User login
An Academic Hurdle
As clinicians and educators, academic hospitalists function within several arenas: They are role models and teachers in the inpatient arena, but they also feel pressure from hospital administration to meet throughput and capacity goals. In addition, hospitalist clinician-educators are expected to be leaders in quality improvement.
But are the rewards for academic hospitalists commensurate with the demands placed upon them? Even as hospitalists prove their worth to hospital administrators, many clinician-educators find themselves pulled between time spent on service and time for the academic pursuits necessary to improve resident education and merit faculty promotions.
“In my current situation, there is difficulty in fitting in the prep work time for teaching rounds,” says Elizabeth A. Schultz, MD, who practices with the Adult Hospitalist Team at Swedish Medical Center in Seattle and is also affiliated with the University of Washington School of Medicine. “There’s really no time for that, other than time on my own—and I’m actually in a really good situation right now where my boss has capped the number of patients I see in a day and afforded me the ability to go to conferences, do teaching rounds, and to really focus on resident and medical student education.”
Dr. Schultz is not alone in struggling to balance clinical and educational duties. Many hospital medicine leaders wrestle with these concerns, aware that growing clinical responsibilities impinge on teaching time and that the sustainability of hospital medicine as a career is at stake.
Confront the Dilemma
An October 2006 survey by the University HealthSystem Consortium confirmed that hospitalists have improved the educational process for residents and medical students, but it also identified impediments to the continuation and growth of hospitalist programs. (The Benchmarking Study, “Role of the Hospitalist,” is available online to University HealthSystem Consortium (UHC) members and registered website users at www.uhc.edu.) The most common barrier is the difficulty in attracting and retaining quality candidates, given the ratio of salary to workload, the potential for burnout, and undefined career paths.
“There is a significant amount of demand on one small group of physicians, and we haven’t necessarily found a way to compensate them for the different roles they play,” reflects Alpesh Amin, MD, MBA, FACP, associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California at Irvine (UCI), where he founded the UCI hospitalist program in 1998 and serves as its executive director. “These three arenas that hospitalists have to constantly keep moving in are not always complementary. How do you spend more time facilitating the teaching mission versus time facilitating the throughput mission or the expanding clinical mission?”
Meeting goals for academic appointments adds yet another layer of role conflict, he notes.
Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston and chair of SHM’s Career Satisfaction Task Force, also acknowledges the tensions between clinical duties and academic pursuits. “If you have 20 patients to see and discharge and yet you also have a grant to write, guess what’s not going to get done?”
To be fair, academic hospitalists experience their situations in different ways. Kathleen Bradford, MD, the inpatient director of the University of North Carolina (UNC) Children’s Hospital, director of the Pediatric Hospitalist Program, and assistant residency director for the Division of General Pediatrics at UNC in Chapel Hill, N.C., has not experienced a huge conflict between her teaching and clinical duties, but she has noticed that there are fewer opportunities for teaching, given the increased clinical demands on physicians and the decreased availability of residents.
“I’ve always felt that medicine—and especially medical teaching—is like an apprenticeship,” she explains. “There are many, many opportunities to teach while doing in an apprenticeship-like fashion. The demands of taking care of patients and [reduced] resident work hours have certainly decreased the ability to do more formal and didactic or classroom-type teaching. However, the opportunities for spontaneous or ‘teach as you go’ education still exist.”
Solutions to the Time Crunch
Dr. Schultz, a member of the Swedish Medical Center’s teaching service who leads a teaching team every month, admits she has no answers to the time crunch academic hospitalists experience. “There just isn’t enough manpower,” she says. “The hospital doesn’t get paid for people to teach, and to pay people to have dedicated time to pursue academic research or prepare lectures just isn’t feasible for most hospitals, as they are already struggling to make ends meet.”
Many hospitals employ both non-teaching and teaching services to ensure night and weekend coverage. But this can create other dilemmas for the academic hospitalist. For instance, Dr. Schultz says her teaching service gets the more complicated and critically ill patients who require more of her time, thus squeezing out, again, the opportunity to prepare lecture notes or conduct research.
At UNC Children’s Hospital, the pediatric hospitalist program is in its infancy, having launched in fall 2006, and the new service is mostly a non-teaching service. Dr. Bradford reports that the teaching and the hospitalist service are assigning patients on a case-by-case basis. “There is [teaching] value in all patients and all cases,” says Dr. Bradford, “but it’s really hard to say which ones have the most value: Should it be the patient who has a short stay with a common illness or a patient who has been chronically ill and in the hospital for 100 days? It’s hard to know.”
At Brigham and Women’s Hospital, Dr. McKean reports the hospitalist group did not want to institute a two-tiered [teaching and non-teaching] hospitalist program, so one of their hospitalists, Chris Roy, MD, created a Physician Assistant Clinician Educator (PACE) service, with a hospitalist supervising two PAs during daytime hours; it’s supplemented by moonlighters at night. Members of this service have teaching responsibilities and are involved in curriculum development for physician assistants and students. Additional research is needed to examine outcomes of educational efforts directed toward the multidisciplinary team in the core competency areas elaborated by the Accreditation Council for Graduate Medical Education, explains Dr. McKean.
Proactive Strategies
Whatever strategies are used to address case workloads, effecting real change for academic hospitalists—ensuring protected time as well as rewards for educational and research pursuits—will require clear-sighted planning from hospitalist leaders. “The bottom line is to proactively manage the program’s direction and growth,” asserts Dr. McKean. “Instead of being everybody’s Band-Aid and being everything to everybody, it’s important to have a strategic plan. You can’t necessarily plan for five years, but you can plan for three, and you could do things in a step-wise manner to increase the academic and research presence.”
This is precisely where SHM’s emphasis on networking and mentoring can come in, believes SHM’s Education Committee Chair Preetha Basaviah, MD, clinical associate professor of medicine and associate course director, Practice of Medicine, at Stanford University School of Medicine, California. SHM has led many initiatives, such as the publication of the Core Competencies and the creation of Web-based quality improvement resource rooms, which help provide curriculum support.
“What we’ve done as an education committee is to help provide some of the resources, support, and advocacy that our members need so that they can go back to their programs and say, ‘These are the national standards and resources provided by an organization that advocates for us.’ ” says Dr. Basaviah.
Creating a network of hospitalists, both regionally and nationally, provides opportunities to gain protected time for research pursuits and recognition from one’s peers, Dr. Basaviah continues. “I think what we’ve done for clinician educators is to promote thinking proactively about your short-term and long-term career goals, including developing an area of expertise, before you take on commitments,” she says.
Input with Curricular Design
Dr. Amin’s role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his role on the Core Competencies Task Force. He believes it is through such initiatives that hospitalists can become leaders in their institutions, participating in curriculum development as well as quality and performance improvement efforts.
“I don’t view myself as just working for the hospital or … for the School [of Medicine]. I view myself as working for the enterprise,” he says. As a result his hospitalist group has taken the lead in designing various residency inpatient curricula. “If you do it right, you could actually design curricula to educate residents about heart failure—teaching them about the pathophysiology and disease management—but then also teach them about core measures, outcomes, and systems-based practice in heart failure,” he says. “When all that comes together, I think you’re making some progress.”
Jeffrey G. Wiese, MD, vice chairman and director of the Internal Medicine Residency Program at Tulane University, New Orleans, is the leader of the SHM Task Force for Integrating Core Competencies into Residency Education. He points to the SHM Academic Task Force’s idea of developing an EVU, or educational value unit, that would define and compensate for amounts of time invested in educational pursuits. He would also like to see SHM take a role in developing standards and recommendations for promotion criteria. These are tools that academic hospitalists could use to “make their case” to medical schools’ residency programs about the value they offer to the institution.
Dr. Wiese is excited about train-the-trainer pre-courses now being designed for SHM’s 2008 annual meeting. These courses, he says, will train academic hospitalists to teach issues that are not only important to residency programs but “right up the alley of the hospitalist: namely, systems of care and practice-based learning.” In this way, he explains, academic hospitalists could have an “exponential effect” on furthering the profession.
Recruitment and Retention
Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine in Atlanta, is “significantly concerned” about attracting academic hospitalists. The 60+ hospitalists in his group staff five community hospitals (two of which have teaching services) in addition to the system’s tertiary care center. At that hospital, he says, patient acuity is appreciably higher, which means hospitalists must spend more time caring for patients and relating to their family members—time that does not translate into more billable relative value units (RVUs). This type of work environment is definitely “a difficult sell” to potential new hires, he notes. “There is … a balance between patient care and teaching in an academic environment, and maintaining that ‘right balance’ is always a challenge.”
System changes to reward educational prep time, such as the EVU Dr. Wiese mentioned, may be one solution to achieving a patient care/teaching time balance, agrees Dr. Dressler. “I think it’s an excellent idea to have some sort of measure that you can utilize to help reward physicians for putting an emphasis on education—actually promoting and executing educational efforts,” he says. Emory’s program is piloting a mechanism that would objectively measure clinicians’ self-identified efforts to set educational standards. Rewards (e.g., financial recognition or awards for “best teacher” and so on) could be built into the effort, he says.
Hospitalists face an uphill battle to secure funding for research, admits Dr. Wiese: “There is not the same level of NIH [National Institutes of Health] funding for quality improvement that there is for basic science research. And the QI funding that is available does not bring the same salary coverage that the basic science researchers are bringing to the department.”
Hospitalists need to be creative in defining their research agenda and funding streams. Dr. Basaviah says that if hospital medicine leaders emphasize the value of their systems-based quality improvement efforts, they may be able to secure funding for QI research efforts from “the hospital/medical center administration, Department of Medicine, QI group/division, or from residency programs, depending on where their efforts are going to be the most closely aligned.”
Avert Burnout
Tapping into SHM’s resources can foster community and allow younger hospitalists a method for charting a career path. Dr. McKean’s Career Satisfaction Task Force will soon release a white paper relating to the four pillars of career satisfaction: control/autonomy, reward/recognition, workload/schedule, and community environment. Questionnaires for individual hospitalists and physician leaders will help both groups identify the best job for an individual or the most appropriate person for a position. Included in the group’s analysis of career sustainability and satisfaction are organizational, system, professional development, and marketing-relationship strategies to help hospitalists assess job satisfaction. It is the task force’s hope that the document can be a useful tool in interactions with hospital administrators as well, to demonstrate the elements necessary for staff satisfaction and retention.
“A surgeon would never operate without a multidisciplinary team in the operating room,” says Dr. McKean. “And yet, because they’ve done order entry, they’ve done resident-level duties, hospitalists across the country are expected to step up without any resources to meet service demands relating to a shortage of residents and high census conditions. Performing residency-level duties not only undermines job satisfaction but also [affects] how efficiently hospitalists can care for a large number of patients. Hospitalists need to be given the tools to be efficient and improve the quality of care in the hospital.”
Fulfillment of Teaching
When asked what keeps him in academics despite lower remuneration rates, Dr. Wiese expresses the same sentiment as his colleagues: “It’s all about fulfillment. I like interacting with people and seeing them get better. If you train residents in the right way and then train them to train others, then suddenly your affect in improving quality of care and education has an exponential effect around the country.”
Dr. Dressler agrees. “Obviously, not everyone wants to do academic medicine, and you must have some interest in teaching and training others,” he says. But more important than financial remuneration, he notes, is “overall job satisfaction and being happy with the people you work with, as well as the patients you’re taking care of and the teaching that you’re doing.” That’s why hospitalists and faculty should work toward building recognition into the system. Hospitalist leaders can advocate for the mechanisms necessary, “to make sure that physicians also have time to have a life, to relax, and to enjoy their profession,” says Dr. Dressler.
“When I hire hospitalists, my goal is to hire people interested not only in good quality, efficient inpatient care but also in teaching,” said Dr. Amin. “I will easily tell them that they can probably make more money and have a better lifestyle working as a community hospitalist if they don’t want to deal with this other mission [of teaching].”
“I think if we view our work as just a job rather than as a career or profession that can be fulfilling, we may be led to paths of potential burnout,” said Dr. Basaviah. “Many of us view the healthcare profession with a notion of service and a vision for a satisfying career. I think that it’s important for all of us to facilitate the ability of our colleagues to thrive in these careers.” TH
Gretchen Henkel has written for The Hospitalist since 2005.
As clinicians and educators, academic hospitalists function within several arenas: They are role models and teachers in the inpatient arena, but they also feel pressure from hospital administration to meet throughput and capacity goals. In addition, hospitalist clinician-educators are expected to be leaders in quality improvement.
But are the rewards for academic hospitalists commensurate with the demands placed upon them? Even as hospitalists prove their worth to hospital administrators, many clinician-educators find themselves pulled between time spent on service and time for the academic pursuits necessary to improve resident education and merit faculty promotions.
“In my current situation, there is difficulty in fitting in the prep work time for teaching rounds,” says Elizabeth A. Schultz, MD, who practices with the Adult Hospitalist Team at Swedish Medical Center in Seattle and is also affiliated with the University of Washington School of Medicine. “There’s really no time for that, other than time on my own—and I’m actually in a really good situation right now where my boss has capped the number of patients I see in a day and afforded me the ability to go to conferences, do teaching rounds, and to really focus on resident and medical student education.”
Dr. Schultz is not alone in struggling to balance clinical and educational duties. Many hospital medicine leaders wrestle with these concerns, aware that growing clinical responsibilities impinge on teaching time and that the sustainability of hospital medicine as a career is at stake.
Confront the Dilemma
An October 2006 survey by the University HealthSystem Consortium confirmed that hospitalists have improved the educational process for residents and medical students, but it also identified impediments to the continuation and growth of hospitalist programs. (The Benchmarking Study, “Role of the Hospitalist,” is available online to University HealthSystem Consortium (UHC) members and registered website users at www.uhc.edu.) The most common barrier is the difficulty in attracting and retaining quality candidates, given the ratio of salary to workload, the potential for burnout, and undefined career paths.
“There is a significant amount of demand on one small group of physicians, and we haven’t necessarily found a way to compensate them for the different roles they play,” reflects Alpesh Amin, MD, MBA, FACP, associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California at Irvine (UCI), where he founded the UCI hospitalist program in 1998 and serves as its executive director. “These three arenas that hospitalists have to constantly keep moving in are not always complementary. How do you spend more time facilitating the teaching mission versus time facilitating the throughput mission or the expanding clinical mission?”
Meeting goals for academic appointments adds yet another layer of role conflict, he notes.
Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston and chair of SHM’s Career Satisfaction Task Force, also acknowledges the tensions between clinical duties and academic pursuits. “If you have 20 patients to see and discharge and yet you also have a grant to write, guess what’s not going to get done?”
To be fair, academic hospitalists experience their situations in different ways. Kathleen Bradford, MD, the inpatient director of the University of North Carolina (UNC) Children’s Hospital, director of the Pediatric Hospitalist Program, and assistant residency director for the Division of General Pediatrics at UNC in Chapel Hill, N.C., has not experienced a huge conflict between her teaching and clinical duties, but she has noticed that there are fewer opportunities for teaching, given the increased clinical demands on physicians and the decreased availability of residents.
“I’ve always felt that medicine—and especially medical teaching—is like an apprenticeship,” she explains. “There are many, many opportunities to teach while doing in an apprenticeship-like fashion. The demands of taking care of patients and [reduced] resident work hours have certainly decreased the ability to do more formal and didactic or classroom-type teaching. However, the opportunities for spontaneous or ‘teach as you go’ education still exist.”
Solutions to the Time Crunch
Dr. Schultz, a member of the Swedish Medical Center’s teaching service who leads a teaching team every month, admits she has no answers to the time crunch academic hospitalists experience. “There just isn’t enough manpower,” she says. “The hospital doesn’t get paid for people to teach, and to pay people to have dedicated time to pursue academic research or prepare lectures just isn’t feasible for most hospitals, as they are already struggling to make ends meet.”
Many hospitals employ both non-teaching and teaching services to ensure night and weekend coverage. But this can create other dilemmas for the academic hospitalist. For instance, Dr. Schultz says her teaching service gets the more complicated and critically ill patients who require more of her time, thus squeezing out, again, the opportunity to prepare lecture notes or conduct research.
At UNC Children’s Hospital, the pediatric hospitalist program is in its infancy, having launched in fall 2006, and the new service is mostly a non-teaching service. Dr. Bradford reports that the teaching and the hospitalist service are assigning patients on a case-by-case basis. “There is [teaching] value in all patients and all cases,” says Dr. Bradford, “but it’s really hard to say which ones have the most value: Should it be the patient who has a short stay with a common illness or a patient who has been chronically ill and in the hospital for 100 days? It’s hard to know.”
At Brigham and Women’s Hospital, Dr. McKean reports the hospitalist group did not want to institute a two-tiered [teaching and non-teaching] hospitalist program, so one of their hospitalists, Chris Roy, MD, created a Physician Assistant Clinician Educator (PACE) service, with a hospitalist supervising two PAs during daytime hours; it’s supplemented by moonlighters at night. Members of this service have teaching responsibilities and are involved in curriculum development for physician assistants and students. Additional research is needed to examine outcomes of educational efforts directed toward the multidisciplinary team in the core competency areas elaborated by the Accreditation Council for Graduate Medical Education, explains Dr. McKean.
Proactive Strategies
Whatever strategies are used to address case workloads, effecting real change for academic hospitalists—ensuring protected time as well as rewards for educational and research pursuits—will require clear-sighted planning from hospitalist leaders. “The bottom line is to proactively manage the program’s direction and growth,” asserts Dr. McKean. “Instead of being everybody’s Band-Aid and being everything to everybody, it’s important to have a strategic plan. You can’t necessarily plan for five years, but you can plan for three, and you could do things in a step-wise manner to increase the academic and research presence.”
This is precisely where SHM’s emphasis on networking and mentoring can come in, believes SHM’s Education Committee Chair Preetha Basaviah, MD, clinical associate professor of medicine and associate course director, Practice of Medicine, at Stanford University School of Medicine, California. SHM has led many initiatives, such as the publication of the Core Competencies and the creation of Web-based quality improvement resource rooms, which help provide curriculum support.
“What we’ve done as an education committee is to help provide some of the resources, support, and advocacy that our members need so that they can go back to their programs and say, ‘These are the national standards and resources provided by an organization that advocates for us.’ ” says Dr. Basaviah.
Creating a network of hospitalists, both regionally and nationally, provides opportunities to gain protected time for research pursuits and recognition from one’s peers, Dr. Basaviah continues. “I think what we’ve done for clinician educators is to promote thinking proactively about your short-term and long-term career goals, including developing an area of expertise, before you take on commitments,” she says.
Input with Curricular Design
Dr. Amin’s role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his role on the Core Competencies Task Force. He believes it is through such initiatives that hospitalists can become leaders in their institutions, participating in curriculum development as well as quality and performance improvement efforts.
“I don’t view myself as just working for the hospital or … for the School [of Medicine]. I view myself as working for the enterprise,” he says. As a result his hospitalist group has taken the lead in designing various residency inpatient curricula. “If you do it right, you could actually design curricula to educate residents about heart failure—teaching them about the pathophysiology and disease management—but then also teach them about core measures, outcomes, and systems-based practice in heart failure,” he says. “When all that comes together, I think you’re making some progress.”
Jeffrey G. Wiese, MD, vice chairman and director of the Internal Medicine Residency Program at Tulane University, New Orleans, is the leader of the SHM Task Force for Integrating Core Competencies into Residency Education. He points to the SHM Academic Task Force’s idea of developing an EVU, or educational value unit, that would define and compensate for amounts of time invested in educational pursuits. He would also like to see SHM take a role in developing standards and recommendations for promotion criteria. These are tools that academic hospitalists could use to “make their case” to medical schools’ residency programs about the value they offer to the institution.
Dr. Wiese is excited about train-the-trainer pre-courses now being designed for SHM’s 2008 annual meeting. These courses, he says, will train academic hospitalists to teach issues that are not only important to residency programs but “right up the alley of the hospitalist: namely, systems of care and practice-based learning.” In this way, he explains, academic hospitalists could have an “exponential effect” on furthering the profession.
Recruitment and Retention
Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine in Atlanta, is “significantly concerned” about attracting academic hospitalists. The 60+ hospitalists in his group staff five community hospitals (two of which have teaching services) in addition to the system’s tertiary care center. At that hospital, he says, patient acuity is appreciably higher, which means hospitalists must spend more time caring for patients and relating to their family members—time that does not translate into more billable relative value units (RVUs). This type of work environment is definitely “a difficult sell” to potential new hires, he notes. “There is … a balance between patient care and teaching in an academic environment, and maintaining that ‘right balance’ is always a challenge.”
System changes to reward educational prep time, such as the EVU Dr. Wiese mentioned, may be one solution to achieving a patient care/teaching time balance, agrees Dr. Dressler. “I think it’s an excellent idea to have some sort of measure that you can utilize to help reward physicians for putting an emphasis on education—actually promoting and executing educational efforts,” he says. Emory’s program is piloting a mechanism that would objectively measure clinicians’ self-identified efforts to set educational standards. Rewards (e.g., financial recognition or awards for “best teacher” and so on) could be built into the effort, he says.
Hospitalists face an uphill battle to secure funding for research, admits Dr. Wiese: “There is not the same level of NIH [National Institutes of Health] funding for quality improvement that there is for basic science research. And the QI funding that is available does not bring the same salary coverage that the basic science researchers are bringing to the department.”
Hospitalists need to be creative in defining their research agenda and funding streams. Dr. Basaviah says that if hospital medicine leaders emphasize the value of their systems-based quality improvement efforts, they may be able to secure funding for QI research efforts from “the hospital/medical center administration, Department of Medicine, QI group/division, or from residency programs, depending on where their efforts are going to be the most closely aligned.”
Avert Burnout
Tapping into SHM’s resources can foster community and allow younger hospitalists a method for charting a career path. Dr. McKean’s Career Satisfaction Task Force will soon release a white paper relating to the four pillars of career satisfaction: control/autonomy, reward/recognition, workload/schedule, and community environment. Questionnaires for individual hospitalists and physician leaders will help both groups identify the best job for an individual or the most appropriate person for a position. Included in the group’s analysis of career sustainability and satisfaction are organizational, system, professional development, and marketing-relationship strategies to help hospitalists assess job satisfaction. It is the task force’s hope that the document can be a useful tool in interactions with hospital administrators as well, to demonstrate the elements necessary for staff satisfaction and retention.
“A surgeon would never operate without a multidisciplinary team in the operating room,” says Dr. McKean. “And yet, because they’ve done order entry, they’ve done resident-level duties, hospitalists across the country are expected to step up without any resources to meet service demands relating to a shortage of residents and high census conditions. Performing residency-level duties not only undermines job satisfaction but also [affects] how efficiently hospitalists can care for a large number of patients. Hospitalists need to be given the tools to be efficient and improve the quality of care in the hospital.”
Fulfillment of Teaching
When asked what keeps him in academics despite lower remuneration rates, Dr. Wiese expresses the same sentiment as his colleagues: “It’s all about fulfillment. I like interacting with people and seeing them get better. If you train residents in the right way and then train them to train others, then suddenly your affect in improving quality of care and education has an exponential effect around the country.”
Dr. Dressler agrees. “Obviously, not everyone wants to do academic medicine, and you must have some interest in teaching and training others,” he says. But more important than financial remuneration, he notes, is “overall job satisfaction and being happy with the people you work with, as well as the patients you’re taking care of and the teaching that you’re doing.” That’s why hospitalists and faculty should work toward building recognition into the system. Hospitalist leaders can advocate for the mechanisms necessary, “to make sure that physicians also have time to have a life, to relax, and to enjoy their profession,” says Dr. Dressler.
“When I hire hospitalists, my goal is to hire people interested not only in good quality, efficient inpatient care but also in teaching,” said Dr. Amin. “I will easily tell them that they can probably make more money and have a better lifestyle working as a community hospitalist if they don’t want to deal with this other mission [of teaching].”
“I think if we view our work as just a job rather than as a career or profession that can be fulfilling, we may be led to paths of potential burnout,” said Dr. Basaviah. “Many of us view the healthcare profession with a notion of service and a vision for a satisfying career. I think that it’s important for all of us to facilitate the ability of our colleagues to thrive in these careers.” TH
Gretchen Henkel has written for The Hospitalist since 2005.
As clinicians and educators, academic hospitalists function within several arenas: They are role models and teachers in the inpatient arena, but they also feel pressure from hospital administration to meet throughput and capacity goals. In addition, hospitalist clinician-educators are expected to be leaders in quality improvement.
But are the rewards for academic hospitalists commensurate with the demands placed upon them? Even as hospitalists prove their worth to hospital administrators, many clinician-educators find themselves pulled between time spent on service and time for the academic pursuits necessary to improve resident education and merit faculty promotions.
“In my current situation, there is difficulty in fitting in the prep work time for teaching rounds,” says Elizabeth A. Schultz, MD, who practices with the Adult Hospitalist Team at Swedish Medical Center in Seattle and is also affiliated with the University of Washington School of Medicine. “There’s really no time for that, other than time on my own—and I’m actually in a really good situation right now where my boss has capped the number of patients I see in a day and afforded me the ability to go to conferences, do teaching rounds, and to really focus on resident and medical student education.”
Dr. Schultz is not alone in struggling to balance clinical and educational duties. Many hospital medicine leaders wrestle with these concerns, aware that growing clinical responsibilities impinge on teaching time and that the sustainability of hospital medicine as a career is at stake.
Confront the Dilemma
An October 2006 survey by the University HealthSystem Consortium confirmed that hospitalists have improved the educational process for residents and medical students, but it also identified impediments to the continuation and growth of hospitalist programs. (The Benchmarking Study, “Role of the Hospitalist,” is available online to University HealthSystem Consortium (UHC) members and registered website users at www.uhc.edu.) The most common barrier is the difficulty in attracting and retaining quality candidates, given the ratio of salary to workload, the potential for burnout, and undefined career paths.
“There is a significant amount of demand on one small group of physicians, and we haven’t necessarily found a way to compensate them for the different roles they play,” reflects Alpesh Amin, MD, MBA, FACP, associate program director for the Internal Medicine Residency Program and the medicine clerkship director at the University of California at Irvine (UCI), where he founded the UCI hospitalist program in 1998 and serves as its executive director. “These three arenas that hospitalists have to constantly keep moving in are not always complementary. How do you spend more time facilitating the teaching mission versus time facilitating the throughput mission or the expanding clinical mission?”
Meeting goals for academic appointments adds yet another layer of role conflict, he notes.
Sylvia Cheney McKean, MD, FACP, medical director of the Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston and chair of SHM’s Career Satisfaction Task Force, also acknowledges the tensions between clinical duties and academic pursuits. “If you have 20 patients to see and discharge and yet you also have a grant to write, guess what’s not going to get done?”
