leave the apartment and have it inspected, we later learned that the fire department was unable to determine the source of the CO. A CO detector was installed and our patient was advised to keep the windows in the apartment open to allow for adequate oxygen flow. One month later she returned to our clinic and reported that her symptoms resolved; serum COHb was negative upon repeat lab tests.
THE TAKEAWAY
Patients who present with headaches, dizziness and/or fatigue should be evaluated for CO poisoning. The patient’s environmental history should be reviewed carefully, especially because CO poisoning is more common during the winter months. Oxygen therapy is the mainstay of treatment. Up to one-third of patients with acute poisoning may develop delayed neuropsychiatric sequelae, including cognitive changes, emotional lability, visual disturbances, disorientation, and depression, that may resolve within one year.
1. Nikkanen H, Skolnik A. Diagnosis and management of carbon monoxide poisoning in the emergency department. Emerg Med Pract. 2011;13:1-14.
2. Hampson NB, Hauff NM. Carboxyhemoglobin levels in carbon monoxide poisoning: do they correlate with the clinical picture? Am J Emerg Med. 2008;26:665-669.
3. Kao LW, Nañagas KA. Toxicity associated with carbon monoxide. Clin Lab Med. 2006;26:99-125.
4. Varon J, Marik PE, Fromm RE Jr, et al. Carbon monoxide poisoning: a review for clinicians. J Emerg Med. 1999;17:87-93.
5. Harper A, Croft-Baker J. Carbon monoxide poisoning: undetected by both patients and their doctors. Age Ageing. 2004;33:105-109.
6. Smollin C, Olson K. Carbon monoxide poisoning (acute). BMJ Clin Evid. 2010;2010. pii:2103.
7. Wright J. Chronic and occult carbon monoxide poisoning: we don’t know what we’re missing. Emerg Med J. 2002;19:366-390.
8. Weaver LK. Clinical practice. Carbon monoxide poisoning. N Engl J Med. 2009;360:1217-1225.
9. Bhatia R, Chacko F, Lal V, et al. Reversible delayed neuropsychiatric syndrome following acute carbon monoxide exposure. Indian J Occup Environ Med. 2007;11:80-82.
THE CASE
One month after moving into her mother’s apartment, a 27-year-old woman sought care at our clinic for fatigue, headache, blurred vision, nausea, and morning vomiting. She had weakness and difficulty sleeping, but denied any fever, rashes, neck stiffness, recent travel, trauma, or tobacco or illicit drug use. She did, however, have a 6-year history of migraines. Her physical exam was normal. She was sent home with a prescription for tramadol 50 mg bid for her headaches.
The patient subsequently went to the emergency department 3 times for the same complaints; none of the treatments she received there (mostly acetaminophen with codeine) relieved her symptoms. Three weeks later she returned to our clinic. She was distressed that the symptoms hadn’t gone away, and noted that her family was now experiencing similar symptoms.
Her temperature was 98.1°F (36.7°C), blood pressure was 131/88 mm Hg, pulse was 85 beats/min, and respiratory rate was 18 breaths/min. Physical and neurologic exams were normal.
THE DIAGNOSIS
Although most of the patient’s lab test results were within normal ranges, her carboxyhemoglobin (COHb) level was 4.2%. COHb levels of >2% to 3% in nonsmokers or >9% to 10% in smokers suggest carbon monoxide (CO) poisoning.1,2 Based on this finding and our patient’s symptoms, we diagnosed unintentional CO poisoning. We recommended that she and her mother vacate the apartment and have it inspected.
