User login
News and Views that Matter to Pediatricians
The leading independent newspaper covering news and commentary in pediatrics.
Topical or intralesional cidofovir an option for recalcitrant warts
HONOLULU – Combining or those located in areas that are challenging to treat, according to John S. Barbieri, MD, MBA.
“There are 5 million office visits per year in the United States for warts and molluscum, and they’re most common in pediatrics,” Dr. Barbieri, of the department of dermatology at Brigham and Women’s Hospital, Boston, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! “In fact, some studies have suggested that one in three children in primary school suffers from warts.”
According to a 2012 Cochrane review of topical therapies for warts, first-line treatments such as salicylic acid, cryotherapy, 5-FU, or Candida antigen injection often have modest efficacy when used alone. For example, the authors found that salicylic acid and cryotherapy cleared warts in about 60%-70% of cases, respectively, but clearance rates were improved by combining the two therapies.
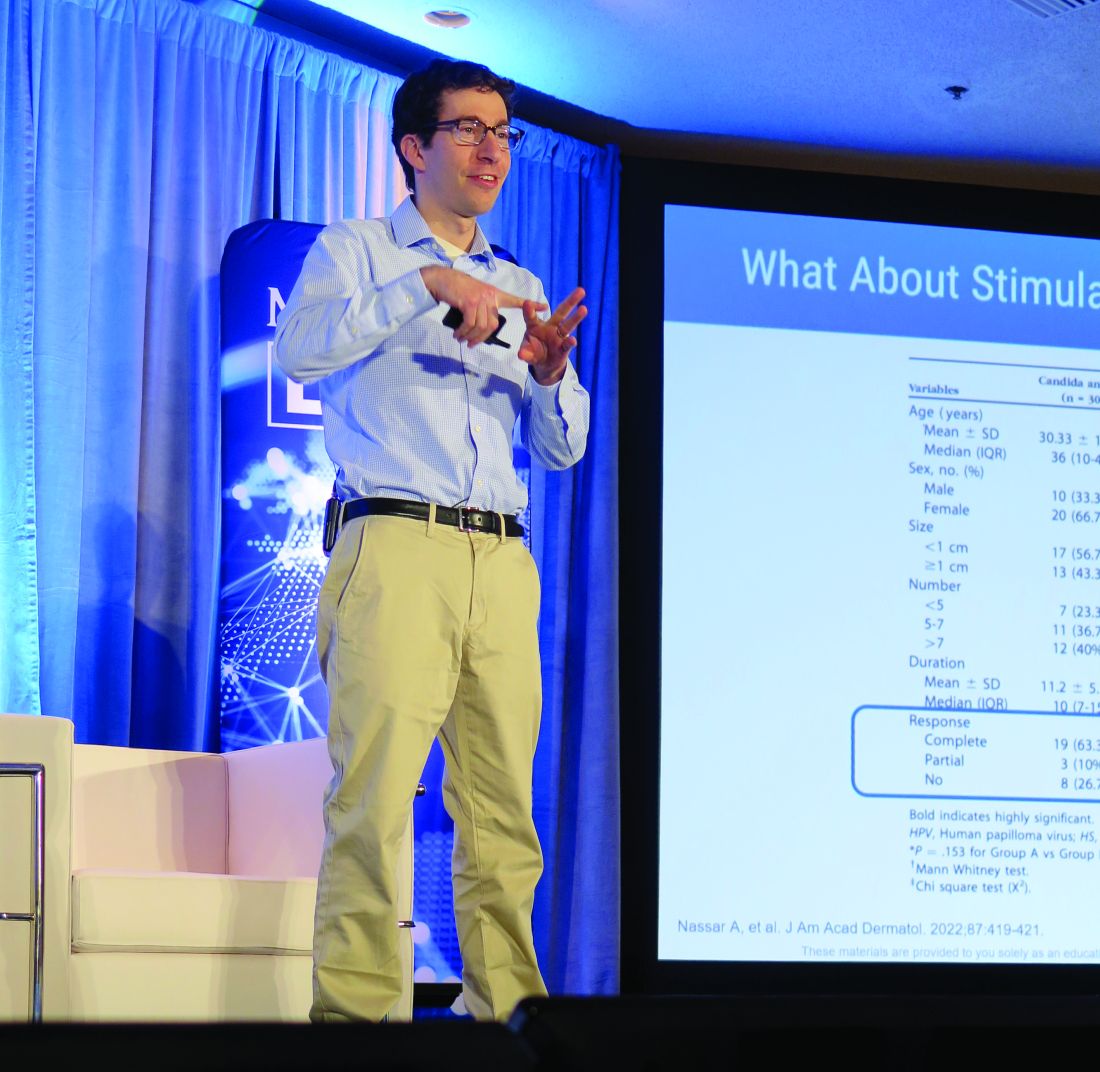
In an earlier literature review and meta-analysis, investigators evaluated the effect of 5-FU plus salicylic acid or salicylic acid alone. The therapeutic effect for common warts across all studies was a 63.4% response rate (complete healing) for 5-FU/SA vversus 23.1% for the 5-FU–free controls, respectively. For plantar warts, the response rate was 63% versus 11%, respectively.
“But what about the person with multiple warts or those in challenging locations where you might worry about destructive treatments hurting the nail fold or causing nail dystrophy?” Dr. Barbieri asked. “Maybe they’ve used salicylic acid or intralesional Candida and they’re still not getting better. What can we do for these patients?”
Emerging research suggests that topical cidofovir can be a valuable option for recalcitrant warts or those in sensitive locations. In a case report of a 10-year-old boy with more than 50 severe verrucous papules on his hands and face that were recalcitrant to multiple conventional therapies, topical 1% cidofovir applied daily for 8 weeks was effective, with no adverse side effects. A young female patient who presented to Dr. Barbieri with multiple warts around the nail matrix of several fingers experienced complete clearance after treatment with topical cidofovir, he said. Other researchers found this approach to be effective for plantar warts as well, in a report of two brothers with severe combined immunodeficiency after hematopoietic stem cell transplantation with persistent warts that did not respond to traditional topical treatments.
“Topical cidofovir is typically a painless treatment, which is nice, especially for our pediatric patients who might be afraid of other therapies like or cryotherapy or intralesional injections,” One limitation is that it is “a bit expensive,” Dr. Barbieri said. “To have topical cidofovir compounded is typically $100-$300, depending on the quantity and strength that you ask for.”
Intralesional cidofovir is another treatment option. In a retrospective study of 58 patients, Dr. Barbieri and colleagues evaluated the outcome of intralesional cidofovir treatment of warts in immunocompromised and nonimmunocompromised patients. Rates of improvement ranged from 98.3% to 100%, while resolution rates ranged from 75.9% to 97.6%.
“Most of the patients had warts for more than 5 years and almost half of them had recalcitrant warts,” Dr. Barbieri said. “These were mostly adult patients, but I think this is a treatment that can work in younger populations as well. About 10%-15% had HIV or cancer or diabetes or were transplant recipients, but despite these challenges and despite these recalcitrant warts, about 100% had improvement.”
He pointed out that cidofovir is available as a 75 mg/mL vial that comes with a 5 mL single-use vial. He dilutes this with normal saline to create a 15 mg/mL solution.
“If you want to be efficient you can try to schedule multiple patients together on the same day as a single vial is sufficient to treat about 25 patients,” assuming about 1 mL is injected per patient, he said. “The challenge with intralesional cidofovir is that it’s painful beyond just the needle part of the injection. Sometimes a nerve block can be helpful. But this can be an effective treatment for patients with recalcitrant warts or those with comorbidities.”
Other intralesional therapies to try for recalcitrant warts, he said, include bleomycin (1 U/mL solution, 1-2 mL per treatment, spaced every 2-4 weeks), and 5-FU (a 4:1 mixture of 5-FU [50 mg/mL] and 2% lidocaine).
Dr. Barbieri disclosed that he receives consulting fees from Dexcel for work unrelated to his presentation. Medscape and this news organization are owned by the same parent company.
HONOLULU – Combining or those located in areas that are challenging to treat, according to John S. Barbieri, MD, MBA.
“There are 5 million office visits per year in the United States for warts and molluscum, and they’re most common in pediatrics,” Dr. Barbieri, of the department of dermatology at Brigham and Women’s Hospital, Boston, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! “In fact, some studies have suggested that one in three children in primary school suffers from warts.”
According to a 2012 Cochrane review of topical therapies for warts, first-line treatments such as salicylic acid, cryotherapy, 5-FU, or Candida antigen injection often have modest efficacy when used alone. For example, the authors found that salicylic acid and cryotherapy cleared warts in about 60%-70% of cases, respectively, but clearance rates were improved by combining the two therapies.
In an earlier literature review and meta-analysis, investigators evaluated the effect of 5-FU plus salicylic acid or salicylic acid alone. The therapeutic effect for common warts across all studies was a 63.4% response rate (complete healing) for 5-FU/SA vversus 23.1% for the 5-FU–free controls, respectively. For plantar warts, the response rate was 63% versus 11%, respectively.
“But what about the person with multiple warts or those in challenging locations where you might worry about destructive treatments hurting the nail fold or causing nail dystrophy?” Dr. Barbieri asked. “Maybe they’ve used salicylic acid or intralesional Candida and they’re still not getting better. What can we do for these patients?”
Emerging research suggests that topical cidofovir can be a valuable option for recalcitrant warts or those in sensitive locations. In a case report of a 10-year-old boy with more than 50 severe verrucous papules on his hands and face that were recalcitrant to multiple conventional therapies, topical 1% cidofovir applied daily for 8 weeks was effective, with no adverse side effects. A young female patient who presented to Dr. Barbieri with multiple warts around the nail matrix of several fingers experienced complete clearance after treatment with topical cidofovir, he said. Other researchers found this approach to be effective for plantar warts as well, in a report of two brothers with severe combined immunodeficiency after hematopoietic stem cell transplantation with persistent warts that did not respond to traditional topical treatments.
“Topical cidofovir is typically a painless treatment, which is nice, especially for our pediatric patients who might be afraid of other therapies like or cryotherapy or intralesional injections,” One limitation is that it is “a bit expensive,” Dr. Barbieri said. “To have topical cidofovir compounded is typically $100-$300, depending on the quantity and strength that you ask for.”
Intralesional cidofovir is another treatment option. In a retrospective study of 58 patients, Dr. Barbieri and colleagues evaluated the outcome of intralesional cidofovir treatment of warts in immunocompromised and nonimmunocompromised patients. Rates of improvement ranged from 98.3% to 100%, while resolution rates ranged from 75.9% to 97.6%.
“Most of the patients had warts for more than 5 years and almost half of them had recalcitrant warts,” Dr. Barbieri said. “These were mostly adult patients, but I think this is a treatment that can work in younger populations as well. About 10%-15% had HIV or cancer or diabetes or were transplant recipients, but despite these challenges and despite these recalcitrant warts, about 100% had improvement.”
He pointed out that cidofovir is available as a 75 mg/mL vial that comes with a 5 mL single-use vial. He dilutes this with normal saline to create a 15 mg/mL solution.
“If you want to be efficient you can try to schedule multiple patients together on the same day as a single vial is sufficient to treat about 25 patients,” assuming about 1 mL is injected per patient, he said. “The challenge with intralesional cidofovir is that it’s painful beyond just the needle part of the injection. Sometimes a nerve block can be helpful. But this can be an effective treatment for patients with recalcitrant warts or those with comorbidities.”
Other intralesional therapies to try for recalcitrant warts, he said, include bleomycin (1 U/mL solution, 1-2 mL per treatment, spaced every 2-4 weeks), and 5-FU (a 4:1 mixture of 5-FU [50 mg/mL] and 2% lidocaine).
Dr. Barbieri disclosed that he receives consulting fees from Dexcel for work unrelated to his presentation. Medscape and this news organization are owned by the same parent company.
HONOLULU – Combining or those located in areas that are challenging to treat, according to John S. Barbieri, MD, MBA.
“There are 5 million office visits per year in the United States for warts and molluscum, and they’re most common in pediatrics,” Dr. Barbieri, of the department of dermatology at Brigham and Women’s Hospital, Boston, said at the Hawaii Dermatology Seminar provided by MedscapeLIVE! “In fact, some studies have suggested that one in three children in primary school suffers from warts.”
According to a 2012 Cochrane review of topical therapies for warts, first-line treatments such as salicylic acid, cryotherapy, 5-FU, or Candida antigen injection often have modest efficacy when used alone. For example, the authors found that salicylic acid and cryotherapy cleared warts in about 60%-70% of cases, respectively, but clearance rates were improved by combining the two therapies.
In an earlier literature review and meta-analysis, investigators evaluated the effect of 5-FU plus salicylic acid or salicylic acid alone. The therapeutic effect for common warts across all studies was a 63.4% response rate (complete healing) for 5-FU/SA vversus 23.1% for the 5-FU–free controls, respectively. For plantar warts, the response rate was 63% versus 11%, respectively.
“But what about the person with multiple warts or those in challenging locations where you might worry about destructive treatments hurting the nail fold or causing nail dystrophy?” Dr. Barbieri asked. “Maybe they’ve used salicylic acid or intralesional Candida and they’re still not getting better. What can we do for these patients?”
Emerging research suggests that topical cidofovir can be a valuable option for recalcitrant warts or those in sensitive locations. In a case report of a 10-year-old boy with more than 50 severe verrucous papules on his hands and face that were recalcitrant to multiple conventional therapies, topical 1% cidofovir applied daily for 8 weeks was effective, with no adverse side effects. A young female patient who presented to Dr. Barbieri with multiple warts around the nail matrix of several fingers experienced complete clearance after treatment with topical cidofovir, he said. Other researchers found this approach to be effective for plantar warts as well, in a report of two brothers with severe combined immunodeficiency after hematopoietic stem cell transplantation with persistent warts that did not respond to traditional topical treatments.
“Topical cidofovir is typically a painless treatment, which is nice, especially for our pediatric patients who might be afraid of other therapies like or cryotherapy or intralesional injections,” One limitation is that it is “a bit expensive,” Dr. Barbieri said. “To have topical cidofovir compounded is typically $100-$300, depending on the quantity and strength that you ask for.”
Intralesional cidofovir is another treatment option. In a retrospective study of 58 patients, Dr. Barbieri and colleagues evaluated the outcome of intralesional cidofovir treatment of warts in immunocompromised and nonimmunocompromised patients. Rates of improvement ranged from 98.3% to 100%, while resolution rates ranged from 75.9% to 97.6%.
“Most of the patients had warts for more than 5 years and almost half of them had recalcitrant warts,” Dr. Barbieri said. “These were mostly adult patients, but I think this is a treatment that can work in younger populations as well. About 10%-15% had HIV or cancer or diabetes or were transplant recipients, but despite these challenges and despite these recalcitrant warts, about 100% had improvement.”
He pointed out that cidofovir is available as a 75 mg/mL vial that comes with a 5 mL single-use vial. He dilutes this with normal saline to create a 15 mg/mL solution.
“If you want to be efficient you can try to schedule multiple patients together on the same day as a single vial is sufficient to treat about 25 patients,” assuming about 1 mL is injected per patient, he said. “The challenge with intralesional cidofovir is that it’s painful beyond just the needle part of the injection. Sometimes a nerve block can be helpful. But this can be an effective treatment for patients with recalcitrant warts or those with comorbidities.”