To be fair, academic hospitalists experience their situations in different ways. Kathleen Bradford, MD, the inpatient director of the University of North Carolina (UNC) Children’s Hospital, director of the Pediatric Hospitalist Program, and assistant residency director for the Division of General Pediatrics at UNC in Chapel Hill, N.C., has not experienced a huge conflict between her teaching and clinical duties, but she has noticed that there are fewer opportunities for teaching, given the increased clinical demands on physicians and the decreased availability of residents.
“I’ve always felt that medicine—and especially medical teaching—is like an apprenticeship,” she explains. “There are many, many opportunities to teach while doing in an apprenticeship-like fashion. The demands of taking care of patients and [reduced] resident work hours have certainly decreased the ability to do more formal and didactic or classroom-type teaching. However, the opportunities for spontaneous or ‘teach as you go’ education still exist.”
Solutions to the Time Crunch
Dr. Schultz, a member of the Swedish Medical Center’s teaching service who leads a teaching team every month, admits she has no answers to the time crunch academic hospitalists experience. “There just isn’t enough manpower,” she says. “The hospital doesn’t get paid for people to teach, and to pay people to have dedicated time to pursue academic research or prepare lectures just isn’t feasible for most hospitals, as they are already struggling to make ends meet.”
Many hospitals employ both non-teaching and teaching services to ensure night and weekend coverage. But this can create other dilemmas for the academic hospitalist. For instance, Dr. Schultz says her teaching service gets the more complicated and critically ill patients who require more of her time, thus squeezing out, again, the opportunity to prepare lecture notes or conduct research.
At UNC Children’s Hospital, the pediatric hospitalist program is in its infancy, having launched in fall 2006, and the new service is mostly a non-teaching service. Dr. Bradford reports that the teaching and the hospitalist service are assigning patients on a case-by-case basis. “There is [teaching] value in all patients and all cases,” says Dr. Bradford, “but it’s really hard to say which ones have the most value: Should it be the patient who has a short stay with a common illness or a patient who has been chronically ill and in the hospital for 100 days? It’s hard to know.”
At Brigham and Women’s Hospital, Dr. McKean reports the hospitalist group did not want to institute a two-tiered [teaching and non-teaching] hospitalist program, so one of their hospitalists, Chris Roy, MD, created a Physician Assistant Clinician Educator (PACE) service, with a hospitalist supervising two PAs during daytime hours; it’s supplemented by moonlighters at night. Members of this service have teaching responsibilities and are involved in curriculum development for physician assistants and students. Additional research is needed to examine outcomes of educational efforts directed toward the multidisciplinary team in the core competency areas elaborated by the Accreditation Council for Graduate Medical Education, explains Dr. McKean.
Proactive Strategies
Whatever strategies are used to address case workloads, effecting real change for academic hospitalists—ensuring protected time as well as rewards for educational and research pursuits—will require clear-sighted planning from hospitalist leaders. “The bottom line is to proactively manage the program’s direction and growth,” asserts Dr. McKean. “Instead of being everybody’s Band-Aid and being everything to everybody, it’s important to have a strategic plan. You can’t necessarily plan for five years, but you can plan for three, and you could do things in a step-wise manner to increase the academic and research presence.”
This is precisely where SHM’s emphasis on networking and mentoring can come in, believes SHM’s Education Committee Chair Preetha Basaviah, MD, clinical associate professor of medicine and associate course director, Practice of Medicine, at Stanford University School of Medicine, California. SHM has led many initiatives, such as the publication of the Core Competencies and the creation of Web-based quality improvement resource rooms, which help provide curriculum support.
“What we’ve done as an education committee is to help provide some of the resources, support, and advocacy that our members need so that they can go back to their programs and say, ‘These are the national standards and resources provided by an organization that advocates for us.’ ” says Dr. Basaviah.
Creating a network of hospitalists, both regionally and nationally, provides opportunities to gain protected time for research pursuits and recognition from one’s peers, Dr. Basaviah continues. “I think what we’ve done for clinician educators is to promote thinking proactively about your short-term and long-term career goals, including developing an area of expertise, before you take on commitments,” she says.
Input with Curricular Design
Dr. Amin’s role in education at his institution informed his active participation in SHM’s Education Committee, which he chaired for four years, and his role on the Core Competencies Task Force. He believes it is through such initiatives that hospitalists can become leaders in their institutions, participating in curriculum development as well as quality and performance improvement efforts.
“I don’t view myself as just working for the hospital or … for the School [of Medicine]. I view myself as working for the enterprise,” he says. As a result his hospitalist group has taken the lead in designing various residency inpatient curricula. “If you do it right, you could actually design curricula to educate residents about heart failure—teaching them about the pathophysiology and disease management—but then also teach them about core measures, outcomes, and systems-based practice in heart failure,” he says. “When all that comes together, I think you’re making some progress.”
Jeffrey G. Wiese, MD, vice chairman and director of the Internal Medicine Residency Program at Tulane University, New Orleans, is the leader of the SHM Task Force for Integrating Core Competencies into Residency Education. He points to the SHM Academic Task Force’s idea of developing an EVU, or educational value unit, that would define and compensate for amounts of time invested in educational pursuits. He would also like to see SHM take a role in developing standards and recommendations for promotion criteria. These are tools that academic hospitalists could use to “make their case” to medical schools’ residency programs about the value they offer to the institution.
Dr. Wiese is excited about train-the-trainer pre-courses now being designed for SHM’s 2008 annual meeting. These courses, he says, will train academic hospitalists to teach issues that are not only important to residency programs but “right up the alley of the hospitalist: namely, systems of care and practice-based learning.” In this way, he explains, academic hospitalists could have an “exponential effect” on furthering the profession.
Recruitment and Retention
Daniel D. Dressler, MD, MSc, director of hospital medicine at Emory University Hospital and assistant professor of medicine at Emory University School of Medicine in Atlanta, is “significantly concerned” about attracting academic hospitalists. The 60+ hospitalists in his group staff five community hospitals (two of which have teaching services) in addition to the system’s tertiary care center. At that hospital, he says, patient acuity is appreciably higher, which means hospitalists must spend more time caring for patients and relating to their family members—time that does not translate into more billable relative value units (RVUs). This type of work environment is definitely “a difficult sell” to potential new hires, he notes. “There is … a balance between patient care and teaching in an academic environment, and maintaining that ‘right balance’ is always a challenge.”
System changes to reward educational prep time, such as the EVU Dr. Wiese mentioned, may be one solution to achieving a patient care/teaching time balance, agrees Dr. Dressler. “I think it’s an excellent idea to have some sort of measure that you can utilize to help reward physicians for putting an emphasis on education—actually promoting and executing educational efforts,” he says. Emory’s program is piloting a mechanism that would objectively measure clinicians’ self-identified efforts to set educational standards. Rewards (e.g., financial recognition or awards for “best teacher” and so on) could be built into the effort, he says.
Hospitalists face an uphill battle to secure funding for research, admits Dr. Wiese: “There is not the same level of NIH [National Institutes of Health] funding for quality improvement that there is for basic science research. And the QI funding that is available does not bring the same salary coverage that the basic science researchers are bringing to the department.”
Hospitalists need to be creative in defining their research agenda and funding streams. Dr. Basaviah says that if hospital medicine leaders emphasize the value of their systems-based quality improvement efforts, they may be able to secure funding for QI research efforts from “the hospital/medical center administration, Department of Medicine, QI group/division, or from residency programs, depending on where their efforts are going to be the most closely aligned.”
Avert Burnout
Tapping into SHM’s resources can foster community and allow younger hospitalists a method for charting a career path. Dr. McKean’s Career Satisfaction Task Force will soon release a white paper relating to the four pillars of career satisfaction: control/autonomy, reward/recognition, workload/schedule, and community environment. Questionnaires for individual hospitalists and physician leaders will help both groups identify the best job for an individual or the most appropriate person for a position. Included in the group’s analysis of career sustainability and satisfaction are organizational, system, professional development, and marketing-relationship strategies to help hospitalists assess job satisfaction. It is the task force’s hope that the document can be a useful tool in interactions with hospital administrators as well, to demonstrate the elements necessary for staff satisfaction and retention.
“A surgeon would never operate without a multidisciplinary team in the operating room,” says Dr. McKean. “And yet, because they’ve done order entry, they’ve done resident-level duties, hospitalists across the country are expected to step up without any resources to meet service demands relating to a shortage of residents and high census conditions. Performing residency-level duties not only undermines job satisfaction but also [affects] how efficiently hospitalists can care for a large number of patients. Hospitalists need to be given the tools to be efficient and improve the quality of care in the hospital.”
Fulfillment of Teaching
When asked what keeps him in academics despite lower remuneration rates, Dr. Wiese expresses the same sentiment as his colleagues: “It’s all about fulfillment. I like interacting with people and seeing them get better. If you train residents in the right way and then train them to train others, then suddenly your affect in improving quality of care and education has an exponential effect around the country.”
Dr. Dressler agrees. “Obviously, not everyone wants to do academic medicine, and you must have some interest in teaching and training others,” he says. But more important than financial remuneration, he notes, is “overall job satisfaction and being happy with the people you work with, as well as the patients you’re taking care of and the teaching that you’re doing.” That’s why hospitalists and faculty should work toward building recognition into the system. Hospitalist leaders can advocate for the mechanisms necessary, “to make sure that physicians also have time to have a life, to relax, and to enjoy their profession,” says Dr. Dressler.
“When I hire hospitalists, my goal is to hire people interested not only in good quality, efficient inpatient care but also in teaching,” said Dr. Amin. “I will easily tell them that they can probably make more money and have a better lifestyle working as a community hospitalist if they don’t want to deal with this other mission [of teaching].”
“I think if we view our work as just a job rather than as a career or profession that can be fulfilling, we may be led to paths of potential burnout,” said Dr. Basaviah. “Many of us view the healthcare profession with a notion of service and a vision for a satisfying career. I think that it’s important for all of us to facilitate the ability of our colleagues to thrive in these careers.” TH
Gretchen Henkel has written for The Hospitalist since 2005.
Dealing with the DTs
Irritability. Tremors. Sweating and a rapid heart rate. Extreme confusion. Fever. Convulsions. These are all symptoms of acute alcohol withdrawal syndrome. A patient may develop acute alcohol withdrawal syndrome when chronic alcohol use is interrupted by hospital admission. Increasingly patients are being treated for alcohol withdrawal on general medical wards.
Acute withdrawal is most safely managed in an inpatient setting if the patient has been using high doses of sedatives, has a history of seizures or delirium tremens, or has co-morbid medical or psychiatric problems.1 The severity of the withdrawal syndrome is affected by concurrent medical illness. Up to 20% of patients develop delirium tremens if left untreated.2 Recognition and effective treatment of alcohol withdrawal are needed to prevent excess mortality or prolonged hospitalization due to complications. It is essential for hospitalists to recognize and effectively treat acute alcohol withdrawal to prevent adverse outcomes in hospitalized patients.
Development of Withdrawal
Hospitalized patients may not be forthcoming about their alcohol consumption for numerous reasons. They may not consider it a problem; they may not recognize that acute withdrawal is a serious and even fatal complication; or they may wish to conceal their alcoholism from family and physicians due to concerns about stigmatization.
Even when patients acknowledge their drinking, they often underestimate the amount, which may be because a patient is minimizing or because alcohol is an amnestic agent, causing drinkers to lose count of how much they have had to drink. It is simplest to ask—in a nonjudgmental manner—all patients admitted to the hospital about drinking and to be alert for signs of acute alcohol withdrawal in all patients.
Not all patients who drink alcohol will develop an acute withdrawal syndrome. Those who drink less frequently—only on weekends with no drinking at all on weekdays, for example—are at lower risk of acute withdrawal. Those who drink on most days of the week are more likely—due to tolerance—to develop withdrawal. Even a habit of two or three drinks each day is enough to set up a person for withdrawal. Not all daily drinkers are guaranteed to develop withdrawal, and it is difficult to predict who will and who will not. The best predictor of whether a patient will develop acute withdrawal while hospitalized is a past history of acute alcohol withdrawal.
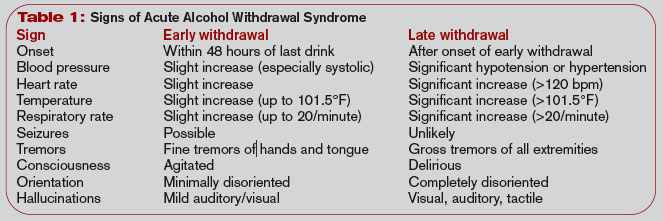
The alcohol withdrawal syndrome has two phases: early withdrawal and late withdrawal. (See Table 1, below.) The signs and symptoms of early withdrawal usually occur within 48 hours of the last drink. The initial indication is an elevation of vital signs: heart rate, blood pressure, and temperature. Tremors develop next—first a fine tremor of the hands and fasciculation of the tongue, then gross tremors of the extremities. As the syndrome progresses, disorientation and mild hallucinations (often auditory but occasionally visual) develop, accompanied by diaphoresis. Seizures are an early sign of alcohol withdrawal and may even be the presenting symptom.
Late alcohol withdrawal is also known as delirium tremens—the DTs—and consists of the worsening autonomic dysregulation that is responsible for the morbidity and mortality attributed to alcohol withdrawal. It begins after early withdrawal—usually 72 hours or more after the last drink. Some patients do not progress from early to late withdrawal, and their symptoms simply subside after a few days, with or without treatment. But it is impossible to predict which patients will progress and which will not. The signs of late withdrawal consist of worsening diaphoresis, nausea, and vomiting (which may result in aspiration pneumonia), delirium with frank hallucinations, and rapid, severe fluctuation in vital signs. Sudden changes in blood pressure and heart rate may result in complications such as myocardial infarction or a cerebrovascular event. Untreated late withdrawal results in significant morbidity and even death.3 Adequate treatment of early withdrawal prevents progression to late withdrawal.
Assessment
When you or a colleague suspect that a hospitalized patient may develop alcohol withdrawal, regularly assess the patient for signs of early withdrawal. Use a validated assessment scale to quantify the severity of the withdrawal syndrome, and initiate treatment decisions such as the dose of medication. If no withdrawal signs manifest after 48 hours, then it is usually safe to discontinue monitoring for withdrawal. Monitor patients for whom alcohol withdrawal is not considered but who then develop withdrawal signs using an assessment scale.
The revised Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) is commonly used to assess severity of withdrawal.4 Competent nurses can give it in less than five minutes. A CIWA-Ar score less than 5 indicates minimal withdrawal with no need for pharmacotherapy, whereas a score that falls in the range of 6-19 indicates mild withdrawal that may benefit from medical treatment. A score greater than 30 indicates severe withdrawal that requires close monitoring due to the risk for complications such as seizures and autonomic instability.5
The CIWA-Ar is just as useful for evaluating and treating withdrawal in hospitalized patients on general medical wards as it is for use in chemical dependency units. It can also be used to determine an appropriate pharmacotherapy dose for patients in withdrawal who also have other medical illnesses.6
Monitor patients every few hours, with the frequency of evaluation varying by severity of withdrawal signs. Every four hours is sufficient for most patients, but those who have developed late withdrawal or those with CIWA-Ar scores greater than 30 should be monitored hourly to prevent complications. Continue regular assessment until the withdrawal syndrome has been under control (CIWA-Ar score less than 6) for at least 24 hours.
Treatment
Medications: Pharmacotherapy is indicated for the management of moderate to severe withdrawal. Any cross-tolerant medication may be used; benzodiazepines or barbiturates are most commonly prescribed. It is inappropriate to use beverage alcohol to prevent or treat alcohol withdrawal. Use of intravenous alcohol infusion is reserved for poisoning with methanol, isopropanol, or ethylene glycol. It should not be given for treatment of acute alcohol withdrawal due to potential complications such as intoxication with delirium and development of gastritis.
Both benzodiazepines and barbiturates, which are different classes of sedative-hypnotic medications, are cross-tolerant with alcohol and effectively treat alcohol withdrawal.7 Acute alcohol withdrawal in the United States is most often managed with benzodiazepines.8 There are a variety of benzodiazepines available, from ultra-short-acting to long-acting, as well as parenteral and oral forms. Diazepam has been used extensively due to rapid onset of action when given intravenously and long duration of action when given orally.
For similar reasons, chlordiazepoxide is also used widely. Lorazepam, an intermediate-acting benzodiazepine that can be given orally or parenterally, has been used extensively for treatment of acute alcohol withdrawal, especially in hospitalized patients, because it has fewer active metabolites than other benzodiazepines. This makes it safer to use in treating patients with severe liver disease, which is important when treating chronic alcoholics. Benzodiazepines have a relatively high therapeutic index when used to treat patients with illnesses in addition to acute withdrawal. This makes benzodiazepines an excellent choice for the treatment of acute withdrawal in patients on general medical wards.
Barbiturates have been used successfully to treat acute alcohol withdrawal syndrome in general medical inpatients, with phenobarbital the most common choice.9,10 Phenobarbital may be preferable to other sedative-hypnotics; with its longer half-life, patients rarely achieve a “high” as they do with other sedatives, and it is available in multiple dosage forms.11
A number of alternative non-sedative-hypnotic medications exist to treat acute alcohol withdrawal. Beta-adrenergic blockers (atenolol, propranolol), clonidine, and anticonvulsant agents (carbamazepine, valproate) decrease alcohol withdrawal symptoms and have been used successfully in the treatment of mild withdrawal. They are not cross-tolerant with alcohol, however, and may result in progression of the withdrawal syndrome. These alternative medications are not appropriate to use as single agents in the treatment of withdrawal in a general medical setting.

Dosing regimens: There are no standard protocols for withdrawal management in widespread use.12 A fixed dosing schedule is commonly used for treatment of acute withdrawal, but either fixed-schedule or symptom-triggered dosing—medication given as needed for withdrawal signs—is efficacious in the treatment of withdrawal, even in patients with medical comorbidity.6
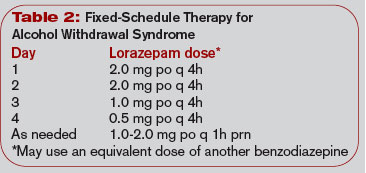
Fixed-schedule dosing is a one-size-fits-all approach for treating alcohol withdrawal. It uses the same dose of cross-tolerant medication on a fixed schedule for all patients for 24-48 hours; the dose is then tapered if the patient is stable. (See Table 2, left.) Reducing the dose by 10%-20% of the initial dose each day over five to 10 days provides a comfortable taper—especially in patients who initially required higher doses of medication to control the withdrawal. Fixed-schedule dosing offers less flexibility for individual patients, but it is a simple approach that can be applied in many settings.
Symptom-triggered therapy occurs when cross-tolerant medication is given only for symptoms of withdrawal rather than on a schedule. (See Table 3, p. 25.) Patients are monitored closely and assessed regularly using a tool such as the CIWA-Ar. The dose of cross-tolerant medication prescribed is based on the severity of withdrawal symptoms as measured by the CIWA-Ar score. This approach is similar to the sliding scale of insulin dosing used to treat hyperglycemia. Symptom-triggered therapy provides individualized treatment for withdrawal without overmedicating or underdosing, but it is a complex system to carry out on a general medical unit.
Severe withdrawal: Treat severe DTs manifested by abnormal and fluctuating vital signs and/or delirium aggressively in an ICU environment with sufficiently large doses of medication to suppress the withdrawal.11 Use IV medications with a rapid onset of action for immediate effect. Lorazepam and diazepam have a rapid onset of action when given intravenously, although the duration of action is shorter than when given orally.
For example, give lorazepam in a dose of one to four mg every 10-30 minutes until the patient is calm but awake and the heart rate is below 120 beats per minute. A continuous intravenous infusion may be warranted to control withdrawal symptoms, and the rate can be titrated to the desired level of consciousness. After stabilization, the patient can be changed to an equivalent dose of a long-acting sedative-hypnotic and tapered as above.
Assessing and medicating acute withdrawal remain necessary first steps in the treatment of the disease of alcohol dependence. After acute detoxification has begun, long-term treatment of alcoholism is necessary to prevent readmission for continuing medical problems due to alcohol consumption. Refer patients who have been treated for alcohol withdrawal for long-term treatment of alcoholism. This may include Alcoholics Anonymous, outpatient counseling, and other treatment modalities.
Conclusion
Ask all patients admitted to the hospital about drinking alcohol and be alert for signs of acute alcohol withdrawal in any patient. The best predictor of whether a patient will develop acute withdrawal is a past history of withdrawal. Signs of withdrawal usually occur within 48 hours of the last drink. Untreated withdrawal may result in significant morbidity and mortality.
Patients in withdrawal should be monitored closely and given appropriate doses of benzodiazepines or barbiturates to treat withdrawal signs. Cross-tolerant medication may be given on a fixed schedule or as symptom-triggered therapy. Severe withdrawal may require a continuous intravenous infusion in an ICU. Recognition and effective treatment of alcohol withdrawal can prevent significant complications in hospitalized patients. TH
Dr. Weaver is associate professor of internal medicine and psychiatry at Virginia Commonwealth University, Richmond.
References
- Saitz R. Introduction to alcohol withdrawal. Alcohol Health Res World. 1998;22(1):5-12.
- Cross GM, Hennessey PT. Principles and practice of detoxification. Prim Care. 1993;20(1):81-93.
- Cutshall BJ. The Saunderssutton syndrome: an analysis of delirium tremens. Q J Stud Alcohol. 1965;26(3):423-448.
- Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict. 1989;84:1353-1357.
- Foy A, March S, Drinkwater V. Use of an objective clinical scale in the assessment and management of alcohol withdrawal in a large general hospital. Alcohol Clin Exp Res. 1988;12(3):360-364.
- Weaver MF, Hoffman HJ, Johnson RE. Alcohol withdrawal pharmacotherapy for inpatients with medical comorbidity. J Addict Dis. 2006;25(2):17-24.
- Mayo-Smith MF. Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278(2):144-151.
- Saitz R, Mayo-Smith MF, Roberts MS, et al. Individualized treatment for alcohol withdrawal. A randomized double-blind controlled trial. JAMA. 1994;272(7):519-523.
- Yeh HS, Dhopesh V, Maany I. Seizures during detoxification. J Gen Intern Med. 1992;7(1):123.
- Young GP, Rores C, Murphy C, et al. Intravenous phenobarbital for alcohol withdrawal and convulsions. Ann Emerg Med. 1987;16(8):847-850.
- Weaver MF, Jarvis MA, Schnoll SH. Role of the primary care physician in problems of substance abuse. Arch Intern Med. 1999;159(9):913-924.
Irritability. Tremors. Sweating and a rapid heart rate. Extreme confusion. Fever. Convulsions. These are all symptoms of acute alcohol withdrawal syndrome. A patient may develop acute alcohol withdrawal syndrome when chronic alcohol use is interrupted by hospital admission. Increasingly patients are being treated for alcohol withdrawal on general medical wards.
Acute withdrawal is most safely managed in an inpatient setting if the patient has been using high doses of sedatives, has a history of seizures or delirium tremens, or has co-morbid medical or psychiatric problems.1 The severity of the withdrawal syndrome is affected by concurrent medical illness. Up to 20% of patients develop delirium tremens if left untreated.2 Recognition and effective treatment of alcohol withdrawal are needed to prevent excess mortality or prolonged hospitalization due to complications. It is essential for hospitalists to recognize and effectively treat acute alcohol withdrawal to prevent adverse outcomes in hospitalized patients.
Development of Withdrawal
Hospitalized patients may not be forthcoming about their alcohol consumption for numerous reasons. They may not consider it a problem; they may not recognize that acute withdrawal is a serious and even fatal complication; or they may wish to conceal their alcoholism from family and physicians due to concerns about stigmatization.
Even when patients acknowledge their drinking, they often underestimate the amount, which may be because a patient is minimizing or because alcohol is an amnestic agent, causing drinkers to lose count of how much they have had to drink. It is simplest to ask—in a nonjudgmental manner—all patients admitted to the hospital about drinking and to be alert for signs of acute alcohol withdrawal in all patients.
Not all patients who drink alcohol will develop an acute withdrawal syndrome. Those who drink less frequently—only on weekends with no drinking at all on weekdays, for example—are at lower risk of acute withdrawal. Those who drink on most days of the week are more likely—due to tolerance—to develop withdrawal. Even a habit of two or three drinks each day is enough to set up a person for withdrawal. Not all daily drinkers are guaranteed to develop withdrawal, and it is difficult to predict who will and who will not. The best predictor of whether a patient will develop acute withdrawal while hospitalized is a past history of acute alcohol withdrawal.
The alcohol withdrawal syndrome has two phases: early withdrawal and late withdrawal. (See Table 1, below.) The signs and symptoms of early withdrawal usually occur within 48 hours of the last drink. The initial indication is an elevation of vital signs: heart rate, blood pressure, and temperature. Tremors develop next—first a fine tremor of the hands and fasciculation of the tongue, then gross tremors of the extremities. As the syndrome progresses, disorientation and mild hallucinations (often auditory but occasionally visual) develop, accompanied by diaphoresis. Seizures are an early sign of alcohol withdrawal and may even be the presenting symptom.
Late alcohol withdrawal is also known as delirium tremens—the DTs—and consists of the worsening autonomic dysregulation that is responsible for the morbidity and mortality attributed to alcohol withdrawal. It begins after early withdrawal—usually 72 hours or more after the last drink. Some patients do not progress from early to late withdrawal, and their symptoms simply subside after a few days, with or without treatment. But it is impossible to predict which patients will progress and which will not. The signs of late withdrawal consist of worsening diaphoresis, nausea, and vomiting (which may result in aspiration pneumonia), delirium with frank hallucinations, and rapid, severe fluctuation in vital signs. Sudden changes in blood pressure and heart rate may result in complications such as myocardial infarction or a cerebrovascular event. Untreated late withdrawal results in significant morbidity and even death.3 Adequate treatment of early withdrawal prevents progression to late withdrawal.
Assessment
When you or a colleague suspect that a hospitalized patient may develop alcohol withdrawal, regularly assess the patient for signs of early withdrawal. Use a validated assessment scale to quantify the severity of the withdrawal syndrome, and initiate treatment decisions such as the dose of medication. If no withdrawal signs manifest after 48 hours, then it is usually safe to discontinue monitoring for withdrawal. Monitor patients for whom alcohol withdrawal is not considered but who then develop withdrawal signs using an assessment scale.
