User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
T-DXd active in many solid tumors; ‘shift in thinking’
CHICAGO – Trastuzumab deruxtecan (T-DXd) (Enhertu) already has proven efficacy against HER2-expressing metastatic breast, gastroesophageal, and lung cancers.
including malignancies of the cervix, endometrium, ovaries, bladder, and other sites.
The findings come from the ongoing DESTINY-PanTumor02 trial. Among 267 patients with solid tumors at various organ sites, the investigator-assessed objective response rate among all patients was 37.1%, and ranged from as high as 57.5% for patients with endometrial cancers to as low as 4% for patients with pancreatic cancer, reported Funda Meric-Bernstam, MD, from the University of Texas MD Anderson Cancer Center, Houston.
For patients with tumors that had HER2 immunohistochemistry (IHC) scores of 3+, the highest level of HER2 expression, the overall response rate was 61.3%..
The responses were also durable, with a median duration of 11.8 months among all patients and 22.1 months among patients with IHC 3+ scores.
“Our data to date showed that T-DXd had clinically meaningful activity across a variety of tumor types,” she said in a briefing held prior to her presentation of the data at the annual meeting of the American Society of Clinical Oncology.
“HER2 expression has been around a long time. We think about this all the time in breast cancer and drugs are approved there, but HER2 is expressed in other tumors as well, and that really represents an unmet need, because we have limited options in this situation” commented ASCO expert Bradley Alexander McGregor, MD, from the Dana-Farber Cancer Institute, Boston, an invited discussant at the briefing.
“Aside from pancreatic cancer we saw really, really encouraging results with no new safety signals, so while early I think this really exciting and represents a shift in how we think about cancer care,” he added.
After the presentation, invited discussant Kohei Shitara, MD, of National Cancer Center Hospital East, Kashiwa, Japan, said that he agrees with authors that T-DXd is a potential new treatment option for patients with HER2-expressing solid tumors, and that the evidence suggests the potential for further tumor-agnostic development of the agent.
He cautioned, however, that there is a lack of concordance between local and central assessment of HER2 IHC, and that quality assurance will be required to ensure that the HER2 status of solid tumors is accurately characterized.
At a press briefing, Dr. Meric-Bernstam was asked how she envisioned using T-DXd in therapy for various HER2-expressing tumors.
“I think the activity we’ve seen is quite compelling, and one hopes that eventually this will be a drug that’s accessible for patients that are HER2-expressing across tumor types. Clearly, the activity is very compelling in some of the diseases to think about doing studies for earlier lines,” she said.
“The data indicate that there is tumor-agnostic activity across the board,” she said, but noted that tumors with epithelial components such as ovarian and breast cancers appear to have the highest responses to T-DXd therapy.
Briefing moderator Julie R. Gralow, MD, chief medical officer and executive vice president of ASCO, asked Dr. McGregor whether, in the light of this new data, oncologists should test more patients for HER2 expression.
“We have some cancers where we know HER2 expression is there. I think the good thing about HER2 testing is that it’s an IHC test, so this is something that can be easily done in local pathology [labs],” he said. As more evidence mounts of potential benefit of T-DXd in HER2 expressing tumors, clinicians will need to consider more routine HER2 testing.
A rendezvous with DESTINY
The DESTINY-PanTumor02 trial is a phase 2, open-label, multicenter study looking at T-DXd in patients with advanced solid tumors who are not eligible for therapy with curative intent.
All patients had disease progression after at least two prior lines of therapy, and had tumors with HER2 expression of IHC 3+ or 2+ either by local or central testing. Patients were allowed to have previously received HER2-targeting therapy. Patients also had to have good performance status (Eastern Cooperative Oncology Group/World Health Organization performance status 0 or 1).
The investigators planned to enroll 40 patients in each cohort, including patients with cervical, endometrial, ovarian, biliary tract, pancreatic, or bladder cancers, as well those with other tumors expressing HER2 who were not included in the other cohorts.
Under the protocol, cohorts in which none of the first 15 patients had objective responses would be closed, as happened with the pancreatic cancer cohort.
At a median follow-up of 9.7 months, an objective response was seen in 99 patients out of the 267 in the entire study population (ORR, 37.1%). This ORR consisted of 15 complete responses and 84 partial responses. An additional 123 patients had stable disease.
An analysis of ORR by HER2 expression showed that IHC 3+ expressing tumors had rates ranging from 84.6% in endometrial cancers, 75% in cervical cancer, 63.6% in ovarian cancers, and 56.3% in bladder cancers, down to zero in IHC 3+ expressing pancreatic cancer.
The T-DXd safety profile was consistent with that seen in other clinical trials, with most common adverse events being nausea, fatigue, neutropenia, anemia, diarrhea, and thrombocytopenia. There were 20 cases of interstitial lung disease, one of which was fatal.
The trial is ongoing, and investigators plan to report overall survival and progression-free survival results with additional follow-up.
DESTINY-PanTumor02 is funded by Daiichi Sankyo. Dr. Meric-Bernstam disclosed a consulting/advisory role with multiple pharmaceutical companies, research funding to her institution from Daiichi Sankyo and others, and travel expenses from ESMO and EORTC. Dr. McGregor disclosed a consulting/advisory role and institutional research funding with multiple companies, not including the study’s funder. Dr. Gralow disclosed a consulting or advisory role with Genentech and Roche.
A version of this article first appeared on Medscape.com.
CHICAGO – Trastuzumab deruxtecan (T-DXd) (Enhertu) already has proven efficacy against HER2-expressing metastatic breast, gastroesophageal, and lung cancers.
including malignancies of the cervix, endometrium, ovaries, bladder, and other sites.
The findings come from the ongoing DESTINY-PanTumor02 trial. Among 267 patients with solid tumors at various organ sites, the investigator-assessed objective response rate among all patients was 37.1%, and ranged from as high as 57.5% for patients with endometrial cancers to as low as 4% for patients with pancreatic cancer, reported Funda Meric-Bernstam, MD, from the University of Texas MD Anderson Cancer Center, Houston.
For patients with tumors that had HER2 immunohistochemistry (IHC) scores of 3+, the highest level of HER2 expression, the overall response rate was 61.3%..
The responses were also durable, with a median duration of 11.8 months among all patients and 22.1 months among patients with IHC 3+ scores.
“Our data to date showed that T-DXd had clinically meaningful activity across a variety of tumor types,” she said in a briefing held prior to her presentation of the data at the annual meeting of the American Society of Clinical Oncology.
“HER2 expression has been around a long time. We think about this all the time in breast cancer and drugs are approved there, but HER2 is expressed in other tumors as well, and that really represents an unmet need, because we have limited options in this situation” commented ASCO expert Bradley Alexander McGregor, MD, from the Dana-Farber Cancer Institute, Boston, an invited discussant at the briefing.
“Aside from pancreatic cancer we saw really, really encouraging results with no new safety signals, so while early I think this really exciting and represents a shift in how we think about cancer care,” he added.
After the presentation, invited discussant Kohei Shitara, MD, of National Cancer Center Hospital East, Kashiwa, Japan, said that he agrees with authors that T-DXd is a potential new treatment option for patients with HER2-expressing solid tumors, and that the evidence suggests the potential for further tumor-agnostic development of the agent.
He cautioned, however, that there is a lack of concordance between local and central assessment of HER2 IHC, and that quality assurance will be required to ensure that the HER2 status of solid tumors is accurately characterized.
At a press briefing, Dr. Meric-Bernstam was asked how she envisioned using T-DXd in therapy for various HER2-expressing tumors.
“I think the activity we’ve seen is quite compelling, and one hopes that eventually this will be a drug that’s accessible for patients that are HER2-expressing across tumor types. Clearly, the activity is very compelling in some of the diseases to think about doing studies for earlier lines,” she said.
“The data indicate that there is tumor-agnostic activity across the board,” she said, but noted that tumors with epithelial components such as ovarian and breast cancers appear to have the highest responses to T-DXd therapy.
Briefing moderator Julie R. Gralow, MD, chief medical officer and executive vice president of ASCO, asked Dr. McGregor whether, in the light of this new data, oncologists should test more patients for HER2 expression.
“We have some cancers where we know HER2 expression is there. I think the good thing about HER2 testing is that it’s an IHC test, so this is something that can be easily done in local pathology [labs],” he said. As more evidence mounts of potential benefit of T-DXd in HER2 expressing tumors, clinicians will need to consider more routine HER2 testing.
A rendezvous with DESTINY
The DESTINY-PanTumor02 trial is a phase 2, open-label, multicenter study looking at T-DXd in patients with advanced solid tumors who are not eligible for therapy with curative intent.
All patients had disease progression after at least two prior lines of therapy, and had tumors with HER2 expression of IHC 3+ or 2+ either by local or central testing. Patients were allowed to have previously received HER2-targeting therapy. Patients also had to have good performance status (Eastern Cooperative Oncology Group/World Health Organization performance status 0 or 1).
The investigators planned to enroll 40 patients in each cohort, including patients with cervical, endometrial, ovarian, biliary tract, pancreatic, or bladder cancers, as well those with other tumors expressing HER2 who were not included in the other cohorts.
Under the protocol, cohorts in which none of the first 15 patients had objective responses would be closed, as happened with the pancreatic cancer cohort.
At a median follow-up of 9.7 months, an objective response was seen in 99 patients out of the 267 in the entire study population (ORR, 37.1%). This ORR consisted of 15 complete responses and 84 partial responses. An additional 123 patients had stable disease.
An analysis of ORR by HER2 expression showed that IHC 3+ expressing tumors had rates ranging from 84.6% in endometrial cancers, 75% in cervical cancer, 63.6% in ovarian cancers, and 56.3% in bladder cancers, down to zero in IHC 3+ expressing pancreatic cancer.
The T-DXd safety profile was consistent with that seen in other clinical trials, with most common adverse events being nausea, fatigue, neutropenia, anemia, diarrhea, and thrombocytopenia. There were 20 cases of interstitial lung disease, one of which was fatal.
The trial is ongoing, and investigators plan to report overall survival and progression-free survival results with additional follow-up.
DESTINY-PanTumor02 is funded by Daiichi Sankyo. Dr. Meric-Bernstam disclosed a consulting/advisory role with multiple pharmaceutical companies, research funding to her institution from Daiichi Sankyo and others, and travel expenses from ESMO and EORTC. Dr. McGregor disclosed a consulting/advisory role and institutional research funding with multiple companies, not including the study’s funder. Dr. Gralow disclosed a consulting or advisory role with Genentech and Roche.
A version of this article first appeared on Medscape.com.
CHICAGO – Trastuzumab deruxtecan (T-DXd) (Enhertu) already has proven efficacy against HER2-expressing metastatic breast, gastroesophageal, and lung cancers.
including malignancies of the cervix, endometrium, ovaries, bladder, and other sites.
The findings come from the ongoing DESTINY-PanTumor02 trial. Among 267 patients with solid tumors at various organ sites, the investigator-assessed objective response rate among all patients was 37.1%, and ranged from as high as 57.5% for patients with endometrial cancers to as low as 4% for patients with pancreatic cancer, reported Funda Meric-Bernstam, MD, from the University of Texas MD Anderson Cancer Center, Houston.
For patients with tumors that had HER2 immunohistochemistry (IHC) scores of 3+, the highest level of HER2 expression, the overall response rate was 61.3%..
The responses were also durable, with a median duration of 11.8 months among all patients and 22.1 months among patients with IHC 3+ scores.
“Our data to date showed that T-DXd had clinically meaningful activity across a variety of tumor types,” she said in a briefing held prior to her presentation of the data at the annual meeting of the American Society of Clinical Oncology.
“HER2 expression has been around a long time. We think about this all the time in breast cancer and drugs are approved there, but HER2 is expressed in other tumors as well, and that really represents an unmet need, because we have limited options in this situation” commented ASCO expert Bradley Alexander McGregor, MD, from the Dana-Farber Cancer Institute, Boston, an invited discussant at the briefing.
“Aside from pancreatic cancer we saw really, really encouraging results with no new safety signals, so while early I think this really exciting and represents a shift in how we think about cancer care,” he added.
After the presentation, invited discussant Kohei Shitara, MD, of National Cancer Center Hospital East, Kashiwa, Japan, said that he agrees with authors that T-DXd is a potential new treatment option for patients with HER2-expressing solid tumors, and that the evidence suggests the potential for further tumor-agnostic development of the agent.
He cautioned, however, that there is a lack of concordance between local and central assessment of HER2 IHC, and that quality assurance will be required to ensure that the HER2 status of solid tumors is accurately characterized.
At a press briefing, Dr. Meric-Bernstam was asked how she envisioned using T-DXd in therapy for various HER2-expressing tumors.
“I think the activity we’ve seen is quite compelling, and one hopes that eventually this will be a drug that’s accessible for patients that are HER2-expressing across tumor types. Clearly, the activity is very compelling in some of the diseases to think about doing studies for earlier lines,” she said.
“The data indicate that there is tumor-agnostic activity across the board,” she said, but noted that tumors with epithelial components such as ovarian and breast cancers appear to have the highest responses to T-DXd therapy.
Briefing moderator Julie R. Gralow, MD, chief medical officer and executive vice president of ASCO, asked Dr. McGregor whether, in the light of this new data, oncologists should test more patients for HER2 expression.
“We have some cancers where we know HER2 expression is there. I think the good thing about HER2 testing is that it’s an IHC test, so this is something that can be easily done in local pathology [labs],” he said. As more evidence mounts of potential benefit of T-DXd in HER2 expressing tumors, clinicians will need to consider more routine HER2 testing.
A rendezvous with DESTINY
The DESTINY-PanTumor02 trial is a phase 2, open-label, multicenter study looking at T-DXd in patients with advanced solid tumors who are not eligible for therapy with curative intent.
All patients had disease progression after at least two prior lines of therapy, and had tumors with HER2 expression of IHC 3+ or 2+ either by local or central testing. Patients were allowed to have previously received HER2-targeting therapy. Patients also had to have good performance status (Eastern Cooperative Oncology Group/World Health Organization performance status 0 or 1).
The investigators planned to enroll 40 patients in each cohort, including patients with cervical, endometrial, ovarian, biliary tract, pancreatic, or bladder cancers, as well those with other tumors expressing HER2 who were not included in the other cohorts.
Under the protocol, cohorts in which none of the first 15 patients had objective responses would be closed, as happened with the pancreatic cancer cohort.
At a median follow-up of 9.7 months, an objective response was seen in 99 patients out of the 267 in the entire study population (ORR, 37.1%). This ORR consisted of 15 complete responses and 84 partial responses. An additional 123 patients had stable disease.
An analysis of ORR by HER2 expression showed that IHC 3+ expressing tumors had rates ranging from 84.6% in endometrial cancers, 75% in cervical cancer, 63.6% in ovarian cancers, and 56.3% in bladder cancers, down to zero in IHC 3+ expressing pancreatic cancer.
The T-DXd safety profile was consistent with that seen in other clinical trials, with most common adverse events being nausea, fatigue, neutropenia, anemia, diarrhea, and thrombocytopenia. There were 20 cases of interstitial lung disease, one of which was fatal.
The trial is ongoing, and investigators plan to report overall survival and progression-free survival results with additional follow-up.
DESTINY-PanTumor02 is funded by Daiichi Sankyo. Dr. Meric-Bernstam disclosed a consulting/advisory role with multiple pharmaceutical companies, research funding to her institution from Daiichi Sankyo and others, and travel expenses from ESMO and EORTC. Dr. McGregor disclosed a consulting/advisory role and institutional research funding with multiple companies, not including the study’s funder. Dr. Gralow disclosed a consulting or advisory role with Genentech and Roche.
A version of this article first appeared on Medscape.com.
AT ASCO 2023
Does ‘skeletal age’ describe fracture impact on mortality?
Thach Tran, MD, and colleagues introduced the concept of “skeletal age” in a recently published paper that aims to incorporate the impact of fragility, or low trauma, fractures – which can occur in patients with osteoporosis – on mortality risk.
They defined “skeletal age” as the age of the skeleton following a fragility fracture. This is calculated as the chronological age of the individual plus the number of years of “life lost” as a consequence of the specific fracture.
The risk for premature death following fragility fractures is concerning, with 22%-58% of patients with hip fracture dying within a year (Brauer et al.; Rapp et al.). Thus, it’s important to treat osteoporosis in a timely fashion to reduce the risk for such fractures and the excess mortality risk associated with them.
Implementation and uptake of such treatment, however, either before or after a fragility fracture, is far from optimal (Solomon et al). This may be because patients don’t fully understand the consequence of such a fracture, and outcomes measures currently in use (such as relative risk or hazard of mortality) are difficult to communicate to patients.
In the recent paper by Dr. Tran and colleagues, the authors examined the association between fractures and mortality based on sex, age, associated comorbidities, and fracture site. They pooled this information to create a “skeletal age” for each fracture site, using data from the Danish National Hospital Discharge Registry, which documents fractures and related mortality for all Danish people.
They examined mortality over a period of at least 2 years following a fragility fracture in individuals aged 50 or older, and reported that occurrence of any fragility fracture is associated with a 30%-45% increased risk for death, with the highest risk noted for hip and femur fractures (twofold increase). Fractures of the pelvis, vertebrae, humerus, ribs, clavicle, and lower leg were also associated with increased mortality risk, but no increase was seen with fractures of the forearm, knee, ankle, hand, or foot.
The number of years of life lost at any age depending on the fracture site is represented as a linear graph of skeletal age for any chronological age, for specific fracture sites, separated by sex.
For example, the skeletal age of a 50-year-old man who has a hip fracture is 57 years (7 years of life lost as a consequence of the fracture), while that for a 70-year-old man with the same fracture is 75 years (5 years of life lost because of the fracture). Similarly, the skeletal age of a 50-year-old man with a fracture of the pelvis, femur, vertebrae, and humerus is 55 years (5 years of life lost). Fractures of the lower leg, humerus, and clavicle lead to fewer lost years of life.
The authors are to be commended for creating a simple strategy to quantify mortality risk following low-impact or fragility fractures in older individuals; this could enable providers to communicate the importance of osteoporosis treatment more effectively to patients on the basis of their skeletal age, and for patients to better understand this information.
The study design appears reasonably robust as the authors considered many factors that might affect mortality risk, such as sex, age, and comorbidities, and the results are based on information from a very large number of people – 1.6 million.
However, there’s a major issue with the concept of “skeletal age” as proposed by Dr. Tran and colleagues. The term is already in use and defines the maturity of bones in children and adolescents, also called “bone age” (Greulich and Pyle 1959; Skeletal Age, Radiology Key). This is a real oversight and could cause confusion in interpreting “skeletal age.”
Skeletal age as currently defined in children and adolescents is influenced by chronological age, exposure to certain hormones, nutritional deficiencies, and systemic diseases, and is a predictor of adult height based on the skeletal age and current height. This concept is completely different from that being proposed by the authors in this paper. Dr. Tran and colleagues (and the reviewers of this paper) are probably not familiar with the use of the terminology in youth, which is a major oversight; they should consider changing the terminology given this overlap.
Further, fragility fractures can occur from osteoporosis at any age, and this study doesn’t provide information regarding years of life lost from occurrence of fragility fractures at younger ages, or the age at which mortality risk starts to increase (as the study was performed only in those aged 50 or older).
While the study takes into account general comorbidities in developing the model to define years of life lost, it doesn’t account for other factors that can influence fracture risk, such as lifestyle factors, activity level, and genetic risk (family history of osteoporosis, for example). Of note, the impact of additional fractures isn’t considered either and should be factored into future investigations.
Overall, the study is robust and important and provides valuable information regarding mortality risk from a fragility fracture in older people. However, there are some flaws that need to be considered and addressed, the most serious of which is that the term “skeletal age” has been in existence for decades, applied to a much younger age group, and its implications are completely different from those being proposed by the authors here.
A version of this article first appeared on Medscape.com.
Thach Tran, MD, and colleagues introduced the concept of “skeletal age” in a recently published paper that aims to incorporate the impact of fragility, or low trauma, fractures – which can occur in patients with osteoporosis – on mortality risk.
They defined “skeletal age” as the age of the skeleton following a fragility fracture. This is calculated as the chronological age of the individual plus the number of years of “life lost” as a consequence of the specific fracture.
The risk for premature death following fragility fractures is concerning, with 22%-58% of patients with hip fracture dying within a year (Brauer et al.; Rapp et al.). Thus, it’s important to treat osteoporosis in a timely fashion to reduce the risk for such fractures and the excess mortality risk associated with them.
Implementation and uptake of such treatment, however, either before or after a fragility fracture, is far from optimal (Solomon et al). This may be because patients don’t fully understand the consequence of such a fracture, and outcomes measures currently in use (such as relative risk or hazard of mortality) are difficult to communicate to patients.
In the recent paper by Dr. Tran and colleagues, the authors examined the association between fractures and mortality based on sex, age, associated comorbidities, and fracture site. They pooled this information to create a “skeletal age” for each fracture site, using data from the Danish National Hospital Discharge Registry, which documents fractures and related mortality for all Danish people.
They examined mortality over a period of at least 2 years following a fragility fracture in individuals aged 50 or older, and reported that occurrence of any fragility fracture is associated with a 30%-45% increased risk for death, with the highest risk noted for hip and femur fractures (twofold increase). Fractures of the pelvis, vertebrae, humerus, ribs, clavicle, and lower leg were also associated with increased mortality risk, but no increase was seen with fractures of the forearm, knee, ankle, hand, or foot.
The number of years of life lost at any age depending on the fracture site is represented as a linear graph of skeletal age for any chronological age, for specific fracture sites, separated by sex.
For example, the skeletal age of a 50-year-old man who has a hip fracture is 57 years (7 years of life lost as a consequence of the fracture), while that for a 70-year-old man with the same fracture is 75 years (5 years of life lost because of the fracture). Similarly, the skeletal age of a 50-year-old man with a fracture of the pelvis, femur, vertebrae, and humerus is 55 years (5 years of life lost). Fractures of the lower leg, humerus, and clavicle lead to fewer lost years of life.
The authors are to be commended for creating a simple strategy to quantify mortality risk following low-impact or fragility fractures in older individuals; this could enable providers to communicate the importance of osteoporosis treatment more effectively to patients on the basis of their skeletal age, and for patients to better understand this information.
The study design appears reasonably robust as the authors considered many factors that might affect mortality risk, such as sex, age, and comorbidities, and the results are based on information from a very large number of people – 1.6 million.
However, there’s a major issue with the concept of “skeletal age” as proposed by Dr. Tran and colleagues. The term is already in use and defines the maturity of bones in children and adolescents, also called “bone age” (Greulich and Pyle 1959; Skeletal Age, Radiology Key). This is a real oversight and could cause confusion in interpreting “skeletal age.”
Skeletal age as currently defined in children and adolescents is influenced by chronological age, exposure to certain hormones, nutritional deficiencies, and systemic diseases, and is a predictor of adult height based on the skeletal age and current height. This concept is completely different from that being proposed by the authors in this paper. Dr. Tran and colleagues (and the reviewers of this paper) are probably not familiar with the use of the terminology in youth, which is a major oversight; they should consider changing the terminology given this overlap.
Further, fragility fractures can occur from osteoporosis at any age, and this study doesn’t provide information regarding years of life lost from occurrence of fragility fractures at younger ages, or the age at which mortality risk starts to increase (as the study was performed only in those aged 50 or older).
While the study takes into account general comorbidities in developing the model to define years of life lost, it doesn’t account for other factors that can influence fracture risk, such as lifestyle factors, activity level, and genetic risk (family history of osteoporosis, for example). Of note, the impact of additional fractures isn’t considered either and should be factored into future investigations.
Overall, the study is robust and important and provides valuable information regarding mortality risk from a fragility fracture in older people. However, there are some flaws that need to be considered and addressed, the most serious of which is that the term “skeletal age” has been in existence for decades, applied to a much younger age group, and its implications are completely different from those being proposed by the authors here.
A version of this article first appeared on Medscape.com.
Thach Tran, MD, and colleagues introduced the concept of “skeletal age” in a recently published paper that aims to incorporate the impact of fragility, or low trauma, fractures – which can occur in patients with osteoporosis – on mortality risk.
They defined “skeletal age” as the age of the skeleton following a fragility fracture. This is calculated as the chronological age of the individual plus the number of years of “life lost” as a consequence of the specific fracture.
The risk for premature death following fragility fractures is concerning, with 22%-58% of patients with hip fracture dying within a year (Brauer et al.; Rapp et al.). Thus, it’s important to treat osteoporosis in a timely fashion to reduce the risk for such fractures and the excess mortality risk associated with them.
Implementation and uptake of such treatment, however, either before or after a fragility fracture, is far from optimal (Solomon et al). This may be because patients don’t fully understand the consequence of such a fracture, and outcomes measures currently in use (such as relative risk or hazard of mortality) are difficult to communicate to patients.
In the recent paper by Dr. Tran and colleagues, the authors examined the association between fractures and mortality based on sex, age, associated comorbidities, and fracture site. They pooled this information to create a “skeletal age” for each fracture site, using data from the Danish National Hospital Discharge Registry, which documents fractures and related mortality for all Danish people.
They examined mortality over a period of at least 2 years following a fragility fracture in individuals aged 50 or older, and reported that occurrence of any fragility fracture is associated with a 30%-45% increased risk for death, with the highest risk noted for hip and femur fractures (twofold increase). Fractures of the pelvis, vertebrae, humerus, ribs, clavicle, and lower leg were also associated with increased mortality risk, but no increase was seen with fractures of the forearm, knee, ankle, hand, or foot.
The number of years of life lost at any age depending on the fracture site is represented as a linear graph of skeletal age for any chronological age, for specific fracture sites, separated by sex.
For example, the skeletal age of a 50-year-old man who has a hip fracture is 57 years (7 years of life lost as a consequence of the fracture), while that for a 70-year-old man with the same fracture is 75 years (5 years of life lost because of the fracture). Similarly, the skeletal age of a 50-year-old man with a fracture of the pelvis, femur, vertebrae, and humerus is 55 years (5 years of life lost). Fractures of the lower leg, humerus, and clavicle lead to fewer lost years of life.
The authors are to be commended for creating a simple strategy to quantify mortality risk following low-impact or fragility fractures in older individuals; this could enable providers to communicate the importance of osteoporosis treatment more effectively to patients on the basis of their skeletal age, and for patients to better understand this information.
The study design appears reasonably robust as the authors considered many factors that might affect mortality risk, such as sex, age, and comorbidities, and the results are based on information from a very large number of people – 1.6 million.
