User login
Trends in Inpatient Continuity of Care
Continuity of care is considered by many physicians to be of critical importance in providing high‐quality patient care. Most of the research to date has focused on continuity in outpatient primary care. Research on outpatient continuity of care has been facilitated by the fact that a number of measurement tools for outpatient continuity exist.1 Outpatient continuity of care has been linked to better quality of life scores,2 lower costs,3 and less emergency room use.4 As hospital medicine has taken on more and more of the responsibility of inpatient care, primary care doctors have voiced concerns about the impact of hospitalists on overall continuity of care5 and the quality of the doctorpatient relationship.6
Recently, continuity of care in the hospital setting has also received attention. When the Accreditation Council for Graduate Medical Education (ACGME) first proposed restrictions to resident duty hours, the importance of continuity of inpatient care began to be debated in earnest in large part because of the increase in hand‐offs which accompanies discontinuity.7, 8 A recent study of hospitalist communication documented that as many as 13% of hand‐offs at the time of service changes are judged as incomplete by the receiving physician. These incomplete hand‐offs were more likely to be associated with uncertainty regarding the plan of care, as well as perceived near misses or adverse events.9 In addition, several case reports and studies suggest that systems with less continuity may have poorer outcomes.7, 1015
Continuity in the hospital setting is likely to be important for several reasons. First, the acuity of a patient's problem during a hospitalization is likely greater than during an outpatient visit. Thus the complexity of information to be transferred between physicians during a hospital stay is correspondingly greater. Second, the diagnostic uncertainty surrounding many admissions leads to complex thought processes that may be difficult to recreate when handing off patient care to another physician. Finally, knowledge of a patient's hospital course and the likely trajectory of care is facilitated by firsthand knowledge of where the patient has been. All this information can be difficult to distill into a brief sign‐out to another physician who assumes care of the patient.
In the current study, we sought to examine the trends over time in continuity of inpatient care. We chose patients likely to be cared for by general internists: those hospitalized for chronic obstructive pulmonary disease (COPD), pneumonia, and congestive heart failure (CHF). The general internists caring for patients in the hospital could be the patient's primary care physician (PCP), a physician covering for the patient's PCP, a physician assigned at admission by the hospital, or a hospitalist. Our goals were to describe the current level of continuity of care in the hospital setting, to examine whether continuity has changed over time, and to determine factors affecting continuity of care.
Methods
We used a 5% national sample of claims data from Medicare beneficiaries for the years 19962006.16 This included Medicare enrollment files, Medicare Provider Analysis and Review (MEDPAR) files, Medicare Carrier files, and Provider of Services (POS) files.17, 18
Establishment of the Study Cohort
Hospital admissions for COPD (Diagnosis Related Group [DRG] 088), pneumonia (DRG 089, 090), and CHF (DRG 127) from 1996 to 2006 for patients older than 66 years in MEDPAR were selected (n = 781,348). We excluded admissions for patients enrolled in health maintenance organizations (HMOs) or who did not have Medicare Parts A and B for the entire year prior to admission (n = 57,558). Admissions with a length of stay >18 days (n = 10,688) were considered outliers (exceeding the 99th percentile) and were excluded. Only admissions cared for by a general internist, family physician, general practitioner, or geriatrician were included (n = 528,453).
Measures
We categorized patients by age, gender, and ethnicity using Medicare enrollment files. We used the Medicaid indicator in the Medicare file as a proxy of low socioeconomic status. We used MEDPAR files to determine the origin of the admission (via the emergency department vs other), weekend versus weekday admission, and DRG. A comorbidity score was generated using the Elixhauser comorbidity scale using inpatient and outpatient billing data.19 In analyses, we listed the total number of comorbidities identified. The specialty of each physician was determined from the codes in the Medicare Carrier files. The 2004 POS files provided hospital‐level information such as zip code, metropolitan size, state, total number of beds, type of hospital, and medical school affiliation. We divided metropolitan size and total number of hospital beds into quartiles. We categorized hospitals as nonprofit, for profit, or public; medical school affiliation was categorized as non, minor, or major.
Determination of Primary Care Physician (PCP)
We identified outpatient visits using American Medical AssociationCommon Procedure Terminology (CPT) evaluation and management codes 99201 to 99205 (new patient) and 99221 to 99215 (established patient encounters). Individual providers were differentiated by using their Unique Provider Identification Number (UPIN). We defined a PCP as a general practitioner, family physician, internist, or geriatrician. Patients had to make at least 3 visits on different days to the same PCP within a year prior to the hospitalization to be categorized as having a PCP.20
Identification of Hospitalists Versus Other Generalist Physicians
As previously described, we defined hospitalists as general internal medicine physicians who derive at least 90% of their Medicare claims for Evaluation and Management services from care provided to hospitalized patients.21 Non‐hospitalist generalist physicians were those generalists who met the criteria for generalists but did not derive at least 90% of their Medicare claims from inpatient medicine.
Definition of Inpatient Continuity of Care
We measured inpatient continuity of care by number of generalist physicians (including hospitalists) who provided care during a hospitalization, through all inpatient claims made during that hospitalization. We considered patients to have had inpatient continuity of care if all billing by generalist physicians was done by one physician during the entire hospitalization.
Statistical Analyses
We calculated the percentage of admissions that received care from 1, 2, or 3 or more generalist physicians during the hospitalization, and stratified by selected patient and hospital characteristics. These proportions were also stratified by whether the patients were cared for by their outpatient PCP or not, and whether they were cared for by hospitalists or not. Based on who cared for the patient during the hospitalization, all admissions were classified as receiving care from: 1) non‐hospitalist generalist physicians, 2) a combination of generalist physicians and hospitalists, and 3) hospitalists only. The effect of patient and hospital characteristics on whether a patient experienced inpatient continuity was evaluated using a hierarchical generalized linear model (HGLM) with a logistic link, adjusting for clustering of admissions within hospitals and all covariates. We repeated our analyses using HGLM with an ordinal logit link to explore the factors associated with number of generalists seen in the hospital. All analyses were performed with SAS version 9.1 (SAS Inc, Cary, NC). The SAS GLIMMIX procedure was used to conduct multilevel analyses.
Results
Between 1996 and 2006, 528,453 patients hospitalized for COPD, pneumonia, and CHF received care by a generalist physician during their hospital stay. Of these, 64.3% were seen by one generalist physician, 26.9% by two generalist physicians, and 8.8% by three or more generalist physicians during hospitalization.
Figure 1 shows the percentage of all patients seen by 1, 2, and 3 or more generalist physicians between 1996 and 2006. The percentage of patients receiving care from one generalist physician declined from 70.7% in 1996 to 59.4% in 2006 (P < 0.001). During the same period, the percentage of patients receiving care from 3 or more generalist physicians increased from 6.5% to 10.7% (P < 0.001). Similar trends were seen for each of the 3 conditions. There was a decrease in overall length of stay during this period, from a mean of 5.7 to 4.9 days (P < 0.001). The increase in the number of generalist physicians providing care during the hospital stay did not correspond to an increase in total number of visits during the hospitalization. The average number of daily visits from a generalist physician was 0.94 (0.30) in 1996 and 0.96 (0.35) in 2006.
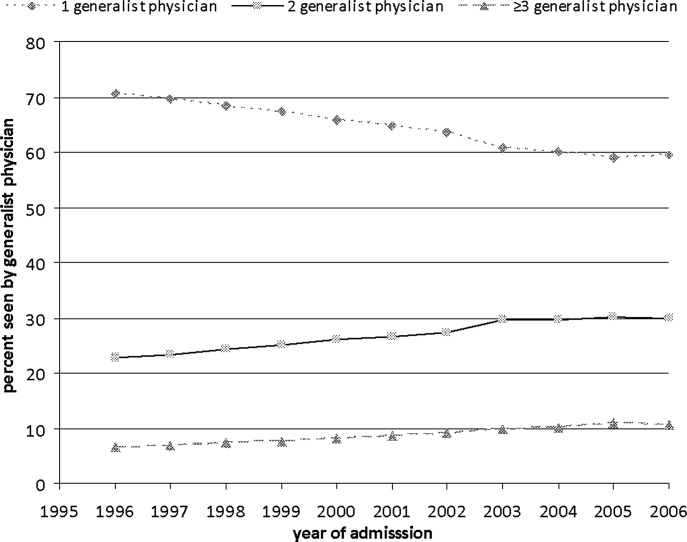
Table 1 presents the percentage of patients receiving care from 1, 2, and 3 or more generalist physicians during hospitalization stratified by patient and hospital characteristics. Older adults, females, non‐Hispanic whites, those with higher socioeconomic status, and those with more comorbidities were more likely to receive care by multiple generalist physicians. There was also large variation by geographic region, metropolitan area size, and hospital characteristics. All of these differences were significant at the P < 0.0001 level.
| No. of Generalist Physicians Seen During Hospitalization | ||||
|---|---|---|---|---|
| Characteristic | N | 1 | 2 | 3 (Percentage of Patients) |
| ||||
| Age at admission | ||||
| 6674 | 152,488 | 66.4 | 25.6 | 8.0 |
| 7584 | 226,802 | 63.8 | 27.3 | 8.9 |
| 85+ | 149,163 | 63.0 | 27.7 | 9.3 |
| Gender | ||||
| Male | 216,602 | 65.3 | 26.4 | 8.3 |
| Female | 311,851 | 63.6 | 27.3 | 9.1 |
| Ethnicity | ||||
| White | 461,543 | 63.7 | 27.4 | 9.0 |
| Black | 46,960 | 68.6 | 23.8 | 7.6 |
| Other | 19,950 | 67.9 | 24.5 | 7.6 |
| Low socioeconomic status | ||||
| No | 366,392 | 63.4 | 27.5 | 9.1 |
| Yes | 162,061 | 66.3 | 25.7 | 8.0 |
| Emergency admission | ||||
| No | 188,354 | 66.8 | 25.6 | 7.6 |
| Yes | 340,099 | 62.9 | 27.7 | 9.4 |
| Weekend admission | ||||
| No | 392,150 | 65.7 | 25.8 | 8.5 |
| Yes | 136,303 | 60.1 | 30.3 | 9.6 |
| Diagnosis‐related groups | ||||
| CHF | 213,914 | 65.0 | 26.3 | 8.7 |
| Pneumonia | 195,430 | 62.5 | 28.0 | 9.5 |
| COPD | 119,109 | 66.1 | 26.2 | 7.7 |
| Had a PCP | ||||
| No | 201,016 | 66.5 | 25.4 | 8.0 |
| Yes | 327,437 | 62.9 | 27.9 | 9.2 |
| Seen hospitalist | ||||
| No | 431,784 | 67.8 | 25.1 | 7.0 |
| Yes | 96,669 | 48.5 | 34.9 | 16.6 |
| Charlson comorbidity score | ||||
| 0 | 127,385 | 64.0 | 27.2 | 8.8 |
| 1 | 131,402 | 65.1 | 26.8 | 8.1 |
| 2 | 105,831 | 64.9 | 26.6 | 8.5 |
| 3 | 163,835 | 63.4 | 27.1 | 9.5 |
| ICU use | ||||
| No | 431,462 | 65.3 | 26.5 | 8.2 |
| Yes | 96,991 | 60.1 | 28.7 | 11.2 |
| Length of stay (in days) | ||||
| Mean (SD) | 4.7 (2.9) | 5.8 (3.1) | 8.1 (3.7) | |
| Geographic region | ||||
| New England | 23,572 | 55.7 | 30.8 | 13.5 |
| Middle Atlantic | 78,181 | 60.8 | 27.8 | 11.4 |
| East North Central | 98,072 | 65.7 | 26.3 | 8.0 |
| West North Central | 44,785 | 59.6 | 30.5 | 9.9 |
| South Atlantic | 104,894 | 63.8 | 27.0 | 9.2 |
| East South Central | 51,450 | 67.8 | 24.6 | 7.6 |
| West South Central | 63,493 | 69.2 | 24.8 | 6.0 |
| Mountain | 20,310 | 61.9 | 29.4 | 8.7 |
| Pacific | 36,484 | 66.7 | 26.3 | 7.0 |
| Size of metropolitan area* | ||||
| 1,000,000 | 229,145 | 63.7 | 26.5 | 9.8 |
| 250,000999,999 | 114,448 | 61.0 | 29.2 | 9.8 |
| 100,000249,999 | 11,448 | 61.3 | 30.4 | 8.3 |
| <100,000 | 171,585 | 67.4 | 25.8 | 6.8 |
| Medical school affiliation* | ||||
| Major | 77,605 | 62.9 | 26.8 | 10.3 |
| Minor | 107,144 | 61.5 | 28.4 | 10.1 |
| Non | 341,874 | 65.5 | 26.5 | 8.0 |
| Type of hospital* | ||||
| Nonprofit | 375,888 | 62.7 | 27.8 | 9.5 |
| For profit | 63,898 | 67.5 | 25.5 | 7.0 |
| Public | 86,837 | 68.9 | 24.2 | 6.9 |
| Hospital size* | . | . | . | |
| <200 beds | 232,869 | 67.2 | 25.7 | 7.1 |
| 200349 beds | 135,954 | 62.6 | 27.9 | 9.5 |
| 350499 beds | 77,080 | 61.1 | 28.3 | 10.6 |
| 500 beds | 80,723 | 61.7 | 27.6 | 10.7 |
| Discharge location | ||||
| Home | 361,893 | 66.6 | 26.0 | 7.4 |
| SNF | 94,723 | 57.6 | 30.1 | 12.3 |
| Rehab | 3,030 | 45.7 | 34.2 | 20.1 |
| Death | 22,133 | 63.1 | 25.4 | 11.5 |
| Other | 46,674 | 61.8 | 28.1 | 10.1 |
Table 2 presents the results of a multivariable analysis of factors independently associated with experiencing continuity of care. In this analysis, continuity of care was defined as receiving inpatient care from one generalist physician (vs two or more). In the unadjusted models, the odds of experiencing continuity of care decreased by 5.5% per year from 1996 through 2006, and this decrease did not substantially change after adjusting for all other variables (4.8% yearly decrease). Younger patients, females, black patients, and those with low socioeconomic status were slightly more likely to experience continuity of care. As expected, patients admitted on weekends, emergency admissions, and those with intensive care unit (ICU) stays were less likely to experience continuity. There were marked geographic variations in continuity, with continuity approximately half as likely in New England as in the South. Continuity was greatest in smaller metropolitan areas versus rural and large metropolitan areas. Hospital size and teaching status produced only minor variation.
| Characteristic | Odds Ratio (95% CI) |
|---|---|
| |
| Admission year (increase by year) | 0.952 (0.9500.954) |
| Length of stay (increase by day) | 0.822 (0.8200.823) |
| Had a PCP | |
| No | 1.0 |
| Yes | 0.762 (0.7520.773) |
| Seen by a hospitalist | |
| No | 1.0 |
| Yes | 0.391 (0.3840.398) |
| Age | |
| 6674 | 1.0 |
| 7584 | 0.959 (0.9440.973) |
| 85+ | 0.946 (0.9300.962) |
| Gender | |
| Male | 1.0 |
| Female | 1.047 (1.0331.060) |
| Ethnicity | |
| White | 1.0 |
| Black | 1.126 (1.0971.155) |
| Other | 1.062 (1.0231.103) |
| Low socioeconomic status | |
| No | 1.0 |
| Yes | 1.036 (1.0201.051) |
| Emergency admission | |
| No | 1.0 |
| Yes | 0.864 (0.8510.878) |
| Weekend admission | |
| No | 1.0 |
| Yes | 0.778 (0.7680.789) |
| Diagnosis‐related group | |
| CHF | 1.0 |
| Pneumonia | 0.964 (0.9500.978) |
| COPD | 1.002 (0.9851.019) |
| Charlson comorbidity score | |
| 0 | 1.0 |
| 1 | 1.053 (1.0351.072) |
| 2 | 1.062 (1.0421.083) |
| 3 | 1.040 (1.0221.058) |
| ICU use | |
| No | 1.0 |
| Yes | 0.918 (0.9020.935) |
| Geographic region | |
| Middle Atlantic | 1.0 |
| New England | 0.714 (0.6210.822) |
| East North Central | 1.015 (0.9221.119) |
| West North Central | 0.791 (0.7110.879) |
| South Atlantic | 1.074 (0.9711.186) |
| East South Central | 1.250 (1.1131.403) |
| West South Central | 1.377 (1.2401.530) |
| Mountain | 0.839 (0.7400.951) |
| Pacific | 0.985 (0.8841.097) |
| Size of metropolitan area | |
| 1,000,000 | 1.0 |
| 250,000999,999 | 0.743 (0.6910.798) |
| 100,000249,999 | 0.651 (0.5380.789) |
| <100,000 | 1.062 (0.9911.138) |
| Medical school affiliation | |
| None | 1.0 |
| Minor | 0.889 (0.8270.956) |
| Major | 1.048 (0.9521.154) |
| Type of hospital | |
| Nonprofit | 1.0 |
| For profit | 1.194 (1.1061.289) |
| Public | 1.394 (1.3091.484) |
| Size of hospital | |
| <200 beds | 1.0 |
| 200349 beds | 0.918 (0.8550.986) |
| 350499 beds | 0.962 (0.8721.061) |
| 500 beds | 1.000 (0.8931.119) |
In Table 2 we also show that patients with an established PCP and those who received care from a hospitalist in the hospital were substantially less likely to experience continuity of care. There are several possible interpretations for that finding. For example, it might be that patients admitted to a hospitalist service were likely to see multiple hospitalists. Alternatively, the decreased continuity associated with hospitalists could reflect the fact that some patients cared for predominantly by non‐hospitalists may have seen a hospitalist on call for a sudden change in health status. To further explore these possible explanatory pathways, we constructed three new cohorts: 1) patients receiving all their care from non‐hospitalists, 2) patients receiving all their care from hospitalists, and 3) patients seen by both. As shown in Table 3, in patients seen by non‐hospitalists only, the mean number of generalist physicians seen during hospitalization was slightly greater than in patients cared for only by hospitalists.
| Received Care During Entire Hospitalization | No. of Admissions | Mean (SD) No. of Generalist Physicians Seen During Hospitalization |
|---|---|---|
| ||
| Non‐hospitalist physician | 431,784 | 1.41 (0.68)* |
| Hospitalist physician | 64,662 | 1.34 (0.62)* |
| Both | 32,007 | 2.55 (0.83)* |
We also tested for interactions in Table 2 between admission year and other factors. There was a significant interaction between admission year and having an identifiable PCP in the year prior to admission (Table 2). The odds of experiencing continuity of care decreased more rapidly for patients who did not have a PCP (5.5% per year; 95% CI: 5.2%5.8%) than for those who had one (4.3% per year; 95% CI: 4.1%4.6%).
