User login
ONLINE EXCLUSIVE: The Case Against a Common Denominator for Urinary Tract Infections
The recent surge in attention to catheter-associated urinary tract infections (CAUTIs) has increased the focus on both preventing and removing inappropriate catheterizations. Ironically, one outcome rate currently reported by hospitals—the number of infections per 1,000 catheter days—could unfairly punish those facilities that are doing the most to address the problem.

—Sanjay Saint, MD, MPH, FHM, professor of internal medicine, University of Michigan, Ann Arbor VA Medical Center
“If your focus is on not putting in the catheter or removing a catheter as soon as possible, you now reduce that denominator of catheter days,” explains Sanjay Saint, MD, MPH, FHM, professor of internal medicine at the University of Michigan and the Ann Arbor VA Medical Center. “The only people who now get a catheter in your hospital are those who are pretty sick; therefore, they need a catheter. These people, because of their underlying sickness, are more likely to have an infection, so you may end up having a paradoxical increased rate of CAUTI after your successful initiative has reduced catheter use.”
Using the wrong denominator, in other words, could defeat the whole point: reducing infections by reducing catheter use.
“If we’re going to publicly report data, we have to make sure that the data we’re reporting and the metrics that we’re using are actually the best metrics for the intended purpose,” Dr. Saint says.
For quality-improvement (QI) efforts, his recommendation is to use 10,000 patient days as a more appropriate denominator.
The recent surge in attention to catheter-associated urinary tract infections (CAUTIs) has increased the focus on both preventing and removing inappropriate catheterizations. Ironically, one outcome rate currently reported by hospitals—the number of infections per 1,000 catheter days—could unfairly punish those facilities that are doing the most to address the problem.
—Sanjay Saint, MD, MPH, FHM, professor of internal medicine, University of Michigan, Ann Arbor VA Medical Center
“If your focus is on not putting in the catheter or removing a catheter as soon as possible, you now reduce that denominator of catheter days,” explains Sanjay Saint, MD, MPH, FHM, professor of internal medicine at the University of Michigan and the Ann Arbor VA Medical Center. “The only people who now get a catheter in your hospital are those who are pretty sick; therefore, they need a catheter. These people, because of their underlying sickness, are more likely to have an infection, so you may end up having a paradoxical increased rate of CAUTI after your successful initiative has reduced catheter use.”
Using the wrong denominator, in other words, could defeat the whole point: reducing infections by reducing catheter use.
“If we’re going to publicly report data, we have to make sure that the data we’re reporting and the metrics that we’re using are actually the best metrics for the intended purpose,” Dr. Saint says.
For quality-improvement (QI) efforts, his recommendation is to use 10,000 patient days as a more appropriate denominator.
The recent surge in attention to catheter-associated urinary tract infections (CAUTIs) has increased the focus on both preventing and removing inappropriate catheterizations. Ironically, one outcome rate currently reported by hospitals—the number of infections per 1,000 catheter days—could unfairly punish those facilities that are doing the most to address the problem.
—Sanjay Saint, MD, MPH, FHM, professor of internal medicine, University of Michigan, Ann Arbor VA Medical Center
“If your focus is on not putting in the catheter or removing a catheter as soon as possible, you now reduce that denominator of catheter days,” explains Sanjay Saint, MD, MPH, FHM, professor of internal medicine at the University of Michigan and the Ann Arbor VA Medical Center. “The only people who now get a catheter in your hospital are those who are pretty sick; therefore, they need a catheter. These people, because of their underlying sickness, are more likely to have an infection, so you may end up having a paradoxical increased rate of CAUTI after your successful initiative has reduced catheter use.”
Using the wrong denominator, in other words, could defeat the whole point: reducing infections by reducing catheter use.
“If we’re going to publicly report data, we have to make sure that the data we’re reporting and the metrics that we’re using are actually the best metrics for the intended purpose,” Dr. Saint says.
For quality-improvement (QI) efforts, his recommendation is to use 10,000 patient days as a more appropriate denominator.
ONLINE EXCLUSIVE: Patient Engagement Critical
Because “med rec” is a responsibility shared by providers, patients, and families, it’s important to engage everyone in the process.
Although the patient is—and should be, if capable—the ultimate owner of the correct healthcare record, “We have a responsibility as healthcare providers to help them be successful,” says Blake Lesselroth, MD, assistant professor of medicine at Oregon Health Sciences University and director of the Portland Patient Safety Center of Inquiry at the Portland VA Medical Center. “We haven’t done that.”