Other intralesional therapies to try for recalcitrant warts, he said, include bleomycin (1 U/mL solution, 1-2 mL per treatment, spaced every 2-4 weeks), and 5-FU (a 4:1 mixture of 5-FU [50 mg/mL] and 2% lidocaine).
Dr. Barbieri disclosed that he receives consulting fees from Dexcel for work unrelated to his presentation. Medscape and this news organization are owned by the same parent company.
AT THE MEDSCAPELIVE! HAWAII DERMATOLOGY SEMINAR
Too many screenings, too little time, not enough payment
Pediatricians have long charted the vitals of children and adolescents – height, weight, blood pressure – to ensure that kids are healthy and developing as they should. This is the core of the profession. But today the American Academy of Pediatrics recommends that pediatricians also perform maternal depression screenings, childhood depression screenings, autism screenings, and suicide risk screenings once children become 12 years old in addition to other screenings. Specific screening tools might include the Modified Checklist for Autism in Toddlers (MCHAT) for autism screening, the PHQ2 and PHQ9 (part of the longer Patient Health Questionnaire) for depression screening, and the Suicide Behavior Questionnaire Revised (SBQ-R) for suicide screening.
The AAP’s list of recommended screenings – which are developed by various research groups and endorsed by AAP – includes approximately 30 screenings in all, which vary somewhat depending on age. Seven screenings are mental and behavioral health assessments that would, depending on the screening results, require other expertise to address.

“We all want to keep [children] healthy. We actually do want to do these screenings, because they can be very helpful,” said Herschel Lessin, MD, of the Children’s Medical Group in Hopewell Junction, N.Y. Dr. Lessin’s concern is that he may not have anywhere to refer children and their families if he conducts a screening that flags something concerning such as a deeply depressed teenager. Sometimes first appointments with mental health professionals are not available for months.
“Sure – they want us to screen for depression, they want us to screen for anxiety. OK, you get a positive. What do you do? Well, guess what – there are no resources for children and mental health in this country,” Dr. Lessin said.
In Dr. Lessin’s view, economic realities prevent pediatricians from performing detailed psychological screenings anyway – no matter how useful or evidence based they might be, even if mental health support was abundant. He estimates that his practice conducts 20-25 visits a day, around 20 minutes each, of which maybe a dozen are well-child visits, just to keep the doors open. If he thoroughly screened every child or adolescent in the manner recommended by the AAP, Dr. Lessin said, he could do a fraction of that volume and would have to close his doors as a result.
Beside the time burden, insurers reimburse developmental and psychological screenings at low rates, Dr. Lessin said, even with claims that accurately itemize every screening delivered.
“Insurance companies refuse to pay adequately for any of this stuff. They expect me to do it for free, or do it for pennies,” Dr. Lessin said. He said that the natural result of such an arrangement is that some pediatricians stop taking insurance and only work with families that can afford their rates, further entrenching unequal health care by catering to wealthy families who can afford to pay for longer visits. Other pediatricians just don’t do all of the recommended screenings.
“I don’t want it to sound like I’m whining about being paid. They don’t adequately resource what they expect us to do, which is to be society’s social worker,” Dr. Lessin said.
Practical advice for interpreting and prioritizing screenings
Other pediatricians called for screening developers to include guidance for pediatricians about how to counsel families when a screening turns up a concerning result.

“What can we do as pediatricians in that moment to help that family?” asked Karalyn Kinsella, MD, of Pediatric Associates of Cheshire in Cheshire, Conn.
Sometimes the path forward is clear, as with an autism screening; in those cases, Dr. Kinsella said, Connecticut requires referral for a full autism evaluation from birth to age 3. But for other situations, such as an anxiety screening, it is less clear how to proceed.
Dr. Kinsella said that in her experience in-person appointments with a mental health professional, compared with telehealth, work best for her patients. This enables the teenager to find a good fit with a therapist, which can take time when first appointments are so elusive. Any support for pediatricians to bridge the gap until therapy is established is welcome.
“It would be great if it came along with some training – just a brief training – of some ways we can help families before they get into a therapist, or before it gets to the point that they need therapy,” Dr. Kinsella said.
Dr. Kinsella stressed that pediatricians need to use their own judgment when interpreting screening results. Sometimes the MCHAT will miss cases of autism, for example, or the PHQ9 will flag a teenager for depression who is actually just fidgety and having some trouble sleeping.
In her view, the existence of such screens – which might also include screenings for drug abuse, toxic stress, or food insecurity, along with autism, anxiety, and maternal or child depression – is a good development, despite their imperfections and the difficulties of getting help in a timely manner.
“Twenty years ago we really didn’t have any screens,” Dr. Kinsella said.
But it may be that there are now too many recommended screens in pediatrics, even if they all individually have value.

“In the adult world, screenings haven’t mushroomed as in pediatrics” said Dr. Timothy J. Joos, MD, MPH, who practices combined internal medicine and pediatrics at Neighborcare Health in Seattle. Recommended adult health screenings are largely driven by the work of the United States Preventive Services Task Force, which requires a high level of evidence before a screening is recommended. The pediatrics screening world, in Dr. Joos’s view, is populated by a more diffuse set of actors and has therefore inevitably resulted in a profusion of recommended screenings.
Although its main focus is adults, Dr. Joos noted that the USPSTF has evaluated many of the pediatric screenings currently endorsed by AAP. Sometimes there is strong evidence for these screenings, such as universal screening for depression and anxiety in older children. But Dr. Joos noted that per the USPSTF, many of the screenings now recommended by AAP on asymptomatic children for autism, high cholesterol, high blood pressure, or anemia don’t have strong evidence on a population level.
“In many cases, we have a good screen, but it just lacks the research,” Dr. Joos said. Nonetheless, every screening is recommended with “equal weight,” Dr. Joos said, calling for AAP to offer a more prioritized approach to screening rather than an “all comers” approach.
“If you don’t set priorities, you don’t have priorities,” Dr. Joos said, which leads to untenable expectations for what can be accomplished during short visits.
AAP responds
Susan Kressly, MD, who chairs AAP’s Section on Administration and Practice and is a consultant based in Sanibel, Fla., said that we know that using targeting screenings will miss a significant proportion of patients whom you could better assist and care for; for example, if you just go by your gut feeling about whether kids are using drugs or alcohol and just screen those kids. Every screening endorsed by AAP has some degree of evidence for use at a population level rather than case by case, Dr. Kressly noted.
This doesn’t mean that every single screening must be done at each and every recommended interval, she emphasized.
“The first priority is what’s important to the patient and the family. While we understand that screening is at a population health level, there should be some intelligent use and prioritization of these screening tools,” Dr. Kressly said. As examples, Dr. Kressly noted that there is no need to keep administering autism screenings in families whose children already receive autism services, or to ask a teenager questions about anxiety they had answered 6 weeks earlier.
The screenings should be seen as a tool for enhancing relationships with children and their families, not as a series of endless tasks, Dr. Kressly concluded.
Dr. Lessin’s priority is that pediatricians get more support – time, money, training, adequately resourced mental health care – to carry out their expanded role.
“Pediatricians are pretty nice. We want to do the right thing, but everything blocks us from doing it,” Dr. Lessin said.
Dr. Joos, Dr. Kinsella, and Dr. Lessin are on the MDedge Pediatric News Editorial Advisory Board.
Pediatricians have long charted the vitals of children and adolescents – height, weight, blood pressure – to ensure that kids are healthy and developing as they should. This is the core of the profession. But today the American Academy of Pediatrics recommends that pediatricians also perform maternal depression screenings, childhood depression screenings, autism screenings, and suicide risk screenings once children become 12 years old in addition to other screenings. Specific screening tools might include the Modified Checklist for Autism in Toddlers (MCHAT) for autism screening, the PHQ2 and PHQ9 (part of the longer Patient Health Questionnaire) for depression screening, and the Suicide Behavior Questionnaire Revised (SBQ-R) for suicide screening.
The AAP’s list of recommended screenings – which are developed by various research groups and endorsed by AAP – includes approximately 30 screenings in all, which vary somewhat depending on age. Seven screenings are mental and behavioral health assessments that would, depending on the screening results, require other expertise to address.
“We all want to keep [children] healthy. We actually do want to do these screenings, because they can be very helpful,” said Herschel Lessin, MD, of the Children’s Medical Group in Hopewell Junction, N.Y. Dr. Lessin’s concern is that he may not have anywhere to refer children and their families if he conducts a screening that flags something concerning such as a deeply depressed teenager. Sometimes first appointments with mental health professionals are not available for months.
“Sure – they want us to screen for depression, they want us to screen for anxiety. OK, you get a positive. What do you do? Well, guess what – there are no resources for children and mental health in this country,” Dr. Lessin said.
In Dr. Lessin’s view, economic realities prevent pediatricians from performing detailed psychological screenings anyway – no matter how useful or evidence based they might be, even if mental health support was abundant. He estimates that his practice conducts 20-25 visits a day, around 20 minutes each, of which maybe a dozen are well-child visits, just to keep the doors open. If he thoroughly screened every child or adolescent in the manner recommended by the AAP, Dr. Lessin said, he could do a fraction of that volume and would have to close his doors as a result.
Beside the time burden, insurers reimburse developmental and psychological screenings at low rates, Dr. Lessin said, even with claims that accurately itemize every screening delivered.
“Insurance companies refuse to pay adequately for any of this stuff. They expect me to do it for free, or do it for pennies,” Dr. Lessin said. He said that the natural result of such an arrangement is that some pediatricians stop taking insurance and only work with families that can afford their rates, further entrenching unequal health care by catering to wealthy families who can afford to pay for longer visits. Other pediatricians just don’t do all of the recommended screenings.
“I don’t want it to sound like I’m whining about being paid. They don’t adequately resource what they expect us to do, which is to be society’s social worker,” Dr. Lessin said.
Practical advice for interpreting and prioritizing screenings
Other pediatricians called for screening developers to include guidance for pediatricians about how to counsel families when a screening turns up a concerning result.
“What can we do as pediatricians in that moment to help that family?” asked Karalyn Kinsella, MD, of Pediatric Associates of Cheshire in Cheshire, Conn.
Sometimes the path forward is clear, as with an autism screening; in those cases, Dr. Kinsella said, Connecticut requires referral for a full autism evaluation from birth to age 3. But for other situations, such as an anxiety screening, it is less clear how to proceed.
Dr. Kinsella said that in her experience in-person appointments with a mental health professional, compared with telehealth, work best for her patients. This enables the teenager to find a good fit with a therapist, which can take time when first appointments are so elusive. Any support for pediatricians to bridge the gap until therapy is established is welcome.
“It would be great if it came along with some training – just a brief training – of some ways we can help families before they get into a therapist, or before it gets to the point that they need therapy,” Dr. Kinsella said.
Dr. Kinsella stressed that pediatricians need to use their own judgment when interpreting screening results. Sometimes the MCHAT will miss cases of autism, for example, or the PHQ9 will flag a teenager for depression who is actually just fidgety and having some trouble sleeping.
In her view, the existence of such screens – which might also include screenings for drug abuse, toxic stress, or food insecurity, along with autism, anxiety, and maternal or child depression – is a good development, despite their imperfections and the difficulties of getting help in a timely manner.
“Twenty years ago we really didn’t have any screens,” Dr. Kinsella said.
But it may be that there are now too many recommended screens in pediatrics, even if they all individually have value.
“In the adult world, screenings haven’t mushroomed as in pediatrics” said Dr. Timothy J. Joos, MD, MPH, who practices combined internal medicine and pediatrics at Neighborcare Health in Seattle. Recommended adult health screenings are largely driven by the work of the United States Preventive Services Task Force, which requires a high level of evidence before a screening is recommended. The pediatrics screening world, in Dr. Joos’s view, is populated by a more diffuse set of actors and has therefore inevitably resulted in a profusion of recommended screenings.
Although its main focus is adults, Dr. Joos noted that the USPSTF has evaluated many of the pediatric screenings currently endorsed by AAP. Sometimes there is strong evidence for these screenings, such as universal screening for depression and anxiety in older children. But Dr. Joos noted that per the USPSTF, many of the screenings now recommended by AAP on asymptomatic children for autism, high cholesterol, high blood pressure, or anemia don’t have strong evidence on a population level.
“In many cases, we have a good screen, but it just lacks the research,” Dr. Joos said. Nonetheless, every screening is recommended with “equal weight,” Dr. Joos said, calling for AAP to offer a more prioritized approach to screening rather than an “all comers” approach.
“If you don’t set priorities, you don’t have priorities,” Dr. Joos said, which leads to untenable expectations for what can be accomplished during short visits.
AAP responds
Susan Kressly, MD, who chairs AAP’s Section on Administration and Practice and is a consultant based in Sanibel, Fla., said that we know that using targeting screenings will miss a significant proportion of patients whom you could better assist and care for; for example, if you just go by your gut feeling about whether kids are using drugs or alcohol and just screen those kids. Every screening endorsed by AAP has some degree of evidence for use at a population level rather than case by case, Dr. Kressly noted.
This doesn’t mean that every single screening must be done at each and every recommended interval, she emphasized.
“The first priority is what’s important to the patient and the family. While we understand that screening is at a population health level, there should be some intelligent use and prioritization of these screening tools,” Dr. Kressly said. As examples, Dr. Kressly noted that there is no need to keep administering autism screenings in families whose children already receive autism services, or to ask a teenager questions about anxiety they had answered 6 weeks earlier.
The screenings should be seen as a tool for enhancing relationships with children and their families, not as a series of endless tasks, Dr. Kressly concluded.
Dr. Lessin’s priority is that pediatricians get more support – time, money, training, adequately resourced mental health care – to carry out their expanded role.
“Pediatricians are pretty nice. We want to do the right thing, but everything blocks us from doing it,” Dr. Lessin said.
Dr. Joos, Dr. Kinsella, and Dr. Lessin are on the MDedge Pediatric News Editorial Advisory Board.
Pediatricians have long charted the vitals of children and adolescents – height, weight, blood pressure – to ensure that kids are healthy and developing as they should. This is the core of the profession. But today the American Academy of Pediatrics recommends that pediatricians also perform maternal depression screenings, childhood depression screenings, autism screenings, and suicide risk screenings once children become 12 years old in addition to other screenings. Specific screening tools might include the Modified Checklist for Autism in Toddlers (MCHAT) for autism screening, the PHQ2 and PHQ9 (part of the longer Patient Health Questionnaire) for depression screening, and the Suicide Behavior Questionnaire Revised (SBQ-R) for suicide screening.
The AAP’s list of recommended screenings – which are developed by various research groups and endorsed by AAP – includes approximately 30 screenings in all, which vary somewhat depending on age. Seven screenings are mental and behavioral health assessments that would, depending on the screening results, require other expertise to address.
“We all want to keep [children] healthy. We actually do want to do these screenings, because they can be very helpful,” said Herschel Lessin, MD, of the Children’s Medical Group in Hopewell Junction, N.Y. Dr. Lessin’s concern is that he may not have anywhere to refer children and their families if he conducts a screening that flags something concerning such as a deeply depressed teenager. Sometimes first appointments with mental health professionals are not available for months.
“Sure – they want us to screen for depression, they want us to screen for anxiety. OK, you get a positive. What do you do? Well, guess what – there are no resources for children and mental health in this country,” Dr. Lessin said.