Discussion
We conducted this study to better understand the degree to which hospitalized patients experience discontinuity of care within a hospital stay and to determine which patients are most likely to experience discontinuity. In our study, we specifically chose admission conditions that would likely be followed primarily by generalist physicians. We found that, over the past decade, discontinuity of care for hospitalized patients has increased substantially, as indicated by the proportion of patients taken care of by more than one generalist physician during a single hospital stay. This occurred even though overall length of stay was decreasing in this same period.
It is perhaps not surprising that inpatient continuity of care has been decreasing in the past 10 years. Outpatient practices are becoming busier, and more doctors are practicing in large group practices, which could lead to several different physicians in the same practice rounding on a hospitalized patient. We have previously demonstrated that hospitalists are caring for an increasing number of patients over this same time period,21 so another possibility is that hospitalist services are being used more often because of this heavy outpatient workload. Our analyses allowed us to test the hypothesis that having hospitalists involved in patient care increases discontinuity.
At first glance, it appears that being cared for by hospitalists may result in worse continuity of care. However, closer scrutiny of the data reveals that the discontinuity ascribed to the hospitalists in the multivariable model appears to be an artifact of defining the hospitalist variable as having been seen by any hospitalist during the hospital stay. This would include patients who saw a hospitalist in addition to their PCP or another non‐hospitalist generalist. When we compared hospitalist‐only care to other generalist care, we could not detect a difference in discontinuity. We know that generalist visits per day to patients has not substantially increased over time, so this discontinuity trend is not explained by having visits by both a hospitalist and the PCP. Therefore, this combination of findings suggests that the increased discontinuity associated with having a hospitalist involved in patient care is likely the result of system issues rather than hospitalist care per se. In fact, patients seem to experience slightly better continuity when they see only hospitalists as opposed to only non‐hospitalists.
What types of systems issues might lead to this finding? Generalists in most settings could choose to involve a hospitalist at any point in the patient's hospital stay. This could occur because of a change in patient acuity requiring the involvement of hospitalists who are present in the hospital more. It is also possible that hospitalists' schedules are created to maximize inpatient continuity of care with individual hospitalists. Even though hospitalists clearly work shifts, the 7 on, 7 off model22 likely results in patients seeing the same physician each day until the switch day. This is in contrast to outpatient primary care doctors whose concentration may be on maintaining continuity within their practice.
As the field of hospital medicine was emerging, many internal medicine physicians from various specialties were concerned about the impact of hospitalists on patient care. In one study, 73% of internal medicine physicians who were not hospitalists thought that hospitalists would worsen continuity of care.23 Primary care and subspecialist internal medicine physicians also expressed the concern that hospitalists could hurt their own relationships with patients,6 presumably because of lost continuity between the inpatient and outpatient settings. However, this fear seems to diminish once hospitalist programs are implemented and primary care doctors have experience with them.23 Our study suggests that the decrease in continuity that has occurred since these studies were published is not likely due to the emergence of hospital medicine, but rather due to other factors that influence who cares for hospitalized patients.
This study had some limitations. Length of stay is an obvious mediator of number of generalist physicians seen. Therefore, the sickest patients are likely to have both a long length of stay and low continuity. We adjusted for this in the multivariable modeling. In addition, given that this study used a large database, certain details are not discernable. For example, we chose to operationalize discontinuity as visits from multiple generalists during a single hospital stay. That is not a perfect definition, but it does represent multiple physicians directing the care of a patient. Importantly, this does not appear to represent continuity with one physician with extra visits from another, as the total number of generalist visits per day did not change over time. It is also possible that patients in the non‐hospitalist group saw physicians only from a single practice, but those details are not included in the database. Finally, we cannot tell what type of hand‐offs were occurring for individual patients during each hospital stay. Despite these disadvantages, using a large database like this one allows for detection of fairly small differences that could still be clinically important.
In summary, hospitalized patients appear to experience less continuity now than 10 years ago. However, the hospitalist model does not appear to play a role in this discontinuity. It is worth exploring in more detail why patients would see both hospitalists and other generalists. This pattern is not surprising, but may have some repercussions in terms of increasing the number of hand‐offs experienced by patients. These could lead to problems with patient safety and quality of care. Future work should explore the reasons for this discontinuity and look at the relationship between inpatient discontinuity outcomes such as quality of care and the doctorpatient relationship.
Acknowledgements
The authors thank Sarah Toombs Smith, PhD, for help in preparation of the manuscript.
- .Defining and measuring interpersonal continuity of care.Ann Fam Med.2003;1(3):134–143.
- ,,.Good continuity of care may improve quality of life in Type 2 diabetes.Diabetes Res Clin Pract.2001;51(1):21–27.
- ,,,.Provider continuity in family medicine: Does it make a difference for total health care costs?Ann Fam Med.2003;1(3):144–148.
- ,,.The effect of continuity of care on emergency department use.Arch Fam Med.2000;9(4):333–338.
- ,,,,,.Physician attitudes toward and prevalence of the hospitalist model of care: Results of a national survey.Am J Med.2000;109(8):648–653.
- ,,.Physician views on caring for hospitalized patients and the hospitalist model of inpatient care.J Gen Intern Med.2001;16(2):116–119.
- ,,,,,.Systematic review: Effects of resident work hours on patient safety.Ann Intern Med.2004;141(11):851–857.
- ,,.Balancing continuity of care with residents' limited work hours: Defining the implications.Acad Med.2005;80(1):39–43.
- ,,.Understanding communication during hospitalist sevice changes: A mixed methods study.J Hosp Med.2009;4:535–540.
- ,,,Center for Safety in Emergency C. Profiles in patient safety: Emergency care transitions.Acad Emerg Med.2003;10(4):364–367.
- .Fumbled handoffs: One dropped ball after another.Ann Intern Med.2005;142(5):352–358.
- Agency for Healthcare Research and Quality. Fumbled handoff.2004. Available at: http://www.webmm.ahrq.gov/printview.aspx?caseID=55. Accessed December 27, 2005.
- ,,.Graduate medical education and patient safety: A busy—and occasionally hazardous—intersection.Ann Intern Med.2006;145(8):592–598.
- ,,,,.Does housestaff discontinuity of care increase the risk for preventable adverse events?Ann Intern Med.1994;121(11):866–872.
- ,,,.The impact of a regulation restricting medical house staff working hours on the quality of patient care.JAMA.1993;269(3):374–378.
- Centers for Medicare and Medicaid Services. Standard analytical files. Available at: http://www.cms.hhs.gov/IdentifiableDataFiles/02_Standard AnalyticalFiles.asp. Accessed March 1,2009.
- Centers for Medicare and Medicaid Services. Nonidentifiable data files: Provider of services files. Available at: http://www.cms.hhs.gov/NonIdentifiableDataFiles/04_ProviderofSerrvicesFile.asp. Accessed March 1,2009.
- Research Data Assistance Center. Medicare data file description. Available at: http://www.resdac.umn.edu/Medicare/file_descriptions.asp. Accessed March 1,2009.
- ,,,.Effect of comorbidity adjustment on CMS criteria for kidney transplant center performance.Am J Transplant.2009;9:506–516.
- ,,,,,.Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults.JAMA.2009;301:1671–1680.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med. 2009;360:1102–1112.
- HCPro Inc.Medical Staff Leader blog.2010. Available at: http://blogs. hcpro.com/medicalstaff/2010/01/free‐form‐example‐seven‐day‐on‐seven‐day‐off‐hospitalist‐schedule/. Accessed November 20, 2010.
- ,,,.How physicians perceive hospitalist services after implementation: Anticipation vs reality.Arch Intern Med.2003;163(19):2330–2336.
Continuity of care is considered by many physicians to be of critical importance in providing high‐quality patient care. Most of the research to date has focused on continuity in outpatient primary care. Research on outpatient continuity of care has been facilitated by the fact that a number of measurement tools for outpatient continuity exist.1 Outpatient continuity of care has been linked to better quality of life scores,2 lower costs,3 and less emergency room use.4 As hospital medicine has taken on more and more of the responsibility of inpatient care, primary care doctors have voiced concerns about the impact of hospitalists on overall continuity of care5 and the quality of the doctorpatient relationship.6
Recently, continuity of care in the hospital setting has also received attention. When the Accreditation Council for Graduate Medical Education (ACGME) first proposed restrictions to resident duty hours, the importance of continuity of inpatient care began to be debated in earnest in large part because of the increase in hand‐offs which accompanies discontinuity.7, 8 A recent study of hospitalist communication documented that as many as 13% of hand‐offs at the time of service changes are judged as incomplete by the receiving physician. These incomplete hand‐offs were more likely to be associated with uncertainty regarding the plan of care, as well as perceived near misses or adverse events.9 In addition, several case reports and studies suggest that systems with less continuity may have poorer outcomes.7, 1015
Continuity in the hospital setting is likely to be important for several reasons. First, the acuity of a patient's problem during a hospitalization is likely greater than during an outpatient visit. Thus the complexity of information to be transferred between physicians during a hospital stay is correspondingly greater. Second, the diagnostic uncertainty surrounding many admissions leads to complex thought processes that may be difficult to recreate when handing off patient care to another physician. Finally, knowledge of a patient's hospital course and the likely trajectory of care is facilitated by firsthand knowledge of where the patient has been. All this information can be difficult to distill into a brief sign‐out to another physician who assumes care of the patient.
In the current study, we sought to examine the trends over time in continuity of inpatient care. We chose patients likely to be cared for by general internists: those hospitalized for chronic obstructive pulmonary disease (COPD), pneumonia, and congestive heart failure (CHF). The general internists caring for patients in the hospital could be the patient's primary care physician (PCP), a physician covering for the patient's PCP, a physician assigned at admission by the hospital, or a hospitalist. Our goals were to describe the current level of continuity of care in the hospital setting, to examine whether continuity has changed over time, and to determine factors affecting continuity of care.
Methods
We used a 5% national sample of claims data from Medicare beneficiaries for the years 19962006.16 This included Medicare enrollment files, Medicare Provider Analysis and Review (MEDPAR) files, Medicare Carrier files, and Provider of Services (POS) files.17, 18
Establishment of the Study Cohort
Hospital admissions for COPD (Diagnosis Related Group [DRG] 088), pneumonia (DRG 089, 090), and CHF (DRG 127) from 1996 to 2006 for patients older than 66 years in MEDPAR were selected (n = 781,348). We excluded admissions for patients enrolled in health maintenance organizations (HMOs) or who did not have Medicare Parts A and B for the entire year prior to admission (n = 57,558). Admissions with a length of stay >18 days (n = 10,688) were considered outliers (exceeding the 99th percentile) and were excluded. Only admissions cared for by a general internist, family physician, general practitioner, or geriatrician were included (n = 528,453).
Measures
We categorized patients by age, gender, and ethnicity using Medicare enrollment files. We used the Medicaid indicator in the Medicare file as a proxy of low socioeconomic status. We used MEDPAR files to determine the origin of the admission (via the emergency department vs other), weekend versus weekday admission, and DRG. A comorbidity score was generated using the Elixhauser comorbidity scale using inpatient and outpatient billing data.19 In analyses, we listed the total number of comorbidities identified. The specialty of each physician was determined from the codes in the Medicare Carrier files. The 2004 POS files provided hospital‐level information such as zip code, metropolitan size, state, total number of beds, type of hospital, and medical school affiliation. We divided metropolitan size and total number of hospital beds into quartiles. We categorized hospitals as nonprofit, for profit, or public; medical school affiliation was categorized as non, minor, or major.
Determination of Primary Care Physician (PCP)
We identified outpatient visits using American Medical AssociationCommon Procedure Terminology (CPT) evaluation and management codes 99201 to 99205 (new patient) and 99221 to 99215 (established patient encounters). Individual providers were differentiated by using their Unique Provider Identification Number (UPIN). We defined a PCP as a general practitioner, family physician, internist, or geriatrician. Patients had to make at least 3 visits on different days to the same PCP within a year prior to the hospitalization to be categorized as having a PCP.20
Identification of Hospitalists Versus Other Generalist Physicians
As previously described, we defined hospitalists as general internal medicine physicians who derive at least 90% of their Medicare claims for Evaluation and Management services from care provided to hospitalized patients.21 Non‐hospitalist generalist physicians were those generalists who met the criteria for generalists but did not derive at least 90% of their Medicare claims from inpatient medicine.
Definition of Inpatient Continuity of Care
We measured inpatient continuity of care by number of generalist physicians (including hospitalists) who provided care during a hospitalization, through all inpatient claims made during that hospitalization. We considered patients to have had inpatient continuity of care if all billing by generalist physicians was done by one physician during the entire hospitalization.
Statistical Analyses
We calculated the percentage of admissions that received care from 1, 2, or 3 or more generalist physicians during the hospitalization, and stratified by selected patient and hospital characteristics. These proportions were also stratified by whether the patients were cared for by their outpatient PCP or not, and whether they were cared for by hospitalists or not. Based on who cared for the patient during the hospitalization, all admissions were classified as receiving care from: 1) non‐hospitalist generalist physicians, 2) a combination of generalist physicians and hospitalists, and 3) hospitalists only. The effect of patient and hospital characteristics on whether a patient experienced inpatient continuity was evaluated using a hierarchical generalized linear model (HGLM) with a logistic link, adjusting for clustering of admissions within hospitals and all covariates. We repeated our analyses using HGLM with an ordinal logit link to explore the factors associated with number of generalists seen in the hospital. All analyses were performed with SAS version 9.1 (SAS Inc, Cary, NC). The SAS GLIMMIX procedure was used to conduct multilevel analyses.
Results
Between 1996 and 2006, 528,453 patients hospitalized for COPD, pneumonia, and CHF received care by a generalist physician during their hospital stay. Of these, 64.3% were seen by one generalist physician, 26.9% by two generalist physicians, and 8.8% by three or more generalist physicians during hospitalization.
Figure 1 shows the percentage of all patients seen by 1, 2, and 3 or more generalist physicians between 1996 and 2006. The percentage of patients receiving care from one generalist physician declined from 70.7% in 1996 to 59.4% in 2006 (P < 0.001). During the same period, the percentage of patients receiving care from 3 or more generalist physicians increased from 6.5% to 10.7% (P < 0.001). Similar trends were seen for each of the 3 conditions. There was a decrease in overall length of stay during this period, from a mean of 5.7 to 4.9 days (P < 0.001). The increase in the number of generalist physicians providing care during the hospital stay did not correspond to an increase in total number of visits during the hospitalization. The average number of daily visits from a generalist physician was 0.94 (0.30) in 1996 and 0.96 (0.35) in 2006.
