User login
Constructive Criticism, Part 2

This is the second in a two-part series on providing constructive criticism to your hospitalist peers. Part 1 appeared in the March issue on p. 12.
Have concerns about a colleague’s work performance? Then you have two main options: You can bring it up in a formal peer review (if it’s a clinical issue) or you can approach the individual yourself.
“Medicine is an art and a science. Many problems relate to the art side—communications and relationships, primarily,” says Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Conn. “You may need to talk to a colleague about how they approach family members or how they communicate with patients. In this instance, you’d offer more of a coaching comment.”
While you may hesitate to point out another hospitalist’s problem areas, keep in mind that it is constructive criticism.
“Physicians love to run things past colleagues,” says Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Informal feedback can provide an unbiased and objective perspective, as opposed to [a formal peer review].”
When to Offer Constructive Criticism
In some practices, or for some individuals, sharing constructive criticism with peers is part of the job. “Informal peer discussions should take place every day,” advises Dr. Rohr. “While handoffs pose a risk for losing vital information, they are also an opportunity to consider alternatives for diagnosis and treatment that may benefit patients greatly.”
If this seems like a natural thing to do within your hospital medicine group, follow Dr. Rohr’s advice: “These discussions should be frank but nonjudgmental. If someone has a problem discussing cases in this manner, then the group leader needs to get involved. If a life-threatening error is exposed, then the formal peer review system needs to be activated.”
Providing Peer Feedback
When there is no personal conflict, you may still consider offering constructive criticism if you feel it’s warranted. “I think [peer feedback] is extremely important—if it’s done correctly,” says Dr. Simone. “It provides a safe haven for discussion and can contribute to professional growth.”
According to Dr. Simone, appropriate topics to discuss regarding a colleague’s performance include logistical problems within the practice, such as a doctor who is chronically late for morning rounds; continuity issues, such as a physician who fails to provide detailed information when handing off patients; communication breakdowns, such as forgetting to check out the labs pending on a newly admitted unit-patient with chest pain; behavioral issues, such as a physician who’s verbally abusive to the nurses or disruptive at morning rounds; problems with work ethic, responsiveness, or availability, such as the doctor who never responds to his/her beeper (necessitating a call from nursing to an accommodating provider who’s always willing and available to help); and general team play.
If you believe you need to address one of these topics regarding a colleague’s performance, plan the logistics of the discussion. “This is a conversation best held one on one—in private,” stresses Dr. Simone. “Don’t discuss these issues in front of colleagues, nurses, patients, families … and don’t do it at the end of a long, difficult day.
“Ideally, do it after hours and out of the workplace, though that can be difficult. Remove the person from the hospital floor or the office, and the emotions and adrenaline associated with work,” continues Dr. Simone. “If the environment is stressful, it will raise their defenses, making them more likely to be resistant and argumentative.”
Talking Points
When you offer constructive criticism, approach the topic carefully. “Take a non-confrontational approach,” says Dr. Simone. “Don’t raise your voice, and don’t take the discussion to a personal level. Use objective data as much as possible. Avoid saying ‘I feel that you’re …’ and instead use ‘Coming in 15 minutes late throws everyone’s schedule off.’ ”
Keep the conversation as casual and as light as possible. “This is not a peer review meeting,” Dr. Simone stresses. “Use a soft approach, and you might have greater success. Stay away from power words such as ‘you shouldn’t’ or ‘don’t.’ ”
Some phrases you might use include:
- “I find it helpful if I … ”
- “This has worked for me.”
- “Have you considered … ?”
Even if you use careful wording, don’t be surprised if the other hospitalist doesn’t react well—at least initially. “Unless you’re seasoned at doing this, the individual may get defensive,” warns Dr. Simone. “If you’re consistent throughout the conversation, show support, and are astute enough to break down their defenses, you should be effective.”
Also, keep your cool: “Don’t respond to defensiveness in like [manner],” says Dr. Simone. Throughout the conversation, show your support. “Convey that your intent is to help the individual—not harm them. Ask if you can be of help, and offer to be a resource” to help them improve.
Also remember that your colleague is part of the conversation. “Allow responses,” adds Dr. Simone. “Give them a chance to express themselves.”
End the conversation with an offer to follow up or suggest a next step. “Offer your personal help or suggest a resource such as the employee assistance program,” advises Dr. Simone. “You can check in with them from time to time, but if you have an unwilling party this may be construed as meddlesome. You must consider the personality involved and if you think they’d be amenable to continued conversations.”
Even without a formal follow-up, be sure to voice your approval if you see their negative behavior change. “If you take the time to provide criticism, you should also offer positive feedback if warranted,” says Dr. Simone. “Tell them they’re doing a great job.”
One final piece of advice regarding informal peer feedback: “Avoid writing anything down,” says Dr. Simone. “This may make it discoverable in a court of law, and it’s not your place to put the discussion in writing. If the issue is that serious, take it to the powers that be.” TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the second in a two-part series on providing constructive criticism to your hospitalist peers. Part 1 appeared in the March issue on p. 12.
Have concerns about a colleague’s work performance? Then you have two main options: You can bring it up in a formal peer review (if it’s a clinical issue) or you can approach the individual yourself.
“Medicine is an art and a science. Many problems relate to the art side—communications and relationships, primarily,” says Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Conn. “You may need to talk to a colleague about how they approach family members or how they communicate with patients. In this instance, you’d offer more of a coaching comment.”
While you may hesitate to point out another hospitalist’s problem areas, keep in mind that it is constructive criticism.
“Physicians love to run things past colleagues,” says Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Informal feedback can provide an unbiased and objective perspective, as opposed to [a formal peer review].”
When to Offer Constructive Criticism
In some practices, or for some individuals, sharing constructive criticism with peers is part of the job. “Informal peer discussions should take place every day,” advises Dr. Rohr. “While handoffs pose a risk for losing vital information, they are also an opportunity to consider alternatives for diagnosis and treatment that may benefit patients greatly.”
If this seems like a natural thing to do within your hospital medicine group, follow Dr. Rohr’s advice: “These discussions should be frank but nonjudgmental. If someone has a problem discussing cases in this manner, then the group leader needs to get involved. If a life-threatening error is exposed, then the formal peer review system needs to be activated.”
Providing Peer Feedback
When there is no personal conflict, you may still consider offering constructive criticism if you feel it’s warranted. “I think [peer feedback] is extremely important—if it’s done correctly,” says Dr. Simone. “It provides a safe haven for discussion and can contribute to professional growth.”
According to Dr. Simone, appropriate topics to discuss regarding a colleague’s performance include logistical problems within the practice, such as a doctor who is chronically late for morning rounds; continuity issues, such as a physician who fails to provide detailed information when handing off patients; communication breakdowns, such as forgetting to check out the labs pending on a newly admitted unit-patient with chest pain; behavioral issues, such as a physician who’s verbally abusive to the nurses or disruptive at morning rounds; problems with work ethic, responsiveness, or availability, such as the doctor who never responds to his/her beeper (necessitating a call from nursing to an accommodating provider who’s always willing and available to help); and general team play.
If you believe you need to address one of these topics regarding a colleague’s performance, plan the logistics of the discussion. “This is a conversation best held one on one—in private,” stresses Dr. Simone. “Don’t discuss these issues in front of colleagues, nurses, patients, families … and don’t do it at the end of a long, difficult day.
“Ideally, do it after hours and out of the workplace, though that can be difficult. Remove the person from the hospital floor or the office, and the emotions and adrenaline associated with work,” continues Dr. Simone. “If the environment is stressful, it will raise their defenses, making them more likely to be resistant and argumentative.”
Talking Points
When you offer constructive criticism, approach the topic carefully. “Take a non-confrontational approach,” says Dr. Simone. “Don’t raise your voice, and don’t take the discussion to a personal level. Use objective data as much as possible. Avoid saying ‘I feel that you’re …’ and instead use ‘Coming in 15 minutes late throws everyone’s schedule off.’ ”
Keep the conversation as casual and as light as possible. “This is not a peer review meeting,” Dr. Simone stresses. “Use a soft approach, and you might have greater success. Stay away from power words such as ‘you shouldn’t’ or ‘don’t.’ ”
Some phrases you might use include:
- “I find it helpful if I … ”
- “This has worked for me.”
- “Have you considered … ?”
Even if you use careful wording, don’t be surprised if the other hospitalist doesn’t react well—at least initially. “Unless you’re seasoned at doing this, the individual may get defensive,” warns Dr. Simone. “If you’re consistent throughout the conversation, show support, and are astute enough to break down their defenses, you should be effective.”
Also, keep your cool: “Don’t respond to defensiveness in like [manner],” says Dr. Simone. Throughout the conversation, show your support. “Convey that your intent is to help the individual—not harm them. Ask if you can be of help, and offer to be a resource” to help them improve.
Also remember that your colleague is part of the conversation. “Allow responses,” adds Dr. Simone. “Give them a chance to express themselves.”
End the conversation with an offer to follow up or suggest a next step. “Offer your personal help or suggest a resource such as the employee assistance program,” advises Dr. Simone. “You can check in with them from time to time, but if you have an unwilling party this may be construed as meddlesome. You must consider the personality involved and if you think they’d be amenable to continued conversations.”
Even without a formal follow-up, be sure to voice your approval if you see their negative behavior change. “If you take the time to provide criticism, you should also offer positive feedback if warranted,” says Dr. Simone. “Tell them they’re doing a great job.”
One final piece of advice regarding informal peer feedback: “Avoid writing anything down,” says Dr. Simone. “This may make it discoverable in a court of law, and it’s not your place to put the discussion in writing. If the issue is that serious, take it to the powers that be.” TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the second in a two-part series on providing constructive criticism to your hospitalist peers. Part 1 appeared in the March issue on p. 12.
Have concerns about a colleague’s work performance? Then you have two main options: You can bring it up in a formal peer review (if it’s a clinical issue) or you can approach the individual yourself.
“Medicine is an art and a science. Many problems relate to the art side—communications and relationships, primarily,” says Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Conn. “You may need to talk to a colleague about how they approach family members or how they communicate with patients. In this instance, you’d offer more of a coaching comment.”
While you may hesitate to point out another hospitalist’s problem areas, keep in mind that it is constructive criticism.
“Physicians love to run things past colleagues,” says Kenneth G. Simone, DO, founder and president of Hospitalist and Practice Solutions, Veazie, Maine, and a consultant to hospital medicine groups. “Informal feedback can provide an unbiased and objective perspective, as opposed to [a formal peer review].”
When to Offer Constructive Criticism
In some practices, or for some individuals, sharing constructive criticism with peers is part of the job. “Informal peer discussions should take place every day,” advises Dr. Rohr. “While handoffs pose a risk for losing vital information, they are also an opportunity to consider alternatives for diagnosis and treatment that may benefit patients greatly.”
If this seems like a natural thing to do within your hospital medicine group, follow Dr. Rohr’s advice: “These discussions should be frank but nonjudgmental. If someone has a problem discussing cases in this manner, then the group leader needs to get involved. If a life-threatening error is exposed, then the formal peer review system needs to be activated.”
Providing Peer Feedback
When there is no personal conflict, you may still consider offering constructive criticism if you feel it’s warranted. “I think [peer feedback] is extremely important—if it’s done correctly,” says Dr. Simone. “It provides a safe haven for discussion and can contribute to professional growth.”
According to Dr. Simone, appropriate topics to discuss regarding a colleague’s performance include logistical problems within the practice, such as a doctor who is chronically late for morning rounds; continuity issues, such as a physician who fails to provide detailed information when handing off patients; communication breakdowns, such as forgetting to check out the labs pending on a newly admitted unit-patient with chest pain; behavioral issues, such as a physician who’s verbally abusive to the nurses or disruptive at morning rounds; problems with work ethic, responsiveness, or availability, such as the doctor who never responds to his/her beeper (necessitating a call from nursing to an accommodating provider who’s always willing and available to help); and general team play.
If you believe you need to address one of these topics regarding a colleague’s performance, plan the logistics of the discussion. “This is a conversation best held one on one—in private,” stresses Dr. Simone. “Don’t discuss these issues in front of colleagues, nurses, patients, families … and don’t do it at the end of a long, difficult day.
“Ideally, do it after hours and out of the workplace, though that can be difficult. Remove the person from the hospital floor or the office, and the emotions and adrenaline associated with work,” continues Dr. Simone. “If the environment is stressful, it will raise their defenses, making them more likely to be resistant and argumentative.”
Talking Points
When you offer constructive criticism, approach the topic carefully. “Take a non-confrontational approach,” says Dr. Simone. “Don’t raise your voice, and don’t take the discussion to a personal level. Use objective data as much as possible. Avoid saying ‘I feel that you’re …’ and instead use ‘Coming in 15 minutes late throws everyone’s schedule off.’ ”
Keep the conversation as casual and as light as possible. “This is not a peer review meeting,” Dr. Simone stresses. “Use a soft approach, and you might have greater success. Stay away from power words such as ‘you shouldn’t’ or ‘don’t.’ ”
Some phrases you might use include:
- “I find it helpful if I … ”
- “This has worked for me.”
- “Have you considered … ?”
Even if you use careful wording, don’t be surprised if the other hospitalist doesn’t react well—at least initially. “Unless you’re seasoned at doing this, the individual may get defensive,” warns Dr. Simone. “If you’re consistent throughout the conversation, show support, and are astute enough to break down their defenses, you should be effective.”
Also, keep your cool: “Don’t respond to defensiveness in like [manner],” says Dr. Simone. Throughout the conversation, show your support. “Convey that your intent is to help the individual—not harm them. Ask if you can be of help, and offer to be a resource” to help them improve.
Also remember that your colleague is part of the conversation. “Allow responses,” adds Dr. Simone. “Give them a chance to express themselves.”
End the conversation with an offer to follow up or suggest a next step. “Offer your personal help or suggest a resource such as the employee assistance program,” advises Dr. Simone. “You can check in with them from time to time, but if you have an unwilling party this may be construed as meddlesome. You must consider the personality involved and if you think they’d be amenable to continued conversations.”
Even without a formal follow-up, be sure to voice your approval if you see their negative behavior change. “If you take the time to provide criticism, you should also offer positive feedback if warranted,” says Dr. Simone. “Tell them they’re doing a great job.”
One final piece of advice regarding informal peer feedback: “Avoid writing anything down,” says Dr. Simone. “This may make it discoverable in a court of law, and it’s not your place to put the discussion in writing. If the issue is that serious, take it to the powers that be.” TH
Jane Jerrard has written for The Hospitalist since 2005.
Medicare Prepares to “Pay for Performance”

This year, interested physicians will participate in Medicare’s first ever pay-for-performance program. Legislation passed in late 2006 calls for a voluntary Medicare quality reporting program that financially rewards physicians reporting on specific quality measures. Those physicians may receive a bonus of 1.5% of their total Medicare payments during the reporting period. This adds a pay-for-performance component to the current Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid Services (CMS) established in January 2006.
“Medicare is really serious about improving quality of care for beneficiaries, and they’re committed to pay for performance as the way to go about it,” says Patrick Torcson, MD, MMM, FACP, medical director, Hospital Medicine, St. Tammany Parish Hospital, Covington, La.
Performance Measures in the Works
The pay-for-performance quality reporting program will use the 66 unique clinical measures CMS announced in December 2006, with additional modifications to be made through April 2007 using a consensus process.
“From looking at the proposed list of 66 performance measures, we’ve identified seven that are going to be available to hospitalists to report,” says Dr. Torcson. “The seven involve stroke and [myocardial infarction] care.”
Most of the internal medicine-related measures of the 16 included in the original PVRP were designed for an outpatient, office-based practice, and that seems true of the expanded list as well.
The current 66 measures are slightly more relevant to the hospital setting and can potentially be reported by hospitalists, as Dr. Torcson specified. Specifically, quality measures have been added for giving beta-blockers upon admission (quality measure #29) and for stroke and stroke rehabilitation (quality measures #31-#36).
Other measures are expected to be added before the July implementation date, and some may be reportable by hospitalists. These include creation of an advance care plan (#47) and measures for emergency medicine services (#54-#59).
“Medicare plans to have specific performance measures for each of the 39 specialties that they recognize,” explains Dr. Torcson. “Hospital medicine is not yet a CMS-recognized specialty; we’re typically lumped under general internal medicine.”