DISCUSSION
CO is the leading cause of poisoning mortality in the United States, and causes half of all fatal poisonings worldwide.1,3,4 It is a colorless, odorless, and tasteless gas that is produced by the incomplete combustion of carbon-based products, such as coal or gas.5,6 Exposure can occur from car exhaust fumes, faulty room heaters, and other sources (TABLE 1).6 The incidence of CO poisoning is higher during the winter months and after natural disasters. Individuals who have a lowered oxygen capacity, such as older adults, pregnant women (and their fetuses), infants, and patients with anemia, cardiovascular disease, or cerebrovascular disease, are more susceptible to CO poisoning.5,6
COHb, a stable complex of CO that forms in red blood cells when CO is inhaled, impairs oxygen delivery and peripheral utilization, resulting in cellular hypoxia.1 Signs and symptoms of CO poisoning are nonspecific and require a high degree of clinical suspicion for early diagnosis and treatment. Although cherry-red lips, peripheral cyanosis, and retinal hemorrhages are often described as “classic” symptoms of CO poisoning, these are rarely seen.6 The most common symptoms are actually headache (90%), dizziness (82%), and weakness (53%).7 Other symptoms include nausea, vomiting, confusion, visual disturbances, loss of consciousness, angina, seizure, and fatigue.6,7 Symptoms of chronic CO poisoning may differ from those of acute poisoning and can include chronic fatigue, neuropathy, and memory deficit.8
The differential diagnosis for CO poisoning includes flu-like syndrome/influenza/other viral illnesses, migraine or tension headaches, depression, transient ischemic attack, encephalitis, coronary artery disease, gastroenteritis or food poisoning, seizures, and dysrhythmias.1,4 Lab testing for COHb can help narrow the diagnosis. CO poisoning can be classified as mild, moderate, or severe based on COHb levels and the patient’s signs and symptoms (TABLE 2).6 However, COHb level is a poor predictor of clinical presentation and should not be used to dictate management.2,7
Oxygen therapy is the recommended treatment
Early treatment with supplemental oxygen is recommended to reduce the length of time red blood cells are exposed to CO.1 A COHb level >25% is the criterion for hyperbaric oxygen therapy.1,3 Patients should receive treatment until their symptoms become less intense.
Delayed neuropsychiatric sequelae (DNS) can occur in up to one-third of patients with acute CO poisoning more than a month after apparent recovery.1,6,9 DNS symptoms include cognitive changes, emotional lability, visual disturbances, disorientation, depression, dementia, psychotic behavior, parkinsonism, amnesia, and incontinence.1,6,9 Approximately 50% to 75% of patients with DNS recover spontaneously within a year with symptomatic treatment.1,6,9
Our patient
After recommending that our patient (and her mother) leave the apartment and have it inspected, we later learned that the fire department was unable to determine the source of the CO. A CO detector was installed and our patient was advised to keep the windows in the apartment open to allow for adequate oxygen flow. One month later she returned to our clinic and reported that her symptoms resolved; serum COHb was negative upon repeat lab tests.
THE TAKEAWAY
Patients who present with headaches, dizziness and/or fatigue should be evaluated for CO poisoning. The patient’s environmental history should be reviewed carefully, especially because CO poisoning is more common during the winter months. Oxygen therapy is the mainstay of treatment. Up to one-third of patients with acute poisoning may develop delayed neuropsychiatric sequelae, including cognitive changes, emotional lability, visual disturbances, disorientation, and depression, that may resolve within one year.
THE CASE
One month after moving into her mother’s apartment, a 27-year-old woman sought care at our clinic for fatigue, headache, blurred vision, nausea, and morning vomiting. She had weakness and difficulty sleeping, but denied any fever, rashes, neck stiffness, recent travel, trauma, or tobacco or illicit drug use. She did, however, have a 6-year history of migraines. Her physical exam was normal. She was sent home with a prescription for tramadol 50 mg bid for her headaches.
The patient subsequently went to the emergency department 3 times for the same complaints; none of the treatments she received there (mostly acetaminophen with codeine) relieved her symptoms. Three weeks later she returned to our clinic. She was distressed that the symptoms hadn’t gone away, and noted that her family was now experiencing similar symptoms.
Her temperature was 98.1°F (36.7°C), blood pressure was 131/88 mm Hg, pulse was 85 beats/min, and respiratory rate was 18 breaths/min. Physical and neurologic exams were normal.
THE DIAGNOSIS
Although most of the patient’s lab test results were within normal ranges, her carboxyhemoglobin (COHb) level was 4.2%. COHb levels of >2% to 3% in nonsmokers or >9% to 10% in smokers suggest carbon monoxide (CO) poisoning.1,2 Based on this finding and our patient’s symptoms, we diagnosed unintentional CO poisoning. We recommended that she and her mother vacate the apartment and have it inspected.