Table 1 presents the percentage of patients receiving care from 1, 2, and 3 or more generalist physicians during hospitalization stratified by patient and hospital characteristics. Older adults, females, non‐Hispanic whites, those with higher socioeconomic status, and those with more comorbidities were more likely to receive care by multiple generalist physicians. There was also large variation by geographic region, metropolitan area size, and hospital characteristics. All of these differences were significant at the P < 0.0001 level.
| No. of Generalist Physicians Seen During Hospitalization | ||||
|---|---|---|---|---|
| Characteristic | N | 1 | 2 | 3 (Percentage of Patients) |
| ||||
| Age at admission | ||||
| 6674 | 152,488 | 66.4 | 25.6 | 8.0 |
| 7584 | 226,802 | 63.8 | 27.3 | 8.9 |
| 85+ | 149,163 | 63.0 | 27.7 | 9.3 |
| Gender | ||||
| Male | 216,602 | 65.3 | 26.4 | 8.3 |
| Female | 311,851 | 63.6 | 27.3 | 9.1 |
| Ethnicity | ||||
| White | 461,543 | 63.7 | 27.4 | 9.0 |
| Black | 46,960 | 68.6 | 23.8 | 7.6 |
| Other | 19,950 | 67.9 | 24.5 | 7.6 |
| Low socioeconomic status | ||||
| No | 366,392 | 63.4 | 27.5 | 9.1 |
| Yes | 162,061 | 66.3 | 25.7 | 8.0 |
| Emergency admission | ||||
| No | 188,354 | 66.8 | 25.6 | 7.6 |
| Yes | 340,099 | 62.9 | 27.7 | 9.4 |
| Weekend admission | ||||
| No | 392,150 | 65.7 | 25.8 | 8.5 |
| Yes | 136,303 | 60.1 | 30.3 | 9.6 |
| Diagnosis‐related groups | ||||
| CHF | 213,914 | 65.0 | 26.3 | 8.7 |
| Pneumonia | 195,430 | 62.5 | 28.0 | 9.5 |
| COPD | 119,109 | 66.1 | 26.2 | 7.7 |
| Had a PCP | ||||
| No | 201,016 | 66.5 | 25.4 | 8.0 |
| Yes | 327,437 | 62.9 | 27.9 | 9.2 |
| Seen hospitalist | ||||
| No | 431,784 | 67.8 | 25.1 | 7.0 |
| Yes | 96,669 | 48.5 | 34.9 | 16.6 |
| Charlson comorbidity score | ||||
| 0 | 127,385 | 64.0 | 27.2 | 8.8 |
| 1 | 131,402 | 65.1 | 26.8 | 8.1 |
| 2 | 105,831 | 64.9 | 26.6 | 8.5 |
| 3 | 163,835 | 63.4 | 27.1 | 9.5 |
| ICU use | ||||
| No | 431,462 | 65.3 | 26.5 | 8.2 |
| Yes | 96,991 | 60.1 | 28.7 | 11.2 |
| Length of stay (in days) | ||||
| Mean (SD) | 4.7 (2.9) | 5.8 (3.1) | 8.1 (3.7) | |
| Geographic region | ||||
| New England | 23,572 | 55.7 | 30.8 | 13.5 |
| Middle Atlantic | 78,181 | 60.8 | 27.8 | 11.4 |
| East North Central | 98,072 | 65.7 | 26.3 | 8.0 |
| West North Central | 44,785 | 59.6 | 30.5 | 9.9 |
| South Atlantic | 104,894 | 63.8 | 27.0 | 9.2 |
| East South Central | 51,450 | 67.8 | 24.6 | 7.6 |
| West South Central | 63,493 | 69.2 | 24.8 | 6.0 |
| Mountain | 20,310 | 61.9 | 29.4 | 8.7 |
| Pacific | 36,484 | 66.7 | 26.3 | 7.0 |
| Size of metropolitan area* | ||||
| 1,000,000 | 229,145 | 63.7 | 26.5 | 9.8 |
| 250,000999,999 | 114,448 | 61.0 | 29.2 | 9.8 |
| 100,000249,999 | 11,448 | 61.3 | 30.4 | 8.3 |
| <100,000 | 171,585 | 67.4 | 25.8 | 6.8 |
| Medical school affiliation* | ||||
| Major | 77,605 | 62.9 | 26.8 | 10.3 |
| Minor | 107,144 | 61.5 | 28.4 | 10.1 |
| Non | 341,874 | 65.5 | 26.5 | 8.0 |
| Type of hospital* | ||||
| Nonprofit | 375,888 | 62.7 | 27.8 | 9.5 |
| For profit | 63,898 | 67.5 | 25.5 | 7.0 |
| Public | 86,837 | 68.9 | 24.2 | 6.9 |
| Hospital size* | . | . | . | |
| <200 beds | 232,869 | 67.2 | 25.7 | 7.1 |
| 200349 beds | 135,954 | 62.6 | 27.9 | 9.5 |
| 350499 beds | 77,080 | 61.1 | 28.3 | 10.6 |
| 500 beds | 80,723 | 61.7 | 27.6 | 10.7 |
| Discharge location | ||||
| Home | 361,893 | 66.6 | 26.0 | 7.4 |
| SNF | 94,723 | 57.6 | 30.1 | 12.3 |
| Rehab | 3,030 | 45.7 | 34.2 | 20.1 |
| Death | 22,133 | 63.1 | 25.4 | 11.5 |
| Other | 46,674 | 61.8 | 28.1 | 10.1 |
Table 2 presents the results of a multivariable analysis of factors independently associated with experiencing continuity of care. In this analysis, continuity of care was defined as receiving inpatient care from one generalist physician (vs two or more). In the unadjusted models, the odds of experiencing continuity of care decreased by 5.5% per year from 1996 through 2006, and this decrease did not substantially change after adjusting for all other variables (4.8% yearly decrease). Younger patients, females, black patients, and those with low socioeconomic status were slightly more likely to experience continuity of care. As expected, patients admitted on weekends, emergency admissions, and those with intensive care unit (ICU) stays were less likely to experience continuity. There were marked geographic variations in continuity, with continuity approximately half as likely in New England as in the South. Continuity was greatest in smaller metropolitan areas versus rural and large metropolitan areas. Hospital size and teaching status produced only minor variation.
| Characteristic | Odds Ratio (95% CI) |
|---|---|
| |
| Admission year (increase by year) | 0.952 (0.9500.954) |
| Length of stay (increase by day) | 0.822 (0.8200.823) |
| Had a PCP | |
| No | 1.0 |
| Yes | 0.762 (0.7520.773) |
| Seen by a hospitalist | |
| No | 1.0 |
| Yes | 0.391 (0.3840.398) |
| Age | |
| 6674 | 1.0 |
| 7584 | 0.959 (0.9440.973) |
| 85+ | 0.946 (0.9300.962) |
| Gender | |
| Male | 1.0 |
| Female | 1.047 (1.0331.060) |
| Ethnicity | |
| White | 1.0 |
| Black | 1.126 (1.0971.155) |
| Other | 1.062 (1.0231.103) |
| Low socioeconomic status | |
| No | 1.0 |
| Yes | 1.036 (1.0201.051) |
| Emergency admission | |
| No | 1.0 |
| Yes | 0.864 (0.8510.878) |
| Weekend admission | |
| No | 1.0 |
| Yes | 0.778 (0.7680.789) |
| Diagnosis‐related group | |
| CHF | 1.0 |
| Pneumonia | 0.964 (0.9500.978) |
| COPD | 1.002 (0.9851.019) |
| Charlson comorbidity score | |
| 0 | 1.0 |
| 1 | 1.053 (1.0351.072) |
| 2 | 1.062 (1.0421.083) |
| 3 | 1.040 (1.0221.058) |
| ICU use | |
| No | 1.0 |
| Yes | 0.918 (0.9020.935) |
| Geographic region | |
| Middle Atlantic | 1.0 |
| New England | 0.714 (0.6210.822) |
| East North Central | 1.015 (0.9221.119) |
| West North Central | 0.791 (0.7110.879) |
| South Atlantic | 1.074 (0.9711.186) |
| East South Central | 1.250 (1.1131.403) |
| West South Central | 1.377 (1.2401.530) |
| Mountain | 0.839 (0.7400.951) |
| Pacific | 0.985 (0.8841.097) |
| Size of metropolitan area | |
| 1,000,000 | 1.0 |
| 250,000999,999 | 0.743 (0.6910.798) |
| 100,000249,999 | 0.651 (0.5380.789) |
| <100,000 | 1.062 (0.9911.138) |
| Medical school affiliation | |
| None | 1.0 |
| Minor | 0.889 (0.8270.956) |
| Major | 1.048 (0.9521.154) |
| Type of hospital | |
| Nonprofit | 1.0 |
| For profit | 1.194 (1.1061.289) |
| Public | 1.394 (1.3091.484) |
| Size of hospital | |
| <200 beds | 1.0 |
| 200349 beds | 0.918 (0.8550.986) |
| 350499 beds | 0.962 (0.8721.061) |
| 500 beds | 1.000 (0.8931.119) |
In Table 2 we also show that patients with an established PCP and those who received care from a hospitalist in the hospital were substantially less likely to experience continuity of care. There are several possible interpretations for that finding. For example, it might be that patients admitted to a hospitalist service were likely to see multiple hospitalists. Alternatively, the decreased continuity associated with hospitalists could reflect the fact that some patients cared for predominantly by non‐hospitalists may have seen a hospitalist on call for a sudden change in health status. To further explore these possible explanatory pathways, we constructed three new cohorts: 1) patients receiving all their care from non‐hospitalists, 2) patients receiving all their care from hospitalists, and 3) patients seen by both. As shown in Table 3, in patients seen by non‐hospitalists only, the mean number of generalist physicians seen during hospitalization was slightly greater than in patients cared for only by hospitalists.
| Received Care During Entire Hospitalization | No. of Admissions | Mean (SD) No. of Generalist Physicians Seen During Hospitalization |
|---|---|---|
| ||
| Non‐hospitalist physician | 431,784 | 1.41 (0.68)* |
| Hospitalist physician | 64,662 | 1.34 (0.62)* |
| Both | 32,007 | 2.55 (0.83)* |
We also tested for interactions in Table 2 between admission year and other factors. There was a significant interaction between admission year and having an identifiable PCP in the year prior to admission (Table 2). The odds of experiencing continuity of care decreased more rapidly for patients who did not have a PCP (5.5% per year; 95% CI: 5.2%5.8%) than for those who had one (4.3% per year; 95% CI: 4.1%4.6%).
Discussion
We conducted this study to better understand the degree to which hospitalized patients experience discontinuity of care within a hospital stay and to determine which patients are most likely to experience discontinuity. In our study, we specifically chose admission conditions that would likely be followed primarily by generalist physicians. We found that, over the past decade, discontinuity of care for hospitalized patients has increased substantially, as indicated by the proportion of patients taken care of by more than one generalist physician during a single hospital stay. This occurred even though overall length of stay was decreasing in this same period.
It is perhaps not surprising that inpatient continuity of care has been decreasing in the past 10 years. Outpatient practices are becoming busier, and more doctors are practicing in large group practices, which could lead to several different physicians in the same practice rounding on a hospitalized patient. We have previously demonstrated that hospitalists are caring for an increasing number of patients over this same time period,21 so another possibility is that hospitalist services are being used more often because of this heavy outpatient workload. Our analyses allowed us to test the hypothesis that having hospitalists involved in patient care increases discontinuity.
At first glance, it appears that being cared for by hospitalists may result in worse continuity of care. However, closer scrutiny of the data reveals that the discontinuity ascribed to the hospitalists in the multivariable model appears to be an artifact of defining the hospitalist variable as having been seen by any hospitalist during the hospital stay. This would include patients who saw a hospitalist in addition to their PCP or another non‐hospitalist generalist. When we compared hospitalist‐only care to other generalist care, we could not detect a difference in discontinuity. We know that generalist visits per day to patients has not substantially increased over time, so this discontinuity trend is not explained by having visits by both a hospitalist and the PCP. Therefore, this combination of findings suggests that the increased discontinuity associated with having a hospitalist involved in patient care is likely the result of system issues rather than hospitalist care per se. In fact, patients seem to experience slightly better continuity when they see only hospitalists as opposed to only non‐hospitalists.
What types of systems issues might lead to this finding? Generalists in most settings could choose to involve a hospitalist at any point in the patient's hospital stay. This could occur because of a change in patient acuity requiring the involvement of hospitalists who are present in the hospital more. It is also possible that hospitalists' schedules are created to maximize inpatient continuity of care with individual hospitalists. Even though hospitalists clearly work shifts, the 7 on, 7 off model22 likely results in patients seeing the same physician each day until the switch day. This is in contrast to outpatient primary care doctors whose concentration may be on maintaining continuity within their practice.
As the field of hospital medicine was emerging, many internal medicine physicians from various specialties were concerned about the impact of hospitalists on patient care. In one study, 73% of internal medicine physicians who were not hospitalists thought that hospitalists would worsen continuity of care.23 Primary care and subspecialist internal medicine physicians also expressed the concern that hospitalists could hurt their own relationships with patients,6 presumably because of lost continuity between the inpatient and outpatient settings. However, this fear seems to diminish once hospitalist programs are implemented and primary care doctors have experience with them.23 Our study suggests that the decrease in continuity that has occurred since these studies were published is not likely due to the emergence of hospital medicine, but rather due to other factors that influence who cares for hospitalized patients.
This study had some limitations. Length of stay is an obvious mediator of number of generalist physicians seen. Therefore, the sickest patients are likely to have both a long length of stay and low continuity. We adjusted for this in the multivariable modeling. In addition, given that this study used a large database, certain details are not discernable. For example, we chose to operationalize discontinuity as visits from multiple generalists during a single hospital stay. That is not a perfect definition, but it does represent multiple physicians directing the care of a patient. Importantly, this does not appear to represent continuity with one physician with extra visits from another, as the total number of generalist visits per day did not change over time. It is also possible that patients in the non‐hospitalist group saw physicians only from a single practice, but those details are not included in the database. Finally, we cannot tell what type of hand‐offs were occurring for individual patients during each hospital stay. Despite these disadvantages, using a large database like this one allows for detection of fairly small differences that could still be clinically important.
In summary, hospitalized patients appear to experience less continuity now than 10 years ago. However, the hospitalist model does not appear to play a role in this discontinuity. It is worth exploring in more detail why patients would see both hospitalists and other generalists. This pattern is not surprising, but may have some repercussions in terms of increasing the number of hand‐offs experienced by patients. These could lead to problems with patient safety and quality of care. Future work should explore the reasons for this discontinuity and look at the relationship between inpatient discontinuity outcomes such as quality of care and the doctorpatient relationship.
Acknowledgements
The authors thank Sarah Toombs Smith, PhD, for help in preparation of the manuscript.
Continuity of care is considered by many physicians to be of critical importance in providing high‐quality patient care. Most of the research to date has focused on continuity in outpatient primary care. Research on outpatient continuity of care has been facilitated by the fact that a number of measurement tools for outpatient continuity exist.1 Outpatient continuity of care has been linked to better quality of life scores,2 lower costs,3 and less emergency room use.4 As hospital medicine has taken on more and more of the responsibility of inpatient care, primary care doctors have voiced concerns about the impact of hospitalists on overall continuity of care5 and the quality of the doctorpatient relationship.6
Recently, continuity of care in the hospital setting has also received attention. When the Accreditation Council for Graduate Medical Education (ACGME) first proposed restrictions to resident duty hours, the importance of continuity of inpatient care began to be debated in earnest in large part because of the increase in hand‐offs which accompanies discontinuity.7, 8 A recent study of hospitalist communication documented that as many as 13% of hand‐offs at the time of service changes are judged as incomplete by the receiving physician. These incomplete hand‐offs were more likely to be associated with uncertainty regarding the plan of care, as well as perceived near misses or adverse events.9 In addition, several case reports and studies suggest that systems with less continuity may have poorer outcomes.7, 1015
Continuity in the hospital setting is likely to be important for several reasons. First, the acuity of a patient's problem during a hospitalization is likely greater than during an outpatient visit. Thus the complexity of information to be transferred between physicians during a hospital stay is correspondingly greater. Second, the diagnostic uncertainty surrounding many admissions leads to complex thought processes that may be difficult to recreate when handing off patient care to another physician. Finally, knowledge of a patient's hospital course and the likely trajectory of care is facilitated by firsthand knowledge of where the patient has been. All this information can be difficult to distill into a brief sign‐out to another physician who assumes care of the patient.
