User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Risk factors for intrauterine tamponade failure in women with postpartum hemorrhage
Key clinical point: Cesarean delivery, preeclampsia, and uterine rupture were independently associated with a higher risk for intrauterine tamponade failure in women with deliveries complicated by postpartum hemorrhage.
Major finding: Intrauterine tamponade failure rate was 11.1%. The risk for intrauterine tamponade failure was higher in women with cesarean delivery (adjusted odds ratio [aOR] 4.2; 95% CI 2.9-6.0), preeclampsia (aOR 2.3; 95% CI 1.3-3.9), and uterine rupture (aOR 14.1; 95% CI 2.4-83.0).
Study details: Findings are from a population-based retrospective cohort study including 1761 women with deliveries complicated by postpartum hemorrhage who underwent intrauterine tamponade within 24 hours of postpartum hemorrhage to manage persistent bleeding.
Disclosures: This study did not report any source of funding. No conflicts of interest were declared.
Source: Gibier M et al. Risk factors for intrauterine tamponade failure in postpartum hemorrhage. Obstet Gynecol. 2022;140(3):439-446 (Aug 3). Doi: 10.1097/AOG.0000000000004888
Key clinical point: Cesarean delivery, preeclampsia, and uterine rupture were independently associated with a higher risk for intrauterine tamponade failure in women with deliveries complicated by postpartum hemorrhage.
Major finding: Intrauterine tamponade failure rate was 11.1%. The risk for intrauterine tamponade failure was higher in women with cesarean delivery (adjusted odds ratio [aOR] 4.2; 95% CI 2.9-6.0), preeclampsia (aOR 2.3; 95% CI 1.3-3.9), and uterine rupture (aOR 14.1; 95% CI 2.4-83.0).
Study details: Findings are from a population-based retrospective cohort study including 1761 women with deliveries complicated by postpartum hemorrhage who underwent intrauterine tamponade within 24 hours of postpartum hemorrhage to manage persistent bleeding.
Disclosures: This study did not report any source of funding. No conflicts of interest were declared.
Source: Gibier M et al. Risk factors for intrauterine tamponade failure in postpartum hemorrhage. Obstet Gynecol. 2022;140(3):439-446 (Aug 3). Doi: 10.1097/AOG.0000000000004888
Key clinical point: Cesarean delivery, preeclampsia, and uterine rupture were independently associated with a higher risk for intrauterine tamponade failure in women with deliveries complicated by postpartum hemorrhage.
Major finding: Intrauterine tamponade failure rate was 11.1%. The risk for intrauterine tamponade failure was higher in women with cesarean delivery (adjusted odds ratio [aOR] 4.2; 95% CI 2.9-6.0), preeclampsia (aOR 2.3; 95% CI 1.3-3.9), and uterine rupture (aOR 14.1; 95% CI 2.4-83.0).
Study details: Findings are from a population-based retrospective cohort study including 1761 women with deliveries complicated by postpartum hemorrhage who underwent intrauterine tamponade within 24 hours of postpartum hemorrhage to manage persistent bleeding.
Disclosures: This study did not report any source of funding. No conflicts of interest were declared.
Source: Gibier M et al. Risk factors for intrauterine tamponade failure in postpartum hemorrhage. Obstet Gynecol. 2022;140(3):439-446 (Aug 3). Doi: 10.1097/AOG.0000000000004888
Labetalol vs nifedipine associated with higher rates of postpartum readmission for hypertension
Key clinical point: The chances of postpartum readmission for hypertension were significantly higher among patients discharged with labetalol vs nifedipine after delivery, irrespective of the severity of their hypertensive disorder of pregnancy.
Major finding: Compared with nifedipine, the chances of postpartum readmission for hypertension were higher with labetalol (adjusted odds ratio [aOR] 1.63, 95% CI 1.43-1.85), with the risk being persistent among patients with mild (aOR 1.57; 95% CI 1.29-1.93) and severe (aOR 1.63, 95% CI 1.43-1.85) hypertensive disorders.
Study details: This study evaluated 24,477 patients who were discharged with nifedipine (36.8%), labetalol (57.7%), or both medications (5.6%) after delivery.
Disclosures: This study did not report any source of funding. DJ Lyell declared receiving payment from various sources.
Source: Do SC et al. Postpartum readmission for hypertension after discharge on labetalol or nifedipine. Obstet Gynecol. 2022;140(4):591-598 (Sep 8). Doi: 10.1097/AOG.0000000000004918
Key clinical point: The chances of postpartum readmission for hypertension were significantly higher among patients discharged with labetalol vs nifedipine after delivery, irrespective of the severity of their hypertensive disorder of pregnancy.
Major finding: Compared with nifedipine, the chances of postpartum readmission for hypertension were higher with labetalol (adjusted odds ratio [aOR] 1.63, 95% CI 1.43-1.85), with the risk being persistent among patients with mild (aOR 1.57; 95% CI 1.29-1.93) and severe (aOR 1.63, 95% CI 1.43-1.85) hypertensive disorders.
Study details: This study evaluated 24,477 patients who were discharged with nifedipine (36.8%), labetalol (57.7%), or both medications (5.6%) after delivery.
Disclosures: This study did not report any source of funding. DJ Lyell declared receiving payment from various sources.
Source: Do SC et al. Postpartum readmission for hypertension after discharge on labetalol or nifedipine. Obstet Gynecol. 2022;140(4):591-598 (Sep 8). Doi: 10.1097/AOG.0000000000004918
Key clinical point: The chances of postpartum readmission for hypertension were significantly higher among patients discharged with labetalol vs nifedipine after delivery, irrespective of the severity of their hypertensive disorder of pregnancy.
Major finding: Compared with nifedipine, the chances of postpartum readmission for hypertension were higher with labetalol (adjusted odds ratio [aOR] 1.63, 95% CI 1.43-1.85), with the risk being persistent among patients with mild (aOR 1.57; 95% CI 1.29-1.93) and severe (aOR 1.63, 95% CI 1.43-1.85) hypertensive disorders.
Study details: This study evaluated 24,477 patients who were discharged with nifedipine (36.8%), labetalol (57.7%), or both medications (5.6%) after delivery.
Disclosures: This study did not report any source of funding. DJ Lyell declared receiving payment from various sources.
Source: Do SC et al. Postpartum readmission for hypertension after discharge on labetalol or nifedipine. Obstet Gynecol. 2022;140(4):591-598 (Sep 8). Doi: 10.1097/AOG.0000000000004918
Simulation training on management of shoulder dystocia reduces incidence of permanent BPBI
Key clinical point: Weekly 3-hour simulation-based training of midwives and doctors on shoulder dystocia (SD) management significantly reduced the incidence of permanent brachial plexus birth injury (BPBI).
Major finding: Despite an increase in the incidence of SD cases (0.1% vs 0.3%; P < .001) and risk factors in pre-training vs post-training period, the incidence of permanent BPBI decreased significantly (0.05% vs 0.02%; P < .001), with the risk for permanent BPBI among those with SD reducing (43.5% vs 6.0%; P < .001) and the rate of successful posterior arm delivery increasing (11.3% vs 23.4%; P = .04) significantly after the implementation of systematic simulation-based training.
Study details: Findings are from a retrospective observational study including 113,785 vertex deliveries performed by a team of doctors and midwives after receiving the weekly 3-hour simulation-based training.
Disclosures: This study was funded by Helsinki University State Research Funding. No conflicts of interest were declared.
Source: Kaijomaa M et al. Impact of simulation training on the management of shoulder dystocia and incidence of permanent brachial plexus birth injury: An observational study. BJOG. 2022 (Aug 10). Doi: 10.1111/1471-0528.17278
Key clinical point: Weekly 3-hour simulation-based training of midwives and doctors on shoulder dystocia (SD) management significantly reduced the incidence of permanent brachial plexus birth injury (BPBI).
Major finding: Despite an increase in the incidence of SD cases (0.1% vs 0.3%; P < .001) and risk factors in pre-training vs post-training period, the incidence of permanent BPBI decreased significantly (0.05% vs 0.02%; P < .001), with the risk for permanent BPBI among those with SD reducing (43.5% vs 6.0%; P < .001) and the rate of successful posterior arm delivery increasing (11.3% vs 23.4%; P = .04) significantly after the implementation of systematic simulation-based training.
Study details: Findings are from a retrospective observational study including 113,785 vertex deliveries performed by a team of doctors and midwives after receiving the weekly 3-hour simulation-based training.
Disclosures: This study was funded by Helsinki University State Research Funding. No conflicts of interest were declared.
Source: Kaijomaa M et al. Impact of simulation training on the management of shoulder dystocia and incidence of permanent brachial plexus birth injury: An observational study. BJOG. 2022 (Aug 10). Doi: 10.1111/1471-0528.17278
Key clinical point: Weekly 3-hour simulation-based training of midwives and doctors on shoulder dystocia (SD) management significantly reduced the incidence of permanent brachial plexus birth injury (BPBI).
Major finding: Despite an increase in the incidence of SD cases (0.1% vs 0.3%; P < .001) and risk factors in pre-training vs post-training period, the incidence of permanent BPBI decreased significantly (0.05% vs 0.02%; P < .001), with the risk for permanent BPBI among those with SD reducing (43.5% vs 6.0%; P < .001) and the rate of successful posterior arm delivery increasing (11.3% vs 23.4%; P = .04) significantly after the implementation of systematic simulation-based training.
Study details: Findings are from a retrospective observational study including 113,785 vertex deliveries performed by a team of doctors and midwives after receiving the weekly 3-hour simulation-based training.
Disclosures: This study was funded by Helsinki University State Research Funding. No conflicts of interest were declared.
Source: Kaijomaa M et al. Impact of simulation training on the management of shoulder dystocia and incidence of permanent brachial plexus birth injury: An observational study. BJOG. 2022 (Aug 10). Doi: 10.1111/1471-0528.17278
The role of repeat uterine curettage in postmolar gestational trophoblastic neoplasia
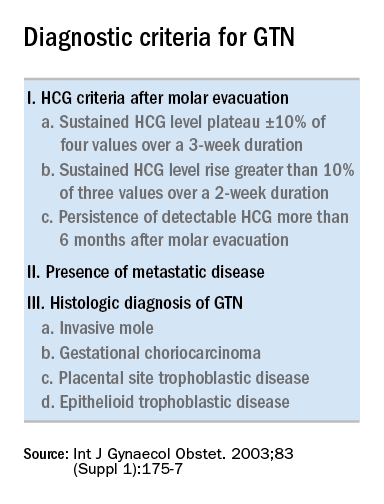
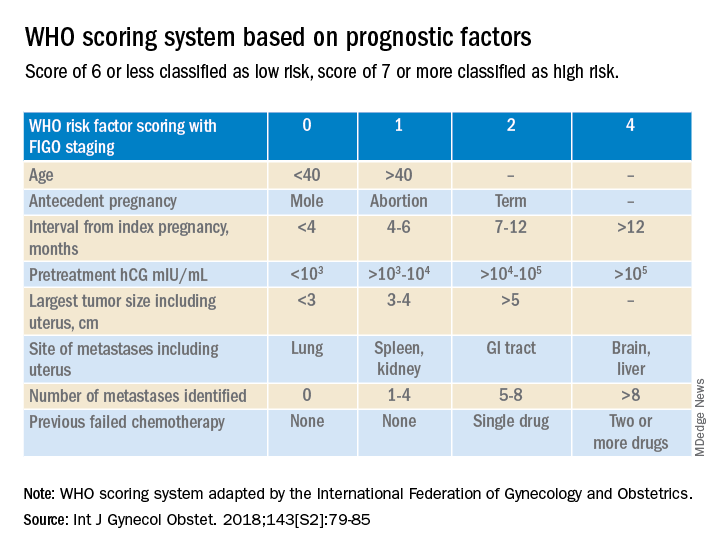
Trophoblastic tissue is responsible for formation of the placenta during pregnancy. Gestational trophoblastic disease (GTD), a group comprising benign (hydatidiform moles) and malignant tumors, occurs when gestational trophoblastic tissue behaves in an abnormal manner. Hydatidiform moles, which are thought to be caused by errors in fertilization, occur in approximately 1 in 1,200 pregnancies in the United States. Gestational trophoblastic neoplasia (GTN) refers to the subgroup of these trophoblastic or placental tumors with malignant behavior and includes postmolar GTN, invasive mole, gestational choriocarcinoma, placental-site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor. Postmolar GTN arises after evacuation of a molar pregnancy and is most frequently diagnosed by a plateau or increase in human chorionic gonadotropin (hCG).1 The risk of postmolar GTN is much higher after a complete mole (7%-30%) compared with a partial mole (2.5%-7.5%).2 Once postmolar GTN is diagnosed, a World Health Organization score is assigned to determine if patients have low- or high-risk disease.3 The primary treatment for most GTN is chemotherapy. A patient’s WHO score helps determine whether they would benefit from single-agent or multiagent chemotherapy. The standard of care for low-risk disease is single-agent chemotherapy with either methotrexate or actinomycin D.
The role of a second uterine curettage, after the diagnosis of low-risk postmolar GTN, has been controversial because of the limited data and disparate outcomes reported. In older retrospective series, a second curettage affected treatment or produced remission in only 9%-20% of patients and caused uterine perforation or major hemorrhage in 5%-8% of patients.4,5 Given relatively high rates of major complications compared with surgical cure or decreased chemotherapy cycles needed, only a limited number of patients seemed to benefit from a second procedure. On the other hand, an observational study of 544 patients who underwent second uterine evacuation after a presumed diagnosis of persistent GTD found that up to 60% of patients did not require chemotherapy afterward.6 Those with hCG levels greater than 1,500 IU/L or histologic evidence of GTD were less likely to have a surgical cure after second curettage. The indications for uterine evacuations were varied across these studies and make it nearly impossible to compare their results.

More recently, there have been two prospective trials that have tackled the question of the utility of second uterine evacuation in low-risk, nonmetastatic GTN. The Gynecologic Oncology Group performed a single-arm prospective study in the United States that enrolled patients with postmolar GTN to undergo second curettage as initial treatment of their disease.7 Of 60 eligible patients, 40% had a surgical cure (defined as normalization of hCG followed by at least 6 months of subsequent normal hCG values). Overall, 47% of patients were able to avoid chemotherapy. All surgical cures were seen in patients with WHO scores between 0 and 4. Importantly, three women were diagnosed with PSTT, which tends to be resistant to methotrexate and actinomycin D (treatment for nonmetastatic PSTT is definitive surgery with hysterectomy). The study found that hCG was a poor discriminator for achieving surgical cure. While age appeared to have an association with surgical cure (cure less likely for younger and older ages, younger than 19 and older than 40), patient numbers were too small to make a statistical conclusion. There were no uterine perforations and one patient had a grade 3 hemorrhage (requiring transfusion).
In the second prospective trial, performed in Iran, 62 patients were randomized to either second uterine evacuation or standard treatment after diagnosis of postmolar GTN.8 All patients in the surgical arm received a cervical ripening agent prior to their procedure, had their procedure under ultrasound guidance, and received misoprostol afterward to prevent uterine bleeding. Among those undergoing second uterine evacuation, 50% were cured (no need for chemotherapy). Among those needing chemotherapy after surgery, the mean number of cycles of chemotherapy needed (3.07 vs. 6.69) and the time it took to achieve negative hCG (3.23 vs. 9.19 weeks) were significantly less compared with patients who did not undergo surgery. hCG prior to second uterine evacuation could distinguish response to surgery compared with those needing chemotherapy (hCG of 1,983 IU/L or less was the level determined to best predict response). No complications related to surgery were reported.
Given prospective data available, second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be considered and discussed with patients given the potential to avoid chemotherapy or decrease the number of cycles needed. It may be prudent to limit the procedure to patients with an hCG less than 1,500-2,000 IU/L and to those between the ages of 20 and 40. While uterine hemorrhage and perforation have been reported in the literature, more recent data suggest low rates of these complications. Unfortunately, given the rarity of the disease and the historically controversial use of second curettage, little is known about the effects on future fertility that this procedure may have, including the development of uterine synechiae.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Ngan HY et al, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2003 Oct;83 Suppl 1:175-7. Erratum in: Int J Gynaecol Obstet. 2021 Dec;155(3):563.
