User login
ONLINE EXCLUSIVE: Listen to JHM's first editor-in-chief talk about HM's only peer-reviewed journal
Click here to listen to Dr. Williams
Click here to listen to Dr. Williams
Click here to listen to Dr. Williams
Business Drivers
MIAMI BEACH, Fla.—Muralidharan Reddy, MD, had just finished a five-hour class on the business concepts behind running a hospital and how a hospital CEO thinks—part of the entry-level curriculum at SHM’s Leadership Academy. As he stood up from the round table in a room still buzzing with conversation, he was glad he had signed up—in fact, he had been one of the first to arrive for the 7:30 a.m. session at the Fontainebleau resort.
“It improves my CV, number one,” says Dr. Reddy, a hospitalist at New England Baptist Hospital in Boston. “And it’s not just the CV, but I need the experience to guide me to work as a leader in a hospital group, or even plan on starting a group, or things like that. If I’m going to be a hospitalist, I have to work on trying to get those skills.”
A big plus, he adds, is “you get to learn from experts.”
The four-day academy provides hospitalists an intense learning experience. “Some of these skills, people learn it on the job or you get it through Academy,” Dr. Reddy says. “So I do both.”
Hospitalists who participate in the session repeatedly express concerns that if they don’t hone their understanding of the business aspects of the hospital and refine their skills in interacting with colleagues, they could be left behind in a fast-moving environment.
“I think it’s important,” said Mana Goshtasbi, MD, a hospitalist with Cogent HMG who has worked for two years at St. Joseph’s Hospital in Tampa, Fla. “I think that’s the direction. I think you have to know this stuff because of all the changes.”
Leadership Academy courses come in three levels, which build on one another: Foundations for Effective Leadership, Personal Leadership Excellence, and Strengthening Your Organization. Those who have completed the three levels can apply for certification, which requires completion of a pre-approved leadership project.
Know Your Value, Know Your Customers

In his first-level session, instructor Michael Guthrie, MD, MBA, executive in residence and adjunct professor at the University of Colorado Denver School of Business’ program in health administration, spent most of his presentation on his feet, wending his way among the tables, challenging the physician-students to think differently from the ways they’ve been trained to think about healthcare. That starts with stepping outside of themselves and taking a look at how they are viewed in terms of the hospital they’re working with as hospitalists, says Dr. Guthrie, former CEO of the Good Samaritan Health System in San Jose, Calif., and former COO for the Penrose-St. Francis Healthcare System in Colorado.
“What’s affecting the organization that you operate in, and what does that mean about the kinds of demands that are being made of you and requests that are being made of you?” he asks the attendees. “What does it mean about the value that’s received from the work that you do in that organization?”
A hospitalists’ value is a common theme. “What is it that you offer as hospitalists that has created a group of enthusiasts?” he asks. “What is it that you offer to any customer that’s of value to them that they would give up their hard-earned money in exchange for it? Who are your customers?”
A key “customer” group is primary-care physicians (PCPs) whose patients end up under a hospitalist’s care, he explains. They get value from the hospitalist in a variety of ways.
“That’s a more effective way for them to spend their life [at their own clinic],” he says. “They get to manage their schedule differently, they don’t have to drive. They are all exchange values. … There’s a very definite exchange going on here. If you fail in that exchange, we all know what would happen, right? They’d stop sending you patients.”
A physician chimes in: “If you’re the only hospitalist there, they don’t have a choice.”
Dr. Guthrie, quick to seize upon what he sees as a teaching moment, tells the group to “be careful.”
“In the short term, that’s absolutely true,” he says. “In the long term, there are a lot of other alternatives. And if there aren’t, someone will invent one. You see that’s the thing about our society—if there’s an opportunity with a whole, big, dissatisfied customer segment, somebody will notice and invent the way to satisfy their needs. That’s called capitalism.”
It’s what happened with the late Steve Jobs and the iPod, when he realized customers needed a way to easily access their music collections, Dr. Guthrie points out.
“He understood the dissatisfactions of the market,” he continues. “Before that, they didn’t have any choices.
“Healthcare is the same. But it’s a little more difficult to develop those choices. It’s hard to build a new hospital right in the middle of someplace where there’s only one hospital. So they invent other ways to do it, ways to get their patients taken care of: They travel.”
About 700,000 people flew to Southeast Asia last year for medical procedures, he says, making the point that American patients have options.
“Somewhat difficult, but they do have alternatives,” he says. “Customers will, when pushed hard enough, if dissatisfied enough, leave you, even when you think you have them trapped.”
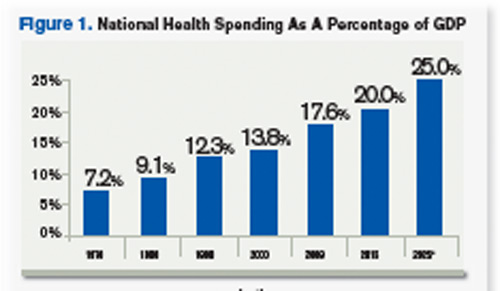
Source: Hartman, M: Martin, A; McDonnell, P et al. (2009). National Helath Spending In 2007: Slower Drug Spending Contributes To Lowest Rate Of Overall Growth Since 1998. Health Affairs, Jan/Feb., p 247. www.healthaffairs.org). See also, Orzag, Peter; Congressional Budget Office (2008). Growth in Health Care Costs, testimony before the Sentae Budget Committee, Jan. 31, p.1. (www.cbo.gov/doc.cfm?index-8948). Center for Medicare & Medicaid Services, January 2011.
Think Tanks
A key part of the session is time set aside for group work, in which Dr. Guthrie gives the class an assignment and attendees tackle it at their tables as a unit. The first task is to identify business drivers at hospitals, what the objectives of the hospital should be in response to those things, and how those objectives affect the work of hospitalists.
Then the groups go to work. A few minutes later, though, Dr. Guthrie speaks up through the chatter.
“Let’s stop for a minute. I want to tell you that most of you are on completely the wrong track,” he says, drawing chuckles. “But this is part of the reason we do it this way. The idea here is to get outside of your head.”
One group lists “profit” as a business driver.
“Profit is not a business driver,” he says. “I know you’re sort of raised to think that way. It isn’t. It’s a measurement. It’s like blood pressure. So it is not a business driver. We use it as a measurement of the success with which we’re synthesizing the business drivers and the environment and meeting the objectives of those drivers, or those trends.”
Business drivers are more along the lines of government mandates and an aging population, which some of the groups had mentioned. “That’s the level of abstraction I want you get to,” he says. “Think out in the marketplace.”
When it comes down to it, Dr. Guthrie explains, the hospitalist plays a role in just about every measurement used to determine excellence at a hospital—from quality to customer loyalty, from retention of patients to productivity.
He also emphasizes the difference between how a doctor has been trained essentially to be an individual expert—patient presents a problem, doctor presents a solution—and how those trained to be managers and leaders operate through other people.
Leaders of the Future
Daniel Duzan, MD, a hospitalist for TeamHealth at Fort Loudoun Medical Center in Lenoir City, Tenn., southwest of Knoxville, says doctors he knows recommended the academy. He says it made sense to him because he’s “migrating toward a leadership role in my own hospital.”
“My goal for coming was to kind of lay some foundation for skills and requirements that it takes to kind of migrate from just being a regular hospitalist to being one that’s got some extra responsibility,” Dr. Duzan says.
He was happy to learn more about “some of the jargon, lingo, that’s getting pushed our direction in terms of business drivers and the objectives” as well as “what would it be like to be the CEO, etc., and kind of putting us in their shoes, hearing things, seeing things and how they think about things, then developing plans.”
Jeet Gujral, MD, a hospitalist at Southside Hospital on Long Island, N.Y., says her motivation to learn about practice management is due in part to the new demands she is feeling because of the business considerations of the hospital. Talking with other hospitalists about their experiences was a big help, she says. In fact, she adds, that was probably even more helpful than the actual content of the session.
“I think what I’m getting more out of it [is that] there are several who are feeling the same heat,” she says. “It’s nice not feeling alone.”
Tom Collins is a freelance writer based in Florida.
MIAMI BEACH, Fla.—Muralidharan Reddy, MD, had just finished a five-hour class on the business concepts behind running a hospital and how a hospital CEO thinks—part of the entry-level curriculum at SHM’s Leadership Academy. As he stood up from the round table in a room still buzzing with conversation, he was glad he had signed up—in fact, he had been one of the first to arrive for the 7:30 a.m. session at the Fontainebleau resort.
“It improves my CV, number one,” says Dr. Reddy, a hospitalist at New England Baptist Hospital in Boston. “And it’s not just the CV, but I need the experience to guide me to work as a leader in a hospital group, or even plan on starting a group, or things like that. If I’m going to be a hospitalist, I have to work on trying to get those skills.”
A big plus, he adds, is “you get to learn from experts.”
The four-day academy provides hospitalists an intense learning experience. “Some of these skills, people learn it on the job or you get it through Academy,” Dr. Reddy says. “So I do both.”
Hospitalists who participate in the session repeatedly express concerns that if they don’t hone their understanding of the business aspects of the hospital and refine their skills in interacting with colleagues, they could be left behind in a fast-moving environment.
“I think it’s important,” said Mana Goshtasbi, MD, a hospitalist with Cogent HMG who has worked for two years at St. Joseph’s Hospital in Tampa, Fla. “I think that’s the direction. I think you have to know this stuff because of all the changes.”
Leadership Academy courses come in three levels, which build on one another: Foundations for Effective Leadership, Personal Leadership Excellence, and Strengthening Your Organization. Those who have completed the three levels can apply for certification, which requires completion of a pre-approved leadership project.
Know Your Value, Know Your Customers
In his first-level session, instructor Michael Guthrie, MD, MBA, executive in residence and adjunct professor at the University of Colorado Denver School of Business’ program in health administration, spent most of his presentation on his feet, wending his way among the tables, challenging the physician-students to think differently from the ways they’ve been trained to think about healthcare. That starts with stepping outside of themselves and taking a look at how they are viewed in terms of the hospital they’re working with as hospitalists, says Dr. Guthrie, former CEO of the Good Samaritan Health System in San Jose, Calif., and former COO for the Penrose-St. Francis Healthcare System in Colorado.
“What’s affecting the organization that you operate in, and what does that mean about the kinds of demands that are being made of you and requests that are being made of you?” he asks the attendees. “What does it mean about the value that’s received from the work that you do in that organization?”
A hospitalists’ value is a common theme. “What is it that you offer as hospitalists that has created a group of enthusiasts?” he asks. “What is it that you offer to any customer that’s of value to them that they would give up their hard-earned money in exchange for it? Who are your customers?”
A key “customer” group is primary-care physicians (PCPs) whose patients end up under a hospitalist’s care, he explains. They get value from the hospitalist in a variety of ways.
“That’s a more effective way for them to spend their life [at their own clinic],” he says. “They get to manage their schedule differently, they don’t have to drive. They are all exchange values. … There’s a very definite exchange going on here. If you fail in that exchange, we all know what would happen, right? They’d stop sending you patients.”
A physician chimes in: “If you’re the only hospitalist there, they don’t have a choice.”
Dr. Guthrie, quick to seize upon what he sees as a teaching moment, tells the group to “be careful.”
“In the short term, that’s absolutely true,” he says. “In the long term, there are a lot of other alternatives. And if there aren’t, someone will invent one. You see that’s the thing about our society—if there’s an opportunity with a whole, big, dissatisfied customer segment, somebody will notice and invent the way to satisfy their needs. That’s called capitalism.”
It’s what happened with the late Steve Jobs and the iPod, when he realized customers needed a way to easily access their music collections, Dr. Guthrie points out.
“He understood the dissatisfactions of the market,” he continues. “Before that, they didn’t have any choices.
“Healthcare is the same. But it’s a little more difficult to develop those choices. It’s hard to build a new hospital right in the middle of someplace where there’s only one hospital. So they invent other ways to do it, ways to get their patients taken care of: They travel.”
About 700,000 people flew to Southeast Asia last year for medical procedures, he says, making the point that American patients have options.
“Somewhat difficult, but they do have alternatives,” he says. “Customers will, when pushed hard enough, if dissatisfied enough, leave you, even when you think you have them trapped.”
Source: Hartman, M: Martin, A; McDonnell, P et al. (2009). National Helath Spending In 2007: Slower Drug Spending Contributes To Lowest Rate Of Overall Growth Since 1998. Health Affairs, Jan/Feb., p 247. www.healthaffairs.org). See also, Orzag, Peter; Congressional Budget Office (2008). Growth in Health Care Costs, testimony before the Sentae Budget Committee, Jan. 31, p.1. (www.cbo.gov/doc.cfm?index-8948). Center for Medicare & Medicaid Services, January 2011.
