User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
NPs, PAs, and physicians hope to join doctors’ union in rare alliance
Advanced practice providers (APPs) such as nurse practitioners (NPs) and physician assistants (PAs) have long been at odds with doctor groups over scope of practice issues. But in a rare alliance, in late September. If successful, the Allina group will join the Doctors Council SEIU, Local 10MD.
The Allina health care providers share concerns about their working conditions, such as understaffing and inadequate resources, limited decision-making authority, and health systems valuing productivity and profit over patient care.
Although doctors and APPs have said that they generally work well together, the relationship has been strained in recent years as APPs argue for greater scope of practice. Meanwhile, physician groups, such as the American Medical Association, believe that APPs need more oversight.
An Allina union organizer, Britta V. Kasmarik, CNP, acknowledges the tension between physicians and APPs. But she said in an interview that the union effort helped bond this group of health care providers. “We share common goals of providing high-quality care for patients in a safe way, and we see the same things day in and day out with our patients.”
Matt Hoffman, MD, a primary care physician at Allina, told this news organization that APPs in his specialty perform the same job as doctors “and the working conditions are really identical. In our view, that means we should be unionizing together.”
The decision to hold a union vote follows similar action by nearly 150 Allina Mercy Hospital physicians in March. Allina Health appealed the vote.
In response to a New York Times investigation, the Minnesota Attorney General’s office began reviewing reports of aggressive billing practices and denied care at Allina Health.
The Allina Health system, which reports $4 billion in annual revenue, cut off nonemergency services to patients, including children, if their medical debt exceeded $4,500, according to the New York Times article. For Allina’s physicians and APPs, that meant leaving patients’ illnesses untreated.
Less than a week after the attorney general announced its investigation, the health system ended this practice.
In a prepared statement to this news organization, Allina Health said that its providers are “critical members of our teams. … We deeply value and share their commitment to providing high-quality care to our patients.”
The health system said it planned to make operational improvements, implement new communication tools, and provide additional well-being resources and enhanced employee benefits “to improve the provider experience.” In addition, it hoped to continue to “foster a culture of collaboration with all our employees.”
Having a union will allow health care providers to advocate for their patients and give health care providers more decision-making power instead of corporate leaders maintaining full authority, Ms. Kasmarik told this news organization.
Union organizers are also concerned with changes to the daily practice of medicine. “We don’t want to be spending our time doing paperwork and calling insurance companies and filling out forms,” said Dr. Hoffman. “We want to be in the exam room with a patient.”
The Allina providers organized after multiple requests to corporate managers failed to address their concerns. Their demands include increased staffing and help with nonclinical work so that clinicians can spend more time with their patients.
“What I’m really excited about is that we will be able to work with the other unionized groups to make change ... by being involved in health care policy at a state or national level,” Dr. Hoffman said. For example, that involvement might include challenging insurance company decisions.
Doctors Council bills itself as the largest union for attending physicians in the country, with 3,500 members, according to Joe Crane, national organizing director.
Despite an increase in union efforts since the pandemic, health care workers – particularly doctors – have been slow to join unions. Mr. Crane estimated that only about 3% of U.S. physicians are currently union members. He cited union campaigns in Massachusetts, New York, and Washington, DC. For comparison, a minority of advanced practice registered nurses (APRNs) (9%) report union membership, according to Medscape’s APRN compensation report last year.
Dr. Hoffman is confident the Allina health care providers will have enough votes to win the election to join the union. “We should have done this years ago.”
A version of this article appeared on Medscape.com.
Advanced practice providers (APPs) such as nurse practitioners (NPs) and physician assistants (PAs) have long been at odds with doctor groups over scope of practice issues. But in a rare alliance, in late September. If successful, the Allina group will join the Doctors Council SEIU, Local 10MD.
The Allina health care providers share concerns about their working conditions, such as understaffing and inadequate resources, limited decision-making authority, and health systems valuing productivity and profit over patient care.
Although doctors and APPs have said that they generally work well together, the relationship has been strained in recent years as APPs argue for greater scope of practice. Meanwhile, physician groups, such as the American Medical Association, believe that APPs need more oversight.
An Allina union organizer, Britta V. Kasmarik, CNP, acknowledges the tension between physicians and APPs. But she said in an interview that the union effort helped bond this group of health care providers. “We share common goals of providing high-quality care for patients in a safe way, and we see the same things day in and day out with our patients.”
Matt Hoffman, MD, a primary care physician at Allina, told this news organization that APPs in his specialty perform the same job as doctors “and the working conditions are really identical. In our view, that means we should be unionizing together.”
The decision to hold a union vote follows similar action by nearly 150 Allina Mercy Hospital physicians in March. Allina Health appealed the vote.
In response to a New York Times investigation, the Minnesota Attorney General’s office began reviewing reports of aggressive billing practices and denied care at Allina Health.
The Allina Health system, which reports $4 billion in annual revenue, cut off nonemergency services to patients, including children, if their medical debt exceeded $4,500, according to the New York Times article. For Allina’s physicians and APPs, that meant leaving patients’ illnesses untreated.
Less than a week after the attorney general announced its investigation, the health system ended this practice.
In a prepared statement to this news organization, Allina Health said that its providers are “critical members of our teams. … We deeply value and share their commitment to providing high-quality care to our patients.”
The health system said it planned to make operational improvements, implement new communication tools, and provide additional well-being resources and enhanced employee benefits “to improve the provider experience.” In addition, it hoped to continue to “foster a culture of collaboration with all our employees.”
Having a union will allow health care providers to advocate for their patients and give health care providers more decision-making power instead of corporate leaders maintaining full authority, Ms. Kasmarik told this news organization.
Union organizers are also concerned with changes to the daily practice of medicine. “We don’t want to be spending our time doing paperwork and calling insurance companies and filling out forms,” said Dr. Hoffman. “We want to be in the exam room with a patient.”
The Allina providers organized after multiple requests to corporate managers failed to address their concerns. Their demands include increased staffing and help with nonclinical work so that clinicians can spend more time with their patients.
“What I’m really excited about is that we will be able to work with the other unionized groups to make change ... by being involved in health care policy at a state or national level,” Dr. Hoffman said. For example, that involvement might include challenging insurance company decisions.
Doctors Council bills itself as the largest union for attending physicians in the country, with 3,500 members, according to Joe Crane, national organizing director.
Despite an increase in union efforts since the pandemic, health care workers – particularly doctors – have been slow to join unions. Mr. Crane estimated that only about 3% of U.S. physicians are currently union members. He cited union campaigns in Massachusetts, New York, and Washington, DC. For comparison, a minority of advanced practice registered nurses (APRNs) (9%) report union membership, according to Medscape’s APRN compensation report last year.
Dr. Hoffman is confident the Allina health care providers will have enough votes to win the election to join the union. “We should have done this years ago.”
A version of this article appeared on Medscape.com.
Advanced practice providers (APPs) such as nurse practitioners (NPs) and physician assistants (PAs) have long been at odds with doctor groups over scope of practice issues. But in a rare alliance, in late September. If successful, the Allina group will join the Doctors Council SEIU, Local 10MD.
The Allina health care providers share concerns about their working conditions, such as understaffing and inadequate resources, limited decision-making authority, and health systems valuing productivity and profit over patient care.
Although doctors and APPs have said that they generally work well together, the relationship has been strained in recent years as APPs argue for greater scope of practice. Meanwhile, physician groups, such as the American Medical Association, believe that APPs need more oversight.
An Allina union organizer, Britta V. Kasmarik, CNP, acknowledges the tension between physicians and APPs. But she said in an interview that the union effort helped bond this group of health care providers. “We share common goals of providing high-quality care for patients in a safe way, and we see the same things day in and day out with our patients.”
Matt Hoffman, MD, a primary care physician at Allina, told this news organization that APPs in his specialty perform the same job as doctors “and the working conditions are really identical. In our view, that means we should be unionizing together.”
The decision to hold a union vote follows similar action by nearly 150 Allina Mercy Hospital physicians in March. Allina Health appealed the vote.
In response to a New York Times investigation, the Minnesota Attorney General’s office began reviewing reports of aggressive billing practices and denied care at Allina Health.
The Allina Health system, which reports $4 billion in annual revenue, cut off nonemergency services to patients, including children, if their medical debt exceeded $4,500, according to the New York Times article. For Allina’s physicians and APPs, that meant leaving patients’ illnesses untreated.
Less than a week after the attorney general announced its investigation, the health system ended this practice.
In a prepared statement to this news organization, Allina Health said that its providers are “critical members of our teams. … We deeply value and share their commitment to providing high-quality care to our patients.”
The health system said it planned to make operational improvements, implement new communication tools, and provide additional well-being resources and enhanced employee benefits “to improve the provider experience.” In addition, it hoped to continue to “foster a culture of collaboration with all our employees.”
Having a union will allow health care providers to advocate for their patients and give health care providers more decision-making power instead of corporate leaders maintaining full authority, Ms. Kasmarik told this news organization.
Union organizers are also concerned with changes to the daily practice of medicine. “We don’t want to be spending our time doing paperwork and calling insurance companies and filling out forms,” said Dr. Hoffman. “We want to be in the exam room with a patient.”
The Allina providers organized after multiple requests to corporate managers failed to address their concerns. Their demands include increased staffing and help with nonclinical work so that clinicians can spend more time with their patients.
“What I’m really excited about is that we will be able to work with the other unionized groups to make change ... by being involved in health care policy at a state or national level,” Dr. Hoffman said. For example, that involvement might include challenging insurance company decisions.
Doctors Council bills itself as the largest union for attending physicians in the country, with 3,500 members, according to Joe Crane, national organizing director.
Despite an increase in union efforts since the pandemic, health care workers – particularly doctors – have been slow to join unions. Mr. Crane estimated that only about 3% of U.S. physicians are currently union members. He cited union campaigns in Massachusetts, New York, and Washington, DC. For comparison, a minority of advanced practice registered nurses (APRNs) (9%) report union membership, according to Medscape’s APRN compensation report last year.
Dr. Hoffman is confident the Allina health care providers will have enough votes to win the election to join the union. “We should have done this years ago.”
A version of this article appeared on Medscape.com.
One in five men carries high-risk HPV in international study
Findings from a meta-analysis of 65 studies conducted in 35 countries indicate that These estimates provide further weight to arguments in favor of vaccinating boys against HPV to prevent certain types of cancer.
“Our results support that sexually active men, regardless of age, are an important reservoir of HPV genital infection,” wrote the authors in The Lancet Global Health . “These estimates emphasize the importance of incorporating men into comprehensive HPV prevention strategies to reduce HPV-related morbidity and mortality in men and ultimately achieve elimination of cervical cancer and other HPV-related diseases.”
Literature review
HPV infection is the most common sexually transmitted viral infection worldwide. More than 200 HPV types can be transmitted sexually, and at least 12 types are oncogenic. Previous studies have shown that most sexually active men and women acquire at least one genital HPV infection during their lifetime.
Although most HPV infections are asymptomatic, they can lead to cancer. Indeed, HPV is involved in the development of cervical, vulval, and vaginal cancers, as well as oropharyngeal and anal cancers, which also affect the male population. More than 25% of cancers caused by HPV occur in men.
Despite these observations, fewer epidemiologic studies have assessed HPV infection in men than in women. To determine the prevalence of HPV infection in the male population, Laia Bruni, MD, MPH, PhD, an epidemiologist at the Catalan Institute of Oncology in Barcelona, and her colleagues collated data from 65 studies conducted in 35 countries pertaining to males older than 15 years.
In this literature review, the researchers selected studies that reported infection rates in males without HPV-related symptoms. Studies conducted exclusively in populations that were considered at increased risk for sexually transmitted infections (STIs) were excluded. Overall, the analysis included close to 45,000 men.
Prevalent HPV genotype
Testing for HPV was conducted on samples collected from the anus and genitals. The results show a global pooled prevalence of HPV infection in males older than 15 years of 31% for any HPV and 21% for HR-HPV. One of these viruses, HPV-16, was the most prevalent HPV genotype (5% prevalence).
HPV prevalence was highest among young adults. It stabilized and decreased from age 50 years. Between ages 25 and 29 years, 35% of men are infected with HPV. It should be noted that prevalence is already high in the youngest group, reaching 28% in males between the ages of 15 and 19 years. The variations are similar for HR-HPV infections.
This age-related change is different from rates in women. Among the female population, HPV prevalence peaks soon after first sexual activity and declines with age, with a slight rebound after ages 50–55 years (i.e., often after or around the time of menopause), wrote the researchers.
The results also show country- and region-based disparities. The pooled prevalence for any HPV was highest in Sub-Saharan Africa (37%), followed by Europe and Northern America (36%). The lowest prevalence was in East and Southeast Asia (15%). Here again, the trends are similar with high-risk HPV.
Preventive measures
“Our study draws attention to the high prevalence, ranging from 20% to 30% for HR-HPV in men across most regions, and the need for strengthening HPV prevention within overall STI control efforts,” wrote the authors.
“Future epidemiological studies are needed to monitor trends in prevalence in men, especially considering the roll-out of HPV vaccination in girls and young women and that many countries are beginning to vaccinate boys.”
In France, the HPV vaccination program was extended in 2021 to include all boys between the ages of 11 and 14 years (two-dose schedule), with a catch-up course in males up to age 19 years (three-dose schedule). This is the same vaccine program as for girls. It is also recommended for men up to age 26 years who have sex with other men.
The 2023 return to school will see the launch of a general vaccination campaign aimed at seventh-grade students, both boys and girls, with parental consent, to increase vaccine coverage. In 2021, vaccine uptake was 43.6% in girls between the ages of 15 and 18 years and scarcely 6% in boys, according to Public Health France.
Two vaccines are in use: the bivalent Cervarix vaccine, which is effective against HPV-16 and HPV-18, and the nonavalent Gardasil 9, which is effective against types 16, 18, 31, 33, 45, 52, and 58. Both provide protection against HPV-16, the type most common in men, which is responsible for more than half of cases of cervical cancer.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
Findings from a meta-analysis of 65 studies conducted in 35 countries indicate that These estimates provide further weight to arguments in favor of vaccinating boys against HPV to prevent certain types of cancer.
“Our results support that sexually active men, regardless of age, are an important reservoir of HPV genital infection,” wrote the authors in The Lancet Global Health . “These estimates emphasize the importance of incorporating men into comprehensive HPV prevention strategies to reduce HPV-related morbidity and mortality in men and ultimately achieve elimination of cervical cancer and other HPV-related diseases.”
Literature review
HPV infection is the most common sexually transmitted viral infection worldwide. More than 200 HPV types can be transmitted sexually, and at least 12 types are oncogenic. Previous studies have shown that most sexually active men and women acquire at least one genital HPV infection during their lifetime.
Although most HPV infections are asymptomatic, they can lead to cancer. Indeed, HPV is involved in the development of cervical, vulval, and vaginal cancers, as well as oropharyngeal and anal cancers, which also affect the male population. More than 25% of cancers caused by HPV occur in men.
Despite these observations, fewer epidemiologic studies have assessed HPV infection in men than in women. To determine the prevalence of HPV infection in the male population, Laia Bruni, MD, MPH, PhD, an epidemiologist at the Catalan Institute of Oncology in Barcelona, and her colleagues collated data from 65 studies conducted in 35 countries pertaining to males older than 15 years.
In this literature review, the researchers selected studies that reported infection rates in males without HPV-related symptoms. Studies conducted exclusively in populations that were considered at increased risk for sexually transmitted infections (STIs) were excluded. Overall, the analysis included close to 45,000 men.
Prevalent HPV genotype
Testing for HPV was conducted on samples collected from the anus and genitals. The results show a global pooled prevalence of HPV infection in males older than 15 years of 31% for any HPV and 21% for HR-HPV. One of these viruses, HPV-16, was the most prevalent HPV genotype (5% prevalence).
HPV prevalence was highest among young adults. It stabilized and decreased from age 50 years. Between ages 25 and 29 years, 35% of men are infected with HPV. It should be noted that prevalence is already high in the youngest group, reaching 28% in males between the ages of 15 and 19 years. The variations are similar for HR-HPV infections.