However, there’s a major issue with the concept of “skeletal age” as proposed by Dr. Tran and colleagues. The term is already in use and defines the maturity of bones in children and adolescents, also called “bone age” (Greulich and Pyle 1959; Skeletal Age, Radiology Key). This is a real oversight and could cause confusion in interpreting “skeletal age.”
Skeletal age as currently defined in children and adolescents is influenced by chronological age, exposure to certain hormones, nutritional deficiencies, and systemic diseases, and is a predictor of adult height based on the skeletal age and current height. This concept is completely different from that being proposed by the authors in this paper. Dr. Tran and colleagues (and the reviewers of this paper) are probably not familiar with the use of the terminology in youth, which is a major oversight; they should consider changing the terminology given this overlap.
Further, fragility fractures can occur from osteoporosis at any age, and this study doesn’t provide information regarding years of life lost from occurrence of fragility fractures at younger ages, or the age at which mortality risk starts to increase (as the study was performed only in those aged 50 or older).
While the study takes into account general comorbidities in developing the model to define years of life lost, it doesn’t account for other factors that can influence fracture risk, such as lifestyle factors, activity level, and genetic risk (family history of osteoporosis, for example). Of note, the impact of additional fractures isn’t considered either and should be factored into future investigations.
Overall, the study is robust and important and provides valuable information regarding mortality risk from a fragility fracture in older people. However, there are some flaws that need to be considered and addressed, the most serious of which is that the term “skeletal age” has been in existence for decades, applied to a much younger age group, and its implications are completely different from those being proposed by the authors here.
A version of this article first appeared on Medscape.com.
Drugmakers are abandoning cheap generics, and now U.S. cancer patients can’t get meds
On Nov. 22, three Food and Drug Administration inspectors arrived at the sprawling Intas Pharmaceuticals plant south of Ahmedabad, India, and found hundreds of trash bags full of shredded documents tossed into a garbage truck. Over the next 10 days, the inspectors assessed what looked like a systematic effort to conceal quality problems at the plant, which provided more than half of the U.S. supply of generic cisplatin and carboplatin, two cheap drugs used to treat as many as 500,000 new cancer cases every year.
Their decisions are likely to result in preventable deaths.
Cisplatin and carboplatin are among scores of drugs in shortage, including 12 other cancer drugs, ADHD pills, blood thinners, and antibiotics. COVID-hangover supply chain issues and limited FDA oversight are part of the problem, but the main cause, experts agree, is the underlying weakness of the generic drug industry. Made mostly overseas, these old but crucial drugs are often sold at a loss or for little profit. Domestic manufacturers have little interest in making them, setting their sights instead on high-priced drugs with plump profit margins.
The problem isn’t new, and that’s particularly infuriating to many clinicians. President Joe Biden, whose son Beau died of an aggressive brain cancer, has focused his Cancer Moonshot on discovering cures – undoubtedly expensive ones. Indeed, existing brand-name cancer drugs often cost tens of thousands of dollars a year.
But what about the thousands of patients today who can’t get a drug like cisplatin, approved by the FDA in 1978 and costing as little as $6 a dose?
“It’s just insane,” said Mark Ratain, MD, a cancer doctor and pharmacologist at the University of Chicago. “Your roof is caving in, but you want to build a basketball court in the backyard because your wife is pregnant with twin boys and you want them to be NBA stars when they grow up?”
“It’s just a travesty that this is the level of health care in the United States of America right now,” said Stephen Divers, MD, an oncologist in Hot Springs, Ark., who in recent weeks has had to delay or change treatment for numerous bladder, breast, and ovarian cancer patients because his clinic cannot find enough cisplatin and carboplatin. Results from a survey of academic cancer centers released June 7 found 93% couldn’t find enough carboplatin and 70% had cisplatin shortages.
“All day, in between patients, we hold staff meetings trying to figure this out,” said Bonny Moore, MD, an oncologist in Fredericksburg, Virginia. “It’s the most nauseous I’ve ever felt. Our office stayed open during COVID; we never had to stop treating patients. We got them vaccinated, kept them safe, and now I can’t get them a $10 drug.”
The cancer clinicians KFF Health News interviewed for this story said that, given current shortages, they prioritize patients who can be cured over later-stage patients, in whom the drugs generally can only slow the disease, and for whom alternatives – though sometimes less effective and often with more side effects – are available. But some doctors are even rationing doses intended to cure.
Isabella McDonald, then a junior at Utah Valley University, was diagnosed in April with a rare, often fatal bone cancer, whose sole treatment for young adults includes the drug methotrexate. When Isabella’s second cycle of treatment began June 5, clinicians advised that she would be getting less than the full dose because of a methotrexate shortage, said her father, Brent.
“They don’t think it will have a negative impact on her treatment, but as far as I am aware, there isn’t any scientific basis to make that conclusion,” he said. “As you can imagine, when they gave us such low odds of her beating this cancer, it feels like we want to give it everything we can and not something short of the standard.”
Mr. McDonald stressed that he didn’t blame the staffers at Intermountain Health who take care of Isabella. The family – his other daughter, Cate, made a TikTok video about her sister’s plight – were simply stunned at such a basic flaw in the health care system.
At Dr. Moore’s practice, in Virginia, clinicians gave 60% of the optimal dose of carboplatin to some uterine cancer patients during the week of May 16, then shifted to 80% after a small shipment came in the following week. The doctors had to omit carboplatin from normal combination treatments for patients with recurrent disease, she said.
On June 2, Dr. Moore and colleagues were glued to their drug distributor’s website, anxious as teenagers waiting for Taylor Swift tickets to go on sale – only with mortal consequences at stake.
She later emailed KFF Health News: “Carboplatin did NOT come back in stock today. Neither did cisplatin.”
Doses remained at 80%, she said. Things hadn’t changed 10 days later.
Generics manufacturers are pulling out
The causes of shortages are well established. Everyone wants to pay less, and the middlemen who procure and distribute generics keep driving down wholesale prices. The average net price of generic drugs fell by more than half between 2016 and 2022, according to research by Anthony Sardella, a business professor at Washington University in St. Louis.
As generics manufacturers compete to win sales contracts with the big negotiators of such purchases, such as Vizient and Premier, their profits sink. Some are going out of business. Akorn, which made 75 common generics, went bankrupt and closed in February. Israeli generics giant Teva, which has a portfolio of 3,600 medicines, announced May 18 it was shifting to brand-name drugs and “high-value generics.” Lannett, with about 120 generics, announced a Chapter 11 reorganization amid declining revenue. Other companies are in trouble too, said David Gaugh, interim CEO of the Association for Accessible Medicines, the leading generics trade group.
The generics industry used to lose money on about a third of the drugs it produced, but now it’s more like half, Mr. Gaugh said. So when a company stops making a drug, others do not necessarily step up, he said. Officials at Fresenius Kabi and Pfizer said they have increased their carboplatin production since March, but not enough to end the shortage. On June 2, FDA Commissioner Robert Califf announced the agency had given emergency authorization for Chinese-made cisplatin to enter the U.S. market, but the impact of the move wasn’t immediately clear.
Cisplatin and carboplatin are made in special production lines under sterile conditions, and expanding or changing the lines requires FDA approval. Bargain-basement prices have pushed production overseas, where it’s harder for the FDA to track quality standards. The Intas plant inspection was a relative rarity in India, where the FDA in 2022 reportedly inspected only 3% of sites that make drugs for the U.S. market. Mr. Sardella testified in May that a quarter of all U.S. drug prescriptions are filled by companies that received FDA warning letters in the past 26 months. And pharmaceutical industry product recalls are at their highest level in 18 years, reflecting fragile supply conditions.
The FDA listed 137 drugs in shortage as of June 13, including many essential medicines made by few companies.
Intas voluntarily shut down its Ahmedabad plant after the FDA inspection, and the agency posted its shocking inspection report in January. Accord Healthcare, the U.S. subsidiary of Intas, said in mid-June it had no date for restarting production.
Asked why it waited 2 months after its inspection to announce the cisplatin shortage, given that Intas supplied more than half the U.S. market for the drug, the FDA said via email that it doesn’t list a drug in shortage until it has “confirmed that overall market demand is not being met.”
Prices for carboplatin, cisplatin, and other drugs have skyrocketed on the so-called gray market, where speculators sell medicines they snapped up in anticipation of shortages. A 600-mg bottle of carboplatin, normally available for $30, was going for $185 in early May and $345 a week later, said Richard Scanlon, the pharmacist at dr. Moore’s clinic.
“It’s hard to have these conversations with patients – ‘I have your dose for this cycle, but not sure about next cycle,’” said Mark Einstein, MD, chair of the department of obstetrics, gynecology and reproductive health at New Jersey Medical School, Newark.
Should government step in?
Despite a drug shortage task force and numerous congressional hearings, progress has been slow at best. The 2020 CARES Act gave the FDA the power to require companies to have contingency plans enabling them to respond to shortages, but the agency has not yet implemented guidance to enforce the provisions.
As a result, neither Accord nor other cisplatin makers had a response plan in place when Intas’ plant was shut down, said Soumi Saha, senior vice president of government affairs for Premier, which arranges wholesale drug purchases for more than 4,400 hospitals and health systems.
Premier understood in December that the shutdown endangered the U.S. supply of cisplatin and carboplatin, but it also didn’t issue an immediate alarm. “It’s a fine balance,” she said. “You don’t want to create panic-buying or hoarding.”
More lasting solutions are under discussion. Mr. Sardella and others have proposed government subsidies to get U.S. generics plants running full time. Their capacity is now half-idle. If federal agencies like the Centers for Medicare & Medicaid Services paid more for more safely and efficiently produced drugs, it would promote a more stable supply chain, he said.
“At a certain point the system needs to recognize there’s a high cost to low-cost drugs,” said Allan Coukell, senior vice president for public policy at Civica Rx, a nonprofit funded by health systems, foundations, and the federal government that provides about 80 drugs to hospitals in its network. Civica is building a $140 million factory near Petersburg, Va., that will produce dozens more, Mr. Coukell said.
Dr. Ratain and his University of Chicago colleague Satyajit Kosuri, MD, recently called for the creation of a strategic inventory buffer for generic medications, something like the Strategic Petroleum Reserve, set up in 1975 in response to the OPEC oil crisis.
In fact, Dr. Ratain reckons, selling a quarter-million barrels of oil would probably generate enough cash to make and store 2 years’ worth of carboplatin and cisplatin.
“It would almost literally be a drop in the bucket.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – an independent source of health policy research, polling, and journalism. Learn more about KFF.
On Nov. 22, three Food and Drug Administration inspectors arrived at the sprawling Intas Pharmaceuticals plant south of Ahmedabad, India, and found hundreds of trash bags full of shredded documents tossed into a garbage truck. Over the next 10 days, the inspectors assessed what looked like a systematic effort to conceal quality problems at the plant, which provided more than half of the U.S. supply of generic cisplatin and carboplatin, two cheap drugs used to treat as many as 500,000 new cancer cases every year.
Their decisions are likely to result in preventable deaths.
Cisplatin and carboplatin are among scores of drugs in shortage, including 12 other cancer drugs, ADHD pills, blood thinners, and antibiotics. COVID-hangover supply chain issues and limited FDA oversight are part of the problem, but the main cause, experts agree, is the underlying weakness of the generic drug industry. Made mostly overseas, these old but crucial drugs are often sold at a loss or for little profit. Domestic manufacturers have little interest in making them, setting their sights instead on high-priced drugs with plump profit margins.
The problem isn’t new, and that’s particularly infuriating to many clinicians. President Joe Biden, whose son Beau died of an aggressive brain cancer, has focused his Cancer Moonshot on discovering cures – undoubtedly expensive ones. Indeed, existing brand-name cancer drugs often cost tens of thousands of dollars a year.
But what about the thousands of patients today who can’t get a drug like cisplatin, approved by the FDA in 1978 and costing as little as $6 a dose?
“It’s just insane,” said Mark Ratain, MD, a cancer doctor and pharmacologist at the University of Chicago. “Your roof is caving in, but you want to build a basketball court in the backyard because your wife is pregnant with twin boys and you want them to be NBA stars when they grow up?”
“It’s just a travesty that this is the level of health care in the United States of America right now,” said Stephen Divers, MD, an oncologist in Hot Springs, Ark., who in recent weeks has had to delay or change treatment for numerous bladder, breast, and ovarian cancer patients because his clinic cannot find enough cisplatin and carboplatin. Results from a survey of academic cancer centers released June 7 found 93% couldn’t find enough carboplatin and 70% had cisplatin shortages.
“All day, in between patients, we hold staff meetings trying to figure this out,” said Bonny Moore, MD, an oncologist in Fredericksburg, Virginia. “It’s the most nauseous I’ve ever felt. Our office stayed open during COVID; we never had to stop treating patients. We got them vaccinated, kept them safe, and now I can’t get them a $10 drug.”
The cancer clinicians KFF Health News interviewed for this story said that, given current shortages, they prioritize patients who can be cured over later-stage patients, in whom the drugs generally can only slow the disease, and for whom alternatives – though sometimes less effective and often with more side effects – are available. But some doctors are even rationing doses intended to cure.
Isabella McDonald, then a junior at Utah Valley University, was diagnosed in April with a rare, often fatal bone cancer, whose sole treatment for young adults includes the drug methotrexate. When Isabella’s second cycle of treatment began June 5, clinicians advised that she would be getting less than the full dose because of a methotrexate shortage, said her father, Brent.
“They don’t think it will have a negative impact on her treatment, but as far as I am aware, there isn’t any scientific basis to make that conclusion,” he said. “As you can imagine, when they gave us such low odds of her beating this cancer, it feels like we want to give it everything we can and not something short of the standard.”
Mr. McDonald stressed that he didn’t blame the staffers at Intermountain Health who take care of Isabella. The family – his other daughter, Cate, made a TikTok video about her sister’s plight – were simply stunned at such a basic flaw in the health care system.
At Dr. Moore’s practice, in Virginia, clinicians gave 60% of the optimal dose of carboplatin to some uterine cancer patients during the week of May 16, then shifted to 80% after a small shipment came in the following week. The doctors had to omit carboplatin from normal combination treatments for patients with recurrent disease, she said.
On June 2, Dr. Moore and colleagues were glued to their drug distributor’s website, anxious as teenagers waiting for Taylor Swift tickets to go on sale – only with mortal consequences at stake.
She later emailed KFF Health News: “Carboplatin did NOT come back in stock today. Neither did cisplatin.”
Doses remained at 80%, she said. Things hadn’t changed 10 days later.
Generics manufacturers are pulling out
The causes of shortages are well established. Everyone wants to pay less, and the middlemen who procure and distribute generics keep driving down wholesale prices. The average net price of generic drugs fell by more than half between 2016 and 2022, according to research by Anthony Sardella, a business professor at Washington University in St. Louis.
As generics manufacturers compete to win sales contracts with the big negotiators of such purchases, such as Vizient and Premier, their profits sink. Some are going out of business. Akorn, which made 75 common generics, went bankrupt and closed in February. Israeli generics giant Teva, which has a portfolio of 3,600 medicines, announced May 18 it was shifting to brand-name drugs and “high-value generics.” Lannett, with about 120 generics, announced a Chapter 11 reorganization amid declining revenue. Other companies are in trouble too, said David Gaugh, interim CEO of the Association for Accessible Medicines, the leading generics trade group.
The generics industry used to lose money on about a third of the drugs it produced, but now it’s more like half, Mr. Gaugh said. So when a company stops making a drug, others do not necessarily step up, he said. Officials at Fresenius Kabi and Pfizer said they have increased their carboplatin production since March, but not enough to end the shortage. On June 2, FDA Commissioner Robert Califf announced the agency had given emergency authorization for Chinese-made cisplatin to enter the U.S. market, but the impact of the move wasn’t immediately clear.
Cisplatin and carboplatin are made in special production lines under sterile conditions, and expanding or changing the lines requires FDA approval. Bargain-basement prices have pushed production overseas, where it’s harder for the FDA to track quality standards. The Intas plant inspection was a relative rarity in India, where the FDA in 2022 reportedly inspected only 3% of sites that make drugs for the U.S. market. Mr. Sardella testified in May that a quarter of all U.S. drug prescriptions are filled by companies that received FDA warning letters in the past 26 months. And pharmaceutical industry product recalls are at their highest level in 18 years, reflecting fragile supply conditions.
The FDA listed 137 drugs in shortage as of June 13, including many essential medicines made by few companies.
Intas voluntarily shut down its Ahmedabad plant after the FDA inspection, and the agency posted its shocking inspection report in January. Accord Healthcare, the U.S. subsidiary of Intas, said in mid-June it had no date for restarting production.
Asked why it waited 2 months after its inspection to announce the cisplatin shortage, given that Intas supplied more than half the U.S. market for the drug, the FDA said via email that it doesn’t list a drug in shortage until it has “confirmed that overall market demand is not being met.”
Prices for carboplatin, cisplatin, and other drugs have skyrocketed on the so-called gray market, where speculators sell medicines they snapped up in anticipation of shortages. A 600-mg bottle of carboplatin, normally available for $30, was going for $185 in early May and $345 a week later, said Richard Scanlon, the pharmacist at dr. Moore’s clinic.
“It’s hard to have these conversations with patients – ‘I have your dose for this cycle, but not sure about next cycle,’” said Mark Einstein, MD, chair of the department of obstetrics, gynecology and reproductive health at New Jersey Medical School, Newark.
Should government step in?
Despite a drug shortage task force and numerous congressional hearings, progress has been slow at best. The 2020 CARES Act gave the FDA the power to require companies to have contingency plans enabling them to respond to shortages, but the agency has not yet implemented guidance to enforce the provisions.
As a result, neither Accord nor other cisplatin makers had a response plan in place when Intas’ plant was shut down, said Soumi Saha, senior vice president of government affairs for Premier, which arranges wholesale drug purchases for more than 4,400 hospitals and health systems.
Premier understood in December that the shutdown endangered the U.S. supply of cisplatin and carboplatin, but it also didn’t issue an immediate alarm. “It’s a fine balance,” she said. “You don’t want to create panic-buying or hoarding.”
More lasting solutions are under discussion. Mr. Sardella and others have proposed government subsidies to get U.S. generics plants running full time. Their capacity is now half-idle. If federal agencies like the Centers for Medicare & Medicaid Services paid more for more safely and efficiently produced drugs, it would promote a more stable supply chain, he said.
“At a certain point the system needs to recognize there’s a high cost to low-cost drugs,” said Allan Coukell, senior vice president for public policy at Civica Rx, a nonprofit funded by health systems, foundations, and the federal government that provides about 80 drugs to hospitals in its network. Civica is building a $140 million factory near Petersburg, Va., that will produce dozens more, Mr. Coukell said.
Dr. Ratain and his University of Chicago colleague Satyajit Kosuri, MD, recently called for the creation of a strategic inventory buffer for generic medications, something like the Strategic Petroleum Reserve, set up in 1975 in response to the OPEC oil crisis.
In fact, Dr. Ratain reckons, selling a quarter-million barrels of oil would probably generate enough cash to make and store 2 years’ worth of carboplatin and cisplatin.
“It would almost literally be a drop in the bucket.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – an independent source of health policy research, polling, and journalism. Learn more about KFF.
On Nov. 22, three Food and Drug Administration inspectors arrived at the sprawling Intas Pharmaceuticals plant south of Ahmedabad, India, and found hundreds of trash bags full of shredded documents tossed into a garbage truck. Over the next 10 days, the inspectors assessed what looked like a systematic effort to conceal quality problems at the plant, which provided more than half of the U.S. supply of generic cisplatin and carboplatin, two cheap drugs used to treat as many as 500,000 new cancer cases every year.
Their decisions are likely to result in preventable deaths.
Cisplatin and carboplatin are among scores of drugs in shortage, including 12 other cancer drugs, ADHD pills, blood thinners, and antibiotics. COVID-hangover supply chain issues and limited FDA oversight are part of the problem, but the main cause, experts agree, is the underlying weakness of the generic drug industry. Made mostly overseas, these old but crucial drugs are often sold at a loss or for little profit. Domestic manufacturers have little interest in making them, setting their sights instead on high-priced drugs with plump profit margins.
The problem isn’t new, and that’s particularly infuriating to many clinicians. President Joe Biden, whose son Beau died of an aggressive brain cancer, has focused his Cancer Moonshot on discovering cures – undoubtedly expensive ones. Indeed, existing brand-name cancer drugs often cost tens of thousands of dollars a year.
But what about the thousands of patients today who can’t get a drug like cisplatin, approved by the FDA in 1978 and costing as little as $6 a dose?
“It’s just insane,” said Mark Ratain, MD, a cancer doctor and pharmacologist at the University of Chicago. “Your roof is caving in, but you want to build a basketball court in the backyard because your wife is pregnant with twin boys and you want them to be NBA stars when they grow up?”
“It’s just a travesty that this is the level of health care in the United States of America right now,” said Stephen Divers, MD, an oncologist in Hot Springs, Ark., who in recent weeks has had to delay or change treatment for numerous bladder, breast, and ovarian cancer patients because his clinic cannot find enough cisplatin and carboplatin. Results from a survey of academic cancer centers released June 7 found 93% couldn’t find enough carboplatin and 70% had cisplatin shortages.
“All day, in between patients, we hold staff meetings trying to figure this out,” said Bonny Moore, MD, an oncologist in Fredericksburg, Virginia. “It’s the most nauseous I’ve ever felt. Our office stayed open during COVID; we never had to stop treating patients. We got them vaccinated, kept them safe, and now I can’t get them a $10 drug.”
The cancer clinicians KFF Health News interviewed for this story said that, given current shortages, they prioritize patients who can be cured over later-stage patients, in whom the drugs generally can only slow the disease, and for whom alternatives – though sometimes less effective and often with more side effects – are available. But some doctors are even rationing doses intended to cure.
Isabella McDonald, then a junior at Utah Valley University, was diagnosed in April with a rare, often fatal bone cancer, whose sole treatment for young adults includes the drug methotrexate. When Isabella’s second cycle of treatment began June 5, clinicians advised that she would be getting less than the full dose because of a methotrexate shortage, said her father, Brent.
“They don’t think it will have a negative impact on her treatment, but as far as I am aware, there isn’t any scientific basis to make that conclusion,” he said. “As you can imagine, when they gave us such low odds of her beating this cancer, it feels like we want to give it everything we can and not something short of the standard.”
Mr. McDonald stressed that he didn’t blame the staffers at Intermountain Health who take care of Isabella. The family – his other daughter, Cate, made a TikTok video about her sister’s plight – were simply stunned at such a basic flaw in the health care system.
At Dr. Moore’s practice, in Virginia, clinicians gave 60% of the optimal dose of carboplatin to some uterine cancer patients during the week of May 16, then shifted to 80% after a small shipment came in the following week. The doctors had to omit carboplatin from normal combination treatments for patients with recurrent disease, she said.
On June 2, Dr. Moore and colleagues were glued to their drug distributor’s website, anxious as teenagers waiting for Taylor Swift tickets to go on sale – only with mortal consequences at stake.
She later emailed KFF Health News: “Carboplatin did NOT come back in stock today. Neither did cisplatin.”
Doses remained at 80%, she said. Things hadn’t changed 10 days later.
Generics manufacturers are pulling out
The causes of shortages are well established. Everyone wants to pay less, and the middlemen who procure and distribute generics keep driving down wholesale prices. The average net price of generic drugs fell by more than half between 2016 and 2022, according to research by Anthony Sardella, a business professor at Washington University in St. Louis.
As generics manufacturers compete to win sales contracts with the big negotiators of such purchases, such as Vizient and Premier, their profits sink. Some are going out of business. Akorn, which made 75 common generics, went bankrupt and closed in February. Israeli generics giant Teva, which has a portfolio of 3,600 medicines, announced May 18 it was shifting to brand-name drugs and “high-value generics.” Lannett, with about 120 generics, announced a Chapter 11 reorganization amid declining revenue. Other companies are in trouble too, said David Gaugh, interim CEO of the Association for Accessible Medicines, the leading generics trade group.
The generics industry used to lose money on about a third of the drugs it produced, but now it’s more like half, Mr. Gaugh said. So when a company stops making a drug, others do not necessarily step up, he said. Officials at Fresenius Kabi and Pfizer said they have increased their carboplatin production since March, but not enough to end the shortage. On June 2, FDA Commissioner Robert Califf announced the agency had given emergency authorization for Chinese-made cisplatin to enter the U.S. market, but the impact of the move wasn’t immediately clear.
Cisplatin and carboplatin are made in special production lines under sterile conditions, and expanding or changing the lines requires FDA approval. Bargain-basement prices have pushed production overseas, where it’s harder for the FDA to track quality standards. The Intas plant inspection was a relative rarity in India, where the FDA in 2022 reportedly inspected only 3% of sites that make drugs for the U.S. market. Mr. Sardella testified in May that a quarter of all U.S. drug prescriptions are filled by companies that received FDA warning letters in the past 26 months. And pharmaceutical industry product recalls are at their highest level in 18 years, reflecting fragile supply conditions.
The FDA listed 137 drugs in shortage as of June 13, including many essential medicines made by few companies.
Intas voluntarily shut down its Ahmedabad plant after the FDA inspection, and the agency posted its shocking inspection report in January. Accord Healthcare, the U.S. subsidiary of Intas, said in mid-June it had no date for restarting production.
Asked why it waited 2 months after its inspection to announce the cisplatin shortage, given that Intas supplied more than half the U.S. market for the drug, the FDA said via email that it doesn’t list a drug in shortage until it has “confirmed that overall market demand is not being met.”
Prices for carboplatin, cisplatin, and other drugs have skyrocketed on the so-called gray market, where speculators sell medicines they snapped up in anticipation of shortages. A 600-mg bottle of carboplatin, normally available for $30, was going for $185 in early May and $345 a week later, said Richard Scanlon, the pharmacist at dr. Moore’s clinic.
“It’s hard to have these conversations with patients – ‘I have your dose for this cycle, but not sure about next cycle,’” said Mark Einstein, MD, chair of the department of obstetrics, gynecology and reproductive health at New Jersey Medical School, Newark.
Should government step in?
Despite a drug shortage task force and numerous congressional hearings, progress has been slow at best. The 2020 CARES Act gave the FDA the power to require companies to have contingency plans enabling them to respond to shortages, but the agency has not yet implemented guidance to enforce the provisions.
As a result, neither Accord nor other cisplatin makers had a response plan in place when Intas’ plant was shut down, said Soumi Saha, senior vice president of government affairs for Premier, which arranges wholesale drug purchases for more than 4,400 hospitals and health systems.
Premier understood in December that the shutdown endangered the U.S. supply of cisplatin and carboplatin, but it also didn’t issue an immediate alarm. “It’s a fine balance,” she said. “You don’t want to create panic-buying or hoarding.”