In Dr. Lessin’s view, economic realities prevent pediatricians from performing detailed psychological screenings anyway – no matter how useful or evidence based they might be, even if mental health support was abundant. He estimates that his practice conducts 20-25 visits a day, around 20 minutes each, of which maybe a dozen are well-child visits, just to keep the doors open. If he thoroughly screened every child or adolescent in the manner recommended by the AAP, Dr. Lessin said, he could do a fraction of that volume and would have to close his doors as a result.
Beside the time burden, insurers reimburse developmental and psychological screenings at low rates, Dr. Lessin said, even with claims that accurately itemize every screening delivered.
“Insurance companies refuse to pay adequately for any of this stuff. They expect me to do it for free, or do it for pennies,” Dr. Lessin said. He said that the natural result of such an arrangement is that some pediatricians stop taking insurance and only work with families that can afford their rates, further entrenching unequal health care by catering to wealthy families who can afford to pay for longer visits. Other pediatricians just don’t do all of the recommended screenings.
“I don’t want it to sound like I’m whining about being paid. They don’t adequately resource what they expect us to do, which is to be society’s social worker,” Dr. Lessin said.
Practical advice for interpreting and prioritizing screenings
Other pediatricians called for screening developers to include guidance for pediatricians about how to counsel families when a screening turns up a concerning result.
“What can we do as pediatricians in that moment to help that family?” asked Karalyn Kinsella, MD, of Pediatric Associates of Cheshire in Cheshire, Conn.
Sometimes the path forward is clear, as with an autism screening; in those cases, Dr. Kinsella said, Connecticut requires referral for a full autism evaluation from birth to age 3. But for other situations, such as an anxiety screening, it is less clear how to proceed.
Dr. Kinsella said that in her experience in-person appointments with a mental health professional, compared with telehealth, work best for her patients. This enables the teenager to find a good fit with a therapist, which can take time when first appointments are so elusive. Any support for pediatricians to bridge the gap until therapy is established is welcome.
“It would be great if it came along with some training – just a brief training – of some ways we can help families before they get into a therapist, or before it gets to the point that they need therapy,” Dr. Kinsella said.
Dr. Kinsella stressed that pediatricians need to use their own judgment when interpreting screening results. Sometimes the MCHAT will miss cases of autism, for example, or the PHQ9 will flag a teenager for depression who is actually just fidgety and having some trouble sleeping.
In her view, the existence of such screens – which might also include screenings for drug abuse, toxic stress, or food insecurity, along with autism, anxiety, and maternal or child depression – is a good development, despite their imperfections and the difficulties of getting help in a timely manner.
“Twenty years ago we really didn’t have any screens,” Dr. Kinsella said.
But it may be that there are now too many recommended screens in pediatrics, even if they all individually have value.
“In the adult world, screenings haven’t mushroomed as in pediatrics” said Dr. Timothy J. Joos, MD, MPH, who practices combined internal medicine and pediatrics at Neighborcare Health in Seattle. Recommended adult health screenings are largely driven by the work of the United States Preventive Services Task Force, which requires a high level of evidence before a screening is recommended. The pediatrics screening world, in Dr. Joos’s view, is populated by a more diffuse set of actors and has therefore inevitably resulted in a profusion of recommended screenings.
Although its main focus is adults, Dr. Joos noted that the USPSTF has evaluated many of the pediatric screenings currently endorsed by AAP. Sometimes there is strong evidence for these screenings, such as universal screening for depression and anxiety in older children. But Dr. Joos noted that per the USPSTF, many of the screenings now recommended by AAP on asymptomatic children for autism, high cholesterol, high blood pressure, or anemia don’t have strong evidence on a population level.
“In many cases, we have a good screen, but it just lacks the research,” Dr. Joos said. Nonetheless, every screening is recommended with “equal weight,” Dr. Joos said, calling for AAP to offer a more prioritized approach to screening rather than an “all comers” approach.
“If you don’t set priorities, you don’t have priorities,” Dr. Joos said, which leads to untenable expectations for what can be accomplished during short visits.
AAP responds
Susan Kressly, MD, who chairs AAP’s Section on Administration and Practice and is a consultant based in Sanibel, Fla., said that we know that using targeting screenings will miss a significant proportion of patients whom you could better assist and care for; for example, if you just go by your gut feeling about whether kids are using drugs or alcohol and just screen those kids. Every screening endorsed by AAP has some degree of evidence for use at a population level rather than case by case, Dr. Kressly noted.
This doesn’t mean that every single screening must be done at each and every recommended interval, she emphasized.
“The first priority is what’s important to the patient and the family. While we understand that screening is at a population health level, there should be some intelligent use and prioritization of these screening tools,” Dr. Kressly said. As examples, Dr. Kressly noted that there is no need to keep administering autism screenings in families whose children already receive autism services, or to ask a teenager questions about anxiety they had answered 6 weeks earlier.
The screenings should be seen as a tool for enhancing relationships with children and their families, not as a series of endless tasks, Dr. Kressly concluded.
Dr. Lessin’s priority is that pediatricians get more support – time, money, training, adequately resourced mental health care – to carry out their expanded role.
“Pediatricians are pretty nice. We want to do the right thing, but everything blocks us from doing it,” Dr. Lessin said.
Dr. Joos, Dr. Kinsella, and Dr. Lessin are on the MDedge Pediatric News Editorial Advisory Board.
‘Forever chemicals’ disrupt biological processes in children: Study
Exposure to “forever chemicals” widely used in consumer products disrupts important biological processes in children and young adults, a new study says.
That could leave children vulnerable to numerous diseases later in life, including diabetes, cardiovascular disease, and cancer, the study said.
Another important finding was that the disruption appeared to be caused by a mixture of PFAS, rather than a single chemical of that type.
PFAS are known as “forever chemicals” because they don’t break down easily over time and persist in water, soil, and the body. They’re used in numerous consumer products, such as nonstick cookware, stain-resistant carpeting, cosmetics, and water-repellent clothing.
PFAS have previously been linked to a host of health issues, including decreased birth weights and immune system problems. To the study authors’ knowledge, this study is the first to evaluate which biological processes are altered by exposure to multiple PFAS, said a news release from the University of Southern California, Los Angeles.
Researchers studied blood samples from 312 children from the Study of Latino Adolescents at Risk and 137 children from the Southern California Children’s Health Study. All the children had a mixture of common PFAS in their blood, including PFOS, PFHxS, PFHpS, PFOA, and PFNA.
“While current interventions have focused on phasing out the use of individual PFAS, such as PFOS and PFOA, this research shows why the focus should be on reducing exposure to all PFAS chemicals,” said Leda Chatzi, MD, a professor of population and public health sciences at the University of Southern California, Los Angeles. Dr. Chatzi is also one of the study authors.
In October 2021, the Biden administration announced a plan to reduce the amount of PFAS released into the air, drinking and ground water, and food supply chain.
A version of this article first appeared on WebMD.com.
Exposure to “forever chemicals” widely used in consumer products disrupts important biological processes in children and young adults, a new study says.
That could leave children vulnerable to numerous diseases later in life, including diabetes, cardiovascular disease, and cancer, the study said.
Another important finding was that the disruption appeared to be caused by a mixture of PFAS, rather than a single chemical of that type.
PFAS are known as “forever chemicals” because they don’t break down easily over time and persist in water, soil, and the body. They’re used in numerous consumer products, such as nonstick cookware, stain-resistant carpeting, cosmetics, and water-repellent clothing.
PFAS have previously been linked to a host of health issues, including decreased birth weights and immune system problems. To the study authors’ knowledge, this study is the first to evaluate which biological processes are altered by exposure to multiple PFAS, said a news release from the University of Southern California, Los Angeles.
Researchers studied blood samples from 312 children from the Study of Latino Adolescents at Risk and 137 children from the Southern California Children’s Health Study. All the children had a mixture of common PFAS in their blood, including PFOS, PFHxS, PFHpS, PFOA, and PFNA.
“While current interventions have focused on phasing out the use of individual PFAS, such as PFOS and PFOA, this research shows why the focus should be on reducing exposure to all PFAS chemicals,” said Leda Chatzi, MD, a professor of population and public health sciences at the University of Southern California, Los Angeles. Dr. Chatzi is also one of the study authors.
In October 2021, the Biden administration announced a plan to reduce the amount of PFAS released into the air, drinking and ground water, and food supply chain.
A version of this article first appeared on WebMD.com.
Exposure to “forever chemicals” widely used in consumer products disrupts important biological processes in children and young adults, a new study says.
That could leave children vulnerable to numerous diseases later in life, including diabetes, cardiovascular disease, and cancer, the study said.
Another important finding was that the disruption appeared to be caused by a mixture of PFAS, rather than a single chemical of that type.
PFAS are known as “forever chemicals” because they don’t break down easily over time and persist in water, soil, and the body. They’re used in numerous consumer products, such as nonstick cookware, stain-resistant carpeting, cosmetics, and water-repellent clothing.
PFAS have previously been linked to a host of health issues, including decreased birth weights and immune system problems. To the study authors’ knowledge, this study is the first to evaluate which biological processes are altered by exposure to multiple PFAS, said a news release from the University of Southern California, Los Angeles.
Researchers studied blood samples from 312 children from the Study of Latino Adolescents at Risk and 137 children from the Southern California Children’s Health Study. All the children had a mixture of common PFAS in their blood, including PFOS, PFHxS, PFHpS, PFOA, and PFNA.
“While current interventions have focused on phasing out the use of individual PFAS, such as PFOS and PFOA, this research shows why the focus should be on reducing exposure to all PFAS chemicals,” said Leda Chatzi, MD, a professor of population and public health sciences at the University of Southern California, Los Angeles. Dr. Chatzi is also one of the study authors.
In October 2021, the Biden administration announced a plan to reduce the amount of PFAS released into the air, drinking and ground water, and food supply chain.
A version of this article first appeared on WebMD.com.
FROM ENVIRONMENTAL HEALTH PERSPECTIVES
Myths about smoking, diet, alcohol, and cancer persist
FRANCE – Conducted every 5 years since 2005, the Cancer Survey documents the knowledge, perceptions, and way of life of the French people in relation to cancer. The researchers analyzed responses to telephone interviews of a representative sample of almost 5,000 individuals aged 15-85 years.
This study shows how thinking has changed over time and how difficult it is to alter preconceived notions.
Is cancer hereditary?
The report shows that 67.7% of respondents believe that cancer is a hereditary disease. Respondents were asked to explain their answer. “Data show that medical practices for cancer treatment substantiate this belief [that cancer is hereditary],” wrote the authors of the report.
“Indeed, health care professionals almost systematically ask questions about family history of breast cancer and, when a family member has been diagnosed with cancer, medical monitoring of other family members is often sought out, thus reinforcing the belief that cancer is hereditary,” they said.
Furthermore, there seems to be confusion regarding the role of genes in the development of cancer. A person can inherit cancer-predisposing genes, not cancer itself. The authors highlighted their concern that this confusion may “lead people to think that prevention measures are unnecessary because cancer is inherited.”
Misconceptions about smoking
About 41% of smokers think that the length of time one has been smoking is the biggest determining factor for developing cancer; 58.1% think the number of cigarettes smoked per day has a bigger impact.
Experts at InCA and SPF put the debate to rest, stating that prolonged exposure to carcinogenic substances is far more toxic. As for the danger threshold concerning the number of cigarettes smoked per day, respondents believed this to be 9.2 cigarettes per day, on average. They believed that the danger threshold for the number of years as an active smoker is 13.4, on average.
“The [survey] respondents clearly understand that smoking carries a risk, but many smokers think that light smoking or smoking for a short period of time doesn’t carry any risks.” Yet it is understood that even occasional tobacco consumption increases mortality.
This was not the only misconception regarding smoking and its relationship with cancer. About 34% of survey respondents agreed with the following statement: “Smoking doesn’t cause cancer unless you’re a heavy smoker and have smoked for a long time.” Furthermore, 43.3% agreed with the statement, “Pollution is more likely to cause cancer than smoking,” 54.6% think that “exercising cleans your lungs of tobacco,” and 61.6% think that “a smoker can prevent developing cancer caused by smoking if they know to quit on time.”
Overweight and obesity
Although diet and excess weight represent the third and fourth biggest avoidable cancer risk factors, after smoking and alcohol, only 30% of survey respondents knew of this link.
“Among the causes of cancer known and cited by respondents without prompting, excessive weight and obesity were mentioned only 100 times out of 12,558 responses,” highlighted the authors of the report. The explanation put forward by the authors is that discourse about diet has been more focused on diet as a protective health factor, especially in preventing cardiovascular diseases. “The link between cancer and diet is less prominent in the public space,” they noted.
Breastfeeding and cancer
About 63% of survey respondents, which for the first time included both women and men, believe that breastfeeding does not affect mothers’ risk of breast cancer, but this is a misconception. And almost 1 in 3 respondents said that breastfeeding provides health benefits for the mother.
Artificial UV rays
Exposure to UV rays, whether of natural or artificial origin, is a major risk factor for skin cancer. However, 1 in 5 people (20.9%) think that a session in a tanning bed is less harmful than sun exposure.
Daily stress
Regarding psychological factors linked to cancer, the authors noted that risk factors not supported by scientific evidence were, ironically, cited more often by respondents than proven risk factors. There is a real knowledge gap between scientific data and the beliefs of the French people. For example, “working at night” is largely not seen as a risk factor, but data show that it presents a clear risk. However, “not being able to express one’s feelings,” “having been weakened by traumatic experiences,” and “being exposed to the stress of modern life” are seen as risk factors of cancer, without any scientific evidence.
Cigarettes and e-cigarettes
About 53% of respondents agreed that “e-cigarettes are just as harmful or more harmful than traditional cigarettes.” Nicotine and the flavors in e-cigarettes are largely perceived as “very” or “extremely” harmful to the health of a person. However, the authors note that “no published study on nicotine substitutes has shown harmful effects on the health of a person, let alone determined it a risk factor for cancer. The nicotine doses in e-cigarettes are similar to traditional nicotine substitutes, and no cytotoxic effect of nicotine in its inhaled form has been found.” There seems to be confusion between dependence and risk of cancer.
Alcohol consumption
Eight of 10 respondents believe that “some people can drink a lot of alcohol all their life without ever getting cancer,” which goes against the scientific literature. The authors of the report state that the negative effects of alcohol on health seem poorly understood. Although alcohol is the second biggest cause of cancer, only a third of survey respondents cited it without having been prompted as one of the main causes of cancer. And 23.5% even think that “in terms of decreasing your risk of cancer, it’s better to drink a little wine than to drink no wine at all.”
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
FRANCE – Conducted every 5 years since 2005, the Cancer Survey documents the knowledge, perceptions, and way of life of the French people in relation to cancer. The researchers analyzed responses to telephone interviews of a representative sample of almost 5,000 individuals aged 15-85 years.
This study shows how thinking has changed over time and how difficult it is to alter preconceived notions.
Is cancer hereditary?
The report shows that 67.7% of respondents believe that cancer is a hereditary disease. Respondents were asked to explain their answer. “Data show that medical practices for cancer treatment substantiate this belief [that cancer is hereditary],” wrote the authors of the report.