Hospitals and healthcare systems use varied strategies for including and empowering patients in the med-rec process:
- The Joint Commission launched its “Speak Up” program (PDF), which gives patients tools to help avoid mistakes with their medications.
- Last year, Southern California Kaiser Permanente rolled out its “medicine in a bag” initiative, according to hospitalist David Wong, MD. Patients are instructed to bring all of their medications (in their respective containers) to the hospital when they are admitted. Then, as the med-rec process is completed, medications are placed in green (take these meds), red (stop these meds), and yellow bags (which may include herbal supplements or other questionable items). In addition, orders are written and explained in simple language: i.e., “twice per day” instead of b.i.d. When patients visit their PCP after discharge, they are instructed to bring the color-coded bags so that the PCPs can verify the coherence of the orders. Clarity reports are filed for each physician, allowing a feedback mechanism to make sure that med rec is taking place.
- Open charting at Griffin Hospital in Derby, Conn., in affiliation with the principles of the nonprofit, patient-centered Planetree organization, supplies another means of double-checking the veracity of patients’ medication lists. It also allows for meaningful patient education and dialogue about treatment and discharge plans, says Dorothea Wild, MD, Griffin Hospital’s chief hospitalist.
Gretchen Henkel is a freelance writer based in California.
Because “med rec” is a responsibility shared by providers, patients, and families, it’s important to engage everyone in the process.
Although the patient is—and should be, if capable—the ultimate owner of the correct healthcare record, “We have a responsibility as healthcare providers to help them be successful,” says Blake Lesselroth, MD, assistant professor of medicine at Oregon Health Sciences University and director of the Portland Patient Safety Center of Inquiry at the Portland VA Medical Center. “We haven’t done that.”
Hospitals and healthcare systems use varied strategies for including and empowering patients in the med-rec process:
- The Joint Commission launched its “Speak Up” program (PDF), which gives patients tools to help avoid mistakes with their medications.
- Last year, Southern California Kaiser Permanente rolled out its “medicine in a bag” initiative, according to hospitalist David Wong, MD. Patients are instructed to bring all of their medications (in their respective containers) to the hospital when they are admitted. Then, as the med-rec process is completed, medications are placed in green (take these meds), red (stop these meds), and yellow bags (which may include herbal supplements or other questionable items). In addition, orders are written and explained in simple language: i.e., “twice per day” instead of b.i.d. When patients visit their PCP after discharge, they are instructed to bring the color-coded bags so that the PCPs can verify the coherence of the orders. Clarity reports are filed for each physician, allowing a feedback mechanism to make sure that med rec is taking place.
- Open charting at Griffin Hospital in Derby, Conn., in affiliation with the principles of the nonprofit, patient-centered Planetree organization, supplies another means of double-checking the veracity of patients’ medication lists. It also allows for meaningful patient education and dialogue about treatment and discharge plans, says Dorothea Wild, MD, Griffin Hospital’s chief hospitalist.
Gretchen Henkel is a freelance writer based in California.
Because “med rec” is a responsibility shared by providers, patients, and families, it’s important to engage everyone in the process.
Although the patient is—and should be, if capable—the ultimate owner of the correct healthcare record, “We have a responsibility as healthcare providers to help them be successful,” says Blake Lesselroth, MD, assistant professor of medicine at Oregon Health Sciences University and director of the Portland Patient Safety Center of Inquiry at the Portland VA Medical Center. “We haven’t done that.”
Hospitals and healthcare systems use varied strategies for including and empowering patients in the med-rec process:
- The Joint Commission launched its “Speak Up” program (PDF), which gives patients tools to help avoid mistakes with their medications.
- Last year, Southern California Kaiser Permanente rolled out its “medicine in a bag” initiative, according to hospitalist David Wong, MD. Patients are instructed to bring all of their medications (in their respective containers) to the hospital when they are admitted. Then, as the med-rec process is completed, medications are placed in green (take these meds), red (stop these meds), and yellow bags (which may include herbal supplements or other questionable items). In addition, orders are written and explained in simple language: i.e., “twice per day” instead of b.i.d. When patients visit their PCP after discharge, they are instructed to bring the color-coded bags so that the PCPs can verify the coherence of the orders. Clarity reports are filed for each physician, allowing a feedback mechanism to make sure that med rec is taking place.
- Open charting at Griffin Hospital in Derby, Conn., in affiliation with the principles of the nonprofit, patient-centered Planetree organization, supplies another means of double-checking the veracity of patients’ medication lists. It also allows for meaningful patient education and dialogue about treatment and discharge plans, says Dorothea Wild, MD, Griffin Hospital’s chief hospitalist.