You can view all the measures at www.cms.hhs.gov/PVRP/01_overview.asp.
How the Program Will Work
The initial reporting period set by the legislation is July 1 through December 31, 2007, and there will be an enrollment period before that for physicians who wish to participate. When a physician enrolls in the program, she will identify which measures apply to her. At that point, CMS will determine if a measure applies.
If less than three quality measures apply for a physician, then 80% reporting on those applicable measures is required to be eligible for the bonus. If four or more measures apply, the physician must report on at least three in order to be eligible.
Bonuses for voluntary reporting would be in a lump sum and won’t be paid until the first quarter of 2008. The method of payment may be subject to certain limits—and it may not offset the physicians’ administrative costs for reporting. Hospital medicine programs will have to consider whether the costs of reporting are worth the bonus.
SHM Involvement
SHM’s Public Policy Committee (PPC) and its Performance and Standards Task Force (PSTF) have been actively involved in getting measures included on the PRVP list that are applicable to hospitalists.
“SHM is a member of the AMA’s Physician Consortium for Performance Improvement (PCPI) and has representatives on work groups that have developed performance measures and will be revising and maintaining measures over time,” says Dr. Torcson. “We hope to eventually include measures that are specific to hospitalized patients.”
In addition to the PCPI, SHM is represented and has influence in the National Quality Forum and the Ambulatory Care Quality Alliance.
“SHM leadership—CEO Larry Wellikson, Eric Siegal, Public Policy chair, and Lakshmi Halasyamani, chair of the Hospital Quality and Patient Safety (HQPS) Committee—have been proactive in positioning SHM to be very involved in the national quality improvement agenda,” says Dr. Torcson. “It’s really a work in progress, but SHM is part of the work groups that are driving this process.”
The Effect on Hospitalists
As they can with the original PVRP, hospitalists can find a few applicable performance measures to report on, so they are eligible to participate—and SHM encourages them to do so.
“The amount of money will be small and the number of [applicable] measures will be limited and not truly representative of a hospitalist’s practice,” says Dr. Torcson, “but performance reporting should be something that every physician, including hospitalists, has as a skill set as their practice moves into the future.”
Moving Ahead
Details on the new program still need to be clarified by CMS in the first half of 2007. Regardless of the details still to be determined for this first major foray into Medicare pay for performance, one thing is clear: CMS is dedicated to the idea of tying financial reward to quality care. And they aren’t the only ones.
“Medicare is not as far along as private insurers,” says Dr. Torcson. “Commercial insurers are much more aggressive about pursuing physician-level performance and efficiency—I think we’ll see more impactful pay-for-performance plans from them first. However, the CMS model will affect 70 million patients, and commercial insurers have tended to use the CMS model for physician reimbursement.”
Dr. Torcson believes this program is simply a first step on that road. “We’re in the infancy of pay-for-performance models for physician reimbursement,” he says. “I think the ultimate model for physician-level value-based purchasing is going to look a lot different than the proposed CMS payment for reporting and payment for performance.”
In the immediate future, the PPC and PSTF will continue to participate in formulating the final quality measures for the CMS voluntary reporting program. Watch the SHM Web site for updates on the status of the program. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
This year, interested physicians will participate in Medicare’s first ever pay-for-performance program. Legislation passed in late 2006 calls for a voluntary Medicare quality reporting program that financially rewards physicians reporting on specific quality measures. Those physicians may receive a bonus of 1.5% of their total Medicare payments during the reporting period. This adds a pay-for-performance component to the current Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid Services (CMS) established in January 2006.
“Medicare is really serious about improving quality of care for beneficiaries, and they’re committed to pay for performance as the way to go about it,” says Patrick Torcson, MD, MMM, FACP, medical director, Hospital Medicine, St. Tammany Parish Hospital, Covington, La.
Performance Measures in the Works
The pay-for-performance quality reporting program will use the 66 unique clinical measures CMS announced in December 2006, with additional modifications to be made through April 2007 using a consensus process.
“From looking at the proposed list of 66 performance measures, we’ve identified seven that are going to be available to hospitalists to report,” says Dr. Torcson. “The seven involve stroke and [myocardial infarction] care.”
Most of the internal medicine-related measures of the 16 included in the original PVRP were designed for an outpatient, office-based practice, and that seems true of the expanded list as well.
The current 66 measures are slightly more relevant to the hospital setting and can potentially be reported by hospitalists, as Dr. Torcson specified. Specifically, quality measures have been added for giving beta-blockers upon admission (quality measure #29) and for stroke and stroke rehabilitation (quality measures #31-#36).
Other measures are expected to be added before the July implementation date, and some may be reportable by hospitalists. These include creation of an advance care plan (#47) and measures for emergency medicine services (#54-#59).
“Medicare plans to have specific performance measures for each of the 39 specialties that they recognize,” explains Dr. Torcson. “Hospital medicine is not yet a CMS-recognized specialty; we’re typically lumped under general internal medicine.”
You can view all the measures at www.cms.hhs.gov/PVRP/01_overview.asp.
How the Program Will Work
The initial reporting period set by the legislation is July 1 through December 31, 2007, and there will be an enrollment period before that for physicians who wish to participate. When a physician enrolls in the program, she will identify which measures apply to her. At that point, CMS will determine if a measure applies.
If less than three quality measures apply for a physician, then 80% reporting on those applicable measures is required to be eligible for the bonus. If four or more measures apply, the physician must report on at least three in order to be eligible.
Bonuses for voluntary reporting would be in a lump sum and won’t be paid until the first quarter of 2008. The method of payment may be subject to certain limits—and it may not offset the physicians’ administrative costs for reporting. Hospital medicine programs will have to consider whether the costs of reporting are worth the bonus.
SHM Involvement
SHM’s Public Policy Committee (PPC) and its Performance and Standards Task Force (PSTF) have been actively involved in getting measures included on the PRVP list that are applicable to hospitalists.
“SHM is a member of the AMA’s Physician Consortium for Performance Improvement (PCPI) and has representatives on work groups that have developed performance measures and will be revising and maintaining measures over time,” says Dr. Torcson. “We hope to eventually include measures that are specific to hospitalized patients.”
In addition to the PCPI, SHM is represented and has influence in the National Quality Forum and the Ambulatory Care Quality Alliance.
“SHM leadership—CEO Larry Wellikson, Eric Siegal, Public Policy chair, and Lakshmi Halasyamani, chair of the Hospital Quality and Patient Safety (HQPS) Committee—have been proactive in positioning SHM to be very involved in the national quality improvement agenda,” says Dr. Torcson. “It’s really a work in progress, but SHM is part of the work groups that are driving this process.”
The Effect on Hospitalists
As they can with the original PVRP, hospitalists can find a few applicable performance measures to report on, so they are eligible to participate—and SHM encourages them to do so.
“The amount of money will be small and the number of [applicable] measures will be limited and not truly representative of a hospitalist’s practice,” says Dr. Torcson, “but performance reporting should be something that every physician, including hospitalists, has as a skill set as their practice moves into the future.”
Moving Ahead
Details on the new program still need to be clarified by CMS in the first half of 2007. Regardless of the details still to be determined for this first major foray into Medicare pay for performance, one thing is clear: CMS is dedicated to the idea of tying financial reward to quality care. And they aren’t the only ones.
“Medicare is not as far along as private insurers,” says Dr. Torcson. “Commercial insurers are much more aggressive about pursuing physician-level performance and efficiency—I think we’ll see more impactful pay-for-performance plans from them first. However, the CMS model will affect 70 million patients, and commercial insurers have tended to use the CMS model for physician reimbursement.”
Dr. Torcson believes this program is simply a first step on that road. “We’re in the infancy of pay-for-performance models for physician reimbursement,” he says. “I think the ultimate model for physician-level value-based purchasing is going to look a lot different than the proposed CMS payment for reporting and payment for performance.”
In the immediate future, the PPC and PSTF will continue to participate in formulating the final quality measures for the CMS voluntary reporting program. Watch the SHM Web site for updates on the status of the program. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
This year, interested physicians will participate in Medicare’s first ever pay-for-performance program. Legislation passed in late 2006 calls for a voluntary Medicare quality reporting program that financially rewards physicians reporting on specific quality measures. Those physicians may receive a bonus of 1.5% of their total Medicare payments during the reporting period. This adds a pay-for-performance component to the current Physician Voluntary Reporting Program (PVRP) that the Centers for Medicare and Medicaid Services (CMS) established in January 2006.
“Medicare is really serious about improving quality of care for beneficiaries, and they’re committed to pay for performance as the way to go about it,” says Patrick Torcson, MD, MMM, FACP, medical director, Hospital Medicine, St. Tammany Parish Hospital, Covington, La.
Performance Measures in the Works
The pay-for-performance quality reporting program will use the 66 unique clinical measures CMS announced in December 2006, with additional modifications to be made through April 2007 using a consensus process.
“From looking at the proposed list of 66 performance measures, we’ve identified seven that are going to be available to hospitalists to report,” says Dr. Torcson. “The seven involve stroke and [myocardial infarction] care.”
Most of the internal medicine-related measures of the 16 included in the original PVRP were designed for an outpatient, office-based practice, and that seems true of the expanded list as well.
The current 66 measures are slightly more relevant to the hospital setting and can potentially be reported by hospitalists, as Dr. Torcson specified. Specifically, quality measures have been added for giving beta-blockers upon admission (quality measure #29) and for stroke and stroke rehabilitation (quality measures #31-#36).
Other measures are expected to be added before the July implementation date, and some may be reportable by hospitalists. These include creation of an advance care plan (#47) and measures for emergency medicine services (#54-#59).
“Medicare plans to have specific performance measures for each of the 39 specialties that they recognize,” explains Dr. Torcson. “Hospital medicine is not yet a CMS-recognized specialty; we’re typically lumped under general internal medicine.”
You can view all the measures at www.cms.hhs.gov/PVRP/01_overview.asp.
How the Program Will Work
The initial reporting period set by the legislation is July 1 through December 31, 2007, and there will be an enrollment period before that for physicians who wish to participate. When a physician enrolls in the program, she will identify which measures apply to her. At that point, CMS will determine if a measure applies.
If less than three quality measures apply for a physician, then 80% reporting on those applicable measures is required to be eligible for the bonus. If four or more measures apply, the physician must report on at least three in order to be eligible.
Bonuses for voluntary reporting would be in a lump sum and won’t be paid until the first quarter of 2008. The method of payment may be subject to certain limits—and it may not offset the physicians’ administrative costs for reporting. Hospital medicine programs will have to consider whether the costs of reporting are worth the bonus.
SHM Involvement
SHM’s Public Policy Committee (PPC) and its Performance and Standards Task Force (PSTF) have been actively involved in getting measures included on the PRVP list that are applicable to hospitalists.
“SHM is a member of the AMA’s Physician Consortium for Performance Improvement (PCPI) and has representatives on work groups that have developed performance measures and will be revising and maintaining measures over time,” says Dr. Torcson. “We hope to eventually include measures that are specific to hospitalized patients.”
In addition to the PCPI, SHM is represented and has influence in the National Quality Forum and the Ambulatory Care Quality Alliance.
“SHM leadership—CEO Larry Wellikson, Eric Siegal, Public Policy chair, and Lakshmi Halasyamani, chair of the Hospital Quality and Patient Safety (HQPS) Committee—have been proactive in positioning SHM to be very involved in the national quality improvement agenda,” says Dr. Torcson. “It’s really a work in progress, but SHM is part of the work groups that are driving this process.”
The Effect on Hospitalists
As they can with the original PVRP, hospitalists can find a few applicable performance measures to report on, so they are eligible to participate—and SHM encourages them to do so.
“The amount of money will be small and the number of [applicable] measures will be limited and not truly representative of a hospitalist’s practice,” says Dr. Torcson, “but performance reporting should be something that every physician, including hospitalists, has as a skill set as their practice moves into the future.”
Moving Ahead
Details on the new program still need to be clarified by CMS in the first half of 2007. Regardless of the details still to be determined for this first major foray into Medicare pay for performance, one thing is clear: CMS is dedicated to the idea of tying financial reward to quality care. And they aren’t the only ones.
“Medicare is not as far along as private insurers,” says Dr. Torcson. “Commercial insurers are much more aggressive about pursuing physician-level performance and efficiency—I think we’ll see more impactful pay-for-performance plans from them first. However, the CMS model will affect 70 million patients, and commercial insurers have tended to use the CMS model for physician reimbursement.”
Dr. Torcson believes this program is simply a first step on that road. “We’re in the infancy of pay-for-performance models for physician reimbursement,” he says. “I think the ultimate model for physician-level value-based purchasing is going to look a lot different than the proposed CMS payment for reporting and payment for performance.”
In the immediate future, the PPC and PSTF will continue to participate in formulating the final quality measures for the CMS voluntary reporting program. Watch the SHM Web site for updates on the status of the program. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Sinus Infection, Headache, and Diplopia

A 36-year-old female with a recently treated sinus infection presents with an 18-hour history of severe right-sided headache and new-onset diplopia. Examination reveals the finding pictured below. Aside from tenderness on palpation over the frontal and maxillary sinuses, the remainder of her physical and neurologic exam is unremarkable. TH

What is the physical exam finding?
a) Anisocoria;
b) Facial nerve palsy;
c) Horner Syndrome;
d) Abducens palsy; or
e) Intranuclear ophthalmoplegia.
Discussion
The answer is D: Abducens palsy, or isolated right cranial nerve VI palsy. Extraocular muscle dysfunction results from insults to the muscle itself or from lesions of the motor nerve innervating the muscle. In this case, the lesion responsible is a cranial nerve VI palsy.
Cranial nerve VI innervates the lateral rectus muscle, which is responsible for eye abduction, or temporal gaze. Patients with dysfunction of the sixth cranial nerve complain of horizontal, binocular diplopia. Impaired abduction often indicates an ipsilateral cranial nerve VI lesion.
The sixth cranial nerve arises from the pons and courses through the subarachnoid space until it ascends the clivus and enters the cavernous sinus before exiting to the lateral rectus muscle. Palsies of the sixth cranial nerve may result from lesions anywhere along the anatomic course of the nerve. The most common cause of isolated sixth cranial nerve palsy in adults is ischemic injury—most often related to hypertension and/or diabetes. This is particularly true for older adults. In younger adults and children, it often occurs as a post-viral manifestation.
Isolated cranial nerve VI palsies occurring in adults over 50 require workup for ischemic vascular diseases or temporal arteritis. In patients younger than 50, MRI imaging is necessary to rule out intracranial processes. The majority of cranial nerve VI palsies that arise from ischemic or idiopathic causes will resolve spontaneously over a course of several months.
In this case, the cranial nerve VI palsy was caused by cavernous sinus thrombosis secondary to extension of a pre-existing sinus infection. Contents of the cavernous sinus include cranial nerves III, IV, and VI; the ophthalmic and maxillary divisions of cranial nerve V; and the internal carotid artery. Cavernous sinus thrombosis is usually the result of the extension of dental, sinus, or orbital infections, with the most common causative organism being Staphylococcus aureus, followed by anaerobes, Streptococcus species, and fungi.
Headache is the most common presenting symptom of cavernous sinus thrombosis, with later complaints including fever and cranial nerve involvement. Cavernous sinus thrombosis is a medical emergency requiring aggressive antimicrobial therapy and early surgical involvement. Patients with sinus infections may require urgent debridement of infected sinuses by ear, nose, and throat surgeons. The role of anticoagulation in cavernous sinus thrombosis is somewhat controversial, though it may be implemented to prevent clot propagation.
Although it is somewhat unusual for patients with cavernous sinus thrombosis to present with a mononeuropathy instead of multiple cranial nerve deficits, cavernous sinus thrombosis should be suspected in any patient complaining of a unilateral headache and horizontal diplopia, particularly in the setting of a sinus or dental infection. TH
A 36-year-old female with a recently treated sinus infection presents with an 18-hour history of severe right-sided headache and new-onset diplopia. Examination reveals the finding pictured below. Aside from tenderness on palpation over the frontal and maxillary sinuses, the remainder of her physical and neurologic exam is unremarkable. TH
What is the physical exam finding?
a) Anisocoria;
b) Facial nerve palsy;
c) Horner Syndrome;
d) Abducens palsy; or
e) Intranuclear ophthalmoplegia.
