User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Clinic and doc must pay millions after faulty hernia surgery
reports a story in the Bowling Green Daily News.
On May 31, 2013, Alice Duff went to Graves-Gilbert Clinic, a multispecialty group whose main campus is in Bowling Green, for hernia surgery. Her surgeon for the procedure at a nearby facility was Tage Haase, MD, a member of the clinic.
Originally, Mrs. Duff was expected to remain in the facility for 23 hours following the procedure. But her recovery didn’t proceed as expected, and that initial period was extended by roughly 3 days. During this time, Ms. Duff’s husband, Lloyd, allegedly requested multiple times that doctors order a CT scan for his wife.
Ten days after the procedure, and with Ms. Duff out of the hospital, the Duffs successfully urged their family physician to order a CT scan. It showed large amounts of free air in Alice’s abdomen, a condition that’s known as pneumoperitoneum.
On June 10, 2013, Mrs. Duff underwent a second surgery, during which doctors discovered that she had sustained a perforated bowel during the first procedure. As a result, her bowel contents had spilled into her abdomen, causing an infection that required an extended hospital stay and five additional surgeries. The infection also led to retinal damage that has left her legally blind.
In their claim against Graves-Gilbert and Dr. Haase, the Duffs argued that Dr. Haase and an assistant doctor who was not named in the suit had failed to meet the standard of care. Specifically, argued the Duffs, because bowel perforation is a known complication in hernia surgeries, Dr. Haase was negligent in not diagnosing and treating Ms. Duff’s problem earlier.
For their part, Graves-Gilbert and Dr. Haase maintained that there was no indication before the second surgery that Mrs. Duff was demonstrating symptoms that necessitated a follow-up procedure. Dr. Haase further argued that Mrs. Duff’s bowel perforation was probably caused by the sawblade-like effect of the suture material he had used to close her incision.
The jury didn’t see it this way, however. It awarded approximately $1.3 million to Mrs. Duff for past medical expenses, plus another $12 million for pain and suffering. Her husband, Lloyd, received an additional $8 million in damages.
The attorney representing the clinic and Dr. Haase has vowed to pursue “all available remedies to have the verdict vacated and the case set for a new trial.”
Case hinged on proper use of a ‘power morcellator’
A claim for punitive damages has been thrown out against a New Jersey doctor and the hospital he’s affiliated with, in a ruling that could help to clarify the standards for such damages in medical malpractice cases, according to a story first reported on NorthJersey.com.
In October 2014, Howard H. Jones, MD, director of minimally invasive gynecologic surgery at The Valley Hospital, in Ridgewood, N.J., treated a patient from nearby Nyack, N.Y., for uterine fibroid tumors. As part of that treatment at the hospital, Dr. Jones used a “laparoscopic power morcellator,” which during a myomectomy procedure cuts, or morcellates, fibroid tumors into pieces small enough to be removed through an incision that’s generally 2 cm or fewer.
While use of the device offers doctors an alternative to open surgery and its longer recovery times, it also risks spreading previously undiagnosed cancer cells throughout the abdomen, thereby shortening a patient’s life. Because of this risk, which has given rise to a number of malpractice cases around the country, the Food and Drug Administration issued a draft guidance in the spring of 2022 for the use of power morcellators.
One recommendation is that physicians employ a “compatible” containment system to catch morcellated tissue, including any with cancer cells. Another is that the device be used selectively, which is to say on patients who have a minimal cancer risk and who have been informed of the procedure’s possible side effects beforehand.
Within a month of the procedure, the patient was diagnosed with metastatic leiomyosarcoma and died in September 2015. Following her death, her sister, the executor of her estate, sued both The Valley Hospital and Dr. Jones. In her suit, the sister argued that the defendants knew, or should have known, the risks involved in using a power morcellator because of both an earlier (2014) FDA “safety communication” discouraging the use of the device and the death of another of Dr. Jones’ patients following a similar procedure the year before.
The suit further alleged that, even after the FDA had issued its safety caution, the hospital had used the device on 37 other patients, “without informing them of the [FDA] letter or obtaining their informed consent to use the device.”
In light of these alleged lapses, Mirian Rivera, the patient’s sister, sought both compensatory and punitive damages. Historically, punitive damages have been limited to the small number of med-mal cases where a doctor or hospital has been found to have acted with actual malice or “wanton and willful disregard.”
Both Valley and Dr. Jones strongly disagreed with Ms. Rivera’s claim, arguing that prior to the procedure Dr. Jones had in fact met with the patient several times and had conducted the proper cancer-detecting tests. Moreover, the defendants emphasized, the request for punitive damages in the absence of actual malice or other factors would almost certainly establish a dangerous legal precedent. Several industry groups – including the American Medical Association, the Medical Society of New Jersey, and the New Jersey Hospital Association – agreed and filed friend-of-court briefs in support of Valley Hospital and Dr. Jones.
But two lower courts refused to dismiss the plaintiff’s claims for punitive damages. That’s when attorneys for Valley and Dr. Jones appealed to the New Jersey Supreme Court. (Claims against the device manufacturer, a German company, had already been resolved.)
Ruling unanimously, the high court sided with the defendants: “As a matter of law, the evidence presented, even affording plaintiffs all favorable inferences, does not establish that defendants’ acts or omissions were motivated by actual malice or accompanied by wanton and willful disregard for the patient’s health and safety.”
The court also found that Valley had in fact reviewed hospital policy and drafted a patient-consent form after the release of the 2014 FDA safety communication on power morcellators. (The consent form had not been adopted before the surgery in question, however.)
The suit will now go back to Superior Court in Bergen County, New Jersey; unless a settlement is reached beforehand, the jury will weigh claims of negligence and compensatory damages.
At press time, no trial date had been set.
Will med-mal cases get tougher to defend in this state?
Late in August, the Pennsylvania Supreme Court reversed its own longstanding rule that required that medical malpractice cases be filed in the county where the alleged injury occurred, as an Associated Press story on NBCPhiladelphia.com, among other news sites, reports.
More than 2 decades ago, in response to what was then seen as a crisis in the med-mal system, the state legislature overwhelmingly passed MCARE (the Medical Care Availability and Reduction of Error Fund), which among other things restricted the venue of medical suits. The legislation was signed into law in March 2002 by then-Gov. Mark Schweiker.
The following year, the state’s high court adopted a similar venue rule.
Over the years, doctor and hospital groups have been big supporters of the rule, arguing that any attempt to shift cases back to allegedly more plaintiff-friendly courts in Philadelphia and other cities would likely retrigger a crisis of higher med-mal premiums, doctor flight, and worse health care.
But a 2020 report by Pennsylvania’s nonpartisan Legislative Budget and Finance Committee took issue with these conclusions. It said that, following a national trend, the cost of medical professional liability insurance had fallen in the state since 2007. The report concluded that nothing in the available data supports the “conclusion that changes in the availability, cost, and affordability of medical professional liability insurance are the result of changes in Pennsylvania law.”
A more recent report by the high court’s Civil Procedural Rules Committee reached a similar conclusion, noting that med-mal cases should be subject to the same rules as any other type of civil litigation. A majority of the high court agreed.
Predictably, this decision sits well with patient groups and officials representing trial attorneys in the Keystone State.
“Cases should be heard before 12 jurors that do not have a connection to a hospital or surgical center that is often times the largest employer in the county,” said Kila Baldwin, president of the Pennsylvania Association for Justice. “The new rule levels the playing field and will improve access to justice for all Pennsylvanians.”
Doctors, hospitals, and other health care providers, however, have predicted a “ruinous path” ahead.
A version of this article first appeared on Medscape.com.
reports a story in the Bowling Green Daily News.
On May 31, 2013, Alice Duff went to Graves-Gilbert Clinic, a multispecialty group whose main campus is in Bowling Green, for hernia surgery. Her surgeon for the procedure at a nearby facility was Tage Haase, MD, a member of the clinic.
Originally, Mrs. Duff was expected to remain in the facility for 23 hours following the procedure. But her recovery didn’t proceed as expected, and that initial period was extended by roughly 3 days. During this time, Ms. Duff’s husband, Lloyd, allegedly requested multiple times that doctors order a CT scan for his wife.
Ten days after the procedure, and with Ms. Duff out of the hospital, the Duffs successfully urged their family physician to order a CT scan. It showed large amounts of free air in Alice’s abdomen, a condition that’s known as pneumoperitoneum.
On June 10, 2013, Mrs. Duff underwent a second surgery, during which doctors discovered that she had sustained a perforated bowel during the first procedure. As a result, her bowel contents had spilled into her abdomen, causing an infection that required an extended hospital stay and five additional surgeries. The infection also led to retinal damage that has left her legally blind.
In their claim against Graves-Gilbert and Dr. Haase, the Duffs argued that Dr. Haase and an assistant doctor who was not named in the suit had failed to meet the standard of care. Specifically, argued the Duffs, because bowel perforation is a known complication in hernia surgeries, Dr. Haase was negligent in not diagnosing and treating Ms. Duff’s problem earlier.
For their part, Graves-Gilbert and Dr. Haase maintained that there was no indication before the second surgery that Mrs. Duff was demonstrating symptoms that necessitated a follow-up procedure. Dr. Haase further argued that Mrs. Duff’s bowel perforation was probably caused by the sawblade-like effect of the suture material he had used to close her incision.
The jury didn’t see it this way, however. It awarded approximately $1.3 million to Mrs. Duff for past medical expenses, plus another $12 million for pain and suffering. Her husband, Lloyd, received an additional $8 million in damages.
The attorney representing the clinic and Dr. Haase has vowed to pursue “all available remedies to have the verdict vacated and the case set for a new trial.”
Case hinged on proper use of a ‘power morcellator’
A claim for punitive damages has been thrown out against a New Jersey doctor and the hospital he’s affiliated with, in a ruling that could help to clarify the standards for such damages in medical malpractice cases, according to a story first reported on NorthJersey.com.
In October 2014, Howard H. Jones, MD, director of minimally invasive gynecologic surgery at The Valley Hospital, in Ridgewood, N.J., treated a patient from nearby Nyack, N.Y., for uterine fibroid tumors. As part of that treatment at the hospital, Dr. Jones used a “laparoscopic power morcellator,” which during a myomectomy procedure cuts, or morcellates, fibroid tumors into pieces small enough to be removed through an incision that’s generally 2 cm or fewer.
While use of the device offers doctors an alternative to open surgery and its longer recovery times, it also risks spreading previously undiagnosed cancer cells throughout the abdomen, thereby shortening a patient’s life. Because of this risk, which has given rise to a number of malpractice cases around the country, the Food and Drug Administration issued a draft guidance in the spring of 2022 for the use of power morcellators.
One recommendation is that physicians employ a “compatible” containment system to catch morcellated tissue, including any with cancer cells. Another is that the device be used selectively, which is to say on patients who have a minimal cancer risk and who have been informed of the procedure’s possible side effects beforehand.
Within a month of the procedure, the patient was diagnosed with metastatic leiomyosarcoma and died in September 2015. Following her death, her sister, the executor of her estate, sued both The Valley Hospital and Dr. Jones. In her suit, the sister argued that the defendants knew, or should have known, the risks involved in using a power morcellator because of both an earlier (2014) FDA “safety communication” discouraging the use of the device and the death of another of Dr. Jones’ patients following a similar procedure the year before.
The suit further alleged that, even after the FDA had issued its safety caution, the hospital had used the device on 37 other patients, “without informing them of the [FDA] letter or obtaining their informed consent to use the device.”
In light of these alleged lapses, Mirian Rivera, the patient’s sister, sought both compensatory and punitive damages. Historically, punitive damages have been limited to the small number of med-mal cases where a doctor or hospital has been found to have acted with actual malice or “wanton and willful disregard.”
Both Valley and Dr. Jones strongly disagreed with Ms. Rivera’s claim, arguing that prior to the procedure Dr. Jones had in fact met with the patient several times and had conducted the proper cancer-detecting tests. Moreover, the defendants emphasized, the request for punitive damages in the absence of actual malice or other factors would almost certainly establish a dangerous legal precedent. Several industry groups – including the American Medical Association, the Medical Society of New Jersey, and the New Jersey Hospital Association – agreed and filed friend-of-court briefs in support of Valley Hospital and Dr. Jones.
But two lower courts refused to dismiss the plaintiff’s claims for punitive damages. That’s when attorneys for Valley and Dr. Jones appealed to the New Jersey Supreme Court. (Claims against the device manufacturer, a German company, had already been resolved.)
Ruling unanimously, the high court sided with the defendants: “As a matter of law, the evidence presented, even affording plaintiffs all favorable inferences, does not establish that defendants’ acts or omissions were motivated by actual malice or accompanied by wanton and willful disregard for the patient’s health and safety.”
The court also found that Valley had in fact reviewed hospital policy and drafted a patient-consent form after the release of the 2014 FDA safety communication on power morcellators. (The consent form had not been adopted before the surgery in question, however.)
The suit will now go back to Superior Court in Bergen County, New Jersey; unless a settlement is reached beforehand, the jury will weigh claims of negligence and compensatory damages.
At press time, no trial date had been set.
Will med-mal cases get tougher to defend in this state?
Late in August, the Pennsylvania Supreme Court reversed its own longstanding rule that required that medical malpractice cases be filed in the county where the alleged injury occurred, as an Associated Press story on NBCPhiladelphia.com, among other news sites, reports.
More than 2 decades ago, in response to what was then seen as a crisis in the med-mal system, the state legislature overwhelmingly passed MCARE (the Medical Care Availability and Reduction of Error Fund), which among other things restricted the venue of medical suits. The legislation was signed into law in March 2002 by then-Gov. Mark Schweiker.
The following year, the state’s high court adopted a similar venue rule.
Over the years, doctor and hospital groups have been big supporters of the rule, arguing that any attempt to shift cases back to allegedly more plaintiff-friendly courts in Philadelphia and other cities would likely retrigger a crisis of higher med-mal premiums, doctor flight, and worse health care.
But a 2020 report by Pennsylvania’s nonpartisan Legislative Budget and Finance Committee took issue with these conclusions. It said that, following a national trend, the cost of medical professional liability insurance had fallen in the state since 2007. The report concluded that nothing in the available data supports the “conclusion that changes in the availability, cost, and affordability of medical professional liability insurance are the result of changes in Pennsylvania law.”
A more recent report by the high court’s Civil Procedural Rules Committee reached a similar conclusion, noting that med-mal cases should be subject to the same rules as any other type of civil litigation. A majority of the high court agreed.
Predictably, this decision sits well with patient groups and officials representing trial attorneys in the Keystone State.
“Cases should be heard before 12 jurors that do not have a connection to a hospital or surgical center that is often times the largest employer in the county,” said Kila Baldwin, president of the Pennsylvania Association for Justice. “The new rule levels the playing field and will improve access to justice for all Pennsylvanians.”
Doctors, hospitals, and other health care providers, however, have predicted a “ruinous path” ahead.
A version of this article first appeared on Medscape.com.
reports a story in the Bowling Green Daily News.
On May 31, 2013, Alice Duff went to Graves-Gilbert Clinic, a multispecialty group whose main campus is in Bowling Green, for hernia surgery. Her surgeon for the procedure at a nearby facility was Tage Haase, MD, a member of the clinic.
Originally, Mrs. Duff was expected to remain in the facility for 23 hours following the procedure. But her recovery didn’t proceed as expected, and that initial period was extended by roughly 3 days. During this time, Ms. Duff’s husband, Lloyd, allegedly requested multiple times that doctors order a CT scan for his wife.
Ten days after the procedure, and with Ms. Duff out of the hospital, the Duffs successfully urged their family physician to order a CT scan. It showed large amounts of free air in Alice’s abdomen, a condition that’s known as pneumoperitoneum.
On June 10, 2013, Mrs. Duff underwent a second surgery, during which doctors discovered that she had sustained a perforated bowel during the first procedure. As a result, her bowel contents had spilled into her abdomen, causing an infection that required an extended hospital stay and five additional surgeries. The infection also led to retinal damage that has left her legally blind.
In their claim against Graves-Gilbert and Dr. Haase, the Duffs argued that Dr. Haase and an assistant doctor who was not named in the suit had failed to meet the standard of care. Specifically, argued the Duffs, because bowel perforation is a known complication in hernia surgeries, Dr. Haase was negligent in not diagnosing and treating Ms. Duff’s problem earlier.
For their part, Graves-Gilbert and Dr. Haase maintained that there was no indication before the second surgery that Mrs. Duff was demonstrating symptoms that necessitated a follow-up procedure. Dr. Haase further argued that Mrs. Duff’s bowel perforation was probably caused by the sawblade-like effect of the suture material he had used to close her incision.