2. Soper JT. Obstet Gynecol. 2021 Feb.;137(2):355-70.
3. Ngan HY et al. Int J Gynecol Obstet. 2018;143:79-85.
4. Schlaerth JB et al. Am J Obstet Gynecol. 1990 Jun;162(6):1465-70.
5. van Trommel NE et al. Gynecol Oncol. 2005 Oct;99(1):6-13.
6. Pezeshki M et al. Gynecol Oncol. 2004 Dec;95(3):423-9.
7. Osborne RJ et al. Obstet Gynecol. 2016 Sep;128(3):535-42.
8. Ayatollahi H et al. Int J Womens Health. 2017 Sep 21;9:665-71.
Trophoblastic tissue is responsible for formation of the placenta during pregnancy. Gestational trophoblastic disease (GTD), a group comprising benign (hydatidiform moles) and malignant tumors, occurs when gestational trophoblastic tissue behaves in an abnormal manner. Hydatidiform moles, which are thought to be caused by errors in fertilization, occur in approximately 1 in 1,200 pregnancies in the United States. Gestational trophoblastic neoplasia (GTN) refers to the subgroup of these trophoblastic or placental tumors with malignant behavior and includes postmolar GTN, invasive mole, gestational choriocarcinoma, placental-site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor. Postmolar GTN arises after evacuation of a molar pregnancy and is most frequently diagnosed by a plateau or increase in human chorionic gonadotropin (hCG).1 The risk of postmolar GTN is much higher after a complete mole (7%-30%) compared with a partial mole (2.5%-7.5%).2 Once postmolar GTN is diagnosed, a World Health Organization score is assigned to determine if patients have low- or high-risk disease.3 The primary treatment for most GTN is chemotherapy. A patient’s WHO score helps determine whether they would benefit from single-agent or multiagent chemotherapy. The standard of care for low-risk disease is single-agent chemotherapy with either methotrexate or actinomycin D.
The role of a second uterine curettage, after the diagnosis of low-risk postmolar GTN, has been controversial because of the limited data and disparate outcomes reported. In older retrospective series, a second curettage affected treatment or produced remission in only 9%-20% of patients and caused uterine perforation or major hemorrhage in 5%-8% of patients.4,5 Given relatively high rates of major complications compared with surgical cure or decreased chemotherapy cycles needed, only a limited number of patients seemed to benefit from a second procedure. On the other hand, an observational study of 544 patients who underwent second uterine evacuation after a presumed diagnosis of persistent GTD found that up to 60% of patients did not require chemotherapy afterward.6 Those with hCG levels greater than 1,500 IU/L or histologic evidence of GTD were less likely to have a surgical cure after second curettage. The indications for uterine evacuations were varied across these studies and make it nearly impossible to compare their results.
More recently, there have been two prospective trials that have tackled the question of the utility of second uterine evacuation in low-risk, nonmetastatic GTN. The Gynecologic Oncology Group performed a single-arm prospective study in the United States that enrolled patients with postmolar GTN to undergo second curettage as initial treatment of their disease.7 Of 60 eligible patients, 40% had a surgical cure (defined as normalization of hCG followed by at least 6 months of subsequent normal hCG values). Overall, 47% of patients were able to avoid chemotherapy. All surgical cures were seen in patients with WHO scores between 0 and 4. Importantly, three women were diagnosed with PSTT, which tends to be resistant to methotrexate and actinomycin D (treatment for nonmetastatic PSTT is definitive surgery with hysterectomy). The study found that hCG was a poor discriminator for achieving surgical cure. While age appeared to have an association with surgical cure (cure less likely for younger and older ages, younger than 19 and older than 40), patient numbers were too small to make a statistical conclusion. There were no uterine perforations and one patient had a grade 3 hemorrhage (requiring transfusion).
In the second prospective trial, performed in Iran, 62 patients were randomized to either second uterine evacuation or standard treatment after diagnosis of postmolar GTN.8 All patients in the surgical arm received a cervical ripening agent prior to their procedure, had their procedure under ultrasound guidance, and received misoprostol afterward to prevent uterine bleeding. Among those undergoing second uterine evacuation, 50% were cured (no need for chemotherapy). Among those needing chemotherapy after surgery, the mean number of cycles of chemotherapy needed (3.07 vs. 6.69) and the time it took to achieve negative hCG (3.23 vs. 9.19 weeks) were significantly less compared with patients who did not undergo surgery. hCG prior to second uterine evacuation could distinguish response to surgery compared with those needing chemotherapy (hCG of 1,983 IU/L or less was the level determined to best predict response). No complications related to surgery were reported.
Given prospective data available, second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be considered and discussed with patients given the potential to avoid chemotherapy or decrease the number of cycles needed. It may be prudent to limit the procedure to patients with an hCG less than 1,500-2,000 IU/L and to those between the ages of 20 and 40. While uterine hemorrhage and perforation have been reported in the literature, more recent data suggest low rates of these complications. Unfortunately, given the rarity of the disease and the historically controversial use of second curettage, little is known about the effects on future fertility that this procedure may have, including the development of uterine synechiae.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Ngan HY et al, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2003 Oct;83 Suppl 1:175-7. Erratum in: Int J Gynaecol Obstet. 2021 Dec;155(3):563.
2. Soper JT. Obstet Gynecol. 2021 Feb.;137(2):355-70.
3. Ngan HY et al. Int J Gynecol Obstet. 2018;143:79-85.
4. Schlaerth JB et al. Am J Obstet Gynecol. 1990 Jun;162(6):1465-70.
5. van Trommel NE et al. Gynecol Oncol. 2005 Oct;99(1):6-13.
6. Pezeshki M et al. Gynecol Oncol. 2004 Dec;95(3):423-9.
7. Osborne RJ et al. Obstet Gynecol. 2016 Sep;128(3):535-42.
8. Ayatollahi H et al. Int J Womens Health. 2017 Sep 21;9:665-71.
Trophoblastic tissue is responsible for formation of the placenta during pregnancy. Gestational trophoblastic disease (GTD), a group comprising benign (hydatidiform moles) and malignant tumors, occurs when gestational trophoblastic tissue behaves in an abnormal manner. Hydatidiform moles, which are thought to be caused by errors in fertilization, occur in approximately 1 in 1,200 pregnancies in the United States. Gestational trophoblastic neoplasia (GTN) refers to the subgroup of these trophoblastic or placental tumors with malignant behavior and includes postmolar GTN, invasive mole, gestational choriocarcinoma, placental-site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor. Postmolar GTN arises after evacuation of a molar pregnancy and is most frequently diagnosed by a plateau or increase in human chorionic gonadotropin (hCG).1 The risk of postmolar GTN is much higher after a complete mole (7%-30%) compared with a partial mole (2.5%-7.5%).2 Once postmolar GTN is diagnosed, a World Health Organization score is assigned to determine if patients have low- or high-risk disease.3 The primary treatment for most GTN is chemotherapy. A patient’s WHO score helps determine whether they would benefit from single-agent or multiagent chemotherapy. The standard of care for low-risk disease is single-agent chemotherapy with either methotrexate or actinomycin D.
The role of a second uterine curettage, after the diagnosis of low-risk postmolar GTN, has been controversial because of the limited data and disparate outcomes reported. In older retrospective series, a second curettage affected treatment or produced remission in only 9%-20% of patients and caused uterine perforation or major hemorrhage in 5%-8% of patients.4,5 Given relatively high rates of major complications compared with surgical cure or decreased chemotherapy cycles needed, only a limited number of patients seemed to benefit from a second procedure. On the other hand, an observational study of 544 patients who underwent second uterine evacuation after a presumed diagnosis of persistent GTD found that up to 60% of patients did not require chemotherapy afterward.6 Those with hCG levels greater than 1,500 IU/L or histologic evidence of GTD were less likely to have a surgical cure after second curettage. The indications for uterine evacuations were varied across these studies and make it nearly impossible to compare their results.
More recently, there have been two prospective trials that have tackled the question of the utility of second uterine evacuation in low-risk, nonmetastatic GTN. The Gynecologic Oncology Group performed a single-arm prospective study in the United States that enrolled patients with postmolar GTN to undergo second curettage as initial treatment of their disease.7 Of 60 eligible patients, 40% had a surgical cure (defined as normalization of hCG followed by at least 6 months of subsequent normal hCG values). Overall, 47% of patients were able to avoid chemotherapy. All surgical cures were seen in patients with WHO scores between 0 and 4. Importantly, three women were diagnosed with PSTT, which tends to be resistant to methotrexate and actinomycin D (treatment for nonmetastatic PSTT is definitive surgery with hysterectomy). The study found that hCG was a poor discriminator for achieving surgical cure. While age appeared to have an association with surgical cure (cure less likely for younger and older ages, younger than 19 and older than 40), patient numbers were too small to make a statistical conclusion. There were no uterine perforations and one patient had a grade 3 hemorrhage (requiring transfusion).
In the second prospective trial, performed in Iran, 62 patients were randomized to either second uterine evacuation or standard treatment after diagnosis of postmolar GTN.8 All patients in the surgical arm received a cervical ripening agent prior to their procedure, had their procedure under ultrasound guidance, and received misoprostol afterward to prevent uterine bleeding. Among those undergoing second uterine evacuation, 50% were cured (no need for chemotherapy). Among those needing chemotherapy after surgery, the mean number of cycles of chemotherapy needed (3.07 vs. 6.69) and the time it took to achieve negative hCG (3.23 vs. 9.19 weeks) were significantly less compared with patients who did not undergo surgery. hCG prior to second uterine evacuation could distinguish response to surgery compared with those needing chemotherapy (hCG of 1,983 IU/L or less was the level determined to best predict response). No complications related to surgery were reported.
Given prospective data available, second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be considered and discussed with patients given the potential to avoid chemotherapy or decrease the number of cycles needed. It may be prudent to limit the procedure to patients with an hCG less than 1,500-2,000 IU/L and to those between the ages of 20 and 40. While uterine hemorrhage and perforation have been reported in the literature, more recent data suggest low rates of these complications. Unfortunately, given the rarity of the disease and the historically controversial use of second curettage, little is known about the effects on future fertility that this procedure may have, including the development of uterine synechiae.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Ngan HY et al, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2003 Oct;83 Suppl 1:175-7. Erratum in: Int J Gynaecol Obstet. 2021 Dec;155(3):563.
2. Soper JT. Obstet Gynecol. 2021 Feb.;137(2):355-70.
3. Ngan HY et al. Int J Gynecol Obstet. 2018;143:79-85.
4. Schlaerth JB et al. Am J Obstet Gynecol. 1990 Jun;162(6):1465-70.
5. van Trommel NE et al. Gynecol Oncol. 2005 Oct;99(1):6-13.
6. Pezeshki M et al. Gynecol Oncol. 2004 Dec;95(3):423-9.
7. Osborne RJ et al. Obstet Gynecol. 2016 Sep;128(3):535-42.
8. Ayatollahi H et al. Int J Womens Health. 2017 Sep 21;9:665-71.
Gender-affirming mastectomy boosts image and quality of life in gender-diverse youth
Adolescents and young adults who undergo “top surgery” for gender dysphoria overwhelmingly report being satisfied with the procedure in the near-term, new research shows.
The results of the prospective cohort study, reported recently in JAMA Pediatrics, suggest that the surgery can help facilitate gender congruence and comfort with body image for transmasculine and nonbinary youth. The authors, from Northwestern University, Chicago, said the findings may “help dispel misconceptions that gender-affirming treatment is experimental and support evidence-based practices of top surgery.”

Sumanas Jordan, MD, PhD, assistant professor of plastic surgery at Northwestern University, Chicago, and a coauthor of the study, said the study was the first prospective, matched cohort analysis showing that chest surgery improves outcomes in this age group.
“We focused our study on chest dysphoria, the distress due to the presence of breasts, and gender congruence, the feeling of alignment between identity and physical characteristics,” Dr. Jordan said. “We will continue to study the effect of surgery in other areas of health, such as physical functioning and quality of life, and follow our patients longer term.”
As many as 9% of adolescents and young adults identify as transgender or nonbinary - a group underrepresented in the pediatric literature, Dr. Jordan’s group said. Chest dysphoria often is associated with psychosocial issues such as depression and anxiety.
“Dysphoria can lead to a range of negative physical and emotional consequences, such as avoidance of exercise and sports, harmful chest-binding practices, functional limitations, and suicidal ideation, said M. Brett Cooper, MD, MEd, assistant professor of pediatrics, and adolescent and young adult medicine, at UT Southwestern Medical Center/Children’s Health, Dallas. “These young people often bind for several hours a day to reduce the presence of their chest.”

The study
The Northwestern team recruited 81 patients with a mean age of 18.6 years whose sex at birth was assigned female. Patients were overwhelmingly White (89%), and the majority (59%) were transgender male, the remaining patients nonbinary.
The population sample included patients aged 13-24 who underwent top surgery from December 2019 to April 2021 and a matched control group of those who did not have surgery.
Outcomes measures were assessed preoperatively and 3 months after surgery.
Thirty-six surgical patients and 34 of those in the control arm completed the outcomes measures. Surgical complications were minimal. Propensity analyses suggested an association between surgery and substantial improvements in scores on the following study endpoints:
- Chest dysphoria measure (–25.58 points, 95% confidence interval [CI], –29.18 to –21.98).
- Transgender congruence scale (7.78 points, 95%: CI, 6.06-9.50)
- Body image scale (–7.20 points, 95% CI, –11.68 to –2.72).
The patients who underwent top surgery reported significant improvements in scores of chest dysphoria, transgender congruence, and body image. The results for patients younger than age 18 paralleled those for older participants in the study.
While the results corroborate other studies showing that gender-affirming therapy improves mental health and quality of life among these young people, the researchers cautioned that some insurers require testosterone therapy for 1 year before their plans will cover the costs of gender-affirming surgery.
This may negatively affect those nonbinary patients who do not undergo hormone therapy,” the researchers wrote. They are currently collecting 1-year follow-up data to determine the long-term effects of top surgery on chest dysphoria, gender congruence, and body image.
As surgical patients progress through adult life, does the risk of regret increase? “We did not address regret in this short-term study,” Dr. Jordan said. “However, previous studies have shown very low levels of regret.”
An accompanying editorial concurred that top surgery is effective and medically necessary in this population of young people.
Calling the study “an important milestone in gender affirmation research,” Kishan M. Thadikonda, MD, and Katherine M. Gast, MD, MS, of the school of medicine and public health at the University of Wisconsin in Madison, said it will be important to follow this young cohort to prove these benefits will endure as patients age.
They cautioned, however, that nonbinary patients represented just 13% of the patient total and only 8% of the surgical cohort. Nonbinary patients are not well understood as a patient population when it comes to gender-affirmation surgery and are often included in studies with transgender patients despite clear differences, they noted.
Current setbacks
According to Dr. Cooper, politics is already affecting care in Texas. “Due to the sociopolitical climate in my state in regard to gender-affirming care, I have also seen a few young people have their surgeries either canceled or postponed by their parents,” he said. “This has led to a worsening of mental health in these patients.”
Dr. Cooper stressed the need for more research on the perspective of non-White and socioeconomically disadvantaged youth.
“This study also highlights the disparity between patients who have commercial insurance versus those who are on Medicaid,” he said. “Medicaid plans often do not cover this, so those patients usually have to continue to suffer or pay for this surgery out of their own pocket.”
This study was supported by the Northwestern University Clinical and Translational Sciences Institute, funded in part by the National Institutes of Health. Funding also came from the Plastic Surgery Foundation and American Association of Pediatric Plastic Surgery. Dr. Jordan received grants from the Plastic Surgery Foundation during the study. One coauthor reported consultant fees from CVS Caremark for consulting outside the submitted work, and another reported grants from the National Institutes of Health outside the submitted work. Dr. Cooper disclosed no competing interests relevant to his comments. The editorial commentators disclosed no conflicts of interest.