Discussion
The answer is D: Abducens palsy, or isolated right cranial nerve VI palsy. Extraocular muscle dysfunction results from insults to the muscle itself or from lesions of the motor nerve innervating the muscle. In this case, the lesion responsible is a cranial nerve VI palsy.
Cranial nerve VI innervates the lateral rectus muscle, which is responsible for eye abduction, or temporal gaze. Patients with dysfunction of the sixth cranial nerve complain of horizontal, binocular diplopia. Impaired abduction often indicates an ipsilateral cranial nerve VI lesion.
The sixth cranial nerve arises from the pons and courses through the subarachnoid space until it ascends the clivus and enters the cavernous sinus before exiting to the lateral rectus muscle. Palsies of the sixth cranial nerve may result from lesions anywhere along the anatomic course of the nerve. The most common cause of isolated sixth cranial nerve palsy in adults is ischemic injury—most often related to hypertension and/or diabetes. This is particularly true for older adults. In younger adults and children, it often occurs as a post-viral manifestation.
Isolated cranial nerve VI palsies occurring in adults over 50 require workup for ischemic vascular diseases or temporal arteritis. In patients younger than 50, MRI imaging is necessary to rule out intracranial processes. The majority of cranial nerve VI palsies that arise from ischemic or idiopathic causes will resolve spontaneously over a course of several months.
In this case, the cranial nerve VI palsy was caused by cavernous sinus thrombosis secondary to extension of a pre-existing sinus infection. Contents of the cavernous sinus include cranial nerves III, IV, and VI; the ophthalmic and maxillary divisions of cranial nerve V; and the internal carotid artery. Cavernous sinus thrombosis is usually the result of the extension of dental, sinus, or orbital infections, with the most common causative organism being Staphylococcus aureus, followed by anaerobes, Streptococcus species, and fungi.
Headache is the most common presenting symptom of cavernous sinus thrombosis, with later complaints including fever and cranial nerve involvement. Cavernous sinus thrombosis is a medical emergency requiring aggressive antimicrobial therapy and early surgical involvement. Patients with sinus infections may require urgent debridement of infected sinuses by ear, nose, and throat surgeons. The role of anticoagulation in cavernous sinus thrombosis is somewhat controversial, though it may be implemented to prevent clot propagation.
Although it is somewhat unusual for patients with cavernous sinus thrombosis to present with a mononeuropathy instead of multiple cranial nerve deficits, cavernous sinus thrombosis should be suspected in any patient complaining of a unilateral headache and horizontal diplopia, particularly in the setting of a sinus or dental infection. TH
A 36-year-old female with a recently treated sinus infection presents with an 18-hour history of severe right-sided headache and new-onset diplopia. Examination reveals the finding pictured below. Aside from tenderness on palpation over the frontal and maxillary sinuses, the remainder of her physical and neurologic exam is unremarkable. TH
What is the physical exam finding?
a) Anisocoria;
b) Facial nerve palsy;
c) Horner Syndrome;
d) Abducens palsy; or
e) Intranuclear ophthalmoplegia.
Discussion
The answer is D: Abducens palsy, or isolated right cranial nerve VI palsy. Extraocular muscle dysfunction results from insults to the muscle itself or from lesions of the motor nerve innervating the muscle. In this case, the lesion responsible is a cranial nerve VI palsy.
Cranial nerve VI innervates the lateral rectus muscle, which is responsible for eye abduction, or temporal gaze. Patients with dysfunction of the sixth cranial nerve complain of horizontal, binocular diplopia. Impaired abduction often indicates an ipsilateral cranial nerve VI lesion.
The sixth cranial nerve arises from the pons and courses through the subarachnoid space until it ascends the clivus and enters the cavernous sinus before exiting to the lateral rectus muscle. Palsies of the sixth cranial nerve may result from lesions anywhere along the anatomic course of the nerve. The most common cause of isolated sixth cranial nerve palsy in adults is ischemic injury—most often related to hypertension and/or diabetes. This is particularly true for older adults. In younger adults and children, it often occurs as a post-viral manifestation.
Isolated cranial nerve VI palsies occurring in adults over 50 require workup for ischemic vascular diseases or temporal arteritis. In patients younger than 50, MRI imaging is necessary to rule out intracranial processes. The majority of cranial nerve VI palsies that arise from ischemic or idiopathic causes will resolve spontaneously over a course of several months.
In this case, the cranial nerve VI palsy was caused by cavernous sinus thrombosis secondary to extension of a pre-existing sinus infection. Contents of the cavernous sinus include cranial nerves III, IV, and VI; the ophthalmic and maxillary divisions of cranial nerve V; and the internal carotid artery. Cavernous sinus thrombosis is usually the result of the extension of dental, sinus, or orbital infections, with the most common causative organism being Staphylococcus aureus, followed by anaerobes, Streptococcus species, and fungi.
Headache is the most common presenting symptom of cavernous sinus thrombosis, with later complaints including fever and cranial nerve involvement. Cavernous sinus thrombosis is a medical emergency requiring aggressive antimicrobial therapy and early surgical involvement. Patients with sinus infections may require urgent debridement of infected sinuses by ear, nose, and throat surgeons. The role of anticoagulation in cavernous sinus thrombosis is somewhat controversial, though it may be implemented to prevent clot propagation.
Although it is somewhat unusual for patients with cavernous sinus thrombosis to present with a mononeuropathy instead of multiple cranial nerve deficits, cavernous sinus thrombosis should be suspected in any patient complaining of a unilateral headache and horizontal diplopia, particularly in the setting of a sinus or dental infection. TH
SHM’s VTE Prevention Collaborative

The problem of hospital-acquired venous thromboembolism (VTE): Venous thromboembolic disease, ranging from asymptomatic deep vein thrombosis (DVT) to massive pulmonary embolism (PE), is a significant cause of morbidity and mortality in hospitalized patients. Almost all hospitalized patients are at risk for VTE, and the literature suggests that approximately half of all cases of VTE are hospital-acquired.1-4 PE is recognized as the cause of death for more than 100,000 hospitalized patients in the United States every year and is considered a contributing factor in the death of 100,000 more patients.1
Multiple clinical trials have provided irrefutable evidence that primary thromboprophylaxis reduces the incidence of DVT and PE.5 Unfortunately, numerous studies have also shown that the majority of hospitalized patients with risk factors for DVT do not receive appropriate prophylaxis.6-8
Hospitalists are ideally positioned to reduce the incidence of preventable VTE, both by using known best practices to improve care delivered to their own patients, and, more importantly, by leading hospital-wide QI efforts that improve care for all patients at their home institutions.
SHM is now accepting applications for the VTE Prevention Collaborative, a program that offers individualized assistance to hospitalists who wish to take the lead on this critical quality and patient safety issue. Participants can choose the option that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The SHM Mentoring Program
The Mentoring Program is the perfect option for individuals who are interested in securing ongoing support for their planned or active VTE prevention projects. SHM mentors with VTE and QI experts who work with participants to tackle site-specific issues using proven QI techniques. Instruction is organized around the VTE QI Workbook, SHM’s step-by-step guide for developing a VTE prevention program. Mentoring occurs in eight telephone calls scheduled throughout the yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. As needed, participants can also interact with their mentors through e-mail and in ad hoc telephone calls. Participants receive assistance with:
- Securing institutional support for the project;
- Assembling and leading the project team;
- Developing project goals and aims;
- Mapping current processes for assessing VTE risk and bleeding risk;
- Evaluating current prophylaxis recommendations;
- Developing evidence-based risk assessment and prophylaxis recommendations;
- Redesigning care delivery processes to include high-reliability features that promote adherence to best practices;
- Developing educational/outreach plans to ensure buy-in from key stakeholders; and
- Collecting, analyzing, and reporting outcome data.
Individuals with relatively little QI leadership experience, as well as those whose VTE prevention projects are in the early planning stages, are encouraged to apply for the SHM Mentoring Program.
The SHM On-site Consultation Program
The On-site Consultation Program is the perfect option for individuals who are interested in securing expert evaluation and input on a VTE prevention program but don’t feel they need ongoing, longitudinal support. Through the SHM On-site Consultation Program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits will be especially helpful to participants who have existing VTE prevention programs they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, any potential barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation visit activities will vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools.
Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation, which will occur 60-90 days after the visit.
SHM On-site Consultation Program visits will be available starting in May 2007, though interested parties are encouraged to apply early; enrollment is limited, and available slots are expected to fill quickly.
Which Option Is Right for You?
SHM welcomes participation from hospitalists who work in all types of facilities (large and small community hospitals, academic medical centers, public hospitals, and others) and all types of practice settings, including acute care hospitals, skilled nursing facilities, and rehabilitation hospitals. Both VTE Prevention Collaborative programs are appropriate for individuals with all levels of QI experience, from the novice embarking on his or her first QI project to the seasoned QI leader. Individuals who have not yet begun working on a VTE prevention project are encouraged to apply, as are those who wish to expand or improve upon an existing project.
There are no rigid prerequisites for either program, though we expect individuals whose local VTE prevention efforts are already partially developed to derive more benefit from the On-site Consultation option than would an applicant who has yet to start his or her project. Individuals who have not yet begun working on a VTE prevention project are encouraged to apply for the Mentoring Program, which will ensure access to expert assistance during key development and implementation tasks.
How to Apply
Participation in both the Mentoring and On-site Consultation programs is open to hospitalists who are leading proposed or active VTE prevention projects. Participation is free, but enrollment is limited; interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct questions about VTE Prevention Collaborative programs to [email protected].
References
- Goldhaber SZ, Tapson VF. DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93:259-262.
- Guidelines on diagnosis and management of acute pulmonary embolism. Task Force on Pulmonary Embolism, European Society of Cardiology. Eur Heart J. 2000 Aug;21(16):1301-1336. Comment in: Eur Heart J. 2000 Aug; 21(16): 1289-1290.
- Stein PD, Huang H, Afzal A, et al. Incidence of acute pulmonary embolism in a general hospital: relation to age, sex, and race. Chest. 1999 Oct;116(4):909-913.
- Silverstein MD, Heit JA, Mohr DN, et al. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998 Mar 23;158(6):585-593.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Comment in: Chest. 2005 Jun; 127(6):2297-2298.
- Stratton MA, Anderson FA, Bussey HI, et al. Prevention of venous thromboembolism: adherence to the 1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med. 2000;160:334-340.
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. Changing clinical practice. Prospective study of the impact of continuing medical education and quality assurance programs on use of prophylaxis for venous thromboembolism. Arch Intern Med. 1994 Mar 28;154(6):669-677.
- Walker A, Campbell S, Grimshaw J. Implementation of a national guideline on prophylaxis of venous thromboembolism: a survey of acute services in Scotland. Thromboembolism Prevention Evaluation Study Group. Health Bull (Edinb). 1999 Mar;57(2):141-147.
Benchmarks Committee Update
By Burke Kealey, MD, chair, SHM Benchmarks Committee
The SHM Benchmarks Committee has had a busy schedule with its new special issues survey and wrapping up work on The Dashboard Project, a first-of-its-kind undertaking. Committee members (under the guidance of Editor Leslie Flores) wrote summaries of 10 sample performance metrics. Each article is designed around a given metric and includes an in-depth discussion of why it is important and where to obtain the necessary data. Sample graphs from other programs will also be included.
The intent is for hospitalist leaders and program managers to use The Dashboard Project to learn what kind of metrics their peers use to manage their respective programs. The final draft was reviewed by the entire committee and circulated to SHM leaders, including the board of directors. It will be published through SHM’s publication, The Hospitalist, and promoted at the SHM Annual Meeting in Dallas in May.
In a break from recent tradition, the SHM Benchmarks Committee (with approval from the SHM Board) has changed how it conducts surveys. The committee will now produce shorter, simpler surveys annually—rather than producing a mega-survey every other year. The committee will conduct an individual hospitalist compensation and productivity survey every other year (including later in 2007); in the alternate year (along with baseline practice demographics) the committee will address the special topics of interest discussed below.
With input from SHM’s Palliative Care Task Force, this year’s special interest survey (which was conducted in November and December of 2006) included questions on palliative care and its growing place in the world of hospital medicine. Night and off-hours coverage continue to be topics of interest for membership. Questions in this section examined the scope of night coverage, including providing ICU coverage for intensivists and getting paid for as well as paying providers for this work.
Issues for family medicine hospitalists are also addressed. Anecdotally, the Benchmarks Committee has heard of family medicine hospitalists running into difficulties securing work because they have been barred by hospital contracts and/or bylaws stating that only internal medicine or pediatrics board-certified physicians can occupy those slots. The survey was designed to capture the pervasiveness of this practice.
Finally, in this era of pay for performance and open reporting, quality measures and their relationship to physician revenue and compensation is a topic that every hospital medicine leader needs to understand. The survey contained a section that looked at the degree to which pay-for-performance programs are actually being seen in the hospitals we practice at, and then, even more important, how those dollars are tied to quality incentive programs between hospitals and hospital medicine groups.
The results of this special interest survey are currently being analyzed and will be published later this spring. TH
SHM is now accepting applications for the VTE Prevention Collaborative, a program that offers individualized assistance to hospitalists wishing to take the lead on this critical quality and patient safety issue.
SHM Behind the Scenes
Making your membership easier to manage: changes to shm’s renewal process to take effect in april
By Todd Von Deak

I’m excited to let you know about a change to SHM’s membership structure that was recently approved by the SHM Board of Directors. This is a change our Membership and Marketing Department recommended to the Board, one that we feel will be a positive development over the coming years.
These changes, which take effect on April 1, affect how membership renewals are handled and processed.
Under the new structure, memberships will be renewed 12 months from when a member last paid dues in order for the member to remain in good standing. In the previous system, memberships were renewed each year between July 1 and September 30—regardless of when the last membership payment had been made.
There were two key factors that led to this change:
- The need to simplify a membership structure in which it was possible for a member who joined on July 1 and another who joined on December 24 to pay the same dues rate; and
- A survey of those whose memberships had recently lapsed in which 46% of respondents indicated that they did not know that their membership had lapsed.
There were three underlying themes to this change. We believe you should expect all three of these themes from any membership organization that you belong to.
- Transparency: We wanted to clear up any confusion surrounding how your membership works. Simplifying the current structure will reduce confusion;
- Fairness: A $230 dues payment in December should result in the same 12 months of benefits as a $230 dues payment in July; and
- Ease of understanding: With membership renewals now due exactly one year from when you last paid, it should be easier to keep track of your membership and to keep it current.
Current members shouldn’t see a major difference as a result of this change. Renewal notices will be sent during the first part of April, with payment required by July 31 in order to keep your membership current.
New members will be most affected by the change. Beginning in April, new members will renew 12 months from when they join—as opposed to the past practice of renewing between July and September.
Over the coming year, we plan to introduce even more benefits to membership in SHM, the only professional society devoted solely to hospital medicine. These benefits will utilize emerging technologies such as podcasting and will make it even easier to access the vital educational content for which SHM has become well respected over the course of the last 10 years.
Stay tuned to The Hospitalist, as well as to SHM’s e-Newsletter, over the next several months for more details of the switch to an anniversary membership structure and how it will impact you. Of course, if you have any questions, please do not hesitate to contact us at (800) 843-3360 or online at [email protected]. TH
The problem of hospital-acquired venous thromboembolism (VTE): Venous thromboembolic disease, ranging from asymptomatic deep vein thrombosis (DVT) to massive pulmonary embolism (PE), is a significant cause of morbidity and mortality in hospitalized patients. Almost all hospitalized patients are at risk for VTE, and the literature suggests that approximately half of all cases of VTE are hospital-acquired.1-4 PE is recognized as the cause of death for more than 100,000 hospitalized patients in the United States every year and is considered a contributing factor in the death of 100,000 more patients.1
Multiple clinical trials have provided irrefutable evidence that primary thromboprophylaxis reduces the incidence of DVT and PE.5 Unfortunately, numerous studies have also shown that the majority of hospitalized patients with risk factors for DVT do not receive appropriate prophylaxis.6-8
Hospitalists are ideally positioned to reduce the incidence of preventable VTE, both by using known best practices to improve care delivered to their own patients, and, more importantly, by leading hospital-wide QI efforts that improve care for all patients at their home institutions.
