User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Cardiologists concerned for patient safety after abortion ruling
Pregnancy termination for medical reasons had been part of the fabric of everyday health care in the United States since the Supreme Court’s 1973 Roe v. Wade decision, which the current high court overturned in a ruling announced on June 24.
That means many clinicians across specialties are entering uncharted territory with the country’s new patchwork of abortion legality. Some specialties, cardiology among them, may feel the impact more than others.

“We know that the rising maternal mortality rate is predominantly driven by cardiovascular disease, women having children at older ages, and ... risk factors like hypertension, diabetes, and obesity,” Jennifer H. Haythe, MD, told this news organization.
So the high court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and leaves the legality of abortion up to the 50 separate state legislatures, “is very relevant to cardiologists specifically,” said Dr. Haythe, who is director of cardiology in the cardio-obstetrics program at New York-Presbyterian/Columbia University Irving Medical Center, New York.
The ruling “is going to have a huge effect on women who may not be able to tolerate pregnancy,” she said. Whether to terminate a pregnancy “is a relatively common discussion I have with women with bad heart failure about their risk of further decompensation, death, or needing a heart transplant or heart pump after delivery, or the risk of death in women with pulmonary hypertension.”
The high court’s decision “is a direct attack on the practice of medicine and really the sanctity of the patient-clinician relationship,” Rachel M. Bond, MD, director of Women’s Heart Health Systems Dignity Health of Arizona, told this news organization.
Physicians take an oath “that we should do no harm to our patients, and once the law or governance impacts that, it places us in a very vulnerable situation,” Dr. Bond said. “As a cardiologist who focuses a lot on high-risk pregnancies, I am worried and hesitant to give guidance to many of these patients in the states that may not have access to something that is a medical right, which at times is an abortion.”
She has colleagues in obstetrics in states where abortion is newly illegal who “don’t know what to do,” Dr. Bond said. Many have sought guidance from their legal teams, she said, “and many of them are now trying to figure out what is the best path.”
Pregnancy is “a very significant cardiovascular stress test, and women who may tolerate certain conditions reasonably well outside of the setting of pregnancy may have severe issues, not just for the mother, but for the baby as well,” Ki Park, MD, University of Florida Health, Gainesville, said in an interview.
“As clinicians, none of us like recommending a medically indicated abortion. But it is health care, just like any other medication or treatment that we advise to our patients in cases where the risk of the mother is excessively high and mortality risk is elevated,” said Dr. Park, who is cochair of the American College of Cardiology Cardio-Obstetrics Work Group.
Some conditions, such as pulmonary hypertension and severe aortic valve stenosis, during pregnancy are well recognized as very high risk, and there are various scoring systems to help clinicians with risk stratification, she observed. “But there are also a lot of gray areas where patients don’t necessarily fit into these risk scores that we use.”
So physician-patient discussions in high-risk pregnancies “are already complicated,” Dr. Park said. “Patients want to have options, and they look to us as physicians for guidance with regard to their risks. And if abortion is not available as an option, then part of our toolbox is no longer available to help us care for the mother.”
In the new legal climate, clinicians in states where abortion is illegal may well want to put more emphasis on preconception counseling, so more of their patients with high-risk conditions are aware of the new barriers to pregnancy termination.
“Unfortunately,” Dr. Haythe said, “many of the states that are going to make or have made abortion illegal are not providing that kind of preconception counseling or good prenatal care to women.”
Cardiologists can provide such counseling to their female patients of childbearing age who have high-risk cardiac conditions, “but not everybody knows that they have a heart problem when they get pregnant, and not everybody is getting screened for heart problems when they’re of childbearing age,” Dr. Haythe said.
“Sometimes it’s not clear whether the problems could have been picked up until a woman is pregnant and has started to have symptoms.” For example, “a lot of women with poor access to health care have rheumatic heart disease. They may have no idea that they have severe aortic stenosis, and it’s not until their second trimester that they start to feel really short of breath.” Often that can be treated in the cath lab, “but again, that’s putting the woman and the baby at risk.”
Cardiologists in states where abortion is illegal will still present the option to their patients with high-risk pregnancies, noted Dr. Haythe. But the conversation may sound something like, “you are at very high risk, termination of the pregnancy takes that risk away, but you’ll have to find a state where it’s legal to do that.”
Dr. Park said such a situation, when abortion is recommended but locally unavailable, is much like any other in cardiology for which the patient may want a second opinion. If a center “doesn’t have the capability or the technology to offer a certain treatment, the patient can opt to seek another opinion at another center,” she said. “Patients will often travel out of state to get the care they need.”
A requirement for out-of-state travel to obtain abortions is likely to worsen socioeconomic disparities in health care, Dr. Bond observed, “because we know that those who are low-income won’t be able to afford that travel.”
Dr. Bond is cosignatory on a statement from the Association of Black Cardiologists (ABC) responding to the high court’s ruling in Dobbs v. Jackson. “This decision will isolate the poor, socioeconomically disadvantaged, and minority populations specifically, widening the already large gaps in health care for our most vulnerable communities,” it states.
“The loss of broad protections supporting the medical and often lifesaving procedure of abortions is likely to have a real impact on the maternal mortality rate, especially in those with congenital and/or acquired cardiovascular conditions where evidence-based guidelines advise at times on termination of such high-risk pregnancies.”
The ABC, it states, “believes that every woman, and every person, should be afforded the right to safe, accessible, legal, timely, patient-centered, equitable, and affordable health care.”
The American College of Cardiology (ACC) released a statement on the matter June 24, signed by its president, Edward T.A. Fry, MD, along with five former ACC presidents. “While the ACC has no official policy on abortion, clinical practice guidelines and other clinical guidance tools address the dangers of pregnancy in certain patient populations at higher risk of death or serious cardiac events.”
The college, it states, is “deeply concerned about the potential implications of the Supreme Court decision regarding Roe vs. Wade on the ability of patients and clinicians to engage in important shared discussions about maternal health, or to remove previously available health care options.”
Dr. Bond proposed that a “vocal stance” from medical societies involved in women’s health, “perhaps even a collective stance from our cardiovascular societies and our obstetrics societies,” would also perhaps reach “the masses of doctors in private practice who are dealing with these patients.”
A version of this article first appeared on Medscape.com.
Pregnancy termination for medical reasons had been part of the fabric of everyday health care in the United States since the Supreme Court’s 1973 Roe v. Wade decision, which the current high court overturned in a ruling announced on June 24.
That means many clinicians across specialties are entering uncharted territory with the country’s new patchwork of abortion legality. Some specialties, cardiology among them, may feel the impact more than others.
“We know that the rising maternal mortality rate is predominantly driven by cardiovascular disease, women having children at older ages, and ... risk factors like hypertension, diabetes, and obesity,” Jennifer H. Haythe, MD, told this news organization.
So the high court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and leaves the legality of abortion up to the 50 separate state legislatures, “is very relevant to cardiologists specifically,” said Dr. Haythe, who is director of cardiology in the cardio-obstetrics program at New York-Presbyterian/Columbia University Irving Medical Center, New York.
The ruling “is going to have a huge effect on women who may not be able to tolerate pregnancy,” she said. Whether to terminate a pregnancy “is a relatively common discussion I have with women with bad heart failure about their risk of further decompensation, death, or needing a heart transplant or heart pump after delivery, or the risk of death in women with pulmonary hypertension.”
The high court’s decision “is a direct attack on the practice of medicine and really the sanctity of the patient-clinician relationship,” Rachel M. Bond, MD, director of Women’s Heart Health Systems Dignity Health of Arizona, told this news organization.
Physicians take an oath “that we should do no harm to our patients, and once the law or governance impacts that, it places us in a very vulnerable situation,” Dr. Bond said. “As a cardiologist who focuses a lot on high-risk pregnancies, I am worried and hesitant to give guidance to many of these patients in the states that may not have access to something that is a medical right, which at times is an abortion.”
She has colleagues in obstetrics in states where abortion is newly illegal who “don’t know what to do,” Dr. Bond said. Many have sought guidance from their legal teams, she said, “and many of them are now trying to figure out what is the best path.”
Pregnancy is “a very significant cardiovascular stress test, and women who may tolerate certain conditions reasonably well outside of the setting of pregnancy may have severe issues, not just for the mother, but for the baby as well,” Ki Park, MD, University of Florida Health, Gainesville, said in an interview.
“As clinicians, none of us like recommending a medically indicated abortion. But it is health care, just like any other medication or treatment that we advise to our patients in cases where the risk of the mother is excessively high and mortality risk is elevated,” said Dr. Park, who is cochair of the American College of Cardiology Cardio-Obstetrics Work Group.
Some conditions, such as pulmonary hypertension and severe aortic valve stenosis, during pregnancy are well recognized as very high risk, and there are various scoring systems to help clinicians with risk stratification, she observed. “But there are also a lot of gray areas where patients don’t necessarily fit into these risk scores that we use.”
So physician-patient discussions in high-risk pregnancies “are already complicated,” Dr. Park said. “Patients want to have options, and they look to us as physicians for guidance with regard to their risks. And if abortion is not available as an option, then part of our toolbox is no longer available to help us care for the mother.”
In the new legal climate, clinicians in states where abortion is illegal may well want to put more emphasis on preconception counseling, so more of their patients with high-risk conditions are aware of the new barriers to pregnancy termination.
“Unfortunately,” Dr. Haythe said, “many of the states that are going to make or have made abortion illegal are not providing that kind of preconception counseling or good prenatal care to women.”
Cardiologists can provide such counseling to their female patients of childbearing age who have high-risk cardiac conditions, “but not everybody knows that they have a heart problem when they get pregnant, and not everybody is getting screened for heart problems when they’re of childbearing age,” Dr. Haythe said.
“Sometimes it’s not clear whether the problems could have been picked up until a woman is pregnant and has started to have symptoms.” For example, “a lot of women with poor access to health care have rheumatic heart disease. They may have no idea that they have severe aortic stenosis, and it’s not until their second trimester that they start to feel really short of breath.” Often that can be treated in the cath lab, “but again, that’s putting the woman and the baby at risk.”
Cardiologists in states where abortion is illegal will still present the option to their patients with high-risk pregnancies, noted Dr. Haythe. But the conversation may sound something like, “you are at very high risk, termination of the pregnancy takes that risk away, but you’ll have to find a state where it’s legal to do that.”
Dr. Park said such a situation, when abortion is recommended but locally unavailable, is much like any other in cardiology for which the patient may want a second opinion. If a center “doesn’t have the capability or the technology to offer a certain treatment, the patient can opt to seek another opinion at another center,” she said. “Patients will often travel out of state to get the care they need.”
A requirement for out-of-state travel to obtain abortions is likely to worsen socioeconomic disparities in health care, Dr. Bond observed, “because we know that those who are low-income won’t be able to afford that travel.”
Dr. Bond is cosignatory on a statement from the Association of Black Cardiologists (ABC) responding to the high court’s ruling in Dobbs v. Jackson. “This decision will isolate the poor, socioeconomically disadvantaged, and minority populations specifically, widening the already large gaps in health care for our most vulnerable communities,” it states.
“The loss of broad protections supporting the medical and often lifesaving procedure of abortions is likely to have a real impact on the maternal mortality rate, especially in those with congenital and/or acquired cardiovascular conditions where evidence-based guidelines advise at times on termination of such high-risk pregnancies.”
The ABC, it states, “believes that every woman, and every person, should be afforded the right to safe, accessible, legal, timely, patient-centered, equitable, and affordable health care.”
The American College of Cardiology (ACC) released a statement on the matter June 24, signed by its president, Edward T.A. Fry, MD, along with five former ACC presidents. “While the ACC has no official policy on abortion, clinical practice guidelines and other clinical guidance tools address the dangers of pregnancy in certain patient populations at higher risk of death or serious cardiac events.”
The college, it states, is “deeply concerned about the potential implications of the Supreme Court decision regarding Roe vs. Wade on the ability of patients and clinicians to engage in important shared discussions about maternal health, or to remove previously available health care options.”
Dr. Bond proposed that a “vocal stance” from medical societies involved in women’s health, “perhaps even a collective stance from our cardiovascular societies and our obstetrics societies,” would also perhaps reach “the masses of doctors in private practice who are dealing with these patients.”
A version of this article first appeared on Medscape.com.
Pregnancy termination for medical reasons had been part of the fabric of everyday health care in the United States since the Supreme Court’s 1973 Roe v. Wade decision, which the current high court overturned in a ruling announced on June 24.
That means many clinicians across specialties are entering uncharted territory with the country’s new patchwork of abortion legality. Some specialties, cardiology among them, may feel the impact more than others.
“We know that the rising maternal mortality rate is predominantly driven by cardiovascular disease, women having children at older ages, and ... risk factors like hypertension, diabetes, and obesity,” Jennifer H. Haythe, MD, told this news organization.
So the high court’s decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and leaves the legality of abortion up to the 50 separate state legislatures, “is very relevant to cardiologists specifically,” said Dr. Haythe, who is director of cardiology in the cardio-obstetrics program at New York-Presbyterian/Columbia University Irving Medical Center, New York.
The ruling “is going to have a huge effect on women who may not be able to tolerate pregnancy,” she said. Whether to terminate a pregnancy “is a relatively common discussion I have with women with bad heart failure about their risk of further decompensation, death, or needing a heart transplant or heart pump after delivery, or the risk of death in women with pulmonary hypertension.”
The high court’s decision “is a direct attack on the practice of medicine and really the sanctity of the patient-clinician relationship,” Rachel M. Bond, MD, director of Women’s Heart Health Systems Dignity Health of Arizona, told this news organization.
Physicians take an oath “that we should do no harm to our patients, and once the law or governance impacts that, it places us in a very vulnerable situation,” Dr. Bond said. “As a cardiologist who focuses a lot on high-risk pregnancies, I am worried and hesitant to give guidance to many of these patients in the states that may not have access to something that is a medical right, which at times is an abortion.”
She has colleagues in obstetrics in states where abortion is newly illegal who “don’t know what to do,” Dr. Bond said. Many have sought guidance from their legal teams, she said, “and many of them are now trying to figure out what is the best path.”
Pregnancy is “a very significant cardiovascular stress test, and women who may tolerate certain conditions reasonably well outside of the setting of pregnancy may have severe issues, not just for the mother, but for the baby as well,” Ki Park, MD, University of Florida Health, Gainesville, said in an interview.
“As clinicians, none of us like recommending a medically indicated abortion. But it is health care, just like any other medication or treatment that we advise to our patients in cases where the risk of the mother is excessively high and mortality risk is elevated,” said Dr. Park, who is cochair of the American College of Cardiology Cardio-Obstetrics Work Group.
Some conditions, such as pulmonary hypertension and severe aortic valve stenosis, during pregnancy are well recognized as very high risk, and there are various scoring systems to help clinicians with risk stratification, she observed. “But there are also a lot of gray areas where patients don’t necessarily fit into these risk scores that we use.”
So physician-patient discussions in high-risk pregnancies “are already complicated,” Dr. Park said. “Patients want to have options, and they look to us as physicians for guidance with regard to their risks. And if abortion is not available as an option, then part of our toolbox is no longer available to help us care for the mother.”
In the new legal climate, clinicians in states where abortion is illegal may well want to put more emphasis on preconception counseling, so more of their patients with high-risk conditions are aware of the new barriers to pregnancy termination.
“Unfortunately,” Dr. Haythe said, “many of the states that are going to make or have made abortion illegal are not providing that kind of preconception counseling or good prenatal care to women.”
Cardiologists can provide such counseling to their female patients of childbearing age who have high-risk cardiac conditions, “but not everybody knows that they have a heart problem when they get pregnant, and not everybody is getting screened for heart problems when they’re of childbearing age,” Dr. Haythe said.
“Sometimes it’s not clear whether the problems could have been picked up until a woman is pregnant and has started to have symptoms.” For example, “a lot of women with poor access to health care have rheumatic heart disease. They may have no idea that they have severe aortic stenosis, and it’s not until their second trimester that they start to feel really short of breath.” Often that can be treated in the cath lab, “but again, that’s putting the woman and the baby at risk.”
Cardiologists in states where abortion is illegal will still present the option to their patients with high-risk pregnancies, noted Dr. Haythe. But the conversation may sound something like, “you are at very high risk, termination of the pregnancy takes that risk away, but you’ll have to find a state where it’s legal to do that.”
Dr. Park said such a situation, when abortion is recommended but locally unavailable, is much like any other in cardiology for which the patient may want a second opinion. If a center “doesn’t have the capability or the technology to offer a certain treatment, the patient can opt to seek another opinion at another center,” she said. “Patients will often travel out of state to get the care they need.”
A requirement for out-of-state travel to obtain abortions is likely to worsen socioeconomic disparities in health care, Dr. Bond observed, “because we know that those who are low-income won’t be able to afford that travel.”
Dr. Bond is cosignatory on a statement from the Association of Black Cardiologists (ABC) responding to the high court’s ruling in Dobbs v. Jackson. “This decision will isolate the poor, socioeconomically disadvantaged, and minority populations specifically, widening the already large gaps in health care for our most vulnerable communities,” it states.
“The loss of broad protections supporting the medical and often lifesaving procedure of abortions is likely to have a real impact on the maternal mortality rate, especially in those with congenital and/or acquired cardiovascular conditions where evidence-based guidelines advise at times on termination of such high-risk pregnancies.”
The ABC, it states, “believes that every woman, and every person, should be afforded the right to safe, accessible, legal, timely, patient-centered, equitable, and affordable health care.”
The American College of Cardiology (ACC) released a statement on the matter June 24, signed by its president, Edward T.A. Fry, MD, along with five former ACC presidents. “While the ACC has no official policy on abortion, clinical practice guidelines and other clinical guidance tools address the dangers of pregnancy in certain patient populations at higher risk of death or serious cardiac events.”
The college, it states, is “deeply concerned about the potential implications of the Supreme Court decision regarding Roe vs. Wade on the ability of patients and clinicians to engage in important shared discussions about maternal health, or to remove previously available health care options.”
Dr. Bond proposed that a “vocal stance” from medical societies involved in women’s health, “perhaps even a collective stance from our cardiovascular societies and our obstetrics societies,” would also perhaps reach “the masses of doctors in private practice who are dealing with these patients.”
A version of this article first appeared on Medscape.com.
Ob.gyns. on the day that Roe v. Wade was overturned
“I’m happy to contribute, but can you keep it anonymous? It’s a safety concern for me.”
On the day that the Supreme Court of the United States voted to strike down Roe v. Wade, I reached out to ob.gyn.s across the country, wanting to hear their reactions. My own response, like that of many doctors and women, was a visceral mix of anger, fear, and grief. I could only begin to imagine what the real experts on reproductive health care were going through.
When the first ob.gyn. responded to my request by expressing concerns around anonymity and personal safety, I was shocked – but I shouldn’t have been. For starters, there is already a storied history in this country of deadly attacks on abortion providers. David Gunn, MD; Barnett Slepian, MD; and George Tiller, MD, were all tragically murdered by antiabortion extremists. Then, there’s the existence of websites that keep logs of abortion providers and sometimes include photos, office contact information, or even home addresses.