The jury didn’t see it this way, however. It awarded approximately $1.3 million to Mrs. Duff for past medical expenses, plus another $12 million for pain and suffering. Her husband, Lloyd, received an additional $8 million in damages.
The attorney representing the clinic and Dr. Haase has vowed to pursue “all available remedies to have the verdict vacated and the case set for a new trial.”
Case hinged on proper use of a ‘power morcellator’
A claim for punitive damages has been thrown out against a New Jersey doctor and the hospital he’s affiliated with, in a ruling that could help to clarify the standards for such damages in medical malpractice cases, according to a story first reported on NorthJersey.com.
In October 2014, Howard H. Jones, MD, director of minimally invasive gynecologic surgery at The Valley Hospital, in Ridgewood, N.J., treated a patient from nearby Nyack, N.Y., for uterine fibroid tumors. As part of that treatment at the hospital, Dr. Jones used a “laparoscopic power morcellator,” which during a myomectomy procedure cuts, or morcellates, fibroid tumors into pieces small enough to be removed through an incision that’s generally 2 cm or fewer.
While use of the device offers doctors an alternative to open surgery and its longer recovery times, it also risks spreading previously undiagnosed cancer cells throughout the abdomen, thereby shortening a patient’s life. Because of this risk, which has given rise to a number of malpractice cases around the country, the Food and Drug Administration issued a draft guidance in the spring of 2022 for the use of power morcellators.
One recommendation is that physicians employ a “compatible” containment system to catch morcellated tissue, including any with cancer cells. Another is that the device be used selectively, which is to say on patients who have a minimal cancer risk and who have been informed of the procedure’s possible side effects beforehand.
Within a month of the procedure, the patient was diagnosed with metastatic leiomyosarcoma and died in September 2015. Following her death, her sister, the executor of her estate, sued both The Valley Hospital and Dr. Jones. In her suit, the sister argued that the defendants knew, or should have known, the risks involved in using a power morcellator because of both an earlier (2014) FDA “safety communication” discouraging the use of the device and the death of another of Dr. Jones’ patients following a similar procedure the year before.
The suit further alleged that, even after the FDA had issued its safety caution, the hospital had used the device on 37 other patients, “without informing them of the [FDA] letter or obtaining their informed consent to use the device.”
In light of these alleged lapses, Mirian Rivera, the patient’s sister, sought both compensatory and punitive damages. Historically, punitive damages have been limited to the small number of med-mal cases where a doctor or hospital has been found to have acted with actual malice or “wanton and willful disregard.”
Both Valley and Dr. Jones strongly disagreed with Ms. Rivera’s claim, arguing that prior to the procedure Dr. Jones had in fact met with the patient several times and had conducted the proper cancer-detecting tests. Moreover, the defendants emphasized, the request for punitive damages in the absence of actual malice or other factors would almost certainly establish a dangerous legal precedent. Several industry groups – including the American Medical Association, the Medical Society of New Jersey, and the New Jersey Hospital Association – agreed and filed friend-of-court briefs in support of Valley Hospital and Dr. Jones.
But two lower courts refused to dismiss the plaintiff’s claims for punitive damages. That’s when attorneys for Valley and Dr. Jones appealed to the New Jersey Supreme Court. (Claims against the device manufacturer, a German company, had already been resolved.)
Ruling unanimously, the high court sided with the defendants: “As a matter of law, the evidence presented, even affording plaintiffs all favorable inferences, does not establish that defendants’ acts or omissions were motivated by actual malice or accompanied by wanton and willful disregard for the patient’s health and safety.”
The court also found that Valley had in fact reviewed hospital policy and drafted a patient-consent form after the release of the 2014 FDA safety communication on power morcellators. (The consent form had not been adopted before the surgery in question, however.)
The suit will now go back to Superior Court in Bergen County, New Jersey; unless a settlement is reached beforehand, the jury will weigh claims of negligence and compensatory damages.
At press time, no trial date had been set.
Will med-mal cases get tougher to defend in this state?
Late in August, the Pennsylvania Supreme Court reversed its own longstanding rule that required that medical malpractice cases be filed in the county where the alleged injury occurred, as an Associated Press story on NBCPhiladelphia.com, among other news sites, reports.
More than 2 decades ago, in response to what was then seen as a crisis in the med-mal system, the state legislature overwhelmingly passed MCARE (the Medical Care Availability and Reduction of Error Fund), which among other things restricted the venue of medical suits. The legislation was signed into law in March 2002 by then-Gov. Mark Schweiker.
The following year, the state’s high court adopted a similar venue rule.
Over the years, doctor and hospital groups have been big supporters of the rule, arguing that any attempt to shift cases back to allegedly more plaintiff-friendly courts in Philadelphia and other cities would likely retrigger a crisis of higher med-mal premiums, doctor flight, and worse health care.
But a 2020 report by Pennsylvania’s nonpartisan Legislative Budget and Finance Committee took issue with these conclusions. It said that, following a national trend, the cost of medical professional liability insurance had fallen in the state since 2007. The report concluded that nothing in the available data supports the “conclusion that changes in the availability, cost, and affordability of medical professional liability insurance are the result of changes in Pennsylvania law.”
A more recent report by the high court’s Civil Procedural Rules Committee reached a similar conclusion, noting that med-mal cases should be subject to the same rules as any other type of civil litigation. A majority of the high court agreed.
Predictably, this decision sits well with patient groups and officials representing trial attorneys in the Keystone State.
“Cases should be heard before 12 jurors that do not have a connection to a hospital or surgical center that is often times the largest employer in the county,” said Kila Baldwin, president of the Pennsylvania Association for Justice. “The new rule levels the playing field and will improve access to justice for all Pennsylvanians.”
Doctors, hospitals, and other health care providers, however, have predicted a “ruinous path” ahead.
A version of this article first appeared on Medscape.com.
Desperate long COVID patients turn to unproven alternative therapies
Entrepreneur Maya McNulty, 49, was one of the first victims of the COVID-19 pandemic. The Schenectady, N.Y., businesswoman spent 2 months in the hospital after catching the disease in March 2020. That September, she was diagnosed with long COVID.
“Even a simple task such as unloading the dishwasher became a major challenge,” she says.
Over the next several months, Ms. McNulty saw a range of specialists, including neurologists, pulmonologists, and cardiologists. She had months of physical therapy and respiratory therapy to help regain strength and lung function. While many of the doctors she saw were sympathetic to what she was going through, not all were.
“I saw one neurologist who told me to my face that she didn’t believe in long COVID,” she recalls. “It was particularly astonishing since the hospital they were affiliated with had a long COVID clinic.”
Ms. McNulty began to connect with other patients with long COVID through a support group she created at the end of 2020 on the social media app Clubhouse. They exchanged ideas and stories about what had helped one another, which led her to try, over the next year, a plant-based diet, Chinese medicine, and vitamin C supplements, among other treatments.
She also acted on unscientific reports she found online and did her own research, which led her to discover claims that some asthma patients with chronic coughing responded well to halotherapy, or dry salt therapy, during which patients inhale micro-particles of salt into their lungs to reduce inflammation, widen airways, and thin mucus. She’s been doing this procedure at a clinic near her home for over a year and credits it with helping with her chronic cough, especially as she recovers from her second bout of COVID-19.
It’s not cheap – a single half-hour session can cost up to $50 and isn’t covered by insurance. There’s also no good research to suggest that it can help with long COVID, according to the Cleveland Clinic.
Ms. McNulty understands that but says many people who live with long COVID turn to these treatments out of a sense of desperation.
“When it comes to this condition, we kind of have to be our own advocates. People are so desperate and feel so gaslit by doctors who don’t believe in their symptoms that they play Russian roulette with their body,” she says. “Most just want some hope and a way to relieve pain.”
Across the country, 16 million Americans have long COVID, according to the Brookings Institution’s analysis of a 2022 Census Bureau report. The report also estimated that up to a quarter of them have such debilitating symptoms that they are no longer able to work. While long COVID centers may offer therapies to help relieve symptoms, “there are no evidence-based established treatments for long COVID at this point,” says Andrew Schamess, MD, a professor of internal medicine at Ohio State Wexner Medical Center, who runs its Post-COVID Recovery Program. “You can’t blame patients for looking for alternative remedies to help them. Unfortunately, there are also a lot of people out to make a buck who are selling unproven and disproven therapies.”
Sniffing out the snake oil
With few evidence-based treatments for long COVID, patients with debilitating symptoms can be tempted by unproven options. One that has gotten a lot of attention is hyperbaric oxygen. This therapy has traditionally been used to treat divers who have decompression sickness, or “the bends.” It’s also being touted by some clinics as an effective treatment for long COVID.
A very small trial of 73 patients with long COVID, published in the journal Scientific Reports, found that those treated in a high-pressure oxygen system 5 days a week for 2 months showed improvements in brain fog, pain, energy, sleep, anxiety, and depression, compared with similar patients who got sham treatments. But larger studies are needed to show how well it works, notes Dr. Schamess.
“It’s very expensive – roughly $120 per session – and there just isn’t the evidence there to support its use,” he says.
In addition, the therapy itself carries risks, such as ear and sinus pain, middle ear injury, temporary vision changes, and, very rarely, lung collapse, according to the U.S. Food and Drug Administration.
One “particularly troubling” treatment being offered, says Kathleen Bell, MD, chair of the department of physical medicine and rehabilitation at the University of Texas Southwestern Medical Center, is stem cell therapy. This therapy is still in its infancy, but it’s being marketed by some clinics as a way to prevent COVID-19 and also treat long-haul symptoms.
The FDA has issued advisories that there are no products approved to treat long COVID and recommends against their use, except in a clinical trial.
“There’s absolutely no regulation – you don’t know what you’re getting, and there’s no research to suggest this therapy even works,” says Dr. Bell. It’s also prohibitively expensive – one Cayman Islands–based company advertises its treatment for as much as $25,000.
Patients with long COVID are even traveling as far as Cyprus, Germany, and Switzerland for a procedure known as blood washing, in which large needles are inserted into veins to filter blood and remove lipids and inflammatory proteins, the British Medical Journal reported in July. Some patients are also prescribed blood thinners to remove microscopic blood clots that may contribute to long COVID. But this treatment is also expensive, with many people paying $10,000-$15,000 out of pocket, and there’s no published evidence to suggest it works, according to the BMJ.
It can be particularly hard to discern what may work and what’s unproven, since many primary care providers are themselves unfamiliar with even traditional long COVID treatments, Dr. Bell says.
Sorting through supplements
Yufang Lin, MD, an integrative specialist at the Cleveland Clinic, says many patients with long COVID enter her office with bags of supplements.
“There’s no data on them, and in large quantities, they may even be harmful,” she says.
Instead, she works closely with the Cleveland Clinic’s long COVID center to do a thorough workup of each patient, which often includes screening for certain nutritional deficiencies.
“Anecdotally, we do see many patients with long COVID who are deficient in these vitamins and minerals,” says Dr. Lin. “If someone is low, we will suggest the appropriate supplement. Otherwise, we work with them to institute some dietary changes.”
This usually involves a plant-based, anti-inflammatory eating pattern such as the Mediterranean diet, which is rich in fruits, vegetables, whole grains, nuts, fatty fish, and healthy fats such as olive oil and avocados.
Other supplements some doctors recommend for patients with long COVID are meant to treat inflammation, Dr. Bell says, although there’s not good evidence they work. One is the antioxidant coenzyme Q10.
But a small preprint study published in The Lancet, of 121 patients with long COVID who took 500 milligrams a day of coenzyme Q10 for 6 weeks saw no differences in recovery, compared with those who took a placebo. Because the study is still a preprint, it has not been peer-reviewed.
Another is probiotics. A small study, published in the journal Infectious Diseases Diagnosis & Treatment, found that a blend of five lactobacillus probiotics, along with a prebiotic called inulin, taken for 30 days, helped with long-term COVID symptoms such as coughing and fatigue. But larger studies need to be done to support their use.
One that may have more promise is omega-3 fatty acids. Like many other supplements, these may help with long COVID by easing inflammation, says Steven Flanagan, MD, a rehabilitation medicine specialist at NYU Langone who works with long COVID patients. Researchers at the Mount Sinai School of Medicine, New York, are studying whether a supplement can help patients who have lost their sense of taste or smell after an infection, but results aren’t yet available.
Among the few alternatives that have been shown to help patients are mindfulness-based therapies – in particular, mindfulness-based forms of exercise such as tai chi and qi gong may be helpful, as they combine a gentle workout with stress reduction.
“Both incorporate meditation, which helps not only to relieve some of the anxiety associated with long COVID but allows patients to redirect their thought process so that they can cope with symptoms better,” says Dr. Flanagan.
A 2022 study, published in BMJ Open, found that these two activities reduced inflammatory markers and improved respiratory muscle strength and function in patients recovering from COVID-19.
“I recommend these activities to all my long COVID patients, as it’s inexpensive and easy to find classes to do either at home or in their community,” he says. “Even if it doesn’t improve their long COVID symptoms, it has other benefits such as increased strength and flexibility that can boost their overall health.”
A version of this article first appeared on WebMD.com.
Entrepreneur Maya McNulty, 49, was one of the first victims of the COVID-19 pandemic. The Schenectady, N.Y., businesswoman spent 2 months in the hospital after catching the disease in March 2020. That September, she was diagnosed with long COVID.
“Even a simple task such as unloading the dishwasher became a major challenge,” she says.
Over the next several months, Ms. McNulty saw a range of specialists, including neurologists, pulmonologists, and cardiologists. She had months of physical therapy and respiratory therapy to help regain strength and lung function. While many of the doctors she saw were sympathetic to what she was going through, not all were.
“I saw one neurologist who told me to my face that she didn’t believe in long COVID,” she recalls. “It was particularly astonishing since the hospital they were affiliated with had a long COVID clinic.”
Ms. McNulty began to connect with other patients with long COVID through a support group she created at the end of 2020 on the social media app Clubhouse. They exchanged ideas and stories about what had helped one another, which led her to try, over the next year, a plant-based diet, Chinese medicine, and vitamin C supplements, among other treatments.
She also acted on unscientific reports she found online and did her own research, which led her to discover claims that some asthma patients with chronic coughing responded well to halotherapy, or dry salt therapy, during which patients inhale micro-particles of salt into their lungs to reduce inflammation, widen airways, and thin mucus. She’s been doing this procedure at a clinic near her home for over a year and credits it with helping with her chronic cough, especially as she recovers from her second bout of COVID-19.
It’s not cheap – a single half-hour session can cost up to $50 and isn’t covered by insurance. There’s also no good research to suggest that it can help with long COVID, according to the Cleveland Clinic.
Ms. McNulty understands that but says many people who live with long COVID turn to these treatments out of a sense of desperation.
“When it comes to this condition, we kind of have to be our own advocates. People are so desperate and feel so gaslit by doctors who don’t believe in their symptoms that they play Russian roulette with their body,” she says. “Most just want some hope and a way to relieve pain.”
Across the country, 16 million Americans have long COVID, according to the Brookings Institution’s analysis of a 2022 Census Bureau report. The report also estimated that up to a quarter of them have such debilitating symptoms that they are no longer able to work. While long COVID centers may offer therapies to help relieve symptoms, “there are no evidence-based established treatments for long COVID at this point,” says Andrew Schamess, MD, a professor of internal medicine at Ohio State Wexner Medical Center, who runs its Post-COVID Recovery Program. “You can’t blame patients for looking for alternative remedies to help them. Unfortunately, there are also a lot of people out to make a buck who are selling unproven and disproven therapies.”
Sniffing out the snake oil
With few evidence-based treatments for long COVID, patients with debilitating symptoms can be tempted by unproven options. One that has gotten a lot of attention is hyperbaric oxygen. This therapy has traditionally been used to treat divers who have decompression sickness, or “the bends.” It’s also being touted by some clinics as an effective treatment for long COVID.
A very small trial of 73 patients with long COVID, published in the journal Scientific Reports, found that those treated in a high-pressure oxygen system 5 days a week for 2 months showed improvements in brain fog, pain, energy, sleep, anxiety, and depression, compared with similar patients who got sham treatments. But larger studies are needed to show how well it works, notes Dr. Schamess.
“It’s very expensive – roughly $120 per session – and there just isn’t the evidence there to support its use,” he says.
In addition, the therapy itself carries risks, such as ear and sinus pain, middle ear injury, temporary vision changes, and, very rarely, lung collapse, according to the U.S. Food and Drug Administration.
One “particularly troubling” treatment being offered, says Kathleen Bell, MD, chair of the department of physical medicine and rehabilitation at the University of Texas Southwestern Medical Center, is stem cell therapy. This therapy is still in its infancy, but it’s being marketed by some clinics as a way to prevent COVID-19 and also treat long-haul symptoms.