Think Tanks
A key part of the session is time set aside for group work, in which Dr. Guthrie gives the class an assignment and attendees tackle it at their tables as a unit. The first task is to identify business drivers at hospitals, what the objectives of the hospital should be in response to those things, and how those objectives affect the work of hospitalists.
Then the groups go to work. A few minutes later, though, Dr. Guthrie speaks up through the chatter.
“Let’s stop for a minute. I want to tell you that most of you are on completely the wrong track,” he says, drawing chuckles. “But this is part of the reason we do it this way. The idea here is to get outside of your head.”
One group lists “profit” as a business driver.
“Profit is not a business driver,” he says. “I know you’re sort of raised to think that way. It isn’t. It’s a measurement. It’s like blood pressure. So it is not a business driver. We use it as a measurement of the success with which we’re synthesizing the business drivers and the environment and meeting the objectives of those drivers, or those trends.”
Business drivers are more along the lines of government mandates and an aging population, which some of the groups had mentioned. “That’s the level of abstraction I want you get to,” he says. “Think out in the marketplace.”
When it comes down to it, Dr. Guthrie explains, the hospitalist plays a role in just about every measurement used to determine excellence at a hospital—from quality to customer loyalty, from retention of patients to productivity.
He also emphasizes the difference between how a doctor has been trained essentially to be an individual expert—patient presents a problem, doctor presents a solution—and how those trained to be managers and leaders operate through other people.
Leaders of the Future
Daniel Duzan, MD, a hospitalist for TeamHealth at Fort Loudoun Medical Center in Lenoir City, Tenn., southwest of Knoxville, says doctors he knows recommended the academy. He says it made sense to him because he’s “migrating toward a leadership role in my own hospital.”
“My goal for coming was to kind of lay some foundation for skills and requirements that it takes to kind of migrate from just being a regular hospitalist to being one that’s got some extra responsibility,” Dr. Duzan says.
He was happy to learn more about “some of the jargon, lingo, that’s getting pushed our direction in terms of business drivers and the objectives” as well as “what would it be like to be the CEO, etc., and kind of putting us in their shoes, hearing things, seeing things and how they think about things, then developing plans.”
Jeet Gujral, MD, a hospitalist at Southside Hospital on Long Island, N.Y., says her motivation to learn about practice management is due in part to the new demands she is feeling because of the business considerations of the hospital. Talking with other hospitalists about their experiences was a big help, she says. In fact, she adds, that was probably even more helpful than the actual content of the session.
“I think what I’m getting more out of it [is that] there are several who are feeling the same heat,” she says. “It’s nice not feeling alone.”
Tom Collins is a freelance writer based in Florida.
MIAMI BEACH, Fla.—Muralidharan Reddy, MD, had just finished a five-hour class on the business concepts behind running a hospital and how a hospital CEO thinks—part of the entry-level curriculum at SHM’s Leadership Academy. As he stood up from the round table in a room still buzzing with conversation, he was glad he had signed up—in fact, he had been one of the first to arrive for the 7:30 a.m. session at the Fontainebleau resort.
“It improves my CV, number one,” says Dr. Reddy, a hospitalist at New England Baptist Hospital in Boston. “And it’s not just the CV, but I need the experience to guide me to work as a leader in a hospital group, or even plan on starting a group, or things like that. If I’m going to be a hospitalist, I have to work on trying to get those skills.”
A big plus, he adds, is “you get to learn from experts.”
The four-day academy provides hospitalists an intense learning experience. “Some of these skills, people learn it on the job or you get it through Academy,” Dr. Reddy says. “So I do both.”
Hospitalists who participate in the session repeatedly express concerns that if they don’t hone their understanding of the business aspects of the hospital and refine their skills in interacting with colleagues, they could be left behind in a fast-moving environment.
“I think it’s important,” said Mana Goshtasbi, MD, a hospitalist with Cogent HMG who has worked for two years at St. Joseph’s Hospital in Tampa, Fla. “I think that’s the direction. I think you have to know this stuff because of all the changes.”
Leadership Academy courses come in three levels, which build on one another: Foundations for Effective Leadership, Personal Leadership Excellence, and Strengthening Your Organization. Those who have completed the three levels can apply for certification, which requires completion of a pre-approved leadership project.
Know Your Value, Know Your Customers
In his first-level session, instructor Michael Guthrie, MD, MBA, executive in residence and adjunct professor at the University of Colorado Denver School of Business’ program in health administration, spent most of his presentation on his feet, wending his way among the tables, challenging the physician-students to think differently from the ways they’ve been trained to think about healthcare. That starts with stepping outside of themselves and taking a look at how they are viewed in terms of the hospital they’re working with as hospitalists, says Dr. Guthrie, former CEO of the Good Samaritan Health System in San Jose, Calif., and former COO for the Penrose-St. Francis Healthcare System in Colorado.
“What’s affecting the organization that you operate in, and what does that mean about the kinds of demands that are being made of you and requests that are being made of you?” he asks the attendees. “What does it mean about the value that’s received from the work that you do in that organization?”
A hospitalists’ value is a common theme. “What is it that you offer as hospitalists that has created a group of enthusiasts?” he asks. “What is it that you offer to any customer that’s of value to them that they would give up their hard-earned money in exchange for it? Who are your customers?”
A key “customer” group is primary-care physicians (PCPs) whose patients end up under a hospitalist’s care, he explains. They get value from the hospitalist in a variety of ways.
“That’s a more effective way for them to spend their life [at their own clinic],” he says. “They get to manage their schedule differently, they don’t have to drive. They are all exchange values. … There’s a very definite exchange going on here. If you fail in that exchange, we all know what would happen, right? They’d stop sending you patients.”
A physician chimes in: “If you’re the only hospitalist there, they don’t have a choice.”
Dr. Guthrie, quick to seize upon what he sees as a teaching moment, tells the group to “be careful.”
“In the short term, that’s absolutely true,” he says. “In the long term, there are a lot of other alternatives. And if there aren’t, someone will invent one. You see that’s the thing about our society—if there’s an opportunity with a whole, big, dissatisfied customer segment, somebody will notice and invent the way to satisfy their needs. That’s called capitalism.”
It’s what happened with the late Steve Jobs and the iPod, when he realized customers needed a way to easily access their music collections, Dr. Guthrie points out.
“He understood the dissatisfactions of the market,” he continues. “Before that, they didn’t have any choices.
“Healthcare is the same. But it’s a little more difficult to develop those choices. It’s hard to build a new hospital right in the middle of someplace where there’s only one hospital. So they invent other ways to do it, ways to get their patients taken care of: They travel.”
About 700,000 people flew to Southeast Asia last year for medical procedures, he says, making the point that American patients have options.
“Somewhat difficult, but they do have alternatives,” he says. “Customers will, when pushed hard enough, if dissatisfied enough, leave you, even when you think you have them trapped.”
Source: Hartman, M: Martin, A; McDonnell, P et al. (2009). National Helath Spending In 2007: Slower Drug Spending Contributes To Lowest Rate Of Overall Growth Since 1998. Health Affairs, Jan/Feb., p 247. www.healthaffairs.org). See also, Orzag, Peter; Congressional Budget Office (2008). Growth in Health Care Costs, testimony before the Sentae Budget Committee, Jan. 31, p.1. (www.cbo.gov/doc.cfm?index-8948). Center for Medicare & Medicaid Services, January 2011.
Think Tanks
A key part of the session is time set aside for group work, in which Dr. Guthrie gives the class an assignment and attendees tackle it at their tables as a unit. The first task is to identify business drivers at hospitals, what the objectives of the hospital should be in response to those things, and how those objectives affect the work of hospitalists.
Then the groups go to work. A few minutes later, though, Dr. Guthrie speaks up through the chatter.
“Let’s stop for a minute. I want to tell you that most of you are on completely the wrong track,” he says, drawing chuckles. “But this is part of the reason we do it this way. The idea here is to get outside of your head.”
One group lists “profit” as a business driver.
“Profit is not a business driver,” he says. “I know you’re sort of raised to think that way. It isn’t. It’s a measurement. It’s like blood pressure. So it is not a business driver. We use it as a measurement of the success with which we’re synthesizing the business drivers and the environment and meeting the objectives of those drivers, or those trends.”
Business drivers are more along the lines of government mandates and an aging population, which some of the groups had mentioned. “That’s the level of abstraction I want you get to,” he says. “Think out in the marketplace.”
When it comes down to it, Dr. Guthrie explains, the hospitalist plays a role in just about every measurement used to determine excellence at a hospital—from quality to customer loyalty, from retention of patients to productivity.
He also emphasizes the difference between how a doctor has been trained essentially to be an individual expert—patient presents a problem, doctor presents a solution—and how those trained to be managers and leaders operate through other people.
Leaders of the Future
Daniel Duzan, MD, a hospitalist for TeamHealth at Fort Loudoun Medical Center in Lenoir City, Tenn., southwest of Knoxville, says doctors he knows recommended the academy. He says it made sense to him because he’s “migrating toward a leadership role in my own hospital.”
“My goal for coming was to kind of lay some foundation for skills and requirements that it takes to kind of migrate from just being a regular hospitalist to being one that’s got some extra responsibility,” Dr. Duzan says.
He was happy to learn more about “some of the jargon, lingo, that’s getting pushed our direction in terms of business drivers and the objectives” as well as “what would it be like to be the CEO, etc., and kind of putting us in their shoes, hearing things, seeing things and how they think about things, then developing plans.”
Jeet Gujral, MD, a hospitalist at Southside Hospital on Long Island, N.Y., says her motivation to learn about practice management is due in part to the new demands she is feeling because of the business considerations of the hospital. Talking with other hospitalists about their experiences was a big help, she says. In fact, she adds, that was probably even more helpful than the actual content of the session.
“I think what I’m getting more out of it [is that] there are several who are feeling the same heat,” she says. “It’s nice not feeling alone.”
Tom Collins is a freelance writer based in Florida.
Survey Insights
SHM and the Medical Group Management Association (MGMA) have enjoyed a successful survey collaboration for the past two years. Working together under a survey collaboration agreement to jointly conduct comprehensive annual surveys of HM groups, the two entities have been able to provide an unprecedented amount of high-quality information for members—not only data about hospitalist compensation and productivity, but also about many other aspects of the ways hospitalists and HM groups function.
And while SHM’s relationship with MGMA remains strong, all good things must come to an end—or at least change considerably.
MGMA is headed in new strategic directions that require a reallocation of its existing survey operations department resources. As a result, SHM and MGMA have agreed to change the way they work together, and this will have some important implications for the types of compensation and productivity data that will be available to hospitalists in the future.
MGMA will continue to conduct its regular surveys, including capturing compensation and productivity data for hospitalists. But instead of incorporating a hospital medicine supplement as it has for the last two years, SHM will instead conduct a separate survey each year to collect additional information about the characteristics of HM practices.
The SHM survey will be launched in January to coincide with the launch of MGMA’s Physician Compensation and Production Survey; in fact, academic groups that participated in MGMA’s Academic Practice Compensation and Production Survey for Faculty and Management this fall might already have noticed that the survey no longer included a hospital medicine supplement. SHM is encouraging hospitalists to participate in both the applicable MGMA survey and the companion SHM survey.
SHM will then license MGMA’s compensation and productivity data for both academic and nonacademic hospitalists, then will combine it with the results of its separate SHM survey to create the 2012 State of Hospital Medicine report.
The good news is that this approach will enable SHM to have greater flexibility to design surveys and analyze results in ways that best meet the needs of its constituents, and SHM will also be able to continue to provide survey information annually, rather than going back to the old biannual format.
However, some of the more detailed looks at compensation and productivity data will be lost; those data glimpses only were possible when the supplemental survey was integrated with MGMA’s survey instruments. Such data for 2012 will only be available for national, hospital-employed vs. not-hospital-employed, and geographic region cohorts.
Like the hospitalists it surveys, this report has changed every time it has been conducted. And SHM depends on its members to make sure it is delivering the kind of information that effectively, efficiently, and profitably guides hospitalists’ decisions.
Together, SHM and MGMA have been working to find the right balance that enables MGMA to pursue new strategies and still gives hospitalists the data they need. Ultimately, hospitalists will be the judges of whether the right balance has been struck.
Please send your thoughts and feedback to [email protected].
SHM and the Medical Group Management Association (MGMA) have enjoyed a successful survey collaboration for the past two years. Working together under a survey collaboration agreement to jointly conduct comprehensive annual surveys of HM groups, the two entities have been able to provide an unprecedented amount of high-quality information for members—not only data about hospitalist compensation and productivity, but also about many other aspects of the ways hospitalists and HM groups function.
And while SHM’s relationship with MGMA remains strong, all good things must come to an end—or at least change considerably.