The idea that any reproductive health care provider should have to think twice before offering their uniquely qualified opinion is profoundly disturbing, nearly as disturbing as the Supreme Court’s decision itself. But it’s more critical than ever for ob.gyn. voices to be amplified. This is the time for the healthcare community to rally around women’s health providers, to learn from them, to support them.
I asked ob.gyns. around the country to tell me what they were thinking and feeling on the day that Roe v. Wade was overturned. We agreed to keep the responses anonymous, given that several people expressed very understandable safety concerns.
Here’s what they had to say.
Tennessee ob.gyn.
“Today is an emotionally charged day for many people in this country, yet as I type this, with my ob.gyn. practice continuing around me, with my own almost 10-week pregnancy growing inside me, I feel quite blunted. I feel powerless to answer questions that are variations on ‘what next?’ or ‘how do we fight back?’ All I can think of is, I am so glad I do not have anyone on my schedule right now who does not want to be pregnant. But what will happen when that eventually changes? What about my colleagues who do have these patients on their schedules today? On a personal level, what if my prenatal genetic testing comes back abnormal? How can we so blatantly disregard a separation of church and state in this country? What ways will our government interfere with my practice next? My head is spinning, but I have to go see my next patient. She is a 25-year-old who is here to have an IUD placed, and that seems like the most important thing I can do today.”
South Carolina ob.gyn.
“I’m really scared. For my patients and for myself. I don’t know how to be a good ob.gyn. if my ability to offer safe and accessible abortion care is being threatened.”
Massachusetts ob.gyn.
“Livid and devastated and sad and terrified.”
California family planning specialist
“The fact is that about one in four people with uteruses have had an abortion. I can’t tell you how many abortions I’ve provided for people who say that they don’t ‘believe’ in them or that they thought they’d never be in this situation. ... The fact is that pregnancy is a life-threatening condition in and of itself. I am an ob.gyn., a medical doctor, and an abortion provider. I will not stop providing abortions or helping people access them. I will dedicate my life to ensuring this right to bodily autonomy. Today I am devastated by the Supreme Court’s decision to force parenthood that will result in increased maternal mortality. I am broken, but I have never been more proud to be an abortion provider.”
New York ob.gyn.
“Grateful to live in a state and work for a hospital where I can provide abortions but feel terrible for so many people less fortunate and underserved.”
Illinois maternal-fetal medicine specialist
“As a maternal-fetal medicine specialist, I fear for my patients who are at the highest risk of pregnancy complications having their freedom taken away. For the tragic ultrasound findings that make a pregnant person carry a baby who will never live. For the patients who cannot use most forms of contraception because of their medical comorbidities. For the patients who are victims of intimate partner violence or under the influence of their culture, to continue having children regardless of their desires or their health. ... The freedom to prevent or end a pregnancy has enabled women to become independent and productive members of society on their own terms, with or without children. My heart breaks for the children and adolescents and adults who are being told they are second-class citizens, not worthy of making their own decisions. Politicians and Supreme Court justices are not in the clinic room, ultrasound suite, operating room, or delivery room when we have these intense conversations and pregnancy outcomes. They have no idea that of which they speak, and it’s unconscionable that they can determine what healthcare decisions my patients can make for their own lives. Nobody knows a body better than the patient themselves.”
Texas ob.gyn.
“In the area where I live and practice, it feels like guns and the people who use them have more legal rights than people with uteruses in desperate or life-threatening situations. I’m afraid for my personal safety as a women’s health practitioner in this political climate. I feel helpless, but I’m supposed to be able to help my patients.”
Missouri family planning specialist
“Abortion is an essential part of healthcare, and the only people that should get a say in it are the patient and their doctor. Period. The fact that some far-off court without any medical expertise can insert itself into individual medical decisions is oppressive and unethical.”
Georgia ob.gyn.
“I can’t even think straight right now. I feel sick. Honestly, I’ve been thinking about moving for a long time now. Somewhere where I would actually be able to offer good, comprehensive care.”
New York ob.gyn.
“I graduated from my ob.gyn. residency hours after the Roe v. Wade news broke. It was so emotional for me. I’ve dedicated my life to caring for people with uteruses and I will not let this heartbreaking news change that. I feel more committed than ever to women’s health. I fully plan to continue delivering babies, providing contraception, and performing abortions. I will be there to help women with desired pregnancies who received unspeakably bad news about fetal anomalies. I will be there to help women with life-threatening pregnancy complications before fetal viability. I will be there to help women with ectopic pregnancies. I will be there to help women who were raped or otherwise forced into pregnancy. I will always be there to help women.”
Dr. Croll is a neurovascular fellow at New York University Langone Health. She disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
“I’m happy to contribute, but can you keep it anonymous? It’s a safety concern for me.”
On the day that the Supreme Court of the United States voted to strike down Roe v. Wade, I reached out to ob.gyn.s across the country, wanting to hear their reactions. My own response, like that of many doctors and women, was a visceral mix of anger, fear, and grief. I could only begin to imagine what the real experts on reproductive health care were going through.
When the first ob.gyn. responded to my request by expressing concerns around anonymity and personal safety, I was shocked – but I shouldn’t have been. For starters, there is already a storied history in this country of deadly attacks on abortion providers. David Gunn, MD; Barnett Slepian, MD; and George Tiller, MD, were all tragically murdered by antiabortion extremists. Then, there’s the existence of websites that keep logs of abortion providers and sometimes include photos, office contact information, or even home addresses.
The idea that any reproductive health care provider should have to think twice before offering their uniquely qualified opinion is profoundly disturbing, nearly as disturbing as the Supreme Court’s decision itself. But it’s more critical than ever for ob.gyn. voices to be amplified. This is the time for the healthcare community to rally around women’s health providers, to learn from them, to support them.
I asked ob.gyns. around the country to tell me what they were thinking and feeling on the day that Roe v. Wade was overturned. We agreed to keep the responses anonymous, given that several people expressed very understandable safety concerns.
Here’s what they had to say.
Tennessee ob.gyn.
“Today is an emotionally charged day for many people in this country, yet as I type this, with my ob.gyn. practice continuing around me, with my own almost 10-week pregnancy growing inside me, I feel quite blunted. I feel powerless to answer questions that are variations on ‘what next?’ or ‘how do we fight back?’ All I can think of is, I am so glad I do not have anyone on my schedule right now who does not want to be pregnant. But what will happen when that eventually changes? What about my colleagues who do have these patients on their schedules today? On a personal level, what if my prenatal genetic testing comes back abnormal? How can we so blatantly disregard a separation of church and state in this country? What ways will our government interfere with my practice next? My head is spinning, but I have to go see my next patient. She is a 25-year-old who is here to have an IUD placed, and that seems like the most important thing I can do today.”
South Carolina ob.gyn.
“I’m really scared. For my patients and for myself. I don’t know how to be a good ob.gyn. if my ability to offer safe and accessible abortion care is being threatened.”
Massachusetts ob.gyn.
“Livid and devastated and sad and terrified.”
California family planning specialist
“The fact is that about one in four people with uteruses have had an abortion. I can’t tell you how many abortions I’ve provided for people who say that they don’t ‘believe’ in them or that they thought they’d never be in this situation. ... The fact is that pregnancy is a life-threatening condition in and of itself. I am an ob.gyn., a medical doctor, and an abortion provider. I will not stop providing abortions or helping people access them. I will dedicate my life to ensuring this right to bodily autonomy. Today I am devastated by the Supreme Court’s decision to force parenthood that will result in increased maternal mortality. I am broken, but I have never been more proud to be an abortion provider.”
New York ob.gyn.
“Grateful to live in a state and work for a hospital where I can provide abortions but feel terrible for so many people less fortunate and underserved.”
Illinois maternal-fetal medicine specialist
“As a maternal-fetal medicine specialist, I fear for my patients who are at the highest risk of pregnancy complications having their freedom taken away. For the tragic ultrasound findings that make a pregnant person carry a baby who will never live. For the patients who cannot use most forms of contraception because of their medical comorbidities. For the patients who are victims of intimate partner violence or under the influence of their culture, to continue having children regardless of their desires or their health. ... The freedom to prevent or end a pregnancy has enabled women to become independent and productive members of society on their own terms, with or without children. My heart breaks for the children and adolescents and adults who are being told they are second-class citizens, not worthy of making their own decisions. Politicians and Supreme Court justices are not in the clinic room, ultrasound suite, operating room, or delivery room when we have these intense conversations and pregnancy outcomes. They have no idea that of which they speak, and it’s unconscionable that they can determine what healthcare decisions my patients can make for their own lives. Nobody knows a body better than the patient themselves.”
Texas ob.gyn.
“In the area where I live and practice, it feels like guns and the people who use them have more legal rights than people with uteruses in desperate or life-threatening situations. I’m afraid for my personal safety as a women’s health practitioner in this political climate. I feel helpless, but I’m supposed to be able to help my patients.”
Missouri family planning specialist
“Abortion is an essential part of healthcare, and the only people that should get a say in it are the patient and their doctor. Period. The fact that some far-off court without any medical expertise can insert itself into individual medical decisions is oppressive and unethical.”
Georgia ob.gyn.
“I can’t even think straight right now. I feel sick. Honestly, I’ve been thinking about moving for a long time now. Somewhere where I would actually be able to offer good, comprehensive care.”
New York ob.gyn.
“I graduated from my ob.gyn. residency hours after the Roe v. Wade news broke. It was so emotional for me. I’ve dedicated my life to caring for people with uteruses and I will not let this heartbreaking news change that. I feel more committed than ever to women’s health. I fully plan to continue delivering babies, providing contraception, and performing abortions. I will be there to help women with desired pregnancies who received unspeakably bad news about fetal anomalies. I will be there to help women with life-threatening pregnancy complications before fetal viability. I will be there to help women with ectopic pregnancies. I will be there to help women who were raped or otherwise forced into pregnancy. I will always be there to help women.”
Dr. Croll is a neurovascular fellow at New York University Langone Health. She disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
“I’m happy to contribute, but can you keep it anonymous? It’s a safety concern for me.”
On the day that the Supreme Court of the United States voted to strike down Roe v. Wade, I reached out to ob.gyn.s across the country, wanting to hear their reactions. My own response, like that of many doctors and women, was a visceral mix of anger, fear, and grief. I could only begin to imagine what the real experts on reproductive health care were going through.
When the first ob.gyn. responded to my request by expressing concerns around anonymity and personal safety, I was shocked – but I shouldn’t have been. For starters, there is already a storied history in this country of deadly attacks on abortion providers. David Gunn, MD; Barnett Slepian, MD; and George Tiller, MD, were all tragically murdered by antiabortion extremists. Then, there’s the existence of websites that keep logs of abortion providers and sometimes include photos, office contact information, or even home addresses.
The idea that any reproductive health care provider should have to think twice before offering their uniquely qualified opinion is profoundly disturbing, nearly as disturbing as the Supreme Court’s decision itself. But it’s more critical than ever for ob.gyn. voices to be amplified. This is the time for the healthcare community to rally around women’s health providers, to learn from them, to support them.
I asked ob.gyns. around the country to tell me what they were thinking and feeling on the day that Roe v. Wade was overturned. We agreed to keep the responses anonymous, given that several people expressed very understandable safety concerns.
Here’s what they had to say.
Tennessee ob.gyn.
“Today is an emotionally charged day for many people in this country, yet as I type this, with my ob.gyn. practice continuing around me, with my own almost 10-week pregnancy growing inside me, I feel quite blunted. I feel powerless to answer questions that are variations on ‘what next?’ or ‘how do we fight back?’ All I can think of is, I am so glad I do not have anyone on my schedule right now who does not want to be pregnant. But what will happen when that eventually changes? What about my colleagues who do have these patients on their schedules today? On a personal level, what if my prenatal genetic testing comes back abnormal? How can we so blatantly disregard a separation of church and state in this country? What ways will our government interfere with my practice next? My head is spinning, but I have to go see my next patient. She is a 25-year-old who is here to have an IUD placed, and that seems like the most important thing I can do today.”
South Carolina ob.gyn.
“I’m really scared. For my patients and for myself. I don’t know how to be a good ob.gyn. if my ability to offer safe and accessible abortion care is being threatened.”
Massachusetts ob.gyn.
“Livid and devastated and sad and terrified.”
California family planning specialist
“The fact is that about one in four people with uteruses have had an abortion. I can’t tell you how many abortions I’ve provided for people who say that they don’t ‘believe’ in them or that they thought they’d never be in this situation. ... The fact is that pregnancy is a life-threatening condition in and of itself. I am an ob.gyn., a medical doctor, and an abortion provider. I will not stop providing abortions or helping people access them. I will dedicate my life to ensuring this right to bodily autonomy. Today I am devastated by the Supreme Court’s decision to force parenthood that will result in increased maternal mortality. I am broken, but I have never been more proud to be an abortion provider.”
New York ob.gyn.
“Grateful to live in a state and work for a hospital where I can provide abortions but feel terrible for so many people less fortunate and underserved.”
Illinois maternal-fetal medicine specialist
“As a maternal-fetal medicine specialist, I fear for my patients who are at the highest risk of pregnancy complications having their freedom taken away. For the tragic ultrasound findings that make a pregnant person carry a baby who will never live. For the patients who cannot use most forms of contraception because of their medical comorbidities. For the patients who are victims of intimate partner violence or under the influence of their culture, to continue having children regardless of their desires or their health. ... The freedom to prevent or end a pregnancy has enabled women to become independent and productive members of society on their own terms, with or without children. My heart breaks for the children and adolescents and adults who are being told they are second-class citizens, not worthy of making their own decisions. Politicians and Supreme Court justices are not in the clinic room, ultrasound suite, operating room, or delivery room when we have these intense conversations and pregnancy outcomes. They have no idea that of which they speak, and it’s unconscionable that they can determine what healthcare decisions my patients can make for their own lives. Nobody knows a body better than the patient themselves.”
Texas ob.gyn.
“In the area where I live and practice, it feels like guns and the people who use them have more legal rights than people with uteruses in desperate or life-threatening situations. I’m afraid for my personal safety as a women’s health practitioner in this political climate. I feel helpless, but I’m supposed to be able to help my patients.”
Missouri family planning specialist
“Abortion is an essential part of healthcare, and the only people that should get a say in it are the patient and their doctor. Period. The fact that some far-off court without any medical expertise can insert itself into individual medical decisions is oppressive and unethical.”
Georgia ob.gyn.
“I can’t even think straight right now. I feel sick. Honestly, I’ve been thinking about moving for a long time now. Somewhere where I would actually be able to offer good, comprehensive care.”
New York ob.gyn.
“I graduated from my ob.gyn. residency hours after the Roe v. Wade news broke. It was so emotional for me. I’ve dedicated my life to caring for people with uteruses and I will not let this heartbreaking news change that. I feel more committed than ever to women’s health. I fully plan to continue delivering babies, providing contraception, and performing abortions. I will be there to help women with desired pregnancies who received unspeakably bad news about fetal anomalies. I will be there to help women with life-threatening pregnancy complications before fetal viability. I will be there to help women with ectopic pregnancies. I will be there to help women who were raped or otherwise forced into pregnancy. I will always be there to help women.”
Dr. Croll is a neurovascular fellow at New York University Langone Health. She disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
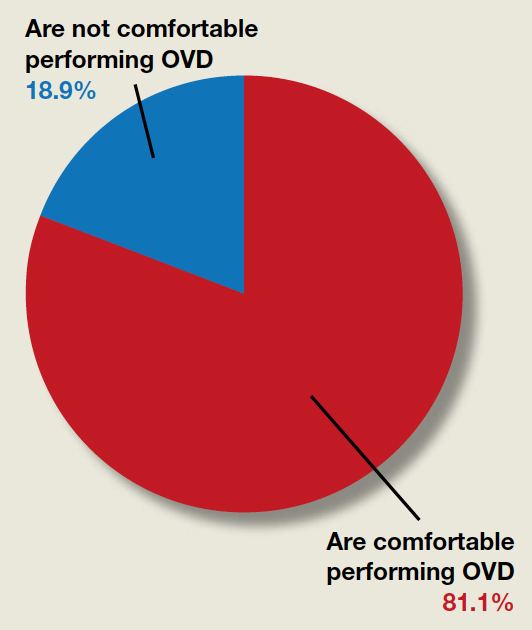
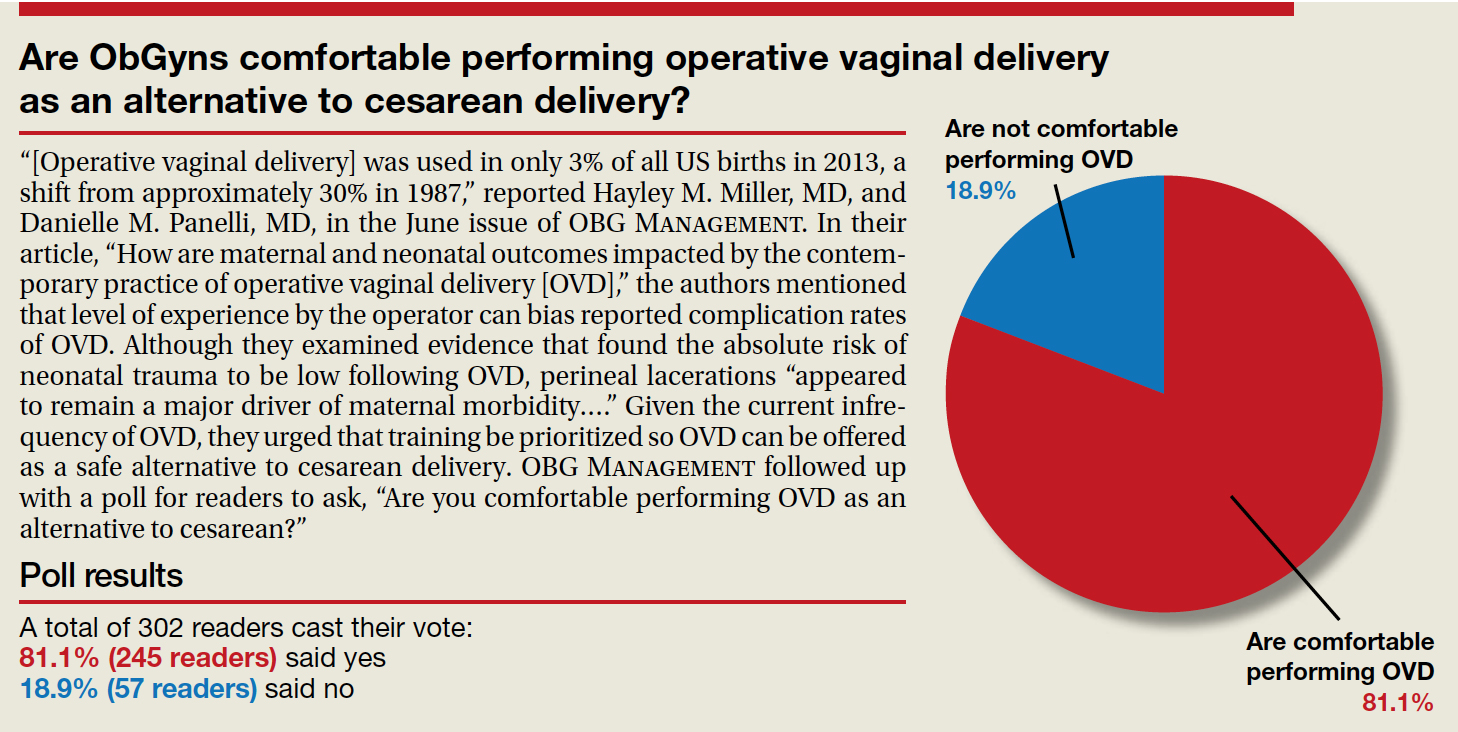
Are ObGyns comfortable performing operative vaginal delivery as an alternative to cesarean delivery?