In the current study, we sought to examine the trends over time in continuity of inpatient care. We chose patients likely to be cared for by general internists: those hospitalized for chronic obstructive pulmonary disease (COPD), pneumonia, and congestive heart failure (CHF). The general internists caring for patients in the hospital could be the patient's primary care physician (PCP), a physician covering for the patient's PCP, a physician assigned at admission by the hospital, or a hospitalist. Our goals were to describe the current level of continuity of care in the hospital setting, to examine whether continuity has changed over time, and to determine factors affecting continuity of care.
Methods
We used a 5% national sample of claims data from Medicare beneficiaries for the years 19962006.16 This included Medicare enrollment files, Medicare Provider Analysis and Review (MEDPAR) files, Medicare Carrier files, and Provider of Services (POS) files.17, 18
Establishment of the Study Cohort
Hospital admissions for COPD (Diagnosis Related Group [DRG] 088), pneumonia (DRG 089, 090), and CHF (DRG 127) from 1996 to 2006 for patients older than 66 years in MEDPAR were selected (n = 781,348). We excluded admissions for patients enrolled in health maintenance organizations (HMOs) or who did not have Medicare Parts A and B for the entire year prior to admission (n = 57,558). Admissions with a length of stay >18 days (n = 10,688) were considered outliers (exceeding the 99th percentile) and were excluded. Only admissions cared for by a general internist, family physician, general practitioner, or geriatrician were included (n = 528,453).
Measures
We categorized patients by age, gender, and ethnicity using Medicare enrollment files. We used the Medicaid indicator in the Medicare file as a proxy of low socioeconomic status. We used MEDPAR files to determine the origin of the admission (via the emergency department vs other), weekend versus weekday admission, and DRG. A comorbidity score was generated using the Elixhauser comorbidity scale using inpatient and outpatient billing data.19 In analyses, we listed the total number of comorbidities identified. The specialty of each physician was determined from the codes in the Medicare Carrier files. The 2004 POS files provided hospital‐level information such as zip code, metropolitan size, state, total number of beds, type of hospital, and medical school affiliation. We divided metropolitan size and total number of hospital beds into quartiles. We categorized hospitals as nonprofit, for profit, or public; medical school affiliation was categorized as non, minor, or major.
Determination of Primary Care Physician (PCP)
We identified outpatient visits using American Medical AssociationCommon Procedure Terminology (CPT) evaluation and management codes 99201 to 99205 (new patient) and 99221 to 99215 (established patient encounters). Individual providers were differentiated by using their Unique Provider Identification Number (UPIN). We defined a PCP as a general practitioner, family physician, internist, or geriatrician. Patients had to make at least 3 visits on different days to the same PCP within a year prior to the hospitalization to be categorized as having a PCP.20
Identification of Hospitalists Versus Other Generalist Physicians
As previously described, we defined hospitalists as general internal medicine physicians who derive at least 90% of their Medicare claims for Evaluation and Management services from care provided to hospitalized patients.21 Non‐hospitalist generalist physicians were those generalists who met the criteria for generalists but did not derive at least 90% of their Medicare claims from inpatient medicine.
Definition of Inpatient Continuity of Care
We measured inpatient continuity of care by number of generalist physicians (including hospitalists) who provided care during a hospitalization, through all inpatient claims made during that hospitalization. We considered patients to have had inpatient continuity of care if all billing by generalist physicians was done by one physician during the entire hospitalization.
Statistical Analyses
We calculated the percentage of admissions that received care from 1, 2, or 3 or more generalist physicians during the hospitalization, and stratified by selected patient and hospital characteristics. These proportions were also stratified by whether the patients were cared for by their outpatient PCP or not, and whether they were cared for by hospitalists or not. Based on who cared for the patient during the hospitalization, all admissions were classified as receiving care from: 1) non‐hospitalist generalist physicians, 2) a combination of generalist physicians and hospitalists, and 3) hospitalists only. The effect of patient and hospital characteristics on whether a patient experienced inpatient continuity was evaluated using a hierarchical generalized linear model (HGLM) with a logistic link, adjusting for clustering of admissions within hospitals and all covariates. We repeated our analyses using HGLM with an ordinal logit link to explore the factors associated with number of generalists seen in the hospital. All analyses were performed with SAS version 9.1 (SAS Inc, Cary, NC). The SAS GLIMMIX procedure was used to conduct multilevel analyses.
Results
Between 1996 and 2006, 528,453 patients hospitalized for COPD, pneumonia, and CHF received care by a generalist physician during their hospital stay. Of these, 64.3% were seen by one generalist physician, 26.9% by two generalist physicians, and 8.8% by three or more generalist physicians during hospitalization.
Figure 1 shows the percentage of all patients seen by 1, 2, and 3 or more generalist physicians between 1996 and 2006. The percentage of patients receiving care from one generalist physician declined from 70.7% in 1996 to 59.4% in 2006 (P < 0.001). During the same period, the percentage of patients receiving care from 3 or more generalist physicians increased from 6.5% to 10.7% (P < 0.001). Similar trends were seen for each of the 3 conditions. There was a decrease in overall length of stay during this period, from a mean of 5.7 to 4.9 days (P < 0.001). The increase in the number of generalist physicians providing care during the hospital stay did not correspond to an increase in total number of visits during the hospitalization. The average number of daily visits from a generalist physician was 0.94 (0.30) in 1996 and 0.96 (0.35) in 2006.
Table 1 presents the percentage of patients receiving care from 1, 2, and 3 or more generalist physicians during hospitalization stratified by patient and hospital characteristics. Older adults, females, non‐Hispanic whites, those with higher socioeconomic status, and those with more comorbidities were more likely to receive care by multiple generalist physicians. There was also large variation by geographic region, metropolitan area size, and hospital characteristics. All of these differences were significant at the P < 0.0001 level.
| No. of Generalist Physicians Seen During Hospitalization | ||||
|---|---|---|---|---|
| Characteristic | N | 1 | 2 | 3 (Percentage of Patients) |
| ||||
| Age at admission | ||||
| 6674 | 152,488 | 66.4 | 25.6 | 8.0 |
| 7584 | 226,802 | 63.8 | 27.3 | 8.9 |
| 85+ | 149,163 | 63.0 | 27.7 | 9.3 |
| Gender | ||||
| Male | 216,602 | 65.3 | 26.4 | 8.3 |
| Female | 311,851 | 63.6 | 27.3 | 9.1 |
| Ethnicity | ||||
| White | 461,543 | 63.7 | 27.4 | 9.0 |
| Black | 46,960 | 68.6 | 23.8 | 7.6 |
| Other | 19,950 | 67.9 | 24.5 | 7.6 |
| Low socioeconomic status | ||||
| No | 366,392 | 63.4 | 27.5 | 9.1 |
| Yes | 162,061 | 66.3 | 25.7 | 8.0 |
| Emergency admission | ||||
| No | 188,354 | 66.8 | 25.6 | 7.6 |
| Yes | 340,099 | 62.9 | 27.7 | 9.4 |
| Weekend admission | ||||
| No | 392,150 | 65.7 | 25.8 | 8.5 |
| Yes | 136,303 | 60.1 | 30.3 | 9.6 |
| Diagnosis‐related groups | ||||
| CHF | 213,914 | 65.0 | 26.3 | 8.7 |
| Pneumonia | 195,430 | 62.5 | 28.0 | 9.5 |
| COPD | 119,109 | 66.1 | 26.2 | 7.7 |
| Had a PCP | ||||
| No | 201,016 | 66.5 | 25.4 | 8.0 |
| Yes | 327,437 | 62.9 | 27.9 | 9.2 |
| Seen hospitalist | ||||
| No | 431,784 | 67.8 | 25.1 | 7.0 |
| Yes | 96,669 | 48.5 | 34.9 | 16.6 |
| Charlson comorbidity score | ||||
| 0 | 127,385 | 64.0 | 27.2 | 8.8 |
| 1 | 131,402 | 65.1 | 26.8 | 8.1 |
| 2 | 105,831 | 64.9 | 26.6 | 8.5 |
| 3 | 163,835 | 63.4 | 27.1 | 9.5 |
| ICU use | ||||
| No | 431,462 | 65.3 | 26.5 | 8.2 |
| Yes | 96,991 | 60.1 | 28.7 | 11.2 |
| Length of stay (in days) | ||||
| Mean (SD) | 4.7 (2.9) | 5.8 (3.1) | 8.1 (3.7) | |
| Geographic region | ||||
| New England | 23,572 | 55.7 | 30.8 | 13.5 |
| Middle Atlantic | 78,181 | 60.8 | 27.8 | 11.4 |
| East North Central | 98,072 | 65.7 | 26.3 | 8.0 |
| West North Central | 44,785 | 59.6 | 30.5 | 9.9 |
| South Atlantic | 104,894 | 63.8 | 27.0 | 9.2 |
| East South Central | 51,450 | 67.8 | 24.6 | 7.6 |
| West South Central | 63,493 | 69.2 | 24.8 | 6.0 |
| Mountain | 20,310 | 61.9 | 29.4 | 8.7 |
| Pacific | 36,484 | 66.7 | 26.3 | 7.0 |
| Size of metropolitan area* | ||||
| 1,000,000 | 229,145 | 63.7 | 26.5 | 9.8 |
| 250,000999,999 | 114,448 | 61.0 | 29.2 | 9.8 |
| 100,000249,999 | 11,448 | 61.3 | 30.4 | 8.3 |
| <100,000 | 171,585 | 67.4 | 25.8 | 6.8 |
| Medical school affiliation* | ||||
| Major | 77,605 | 62.9 | 26.8 | 10.3 |
| Minor | 107,144 | 61.5 | 28.4 | 10.1 |
| Non | 341,874 | 65.5 | 26.5 | 8.0 |
| Type of hospital* | ||||
| Nonprofit | 375,888 | 62.7 | 27.8 | 9.5 |
| For profit | 63,898 | 67.5 | 25.5 | 7.0 |
| Public | 86,837 | 68.9 | 24.2 | 6.9 |
| Hospital size* | . | . | . | |
| <200 beds | 232,869 | 67.2 | 25.7 | 7.1 |
| 200349 beds | 135,954 | 62.6 | 27.9 | 9.5 |
| 350499 beds | 77,080 | 61.1 | 28.3 | 10.6 |
| 500 beds | 80,723 | 61.7 | 27.6 | 10.7 |
| Discharge location | ||||
| Home | 361,893 | 66.6 | 26.0 | 7.4 |
| SNF | 94,723 | 57.6 | 30.1 | 12.3 |
| Rehab | 3,030 | 45.7 | 34.2 | 20.1 |
| Death | 22,133 | 63.1 | 25.4 | 11.5 |
| Other | 46,674 | 61.8 | 28.1 | 10.1 |
Table 2 presents the results of a multivariable analysis of factors independently associated with experiencing continuity of care. In this analysis, continuity of care was defined as receiving inpatient care from one generalist physician (vs two or more). In the unadjusted models, the odds of experiencing continuity of care decreased by 5.5% per year from 1996 through 2006, and this decrease did not substantially change after adjusting for all other variables (4.8% yearly decrease). Younger patients, females, black patients, and those with low socioeconomic status were slightly more likely to experience continuity of care. As expected, patients admitted on weekends, emergency admissions, and those with intensive care unit (ICU) stays were less likely to experience continuity. There were marked geographic variations in continuity, with continuity approximately half as likely in New England as in the South. Continuity was greatest in smaller metropolitan areas versus rural and large metropolitan areas. Hospital size and teaching status produced only minor variation.
| Characteristic | Odds Ratio (95% CI) |
|---|---|
| |
| Admission year (increase by year) | 0.952 (0.9500.954) |
| Length of stay (increase by day) | 0.822 (0.8200.823) |
| Had a PCP | |
| No | 1.0 |
| Yes | 0.762 (0.7520.773) |
| Seen by a hospitalist | |
| No | 1.0 |
| Yes | 0.391 (0.3840.398) |
| Age | |
| 6674 | 1.0 |
| 7584 | 0.959 (0.9440.973) |
| 85+ | 0.946 (0.9300.962) |
| Gender | |
| Male | 1.0 |
| Female | 1.047 (1.0331.060) |
| Ethnicity | |
| White | 1.0 |
| Black | 1.126 (1.0971.155) |
| Other | 1.062 (1.0231.103) |
| Low socioeconomic status | |
| No | 1.0 |
| Yes | 1.036 (1.0201.051) |
| Emergency admission | |
| No | 1.0 |
| Yes | 0.864 (0.8510.878) |
| Weekend admission | |
| No | 1.0 |
| Yes | 0.778 (0.7680.789) |
| Diagnosis‐related group | |
| CHF | 1.0 |
| Pneumonia | 0.964 (0.9500.978) |
| COPD | 1.002 (0.9851.019) |
| Charlson comorbidity score | |
| 0 | 1.0 |
| 1 | 1.053 (1.0351.072) |
| 2 | 1.062 (1.0421.083) |
| 3 | 1.040 (1.0221.058) |
| ICU use | |
| No | 1.0 |
| Yes | 0.918 (0.9020.935) |
| Geographic region | |
| Middle Atlantic | 1.0 |
| New England | 0.714 (0.6210.822) |
| East North Central | 1.015 (0.9221.119) |
| West North Central | 0.791 (0.7110.879) |
| South Atlantic | 1.074 (0.9711.186) |
| East South Central | 1.250 (1.1131.403) |
| West South Central | 1.377 (1.2401.530) |
| Mountain | 0.839 (0.7400.951) |
| Pacific | 0.985 (0.8841.097) |
| Size of metropolitan area | |
| 1,000,000 | 1.0 |
| 250,000999,999 | 0.743 (0.6910.798) |
| 100,000249,999 | 0.651 (0.5380.789) |
| <100,000 | 1.062 (0.9911.138) |
| Medical school affiliation | |
| None | 1.0 |
| Minor | 0.889 (0.8270.956) |
| Major | 1.048 (0.9521.154) |
| Type of hospital | |
| Nonprofit | 1.0 |
| For profit | 1.194 (1.1061.289) |
| Public | 1.394 (1.3091.484) |
| Size of hospital | |
| <200 beds | 1.0 |
| 200349 beds | 0.918 (0.8550.986) |
| 350499 beds | 0.962 (0.8721.061) |
| 500 beds | 1.000 (0.8931.119) |
In Table 2 we also show that patients with an established PCP and those who received care from a hospitalist in the hospital were substantially less likely to experience continuity of care. There are several possible interpretations for that finding. For example, it might be that patients admitted to a hospitalist service were likely to see multiple hospitalists. Alternatively, the decreased continuity associated with hospitalists could reflect the fact that some patients cared for predominantly by non‐hospitalists may have seen a hospitalist on call for a sudden change in health status. To further explore these possible explanatory pathways, we constructed three new cohorts: 1) patients receiving all their care from non‐hospitalists, 2) patients receiving all their care from hospitalists, and 3) patients seen by both. As shown in Table 3, in patients seen by non‐hospitalists only, the mean number of generalist physicians seen during hospitalization was slightly greater than in patients cared for only by hospitalists.
| Received Care During Entire Hospitalization | No. of Admissions | Mean (SD) No. of Generalist Physicians Seen During Hospitalization |
|---|---|---|
| ||
| Non‐hospitalist physician | 431,784 | 1.41 (0.68)* |
| Hospitalist physician | 64,662 | 1.34 (0.62)* |
| Both | 32,007 | 2.55 (0.83)* |
We also tested for interactions in Table 2 between admission year and other factors. There was a significant interaction between admission year and having an identifiable PCP in the year prior to admission (Table 2). The odds of experiencing continuity of care decreased more rapidly for patients who did not have a PCP (5.5% per year; 95% CI: 5.2%5.8%) than for those who had one (4.3% per year; 95% CI: 4.1%4.6%).
Discussion
We conducted this study to better understand the degree to which hospitalized patients experience discontinuity of care within a hospital stay and to determine which patients are most likely to experience discontinuity. In our study, we specifically chose admission conditions that would likely be followed primarily by generalist physicians. We found that, over the past decade, discontinuity of care for hospitalized patients has increased substantially, as indicated by the proportion of patients taken care of by more than one generalist physician during a single hospital stay. This occurred even though overall length of stay was decreasing in this same period.