SHM is now accepting applications for the VTE Prevention Collaborative, a program that offers individualized assistance to hospitalists who wish to take the lead on this critical quality and patient safety issue. Participants can choose the option that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The SHM Mentoring Program
The Mentoring Program is the perfect option for individuals who are interested in securing ongoing support for their planned or active VTE prevention projects. SHM mentors with VTE and QI experts who work with participants to tackle site-specific issues using proven QI techniques. Instruction is organized around the VTE QI Workbook, SHM’s step-by-step guide for developing a VTE prevention program. Mentoring occurs in eight telephone calls scheduled throughout the yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. As needed, participants can also interact with their mentors through e-mail and in ad hoc telephone calls. Participants receive assistance with:
- Securing institutional support for the project;
- Assembling and leading the project team;
- Developing project goals and aims;
- Mapping current processes for assessing VTE risk and bleeding risk;
- Evaluating current prophylaxis recommendations;
- Developing evidence-based risk assessment and prophylaxis recommendations;
- Redesigning care delivery processes to include high-reliability features that promote adherence to best practices;
- Developing educational/outreach plans to ensure buy-in from key stakeholders; and
- Collecting, analyzing, and reporting outcome data.
Individuals with relatively little QI leadership experience, as well as those whose VTE prevention projects are in the early planning stages, are encouraged to apply for the SHM Mentoring Program.
The SHM On-site Consultation Program
The On-site Consultation Program is the perfect option for individuals who are interested in securing expert evaluation and input on a VTE prevention program but don’t feel they need ongoing, longitudinal support. Through the SHM On-site Consultation Program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits will be especially helpful to participants who have existing VTE prevention programs they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, any potential barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation visit activities will vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools.
Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation, which will occur 60-90 days after the visit.
SHM On-site Consultation Program visits will be available starting in May 2007, though interested parties are encouraged to apply early; enrollment is limited, and available slots are expected to fill quickly.
Which Option Is Right for You?
SHM welcomes participation from hospitalists who work in all types of facilities (large and small community hospitals, academic medical centers, public hospitals, and others) and all types of practice settings, including acute care hospitals, skilled nursing facilities, and rehabilitation hospitals. Both VTE Prevention Collaborative programs are appropriate for individuals with all levels of QI experience, from the novice embarking on his or her first QI project to the seasoned QI leader. Individuals who have not yet begun working on a VTE prevention project are encouraged to apply, as are those who wish to expand or improve upon an existing project.
There are no rigid prerequisites for either program, though we expect individuals whose local VTE prevention efforts are already partially developed to derive more benefit from the On-site Consultation option than would an applicant who has yet to start his or her project. Individuals who have not yet begun working on a VTE prevention project are encouraged to apply for the Mentoring Program, which will ensure access to expert assistance during key development and implementation tasks.
How to Apply
Participation in both the Mentoring and On-site Consultation programs is open to hospitalists who are leading proposed or active VTE prevention projects. Participation is free, but enrollment is limited; interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct questions about VTE Prevention Collaborative programs to [email protected].
References
- Goldhaber SZ, Tapson VF. DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93:259-262.
- Guidelines on diagnosis and management of acute pulmonary embolism. Task Force on Pulmonary Embolism, European Society of Cardiology. Eur Heart J. 2000 Aug;21(16):1301-1336. Comment in: Eur Heart J. 2000 Aug; 21(16): 1289-1290.
- Stein PD, Huang H, Afzal A, et al. Incidence of acute pulmonary embolism in a general hospital: relation to age, sex, and race. Chest. 1999 Oct;116(4):909-913.
- Silverstein MD, Heit JA, Mohr DN, et al. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998 Mar 23;158(6):585-593.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Comment in: Chest. 2005 Jun; 127(6):2297-2298.
- Stratton MA, Anderson FA, Bussey HI, et al. Prevention of venous thromboembolism: adherence to the 1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med. 2000;160:334-340.
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. Changing clinical practice. Prospective study of the impact of continuing medical education and quality assurance programs on use of prophylaxis for venous thromboembolism. Arch Intern Med. 1994 Mar 28;154(6):669-677.
- Walker A, Campbell S, Grimshaw J. Implementation of a national guideline on prophylaxis of venous thromboembolism: a survey of acute services in Scotland. Thromboembolism Prevention Evaluation Study Group. Health Bull (Edinb). 1999 Mar;57(2):141-147.
Benchmarks Committee Update
By Burke Kealey, MD, chair, SHM Benchmarks Committee
The SHM Benchmarks Committee has had a busy schedule with its new special issues survey and wrapping up work on The Dashboard Project, a first-of-its-kind undertaking. Committee members (under the guidance of Editor Leslie Flores) wrote summaries of 10 sample performance metrics. Each article is designed around a given metric and includes an in-depth discussion of why it is important and where to obtain the necessary data. Sample graphs from other programs will also be included.
The intent is for hospitalist leaders and program managers to use The Dashboard Project to learn what kind of metrics their peers use to manage their respective programs. The final draft was reviewed by the entire committee and circulated to SHM leaders, including the board of directors. It will be published through SHM’s publication, The Hospitalist, and promoted at the SHM Annual Meeting in Dallas in May.
In a break from recent tradition, the SHM Benchmarks Committee (with approval from the SHM Board) has changed how it conducts surveys. The committee will now produce shorter, simpler surveys annually—rather than producing a mega-survey every other year. The committee will conduct an individual hospitalist compensation and productivity survey every other year (including later in 2007); in the alternate year (along with baseline practice demographics) the committee will address the special topics of interest discussed below.
With input from SHM’s Palliative Care Task Force, this year’s special interest survey (which was conducted in November and December of 2006) included questions on palliative care and its growing place in the world of hospital medicine. Night and off-hours coverage continue to be topics of interest for membership. Questions in this section examined the scope of night coverage, including providing ICU coverage for intensivists and getting paid for as well as paying providers for this work.
Issues for family medicine hospitalists are also addressed. Anecdotally, the Benchmarks Committee has heard of family medicine hospitalists running into difficulties securing work because they have been barred by hospital contracts and/or bylaws stating that only internal medicine or pediatrics board-certified physicians can occupy those slots. The survey was designed to capture the pervasiveness of this practice.
Finally, in this era of pay for performance and open reporting, quality measures and their relationship to physician revenue and compensation is a topic that every hospital medicine leader needs to understand. The survey contained a section that looked at the degree to which pay-for-performance programs are actually being seen in the hospitals we practice at, and then, even more important, how those dollars are tied to quality incentive programs between hospitals and hospital medicine groups.
The results of this special interest survey are currently being analyzed and will be published later this spring. TH
SHM is now accepting applications for the VTE Prevention Collaborative, a program that offers individualized assistance to hospitalists wishing to take the lead on this critical quality and patient safety issue.
SHM Behind the Scenes
Making your membership easier to manage: changes to shm’s renewal process to take effect in april
By Todd Von Deak
I’m excited to let you know about a change to SHM’s membership structure that was recently approved by the SHM Board of Directors. This is a change our Membership and Marketing Department recommended to the Board, one that we feel will be a positive development over the coming years.
These changes, which take effect on April 1, affect how membership renewals are handled and processed.
Under the new structure, memberships will be renewed 12 months from when a member last paid dues in order for the member to remain in good standing. In the previous system, memberships were renewed each year between July 1 and September 30—regardless of when the last membership payment had been made.
There were two key factors that led to this change:
- The need to simplify a membership structure in which it was possible for a member who joined on July 1 and another who joined on December 24 to pay the same dues rate; and
- A survey of those whose memberships had recently lapsed in which 46% of respondents indicated that they did not know that their membership had lapsed.
There were three underlying themes to this change. We believe you should expect all three of these themes from any membership organization that you belong to.
- Transparency: We wanted to clear up any confusion surrounding how your membership works. Simplifying the current structure will reduce confusion;
- Fairness: A $230 dues payment in December should result in the same 12 months of benefits as a $230 dues payment in July; and
- Ease of understanding: With membership renewals now due exactly one year from when you last paid, it should be easier to keep track of your membership and to keep it current.
Current members shouldn’t see a major difference as a result of this change. Renewal notices will be sent during the first part of April, with payment required by July 31 in order to keep your membership current.
New members will be most affected by the change. Beginning in April, new members will renew 12 months from when they join—as opposed to the past practice of renewing between July and September.
Over the coming year, we plan to introduce even more benefits to membership in SHM, the only professional society devoted solely to hospital medicine. These benefits will utilize emerging technologies such as podcasting and will make it even easier to access the vital educational content for which SHM has become well respected over the course of the last 10 years.
Stay tuned to The Hospitalist, as well as to SHM’s e-Newsletter, over the next several months for more details of the switch to an anniversary membership structure and how it will impact you. Of course, if you have any questions, please do not hesitate to contact us at (800) 843-3360 or online at [email protected]. TH
The problem of hospital-acquired venous thromboembolism (VTE): Venous thromboembolic disease, ranging from asymptomatic deep vein thrombosis (DVT) to massive pulmonary embolism (PE), is a significant cause of morbidity and mortality in hospitalized patients. Almost all hospitalized patients are at risk for VTE, and the literature suggests that approximately half of all cases of VTE are hospital-acquired.1-4 PE is recognized as the cause of death for more than 100,000 hospitalized patients in the United States every year and is considered a contributing factor in the death of 100,000 more patients.1
Multiple clinical trials have provided irrefutable evidence that primary thromboprophylaxis reduces the incidence of DVT and PE.5 Unfortunately, numerous studies have also shown that the majority of hospitalized patients with risk factors for DVT do not receive appropriate prophylaxis.6-8
Hospitalists are ideally positioned to reduce the incidence of preventable VTE, both by using known best practices to improve care delivered to their own patients, and, more importantly, by leading hospital-wide QI efforts that improve care for all patients at their home institutions.
SHM is now accepting applications for the VTE Prevention Collaborative, a program that offers individualized assistance to hospitalists who wish to take the lead on this critical quality and patient safety issue. Participants can choose the option that best fits their needs: a full year of distance mentoring or a one-day evaluation and consultation visit to their site.
The SHM Mentoring Program
The Mentoring Program is the perfect option for individuals who are interested in securing ongoing support for their planned or active VTE prevention projects. SHM mentors with VTE and QI experts who work with participants to tackle site-specific issues using proven QI techniques. Instruction is organized around the VTE QI Workbook, SHM’s step-by-step guide for developing a VTE prevention program. Mentoring occurs in eight telephone calls scheduled throughout the yearlong mentoring period. During the calls, mentors offer individualized assistance on any topics, tasks, and barriers that are encountered in the course of designing, implementing, and evaluating a VTE prevention project. As needed, participants can also interact with their mentors through e-mail and in ad hoc telephone calls. Participants receive assistance with:
- Securing institutional support for the project;
- Assembling and leading the project team;
- Developing project goals and aims;
- Mapping current processes for assessing VTE risk and bleeding risk;
- Evaluating current prophylaxis recommendations;
- Developing evidence-based risk assessment and prophylaxis recommendations;
- Redesigning care delivery processes to include high-reliability features that promote adherence to best practices;
- Developing educational/outreach plans to ensure buy-in from key stakeholders; and
- Collecting, analyzing, and reporting outcome data.
Individuals with relatively little QI leadership experience, as well as those whose VTE prevention projects are in the early planning stages, are encouraged to apply for the SHM Mentoring Program.
The SHM On-site Consultation Program
The On-site Consultation Program is the perfect option for individuals who are interested in securing expert evaluation and input on a VTE prevention program but don’t feel they need ongoing, longitudinal support. Through the SHM On-site Consultation Program, SHM consultants with VTE and QI expertise visit applicants’ hospitals to evaluate active or planned VTE prevention programs. The visits will be especially helpful to participants who have existing VTE prevention programs they wish to expand or improve upon.
The consultation visits feature a structured evaluation of the site’s strengths and resources, any potential barriers to improvement, and the design and functioning of active or proposed VTE prevention interventions. Specific consultation visit activities will vary according to participant goals and needs but may include meeting with the local project team, QI leaders, hospital administrators, and hospital medicine group leaders, as well as reviewing project documents—order sets, policies, and procedures—data, and data collection/management tools.
Following the visits, SHM consultants provide participants with a written report of findings and recommendations. Participants also receive one follow-up telephone consultation, which will occur 60-90 days after the visit.
SHM On-site Consultation Program visits will be available starting in May 2007, though interested parties are encouraged to apply early; enrollment is limited, and available slots are expected to fill quickly.
Which Option Is Right for You?
SHM welcomes participation from hospitalists who work in all types of facilities (large and small community hospitals, academic medical centers, public hospitals, and others) and all types of practice settings, including acute care hospitals, skilled nursing facilities, and rehabilitation hospitals. Both VTE Prevention Collaborative programs are appropriate for individuals with all levels of QI experience, from the novice embarking on his or her first QI project to the seasoned QI leader. Individuals who have not yet begun working on a VTE prevention project are encouraged to apply, as are those who wish to expand or improve upon an existing project.
There are no rigid prerequisites for either program, though we expect individuals whose local VTE prevention efforts are already partially developed to derive more benefit from the On-site Consultation option than would an applicant who has yet to start his or her project. Individuals who have not yet begun working on a VTE prevention project are encouraged to apply for the Mentoring Program, which will ensure access to expert assistance during key development and implementation tasks.
How to Apply
Participation in both the Mentoring and On-site Consultation programs is open to hospitalists who are leading proposed or active VTE prevention projects. Participation is free, but enrollment is limited; interested individuals are encouraged to apply early. SHM members can apply to either program by completing the online application available on the VTE Prevention Collaborative Web site: www.hospitalmedicine.org/vte-pc.
Direct questions about VTE Prevention Collaborative programs to [email protected].
References
- Goldhaber SZ, Tapson VF. DVT FREE Steering Committee. A prospective registry of 5,451 patients with ultrasound-confirmed deep vein thrombosis. Am J Cardiol. 2004;93:259-262.
- Guidelines on diagnosis and management of acute pulmonary embolism. Task Force on Pulmonary Embolism, European Society of Cardiology. Eur Heart J. 2000 Aug;21(16):1301-1336. Comment in: Eur Heart J. 2000 Aug; 21(16): 1289-1290.
- Stein PD, Huang H, Afzal A, et al. Incidence of acute pulmonary embolism in a general hospital: relation to age, sex, and race. Chest. 1999 Oct;116(4):909-913.
- Silverstein MD, Heit JA, Mohr DN, et al. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998 Mar 23;158(6):585-593.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004 Sep;126(3 Suppl):338S-400S. Comment in: Chest. 2005 Jun; 127(6):2297-2298.
- Stratton MA, Anderson FA, Bussey HI, et al. Prevention of venous thromboembolism: adherence to the 1995 American College of Chest Physicians consensus guidelines for surgical patients. Arch Intern Med. 2000;160:334-340.
- Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. Changing clinical practice. Prospective study of the impact of continuing medical education and quality assurance programs on use of prophylaxis for venous thromboembolism. Arch Intern Med. 1994 Mar 28;154(6):669-677.
- Walker A, Campbell S, Grimshaw J. Implementation of a national guideline on prophylaxis of venous thromboembolism: a survey of acute services in Scotland. Thromboembolism Prevention Evaluation Study Group. Health Bull (Edinb). 1999 Mar;57(2):141-147.
Benchmarks Committee Update
By Burke Kealey, MD, chair, SHM Benchmarks Committee
The SHM Benchmarks Committee has had a busy schedule with its new special issues survey and wrapping up work on The Dashboard Project, a first-of-its-kind undertaking. Committee members (under the guidance of Editor Leslie Flores) wrote summaries of 10 sample performance metrics. Each article is designed around a given metric and includes an in-depth discussion of why it is important and where to obtain the necessary data. Sample graphs from other programs will also be included.
The intent is for hospitalist leaders and program managers to use The Dashboard Project to learn what kind of metrics their peers use to manage their respective programs. The final draft was reviewed by the entire committee and circulated to SHM leaders, including the board of directors. It will be published through SHM’s publication, The Hospitalist, and promoted at the SHM Annual Meeting in Dallas in May.
In a break from recent tradition, the SHM Benchmarks Committee (with approval from the SHM Board) has changed how it conducts surveys. The committee will now produce shorter, simpler surveys annually—rather than producing a mega-survey every other year. The committee will conduct an individual hospitalist compensation and productivity survey every other year (including later in 2007); in the alternate year (along with baseline practice demographics) the committee will address the special topics of interest discussed below.