“[Operative vaginal delivery] was used in only 3% of all US births in 2013, a shift from approximately 30% in 1987,” reported Hayley M. Miller, MD, and Danielle M. Panelli, MD, in the June issue of OBG Management. In their article, “How are maternal and neonatal outcomes impacted by the contemporary practice of operative vaginal delivery [OVD],” the authors mentioned that level of experience by the operator can bias reported complication rates of OVD. Although they examined evidence that found the absolute risk of neonatal trauma to be low following OVD, perineal lacerations “appeared to remain a major driver of maternal morbidity….” Given the current infrequency of OVD, they urged that training be prioritized so OVD can be offered as a safe alternative to cesarean delivery. OBG Management followed up with a poll for readers to ask, “Are you comfortable performing OVD as an alternative to cesarean?”
A total of 302 readers cast their vote:
81.1% (245 readers) said yes
18.9% (57 readers) said no
“[Operative vaginal delivery] was used in only 3% of all US births in 2013, a shift from approximately 30% in 1987,” reported Hayley M. Miller, MD, and Danielle M. Panelli, MD, in the June issue of OBG Management. In their article, “How are maternal and neonatal outcomes impacted by the contemporary practice of operative vaginal delivery [OVD],” the authors mentioned that level of experience by the operator can bias reported complication rates of OVD. Although they examined evidence that found the absolute risk of neonatal trauma to be low following OVD, perineal lacerations “appeared to remain a major driver of maternal morbidity….” Given the current infrequency of OVD, they urged that training be prioritized so OVD can be offered as a safe alternative to cesarean delivery. OBG Management followed up with a poll for readers to ask, “Are you comfortable performing OVD as an alternative to cesarean?”
A total of 302 readers cast their vote:
81.1% (245 readers) said yes
18.9% (57 readers) said no
“[Operative vaginal delivery] was used in only 3% of all US births in 2013, a shift from approximately 30% in 1987,” reported Hayley M. Miller, MD, and Danielle M. Panelli, MD, in the June issue of OBG Management. In their article, “How are maternal and neonatal outcomes impacted by the contemporary practice of operative vaginal delivery [OVD],” the authors mentioned that level of experience by the operator can bias reported complication rates of OVD. Although they examined evidence that found the absolute risk of neonatal trauma to be low following OVD, perineal lacerations “appeared to remain a major driver of maternal morbidity….” Given the current infrequency of OVD, they urged that training be prioritized so OVD can be offered as a safe alternative to cesarean delivery. OBG Management followed up with a poll for readers to ask, “Are you comfortable performing OVD as an alternative to cesarean?”
A total of 302 readers cast their vote:
81.1% (245 readers) said yes
18.9% (57 readers) said no
Racial/ethnic disparities exacerbated maternal death rise during 2020 pandemic.
U.S. maternal deaths – those during pregnancy or within 42 days of pregnancy – increased substantially by 33.3% after March 2020 corresponding to the COVID-19 pandemic onset, according to new research published in JAMA Network Open.
Data from the National Center for Health Statistics (NCHS) revealed this rise in maternal deaths was higher than the 22% overall excess death estimate associated with the pandemic in 2020.

Increases were highest for Hispanic and non-Hispanic Black women, exacerbating already high rates of disparity in comparison with White women, wrote Marie E. Thoma, PhD, an associate professor at the University of Maryland, College Park, and Eugene R. Declercq, PhD, a professor at Boston University.
The authors noted that this spike in maternal deaths might be caused either by conditions directly related to COVID-19, such as respiratory or viral infections, or by conditions worsened by pandemic-associated health care disruptions including those for diabetes or cardiovascular disease.
The precise causes, however, could not be discerned from the data, the authors noted.
The NCHS reported an 18.4% increase in U.S. maternal mortality from 2019 to 2020. The relative increase was 44.4% among Hispanic, 25.7% among non-Hispanic Black, and 6.1% among non-Hispanic White women.
“The rise in maternal mortality among Hispanic women was unprecedented,” Dr. Thoma said in an interview. Given a 16.8% increase in overall U.S. mortality in 2020, largely attributed to the COVID-19 pandemic, the authors examined the pandemic’s role in [the higher] maternal death rates for 2020.
“Prior to this report, the NCHS released an e-report that there had been a rise in maternal mortality in 2020, but questions remained about the role of the pandemic in this rise that their report hadn’t addressed,” Dr. Thoma said in an interview “So we decided to look at the data further to assess whether the rise coincided with the pandemic and how this differed by race/ethnicity, whether there were changes in the causes of maternal death, and how often COVID-19 was listed as a contributory factor in those deaths.”
A total of 1,588 maternal deaths (18.8 per 100,000 live births) occurred before the pandemic versus 684 deaths (25.1 per 100,000 live births) during the 2020 phase of the pandemic, for a relative increase of 33.3%.
Direct obstetrical causes of death included diabetes, hypertensive and liver disorders, pregnancy-related infections, and obstetrical hemorrhage and embolism. Indirect causes comprised, among others, nonobstetrical infections and diseases of the circulatory and respiratory systems as well as mental and nervous disorders.
Relative increases in direct causes (27.7%) were mostly associated with diabetes (95.9%), hypertensive disorders (39.0%), and other specified pregnancy-related conditions (48.0%).
COVID-19 was commonly listed as a lethal condition along with other viral diseases (16 of 16 deaths and diseases of the respiratory system (11 of 19 deaths).
Late maternal mortality – defined as more than 42 days but less than 1 year after pregnancy – increased by 41%. “This was surprising as we might anticipate risk being higher during pregnancy given that pregnant women may be more susceptible, but we see that this rise was also found among people in the later postpartum period,” Dr. Thoma said.
Absolute and relative changes were highest for Hispanic women (8.9 per 100,000 live births and 74.2%, respectively) and non-Hispanic Black women (16.8 per 100,000 live births and 40.2%). In contrast, non-Hispanic White women saw increases of just 2.9 per 100,000 live births and 17.2%.
“Overall, we found the rise in maternal mortality in 2020 was concentrated after the start of pandemic, particularly for non-Hispanic Black and Hispanic women, and we saw a dramatic rise in respiratory-related conditions,” Dr. Thoma said.

In a comment, Steven Woolf, MD, MPH, director emeritus of the Center on Society and Health at Virginia Commonwealth University, Richmond, said the findings are very consistent with his and others research showing dramatic increases in overall death rates from many causes during the pandemic, with these ranging from COVID-19 leading conditions such as diabetes, cardiovascular and Alzheimer’s disease to less-studied causes such as drug overdoses and alcoholism caused by the stresses of the pandemic. Again, deaths were likely caused by both COVID-19 infections and disruptions in diagnosis and care.
“So a rise in maternal mortality would unfortunately also be expected, and these researchers have shown that,” he said in an interview. In addition, they have confirmed “the pattern of stark health disparities in the Hispanic and Black populations relative to the White. Our group has shown marked decreases in the life expectancies of the Black and Hispanic populations relative to the White population.”
While he might take issue with the study’s research methodology, Dr. Woolf said, “The work is useful partly because we need to work out the best research methods to do this kind of analysis because we really need to understand the effects on maternal mortality.”
He said sorting out the best way to do this type of research will be important for looking at excess deaths and maternal mortality following other events, for example, in the wake of the Supreme Court’s recent decision to reverse Roe v. Wade.
The authors acknowledged certain study limitations, including the large percentage of COVID-19 cases with a nonspecific underlying cause. According to Dr. Thoma and Dr. Declercq, that reflects a maternal death coding problem that needs to be addressed, as well as a partitioning of data. The latter resulted in small numbers for some categories, with rates suppressed for fewer than 16 deaths because of reduced reliability.
“We found that more specific information is often available on death certificates but is lost in the process of coding,” said Dr. Thoma. “We were able to reclassify many of these causes to a more specific cause that we attributed to be the primary cause of death.”
The authors said future studies of maternal death should examine the contribution of the pandemic to racial and ethnic disparities and should identify specific causes of maternal deaths overall and associated with COVID-19.
In earlier research, the authors previously warned of possible misclassifications of maternal deaths.
They found evidence of both underreporting and overreporting of deaths, with possible overreporting predominant, whereas accurate data are essential for measuring the effectiveness of maternal mortality reduction programs.
Dr. Thoma’s group will continue to monitor mortality trends with the release of 2021 data. “We hope we will see improvements in 2021 given greater access to vaccines, treatments, and fewer health care disruptions,” Dr. Thoma said. “It will be important to continue to stress the importance of COVID-19 vaccines for pregnant and postpartum people.”
This study had no external funding. The authors disclosed no competing interests. Dr. Woolf declared no conflicts of interest.
U.S. maternal deaths – those during pregnancy or within 42 days of pregnancy – increased substantially by 33.3% after March 2020 corresponding to the COVID-19 pandemic onset, according to new research published in JAMA Network Open.
Data from the National Center for Health Statistics (NCHS) revealed this rise in maternal deaths was higher than the 22% overall excess death estimate associated with the pandemic in 2020.
Increases were highest for Hispanic and non-Hispanic Black women, exacerbating already high rates of disparity in comparison with White women, wrote Marie E. Thoma, PhD, an associate professor at the University of Maryland, College Park, and Eugene R. Declercq, PhD, a professor at Boston University.
The authors noted that this spike in maternal deaths might be caused either by conditions directly related to COVID-19, such as respiratory or viral infections, or by conditions worsened by pandemic-associated health care disruptions including those for diabetes or cardiovascular disease.
The precise causes, however, could not be discerned from the data, the authors noted.
The NCHS reported an 18.4% increase in U.S. maternal mortality from 2019 to 2020. The relative increase was 44.4% among Hispanic, 25.7% among non-Hispanic Black, and 6.1% among non-Hispanic White women.
“The rise in maternal mortality among Hispanic women was unprecedented,” Dr. Thoma said in an interview. Given a 16.8% increase in overall U.S. mortality in 2020, largely attributed to the COVID-19 pandemic, the authors examined the pandemic’s role in [the higher] maternal death rates for 2020.
“Prior to this report, the NCHS released an e-report that there had been a rise in maternal mortality in 2020, but questions remained about the role of the pandemic in this rise that their report hadn’t addressed,” Dr. Thoma said in an interview “So we decided to look at the data further to assess whether the rise coincided with the pandemic and how this differed by race/ethnicity, whether there were changes in the causes of maternal death, and how often COVID-19 was listed as a contributory factor in those deaths.”
A total of 1,588 maternal deaths (18.8 per 100,000 live births) occurred before the pandemic versus 684 deaths (25.1 per 100,000 live births) during the 2020 phase of the pandemic, for a relative increase of 33.3%.
Direct obstetrical causes of death included diabetes, hypertensive and liver disorders, pregnancy-related infections, and obstetrical hemorrhage and embolism. Indirect causes comprised, among others, nonobstetrical infections and diseases of the circulatory and respiratory systems as well as mental and nervous disorders.
Relative increases in direct causes (27.7%) were mostly associated with diabetes (95.9%), hypertensive disorders (39.0%), and other specified pregnancy-related conditions (48.0%).
COVID-19 was commonly listed as a lethal condition along with other viral diseases (16 of 16 deaths and diseases of the respiratory system (11 of 19 deaths).
Late maternal mortality – defined as more than 42 days but less than 1 year after pregnancy – increased by 41%. “This was surprising as we might anticipate risk being higher during pregnancy given that pregnant women may be more susceptible, but we see that this rise was also found among people in the later postpartum period,” Dr. Thoma said.
Absolute and relative changes were highest for Hispanic women (8.9 per 100,000 live births and 74.2%, respectively) and non-Hispanic Black women (16.8 per 100,000 live births and 40.2%). In contrast, non-Hispanic White women saw increases of just 2.9 per 100,000 live births and 17.2%.
“Overall, we found the rise in maternal mortality in 2020 was concentrated after the start of pandemic, particularly for non-Hispanic Black and Hispanic women, and we saw a dramatic rise in respiratory-related conditions,” Dr. Thoma said.
In a comment, Steven Woolf, MD, MPH, director emeritus of the Center on Society and Health at Virginia Commonwealth University, Richmond, said the findings are very consistent with his and others research showing dramatic increases in overall death rates from many causes during the pandemic, with these ranging from COVID-19 leading conditions such as diabetes, cardiovascular and Alzheimer’s disease to less-studied causes such as drug overdoses and alcoholism caused by the stresses of the pandemic. Again, deaths were likely caused by both COVID-19 infections and disruptions in diagnosis and care.
“So a rise in maternal mortality would unfortunately also be expected, and these researchers have shown that,” he said in an interview. In addition, they have confirmed “the pattern of stark health disparities in the Hispanic and Black populations relative to the White. Our group has shown marked decreases in the life expectancies of the Black and Hispanic populations relative to the White population.”
While he might take issue with the study’s research methodology, Dr. Woolf said, “The work is useful partly because we need to work out the best research methods to do this kind of analysis because we really need to understand the effects on maternal mortality.”
He said sorting out the best way to do this type of research will be important for looking at excess deaths and maternal mortality following other events, for example, in the wake of the Supreme Court’s recent decision to reverse Roe v. Wade.
The authors acknowledged certain study limitations, including the large percentage of COVID-19 cases with a nonspecific underlying cause. According to Dr. Thoma and Dr. Declercq, that reflects a maternal death coding problem that needs to be addressed, as well as a partitioning of data. The latter resulted in small numbers for some categories, with rates suppressed for fewer than 16 deaths because of reduced reliability.
“We found that more specific information is often available on death certificates but is lost in the process of coding,” said Dr. Thoma. “We were able to reclassify many of these causes to a more specific cause that we attributed to be the primary cause of death.”
The authors said future studies of maternal death should examine the contribution of the pandemic to racial and ethnic disparities and should identify specific causes of maternal deaths overall and associated with COVID-19.
In earlier research, the authors previously warned of possible misclassifications of maternal deaths.
They found evidence of both underreporting and overreporting of deaths, with possible overreporting predominant, whereas accurate data are essential for measuring the effectiveness of maternal mortality reduction programs.
Dr. Thoma’s group will continue to monitor mortality trends with the release of 2021 data. “We hope we will see improvements in 2021 given greater access to vaccines, treatments, and fewer health care disruptions,” Dr. Thoma said. “It will be important to continue to stress the importance of COVID-19 vaccines for pregnant and postpartum people.”
This study had no external funding. The authors disclosed no competing interests. Dr. Woolf declared no conflicts of interest.
U.S. maternal deaths – those during pregnancy or within 42 days of pregnancy – increased substantially by 33.3% after March 2020 corresponding to the COVID-19 pandemic onset, according to new research published in JAMA Network Open.
Data from the National Center for Health Statistics (NCHS) revealed this rise in maternal deaths was higher than the 22% overall excess death estimate associated with the pandemic in 2020.
Increases were highest for Hispanic and non-Hispanic Black women, exacerbating already high rates of disparity in comparison with White women, wrote Marie E. Thoma, PhD, an associate professor at the University of Maryland, College Park, and Eugene R. Declercq, PhD, a professor at Boston University.
The authors noted that this spike in maternal deaths might be caused either by conditions directly related to COVID-19, such as respiratory or viral infections, or by conditions worsened by pandemic-associated health care disruptions including those for diabetes or cardiovascular disease.
The precise causes, however, could not be discerned from the data, the authors noted.
The NCHS reported an 18.4% increase in U.S. maternal mortality from 2019 to 2020. The relative increase was 44.4% among Hispanic, 25.7% among non-Hispanic Black, and 6.1% among non-Hispanic White women.
“The rise in maternal mortality among Hispanic women was unprecedented,” Dr. Thoma said in an interview. Given a 16.8% increase in overall U.S. mortality in 2020, largely attributed to the COVID-19 pandemic, the authors examined the pandemic’s role in [the higher] maternal death rates for 2020.
“Prior to this report, the NCHS released an e-report that there had been a rise in maternal mortality in 2020, but questions remained about the role of the pandemic in this rise that their report hadn’t addressed,” Dr. Thoma said in an interview “So we decided to look at the data further to assess whether the rise coincided with the pandemic and how this differed by race/ethnicity, whether there were changes in the causes of maternal death, and how often COVID-19 was listed as a contributory factor in those deaths.”
A total of 1,588 maternal deaths (18.8 per 100,000 live births) occurred before the pandemic versus 684 deaths (25.1 per 100,000 live births) during the 2020 phase of the pandemic, for a relative increase of 33.3%.
Direct obstetrical causes of death included diabetes, hypertensive and liver disorders, pregnancy-related infections, and obstetrical hemorrhage and embolism. Indirect causes comprised, among others, nonobstetrical infections and diseases of the circulatory and respiratory systems as well as mental and nervous disorders.
Relative increases in direct causes (27.7%) were mostly associated with diabetes (95.9%), hypertensive disorders (39.0%), and other specified pregnancy-related conditions (48.0%).
COVID-19 was commonly listed as a lethal condition along with other viral diseases (16 of 16 deaths and diseases of the respiratory system (11 of 19 deaths).
Late maternal mortality – defined as more than 42 days but less than 1 year after pregnancy – increased by 41%. “This was surprising as we might anticipate risk being higher during pregnancy given that pregnant women may be more susceptible, but we see that this rise was also found among people in the later postpartum period,” Dr. Thoma said.
Absolute and relative changes were highest for Hispanic women (8.9 per 100,000 live births and 74.2%, respectively) and non-Hispanic Black women (16.8 per 100,000 live births and 40.2%). In contrast, non-Hispanic White women saw increases of just 2.9 per 100,000 live births and 17.2%.
“Overall, we found the rise in maternal mortality in 2020 was concentrated after the start of pandemic, particularly for non-Hispanic Black and Hispanic women, and we saw a dramatic rise in respiratory-related conditions,” Dr. Thoma said.