The FDA has issued advisories that there are no products approved to treat long COVID and recommends against their use, except in a clinical trial.
“There’s absolutely no regulation – you don’t know what you’re getting, and there’s no research to suggest this therapy even works,” says Dr. Bell. It’s also prohibitively expensive – one Cayman Islands–based company advertises its treatment for as much as $25,000.
Patients with long COVID are even traveling as far as Cyprus, Germany, and Switzerland for a procedure known as blood washing, in which large needles are inserted into veins to filter blood and remove lipids and inflammatory proteins, the British Medical Journal reported in July. Some patients are also prescribed blood thinners to remove microscopic blood clots that may contribute to long COVID. But this treatment is also expensive, with many people paying $10,000-$15,000 out of pocket, and there’s no published evidence to suggest it works, according to the BMJ.
It can be particularly hard to discern what may work and what’s unproven, since many primary care providers are themselves unfamiliar with even traditional long COVID treatments, Dr. Bell says.
Sorting through supplements
Yufang Lin, MD, an integrative specialist at the Cleveland Clinic, says many patients with long COVID enter her office with bags of supplements.
“There’s no data on them, and in large quantities, they may even be harmful,” she says.
Instead, she works closely with the Cleveland Clinic’s long COVID center to do a thorough workup of each patient, which often includes screening for certain nutritional deficiencies.
“Anecdotally, we do see many patients with long COVID who are deficient in these vitamins and minerals,” says Dr. Lin. “If someone is low, we will suggest the appropriate supplement. Otherwise, we work with them to institute some dietary changes.”
This usually involves a plant-based, anti-inflammatory eating pattern such as the Mediterranean diet, which is rich in fruits, vegetables, whole grains, nuts, fatty fish, and healthy fats such as olive oil and avocados.
Other supplements some doctors recommend for patients with long COVID are meant to treat inflammation, Dr. Bell says, although there’s not good evidence they work. One is the antioxidant coenzyme Q10.
But a small preprint study published in The Lancet, of 121 patients with long COVID who took 500 milligrams a day of coenzyme Q10 for 6 weeks saw no differences in recovery, compared with those who took a placebo. Because the study is still a preprint, it has not been peer-reviewed.
Another is probiotics. A small study, published in the journal Infectious Diseases Diagnosis & Treatment, found that a blend of five lactobacillus probiotics, along with a prebiotic called inulin, taken for 30 days, helped with long-term COVID symptoms such as coughing and fatigue. But larger studies need to be done to support their use.
One that may have more promise is omega-3 fatty acids. Like many other supplements, these may help with long COVID by easing inflammation, says Steven Flanagan, MD, a rehabilitation medicine specialist at NYU Langone who works with long COVID patients. Researchers at the Mount Sinai School of Medicine, New York, are studying whether a supplement can help patients who have lost their sense of taste or smell after an infection, but results aren’t yet available.
Among the few alternatives that have been shown to help patients are mindfulness-based therapies – in particular, mindfulness-based forms of exercise such as tai chi and qi gong may be helpful, as they combine a gentle workout with stress reduction.
“Both incorporate meditation, which helps not only to relieve some of the anxiety associated with long COVID but allows patients to redirect their thought process so that they can cope with symptoms better,” says Dr. Flanagan.
A 2022 study, published in BMJ Open, found that these two activities reduced inflammatory markers and improved respiratory muscle strength and function in patients recovering from COVID-19.
“I recommend these activities to all my long COVID patients, as it’s inexpensive and easy to find classes to do either at home or in their community,” he says. “Even if it doesn’t improve their long COVID symptoms, it has other benefits such as increased strength and flexibility that can boost their overall health.”
A version of this article first appeared on WebMD.com.
Entrepreneur Maya McNulty, 49, was one of the first victims of the COVID-19 pandemic. The Schenectady, N.Y., businesswoman spent 2 months in the hospital after catching the disease in March 2020. That September, she was diagnosed with long COVID.
“Even a simple task such as unloading the dishwasher became a major challenge,” she says.
Over the next several months, Ms. McNulty saw a range of specialists, including neurologists, pulmonologists, and cardiologists. She had months of physical therapy and respiratory therapy to help regain strength and lung function. While many of the doctors she saw were sympathetic to what she was going through, not all were.
“I saw one neurologist who told me to my face that she didn’t believe in long COVID,” she recalls. “It was particularly astonishing since the hospital they were affiliated with had a long COVID clinic.”
Ms. McNulty began to connect with other patients with long COVID through a support group she created at the end of 2020 on the social media app Clubhouse. They exchanged ideas and stories about what had helped one another, which led her to try, over the next year, a plant-based diet, Chinese medicine, and vitamin C supplements, among other treatments.
She also acted on unscientific reports she found online and did her own research, which led her to discover claims that some asthma patients with chronic coughing responded well to halotherapy, or dry salt therapy, during which patients inhale micro-particles of salt into their lungs to reduce inflammation, widen airways, and thin mucus. She’s been doing this procedure at a clinic near her home for over a year and credits it with helping with her chronic cough, especially as she recovers from her second bout of COVID-19.
It’s not cheap – a single half-hour session can cost up to $50 and isn’t covered by insurance. There’s also no good research to suggest that it can help with long COVID, according to the Cleveland Clinic.
Ms. McNulty understands that but says many people who live with long COVID turn to these treatments out of a sense of desperation.
“When it comes to this condition, we kind of have to be our own advocates. People are so desperate and feel so gaslit by doctors who don’t believe in their symptoms that they play Russian roulette with their body,” she says. “Most just want some hope and a way to relieve pain.”
Across the country, 16 million Americans have long COVID, according to the Brookings Institution’s analysis of a 2022 Census Bureau report. The report also estimated that up to a quarter of them have such debilitating symptoms that they are no longer able to work. While long COVID centers may offer therapies to help relieve symptoms, “there are no evidence-based established treatments for long COVID at this point,” says Andrew Schamess, MD, a professor of internal medicine at Ohio State Wexner Medical Center, who runs its Post-COVID Recovery Program. “You can’t blame patients for looking for alternative remedies to help them. Unfortunately, there are also a lot of people out to make a buck who are selling unproven and disproven therapies.”
Sniffing out the snake oil
With few evidence-based treatments for long COVID, patients with debilitating symptoms can be tempted by unproven options. One that has gotten a lot of attention is hyperbaric oxygen. This therapy has traditionally been used to treat divers who have decompression sickness, or “the bends.” It’s also being touted by some clinics as an effective treatment for long COVID.
A very small trial of 73 patients with long COVID, published in the journal Scientific Reports, found that those treated in a high-pressure oxygen system 5 days a week for 2 months showed improvements in brain fog, pain, energy, sleep, anxiety, and depression, compared with similar patients who got sham treatments. But larger studies are needed to show how well it works, notes Dr. Schamess.
“It’s very expensive – roughly $120 per session – and there just isn’t the evidence there to support its use,” he says.
In addition, the therapy itself carries risks, such as ear and sinus pain, middle ear injury, temporary vision changes, and, very rarely, lung collapse, according to the U.S. Food and Drug Administration.
One “particularly troubling” treatment being offered, says Kathleen Bell, MD, chair of the department of physical medicine and rehabilitation at the University of Texas Southwestern Medical Center, is stem cell therapy. This therapy is still in its infancy, but it’s being marketed by some clinics as a way to prevent COVID-19 and also treat long-haul symptoms.
The FDA has issued advisories that there are no products approved to treat long COVID and recommends against their use, except in a clinical trial.
“There’s absolutely no regulation – you don’t know what you’re getting, and there’s no research to suggest this therapy even works,” says Dr. Bell. It’s also prohibitively expensive – one Cayman Islands–based company advertises its treatment for as much as $25,000.
Patients with long COVID are even traveling as far as Cyprus, Germany, and Switzerland for a procedure known as blood washing, in which large needles are inserted into veins to filter blood and remove lipids and inflammatory proteins, the British Medical Journal reported in July. Some patients are also prescribed blood thinners to remove microscopic blood clots that may contribute to long COVID. But this treatment is also expensive, with many people paying $10,000-$15,000 out of pocket, and there’s no published evidence to suggest it works, according to the BMJ.
It can be particularly hard to discern what may work and what’s unproven, since many primary care providers are themselves unfamiliar with even traditional long COVID treatments, Dr. Bell says.
Sorting through supplements
Yufang Lin, MD, an integrative specialist at the Cleveland Clinic, says many patients with long COVID enter her office with bags of supplements.
“There’s no data on them, and in large quantities, they may even be harmful,” she says.
Instead, she works closely with the Cleveland Clinic’s long COVID center to do a thorough workup of each patient, which often includes screening for certain nutritional deficiencies.
“Anecdotally, we do see many patients with long COVID who are deficient in these vitamins and minerals,” says Dr. Lin. “If someone is low, we will suggest the appropriate supplement. Otherwise, we work with them to institute some dietary changes.”
This usually involves a plant-based, anti-inflammatory eating pattern such as the Mediterranean diet, which is rich in fruits, vegetables, whole grains, nuts, fatty fish, and healthy fats such as olive oil and avocados.
Other supplements some doctors recommend for patients with long COVID are meant to treat inflammation, Dr. Bell says, although there’s not good evidence they work. One is the antioxidant coenzyme Q10.
But a small preprint study published in The Lancet, of 121 patients with long COVID who took 500 milligrams a day of coenzyme Q10 for 6 weeks saw no differences in recovery, compared with those who took a placebo. Because the study is still a preprint, it has not been peer-reviewed.
Another is probiotics. A small study, published in the journal Infectious Diseases Diagnosis & Treatment, found that a blend of five lactobacillus probiotics, along with a prebiotic called inulin, taken for 30 days, helped with long-term COVID symptoms such as coughing and fatigue. But larger studies need to be done to support their use.
One that may have more promise is omega-3 fatty acids. Like many other supplements, these may help with long COVID by easing inflammation, says Steven Flanagan, MD, a rehabilitation medicine specialist at NYU Langone who works with long COVID patients. Researchers at the Mount Sinai School of Medicine, New York, are studying whether a supplement can help patients who have lost their sense of taste or smell after an infection, but results aren’t yet available.
Among the few alternatives that have been shown to help patients are mindfulness-based therapies – in particular, mindfulness-based forms of exercise such as tai chi and qi gong may be helpful, as they combine a gentle workout with stress reduction.
“Both incorporate meditation, which helps not only to relieve some of the anxiety associated with long COVID but allows patients to redirect their thought process so that they can cope with symptoms better,” says Dr. Flanagan.
A 2022 study, published in BMJ Open, found that these two activities reduced inflammatory markers and improved respiratory muscle strength and function in patients recovering from COVID-19.
“I recommend these activities to all my long COVID patients, as it’s inexpensive and easy to find classes to do either at home or in their community,” he says. “Even if it doesn’t improve their long COVID symptoms, it has other benefits such as increased strength and flexibility that can boost their overall health.”
A version of this article first appeared on WebMD.com.
Early age at hysterectomy ups type 2 diabetes risk
Data from a large French cohort study suggest that women who have a hysterectomy before 40-45 years of age may be at particular risk of subsequently developing type 2 diabetes.
A 20% increase in the risk for incident diabetes was found comparing women of all ages who had and had not had a hysterectomy (P = .0003).
This risk jumped to a 52% increase when only women below the age of 45 were considered (P < .0001) and was still 38% higher if only women under 40 years were analyzed (P = .005).

“Our findings clearly show that hysterectomy is a risk marker for diabetes,” Fabrice Bonnet, MD, PhD, of Centre Hospitalier Universitaire (CHU) de Rennes (France), said at the annual meeting of the European Association for the Study of Diabetes.
Importantly, this risk appears to occur “independently of any hormonal therapy, any reproductive factors, physical activity, and diet,” Dr. Bonnet added.
Findings challenged
“I would like to challenge your findings,” said Peter Nilsson, MD, PhD, a professor at Lund (Sweden) University, during the postpresentation discussion period.
“Could there be a detection bias?” queried Dr. Nilsson. “If you undergo surgery like this, there will be several postoperative visits to a physician and there’s a higher likelihood of somebody taking blood samples and detecting diabetes.
“So, if this is true, it could mean that postoperative controls of goiter or thyroid surgery would bring the same findings,” Dr. Nilsson suggested.
“It is an epidemiological cohort of woman followed for a long time,” Dr. Bonnet responded. “So of course, there probably was more blood testing than in the usual population, but we did not observe the association for another type of surgery and type 2 diabetes.”
Clarifying further, Dr. Bonnet said that they had looked at thyroid surgery but not any other types of abdominal surgery.
Assessing the risk of incident diabetes
Hysterectomy is a common surgery among women – more than 400,000 are estimated to be performed every year in the United States, and 80,000 in France, with a rising rate in developing countries, Dr. Bonnet said in an interview.
“We don’t know exactly why that is, but it could have long-term consequences in terms of metabolic effects and the incidence of diabetes,” he said.
Prior research has linked having a hysterectomy with an increased rate of hypertension and cardiovascular risk, and there have also been a few studies linking it to diabetes.
“Our aim was to analyze the relationship between the past history of hysterectomies and the risk of incident diabetes; and specifically, we assessed the influence of age,” Dr. Bonnet said.
To do so, data on more than 83,000 women who had participated in The French E3N Prospective Cohort Study (E3N) were obtained. This large epidemiologic study is the French component of the long-running EPIC study.
For inclusion in the analysis, women had to have no diabetes at baseline, to have had their uterus, ovaries, or both removed for benign gynecologic reasons, and to have had their surgeries performed before any diagnosis of diabetes had been made. A diagnosis of diabetes was identified through the women’s responses to self-report questionnaires and prescriptions for antidiabetic medications.
In all, 2,672 women were found to have developed diabetes during the 16-year follow-up period.
The hazard ratio for the risk of diabetes in women who had and had not had a hysterectomy was 1.30 (95% confidence interval, 1.17-1.43; P < .0001), taking age into account and stratifying for birth generation.
The association held, when there was adjustment for other factors such as smoking status, physical activity, history of diabetes, weight, and adherence to a Mediterranean diet (HR 1.27; 95% CI 1.02-1.05; P = .02).
And, after adjustment for age at menarche, menopausal status, age at which menopause was reached, oral contraceptive and hormone therapy use, and the number of pregnancies, the risk for type 2 diabetes was still apparent in those who had undergoing a hysterectomy (HR, 1.20; 95% CI, 1.09-1.33; P = .0003).
Risk increased with oophorectomy
“Women who had both hysterectomy with bilateral oophorectomy had the highest rates of incident diabetes, as compared to women without hysterectomy and no oophorectomy,” said Dr. Bonnet (HR, 1.26; 95% CI, 1.11-1.42; P = .0003).
“This suggests preserving ovarian function is of importance,” he added. “Try to keep the ovaries in place, so just have hysterectomy alone,” he suggested might be the advice to fellow clinicians.
“So, identifying women at higher risk could be followed by a prevention program,” he suggested. “We do this for women who have gestational diabetes,” but for women who have had a hysterectomy, “we didn’t pay attention to this until now.”
No increased risk for endometriosis
While hysterectomy appears to up the risk for diabetes, having endometriosis does not. In a separate analysis of data from the E3N cohort, no effect was seen despite the association between endometriosis and other cardiometabolic risk factors.
The HR for incident type 2 diabetes comparing women with and without endometriosis was 10.06 in a fully adjusted statistical model (95% CI, 0.87-1.29). While there was an increase in the risk for diabetes if a woman had endometriosis and had also had a hysterectomy, this was not significant (HR, 1.22; 95% CI, 0.96-1.54).
The E3N study was sponsored by the French Institute for Health and Research. Dr. Bonnet and Dr. Nilsson had no relevant conflicts of interest to disclose.
Data from a large French cohort study suggest that women who have a hysterectomy before 40-45 years of age may be at particular risk of subsequently developing type 2 diabetes.
A 20% increase in the risk for incident diabetes was found comparing women of all ages who had and had not had a hysterectomy (P = .0003).
This risk jumped to a 52% increase when only women below the age of 45 were considered (P < .0001) and was still 38% higher if only women under 40 years were analyzed (P = .005).
“Our findings clearly show that hysterectomy is a risk marker for diabetes,” Fabrice Bonnet, MD, PhD, of Centre Hospitalier Universitaire (CHU) de Rennes (France), said at the annual meeting of the European Association for the Study of Diabetes.
Importantly, this risk appears to occur “independently of any hormonal therapy, any reproductive factors, physical activity, and diet,” Dr. Bonnet added.
Findings challenged
“I would like to challenge your findings,” said Peter Nilsson, MD, PhD, a professor at Lund (Sweden) University, during the postpresentation discussion period.