DISCUSSION
CO is the leading cause of poisoning mortality in the United States, and causes half of all fatal poisonings worldwide.1,3,4 It is a colorless, odorless, and tasteless gas that is produced by the incomplete combustion of carbon-based products, such as coal or gas.5,6 Exposure can occur from car exhaust fumes, faulty room heaters, and other sources (TABLE 1).6 The incidence of CO poisoning is higher during the winter months and after natural disasters. Individuals who have a lowered oxygen capacity, such as older adults, pregnant women (and their fetuses), infants, and patients with anemia, cardiovascular disease, or cerebrovascular disease, are more susceptible to CO poisoning.5,6
COHb, a stable complex of CO that forms in red blood cells when CO is inhaled, impairs oxygen delivery and peripheral utilization, resulting in cellular hypoxia.1 Signs and symptoms of CO poisoning are nonspecific and require a high degree of clinical suspicion for early diagnosis and treatment. Although cherry-red lips, peripheral cyanosis, and retinal hemorrhages are often described as “classic” symptoms of CO poisoning, these are rarely seen.6 The most common symptoms are actually headache (90%), dizziness (82%), and weakness (53%).7 Other symptoms include nausea, vomiting, confusion, visual disturbances, loss of consciousness, angina, seizure, and fatigue.6,7 Symptoms of chronic CO poisoning may differ from those of acute poisoning and can include chronic fatigue, neuropathy, and memory deficit.8
The differential diagnosis for CO poisoning includes flu-like syndrome/influenza/other viral illnesses, migraine or tension headaches, depression, transient ischemic attack, encephalitis, coronary artery disease, gastroenteritis or food poisoning, seizures, and dysrhythmias.1,4 Lab testing for COHb can help narrow the diagnosis. CO poisoning can be classified as mild, moderate, or severe based on COHb levels and the patient’s signs and symptoms (TABLE 2).6 However, COHb level is a poor predictor of clinical presentation and should not be used to dictate management.2,7
Oxygen therapy is the recommended treatment
Early treatment with supplemental oxygen is recommended to reduce the length of time red blood cells are exposed to CO.1 A COHb level >25% is the criterion for hyperbaric oxygen therapy.1,3 Patients should receive treatment until their symptoms become less intense.
Delayed neuropsychiatric sequelae (DNS) can occur in up to one-third of patients with acute CO poisoning more than a month after apparent recovery.1,6,9 DNS symptoms include cognitive changes, emotional lability, visual disturbances, disorientation, depression, dementia, psychotic behavior, parkinsonism, amnesia, and incontinence.1,6,9 Approximately 50% to 75% of patients with DNS recover spontaneously within a year with symptomatic treatment.1,6,9
Our patient
After recommending that our patient (and her mother) leave the apartment and have it inspected, we later learned that the fire department was unable to determine the source of the CO. A CO detector was installed and our patient was advised to keep the windows in the apartment open to allow for adequate oxygen flow. One month later she returned to our clinic and reported that her symptoms resolved; serum COHb was negative upon repeat lab tests.
THE TAKEAWAY
Patients who present with headaches, dizziness and/or fatigue should be evaluated for CO poisoning. The patient’s environmental history should be reviewed carefully, especially because CO poisoning is more common during the winter months. Oxygen therapy is the mainstay of treatment. Up to one-third of patients with acute poisoning may develop delayed neuropsychiatric sequelae, including cognitive changes, emotional lability, visual disturbances, disorientation, and depression, that may resolve within one year.
1. Nikkanen H, Skolnik A. Diagnosis and management of carbon monoxide poisoning in the emergency department. Emerg Med Pract. 2011;13:1-14.
2. Hampson NB, Hauff NM. Carboxyhemoglobin levels in carbon monoxide poisoning: do they correlate with the clinical picture? Am J Emerg Med. 2008;26:665-669.
3. Kao LW, Nañagas KA. Toxicity associated with carbon monoxide. Clin Lab Med. 2006;26:99-125.
4. Varon J, Marik PE, Fromm RE Jr, et al. Carbon monoxide poisoning: a review for clinicians. J Emerg Med. 1999;17:87-93.
5. Harper A, Croft-Baker J. Carbon monoxide poisoning: undetected by both patients and their doctors. Age Ageing. 2004;33:105-109.