“Indeed, health care professionals almost systematically ask questions about family history of breast cancer and, when a family member has been diagnosed with cancer, medical monitoring of other family members is often sought out, thus reinforcing the belief that cancer is hereditary,” they said.
Furthermore, there seems to be confusion regarding the role of genes in the development of cancer. A person can inherit cancer-predisposing genes, not cancer itself. The authors highlighted their concern that this confusion may “lead people to think that prevention measures are unnecessary because cancer is inherited.”
Misconceptions about smoking
About 41% of smokers think that the length of time one has been smoking is the biggest determining factor for developing cancer; 58.1% think the number of cigarettes smoked per day has a bigger impact.
Experts at InCA and SPF put the debate to rest, stating that prolonged exposure to carcinogenic substances is far more toxic. As for the danger threshold concerning the number of cigarettes smoked per day, respondents believed this to be 9.2 cigarettes per day, on average. They believed that the danger threshold for the number of years as an active smoker is 13.4, on average.
“The [survey] respondents clearly understand that smoking carries a risk, but many smokers think that light smoking or smoking for a short period of time doesn’t carry any risks.” Yet it is understood that even occasional tobacco consumption increases mortality.
This was not the only misconception regarding smoking and its relationship with cancer. About 34% of survey respondents agreed with the following statement: “Smoking doesn’t cause cancer unless you’re a heavy smoker and have smoked for a long time.” Furthermore, 43.3% agreed with the statement, “Pollution is more likely to cause cancer than smoking,” 54.6% think that “exercising cleans your lungs of tobacco,” and 61.6% think that “a smoker can prevent developing cancer caused by smoking if they know to quit on time.”
Overweight and obesity
Although diet and excess weight represent the third and fourth biggest avoidable cancer risk factors, after smoking and alcohol, only 30% of survey respondents knew of this link.
“Among the causes of cancer known and cited by respondents without prompting, excessive weight and obesity were mentioned only 100 times out of 12,558 responses,” highlighted the authors of the report. The explanation put forward by the authors is that discourse about diet has been more focused on diet as a protective health factor, especially in preventing cardiovascular diseases. “The link between cancer and diet is less prominent in the public space,” they noted.
Breastfeeding and cancer
About 63% of survey respondents, which for the first time included both women and men, believe that breastfeeding does not affect mothers’ risk of breast cancer, but this is a misconception. And almost 1 in 3 respondents said that breastfeeding provides health benefits for the mother.
Artificial UV rays
Exposure to UV rays, whether of natural or artificial origin, is a major risk factor for skin cancer. However, 1 in 5 people (20.9%) think that a session in a tanning bed is less harmful than sun exposure.
Daily stress
Regarding psychological factors linked to cancer, the authors noted that risk factors not supported by scientific evidence were, ironically, cited more often by respondents than proven risk factors. There is a real knowledge gap between scientific data and the beliefs of the French people. For example, “working at night” is largely not seen as a risk factor, but data show that it presents a clear risk. However, “not being able to express one’s feelings,” “having been weakened by traumatic experiences,” and “being exposed to the stress of modern life” are seen as risk factors of cancer, without any scientific evidence.
Cigarettes and e-cigarettes
About 53% of respondents agreed that “e-cigarettes are just as harmful or more harmful than traditional cigarettes.” Nicotine and the flavors in e-cigarettes are largely perceived as “very” or “extremely” harmful to the health of a person. However, the authors note that “no published study on nicotine substitutes has shown harmful effects on the health of a person, let alone determined it a risk factor for cancer. The nicotine doses in e-cigarettes are similar to traditional nicotine substitutes, and no cytotoxic effect of nicotine in its inhaled form has been found.” There seems to be confusion between dependence and risk of cancer.
Alcohol consumption
Eight of 10 respondents believe that “some people can drink a lot of alcohol all their life without ever getting cancer,” which goes against the scientific literature. The authors of the report state that the negative effects of alcohol on health seem poorly understood. Although alcohol is the second biggest cause of cancer, only a third of survey respondents cited it without having been prompted as one of the main causes of cancer. And 23.5% even think that “in terms of decreasing your risk of cancer, it’s better to drink a little wine than to drink no wine at all.”
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
FRANCE – Conducted every 5 years since 2005, the Cancer Survey documents the knowledge, perceptions, and way of life of the French people in relation to cancer. The researchers analyzed responses to telephone interviews of a representative sample of almost 5,000 individuals aged 15-85 years.
This study shows how thinking has changed over time and how difficult it is to alter preconceived notions.
Is cancer hereditary?
The report shows that 67.7% of respondents believe that cancer is a hereditary disease. Respondents were asked to explain their answer. “Data show that medical practices for cancer treatment substantiate this belief [that cancer is hereditary],” wrote the authors of the report.
“Indeed, health care professionals almost systematically ask questions about family history of breast cancer and, when a family member has been diagnosed with cancer, medical monitoring of other family members is often sought out, thus reinforcing the belief that cancer is hereditary,” they said.
Furthermore, there seems to be confusion regarding the role of genes in the development of cancer. A person can inherit cancer-predisposing genes, not cancer itself. The authors highlighted their concern that this confusion may “lead people to think that prevention measures are unnecessary because cancer is inherited.”
Misconceptions about smoking
About 41% of smokers think that the length of time one has been smoking is the biggest determining factor for developing cancer; 58.1% think the number of cigarettes smoked per day has a bigger impact.
Experts at InCA and SPF put the debate to rest, stating that prolonged exposure to carcinogenic substances is far more toxic. As for the danger threshold concerning the number of cigarettes smoked per day, respondents believed this to be 9.2 cigarettes per day, on average. They believed that the danger threshold for the number of years as an active smoker is 13.4, on average.
“The [survey] respondents clearly understand that smoking carries a risk, but many smokers think that light smoking or smoking for a short period of time doesn’t carry any risks.” Yet it is understood that even occasional tobacco consumption increases mortality.
This was not the only misconception regarding smoking and its relationship with cancer. About 34% of survey respondents agreed with the following statement: “Smoking doesn’t cause cancer unless you’re a heavy smoker and have smoked for a long time.” Furthermore, 43.3% agreed with the statement, “Pollution is more likely to cause cancer than smoking,” 54.6% think that “exercising cleans your lungs of tobacco,” and 61.6% think that “a smoker can prevent developing cancer caused by smoking if they know to quit on time.”
Overweight and obesity
Although diet and excess weight represent the third and fourth biggest avoidable cancer risk factors, after smoking and alcohol, only 30% of survey respondents knew of this link.
“Among the causes of cancer known and cited by respondents without prompting, excessive weight and obesity were mentioned only 100 times out of 12,558 responses,” highlighted the authors of the report. The explanation put forward by the authors is that discourse about diet has been more focused on diet as a protective health factor, especially in preventing cardiovascular diseases. “The link between cancer and diet is less prominent in the public space,” they noted.
Breastfeeding and cancer
About 63% of survey respondents, which for the first time included both women and men, believe that breastfeeding does not affect mothers’ risk of breast cancer, but this is a misconception. And almost 1 in 3 respondents said that breastfeeding provides health benefits for the mother.
Artificial UV rays
Exposure to UV rays, whether of natural or artificial origin, is a major risk factor for skin cancer. However, 1 in 5 people (20.9%) think that a session in a tanning bed is less harmful than sun exposure.
Daily stress
Regarding psychological factors linked to cancer, the authors noted that risk factors not supported by scientific evidence were, ironically, cited more often by respondents than proven risk factors. There is a real knowledge gap between scientific data and the beliefs of the French people. For example, “working at night” is largely not seen as a risk factor, but data show that it presents a clear risk. However, “not being able to express one’s feelings,” “having been weakened by traumatic experiences,” and “being exposed to the stress of modern life” are seen as risk factors of cancer, without any scientific evidence.
Cigarettes and e-cigarettes
About 53% of respondents agreed that “e-cigarettes are just as harmful or more harmful than traditional cigarettes.” Nicotine and the flavors in e-cigarettes are largely perceived as “very” or “extremely” harmful to the health of a person. However, the authors note that “no published study on nicotine substitutes has shown harmful effects on the health of a person, let alone determined it a risk factor for cancer. The nicotine doses in e-cigarettes are similar to traditional nicotine substitutes, and no cytotoxic effect of nicotine in its inhaled form has been found.” There seems to be confusion between dependence and risk of cancer.
Alcohol consumption
Eight of 10 respondents believe that “some people can drink a lot of alcohol all their life without ever getting cancer,” which goes against the scientific literature. The authors of the report state that the negative effects of alcohol on health seem poorly understood. Although alcohol is the second biggest cause of cancer, only a third of survey respondents cited it without having been prompted as one of the main causes of cancer. And 23.5% even think that “in terms of decreasing your risk of cancer, it’s better to drink a little wine than to drink no wine at all.”
This article was translated from the Medscape French edition. A version of this article appeared on Medscape.com.
Physician pleads guilty to 52 counts in opioid scheme
Jeffrey B. Sutton, DO, a neuromuscular medicine specialist, pled guilty on January 30 in federal court to 31 counts of illegally prescribing opioids and other controlled substances, 1 count of illegally distributing controlled substances, and 20 counts of health care fraud.
Prosecutors said Dr. Sutton admitted that he ignored warnings from prescription drug management organizations, insurers, and state authorities that he was prescribing excessively high dosages of opioids.
Dr. Sutton also admitted to ignoring patient requests to lower dosages and that he also ignored signs that patients were selling prescribed medications or otherwise engaging in illicit activity, including violations of a “pain management agreement” that he required them to sign.
The fraud counts pertained to Dr. Sutton billing Medicare, Medicaid, and other insurers for medically unnecessary visits that he required of patients so that he could prescribe inappropriate or unnecessary opioids.
In the charging document shared with this news organization, prosecutors said Dr. Sutton had sex with at least three patients, including during office visits and outside of the office. Occasionally, the physician would give opioids or other controlled substances – often benzodiazepines – to these patients, without a prescription or valid medical need.
Dr. Sutton escalated the dosage for one of those patients, even as the subjective pain score did not improve and when the patient’s urine tests showed the presence of THC and buprenorphine, but not any of the prescribed medications.
Another patient came to Dr. Sutton in 2007 with a warning that she had a history of “narcotic-seeking” behavior and diagnoses of depression, anxiety, paranoid schizophrenia, and obsessive-compulsive disorder.
The patient was hospitalized in 2018 for complications from benzodiazepine use (prescribed by Dr. Sutton). She weighed 80 pounds at the time. Dr. Sutton continued to prescribe benzodiazepines and extreme doses of opioids – in excess of 2,000 morphine equivalent dose – “despite recognizing and documenting repeated instances of noncompliance with treatment for psychiatric conditions, and despite the known contraindications of long-term opioid use for patients with these mental illnesses,” according to the charging document.
Dr. Sutton continued to prescribe opioids despite two hospitalizations for overdoses, more than 20 failed urine drug screens that showed presence of illicit drugs such as cocaine, and documented excessive use of alprazolam (Xanax) and methadone.
The physician surrendered his Drug Enforcement Administration Certificate of Registration of Controlled Substances Privileges in February 2022 “as an indication of your good faith in desiring to remedy any incorrect or unlawful practices on your part,” according to a letter to Dr. Sutton from the State Medical Board of Ohio. In that September 2022 letter, the Board notified Dr. Sutton of its intention to possibly suspend or revoke his license.
Dr. Sutton did not request a hearing, and the Board permanently revoked his medical license on January 16.
The court will sentence Dr. Sutton on May 23, according to a report by WFMJ.
A version of this article originally appeared on Medscape.com.
Jeffrey B. Sutton, DO, a neuromuscular medicine specialist, pled guilty on January 30 in federal court to 31 counts of illegally prescribing opioids and other controlled substances, 1 count of illegally distributing controlled substances, and 20 counts of health care fraud.
Prosecutors said Dr. Sutton admitted that he ignored warnings from prescription drug management organizations, insurers, and state authorities that he was prescribing excessively high dosages of opioids.
Dr. Sutton also admitted to ignoring patient requests to lower dosages and that he also ignored signs that patients were selling prescribed medications or otherwise engaging in illicit activity, including violations of a “pain management agreement” that he required them to sign.
The fraud counts pertained to Dr. Sutton billing Medicare, Medicaid, and other insurers for medically unnecessary visits that he required of patients so that he could prescribe inappropriate or unnecessary opioids.
In the charging document shared with this news organization, prosecutors said Dr. Sutton had sex with at least three patients, including during office visits and outside of the office. Occasionally, the physician would give opioids or other controlled substances – often benzodiazepines – to these patients, without a prescription or valid medical need.
Dr. Sutton escalated the dosage for one of those patients, even as the subjective pain score did not improve and when the patient’s urine tests showed the presence of THC and buprenorphine, but not any of the prescribed medications.
Another patient came to Dr. Sutton in 2007 with a warning that she had a history of “narcotic-seeking” behavior and diagnoses of depression, anxiety, paranoid schizophrenia, and obsessive-compulsive disorder.
The patient was hospitalized in 2018 for complications from benzodiazepine use (prescribed by Dr. Sutton). She weighed 80 pounds at the time. Dr. Sutton continued to prescribe benzodiazepines and extreme doses of opioids – in excess of 2,000 morphine equivalent dose – “despite recognizing and documenting repeated instances of noncompliance with treatment for psychiatric conditions, and despite the known contraindications of long-term opioid use for patients with these mental illnesses,” according to the charging document.
Dr. Sutton continued to prescribe opioids despite two hospitalizations for overdoses, more than 20 failed urine drug screens that showed presence of illicit drugs such as cocaine, and documented excessive use of alprazolam (Xanax) and methadone.
The physician surrendered his Drug Enforcement Administration Certificate of Registration of Controlled Substances Privileges in February 2022 “as an indication of your good faith in desiring to remedy any incorrect or unlawful practices on your part,” according to a letter to Dr. Sutton from the State Medical Board of Ohio. In that September 2022 letter, the Board notified Dr. Sutton of its intention to possibly suspend or revoke his license.
Dr. Sutton did not request a hearing, and the Board permanently revoked his medical license on January 16.
The court will sentence Dr. Sutton on May 23, according to a report by WFMJ.
A version of this article originally appeared on Medscape.com.
Jeffrey B. Sutton, DO, a neuromuscular medicine specialist, pled guilty on January 30 in federal court to 31 counts of illegally prescribing opioids and other controlled substances, 1 count of illegally distributing controlled substances, and 20 counts of health care fraud.
Prosecutors said Dr. Sutton admitted that he ignored warnings from prescription drug management organizations, insurers, and state authorities that he was prescribing excessively high dosages of opioids.
Dr. Sutton also admitted to ignoring patient requests to lower dosages and that he also ignored signs that patients were selling prescribed medications or otherwise engaging in illicit activity, including violations of a “pain management agreement” that he required them to sign.
The fraud counts pertained to Dr. Sutton billing Medicare, Medicaid, and other insurers for medically unnecessary visits that he required of patients so that he could prescribe inappropriate or unnecessary opioids.
In the charging document shared with this news organization, prosecutors said Dr. Sutton had sex with at least three patients, including during office visits and outside of the office. Occasionally, the physician would give opioids or other controlled substances – often benzodiazepines – to these patients, without a prescription or valid medical need.
Dr. Sutton escalated the dosage for one of those patients, even as the subjective pain score did not improve and when the patient’s urine tests showed the presence of THC and buprenorphine, but not any of the prescribed medications.