Adolescents and young adults who undergo “top surgery” for gender dysphoria overwhelmingly report being satisfied with the procedure in the near-term, new research shows.
The results of the prospective cohort study, reported recently in JAMA Pediatrics, suggest that the surgery can help facilitate gender congruence and comfort with body image for transmasculine and nonbinary youth. The authors, from Northwestern University, Chicago, said the findings may “help dispel misconceptions that gender-affirming treatment is experimental and support evidence-based practices of top surgery.”
Sumanas Jordan, MD, PhD, assistant professor of plastic surgery at Northwestern University, Chicago, and a coauthor of the study, said the study was the first prospective, matched cohort analysis showing that chest surgery improves outcomes in this age group.
“We focused our study on chest dysphoria, the distress due to the presence of breasts, and gender congruence, the feeling of alignment between identity and physical characteristics,” Dr. Jordan said. “We will continue to study the effect of surgery in other areas of health, such as physical functioning and quality of life, and follow our patients longer term.”
As many as 9% of adolescents and young adults identify as transgender or nonbinary - a group underrepresented in the pediatric literature, Dr. Jordan’s group said. Chest dysphoria often is associated with psychosocial issues such as depression and anxiety.
“Dysphoria can lead to a range of negative physical and emotional consequences, such as avoidance of exercise and sports, harmful chest-binding practices, functional limitations, and suicidal ideation, said M. Brett Cooper, MD, MEd, assistant professor of pediatrics, and adolescent and young adult medicine, at UT Southwestern Medical Center/Children’s Health, Dallas. “These young people often bind for several hours a day to reduce the presence of their chest.”
The study
The Northwestern team recruited 81 patients with a mean age of 18.6 years whose sex at birth was assigned female. Patients were overwhelmingly White (89%), and the majority (59%) were transgender male, the remaining patients nonbinary.
The population sample included patients aged 13-24 who underwent top surgery from December 2019 to April 2021 and a matched control group of those who did not have surgery.
Outcomes measures were assessed preoperatively and 3 months after surgery.
Thirty-six surgical patients and 34 of those in the control arm completed the outcomes measures. Surgical complications were minimal. Propensity analyses suggested an association between surgery and substantial improvements in scores on the following study endpoints:
- Chest dysphoria measure (–25.58 points, 95% confidence interval [CI], –29.18 to –21.98).
- Transgender congruence scale (7.78 points, 95%: CI, 6.06-9.50)
- Body image scale (–7.20 points, 95% CI, –11.68 to –2.72).
The patients who underwent top surgery reported significant improvements in scores of chest dysphoria, transgender congruence, and body image. The results for patients younger than age 18 paralleled those for older participants in the study.
While the results corroborate other studies showing that gender-affirming therapy improves mental health and quality of life among these young people, the researchers cautioned that some insurers require testosterone therapy for 1 year before their plans will cover the costs of gender-affirming surgery.
This may negatively affect those nonbinary patients who do not undergo hormone therapy,” the researchers wrote. They are currently collecting 1-year follow-up data to determine the long-term effects of top surgery on chest dysphoria, gender congruence, and body image.
As surgical patients progress through adult life, does the risk of regret increase? “We did not address regret in this short-term study,” Dr. Jordan said. “However, previous studies have shown very low levels of regret.”
An accompanying editorial concurred that top surgery is effective and medically necessary in this population of young people.
Calling the study “an important milestone in gender affirmation research,” Kishan M. Thadikonda, MD, and Katherine M. Gast, MD, MS, of the school of medicine and public health at the University of Wisconsin in Madison, said it will be important to follow this young cohort to prove these benefits will endure as patients age.
They cautioned, however, that nonbinary patients represented just 13% of the patient total and only 8% of the surgical cohort. Nonbinary patients are not well understood as a patient population when it comes to gender-affirmation surgery and are often included in studies with transgender patients despite clear differences, they noted.
Current setbacks
According to Dr. Cooper, politics is already affecting care in Texas. “Due to the sociopolitical climate in my state in regard to gender-affirming care, I have also seen a few young people have their surgeries either canceled or postponed by their parents,” he said. “This has led to a worsening of mental health in these patients.”
Dr. Cooper stressed the need for more research on the perspective of non-White and socioeconomically disadvantaged youth.
“This study also highlights the disparity between patients who have commercial insurance versus those who are on Medicaid,” he said. “Medicaid plans often do not cover this, so those patients usually have to continue to suffer or pay for this surgery out of their own pocket.”
This study was supported by the Northwestern University Clinical and Translational Sciences Institute, funded in part by the National Institutes of Health. Funding also came from the Plastic Surgery Foundation and American Association of Pediatric Plastic Surgery. Dr. Jordan received grants from the Plastic Surgery Foundation during the study. One coauthor reported consultant fees from CVS Caremark for consulting outside the submitted work, and another reported grants from the National Institutes of Health outside the submitted work. Dr. Cooper disclosed no competing interests relevant to his comments. The editorial commentators disclosed no conflicts of interest.
Adolescents and young adults who undergo “top surgery” for gender dysphoria overwhelmingly report being satisfied with the procedure in the near-term, new research shows.
The results of the prospective cohort study, reported recently in JAMA Pediatrics, suggest that the surgery can help facilitate gender congruence and comfort with body image for transmasculine and nonbinary youth. The authors, from Northwestern University, Chicago, said the findings may “help dispel misconceptions that gender-affirming treatment is experimental and support evidence-based practices of top surgery.”
Sumanas Jordan, MD, PhD, assistant professor of plastic surgery at Northwestern University, Chicago, and a coauthor of the study, said the study was the first prospective, matched cohort analysis showing that chest surgery improves outcomes in this age group.
“We focused our study on chest dysphoria, the distress due to the presence of breasts, and gender congruence, the feeling of alignment between identity and physical characteristics,” Dr. Jordan said. “We will continue to study the effect of surgery in other areas of health, such as physical functioning and quality of life, and follow our patients longer term.”
As many as 9% of adolescents and young adults identify as transgender or nonbinary - a group underrepresented in the pediatric literature, Dr. Jordan’s group said. Chest dysphoria often is associated with psychosocial issues such as depression and anxiety.
“Dysphoria can lead to a range of negative physical and emotional consequences, such as avoidance of exercise and sports, harmful chest-binding practices, functional limitations, and suicidal ideation, said M. Brett Cooper, MD, MEd, assistant professor of pediatrics, and adolescent and young adult medicine, at UT Southwestern Medical Center/Children’s Health, Dallas. “These young people often bind for several hours a day to reduce the presence of their chest.”
The study
The Northwestern team recruited 81 patients with a mean age of 18.6 years whose sex at birth was assigned female. Patients were overwhelmingly White (89%), and the majority (59%) were transgender male, the remaining patients nonbinary.
The population sample included patients aged 13-24 who underwent top surgery from December 2019 to April 2021 and a matched control group of those who did not have surgery.
Outcomes measures were assessed preoperatively and 3 months after surgery.
Thirty-six surgical patients and 34 of those in the control arm completed the outcomes measures. Surgical complications were minimal. Propensity analyses suggested an association between surgery and substantial improvements in scores on the following study endpoints:
- Chest dysphoria measure (–25.58 points, 95% confidence interval [CI], –29.18 to –21.98).
- Transgender congruence scale (7.78 points, 95%: CI, 6.06-9.50)
- Body image scale (–7.20 points, 95% CI, –11.68 to –2.72).
The patients who underwent top surgery reported significant improvements in scores of chest dysphoria, transgender congruence, and body image. The results for patients younger than age 18 paralleled those for older participants in the study.
While the results corroborate other studies showing that gender-affirming therapy improves mental health and quality of life among these young people, the researchers cautioned that some insurers require testosterone therapy for 1 year before their plans will cover the costs of gender-affirming surgery.
This may negatively affect those nonbinary patients who do not undergo hormone therapy,” the researchers wrote. They are currently collecting 1-year follow-up data to determine the long-term effects of top surgery on chest dysphoria, gender congruence, and body image.
As surgical patients progress through adult life, does the risk of regret increase? “We did not address regret in this short-term study,” Dr. Jordan said. “However, previous studies have shown very low levels of regret.”
An accompanying editorial concurred that top surgery is effective and medically necessary in this population of young people.
Calling the study “an important milestone in gender affirmation research,” Kishan M. Thadikonda, MD, and Katherine M. Gast, MD, MS, of the school of medicine and public health at the University of Wisconsin in Madison, said it will be important to follow this young cohort to prove these benefits will endure as patients age.
They cautioned, however, that nonbinary patients represented just 13% of the patient total and only 8% of the surgical cohort. Nonbinary patients are not well understood as a patient population when it comes to gender-affirmation surgery and are often included in studies with transgender patients despite clear differences, they noted.
Current setbacks
According to Dr. Cooper, politics is already affecting care in Texas. “Due to the sociopolitical climate in my state in regard to gender-affirming care, I have also seen a few young people have their surgeries either canceled or postponed by their parents,” he said. “This has led to a worsening of mental health in these patients.”
Dr. Cooper stressed the need for more research on the perspective of non-White and socioeconomically disadvantaged youth.
“This study also highlights the disparity between patients who have commercial insurance versus those who are on Medicaid,” he said. “Medicaid plans often do not cover this, so those patients usually have to continue to suffer or pay for this surgery out of their own pocket.”
This study was supported by the Northwestern University Clinical and Translational Sciences Institute, funded in part by the National Institutes of Health. Funding also came from the Plastic Surgery Foundation and American Association of Pediatric Plastic Surgery. Dr. Jordan received grants from the Plastic Surgery Foundation during the study. One coauthor reported consultant fees from CVS Caremark for consulting outside the submitted work, and another reported grants from the National Institutes of Health outside the submitted work. Dr. Cooper disclosed no competing interests relevant to his comments. The editorial commentators disclosed no conflicts of interest.
FROM JAMA PEDIATRICS
Under 2% of eligible have gotten newest COVID booster shot
The newest booster became available to the public around Labor Day weekend, and about 4.4 million people have gotten it as of Sept. 21, according to Centers for Disease Control and Prevention data. That figure represents about 1.5% of the people eligible to receive the booster, NBC News reported.
The White House has said the total is probably closer to 5 million people. The CDC totals don’t yet include Texas and Idaho, which use an aggregate vaccination record reporting method for the Pfizer vaccine.
Scott Roberts, MD, a Yale Medicine infectious disease specialist in New Haven, Conn., told NBC News the low numbers are “demoralizing.”
“I would expect a much higher proportion of Americans to have gotten the booster by this point,” he said. “The fact that this booster came out days before Biden said the pandemic is over is a huge mixed message. Now it’s going to be that much harder to convince those at risk who are on the fence to get a booster.”
White House COVID-19 coordinator Ashish Jha, MD, says he thinks demand will pick up in the coming weeks.
“We’ve been thinking and talking about this as an annual vaccine like the flu vaccine. Flu vaccine season picks up in late September and early October. We’re just getting our education campaign going. So we expect to see, despite the fact that this was a strong start, we actually expect this to ramp up stronger,” Dr. Jha said.
The new booster is the third one authorized by the federal government and was redesigned to protect against the currently circulating subvariants BA.4 and BA.5 of the Omicron strain. People who have received a primary vaccine series or a booster at least 2 months before can receive it.
The new Pfizer booster is available for people 12 and up and the Moderna version for people 18 and up. The vaccines can be mixed and matched.
A version of this article first appeared on WebMD.com.
The newest booster became available to the public around Labor Day weekend, and about 4.4 million people have gotten it as of Sept. 21, according to Centers for Disease Control and Prevention data. That figure represents about 1.5% of the people eligible to receive the booster, NBC News reported.
The White House has said the total is probably closer to 5 million people. The CDC totals don’t yet include Texas and Idaho, which use an aggregate vaccination record reporting method for the Pfizer vaccine.
Scott Roberts, MD, a Yale Medicine infectious disease specialist in New Haven, Conn., told NBC News the low numbers are “demoralizing.”
“I would expect a much higher proportion of Americans to have gotten the booster by this point,” he said. “The fact that this booster came out days before Biden said the pandemic is over is a huge mixed message. Now it’s going to be that much harder to convince those at risk who are on the fence to get a booster.”
White House COVID-19 coordinator Ashish Jha, MD, says he thinks demand will pick up in the coming weeks.
“We’ve been thinking and talking about this as an annual vaccine like the flu vaccine. Flu vaccine season picks up in late September and early October. We’re just getting our education campaign going. So we expect to see, despite the fact that this was a strong start, we actually expect this to ramp up stronger,” Dr. Jha said.
The new booster is the third one authorized by the federal government and was redesigned to protect against the currently circulating subvariants BA.4 and BA.5 of the Omicron strain. People who have received a primary vaccine series or a booster at least 2 months before can receive it.
The new Pfizer booster is available for people 12 and up and the Moderna version for people 18 and up. The vaccines can be mixed and matched.
A version of this article first appeared on WebMD.com.
The newest booster became available to the public around Labor Day weekend, and about 4.4 million people have gotten it as of Sept. 21, according to Centers for Disease Control and Prevention data. That figure represents about 1.5% of the people eligible to receive the booster, NBC News reported.
The White House has said the total is probably closer to 5 million people. The CDC totals don’t yet include Texas and Idaho, which use an aggregate vaccination record reporting method for the Pfizer vaccine.
Scott Roberts, MD, a Yale Medicine infectious disease specialist in New Haven, Conn., told NBC News the low numbers are “demoralizing.”
“I would expect a much higher proportion of Americans to have gotten the booster by this point,” he said. “The fact that this booster came out days before Biden said the pandemic is over is a huge mixed message. Now it’s going to be that much harder to convince those at risk who are on the fence to get a booster.”
White House COVID-19 coordinator Ashish Jha, MD, says he thinks demand will pick up in the coming weeks.
“We’ve been thinking and talking about this as an annual vaccine like the flu vaccine. Flu vaccine season picks up in late September and early October. We’re just getting our education campaign going. So we expect to see, despite the fact that this was a strong start, we actually expect this to ramp up stronger,” Dr. Jha said.
The new booster is the third one authorized by the federal government and was redesigned to protect against the currently circulating subvariants BA.4 and BA.5 of the Omicron strain. People who have received a primary vaccine series or a booster at least 2 months before can receive it.
The new Pfizer booster is available for people 12 and up and the Moderna version for people 18 and up. The vaccines can be mixed and matched.
A version of this article first appeared on WebMD.com.
Postpartum sexual enjoyment: Does mode of delivery matter?
For some parents, resuming sexual intimacy after having a baby is a top priority. For others, not so much – and late-night feedings and diaper changes may not be the only hang-ups.
Dyspareunia – pain during sex – occurs in a substantial number of women after childbirth, and recent research sheds light on how psychological and biomedical factors relate to this condition.
Mode of delivery, for instance, may have less of an effect on sexual well-being than some people suspect.
Despite a perception that cesarean delivery might affect sexual function less than vaginal delivery does, how mothers delivered did not affect how often they had sex postpartum or the amount of enjoyment they got from it, according to research published in BJOG.
Eleven years after delivery, however, cesarean delivery was associated with a 74% increased likelihood of pain in the vagina during sex, compared with vaginal delivery, the researchers found (odds ratio, 1.74; 95% confidence interval, 1.46-2.08).
The results suggest that cesarean delivery “may not help protect against sexual dysfunction, as previously thought,” Flo Martin, a PhD student in epidemiology at the University of Bristol, United Kingdom, and lead author of the study, said in a news release.
For their study, Ms. Martin and her colleagues analyzed data from more than 10,300 participants in the Avon Longitudinal Study of Parents and Children, which recruited women in the United Kingdom who were pregnant in 1991 and 1992.
The researchers had data about pain during sex at 11 years. They had data about sexual enjoyment and frequency at 33 months, 5 years, 12 years, and 18 years after delivery.
If women experienced pain during sex years after cesarean delivery, uterine scarring might have been a cause, Ms. Martin and colleagues suggested. Alternatively, women with dyspareunia before delivery may be more likely to have cesarean surgery, which also could explain the association.