In a comment, Steven Woolf, MD, MPH, director emeritus of the Center on Society and Health at Virginia Commonwealth University, Richmond, said the findings are very consistent with his and others research showing dramatic increases in overall death rates from many causes during the pandemic, with these ranging from COVID-19 leading conditions such as diabetes, cardiovascular and Alzheimer’s disease to less-studied causes such as drug overdoses and alcoholism caused by the stresses of the pandemic. Again, deaths were likely caused by both COVID-19 infections and disruptions in diagnosis and care.
“So a rise in maternal mortality would unfortunately also be expected, and these researchers have shown that,” he said in an interview. In addition, they have confirmed “the pattern of stark health disparities in the Hispanic and Black populations relative to the White. Our group has shown marked decreases in the life expectancies of the Black and Hispanic populations relative to the White population.”
While he might take issue with the study’s research methodology, Dr. Woolf said, “The work is useful partly because we need to work out the best research methods to do this kind of analysis because we really need to understand the effects on maternal mortality.”
He said sorting out the best way to do this type of research will be important for looking at excess deaths and maternal mortality following other events, for example, in the wake of the Supreme Court’s recent decision to reverse Roe v. Wade.
The authors acknowledged certain study limitations, including the large percentage of COVID-19 cases with a nonspecific underlying cause. According to Dr. Thoma and Dr. Declercq, that reflects a maternal death coding problem that needs to be addressed, as well as a partitioning of data. The latter resulted in small numbers for some categories, with rates suppressed for fewer than 16 deaths because of reduced reliability.
“We found that more specific information is often available on death certificates but is lost in the process of coding,” said Dr. Thoma. “We were able to reclassify many of these causes to a more specific cause that we attributed to be the primary cause of death.”
The authors said future studies of maternal death should examine the contribution of the pandemic to racial and ethnic disparities and should identify specific causes of maternal deaths overall and associated with COVID-19.
In earlier research, the authors previously warned of possible misclassifications of maternal deaths.
They found evidence of both underreporting and overreporting of deaths, with possible overreporting predominant, whereas accurate data are essential for measuring the effectiveness of maternal mortality reduction programs.
Dr. Thoma’s group will continue to monitor mortality trends with the release of 2021 data. “We hope we will see improvements in 2021 given greater access to vaccines, treatments, and fewer health care disruptions,” Dr. Thoma said. “It will be important to continue to stress the importance of COVID-19 vaccines for pregnant and postpartum people.”
This study had no external funding. The authors disclosed no competing interests. Dr. Woolf declared no conflicts of interest.
FROM JAMA NETWORK OPEN
Abortion pills over the counter? Experts see major hurdles in widening U.S. access
WASHINGTON (Reuters) – A pill used to terminate early pregnancies is unlikely to become available without a prescription for years, if ever, experts told Reuters, as the conservative-leaning U.S. Supreme Court dramatically curbed abortion rights.
The Supreme Court on June 24 overturned the landmark 1973 Roe v. Wade ruling that recognized the constitutional right to an abortion and legalized it nationwide. The new ruling stung abortion rights advocates and was a momentous victory to Republicans and religious conservatives.
Many U.S. states are expected to severely limit or outright ban abortions following the Supreme Court ruling. President Joe Biden’s administration is considering options to increase access to so-called medication abortions, which can be administered at home.
“Today I am directing the Department of Health & Human Services to take steps to ensure these critical medications are available to the fullest extent possible,” Mr. Biden said in remarks from the White House.
The pill, mifepristone, is used in combination with a second drug called misoprostol to induce an abortion up to 10 weeks into a pregnancy and is heavily restricted – only available through a certified doctor’s prescription. Abortion rights activists have stepped up calls to make it available for anyone to buy at pharmacies without a prescription.
“We will double down and use every lever we have to protect access to abortion care,” Secretary of Health and Human Services Xavier Becerra said in a statement, adding the department was committed to ensuring access to “medication abortion that has been approved by the FDA for over 20 years.”
Neither Mr. Biden nor Mr. Becerra addressed making the pills available over-the-counter, a process that could take years according to medical and regulatory experts interviewed by Reuters. They said drugmakers would need to conduct new studies showing directions on the product’s packaging would enable a consumer to safely use it without professional medical guidance.
The two companies that make the pill for the U.S. market have shown no interest in conducting the research. Should they do so, any Food and Drug Administration approval would become a target for lawsuits from abortion opponents that could delay implementation for years, experts said.
“The hard part that I see is getting the evidence or the agreement that no prescriber is needed at all,” said Susan Wood, a former Assistant Commissioner for Women’s Health at the FDA.
“I personally don’t see it happening in the next couple of years,” said Ms. Wood, now director of George Washington University’s Jacobs Institute of Women’s Health.
The next battle
Access to abortion pills is expected to become the next big battle, as their use is harder to track. The FDA has already relaxed some restrictions, making it easier for certified doctors to prescribe them.
The agency now allows doctors to prescribe mifepristone after a telehealth visit rather than in-person. Patients can receive it by mail, making it easier for women in U.S. states that already restrict its use.
The White House has already considered making abortion pills available online and from pharmacies abroad, with a prescription. However, the import possibility has been curtailed by Congress in broader legislation about drug regulation.
An over-the-counter designation would make it much easier for pregnant women to access the pills in states that seek to restrict their use. For example, they could more easily be mailed to a patient from a friend or supporter in a state where they are not banned.
An FDA spokesperson declined to comment on whether over-the-counter use of abortion pills has been considered. A spokesperson for Danco Laboratories, a manufacturer of mifepristone, said that it does not plan to seek over-the-counter approval. GenBioPro, the second maker of mifepristone for the U.S. market, did not respond to requests for comment.
Are they safe?
Medication abortion involves two drugs, taken over a day or two. The first, mifepristone, blocks the pregnancy-sustaining hormone progesterone. The second, misoprostol, induces uterine contractions.
When taken together, the pills halt the pregnancy and prompt cramping and bleeding to empty the uterus, in a process similar to miscarriage.
Abortion rights activists say the pills have a long track record of being safe and effective, with no risk of overdose or addiction. In several countries, including India and Mexico, women can buy mifepristone and misoprostol without a prescription to induce abortion.
“Medication abortion really does meet all the FDA criteria for an over-the-counter switch,” said Antonia Biggs, associate professor at the University of California, San Francisco’s obstetrics, gynecology and reproductive sciences department.
A recent study by Ms. Biggs and colleagues found that the majority of participants would understand a medication abortion over-the-counter label. Ms. Biggs said she was not in talks with drugmakers over her research.
The Charlotte Lozier Institute and Susan B. Anthony List, which advocate against abortion, have said that the FDA decision to relax restrictions on mifepristone ignored data on complications and put women at risk.
Others point to the decade-long legal fight for over-the-counter Plan B, a form of emergency contraception taken within days of sexual intercourse to prevent a pregnancy. Approval for women 18 and over was granted in 2006 and for use by women of all ages in 2013.
“There was very strong support that you did not need a prescriber,” said Ms. Wood, who resigned from the FDA in 2005 over the delay. “Everybody under the sun agreed except for a small group of people who somehow had an enormous political influence.”
Reuters Health Information © 2022
WASHINGTON (Reuters) – A pill used to terminate early pregnancies is unlikely to become available without a prescription for years, if ever, experts told Reuters, as the conservative-leaning U.S. Supreme Court dramatically curbed abortion rights.
The Supreme Court on June 24 overturned the landmark 1973 Roe v. Wade ruling that recognized the constitutional right to an abortion and legalized it nationwide. The new ruling stung abortion rights advocates and was a momentous victory to Republicans and religious conservatives.
Many U.S. states are expected to severely limit or outright ban abortions following the Supreme Court ruling. President Joe Biden’s administration is considering options to increase access to so-called medication abortions, which can be administered at home.
“Today I am directing the Department of Health & Human Services to take steps to ensure these critical medications are available to the fullest extent possible,” Mr. Biden said in remarks from the White House.
The pill, mifepristone, is used in combination with a second drug called misoprostol to induce an abortion up to 10 weeks into a pregnancy and is heavily restricted – only available through a certified doctor’s prescription. Abortion rights activists have stepped up calls to make it available for anyone to buy at pharmacies without a prescription.
“We will double down and use every lever we have to protect access to abortion care,” Secretary of Health and Human Services Xavier Becerra said in a statement, adding the department was committed to ensuring access to “medication abortion that has been approved by the FDA for over 20 years.”
Neither Mr. Biden nor Mr. Becerra addressed making the pills available over-the-counter, a process that could take years according to medical and regulatory experts interviewed by Reuters. They said drugmakers would need to conduct new studies showing directions on the product’s packaging would enable a consumer to safely use it without professional medical guidance.
The two companies that make the pill for the U.S. market have shown no interest in conducting the research. Should they do so, any Food and Drug Administration approval would become a target for lawsuits from abortion opponents that could delay implementation for years, experts said.
“The hard part that I see is getting the evidence or the agreement that no prescriber is needed at all,” said Susan Wood, a former Assistant Commissioner for Women’s Health at the FDA.
“I personally don’t see it happening in the next couple of years,” said Ms. Wood, now director of George Washington University’s Jacobs Institute of Women’s Health.
The next battle
Access to abortion pills is expected to become the next big battle, as their use is harder to track. The FDA has already relaxed some restrictions, making it easier for certified doctors to prescribe them.
The agency now allows doctors to prescribe mifepristone after a telehealth visit rather than in-person. Patients can receive it by mail, making it easier for women in U.S. states that already restrict its use.
The White House has already considered making abortion pills available online and from pharmacies abroad, with a prescription. However, the import possibility has been curtailed by Congress in broader legislation about drug regulation.
An over-the-counter designation would make it much easier for pregnant women to access the pills in states that seek to restrict their use. For example, they could more easily be mailed to a patient from a friend or supporter in a state where they are not banned.
An FDA spokesperson declined to comment on whether over-the-counter use of abortion pills has been considered. A spokesperson for Danco Laboratories, a manufacturer of mifepristone, said that it does not plan to seek over-the-counter approval. GenBioPro, the second maker of mifepristone for the U.S. market, did not respond to requests for comment.
Are they safe?
Medication abortion involves two drugs, taken over a day or two. The first, mifepristone, blocks the pregnancy-sustaining hormone progesterone. The second, misoprostol, induces uterine contractions.
When taken together, the pills halt the pregnancy and prompt cramping and bleeding to empty the uterus, in a process similar to miscarriage.
Abortion rights activists say the pills have a long track record of being safe and effective, with no risk of overdose or addiction. In several countries, including India and Mexico, women can buy mifepristone and misoprostol without a prescription to induce abortion.
“Medication abortion really does meet all the FDA criteria for an over-the-counter switch,” said Antonia Biggs, associate professor at the University of California, San Francisco’s obstetrics, gynecology and reproductive sciences department.
A recent study by Ms. Biggs and colleagues found that the majority of participants would understand a medication abortion over-the-counter label. Ms. Biggs said she was not in talks with drugmakers over her research.
The Charlotte Lozier Institute and Susan B. Anthony List, which advocate against abortion, have said that the FDA decision to relax restrictions on mifepristone ignored data on complications and put women at risk.
Others point to the decade-long legal fight for over-the-counter Plan B, a form of emergency contraception taken within days of sexual intercourse to prevent a pregnancy. Approval for women 18 and over was granted in 2006 and for use by women of all ages in 2013.
“There was very strong support that you did not need a prescriber,” said Ms. Wood, who resigned from the FDA in 2005 over the delay. “Everybody under the sun agreed except for a small group of people who somehow had an enormous political influence.”
Reuters Health Information © 2022
WASHINGTON (Reuters) – A pill used to terminate early pregnancies is unlikely to become available without a prescription for years, if ever, experts told Reuters, as the conservative-leaning U.S. Supreme Court dramatically curbed abortion rights.
The Supreme Court on June 24 overturned the landmark 1973 Roe v. Wade ruling that recognized the constitutional right to an abortion and legalized it nationwide. The new ruling stung abortion rights advocates and was a momentous victory to Republicans and religious conservatives.
Many U.S. states are expected to severely limit or outright ban abortions following the Supreme Court ruling. President Joe Biden’s administration is considering options to increase access to so-called medication abortions, which can be administered at home.
“Today I am directing the Department of Health & Human Services to take steps to ensure these critical medications are available to the fullest extent possible,” Mr. Biden said in remarks from the White House.
The pill, mifepristone, is used in combination with a second drug called misoprostol to induce an abortion up to 10 weeks into a pregnancy and is heavily restricted – only available through a certified doctor’s prescription. Abortion rights activists have stepped up calls to make it available for anyone to buy at pharmacies without a prescription.
“We will double down and use every lever we have to protect access to abortion care,” Secretary of Health and Human Services Xavier Becerra said in a statement, adding the department was committed to ensuring access to “medication abortion that has been approved by the FDA for over 20 years.”
Neither Mr. Biden nor Mr. Becerra addressed making the pills available over-the-counter, a process that could take years according to medical and regulatory experts interviewed by Reuters. They said drugmakers would need to conduct new studies showing directions on the product’s packaging would enable a consumer to safely use it without professional medical guidance.
The two companies that make the pill for the U.S. market have shown no interest in conducting the research. Should they do so, any Food and Drug Administration approval would become a target for lawsuits from abortion opponents that could delay implementation for years, experts said.
“The hard part that I see is getting the evidence or the agreement that no prescriber is needed at all,” said Susan Wood, a former Assistant Commissioner for Women’s Health at the FDA.
“I personally don’t see it happening in the next couple of years,” said Ms. Wood, now director of George Washington University’s Jacobs Institute of Women’s Health.
The next battle
Access to abortion pills is expected to become the next big battle, as their use is harder to track. The FDA has already relaxed some restrictions, making it easier for certified doctors to prescribe them.
The agency now allows doctors to prescribe mifepristone after a telehealth visit rather than in-person. Patients can receive it by mail, making it easier for women in U.S. states that already restrict its use.
The White House has already considered making abortion pills available online and from pharmacies abroad, with a prescription. However, the import possibility has been curtailed by Congress in broader legislation about drug regulation.
An over-the-counter designation would make it much easier for pregnant women to access the pills in states that seek to restrict their use. For example, they could more easily be mailed to a patient from a friend or supporter in a state where they are not banned.
An FDA spokesperson declined to comment on whether over-the-counter use of abortion pills has been considered. A spokesperson for Danco Laboratories, a manufacturer of mifepristone, said that it does not plan to seek over-the-counter approval. GenBioPro, the second maker of mifepristone for the U.S. market, did not respond to requests for comment.
Are they safe?
Medication abortion involves two drugs, taken over a day or two. The first, mifepristone, blocks the pregnancy-sustaining hormone progesterone. The second, misoprostol, induces uterine contractions.
When taken together, the pills halt the pregnancy and prompt cramping and bleeding to empty the uterus, in a process similar to miscarriage.
Abortion rights activists say the pills have a long track record of being safe and effective, with no risk of overdose or addiction. In several countries, including India and Mexico, women can buy mifepristone and misoprostol without a prescription to induce abortion.
“Medication abortion really does meet all the FDA criteria for an over-the-counter switch,” said Antonia Biggs, associate professor at the University of California, San Francisco’s obstetrics, gynecology and reproductive sciences department.
A recent study by Ms. Biggs and colleagues found that the majority of participants would understand a medication abortion over-the-counter label. Ms. Biggs said she was not in talks with drugmakers over her research.
The Charlotte Lozier Institute and Susan B. Anthony List, which advocate against abortion, have said that the FDA decision to relax restrictions on mifepristone ignored data on complications and put women at risk.
Others point to the decade-long legal fight for over-the-counter Plan B, a form of emergency contraception taken within days of sexual intercourse to prevent a pregnancy. Approval for women 18 and over was granted in 2006 and for use by women of all ages in 2013.
“There was very strong support that you did not need a prescriber,” said Ms. Wood, who resigned from the FDA in 2005 over the delay. “Everybody under the sun agreed except for a small group of people who somehow had an enormous political influence.”
Reuters Health Information © 2022
LGBTQ students would get new protections under Biden plan
On the 50th anniversary of Title IX’s inception, the Biden administration has proposed changes to the law that would protect transgender students and assault survivors on college and university campuses.
With these changes, the protections provided by Title IX – a civil rights law that prohibits sex-based discrimination in schools that receive federal funding – would now be extended to students who identify as trans. The update would ensure that government-funded schools make proper accommodations for a trans student population, such as allowing students to use bathrooms and other facilities that align with their gender identity, and enforcing the use of students’ correct pronouns.
The revisions also seek to undo amendments made to the law by Betsy DeVos, who was secretary of education during the Trump presidency, which strengthened due process protections for students accused of sexual assault and narrowed the definition of sexual harassment. These rules “weakened protections for survivors of sexual assault and diminished the promise of an education free from discrimination,” the Biden administration said.
“Our proposed changes will allow us to continue that progress and ensure all our nation’s students – no matter where they live, who they are, or whom they love – can learn, grow, and thrive in school,” Education Secretary Miguel Cardona, PhD, said in a news release. “We welcome public comment on these critical regulations so we can further the Biden-Harris Administration’s mission of creating educational environments free from sex discrimination and sexual violence.”
The revisions will go through a long period of public comment before they are set into law. Still, the proposed changes mark a way forward for trans students who are not explicitly protected under Title IX, and they offer solace to assault survivors who may have felt discouraged to come forward and report under Ms. DeVos’s rules.
“The proposed regulations reflect the [Education] Department’s commitment to give full effect to Title IX, ensuring that no person experiences sex discrimination in education, and that school procedures for addressing complaints of sex discrimination, including sexual violence and other forms of sex-based harassment, are clear, effective, and fair to all involved,” said Catherine Lhamon, JD, assistant secretary for the Education Department’s Office Of Civil Rights.
More specific rules about transgender students’ participation in school sports are still to come.
A version of this article first appeared on WebMD.com.
On the 50th anniversary of Title IX’s inception, the Biden administration has proposed changes to the law that would protect transgender students and assault survivors on college and university campuses.
With these changes, the protections provided by Title IX – a civil rights law that prohibits sex-based discrimination in schools that receive federal funding – would now be extended to students who identify as trans. The update would ensure that government-funded schools make proper accommodations for a trans student population, such as allowing students to use bathrooms and other facilities that align with their gender identity, and enforcing the use of students’ correct pronouns.
The revisions also seek to undo amendments made to the law by Betsy DeVos, who was secretary of education during the Trump presidency, which strengthened due process protections for students accused of sexual assault and narrowed the definition of sexual harassment. These rules “weakened protections for survivors of sexual assault and diminished the promise of an education free from discrimination,” the Biden administration said.
“Our proposed changes will allow us to continue that progress and ensure all our nation’s students – no matter where they live, who they are, or whom they love – can learn, grow, and thrive in school,” Education Secretary Miguel Cardona, PhD, said in a news release. “We welcome public comment on these critical regulations so we can further the Biden-Harris Administration’s mission of creating educational environments free from sex discrimination and sexual violence.”
The revisions will go through a long period of public comment before they are set into law. Still, the proposed changes mark a way forward for trans students who are not explicitly protected under Title IX, and they offer solace to assault survivors who may have felt discouraged to come forward and report under Ms. DeVos’s rules.
