User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
COVID-19–related HCQ shortages affected rheumatology patients worldwide
New data document the global fallout for rheumatology patients when hydroxychloroquine (HCQ) supplies were being diverted to hospitals for COVID-19 patients.
Demand for HCQ soared on evidence-lacking claims that the drug was effective in treating and preventing SARS-CoV-2 infection. Further research has since shown HCQ to be ineffective for COVID-19 and potentially harmful to patients.
But during the height of the COVID-19-related hype, patients worldwide with autoimmune diseases, particularly lupus and rheumatoid arthritis, had trouble getting the pills at all or couldn’t get as many as they needed for their chronic conditions.
Emily Sirotich, MSc, a PhD student at McMaster University in Hamilton, Ont., presented data at the virtual annual meeting of the American College of Rheumatology demonstrating that the severity of shortages differed widely.
Whereas 26.7% of rheumatology patients in Africa and 21.4% in southeast Asia said their pharmacy ran short of HCQ – which was originally developed as an antimalarial drug but has been found effective in treating some rheumatic diseases – only 6.8% of patients in the Americas and 2.1% in European regions reported the shortages.
“There are large regional disparities in access to antimalarials whether they were caused by the COVID-19 pandemic or already existed,” she said in an interview.
Global survey polled patient experience
Ms. Sirotich’s team analyzed data from the Global Rheumatology Alliance Patient Experience Survey.
They found that from 9,393 respondents (average age 46.1 years and 90% female), 3,872 (41.2%) were taking antimalarials. Of these, 230 (6.2% globally) were unable to keep taking the drugs because their pharmacy ran out.
Researchers evaluated the effect of drug shortages on disease activity, mental health, and physical health by comparing mean values with two-sided independent t-tests to identify significant differences.
They found that patients who were unable to obtain antimalarials had significantly higher levels of rheumatic disease activity as well as poorer mental and physical health (all P < .001).
The survey was distributed online through patient support groups and on social media. Patients with rheumatic diseases or their parents anonymously entered data including their rheumatic disease diagnosis, medications, COVID-19 status, and disease outcomes.
Ms. Sirotich said they are currently gathering new data to see if the gaps in access to HCQ persist and whether the physical and mental consequences of not having the medications continue.
Hospitals stockpiled HCQ in the U.S.
Michael Ganio, PharmD, senior director of pharmacy practice and quality at the American Society of Health-System Pharmacists (ASHP), said in an interview that hospitals in the United States received large amounts of HCQ in late spring and early summer, donated by pharmaceutical companies for COVID-19 before the lack of evidence for efficacy became clear.
Hospitals found themselves sitting on large quantities of HCQ they couldn’t use while prescriptions for rheumatology outpatients were going unfilled.
It is only in recent months that the U.S. Department of Health and Human Services has given clear direction to hospitals on how to redistribute those supplies, Dr. Ganio said.
“There’s no good real good way to move a product from a hospital to a [drug store] down the street,” he said.
The Food and Drug Administration now lists the HCQ shortages as resolved.
Declined prescriptions have frustrated physicians
Brett Smith, DO, a pediatric and adult rheumatologist in Alcoa, Tenn., said he was frustrated by pharmacies declining his prescriptions for HCQ for patients with rheumatoid arthritis.
“I got notes from pharmacies that I should consider alternative agents,” he said in an interview. But the safety profiles of the alternatives were not as good, he said.
“Hydroxychloroquine has no risk of infection and no risk of malignancy, and they were proposing alternative agents that carry those risks,” he said.
“I had some people with RA who couldn’t get [HCQ] who had a substantial increase in swollen joints and pain without it,” he said.
Dr. Smith said some patients who use HCQ for off-label uses such as certain skin disorders still aren’t getting the drug, as off-label use has been discouraged to make sure those with lupus and RA have enough, he said.
Saira Sheikh, MD, director of the University of North Carolina Rheumatology Lupus Clinic in Chapel Hill, said in an interview that during the summer months pharmacists required additional documentation of the diagnosis of autoimmune disease, resulting in unnecessary delays even when patients had been on the medication for many years.
She said emerging research has found patient-reported barriers to filling prescriptions, interruptions in HCQ treatment, and reported emotional stress and anxiety related to medication access during the COVID-19 pandemic.
“This experience with HCQ during the COVID-19 pandemic teaches us that while swift action and progress to address the immediate threats of the pandemic should be commended, it is important that we move forward in a conscious manner, guided by an evidence base that comes from high-quality research, not from rushed judgments based on preliminary studies, or pressure from political leaders,” Dr. Sheikh said.
Ms. Sirotich, Dr. Smith, Dr. Sheikh, and Dr. Ganio have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
New data document the global fallout for rheumatology patients when hydroxychloroquine (HCQ) supplies were being diverted to hospitals for COVID-19 patients.
Demand for HCQ soared on evidence-lacking claims that the drug was effective in treating and preventing SARS-CoV-2 infection. Further research has since shown HCQ to be ineffective for COVID-19 and potentially harmful to patients.
But during the height of the COVID-19-related hype, patients worldwide with autoimmune diseases, particularly lupus and rheumatoid arthritis, had trouble getting the pills at all or couldn’t get as many as they needed for their chronic conditions.
Emily Sirotich, MSc, a PhD student at McMaster University in Hamilton, Ont., presented data at the virtual annual meeting of the American College of Rheumatology demonstrating that the severity of shortages differed widely.
Whereas 26.7% of rheumatology patients in Africa and 21.4% in southeast Asia said their pharmacy ran short of HCQ – which was originally developed as an antimalarial drug but has been found effective in treating some rheumatic diseases – only 6.8% of patients in the Americas and 2.1% in European regions reported the shortages.
“There are large regional disparities in access to antimalarials whether they were caused by the COVID-19 pandemic or already existed,” she said in an interview.
Global survey polled patient experience
Ms. Sirotich’s team analyzed data from the Global Rheumatology Alliance Patient Experience Survey.
They found that from 9,393 respondents (average age 46.1 years and 90% female), 3,872 (41.2%) were taking antimalarials. Of these, 230 (6.2% globally) were unable to keep taking the drugs because their pharmacy ran out.
Researchers evaluated the effect of drug shortages on disease activity, mental health, and physical health by comparing mean values with two-sided independent t-tests to identify significant differences.
They found that patients who were unable to obtain antimalarials had significantly higher levels of rheumatic disease activity as well as poorer mental and physical health (all P < .001).
The survey was distributed online through patient support groups and on social media. Patients with rheumatic diseases or their parents anonymously entered data including their rheumatic disease diagnosis, medications, COVID-19 status, and disease outcomes.
Ms. Sirotich said they are currently gathering new data to see if the gaps in access to HCQ persist and whether the physical and mental consequences of not having the medications continue.
Hospitals stockpiled HCQ in the U.S.
Michael Ganio, PharmD, senior director of pharmacy practice and quality at the American Society of Health-System Pharmacists (ASHP), said in an interview that hospitals in the United States received large amounts of HCQ in late spring and early summer, donated by pharmaceutical companies for COVID-19 before the lack of evidence for efficacy became clear.
Hospitals found themselves sitting on large quantities of HCQ they couldn’t use while prescriptions for rheumatology outpatients were going unfilled.
It is only in recent months that the U.S. Department of Health and Human Services has given clear direction to hospitals on how to redistribute those supplies, Dr. Ganio said.
“There’s no good real good way to move a product from a hospital to a [drug store] down the street,” he said.
The Food and Drug Administration now lists the HCQ shortages as resolved.
Declined prescriptions have frustrated physicians
Brett Smith, DO, a pediatric and adult rheumatologist in Alcoa, Tenn., said he was frustrated by pharmacies declining his prescriptions for HCQ for patients with rheumatoid arthritis.
“I got notes from pharmacies that I should consider alternative agents,” he said in an interview. But the safety profiles of the alternatives were not as good, he said.
“Hydroxychloroquine has no risk of infection and no risk of malignancy, and they were proposing alternative agents that carry those risks,” he said.
“I had some people with RA who couldn’t get [HCQ] who had a substantial increase in swollen joints and pain without it,” he said.
Dr. Smith said some patients who use HCQ for off-label uses such as certain skin disorders still aren’t getting the drug, as off-label use has been discouraged to make sure those with lupus and RA have enough, he said.
Saira Sheikh, MD, director of the University of North Carolina Rheumatology Lupus Clinic in Chapel Hill, said in an interview that during the summer months pharmacists required additional documentation of the diagnosis of autoimmune disease, resulting in unnecessary delays even when patients had been on the medication for many years.
She said emerging research has found patient-reported barriers to filling prescriptions, interruptions in HCQ treatment, and reported emotional stress and anxiety related to medication access during the COVID-19 pandemic.
“This experience with HCQ during the COVID-19 pandemic teaches us that while swift action and progress to address the immediate threats of the pandemic should be commended, it is important that we move forward in a conscious manner, guided by an evidence base that comes from high-quality research, not from rushed judgments based on preliminary studies, or pressure from political leaders,” Dr. Sheikh said.
Ms. Sirotich, Dr. Smith, Dr. Sheikh, and Dr. Ganio have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
New data document the global fallout for rheumatology patients when hydroxychloroquine (HCQ) supplies were being diverted to hospitals for COVID-19 patients.
Demand for HCQ soared on evidence-lacking claims that the drug was effective in treating and preventing SARS-CoV-2 infection. Further research has since shown HCQ to be ineffective for COVID-19 and potentially harmful to patients.
But during the height of the COVID-19-related hype, patients worldwide with autoimmune diseases, particularly lupus and rheumatoid arthritis, had trouble getting the pills at all or couldn’t get as many as they needed for their chronic conditions.
Emily Sirotich, MSc, a PhD student at McMaster University in Hamilton, Ont., presented data at the virtual annual meeting of the American College of Rheumatology demonstrating that the severity of shortages differed widely.
Whereas 26.7% of rheumatology patients in Africa and 21.4% in southeast Asia said their pharmacy ran short of HCQ – which was originally developed as an antimalarial drug but has been found effective in treating some rheumatic diseases – only 6.8% of patients in the Americas and 2.1% in European regions reported the shortages.
“There are large regional disparities in access to antimalarials whether they were caused by the COVID-19 pandemic or already existed,” she said in an interview.
Global survey polled patient experience
Ms. Sirotich’s team analyzed data from the Global Rheumatology Alliance Patient Experience Survey.
They found that from 9,393 respondents (average age 46.1 years and 90% female), 3,872 (41.2%) were taking antimalarials. Of these, 230 (6.2% globally) were unable to keep taking the drugs because their pharmacy ran out.
Researchers evaluated the effect of drug shortages on disease activity, mental health, and physical health by comparing mean values with two-sided independent t-tests to identify significant differences.
They found that patients who were unable to obtain antimalarials had significantly higher levels of rheumatic disease activity as well as poorer mental and physical health (all P < .001).
The survey was distributed online through patient support groups and on social media. Patients with rheumatic diseases or their parents anonymously entered data including their rheumatic disease diagnosis, medications, COVID-19 status, and disease outcomes.
Ms. Sirotich said they are currently gathering new data to see if the gaps in access to HCQ persist and whether the physical and mental consequences of not having the medications continue.
Hospitals stockpiled HCQ in the U.S.
Michael Ganio, PharmD, senior director of pharmacy practice and quality at the American Society of Health-System Pharmacists (ASHP), said in an interview that hospitals in the United States received large amounts of HCQ in late spring and early summer, donated by pharmaceutical companies for COVID-19 before the lack of evidence for efficacy became clear.
Hospitals found themselves sitting on large quantities of HCQ they couldn’t use while prescriptions for rheumatology outpatients were going unfilled.
It is only in recent months that the U.S. Department of Health and Human Services has given clear direction to hospitals on how to redistribute those supplies, Dr. Ganio said.
“There’s no good real good way to move a product from a hospital to a [drug store] down the street,” he said.
The Food and Drug Administration now lists the HCQ shortages as resolved.
Declined prescriptions have frustrated physicians
Brett Smith, DO, a pediatric and adult rheumatologist in Alcoa, Tenn., said he was frustrated by pharmacies declining his prescriptions for HCQ for patients with rheumatoid arthritis.
“I got notes from pharmacies that I should consider alternative agents,” he said in an interview. But the safety profiles of the alternatives were not as good, he said.
“Hydroxychloroquine has no risk of infection and no risk of malignancy, and they were proposing alternative agents that carry those risks,” he said.
“I had some people with RA who couldn’t get [HCQ] who had a substantial increase in swollen joints and pain without it,” he said.
Dr. Smith said some patients who use HCQ for off-label uses such as certain skin disorders still aren’t getting the drug, as off-label use has been discouraged to make sure those with lupus and RA have enough, he said.
Saira Sheikh, MD, director of the University of North Carolina Rheumatology Lupus Clinic in Chapel Hill, said in an interview that during the summer months pharmacists required additional documentation of the diagnosis of autoimmune disease, resulting in unnecessary delays even when patients had been on the medication for many years.
She said emerging research has found patient-reported barriers to filling prescriptions, interruptions in HCQ treatment, and reported emotional stress and anxiety related to medication access during the COVID-19 pandemic.
“This experience with HCQ during the COVID-19 pandemic teaches us that while swift action and progress to address the immediate threats of the pandemic should be commended, it is important that we move forward in a conscious manner, guided by an evidence base that comes from high-quality research, not from rushed judgments based on preliminary studies, or pressure from political leaders,” Dr. Sheikh said.
Ms. Sirotich, Dr. Smith, Dr. Sheikh, and Dr. Ganio have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Who’s at risk for depression on isotretinoin?
A Sanaa Butt, MD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.

This was, however, the sole identifiable risk factor for treatment-limiting depressive symptoms in acne patients on isotretinoin in the study of 3,151 consecutive acne patients taking isotretinoin. There was no significant difference between those who did or did not develop depression on the oral retinoid in terms of age, gender, or daily dose of the drug at the time it was discontinued.
“Depressive symptoms occurred at any time from the date of initiation of isotretinoin up to 6 months into therapy, with no identifiable peak time period,” said Dr. Butt, a dermatologist with the U.K. National Health Service Tayside district at Ninewells Hospital, Dundee, Scotland. “Lower doses appear not to be protective,” she added.
The Tayside district has a catchment of roughly 450,000 people. The local population tends to stay put because Tayside is an economically disadvantaged and remote part of Scotland. There are very few private practice dermatologists in the area, so Dr. Butt and coinvestigators are confident their observational study of NHS patients captured the great majority of isotretinoin users in northern Scotland.
The investigators utilized software to analyze the contents of more than 8,000 digitized letters exchanged between NHS Tayside dermatologists and general practitioners during 2005-2018, zeroing in on 3,151 consecutive patients on isotretinoin for acne and 158 on the drug for other conditions, most often rosacea or folliculitis. They then drilled down further through the letters, electronically searching for key words such as suicide, depression, and anxiety. In this way, they ultimately identified 30 patients who discontinued the drug because they developed depressive symptoms. All 30 were on the drug for acne.
The annual incidence of treatment-limiting depressive mood changes was 0.96%, a figure that remained steady over the 13-year study period, even though prescribing of isotretinoin increased over time. This flat incidence rate effectively rules out the potential for confounding because of assessor bias, especially since many different NHS dermatologists were prescribing the drug, Dr. Butt said.
Half of acne patients prescribed isotretinoin were female and 50% were male. And 15 cases of treatment discontinuation caused by development of depressive symptoms occurred in females, 15 in males. A history of past depressive illness was present in 9.3% of females who started on isotretinoin and in 4.5% of the males. The relative risk of treatment-limiting depressive mood changes was increased 790% among females with a prior history of depressive illness and 440% in males with such a history.
Dr. Butt reported having no financial conflicts regarding her NHS-funded study.
A Sanaa Butt, MD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
This was, however, the sole identifiable risk factor for treatment-limiting depressive symptoms in acne patients on isotretinoin in the study of 3,151 consecutive acne patients taking isotretinoin. There was no significant difference between those who did or did not develop depression on the oral retinoid in terms of age, gender, or daily dose of the drug at the time it was discontinued.
“Depressive symptoms occurred at any time from the date of initiation of isotretinoin up to 6 months into therapy, with no identifiable peak time period,” said Dr. Butt, a dermatologist with the U.K. National Health Service Tayside district at Ninewells Hospital, Dundee, Scotland. “Lower doses appear not to be protective,” she added.
The Tayside district has a catchment of roughly 450,000 people. The local population tends to stay put because Tayside is an economically disadvantaged and remote part of Scotland. There are very few private practice dermatologists in the area, so Dr. Butt and coinvestigators are confident their observational study of NHS patients captured the great majority of isotretinoin users in northern Scotland.
The investigators utilized software to analyze the contents of more than 8,000 digitized letters exchanged between NHS Tayside dermatologists and general practitioners during 2005-2018, zeroing in on 3,151 consecutive patients on isotretinoin for acne and 158 on the drug for other conditions, most often rosacea or folliculitis. They then drilled down further through the letters, electronically searching for key words such as suicide, depression, and anxiety. In this way, they ultimately identified 30 patients who discontinued the drug because they developed depressive symptoms. All 30 were on the drug for acne.