This age-related change is different from rates in women. Among the female population, HPV prevalence peaks soon after first sexual activity and declines with age, with a slight rebound after ages 50–55 years (i.e., often after or around the time of menopause), wrote the researchers.
The results also show country- and region-based disparities. The pooled prevalence for any HPV was highest in Sub-Saharan Africa (37%), followed by Europe and Northern America (36%). The lowest prevalence was in East and Southeast Asia (15%). Here again, the trends are similar with high-risk HPV.
Preventive measures
“Our study draws attention to the high prevalence, ranging from 20% to 30% for HR-HPV in men across most regions, and the need for strengthening HPV prevention within overall STI control efforts,” wrote the authors.
“Future epidemiological studies are needed to monitor trends in prevalence in men, especially considering the roll-out of HPV vaccination in girls and young women and that many countries are beginning to vaccinate boys.”
In France, the HPV vaccination program was extended in 2021 to include all boys between the ages of 11 and 14 years (two-dose schedule), with a catch-up course in males up to age 19 years (three-dose schedule). This is the same vaccine program as for girls. It is also recommended for men up to age 26 years who have sex with other men.
The 2023 return to school will see the launch of a general vaccination campaign aimed at seventh-grade students, both boys and girls, with parental consent, to increase vaccine coverage. In 2021, vaccine uptake was 43.6% in girls between the ages of 15 and 18 years and scarcely 6% in boys, according to Public Health France.
Two vaccines are in use: the bivalent Cervarix vaccine, which is effective against HPV-16 and HPV-18, and the nonavalent Gardasil 9, which is effective against types 16, 18, 31, 33, 45, 52, and 58. Both provide protection against HPV-16, the type most common in men, which is responsible for more than half of cases of cervical cancer.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
Findings from a meta-analysis of 65 studies conducted in 35 countries indicate that These estimates provide further weight to arguments in favor of vaccinating boys against HPV to prevent certain types of cancer.
“Our results support that sexually active men, regardless of age, are an important reservoir of HPV genital infection,” wrote the authors in The Lancet Global Health . “These estimates emphasize the importance of incorporating men into comprehensive HPV prevention strategies to reduce HPV-related morbidity and mortality in men and ultimately achieve elimination of cervical cancer and other HPV-related diseases.”
Literature review
HPV infection is the most common sexually transmitted viral infection worldwide. More than 200 HPV types can be transmitted sexually, and at least 12 types are oncogenic. Previous studies have shown that most sexually active men and women acquire at least one genital HPV infection during their lifetime.
Although most HPV infections are asymptomatic, they can lead to cancer. Indeed, HPV is involved in the development of cervical, vulval, and vaginal cancers, as well as oropharyngeal and anal cancers, which also affect the male population. More than 25% of cancers caused by HPV occur in men.
Despite these observations, fewer epidemiologic studies have assessed HPV infection in men than in women. To determine the prevalence of HPV infection in the male population, Laia Bruni, MD, MPH, PhD, an epidemiologist at the Catalan Institute of Oncology in Barcelona, and her colleagues collated data from 65 studies conducted in 35 countries pertaining to males older than 15 years.
In this literature review, the researchers selected studies that reported infection rates in males without HPV-related symptoms. Studies conducted exclusively in populations that were considered at increased risk for sexually transmitted infections (STIs) were excluded. Overall, the analysis included close to 45,000 men.
Prevalent HPV genotype
Testing for HPV was conducted on samples collected from the anus and genitals. The results show a global pooled prevalence of HPV infection in males older than 15 years of 31% for any HPV and 21% for HR-HPV. One of these viruses, HPV-16, was the most prevalent HPV genotype (5% prevalence).
HPV prevalence was highest among young adults. It stabilized and decreased from age 50 years. Between ages 25 and 29 years, 35% of men are infected with HPV. It should be noted that prevalence is already high in the youngest group, reaching 28% in males between the ages of 15 and 19 years. The variations are similar for HR-HPV infections.
This age-related change is different from rates in women. Among the female population, HPV prevalence peaks soon after first sexual activity and declines with age, with a slight rebound after ages 50–55 years (i.e., often after or around the time of menopause), wrote the researchers.
The results also show country- and region-based disparities. The pooled prevalence for any HPV was highest in Sub-Saharan Africa (37%), followed by Europe and Northern America (36%). The lowest prevalence was in East and Southeast Asia (15%). Here again, the trends are similar with high-risk HPV.
Preventive measures
“Our study draws attention to the high prevalence, ranging from 20% to 30% for HR-HPV in men across most regions, and the need for strengthening HPV prevention within overall STI control efforts,” wrote the authors.
“Future epidemiological studies are needed to monitor trends in prevalence in men, especially considering the roll-out of HPV vaccination in girls and young women and that many countries are beginning to vaccinate boys.”
In France, the HPV vaccination program was extended in 2021 to include all boys between the ages of 11 and 14 years (two-dose schedule), with a catch-up course in males up to age 19 years (three-dose schedule). This is the same vaccine program as for girls. It is also recommended for men up to age 26 years who have sex with other men.
The 2023 return to school will see the launch of a general vaccination campaign aimed at seventh-grade students, both boys and girls, with parental consent, to increase vaccine coverage. In 2021, vaccine uptake was 43.6% in girls between the ages of 15 and 18 years and scarcely 6% in boys, according to Public Health France.
Two vaccines are in use: the bivalent Cervarix vaccine, which is effective against HPV-16 and HPV-18, and the nonavalent Gardasil 9, which is effective against types 16, 18, 31, 33, 45, 52, and 58. Both provide protection against HPV-16, the type most common in men, which is responsible for more than half of cases of cervical cancer.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
FROM THE LANCET GLOBAL HEALTH
Five questions for COVID experts: How concerned should we be?
COVID-19 hospitalizations have been on the rise for weeks as summer nears its end, but how concerned should you be? SARS-CoV-2, the virus behind COVID, continues to evolve and surprise us. So COVID transmission, hospitalization, and death rates can be difficult to predict.
, especially now that testing and vaccinations are no longer free of charge.
Question 1: Are you expecting an end-of-summer COVID wave to be substantial?
Eric Topol, MD: “This wave won’t likely be substantial and could be more of a ‘wavelet.’ I’m not thinking that physicians are too concerned,” said Dr. Topol, founder and director of Scripps Research Translational Institute in La Jolla, Calif.
Thomas Gut, DO: “It’s always impossible to predict the severity of COVID waves. Although the virus has generally mutated in ways that favor easier transmission and milder illness, there have been a handful of surprising mutations that were more dangerous and deadly than the preceding strain,” said Dr. Gut, associate chair of medicine at Staten Island University Hospital/Northwell Health in New York.
Robert Atmar, MD: “I’ll start with the caveat that prognosticating for SARS-CoV-2 is a bit hazardous as we remain in unknown territory for some aspects of its epidemiology and evolution,” said Dr. Atmar, a professor of infectious diseases at Baylor College of Medicine in Houston. “It depends on your definition of substantial. We, at least in Houston, are already in the midst of a substantial surge in the burden of infection, at least as monitored through wastewater surveillance. The amount of virus in the wastewater already exceeds the peak level we saw last winter. That said, the increased infection burden has not translated into large increases in hospitalizations for COVID-19. Most persons hospitalized in our hospital are admitted with infection, not for the consequences of infection.”
Stuart Campbell Ray, MD: “It looks like there is a rise in infections, but the proportional rise in hospitalizations from severe cases is lower than in the past, suggesting that folks are protected by the immunity we’ve gained over the past few years through vaccination and prior infections. Of course, we should be thinking about how that applies to each of us – how recently we had a vaccine or COVID-19, and whether we might see more severe infections as immunity wanes,” said Dr. Ray, who is a professor of medicine in the division of infectious diseases at Johns Hopkins University in Baltimore.
Question 2: Is a return to masks or mask mandates coming this fall or winter?
Dr. Topol: “Mandating masks doesn’t work very well, but we may see wide use again if a descendant of [variant] BA.2.86 takes off.”
Dr. Gut: “It’s difficult to predict if there are any mask mandates returning at any point. Ever since the Omicron strains emerged, COVID has been relatively mild, compared to previous strains, so there probably won’t be any plan to start masking in public unless a more deadly strain appears.”
Dr. Atmar: “I do not think we will see a return to mask mandates this fall or winter for a variety of reasons. The primary one is that I don’t think the public will accept mask mandates. However, I think masking can continue to be an adjunctive measure to enhance protection from infection, along with booster vaccination.”
Dr. Ray: “Some people will choose to wear masks during a surge, particularly in situations like commuting where they don’t interfere with what they’re doing. They will wear masks particularly if they want to avoid infection due to concerns about others they care about, disruption of work or travel plans, or concerns about long-term consequences of repeated COVID-19.”
Question 3: Now that COVID testing and vaccinations are no longer free of charge, how might that affect their use?
Dr. Topol: “It was already low, and this will undoubtedly further compromise their uptake.”
Dr. Gut: “I do expect that testing will become less common now that tests are no longer free. I’m sure there will be a lower amount of detection in patients with milder or asymptomatic disease compared to what we had previously.”
Dr. Atmar: “If there are out-of-pocket costs for the SARS-CoV-2 vaccine, or if the administrative paperwork attached to getting a vaccine is increased, the uptake of SARS-CoV-2 vaccines will likely decrease. It will be important to communicate to the populations targeted for vaccination the potential benefits of such vaccination.”
Dr. Ray: “A challenge with COVID-19, all along, has been disparities in access to care, and this will be worse without public support for prevention and testing. This applies to everyone but is especially burdensome for those who are often marginalized in our health care system and society in general. I hope that we’ll find ways to ensure that people who need tests and vaccinations are able to access them, as good health is in everyone’s interest.”
Question 4: Will the new vaccines against COVID work for the currently circulating variants?
Dr. Topol: “The XBB.1.5 boosters will be out Sept. 14. They should help versus EG.5.1 and FL.1.5.1. The FL.1.5.1 variant is gaining now.”
Dr. Gut: “In the next several weeks, we expect the newer monovalent XBB-based vaccines to be offered that offer good protection against current circulating COVID variants along with the new Eris variant.”
Dr. Atmar: “The vaccines are expected to induce immune responses to the currently circulating variants, most of which are strains that evolved from the vaccine strain. The vaccine is expected to be most effective in preventing severe illness and will likely be less effective in preventing infection and mild illness.”
Dr. Ray: “Yes, the updated vaccine design has a spike antigen (XBB.1.5) nearly identical to the current dominant variant (EG.5). Even as variants change, the boosters stimulate B cells and T cells to help protect in a way that is safer than getting COVID-19 infection.”
Question 5: Is there anything we should watch out for regarding the BA.2.86 variant in particular?
Dr. Topol: “The scenario could change if there are new functional mutations added to it.”
Dr. Gut: “BA.2.86 is still fairly uncommon and does not have much data to directly make any informed guesses. However, in general, people that have been exposed to more recent mutations of the COVID virus have been shown to have more protection from newer upcoming mutations. It’s fair to guess that people that have not had recent infection from COVID, or have not had a recent booster, are at higher risk for being infected by any XBB- or BA.2-based strains.”
Dr. Atmar: BA.2.86 has been designated as a variant under monitoring. We will want to see whether it becomes more common and if there are any unexpected characteristics associated with infection by this variant.”
Dr. Ray: “It’s still rare, but it’s been seen in geographically dispersed places, so it’s got legs. The question is how effectively it will bypass some of the immunity we’ve gained. T cells are likely to remain protective, because they target so many parts of the virus that change more slowly, but antibodies from B cells to spike protein may have more trouble recognizing BA.2.86, whether those antibodies were made to a vaccine or a prior variant.”
A version of this article first appeared on WebMD.com.
COVID-19 hospitalizations have been on the rise for weeks as summer nears its end, but how concerned should you be? SARS-CoV-2, the virus behind COVID, continues to evolve and surprise us. So COVID transmission, hospitalization, and death rates can be difficult to predict.
, especially now that testing and vaccinations are no longer free of charge.
Question 1: Are you expecting an end-of-summer COVID wave to be substantial?
Eric Topol, MD: “This wave won’t likely be substantial and could be more of a ‘wavelet.’ I’m not thinking that physicians are too concerned,” said Dr. Topol, founder and director of Scripps Research Translational Institute in La Jolla, Calif.
Thomas Gut, DO: “It’s always impossible to predict the severity of COVID waves. Although the virus has generally mutated in ways that favor easier transmission and milder illness, there have been a handful of surprising mutations that were more dangerous and deadly than the preceding strain,” said Dr. Gut, associate chair of medicine at Staten Island University Hospital/Northwell Health in New York.
Robert Atmar, MD: “I’ll start with the caveat that prognosticating for SARS-CoV-2 is a bit hazardous as we remain in unknown territory for some aspects of its epidemiology and evolution,” said Dr. Atmar, a professor of infectious diseases at Baylor College of Medicine in Houston. “It depends on your definition of substantial. We, at least in Houston, are already in the midst of a substantial surge in the burden of infection, at least as monitored through wastewater surveillance. The amount of virus in the wastewater already exceeds the peak level we saw last winter. That said, the increased infection burden has not translated into large increases in hospitalizations for COVID-19. Most persons hospitalized in our hospital are admitted with infection, not for the consequences of infection.”
Stuart Campbell Ray, MD: “It looks like there is a rise in infections, but the proportional rise in hospitalizations from severe cases is lower than in the past, suggesting that folks are protected by the immunity we’ve gained over the past few years through vaccination and prior infections. Of course, we should be thinking about how that applies to each of us – how recently we had a vaccine or COVID-19, and whether we might see more severe infections as immunity wanes,” said Dr. Ray, who is a professor of medicine in the division of infectious diseases at Johns Hopkins University in Baltimore.
Question 2: Is a return to masks or mask mandates coming this fall or winter?
Dr. Topol: “Mandating masks doesn’t work very well, but we may see wide use again if a descendant of [variant] BA.2.86 takes off.”
Dr. Gut: “It’s difficult to predict if there are any mask mandates returning at any point. Ever since the Omicron strains emerged, COVID has been relatively mild, compared to previous strains, so there probably won’t be any plan to start masking in public unless a more deadly strain appears.”
Dr. Atmar: “I do not think we will see a return to mask mandates this fall or winter for a variety of reasons. The primary one is that I don’t think the public will accept mask mandates. However, I think masking can continue to be an adjunctive measure to enhance protection from infection, along with booster vaccination.”
Dr. Ray: “Some people will choose to wear masks during a surge, particularly in situations like commuting where they don’t interfere with what they’re doing. They will wear masks particularly if they want to avoid infection due to concerns about others they care about, disruption of work or travel plans, or concerns about long-term consequences of repeated COVID-19.”
Question 3: Now that COVID testing and vaccinations are no longer free of charge, how might that affect their use?
Dr. Topol: “It was already low, and this will undoubtedly further compromise their uptake.”
Dr. Gut: “I do expect that testing will become less common now that tests are no longer free. I’m sure there will be a lower amount of detection in patients with milder or asymptomatic disease compared to what we had previously.”
Dr. Atmar: “If there are out-of-pocket costs for the SARS-CoV-2 vaccine, or if the administrative paperwork attached to getting a vaccine is increased, the uptake of SARS-CoV-2 vaccines will likely decrease. It will be important to communicate to the populations targeted for vaccination the potential benefits of such vaccination.”
Dr. Ray: “A challenge with COVID-19, all along, has been disparities in access to care, and this will be worse without public support for prevention and testing. This applies to everyone but is especially burdensome for those who are often marginalized in our health care system and society in general. I hope that we’ll find ways to ensure that people who need tests and vaccinations are able to access them, as good health is in everyone’s interest.”
Question 4: Will the new vaccines against COVID work for the currently circulating variants?
Dr. Topol: “The XBB.1.5 boosters will be out Sept. 14. They should help versus EG.5.1 and FL.1.5.1. The FL.1.5.1 variant is gaining now.”
Dr. Gut: “In the next several weeks, we expect the newer monovalent XBB-based vaccines to be offered that offer good protection against current circulating COVID variants along with the new Eris variant.”