Gretchen Henkel is a freelance writer based in California.
ONLINE EXCLUSIVE: The Culture of Medicine Must Change, Watchdog Group Says
ONLINE EXCLUSIVE: Med-Rec Experts Discuss Prevention Strategies
Click here to listen to Dr. Tsomides
Click here to listen to Dr. Lesselroth
Click here to listen to Dr. Tsomides
Click here to listen to Dr. Lesselroth
Click here to listen to Dr. Tsomides
Click here to listen to Dr. Lesselroth
Family and Caregiver Needs Over the Course of the Cancer Trajectory
When a patient is diagnosed with cancer, family members often assume responsibility for providing care. They are typically involved not only with the diagnostic and treatment phases of care but also across the care trajectory and into survivorship. These caregivers are a primary source of support to individuals with cancer. The purpose of this article is to present an overview of the challenges, needs, and roles of family caregivers over the course of the cancer treatment trajectory and to discuss what support the professionals can provide.
Click of the PDF icon at the top of this introduction to read the full article.
When a patient is diagnosed with cancer, family members often assume responsibility for providing care. They are typically involved not only with the diagnostic and treatment phases of care but also across the care trajectory and into survivorship. These caregivers are a primary source of support to individuals with cancer. The purpose of this article is to present an overview of the challenges, needs, and roles of family caregivers over the course of the cancer treatment trajectory and to discuss what support the professionals can provide.
Click of the PDF icon at the top of this introduction to read the full article.
When a patient is diagnosed with cancer, family members often assume responsibility for providing care. They are typically involved not only with the diagnostic and treatment phases of care but also across the care trajectory and into survivorship. These caregivers are a primary source of support to individuals with cancer. The purpose of this article is to present an overview of the challenges, needs, and roles of family caregivers over the course of the cancer treatment trajectory and to discuss what support the professionals can provide.
Click of the PDF icon at the top of this introduction to read the full article.
'Best Results' Yet for Poor-Prognosis Elderly With DLBCL
SAN DIEGO – Stretching out the delivery of rituximab significantly improved overall and event-free survival among older patients with poor-prognosis diffuse large B-cell lymphoma, German investigators reported.
Patients older than 60 years who had diffuse large B-cell lymphoma (DLBCL) were treated with the CHOP regimen and rituximab (Rituxan) on days 4 and 1 before CHOP and at increasing intervals thereafter, in the SMARTE-R-CHOP-14 trial.
Those with poor-prognosis disease had an overall survival rate of 80% at 37 months, compared with 67% for similar patients treated with CHOP and biweekly rituximab in an earlier trial (P = .034), reported Dr. Michael Pfreundschuh on behalf of his colleagues in the German High-Grade Non-Hodgkin's Lymphoma Study Group.
Event-free survival rates among poor-prognosis patients (defined as those with an International Prognostic Index [IPI] score higher than 2) were also significantly higher with the extended rituximab–dosing schedule, dubbed SMARTE-R-CHOP-14, at 67% vs. 54% for patients who received biweekly rituximab in the previous RICOVER-60 trial (P = .030).
"SMARTE-R-CHOP 14 has achieved by far the best results reported to date for elderly patients with poor prognosis," said Dr. Pfreundschuh of Saarland University in Homburg, Germany, at the annual meeting of the American Society of Hematology (ASH).
Giving rituximab every 3 weeks after 2 pre-CHOP doses maintains serum levels of rituximab over a longer period than when it is given every other week, he said.
Patients with good- or moderate-prognosis disease (defined as an IPI of 1 or 2) also had numerically better event-free and overall survival rates, compared with patients treated with biweekly rituximab, he noted, but the differences were not significant.
Although CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) given every 14 days (CHOP-14) had been shown to be superior to CHOP given every 21 days (CHOP-21), the same could not be said when rituximab was added (R-CHOP-14 vs. R-CHOP-21). Presentations at ASH in 2009 and at the American Society of Clinical Oncology annual meeting in 2011 suggested that biweekly rituximab dosing was suboptimal, Dr. Freundschuh said.
In the SMARTE-R-CHOP-14 study, Dr. Pfreundschuh and colleagues treated 190 patients with DLBCL with six cycles of CHOP-14. combined with eight cycles of rituximab 375 mg/m2. The first three rituximab cycles were given in a dose-dense fashion on days 1 and 4 before CHOP, followed by infusions on days 10, 29, 57, 99, 155, and 239. Patients also received prophylaxis against infections with levofloxacin, acyclovir, and cotrimoxazole. One patient did not give informed consent for the trial, and was not included in the final analysis.