Another patient came to Dr. Sutton in 2007 with a warning that she had a history of “narcotic-seeking” behavior and diagnoses of depression, anxiety, paranoid schizophrenia, and obsessive-compulsive disorder.
The patient was hospitalized in 2018 for complications from benzodiazepine use (prescribed by Dr. Sutton). She weighed 80 pounds at the time. Dr. Sutton continued to prescribe benzodiazepines and extreme doses of opioids – in excess of 2,000 morphine equivalent dose – “despite recognizing and documenting repeated instances of noncompliance with treatment for psychiatric conditions, and despite the known contraindications of long-term opioid use for patients with these mental illnesses,” according to the charging document.
Dr. Sutton continued to prescribe opioids despite two hospitalizations for overdoses, more than 20 failed urine drug screens that showed presence of illicit drugs such as cocaine, and documented excessive use of alprazolam (Xanax) and methadone.
The physician surrendered his Drug Enforcement Administration Certificate of Registration of Controlled Substances Privileges in February 2022 “as an indication of your good faith in desiring to remedy any incorrect or unlawful practices on your part,” according to a letter to Dr. Sutton from the State Medical Board of Ohio. In that September 2022 letter, the Board notified Dr. Sutton of its intention to possibly suspend or revoke his license.
Dr. Sutton did not request a hearing, and the Board permanently revoked his medical license on January 16.
The court will sentence Dr. Sutton on May 23, according to a report by WFMJ.
A version of this article originally appeared on Medscape.com.
Regular laxative use tied to increased dementia risk
Among more than 500,000 middle-aged or older adults in the UK Biobank, those who reported regular laxative use had a 51% increased risk of dementia due to any cause, compared with their counterparts who did not regularly use laxatives.
Individuals who used only osmotic laxatives had a 64% increased risk, compared with peers who did not use laxatives, while those using one or more types of laxatives, including bulk-forming, stool-softening, or stimulating laxatives, had a 90% increased risk.
“Constipation and laxative use are common among middle-aged and older adults,” study investigator Feng Sha, PhD, with the Chinese Academy of Sciences in Guangdong, China, said in a news release.
“However, regular laxative use may change the microbiome of the gut, possibly affecting nerve signaling from the gut to the brain or increasing the production of intestinal toxins that may affect the brain,” Dr. Sha noted.
The study was published online in Neurology.
Robust link
The findings are based on 502,229 people (54% women; mean age, 57 at baseline) from the UK biobank database. All were dementia-free at baseline.
A total of 18,235 participants (3.6%) said they used over-the-counter laxatives regularly, which was defined as using them most days of the week during the month before the study.
Over an average of 9.8 years, dementia was recorded in 218 (1.3%) of those who regularly used laxatives and in 1,969 (0.4%) of those did not.
After adjusting for factors such as age, sex, education, other illnesses, medication use, and a family history of dementia, regular use of laxatives was significantly associated with increased risk of all-cause dementia (adjusted hazard ratio, 1.51; 95% confidence interval, 1.30-1.75) and vascular dementia (aHR, 1.65; 95% CI, 1.21-2.27), with no significant association observed for Alzheimer’s disease (aHR, 1.05; 95% CI, 0.79-1.40).
The risk of dementia also increased with the number of laxative types used. All-cause dementia risk increased by 28% (aHR, 1.28; 95% CI, 1.03-1.61) for those using a single laxative type and by 90% (aHR, 1.90; 95% CI, 1.20-3.01) for those using two or more types, compared with nonuse.
Among those who reported using only one type of laxative, only those using osmotic laxatives had a statistically significant higher risk of all-cause dementia (aHR, 1.64; 95% CI, 1.20-2.24) and vascular dementia (aHR, 1.97; 95% CI, 1.04-3.75).
“These results remained robust in various subgroup and sensitivity analyses,” the investigators report.
They caution that they had no data on laxative dosage and so they were unable to explore the relationship between various laxative dosages and dementia risk.
Interpret with caution
Commenting on the findings for this news organization, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, said the results are “interesting and demonstrate an association between laxative use and later life risk of dementia.”
However, “there is no proven causation, and there are some caveats,” Dr. Snyder said. “It’s unclear what may be driving this association, though other lines of research have suggested a linkage between our overall gut health, our immune system, and our brain health.”
Dr. Snyder said it’s also worth noting that the data came from the UK Biobank, which, “while a wealth of information for research purposes, is not representative of other countries. More research is needed.”
The Alzheimer’s Association is leading a 2-year clinical trial, U.S. Pointer, to examine the impact of behavioral interventions on the gut-brain axis to “better understand how our gut health may affect our brains,” Dr. Snyder told this news organization.
“While we await the results of that study, people should talk to their doctor about the risks and benefits of laxatives for their health, as well as discuss alternative methods of alleviating constipation, such as increasing dietary fiber and drinking more water,” she advised.
The study was funded by the National Natural Science Foundation of China, Shenzhen Science and Technology Program, and the Chinese Academy of Sciences. The authors and Dr. Snyder have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among more than 500,000 middle-aged or older adults in the UK Biobank, those who reported regular laxative use had a 51% increased risk of dementia due to any cause, compared with their counterparts who did not regularly use laxatives.
Individuals who used only osmotic laxatives had a 64% increased risk, compared with peers who did not use laxatives, while those using one or more types of laxatives, including bulk-forming, stool-softening, or stimulating laxatives, had a 90% increased risk.
“Constipation and laxative use are common among middle-aged and older adults,” study investigator Feng Sha, PhD, with the Chinese Academy of Sciences in Guangdong, China, said in a news release.
“However, regular laxative use may change the microbiome of the gut, possibly affecting nerve signaling from the gut to the brain or increasing the production of intestinal toxins that may affect the brain,” Dr. Sha noted.
The study was published online in Neurology.
Robust link
The findings are based on 502,229 people (54% women; mean age, 57 at baseline) from the UK biobank database. All were dementia-free at baseline.
A total of 18,235 participants (3.6%) said they used over-the-counter laxatives regularly, which was defined as using them most days of the week during the month before the study.
Over an average of 9.8 years, dementia was recorded in 218 (1.3%) of those who regularly used laxatives and in 1,969 (0.4%) of those did not.
After adjusting for factors such as age, sex, education, other illnesses, medication use, and a family history of dementia, regular use of laxatives was significantly associated with increased risk of all-cause dementia (adjusted hazard ratio, 1.51; 95% confidence interval, 1.30-1.75) and vascular dementia (aHR, 1.65; 95% CI, 1.21-2.27), with no significant association observed for Alzheimer’s disease (aHR, 1.05; 95% CI, 0.79-1.40).
The risk of dementia also increased with the number of laxative types used. All-cause dementia risk increased by 28% (aHR, 1.28; 95% CI, 1.03-1.61) for those using a single laxative type and by 90% (aHR, 1.90; 95% CI, 1.20-3.01) for those using two or more types, compared with nonuse.
Among those who reported using only one type of laxative, only those using osmotic laxatives had a statistically significant higher risk of all-cause dementia (aHR, 1.64; 95% CI, 1.20-2.24) and vascular dementia (aHR, 1.97; 95% CI, 1.04-3.75).
“These results remained robust in various subgroup and sensitivity analyses,” the investigators report.
They caution that they had no data on laxative dosage and so they were unable to explore the relationship between various laxative dosages and dementia risk.
Interpret with caution
Commenting on the findings for this news organization, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, said the results are “interesting and demonstrate an association between laxative use and later life risk of dementia.”
However, “there is no proven causation, and there are some caveats,” Dr. Snyder said. “It’s unclear what may be driving this association, though other lines of research have suggested a linkage between our overall gut health, our immune system, and our brain health.”
Dr. Snyder said it’s also worth noting that the data came from the UK Biobank, which, “while a wealth of information for research purposes, is not representative of other countries. More research is needed.”
The Alzheimer’s Association is leading a 2-year clinical trial, U.S. Pointer, to examine the impact of behavioral interventions on the gut-brain axis to “better understand how our gut health may affect our brains,” Dr. Snyder told this news organization.
“While we await the results of that study, people should talk to their doctor about the risks and benefits of laxatives for their health, as well as discuss alternative methods of alleviating constipation, such as increasing dietary fiber and drinking more water,” she advised.
The study was funded by the National Natural Science Foundation of China, Shenzhen Science and Technology Program, and the Chinese Academy of Sciences. The authors and Dr. Snyder have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among more than 500,000 middle-aged or older adults in the UK Biobank, those who reported regular laxative use had a 51% increased risk of dementia due to any cause, compared with their counterparts who did not regularly use laxatives.
Individuals who used only osmotic laxatives had a 64% increased risk, compared with peers who did not use laxatives, while those using one or more types of laxatives, including bulk-forming, stool-softening, or stimulating laxatives, had a 90% increased risk.
“Constipation and laxative use are common among middle-aged and older adults,” study investigator Feng Sha, PhD, with the Chinese Academy of Sciences in Guangdong, China, said in a news release.
“However, regular laxative use may change the microbiome of the gut, possibly affecting nerve signaling from the gut to the brain or increasing the production of intestinal toxins that may affect the brain,” Dr. Sha noted.
The study was published online in Neurology.
Robust link
The findings are based on 502,229 people (54% women; mean age, 57 at baseline) from the UK biobank database. All were dementia-free at baseline.
A total of 18,235 participants (3.6%) said they used over-the-counter laxatives regularly, which was defined as using them most days of the week during the month before the study.
Over an average of 9.8 years, dementia was recorded in 218 (1.3%) of those who regularly used laxatives and in 1,969 (0.4%) of those did not.
After adjusting for factors such as age, sex, education, other illnesses, medication use, and a family history of dementia, regular use of laxatives was significantly associated with increased risk of all-cause dementia (adjusted hazard ratio, 1.51; 95% confidence interval, 1.30-1.75) and vascular dementia (aHR, 1.65; 95% CI, 1.21-2.27), with no significant association observed for Alzheimer’s disease (aHR, 1.05; 95% CI, 0.79-1.40).
The risk of dementia also increased with the number of laxative types used. All-cause dementia risk increased by 28% (aHR, 1.28; 95% CI, 1.03-1.61) for those using a single laxative type and by 90% (aHR, 1.90; 95% CI, 1.20-3.01) for those using two or more types, compared with nonuse.
Among those who reported using only one type of laxative, only those using osmotic laxatives had a statistically significant higher risk of all-cause dementia (aHR, 1.64; 95% CI, 1.20-2.24) and vascular dementia (aHR, 1.97; 95% CI, 1.04-3.75).
“These results remained robust in various subgroup and sensitivity analyses,” the investigators report.
They caution that they had no data on laxative dosage and so they were unable to explore the relationship between various laxative dosages and dementia risk.
Interpret with caution
Commenting on the findings for this news organization, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, said the results are “interesting and demonstrate an association between laxative use and later life risk of dementia.”
However, “there is no proven causation, and there are some caveats,” Dr. Snyder said. “It’s unclear what may be driving this association, though other lines of research have suggested a linkage between our overall gut health, our immune system, and our brain health.”
Dr. Snyder said it’s also worth noting that the data came from the UK Biobank, which, “while a wealth of information for research purposes, is not representative of other countries. More research is needed.”
The Alzheimer’s Association is leading a 2-year clinical trial, U.S. Pointer, to examine the impact of behavioral interventions on the gut-brain axis to “better understand how our gut health may affect our brains,” Dr. Snyder told this news organization.
“While we await the results of that study, people should talk to their doctor about the risks and benefits of laxatives for their health, as well as discuss alternative methods of alleviating constipation, such as increasing dietary fiber and drinking more water,” she advised.
The study was funded by the National Natural Science Foundation of China, Shenzhen Science and Technology Program, and the Chinese Academy of Sciences. The authors and Dr. Snyder have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM NEUROLOGY
Returning to normal after concussion
Last night I invested an hour and a half watching the first half of the Super Bowl ... because ... well, just because. As exciting as it might have been to watch, investing another 2 hours on the second half would have kept me up well past my bedtime. As I lay in bed with the thwack-thwack-thud of helmets hitting pads still reverberating in my ears, my thoughts drifted to the ever-shifting landscape of concussion management.
More than 2 decades ago, concussions were just beginning to exit the dark ages when loss of consciousness was the defining symptom or sign that most folks (and here I am including physicians) used to separate the run-of-the-mill stinger or bell-ringer from a “real” concussion.
The new era dawned with the appearance of clinics devoted to concussion management and the development of protocols that limited everything from physical exertion to reading and screen time. Schools were coaxed into subjecting their athletes to preparticipation testing sessions with the hope that creating a baseline cognitive assessment would somehow make the diagnosis and management of concussion feel more scientific. Many of the recommended management strategies were based on the intuitive but flawed notion of “brain rest.” If reading or bright lights aggravate patient’s symptoms, they should be avoided but otherwise resting the brain doesn’t seem to make sense.

Fortunately, there were, and hopefully will continue to be, clinicians willing to question hastily developed management protocols. One recent cohort study from Canada has found that, surprisingly, (to some experts), “early return to school was associated with a lower symptom burden” This association held true for both age groups the researches studied (8-12 years and 13-18 years). The authors conclude that delayed return to school “may be detrimental to recovery.” In this study, early return to school was defined as less than 3 days.
In another study, this one in the journal Pediatrics, the authors found that “the association of early screen time with postconcussion symptoms is not linear.” Their conclusion was that the best approach to clinical management of concussion should include a moderate amount of screen time.
After reading both of these studies I am heartened that we are now hearing voices suggesting a return to concussion management based on careful observation of the individual patient and common sense. A concussed brain is not a torn hamstring or a broken clavicle that under most circumstances will heal in a predictable amount of time. It is prudent to exclude the concussed patient from activities that carry a significant risk of reinjury until the symptoms have subsided. However, postconcussion symptoms are often vague and can be mistaken for or aggravated by a host of other conditions including learning disabilities, anxiety, and depression.
I hope that our experience with the COVID pandemic has taught us that removing children from school and their usual activities can have a serious negative effect on their emotional health and academic achievement. This seems to be particularly true for the young people who were already struggling to adjust to being a student. Getting out of the habit of going to school often intensifies the anxieties of an emotionally or academically challenged student. Each day away from the school atmosphere can compound the symptoms that may or may not have been triggered by the concussion.
The message here is clear that, whether we are talking about concussions or appendectomies or mononucleosis, the sooner we can return the child to something close to their old normal the more successful we will be in a helping them adjust to the new normal.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Last night I invested an hour and a half watching the first half of the Super Bowl ... because ... well, just because. As exciting as it might have been to watch, investing another 2 hours on the second half would have kept me up well past my bedtime. As I lay in bed with the thwack-thwack-thud of helmets hitting pads still reverberating in my ears, my thoughts drifted to the ever-shifting landscape of concussion management.
More than 2 decades ago, concussions were just beginning to exit the dark ages when loss of consciousness was the defining symptom or sign that most folks (and here I am including physicians) used to separate the run-of-the-mill stinger or bell-ringer from a “real” concussion.