Other studies have likewise found that different modes of delivery generally lead to similar outcomes of sexual well-being after birth.
“Several of my own longitudinal studies have shown limited associations between mode of delivery and various aspects of sexual well-being, including sexual satisfaction, sexual function, and sexual desire,” said Natalie O. Rosen, PhD, director of the Couples and Sexual Health Laboratory at Dalhousie University, Halifax, N.S.
Nevertheless, other published studies have yielded conflicting results, so the question warrants further study, she said.
Pain catastrophizing
One study by Dr. Rosen’s group, published in Obstetrics & Gynecology, tracked sexual pain in 582 people from mid-pregnancy to 2 years postpartum.
About 21% of participants experienced moderate pain during sex, as determined by an average pain score greater than 4 on scale of 0-10 points. The rest were classified as having “minimal dyspareunia.”
Pain tended to peak at 3 months postpartum and then steadily decrease in both the moderate and minimal pain groups.
Mode of delivery did not affect the odds that a participant would have moderate dyspareunia. Neither did breastfeeding or prior chronic pain.
“But we did find one key thing to look out for: Those who reported a lot of negative thoughts and feelings about pain, something called pain catastrophizing, were more likely to experience moderate persistent pain during sex,” the researchers said in a video about their findings.
Pain catastrophizing 3 months after delivery was associated with significantly increased odds of following a moderate pain trajectory (odds ratio, 1.09; 95% confidence interval, 1.04-1.15).
Let’s talk about #postbabyhankypanky
Caring for a newborn while maintaining a romantic relationship can be challenging, and “there is a lack of evidence-based research aimed at helping couples prevent and navigate changes to their sexual well-being postpartum,” Dr. Rosen said.
During the 2-year study, a growing number of participants reported having sex less often over time. The percentage of women who had engaged in sexual activity in the past 4 weeks was 99% at baseline (20-24 weeks of gestation), 83.5% at 32 weeks of gestation, 73.9% at 3 months postpartum, and 69.6% at 2 years postpartum.
“One crucial way that couples sustain their connection is through their sexuality,” Dr. Rosen said. “Unfortunately, most new parents experience significant disruptions to their sexual function,” such as lower sexual desire or more pain during intercourse.
Dr. Rosen’s group has created a series of videos related to this topic dubbed #postbabyhankypanky to facilitate communication about sex postpartum. She encourages women with dyspareunia to talk with a health care provider because treatments such as cognitive-behavioral therapy, pelvic floor physical therapy, and topical medications can help manage pain.
‘Reassuring’ data
Veronica Gillispie-Bell, MD, MAS, director of quality for women’s services at the Ochsner Health System, New Orleans, said that she sees patients with postpartum sexual pain frequently.
Patients typically are instructed to have pelvic rest from delivery until 6 weeks after.
At the 6-week appointment, she tells patients to make sure that they are using lots of lubrication, because vaginal dryness related to hormonal changes during pregnancy and breastfeeding can make sex more painful, regardless of mode of delivery.
For many patients, she also recommends pelvic floor physical therapy.
As the medical director for the Louisiana Perinatal Quality Collaborative – a network of care providers, public health officials, and advocates that aims to improve outcomes for birthing persons, families, and newborns – Dr. Gillispie-Bell also is focused on reducing the rate of cesarean deliveries in the state. The BJOG study showing an increased risk for dyspareunia after a cesarean surgery serves as a reminder that there may be “long-term effects of having a C-section that may not be as obvious,” she said.
“C-sections are life-saving procedures, but they are not without risk,” Dr. Gillispie-Bell said.
Leila Frodsham, MBChB, a spokesperson for the Royal College of Obstetricians and Gynaecologists, told Medscape UK that it was “reassuring” to see “no difference in sexual enjoyment or sexual frequency at any time point postpartum between women who gave birth via cesarean section and those who delivered vaginally.”
“Women should be supported to make informed decisions about how they plan to give birth, and it is vital that health care professionals respect their preferences,” Dr. Frodsham added.
Clinicians should also remain aware that sexual pain is also common during periods of subfertility, perimenopause, and initiation of sexual activity.
Combinations of biological, psychological, and social factors can influence pain during sex, and there is an interpersonal element to keep in mind as well, Dr. Rosen noted.
“Pain during sex is typically elicited in the context of a partnered relationship,” Dr. Rosen said. “This means that this is an inherently interpersonal issue – let’s not forget about the partner who is both impacted by and can impact the pain through their own responses.”
A version of this article first appeared on Medscape.com.
For some parents, resuming sexual intimacy after having a baby is a top priority. For others, not so much – and late-night feedings and diaper changes may not be the only hang-ups.
Dyspareunia – pain during sex – occurs in a substantial number of women after childbirth, and recent research sheds light on how psychological and biomedical factors relate to this condition.
Mode of delivery, for instance, may have less of an effect on sexual well-being than some people suspect.
Despite a perception that cesarean delivery might affect sexual function less than vaginal delivery does, how mothers delivered did not affect how often they had sex postpartum or the amount of enjoyment they got from it, according to research published in BJOG.
Eleven years after delivery, however, cesarean delivery was associated with a 74% increased likelihood of pain in the vagina during sex, compared with vaginal delivery, the researchers found (odds ratio, 1.74; 95% confidence interval, 1.46-2.08).
The results suggest that cesarean delivery “may not help protect against sexual dysfunction, as previously thought,” Flo Martin, a PhD student in epidemiology at the University of Bristol, United Kingdom, and lead author of the study, said in a news release.
For their study, Ms. Martin and her colleagues analyzed data from more than 10,300 participants in the Avon Longitudinal Study of Parents and Children, which recruited women in the United Kingdom who were pregnant in 1991 and 1992.
The researchers had data about pain during sex at 11 years. They had data about sexual enjoyment and frequency at 33 months, 5 years, 12 years, and 18 years after delivery.
If women experienced pain during sex years after cesarean delivery, uterine scarring might have been a cause, Ms. Martin and colleagues suggested. Alternatively, women with dyspareunia before delivery may be more likely to have cesarean surgery, which also could explain the association.
Other studies have likewise found that different modes of delivery generally lead to similar outcomes of sexual well-being after birth.
“Several of my own longitudinal studies have shown limited associations between mode of delivery and various aspects of sexual well-being, including sexual satisfaction, sexual function, and sexual desire,” said Natalie O. Rosen, PhD, director of the Couples and Sexual Health Laboratory at Dalhousie University, Halifax, N.S.
Nevertheless, other published studies have yielded conflicting results, so the question warrants further study, she said.
Pain catastrophizing
One study by Dr. Rosen’s group, published in Obstetrics & Gynecology, tracked sexual pain in 582 people from mid-pregnancy to 2 years postpartum.
About 21% of participants experienced moderate pain during sex, as determined by an average pain score greater than 4 on scale of 0-10 points. The rest were classified as having “minimal dyspareunia.”
Pain tended to peak at 3 months postpartum and then steadily decrease in both the moderate and minimal pain groups.
Mode of delivery did not affect the odds that a participant would have moderate dyspareunia. Neither did breastfeeding or prior chronic pain.
“But we did find one key thing to look out for: Those who reported a lot of negative thoughts and feelings about pain, something called pain catastrophizing, were more likely to experience moderate persistent pain during sex,” the researchers said in a video about their findings.
Pain catastrophizing 3 months after delivery was associated with significantly increased odds of following a moderate pain trajectory (odds ratio, 1.09; 95% confidence interval, 1.04-1.15).
Let’s talk about #postbabyhankypanky
Caring for a newborn while maintaining a romantic relationship can be challenging, and “there is a lack of evidence-based research aimed at helping couples prevent and navigate changes to their sexual well-being postpartum,” Dr. Rosen said.
During the 2-year study, a growing number of participants reported having sex less often over time. The percentage of women who had engaged in sexual activity in the past 4 weeks was 99% at baseline (20-24 weeks of gestation), 83.5% at 32 weeks of gestation, 73.9% at 3 months postpartum, and 69.6% at 2 years postpartum.
“One crucial way that couples sustain their connection is through their sexuality,” Dr. Rosen said. “Unfortunately, most new parents experience significant disruptions to their sexual function,” such as lower sexual desire or more pain during intercourse.
Dr. Rosen’s group has created a series of videos related to this topic dubbed #postbabyhankypanky to facilitate communication about sex postpartum. She encourages women with dyspareunia to talk with a health care provider because treatments such as cognitive-behavioral therapy, pelvic floor physical therapy, and topical medications can help manage pain.
‘Reassuring’ data
Veronica Gillispie-Bell, MD, MAS, director of quality for women’s services at the Ochsner Health System, New Orleans, said that she sees patients with postpartum sexual pain frequently.
Patients typically are instructed to have pelvic rest from delivery until 6 weeks after.
At the 6-week appointment, she tells patients to make sure that they are using lots of lubrication, because vaginal dryness related to hormonal changes during pregnancy and breastfeeding can make sex more painful, regardless of mode of delivery.
For many patients, she also recommends pelvic floor physical therapy.
As the medical director for the Louisiana Perinatal Quality Collaborative – a network of care providers, public health officials, and advocates that aims to improve outcomes for birthing persons, families, and newborns – Dr. Gillispie-Bell also is focused on reducing the rate of cesarean deliveries in the state. The BJOG study showing an increased risk for dyspareunia after a cesarean surgery serves as a reminder that there may be “long-term effects of having a C-section that may not be as obvious,” she said.
“C-sections are life-saving procedures, but they are not without risk,” Dr. Gillispie-Bell said.
Leila Frodsham, MBChB, a spokesperson for the Royal College of Obstetricians and Gynaecologists, told Medscape UK that it was “reassuring” to see “no difference in sexual enjoyment or sexual frequency at any time point postpartum between women who gave birth via cesarean section and those who delivered vaginally.”
“Women should be supported to make informed decisions about how they plan to give birth, and it is vital that health care professionals respect their preferences,” Dr. Frodsham added.
Clinicians should also remain aware that sexual pain is also common during periods of subfertility, perimenopause, and initiation of sexual activity.
Combinations of biological, psychological, and social factors can influence pain during sex, and there is an interpersonal element to keep in mind as well, Dr. Rosen noted.
“Pain during sex is typically elicited in the context of a partnered relationship,” Dr. Rosen said. “This means that this is an inherently interpersonal issue – let’s not forget about the partner who is both impacted by and can impact the pain through their own responses.”
A version of this article first appeared on Medscape.com.
For some parents, resuming sexual intimacy after having a baby is a top priority. For others, not so much – and late-night feedings and diaper changes may not be the only hang-ups.
Dyspareunia – pain during sex – occurs in a substantial number of women after childbirth, and recent research sheds light on how psychological and biomedical factors relate to this condition.
Mode of delivery, for instance, may have less of an effect on sexual well-being than some people suspect.
Despite a perception that cesarean delivery might affect sexual function less than vaginal delivery does, how mothers delivered did not affect how often they had sex postpartum or the amount of enjoyment they got from it, according to research published in BJOG.
Eleven years after delivery, however, cesarean delivery was associated with a 74% increased likelihood of pain in the vagina during sex, compared with vaginal delivery, the researchers found (odds ratio, 1.74; 95% confidence interval, 1.46-2.08).
The results suggest that cesarean delivery “may not help protect against sexual dysfunction, as previously thought,” Flo Martin, a PhD student in epidemiology at the University of Bristol, United Kingdom, and lead author of the study, said in a news release.
For their study, Ms. Martin and her colleagues analyzed data from more than 10,300 participants in the Avon Longitudinal Study of Parents and Children, which recruited women in the United Kingdom who were pregnant in 1991 and 1992.
The researchers had data about pain during sex at 11 years. They had data about sexual enjoyment and frequency at 33 months, 5 years, 12 years, and 18 years after delivery.
If women experienced pain during sex years after cesarean delivery, uterine scarring might have been a cause, Ms. Martin and colleagues suggested. Alternatively, women with dyspareunia before delivery may be more likely to have cesarean surgery, which also could explain the association.
Other studies have likewise found that different modes of delivery generally lead to similar outcomes of sexual well-being after birth.
“Several of my own longitudinal studies have shown limited associations between mode of delivery and various aspects of sexual well-being, including sexual satisfaction, sexual function, and sexual desire,” said Natalie O. Rosen, PhD, director of the Couples and Sexual Health Laboratory at Dalhousie University, Halifax, N.S.
Nevertheless, other published studies have yielded conflicting results, so the question warrants further study, she said.
Pain catastrophizing
One study by Dr. Rosen’s group, published in Obstetrics & Gynecology, tracked sexual pain in 582 people from mid-pregnancy to 2 years postpartum.
About 21% of participants experienced moderate pain during sex, as determined by an average pain score greater than 4 on scale of 0-10 points. The rest were classified as having “minimal dyspareunia.”
Pain tended to peak at 3 months postpartum and then steadily decrease in both the moderate and minimal pain groups.
Mode of delivery did not affect the odds that a participant would have moderate dyspareunia. Neither did breastfeeding or prior chronic pain.
“But we did find one key thing to look out for: Those who reported a lot of negative thoughts and feelings about pain, something called pain catastrophizing, were more likely to experience moderate persistent pain during sex,” the researchers said in a video about their findings.
Pain catastrophizing 3 months after delivery was associated with significantly increased odds of following a moderate pain trajectory (odds ratio, 1.09; 95% confidence interval, 1.04-1.15).
Let’s talk about #postbabyhankypanky
Caring for a newborn while maintaining a romantic relationship can be challenging, and “there is a lack of evidence-based research aimed at helping couples prevent and navigate changes to their sexual well-being postpartum,” Dr. Rosen said.
During the 2-year study, a growing number of participants reported having sex less often over time. The percentage of women who had engaged in sexual activity in the past 4 weeks was 99% at baseline (20-24 weeks of gestation), 83.5% at 32 weeks of gestation, 73.9% at 3 months postpartum, and 69.6% at 2 years postpartum.
“One crucial way that couples sustain their connection is through their sexuality,” Dr. Rosen said. “Unfortunately, most new parents experience significant disruptions to their sexual function,” such as lower sexual desire or more pain during intercourse.
Dr. Rosen’s group has created a series of videos related to this topic dubbed #postbabyhankypanky to facilitate communication about sex postpartum. She encourages women with dyspareunia to talk with a health care provider because treatments such as cognitive-behavioral therapy, pelvic floor physical therapy, and topical medications can help manage pain.
‘Reassuring’ data
Veronica Gillispie-Bell, MD, MAS, director of quality for women’s services at the Ochsner Health System, New Orleans, said that she sees patients with postpartum sexual pain frequently.
Patients typically are instructed to have pelvic rest from delivery until 6 weeks after.
At the 6-week appointment, she tells patients to make sure that they are using lots of lubrication, because vaginal dryness related to hormonal changes during pregnancy and breastfeeding can make sex more painful, regardless of mode of delivery.
For many patients, she also recommends pelvic floor physical therapy.
As the medical director for the Louisiana Perinatal Quality Collaborative – a network of care providers, public health officials, and advocates that aims to improve outcomes for birthing persons, families, and newborns – Dr. Gillispie-Bell also is focused on reducing the rate of cesarean deliveries in the state. The BJOG study showing an increased risk for dyspareunia after a cesarean surgery serves as a reminder that there may be “long-term effects of having a C-section that may not be as obvious,” she said.
“C-sections are life-saving procedures, but they are not without risk,” Dr. Gillispie-Bell said.
Leila Frodsham, MBChB, a spokesperson for the Royal College of Obstetricians and Gynaecologists, told Medscape UK that it was “reassuring” to see “no difference in sexual enjoyment or sexual frequency at any time point postpartum between women who gave birth via cesarean section and those who delivered vaginally.”
“Women should be supported to make informed decisions about how they plan to give birth, and it is vital that health care professionals respect their preferences,” Dr. Frodsham added.
Clinicians should also remain aware that sexual pain is also common during periods of subfertility, perimenopause, and initiation of sexual activity.