The annual incidence of treatment-limiting depressive mood changes was 0.96%, a figure that remained steady over the 13-year study period, even though prescribing of isotretinoin increased over time. This flat incidence rate effectively rules out the potential for confounding because of assessor bias, especially since many different NHS dermatologists were prescribing the drug, Dr. Butt said.
Half of acne patients prescribed isotretinoin were female and 50% were male. And 15 cases of treatment discontinuation caused by development of depressive symptoms occurred in females, 15 in males. A history of past depressive illness was present in 9.3% of females who started on isotretinoin and in 4.5% of the males. The relative risk of treatment-limiting depressive mood changes was increased 790% among females with a prior history of depressive illness and 440% in males with such a history.
Dr. Butt reported having no financial conflicts regarding her NHS-funded study.
A Sanaa Butt, MD, reported at the virtual annual congress of the European Academy of Dermatology and Venereology.
This was, however, the sole identifiable risk factor for treatment-limiting depressive symptoms in acne patients on isotretinoin in the study of 3,151 consecutive acne patients taking isotretinoin. There was no significant difference between those who did or did not develop depression on the oral retinoid in terms of age, gender, or daily dose of the drug at the time it was discontinued.
“Depressive symptoms occurred at any time from the date of initiation of isotretinoin up to 6 months into therapy, with no identifiable peak time period,” said Dr. Butt, a dermatologist with the U.K. National Health Service Tayside district at Ninewells Hospital, Dundee, Scotland. “Lower doses appear not to be protective,” she added.
The Tayside district has a catchment of roughly 450,000 people. The local population tends to stay put because Tayside is an economically disadvantaged and remote part of Scotland. There are very few private practice dermatologists in the area, so Dr. Butt and coinvestigators are confident their observational study of NHS patients captured the great majority of isotretinoin users in northern Scotland.
The investigators utilized software to analyze the contents of more than 8,000 digitized letters exchanged between NHS Tayside dermatologists and general practitioners during 2005-2018, zeroing in on 3,151 consecutive patients on isotretinoin for acne and 158 on the drug for other conditions, most often rosacea or folliculitis. They then drilled down further through the letters, electronically searching for key words such as suicide, depression, and anxiety. In this way, they ultimately identified 30 patients who discontinued the drug because they developed depressive symptoms. All 30 were on the drug for acne.
The annual incidence of treatment-limiting depressive mood changes was 0.96%, a figure that remained steady over the 13-year study period, even though prescribing of isotretinoin increased over time. This flat incidence rate effectively rules out the potential for confounding because of assessor bias, especially since many different NHS dermatologists were prescribing the drug, Dr. Butt said.
Half of acne patients prescribed isotretinoin were female and 50% were male. And 15 cases of treatment discontinuation caused by development of depressive symptoms occurred in females, 15 in males. A history of past depressive illness was present in 9.3% of females who started on isotretinoin and in 4.5% of the males. The relative risk of treatment-limiting depressive mood changes was increased 790% among females with a prior history of depressive illness and 440% in males with such a history.
Dr. Butt reported having no financial conflicts regarding her NHS-funded study.
FROM THE EADV CONGRESS
Sparse Hair on the Scalp
The Diagnosis: Monilethrix
Trichoscopy showed a beaded appearance of the hair shafts (Figure, A). Light microscopy demonstrated normal medullated nodes of hair coupled with internodal, thin, nonmedullated hair at regular intervals (Figure, B). Clinical and trichoscopic findings led to a diagnosis of monilethrix.
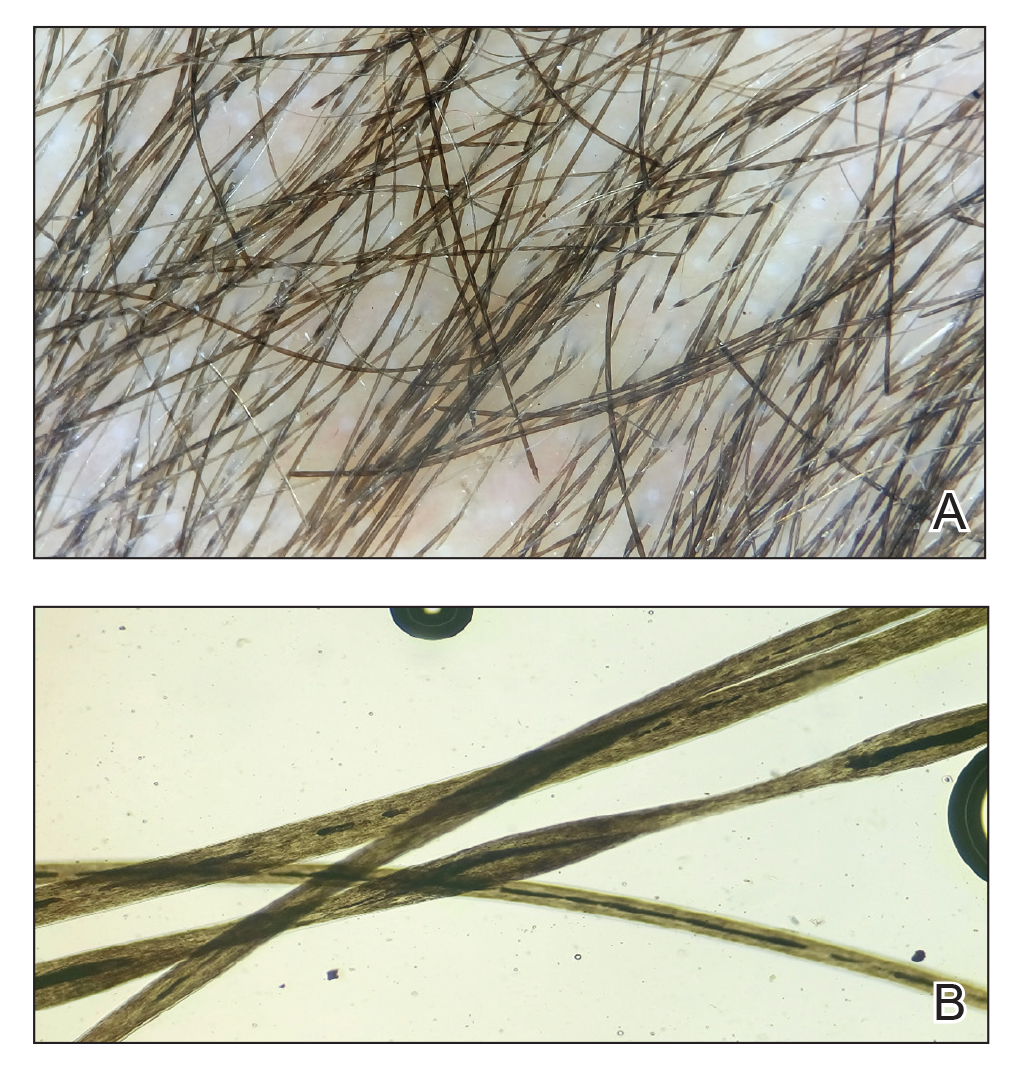
Monilethrix is a genetic hair disorder characterized by regular periodic thinning of the hair shafts, giving the strands a beaded appearance. The hair tends to break at these constricted parts, resulting in short hairs. Nodosities represent the normal hair shaft, whereas the constricted points are the site of the defect. The hair tends to be normal at birth and then becomes short, fragile, and brittle within months, leading to hypotrichosis, particularly on the occipital scalp.1 Monilethrix also may involve the eyebrows and eyelashes in addition to scalp hair. Follicular hyperkeratotic papules with perifollicular erythema frequently are noted on the occipital area. Monilethrix can be inherited in an autosomal-dominant fashion with mutations involving KRT81, KRT83, and KRT86, which code for the type II hair keratins Hb1, Hb3, and Hb6, respectively. The autosomal-recessive form is caused by mutations in the DSG4 gene, coding for the desmoglein 4 protein.2 Trichoscopy or light microscopy is essential to establish a diagnosis of monilethrix. Trichoscopy is an easy and rapid tool that is utilized to illustrate the beaded appearance of the hair shafts.3 Light microscopy shows the distinctive nodes that are medullated, with a normal hair diameter alternating with the internodes, or constrictions, that are nonmedullated and represent the sites of fracture.1 Monilethrix can improve by puberty. There is no definitive treatment; however, some patients show considerable improvement on minoxidil.4 Treatment with minoxidil was initiated in this patient; however, she was lost to follow-up.
Genetic hair disorders are rare and can be an isolated phenomenon or part of concurrent genetic syndromes. Therefore, thorough clinical examination of other ectodermal structures such as the nails and teeth is crucial as well as obtaining a detailed family history and review of systems to exclude other syndromes.2 Hypotrichosis simplex is characterized by hair loss exclusively on the scalp, sparing other ectodermal structures and with no systemic abnormalities. Ectodermal dysplasia is a heterogeneous group of disorders affecting not only the hair but also the teeth, nails, and sweat glands.2 Pili torti is another rare genetic hair disorder that is characterized by twisting of the hair fiber on its own axis. It presents clinically as sparse, depigmented, lusterless hair that is easily broken. Light microscopy demonstrates twists of hair at irregular intervals. Pili annulati is characterized by bright and dark bands when viewed with reflected light. Unlike monilethrix, there is no fragility, and the hair can grow long.5
- Mirmirani P, Huang KP, Price VH. A practical, algorithmic approach to diagnosing hair shaft disorders. Int J Dermatol. 2011;50:1-12.
- Ahmed A, Almohanna H, Griggs J, et al. Genetic hair disorders: a review. Dermatol Ther. 2019;9:421-448.
- Liu C-I, Hsu C-H. Rapid diagnosis of monilethrix using dermoscopy. Br J Dermatol. 2008;159:741-743.
- Rossi A, Iorio A, Fortuna MC, et al. Monilethrix treated with minoxidil. Int J Immunopathol Pharmacol. 2011;24:239-242.
- Singh G, Miteva M. Prognosis and management of congenital hair shaft disorders with fragility—part I. Pediatr Dermatol. 2016;33:473-480.
The Diagnosis: Monilethrix
Trichoscopy showed a beaded appearance of the hair shafts (Figure, A). Light microscopy demonstrated normal medullated nodes of hair coupled with internodal, thin, nonmedullated hair at regular intervals (Figure, B). Clinical and trichoscopic findings led to a diagnosis of monilethrix.
Monilethrix is a genetic hair disorder characterized by regular periodic thinning of the hair shafts, giving the strands a beaded appearance. The hair tends to break at these constricted parts, resulting in short hairs. Nodosities represent the normal hair shaft, whereas the constricted points are the site of the defect. The hair tends to be normal at birth and then becomes short, fragile, and brittle within months, leading to hypotrichosis, particularly on the occipital scalp.1 Monilethrix also may involve the eyebrows and eyelashes in addition to scalp hair. Follicular hyperkeratotic papules with perifollicular erythema frequently are noted on the occipital area. Monilethrix can be inherited in an autosomal-dominant fashion with mutations involving KRT81, KRT83, and KRT86, which code for the type II hair keratins Hb1, Hb3, and Hb6, respectively. The autosomal-recessive form is caused by mutations in the DSG4 gene, coding for the desmoglein 4 protein.2 Trichoscopy or light microscopy is essential to establish a diagnosis of monilethrix. Trichoscopy is an easy and rapid tool that is utilized to illustrate the beaded appearance of the hair shafts.3 Light microscopy shows the distinctive nodes that are medullated, with a normal hair diameter alternating with the internodes, or constrictions, that are nonmedullated and represent the sites of fracture.1 Monilethrix can improve by puberty. There is no definitive treatment; however, some patients show considerable improvement on minoxidil.4 Treatment with minoxidil was initiated in this patient; however, she was lost to follow-up.
Genetic hair disorders are rare and can be an isolated phenomenon or part of concurrent genetic syndromes. Therefore, thorough clinical examination of other ectodermal structures such as the nails and teeth is crucial as well as obtaining a detailed family history and review of systems to exclude other syndromes.2 Hypotrichosis simplex is characterized by hair loss exclusively on the scalp, sparing other ectodermal structures and with no systemic abnormalities. Ectodermal dysplasia is a heterogeneous group of disorders affecting not only the hair but also the teeth, nails, and sweat glands.2 Pili torti is another rare genetic hair disorder that is characterized by twisting of the hair fiber on its own axis. It presents clinically as sparse, depigmented, lusterless hair that is easily broken. Light microscopy demonstrates twists of hair at irregular intervals. Pili annulati is characterized by bright and dark bands when viewed with reflected light. Unlike monilethrix, there is no fragility, and the hair can grow long.5
The Diagnosis: Monilethrix
Trichoscopy showed a beaded appearance of the hair shafts (Figure, A). Light microscopy demonstrated normal medullated nodes of hair coupled with internodal, thin, nonmedullated hair at regular intervals (Figure, B). Clinical and trichoscopic findings led to a diagnosis of monilethrix.
Monilethrix is a genetic hair disorder characterized by regular periodic thinning of the hair shafts, giving the strands a beaded appearance. The hair tends to break at these constricted parts, resulting in short hairs. Nodosities represent the normal hair shaft, whereas the constricted points are the site of the defect. The hair tends to be normal at birth and then becomes short, fragile, and brittle within months, leading to hypotrichosis, particularly on the occipital scalp.1 Monilethrix also may involve the eyebrows and eyelashes in addition to scalp hair. Follicular hyperkeratotic papules with perifollicular erythema frequently are noted on the occipital area. Monilethrix can be inherited in an autosomal-dominant fashion with mutations involving KRT81, KRT83, and KRT86, which code for the type II hair keratins Hb1, Hb3, and Hb6, respectively. The autosomal-recessive form is caused by mutations in the DSG4 gene, coding for the desmoglein 4 protein.2 Trichoscopy or light microscopy is essential to establish a diagnosis of monilethrix. Trichoscopy is an easy and rapid tool that is utilized to illustrate the beaded appearance of the hair shafts.3 Light microscopy shows the distinctive nodes that are medullated, with a normal hair diameter alternating with the internodes, or constrictions, that are nonmedullated and represent the sites of fracture.1 Monilethrix can improve by puberty. There is no definitive treatment; however, some patients show considerable improvement on minoxidil.4 Treatment with minoxidil was initiated in this patient; however, she was lost to follow-up.
Genetic hair disorders are rare and can be an isolated phenomenon or part of concurrent genetic syndromes. Therefore, thorough clinical examination of other ectodermal structures such as the nails and teeth is crucial as well as obtaining a detailed family history and review of systems to exclude other syndromes.2 Hypotrichosis simplex is characterized by hair loss exclusively on the scalp, sparing other ectodermal structures and with no systemic abnormalities. Ectodermal dysplasia is a heterogeneous group of disorders affecting not only the hair but also the teeth, nails, and sweat glands.2 Pili torti is another rare genetic hair disorder that is characterized by twisting of the hair fiber on its own axis. It presents clinically as sparse, depigmented, lusterless hair that is easily broken. Light microscopy demonstrates twists of hair at irregular intervals. Pili annulati is characterized by bright and dark bands when viewed with reflected light. Unlike monilethrix, there is no fragility, and the hair can grow long.5
- Mirmirani P, Huang KP, Price VH. A practical, algorithmic approach to diagnosing hair shaft disorders. Int J Dermatol. 2011;50:1-12.
- Ahmed A, Almohanna H, Griggs J, et al. Genetic hair disorders: a review. Dermatol Ther. 2019;9:421-448.
- Liu C-I, Hsu C-H. Rapid diagnosis of monilethrix using dermoscopy. Br J Dermatol. 2008;159:741-743.
- Rossi A, Iorio A, Fortuna MC, et al. Monilethrix treated with minoxidil. Int J Immunopathol Pharmacol. 2011;24:239-242.
- Singh G, Miteva M. Prognosis and management of congenital hair shaft disorders with fragility—part I. Pediatr Dermatol. 2016;33:473-480.
- Mirmirani P, Huang KP, Price VH. A practical, algorithmic approach to diagnosing hair shaft disorders. Int J Dermatol. 2011;50:1-12.
- Ahmed A, Almohanna H, Griggs J, et al. Genetic hair disorders: a review. Dermatol Ther. 2019;9:421-448.
- Liu C-I, Hsu C-H. Rapid diagnosis of monilethrix using dermoscopy. Br J Dermatol. 2008;159:741-743.
- Rossi A, Iorio A, Fortuna MC, et al. Monilethrix treated with minoxidil. Int J Immunopathol Pharmacol. 2011;24:239-242.
- Singh G, Miteva M. Prognosis and management of congenital hair shaft disorders with fragility—part I. Pediatr Dermatol. 2016;33:473-480.