6. Smollin C, Olson K. Carbon monoxide poisoning (acute). BMJ Clin Evid. 2010;2010. pii:2103.
7. Wright J. Chronic and occult carbon monoxide poisoning: we don’t know what we’re missing. Emerg Med J. 2002;19:366-390.
8. Weaver LK. Clinical practice. Carbon monoxide poisoning. N Engl J Med. 2009;360:1217-1225.
9. Bhatia R, Chacko F, Lal V, et al. Reversible delayed neuropsychiatric syndrome following acute carbon monoxide exposure. Indian J Occup Environ Med. 2007;11:80-82.
1. Nikkanen H, Skolnik A. Diagnosis and management of carbon monoxide poisoning in the emergency department. Emerg Med Pract. 2011;13:1-14.
2. Hampson NB, Hauff NM. Carboxyhemoglobin levels in carbon monoxide poisoning: do they correlate with the clinical picture? Am J Emerg Med. 2008;26:665-669.
3. Kao LW, Nañagas KA. Toxicity associated with carbon monoxide. Clin Lab Med. 2006;26:99-125.
4. Varon J, Marik PE, Fromm RE Jr, et al. Carbon monoxide poisoning: a review for clinicians. J Emerg Med. 1999;17:87-93.
5. Harper A, Croft-Baker J. Carbon monoxide poisoning: undetected by both patients and their doctors. Age Ageing. 2004;33:105-109.
6. Smollin C, Olson K. Carbon monoxide poisoning (acute). BMJ Clin Evid. 2010;2010. pii:2103.
7. Wright J. Chronic and occult carbon monoxide poisoning: we don’t know what we’re missing. Emerg Med J. 2002;19:366-390.
8. Weaver LK. Clinical practice. Carbon monoxide poisoning. N Engl J Med. 2009;360:1217-1225.
9. Bhatia R, Chacko F, Lal V, et al. Reversible delayed neuropsychiatric syndrome following acute carbon monoxide exposure. Indian J Occup Environ Med. 2007;11:80-82.

U.S. grants drug company $12 million to develop Ebola drug
The federal government has taken its first step toward supporting an experimental drug for treating Ebola.
The U.S. Department of Health & Human Services’ Office of the Assistant Secretary for Preparedness and Response committed to funding BioCryst Pharmaceuticals’ development and manufacturing of such a drug, according to a written statement issued by the agency March 31.
The Office awarded approximately $12 million to the North Carolina–based drug company, but the size of the grant could grow to $35 million.
The drug, BCX4430, is a small-molecule drug that prevents the Ebola virus from reproducing in the body. BioCryst is currently using money from the National Institutes of Health to conduct phase I safety studies of the drug in healthy volunteers.
The drug’s effectiveness at treating both the Ebola and Marburg viruses in nonhuman primates indicates that “BCX4430 may be useful as a broad spectrum antiviral drug,” according to the statement.
The federal government has taken its first step toward supporting an experimental drug for treating Ebola.
The U.S. Department of Health & Human Services’ Office of the Assistant Secretary for Preparedness and Response committed to funding BioCryst Pharmaceuticals’ development and manufacturing of such a drug, according to a written statement issued by the agency March 31.
The Office awarded approximately $12 million to the North Carolina–based drug company, but the size of the grant could grow to $35 million.
The drug, BCX4430, is a small-molecule drug that prevents the Ebola virus from reproducing in the body. BioCryst is currently using money from the National Institutes of Health to conduct phase I safety studies of the drug in healthy volunteers.
The drug’s effectiveness at treating both the Ebola and Marburg viruses in nonhuman primates indicates that “BCX4430 may be useful as a broad spectrum antiviral drug,” according to the statement.
The federal government has taken its first step toward supporting an experimental drug for treating Ebola.
The U.S. Department of Health & Human Services’ Office of the Assistant Secretary for Preparedness and Response committed to funding BioCryst Pharmaceuticals’ development and manufacturing of such a drug, according to a written statement issued by the agency March 31.
The Office awarded approximately $12 million to the North Carolina–based drug company, but the size of the grant could grow to $35 million.
The drug, BCX4430, is a small-molecule drug that prevents the Ebola virus from reproducing in the body. BioCryst is currently using money from the National Institutes of Health to conduct phase I safety studies of the drug in healthy volunteers.