Combinations of biological, psychological, and social factors can influence pain during sex, and there is an interpersonal element to keep in mind as well, Dr. Rosen noted.
“Pain during sex is typically elicited in the context of a partnered relationship,” Dr. Rosen said. “This means that this is an inherently interpersonal issue – let’s not forget about the partner who is both impacted by and can impact the pain through their own responses.”
A version of this article first appeared on Medscape.com.
COMMENT & CONTROVERSY
CAN WE RETURN TO THE ABCS OF CRAFTING A MEDICAL RECORD NOTE?
ROBERT L. BARBIERI, MD (OCTOBER 2021)
Physicians can help provide EMR fixes
I appreciate Dr. Barbieri’s editorials and insight on many issues facing our profession. I would like to offer my comments on a recent article.
If you want your brakes fixed, don’t go to a shoe maker. Physicians seem to have lost our sense of who is most competent in determining the best way to practice and communicate medical care. Somehow we have turned this over to the bureaucrats, who seem to find ways to complicate the lives of both providers and patients. Maybe we are too busy caring for patients and trying to find ways to alleviate the burden placed on our time by the electronic medical record (EMR) system, which was touted as an improvement in medical care and increasing provider efficiency. Most of the time I hear my colleagues describing ways to “work around” an EMR system that has immense deficiencies in providing accurate information in a way that is easily digested by whomever is viewing the record. The universal ability to transfer information is simply not true. One colleague had the same office version of Cerner as was used in the hospital setting but was unable to send information back and forth due to the danger of the potential to corrupt the system.
Dr. Barbieri mentioned his work around to make the record easier for the patient to read. I ask, what about the coding descriptions, which most systems are now requiring physicians to put in at the time of the encounter? In the past this was done by certified coders, who undergo a 1- to 2-year training program, and is now being performed by physicians who have minimal to no training in coding. (And who, by the way, can be fined for both under- and over coding.) The example Dr. Barbieri put forth for obesity comes to mind and is part of the medical record in all cases. The terminology used by ICD10 is not so kind and requires some imagination when trying to find the right code for many diagnoses.
When will we stop allowing others, who know little about medicine and caring for patients, to tell us how to provide the care that we have trained for 7-12 years on how best to deliver?
William Sutton, MD
Muncie, Indiana
Dr. Barbieri responds
I thank Dr. Sutton for providing his experience with the electronic medical record. I agree with him that bureaucrats often create health care rules that do more to hinder than help patients. With regard to coding and billing, I use ICD-10 codes and usually bill based on time, which includes both face-to-face time with the patient and time spent reviewing the patient’s medical records. Now that federal regulations require medical notes to be shared with patients, I craft my history, assessment, and plan with language that is easy for a patient to accept and understand, avoiding medical terms that patients might misinterpret.
Should microscopy be replaced?
I agree with many points Dr. Barbieri made in his editorial. However, I do not agree that the microscopic examination of the vaginal discharge should be replaced. NAAT offers some advantages, but it does not offer a complete assessment of the vaginal ecosystem and microbiome. I believe that NAAT should be used in conjunction with the pelvic examination and microscopic examination of the vaginal discharge.
Microscopic examination of the vaginal discharge can reveal:
- whether or not the squamous epithelial cells are estrogenized. The absence of estrogen will, along with physical findings, indicate the possibility that the patient is experiencing atrophic vaginitis.
- the presence of estrogenized squamous epithelial cells. Plus, a finding of erythema of the vaginal epithelium indicates that the patient has an inflammatory condition and vaginitis, suggesting a possible infection in addition to vaginitis.
- the presence of white blood cells >5/40X magnification, which indicates the possible presence of infection in addition to vaginitis (eg, BV).
I agree that NAAT can confirm an initial diagnosis or refute it. In the latter case, the physician can change treatment accordingly. In the absence or in conjunction with the presence of a sexually transmitted infection, the composition of the vaginal microbiome is significant (ie, determining if vaginal dysbiosis is present). Performing a comprehensive evaluation, determining if the most common pathogens are present in aerobic vaginitis and/or BV, plus completing a Lactobacillus panel can be expensive. If insurance companies do not pay for such testing, patients will be reluctant to pay out of pocket for these tests.
My final comment addresses the administration of NAAT for aerobic vaginitis, and for BV, it is probably an ineffective treatment. Vaginal dysbiosis is based on whether the appropriate species of Lactobacillus is present, and the concentration. Treatment most likely will be based on replenishing or restoring the appropriate species of Lactobacillus to dominance.
Sebastian Faro, MD, PhD
Houston, Texas
Dr. Barbieri responds
I agree with Dr. Faro; when used by highly trained clinicians, microscopy is an excellent tool for evaluating vaginal specimens. Expert clinicians, such as Dr. Faro, with a focus on infectious diseases do not need to rely on NAAT testing except for identifying cases of T vaginalis infection. However, in standard clinical practice, microscopy performs poorly, resulting in misdiagnosis.1 In the average clinical practice, NAAT testing may help improve patient outcomes.
1. Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
A note of thanks
I am a 74-year-old ObGyn who finished training at the University of North Carolina in 1979. Currently, I am working at a rural health group 2 days a week as a source of in-house gyn referral for 17 primary care physicians and mid-level providers. Our patients are almost all underserved and self-pay. The bulk of my work is related to evaluating abnormal uterine bleeding and abnormal Pap tests. Your publication of OBG Management serves now as one of my main sources of information. I just wanted to thank you and let you know that the publication is important. Keep up the good work and best wishes.
Julian Brantley, MD
Rocky Mountain, North Carolina
Dr. Barbieri responds
I thank Dr. Brantley for taking time from a busy practice to write about how OBG Management provides practical information relevant to practice. Each issue of OBG Management is built on a foundation of insights from expert clinicians, which is crafted into a finished product by a superb editorial team. Our goal is to enhance the quality of women’s health care and the professional development of obstetrician-gynecologists and all women’s health care clinicians. ●
CAN WE RETURN TO THE ABCS OF CRAFTING A MEDICAL RECORD NOTE?
ROBERT L. BARBIERI, MD (OCTOBER 2021)
Physicians can help provide EMR fixes
I appreciate Dr. Barbieri’s editorials and insight on many issues facing our profession. I would like to offer my comments on a recent article.
If you want your brakes fixed, don’t go to a shoe maker. Physicians seem to have lost our sense of who is most competent in determining the best way to practice and communicate medical care. Somehow we have turned this over to the bureaucrats, who seem to find ways to complicate the lives of both providers and patients. Maybe we are too busy caring for patients and trying to find ways to alleviate the burden placed on our time by the electronic medical record (EMR) system, which was touted as an improvement in medical care and increasing provider efficiency. Most of the time I hear my colleagues describing ways to “work around” an EMR system that has immense deficiencies in providing accurate information in a way that is easily digested by whomever is viewing the record. The universal ability to transfer information is simply not true. One colleague had the same office version of Cerner as was used in the hospital setting but was unable to send information back and forth due to the danger of the potential to corrupt the system.
Dr. Barbieri mentioned his work around to make the record easier for the patient to read. I ask, what about the coding descriptions, which most systems are now requiring physicians to put in at the time of the encounter? In the past this was done by certified coders, who undergo a 1- to 2-year training program, and is now being performed by physicians who have minimal to no training in coding. (And who, by the way, can be fined for both under- and over coding.) The example Dr. Barbieri put forth for obesity comes to mind and is part of the medical record in all cases. The terminology used by ICD10 is not so kind and requires some imagination when trying to find the right code for many diagnoses.
When will we stop allowing others, who know little about medicine and caring for patients, to tell us how to provide the care that we have trained for 7-12 years on how best to deliver?
William Sutton, MD
Muncie, Indiana
Dr. Barbieri responds
I thank Dr. Sutton for providing his experience with the electronic medical record. I agree with him that bureaucrats often create health care rules that do more to hinder than help patients. With regard to coding and billing, I use ICD-10 codes and usually bill based on time, which includes both face-to-face time with the patient and time spent reviewing the patient’s medical records. Now that federal regulations require medical notes to be shared with patients, I craft my history, assessment, and plan with language that is easy for a patient to accept and understand, avoiding medical terms that patients might misinterpret.
Should microscopy be replaced?
I agree with many points Dr. Barbieri made in his editorial. However, I do not agree that the microscopic examination of the vaginal discharge should be replaced. NAAT offers some advantages, but it does not offer a complete assessment of the vaginal ecosystem and microbiome. I believe that NAAT should be used in conjunction with the pelvic examination and microscopic examination of the vaginal discharge.
Microscopic examination of the vaginal discharge can reveal:
- whether or not the squamous epithelial cells are estrogenized. The absence of estrogen will, along with physical findings, indicate the possibility that the patient is experiencing atrophic vaginitis.
- the presence of estrogenized squamous epithelial cells. Plus, a finding of erythema of the vaginal epithelium indicates that the patient has an inflammatory condition and vaginitis, suggesting a possible infection in addition to vaginitis.
- the presence of white blood cells >5/40X magnification, which indicates the possible presence of infection in addition to vaginitis (eg, BV).
I agree that NAAT can confirm an initial diagnosis or refute it. In the latter case, the physician can change treatment accordingly. In the absence or in conjunction with the presence of a sexually transmitted infection, the composition of the vaginal microbiome is significant (ie, determining if vaginal dysbiosis is present). Performing a comprehensive evaluation, determining if the most common pathogens are present in aerobic vaginitis and/or BV, plus completing a Lactobacillus panel can be expensive. If insurance companies do not pay for such testing, patients will be reluctant to pay out of pocket for these tests.
My final comment addresses the administration of NAAT for aerobic vaginitis, and for BV, it is probably an ineffective treatment. Vaginal dysbiosis is based on whether the appropriate species of Lactobacillus is present, and the concentration. Treatment most likely will be based on replenishing or restoring the appropriate species of Lactobacillus to dominance.
Sebastian Faro, MD, PhD
Houston, Texas
Dr. Barbieri responds
I agree with Dr. Faro; when used by highly trained clinicians, microscopy is an excellent tool for evaluating vaginal specimens. Expert clinicians, such as Dr. Faro, with a focus on infectious diseases do not need to rely on NAAT testing except for identifying cases of T vaginalis infection. However, in standard clinical practice, microscopy performs poorly, resulting in misdiagnosis.1 In the average clinical practice, NAAT testing may help improve patient outcomes.
1. Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
A note of thanks
I am a 74-year-old ObGyn who finished training at the University of North Carolina in 1979. Currently, I am working at a rural health group 2 days a week as a source of in-house gyn referral for 17 primary care physicians and mid-level providers. Our patients are almost all underserved and self-pay. The bulk of my work is related to evaluating abnormal uterine bleeding and abnormal Pap tests. Your publication of OBG Management serves now as one of my main sources of information. I just wanted to thank you and let you know that the publication is important. Keep up the good work and best wishes.
Julian Brantley, MD
Rocky Mountain, North Carolina
Dr. Barbieri responds
I thank Dr. Brantley for taking time from a busy practice to write about how OBG Management provides practical information relevant to practice. Each issue of OBG Management is built on a foundation of insights from expert clinicians, which is crafted into a finished product by a superb editorial team. Our goal is to enhance the quality of women’s health care and the professional development of obstetrician-gynecologists and all women’s health care clinicians. ●
CAN WE RETURN TO THE ABCS OF CRAFTING A MEDICAL RECORD NOTE?
ROBERT L. BARBIERI, MD (OCTOBER 2021)
Physicians can help provide EMR fixes
I appreciate Dr. Barbieri’s editorials and insight on many issues facing our profession. I would like to offer my comments on a recent article.
If you want your brakes fixed, don’t go to a shoe maker. Physicians seem to have lost our sense of who is most competent in determining the best way to practice and communicate medical care. Somehow we have turned this over to the bureaucrats, who seem to find ways to complicate the lives of both providers and patients. Maybe we are too busy caring for patients and trying to find ways to alleviate the burden placed on our time by the electronic medical record (EMR) system, which was touted as an improvement in medical care and increasing provider efficiency. Most of the time I hear my colleagues describing ways to “work around” an EMR system that has immense deficiencies in providing accurate information in a way that is easily digested by whomever is viewing the record. The universal ability to transfer information is simply not true. One colleague had the same office version of Cerner as was used in the hospital setting but was unable to send information back and forth due to the danger of the potential to corrupt the system.
Dr. Barbieri mentioned his work around to make the record easier for the patient to read. I ask, what about the coding descriptions, which most systems are now requiring physicians to put in at the time of the encounter? In the past this was done by certified coders, who undergo a 1- to 2-year training program, and is now being performed by physicians who have minimal to no training in coding. (And who, by the way, can be fined for both under- and over coding.) The example Dr. Barbieri put forth for obesity comes to mind and is part of the medical record in all cases. The terminology used by ICD10 is not so kind and requires some imagination when trying to find the right code for many diagnoses.
When will we stop allowing others, who know little about medicine and caring for patients, to tell us how to provide the care that we have trained for 7-12 years on how best to deliver?
William Sutton, MD
Muncie, Indiana
Dr. Barbieri responds
I thank Dr. Sutton for providing his experience with the electronic medical record. I agree with him that bureaucrats often create health care rules that do more to hinder than help patients. With regard to coding and billing, I use ICD-10 codes and usually bill based on time, which includes both face-to-face time with the patient and time spent reviewing the patient’s medical records. Now that federal regulations require medical notes to be shared with patients, I craft my history, assessment, and plan with language that is easy for a patient to accept and understand, avoiding medical terms that patients might misinterpret.
Should microscopy be replaced?
I agree with many points Dr. Barbieri made in his editorial. However, I do not agree that the microscopic examination of the vaginal discharge should be replaced. NAAT offers some advantages, but it does not offer a complete assessment of the vaginal ecosystem and microbiome. I believe that NAAT should be used in conjunction with the pelvic examination and microscopic examination of the vaginal discharge.
Microscopic examination of the vaginal discharge can reveal:
- whether or not the squamous epithelial cells are estrogenized. The absence of estrogen will, along with physical findings, indicate the possibility that the patient is experiencing atrophic vaginitis.
- the presence of estrogenized squamous epithelial cells. Plus, a finding of erythema of the vaginal epithelium indicates that the patient has an inflammatory condition and vaginitis, suggesting a possible infection in addition to vaginitis.
- the presence of white blood cells >5/40X magnification, which indicates the possible presence of infection in addition to vaginitis (eg, BV).
I agree that NAAT can confirm an initial diagnosis or refute it. In the latter case, the physician can change treatment accordingly. In the absence or in conjunction with the presence of a sexually transmitted infection, the composition of the vaginal microbiome is significant (ie, determining if vaginal dysbiosis is present). Performing a comprehensive evaluation, determining if the most common pathogens are present in aerobic vaginitis and/or BV, plus completing a Lactobacillus panel can be expensive. If insurance companies do not pay for such testing, patients will be reluctant to pay out of pocket for these tests.
My final comment addresses the administration of NAAT for aerobic vaginitis, and for BV, it is probably an ineffective treatment. Vaginal dysbiosis is based on whether the appropriate species of Lactobacillus is present, and the concentration. Treatment most likely will be based on replenishing or restoring the appropriate species of Lactobacillus to dominance.
Sebastian Faro, MD, PhD
Houston, Texas
Dr. Barbieri responds
I agree with Dr. Faro; when used by highly trained clinicians, microscopy is an excellent tool for evaluating vaginal specimens. Expert clinicians, such as Dr. Faro, with a focus on infectious diseases do not need to rely on NAAT testing except for identifying cases of T vaginalis infection. However, in standard clinical practice, microscopy performs poorly, resulting in misdiagnosis.1 In the average clinical practice, NAAT testing may help improve patient outcomes.
1. Gaydos CA, Beqaj S, Schwebke JR, et al. Clinical validation of a test for the diagnosis of vaginitis. Obstet Gynecol. 2017;130:181-189.