It is perhaps not surprising that inpatient continuity of care has been decreasing in the past 10 years. Outpatient practices are becoming busier, and more doctors are practicing in large group practices, which could lead to several different physicians in the same practice rounding on a hospitalized patient. We have previously demonstrated that hospitalists are caring for an increasing number of patients over this same time period,21 so another possibility is that hospitalist services are being used more often because of this heavy outpatient workload. Our analyses allowed us to test the hypothesis that having hospitalists involved in patient care increases discontinuity.
At first glance, it appears that being cared for by hospitalists may result in worse continuity of care. However, closer scrutiny of the data reveals that the discontinuity ascribed to the hospitalists in the multivariable model appears to be an artifact of defining the hospitalist variable as having been seen by any hospitalist during the hospital stay. This would include patients who saw a hospitalist in addition to their PCP or another non‐hospitalist generalist. When we compared hospitalist‐only care to other generalist care, we could not detect a difference in discontinuity. We know that generalist visits per day to patients has not substantially increased over time, so this discontinuity trend is not explained by having visits by both a hospitalist and the PCP. Therefore, this combination of findings suggests that the increased discontinuity associated with having a hospitalist involved in patient care is likely the result of system issues rather than hospitalist care per se. In fact, patients seem to experience slightly better continuity when they see only hospitalists as opposed to only non‐hospitalists.
What types of systems issues might lead to this finding? Generalists in most settings could choose to involve a hospitalist at any point in the patient's hospital stay. This could occur because of a change in patient acuity requiring the involvement of hospitalists who are present in the hospital more. It is also possible that hospitalists' schedules are created to maximize inpatient continuity of care with individual hospitalists. Even though hospitalists clearly work shifts, the 7 on, 7 off model22 likely results in patients seeing the same physician each day until the switch day. This is in contrast to outpatient primary care doctors whose concentration may be on maintaining continuity within their practice.
As the field of hospital medicine was emerging, many internal medicine physicians from various specialties were concerned about the impact of hospitalists on patient care. In one study, 73% of internal medicine physicians who were not hospitalists thought that hospitalists would worsen continuity of care.23 Primary care and subspecialist internal medicine physicians also expressed the concern that hospitalists could hurt their own relationships with patients,6 presumably because of lost continuity between the inpatient and outpatient settings. However, this fear seems to diminish once hospitalist programs are implemented and primary care doctors have experience with them.23 Our study suggests that the decrease in continuity that has occurred since these studies were published is not likely due to the emergence of hospital medicine, but rather due to other factors that influence who cares for hospitalized patients.
This study had some limitations. Length of stay is an obvious mediator of number of generalist physicians seen. Therefore, the sickest patients are likely to have both a long length of stay and low continuity. We adjusted for this in the multivariable modeling. In addition, given that this study used a large database, certain details are not discernable. For example, we chose to operationalize discontinuity as visits from multiple generalists during a single hospital stay. That is not a perfect definition, but it does represent multiple physicians directing the care of a patient. Importantly, this does not appear to represent continuity with one physician with extra visits from another, as the total number of generalist visits per day did not change over time. It is also possible that patients in the non‐hospitalist group saw physicians only from a single practice, but those details are not included in the database. Finally, we cannot tell what type of hand‐offs were occurring for individual patients during each hospital stay. Despite these disadvantages, using a large database like this one allows for detection of fairly small differences that could still be clinically important.
In summary, hospitalized patients appear to experience less continuity now than 10 years ago. However, the hospitalist model does not appear to play a role in this discontinuity. It is worth exploring in more detail why patients would see both hospitalists and other generalists. This pattern is not surprising, but may have some repercussions in terms of increasing the number of hand‐offs experienced by patients. These could lead to problems with patient safety and quality of care. Future work should explore the reasons for this discontinuity and look at the relationship between inpatient discontinuity outcomes such as quality of care and the doctorpatient relationship.
Acknowledgements
The authors thank Sarah Toombs Smith, PhD, for help in preparation of the manuscript.
- .Defining and measuring interpersonal continuity of care.Ann Fam Med.2003;1(3):134–143.
- ,,.Good continuity of care may improve quality of life in Type 2 diabetes.Diabetes Res Clin Pract.2001;51(1):21–27.
- ,,,.Provider continuity in family medicine: Does it make a difference for total health care costs?Ann Fam Med.2003;1(3):144–148.
- ,,.The effect of continuity of care on emergency department use.Arch Fam Med.2000;9(4):333–338.
- ,,,,,.Physician attitudes toward and prevalence of the hospitalist model of care: Results of a national survey.Am J Med.2000;109(8):648–653.
- ,,.Physician views on caring for hospitalized patients and the hospitalist model of inpatient care.J Gen Intern Med.2001;16(2):116–119.
- ,,,,,.Systematic review: Effects of resident work hours on patient safety.Ann Intern Med.2004;141(11):851–857.
- ,,.Balancing continuity of care with residents' limited work hours: Defining the implications.Acad Med.2005;80(1):39–43.
- ,,.Understanding communication during hospitalist sevice changes: A mixed methods study.J Hosp Med.2009;4:535–540.
- ,,,Center for Safety in Emergency C. Profiles in patient safety: Emergency care transitions.Acad Emerg Med.2003;10(4):364–367.
- .Fumbled handoffs: One dropped ball after another.Ann Intern Med.2005;142(5):352–358.
- Agency for Healthcare Research and Quality. Fumbled handoff.2004. Available at: http://www.webmm.ahrq.gov/printview.aspx?caseID=55. Accessed December 27, 2005.
- ,,.Graduate medical education and patient safety: A busy—and occasionally hazardous—intersection.Ann Intern Med.2006;145(8):592–598.
- ,,,,.Does housestaff discontinuity of care increase the risk for preventable adverse events?Ann Intern Med.1994;121(11):866–872.
- ,,,.The impact of a regulation restricting medical house staff working hours on the quality of patient care.JAMA.1993;269(3):374–378.
- Centers for Medicare and Medicaid Services. Standard analytical files. Available at: http://www.cms.hhs.gov/IdentifiableDataFiles/02_Standard AnalyticalFiles.asp. Accessed March 1,2009.
- Centers for Medicare and Medicaid Services. Nonidentifiable data files: Provider of services files. Available at: http://www.cms.hhs.gov/NonIdentifiableDataFiles/04_ProviderofSerrvicesFile.asp. Accessed March 1,2009.
- Research Data Assistance Center. Medicare data file description. Available at: http://www.resdac.umn.edu/Medicare/file_descriptions.asp. Accessed March 1,2009.
- ,,,.Effect of comorbidity adjustment on CMS criteria for kidney transplant center performance.Am J Transplant.2009;9:506–516.
- ,,,,,.Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults.JAMA.2009;301:1671–1680.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med. 2009;360:1102–1112.
- HCPro Inc.Medical Staff Leader blog.2010. Available at: http://blogs. hcpro.com/medicalstaff/2010/01/free‐form‐example‐seven‐day‐on‐seven‐day‐off‐hospitalist‐schedule/. Accessed November 20, 2010.
- ,,,.How physicians perceive hospitalist services after implementation: Anticipation vs reality.Arch Intern Med.2003;163(19):2330–2336.
- .Defining and measuring interpersonal continuity of care.Ann Fam Med.2003;1(3):134–143.
- ,,.Good continuity of care may improve quality of life in Type 2 diabetes.Diabetes Res Clin Pract.2001;51(1):21–27.
- ,,,.Provider continuity in family medicine: Does it make a difference for total health care costs?Ann Fam Med.2003;1(3):144–148.
- ,,.The effect of continuity of care on emergency department use.Arch Fam Med.2000;9(4):333–338.
- ,,,,,.Physician attitudes toward and prevalence of the hospitalist model of care: Results of a national survey.Am J Med.2000;109(8):648–653.
- ,,.Physician views on caring for hospitalized patients and the hospitalist model of inpatient care.J Gen Intern Med.2001;16(2):116–119.
- ,,,,,.Systematic review: Effects of resident work hours on patient safety.Ann Intern Med.2004;141(11):851–857.
- ,,.Balancing continuity of care with residents' limited work hours: Defining the implications.Acad Med.2005;80(1):39–43.
- ,,.Understanding communication during hospitalist sevice changes: A mixed methods study.J Hosp Med.2009;4:535–540.
- ,,,Center for Safety in Emergency C. Profiles in patient safety: Emergency care transitions.Acad Emerg Med.2003;10(4):364–367.
- .Fumbled handoffs: One dropped ball after another.Ann Intern Med.2005;142(5):352–358.
- Agency for Healthcare Research and Quality. Fumbled handoff.2004. Available at: http://www.webmm.ahrq.gov/printview.aspx?caseID=55. Accessed December 27, 2005.
- ,,.Graduate medical education and patient safety: A busy—and occasionally hazardous—intersection.Ann Intern Med.2006;145(8):592–598.
- ,,,,.Does housestaff discontinuity of care increase the risk for preventable adverse events?Ann Intern Med.1994;121(11):866–872.
- ,,,.The impact of a regulation restricting medical house staff working hours on the quality of patient care.JAMA.1993;269(3):374–378.
- Centers for Medicare and Medicaid Services. Standard analytical files. Available at: http://www.cms.hhs.gov/IdentifiableDataFiles/02_Standard AnalyticalFiles.asp. Accessed March 1,2009.
- Centers for Medicare and Medicaid Services. Nonidentifiable data files: Provider of services files. Available at: http://www.cms.hhs.gov/NonIdentifiableDataFiles/04_ProviderofSerrvicesFile.asp. Accessed March 1,2009.
- Research Data Assistance Center. Medicare data file description. Available at: http://www.resdac.umn.edu/Medicare/file_descriptions.asp. Accessed March 1,2009.
- ,,,.Effect of comorbidity adjustment on CMS criteria for kidney transplant center performance.Am J Transplant.2009;9:506–516.
- ,,,,,.Continuity of outpatient and inpatient care by primary care physicians for hospitalized older adults.JAMA.2009;301:1671–1680.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med. 2009;360:1102–1112.
- HCPro Inc.Medical Staff Leader blog.2010. Available at: http://blogs. hcpro.com/medicalstaff/2010/01/free‐form‐example‐seven‐day‐on‐seven‐day‐off‐hospitalist‐schedule/. Accessed November 20, 2010.
- ,,,.How physicians perceive hospitalist services after implementation: Anticipation vs reality.Arch Intern Med.2003;163(19):2330–2336.
Copyright © 2011 Society of Hospital Medicine
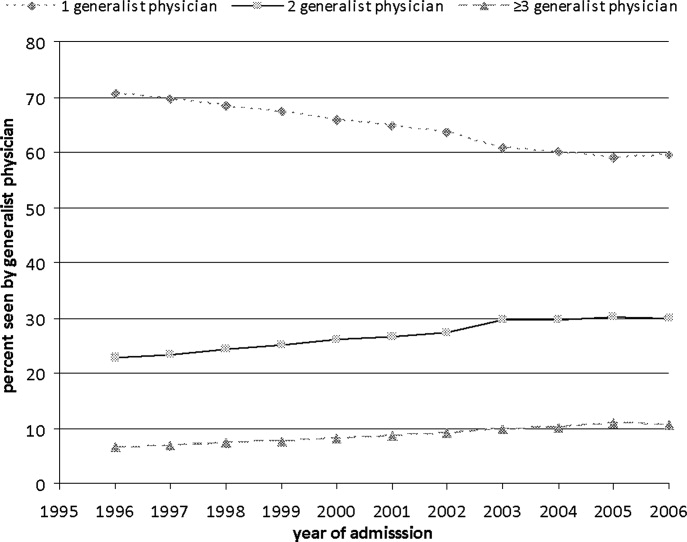
Continuing Medical Education Program in
If you wish to receive credit for this activity, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this journal‐based CME activity for a maximum of 1 AMA PRA Category 1 Credit.. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
The objectives need to be changed. Please remove the existing ones, and include these two:
-
Identify recent changes to the Joint Commission accreditation process.
-
Interpret the association between accreditation status and hospital performance in three common clinical conditions.
This manuscript underwent peer review in line with the standards of editorial integrity and publication ethics maintained by Journal of Hospital Medicine. The peer reviewers have no relevant financial relationships. The peer review process for Journal of Hospital Medicine is single‐blinded. As such, the identities of the reviewers are not disclosed in line with the standard accepted practices of medical journal peer review.
Conflicts of interest have been identified and resolved in accordance with Blackwell Futura Media Services's Policy on Activity Disclosure and Conflict of Interest. The primary resolution method used was peer review and review by a non‐conflicted expert.
Instructions on Receiving Credit
For information on applicability and acceptance of CME credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within an hour; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period, which is up to two years from initial publication.
Follow these steps to earn credit:
-
Log on to
www.wileyblackwellcme.com -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
This activity will be available for CME credit for twelve months following its publication date. At that time, it will be reviewed and potentially updated and extended for an additional twelve months.
If you wish to receive credit for this activity, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this journal‐based CME activity for a maximum of 1 AMA PRA Category 1 Credit.. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
The objectives need to be changed. Please remove the existing ones, and include these two:
-
Identify recent changes to the Joint Commission accreditation process.
-
Interpret the association between accreditation status and hospital performance in three common clinical conditions.
This manuscript underwent peer review in line with the standards of editorial integrity and publication ethics maintained by Journal of Hospital Medicine. The peer reviewers have no relevant financial relationships. The peer review process for Journal of Hospital Medicine is single‐blinded. As such, the identities of the reviewers are not disclosed in line with the standard accepted practices of medical journal peer review.
Conflicts of interest have been identified and resolved in accordance with Blackwell Futura Media Services's Policy on Activity Disclosure and Conflict of Interest. The primary resolution method used was peer review and review by a non‐conflicted expert.
Instructions on Receiving Credit
For information on applicability and acceptance of CME credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within an hour; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period, which is up to two years from initial publication.
Follow these steps to earn credit:
-
Log on to
www.wileyblackwellcme.com -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
This activity will be available for CME credit for twelve months following its publication date. At that time, it will be reviewed and potentially updated and extended for an additional twelve months.
If you wish to receive credit for this activity, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this journal‐based CME activity for a maximum of 1 AMA PRA Category 1 Credit.. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
The objectives need to be changed. Please remove the existing ones, and include these two:
-
Identify recent changes to the Joint Commission accreditation process.
-
Interpret the association between accreditation status and hospital performance in three common clinical conditions.
This manuscript underwent peer review in line with the standards of editorial integrity and publication ethics maintained by Journal of Hospital Medicine. The peer reviewers have no relevant financial relationships. The peer review process for Journal of Hospital Medicine is single‐blinded. As such, the identities of the reviewers are not disclosed in line with the standard accepted practices of medical journal peer review.
Conflicts of interest have been identified and resolved in accordance with Blackwell Futura Media Services's Policy on Activity Disclosure and Conflict of Interest. The primary resolution method used was peer review and review by a non‐conflicted expert.
Instructions on Receiving Credit
For information on applicability and acceptance of CME credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within an hour; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period, which is up to two years from initial publication.
Follow these steps to earn credit:
-
Log on to
www.wileyblackwellcme.com -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
This activity will be available for CME credit for twelve months following its publication date. At that time, it will be reviewed and potentially updated and extended for an additional twelve months.
Similar Survival in VLBW Infants with Delayed Surgery
PHILADELPHIA – When a very low birth weight (VLWBW) infant has congenital heart disease needing surgical repair, the two opposing strategies of immediate surgery or delaying surgery for several weeks until the newborn grows larger work equally well for survival. Survival rates after both approaches tracked nearly identically during 3 years of follow-up, in a single center review of 80 cases.
Because the review included a relatively small number of VLBW newborns, the analysis could not determine which benefited most from immediate surgery and which did better with a delayed operation. "But we were reassured that delay did not lead to excess risk," Dr. Edward J. Hickey said at the annual meeting of the American Association for Thoracic Surgery.
Results from a second, related analysis that he reported showed that birth weight surpassed gestational age as a predictor of survival in newborns with congenital heart disease. "Birth weight is a more reliable, independent risk factor for death," said Dr. Hickey, a cardiothoracic surgeon at the Hospital for Sick Children in Toronto. The analysis showed that the highest risk for survival occurred in newborns who weighed less than 2.0 kg at birth. As a result of this finding, Dr. Hickey’s comparison of immediate and delayed surgical repair focused on the 80 newborns in the series who weighed less than 2.0 kg and required prompt intervention.