In the RICOVER-60 trial that was used for comparison, patients received six cycles of CHOP plus rituximab given on days 1, 15, 29, 43, 57, 71, 85, and 99. The baseline characteristics of patients were similar between the trials, except that significantly more patients in SMARTE-R-CHOP-14 had high-risk disease (P = .015).
Complete response rates overall were not significantly different (85% in SMARTE-R and 78% in RICOVER-60). Among patients with IPI scores less than 2, the respective rates were 90% and 84%, also not significantly different. Among patients with an IPI greater than 2, however, the complete response rate in SMARTE-R-CHOP-14 was 81%, compared with 68% in RICOVER-60 (P = .035).
Overall survival did not differ significantly between the trials, at 84% in SMARTE-R and 78% in RICOVER. When patients stratified by risk were considered, there were no between-trial differences for low-risk patients.
Overall event-free survival was 71% at 37 months’ median follow-up in SMARTE-R, and 66% at 34 months in RICOVER; this difference was not significant, nor was the difference between the trials among patients with low-risk disease.
"The pharmacokinetics of eight biweekly applications of rituximab are adequate for elderly patients with good prognosis, meaning patients with IP1 1 or 2, or low tumor burden diffuse large B-cell lymphoma, but not for higher tumor loads," Dr. Pfreundschuh said.
The investigators are exploring the SMARTE-R treatment strategy in a prospective trial, labeled "OPTIMAL Greater Than 60."
The trial was supported by Deutsche Krebshilfe and Roche. Dr. Pfreundschuh disclosed serving on a Roche board of directors or advisory committee, and receiving research funding from that company and from Amgen.
SAN DIEGO – Stretching out the delivery of rituximab significantly improved overall and event-free survival among older patients with poor-prognosis diffuse large B-cell lymphoma, German investigators reported.
Patients older than 60 years who had diffuse large B-cell lymphoma (DLBCL) were treated with the CHOP regimen and rituximab (Rituxan) on days 4 and 1 before CHOP and at increasing intervals thereafter, in the SMARTE-R-CHOP-14 trial.
Those with poor-prognosis disease had an overall survival rate of 80% at 37 months, compared with 67% for similar patients treated with CHOP and biweekly rituximab in an earlier trial (P = .034), reported Dr. Michael Pfreundschuh on behalf of his colleagues in the German High-Grade Non-Hodgkin's Lymphoma Study Group.
Event-free survival rates among poor-prognosis patients (defined as those with an International Prognostic Index [IPI] score higher than 2) were also significantly higher with the extended rituximab–dosing schedule, dubbed SMARTE-R-CHOP-14, at 67% vs. 54% for patients who received biweekly rituximab in the previous RICOVER-60 trial (P = .030).
"SMARTE-R-CHOP 14 has achieved by far the best results reported to date for elderly patients with poor prognosis," said Dr. Pfreundschuh of Saarland University in Homburg, Germany, at the annual meeting of the American Society of Hematology (ASH).
Giving rituximab every 3 weeks after 2 pre-CHOP doses maintains serum levels of rituximab over a longer period than when it is given every other week, he said.
Patients with good- or moderate-prognosis disease (defined as an IPI of 1 or 2) also had numerically better event-free and overall survival rates, compared with patients treated with biweekly rituximab, he noted, but the differences were not significant.
Although CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) given every 14 days (CHOP-14) had been shown to be superior to CHOP given every 21 days (CHOP-21), the same could not be said when rituximab was added (R-CHOP-14 vs. R-CHOP-21). Presentations at ASH in 2009 and at the American Society of Clinical Oncology annual meeting in 2011 suggested that biweekly rituximab dosing was suboptimal, Dr. Freundschuh said.
In the SMARTE-R-CHOP-14 study, Dr. Pfreundschuh and colleagues treated 190 patients with DLBCL with six cycles of CHOP-14. combined with eight cycles of rituximab 375 mg/m2. The first three rituximab cycles were given in a dose-dense fashion on days 1 and 4 before CHOP, followed by infusions on days 10, 29, 57, 99, 155, and 239. Patients also received prophylaxis against infections with levofloxacin, acyclovir, and cotrimoxazole. One patient did not give informed consent for the trial, and was not included in the final analysis.