With input from SHM’s Palliative Care Task Force, this year’s special interest survey (which was conducted in November and December of 2006) included questions on palliative care and its growing place in the world of hospital medicine. Night and off-hours coverage continue to be topics of interest for membership. Questions in this section examined the scope of night coverage, including providing ICU coverage for intensivists and getting paid for as well as paying providers for this work.
Issues for family medicine hospitalists are also addressed. Anecdotally, the Benchmarks Committee has heard of family medicine hospitalists running into difficulties securing work because they have been barred by hospital contracts and/or bylaws stating that only internal medicine or pediatrics board-certified physicians can occupy those slots. The survey was designed to capture the pervasiveness of this practice.
Finally, in this era of pay for performance and open reporting, quality measures and their relationship to physician revenue and compensation is a topic that every hospital medicine leader needs to understand. The survey contained a section that looked at the degree to which pay-for-performance programs are actually being seen in the hospitals we practice at, and then, even more important, how those dollars are tied to quality incentive programs between hospitals and hospital medicine groups.
The results of this special interest survey are currently being analyzed and will be published later this spring. TH
SHM is now accepting applications for the VTE Prevention Collaborative, a program that offers individualized assistance to hospitalists wishing to take the lead on this critical quality and patient safety issue.
SHM Behind the Scenes
Making your membership easier to manage: changes to shm’s renewal process to take effect in april
By Todd Von Deak
I’m excited to let you know about a change to SHM’s membership structure that was recently approved by the SHM Board of Directors. This is a change our Membership and Marketing Department recommended to the Board, one that we feel will be a positive development over the coming years.
These changes, which take effect on April 1, affect how membership renewals are handled and processed.
Under the new structure, memberships will be renewed 12 months from when a member last paid dues in order for the member to remain in good standing. In the previous system, memberships were renewed each year between July 1 and September 30—regardless of when the last membership payment had been made.
There were two key factors that led to this change:
- The need to simplify a membership structure in which it was possible for a member who joined on July 1 and another who joined on December 24 to pay the same dues rate; and
- A survey of those whose memberships had recently lapsed in which 46% of respondents indicated that they did not know that their membership had lapsed.
There were three underlying themes to this change. We believe you should expect all three of these themes from any membership organization that you belong to.
- Transparency: We wanted to clear up any confusion surrounding how your membership works. Simplifying the current structure will reduce confusion;
- Fairness: A $230 dues payment in December should result in the same 12 months of benefits as a $230 dues payment in July; and
- Ease of understanding: With membership renewals now due exactly one year from when you last paid, it should be easier to keep track of your membership and to keep it current.
Current members shouldn’t see a major difference as a result of this change. Renewal notices will be sent during the first part of April, with payment required by July 31 in order to keep your membership current.
New members will be most affected by the change. Beginning in April, new members will renew 12 months from when they join—as opposed to the past practice of renewing between July and September.
Over the coming year, we plan to introduce even more benefits to membership in SHM, the only professional society devoted solely to hospital medicine. These benefits will utilize emerging technologies such as podcasting and will make it even easier to access the vital educational content for which SHM has become well respected over the course of the last 10 years.
Stay tuned to The Hospitalist, as well as to SHM’s e-Newsletter, over the next several months for more details of the switch to an anniversary membership structure and how it will impact you. Of course, if you have any questions, please do not hesitate to contact us at (800) 843-3360 or online at [email protected]. TH
The Front Line of Change

We are in the midst of a true evolution of how hospitals will approach creating a culture of quality. The drivers for process improvement and management of resources have traditionally been more concerned with full occupancy and risk management, but now many external forces are raising quality improvement as a potential core competency for our nation’s hospitals.
With the push of the Institute for Healthcare Improvement (IHI), Leapfrog, and even Medicare, hospitals now must grapple with a culture change—one in which measurement and reporting of outcomes and processes will become, if not truly job one, at least in the top five. The fact that a hospital’s revenue stream through pay-for-performance (P4P) bonuses and its reputation by public reporting are at stake only serve to create a real immediacy in the coming years.
A recent SHM survey of the leaders of hospital medicine groups (HMGs) has shown that, once again, hospitalists find themselves right smack in the middle of quality improvement.
Survey Says
More than 41% of hospitalist leaders report that their HMG has a quality incentive program. This is even more prevalent at hospitals participating in P4P programs, where 60% of HMGs have quality incentives to align priorities. It is a hallmark of hospitalist groups to place a particular emphasis on the process and system improvement necessary for true measurable quality improvement. Many times, this improvement takes time away from direct and billable patient care.
Pointing to the relatively early stage in the adoption of P4P, this same survey reported that only 29% of HMGs were working in hospitals that participated in P4P programs, while 56% report their hospital did not have any P4P programs in place.
As we enter 2007, it is clear that while a small percentage of hospitals have embraced P4P the majority of hospitals are—at best—on the sidelines or still in planning mode. But those who are active in P4P have engaged their hospitalists to help them meet their goals. And everything that is coming out in the literature commonly read by the hospital C-suite promotes the promise of more reimbursement from the insurance industry and Medicare, leading to the conclusion that P4P and rewarding performance will increase in the near term.
What Can SHM Do for You?
Positioning hospitalists to play a key role in quality improvement, SHM has launched a number of initiatives and partnerships to provide hospitalists with the tools they need to help their hospitals to succeed.
As a framework of tools, SHM has now built six Web-based Quality Improvement Resource Rooms in VTE, Heart Failure, Stroke, Glycemic Control, Care Transitions in the Elderly, and Antibiotic Resistance. These practical tools and references are now available on the SHM Web site (www.hospitalmedicine.org) as are, in many cases, a comprehensive workbook that helps hospitalists to be the leaders of quality improvement change at their hospitals.
SHM realizes that, while this approach may work for the savvy, experienced quality improvement (QI) implementer, most young hospitalist leaders need a more personal, hands-on approach. With this in mind, SHM has launched its Mentored QI Implementation project. Centered around VTE prevention and supported by funding from Sanofi-Aventis, two senior hospitalist mentors will each work with 15 HMG leaders to take them step by step through the process of implementing a quality improvement process in 2007 and 2008.
To take this hands-on, supportive approach to the next level SHM (with support from a Kettering Foundation grant) will add the capability for on-site consultation—sort of a QI SWAT team that can show up at your hospital and work shoulder to shoulder with hospitalists and other members of the healthcare team to develop and implement processes that will improve patient care.
To further educate and energize hospitalist leaders who have been charged with leading this change, SHM developed the Leadership Academy. To date more than 400 hospitalist leaders have been trained in sold-out small-group sessions during the past two years. The most recent academy was held last month in Orlando, Fla.
SHM provides additional training for those who will implement quality improvement at the Quality Training precourse at the SHM Annual Meeting. In the precourse up to 100 change leaders get hands-on direction, tools, and tricks of the trade to allow them to succeed in their local efforts. The next Quality Training Precourse will be held in small group sessions on May 23, 2007, in Dallas.
The SHM Annual Meeting has consistently been a venue that allows hospitalists to hear from national thought leaders in the quality revolution. In 2006, hospitalists heard from Carolyn Clancy, MD, CEO of the Agency for Healthcare Research and Quality, and Jack Rowe, MD, CEO of Aetna Insurance Company.
At this year’s meeting Jonathan Perlin, MD, PhD, who led the cutting edge QI efforts at Veterans Affairs and who is now bringing innovation to HCA (Nashville, Tenn.), the nation’s largest hospital company, will share his ideas with us. In addition, hospitalists will hear from David Brailer, MD, PhD, President George W. Bush’s first appointee to head up national efforts for health information technology. In addition, SHM’s Bob Wachter, MD, a nationally recognized leader in QI and patient safety, will share his perspectives on hospital medicine. With Drs. Perlin, Brailer, and Wachter, SHM continues its tradition of placing innovations that are changing healthcare for the better front and center at our annual meeting.
As for the future, SHM has submitted a multi-year grant application to the Hartford Foundation (Conn.) to expand our efforts—specifically in developing implementation strategies to improve the care processes and outcomes for the senior population.
One of the key areas that emerged from SHM’s work with the Hartford Foundation is the importance of improving the transitions of care and better coordinating healthcare from the patient’s point of view. This has led SHM to partner with several national organizations to make sense of what has been a squishy subject. SHM is working closely with the American Board of Internal Medicine (ABIM) Foundation on its Stepping Up to the Plate consortium, a group of specialty physicians focusing on best practice strategies in patient-centered transitions, hand-offs, and information transfer.
In addition, SHM is working with the American College of Physicians, the AHRQ, the ABIM, the American Geriatrics Society (AGS), and the Society of General Internal Medicine to hold a National Consensus Conference in 2007 to establish policy on transitions of care. The conference will involve a broad range of stakeholders and may very well lead to the establishment of performance standards that can be applied directly to patient care.
Also SHM has been working with the Case Management Society of America to bring together the broader healthcare team on its National Transitions of Care Coalition (NTOCC) project. NTOCC includes pharmacists (American Society of Health-System Pharmacists), the C-suite (American College of Healthcare Executives), social workers (National Association of Social Workers), geriatricians (the AGS), the Joint Commission on Accreditation of Healthcare Organizations, and others. NTOCC plans to develop clear tools, guidelines, and pathways for consistent communication among patients, providers, and payers throughout the care continuum, and to look at aligning incentives for use of these tools and resources.
SHM has also worked with recognized leaders in action-oriented campaigns in QI, including the IHI—first on its “100,000 Lives Campaign,” and more recently on its “5 Million Lives Campaign.” In fact, leadership from only one medical professional society—SHM—was on the stage with Don Berwick for IHI’s national announcement at the December 2006 IHI national meeting in Orlando.
Hospitalists Lead the Charge
It is clear that our nation’s hospitals will be incentivized and mandated to create processes and produce outcomes based on national performance standards and data. This will require a re-engineering of the hospitals and their medical staffs. Hospitalists will be charged (as part of their job description) to be physician leaders in making this happen. Unfortunately, their training in medical school or residency has not provided them with all the skills in QI measurement or implementation that they will need. That is where SHM comes in.
Whether developing tools and workbooks or developing educational and implementation strategies, SHM will be innovative and on the cutting edge. Just as importantly, SHM will be on the lookout for like-minded organizations to partner with to raise the visibility and necessity of QI. We will not shy away from helping to set performance standards just because they may create initial discomfort with some of our members. We will not back off from developing creative strategies to push QI down to more than 4,000 acute care hospitals just because it is difficult and at times daunting.
Hospitalists are on the front line of change. Our patients, our institutions, our fellow physicians, and the other members of the healthcare team want and need a better system. There is no standing still. There is no turning back. The time is now. It is our turn, and hospitalists, with SHM’s help, are ready to step up and make it happen. TH
Dr. Wellikson has been CEO of SHM since 2000.
We are in the midst of a true evolution of how hospitals will approach creating a culture of quality. The drivers for process improvement and management of resources have traditionally been more concerned with full occupancy and risk management, but now many external forces are raising quality improvement as a potential core competency for our nation’s hospitals.
With the push of the Institute for Healthcare Improvement (IHI), Leapfrog, and even Medicare, hospitals now must grapple with a culture change—one in which measurement and reporting of outcomes and processes will become, if not truly job one, at least in the top five. The fact that a hospital’s revenue stream through pay-for-performance (P4P) bonuses and its reputation by public reporting are at stake only serve to create a real immediacy in the coming years.
A recent SHM survey of the leaders of hospital medicine groups (HMGs) has shown that, once again, hospitalists find themselves right smack in the middle of quality improvement.
Survey Says
More than 41% of hospitalist leaders report that their HMG has a quality incentive program. This is even more prevalent at hospitals participating in P4P programs, where 60% of HMGs have quality incentives to align priorities. It is a hallmark of hospitalist groups to place a particular emphasis on the process and system improvement necessary for true measurable quality improvement. Many times, this improvement takes time away from direct and billable patient care.
Pointing to the relatively early stage in the adoption of P4P, this same survey reported that only 29% of HMGs were working in hospitals that participated in P4P programs, while 56% report their hospital did not have any P4P programs in place.
As we enter 2007, it is clear that while a small percentage of hospitals have embraced P4P the majority of hospitals are—at best—on the sidelines or still in planning mode. But those who are active in P4P have engaged their hospitalists to help them meet their goals. And everything that is coming out in the literature commonly read by the hospital C-suite promotes the promise of more reimbursement from the insurance industry and Medicare, leading to the conclusion that P4P and rewarding performance will increase in the near term.
What Can SHM Do for You?
Positioning hospitalists to play a key role in quality improvement, SHM has launched a number of initiatives and partnerships to provide hospitalists with the tools they need to help their hospitals to succeed.
As a framework of tools, SHM has now built six Web-based Quality Improvement Resource Rooms in VTE, Heart Failure, Stroke, Glycemic Control, Care Transitions in the Elderly, and Antibiotic Resistance. These practical tools and references are now available on the SHM Web site (www.hospitalmedicine.org) as are, in many cases, a comprehensive workbook that helps hospitalists to be the leaders of quality improvement change at their hospitals.
SHM realizes that, while this approach may work for the savvy, experienced quality improvement (QI) implementer, most young hospitalist leaders need a more personal, hands-on approach. With this in mind, SHM has launched its Mentored QI Implementation project. Centered around VTE prevention and supported by funding from Sanofi-Aventis, two senior hospitalist mentors will each work with 15 HMG leaders to take them step by step through the process of implementing a quality improvement process in 2007 and 2008.
To take this hands-on, supportive approach to the next level SHM (with support from a Kettering Foundation grant) will add the capability for on-site consultation—sort of a QI SWAT team that can show up at your hospital and work shoulder to shoulder with hospitalists and other members of the healthcare team to develop and implement processes that will improve patient care.
To further educate and energize hospitalist leaders who have been charged with leading this change, SHM developed the Leadership Academy. To date more than 400 hospitalist leaders have been trained in sold-out small-group sessions during the past two years. The most recent academy was held last month in Orlando, Fla.
SHM provides additional training for those who will implement quality improvement at the Quality Training precourse at the SHM Annual Meeting. In the precourse up to 100 change leaders get hands-on direction, tools, and tricks of the trade to allow them to succeed in their local efforts. The next Quality Training Precourse will be held in small group sessions on May 23, 2007, in Dallas.
The SHM Annual Meeting has consistently been a venue that allows hospitalists to hear from national thought leaders in the quality revolution. In 2006, hospitalists heard from Carolyn Clancy, MD, CEO of the Agency for Healthcare Research and Quality, and Jack Rowe, MD, CEO of Aetna Insurance Company.
At this year’s meeting Jonathan Perlin, MD, PhD, who led the cutting edge QI efforts at Veterans Affairs and who is now bringing innovation to HCA (Nashville, Tenn.), the nation’s largest hospital company, will share his ideas with us. In addition, hospitalists will hear from David Brailer, MD, PhD, President George W. Bush’s first appointee to head up national efforts for health information technology. In addition, SHM’s Bob Wachter, MD, a nationally recognized leader in QI and patient safety, will share his perspectives on hospital medicine. With Drs. Perlin, Brailer, and Wachter, SHM continues its tradition of placing innovations that are changing healthcare for the better front and center at our annual meeting.
As for the future, SHM has submitted a multi-year grant application to the Hartford Foundation (Conn.) to expand our efforts—specifically in developing implementation strategies to improve the care processes and outcomes for the senior population.
One of the key areas that emerged from SHM’s work with the Hartford Foundation is the importance of improving the transitions of care and better coordinating healthcare from the patient’s point of view. This has led SHM to partner with several national organizations to make sense of what has been a squishy subject. SHM is working closely with the American Board of Internal Medicine (ABIM) Foundation on its Stepping Up to the Plate consortium, a group of specialty physicians focusing on best practice strategies in patient-centered transitions, hand-offs, and information transfer.
In addition, SHM is working with the American College of Physicians, the AHRQ, the ABIM, the American Geriatrics Society (AGS), and the Society of General Internal Medicine to hold a National Consensus Conference in 2007 to establish policy on transitions of care. The conference will involve a broad range of stakeholders and may very well lead to the establishment of performance standards that can be applied directly to patient care.