“Could there be a detection bias?” queried Dr. Nilsson. “If you undergo surgery like this, there will be several postoperative visits to a physician and there’s a higher likelihood of somebody taking blood samples and detecting diabetes.
“So, if this is true, it could mean that postoperative controls of goiter or thyroid surgery would bring the same findings,” Dr. Nilsson suggested.
“It is an epidemiological cohort of woman followed for a long time,” Dr. Bonnet responded. “So of course, there probably was more blood testing than in the usual population, but we did not observe the association for another type of surgery and type 2 diabetes.”
Clarifying further, Dr. Bonnet said that they had looked at thyroid surgery but not any other types of abdominal surgery.
Assessing the risk of incident diabetes
Hysterectomy is a common surgery among women – more than 400,000 are estimated to be performed every year in the United States, and 80,000 in France, with a rising rate in developing countries, Dr. Bonnet said in an interview.
“We don’t know exactly why that is, but it could have long-term consequences in terms of metabolic effects and the incidence of diabetes,” he said.
Prior research has linked having a hysterectomy with an increased rate of hypertension and cardiovascular risk, and there have also been a few studies linking it to diabetes.
“Our aim was to analyze the relationship between the past history of hysterectomies and the risk of incident diabetes; and specifically, we assessed the influence of age,” Dr. Bonnet said.
To do so, data on more than 83,000 women who had participated in The French E3N Prospective Cohort Study (E3N) were obtained. This large epidemiologic study is the French component of the long-running EPIC study.
For inclusion in the analysis, women had to have no diabetes at baseline, to have had their uterus, ovaries, or both removed for benign gynecologic reasons, and to have had their surgeries performed before any diagnosis of diabetes had been made. A diagnosis of diabetes was identified through the women’s responses to self-report questionnaires and prescriptions for antidiabetic medications.
In all, 2,672 women were found to have developed diabetes during the 16-year follow-up period.
The hazard ratio for the risk of diabetes in women who had and had not had a hysterectomy was 1.30 (95% confidence interval, 1.17-1.43; P < .0001), taking age into account and stratifying for birth generation.
The association held, when there was adjustment for other factors such as smoking status, physical activity, history of diabetes, weight, and adherence to a Mediterranean diet (HR 1.27; 95% CI 1.02-1.05; P = .02).
And, after adjustment for age at menarche, menopausal status, age at which menopause was reached, oral contraceptive and hormone therapy use, and the number of pregnancies, the risk for type 2 diabetes was still apparent in those who had undergoing a hysterectomy (HR, 1.20; 95% CI, 1.09-1.33; P = .0003).
Risk increased with oophorectomy
“Women who had both hysterectomy with bilateral oophorectomy had the highest rates of incident diabetes, as compared to women without hysterectomy and no oophorectomy,” said Dr. Bonnet (HR, 1.26; 95% CI, 1.11-1.42; P = .0003).
“This suggests preserving ovarian function is of importance,” he added. “Try to keep the ovaries in place, so just have hysterectomy alone,” he suggested might be the advice to fellow clinicians.
“So, identifying women at higher risk could be followed by a prevention program,” he suggested. “We do this for women who have gestational diabetes,” but for women who have had a hysterectomy, “we didn’t pay attention to this until now.”
No increased risk for endometriosis
While hysterectomy appears to up the risk for diabetes, having endometriosis does not. In a separate analysis of data from the E3N cohort, no effect was seen despite the association between endometriosis and other cardiometabolic risk factors.
The HR for incident type 2 diabetes comparing women with and without endometriosis was 10.06 in a fully adjusted statistical model (95% CI, 0.87-1.29). While there was an increase in the risk for diabetes if a woman had endometriosis and had also had a hysterectomy, this was not significant (HR, 1.22; 95% CI, 0.96-1.54).
The E3N study was sponsored by the French Institute for Health and Research. Dr. Bonnet and Dr. Nilsson had no relevant conflicts of interest to disclose.
Data from a large French cohort study suggest that women who have a hysterectomy before 40-45 years of age may be at particular risk of subsequently developing type 2 diabetes.
A 20% increase in the risk for incident diabetes was found comparing women of all ages who had and had not had a hysterectomy (P = .0003).
This risk jumped to a 52% increase when only women below the age of 45 were considered (P < .0001) and was still 38% higher if only women under 40 years were analyzed (P = .005).
“Our findings clearly show that hysterectomy is a risk marker for diabetes,” Fabrice Bonnet, MD, PhD, of Centre Hospitalier Universitaire (CHU) de Rennes (France), said at the annual meeting of the European Association for the Study of Diabetes.
Importantly, this risk appears to occur “independently of any hormonal therapy, any reproductive factors, physical activity, and diet,” Dr. Bonnet added.
Findings challenged
“I would like to challenge your findings,” said Peter Nilsson, MD, PhD, a professor at Lund (Sweden) University, during the postpresentation discussion period.
“Could there be a detection bias?” queried Dr. Nilsson. “If you undergo surgery like this, there will be several postoperative visits to a physician and there’s a higher likelihood of somebody taking blood samples and detecting diabetes.
“So, if this is true, it could mean that postoperative controls of goiter or thyroid surgery would bring the same findings,” Dr. Nilsson suggested.
“It is an epidemiological cohort of woman followed for a long time,” Dr. Bonnet responded. “So of course, there probably was more blood testing than in the usual population, but we did not observe the association for another type of surgery and type 2 diabetes.”
Clarifying further, Dr. Bonnet said that they had looked at thyroid surgery but not any other types of abdominal surgery.
Assessing the risk of incident diabetes
Hysterectomy is a common surgery among women – more than 400,000 are estimated to be performed every year in the United States, and 80,000 in France, with a rising rate in developing countries, Dr. Bonnet said in an interview.
“We don’t know exactly why that is, but it could have long-term consequences in terms of metabolic effects and the incidence of diabetes,” he said.
Prior research has linked having a hysterectomy with an increased rate of hypertension and cardiovascular risk, and there have also been a few studies linking it to diabetes.
“Our aim was to analyze the relationship between the past history of hysterectomies and the risk of incident diabetes; and specifically, we assessed the influence of age,” Dr. Bonnet said.
To do so, data on more than 83,000 women who had participated in The French E3N Prospective Cohort Study (E3N) were obtained. This large epidemiologic study is the French component of the long-running EPIC study.
For inclusion in the analysis, women had to have no diabetes at baseline, to have had their uterus, ovaries, or both removed for benign gynecologic reasons, and to have had their surgeries performed before any diagnosis of diabetes had been made. A diagnosis of diabetes was identified through the women’s responses to self-report questionnaires and prescriptions for antidiabetic medications.
In all, 2,672 women were found to have developed diabetes during the 16-year follow-up period.
The hazard ratio for the risk of diabetes in women who had and had not had a hysterectomy was 1.30 (95% confidence interval, 1.17-1.43; P < .0001), taking age into account and stratifying for birth generation.
The association held, when there was adjustment for other factors such as smoking status, physical activity, history of diabetes, weight, and adherence to a Mediterranean diet (HR 1.27; 95% CI 1.02-1.05; P = .02).
And, after adjustment for age at menarche, menopausal status, age at which menopause was reached, oral contraceptive and hormone therapy use, and the number of pregnancies, the risk for type 2 diabetes was still apparent in those who had undergoing a hysterectomy (HR, 1.20; 95% CI, 1.09-1.33; P = .0003).
Risk increased with oophorectomy
“Women who had both hysterectomy with bilateral oophorectomy had the highest rates of incident diabetes, as compared to women without hysterectomy and no oophorectomy,” said Dr. Bonnet (HR, 1.26; 95% CI, 1.11-1.42; P = .0003).
“This suggests preserving ovarian function is of importance,” he added. “Try to keep the ovaries in place, so just have hysterectomy alone,” he suggested might be the advice to fellow clinicians.
“So, identifying women at higher risk could be followed by a prevention program,” he suggested. “We do this for women who have gestational diabetes,” but for women who have had a hysterectomy, “we didn’t pay attention to this until now.”
No increased risk for endometriosis
While hysterectomy appears to up the risk for diabetes, having endometriosis does not. In a separate analysis of data from the E3N cohort, no effect was seen despite the association between endometriosis and other cardiometabolic risk factors.
The HR for incident type 2 diabetes comparing women with and without endometriosis was 10.06 in a fully adjusted statistical model (95% CI, 0.87-1.29). While there was an increase in the risk for diabetes if a woman had endometriosis and had also had a hysterectomy, this was not significant (HR, 1.22; 95% CI, 0.96-1.54).
The E3N study was sponsored by the French Institute for Health and Research. Dr. Bonnet and Dr. Nilsson had no relevant conflicts of interest to disclose.
FROM EASD 2022
Genetic tests create treatment opportunities and confusion for breast cancer patients
The past decade has witnessed a rapid expansion of genetic tests, including new instruments to inform patients who have been diagnosed with breast cancer about the risk of recurrence and to guide their treatment.
Patients are sometimes left paying out-of-pocket for exams that are not yet the standard of care, and even the most up-to-date oncologists may be uncertain how to incorporate the flood of new information into what used to be standard treatment protocols.
A quarter-century ago, Myriad Genetics introduced the first breast cancer genetic test for BRCA mutations, two genes associated with a substantially elevated risk of getting breast cancer, opening the door to a new era in genetic testing. BRCA1 and BRCA2 mutations account for as many as half of all hereditary breast cancers, and people with a problematic mutation on one of those genes have a 45%-72% chance of developing breast cancer during their lifetimes. They may also be at higher risk for ovarian and other cancers than people without harmful BRCA mutations.
But the clinical significance is murkier for many other genetic tests.
Testing for BRCA1 and BRCA2 genes used to cost thousands of dollars. Now, for a fraction of that, doctors can order multigene test panels from commercial labs that look for mutations in dozens of genes. Some direct-to-consumer companies offer screening panels for a few hundred dollars, though their reliability varies.
When Jen Carbary was diagnosed with breast cancer in 2017 at age 44, genetic testing identified a mutation in a gene called PALB2 that significantly increases the risk of developing breast cancer. Guidelines suggest that breast cancer patients with a PALB2 mutation, much like those with BRCA1 and BRCA2 mutations, consider having a mastectomy to reduce the chance of a breast cancer recurrence.
“I wish genetic testing was the standard of care,” said Ms. Carbary, who owed nothing for the test because her insurer covered the cost.
Ms. Carbary, who lives in Sterling Heights, Mich., said the test results affirmed the decision she had already made to have a double mastectomy and provided important information for family members, including her 21-year-old daughter and 18-year-old son, who will likely be tested in their mid-20s or early 30s.
But some breast cancer experts are concerned that widespread testing may also identify genetic mutations whose impact is unclear, creating anxiety and leading to further testing and to treatment of questionable value that could raise costs for the health care system.
It can also confuse patients.
“It happens a lot, that patients find their way to us after getting confusing results elsewhere,” said Mark Robson, MD, chief of the breast medicine service at Memorial Sloan Kettering Cancer Center, New York. Robson said the cancer center has a clinical genetics service, staffed by doctors and genetic counselors, that helps people make decisions about how to manage genetic testing results.
For people diagnosed with breast cancer, many professional groups, including the influential National Comprehensive Cancer Network, recommend limiting testing to certain people, including those with high-risk factors, such as a family history of breast cancer; those who are 45 or younger when they’re diagnosed; and those with Ashkenazi Jewish ancestry.
But in 2019, the American Society of Breast Surgeons recommended a different approach: Offer genetic testing to all patients who are diagnosed with or have a personal history of breast cancer. The recommendation was controversial.
“The NCCN guidelines [cover] most of the women who needed testing, but we wanted to get them all,” said Eric Manahan, MD, a general surgeon in Dalton, Georgia, and a member of the surgeons group’s board of directors.
Mutations on other genes that are associated with breast cancer are much less common than BRCA1 and BRCA2 mutations and generally don’t increase the risk of developing breast cancer as much. The cancer-causing impact of these genes may be less clear than that of the BRCA genes, which have been tested for since the mid-1990s.
And the appropriate response to the less common mutations – whether to consider a risk-reducing mastectomy or stepped-up screening – is often unclear.
“Things get sloppier and sloppier when you look at other genes,” said Steven Katz, MD, MPH, a professor of medicine and health management and policy at the University of Michigan. “The risks tend to be lower for different cancers, and less certain and more variable. You might walk away wondering: ‘Why’d I have to know that?’ ”
After people are diagnosed with breast cancer, genetic testing can help inform their decisions about the types of surgery to pursue – for example, a high risk of recurrence or a new breast cancer might persuade some to opt for more extensive surgery, such as a double mastectomy. Testing can also provide important information to family members about their potential cancer risk.
(This type of “germline” genetic testing, as it’s called, looks at mutations in the genes that people inherit from their parents. It is different from genomic tumor tests that look at specific genes or proteins in the cancer cells and can help doctors understand the rate at which the cancer cells are dividing, for example, and the likelihood of a cancer recurrence.)
Increasingly, germline genetic testing can also help guide other treatment decisions. Some patients with metastatic breast cancer who have BRCA1 or BRCA2 mutations may be good candidates for poly (ADP-ribose) polymerase inhibitors, cancer drugs that target tumors with mutations in those genes.
But genetic testing that uncovers inherited mutations in many other genes yields less clearly actionable information, even though positive results may alarm people.
At Memorial Sloan Kettering, cancer specialists focus on “therapeutic actionability,” said Dr. Robson. Will testing help someone decide whether she should get a double mastectomy or provide other important guidance? “A policy of testing everyone will identify very few additional BRCA breast mutations but will cost a lot.”
As a result, doctors are debating how best to deploy and incorporate new genetic knowledge. Insurers are trying to figure out which to pay for.
There is both underuse of tests that science says are relevant and overuse of tests that experts say provide information that can’t be interpreted with any scientific certainty.
The result may be confusion for patients newly diagnosed with breast cancer as they confront the expense of genetic tests and sometimes little guidance on the proper treatment.
Some doctors say the first step is to make sure that the small group of people who would clearly benefit are getting the genetic tests whose meaning is clearly understood. Only 15% of breast cancer patients who met select NCCN testing guidelines for inherited cancer received genetic testing, according to a 2017 study that examined data from a national household health survey between 2005 and 2015.
“I would argue that our focus needs to be on the people who are at high risk for breast cancer that aren’t even identified yet,” said Tuya Pal, MD, associate director for cancer health disparities at Vanderbilt-Ingram Cancer Center and vice chair of the NCCN guidelines panel for genetic/familial high-risk assessment of breast, ovarian, and pancreatic cancers.
Patients may fall through the cracks because no one tells them they should be tested. In one analysis, 56% of high-risk breast cancer patients who didn’t get genetic testing said their doctors didn’t recommend it.
Even if doctors recommend genetic testing, they may lack the expertise to determine which tests people need and how to interpret the results. That’s the role of genetic counselors, but their ranks are stretched thin.
The consequences can be serious. In a study of 666 breast cancer patients who received genetic testing, half of those at average risk for inherited cancer got double mastectomies based on test results that found “variants of uncertain significance,” which aren’t clinically actionable. As many as half of surgeons reported managing such patients the same way as those with cancer-causing mutations.
“The bulk of our research would say that there is still room for improvement in terms of clinicians getting the understanding they need,” said Allison Kurian, MD, director of the women’s clinical cancer genetics program at Stanford (Calif.) University and a coauthor of the study.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
The past decade has witnessed a rapid expansion of genetic tests, including new instruments to inform patients who have been diagnosed with breast cancer about the risk of recurrence and to guide their treatment.
Patients are sometimes left paying out-of-pocket for exams that are not yet the standard of care, and even the most up-to-date oncologists may be uncertain how to incorporate the flood of new information into what used to be standard treatment protocols.
A quarter-century ago, Myriad Genetics introduced the first breast cancer genetic test for BRCA mutations, two genes associated with a substantially elevated risk of getting breast cancer, opening the door to a new era in genetic testing. BRCA1 and BRCA2 mutations account for as many as half of all hereditary breast cancers, and people with a problematic mutation on one of those genes have a 45%-72% chance of developing breast cancer during their lifetimes. They may also be at higher risk for ovarian and other cancers than people without harmful BRCA mutations.
But the clinical significance is murkier for many other genetic tests.
Testing for BRCA1 and BRCA2 genes used to cost thousands of dollars. Now, for a fraction of that, doctors can order multigene test panels from commercial labs that look for mutations in dozens of genes. Some direct-to-consumer companies offer screening panels for a few hundred dollars, though their reliability varies.
When Jen Carbary was diagnosed with breast cancer in 2017 at age 44, genetic testing identified a mutation in a gene called PALB2 that significantly increases the risk of developing breast cancer. Guidelines suggest that breast cancer patients with a PALB2 mutation, much like those with BRCA1 and BRCA2 mutations, consider having a mastectomy to reduce the chance of a breast cancer recurrence.