MGMA is headed in new strategic directions that require a reallocation of its existing survey operations department resources. As a result, SHM and MGMA have agreed to change the way they work together, and this will have some important implications for the types of compensation and productivity data that will be available to hospitalists in the future.
MGMA will continue to conduct its regular surveys, including capturing compensation and productivity data for hospitalists. But instead of incorporating a hospital medicine supplement as it has for the last two years, SHM will instead conduct a separate survey each year to collect additional information about the characteristics of HM practices.
The SHM survey will be launched in January to coincide with the launch of MGMA’s Physician Compensation and Production Survey; in fact, academic groups that participated in MGMA’s Academic Practice Compensation and Production Survey for Faculty and Management this fall might already have noticed that the survey no longer included a hospital medicine supplement. SHM is encouraging hospitalists to participate in both the applicable MGMA survey and the companion SHM survey.
SHM will then license MGMA’s compensation and productivity data for both academic and nonacademic hospitalists, then will combine it with the results of its separate SHM survey to create the 2012 State of Hospital Medicine report.
The good news is that this approach will enable SHM to have greater flexibility to design surveys and analyze results in ways that best meet the needs of its constituents, and SHM will also be able to continue to provide survey information annually, rather than going back to the old biannual format.
However, some of the more detailed looks at compensation and productivity data will be lost; those data glimpses only were possible when the supplemental survey was integrated with MGMA’s survey instruments. Such data for 2012 will only be available for national, hospital-employed vs. not-hospital-employed, and geographic region cohorts.
Like the hospitalists it surveys, this report has changed every time it has been conducted. And SHM depends on its members to make sure it is delivering the kind of information that effectively, efficiently, and profitably guides hospitalists’ decisions.
Together, SHM and MGMA have been working to find the right balance that enables MGMA to pursue new strategies and still gives hospitalists the data they need. Ultimately, hospitalists will be the judges of whether the right balance has been struck.
Please send your thoughts and feedback to [email protected].
SHM and the Medical Group Management Association (MGMA) have enjoyed a successful survey collaboration for the past two years. Working together under a survey collaboration agreement to jointly conduct comprehensive annual surveys of HM groups, the two entities have been able to provide an unprecedented amount of high-quality information for members—not only data about hospitalist compensation and productivity, but also about many other aspects of the ways hospitalists and HM groups function.
And while SHM’s relationship with MGMA remains strong, all good things must come to an end—or at least change considerably.
MGMA is headed in new strategic directions that require a reallocation of its existing survey operations department resources. As a result, SHM and MGMA have agreed to change the way they work together, and this will have some important implications for the types of compensation and productivity data that will be available to hospitalists in the future.
MGMA will continue to conduct its regular surveys, including capturing compensation and productivity data for hospitalists. But instead of incorporating a hospital medicine supplement as it has for the last two years, SHM will instead conduct a separate survey each year to collect additional information about the characteristics of HM practices.
The SHM survey will be launched in January to coincide with the launch of MGMA’s Physician Compensation and Production Survey; in fact, academic groups that participated in MGMA’s Academic Practice Compensation and Production Survey for Faculty and Management this fall might already have noticed that the survey no longer included a hospital medicine supplement. SHM is encouraging hospitalists to participate in both the applicable MGMA survey and the companion SHM survey.
SHM will then license MGMA’s compensation and productivity data for both academic and nonacademic hospitalists, then will combine it with the results of its separate SHM survey to create the 2012 State of Hospital Medicine report.
The good news is that this approach will enable SHM to have greater flexibility to design surveys and analyze results in ways that best meet the needs of its constituents, and SHM will also be able to continue to provide survey information annually, rather than going back to the old biannual format.
However, some of the more detailed looks at compensation and productivity data will be lost; those data glimpses only were possible when the supplemental survey was integrated with MGMA’s survey instruments. Such data for 2012 will only be available for national, hospital-employed vs. not-hospital-employed, and geographic region cohorts.
Like the hospitalists it surveys, this report has changed every time it has been conducted. And SHM depends on its members to make sure it is delivering the kind of information that effectively, efficiently, and profitably guides hospitalists’ decisions.
Together, SHM and MGMA have been working to find the right balance that enables MGMA to pursue new strategies and still gives hospitalists the data they need. Ultimately, hospitalists will be the judges of whether the right balance has been struck.
Please send your thoughts and feedback to [email protected].
Bayes Theorem? There's an App for That
A hospitalist at Beth Israel Deaconess Medical Center in Boston has created an iPhone application to help give academic HM groups fingertip access to Bayesian nomograms and real-time research.
Hospitalist Elizabeth Farrell, MD, says an app dubbed Medicine Toolkit (www.medicinetoolkit.com) should be available for download in a matter of weeks. The app has two components. The first is Bayes at the Bedside, a database of likelihood ratios (LRs) for more than 150 commonly used physical exam findings, labs, and imaging studies paired with an automated Bayesian nomogram to visually display the theorem and its application to clinical decision-making. The second piece of the program is Pocket Evidence, a compilation of more than 300 review articles, consensus guidelines, meta-analyses, and new and notable articles. Both components will be updated monthly.
“I really am envisioning it as a teaching tool and one that could be used by attendings to teach residents, interns, and medical students alike to facilitate critical thinking and evidence-based medicine,” Dr. Farrell says. “It can be used on rounds, in the clinic, or in the classroom.”
Dr. Farrell, a hospitalist for two years, had the idea to develop the application after printing out nomograms on index cards to use on rounds. She gave cards to team members and printed LRs on the back.
“It was a lot of fun, the team loved it, it worked great,” Dr. Farrell says. “But a lot of times I’d find that I ran out of the index cards, or someone on the team left theirs back in the workroom, or we didn’t have the LR for the test we were talking about. It resulted in a lot of missed teaching opportunities.”
A hospitalist at Beth Israel Deaconess Medical Center in Boston has created an iPhone application to help give academic HM groups fingertip access to Bayesian nomograms and real-time research.
Hospitalist Elizabeth Farrell, MD, says an app dubbed Medicine Toolkit (www.medicinetoolkit.com) should be available for download in a matter of weeks. The app has two components. The first is Bayes at the Bedside, a database of likelihood ratios (LRs) for more than 150 commonly used physical exam findings, labs, and imaging studies paired with an automated Bayesian nomogram to visually display the theorem and its application to clinical decision-making. The second piece of the program is Pocket Evidence, a compilation of more than 300 review articles, consensus guidelines, meta-analyses, and new and notable articles. Both components will be updated monthly.
“I really am envisioning it as a teaching tool and one that could be used by attendings to teach residents, interns, and medical students alike to facilitate critical thinking and evidence-based medicine,” Dr. Farrell says. “It can be used on rounds, in the clinic, or in the classroom.”
Dr. Farrell, a hospitalist for two years, had the idea to develop the application after printing out nomograms on index cards to use on rounds. She gave cards to team members and printed LRs on the back.
“It was a lot of fun, the team loved it, it worked great,” Dr. Farrell says. “But a lot of times I’d find that I ran out of the index cards, or someone on the team left theirs back in the workroom, or we didn’t have the LR for the test we were talking about. It resulted in a lot of missed teaching opportunities.”
A hospitalist at Beth Israel Deaconess Medical Center in Boston has created an iPhone application to help give academic HM groups fingertip access to Bayesian nomograms and real-time research.
Hospitalist Elizabeth Farrell, MD, says an app dubbed Medicine Toolkit (www.medicinetoolkit.com) should be available for download in a matter of weeks. The app has two components. The first is Bayes at the Bedside, a database of likelihood ratios (LRs) for more than 150 commonly used physical exam findings, labs, and imaging studies paired with an automated Bayesian nomogram to visually display the theorem and its application to clinical decision-making. The second piece of the program is Pocket Evidence, a compilation of more than 300 review articles, consensus guidelines, meta-analyses, and new and notable articles. Both components will be updated monthly.
“I really am envisioning it as a teaching tool and one that could be used by attendings to teach residents, interns, and medical students alike to facilitate critical thinking and evidence-based medicine,” Dr. Farrell says. “It can be used on rounds, in the clinic, or in the classroom.”
Dr. Farrell, a hospitalist for two years, had the idea to develop the application after printing out nomograms on index cards to use on rounds. She gave cards to team members and printed LRs on the back.
“It was a lot of fun, the team loved it, it worked great,” Dr. Farrell says. “But a lot of times I’d find that I ran out of the index cards, or someone on the team left theirs back in the workroom, or we didn’t have the LR for the test we were talking about. It resulted in a lot of missed teaching opportunities.”
ONLINE EXCLUSIVE: New Journal Chief Faces Myriad Challenges
Enter text here
Enter text here
Enter text here
ONLINE EXCLUSIVE: A Loss of Meaning Vs. a Sense of Calling
Enter text here
Enter text here
Enter text here
Policy Corner
Payment bundling may create new opportunities for hospitalists to start an important discussion with hospital executives. And forward-looking hospitalist leaders will use the new model to shape their own financial destinies.
The concept of payment bundling broadly means paying for healthcare with a single, comprehensive payment, which is intended to cover all services received by a patient. Due to the promise bundling holds when it comes to both cost containment and quality, the Affordable Care Act (ACA) includes a provision requiring the establishment of a voluntary national pilot program on payment bundling. This provision calls for bundled payments for 10 unnamed conditions by Jan. 1, 2013, and states that payment for each bundle will surround an episode of care consisting of three days prior to admission and 30 days post-hospital discharge. There is some flexibility built in because the ACA also allows for different episodes of care to be defined by the secretary of Health and Human Services.
Due to this flexibility, the discussion at SHM is probably similar to that of other forward-thinking organizations: What conditions would benefit from a hospitalist-led bundle and what is the appropriate episode of care?
In late August, the Centers for Medicare & Medicaid Services (CMS) and the Center for Medicare and Medicaid Innovation (CMMI) answered these questions with the introduction of the Bundled Payments for Care Improvement initiative. This initiative outlines four models as options for the bundling pilot while maintaining a degree of flexibility in the details for participating providers to define:
- The first model will cover all Medicare DRGs for inpatient hospital services.
- Model two will include hospital and physician inpatient and post-discharge services.
- Model three will be for post-discharge services only.
- Under the fourth model, CMS would make a single, prospective bundled payment that would encompass all services furnished during an inpatient stay by the hospital, physicians, and other practitioners.
With the exception of the first model, providers wishing to participate may propose the condition (or conditions) their bundle will cover, the episode of care, and even the measures they will use for quality purposes.
CMMI clearly is aiming for a high level of provider involvement in developing bundling models that will work, and the inpatient focus for three out of four bundling models means that hospitalists should be prepared to play a part. For example, at press time, a tight application deadline and an unclear return on investment posed potential barriers.
Nevertheless, the inpatient focus for three out of four bundling models means that hospitalists should be prepared to play a part. At a minimum, hospitalists should be prepared to negotiate their level of involvement and how they will get paid for their work, should their institutions participate. But there is nothing preventing hospitalists from taking the lead in bringing bundled payments to their institutions by approaching hospital administrators with their own bundle for a condition they will manage.
If your group or institution is planning to participate in the bundled payments initiative, please let us know by emailing [email protected].
Payment bundling may create new opportunities for hospitalists to start an important discussion with hospital executives. And forward-looking hospitalist leaders will use the new model to shape their own financial destinies.
The concept of payment bundling broadly means paying for healthcare with a single, comprehensive payment, which is intended to cover all services received by a patient. Due to the promise bundling holds when it comes to both cost containment and quality, the Affordable Care Act (ACA) includes a provision requiring the establishment of a voluntary national pilot program on payment bundling. This provision calls for bundled payments for 10 unnamed conditions by Jan. 1, 2013, and states that payment for each bundle will surround an episode of care consisting of three days prior to admission and 30 days post-hospital discharge. There is some flexibility built in because the ACA also allows for different episodes of care to be defined by the secretary of Health and Human Services.
Due to this flexibility, the discussion at SHM is probably similar to that of other forward-thinking organizations: What conditions would benefit from a hospitalist-led bundle and what is the appropriate episode of care?
In late August, the Centers for Medicare & Medicaid Services (CMS) and the Center for Medicare and Medicaid Innovation (CMMI) answered these questions with the introduction of the Bundled Payments for Care Improvement initiative. This initiative outlines four models as options for the bundling pilot while maintaining a degree of flexibility in the details for participating providers to define:
- The first model will cover all Medicare DRGs for inpatient hospital services.
- Model two will include hospital and physician inpatient and post-discharge services.
- Model three will be for post-discharge services only.
- Under the fourth model, CMS would make a single, prospective bundled payment that would encompass all services furnished during an inpatient stay by the hospital, physicians, and other practitioners.
With the exception of the first model, providers wishing to participate may propose the condition (or conditions) their bundle will cover, the episode of care, and even the measures they will use for quality purposes.