More lasting solutions are under discussion. Mr. Sardella and others have proposed government subsidies to get U.S. generics plants running full time. Their capacity is now half-idle. If federal agencies like the Centers for Medicare & Medicaid Services paid more for more safely and efficiently produced drugs, it would promote a more stable supply chain, he said.
“At a certain point the system needs to recognize there’s a high cost to low-cost drugs,” said Allan Coukell, senior vice president for public policy at Civica Rx, a nonprofit funded by health systems, foundations, and the federal government that provides about 80 drugs to hospitals in its network. Civica is building a $140 million factory near Petersburg, Va., that will produce dozens more, Mr. Coukell said.
Dr. Ratain and his University of Chicago colleague Satyajit Kosuri, MD, recently called for the creation of a strategic inventory buffer for generic medications, something like the Strategic Petroleum Reserve, set up in 1975 in response to the OPEC oil crisis.
In fact, Dr. Ratain reckons, selling a quarter-million barrels of oil would probably generate enough cash to make and store 2 years’ worth of carboplatin and cisplatin.
“It would almost literally be a drop in the bucket.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – an independent source of health policy research, polling, and journalism. Learn more about KFF.
Product updates and reviews
REVIEW
Butterfly iQ+: Offering day-to-day portable ultrasound tech

The Butterfly iQ+ app with an ultrasound probe and cable is available from Butterfly Network, Inc, in Guilford, Connecticut.
Background. It could be reasonably argued that ultrasonography has surpassed the speculum as the single most important tool in ObGyn. From its origins in 1949 with the pioneering work of George Ludwig using A-mode (amplitude-mode) ultrasound and the first publication of its use in pregnancy using B-mode (brightness-mode) ultrasound in Lancet in 1958 by Donald and colleagues, this technology has become so ingrained into ObGyn that it is often frustrating to practice comfortably without it. Thus, today, the biggest question facing most practitioners is not whether or not to have an ultrasound in their practice but which one to have.
Given the wide range of quality, functionality, and price within the ultrasound device space, choosing the right technology can feel as daunting as choosing the perfect restaurant in New York City. That said, when looking for entry-level ultrasound technology to address the day-to-day basic needs of your average ObGyn, the Butterfly iQ+ may be an easy choice.
Design/Functionality. The Butterfly iQ+ app does not come with a screen. Rather, the device is compatible with both iOS and Android systems and readily connects to a vast array of easily purchased devices, with either lightening or USB-C ports. In our office, we use an iPad mini. The probe is lightweight (309 g) and contains a rechargeable 2600 mAh lithium ion battery, so that its power source is independent of the device to which it is attached. The probe is a 2D array with 9000 micro-machined sensors. It allows for imaging using M-mode, B-mode, Color Doppler, Power Doppler, and Pulsed Wave Doppler. (I don’t know what the last two are or what they are used for, but they sound important.) It has a scan depth range of 1 cm to 30 cm. The downloadable Butterfly iQ+ app that has the software that makes the probe functional has more tools, controls, and presets than anyone could ever need. But that’s not all. The App has data encrypted HIPAA/HITECH-compliant Cloud-based connectivity that offers unlimited image storage, access to reports, and embedded CPT codes should billing capabilities be needed.
The true beauty of the Butterfly iQ+ is that the image quality is awesome and it is really easy to use. The software is mostly intuitive and takes only a minimal effort to learn. The device holds its charge more than adequately for a day in the office and the recharging process is fast and easy. When it comes to the device’s design and functionality–as a Capricorn–I am still looking for its flaws.
Innovation. The real innovations of the Butterfly iQ+ are its “ultrasound-on-a-chip”™ technology and its incorporation of a rechargeable battery into the probe. This combination allows for crystal clear imaging in a cordless, portable device. While most other similar technologies waste their time, technology, space, and cost on the screen, the Butterfly iQ+ punted on that challenge and put all their efforts into the probe and the software. It was a great choice.
Summary. In our office, the Butterfly iQ+ has changed the way we practice. Our trusty fetal dopplers are mostly gone, having been replaced by the Butterfly iQ+. At almost every prenatal visit, patients can now see their baby rather than just hear the heartbeat (and they can hear it too if they want by using the M-mode functionality on the device). Patients love it, and so do the doctors. Instead of just hearing heart beats, fetal position and quick fluid checks are now routine, so we think our care is actually a little better than it was. The Butterfly iQ+ is also great for confirming IUD locations after placement or when the strings are not visible. All-in-all, I love this product. Who doesn’t love butterflies?!
For more information, visit https://www.butterflynetwork.com
The views of the author are personal opinions and do not necessarily represent the views of OBG
References
- Kaproth-Joslin KA, Nicola R, Dogra VS. The History of US: from bats and boats to the bedside and beyond: RSNA centennial article. Radiographics. 2015;35:960-970.
- Donald I, MacVicar J, Brown TG. Investigation of abdominal masses by pulsed ultrasound. Lancet. 1958;1:1188-1195.
REVIEW
Butterfly iQ+: Offering day-to-day portable ultrasound tech
The Butterfly iQ+ app with an ultrasound probe and cable is available from Butterfly Network, Inc, in Guilford, Connecticut.
Background. It could be reasonably argued that ultrasonography has surpassed the speculum as the single most important tool in ObGyn. From its origins in 1949 with the pioneering work of George Ludwig using A-mode (amplitude-mode) ultrasound and the first publication of its use in pregnancy using B-mode (brightness-mode) ultrasound in Lancet in 1958 by Donald and colleagues, this technology has become so ingrained into ObGyn that it is often frustrating to practice comfortably without it. Thus, today, the biggest question facing most practitioners is not whether or not to have an ultrasound in their practice but which one to have.
Given the wide range of quality, functionality, and price within the ultrasound device space, choosing the right technology can feel as daunting as choosing the perfect restaurant in New York City. That said, when looking for entry-level ultrasound technology to address the day-to-day basic needs of your average ObGyn, the Butterfly iQ+ may be an easy choice.
Design/Functionality. The Butterfly iQ+ app does not come with a screen. Rather, the device is compatible with both iOS and Android systems and readily connects to a vast array of easily purchased devices, with either lightening or USB-C ports. In our office, we use an iPad mini. The probe is lightweight (309 g) and contains a rechargeable 2600 mAh lithium ion battery, so that its power source is independent of the device to which it is attached. The probe is a 2D array with 9000 micro-machined sensors. It allows for imaging using M-mode, B-mode, Color Doppler, Power Doppler, and Pulsed Wave Doppler. (I don’t know what the last two are or what they are used for, but they sound important.) It has a scan depth range of 1 cm to 30 cm. The downloadable Butterfly iQ+ app that has the software that makes the probe functional has more tools, controls, and presets than anyone could ever need. But that’s not all. The App has data encrypted HIPAA/HITECH-compliant Cloud-based connectivity that offers unlimited image storage, access to reports, and embedded CPT codes should billing capabilities be needed.
The true beauty of the Butterfly iQ+ is that the image quality is awesome and it is really easy to use. The software is mostly intuitive and takes only a minimal effort to learn. The device holds its charge more than adequately for a day in the office and the recharging process is fast and easy. When it comes to the device’s design and functionality–as a Capricorn–I am still looking for its flaws.
Innovation. The real innovations of the Butterfly iQ+ are its “ultrasound-on-a-chip”™ technology and its incorporation of a rechargeable battery into the probe. This combination allows for crystal clear imaging in a cordless, portable device. While most other similar technologies waste their time, technology, space, and cost on the screen, the Butterfly iQ+ punted on that challenge and put all their efforts into the probe and the software. It was a great choice.
Summary. In our office, the Butterfly iQ+ has changed the way we practice. Our trusty fetal dopplers are mostly gone, having been replaced by the Butterfly iQ+. At almost every prenatal visit, patients can now see their baby rather than just hear the heartbeat (and they can hear it too if they want by using the M-mode functionality on the device). Patients love it, and so do the doctors. Instead of just hearing heart beats, fetal position and quick fluid checks are now routine, so we think our care is actually a little better than it was. The Butterfly iQ+ is also great for confirming IUD locations after placement or when the strings are not visible. All-in-all, I love this product. Who doesn’t love butterflies?!
For more information, visit https://www.butterflynetwork.com
The views of the author are personal opinions and do not necessarily represent the views of OBG
References
- Kaproth-Joslin KA, Nicola R, Dogra VS. The History of US: from bats and boats to the bedside and beyond: RSNA centennial article. Radiographics. 2015;35:960-970.
- Donald I, MacVicar J, Brown TG. Investigation of abdominal masses by pulsed ultrasound. Lancet. 1958;1:1188-1195.
REVIEW
Butterfly iQ+: Offering day-to-day portable ultrasound tech
The Butterfly iQ+ app with an ultrasound probe and cable is available from Butterfly Network, Inc, in Guilford, Connecticut.
Background. It could be reasonably argued that ultrasonography has surpassed the speculum as the single most important tool in ObGyn. From its origins in 1949 with the pioneering work of George Ludwig using A-mode (amplitude-mode) ultrasound and the first publication of its use in pregnancy using B-mode (brightness-mode) ultrasound in Lancet in 1958 by Donald and colleagues, this technology has become so ingrained into ObGyn that it is often frustrating to practice comfortably without it. Thus, today, the biggest question facing most practitioners is not whether or not to have an ultrasound in their practice but which one to have.
Given the wide range of quality, functionality, and price within the ultrasound device space, choosing the right technology can feel as daunting as choosing the perfect restaurant in New York City. That said, when looking for entry-level ultrasound technology to address the day-to-day basic needs of your average ObGyn, the Butterfly iQ+ may be an easy choice.
Design/Functionality. The Butterfly iQ+ app does not come with a screen. Rather, the device is compatible with both iOS and Android systems and readily connects to a vast array of easily purchased devices, with either lightening or USB-C ports. In our office, we use an iPad mini. The probe is lightweight (309 g) and contains a rechargeable 2600 mAh lithium ion battery, so that its power source is independent of the device to which it is attached. The probe is a 2D array with 9000 micro-machined sensors. It allows for imaging using M-mode, B-mode, Color Doppler, Power Doppler, and Pulsed Wave Doppler. (I don’t know what the last two are or what they are used for, but they sound important.) It has a scan depth range of 1 cm to 30 cm. The downloadable Butterfly iQ+ app that has the software that makes the probe functional has more tools, controls, and presets than anyone could ever need. But that’s not all. The App has data encrypted HIPAA/HITECH-compliant Cloud-based connectivity that offers unlimited image storage, access to reports, and embedded CPT codes should billing capabilities be needed.
The true beauty of the Butterfly iQ+ is that the image quality is awesome and it is really easy to use. The software is mostly intuitive and takes only a minimal effort to learn. The device holds its charge more than adequately for a day in the office and the recharging process is fast and easy. When it comes to the device’s design and functionality–as a Capricorn–I am still looking for its flaws.
Innovation. The real innovations of the Butterfly iQ+ are its “ultrasound-on-a-chip”™ technology and its incorporation of a rechargeable battery into the probe. This combination allows for crystal clear imaging in a cordless, portable device. While most other similar technologies waste their time, technology, space, and cost on the screen, the Butterfly iQ+ punted on that challenge and put all their efforts into the probe and the software. It was a great choice.
Summary. In our office, the Butterfly iQ+ has changed the way we practice. Our trusty fetal dopplers are mostly gone, having been replaced by the Butterfly iQ+. At almost every prenatal visit, patients can now see their baby rather than just hear the heartbeat (and they can hear it too if they want by using the M-mode functionality on the device). Patients love it, and so do the doctors. Instead of just hearing heart beats, fetal position and quick fluid checks are now routine, so we think our care is actually a little better than it was. The Butterfly iQ+ is also great for confirming IUD locations after placement or when the strings are not visible. All-in-all, I love this product. Who doesn’t love butterflies?!
For more information, visit https://www.butterflynetwork.com
The views of the author are personal opinions and do not necessarily represent the views of OBG
References
- Kaproth-Joslin KA, Nicola R, Dogra VS. The History of US: from bats and boats to the bedside and beyond: RSNA centennial article. Radiographics. 2015;35:960-970.
- Donald I, MacVicar J, Brown TG. Investigation of abdominal masses by pulsed ultrasound. Lancet. 1958;1:1188-1195.

Should you dismiss a difficult patient?
Some patients continually cancel their appointments, ignore your medical directions, treat your staff rudely, or send you harassing emails.
Do you have to tolerate their behavior?
No, these are all appropriate reasons to terminate patients, attorneys say. Patients also can be dismissed for misleading doctors about their past medical history, chronic drug-seeking, displaying threatening or seductive behavior toward staff members or physicians, or any criminal behavior in the office, experts say.
But even if a reason seems legitimate, that doesn’t make it legal. Doctors should consider whether the reason is legal, said Chicago-area attorney Ericka Adler, JD, a partner at Roetzel & Andress, who advises doctors about terminating patients.
Ms. Adler said.
Terminating patients for an “illegal” reason such as discrimination based on race or gender or sexual orientation – even if couched as a legitimate patient issue – could open the practice to a lawsuit, Ms. Adler said.
Doctors also want to avoid patient abandonment claims by talking to the patient about problems and documenting them as they arise. If they can’t be resolved, doctors should ensure that there’s continuity of care when patients change physicians, said Ms. Adler.
About 90% of physicians have dismissed at least one patient during their career, according to a study of nearly 800 primary care practices. The most common reasons were legitimate: a patient was “extremely disruptive and/or behaved inappropriately toward clinicians or staff”; a patient had “violated chronic pain and controlled substance policies”; and a patient had “repeatedly missed appointments.”
Jacqui O’Kane, DO, a family physician at South Georgia Medical Center in rural Nashville, said she has dismissed about 15 of 3,000 patients she has seen in the past 3 years at the clinic. Before she dismisses a patient, she looks at whether there has been a pattern of behavior and tries to talk to them about the problem first to find out if there are other reasons for it.
She also gives patients a warning: If the unacceptable behavior continues, it will lead to their dismissal.
When patients cross a line
Dr. O’Kane warned an elderly man who used the N-word with her that she wouldn’t tolerate that language in her office. Then, when he later called her front office employee the N-word, she decided to dismiss him.
“I said, ‘That’s it, you can’t say that to someone in this office. I already told you once, and you did it again. I’m sorry, you have to find another doctor,’ ” said Dr. O’Kane.
Another patient crossed a line when she missed four appointments, refused to come in, and kept sending Dr. O’Kane long messages on MyChart demanding medications and advice. One message was fairly obtrusive: “If you don’t give me something stronger for my nerves TODAY, I am going to LOSE MY MIND!!!” Dr. O’Kane said the patient wrote.
“I then told her that’s not how I run my practice and that she needed to find someone else.”
Another common reason doctors dismiss patients is for nonpayment, says Ms. Adler.
Recently, however, some patients have also begun demanding their money back from doctors for services already received and billed because they were unhappy about something that occurred at the doctor’s office, said Ms. Adler.
“I advise doctors to respond: ‘We disagree that you didn’t get the service, but we will give you your money back, and we’re also terminating you from our practice.’ At that point, the doctor-patient relationship has become impossible,” said Ms. Adler.
How to dismiss difficult patients ethically and legally
According to the AMA’s Council on Ethical and Judicial Affairs, a physician may not discontinue treatment of a patient if further treatment is medically indicated without giving the patient reasonable notice and sufficient opportunity to make alternative arrangements for care.
Terminating a patient abruptly without transferring their care could lead to a claim of patient abandonment and the physician being called before a licensing board for potentially violating the state’s Medical Practice Act, said Ms. Adler.
Doctors can take these six steps to set the stage for dismissal and avoid a claim of patient abandonment.
1. Create written policies. Medical practices can describe the rules and behavior they expect from patients in these policies, which can cover, for example, payment, treating staff with courtesy, and medications. “When the rules are in writing and patients sign off on them, that gives doctors a certain comfort level in being able to refer to them and say that the patient hasn’t been compliant,” said Ms. Adler.
She also recommends that your practice create a policy that doctors should let the patient know about their concerns and meet with them to discuss the problem before receiving a termination letter.
2. Document any consistent problems you’re having with a patient. When you start having problems with a patient, you should document when the problem occurred, how often it occurred, any discussions with the patient about the problem, warnings you gave the patient, and if and when you decided to terminate the patient.
3. Meet with the patient to discuss the problem. “Talking and meeting with a patient also allows the physician to assess whether there’s another issue. For example, is there a mental health concern? Is there a financial reason for nonpayment or no-shows? There are multiple benefits to finding out what the problem is,” said Ms. Adler.
Once you’ve decided to terminate a patient, here’s what you should do:
4. Allow enough time for the patient to find alternative care. Ms. Adler recommends giving patients 30 days’ notice and that physicians offer to provide emergency care during that time. However, if the patient is undergoing treatment or has other challenges, more time may be needed to transfer care.
“It’s important to consider the patient’s context – if the patient is receiving cancer treatment, or is in a late stage of pregnancy, or lives in a rural area where few specialists are available, you may want to treat them longer – at least until they finish their treatment,” said Ms. Adler. Also, states may have their own requirements about minimum notice periods, she said.
5. Provide patients with written notice that you intend to terminate their care. Ms. Adler recommends that each letter be tailored to the patient’s specific circumstances. “You could spell out a patient’s history of noncompliance or nonpayment or inappropriate conduct because it’s been documented and the patient is already aware of it from a previous discussion,” she said.
Ms. Adler also recommends that doctors consult with legal counsel when in doubt or if contacted by the patient’s lawyer. Some lawyers will draft the termination letters, she said.
6. Include the following information in the written letter: The date that they will no longer receive care, how they can obtain copies of their medical records, and how they can find a new physician by providing contact information for a state medical association or similar organization, which often maintains a database of clinicians by specialty and location.
The letter should also state that the doctor will provide emergency care during the 30 days. Ms. Adler also recommends sending the notice by certified mail.
Dr. O’Kane said she may be more likely to give patients a second chance because she practices in a rural underserved area, and she understands that her patients don’t have many other options for health care. She also has developed a reputation for being willing to take on difficult patients that other physicians didn’t want to deal with, she said.
She encourages physicians to talk to patients to find out why, for example, they may not be compliant with medications.
“The patient may say, ‘I had to choose between paying for medications and putting food on the table,’ ” said Dr. O’Kane.
A version of this article first appeared on Medscape.com.
Some patients continually cancel their appointments, ignore your medical directions, treat your staff rudely, or send you harassing emails.
Do you have to tolerate their behavior?
No, these are all appropriate reasons to terminate patients, attorneys say. Patients also can be dismissed for misleading doctors about their past medical history, chronic drug-seeking, displaying threatening or seductive behavior toward staff members or physicians, or any criminal behavior in the office, experts say.
But even if a reason seems legitimate, that doesn’t make it legal. Doctors should consider whether the reason is legal, said Chicago-area attorney Ericka Adler, JD, a partner at Roetzel & Andress, who advises doctors about terminating patients.
Ms. Adler said.
Terminating patients for an “illegal” reason such as discrimination based on race or gender or sexual orientation – even if couched as a legitimate patient issue – could open the practice to a lawsuit, Ms. Adler said.
Doctors also want to avoid patient abandonment claims by talking to the patient about problems and documenting them as they arise. If they can’t be resolved, doctors should ensure that there’s continuity of care when patients change physicians, said Ms. Adler.
About 90% of physicians have dismissed at least one patient during their career, according to a study of nearly 800 primary care practices. The most common reasons were legitimate: a patient was “extremely disruptive and/or behaved inappropriately toward clinicians or staff”; a patient had “violated chronic pain and controlled substance policies”; and a patient had “repeatedly missed appointments.”
Jacqui O’Kane, DO, a family physician at South Georgia Medical Center in rural Nashville, said she has dismissed about 15 of 3,000 patients she has seen in the past 3 years at the clinic. Before she dismisses a patient, she looks at whether there has been a pattern of behavior and tries to talk to them about the problem first to find out if there are other reasons for it.
She also gives patients a warning: If the unacceptable behavior continues, it will lead to their dismissal.
When patients cross a line
Dr. O’Kane warned an elderly man who used the N-word with her that she wouldn’t tolerate that language in her office. Then, when he later called her front office employee the N-word, she decided to dismiss him.
“I said, ‘That’s it, you can’t say that to someone in this office. I already told you once, and you did it again. I’m sorry, you have to find another doctor,’ ” said Dr. O’Kane.
Another patient crossed a line when she missed four appointments, refused to come in, and kept sending Dr. O’Kane long messages on MyChart demanding medications and advice. One message was fairly obtrusive: “If you don’t give me something stronger for my nerves TODAY, I am going to LOSE MY MIND!!!” Dr. O’Kane said the patient wrote.
“I then told her that’s not how I run my practice and that she needed to find someone else.”
Another common reason doctors dismiss patients is for nonpayment, says Ms. Adler.
Recently, however, some patients have also begun demanding their money back from doctors for services already received and billed because they were unhappy about something that occurred at the doctor’s office, said Ms. Adler.
“I advise doctors to respond: ‘We disagree that you didn’t get the service, but we will give you your money back, and we’re also terminating you from our practice.’ At that point, the doctor-patient relationship has become impossible,” said Ms. Adler.
How to dismiss difficult patients ethically and legally
According to the AMA’s Council on Ethical and Judicial Affairs, a physician may not discontinue treatment of a patient if further treatment is medically indicated without giving the patient reasonable notice and sufficient opportunity to make alternative arrangements for care.
Terminating a patient abruptly without transferring their care could lead to a claim of patient abandonment and the physician being called before a licensing board for potentially violating the state’s Medical Practice Act, said Ms. Adler.
Doctors can take these six steps to set the stage for dismissal and avoid a claim of patient abandonment.
1. Create written policies. Medical practices can describe the rules and behavior they expect from patients in these policies, which can cover, for example, payment, treating staff with courtesy, and medications. “When the rules are in writing and patients sign off on them, that gives doctors a certain comfort level in being able to refer to them and say that the patient hasn’t been compliant,” said Ms. Adler.
She also recommends that your practice create a policy that doctors should let the patient know about their concerns and meet with them to discuss the problem before receiving a termination letter.
2. Document any consistent problems you’re having with a patient. When you start having problems with a patient, you should document when the problem occurred, how often it occurred, any discussions with the patient about the problem, warnings you gave the patient, and if and when you decided to terminate the patient.
3. Meet with the patient to discuss the problem. “Talking and meeting with a patient also allows the physician to assess whether there’s another issue. For example, is there a mental health concern? Is there a financial reason for nonpayment or no-shows? There are multiple benefits to finding out what the problem is,” said Ms. Adler.
Once you’ve decided to terminate a patient, here’s what you should do:
4. Allow enough time for the patient to find alternative care. Ms. Adler recommends giving patients 30 days’ notice and that physicians offer to provide emergency care during that time. However, if the patient is undergoing treatment or has other challenges, more time may be needed to transfer care.
“It’s important to consider the patient’s context – if the patient is receiving cancer treatment, or is in a late stage of pregnancy, or lives in a rural area where few specialists are available, you may want to treat them longer – at least until they finish their treatment,” said Ms. Adler. Also, states may have their own requirements about minimum notice periods, she said.
5. Provide patients with written notice that you intend to terminate their care. Ms. Adler recommends that each letter be tailored to the patient’s specific circumstances. “You could spell out a patient’s history of noncompliance or nonpayment or inappropriate conduct because it’s been documented and the patient is already aware of it from a previous discussion,” she said.
Ms. Adler also recommends that doctors consult with legal counsel when in doubt or if contacted by the patient’s lawyer. Some lawyers will draft the termination letters, she said.
6. Include the following information in the written letter: The date that they will no longer receive care, how they can obtain copies of their medical records, and how they can find a new physician by providing contact information for a state medical association or similar organization, which often maintains a database of clinicians by specialty and location.
The letter should also state that the doctor will provide emergency care during the 30 days. Ms. Adler also recommends sending the notice by certified mail.
Dr. O’Kane said she may be more likely to give patients a second chance because she practices in a rural underserved area, and she understands that her patients don’t have many other options for health care. She also has developed a reputation for being willing to take on difficult patients that other physicians didn’t want to deal with, she said.
She encourages physicians to talk to patients to find out why, for example, they may not be compliant with medications.
“The patient may say, ‘I had to choose between paying for medications and putting food on the table,’ ” said Dr. O’Kane.
A version of this article first appeared on Medscape.com.
Some patients continually cancel their appointments, ignore your medical directions, treat your staff rudely, or send you harassing emails.
Do you have to tolerate their behavior?
No, these are all appropriate reasons to terminate patients, attorneys say. Patients also can be dismissed for misleading doctors about their past medical history, chronic drug-seeking, displaying threatening or seductive behavior toward staff members or physicians, or any criminal behavior in the office, experts say.
But even if a reason seems legitimate, that doesn’t make it legal. Doctors should consider whether the reason is legal, said Chicago-area attorney Ericka Adler, JD, a partner at Roetzel & Andress, who advises doctors about terminating patients.
Ms. Adler said.
Terminating patients for an “illegal” reason such as discrimination based on race or gender or sexual orientation – even if couched as a legitimate patient issue – could open the practice to a lawsuit, Ms. Adler said.
Doctors also want to avoid patient abandonment claims by talking to the patient about problems and documenting them as they arise. If they can’t be resolved, doctors should ensure that there’s continuity of care when patients change physicians, said Ms. Adler.
About 90% of physicians have dismissed at least one patient during their career, according to a study of nearly 800 primary care practices. The most common reasons were legitimate: a patient was “extremely disruptive and/or behaved inappropriately toward clinicians or staff”; a patient had “violated chronic pain and controlled substance policies”; and a patient had “repeatedly missed appointments.”
Jacqui O’Kane, DO, a family physician at South Georgia Medical Center in rural Nashville, said she has dismissed about 15 of 3,000 patients she has seen in the past 3 years at the clinic. Before she dismisses a patient, she looks at whether there has been a pattern of behavior and tries to talk to them about the problem first to find out if there are other reasons for it.
She also gives patients a warning: If the unacceptable behavior continues, it will lead to their dismissal.
When patients cross a line
Dr. O’Kane warned an elderly man who used the N-word with her that she wouldn’t tolerate that language in her office. Then, when he later called her front office employee the N-word, she decided to dismiss him.
“I said, ‘That’s it, you can’t say that to someone in this office. I already told you once, and you did it again. I’m sorry, you have to find another doctor,’ ” said Dr. O’Kane.
Another patient crossed a line when she missed four appointments, refused to come in, and kept sending Dr. O’Kane long messages on MyChart demanding medications and advice. One message was fairly obtrusive: “If you don’t give me something stronger for my nerves TODAY, I am going to LOSE MY MIND!!!” Dr. O’Kane said the patient wrote.