“I wish genetic testing was the standard of care,” said Ms. Carbary, who owed nothing for the test because her insurer covered the cost.
Ms. Carbary, who lives in Sterling Heights, Mich., said the test results affirmed the decision she had already made to have a double mastectomy and provided important information for family members, including her 21-year-old daughter and 18-year-old son, who will likely be tested in their mid-20s or early 30s.
But some breast cancer experts are concerned that widespread testing may also identify genetic mutations whose impact is unclear, creating anxiety and leading to further testing and to treatment of questionable value that could raise costs for the health care system.
It can also confuse patients.
“It happens a lot, that patients find their way to us after getting confusing results elsewhere,” said Mark Robson, MD, chief of the breast medicine service at Memorial Sloan Kettering Cancer Center, New York. Robson said the cancer center has a clinical genetics service, staffed by doctors and genetic counselors, that helps people make decisions about how to manage genetic testing results.
For people diagnosed with breast cancer, many professional groups, including the influential National Comprehensive Cancer Network, recommend limiting testing to certain people, including those with high-risk factors, such as a family history of breast cancer; those who are 45 or younger when they’re diagnosed; and those with Ashkenazi Jewish ancestry.
But in 2019, the American Society of Breast Surgeons recommended a different approach: Offer genetic testing to all patients who are diagnosed with or have a personal history of breast cancer. The recommendation was controversial.
“The NCCN guidelines [cover] most of the women who needed testing, but we wanted to get them all,” said Eric Manahan, MD, a general surgeon in Dalton, Georgia, and a member of the surgeons group’s board of directors.
Mutations on other genes that are associated with breast cancer are much less common than BRCA1 and BRCA2 mutations and generally don’t increase the risk of developing breast cancer as much. The cancer-causing impact of these genes may be less clear than that of the BRCA genes, which have been tested for since the mid-1990s.
And the appropriate response to the less common mutations – whether to consider a risk-reducing mastectomy or stepped-up screening – is often unclear.
“Things get sloppier and sloppier when you look at other genes,” said Steven Katz, MD, MPH, a professor of medicine and health management and policy at the University of Michigan. “The risks tend to be lower for different cancers, and less certain and more variable. You might walk away wondering: ‘Why’d I have to know that?’ ”
After people are diagnosed with breast cancer, genetic testing can help inform their decisions about the types of surgery to pursue – for example, a high risk of recurrence or a new breast cancer might persuade some to opt for more extensive surgery, such as a double mastectomy. Testing can also provide important information to family members about their potential cancer risk.
(This type of “germline” genetic testing, as it’s called, looks at mutations in the genes that people inherit from their parents. It is different from genomic tumor tests that look at specific genes or proteins in the cancer cells and can help doctors understand the rate at which the cancer cells are dividing, for example, and the likelihood of a cancer recurrence.)
Increasingly, germline genetic testing can also help guide other treatment decisions. Some patients with metastatic breast cancer who have BRCA1 or BRCA2 mutations may be good candidates for poly (ADP-ribose) polymerase inhibitors, cancer drugs that target tumors with mutations in those genes.
But genetic testing that uncovers inherited mutations in many other genes yields less clearly actionable information, even though positive results may alarm people.
At Memorial Sloan Kettering, cancer specialists focus on “therapeutic actionability,” said Dr. Robson. Will testing help someone decide whether she should get a double mastectomy or provide other important guidance? “A policy of testing everyone will identify very few additional BRCA breast mutations but will cost a lot.”
As a result, doctors are debating how best to deploy and incorporate new genetic knowledge. Insurers are trying to figure out which to pay for.
There is both underuse of tests that science says are relevant and overuse of tests that experts say provide information that can’t be interpreted with any scientific certainty.
The result may be confusion for patients newly diagnosed with breast cancer as they confront the expense of genetic tests and sometimes little guidance on the proper treatment.
Some doctors say the first step is to make sure that the small group of people who would clearly benefit are getting the genetic tests whose meaning is clearly understood. Only 15% of breast cancer patients who met select NCCN testing guidelines for inherited cancer received genetic testing, according to a 2017 study that examined data from a national household health survey between 2005 and 2015.
“I would argue that our focus needs to be on the people who are at high risk for breast cancer that aren’t even identified yet,” said Tuya Pal, MD, associate director for cancer health disparities at Vanderbilt-Ingram Cancer Center and vice chair of the NCCN guidelines panel for genetic/familial high-risk assessment of breast, ovarian, and pancreatic cancers.
Patients may fall through the cracks because no one tells them they should be tested. In one analysis, 56% of high-risk breast cancer patients who didn’t get genetic testing said their doctors didn’t recommend it.
Even if doctors recommend genetic testing, they may lack the expertise to determine which tests people need and how to interpret the results. That’s the role of genetic counselors, but their ranks are stretched thin.
The consequences can be serious. In a study of 666 breast cancer patients who received genetic testing, half of those at average risk for inherited cancer got double mastectomies based on test results that found “variants of uncertain significance,” which aren’t clinically actionable. As many as half of surgeons reported managing such patients the same way as those with cancer-causing mutations.
“The bulk of our research would say that there is still room for improvement in terms of clinicians getting the understanding they need,” said Allison Kurian, MD, director of the women’s clinical cancer genetics program at Stanford (Calif.) University and a coauthor of the study.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
The past decade has witnessed a rapid expansion of genetic tests, including new instruments to inform patients who have been diagnosed with breast cancer about the risk of recurrence and to guide their treatment.
Patients are sometimes left paying out-of-pocket for exams that are not yet the standard of care, and even the most up-to-date oncologists may be uncertain how to incorporate the flood of new information into what used to be standard treatment protocols.
A quarter-century ago, Myriad Genetics introduced the first breast cancer genetic test for BRCA mutations, two genes associated with a substantially elevated risk of getting breast cancer, opening the door to a new era in genetic testing. BRCA1 and BRCA2 mutations account for as many as half of all hereditary breast cancers, and people with a problematic mutation on one of those genes have a 45%-72% chance of developing breast cancer during their lifetimes. They may also be at higher risk for ovarian and other cancers than people without harmful BRCA mutations.
But the clinical significance is murkier for many other genetic tests.
Testing for BRCA1 and BRCA2 genes used to cost thousands of dollars. Now, for a fraction of that, doctors can order multigene test panels from commercial labs that look for mutations in dozens of genes. Some direct-to-consumer companies offer screening panels for a few hundred dollars, though their reliability varies.
When Jen Carbary was diagnosed with breast cancer in 2017 at age 44, genetic testing identified a mutation in a gene called PALB2 that significantly increases the risk of developing breast cancer. Guidelines suggest that breast cancer patients with a PALB2 mutation, much like those with BRCA1 and BRCA2 mutations, consider having a mastectomy to reduce the chance of a breast cancer recurrence.
“I wish genetic testing was the standard of care,” said Ms. Carbary, who owed nothing for the test because her insurer covered the cost.
Ms. Carbary, who lives in Sterling Heights, Mich., said the test results affirmed the decision she had already made to have a double mastectomy and provided important information for family members, including her 21-year-old daughter and 18-year-old son, who will likely be tested in their mid-20s or early 30s.
But some breast cancer experts are concerned that widespread testing may also identify genetic mutations whose impact is unclear, creating anxiety and leading to further testing and to treatment of questionable value that could raise costs for the health care system.
It can also confuse patients.
“It happens a lot, that patients find their way to us after getting confusing results elsewhere,” said Mark Robson, MD, chief of the breast medicine service at Memorial Sloan Kettering Cancer Center, New York. Robson said the cancer center has a clinical genetics service, staffed by doctors and genetic counselors, that helps people make decisions about how to manage genetic testing results.
For people diagnosed with breast cancer, many professional groups, including the influential National Comprehensive Cancer Network, recommend limiting testing to certain people, including those with high-risk factors, such as a family history of breast cancer; those who are 45 or younger when they’re diagnosed; and those with Ashkenazi Jewish ancestry.
But in 2019, the American Society of Breast Surgeons recommended a different approach: Offer genetic testing to all patients who are diagnosed with or have a personal history of breast cancer. The recommendation was controversial.
“The NCCN guidelines [cover] most of the women who needed testing, but we wanted to get them all,” said Eric Manahan, MD, a general surgeon in Dalton, Georgia, and a member of the surgeons group’s board of directors.
Mutations on other genes that are associated with breast cancer are much less common than BRCA1 and BRCA2 mutations and generally don’t increase the risk of developing breast cancer as much. The cancer-causing impact of these genes may be less clear than that of the BRCA genes, which have been tested for since the mid-1990s.
And the appropriate response to the less common mutations – whether to consider a risk-reducing mastectomy or stepped-up screening – is often unclear.
“Things get sloppier and sloppier when you look at other genes,” said Steven Katz, MD, MPH, a professor of medicine and health management and policy at the University of Michigan. “The risks tend to be lower for different cancers, and less certain and more variable. You might walk away wondering: ‘Why’d I have to know that?’ ”
After people are diagnosed with breast cancer, genetic testing can help inform their decisions about the types of surgery to pursue – for example, a high risk of recurrence or a new breast cancer might persuade some to opt for more extensive surgery, such as a double mastectomy. Testing can also provide important information to family members about their potential cancer risk.
(This type of “germline” genetic testing, as it’s called, looks at mutations in the genes that people inherit from their parents. It is different from genomic tumor tests that look at specific genes or proteins in the cancer cells and can help doctors understand the rate at which the cancer cells are dividing, for example, and the likelihood of a cancer recurrence.)
Increasingly, germline genetic testing can also help guide other treatment decisions. Some patients with metastatic breast cancer who have BRCA1 or BRCA2 mutations may be good candidates for poly (ADP-ribose) polymerase inhibitors, cancer drugs that target tumors with mutations in those genes.
But genetic testing that uncovers inherited mutations in many other genes yields less clearly actionable information, even though positive results may alarm people.
At Memorial Sloan Kettering, cancer specialists focus on “therapeutic actionability,” said Dr. Robson. Will testing help someone decide whether she should get a double mastectomy or provide other important guidance? “A policy of testing everyone will identify very few additional BRCA breast mutations but will cost a lot.”
As a result, doctors are debating how best to deploy and incorporate new genetic knowledge. Insurers are trying to figure out which to pay for.
There is both underuse of tests that science says are relevant and overuse of tests that experts say provide information that can’t be interpreted with any scientific certainty.
The result may be confusion for patients newly diagnosed with breast cancer as they confront the expense of genetic tests and sometimes little guidance on the proper treatment.
Some doctors say the first step is to make sure that the small group of people who would clearly benefit are getting the genetic tests whose meaning is clearly understood. Only 15% of breast cancer patients who met select NCCN testing guidelines for inherited cancer received genetic testing, according to a 2017 study that examined data from a national household health survey between 2005 and 2015.
“I would argue that our focus needs to be on the people who are at high risk for breast cancer that aren’t even identified yet,” said Tuya Pal, MD, associate director for cancer health disparities at Vanderbilt-Ingram Cancer Center and vice chair of the NCCN guidelines panel for genetic/familial high-risk assessment of breast, ovarian, and pancreatic cancers.
Patients may fall through the cracks because no one tells them they should be tested. In one analysis, 56% of high-risk breast cancer patients who didn’t get genetic testing said their doctors didn’t recommend it.
Even if doctors recommend genetic testing, they may lack the expertise to determine which tests people need and how to interpret the results. That’s the role of genetic counselors, but their ranks are stretched thin.
The consequences can be serious. In a study of 666 breast cancer patients who received genetic testing, half of those at average risk for inherited cancer got double mastectomies based on test results that found “variants of uncertain significance,” which aren’t clinically actionable. As many as half of surgeons reported managing such patients the same way as those with cancer-causing mutations.
“The bulk of our research would say that there is still room for improvement in terms of clinicians getting the understanding they need,” said Allison Kurian, MD, director of the women’s clinical cancer genetics program at Stanford (Calif.) University and a coauthor of the study.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Early bird gets the worm, night owl gets the diabetes
Metabolism a player in circadian rhythm section
Are you an early bird, or do you wake up and stare at your phone, wondering why you were up watching “The Crown” until 3 a.m.? Recent research suggests that people who wake up earlier tend to be more active during the day and burn more fat than those who sleep in. Fat builds up in the night owls, putting them at higher risk of type 2 diabetes and heart disease.
The study gives physicians something to think about when assessing a patient’s risk factors. “This could help medical professionals consider another behavioral factor contributing to disease risk,” Steven Malin, PhD, lead author of the study and expert in metabolism at Rutgers University in New Brunswick, N.J., said in The Guardian.
For the research, 51 participants were divided into night owls and early birds, depending on their answers to a questionnaire. They were examined, monitored for a week, and assessed while doing various activities. Those who woke up early tended to be more sensitive to insulin and burned off fat faster than those who woke up late, the researchers explained.
“Night owls are reported to have a higher risk of obesity, type 2 diabetes, and cardiovascular disease when compared with early birds,” Dr. Malin said. “A potential explanation is they become misaligned with their circadian rhythm for various reasons, but most notably among adults would be work.”
We all know that we may not be at our best when we throw off our internal clocks by going to sleep late and waking up early. Think about that next time you start another episode on Netflix at 2:57 a.m.
Mosquitoes, chemical cocktails, and glass sock beads
We all know that mosquitoes are annoying little disease vectors with a taste for human blood. One of the less-known things about mosquitoes is what attracts them to humans in the first place. It’s so less known that, until now, it was unknown. Oh sure, we knew that odor was involved, and that lactic acid was part of the odor equation, but what are the specific chemicals? Well, there’s carbon dioxide … and ammonia. Those were already known.
Ring Cardé, PhD, an entomologist at the University of California, Riverside, wasn’t convinced. “I suspected there was something undiscovered about the chemistry of odors luring the yellow fever mosquito. I wanted to nail down the exact blend,” he said in a statement from the university.
Dr. Cardé and his associates eventually figured out that the exact chemical cocktail attracting female Aedes aegypti mosquitoes was a combination of carbon dioxide plus two chemicals, 2-ketoglutaric acid and lactic acid. The odor from these chemicals enables mosquitoes to locate and land on their victim and “also encourages probing, the use of piercing mouthparts to find blood,” the university said.
This amazing destination of science is important, but we have to acknowledge the journey as well. To do that we turn to one of Dr. Cardé’s associates, Jan Bello, PhD, formerly of Cal-Riverside and now with insect pest control company Provivi. Turns out that 2-ketoglutaric acid is tricky stuff because the methods typically used to identify chemicals don’t work on it.
Dr. Bello employed a somewhat unorthodox chemical extraction method: He filled his socks with glass beads and walked around with the beads in his socks. 
“Wearing the beads felt almost like a massage, like squeezing stress balls full of sand, but with your feet,” Dr. Bello said. “The most frustrating part of doing it for a long time is that they would get stuck in between your toes, so it would be uncomfortable after a while.”
We hate when science gets stuck between our toes, but we love it when scientists write their own punchlines.
The MS drugs are better down where it’s wetter, take it from me
The myth of the mermaid is one with hundreds, if not thousands, of years of history. The ancient Greeks had the mythological siren, while the Babylonians depicted kulullû (which were mermen – never let the Babylonians be known as noninclusive) in artwork as far back as 1600 BC. Cultures as far flung as Japan, southern Africa, and New Zealand have folkloric figures similar to the mermaid. It is most decidedly not a creation of western Europe, Hans Christian Andersen, or Disney.