“The proposed regulations reflect the [Education] Department’s commitment to give full effect to Title IX, ensuring that no person experiences sex discrimination in education, and that school procedures for addressing complaints of sex discrimination, including sexual violence and other forms of sex-based harassment, are clear, effective, and fair to all involved,” said Catherine Lhamon, JD, assistant secretary for the Education Department’s Office Of Civil Rights.
More specific rules about transgender students’ participation in school sports are still to come.
A version of this article first appeared on WebMD.com.
On the 50th anniversary of Title IX’s inception, the Biden administration has proposed changes to the law that would protect transgender students and assault survivors on college and university campuses.
With these changes, the protections provided by Title IX – a civil rights law that prohibits sex-based discrimination in schools that receive federal funding – would now be extended to students who identify as trans. The update would ensure that government-funded schools make proper accommodations for a trans student population, such as allowing students to use bathrooms and other facilities that align with their gender identity, and enforcing the use of students’ correct pronouns.
The revisions also seek to undo amendments made to the law by Betsy DeVos, who was secretary of education during the Trump presidency, which strengthened due process protections for students accused of sexual assault and narrowed the definition of sexual harassment. These rules “weakened protections for survivors of sexual assault and diminished the promise of an education free from discrimination,” the Biden administration said.
“Our proposed changes will allow us to continue that progress and ensure all our nation’s students – no matter where they live, who they are, or whom they love – can learn, grow, and thrive in school,” Education Secretary Miguel Cardona, PhD, said in a news release. “We welcome public comment on these critical regulations so we can further the Biden-Harris Administration’s mission of creating educational environments free from sex discrimination and sexual violence.”
The revisions will go through a long period of public comment before they are set into law. Still, the proposed changes mark a way forward for trans students who are not explicitly protected under Title IX, and they offer solace to assault survivors who may have felt discouraged to come forward and report under Ms. DeVos’s rules.
“The proposed regulations reflect the [Education] Department’s commitment to give full effect to Title IX, ensuring that no person experiences sex discrimination in education, and that school procedures for addressing complaints of sex discrimination, including sexual violence and other forms of sex-based harassment, are clear, effective, and fair to all involved,” said Catherine Lhamon, JD, assistant secretary for the Education Department’s Office Of Civil Rights.
More specific rules about transgender students’ participation in school sports are still to come.
A version of this article first appeared on WebMD.com.
Both parents at risk for depression following birth
Physicians have screened new and expectant mothers for perinatal depression for years. But what about fathers?
A new systematic review and meta-analysis suggests it’s time for health care providers to ask both parents about any mental health symptoms before and after their baby is born.
“We are screening most mothers for signs of perinatal depression,” said Kara Smythe, MD, at the department of primary care and population health and Institute of Epidemiology and Health Care at the University College London, who is the lead author of the study. “But we aren’t always asking about the relationship between them and the person helping them care for this newborn. If we don’t consider the experience of new fathers, we’re doing a disservice to everyone.”
Without screening both parents, health care providers can miss important clues to why child and parents experience adverse health outcomes post birth.
The study, published in JAMA Network Open, found that for 3.18% of couples, both parents concurrently experienced depression before and following a birth. The mental illness was more common in the late postnatal period (3-12 months).
According to the Centers for Disease Control and Prevention, about 1 in 8 women experience symptoms of postpartum depression. Other sources indicate the incidence may be much higher. Findings from a mobile app using the Edinburgh Postnatal Depression Scale presented at the American Psychiatric Association’s annual meeting in 2019 indicated more than half of the 164,237 women who used the free app reported symptoms of depression for up to a year following the birth of their baby.
The findings
Dr. Smythe and her team reviewed previously published observational studies on the prevalence of perinatal depression or anxiety in couples from the Ovid and Web of Science between Jan. 1, 1990, and June 8, 2021.
They ultimately included 23 studies with data from 29,286 couples. They broke the data into subgroups of persons with antenatal depression, early postnatal depression (0-12 weeks), late postnatal depression (3-13 months), and perinatal anxiety.
About 1.7% (P < .001) of couples experienced antenatal depression, and about 2.4% (P < .001) experienced early postnatal depression. About 3.2% (P < .001) experienced late postnatal depression. The data on perinatal anxiety were insufficient, they write.
The vast majority of couples included in the samples were White, heterosexual, and highly educated with a middle to high socioeconomic background. The pregnancies were reportedly wanted, if not planned. The majority of the studies – 21 – included in the analysis were from countries other than the United States.
According to the study, evidence suggests that paternal depression can lead to increased symptoms of depression in mothers during pregnancy and the following 6 months. Men reported perinatal depression at similar rates as women, and Dr. Smythe said it’s becoming clear that men experience similar struggles as they transition into fatherhood.
J. J. Parker, MD, a pediatric and internal attending physician at Lurie Children’s Hospital of Chicago and Northwestern Medicine, said the findings solidify what he has observed from his own experience as a new father and resident.
“You’re at higher risk of having depression if your partner has depression, but it’s important to see that in the numbers,” Dr. Parker told this news organization. “I think from a clinician standpoint, this demonstrates that 3% of infants are living in households where both parents are depressed, and that has major implications for the development and health of those children.”
Dr. Smythe and her colleagues found that if even one parent is experiencing a mood disorder such as depression or anxiety, the newborn can experience impaired bonding, behavioral problems, and other harms later in life.
If both parents are experiencing perinatal depression, those negative outcomes could be amplified, although Dr. Smythe said more research is needed to solidify the link.
“I think one quick takeaway for pediatricians, clinicians, and any other health care providers taking care of mothers and infants is to ask about the nonbirthing parent,” Dr. Parker said. “All clinicians can do that right away, even if the mother does not have depression.”
The study was independently supported. Dr. Smythe and her colleagues report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physicians have screened new and expectant mothers for perinatal depression for years. But what about fathers?
A new systematic review and meta-analysis suggests it’s time for health care providers to ask both parents about any mental health symptoms before and after their baby is born.
“We are screening most mothers for signs of perinatal depression,” said Kara Smythe, MD, at the department of primary care and population health and Institute of Epidemiology and Health Care at the University College London, who is the lead author of the study. “But we aren’t always asking about the relationship between them and the person helping them care for this newborn. If we don’t consider the experience of new fathers, we’re doing a disservice to everyone.”
Without screening both parents, health care providers can miss important clues to why child and parents experience adverse health outcomes post birth.
The study, published in JAMA Network Open, found that for 3.18% of couples, both parents concurrently experienced depression before and following a birth. The mental illness was more common in the late postnatal period (3-12 months).
According to the Centers for Disease Control and Prevention, about 1 in 8 women experience symptoms of postpartum depression. Other sources indicate the incidence may be much higher. Findings from a mobile app using the Edinburgh Postnatal Depression Scale presented at the American Psychiatric Association’s annual meeting in 2019 indicated more than half of the 164,237 women who used the free app reported symptoms of depression for up to a year following the birth of their baby.
The findings
Dr. Smythe and her team reviewed previously published observational studies on the prevalence of perinatal depression or anxiety in couples from the Ovid and Web of Science between Jan. 1, 1990, and June 8, 2021.
They ultimately included 23 studies with data from 29,286 couples. They broke the data into subgroups of persons with antenatal depression, early postnatal depression (0-12 weeks), late postnatal depression (3-13 months), and perinatal anxiety.
About 1.7% (P < .001) of couples experienced antenatal depression, and about 2.4% (P < .001) experienced early postnatal depression. About 3.2% (P < .001) experienced late postnatal depression. The data on perinatal anxiety were insufficient, they write.
The vast majority of couples included in the samples were White, heterosexual, and highly educated with a middle to high socioeconomic background. The pregnancies were reportedly wanted, if not planned. The majority of the studies – 21 – included in the analysis were from countries other than the United States.
According to the study, evidence suggests that paternal depression can lead to increased symptoms of depression in mothers during pregnancy and the following 6 months. Men reported perinatal depression at similar rates as women, and Dr. Smythe said it’s becoming clear that men experience similar struggles as they transition into fatherhood.
J. J. Parker, MD, a pediatric and internal attending physician at Lurie Children’s Hospital of Chicago and Northwestern Medicine, said the findings solidify what he has observed from his own experience as a new father and resident.
“You’re at higher risk of having depression if your partner has depression, but it’s important to see that in the numbers,” Dr. Parker told this news organization. “I think from a clinician standpoint, this demonstrates that 3% of infants are living in households where both parents are depressed, and that has major implications for the development and health of those children.”
Dr. Smythe and her colleagues found that if even one parent is experiencing a mood disorder such as depression or anxiety, the newborn can experience impaired bonding, behavioral problems, and other harms later in life.
If both parents are experiencing perinatal depression, those negative outcomes could be amplified, although Dr. Smythe said more research is needed to solidify the link.
“I think one quick takeaway for pediatricians, clinicians, and any other health care providers taking care of mothers and infants is to ask about the nonbirthing parent,” Dr. Parker said. “All clinicians can do that right away, even if the mother does not have depression.”
The study was independently supported. Dr. Smythe and her colleagues report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physicians have screened new and expectant mothers for perinatal depression for years. But what about fathers?
A new systematic review and meta-analysis suggests it’s time for health care providers to ask both parents about any mental health symptoms before and after their baby is born.
“We are screening most mothers for signs of perinatal depression,” said Kara Smythe, MD, at the department of primary care and population health and Institute of Epidemiology and Health Care at the University College London, who is the lead author of the study. “But we aren’t always asking about the relationship between them and the person helping them care for this newborn. If we don’t consider the experience of new fathers, we’re doing a disservice to everyone.”
Without screening both parents, health care providers can miss important clues to why child and parents experience adverse health outcomes post birth.
The study, published in JAMA Network Open, found that for 3.18% of couples, both parents concurrently experienced depression before and following a birth. The mental illness was more common in the late postnatal period (3-12 months).
According to the Centers for Disease Control and Prevention, about 1 in 8 women experience symptoms of postpartum depression. Other sources indicate the incidence may be much higher. Findings from a mobile app using the Edinburgh Postnatal Depression Scale presented at the American Psychiatric Association’s annual meeting in 2019 indicated more than half of the 164,237 women who used the free app reported symptoms of depression for up to a year following the birth of their baby.
The findings
Dr. Smythe and her team reviewed previously published observational studies on the prevalence of perinatal depression or anxiety in couples from the Ovid and Web of Science between Jan. 1, 1990, and June 8, 2021.
They ultimately included 23 studies with data from 29,286 couples. They broke the data into subgroups of persons with antenatal depression, early postnatal depression (0-12 weeks), late postnatal depression (3-13 months), and perinatal anxiety.
About 1.7% (P < .001) of couples experienced antenatal depression, and about 2.4% (P < .001) experienced early postnatal depression. About 3.2% (P < .001) experienced late postnatal depression. The data on perinatal anxiety were insufficient, they write.
The vast majority of couples included in the samples were White, heterosexual, and highly educated with a middle to high socioeconomic background. The pregnancies were reportedly wanted, if not planned. The majority of the studies – 21 – included in the analysis were from countries other than the United States.
According to the study, evidence suggests that paternal depression can lead to increased symptoms of depression in mothers during pregnancy and the following 6 months. Men reported perinatal depression at similar rates as women, and Dr. Smythe said it’s becoming clear that men experience similar struggles as they transition into fatherhood.
J. J. Parker, MD, a pediatric and internal attending physician at Lurie Children’s Hospital of Chicago and Northwestern Medicine, said the findings solidify what he has observed from his own experience as a new father and resident.
“You’re at higher risk of having depression if your partner has depression, but it’s important to see that in the numbers,” Dr. Parker told this news organization. “I think from a clinician standpoint, this demonstrates that 3% of infants are living in households where both parents are depressed, and that has major implications for the development and health of those children.”
Dr. Smythe and her colleagues found that if even one parent is experiencing a mood disorder such as depression or anxiety, the newborn can experience impaired bonding, behavioral problems, and other harms later in life.
If both parents are experiencing perinatal depression, those negative outcomes could be amplified, although Dr. Smythe said more research is needed to solidify the link.
“I think one quick takeaway for pediatricians, clinicians, and any other health care providers taking care of mothers and infants is to ask about the nonbirthing parent,” Dr. Parker said. “All clinicians can do that right away, even if the mother does not have depression.”
The study was independently supported. Dr. Smythe and her colleagues report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Roe v. Wade: Medical groups react to Supreme Court decision
The country’s top medical organizations condemned the overturning of Roe v. Wade, saying the removal of federal protections for women to access abortion services marks a “dark day.”
“It is unfathomable. It is unfair. It is wrong,” said the President of the American College of Obstetricians and Gynecologists (ACOG) Iffath Abbasi Hoskins, MD.
“Today is a very dark day in health care. It is a dark day, indeed, for the tens of millions of patients who have suddenly and unfairly lost access to safe legal and evidence-based abortion care,” Dr. Hoskins said at a press conference June 24 sponsored by ACOG.
“It is dark for the thousands of clinicians who now, instead of focusing on providing health care to their patients, have to live with the threats of legal, civil, and even professional penalties,” Dr. Hoskins added.
ACOG has 62,000 members and is the leading group of doctors that provides obstetric and gynecologic care.
Dilemma for some doctors?
“I’d like to take a moment to talk about the future of the medical profession,” said ACOG Chief Executive Officer Maureen G. Phipps, MD, MPH. “[The] decision is, as Dr. Hoskins clearly said, a tragic one for our patients in states across the country, but the harm does not end there.”
Dr. Phipps described overturning Roe v. Wade as “the boldest act of legislative interference that we have seen in this country. It will allow state legislators to tell physicians what care they can and cannot provide to their patients.”
“It will leave physicians looking over our shoulders, wondering if a patient is in enough of a crisis to permit an exception to a law,” Dr. Phipps added. “This is an affront to all that drew my colleagues and me into medicine.”
Although the impact on doctor training remains to be seen, she said 44% of ob.gyn. residents are trained in states now empowered to ban abortions.
The effect of the Supreme Court decision on miscarriage management is another unknown.
“It’s going to be very difficult for us, the clinicians, to manage miscarriage,” Dr. Hoskins said. “Many miscarriages could be what we call ‘incomplete’ in the beginning,” where there is still a heartbeat and the patient is cramping and/or bleeding.
In that instance, Dr. Hoskins said, clinicians may be thinking that they have to wait.
“They may be needing to get additional opinions, whether it’s a legal opinion ... or another medical opinion.”
“It’s going to have a devastating effect on every aspect of a woman’s health care, including if she is spontaneously miscarrying,” Dr. Hoskins predicted.
Physician protect thyself?
To what extent doctors can shield themselves from potential prosecution “is a hard question to answer,” Molly Meegan, JD, ACOG’s chief legal officer and general counsel, said.
Ms. Meegan recommended members speak to the risk managers at their individual institutions for guidance.
“It is a real patchwork [of laws] out there, she said. “And that patchwork itself is a danger to people as they seek essential reproductive health care.”
Also, she added, “If a doctor can’t tell what the law is at the time they’re trying to provide the care, it has a terribly chilling effect on medical care.”
Another potential threat to doctors in states that still allow abortion services is action from a neighboring state.
“We are going to be advocating very strongly that states do not have extra-territorial jurisdiction to reach beyond the edges of their state.”
The worry is if a doctor in New Mexico, where abortion is legal, performs an abortion for a person from Texas, where it will soon be illegal, is then prosecuted by Texas, for example.
Medication abortion
Asked about any potential effects on medication abortions, ACOG’s Jen Villavicencio, MD, said it remains to be seen.
“Certainly many of the laws that we have seen, including trigger ban laws, encompass medication abortion,” she said. Several states have these so-called trigger laws, which put into effect laws passed to ban abortion in case Roe was overturned.
This means, she said, that any abortion option, whether it’s procedural or medication, could be and will be banned in some of these states.
Ms. Meegan added that ACOG will continue to support access to medication abortion and that it should be decided by the U.S. Food and Drug Administration and not individual states.
Maternal mortality may rise
“Maternal mortality in and of itself is a very difficult topic,” Dr. Hoskins said, but [the] decision amplifies the implications. “I think of the patients who will have to manage severe complications and mental health challenges while they are carrying a pregnancy that they are forced to carry.”
“I also think of the patients who need to end their pregnancies in order to save their own lives,” Dr. Hoskins added.
Dr. Hoskins said the United States already has a high maternal mortality rate. This new law, she added, could force women into higher-risk situations if they experience high blood pressure, preeclampsia, or bleeding after the birth of the baby.
Growing inequality possible?
“The grievous inequities that exist in this country will grow and expand unchecked without safe access to legal abortion,” Dr. Phipps said.
She noted that women, based on location, will continue “to have protected access to safe evidence-based abortion. Others will have the means and resources and opportunities to secure the care.”
But the same may not be true for women in underserved or disadvantaged communities, Dr. Phipps added.
American Medical Association
ACOG was not the only group to react. “The American Medical Association is deeply disturbed by the U.S. Supreme Court’s decision to overturn nearly a half century of precedent protecting patients’ right to critical reproductive health care,” President Jack Resneck Jr., MD, said in a statement.
The decision represents “an egregious allowance of government intrusion into the medical examination room, a direct attack on the practice of medicine and the patient-physician relationship, and a brazen violation of patients’ rights to evidence-based reproductive health services.”
American Academy of Family Physicians
“The American Academy of Family Physicians is disappointed and disheartened by the Supreme Court’s decision to strike down longstanding protections afforded by Roe v. Wade and Planned Parenthood v. Casey,” President Sterling N. Ransone Jr., MD, said in a statement.
The organization has 127,600 physician and medical student members.
“This decision negatively impacts our practices and our patients by undermining the patient-physician relationship and potentially criminalizing evidence-based medical care,” added Dr. Ransone.
American College of Physicians
“A patient’s decision about whether to continue a pregnancy should be a private decision made in consultation with a physician or other health care professional, without interference from the government,” President Ryan D. Mire, MD, said in a statement. “We strongly oppose medically unnecessary government restrictions on any health care services,” added Dr. Mire on behalf of the group’s 161,000 members.
American Academy of Pediatrics
“This decision carries grave consequences for our adolescent patients, who already face many more barriers than adults in accessing comprehensive reproductive health care services and abortion care,” President Moira Szilagyi, MD, PhD, said in a statement.
“In the wake of this ruling, the American Academy of Pediatrics will continue to support our chapters as states consider policies affecting access to abortion care, and pediatricians will continue to support our patients,” Dr. Szilagyi added.
American Public Health Association
The court’s decision “is a catastrophic judicial failure that will reverberate differently in each state and portends to jeopardize the health and lives of all Americans,” Executive Director Georges C. Benjamin, MD, said in a statement.
American Urogynecologic Society
“The American Urogynecologic Society opposes any ruling that restricts a person’s access to health care and criminalizes the practice of medicine,” the group said in a statement. “This ruling ultimately poses a serious threat to the patient-provider relationship and subsequent decisionmaking necessary to ensure optimal outcomes for patients. As practitioners, we should be free to provide what is in the best interest of our patients.”