Also SHM has been working with the Case Management Society of America to bring together the broader healthcare team on its National Transitions of Care Coalition (NTOCC) project. NTOCC includes pharmacists (American Society of Health-System Pharmacists), the C-suite (American College of Healthcare Executives), social workers (National Association of Social Workers), geriatricians (the AGS), the Joint Commission on Accreditation of Healthcare Organizations, and others. NTOCC plans to develop clear tools, guidelines, and pathways for consistent communication among patients, providers, and payers throughout the care continuum, and to look at aligning incentives for use of these tools and resources.
SHM has also worked with recognized leaders in action-oriented campaigns in QI, including the IHI—first on its “100,000 Lives Campaign,” and more recently on its “5 Million Lives Campaign.” In fact, leadership from only one medical professional society—SHM—was on the stage with Don Berwick for IHI’s national announcement at the December 2006 IHI national meeting in Orlando.
Hospitalists Lead the Charge
It is clear that our nation’s hospitals will be incentivized and mandated to create processes and produce outcomes based on national performance standards and data. This will require a re-engineering of the hospitals and their medical staffs. Hospitalists will be charged (as part of their job description) to be physician leaders in making this happen. Unfortunately, their training in medical school or residency has not provided them with all the skills in QI measurement or implementation that they will need. That is where SHM comes in.
Whether developing tools and workbooks or developing educational and implementation strategies, SHM will be innovative and on the cutting edge. Just as importantly, SHM will be on the lookout for like-minded organizations to partner with to raise the visibility and necessity of QI. We will not shy away from helping to set performance standards just because they may create initial discomfort with some of our members. We will not back off from developing creative strategies to push QI down to more than 4,000 acute care hospitals just because it is difficult and at times daunting.
Hospitalists are on the front line of change. Our patients, our institutions, our fellow physicians, and the other members of the healthcare team want and need a better system. There is no standing still. There is no turning back. The time is now. It is our turn, and hospitalists, with SHM’s help, are ready to step up and make it happen. TH
Dr. Wellikson has been CEO of SHM since 2000.
We are in the midst of a true evolution of how hospitals will approach creating a culture of quality. The drivers for process improvement and management of resources have traditionally been more concerned with full occupancy and risk management, but now many external forces are raising quality improvement as a potential core competency for our nation’s hospitals.
With the push of the Institute for Healthcare Improvement (IHI), Leapfrog, and even Medicare, hospitals now must grapple with a culture change—one in which measurement and reporting of outcomes and processes will become, if not truly job one, at least in the top five. The fact that a hospital’s revenue stream through pay-for-performance (P4P) bonuses and its reputation by public reporting are at stake only serve to create a real immediacy in the coming years.
A recent SHM survey of the leaders of hospital medicine groups (HMGs) has shown that, once again, hospitalists find themselves right smack in the middle of quality improvement.
Survey Says
More than 41% of hospitalist leaders report that their HMG has a quality incentive program. This is even more prevalent at hospitals participating in P4P programs, where 60% of HMGs have quality incentives to align priorities. It is a hallmark of hospitalist groups to place a particular emphasis on the process and system improvement necessary for true measurable quality improvement. Many times, this improvement takes time away from direct and billable patient care.
Pointing to the relatively early stage in the adoption of P4P, this same survey reported that only 29% of HMGs were working in hospitals that participated in P4P programs, while 56% report their hospital did not have any P4P programs in place.
As we enter 2007, it is clear that while a small percentage of hospitals have embraced P4P the majority of hospitals are—at best—on the sidelines or still in planning mode. But those who are active in P4P have engaged their hospitalists to help them meet their goals. And everything that is coming out in the literature commonly read by the hospital C-suite promotes the promise of more reimbursement from the insurance industry and Medicare, leading to the conclusion that P4P and rewarding performance will increase in the near term.
What Can SHM Do for You?
Positioning hospitalists to play a key role in quality improvement, SHM has launched a number of initiatives and partnerships to provide hospitalists with the tools they need to help their hospitals to succeed.
As a framework of tools, SHM has now built six Web-based Quality Improvement Resource Rooms in VTE, Heart Failure, Stroke, Glycemic Control, Care Transitions in the Elderly, and Antibiotic Resistance. These practical tools and references are now available on the SHM Web site (www.hospitalmedicine.org) as are, in many cases, a comprehensive workbook that helps hospitalists to be the leaders of quality improvement change at their hospitals.
SHM realizes that, while this approach may work for the savvy, experienced quality improvement (QI) implementer, most young hospitalist leaders need a more personal, hands-on approach. With this in mind, SHM has launched its Mentored QI Implementation project. Centered around VTE prevention and supported by funding from Sanofi-Aventis, two senior hospitalist mentors will each work with 15 HMG leaders to take them step by step through the process of implementing a quality improvement process in 2007 and 2008.
To take this hands-on, supportive approach to the next level SHM (with support from a Kettering Foundation grant) will add the capability for on-site consultation—sort of a QI SWAT team that can show up at your hospital and work shoulder to shoulder with hospitalists and other members of the healthcare team to develop and implement processes that will improve patient care.
To further educate and energize hospitalist leaders who have been charged with leading this change, SHM developed the Leadership Academy. To date more than 400 hospitalist leaders have been trained in sold-out small-group sessions during the past two years. The most recent academy was held last month in Orlando, Fla.
SHM provides additional training for those who will implement quality improvement at the Quality Training precourse at the SHM Annual Meeting. In the precourse up to 100 change leaders get hands-on direction, tools, and tricks of the trade to allow them to succeed in their local efforts. The next Quality Training Precourse will be held in small group sessions on May 23, 2007, in Dallas.
The SHM Annual Meeting has consistently been a venue that allows hospitalists to hear from national thought leaders in the quality revolution. In 2006, hospitalists heard from Carolyn Clancy, MD, CEO of the Agency for Healthcare Research and Quality, and Jack Rowe, MD, CEO of Aetna Insurance Company.
At this year’s meeting Jonathan Perlin, MD, PhD, who led the cutting edge QI efforts at Veterans Affairs and who is now bringing innovation to HCA (Nashville, Tenn.), the nation’s largest hospital company, will share his ideas with us. In addition, hospitalists will hear from David Brailer, MD, PhD, President George W. Bush’s first appointee to head up national efforts for health information technology. In addition, SHM’s Bob Wachter, MD, a nationally recognized leader in QI and patient safety, will share his perspectives on hospital medicine. With Drs. Perlin, Brailer, and Wachter, SHM continues its tradition of placing innovations that are changing healthcare for the better front and center at our annual meeting.
As for the future, SHM has submitted a multi-year grant application to the Hartford Foundation (Conn.) to expand our efforts—specifically in developing implementation strategies to improve the care processes and outcomes for the senior population.
One of the key areas that emerged from SHM’s work with the Hartford Foundation is the importance of improving the transitions of care and better coordinating healthcare from the patient’s point of view. This has led SHM to partner with several national organizations to make sense of what has been a squishy subject. SHM is working closely with the American Board of Internal Medicine (ABIM) Foundation on its Stepping Up to the Plate consortium, a group of specialty physicians focusing on best practice strategies in patient-centered transitions, hand-offs, and information transfer.
In addition, SHM is working with the American College of Physicians, the AHRQ, the ABIM, the American Geriatrics Society (AGS), and the Society of General Internal Medicine to hold a National Consensus Conference in 2007 to establish policy on transitions of care. The conference will involve a broad range of stakeholders and may very well lead to the establishment of performance standards that can be applied directly to patient care.
Also SHM has been working with the Case Management Society of America to bring together the broader healthcare team on its National Transitions of Care Coalition (NTOCC) project. NTOCC includes pharmacists (American Society of Health-System Pharmacists), the C-suite (American College of Healthcare Executives), social workers (National Association of Social Workers), geriatricians (the AGS), the Joint Commission on Accreditation of Healthcare Organizations, and others. NTOCC plans to develop clear tools, guidelines, and pathways for consistent communication among patients, providers, and payers throughout the care continuum, and to look at aligning incentives for use of these tools and resources.
SHM has also worked with recognized leaders in action-oriented campaigns in QI, including the IHI—first on its “100,000 Lives Campaign,” and more recently on its “5 Million Lives Campaign.” In fact, leadership from only one medical professional society—SHM—was on the stage with Don Berwick for IHI’s national announcement at the December 2006 IHI national meeting in Orlando.
Hospitalists Lead the Charge
It is clear that our nation’s hospitals will be incentivized and mandated to create processes and produce outcomes based on national performance standards and data. This will require a re-engineering of the hospitals and their medical staffs. Hospitalists will be charged (as part of their job description) to be physician leaders in making this happen. Unfortunately, their training in medical school or residency has not provided them with all the skills in QI measurement or implementation that they will need. That is where SHM comes in.
Whether developing tools and workbooks or developing educational and implementation strategies, SHM will be innovative and on the cutting edge. Just as importantly, SHM will be on the lookout for like-minded organizations to partner with to raise the visibility and necessity of QI. We will not shy away from helping to set performance standards just because they may create initial discomfort with some of our members. We will not back off from developing creative strategies to push QI down to more than 4,000 acute care hospitals just because it is difficult and at times daunting.
Hospitalists are on the front line of change. Our patients, our institutions, our fellow physicians, and the other members of the healthcare team want and need a better system. There is no standing still. There is no turning back. The time is now. It is our turn, and hospitalists, with SHM’s help, are ready to step up and make it happen. TH
Dr. Wellikson has been CEO of SHM since 2000.
A Fine Formation
In the football-loving state of Michigan, legendary athletes take their cues from a coach and map their strategies for one big group effort. But Michigan is also home to what may be the first-ever homegrown regional consortium for patient safety and quality improvement—and in this case—after a huddle each team member gets to call his own plays.
The Hospitalists as Emerging Leaders in Patient Safety (HELPS) Consortium of Southeastern Michigan (funded by a grant from the Blue Cross Blue Shield of Michigan Foundation) includes representatives from nine regional hospitalist programs representing 11 hospitals and approximately 75,000 patients.1
The participants in this program identify proven patient safety practices and facilitate widespread dissemination of those practices among hospitalists.
The member institutions include academic medical centers, large private teaching and non-teaching hospitals, federal facilities, and urban and rural hospitals.
Each institution is represented by a hospitalist—usually the director of the hospitalist program or the individual most interested in and familiar with quality improvement—and a representative from quality improvement or patient safety. The issues they have addressed, which emerged from a variety of sources, such as the Agency of Healthcare Research and Quality, the National Quality Forum, and the Joint Commission on Accreditation of Healthcare Organizations, are those that are commonly encountered in hospitalist practice. These physicians “are bridging the gap between that which they know to be effective and that which is actually practiced.”1
HELPS builds on the experience of medical professionals who have united geographically dispersed physicians from the same specialty to boost quality. The HELPS consortium also aids participating institutions in evaluating outcomes after implementing a targeted patient safety practice, thereby allowing rapid cycle improvement while identifying factors associated with success.
“We have gotten the work that is being done by these different organizations out there, brought it up a notch in certain situations—we like to think—and have gotten it effectively disseminated to a larger group of hospitalists,” says Scott Flanders, MD, an associate professor of medicine at the University of Michigan (Ann Arbor), director of the hospital medicine program there, and an SHM board member.
Where They Are
The consortium is about three-quarters of the way through its overall estimated project period, says Dr. Flanders. It originally planned to have nine gatherings over two years. (See Table 1, p. 35.) To date the consortium has held seven of those sessions and have met roughly every two to three months. End-of-life care and the final wrap-up are the only sessions still to be completed.
The individual sites took on projects that included reducing errors with heparin use in hospitalized patients, reducing falls in hospitalized patients, improving care transitions (a collaborative multidisciplinary approach), reducing unnecessary ICU admission and preventing in-hospital cardiac arrests, reducing urinary catheter infections, improving rates of appropriate deep vein thrombosis prophylaxis, and implementing best practices for reducing central line infections. A national expert conducted a session on implementing a program to reduce perioperative cardiovascular events while ensuring the appropriate use of perioperative beta-blockers.
Challenges and Lessons Learned
From the outset, the HELPS group knew that its primary challenge would be to fulfill the intention to meet as a complete group four or five times per year. “There aren’t a lot of hospitalists who have big parts of their jobs carved out for dedicated time to work on quality improvement research or patient safety,” says Dr. Flanders. “It’s part of what we do in our day, but in terms of taking on a big project, designing it, implementing it, and measuring its effect, it is hard to do in the day-to-day job of most hospitalist groups.”
He suspects that hospitalists frequently help steering committees address certain issues, “but it may not be the individual hospitalist group that is managing or driving the quality issue for an entire hospital or health system.” The HELPS physicians knew that if they could surmount the scheduling challenge, however, they would have a terrific opportunity to learn from each other and move their individual institutional patient safety initiatives forward.
They also knew that the majority of hospitalized patients receive care in community hospitals and that the culture of a community hospital differed dramatically from a tertiary-care academic medical center. Interventions would need to be tried at varied settings, and HELPS would allow that to happen. In addition, few clinically active hospitalists have developed the research expertise to evaluate an intervention rigorously at their own institution, yet decision makers often require such an evaluation when they are considering adopting a new intervention. Using the resources of an academic center such as the University of Michigan, where evaluative and methodologic expertise is available, allowed them to facilitate a resolution for that problem. “As physicians, we are helping [smaller hospitals] by facilitating data collection and data analysis for their ongoing projects,” says Dr. Flanders.
Another challenge the hospitalists faced pertained to the relative instability of hospital medicine compared with other specialties. For instance, it is probably far easier for the members of the consortium of cardiology groups working on best practices for managing acute myocardial infarction to find time to work together. In contrast, because hospital medicine is a relatively new specialty, “we are seeing a certain amount of instability,” explains Dr. Flanders. “Of our nine involved health systems, at least two had dramatic organizational and structural changes within their hospital medicine group over the last year and a half.” One hospital medicine director left, with repercussions in several areas, and, in another group, the practice was sold to a large physician management company, which meant that the HELPS data that had been collected was no longer owned by the [original] group, making their activities more complex.
What They’ve Done So Far
Dr. Flanders is not aware of any other groups of physicians from another state who have undertaken such a project. The Institute for Healthcare Improvement’s “100,000 Lives Campaign” may be similar in some ways, focusing on a few key topic areas. The Michigan Keystone Project, which concentrated on various ICU patient safety topics, is another example of a regional consortium. “But the difference is that they basically drive the agenda,” he says. “They say, ‘This is what we want you all to do, and let’s figure out how we can all do it.’ In our case, we focused on some key areas, but we did not dictate what the project was.”
The following brief recaps represent some of the projects undertaken by consortium member sites.
Falls
The University of Michigan-affiliated Ann Arbor Veterans Affairs (VA) Hospital, where Sanjay Saint, MD, MPH, is a hospitalist, has many elderly and cognitively impaired patients, so preventing falls is a big issue. “My responsibility isn’t to prevent falls but to share these best practices with others in my organization,” he says. “In fact, each project team points out where to look with a certain problem but not necessarily what to do.”
Dr. Saint brought up the issue of mattresses with lipped/raised edges to prevent patients from rolling out of bed. Following that, at least one other consortium hospital suggested to its fall prevention group that they explore the use of these lipped mattresses.
Bed alarms were another problem. Participants shared a common problem: Often, nurses wouldn’t hear a patient’s alarm go off. Other providers might reset them, but if they neglected to let the assigned nurse know the patient was calling, the patient might get tired of waiting, attempt to get out of bed, and sustain a fall. Consequently, providers in most institutions thought the alarms were not useful. But one institution identified a novel way to use bed alarms: attaching them to the nurse’s pager. Now, when the alarm goes off, it alerts the appropriate nurse directly, and because that nurse is responsible for resetting the alarm, she knows that the patient has called and needs help.
Changing Names: CARE Assistants
To avoid the use of physical or chemical restraints, many institutions have resorted to hiring “sitters” who stay at the bedside of confused or delirious patients to calm them; if patients try to get out of bed, sitters are there to coax them back in. A number of HELPS institutions shared the idea that using the term “sitter” might have been inadvertently encouraging inactivity: Too many sitters were doing just that, sitting all day, often watching television.