The revised Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) is commonly used to assess severity of withdrawal.4 Competent nurses can give it in less than five minutes. A CIWA-Ar score less than 5 indicates minimal withdrawal with no need for pharmacotherapy, whereas a score that falls in the range of 6-19 indicates mild withdrawal that may benefit from medical treatment. A score greater than 30 indicates severe withdrawal that requires close monitoring due to the risk for complications such as seizures and autonomic instability.5
The CIWA-Ar is just as useful for evaluating and treating withdrawal in hospitalized patients on general medical wards as it is for use in chemical dependency units. It can also be used to determine an appropriate pharmacotherapy dose for patients in withdrawal who also have other medical illnesses.6
Monitor patients every few hours, with the frequency of evaluation varying by severity of withdrawal signs. Every four hours is sufficient for most patients, but those who have developed late withdrawal or those with CIWA-Ar scores greater than 30 should be monitored hourly to prevent complications. Continue regular assessment until the withdrawal syndrome has been under control (CIWA-Ar score less than 6) for at least 24 hours.
Treatment
Medications: Pharmacotherapy is indicated for the management of moderate to severe withdrawal. Any cross-tolerant medication may be used; benzodiazepines or barbiturates are most commonly prescribed. It is inappropriate to use beverage alcohol to prevent or treat alcohol withdrawal. Use of intravenous alcohol infusion is reserved for poisoning with methanol, isopropanol, or ethylene glycol. It should not be given for treatment of acute alcohol withdrawal due to potential complications such as intoxication with delirium and development of gastritis.
Both benzodiazepines and barbiturates, which are different classes of sedative-hypnotic medications, are cross-tolerant with alcohol and effectively treat alcohol withdrawal.7 Acute alcohol withdrawal in the United States is most often managed with benzodiazepines.8 There are a variety of benzodiazepines available, from ultra-short-acting to long-acting, as well as parenteral and oral forms. Diazepam has been used extensively due to rapid onset of action when given intravenously and long duration of action when given orally.
For similar reasons, chlordiazepoxide is also used widely. Lorazepam, an intermediate-acting benzodiazepine that can be given orally or parenterally, has been used extensively for treatment of acute alcohol withdrawal, especially in hospitalized patients, because it has fewer active metabolites than other benzodiazepines. This makes it safer to use in treating patients with severe liver disease, which is important when treating chronic alcoholics. Benzodiazepines have a relatively high therapeutic index when used to treat patients with illnesses in addition to acute withdrawal. This makes benzodiazepines an excellent choice for the treatment of acute withdrawal in patients on general medical wards.
Barbiturates have been used successfully to treat acute alcohol withdrawal syndrome in general medical inpatients, with phenobarbital the most common choice.9,10 Phenobarbital may be preferable to other sedative-hypnotics; with its longer half-life, patients rarely achieve a “high” as they do with other sedatives, and it is available in multiple dosage forms.11
A number of alternative non-sedative-hypnotic medications exist to treat acute alcohol withdrawal. Beta-adrenergic blockers (atenolol, propranolol), clonidine, and anticonvulsant agents (carbamazepine, valproate) decrease alcohol withdrawal symptoms and have been used successfully in the treatment of mild withdrawal. They are not cross-tolerant with alcohol, however, and may result in progression of the withdrawal syndrome. These alternative medications are not appropriate to use as single agents in the treatment of withdrawal in a general medical setting.
Dosing regimens: There are no standard protocols for withdrawal management in widespread use.12 A fixed dosing schedule is commonly used for treatment of acute withdrawal, but either fixed-schedule or symptom-triggered dosing—medication given as needed for withdrawal signs—is efficacious in the treatment of withdrawal, even in patients with medical comorbidity.6
Fixed-schedule dosing is a one-size-fits-all approach for treating alcohol withdrawal. It uses the same dose of cross-tolerant medication on a fixed schedule for all patients for 24-48 hours; the dose is then tapered if the patient is stable. (See Table 2, left.) Reducing the dose by 10%-20% of the initial dose each day over five to 10 days provides a comfortable taper—especially in patients who initially required higher doses of medication to control the withdrawal. Fixed-schedule dosing offers less flexibility for individual patients, but it is a simple approach that can be applied in many settings.
Symptom-triggered therapy occurs when cross-tolerant medication is given only for symptoms of withdrawal rather than on a schedule. (See Table 3, p. 25.) Patients are monitored closely and assessed regularly using a tool such as the CIWA-Ar. The dose of cross-tolerant medication prescribed is based on the severity of withdrawal symptoms as measured by the CIWA-Ar score. This approach is similar to the sliding scale of insulin dosing used to treat hyperglycemia. Symptom-triggered therapy provides individualized treatment for withdrawal without overmedicating or underdosing, but it is a complex system to carry out on a general medical unit.
Severe withdrawal: Treat severe DTs manifested by abnormal and fluctuating vital signs and/or delirium aggressively in an ICU environment with sufficiently large doses of medication to suppress the withdrawal.11 Use IV medications with a rapid onset of action for immediate effect. Lorazepam and diazepam have a rapid onset of action when given intravenously, although the duration of action is shorter than when given orally.
For example, give lorazepam in a dose of one to four mg every 10-30 minutes until the patient is calm but awake and the heart rate is below 120 beats per minute. A continuous intravenous infusion may be warranted to control withdrawal symptoms, and the rate can be titrated to the desired level of consciousness. After stabilization, the patient can be changed to an equivalent dose of a long-acting sedative-hypnotic and tapered as above.
Assessing and medicating acute withdrawal remain necessary first steps in the treatment of the disease of alcohol dependence. After acute detoxification has begun, long-term treatment of alcoholism is necessary to prevent readmission for continuing medical problems due to alcohol consumption. Refer patients who have been treated for alcohol withdrawal for long-term treatment of alcoholism. This may include Alcoholics Anonymous, outpatient counseling, and other treatment modalities.
Conclusion
Ask all patients admitted to the hospital about drinking alcohol and be alert for signs of acute alcohol withdrawal in any patient. The best predictor of whether a patient will develop acute withdrawal is a past history of withdrawal. Signs of withdrawal usually occur within 48 hours of the last drink. Untreated withdrawal may result in significant morbidity and mortality.
Patients in withdrawal should be monitored closely and given appropriate doses of benzodiazepines or barbiturates to treat withdrawal signs. Cross-tolerant medication may be given on a fixed schedule or as symptom-triggered therapy. Severe withdrawal may require a continuous intravenous infusion in an ICU. Recognition and effective treatment of alcohol withdrawal can prevent significant complications in hospitalized patients. TH
Dr. Weaver is associate professor of internal medicine and psychiatry at Virginia Commonwealth University, Richmond.
References
- Saitz R. Introduction to alcohol withdrawal. Alcohol Health Res World. 1998;22(1):5-12.
- Cross GM, Hennessey PT. Principles and practice of detoxification. Prim Care. 1993;20(1):81-93.
- Cutshall BJ. The Saunderssutton syndrome: an analysis of delirium tremens. Q J Stud Alcohol. 1965;26(3):423-448.
- Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict. 1989;84:1353-1357.
- Foy A, March S, Drinkwater V. Use of an objective clinical scale in the assessment and management of alcohol withdrawal in a large general hospital. Alcohol Clin Exp Res. 1988;12(3):360-364.
- Weaver MF, Hoffman HJ, Johnson RE. Alcohol withdrawal pharmacotherapy for inpatients with medical comorbidity. J Addict Dis. 2006;25(2):17-24.
- Mayo-Smith MF. Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278(2):144-151.
- Saitz R, Mayo-Smith MF, Roberts MS, et al. Individualized treatment for alcohol withdrawal. A randomized double-blind controlled trial. JAMA. 1994;272(7):519-523.
- Yeh HS, Dhopesh V, Maany I. Seizures during detoxification. J Gen Intern Med. 1992;7(1):123.
- Young GP, Rores C, Murphy C, et al. Intravenous phenobarbital for alcohol withdrawal and convulsions. Ann Emerg Med. 1987;16(8):847-850.
- Weaver MF, Jarvis MA, Schnoll SH. Role of the primary care physician in problems of substance abuse. Arch Intern Med. 1999;159(9):913-924.
Irritability. Tremors. Sweating and a rapid heart rate. Extreme confusion. Fever. Convulsions. These are all symptoms of acute alcohol withdrawal syndrome. A patient may develop acute alcohol withdrawal syndrome when chronic alcohol use is interrupted by hospital admission. Increasingly patients are being treated for alcohol withdrawal on general medical wards.
Acute withdrawal is most safely managed in an inpatient setting if the patient has been using high doses of sedatives, has a history of seizures or delirium tremens, or has co-morbid medical or psychiatric problems.1 The severity of the withdrawal syndrome is affected by concurrent medical illness. Up to 20% of patients develop delirium tremens if left untreated.2 Recognition and effective treatment of alcohol withdrawal are needed to prevent excess mortality or prolonged hospitalization due to complications. It is essential for hospitalists to recognize and effectively treat acute alcohol withdrawal to prevent adverse outcomes in hospitalized patients.
Development of Withdrawal
Hospitalized patients may not be forthcoming about their alcohol consumption for numerous reasons. They may not consider it a problem; they may not recognize that acute withdrawal is a serious and even fatal complication; or they may wish to conceal their alcoholism from family and physicians due to concerns about stigmatization.
Even when patients acknowledge their drinking, they often underestimate the amount, which may be because a patient is minimizing or because alcohol is an amnestic agent, causing drinkers to lose count of how much they have had to drink. It is simplest to ask—in a nonjudgmental manner—all patients admitted to the hospital about drinking and to be alert for signs of acute alcohol withdrawal in all patients.
Not all patients who drink alcohol will develop an acute withdrawal syndrome. Those who drink less frequently—only on weekends with no drinking at all on weekdays, for example—are at lower risk of acute withdrawal. Those who drink on most days of the week are more likely—due to tolerance—to develop withdrawal. Even a habit of two or three drinks each day is enough to set up a person for withdrawal. Not all daily drinkers are guaranteed to develop withdrawal, and it is difficult to predict who will and who will not. The best predictor of whether a patient will develop acute withdrawal while hospitalized is a past history of acute alcohol withdrawal.
The alcohol withdrawal syndrome has two phases: early withdrawal and late withdrawal. (See Table 1, below.) The signs and symptoms of early withdrawal usually occur within 48 hours of the last drink. The initial indication is an elevation of vital signs: heart rate, blood pressure, and temperature. Tremors develop next—first a fine tremor of the hands and fasciculation of the tongue, then gross tremors of the extremities. As the syndrome progresses, disorientation and mild hallucinations (often auditory but occasionally visual) develop, accompanied by diaphoresis. Seizures are an early sign of alcohol withdrawal and may even be the presenting symptom.
Late alcohol withdrawal is also known as delirium tremens—the DTs—and consists of the worsening autonomic dysregulation that is responsible for the morbidity and mortality attributed to alcohol withdrawal. It begins after early withdrawal—usually 72 hours or more after the last drink. Some patients do not progress from early to late withdrawal, and their symptoms simply subside after a few days, with or without treatment. But it is impossible to predict which patients will progress and which will not. The signs of late withdrawal consist of worsening diaphoresis, nausea, and vomiting (which may result in aspiration pneumonia), delirium with frank hallucinations, and rapid, severe fluctuation in vital signs. Sudden changes in blood pressure and heart rate may result in complications such as myocardial infarction or a cerebrovascular event. Untreated late withdrawal results in significant morbidity and even death.3 Adequate treatment of early withdrawal prevents progression to late withdrawal.
Assessment
When you or a colleague suspect that a hospitalized patient may develop alcohol withdrawal, regularly assess the patient for signs of early withdrawal. Use a validated assessment scale to quantify the severity of the withdrawal syndrome, and initiate treatment decisions such as the dose of medication. If no withdrawal signs manifest after 48 hours, then it is usually safe to discontinue monitoring for withdrawal. Monitor patients for whom alcohol withdrawal is not considered but who then develop withdrawal signs using an assessment scale.
The revised Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) is commonly used to assess severity of withdrawal.4 Competent nurses can give it in less than five minutes. A CIWA-Ar score less than 5 indicates minimal withdrawal with no need for pharmacotherapy, whereas a score that falls in the range of 6-19 indicates mild withdrawal that may benefit from medical treatment. A score greater than 30 indicates severe withdrawal that requires close monitoring due to the risk for complications such as seizures and autonomic instability.5
The CIWA-Ar is just as useful for evaluating and treating withdrawal in hospitalized patients on general medical wards as it is for use in chemical dependency units. It can also be used to determine an appropriate pharmacotherapy dose for patients in withdrawal who also have other medical illnesses.6
Monitor patients every few hours, with the frequency of evaluation varying by severity of withdrawal signs. Every four hours is sufficient for most patients, but those who have developed late withdrawal or those with CIWA-Ar scores greater than 30 should be monitored hourly to prevent complications. Continue regular assessment until the withdrawal syndrome has been under control (CIWA-Ar score less than 6) for at least 24 hours.
Treatment
Medications: Pharmacotherapy is indicated for the management of moderate to severe withdrawal. Any cross-tolerant medication may be used; benzodiazepines or barbiturates are most commonly prescribed. It is inappropriate to use beverage alcohol to prevent or treat alcohol withdrawal. Use of intravenous alcohol infusion is reserved for poisoning with methanol, isopropanol, or ethylene glycol. It should not be given for treatment of acute alcohol withdrawal due to potential complications such as intoxication with delirium and development of gastritis.
Both benzodiazepines and barbiturates, which are different classes of sedative-hypnotic medications, are cross-tolerant with alcohol and effectively treat alcohol withdrawal.7 Acute alcohol withdrawal in the United States is most often managed with benzodiazepines.8 There are a variety of benzodiazepines available, from ultra-short-acting to long-acting, as well as parenteral and oral forms. Diazepam has been used extensively due to rapid onset of action when given intravenously and long duration of action when given orally.
For similar reasons, chlordiazepoxide is also used widely. Lorazepam, an intermediate-acting benzodiazepine that can be given orally or parenterally, has been used extensively for treatment of acute alcohol withdrawal, especially in hospitalized patients, because it has fewer active metabolites than other benzodiazepines. This makes it safer to use in treating patients with severe liver disease, which is important when treating chronic alcoholics. Benzodiazepines have a relatively high therapeutic index when used to treat patients with illnesses in addition to acute withdrawal. This makes benzodiazepines an excellent choice for the treatment of acute withdrawal in patients on general medical wards.
Barbiturates have been used successfully to treat acute alcohol withdrawal syndrome in general medical inpatients, with phenobarbital the most common choice.9,10 Phenobarbital may be preferable to other sedative-hypnotics; with its longer half-life, patients rarely achieve a “high” as they do with other sedatives, and it is available in multiple dosage forms.11
A number of alternative non-sedative-hypnotic medications exist to treat acute alcohol withdrawal. Beta-adrenergic blockers (atenolol, propranolol), clonidine, and anticonvulsant agents (carbamazepine, valproate) decrease alcohol withdrawal symptoms and have been used successfully in the treatment of mild withdrawal. They are not cross-tolerant with alcohol, however, and may result in progression of the withdrawal syndrome. These alternative medications are not appropriate to use as single agents in the treatment of withdrawal in a general medical setting.
Dosing regimens: There are no standard protocols for withdrawal management in widespread use.12 A fixed dosing schedule is commonly used for treatment of acute withdrawal, but either fixed-schedule or symptom-triggered dosing—medication given as needed for withdrawal signs—is efficacious in the treatment of withdrawal, even in patients with medical comorbidity.6
Fixed-schedule dosing is a one-size-fits-all approach for treating alcohol withdrawal. It uses the same dose of cross-tolerant medication on a fixed schedule for all patients for 24-48 hours; the dose is then tapered if the patient is stable. (See Table 2, left.) Reducing the dose by 10%-20% of the initial dose each day over five to 10 days provides a comfortable taper—especially in patients who initially required higher doses of medication to control the withdrawal. Fixed-schedule dosing offers less flexibility for individual patients, but it is a simple approach that can be applied in many settings.
Symptom-triggered therapy occurs when cross-tolerant medication is given only for symptoms of withdrawal rather than on a schedule. (See Table 3, p. 25.) Patients are monitored closely and assessed regularly using a tool such as the CIWA-Ar. The dose of cross-tolerant medication prescribed is based on the severity of withdrawal symptoms as measured by the CIWA-Ar score. This approach is similar to the sliding scale of insulin dosing used to treat hyperglycemia. Symptom-triggered therapy provides individualized treatment for withdrawal without overmedicating or underdosing, but it is a complex system to carry out on a general medical unit.
Severe withdrawal: Treat severe DTs manifested by abnormal and fluctuating vital signs and/or delirium aggressively in an ICU environment with sufficiently large doses of medication to suppress the withdrawal.11 Use IV medications with a rapid onset of action for immediate effect. Lorazepam and diazepam have a rapid onset of action when given intravenously, although the duration of action is shorter than when given orally.
For example, give lorazepam in a dose of one to four mg every 10-30 minutes until the patient is calm but awake and the heart rate is below 120 beats per minute. A continuous intravenous infusion may be warranted to control withdrawal symptoms, and the rate can be titrated to the desired level of consciousness. After stabilization, the patient can be changed to an equivalent dose of a long-acting sedative-hypnotic and tapered as above.
Assessing and medicating acute withdrawal remain necessary first steps in the treatment of the disease of alcohol dependence. After acute detoxification has begun, long-term treatment of alcoholism is necessary to prevent readmission for continuing medical problems due to alcohol consumption. Refer patients who have been treated for alcohol withdrawal for long-term treatment of alcoholism. This may include Alcoholics Anonymous, outpatient counseling, and other treatment modalities.
Conclusion
Ask all patients admitted to the hospital about drinking alcohol and be alert for signs of acute alcohol withdrawal in any patient. The best predictor of whether a patient will develop acute withdrawal is a past history of withdrawal. Signs of withdrawal usually occur within 48 hours of the last drink. Untreated withdrawal may result in significant morbidity and mortality.
Patients in withdrawal should be monitored closely and given appropriate doses of benzodiazepines or barbiturates to treat withdrawal signs. Cross-tolerant medication may be given on a fixed schedule or as symptom-triggered therapy. Severe withdrawal may require a continuous intravenous infusion in an ICU. Recognition and effective treatment of alcohol withdrawal can prevent significant complications in hospitalized patients. TH
Dr. Weaver is associate professor of internal medicine and psychiatry at Virginia Commonwealth University, Richmond.
References
- Saitz R. Introduction to alcohol withdrawal. Alcohol Health Res World. 1998;22(1):5-12.
- Cross GM, Hennessey PT. Principles and practice of detoxification. Prim Care. 1993;20(1):81-93.
- Cutshall BJ. The Saunderssutton syndrome: an analysis of delirium tremens. Q J Stud Alcohol. 1965;26(3):423-448.
- Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict. 1989;84:1353-1357.
- Foy A, March S, Drinkwater V. Use of an objective clinical scale in the assessment and management of alcohol withdrawal in a large general hospital. Alcohol Clin Exp Res. 1988;12(3):360-364.
- Weaver MF, Hoffman HJ, Johnson RE. Alcohol withdrawal pharmacotherapy for inpatients with medical comorbidity. J Addict Dis. 2006;25(2):17-24.
- Mayo-Smith MF. Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278(2):144-151.
- Saitz R, Mayo-Smith MF, Roberts MS, et al. Individualized treatment for alcohol withdrawal. A randomized double-blind controlled trial. JAMA. 1994;272(7):519-523.
- Yeh HS, Dhopesh V, Maany I. Seizures during detoxification. J Gen Intern Med. 1992;7(1):123.
- Young GP, Rores C, Murphy C, et al. Intravenous phenobarbital for alcohol withdrawal and convulsions. Ann Emerg Med. 1987;16(8):847-850.
- Weaver MF, Jarvis MA, Schnoll SH. Role of the primary care physician in problems of substance abuse. Arch Intern Med. 1999;159(9):913-924.
From Weapon to Wonder Drug

Gas! Gas! Quick, boys! An ecstasy of fumbling, Fitting the clumsy helmets just in time; But someone still was yelling out and stumbling And flound’ring like a man in fire or lime.
—Wilfred Owen, Dulce et Decorum Est (1917)
In virtually every hospital around the world, oncology patients are treated with constantly evolving life- and limb-saving protocols. Cancer has plagued mankind for thousands of years. Records of cancer exist from as early as the ancient Egyptian era. The famous Edwin Smith Surgical Papyrus, dating to 1,600 B.C., describes a man with “bulging tumors on his breast.” The translation of the treatment for this case simply reads: “There is no treatment.” Unfortunately, the history of chemotherapy lags behind that of the disease it treats by at least 4,000 years. And ironically, the first modern day anticancer drug was spawned from a deadly World War I weapon.
Sulfur mustard, or mustard gas, has the dubious distinction of being one of the original chemical weapons. Bis-(2-chloroethyl) sulfide was first synthesized by London Institute of Physics Co-founder Frederick Guthrie in 1860. Guthrie, a profound believer in the advancement of science through experimentation rather than discussion, first documented the toxic effects of mustard gas by applying his mixture of ethylene and sulfur dichloride to his own skin, thus joining other notables in the halls of self-experimentation.
Mustard gas was mass-produced under the name LOST (an acronym fashioned from the names of its developers) for the German company Bayer AG during the first decade of the 20th century. Unfortunately, this proved to be perfect timing for the introduction of chemical warfare by the German army in 1917. The first strike was against Canadian troops. One year later the British used the same agent to destroy the “impregnable” Hindenburg Line. This culmination of the storied allied forces’ 100 Days Offensive ultimately led to the end of the First World War.
Various permutations of this compound were used sporadically by numerous world powers over the next 25 years. The malevolent use of mustard gas may be responsible for nearly 100,000 deaths and approximately five times as many wartime injuries. In fact, sulfur mustard gas—not a gas or a mustard, but rather a yellowish-brown vaporized liquid with a mustard seed-like odor—is known primarily as an incapacitant rather than as a lethal weapon. The effects of this poison may remain hidden for two to 24 hours after exposure.
Sulfur mustard is a vesicant. It exerts its effects on the body’s mucous membranes. The skin and the eyes are among the first organs to be affected. The toxicity of this agent is dose-dependent. While lower concentrations can cause symptoms as minor as skin irritation and conjunctivitis, higher titers can lead to morbid consequences such as necrotic ulcerations of the skin and blindness. At still higher concentrations, inhaled vapors can damage the mucous membrane lining of the respiratory tract, leading to hemorrhagic pulmonary edema.
Sulfur mustard also causes chronic sequelae. After exposure, surviving victims might exhibit nausea, vomiting, alopecia, and increased vulnerability to infection. These later symptoms are the result of the poison’s ability to act as an alkylating agent, cross-linking DNA and preventing the normal sequence of DNA replication. The organs primarily affected are the lining of the gastrointestinal tract and the bone marrow, due to their inherent high mitotic activity.
Despite its sinister history, mustard gas has played a key role in the development of anti-cancer chemotherapeutic agents and may justly be referred to as the egg from which medical oncology has hatched. The history of medicine contains many tales of accidental discovery, but how did a deadly gas become the first effective chemotherapeutic agent?
Fast forward 30 years to the Second World War. The interwar period resulted in numerous provisions—including the Geneva Protocol of 1929—to ban the use of chemical weapons. It was also a time during which many nations—both purposefully and accidentally—developed and stockpiled chemical agents. Thankfully, chemical weapons, including mustard gas, were not used extensively by either side during World War II. This was a period of intense—and justified—paranoia, however. General Dwight D. Eisenhower had made provisions for a stockpile of 100 tons of mustard gas on the S.S. John Harvey, which was stationed in Italy’s Bari Harbor. In December 1943, Nazi air strikes destroyed the John Harvey, among other ships, resulting in surprisingly few casualties despite the impressive amount of fire and destruction.
In the days and weeks following this catastrophe, however, survivors began to develop the familiar signs of mustard gas exposure. Lt. Col. Stewart Francis Alexander, an expert in chemical warfare, suspected exposure to the famous vapor. Autopsies of the victims reported profound lymphopenia as well as suppression of myeloid cell lines. This prompted the United States to lift the Office of Scientific Research and Development publication ban in 1946. At this time, numerous accounts were uncovered of mustard gas and its derivatives in experimental trials involving humans and cloned mice.
The first clinical trial, conducted by Louis Goodman and Alfred Gilman, involved the use of nitrogen mustard on a patient with advanced lymphosarcoma. After just four days of therapy, the patient’s tumor mass receded remarkably. Unfortunately, withdrawal of the medication due to profound neutropenia resulted in an abrupt return of the tumors. A second, shorter course resulted in a less profound reduction in tumor bulk, and a third try had no effect at all.

Interestingly, this temporary miracle with its subsequent failure illustrates two paradigms faced by medical oncologists today. Chemotherapeutic agents exert a toxic toll on the host, and tumor cells eventually develop resistance to circumvent the effects of these same medications. This is exactly why complicated protocols are used to treat patients with cancer.
Goodman and Gilman, authors of the famous medical pharmacology textbook The Pharmacological Basis of Therapeutics, used nitrogen mustard, a derivative of sulfur mustard, for their experiment. This compound, also known as mechlorethamine, is the first in-class alkylating agent, and is still used as a topical ointment in the treatment of cutaneous lymphomas. Other alkylating agents, such as cyclophosphamide, ifosfamide, and cisplatin, are used in cancer protocols worldwide.
We have not seen the last of mustard gas, which made its last acknowledged appearance in the Iran-Iraq war. Frequently, those things that are most destructive can be tamed for medical use.
The next time you have a patient receiving chemotherapy, think back to the roots of the cure. TH
References
- Pratt WB, Ruddon RW, Ensminger WD, et al. The Anticancer Drugs. 2nd ed. New York: Oxford University Press; 1994.
- Faguet GB. The War on Cancer: An Anatomy of Failure, a Blueprint for the Future. Dordrecht, Netherlands: Springer Press; 2005.
- Baguley BC, Kerr DJ, eds. Anticancer Drug Development. New York: Academic Press; 2002.
- Goodman LS, Wintrobe MM, Dameshek W, et al. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl)amine hydrochloride and tris(beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA. 1984;251:2255-2261.
- Kazin RA, Lowitt NR, Lowitt MH. Update in dermatology. Ann Intern Med. 2001;135:124-132.
Gas! Gas! Quick, boys! An ecstasy of fumbling, Fitting the clumsy helmets just in time; But someone still was yelling out and stumbling And flound’ring like a man in fire or lime.
—Wilfred Owen, Dulce et Decorum Est (1917)
In virtually every hospital around the world, oncology patients are treated with constantly evolving life- and limb-saving protocols. Cancer has plagued mankind for thousands of years. Records of cancer exist from as early as the ancient Egyptian era. The famous Edwin Smith Surgical Papyrus, dating to 1,600 B.C., describes a man with “bulging tumors on his breast.” The translation of the treatment for this case simply reads: “There is no treatment.” Unfortunately, the history of chemotherapy lags behind that of the disease it treats by at least 4,000 years. And ironically, the first modern day anticancer drug was spawned from a deadly World War I weapon.