Dr. Atmar: “The vaccines are expected to induce immune responses to the currently circulating variants, most of which are strains that evolved from the vaccine strain. The vaccine is expected to be most effective in preventing severe illness and will likely be less effective in preventing infection and mild illness.”
Dr. Ray: “Yes, the updated vaccine design has a spike antigen (XBB.1.5) nearly identical to the current dominant variant (EG.5). Even as variants change, the boosters stimulate B cells and T cells to help protect in a way that is safer than getting COVID-19 infection.”
Question 5: Is there anything we should watch out for regarding the BA.2.86 variant in particular?
Dr. Topol: “The scenario could change if there are new functional mutations added to it.”
Dr. Gut: “BA.2.86 is still fairly uncommon and does not have much data to directly make any informed guesses. However, in general, people that have been exposed to more recent mutations of the COVID virus have been shown to have more protection from newer upcoming mutations. It’s fair to guess that people that have not had recent infection from COVID, or have not had a recent booster, are at higher risk for being infected by any XBB- or BA.2-based strains.”
Dr. Atmar: BA.2.86 has been designated as a variant under monitoring. We will want to see whether it becomes more common and if there are any unexpected characteristics associated with infection by this variant.”
Dr. Ray: “It’s still rare, but it’s been seen in geographically dispersed places, so it’s got legs. The question is how effectively it will bypass some of the immunity we’ve gained. T cells are likely to remain protective, because they target so many parts of the virus that change more slowly, but antibodies from B cells to spike protein may have more trouble recognizing BA.2.86, whether those antibodies were made to a vaccine or a prior variant.”
A version of this article first appeared on WebMD.com.
COVID-19 hospitalizations have been on the rise for weeks as summer nears its end, but how concerned should you be? SARS-CoV-2, the virus behind COVID, continues to evolve and surprise us. So COVID transmission, hospitalization, and death rates can be difficult to predict.
, especially now that testing and vaccinations are no longer free of charge.
Question 1: Are you expecting an end-of-summer COVID wave to be substantial?
Eric Topol, MD: “This wave won’t likely be substantial and could be more of a ‘wavelet.’ I’m not thinking that physicians are too concerned,” said Dr. Topol, founder and director of Scripps Research Translational Institute in La Jolla, Calif.
Thomas Gut, DO: “It’s always impossible to predict the severity of COVID waves. Although the virus has generally mutated in ways that favor easier transmission and milder illness, there have been a handful of surprising mutations that were more dangerous and deadly than the preceding strain,” said Dr. Gut, associate chair of medicine at Staten Island University Hospital/Northwell Health in New York.
Robert Atmar, MD: “I’ll start with the caveat that prognosticating for SARS-CoV-2 is a bit hazardous as we remain in unknown territory for some aspects of its epidemiology and evolution,” said Dr. Atmar, a professor of infectious diseases at Baylor College of Medicine in Houston. “It depends on your definition of substantial. We, at least in Houston, are already in the midst of a substantial surge in the burden of infection, at least as monitored through wastewater surveillance. The amount of virus in the wastewater already exceeds the peak level we saw last winter. That said, the increased infection burden has not translated into large increases in hospitalizations for COVID-19. Most persons hospitalized in our hospital are admitted with infection, not for the consequences of infection.”
Stuart Campbell Ray, MD: “It looks like there is a rise in infections, but the proportional rise in hospitalizations from severe cases is lower than in the past, suggesting that folks are protected by the immunity we’ve gained over the past few years through vaccination and prior infections. Of course, we should be thinking about how that applies to each of us – how recently we had a vaccine or COVID-19, and whether we might see more severe infections as immunity wanes,” said Dr. Ray, who is a professor of medicine in the division of infectious diseases at Johns Hopkins University in Baltimore.
Question 2: Is a return to masks or mask mandates coming this fall or winter?
Dr. Topol: “Mandating masks doesn’t work very well, but we may see wide use again if a descendant of [variant] BA.2.86 takes off.”
Dr. Gut: “It’s difficult to predict if there are any mask mandates returning at any point. Ever since the Omicron strains emerged, COVID has been relatively mild, compared to previous strains, so there probably won’t be any plan to start masking in public unless a more deadly strain appears.”
Dr. Atmar: “I do not think we will see a return to mask mandates this fall or winter for a variety of reasons. The primary one is that I don’t think the public will accept mask mandates. However, I think masking can continue to be an adjunctive measure to enhance protection from infection, along with booster vaccination.”
Dr. Ray: “Some people will choose to wear masks during a surge, particularly in situations like commuting where they don’t interfere with what they’re doing. They will wear masks particularly if they want to avoid infection due to concerns about others they care about, disruption of work or travel plans, or concerns about long-term consequences of repeated COVID-19.”
Question 3: Now that COVID testing and vaccinations are no longer free of charge, how might that affect their use?
Dr. Topol: “It was already low, and this will undoubtedly further compromise their uptake.”
Dr. Gut: “I do expect that testing will become less common now that tests are no longer free. I’m sure there will be a lower amount of detection in patients with milder or asymptomatic disease compared to what we had previously.”
Dr. Atmar: “If there are out-of-pocket costs for the SARS-CoV-2 vaccine, or if the administrative paperwork attached to getting a vaccine is increased, the uptake of SARS-CoV-2 vaccines will likely decrease. It will be important to communicate to the populations targeted for vaccination the potential benefits of such vaccination.”
Dr. Ray: “A challenge with COVID-19, all along, has been disparities in access to care, and this will be worse without public support for prevention and testing. This applies to everyone but is especially burdensome for those who are often marginalized in our health care system and society in general. I hope that we’ll find ways to ensure that people who need tests and vaccinations are able to access them, as good health is in everyone’s interest.”
Question 4: Will the new vaccines against COVID work for the currently circulating variants?
Dr. Topol: “The XBB.1.5 boosters will be out Sept. 14. They should help versus EG.5.1 and FL.1.5.1. The FL.1.5.1 variant is gaining now.”
Dr. Gut: “In the next several weeks, we expect the newer monovalent XBB-based vaccines to be offered that offer good protection against current circulating COVID variants along with the new Eris variant.”
Dr. Atmar: “The vaccines are expected to induce immune responses to the currently circulating variants, most of which are strains that evolved from the vaccine strain. The vaccine is expected to be most effective in preventing severe illness and will likely be less effective in preventing infection and mild illness.”
Dr. Ray: “Yes, the updated vaccine design has a spike antigen (XBB.1.5) nearly identical to the current dominant variant (EG.5). Even as variants change, the boosters stimulate B cells and T cells to help protect in a way that is safer than getting COVID-19 infection.”
Question 5: Is there anything we should watch out for regarding the BA.2.86 variant in particular?
Dr. Topol: “The scenario could change if there are new functional mutations added to it.”
Dr. Gut: “BA.2.86 is still fairly uncommon and does not have much data to directly make any informed guesses. However, in general, people that have been exposed to more recent mutations of the COVID virus have been shown to have more protection from newer upcoming mutations. It’s fair to guess that people that have not had recent infection from COVID, or have not had a recent booster, are at higher risk for being infected by any XBB- or BA.2-based strains.”
Dr. Atmar: BA.2.86 has been designated as a variant under monitoring. We will want to see whether it becomes more common and if there are any unexpected characteristics associated with infection by this variant.”
Dr. Ray: “It’s still rare, but it’s been seen in geographically dispersed places, so it’s got legs. The question is how effectively it will bypass some of the immunity we’ve gained. T cells are likely to remain protective, because they target so many parts of the virus that change more slowly, but antibodies from B cells to spike protein may have more trouble recognizing BA.2.86, whether those antibodies were made to a vaccine or a prior variant.”
A version of this article first appeared on WebMD.com.
FDA to step up oversight of cosmetics, assess ‘forever chemicals’
They are also preparing to assess potential risks of so-called forever chemicals in these products.
The Food and Drug Administration last year gained new authority over cosmetics when Congress passed the Modernization of Cosmetics Regulation Act of 2022 (MoCRA) by adding this bill to a December budget package.
“On average, consumers in the U.S. use six to 12 cosmetics products daily. But, until recently the FDA didn’t have the authority to require manufacturers to submit cosmetic product listings, including a list of ingredients used in these products, or register the facilities where they were produced,” Namandjé Bumpus, PhD, FDA’s chief scientist, said in a press release.
In the statement, the FDA announced the release of a draft guidance document that is intended to help companies comply with the transparency requirements slated to kick in this December. The agency is accepting comments on this draft guidance through Sept. 7.
“Later this year, registration and listing of cosmetic product facilities and products will become a requirement, making information about cosmetic products, including the ingredients used in products and the facilities where they are produced, readily available to the agency,” Dr. Bumpus said.
The products, according to the FDA statement, include makeup, nail polishes, shaving creams, other grooming products, perfumes, face and body cleansers, hair products, moisturizers, and other skin care items.
MoCRA “represents a sea change in how FDA regulates the cosmetics industry,” attorneys Frederick R. Ball, Alyson Walker Lotman, and Kelly A. Bonner, wrote in an article for the Food and Drug Law Institute published in spring 2023.
The FDA has called the MoCRA law “the most significant expansion” of its authority to regulate cosmetics since the Federal Food, Drug, and Cosmetic Act was passed in 1938.
The agency is in the process of expanding its staff to carry out newly authorized duties, including the tracking of adverse events. The FDA budget request for fiscal 2024, which begins Oct. 1, seeks $5 million for work needed to implement MoCRA.
PFAS, or ‘forever chemicals’
Some of the requested FDA funding is intended to prepare the agency to assess the use of per-and polyfluoroalkyl substances (PFAS) in cosmetics.
MoCRA sets a 3-year deadline for the FDA to issue an assessment of the use and potential risks of PFAS in cosmetics products. PFAS are sometimes added as ingredients in some cosmetic products, including lotions, cleansers, nail polish, shaving cream, foundation, lipstick, eyeliner, eyeshadow, and mascara, according to the FDA. Sometimes the presence of PFAS in cosmetics is unintentional and is the result of impurities in raw materials or is due to the breakdown of ingredients, the FDA said.
The FDA’s website says that so far, the available research doesn’t allow for “definitive conclusions about the potential health risks of PFAS in cosmetics.”
The Centers for Disease Control and Prevention has stated that research has suggested potential links between high levels of certain PFAS, in general, with increased cholesterol levels, changes in liver enzyme levels, increased risk of hypertension or preeclampsia in pregnant women, and increased risk of kidney or testicular cancer.
PFAS compounds often are used to resist grease, oil, water, and heat in industrial settings. They are used in thousands of products, from nonstick cookware to firefighting foams and protective gear, because they can reduce friction, according to a National Academies of Sciences, Engineering, and Medicine report on PFAS that was issued last year.
PFAS are known as “forever chemicals” because they contain a carbon-fluorine bond, which does not break naturally. Even when PFAS are transformed in the body, they can assume other forms of PFAS that preserve the troublesome carbon-fluorine bond. With PFAS, the human body is confronted with a substance it doesn’t have the tools to process.
This is in contrast to proteins and carbohydrates, which are in a sense prepackaged for relatively easy disassembly in the human body. Many of these compounds have weak links that enzymes and stomach acid can take apart, such as sulfur-to-sulfur (disulfide) bonds. That’s why protein-based biotech drugs are injected instead of administered as pills. The ultimate goal of this digestion is for the body to gain energy from these compounds.
But with PFAS, the body faces the challenge of carbon-fluorine bonds that are very hard to break down, and there is no payoff for these efforts, Graham F. Peaslee, PhD, professor of physics at the University of Notre Dame (Indiana), told this news organization.
“Nothing will naturally eat it because when you break the bond, it’s like eating celery,” he said. “You use more calories to eat the celery than you gain back from it.”
Interest from a U.S. senator
Dr. Peaslee was one of the authors of a 2021 article about PFAS in cosmetics that appeared in the journal Environmental Science and Technology Letters.
In the article, Dr. Peaslee and colleagues reported on their screening of 231 cosmetic products purchased in the United States and Canada using particle-induced gamma-ray emission spectroscopy. They found cases of undisclosed PFAS in cosmetic products. Foundations, mascaras, and lip products were noted as being especially problematic.
Sen. Susan Collins (R-ME) cited Dr. Peaslee’s article in a 2021 floor speech as she argued for having the FDA ban the intentional addition of PFAS to cosmetics.
“The findings of this study are particularly alarming, as many of these products are subject to direct human exposure,” Sen. Collins said. “For example, lipstick is often inadvertently ingested, and mascara is sometimes absorbed through tear ducts.”
In addition, workers at cosmetics plants may be exposed to PFAS and discarded cosmetics that have these compounds, which could potentially contaminate drinking water, Sen. Collins said. In 2021, she introduced legislation seeking a ban on PFAS that are intentionally added to cosmetics. That legislation did not advance through the Senate.
But the Senate Appropriations Committee, on which Sen. Collins is the ranking Republican, wants the FDA to keep a ban on PFAS in mind.
The Senate Agriculture Appropriations subcommittee, which oversees the FDA’s budget, raised the issue of PFAS and cosmetics in a June report. The FDA should develop a plan outlining research needed to inform “regulatory decision making, including potential development of a proposed rule to ban intentionally added PFAS substances in cosmetics,” the subcommittee said.
A version of this article first appeared on Medscape.com.
They are also preparing to assess potential risks of so-called forever chemicals in these products.
The Food and Drug Administration last year gained new authority over cosmetics when Congress passed the Modernization of Cosmetics Regulation Act of 2022 (MoCRA) by adding this bill to a December budget package.
“On average, consumers in the U.S. use six to 12 cosmetics products daily. But, until recently the FDA didn’t have the authority to require manufacturers to submit cosmetic product listings, including a list of ingredients used in these products, or register the facilities where they were produced,” Namandjé Bumpus, PhD, FDA’s chief scientist, said in a press release.
In the statement, the FDA announced the release of a draft guidance document that is intended to help companies comply with the transparency requirements slated to kick in this December. The agency is accepting comments on this draft guidance through Sept. 7.
“Later this year, registration and listing of cosmetic product facilities and products will become a requirement, making information about cosmetic products, including the ingredients used in products and the facilities where they are produced, readily available to the agency,” Dr. Bumpus said.
The products, according to the FDA statement, include makeup, nail polishes, shaving creams, other grooming products, perfumes, face and body cleansers, hair products, moisturizers, and other skin care items.
MoCRA “represents a sea change in how FDA regulates the cosmetics industry,” attorneys Frederick R. Ball, Alyson Walker Lotman, and Kelly A. Bonner, wrote in an article for the Food and Drug Law Institute published in spring 2023.
The FDA has called the MoCRA law “the most significant expansion” of its authority to regulate cosmetics since the Federal Food, Drug, and Cosmetic Act was passed in 1938.
The agency is in the process of expanding its staff to carry out newly authorized duties, including the tracking of adverse events. The FDA budget request for fiscal 2024, which begins Oct. 1, seeks $5 million for work needed to implement MoCRA.
PFAS, or ‘forever chemicals’
Some of the requested FDA funding is intended to prepare the agency to assess the use of per-and polyfluoroalkyl substances (PFAS) in cosmetics.
MoCRA sets a 3-year deadline for the FDA to issue an assessment of the use and potential risks of PFAS in cosmetics products. PFAS are sometimes added as ingredients in some cosmetic products, including lotions, cleansers, nail polish, shaving cream, foundation, lipstick, eyeliner, eyeshadow, and mascara, according to the FDA. Sometimes the presence of PFAS in cosmetics is unintentional and is the result of impurities in raw materials or is due to the breakdown of ingredients, the FDA said.
The FDA’s website says that so far, the available research doesn’t allow for “definitive conclusions about the potential health risks of PFAS in cosmetics.”
The Centers for Disease Control and Prevention has stated that research has suggested potential links between high levels of certain PFAS, in general, with increased cholesterol levels, changes in liver enzyme levels, increased risk of hypertension or preeclampsia in pregnant women, and increased risk of kidney or testicular cancer.