Among these 80 infants, 34 had "immediate surgery," which meant they had their operation as soon as it could be scheduled and performed, generally within 3 weeks of birth. Surgery for the other 46 was an average of 8 weeks after birth. These differences reflected the way surgeons at Sick Children managed each case.
Among the delayed surgery cases, infants with truncus or coarctation had the slowest growth, with as little as 50 g gained per week. In contrast, infants with an atrial septal defect, tetralogy, or a total anomalous pulmonary venous connection had growth rates above average, often at a pace of more than 150 g/week.
"I was most struck by the infants with coarctation, who seemed to grow at very low rates. That suggests to us that these patients are the ones we should repair early," because it is less likely that a delay would lead to much weight gain and improved surgical prospects, Dr. Hickey said. Based on these findings, he and his associates now perform coarctation repairs in infants whose weight is as low as 1.4 kg, he said. But Dr. Hickey also stressed that the timing of surgical repair must be individualized for each patient.
The two analyses done by Dr. Hickey and his associates involved 1,557 children with congenital heart disease admitted to the Hospital for Sick Children at age 30 days or younger who underwent active management during a 10-year period. Overall survival in this group was 91% at 3 months after admission, 88% after 6 months, and 86% after 5 years.
They evaluated the impact of both gestational age and birth weight on survival among these children, and found that both parameters were linked to mortality. Infants born at 28 weeks’ gestational age had a roughly 40% survival rate after 1 year, those born at 32 weeks had about a 60% survival rate to 1 year, and those born at 36 weeks had about an 80% survival rate at 1 year.
When analyzed by birth weight, those born at 3.5 kg or larger had a greater than 90% 1-year survival rate, those born with a weight of 2.0 kg had about an 80% 1-year survival, and those born weighing 1.5 kg had about a 60% survival to 1 year. These data identified an inflection point where infants born weighing less than 2.0 kg had a substantially worse survival than those who weighed 2.0 kg or more. Additional analysis that compared the relative contributions of gestational age and birth weight also showed that birth weight was the much stronger factor influencing 1-year survival.
The series included 149 infants born at less than 2.0 kg, highlighting how uncommon it is for surgeons to face the question of how to manage VLBW infants with congenital heart disease. Eighty-five of these infants (57%) weighed 1.5-1.9 kg at birth, while the remainder weighed less than 1.5 kg. Thirty did not require immediate surgical intervention, 12 had other, noncardiovascular complications requiring initial intervention, and 27 received comfort care only, leaving 80 candidates that became part of the immediate – versus delayed – surgery analysis.
Among the 46 infants whose surgery was delayed for an average of 8 weeks, 18 (39%) had a total of 33 complications. Six of these 18 children died while awaiting surgery. "Despite this high complication rate, we see roughly equivalent survival" between the immediate and delayed surgery groups. That observation, coupled with the finding that many infants gained weight at an "acceptable" rate during the period of surgical delay, led to the conclusion that either strategy is reasonable and should depend on the specific features of each case, he said.
Dr. Hickey had no disclosures. ☐
PHILADELPHIA – When a very low birth weight (VLWBW) infant has congenital heart disease needing surgical repair, the two opposing strategies of immediate surgery or delaying surgery for several weeks until the newborn grows larger work equally well for survival. Survival rates after both approaches tracked nearly identically during 3 years of follow-up, in a single center review of 80 cases.
Because the review included a relatively small number of VLBW newborns, the analysis could not determine which benefited most from immediate surgery and which did better with a delayed operation. "But we were reassured that delay did not lead to excess risk," Dr. Edward J. Hickey said at the annual meeting of the American Association for Thoracic Surgery.
Results from a second, related analysis that he reported showed that birth weight surpassed gestational age as a predictor of survival in newborns with congenital heart disease. "Birth weight is a more reliable, independent risk factor for death," said Dr. Hickey, a cardiothoracic surgeon at the Hospital for Sick Children in Toronto. The analysis showed that the highest risk for survival occurred in newborns who weighed less than 2.0 kg at birth. As a result of this finding, Dr. Hickey’s comparison of immediate and delayed surgical repair focused on the 80 newborns in the series who weighed less than 2.0 kg and required prompt intervention.
Among these 80 infants, 34 had "immediate surgery," which meant they had their operation as soon as it could be scheduled and performed, generally within 3 weeks of birth. Surgery for the other 46 was an average of 8 weeks after birth. These differences reflected the way surgeons at Sick Children managed each case.
Among the delayed surgery cases, infants with truncus or coarctation had the slowest growth, with as little as 50 g gained per week. In contrast, infants with an atrial septal defect, tetralogy, or a total anomalous pulmonary venous connection had growth rates above average, often at a pace of more than 150 g/week.
"I was most struck by the infants with coarctation, who seemed to grow at very low rates. That suggests to us that these patients are the ones we should repair early," because it is less likely that a delay would lead to much weight gain and improved surgical prospects, Dr. Hickey said. Based on these findings, he and his associates now perform coarctation repairs in infants whose weight is as low as 1.4 kg, he said. But Dr. Hickey also stressed that the timing of surgical repair must be individualized for each patient.
The two analyses done by Dr. Hickey and his associates involved 1,557 children with congenital heart disease admitted to the Hospital for Sick Children at age 30 days or younger who underwent active management during a 10-year period. Overall survival in this group was 91% at 3 months after admission, 88% after 6 months, and 86% after 5 years.
They evaluated the impact of both gestational age and birth weight on survival among these children, and found that both parameters were linked to mortality. Infants born at 28 weeks’ gestational age had a roughly 40% survival rate after 1 year, those born at 32 weeks had about a 60% survival rate to 1 year, and those born at 36 weeks had about an 80% survival rate at 1 year.
When analyzed by birth weight, those born at 3.5 kg or larger had a greater than 90% 1-year survival rate, those born with a weight of 2.0 kg had about an 80% 1-year survival, and those born weighing 1.5 kg had about a 60% survival to 1 year. These data identified an inflection point where infants born weighing less than 2.0 kg had a substantially worse survival than those who weighed 2.0 kg or more. Additional analysis that compared the relative contributions of gestational age and birth weight also showed that birth weight was the much stronger factor influencing 1-year survival.
The series included 149 infants born at less than 2.0 kg, highlighting how uncommon it is for surgeons to face the question of how to manage VLBW infants with congenital heart disease. Eighty-five of these infants (57%) weighed 1.5-1.9 kg at birth, while the remainder weighed less than 1.5 kg. Thirty did not require immediate surgical intervention, 12 had other, noncardiovascular complications requiring initial intervention, and 27 received comfort care only, leaving 80 candidates that became part of the immediate – versus delayed – surgery analysis.
Among the 46 infants whose surgery was delayed for an average of 8 weeks, 18 (39%) had a total of 33 complications. Six of these 18 children died while awaiting surgery. "Despite this high complication rate, we see roughly equivalent survival" between the immediate and delayed surgery groups. That observation, coupled with the finding that many infants gained weight at an "acceptable" rate during the period of surgical delay, led to the conclusion that either strategy is reasonable and should depend on the specific features of each case, he said.
Dr. Hickey had no disclosures. ☐
PHILADELPHIA – When a very low birth weight (VLWBW) infant has congenital heart disease needing surgical repair, the two opposing strategies of immediate surgery or delaying surgery for several weeks until the newborn grows larger work equally well for survival. Survival rates after both approaches tracked nearly identically during 3 years of follow-up, in a single center review of 80 cases.
Because the review included a relatively small number of VLBW newborns, the analysis could not determine which benefited most from immediate surgery and which did better with a delayed operation. "But we were reassured that delay did not lead to excess risk," Dr. Edward J. Hickey said at the annual meeting of the American Association for Thoracic Surgery.
Results from a second, related analysis that he reported showed that birth weight surpassed gestational age as a predictor of survival in newborns with congenital heart disease. "Birth weight is a more reliable, independent risk factor for death," said Dr. Hickey, a cardiothoracic surgeon at the Hospital for Sick Children in Toronto. The analysis showed that the highest risk for survival occurred in newborns who weighed less than 2.0 kg at birth. As a result of this finding, Dr. Hickey’s comparison of immediate and delayed surgical repair focused on the 80 newborns in the series who weighed less than 2.0 kg and required prompt intervention.
Among these 80 infants, 34 had "immediate surgery," which meant they had their operation as soon as it could be scheduled and performed, generally within 3 weeks of birth. Surgery for the other 46 was an average of 8 weeks after birth. These differences reflected the way surgeons at Sick Children managed each case.
Among the delayed surgery cases, infants with truncus or coarctation had the slowest growth, with as little as 50 g gained per week. In contrast, infants with an atrial septal defect, tetralogy, or a total anomalous pulmonary venous connection had growth rates above average, often at a pace of more than 150 g/week.
"I was most struck by the infants with coarctation, who seemed to grow at very low rates. That suggests to us that these patients are the ones we should repair early," because it is less likely that a delay would lead to much weight gain and improved surgical prospects, Dr. Hickey said. Based on these findings, he and his associates now perform coarctation repairs in infants whose weight is as low as 1.4 kg, he said. But Dr. Hickey also stressed that the timing of surgical repair must be individualized for each patient.
The two analyses done by Dr. Hickey and his associates involved 1,557 children with congenital heart disease admitted to the Hospital for Sick Children at age 30 days or younger who underwent active management during a 10-year period. Overall survival in this group was 91% at 3 months after admission, 88% after 6 months, and 86% after 5 years.
They evaluated the impact of both gestational age and birth weight on survival among these children, and found that both parameters were linked to mortality. Infants born at 28 weeks’ gestational age had a roughly 40% survival rate after 1 year, those born at 32 weeks had about a 60% survival rate to 1 year, and those born at 36 weeks had about an 80% survival rate at 1 year.
When analyzed by birth weight, those born at 3.5 kg or larger had a greater than 90% 1-year survival rate, those born with a weight of 2.0 kg had about an 80% 1-year survival, and those born weighing 1.5 kg had about a 60% survival to 1 year. These data identified an inflection point where infants born weighing less than 2.0 kg had a substantially worse survival than those who weighed 2.0 kg or more. Additional analysis that compared the relative contributions of gestational age and birth weight also showed that birth weight was the much stronger factor influencing 1-year survival.
The series included 149 infants born at less than 2.0 kg, highlighting how uncommon it is for surgeons to face the question of how to manage VLBW infants with congenital heart disease. Eighty-five of these infants (57%) weighed 1.5-1.9 kg at birth, while the remainder weighed less than 1.5 kg. Thirty did not require immediate surgical intervention, 12 had other, noncardiovascular complications requiring initial intervention, and 27 received comfort care only, leaving 80 candidates that became part of the immediate – versus delayed – surgery analysis.
Among the 46 infants whose surgery was delayed for an average of 8 weeks, 18 (39%) had a total of 33 complications. Six of these 18 children died while awaiting surgery. "Despite this high complication rate, we see roughly equivalent survival" between the immediate and delayed surgery groups. That observation, coupled with the finding that many infants gained weight at an "acceptable" rate during the period of surgical delay, led to the conclusion that either strategy is reasonable and should depend on the specific features of each case, he said.
Dr. Hickey had no disclosures. ☐
Major Finding: In infants with congenital heart disease with a birth weight below 2.0 kg who required surgical intervention, immediate surgery or surgery delayed for an average of 8 weeks led to similar survival rates during the following 3 years.
Data Source: Review of 80 VLBW infants who required surgery for congenital heart disease at one center during a 10-year period.
Disclosures: Dr. Hickey said that he had no disclosures.
FDA Approves Juvisync for Diabetes, High Cholesterol
The Food and Drug Administration on Oct. 7 announced the approval of a combination pill containing fixed doses of sitagliptin and simvastatin for people in whom treatment with both drugs is indicated.
The combination product, which will be marketed as Juvisync, is the first product that combines in a single tablet a drug approved for treating type 2 diabetes with a cholesterol-lowering drug, according to an agency statement announcing the approval.
Sitagliptin is a dipeptidyl peptidase 4 (DPP-4) inhibitor approved for use in combination with diet and exercise to improve glycemic control in adults with type 2 diabetes; it is marketed as Januvia (and as Janumet in combination with metformin). Simvastatin is an HMG-CoA reductase inhibitor approved for use with diet and exercise to lower low-density lipoprotein cholesterol and is marketed as Zocor and is available in generic formulations (and in combination with niacin and with ezetimibe).
Approval of Juvisync is based on the "substantial experience" with both drugs separately, "and the ability of the single tablet to deliver similar amounts of the drugs to the bloodstream as when sitagliptin and simvastatin are taken separately," according to the statement, which describes Juvisync as a "convenience combination" that should only be prescribed "when it is appropriate for a patient to be placed on both of these drugs."
"To ensure safe and effective use of this product, tablets containing different doses of sitagliptin and simvastatin in fixed-dose combination have been developed to meet the different needs of individual patients," Dr. Mary H. Parks, director of the Division of Metabolism and Endocrinology Products in the FDA’s Center for Drug Evaluation and Research said in the statement.
The approved dosage strengths of the sitagliptin/simvastatin combination are 100 mg/10 mg, 100 mg/20 mg, and 100 mg/40 mg, all of which are taken as a single dose in the evening, according to the prescribing information.
The manufacturer has committed to developing combined tablets containing the 50 mg sitagliptin dose, with 10 mg, 20 mg and 40 mg of simvastatin, but until these are available, patients who need the 50-mg dose of sitagliptin should be prescribed the single-ingredient tablet. There are no plans to develop a combination tablet with the 25-mg sitagliptin dose, which is not used very much, or with the 80-mg dose of simvastatin, because of recent restrictions on the use of this dose because it is associated with an increased risk of muscle toxicity, the statement said.
The statement says that the agency has recently become aware of the potential for statins to increase serum glucose levels in patients with type 2 diabetes, although the risk "appears very small and is outweighed by the benefits of statins for reducing heart disease in diabetes." To assess this risk further, the FDA is requiring that the manufacturer conduct a postmarketing clinical study. The FDA’s approval letter for Juvisync says that the trial should be a randomized, double-blind, active-controlled study that compares the effect of sitagliptin and simvastatin fixed-dose combination with sitagliptin on glycemic control in type 2 diabetic patients on background metformin therapy.
Juvisync is manufactured by MSD International GmbH Clonmel Co., based in Tipperary, Ireland.
The Food and Drug Administration on Oct. 7 announced the approval of a combination pill containing fixed doses of sitagliptin and simvastatin for people in whom treatment with both drugs is indicated.
The combination product, which will be marketed as Juvisync, is the first product that combines in a single tablet a drug approved for treating type 2 diabetes with a cholesterol-lowering drug, according to an agency statement announcing the approval.
Sitagliptin is a dipeptidyl peptidase 4 (DPP-4) inhibitor approved for use in combination with diet and exercise to improve glycemic control in adults with type 2 diabetes; it is marketed as Januvia (and as Janumet in combination with metformin). Simvastatin is an HMG-CoA reductase inhibitor approved for use with diet and exercise to lower low-density lipoprotein cholesterol and is marketed as Zocor and is available in generic formulations (and in combination with niacin and with ezetimibe).
Approval of Juvisync is based on the "substantial experience" with both drugs separately, "and the ability of the single tablet to deliver similar amounts of the drugs to the bloodstream as when sitagliptin and simvastatin are taken separately," according to the statement, which describes Juvisync as a "convenience combination" that should only be prescribed "when it is appropriate for a patient to be placed on both of these drugs."
"To ensure safe and effective use of this product, tablets containing different doses of sitagliptin and simvastatin in fixed-dose combination have been developed to meet the different needs of individual patients," Dr. Mary H. Parks, director of the Division of Metabolism and Endocrinology Products in the FDA’s Center for Drug Evaluation and Research said in the statement.
The approved dosage strengths of the sitagliptin/simvastatin combination are 100 mg/10 mg, 100 mg/20 mg, and 100 mg/40 mg, all of which are taken as a single dose in the evening, according to the prescribing information.
The manufacturer has committed to developing combined tablets containing the 50 mg sitagliptin dose, with 10 mg, 20 mg and 40 mg of simvastatin, but until these are available, patients who need the 50-mg dose of sitagliptin should be prescribed the single-ingredient tablet. There are no plans to develop a combination tablet with the 25-mg sitagliptin dose, which is not used very much, or with the 80-mg dose of simvastatin, because of recent restrictions on the use of this dose because it is associated with an increased risk of muscle toxicity, the statement said.