The drug’s effectiveness at treating both the Ebola and Marburg viruses in nonhuman primates indicates that “BCX4430 may be useful as a broad spectrum antiviral drug,” according to the statement.
Sitting while watching television tied to poor sleep, obstructive sleep apnea risk
Every extra hour per day spent sitting while watching television increased the odds of sleep problems and obstructive sleep apnea (OSA) risk by about 12%-15%, even after accounting for body mass index and physical activity, researchers reported in the March issue of Chest.
“Overall, this investigation represents a first step in understanding the relationship between sitting and sleep,” said Matthew Burman, Ph.D., at the Arizona State University in Phoenix and his associates. “To our knowledge, no studies in adults have explored the relationship between sitting, sleep disturbance, and obstructive sleep apnea. Sitting time and television viewing appear to be novel and important risk factors for sleep quality and OSA risk.”

The cross-sectional study analyzed data on 1,000 adults aged 23-60 years who had responded to the National Sleep Foundation’s 2013 Sleep in America poll. The researchers examined associations between daily time sitting, time sitting while watching television, and quality and amount of sleep, daytime sleepiness, and OSA. To avoid overreporting television viewing, they looked at time spent sitting during activities such as using a computer, reading, socializing, and traveling.
After controlling for factors such as body mass index and physical activity, every extra hour per day of sitting was tied to a 6% rise in the odds of poor sleep quality (odds ratio, 1.06; 95% confidence interval, 1.01-1.11), But overall sitting time was not linked with sleep duration, OSA risk category, or daytime sleepiness, said the researchers.
However, when they look specifically at time spent sitting watching television, they found that every extra hour a day significantly increased the odds of taking at least 30 minutes to fall asleep (OR, 1.15; 95% CI, 1.04-1.27), waking up too early in the morning (OR, 1.12; 95% CI, 1.03-1.23), sleeping poorly (OR, 1.12; 95% CI, 1.02-1.24), and being at high risk for OSA (OR, 1.15; 95% CI, 1.04-1.28) based on the STOP (snoring, tiredness during the daytime, observed apnea, and reported high blood pressure) measure.
Notably, regular physical activity helped mitigate the risk of OSA associated with watching television (P = .04). “The relationship between television viewing and OSA risk was not as strong among physically active individuals as it was among physically inactive individuals,” said the investigators.
The study did not look at the timing of sitting relative to bedtime, the researchers said. “Sitting time increases throughout the day, and it is possible that excess sitting close to bedtime may have more harmful effects on sleep. Future studies should examine the association of timing of sitting with sleep. Being physically active rather than sitting near bedtime might be associated with reduction in some risks,” they added.
The National Sleep Foundation and the National Institutes of Health funded the study. The authors declared no relevant conflicts of interest.
Every extra hour per day spent sitting while watching television increased the odds of sleep problems and obstructive sleep apnea (OSA) risk by about 12%-15%, even after accounting for body mass index and physical activity, researchers reported in the March issue of Chest.
“Overall, this investigation represents a first step in understanding the relationship between sitting and sleep,” said Matthew Burman, Ph.D., at the Arizona State University in Phoenix and his associates. “To our knowledge, no studies in adults have explored the relationship between sitting, sleep disturbance, and obstructive sleep apnea. Sitting time and television viewing appear to be novel and important risk factors for sleep quality and OSA risk.”
The cross-sectional study analyzed data on 1,000 adults aged 23-60 years who had responded to the National Sleep Foundation’s 2013 Sleep in America poll. The researchers examined associations between daily time sitting, time sitting while watching television, and quality and amount of sleep, daytime sleepiness, and OSA. To avoid overreporting television viewing, they looked at time spent sitting during activities such as using a computer, reading, socializing, and traveling.
After controlling for factors such as body mass index and physical activity, every extra hour per day of sitting was tied to a 6% rise in the odds of poor sleep quality (odds ratio, 1.06; 95% confidence interval, 1.01-1.11), But overall sitting time was not linked with sleep duration, OSA risk category, or daytime sleepiness, said the researchers.