A 5-year-old girl presented to our clinic with sparse scalp hair. Her mother reported thinning of the hair and breakage that appeared shortly after birth. She also reported that the patient’s hair was dull, dry, and unable to be grown long. The patient was otherwise healthy. She was born to nonconsanguineous parents, and her family history was unremarkable. Physical examination revealed dry, brittle, and short hairs. The hair was sparser on the occipital area of the scalp, and multiple keratotic papules were noted in this area. No abnormalities were detected on the teeth or nails, and a review of systems was unremarkable. Trichoscopy and light microscopy were performed.

COVID-19 in pregnancy raises risk of preterm birth and severe disease
based on data from two studies published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
In a study of birth and infant outcomes, rates of preterm birth (less than 37 weeks’ gestational age) were higher among women with confirmed SARS-CoV-2 infections compared with the national average (12.9% vs. 10.2%) wrote Kate R. Woodworth, MD, and colleagues of the CDC COVID-19 Response Pregnancy and Linked Outcomes Team.
The researchers collected information on pregnancy and infant outcomes from 16 jurisdictions through the Surveillance for Emerging Threats to Mothers and Babies Network (SET-NET). The study included 5,252 women with laboratory-confirmed SARS-CoV-2 infection reported during March 29–Oct. 14, 2020.
Overall, 12.9% of the 3,912 live births with known gestational age were preterm. A total of 610 infants were tested for SARS-CoV-2, and 2.6% were positive. Most of these perinatal infections (85%) occurred among infants born to women with SARS-CoV-2 infection within 1 week of delivery.
Half of the infants with positive test results were preterm, possibly reflecting higher screening rates in the ICU, the researchers said. “These findings also support the growing evidence that although severe COVID-19 does occur in neonates the majority of term neonates experience asymptomatic infection or mild disease; however, information on long term outcomes among exposed infants is unknown.”
Address disparities that amplify risk
The study findings were limited by several factors including inconsistent symptom reporting, overrepresentation of Hispanic women, and incomplete information on pregnancy loss, Dr. Woodworth and associates noted. However, the results add to the knowledge about the impact of COVID-19 disease on pregnancy by providing a large, population-based cohort with completed pregnancy outcomes as well as infant testing.
“SET-NET will continue to follow pregnancies affected by SARS-CoV-2 through completion of pregnancy and infants until age 6 months to guide clinical and public health practice,” the researchers noted. “Longer-term investigation into solutions to alleviate underlying inequities in social determinants of health associated with disparities in maternal morbidity, mortality, and adverse pregnancy outcomes, and effectively addressing these inequities, could reduce the prevalence of conditions and experiences that might amplify risks from COVID-19,” they added.
Severe disease and death increased in pregnant women
In a second study published in the MMWR, Laura D. Zambrano, PhD, and colleagues, also of the CDC COVID-19 Response Pregnancy and Linked Outcomes Team, compared data on 23,434 reportedly pregnant and 386,028 nonpregnant women of reproductive age (15-44 years) with confirmed and symptomatic SARS-CoV-2 infections reported to the CDC between Jan. 22, 2020, and Oct. 3, 2020.
After adjustment for age, race, and underlying medical conditions, pregnant women with COVID-19 disease were significantly more likely than were nonpregnant women to be admitted to intensive care (10.5 per 1,000 cases vs. 3.9 per 1,000 cases), to receive invasive ventilation (2.9 vs. 1.1), receive extracorporeal membrane oxygenation (0.7 vs. 0.3) and to die (1.5 vs. 1.2).
“Irrespective of pregnancy status, ICU admissions, receipt of invasive ventilation, and death occurred more often among women aged 35-44 years than among those aged 15-24 years,” Dr. Zambrano and associates noted. In addition, non-Hispanic Black and Black women comprised 14.1% of the study population but accounted for 36.6% of deaths overall (9 in pregnant women and 167 in nonpregnant women).
The findings in the study of characteristics were limited by several factors including the voluntary reporting of COVID-19 cases, potential reporting bias, and inadequate time to assess severe cases, the researchers noted. However, “data from previous influenza pandemics, including 2009 H1N1, have shown that pregnant women are at increased risk for severe outcomes including death and the absolute risks for severe outcomes were higher than in this study of COVID-19 during pregnancy.”
“Pregnant women should be informed of their risk for severe COVID-19–associated illness and the warning signs of severe COVID-19,” Dr. Zambrano and associates said. “Providers who care for pregnant women should be familiar with guidelines for medical management of COVID-19, including considerations for management of COVID-19 in pregnancy.”
More data needed for informed counseling
“It is important to conduct research trials involving pregnant women so that we have reliable data regarding outcomes with which to counsel women,” Angela Bianco, MD, a maternal fetal medicine specialist at Mount Sinai Hospital in New York, said in an interview.
“Often pregnant women are excluded from research trials, but the impact of the current public health crisis affects all persons regardless of pregnancy status,” she said.
Dr. Bianco said that she was not surprised by the findings of either study. “In fact, our own research produced similar results.”
“These recent publications found that age-matched pregnant versus nonpregnant women had more severe manifestations of COVID-19, and specifically that pregnant women had a higher risk of requiring ventilation and intensive care admission, as well as higher risk of death,” she said. “Previous studies examining the effect of other SARS viruses have demonstrated that pregnancy is associated with worse outcomes; these findings are likely attributable to the relative state of immunosuppression in pregnancy.” Also, “one of these trials found a greater risk of premature birth in women with COVID-19; this may largely be attributable to iatrogenic delivery due to maternal illness as opposed to spontaneous preterm birth,” Dr. Bianco explained.
“Data are emerging regarding the impact of SARS-CoV-2 on pregnancy outcomes, however information remains limited,” Dr. Bianco noted. “Clinicians need to make patients aware that SARS-CoV-2 infection during pregnancy is associated with a greater risk of severe illness requiring intensive care and/or ventilatory support and even death; however, the precise rates remain unknown. “COVID-19 during pregnancy may result in a preterm birth, but at this time the rate of fetal infection remains unknown,” she said. “Clinicians need to reinforce the importance of physical distancing, mask use, and proper hand hygiene, particularly in this vulnerable population.”
Dr. Bianco emphasized: “Longitudinal studies assessing the impact of SARS-CoV-2 infection at various gestational age periods are needed, as at this time most of the available data includes women with SARS-CoV-2 infection around the time of delivery. Long-term infant outcomes are needed, as well as studies assessing the risk of fetal infection.”
The studies were supported by the Centers for Disease Control and Prevention. The researchers had no financial conflicts to disclose. Dr. Bianco had no relevant financial disclosures.
SOURCE: Woodworth KR et al. MMWR. 2020 Nov 2. doi: 10.15585/mmwr.mm6944e2; Zambrano LD et al. MMWR. 2020 Nov 2. doi: 10.15585/mmwr.mm6944e3.
based on data from two studies published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
In a study of birth and infant outcomes, rates of preterm birth (less than 37 weeks’ gestational age) were higher among women with confirmed SARS-CoV-2 infections compared with the national average (12.9% vs. 10.2%) wrote Kate R. Woodworth, MD, and colleagues of the CDC COVID-19 Response Pregnancy and Linked Outcomes Team.
The researchers collected information on pregnancy and infant outcomes from 16 jurisdictions through the Surveillance for Emerging Threats to Mothers and Babies Network (SET-NET). The study included 5,252 women with laboratory-confirmed SARS-CoV-2 infection reported during March 29–Oct. 14, 2020.
Overall, 12.9% of the 3,912 live births with known gestational age were preterm. A total of 610 infants were tested for SARS-CoV-2, and 2.6% were positive. Most of these perinatal infections (85%) occurred among infants born to women with SARS-CoV-2 infection within 1 week of delivery.
Half of the infants with positive test results were preterm, possibly reflecting higher screening rates in the ICU, the researchers said. “These findings also support the growing evidence that although severe COVID-19 does occur in neonates the majority of term neonates experience asymptomatic infection or mild disease; however, information on long term outcomes among exposed infants is unknown.”
Address disparities that amplify risk
The study findings were limited by several factors including inconsistent symptom reporting, overrepresentation of Hispanic women, and incomplete information on pregnancy loss, Dr. Woodworth and associates noted. However, the results add to the knowledge about the impact of COVID-19 disease on pregnancy by providing a large, population-based cohort with completed pregnancy outcomes as well as infant testing.
“SET-NET will continue to follow pregnancies affected by SARS-CoV-2 through completion of pregnancy and infants until age 6 months to guide clinical and public health practice,” the researchers noted. “Longer-term investigation into solutions to alleviate underlying inequities in social determinants of health associated with disparities in maternal morbidity, mortality, and adverse pregnancy outcomes, and effectively addressing these inequities, could reduce the prevalence of conditions and experiences that might amplify risks from COVID-19,” they added.
Severe disease and death increased in pregnant women
In a second study published in the MMWR, Laura D. Zambrano, PhD, and colleagues, also of the CDC COVID-19 Response Pregnancy and Linked Outcomes Team, compared data on 23,434 reportedly pregnant and 386,028 nonpregnant women of reproductive age (15-44 years) with confirmed and symptomatic SARS-CoV-2 infections reported to the CDC between Jan. 22, 2020, and Oct. 3, 2020.
After adjustment for age, race, and underlying medical conditions, pregnant women with COVID-19 disease were significantly more likely than were nonpregnant women to be admitted to intensive care (10.5 per 1,000 cases vs. 3.9 per 1,000 cases), to receive invasive ventilation (2.9 vs. 1.1), receive extracorporeal membrane oxygenation (0.7 vs. 0.3) and to die (1.5 vs. 1.2).
“Irrespective of pregnancy status, ICU admissions, receipt of invasive ventilation, and death occurred more often among women aged 35-44 years than among those aged 15-24 years,” Dr. Zambrano and associates noted. In addition, non-Hispanic Black and Black women comprised 14.1% of the study population but accounted for 36.6% of deaths overall (9 in pregnant women and 167 in nonpregnant women).
The findings in the study of characteristics were limited by several factors including the voluntary reporting of COVID-19 cases, potential reporting bias, and inadequate time to assess severe cases, the researchers noted. However, “data from previous influenza pandemics, including 2009 H1N1, have shown that pregnant women are at increased risk for severe outcomes including death and the absolute risks for severe outcomes were higher than in this study of COVID-19 during pregnancy.”
“Pregnant women should be informed of their risk for severe COVID-19–associated illness and the warning signs of severe COVID-19,” Dr. Zambrano and associates said. “Providers who care for pregnant women should be familiar with guidelines for medical management of COVID-19, including considerations for management of COVID-19 in pregnancy.”
More data needed for informed counseling
“It is important to conduct research trials involving pregnant women so that we have reliable data regarding outcomes with which to counsel women,” Angela Bianco, MD, a maternal fetal medicine specialist at Mount Sinai Hospital in New York, said in an interview.
“Often pregnant women are excluded from research trials, but the impact of the current public health crisis affects all persons regardless of pregnancy status,” she said.
Dr. Bianco said that she was not surprised by the findings of either study. “In fact, our own research produced similar results.”
“These recent publications found that age-matched pregnant versus nonpregnant women had more severe manifestations of COVID-19, and specifically that pregnant women had a higher risk of requiring ventilation and intensive care admission, as well as higher risk of death,” she said. “Previous studies examining the effect of other SARS viruses have demonstrated that pregnancy is associated with worse outcomes; these findings are likely attributable to the relative state of immunosuppression in pregnancy.” Also, “one of these trials found a greater risk of premature birth in women with COVID-19; this may largely be attributable to iatrogenic delivery due to maternal illness as opposed to spontaneous preterm birth,” Dr. Bianco explained.
“Data are emerging regarding the impact of SARS-CoV-2 on pregnancy outcomes, however information remains limited,” Dr. Bianco noted. “Clinicians need to make patients aware that SARS-CoV-2 infection during pregnancy is associated with a greater risk of severe illness requiring intensive care and/or ventilatory support and even death; however, the precise rates remain unknown. “COVID-19 during pregnancy may result in a preterm birth, but at this time the rate of fetal infection remains unknown,” she said. “Clinicians need to reinforce the importance of physical distancing, mask use, and proper hand hygiene, particularly in this vulnerable population.”
Dr. Bianco emphasized: “Longitudinal studies assessing the impact of SARS-CoV-2 infection at various gestational age periods are needed, as at this time most of the available data includes women with SARS-CoV-2 infection around the time of delivery. Long-term infant outcomes are needed, as well as studies assessing the risk of fetal infection.”
The studies were supported by the Centers for Disease Control and Prevention. The researchers had no financial conflicts to disclose. Dr. Bianco had no relevant financial disclosures.
SOURCE: Woodworth KR et al. MMWR. 2020 Nov 2. doi: 10.15585/mmwr.mm6944e2; Zambrano LD et al. MMWR. 2020 Nov 2. doi: 10.15585/mmwr.mm6944e3.
based on data from two studies published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
In a study of birth and infant outcomes, rates of preterm birth (less than 37 weeks’ gestational age) were higher among women with confirmed SARS-CoV-2 infections compared with the national average (12.9% vs. 10.2%) wrote Kate R. Woodworth, MD, and colleagues of the CDC COVID-19 Response Pregnancy and Linked Outcomes Team.
The researchers collected information on pregnancy and infant outcomes from 16 jurisdictions through the Surveillance for Emerging Threats to Mothers and Babies Network (SET-NET). The study included 5,252 women with laboratory-confirmed SARS-CoV-2 infection reported during March 29–Oct. 14, 2020.
Overall, 12.9% of the 3,912 live births with known gestational age were preterm. A total of 610 infants were tested for SARS-CoV-2, and 2.6% were positive. Most of these perinatal infections (85%) occurred among infants born to women with SARS-CoV-2 infection within 1 week of delivery.
Half of the infants with positive test results were preterm, possibly reflecting higher screening rates in the ICU, the researchers said. “These findings also support the growing evidence that although severe COVID-19 does occur in neonates the majority of term neonates experience asymptomatic infection or mild disease; however, information on long term outcomes among exposed infants is unknown.”
Address disparities that amplify risk
The study findings were limited by several factors including inconsistent symptom reporting, overrepresentation of Hispanic women, and incomplete information on pregnancy loss, Dr. Woodworth and associates noted. However, the results add to the knowledge about the impact of COVID-19 disease on pregnancy by providing a large, population-based cohort with completed pregnancy outcomes as well as infant testing.
“SET-NET will continue to follow pregnancies affected by SARS-CoV-2 through completion of pregnancy and infants until age 6 months to guide clinical and public health practice,” the researchers noted. “Longer-term investigation into solutions to alleviate underlying inequities in social determinants of health associated with disparities in maternal morbidity, mortality, and adverse pregnancy outcomes, and effectively addressing these inequities, could reduce the prevalence of conditions and experiences that might amplify risks from COVID-19,” they added.
Severe disease and death increased in pregnant women
In a second study published in the MMWR, Laura D. Zambrano, PhD, and colleagues, also of the CDC COVID-19 Response Pregnancy and Linked Outcomes Team, compared data on 23,434 reportedly pregnant and 386,028 nonpregnant women of reproductive age (15-44 years) with confirmed and symptomatic SARS-CoV-2 infections reported to the CDC between Jan. 22, 2020, and Oct. 3, 2020.
After adjustment for age, race, and underlying medical conditions, pregnant women with COVID-19 disease were significantly more likely than were nonpregnant women to be admitted to intensive care (10.5 per 1,000 cases vs. 3.9 per 1,000 cases), to receive invasive ventilation (2.9 vs. 1.1), receive extracorporeal membrane oxygenation (0.7 vs. 0.3) and to die (1.5 vs. 1.2).
“Irrespective of pregnancy status, ICU admissions, receipt of invasive ventilation, and death occurred more often among women aged 35-44 years than among those aged 15-24 years,” Dr. Zambrano and associates noted. In addition, non-Hispanic Black and Black women comprised 14.1% of the study population but accounted for 36.6% of deaths overall (9 in pregnant women and 167 in nonpregnant women).
The findings in the study of characteristics were limited by several factors including the voluntary reporting of COVID-19 cases, potential reporting bias, and inadequate time to assess severe cases, the researchers noted. However, “data from previous influenza pandemics, including 2009 H1N1, have shown that pregnant women are at increased risk for severe outcomes including death and the absolute risks for severe outcomes were higher than in this study of COVID-19 during pregnancy.”
“Pregnant women should be informed of their risk for severe COVID-19–associated illness and the warning signs of severe COVID-19,” Dr. Zambrano and associates said. “Providers who care for pregnant women should be familiar with guidelines for medical management of COVID-19, including considerations for management of COVID-19 in pregnancy.”
More data needed for informed counseling
“It is important to conduct research trials involving pregnant women so that we have reliable data regarding outcomes with which to counsel women,” Angela Bianco, MD, a maternal fetal medicine specialist at Mount Sinai Hospital in New York, said in an interview.
“Often pregnant women are excluded from research trials, but the impact of the current public health crisis affects all persons regardless of pregnancy status,” she said.
Dr. Bianco said that she was not surprised by the findings of either study. “In fact, our own research produced similar results.”