One of the collaborative sites now calls these employees CARE assistants, an acronym for Caring Alternative to a Restraint-free Environment. The group has predicted that calling them something different will inspire these people to “do more caring and less sitting,” says Dr. Saint. After a HELPS session, Dr. Saint submitted this idea to the key decision makers at the VA. “I could have tried by myself to resolve this dilemma for years and not come up with that idea,” he says. “Why not just take what they’ve done and modify it to suit your own environment?”
Weighty Problem: Heparin Dosing
One hospital in the consortium conducted a project on medication safety that focused on appropriate use of heparin in hospitalized patients. When the site’s hospitalists began studying the problems they were having, they realized that the weights they were using for dosing decisions were being generated in the emergency department (ED). Studying it further, they saw that, most of the time, those patients weren’t actually being weighed; nurses were simply estimating their weights. Having traced the problem to the ED, they were then able to intervene, fix the problem, and show that by doing so their rates of bleeding complications from inappropriate dosing of anticoagulants improved.
At his own institution, Dr. Flanders was participating in a group committee meeting discussing this problem. Consequently, “I was able to ask, ‘Have we looked at weights [being assessed] in the emergency department?’ Everyone involved with that project said, ‘No, why?’ And, sure enough, a similar problem existed.”
Care Transitions and Multidisciplinary Rounding
One member-team of the consortium was able to come up with a multidisciplinary team that met and rounded on patients each day and focused on the care transitions. They were able to dramatically improve staff communication, the overall discharge process, and patient satisfaction. As a result of what he learned of their successes, Dr. Flanders’ institution plans to use a similar strategy to enhance communication among healthcare providers involved in the discharge process on their hospitalist unit.
Rapid Response Teams and Input from Residents
“It’s very helpful to hear, from another site, the challenges and benefits of having hospitalists involved with the rapid response teams,” says Dr. Saint. “How did they operationalize it? What were the remaining challenges? What outcome measures did they use? How do you assess whether it’s worth the cost? What do residents think about this?
This last point turned out to be a valuable question to ask. The group included some residents at the site where this project was piloted and had a fruitful discussion. Adding the perspective of residents along with faculty, says Dr. Saint, as well as a couple of nurses and quality care managers, allows a synergy and combination of ideas that led to effective solutions. “Those are exactly the individuals who need to be around a table to overcome some of the challenges.” They have also considered inviting nursing students. “Before they get inculcated in thinking a certain way,” he says, “why not hear what they have to say?”
Dr. Saint believes, however, that this is not a step to be taken lightly. If you are going to include people, “then you have to act on their suggestions or at least hear them out and say why you’re not going to take their suggestions because a good way to get people to become jaded is to listen to their feedback and then just ignore it.”
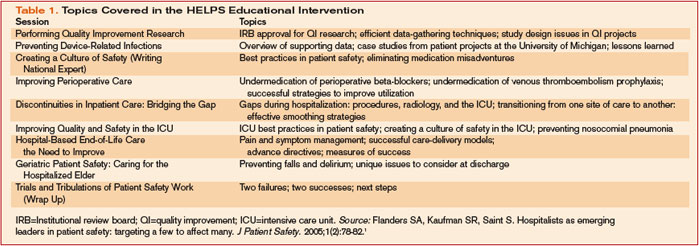
Calling in Outside Experts
To focus on the issue of preventing hospital-acquired urinary tract infections (UTIs), the consortium invited Russell Olmstead, MPH, an infection control expert and epidemiologist at one of the HELPS sites and past president of the Michigan Society of Infection Control.
“We’d like to do a Keystone[-type] UTI project,” says Dr. Saint, referring to the federally funded statewide three-year initiative, conducted in collaboration with the Michigan Hospital Association and Johns Hopkins Research and Safety Group, that focused on applying evidence-based medicine and quality improvement efforts to prevent ventilator-associated pneumonia and central line-related infections. “We’ve called it the Bladder Bundle; that is, you bundle a group of practices together, and you give the hospitalists who want to participate a toolkit in order to roll this out.”
Although the details still need to be finalized, the project would include ensuring that patients have appropriate indication for an indwelling catheter, that the indwelling catheter is inserted in an aseptic manner, that there was some type of assessment of discontinuation after a certain amount of time, and that alternatives to an indwelling catheter are considered.
Another expert consulting with the consortium was Peter Lindenauer, MD, MSc, with the Division of Healthcare Quality, Baystate Medical Center, Springfield, Mass., and the Department of Medicine, Tufts University School of Medicine, Boston. Dr. Lindenauer came to discuss lessons he and his colleagues have learned from efforts to improve appropriate perioperative beta blocker use.
The final HELPS wrap-up session for the group will include another nationally renowned expert in patient safety.
SHARP: Research Translated into Practice
Another project initiated by the Michigan hospitalists will generate and disseminate new knowledge in the realm of clinical research. The Specialist-Hospitalist Allied Research Program (SHARP), directed by Dr. Flanders and Brahmajee Nallamothu, MD, MPH, an interventional cardiologist, is the first specialist-hospitalist clinical research program in the United States. This hospitalist delivery model alters the way clinical problems are approached and creates opportunities and challenges in implementing best practices, including those surrounding drugs and devices. A successful clinical and translational research program will combine specialists and hospitalists working collaboratively to better understand the best ways to care for inpatients.
This project is similar to what cardiology and oncology specialties have done over the last several decades, says Dr. Saint. In the future, he foresees that the NIH will increasingly focus on translating research into practice in diverse settings. Both specialists and hospitalists who work in a particular area together—such as prevention of lower extremity clots or of nosocomial infections—can use the health consortium to roll out protocols and studies in order to tackle some of the important inpatient topics.
SHARP was awarded funding through the University of Michigan Department of Medicine and was scheduled to take off in February. “Our hope is that we will be able to take advantage of and build upon the health collaborative that we have and bring in our subspecialty expertise to help inform clinical investigations,” says Dr. Saint.
Where They’re Going
Both Dr. Flanders and Dr. Saint are pleased about the HELPS consortium’s progress so far. They believe that they have found a group of people who are interested in patient safety and are willing to learn from one another and that they have done an excellent job of disseminating the best practices they have been exploring.
Ultimately, their goal is to grow this into a “more robust clinical research consortium,” says Dr. Flanders. Instead of disseminating best practices and focusing on just a few targeted patient safety quality improvement areas, they will begin to take on studies that could center around patient safety and quality improvement but will also move toward multi-center projects that might address issues related to management of common clinical problems that hospitalists are now managing and focusing on.
“We’re really excited about what we have been able to accomplish,” he says. “We’ve learned a lot about the challenges of doing this, and of course it’s never perfect. We wish we could always do more, but we’ve learned why we can’t. That will be helpful in future projects and helpful for others who are trying to tackle this same problem.” TH
Reference
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005;1(2):78-82.
In the football-loving state of Michigan, legendary athletes take their cues from a coach and map their strategies for one big group effort. But Michigan is also home to what may be the first-ever homegrown regional consortium for patient safety and quality improvement—and in this case—after a huddle each team member gets to call his own plays.
The Hospitalists as Emerging Leaders in Patient Safety (HELPS) Consortium of Southeastern Michigan (funded by a grant from the Blue Cross Blue Shield of Michigan Foundation) includes representatives from nine regional hospitalist programs representing 11 hospitals and approximately 75,000 patients.1
The participants in this program identify proven patient safety practices and facilitate widespread dissemination of those practices among hospitalists.
The member institutions include academic medical centers, large private teaching and non-teaching hospitals, federal facilities, and urban and rural hospitals.
Each institution is represented by a hospitalist—usually the director of the hospitalist program or the individual most interested in and familiar with quality improvement—and a representative from quality improvement or patient safety. The issues they have addressed, which emerged from a variety of sources, such as the Agency of Healthcare Research and Quality, the National Quality Forum, and the Joint Commission on Accreditation of Healthcare Organizations, are those that are commonly encountered in hospitalist practice. These physicians “are bridging the gap between that which they know to be effective and that which is actually practiced.”1
HELPS builds on the experience of medical professionals who have united geographically dispersed physicians from the same specialty to boost quality. The HELPS consortium also aids participating institutions in evaluating outcomes after implementing a targeted patient safety practice, thereby allowing rapid cycle improvement while identifying factors associated with success.
“We have gotten the work that is being done by these different organizations out there, brought it up a notch in certain situations—we like to think—and have gotten it effectively disseminated to a larger group of hospitalists,” says Scott Flanders, MD, an associate professor of medicine at the University of Michigan (Ann Arbor), director of the hospital medicine program there, and an SHM board member.
Where They Are
The consortium is about three-quarters of the way through its overall estimated project period, says Dr. Flanders. It originally planned to have nine gatherings over two years. (See Table 1, p. 35.) To date the consortium has held seven of those sessions and have met roughly every two to three months. End-of-life care and the final wrap-up are the only sessions still to be completed.
The individual sites took on projects that included reducing errors with heparin use in hospitalized patients, reducing falls in hospitalized patients, improving care transitions (a collaborative multidisciplinary approach), reducing unnecessary ICU admission and preventing in-hospital cardiac arrests, reducing urinary catheter infections, improving rates of appropriate deep vein thrombosis prophylaxis, and implementing best practices for reducing central line infections. A national expert conducted a session on implementing a program to reduce perioperative cardiovascular events while ensuring the appropriate use of perioperative beta-blockers.
Challenges and Lessons Learned
From the outset, the HELPS group knew that its primary challenge would be to fulfill the intention to meet as a complete group four or five times per year. “There aren’t a lot of hospitalists who have big parts of their jobs carved out for dedicated time to work on quality improvement research or patient safety,” says Dr. Flanders. “It’s part of what we do in our day, but in terms of taking on a big project, designing it, implementing it, and measuring its effect, it is hard to do in the day-to-day job of most hospitalist groups.”
He suspects that hospitalists frequently help steering committees address certain issues, “but it may not be the individual hospitalist group that is managing or driving the quality issue for an entire hospital or health system.” The HELPS physicians knew that if they could surmount the scheduling challenge, however, they would have a terrific opportunity to learn from each other and move their individual institutional patient safety initiatives forward.
They also knew that the majority of hospitalized patients receive care in community hospitals and that the culture of a community hospital differed dramatically from a tertiary-care academic medical center. Interventions would need to be tried at varied settings, and HELPS would allow that to happen. In addition, few clinically active hospitalists have developed the research expertise to evaluate an intervention rigorously at their own institution, yet decision makers often require such an evaluation when they are considering adopting a new intervention. Using the resources of an academic center such as the University of Michigan, where evaluative and methodologic expertise is available, allowed them to facilitate a resolution for that problem. “As physicians, we are helping [smaller hospitals] by facilitating data collection and data analysis for their ongoing projects,” says Dr. Flanders.
Another challenge the hospitalists faced pertained to the relative instability of hospital medicine compared with other specialties. For instance, it is probably far easier for the members of the consortium of cardiology groups working on best practices for managing acute myocardial infarction to find time to work together. In contrast, because hospital medicine is a relatively new specialty, “we are seeing a certain amount of instability,” explains Dr. Flanders. “Of our nine involved health systems, at least two had dramatic organizational and structural changes within their hospital medicine group over the last year and a half.” One hospital medicine director left, with repercussions in several areas, and, in another group, the practice was sold to a large physician management company, which meant that the HELPS data that had been collected was no longer owned by the [original] group, making their activities more complex.
What They’ve Done So Far
Dr. Flanders is not aware of any other groups of physicians from another state who have undertaken such a project. The Institute for Healthcare Improvement’s “100,000 Lives Campaign” may be similar in some ways, focusing on a few key topic areas. The Michigan Keystone Project, which concentrated on various ICU patient safety topics, is another example of a regional consortium. “But the difference is that they basically drive the agenda,” he says. “They say, ‘This is what we want you all to do, and let’s figure out how we can all do it.’ In our case, we focused on some key areas, but we did not dictate what the project was.”
The following brief recaps represent some of the projects undertaken by consortium member sites.
Falls
The University of Michigan-affiliated Ann Arbor Veterans Affairs (VA) Hospital, where Sanjay Saint, MD, MPH, is a hospitalist, has many elderly and cognitively impaired patients, so preventing falls is a big issue. “My responsibility isn’t to prevent falls but to share these best practices with others in my organization,” he says. “In fact, each project team points out where to look with a certain problem but not necessarily what to do.”
Dr. Saint brought up the issue of mattresses with lipped/raised edges to prevent patients from rolling out of bed. Following that, at least one other consortium hospital suggested to its fall prevention group that they explore the use of these lipped mattresses.
Bed alarms were another problem. Participants shared a common problem: Often, nurses wouldn’t hear a patient’s alarm go off. Other providers might reset them, but if they neglected to let the assigned nurse know the patient was calling, the patient might get tired of waiting, attempt to get out of bed, and sustain a fall. Consequently, providers in most institutions thought the alarms were not useful. But one institution identified a novel way to use bed alarms: attaching them to the nurse’s pager. Now, when the alarm goes off, it alerts the appropriate nurse directly, and because that nurse is responsible for resetting the alarm, she knows that the patient has called and needs help.
Changing Names: CARE Assistants
To avoid the use of physical or chemical restraints, many institutions have resorted to hiring “sitters” who stay at the bedside of confused or delirious patients to calm them; if patients try to get out of bed, sitters are there to coax them back in. A number of HELPS institutions shared the idea that using the term “sitter” might have been inadvertently encouraging inactivity: Too many sitters were doing just that, sitting all day, often watching television.
One of the collaborative sites now calls these employees CARE assistants, an acronym for Caring Alternative to a Restraint-free Environment. The group has predicted that calling them something different will inspire these people to “do more caring and less sitting,” says Dr. Saint. After a HELPS session, Dr. Saint submitted this idea to the key decision makers at the VA. “I could have tried by myself to resolve this dilemma for years and not come up with that idea,” he says. “Why not just take what they’ve done and modify it to suit your own environment?”
Weighty Problem: Heparin Dosing
One hospital in the consortium conducted a project on medication safety that focused on appropriate use of heparin in hospitalized patients. When the site’s hospitalists began studying the problems they were having, they realized that the weights they were using for dosing decisions were being generated in the emergency department (ED). Studying it further, they saw that, most of the time, those patients weren’t actually being weighed; nurses were simply estimating their weights. Having traced the problem to the ED, they were then able to intervene, fix the problem, and show that by doing so their rates of bleeding complications from inappropriate dosing of anticoagulants improved.
At his own institution, Dr. Flanders was participating in a group committee meeting discussing this problem. Consequently, “I was able to ask, ‘Have we looked at weights [being assessed] in the emergency department?’ Everyone involved with that project said, ‘No, why?’ And, sure enough, a similar problem existed.”
Care Transitions and Multidisciplinary Rounding
One member-team of the consortium was able to come up with a multidisciplinary team that met and rounded on patients each day and focused on the care transitions. They were able to dramatically improve staff communication, the overall discharge process, and patient satisfaction. As a result of what he learned of their successes, Dr. Flanders’ institution plans to use a similar strategy to enhance communication among healthcare providers involved in the discharge process on their hospitalist unit.
Rapid Response Teams and Input from Residents
“It’s very helpful to hear, from another site, the challenges and benefits of having hospitalists involved with the rapid response teams,” says Dr. Saint. “How did they operationalize it? What were the remaining challenges? What outcome measures did they use? How do you assess whether it’s worth the cost? What do residents think about this?
This last point turned out to be a valuable question to ask. The group included some residents at the site where this project was piloted and had a fruitful discussion. Adding the perspective of residents along with faculty, says Dr. Saint, as well as a couple of nurses and quality care managers, allows a synergy and combination of ideas that led to effective solutions. “Those are exactly the individuals who need to be around a table to overcome some of the challenges.” They have also considered inviting nursing students. “Before they get inculcated in thinking a certain way,” he says, “why not hear what they have to say?”
Dr. Saint believes, however, that this is not a step to be taken lightly. If you are going to include people, “then you have to act on their suggestions or at least hear them out and say why you’re not going to take their suggestions because a good way to get people to become jaded is to listen to their feedback and then just ignore it.”
Calling in Outside Experts
To focus on the issue of preventing hospital-acquired urinary tract infections (UTIs), the consortium invited Russell Olmstead, MPH, an infection control expert and epidemiologist at one of the HELPS sites and past president of the Michigan Society of Infection Control.