A note of thanks
I am a 74-year-old ObGyn who finished training at the University of North Carolina in 1979. Currently, I am working at a rural health group 2 days a week as a source of in-house gyn referral for 17 primary care physicians and mid-level providers. Our patients are almost all underserved and self-pay. The bulk of my work is related to evaluating abnormal uterine bleeding and abnormal Pap tests. Your publication of OBG Management serves now as one of my main sources of information. I just wanted to thank you and let you know that the publication is important. Keep up the good work and best wishes.
Julian Brantley, MD
Rocky Mountain, North Carolina
Dr. Barbieri responds
I thank Dr. Brantley for taking time from a busy practice to write about how OBG Management provides practical information relevant to practice. Each issue of OBG Management is built on a foundation of insights from expert clinicians, which is crafted into a finished product by a superb editorial team. Our goal is to enhance the quality of women’s health care and the professional development of obstetrician-gynecologists and all women’s health care clinicians. ●
Docs gain new flexibility treating osteoporosis from steroids
Doctors caring for patients taking steroids now have broader flexibility for which drugs to use to prevent osteoporosis associated with the medications.
The American College of Rheumatology (ACR) has released an updated guideline that advises treatment providers on when and how long to prescribe therapies that prevent or treat glucocorticoid-induced osteoporosis (GIOP). Since the ACR last updated the guideline in 2017, the Food and Drug Administration has approved new treatments for osteoporosis, which are now included in the recommendations.
The new guideline also advises physicians that they may need to transition patients to a second treatment after concluding a first course – so-called sequential therapy – to better protect them against bone loss and fracture. It also offers detailed instructions for which drugs to use, when, and how long these medications should be administered for patients taking glucocorticoids over a long period of time.
The guideline’s inclusion of sequential therapy is significant and will be helpful to practicing clinicians, according to S.B. Tanner IV, MD, director of the Osteoporosis Clinic at Vanderbilt Health, Nashville, Tenn.
“For the first time, the ACR has offered guidance for starting and stopping treatments,” Dr. Tanner said. “This guideline supports awareness that osteoporosis is lifelong – something that will consistently need monitoring.”
An estimated 2.5 million Americans use glucocorticoids, according to a 2013 study in Arthritis Care & Research. Meanwhile, a 2019 study of residents in Denmark found 3% of people in the country were prescribed glucocorticoids annually. That study estimated 54% of glucocorticoid users were female and found the percentage of people taking glucocorticoids increased with age.
Glucocorticoids are used to treat a variety of inflammatory conditions, from multiple sclerosis to lupus, and often are prescribed to transplant patients to prevent their immune systems from rejecting new organs. When taken over time these medications can cause osteoporosis, which in turn raises the risk of fracture.
More than 10% of patients who receive long-term glucocorticoid treatment are diagnosed with clinical fractures. In addition, even low-dose glucocorticoid therapy is associated with a bone loss rate of 10% per year for a patient.
Osteoporosis prevention
After stopping some prevention therapies for GIOP, a high risk of bone loss or fracture still persists, according to Linda A. Russell, MD, director of the Osteoporosis and Metabolic Bone Health Center for the Hospital for Special Surgery, New York, and co-principal investigator of the new guideline.

“We wanted to be sure the need for sequential treatment is adequately communicated, including to patients who might not know they need to start a second medication,” Dr. Russell said.
Physicians and patients must be aware that when completing a course of one GIOP treatment, another drug for the condition should be started, as specified in the guideline.
“Early intervention can prevent glucocorticoid-induced fractures that can lead to substantial morbidity and increased mortality,” said Mary Beth Humphrey, MD, PhD, interim vice president for research at the University of Oklahoma Health Sciences Center in Oklahoma City and co-principal investigator of the ACR guideline.

Janet Rubin, MD, vice chair for research in the Department of medicine at the University of North Carolina at Chapel Hill, said she is hopeful the guideline will change practice.”The risk of bone loss, fractures, and osteoporosis due to glucocorticoids has been known since the beginning of time, but the guideline reinforces the risk and treatment strategies for rheumatologists,” she said. “Such recommendations are known to influence doctor prescribing habits.”

Anyone can fracture
While age and other risk factors, including menopause, increase the risk of developing GIOP, bone loss can occur rapidly for a patient of any age.
Even a glucocorticoid dose as low as 2.5 mg will increase the risk of vertebral fractures, with some occurring as soon as 3 months after treatment starts, Dr. Humphrey said. For patients taking up to 7.5 mg daily, the risk of vertebral fracture doubles. Doses greater than 10 mg daily for more than 3 months raise the likelihood of a vertebral fracture by a factor of 14, and result in a 300% increase in the likelihood of hip fractures, according to Dr. Humphrey.
“When on steroids, even patients with high bone density scores can fracture,” Dr. Tanner said. “The 2017 guideline was almost too elaborate in its effort to calculate risk. The updated guideline acknowledges moderate risk and suggests that this is a group of patients who need treatment.”
Rank ordering adds flexibility
The updated ACR guideline no longer ranks medications based on patient fracture data, side effects, cost care, and whether the drug is provided through injection, pill, or IV.
All of the preventive treatments the panel recommends reduce the risk of steroid-induced bone loss, Dr. Humphrey said.
“We thought the 2017 guideline was too restrictive,” Dr. Russell said. “We’re giving physicians and patients more leeway to choose a medication based on their preferences.”
Patient preference of delivery mechanism – such as a desire for pills only – can now be weighed more heavily into drug treatment decisions.
“In the exam room, there are three dynamics going on: What the patient wants, what the doctor knows is most effective, and what the insurer will pay,” Dr. Tanner said. “Doing away with rank ordering opens up the conversation beyond cost to consider all those factors.”
The guideline team conducted a systematic literature review for clinical questions on nonpharmacologic and pharmacologic treatment addressed in the 2017 guideline, and for questions on new pharmacologic treatments, discontinuation of medications, and sequential and combination therapy. The voting panel consisted of two patient representatives and 13 experts representing adult and pediatric rheumatology and endocrinology, nephrology, and gastroenterology.
A full manuscript has been submitted for publication in Arthritis & Rheumatology and Arthritis Care and Research for peer review, and is expected to publish in early 2023.
Dr. Humphrey and Dr. Russell, the co-principal investigators for the guideline, and Dr. Rubin have disclosed no relevant financial relationships. Dr. Tanner reported a current research grant funded by Amgen through the University of Alabama at Birmingham and being a paid course instructor for the International Society for Clinical Densitometry bone density course, Osteoporosis Essentials.
A version of this article first appeared on Medscape.com.
Doctors caring for patients taking steroids now have broader flexibility for which drugs to use to prevent osteoporosis associated with the medications.
The American College of Rheumatology (ACR) has released an updated guideline that advises treatment providers on when and how long to prescribe therapies that prevent or treat glucocorticoid-induced osteoporosis (GIOP). Since the ACR last updated the guideline in 2017, the Food and Drug Administration has approved new treatments for osteoporosis, which are now included in the recommendations.
The new guideline also advises physicians that they may need to transition patients to a second treatment after concluding a first course – so-called sequential therapy – to better protect them against bone loss and fracture. It also offers detailed instructions for which drugs to use, when, and how long these medications should be administered for patients taking glucocorticoids over a long period of time.
The guideline’s inclusion of sequential therapy is significant and will be helpful to practicing clinicians, according to S.B. Tanner IV, MD, director of the Osteoporosis Clinic at Vanderbilt Health, Nashville, Tenn.
“For the first time, the ACR has offered guidance for starting and stopping treatments,” Dr. Tanner said. “This guideline supports awareness that osteoporosis is lifelong – something that will consistently need monitoring.”
An estimated 2.5 million Americans use glucocorticoids, according to a 2013 study in Arthritis Care & Research. Meanwhile, a 2019 study of residents in Denmark found 3% of people in the country were prescribed glucocorticoids annually. That study estimated 54% of glucocorticoid users were female and found the percentage of people taking glucocorticoids increased with age.
Glucocorticoids are used to treat a variety of inflammatory conditions, from multiple sclerosis to lupus, and often are prescribed to transplant patients to prevent their immune systems from rejecting new organs. When taken over time these medications can cause osteoporosis, which in turn raises the risk of fracture.
More than 10% of patients who receive long-term glucocorticoid treatment are diagnosed with clinical fractures. In addition, even low-dose glucocorticoid therapy is associated with a bone loss rate of 10% per year for a patient.
Osteoporosis prevention
After stopping some prevention therapies for GIOP, a high risk of bone loss or fracture still persists, according to Linda A. Russell, MD, director of the Osteoporosis and Metabolic Bone Health Center for the Hospital for Special Surgery, New York, and co-principal investigator of the new guideline.
“We wanted to be sure the need for sequential treatment is adequately communicated, including to patients who might not know they need to start a second medication,” Dr. Russell said.
Physicians and patients must be aware that when completing a course of one GIOP treatment, another drug for the condition should be started, as specified in the guideline.
“Early intervention can prevent glucocorticoid-induced fractures that can lead to substantial morbidity and increased mortality,” said Mary Beth Humphrey, MD, PhD, interim vice president for research at the University of Oklahoma Health Sciences Center in Oklahoma City and co-principal investigator of the ACR guideline.
Janet Rubin, MD, vice chair for research in the Department of medicine at the University of North Carolina at Chapel Hill, said she is hopeful the guideline will change practice.”The risk of bone loss, fractures, and osteoporosis due to glucocorticoids has been known since the beginning of time, but the guideline reinforces the risk and treatment strategies for rheumatologists,” she said. “Such recommendations are known to influence doctor prescribing habits.”
Anyone can fracture
While age and other risk factors, including menopause, increase the risk of developing GIOP, bone loss can occur rapidly for a patient of any age.
Even a glucocorticoid dose as low as 2.5 mg will increase the risk of vertebral fractures, with some occurring as soon as 3 months after treatment starts, Dr. Humphrey said. For patients taking up to 7.5 mg daily, the risk of vertebral fracture doubles. Doses greater than 10 mg daily for more than 3 months raise the likelihood of a vertebral fracture by a factor of 14, and result in a 300% increase in the likelihood of hip fractures, according to Dr. Humphrey.
“When on steroids, even patients with high bone density scores can fracture,” Dr. Tanner said. “The 2017 guideline was almost too elaborate in its effort to calculate risk. The updated guideline acknowledges moderate risk and suggests that this is a group of patients who need treatment.”
Rank ordering adds flexibility
The updated ACR guideline no longer ranks medications based on patient fracture data, side effects, cost care, and whether the drug is provided through injection, pill, or IV.
All of the preventive treatments the panel recommends reduce the risk of steroid-induced bone loss, Dr. Humphrey said.
“We thought the 2017 guideline was too restrictive,” Dr. Russell said. “We’re giving physicians and patients more leeway to choose a medication based on their preferences.”
Patient preference of delivery mechanism – such as a desire for pills only – can now be weighed more heavily into drug treatment decisions.
“In the exam room, there are three dynamics going on: What the patient wants, what the doctor knows is most effective, and what the insurer will pay,” Dr. Tanner said. “Doing away with rank ordering opens up the conversation beyond cost to consider all those factors.”
The guideline team conducted a systematic literature review for clinical questions on nonpharmacologic and pharmacologic treatment addressed in the 2017 guideline, and for questions on new pharmacologic treatments, discontinuation of medications, and sequential and combination therapy. The voting panel consisted of two patient representatives and 13 experts representing adult and pediatric rheumatology and endocrinology, nephrology, and gastroenterology.
A full manuscript has been submitted for publication in Arthritis & Rheumatology and Arthritis Care and Research for peer review, and is expected to publish in early 2023.
Dr. Humphrey and Dr. Russell, the co-principal investigators for the guideline, and Dr. Rubin have disclosed no relevant financial relationships. Dr. Tanner reported a current research grant funded by Amgen through the University of Alabama at Birmingham and being a paid course instructor for the International Society for Clinical Densitometry bone density course, Osteoporosis Essentials.
A version of this article first appeared on Medscape.com.
Doctors caring for patients taking steroids now have broader flexibility for which drugs to use to prevent osteoporosis associated with the medications.
The American College of Rheumatology (ACR) has released an updated guideline that advises treatment providers on when and how long to prescribe therapies that prevent or treat glucocorticoid-induced osteoporosis (GIOP). Since the ACR last updated the guideline in 2017, the Food and Drug Administration has approved new treatments for osteoporosis, which are now included in the recommendations.
The new guideline also advises physicians that they may need to transition patients to a second treatment after concluding a first course – so-called sequential therapy – to better protect them against bone loss and fracture. It also offers detailed instructions for which drugs to use, when, and how long these medications should be administered for patients taking glucocorticoids over a long period of time.
The guideline’s inclusion of sequential therapy is significant and will be helpful to practicing clinicians, according to S.B. Tanner IV, MD, director of the Osteoporosis Clinic at Vanderbilt Health, Nashville, Tenn.
“For the first time, the ACR has offered guidance for starting and stopping treatments,” Dr. Tanner said. “This guideline supports awareness that osteoporosis is lifelong – something that will consistently need monitoring.”
An estimated 2.5 million Americans use glucocorticoids, according to a 2013 study in Arthritis Care & Research. Meanwhile, a 2019 study of residents in Denmark found 3% of people in the country were prescribed glucocorticoids annually. That study estimated 54% of glucocorticoid users were female and found the percentage of people taking glucocorticoids increased with age.
Glucocorticoids are used to treat a variety of inflammatory conditions, from multiple sclerosis to lupus, and often are prescribed to transplant patients to prevent their immune systems from rejecting new organs. When taken over time these medications can cause osteoporosis, which in turn raises the risk of fracture.
More than 10% of patients who receive long-term glucocorticoid treatment are diagnosed with clinical fractures. In addition, even low-dose glucocorticoid therapy is associated with a bone loss rate of 10% per year for a patient.
Osteoporosis prevention
After stopping some prevention therapies for GIOP, a high risk of bone loss or fracture still persists, according to Linda A. Russell, MD, director of the Osteoporosis and Metabolic Bone Health Center for the Hospital for Special Surgery, New York, and co-principal investigator of the new guideline.
“We wanted to be sure the need for sequential treatment is adequately communicated, including to patients who might not know they need to start a second medication,” Dr. Russell said.
Physicians and patients must be aware that when completing a course of one GIOP treatment, another drug for the condition should be started, as specified in the guideline.
“Early intervention can prevent glucocorticoid-induced fractures that can lead to substantial morbidity and increased mortality,” said Mary Beth Humphrey, MD, PhD, interim vice president for research at the University of Oklahoma Health Sciences Center in Oklahoma City and co-principal investigator of the ACR guideline.
Janet Rubin, MD, vice chair for research in the Department of medicine at the University of North Carolina at Chapel Hill, said she is hopeful the guideline will change practice.”The risk of bone loss, fractures, and osteoporosis due to glucocorticoids has been known since the beginning of time, but the guideline reinforces the risk and treatment strategies for rheumatologists,” she said. “Such recommendations are known to influence doctor prescribing habits.”
Anyone can fracture
While age and other risk factors, including menopause, increase the risk of developing GIOP, bone loss can occur rapidly for a patient of any age.
Even a glucocorticoid dose as low as 2.5 mg will increase the risk of vertebral fractures, with some occurring as soon as 3 months after treatment starts, Dr. Humphrey said. For patients taking up to 7.5 mg daily, the risk of vertebral fracture doubles. Doses greater than 10 mg daily for more than 3 months raise the likelihood of a vertebral fracture by a factor of 14, and result in a 300% increase in the likelihood of hip fractures, according to Dr. Humphrey.
“When on steroids, even patients with high bone density scores can fracture,” Dr. Tanner said. “The 2017 guideline was almost too elaborate in its effort to calculate risk. The updated guideline acknowledges moderate risk and suggests that this is a group of patients who need treatment.”
Rank ordering adds flexibility
The updated ACR guideline no longer ranks medications based on patient fracture data, side effects, cost care, and whether the drug is provided through injection, pill, or IV.
All of the preventive treatments the panel recommends reduce the risk of steroid-induced bone loss, Dr. Humphrey said.
“We thought the 2017 guideline was too restrictive,” Dr. Russell said. “We’re giving physicians and patients more leeway to choose a medication based on their preferences.”