“These recent publications found that age-matched pregnant versus nonpregnant women had more severe manifestations of COVID-19, and specifically that pregnant women had a higher risk of requiring ventilation and intensive care admission, as well as higher risk of death,” she said. “Previous studies examining the effect of other SARS viruses have demonstrated that pregnancy is associated with worse outcomes; these findings are likely attributable to the relative state of immunosuppression in pregnancy.” Also, “one of these trials found a greater risk of premature birth in women with COVID-19; this may largely be attributable to iatrogenic delivery due to maternal illness as opposed to spontaneous preterm birth,” Dr. Bianco explained.
“Data are emerging regarding the impact of SARS-CoV-2 on pregnancy outcomes, however information remains limited,” Dr. Bianco noted. “Clinicians need to make patients aware that SARS-CoV-2 infection during pregnancy is associated with a greater risk of severe illness requiring intensive care and/or ventilatory support and even death; however, the precise rates remain unknown. “COVID-19 during pregnancy may result in a preterm birth, but at this time the rate of fetal infection remains unknown,” she said. “Clinicians need to reinforce the importance of physical distancing, mask use, and proper hand hygiene, particularly in this vulnerable population.”
Dr. Bianco emphasized: “Longitudinal studies assessing the impact of SARS-CoV-2 infection at various gestational age periods are needed, as at this time most of the available data includes women with SARS-CoV-2 infection around the time of delivery. Long-term infant outcomes are needed, as well as studies assessing the risk of fetal infection.”
The studies were supported by the Centers for Disease Control and Prevention. The researchers had no financial conflicts to disclose. Dr. Bianco had no relevant financial disclosures.
SOURCE: Woodworth KR et al. MMWR. 2020 Nov 2. doi: 10.15585/mmwr.mm6944e2; Zambrano LD et al. MMWR. 2020 Nov 2. doi: 10.15585/mmwr.mm6944e3.
FROM MMWR
Gene-replacement therapy shows promise in X-linked myotubular myopathy
, according to research presented at the 2020 CNS-ICNA Conjoint Meeting, which was held virtually this year. The treatment also appears to improve patients’ motor function significantly and help them to achieve motor milestones.

The results come from a phase 1/2 study of two doses of AT132. Three of 17 patients who received the higher dose had fatal liver dysfunction. The researchers are investigating these cases and will communicate their findings.
X-linked myotubular myopathy is a rare and often fatal neuromuscular disease. Mutations in MTM1, which encodes the myotubularin enzyme that is required for the development and function of skeletal muscle, cause the disease, which affects about one in 50,000 to one in 40,000 newborn boys. The disease is associated with profound muscle weakness and impairment of neuromuscular and respiratory function. Patients with X-linked myotubular myopathy achieve motor milestones much later or not at all, and most require a ventilator or a feeding tube. The mortality by age 18 months is approximately 50%.
The ASPIRO trial
Investigators theorized that muscle tissue would be an appropriate therapeutic target because it does not display dystrophic or inflammatory changes in most patients. They identified adeno-associated virus AAV8 as a potential carrier for gene therapy, since it targets skeletal muscle effectively.
Nancy L. Kuntz, MD, an attending physician at Ann and Robert H. Lurie Children’s Hospital of Chicago, and colleagues conducted the ASPIRO trial to examine AT132 as a potential treatment for X-linked myotubular myopathy. Eligible patients were younger than 5 years or had previously enrolled in a natural history study of the disease, required ventilator support at baseline, and had no clinically significant underlying liver disease. Patients were randomly assigned to 1 × 1014 vg/kg of AAT132, 3 × 1014 vg/kg of AT132, or delayed treatment. Participants assigned to delayed treatment served as the study’s control group.
The study’s primary end points were safety and change in hours of daily ventilator support from baseline to week 24 after dosing. The investigators also examined a respiratory endpoint (i.e., maximal inspiratory pressure [MIP]) and neuromuscular endpoints (i.e., motor milestones, CHOP INTEND score, and muscle biopsy).
Treatment improved respiratory function
As of July 28, Dr. Kuntz and colleagues had enrolled 23 patients in the trial. Six participants received the lower dose of therapy, and 17 received the higher dose. Median age was 1.7 years for the low-dose group and 2.6 years for the high-dose group.
Patients assigned to receive the higher dose of therapy received treatment more recently than the low-dose group, and not all of the former have reached 48 weeks since treatment, said Dr. Kuntz. Fewer efficacy data are thus available for the high-dose group.
Each dose of AT132 was associated with a significantly greater decrease from baseline in least squares mean daily hours of ventilator dependence, compared with the control condition. At week 48, the mean reduction was approximately 19 hours/day for patients receiving 1 × 1014 vg/kg of AAT132 and approximately 13 hours per day for patients receiving 3 × 1014 vg/kg of AT132. The investigators did not perform a statistical comparison of the two doses because of differing protocols for ventilator weaning between groups. All six patients who received the lower dose achieved ventilator independence, as did one patient who received the higher dose.
In addition, all treated patients had significantly greater increases from baseline in least squares mean MIP, compared with controls. The mean increase was 45.7 cmH2O for the low-dose group, 46.1 cmH2O for the high-dose group, and −8.0 cmH2O for controls.
Before treatment, most patients had not achieved any of the motor milestones that investigators assessed. After treatment, five of six patients receiving the low dose achieved independent walking, as did one in 10 patients receiving the high dose. No controls achieved this milestone. Treated patients also had significantly greater increases from baseline in least squares mean CHOP INTEND scores, compared with controls. At least at one time point, five of six patients receiving the low dose, six of 10 patients receiving the high dose, and one control patient achieved the mean score observed in healthy infants.
Patients in both treatment arms had improvements in muscle pathology at weeks 24 and 48, including improvements in organelle localization and fiber size. In addition, patients in both treatment arms had continued detectable vector copies and myotubularin protein expression at both time points.
Deaths under investigation
In the low-dose group, one patient had four serious treatment-emergent adverse events, and in the high-dose group, eight patients had 27 serious treatment-emergent adverse events. The three patients in the high-dose group who developed fatal liver dysfunction were among the older, heavier patients in the study and, consequently, received among the highest total doses of treatment. These patients had evidence of likely preexisting intrahepatic cholestasis.
“This clinical trial is on hold pending discussions between regulatory agencies and the study sponsor regarding additional recruitment and the duration of follow-up,” said Dr. Kuntz.
Audentes Therapeutics, which is developing AT132, funded the trial. Dr. Kuntz had no conflicts of interest.
SOURCE: Bönnemann CG et al. CNS-ICNA 2020, Abstract P.62.
, according to research presented at the 2020 CNS-ICNA Conjoint Meeting, which was held virtually this year. The treatment also appears to improve patients’ motor function significantly and help them to achieve motor milestones.
The results come from a phase 1/2 study of two doses of AT132. Three of 17 patients who received the higher dose had fatal liver dysfunction. The researchers are investigating these cases and will communicate their findings.
X-linked myotubular myopathy is a rare and often fatal neuromuscular disease. Mutations in MTM1, which encodes the myotubularin enzyme that is required for the development and function of skeletal muscle, cause the disease, which affects about one in 50,000 to one in 40,000 newborn boys. The disease is associated with profound muscle weakness and impairment of neuromuscular and respiratory function. Patients with X-linked myotubular myopathy achieve motor milestones much later or not at all, and most require a ventilator or a feeding tube. The mortality by age 18 months is approximately 50%.
The ASPIRO trial
Investigators theorized that muscle tissue would be an appropriate therapeutic target because it does not display dystrophic or inflammatory changes in most patients. They identified adeno-associated virus AAV8 as a potential carrier for gene therapy, since it targets skeletal muscle effectively.
Nancy L. Kuntz, MD, an attending physician at Ann and Robert H. Lurie Children’s Hospital of Chicago, and colleagues conducted the ASPIRO trial to examine AT132 as a potential treatment for X-linked myotubular myopathy. Eligible patients were younger than 5 years or had previously enrolled in a natural history study of the disease, required ventilator support at baseline, and had no clinically significant underlying liver disease. Patients were randomly assigned to 1 × 1014 vg/kg of AAT132, 3 × 1014 vg/kg of AT132, or delayed treatment. Participants assigned to delayed treatment served as the study’s control group.
The study’s primary end points were safety and change in hours of daily ventilator support from baseline to week 24 after dosing. The investigators also examined a respiratory endpoint (i.e., maximal inspiratory pressure [MIP]) and neuromuscular endpoints (i.e., motor milestones, CHOP INTEND score, and muscle biopsy).
Treatment improved respiratory function
As of July 28, Dr. Kuntz and colleagues had enrolled 23 patients in the trial. Six participants received the lower dose of therapy, and 17 received the higher dose. Median age was 1.7 years for the low-dose group and 2.6 years for the high-dose group.
Patients assigned to receive the higher dose of therapy received treatment more recently than the low-dose group, and not all of the former have reached 48 weeks since treatment, said Dr. Kuntz. Fewer efficacy data are thus available for the high-dose group.
Each dose of AT132 was associated with a significantly greater decrease from baseline in least squares mean daily hours of ventilator dependence, compared with the control condition. At week 48, the mean reduction was approximately 19 hours/day for patients receiving 1 × 1014 vg/kg of AAT132 and approximately 13 hours per day for patients receiving 3 × 1014 vg/kg of AT132. The investigators did not perform a statistical comparison of the two doses because of differing protocols for ventilator weaning between groups. All six patients who received the lower dose achieved ventilator independence, as did one patient who received the higher dose.
In addition, all treated patients had significantly greater increases from baseline in least squares mean MIP, compared with controls. The mean increase was 45.7 cmH2O for the low-dose group, 46.1 cmH2O for the high-dose group, and −8.0 cmH2O for controls.
Before treatment, most patients had not achieved any of the motor milestones that investigators assessed. After treatment, five of six patients receiving the low dose achieved independent walking, as did one in 10 patients receiving the high dose. No controls achieved this milestone. Treated patients also had significantly greater increases from baseline in least squares mean CHOP INTEND scores, compared with controls. At least at one time point, five of six patients receiving the low dose, six of 10 patients receiving the high dose, and one control patient achieved the mean score observed in healthy infants.
Patients in both treatment arms had improvements in muscle pathology at weeks 24 and 48, including improvements in organelle localization and fiber size. In addition, patients in both treatment arms had continued detectable vector copies and myotubularin protein expression at both time points.
Deaths under investigation
In the low-dose group, one patient had four serious treatment-emergent adverse events, and in the high-dose group, eight patients had 27 serious treatment-emergent adverse events. The three patients in the high-dose group who developed fatal liver dysfunction were among the older, heavier patients in the study and, consequently, received among the highest total doses of treatment. These patients had evidence of likely preexisting intrahepatic cholestasis.
“This clinical trial is on hold pending discussions between regulatory agencies and the study sponsor regarding additional recruitment and the duration of follow-up,” said Dr. Kuntz.
Audentes Therapeutics, which is developing AT132, funded the trial. Dr. Kuntz had no conflicts of interest.
SOURCE: Bönnemann CG et al. CNS-ICNA 2020, Abstract P.62.
, according to research presented at the 2020 CNS-ICNA Conjoint Meeting, which was held virtually this year. The treatment also appears to improve patients’ motor function significantly and help them to achieve motor milestones.
The results come from a phase 1/2 study of two doses of AT132. Three of 17 patients who received the higher dose had fatal liver dysfunction. The researchers are investigating these cases and will communicate their findings.
X-linked myotubular myopathy is a rare and often fatal neuromuscular disease. Mutations in MTM1, which encodes the myotubularin enzyme that is required for the development and function of skeletal muscle, cause the disease, which affects about one in 50,000 to one in 40,000 newborn boys. The disease is associated with profound muscle weakness and impairment of neuromuscular and respiratory function. Patients with X-linked myotubular myopathy achieve motor milestones much later or not at all, and most require a ventilator or a feeding tube. The mortality by age 18 months is approximately 50%.
The ASPIRO trial
Investigators theorized that muscle tissue would be an appropriate therapeutic target because it does not display dystrophic or inflammatory changes in most patients. They identified adeno-associated virus AAV8 as a potential carrier for gene therapy, since it targets skeletal muscle effectively.
Nancy L. Kuntz, MD, an attending physician at Ann and Robert H. Lurie Children’s Hospital of Chicago, and colleagues conducted the ASPIRO trial to examine AT132 as a potential treatment for X-linked myotubular myopathy. Eligible patients were younger than 5 years or had previously enrolled in a natural history study of the disease, required ventilator support at baseline, and had no clinically significant underlying liver disease. Patients were randomly assigned to 1 × 1014 vg/kg of AAT132, 3 × 1014 vg/kg of AT132, or delayed treatment. Participants assigned to delayed treatment served as the study’s control group.
The study’s primary end points were safety and change in hours of daily ventilator support from baseline to week 24 after dosing. The investigators also examined a respiratory endpoint (i.e., maximal inspiratory pressure [MIP]) and neuromuscular endpoints (i.e., motor milestones, CHOP INTEND score, and muscle biopsy).
Treatment improved respiratory function
As of July 28, Dr. Kuntz and colleagues had enrolled 23 patients in the trial. Six participants received the lower dose of therapy, and 17 received the higher dose. Median age was 1.7 years for the low-dose group and 2.6 years for the high-dose group.
Patients assigned to receive the higher dose of therapy received treatment more recently than the low-dose group, and not all of the former have reached 48 weeks since treatment, said Dr. Kuntz. Fewer efficacy data are thus available for the high-dose group.
Each dose of AT132 was associated with a significantly greater decrease from baseline in least squares mean daily hours of ventilator dependence, compared with the control condition. At week 48, the mean reduction was approximately 19 hours/day for patients receiving 1 × 1014 vg/kg of AAT132 and approximately 13 hours per day for patients receiving 3 × 1014 vg/kg of AT132. The investigators did not perform a statistical comparison of the two doses because of differing protocols for ventilator weaning between groups. All six patients who received the lower dose achieved ventilator independence, as did one patient who received the higher dose.
In addition, all treated patients had significantly greater increases from baseline in least squares mean MIP, compared with controls. The mean increase was 45.7 cmH2O for the low-dose group, 46.1 cmH2O for the high-dose group, and −8.0 cmH2O for controls.
Before treatment, most patients had not achieved any of the motor milestones that investigators assessed. After treatment, five of six patients receiving the low dose achieved independent walking, as did one in 10 patients receiving the high dose. No controls achieved this milestone. Treated patients also had significantly greater increases from baseline in least squares mean CHOP INTEND scores, compared with controls. At least at one time point, five of six patients receiving the low dose, six of 10 patients receiving the high dose, and one control patient achieved the mean score observed in healthy infants.
Patients in both treatment arms had improvements in muscle pathology at weeks 24 and 48, including improvements in organelle localization and fiber size. In addition, patients in both treatment arms had continued detectable vector copies and myotubularin protein expression at both time points.
Deaths under investigation
In the low-dose group, one patient had four serious treatment-emergent adverse events, and in the high-dose group, eight patients had 27 serious treatment-emergent adverse events. The three patients in the high-dose group who developed fatal liver dysfunction were among the older, heavier patients in the study and, consequently, received among the highest total doses of treatment. These patients had evidence of likely preexisting intrahepatic cholestasis.
“This clinical trial is on hold pending discussions between regulatory agencies and the study sponsor regarding additional recruitment and the duration of follow-up,” said Dr. Kuntz.
Audentes Therapeutics, which is developing AT132, funded the trial. Dr. Kuntz had no conflicts of interest.
SOURCE: Bönnemann CG et al. CNS-ICNA 2020, Abstract P.62.
FROM CNS-ICNA 2020
New case suggestive of in utero SARS-CoV-2 transmission
A new report of mother-to-fetus transmission of SARS-CoV-2 through umbilical cord blood adds to a small but growing body of evidence that the virus can be transmitted in utero.
Further,
The data
In a report published in the Journal of The Pediatric Infectious Diseases Society, Isabelle Von Kohorn, MD, PhD, of Holy Cross Health in Silver Spring, Md., and colleagues, described a case of neonatal infection with SARS-CoV-2 in a boy delivered by C-section at 34 weeks to a mother diagnosed with COVID-19 some 14 hours before. The newborn was immediately removed to a neonatal ICU and reunited with his mother a week later, once the mother had recovered.
Dr. Von Kohorn and colleagues reported that, while the infant’s nasopharyngeal swab test for SARS-CoV-2 was negative at 24 hours after birth, repeat molecular tests (using different assays) from 49 hours on were positive and indicated an increasing viral burden, although the infant never developed symptoms of COVID-19. In addition to being found in the nasopharynx, viral RNA also was detected in cord blood and in urine. No viral RNA was found in the placenta.
The circumstances of the birth, and the care taken to keep mother and her infant at a safe distance along with masking of the mother, made it “extremely unlikely” that the infant acquired his infection by the respiratory route, Dr. Von Kohorn and colleagues wrote.
“While we cannot rule out microscopic maternal blood contamination of cord blood in this or any other delivery, cord blood collection procedures are designed to avoid gross contamination with maternal blood. Microscopic contamination would not explain the RNA levels observed in our patient’s cord blood,” they wrote.