“I then told her that’s not how I run my practice and that she needed to find someone else.”
Another common reason doctors dismiss patients is for nonpayment, says Ms. Adler.
Recently, however, some patients have also begun demanding their money back from doctors for services already received and billed because they were unhappy about something that occurred at the doctor’s office, said Ms. Adler.
“I advise doctors to respond: ‘We disagree that you didn’t get the service, but we will give you your money back, and we’re also terminating you from our practice.’ At that point, the doctor-patient relationship has become impossible,” said Ms. Adler.
How to dismiss difficult patients ethically and legally
According to the AMA’s Council on Ethical and Judicial Affairs, a physician may not discontinue treatment of a patient if further treatment is medically indicated without giving the patient reasonable notice and sufficient opportunity to make alternative arrangements for care.
Terminating a patient abruptly without transferring their care could lead to a claim of patient abandonment and the physician being called before a licensing board for potentially violating the state’s Medical Practice Act, said Ms. Adler.
Doctors can take these six steps to set the stage for dismissal and avoid a claim of patient abandonment.
1. Create written policies. Medical practices can describe the rules and behavior they expect from patients in these policies, which can cover, for example, payment, treating staff with courtesy, and medications. “When the rules are in writing and patients sign off on them, that gives doctors a certain comfort level in being able to refer to them and say that the patient hasn’t been compliant,” said Ms. Adler.
She also recommends that your practice create a policy that doctors should let the patient know about their concerns and meet with them to discuss the problem before receiving a termination letter.
2. Document any consistent problems you’re having with a patient. When you start having problems with a patient, you should document when the problem occurred, how often it occurred, any discussions with the patient about the problem, warnings you gave the patient, and if and when you decided to terminate the patient.
3. Meet with the patient to discuss the problem. “Talking and meeting with a patient also allows the physician to assess whether there’s another issue. For example, is there a mental health concern? Is there a financial reason for nonpayment or no-shows? There are multiple benefits to finding out what the problem is,” said Ms. Adler.
Once you’ve decided to terminate a patient, here’s what you should do:
4. Allow enough time for the patient to find alternative care. Ms. Adler recommends giving patients 30 days’ notice and that physicians offer to provide emergency care during that time. However, if the patient is undergoing treatment or has other challenges, more time may be needed to transfer care.
“It’s important to consider the patient’s context – if the patient is receiving cancer treatment, or is in a late stage of pregnancy, or lives in a rural area where few specialists are available, you may want to treat them longer – at least until they finish their treatment,” said Ms. Adler. Also, states may have their own requirements about minimum notice periods, she said.
5. Provide patients with written notice that you intend to terminate their care. Ms. Adler recommends that each letter be tailored to the patient’s specific circumstances. “You could spell out a patient’s history of noncompliance or nonpayment or inappropriate conduct because it’s been documented and the patient is already aware of it from a previous discussion,” she said.
Ms. Adler also recommends that doctors consult with legal counsel when in doubt or if contacted by the patient’s lawyer. Some lawyers will draft the termination letters, she said.
6. Include the following information in the written letter: The date that they will no longer receive care, how they can obtain copies of their medical records, and how they can find a new physician by providing contact information for a state medical association or similar organization, which often maintains a database of clinicians by specialty and location.
The letter should also state that the doctor will provide emergency care during the 30 days. Ms. Adler also recommends sending the notice by certified mail.
Dr. O’Kane said she may be more likely to give patients a second chance because she practices in a rural underserved area, and she understands that her patients don’t have many other options for health care. She also has developed a reputation for being willing to take on difficult patients that other physicians didn’t want to deal with, she said.
She encourages physicians to talk to patients to find out why, for example, they may not be compliant with medications.
“The patient may say, ‘I had to choose between paying for medications and putting food on the table,’ ” said Dr. O’Kane.
A version of this article first appeared on Medscape.com.
Low-calorie tastes sweeter with a little salt
Low-calorie tastes sweeter with a little salt
Diet and sugar-free foods and drinks seem like a good idea, but it’s hard to get past that strange aftertaste, right? It’s the calling card for the noncaloric aspartame- and stevia-containing sweeteners that we consume to make us feel like we can have the best of both worlds.
That weird lingering taste can be a total turn-off for some (raises hand), but researchers have found an almost facepalm solution to the not-so-sweet problem, and it’s salt.
Now, the concept of sweet and salty is not a far-fetched partnership when it comes to snack consumption (try M&Ms in your popcorn). The researchers at Almendra, a manufacturer of stevia sweeteners, put that iconic flavor pair to the test by adding mineral salts that have some nutritional value to lessen the effect of a stevia compound, rebaudioside A, found in noncaloric sweeteners.
The researchers added in magnesium chloride, calcium chloride, and potassium chloride separately to lessen rebaudioside A’s intensity, but they needed so much salt that it killed the sweet taste completely. A blend of the three mineral salts, however, reduced the lingering taste by 79% and improved the real sugar-like taste. The researchers tried this blend in reduced-calorie orange juice and a citrus-flavored soft drink, improving the taste in both.
The salty and sweet match comes in for the win once again. This time helping against the fight of obesity instead of making it worse.
Pseudomonas’ Achilles’ heel is more of an Achilles’ genetic switch
Today, on the long-awaited return of “Bacteria vs. the World,” we meet one of the rock stars of infectious disease.
LOTME: Through the use of imaginary technology, we’re talking to Pseudomonas aeruginosa. Thanks for joining us on such short notice, after Neisseria gonorrhoeae canceled at the last minute.
P. aeruginosa: No problem. I think we can all guess what that little devil is up to.
LOTME: Bacterial resistance to antibiotics is a huge problem for our species. What makes you so hard to fight?
P. aeruginosa: We’ve been trying to keep that a secret, actually, but now that researchers in Switzerland and Denmark seem to have figured it out, I guess it’s okay for me to spill the beans.
LOTME: Beans? What do beans have to do with it?
P. aeruginosa: Nothing, it’s just a colloquial expression that means I’m sharing previously private information.
LOTME: Sure, we knew that. Please, continue your spilling.
P. aeruginosa: The secret is … Well, let’s just say we were a little worried when the Clash released “Should I Stay or Should I Go” back in the 1980s.
LOTME: The Clash? Now we’re really confused.
P. aeruginosa: The answer to their question, “Should I stay or should I go? is yes. Successful invasion of a human is all about division of labor. “While one fraction of the bacterial population adheres to the mucosal surface and forms a biofilm, the other subpopulation spreads to distant tissue sites,” is how the investigators described it. We can increase surface colonization by using a “job-sharing” process, they said, and even resist antibiotics because most of us remain in the protective biofilm.
LOTME: And they say you guys don’t have brains.
P. aeruginosa: But wait, there’s more. We don’t just divide the labor randomly. After the initial colonization we form two functionally distinct subpopulations. One has high levels of the bacterial signaling molecule c-di-GMP and stays put to work on the biofilm. The other group, with low levels of c-di-GMP, heads out to the surrounding tissue to continue the colonization. As project leader Urs Jenal put it, “By identifying the genetic switch, we have tracked down the Achilles heel of the pathogen.”
LOTME: Pretty clever stuff, for humans, anyway.
P. aeruginosa: We agree, but now that you know our secret, we can’t let you share it.
LOTME: Wait! The journal article’s already been published. Your secret is out. You can’t stop that by infecting me.
P. aeruginosa: True enough, but are you familiar with the fable of the scorpion and the frog? It’s our nature.
LOTME: Nooooo! N. gonorrhoeae wouldn’t have done this!
What a pain in the Butt
Businesses rise and businesses fall. We all know that one cursed location, that spot in town where we see businesses move in and close up in a matter of months. At the same time, though, there are also businesses that have been around as long as anyone can remember, pillars of the community.
Corydon, IN., likely has a few such long-lived shops, but it is officially down one 70-year-old family business as of late April, with the unfortunate passing of beloved local pharmacy Butt Drugs. Prescription pick-up in rear.
The business dates back to 1952, when it was founded as William H. Butt Drugs. We’re sure William Butt was never teased about his last name. Nope. No one would ever do that. After he passed the store to his children, it underwent a stint as Butt Rexall Drugs. When the shop was passed down to its third-generation and ultimately final owner, Katie Butt Beckort, she decided to simplify the name. Get right down to the bottom of things, as it were.
Butt Drugs was a popular spot, featuring an old-school soda fountain and themed souvenirs. According to Ms. Butt Beckort, people would come from miles away to buy “I love Butt Drugs” T-shirts, magnets, and so on. Yes, they knew perfectly well what they were sitting on.
So, if was such a hit, why did it close? Butt Drugs may have a hilarious name and merchandise to match, but the pharmacy portion of the pharmacy had been losing money for years. You know, the actual point of the business. As with so many things, we can blame it on the insurance companies. More than half the drugs that passed through Butt Drugs’ doors were sold at a loss, because the insurance companies refused to reimburse the store more than the wholesale price of the drug. Not even a good butt drug could clear up that financial diarrhea.
And so, we’ve lost Butt Drugs forever. Spicy food enthusiasts, coffee drinkers, and all patrons of Taco Bell, take a moment to reflect and mourn on what you’ve lost. No more Butt Drugs to relieve your suffering. A true kick in the butt indeed.
Low-calorie tastes sweeter with a little salt
Diet and sugar-free foods and drinks seem like a good idea, but it’s hard to get past that strange aftertaste, right? It’s the calling card for the noncaloric aspartame- and stevia-containing sweeteners that we consume to make us feel like we can have the best of both worlds.
That weird lingering taste can be a total turn-off for some (raises hand), but researchers have found an almost facepalm solution to the not-so-sweet problem, and it’s salt.
Now, the concept of sweet and salty is not a far-fetched partnership when it comes to snack consumption (try M&Ms in your popcorn). The researchers at Almendra, a manufacturer of stevia sweeteners, put that iconic flavor pair to the test by adding mineral salts that have some nutritional value to lessen the effect of a stevia compound, rebaudioside A, found in noncaloric sweeteners.
The researchers added in magnesium chloride, calcium chloride, and potassium chloride separately to lessen rebaudioside A’s intensity, but they needed so much salt that it killed the sweet taste completely. A blend of the three mineral salts, however, reduced the lingering taste by 79% and improved the real sugar-like taste. The researchers tried this blend in reduced-calorie orange juice and a citrus-flavored soft drink, improving the taste in both.
The salty and sweet match comes in for the win once again. This time helping against the fight of obesity instead of making it worse.
Pseudomonas’ Achilles’ heel is more of an Achilles’ genetic switch
Today, on the long-awaited return of “Bacteria vs. the World,” we meet one of the rock stars of infectious disease.
LOTME: Through the use of imaginary technology, we’re talking to Pseudomonas aeruginosa. Thanks for joining us on such short notice, after Neisseria gonorrhoeae canceled at the last minute.
P. aeruginosa: No problem. I think we can all guess what that little devil is up to.
LOTME: Bacterial resistance to antibiotics is a huge problem for our species. What makes you so hard to fight?
P. aeruginosa: We’ve been trying to keep that a secret, actually, but now that researchers in Switzerland and Denmark seem to have figured it out, I guess it’s okay for me to spill the beans.
LOTME: Beans? What do beans have to do with it?
P. aeruginosa: Nothing, it’s just a colloquial expression that means I’m sharing previously private information.
LOTME: Sure, we knew that. Please, continue your spilling.
P. aeruginosa: The secret is … Well, let’s just say we were a little worried when the Clash released “Should I Stay or Should I Go” back in the 1980s.
LOTME: The Clash? Now we’re really confused.
P. aeruginosa: The answer to their question, “Should I stay or should I go? is yes. Successful invasion of a human is all about division of labor. “While one fraction of the bacterial population adheres to the mucosal surface and forms a biofilm, the other subpopulation spreads to distant tissue sites,” is how the investigators described it. We can increase surface colonization by using a “job-sharing” process, they said, and even resist antibiotics because most of us remain in the protective biofilm.
LOTME: And they say you guys don’t have brains.
P. aeruginosa: But wait, there’s more. We don’t just divide the labor randomly. After the initial colonization we form two functionally distinct subpopulations. One has high levels of the bacterial signaling molecule c-di-GMP and stays put to work on the biofilm. The other group, with low levels of c-di-GMP, heads out to the surrounding tissue to continue the colonization. As project leader Urs Jenal put it, “By identifying the genetic switch, we have tracked down the Achilles heel of the pathogen.”
LOTME: Pretty clever stuff, for humans, anyway.
P. aeruginosa: We agree, but now that you know our secret, we can’t let you share it.
LOTME: Wait! The journal article’s already been published. Your secret is out. You can’t stop that by infecting me.
P. aeruginosa: True enough, but are you familiar with the fable of the scorpion and the frog? It’s our nature.
LOTME: Nooooo! N. gonorrhoeae wouldn’t have done this!
What a pain in the Butt
Businesses rise and businesses fall. We all know that one cursed location, that spot in town where we see businesses move in and close up in a matter of months. At the same time, though, there are also businesses that have been around as long as anyone can remember, pillars of the community.
Corydon, IN., likely has a few such long-lived shops, but it is officially down one 70-year-old family business as of late April, with the unfortunate passing of beloved local pharmacy Butt Drugs. Prescription pick-up in rear.
The business dates back to 1952, when it was founded as William H. Butt Drugs. We’re sure William Butt was never teased about his last name. Nope. No one would ever do that. After he passed the store to his children, it underwent a stint as Butt Rexall Drugs. When the shop was passed down to its third-generation and ultimately final owner, Katie Butt Beckort, she decided to simplify the name. Get right down to the bottom of things, as it were.
Butt Drugs was a popular spot, featuring an old-school soda fountain and themed souvenirs. According to Ms. Butt Beckort, people would come from miles away to buy “I love Butt Drugs” T-shirts, magnets, and so on. Yes, they knew perfectly well what they were sitting on.
So, if was such a hit, why did it close? Butt Drugs may have a hilarious name and merchandise to match, but the pharmacy portion of the pharmacy had been losing money for years. You know, the actual point of the business. As with so many things, we can blame it on the insurance companies. More than half the drugs that passed through Butt Drugs’ doors were sold at a loss, because the insurance companies refused to reimburse the store more than the wholesale price of the drug. Not even a good butt drug could clear up that financial diarrhea.
And so, we’ve lost Butt Drugs forever. Spicy food enthusiasts, coffee drinkers, and all patrons of Taco Bell, take a moment to reflect and mourn on what you’ve lost. No more Butt Drugs to relieve your suffering. A true kick in the butt indeed.
Low-calorie tastes sweeter with a little salt
Diet and sugar-free foods and drinks seem like a good idea, but it’s hard to get past that strange aftertaste, right? It’s the calling card for the noncaloric aspartame- and stevia-containing sweeteners that we consume to make us feel like we can have the best of both worlds.
That weird lingering taste can be a total turn-off for some (raises hand), but researchers have found an almost facepalm solution to the not-so-sweet problem, and it’s salt.
Now, the concept of sweet and salty is not a far-fetched partnership when it comes to snack consumption (try M&Ms in your popcorn). The researchers at Almendra, a manufacturer of stevia sweeteners, put that iconic flavor pair to the test by adding mineral salts that have some nutritional value to lessen the effect of a stevia compound, rebaudioside A, found in noncaloric sweeteners.
The researchers added in magnesium chloride, calcium chloride, and potassium chloride separately to lessen rebaudioside A’s intensity, but they needed so much salt that it killed the sweet taste completely. A blend of the three mineral salts, however, reduced the lingering taste by 79% and improved the real sugar-like taste. The researchers tried this blend in reduced-calorie orange juice and a citrus-flavored soft drink, improving the taste in both.
The salty and sweet match comes in for the win once again. This time helping against the fight of obesity instead of making it worse.
Pseudomonas’ Achilles’ heel is more of an Achilles’ genetic switch
Today, on the long-awaited return of “Bacteria vs. the World,” we meet one of the rock stars of infectious disease.
LOTME: Through the use of imaginary technology, we’re talking to Pseudomonas aeruginosa. Thanks for joining us on such short notice, after Neisseria gonorrhoeae canceled at the last minute.
P. aeruginosa: No problem. I think we can all guess what that little devil is up to.
LOTME: Bacterial resistance to antibiotics is a huge problem for our species. What makes you so hard to fight?
P. aeruginosa: We’ve been trying to keep that a secret, actually, but now that researchers in Switzerland and Denmark seem to have figured it out, I guess it’s okay for me to spill the beans.
LOTME: Beans? What do beans have to do with it?
P. aeruginosa: Nothing, it’s just a colloquial expression that means I’m sharing previously private information.
LOTME: Sure, we knew that. Please, continue your spilling.
P. aeruginosa: The secret is … Well, let’s just say we were a little worried when the Clash released “Should I Stay or Should I Go” back in the 1980s.
LOTME: The Clash? Now we’re really confused.
P. aeruginosa: The answer to their question, “Should I stay or should I go? is yes. Successful invasion of a human is all about division of labor. “While one fraction of the bacterial population adheres to the mucosal surface and forms a biofilm, the other subpopulation spreads to distant tissue sites,” is how the investigators described it. We can increase surface colonization by using a “job-sharing” process, they said, and even resist antibiotics because most of us remain in the protective biofilm.
LOTME: And they say you guys don’t have brains.
P. aeruginosa: But wait, there’s more. We don’t just divide the labor randomly. After the initial colonization we form two functionally distinct subpopulations. One has high levels of the bacterial signaling molecule c-di-GMP and stays put to work on the biofilm. The other group, with low levels of c-di-GMP, heads out to the surrounding tissue to continue the colonization. As project leader Urs Jenal put it, “By identifying the genetic switch, we have tracked down the Achilles heel of the pathogen.”
LOTME: Pretty clever stuff, for humans, anyway.
P. aeruginosa: We agree, but now that you know our secret, we can’t let you share it.
LOTME: Wait! The journal article’s already been published. Your secret is out. You can’t stop that by infecting me.
P. aeruginosa: True enough, but are you familiar with the fable of the scorpion and the frog? It’s our nature.
LOTME: Nooooo! N. gonorrhoeae wouldn’t have done this!
What a pain in the Butt
Businesses rise and businesses fall. We all know that one cursed location, that spot in town where we see businesses move in and close up in a matter of months. At the same time, though, there are also businesses that have been around as long as anyone can remember, pillars of the community.
Corydon, IN., likely has a few such long-lived shops, but it is officially down one 70-year-old family business as of late April, with the unfortunate passing of beloved local pharmacy Butt Drugs. Prescription pick-up in rear.
The business dates back to 1952, when it was founded as William H. Butt Drugs. We’re sure William Butt was never teased about his last name. Nope. No one would ever do that. After he passed the store to his children, it underwent a stint as Butt Rexall Drugs. When the shop was passed down to its third-generation and ultimately final owner, Katie Butt Beckort, she decided to simplify the name. Get right down to the bottom of things, as it were.
Butt Drugs was a popular spot, featuring an old-school soda fountain and themed souvenirs. According to Ms. Butt Beckort, people would come from miles away to buy “I love Butt Drugs” T-shirts, magnets, and so on. Yes, they knew perfectly well what they were sitting on.
So, if was such a hit, why did it close? Butt Drugs may have a hilarious name and merchandise to match, but the pharmacy portion of the pharmacy had been losing money for years. You know, the actual point of the business. As with so many things, we can blame it on the insurance companies. More than half the drugs that passed through Butt Drugs’ doors were sold at a loss, because the insurance companies refused to reimburse the store more than the wholesale price of the drug. Not even a good butt drug could clear up that financial diarrhea.
And so, we’ve lost Butt Drugs forever. Spicy food enthusiasts, coffee drinkers, and all patrons of Taco Bell, take a moment to reflect and mourn on what you’ve lost. No more Butt Drugs to relieve your suffering. A true kick in the butt indeed.
How not to establish rapport with your patient
1. Stride confidently into the room to greet your 84-year-old female patient.
2. Introduce yourself saying, “Hi, I’m Dr. Jeff Benabio.”
3. Extend your clenched fist toward her chest and wait for her to reciprocate.
4. Smile awkwardly behind your mask while you wait.
5. Advise that you are doing a fist bump instead of a handshake to prevent the spread of viruses.
6. Wait.
7. Explain that she can bump, also known as “dap,” you back by extending her clenched fist and bumping into yours.
8. Wait a bit more.
9. Lower your fist and pat her on the shoulder with your left hand. Do so gently so it doesn’t seem like you just did a quick right jab followed by a left hook.
10. Sit down diffidently and pray that you can help her so this office visit is not an utter disaster.
It seemed a good idea for 2020: Let’s stop shaking hands while we wait out this viral apocalypse. Sensible, but entering a patient room and just sitting down didn’t work. It felt cold, impolite – this isn’t the DMV. In medicine, a complete stranger has to trust us to get naked, tell intimate secrets, even be stuck by needles all within minutes of meeting. We needed a trust-building substitute greeting.

There was the Muslim hand-on-my-heart greeting. Or the Hindu “namaste” or Buddhist “amituofo” folded hands. Or perhaps the paternalistic shoulder pat? I went with the fist bump. With some of my partner docs, my old MBA squad, my neighbor, the fist bump felt natural, reciprocated without hesitation. But it fails with many patients. To understand why, it’s helpful to know the history of the fist bump, also known as the dap.
Dap is an acronym for Dignity And Pride. It’s a variation of a handshake that originated among Black soldiers in the Vietnam war as a means of showing fraternity and establishing connectedness. In Vietnam, 30% of the combat battalions were Black. Marginalized in the military and at home, they created a greeting that was meaningful and unique. The dap was a series of shakes, bumps, slaps, and hugs that was symbolic. It was a means of showing respect and humility, that no one is above others, that I’ve got your back and you’ve got mine. It was a powerful recognition of humanity and effective means of personal connection. It spread from the Black community to the general population and it exists still today. The choreographed pregame handshake you see so many NBA players engage in is a descendant of the dap. Like many rituals, it reinforces bonds with those who are your people, your team, those you trust.
The more generalized version is the simple fist bump. It is widely used, notably by President Obama, and in the appropriate circumstance, will almost always be reciprocated. But it doesn’t work well to create trust with a stranger. With a patient for example, you are not showing them respect for some accomplishment. Nor are we connecting with them as a member of your team. Unless this is a patient whom you’ve seen many times before, a fist bump attempt might be met with “are you serious?” In fact, a survey done in 2016 asking infectious disease professionals what they thought of fist bumps as a greeting, very few replied it was a good idea. Most felt it was unprofessional. Not to mention that a fist bump does not symbolize an agreement in the way that a handshake does (and has done since at least the 9th century BC).
With COVID waning and masks doffed, I’ve found myself back to handshaking. Yes, I sanitize before and after, another ritual that has symbolic as well as practical significance. I get fewer sideways glances from my geriatric patients for sure. But I do still offer a little dap for my liquid nitrogen–survivor kids and for the occasional fellow Gen Xer. “Wonder Twin powers, activate!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]
1. Stride confidently into the room to greet your 84-year-old female patient.
2. Introduce yourself saying, “Hi, I’m Dr. Jeff Benabio.”
3. Extend your clenched fist toward her chest and wait for her to reciprocate.
4. Smile awkwardly behind your mask while you wait.
5. Advise that you are doing a fist bump instead of a handshake to prevent the spread of viruses.
6. Wait.
7. Explain that she can bump, also known as “dap,” you back by extending her clenched fist and bumping into yours.
8. Wait a bit more.
9. Lower your fist and pat her on the shoulder with your left hand. Do so gently so it doesn’t seem like you just did a quick right jab followed by a left hook.
10. Sit down diffidently and pray that you can help her so this office visit is not an utter disaster.
It seemed a good idea for 2020: Let’s stop shaking hands while we wait out this viral apocalypse. Sensible, but entering a patient room and just sitting down didn’t work. It felt cold, impolite – this isn’t the DMV. In medicine, a complete stranger has to trust us to get naked, tell intimate secrets, even be stuck by needles all within minutes of meeting. We needed a trust-building substitute greeting.
There was the Muslim hand-on-my-heart greeting. Or the Hindu “namaste” or Buddhist “amituofo” folded hands. Or perhaps the paternalistic shoulder pat? I went with the fist bump. With some of my partner docs, my old MBA squad, my neighbor, the fist bump felt natural, reciprocated without hesitation. But it fails with many patients. To understand why, it’s helpful to know the history of the fist bump, also known as the dap.
Dap is an acronym for Dignity And Pride. It’s a variation of a handshake that originated among Black soldiers in the Vietnam war as a means of showing fraternity and establishing connectedness. In Vietnam, 30% of the combat battalions were Black. Marginalized in the military and at home, they created a greeting that was meaningful and unique. The dap was a series of shakes, bumps, slaps, and hugs that was symbolic. It was a means of showing respect and humility, that no one is above others, that I’ve got your back and you’ve got mine. It was a powerful recognition of humanity and effective means of personal connection. It spread from the Black community to the general population and it exists still today. The choreographed pregame handshake you see so many NBA players engage in is a descendant of the dap. Like many rituals, it reinforces bonds with those who are your people, your team, those you trust.
The more generalized version is the simple fist bump. It is widely used, notably by President Obama, and in the appropriate circumstance, will almost always be reciprocated. But it doesn’t work well to create trust with a stranger. With a patient for example, you are not showing them respect for some accomplishment. Nor are we connecting with them as a member of your team. Unless this is a patient whom you’ve seen many times before, a fist bump attempt might be met with “are you serious?” In fact, a survey done in 2016 asking infectious disease professionals what they thought of fist bumps as a greeting, very few replied it was a good idea. Most felt it was unprofessional. Not to mention that a fist bump does not symbolize an agreement in the way that a handshake does (and has done since at least the 9th century BC).
With COVID waning and masks doffed, I’ve found myself back to handshaking. Yes, I sanitize before and after, another ritual that has symbolic as well as practical significance. I get fewer sideways glances from my geriatric patients for sure. But I do still offer a little dap for my liquid nitrogen–survivor kids and for the occasional fellow Gen Xer. “Wonder Twin powers, activate!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]
1. Stride confidently into the room to greet your 84-year-old female patient.
2. Introduce yourself saying, “Hi, I’m Dr. Jeff Benabio.”
3. Extend your clenched fist toward her chest and wait for her to reciprocate.
4. Smile awkwardly behind your mask while you wait.
5. Advise that you are doing a fist bump instead of a handshake to prevent the spread of viruses.
6. Wait.
7. Explain that she can bump, also known as “dap,” you back by extending her clenched fist and bumping into yours.
8. Wait a bit more.
9. Lower your fist and pat her on the shoulder with your left hand. Do so gently so it doesn’t seem like you just did a quick right jab followed by a left hook.