Patient preference of delivery mechanism – such as a desire for pills only – can now be weighed more heavily into drug treatment decisions.
“In the exam room, there are three dynamics going on: What the patient wants, what the doctor knows is most effective, and what the insurer will pay,” Dr. Tanner said. “Doing away with rank ordering opens up the conversation beyond cost to consider all those factors.”
The guideline team conducted a systematic literature review for clinical questions on nonpharmacologic and pharmacologic treatment addressed in the 2017 guideline, and for questions on new pharmacologic treatments, discontinuation of medications, and sequential and combination therapy. The voting panel consisted of two patient representatives and 13 experts representing adult and pediatric rheumatology and endocrinology, nephrology, and gastroenterology.
A full manuscript has been submitted for publication in Arthritis & Rheumatology and Arthritis Care and Research for peer review, and is expected to publish in early 2023.
Dr. Humphrey and Dr. Russell, the co-principal investigators for the guideline, and Dr. Rubin have disclosed no relevant financial relationships. Dr. Tanner reported a current research grant funded by Amgen through the University of Alabama at Birmingham and being a paid course instructor for the International Society for Clinical Densitometry bone density course, Osteoporosis Essentials.
A version of this article first appeared on Medscape.com.
Dr. Birds-n-Bees: How physicians are taking up the sex ed slack
An athletic coach stands in front of a packed gym full of high school students.
“Don’t have sex,” he instructs, “because you will get pregnant and die. Don’t have sex in the missionary position. Don’t have sex standing up. Just don’t do it, promise? Okay, everybody take some rubbers.”
Sad to say, this scene from the 2004 movie “Mean Girls” bears a striking resemblance to the actual sex education courses taught in schools across the United States today. In fact, things may have gotten measurably worse.
National data recently published by the Guttmacher Institute showed that adolescents were less likely to receive adequate sex education from 2015 to 2019 than they were in 1995. Only half of kids aged 15-19 received sex education that met minimum standards recommended by the Department of Health & Human Services, and fewer than half were given this information before having sex for the first time. With such a vast learning gap, it is no surprise that the United States has some of the highest rates of teenage pregnancy and sexually transmitted infections in the developed world.
Concerned and motivated by this need for sex education, physicians and other medical professionals are stepping in to fill the void, offering sexual health information through a range of methods to students of all ages (some a lot older than one may think). It is a calling that takes them outside their hospitals and exam rooms into workshops and through educational materials, video, and social media content created from scratch.
“The fact that we’re able to go in and provide factual, scientific, important information that can affect the trajectory of someone’s life is powerful,” said Julia Rossen, part of a contingent of med students at Brown University, Providence, R.I., who now teach sex ed as an elective.
Their goals are not just about protecting health. Many are also teaching about other topics commonly ignored in sex education classes, such as consent, pleasure, LGBTQ+ identities, and cultural competence. There is a mutually beneficial relationship, they say, between their sex education work and their medical practice.
Changing the status quo
A jumble of state laws govern how and when schools should offer sex education courses. Individual school districts often make the final decisions about their content, creating even more inconsistent standards. Only 29 states and the District of Columbia mandate sex education, and 13 of those do not require that it be medically accurate. Abstinence-only education, which has been shown to be ineffective, is exclusively taught in 16 states.
Without formal instruction, many young people must learn about sex from family members, who may be unwilling, or they may share knowledge between themselves, which is often incorrect, or navigate the limitless information and misinformation available on the internet.
The consequences of this were apparent to several medical students at Brown University in 2013. At the time, the rate of teenage pregnancy across Rhode Island was 1 in 100, but in the small city of Central Falls, it was 1 in 25. Aiming to improve this, the group created a comprehensive sex education program for a Central Falls middle school that was taught by medical student volunteers.
The Sex Ed by Brown Med program continues today. It consists of eight in-person sessions. Topics include anatomy, contraception, STIs, sexual decision-making, consent, sexual violence, and sexual and gender identity. Through this program, as well as other factors, the Central Falls teenage pregnancy rate declined to 1.6 in 100 from 2016 to 2020, according to the Rhode Island Department of Health.
“Historically, sexual education has been politicized,” said Ms. Rossen, one of the current program leaders. “It’s been at the discretion of a lot of different factors that aren’t under the control of the communities that are actually receiving the education.”
Among seventh graders, the teachers say they encounter different levels of maturity. But they feel that the kids are more receptive and open with younger adults who, like them, are still students. Some volunteers recall the flaws in their own sex education, particularly regarding topics such as consent and gender and sexual identity, and they believe middle school is the time to begin the sexual health conversation. “By the time you’re talking to college-age students, it’s pretty much too late,” said another group leader, Benjamin Stone.
Mr. Stone feels that practicing having these often-awkward discussions enhances their clinical skills as physicians. “Sex and sexual history are part of the comprehensive medical interview. People want to have these conversations, and they’re looking for someone to open the door. The kids are excited that we’re opening that door for them. And I think patients feel the same way.”
Conquering social media
Opening the door has been more like releasing a floodgate for Danielle Jones, MD, an ob.gyn. physician who is originally from Texas but who moved to New Zealand in 2021. Known on social media as “Mama Doctor Jones,” she has garnered more than 3 million followers across YouTube, TikTok, Twitter, Instagram, and Facebook. Dr. Jones produces short, friendly, entertaining videos on a range of reproductive health and sex education topics. They appeal to an adolescent audience hungry for a trustworthy voice on issues such as,: “5 ‘Strange’ Things Your Vagina Does That Are NORMAL” and “Condom Broke ... Now What?”
Dr. Jones uses her platform to debunk some of the misleading and inaccurate sexual health information being taught in classrooms, by other social media influencers, and that is found on the internet in general. Her no-nonsense-style videos call out such myths as being unable to pee with a tampon in, Plan B emergency contraception causing abortions, and COVID-19 vaccines damaging fertility.
“The way sex ed is done in the U.S. in most places is continuing the taboo by making it a one-time discussion or health class,” said Dr. Jones, “particularly if boys and girls are separated. That doesn’t further communication between people or foster an environment where it’s okay to discuss your body and puberty and changes in sexual health in general. And if you can’t talk about it in educational spaces, you’re certainly not going to be comfortable talking about that in a one-on-one situation with another 16-year-old.”
Taking on other taboos, Dr. Jones has been outspoken about abortion and the consequences of the recent Supreme Court decision, both as an ethical issue and a medical one that endangers lives. Raised in a deeply religious family, Dr. Jones said she was indoctrinated with antiabortion views, and it took time for her thinking to evolve “from a scientific and humanistic standpoint.” While working in a Texas private practice, Dr. Jones described being unable to mention abortion online because of fear of losing her patients and for her own safety.
Now free of those constraints, Dr. Jones feels that her videos can be important resources for teachers who may have little health training. And she is enthusiastic about the complementary relationship between her social media work and her clinical practice. “There are conversations I have all the time in the clinic where patients tell me: ‘Nobody’s ever really had this conversation in this way with me. Thank you for explaining that,’ ” said Dr. Jones. “And then I think: ‘Well, now I’ll have it with a hundred thousand other people too.’ ”
Promoting pleasure
While not an ob.gyn., discussing sexuality with patients has become a focus for Evelin Dacker, MD, a family physician in Salem, Ore. Dr. Dacker is certified in functional medicine, which takes a holistic and integrative approach. During her training she had a sudden realization: Sexuality had not been discussed at any point during her medical education.
“I recognized that this was a huge gap in how we deal with a person as a human,” Dr. Dacker explained. “Since sexuality plays a role in so many aspects of our humanness, not just having sex.”
Dr. Dacker believes in rethinking sexuality as a fundamental part of overall health, as vital as nutrition or blood pressure. Outside her medical practice, she teaches classes and workshops on sexual health and sex positivity for young adults and other physicians. She has also developed an educational framework for sexual health topics. Dr. Dacker said she frequently confronts the idea that sexuality is only about engaging with another person. She disagrees. Using food as a metaphor, she argues that just as the pleasure of eating something is purely for oneself, sexuality belongs to the individual.
Sexuality can also be a tool for pleasure, which Dr. Dacker believes plays an essential role in physical health. “Pleasure is a medicine,” Dr. Dacker said. “I actually prescribe self-pleasure practices to my patients, so they can start owning it within themselves. Make sure you get 7-8 hours of sleep, do some breathing exercises to help bring down your stress, and do self-pleasure so that you can integrate into your body better.”
She added that the impact of prioritizing one’s own desires, needs, and boundaries can transform how people view their sexuality. Her adult students frequently ask: “Why wasn’t I taught this as a teenager?”
Speaking of adult students – An older generation learns new tricks
While the teen cohort is usually the focus, the lack of sex education in previous decades – and the way sexual culture has evolved in that time – have an impact on older groups. Among U.S. adults aged 55 and older, the rate of STIs has more than doubled in the past 10 years, according to the Centers for Disease Control and Prevention. While the majority of STI cases still occur among teenagers and young adults, the consistent increase in STIs among older persons is cause for concern among physicians and researchers.
The issue worries Shannon Dowler, MD, a family physician in western North Carolina and chief medical officer for North Carolina Medicaid. Dr. Dowler, who has practiced in an STI clinic throughout her career, began seeing more and more older adults with chlamydia, herpes, and other STIs. Dowler cites several factors behind the rise, including the growing retirement community population, the availability of pharmaceuticals for sexual dysfunction, and the “hook-up culture” that is active on dating apps, which research shows are regularly used by more than a third of adults older than 55.
Dr. Dowler also sees a lack of communication about sexual health between physicians and their older patients. “Older adults are more likely to be in relationship with their physician outside the exam room, especially if they’re in a small community,” Dr. Dowler said. “Sometimes they aren’t as comfortable sharing what their risks are. But we are guilty in medicine all the time of not asking. We assume someone’s older so they’re not having sex anymore. But, in fact, they are, and we’re not taking the time to say: ‘Let’s talk about your sex life. Are you at risk for anything? Are you having any difficulties with sex?’ We tend to avoid it as a health care culture.”
In contrast, Dr. Dowler said she talks about sexual health with anyone who will listen. She teaches classes in private schools and universities and for church youth groups and other physicians. She often finds that public schools are not interested, which she attributes to fear of her discussing things “outside the rule book.”
Dr. Dowler takes creative approaches. In 2017, she released a hip-hop video, “STD’s Never Get Old,” in which she raps about safe sex for older adults. Her video went viral, was mentioned by several news outlets, and received over 50,000 views on YouTube. Dr. Dowler’s latest project is a book, “Never Too Late: Your Guide to Safer Sex after 60,” which is scheduled for publication on Valentine’s Day, 2023.
“It’s sex ed for seniors,” she explained. “It’s that gym class that some people got – I won’t say everyone got – in high school. This is the version for older adults who didn’t get that. There are new infections now that didn’t exist when they had sex education, if they had sex education.”
A big subject requires a big mission
For others in the sex education field, physicians are allies in their fight against agendas designed to obstruct or erode sex education. Alison Macklin, director of policy and advocacy at SIECUS: Sex Ed for Social Change, formerly the Sexuality Information and Education Council of the United States, sees this struggle playing out in school boards and state legislatures across the country. For every comprehensive sex education bill passed or school district victory, there is yet another blocked proposal or restrictive law somewhere else.
Ms. Macklin urged doctors to get more involved locally and to expand their knowledge of sexual health issues by reaching out to organizations such as Planned Parenthood and to be “hyper vigilant” in their own communities.
“Doctors are trusted. People really respect what they have to say,” Ms. Macklin said. “And this is an important time for them to speak up.”
A version of this article first appeared on Medscape.com.
An athletic coach stands in front of a packed gym full of high school students.
“Don’t have sex,” he instructs, “because you will get pregnant and die. Don’t have sex in the missionary position. Don’t have sex standing up. Just don’t do it, promise? Okay, everybody take some rubbers.”
Sad to say, this scene from the 2004 movie “Mean Girls” bears a striking resemblance to the actual sex education courses taught in schools across the United States today. In fact, things may have gotten measurably worse.
National data recently published by the Guttmacher Institute showed that adolescents were less likely to receive adequate sex education from 2015 to 2019 than they were in 1995. Only half of kids aged 15-19 received sex education that met minimum standards recommended by the Department of Health & Human Services, and fewer than half were given this information before having sex for the first time. With such a vast learning gap, it is no surprise that the United States has some of the highest rates of teenage pregnancy and sexually transmitted infections in the developed world.
Concerned and motivated by this need for sex education, physicians and other medical professionals are stepping in to fill the void, offering sexual health information through a range of methods to students of all ages (some a lot older than one may think). It is a calling that takes them outside their hospitals and exam rooms into workshops and through educational materials, video, and social media content created from scratch.
“The fact that we’re able to go in and provide factual, scientific, important information that can affect the trajectory of someone’s life is powerful,” said Julia Rossen, part of a contingent of med students at Brown University, Providence, R.I., who now teach sex ed as an elective.
Their goals are not just about protecting health. Many are also teaching about other topics commonly ignored in sex education classes, such as consent, pleasure, LGBTQ+ identities, and cultural competence. There is a mutually beneficial relationship, they say, between their sex education work and their medical practice.
Changing the status quo
A jumble of state laws govern how and when schools should offer sex education courses. Individual school districts often make the final decisions about their content, creating even more inconsistent standards. Only 29 states and the District of Columbia mandate sex education, and 13 of those do not require that it be medically accurate. Abstinence-only education, which has been shown to be ineffective, is exclusively taught in 16 states.
Without formal instruction, many young people must learn about sex from family members, who may be unwilling, or they may share knowledge between themselves, which is often incorrect, or navigate the limitless information and misinformation available on the internet.
The consequences of this were apparent to several medical students at Brown University in 2013. At the time, the rate of teenage pregnancy across Rhode Island was 1 in 100, but in the small city of Central Falls, it was 1 in 25. Aiming to improve this, the group created a comprehensive sex education program for a Central Falls middle school that was taught by medical student volunteers.
The Sex Ed by Brown Med program continues today. It consists of eight in-person sessions. Topics include anatomy, contraception, STIs, sexual decision-making, consent, sexual violence, and sexual and gender identity. Through this program, as well as other factors, the Central Falls teenage pregnancy rate declined to 1.6 in 100 from 2016 to 2020, according to the Rhode Island Department of Health.
“Historically, sexual education has been politicized,” said Ms. Rossen, one of the current program leaders. “It’s been at the discretion of a lot of different factors that aren’t under the control of the communities that are actually receiving the education.”
Among seventh graders, the teachers say they encounter different levels of maturity. But they feel that the kids are more receptive and open with younger adults who, like them, are still students. Some volunteers recall the flaws in their own sex education, particularly regarding topics such as consent and gender and sexual identity, and they believe middle school is the time to begin the sexual health conversation. “By the time you’re talking to college-age students, it’s pretty much too late,” said another group leader, Benjamin Stone.
Mr. Stone feels that practicing having these often-awkward discussions enhances their clinical skills as physicians. “Sex and sexual history are part of the comprehensive medical interview. People want to have these conversations, and they’re looking for someone to open the door. The kids are excited that we’re opening that door for them. And I think patients feel the same way.”
Conquering social media
Opening the door has been more like releasing a floodgate for Danielle Jones, MD, an ob.gyn. physician who is originally from Texas but who moved to New Zealand in 2021. Known on social media as “Mama Doctor Jones,” she has garnered more than 3 million followers across YouTube, TikTok, Twitter, Instagram, and Facebook. Dr. Jones produces short, friendly, entertaining videos on a range of reproductive health and sex education topics. They appeal to an adolescent audience hungry for a trustworthy voice on issues such as,: “5 ‘Strange’ Things Your Vagina Does That Are NORMAL” and “Condom Broke ... Now What?”
Dr. Jones uses her platform to debunk some of the misleading and inaccurate sexual health information being taught in classrooms, by other social media influencers, and that is found on the internet in general. Her no-nonsense-style videos call out such myths as being unable to pee with a tampon in, Plan B emergency contraception causing abortions, and COVID-19 vaccines damaging fertility.