CMMI clearly is aiming for a high level of provider involvement in developing bundling models that will work, and the inpatient focus for three out of four bundling models means that hospitalists should be prepared to play a part. For example, at press time, a tight application deadline and an unclear return on investment posed potential barriers.
Nevertheless, the inpatient focus for three out of four bundling models means that hospitalists should be prepared to play a part. At a minimum, hospitalists should be prepared to negotiate their level of involvement and how they will get paid for their work, should their institutions participate. But there is nothing preventing hospitalists from taking the lead in bringing bundled payments to their institutions by approaching hospital administrators with their own bundle for a condition they will manage.
If your group or institution is planning to participate in the bundled payments initiative, please let us know by emailing [email protected].
Payment bundling may create new opportunities for hospitalists to start an important discussion with hospital executives. And forward-looking hospitalist leaders will use the new model to shape their own financial destinies.
The concept of payment bundling broadly means paying for healthcare with a single, comprehensive payment, which is intended to cover all services received by a patient. Due to the promise bundling holds when it comes to both cost containment and quality, the Affordable Care Act (ACA) includes a provision requiring the establishment of a voluntary national pilot program on payment bundling. This provision calls for bundled payments for 10 unnamed conditions by Jan. 1, 2013, and states that payment for each bundle will surround an episode of care consisting of three days prior to admission and 30 days post-hospital discharge. There is some flexibility built in because the ACA also allows for different episodes of care to be defined by the secretary of Health and Human Services.
Due to this flexibility, the discussion at SHM is probably similar to that of other forward-thinking organizations: What conditions would benefit from a hospitalist-led bundle and what is the appropriate episode of care?
In late August, the Centers for Medicare & Medicaid Services (CMS) and the Center for Medicare and Medicaid Innovation (CMMI) answered these questions with the introduction of the Bundled Payments for Care Improvement initiative. This initiative outlines four models as options for the bundling pilot while maintaining a degree of flexibility in the details for participating providers to define:
- The first model will cover all Medicare DRGs for inpatient hospital services.
- Model two will include hospital and physician inpatient and post-discharge services.
- Model three will be for post-discharge services only.
- Under the fourth model, CMS would make a single, prospective bundled payment that would encompass all services furnished during an inpatient stay by the hospital, physicians, and other practitioners.
With the exception of the first model, providers wishing to participate may propose the condition (or conditions) their bundle will cover, the episode of care, and even the measures they will use for quality purposes.
CMMI clearly is aiming for a high level of provider involvement in developing bundling models that will work, and the inpatient focus for three out of four bundling models means that hospitalists should be prepared to play a part. For example, at press time, a tight application deadline and an unclear return on investment posed potential barriers.
Nevertheless, the inpatient focus for three out of four bundling models means that hospitalists should be prepared to play a part. At a minimum, hospitalists should be prepared to negotiate their level of involvement and how they will get paid for their work, should their institutions participate. But there is nothing preventing hospitalists from taking the lead in bringing bundled payments to their institutions by approaching hospital administrators with their own bundle for a condition they will manage.
If your group or institution is planning to participate in the bundled payments initiative, please let us know by emailing [email protected].
Academic Opportunity
Academic hospitalists will find new opportunities to learn, network, and showcase their own insights at HM12, SHM’s annual meeting April 1-4 in San Diego.
This year, poster presenters will have even more time to present cutting-edge topics in hospital medicine. The popular Research, Innovation, and Clinical Vignettes (RIV) poster sessions will be split into two days.
The Research and Innovations poster reception will be held 5 to 7 p.m. April 2, while the Vignettes poster session will be held during lunch the next day. However, some things about the receptions won’t change: Sessions will be held in the exhibit hall.
The move to two poster receptions was in response to previous attendee feedback. As the numbers of attendees and poster presenters has grown, visiting all the posters and having meaningful conversations with the presenters became increasingly difficult. Now attendees—both academic and community-based hospitalist—can take their time and soak in more of the best thinking in the specialty.
If you’re thinking about submitting a poster for any of the three categories, now is the time to act: The submission deadline for abstracts is Dec. 2.
Poster sessions aren’t the only new chances for academic hospitalists to find valuable face time at HM12, either. This year’s program includes new opportunities to collaborate and connect with other academic hospitalists—and hospitalists from other backgrounds as well.
And the HM12 schedule will feature valuable courses specifically chosen for the unique needs and challenges of the academic hospitalist’s career.
Brendon Shank is SHM’s associate vice president of communications.
Academic hospitalists will find new opportunities to learn, network, and showcase their own insights at HM12, SHM’s annual meeting April 1-4 in San Diego.
This year, poster presenters will have even more time to present cutting-edge topics in hospital medicine. The popular Research, Innovation, and Clinical Vignettes (RIV) poster sessions will be split into two days.
The Research and Innovations poster reception will be held 5 to 7 p.m. April 2, while the Vignettes poster session will be held during lunch the next day. However, some things about the receptions won’t change: Sessions will be held in the exhibit hall.
The move to two poster receptions was in response to previous attendee feedback. As the numbers of attendees and poster presenters has grown, visiting all the posters and having meaningful conversations with the presenters became increasingly difficult. Now attendees—both academic and community-based hospitalist—can take their time and soak in more of the best thinking in the specialty.
If you’re thinking about submitting a poster for any of the three categories, now is the time to act: The submission deadline for abstracts is Dec. 2.
Poster sessions aren’t the only new chances for academic hospitalists to find valuable face time at HM12, either. This year’s program includes new opportunities to collaborate and connect with other academic hospitalists—and hospitalists from other backgrounds as well.
And the HM12 schedule will feature valuable courses specifically chosen for the unique needs and challenges of the academic hospitalist’s career.
Brendon Shank is SHM’s associate vice president of communications.
Academic hospitalists will find new opportunities to learn, network, and showcase their own insights at HM12, SHM’s annual meeting April 1-4 in San Diego.
This year, poster presenters will have even more time to present cutting-edge topics in hospital medicine. The popular Research, Innovation, and Clinical Vignettes (RIV) poster sessions will be split into two days.
The Research and Innovations poster reception will be held 5 to 7 p.m. April 2, while the Vignettes poster session will be held during lunch the next day. However, some things about the receptions won’t change: Sessions will be held in the exhibit hall.
The move to two poster receptions was in response to previous attendee feedback. As the numbers of attendees and poster presenters has grown, visiting all the posters and having meaningful conversations with the presenters became increasingly difficult. Now attendees—both academic and community-based hospitalist—can take their time and soak in more of the best thinking in the specialty.
If you’re thinking about submitting a poster for any of the three categories, now is the time to act: The submission deadline for abstracts is Dec. 2.
Poster sessions aren’t the only new chances for academic hospitalists to find valuable face time at HM12, either. This year’s program includes new opportunities to collaborate and connect with other academic hospitalists—and hospitalists from other backgrounds as well.
And the HM12 schedule will feature valuable courses specifically chosen for the unique needs and challenges of the academic hospitalist’s career.
Brendon Shank is SHM’s associate vice president of communications.
In the Literature: The latest research you need to know
In This Edition
Literature At A Glance
A guide to this month’s studies
- Use of a Care-Transitions Intervention Reduces 30-Day Hospital Readmissions
- Routine Chest Radiographs after Pneumonia to Rule Out Lung Cancer Have Low Diagnostic Yield
- Hospitalist Care Shifts Costs to the Outpatient Environment
- Stopping Smoking at Any Time before Surgery Is Safe
- Hospitalization for Infection Increases Risk of Stroke
- Longer Duration of Perioperative Antibiotics May Be Beneficial after Cardiac Surgery
- Stroke Unit Care Combined with Early Supported Discharge Improves Outcomes
- Criteria May Help Identify Patients at Risk for Infective Endocarditis
Use of a Care-Transitions Intervention Reduces 30-Day Hospital Readmissions
Clinical question: Does use of a specific care-transitions intervention (CTI) reduce 30-day hospital readmissions in a nonintegrated healthcare system?
Background: Previous interventions addressing improved communication between members of the healthcare team, patients, and families at time of discharge show promise for reducing hospital readmissions. Although these interventions revealed positive results, no research has been completed within a system where healthcare is integrated across settings.
Study design: Quasi-experimental prospective cohort study.
Setting: Six Rhode Island acute-care hospitals, including two community hospitals, three teaching hospitals, and a tertiary-care center and teaching hospital. Facilities ranged from 129 beds to 719 beds.
Synopsis: The CTI is a patient-centered intervention occurring across 30 days. The intervention includes a home visit by a coach within three days of hospital discharge, a telephone call within seven to 10 days of discharge, and a final telephone call no later than 30 days after admission. During these contacts, coaches encourage patient and family participation in care, and active communication with their primary-care provider regarding their disease state. A convenience sample of fee-for-service Medicare beneficiaries was identified by admission diagnoses of acute myocardial infarction, congestive heart failure, or specific pulmonary conditions. Overall, 74% participants completed the entire intervention. The odds of a hospital readmission were significantly lower in the intervention population compared with those who did not receive the intervention (OR 0.61; 95% CI, 0.42-0.88).
Study design: Study design was limited by ability to provide coaching (only 8% of total population was approached), and therefore may not be representative of a typical integrated healthcare setting. In addition, the sample consisted of a convenience sample, which may limit generalizability.
Bottom line: The CTI appears to decrease the rate of 30-day hospital readmissions in Medicare patients with certain cardiac and pulmonary diagnoses.
Citation: Voss R, Gardner R, Baier R, Butterfield K, Lehrman S, Gravenstein S. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171:1232-1237.
Routine Chest Radiographs after Pneumonia to Rule Out Lung Cancer Have Low Diagnostic Yield
Clinical question: What is the incidence of new lung cancer detected on routine post-pneumonia chest radiographs?
Background: Routine chest radiographs have been recommended four to eight weeks after resolution of pneumonia to exclude underlying lung cancer. The diagnostic yield of this practice is uncertain.
Study design: Population-based cohort.
Setting: Seven emergency departments and six hospitals in Edmonton, Alberta, Canada.
Synopsis: Authors enrolled 3,398 patients with clinical and radiographic evidence of pneumonia. Of these, 59% were aged 50 and older, 52% were male, 17% were current smokers, 18% had COPD, and 49% were treated as inpatients. At 90-day follow-up, 1.1% of patients received a new diagnosis of lung cancer, with incidence steadily increasing to 2.2% at three-year follow-up. In multivariate analysis, age 50 and older, male sex, and current smoking were independent predictors of post-pneumonia new lung cancer diagnosis. Limiting follow-up chest radiographs to patients aged 50 and older would have detected 98% of new lung cancers and improved diagnostic yield to 2.8%.
Bottom line: Routine post-pneumonia chest radiographs for lung cancer screening have low diagnostic yield that is only marginally improved by selecting high-risk populations.
Citation: Tang KL, Eurich DT, Minhas-Sandhu JK, Marrie TJ, Majumdar SR. Incidence, correlates, and chest radiographic yield of new lung cancer diagnosis in 3398 patients with pneumonia. Arch Intern Med. 2011;171:1193-1198.
Hospitalist Care Shifts Costs to the Outpatient Environment
Clinical question: How does hospitalist care affect medical utilization costs after hospital discharge?
Background: The number of patients cared for by hospitalists is growing rapidly. Some studies have shown hospitalists to decrease length of stay and inpatient costs. The impact of shorter hospitalization on outpatient medical utilization and costs is not known.
Study design: Population-based national cohort.
Setting: Hospitalized Medicare patients.
Synopsis: In this study of 58,125 Medicare admissions at 454 hospitals, hospitalist care was associated with a 0.64-day shorter adjusted length of stay and $282 lower hospital charges compared with patients cared for by their primary-care physicians (PCPs). This was offset by $332 higher Medicare spending in the 30 days following hospitalization. Patients cared for by hospitalists were less likely to be discharged home (OR 0.82, 95% CI, 0.78-0.86), and were more likely to require emergency department visits (OR 1.18, 95% CI, 1.12-1.24) and readmissions (OR 1.08, 95% CI, 1.02-1.14). The authors postulate that shorter length of stay associated with hospitalist care is achieved at the expense of shifting costs to the outpatient environment. The discharged patients are sicker and, as a result, require more skilled care and repeat hospital visits.
Bottom line: Hospitalist care may be associated with higher overall costs and more medical utilization.
Citation: Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155:152-159.
Stopping Smoking at Any Time before Surgery Is Safe
Clinical question: Is smoking cessation within eight weeks of surgery safe?
Background: Smoking cessation before surgery can decrease the risk of surgical complications. However, several studies found increased risk for perioperative complications when smoking was stopped within eight weeks of surgery. These findings created uncertainty about general safety of tobacco cessation counseling before surgery.
Study design: Systematic review and meta-analysis.