PFAS compounds often are used to resist grease, oil, water, and heat in industrial settings. They are used in thousands of products, from nonstick cookware to firefighting foams and protective gear, because they can reduce friction, according to a National Academies of Sciences, Engineering, and Medicine report on PFAS that was issued last year.
PFAS are known as “forever chemicals” because they contain a carbon-fluorine bond, which does not break naturally. Even when PFAS are transformed in the body, they can assume other forms of PFAS that preserve the troublesome carbon-fluorine bond. With PFAS, the human body is confronted with a substance it doesn’t have the tools to process.
This is in contrast to proteins and carbohydrates, which are in a sense prepackaged for relatively easy disassembly in the human body. Many of these compounds have weak links that enzymes and stomach acid can take apart, such as sulfur-to-sulfur (disulfide) bonds. That’s why protein-based biotech drugs are injected instead of administered as pills. The ultimate goal of this digestion is for the body to gain energy from these compounds.
But with PFAS, the body faces the challenge of carbon-fluorine bonds that are very hard to break down, and there is no payoff for these efforts, Graham F. Peaslee, PhD, professor of physics at the University of Notre Dame (Indiana), told this news organization.
“Nothing will naturally eat it because when you break the bond, it’s like eating celery,” he said. “You use more calories to eat the celery than you gain back from it.”
Interest from a U.S. senator
Dr. Peaslee was one of the authors of a 2021 article about PFAS in cosmetics that appeared in the journal Environmental Science and Technology Letters.
In the article, Dr. Peaslee and colleagues reported on their screening of 231 cosmetic products purchased in the United States and Canada using particle-induced gamma-ray emission spectroscopy. They found cases of undisclosed PFAS in cosmetic products. Foundations, mascaras, and lip products were noted as being especially problematic.
Sen. Susan Collins (R-ME) cited Dr. Peaslee’s article in a 2021 floor speech as she argued for having the FDA ban the intentional addition of PFAS to cosmetics.
“The findings of this study are particularly alarming, as many of these products are subject to direct human exposure,” Sen. Collins said. “For example, lipstick is often inadvertently ingested, and mascara is sometimes absorbed through tear ducts.”
In addition, workers at cosmetics plants may be exposed to PFAS and discarded cosmetics that have these compounds, which could potentially contaminate drinking water, Sen. Collins said. In 2021, she introduced legislation seeking a ban on PFAS that are intentionally added to cosmetics. That legislation did not advance through the Senate.
But the Senate Appropriations Committee, on which Sen. Collins is the ranking Republican, wants the FDA to keep a ban on PFAS in mind.
The Senate Agriculture Appropriations subcommittee, which oversees the FDA’s budget, raised the issue of PFAS and cosmetics in a June report. The FDA should develop a plan outlining research needed to inform “regulatory decision making, including potential development of a proposed rule to ban intentionally added PFAS substances in cosmetics,” the subcommittee said.
A version of this article first appeared on Medscape.com.
They are also preparing to assess potential risks of so-called forever chemicals in these products.
The Food and Drug Administration last year gained new authority over cosmetics when Congress passed the Modernization of Cosmetics Regulation Act of 2022 (MoCRA) by adding this bill to a December budget package.
“On average, consumers in the U.S. use six to 12 cosmetics products daily. But, until recently the FDA didn’t have the authority to require manufacturers to submit cosmetic product listings, including a list of ingredients used in these products, or register the facilities where they were produced,” Namandjé Bumpus, PhD, FDA’s chief scientist, said in a press release.
In the statement, the FDA announced the release of a draft guidance document that is intended to help companies comply with the transparency requirements slated to kick in this December. The agency is accepting comments on this draft guidance through Sept. 7.
“Later this year, registration and listing of cosmetic product facilities and products will become a requirement, making information about cosmetic products, including the ingredients used in products and the facilities where they are produced, readily available to the agency,” Dr. Bumpus said.
The products, according to the FDA statement, include makeup, nail polishes, shaving creams, other grooming products, perfumes, face and body cleansers, hair products, moisturizers, and other skin care items.
MoCRA “represents a sea change in how FDA regulates the cosmetics industry,” attorneys Frederick R. Ball, Alyson Walker Lotman, and Kelly A. Bonner, wrote in an article for the Food and Drug Law Institute published in spring 2023.
The FDA has called the MoCRA law “the most significant expansion” of its authority to regulate cosmetics since the Federal Food, Drug, and Cosmetic Act was passed in 1938.
The agency is in the process of expanding its staff to carry out newly authorized duties, including the tracking of adverse events. The FDA budget request for fiscal 2024, which begins Oct. 1, seeks $5 million for work needed to implement MoCRA.
PFAS, or ‘forever chemicals’
Some of the requested FDA funding is intended to prepare the agency to assess the use of per-and polyfluoroalkyl substances (PFAS) in cosmetics.
MoCRA sets a 3-year deadline for the FDA to issue an assessment of the use and potential risks of PFAS in cosmetics products. PFAS are sometimes added as ingredients in some cosmetic products, including lotions, cleansers, nail polish, shaving cream, foundation, lipstick, eyeliner, eyeshadow, and mascara, according to the FDA. Sometimes the presence of PFAS in cosmetics is unintentional and is the result of impurities in raw materials or is due to the breakdown of ingredients, the FDA said.
The FDA’s website says that so far, the available research doesn’t allow for “definitive conclusions about the potential health risks of PFAS in cosmetics.”
The Centers for Disease Control and Prevention has stated that research has suggested potential links between high levels of certain PFAS, in general, with increased cholesterol levels, changes in liver enzyme levels, increased risk of hypertension or preeclampsia in pregnant women, and increased risk of kidney or testicular cancer.
PFAS compounds often are used to resist grease, oil, water, and heat in industrial settings. They are used in thousands of products, from nonstick cookware to firefighting foams and protective gear, because they can reduce friction, according to a National Academies of Sciences, Engineering, and Medicine report on PFAS that was issued last year.
PFAS are known as “forever chemicals” because they contain a carbon-fluorine bond, which does not break naturally. Even when PFAS are transformed in the body, they can assume other forms of PFAS that preserve the troublesome carbon-fluorine bond. With PFAS, the human body is confronted with a substance it doesn’t have the tools to process.
This is in contrast to proteins and carbohydrates, which are in a sense prepackaged for relatively easy disassembly in the human body. Many of these compounds have weak links that enzymes and stomach acid can take apart, such as sulfur-to-sulfur (disulfide) bonds. That’s why protein-based biotech drugs are injected instead of administered as pills. The ultimate goal of this digestion is for the body to gain energy from these compounds.
But with PFAS, the body faces the challenge of carbon-fluorine bonds that are very hard to break down, and there is no payoff for these efforts, Graham F. Peaslee, PhD, professor of physics at the University of Notre Dame (Indiana), told this news organization.
“Nothing will naturally eat it because when you break the bond, it’s like eating celery,” he said. “You use more calories to eat the celery than you gain back from it.”
Interest from a U.S. senator
Dr. Peaslee was one of the authors of a 2021 article about PFAS in cosmetics that appeared in the journal Environmental Science and Technology Letters.
In the article, Dr. Peaslee and colleagues reported on their screening of 231 cosmetic products purchased in the United States and Canada using particle-induced gamma-ray emission spectroscopy. They found cases of undisclosed PFAS in cosmetic products. Foundations, mascaras, and lip products were noted as being especially problematic.
Sen. Susan Collins (R-ME) cited Dr. Peaslee’s article in a 2021 floor speech as she argued for having the FDA ban the intentional addition of PFAS to cosmetics.
“The findings of this study are particularly alarming, as many of these products are subject to direct human exposure,” Sen. Collins said. “For example, lipstick is often inadvertently ingested, and mascara is sometimes absorbed through tear ducts.”
In addition, workers at cosmetics plants may be exposed to PFAS and discarded cosmetics that have these compounds, which could potentially contaminate drinking water, Sen. Collins said. In 2021, she introduced legislation seeking a ban on PFAS that are intentionally added to cosmetics. That legislation did not advance through the Senate.
But the Senate Appropriations Committee, on which Sen. Collins is the ranking Republican, wants the FDA to keep a ban on PFAS in mind.
The Senate Agriculture Appropriations subcommittee, which oversees the FDA’s budget, raised the issue of PFAS and cosmetics in a June report. The FDA should develop a plan outlining research needed to inform “regulatory decision making, including potential development of a proposed rule to ban intentionally added PFAS substances in cosmetics,” the subcommittee said.
A version of this article first appeared on Medscape.com.
Making one key connection may increase HPV vax uptake
The understanding that human papillomavirus (HPV) causes oropharyngeal squamous cell carcinoma (OPSCC) has been linked with increased likelihood of adults having been vaccinated for HPV, new research indicates.
In a study published online in JAMA Otolaryngology–Head and Neck Surgery, most of the 288 adults surveyed with validated questions were not aware that HPV causes OPSCC and had not been told of the relationship by their health care provider.
Researchers found that when participants knew about the relationship between HPV infection and OPSCC they were more than three times as likely to be vaccinated (odds ratio, 3.7; 95% confidence interval, 1.8-7.6) as those without the knowledge.
The survey was paired with a novel point-of-care adult vaccination program within an otolaryngology clinic.
“Targeted education aimed at unvaccinated adults establishing the relationship between HPV infection and OPSCC, paired with point-of-care vaccination, may be an innovative strategy for increasing HPV vaccination rates in adults,” write the authors, led by Jacob C. Bloom, MD, with the department of otolaryngology–head and neck surgery at Boston Medical Center.
Current HPV vaccination recommendations include three parts:
- Routine vaccination at age 11 or 12 years
- Catch-up vaccination at ages 13-26 years if not adequately vaccinated
- Shared clinical decision-making in adults aged 27-45 years if the vaccine series has not been completed.
Despite proven efficacy and safety of the HPV vaccine, vaccination rates are low for adults. Although 75% of adolescents aged 13-17 years have initiated the HPV vaccine, recent studies show only 16% of U.S. men aged 18-21 years have received at least 1 dose of the HPV vaccine, the authors write.
Christiana Zhang, MD, with the division of internal medicine at Johns Hopkins University in Baltimore, who was not part of the study, said she was not surprised by the lack of knowledge about the HPV-OPSCC link.
Patients are often counseled on the relationship between HPV and genital warts or anogenital cancers like cervical cancer, she says, but there is less patient education surrounding the relationship between HPV and oropharyngeal cancers.
She says she does counsel patients on the link with OPSCC, but not all providers do and provider knowledge in general surrounding HPV is low.
“Research has shown that knowledge and confidence among health care providers surrounding HPV vaccination is generally low, and this corresponds with a low vaccination recommendation rate,” she says.
She adds, “Patient education on HPV infection and its relationship with OPSCC, paired with point-of-care vaccination for qualifying patients, is a great approach.”
But the education needs to go beyond patients, she says.
“Given the important role that health care providers play in vaccine uptake, I think further efforts are needed to educate providers on HPV vaccination as well,” she says.
The study included patients aged 18-45 years who sought routine outpatient care at the otolaryngology clinic at Boston Medical Center from Sept. 1, 2020, to May 19, 2021.
Limitations of this study include studying a population from a single otolaryngology clinic in an urban, academic medical center. The population was more racially and ethnically diverse than the U.S. population with 60.3% identifying as racial and ethnic minorities. Gender and educational levels were also not reflective of U.S. demographics as half (50.8%) of the participants had a college degree or higher and 58.3% were women.
Dr. Bloom reports grants from the American Head and Neck Cancer Society during the conduct of the study. Coauthor Dr. Faden reports personal fees from Merck, Neotic, Focus, BMS, Chrystalis Biomedical Advisors, and Guidepoint; receiving nonfinancial support from BostonGene and Predicine; and receiving grants from Calico outside the submitted work. Dr. Zhang reports no relevant financial relationships.
The understanding that human papillomavirus (HPV) causes oropharyngeal squamous cell carcinoma (OPSCC) has been linked with increased likelihood of adults having been vaccinated for HPV, new research indicates.
In a study published online in JAMA Otolaryngology–Head and Neck Surgery, most of the 288 adults surveyed with validated questions were not aware that HPV causes OPSCC and had not been told of the relationship by their health care provider.
Researchers found that when participants knew about the relationship between HPV infection and OPSCC they were more than three times as likely to be vaccinated (odds ratio, 3.7; 95% confidence interval, 1.8-7.6) as those without the knowledge.
The survey was paired with a novel point-of-care adult vaccination program within an otolaryngology clinic.
“Targeted education aimed at unvaccinated adults establishing the relationship between HPV infection and OPSCC, paired with point-of-care vaccination, may be an innovative strategy for increasing HPV vaccination rates in adults,” write the authors, led by Jacob C. Bloom, MD, with the department of otolaryngology–head and neck surgery at Boston Medical Center.
Current HPV vaccination recommendations include three parts:
- Routine vaccination at age 11 or 12 years
- Catch-up vaccination at ages 13-26 years if not adequately vaccinated
- Shared clinical decision-making in adults aged 27-45 years if the vaccine series has not been completed.
Despite proven efficacy and safety of the HPV vaccine, vaccination rates are low for adults. Although 75% of adolescents aged 13-17 years have initiated the HPV vaccine, recent studies show only 16% of U.S. men aged 18-21 years have received at least 1 dose of the HPV vaccine, the authors write.
Christiana Zhang, MD, with the division of internal medicine at Johns Hopkins University in Baltimore, who was not part of the study, said she was not surprised by the lack of knowledge about the HPV-OPSCC link.
Patients are often counseled on the relationship between HPV and genital warts or anogenital cancers like cervical cancer, she says, but there is less patient education surrounding the relationship between HPV and oropharyngeal cancers.
She says she does counsel patients on the link with OPSCC, but not all providers do and provider knowledge in general surrounding HPV is low.
“Research has shown that knowledge and confidence among health care providers surrounding HPV vaccination is generally low, and this corresponds with a low vaccination recommendation rate,” she says.
She adds, “Patient education on HPV infection and its relationship with OPSCC, paired with point-of-care vaccination for qualifying patients, is a great approach.”
But the education needs to go beyond patients, she says.
“Given the important role that health care providers play in vaccine uptake, I think further efforts are needed to educate providers on HPV vaccination as well,” she says.
The study included patients aged 18-45 years who sought routine outpatient care at the otolaryngology clinic at Boston Medical Center from Sept. 1, 2020, to May 19, 2021.
Limitations of this study include studying a population from a single otolaryngology clinic in an urban, academic medical center. The population was more racially and ethnically diverse than the U.S. population with 60.3% identifying as racial and ethnic minorities. Gender and educational levels were also not reflective of U.S. demographics as half (50.8%) of the participants had a college degree or higher and 58.3% were women.
Dr. Bloom reports grants from the American Head and Neck Cancer Society during the conduct of the study. Coauthor Dr. Faden reports personal fees from Merck, Neotic, Focus, BMS, Chrystalis Biomedical Advisors, and Guidepoint; receiving nonfinancial support from BostonGene and Predicine; and receiving grants from Calico outside the submitted work. Dr. Zhang reports no relevant financial relationships.
The understanding that human papillomavirus (HPV) causes oropharyngeal squamous cell carcinoma (OPSCC) has been linked with increased likelihood of adults having been vaccinated for HPV, new research indicates.
In a study published online in JAMA Otolaryngology–Head and Neck Surgery, most of the 288 adults surveyed with validated questions were not aware that HPV causes OPSCC and had not been told of the relationship by their health care provider.
Researchers found that when participants knew about the relationship between HPV infection and OPSCC they were more than three times as likely to be vaccinated (odds ratio, 3.7; 95% confidence interval, 1.8-7.6) as those without the knowledge.
The survey was paired with a novel point-of-care adult vaccination program within an otolaryngology clinic.
“Targeted education aimed at unvaccinated adults establishing the relationship between HPV infection and OPSCC, paired with point-of-care vaccination, may be an innovative strategy for increasing HPV vaccination rates in adults,” write the authors, led by Jacob C. Bloom, MD, with the department of otolaryngology–head and neck surgery at Boston Medical Center.