However, when they look specifically at time spent sitting watching television, they found that every extra hour a day significantly increased the odds of taking at least 30 minutes to fall asleep (OR, 1.15; 95% CI, 1.04-1.27), waking up too early in the morning (OR, 1.12; 95% CI, 1.03-1.23), sleeping poorly (OR, 1.12; 95% CI, 1.02-1.24), and being at high risk for OSA (OR, 1.15; 95% CI, 1.04-1.28) based on the STOP (snoring, tiredness during the daytime, observed apnea, and reported high blood pressure) measure.
Notably, regular physical activity helped mitigate the risk of OSA associated with watching television (P = .04). “The relationship between television viewing and OSA risk was not as strong among physically active individuals as it was among physically inactive individuals,” said the investigators.
The study did not look at the timing of sitting relative to bedtime, the researchers said. “Sitting time increases throughout the day, and it is possible that excess sitting close to bedtime may have more harmful effects on sleep. Future studies should examine the association of timing of sitting with sleep. Being physically active rather than sitting near bedtime might be associated with reduction in some risks,” they added.
The National Sleep Foundation and the National Institutes of Health funded the study. The authors declared no relevant conflicts of interest.
Every extra hour per day spent sitting while watching television increased the odds of sleep problems and obstructive sleep apnea (OSA) risk by about 12%-15%, even after accounting for body mass index and physical activity, researchers reported in the March issue of Chest.
“Overall, this investigation represents a first step in understanding the relationship between sitting and sleep,” said Matthew Burman, Ph.D., at the Arizona State University in Phoenix and his associates. “To our knowledge, no studies in adults have explored the relationship between sitting, sleep disturbance, and obstructive sleep apnea. Sitting time and television viewing appear to be novel and important risk factors for sleep quality and OSA risk.”
The cross-sectional study analyzed data on 1,000 adults aged 23-60 years who had responded to the National Sleep Foundation’s 2013 Sleep in America poll. The researchers examined associations between daily time sitting, time sitting while watching television, and quality and amount of sleep, daytime sleepiness, and OSA. To avoid overreporting television viewing, they looked at time spent sitting during activities such as using a computer, reading, socializing, and traveling.
After controlling for factors such as body mass index and physical activity, every extra hour per day of sitting was tied to a 6% rise in the odds of poor sleep quality (odds ratio, 1.06; 95% confidence interval, 1.01-1.11), But overall sitting time was not linked with sleep duration, OSA risk category, or daytime sleepiness, said the researchers.
However, when they look specifically at time spent sitting watching television, they found that every extra hour a day significantly increased the odds of taking at least 30 minutes to fall asleep (OR, 1.15; 95% CI, 1.04-1.27), waking up too early in the morning (OR, 1.12; 95% CI, 1.03-1.23), sleeping poorly (OR, 1.12; 95% CI, 1.02-1.24), and being at high risk for OSA (OR, 1.15; 95% CI, 1.04-1.28) based on the STOP (snoring, tiredness during the daytime, observed apnea, and reported high blood pressure) measure.
Notably, regular physical activity helped mitigate the risk of OSA associated with watching television (P = .04). “The relationship between television viewing and OSA risk was not as strong among physically active individuals as it was among physically inactive individuals,” said the investigators.
The study did not look at the timing of sitting relative to bedtime, the researchers said. “Sitting time increases throughout the day, and it is possible that excess sitting close to bedtime may have more harmful effects on sleep. Future studies should examine the association of timing of sitting with sleep. Being physically active rather than sitting near bedtime might be associated with reduction in some risks,” they added.
The National Sleep Foundation and the National Institutes of Health funded the study. The authors declared no relevant conflicts of interest.
Key clinical point: Sitting while watching television appears to increase the risk of sleep disturbances and obstructive sleep apnea.
Major finding: Every extra hour per day spent sitting while watching television increased the odds of sleep problems and OSA risk by about 12%-15%.
Data source: Multiregional cross-sectional study of 1,000 adults.
Disclosures: The National Sleep Foundation and the National Institutes of Health funded the study. The authors declared no relevant conflicts of interest.

Executive function deficits linked to e-cigarette use in early adolescents
Adolescents with deficits in executive function were almost five times more likely to use e-cigarettes than were those without deficits, Dr. Mary Ann Pentz and her coauthors from the University of Southern, Los Angeles, reported.