Setting: Smokers undergoing any type of surgery.
Synopsis: The authors identified nine studies involving 889 patients that compared smokers who quit within eight weeks of surgery with those who continued to smoke. There was considerable heterogeneity in the studies but no overall difference in perioperative complications between those who quit smoking and those who continued to smoke (OR 0.78, 95% CI, 0.57-1.07). The subset of studies examining pulmonary complications also found no difference (OR 1.18, 95% CI, 0.95-1.46).
Bottom line: Smoking cessation at any time before surgery appears to be safe.
Citation: Myers K, Hajek P, Hinds C, McRobbie H. Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis. Arch Intern Med. 2011;171:983-989.
Hospitalization for Infection Increases Risk of Stroke
Clinical question: Can infection act as a precipitant for acute ischemic stroke?
Background: Little is known about precipitants of acute ischemic stroke. Severe infections have been shown to promote hypercoagulability and platelet activation, and to induce endothelial dysfunction. Authors postulated that infections severe enough to warrant hospitalization might transiently increase the risk for stroke.
Study design: Case-crossover analysis of data from a multicenter prospective cohort (Cardiovascular Health Study).
Setting: Medicare patients in four communities.
Synopsis: During a median follow-up of 12.2 years, 669 strokes occurred in 5,639 study participants. Hospitalization for infection within 14 days was associated with increased risk of stroke (OR 8.0, 95% CI, 1.6-77.3), and the risk remained elevated for hospitalizations within 90 days (OR 3.4, 95% CI, 1.8-6.5). The findings remained significant after adjusting for comorbidities, including age, sex, race, smoking, and diabetes. The number of patients hospitalized for infection before stroke was small—eight within 14 days, and 29 within 90 days.
Bottom line: Infection severe enough to require hospitalization may act as a trigger for acute ischemic stroke.
Citation: Elkind MS, Carty CL, O’Meara ES, et al. Hospitalization for infection and risk of acute ischemic stroke: the Cardiovascular Health Study. Stroke. 2011;42:1851-1856.
Longer Duration of Perioperative Antibiotics May Be Beneficial after Cardiac Surgery
Clinical question: Is antibiotic prophylaxis for 24 or more hours better than shorter duration of treatment after cardiac surgery?
Background: Sternal surgical site infections are a serious complication of cardiac surgery. The optimal duration of perioperative antibiotic prophylaxis is not known, with recommendations ranging from a single dose to 72 hours. The Society of Thoracic Surgeons’ recommendation for 24 to 72 hours of prophylaxis is not based on a systematic review and meta-analysis.
Study design: Systematic review and meta-analysis.
Setting: Adult patients undergoing open-heart surgery who received perioperative antibiotic prophylaxis.
Synopsis: Authors identified 12 trials encompassing 7,893 patients. Compared with prophylaxis of ≥24 hours, prophylaxis of <24 hours was associated with a higher risk of sternal surgical site infections (RR 1.38, 95% CI, 1.13-1.69) and deep infections (RR 1.68, 95% CI, 1.12-2.53). There was no difference in mortality, other infections, or adverse events. Most studies had methodological limitations with a high risk for bias.
Bottom line: Perioperative antibiotic prophylaxis of ≥24 hours reduces sternal surgical infections.
Citation: Mertz D, Johnstone J, Loeb M. Does duration of perioperative antibiotic prophylaxis matter in cardiac surgery? A systematic review and meta-analysis. Ann Surg. 2011;254:48-54.
Stroke Unit Care Combined with Early Supported Discharge Improves Outcomes
Clinical question: Does early supported discharge (ESD) improve outcomes more than conventional follow-up in stroke patients?
Background: ESD is a mobile team that coordinates follow-up and rehabilitation. Previous studies have shown it to be beneficial in patients with mild to moderate disability at one year, but long-term effects of ESD are not known.
Study design: Randomized controlled trial.
Setting: Single center in Norway.
Synopsis: Stroke-unit patients were recruited and received standard care or ESD after discharge. All 320 patients received standard acute care. The proportion of patients with modified Rankin Score (mRS) of ≤2 was not significantly different in the two groups but identified a trend toward improvement in the intervention group (38% vs. 30%, P=0.106). More patients receiving conventional follow-up died or were institutionalized (P=0.032) but mortality rates at five years were similar (ESD 46% vs. 51%). Secondary outcomes (Scandinavian Stroke Scale, Barthel Index, Frenchay Activity Index, and Mini Mental Status Examination) were not statistically different. Predictors of good outcome in the ESD group included young age, low mRS, and living with others.
This study recruited patients from 1995 to 1997 and followed the patients for five years. Limitations to the applicability include advances in stroke rehabilitation in the last 10 years. The cost of a mobile multidisciplinary team consisting of a physiotherapist, occupational therapist, nurse, and part-time physician was not discussed and may limit the availability to many patients.
Bottom line: Early supported discharge may increase the proportion of patients living at home five years after stroke.
Citation: Fjaertoft H, Rohweder G, Indredavik B. Stroke unit care combined with early supported discharge improves 5-year outcome: a randomized controlled trial. Stroke. 2011;42:1707-1711.
Criteria May Help Identify Patients at Risk for Infective Endocarditis
Clinical question: Which patients with Staphylococcus aureus bacteremia benefit the most from transesophageal echocardiography?
Background: Infective endocarditis is a serious complication of S. aureus bacteremia (SAB), occurring in 5% to 17% of patients with documented SAB. It has been recommended to perform transesophageal echocardiography (TEE) in all patients with SAB. Large variation exists in rates of TEE, and identifying patients at low risk for endocarditis may help with more appropriate utilization of this test.
Study design: Retrospective cohort analysis.
Setting: Two university-based German tertiary hospitals (INSTINCT cohort) and one North American university-based hospital from October 1994 to December 2009 (SABG cohort).
Synopsis: A total of 736 cases of nosocomial SAB were analyzed. Age, source of infection, and 30-day and 90-day case fatality rates were similar between the two cohorts. Patients were followed during the index hospitalization and for three months after discharge.
Patients with infective endocarditis were more likely to have prolonged bacteremia; a permanent intracardiac device, such as a pacemaker or a heart valve; be recipients of hemodialysis; and have osteomyelitis. Of the 83 patients who did not fulfill any of the prediction criteria, no cases of infective endocarditis were found.
Bottom line: A set of simple criteria may help identify patients with nosocomial SAB who are at risk for infective endocarditis. The subset of patients who do not meet any of these criteria may not need diagnostic evaluation with TEE.
Citation: Kaasch, AJ, Fowler VG Jr., Rieg S, et al. Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia. Clin Infect Dis. 2011;53:1-9.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Use of a Care-Transitions Intervention Reduces 30-Day Hospital Readmissions
- Routine Chest Radiographs after Pneumonia to Rule Out Lung Cancer Have Low Diagnostic Yield
- Hospitalist Care Shifts Costs to the Outpatient Environment
- Stopping Smoking at Any Time before Surgery Is Safe
- Hospitalization for Infection Increases Risk of Stroke
- Longer Duration of Perioperative Antibiotics May Be Beneficial after Cardiac Surgery
- Stroke Unit Care Combined with Early Supported Discharge Improves Outcomes
- Criteria May Help Identify Patients at Risk for Infective Endocarditis
Use of a Care-Transitions Intervention Reduces 30-Day Hospital Readmissions
Clinical question: Does use of a specific care-transitions intervention (CTI) reduce 30-day hospital readmissions in a nonintegrated healthcare system?
Background: Previous interventions addressing improved communication between members of the healthcare team, patients, and families at time of discharge show promise for reducing hospital readmissions. Although these interventions revealed positive results, no research has been completed within a system where healthcare is integrated across settings.
Study design: Quasi-experimental prospective cohort study.
Setting: Six Rhode Island acute-care hospitals, including two community hospitals, three teaching hospitals, and a tertiary-care center and teaching hospital. Facilities ranged from 129 beds to 719 beds.
Synopsis: The CTI is a patient-centered intervention occurring across 30 days. The intervention includes a home visit by a coach within three days of hospital discharge, a telephone call within seven to 10 days of discharge, and a final telephone call no later than 30 days after admission. During these contacts, coaches encourage patient and family participation in care, and active communication with their primary-care provider regarding their disease state. A convenience sample of fee-for-service Medicare beneficiaries was identified by admission diagnoses of acute myocardial infarction, congestive heart failure, or specific pulmonary conditions. Overall, 74% participants completed the entire intervention. The odds of a hospital readmission were significantly lower in the intervention population compared with those who did not receive the intervention (OR 0.61; 95% CI, 0.42-0.88).
Study design: Study design was limited by ability to provide coaching (only 8% of total population was approached), and therefore may not be representative of a typical integrated healthcare setting. In addition, the sample consisted of a convenience sample, which may limit generalizability.
Bottom line: The CTI appears to decrease the rate of 30-day hospital readmissions in Medicare patients with certain cardiac and pulmonary diagnoses.
Citation: Voss R, Gardner R, Baier R, Butterfield K, Lehrman S, Gravenstein S. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171:1232-1237.
Routine Chest Radiographs after Pneumonia to Rule Out Lung Cancer Have Low Diagnostic Yield
Clinical question: What is the incidence of new lung cancer detected on routine post-pneumonia chest radiographs?
Background: Routine chest radiographs have been recommended four to eight weeks after resolution of pneumonia to exclude underlying lung cancer. The diagnostic yield of this practice is uncertain.
Study design: Population-based cohort.
Setting: Seven emergency departments and six hospitals in Edmonton, Alberta, Canada.
Synopsis: Authors enrolled 3,398 patients with clinical and radiographic evidence of pneumonia. Of these, 59% were aged 50 and older, 52% were male, 17% were current smokers, 18% had COPD, and 49% were treated as inpatients. At 90-day follow-up, 1.1% of patients received a new diagnosis of lung cancer, with incidence steadily increasing to 2.2% at three-year follow-up. In multivariate analysis, age 50 and older, male sex, and current smoking were independent predictors of post-pneumonia new lung cancer diagnosis. Limiting follow-up chest radiographs to patients aged 50 and older would have detected 98% of new lung cancers and improved diagnostic yield to 2.8%.
Bottom line: Routine post-pneumonia chest radiographs for lung cancer screening have low diagnostic yield that is only marginally improved by selecting high-risk populations.
Citation: Tang KL, Eurich DT, Minhas-Sandhu JK, Marrie TJ, Majumdar SR. Incidence, correlates, and chest radiographic yield of new lung cancer diagnosis in 3398 patients with pneumonia. Arch Intern Med. 2011;171:1193-1198.
Hospitalist Care Shifts Costs to the Outpatient Environment
Clinical question: How does hospitalist care affect medical utilization costs after hospital discharge?
Background: The number of patients cared for by hospitalists is growing rapidly. Some studies have shown hospitalists to decrease length of stay and inpatient costs. The impact of shorter hospitalization on outpatient medical utilization and costs is not known.
Study design: Population-based national cohort.
Setting: Hospitalized Medicare patients.
Synopsis: In this study of 58,125 Medicare admissions at 454 hospitals, hospitalist care was associated with a 0.64-day shorter adjusted length of stay and $282 lower hospital charges compared with patients cared for by their primary-care physicians (PCPs). This was offset by $332 higher Medicare spending in the 30 days following hospitalization. Patients cared for by hospitalists were less likely to be discharged home (OR 0.82, 95% CI, 0.78-0.86), and were more likely to require emergency department visits (OR 1.18, 95% CI, 1.12-1.24) and readmissions (OR 1.08, 95% CI, 1.02-1.14). The authors postulate that shorter length of stay associated with hospitalist care is achieved at the expense of shifting costs to the outpatient environment. The discharged patients are sicker and, as a result, require more skilled care and repeat hospital visits.
Bottom line: Hospitalist care may be associated with higher overall costs and more medical utilization.
Citation: Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155:152-159.
Stopping Smoking at Any Time before Surgery Is Safe
Clinical question: Is smoking cessation within eight weeks of surgery safe?
Background: Smoking cessation before surgery can decrease the risk of surgical complications. However, several studies found increased risk for perioperative complications when smoking was stopped within eight weeks of surgery. These findings created uncertainty about general safety of tobacco cessation counseling before surgery.
Study design: Systematic review and meta-analysis.
Setting: Smokers undergoing any type of surgery.
Synopsis: The authors identified nine studies involving 889 patients that compared smokers who quit within eight weeks of surgery with those who continued to smoke. There was considerable heterogeneity in the studies but no overall difference in perioperative complications between those who quit smoking and those who continued to smoke (OR 0.78, 95% CI, 0.57-1.07). The subset of studies examining pulmonary complications also found no difference (OR 1.18, 95% CI, 0.95-1.46).
Bottom line: Smoking cessation at any time before surgery appears to be safe.