Sulfur mustard, or mustard gas, has the dubious distinction of being one of the original chemical weapons. Bis-(2-chloroethyl) sulfide was first synthesized by London Institute of Physics Co-founder Frederick Guthrie in 1860. Guthrie, a profound believer in the advancement of science through experimentation rather than discussion, first documented the toxic effects of mustard gas by applying his mixture of ethylene and sulfur dichloride to his own skin, thus joining other notables in the halls of self-experimentation.
Mustard gas was mass-produced under the name LOST (an acronym fashioned from the names of its developers) for the German company Bayer AG during the first decade of the 20th century. Unfortunately, this proved to be perfect timing for the introduction of chemical warfare by the German army in 1917. The first strike was against Canadian troops. One year later the British used the same agent to destroy the “impregnable” Hindenburg Line. This culmination of the storied allied forces’ 100 Days Offensive ultimately led to the end of the First World War.
Various permutations of this compound were used sporadically by numerous world powers over the next 25 years. The malevolent use of mustard gas may be responsible for nearly 100,000 deaths and approximately five times as many wartime injuries. In fact, sulfur mustard gas—not a gas or a mustard, but rather a yellowish-brown vaporized liquid with a mustard seed-like odor—is known primarily as an incapacitant rather than as a lethal weapon. The effects of this poison may remain hidden for two to 24 hours after exposure.
Sulfur mustard is a vesicant. It exerts its effects on the body’s mucous membranes. The skin and the eyes are among the first organs to be affected. The toxicity of this agent is dose-dependent. While lower concentrations can cause symptoms as minor as skin irritation and conjunctivitis, higher titers can lead to morbid consequences such as necrotic ulcerations of the skin and blindness. At still higher concentrations, inhaled vapors can damage the mucous membrane lining of the respiratory tract, leading to hemorrhagic pulmonary edema.
Sulfur mustard also causes chronic sequelae. After exposure, surviving victims might exhibit nausea, vomiting, alopecia, and increased vulnerability to infection. These later symptoms are the result of the poison’s ability to act as an alkylating agent, cross-linking DNA and preventing the normal sequence of DNA replication. The organs primarily affected are the lining of the gastrointestinal tract and the bone marrow, due to their inherent high mitotic activity.
Despite its sinister history, mustard gas has played a key role in the development of anti-cancer chemotherapeutic agents and may justly be referred to as the egg from which medical oncology has hatched. The history of medicine contains many tales of accidental discovery, but how did a deadly gas become the first effective chemotherapeutic agent?
Fast forward 30 years to the Second World War. The interwar period resulted in numerous provisions—including the Geneva Protocol of 1929—to ban the use of chemical weapons. It was also a time during which many nations—both purposefully and accidentally—developed and stockpiled chemical agents. Thankfully, chemical weapons, including mustard gas, were not used extensively by either side during World War II. This was a period of intense—and justified—paranoia, however. General Dwight D. Eisenhower had made provisions for a stockpile of 100 tons of mustard gas on the S.S. John Harvey, which was stationed in Italy’s Bari Harbor. In December 1943, Nazi air strikes destroyed the John Harvey, among other ships, resulting in surprisingly few casualties despite the impressive amount of fire and destruction.
In the days and weeks following this catastrophe, however, survivors began to develop the familiar signs of mustard gas exposure. Lt. Col. Stewart Francis Alexander, an expert in chemical warfare, suspected exposure to the famous vapor. Autopsies of the victims reported profound lymphopenia as well as suppression of myeloid cell lines. This prompted the United States to lift the Office of Scientific Research and Development publication ban in 1946. At this time, numerous accounts were uncovered of mustard gas and its derivatives in experimental trials involving humans and cloned mice.
The first clinical trial, conducted by Louis Goodman and Alfred Gilman, involved the use of nitrogen mustard on a patient with advanced lymphosarcoma. After just four days of therapy, the patient’s tumor mass receded remarkably. Unfortunately, withdrawal of the medication due to profound neutropenia resulted in an abrupt return of the tumors. A second, shorter course resulted in a less profound reduction in tumor bulk, and a third try had no effect at all.
Interestingly, this temporary miracle with its subsequent failure illustrates two paradigms faced by medical oncologists today. Chemotherapeutic agents exert a toxic toll on the host, and tumor cells eventually develop resistance to circumvent the effects of these same medications. This is exactly why complicated protocols are used to treat patients with cancer.
Goodman and Gilman, authors of the famous medical pharmacology textbook The Pharmacological Basis of Therapeutics, used nitrogen mustard, a derivative of sulfur mustard, for their experiment. This compound, also known as mechlorethamine, is the first in-class alkylating agent, and is still used as a topical ointment in the treatment of cutaneous lymphomas. Other alkylating agents, such as cyclophosphamide, ifosfamide, and cisplatin, are used in cancer protocols worldwide.
We have not seen the last of mustard gas, which made its last acknowledged appearance in the Iran-Iraq war. Frequently, those things that are most destructive can be tamed for medical use.
The next time you have a patient receiving chemotherapy, think back to the roots of the cure. TH
References
- Pratt WB, Ruddon RW, Ensminger WD, et al. The Anticancer Drugs. 2nd ed. New York: Oxford University Press; 1994.
- Faguet GB. The War on Cancer: An Anatomy of Failure, a Blueprint for the Future. Dordrecht, Netherlands: Springer Press; 2005.
- Baguley BC, Kerr DJ, eds. Anticancer Drug Development. New York: Academic Press; 2002.
- Goodman LS, Wintrobe MM, Dameshek W, et al. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl)amine hydrochloride and tris(beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA. 1984;251:2255-2261.
- Kazin RA, Lowitt NR, Lowitt MH. Update in dermatology. Ann Intern Med. 2001;135:124-132.
Gas! Gas! Quick, boys! An ecstasy of fumbling, Fitting the clumsy helmets just in time; But someone still was yelling out and stumbling And flound’ring like a man in fire or lime.
—Wilfred Owen, Dulce et Decorum Est (1917)
In virtually every hospital around the world, oncology patients are treated with constantly evolving life- and limb-saving protocols. Cancer has plagued mankind for thousands of years. Records of cancer exist from as early as the ancient Egyptian era. The famous Edwin Smith Surgical Papyrus, dating to 1,600 B.C., describes a man with “bulging tumors on his breast.” The translation of the treatment for this case simply reads: “There is no treatment.” Unfortunately, the history of chemotherapy lags behind that of the disease it treats by at least 4,000 years. And ironically, the first modern day anticancer drug was spawned from a deadly World War I weapon.
Sulfur mustard, or mustard gas, has the dubious distinction of being one of the original chemical weapons. Bis-(2-chloroethyl) sulfide was first synthesized by London Institute of Physics Co-founder Frederick Guthrie in 1860. Guthrie, a profound believer in the advancement of science through experimentation rather than discussion, first documented the toxic effects of mustard gas by applying his mixture of ethylene and sulfur dichloride to his own skin, thus joining other notables in the halls of self-experimentation.
Mustard gas was mass-produced under the name LOST (an acronym fashioned from the names of its developers) for the German company Bayer AG during the first decade of the 20th century. Unfortunately, this proved to be perfect timing for the introduction of chemical warfare by the German army in 1917. The first strike was against Canadian troops. One year later the British used the same agent to destroy the “impregnable” Hindenburg Line. This culmination of the storied allied forces’ 100 Days Offensive ultimately led to the end of the First World War.
Various permutations of this compound were used sporadically by numerous world powers over the next 25 years. The malevolent use of mustard gas may be responsible for nearly 100,000 deaths and approximately five times as many wartime injuries. In fact, sulfur mustard gas—not a gas or a mustard, but rather a yellowish-brown vaporized liquid with a mustard seed-like odor—is known primarily as an incapacitant rather than as a lethal weapon. The effects of this poison may remain hidden for two to 24 hours after exposure.
Sulfur mustard is a vesicant. It exerts its effects on the body’s mucous membranes. The skin and the eyes are among the first organs to be affected. The toxicity of this agent is dose-dependent. While lower concentrations can cause symptoms as minor as skin irritation and conjunctivitis, higher titers can lead to morbid consequences such as necrotic ulcerations of the skin and blindness. At still higher concentrations, inhaled vapors can damage the mucous membrane lining of the respiratory tract, leading to hemorrhagic pulmonary edema.
Sulfur mustard also causes chronic sequelae. After exposure, surviving victims might exhibit nausea, vomiting, alopecia, and increased vulnerability to infection. These later symptoms are the result of the poison’s ability to act as an alkylating agent, cross-linking DNA and preventing the normal sequence of DNA replication. The organs primarily affected are the lining of the gastrointestinal tract and the bone marrow, due to their inherent high mitotic activity.
Despite its sinister history, mustard gas has played a key role in the development of anti-cancer chemotherapeutic agents and may justly be referred to as the egg from which medical oncology has hatched. The history of medicine contains many tales of accidental discovery, but how did a deadly gas become the first effective chemotherapeutic agent?
Fast forward 30 years to the Second World War. The interwar period resulted in numerous provisions—including the Geneva Protocol of 1929—to ban the use of chemical weapons. It was also a time during which many nations—both purposefully and accidentally—developed and stockpiled chemical agents. Thankfully, chemical weapons, including mustard gas, were not used extensively by either side during World War II. This was a period of intense—and justified—paranoia, however. General Dwight D. Eisenhower had made provisions for a stockpile of 100 tons of mustard gas on the S.S. John Harvey, which was stationed in Italy’s Bari Harbor. In December 1943, Nazi air strikes destroyed the John Harvey, among other ships, resulting in surprisingly few casualties despite the impressive amount of fire and destruction.
In the days and weeks following this catastrophe, however, survivors began to develop the familiar signs of mustard gas exposure. Lt. Col. Stewart Francis Alexander, an expert in chemical warfare, suspected exposure to the famous vapor. Autopsies of the victims reported profound lymphopenia as well as suppression of myeloid cell lines. This prompted the United States to lift the Office of Scientific Research and Development publication ban in 1946. At this time, numerous accounts were uncovered of mustard gas and its derivatives in experimental trials involving humans and cloned mice.
The first clinical trial, conducted by Louis Goodman and Alfred Gilman, involved the use of nitrogen mustard on a patient with advanced lymphosarcoma. After just four days of therapy, the patient’s tumor mass receded remarkably. Unfortunately, withdrawal of the medication due to profound neutropenia resulted in an abrupt return of the tumors. A second, shorter course resulted in a less profound reduction in tumor bulk, and a third try had no effect at all.
Interestingly, this temporary miracle with its subsequent failure illustrates two paradigms faced by medical oncologists today. Chemotherapeutic agents exert a toxic toll on the host, and tumor cells eventually develop resistance to circumvent the effects of these same medications. This is exactly why complicated protocols are used to treat patients with cancer.
Goodman and Gilman, authors of the famous medical pharmacology textbook The Pharmacological Basis of Therapeutics, used nitrogen mustard, a derivative of sulfur mustard, for their experiment. This compound, also known as mechlorethamine, is the first in-class alkylating agent, and is still used as a topical ointment in the treatment of cutaneous lymphomas. Other alkylating agents, such as cyclophosphamide, ifosfamide, and cisplatin, are used in cancer protocols worldwide.
We have not seen the last of mustard gas, which made its last acknowledged appearance in the Iran-Iraq war. Frequently, those things that are most destructive can be tamed for medical use.
The next time you have a patient receiving chemotherapy, think back to the roots of the cure. TH
References
- Pratt WB, Ruddon RW, Ensminger WD, et al. The Anticancer Drugs. 2nd ed. New York: Oxford University Press; 1994.
- Faguet GB. The War on Cancer: An Anatomy of Failure, a Blueprint for the Future. Dordrecht, Netherlands: Springer Press; 2005.
- Baguley BC, Kerr DJ, eds. Anticancer Drug Development. New York: Academic Press; 2002.
- Goodman LS, Wintrobe MM, Dameshek W, et al. Landmark article Sept. 21, 1946: Nitrogen mustard therapy. Use of methyl-bis(beta-chloroethyl)amine hydrochloride and tris(beta-chloroethyl)amine hydrochloride for Hodgkin’s disease, lymphosarcoma, leukemia and certain allied and miscellaneous disorders. JAMA. 1984;251:2255-2261.
- Kazin RA, Lowitt NR, Lowitt MH. Update in dermatology. Ann Intern Med. 2001;135:124-132.
Safety after Surgery
An 86-year-old female with Alzheimer’s dementia, hypertension, type 2 diabetes, and chronic obstructive pulmonary disease was admitted with lethargy, fever, and vomiting. After she was diagnosed with necrotizing cholecystitis, she underwent an emergent cholecystectomy. Three days later the patient was short of breath, confused, and hadn’t urinated since the indwelling catheter was removed.
Sound familiar? If this scenario doesn’t ring a bell now, then it soon will. The 65-and-up age group is the fastest growing section of the United States population. A recent poll found that elderly patients now account for more than 60% of most general surgeons’ practices. Additionally, the use of minimally invasive surgical techniques and advanced perioperative monitoring has permitted elderly patients who were previously considered too debilitated to now become surgical candidates.
Though patients and their families most often worry about events in the operating room, the vast majority of complications occur in the postoperative period. Morbidity and mortality rates double during the first 24 hours after surgery and are tenfold higher over the remainder of the first postoperative week. In a recent study of more than 500 elderly general surgery patients, 21% experienced complications during this period.
The most common postoperative complications in the geriatric population include delirium, ileus, nutritional deficiencies, respiratory complications—including pulmonary embolism—and urinary retention. The goal in managing any elderly patient is to preserve cognitive and physical function. Maintaining this goal in the postoperative setting requires the early implementation of preventive measures, as well as an understanding of when age-appropriate intervention is necessary.
Hospitalists are often the first line of defense for postoperative situations in medically ill patients, and an amplification of issues unique to the geriatric patient follows.
Delirium
Postoperative delirium occurs in 10%-15% of older general surgery patients and in 30%-60% of older patients who undergo orthopedic procedures. The most common presentation of delirium in the elderly postoperative patient is a “quiet confusion” that is more pronounced in the evening—otherwise known as sundowning. An acute change in mental status, manifested as a fluctuating level of consciousness or a cognitive deficit, is also common. Though delirium may result solely from the acute stress of the operation, other medically relevant causes include metabolic abnormalities, abnormal respiratory parameters, infections, and medications, and these causes should be aggressively investigated and treated.
After potential medical etiologies have been addressed, focus the treatment of delirium in the elderly postoperative patient on interventions to restore mental and physical function as well as pharmacotherapy. Measures to restore function, such as early mobilization and ambulation, sleep hygiene, volume repletion, and restoration of vision and hearing with appropriate devices, have been shown to decrease the duration of the delirium episode. Other non-pharmacologic interventions, including placing a patient near the nurses’ station, encouraging social visits with caregivers, and avoiding the use of physical restraints (which can aggravate agitation) may also prove helpful.
Avoid the use of psychoactive medications (e.g., antiarrhythmic agents, tricyclic antidepressants, neuroleptics, gastrointestinal medications, antihistamines, ciprofloxacin, nonsteroidal anti-inflammatory drugs, meperidine, and cimetidine) as much as possible during the acute confusional state.
Pharmacologic treatment of delirium may be warranted in patients experiencing symptoms of psychosis or in those exhibiting signs of physical aggression or severe personal distress. Haloperidol and risperidol are the medications of choice, though the FDA has approved neither drug specifically for this indication. High doses of these medications are associated with extrapyramidal effects, dystonic reactions, and torsade de pointe. Once the delirium begins to resolve, doses should be tapered gradually over several days.
Ileus
Postsurgical ileus can cause profound clinical consequences in elderly patients. This complication is associated with delayed enteral feeding and malnutrition, increased length of hospital stay, and increased risk of pulmonary complications. Patients present with abdominal distension, nausea and vomiting, limited flatus, and a decreased presence of bowel sounds on auscultation. In cases of prolonged postsurgical ileus, consider pseudo-obstruction (Ogilvie’s syndrome) and mechanical obstruction.
Intravenous hydration and nutrition (in prolonged cases), assisted ambulation, and the avoidance of opiates remain the mainstays of treatment. Nasogastric tubes may provide symptomatic relief in patients with nausea and vomiting, but studies don’t support the use of this intervention to enhance resolution of the ileus. Many prokinetic agents have been examined for this use, including neostigmine and cisapride, but the results have been mixed, and the side effect profiles are generally unacceptable for elderly patients. Delay oral feeding until satisfactory bowel function has been restored.
Nutritional Care
An estimated 12%-50% of geriatric patients are found to be malnourished in the acute hospital setting. The adverse effects of malnutrition include delayed wound healing, greater risk of sepsis and wound infections, deterioration of functional status secondary to muscle wasting, and increased mortality.
Early identification of the patient’s feeding limitations is the key to preventing adverse outcomes. If a patient is restricted from oral or enteral feeding, parenteral nutrition should be started within 48 hours. When volitional food intake is permitted, the addition of canned nutritional supplements, fortified meals, and between-meal snacks may improve elderly patients’ energy and protein intake.
Initiate enteral feeding in patients for whom voluntary food intake is decreased. Parenteral nutrition may still be required until enteral feeding is established, however, and prescribed nutrients can be administered enterally. Because glucose tolerance diminishes with normal aging and may be further reduced in a state of acute illness, initiation of insulin therapy may be necessary in patients receiving either enteral or parenteral supplementation. Additionally, supplementation with a zinc-containing daily multivitamin has been shown to enhance immune function and prevent infections.
Respiratory Care
Respiratory function may be diminished in elderly patients due to age-related changes in the upper and lower respiratory tracts. Factors that contribute to an increased rate of pulmonary postoperative complications include diminished protective mechanisms like coughing and swallowing, decreased compliance of the chest wall and lung tissue, inadequate mucociliary transport, and a blunted ventilatory response to hypoxia and hypercapnia. Postoperative respiratory complications, including pneumonia, hypoxemia, hypoventilation, and atelectasis, occur in 2.1%-10.2% of elderly patients. These complications are associated with increased length of stay and a higher risk of long-term mortality.
Respiratory function may be preserved in the postoperative geriatric patient using a variety of measures. Effective pain control is essential in maintaining adequate lung volumes, and regional analgesia is associated with less-severe postoperative decreases in vital capacity and functional residual capacity (FRC). Once postoperative pain has been controlled, encourage the early resumption of physical activity (with appropriate assistance). Positioning patients in a seated position increases FRC and improves gas exchange in those recovering from abdominal procedures. Additionally, incentive spirometers, breathing exercises, and intermittent positive-pressure breathing may reduce the incidence of pulmonary complications after upper-abdominal operations, shortening the length of hospital stay.
Thromboembolic Disease
Fatal pulmonary embolism accounts for a large proportion of postoperative deaths in the elderly population. Between 20%-30% of patients undergoing general surgery without prophylaxis develop deep vein thrombosis, and the incidence is as high as 40% in those undergoing orthopedic surgeries, gynecologic cancer operations, and major neurosurgical procedures.
The Fifth American College of Chest Physicians Consensus Conference on Antithrombotic Therapy recommends the following postoperative interventions for older surgical patients:
- General surgery without clinical risk factors for thrombosis: Give low-dose unfractionated heparin two hours before and every 12 hours after the operation;
- General surgery with any clinical risk factors such as prolonged immobilization or paralysis, obesity, varicose veins, congestive heart failure, or pelvic or leg fractures: Administer low molecular weight heparin (LMWH) or low-dose unfractionated heparin every eight hours. If the patient is also prone to bleeding or infection, intermittent pneumatic compression (IPC) can be used instead;
- General surgery with multiple clinical risk factors or with a history of previous deep vein thrombosis, malignancy, stroke, spinal cord injury, or hip fracture: Use low dose unfractionated heparin or LMWH combined with intermittent pneumatic compression; for very high risk patients, perioperative warfarin is an alternative;
- Total hip replacement: Give postoperative LMWH every 12 hours; initiate low-intensity warfarin therapy—to keep International Normalized Ratio of 2-3—preoperatively or immediately postoperatively;
- Total knee replacement: Administer postoperative LMWH every 12 hours. IPC is the most effective non-pharmacologic regimen and is comparable to LMWH. Low-intensity warfarin can also be used; and
- Hip fracture repair: Start preoperative fixed-dose LMWH or low-intensity warfarin.
Urinary Retention
The incidence of postoperative urinary retention in elderly patients has been reported to be as high as 87%. Factors contributing to the development of this complication include immobility, analgesics and opiates, intravenous hydration, and general anesthesia. Urinary retention can lead to overflow incontinence and urinary tract infection and is associated with a decline in function and nursing home placement. The first indication of urinary retention may be a diminished urinary output after removal of an indwelling catheter, overflow incontinence, or the frequent voiding of small amounts of urine.
Urinary retention is treated with catheterization. This prevents bladder distension, which leads to reduced detrusor contractile function, and helps restore preoperative bladder function.
Recent studies have found that normal voiding resumes earlier with the use of intermittent catheterization (if begun at the onset of urinary retention and repeated every six to eight hours) than with the use of an indwelling catheter. Additionally, the use of indwelling catheters in the elderly after the immediate perioperative period is associated with an increased risk of urosepsis and a more dependent postoperative functional status.
Conclusion
The 65-and-up age group is the fastest growing section of the United States population. The vast majority of complications for this age group occur in the postoperative period. It’s important for hospitalists to remain involved in key areas of postoperative complications in the geriatric population—specifically, delirium, ileus, nutritional deficiencies, respiratory complications—including pulmonary embolism—and urinary retention. TH
Jill Landis is a frequent contributor to The Hospitalist.
References
- Souders JE, Rooke GA. Perioperative care for geriatric patients. Ann Long Term Care. 2005;13(6):17-29.
- Williams SL, Jones PB, Pofahl WE. Preoperative management of the older patient—a surgeon’s perspective: part I. Ann Long Term Care. 2006;14(6):24-30.
- Palmer RM. Management of common clinical disorders in geriatric patients: delirium. ACP Medicine Online. June 7, 2006. Available at: www.medscape.com/viewarticle/534766. Last accessed January 11, 2007.
- Manku K, Bacchetti P, Leung JM. Prognostic significance of postoperative in-hospital complications in elderly patients. I. Long-term survival. Anesth Analg. 2003 Feb;96(2):583-589.
- Watters JM, McClaran JC, Man-Son-Hing M. The elderly surgical patient: introduction. ACS Surgery Online. June 7, 2006. Available at: www.medscape.com/viewarticle/535461?rss. Last accessed January 11, 2006.
- Skelly JM, Guyatt GH, Kalbfleisch R, et al. Management of urinary retention after surgical repair of hip fracture. CMAJ. 1992 Apr 1;146(7):1185-1189.
- Wittbrodt E. The impact of postoperative ileus and emerging therapies. Pharm Treatment. 2006 Jan;31(1):39-59.
An 86-year-old female with Alzheimer’s dementia, hypertension, type 2 diabetes, and chronic obstructive pulmonary disease was admitted with lethargy, fever, and vomiting. After she was diagnosed with necrotizing cholecystitis, she underwent an emergent cholecystectomy. Three days later the patient was short of breath, confused, and hadn’t urinated since the indwelling catheter was removed.
Sound familiar? If this scenario doesn’t ring a bell now, then it soon will. The 65-and-up age group is the fastest growing section of the United States population. A recent poll found that elderly patients now account for more than 60% of most general surgeons’ practices. Additionally, the use of minimally invasive surgical techniques and advanced perioperative monitoring has permitted elderly patients who were previously considered too debilitated to now become surgical candidates.
Though patients and their families most often worry about events in the operating room, the vast majority of complications occur in the postoperative period. Morbidity and mortality rates double during the first 24 hours after surgery and are tenfold higher over the remainder of the first postoperative week. In a recent study of more than 500 elderly general surgery patients, 21% experienced complications during this period.
The most common postoperative complications in the geriatric population include delirium, ileus, nutritional deficiencies, respiratory complications—including pulmonary embolism—and urinary retention. The goal in managing any elderly patient is to preserve cognitive and physical function. Maintaining this goal in the postoperative setting requires the early implementation of preventive measures, as well as an understanding of when age-appropriate intervention is necessary.
Hospitalists are often the first line of defense for postoperative situations in medically ill patients, and an amplification of issues unique to the geriatric patient follows.
Delirium
Postoperative delirium occurs in 10%-15% of older general surgery patients and in 30%-60% of older patients who undergo orthopedic procedures. The most common presentation of delirium in the elderly postoperative patient is a “quiet confusion” that is more pronounced in the evening—otherwise known as sundowning. An acute change in mental status, manifested as a fluctuating level of consciousness or a cognitive deficit, is also common. Though delirium may result solely from the acute stress of the operation, other medically relevant causes include metabolic abnormalities, abnormal respiratory parameters, infections, and medications, and these causes should be aggressively investigated and treated.
After potential medical etiologies have been addressed, focus the treatment of delirium in the elderly postoperative patient on interventions to restore mental and physical function as well as pharmacotherapy. Measures to restore function, such as early mobilization and ambulation, sleep hygiene, volume repletion, and restoration of vision and hearing with appropriate devices, have been shown to decrease the duration of the delirium episode. Other non-pharmacologic interventions, including placing a patient near the nurses’ station, encouraging social visits with caregivers, and avoiding the use of physical restraints (which can aggravate agitation) may also prove helpful.
Avoid the use of psychoactive medications (e.g., antiarrhythmic agents, tricyclic antidepressants, neuroleptics, gastrointestinal medications, antihistamines, ciprofloxacin, nonsteroidal anti-inflammatory drugs, meperidine, and cimetidine) as much as possible during the acute confusional state.
Pharmacologic treatment of delirium may be warranted in patients experiencing symptoms of psychosis or in those exhibiting signs of physical aggression or severe personal distress. Haloperidol and risperidol are the medications of choice, though the FDA has approved neither drug specifically for this indication. High doses of these medications are associated with extrapyramidal effects, dystonic reactions, and torsade de pointe. Once the delirium begins to resolve, doses should be tapered gradually over several days.
Ileus
Postsurgical ileus can cause profound clinical consequences in elderly patients. This complication is associated with delayed enteral feeding and malnutrition, increased length of hospital stay, and increased risk of pulmonary complications. Patients present with abdominal distension, nausea and vomiting, limited flatus, and a decreased presence of bowel sounds on auscultation. In cases of prolonged postsurgical ileus, consider pseudo-obstruction (Ogilvie’s syndrome) and mechanical obstruction.
Intravenous hydration and nutrition (in prolonged cases), assisted ambulation, and the avoidance of opiates remain the mainstays of treatment. Nasogastric tubes may provide symptomatic relief in patients with nausea and vomiting, but studies don’t support the use of this intervention to enhance resolution of the ileus. Many prokinetic agents have been examined for this use, including neostigmine and cisapride, but the results have been mixed, and the side effect profiles are generally unacceptable for elderly patients. Delay oral feeding until satisfactory bowel function has been restored.