Current HPV vaccination recommendations include three parts:
- Routine vaccination at age 11 or 12 years
- Catch-up vaccination at ages 13-26 years if not adequately vaccinated
- Shared clinical decision-making in adults aged 27-45 years if the vaccine series has not been completed.
Despite proven efficacy and safety of the HPV vaccine, vaccination rates are low for adults. Although 75% of adolescents aged 13-17 years have initiated the HPV vaccine, recent studies show only 16% of U.S. men aged 18-21 years have received at least 1 dose of the HPV vaccine, the authors write.
Christiana Zhang, MD, with the division of internal medicine at Johns Hopkins University in Baltimore, who was not part of the study, said she was not surprised by the lack of knowledge about the HPV-OPSCC link.
Patients are often counseled on the relationship between HPV and genital warts or anogenital cancers like cervical cancer, she says, but there is less patient education surrounding the relationship between HPV and oropharyngeal cancers.
She says she does counsel patients on the link with OPSCC, but not all providers do and provider knowledge in general surrounding HPV is low.
“Research has shown that knowledge and confidence among health care providers surrounding HPV vaccination is generally low, and this corresponds with a low vaccination recommendation rate,” she says.
She adds, “Patient education on HPV infection and its relationship with OPSCC, paired with point-of-care vaccination for qualifying patients, is a great approach.”
But the education needs to go beyond patients, she says.
“Given the important role that health care providers play in vaccine uptake, I think further efforts are needed to educate providers on HPV vaccination as well,” she says.
The study included patients aged 18-45 years who sought routine outpatient care at the otolaryngology clinic at Boston Medical Center from Sept. 1, 2020, to May 19, 2021.
Limitations of this study include studying a population from a single otolaryngology clinic in an urban, academic medical center. The population was more racially and ethnically diverse than the U.S. population with 60.3% identifying as racial and ethnic minorities. Gender and educational levels were also not reflective of U.S. demographics as half (50.8%) of the participants had a college degree or higher and 58.3% were women.
Dr. Bloom reports grants from the American Head and Neck Cancer Society during the conduct of the study. Coauthor Dr. Faden reports personal fees from Merck, Neotic, Focus, BMS, Chrystalis Biomedical Advisors, and Guidepoint; receiving nonfinancial support from BostonGene and Predicine; and receiving grants from Calico outside the submitted work. Dr. Zhang reports no relevant financial relationships.
FROM JAMA OTOLARYNGOLOGY–HEAD AND NECK SURGERY
Gender-affirming surgeries nearly tripled between 2016 and 2019: Study
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).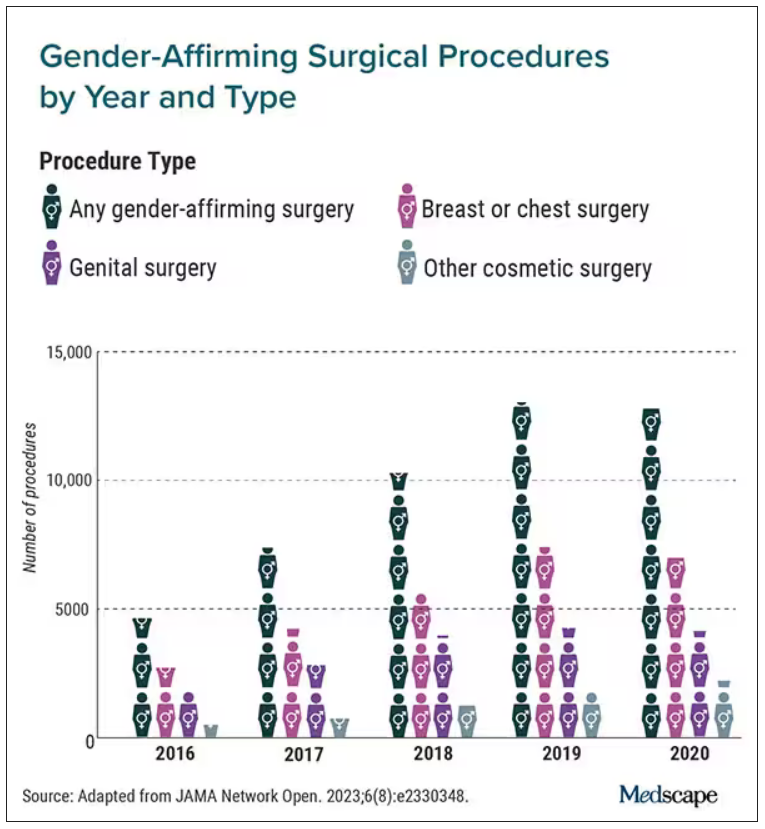
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
a new study published in JAMA Network Open found.
Breast and chest surgeries were the most common procedures performed, and the number of surgical procedures carried out increased with age. The researchers said that, in addition to legal shifts, the established safety of the surgeries and resulting increase in quality of life may also help explain the increase.
“The point of this is to raise awareness and to really document the patterns of care in the United States,” said Jason Wright, MD, an associate professor at Columbia University, New York. “We hope that people understand that these procedures are being performed more commonly and they’re out there.”
A study published in 2022 in JAMA Pediatrics found that the number of chest reconstruction surgeries among U.S. adolescents rose fourfold between 2016 and 2019.
The new study included data from 2016 to 2020 in the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample. More than 48,000 patients with diagnosis codes for gender identity disorder, transsexualism, or a personal history of sex reassignment were identified. Age ranges were grouped as 12-18 (7.7%), 19-30 (52.3%), and 31-40 (21.8%).
The number of gender-affirming procedures rose from 4,552 in 2016 to a peak of 13,011 in 2019. (A slight decline to 12,818 procedures in 2020 was attributed to the COVID-19 pandemic.) The surgeries were grouped into three categories: breast and chest procedures, which occurred in 56.6% of patients; genital reconstructive surgeries (35.1%), and other facial cosmetic procedures (13.9%).
“We really wanted to try to make this as representative as we could,” Dr. Wright said. “I think this is really the best estimates that are available to date.”
Chest and breast procedures made up a higher percentage of surgeries in younger patients, while genital surgical procedures made up a higher percentage in older patients. For example, patients aged 19-30 made up 59.1% of breast or chest surgeries and 44.2% of genital surgeries. However, those aged 31-40 accounted for 26.2% of genital surgeries and 18.1% of breast or chest surgeries. For ages 41-50, the spread was more than double, accounting for 12.8% of genital surgeries and only 6.1% of breast or chest surgeries, according to the researchers.
Undocumented uptick
In addition to more inclusive health insurance, Dr. Wright said the increase in these procedures can also be attributed to studies showing their safety and the long-term association with high patient satisfaction.
Kevin Wang, MD, medical director of Providence–Swedish Health Services’ LGBTQIA+ program in Seattle, agreed that changes in health insurance coverage for gender-affirming surgery likely account in part for their increase. But he added that more clinicians are performing these procedures.
He said gender-affirming surgeries improve quality of life for the people who undergo them. The American Academy of Pediatrics has said it would be conducting a thorough review of the effects of transgender care on youth. A 2018 policy statement from the group said transgender youth should “have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space.”
Dr. Wright cited several limitations to his group’s study that may result in the undercapture of transgender individuals and gender-affirming surgery; in particular, while the study captured inpatient and ambulatory surgical procedures in large, nationwide datasets, a small number of the procedures could have been performed in other settings.
Guiding a patient through gender-affirming care and surgical procedures can be an arduous process, including understanding their goals, using hormone therapy, and making referrals to specialists. Dr. Wang said he works to maximize his patients’ physical, mental, and emotional health, and helps them understand the risks.
He cited the double standard of a cisgender woman wanting breast augmentation without justification, but someone who identifies as transgender has many more boxes to check – for example, seeing a behavior health specialist to demonstrate they understand the risks and securing a letter of support from their primary care physician to undergo a similar procedure.
“It’s just interesting how the transgender community has to jump through so many more barriers and hoops for affirming, lifesaving procedures where you have other people who are doing it for aesthetic purposes and do not require any type of authorization,” Dr. Wang said.
Dr. Wright said he hopes the findings call attention to the need for more professionals working in the gender-affirming care field.
“I think for the medical community, it’s important to raise the idea that these procedures are becoming more common,” Dr. Wright said. “We are going to need specialists who have expertise in transgender care and surgeons who have the ability to perform these operations. Hopefully, this sheds light on the resources that are going to be required to care for these patients going forward.”
Dr. Wright reported receiving grants from Merck and personal fees from UpToDate outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Really? Cancer screening doesn’t save lives?
This transcript from Impact Factor has been edited for clarity.
If you are my age or older, and like me, you are something of a rule follower, then you’re getting screened for various cancers.
Colonoscopies, mammograms, cervical cancer screening, chest CTs for people with a significant smoking history. The tests are done and usually, but not always, they are negative. And if positive, usually, but not always, follow-up tests are negative, and if they aren’t and a new cancer is diagnosed you tell yourself, Well, at least we caught it early. Isn’t it good that I’m a rule follower? My life was just saved.
But it turns out, proving that cancer screening actually saves lives is quite difficult. Is it possible that all this screening is for nothing?
The benefits, risks, or perhaps futility of cancer screening is in the news this week because of this article, appearing in JAMA Internal Medicine.
It’s a meta-analysis of very specific randomized trials of cancer screening modalities and concludes that, with the exception of sigmoidoscopy for colon cancer screening, none of them meaningfully change life expectancy.
Now – a bit of inside baseball here – I almost never choose to discuss meta-analyses on Impact Factor. It’s hard enough to dig deep into the methodology of a single study, but with a meta-analysis, you’re sort of obligated to review all the included studies, and, what’s worse, the studies that were not included but might bear on the central question.
In this case, though, the topic is important enough to think about a bit more, and the conclusions have large enough implications for public health that we should question them a bit.
First, let’s run down the study as presented.
The authors searched for randomized trials of cancer screening modalities. This is important, and I think appropriate. They wanted studies that took some people and assigned them to screening, and some people to no screening – avoiding the confounding that would come from observational data (rule followers like me tend to live longer owing to a variety of healthful behaviors, not just cancer screening).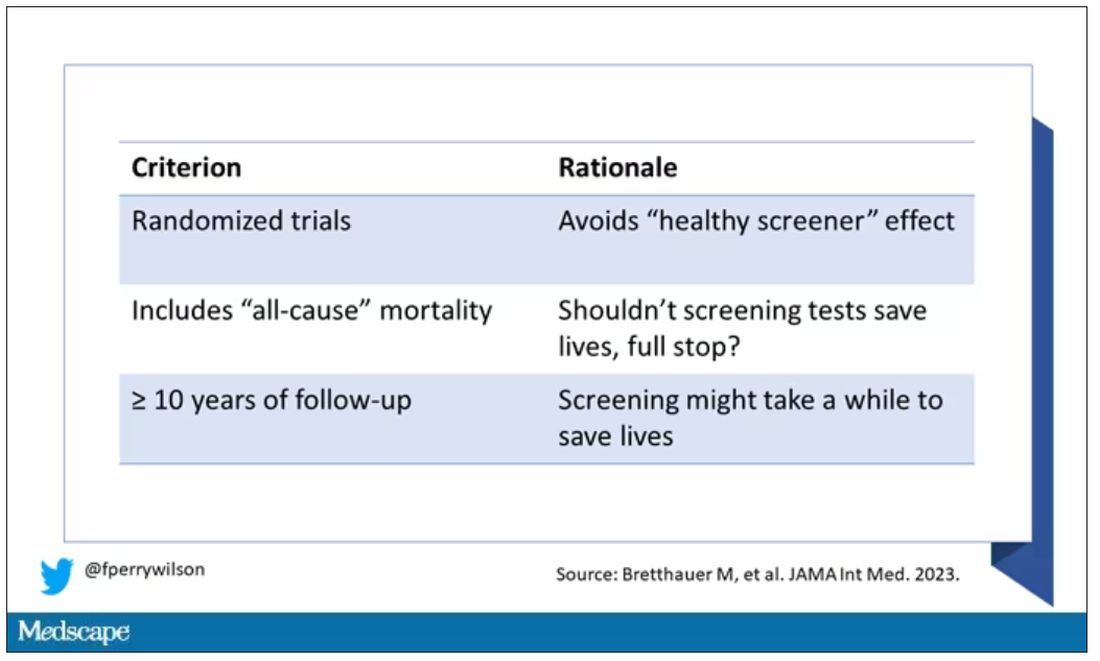
They didn’t stop at just randomized trials, though. They wanted trials that reported on all-cause, not cancer-specific, mortality. We’ll dig into the distinction in a sec. Finally, they wanted trials with at least 10 years of follow-up time.
These are pretty strict criteria – and after applying that filter, we are left with a grand total of 18 studies to analyze. Most were in the colon cancer space; only two studies met criteria for mammography screening.
Right off the bat, this raises concerns to me. In the universe of high-quality studies of cancer screening modalities, this is just the tip of the iceberg. And the results of meta-analyses are always dependent on the included studies – definitionally.
The results as presented are compelling.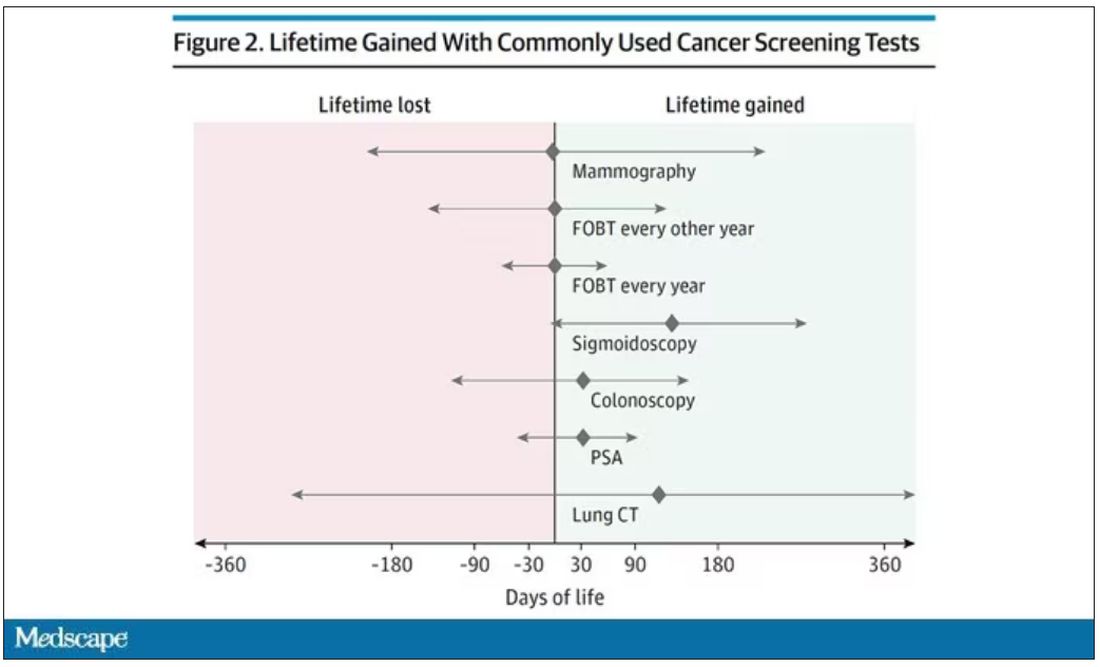
(Side note: Averages are tricky here. It’s not like everyone who gets screened gets 110 extra days. Most people get nothing, and some people – those whose colon cancer was detected early – get a bunch of extra days.)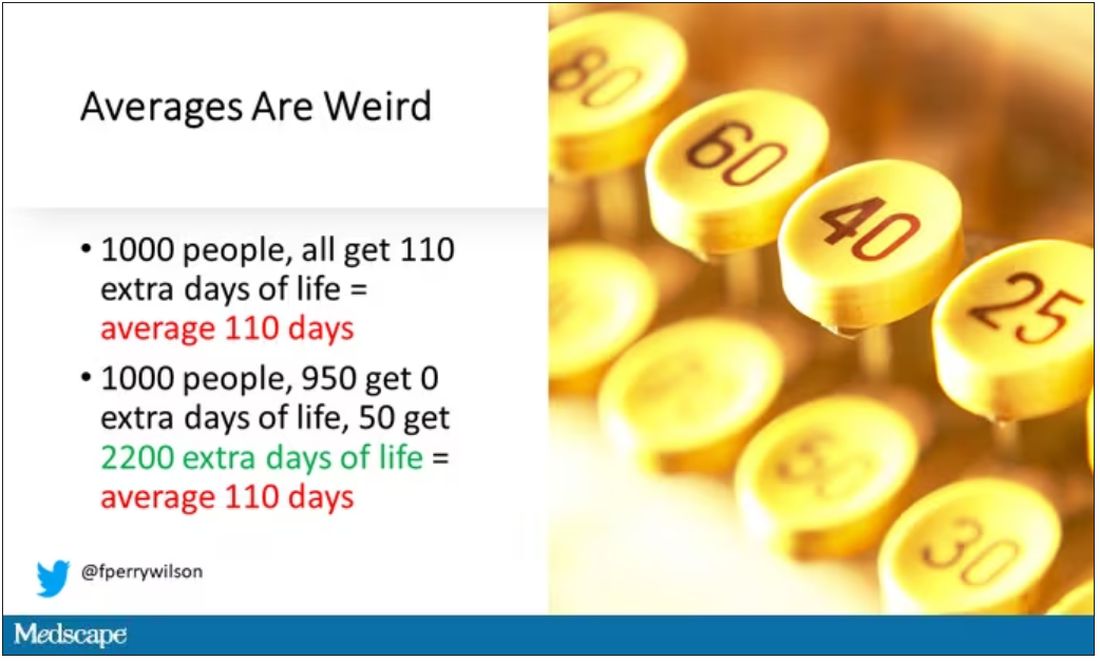
And a thing about meta-analysis: Meeting the criteria to be included in a meta-analysis does not necessarily mean the study was a good one. For example, one of the two mammography screening studies included is this one, from Miller and colleagues.