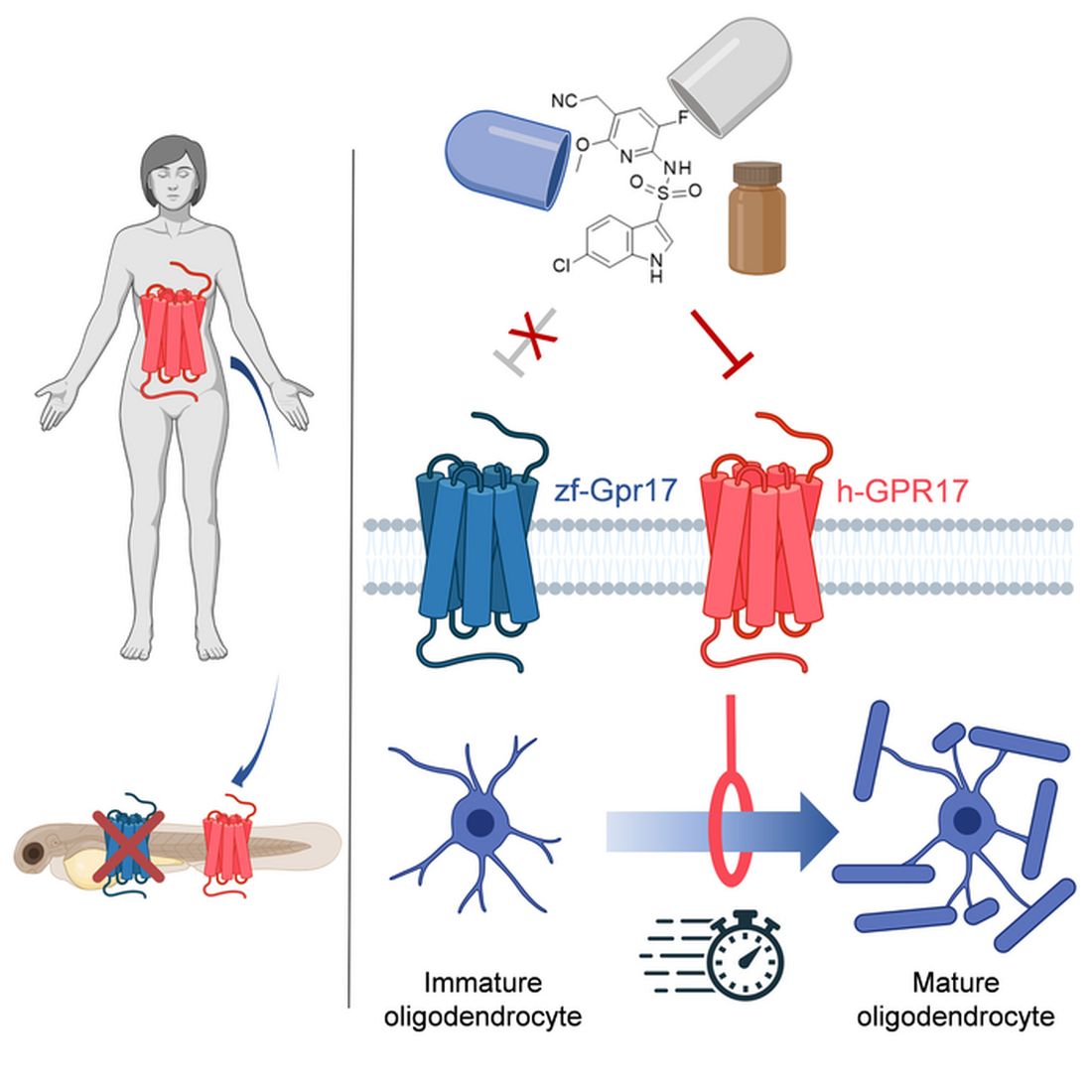
With that mild rant out of the way, let’s move to Germany and a group of researchers from the University of Bonn, who have not created a mermaid. They did, however, add human genes to a zebrafish for research purposes, which feels uncomfortably close. Nothing better than unholy animal-human hybrids, right?
Stick with us here, because the researchers did have a good reason for their gene splicing. Zebrafish and humans both have the GPR17 receptor, which is highly active in nerve tissue. When GPR17 is overactivated, diseases such as multiple sclerosis can develop. Because the zebrafish has this receptor, which performs the same function in its body as in ours, it’s a prime candidate for replacement. Also, zebrafish larvae are transparent, which makes it very easy to observe a drug working.
That said, fish and humans are very far apart, genetically speaking. Big shock right there. But by replacing their GPR17 receptor with ours, the scientists have created a fish that we could test drug candidates on and be assured that they would also work on humans. Actually testing drugs for MS on these humanized zebrafish was beyond the scope of the study, but the researchers said that the new genes function normally in the fish larvae, making them a promising new avenue for MS drug development.
Can we all promise not to tell Disney that human DNA can be spliced into a fish without consequence? Otherwise, we’re just going to have to sit through another “Little Mermaid” adaptation in 30 years, this one in super live-action featuring actual, real-life mermaids. And we’re not ready for that level of man-made horror just yet.
Beware of the fly vomit
Picture this: You’re outside at a picnic or barbecue, loading a plate with food. In a brief moment of conversation a fly lands right on top of your sandwich. You shoo it away and think nothing more of it, eating the sandwich anyway. We’ve all been there.
A recent study is making us think again.
John Stoffolano, an entomology professor at the University of Massachusetts, Amherst, claims that too much attention has been focused on pathogen transmission by the biting, blood-feeding flies when really we should be taking note of the nonbiting, or synanthropic, flies we live with, which may have a greater impact on the transmission of pathogens right in our own homes.

Sure, blood-feeding flies can spread pathogens directly, but house flies vomit every time they land on something. Think about that.
The fly that sneakily swooped into your house from a tear in your window screen has just been outside in the neighbor’s garbage or sitting on dog poop and now has who knows what filling its crop, the tank in their body that serves as “a place to store food before it makes its way into the digestive tract where it will get turned into energy for the fly,” Dr. Stoffolano explained in a written statement.
Did that fly land right on the baked potato you were prepping for dinner before you shooed it away? Guess what? Before flying off it emitted excess water that has pathogens from whatever was in its crop. We don’t want to say your potato might have dog poop on it, but you get the idea. The crop doesn’t have a ton of digestive enzymes that would help neutralize pathogens, so whatever that fly regurgitated before buzzing off is still around for you to ingest and there’s not much you can do about it.
More research needs to be done about flies, but at the very least this study should make you think twice before eating that baked potato after a fly has been there.
Metabolism a player in circadian rhythm section
Are you an early bird, or do you wake up and stare at your phone, wondering why you were up watching “The Crown” until 3 a.m.? Recent research suggests that people who wake up earlier tend to be more active during the day and burn more fat than those who sleep in. Fat builds up in the night owls, putting them at higher risk of type 2 diabetes and heart disease.
The study gives physicians something to think about when assessing a patient’s risk factors. “This could help medical professionals consider another behavioral factor contributing to disease risk,” Steven Malin, PhD, lead author of the study and expert in metabolism at Rutgers University in New Brunswick, N.J., said in The Guardian.
For the research, 51 participants were divided into night owls and early birds, depending on their answers to a questionnaire. They were examined, monitored for a week, and assessed while doing various activities. Those who woke up early tended to be more sensitive to insulin and burned off fat faster than those who woke up late, the researchers explained.
“Night owls are reported to have a higher risk of obesity, type 2 diabetes, and cardiovascular disease when compared with early birds,” Dr. Malin said. “A potential explanation is they become misaligned with their circadian rhythm for various reasons, but most notably among adults would be work.”
We all know that we may not be at our best when we throw off our internal clocks by going to sleep late and waking up early. Think about that next time you start another episode on Netflix at 2:57 a.m.
Mosquitoes, chemical cocktails, and glass sock beads
We all know that mosquitoes are annoying little disease vectors with a taste for human blood. One of the less-known things about mosquitoes is what attracts them to humans in the first place. It’s so less known that, until now, it was unknown. Oh sure, we knew that odor was involved, and that lactic acid was part of the odor equation, but what are the specific chemicals? Well, there’s carbon dioxide … and ammonia. Those were already known.
Ring Cardé, PhD, an entomologist at the University of California, Riverside, wasn’t convinced. “I suspected there was something undiscovered about the chemistry of odors luring the yellow fever mosquito. I wanted to nail down the exact blend,” he said in a statement from the university.
Dr. Cardé and his associates eventually figured out that the exact chemical cocktail attracting female Aedes aegypti mosquitoes was a combination of carbon dioxide plus two chemicals, 2-ketoglutaric acid and lactic acid. The odor from these chemicals enables mosquitoes to locate and land on their victim and “also encourages probing, the use of piercing mouthparts to find blood,” the university said.
This amazing destination of science is important, but we have to acknowledge the journey as well. To do that we turn to one of Dr. Cardé’s associates, Jan Bello, PhD, formerly of Cal-Riverside and now with insect pest control company Provivi. Turns out that 2-ketoglutaric acid is tricky stuff because the methods typically used to identify chemicals don’t work on it.
Dr. Bello employed a somewhat unorthodox chemical extraction method: He filled his socks with glass beads and walked around with the beads in his socks.
“Wearing the beads felt almost like a massage, like squeezing stress balls full of sand, but with your feet,” Dr. Bello said. “The most frustrating part of doing it for a long time is that they would get stuck in between your toes, so it would be uncomfortable after a while.”
We hate when science gets stuck between our toes, but we love it when scientists write their own punchlines.
The MS drugs are better down where it’s wetter, take it from me
The myth of the mermaid is one with hundreds, if not thousands, of years of history. The ancient Greeks had the mythological siren, while the Babylonians depicted kulullû (which were mermen – never let the Babylonians be known as noninclusive) in artwork as far back as 1600 BC. Cultures as far flung as Japan, southern Africa, and New Zealand have folkloric figures similar to the mermaid. It is most decidedly not a creation of western Europe, Hans Christian Andersen, or Disney.
With that mild rant out of the way, let’s move to Germany and a group of researchers from the University of Bonn, who have not created a mermaid. They did, however, add human genes to a zebrafish for research purposes, which feels uncomfortably close. Nothing better than unholy animal-human hybrids, right?
Stick with us here, because the researchers did have a good reason for their gene splicing. Zebrafish and humans both have the GPR17 receptor, which is highly active in nerve tissue. When GPR17 is overactivated, diseases such as multiple sclerosis can develop. Because the zebrafish has this receptor, which performs the same function in its body as in ours, it’s a prime candidate for replacement. Also, zebrafish larvae are transparent, which makes it very easy to observe a drug working.
That said, fish and humans are very far apart, genetically speaking. Big shock right there. But by replacing their GPR17 receptor with ours, the scientists have created a fish that we could test drug candidates on and be assured that they would also work on humans. Actually testing drugs for MS on these humanized zebrafish was beyond the scope of the study, but the researchers said that the new genes function normally in the fish larvae, making them a promising new avenue for MS drug development.
Can we all promise not to tell Disney that human DNA can be spliced into a fish without consequence? Otherwise, we’re just going to have to sit through another “Little Mermaid” adaptation in 30 years, this one in super live-action featuring actual, real-life mermaids. And we’re not ready for that level of man-made horror just yet.
Beware of the fly vomit
Picture this: You’re outside at a picnic or barbecue, loading a plate with food. In a brief moment of conversation a fly lands right on top of your sandwich. You shoo it away and think nothing more of it, eating the sandwich anyway. We’ve all been there.
A recent study is making us think again.
John Stoffolano, an entomology professor at the University of Massachusetts, Amherst, claims that too much attention has been focused on pathogen transmission by the biting, blood-feeding flies when really we should be taking note of the nonbiting, or synanthropic, flies we live with, which may have a greater impact on the transmission of pathogens right in our own homes.
Sure, blood-feeding flies can spread pathogens directly, but house flies vomit every time they land on something. Think about that.
The fly that sneakily swooped into your house from a tear in your window screen has just been outside in the neighbor’s garbage or sitting on dog poop and now has who knows what filling its crop, the tank in their body that serves as “a place to store food before it makes its way into the digestive tract where it will get turned into energy for the fly,” Dr. Stoffolano explained in a written statement.
Did that fly land right on the baked potato you were prepping for dinner before you shooed it away? Guess what? Before flying off it emitted excess water that has pathogens from whatever was in its crop. We don’t want to say your potato might have dog poop on it, but you get the idea. The crop doesn’t have a ton of digestive enzymes that would help neutralize pathogens, so whatever that fly regurgitated before buzzing off is still around for you to ingest and there’s not much you can do about it.
More research needs to be done about flies, but at the very least this study should make you think twice before eating that baked potato after a fly has been there.
Metabolism a player in circadian rhythm section
Are you an early bird, or do you wake up and stare at your phone, wondering why you were up watching “The Crown” until 3 a.m.? Recent research suggests that people who wake up earlier tend to be more active during the day and burn more fat than those who sleep in. Fat builds up in the night owls, putting them at higher risk of type 2 diabetes and heart disease.
The study gives physicians something to think about when assessing a patient’s risk factors. “This could help medical professionals consider another behavioral factor contributing to disease risk,” Steven Malin, PhD, lead author of the study and expert in metabolism at Rutgers University in New Brunswick, N.J., said in The Guardian.
For the research, 51 participants were divided into night owls and early birds, depending on their answers to a questionnaire. They were examined, monitored for a week, and assessed while doing various activities. Those who woke up early tended to be more sensitive to insulin and burned off fat faster than those who woke up late, the researchers explained.
“Night owls are reported to have a higher risk of obesity, type 2 diabetes, and cardiovascular disease when compared with early birds,” Dr. Malin said. “A potential explanation is they become misaligned with their circadian rhythm for various reasons, but most notably among adults would be work.”
We all know that we may not be at our best when we throw off our internal clocks by going to sleep late and waking up early. Think about that next time you start another episode on Netflix at 2:57 a.m.
Mosquitoes, chemical cocktails, and glass sock beads
We all know that mosquitoes are annoying little disease vectors with a taste for human blood. One of the less-known things about mosquitoes is what attracts them to humans in the first place. It’s so less known that, until now, it was unknown. Oh sure, we knew that odor was involved, and that lactic acid was part of the odor equation, but what are the specific chemicals? Well, there’s carbon dioxide … and ammonia. Those were already known.
Ring Cardé, PhD, an entomologist at the University of California, Riverside, wasn’t convinced. “I suspected there was something undiscovered about the chemistry of odors luring the yellow fever mosquito. I wanted to nail down the exact blend,” he said in a statement from the university.
Dr. Cardé and his associates eventually figured out that the exact chemical cocktail attracting female Aedes aegypti mosquitoes was a combination of carbon dioxide plus two chemicals, 2-ketoglutaric acid and lactic acid. The odor from these chemicals enables mosquitoes to locate and land on their victim and “also encourages probing, the use of piercing mouthparts to find blood,” the university said.
This amazing destination of science is important, but we have to acknowledge the journey as well. To do that we turn to one of Dr. Cardé’s associates, Jan Bello, PhD, formerly of Cal-Riverside and now with insect pest control company Provivi. Turns out that 2-ketoglutaric acid is tricky stuff because the methods typically used to identify chemicals don’t work on it.
Dr. Bello employed a somewhat unorthodox chemical extraction method: He filled his socks with glass beads and walked around with the beads in his socks.
“Wearing the beads felt almost like a massage, like squeezing stress balls full of sand, but with your feet,” Dr. Bello said. “The most frustrating part of doing it for a long time is that they would get stuck in between your toes, so it would be uncomfortable after a while.”
We hate when science gets stuck between our toes, but we love it when scientists write their own punchlines.
The MS drugs are better down where it’s wetter, take it from me
The myth of the mermaid is one with hundreds, if not thousands, of years of history. The ancient Greeks had the mythological siren, while the Babylonians depicted kulullû (which were mermen – never let the Babylonians be known as noninclusive) in artwork as far back as 1600 BC. Cultures as far flung as Japan, southern Africa, and New Zealand have folkloric figures similar to the mermaid. It is most decidedly not a creation of western Europe, Hans Christian Andersen, or Disney.
With that mild rant out of the way, let’s move to Germany and a group of researchers from the University of Bonn, who have not created a mermaid. They did, however, add human genes to a zebrafish for research purposes, which feels uncomfortably close. Nothing better than unholy animal-human hybrids, right?
Stick with us here, because the researchers did have a good reason for their gene splicing. Zebrafish and humans both have the GPR17 receptor, which is highly active in nerve tissue. When GPR17 is overactivated, diseases such as multiple sclerosis can develop. Because the zebrafish has this receptor, which performs the same function in its body as in ours, it’s a prime candidate for replacement. Also, zebrafish larvae are transparent, which makes it very easy to observe a drug working.
That said, fish and humans are very far apart, genetically speaking. Big shock right there. But by replacing their GPR17 receptor with ours, the scientists have created a fish that we could test drug candidates on and be assured that they would also work on humans. Actually testing drugs for MS on these humanized zebrafish was beyond the scope of the study, but the researchers said that the new genes function normally in the fish larvae, making them a promising new avenue for MS drug development.
Can we all promise not to tell Disney that human DNA can be spliced into a fish without consequence? Otherwise, we’re just going to have to sit through another “Little Mermaid” adaptation in 30 years, this one in super live-action featuring actual, real-life mermaids. And we’re not ready for that level of man-made horror just yet.
Beware of the fly vomit
Picture this: You’re outside at a picnic or barbecue, loading a plate with food. In a brief moment of conversation a fly lands right on top of your sandwich. You shoo it away and think nothing more of it, eating the sandwich anyway. We’ve all been there.
A recent study is making us think again.