Nutritional Care
An estimated 12%-50% of geriatric patients are found to be malnourished in the acute hospital setting. The adverse effects of malnutrition include delayed wound healing, greater risk of sepsis and wound infections, deterioration of functional status secondary to muscle wasting, and increased mortality.
Early identification of the patient’s feeding limitations is the key to preventing adverse outcomes. If a patient is restricted from oral or enteral feeding, parenteral nutrition should be started within 48 hours. When volitional food intake is permitted, the addition of canned nutritional supplements, fortified meals, and between-meal snacks may improve elderly patients’ energy and protein intake.
Initiate enteral feeding in patients for whom voluntary food intake is decreased. Parenteral nutrition may still be required until enteral feeding is established, however, and prescribed nutrients can be administered enterally. Because glucose tolerance diminishes with normal aging and may be further reduced in a state of acute illness, initiation of insulin therapy may be necessary in patients receiving either enteral or parenteral supplementation. Additionally, supplementation with a zinc-containing daily multivitamin has been shown to enhance immune function and prevent infections.
Respiratory Care
Respiratory function may be diminished in elderly patients due to age-related changes in the upper and lower respiratory tracts. Factors that contribute to an increased rate of pulmonary postoperative complications include diminished protective mechanisms like coughing and swallowing, decreased compliance of the chest wall and lung tissue, inadequate mucociliary transport, and a blunted ventilatory response to hypoxia and hypercapnia. Postoperative respiratory complications, including pneumonia, hypoxemia, hypoventilation, and atelectasis, occur in 2.1%-10.2% of elderly patients. These complications are associated with increased length of stay and a higher risk of long-term mortality.
Respiratory function may be preserved in the postoperative geriatric patient using a variety of measures. Effective pain control is essential in maintaining adequate lung volumes, and regional analgesia is associated with less-severe postoperative decreases in vital capacity and functional residual capacity (FRC). Once postoperative pain has been controlled, encourage the early resumption of physical activity (with appropriate assistance). Positioning patients in a seated position increases FRC and improves gas exchange in those recovering from abdominal procedures. Additionally, incentive spirometers, breathing exercises, and intermittent positive-pressure breathing may reduce the incidence of pulmonary complications after upper-abdominal operations, shortening the length of hospital stay.
Thromboembolic Disease
Fatal pulmonary embolism accounts for a large proportion of postoperative deaths in the elderly population. Between 20%-30% of patients undergoing general surgery without prophylaxis develop deep vein thrombosis, and the incidence is as high as 40% in those undergoing orthopedic surgeries, gynecologic cancer operations, and major neurosurgical procedures.
The Fifth American College of Chest Physicians Consensus Conference on Antithrombotic Therapy recommends the following postoperative interventions for older surgical patients:
- General surgery without clinical risk factors for thrombosis: Give low-dose unfractionated heparin two hours before and every 12 hours after the operation;
- General surgery with any clinical risk factors such as prolonged immobilization or paralysis, obesity, varicose veins, congestive heart failure, or pelvic or leg fractures: Administer low molecular weight heparin (LMWH) or low-dose unfractionated heparin every eight hours. If the patient is also prone to bleeding or infection, intermittent pneumatic compression (IPC) can be used instead;
- General surgery with multiple clinical risk factors or with a history of previous deep vein thrombosis, malignancy, stroke, spinal cord injury, or hip fracture: Use low dose unfractionated heparin or LMWH combined with intermittent pneumatic compression; for very high risk patients, perioperative warfarin is an alternative;
- Total hip replacement: Give postoperative LMWH every 12 hours; initiate low-intensity warfarin therapy—to keep International Normalized Ratio of 2-3—preoperatively or immediately postoperatively;
- Total knee replacement: Administer postoperative LMWH every 12 hours. IPC is the most effective non-pharmacologic regimen and is comparable to LMWH. Low-intensity warfarin can also be used; and
- Hip fracture repair: Start preoperative fixed-dose LMWH or low-intensity warfarin.
Urinary Retention
The incidence of postoperative urinary retention in elderly patients has been reported to be as high as 87%. Factors contributing to the development of this complication include immobility, analgesics and opiates, intravenous hydration, and general anesthesia. Urinary retention can lead to overflow incontinence and urinary tract infection and is associated with a decline in function and nursing home placement. The first indication of urinary retention may be a diminished urinary output after removal of an indwelling catheter, overflow incontinence, or the frequent voiding of small amounts of urine.
Urinary retention is treated with catheterization. This prevents bladder distension, which leads to reduced detrusor contractile function, and helps restore preoperative bladder function.
Recent studies have found that normal voiding resumes earlier with the use of intermittent catheterization (if begun at the onset of urinary retention and repeated every six to eight hours) than with the use of an indwelling catheter. Additionally, the use of indwelling catheters in the elderly after the immediate perioperative period is associated with an increased risk of urosepsis and a more dependent postoperative functional status.
Conclusion
The 65-and-up age group is the fastest growing section of the United States population. The vast majority of complications for this age group occur in the postoperative period. It’s important for hospitalists to remain involved in key areas of postoperative complications in the geriatric population—specifically, delirium, ileus, nutritional deficiencies, respiratory complications—including pulmonary embolism—and urinary retention. TH
Jill Landis is a frequent contributor to The Hospitalist.
References
- Souders JE, Rooke GA. Perioperative care for geriatric patients. Ann Long Term Care. 2005;13(6):17-29.
- Williams SL, Jones PB, Pofahl WE. Preoperative management of the older patient—a surgeon’s perspective: part I. Ann Long Term Care. 2006;14(6):24-30.
- Palmer RM. Management of common clinical disorders in geriatric patients: delirium. ACP Medicine Online. June 7, 2006. Available at: www.medscape.com/viewarticle/534766. Last accessed January 11, 2007.
- Manku K, Bacchetti P, Leung JM. Prognostic significance of postoperative in-hospital complications in elderly patients. I. Long-term survival. Anesth Analg. 2003 Feb;96(2):583-589.
- Watters JM, McClaran JC, Man-Son-Hing M. The elderly surgical patient: introduction. ACS Surgery Online. June 7, 2006. Available at: www.medscape.com/viewarticle/535461?rss. Last accessed January 11, 2006.
- Skelly JM, Guyatt GH, Kalbfleisch R, et al. Management of urinary retention after surgical repair of hip fracture. CMAJ. 1992 Apr 1;146(7):1185-1189.
- Wittbrodt E. The impact of postoperative ileus and emerging therapies. Pharm Treatment. 2006 Jan;31(1):39-59.
An 86-year-old female with Alzheimer’s dementia, hypertension, type 2 diabetes, and chronic obstructive pulmonary disease was admitted with lethargy, fever, and vomiting. After she was diagnosed with necrotizing cholecystitis, she underwent an emergent cholecystectomy. Three days later the patient was short of breath, confused, and hadn’t urinated since the indwelling catheter was removed.
Sound familiar? If this scenario doesn’t ring a bell now, then it soon will. The 65-and-up age group is the fastest growing section of the United States population. A recent poll found that elderly patients now account for more than 60% of most general surgeons’ practices. Additionally, the use of minimally invasive surgical techniques and advanced perioperative monitoring has permitted elderly patients who were previously considered too debilitated to now become surgical candidates.
Though patients and their families most often worry about events in the operating room, the vast majority of complications occur in the postoperative period. Morbidity and mortality rates double during the first 24 hours after surgery and are tenfold higher over the remainder of the first postoperative week. In a recent study of more than 500 elderly general surgery patients, 21% experienced complications during this period.
The most common postoperative complications in the geriatric population include delirium, ileus, nutritional deficiencies, respiratory complications—including pulmonary embolism—and urinary retention. The goal in managing any elderly patient is to preserve cognitive and physical function. Maintaining this goal in the postoperative setting requires the early implementation of preventive measures, as well as an understanding of when age-appropriate intervention is necessary.
Hospitalists are often the first line of defense for postoperative situations in medically ill patients, and an amplification of issues unique to the geriatric patient follows.
Delirium
Postoperative delirium occurs in 10%-15% of older general surgery patients and in 30%-60% of older patients who undergo orthopedic procedures. The most common presentation of delirium in the elderly postoperative patient is a “quiet confusion” that is more pronounced in the evening—otherwise known as sundowning. An acute change in mental status, manifested as a fluctuating level of consciousness or a cognitive deficit, is also common. Though delirium may result solely from the acute stress of the operation, other medically relevant causes include metabolic abnormalities, abnormal respiratory parameters, infections, and medications, and these causes should be aggressively investigated and treated.
After potential medical etiologies have been addressed, focus the treatment of delirium in the elderly postoperative patient on interventions to restore mental and physical function as well as pharmacotherapy. Measures to restore function, such as early mobilization and ambulation, sleep hygiene, volume repletion, and restoration of vision and hearing with appropriate devices, have been shown to decrease the duration of the delirium episode. Other non-pharmacologic interventions, including placing a patient near the nurses’ station, encouraging social visits with caregivers, and avoiding the use of physical restraints (which can aggravate agitation) may also prove helpful.
Avoid the use of psychoactive medications (e.g., antiarrhythmic agents, tricyclic antidepressants, neuroleptics, gastrointestinal medications, antihistamines, ciprofloxacin, nonsteroidal anti-inflammatory drugs, meperidine, and cimetidine) as much as possible during the acute confusional state.
Pharmacologic treatment of delirium may be warranted in patients experiencing symptoms of psychosis or in those exhibiting signs of physical aggression or severe personal distress. Haloperidol and risperidol are the medications of choice, though the FDA has approved neither drug specifically for this indication. High doses of these medications are associated with extrapyramidal effects, dystonic reactions, and torsade de pointe. Once the delirium begins to resolve, doses should be tapered gradually over several days.
Ileus
Postsurgical ileus can cause profound clinical consequences in elderly patients. This complication is associated with delayed enteral feeding and malnutrition, increased length of hospital stay, and increased risk of pulmonary complications. Patients present with abdominal distension, nausea and vomiting, limited flatus, and a decreased presence of bowel sounds on auscultation. In cases of prolonged postsurgical ileus, consider pseudo-obstruction (Ogilvie’s syndrome) and mechanical obstruction.
Intravenous hydration and nutrition (in prolonged cases), assisted ambulation, and the avoidance of opiates remain the mainstays of treatment. Nasogastric tubes may provide symptomatic relief in patients with nausea and vomiting, but studies don’t support the use of this intervention to enhance resolution of the ileus. Many prokinetic agents have been examined for this use, including neostigmine and cisapride, but the results have been mixed, and the side effect profiles are generally unacceptable for elderly patients. Delay oral feeding until satisfactory bowel function has been restored.
Nutritional Care
An estimated 12%-50% of geriatric patients are found to be malnourished in the acute hospital setting. The adverse effects of malnutrition include delayed wound healing, greater risk of sepsis and wound infections, deterioration of functional status secondary to muscle wasting, and increased mortality.
Early identification of the patient’s feeding limitations is the key to preventing adverse outcomes. If a patient is restricted from oral or enteral feeding, parenteral nutrition should be started within 48 hours. When volitional food intake is permitted, the addition of canned nutritional supplements, fortified meals, and between-meal snacks may improve elderly patients’ energy and protein intake.
Initiate enteral feeding in patients for whom voluntary food intake is decreased. Parenteral nutrition may still be required until enteral feeding is established, however, and prescribed nutrients can be administered enterally. Because glucose tolerance diminishes with normal aging and may be further reduced in a state of acute illness, initiation of insulin therapy may be necessary in patients receiving either enteral or parenteral supplementation. Additionally, supplementation with a zinc-containing daily multivitamin has been shown to enhance immune function and prevent infections.
Respiratory Care
Respiratory function may be diminished in elderly patients due to age-related changes in the upper and lower respiratory tracts. Factors that contribute to an increased rate of pulmonary postoperative complications include diminished protective mechanisms like coughing and swallowing, decreased compliance of the chest wall and lung tissue, inadequate mucociliary transport, and a blunted ventilatory response to hypoxia and hypercapnia. Postoperative respiratory complications, including pneumonia, hypoxemia, hypoventilation, and atelectasis, occur in 2.1%-10.2% of elderly patients. These complications are associated with increased length of stay and a higher risk of long-term mortality.
Respiratory function may be preserved in the postoperative geriatric patient using a variety of measures. Effective pain control is essential in maintaining adequate lung volumes, and regional analgesia is associated with less-severe postoperative decreases in vital capacity and functional residual capacity (FRC). Once postoperative pain has been controlled, encourage the early resumption of physical activity (with appropriate assistance). Positioning patients in a seated position increases FRC and improves gas exchange in those recovering from abdominal procedures. Additionally, incentive spirometers, breathing exercises, and intermittent positive-pressure breathing may reduce the incidence of pulmonary complications after upper-abdominal operations, shortening the length of hospital stay.
Thromboembolic Disease
Fatal pulmonary embolism accounts for a large proportion of postoperative deaths in the elderly population. Between 20%-30% of patients undergoing general surgery without prophylaxis develop deep vein thrombosis, and the incidence is as high as 40% in those undergoing orthopedic surgeries, gynecologic cancer operations, and major neurosurgical procedures.
The Fifth American College of Chest Physicians Consensus Conference on Antithrombotic Therapy recommends the following postoperative interventions for older surgical patients:
- General surgery without clinical risk factors for thrombosis: Give low-dose unfractionated heparin two hours before and every 12 hours after the operation;
- General surgery with any clinical risk factors such as prolonged immobilization or paralysis, obesity, varicose veins, congestive heart failure, or pelvic or leg fractures: Administer low molecular weight heparin (LMWH) or low-dose unfractionated heparin every eight hours. If the patient is also prone to bleeding or infection, intermittent pneumatic compression (IPC) can be used instead;
- General surgery with multiple clinical risk factors or with a history of previous deep vein thrombosis, malignancy, stroke, spinal cord injury, or hip fracture: Use low dose unfractionated heparin or LMWH combined with intermittent pneumatic compression; for very high risk patients, perioperative warfarin is an alternative;
- Total hip replacement: Give postoperative LMWH every 12 hours; initiate low-intensity warfarin therapy—to keep International Normalized Ratio of 2-3—preoperatively or immediately postoperatively;
- Total knee replacement: Administer postoperative LMWH every 12 hours. IPC is the most effective non-pharmacologic regimen and is comparable to LMWH. Low-intensity warfarin can also be used; and
- Hip fracture repair: Start preoperative fixed-dose LMWH or low-intensity warfarin.
Urinary Retention
The incidence of postoperative urinary retention in elderly patients has been reported to be as high as 87%. Factors contributing to the development of this complication include immobility, analgesics and opiates, intravenous hydration, and general anesthesia. Urinary retention can lead to overflow incontinence and urinary tract infection and is associated with a decline in function and nursing home placement. The first indication of urinary retention may be a diminished urinary output after removal of an indwelling catheter, overflow incontinence, or the frequent voiding of small amounts of urine.
Urinary retention is treated with catheterization. This prevents bladder distension, which leads to reduced detrusor contractile function, and helps restore preoperative bladder function.
Recent studies have found that normal voiding resumes earlier with the use of intermittent catheterization (if begun at the onset of urinary retention and repeated every six to eight hours) than with the use of an indwelling catheter. Additionally, the use of indwelling catheters in the elderly after the immediate perioperative period is associated with an increased risk of urosepsis and a more dependent postoperative functional status.
Conclusion
The 65-and-up age group is the fastest growing section of the United States population. The vast majority of complications for this age group occur in the postoperative period. It’s important for hospitalists to remain involved in key areas of postoperative complications in the geriatric population—specifically, delirium, ileus, nutritional deficiencies, respiratory complications—including pulmonary embolism—and urinary retention. TH
Jill Landis is a frequent contributor to The Hospitalist.
References
- Souders JE, Rooke GA. Perioperative care for geriatric patients. Ann Long Term Care. 2005;13(6):17-29.
- Williams SL, Jones PB, Pofahl WE. Preoperative management of the older patient—a surgeon’s perspective: part I. Ann Long Term Care. 2006;14(6):24-30.
- Palmer RM. Management of common clinical disorders in geriatric patients: delirium. ACP Medicine Online. June 7, 2006. Available at: www.medscape.com/viewarticle/534766. Last accessed January 11, 2007.
- Manku K, Bacchetti P, Leung JM. Prognostic significance of postoperative in-hospital complications in elderly patients. I. Long-term survival. Anesth Analg. 2003 Feb;96(2):583-589.
- Watters JM, McClaran JC, Man-Son-Hing M. The elderly surgical patient: introduction. ACS Surgery Online. June 7, 2006. Available at: www.medscape.com/viewarticle/535461?rss. Last accessed January 11, 2006.
- Skelly JM, Guyatt GH, Kalbfleisch R, et al. Management of urinary retention after surgical repair of hip fracture. CMAJ. 1992 Apr 1;146(7):1185-1189.
- Wittbrodt E. The impact of postoperative ileus and emerging therapies. Pharm Treatment. 2006 Jan;31(1):39-59.
Constructive Criticism

This is the first in a two-part series about how to provide constructive criticism to your hospitalist peers.
Part of improving your performance is learning from other hospitalists on a regular basis. You can do this through observation or discussion, and—when appropriate—by offering or receiving constructive criticism.
There are two types of physician-to-physician constructive criticism: When discussing perceived poor handling of a patient’s case, comments should take place within a formal peer review. Concerns about a physician’s non-clinical performance, such as communications problems or lack of availability, can be handled in a one-on-one conversation. Herein we’ll examine the peer review process; next month we’ll take a look at how and when to give constructive criticism to a peer informally.
Why Use Peer Review?
When a hospitalist notices a colleague’s clinical error or lack of judgment, it should be addressed in the program’s next peer review meeting, both for legal and procedural reasons.
“The key thing to understand is that ‘peer review’ offers certain protections for physicians and their colleagues,” explains Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Milford, Conn. “Ordinarily, if I discuss [another physician’s] case and render my opinion, then—in principle—if that patient were to file a lawsuit, they could subpoena me to testify about what I thought about their case. In the past, this had a chilling effect on peer review.”
Due to state laws passed years ago, peer review meetings now offer protection against subpoena. “Peer review meetings are protected,” says Dr. Rohr. “They can’t be used in court, and this makes it possible to have an organized peer review where you look at physicians’ work and provide an opinion about that work without fear of being drawn into a legal situation.”
The bottom line: “If you want to talk to another physician about their case, do so within [the peer review structure] so you’re legally protected,” says Dr. Rohr.
Focus on Improvement
When discussing a specific case or physician, remember that the reason for doing so is to improve quality of care. “Every practice should sit down, look at specific cases, and talk about possible areas of improvement,” says Dr. Rohr. “You need to take minutes of these meetings that are marked as confidential.”
The key to improvement is having an open discussion in each peer review meeting. “A good meeting is educational,” says Dr. Rohr. “The objective is to support each other and improve performance. A lot depends on the attitude that people bring to it. You have to not be afraid to say something; you must be willing to express opinions, or you’ll have a wasted meeting.”
Sometimes you may find that the problem goes beyond a single physician’s actions on a case. “If there is a problem with a case, find out whether it’s an aberration or if the problem needs to be addressed,” says Dr. Rohr. “Some things are not a physician’s fault, so much as [they are] signs that a medical system doesn’t work as effectively as it should or [that there is] a general lack of training. For example, an ER [emergency room] doctor misses a fracture. Was finding that fracture outside his competency? Does he need training reading X-rays, or can you manage to get radiologists in to check X-rays fast enough to become part of the process?”
Use a Set Structure
It’s up to the hospital medicine program director to set up a peer review process, which should be done within the structure established by the hospital. Peer review meetings “should be done on a regular basis,” advises Dr. Rohr. “How often depends on the volume of the program, but a typical group should meet monthly. You’ll probably look at three or four cases, which is a reasonable number to cover in one meeting. Look at unexpected mortalities or complications—you have a responsibility to the public to examine these.”
You might do best by bringing in an outside facilitator for the meetings. This creates an impartial atmosphere for discussions. “We bring in an external facilitator from a local teaching hospital,” says Dr. Rohr. “It’s good to have an educator lead the meeting; someone from academia will have a greater fund of knowledge and [a stronger] grasp of the medical literature, which helps bring the discussion to a more educational level. Everyone respects medical science.”
Note that the facilitator may need to be credentialed as a member of the medical staff in order for the proceedings to be protected from legal discovery.
“Peer review is difficult in smaller practices, because everyone knows everyone and they may be uncomfortable addressing problems,” explains Dr. Rohr. “Here, it’s especially helpful to have a leader from the outside who can render opinions and get everyone to chime in and render their own opinions.”
Remember that your peer review system is reportable. “As part of the hospital’s peer review structure, you’ll have to report findings from the meetings,” adds Dr. Rohr. “If someone is showing a pattern, these things have to be trended. Do they need training, or should they be dismissed?”
Giving Feedback through Peer Review
When you participate in a peer review discussion, don’t let your comments get too personal or subjective. “The most important thing is to keep it professional and make it educational to the greatest extent possible,” says Dr. Rohr. “Reference facts in the medical literature as often as possible. Point to something that’s been published to support your opinion. Base your comments on what’s known, and apply that to your analysis of the case.”
An evidence-based opinion doesn’t have to cite specific details; as long as you’re aware of major papers on the topic, you should have a grounded opinion.
Finally, as a physician participating in a peer review discussion, think before you speak. “Peer review works best when you have a basic respect for each other, as well as basic humility,” he says. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the first in a two-part series about how to provide constructive criticism to your hospitalist peers.
Part of improving your performance is learning from other hospitalists on a regular basis. You can do this through observation or discussion, and—when appropriate—by offering or receiving constructive criticism.
There are two types of physician-to-physician constructive criticism: When discussing perceived poor handling of a patient’s case, comments should take place within a formal peer review. Concerns about a physician’s non-clinical performance, such as communications problems or lack of availability, can be handled in a one-on-one conversation. Herein we’ll examine the peer review process; next month we’ll take a look at how and when to give constructive criticism to a peer informally.
Why Use Peer Review?
When a hospitalist notices a colleague’s clinical error or lack of judgment, it should be addressed in the program’s next peer review meeting, both for legal and procedural reasons.
“The key thing to understand is that ‘peer review’ offers certain protections for physicians and their colleagues,” explains Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Milford, Conn. “Ordinarily, if I discuss [another physician’s] case and render my opinion, then—in principle—if that patient were to file a lawsuit, they could subpoena me to testify about what I thought about their case. In the past, this had a chilling effect on peer review.”
Due to state laws passed years ago, peer review meetings now offer protection against subpoena. “Peer review meetings are protected,” says Dr. Rohr. “They can’t be used in court, and this makes it possible to have an organized peer review where you look at physicians’ work and provide an opinion about that work without fear of being drawn into a legal situation.”
The bottom line: “If you want to talk to another physician about their case, do so within [the peer review structure] so you’re legally protected,” says Dr. Rohr.
Focus on Improvement
When discussing a specific case or physician, remember that the reason for doing so is to improve quality of care. “Every practice should sit down, look at specific cases, and talk about possible areas of improvement,” says Dr. Rohr. “You need to take minutes of these meetings that are marked as confidential.”
The key to improvement is having an open discussion in each peer review meeting. “A good meeting is educational,” says Dr. Rohr. “The objective is to support each other and improve performance. A lot depends on the attitude that people bring to it. You have to not be afraid to say something; you must be willing to express opinions, or you’ll have a wasted meeting.”
Sometimes you may find that the problem goes beyond a single physician’s actions on a case. “If there is a problem with a case, find out whether it’s an aberration or if the problem needs to be addressed,” says Dr. Rohr. “Some things are not a physician’s fault, so much as [they are] signs that a medical system doesn’t work as effectively as it should or [that there is] a general lack of training. For example, an ER [emergency room] doctor misses a fracture. Was finding that fracture outside his competency? Does he need training reading X-rays, or can you manage to get radiologists in to check X-rays fast enough to become part of the process?”
Use a Set Structure
It’s up to the hospital medicine program director to set up a peer review process, which should be done within the structure established by the hospital. Peer review meetings “should be done on a regular basis,” advises Dr. Rohr. “How often depends on the volume of the program, but a typical group should meet monthly. You’ll probably look at three or four cases, which is a reasonable number to cover in one meeting. Look at unexpected mortalities or complications—you have a responsibility to the public to examine these.”
You might do best by bringing in an outside facilitator for the meetings. This creates an impartial atmosphere for discussions. “We bring in an external facilitator from a local teaching hospital,” says Dr. Rohr. “It’s good to have an educator lead the meeting; someone from academia will have a greater fund of knowledge and [a stronger] grasp of the medical literature, which helps bring the discussion to a more educational level. Everyone respects medical science.”
Note that the facilitator may need to be credentialed as a member of the medical staff in order for the proceedings to be protected from legal discovery.
“Peer review is difficult in smaller practices, because everyone knows everyone and they may be uncomfortable addressing problems,” explains Dr. Rohr. “Here, it’s especially helpful to have a leader from the outside who can render opinions and get everyone to chime in and render their own opinions.”
Remember that your peer review system is reportable. “As part of the hospital’s peer review structure, you’ll have to report findings from the meetings,” adds Dr. Rohr. “If someone is showing a pattern, these things have to be trended. Do they need training, or should they be dismissed?”
Giving Feedback through Peer Review
When you participate in a peer review discussion, don’t let your comments get too personal or subjective. “The most important thing is to keep it professional and make it educational to the greatest extent possible,” says Dr. Rohr. “Reference facts in the medical literature as often as possible. Point to something that’s been published to support your opinion. Base your comments on what’s known, and apply that to your analysis of the case.”
An evidence-based opinion doesn’t have to cite specific details; as long as you’re aware of major papers on the topic, you should have a grounded opinion.
Finally, as a physician participating in a peer review discussion, think before you speak. “Peer review works best when you have a basic respect for each other, as well as basic humility,” he says. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the first in a two-part series about how to provide constructive criticism to your hospitalist peers.
Part of improving your performance is learning from other hospitalists on a regular basis. You can do this through observation or discussion, and—when appropriate—by offering or receiving constructive criticism.
There are two types of physician-to-physician constructive criticism: When discussing perceived poor handling of a patient’s case, comments should take place within a formal peer review. Concerns about a physician’s non-clinical performance, such as communications problems or lack of availability, can be handled in a one-on-one conversation. Herein we’ll examine the peer review process; next month we’ll take a look at how and when to give constructive criticism to a peer informally.
Why Use Peer Review?
When a hospitalist notices a colleague’s clinical error or lack of judgment, it should be addressed in the program’s next peer review meeting, both for legal and procedural reasons.
“The key thing to understand is that ‘peer review’ offers certain protections for physicians and their colleagues,” explains Richard Rohr, MD, director, Hospitalist Service, Milford Hospital, Milford, Conn. “Ordinarily, if I discuss [another physician’s] case and render my opinion, then—in principle—if that patient were to file a lawsuit, they could subpoena me to testify about what I thought about their case. In the past, this had a chilling effect on peer review.”