“The way sex ed is done in the U.S. in most places is continuing the taboo by making it a one-time discussion or health class,” said Dr. Jones, “particularly if boys and girls are separated. That doesn’t further communication between people or foster an environment where it’s okay to discuss your body and puberty and changes in sexual health in general. And if you can’t talk about it in educational spaces, you’re certainly not going to be comfortable talking about that in a one-on-one situation with another 16-year-old.”
Taking on other taboos, Dr. Jones has been outspoken about abortion and the consequences of the recent Supreme Court decision, both as an ethical issue and a medical one that endangers lives. Raised in a deeply religious family, Dr. Jones said she was indoctrinated with antiabortion views, and it took time for her thinking to evolve “from a scientific and humanistic standpoint.” While working in a Texas private practice, Dr. Jones described being unable to mention abortion online because of fear of losing her patients and for her own safety.
Now free of those constraints, Dr. Jones feels that her videos can be important resources for teachers who may have little health training. And she is enthusiastic about the complementary relationship between her social media work and her clinical practice. “There are conversations I have all the time in the clinic where patients tell me: ‘Nobody’s ever really had this conversation in this way with me. Thank you for explaining that,’ ” said Dr. Jones. “And then I think: ‘Well, now I’ll have it with a hundred thousand other people too.’ ”
Promoting pleasure
While not an ob.gyn., discussing sexuality with patients has become a focus for Evelin Dacker, MD, a family physician in Salem, Ore. Dr. Dacker is certified in functional medicine, which takes a holistic and integrative approach. During her training she had a sudden realization: Sexuality had not been discussed at any point during her medical education.
“I recognized that this was a huge gap in how we deal with a person as a human,” Dr. Dacker explained. “Since sexuality plays a role in so many aspects of our humanness, not just having sex.”
Dr. Dacker believes in rethinking sexuality as a fundamental part of overall health, as vital as nutrition or blood pressure. Outside her medical practice, she teaches classes and workshops on sexual health and sex positivity for young adults and other physicians. She has also developed an educational framework for sexual health topics. Dr. Dacker said she frequently confronts the idea that sexuality is only about engaging with another person. She disagrees. Using food as a metaphor, she argues that just as the pleasure of eating something is purely for oneself, sexuality belongs to the individual.
Sexuality can also be a tool for pleasure, which Dr. Dacker believes plays an essential role in physical health. “Pleasure is a medicine,” Dr. Dacker said. “I actually prescribe self-pleasure practices to my patients, so they can start owning it within themselves. Make sure you get 7-8 hours of sleep, do some breathing exercises to help bring down your stress, and do self-pleasure so that you can integrate into your body better.”
She added that the impact of prioritizing one’s own desires, needs, and boundaries can transform how people view their sexuality. Her adult students frequently ask: “Why wasn’t I taught this as a teenager?”
Speaking of adult students – An older generation learns new tricks
While the teen cohort is usually the focus, the lack of sex education in previous decades – and the way sexual culture has evolved in that time – have an impact on older groups. Among U.S. adults aged 55 and older, the rate of STIs has more than doubled in the past 10 years, according to the Centers for Disease Control and Prevention. While the majority of STI cases still occur among teenagers and young adults, the consistent increase in STIs among older persons is cause for concern among physicians and researchers.
The issue worries Shannon Dowler, MD, a family physician in western North Carolina and chief medical officer for North Carolina Medicaid. Dr. Dowler, who has practiced in an STI clinic throughout her career, began seeing more and more older adults with chlamydia, herpes, and other STIs. Dowler cites several factors behind the rise, including the growing retirement community population, the availability of pharmaceuticals for sexual dysfunction, and the “hook-up culture” that is active on dating apps, which research shows are regularly used by more than a third of adults older than 55.
Dr. Dowler also sees a lack of communication about sexual health between physicians and their older patients. “Older adults are more likely to be in relationship with their physician outside the exam room, especially if they’re in a small community,” Dr. Dowler said. “Sometimes they aren’t as comfortable sharing what their risks are. But we are guilty in medicine all the time of not asking. We assume someone’s older so they’re not having sex anymore. But, in fact, they are, and we’re not taking the time to say: ‘Let’s talk about your sex life. Are you at risk for anything? Are you having any difficulties with sex?’ We tend to avoid it as a health care culture.”
In contrast, Dr. Dowler said she talks about sexual health with anyone who will listen. She teaches classes in private schools and universities and for church youth groups and other physicians. She often finds that public schools are not interested, which she attributes to fear of her discussing things “outside the rule book.”
Dr. Dowler takes creative approaches. In 2017, she released a hip-hop video, “STD’s Never Get Old,” in which she raps about safe sex for older adults. Her video went viral, was mentioned by several news outlets, and received over 50,000 views on YouTube. Dr. Dowler’s latest project is a book, “Never Too Late: Your Guide to Safer Sex after 60,” which is scheduled for publication on Valentine’s Day, 2023.
“It’s sex ed for seniors,” she explained. “It’s that gym class that some people got – I won’t say everyone got – in high school. This is the version for older adults who didn’t get that. There are new infections now that didn’t exist when they had sex education, if they had sex education.”
A big subject requires a big mission
For others in the sex education field, physicians are allies in their fight against agendas designed to obstruct or erode sex education. Alison Macklin, director of policy and advocacy at SIECUS: Sex Ed for Social Change, formerly the Sexuality Information and Education Council of the United States, sees this struggle playing out in school boards and state legislatures across the country. For every comprehensive sex education bill passed or school district victory, there is yet another blocked proposal or restrictive law somewhere else.
Ms. Macklin urged doctors to get more involved locally and to expand their knowledge of sexual health issues by reaching out to organizations such as Planned Parenthood and to be “hyper vigilant” in their own communities.
“Doctors are trusted. People really respect what they have to say,” Ms. Macklin said. “And this is an important time for them to speak up.”
A version of this article first appeared on Medscape.com.
An athletic coach stands in front of a packed gym full of high school students.
“Don’t have sex,” he instructs, “because you will get pregnant and die. Don’t have sex in the missionary position. Don’t have sex standing up. Just don’t do it, promise? Okay, everybody take some rubbers.”
Sad to say, this scene from the 2004 movie “Mean Girls” bears a striking resemblance to the actual sex education courses taught in schools across the United States today. In fact, things may have gotten measurably worse.
National data recently published by the Guttmacher Institute showed that adolescents were less likely to receive adequate sex education from 2015 to 2019 than they were in 1995. Only half of kids aged 15-19 received sex education that met minimum standards recommended by the Department of Health & Human Services, and fewer than half were given this information before having sex for the first time. With such a vast learning gap, it is no surprise that the United States has some of the highest rates of teenage pregnancy and sexually transmitted infections in the developed world.
Concerned and motivated by this need for sex education, physicians and other medical professionals are stepping in to fill the void, offering sexual health information through a range of methods to students of all ages (some a lot older than one may think). It is a calling that takes them outside their hospitals and exam rooms into workshops and through educational materials, video, and social media content created from scratch.
“The fact that we’re able to go in and provide factual, scientific, important information that can affect the trajectory of someone’s life is powerful,” said Julia Rossen, part of a contingent of med students at Brown University, Providence, R.I., who now teach sex ed as an elective.
Their goals are not just about protecting health. Many are also teaching about other topics commonly ignored in sex education classes, such as consent, pleasure, LGBTQ+ identities, and cultural competence. There is a mutually beneficial relationship, they say, between their sex education work and their medical practice.
Changing the status quo
A jumble of state laws govern how and when schools should offer sex education courses. Individual school districts often make the final decisions about their content, creating even more inconsistent standards. Only 29 states and the District of Columbia mandate sex education, and 13 of those do not require that it be medically accurate. Abstinence-only education, which has been shown to be ineffective, is exclusively taught in 16 states.
Without formal instruction, many young people must learn about sex from family members, who may be unwilling, or they may share knowledge between themselves, which is often incorrect, or navigate the limitless information and misinformation available on the internet.
The consequences of this were apparent to several medical students at Brown University in 2013. At the time, the rate of teenage pregnancy across Rhode Island was 1 in 100, but in the small city of Central Falls, it was 1 in 25. Aiming to improve this, the group created a comprehensive sex education program for a Central Falls middle school that was taught by medical student volunteers.
The Sex Ed by Brown Med program continues today. It consists of eight in-person sessions. Topics include anatomy, contraception, STIs, sexual decision-making, consent, sexual violence, and sexual and gender identity. Through this program, as well as other factors, the Central Falls teenage pregnancy rate declined to 1.6 in 100 from 2016 to 2020, according to the Rhode Island Department of Health.
“Historically, sexual education has been politicized,” said Ms. Rossen, one of the current program leaders. “It’s been at the discretion of a lot of different factors that aren’t under the control of the communities that are actually receiving the education.”
Among seventh graders, the teachers say they encounter different levels of maturity. But they feel that the kids are more receptive and open with younger adults who, like them, are still students. Some volunteers recall the flaws in their own sex education, particularly regarding topics such as consent and gender and sexual identity, and they believe middle school is the time to begin the sexual health conversation. “By the time you’re talking to college-age students, it’s pretty much too late,” said another group leader, Benjamin Stone.
Mr. Stone feels that practicing having these often-awkward discussions enhances their clinical skills as physicians. “Sex and sexual history are part of the comprehensive medical interview. People want to have these conversations, and they’re looking for someone to open the door. The kids are excited that we’re opening that door for them. And I think patients feel the same way.”
Conquering social media
Opening the door has been more like releasing a floodgate for Danielle Jones, MD, an ob.gyn. physician who is originally from Texas but who moved to New Zealand in 2021. Known on social media as “Mama Doctor Jones,” she has garnered more than 3 million followers across YouTube, TikTok, Twitter, Instagram, and Facebook. Dr. Jones produces short, friendly, entertaining videos on a range of reproductive health and sex education topics. They appeal to an adolescent audience hungry for a trustworthy voice on issues such as,: “5 ‘Strange’ Things Your Vagina Does That Are NORMAL” and “Condom Broke ... Now What?”
Dr. Jones uses her platform to debunk some of the misleading and inaccurate sexual health information being taught in classrooms, by other social media influencers, and that is found on the internet in general. Her no-nonsense-style videos call out such myths as being unable to pee with a tampon in, Plan B emergency contraception causing abortions, and COVID-19 vaccines damaging fertility.
“The way sex ed is done in the U.S. in most places is continuing the taboo by making it a one-time discussion or health class,” said Dr. Jones, “particularly if boys and girls are separated. That doesn’t further communication between people or foster an environment where it’s okay to discuss your body and puberty and changes in sexual health in general. And if you can’t talk about it in educational spaces, you’re certainly not going to be comfortable talking about that in a one-on-one situation with another 16-year-old.”
Taking on other taboos, Dr. Jones has been outspoken about abortion and the consequences of the recent Supreme Court decision, both as an ethical issue and a medical one that endangers lives. Raised in a deeply religious family, Dr. Jones said she was indoctrinated with antiabortion views, and it took time for her thinking to evolve “from a scientific and humanistic standpoint.” While working in a Texas private practice, Dr. Jones described being unable to mention abortion online because of fear of losing her patients and for her own safety.
Now free of those constraints, Dr. Jones feels that her videos can be important resources for teachers who may have little health training. And she is enthusiastic about the complementary relationship between her social media work and her clinical practice. “There are conversations I have all the time in the clinic where patients tell me: ‘Nobody’s ever really had this conversation in this way with me. Thank you for explaining that,’ ” said Dr. Jones. “And then I think: ‘Well, now I’ll have it with a hundred thousand other people too.’ ”
Promoting pleasure
While not an ob.gyn., discussing sexuality with patients has become a focus for Evelin Dacker, MD, a family physician in Salem, Ore. Dr. Dacker is certified in functional medicine, which takes a holistic and integrative approach. During her training she had a sudden realization: Sexuality had not been discussed at any point during her medical education.
“I recognized that this was a huge gap in how we deal with a person as a human,” Dr. Dacker explained. “Since sexuality plays a role in so many aspects of our humanness, not just having sex.”
Dr. Dacker believes in rethinking sexuality as a fundamental part of overall health, as vital as nutrition or blood pressure. Outside her medical practice, she teaches classes and workshops on sexual health and sex positivity for young adults and other physicians. She has also developed an educational framework for sexual health topics. Dr. Dacker said she frequently confronts the idea that sexuality is only about engaging with another person. She disagrees. Using food as a metaphor, she argues that just as the pleasure of eating something is purely for oneself, sexuality belongs to the individual.
Sexuality can also be a tool for pleasure, which Dr. Dacker believes plays an essential role in physical health. “Pleasure is a medicine,” Dr. Dacker said. “I actually prescribe self-pleasure practices to my patients, so they can start owning it within themselves. Make sure you get 7-8 hours of sleep, do some breathing exercises to help bring down your stress, and do self-pleasure so that you can integrate into your body better.”
She added that the impact of prioritizing one’s own desires, needs, and boundaries can transform how people view their sexuality. Her adult students frequently ask: “Why wasn’t I taught this as a teenager?”
Speaking of adult students – An older generation learns new tricks
While the teen cohort is usually the focus, the lack of sex education in previous decades – and the way sexual culture has evolved in that time – have an impact on older groups. Among U.S. adults aged 55 and older, the rate of STIs has more than doubled in the past 10 years, according to the Centers for Disease Control and Prevention. While the majority of STI cases still occur among teenagers and young adults, the consistent increase in STIs among older persons is cause for concern among physicians and researchers.
The issue worries Shannon Dowler, MD, a family physician in western North Carolina and chief medical officer for North Carolina Medicaid. Dr. Dowler, who has practiced in an STI clinic throughout her career, began seeing more and more older adults with chlamydia, herpes, and other STIs. Dowler cites several factors behind the rise, including the growing retirement community population, the availability of pharmaceuticals for sexual dysfunction, and the “hook-up culture” that is active on dating apps, which research shows are regularly used by more than a third of adults older than 55.
Dr. Dowler also sees a lack of communication about sexual health between physicians and their older patients. “Older adults are more likely to be in relationship with their physician outside the exam room, especially if they’re in a small community,” Dr. Dowler said. “Sometimes they aren’t as comfortable sharing what their risks are. But we are guilty in medicine all the time of not asking. We assume someone’s older so they’re not having sex anymore. But, in fact, they are, and we’re not taking the time to say: ‘Let’s talk about your sex life. Are you at risk for anything? Are you having any difficulties with sex?’ We tend to avoid it as a health care culture.”
In contrast, Dr. Dowler said she talks about sexual health with anyone who will listen. She teaches classes in private schools and universities and for church youth groups and other physicians. She often finds that public schools are not interested, which she attributes to fear of her discussing things “outside the rule book.”
Dr. Dowler takes creative approaches. In 2017, she released a hip-hop video, “STD’s Never Get Old,” in which she raps about safe sex for older adults. Her video went viral, was mentioned by several news outlets, and received over 50,000 views on YouTube. Dr. Dowler’s latest project is a book, “Never Too Late: Your Guide to Safer Sex after 60,” which is scheduled for publication on Valentine’s Day, 2023.
“It’s sex ed for seniors,” she explained. “It’s that gym class that some people got – I won’t say everyone got – in high school. This is the version for older adults who didn’t get that. There are new infections now that didn’t exist when they had sex education, if they had sex education.”
A big subject requires a big mission
For others in the sex education field, physicians are allies in their fight against agendas designed to obstruct or erode sex education. Alison Macklin, director of policy and advocacy at SIECUS: Sex Ed for Social Change, formerly the Sexuality Information and Education Council of the United States, sees this struggle playing out in school boards and state legislatures across the country. For every comprehensive sex education bill passed or school district victory, there is yet another blocked proposal or restrictive law somewhere else.
Ms. Macklin urged doctors to get more involved locally and to expand their knowledge of sexual health issues by reaching out to organizations such as Planned Parenthood and to be “hyper vigilant” in their own communities.
“Doctors are trusted. People really respect what they have to say,” Ms. Macklin said. “And this is an important time for them to speak up.”
A version of this article first appeared on Medscape.com.