Clinicians should note that a neonate born to a mother with COVID-19 may take time to test positive for SARS-CoV-2 , the investigators argued, though the current recommendation of the American Academy of Pediatrics is to test nasopharyngeal secretions of well newborns at 24 and 48 hours but not again in the absence of symptoms. “This case suggests that some cases of SARS-CoV-2 in newborns may be detectable only after 48 hours of life.”
The authors hypothesized that virus transmitted by cord blood “seeded the nasopharynx and required 2 days for incubation and replication sufficient for detection.”
Some perspective
In an interview, Andrea Edlow, MD, A maternal-fetal medicine specialist at Massachusetts General Hospital in Boston, called the findings provocative if not definitive in establishing in utero or vertical transmission of SARS-CoV-2 in the same way that a Nature Communications case report did in July 2020. In that case, of a baby born to a mother with COVID-19, virus was seen at high levels in the placenta.
With the current case, “the absence of detectable virus in the placenta is certainly inconsistent/confusing if the authors claim hematogenous spread from mother to baby,” Dr. Edlow commented, “but the authors do offer plausible explanations, such as examination of limited areas within the placenta (when we know infection is likely to be patchy) and possible degradation of RNA prior to attempting to measure placental viral presence.”
Dr. Von Kohorn and colleagues’ study was funded by the National Institutes of Health, and the investigators disclosed no financial conflicts of interest. Dr. Edlow had no relevant financial disclosures.
SOURCE: Von Kohorn I et al. J Pediat Inf Dis Soc. 2020 Oct 22. doi: 10.1093/jpids/piaa127
A new report of mother-to-fetus transmission of SARS-CoV-2 through umbilical cord blood adds to a small but growing body of evidence that the virus can be transmitted in utero.
Further,
The data
In a report published in the Journal of The Pediatric Infectious Diseases Society, Isabelle Von Kohorn, MD, PhD, of Holy Cross Health in Silver Spring, Md., and colleagues, described a case of neonatal infection with SARS-CoV-2 in a boy delivered by C-section at 34 weeks to a mother diagnosed with COVID-19 some 14 hours before. The newborn was immediately removed to a neonatal ICU and reunited with his mother a week later, once the mother had recovered.
Dr. Von Kohorn and colleagues reported that, while the infant’s nasopharyngeal swab test for SARS-CoV-2 was negative at 24 hours after birth, repeat molecular tests (using different assays) from 49 hours on were positive and indicated an increasing viral burden, although the infant never developed symptoms of COVID-19. In addition to being found in the nasopharynx, viral RNA also was detected in cord blood and in urine. No viral RNA was found in the placenta.
The circumstances of the birth, and the care taken to keep mother and her infant at a safe distance along with masking of the mother, made it “extremely unlikely” that the infant acquired his infection by the respiratory route, Dr. Von Kohorn and colleagues wrote.
“While we cannot rule out microscopic maternal blood contamination of cord blood in this or any other delivery, cord blood collection procedures are designed to avoid gross contamination with maternal blood. Microscopic contamination would not explain the RNA levels observed in our patient’s cord blood,” they wrote.
Clinicians should note that a neonate born to a mother with COVID-19 may take time to test positive for SARS-CoV-2 , the investigators argued, though the current recommendation of the American Academy of Pediatrics is to test nasopharyngeal secretions of well newborns at 24 and 48 hours but not again in the absence of symptoms. “This case suggests that some cases of SARS-CoV-2 in newborns may be detectable only after 48 hours of life.”
The authors hypothesized that virus transmitted by cord blood “seeded the nasopharynx and required 2 days for incubation and replication sufficient for detection.”
Some perspective
In an interview, Andrea Edlow, MD, A maternal-fetal medicine specialist at Massachusetts General Hospital in Boston, called the findings provocative if not definitive in establishing in utero or vertical transmission of SARS-CoV-2 in the same way that a Nature Communications case report did in July 2020. In that case, of a baby born to a mother with COVID-19, virus was seen at high levels in the placenta.
With the current case, “the absence of detectable virus in the placenta is certainly inconsistent/confusing if the authors claim hematogenous spread from mother to baby,” Dr. Edlow commented, “but the authors do offer plausible explanations, such as examination of limited areas within the placenta (when we know infection is likely to be patchy) and possible degradation of RNA prior to attempting to measure placental viral presence.”
Dr. Von Kohorn and colleagues’ study was funded by the National Institutes of Health, and the investigators disclosed no financial conflicts of interest. Dr. Edlow had no relevant financial disclosures.
SOURCE: Von Kohorn I et al. J Pediat Inf Dis Soc. 2020 Oct 22. doi: 10.1093/jpids/piaa127
A new report of mother-to-fetus transmission of SARS-CoV-2 through umbilical cord blood adds to a small but growing body of evidence that the virus can be transmitted in utero.
Further,
The data
In a report published in the Journal of The Pediatric Infectious Diseases Society, Isabelle Von Kohorn, MD, PhD, of Holy Cross Health in Silver Spring, Md., and colleagues, described a case of neonatal infection with SARS-CoV-2 in a boy delivered by C-section at 34 weeks to a mother diagnosed with COVID-19 some 14 hours before. The newborn was immediately removed to a neonatal ICU and reunited with his mother a week later, once the mother had recovered.
Dr. Von Kohorn and colleagues reported that, while the infant’s nasopharyngeal swab test for SARS-CoV-2 was negative at 24 hours after birth, repeat molecular tests (using different assays) from 49 hours on were positive and indicated an increasing viral burden, although the infant never developed symptoms of COVID-19. In addition to being found in the nasopharynx, viral RNA also was detected in cord blood and in urine. No viral RNA was found in the placenta.
The circumstances of the birth, and the care taken to keep mother and her infant at a safe distance along with masking of the mother, made it “extremely unlikely” that the infant acquired his infection by the respiratory route, Dr. Von Kohorn and colleagues wrote.
“While we cannot rule out microscopic maternal blood contamination of cord blood in this or any other delivery, cord blood collection procedures are designed to avoid gross contamination with maternal blood. Microscopic contamination would not explain the RNA levels observed in our patient’s cord blood,” they wrote.
Clinicians should note that a neonate born to a mother with COVID-19 may take time to test positive for SARS-CoV-2 , the investigators argued, though the current recommendation of the American Academy of Pediatrics is to test nasopharyngeal secretions of well newborns at 24 and 48 hours but not again in the absence of symptoms. “This case suggests that some cases of SARS-CoV-2 in newborns may be detectable only after 48 hours of life.”
The authors hypothesized that virus transmitted by cord blood “seeded the nasopharynx and required 2 days for incubation and replication sufficient for detection.”
Some perspective
In an interview, Andrea Edlow, MD, A maternal-fetal medicine specialist at Massachusetts General Hospital in Boston, called the findings provocative if not definitive in establishing in utero or vertical transmission of SARS-CoV-2 in the same way that a Nature Communications case report did in July 2020. In that case, of a baby born to a mother with COVID-19, virus was seen at high levels in the placenta.
With the current case, “the absence of detectable virus in the placenta is certainly inconsistent/confusing if the authors claim hematogenous spread from mother to baby,” Dr. Edlow commented, “but the authors do offer plausible explanations, such as examination of limited areas within the placenta (when we know infection is likely to be patchy) and possible degradation of RNA prior to attempting to measure placental viral presence.”
Dr. Von Kohorn and colleagues’ study was funded by the National Institutes of Health, and the investigators disclosed no financial conflicts of interest. Dr. Edlow had no relevant financial disclosures.
SOURCE: Von Kohorn I et al. J Pediat Inf Dis Soc. 2020 Oct 22. doi: 10.1093/jpids/piaa127
FROM THE JOURNAL OF THE PEDIATRIC INFECTIOUS DISEASES SOCIETY
Home spirometry improved monitoring of cystic fibrosis patients during COVID-19 pandemic
Home spirometry has become increasingly used among cystic fibrosis patients during the COVID-19 pandemic, and new research suggests that home devices perform reasonably well. Forced expiratory volume in 1 second (FEV1) values were a bit lower than values seen in clinical spirometry performed in the same patient at a nearby time point, but the procedure reliably picked up decreases in FEV1, potentially helping patients and clinicians spot exacerbations early.
“Home spirometry was sort of a curiosity that was slowly working its way into cystic fibrosis research in 2019, and then all of a sudden in 2020 it became front and center as the only way to continue with clinical monitoring and research in many cases,” Alexander Paynter, MS, a biostatistician at the Cystic Fibrosis Foundation’s Therapeutic Development Network Coordinating Center, said during a talk at the virtual North American Cystic Fibrosis Conference.
To better determine how closely home spirometry matches clinical spirometry, Mr. Paynter and his colleagues analyzed data from the eICE study, which included 267 cystic fibrosis patients aged 14 and over at 14 cystic fibrosis centers. They were randomized to use home spirometry as an early intervention to detect exacerbations, or to continue usual clinic care with visits to the clinic every 3 months. The dataset includes twice-weekly home spirometry values, with a full-year of follow-up data. The researchers compared the home spirometry data to the clinical data closest in time to it. Clinic spirometry data with no corresponding home data within 7 days were discarded.
There was an estimated difference of –2.01 mL between home and clinic tests, with home spirometry producing lower values (95% confidence interval, –3.56 to –0.45). “There is actually a bias in home spirometry as compared to clinic spirometry,” concluded Mr. Paynter.
One explanation for lower values in home spirometry is that users are inexperienced with the device. If that’s true, then agreement should improve over time, but the researchers didn’t see strong evidence of that. Among 44 patients who completed five clinical visits, there was a difference of –2.97 (standard deviation [SD], 10.51) at baseline, –1.66 at 3 months (SD, 13.49), –3.7 at 6 months (SD, 12.44), –0.86 at 9 months (SD, 13.73), and –0.53 at 12 months (SD, 13.35). Though there was improvement over time, “we don’t find a lot of evidence that this bias completely resolves,” said Mr. Paynter.
In fact, a more likely explanation is the presence of coaching by a technician during clinical spirometry, according to Robert J. Giusti, MD, clinical professor of pediatrics and director of the Pediatric Cystic Fibrosis Center at New York University. “When they’re doing it at home, they don’t do it with the same effort, so I think that coaching through telemedicine during the home spirometry would make that difference disappear,” he said when asked to comment on the study.

The researchers found that change-based endpoints were similar between clinic and at-home spirometry. Compared to baseline, the two showed similar declines over time. “The clinic and home observations tend to track each other pretty well. At 6 months, for instance, it’s about a change of three points decrease (in both). But the bad news is that the variability is much greater in home devices,” said Mr. Paynter, noting larger confidence intervals and standard deviation values associated with home spirometry. That could influence future clinical designs that may rely on home spirometry, since a larger confidence interval means reduced power, which could double or even quadruple the number of participants needed to achieve the required power, he said.
But from a clinical standpoint, the ability of home spirometry to consistently detect a change from baseline could be quite valuable to future patient management, according to Dr. Giusti. “It looks like home spirometry will show that kind of a decrease, so that it’s still sensitive to pick up the concern that a patient is getting worse at home,” he said.
That could be useful even after the COVID-19 pandemic passes, as patients continue to embrace home monitoring. Physicians could keep track of patients and keep them focused on their care and treatment through frequent telemedicine visits combined with home spirometry. “I really think home spirometry will keep us more focused on how the patients are doing and make for better outcomes,” said Dr. Giusti.
Mr. Paynter and Dr. Giusti have no relevant financial disclosures.
SOURCE: Alex Paynter et al. NACFC 2020. Poster 643.
Home spirometry has become increasingly used among cystic fibrosis patients during the COVID-19 pandemic, and new research suggests that home devices perform reasonably well. Forced expiratory volume in 1 second (FEV1) values were a bit lower than values seen in clinical spirometry performed in the same patient at a nearby time point, but the procedure reliably picked up decreases in FEV1, potentially helping patients and clinicians spot exacerbations early.
“Home spirometry was sort of a curiosity that was slowly working its way into cystic fibrosis research in 2019, and then all of a sudden in 2020 it became front and center as the only way to continue with clinical monitoring and research in many cases,” Alexander Paynter, MS, a biostatistician at the Cystic Fibrosis Foundation’s Therapeutic Development Network Coordinating Center, said during a talk at the virtual North American Cystic Fibrosis Conference.
To better determine how closely home spirometry matches clinical spirometry, Mr. Paynter and his colleagues analyzed data from the eICE study, which included 267 cystic fibrosis patients aged 14 and over at 14 cystic fibrosis centers. They were randomized to use home spirometry as an early intervention to detect exacerbations, or to continue usual clinic care with visits to the clinic every 3 months. The dataset includes twice-weekly home spirometry values, with a full-year of follow-up data. The researchers compared the home spirometry data to the clinical data closest in time to it. Clinic spirometry data with no corresponding home data within 7 days were discarded.
There was an estimated difference of –2.01 mL between home and clinic tests, with home spirometry producing lower values (95% confidence interval, –3.56 to –0.45). “There is actually a bias in home spirometry as compared to clinic spirometry,” concluded Mr. Paynter.
One explanation for lower values in home spirometry is that users are inexperienced with the device. If that’s true, then agreement should improve over time, but the researchers didn’t see strong evidence of that. Among 44 patients who completed five clinical visits, there was a difference of –2.97 (standard deviation [SD], 10.51) at baseline, –1.66 at 3 months (SD, 13.49), –3.7 at 6 months (SD, 12.44), –0.86 at 9 months (SD, 13.73), and –0.53 at 12 months (SD, 13.35). Though there was improvement over time, “we don’t find a lot of evidence that this bias completely resolves,” said Mr. Paynter.
In fact, a more likely explanation is the presence of coaching by a technician during clinical spirometry, according to Robert J. Giusti, MD, clinical professor of pediatrics and director of the Pediatric Cystic Fibrosis Center at New York University. “When they’re doing it at home, they don’t do it with the same effort, so I think that coaching through telemedicine during the home spirometry would make that difference disappear,” he said when asked to comment on the study.
The researchers found that change-based endpoints were similar between clinic and at-home spirometry. Compared to baseline, the two showed similar declines over time. “The clinic and home observations tend to track each other pretty well. At 6 months, for instance, it’s about a change of three points decrease (in both). But the bad news is that the variability is much greater in home devices,” said Mr. Paynter, noting larger confidence intervals and standard deviation values associated with home spirometry. That could influence future clinical designs that may rely on home spirometry, since a larger confidence interval means reduced power, which could double or even quadruple the number of participants needed to achieve the required power, he said.
But from a clinical standpoint, the ability of home spirometry to consistently detect a change from baseline could be quite valuable to future patient management, according to Dr. Giusti. “It looks like home spirometry will show that kind of a decrease, so that it’s still sensitive to pick up the concern that a patient is getting worse at home,” he said.
That could be useful even after the COVID-19 pandemic passes, as patients continue to embrace home monitoring. Physicians could keep track of patients and keep them focused on their care and treatment through frequent telemedicine visits combined with home spirometry. “I really think home spirometry will keep us more focused on how the patients are doing and make for better outcomes,” said Dr. Giusti.
Mr. Paynter and Dr. Giusti have no relevant financial disclosures.
SOURCE: Alex Paynter et al. NACFC 2020. Poster 643.
Home spirometry has become increasingly used among cystic fibrosis patients during the COVID-19 pandemic, and new research suggests that home devices perform reasonably well. Forced expiratory volume in 1 second (FEV1) values were a bit lower than values seen in clinical spirometry performed in the same patient at a nearby time point, but the procedure reliably picked up decreases in FEV1, potentially helping patients and clinicians spot exacerbations early.
“Home spirometry was sort of a curiosity that was slowly working its way into cystic fibrosis research in 2019, and then all of a sudden in 2020 it became front and center as the only way to continue with clinical monitoring and research in many cases,” Alexander Paynter, MS, a biostatistician at the Cystic Fibrosis Foundation’s Therapeutic Development Network Coordinating Center, said during a talk at the virtual North American Cystic Fibrosis Conference.
To better determine how closely home spirometry matches clinical spirometry, Mr. Paynter and his colleagues analyzed data from the eICE study, which included 267 cystic fibrosis patients aged 14 and over at 14 cystic fibrosis centers. They were randomized to use home spirometry as an early intervention to detect exacerbations, or to continue usual clinic care with visits to the clinic every 3 months. The dataset includes twice-weekly home spirometry values, with a full-year of follow-up data. The researchers compared the home spirometry data to the clinical data closest in time to it. Clinic spirometry data with no corresponding home data within 7 days were discarded.
There was an estimated difference of –2.01 mL between home and clinic tests, with home spirometry producing lower values (95% confidence interval, –3.56 to –0.45). “There is actually a bias in home spirometry as compared to clinic spirometry,” concluded Mr. Paynter.
One explanation for lower values in home spirometry is that users are inexperienced with the device. If that’s true, then agreement should improve over time, but the researchers didn’t see strong evidence of that. Among 44 patients who completed five clinical visits, there was a difference of –2.97 (standard deviation [SD], 10.51) at baseline, –1.66 at 3 months (SD, 13.49), –3.7 at 6 months (SD, 12.44), –0.86 at 9 months (SD, 13.73), and –0.53 at 12 months (SD, 13.35). Though there was improvement over time, “we don’t find a lot of evidence that this bias completely resolves,” said Mr. Paynter.