In the RICOVER-60 trial that was used for comparison, patients received six cycles of CHOP plus rituximab given on days 1, 15, 29, 43, 57, 71, 85, and 99. The baseline characteristics of patients were similar between the trials, except that significantly more patients in SMARTE-R-CHOP-14 had high-risk disease (P = .015).
Complete response rates overall were not significantly different (85% in SMARTE-R and 78% in RICOVER-60). Among patients with IPI scores less than 2, the respective rates were 90% and 84%, also not significantly different. Among patients with an IPI greater than 2, however, the complete response rate in SMARTE-R-CHOP-14 was 81%, compared with 68% in RICOVER-60 (P = .035).
Overall survival did not differ significantly between the trials, at 84% in SMARTE-R and 78% in RICOVER. When patients stratified by risk were considered, there were no between-trial differences for low-risk patients.
Overall event-free survival was 71% at 37 months’ median follow-up in SMARTE-R, and 66% at 34 months in RICOVER; this difference was not significant, nor was the difference between the trials among patients with low-risk disease.
"The pharmacokinetics of eight biweekly applications of rituximab are adequate for elderly patients with good prognosis, meaning patients with IP1 1 or 2, or low tumor burden diffuse large B-cell lymphoma, but not for higher tumor loads," Dr. Pfreundschuh said.
The investigators are exploring the SMARTE-R treatment strategy in a prospective trial, labeled "OPTIMAL Greater Than 60."
The trial was supported by Deutsche Krebshilfe and Roche. Dr. Pfreundschuh disclosed serving on a Roche board of directors or advisory committee, and receiving research funding from that company and from Amgen.
SAN DIEGO – Stretching out the delivery of rituximab significantly improved overall and event-free survival among older patients with poor-prognosis diffuse large B-cell lymphoma, German investigators reported.
Patients older than 60 years who had diffuse large B-cell lymphoma (DLBCL) were treated with the CHOP regimen and rituximab (Rituxan) on days 4 and 1 before CHOP and at increasing intervals thereafter, in the SMARTE-R-CHOP-14 trial.
Those with poor-prognosis disease had an overall survival rate of 80% at 37 months, compared with 67% for similar patients treated with CHOP and biweekly rituximab in an earlier trial (P = .034), reported Dr. Michael Pfreundschuh on behalf of his colleagues in the German High-Grade Non-Hodgkin's Lymphoma Study Group.
Event-free survival rates among poor-prognosis patients (defined as those with an International Prognostic Index [IPI] score higher than 2) were also significantly higher with the extended rituximab–dosing schedule, dubbed SMARTE-R-CHOP-14, at 67% vs. 54% for patients who received biweekly rituximab in the previous RICOVER-60 trial (P = .030).
"SMARTE-R-CHOP 14 has achieved by far the best results reported to date for elderly patients with poor prognosis," said Dr. Pfreundschuh of Saarland University in Homburg, Germany, at the annual meeting of the American Society of Hematology (ASH).
Giving rituximab every 3 weeks after 2 pre-CHOP doses maintains serum levels of rituximab over a longer period than when it is given every other week, he said.
Patients with good- or moderate-prognosis disease (defined as an IPI of 1 or 2) also had numerically better event-free and overall survival rates, compared with patients treated with biweekly rituximab, he noted, but the differences were not significant.
Although CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) given every 14 days (CHOP-14) had been shown to be superior to CHOP given every 21 days (CHOP-21), the same could not be said when rituximab was added (R-CHOP-14 vs. R-CHOP-21). Presentations at ASH in 2009 and at the American Society of Clinical Oncology annual meeting in 2011 suggested that biweekly rituximab dosing was suboptimal, Dr. Freundschuh said.
In the SMARTE-R-CHOP-14 study, Dr. Pfreundschuh and colleagues treated 190 patients with DLBCL with six cycles of CHOP-14. combined with eight cycles of rituximab 375 mg/m2. The first three rituximab cycles were given in a dose-dense fashion on days 1 and 4 before CHOP, followed by infusions on days 10, 29, 57, 99, 155, and 239. Patients also received prophylaxis against infections with levofloxacin, acyclovir, and cotrimoxazole. One patient did not give informed consent for the trial, and was not included in the final analysis.
In the RICOVER-60 trial that was used for comparison, patients received six cycles of CHOP plus rituximab given on days 1, 15, 29, 43, 57, 71, 85, and 99. The baseline characteristics of patients were similar between the trials, except that significantly more patients in SMARTE-R-CHOP-14 had high-risk disease (P = .015).