The new era dawned with the appearance of clinics devoted to concussion management and the development of protocols that limited everything from physical exertion to reading and screen time. Schools were coaxed into subjecting their athletes to preparticipation testing sessions with the hope that creating a baseline cognitive assessment would somehow make the diagnosis and management of concussion feel more scientific. Many of the recommended management strategies were based on the intuitive but flawed notion of “brain rest.” If reading or bright lights aggravate patient’s symptoms, they should be avoided but otherwise resting the brain doesn’t seem to make sense.
Fortunately, there were, and hopefully will continue to be, clinicians willing to question hastily developed management protocols. One recent cohort study from Canada has found that, surprisingly, (to some experts), “early return to school was associated with a lower symptom burden” This association held true for both age groups the researches studied (8-12 years and 13-18 years). The authors conclude that delayed return to school “may be detrimental to recovery.” In this study, early return to school was defined as less than 3 days.
In another study, this one in the journal Pediatrics, the authors found that “the association of early screen time with postconcussion symptoms is not linear.” Their conclusion was that the best approach to clinical management of concussion should include a moderate amount of screen time.
After reading both of these studies I am heartened that we are now hearing voices suggesting a return to concussion management based on careful observation of the individual patient and common sense. A concussed brain is not a torn hamstring or a broken clavicle that under most circumstances will heal in a predictable amount of time. It is prudent to exclude the concussed patient from activities that carry a significant risk of reinjury until the symptoms have subsided. However, postconcussion symptoms are often vague and can be mistaken for or aggravated by a host of other conditions including learning disabilities, anxiety, and depression.
I hope that our experience with the COVID pandemic has taught us that removing children from school and their usual activities can have a serious negative effect on their emotional health and academic achievement. This seems to be particularly true for the young people who were already struggling to adjust to being a student. Getting out of the habit of going to school often intensifies the anxieties of an emotionally or academically challenged student. Each day away from the school atmosphere can compound the symptoms that may or may not have been triggered by the concussion.
The message here is clear that, whether we are talking about concussions or appendectomies or mononucleosis, the sooner we can return the child to something close to their old normal the more successful we will be in a helping them adjust to the new normal.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Last night I invested an hour and a half watching the first half of the Super Bowl ... because ... well, just because. As exciting as it might have been to watch, investing another 2 hours on the second half would have kept me up well past my bedtime. As I lay in bed with the thwack-thwack-thud of helmets hitting pads still reverberating in my ears, my thoughts drifted to the ever-shifting landscape of concussion management.
More than 2 decades ago, concussions were just beginning to exit the dark ages when loss of consciousness was the defining symptom or sign that most folks (and here I am including physicians) used to separate the run-of-the-mill stinger or bell-ringer from a “real” concussion.
The new era dawned with the appearance of clinics devoted to concussion management and the development of protocols that limited everything from physical exertion to reading and screen time. Schools were coaxed into subjecting their athletes to preparticipation testing sessions with the hope that creating a baseline cognitive assessment would somehow make the diagnosis and management of concussion feel more scientific. Many of the recommended management strategies were based on the intuitive but flawed notion of “brain rest.” If reading or bright lights aggravate patient’s symptoms, they should be avoided but otherwise resting the brain doesn’t seem to make sense.
Fortunately, there were, and hopefully will continue to be, clinicians willing to question hastily developed management protocols. One recent cohort study from Canada has found that, surprisingly, (to some experts), “early return to school was associated with a lower symptom burden” This association held true for both age groups the researches studied (8-12 years and 13-18 years). The authors conclude that delayed return to school “may be detrimental to recovery.” In this study, early return to school was defined as less than 3 days.
In another study, this one in the journal Pediatrics, the authors found that “the association of early screen time with postconcussion symptoms is not linear.” Their conclusion was that the best approach to clinical management of concussion should include a moderate amount of screen time.
After reading both of these studies I am heartened that we are now hearing voices suggesting a return to concussion management based on careful observation of the individual patient and common sense. A concussed brain is not a torn hamstring or a broken clavicle that under most circumstances will heal in a predictable amount of time. It is prudent to exclude the concussed patient from activities that carry a significant risk of reinjury until the symptoms have subsided. However, postconcussion symptoms are often vague and can be mistaken for or aggravated by a host of other conditions including learning disabilities, anxiety, and depression.
I hope that our experience with the COVID pandemic has taught us that removing children from school and their usual activities can have a serious negative effect on their emotional health and academic achievement. This seems to be particularly true for the young people who were already struggling to adjust to being a student. Getting out of the habit of going to school often intensifies the anxieties of an emotionally or academically challenged student. Each day away from the school atmosphere can compound the symptoms that may or may not have been triggered by the concussion.
The message here is clear that, whether we are talking about concussions or appendectomies or mononucleosis, the sooner we can return the child to something close to their old normal the more successful we will be in a helping them adjust to the new normal.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Toxic chemicals we consume without knowing it
Life expectancy is falling precipitously. Three-fourths of Americans are overweight or obese, half have diabetes or prediabetes, and a majority are metabolically unhealthy. Furthermore, the rates of allergic, inflammatory, and autoimmune diseases are rising at rates of 3%-9% per year in the West, far faster than the speed of genetic change in this population.
Of course, diet and lifestyle are major factors behind such trends, but a grossly underappreciated driver in what ails us is the role of environmental toxins and endocrine-disrupting chemicals. In years past, these factors have largely evaded the traditional Western medical establishment; however, mounting evidence now supports their significance in fertility, metabolic health, and cancer.
Although several industrial chemicals and toxins have been identified as carcinogens and have subsequently been regulated, many more remain persistent in the environment and continue to be freely used. It is therefore incumbent upon both the general public and clinicians to be knowledgeable about these exposures. Here, we review some of the most common exposures and the substantial health risks associated with them, along with some general guidance around best practices for how to minimize exposure.
Microplastics
“Microplastics” is a term used to describe small fragments or particles of plastic breakdown or microbeads from household or personal care products, measuring less than 5 mm in length.
Plastic waste is accumulating at alarming and devastating proportions – by 2050, it is estimated that by weight, there will be more plastic than fish in the oceans. That translates into hundreds of thousands of tons of microplastics and trillions of these particles in the seas. A recent study demonstrated that microplastics were present in the bloodstream in the majority of 22 otherwise healthy participants.
Since the 1950s, plastic exposure has been shown to promote tumorigenesis in animal studies, and in vitro studies have demonstrated the toxicity of microplastics at the cellular level. However, it is not well known whether the plastic itself is toxic or if it simply serves as a carrier for other environmental toxins to bioaccumulate.
According to Tasha Stoiber, a senior scientist at the Environmental Working Group, “Microplastics have been widely detected in fish and seafood, as well as other products like bottled water, beer, honey, and tap water.” The EWG states there are no formal advisories on fish consumption to avoid exposure to microplastics at the moment.
Pressure also is mounting for a ban on microbeads in personal care products.
Until such bans are put in place, it is advised to avoid single-use plastics, favor reusable tote bags for grocery shopping rather than plastic bags, and opt for loose leaf tea or paper tea bags rather than mesh-based alternatives.
Phthalates
Phthalates are chemicals used to make plastics soft and durable, as well as to bind fragrances. They are commonly found in household items such as vinyl (for example, flooring, shower curtains) and fragrances, air fresheners, and perfumes.
Phthalates are known hormone-disrupting chemicals, exposure to which has been associated with abnormal sexual and brain development in children, as well as lower levels of testosterone in men. Exposures are thought to occur via inhalation, ingestion, and skin contact; however, fasting studies demonstrate that a majority of exposure is probably food related.
To avoid phthalate exposures, recommendations include avoiding polyvinyl chloride plastics (particularly food containers, plastic wrap, and children’s toys), which are identifiable by the recycle code number 3, as well as air fresheners and fragranced products.
The EWG’s Skin Deep database provides an important resource on phthalate-free personal care products.
Despite pressure from consumer advocacy groups, the U.S. Food and Drug Administration has not yet banned phthalates in food packaging.
Bisphenol A (BPA)
BPA is a chemical additive used to make clear and hard polycarbonate plastics, as well as epoxy and thermal papers. BPA is one of the highest-volume chemicals, with roughly 6 billion pounds produced each year. BPA is traditionally found in many clear plastic bottles and sippy cups, as well as in the lining of canned foods.
Structurally, BPA acts as an estrogen mimetic and has been associated with cardiovascular disease, obesity, and male sexual dysfunction. Since 2012, BPA has been banned in sippy cups and baby bottles, but there is some debate as to whether its replacements (bisphenol S and bisphenol F) are any safer; they appear to have similar hormonal effects as BPA.
As with phthalates, the majority of ingestion is thought to be food related. BPA has been found in more than 90% of a representative study population in the United States.
Guidance advises avoiding polycarbonate plastics (identifiable with the recycling code number 7), as well as avoiding handling thermal papers such as tickets and receipts, if possible. Food and beverages should be stored in glass or stainless steel. If plastic must be used, opt for polycarbonate- and polyvinyl chloride–free plastics, and food and beverages should never be reheated in plastic containers or wrapping. Canned foods should ideally be avoided, particularly canned tunas and condensed soups. If canned products are bought, they should ideally be BPA free.
Dioxins and polychlorinated biphenyls (PCBs)
Dioxins are mainly the byproducts of industrial practices; they are released after incineration, trash burning, and fires. PCBs, which are somewhat structurally related to dioxins, were previously found in products such as flame retardants and coolants. Dioxins and PCBs are often grouped in the same category under the umbrella term “persistent organic pollutants” because they break down slowly and remain in the environment even after emissions have been curbed.
Tetrachlorodibenzodioxin, perhaps the best-known dioxin, is a known carcinogen. Dioxins also have been associated with a host of health implications in development, immunity, and reproductive and endocrine systems. Higher levels of PCB exposure have also been associated with an increased risk for mortality from cardiovascular disease.
Notably, dioxin emissions have been reduced by 90% since the 1980s, and the U.S. Environmental Protection Agency has banned the use of PCBs in industrial manufacturing since 1979. However, environmental dioxins and PCBs still enter the food chain and accumulate in fat.
The best ways to avoid exposures are through limiting meat, fish, and dairy consumption and trimming the skin and fat from meats. The level of dioxins and PCBs found in meat, eggs, fish, and dairy are approximately 5-10 times higher than they are in plant-based foods. Research has shown that farmed salmon is likely to be the most PCB-contaminated protein source in the U.S. diet; however, newer forms of land-based and sustainable aquaculture probably avoid this exposure.
Pesticides
The growth of modern monoculture agriculture in the United States over the past century has coincided with a dramatic surge in the use of industrial pesticides. In fact, over 90% of the U.S. population have pesticides in their urine and blood, regardless of where they live. Exposures are thought to be food related.
Approximately 1 billion pounds of pesticides are used annually in the United States, including nearly 300 million pounds of glyphosate, which has been identified as a probable carcinogen by European agencies. The EPA has not yet reached this conclusion, although the matter is currently being litigated.
A large European prospective cohort trial demonstrated a lower risk for cancer in those with a greater frequency of self-reported organic food consumption. In addition to cancer risk, relatively elevated blood levels of a pesticide known as beta-hexachlorocyclohexane (B-HCH) are associated with higher all-cause mortality. Also, exposure to DDE – a metabolite of DDT, a chlorinated pesticide heavily used in the 1940s-1960s that still persists in the environment today – has been shown to increase the risk for Alzheimer’s-type dementia as well as overall cognitive decline.
Because these chlorinated pesticides are often fat soluble, they seem to accumulate in animal products. Therefore, people consuming a vegetarian diet have been found to have lower levels of B-HCH. This has led to the recommendation that consumers of produce should favor organic over conventional, if possible. Here too, the EWG provides an important resource to consumers in the form of shopper guides regarding pesticides in produce.
Per- and polyfluoroalkyl substances (PFAS)
PFAS are a group of fluorinated compounds discovered in the 1930s. Their chemical composition includes a durable carbon-fluoride bond, giving them a persistence within the environment that has led to their being referred to as “forever chemicals.”
PFAS have been detected in the blood of 98% of Americans, and in the rainwater of locations as far afield as Tibet and Antarctica. Even low levels of exposure have been associated with an increased risk for cancer, liver disease, low birth weight, and hormonal disruption.
The properties of PFAS also make them both durable at very high heat and water repellent. Notoriously, the chemical was used by 3M to make Scotchgard for carpets and fabrics and by Dupont to make Teflon for nonstick coating of pots and pans. Although perfluorooctanoic acid (PFOA) was removed from nonstick cookware in 2013, PFAS – a family of thousands of synthetic compounds – remain common in fast-food packaging, water- and stain-repellent clothing, firefighting foam, and personal care products. PFAS are released into the environment during the breakdown of these consumer and industrial products, as well as from dumping from waste facilities.
Alarmingly, the EWG notes that up to 200 million Americans may be exposed to PFAS in their drinking water. In March 2021, the EPA announced that they will be regulating PFAS in drinking water; however, the regulations have not been finalized. Currently, it is up to individual states to test for its presence in the water. The EWG has compiled a map of all known PFAS contamination sites.
To avoid or prevent exposures from PFAS, recommendations include filtering tap water with either reverse osmosis or activated carbon filters, as well as avoiding fast food and carry-out food, if possible, and consumer products labeled as “water resistant,” “stain-resistant,” and “nonstick.”
In a testament to how harmful these chemicals are, the EPA recently revised their lifetime health advisories for PFAS, such as PFOA, to 0.004 parts per trillion, which is more than 10,000 times smaller than the previous limit of 70 parts per trillion. The EPA also has proposed formally designating certain PFAS chemicals as “hazardous substances.”
Dr. Goel, clinical assistant professor of medicine at Weill Cornell Medicine, New York, has disclosed no relevant financial relationships. A version of this article originally appeared on Medscape.com.
Life expectancy is falling precipitously. Three-fourths of Americans are overweight or obese, half have diabetes or prediabetes, and a majority are metabolically unhealthy. Furthermore, the rates of allergic, inflammatory, and autoimmune diseases are rising at rates of 3%-9% per year in the West, far faster than the speed of genetic change in this population.
Of course, diet and lifestyle are major factors behind such trends, but a grossly underappreciated driver in what ails us is the role of environmental toxins and endocrine-disrupting chemicals. In years past, these factors have largely evaded the traditional Western medical establishment; however, mounting evidence now supports their significance in fertility, metabolic health, and cancer.
Although several industrial chemicals and toxins have been identified as carcinogens and have subsequently been regulated, many more remain persistent in the environment and continue to be freely used. It is therefore incumbent upon both the general public and clinicians to be knowledgeable about these exposures. Here, we review some of the most common exposures and the substantial health risks associated with them, along with some general guidance around best practices for how to minimize exposure.
Microplastics
“Microplastics” is a term used to describe small fragments or particles of plastic breakdown or microbeads from household or personal care products, measuring less than 5 mm in length.
Plastic waste is accumulating at alarming and devastating proportions – by 2050, it is estimated that by weight, there will be more plastic than fish in the oceans. That translates into hundreds of thousands of tons of microplastics and trillions of these particles in the seas. A recent study demonstrated that microplastics were present in the bloodstream in the majority of 22 otherwise healthy participants.
Since the 1950s, plastic exposure has been shown to promote tumorigenesis in animal studies, and in vitro studies have demonstrated the toxicity of microplastics at the cellular level. However, it is not well known whether the plastic itself is toxic or if it simply serves as a carrier for other environmental toxins to bioaccumulate.