In fact, a more likely explanation is the presence of coaching by a technician during clinical spirometry, according to Robert J. Giusti, MD, clinical professor of pediatrics and director of the Pediatric Cystic Fibrosis Center at New York University. “When they’re doing it at home, they don’t do it with the same effort, so I think that coaching through telemedicine during the home spirometry would make that difference disappear,” he said when asked to comment on the study.
The researchers found that change-based endpoints were similar between clinic and at-home spirometry. Compared to baseline, the two showed similar declines over time. “The clinic and home observations tend to track each other pretty well. At 6 months, for instance, it’s about a change of three points decrease (in both). But the bad news is that the variability is much greater in home devices,” said Mr. Paynter, noting larger confidence intervals and standard deviation values associated with home spirometry. That could influence future clinical designs that may rely on home spirometry, since a larger confidence interval means reduced power, which could double or even quadruple the number of participants needed to achieve the required power, he said.
But from a clinical standpoint, the ability of home spirometry to consistently detect a change from baseline could be quite valuable to future patient management, according to Dr. Giusti. “It looks like home spirometry will show that kind of a decrease, so that it’s still sensitive to pick up the concern that a patient is getting worse at home,” he said.
That could be useful even after the COVID-19 pandemic passes, as patients continue to embrace home monitoring. Physicians could keep track of patients and keep them focused on their care and treatment through frequent telemedicine visits combined with home spirometry. “I really think home spirometry will keep us more focused on how the patients are doing and make for better outcomes,” said Dr. Giusti.
Mr. Paynter and Dr. Giusti have no relevant financial disclosures.
SOURCE: Alex Paynter et al. NACFC 2020. Poster 643.
FROM NACFC 2020
Lions and tigers and anteaters? U.S. scientists scan the menagerie for COVID
As COVID-19 cases surge in the United States, one Texas veterinarian has been quietly tracking the spread of the disease – not in people, but in their pets.
Since June, Dr. Sarah Hamer and her team at Texas A&M University have tested hundreds of animals from area households where humans contracted COVID-19. They’ve swabbed dogs and cats, sure, but also pet hamsters and guinea pigs, looking for signs of infection. “We’re open to all of it,” said Dr. Hamer, a professor of epidemiology, who has found at least 19 cases of infection.
One pet that tested positive was Phoenix, a 7-year-old part Siamese cat owned by Kaitlyn Romoser, who works in a university lab. Ms. Romoser, 23, was confirmed to have COVID-19 twice, once in March and again in September. The second time she was much sicker, she said, and Phoenix was her constant companion.
“If I would have known animals were just getting it everywhere, I would have tried to distance myself, but he will not distance himself from me,” Ms. Romoser said. “He sleeps in my bed with me. There was absolutely no social distancing.”
Across the country, veterinarians and other researchers are scouring the animal kingdom for signs of the virus that causes COVID-19. At least 2,000 animals in the U.S. have been tested for the coronavirus since the pandemic began, according to federal records. Cats and dogs that were exposed to sick owners represent most of the animals tested and 80% of the positive cases found.
But scientists have cast a wide net investigating other animals that could be at risk. In states from California to Florida, researchers have tested species ranging from farmed minks and zoo cats to unexpected critters like dolphins, armadillos, and anteaters.
The U.S. Department of Agriculture keeps an official tally of confirmed animal COVID cases that stands at several dozen. But that list is a vast undercount of actual infections. In Utah and Wisconsin, for instance, more than 14,000 minks died in recent weeks after contracting COVID infections initially spread by humans.
So far, there’s limited evidence that animals are transmitting the virus to people. Veterinarians emphasize that pet owners appear to be in no danger from their animal companions and should continue to love and care for them. But scientists say continued testing is one way to remain vigilant in the face of a previously unknown pathogen.
“We just know that coronaviruses, as a family, infect a lot of species, mostly mammals,” said Dr. Peter Rabinowitz, a professor of environmental and occupational health sciences and the director of the University of Washington Center for One Health Research in Seattle. “It makes sense to take a species-spanning approach and look at a wide spectrum.”
Much of the testing has been rooted in scientific curiosity. Since the pandemic began, a major puzzle has been how the virus, which likely originated in bats, spread to humans. A leading theory is that it jumped to an intermediate species, still unknown, and then to people.
In April, a 4-year-old Malayan tiger at the Bronx Zoo tested positive for COVID-19 in a first-of-its-kind case after seven big cats showed signs of respiratory illness. The tiger, Nadia, contracted the virus from a caretaker, federal health officials said. Four other tigers and three African lions were also confirmed to be infected.
In Washington state, the site of the first U.S. outbreak in humans, scientists rushed to design a COVID test for animals in March, said Charlie Powell, a spokesperson for the Washington State University College of Veterinary Medicine, Pullman. “We knew with warm-blooded animals, housed together, there’s going to be some cross-infection,” he said. Tests for animals use different reagent compounds than those used for tests in people, so they don’t deplete the human supply, Mr. Powell added.
Since spring, the Washington Animal Disease Diagnostic Laboratory has tested nearly 80 animals, including 38 dogs, 29 cats, 2 ferrets, a camel, and 2 tamanduas, a type of anteater. The lab also tested six minks from the outbreak in Utah, five of which accounted for the lab’s only positive tests.
All told, nearly 1,400 animals have been tested for COVID-19 through the National Animal Health Laboratory Network or private labs, said Lyndsay Cole, a spokesperson for the USDA’s Animal and Plant Health Inspection Service. More than 400 animals have been tested through the National Veterinary Services Laboratories. At least 250 more have been tested through academic research projects.
Most of the tests have been in household cats and dogs with suspicious respiratory symptoms. In June, the USDA reported that a dog in New York was the first pet dog to test positive for the coronavirus after falling ill and struggling to breathe. The dog, a 7-year-old German shepherd named Buddy, later died. Officials determined he’d contracted the virus from his owner.
Neither the Centers for Disease Control and Prevention nor the USDA recommends routine testing for house pets or other animals – but that hasn’t stopped owners from asking, said Dr. Douglas Kratt, president of the American Veterinary Medical Association.
“The questions have become a little more consistent at my practice,” he said. “People do want to know about COVID-19 and their pets. Can their pet pick it up at a clinic or boarding or in doggie day care?”
The answer, so far, is that humans are the primary source of infection in pets. In September, a small, unpublished study from the University of Guelph in Canada found that companion cats and dogs appeared to be infected by their sick owners, judging by antibodies to the coronavirus detected in their blood.
In Texas, Dr. Hamer started testing animals from households where someone had contracted COVID-19 to learn more about transmission pathways. “Right now, we’re very much trying to describe what’s happening in nature,” she said.
So far, most of the animals – including Phoenix, Ms. Romoser’s cat – have shown no signs of illness or disease. That’s true so far for many species of animals tested for COVID-19, veterinarians said. Most nonhuman creatures appear to weather COVID infection with mild symptoms like sniffles and lethargy, if any.
Still, owners should apply best practices for avoiding COVID infection to pets, too, Dr. Kratt said. Don’t let pets come into contact with unfamiliar animals, he suggested. Owners should wash their hands frequently and avoid nuzzling and other very close contact, if possible.
Cats appear to be more susceptible to COVID-19 than dogs, researchers said. And minks, which are farmed in the U.S. and elsewhere for their fur, appear quite vulnerable.
In the meantime, the list of creatures tested for COVID-19 – whether for illness or science – is growing. In Florida, 22 animals had been tested as of early October, including 3 wild dolphins, 2 civets, 2 clouded leopards, a gorilla, an orangutan, an alpaca, and a bush baby, state officials said.
In California, 29 animals had been tested by the end of September, including a meerkat, a monkey, and a coatimundi, a member of the raccoon family.
In Seattle, a plan to test orcas, or killer whales, in Puget Sound was called off at the last minute after a member of the scientific team was exposed to COVID-19 and had to quarantine, said Dr. Joe Gaydos, a senior wildlife veterinarian and science director for the SeaDoc Society, a conservation program at the University of California-Davis. The group missed its September window to locate the animals and obtain breath and fecal samples for analysis.
No one thinks marine animals will play a big role in the pandemic decimating the human population, Dr. Gaydos said. But testing many creatures on both land and sea is vital.
“We don’t know what this virus is going to do or can do,” Dr. Gaydos said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
As COVID-19 cases surge in the United States, one Texas veterinarian has been quietly tracking the spread of the disease – not in people, but in their pets.
Since June, Dr. Sarah Hamer and her team at Texas A&M University have tested hundreds of animals from area households where humans contracted COVID-19. They’ve swabbed dogs and cats, sure, but also pet hamsters and guinea pigs, looking for signs of infection. “We’re open to all of it,” said Dr. Hamer, a professor of epidemiology, who has found at least 19 cases of infection.
One pet that tested positive was Phoenix, a 7-year-old part Siamese cat owned by Kaitlyn Romoser, who works in a university lab. Ms. Romoser, 23, was confirmed to have COVID-19 twice, once in March and again in September. The second time she was much sicker, she said, and Phoenix was her constant companion.
“If I would have known animals were just getting it everywhere, I would have tried to distance myself, but he will not distance himself from me,” Ms. Romoser said. “He sleeps in my bed with me. There was absolutely no social distancing.”
Across the country, veterinarians and other researchers are scouring the animal kingdom for signs of the virus that causes COVID-19. At least 2,000 animals in the U.S. have been tested for the coronavirus since the pandemic began, according to federal records. Cats and dogs that were exposed to sick owners represent most of the animals tested and 80% of the positive cases found.
But scientists have cast a wide net investigating other animals that could be at risk. In states from California to Florida, researchers have tested species ranging from farmed minks and zoo cats to unexpected critters like dolphins, armadillos, and anteaters.
The U.S. Department of Agriculture keeps an official tally of confirmed animal COVID cases that stands at several dozen. But that list is a vast undercount of actual infections. In Utah and Wisconsin, for instance, more than 14,000 minks died in recent weeks after contracting COVID infections initially spread by humans.
So far, there’s limited evidence that animals are transmitting the virus to people. Veterinarians emphasize that pet owners appear to be in no danger from their animal companions and should continue to love and care for them. But scientists say continued testing is one way to remain vigilant in the face of a previously unknown pathogen.
“We just know that coronaviruses, as a family, infect a lot of species, mostly mammals,” said Dr. Peter Rabinowitz, a professor of environmental and occupational health sciences and the director of the University of Washington Center for One Health Research in Seattle. “It makes sense to take a species-spanning approach and look at a wide spectrum.”
Much of the testing has been rooted in scientific curiosity. Since the pandemic began, a major puzzle has been how the virus, which likely originated in bats, spread to humans. A leading theory is that it jumped to an intermediate species, still unknown, and then to people.
In April, a 4-year-old Malayan tiger at the Bronx Zoo tested positive for COVID-19 in a first-of-its-kind case after seven big cats showed signs of respiratory illness. The tiger, Nadia, contracted the virus from a caretaker, federal health officials said. Four other tigers and three African lions were also confirmed to be infected.
In Washington state, the site of the first U.S. outbreak in humans, scientists rushed to design a COVID test for animals in March, said Charlie Powell, a spokesperson for the Washington State University College of Veterinary Medicine, Pullman. “We knew with warm-blooded animals, housed together, there’s going to be some cross-infection,” he said. Tests for animals use different reagent compounds than those used for tests in people, so they don’t deplete the human supply, Mr. Powell added.
Since spring, the Washington Animal Disease Diagnostic Laboratory has tested nearly 80 animals, including 38 dogs, 29 cats, 2 ferrets, a camel, and 2 tamanduas, a type of anteater. The lab also tested six minks from the outbreak in Utah, five of which accounted for the lab’s only positive tests.
All told, nearly 1,400 animals have been tested for COVID-19 through the National Animal Health Laboratory Network or private labs, said Lyndsay Cole, a spokesperson for the USDA’s Animal and Plant Health Inspection Service. More than 400 animals have been tested through the National Veterinary Services Laboratories. At least 250 more have been tested through academic research projects.
Most of the tests have been in household cats and dogs with suspicious respiratory symptoms. In June, the USDA reported that a dog in New York was the first pet dog to test positive for the coronavirus after falling ill and struggling to breathe. The dog, a 7-year-old German shepherd named Buddy, later died. Officials determined he’d contracted the virus from his owner.
Neither the Centers for Disease Control and Prevention nor the USDA recommends routine testing for house pets or other animals – but that hasn’t stopped owners from asking, said Dr. Douglas Kratt, president of the American Veterinary Medical Association.
“The questions have become a little more consistent at my practice,” he said. “People do want to know about COVID-19 and their pets. Can their pet pick it up at a clinic or boarding or in doggie day care?”
The answer, so far, is that humans are the primary source of infection in pets. In September, a small, unpublished study from the University of Guelph in Canada found that companion cats and dogs appeared to be infected by their sick owners, judging by antibodies to the coronavirus detected in their blood.
In Texas, Dr. Hamer started testing animals from households where someone had contracted COVID-19 to learn more about transmission pathways. “Right now, we’re very much trying to describe what’s happening in nature,” she said.
So far, most of the animals – including Phoenix, Ms. Romoser’s cat – have shown no signs of illness or disease. That’s true so far for many species of animals tested for COVID-19, veterinarians said. Most nonhuman creatures appear to weather COVID infection with mild symptoms like sniffles and lethargy, if any.
Still, owners should apply best practices for avoiding COVID infection to pets, too, Dr. Kratt said. Don’t let pets come into contact with unfamiliar animals, he suggested. Owners should wash their hands frequently and avoid nuzzling and other very close contact, if possible.
Cats appear to be more susceptible to COVID-19 than dogs, researchers said. And minks, which are farmed in the U.S. and elsewhere for their fur, appear quite vulnerable.
In the meantime, the list of creatures tested for COVID-19 – whether for illness or science – is growing. In Florida, 22 animals had been tested as of early October, including 3 wild dolphins, 2 civets, 2 clouded leopards, a gorilla, an orangutan, an alpaca, and a bush baby, state officials said.
In California, 29 animals had been tested by the end of September, including a meerkat, a monkey, and a coatimundi, a member of the raccoon family.
In Seattle, a plan to test orcas, or killer whales, in Puget Sound was called off at the last minute after a member of the scientific team was exposed to COVID-19 and had to quarantine, said Dr. Joe Gaydos, a senior wildlife veterinarian and science director for the SeaDoc Society, a conservation program at the University of California-Davis. The group missed its September window to locate the animals and obtain breath and fecal samples for analysis.
No one thinks marine animals will play a big role in the pandemic decimating the human population, Dr. Gaydos said. But testing many creatures on both land and sea is vital.
“We don’t know what this virus is going to do or can do,” Dr. Gaydos said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
As COVID-19 cases surge in the United States, one Texas veterinarian has been quietly tracking the spread of the disease – not in people, but in their pets.
Since June, Dr. Sarah Hamer and her team at Texas A&M University have tested hundreds of animals from area households where humans contracted COVID-19. They’ve swabbed dogs and cats, sure, but also pet hamsters and guinea pigs, looking for signs of infection. “We’re open to all of it,” said Dr. Hamer, a professor of epidemiology, who has found at least 19 cases of infection.
One pet that tested positive was Phoenix, a 7-year-old part Siamese cat owned by Kaitlyn Romoser, who works in a university lab. Ms. Romoser, 23, was confirmed to have COVID-19 twice, once in March and again in September. The second time she was much sicker, she said, and Phoenix was her constant companion.
“If I would have known animals were just getting it everywhere, I would have tried to distance myself, but he will not distance himself from me,” Ms. Romoser said. “He sleeps in my bed with me. There was absolutely no social distancing.”
Across the country, veterinarians and other researchers are scouring the animal kingdom for signs of the virus that causes COVID-19. At least 2,000 animals in the U.S. have been tested for the coronavirus since the pandemic began, according to federal records. Cats and dogs that were exposed to sick owners represent most of the animals tested and 80% of the positive cases found.
But scientists have cast a wide net investigating other animals that could be at risk. In states from California to Florida, researchers have tested species ranging from farmed minks and zoo cats to unexpected critters like dolphins, armadillos, and anteaters.
The U.S. Department of Agriculture keeps an official tally of confirmed animal COVID cases that stands at several dozen. But that list is a vast undercount of actual infections. In Utah and Wisconsin, for instance, more than 14,000 minks died in recent weeks after contracting COVID infections initially spread by humans.
So far, there’s limited evidence that animals are transmitting the virus to people. Veterinarians emphasize that pet owners appear to be in no danger from their animal companions and should continue to love and care for them. But scientists say continued testing is one way to remain vigilant in the face of a previously unknown pathogen.
“We just know that coronaviruses, as a family, infect a lot of species, mostly mammals,” said Dr. Peter Rabinowitz, a professor of environmental and occupational health sciences and the director of the University of Washington Center for One Health Research in Seattle. “It makes sense to take a species-spanning approach and look at a wide spectrum.”