On the surface, it looks good – a large randomized trial of mammography screening in Canada, with long-term follow-up including all-cause mortality. Showing, by the way, no effect of screening on either breast cancer–specific or all-cause mortality.
But that study came under a lot of criticism owing to allegations that randomization was broken and women with palpable breast masses were preferentially put into the mammography group, making those outcomes worse.
The authors of the current meta-analysis don’t mention this. Indeed, they state that they don’t perform any assessments of the quality of the included studies.
But I don’t want to criticize all the included studies. Let’s think bigger picture.
Randomized trials of screening for cancers like colon, breast, and lung cancer in smokers have generally shown that those randomized to screening had lower target-cancer–specific mortality. Across all the randomized mammography studies, for example, women randomized to mammography were about 20% less likely to die of breast cancer than were those who were randomized to not be screened – particularly among those above age 50.
But it’s true that all-cause mortality, on the whole, has not differed statistically between those randomized to mammography vs. no mammography. What’s the deal?
Well, the authors of the meta-analysis engage in some zero-sum thinking here. They say that if it is true that screening tests reduce cancer-specific deaths, but all-cause mortality is not different, screening tests must increase mortality due to other causes. How? They cite colonic perforation during colonoscopy as an example of a harm that could lead to earlier death, which makes some sense. For mammogram and other less invasive screening modalities, they suggest that the stress and anxiety associated with screening might increase the risk for death – this is a bit harder for me to defend.
The thing is, statistics really isn’t a zero-sum game. It’s a question of signal vs. noise. Take breast cancer, for example. Without screening, about 3.2% of women in this country would die of breast cancer. With screening, 2.8% would die (that’s a 20% reduction on the relative scale). The truth is, most women don’t die of breast cancer. Most people don’t die of colon cancer. Even most smokers don’t die of lung cancer. Most people die of heart disease. And then cancer – but there are a lot of cancers out there, and only a handful have decent screening tests.
In other words, the screening tests are unlikely to help most people because most people will not die of the particular type of cancer being screened for. But it will help some small number of those people being screened a lot, potentially saving their lives. If we knew who those people were in advance, it would be great, but then I suppose we wouldn’t need the screening test in the first place.
It’s not fair, then, to say that mammography increases non–breast cancer causes of death. In reality, it’s just that the impact of mammography on all-cause mortality is washed out by the random noise inherent to studying a sample of individuals rather than the entire population.
I’m reminded of that old story about the girl on the beach after a storm, throwing beached starfish back into the water. Someone comes by and says, “Why are you doing that? There are millions of starfish here – it doesn’t matter if you throw a few back.” And she says, “It matters for this one.”
There are other issues with aggregating data like these and concluding that there is no effect on all-cause mortality. For one, it assumes the people randomized to no screening never got screening. Most of these studies lasted 5-10 years, some with longer follow-up, but many people in the no-screening arm may have been screened as recommendations have changed. That would tend to bias the results against screening because the so-called control group, well, isn’t.
It also fails to acknowledge the reality that screening for disease can be thought of as a package deal. Instead of asking whether screening for breast cancer, and colon cancer, and lung cancer individually saves lives, the real relevant question is whether a policy of screening for cancer in general saves lives. And that hasn’t been studied very broadly, except in one trial looking at screening for four cancers. That study is in this meta-analysis and, interestingly, seems to suggest that the policy does extend life – by 123 days. Again, be careful how you think about that average.
I don’t want to be an absolutist here. Whether these screening tests are a good idea or not is actually a moving target. As treatment for cancer gets better, detecting cancer early may not be as important. As new screening modalities emerge, older ones may not be preferable any longer. Better testing, genetic or otherwise, might allow us to tailor screening more narrowly than the population-based approach we have now.
But I worry that a meta-analysis like this, which concludes that screening doesn’t help on the basis of a handful of studies – without acknowledgment of the signal-to-noise problem, without accounting for screening in the control group, without acknowledging that screening should be thought of as a package – will lead some people to make the decision to forgo screening. for, say, 49 out of 50 of them, that may be fine. But for 1 out of 50 or so, well, it matters for that one.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript from Impact Factor has been edited for clarity.
If you are my age or older, and like me, you are something of a rule follower, then you’re getting screened for various cancers.
Colonoscopies, mammograms, cervical cancer screening, chest CTs for people with a significant smoking history. The tests are done and usually, but not always, they are negative. And if positive, usually, but not always, follow-up tests are negative, and if they aren’t and a new cancer is diagnosed you tell yourself, Well, at least we caught it early. Isn’t it good that I’m a rule follower? My life was just saved.
But it turns out, proving that cancer screening actually saves lives is quite difficult. Is it possible that all this screening is for nothing?
The benefits, risks, or perhaps futility of cancer screening is in the news this week because of this article, appearing in JAMA Internal Medicine.
It’s a meta-analysis of very specific randomized trials of cancer screening modalities and concludes that, with the exception of sigmoidoscopy for colon cancer screening, none of them meaningfully change life expectancy.
Now – a bit of inside baseball here – I almost never choose to discuss meta-analyses on Impact Factor. It’s hard enough to dig deep into the methodology of a single study, but with a meta-analysis, you’re sort of obligated to review all the included studies, and, what’s worse, the studies that were not included but might bear on the central question.
In this case, though, the topic is important enough to think about a bit more, and the conclusions have large enough implications for public health that we should question them a bit.
First, let’s run down the study as presented.
The authors searched for randomized trials of cancer screening modalities. This is important, and I think appropriate. They wanted studies that took some people and assigned them to screening, and some people to no screening – avoiding the confounding that would come from observational data (rule followers like me tend to live longer owing to a variety of healthful behaviors, not just cancer screening).
They didn’t stop at just randomized trials, though. They wanted trials that reported on all-cause, not cancer-specific, mortality. We’ll dig into the distinction in a sec. Finally, they wanted trials with at least 10 years of follow-up time.
These are pretty strict criteria – and after applying that filter, we are left with a grand total of 18 studies to analyze. Most were in the colon cancer space; only two studies met criteria for mammography screening.
Right off the bat, this raises concerns to me. In the universe of high-quality studies of cancer screening modalities, this is just the tip of the iceberg. And the results of meta-analyses are always dependent on the included studies – definitionally.
The results as presented are compelling.
(Side note: Averages are tricky here. It’s not like everyone who gets screened gets 110 extra days. Most people get nothing, and some people – those whose colon cancer was detected early – get a bunch of extra days.)
And a thing about meta-analysis: Meeting the criteria to be included in a meta-analysis does not necessarily mean the study was a good one. For example, one of the two mammography screening studies included is this one, from Miller and colleagues.
On the surface, it looks good – a large randomized trial of mammography screening in Canada, with long-term follow-up including all-cause mortality. Showing, by the way, no effect of screening on either breast cancer–specific or all-cause mortality.
But that study came under a lot of criticism owing to allegations that randomization was broken and women with palpable breast masses were preferentially put into the mammography group, making those outcomes worse.
The authors of the current meta-analysis don’t mention this. Indeed, they state that they don’t perform any assessments of the quality of the included studies.
But I don’t want to criticize all the included studies. Let’s think bigger picture.
Randomized trials of screening for cancers like colon, breast, and lung cancer in smokers have generally shown that those randomized to screening had lower target-cancer–specific mortality. Across all the randomized mammography studies, for example, women randomized to mammography were about 20% less likely to die of breast cancer than were those who were randomized to not be screened – particularly among those above age 50.
But it’s true that all-cause mortality, on the whole, has not differed statistically between those randomized to mammography vs. no mammography. What’s the deal?
Well, the authors of the meta-analysis engage in some zero-sum thinking here. They say that if it is true that screening tests reduce cancer-specific deaths, but all-cause mortality is not different, screening tests must increase mortality due to other causes. How? They cite colonic perforation during colonoscopy as an example of a harm that could lead to earlier death, which makes some sense. For mammogram and other less invasive screening modalities, they suggest that the stress and anxiety associated with screening might increase the risk for death – this is a bit harder for me to defend.
The thing is, statistics really isn’t a zero-sum game. It’s a question of signal vs. noise. Take breast cancer, for example. Without screening, about 3.2% of women in this country would die of breast cancer. With screening, 2.8% would die (that’s a 20% reduction on the relative scale). The truth is, most women don’t die of breast cancer. Most people don’t die of colon cancer. Even most smokers don’t die of lung cancer. Most people die of heart disease. And then cancer – but there are a lot of cancers out there, and only a handful have decent screening tests.
In other words, the screening tests are unlikely to help most people because most people will not die of the particular type of cancer being screened for. But it will help some small number of those people being screened a lot, potentially saving their lives. If we knew who those people were in advance, it would be great, but then I suppose we wouldn’t need the screening test in the first place.
It’s not fair, then, to say that mammography increases non–breast cancer causes of death. In reality, it’s just that the impact of mammography on all-cause mortality is washed out by the random noise inherent to studying a sample of individuals rather than the entire population.
I’m reminded of that old story about the girl on the beach after a storm, throwing beached starfish back into the water. Someone comes by and says, “Why are you doing that? There are millions of starfish here – it doesn’t matter if you throw a few back.” And she says, “It matters for this one.”
There are other issues with aggregating data like these and concluding that there is no effect on all-cause mortality. For one, it assumes the people randomized to no screening never got screening. Most of these studies lasted 5-10 years, some with longer follow-up, but many people in the no-screening arm may have been screened as recommendations have changed. That would tend to bias the results against screening because the so-called control group, well, isn’t.
It also fails to acknowledge the reality that screening for disease can be thought of as a package deal. Instead of asking whether screening for breast cancer, and colon cancer, and lung cancer individually saves lives, the real relevant question is whether a policy of screening for cancer in general saves lives. And that hasn’t been studied very broadly, except in one trial looking at screening for four cancers. That study is in this meta-analysis and, interestingly, seems to suggest that the policy does extend life – by 123 days. Again, be careful how you think about that average.
I don’t want to be an absolutist here. Whether these screening tests are a good idea or not is actually a moving target. As treatment for cancer gets better, detecting cancer early may not be as important. As new screening modalities emerge, older ones may not be preferable any longer. Better testing, genetic or otherwise, might allow us to tailor screening more narrowly than the population-based approach we have now.
But I worry that a meta-analysis like this, which concludes that screening doesn’t help on the basis of a handful of studies – without acknowledgment of the signal-to-noise problem, without accounting for screening in the control group, without acknowledging that screening should be thought of as a package – will lead some people to make the decision to forgo screening. for, say, 49 out of 50 of them, that may be fine. But for 1 out of 50 or so, well, it matters for that one.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript from Impact Factor has been edited for clarity.
If you are my age or older, and like me, you are something of a rule follower, then you’re getting screened for various cancers.
Colonoscopies, mammograms, cervical cancer screening, chest CTs for people with a significant smoking history. The tests are done and usually, but not always, they are negative. And if positive, usually, but not always, follow-up tests are negative, and if they aren’t and a new cancer is diagnosed you tell yourself, Well, at least we caught it early. Isn’t it good that I’m a rule follower? My life was just saved.
But it turns out, proving that cancer screening actually saves lives is quite difficult. Is it possible that all this screening is for nothing?
The benefits, risks, or perhaps futility of cancer screening is in the news this week because of this article, appearing in JAMA Internal Medicine.
It’s a meta-analysis of very specific randomized trials of cancer screening modalities and concludes that, with the exception of sigmoidoscopy for colon cancer screening, none of them meaningfully change life expectancy.
Now – a bit of inside baseball here – I almost never choose to discuss meta-analyses on Impact Factor. It’s hard enough to dig deep into the methodology of a single study, but with a meta-analysis, you’re sort of obligated to review all the included studies, and, what’s worse, the studies that were not included but might bear on the central question.
In this case, though, the topic is important enough to think about a bit more, and the conclusions have large enough implications for public health that we should question them a bit.
First, let’s run down the study as presented.
The authors searched for randomized trials of cancer screening modalities. This is important, and I think appropriate. They wanted studies that took some people and assigned them to screening, and some people to no screening – avoiding the confounding that would come from observational data (rule followers like me tend to live longer owing to a variety of healthful behaviors, not just cancer screening).
They didn’t stop at just randomized trials, though. They wanted trials that reported on all-cause, not cancer-specific, mortality. We’ll dig into the distinction in a sec. Finally, they wanted trials with at least 10 years of follow-up time.
These are pretty strict criteria – and after applying that filter, we are left with a grand total of 18 studies to analyze. Most were in the colon cancer space; only two studies met criteria for mammography screening.
Right off the bat, this raises concerns to me. In the universe of high-quality studies of cancer screening modalities, this is just the tip of the iceberg. And the results of meta-analyses are always dependent on the included studies – definitionally.
The results as presented are compelling.
(Side note: Averages are tricky here. It’s not like everyone who gets screened gets 110 extra days. Most people get nothing, and some people – those whose colon cancer was detected early – get a bunch of extra days.)
And a thing about meta-analysis: Meeting the criteria to be included in a meta-analysis does not necessarily mean the study was a good one. For example, one of the two mammography screening studies included is this one, from Miller and colleagues.
On the surface, it looks good – a large randomized trial of mammography screening in Canada, with long-term follow-up including all-cause mortality. Showing, by the way, no effect of screening on either breast cancer–specific or all-cause mortality.
But that study came under a lot of criticism owing to allegations that randomization was broken and women with palpable breast masses were preferentially put into the mammography group, making those outcomes worse.
The authors of the current meta-analysis don’t mention this. Indeed, they state that they don’t perform any assessments of the quality of the included studies.
But I don’t want to criticize all the included studies. Let’s think bigger picture.
Randomized trials of screening for cancers like colon, breast, and lung cancer in smokers have generally shown that those randomized to screening had lower target-cancer–specific mortality. Across all the randomized mammography studies, for example, women randomized to mammography were about 20% less likely to die of breast cancer than were those who were randomized to not be screened – particularly among those above age 50.
But it’s true that all-cause mortality, on the whole, has not differed statistically between those randomized to mammography vs. no mammography. What’s the deal?