Citation: Myers K, Hajek P, Hinds C, McRobbie H. Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis. Arch Intern Med. 2011;171:983-989.
Hospitalization for Infection Increases Risk of Stroke
Clinical question: Can infection act as a precipitant for acute ischemic stroke?
Background: Little is known about precipitants of acute ischemic stroke. Severe infections have been shown to promote hypercoagulability and platelet activation, and to induce endothelial dysfunction. Authors postulated that infections severe enough to warrant hospitalization might transiently increase the risk for stroke.
Study design: Case-crossover analysis of data from a multicenter prospective cohort (Cardiovascular Health Study).
Setting: Medicare patients in four communities.
Synopsis: During a median follow-up of 12.2 years, 669 strokes occurred in 5,639 study participants. Hospitalization for infection within 14 days was associated with increased risk of stroke (OR 8.0, 95% CI, 1.6-77.3), and the risk remained elevated for hospitalizations within 90 days (OR 3.4, 95% CI, 1.8-6.5). The findings remained significant after adjusting for comorbidities, including age, sex, race, smoking, and diabetes. The number of patients hospitalized for infection before stroke was small—eight within 14 days, and 29 within 90 days.
Bottom line: Infection severe enough to require hospitalization may act as a trigger for acute ischemic stroke.
Citation: Elkind MS, Carty CL, O’Meara ES, et al. Hospitalization for infection and risk of acute ischemic stroke: the Cardiovascular Health Study. Stroke. 2011;42:1851-1856.
Longer Duration of Perioperative Antibiotics May Be Beneficial after Cardiac Surgery
Clinical question: Is antibiotic prophylaxis for 24 or more hours better than shorter duration of treatment after cardiac surgery?
Background: Sternal surgical site infections are a serious complication of cardiac surgery. The optimal duration of perioperative antibiotic prophylaxis is not known, with recommendations ranging from a single dose to 72 hours. The Society of Thoracic Surgeons’ recommendation for 24 to 72 hours of prophylaxis is not based on a systematic review and meta-analysis.
Study design: Systematic review and meta-analysis.
Setting: Adult patients undergoing open-heart surgery who received perioperative antibiotic prophylaxis.
Synopsis: Authors identified 12 trials encompassing 7,893 patients. Compared with prophylaxis of ≥24 hours, prophylaxis of <24 hours was associated with a higher risk of sternal surgical site infections (RR 1.38, 95% CI, 1.13-1.69) and deep infections (RR 1.68, 95% CI, 1.12-2.53). There was no difference in mortality, other infections, or adverse events. Most studies had methodological limitations with a high risk for bias.
Bottom line: Perioperative antibiotic prophylaxis of ≥24 hours reduces sternal surgical infections.
Citation: Mertz D, Johnstone J, Loeb M. Does duration of perioperative antibiotic prophylaxis matter in cardiac surgery? A systematic review and meta-analysis. Ann Surg. 2011;254:48-54.
Stroke Unit Care Combined with Early Supported Discharge Improves Outcomes
Clinical question: Does early supported discharge (ESD) improve outcomes more than conventional follow-up in stroke patients?
Background: ESD is a mobile team that coordinates follow-up and rehabilitation. Previous studies have shown it to be beneficial in patients with mild to moderate disability at one year, but long-term effects of ESD are not known.
Study design: Randomized controlled trial.
Setting: Single center in Norway.
Synopsis: Stroke-unit patients were recruited and received standard care or ESD after discharge. All 320 patients received standard acute care. The proportion of patients with modified Rankin Score (mRS) of ≤2 was not significantly different in the two groups but identified a trend toward improvement in the intervention group (38% vs. 30%, P=0.106). More patients receiving conventional follow-up died or were institutionalized (P=0.032) but mortality rates at five years were similar (ESD 46% vs. 51%). Secondary outcomes (Scandinavian Stroke Scale, Barthel Index, Frenchay Activity Index, and Mini Mental Status Examination) were not statistically different. Predictors of good outcome in the ESD group included young age, low mRS, and living with others.
This study recruited patients from 1995 to 1997 and followed the patients for five years. Limitations to the applicability include advances in stroke rehabilitation in the last 10 years. The cost of a mobile multidisciplinary team consisting of a physiotherapist, occupational therapist, nurse, and part-time physician was not discussed and may limit the availability to many patients.
Bottom line: Early supported discharge may increase the proportion of patients living at home five years after stroke.
Citation: Fjaertoft H, Rohweder G, Indredavik B. Stroke unit care combined with early supported discharge improves 5-year outcome: a randomized controlled trial. Stroke. 2011;42:1707-1711.
Criteria May Help Identify Patients at Risk for Infective Endocarditis
Clinical question: Which patients with Staphylococcus aureus bacteremia benefit the most from transesophageal echocardiography?
Background: Infective endocarditis is a serious complication of S. aureus bacteremia (SAB), occurring in 5% to 17% of patients with documented SAB. It has been recommended to perform transesophageal echocardiography (TEE) in all patients with SAB. Large variation exists in rates of TEE, and identifying patients at low risk for endocarditis may help with more appropriate utilization of this test.
Study design: Retrospective cohort analysis.
Setting: Two university-based German tertiary hospitals (INSTINCT cohort) and one North American university-based hospital from October 1994 to December 2009 (SABG cohort).
Synopsis: A total of 736 cases of nosocomial SAB were analyzed. Age, source of infection, and 30-day and 90-day case fatality rates were similar between the two cohorts. Patients were followed during the index hospitalization and for three months after discharge.
Patients with infective endocarditis were more likely to have prolonged bacteremia; a permanent intracardiac device, such as a pacemaker or a heart valve; be recipients of hemodialysis; and have osteomyelitis. Of the 83 patients who did not fulfill any of the prediction criteria, no cases of infective endocarditis were found.
Bottom line: A set of simple criteria may help identify patients with nosocomial SAB who are at risk for infective endocarditis. The subset of patients who do not meet any of these criteria may not need diagnostic evaluation with TEE.
Citation: Kaasch, AJ, Fowler VG Jr., Rieg S, et al. Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia. Clin Infect Dis. 2011;53:1-9.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Use of a Care-Transitions Intervention Reduces 30-Day Hospital Readmissions
- Routine Chest Radiographs after Pneumonia to Rule Out Lung Cancer Have Low Diagnostic Yield
- Hospitalist Care Shifts Costs to the Outpatient Environment
- Stopping Smoking at Any Time before Surgery Is Safe
- Hospitalization for Infection Increases Risk of Stroke
- Longer Duration of Perioperative Antibiotics May Be Beneficial after Cardiac Surgery
- Stroke Unit Care Combined with Early Supported Discharge Improves Outcomes
- Criteria May Help Identify Patients at Risk for Infective Endocarditis
Use of a Care-Transitions Intervention Reduces 30-Day Hospital Readmissions
Clinical question: Does use of a specific care-transitions intervention (CTI) reduce 30-day hospital readmissions in a nonintegrated healthcare system?
Background: Previous interventions addressing improved communication between members of the healthcare team, patients, and families at time of discharge show promise for reducing hospital readmissions. Although these interventions revealed positive results, no research has been completed within a system where healthcare is integrated across settings.
Study design: Quasi-experimental prospective cohort study.
Setting: Six Rhode Island acute-care hospitals, including two community hospitals, three teaching hospitals, and a tertiary-care center and teaching hospital. Facilities ranged from 129 beds to 719 beds.
Synopsis: The CTI is a patient-centered intervention occurring across 30 days. The intervention includes a home visit by a coach within three days of hospital discharge, a telephone call within seven to 10 days of discharge, and a final telephone call no later than 30 days after admission. During these contacts, coaches encourage patient and family participation in care, and active communication with their primary-care provider regarding their disease state. A convenience sample of fee-for-service Medicare beneficiaries was identified by admission diagnoses of acute myocardial infarction, congestive heart failure, or specific pulmonary conditions. Overall, 74% participants completed the entire intervention. The odds of a hospital readmission were significantly lower in the intervention population compared with those who did not receive the intervention (OR 0.61; 95% CI, 0.42-0.88).
Study design: Study design was limited by ability to provide coaching (only 8% of total population was approached), and therefore may not be representative of a typical integrated healthcare setting. In addition, the sample consisted of a convenience sample, which may limit generalizability.
Bottom line: The CTI appears to decrease the rate of 30-day hospital readmissions in Medicare patients with certain cardiac and pulmonary diagnoses.
Citation: Voss R, Gardner R, Baier R, Butterfield K, Lehrman S, Gravenstein S. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171:1232-1237.
Routine Chest Radiographs after Pneumonia to Rule Out Lung Cancer Have Low Diagnostic Yield
Clinical question: What is the incidence of new lung cancer detected on routine post-pneumonia chest radiographs?
Background: Routine chest radiographs have been recommended four to eight weeks after resolution of pneumonia to exclude underlying lung cancer. The diagnostic yield of this practice is uncertain.
Study design: Population-based cohort.
Setting: Seven emergency departments and six hospitals in Edmonton, Alberta, Canada.
Synopsis: Authors enrolled 3,398 patients with clinical and radiographic evidence of pneumonia. Of these, 59% were aged 50 and older, 52% were male, 17% were current smokers, 18% had COPD, and 49% were treated as inpatients. At 90-day follow-up, 1.1% of patients received a new diagnosis of lung cancer, with incidence steadily increasing to 2.2% at three-year follow-up. In multivariate analysis, age 50 and older, male sex, and current smoking were independent predictors of post-pneumonia new lung cancer diagnosis. Limiting follow-up chest radiographs to patients aged 50 and older would have detected 98% of new lung cancers and improved diagnostic yield to 2.8%.
Bottom line: Routine post-pneumonia chest radiographs for lung cancer screening have low diagnostic yield that is only marginally improved by selecting high-risk populations.
Citation: Tang KL, Eurich DT, Minhas-Sandhu JK, Marrie TJ, Majumdar SR. Incidence, correlates, and chest radiographic yield of new lung cancer diagnosis in 3398 patients with pneumonia. Arch Intern Med. 2011;171:1193-1198.
Hospitalist Care Shifts Costs to the Outpatient Environment
Clinical question: How does hospitalist care affect medical utilization costs after hospital discharge?
Background: The number of patients cared for by hospitalists is growing rapidly. Some studies have shown hospitalists to decrease length of stay and inpatient costs. The impact of shorter hospitalization on outpatient medical utilization and costs is not known.
Study design: Population-based national cohort.
Setting: Hospitalized Medicare patients.
Synopsis: In this study of 58,125 Medicare admissions at 454 hospitals, hospitalist care was associated with a 0.64-day shorter adjusted length of stay and $282 lower hospital charges compared with patients cared for by their primary-care physicians (PCPs). This was offset by $332 higher Medicare spending in the 30 days following hospitalization. Patients cared for by hospitalists were less likely to be discharged home (OR 0.82, 95% CI, 0.78-0.86), and were more likely to require emergency department visits (OR 1.18, 95% CI, 1.12-1.24) and readmissions (OR 1.08, 95% CI, 1.02-1.14). The authors postulate that shorter length of stay associated with hospitalist care is achieved at the expense of shifting costs to the outpatient environment. The discharged patients are sicker and, as a result, require more skilled care and repeat hospital visits.
Bottom line: Hospitalist care may be associated with higher overall costs and more medical utilization.
Citation: Kuo YF, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155:152-159.
Stopping Smoking at Any Time before Surgery Is Safe
Clinical question: Is smoking cessation within eight weeks of surgery safe?
Background: Smoking cessation before surgery can decrease the risk of surgical complications. However, several studies found increased risk for perioperative complications when smoking was stopped within eight weeks of surgery. These findings created uncertainty about general safety of tobacco cessation counseling before surgery.
Study design: Systematic review and meta-analysis.
Setting: Smokers undergoing any type of surgery.
Synopsis: The authors identified nine studies involving 889 patients that compared smokers who quit within eight weeks of surgery with those who continued to smoke. There was considerable heterogeneity in the studies but no overall difference in perioperative complications between those who quit smoking and those who continued to smoke (OR 0.78, 95% CI, 0.57-1.07). The subset of studies examining pulmonary complications also found no difference (OR 1.18, 95% CI, 0.95-1.46).
Bottom line: Smoking cessation at any time before surgery appears to be safe.
Citation: Myers K, Hajek P, Hinds C, McRobbie H. Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis. Arch Intern Med. 2011;171:983-989.
Hospitalization for Infection Increases Risk of Stroke
Clinical question: Can infection act as a precipitant for acute ischemic stroke?
Background: Little is known about precipitants of acute ischemic stroke. Severe infections have been shown to promote hypercoagulability and platelet activation, and to induce endothelial dysfunction. Authors postulated that infections severe enough to warrant hospitalization might transiently increase the risk for stroke.