Due to state laws passed years ago, peer review meetings now offer protection against subpoena. “Peer review meetings are protected,” says Dr. Rohr. “They can’t be used in court, and this makes it possible to have an organized peer review where you look at physicians’ work and provide an opinion about that work without fear of being drawn into a legal situation.”
The bottom line: “If you want to talk to another physician about their case, do so within [the peer review structure] so you’re legally protected,” says Dr. Rohr.
Focus on Improvement
When discussing a specific case or physician, remember that the reason for doing so is to improve quality of care. “Every practice should sit down, look at specific cases, and talk about possible areas of improvement,” says Dr. Rohr. “You need to take minutes of these meetings that are marked as confidential.”
The key to improvement is having an open discussion in each peer review meeting. “A good meeting is educational,” says Dr. Rohr. “The objective is to support each other and improve performance. A lot depends on the attitude that people bring to it. You have to not be afraid to say something; you must be willing to express opinions, or you’ll have a wasted meeting.”
Sometimes you may find that the problem goes beyond a single physician’s actions on a case. “If there is a problem with a case, find out whether it’s an aberration or if the problem needs to be addressed,” says Dr. Rohr. “Some things are not a physician’s fault, so much as [they are] signs that a medical system doesn’t work as effectively as it should or [that there is] a general lack of training. For example, an ER [emergency room] doctor misses a fracture. Was finding that fracture outside his competency? Does he need training reading X-rays, or can you manage to get radiologists in to check X-rays fast enough to become part of the process?”
Use a Set Structure
It’s up to the hospital medicine program director to set up a peer review process, which should be done within the structure established by the hospital. Peer review meetings “should be done on a regular basis,” advises Dr. Rohr. “How often depends on the volume of the program, but a typical group should meet monthly. You’ll probably look at three or four cases, which is a reasonable number to cover in one meeting. Look at unexpected mortalities or complications—you have a responsibility to the public to examine these.”
You might do best by bringing in an outside facilitator for the meetings. This creates an impartial atmosphere for discussions. “We bring in an external facilitator from a local teaching hospital,” says Dr. Rohr. “It’s good to have an educator lead the meeting; someone from academia will have a greater fund of knowledge and [a stronger] grasp of the medical literature, which helps bring the discussion to a more educational level. Everyone respects medical science.”
Note that the facilitator may need to be credentialed as a member of the medical staff in order for the proceedings to be protected from legal discovery.
“Peer review is difficult in smaller practices, because everyone knows everyone and they may be uncomfortable addressing problems,” explains Dr. Rohr. “Here, it’s especially helpful to have a leader from the outside who can render opinions and get everyone to chime in and render their own opinions.”
Remember that your peer review system is reportable. “As part of the hospital’s peer review structure, you’ll have to report findings from the meetings,” adds Dr. Rohr. “If someone is showing a pattern, these things have to be trended. Do they need training, or should they be dismissed?”
Giving Feedback through Peer Review
When you participate in a peer review discussion, don’t let your comments get too personal or subjective. “The most important thing is to keep it professional and make it educational to the greatest extent possible,” says Dr. Rohr. “Reference facts in the medical literature as often as possible. Point to something that’s been published to support your opinion. Base your comments on what’s known, and apply that to your analysis of the case.”
An evidence-based opinion doesn’t have to cite specific details; as long as you’re aware of major papers on the topic, you should have a grounded opinion.
Finally, as a physician participating in a peer review discussion, think before you speak. “Peer review works best when you have a basic respect for each other, as well as basic humility,” he says. TH
Jane Jerrard has written for The Hospitalist since 2005.
Fibromuscular Dysplasia

Brief history: 52-year-old female with uncontrolled hypertension.
Salient findings: The middle third of the arteries are involved with a “string of pearls” appearance of alternating webs and stenoses. This appearance is classic for fibromuscular dysplasia (FMD) (white arrow, above). The patient also has a 1.8-cm right renal artery aneurysm at the trifurcation of her first order renal artery branches (black arrow, above).
Patient population and natural history of disease: FMD is most common in young adult females, and its etiology is unknown. An association with alpha-1 antitrypsin deficiency has been reported in the literature. FMD is a leading cause of curable hypertension. Clinical manifestations of FMD include distal embolization of thrombus formed in small aneurysms, hypertension/ischemia due to obstruction by webs, and occlusion/infarct via spontaneous dissection. The natural prevalence of renal artery aneurysms is low—0.1% in all angiography patients—and its natural course is not well established. Renal artery aneurysms are most common in FMD, vasculitides, neoplasm, trauma, and Ehlers-Danlos Syndrome; they may be iatrogenic or idiopathic.
Management: Symptomatic medial fibroplasia-type FMD responds well to balloon angioplasty. Renal artery aneurysms may be managed medically or surgically, depending on risk factors. Indications for repair of renal artery aneurysms include a size of 2 cm or greater, pregnancy, expansion, renovascular hypertension, distal embolization, and rupture. Mortality from ruptured renal artery aneurysms is 10% in nonpregnant patients and 55% during pregnancy.
This patient had a good response to balloon angioplasty of the left renal artery. The right renal artery could not be angioplastied secondary to increased risk of aneurysm rupture with restoration of arterial blood flow due to increased pressure on the walls of the aneurysm. Hence, physicians surgically resected the right renal artery aneurysm and performed a bypass to the aorta.

Take Home Points
- FMD is most common in young or middle-age women;
- FMD is a type of curable hypertension, treated by renal artery angioplasty;
- FMD is diagnosed by an angiographic study—in classic cases, the involved artery has a string of pearls appearance; and
- FMD is associated with renal artery aneurysms. Consider surgical intervention in aneurysms greater than 2 cm. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
Bibliography
- Kaufman JA, Lee MJ. Vascular and Interventional Radiology: The Requisites. Philadelphia: Mosby; 2004.
- Bisschops RH, Popma JJ, Meyerovitz MF. Treatment of fibromuscular dysplasia and renal artery aneurysm with use of a stent-graft. J Vasc Interv Radiol. 2001 Jun;12(6):757-760.
- Luscher TF, Lie JT, Stanson AW, et al. Arterial fibromuscular dysplasia. Mayo Clin Proc. 1987;62:931-952.
Brief history: 52-year-old female with uncontrolled hypertension.
Salient findings: The middle third of the arteries are involved with a “string of pearls” appearance of alternating webs and stenoses. This appearance is classic for fibromuscular dysplasia (FMD) (white arrow, above). The patient also has a 1.8-cm right renal artery aneurysm at the trifurcation of her first order renal artery branches (black arrow, above).
Patient population and natural history of disease: FMD is most common in young adult females, and its etiology is unknown. An association with alpha-1 antitrypsin deficiency has been reported in the literature. FMD is a leading cause of curable hypertension. Clinical manifestations of FMD include distal embolization of thrombus formed in small aneurysms, hypertension/ischemia due to obstruction by webs, and occlusion/infarct via spontaneous dissection. The natural prevalence of renal artery aneurysms is low—0.1% in all angiography patients—and its natural course is not well established. Renal artery aneurysms are most common in FMD, vasculitides, neoplasm, trauma, and Ehlers-Danlos Syndrome; they may be iatrogenic or idiopathic.
Management: Symptomatic medial fibroplasia-type FMD responds well to balloon angioplasty. Renal artery aneurysms may be managed medically or surgically, depending on risk factors. Indications for repair of renal artery aneurysms include a size of 2 cm or greater, pregnancy, expansion, renovascular hypertension, distal embolization, and rupture. Mortality from ruptured renal artery aneurysms is 10% in nonpregnant patients and 55% during pregnancy.
This patient had a good response to balloon angioplasty of the left renal artery. The right renal artery could not be angioplastied secondary to increased risk of aneurysm rupture with restoration of arterial blood flow due to increased pressure on the walls of the aneurysm. Hence, physicians surgically resected the right renal artery aneurysm and performed a bypass to the aorta.
Take Home Points
- FMD is most common in young or middle-age women;
- FMD is a type of curable hypertension, treated by renal artery angioplasty;
- FMD is diagnosed by an angiographic study—in classic cases, the involved artery has a string of pearls appearance; and
- FMD is associated with renal artery aneurysms. Consider surgical intervention in aneurysms greater than 2 cm. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
Bibliography
- Kaufman JA, Lee MJ. Vascular and Interventional Radiology: The Requisites. Philadelphia: Mosby; 2004.
- Bisschops RH, Popma JJ, Meyerovitz MF. Treatment of fibromuscular dysplasia and renal artery aneurysm with use of a stent-graft. J Vasc Interv Radiol. 2001 Jun;12(6):757-760.
- Luscher TF, Lie JT, Stanson AW, et al. Arterial fibromuscular dysplasia. Mayo Clin Proc. 1987;62:931-952.
Brief history: 52-year-old female with uncontrolled hypertension.
Salient findings: The middle third of the arteries are involved with a “string of pearls” appearance of alternating webs and stenoses. This appearance is classic for fibromuscular dysplasia (FMD) (white arrow, above). The patient also has a 1.8-cm right renal artery aneurysm at the trifurcation of her first order renal artery branches (black arrow, above).
Patient population and natural history of disease: FMD is most common in young adult females, and its etiology is unknown. An association with alpha-1 antitrypsin deficiency has been reported in the literature. FMD is a leading cause of curable hypertension. Clinical manifestations of FMD include distal embolization of thrombus formed in small aneurysms, hypertension/ischemia due to obstruction by webs, and occlusion/infarct via spontaneous dissection. The natural prevalence of renal artery aneurysms is low—0.1% in all angiography patients—and its natural course is not well established. Renal artery aneurysms are most common in FMD, vasculitides, neoplasm, trauma, and Ehlers-Danlos Syndrome; they may be iatrogenic or idiopathic.
Management: Symptomatic medial fibroplasia-type FMD responds well to balloon angioplasty. Renal artery aneurysms may be managed medically or surgically, depending on risk factors. Indications for repair of renal artery aneurysms include a size of 2 cm or greater, pregnancy, expansion, renovascular hypertension, distal embolization, and rupture. Mortality from ruptured renal artery aneurysms is 10% in nonpregnant patients and 55% during pregnancy.
This patient had a good response to balloon angioplasty of the left renal artery. The right renal artery could not be angioplastied secondary to increased risk of aneurysm rupture with restoration of arterial blood flow due to increased pressure on the walls of the aneurysm. Hence, physicians surgically resected the right renal artery aneurysm and performed a bypass to the aorta.
Take Home Points
- FMD is most common in young or middle-age women;
- FMD is a type of curable hypertension, treated by renal artery angioplasty;
- FMD is diagnosed by an angiographic study—in classic cases, the involved artery has a string of pearls appearance; and
- FMD is associated with renal artery aneurysms. Consider surgical intervention in aneurysms greater than 2 cm. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
Bibliography
- Kaufman JA, Lee MJ. Vascular and Interventional Radiology: The Requisites. Philadelphia: Mosby; 2004.
- Bisschops RH, Popma JJ, Meyerovitz MF. Treatment of fibromuscular dysplasia and renal artery aneurysm with use of a stent-graft. J Vasc Interv Radiol. 2001 Jun;12(6):757-760.
- Luscher TF, Lie JT, Stanson AW, et al. Arterial fibromuscular dysplasia. Mayo Clin Proc. 1987;62:931-952.
New Party in Power

Due to an overwhelming number of Democratic victories in last November’s midterm elections, the 110th Congress, which took office early this year, has new leaders and a new agenda that could bode well for healthcare legislation.
In this article, Laura Allendorf, SHM’s senior advisor for advocacy and government affairs, explains what the changes in Congress could mean for the near future of healthcare and for the legislation and issues that SHM strongly supports. Based in Washington, D.C., Allendorf is responsible for providing government relations services for SHM. She advises the organization on key legislative and regulatory healthcare issues before Congress and the Bush administration, and she works with SHM leaders and staff on policy development and advocacy strategies.
Majority Rules
The midterm elections brought about a shift in power that goes deeper than numbers of bodies on each side of the aisle. “The Democrats are now the majority in both chambers. This is significant, because they’ve been the minority since 1994, says Allendorf. “As the majority, they control the agenda now—on healthcare and other issues—and they also head the key committees.”
What can we expect to see from the Democratic Congress? “We should expect to see a more expansionist agenda” in general, according to Allendorf. “We’re going to see more activism in the area of healthcare, but whether anything gets done remains to be seen. There’s only a slim majority in the Senate, and President Bush can wield his veto pen. For example, the Democrats would like to give [the Department of] Health and Human Services the power to negotiate drug prices with pharmaceutical companies, specifically on Medicare Part D, but Bush won’t like that.”
Much depends on the issues at hand, as well as on how much bipartisan support exists for each specific bill.
Changing of the Guard
Anyone who glances at the newspaper knows that Democrat Nancy Pelosi (Calif.) is now the Speaker of the House. But Democratic leadership goes much deeper than that because the ruling party has also taken over leadership of Congressional committees. These committees shape the legislation introduced in the House and Senate.
As of press time, Congressional committee assignments had not been formally decided—at least not in the Senate—but many assignments were certain. “Typically, the highest-ranking Democrat [House or Senate] on a committee will become the new head, though Nancy Pelosi isn’t sticking to that,” explains Allendorf. “Pete Stark (D-Calif.) will likely chair the Ways and Means Committee’s Subcommittee on Health, and Charles Rangel (D-N.Y.) will head the House Ways and Means Committee. John Dingell (D-Mich.) will chair the House Energy and Commerce Committee.” (For more on committee chairs, visit http://media-newswire.com/release_1040623.html.)
For a complete list of committee members, visit SHM’s new Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. See “New Advocacy Tool Available,” for more information on the Legislative Action Center, above.)
Starting Over on Key Issues
Many of the bills introduced in 2006—particularly spending bills—were not voted on by the end of the lame duck session last fall. That means that these bills must be reintroduced in the new year. Bills that recommend funding changes are frozen, so agencies continue to receive 2006 funding until the new Congress votes to change their budget.
“All bills have to be reintroduced in the 110th,” stresses Allendorf. “It will take some time—how much depends on the issue. The Democrats may want to hold hearings on legislation, or they may simply dust off legislation that was introduced last year.”
The Democrats are expected to move on many of the issues that SHM has been lobbying for. “They’ve said that they want to reform the healthcare system,” says Allendorf. “Top issues include providing coverage to the uninsured, reforming Medicare Part D, and resolving the physician payment issue.”
Allendorf believes that there will be a bipartisan effort to push through physician payment reform. “There are some 265 members of Congress who requested action on this issue this year [in 2006],” she points out. “There’s a genuine interest and desire to address physician payment reform and pay-for-performance as well. They may differ on how quickly they want to move on some of these.”
The news is not so good on the issue of gainsharing, where physicians are allowed to share the profits realized by a hospital’s cost reductions when linked to specific best practices. “Representative Nancy Johnson (R-Conn.) was a big proponent of this issue in the House, and she was not re-elected,” says Allendorf. “Stark is an opponent of gainsharing, so there may not be the same Congressional push behind it—at least in the House.”
However, the unexpected gainsharing demonstration projects approved in 2006 are underway, and Congress will hear reports on those in several years, once the projects have been analyzed.
Another issue that may not be addressed is liability. “Medical liability reform will be on the back burner,” warns Allendorf. “It’s generally not supported by the Democrats.”
In 2006, SHM supported increased funding for the Agency for Healthcare Research and Quality (AHRQ)—this was one of the major issues addressed by members during Legislative Advocacy Day during the Annual Meeting in Washington, D.C. Whether the next budget includes more money for the agency remains to be seen. “The Democrats support increased funding for NIH (National Institutes of Health), AHRQ, and other healthcare agencies,” says Allendorf. “There’s certainly political will, but where is the money going to come from?”
New Congress, New Issues
What about new issues? “Democrats have signaled that healthcare access for the uninsured will be a priority,” says Allendorf. “I think that we’ll see new legislation with a renewed emphasis on access to care.”
SHM’s Public Policy Committee will be waiting for the first legislation to be introduced regarding coverage for uninsured Americans. “This is an issue that SHM is strongly in favor of,” explains Allendorf. “SHM will look at any bills that come out on this issue and then form a policy.”
Regardless of which healthcare issues come to the forefront first, SHM’s Public Policy Committee, staff, and members are likely to be more active than ever. “I see a very busy year legislatively for SHM,” says Allendorf. TH
Jane Jerrard regularly writes “Public Policy” for The Hospitalist.
Due to an overwhelming number of Democratic victories in last November’s midterm elections, the 110th Congress, which took office early this year, has new leaders and a new agenda that could bode well for healthcare legislation.
In this article, Laura Allendorf, SHM’s senior advisor for advocacy and government affairs, explains what the changes in Congress could mean for the near future of healthcare and for the legislation and issues that SHM strongly supports. Based in Washington, D.C., Allendorf is responsible for providing government relations services for SHM. She advises the organization on key legislative and regulatory healthcare issues before Congress and the Bush administration, and she works with SHM leaders and staff on policy development and advocacy strategies.
Majority Rules
The midterm elections brought about a shift in power that goes deeper than numbers of bodies on each side of the aisle. “The Democrats are now the majority in both chambers. This is significant, because they’ve been the minority since 1994, says Allendorf. “As the majority, they control the agenda now—on healthcare and other issues—and they also head the key committees.”
What can we expect to see from the Democratic Congress? “We should expect to see a more expansionist agenda” in general, according to Allendorf. “We’re going to see more activism in the area of healthcare, but whether anything gets done remains to be seen. There’s only a slim majority in the Senate, and President Bush can wield his veto pen. For example, the Democrats would like to give [the Department of] Health and Human Services the power to negotiate drug prices with pharmaceutical companies, specifically on Medicare Part D, but Bush won’t like that.”
Much depends on the issues at hand, as well as on how much bipartisan support exists for each specific bill.
Changing of the Guard
Anyone who glances at the newspaper knows that Democrat Nancy Pelosi (Calif.) is now the Speaker of the House. But Democratic leadership goes much deeper than that because the ruling party has also taken over leadership of Congressional committees. These committees shape the legislation introduced in the House and Senate.
As of press time, Congressional committee assignments had not been formally decided—at least not in the Senate—but many assignments were certain. “Typically, the highest-ranking Democrat [House or Senate] on a committee will become the new head, though Nancy Pelosi isn’t sticking to that,” explains Allendorf. “Pete Stark (D-Calif.) will likely chair the Ways and Means Committee’s Subcommittee on Health, and Charles Rangel (D-N.Y.) will head the House Ways and Means Committee. John Dingell (D-Mich.) will chair the House Energy and Commerce Committee.” (For more on committee chairs, visit http://media-newswire.com/release_1040623.html.)
For a complete list of committee members, visit SHM’s new Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. See “New Advocacy Tool Available,” for more information on the Legislative Action Center, above.)
Starting Over on Key Issues
Many of the bills introduced in 2006—particularly spending bills—were not voted on by the end of the lame duck session last fall. That means that these bills must be reintroduced in the new year. Bills that recommend funding changes are frozen, so agencies continue to receive 2006 funding until the new Congress votes to change their budget.
“All bills have to be reintroduced in the 110th,” stresses Allendorf. “It will take some time—how much depends on the issue. The Democrats may want to hold hearings on legislation, or they may simply dust off legislation that was introduced last year.”
The Democrats are expected to move on many of the issues that SHM has been lobbying for. “They’ve said that they want to reform the healthcare system,” says Allendorf. “Top issues include providing coverage to the uninsured, reforming Medicare Part D, and resolving the physician payment issue.”
Allendorf believes that there will be a bipartisan effort to push through physician payment reform. “There are some 265 members of Congress who requested action on this issue this year [in 2006],” she points out. “There’s a genuine interest and desire to address physician payment reform and pay-for-performance as well. They may differ on how quickly they want to move on some of these.”
The news is not so good on the issue of gainsharing, where physicians are allowed to share the profits realized by a hospital’s cost reductions when linked to specific best practices. “Representative Nancy Johnson (R-Conn.) was a big proponent of this issue in the House, and she was not re-elected,” says Allendorf. “Stark is an opponent of gainsharing, so there may not be the same Congressional push behind it—at least in the House.”
However, the unexpected gainsharing demonstration projects approved in 2006 are underway, and Congress will hear reports on those in several years, once the projects have been analyzed.
Another issue that may not be addressed is liability. “Medical liability reform will be on the back burner,” warns Allendorf. “It’s generally not supported by the Democrats.”
In 2006, SHM supported increased funding for the Agency for Healthcare Research and Quality (AHRQ)—this was one of the major issues addressed by members during Legislative Advocacy Day during the Annual Meeting in Washington, D.C. Whether the next budget includes more money for the agency remains to be seen. “The Democrats support increased funding for NIH (National Institutes of Health), AHRQ, and other healthcare agencies,” says Allendorf. “There’s certainly political will, but where is the money going to come from?”
New Congress, New Issues
What about new issues? “Democrats have signaled that healthcare access for the uninsured will be a priority,” says Allendorf. “I think that we’ll see new legislation with a renewed emphasis on access to care.”
SHM’s Public Policy Committee will be waiting for the first legislation to be introduced regarding coverage for uninsured Americans. “This is an issue that SHM is strongly in favor of,” explains Allendorf. “SHM will look at any bills that come out on this issue and then form a policy.”
Regardless of which healthcare issues come to the forefront first, SHM’s Public Policy Committee, staff, and members are likely to be more active than ever. “I see a very busy year legislatively for SHM,” says Allendorf. TH
Jane Jerrard regularly writes “Public Policy” for The Hospitalist.
Due to an overwhelming number of Democratic victories in last November’s midterm elections, the 110th Congress, which took office early this year, has new leaders and a new agenda that could bode well for healthcare legislation.
In this article, Laura Allendorf, SHM’s senior advisor for advocacy and government affairs, explains what the changes in Congress could mean for the near future of healthcare and for the legislation and issues that SHM strongly supports. Based in Washington, D.C., Allendorf is responsible for providing government relations services for SHM. She advises the organization on key legislative and regulatory healthcare issues before Congress and the Bush administration, and she works with SHM leaders and staff on policy development and advocacy strategies.
Majority Rules
The midterm elections brought about a shift in power that goes deeper than numbers of bodies on each side of the aisle. “The Democrats are now the majority in both chambers. This is significant, because they’ve been the minority since 1994, says Allendorf. “As the majority, they control the agenda now—on healthcare and other issues—and they also head the key committees.”
What can we expect to see from the Democratic Congress? “We should expect to see a more expansionist agenda” in general, according to Allendorf. “We’re going to see more activism in the area of healthcare, but whether anything gets done remains to be seen. There’s only a slim majority in the Senate, and President Bush can wield his veto pen. For example, the Democrats would like to give [the Department of] Health and Human Services the power to negotiate drug prices with pharmaceutical companies, specifically on Medicare Part D, but Bush won’t like that.”
Much depends on the issues at hand, as well as on how much bipartisan support exists for each specific bill.
Changing of the Guard
Anyone who glances at the newspaper knows that Democrat Nancy Pelosi (Calif.) is now the Speaker of the House. But Democratic leadership goes much deeper than that because the ruling party has also taken over leadership of Congressional committees. These committees shape the legislation introduced in the House and Senate.
As of press time, Congressional committee assignments had not been formally decided—at least not in the Senate—but many assignments were certain. “Typically, the highest-ranking Democrat [House or Senate] on a committee will become the new head, though Nancy Pelosi isn’t sticking to that,” explains Allendorf. “Pete Stark (D-Calif.) will likely chair the Ways and Means Committee’s Subcommittee on Health, and Charles Rangel (D-N.Y.) will head the House Ways and Means Committee. John Dingell (D-Mich.) will chair the House Energy and Commerce Committee.” (For more on committee chairs, visit http://media-newswire.com/release_1040623.html.)
For a complete list of committee members, visit SHM’s new Legislative Action Center at http://capwiz.com/hospitalmedicine/home/. See “New Advocacy Tool Available,” for more information on the Legislative Action Center, above.)
Starting Over on Key Issues
Many of the bills introduced in 2006—particularly spending bills—were not voted on by the end of the lame duck session last fall. That means that these bills must be reintroduced in the new year. Bills that recommend funding changes are frozen, so agencies continue to receive 2006 funding until the new Congress votes to change their budget.
“All bills have to be reintroduced in the 110th,” stresses Allendorf. “It will take some time—how much depends on the issue. The Democrats may want to hold hearings on legislation, or they may simply dust off legislation that was introduced last year.”
The Democrats are expected to move on many of the issues that SHM has been lobbying for. “They’ve said that they want to reform the healthcare system,” says Allendorf. “Top issues include providing coverage to the uninsured, reforming Medicare Part D, and resolving the physician payment issue.”
Allendorf believes that there will be a bipartisan effort to push through physician payment reform. “There are some 265 members of Congress who requested action on this issue this year [in 2006],” she points out. “There’s a genuine interest and desire to address physician payment reform and pay-for-performance as well. They may differ on how quickly they want to move on some of these.”
The news is not so good on the issue of gainsharing, where physicians are allowed to share the profits realized by a hospital’s cost reductions when linked to specific best practices. “Representative Nancy Johnson (R-Conn.) was a big proponent of this issue in the House, and she was not re-elected,” says Allendorf. “Stark is an opponent of gainsharing, so there may not be the same Congressional push behind it—at least in the House.”
However, the unexpected gainsharing demonstration projects approved in 2006 are underway, and Congress will hear reports on those in several years, once the projects have been analyzed.
Another issue that may not be addressed is liability. “Medical liability reform will be on the back burner,” warns Allendorf. “It’s generally not supported by the Democrats.”
In 2006, SHM supported increased funding for the Agency for Healthcare Research and Quality (AHRQ)—this was one of the major issues addressed by members during Legislative Advocacy Day during the Annual Meeting in Washington, D.C. Whether the next budget includes more money for the agency remains to be seen. “The Democrats support increased funding for NIH (National Institutes of Health), AHRQ, and other healthcare agencies,” says Allendorf. “There’s certainly political will, but where is the money going to come from?”
New Congress, New Issues
What about new issues? “Democrats have signaled that healthcare access for the uninsured will be a priority,” says Allendorf. “I think that we’ll see new legislation with a renewed emphasis on access to care.”
SHM’s Public Policy Committee will be waiting for the first legislation to be introduced regarding coverage for uninsured Americans. “This is an issue that SHM is strongly in favor of,” explains Allendorf. “SHM will look at any bills that come out on this issue and then form a policy.”
Regardless of which healthcare issues come to the forefront first, SHM’s Public Policy Committee, staff, and members are likely to be more active than ever. “I see a very busy year legislatively for SHM,” says Allendorf. TH
Jane Jerrard regularly writes “Public Policy” for The Hospitalist.