Well, the authors of the meta-analysis engage in some zero-sum thinking here. They say that if it is true that screening tests reduce cancer-specific deaths, but all-cause mortality is not different, screening tests must increase mortality due to other causes. How? They cite colonic perforation during colonoscopy as an example of a harm that could lead to earlier death, which makes some sense. For mammogram and other less invasive screening modalities, they suggest that the stress and anxiety associated with screening might increase the risk for death – this is a bit harder for me to defend.
The thing is, statistics really isn’t a zero-sum game. It’s a question of signal vs. noise. Take breast cancer, for example. Without screening, about 3.2% of women in this country would die of breast cancer. With screening, 2.8% would die (that’s a 20% reduction on the relative scale). The truth is, most women don’t die of breast cancer. Most people don’t die of colon cancer. Even most smokers don’t die of lung cancer. Most people die of heart disease. And then cancer – but there are a lot of cancers out there, and only a handful have decent screening tests.
In other words, the screening tests are unlikely to help most people because most people will not die of the particular type of cancer being screened for. But it will help some small number of those people being screened a lot, potentially saving their lives. If we knew who those people were in advance, it would be great, but then I suppose we wouldn’t need the screening test in the first place.
It’s not fair, then, to say that mammography increases non–breast cancer causes of death. In reality, it’s just that the impact of mammography on all-cause mortality is washed out by the random noise inherent to studying a sample of individuals rather than the entire population.
I’m reminded of that old story about the girl on the beach after a storm, throwing beached starfish back into the water. Someone comes by and says, “Why are you doing that? There are millions of starfish here – it doesn’t matter if you throw a few back.” And she says, “It matters for this one.”
There are other issues with aggregating data like these and concluding that there is no effect on all-cause mortality. For one, it assumes the people randomized to no screening never got screening. Most of these studies lasted 5-10 years, some with longer follow-up, but many people in the no-screening arm may have been screened as recommendations have changed. That would tend to bias the results against screening because the so-called control group, well, isn’t.
It also fails to acknowledge the reality that screening for disease can be thought of as a package deal. Instead of asking whether screening for breast cancer, and colon cancer, and lung cancer individually saves lives, the real relevant question is whether a policy of screening for cancer in general saves lives. And that hasn’t been studied very broadly, except in one trial looking at screening for four cancers. That study is in this meta-analysis and, interestingly, seems to suggest that the policy does extend life – by 123 days. Again, be careful how you think about that average.
I don’t want to be an absolutist here. Whether these screening tests are a good idea or not is actually a moving target. As treatment for cancer gets better, detecting cancer early may not be as important. As new screening modalities emerge, older ones may not be preferable any longer. Better testing, genetic or otherwise, might allow us to tailor screening more narrowly than the population-based approach we have now.
But I worry that a meta-analysis like this, which concludes that screening doesn’t help on the basis of a handful of studies – without acknowledgment of the signal-to-noise problem, without accounting for screening in the control group, without acknowledging that screening should be thought of as a package – will lead some people to make the decision to forgo screening. for, say, 49 out of 50 of them, that may be fine. But for 1 out of 50 or so, well, it matters for that one.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Severe COVID may cause long-term cellular changes: Study
The small study, published in Cell and funded by the National Institutes of Health, details how immune cells were analyzed through blood samples collected from 38 patients recovering from severe COVID and other critical illnesses, and from 19 healthy people. Researchers from Weill Cornell Medicine, New York, and The Jackson Laboratory for Genomic Medicine, Farmington, Conn., found through isolating hematopoietic stem cells that people recovering from severe bouts of COVID had changes to their DNA that were passed down to offspring cells.
The research team, led by Steven Josefowicz, PhD, of Weill Cornell’s pathology department, and Duygu Ucar, PhD, associate professor at The Jackson Laboratory for Genomic Medicine, discovered that this chain reaction of stem cell changes caused a boost in the production of monocytes. The authors found that, due to the innate cellular changes from a severe case of COVID, patients in recovery ended up producing a larger amount of inflammatory cytokines, rather than monocytes – distinct from samples collected from healthy patients and those recovering from other critical illnesses.
These changes to patients’ epigenetic landscapes were observed even a year after the initial COVID-19 infection. While the small participant pool meant that the research team could not establish a direct line between these innate changes and any ensuing health outcomes, the research provides us with clues as to why patients continue to struggle with inflammation and long COVID symptoms well after they recover.
While the authors reiterate the study’s limitations and hesitate to make any clear-cut associations between the results and long-term health outcomes, Wolfgang Leitner, PhD, from the NIH’s National Institute of Allergy and Infectious Diseases, predicts that long COVID can, at least in part, be explained by the changes in innate immune responses.
“Ideally, the authors would have had cells from each patient before they got infected, as a comparator, to see what the epigenetic landscape was before COVID changed it,” said Dr. Leitner. “Clear links between the severity of COVID and genetics were discovered already early in the pandemic and this paper should prompt follow-up studies that link mutations in immune genes with the epigenetic changes described here.”
Dr. Leitner said he had some initial predictions about the long-term impact of COVID-19, but he had not anticipated some of what the study’s findings now show.
“Unlike in the case of, for example, influenza, where the lungs go into ‘repair mode’ after the infection has been resolved – which leaves people susceptible to secondary infections for up to several months – this study shows that after severe COVID, the immune system remains in ‘emergency mode’ and in a heightened state of inflammation,” said Dr. Leitner.
“That further aggravates the problem the initial strong inflammation causes: even higher risk of autoimmune disease, but also, cancer.”
Commenting on the findings, Eric Topol, MD, editor-in-chief of Medscape Medical News, said the study presents “evidence that a key line of immune cells are essentially irrevocably, epigenetically altered and activated.
“You do not want to have this [COVID],” he added.
The study also highlights the researchers’ novel approach to isolating hematopoietic stem cells, found largely in bone marrow. This type of research has been limited in the past because of how costly and invasive it can be to analyze cells in bone marrow. But, by isolating and enriching hematopoietic stem cells, the team can decipher the full cellular diversity of the cells’ bone marrow counterparts.
“This revelation opened the doors to study, at single-cell resolution, how stem cells are affected upon infection and vaccination with a simple blood draw,” representatives from the Jackson lab said in a press release.
A version of this article appeared on Medscape.com.
The small study, published in Cell and funded by the National Institutes of Health, details how immune cells were analyzed through blood samples collected from 38 patients recovering from severe COVID and other critical illnesses, and from 19 healthy people. Researchers from Weill Cornell Medicine, New York, and The Jackson Laboratory for Genomic Medicine, Farmington, Conn., found through isolating hematopoietic stem cells that people recovering from severe bouts of COVID had changes to their DNA that were passed down to offspring cells.
The research team, led by Steven Josefowicz, PhD, of Weill Cornell’s pathology department, and Duygu Ucar, PhD, associate professor at The Jackson Laboratory for Genomic Medicine, discovered that this chain reaction of stem cell changes caused a boost in the production of monocytes. The authors found that, due to the innate cellular changes from a severe case of COVID, patients in recovery ended up producing a larger amount of inflammatory cytokines, rather than monocytes – distinct from samples collected from healthy patients and those recovering from other critical illnesses.
These changes to patients’ epigenetic landscapes were observed even a year after the initial COVID-19 infection. While the small participant pool meant that the research team could not establish a direct line between these innate changes and any ensuing health outcomes, the research provides us with clues as to why patients continue to struggle with inflammation and long COVID symptoms well after they recover.
While the authors reiterate the study’s limitations and hesitate to make any clear-cut associations between the results and long-term health outcomes, Wolfgang Leitner, PhD, from the NIH’s National Institute of Allergy and Infectious Diseases, predicts that long COVID can, at least in part, be explained by the changes in innate immune responses.
“Ideally, the authors would have had cells from each patient before they got infected, as a comparator, to see what the epigenetic landscape was before COVID changed it,” said Dr. Leitner. “Clear links between the severity of COVID and genetics were discovered already early in the pandemic and this paper should prompt follow-up studies that link mutations in immune genes with the epigenetic changes described here.”
Dr. Leitner said he had some initial predictions about the long-term impact of COVID-19, but he had not anticipated some of what the study’s findings now show.
“Unlike in the case of, for example, influenza, where the lungs go into ‘repair mode’ after the infection has been resolved – which leaves people susceptible to secondary infections for up to several months – this study shows that after severe COVID, the immune system remains in ‘emergency mode’ and in a heightened state of inflammation,” said Dr. Leitner.
“That further aggravates the problem the initial strong inflammation causes: even higher risk of autoimmune disease, but also, cancer.”
Commenting on the findings, Eric Topol, MD, editor-in-chief of Medscape Medical News, said the study presents “evidence that a key line of immune cells are essentially irrevocably, epigenetically altered and activated.
“You do not want to have this [COVID],” he added.
The study also highlights the researchers’ novel approach to isolating hematopoietic stem cells, found largely in bone marrow. This type of research has been limited in the past because of how costly and invasive it can be to analyze cells in bone marrow. But, by isolating and enriching hematopoietic stem cells, the team can decipher the full cellular diversity of the cells’ bone marrow counterparts.
“This revelation opened the doors to study, at single-cell resolution, how stem cells are affected upon infection and vaccination with a simple blood draw,” representatives from the Jackson lab said in a press release.
A version of this article appeared on Medscape.com.
The small study, published in Cell and funded by the National Institutes of Health, details how immune cells were analyzed through blood samples collected from 38 patients recovering from severe COVID and other critical illnesses, and from 19 healthy people. Researchers from Weill Cornell Medicine, New York, and The Jackson Laboratory for Genomic Medicine, Farmington, Conn., found through isolating hematopoietic stem cells that people recovering from severe bouts of COVID had changes to their DNA that were passed down to offspring cells.
The research team, led by Steven Josefowicz, PhD, of Weill Cornell’s pathology department, and Duygu Ucar, PhD, associate professor at The Jackson Laboratory for Genomic Medicine, discovered that this chain reaction of stem cell changes caused a boost in the production of monocytes. The authors found that, due to the innate cellular changes from a severe case of COVID, patients in recovery ended up producing a larger amount of inflammatory cytokines, rather than monocytes – distinct from samples collected from healthy patients and those recovering from other critical illnesses.
These changes to patients’ epigenetic landscapes were observed even a year after the initial COVID-19 infection. While the small participant pool meant that the research team could not establish a direct line between these innate changes and any ensuing health outcomes, the research provides us with clues as to why patients continue to struggle with inflammation and long COVID symptoms well after they recover.
While the authors reiterate the study’s limitations and hesitate to make any clear-cut associations between the results and long-term health outcomes, Wolfgang Leitner, PhD, from the NIH’s National Institute of Allergy and Infectious Diseases, predicts that long COVID can, at least in part, be explained by the changes in innate immune responses.
“Ideally, the authors would have had cells from each patient before they got infected, as a comparator, to see what the epigenetic landscape was before COVID changed it,” said Dr. Leitner. “Clear links between the severity of COVID and genetics were discovered already early in the pandemic and this paper should prompt follow-up studies that link mutations in immune genes with the epigenetic changes described here.”
Dr. Leitner said he had some initial predictions about the long-term impact of COVID-19, but he had not anticipated some of what the study’s findings now show.
“Unlike in the case of, for example, influenza, where the lungs go into ‘repair mode’ after the infection has been resolved – which leaves people susceptible to secondary infections for up to several months – this study shows that after severe COVID, the immune system remains in ‘emergency mode’ and in a heightened state of inflammation,” said Dr. Leitner.
“That further aggravates the problem the initial strong inflammation causes: even higher risk of autoimmune disease, but also, cancer.”
Commenting on the findings, Eric Topol, MD, editor-in-chief of Medscape Medical News, said the study presents “evidence that a key line of immune cells are essentially irrevocably, epigenetically altered and activated.
“You do not want to have this [COVID],” he added.
The study also highlights the researchers’ novel approach to isolating hematopoietic stem cells, found largely in bone marrow. This type of research has been limited in the past because of how costly and invasive it can be to analyze cells in bone marrow. But, by isolating and enriching hematopoietic stem cells, the team can decipher the full cellular diversity of the cells’ bone marrow counterparts.
“This revelation opened the doors to study, at single-cell resolution, how stem cells are affected upon infection and vaccination with a simple blood draw,” representatives from the Jackson lab said in a press release.
A version of this article appeared on Medscape.com.
FROM CELL
Cruel summer for medical students and Taylor Swift fans
Most medical students won’t see Taylor Swift perform her hit song “Cruel Summer,” but they will spend thousands of dollars on ERAS as they prepare for the 2024 residency match. Medical students applying for residency tend to be as stressed out as Swifties trying to score concert tickets. Aside from the expenses of residency applications, students also face an increasingly complex application process: a match algorithm many of them do not understand and major changes to the application process that most learn about right before the application cycle begins.
I have gone through two matches myself, one for internal medicine and one for neurology, and I have also guided students through the process for almost a decade as a dean of student affairs at a medical school. Every summer, the application process is filled with numerous changes, often with little, if any, warning for the students. One year, for example, a specialty required additional essays tailored to each program. Though this requirement may have helped programs discern which students are most enthusiastic about their programs, it also disadvantaged students working on busier rotations, strapped for time to write as many as 70 additional essays in a matter of weeks.
Other recent changes have included “signaling” programs, selecting preferred regions, and preinterview recordings for some specialties. In 2023, students cannot include more than 10 activities on their ERAS application. I have spoken to students at numerous medical schools concerned about the difficulty of selecting 10 activities out of dozens of meaningful pursuits throughout their journeys; this challenge is particularly acute for students who had other careers before entering medical school.
The stress continues to mount even after residency applications have been submitted. Students often feel tied to their phones because offers for residency interviews roll in day and night by email, and if they wait more than a few hours to respond, they’re often moved to a waiting list for their preferred interview date. One year, while we were rounding on patients, a student stepped away to schedule an interview; while doing so, he missed out on managing a patient who developed a neurologic emergency. Thankfully, many but not all specialties have put rules in place to allow students more time to think through interview offers. Having more time to think, even if it’s just 48 hours, may decrease stress, limit the negative impacts on medical education, and promote informed decisions during interview season.
To be sure, most changes are being made in an effort to improve the experience of the students and programs. But as with anything, the result has been a mix of good and bad. The transition to virtual interviews allowed students to apply more broadly to programs without worrying about travel costs. The move also benefits students with disabilities who face accessibility and other challenges with traveling. However, virtual interviews came with several downsides, including but not limited to an increased number of applications submitted (recall that this was also a benefit), interview hoarding, and challenges of connecting personally via virtual platform. Despite the virtual format, applicants increasingly are doing in-person second looks, which some worry may give those applicants an additional advantage over applicants who do not have the time or financial resources to travel for a second look. Despite these shortcomings, it is important that virtual interviews remain an option for those applicants who need it.
Another change, which has been extensively debated in medical education in recent years, was the switch to pass/fail on the USMLE Step 1 exam. Though this move decreased the stress students experienced in the first 2 years of medical school, it has resulted in a new challenge as many residency programs put more emphasis on USMLE Step 2. Many medical students feel they do not have a good gauge of their competitiveness until a few weeks before they submit their application, particularly those applicants attending medical schools that do not provide them with information regarding their class standing until right before they submit their applications.
By the time Swift’s Eras Tour ends in the summer of 2024, medical students will already have matched and started their residency programs. At the same time, a new batch of students will be entering the next year’s match. Though the number of anticipated changes may not reach the level of seismic activity caused by the Swifties at her Seattle concert, many medical students fear that the changes may be just like tectonic plates shifting the match process away from its original purpose: to provide an orderly and fair mechanism for matching the preferences of applicants for U.S. residency positions with the preferences of residency program directors.
Dr. Etienne is with WMCHealth Good Samaritan Hospital, New York, and New York Medical College. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Most medical students won’t see Taylor Swift perform her hit song “Cruel Summer,” but they will spend thousands of dollars on ERAS as they prepare for the 2024 residency match. Medical students applying for residency tend to be as stressed out as Swifties trying to score concert tickets. Aside from the expenses of residency applications, students also face an increasingly complex application process: a match algorithm many of them do not understand and major changes to the application process that most learn about right before the application cycle begins.