Much of the testing has been rooted in scientific curiosity. Since the pandemic began, a major puzzle has been how the virus, which likely originated in bats, spread to humans. A leading theory is that it jumped to an intermediate species, still unknown, and then to people.
In April, a 4-year-old Malayan tiger at the Bronx Zoo tested positive for COVID-19 in a first-of-its-kind case after seven big cats showed signs of respiratory illness. The tiger, Nadia, contracted the virus from a caretaker, federal health officials said. Four other tigers and three African lions were also confirmed to be infected.
In Washington state, the site of the first U.S. outbreak in humans, scientists rushed to design a COVID test for animals in March, said Charlie Powell, a spokesperson for the Washington State University College of Veterinary Medicine, Pullman. “We knew with warm-blooded animals, housed together, there’s going to be some cross-infection,” he said. Tests for animals use different reagent compounds than those used for tests in people, so they don’t deplete the human supply, Mr. Powell added.
Since spring, the Washington Animal Disease Diagnostic Laboratory has tested nearly 80 animals, including 38 dogs, 29 cats, 2 ferrets, a camel, and 2 tamanduas, a type of anteater. The lab also tested six minks from the outbreak in Utah, five of which accounted for the lab’s only positive tests.
All told, nearly 1,400 animals have been tested for COVID-19 through the National Animal Health Laboratory Network or private labs, said Lyndsay Cole, a spokesperson for the USDA’s Animal and Plant Health Inspection Service. More than 400 animals have been tested through the National Veterinary Services Laboratories. At least 250 more have been tested through academic research projects.
Most of the tests have been in household cats and dogs with suspicious respiratory symptoms. In June, the USDA reported that a dog in New York was the first pet dog to test positive for the coronavirus after falling ill and struggling to breathe. The dog, a 7-year-old German shepherd named Buddy, later died. Officials determined he’d contracted the virus from his owner.
Neither the Centers for Disease Control and Prevention nor the USDA recommends routine testing for house pets or other animals – but that hasn’t stopped owners from asking, said Dr. Douglas Kratt, president of the American Veterinary Medical Association.
“The questions have become a little more consistent at my practice,” he said. “People do want to know about COVID-19 and their pets. Can their pet pick it up at a clinic or boarding or in doggie day care?”
The answer, so far, is that humans are the primary source of infection in pets. In September, a small, unpublished study from the University of Guelph in Canada found that companion cats and dogs appeared to be infected by their sick owners, judging by antibodies to the coronavirus detected in their blood.
In Texas, Dr. Hamer started testing animals from households where someone had contracted COVID-19 to learn more about transmission pathways. “Right now, we’re very much trying to describe what’s happening in nature,” she said.
So far, most of the animals – including Phoenix, Ms. Romoser’s cat – have shown no signs of illness or disease. That’s true so far for many species of animals tested for COVID-19, veterinarians said. Most nonhuman creatures appear to weather COVID infection with mild symptoms like sniffles and lethargy, if any.
Still, owners should apply best practices for avoiding COVID infection to pets, too, Dr. Kratt said. Don’t let pets come into contact with unfamiliar animals, he suggested. Owners should wash their hands frequently and avoid nuzzling and other very close contact, if possible.
Cats appear to be more susceptible to COVID-19 than dogs, researchers said. And minks, which are farmed in the U.S. and elsewhere for their fur, appear quite vulnerable.
In the meantime, the list of creatures tested for COVID-19 – whether for illness or science – is growing. In Florida, 22 animals had been tested as of early October, including 3 wild dolphins, 2 civets, 2 clouded leopards, a gorilla, an orangutan, an alpaca, and a bush baby, state officials said.
In California, 29 animals had been tested by the end of September, including a meerkat, a monkey, and a coatimundi, a member of the raccoon family.
In Seattle, a plan to test orcas, or killer whales, in Puget Sound was called off at the last minute after a member of the scientific team was exposed to COVID-19 and had to quarantine, said Dr. Joe Gaydos, a senior wildlife veterinarian and science director for the SeaDoc Society, a conservation program at the University of California-Davis. The group missed its September window to locate the animals and obtain breath and fecal samples for analysis.
No one thinks marine animals will play a big role in the pandemic decimating the human population, Dr. Gaydos said. But testing many creatures on both land and sea is vital.
“We don’t know what this virus is going to do or can do,” Dr. Gaydos said.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Poor and minority children with food allergies overlooked and in danger
As Emily Brown stood in a food pantry looking at her options, she felt alone. Up to that point, she had never struggled financially. But there she was, desperate to find safe food for her young daughter with food allergies. What she found was a jar of salsa and some potatoes.
“That was all that was available,” said Ms. Brown, who lives in Kansas City, Kansas. “It was just a desperate place.”
When she became a parent, Ms. Brown left her job for lack of child care that would accommodate her daughter’s allergies to peanuts, tree nuts, milk, eggs, wheat, and soy. When she and her husband then turned to a federal food assistance program, they found few allowable allergy substitutions. The closest allergy support group she could find was an hour away. She was almost always the only Black parent, and the only poor parent, there.
Ms. Brown called national food allergy advocacy organizations to ask for guidance to help poor families find safe food and medical resources, but she said she was told that wasn’t their focus. Support groups, fundraising activities, and advocacy efforts, plus clinical and research outreach, were targeted at wealthier – and White – families. Advertising rarely reflected families that looked like hers. She felt unseen.
“In many ways, food allergy is an invisible disease. The burden of the disease, the activities and energy it takes to avoid allergens, are mostly invisible to those not impacted,” Ms. Brown said. “Black and other minority patients often lack voice and visibility in the health care system. Add the additional burden of an invisible condition and you are in a really vulnerable position.”
An estimated 6 million children in the United States have food allergies, 40% of them with more than one. Though limited research has been done on race and class breakdowns, recent studies show that poor children and some groups of minority children not only have a higher incidence of food allergies than White children, but their families also have more difficulty accessing appropriate child care, safe food, medical care, and lifesaving medicine like epinephrine for them.
Black children are 7% more likely to have food allergies than white children, according to a 2020 study by Dr. Ruchi Gupta, MD, at Northwestern University, Chicago. To be sure, the study shows that Asian children are 24% more likely than White children to have food allergies. But Black and Hispanic children are disproportionately more likely to live in poor communities, to have asthma, and to suffer from systemic racism in the delivery of medical care.
“Many times, a mother is frank and says: ‘I have $20-$40 to buy groceries for the week, and if I buy these foods that you are telling me to buy, I will not be able to feed my entire family,’” said Carla Davis, MD, director of the food allergy program at Houston’s Texas Children’s Hospital. “If you are diagnosed with a food allergy and you don’t have disposable income or disposable time, there is really no way that you will be able to alter your diet in a way that your child is going to stay away from their allergen.”
Fed up with the lack of support, Ms. Brown founded the Food Equality Initiative advocacy organization in 2014. It offers an online marketplace to income-eligible families in Kansas and Missouri who, with a doctor’s note about the allergy, can order free allergy-safe food to fit their needs.
Nationwide, though, families’ needs far outstrip what her group can offer – and the problem has gotten worse amid the economic squeeze of the COVID pandemic. Job losses and business closures have exacerbated the barriers to finding and affording nutritious food, according to a report from Feeding America, an association of food banks.
Ms. Brown said her organization more than doubled its clientele in March through August, compared with the same period in 2019. And though it currently serves only Missouri and Kansas, she said the organization has been fielding an increasing number of calls from across the country since the pandemic began.
For low-income minorities, who live disproportionately in food deserts, fresh and allergy-friendly foods can be especially expensive and difficult to find in the best of times.
Food assistance programs are heavily weighted to prepackaged and processed foods, which often include the very ingredients that are problematic. Black children are more likely to be allergic to wheat and soy than White children, and both Black and Hispanic children are more likely to be allergic to corn, shellfish, and fish, according to a 2016 study.
Some programs allow few allergy substitutions. For example, the federal Special Supplemental Nutrition Program for Women, Infants, and Children allows only canned beans as a substitute for peanut butter. While nutritionally similar, beans are not as easy to pack for a kid’s lunch. Ms. Brown questions why WIC won’t allow a seed butter, such as sunflower butter, instead. She said they are nutritionally and functionally similar and are offered as allergy substitutions in other food programs.
Making matters worse, low-income households pay more than twice as much as higher-income families for the emergency medical care their children receive for their allergies, according to a 2016 study by Dr. Gupta. The kids often arrive at the hospital in more distress because they lack safe food and allergy medications – and because asthma, which disproportionately hits Black and Puerto Rican children and low-income communities, complicates allergic reactions.
“So, in these vulnerable populations, it’s like a double whammy, and we see that reflected in the data,” said Lakiea Wright-Bello, MD, a medical director in specialty diagnostics at Thermo Fisher Scientific and an allergist at Brigham and Women’s Hospital in Boston.
Thomas and Dina Silvera, who are Black and Latina, lived this horror firsthand. After their 3-year-old son, Elijah-Alavi, died as a result of a dairy allergy when fed a grilled cheese instead of his allergen-free food at his preschool, they launched the Elijah-Alavi Foundation to address the dearth of information about food allergies and the critical lack of culturally sensitive medical care in low-income communities.
“We started it for a cause, not because we wanted to, but because we had to,” said Thomas Silvera. “Our main focus is to bring to underserved communities – especially communities of color – this information at no cost to them.”
Recently, other advocacy groups, including Food Allergy Research & Education, a national advocacy organization, also have started to turn their attention to a lack of access and support in poor and minority communities. When Lisa Gable, who is White, took over at the group known as FARE in 2018, she began to diversify the organization internally and to make it more inclusive.
“There wasn’t a big tent when I walked in the door,” said Ms. Gable. “What we have been focused on doing is trying to find partners and relationships that will allow us to diversify those engaged in the community, because it has not been a diverse community.”
FARE has funded research into the cost of food allergies. It is also expanding its patient registry, which collects data for research, as well as its clinical network of medical institutions to include more diverse communities.
Dr. Gupta is now leading one of the first studies funded by the National Institutes of Health to investigate food allergy in children by race and ethnicity. It looks at all aspects of food allergies, including family life, management, access to care, and genetics.
“That’s a big deal,” said Dr. Gupta. “Because if we really want to improve food allergy management, care and understanding, we really need to understand how it impacts different groups. And that hasn’t been done.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
As Emily Brown stood in a food pantry looking at her options, she felt alone. Up to that point, she had never struggled financially. But there she was, desperate to find safe food for her young daughter with food allergies. What she found was a jar of salsa and some potatoes.
“That was all that was available,” said Ms. Brown, who lives in Kansas City, Kansas. “It was just a desperate place.”
When she became a parent, Ms. Brown left her job for lack of child care that would accommodate her daughter’s allergies to peanuts, tree nuts, milk, eggs, wheat, and soy. When she and her husband then turned to a federal food assistance program, they found few allowable allergy substitutions. The closest allergy support group she could find was an hour away. She was almost always the only Black parent, and the only poor parent, there.
Ms. Brown called national food allergy advocacy organizations to ask for guidance to help poor families find safe food and medical resources, but she said she was told that wasn’t their focus. Support groups, fundraising activities, and advocacy efforts, plus clinical and research outreach, were targeted at wealthier – and White – families. Advertising rarely reflected families that looked like hers. She felt unseen.
“In many ways, food allergy is an invisible disease. The burden of the disease, the activities and energy it takes to avoid allergens, are mostly invisible to those not impacted,” Ms. Brown said. “Black and other minority patients often lack voice and visibility in the health care system. Add the additional burden of an invisible condition and you are in a really vulnerable position.”
An estimated 6 million children in the United States have food allergies, 40% of them with more than one. Though limited research has been done on race and class breakdowns, recent studies show that poor children and some groups of minority children not only have a higher incidence of food allergies than White children, but their families also have more difficulty accessing appropriate child care, safe food, medical care, and lifesaving medicine like epinephrine for them.
Black children are 7% more likely to have food allergies than white children, according to a 2020 study by Dr. Ruchi Gupta, MD, at Northwestern University, Chicago. To be sure, the study shows that Asian children are 24% more likely than White children to have food allergies. But Black and Hispanic children are disproportionately more likely to live in poor communities, to have asthma, and to suffer from systemic racism in the delivery of medical care.
“Many times, a mother is frank and says: ‘I have $20-$40 to buy groceries for the week, and if I buy these foods that you are telling me to buy, I will not be able to feed my entire family,’” said Carla Davis, MD, director of the food allergy program at Houston’s Texas Children’s Hospital. “If you are diagnosed with a food allergy and you don’t have disposable income or disposable time, there is really no way that you will be able to alter your diet in a way that your child is going to stay away from their allergen.”
Fed up with the lack of support, Ms. Brown founded the Food Equality Initiative advocacy organization in 2014. It offers an online marketplace to income-eligible families in Kansas and Missouri who, with a doctor’s note about the allergy, can order free allergy-safe food to fit their needs.
Nationwide, though, families’ needs far outstrip what her group can offer – and the problem has gotten worse amid the economic squeeze of the COVID pandemic. Job losses and business closures have exacerbated the barriers to finding and affording nutritious food, according to a report from Feeding America, an association of food banks.
Ms. Brown said her organization more than doubled its clientele in March through August, compared with the same period in 2019. And though it currently serves only Missouri and Kansas, she said the organization has been fielding an increasing number of calls from across the country since the pandemic began.
For low-income minorities, who live disproportionately in food deserts, fresh and allergy-friendly foods can be especially expensive and difficult to find in the best of times.
Food assistance programs are heavily weighted to prepackaged and processed foods, which often include the very ingredients that are problematic. Black children are more likely to be allergic to wheat and soy than White children, and both Black and Hispanic children are more likely to be allergic to corn, shellfish, and fish, according to a 2016 study.
Some programs allow few allergy substitutions. For example, the federal Special Supplemental Nutrition Program for Women, Infants, and Children allows only canned beans as a substitute for peanut butter. While nutritionally similar, beans are not as easy to pack for a kid’s lunch. Ms. Brown questions why WIC won’t allow a seed butter, such as sunflower butter, instead. She said they are nutritionally and functionally similar and are offered as allergy substitutions in other food programs.
Making matters worse, low-income households pay more than twice as much as higher-income families for the emergency medical care their children receive for their allergies, according to a 2016 study by Dr. Gupta. The kids often arrive at the hospital in more distress because they lack safe food and allergy medications – and because asthma, which disproportionately hits Black and Puerto Rican children and low-income communities, complicates allergic reactions.
“So, in these vulnerable populations, it’s like a double whammy, and we see that reflected in the data,” said Lakiea Wright-Bello, MD, a medical director in specialty diagnostics at Thermo Fisher Scientific and an allergist at Brigham and Women’s Hospital in Boston.
Thomas and Dina Silvera, who are Black and Latina, lived this horror firsthand. After their 3-year-old son, Elijah-Alavi, died as a result of a dairy allergy when fed a grilled cheese instead of his allergen-free food at his preschool, they launched the Elijah-Alavi Foundation to address the dearth of information about food allergies and the critical lack of culturally sensitive medical care in low-income communities.
“We started it for a cause, not because we wanted to, but because we had to,” said Thomas Silvera. “Our main focus is to bring to underserved communities – especially communities of color – this information at no cost to them.”
Recently, other advocacy groups, including Food Allergy Research & Education, a national advocacy organization, also have started to turn their attention to a lack of access and support in poor and minority communities. When Lisa Gable, who is White, took over at the group known as FARE in 2018, she began to diversify the organization internally and to make it more inclusive.
“There wasn’t a big tent when I walked in the door,” said Ms. Gable. “What we have been focused on doing is trying to find partners and relationships that will allow us to diversify those engaged in the community, because it has not been a diverse community.”
FARE has funded research into the cost of food allergies. It is also expanding its patient registry, which collects data for research, as well as its clinical network of medical institutions to include more diverse communities.
Dr. Gupta is now leading one of the first studies funded by the National Institutes of Health to investigate food allergy in children by race and ethnicity. It looks at all aspects of food allergies, including family life, management, access to care, and genetics.
“That’s a big deal,” said Dr. Gupta. “Because if we really want to improve food allergy management, care and understanding, we really need to understand how it impacts different groups. And that hasn’t been done.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
As Emily Brown stood in a food pantry looking at her options, she felt alone. Up to that point, she had never struggled financially. But there she was, desperate to find safe food for her young daughter with food allergies. What she found was a jar of salsa and some potatoes.
“That was all that was available,” said Ms. Brown, who lives in Kansas City, Kansas. “It was just a desperate place.”
When she became a parent, Ms. Brown left her job for lack of child care that would accommodate her daughter’s allergies to peanuts, tree nuts, milk, eggs, wheat, and soy. When she and her husband then turned to a federal food assistance program, they found few allowable allergy substitutions. The closest allergy support group she could find was an hour away. She was almost always the only Black parent, and the only poor parent, there.