According to Tasha Stoiber, a senior scientist at the Environmental Working Group, “Microplastics have been widely detected in fish and seafood, as well as other products like bottled water, beer, honey, and tap water.” The EWG states there are no formal advisories on fish consumption to avoid exposure to microplastics at the moment.
Pressure also is mounting for a ban on microbeads in personal care products.
Until such bans are put in place, it is advised to avoid single-use plastics, favor reusable tote bags for grocery shopping rather than plastic bags, and opt for loose leaf tea or paper tea bags rather than mesh-based alternatives.
Phthalates
Phthalates are chemicals used to make plastics soft and durable, as well as to bind fragrances. They are commonly found in household items such as vinyl (for example, flooring, shower curtains) and fragrances, air fresheners, and perfumes.
Phthalates are known hormone-disrupting chemicals, exposure to which has been associated with abnormal sexual and brain development in children, as well as lower levels of testosterone in men. Exposures are thought to occur via inhalation, ingestion, and skin contact; however, fasting studies demonstrate that a majority of exposure is probably food related.
To avoid phthalate exposures, recommendations include avoiding polyvinyl chloride plastics (particularly food containers, plastic wrap, and children’s toys), which are identifiable by the recycle code number 3, as well as air fresheners and fragranced products.
The EWG’s Skin Deep database provides an important resource on phthalate-free personal care products.
Despite pressure from consumer advocacy groups, the U.S. Food and Drug Administration has not yet banned phthalates in food packaging.
Bisphenol A (BPA)
BPA is a chemical additive used to make clear and hard polycarbonate plastics, as well as epoxy and thermal papers. BPA is one of the highest-volume chemicals, with roughly 6 billion pounds produced each year. BPA is traditionally found in many clear plastic bottles and sippy cups, as well as in the lining of canned foods.
Structurally, BPA acts as an estrogen mimetic and has been associated with cardiovascular disease, obesity, and male sexual dysfunction. Since 2012, BPA has been banned in sippy cups and baby bottles, but there is some debate as to whether its replacements (bisphenol S and bisphenol F) are any safer; they appear to have similar hormonal effects as BPA.
As with phthalates, the majority of ingestion is thought to be food related. BPA has been found in more than 90% of a representative study population in the United States.
Guidance advises avoiding polycarbonate plastics (identifiable with the recycling code number 7), as well as avoiding handling thermal papers such as tickets and receipts, if possible. Food and beverages should be stored in glass or stainless steel. If plastic must be used, opt for polycarbonate- and polyvinyl chloride–free plastics, and food and beverages should never be reheated in plastic containers or wrapping. Canned foods should ideally be avoided, particularly canned tunas and condensed soups. If canned products are bought, they should ideally be BPA free.
Dioxins and polychlorinated biphenyls (PCBs)
Dioxins are mainly the byproducts of industrial practices; they are released after incineration, trash burning, and fires. PCBs, which are somewhat structurally related to dioxins, were previously found in products such as flame retardants and coolants. Dioxins and PCBs are often grouped in the same category under the umbrella term “persistent organic pollutants” because they break down slowly and remain in the environment even after emissions have been curbed.
Tetrachlorodibenzodioxin, perhaps the best-known dioxin, is a known carcinogen. Dioxins also have been associated with a host of health implications in development, immunity, and reproductive and endocrine systems. Higher levels of PCB exposure have also been associated with an increased risk for mortality from cardiovascular disease.
Notably, dioxin emissions have been reduced by 90% since the 1980s, and the U.S. Environmental Protection Agency has banned the use of PCBs in industrial manufacturing since 1979. However, environmental dioxins and PCBs still enter the food chain and accumulate in fat.
The best ways to avoid exposures are through limiting meat, fish, and dairy consumption and trimming the skin and fat from meats. The level of dioxins and PCBs found in meat, eggs, fish, and dairy are approximately 5-10 times higher than they are in plant-based foods. Research has shown that farmed salmon is likely to be the most PCB-contaminated protein source in the U.S. diet; however, newer forms of land-based and sustainable aquaculture probably avoid this exposure.
Pesticides
The growth of modern monoculture agriculture in the United States over the past century has coincided with a dramatic surge in the use of industrial pesticides. In fact, over 90% of the U.S. population have pesticides in their urine and blood, regardless of where they live. Exposures are thought to be food related.
Approximately 1 billion pounds of pesticides are used annually in the United States, including nearly 300 million pounds of glyphosate, which has been identified as a probable carcinogen by European agencies. The EPA has not yet reached this conclusion, although the matter is currently being litigated.
A large European prospective cohort trial demonstrated a lower risk for cancer in those with a greater frequency of self-reported organic food consumption. In addition to cancer risk, relatively elevated blood levels of a pesticide known as beta-hexachlorocyclohexane (B-HCH) are associated with higher all-cause mortality. Also, exposure to DDE – a metabolite of DDT, a chlorinated pesticide heavily used in the 1940s-1960s that still persists in the environment today – has been shown to increase the risk for Alzheimer’s-type dementia as well as overall cognitive decline.
Because these chlorinated pesticides are often fat soluble, they seem to accumulate in animal products. Therefore, people consuming a vegetarian diet have been found to have lower levels of B-HCH. This has led to the recommendation that consumers of produce should favor organic over conventional, if possible. Here too, the EWG provides an important resource to consumers in the form of shopper guides regarding pesticides in produce.
Per- and polyfluoroalkyl substances (PFAS)
PFAS are a group of fluorinated compounds discovered in the 1930s. Their chemical composition includes a durable carbon-fluoride bond, giving them a persistence within the environment that has led to their being referred to as “forever chemicals.”
PFAS have been detected in the blood of 98% of Americans, and in the rainwater of locations as far afield as Tibet and Antarctica. Even low levels of exposure have been associated with an increased risk for cancer, liver disease, low birth weight, and hormonal disruption.
The properties of PFAS also make them both durable at very high heat and water repellent. Notoriously, the chemical was used by 3M to make Scotchgard for carpets and fabrics and by Dupont to make Teflon for nonstick coating of pots and pans. Although perfluorooctanoic acid (PFOA) was removed from nonstick cookware in 2013, PFAS – a family of thousands of synthetic compounds – remain common in fast-food packaging, water- and stain-repellent clothing, firefighting foam, and personal care products. PFAS are released into the environment during the breakdown of these consumer and industrial products, as well as from dumping from waste facilities.
Alarmingly, the EWG notes that up to 200 million Americans may be exposed to PFAS in their drinking water. In March 2021, the EPA announced that they will be regulating PFAS in drinking water; however, the regulations have not been finalized. Currently, it is up to individual states to test for its presence in the water. The EWG has compiled a map of all known PFAS contamination sites.
To avoid or prevent exposures from PFAS, recommendations include filtering tap water with either reverse osmosis or activated carbon filters, as well as avoiding fast food and carry-out food, if possible, and consumer products labeled as “water resistant,” “stain-resistant,” and “nonstick.”
In a testament to how harmful these chemicals are, the EPA recently revised their lifetime health advisories for PFAS, such as PFOA, to 0.004 parts per trillion, which is more than 10,000 times smaller than the previous limit of 70 parts per trillion. The EPA also has proposed formally designating certain PFAS chemicals as “hazardous substances.”
Dr. Goel, clinical assistant professor of medicine at Weill Cornell Medicine, New York, has disclosed no relevant financial relationships. A version of this article originally appeared on Medscape.com.
Life expectancy is falling precipitously. Three-fourths of Americans are overweight or obese, half have diabetes or prediabetes, and a majority are metabolically unhealthy. Furthermore, the rates of allergic, inflammatory, and autoimmune diseases are rising at rates of 3%-9% per year in the West, far faster than the speed of genetic change in this population.
Of course, diet and lifestyle are major factors behind such trends, but a grossly underappreciated driver in what ails us is the role of environmental toxins and endocrine-disrupting chemicals. In years past, these factors have largely evaded the traditional Western medical establishment; however, mounting evidence now supports their significance in fertility, metabolic health, and cancer.
Although several industrial chemicals and toxins have been identified as carcinogens and have subsequently been regulated, many more remain persistent in the environment and continue to be freely used. It is therefore incumbent upon both the general public and clinicians to be knowledgeable about these exposures. Here, we review some of the most common exposures and the substantial health risks associated with them, along with some general guidance around best practices for how to minimize exposure.
Microplastics
“Microplastics” is a term used to describe small fragments or particles of plastic breakdown or microbeads from household or personal care products, measuring less than 5 mm in length.
Plastic waste is accumulating at alarming and devastating proportions – by 2050, it is estimated that by weight, there will be more plastic than fish in the oceans. That translates into hundreds of thousands of tons of microplastics and trillions of these particles in the seas. A recent study demonstrated that microplastics were present in the bloodstream in the majority of 22 otherwise healthy participants.
Since the 1950s, plastic exposure has been shown to promote tumorigenesis in animal studies, and in vitro studies have demonstrated the toxicity of microplastics at the cellular level. However, it is not well known whether the plastic itself is toxic or if it simply serves as a carrier for other environmental toxins to bioaccumulate.
According to Tasha Stoiber, a senior scientist at the Environmental Working Group, “Microplastics have been widely detected in fish and seafood, as well as other products like bottled water, beer, honey, and tap water.” The EWG states there are no formal advisories on fish consumption to avoid exposure to microplastics at the moment.
Pressure also is mounting for a ban on microbeads in personal care products.
Until such bans are put in place, it is advised to avoid single-use plastics, favor reusable tote bags for grocery shopping rather than plastic bags, and opt for loose leaf tea or paper tea bags rather than mesh-based alternatives.
Phthalates
Phthalates are chemicals used to make plastics soft and durable, as well as to bind fragrances. They are commonly found in household items such as vinyl (for example, flooring, shower curtains) and fragrances, air fresheners, and perfumes.
Phthalates are known hormone-disrupting chemicals, exposure to which has been associated with abnormal sexual and brain development in children, as well as lower levels of testosterone in men. Exposures are thought to occur via inhalation, ingestion, and skin contact; however, fasting studies demonstrate that a majority of exposure is probably food related.
To avoid phthalate exposures, recommendations include avoiding polyvinyl chloride plastics (particularly food containers, plastic wrap, and children’s toys), which are identifiable by the recycle code number 3, as well as air fresheners and fragranced products.
The EWG’s Skin Deep database provides an important resource on phthalate-free personal care products.
Despite pressure from consumer advocacy groups, the U.S. Food and Drug Administration has not yet banned phthalates in food packaging.
Bisphenol A (BPA)
BPA is a chemical additive used to make clear and hard polycarbonate plastics, as well as epoxy and thermal papers. BPA is one of the highest-volume chemicals, with roughly 6 billion pounds produced each year. BPA is traditionally found in many clear plastic bottles and sippy cups, as well as in the lining of canned foods.
Structurally, BPA acts as an estrogen mimetic and has been associated with cardiovascular disease, obesity, and male sexual dysfunction. Since 2012, BPA has been banned in sippy cups and baby bottles, but there is some debate as to whether its replacements (bisphenol S and bisphenol F) are any safer; they appear to have similar hormonal effects as BPA.
As with phthalates, the majority of ingestion is thought to be food related. BPA has been found in more than 90% of a representative study population in the United States.
Guidance advises avoiding polycarbonate plastics (identifiable with the recycling code number 7), as well as avoiding handling thermal papers such as tickets and receipts, if possible. Food and beverages should be stored in glass or stainless steel. If plastic must be used, opt for polycarbonate- and polyvinyl chloride–free plastics, and food and beverages should never be reheated in plastic containers or wrapping. Canned foods should ideally be avoided, particularly canned tunas and condensed soups. If canned products are bought, they should ideally be BPA free.
Dioxins and polychlorinated biphenyls (PCBs)
Dioxins are mainly the byproducts of industrial practices; they are released after incineration, trash burning, and fires. PCBs, which are somewhat structurally related to dioxins, were previously found in products such as flame retardants and coolants. Dioxins and PCBs are often grouped in the same category under the umbrella term “persistent organic pollutants” because they break down slowly and remain in the environment even after emissions have been curbed.
Tetrachlorodibenzodioxin, perhaps the best-known dioxin, is a known carcinogen. Dioxins also have been associated with a host of health implications in development, immunity, and reproductive and endocrine systems. Higher levels of PCB exposure have also been associated with an increased risk for mortality from cardiovascular disease.
Notably, dioxin emissions have been reduced by 90% since the 1980s, and the U.S. Environmental Protection Agency has banned the use of PCBs in industrial manufacturing since 1979. However, environmental dioxins and PCBs still enter the food chain and accumulate in fat.
The best ways to avoid exposures are through limiting meat, fish, and dairy consumption and trimming the skin and fat from meats. The level of dioxins and PCBs found in meat, eggs, fish, and dairy are approximately 5-10 times higher than they are in plant-based foods. Research has shown that farmed salmon is likely to be the most PCB-contaminated protein source in the U.S. diet; however, newer forms of land-based and sustainable aquaculture probably avoid this exposure.
Pesticides
The growth of modern monoculture agriculture in the United States over the past century has coincided with a dramatic surge in the use of industrial pesticides. In fact, over 90% of the U.S. population have pesticides in their urine and blood, regardless of where they live. Exposures are thought to be food related.
Approximately 1 billion pounds of pesticides are used annually in the United States, including nearly 300 million pounds of glyphosate, which has been identified as a probable carcinogen by European agencies. The EPA has not yet reached this conclusion, although the matter is currently being litigated.
A large European prospective cohort trial demonstrated a lower risk for cancer in those with a greater frequency of self-reported organic food consumption. In addition to cancer risk, relatively elevated blood levels of a pesticide known as beta-hexachlorocyclohexane (B-HCH) are associated with higher all-cause mortality. Also, exposure to DDE – a metabolite of DDT, a chlorinated pesticide heavily used in the 1940s-1960s that still persists in the environment today – has been shown to increase the risk for Alzheimer’s-type dementia as well as overall cognitive decline.
Because these chlorinated pesticides are often fat soluble, they seem to accumulate in animal products. Therefore, people consuming a vegetarian diet have been found to have lower levels of B-HCH. This has led to the recommendation that consumers of produce should favor organic over conventional, if possible. Here too, the EWG provides an important resource to consumers in the form of shopper guides regarding pesticides in produce.
Per- and polyfluoroalkyl substances (PFAS)
PFAS are a group of fluorinated compounds discovered in the 1930s. Their chemical composition includes a durable carbon-fluoride bond, giving them a persistence within the environment that has led to their being referred to as “forever chemicals.”
PFAS have been detected in the blood of 98% of Americans, and in the rainwater of locations as far afield as Tibet and Antarctica. Even low levels of exposure have been associated with an increased risk for cancer, liver disease, low birth weight, and hormonal disruption.
The properties of PFAS also make them both durable at very high heat and water repellent. Notoriously, the chemical was used by 3M to make Scotchgard for carpets and fabrics and by Dupont to make Teflon for nonstick coating of pots and pans. Although perfluorooctanoic acid (PFOA) was removed from nonstick cookware in 2013, PFAS – a family of thousands of synthetic compounds – remain common in fast-food packaging, water- and stain-repellent clothing, firefighting foam, and personal care products. PFAS are released into the environment during the breakdown of these consumer and industrial products, as well as from dumping from waste facilities.