A version of this article first appeared on Medscape.com.
The country’s top medical organizations condemned the overturning of Roe v. Wade, saying the removal of federal protections for women to access abortion services marks a “dark day.”
“It is unfathomable. It is unfair. It is wrong,” said the President of the American College of Obstetricians and Gynecologists (ACOG) Iffath Abbasi Hoskins, MD.
“Today is a very dark day in health care. It is a dark day, indeed, for the tens of millions of patients who have suddenly and unfairly lost access to safe legal and evidence-based abortion care,” Dr. Hoskins said at a press conference June 24 sponsored by ACOG.
“It is dark for the thousands of clinicians who now, instead of focusing on providing health care to their patients, have to live with the threats of legal, civil, and even professional penalties,” Dr. Hoskins added.
ACOG has 62,000 members and is the leading group of doctors that provides obstetric and gynecologic care.
Dilemma for some doctors?
“I’d like to take a moment to talk about the future of the medical profession,” said ACOG Chief Executive Officer Maureen G. Phipps, MD, MPH. “[The] decision is, as Dr. Hoskins clearly said, a tragic one for our patients in states across the country, but the harm does not end there.”
Dr. Phipps described overturning Roe v. Wade as “the boldest act of legislative interference that we have seen in this country. It will allow state legislators to tell physicians what care they can and cannot provide to their patients.”
“It will leave physicians looking over our shoulders, wondering if a patient is in enough of a crisis to permit an exception to a law,” Dr. Phipps added. “This is an affront to all that drew my colleagues and me into medicine.”
Although the impact on doctor training remains to be seen, she said 44% of ob.gyn. residents are trained in states now empowered to ban abortions.
The effect of the Supreme Court decision on miscarriage management is another unknown.
“It’s going to be very difficult for us, the clinicians, to manage miscarriage,” Dr. Hoskins said. “Many miscarriages could be what we call ‘incomplete’ in the beginning,” where there is still a heartbeat and the patient is cramping and/or bleeding.
In that instance, Dr. Hoskins said, clinicians may be thinking that they have to wait.
“They may be needing to get additional opinions, whether it’s a legal opinion ... or another medical opinion.”
“It’s going to have a devastating effect on every aspect of a woman’s health care, including if she is spontaneously miscarrying,” Dr. Hoskins predicted.
Physician protect thyself?
To what extent doctors can shield themselves from potential prosecution “is a hard question to answer,” Molly Meegan, JD, ACOG’s chief legal officer and general counsel, said.
Ms. Meegan recommended members speak to the risk managers at their individual institutions for guidance.
“It is a real patchwork [of laws] out there, she said. “And that patchwork itself is a danger to people as they seek essential reproductive health care.”
Also, she added, “If a doctor can’t tell what the law is at the time they’re trying to provide the care, it has a terribly chilling effect on medical care.”
Another potential threat to doctors in states that still allow abortion services is action from a neighboring state.
“We are going to be advocating very strongly that states do not have extra-territorial jurisdiction to reach beyond the edges of their state.”
The worry is if a doctor in New Mexico, where abortion is legal, performs an abortion for a person from Texas, where it will soon be illegal, is then prosecuted by Texas, for example.
Medication abortion
Asked about any potential effects on medication abortions, ACOG’s Jen Villavicencio, MD, said it remains to be seen.
“Certainly many of the laws that we have seen, including trigger ban laws, encompass medication abortion,” she said. Several states have these so-called trigger laws, which put into effect laws passed to ban abortion in case Roe was overturned.
This means, she said, that any abortion option, whether it’s procedural or medication, could be and will be banned in some of these states.
Ms. Meegan added that ACOG will continue to support access to medication abortion and that it should be decided by the U.S. Food and Drug Administration and not individual states.
Maternal mortality may rise
“Maternal mortality in and of itself is a very difficult topic,” Dr. Hoskins said, but [the] decision amplifies the implications. “I think of the patients who will have to manage severe complications and mental health challenges while they are carrying a pregnancy that they are forced to carry.”
“I also think of the patients who need to end their pregnancies in order to save their own lives,” Dr. Hoskins added.
Dr. Hoskins said the United States already has a high maternal mortality rate. This new law, she added, could force women into higher-risk situations if they experience high blood pressure, preeclampsia, or bleeding after the birth of the baby.
Growing inequality possible?
“The grievous inequities that exist in this country will grow and expand unchecked without safe access to legal abortion,” Dr. Phipps said.
She noted that women, based on location, will continue “to have protected access to safe evidence-based abortion. Others will have the means and resources and opportunities to secure the care.”
But the same may not be true for women in underserved or disadvantaged communities, Dr. Phipps added.
American Medical Association
ACOG was not the only group to react. “The American Medical Association is deeply disturbed by the U.S. Supreme Court’s decision to overturn nearly a half century of precedent protecting patients’ right to critical reproductive health care,” President Jack Resneck Jr., MD, said in a statement.
The decision represents “an egregious allowance of government intrusion into the medical examination room, a direct attack on the practice of medicine and the patient-physician relationship, and a brazen violation of patients’ rights to evidence-based reproductive health services.”
American Academy of Family Physicians
“The American Academy of Family Physicians is disappointed and disheartened by the Supreme Court’s decision to strike down longstanding protections afforded by Roe v. Wade and Planned Parenthood v. Casey,” President Sterling N. Ransone Jr., MD, said in a statement.
The organization has 127,600 physician and medical student members.
“This decision negatively impacts our practices and our patients by undermining the patient-physician relationship and potentially criminalizing evidence-based medical care,” added Dr. Ransone.
American College of Physicians
“A patient’s decision about whether to continue a pregnancy should be a private decision made in consultation with a physician or other health care professional, without interference from the government,” President Ryan D. Mire, MD, said in a statement. “We strongly oppose medically unnecessary government restrictions on any health care services,” added Dr. Mire on behalf of the group’s 161,000 members.
American Academy of Pediatrics
“This decision carries grave consequences for our adolescent patients, who already face many more barriers than adults in accessing comprehensive reproductive health care services and abortion care,” President Moira Szilagyi, MD, PhD, said in a statement.
“In the wake of this ruling, the American Academy of Pediatrics will continue to support our chapters as states consider policies affecting access to abortion care, and pediatricians will continue to support our patients,” Dr. Szilagyi added.
American Public Health Association
The court’s decision “is a catastrophic judicial failure that will reverberate differently in each state and portends to jeopardize the health and lives of all Americans,” Executive Director Georges C. Benjamin, MD, said in a statement.
American Urogynecologic Society
“The American Urogynecologic Society opposes any ruling that restricts a person’s access to health care and criminalizes the practice of medicine,” the group said in a statement. “This ruling ultimately poses a serious threat to the patient-provider relationship and subsequent decisionmaking necessary to ensure optimal outcomes for patients. As practitioners, we should be free to provide what is in the best interest of our patients.”
A version of this article first appeared on Medscape.com.
The country’s top medical organizations condemned the overturning of Roe v. Wade, saying the removal of federal protections for women to access abortion services marks a “dark day.”
“It is unfathomable. It is unfair. It is wrong,” said the President of the American College of Obstetricians and Gynecologists (ACOG) Iffath Abbasi Hoskins, MD.
“Today is a very dark day in health care. It is a dark day, indeed, for the tens of millions of patients who have suddenly and unfairly lost access to safe legal and evidence-based abortion care,” Dr. Hoskins said at a press conference June 24 sponsored by ACOG.
“It is dark for the thousands of clinicians who now, instead of focusing on providing health care to their patients, have to live with the threats of legal, civil, and even professional penalties,” Dr. Hoskins added.
ACOG has 62,000 members and is the leading group of doctors that provides obstetric and gynecologic care.
Dilemma for some doctors?
“I’d like to take a moment to talk about the future of the medical profession,” said ACOG Chief Executive Officer Maureen G. Phipps, MD, MPH. “[The] decision is, as Dr. Hoskins clearly said, a tragic one for our patients in states across the country, but the harm does not end there.”
Dr. Phipps described overturning Roe v. Wade as “the boldest act of legislative interference that we have seen in this country. It will allow state legislators to tell physicians what care they can and cannot provide to their patients.”
“It will leave physicians looking over our shoulders, wondering if a patient is in enough of a crisis to permit an exception to a law,” Dr. Phipps added. “This is an affront to all that drew my colleagues and me into medicine.”
Although the impact on doctor training remains to be seen, she said 44% of ob.gyn. residents are trained in states now empowered to ban abortions.
The effect of the Supreme Court decision on miscarriage management is another unknown.
“It’s going to be very difficult for us, the clinicians, to manage miscarriage,” Dr. Hoskins said. “Many miscarriages could be what we call ‘incomplete’ in the beginning,” where there is still a heartbeat and the patient is cramping and/or bleeding.
In that instance, Dr. Hoskins said, clinicians may be thinking that they have to wait.
“They may be needing to get additional opinions, whether it’s a legal opinion ... or another medical opinion.”
“It’s going to have a devastating effect on every aspect of a woman’s health care, including if she is spontaneously miscarrying,” Dr. Hoskins predicted.
Physician protect thyself?
To what extent doctors can shield themselves from potential prosecution “is a hard question to answer,” Molly Meegan, JD, ACOG’s chief legal officer and general counsel, said.
Ms. Meegan recommended members speak to the risk managers at their individual institutions for guidance.
“It is a real patchwork [of laws] out there, she said. “And that patchwork itself is a danger to people as they seek essential reproductive health care.”
Also, she added, “If a doctor can’t tell what the law is at the time they’re trying to provide the care, it has a terribly chilling effect on medical care.”
Another potential threat to doctors in states that still allow abortion services is action from a neighboring state.
“We are going to be advocating very strongly that states do not have extra-territorial jurisdiction to reach beyond the edges of their state.”
The worry is if a doctor in New Mexico, where abortion is legal, performs an abortion for a person from Texas, where it will soon be illegal, is then prosecuted by Texas, for example.
Medication abortion
Asked about any potential effects on medication abortions, ACOG’s Jen Villavicencio, MD, said it remains to be seen.
“Certainly many of the laws that we have seen, including trigger ban laws, encompass medication abortion,” she said. Several states have these so-called trigger laws, which put into effect laws passed to ban abortion in case Roe was overturned.
This means, she said, that any abortion option, whether it’s procedural or medication, could be and will be banned in some of these states.
Ms. Meegan added that ACOG will continue to support access to medication abortion and that it should be decided by the U.S. Food and Drug Administration and not individual states.
Maternal mortality may rise
“Maternal mortality in and of itself is a very difficult topic,” Dr. Hoskins said, but [the] decision amplifies the implications. “I think of the patients who will have to manage severe complications and mental health challenges while they are carrying a pregnancy that they are forced to carry.”
“I also think of the patients who need to end their pregnancies in order to save their own lives,” Dr. Hoskins added.
Dr. Hoskins said the United States already has a high maternal mortality rate. This new law, she added, could force women into higher-risk situations if they experience high blood pressure, preeclampsia, or bleeding after the birth of the baby.
Growing inequality possible?
“The grievous inequities that exist in this country will grow and expand unchecked without safe access to legal abortion,” Dr. Phipps said.
She noted that women, based on location, will continue “to have protected access to safe evidence-based abortion. Others will have the means and resources and opportunities to secure the care.”
But the same may not be true for women in underserved or disadvantaged communities, Dr. Phipps added.
American Medical Association
ACOG was not the only group to react. “The American Medical Association is deeply disturbed by the U.S. Supreme Court’s decision to overturn nearly a half century of precedent protecting patients’ right to critical reproductive health care,” President Jack Resneck Jr., MD, said in a statement.
The decision represents “an egregious allowance of government intrusion into the medical examination room, a direct attack on the practice of medicine and the patient-physician relationship, and a brazen violation of patients’ rights to evidence-based reproductive health services.”
American Academy of Family Physicians
“The American Academy of Family Physicians is disappointed and disheartened by the Supreme Court’s decision to strike down longstanding protections afforded by Roe v. Wade and Planned Parenthood v. Casey,” President Sterling N. Ransone Jr., MD, said in a statement.
The organization has 127,600 physician and medical student members.
“This decision negatively impacts our practices and our patients by undermining the patient-physician relationship and potentially criminalizing evidence-based medical care,” added Dr. Ransone.
American College of Physicians
“A patient’s decision about whether to continue a pregnancy should be a private decision made in consultation with a physician or other health care professional, without interference from the government,” President Ryan D. Mire, MD, said in a statement. “We strongly oppose medically unnecessary government restrictions on any health care services,” added Dr. Mire on behalf of the group’s 161,000 members.
American Academy of Pediatrics
“This decision carries grave consequences for our adolescent patients, who already face many more barriers than adults in accessing comprehensive reproductive health care services and abortion care,” President Moira Szilagyi, MD, PhD, said in a statement.
“In the wake of this ruling, the American Academy of Pediatrics will continue to support our chapters as states consider policies affecting access to abortion care, and pediatricians will continue to support our patients,” Dr. Szilagyi added.
American Public Health Association
The court’s decision “is a catastrophic judicial failure that will reverberate differently in each state and portends to jeopardize the health and lives of all Americans,” Executive Director Georges C. Benjamin, MD, said in a statement.
American Urogynecologic Society
“The American Urogynecologic Society opposes any ruling that restricts a person’s access to health care and criminalizes the practice of medicine,” the group said in a statement. “This ruling ultimately poses a serious threat to the patient-provider relationship and subsequent decisionmaking necessary to ensure optimal outcomes for patients. As practitioners, we should be free to provide what is in the best interest of our patients.”
A version of this article first appeared on Medscape.com.
Stroke risk rises for women with history of infertility, miscarriage, stillbirth
Infertility, pregnancy loss, and stillbirth increased women’s later risk of both nonfatal and fatal stroke, based on data from more than 600,000 women.
“To date, multiple studies have generated an expanding body of evidence on the association between pregnancy complications (e.g., gestational diabetes and preeclampsia) and the long-term risk of stroke, but studies on associations with infertility, miscarriage, or stillbirth have produced mixed evidence,” Chen Liang, a PhD candidate at the University of Queensland, Brisbane, Australia, and colleagues wrote.
In a study published in the BMJ, the researchers reviewed data from eight observational cohort studies across seven countries (Australia, China, Japan, the Netherlands, Sweden, the United Kingdom, and the United States). The participants were part of the InterLACE (International Collaboration for a Life Course Approach to Reproductive Health and Chronic Disease Events) consortium established in 2021. Most observational studies included in the analysis began between 1990 and 2000.
The study population included 618,851 women aged 32-73 years at baseline for whom data on infertility, miscarriage, or stillbirth, were available. The primary outcome was the association of infertility, recurrent miscarriage, and stillbirth with risk of first fatal or nonfatal stroke, and the results were further stratified by subtype. Stroke was identified through self-reports, linked hospital data, national patient registers, or death registry data. Baseline was defined as the first incidence of infertility, miscarriage, or stillbirth. The exception was the National Survey of Health and Development, a British birth cohort started in 1946, that collected data retrospectively.
The median follow-up period was 13 years for nonfatal stroke and 9.4 years for fatal stroke.
Overall, 17.2%, 16.6%, and 4.6% of the women experienced infertility, miscarriage, and stillbirth, respectively.
Women with a history of infertility had a significantly higher nonfatal stroke risk, compared with those without infertility (hazard ratio, 1.14). Further analysis by stroke subtypes showed an increased association between miscarriage and ischemic stroke (HR, 1.15).
Those with a history of miscarriage also had an increased risk of nonfatal stroke, compared with those without miscarriages (HR, 1.11). In the miscarriage group, the risk of stroke increased with the number of miscarriages, with adjusted HRs of 1.07, 1.12, and 1.35 for women with one, two, and three or more miscarriages, respectively. When stratified by stroke subtype, women with three or more miscarriages were more likely than women with no miscarriages to experience ischemic and hemorrhagic nonfatal strokes.
Associations were similar between miscarriage history and fatal stroke risk. Women with one, two, and three or more miscarriages had increased risk of fatal stroke, compared with those with no miscarriages (aHR, 1.08, 1.26, and 1.82, respectively, and women with three or more miscarriages had a higher risk of ischemic and hemorrhagic stroke (aHR, 1.83 and 1.84, respectively).
Women with a history of stillbirth had an approximately 31% increased risk of nonfatal stroke, compared with those with no history of stillbirth, with aHRs similar for single and recurrent stillbirths (1.32 and 1.29, respectively). Ischemic nonfatal stroke risk was higher in women with any stillbirth, compared with those without stillbirth (aHR, 1.77). Fatal stroke risk also was higher in women with any stillbirth, compared with those without, and this risk increased with the number of stillbirths (HR, 0.97 and HR, 1.26 for those with one stillbirth and two or more, respectively).
“The increased risk of stroke associated with infertility or recurrent stillbirths was mainly driven by a single subtype of stroke (nonfatal ischemic stroke or fatal hemorrhagic stroke, respectively), whereas the risk of stroke associated with recurrent miscarriages was driven by both subtypes,” the researchers wrote.
The researchers cited endothelial dysfunction as a potential underlying mechanism for increased stroke risk associated with pregnancy complications. “Endothelial dysfunction might lead to pregnancy loss through placentation-related defects, persist after a complicated pregnancy, and contribute to the development of stroke through reduced vasodilation, proinflammatory status, and prothrombic properties,” and that history of recurrent pregnancy loss might be a female-specific risk factor for stroke.
To mitigate this risk, they advised early monitoring of women with a history of recurrent miscarriages and stillbirths for stroke risk factors such as high blood pressure, blood sugar levels, and lipid levels.
The study findings were limited by several factors including the use of questionnaires to collect information on infertility, miscarriage, and stillbirth, and the potential variation in definitions of infertility, miscarriage, and stillbirth across the included studies, and a lack of data on the effect of different causes or treatments based on reproductive histories, the researchers noted. Other limitations include incomplete data on stroke subtypes and inability to adjust for all covariates such as thyroid disorders and endometriosis. However, the results were strengthened by the large study size and geographically and racially diverse population, extend the current knowledge on associations between infertility, miscarriage, and stillbirth with stroke, and highlight the need for more research on underlying mechanisms.
Data support gender-specific stroke risk stratification
“Studies that seek to understand gender differences and disparities in adverse outcomes, such as stroke risk, are extremely important given that women historically were excluded from research studies,” Catherine M. Albright, MD, of the University of Washington, Seattle, said in an interview. “By doing these studies, we are able to better risk stratify people in order to better predict and modify risks,” added Dr. Albright, who was not involved in the current study.
“It is well known than adverse pregnancy outcomes such as hypertension in pregnancy, fetal growth restriction, and preterm birth, lead to increased risk of cardiovascular disease and stroke later in life, so the general findings of an association between other adverse reproductive and pregnancy outcomes leads to increased stroke risk are not surprising,” she said.