Hospital Medicine 2007

This year marks the 10-year anniversary of Robert Wachter’s coining of the term “hospitalist,” as well as the celebration of the decade-old SHM. The celebration culminates in a stellar annual meeting that epitomizes the growth of hospital medicine.
The SHM Annual Meeting attendance has grown from just a handful of participants to more than 1,200 expected at the 2007 Annual Meeting. More importantly, as the role of hospitalists has changed from primarily focusing on providing care to the hospitalized patient to serving as the leader of quality improvement, a key staff educator, and a facilitator of care transitions, so have their educational needs. Thus, the annual meeting has evolved in order to provide an educational experience that has relevance on a practical level.
The SHM 2007 Annual Meeting Committee (AMC), led by Course Director Chad Whelan, MD, challenged itself to develop a program that will meet the needs of a diverse audience that includes community-based and academic-based hospitalists; research-oriented and clinician-focused seasoned veteran physicians and early career hospitalists; as well as pediatric, geriatric, and family practice hospitalists. Such an effort begins with the big picture: What is happening in the environment that will impact healthcare today and in the future?
The answer is found in the role of information technology, and SHM will welcome two renowned speakers to provide current and future perspectives. David Brailer, MD, PhD, the first National Coordinator for Health Information Technology (2004-2006), will examine the forces driving health information technology and how technology affects pressures on the quality and cost of care. Jonathan Perlin, MD, PhD, chief medical officer and senior vice president for Quality for Hospital Corporation of America, will look to healthcare’s challenges and opportunities in the decade ahead, with a focus on health IT and performance and the role of hospital medicine as it relates to care improvement.
The 2007 Annual Meeting will again feature Robert Wachter, MD, as the keynote speaker in the closing plenary session. Dr. Wachter is sure to entertain as he examines “The Hospitalist Movement a Decade Later: Life as a Swiss Army Knife.”
The goal of a broad-based program will be achieved through separate breakout sessions and workshops, divided into seven tracks. Though the format is similar to other years, the 2007 program has some new twists. One clinical track focuses on “Things You Didn’t Learn in Medical School,” and a palliative care track has been added. Relevant sessions have been selected using the Core Competencies in Hospital Medicine and collaborating with SHM’s committees, which serve the interests of all of the groups.
The connection between the program and SHM’s committees will be strong. The committees will focus their efforts on topics and goals that are important to our members. The AMC solicits ideas for breakout sessions from the committees; it also profiles the output of a committee that has significance to attendees in their daily responsibilities.
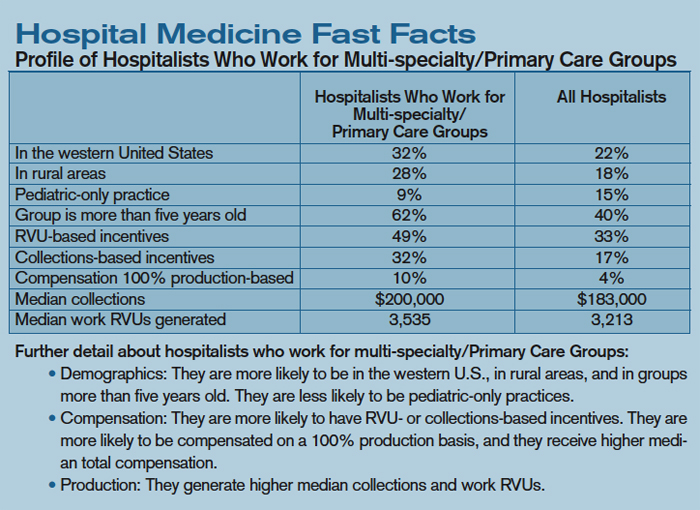
Suggestions from the committees have resulted in a combination of pertinent and innovative sessions. Here are just a few to whet your appetite for the complete program:
- A workshop jointly planned by the Hospital Quality and Patient Safety (HQPS) and Education Committees, designed to obtain input and consensus on SHM-developed communication and hand-off standards;
- An Academic Track, intended to appeal to those hospitalists focused on teaching, quality improvement, research, and growing a hospital medicine program;
- A workshop, proposed by the Career Satisfaction Task Force, that addresses relevant career issues from the leaders’ and hospitalists’ perspectives;
- A Quality Track defined by the HQPS Committee that, in addition to the consensus-building workshop, features medication reconciliation and Toyota Methods sessions;
- A Pediatric Track, designed to address the needs of our fastest growing member segment, features a range of clinical and leadership topics, including electronic health records, the prevention of the transmission of infectious agents, and the utilization of dashboards to improve care;
- The work of the Benchmarks Committee will be profiled in a session that will demonstrate how to use key performance metrics to improve hospital medicine and the care of the hospitalized patient;
- The Public Policy Committee has recommended a pay-for-performance (P4P) breakout session, because P4P has been identified as an important issue in hospital medicine;
- A Palliative Care Track, proposed and developed by the Palliative Care Task Force, includes relevant topics such as pain management, the ethical and legal considerations of palliative care, and communications skills; and
- A visiting professor, Stephan Fihn, MD, MPH, will conduct poster rounds, lead a workshop, and participate in “Breakfast with Leaders in Hospital Medicine.”
The Annual Meeting Committee focused on identifying faculty members who can share their experience and expertise in an entertaining and elucidating way. We anticipate that you will enjoy presentations by experts new to the SHM Annual Meeting, as well as return engagements by past faculty.
Letters
Correction

On p. 6 of the January 2007 issue the “Profile of Academic Hospitalists” contained errors inadvertently introduced in the editing process.
Line 4 of the table should read: “Clinical Full Time Equivalency—Academic Hospitalists .69, All Hospitalists .89.”
Line 8 of the table should read “Nurse Practitioners Per Group—Academic Hospitalists .82, All Hospitalists .43.”
The SHM Annual Meeting traditionally offers networking opportunities with more than 1,100 hospitalists. Special Interest Forums provide each attendee not only with a unique occasion to meet with hospitalists who share similar interests but also with the venue to express their opinions on a national level. SHM utilizes the input to change and grow the organization and hospital medicine. Planned Special Interest Forums include:
- Research;
- Community-based hospitalists;
- Pediatric hospitalists;
- Medical directors and leadership;
- Family practice hospitalists;
- Geriatric hospitalists;
- Nurse practitioners and physician assistants;
- Women in hospital medicine;
- Early career hospitalists;
- Education;
- Curriculum/fellowship;
- Public policy; and
- History of medicine.
Other networking mainstays of the Annual Meeting, including the Research, Innovations, and Clinical Vignettes Competition; Exhibits; President’s Lunch; and Town Meeting, will again be featured. Satellite symposia are planned, as well as the following pre-courses:
- Inpatient Coding and Documentation: Getting Paid What You Deserve;
- Best Practices in Managing a Hospital Medicine Program;
- Critical Care Medicine for the Hospitalist;
- Perioperative Medicine for the Hospitalist; and
- High Impact Quality Improvement: How to Ensure a Successful Project.
Additionally, a PICC Line Placement for Pediatric and Adult Hospitalists pre-course is being proposed by the Pediatrics Committee.
As you can see, 2007 Annual Meeting will present variety and choice; there is something for everyone. Don’t miss this premier educational event for hospitalists and the opportunity to be a part of the hospital medicine movement. The SHM 2007 Annual Meeting will be held at the Gaylord Texan Resort and Convention Center outside Dallas on May 24 and 25, with pre-courses held on May 23. Visit the SHM Web site at www.hospitalmedicine.org/hospitalmedicine2007 for complete program details or to register online. You may also register by calling SHM at (800) 843-3360. Come to Texas and help us celebrate 10 years of improving the quality of healthcare!
SHM: BEHIND THE SCENES
Resolutions
By Tina Budnitz, MPH

This is the time of year when many New Year’s resolutions dissolve. In some cases, people set unrealistic goals. Others lack the tools to succeed or live in an environment that makes change too difficult. In 2006 I resolved to start running each morning before work. I have the determination and the physical ability to meet this goal. Disarming the house alarm at 5 a.m., however, awakens my two toddlers. And detaching two toddlers from my legs proves to be quite a challenge. It also turns out that my tolerance for cold weather is low, while my ability to forgive a missed run is high.
Sustaining quality improvement initiatives at the hospital is lot like sustaining New Year’s resolutions. The best of intentions are often thwarted by a lack of time, resources, or energy to change the system, as well as by those within the system who resist change. For example, SHM members tell me that attempting to introduce a new discharge planning process feels a lot like trying to run through the hospital with two toddlers hanging on to your legs. SHM strives to support hospitalists in their resolutions to implement positive change in the hospital.
My role at SHM is to lead the development of programs, tool kits, and support mechanisms that will enable you, our members, to implement and sustain local quality improvement efforts.
SHM currently supports members in their efforts to improve outcomes for patients with heart failure, stroke, or diabetes; we work to prevent venous thromboembolism (VTE) and hospital-acquired blood-stream infections. We also support members in their efforts to improve the discharge process for older adults, thereby reducing readmission rates and adverse drug events while improving communications with receiving physicians.
We support members in their efforts to implement, evaluate, and sustain QI initiatives using a variety of methodologies. We offer symposia, workshops, and a full-day Annual Meeting Pre-Course on quality improvement; we also provide Leadership Academy Level I and Level II and networking opportunities for members and their mentors. We’ve designed Web-based clinical tool kits around specific disease states and special patient populations. We offer Web-based resource rooms to guide members from start to finish through a new local QI initiative. We have funded demonstration projects to pilot new approaches and tools for use in discharge planning, along with innovative research to improve care for heart failure patients. And we’ve only just begun.
Researching the Approach
For each QI area we address, an advisory board is recruited to represent the best available experts, organizations, and multidisciplinary professionals. For example, the Discharge Planning for Older Adults Advisory Board includes representatives from the American Geriatrics Society (AGS), the Institute for Healthcare Improvement (IHI), the Agency for Healthcare Research and Quality (AHRQ), the Society of General Internal Medicine (SGIM), the Case Management Society of America (CMSA), the National Quality Forum (NQF), and the Association for Health-System Pharmacists (AHSP), in addition to nationally renowned leaders in care transitions, geriatrics, nursing, patient literacy, and pharmacy.
Each Advisory Board conducts a needs assessment and a review of the literature to examine interventions and approaches. The board identifies existing “gaps” in clinical tools and guidelines. Finally, the Advisory Board determines specific, measurable targets for a hospitalist-led intervention and suggests the evidence-based approach(es) that should be most effective.
Implementing an Intervention: Where the Rubber Meets the Road
As I pointed out earlier, resolving what should be done and getting it done are two very different things. In most cases, few people debate the need for the intervention—reducing the incidence of inpatient VTEs, for example—or the validity of the proposed intervention. The challenge arises in changing the system of care so that the intervention becomes the new standard of care. Therefore, after the Advisory Board has determined the aims and intervention(s), SHM develops a “workbook,” a step-by-step field guide for hospitalists that walks them through the process of building a project team, establishing project aims and key metrics, obtaining institutional support, planning the intervention, launching the intervention, measuring impact, and sustaining system improvements.
The workbooks are posted in the SHM Resource Rooms along with other key resources, including slide sets, bedside teaching tools, patient education literature, CME modules, reviews of key literature, interactive “Ask the Expert” discussion boards, and improvement reports detailing the strategies, successes, and setbacks of other institutions. SHM currently offers resource rooms for Preventing VTE, Heart Failure, Stroke, Discharge Planning for the Elderly, Glycemic Control, and Antimicrobial Resistance. To access the resource rooms, visit our Web site at www.hospitalmedicine.org.
Training Leaders
SHM offers its members diverse training opportunities designed to accommodate the range of knowledge, expertise, and resources available at local institutions. The resource rooms and workbooks described above are made freely available to everyone. At the 2007 SHM Annual Meeting, we will offer a quality pre-course for hands-on training to lead a QI initiative for discharge planning, VTE prevention, or glycemic control.
For SHM members who desire additional support, SHM is developing “Mentored Implementation” and “On-Site Consulting” programs. The Mentored Implementation Program provides enrolled sites with all of the tools described above and an additional yearlong training program conducted via monthly conference calls with SHM mentors and/or one-day training programs. The On-Site Consulting Program surveys an institution’s resources and infrastructure. The SHM consultant team reviews the assessment with the site. Following this assessment, the consultant team visits the site to meet with hospital administrators, QI teams, and others to further assess the site and to help build internal support for the QI initiative. Following the visit, each site receives a customized report detailing recommendations and strategies to advance specific local QI initiatives.
SHM recently launched a Mentored Implementation and On-Site Consulting Program for VTE (known as the SHM VTE Collaborative). Similar programs are scheduled to launch for discharge planning this spring. In the coming years, we hope to add training programs in several other key patient safety areas.
Additionally, SHM is engaged in a strategic planning process to determine how best to attract the highest caliber medical students into hospital medicine and to mentor, train, and retain the next generation of leaders.
In summary, I hope the range of training opportunities and educational programs, the depth of SHM tool kits, and the scope of patient safety initiatives are meeting your needs to plan, implement, evaluate, and sustain positive change at your institution. If you are interested in learning more about SHM QI programs or have suggestions on how we might improve them to better meet your needs, please e-mail me at [email protected].
And, in case you were wondering, I’m making progress on my resolution to run. This year my resolution has the support of my department chairs (Jacob, five; Noah, two), with better-defined outcomes (run three times a week for more than 40 minutes each time), and a better tool kit (gloves, ear muffs). In the planning stage, I addressed my biggest barrier (leave the alarm off) and built a support team (my neighbor joins me).
If you see me at the annual meeting, please let me know how your resolutions are working to prevent DVT or to improve the discharge process, glycemic control, or heart failure care. Or better yet, submit those stories to me to share with members in our “Improvement Stories” or resource rooms Web site areas or in print via The Hospitalist or Journal of Hospital Medicine.
Budnitz is senior advisor, quality initiatives, for SHM.
This year marks the 10-year anniversary of Robert Wachter’s coining of the term “hospitalist,” as well as the celebration of the decade-old SHM. The celebration culminates in a stellar annual meeting that epitomizes the growth of hospital medicine.
The SHM Annual Meeting attendance has grown from just a handful of participants to more than 1,200 expected at the 2007 Annual Meeting. More importantly, as the role of hospitalists has changed from primarily focusing on providing care to the hospitalized patient to serving as the leader of quality improvement, a key staff educator, and a facilitator of care transitions, so have their educational needs. Thus, the annual meeting has evolved in order to provide an educational experience that has relevance on a practical level.
The SHM 2007 Annual Meeting Committee (AMC), led by Course Director Chad Whelan, MD, challenged itself to develop a program that will meet the needs of a diverse audience that includes community-based and academic-based hospitalists; research-oriented and clinician-focused seasoned veteran physicians and early career hospitalists; as well as pediatric, geriatric, and family practice hospitalists. Such an effort begins with the big picture: What is happening in the environment that will impact healthcare today and in the future?
The answer is found in the role of information technology, and SHM will welcome two renowned speakers to provide current and future perspectives. David Brailer, MD, PhD, the first National Coordinator for Health Information Technology (2004-2006), will examine the forces driving health information technology and how technology affects pressures on the quality and cost of care. Jonathan Perlin, MD, PhD, chief medical officer and senior vice president for Quality for Hospital Corporation of America, will look to healthcare’s challenges and opportunities in the decade ahead, with a focus on health IT and performance and the role of hospital medicine as it relates to care improvement.
The 2007 Annual Meeting will again feature Robert Wachter, MD, as the keynote speaker in the closing plenary session. Dr. Wachter is sure to entertain as he examines “The Hospitalist Movement a Decade Later: Life as a Swiss Army Knife.”
The goal of a broad-based program will be achieved through separate breakout sessions and workshops, divided into seven tracks. Though the format is similar to other years, the 2007 program has some new twists. One clinical track focuses on “Things You Didn’t Learn in Medical School,” and a palliative care track has been added. Relevant sessions have been selected using the Core Competencies in Hospital Medicine and collaborating with SHM’s committees, which serve the interests of all of the groups.
The connection between the program and SHM’s committees will be strong. The committees will focus their efforts on topics and goals that are important to our members. The AMC solicits ideas for breakout sessions from the committees; it also profiles the output of a committee that has significance to attendees in their daily responsibilities.
Suggestions from the committees have resulted in a combination of pertinent and innovative sessions. Here are just a few to whet your appetite for the complete program:
- A workshop jointly planned by the Hospital Quality and Patient Safety (HQPS) and Education Committees, designed to obtain input and consensus on SHM-developed communication and hand-off standards;
- An Academic Track, intended to appeal to those hospitalists focused on teaching, quality improvement, research, and growing a hospital medicine program;
- A workshop, proposed by the Career Satisfaction Task Force, that addresses relevant career issues from the leaders’ and hospitalists’ perspectives;
- A Quality Track defined by the HQPS Committee that, in addition to the consensus-building workshop, features medication reconciliation and Toyota Methods sessions;
- A Pediatric Track, designed to address the needs of our fastest growing member segment, features a range of clinical and leadership topics, including electronic health records, the prevention of the transmission of infectious agents, and the utilization of dashboards to improve care;
- The work of the Benchmarks Committee will be profiled in a session that will demonstrate how to use key performance metrics to improve hospital medicine and the care of the hospitalized patient;
- The Public Policy Committee has recommended a pay-for-performance (P4P) breakout session, because P4P has been identified as an important issue in hospital medicine;
- A Palliative Care Track, proposed and developed by the Palliative Care Task Force, includes relevant topics such as pain management, the ethical and legal considerations of palliative care, and communications skills; and
- A visiting professor, Stephan Fihn, MD, MPH, will conduct poster rounds, lead a workshop, and participate in “Breakfast with Leaders in Hospital Medicine.”
The Annual Meeting Committee focused on identifying faculty members who can share their experience and expertise in an entertaining and elucidating way. We anticipate that you will enjoy presentations by experts new to the SHM Annual Meeting, as well as return engagements by past faculty.
Letters
Correction
On p. 6 of the January 2007 issue the “Profile of Academic Hospitalists” contained errors inadvertently introduced in the editing process.
Line 4 of the table should read: “Clinical Full Time Equivalency—Academic Hospitalists .69, All Hospitalists .89.”
Line 8 of the table should read “Nurse Practitioners Per Group—Academic Hospitalists .82, All Hospitalists .43.”
The SHM Annual Meeting traditionally offers networking opportunities with more than 1,100 hospitalists. Special Interest Forums provide each attendee not only with a unique occasion to meet with hospitalists who share similar interests but also with the venue to express their opinions on a national level. SHM utilizes the input to change and grow the organization and hospital medicine. Planned Special Interest Forums include:
- Research;
- Community-based hospitalists;
- Pediatric hospitalists;
- Medical directors and leadership;
- Family practice hospitalists;
- Geriatric hospitalists;
- Nurse practitioners and physician assistants;
- Women in hospital medicine;
- Early career hospitalists;
- Education;
- Curriculum/fellowship;
- Public policy; and
- History of medicine.
Other networking mainstays of the Annual Meeting, including the Research, Innovations, and Clinical Vignettes Competition; Exhibits; President’s Lunch; and Town Meeting, will again be featured. Satellite symposia are planned, as well as the following pre-courses:
- Inpatient Coding and Documentation: Getting Paid What You Deserve;
- Best Practices in Managing a Hospital Medicine Program;
- Critical Care Medicine for the Hospitalist;
- Perioperative Medicine for the Hospitalist; and
- High Impact Quality Improvement: How to Ensure a Successful Project.
Additionally, a PICC Line Placement for Pediatric and Adult Hospitalists pre-course is being proposed by the Pediatrics Committee.
As you can see, 2007 Annual Meeting will present variety and choice; there is something for everyone. Don’t miss this premier educational event for hospitalists and the opportunity to be a part of the hospital medicine movement. The SHM 2007 Annual Meeting will be held at the Gaylord Texan Resort and Convention Center outside Dallas on May 24 and 25, with pre-courses held on May 23. Visit the SHM Web site at www.hospitalmedicine.org/hospitalmedicine2007 for complete program details or to register online. You may also register by calling SHM at (800) 843-3360. Come to Texas and help us celebrate 10 years of improving the quality of healthcare!
SHM: BEHIND THE SCENES
Resolutions
By Tina Budnitz, MPH
This is the time of year when many New Year’s resolutions dissolve. In some cases, people set unrealistic goals. Others lack the tools to succeed or live in an environment that makes change too difficult. In 2006 I resolved to start running each morning before work. I have the determination and the physical ability to meet this goal. Disarming the house alarm at 5 a.m., however, awakens my two toddlers. And detaching two toddlers from my legs proves to be quite a challenge. It also turns out that my tolerance for cold weather is low, while my ability to forgive a missed run is high.
Sustaining quality improvement initiatives at the hospital is lot like sustaining New Year’s resolutions. The best of intentions are often thwarted by a lack of time, resources, or energy to change the system, as well as by those within the system who resist change. For example, SHM members tell me that attempting to introduce a new discharge planning process feels a lot like trying to run through the hospital with two toddlers hanging on to your legs. SHM strives to support hospitalists in their resolutions to implement positive change in the hospital.
My role at SHM is to lead the development of programs, tool kits, and support mechanisms that will enable you, our members, to implement and sustain local quality improvement efforts.
SHM currently supports members in their efforts to improve outcomes for patients with heart failure, stroke, or diabetes; we work to prevent venous thromboembolism (VTE) and hospital-acquired blood-stream infections. We also support members in their efforts to improve the discharge process for older adults, thereby reducing readmission rates and adverse drug events while improving communications with receiving physicians.
We support members in their efforts to implement, evaluate, and sustain QI initiatives using a variety of methodologies. We offer symposia, workshops, and a full-day Annual Meeting Pre-Course on quality improvement; we also provide Leadership Academy Level I and Level II and networking opportunities for members and their mentors. We’ve designed Web-based clinical tool kits around specific disease states and special patient populations. We offer Web-based resource rooms to guide members from start to finish through a new local QI initiative. We have funded demonstration projects to pilot new approaches and tools for use in discharge planning, along with innovative research to improve care for heart failure patients. And we’ve only just begun.
Researching the Approach
For each QI area we address, an advisory board is recruited to represent the best available experts, organizations, and multidisciplinary professionals. For example, the Discharge Planning for Older Adults Advisory Board includes representatives from the American Geriatrics Society (AGS), the Institute for Healthcare Improvement (IHI), the Agency for Healthcare Research and Quality (AHRQ), the Society of General Internal Medicine (SGIM), the Case Management Society of America (CMSA), the National Quality Forum (NQF), and the Association for Health-System Pharmacists (AHSP), in addition to nationally renowned leaders in care transitions, geriatrics, nursing, patient literacy, and pharmacy.
Each Advisory Board conducts a needs assessment and a review of the literature to examine interventions and approaches. The board identifies existing “gaps” in clinical tools and guidelines. Finally, the Advisory Board determines specific, measurable targets for a hospitalist-led intervention and suggests the evidence-based approach(es) that should be most effective.
Implementing an Intervention: Where the Rubber Meets the Road
As I pointed out earlier, resolving what should be done and getting it done are two very different things. In most cases, few people debate the need for the intervention—reducing the incidence of inpatient VTEs, for example—or the validity of the proposed intervention. The challenge arises in changing the system of care so that the intervention becomes the new standard of care. Therefore, after the Advisory Board has determined the aims and intervention(s), SHM develops a “workbook,” a step-by-step field guide for hospitalists that walks them through the process of building a project team, establishing project aims and key metrics, obtaining institutional support, planning the intervention, launching the intervention, measuring impact, and sustaining system improvements.
The workbooks are posted in the SHM Resource Rooms along with other key resources, including slide sets, bedside teaching tools, patient education literature, CME modules, reviews of key literature, interactive “Ask the Expert” discussion boards, and improvement reports detailing the strategies, successes, and setbacks of other institutions. SHM currently offers resource rooms for Preventing VTE, Heart Failure, Stroke, Discharge Planning for the Elderly, Glycemic Control, and Antimicrobial Resistance. To access the resource rooms, visit our Web site at www.hospitalmedicine.org.
Training Leaders
SHM offers its members diverse training opportunities designed to accommodate the range of knowledge, expertise, and resources available at local institutions. The resource rooms and workbooks described above are made freely available to everyone. At the 2007 SHM Annual Meeting, we will offer a quality pre-course for hands-on training to lead a QI initiative for discharge planning, VTE prevention, or glycemic control.
For SHM members who desire additional support, SHM is developing “Mentored Implementation” and “On-Site Consulting” programs. The Mentored Implementation Program provides enrolled sites with all of the tools described above and an additional yearlong training program conducted via monthly conference calls with SHM mentors and/or one-day training programs. The On-Site Consulting Program surveys an institution’s resources and infrastructure. The SHM consultant team reviews the assessment with the site. Following this assessment, the consultant team visits the site to meet with hospital administrators, QI teams, and others to further assess the site and to help build internal support for the QI initiative. Following the visit, each site receives a customized report detailing recommendations and strategies to advance specific local QI initiatives.
SHM recently launched a Mentored Implementation and On-Site Consulting Program for VTE (known as the SHM VTE Collaborative). Similar programs are scheduled to launch for discharge planning this spring. In the coming years, we hope to add training programs in several other key patient safety areas.
Additionally, SHM is engaged in a strategic planning process to determine how best to attract the highest caliber medical students into hospital medicine and to mentor, train, and retain the next generation of leaders.
In summary, I hope the range of training opportunities and educational programs, the depth of SHM tool kits, and the scope of patient safety initiatives are meeting your needs to plan, implement, evaluate, and sustain positive change at your institution. If you are interested in learning more about SHM QI programs or have suggestions on how we might improve them to better meet your needs, please e-mail me at [email protected].
And, in case you were wondering, I’m making progress on my resolution to run. This year my resolution has the support of my department chairs (Jacob, five; Noah, two), with better-defined outcomes (run three times a week for more than 40 minutes each time), and a better tool kit (gloves, ear muffs). In the planning stage, I addressed my biggest barrier (leave the alarm off) and built a support team (my neighbor joins me).
If you see me at the annual meeting, please let me know how your resolutions are working to prevent DVT or to improve the discharge process, glycemic control, or heart failure care. Or better yet, submit those stories to me to share with members in our “Improvement Stories” or resource rooms Web site areas or in print via The Hospitalist or Journal of Hospital Medicine.
Budnitz is senior advisor, quality initiatives, for SHM.
This year marks the 10-year anniversary of Robert Wachter’s coining of the term “hospitalist,” as well as the celebration of the decade-old SHM. The celebration culminates in a stellar annual meeting that epitomizes the growth of hospital medicine.