John Stoffolano, an entomology professor at the University of Massachusetts, Amherst, claims that too much attention has been focused on pathogen transmission by the biting, blood-feeding flies when really we should be taking note of the nonbiting, or synanthropic, flies we live with, which may have a greater impact on the transmission of pathogens right in our own homes.
Sure, blood-feeding flies can spread pathogens directly, but house flies vomit every time they land on something. Think about that.
The fly that sneakily swooped into your house from a tear in your window screen has just been outside in the neighbor’s garbage or sitting on dog poop and now has who knows what filling its crop, the tank in their body that serves as “a place to store food before it makes its way into the digestive tract where it will get turned into energy for the fly,” Dr. Stoffolano explained in a written statement.
Did that fly land right on the baked potato you were prepping for dinner before you shooed it away? Guess what? Before flying off it emitted excess water that has pathogens from whatever was in its crop. We don’t want to say your potato might have dog poop on it, but you get the idea. The crop doesn’t have a ton of digestive enzymes that would help neutralize pathogens, so whatever that fly regurgitated before buzzing off is still around for you to ingest and there’s not much you can do about it.
More research needs to be done about flies, but at the very least this study should make you think twice before eating that baked potato after a fly has been there.
Community-level actions could mitigate maternal mortality
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Early trial supports hypofractionated radiotherapy in uterine cancer
Postoperative radiotherapy is a mainstay in the treatment of uterine cancer, but the typical 5-week regimen can be time-consuming and expensive. A pilot study found that delivery of approximately the same dose over just 2.5 weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, who is an associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues, and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in the hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective [compared to standard protocol], and their study cannot answer that at any rate because it was not designed to answer that question,” said Dr. Williams in an interview. She also noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is [equivalent]. Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” Dr. Williams said.
The study’s findings
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 serous or clear cell, 3 carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
Postoperative radiotherapy is a mainstay in the treatment of uterine cancer, but the typical 5-week regimen can be time-consuming and expensive. A pilot study found that delivery of approximately the same dose over just 2.5 weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, who is an associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues, and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in the hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective [compared to standard protocol], and their study cannot answer that at any rate because it was not designed to answer that question,” said Dr. Williams in an interview. She also noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is [equivalent]. Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” Dr. Williams said.
The study’s findings
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 serous or clear cell, 3 carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
Postoperative radiotherapy is a mainstay in the treatment of uterine cancer, but the typical 5-week regimen can be time-consuming and expensive. A pilot study found that delivery of approximately the same dose over just 2.5 weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, who is an associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues, and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in the hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective [compared to standard protocol], and their study cannot answer that at any rate because it was not designed to answer that question,” said Dr. Williams in an interview. She also noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is [equivalent]. Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” Dr. Williams said.
The study’s findings
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 serous or clear cell, 3 carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
FROM JAMA ONCOLOGY
Children born from frozen embryos may have increased cancer risk
, a large registry study suggests.
The results, however, “should be interpreted cautiously,” the authors noted, given the low number of cancer cases reported among children born using FET.
Still, the findings do “raise concerns considering the increasing use of FET, in particular freeze-all strategies without clear medical indications,” the authors concluded.
The study was published online in PLOS Medicine.
The number of children born after FET has increased globally and even exceeds the number of those born after fresh embryo transfer in many countries. In the United States, for instance, the FET rate has doubled since 2015; FETs constituted almost 80% of all embryo transfers using assisted reproductive technology (ART) without a donor in 2019.
Despite the benefits associated with FET, which include improved embryo survival and higher live birth rates, some previous research has hinted at a higher risk of childhood cancer in this population.
In the current study, researchers from the University of Gothenburg, Sweden, wanted to better understand the risk of childhood cancer following FET. The investigators analyzed data from 171,774 children born via ART, including 22,630 born after FET, as well as roughly 7.7 million children born after spontaneous conception in Denmark, Finland, Norway, and Sweden.
After a mean follow-up of about 10 years, the incidence rate of cancer diagnosed before age 18 years was 16.7 per 100,000 person-years for children born after spontaneous conception (16,184 cases) and 19.3 per 100,000 person-years for children born after ART (329 cases).
The researchers found no increased risk of cancer before age 18 years in the group of children conceived via ART compared with those conceived spontaneously.
However, children born after FET had a significantly higher risk of cancer compared with children born after fresh embryo transfer (adjusted hazard ratio [aHR], 1.59) and spontaneous conception (aHR, 1.65). Specifically with regard to ART, the incidence rate for those born after FET was 30.1 per 100,000 person-years – 48 total cases – compared with 18.8 per 1000,000 person-years after fresh embryo transfer.
Adjustment for macrosomia, birth weight, or major birth defects influenced the association only marginally.
For specific cancer types, children born after FET had more than a twofold higher risk for leukemia in comparison with those born after fresh embryo transfer (aHR, 2.25) and spontaneous conception (aHR, 2.22).
Still, the authors said these results should be interpreted “cautiously,” given the small number of children diagnosed with cancer after FET. The researchers also acknowledged that they do not know why children born after FET would face a higher risk of cancer.
These findings, however, do align with those from a 2019 Dutch population-based study. In the Dutch study, which included more than 24,000 ART-conceived children and more than 23,000 naturally conceived children, the risk of cancer after ART was not higher overall, but it was greater when only those conceived after FET were considered (aHR 1.80); this increased risk, however, was not statistically significant.
“Since the use of FET is substantially increasing, it is important to tease out whether the increased cancer risk is a true risk increase due to the ART procedures using FET, or due to chance or confounding by other factors,” authors of the 2019 Dutch study, Mandy Spaan, PhD, and Flora E. van Leeuwen, PhD, said in an interview.
“But, as childhood cancer is (fortunately) a rare disease, it is very difficult to study this research question among ART children due to limited numbers,” said Dr. Spaan and Dr. van Leeuwen, who are with the Netherlands Cancer Institute.
Given this, the two experts call for additional large population-based cohort studies to investigate the risk of cancer after ART, especially FET, and for a subsequent analysis that pools these data. They hope this strategy “will lead to reliable estimates” and provide information on the risks of FET in comparison with approaches that involve fresh embryos.
The current study had no commercial funding. The study authors as well as Dr. Spaan and Dr. van Leeuwen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a large registry study suggests.
The results, however, “should be interpreted cautiously,” the authors noted, given the low number of cancer cases reported among children born using FET.
Still, the findings do “raise concerns considering the increasing use of FET, in particular freeze-all strategies without clear medical indications,” the authors concluded.
The study was published online in PLOS Medicine.
The number of children born after FET has increased globally and even exceeds the number of those born after fresh embryo transfer in many countries. In the United States, for instance, the FET rate has doubled since 2015; FETs constituted almost 80% of all embryo transfers using assisted reproductive technology (ART) without a donor in 2019.
Despite the benefits associated with FET, which include improved embryo survival and higher live birth rates, some previous research has hinted at a higher risk of childhood cancer in this population.
In the current study, researchers from the University of Gothenburg, Sweden, wanted to better understand the risk of childhood cancer following FET. The investigators analyzed data from 171,774 children born via ART, including 22,630 born after FET, as well as roughly 7.7 million children born after spontaneous conception in Denmark, Finland, Norway, and Sweden.
After a mean follow-up of about 10 years, the incidence rate of cancer diagnosed before age 18 years was 16.7 per 100,000 person-years for children born after spontaneous conception (16,184 cases) and 19.3 per 100,000 person-years for children born after ART (329 cases).
The researchers found no increased risk of cancer before age 18 years in the group of children conceived via ART compared with those conceived spontaneously.
However, children born after FET had a significantly higher risk of cancer compared with children born after fresh embryo transfer (adjusted hazard ratio [aHR], 1.59) and spontaneous conception (aHR, 1.65). Specifically with regard to ART, the incidence rate for those born after FET was 30.1 per 100,000 person-years – 48 total cases – compared with 18.8 per 1000,000 person-years after fresh embryo transfer.
Adjustment for macrosomia, birth weight, or major birth defects influenced the association only marginally.
For specific cancer types, children born after FET had more than a twofold higher risk for leukemia in comparison with those born after fresh embryo transfer (aHR, 2.25) and spontaneous conception (aHR, 2.22).
Still, the authors said these results should be interpreted “cautiously,” given the small number of children diagnosed with cancer after FET. The researchers also acknowledged that they do not know why children born after FET would face a higher risk of cancer.
These findings, however, do align with those from a 2019 Dutch population-based study. In the Dutch study, which included more than 24,000 ART-conceived children and more than 23,000 naturally conceived children, the risk of cancer after ART was not higher overall, but it was greater when only those conceived after FET were considered (aHR 1.80); this increased risk, however, was not statistically significant.
“Since the use of FET is substantially increasing, it is important to tease out whether the increased cancer risk is a true risk increase due to the ART procedures using FET, or due to chance or confounding by other factors,” authors of the 2019 Dutch study, Mandy Spaan, PhD, and Flora E. van Leeuwen, PhD, said in an interview.
“But, as childhood cancer is (fortunately) a rare disease, it is very difficult to study this research question among ART children due to limited numbers,” said Dr. Spaan and Dr. van Leeuwen, who are with the Netherlands Cancer Institute.
Given this, the two experts call for additional large population-based cohort studies to investigate the risk of cancer after ART, especially FET, and for a subsequent analysis that pools these data. They hope this strategy “will lead to reliable estimates” and provide information on the risks of FET in comparison with approaches that involve fresh embryos.
The current study had no commercial funding. The study authors as well as Dr. Spaan and Dr. van Leeuwen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a large registry study suggests.
The results, however, “should be interpreted cautiously,” the authors noted, given the low number of cancer cases reported among children born using FET.
Still, the findings do “raise concerns considering the increasing use of FET, in particular freeze-all strategies without clear medical indications,” the authors concluded.
The study was published online in PLOS Medicine.
The number of children born after FET has increased globally and even exceeds the number of those born after fresh embryo transfer in many countries. In the United States, for instance, the FET rate has doubled since 2015; FETs constituted almost 80% of all embryo transfers using assisted reproductive technology (ART) without a donor in 2019.
Despite the benefits associated with FET, which include improved embryo survival and higher live birth rates, some previous research has hinted at a higher risk of childhood cancer in this population.
In the current study, researchers from the University of Gothenburg, Sweden, wanted to better understand the risk of childhood cancer following FET. The investigators analyzed data from 171,774 children born via ART, including 22,630 born after FET, as well as roughly 7.7 million children born after spontaneous conception in Denmark, Finland, Norway, and Sweden.
After a mean follow-up of about 10 years, the incidence rate of cancer diagnosed before age 18 years was 16.7 per 100,000 person-years for children born after spontaneous conception (16,184 cases) and 19.3 per 100,000 person-years for children born after ART (329 cases).
The researchers found no increased risk of cancer before age 18 years in the group of children conceived via ART compared with those conceived spontaneously.
However, children born after FET had a significantly higher risk of cancer compared with children born after fresh embryo transfer (adjusted hazard ratio [aHR], 1.59) and spontaneous conception (aHR, 1.65). Specifically with regard to ART, the incidence rate for those born after FET was 30.1 per 100,000 person-years – 48 total cases – compared with 18.8 per 1000,000 person-years after fresh embryo transfer.
Adjustment for macrosomia, birth weight, or major birth defects influenced the association only marginally.
For specific cancer types, children born after FET had more than a twofold higher risk for leukemia in comparison with those born after fresh embryo transfer (aHR, 2.25) and spontaneous conception (aHR, 2.22).
Still, the authors said these results should be interpreted “cautiously,” given the small number of children diagnosed with cancer after FET. The researchers also acknowledged that they do not know why children born after FET would face a higher risk of cancer.
These findings, however, do align with those from a 2019 Dutch population-based study. In the Dutch study, which included more than 24,000 ART-conceived children and more than 23,000 naturally conceived children, the risk of cancer after ART was not higher overall, but it was greater when only those conceived after FET were considered (aHR 1.80); this increased risk, however, was not statistically significant.
“Since the use of FET is substantially increasing, it is important to tease out whether the increased cancer risk is a true risk increase due to the ART procedures using FET, or due to chance or confounding by other factors,” authors of the 2019 Dutch study, Mandy Spaan, PhD, and Flora E. van Leeuwen, PhD, said in an interview.
“But, as childhood cancer is (fortunately) a rare disease, it is very difficult to study this research question among ART children due to limited numbers,” said Dr. Spaan and Dr. van Leeuwen, who are with the Netherlands Cancer Institute.
Given this, the two experts call for additional large population-based cohort studies to investigate the risk of cancer after ART, especially FET, and for a subsequent analysis that pools these data. They hope this strategy “will lead to reliable estimates” and provide information on the risks of FET in comparison with approaches that involve fresh embryos.
The current study had no commercial funding. The study authors as well as Dr. Spaan and Dr. van Leeuwen have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PLOS MEDICINE
USPSTF recommends anxiety screening in adults younger than 65
For the first time, the task force is recommending screening all adults aged 64 and younger for anxiety – including pregnant and postpartum women.
This “B” recommendation reflects “moderate certainty” evidence that screening for anxiety in this population has a moderate net benefit, the task force notes in a draft recommendation statement posted on its website.
The recommendation applies to adults aged 19-64 years who do not have a diagnosed mental health disorder or are not showing recognized signs or symptoms of anxiety.
Anxiety disorders are common and often go unrecognized in primary care, leading to long delays in treatment, the task force writes. They add that more evidence is needed to identify ideal screening intervals for all populations.
“A pragmatic approach in the absence of data might include screening all adults who have not been screened previously and using clinical judgment in consideration of risk factors, comorbid conditions, and life events to determine if additional screening of high-risk patients is warranted,” they write.
For adults aged 65 and older, the task force found “insufficient” evidence on the benefits and potential harms of screening for anxiety.
“Evidence on the accuracy of screening tools and the benefits and harms of screening and treatment of screen-detected anxiety in older adults is lacking, and the balance of benefits and harms cannot be determined,” they write.
Jury out on screening for suicide risk
The task force is continuing to recommend screening all adults for depression. This “B” recommendation reflects moderate-certainty evidence that screening for major depression in adults has a moderate net benefit.
However, they note there is not enough evidence to recommend for or against screening for suicide risk in all adults.
They therefore issued an “I” statement, indicating that the balance of benefits and harms cannot be determined at present.
“To address the critical need for supporting the mental health of adults in primary care, the Task Force reviewed the evidence on screening for anxiety, depression, and suicide risk,” task force member Lori Pbert, PhD, University of Massachusetts, Worcester, said in a news release.
“The good news is that screening all adults for depression, including those who are pregnant and postpartum, and screening adults younger than 65 for anxiety can help identify these conditions early so people can be connected to care,” Dr. Pbert said.
“Unfortunately, evidence is limited on screening adults 65 or older for anxiety and screening all adults for suicide risk, so we are urgently calling for more research,” added task force member Gbenga Ogedegbe, MD, MPH, founding director of the Institute for Excellence in Health Equity at NYU Langone Health.
Dr. Ogedegbe, also a professor at New York University, noted that “in the absence of evidence, health care professionals should use their judgment based on individual patient circumstances when determining whether or not to screen.”
The public comment period for the draft recommendations runs until Oct. 17.
A version of this article first appeared on Medscape.com.
For the first time, the task force is recommending screening all adults aged 64 and younger for anxiety – including pregnant and postpartum women.
This “B” recommendation reflects “moderate certainty” evidence that screening for anxiety in this population has a moderate net benefit, the task force notes in a draft recommendation statement posted on its website.
The recommendation applies to adults aged 19-64 years who do not have a diagnosed mental health disorder or are not showing recognized signs or symptoms of anxiety.
Anxiety disorders are common and often go unrecognized in primary care, leading to long delays in treatment, the task force writes. They add that more evidence is needed to identify ideal screening intervals for all populations.
“A pragmatic approach in the absence of data might include screening all adults who have not been screened previously and using clinical judgment in consideration of risk factors, comorbid conditions, and life events to determine if additional screening of high-risk patients is warranted,” they write.
For adults aged 65 and older, the task force found “insufficient” evidence on the benefits and potential harms of screening for anxiety.
“Evidence on the accuracy of screening tools and the benefits and harms of screening and treatment of screen-detected anxiety in older adults is lacking, and the balance of benefits and harms cannot be determined,” they write.
Jury out on screening for suicide risk
The task force is continuing to recommend screening all adults for depression. This “B” recommendation reflects moderate-certainty evidence that screening for major depression in adults has a moderate net benefit.
However, they note there is not enough evidence to recommend for or against screening for suicide risk in all adults.
They therefore issued an “I” statement, indicating that the balance of benefits and harms cannot be determined at present.
“To address the critical need for supporting the mental health of adults in primary care, the Task Force reviewed the evidence on screening for anxiety, depression, and suicide risk,” task force member Lori Pbert, PhD, University of Massachusetts, Worcester, said in a news release.