Study design: Case-crossover analysis of data from a multicenter prospective cohort (Cardiovascular Health Study).
Setting: Medicare patients in four communities.
Synopsis: During a median follow-up of 12.2 years, 669 strokes occurred in 5,639 study participants. Hospitalization for infection within 14 days was associated with increased risk of stroke (OR 8.0, 95% CI, 1.6-77.3), and the risk remained elevated for hospitalizations within 90 days (OR 3.4, 95% CI, 1.8-6.5). The findings remained significant after adjusting for comorbidities, including age, sex, race, smoking, and diabetes. The number of patients hospitalized for infection before stroke was small—eight within 14 days, and 29 within 90 days.
Bottom line: Infection severe enough to require hospitalization may act as a trigger for acute ischemic stroke.
Citation: Elkind MS, Carty CL, O’Meara ES, et al. Hospitalization for infection and risk of acute ischemic stroke: the Cardiovascular Health Study. Stroke. 2011;42:1851-1856.
Longer Duration of Perioperative Antibiotics May Be Beneficial after Cardiac Surgery
Clinical question: Is antibiotic prophylaxis for 24 or more hours better than shorter duration of treatment after cardiac surgery?
Background: Sternal surgical site infections are a serious complication of cardiac surgery. The optimal duration of perioperative antibiotic prophylaxis is not known, with recommendations ranging from a single dose to 72 hours. The Society of Thoracic Surgeons’ recommendation for 24 to 72 hours of prophylaxis is not based on a systematic review and meta-analysis.
Study design: Systematic review and meta-analysis.
Setting: Adult patients undergoing open-heart surgery who received perioperative antibiotic prophylaxis.
Synopsis: Authors identified 12 trials encompassing 7,893 patients. Compared with prophylaxis of ≥24 hours, prophylaxis of <24 hours was associated with a higher risk of sternal surgical site infections (RR 1.38, 95% CI, 1.13-1.69) and deep infections (RR 1.68, 95% CI, 1.12-2.53). There was no difference in mortality, other infections, or adverse events. Most studies had methodological limitations with a high risk for bias.
Bottom line: Perioperative antibiotic prophylaxis of ≥24 hours reduces sternal surgical infections.
Citation: Mertz D, Johnstone J, Loeb M. Does duration of perioperative antibiotic prophylaxis matter in cardiac surgery? A systematic review and meta-analysis. Ann Surg. 2011;254:48-54.
Stroke Unit Care Combined with Early Supported Discharge Improves Outcomes
Clinical question: Does early supported discharge (ESD) improve outcomes more than conventional follow-up in stroke patients?
Background: ESD is a mobile team that coordinates follow-up and rehabilitation. Previous studies have shown it to be beneficial in patients with mild to moderate disability at one year, but long-term effects of ESD are not known.
Study design: Randomized controlled trial.
Setting: Single center in Norway.
Synopsis: Stroke-unit patients were recruited and received standard care or ESD after discharge. All 320 patients received standard acute care. The proportion of patients with modified Rankin Score (mRS) of ≤2 was not significantly different in the two groups but identified a trend toward improvement in the intervention group (38% vs. 30%, P=0.106). More patients receiving conventional follow-up died or were institutionalized (P=0.032) but mortality rates at five years were similar (ESD 46% vs. 51%). Secondary outcomes (Scandinavian Stroke Scale, Barthel Index, Frenchay Activity Index, and Mini Mental Status Examination) were not statistically different. Predictors of good outcome in the ESD group included young age, low mRS, and living with others.
This study recruited patients from 1995 to 1997 and followed the patients for five years. Limitations to the applicability include advances in stroke rehabilitation in the last 10 years. The cost of a mobile multidisciplinary team consisting of a physiotherapist, occupational therapist, nurse, and part-time physician was not discussed and may limit the availability to many patients.
Bottom line: Early supported discharge may increase the proportion of patients living at home five years after stroke.
Citation: Fjaertoft H, Rohweder G, Indredavik B. Stroke unit care combined with early supported discharge improves 5-year outcome: a randomized controlled trial. Stroke. 2011;42:1707-1711.
Criteria May Help Identify Patients at Risk for Infective Endocarditis
Clinical question: Which patients with Staphylococcus aureus bacteremia benefit the most from transesophageal echocardiography?
Background: Infective endocarditis is a serious complication of S. aureus bacteremia (SAB), occurring in 5% to 17% of patients with documented SAB. It has been recommended to perform transesophageal echocardiography (TEE) in all patients with SAB. Large variation exists in rates of TEE, and identifying patients at low risk for endocarditis may help with more appropriate utilization of this test.
Study design: Retrospective cohort analysis.
Setting: Two university-based German tertiary hospitals (INSTINCT cohort) and one North American university-based hospital from October 1994 to December 2009 (SABG cohort).
Synopsis: A total of 736 cases of nosocomial SAB were analyzed. Age, source of infection, and 30-day and 90-day case fatality rates were similar between the two cohorts. Patients were followed during the index hospitalization and for three months after discharge.
Patients with infective endocarditis were more likely to have prolonged bacteremia; a permanent intracardiac device, such as a pacemaker or a heart valve; be recipients of hemodialysis; and have osteomyelitis. Of the 83 patients who did not fulfill any of the prediction criteria, no cases of infective endocarditis were found.
Bottom line: A set of simple criteria may help identify patients with nosocomial SAB who are at risk for infective endocarditis. The subset of patients who do not meet any of these criteria may not need diagnostic evaluation with TEE.
Citation: Kaasch, AJ, Fowler VG Jr., Rieg S, et al. Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia. Clin Infect Dis. 2011;53:1-9.
Politics of Medicare Cuts
It reads like a brainteaser from hell: Twelve members of Congress must identify at least $1.2 trillion to cut from the federal budget over the next 10 years. Social Security cuts are a virtual nonstarter with Democrats. Tax hikes on the wealthy are anathema to Republicans. Significant Medicare cuts will invoke the wrath of seniors. The Joint Select Committee on Deficit Reduction, evenly split between both political parties, must somehow reach a majority agreement on what to trim by the Nov. 23 deadline. Then the full Congress must approve the committee’s recommendations by Dec. 23.
Here’s another caveat: In a Sept. 20 letter, SHM and 117 other medical groups urged the deficit reduction “super-committee” to “include a full repeal of the fatally flawed Medicare sustainable growth rate (SGR) formula in its final legislation.” Unless Congress repeals or delays the widely despised SGR mechanism, Medicare reimbursement rates for doctors will be cut by a catastrophic 29.4% in January. A full repeal, however, could cost $300 billion or more over 10 years, according to estimates by the nonpartisan Congressional Budget Office (CBO). If the super-committee takes up the SGR challenge, it will need to find at least $1.5 trillion worth of mutually agreeable cuts.
In a final twist, President Obama has threatened to veto any deficit reduction plan that slashes Medicare benefits and fails to raise taxes on the wealthy. The punchline is that unless the divided super-committee, a polarized Congress, and the president can all agree, $1.2 trillion in domestic and military spending cuts will automatically kick in, giving both political parties a lump of coal just in time for Christmas.
If any solution is possible, it might have to rely on some old numbers regarding potential cuts to Medicare and other federal programs. “There’s no time to develop new policy,” says Joseph Antos, PhD, a health policy expert at the American Enterprise Institute, a conservative think tank. “The old ideas that have been kicking around for years are scorable [by the CBO], and because they’ve been around for so long, it’s easier to write the legislative language.”
Here’s a look at perennial Medicare proposals and the chances of their inclusion in serious deficit-reduction negotiations.
—Joseph Antos, PhD, health policy expert, American Enterprise Institute, Washington, D.C.
Reduced Payments
Obama’s proposal to the super-committee includes $248 billion in Medicare cuts and savings. Of most direct relevance to hospitalists, about $57 billion comes from reduced payments to providers over 10 years. The proposal would reduce Indirect Medical Education add-on payments to teaching hospitals by 10%, end an add-on payment for hospitals and physicians in low-population states, and reduce payments to post-acute-care facilities.
Separately, the Medicare Payment Advisory Commission (MedPAC) released a proposal that would save $233 billion over 10 years—designed in large part to offset the costs necessary for a permanent SGR fix. Among its suggestions, the MedPAC proposal would freeze reimbursements for primary-care providers (PCPs) and trim payments to specialists by 5.9% per year for three years. Despite agreement by virtually everyone that the SGR has to go, groups like the Alliance of Specialty Medicine and American College of Surgeons have expressed concerns with MedPAC’s suggested offsets.
Dr. Antos says MedPAC has adopted the view that preventing the 29.4% cut in Medicare reimbursements will require spreading the pain more generally throughout the health sector. “That makes sense until you realize that politically, when you do that, you just generate lots of resistance from lots of organizations,” he says. So what about the SGR? Dr. Antos sees a permanent fix this year as “extremely unlikely,” especially given the general pessimism over the super-committee’s ability to agree on $1.2 trillion in cuts. Instead, he predicts a two-year fix that would require tens of billions in offsets but delay (yet again) more difficult political choices until after the 2012 elections. “They definitely do not want to be arguing about this next fall,” he says.
Drug Rebates
Under the president’s proposal, Medicare would receive the same rebates as Medicaid’s discount for brand name and generic drugs given to beneficiaries under the Medicare Low-Income Subsidy. This proposal alone is estimated to net some $135 billion in savings over 10 years, an inclusion that Judith Stein, executive director of the Center for Medicare Advocacy, says her organization was “delighted” to see. “We think that’s extremely reasonable, fair, good public policy, and good economic policy,” she says. Left-leaning groups are particularly vehement on this issue, given Medicare’s prohibition against negotiating with pharmaceutical companies on drug prices, a restriction that other bulk buyers, such as the Veterans Administration, don’t face.
Dr. Antos expects some form of the president’s proposal to be taken seriously. “This is something that is easy to do, and I think politically, it’s easier to go after a supplier of products—and drugs are the biggest one—than it is to go after doctors or hospitals,” he says. “And it’s hardest to go after beneficiaries.”
Premium Surcharges
Another element of President Obama’s proposal would save $20 billion by increasing wealthier beneficiaries’ insurance premiums on prescription drugs and doctors’ services. Beginning in 2017, income-based premiums for Medicare Part B and Part D both would rise by 15% for beneficiaries earning more than $85,000 annually.
AARP opposes the idea, and Stein says she’s concerned about the overall notion of basing Medicare premiums on income. “The problem is that we want to keep higher-income people satisfied with the Medicare program, because they’re the ones that get listened to,” Stein says.
Austin Frakt, PhD, a healthcare economist at Boston University, makes a similar point in a recent Health Affairs blog post: “The wealthy are a potential source of revenue for Medicare but also possess the means to finance the most strident challenge to it,” he writes. Even so, Stein says, “it’s easier to swallow than some other things,” especially if drug companies and others are required to share in the sacrifices.
Medicare Eligibility
President Obama’s proposal excludes any discussion about raising the age of Medicare eligibility, signaling a harder line on a change that Republicans and groups like the American Hospital Association have favored and that Obama himself floated as a trial balloon earlier this year. The Democratic base and AARP, however, rebelled against the notion, and Dr. Antos says the idea has “zero” chance of being included in the super-committee’s proposal. “This is the sort of thing that you don’t really want to bring up when you’re running for president, which is why the president backed off, and which is why the Republicans won’t be eager to see it, either,” he says.
Dr. Antos expects the eligible-age proposal to re-emerge in 2013, though he cautions against taking any “extravagant claims for savings” at face value. To be publicly acceptable, Medicare’s minimum age would need to rise slowly, he says, perhaps phased in over 20 years, and in a way that likely wouldn’t save a huge sum of money.
If Medicare raised its minimum age to 67 in 2014, the federal government would save roughly $5.7 billion, according to the nonprofit Center on Budget and Policy Priorities. In an “Incidental Economist” blog post, however, Dr. Frakt points out that the savings would simply shift the cost to beneficiaries, employers, private insurers, and others, a point echoed by Stein.
“All told, the cost to the system of raising the Medicare age to 67 would be $11.4 billion in 2014,” Dr. Frakt writes, “which is a high price to pay for $5.7 billion in federal savings.”
Bryn Nelson is a freelance medical writer based in Seattle.
It reads like a brainteaser from hell: Twelve members of Congress must identify at least $1.2 trillion to cut from the federal budget over the next 10 years. Social Security cuts are a virtual nonstarter with Democrats. Tax hikes on the wealthy are anathema to Republicans. Significant Medicare cuts will invoke the wrath of seniors. The Joint Select Committee on Deficit Reduction, evenly split between both political parties, must somehow reach a majority agreement on what to trim by the Nov. 23 deadline. Then the full Congress must approve the committee’s recommendations by Dec. 23.