The SHM Annual Meeting attendance has grown from just a handful of participants to more than 1,200 expected at the 2007 Annual Meeting. More importantly, as the role of hospitalists has changed from primarily focusing on providing care to the hospitalized patient to serving as the leader of quality improvement, a key staff educator, and a facilitator of care transitions, so have their educational needs. Thus, the annual meeting has evolved in order to provide an educational experience that has relevance on a practical level.
The SHM 2007 Annual Meeting Committee (AMC), led by Course Director Chad Whelan, MD, challenged itself to develop a program that will meet the needs of a diverse audience that includes community-based and academic-based hospitalists; research-oriented and clinician-focused seasoned veteran physicians and early career hospitalists; as well as pediatric, geriatric, and family practice hospitalists. Such an effort begins with the big picture: What is happening in the environment that will impact healthcare today and in the future?
The answer is found in the role of information technology, and SHM will welcome two renowned speakers to provide current and future perspectives. David Brailer, MD, PhD, the first National Coordinator for Health Information Technology (2004-2006), will examine the forces driving health information technology and how technology affects pressures on the quality and cost of care. Jonathan Perlin, MD, PhD, chief medical officer and senior vice president for Quality for Hospital Corporation of America, will look to healthcare’s challenges and opportunities in the decade ahead, with a focus on health IT and performance and the role of hospital medicine as it relates to care improvement.
The 2007 Annual Meeting will again feature Robert Wachter, MD, as the keynote speaker in the closing plenary session. Dr. Wachter is sure to entertain as he examines “The Hospitalist Movement a Decade Later: Life as a Swiss Army Knife.”
The goal of a broad-based program will be achieved through separate breakout sessions and workshops, divided into seven tracks. Though the format is similar to other years, the 2007 program has some new twists. One clinical track focuses on “Things You Didn’t Learn in Medical School,” and a palliative care track has been added. Relevant sessions have been selected using the Core Competencies in Hospital Medicine and collaborating with SHM’s committees, which serve the interests of all of the groups.
The connection between the program and SHM’s committees will be strong. The committees will focus their efforts on topics and goals that are important to our members. The AMC solicits ideas for breakout sessions from the committees; it also profiles the output of a committee that has significance to attendees in their daily responsibilities.
Suggestions from the committees have resulted in a combination of pertinent and innovative sessions. Here are just a few to whet your appetite for the complete program:
- A workshop jointly planned by the Hospital Quality and Patient Safety (HQPS) and Education Committees, designed to obtain input and consensus on SHM-developed communication and hand-off standards;
- An Academic Track, intended to appeal to those hospitalists focused on teaching, quality improvement, research, and growing a hospital medicine program;
- A workshop, proposed by the Career Satisfaction Task Force, that addresses relevant career issues from the leaders’ and hospitalists’ perspectives;
- A Quality Track defined by the HQPS Committee that, in addition to the consensus-building workshop, features medication reconciliation and Toyota Methods sessions;
- A Pediatric Track, designed to address the needs of our fastest growing member segment, features a range of clinical and leadership topics, including electronic health records, the prevention of the transmission of infectious agents, and the utilization of dashboards to improve care;
- The work of the Benchmarks Committee will be profiled in a session that will demonstrate how to use key performance metrics to improve hospital medicine and the care of the hospitalized patient;
- The Public Policy Committee has recommended a pay-for-performance (P4P) breakout session, because P4P has been identified as an important issue in hospital medicine;
- A Palliative Care Track, proposed and developed by the Palliative Care Task Force, includes relevant topics such as pain management, the ethical and legal considerations of palliative care, and communications skills; and
- A visiting professor, Stephan Fihn, MD, MPH, will conduct poster rounds, lead a workshop, and participate in “Breakfast with Leaders in Hospital Medicine.”
The Annual Meeting Committee focused on identifying faculty members who can share their experience and expertise in an entertaining and elucidating way. We anticipate that you will enjoy presentations by experts new to the SHM Annual Meeting, as well as return engagements by past faculty.
Letters
Correction
On p. 6 of the January 2007 issue the “Profile of Academic Hospitalists” contained errors inadvertently introduced in the editing process.
Line 4 of the table should read: “Clinical Full Time Equivalency—Academic Hospitalists .69, All Hospitalists .89.”
Line 8 of the table should read “Nurse Practitioners Per Group—Academic Hospitalists .82, All Hospitalists .43.”
The SHM Annual Meeting traditionally offers networking opportunities with more than 1,100 hospitalists. Special Interest Forums provide each attendee not only with a unique occasion to meet with hospitalists who share similar interests but also with the venue to express their opinions on a national level. SHM utilizes the input to change and grow the organization and hospital medicine. Planned Special Interest Forums include:
- Research;
- Community-based hospitalists;
- Pediatric hospitalists;
- Medical directors and leadership;
- Family practice hospitalists;
- Geriatric hospitalists;
- Nurse practitioners and physician assistants;
- Women in hospital medicine;
- Early career hospitalists;
- Education;
- Curriculum/fellowship;
- Public policy; and
- History of medicine.
Other networking mainstays of the Annual Meeting, including the Research, Innovations, and Clinical Vignettes Competition; Exhibits; President’s Lunch; and Town Meeting, will again be featured. Satellite symposia are planned, as well as the following pre-courses:
- Inpatient Coding and Documentation: Getting Paid What You Deserve;
- Best Practices in Managing a Hospital Medicine Program;
- Critical Care Medicine for the Hospitalist;
- Perioperative Medicine for the Hospitalist; and
- High Impact Quality Improvement: How to Ensure a Successful Project.
Additionally, a PICC Line Placement for Pediatric and Adult Hospitalists pre-course is being proposed by the Pediatrics Committee.
As you can see, 2007 Annual Meeting will present variety and choice; there is something for everyone. Don’t miss this premier educational event for hospitalists and the opportunity to be a part of the hospital medicine movement. The SHM 2007 Annual Meeting will be held at the Gaylord Texan Resort and Convention Center outside Dallas on May 24 and 25, with pre-courses held on May 23. Visit the SHM Web site at www.hospitalmedicine.org/hospitalmedicine2007 for complete program details or to register online. You may also register by calling SHM at (800) 843-3360. Come to Texas and help us celebrate 10 years of improving the quality of healthcare!
SHM: BEHIND THE SCENES
Resolutions
By Tina Budnitz, MPH
This is the time of year when many New Year’s resolutions dissolve. In some cases, people set unrealistic goals. Others lack the tools to succeed or live in an environment that makes change too difficult. In 2006 I resolved to start running each morning before work. I have the determination and the physical ability to meet this goal. Disarming the house alarm at 5 a.m., however, awakens my two toddlers. And detaching two toddlers from my legs proves to be quite a challenge. It also turns out that my tolerance for cold weather is low, while my ability to forgive a missed run is high.
Sustaining quality improvement initiatives at the hospital is lot like sustaining New Year’s resolutions. The best of intentions are often thwarted by a lack of time, resources, or energy to change the system, as well as by those within the system who resist change. For example, SHM members tell me that attempting to introduce a new discharge planning process feels a lot like trying to run through the hospital with two toddlers hanging on to your legs. SHM strives to support hospitalists in their resolutions to implement positive change in the hospital.
My role at SHM is to lead the development of programs, tool kits, and support mechanisms that will enable you, our members, to implement and sustain local quality improvement efforts.
SHM currently supports members in their efforts to improve outcomes for patients with heart failure, stroke, or diabetes; we work to prevent venous thromboembolism (VTE) and hospital-acquired blood-stream infections. We also support members in their efforts to improve the discharge process for older adults, thereby reducing readmission rates and adverse drug events while improving communications with receiving physicians.
We support members in their efforts to implement, evaluate, and sustain QI initiatives using a variety of methodologies. We offer symposia, workshops, and a full-day Annual Meeting Pre-Course on quality improvement; we also provide Leadership Academy Level I and Level II and networking opportunities for members and their mentors. We’ve designed Web-based clinical tool kits around specific disease states and special patient populations. We offer Web-based resource rooms to guide members from start to finish through a new local QI initiative. We have funded demonstration projects to pilot new approaches and tools for use in discharge planning, along with innovative research to improve care for heart failure patients. And we’ve only just begun.
Researching the Approach
For each QI area we address, an advisory board is recruited to represent the best available experts, organizations, and multidisciplinary professionals. For example, the Discharge Planning for Older Adults Advisory Board includes representatives from the American Geriatrics Society (AGS), the Institute for Healthcare Improvement (IHI), the Agency for Healthcare Research and Quality (AHRQ), the Society of General Internal Medicine (SGIM), the Case Management Society of America (CMSA), the National Quality Forum (NQF), and the Association for Health-System Pharmacists (AHSP), in addition to nationally renowned leaders in care transitions, geriatrics, nursing, patient literacy, and pharmacy.
Each Advisory Board conducts a needs assessment and a review of the literature to examine interventions and approaches. The board identifies existing “gaps” in clinical tools and guidelines. Finally, the Advisory Board determines specific, measurable targets for a hospitalist-led intervention and suggests the evidence-based approach(es) that should be most effective.
Implementing an Intervention: Where the Rubber Meets the Road
As I pointed out earlier, resolving what should be done and getting it done are two very different things. In most cases, few people debate the need for the intervention—reducing the incidence of inpatient VTEs, for example—or the validity of the proposed intervention. The challenge arises in changing the system of care so that the intervention becomes the new standard of care. Therefore, after the Advisory Board has determined the aims and intervention(s), SHM develops a “workbook,” a step-by-step field guide for hospitalists that walks them through the process of building a project team, establishing project aims and key metrics, obtaining institutional support, planning the intervention, launching the intervention, measuring impact, and sustaining system improvements.
The workbooks are posted in the SHM Resource Rooms along with other key resources, including slide sets, bedside teaching tools, patient education literature, CME modules, reviews of key literature, interactive “Ask the Expert” discussion boards, and improvement reports detailing the strategies, successes, and setbacks of other institutions. SHM currently offers resource rooms for Preventing VTE, Heart Failure, Stroke, Discharge Planning for the Elderly, Glycemic Control, and Antimicrobial Resistance. To access the resource rooms, visit our Web site at www.hospitalmedicine.org.
Training Leaders
SHM offers its members diverse training opportunities designed to accommodate the range of knowledge, expertise, and resources available at local institutions. The resource rooms and workbooks described above are made freely available to everyone. At the 2007 SHM Annual Meeting, we will offer a quality pre-course for hands-on training to lead a QI initiative for discharge planning, VTE prevention, or glycemic control.
For SHM members who desire additional support, SHM is developing “Mentored Implementation” and “On-Site Consulting” programs. The Mentored Implementation Program provides enrolled sites with all of the tools described above and an additional yearlong training program conducted via monthly conference calls with SHM mentors and/or one-day training programs. The On-Site Consulting Program surveys an institution’s resources and infrastructure. The SHM consultant team reviews the assessment with the site. Following this assessment, the consultant team visits the site to meet with hospital administrators, QI teams, and others to further assess the site and to help build internal support for the QI initiative. Following the visit, each site receives a customized report detailing recommendations and strategies to advance specific local QI initiatives.
SHM recently launched a Mentored Implementation and On-Site Consulting Program for VTE (known as the SHM VTE Collaborative). Similar programs are scheduled to launch for discharge planning this spring. In the coming years, we hope to add training programs in several other key patient safety areas.
Additionally, SHM is engaged in a strategic planning process to determine how best to attract the highest caliber medical students into hospital medicine and to mentor, train, and retain the next generation of leaders.
In summary, I hope the range of training opportunities and educational programs, the depth of SHM tool kits, and the scope of patient safety initiatives are meeting your needs to plan, implement, evaluate, and sustain positive change at your institution. If you are interested in learning more about SHM QI programs or have suggestions on how we might improve them to better meet your needs, please e-mail me at [email protected].
And, in case you were wondering, I’m making progress on my resolution to run. This year my resolution has the support of my department chairs (Jacob, five; Noah, two), with better-defined outcomes (run three times a week for more than 40 minutes each time), and a better tool kit (gloves, ear muffs). In the planning stage, I addressed my biggest barrier (leave the alarm off) and built a support team (my neighbor joins me).
If you see me at the annual meeting, please let me know how your resolutions are working to prevent DVT or to improve the discharge process, glycemic control, or heart failure care. Or better yet, submit those stories to me to share with members in our “Improvement Stories” or resource rooms Web site areas or in print via The Hospitalist or Journal of Hospital Medicine.
Budnitz is senior advisor, quality initiatives, for SHM.
Face the Future

We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
We need not be afraid of the future, for the future will be in our own hands.
—Thomas E. Dewey
Your SHM board recently spent some time on the most comprehensive strategic planning that we have undertaken. Our last strategic planning meeting was almost three years ago. It is reassuring to review those minutes and see that we have accomplished a number of things that we set out to do. We have:
- Enhanced our chapters by making more resources and staff assistance available to them;
- Expanded our leadership training offerings;
- Established relationships with other organizations, such as the American Hospital Association, the Joint Commission on Accreditation of Healthcare Organizations, the Society of Critical Care Medicine, and many others; and
- Explored a credential for the hospitalist that distinguishes our work from other practitioners.
Planning to Plan
In these exciting times, however, we decided it was important to stop and take stock to either confirm that we are on the right track or adjust our direction. To prepare for the meeting, we hired an outside facilitator. We invited all board members and our staff from Philadelphia. Our staff has grown from several people to more than 20. They are a diverse group with a tremendous amount of talent. Their perspective and input remain crucial to our success.
We included some of our key committee chairs as well. These individuals have regular contact with other agencies, our members, and their employees. We surveyed our membership and hospitalist leaders to determine their perspective on the dilemmas that they face. We interviewed 13 “futurists” to obtain their opinions about key trends that will affect hospitalists, including:
- The current environment for hospitalists;
- The implications of future trends in patient populations;
- The regulatory and political environment;
- The competitive forces; and
- Advancements in science, technology, and pharmaceuticals.
Bang for the Buck
The SHM board, when surveyed, expressed a strong interest in better understanding SHM’s customer groups, what they value, and what we can offer to them. We conduct many activities and support many projects through our staff, our volunteer leadership, and our members. We need to know if we are spending our resources in a way that optimizes our impact on our members and our field. Each participant spent two to three hours reviewing materials in preparation for the meeting.
When we gathered for two days, our facilitator worked us hard. We began by reviewing what we are doing and checking that against the needs and directions identified by our members and others. We then attempted to prioritize new initiatives so that we could focus on “bang for the buck.”
As we continued the process of refining our findings and designing our action plans, a few things become apparent. Among them:
- There is and will continue to be a shortage of qualified hospitalists;
- The demands of an aging population, in conjunction with the expectations of healthcare givers, will be a source of pressure;
- It will take more time to deliver care to our incoming group of patients than it did for their grandparents;
- The technology and options that are available continue to expand, as does the need to stay abreast of ongoing changes; and
- There will be more medical information to absorb and more to communicate and organize.
As this pressure increases, the facilities’ search for solutions to the impact on cost will increase. In addition, the transparency of hospital results, as well as pay for performance, will drive a desire to improve quality results. The process improvement changes that will be needed cannot be accomplished without a committed medical staff. Hospitalists are uniquely positioned to take on this role. Thus, the demands on hospitalists for participation and leadership will increase.
Labor Shortage a Key Issue
It appears from our membership survey that the labor shortage is a key worry. Because we have no control over demand and we expect demand to increase, we will need to be creative about impacting supply. SHM may be able to address this issue. One approach is to increase supply in the following ways:
1. Design programs that attract individuals who want to be hospitalists into the primary residencies for hospitalists: internal medicine, pediatrics, and family medicine.
An example:
- Influencing training programs and educators to develop positive experiences for residents.
2. Create a model that includes nursing and physician assistants, as well as others, who can extend physicians’ capabilities
Another approach is to improve retention, a goal that might be accomplished by:
- Educating hospitals on their roles in creating a good working environment with excellent support systems for their hospitalists;
- Training group leaders to manage their programs for success;
- Creating alternative delivery models that enhance the physician lifestyle and practice experience; and
- Training individuals to matching their career goals with the right program.
Leadership Gap
Our members and their leaders seem to feel adequately prepared for clinical decision-making to deliver high quality care, but they see a gap when it comes to how they are equipped to provide leadership in a number of areas. These areas include transitions and coordination of care, resource utilization, and collaboration with multidisciplinary teams. SHM can respond to this need with training and mentoring. Perhaps we can also influence training programs and their curriculum.
Caring for the Uninsured
As many of you experience, hospitalists are increasingly called on to provide care for those without funds. When caring for the uninsured, physicians experience special challenges that create job dissatisfaction and affect the sustainability of the practice. In many cases, hospitals are willing to pay for this care because they are required by government regulation to provide it. As they see their profit margins erode, however, they are reluctant to compensate this work. It is important for SHM to be positioned to participate in these discussions as the payment and care of the uninsured gets increasing attention. Our public policy committee will continue to try to identify our best opportunities to impact this issue. How their mission will change is unclear, but this issue continues to be identified by our members as an important one.
This article only touches briefly on the many topics that SHM continues to explore as we try to see the future and take it into our hands. TH
Dr. Gorman is the president of SHM.
TH NewsAlerts
Hospitalists Prone to Evidence-Based Treatments
Researchers from Harvard Medical School (Boston) and other institutions surveyed 213 pediatric hospitalists and a random sample of 352 community pediatricians. They found that, overall, the hospitalist group showed greater adherence to evidence-based therapies and tests for common pediatric illnesses in hospitalized patients, and relied less on those therapies and tests of unproven benefits.
Hourly Rounding Pays Off
According to a study by the Studer Group (Gulf Breeze, Fl.) and the Alliance for Health Care Research, having nurses round every hour results in an average 8.9-point increase in patient satisfaction, a 50% decrease in patient falls, a reduction in the use of call lights, and an undocumented improvement in clinical outcomes.
SHM Makes Acute Heart Failure a High Priority

SHM, supported in part by funding from Scios, Inc., will undertake a major outreach campaign on quality improvement related to acute heart failure. These initiatives will focus on the “front end” of the acutely decompensated heart failure patient admission, beginning with early diagnosis and aggressive treatment and intervention including emergency department and observation unit care to optimize outcomes.
“Hospitalists manage a significant number of heart failure patients across the hospital continuum,” says Larry Wellikson, MD, CEO of SHM. “Our goal is to improve heart failure care by disseminating the necessary tools and knowledge to hospitalists.”
Google as Diagnostic Tool
The popular Web site Google (Mountain View, Calif.) can help physicians with diagnoses, according to researchers from Princess Alexandria Hospital in Brisbane, Australia. The team “googled” symptoms of 26 mystery cases, and a Web search resulted in a correct diagnosis for 15 of them. The researchers call Google a useful aid for physicians.
SHM Participates in IHI Campaign
When the Institute for Healthcare Improvement (IHI) introduced its “5 Million Lives” campaign recently, SHM was one of the few organizations asked to speak about their part in the campaign.
“We are ready … and could not be more enthusiastic about participating in this landmark campaign,” said Russell Holman, M.D., SHM’s president-elect.
A Winning Team Reaps Rewards
Caritas Good Samaritan Medical Center in Brockton, Mass., and hospital medicine provider Cogent Healthcare (Irvine, Calif.) collaborated to achieve quality of care goals that earned the facility pay-for-performance bonuses from major commercial payers. Cogent used best practices that also helped reduce length of stay and unnecessary re-admissions, and improve patient and physician satisfaction.
A Prevalence of Persistent Pain
The “Health United States 2006” report issued by the National Center for Health Statistics (Hyattsville, Md.) finds a prevalence of pain in the U.S. One in four adults reported a daylong bout of pain in the last month, and one in 10 say they’ve suffered pain for at least a year.

Palliative Medicine Now Official Subspecialty
The American Board of Medical Specialties (ABMS) will establish a subspecialty certificate in Hospice and Palliative Medicine. “[This certification] affirms the concept that specialized knowledge and skills must be learned to care for the increasingly complex-care needs of the dying and their families,” says David Weissman, MD, FACP, editor-in-chief of the Journal of Palliative Medicine.
Busy Shifts Put Elderly Admissions at Risk
Older patients admitted during busy hospital shifts may have a greater mortality rate, according to a study by the University of California San Francisco’s Moffitt-Long Hospital. The retrospective cohort analysis included 5,742 adults admitted to the general medicine service and intensive care unit without cardiovascular, neurologic, or cancer- related primary diagnoses. TH
Hospitalists Prone to Evidence-Based Treatments
Researchers from Harvard Medical School (Boston) and other institutions surveyed 213 pediatric hospitalists and a random sample of 352 community pediatricians. They found that, overall, the hospitalist group showed greater adherence to evidence-based therapies and tests for common pediatric illnesses in hospitalized patients, and relied less on those therapies and tests of unproven benefits.
Hourly Rounding Pays Off
According to a study by the Studer Group (Gulf Breeze, Fl.) and the Alliance for Health Care Research, having nurses round every hour results in an average 8.9-point increase in patient satisfaction, a 50% decrease in patient falls, a reduction in the use of call lights, and an undocumented improvement in clinical outcomes.
SHM Makes Acute Heart Failure a High Priority
SHM, supported in part by funding from Scios, Inc., will undertake a major outreach campaign on quality improvement related to acute heart failure. These initiatives will focus on the “front end” of the acutely decompensated heart failure patient admission, beginning with early diagnosis and aggressive treatment and intervention including emergency department and observation unit care to optimize outcomes.
“Hospitalists manage a significant number of heart failure patients across the hospital continuum,” says Larry Wellikson, MD, CEO of SHM. “Our goal is to improve heart failure care by disseminating the necessary tools and knowledge to hospitalists.”
Google as Diagnostic Tool
The popular Web site Google (Mountain View, Calif.) can help physicians with diagnoses, according to researchers from Princess Alexandria Hospital in Brisbane, Australia. The team “googled” symptoms of 26 mystery cases, and a Web search resulted in a correct diagnosis for 15 of them. The researchers call Google a useful aid for physicians.
SHM Participates in IHI Campaign
When the Institute for Healthcare Improvement (IHI) introduced its “5 Million Lives” campaign recently, SHM was one of the few organizations asked to speak about their part in the campaign.
“We are ready … and could not be more enthusiastic about participating in this landmark campaign,” said Russell Holman, M.D., SHM’s president-elect.
A Winning Team Reaps Rewards
Caritas Good Samaritan Medical Center in Brockton, Mass., and hospital medicine provider Cogent Healthcare (Irvine, Calif.) collaborated to achieve quality of care goals that earned the facility pay-for-performance bonuses from major commercial payers. Cogent used best practices that also helped reduce length of stay and unnecessary re-admissions, and improve patient and physician satisfaction.
A Prevalence of Persistent Pain
The “Health United States 2006” report issued by the National Center for Health Statistics (Hyattsville, Md.) finds a prevalence of pain in the U.S. One in four adults reported a daylong bout of pain in the last month, and one in 10 say they’ve suffered pain for at least a year.
Palliative Medicine Now Official Subspecialty
The American Board of Medical Specialties (ABMS) will establish a subspecialty certificate in Hospice and Palliative Medicine. “[This certification] affirms the concept that specialized knowledge and skills must be learned to care for the increasingly complex-care needs of the dying and their families,” says David Weissman, MD, FACP, editor-in-chief of the Journal of Palliative Medicine.
Busy Shifts Put Elderly Admissions at Risk
Older patients admitted during busy hospital shifts may have a greater mortality rate, according to a study by the University of California San Francisco’s Moffitt-Long Hospital. The retrospective cohort analysis included 5,742 adults admitted to the general medicine service and intensive care unit without cardiovascular, neurologic, or cancer- related primary diagnoses. TH
Hospitalists Prone to Evidence-Based Treatments
Researchers from Harvard Medical School (Boston) and other institutions surveyed 213 pediatric hospitalists and a random sample of 352 community pediatricians. They found that, overall, the hospitalist group showed greater adherence to evidence-based therapies and tests for common pediatric illnesses in hospitalized patients, and relied less on those therapies and tests of unproven benefits.
Hourly Rounding Pays Off
According to a study by the Studer Group (Gulf Breeze, Fl.) and the Alliance for Health Care Research, having nurses round every hour results in an average 8.9-point increase in patient satisfaction, a 50% decrease in patient falls, a reduction in the use of call lights, and an undocumented improvement in clinical outcomes.
SHM Makes Acute Heart Failure a High Priority
SHM, supported in part by funding from Scios, Inc., will undertake a major outreach campaign on quality improvement related to acute heart failure. These initiatives will focus on the “front end” of the acutely decompensated heart failure patient admission, beginning with early diagnosis and aggressive treatment and intervention including emergency department and observation unit care to optimize outcomes.
“Hospitalists manage a significant number of heart failure patients across the hospital continuum,” says Larry Wellikson, MD, CEO of SHM. “Our goal is to improve heart failure care by disseminating the necessary tools and knowledge to hospitalists.”
Google as Diagnostic Tool
The popular Web site Google (Mountain View, Calif.) can help physicians with diagnoses, according to researchers from Princess Alexandria Hospital in Brisbane, Australia. The team “googled” symptoms of 26 mystery cases, and a Web search resulted in a correct diagnosis for 15 of them. The researchers call Google a useful aid for physicians.
SHM Participates in IHI Campaign
When the Institute for Healthcare Improvement (IHI) introduced its “5 Million Lives” campaign recently, SHM was one of the few organizations asked to speak about their part in the campaign.
“We are ready … and could not be more enthusiastic about participating in this landmark campaign,” said Russell Holman, M.D., SHM’s president-elect.
A Winning Team Reaps Rewards
Caritas Good Samaritan Medical Center in Brockton, Mass., and hospital medicine provider Cogent Healthcare (Irvine, Calif.) collaborated to achieve quality of care goals that earned the facility pay-for-performance bonuses from major commercial payers. Cogent used best practices that also helped reduce length of stay and unnecessary re-admissions, and improve patient and physician satisfaction.
A Prevalence of Persistent Pain
The “Health United States 2006” report issued by the National Center for Health Statistics (Hyattsville, Md.) finds a prevalence of pain in the U.S. One in four adults reported a daylong bout of pain in the last month, and one in 10 say they’ve suffered pain for at least a year.
Palliative Medicine Now Official Subspecialty
The American Board of Medical Specialties (ABMS) will establish a subspecialty certificate in Hospice and Palliative Medicine. “[This certification] affirms the concept that specialized knowledge and skills must be learned to care for the increasingly complex-care needs of the dying and their families,” says David Weissman, MD, FACP, editor-in-chief of the Journal of Palliative Medicine.
Busy Shifts Put Elderly Admissions at Risk
Older patients admitted during busy hospital shifts may have a greater mortality rate, according to a study by the University of California San Francisco’s Moffitt-Long Hospital. The retrospective cohort analysis included 5,742 adults admitted to the general medicine service and intensive care unit without cardiovascular, neurologic, or cancer- related primary diagnoses. TH