The statement says that the agency has recently become aware of the potential for statins to increase serum glucose levels in patients with type 2 diabetes, although the risk "appears very small and is outweighed by the benefits of statins for reducing heart disease in diabetes." To assess this risk further, the FDA is requiring that the manufacturer conduct a postmarketing clinical study. The FDA’s approval letter for Juvisync says that the trial should be a randomized, double-blind, active-controlled study that compares the effect of sitagliptin and simvastatin fixed-dose combination with sitagliptin on glycemic control in type 2 diabetic patients on background metformin therapy.
Juvisync is manufactured by MSD International GmbH Clonmel Co., based in Tipperary, Ireland.
The Food and Drug Administration on Oct. 7 announced the approval of a combination pill containing fixed doses of sitagliptin and simvastatin for people in whom treatment with both drugs is indicated.
The combination product, which will be marketed as Juvisync, is the first product that combines in a single tablet a drug approved for treating type 2 diabetes with a cholesterol-lowering drug, according to an agency statement announcing the approval.
Sitagliptin is a dipeptidyl peptidase 4 (DPP-4) inhibitor approved for use in combination with diet and exercise to improve glycemic control in adults with type 2 diabetes; it is marketed as Januvia (and as Janumet in combination with metformin). Simvastatin is an HMG-CoA reductase inhibitor approved for use with diet and exercise to lower low-density lipoprotein cholesterol and is marketed as Zocor and is available in generic formulations (and in combination with niacin and with ezetimibe).
Approval of Juvisync is based on the "substantial experience" with both drugs separately, "and the ability of the single tablet to deliver similar amounts of the drugs to the bloodstream as when sitagliptin and simvastatin are taken separately," according to the statement, which describes Juvisync as a "convenience combination" that should only be prescribed "when it is appropriate for a patient to be placed on both of these drugs."
"To ensure safe and effective use of this product, tablets containing different doses of sitagliptin and simvastatin in fixed-dose combination have been developed to meet the different needs of individual patients," Dr. Mary H. Parks, director of the Division of Metabolism and Endocrinology Products in the FDA’s Center for Drug Evaluation and Research said in the statement.
The approved dosage strengths of the sitagliptin/simvastatin combination are 100 mg/10 mg, 100 mg/20 mg, and 100 mg/40 mg, all of which are taken as a single dose in the evening, according to the prescribing information.
The manufacturer has committed to developing combined tablets containing the 50 mg sitagliptin dose, with 10 mg, 20 mg and 40 mg of simvastatin, but until these are available, patients who need the 50-mg dose of sitagliptin should be prescribed the single-ingredient tablet. There are no plans to develop a combination tablet with the 25-mg sitagliptin dose, which is not used very much, or with the 80-mg dose of simvastatin, because of recent restrictions on the use of this dose because it is associated with an increased risk of muscle toxicity, the statement said.
The statement says that the agency has recently become aware of the potential for statins to increase serum glucose levels in patients with type 2 diabetes, although the risk "appears very small and is outweighed by the benefits of statins for reducing heart disease in diabetes." To assess this risk further, the FDA is requiring that the manufacturer conduct a postmarketing clinical study. The FDA’s approval letter for Juvisync says that the trial should be a randomized, double-blind, active-controlled study that compares the effect of sitagliptin and simvastatin fixed-dose combination with sitagliptin on glycemic control in type 2 diabetic patients on background metformin therapy.
Juvisync is manufactured by MSD International GmbH Clonmel Co., based in Tipperary, Ireland.
Small Changes Count in Type 2 Diabetes Patients
LISBON – Even small changes in hemoglobin A1c and blood pressure could significantly reduce the risk of heart attack, stroke, and other cardiovascular complications in people with type 2 diabetes, according to the findings of a population-based observational study.
A 0.5% decrease in HbA1c and a 10 Hg/mm decrease in systolic blood pressure could avert 10% of such events over 5 years, Dr. Edith Heintjes said at the annual meeting of the European Society for the Study of Diabetes. Greater changes could reduce cardiovascular events by as much as 21%, said Dr. Heintjes of the PHARMO Institute for Drug Research, Utrecht, the Netherlands.
While her study on population attributable risk was albeit theoretical, it still adds weight to the emerging theory that small changes can make a big difference to the health of people with type 2 diabetes.
"Even when we examined only modest incremental reductions, which could be achieved in the clinical setting, we found the possibility of significant benefit," she said. Those patients with the greatest risk factors – elevated HbA1c, high blood pressure, and higher body mass index – stand to gain the most when they improve those factors, she said.
Dr. Heintjes’ analysis included 5,841 Dutch patients with a diagnosis of type 2 diabetes for at least 2 years. The patients were all taking some form of treatment – oral medications, insulin, or both – for at least 6 months to be included in the study. After examining both baseline data and 5-year outcomes, she was able to extrapolate how improvements in the three risk factors might impact the expected number of cardiovascular events.
Patient data were drawn from the PHARMO record linkage system, which includes community pharmaceutical dispensing information, laboratory information, national hospitalization information, and statistics from the Dutch national diabetes monitoring program.
Patients were treated with the aim of achieving the country’s national targets: an HbA1c of below 7%, a systolic blood pressure of 140 mmHg or lower, and a body mass index of 25 kg/m2 or less.
"Even when we examined only modest incremental reductions, we found the possibility of significant benefit."
At baseline, the patients’ average age was 66 years. The average HbA1c was 7%; systolic blood pressure 149 mmHg, and body mass index, 29.5 kg/m2. Most (92%) were taking only oral medications; the remainder was also taking insulin.
Some cardiovascular morbidity was already present in the group, including peripheral artery disease (0.5%), renal impairment (11%), neuropathy (51%), and retinopathy (7%). About half of the group (45%) had a family history of cardiovascular disease.
Dr. Heintjes divided the group according to the number of risk factors each patient exhibited. A quarter (24%) had just one elevated risk factor; 47% had two elevated risk factors, and 26% had elevations in all three risk factors.
A multivariable analysis allowed her to extrapolate that 796 cardiovascular events (heart attack, ischemic heart disease, stroke, and chronic heart failure) would occur if all of the patients were followed for 5 years.
If every patient in this population were able to correct each one of the risk factors to the national recommendations, she said, 687 events would occur – a 14% decrease. Correcting HbA1c and blood pressure accounted for this change, she said; changing BMI did nothing to increase the benefit.
Theoretically, she said, patients with the most risk factors would reap the greatest benefit. The 24% with one elevated risk factor would experience a 5% reduction in cardiovascular events, while those with all three elevated risk factors, upon correcting them, would see a 21% reduction.
Considering the group’s baseline measurements, correcting to national Dutch standards would mean an average HbA1c reduction of 0.8%, a 26-mmHg reduction in systolic blood pressure, and a weight loss of 16 kg (equivalent to a BMI decrease of 5.7 kg/m2). However, Dr. Heintjes said, it might not be realistic to expect such changes. Her second analysis explored the improvements that could arise from smaller changes: a 0.5% reduction in HbA1c, a 10-mmHg reduction in systolic blood pressure and a 10% reduction in total body weight (2.6 kg/m2 decrease in BMI).
"With this analysis, we saw in the overall population that 6% of the risk could be averted," she said. Among those in the subpopulation with three risk factors, applying the smaller changes could cut the number of events by 10%.
It’s not exactly clear how the results can change clinical practice, Dr. Heintjes acknowledged. "But this does allow us to understand how small changes can translate into bigger benefits for people with type 2 diabetes."
Dr. Heintjes reported having no conflicts of interest. Her employer, PHARMO, however, receives funding from numerous pharmaceutical companies, including Astra Zeneca, which sponsored the current study.
LISBON – Even small changes in hemoglobin A1c and blood pressure could significantly reduce the risk of heart attack, stroke, and other cardiovascular complications in people with type 2 diabetes, according to the findings of a population-based observational study.
A 0.5% decrease in HbA1c and a 10 Hg/mm decrease in systolic blood pressure could avert 10% of such events over 5 years, Dr. Edith Heintjes said at the annual meeting of the European Society for the Study of Diabetes. Greater changes could reduce cardiovascular events by as much as 21%, said Dr. Heintjes of the PHARMO Institute for Drug Research, Utrecht, the Netherlands.
While her study on population attributable risk was albeit theoretical, it still adds weight to the emerging theory that small changes can make a big difference to the health of people with type 2 diabetes.
"Even when we examined only modest incremental reductions, which could be achieved in the clinical setting, we found the possibility of significant benefit," she said. Those patients with the greatest risk factors – elevated HbA1c, high blood pressure, and higher body mass index – stand to gain the most when they improve those factors, she said.
Dr. Heintjes’ analysis included 5,841 Dutch patients with a diagnosis of type 2 diabetes for at least 2 years. The patients were all taking some form of treatment – oral medications, insulin, or both – for at least 6 months to be included in the study. After examining both baseline data and 5-year outcomes, she was able to extrapolate how improvements in the three risk factors might impact the expected number of cardiovascular events.
Patient data were drawn from the PHARMO record linkage system, which includes community pharmaceutical dispensing information, laboratory information, national hospitalization information, and statistics from the Dutch national diabetes monitoring program.
Patients were treated with the aim of achieving the country’s national targets: an HbA1c of below 7%, a systolic blood pressure of 140 mmHg or lower, and a body mass index of 25 kg/m2 or less.
"Even when we examined only modest incremental reductions, we found the possibility of significant benefit."
At baseline, the patients’ average age was 66 years. The average HbA1c was 7%; systolic blood pressure 149 mmHg, and body mass index, 29.5 kg/m2. Most (92%) were taking only oral medications; the remainder was also taking insulin.
Some cardiovascular morbidity was already present in the group, including peripheral artery disease (0.5%), renal impairment (11%), neuropathy (51%), and retinopathy (7%). About half of the group (45%) had a family history of cardiovascular disease.
Dr. Heintjes divided the group according to the number of risk factors each patient exhibited. A quarter (24%) had just one elevated risk factor; 47% had two elevated risk factors, and 26% had elevations in all three risk factors.
A multivariable analysis allowed her to extrapolate that 796 cardiovascular events (heart attack, ischemic heart disease, stroke, and chronic heart failure) would occur if all of the patients were followed for 5 years.
If every patient in this population were able to correct each one of the risk factors to the national recommendations, she said, 687 events would occur – a 14% decrease. Correcting HbA1c and blood pressure accounted for this change, she said; changing BMI did nothing to increase the benefit.
Theoretically, she said, patients with the most risk factors would reap the greatest benefit. The 24% with one elevated risk factor would experience a 5% reduction in cardiovascular events, while those with all three elevated risk factors, upon correcting them, would see a 21% reduction.
Considering the group’s baseline measurements, correcting to national Dutch standards would mean an average HbA1c reduction of 0.8%, a 26-mmHg reduction in systolic blood pressure, and a weight loss of 16 kg (equivalent to a BMI decrease of 5.7 kg/m2). However, Dr. Heintjes said, it might not be realistic to expect such changes. Her second analysis explored the improvements that could arise from smaller changes: a 0.5% reduction in HbA1c, a 10-mmHg reduction in systolic blood pressure and a 10% reduction in total body weight (2.6 kg/m2 decrease in BMI).
"With this analysis, we saw in the overall population that 6% of the risk could be averted," she said. Among those in the subpopulation with three risk factors, applying the smaller changes could cut the number of events by 10%.
It’s not exactly clear how the results can change clinical practice, Dr. Heintjes acknowledged. "But this does allow us to understand how small changes can translate into bigger benefits for people with type 2 diabetes."
Dr. Heintjes reported having no conflicts of interest. Her employer, PHARMO, however, receives funding from numerous pharmaceutical companies, including Astra Zeneca, which sponsored the current study.
LISBON – Even small changes in hemoglobin A1c and blood pressure could significantly reduce the risk of heart attack, stroke, and other cardiovascular complications in people with type 2 diabetes, according to the findings of a population-based observational study.
A 0.5% decrease in HbA1c and a 10 Hg/mm decrease in systolic blood pressure could avert 10% of such events over 5 years, Dr. Edith Heintjes said at the annual meeting of the European Society for the Study of Diabetes. Greater changes could reduce cardiovascular events by as much as 21%, said Dr. Heintjes of the PHARMO Institute for Drug Research, Utrecht, the Netherlands.
While her study on population attributable risk was albeit theoretical, it still adds weight to the emerging theory that small changes can make a big difference to the health of people with type 2 diabetes.
"Even when we examined only modest incremental reductions, which could be achieved in the clinical setting, we found the possibility of significant benefit," she said. Those patients with the greatest risk factors – elevated HbA1c, high blood pressure, and higher body mass index – stand to gain the most when they improve those factors, she said.
Dr. Heintjes’ analysis included 5,841 Dutch patients with a diagnosis of type 2 diabetes for at least 2 years. The patients were all taking some form of treatment – oral medications, insulin, or both – for at least 6 months to be included in the study. After examining both baseline data and 5-year outcomes, she was able to extrapolate how improvements in the three risk factors might impact the expected number of cardiovascular events.
Patient data were drawn from the PHARMO record linkage system, which includes community pharmaceutical dispensing information, laboratory information, national hospitalization information, and statistics from the Dutch national diabetes monitoring program.
Patients were treated with the aim of achieving the country’s national targets: an HbA1c of below 7%, a systolic blood pressure of 140 mmHg or lower, and a body mass index of 25 kg/m2 or less.
"Even when we examined only modest incremental reductions, we found the possibility of significant benefit."
At baseline, the patients’ average age was 66 years. The average HbA1c was 7%; systolic blood pressure 149 mmHg, and body mass index, 29.5 kg/m2. Most (92%) were taking only oral medications; the remainder was also taking insulin.
Some cardiovascular morbidity was already present in the group, including peripheral artery disease (0.5%), renal impairment (11%), neuropathy (51%), and retinopathy (7%). About half of the group (45%) had a family history of cardiovascular disease.
Dr. Heintjes divided the group according to the number of risk factors each patient exhibited. A quarter (24%) had just one elevated risk factor; 47% had two elevated risk factors, and 26% had elevations in all three risk factors.
A multivariable analysis allowed her to extrapolate that 796 cardiovascular events (heart attack, ischemic heart disease, stroke, and chronic heart failure) would occur if all of the patients were followed for 5 years.
If every patient in this population were able to correct each one of the risk factors to the national recommendations, she said, 687 events would occur – a 14% decrease. Correcting HbA1c and blood pressure accounted for this change, she said; changing BMI did nothing to increase the benefit.
Theoretically, she said, patients with the most risk factors would reap the greatest benefit. The 24% with one elevated risk factor would experience a 5% reduction in cardiovascular events, while those with all three elevated risk factors, upon correcting them, would see a 21% reduction.
Considering the group’s baseline measurements, correcting to national Dutch standards would mean an average HbA1c reduction of 0.8%, a 26-mmHg reduction in systolic blood pressure, and a weight loss of 16 kg (equivalent to a BMI decrease of 5.7 kg/m2). However, Dr. Heintjes said, it might not be realistic to expect such changes. Her second analysis explored the improvements that could arise from smaller changes: a 0.5% reduction in HbA1c, a 10-mmHg reduction in systolic blood pressure and a 10% reduction in total body weight (2.6 kg/m2 decrease in BMI).
"With this analysis, we saw in the overall population that 6% of the risk could be averted," she said. Among those in the subpopulation with three risk factors, applying the smaller changes could cut the number of events by 10%.
It’s not exactly clear how the results can change clinical practice, Dr. Heintjes acknowledged. "But this does allow us to understand how small changes can translate into bigger benefits for people with type 2 diabetes."
Dr. Heintjes reported having no conflicts of interest. Her employer, PHARMO, however, receives funding from numerous pharmaceutical companies, including Astra Zeneca, which sponsored the current study.
FROM THE ANNUAL MEETING OF THE EUROPEAN ASSOCIATION FOR THE STUDY OF DIABETES
Major Finding: Reducing HbA1c, blood pressure, and weight could avert up to 21% of cardiovascular events in patients with type 2 diabetes.
Data Source: A population-based observational study comprising 5,841 patients.
Disclosures: Dr. Heintjes reported having no conflicts of interest. Her employer, PHARMO, however, receives funding from numerous pharmaceutical companies, including Astra Zeneca, which sponsored the current study.
Temporary Staffing Common in HM, Study Reports
One in 10 hospitalists has worked locum tenens in the past year, according to a study of the practice released this week.
Locum Leaders, a locum tenens staffing agency in Alpharetta, Ga., put the study together this summer to define for the first time just how prevalent the practice of temporary staffing is and what motivates physicians to do the work. The report found that of hospitalists who work as locums tenens, 82% do it in addition to their full-time jobs and 11% do it as their full-time jobs.