10. Sit down diffidently and pray that you can help her so this office visit is not an utter disaster.
It seemed a good idea for 2020: Let’s stop shaking hands while we wait out this viral apocalypse. Sensible, but entering a patient room and just sitting down didn’t work. It felt cold, impolite – this isn’t the DMV. In medicine, a complete stranger has to trust us to get naked, tell intimate secrets, even be stuck by needles all within minutes of meeting. We needed a trust-building substitute greeting.
There was the Muslim hand-on-my-heart greeting. Or the Hindu “namaste” or Buddhist “amituofo” folded hands. Or perhaps the paternalistic shoulder pat? I went with the fist bump. With some of my partner docs, my old MBA squad, my neighbor, the fist bump felt natural, reciprocated without hesitation. But it fails with many patients. To understand why, it’s helpful to know the history of the fist bump, also known as the dap.
Dap is an acronym for Dignity And Pride. It’s a variation of a handshake that originated among Black soldiers in the Vietnam war as a means of showing fraternity and establishing connectedness. In Vietnam, 30% of the combat battalions were Black. Marginalized in the military and at home, they created a greeting that was meaningful and unique. The dap was a series of shakes, bumps, slaps, and hugs that was symbolic. It was a means of showing respect and humility, that no one is above others, that I’ve got your back and you’ve got mine. It was a powerful recognition of humanity and effective means of personal connection. It spread from the Black community to the general population and it exists still today. The choreographed pregame handshake you see so many NBA players engage in is a descendant of the dap. Like many rituals, it reinforces bonds with those who are your people, your team, those you trust.
The more generalized version is the simple fist bump. It is widely used, notably by President Obama, and in the appropriate circumstance, will almost always be reciprocated. But it doesn’t work well to create trust with a stranger. With a patient for example, you are not showing them respect for some accomplishment. Nor are we connecting with them as a member of your team. Unless this is a patient whom you’ve seen many times before, a fist bump attempt might be met with “are you serious?” In fact, a survey done in 2016 asking infectious disease professionals what they thought of fist bumps as a greeting, very few replied it was a good idea. Most felt it was unprofessional. Not to mention that a fist bump does not symbolize an agreement in the way that a handshake does (and has done since at least the 9th century BC).
With COVID waning and masks doffed, I’ve found myself back to handshaking. Yes, I sanitize before and after, another ritual that has symbolic as well as practical significance. I get fewer sideways glances from my geriatric patients for sure. But I do still offer a little dap for my liquid nitrogen–survivor kids and for the occasional fellow Gen Xer. “Wonder Twin powers, activate!”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]
Should you have a chaperone in the exam room? Many say yes
This transcript has been edited for clarity.
I’m Art Caplan, PhD. I’m at the division of medical ethics at NYU’s Grossman School of Medicine.
, such as breasts, genitalia, and the perianal area.
In some institutions, there has been a movement toward saying a chaperone must be present, that it’s mandatory. I know that is true at Yale’s health care centers and clinics. Others do so when the patient requests it. An interesting situation sometimes occurs when the hospital or the clinic requires a chaperone but the patient says, “I don’t want a chaperone. I want my privacy. I want the gynecologist or the urologist only. I don’t want anyone else to be seeing me. I’m not comfortable with anyone other than the doctor in the room.”
Complicating this issue of when is a chaperone appropriate and when can it be refused, if ever, is the fact that the role of chaperone is ill defined. For example, there isn’t really agreement on who can be a chaperone. Could it be a medical student? Could it be a nurse? Could it be another doctor? Should it be someone who at least has finished nursing school or medical school? Can it be a patient representative? There are no standards about who can play the role.
Should the chaperone be available to be seen when they’re in the room? Should they stay behind a curtain or somewhere where they’re not, so to speak, intrusive into what’s going on in the exam room? Do they sit in a chair? Do they stand? How do they behave, if you will? There’s no agreement.
There’s still no agreement on the training that a chaperone should have. Do we charge them with trying to represent what’s going on with the patient or trying to protect the doctor against any accusations that are ill founded about inappropriate conduct? Are they supposed to do both? How do they obtain consent, if they do, from the patient undergoing an examination in a sensitive part of their body or one that they’re sensitive about?
This area really requires some hard thinking if you’re considering having chaperones present. I think there are some online courses that offer some training. I haven’t looked at them, but they might be worth a look to see if they make you more comfortable about getting a chaperone oriented. I think it’s probably important to set a policy saying a chaperone must always be present for these kinds of examinations and list them, or one can be requested no matter what is going on in terms of the kind of exam being conducted.
There needs to be some statement saying that you have permission to either accept them or refuse them – or you don’t. Should they always be present, for example, with patients who are minors, adolescents or children? Does that extend that far out where a guardian, parent, or someone has to give permission?
In this area, I think we can all understand why chaperones have come to the fore, including allegations of misconduct and inappropriate touching, and considering comfort levels of patients to just put them more at ease. It’s obvious that we haven’t, as a nation or a medical profession, thought it through to the degree to which we have to.
I’m certainly not anti-chaperone, and I believe that if patients are more comfortable having one present, or a doctor is more comfortable having one present, or if we all agree that there are certain patients – kids – where certain types of examinations require or ought to expect the chaperone to be present, that’s wonderful.
We’ve got to lay out the rights of the doctors. We’ve got to lay out the rights of the institutions. We’ve got to lay out the rights of the patients. We should agree on who these people are. We should agree on how they’re trained.
We’ve got some work ahead of us if we’re going to have chaperones become a standard part of the medical examination.
Dr. Kaplan reported conflicts of interest with the Franklin Institute, Tengion, Biogen Idec, Johnson & Johnson, and PriCara.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Art Caplan, PhD. I’m at the division of medical ethics at NYU’s Grossman School of Medicine.
, such as breasts, genitalia, and the perianal area.
In some institutions, there has been a movement toward saying a chaperone must be present, that it’s mandatory. I know that is true at Yale’s health care centers and clinics. Others do so when the patient requests it. An interesting situation sometimes occurs when the hospital or the clinic requires a chaperone but the patient says, “I don’t want a chaperone. I want my privacy. I want the gynecologist or the urologist only. I don’t want anyone else to be seeing me. I’m not comfortable with anyone other than the doctor in the room.”
Complicating this issue of when is a chaperone appropriate and when can it be refused, if ever, is the fact that the role of chaperone is ill defined. For example, there isn’t really agreement on who can be a chaperone. Could it be a medical student? Could it be a nurse? Could it be another doctor? Should it be someone who at least has finished nursing school or medical school? Can it be a patient representative? There are no standards about who can play the role.
Should the chaperone be available to be seen when they’re in the room? Should they stay behind a curtain or somewhere where they’re not, so to speak, intrusive into what’s going on in the exam room? Do they sit in a chair? Do they stand? How do they behave, if you will? There’s no agreement.
There’s still no agreement on the training that a chaperone should have. Do we charge them with trying to represent what’s going on with the patient or trying to protect the doctor against any accusations that are ill founded about inappropriate conduct? Are they supposed to do both? How do they obtain consent, if they do, from the patient undergoing an examination in a sensitive part of their body or one that they’re sensitive about?
This area really requires some hard thinking if you’re considering having chaperones present. I think there are some online courses that offer some training. I haven’t looked at them, but they might be worth a look to see if they make you more comfortable about getting a chaperone oriented. I think it’s probably important to set a policy saying a chaperone must always be present for these kinds of examinations and list them, or one can be requested no matter what is going on in terms of the kind of exam being conducted.
There needs to be some statement saying that you have permission to either accept them or refuse them – or you don’t. Should they always be present, for example, with patients who are minors, adolescents or children? Does that extend that far out where a guardian, parent, or someone has to give permission?
In this area, I think we can all understand why chaperones have come to the fore, including allegations of misconduct and inappropriate touching, and considering comfort levels of patients to just put them more at ease. It’s obvious that we haven’t, as a nation or a medical profession, thought it through to the degree to which we have to.
I’m certainly not anti-chaperone, and I believe that if patients are more comfortable having one present, or a doctor is more comfortable having one present, or if we all agree that there are certain patients – kids – where certain types of examinations require or ought to expect the chaperone to be present, that’s wonderful.
We’ve got to lay out the rights of the doctors. We’ve got to lay out the rights of the institutions. We’ve got to lay out the rights of the patients. We should agree on who these people are. We should agree on how they’re trained.
We’ve got some work ahead of us if we’re going to have chaperones become a standard part of the medical examination.
Dr. Kaplan reported conflicts of interest with the Franklin Institute, Tengion, Biogen Idec, Johnson & Johnson, and PriCara.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m Art Caplan, PhD. I’m at the division of medical ethics at NYU’s Grossman School of Medicine.
, such as breasts, genitalia, and the perianal area.
In some institutions, there has been a movement toward saying a chaperone must be present, that it’s mandatory. I know that is true at Yale’s health care centers and clinics. Others do so when the patient requests it. An interesting situation sometimes occurs when the hospital or the clinic requires a chaperone but the patient says, “I don’t want a chaperone. I want my privacy. I want the gynecologist or the urologist only. I don’t want anyone else to be seeing me. I’m not comfortable with anyone other than the doctor in the room.”
Complicating this issue of when is a chaperone appropriate and when can it be refused, if ever, is the fact that the role of chaperone is ill defined. For example, there isn’t really agreement on who can be a chaperone. Could it be a medical student? Could it be a nurse? Could it be another doctor? Should it be someone who at least has finished nursing school or medical school? Can it be a patient representative? There are no standards about who can play the role.
Should the chaperone be available to be seen when they’re in the room? Should they stay behind a curtain or somewhere where they’re not, so to speak, intrusive into what’s going on in the exam room? Do they sit in a chair? Do they stand? How do they behave, if you will? There’s no agreement.
There’s still no agreement on the training that a chaperone should have. Do we charge them with trying to represent what’s going on with the patient or trying to protect the doctor against any accusations that are ill founded about inappropriate conduct? Are they supposed to do both? How do they obtain consent, if they do, from the patient undergoing an examination in a sensitive part of their body or one that they’re sensitive about?
This area really requires some hard thinking if you’re considering having chaperones present. I think there are some online courses that offer some training. I haven’t looked at them, but they might be worth a look to see if they make you more comfortable about getting a chaperone oriented. I think it’s probably important to set a policy saying a chaperone must always be present for these kinds of examinations and list them, or one can be requested no matter what is going on in terms of the kind of exam being conducted.
There needs to be some statement saying that you have permission to either accept them or refuse them – or you don’t. Should they always be present, for example, with patients who are minors, adolescents or children? Does that extend that far out where a guardian, parent, or someone has to give permission?
In this area, I think we can all understand why chaperones have come to the fore, including allegations of misconduct and inappropriate touching, and considering comfort levels of patients to just put them more at ease. It’s obvious that we haven’t, as a nation or a medical profession, thought it through to the degree to which we have to.
I’m certainly not anti-chaperone, and I believe that if patients are more comfortable having one present, or a doctor is more comfortable having one present, or if we all agree that there are certain patients – kids – where certain types of examinations require or ought to expect the chaperone to be present, that’s wonderful.
We’ve got to lay out the rights of the doctors. We’ve got to lay out the rights of the institutions. We’ve got to lay out the rights of the patients. We should agree on who these people are. We should agree on how they’re trained.
We’ve got some work ahead of us if we’re going to have chaperones become a standard part of the medical examination.
Dr. Kaplan reported conflicts of interest with the Franklin Institute, Tengion, Biogen Idec, Johnson & Johnson, and PriCara.
A version of this article first appeared on Medscape.com.
How physician-inventors create new, life-saving products
WakeMed emergency department physician and medical director, Graham Snyder, MD, has seen his fair share of deaths: an average of one or two per day. That’s part of the job. Some of the deaths were the result of risky behavior, ongoing health problems, and other natural causes.
But what he didn’t find acceptable was losing a 6-year-old girl in a backyard pool drowning at what was meant to be a celebratory birthday party and family reunion.
“There were aunts and uncles and brothers and sisters and cousins, and the pool was packed, and they’re having a great time. One of the parents looked over and saw that she was swimming around underneath but acting weird. A relative pulled her up by the arm, and she was dead,” he said. “What nobody could tell me, and what they’ll live with the rest of their life, is how long was she under water?”
So Dr. Snyder invented a solution. The catch: The goal: Improving systemic and “unsolvable” issues that harm society.
The cool part: Any MD with an idea can get in on the game.
Keeping little heads above water
Drowning is the leading cause of death in young children ages 1-4 years, and the second leading cause for children ages 5-14 years. The issue, Dr. Snyder explained, is not that rescuers couldn’t get to these children in time. “It’s that nobody knew to start looking.”
Dr. Snyder created a collar that alerts those around the swimmer that they are in trouble. The SEAL SwimSafe drowning prevention technology sets off an alarm system if a child is under water for too long. The necklace has been used to protect more than 10,000 children, including at larger swim facilities, such as the YMCA.
When Dr. Snyder first started pursuing his invention, he asked himself two key questions: “Has someone already tried this? And if they did, why did they not succeed?” These questions help counteract the potential arrogance, he says, with imagining that you are the first person to have a certain idea. And using whatever reason others didn’t succeed as your “secret sauce” helps lead to more success. He also had to consider obstacles. People might resist wearing a collar or necklace while swimming or putting one on their child, like the reluctance around wearing bicycle helmets when they gained popularity in the 1980s. He concluded that the collars would work best at larger facilities, where they were mandated.
Another obstacle was false alarms. “It was possible to trigger a false alarm, and that could really scare people,” Dr. Snyder said. He is still considering systems to prevent the collars from being stolen or from “13-year-old boys hiding them in the water drain and making everyone really scared when an alarm is going off.”
The demand is real, however, and is based on alarming data. Safe Kids has reported that 66% of natural water drownings and around half of pool drownings happened with an adult supervising. They added, however, that supervision is often lacking or insufficient, such as a parent not being within arm’s reach of a young kid. As Dr. Snyder told reporters in a 2018 story, even the most well-intentioned parents still “miss something” sometimes, and this technology is for that moment.
“This is a completely solvable problem, but not a flip-a-switch, one and done,” he said, pointing to his product as a part of a more comprehensive approach, such as in Europe, where mandated public school swimming lessons are helping to decrease drowning deaths.
The pandemic slowed progress for the SEAL SwimSafe collar, which is currently waiting on a new funder or investor to take the reins. But the concept is alive and well with competitors pursuing related ideas. Dr. Snyder is holding out hope that entrepreneurs, scientists, public health workers, researchers, and others will be interested in continuing this work.
Eliminating the stigma of incontinence
Ever had an accident before making it to the bathroom? So have two-thirds of adult women, and almost one-third of older men. Incontinence is linked to a wide variety of conditions, from pelvic-floor trauma to neurological issues to diabetes, and others. Urologist Jessica Lubahn, MD, in Portland, Ore., saw one too many patients feeling this type of shame, unaware that the condition was so common. In addition, she personally experienced childbirth-related incontinence, and helped a relative who was having incontinence after prostate cancer surgery.
“He had a great result, but he had confided in me ... it was one of the only times in his life that he’s been truly depressed,” Dr. Lubahn said. “It’s not even the amount of leakage, but the smell, the stigma is so embarrassing, that not only is it an inconvenience, but [it affects] your entire psyche.” She thought there had to be a better solution than the “demeaning” act of wearing adult diapers.
Noting the explosion of the period panty industry in the past decade, Dr. Lubahn wanted to “destigmatize” incontinence in the same way menstruation education and products have been. She created ONDR incontinence underwear, specifically meant for urine, to ease the mental and physical burden on her patients and many others.
Dr. Lubahn said a process happens when you decide to start talking about the product you want to make rather than trying to find answers on your own. “A lot of people are so afraid to talk about their ideas because they’re afraid it’s going to get stolen or scooped, or it might fail,” she said. “I just openly discussed it, kind of like cocktail party conversation – ‘Wouldn’t it be funny if you just pee into your underwear?’ ” She noticed each connection led to finding more people to help her along her journey.
Dr. Lubahn studied the apparel industry, learning that overseas manufacturers were more helpful and cost-effective. She navigated issues such as a special stitch that prevented leakage and other details. She was also intent on using eco-friendly products that offset the environmental impact of pads, liners, and diapers. She said there’s a strong entrepreneurship community that can help other physician-inventors get grants, be part of accelerator programs, and receive support.
Six years after the original idea, Dr. Lubahn’s product was released in 2020. She now sells eight types of underwear for women and men’s boxer briefs. She wears them herself daily.
Deterring carjackers, saving lives
In 2022, carjackings tripled in Chicago and Memphis. The areas have the highest rates in 30 cities that the Council on Criminal Justice analyzed in a report on pandemic crime rates. According to the report, nearly 40% of offenders used a firearm, more than a quarter of victims were injured, and only around half of the vehicles taken were recovered. In addition, vehicles are sometimes used in secondary crimes, such as drive-by shootings. William Yates, MD, former trauma surgeon, now turned hair restoration surgeon in Chicago, saw the evidence of those crimes daily.
“I was perplexed by carjacking because there wasn’t any answer, and it just kept getting worse and worse. A lot of innocent people were being affected,” he said. “I was seeing deaths – needless. If you give them any push back at all, they will shoot you.”
As a deterrent to counter this “easy crime,” he invented the Yates Device, an alarm system designed to prevent or interrupt carjacking. The driver can activate a switch located beneath the foot pedal or an app on the phone to trigger a programmed high-decibel alarm. Critically, it allows the carjacker to drive a safe distance away from the victim before it starts going off.
The alarm “turns your car into a very noisy Christmas tree on a time delay,” Dr. Yates explained. An external siren blares “stolen vehicle” repeatedly. A camera records everything in the car. Lights flash. Only the original driver can turn off the system. Later, once the car is abandoned, the police can help recover the vehicle.
In Dr. Yates’ experience, the invention process takes longer than you think. He worked through earlier iterations with strobe lights, but these could lead to bystanders getting hurt if the carjacker couldn’t see, for example. Developing the final product and applying for patents was a two-part process.
“The first is part is a pending patent phase, which secures your place in line,” he said. “After 1 year, we filed the utility patent as the final documentation that the invention is truly unique. That has been in process for a year now and the attorneys say we should receive approval soon.”
The product has initially been tested in seven cars for about 1 year. Dr. Yates is measuring how the system performs in all types of weather, including Chicago’s below-zero temperatures. The product is not available to the public for purchase yet because Dr. Yates is still seeking funding to have it mass produced, but it is currently being evaluated by Korean automakers for their car manufacturers.
“Everybody was saying ‘Let’s do something about this,’ but I didn’t see anybody doing anything yet,” Dr. Yates recalled. In the surgeon’s lounge, everybody has ideas. “You go around the room, and every doctor would have five ideas that would make them the richest doctor, but nobody takes it beyond that stage – talk. You have to synthesize that into a plan, to take action.”
Dr. Yates said that many doctors have the intellect to invent, but they aren’t in a network like entrepreneurs to bring their ideas to life.
For Dr. Yates, it takes a curious mindset to solve these daunting problems. “I’m always curious, always looking for how to improve something, to get better outcomes you have to be asking questions and just never let it go.”
A version of this article originally appeared on Medscape.com.
WakeMed emergency department physician and medical director, Graham Snyder, MD, has seen his fair share of deaths: an average of one or two per day. That’s part of the job. Some of the deaths were the result of risky behavior, ongoing health problems, and other natural causes.
But what he didn’t find acceptable was losing a 6-year-old girl in a backyard pool drowning at what was meant to be a celebratory birthday party and family reunion.
“There were aunts and uncles and brothers and sisters and cousins, and the pool was packed, and they’re having a great time. One of the parents looked over and saw that she was swimming around underneath but acting weird. A relative pulled her up by the arm, and she was dead,” he said. “What nobody could tell me, and what they’ll live with the rest of their life, is how long was she under water?”
So Dr. Snyder invented a solution. The catch: The goal: Improving systemic and “unsolvable” issues that harm society.
The cool part: Any MD with an idea can get in on the game.
Keeping little heads above water
Drowning is the leading cause of death in young children ages 1-4 years, and the second leading cause for children ages 5-14 years. The issue, Dr. Snyder explained, is not that rescuers couldn’t get to these children in time. “It’s that nobody knew to start looking.”
Dr. Snyder created a collar that alerts those around the swimmer that they are in trouble. The SEAL SwimSafe drowning prevention technology sets off an alarm system if a child is under water for too long. The necklace has been used to protect more than 10,000 children, including at larger swim facilities, such as the YMCA.
When Dr. Snyder first started pursuing his invention, he asked himself two key questions: “Has someone already tried this? And if they did, why did they not succeed?” These questions help counteract the potential arrogance, he says, with imagining that you are the first person to have a certain idea. And using whatever reason others didn’t succeed as your “secret sauce” helps lead to more success. He also had to consider obstacles. People might resist wearing a collar or necklace while swimming or putting one on their child, like the reluctance around wearing bicycle helmets when they gained popularity in the 1980s. He concluded that the collars would work best at larger facilities, where they were mandated.
Another obstacle was false alarms. “It was possible to trigger a false alarm, and that could really scare people,” Dr. Snyder said. He is still considering systems to prevent the collars from being stolen or from “13-year-old boys hiding them in the water drain and making everyone really scared when an alarm is going off.”
The demand is real, however, and is based on alarming data. Safe Kids has reported that 66% of natural water drownings and around half of pool drownings happened with an adult supervising. They added, however, that supervision is often lacking or insufficient, such as a parent not being within arm’s reach of a young kid. As Dr. Snyder told reporters in a 2018 story, even the most well-intentioned parents still “miss something” sometimes, and this technology is for that moment.
“This is a completely solvable problem, but not a flip-a-switch, one and done,” he said, pointing to his product as a part of a more comprehensive approach, such as in Europe, where mandated public school swimming lessons are helping to decrease drowning deaths.
The pandemic slowed progress for the SEAL SwimSafe collar, which is currently waiting on a new funder or investor to take the reins. But the concept is alive and well with competitors pursuing related ideas. Dr. Snyder is holding out hope that entrepreneurs, scientists, public health workers, researchers, and others will be interested in continuing this work.
Eliminating the stigma of incontinence
Ever had an accident before making it to the bathroom? So have two-thirds of adult women, and almost one-third of older men. Incontinence is linked to a wide variety of conditions, from pelvic-floor trauma to neurological issues to diabetes, and others. Urologist Jessica Lubahn, MD, in Portland, Ore., saw one too many patients feeling this type of shame, unaware that the condition was so common. In addition, she personally experienced childbirth-related incontinence, and helped a relative who was having incontinence after prostate cancer surgery.
“He had a great result, but he had confided in me ... it was one of the only times in his life that he’s been truly depressed,” Dr. Lubahn said. “It’s not even the amount of leakage, but the smell, the stigma is so embarrassing, that not only is it an inconvenience, but [it affects] your entire psyche.” She thought there had to be a better solution than the “demeaning” act of wearing adult diapers.
Noting the explosion of the period panty industry in the past decade, Dr. Lubahn wanted to “destigmatize” incontinence in the same way menstruation education and products have been. She created ONDR incontinence underwear, specifically meant for urine, to ease the mental and physical burden on her patients and many others.
Dr. Lubahn said a process happens when you decide to start talking about the product you want to make rather than trying to find answers on your own. “A lot of people are so afraid to talk about their ideas because they’re afraid it’s going to get stolen or scooped, or it might fail,” she said. “I just openly discussed it, kind of like cocktail party conversation – ‘Wouldn’t it be funny if you just pee into your underwear?’ ” She noticed each connection led to finding more people to help her along her journey.
Dr. Lubahn studied the apparel industry, learning that overseas manufacturers were more helpful and cost-effective. She navigated issues such as a special stitch that prevented leakage and other details. She was also intent on using eco-friendly products that offset the environmental impact of pads, liners, and diapers. She said there’s a strong entrepreneurship community that can help other physician-inventors get grants, be part of accelerator programs, and receive support.
Six years after the original idea, Dr. Lubahn’s product was released in 2020. She now sells eight types of underwear for women and men’s boxer briefs. She wears them herself daily.
Deterring carjackers, saving lives
In 2022, carjackings tripled in Chicago and Memphis. The areas have the highest rates in 30 cities that the Council on Criminal Justice analyzed in a report on pandemic crime rates. According to the report, nearly 40% of offenders used a firearm, more than a quarter of victims were injured, and only around half of the vehicles taken were recovered. In addition, vehicles are sometimes used in secondary crimes, such as drive-by shootings. William Yates, MD, former trauma surgeon, now turned hair restoration surgeon in Chicago, saw the evidence of those crimes daily.
“I was perplexed by carjacking because there wasn’t any answer, and it just kept getting worse and worse. A lot of innocent people were being affected,” he said. “I was seeing deaths – needless. If you give them any push back at all, they will shoot you.”
As a deterrent to counter this “easy crime,” he invented the Yates Device, an alarm system designed to prevent or interrupt carjacking. The driver can activate a switch located beneath the foot pedal or an app on the phone to trigger a programmed high-decibel alarm. Critically, it allows the carjacker to drive a safe distance away from the victim before it starts going off.
The alarm “turns your car into a very noisy Christmas tree on a time delay,” Dr. Yates explained. An external siren blares “stolen vehicle” repeatedly. A camera records everything in the car. Lights flash. Only the original driver can turn off the system. Later, once the car is abandoned, the police can help recover the vehicle.
In Dr. Yates’ experience, the invention process takes longer than you think. He worked through earlier iterations with strobe lights, but these could lead to bystanders getting hurt if the carjacker couldn’t see, for example. Developing the final product and applying for patents was a two-part process.
“The first is part is a pending patent phase, which secures your place in line,” he said. “After 1 year, we filed the utility patent as the final documentation that the invention is truly unique. That has been in process for a year now and the attorneys say we should receive approval soon.”
The product has initially been tested in seven cars for about 1 year. Dr. Yates is measuring how the system performs in all types of weather, including Chicago’s below-zero temperatures. The product is not available to the public for purchase yet because Dr. Yates is still seeking funding to have it mass produced, but it is currently being evaluated by Korean automakers for their car manufacturers.
“Everybody was saying ‘Let’s do something about this,’ but I didn’t see anybody doing anything yet,” Dr. Yates recalled. In the surgeon’s lounge, everybody has ideas. “You go around the room, and every doctor would have five ideas that would make them the richest doctor, but nobody takes it beyond that stage – talk. You have to synthesize that into a plan, to take action.”
Dr. Yates said that many doctors have the intellect to invent, but they aren’t in a network like entrepreneurs to bring their ideas to life.