Ms. Brown called national food allergy advocacy organizations to ask for guidance to help poor families find safe food and medical resources, but she said she was told that wasn’t their focus. Support groups, fundraising activities, and advocacy efforts, plus clinical and research outreach, were targeted at wealthier – and White – families. Advertising rarely reflected families that looked like hers. She felt unseen.
“In many ways, food allergy is an invisible disease. The burden of the disease, the activities and energy it takes to avoid allergens, are mostly invisible to those not impacted,” Ms. Brown said. “Black and other minority patients often lack voice and visibility in the health care system. Add the additional burden of an invisible condition and you are in a really vulnerable position.”
An estimated 6 million children in the United States have food allergies, 40% of them with more than one. Though limited research has been done on race and class breakdowns, recent studies show that poor children and some groups of minority children not only have a higher incidence of food allergies than White children, but their families also have more difficulty accessing appropriate child care, safe food, medical care, and lifesaving medicine like epinephrine for them.
Black children are 7% more likely to have food allergies than white children, according to a 2020 study by Dr. Ruchi Gupta, MD, at Northwestern University, Chicago. To be sure, the study shows that Asian children are 24% more likely than White children to have food allergies. But Black and Hispanic children are disproportionately more likely to live in poor communities, to have asthma, and to suffer from systemic racism in the delivery of medical care.
“Many times, a mother is frank and says: ‘I have $20-$40 to buy groceries for the week, and if I buy these foods that you are telling me to buy, I will not be able to feed my entire family,’” said Carla Davis, MD, director of the food allergy program at Houston’s Texas Children’s Hospital. “If you are diagnosed with a food allergy and you don’t have disposable income or disposable time, there is really no way that you will be able to alter your diet in a way that your child is going to stay away from their allergen.”
Fed up with the lack of support, Ms. Brown founded the Food Equality Initiative advocacy organization in 2014. It offers an online marketplace to income-eligible families in Kansas and Missouri who, with a doctor’s note about the allergy, can order free allergy-safe food to fit their needs.
Nationwide, though, families’ needs far outstrip what her group can offer – and the problem has gotten worse amid the economic squeeze of the COVID pandemic. Job losses and business closures have exacerbated the barriers to finding and affording nutritious food, according to a report from Feeding America, an association of food banks.
Ms. Brown said her organization more than doubled its clientele in March through August, compared with the same period in 2019. And though it currently serves only Missouri and Kansas, she said the organization has been fielding an increasing number of calls from across the country since the pandemic began.
For low-income minorities, who live disproportionately in food deserts, fresh and allergy-friendly foods can be especially expensive and difficult to find in the best of times.
Food assistance programs are heavily weighted to prepackaged and processed foods, which often include the very ingredients that are problematic. Black children are more likely to be allergic to wheat and soy than White children, and both Black and Hispanic children are more likely to be allergic to corn, shellfish, and fish, according to a 2016 study.
Some programs allow few allergy substitutions. For example, the federal Special Supplemental Nutrition Program for Women, Infants, and Children allows only canned beans as a substitute for peanut butter. While nutritionally similar, beans are not as easy to pack for a kid’s lunch. Ms. Brown questions why WIC won’t allow a seed butter, such as sunflower butter, instead. She said they are nutritionally and functionally similar and are offered as allergy substitutions in other food programs.
Making matters worse, low-income households pay more than twice as much as higher-income families for the emergency medical care their children receive for their allergies, according to a 2016 study by Dr. Gupta. The kids often arrive at the hospital in more distress because they lack safe food and allergy medications – and because asthma, which disproportionately hits Black and Puerto Rican children and low-income communities, complicates allergic reactions.
“So, in these vulnerable populations, it’s like a double whammy, and we see that reflected in the data,” said Lakiea Wright-Bello, MD, a medical director in specialty diagnostics at Thermo Fisher Scientific and an allergist at Brigham and Women’s Hospital in Boston.
Thomas and Dina Silvera, who are Black and Latina, lived this horror firsthand. After their 3-year-old son, Elijah-Alavi, died as a result of a dairy allergy when fed a grilled cheese instead of his allergen-free food at his preschool, they launched the Elijah-Alavi Foundation to address the dearth of information about food allergies and the critical lack of culturally sensitive medical care in low-income communities.
“We started it for a cause, not because we wanted to, but because we had to,” said Thomas Silvera. “Our main focus is to bring to underserved communities – especially communities of color – this information at no cost to them.”
Recently, other advocacy groups, including Food Allergy Research & Education, a national advocacy organization, also have started to turn their attention to a lack of access and support in poor and minority communities. When Lisa Gable, who is White, took over at the group known as FARE in 2018, she began to diversify the organization internally and to make it more inclusive.
“There wasn’t a big tent when I walked in the door,” said Ms. Gable. “What we have been focused on doing is trying to find partners and relationships that will allow us to diversify those engaged in the community, because it has not been a diverse community.”
FARE has funded research into the cost of food allergies. It is also expanding its patient registry, which collects data for research, as well as its clinical network of medical institutions to include more diverse communities.
Dr. Gupta is now leading one of the first studies funded by the National Institutes of Health to investigate food allergy in children by race and ethnicity. It looks at all aspects of food allergies, including family life, management, access to care, and genetics.
“That’s a big deal,” said Dr. Gupta. “Because if we really want to improve food allergy management, care and understanding, we really need to understand how it impacts different groups. And that hasn’t been done.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Common SARS-CoV-2 mutation may be making COVID-19 more contagious
Most SARS-CoV-2 virus strains feature a specific mutation that makes them more transmissible, to the point that these strains now predominate globally, new evidence shows.
In contrast to a greater variety of strains early in the pandemic, now 99.9% of circulating SARS-CoV-2 strains in the study feature the D614G mutation on the spike protein. In addition, people infected with a D614G strain have higher nasopharynx viral loads at diagnosis.
It’s not all bad news. This single-point mutation was not associated with worse clinical COVID-19 severity. Also, the mutation isn’t expected to interfere with the efficacy any of the antibody cocktails, small molecule therapies or vaccines in development.
Furthermore, “as bad as SARS-CoV-2 is, we may have dodged a bullet in terms of how quickly it mutates,” study author Ilya Finkelstein, PhD, said in an interview. This virus mutates much slower than HIV, for example, giving researchers a greater chance to stay one step ahead, he said.
The study was published online Oct. 30 in the journal mBio.
Molecular sleuthing
The research was possible because colleagues at the Houston Methodist Hospital system sequenced the genome of 5085 SARS-CoV-2 strains early in the outbreak and during a second wave of infection over the summer, Dr. Finkelstein said.
The unique data source also includes information from plasma, convalescent plasma, and patient outcomes. Studying a large and diverse population in a major metropolitan area like Houston helps create a “molecular fingerprint” for the virus that will continue to be very useful, said Dr. Finkelstein, a researcher and director of the Finkelstein Lab at the University of Texas, Austin.
D614G was the most common genetic substitution the researchers found, appearing in 82% of SARS-CoV-2 strains during the first wave from March 5 to May 11. The proportion with this mutation jumped to 99.9% by the second wave, defined as occurring between May 12 and July 7 in the study.
The jump in mutation frequency “occurred very rapidly, in a matter of just a few months,” the researchers noted.
The presence of the mutation during the first wave was independently associated with mechanical ventilation days, overall length of stay, and ICU length of stay. However, it was not associated with any significant differences in patient outcomes.
The D614G mutation is now so common worldwide that these viruses are considered reference strains. Researchers believe D614G predominates because it increases the spike protein’s ability to open cells for the virus to enter.
Despite the large number of virus strains evaluated, the samples only represent about 10% of COVID-19 cases in Houston during the study, a potential limitation. Also, some collected samples could not be used for high-quality genome analysis because of limited virus nucleic acid.
Also, it remains unclear if host-virus immune interactions play a significant role. However, the researchers noted in the paper that “available data suggest that, in the aggregate, host genetics does not play an overwhelming role in determining outcome in the great majority of adult patients, once virus infection is established.”
Surveillance ongoing
“The findings will help us to understand the origin, composition, and trajectory of future infection waves and the potential effect of the host immune response and therapeutic maneuvers on SARS-CoV-2 evolution,” the researchers added.
Going forward, the ongoing molecular surveillance of SARS-CoV-2 “may provide critical insights into the origin of the new infection spikes and waves that are occurring as public health constraints are further relaxed, schools and colleges reopen, holidays occur, commercial air travel increases and individuals change their behavior because of COVID-19 ‘fatigue,’ ” the researchers noted.
They added that the genome data will also be useful in assessing ongoing molecular evolution in spike and other proteins “as baseline herd immunity is generated, either by natural exposure to SARS-CoV-2 or by vaccination.”
Further validation warranted
“The study is very interesting and well performed,” Noam Shomron, PhD, a member of the faculty of medicine at Tel Aviv University, said in an interview.
Analyzing the “SARS-CoV-2 molecular evolution in a specific region in the USA … could be viewed as a microcosm of what occurs in other large cities in the USA,” he said.
However, “before jumping to conclusions, this should be further validated,” added Dr. Shomron, who authored a study suggesting differences in genetic alleles could partially explain variations across countries in the infection rates, severity, and mortality associated with SARS-CoV-2.
“We know that many other features and contributors might affect the results – even social constraints could generate a bias in the observations,” he said.
Dr. Finkelstein and Dr. Shomron disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Most SARS-CoV-2 virus strains feature a specific mutation that makes them more transmissible, to the point that these strains now predominate globally, new evidence shows.
In contrast to a greater variety of strains early in the pandemic, now 99.9% of circulating SARS-CoV-2 strains in the study feature the D614G mutation on the spike protein. In addition, people infected with a D614G strain have higher nasopharynx viral loads at diagnosis.
It’s not all bad news. This single-point mutation was not associated with worse clinical COVID-19 severity. Also, the mutation isn’t expected to interfere with the efficacy any of the antibody cocktails, small molecule therapies or vaccines in development.
Furthermore, “as bad as SARS-CoV-2 is, we may have dodged a bullet in terms of how quickly it mutates,” study author Ilya Finkelstein, PhD, said in an interview. This virus mutates much slower than HIV, for example, giving researchers a greater chance to stay one step ahead, he said.
The study was published online Oct. 30 in the journal mBio.
Molecular sleuthing
The research was possible because colleagues at the Houston Methodist Hospital system sequenced the genome of 5085 SARS-CoV-2 strains early in the outbreak and during a second wave of infection over the summer, Dr. Finkelstein said.
The unique data source also includes information from plasma, convalescent plasma, and patient outcomes. Studying a large and diverse population in a major metropolitan area like Houston helps create a “molecular fingerprint” for the virus that will continue to be very useful, said Dr. Finkelstein, a researcher and director of the Finkelstein Lab at the University of Texas, Austin.
D614G was the most common genetic substitution the researchers found, appearing in 82% of SARS-CoV-2 strains during the first wave from March 5 to May 11. The proportion with this mutation jumped to 99.9% by the second wave, defined as occurring between May 12 and July 7 in the study.
The jump in mutation frequency “occurred very rapidly, in a matter of just a few months,” the researchers noted.
The presence of the mutation during the first wave was independently associated with mechanical ventilation days, overall length of stay, and ICU length of stay. However, it was not associated with any significant differences in patient outcomes.
The D614G mutation is now so common worldwide that these viruses are considered reference strains. Researchers believe D614G predominates because it increases the spike protein’s ability to open cells for the virus to enter.
Despite the large number of virus strains evaluated, the samples only represent about 10% of COVID-19 cases in Houston during the study, a potential limitation. Also, some collected samples could not be used for high-quality genome analysis because of limited virus nucleic acid.
Also, it remains unclear if host-virus immune interactions play a significant role. However, the researchers noted in the paper that “available data suggest that, in the aggregate, host genetics does not play an overwhelming role in determining outcome in the great majority of adult patients, once virus infection is established.”
Surveillance ongoing
“The findings will help us to understand the origin, composition, and trajectory of future infection waves and the potential effect of the host immune response and therapeutic maneuvers on SARS-CoV-2 evolution,” the researchers added.
Going forward, the ongoing molecular surveillance of SARS-CoV-2 “may provide critical insights into the origin of the new infection spikes and waves that are occurring as public health constraints are further relaxed, schools and colleges reopen, holidays occur, commercial air travel increases and individuals change their behavior because of COVID-19 ‘fatigue,’ ” the researchers noted.
They added that the genome data will also be useful in assessing ongoing molecular evolution in spike and other proteins “as baseline herd immunity is generated, either by natural exposure to SARS-CoV-2 or by vaccination.”
Further validation warranted
“The study is very interesting and well performed,” Noam Shomron, PhD, a member of the faculty of medicine at Tel Aviv University, said in an interview.
Analyzing the “SARS-CoV-2 molecular evolution in a specific region in the USA … could be viewed as a microcosm of what occurs in other large cities in the USA,” he said.
However, “before jumping to conclusions, this should be further validated,” added Dr. Shomron, who authored a study suggesting differences in genetic alleles could partially explain variations across countries in the infection rates, severity, and mortality associated with SARS-CoV-2.
“We know that many other features and contributors might affect the results – even social constraints could generate a bias in the observations,” he said.
Dr. Finkelstein and Dr. Shomron disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Most SARS-CoV-2 virus strains feature a specific mutation that makes them more transmissible, to the point that these strains now predominate globally, new evidence shows.
In contrast to a greater variety of strains early in the pandemic, now 99.9% of circulating SARS-CoV-2 strains in the study feature the D614G mutation on the spike protein. In addition, people infected with a D614G strain have higher nasopharynx viral loads at diagnosis.
It’s not all bad news. This single-point mutation was not associated with worse clinical COVID-19 severity. Also, the mutation isn’t expected to interfere with the efficacy any of the antibody cocktails, small molecule therapies or vaccines in development.
Furthermore, “as bad as SARS-CoV-2 is, we may have dodged a bullet in terms of how quickly it mutates,” study author Ilya Finkelstein, PhD, said in an interview. This virus mutates much slower than HIV, for example, giving researchers a greater chance to stay one step ahead, he said.
The study was published online Oct. 30 in the journal mBio.
Molecular sleuthing
The research was possible because colleagues at the Houston Methodist Hospital system sequenced the genome of 5085 SARS-CoV-2 strains early in the outbreak and during a second wave of infection over the summer, Dr. Finkelstein said.
The unique data source also includes information from plasma, convalescent plasma, and patient outcomes. Studying a large and diverse population in a major metropolitan area like Houston helps create a “molecular fingerprint” for the virus that will continue to be very useful, said Dr. Finkelstein, a researcher and director of the Finkelstein Lab at the University of Texas, Austin.
D614G was the most common genetic substitution the researchers found, appearing in 82% of SARS-CoV-2 strains during the first wave from March 5 to May 11. The proportion with this mutation jumped to 99.9% by the second wave, defined as occurring between May 12 and July 7 in the study.
The jump in mutation frequency “occurred very rapidly, in a matter of just a few months,” the researchers noted.
The presence of the mutation during the first wave was independently associated with mechanical ventilation days, overall length of stay, and ICU length of stay. However, it was not associated with any significant differences in patient outcomes.
The D614G mutation is now so common worldwide that these viruses are considered reference strains. Researchers believe D614G predominates because it increases the spike protein’s ability to open cells for the virus to enter.
Despite the large number of virus strains evaluated, the samples only represent about 10% of COVID-19 cases in Houston during the study, a potential limitation. Also, some collected samples could not be used for high-quality genome analysis because of limited virus nucleic acid.
Also, it remains unclear if host-virus immune interactions play a significant role. However, the researchers noted in the paper that “available data suggest that, in the aggregate, host genetics does not play an overwhelming role in determining outcome in the great majority of adult patients, once virus infection is established.”
Surveillance ongoing
“The findings will help us to understand the origin, composition, and trajectory of future infection waves and the potential effect of the host immune response and therapeutic maneuvers on SARS-CoV-2 evolution,” the researchers added.
Going forward, the ongoing molecular surveillance of SARS-CoV-2 “may provide critical insights into the origin of the new infection spikes and waves that are occurring as public health constraints are further relaxed, schools and colleges reopen, holidays occur, commercial air travel increases and individuals change their behavior because of COVID-19 ‘fatigue,’ ” the researchers noted.
They added that the genome data will also be useful in assessing ongoing molecular evolution in spike and other proteins “as baseline herd immunity is generated, either by natural exposure to SARS-CoV-2 or by vaccination.”
Further validation warranted
“The study is very interesting and well performed,” Noam Shomron, PhD, a member of the faculty of medicine at Tel Aviv University, said in an interview.
Analyzing the “SARS-CoV-2 molecular evolution in a specific region in the USA … could be viewed as a microcosm of what occurs in other large cities in the USA,” he said.
However, “before jumping to conclusions, this should be further validated,” added Dr. Shomron, who authored a study suggesting differences in genetic alleles could partially explain variations across countries in the infection rates, severity, and mortality associated with SARS-CoV-2.
“We know that many other features and contributors might affect the results – even social constraints could generate a bias in the observations,” he said.
Dr. Finkelstein and Dr. Shomron disclosed no relevant financial relationships.
This article first appeared on Medscape.com.