“We’d like to do a Keystone[-type] UTI project,” says Dr. Saint, referring to the federally funded statewide three-year initiative, conducted in collaboration with the Michigan Hospital Association and Johns Hopkins Research and Safety Group, that focused on applying evidence-based medicine and quality improvement efforts to prevent ventilator-associated pneumonia and central line-related infections. “We’ve called it the Bladder Bundle; that is, you bundle a group of practices together, and you give the hospitalists who want to participate a toolkit in order to roll this out.”
Although the details still need to be finalized, the project would include ensuring that patients have appropriate indication for an indwelling catheter, that the indwelling catheter is inserted in an aseptic manner, that there was some type of assessment of discontinuation after a certain amount of time, and that alternatives to an indwelling catheter are considered.
Another expert consulting with the consortium was Peter Lindenauer, MD, MSc, with the Division of Healthcare Quality, Baystate Medical Center, Springfield, Mass., and the Department of Medicine, Tufts University School of Medicine, Boston. Dr. Lindenauer came to discuss lessons he and his colleagues have learned from efforts to improve appropriate perioperative beta blocker use.
The final HELPS wrap-up session for the group will include another nationally renowned expert in patient safety.
SHARP: Research Translated into Practice
Another project initiated by the Michigan hospitalists will generate and disseminate new knowledge in the realm of clinical research. The Specialist-Hospitalist Allied Research Program (SHARP), directed by Dr. Flanders and Brahmajee Nallamothu, MD, MPH, an interventional cardiologist, is the first specialist-hospitalist clinical research program in the United States. This hospitalist delivery model alters the way clinical problems are approached and creates opportunities and challenges in implementing best practices, including those surrounding drugs and devices. A successful clinical and translational research program will combine specialists and hospitalists working collaboratively to better understand the best ways to care for inpatients.
This project is similar to what cardiology and oncology specialties have done over the last several decades, says Dr. Saint. In the future, he foresees that the NIH will increasingly focus on translating research into practice in diverse settings. Both specialists and hospitalists who work in a particular area together—such as prevention of lower extremity clots or of nosocomial infections—can use the health consortium to roll out protocols and studies in order to tackle some of the important inpatient topics.
SHARP was awarded funding through the University of Michigan Department of Medicine and was scheduled to take off in February. “Our hope is that we will be able to take advantage of and build upon the health collaborative that we have and bring in our subspecialty expertise to help inform clinical investigations,” says Dr. Saint.
Where They’re Going
Both Dr. Flanders and Dr. Saint are pleased about the HELPS consortium’s progress so far. They believe that they have found a group of people who are interested in patient safety and are willing to learn from one another and that they have done an excellent job of disseminating the best practices they have been exploring.
Ultimately, their goal is to grow this into a “more robust clinical research consortium,” says Dr. Flanders. Instead of disseminating best practices and focusing on just a few targeted patient safety quality improvement areas, they will begin to take on studies that could center around patient safety and quality improvement but will also move toward multi-center projects that might address issues related to management of common clinical problems that hospitalists are now managing and focusing on.
“We’re really excited about what we have been able to accomplish,” he says. “We’ve learned a lot about the challenges of doing this, and of course it’s never perfect. We wish we could always do more, but we’ve learned why we can’t. That will be helpful in future projects and helpful for others who are trying to tackle this same problem.” TH
Reference
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005;1(2):78-82.
In the football-loving state of Michigan, legendary athletes take their cues from a coach and map their strategies for one big group effort. But Michigan is also home to what may be the first-ever homegrown regional consortium for patient safety and quality improvement—and in this case—after a huddle each team member gets to call his own plays.
The Hospitalists as Emerging Leaders in Patient Safety (HELPS) Consortium of Southeastern Michigan (funded by a grant from the Blue Cross Blue Shield of Michigan Foundation) includes representatives from nine regional hospitalist programs representing 11 hospitals and approximately 75,000 patients.1
The participants in this program identify proven patient safety practices and facilitate widespread dissemination of those practices among hospitalists.
The member institutions include academic medical centers, large private teaching and non-teaching hospitals, federal facilities, and urban and rural hospitals.
Each institution is represented by a hospitalist—usually the director of the hospitalist program or the individual most interested in and familiar with quality improvement—and a representative from quality improvement or patient safety. The issues they have addressed, which emerged from a variety of sources, such as the Agency of Healthcare Research and Quality, the National Quality Forum, and the Joint Commission on Accreditation of Healthcare Organizations, are those that are commonly encountered in hospitalist practice. These physicians “are bridging the gap between that which they know to be effective and that which is actually practiced.”1
HELPS builds on the experience of medical professionals who have united geographically dispersed physicians from the same specialty to boost quality. The HELPS consortium also aids participating institutions in evaluating outcomes after implementing a targeted patient safety practice, thereby allowing rapid cycle improvement while identifying factors associated with success.
“We have gotten the work that is being done by these different organizations out there, brought it up a notch in certain situations—we like to think—and have gotten it effectively disseminated to a larger group of hospitalists,” says Scott Flanders, MD, an associate professor of medicine at the University of Michigan (Ann Arbor), director of the hospital medicine program there, and an SHM board member.
Where They Are
The consortium is about three-quarters of the way through its overall estimated project period, says Dr. Flanders. It originally planned to have nine gatherings over two years. (See Table 1, p. 35.) To date the consortium has held seven of those sessions and have met roughly every two to three months. End-of-life care and the final wrap-up are the only sessions still to be completed.
The individual sites took on projects that included reducing errors with heparin use in hospitalized patients, reducing falls in hospitalized patients, improving care transitions (a collaborative multidisciplinary approach), reducing unnecessary ICU admission and preventing in-hospital cardiac arrests, reducing urinary catheter infections, improving rates of appropriate deep vein thrombosis prophylaxis, and implementing best practices for reducing central line infections. A national expert conducted a session on implementing a program to reduce perioperative cardiovascular events while ensuring the appropriate use of perioperative beta-blockers.
Challenges and Lessons Learned
From the outset, the HELPS group knew that its primary challenge would be to fulfill the intention to meet as a complete group four or five times per year. “There aren’t a lot of hospitalists who have big parts of their jobs carved out for dedicated time to work on quality improvement research or patient safety,” says Dr. Flanders. “It’s part of what we do in our day, but in terms of taking on a big project, designing it, implementing it, and measuring its effect, it is hard to do in the day-to-day job of most hospitalist groups.”
He suspects that hospitalists frequently help steering committees address certain issues, “but it may not be the individual hospitalist group that is managing or driving the quality issue for an entire hospital or health system.” The HELPS physicians knew that if they could surmount the scheduling challenge, however, they would have a terrific opportunity to learn from each other and move their individual institutional patient safety initiatives forward.
They also knew that the majority of hospitalized patients receive care in community hospitals and that the culture of a community hospital differed dramatically from a tertiary-care academic medical center. Interventions would need to be tried at varied settings, and HELPS would allow that to happen. In addition, few clinically active hospitalists have developed the research expertise to evaluate an intervention rigorously at their own institution, yet decision makers often require such an evaluation when they are considering adopting a new intervention. Using the resources of an academic center such as the University of Michigan, where evaluative and methodologic expertise is available, allowed them to facilitate a resolution for that problem. “As physicians, we are helping [smaller hospitals] by facilitating data collection and data analysis for their ongoing projects,” says Dr. Flanders.
Another challenge the hospitalists faced pertained to the relative instability of hospital medicine compared with other specialties. For instance, it is probably far easier for the members of the consortium of cardiology groups working on best practices for managing acute myocardial infarction to find time to work together. In contrast, because hospital medicine is a relatively new specialty, “we are seeing a certain amount of instability,” explains Dr. Flanders. “Of our nine involved health systems, at least two had dramatic organizational and structural changes within their hospital medicine group over the last year and a half.” One hospital medicine director left, with repercussions in several areas, and, in another group, the practice was sold to a large physician management company, which meant that the HELPS data that had been collected was no longer owned by the [original] group, making their activities more complex.
What They’ve Done So Far
Dr. Flanders is not aware of any other groups of physicians from another state who have undertaken such a project. The Institute for Healthcare Improvement’s “100,000 Lives Campaign” may be similar in some ways, focusing on a few key topic areas. The Michigan Keystone Project, which concentrated on various ICU patient safety topics, is another example of a regional consortium. “But the difference is that they basically drive the agenda,” he says. “They say, ‘This is what we want you all to do, and let’s figure out how we can all do it.’ In our case, we focused on some key areas, but we did not dictate what the project was.”
The following brief recaps represent some of the projects undertaken by consortium member sites.
Falls
The University of Michigan-affiliated Ann Arbor Veterans Affairs (VA) Hospital, where Sanjay Saint, MD, MPH, is a hospitalist, has many elderly and cognitively impaired patients, so preventing falls is a big issue. “My responsibility isn’t to prevent falls but to share these best practices with others in my organization,” he says. “In fact, each project team points out where to look with a certain problem but not necessarily what to do.”
Dr. Saint brought up the issue of mattresses with lipped/raised edges to prevent patients from rolling out of bed. Following that, at least one other consortium hospital suggested to its fall prevention group that they explore the use of these lipped mattresses.
Bed alarms were another problem. Participants shared a common problem: Often, nurses wouldn’t hear a patient’s alarm go off. Other providers might reset them, but if they neglected to let the assigned nurse know the patient was calling, the patient might get tired of waiting, attempt to get out of bed, and sustain a fall. Consequently, providers in most institutions thought the alarms were not useful. But one institution identified a novel way to use bed alarms: attaching them to the nurse’s pager. Now, when the alarm goes off, it alerts the appropriate nurse directly, and because that nurse is responsible for resetting the alarm, she knows that the patient has called and needs help.
Changing Names: CARE Assistants
To avoid the use of physical or chemical restraints, many institutions have resorted to hiring “sitters” who stay at the bedside of confused or delirious patients to calm them; if patients try to get out of bed, sitters are there to coax them back in. A number of HELPS institutions shared the idea that using the term “sitter” might have been inadvertently encouraging inactivity: Too many sitters were doing just that, sitting all day, often watching television.
One of the collaborative sites now calls these employees CARE assistants, an acronym for Caring Alternative to a Restraint-free Environment. The group has predicted that calling them something different will inspire these people to “do more caring and less sitting,” says Dr. Saint. After a HELPS session, Dr. Saint submitted this idea to the key decision makers at the VA. “I could have tried by myself to resolve this dilemma for years and not come up with that idea,” he says. “Why not just take what they’ve done and modify it to suit your own environment?”
Weighty Problem: Heparin Dosing
One hospital in the consortium conducted a project on medication safety that focused on appropriate use of heparin in hospitalized patients. When the site’s hospitalists began studying the problems they were having, they realized that the weights they were using for dosing decisions were being generated in the emergency department (ED). Studying it further, they saw that, most of the time, those patients weren’t actually being weighed; nurses were simply estimating their weights. Having traced the problem to the ED, they were then able to intervene, fix the problem, and show that by doing so their rates of bleeding complications from inappropriate dosing of anticoagulants improved.
At his own institution, Dr. Flanders was participating in a group committee meeting discussing this problem. Consequently, “I was able to ask, ‘Have we looked at weights [being assessed] in the emergency department?’ Everyone involved with that project said, ‘No, why?’ And, sure enough, a similar problem existed.”
Care Transitions and Multidisciplinary Rounding
One member-team of the consortium was able to come up with a multidisciplinary team that met and rounded on patients each day and focused on the care transitions. They were able to dramatically improve staff communication, the overall discharge process, and patient satisfaction. As a result of what he learned of their successes, Dr. Flanders’ institution plans to use a similar strategy to enhance communication among healthcare providers involved in the discharge process on their hospitalist unit.
Rapid Response Teams and Input from Residents
“It’s very helpful to hear, from another site, the challenges and benefits of having hospitalists involved with the rapid response teams,” says Dr. Saint. “How did they operationalize it? What were the remaining challenges? What outcome measures did they use? How do you assess whether it’s worth the cost? What do residents think about this?
This last point turned out to be a valuable question to ask. The group included some residents at the site where this project was piloted and had a fruitful discussion. Adding the perspective of residents along with faculty, says Dr. Saint, as well as a couple of nurses and quality care managers, allows a synergy and combination of ideas that led to effective solutions. “Those are exactly the individuals who need to be around a table to overcome some of the challenges.” They have also considered inviting nursing students. “Before they get inculcated in thinking a certain way,” he says, “why not hear what they have to say?”
Dr. Saint believes, however, that this is not a step to be taken lightly. If you are going to include people, “then you have to act on their suggestions or at least hear them out and say why you’re not going to take their suggestions because a good way to get people to become jaded is to listen to their feedback and then just ignore it.”
Calling in Outside Experts
To focus on the issue of preventing hospital-acquired urinary tract infections (UTIs), the consortium invited Russell Olmstead, MPH, an infection control expert and epidemiologist at one of the HELPS sites and past president of the Michigan Society of Infection Control.
“We’d like to do a Keystone[-type] UTI project,” says Dr. Saint, referring to the federally funded statewide three-year initiative, conducted in collaboration with the Michigan Hospital Association and Johns Hopkins Research and Safety Group, that focused on applying evidence-based medicine and quality improvement efforts to prevent ventilator-associated pneumonia and central line-related infections. “We’ve called it the Bladder Bundle; that is, you bundle a group of practices together, and you give the hospitalists who want to participate a toolkit in order to roll this out.”
Although the details still need to be finalized, the project would include ensuring that patients have appropriate indication for an indwelling catheter, that the indwelling catheter is inserted in an aseptic manner, that there was some type of assessment of discontinuation after a certain amount of time, and that alternatives to an indwelling catheter are considered.
Another expert consulting with the consortium was Peter Lindenauer, MD, MSc, with the Division of Healthcare Quality, Baystate Medical Center, Springfield, Mass., and the Department of Medicine, Tufts University School of Medicine, Boston. Dr. Lindenauer came to discuss lessons he and his colleagues have learned from efforts to improve appropriate perioperative beta blocker use.
The final HELPS wrap-up session for the group will include another nationally renowned expert in patient safety.
SHARP: Research Translated into Practice
Another project initiated by the Michigan hospitalists will generate and disseminate new knowledge in the realm of clinical research. The Specialist-Hospitalist Allied Research Program (SHARP), directed by Dr. Flanders and Brahmajee Nallamothu, MD, MPH, an interventional cardiologist, is the first specialist-hospitalist clinical research program in the United States. This hospitalist delivery model alters the way clinical problems are approached and creates opportunities and challenges in implementing best practices, including those surrounding drugs and devices. A successful clinical and translational research program will combine specialists and hospitalists working collaboratively to better understand the best ways to care for inpatients.
This project is similar to what cardiology and oncology specialties have done over the last several decades, says Dr. Saint. In the future, he foresees that the NIH will increasingly focus on translating research into practice in diverse settings. Both specialists and hospitalists who work in a particular area together—such as prevention of lower extremity clots or of nosocomial infections—can use the health consortium to roll out protocols and studies in order to tackle some of the important inpatient topics.
SHARP was awarded funding through the University of Michigan Department of Medicine and was scheduled to take off in February. “Our hope is that we will be able to take advantage of and build upon the health collaborative that we have and bring in our subspecialty expertise to help inform clinical investigations,” says Dr. Saint.
Where They’re Going
Both Dr. Flanders and Dr. Saint are pleased about the HELPS consortium’s progress so far. They believe that they have found a group of people who are interested in patient safety and are willing to learn from one another and that they have done an excellent job of disseminating the best practices they have been exploring.
Ultimately, their goal is to grow this into a “more robust clinical research consortium,” says Dr. Flanders. Instead of disseminating best practices and focusing on just a few targeted patient safety quality improvement areas, they will begin to take on studies that could center around patient safety and quality improvement but will also move toward multi-center projects that might address issues related to management of common clinical problems that hospitalists are now managing and focusing on.
“We’re really excited about what we have been able to accomplish,” he says. “We’ve learned a lot about the challenges of doing this, and of course it’s never perfect. We wish we could always do more, but we’ve learned why we can’t. That will be helpful in future projects and helpful for others who are trying to tackle this same problem.” TH
Reference
- Flanders SA, Kaufman SR, Saint S. Hospitalists as emerging leaders in patient safety: targeting a few to affect many. J Patient Safety. 2005;1(2):78-82.