For Dr. Yates, it takes a curious mindset to solve these daunting problems. “I’m always curious, always looking for how to improve something, to get better outcomes you have to be asking questions and just never let it go.”
A version of this article originally appeared on Medscape.com.
WakeMed emergency department physician and medical director, Graham Snyder, MD, has seen his fair share of deaths: an average of one or two per day. That’s part of the job. Some of the deaths were the result of risky behavior, ongoing health problems, and other natural causes.
But what he didn’t find acceptable was losing a 6-year-old girl in a backyard pool drowning at what was meant to be a celebratory birthday party and family reunion.
“There were aunts and uncles and brothers and sisters and cousins, and the pool was packed, and they’re having a great time. One of the parents looked over and saw that she was swimming around underneath but acting weird. A relative pulled her up by the arm, and she was dead,” he said. “What nobody could tell me, and what they’ll live with the rest of their life, is how long was she under water?”
So Dr. Snyder invented a solution. The catch: The goal: Improving systemic and “unsolvable” issues that harm society.
The cool part: Any MD with an idea can get in on the game.
Keeping little heads above water
Drowning is the leading cause of death in young children ages 1-4 years, and the second leading cause for children ages 5-14 years. The issue, Dr. Snyder explained, is not that rescuers couldn’t get to these children in time. “It’s that nobody knew to start looking.”
Dr. Snyder created a collar that alerts those around the swimmer that they are in trouble. The SEAL SwimSafe drowning prevention technology sets off an alarm system if a child is under water for too long. The necklace has been used to protect more than 10,000 children, including at larger swim facilities, such as the YMCA.
When Dr. Snyder first started pursuing his invention, he asked himself two key questions: “Has someone already tried this? And if they did, why did they not succeed?” These questions help counteract the potential arrogance, he says, with imagining that you are the first person to have a certain idea. And using whatever reason others didn’t succeed as your “secret sauce” helps lead to more success. He also had to consider obstacles. People might resist wearing a collar or necklace while swimming or putting one on their child, like the reluctance around wearing bicycle helmets when they gained popularity in the 1980s. He concluded that the collars would work best at larger facilities, where they were mandated.
Another obstacle was false alarms. “It was possible to trigger a false alarm, and that could really scare people,” Dr. Snyder said. He is still considering systems to prevent the collars from being stolen or from “13-year-old boys hiding them in the water drain and making everyone really scared when an alarm is going off.”
The demand is real, however, and is based on alarming data. Safe Kids has reported that 66% of natural water drownings and around half of pool drownings happened with an adult supervising. They added, however, that supervision is often lacking or insufficient, such as a parent not being within arm’s reach of a young kid. As Dr. Snyder told reporters in a 2018 story, even the most well-intentioned parents still “miss something” sometimes, and this technology is for that moment.
“This is a completely solvable problem, but not a flip-a-switch, one and done,” he said, pointing to his product as a part of a more comprehensive approach, such as in Europe, where mandated public school swimming lessons are helping to decrease drowning deaths.
The pandemic slowed progress for the SEAL SwimSafe collar, which is currently waiting on a new funder or investor to take the reins. But the concept is alive and well with competitors pursuing related ideas. Dr. Snyder is holding out hope that entrepreneurs, scientists, public health workers, researchers, and others will be interested in continuing this work.
Eliminating the stigma of incontinence
Ever had an accident before making it to the bathroom? So have two-thirds of adult women, and almost one-third of older men. Incontinence is linked to a wide variety of conditions, from pelvic-floor trauma to neurological issues to diabetes, and others. Urologist Jessica Lubahn, MD, in Portland, Ore., saw one too many patients feeling this type of shame, unaware that the condition was so common. In addition, she personally experienced childbirth-related incontinence, and helped a relative who was having incontinence after prostate cancer surgery.
“He had a great result, but he had confided in me ... it was one of the only times in his life that he’s been truly depressed,” Dr. Lubahn said. “It’s not even the amount of leakage, but the smell, the stigma is so embarrassing, that not only is it an inconvenience, but [it affects] your entire psyche.” She thought there had to be a better solution than the “demeaning” act of wearing adult diapers.
Noting the explosion of the period panty industry in the past decade, Dr. Lubahn wanted to “destigmatize” incontinence in the same way menstruation education and products have been. She created ONDR incontinence underwear, specifically meant for urine, to ease the mental and physical burden on her patients and many others.
Dr. Lubahn said a process happens when you decide to start talking about the product you want to make rather than trying to find answers on your own. “A lot of people are so afraid to talk about their ideas because they’re afraid it’s going to get stolen or scooped, or it might fail,” she said. “I just openly discussed it, kind of like cocktail party conversation – ‘Wouldn’t it be funny if you just pee into your underwear?’ ” She noticed each connection led to finding more people to help her along her journey.
Dr. Lubahn studied the apparel industry, learning that overseas manufacturers were more helpful and cost-effective. She navigated issues such as a special stitch that prevented leakage and other details. She was also intent on using eco-friendly products that offset the environmental impact of pads, liners, and diapers. She said there’s a strong entrepreneurship community that can help other physician-inventors get grants, be part of accelerator programs, and receive support.
Six years after the original idea, Dr. Lubahn’s product was released in 2020. She now sells eight types of underwear for women and men’s boxer briefs. She wears them herself daily.
Deterring carjackers, saving lives
In 2022, carjackings tripled in Chicago and Memphis. The areas have the highest rates in 30 cities that the Council on Criminal Justice analyzed in a report on pandemic crime rates. According to the report, nearly 40% of offenders used a firearm, more than a quarter of victims were injured, and only around half of the vehicles taken were recovered. In addition, vehicles are sometimes used in secondary crimes, such as drive-by shootings. William Yates, MD, former trauma surgeon, now turned hair restoration surgeon in Chicago, saw the evidence of those crimes daily.
“I was perplexed by carjacking because there wasn’t any answer, and it just kept getting worse and worse. A lot of innocent people were being affected,” he said. “I was seeing deaths – needless. If you give them any push back at all, they will shoot you.”
As a deterrent to counter this “easy crime,” he invented the Yates Device, an alarm system designed to prevent or interrupt carjacking. The driver can activate a switch located beneath the foot pedal or an app on the phone to trigger a programmed high-decibel alarm. Critically, it allows the carjacker to drive a safe distance away from the victim before it starts going off.
The alarm “turns your car into a very noisy Christmas tree on a time delay,” Dr. Yates explained. An external siren blares “stolen vehicle” repeatedly. A camera records everything in the car. Lights flash. Only the original driver can turn off the system. Later, once the car is abandoned, the police can help recover the vehicle.
In Dr. Yates’ experience, the invention process takes longer than you think. He worked through earlier iterations with strobe lights, but these could lead to bystanders getting hurt if the carjacker couldn’t see, for example. Developing the final product and applying for patents was a two-part process.
“The first is part is a pending patent phase, which secures your place in line,” he said. “After 1 year, we filed the utility patent as the final documentation that the invention is truly unique. That has been in process for a year now and the attorneys say we should receive approval soon.”
The product has initially been tested in seven cars for about 1 year. Dr. Yates is measuring how the system performs in all types of weather, including Chicago’s below-zero temperatures. The product is not available to the public for purchase yet because Dr. Yates is still seeking funding to have it mass produced, but it is currently being evaluated by Korean automakers for their car manufacturers.
“Everybody was saying ‘Let’s do something about this,’ but I didn’t see anybody doing anything yet,” Dr. Yates recalled. In the surgeon’s lounge, everybody has ideas. “You go around the room, and every doctor would have five ideas that would make them the richest doctor, but nobody takes it beyond that stage – talk. You have to synthesize that into a plan, to take action.”
Dr. Yates said that many doctors have the intellect to invent, but they aren’t in a network like entrepreneurs to bring their ideas to life.
For Dr. Yates, it takes a curious mindset to solve these daunting problems. “I’m always curious, always looking for how to improve something, to get better outcomes you have to be asking questions and just never let it go.”
A version of this article originally appeared on Medscape.com.
Raising the bar (and the OR table):Ergonomics in MIGS
Work-related musculoskeletal disorders (WMSDs) are “musculoskeletal disorders (injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs) in which the work environment and performance of work contribute significantly to the condition; and/or the condition is made worse or persists longer due to work conditions.”1 The health care industry has one of the highest rates of WMSDs, even when compared with traditional labor-intensive occupations, such as coal mining. In 2017, the health care industry reported more than a half million incidents of work-related injury and illness.2,3 In particular, surgeons are at increased risk for WMSDs, since they repetitively perform the classic tenets of poor ergonomics, including operating in static, extreme, and awkward positions and for prolonged periods of time.3
Gynecologic surgeons face unique ergonomic challenges. Operating in the pelvis requires an oblique approach that adds complexity and inhibits appropriate ergonomic positioning.4 All modalities of surgery incur their own challenges and risks to the surgeon, including minimally invasive gynecologic surgery (MIGS), which has become the standard of care for most conditions. Although MIGS has several benefits for the patient, a survey of gynecologic oncologists found that 88% of respondents reported discomfort related to MIGS.5 Several factors contribute to the development of WMSDs in surgery, including lack of ergonomic awareness, suboptimal ergonomic education and training,5,6 and ergonomically poor operating room (OR) equipment and instrument design.7 Furthermore, surgical culture does not generally prioritize ergonomics in the OR or requests for ergonomic accommodations.7,8
Within 5 years, a physician workforce shortage is projected for the United States.9 WMSDs contribute to workforce issues as they are associated with decreased productivity; time off needed for pain and treatment, including short-term disability; and possibly early retirement (as those who are older and have more work experience may be more likely to seek medical attention).10 In a 2013 study of vaginal surgeons, 14% missed work; 21% modified their work hours, work type, or amount of surgery; and 29% modified their surgical technique because of injury.10 Work-related pain also can negatively affect mental health, sleep, relationships, and quality of life.6
Recently, awareness has increased regarding WMSDs and their consequences, which has led to significant strides in the study of ergonomics among surgeons, a growing body of research on the topic, and guidance for optimizing ergonomics in the OR.
Risk factors for ergonomic strain
Several factors contribute to ergonomic strain and, subsequently, the development of WMSDs. Recognizing these factors can direct strategies for injury prevention.
Patient factors
The prevalence of obesity in the United States increased from 30.5% in 1999–2000 to 41.9% between 2017 and 2020.11 As the average patient’s body mass index (BMI) has increased, there is concern for a parallel increase in the ergonomic strain on laparoscopic surgeons.
A study of simulated laparoscopic tasks at varying model BMI levels demonstrated increased surgeon postural stress and workload at higher model BMIs (50 kg/m2) when compared with lower model BMIs (20 and 30 kg/m2).11 This result was supported in another study, which demonstrated both increased muscle activity and increased time needed to complete a surgical task with laparoscopic surgery; interestingly, when the same study measured these parameters for robotic surgery, this association was not seen.12 This suggests that a robotic rather than a laparoscopic approach may avoid some of the ergonomic strain associated with increased patient BMI.
Continue to: Surgeon factors...
Surgeon factors
Various surgeon characteristics have been shown to influence ergonomics in the OR. Surgeons with smaller hand sizes, for example, reported greater physical discomfort and demonstrated greater ergonomic workload when operating laparoscopically.13-15 In particular, those with a glove size of 6.5 or smaller have more difficulty using laparoscopic instruments, and those with a glove size smaller than 7 demonstrate a larger decline in grip strength when using laparoscopic instruments repeatedly.14,16
Surgeon height also can affect the amount of time spent in high-risk, nonergonomic positions. In a study that evaluated video recordings of surgeon posture during gynecologic laparoscopy, shorter surgeons were noted to use greater degrees of neck rotation to look at the monitor.17 Furthermore, surgeons with shorter arm lengths experienced more “extreme positions” of the nondominant shoulder and elbow.17 This trend also was seen in open and robotic surgery, where surgeons with a height of 66 cm or less reported increased pain scores after operating.18
Surgical instruments and OR setup
Surgical instrument characteristics can contribute to ergonomic strain, especially when the instruments have been designed with a one-size-fits-all mentality.8,19 In an examination of the anthropometric measurements of surgeon hand sizes and their correlation with difficulty when using a “standard” laparoscopic instrument, surgeons with smaller finger and hand spans had trouble using these instruments.19 Another study compared surgeon grip strength and ergonomic workloads after using 3 laparoscopic advanced bipolar instruments.16 Gender and hand size aside, the authors found that use of several of the laparoscopic devices led to greater decline in grip strength.16
The setup of the OR also can have a profound effect on the surgeon’s ergonomics. Monitor placement, for example, is crucial to ergonomic success. One study found that positioning the monitor directly in front of the surgeon at eye level was associated with the lowest neck muscle activity during a simulated task.20
Route of surgery
Each surgical approach has intrinsic ergonomic risks. With laparoscopy, surgeons often remain in straight head and back positions without much trunk motion, especially when compared with open surgery.21 In one study, laparoscopic surgeons spent more than 60% of a case in a static position and more than 80% of a case in a high-risk, “demanding” neck position.22
Robotic surgery, in contrast to laparoscopy, often has been cited as being more “ergonomic.” While robotic surgery has less of an effect on the neck, shoulders, arms, and legs than laparoscopy23 and often is associated with less physical discomfort than either open or laparoscopic surgery,23,24 robotic surgery still maintains its own innate ergonomic risks. Of robotic surgeons surveyed, 56.1% reported neck stiffness, finger fatigue, and eye symptoms in one study.25 In another survey study, more robotic surgeons (72%) reported physical symptoms than laparoscopic (57%) and open (49%) surgeons.26Vaginal surgery also puts surgeons at ergonomic risk. A majority of surgeons (87.2%) who completed more than 50% of their cases vaginally reported a history of WMSDs.10 Vaginal surgery places surgeons in awkward positions of the neck, shoulder, and trunk frequently and for longer durations.27
Continue to: Strategies for preventing WMSDs...
Strategies for preventing WMSDs
As factors that contribute to the development of WMSDs are identified, preventive strategies can be targeted to these individual factors. Research has focused on appropriate setup of the OR, surgeon posture, intraoperative microbreaks, and stretching both in and outside of the OR.
1. OR setup and positioning of the surgeon by MIGS route
The route of MIGS affects OR setup and surgeon posture. Ergonomic recommendations for laparoscopy, robotic surgery, and vaginal surgery are all unique to the risks posed by each particular approach.
Laparoscopic surgery. Laparoscopic monitors should face the surgeon directly, with the screen just below eye level to maintain the surgeon’s neck in a neutral position.28 The table height should be set for the tallest surgeon, and shorter surgeons should stand on steps as needed.28 The table height also should allow for the surgeon’s hands to be at elbow height, with the elbows bent at 90 degrees with the wrists straight.29 Foot pedals should be placed at the surgeons’ foot level and should be reached easily.28 Additionally, the patient’s arms should be tucked at their sides to allow surgeons a larger operative space.29 When using laparoscopic instruments, locking and ratcheting features should be used whenever possible to reduce prolonged grip or squeeze forces.28 The laparoscopic camera should be held in the palm with the wrist in a neutral position.29
Robotic surgery. Positioning and setup of the robotic console is a main focus of ergonomic recommendations. The surgeon’s chair should be brought as close to the console as possible, and the knees positioned in a 90-degree angle.30 The foot pedals should be brought toward the surgeon to maintain this angle of the knees.30 The console should be rotated toward the surgeon and then the height adjusted so that the surgeon can look through the eyepiece while sitting upright and can maintain the neck in a neutral position.28,30 The surgeon’s forehead should rest comfortably on the headrest.29 The forearms should rest on the armrest while the arms are maintained in a neutral position and the shoulders remain relaxed while the surgeon holds the robotic controls.30 It is important to utilize the armrest often to relieve stress on the arm while operating.28 Frequent use of the clutch function can keep the robotic controls in the center of the workspace.28
Vaginal surgery. Both seated and standing positions are associated with high-risk positioning of the trunk and bilateral shoulders, respectively, in vaginal surgery.31 However, surgeons who stand while operating vaginally reported more discomfort in the bilateral wrists, thighs, and lower legs than those who operated while seated.31 This suggests a potential ergonomic advantage to the seated position for vaginal surgery. Chair height should be adjusted so the surgeon can look straight ahead with the neck in a neutral position.32 Surgeons should consider using a headlamp, as this may prevent repetitive awkward movements to adjust overhead lights.32 For standing surgery, the table height should be adjusted for the tallest surgeon, and shorter surgeons or assistants should use steps as needed.3
Surgical assistants should switch sides during the course of the case to avoid excessive unilateral upper-extremity strain.32 The addition of a table-mounted vaginal retractor system may be useful in relieving physical strain for surgical assistants, but data currently are lacking to demonstrate this ergonomic benefit.33 Further studies are needed, especially since many surgeons take on the role of surgical assist in the teaching environment and subsequently report more WMSDs than their colleagues who do not work in teaching environments.10,34
2. Pain relief from individual ergonomic positioning devices
Apart from adjusting how the OR equipment is arranged or how the surgeons adjust their positioning, several devices that assist with surgeon positioning—including gel mats or insoles, exoskeletons, and “augmented reality” glasses—are being studied.
The use of gel mats or insoles in the OR has mixed evidence in the literature.35-37
Exoskeletons, external devices that support a surgeon’s posture and positioning, have been studied thus far in simulated nonsterile surgical environments. Preliminarily, it appears that use of an exoskeleton can decrease muscle activity and time spent in static positions, with a reported decrease in post-task user discomfort.38,39 More data are needed to determine if exoskeletons can be used in the sterile setting and for longer durations as may occur in actual OR cases.
Augmented reality glasses project the laparoscopic monitor image to the glasses, which frees the surgeon to place the “monitor” in a more neutral, ergonomic position. In one study, use of augmented reality glasses was associated with decreased muscle activity and a reduction in Rapid Entire Body Assessment (REBA) scores when compared with use of the conventional laparoscopic monitor.40More data are needed on these emerging technologies to determine whether adverse effects occur with prolonged use.
Continue to: 3. Implementing intraoperative microbreaks and stretching...
3. Implementing intraoperative microbreaks and stretching
The American College of Surgeons (ACS) recommends that surgeons avoid prolonged static postures during procedures.28 One strategy for preventing sustained positioning is to incorporate breaks with associated stretching routinely during surgery.28
Microbreaks. In a landmark study by Park and colleagues in 2017, 120-second long targeted stretching microbreaks (TSMBs) were completed every 20 to 40 minutes during a surgery, and results demonstrated improved postoperative surgeon pain scores without an associated increase in the length of the case.41 These surgeons reported improved pain in the neck, bilateral shoulders, bilateral hands, and lower back. Eighty-eight percent of surgeons reported either improvement or “no change” in their mental focus, and 100% reported improvement or “no change” in their physical performance after TSMBs were implemented.42 Of surveyed surgeons, 87% wanted TSMBs incorporated routinely.41,42
Stretches. Multiple resources, such as the ACS and the Mayo Clinic, for intraoperative stretches are available. The ACS recommends performing neck and shoulder stretches during intraoperative microbreaks, including a range-of-movement neck exercise, deep cervical flexor training, and standing scapular retraction.28 The ACS also demonstrates lumbrical stretches for the fingers and passive wrist extension exercises to be used intraoperatively (or between cases) (FIGURE 1).28 The Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR Stretch Instructional Video” in which the surgeon is guided through several different short stretches, including shoulder shrugging and side bends, that can be used during surgery.43
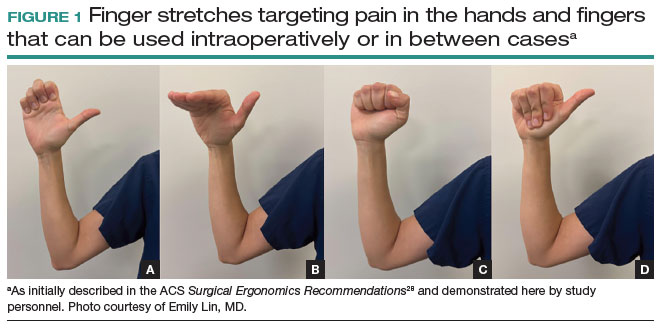
Both the ACS and the Mayo Clinic provide examples of pertinent stretch exercises for use when not in the sterile environment, between cases or after cases are complete. The ACS recommends several neck and shoulder stretches for the trapezius, levator scapulae, and pectoralis and recommends the use of a foam roller to improve thoracic mobility (FIGURE 2).28 As above, the Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR-Stretch Between Surgery Stretches Video” in which the surgeon is guided through several short stretches that are done in a seated position, including stretches for the hamstring, lower back, and arms (FIGURE 3).43
Many of the above-mentioned stretches were designed for use in the context of open, laparoscopic, or robotic surgery. For the vaginal surgeon, the intraoperative ergonomic stressors differ from those of other routes of surgery, and thus stretches tailored to the positioning during vaginal surgery are necessary. In a video recently published by the Society of Gynecologic Surgeons, several stretches are reviewed that target high-risk positions often held by the surgeon or assistant when operating vaginally.44 These stretches include cervical retraction, thoracic extension, external arm rotation, cervical side bending, and lumbar extension (FIGURE 4).44 The recommendation is to complete these exercises 2 times per day, with 8 to 10 repetitions per set.44
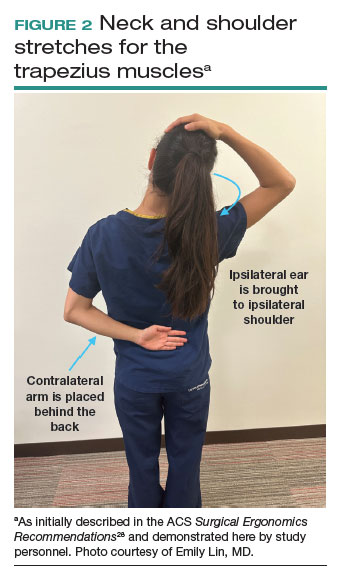
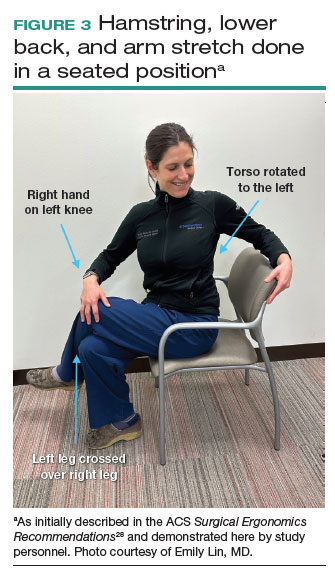
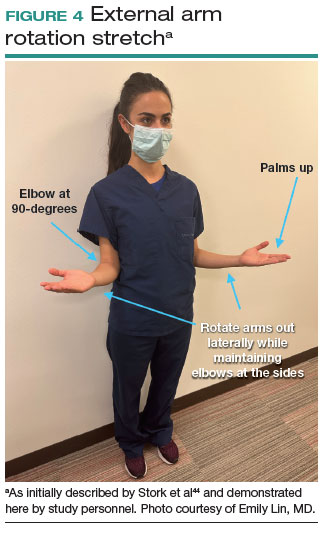
Prioritizing ergonomic awareness and training
As caregivers, it is not uncommon for us to prioritize the needs of others before those of ourselves. However, WMSDs are prevalent, and their downstream effects may cause catastrophic professional and personal losses. Cumulatively, the global impact of WMSDs is a significant issue for the health care workforce and its longevity.
To prevent WMSDs, it is imperative that surgeons are aware of the factors that contribute to injury development and the appropriate, accessible modifications for these factors. While each surgical modality confers its own ergonomic challenges, these risks can be mitigated through increased awareness of OR setup, surgeon positioning, and incorporation of microbreaks and stretching exercises during and after surgical procedures.
Formal training in surgical ergonomics is lacking across specialties, including gynecology.45 Multiple educational interventions have been proposed and studied to help fill this training gap.30,46-49When used, these interventions have been associated with increased knowledge of surgical ergonomic principles or reduction in surgeon pain scores, including trainees.50 As we become more cognizant of WMSDs, standardized resident curricula should be developed in an effort to reduce the prevalence of these potentially career-ending injuries.
In addition to education, cultivating a culture in which ergonomics is prioritized is essential. Although most surgeons report work-related pain, very few report their injuries to occupational health. For example, while 29% of gynecologic oncologists reported seeking treatment for a WMSD, only 1% had reported their injury to their employer.5 In a study of ACS members, only 19% of injuries were reported, 30% of surgeons stated that they did not know how to report an injury, and 21% felt that the resources for surgeons during and after an injury were inadequate.6
As we prioritize the health and safety of our patients, we also need to promote ergonomic awareness in the OR, respect the need for accommodations, encourage injury reporting, support surgeons who need to take time away for medical treatment, and partner with industry to develop new instruments and technology with effective ergonomic features. ●
- Workplace health glossary. Reviewed February 12, 2020. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://www.cdc.gov/workplacehealthpromotion/tools-resources /glossary/glossary.html#W
- Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153:e174947.
- Yurteri-Kaplan LA, Park AJ. Surgical ergonomics and preventing workrelated musculoskeletal disorders. Obstet Gynecol. 2023;141:455-462.
- Symer MM, Keller DS. Human factors in pelvic surgery. Eur J Surg Oncol. 2022;48:2346-2351.
- Franasiak J, Ko EM, Kidd J, et al. Physical strain and urgent need for ergonomic training among gynecologic oncologists who perform minimally invasive surgery. Gynecol Oncol. 2012;126:437-442.
- Davis WT, Fletcher SA, Guillamondegui OD. Musculoskeletal occupational injury among surgeons: effects for patients, providers, and institutions. J Surg Res. 2014;189:207-212.e6.
- Fox M. Surgeons face unique ergonomic challenges. American College of Surgeons. September 1, 2022. Accessed May 22, 2023. https://www.facs.org/for-medical-professionals/news-publications /news-and-articles/bulletin/september-2022-volume-107-issue-9 /surgeons-face-unique-ergonomic-challenges/
- Wong JMK, Carey ET, King C, et al. A call to action for ergonomic surgical devices designed for diverse surgeon end users. Obstet Gynecol. 2023;141:463-466.
- IHS Inc. The Complexities of Physician Supply and Demand: Projections from 2014 to 2025. Association of American Medical Colleges. April 5, 2016.
- Kim-Fine S, Woolley SM, Weaver AL, et al. Work-related musculoskeletal disorders among vaginal surgeons. Int Urogynecol J. 2013;24:1191-1200.
- Sers R, Forrester S, Zecca M, et al. The ergonomic impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl Ergon. 2021;97:103501.