A study of 410 7th-grade students from two Southern California school districts found that both parent ownership of e-cigarettes (odds ratio, 2.29; 95% confidence interval, 1.01-5.15) and executive function deficits (OR, 4.99; 95% CI, 1.80-13.86) were significantly associated with e-cigarette use, the authors reported.
The findings suggest that “substance use prevention programs should include e-cigarette use and emphasize [executive function] skills training that targets emotional regulation, impulse control, goal setting, and planful decision-making,” Dr. Pentz and her associates said.
Read the full article in Addictive Behaviors (2015;42:73-8).
Adolescents with deficits in executive function were almost five times more likely to use e-cigarettes than were those without deficits, Dr. Mary Ann Pentz and her coauthors from the University of Southern, Los Angeles, reported.
A study of 410 7th-grade students from two Southern California school districts found that both parent ownership of e-cigarettes (odds ratio, 2.29; 95% confidence interval, 1.01-5.15) and executive function deficits (OR, 4.99; 95% CI, 1.80-13.86) were significantly associated with e-cigarette use, the authors reported.
The findings suggest that “substance use prevention programs should include e-cigarette use and emphasize [executive function] skills training that targets emotional regulation, impulse control, goal setting, and planful decision-making,” Dr. Pentz and her associates said.
Read the full article in Addictive Behaviors (2015;42:73-8).
Adolescents with deficits in executive function were almost five times more likely to use e-cigarettes than were those without deficits, Dr. Mary Ann Pentz and her coauthors from the University of Southern, Los Angeles, reported.
A study of 410 7th-grade students from two Southern California school districts found that both parent ownership of e-cigarettes (odds ratio, 2.29; 95% confidence interval, 1.01-5.15) and executive function deficits (OR, 4.99; 95% CI, 1.80-13.86) were significantly associated with e-cigarette use, the authors reported.
The findings suggest that “substance use prevention programs should include e-cigarette use and emphasize [executive function] skills training that targets emotional regulation, impulse control, goal setting, and planful decision-making,” Dr. Pentz and her associates said.
Read the full article in Addictive Behaviors (2015;42:73-8).
Identifying as a nonsmoker may help ex-smokers stay abstinent
Former smokers who identify themselves as nonsmokers are more likely to remain abstinent in the medium term, according to Dr. Ildiko Tombor and associates.
Just over 80% of study participants identified as nonsmokers, with younger age and longer abstinence time independently associated. A nonsmoker identity and length of abstinence at baseline was associated with continued abstinence after 3 months; however at 6 months only baseline abstinence was associated.
“Findings from this study suggest that harnessing identity change (towards a nonsmoker identity) as part of behavioral smoking cessation support might improve the lasting success of quit attempts, and future research should explore the set of behavior change techniques that can be effective to help people achieve this by incorporating a nonsmoker self-label into a core part of their identity,” the investigators said.
Find the full study from Addictive Behaviors here.
Former smokers who identify themselves as nonsmokers are more likely to remain abstinent in the medium term, according to Dr. Ildiko Tombor and associates.
Just over 80% of study participants identified as nonsmokers, with younger age and longer abstinence time independently associated. A nonsmoker identity and length of abstinence at baseline was associated with continued abstinence after 3 months; however at 6 months only baseline abstinence was associated.
“Findings from this study suggest that harnessing identity change (towards a nonsmoker identity) as part of behavioral smoking cessation support might improve the lasting success of quit attempts, and future research should explore the set of behavior change techniques that can be effective to help people achieve this by incorporating a nonsmoker self-label into a core part of their identity,” the investigators said.
Find the full study from Addictive Behaviors here.
Former smokers who identify themselves as nonsmokers are more likely to remain abstinent in the medium term, according to Dr. Ildiko Tombor and associates.
Just over 80% of study participants identified as nonsmokers, with younger age and longer abstinence time independently associated. A nonsmoker identity and length of abstinence at baseline was associated with continued abstinence after 3 months; however at 6 months only baseline abstinence was associated.
“Findings from this study suggest that harnessing identity change (towards a nonsmoker identity) as part of behavioral smoking cessation support might improve the lasting success of quit attempts, and future research should explore the set of behavior change techniques that can be effective to help people achieve this by incorporating a nonsmoker self-label into a core part of their identity,” the investigators said.
Find the full study from Addictive Behaviors here.