“The take-home message is that outcomes for pregnancy really do provide a window to future health,” said Dr. Albright. “For clinicians, especially non-ob.gyns., knowing a complete pregnancy history for any new patient is important and can help risk-stratify patients, especially as we continue to gain knowledge like what is shown in this study.”
However, “this study did not evaluate why individual patients may have had infertility, recurrent pregnancy loss, or stillbirth, so research to look further into this association to determine if there is an underlying medical condition that could be treated and therefore possibly reduce both pregnancy complications and future stroke risks would be important,” Dr. Albright noted.
The study was supported by the Australian National Health and Medical Research Council Centres of Research Excellence; one corresponding author was supported by an Australian National Health and Medical Research Council Investigator grant. The researchers had no financial conflicts to disclose. Dr. Albright had no financial conflicts to disclose.
Infertility, pregnancy loss, and stillbirth increased women’s later risk of both nonfatal and fatal stroke, based on data from more than 600,000 women.
“To date, multiple studies have generated an expanding body of evidence on the association between pregnancy complications (e.g., gestational diabetes and preeclampsia) and the long-term risk of stroke, but studies on associations with infertility, miscarriage, or stillbirth have produced mixed evidence,” Chen Liang, a PhD candidate at the University of Queensland, Brisbane, Australia, and colleagues wrote.
In a study published in the BMJ, the researchers reviewed data from eight observational cohort studies across seven countries (Australia, China, Japan, the Netherlands, Sweden, the United Kingdom, and the United States). The participants were part of the InterLACE (International Collaboration for a Life Course Approach to Reproductive Health and Chronic Disease Events) consortium established in 2021. Most observational studies included in the analysis began between 1990 and 2000.
The study population included 618,851 women aged 32-73 years at baseline for whom data on infertility, miscarriage, or stillbirth, were available. The primary outcome was the association of infertility, recurrent miscarriage, and stillbirth with risk of first fatal or nonfatal stroke, and the results were further stratified by subtype. Stroke was identified through self-reports, linked hospital data, national patient registers, or death registry data. Baseline was defined as the first incidence of infertility, miscarriage, or stillbirth. The exception was the National Survey of Health and Development, a British birth cohort started in 1946, that collected data retrospectively.
The median follow-up period was 13 years for nonfatal stroke and 9.4 years for fatal stroke.
Overall, 17.2%, 16.6%, and 4.6% of the women experienced infertility, miscarriage, and stillbirth, respectively.
Women with a history of infertility had a significantly higher nonfatal stroke risk, compared with those without infertility (hazard ratio, 1.14). Further analysis by stroke subtypes showed an increased association between miscarriage and ischemic stroke (HR, 1.15).
Those with a history of miscarriage also had an increased risk of nonfatal stroke, compared with those without miscarriages (HR, 1.11). In the miscarriage group, the risk of stroke increased with the number of miscarriages, with adjusted HRs of 1.07, 1.12, and 1.35 for women with one, two, and three or more miscarriages, respectively. When stratified by stroke subtype, women with three or more miscarriages were more likely than women with no miscarriages to experience ischemic and hemorrhagic nonfatal strokes.
Associations were similar between miscarriage history and fatal stroke risk. Women with one, two, and three or more miscarriages had increased risk of fatal stroke, compared with those with no miscarriages (aHR, 1.08, 1.26, and 1.82, respectively, and women with three or more miscarriages had a higher risk of ischemic and hemorrhagic stroke (aHR, 1.83 and 1.84, respectively).
Women with a history of stillbirth had an approximately 31% increased risk of nonfatal stroke, compared with those with no history of stillbirth, with aHRs similar for single and recurrent stillbirths (1.32 and 1.29, respectively). Ischemic nonfatal stroke risk was higher in women with any stillbirth, compared with those without stillbirth (aHR, 1.77). Fatal stroke risk also was higher in women with any stillbirth, compared with those without, and this risk increased with the number of stillbirths (HR, 0.97 and HR, 1.26 for those with one stillbirth and two or more, respectively).
“The increased risk of stroke associated with infertility or recurrent stillbirths was mainly driven by a single subtype of stroke (nonfatal ischemic stroke or fatal hemorrhagic stroke, respectively), whereas the risk of stroke associated with recurrent miscarriages was driven by both subtypes,” the researchers wrote.
The researchers cited endothelial dysfunction as a potential underlying mechanism for increased stroke risk associated with pregnancy complications. “Endothelial dysfunction might lead to pregnancy loss through placentation-related defects, persist after a complicated pregnancy, and contribute to the development of stroke through reduced vasodilation, proinflammatory status, and prothrombic properties,” and that history of recurrent pregnancy loss might be a female-specific risk factor for stroke.
To mitigate this risk, they advised early monitoring of women with a history of recurrent miscarriages and stillbirths for stroke risk factors such as high blood pressure, blood sugar levels, and lipid levels.
The study findings were limited by several factors including the use of questionnaires to collect information on infertility, miscarriage, and stillbirth, and the potential variation in definitions of infertility, miscarriage, and stillbirth across the included studies, and a lack of data on the effect of different causes or treatments based on reproductive histories, the researchers noted. Other limitations include incomplete data on stroke subtypes and inability to adjust for all covariates such as thyroid disorders and endometriosis. However, the results were strengthened by the large study size and geographically and racially diverse population, extend the current knowledge on associations between infertility, miscarriage, and stillbirth with stroke, and highlight the need for more research on underlying mechanisms.
Data support gender-specific stroke risk stratification
“Studies that seek to understand gender differences and disparities in adverse outcomes, such as stroke risk, are extremely important given that women historically were excluded from research studies,” Catherine M. Albright, MD, of the University of Washington, Seattle, said in an interview. “By doing these studies, we are able to better risk stratify people in order to better predict and modify risks,” added Dr. Albright, who was not involved in the current study.
“It is well known than adverse pregnancy outcomes such as hypertension in pregnancy, fetal growth restriction, and preterm birth, lead to increased risk of cardiovascular disease and stroke later in life, so the general findings of an association between other adverse reproductive and pregnancy outcomes leads to increased stroke risk are not surprising,” she said.
“The take-home message is that outcomes for pregnancy really do provide a window to future health,” said Dr. Albright. “For clinicians, especially non-ob.gyns., knowing a complete pregnancy history for any new patient is important and can help risk-stratify patients, especially as we continue to gain knowledge like what is shown in this study.”
However, “this study did not evaluate why individual patients may have had infertility, recurrent pregnancy loss, or stillbirth, so research to look further into this association to determine if there is an underlying medical condition that could be treated and therefore possibly reduce both pregnancy complications and future stroke risks would be important,” Dr. Albright noted.
The study was supported by the Australian National Health and Medical Research Council Centres of Research Excellence; one corresponding author was supported by an Australian National Health and Medical Research Council Investigator grant. The researchers had no financial conflicts to disclose. Dr. Albright had no financial conflicts to disclose.
Infertility, pregnancy loss, and stillbirth increased women’s later risk of both nonfatal and fatal stroke, based on data from more than 600,000 women.
“To date, multiple studies have generated an expanding body of evidence on the association between pregnancy complications (e.g., gestational diabetes and preeclampsia) and the long-term risk of stroke, but studies on associations with infertility, miscarriage, or stillbirth have produced mixed evidence,” Chen Liang, a PhD candidate at the University of Queensland, Brisbane, Australia, and colleagues wrote.
In a study published in the BMJ, the researchers reviewed data from eight observational cohort studies across seven countries (Australia, China, Japan, the Netherlands, Sweden, the United Kingdom, and the United States). The participants were part of the InterLACE (International Collaboration for a Life Course Approach to Reproductive Health and Chronic Disease Events) consortium established in 2021. Most observational studies included in the analysis began between 1990 and 2000.
The study population included 618,851 women aged 32-73 years at baseline for whom data on infertility, miscarriage, or stillbirth, were available. The primary outcome was the association of infertility, recurrent miscarriage, and stillbirth with risk of first fatal or nonfatal stroke, and the results were further stratified by subtype. Stroke was identified through self-reports, linked hospital data, national patient registers, or death registry data. Baseline was defined as the first incidence of infertility, miscarriage, or stillbirth. The exception was the National Survey of Health and Development, a British birth cohort started in 1946, that collected data retrospectively.
The median follow-up period was 13 years for nonfatal stroke and 9.4 years for fatal stroke.
Overall, 17.2%, 16.6%, and 4.6% of the women experienced infertility, miscarriage, and stillbirth, respectively.
Women with a history of infertility had a significantly higher nonfatal stroke risk, compared with those without infertility (hazard ratio, 1.14). Further analysis by stroke subtypes showed an increased association between miscarriage and ischemic stroke (HR, 1.15).
Those with a history of miscarriage also had an increased risk of nonfatal stroke, compared with those without miscarriages (HR, 1.11). In the miscarriage group, the risk of stroke increased with the number of miscarriages, with adjusted HRs of 1.07, 1.12, and 1.35 for women with one, two, and three or more miscarriages, respectively. When stratified by stroke subtype, women with three or more miscarriages were more likely than women with no miscarriages to experience ischemic and hemorrhagic nonfatal strokes.
Associations were similar between miscarriage history and fatal stroke risk. Women with one, two, and three or more miscarriages had increased risk of fatal stroke, compared with those with no miscarriages (aHR, 1.08, 1.26, and 1.82, respectively, and women with three or more miscarriages had a higher risk of ischemic and hemorrhagic stroke (aHR, 1.83 and 1.84, respectively).
Women with a history of stillbirth had an approximately 31% increased risk of nonfatal stroke, compared with those with no history of stillbirth, with aHRs similar for single and recurrent stillbirths (1.32 and 1.29, respectively). Ischemic nonfatal stroke risk was higher in women with any stillbirth, compared with those without stillbirth (aHR, 1.77). Fatal stroke risk also was higher in women with any stillbirth, compared with those without, and this risk increased with the number of stillbirths (HR, 0.97 and HR, 1.26 for those with one stillbirth and two or more, respectively).
“The increased risk of stroke associated with infertility or recurrent stillbirths was mainly driven by a single subtype of stroke (nonfatal ischemic stroke or fatal hemorrhagic stroke, respectively), whereas the risk of stroke associated with recurrent miscarriages was driven by both subtypes,” the researchers wrote.
The researchers cited endothelial dysfunction as a potential underlying mechanism for increased stroke risk associated with pregnancy complications. “Endothelial dysfunction might lead to pregnancy loss through placentation-related defects, persist after a complicated pregnancy, and contribute to the development of stroke through reduced vasodilation, proinflammatory status, and prothrombic properties,” and that history of recurrent pregnancy loss might be a female-specific risk factor for stroke.
To mitigate this risk, they advised early monitoring of women with a history of recurrent miscarriages and stillbirths for stroke risk factors such as high blood pressure, blood sugar levels, and lipid levels.
The study findings were limited by several factors including the use of questionnaires to collect information on infertility, miscarriage, and stillbirth, and the potential variation in definitions of infertility, miscarriage, and stillbirth across the included studies, and a lack of data on the effect of different causes or treatments based on reproductive histories, the researchers noted. Other limitations include incomplete data on stroke subtypes and inability to adjust for all covariates such as thyroid disorders and endometriosis. However, the results were strengthened by the large study size and geographically and racially diverse population, extend the current knowledge on associations between infertility, miscarriage, and stillbirth with stroke, and highlight the need for more research on underlying mechanisms.
Data support gender-specific stroke risk stratification
“Studies that seek to understand gender differences and disparities in adverse outcomes, such as stroke risk, are extremely important given that women historically were excluded from research studies,” Catherine M. Albright, MD, of the University of Washington, Seattle, said in an interview. “By doing these studies, we are able to better risk stratify people in order to better predict and modify risks,” added Dr. Albright, who was not involved in the current study.
“It is well known than adverse pregnancy outcomes such as hypertension in pregnancy, fetal growth restriction, and preterm birth, lead to increased risk of cardiovascular disease and stroke later in life, so the general findings of an association between other adverse reproductive and pregnancy outcomes leads to increased stroke risk are not surprising,” she said.
“The take-home message is that outcomes for pregnancy really do provide a window to future health,” said Dr. Albright. “For clinicians, especially non-ob.gyns., knowing a complete pregnancy history for any new patient is important and can help risk-stratify patients, especially as we continue to gain knowledge like what is shown in this study.”
However, “this study did not evaluate why individual patients may have had infertility, recurrent pregnancy loss, or stillbirth, so research to look further into this association to determine if there is an underlying medical condition that could be treated and therefore possibly reduce both pregnancy complications and future stroke risks would be important,” Dr. Albright noted.
The study was supported by the Australian National Health and Medical Research Council Centres of Research Excellence; one corresponding author was supported by an Australian National Health and Medical Research Council Investigator grant. The researchers had no financial conflicts to disclose. Dr. Albright had no financial conflicts to disclose.
FROM THE BMJ
‘Can I survive without payments from insurers?’
It took Michael Golden, MD, 5 years to decide to switch to a concierge practice, in which patients pay a monthly or annual fee for more personalized care. Dr. Golden, an internist in Beverly, Mass., changed course in 2021, during the COVID-19 pandemic.
“I’m not sure why I hesitated for so long,” said Dr. Golden.
But taking the plunge is a big step that they sometimes put off for years.
“The main factors for waiting are fear, uncertainty, and doubt,” said Leigh “Jack” Forbush, DO, a family physician who runs a DPC practice in Hampden, Maine, and mentors doctors contemplating the switch.
According to Dr. Forbush, the critical questions doctors ask themselves are, “Will I be able to find enough paying patients?” and – in the case of DPC practices, which cancel insurance – “Can I live without the money I get from insurers?”
Terry Bauer, CEO of Specialdocs Consultants in Highland Park, Ill., which helps doctors move to a concierge practice, said many of his clients put off the decision for as long as 15 years.
“Clients became progressively worn out – or even burnt out – by the demands of fee-for-service medicine,” said Dr. Bauer. “For women, the tipping point can be when their kids ask, ‘Mom, do you like your job better than me?’ For men, it may be more about feeling tired and unsatisfied with their work.”
But once these doctors make the switch, it’s with all their heart. “A client recently told me that if he couldn’t open a concierge practice, he might have to quit medicine,” Dr. Bauer said. “And he’s only 51.”
Few doctors regret switching
A 2020 survey of DPC physicians for the Society of Actuaries found that 99% reported having better or much better overall personal and professional satisfaction.
Retainer-based physicians report feeling much more relaxed after they start a concierge practice. On many workdays, Dr. Golden takes a walk on a trail in the woods behind his office. “That’s something I couldn’t do before,” he said. “And I go to my kids’ soccer games. I’m able to be present in their lives now.”
Since retainer-based doctors have markedly fewer patients, they can form personal relationships with each one. When Dr. Golden switched, he “went from having a couple of thousand patients to a few hundred,” he said.
“I know each patient now,” said Dorothy Cohen Serna, MD, an internist in Cypress, Tex., who moved to concierge in 2017. “I don’t need to look at their chart to know who they are.”
Dr. Serna said patients’ close relationship with her helped them get through the worst months of the pandemic. “They were scared, depressed, and concerned, and they needed a lot of individual attention,” she said.
Because they see fewer patients, concierge doctors can lengthen appointment times to about 30 minutes – or longer, if necessary. They no longer have a problem answering patients’ “doorknob questions” – wholly new concerns brought up at the end of the visit.
“The appointment might be for a sprained ankle, and then the patient might mention they haven’t been sleeping well,” Dr. Golden said. “I have time to talk about that without worrying that my schedule is getting backed up.”
Why patients sign up
Retainer-based practices are still an exotic concept in many areas, but patients are beginning to understand the value, said Shalini Kaneriya, MD, an internist in Herndon, Va,, who switched her practice to concierge in 2018.
Several hundred patients followed her into her new practice because “people realized their care would be better if they had a concierge doctor,” she said. Two years ago, partly because of growing demand, she recruited another physician as an associate.
“People want a relationship with their doctor,” Dr. Serna added. “It’s hard to provide that in a regular practice.”
Todd Granger, MD, an internist who opened a DPC practice in Chapel Hill, N.C., in 2016, said new patients often mention feeling rushed through appointments with their previous doctors. Also, “it’s hard to get to see a doctor around here.”
Scott Bernstein, MD, an internist who runs a DPC practice in Scottsdale, Ariz., said he can arrange to have patients see specialists much faster than if they try to make appointments on their own. “I personally call specialists and then prep my patients on how to deal with the appointment,” he said.
Retainer-based practices tend to have a greater number of older and chronically ill patients, but they also attract patients who need less care. “The healthier patients find value in our proactive approach to prevention and wellness,” Dr. Serna said.
Some concierge physicians charge higher fees to patients who need more care, but many decide this is too complicated and charge everyone the same fee. Dr. Granger said he initially had a variable fee schedule, but when some lower-paying patients began to need more visits, he had to consider charging them extra. “Now I basically have just one fee,” he said.
Not a good fit for many physicians
Dr. Bauer said a lot of physicians are interested in retainer-based practice, but many of them might not make the income they had hoped for. Specialdocs interviews physicians who inquire about the model and ultimately doesn’t contract with 80% of them, Dr. Bauer said.
To be able to sign up and retain enough patients, the doctor’s attitude is important. “You have to be driven by the desire to go deep with patients -- to work hard with them and deal with their issues,” said Erika Bliss, MD, who runs a DPC practice in Seattle.
Dr. Bernstein said retainer-based physicians have to be interested in lifestyle issues, such as diet, exercise, and sleep. “I spend a lot of time dealing with issues like how to incorporate physical activity into daily routines,” he said. “Some doctors wouldn’t enjoy doing that.”
Also, concierge physicians have to be available all the time. “Patients have my cell phone number,” Dr. Granger said. “They could call in the middle of the night, but they usually don’t.”
To ensure that they get some time off, many concierge physicians have partners. Dr. Bernstein and another DPC doctor maintain separate practices but cover for each other. Each takes every other weekend off plus 6 weeks every year.
Can you attract enough patients?
A key challenge is finding enough patients to sustain a concierge practice. Planning the switch involves setting a target number of patients needed for the doctor to make a decent income after paying practice expenses. For example, a doctor charging $300 a month to 250 patients would gross $900,000 per year, and then pay practice expenses from that.
Attracting the target number of patients can take months or even years. After almost 6 years, Dr. Granger said, he has around 240 patients ― well below his target number of 440.
Partly because the practice model is not well known in North Carolina, Dr. Granger set his fee very low, at $60 a month, then raised it to $75. That means his practice has been grossing just $216,000 a year. But he is not about to give up. He plans to raise his fee in July and hopes that word of mouth will add more patients.
If physicians cannot earn enough in their concierge practice, Dr. Bauer said, they may moonlight at a local hospital or work for a telemedicine company. He hasn’t heard of physicians closing their concierge practice and returning to their previous practice model. “They didn’t like what they were doing before,” he said.