I have gone through two matches myself, one for internal medicine and one for neurology, and I have also guided students through the process for almost a decade as a dean of student affairs at a medical school. Every summer, the application process is filled with numerous changes, often with little, if any, warning for the students. One year, for example, a specialty required additional essays tailored to each program. Though this requirement may have helped programs discern which students are most enthusiastic about their programs, it also disadvantaged students working on busier rotations, strapped for time to write as many as 70 additional essays in a matter of weeks.
Other recent changes have included “signaling” programs, selecting preferred regions, and preinterview recordings for some specialties. In 2023, students cannot include more than 10 activities on their ERAS application. I have spoken to students at numerous medical schools concerned about the difficulty of selecting 10 activities out of dozens of meaningful pursuits throughout their journeys; this challenge is particularly acute for students who had other careers before entering medical school.
The stress continues to mount even after residency applications have been submitted. Students often feel tied to their phones because offers for residency interviews roll in day and night by email, and if they wait more than a few hours to respond, they’re often moved to a waiting list for their preferred interview date. One year, while we were rounding on patients, a student stepped away to schedule an interview; while doing so, he missed out on managing a patient who developed a neurologic emergency. Thankfully, many but not all specialties have put rules in place to allow students more time to think through interview offers. Having more time to think, even if it’s just 48 hours, may decrease stress, limit the negative impacts on medical education, and promote informed decisions during interview season.
To be sure, most changes are being made in an effort to improve the experience of the students and programs. But as with anything, the result has been a mix of good and bad. The transition to virtual interviews allowed students to apply more broadly to programs without worrying about travel costs. The move also benefits students with disabilities who face accessibility and other challenges with traveling. However, virtual interviews came with several downsides, including but not limited to an increased number of applications submitted (recall that this was also a benefit), interview hoarding, and challenges of connecting personally via virtual platform. Despite the virtual format, applicants increasingly are doing in-person second looks, which some worry may give those applicants an additional advantage over applicants who do not have the time or financial resources to travel for a second look. Despite these shortcomings, it is important that virtual interviews remain an option for those applicants who need it.
Another change, which has been extensively debated in medical education in recent years, was the switch to pass/fail on the USMLE Step 1 exam. Though this move decreased the stress students experienced in the first 2 years of medical school, it has resulted in a new challenge as many residency programs put more emphasis on USMLE Step 2. Many medical students feel they do not have a good gauge of their competitiveness until a few weeks before they submit their application, particularly those applicants attending medical schools that do not provide them with information regarding their class standing until right before they submit their applications.
By the time Swift’s Eras Tour ends in the summer of 2024, medical students will already have matched and started their residency programs. At the same time, a new batch of students will be entering the next year’s match. Though the number of anticipated changes may not reach the level of seismic activity caused by the Swifties at her Seattle concert, many medical students fear that the changes may be just like tectonic plates shifting the match process away from its original purpose: to provide an orderly and fair mechanism for matching the preferences of applicants for U.S. residency positions with the preferences of residency program directors.
Dr. Etienne is with WMCHealth Good Samaritan Hospital, New York, and New York Medical College. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Most medical students won’t see Taylor Swift perform her hit song “Cruel Summer,” but they will spend thousands of dollars on ERAS as they prepare for the 2024 residency match. Medical students applying for residency tend to be as stressed out as Swifties trying to score concert tickets. Aside from the expenses of residency applications, students also face an increasingly complex application process: a match algorithm many of them do not understand and major changes to the application process that most learn about right before the application cycle begins.
I have gone through two matches myself, one for internal medicine and one for neurology, and I have also guided students through the process for almost a decade as a dean of student affairs at a medical school. Every summer, the application process is filled with numerous changes, often with little, if any, warning for the students. One year, for example, a specialty required additional essays tailored to each program. Though this requirement may have helped programs discern which students are most enthusiastic about their programs, it also disadvantaged students working on busier rotations, strapped for time to write as many as 70 additional essays in a matter of weeks.
Other recent changes have included “signaling” programs, selecting preferred regions, and preinterview recordings for some specialties. In 2023, students cannot include more than 10 activities on their ERAS application. I have spoken to students at numerous medical schools concerned about the difficulty of selecting 10 activities out of dozens of meaningful pursuits throughout their journeys; this challenge is particularly acute for students who had other careers before entering medical school.
The stress continues to mount even after residency applications have been submitted. Students often feel tied to their phones because offers for residency interviews roll in day and night by email, and if they wait more than a few hours to respond, they’re often moved to a waiting list for their preferred interview date. One year, while we were rounding on patients, a student stepped away to schedule an interview; while doing so, he missed out on managing a patient who developed a neurologic emergency. Thankfully, many but not all specialties have put rules in place to allow students more time to think through interview offers. Having more time to think, even if it’s just 48 hours, may decrease stress, limit the negative impacts on medical education, and promote informed decisions during interview season.
To be sure, most changes are being made in an effort to improve the experience of the students and programs. But as with anything, the result has been a mix of good and bad. The transition to virtual interviews allowed students to apply more broadly to programs without worrying about travel costs. The move also benefits students with disabilities who face accessibility and other challenges with traveling. However, virtual interviews came with several downsides, including but not limited to an increased number of applications submitted (recall that this was also a benefit), interview hoarding, and challenges of connecting personally via virtual platform. Despite the virtual format, applicants increasingly are doing in-person second looks, which some worry may give those applicants an additional advantage over applicants who do not have the time or financial resources to travel for a second look. Despite these shortcomings, it is important that virtual interviews remain an option for those applicants who need it.
Another change, which has been extensively debated in medical education in recent years, was the switch to pass/fail on the USMLE Step 1 exam. Though this move decreased the stress students experienced in the first 2 years of medical school, it has resulted in a new challenge as many residency programs put more emphasis on USMLE Step 2. Many medical students feel they do not have a good gauge of their competitiveness until a few weeks before they submit their application, particularly those applicants attending medical schools that do not provide them with information regarding their class standing until right before they submit their applications.
By the time Swift’s Eras Tour ends in the summer of 2024, medical students will already have matched and started their residency programs. At the same time, a new batch of students will be entering the next year’s match. Though the number of anticipated changes may not reach the level of seismic activity caused by the Swifties at her Seattle concert, many medical students fear that the changes may be just like tectonic plates shifting the match process away from its original purpose: to provide an orderly and fair mechanism for matching the preferences of applicants for U.S. residency positions with the preferences of residency program directors.
Dr. Etienne is with WMCHealth Good Samaritan Hospital, New York, and New York Medical College. He disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Number of people with long COVID could be vastly underestimated
It’s been estimated that up to one-third of people who survive acute SARS-CoV-2 infection will suffer a post-viral syndrome with lingering neurologic and other symptoms – now known as long COVID or neurological postacute sequelae of SARS-CoV-2 infection (Neuro-PASC).
However, Researchers found a significant proportion of patients in their small study who had never tested positive for COVID-19 but who were having symptoms of long COVID nevertheless showed evidence of immune responses consistent with previous exposure.
“We estimate that millions of people got COVID in the U.S. during the first year of the pandemic and then developed long COVID, yet they did not get a positive COVID diagnosis because of testing limitations,” Igor J. Koralnik, MD, of Northwestern Medicine Comprehensive COVID-19 Center in Chicago, said in an interview.
He noted that many post-COVID-19 clinics in the United States don’t accept people with long COVID symptoms who do not have a positive test result.
Patients with long COVID symptoms but without laboratory evidence of prior infection, “who have often been rejected and stigmatized, should feel vindicated by the results of our study,” Dr. Koralnik said.
“We think that those patients deserve the same clinical care as those with a positive test, as well as inclusion in research studies. This is what we are doing at Northwestern Medicine’s Comprehensive COVID[-19] Center,” Dr. Koralnik added.
The study was published online in the journal Neurology: Neuroimmunology & Neuroinflammation.
Delayed care
The researchers measured SARS-CoV-2-specific humoral and cell-mediated immune responses against nucleocapsid protein and spike proteins, which indicate a prior COVID-19 infection, in 29 patients with post-viral syndrome after suspected COVID-19, including neurologic symptoms such as cognitive impairment, headache, and fatigue, but who did not have a confirmed positive COVID-19 test.
They did the same in 32 age- and sex-matched COVID long haulers with confirmed Neuro-PASC and 18 healthy controls with none of the symptoms of long COVID and no known exposure to SARS-CoV-2 or positive test result.
They found that 12 of the 29 patients (41%) with post-viral syndrome (but no positive COVID-19 test) had detectable humoral and cellular immune responses consistent with prior exposure to SARS-CoV-2. Three-quarters harbored antinucleocapsid and 50% harbored antispike responses.
“Our data suggest that at least 4 million people with post-viral syndrome similar to long COVID may indeed have detectable immune responses to support a COVID diagnosis,” Dr. Koralnik said in a news release.
The 12 patients with post-viral syndrome but without a confirmed COVID-19 test had neurologic symptoms similar to those of patients with confirmed Neuro-PASC.
However, lack of a confirmed COVID-19 diagnosis likely contributed to the 5-month delay in the median time from symptom onset to clinic visit, the researchers said. They were evaluated at a median of 10.7 months vs. 5.4 months for Neuro-PASC patients.
Dr. Koralnik said in an interview that the “most important take-home message” of the study is that patients with post-viral syndrome often present with clinical manifestations similar to those of confirmed patients with Neuro-PASC, suggesting that a positive result by commercially available SARS-CoV-2 diagnostic test should not be a prerequisite for accessing care.
Patients with post-viral syndrome may benefit from the same clinical care as confirmed patients with Neuro-PASC, and the absence of a positive SARS-CoV-2 test should not preclude or delay treatment, he added.
A version of this article first appeared on Medscape.com .
This article was updated 8/28/23.
It’s been estimated that up to one-third of people who survive acute SARS-CoV-2 infection will suffer a post-viral syndrome with lingering neurologic and other symptoms – now known as long COVID or neurological postacute sequelae of SARS-CoV-2 infection (Neuro-PASC).
However, Researchers found a significant proportion of patients in their small study who had never tested positive for COVID-19 but who were having symptoms of long COVID nevertheless showed evidence of immune responses consistent with previous exposure.
“We estimate that millions of people got COVID in the U.S. during the first year of the pandemic and then developed long COVID, yet they did not get a positive COVID diagnosis because of testing limitations,” Igor J. Koralnik, MD, of Northwestern Medicine Comprehensive COVID-19 Center in Chicago, said in an interview.
He noted that many post-COVID-19 clinics in the United States don’t accept people with long COVID symptoms who do not have a positive test result.
Patients with long COVID symptoms but without laboratory evidence of prior infection, “who have often been rejected and stigmatized, should feel vindicated by the results of our study,” Dr. Koralnik said.
“We think that those patients deserve the same clinical care as those with a positive test, as well as inclusion in research studies. This is what we are doing at Northwestern Medicine’s Comprehensive COVID[-19] Center,” Dr. Koralnik added.
The study was published online in the journal Neurology: Neuroimmunology & Neuroinflammation.
Delayed care
The researchers measured SARS-CoV-2-specific humoral and cell-mediated immune responses against nucleocapsid protein and spike proteins, which indicate a prior COVID-19 infection, in 29 patients with post-viral syndrome after suspected COVID-19, including neurologic symptoms such as cognitive impairment, headache, and fatigue, but who did not have a confirmed positive COVID-19 test.
They did the same in 32 age- and sex-matched COVID long haulers with confirmed Neuro-PASC and 18 healthy controls with none of the symptoms of long COVID and no known exposure to SARS-CoV-2 or positive test result.
They found that 12 of the 29 patients (41%) with post-viral syndrome (but no positive COVID-19 test) had detectable humoral and cellular immune responses consistent with prior exposure to SARS-CoV-2. Three-quarters harbored antinucleocapsid and 50% harbored antispike responses.
“Our data suggest that at least 4 million people with post-viral syndrome similar to long COVID may indeed have detectable immune responses to support a COVID diagnosis,” Dr. Koralnik said in a news release.
The 12 patients with post-viral syndrome but without a confirmed COVID-19 test had neurologic symptoms similar to those of patients with confirmed Neuro-PASC.
However, lack of a confirmed COVID-19 diagnosis likely contributed to the 5-month delay in the median time from symptom onset to clinic visit, the researchers said. They were evaluated at a median of 10.7 months vs. 5.4 months for Neuro-PASC patients.
Dr. Koralnik said in an interview that the “most important take-home message” of the study is that patients with post-viral syndrome often present with clinical manifestations similar to those of confirmed patients with Neuro-PASC, suggesting that a positive result by commercially available SARS-CoV-2 diagnostic test should not be a prerequisite for accessing care.
Patients with post-viral syndrome may benefit from the same clinical care as confirmed patients with Neuro-PASC, and the absence of a positive SARS-CoV-2 test should not preclude or delay treatment, he added.
A version of this article first appeared on Medscape.com .
This article was updated 8/28/23.
It’s been estimated that up to one-third of people who survive acute SARS-CoV-2 infection will suffer a post-viral syndrome with lingering neurologic and other symptoms – now known as long COVID or neurological postacute sequelae of SARS-CoV-2 infection (Neuro-PASC).
However, Researchers found a significant proportion of patients in their small study who had never tested positive for COVID-19 but who were having symptoms of long COVID nevertheless showed evidence of immune responses consistent with previous exposure.
“We estimate that millions of people got COVID in the U.S. during the first year of the pandemic and then developed long COVID, yet they did not get a positive COVID diagnosis because of testing limitations,” Igor J. Koralnik, MD, of Northwestern Medicine Comprehensive COVID-19 Center in Chicago, said in an interview.
He noted that many post-COVID-19 clinics in the United States don’t accept people with long COVID symptoms who do not have a positive test result.
Patients with long COVID symptoms but without laboratory evidence of prior infection, “who have often been rejected and stigmatized, should feel vindicated by the results of our study,” Dr. Koralnik said.
“We think that those patients deserve the same clinical care as those with a positive test, as well as inclusion in research studies. This is what we are doing at Northwestern Medicine’s Comprehensive COVID[-19] Center,” Dr. Koralnik added.
The study was published online in the journal Neurology: Neuroimmunology & Neuroinflammation.
Delayed care
The researchers measured SARS-CoV-2-specific humoral and cell-mediated immune responses against nucleocapsid protein and spike proteins, which indicate a prior COVID-19 infection, in 29 patients with post-viral syndrome after suspected COVID-19, including neurologic symptoms such as cognitive impairment, headache, and fatigue, but who did not have a confirmed positive COVID-19 test.
They did the same in 32 age- and sex-matched COVID long haulers with confirmed Neuro-PASC and 18 healthy controls with none of the symptoms of long COVID and no known exposure to SARS-CoV-2 or positive test result.
They found that 12 of the 29 patients (41%) with post-viral syndrome (but no positive COVID-19 test) had detectable humoral and cellular immune responses consistent with prior exposure to SARS-CoV-2. Three-quarters harbored antinucleocapsid and 50% harbored antispike responses.
“Our data suggest that at least 4 million people with post-viral syndrome similar to long COVID may indeed have detectable immune responses to support a COVID diagnosis,” Dr. Koralnik said in a news release.
The 12 patients with post-viral syndrome but without a confirmed COVID-19 test had neurologic symptoms similar to those of patients with confirmed Neuro-PASC.
However, lack of a confirmed COVID-19 diagnosis likely contributed to the 5-month delay in the median time from symptom onset to clinic visit, the researchers said. They were evaluated at a median of 10.7 months vs. 5.4 months for Neuro-PASC patients.
Dr. Koralnik said in an interview that the “most important take-home message” of the study is that patients with post-viral syndrome often present with clinical manifestations similar to those of confirmed patients with Neuro-PASC, suggesting that a positive result by commercially available SARS-CoV-2 diagnostic test should not be a prerequisite for accessing care.
Patients with post-viral syndrome may benefit from the same clinical care as confirmed patients with Neuro-PASC, and the absence of a positive SARS-CoV-2 test should not preclude or delay treatment, he added.
A version of this article first appeared on Medscape.com .
This article was updated 8/28/23.
FROM NEUROLOGY, NEUROIMMUNOLOGY & NEUROINFLAMMATION