- Moss EL, Sarhanis P, Ind T, et al. Impact of obesity on surgeon ergonomics in robotic and straight-stick laparoscopic surgery. J Minim Invasive Gynecol. 2020;27:1063-1069.
- Sutton E, Irvin M, Zeigler C, et al. The ergonomics of women in surgery. Surg Endosc. 2014;28:1051-1055.
- Berguer R, Hreljac A. The relationship between hand size and difficulty using surgical instruments: a survey of 726 laparoscopic surgeons. Surg Endosc. 2004;18:508-512.
- Bellini MI, Amabile MI, Saullo P, et al. A woman’s place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery. J Clin Med. 2022;11:3496.
- Wong JMK, Moore KJ, Lewis P, et al. Ergonomic assessment of surgeon characteristics and laparoscopic device strain in gynecologic surgery. J Minim Invasive Gynecol. 2022;29:1357-1363.
- Aitchison LP, Cui CK, Arnold A, et al. The ergonomics of laparoscopic surgery: a quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg Endosc. 2016;30:5068-5076.
- Stewart C, Raoof M, Fong Y, et al. Who is hurting? A prospective study of surgeon ergonomics. Surg Endosc. 2022;36:292-299.
- Green SV, Morris DE, Naumann DN, et al. One size does not fit all: impact of hand size on ease of use of instruments for minimally invasive surgery. Surgeon. 2022;S1479-666X(22)00131-7.
- Matern U, Faist M, Kehl K, et al. Monitor position in laparoscopic surgery. Surg Endosc. 2005;19:436-440.
- Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11:139-142.
- Athanasiadis DI, Monfared S, Asadi H, et al. An analysis of the ergonomic risk of surgical trainees and experienced surgeons during laparoscopic procedures. Surgery. 2021;169:496-501.
- Hotton J, Bogart E, Le Deley MC, et al. Ergonomic assessment of the surgeon’s physical workload during robot-assisted versus standard laparoscopy in a French multicenter randomized trial (ROBOGYN-1004 Trial). Ann Surg Oncol. 2023;30:916-923.
- Plerhoples TA, Hernandez-Boussard T, Wren SM. The aching surgeon: a survey of physical discomfort and symptoms following open, laparoscopic, and robotic surgery. J Robot Surg. 2012;6:65-72.
- Lee GI, Lee MR, Green I, et al. Surgeons’ physical discomfort and symptoms during robotic surgery: a comprehensive ergonomic survey study. Surg Endosc. 2017;31:1697-1706.
- McDonald ME, Ramirez PT, Munsell MF, et al. Physician pain and discomfort during minimally invasive gynecologic cancer surgery. Gynecol Oncol. 2014;134:243-247.
- Zhu X, Yurteri-Kaplan LA, Gutman RE, et al. Postural stress experienced by vaginal surgeons. Proc Hum Factors Ergonomics Soc Annu Meet. 2014;58:763-767.
- American College of Surgeons Division of Education and Surgical Ergonomics Committee. Surgical Ergonomics Recommendations. ACS Education. 2022.
- Cardenas-Trowers O, Kjellsson K, Hatch K. Ergonomics: making the OR a comfortable place. Int Urogynecol J. 2018;29:1065-1066.
- Hokenstad ED, Hallbeck MS, Lowndes BR, et al. Ergonomic robotic console configuration in gynecologic surgery: an interventional study. J Minim Invasive Gynecol. 2021;28:850-859.
- Singh R, Yurteri-Kaplan LA, Morrow MM, et al. Sitting versus standing makes a difference in musculoskeletal discomfort and postural load for surgeons performing vaginal surgery. Int Urogynecol J. 2019;30:231-237.
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery: “surgeon protect thyself.” J Pelvic Med Surg. 2009;15:435-439.
- Woodburn KL, Kho RM. Vaginal surgery: don’t get bent out of shape. Am J Obstet Gynecol. 2020;223:762-763.
- Hobson DTG, Meriwether KV, Gaskins JT, et al. Learner satisfaction and experience with a high-definition telescopic camera during vaginal procedures: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2021;27:105-111.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: a systematic review. Appl Ergon. 2018;70:300-334.
- Haramis G, Rosales JC, Palacios JM, et al. Prospective randomized evaluation of FOOT gel pads for operating room staff COMFORT during laparoscopic renal surgery. Urology. 2010;76:1405-1408.
- Voss RK, Chiang YJ, Cromwell KD, et al. Do no harm, except to ourselves? A survey of symptoms and injuries in oncologic surgeons and pilot study of an intraoperative ergonomic intervention. J Am Coll Surg. 2017;224:16-25.e1.
- Marquetand J, Gabriel J, Seibt R, et al. Ergonomics for surgeons—prototype of an external surgeon support system reduces muscular activity and fatigue. J Electromyogr Kinesiol. 2021;60:102586.
- Tetteh E, Hallbeck MS, Mirka GA. Effects of passive exoskeleton support on EMG measures of the neck, shoulder and trunk muscles while holding simulated surgical postures and performing a simulated surgical procedure. Appl Ergon. 2022;100:103646.
- Lim AK, Ryu J, Yoon HM, et al. Ergonomic effects of medical augmented reality glasses in video-assisted surgery. Surg Endosc. 2022;36:988-998.
- Park AE, Zahiri HR, Hallbeck MS, et al. Intraoperative “micro breaks” with targeted stretching enhance surgeon physical function and mental focus: a multicenter cohort study. Ann Surg. 2017;265:340-346.
- Hallbeck MS, Lowndes BR, Bingener J, et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon. 2017;60:334-341.
- Hallbeck Human Factors Engineering Laboratories. OR Stretch Videos. Mayo Clinic, 2018. Accessed May 19, 2023. https://www.mayo .edu/research/labs/human-factors-engineering/or-stretch /or-stretch-videos
- Stork A, Bacon T, Corton M. Prevention of Work-Related Musculoskeletal Disorders in Vaginal Surgery. Video presentation at: Society of Gynecologic Surgeons’ Annual Scientific Meeting 2023, Tucson, AZ. Accessed April 3, 2023. https://sgs.eng.us/category.php?cat=2023 -video-presentations
- Aaron KA, Vaughan J, Gupta R, et al. The risk of ergonomic injury across surgical specialties. PLoS One. 2021;16:e0244868.
- Smith TG, Lowndes BR, Schmida E, et al. Course design and learning outcomes of a practical online ergonomics course for surgical residents. J Surg Educ. 2022;79:1489-1499.
- Franasiak J, Craven R, Mosaly P, et al. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS. 2014;18:e2014.00166.
- Cerier E, Hu A, Goldring A, et al. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. 2022;280:567-574.
- Giagio S, Volpe G, Pillastrini P, et al. A preventive program for workrelated musculoskeletal disorders among surgeons: outcomes of a randomized controlled clinical trial. Ann Surg. 2019;270:969-975.
- Jensen MJ, Liao J, Van Gorp B, et al. Incorporating surgical ergonomics education into surgical residency curriculum. J Surg Educ. 2021;78:1209-1215.
Work-related musculoskeletal disorders (WMSDs) are “musculoskeletal disorders (injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs) in which the work environment and performance of work contribute significantly to the condition; and/or the condition is made worse or persists longer due to work conditions.”1 The health care industry has one of the highest rates of WMSDs, even when compared with traditional labor-intensive occupations, such as coal mining. In 2017, the health care industry reported more than a half million incidents of work-related injury and illness.2,3 In particular, surgeons are at increased risk for WMSDs, since they repetitively perform the classic tenets of poor ergonomics, including operating in static, extreme, and awkward positions and for prolonged periods of time.3
Gynecologic surgeons face unique ergonomic challenges. Operating in the pelvis requires an oblique approach that adds complexity and inhibits appropriate ergonomic positioning.4 All modalities of surgery incur their own challenges and risks to the surgeon, including minimally invasive gynecologic surgery (MIGS), which has become the standard of care for most conditions. Although MIGS has several benefits for the patient, a survey of gynecologic oncologists found that 88% of respondents reported discomfort related to MIGS.5 Several factors contribute to the development of WMSDs in surgery, including lack of ergonomic awareness, suboptimal ergonomic education and training,5,6 and ergonomically poor operating room (OR) equipment and instrument design.7 Furthermore, surgical culture does not generally prioritize ergonomics in the OR or requests for ergonomic accommodations.7,8
Within 5 years, a physician workforce shortage is projected for the United States.9 WMSDs contribute to workforce issues as they are associated with decreased productivity; time off needed for pain and treatment, including short-term disability; and possibly early retirement (as those who are older and have more work experience may be more likely to seek medical attention).10 In a 2013 study of vaginal surgeons, 14% missed work; 21% modified their work hours, work type, or amount of surgery; and 29% modified their surgical technique because of injury.10 Work-related pain also can negatively affect mental health, sleep, relationships, and quality of life.6
Recently, awareness has increased regarding WMSDs and their consequences, which has led to significant strides in the study of ergonomics among surgeons, a growing body of research on the topic, and guidance for optimizing ergonomics in the OR.
Risk factors for ergonomic strain
Several factors contribute to ergonomic strain and, subsequently, the development of WMSDs. Recognizing these factors can direct strategies for injury prevention.
Patient factors
The prevalence of obesity in the United States increased from 30.5% in 1999–2000 to 41.9% between 2017 and 2020.11 As the average patient’s body mass index (BMI) has increased, there is concern for a parallel increase in the ergonomic strain on laparoscopic surgeons.
A study of simulated laparoscopic tasks at varying model BMI levels demonstrated increased surgeon postural stress and workload at higher model BMIs (50 kg/m2) when compared with lower model BMIs (20 and 30 kg/m2).11 This result was supported in another study, which demonstrated both increased muscle activity and increased time needed to complete a surgical task with laparoscopic surgery; interestingly, when the same study measured these parameters for robotic surgery, this association was not seen.12 This suggests that a robotic rather than a laparoscopic approach may avoid some of the ergonomic strain associated with increased patient BMI.
Continue to: Surgeon factors...
Surgeon factors
Various surgeon characteristics have been shown to influence ergonomics in the OR. Surgeons with smaller hand sizes, for example, reported greater physical discomfort and demonstrated greater ergonomic workload when operating laparoscopically.13-15 In particular, those with a glove size of 6.5 or smaller have more difficulty using laparoscopic instruments, and those with a glove size smaller than 7 demonstrate a larger decline in grip strength when using laparoscopic instruments repeatedly.14,16
Surgeon height also can affect the amount of time spent in high-risk, nonergonomic positions. In a study that evaluated video recordings of surgeon posture during gynecologic laparoscopy, shorter surgeons were noted to use greater degrees of neck rotation to look at the monitor.17 Furthermore, surgeons with shorter arm lengths experienced more “extreme positions” of the nondominant shoulder and elbow.17 This trend also was seen in open and robotic surgery, where surgeons with a height of 66 cm or less reported increased pain scores after operating.18
Surgical instruments and OR setup
Surgical instrument characteristics can contribute to ergonomic strain, especially when the instruments have been designed with a one-size-fits-all mentality.8,19 In an examination of the anthropometric measurements of surgeon hand sizes and their correlation with difficulty when using a “standard” laparoscopic instrument, surgeons with smaller finger and hand spans had trouble using these instruments.19 Another study compared surgeon grip strength and ergonomic workloads after using 3 laparoscopic advanced bipolar instruments.16 Gender and hand size aside, the authors found that use of several of the laparoscopic devices led to greater decline in grip strength.16
The setup of the OR also can have a profound effect on the surgeon’s ergonomics. Monitor placement, for example, is crucial to ergonomic success. One study found that positioning the monitor directly in front of the surgeon at eye level was associated with the lowest neck muscle activity during a simulated task.20
Route of surgery
Each surgical approach has intrinsic ergonomic risks. With laparoscopy, surgeons often remain in straight head and back positions without much trunk motion, especially when compared with open surgery.21 In one study, laparoscopic surgeons spent more than 60% of a case in a static position and more than 80% of a case in a high-risk, “demanding” neck position.22
Robotic surgery, in contrast to laparoscopy, often has been cited as being more “ergonomic.” While robotic surgery has less of an effect on the neck, shoulders, arms, and legs than laparoscopy23 and often is associated with less physical discomfort than either open or laparoscopic surgery,23,24 robotic surgery still maintains its own innate ergonomic risks. Of robotic surgeons surveyed, 56.1% reported neck stiffness, finger fatigue, and eye symptoms in one study.25 In another survey study, more robotic surgeons (72%) reported physical symptoms than laparoscopic (57%) and open (49%) surgeons.26Vaginal surgery also puts surgeons at ergonomic risk. A majority of surgeons (87.2%) who completed more than 50% of their cases vaginally reported a history of WMSDs.10 Vaginal surgery places surgeons in awkward positions of the neck, shoulder, and trunk frequently and for longer durations.27
Continue to: Strategies for preventing WMSDs...
Strategies for preventing WMSDs
As factors that contribute to the development of WMSDs are identified, preventive strategies can be targeted to these individual factors. Research has focused on appropriate setup of the OR, surgeon posture, intraoperative microbreaks, and stretching both in and outside of the OR.
1. OR setup and positioning of the surgeon by MIGS route
The route of MIGS affects OR setup and surgeon posture. Ergonomic recommendations for laparoscopy, robotic surgery, and vaginal surgery are all unique to the risks posed by each particular approach.
Laparoscopic surgery. Laparoscopic monitors should face the surgeon directly, with the screen just below eye level to maintain the surgeon’s neck in a neutral position.28 The table height should be set for the tallest surgeon, and shorter surgeons should stand on steps as needed.28 The table height also should allow for the surgeon’s hands to be at elbow height, with the elbows bent at 90 degrees with the wrists straight.29 Foot pedals should be placed at the surgeons’ foot level and should be reached easily.28 Additionally, the patient’s arms should be tucked at their sides to allow surgeons a larger operative space.29 When using laparoscopic instruments, locking and ratcheting features should be used whenever possible to reduce prolonged grip or squeeze forces.28 The laparoscopic camera should be held in the palm with the wrist in a neutral position.29
Robotic surgery. Positioning and setup of the robotic console is a main focus of ergonomic recommendations. The surgeon’s chair should be brought as close to the console as possible, and the knees positioned in a 90-degree angle.30 The foot pedals should be brought toward the surgeon to maintain this angle of the knees.30 The console should be rotated toward the surgeon and then the height adjusted so that the surgeon can look through the eyepiece while sitting upright and can maintain the neck in a neutral position.28,30 The surgeon’s forehead should rest comfortably on the headrest.29 The forearms should rest on the armrest while the arms are maintained in a neutral position and the shoulders remain relaxed while the surgeon holds the robotic controls.30 It is important to utilize the armrest often to relieve stress on the arm while operating.28 Frequent use of the clutch function can keep the robotic controls in the center of the workspace.28
Vaginal surgery. Both seated and standing positions are associated with high-risk positioning of the trunk and bilateral shoulders, respectively, in vaginal surgery.31 However, surgeons who stand while operating vaginally reported more discomfort in the bilateral wrists, thighs, and lower legs than those who operated while seated.31 This suggests a potential ergonomic advantage to the seated position for vaginal surgery. Chair height should be adjusted so the surgeon can look straight ahead with the neck in a neutral position.32 Surgeons should consider using a headlamp, as this may prevent repetitive awkward movements to adjust overhead lights.32 For standing surgery, the table height should be adjusted for the tallest surgeon, and shorter surgeons or assistants should use steps as needed.3
Surgical assistants should switch sides during the course of the case to avoid excessive unilateral upper-extremity strain.32 The addition of a table-mounted vaginal retractor system may be useful in relieving physical strain for surgical assistants, but data currently are lacking to demonstrate this ergonomic benefit.33 Further studies are needed, especially since many surgeons take on the role of surgical assist in the teaching environment and subsequently report more WMSDs than their colleagues who do not work in teaching environments.10,34
2. Pain relief from individual ergonomic positioning devices
Apart from adjusting how the OR equipment is arranged or how the surgeons adjust their positioning, several devices that assist with surgeon positioning—including gel mats or insoles, exoskeletons, and “augmented reality” glasses—are being studied.
The use of gel mats or insoles in the OR has mixed evidence in the literature.35-37
Exoskeletons, external devices that support a surgeon’s posture and positioning, have been studied thus far in simulated nonsterile surgical environments. Preliminarily, it appears that use of an exoskeleton can decrease muscle activity and time spent in static positions, with a reported decrease in post-task user discomfort.38,39 More data are needed to determine if exoskeletons can be used in the sterile setting and for longer durations as may occur in actual OR cases.
Augmented reality glasses project the laparoscopic monitor image to the glasses, which frees the surgeon to place the “monitor” in a more neutral, ergonomic position. In one study, use of augmented reality glasses was associated with decreased muscle activity and a reduction in Rapid Entire Body Assessment (REBA) scores when compared with use of the conventional laparoscopic monitor.40More data are needed on these emerging technologies to determine whether adverse effects occur with prolonged use.
Continue to: 3. Implementing intraoperative microbreaks and stretching...
3. Implementing intraoperative microbreaks and stretching
The American College of Surgeons (ACS) recommends that surgeons avoid prolonged static postures during procedures.28 One strategy for preventing sustained positioning is to incorporate breaks with associated stretching routinely during surgery.28
Microbreaks. In a landmark study by Park and colleagues in 2017, 120-second long targeted stretching microbreaks (TSMBs) were completed every 20 to 40 minutes during a surgery, and results demonstrated improved postoperative surgeon pain scores without an associated increase in the length of the case.41 These surgeons reported improved pain in the neck, bilateral shoulders, bilateral hands, and lower back. Eighty-eight percent of surgeons reported either improvement or “no change” in their mental focus, and 100% reported improvement or “no change” in their physical performance after TSMBs were implemented.42 Of surveyed surgeons, 87% wanted TSMBs incorporated routinely.41,42
Stretches. Multiple resources, such as the ACS and the Mayo Clinic, for intraoperative stretches are available. The ACS recommends performing neck and shoulder stretches during intraoperative microbreaks, including a range-of-movement neck exercise, deep cervical flexor training, and standing scapular retraction.28 The ACS also demonstrates lumbrical stretches for the fingers and passive wrist extension exercises to be used intraoperatively (or between cases) (FIGURE 1).28 The Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR Stretch Instructional Video” in which the surgeon is guided through several different short stretches, including shoulder shrugging and side bends, that can be used during surgery.43
Both the ACS and the Mayo Clinic provide examples of pertinent stretch exercises for use when not in the sterile environment, between cases or after cases are complete. The ACS recommends several neck and shoulder stretches for the trapezius, levator scapulae, and pectoralis and recommends the use of a foam roller to improve thoracic mobility (FIGURE 2).28 As above, the Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR-Stretch Between Surgery Stretches Video” in which the surgeon is guided through several short stretches that are done in a seated position, including stretches for the hamstring, lower back, and arms (FIGURE 3).43
Many of the above-mentioned stretches were designed for use in the context of open, laparoscopic, or robotic surgery. For the vaginal surgeon, the intraoperative ergonomic stressors differ from those of other routes of surgery, and thus stretches tailored to the positioning during vaginal surgery are necessary. In a video recently published by the Society of Gynecologic Surgeons, several stretches are reviewed that target high-risk positions often held by the surgeon or assistant when operating vaginally.44 These stretches include cervical retraction, thoracic extension, external arm rotation, cervical side bending, and lumbar extension (FIGURE 4).44 The recommendation is to complete these exercises 2 times per day, with 8 to 10 repetitions per set.44
Prioritizing ergonomic awareness and training
As caregivers, it is not uncommon for us to prioritize the needs of others before those of ourselves. However, WMSDs are prevalent, and their downstream effects may cause catastrophic professional and personal losses. Cumulatively, the global impact of WMSDs is a significant issue for the health care workforce and its longevity.
To prevent WMSDs, it is imperative that surgeons are aware of the factors that contribute to injury development and the appropriate, accessible modifications for these factors. While each surgical modality confers its own ergonomic challenges, these risks can be mitigated through increased awareness of OR setup, surgeon positioning, and incorporation of microbreaks and stretching exercises during and after surgical procedures.
Formal training in surgical ergonomics is lacking across specialties, including gynecology.45 Multiple educational interventions have been proposed and studied to help fill this training gap.30,46-49When used, these interventions have been associated with increased knowledge of surgical ergonomic principles or reduction in surgeon pain scores, including trainees.50 As we become more cognizant of WMSDs, standardized resident curricula should be developed in an effort to reduce the prevalence of these potentially career-ending injuries.
In addition to education, cultivating a culture in which ergonomics is prioritized is essential. Although most surgeons report work-related pain, very few report their injuries to occupational health. For example, while 29% of gynecologic oncologists reported seeking treatment for a WMSD, only 1% had reported their injury to their employer.5 In a study of ACS members, only 19% of injuries were reported, 30% of surgeons stated that they did not know how to report an injury, and 21% felt that the resources for surgeons during and after an injury were inadequate.6
As we prioritize the health and safety of our patients, we also need to promote ergonomic awareness in the OR, respect the need for accommodations, encourage injury reporting, support surgeons who need to take time away for medical treatment, and partner with industry to develop new instruments and technology with effective ergonomic features. ●
Work-related musculoskeletal disorders (WMSDs) are “musculoskeletal disorders (injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs) in which the work environment and performance of work contribute significantly to the condition; and/or the condition is made worse or persists longer due to work conditions.”1 The health care industry has one of the highest rates of WMSDs, even when compared with traditional labor-intensive occupations, such as coal mining. In 2017, the health care industry reported more than a half million incidents of work-related injury and illness.2,3 In particular, surgeons are at increased risk for WMSDs, since they repetitively perform the classic tenets of poor ergonomics, including operating in static, extreme, and awkward positions and for prolonged periods of time.3
Gynecologic surgeons face unique ergonomic challenges. Operating in the pelvis requires an oblique approach that adds complexity and inhibits appropriate ergonomic positioning.4 All modalities of surgery incur their own challenges and risks to the surgeon, including minimally invasive gynecologic surgery (MIGS), which has become the standard of care for most conditions. Although MIGS has several benefits for the patient, a survey of gynecologic oncologists found that 88% of respondents reported discomfort related to MIGS.5 Several factors contribute to the development of WMSDs in surgery, including lack of ergonomic awareness, suboptimal ergonomic education and training,5,6 and ergonomically poor operating room (OR) equipment and instrument design.7 Furthermore, surgical culture does not generally prioritize ergonomics in the OR or requests for ergonomic accommodations.7,8
Within 5 years, a physician workforce shortage is projected for the United States.9 WMSDs contribute to workforce issues as they are associated with decreased productivity; time off needed for pain and treatment, including short-term disability; and possibly early retirement (as those who are older and have more work experience may be more likely to seek medical attention).10 In a 2013 study of vaginal surgeons, 14% missed work; 21% modified their work hours, work type, or amount of surgery; and 29% modified their surgical technique because of injury.10 Work-related pain also can negatively affect mental health, sleep, relationships, and quality of life.6
Recently, awareness has increased regarding WMSDs and their consequences, which has led to significant strides in the study of ergonomics among surgeons, a growing body of research on the topic, and guidance for optimizing ergonomics in the OR.
Risk factors for ergonomic strain
Several factors contribute to ergonomic strain and, subsequently, the development of WMSDs. Recognizing these factors can direct strategies for injury prevention.
Patient factors
The prevalence of obesity in the United States increased from 30.5% in 1999–2000 to 41.9% between 2017 and 2020.11 As the average patient’s body mass index (BMI) has increased, there is concern for a parallel increase in the ergonomic strain on laparoscopic surgeons.
A study of simulated laparoscopic tasks at varying model BMI levels demonstrated increased surgeon postural stress and workload at higher model BMIs (50 kg/m2) when compared with lower model BMIs (20 and 30 kg/m2).11 This result was supported in another study, which demonstrated both increased muscle activity and increased time needed to complete a surgical task with laparoscopic surgery; interestingly, when the same study measured these parameters for robotic surgery, this association was not seen.12 This suggests that a robotic rather than a laparoscopic approach may avoid some of the ergonomic strain associated with increased patient BMI.
Continue to: Surgeon factors...
Surgeon factors
Various surgeon characteristics have been shown to influence ergonomics in the OR. Surgeons with smaller hand sizes, for example, reported greater physical discomfort and demonstrated greater ergonomic workload when operating laparoscopically.13-15 In particular, those with a glove size of 6.5 or smaller have more difficulty using laparoscopic instruments, and those with a glove size smaller than 7 demonstrate a larger decline in grip strength when using laparoscopic instruments repeatedly.14,16
Surgeon height also can affect the amount of time spent in high-risk, nonergonomic positions. In a study that evaluated video recordings of surgeon posture during gynecologic laparoscopy, shorter surgeons were noted to use greater degrees of neck rotation to look at the monitor.17 Furthermore, surgeons with shorter arm lengths experienced more “extreme positions” of the nondominant shoulder and elbow.17 This trend also was seen in open and robotic surgery, where surgeons with a height of 66 cm or less reported increased pain scores after operating.18
Surgical instruments and OR setup
Surgical instrument characteristics can contribute to ergonomic strain, especially when the instruments have been designed with a one-size-fits-all mentality.8,19 In an examination of the anthropometric measurements of surgeon hand sizes and their correlation with difficulty when using a “standard” laparoscopic instrument, surgeons with smaller finger and hand spans had trouble using these instruments.19 Another study compared surgeon grip strength and ergonomic workloads after using 3 laparoscopic advanced bipolar instruments.16 Gender and hand size aside, the authors found that use of several of the laparoscopic devices led to greater decline in grip strength.16
The setup of the OR also can have a profound effect on the surgeon’s ergonomics. Monitor placement, for example, is crucial to ergonomic success. One study found that positioning the monitor directly in front of the surgeon at eye level was associated with the lowest neck muscle activity during a simulated task.20
Route of surgery
Each surgical approach has intrinsic ergonomic risks. With laparoscopy, surgeons often remain in straight head and back positions without much trunk motion, especially when compared with open surgery.21 In one study, laparoscopic surgeons spent more than 60% of a case in a static position and more than 80% of a case in a high-risk, “demanding” neck position.22
Robotic surgery, in contrast to laparoscopy, often has been cited as being more “ergonomic.” While robotic surgery has less of an effect on the neck, shoulders, arms, and legs than laparoscopy23 and often is associated with less physical discomfort than either open or laparoscopic surgery,23,24 robotic surgery still maintains its own innate ergonomic risks. Of robotic surgeons surveyed, 56.1% reported neck stiffness, finger fatigue, and eye symptoms in one study.25 In another survey study, more robotic surgeons (72%) reported physical symptoms than laparoscopic (57%) and open (49%) surgeons.26Vaginal surgery also puts surgeons at ergonomic risk. A majority of surgeons (87.2%) who completed more than 50% of their cases vaginally reported a history of WMSDs.10 Vaginal surgery places surgeons in awkward positions of the neck, shoulder, and trunk frequently and for longer durations.27
Continue to: Strategies for preventing WMSDs...