Robert Harrington Jr., MD, SFHM, chief medical officer for Locum Leaders and an SHM board member, says the phenomenon allows some hospitalists to learn more about an institution before signing a long-term contract. It also affords other physicians flexibility, higher earning potential, or just the chance to "try something on for size before they buy."
"On the physician side, there are opportunities out there for you to not strain yourself immensely to increase your compensation, to travel to places you may not normally get to go, and to see how different programs are structured and operate," he says. "To see a more worldly view of hospital medicine."
For hospitals, even though locum physicians can cost more in salary, they can provide an opportunity for savings, as the hospital does not have to contribute to healthcare, pensions, or other costs. To wit, locum physicians can gross 30% to 40% more per year for the same number of shifts as a typical FTE hospitalist.
"They're all independent contractors," Dr. Harrington adds. "The increase in compensation that locum tenens physicians are able to demand, for the most part, comes from the difference between having a full-time employee versus an independent contractor."
One in 10 hospitalists has worked locum tenens in the past year, according to a study of the practice released this week.
Locum Leaders, a locum tenens staffing agency in Alpharetta, Ga., put the study together this summer to define for the first time just how prevalent the practice of temporary staffing is and what motivates physicians to do the work. The report found that of hospitalists who work as locums tenens, 82% do it in addition to their full-time jobs and 11% do it as their full-time jobs.
Robert Harrington Jr., MD, SFHM, chief medical officer for Locum Leaders and an SHM board member, says the phenomenon allows some hospitalists to learn more about an institution before signing a long-term contract. It also affords other physicians flexibility, higher earning potential, or just the chance to "try something on for size before they buy."
"On the physician side, there are opportunities out there for you to not strain yourself immensely to increase your compensation, to travel to places you may not normally get to go, and to see how different programs are structured and operate," he says. "To see a more worldly view of hospital medicine."
For hospitals, even though locum physicians can cost more in salary, they can provide an opportunity for savings, as the hospital does not have to contribute to healthcare, pensions, or other costs. To wit, locum physicians can gross 30% to 40% more per year for the same number of shifts as a typical FTE hospitalist.
"They're all independent contractors," Dr. Harrington adds. "The increase in compensation that locum tenens physicians are able to demand, for the most part, comes from the difference between having a full-time employee versus an independent contractor."
One in 10 hospitalists has worked locum tenens in the past year, according to a study of the practice released this week.
Locum Leaders, a locum tenens staffing agency in Alpharetta, Ga., put the study together this summer to define for the first time just how prevalent the practice of temporary staffing is and what motivates physicians to do the work. The report found that of hospitalists who work as locums tenens, 82% do it in addition to their full-time jobs and 11% do it as their full-time jobs.
Robert Harrington Jr., MD, SFHM, chief medical officer for Locum Leaders and an SHM board member, says the phenomenon allows some hospitalists to learn more about an institution before signing a long-term contract. It also affords other physicians flexibility, higher earning potential, or just the chance to "try something on for size before they buy."
"On the physician side, there are opportunities out there for you to not strain yourself immensely to increase your compensation, to travel to places you may not normally get to go, and to see how different programs are structured and operate," he says. "To see a more worldly view of hospital medicine."
For hospitals, even though locum physicians can cost more in salary, they can provide an opportunity for savings, as the hospital does not have to contribute to healthcare, pensions, or other costs. To wit, locum physicians can gross 30% to 40% more per year for the same number of shifts as a typical FTE hospitalist.
"They're all independent contractors," Dr. Harrington adds. "The increase in compensation that locum tenens physicians are able to demand, for the most part, comes from the difference between having a full-time employee versus an independent contractor."
The Appropriate Patient Census
What's the appropriate number of patients that an FTE hospitalist should see in one day? More than half of those surveyed on the-hospitalist.org believe they should see between 11 and 15 patients. According to two members of Team Hospitalist, 10 to 20 patients per day is a reasonable guideline.
"On average, 15 to 18 patients per day is a pretty easy-to-manage number," says Rachel George, MD, MBA, FHM, CPE, chief operating officer for Cogent HMG's west and north-central regions. But daily patient census depends on several factors, such as the types of patients admitted, the length of the doctor's shift, and the level of support from other staff on duty, she explains.
Readers were given one of five choices to respond with: "10 or fewer patients," "11-15," "16-20," "21-25," and "more than 25." Of the 421 responses, 51% felt that the average full-time hospitalist should see from 11 to 15 patients per day, followed by 35% who say they'd prefer to see 16 to 20 patients. Six percent voted for "10 or fewer." Only 4% of respondents said 20 or more patients a day was optimum.
"Honestly, I try not to get fixated on numbers," says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine. As a consultant, he says that rather than trying to expect physicians to attend to a standard census, HM groups should focus on acuity of illness and quality of care, and let patient needs dictate the staff required. Dr. Simone also recalled working with some groups who have delegated one or more staff members to handle admitting and screening, so that hospitalists can concentrate on the patients already in beds.
What's the appropriate number of patients that an FTE hospitalist should see in one day? More than half of those surveyed on the-hospitalist.org believe they should see between 11 and 15 patients. According to two members of Team Hospitalist, 10 to 20 patients per day is a reasonable guideline.
"On average, 15 to 18 patients per day is a pretty easy-to-manage number," says Rachel George, MD, MBA, FHM, CPE, chief operating officer for Cogent HMG's west and north-central regions. But daily patient census depends on several factors, such as the types of patients admitted, the length of the doctor's shift, and the level of support from other staff on duty, she explains.
Readers were given one of five choices to respond with: "10 or fewer patients," "11-15," "16-20," "21-25," and "more than 25." Of the 421 responses, 51% felt that the average full-time hospitalist should see from 11 to 15 patients per day, followed by 35% who say they'd prefer to see 16 to 20 patients. Six percent voted for "10 or fewer." Only 4% of respondents said 20 or more patients a day was optimum.
"Honestly, I try not to get fixated on numbers," says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine. As a consultant, he says that rather than trying to expect physicians to attend to a standard census, HM groups should focus on acuity of illness and quality of care, and let patient needs dictate the staff required. Dr. Simone also recalled working with some groups who have delegated one or more staff members to handle admitting and screening, so that hospitalists can concentrate on the patients already in beds.
What's the appropriate number of patients that an FTE hospitalist should see in one day? More than half of those surveyed on the-hospitalist.org believe they should see between 11 and 15 patients. According to two members of Team Hospitalist, 10 to 20 patients per day is a reasonable guideline.
"On average, 15 to 18 patients per day is a pretty easy-to-manage number," says Rachel George, MD, MBA, FHM, CPE, chief operating officer for Cogent HMG's west and north-central regions. But daily patient census depends on several factors, such as the types of patients admitted, the length of the doctor's shift, and the level of support from other staff on duty, she explains.
Readers were given one of five choices to respond with: "10 or fewer patients," "11-15," "16-20," "21-25," and "more than 25." Of the 421 responses, 51% felt that the average full-time hospitalist should see from 11 to 15 patients per day, followed by 35% who say they'd prefer to see 16 to 20 patients. Six percent voted for "10 or fewer." Only 4% of respondents said 20 or more patients a day was optimum.
"Honestly, I try not to get fixated on numbers," says Ken Simone, DO, SFHM, founder and president of Hospitalist and Practice Solutions in Veazie, Maine. As a consultant, he says that rather than trying to expect physicians to attend to a standard census, HM groups should focus on acuity of illness and quality of care, and let patient needs dictate the staff required. Dr. Simone also recalled working with some groups who have delegated one or more staff members to handle admitting and screening, so that hospitalists can concentrate on the patients already in beds.
By the Numbers: $4,000
According to a new study in American Economic Journal: Applied Economics by MIT economist Joseph Doyle, a $4,000 increase in per-patient hospital expenditures equates to a 1.4% decrease in mortality rates. Doyle studied 37,000 hospitalized patients in Florida who entered through the ED from 1996 to 2003. However, he focused on those visiting from other states in order to identify variation resulting from the level of care itself, not the prior health of the patients. The greater expense—and benefits—of care in the higher-cost hospital appeared to come from the broader application of ICU tools and greater complement of medical personnel, he notes.
“There are smart ways to spend money and ineffective ways to spend money,” he says, “and we’re still trying to figure out which are which, as much as possible.”
According to a new study in American Economic Journal: Applied Economics by MIT economist Joseph Doyle, a $4,000 increase in per-patient hospital expenditures equates to a 1.4% decrease in mortality rates. Doyle studied 37,000 hospitalized patients in Florida who entered through the ED from 1996 to 2003. However, he focused on those visiting from other states in order to identify variation resulting from the level of care itself, not the prior health of the patients. The greater expense—and benefits—of care in the higher-cost hospital appeared to come from the broader application of ICU tools and greater complement of medical personnel, he notes.
“There are smart ways to spend money and ineffective ways to spend money,” he says, “and we’re still trying to figure out which are which, as much as possible.”
According to a new study in American Economic Journal: Applied Economics by MIT economist Joseph Doyle, a $4,000 increase in per-patient hospital expenditures equates to a 1.4% decrease in mortality rates. Doyle studied 37,000 hospitalized patients in Florida who entered through the ED from 1996 to 2003. However, he focused on those visiting from other states in order to identify variation resulting from the level of care itself, not the prior health of the patients. The greater expense—and benefits—of care in the higher-cost hospital appeared to come from the broader application of ICU tools and greater complement of medical personnel, he notes.
“There are smart ways to spend money and ineffective ways to spend money,” he says, “and we’re still trying to figure out which are which, as much as possible.”
Transferring “Boarders” Could Save Millions
A pilot project that transferred “boarded” patients from one hospital’s ED to an inpatient bed at another nearby hospital in the same health system suggests that the concept could save hospitals millions.
“Improvement in Emergency Department Treatment Capacity: A Health System Integration Approach” was the subject of an oral presentation at HM11 in Dallas. Lead researcher Diego Martinez-Vasquez, MD, MPH, FACP, CPE, medical director for clinical resource utilization at Franklin Square Hospital Center in Baltimore, conducted the research in the University of Maryland medical system.
In the project, 265 patients who consented were transferred 1.3 miles to a sister hospital. Without “boarders”—admitted patients held in the ED—Dr. Martinez-Vasquez’s team found that the referring hospital could have regained enough capacity for an additional 2.9 patients per day. The project also showed median net revenue of $520,000 for the referring hospital and $1.9 million for the accepting hospital.
“The hospitalist group at the receiving hospital was the instrument that facilitated this program,” Dr. Martinez-Vasquez says. “But really what kept my attention was that healthcare systems sometimes don’t use resources effectively. So when I looked at the problem that this particular hospital was having regarding increased boarding time and decreased treatment capacity, I said, ‘Well, one way to resolve this issue is to develop a process that connects two system hospitals and their bed resources.’ ”
A pilot project that transferred “boarded” patients from one hospital’s ED to an inpatient bed at another nearby hospital in the same health system suggests that the concept could save hospitals millions.
“Improvement in Emergency Department Treatment Capacity: A Health System Integration Approach” was the subject of an oral presentation at HM11 in Dallas. Lead researcher Diego Martinez-Vasquez, MD, MPH, FACP, CPE, medical director for clinical resource utilization at Franklin Square Hospital Center in Baltimore, conducted the research in the University of Maryland medical system.
In the project, 265 patients who consented were transferred 1.3 miles to a sister hospital. Without “boarders”—admitted patients held in the ED—Dr. Martinez-Vasquez’s team found that the referring hospital could have regained enough capacity for an additional 2.9 patients per day. The project also showed median net revenue of $520,000 for the referring hospital and $1.9 million for the accepting hospital.
“The hospitalist group at the receiving hospital was the instrument that facilitated this program,” Dr. Martinez-Vasquez says. “But really what kept my attention was that healthcare systems sometimes don’t use resources effectively. So when I looked at the problem that this particular hospital was having regarding increased boarding time and decreased treatment capacity, I said, ‘Well, one way to resolve this issue is to develop a process that connects two system hospitals and their bed resources.’ ”
A pilot project that transferred “boarded” patients from one hospital’s ED to an inpatient bed at another nearby hospital in the same health system suggests that the concept could save hospitals millions.
“Improvement in Emergency Department Treatment Capacity: A Health System Integration Approach” was the subject of an oral presentation at HM11 in Dallas. Lead researcher Diego Martinez-Vasquez, MD, MPH, FACP, CPE, medical director for clinical resource utilization at Franklin Square Hospital Center in Baltimore, conducted the research in the University of Maryland medical system.
In the project, 265 patients who consented were transferred 1.3 miles to a sister hospital. Without “boarders”—admitted patients held in the ED—Dr. Martinez-Vasquez’s team found that the referring hospital could have regained enough capacity for an additional 2.9 patients per day. The project also showed median net revenue of $520,000 for the referring hospital and $1.9 million for the accepting hospital.
“The hospitalist group at the receiving hospital was the instrument that facilitated this program,” Dr. Martinez-Vasquez says. “But really what kept my attention was that healthcare systems sometimes don’t use resources effectively. So when I looked at the problem that this particular hospital was having regarding increased boarding time and decreased treatment capacity, I said, ‘Well, one way to resolve this issue is to develop a process that connects two system hospitals and their bed resources.’ ”
High-Performing Hospitals Invest in QI Infrastructure
A new study evaluating outcomes for hospitals participating in the American Heart Association’s Get with the Guidelines program found no correlation between high performance on adhering to measures and care standards for acute myocardial infarction and for heart failure despite overlap between the sets of care processes (J Am Coll Cardio. 2011;58:637-644).
A total of 400,000 heart patients were studied, and 283 participating hospitals were stratified into thirds based on their adherence to core quality measures for each disease, with the upper third labeled superior in performance. Lead author Tracy Wang, MD, MHS, MSc, of the Duke Clinical Research Institute in Durham, N.C., and colleagues found that superior performance for only one of the two diseases led to such end-result outcomes as in-hospital mortality that were no better than for hospitals that were not high performers for either condition. But hospitals with superior performance for both conditions had lower in-hospital mortality rates.
“Perhaps quality is more than just following checklists,” Dr. Wang says. “There’s something special about these high-performing hospitals across the board, with better QI, perhaps a little more investment in infrastructure for quality.”
This result, Dr. Wang says, should give ammunition for hospitalists and other physicians to go to their hospital administrators to request more investment in quality improvement overall, not just for specific conditions.
A new study evaluating outcomes for hospitals participating in the American Heart Association’s Get with the Guidelines program found no correlation between high performance on adhering to measures and care standards for acute myocardial infarction and for heart failure despite overlap between the sets of care processes (J Am Coll Cardio. 2011;58:637-644).
A total of 400,000 heart patients were studied, and 283 participating hospitals were stratified into thirds based on their adherence to core quality measures for each disease, with the upper third labeled superior in performance. Lead author Tracy Wang, MD, MHS, MSc, of the Duke Clinical Research Institute in Durham, N.C., and colleagues found that superior performance for only one of the two diseases led to such end-result outcomes as in-hospital mortality that were no better than for hospitals that were not high performers for either condition. But hospitals with superior performance for both conditions had lower in-hospital mortality rates.
“Perhaps quality is more than just following checklists,” Dr. Wang says. “There’s something special about these high-performing hospitals across the board, with better QI, perhaps a little more investment in infrastructure for quality.”
This result, Dr. Wang says, should give ammunition for hospitalists and other physicians to go to their hospital administrators to request more investment in quality improvement overall, not just for specific conditions.
A new study evaluating outcomes for hospitals participating in the American Heart Association’s Get with the Guidelines program found no correlation between high performance on adhering to measures and care standards for acute myocardial infarction and for heart failure despite overlap between the sets of care processes (J Am Coll Cardio. 2011;58:637-644).
A total of 400,000 heart patients were studied, and 283 participating hospitals were stratified into thirds based on their adherence to core quality measures for each disease, with the upper third labeled superior in performance. Lead author Tracy Wang, MD, MHS, MSc, of the Duke Clinical Research Institute in Durham, N.C., and colleagues found that superior performance for only one of the two diseases led to such end-result outcomes as in-hospital mortality that were no better than for hospitals that were not high performers for either condition. But hospitals with superior performance for both conditions had lower in-hospital mortality rates.
“Perhaps quality is more than just following checklists,” Dr. Wang says. “There’s something special about these high-performing hospitals across the board, with better QI, perhaps a little more investment in infrastructure for quality.”
This result, Dr. Wang says, should give ammunition for hospitalists and other physicians to go to their hospital administrators to request more investment in quality improvement overall, not just for specific conditions.