Alarmingly, the EWG notes that up to 200 million Americans may be exposed to PFAS in their drinking water. In March 2021, the EPA announced that they will be regulating PFAS in drinking water; however, the regulations have not been finalized. Currently, it is up to individual states to test for its presence in the water. The EWG has compiled a map of all known PFAS contamination sites.
To avoid or prevent exposures from PFAS, recommendations include filtering tap water with either reverse osmosis or activated carbon filters, as well as avoiding fast food and carry-out food, if possible, and consumer products labeled as “water resistant,” “stain-resistant,” and “nonstick.”
In a testament to how harmful these chemicals are, the EPA recently revised their lifetime health advisories for PFAS, such as PFOA, to 0.004 parts per trillion, which is more than 10,000 times smaller than the previous limit of 70 parts per trillion. The EPA also has proposed formally designating certain PFAS chemicals as “hazardous substances.”
Dr. Goel, clinical assistant professor of medicine at Weill Cornell Medicine, New York, has disclosed no relevant financial relationships. A version of this article originally appeared on Medscape.com.
Physicians and clinicians should be required to get flu shots: Ethicist
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at New York University’s Grossman School of Medicine, where I’m the director.
I’ve long believed that every health care institution – nursing homes, hospitals, clinics, home care, hospice – should require flu shots for all doctors and all nurses because it is the easiest, cheapest, and most ethical way to protect the workforce, who you need to be in there when flu outbreaks take place, and to protect patients against getting the flu when they come into hospital settings and get exposed to health care workers who may have the flu already but don’t know it.
In a recent poll, I was happy to see that the majority of physicians surveyed agreed with me: 65% said they supported mandatory flu vaccination in hospitals and only 23% said they did not. I think flu vaccination is something that has already been shown to be useful and important, not only in stopping people from getting the flu but also in making sure that they don’t get as sick when they get the flu.
Just like COVID-19 vaccination, it doesn’t always prevent somebody from getting infected, but if you get it, it keeps you from winding up sick at home, or worse – from dying and winding up in the morgue. Flu kills many, many people every year. We don’t want that to happen. A flu vaccine will really help prevent deaths, help prevent the number of symptoms that somebody gets, and will get people back to work. The benefits are pretty clear.
Does the flu vaccine work equally well every year? It does not. Some years, the strains that are picked for the vaccine don’t match the ones that circulate, and we don’t get as much protection as we hoped for. I think the safety side is so strong that it’s worth making the investment and the effort to promote mandatory flu vaccination.
Can you opt out on religious grounds? Well, some hospitals permit that at New York University. You have to go before a committee and make a case that your exemption on religious grounds is based on an authentic set of beliefs that are deeply held, and not just something you thought up the day before flu vaccine requirements went into effect.
There may be room for some exemptions – obviously, for health reasons. If people think that the flu vaccine is dangerous to them and can get a physician to agree and sign off that they are not appropriate to vaccinate, okay.
On the other hand, if you’re working with an especially vulnerable population – newborns, people who are immunosuppressed – then I think you’ve got to be vaccinated and you shouldn’t be working around people who are at huge risk of getting the flu if you refuse to be vaccinated or, for that matter, can’t be vaccinated.
Would I extend these mandates? Yes, I would. I’d extend them to COVID-19 vaccination and to measles vaccination. I think physicians and nurses should be good role models. They should get vaccinated. We know that the best available evidence says that vaccination for infectious disease is safe. It is really the best thing we can do to combat a variety of diseases such as the flu and COVID-19.
It seems to me that, in addition, the data that are out there in terms of risks from flu and COVID-19 – deaths in places like nursing homes – are overwhelming about the importance of trying to get staff vaccinated so they don’t bring flu into an institutionalized population. This is similar for prison health and many other settings where people are kept close together and staff may move from place to place, rotating from institution to institution, spreading infectious disease.
I’m going to go with the poll. Let’s keep pushing for health care workers to do the right thing and to be good role models. Let’s get everybody a flu vaccination. Let’s extend it to a COVID-19 vaccination and its boosters.
Let’s try to show the nation that health care is going to be guided by good science, a duty to one’s own health, and a duty to one’s patients. It shouldn’t be political. It should be based on what works best for the interests of health care providers and those they care for.
I’m Art Caplan at the New York University Grossman School of Medicine. Thanks for watching.
Dr. Caplan has disclosed the following relevant financial relationships: Served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position). Serves as a contributing author and advisor for Medscape. A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at New York University’s Grossman School of Medicine, where I’m the director.
I’ve long believed that every health care institution – nursing homes, hospitals, clinics, home care, hospice – should require flu shots for all doctors and all nurses because it is the easiest, cheapest, and most ethical way to protect the workforce, who you need to be in there when flu outbreaks take place, and to protect patients against getting the flu when they come into hospital settings and get exposed to health care workers who may have the flu already but don’t know it.
In a recent poll, I was happy to see that the majority of physicians surveyed agreed with me: 65% said they supported mandatory flu vaccination in hospitals and only 23% said they did not. I think flu vaccination is something that has already been shown to be useful and important, not only in stopping people from getting the flu but also in making sure that they don’t get as sick when they get the flu.
Just like COVID-19 vaccination, it doesn’t always prevent somebody from getting infected, but if you get it, it keeps you from winding up sick at home, or worse – from dying and winding up in the morgue. Flu kills many, many people every year. We don’t want that to happen. A flu vaccine will really help prevent deaths, help prevent the number of symptoms that somebody gets, and will get people back to work. The benefits are pretty clear.
Does the flu vaccine work equally well every year? It does not. Some years, the strains that are picked for the vaccine don’t match the ones that circulate, and we don’t get as much protection as we hoped for. I think the safety side is so strong that it’s worth making the investment and the effort to promote mandatory flu vaccination.
Can you opt out on religious grounds? Well, some hospitals permit that at New York University. You have to go before a committee and make a case that your exemption on religious grounds is based on an authentic set of beliefs that are deeply held, and not just something you thought up the day before flu vaccine requirements went into effect.
There may be room for some exemptions – obviously, for health reasons. If people think that the flu vaccine is dangerous to them and can get a physician to agree and sign off that they are not appropriate to vaccinate, okay.
On the other hand, if you’re working with an especially vulnerable population – newborns, people who are immunosuppressed – then I think you’ve got to be vaccinated and you shouldn’t be working around people who are at huge risk of getting the flu if you refuse to be vaccinated or, for that matter, can’t be vaccinated.
Would I extend these mandates? Yes, I would. I’d extend them to COVID-19 vaccination and to measles vaccination. I think physicians and nurses should be good role models. They should get vaccinated. We know that the best available evidence says that vaccination for infectious disease is safe. It is really the best thing we can do to combat a variety of diseases such as the flu and COVID-19.
It seems to me that, in addition, the data that are out there in terms of risks from flu and COVID-19 – deaths in places like nursing homes – are overwhelming about the importance of trying to get staff vaccinated so they don’t bring flu into an institutionalized population. This is similar for prison health and many other settings where people are kept close together and staff may move from place to place, rotating from institution to institution, spreading infectious disease.
I’m going to go with the poll. Let’s keep pushing for health care workers to do the right thing and to be good role models. Let’s get everybody a flu vaccination. Let’s extend it to a COVID-19 vaccination and its boosters.
Let’s try to show the nation that health care is going to be guided by good science, a duty to one’s own health, and a duty to one’s patients. It shouldn’t be political. It should be based on what works best for the interests of health care providers and those they care for.
I’m Art Caplan at the New York University Grossman School of Medicine. Thanks for watching.
Dr. Caplan has disclosed the following relevant financial relationships: Served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position). Serves as a contributing author and advisor for Medscape. A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
Hi. I’m Art Caplan. I’m at the Division of Medical Ethics at New York University’s Grossman School of Medicine, where I’m the director.
I’ve long believed that every health care institution – nursing homes, hospitals, clinics, home care, hospice – should require flu shots for all doctors and all nurses because it is the easiest, cheapest, and most ethical way to protect the workforce, who you need to be in there when flu outbreaks take place, and to protect patients against getting the flu when they come into hospital settings and get exposed to health care workers who may have the flu already but don’t know it.
In a recent poll, I was happy to see that the majority of physicians surveyed agreed with me: 65% said they supported mandatory flu vaccination in hospitals and only 23% said they did not. I think flu vaccination is something that has already been shown to be useful and important, not only in stopping people from getting the flu but also in making sure that they don’t get as sick when they get the flu.
Just like COVID-19 vaccination, it doesn’t always prevent somebody from getting infected, but if you get it, it keeps you from winding up sick at home, or worse – from dying and winding up in the morgue. Flu kills many, many people every year. We don’t want that to happen. A flu vaccine will really help prevent deaths, help prevent the number of symptoms that somebody gets, and will get people back to work. The benefits are pretty clear.
Does the flu vaccine work equally well every year? It does not. Some years, the strains that are picked for the vaccine don’t match the ones that circulate, and we don’t get as much protection as we hoped for. I think the safety side is so strong that it’s worth making the investment and the effort to promote mandatory flu vaccination.
Can you opt out on religious grounds? Well, some hospitals permit that at New York University. You have to go before a committee and make a case that your exemption on religious grounds is based on an authentic set of beliefs that are deeply held, and not just something you thought up the day before flu vaccine requirements went into effect.
There may be room for some exemptions – obviously, for health reasons. If people think that the flu vaccine is dangerous to them and can get a physician to agree and sign off that they are not appropriate to vaccinate, okay.
On the other hand, if you’re working with an especially vulnerable population – newborns, people who are immunosuppressed – then I think you’ve got to be vaccinated and you shouldn’t be working around people who are at huge risk of getting the flu if you refuse to be vaccinated or, for that matter, can’t be vaccinated.
Would I extend these mandates? Yes, I would. I’d extend them to COVID-19 vaccination and to measles vaccination. I think physicians and nurses should be good role models. They should get vaccinated. We know that the best available evidence says that vaccination for infectious disease is safe. It is really the best thing we can do to combat a variety of diseases such as the flu and COVID-19.
It seems to me that, in addition, the data that are out there in terms of risks from flu and COVID-19 – deaths in places like nursing homes – are overwhelming about the importance of trying to get staff vaccinated so they don’t bring flu into an institutionalized population. This is similar for prison health and many other settings where people are kept close together and staff may move from place to place, rotating from institution to institution, spreading infectious disease.
I’m going to go with the poll. Let’s keep pushing for health care workers to do the right thing and to be good role models. Let’s get everybody a flu vaccination. Let’s extend it to a COVID-19 vaccination and its boosters.
Let’s try to show the nation that health care is going to be guided by good science, a duty to one’s own health, and a duty to one’s patients. It shouldn’t be political. It should be based on what works best for the interests of health care providers and those they care for.
I’m Art Caplan at the New York University Grossman School of Medicine. Thanks for watching.
Dr. Caplan has disclosed the following relevant financial relationships: Served as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position). Serves as a contributing author and advisor for Medscape. A version of this article originally appeared on Medscape.com.
Concussion burden tied to later hypertension in football players
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
a new study suggests.
Among more than 4,000 participants, 37% had hypertension at a median of 24 years post career and reported a median concussion symptom score (CSS) of 23 on a scale of 0 to 130.
“We have long seen an incompletely explained link between football participation and later-life cardiovascular disease,” Aaron L. Baggish, MD, of Massachusetts Hospital and Harvard Medical School, Boston, told this news organization.
“This study tested [whether] concussion burden during years of active play would be a determinant of later-life hypertension, the most common cause of cardiovascular disease, and indeed found this relationship to be a strong one.”
The study was published online in Circulation.
Link to cognitive decline?
Dr. Baggish and colleagues recruited former professional American-style football (ASF) players to participate in a survey administered by the Football Players Health Study at Harvard University.
Concussion burden was quantified with respect to the occurrence and severity of common concussion symptoms – e.g., headaches, nausea, dizziness, confusion, loss of consciousness (LOC), disorientation, and feeling unsteady on one’s feet – over years of active participation.
Prevalent hypertension was determined either by the participants’ previously receiving from a clinician a recommendation for medication for “high blood pressure” or by the participants’ taking such medication at the time of survey completion. Diabetes status was determined by the participants’ receiving a prior recommendation for or prescription for “diabetes or high blood sugar” medication.
Of 15,070 invited to participate in the study, 4,168 did so. The mean age of the participants was 51.8 years; 39.4% were Black; the mean body mass index was 31.3; and 33.9% were linemen. Participants played for a mean of 6.9 seasons and were surveyed at a median 24.1 years post ASF career completion. The median CSS was 23.
A total of 1,542 participants (37.3%) had hypertension, and 8.8% had diabetes.
After adjustment for established hypertension risk factors, including smoking, race, diabetes, age, and BMI, there was a graded association between CSS category and odds of later-life hypertension and between high CSS exposure and prevalent hypertension.
Results persisted when LOC, a single highly specific severe concussion symptom, was used in isolation as a surrogate for CSS, the investigators noted.
“These results suggest that repetitive early-life brain injury may have later-life implications for cardiovascular health,” they wrote. They also noted that hypertension has been shown to independently increase the risk of cognitive decline.
While premature cognitive decline among ASF players is generally attributed to chronic traumatic encephalopathy, “data from the current study raise the possibility that some element of cognitive decline among former ASF players may be attributable to hypertension,” which is potentially treatable.
“Future studies clarifying associations and causal pathways between brain injury, hypertension, and brain health are warranted,” they concluded.
Dr. Baggish added, “We hope that clinicians will now understand that head injury is an independent risk factor for high blood pressure and will screen vulnerable populations accordingly, as this may lead to better recognition of previously underdiagnosed hypertension with subsequent opportunities for intervention.”
Close monitoring
Commenting on the study, Jonathan Kim, MD, chair-elect of the American College of Cardiology’s Sports–Cardiology Section and chief of sports cardiology at Emory University in Atlanta, said, “They clearly show an independent association, which is not causality but is a new finding that requires more research. To me, it really emphasizes that cardiovascular risk is the most important health consequence that we should be worried about in retired NFL [National Football League] players.
“There are multifactorial reasons – not just repetitive head trauma – why this athletic population is at risk for the development of high blood pressure, even among college players,” he said.
Dr. Kim’s team has shown in studies conducted in collaboration with Dr. Baggish and others that collegiate football players who gain weight and develop increased systolic blood pressure are at risk of developing a “pathologic” cardiovascular phenotype.
Other research from this group showed links between nonsteroidal anti-inflammatory drug use among high school and collegiate ASF players and increased cardiovascular risk, as well as ASF-associated hypertension and ventricular-arterial coupling.
The suggestion that late-life hypertension could play a role in premature cognitive decline among ASF players “warrants further study,” Dr. Kim said, “because we do know that hypertension in the general population can be associated with cognitive decline. So that’s an important future direction.”
He concluded: “It’s a matter of focusing on cardiac prevention.” After their careers, players should be counseled on the importance of losing weight and adopting heart-healthy habits. In addition to some of the traditional concerns that might lead to closer follow-up of these patients, “having a lot of concussions in the history could potentially be another risk factor that should warrant close monitoring of blood pressure and, of course, treatment if necessary.”
The study was supported by Harvard Catalyst/the Harvard Clinical and Translational Science Center and the NFL Players Association. Dr. Baggish and several coauthors have received funding from the NFL Players Association.
A version of this article originally appeared on Medscape.com.
FROM CIRCULATION