Strategies for preventing WMSDs
As factors that contribute to the development of WMSDs are identified, preventive strategies can be targeted to these individual factors. Research has focused on appropriate setup of the OR, surgeon posture, intraoperative microbreaks, and stretching both in and outside of the OR.
1. OR setup and positioning of the surgeon by MIGS route
The route of MIGS affects OR setup and surgeon posture. Ergonomic recommendations for laparoscopy, robotic surgery, and vaginal surgery are all unique to the risks posed by each particular approach.
Laparoscopic surgery. Laparoscopic monitors should face the surgeon directly, with the screen just below eye level to maintain the surgeon’s neck in a neutral position.28 The table height should be set for the tallest surgeon, and shorter surgeons should stand on steps as needed.28 The table height also should allow for the surgeon’s hands to be at elbow height, with the elbows bent at 90 degrees with the wrists straight.29 Foot pedals should be placed at the surgeons’ foot level and should be reached easily.28 Additionally, the patient’s arms should be tucked at their sides to allow surgeons a larger operative space.29 When using laparoscopic instruments, locking and ratcheting features should be used whenever possible to reduce prolonged grip or squeeze forces.28 The laparoscopic camera should be held in the palm with the wrist in a neutral position.29
Robotic surgery. Positioning and setup of the robotic console is a main focus of ergonomic recommendations. The surgeon’s chair should be brought as close to the console as possible, and the knees positioned in a 90-degree angle.30 The foot pedals should be brought toward the surgeon to maintain this angle of the knees.30 The console should be rotated toward the surgeon and then the height adjusted so that the surgeon can look through the eyepiece while sitting upright and can maintain the neck in a neutral position.28,30 The surgeon’s forehead should rest comfortably on the headrest.29 The forearms should rest on the armrest while the arms are maintained in a neutral position and the shoulders remain relaxed while the surgeon holds the robotic controls.30 It is important to utilize the armrest often to relieve stress on the arm while operating.28 Frequent use of the clutch function can keep the robotic controls in the center of the workspace.28
Vaginal surgery. Both seated and standing positions are associated with high-risk positioning of the trunk and bilateral shoulders, respectively, in vaginal surgery.31 However, surgeons who stand while operating vaginally reported more discomfort in the bilateral wrists, thighs, and lower legs than those who operated while seated.31 This suggests a potential ergonomic advantage to the seated position for vaginal surgery. Chair height should be adjusted so the surgeon can look straight ahead with the neck in a neutral position.32 Surgeons should consider using a headlamp, as this may prevent repetitive awkward movements to adjust overhead lights.32 For standing surgery, the table height should be adjusted for the tallest surgeon, and shorter surgeons or assistants should use steps as needed.3
Surgical assistants should switch sides during the course of the case to avoid excessive unilateral upper-extremity strain.32 The addition of a table-mounted vaginal retractor system may be useful in relieving physical strain for surgical assistants, but data currently are lacking to demonstrate this ergonomic benefit.33 Further studies are needed, especially since many surgeons take on the role of surgical assist in the teaching environment and subsequently report more WMSDs than their colleagues who do not work in teaching environments.10,34
2. Pain relief from individual ergonomic positioning devices
Apart from adjusting how the OR equipment is arranged or how the surgeons adjust their positioning, several devices that assist with surgeon positioning—including gel mats or insoles, exoskeletons, and “augmented reality” glasses—are being studied.
The use of gel mats or insoles in the OR has mixed evidence in the literature.35-37
Exoskeletons, external devices that support a surgeon’s posture and positioning, have been studied thus far in simulated nonsterile surgical environments. Preliminarily, it appears that use of an exoskeleton can decrease muscle activity and time spent in static positions, with a reported decrease in post-task user discomfort.38,39 More data are needed to determine if exoskeletons can be used in the sterile setting and for longer durations as may occur in actual OR cases.
Augmented reality glasses project the laparoscopic monitor image to the glasses, which frees the surgeon to place the “monitor” in a more neutral, ergonomic position. In one study, use of augmented reality glasses was associated with decreased muscle activity and a reduction in Rapid Entire Body Assessment (REBA) scores when compared with use of the conventional laparoscopic monitor.40More data are needed on these emerging technologies to determine whether adverse effects occur with prolonged use.
Continue to: 3. Implementing intraoperative microbreaks and stretching...
3. Implementing intraoperative microbreaks and stretching
The American College of Surgeons (ACS) recommends that surgeons avoid prolonged static postures during procedures.28 One strategy for preventing sustained positioning is to incorporate breaks with associated stretching routinely during surgery.28
Microbreaks. In a landmark study by Park and colleagues in 2017, 120-second long targeted stretching microbreaks (TSMBs) were completed every 20 to 40 minutes during a surgery, and results demonstrated improved postoperative surgeon pain scores without an associated increase in the length of the case.41 These surgeons reported improved pain in the neck, bilateral shoulders, bilateral hands, and lower back. Eighty-eight percent of surgeons reported either improvement or “no change” in their mental focus, and 100% reported improvement or “no change” in their physical performance after TSMBs were implemented.42 Of surveyed surgeons, 87% wanted TSMBs incorporated routinely.41,42
Stretches. Multiple resources, such as the ACS and the Mayo Clinic, for intraoperative stretches are available. The ACS recommends performing neck and shoulder stretches during intraoperative microbreaks, including a range-of-movement neck exercise, deep cervical flexor training, and standing scapular retraction.28 The ACS also demonstrates lumbrical stretches for the fingers and passive wrist extension exercises to be used intraoperatively (or between cases) (FIGURE 1).28 The Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR Stretch Instructional Video” in which the surgeon is guided through several different short stretches, including shoulder shrugging and side bends, that can be used during surgery.43
Both the ACS and the Mayo Clinic provide examples of pertinent stretch exercises for use when not in the sterile environment, between cases or after cases are complete. The ACS recommends several neck and shoulder stretches for the trapezius, levator scapulae, and pectoralis and recommends the use of a foam roller to improve thoracic mobility (FIGURE 2).28 As above, the Mayo Clinic Hallbeck Human Factors Engineering Laboratories has a publicly available “OR-Stretch Between Surgery Stretches Video” in which the surgeon is guided through several short stretches that are done in a seated position, including stretches for the hamstring, lower back, and arms (FIGURE 3).43
Many of the above-mentioned stretches were designed for use in the context of open, laparoscopic, or robotic surgery. For the vaginal surgeon, the intraoperative ergonomic stressors differ from those of other routes of surgery, and thus stretches tailored to the positioning during vaginal surgery are necessary. In a video recently published by the Society of Gynecologic Surgeons, several stretches are reviewed that target high-risk positions often held by the surgeon or assistant when operating vaginally.44 These stretches include cervical retraction, thoracic extension, external arm rotation, cervical side bending, and lumbar extension (FIGURE 4).44 The recommendation is to complete these exercises 2 times per day, with 8 to 10 repetitions per set.44
Prioritizing ergonomic awareness and training
As caregivers, it is not uncommon for us to prioritize the needs of others before those of ourselves. However, WMSDs are prevalent, and their downstream effects may cause catastrophic professional and personal losses. Cumulatively, the global impact of WMSDs is a significant issue for the health care workforce and its longevity.
To prevent WMSDs, it is imperative that surgeons are aware of the factors that contribute to injury development and the appropriate, accessible modifications for these factors. While each surgical modality confers its own ergonomic challenges, these risks can be mitigated through increased awareness of OR setup, surgeon positioning, and incorporation of microbreaks and stretching exercises during and after surgical procedures.
Formal training in surgical ergonomics is lacking across specialties, including gynecology.45 Multiple educational interventions have been proposed and studied to help fill this training gap.30,46-49When used, these interventions have been associated with increased knowledge of surgical ergonomic principles or reduction in surgeon pain scores, including trainees.50 As we become more cognizant of WMSDs, standardized resident curricula should be developed in an effort to reduce the prevalence of these potentially career-ending injuries.
In addition to education, cultivating a culture in which ergonomics is prioritized is essential. Although most surgeons report work-related pain, very few report their injuries to occupational health. For example, while 29% of gynecologic oncologists reported seeking treatment for a WMSD, only 1% had reported their injury to their employer.5 In a study of ACS members, only 19% of injuries were reported, 30% of surgeons stated that they did not know how to report an injury, and 21% felt that the resources for surgeons during and after an injury were inadequate.6
As we prioritize the health and safety of our patients, we also need to promote ergonomic awareness in the OR, respect the need for accommodations, encourage injury reporting, support surgeons who need to take time away for medical treatment, and partner with industry to develop new instruments and technology with effective ergonomic features. ●
- Workplace health glossary. Reviewed February 12, 2020. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://www.cdc.gov/workplacehealthpromotion/tools-resources /glossary/glossary.html#W
- Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153:e174947.
- Yurteri-Kaplan LA, Park AJ. Surgical ergonomics and preventing workrelated musculoskeletal disorders. Obstet Gynecol. 2023;141:455-462.
- Symer MM, Keller DS. Human factors in pelvic surgery. Eur J Surg Oncol. 2022;48:2346-2351.
- Franasiak J, Ko EM, Kidd J, et al. Physical strain and urgent need for ergonomic training among gynecologic oncologists who perform minimally invasive surgery. Gynecol Oncol. 2012;126:437-442.
- Davis WT, Fletcher SA, Guillamondegui OD. Musculoskeletal occupational injury among surgeons: effects for patients, providers, and institutions. J Surg Res. 2014;189:207-212.e6.
- Fox M. Surgeons face unique ergonomic challenges. American College of Surgeons. September 1, 2022. Accessed May 22, 2023. https://www.facs.org/for-medical-professionals/news-publications /news-and-articles/bulletin/september-2022-volume-107-issue-9 /surgeons-face-unique-ergonomic-challenges/
- Wong JMK, Carey ET, King C, et al. A call to action for ergonomic surgical devices designed for diverse surgeon end users. Obstet Gynecol. 2023;141:463-466.
- IHS Inc. The Complexities of Physician Supply and Demand: Projections from 2014 to 2025. Association of American Medical Colleges. April 5, 2016.
- Kim-Fine S, Woolley SM, Weaver AL, et al. Work-related musculoskeletal disorders among vaginal surgeons. Int Urogynecol J. 2013;24:1191-1200.
- Sers R, Forrester S, Zecca M, et al. The ergonomic impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl Ergon. 2021;97:103501.
- Moss EL, Sarhanis P, Ind T, et al. Impact of obesity on surgeon ergonomics in robotic and straight-stick laparoscopic surgery. J Minim Invasive Gynecol. 2020;27:1063-1069.
- Sutton E, Irvin M, Zeigler C, et al. The ergonomics of women in surgery. Surg Endosc. 2014;28:1051-1055.
- Berguer R, Hreljac A. The relationship between hand size and difficulty using surgical instruments: a survey of 726 laparoscopic surgeons. Surg Endosc. 2004;18:508-512.
- Bellini MI, Amabile MI, Saullo P, et al. A woman’s place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery. J Clin Med. 2022;11:3496.
- Wong JMK, Moore KJ, Lewis P, et al. Ergonomic assessment of surgeon characteristics and laparoscopic device strain in gynecologic surgery. J Minim Invasive Gynecol. 2022;29:1357-1363.
- Aitchison LP, Cui CK, Arnold A, et al. The ergonomics of laparoscopic surgery: a quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg Endosc. 2016;30:5068-5076.
- Stewart C, Raoof M, Fong Y, et al. Who is hurting? A prospective study of surgeon ergonomics. Surg Endosc. 2022;36:292-299.
- Green SV, Morris DE, Naumann DN, et al. One size does not fit all: impact of hand size on ease of use of instruments for minimally invasive surgery. Surgeon. 2022;S1479-666X(22)00131-7.
- Matern U, Faist M, Kehl K, et al. Monitor position in laparoscopic surgery. Surg Endosc. 2005;19:436-440.
- Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11:139-142.
- Athanasiadis DI, Monfared S, Asadi H, et al. An analysis of the ergonomic risk of surgical trainees and experienced surgeons during laparoscopic procedures. Surgery. 2021;169:496-501.
- Hotton J, Bogart E, Le Deley MC, et al. Ergonomic assessment of the surgeon’s physical workload during robot-assisted versus standard laparoscopy in a French multicenter randomized trial (ROBOGYN-1004 Trial). Ann Surg Oncol. 2023;30:916-923.
- Plerhoples TA, Hernandez-Boussard T, Wren SM. The aching surgeon: a survey of physical discomfort and symptoms following open, laparoscopic, and robotic surgery. J Robot Surg. 2012;6:65-72.
- Lee GI, Lee MR, Green I, et al. Surgeons’ physical discomfort and symptoms during robotic surgery: a comprehensive ergonomic survey study. Surg Endosc. 2017;31:1697-1706.
- McDonald ME, Ramirez PT, Munsell MF, et al. Physician pain and discomfort during minimally invasive gynecologic cancer surgery. Gynecol Oncol. 2014;134:243-247.
- Zhu X, Yurteri-Kaplan LA, Gutman RE, et al. Postural stress experienced by vaginal surgeons. Proc Hum Factors Ergonomics Soc Annu Meet. 2014;58:763-767.
- American College of Surgeons Division of Education and Surgical Ergonomics Committee. Surgical Ergonomics Recommendations. ACS Education. 2022.
- Cardenas-Trowers O, Kjellsson K, Hatch K. Ergonomics: making the OR a comfortable place. Int Urogynecol J. 2018;29:1065-1066.
- Hokenstad ED, Hallbeck MS, Lowndes BR, et al. Ergonomic robotic console configuration in gynecologic surgery: an interventional study. J Minim Invasive Gynecol. 2021;28:850-859.
- Singh R, Yurteri-Kaplan LA, Morrow MM, et al. Sitting versus standing makes a difference in musculoskeletal discomfort and postural load for surgeons performing vaginal surgery. Int Urogynecol J. 2019;30:231-237.
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery: “surgeon protect thyself.” J Pelvic Med Surg. 2009;15:435-439.
- Woodburn KL, Kho RM. Vaginal surgery: don’t get bent out of shape. Am J Obstet Gynecol. 2020;223:762-763.
- Hobson DTG, Meriwether KV, Gaskins JT, et al. Learner satisfaction and experience with a high-definition telescopic camera during vaginal procedures: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2021;27:105-111.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: a systematic review. Appl Ergon. 2018;70:300-334.
- Haramis G, Rosales JC, Palacios JM, et al. Prospective randomized evaluation of FOOT gel pads for operating room staff COMFORT during laparoscopic renal surgery. Urology. 2010;76:1405-1408.
- Voss RK, Chiang YJ, Cromwell KD, et al. Do no harm, except to ourselves? A survey of symptoms and injuries in oncologic surgeons and pilot study of an intraoperative ergonomic intervention. J Am Coll Surg. 2017;224:16-25.e1.
- Marquetand J, Gabriel J, Seibt R, et al. Ergonomics for surgeons—prototype of an external surgeon support system reduces muscular activity and fatigue. J Electromyogr Kinesiol. 2021;60:102586.
- Tetteh E, Hallbeck MS, Mirka GA. Effects of passive exoskeleton support on EMG measures of the neck, shoulder and trunk muscles while holding simulated surgical postures and performing a simulated surgical procedure. Appl Ergon. 2022;100:103646.
- Lim AK, Ryu J, Yoon HM, et al. Ergonomic effects of medical augmented reality glasses in video-assisted surgery. Surg Endosc. 2022;36:988-998.
- Park AE, Zahiri HR, Hallbeck MS, et al. Intraoperative “micro breaks” with targeted stretching enhance surgeon physical function and mental focus: a multicenter cohort study. Ann Surg. 2017;265:340-346.
- Hallbeck MS, Lowndes BR, Bingener J, et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon. 2017;60:334-341.
- Hallbeck Human Factors Engineering Laboratories. OR Stretch Videos. Mayo Clinic, 2018. Accessed May 19, 2023. https://www.mayo .edu/research/labs/human-factors-engineering/or-stretch /or-stretch-videos
- Stork A, Bacon T, Corton M. Prevention of Work-Related Musculoskeletal Disorders in Vaginal Surgery. Video presentation at: Society of Gynecologic Surgeons’ Annual Scientific Meeting 2023, Tucson, AZ. Accessed April 3, 2023. https://sgs.eng.us/category.php?cat=2023 -video-presentations
- Aaron KA, Vaughan J, Gupta R, et al. The risk of ergonomic injury across surgical specialties. PLoS One. 2021;16:e0244868.
- Smith TG, Lowndes BR, Schmida E, et al. Course design and learning outcomes of a practical online ergonomics course for surgical residents. J Surg Educ. 2022;79:1489-1499.
- Franasiak J, Craven R, Mosaly P, et al. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS. 2014;18:e2014.00166.
- Cerier E, Hu A, Goldring A, et al. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. 2022;280:567-574.
- Giagio S, Volpe G, Pillastrini P, et al. A preventive program for workrelated musculoskeletal disorders among surgeons: outcomes of a randomized controlled clinical trial. Ann Surg. 2019;270:969-975.
- Jensen MJ, Liao J, Van Gorp B, et al. Incorporating surgical ergonomics education into surgical residency curriculum. J Surg Educ. 2021;78:1209-1215.
- Workplace health glossary. Reviewed February 12, 2020. Centers for Disease Control and Prevention. Accessed May 18, 2023. https://www.cdc.gov/workplacehealthpromotion/tools-resources /glossary/glossary.html#W
- Epstein S, Sparer EH, Tran BN, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: a systematic review and meta-analysis. JAMA Surg. 2018;153:e174947.
- Yurteri-Kaplan LA, Park AJ. Surgical ergonomics and preventing workrelated musculoskeletal disorders. Obstet Gynecol. 2023;141:455-462.
- Symer MM, Keller DS. Human factors in pelvic surgery. Eur J Surg Oncol. 2022;48:2346-2351.
- Franasiak J, Ko EM, Kidd J, et al. Physical strain and urgent need for ergonomic training among gynecologic oncologists who perform minimally invasive surgery. Gynecol Oncol. 2012;126:437-442.
- Davis WT, Fletcher SA, Guillamondegui OD. Musculoskeletal occupational injury among surgeons: effects for patients, providers, and institutions. J Surg Res. 2014;189:207-212.e6.
- Fox M. Surgeons face unique ergonomic challenges. American College of Surgeons. September 1, 2022. Accessed May 22, 2023. https://www.facs.org/for-medical-professionals/news-publications /news-and-articles/bulletin/september-2022-volume-107-issue-9 /surgeons-face-unique-ergonomic-challenges/
- Wong JMK, Carey ET, King C, et al. A call to action for ergonomic surgical devices designed for diverse surgeon end users. Obstet Gynecol. 2023;141:463-466.
- IHS Inc. The Complexities of Physician Supply and Demand: Projections from 2014 to 2025. Association of American Medical Colleges. April 5, 2016.
- Kim-Fine S, Woolley SM, Weaver AL, et al. Work-related musculoskeletal disorders among vaginal surgeons. Int Urogynecol J. 2013;24:1191-1200.
- Sers R, Forrester S, Zecca M, et al. The ergonomic impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl Ergon. 2021;97:103501.
- Moss EL, Sarhanis P, Ind T, et al. Impact of obesity on surgeon ergonomics in robotic and straight-stick laparoscopic surgery. J Minim Invasive Gynecol. 2020;27:1063-1069.
- Sutton E, Irvin M, Zeigler C, et al. The ergonomics of women in surgery. Surg Endosc. 2014;28:1051-1055.
- Berguer R, Hreljac A. The relationship between hand size and difficulty using surgical instruments: a survey of 726 laparoscopic surgeons. Surg Endosc. 2004;18:508-512.
- Bellini MI, Amabile MI, Saullo P, et al. A woman’s place is in theatre, but are theatres designed with women in mind? A systematic review of ergonomics for women in surgery. J Clin Med. 2022;11:3496.
- Wong JMK, Moore KJ, Lewis P, et al. Ergonomic assessment of surgeon characteristics and laparoscopic device strain in gynecologic surgery. J Minim Invasive Gynecol. 2022;29:1357-1363.
- Aitchison LP, Cui CK, Arnold A, et al. The ergonomics of laparoscopic surgery: a quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg Endosc. 2016;30:5068-5076.
- Stewart C, Raoof M, Fong Y, et al. Who is hurting? A prospective study of surgeon ergonomics. Surg Endosc. 2022;36:292-299.
- Green SV, Morris DE, Naumann DN, et al. One size does not fit all: impact of hand size on ease of use of instruments for minimally invasive surgery. Surgeon. 2022;S1479-666X(22)00131-7.
- Matern U, Faist M, Kehl K, et al. Monitor position in laparoscopic surgery. Surg Endosc. 2005;19:436-440.
- Berguer R, Rab GT, Abu-Ghaida H, et al. A comparison of surgeons’ posture during laparoscopic and open surgical procedures. Surg Endosc. 1997;11:139-142.
- Athanasiadis DI, Monfared S, Asadi H, et al. An analysis of the ergonomic risk of surgical trainees and experienced surgeons during laparoscopic procedures. Surgery. 2021;169:496-501.
- Hotton J, Bogart E, Le Deley MC, et al. Ergonomic assessment of the surgeon’s physical workload during robot-assisted versus standard laparoscopy in a French multicenter randomized trial (ROBOGYN-1004 Trial). Ann Surg Oncol. 2023;30:916-923.
- Plerhoples TA, Hernandez-Boussard T, Wren SM. The aching surgeon: a survey of physical discomfort and symptoms following open, laparoscopic, and robotic surgery. J Robot Surg. 2012;6:65-72.
- Lee GI, Lee MR, Green I, et al. Surgeons’ physical discomfort and symptoms during robotic surgery: a comprehensive ergonomic survey study. Surg Endosc. 2017;31:1697-1706.
- McDonald ME, Ramirez PT, Munsell MF, et al. Physician pain and discomfort during minimally invasive gynecologic cancer surgery. Gynecol Oncol. 2014;134:243-247.
- Zhu X, Yurteri-Kaplan LA, Gutman RE, et al. Postural stress experienced by vaginal surgeons. Proc Hum Factors Ergonomics Soc Annu Meet. 2014;58:763-767.
- American College of Surgeons Division of Education and Surgical Ergonomics Committee. Surgical Ergonomics Recommendations. ACS Education. 2022.
- Cardenas-Trowers O, Kjellsson K, Hatch K. Ergonomics: making the OR a comfortable place. Int Urogynecol J. 2018;29:1065-1066.
- Hokenstad ED, Hallbeck MS, Lowndes BR, et al. Ergonomic robotic console configuration in gynecologic surgery: an interventional study. J Minim Invasive Gynecol. 2021;28:850-859.
- Singh R, Yurteri-Kaplan LA, Morrow MM, et al. Sitting versus standing makes a difference in musculoskeletal discomfort and postural load for surgeons performing vaginal surgery. Int Urogynecol J. 2019;30:231-237.
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery: “surgeon protect thyself.” J Pelvic Med Surg. 2009;15:435-439.
- Woodburn KL, Kho RM. Vaginal surgery: don’t get bent out of shape. Am J Obstet Gynecol. 2020;223:762-763.
- Hobson DTG, Meriwether KV, Gaskins JT, et al. Learner satisfaction and experience with a high-definition telescopic camera during vaginal procedures: a randomized controlled trial. Female Pelvic Med Reconstr Surg. 2021;27:105-111.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: a systematic review. Appl Ergon. 2018;70:300-334.
- Haramis G, Rosales JC, Palacios JM, et al. Prospective randomized evaluation of FOOT gel pads for operating room staff COMFORT during laparoscopic renal surgery. Urology. 2010;76:1405-1408.
- Voss RK, Chiang YJ, Cromwell KD, et al. Do no harm, except to ourselves? A survey of symptoms and injuries in oncologic surgeons and pilot study of an intraoperative ergonomic intervention. J Am Coll Surg. 2017;224:16-25.e1.
- Marquetand J, Gabriel J, Seibt R, et al. Ergonomics for surgeons—prototype of an external surgeon support system reduces muscular activity and fatigue. J Electromyogr Kinesiol. 2021;60:102586.
- Tetteh E, Hallbeck MS, Mirka GA. Effects of passive exoskeleton support on EMG measures of the neck, shoulder and trunk muscles while holding simulated surgical postures and performing a simulated surgical procedure. Appl Ergon. 2022;100:103646.
- Lim AK, Ryu J, Yoon HM, et al. Ergonomic effects of medical augmented reality glasses in video-assisted surgery. Surg Endosc. 2022;36:988-998.
- Park AE, Zahiri HR, Hallbeck MS, et al. Intraoperative “micro breaks” with targeted stretching enhance surgeon physical function and mental focus: a multicenter cohort study. Ann Surg. 2017;265:340-346.
- Hallbeck MS, Lowndes BR, Bingener J, et al. The impact of intraoperative microbreaks with exercises on surgeons: a multi-center cohort study. Appl Ergon. 2017;60:334-341.
- Hallbeck Human Factors Engineering Laboratories. OR Stretch Videos. Mayo Clinic, 2018. Accessed May 19, 2023. https://www.mayo .edu/research/labs/human-factors-engineering/or-stretch /or-stretch-videos
- Stork A, Bacon T, Corton M. Prevention of Work-Related Musculoskeletal Disorders in Vaginal Surgery. Video presentation at: Society of Gynecologic Surgeons’ Annual Scientific Meeting 2023, Tucson, AZ. Accessed April 3, 2023. https://sgs.eng.us/category.php?cat=2023 -video-presentations
- Aaron KA, Vaughan J, Gupta R, et al. The risk of ergonomic injury across surgical specialties. PLoS One. 2021;16:e0244868.
- Smith TG, Lowndes BR, Schmida E, et al. Course design and learning outcomes of a practical online ergonomics course for surgical residents. J Surg Educ. 2022;79:1489-1499.
- Franasiak J, Craven R, Mosaly P, et al. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS. 2014;18:e2014.00166.
- Cerier E, Hu A, Goldring A, et al. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. 2022;280:567-574.
- Giagio S, Volpe G, Pillastrini P, et al. A preventive program for workrelated musculoskeletal disorders among surgeons: outcomes of a randomized controlled clinical trial. Ann Surg. 2019;270:969-975.
- Jensen MJ, Liao J, Van Gorp B, et al. Incorporating surgical ergonomics education into surgical residency curriculum. J Surg Educ. 2021;78:1209-1215.