Here’s another caveat: In a Sept. 20 letter, SHM and 117 other medical groups urged the deficit reduction “super-committee” to “include a full repeal of the fatally flawed Medicare sustainable growth rate (SGR) formula in its final legislation.” Unless Congress repeals or delays the widely despised SGR mechanism, Medicare reimbursement rates for doctors will be cut by a catastrophic 29.4% in January. A full repeal, however, could cost $300 billion or more over 10 years, according to estimates by the nonpartisan Congressional Budget Office (CBO). If the super-committee takes up the SGR challenge, it will need to find at least $1.5 trillion worth of mutually agreeable cuts.
In a final twist, President Obama has threatened to veto any deficit reduction plan that slashes Medicare benefits and fails to raise taxes on the wealthy. The punchline is that unless the divided super-committee, a polarized Congress, and the president can all agree, $1.2 trillion in domestic and military spending cuts will automatically kick in, giving both political parties a lump of coal just in time for Christmas.
If any solution is possible, it might have to rely on some old numbers regarding potential cuts to Medicare and other federal programs. “There’s no time to develop new policy,” says Joseph Antos, PhD, a health policy expert at the American Enterprise Institute, a conservative think tank. “The old ideas that have been kicking around for years are scorable [by the CBO], and because they’ve been around for so long, it’s easier to write the legislative language.”
Here’s a look at perennial Medicare proposals and the chances of their inclusion in serious deficit-reduction negotiations.
—Joseph Antos, PhD, health policy expert, American Enterprise Institute, Washington, D.C.
Reduced Payments
Obama’s proposal to the super-committee includes $248 billion in Medicare cuts and savings. Of most direct relevance to hospitalists, about $57 billion comes from reduced payments to providers over 10 years. The proposal would reduce Indirect Medical Education add-on payments to teaching hospitals by 10%, end an add-on payment for hospitals and physicians in low-population states, and reduce payments to post-acute-care facilities.
Separately, the Medicare Payment Advisory Commission (MedPAC) released a proposal that would save $233 billion over 10 years—designed in large part to offset the costs necessary for a permanent SGR fix. Among its suggestions, the MedPAC proposal would freeze reimbursements for primary-care providers (PCPs) and trim payments to specialists by 5.9% per year for three years. Despite agreement by virtually everyone that the SGR has to go, groups like the Alliance of Specialty Medicine and American College of Surgeons have expressed concerns with MedPAC’s suggested offsets.
Dr. Antos says MedPAC has adopted the view that preventing the 29.4% cut in Medicare reimbursements will require spreading the pain more generally throughout the health sector. “That makes sense until you realize that politically, when you do that, you just generate lots of resistance from lots of organizations,” he says. So what about the SGR? Dr. Antos sees a permanent fix this year as “extremely unlikely,” especially given the general pessimism over the super-committee’s ability to agree on $1.2 trillion in cuts. Instead, he predicts a two-year fix that would require tens of billions in offsets but delay (yet again) more difficult political choices until after the 2012 elections. “They definitely do not want to be arguing about this next fall,” he says.
Drug Rebates
Under the president’s proposal, Medicare would receive the same rebates as Medicaid’s discount for brand name and generic drugs given to beneficiaries under the Medicare Low-Income Subsidy. This proposal alone is estimated to net some $135 billion in savings over 10 years, an inclusion that Judith Stein, executive director of the Center for Medicare Advocacy, says her organization was “delighted” to see. “We think that’s extremely reasonable, fair, good public policy, and good economic policy,” she says. Left-leaning groups are particularly vehement on this issue, given Medicare’s prohibition against negotiating with pharmaceutical companies on drug prices, a restriction that other bulk buyers, such as the Veterans Administration, don’t face.
Dr. Antos expects some form of the president’s proposal to be taken seriously. “This is something that is easy to do, and I think politically, it’s easier to go after a supplier of products—and drugs are the biggest one—than it is to go after doctors or hospitals,” he says. “And it’s hardest to go after beneficiaries.”
Premium Surcharges
Another element of President Obama’s proposal would save $20 billion by increasing wealthier beneficiaries’ insurance premiums on prescription drugs and doctors’ services. Beginning in 2017, income-based premiums for Medicare Part B and Part D both would rise by 15% for beneficiaries earning more than $85,000 annually.
AARP opposes the idea, and Stein says she’s concerned about the overall notion of basing Medicare premiums on income. “The problem is that we want to keep higher-income people satisfied with the Medicare program, because they’re the ones that get listened to,” Stein says.
Austin Frakt, PhD, a healthcare economist at Boston University, makes a similar point in a recent Health Affairs blog post: “The wealthy are a potential source of revenue for Medicare but also possess the means to finance the most strident challenge to it,” he writes. Even so, Stein says, “it’s easier to swallow than some other things,” especially if drug companies and others are required to share in the sacrifices.
Medicare Eligibility
President Obama’s proposal excludes any discussion about raising the age of Medicare eligibility, signaling a harder line on a change that Republicans and groups like the American Hospital Association have favored and that Obama himself floated as a trial balloon earlier this year. The Democratic base and AARP, however, rebelled against the notion, and Dr. Antos says the idea has “zero” chance of being included in the super-committee’s proposal. “This is the sort of thing that you don’t really want to bring up when you’re running for president, which is why the president backed off, and which is why the Republicans won’t be eager to see it, either,” he says.
Dr. Antos expects the eligible-age proposal to re-emerge in 2013, though he cautions against taking any “extravagant claims for savings” at face value. To be publicly acceptable, Medicare’s minimum age would need to rise slowly, he says, perhaps phased in over 20 years, and in a way that likely wouldn’t save a huge sum of money.
If Medicare raised its minimum age to 67 in 2014, the federal government would save roughly $5.7 billion, according to the nonprofit Center on Budget and Policy Priorities. In an “Incidental Economist” blog post, however, Dr. Frakt points out that the savings would simply shift the cost to beneficiaries, employers, private insurers, and others, a point echoed by Stein.
“All told, the cost to the system of raising the Medicare age to 67 would be $11.4 billion in 2014,” Dr. Frakt writes, “which is a high price to pay for $5.7 billion in federal savings.”
Bryn Nelson is a freelance medical writer based in Seattle.
It reads like a brainteaser from hell: Twelve members of Congress must identify at least $1.2 trillion to cut from the federal budget over the next 10 years. Social Security cuts are a virtual nonstarter with Democrats. Tax hikes on the wealthy are anathema to Republicans. Significant Medicare cuts will invoke the wrath of seniors. The Joint Select Committee on Deficit Reduction, evenly split between both political parties, must somehow reach a majority agreement on what to trim by the Nov. 23 deadline. Then the full Congress must approve the committee’s recommendations by Dec. 23.
Here’s another caveat: In a Sept. 20 letter, SHM and 117 other medical groups urged the deficit reduction “super-committee” to “include a full repeal of the fatally flawed Medicare sustainable growth rate (SGR) formula in its final legislation.” Unless Congress repeals or delays the widely despised SGR mechanism, Medicare reimbursement rates for doctors will be cut by a catastrophic 29.4% in January. A full repeal, however, could cost $300 billion or more over 10 years, according to estimates by the nonpartisan Congressional Budget Office (CBO). If the super-committee takes up the SGR challenge, it will need to find at least $1.5 trillion worth of mutually agreeable cuts.
In a final twist, President Obama has threatened to veto any deficit reduction plan that slashes Medicare benefits and fails to raise taxes on the wealthy. The punchline is that unless the divided super-committee, a polarized Congress, and the president can all agree, $1.2 trillion in domestic and military spending cuts will automatically kick in, giving both political parties a lump of coal just in time for Christmas.
If any solution is possible, it might have to rely on some old numbers regarding potential cuts to Medicare and other federal programs. “There’s no time to develop new policy,” says Joseph Antos, PhD, a health policy expert at the American Enterprise Institute, a conservative think tank. “The old ideas that have been kicking around for years are scorable [by the CBO], and because they’ve been around for so long, it’s easier to write the legislative language.”
Here’s a look at perennial Medicare proposals and the chances of their inclusion in serious deficit-reduction negotiations.
—Joseph Antos, PhD, health policy expert, American Enterprise Institute, Washington, D.C.
Reduced Payments
Obama’s proposal to the super-committee includes $248 billion in Medicare cuts and savings. Of most direct relevance to hospitalists, about $57 billion comes from reduced payments to providers over 10 years. The proposal would reduce Indirect Medical Education add-on payments to teaching hospitals by 10%, end an add-on payment for hospitals and physicians in low-population states, and reduce payments to post-acute-care facilities.
Separately, the Medicare Payment Advisory Commission (MedPAC) released a proposal that would save $233 billion over 10 years—designed in large part to offset the costs necessary for a permanent SGR fix. Among its suggestions, the MedPAC proposal would freeze reimbursements for primary-care providers (PCPs) and trim payments to specialists by 5.9% per year for three years. Despite agreement by virtually everyone that the SGR has to go, groups like the Alliance of Specialty Medicine and American College of Surgeons have expressed concerns with MedPAC’s suggested offsets.
Dr. Antos says MedPAC has adopted the view that preventing the 29.4% cut in Medicare reimbursements will require spreading the pain more generally throughout the health sector. “That makes sense until you realize that politically, when you do that, you just generate lots of resistance from lots of organizations,” he says. So what about the SGR? Dr. Antos sees a permanent fix this year as “extremely unlikely,” especially given the general pessimism over the super-committee’s ability to agree on $1.2 trillion in cuts. Instead, he predicts a two-year fix that would require tens of billions in offsets but delay (yet again) more difficult political choices until after the 2012 elections. “They definitely do not want to be arguing about this next fall,” he says.
Drug Rebates
Under the president’s proposal, Medicare would receive the same rebates as Medicaid’s discount for brand name and generic drugs given to beneficiaries under the Medicare Low-Income Subsidy. This proposal alone is estimated to net some $135 billion in savings over 10 years, an inclusion that Judith Stein, executive director of the Center for Medicare Advocacy, says her organization was “delighted” to see. “We think that’s extremely reasonable, fair, good public policy, and good economic policy,” she says. Left-leaning groups are particularly vehement on this issue, given Medicare’s prohibition against negotiating with pharmaceutical companies on drug prices, a restriction that other bulk buyers, such as the Veterans Administration, don’t face.
Dr. Antos expects some form of the president’s proposal to be taken seriously. “This is something that is easy to do, and I think politically, it’s easier to go after a supplier of products—and drugs are the biggest one—than it is to go after doctors or hospitals,” he says. “And it’s hardest to go after beneficiaries.”
Premium Surcharges
Another element of President Obama’s proposal would save $20 billion by increasing wealthier beneficiaries’ insurance premiums on prescription drugs and doctors’ services. Beginning in 2017, income-based premiums for Medicare Part B and Part D both would rise by 15% for beneficiaries earning more than $85,000 annually.
AARP opposes the idea, and Stein says she’s concerned about the overall notion of basing Medicare premiums on income. “The problem is that we want to keep higher-income people satisfied with the Medicare program, because they’re the ones that get listened to,” Stein says.
Austin Frakt, PhD, a healthcare economist at Boston University, makes a similar point in a recent Health Affairs blog post: “The wealthy are a potential source of revenue for Medicare but also possess the means to finance the most strident challenge to it,” he writes. Even so, Stein says, “it’s easier to swallow than some other things,” especially if drug companies and others are required to share in the sacrifices.
Medicare Eligibility
President Obama’s proposal excludes any discussion about raising the age of Medicare eligibility, signaling a harder line on a change that Republicans and groups like the American Hospital Association have favored and that Obama himself floated as a trial balloon earlier this year. The Democratic base and AARP, however, rebelled against the notion, and Dr. Antos says the idea has “zero” chance of being included in the super-committee’s proposal. “This is the sort of thing that you don’t really want to bring up when you’re running for president, which is why the president backed off, and which is why the Republicans won’t be eager to see it, either,” he says.
Dr. Antos expects the eligible-age proposal to re-emerge in 2013, though he cautions against taking any “extravagant claims for savings” at face value. To be publicly acceptable, Medicare’s minimum age would need to rise slowly, he says, perhaps phased in over 20 years, and in a way that likely wouldn’t save a huge sum of money.
If Medicare raised its minimum age to 67 in 2014, the federal government would save roughly $5.7 billion, according to the nonprofit Center on Budget and Policy Priorities. In an “Incidental Economist” blog post, however, Dr. Frakt points out that the savings would simply shift the cost to beneficiaries, employers, private insurers, and others, a point echoed by Stein.
“All told, the cost to the system of raising the Medicare age to 67 would be $11.4 billion in 2014,” Dr. Frakt writes, “which is a high price to pay for $5.7 billion in federal savings.”
Bryn Nelson is a freelance medical writer based in Seattle.