“The good news is that screening all adults for depression, including those who are pregnant and postpartum, and screening adults younger than 65 for anxiety can help identify these conditions early so people can be connected to care,” Dr. Pbert said.
“Unfortunately, evidence is limited on screening adults 65 or older for anxiety and screening all adults for suicide risk, so we are urgently calling for more research,” added task force member Gbenga Ogedegbe, MD, MPH, founding director of the Institute for Excellence in Health Equity at NYU Langone Health.
Dr. Ogedegbe, also a professor at New York University, noted that “in the absence of evidence, health care professionals should use their judgment based on individual patient circumstances when determining whether or not to screen.”
The public comment period for the draft recommendations runs until Oct. 17.
A version of this article first appeared on Medscape.com.
For the first time, the task force is recommending screening all adults aged 64 and younger for anxiety – including pregnant and postpartum women.
This “B” recommendation reflects “moderate certainty” evidence that screening for anxiety in this population has a moderate net benefit, the task force notes in a draft recommendation statement posted on its website.
The recommendation applies to adults aged 19-64 years who do not have a diagnosed mental health disorder or are not showing recognized signs or symptoms of anxiety.
Anxiety disorders are common and often go unrecognized in primary care, leading to long delays in treatment, the task force writes. They add that more evidence is needed to identify ideal screening intervals for all populations.
“A pragmatic approach in the absence of data might include screening all adults who have not been screened previously and using clinical judgment in consideration of risk factors, comorbid conditions, and life events to determine if additional screening of high-risk patients is warranted,” they write.
For adults aged 65 and older, the task force found “insufficient” evidence on the benefits and potential harms of screening for anxiety.
“Evidence on the accuracy of screening tools and the benefits and harms of screening and treatment of screen-detected anxiety in older adults is lacking, and the balance of benefits and harms cannot be determined,” they write.
Jury out on screening for suicide risk
The task force is continuing to recommend screening all adults for depression. This “B” recommendation reflects moderate-certainty evidence that screening for major depression in adults has a moderate net benefit.
However, they note there is not enough evidence to recommend for or against screening for suicide risk in all adults.
They therefore issued an “I” statement, indicating that the balance of benefits and harms cannot be determined at present.
“To address the critical need for supporting the mental health of adults in primary care, the Task Force reviewed the evidence on screening for anxiety, depression, and suicide risk,” task force member Lori Pbert, PhD, University of Massachusetts, Worcester, said in a news release.
“The good news is that screening all adults for depression, including those who are pregnant and postpartum, and screening adults younger than 65 for anxiety can help identify these conditions early so people can be connected to care,” Dr. Pbert said.
“Unfortunately, evidence is limited on screening adults 65 or older for anxiety and screening all adults for suicide risk, so we are urgently calling for more research,” added task force member Gbenga Ogedegbe, MD, MPH, founding director of the Institute for Excellence in Health Equity at NYU Langone Health.
Dr. Ogedegbe, also a professor at New York University, noted that “in the absence of evidence, health care professionals should use their judgment based on individual patient circumstances when determining whether or not to screen.”
The public comment period for the draft recommendations runs until Oct. 17.
A version of this article first appeared on Medscape.com.
‘Cracking’ technology shows promise for reducing environmental inhaled nitrous oxide impacts during labor
New evidence indicates that the use of “cracking” technology can significantly reduce the ambient levels of inhaled nitrous oxide (N2O) during labor, especially when women are coached on how best to use it.
The findings, from a quality improvement study conducted by anesthetists and midwives in the United Kingdom, appear to have implications for minimizing staff exposures and for lowering N2O’s environmental effect overall. The potent greenhouse gas has a carbon footprint that is 265 times larger than carbon dioxide.
“Our results indicate that cracking technology can reduce ambient nitrous oxide levels in the obstetric setting, with potential for reductions in environmental impacts and occupational exposure,” reported Annie Pinder, MBChB, a fellow in sustainable anesthesia at North West School of Anaesthesia, Manchester, England, and colleagues in Anaesthesia.
Proportionally, the United Kingdom is one of the largest users of inhaled N2O during labor, often for first-line pain control. A 2017 survey by the Care Quality Commission estimated that 77% of women in labor used inhaled N2O for pain, and that it didn’t preclude them from using other types of analgesia, including opioids, epidurals, and nonpharmacologic approaches.
Previous research has established the effectiveness of cracking, which uses a catalyst to convert N2O into nitrogen and oxygen. However, little is known about the effectiveness of scavenging devices that minimize waste N2O in a real-world setting, the authors said.
For the study, median ambient N2O levels were recorded for 36 women during the final 30 minutes of uncomplicated labor. Ambient N2O levels were initially recorded in 12 patients without use of three N2O scavenging devices, and then in three groups of eight patients using either a mouthpiece, a facemask with an air-filled cushion, or a low-profile facemask. Women were also coached on how to use the devices, and given feedback.
“Given that a similar magnitude of reduction in nitrous oxide levels was seen with mouthpieces and low-profile face masks, we suggest that pregnant women should be offered the option of either device when cracking is used,” the study authors wrote.
Staff feedback was generally positive, but some found use of the technology cumbersome. Sufficient staff engagement is the key to successful implementation, the researchers pointed out.
The results showed that when women consistently exhaled into the mouthpiece, median ambient N2O levels were 71% lower compared with levels recorded prior to use of the scavenging device. When women exhaled into a lightweight face mask with a flexible seal, median ambient N2O levels were 81% lower compared with baseline.
These data are consistent with the United Kingdom’s goal of achieving a net zero carbon footprint for the National Health Service by 2040, the researchers said. The study findings are also in keeping with predictions that cracking technology could reduce greenhouse gas emissions associated with N2O by an estimated 75%.
“Although cracking may make nitrous oxide ‘greener,’ it does not make it ‘green,’ ” noted Dr. Pinder and coauthor Cliff Shelton, MBChB, in an interview. Dr. Shelton is a senior clinical lecturer in anesthesia at Lancaster (England) University and a consultant anesthetist at Wythenshawe Hospital, Manchester.
Even with the use of cracking technology, the occupational effect of inhaled N2O is likely to remain higher than for other, more effective forms of anesthesia, such as epidurals and remifentanil (Ultiva), Dr. Pinder and Dr. Shelton said. Furthermore, ambient N2O levels are not a direct measure of the proportion of nitrous oxide cracked, “so there is scope for further work to more precisely understand the ‘carbon footprint’ impacts,” they pointed out.
Inhaled N20 is widely used for labor pain in the Scandinavian countries, as well as in Canada, Australia, and New Zealand. It’s also making a comeback in the United States, facilitated by the Food and Drug Administration’s (FDA) approval of a portable N2O delivery system in 2012.
The system, which delivers a mixture of 50% nitrous oxide and 50% oxygen, has offered a new option for laboring mothers, said Robert L. Barbieri, MD, chair of obstetrics and gynecology at Brigham and Women’s Hospital, Boston, and coauthors in a 2014 report.
“Nitrous oxide works really well as an adjunct to other analgesia,” said Laura Goetzl, MD, MPH, professor of obstetrics, gynecology, and reproductive sciences at University of Texas at Houston Health Science Center. Women in labor really like having the option of inhaled N2O to manage pain, she said in an interview. “The more options that we have to offer, the better for women.”
“Not only does nitrous oxide help with perception of pain, it’s also highly effective for reducing patient anxiety,” Dr. Goetzl explained. “If a patient is waiting for an epidural, the use of nitrous oxide can be particularly helpful.”
Dr. Shelton reported that he is executive editor of Anaesthesia Reports. Dr. Pinder and the remaining coauthors disclosed having no conflicts of interest. Dr. Goetzl reported that she is on the medical advisory board of Mirvie.
This story was updated on Sept. 27, 2022.
New evidence indicates that the use of “cracking” technology can significantly reduce the ambient levels of inhaled nitrous oxide (N2O) during labor, especially when women are coached on how best to use it.
The findings, from a quality improvement study conducted by anesthetists and midwives in the United Kingdom, appear to have implications for minimizing staff exposures and for lowering N2O’s environmental effect overall. The potent greenhouse gas has a carbon footprint that is 265 times larger than carbon dioxide.
“Our results indicate that cracking technology can reduce ambient nitrous oxide levels in the obstetric setting, with potential for reductions in environmental impacts and occupational exposure,” reported Annie Pinder, MBChB, a fellow in sustainable anesthesia at North West School of Anaesthesia, Manchester, England, and colleagues in Anaesthesia.
Proportionally, the United Kingdom is one of the largest users of inhaled N2O during labor, often for first-line pain control. A 2017 survey by the Care Quality Commission estimated that 77% of women in labor used inhaled N2O for pain, and that it didn’t preclude them from using other types of analgesia, including opioids, epidurals, and nonpharmacologic approaches.
Previous research has established the effectiveness of cracking, which uses a catalyst to convert N2O into nitrogen and oxygen. However, little is known about the effectiveness of scavenging devices that minimize waste N2O in a real-world setting, the authors said.
For the study, median ambient N2O levels were recorded for 36 women during the final 30 minutes of uncomplicated labor. Ambient N2O levels were initially recorded in 12 patients without use of three N2O scavenging devices, and then in three groups of eight patients using either a mouthpiece, a facemask with an air-filled cushion, or a low-profile facemask. Women were also coached on how to use the devices, and given feedback.
“Given that a similar magnitude of reduction in nitrous oxide levels was seen with mouthpieces and low-profile face masks, we suggest that pregnant women should be offered the option of either device when cracking is used,” the study authors wrote.
Staff feedback was generally positive, but some found use of the technology cumbersome. Sufficient staff engagement is the key to successful implementation, the researchers pointed out.
The results showed that when women consistently exhaled into the mouthpiece, median ambient N2O levels were 71% lower compared with levels recorded prior to use of the scavenging device. When women exhaled into a lightweight face mask with a flexible seal, median ambient N2O levels were 81% lower compared with baseline.
These data are consistent with the United Kingdom’s goal of achieving a net zero carbon footprint for the National Health Service by 2040, the researchers said. The study findings are also in keeping with predictions that cracking technology could reduce greenhouse gas emissions associated with N2O by an estimated 75%.
“Although cracking may make nitrous oxide ‘greener,’ it does not make it ‘green,’ ” noted Dr. Pinder and coauthor Cliff Shelton, MBChB, in an interview. Dr. Shelton is a senior clinical lecturer in anesthesia at Lancaster (England) University and a consultant anesthetist at Wythenshawe Hospital, Manchester.
Even with the use of cracking technology, the occupational effect of inhaled N2O is likely to remain higher than for other, more effective forms of anesthesia, such as epidurals and remifentanil (Ultiva), Dr. Pinder and Dr. Shelton said. Furthermore, ambient N2O levels are not a direct measure of the proportion of nitrous oxide cracked, “so there is scope for further work to more precisely understand the ‘carbon footprint’ impacts,” they pointed out.
Inhaled N20 is widely used for labor pain in the Scandinavian countries, as well as in Canada, Australia, and New Zealand. It’s also making a comeback in the United States, facilitated by the Food and Drug Administration’s (FDA) approval of a portable N2O delivery system in 2012.
The system, which delivers a mixture of 50% nitrous oxide and 50% oxygen, has offered a new option for laboring mothers, said Robert L. Barbieri, MD, chair of obstetrics and gynecology at Brigham and Women’s Hospital, Boston, and coauthors in a 2014 report.
“Nitrous oxide works really well as an adjunct to other analgesia,” said Laura Goetzl, MD, MPH, professor of obstetrics, gynecology, and reproductive sciences at University of Texas at Houston Health Science Center. Women in labor really like having the option of inhaled N2O to manage pain, she said in an interview. “The more options that we have to offer, the better for women.”
“Not only does nitrous oxide help with perception of pain, it’s also highly effective for reducing patient anxiety,” Dr. Goetzl explained. “If a patient is waiting for an epidural, the use of nitrous oxide can be particularly helpful.”
Dr. Shelton reported that he is executive editor of Anaesthesia Reports. Dr. Pinder and the remaining coauthors disclosed having no conflicts of interest. Dr. Goetzl reported that she is on the medical advisory board of Mirvie.
This story was updated on Sept. 27, 2022.
New evidence indicates that the use of “cracking” technology can significantly reduce the ambient levels of inhaled nitrous oxide (N2O) during labor, especially when women are coached on how best to use it.
The findings, from a quality improvement study conducted by anesthetists and midwives in the United Kingdom, appear to have implications for minimizing staff exposures and for lowering N2O’s environmental effect overall. The potent greenhouse gas has a carbon footprint that is 265 times larger than carbon dioxide.
“Our results indicate that cracking technology can reduce ambient nitrous oxide levels in the obstetric setting, with potential for reductions in environmental impacts and occupational exposure,” reported Annie Pinder, MBChB, a fellow in sustainable anesthesia at North West School of Anaesthesia, Manchester, England, and colleagues in Anaesthesia.
Proportionally, the United Kingdom is one of the largest users of inhaled N2O during labor, often for first-line pain control. A 2017 survey by the Care Quality Commission estimated that 77% of women in labor used inhaled N2O for pain, and that it didn’t preclude them from using other types of analgesia, including opioids, epidurals, and nonpharmacologic approaches.
Previous research has established the effectiveness of cracking, which uses a catalyst to convert N2O into nitrogen and oxygen. However, little is known about the effectiveness of scavenging devices that minimize waste N2O in a real-world setting, the authors said.
For the study, median ambient N2O levels were recorded for 36 women during the final 30 minutes of uncomplicated labor. Ambient N2O levels were initially recorded in 12 patients without use of three N2O scavenging devices, and then in three groups of eight patients using either a mouthpiece, a facemask with an air-filled cushion, or a low-profile facemask. Women were also coached on how to use the devices, and given feedback.
“Given that a similar magnitude of reduction in nitrous oxide levels was seen with mouthpieces and low-profile face masks, we suggest that pregnant women should be offered the option of either device when cracking is used,” the study authors wrote.
Staff feedback was generally positive, but some found use of the technology cumbersome. Sufficient staff engagement is the key to successful implementation, the researchers pointed out.
The results showed that when women consistently exhaled into the mouthpiece, median ambient N2O levels were 71% lower compared with levels recorded prior to use of the scavenging device. When women exhaled into a lightweight face mask with a flexible seal, median ambient N2O levels were 81% lower compared with baseline.
These data are consistent with the United Kingdom’s goal of achieving a net zero carbon footprint for the National Health Service by 2040, the researchers said. The study findings are also in keeping with predictions that cracking technology could reduce greenhouse gas emissions associated with N2O by an estimated 75%.
“Although cracking may make nitrous oxide ‘greener,’ it does not make it ‘green,’ ” noted Dr. Pinder and coauthor Cliff Shelton, MBChB, in an interview. Dr. Shelton is a senior clinical lecturer in anesthesia at Lancaster (England) University and a consultant anesthetist at Wythenshawe Hospital, Manchester.
Even with the use of cracking technology, the occupational effect of inhaled N2O is likely to remain higher than for other, more effective forms of anesthesia, such as epidurals and remifentanil (Ultiva), Dr. Pinder and Dr. Shelton said. Furthermore, ambient N2O levels are not a direct measure of the proportion of nitrous oxide cracked, “so there is scope for further work to more precisely understand the ‘carbon footprint’ impacts,” they pointed out.
Inhaled N20 is widely used for labor pain in the Scandinavian countries, as well as in Canada, Australia, and New Zealand. It’s also making a comeback in the United States, facilitated by the Food and Drug Administration’s (FDA) approval of a portable N2O delivery system in 2012.
The system, which delivers a mixture of 50% nitrous oxide and 50% oxygen, has offered a new option for laboring mothers, said Robert L. Barbieri, MD, chair of obstetrics and gynecology at Brigham and Women’s Hospital, Boston, and coauthors in a 2014 report.
“Nitrous oxide works really well as an adjunct to other analgesia,” said Laura Goetzl, MD, MPH, professor of obstetrics, gynecology, and reproductive sciences at University of Texas at Houston Health Science Center. Women in labor really like having the option of inhaled N2O to manage pain, she said in an interview. “The more options that we have to offer, the better for women.”
“Not only does nitrous oxide help with perception of pain, it’s also highly effective for reducing patient anxiety,” Dr. Goetzl explained. “If a patient is waiting for an epidural, the use of nitrous oxide can be particularly helpful.”
Dr. Shelton reported that he is executive editor of Anaesthesia Reports. Dr. Pinder and the remaining coauthors disclosed having no conflicts of interest. Dr. Goetzl reported that she is on the medical advisory board of Mirvie.
This story was updated on Sept. 27, 2022.
FROM ANAESTHESIA