Opening up to lower-income patients
Dr. Granger’s $75 monthly fee is an example of how retainer-based medicine has transformed itself from a gold-plated service for rich people to a service that middle-class and even lower-income people can afford. DPC practices like Dr. Granger’s have dramatically lowered expenses by cutting out the need to bill insurance companies. Some DPC practices further reduce expenses by not having any staff and by renting out office space.
Dr. Forbush’s Pine Tree State patients are mostly blue-collar workers – electricians, plumbers, people who work in small businesses. He charges them $150 a month, which most patients who don’t have health insurance can afford. He said three-quarters of his patients lack health insurance, although some have back-up finances, such as health savings accounts.
Since his patients have to pay out of pocket for tests and specialists, Dr. Forbush keeps referrals in check by handling many problems himself. “Since I have more time to spend with the patient, I can often work out issues that other doctors might ask specialists to deal with,” he said.
He has learned some dermatologic procedures. “There are plenty of things I can handle on my own,” he said.
Dr. Granger adds that by examining patients during longer appointments, expensive diagnostic exams are not always necessary.
The challenges for this model
Many experts warn that retainer-based practices won’t work for doctors who want to leave employment or for doctors fresh out of residency. Not having your own patients to bring into the new practice is a big minus, because this is the best way to start the new practice.
Still, there are other ways to find patients. Dr. Bauer said physicians can advertise online, make themselves known by giving speeches in the community, or contract with small employers to treat their workers.
Dr. Bauer said some of his clients were employed physicians, and he thinks they will become a bigger factor now that fewer doctors remain in private practice. The chief barrier for employed physicians is the restrictive covenant that prevents them from setting up a practice nearby. But Dr. Bauer said some employers are willing to waive restrictive covenants for retainer-based doctors.
New physicians are also adopting the concierge model. Dr. Forbush said physicians straight out of residency have set up DPC practices in Maine. They signed up patients for their new practices even before they graduated, he said.
Retainer-based medicine is still mainly limited to primary care physicians, but according to Dr. Bauer, it can also work for specialists who have long-term relationships with patients, such as cardiologists, ob.gyns., rheumatologists, neurologists, and endocrinologists.
No going back
Most doctors who make the switch to retainer-based practice understand that there’s likely no going back. When Dr. Bernstein switched, he announced the change to patients and canceled insurance contracts. “It was make or break,” he said. “I had no parachute.”
A version of this article first appeared on Medscape.com.
It took Michael Golden, MD, 5 years to decide to switch to a concierge practice, in which patients pay a monthly or annual fee for more personalized care. Dr. Golden, an internist in Beverly, Mass., changed course in 2021, during the COVID-19 pandemic.
“I’m not sure why I hesitated for so long,” said Dr. Golden.
But taking the plunge is a big step that they sometimes put off for years.
“The main factors for waiting are fear, uncertainty, and doubt,” said Leigh “Jack” Forbush, DO, a family physician who runs a DPC practice in Hampden, Maine, and mentors doctors contemplating the switch.
According to Dr. Forbush, the critical questions doctors ask themselves are, “Will I be able to find enough paying patients?” and – in the case of DPC practices, which cancel insurance – “Can I live without the money I get from insurers?”
Terry Bauer, CEO of Specialdocs Consultants in Highland Park, Ill., which helps doctors move to a concierge practice, said many of his clients put off the decision for as long as 15 years.
“Clients became progressively worn out – or even burnt out – by the demands of fee-for-service medicine,” said Dr. Bauer. “For women, the tipping point can be when their kids ask, ‘Mom, do you like your job better than me?’ For men, it may be more about feeling tired and unsatisfied with their work.”
But once these doctors make the switch, it’s with all their heart. “A client recently told me that if he couldn’t open a concierge practice, he might have to quit medicine,” Dr. Bauer said. “And he’s only 51.”
Few doctors regret switching
A 2020 survey of DPC physicians for the Society of Actuaries found that 99% reported having better or much better overall personal and professional satisfaction.
Retainer-based physicians report feeling much more relaxed after they start a concierge practice. On many workdays, Dr. Golden takes a walk on a trail in the woods behind his office. “That’s something I couldn’t do before,” he said. “And I go to my kids’ soccer games. I’m able to be present in their lives now.”
Since retainer-based doctors have markedly fewer patients, they can form personal relationships with each one. When Dr. Golden switched, he “went from having a couple of thousand patients to a few hundred,” he said.
“I know each patient now,” said Dorothy Cohen Serna, MD, an internist in Cypress, Tex., who moved to concierge in 2017. “I don’t need to look at their chart to know who they are.”
Dr. Serna said patients’ close relationship with her helped them get through the worst months of the pandemic. “They were scared, depressed, and concerned, and they needed a lot of individual attention,” she said.
Because they see fewer patients, concierge doctors can lengthen appointment times to about 30 minutes – or longer, if necessary. They no longer have a problem answering patients’ “doorknob questions” – wholly new concerns brought up at the end of the visit.
“The appointment might be for a sprained ankle, and then the patient might mention they haven’t been sleeping well,” Dr. Golden said. “I have time to talk about that without worrying that my schedule is getting backed up.”
Why patients sign up
Retainer-based practices are still an exotic concept in many areas, but patients are beginning to understand the value, said Shalini Kaneriya, MD, an internist in Herndon, Va,, who switched her practice to concierge in 2018.
Several hundred patients followed her into her new practice because “people realized their care would be better if they had a concierge doctor,” she said. Two years ago, partly because of growing demand, she recruited another physician as an associate.
“People want a relationship with their doctor,” Dr. Serna added. “It’s hard to provide that in a regular practice.”
Todd Granger, MD, an internist who opened a DPC practice in Chapel Hill, N.C., in 2016, said new patients often mention feeling rushed through appointments with their previous doctors. Also, “it’s hard to get to see a doctor around here.”
Scott Bernstein, MD, an internist who runs a DPC practice in Scottsdale, Ariz., said he can arrange to have patients see specialists much faster than if they try to make appointments on their own. “I personally call specialists and then prep my patients on how to deal with the appointment,” he said.
Retainer-based practices tend to have a greater number of older and chronically ill patients, but they also attract patients who need less care. “The healthier patients find value in our proactive approach to prevention and wellness,” Dr. Serna said.
Some concierge physicians charge higher fees to patients who need more care, but many decide this is too complicated and charge everyone the same fee. Dr. Granger said he initially had a variable fee schedule, but when some lower-paying patients began to need more visits, he had to consider charging them extra. “Now I basically have just one fee,” he said.
Not a good fit for many physicians
Dr. Bauer said a lot of physicians are interested in retainer-based practice, but many of them might not make the income they had hoped for. Specialdocs interviews physicians who inquire about the model and ultimately doesn’t contract with 80% of them, Dr. Bauer said.
To be able to sign up and retain enough patients, the doctor’s attitude is important. “You have to be driven by the desire to go deep with patients -- to work hard with them and deal with their issues,” said Erika Bliss, MD, who runs a DPC practice in Seattle.
Dr. Bernstein said retainer-based physicians have to be interested in lifestyle issues, such as diet, exercise, and sleep. “I spend a lot of time dealing with issues like how to incorporate physical activity into daily routines,” he said. “Some doctors wouldn’t enjoy doing that.”
Also, concierge physicians have to be available all the time. “Patients have my cell phone number,” Dr. Granger said. “They could call in the middle of the night, but they usually don’t.”
To ensure that they get some time off, many concierge physicians have partners. Dr. Bernstein and another DPC doctor maintain separate practices but cover for each other. Each takes every other weekend off plus 6 weeks every year.
Can you attract enough patients?
A key challenge is finding enough patients to sustain a concierge practice. Planning the switch involves setting a target number of patients needed for the doctor to make a decent income after paying practice expenses. For example, a doctor charging $300 a month to 250 patients would gross $900,000 per year, and then pay practice expenses from that.
Attracting the target number of patients can take months or even years. After almost 6 years, Dr. Granger said, he has around 240 patients ― well below his target number of 440.
Partly because the practice model is not well known in North Carolina, Dr. Granger set his fee very low, at $60 a month, then raised it to $75. That means his practice has been grossing just $216,000 a year. But he is not about to give up. He plans to raise his fee in July and hopes that word of mouth will add more patients.
If physicians cannot earn enough in their concierge practice, Dr. Bauer said, they may moonlight at a local hospital or work for a telemedicine company. He hasn’t heard of physicians closing their concierge practice and returning to their previous practice model. “They didn’t like what they were doing before,” he said.
Opening up to lower-income patients
Dr. Granger’s $75 monthly fee is an example of how retainer-based medicine has transformed itself from a gold-plated service for rich people to a service that middle-class and even lower-income people can afford. DPC practices like Dr. Granger’s have dramatically lowered expenses by cutting out the need to bill insurance companies. Some DPC practices further reduce expenses by not having any staff and by renting out office space.
Dr. Forbush’s Pine Tree State patients are mostly blue-collar workers – electricians, plumbers, people who work in small businesses. He charges them $150 a month, which most patients who don’t have health insurance can afford. He said three-quarters of his patients lack health insurance, although some have back-up finances, such as health savings accounts.
Since his patients have to pay out of pocket for tests and specialists, Dr. Forbush keeps referrals in check by handling many problems himself. “Since I have more time to spend with the patient, I can often work out issues that other doctors might ask specialists to deal with,” he said.
He has learned some dermatologic procedures. “There are plenty of things I can handle on my own,” he said.
Dr. Granger adds that by examining patients during longer appointments, expensive diagnostic exams are not always necessary.
The challenges for this model
Many experts warn that retainer-based practices won’t work for doctors who want to leave employment or for doctors fresh out of residency. Not having your own patients to bring into the new practice is a big minus, because this is the best way to start the new practice.
Still, there are other ways to find patients. Dr. Bauer said physicians can advertise online, make themselves known by giving speeches in the community, or contract with small employers to treat their workers.
Dr. Bauer said some of his clients were employed physicians, and he thinks they will become a bigger factor now that fewer doctors remain in private practice. The chief barrier for employed physicians is the restrictive covenant that prevents them from setting up a practice nearby. But Dr. Bauer said some employers are willing to waive restrictive covenants for retainer-based doctors.
New physicians are also adopting the concierge model. Dr. Forbush said physicians straight out of residency have set up DPC practices in Maine. They signed up patients for their new practices even before they graduated, he said.
Retainer-based medicine is still mainly limited to primary care physicians, but according to Dr. Bauer, it can also work for specialists who have long-term relationships with patients, such as cardiologists, ob.gyns., rheumatologists, neurologists, and endocrinologists.
No going back
Most doctors who make the switch to retainer-based practice understand that there’s likely no going back. When Dr. Bernstein switched, he announced the change to patients and canceled insurance contracts. “It was make or break,” he said. “I had no parachute.”
A version of this article first appeared on Medscape.com.
It took Michael Golden, MD, 5 years to decide to switch to a concierge practice, in which patients pay a monthly or annual fee for more personalized care. Dr. Golden, an internist in Beverly, Mass., changed course in 2021, during the COVID-19 pandemic.
“I’m not sure why I hesitated for so long,” said Dr. Golden.
But taking the plunge is a big step that they sometimes put off for years.
“The main factors for waiting are fear, uncertainty, and doubt,” said Leigh “Jack” Forbush, DO, a family physician who runs a DPC practice in Hampden, Maine, and mentors doctors contemplating the switch.
According to Dr. Forbush, the critical questions doctors ask themselves are, “Will I be able to find enough paying patients?” and – in the case of DPC practices, which cancel insurance – “Can I live without the money I get from insurers?”
Terry Bauer, CEO of Specialdocs Consultants in Highland Park, Ill., which helps doctors move to a concierge practice, said many of his clients put off the decision for as long as 15 years.
“Clients became progressively worn out – or even burnt out – by the demands of fee-for-service medicine,” said Dr. Bauer. “For women, the tipping point can be when their kids ask, ‘Mom, do you like your job better than me?’ For men, it may be more about feeling tired and unsatisfied with their work.”
But once these doctors make the switch, it’s with all their heart. “A client recently told me that if he couldn’t open a concierge practice, he might have to quit medicine,” Dr. Bauer said. “And he’s only 51.”
Few doctors regret switching
A 2020 survey of DPC physicians for the Society of Actuaries found that 99% reported having better or much better overall personal and professional satisfaction.
Retainer-based physicians report feeling much more relaxed after they start a concierge practice. On many workdays, Dr. Golden takes a walk on a trail in the woods behind his office. “That’s something I couldn’t do before,” he said. “And I go to my kids’ soccer games. I’m able to be present in their lives now.”
Since retainer-based doctors have markedly fewer patients, they can form personal relationships with each one. When Dr. Golden switched, he “went from having a couple of thousand patients to a few hundred,” he said.
“I know each patient now,” said Dorothy Cohen Serna, MD, an internist in Cypress, Tex., who moved to concierge in 2017. “I don’t need to look at their chart to know who they are.”
Dr. Serna said patients’ close relationship with her helped them get through the worst months of the pandemic. “They were scared, depressed, and concerned, and they needed a lot of individual attention,” she said.
Because they see fewer patients, concierge doctors can lengthen appointment times to about 30 minutes – or longer, if necessary. They no longer have a problem answering patients’ “doorknob questions” – wholly new concerns brought up at the end of the visit.
“The appointment might be for a sprained ankle, and then the patient might mention they haven’t been sleeping well,” Dr. Golden said. “I have time to talk about that without worrying that my schedule is getting backed up.”
Why patients sign up
Retainer-based practices are still an exotic concept in many areas, but patients are beginning to understand the value, said Shalini Kaneriya, MD, an internist in Herndon, Va,, who switched her practice to concierge in 2018.
Several hundred patients followed her into her new practice because “people realized their care would be better if they had a concierge doctor,” she said. Two years ago, partly because of growing demand, she recruited another physician as an associate.
“People want a relationship with their doctor,” Dr. Serna added. “It’s hard to provide that in a regular practice.”
Todd Granger, MD, an internist who opened a DPC practice in Chapel Hill, N.C., in 2016, said new patients often mention feeling rushed through appointments with their previous doctors. Also, “it’s hard to get to see a doctor around here.”
Scott Bernstein, MD, an internist who runs a DPC practice in Scottsdale, Ariz., said he can arrange to have patients see specialists much faster than if they try to make appointments on their own. “I personally call specialists and then prep my patients on how to deal with the appointment,” he said.
Retainer-based practices tend to have a greater number of older and chronically ill patients, but they also attract patients who need less care. “The healthier patients find value in our proactive approach to prevention and wellness,” Dr. Serna said.
Some concierge physicians charge higher fees to patients who need more care, but many decide this is too complicated and charge everyone the same fee. Dr. Granger said he initially had a variable fee schedule, but when some lower-paying patients began to need more visits, he had to consider charging them extra. “Now I basically have just one fee,” he said.
Not a good fit for many physicians
Dr. Bauer said a lot of physicians are interested in retainer-based practice, but many of them might not make the income they had hoped for. Specialdocs interviews physicians who inquire about the model and ultimately doesn’t contract with 80% of them, Dr. Bauer said.
To be able to sign up and retain enough patients, the doctor’s attitude is important. “You have to be driven by the desire to go deep with patients -- to work hard with them and deal with their issues,” said Erika Bliss, MD, who runs a DPC practice in Seattle.
Dr. Bernstein said retainer-based physicians have to be interested in lifestyle issues, such as diet, exercise, and sleep. “I spend a lot of time dealing with issues like how to incorporate physical activity into daily routines,” he said. “Some doctors wouldn’t enjoy doing that.”
Also, concierge physicians have to be available all the time. “Patients have my cell phone number,” Dr. Granger said. “They could call in the middle of the night, but they usually don’t.”
To ensure that they get some time off, many concierge physicians have partners. Dr. Bernstein and another DPC doctor maintain separate practices but cover for each other. Each takes every other weekend off plus 6 weeks every year.
Can you attract enough patients?
A key challenge is finding enough patients to sustain a concierge practice. Planning the switch involves setting a target number of patients needed for the doctor to make a decent income after paying practice expenses. For example, a doctor charging $300 a month to 250 patients would gross $900,000 per year, and then pay practice expenses from that.
Attracting the target number of patients can take months or even years. After almost 6 years, Dr. Granger said, he has around 240 patients ― well below his target number of 440.
Partly because the practice model is not well known in North Carolina, Dr. Granger set his fee very low, at $60 a month, then raised it to $75. That means his practice has been grossing just $216,000 a year. But he is not about to give up. He plans to raise his fee in July and hopes that word of mouth will add more patients.
If physicians cannot earn enough in their concierge practice, Dr. Bauer said, they may moonlight at a local hospital or work for a telemedicine company. He hasn’t heard of physicians closing their concierge practice and returning to their previous practice model. “They didn’t like what they were doing before,” he said.
Opening up to lower-income patients
Dr. Granger’s $75 monthly fee is an example of how retainer-based medicine has transformed itself from a gold-plated service for rich people to a service that middle-class and even lower-income people can afford. DPC practices like Dr. Granger’s have dramatically lowered expenses by cutting out the need to bill insurance companies. Some DPC practices further reduce expenses by not having any staff and by renting out office space.
Dr. Forbush’s Pine Tree State patients are mostly blue-collar workers – electricians, plumbers, people who work in small businesses. He charges them $150 a month, which most patients who don’t have health insurance can afford. He said three-quarters of his patients lack health insurance, although some have back-up finances, such as health savings accounts.
Since his patients have to pay out of pocket for tests and specialists, Dr. Forbush keeps referrals in check by handling many problems himself. “Since I have more time to spend with the patient, I can often work out issues that other doctors might ask specialists to deal with,” he said.
He has learned some dermatologic procedures. “There are plenty of things I can handle on my own,” he said.
Dr. Granger adds that by examining patients during longer appointments, expensive diagnostic exams are not always necessary.
The challenges for this model
Many experts warn that retainer-based practices won’t work for doctors who want to leave employment or for doctors fresh out of residency. Not having your own patients to bring into the new practice is a big minus, because this is the best way to start the new practice.
Still, there are other ways to find patients. Dr. Bauer said physicians can advertise online, make themselves known by giving speeches in the community, or contract with small employers to treat their workers.
Dr. Bauer said some of his clients were employed physicians, and he thinks they will become a bigger factor now that fewer doctors remain in private practice. The chief barrier for employed physicians is the restrictive covenant that prevents them from setting up a practice nearby. But Dr. Bauer said some employers are willing to waive restrictive covenants for retainer-based doctors.
New physicians are also adopting the concierge model. Dr. Forbush said physicians straight out of residency have set up DPC practices in Maine. They signed up patients for their new practices even before they graduated, he said.
Retainer-based medicine is still mainly limited to primary care physicians, but according to Dr. Bauer, it can also work for specialists who have long-term relationships with patients, such as cardiologists, ob.gyns., rheumatologists, neurologists, and endocrinologists.
No going back
Most doctors who make the switch to retainer-based practice understand that there’s likely no going back. When Dr. Bernstein switched, he announced the change to patients and canceled insurance contracts. “It was make or break,” he said. “I had no parachute.”
A version of this article first appeared on Medscape.com.