Complete response rates overall were not significantly different (85% in SMARTE-R and 78% in RICOVER-60). Among patients with IPI scores less than 2, the respective rates were 90% and 84%, also not significantly different. Among patients with an IPI greater than 2, however, the complete response rate in SMARTE-R-CHOP-14 was 81%, compared with 68% in RICOVER-60 (P = .035).
Overall survival did not differ significantly between the trials, at 84% in SMARTE-R and 78% in RICOVER. When patients stratified by risk were considered, there were no between-trial differences for low-risk patients.
Overall event-free survival was 71% at 37 months’ median follow-up in SMARTE-R, and 66% at 34 months in RICOVER; this difference was not significant, nor was the difference between the trials among patients with low-risk disease.
"The pharmacokinetics of eight biweekly applications of rituximab are adequate for elderly patients with good prognosis, meaning patients with IP1 1 or 2, or low tumor burden diffuse large B-cell lymphoma, but not for higher tumor loads," Dr. Pfreundschuh said.
The investigators are exploring the SMARTE-R treatment strategy in a prospective trial, labeled "OPTIMAL Greater Than 60."
The trial was supported by Deutsche Krebshilfe and Roche. Dr. Pfreundschuh disclosed serving on a Roche board of directors or advisory committee, and receiving research funding from that company and from Amgen.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: Among elderly poor-prognosis patients, treatment with the CHOP regimen and extended rituximab yielded an overall survival rate of 80% at 37 months, compared with 67% for a historical control group treated with a standard rituximab schedule (P = .034).
Data Source: Comparison of two prospective trials in patients older than 60 years with diffuse large B-cell lymphoma.
Disclosures: The trial was supported by Deutsche Krebshilfe and Roche. Dr. Pfreundschuh disclosed serving on a Roche board of directors or advisory committee, and receiving research funding from that company and from Amgen.
Hospitalists' Role in Stewardship
Healthcare‐associated infections (HAIs) are important causes of morbidity and mortality in the United States and other countries.13 Moreover, treatment of HAIs is frequently complicated by involvement of bacterial pathogens resistant to 1 or more antibiotics or antibiotic classes,4 and sometimes bacteria resistant to all or nearly all currently available agents.57 The rapid emergence of resistant bacteria both in and out of the hospital setting can affect empiric antimicrobial choices across all patients. The effort to avoid undertreating or not covering resistant bacteria can lead to overuse of wide‐spectrum antimicrobials. Antimicrobial useand especially antimicrobial overuse or misusehas been linked with increased antimicrobial resistance,817 leading to worsened clinical outcomes with increased length of hospital stay and healthcare costs. Table 1 defines the various lines of evidence supporting a causal relationship between antibiotic use and emergence of antimicrobial resistance.18, 19
|
| Changes in antimicrobial use are paralleled by changes in the prevalence of resistance |
| Antimicrobial resistance is more prevalent in healthcare‐associated bacterial infections vs community‐acquired infections |
| Patients with healthcare‐associated infections caused by resistant strains are more likely than control patients to have received prior antimicrobials |
| Areas within hospitals that have the highest rates of antimicrobial resistance also have the highest rates of antimicrobial use |
| Increasing duration of patient exposure to antimicrobials increases the likelihood of colonization with resistant organisms |
Optimal management of patients with bacterial infections, both HAIs and those that originate in the community, involves a focus on treatment that maximizes clinical outcomes for the individual patient, while also inhibiting or slowing the development of antimicrobial resistance and its spread to other patients. Antimicrobial stewardship is a term describing the various clinical strategies that have been devised to maximize the benefits and minimize the costs of antimicrobial therapy through judicious use of these agents.18, 20, 21 This article examines the developing patterns of resistance among key bacterial pathogens in the hospital and associated healthcare settings, the costs associated with HAIs (specifically, those caused by resistant pathogens), and the various strategies or programs that have been developed by governmental agencies, individual healthcare institutions, and other organizations to optimize the use of antibiotics to improve patient outcomes and minimize healthcare costs. The value that the hospitalist can bring to the development and/or implementation of institutional antimicrobial stewardship programs is explored.
ANTIMICROBIAL RESISTANCE AND HAI TRENDS FOR KEY BACTERIAL PATHOGENS
Bacterial pathogens including Enterobacteriaceae (Klebsiella pneumoniae, Enterobacter spp, Escherichia coli, and Proteus spp, among others), Acinetobacter baumannii, Pseudomonas aeruginosa, Staphylococcus aureus, and Enterococcus faecium22, 23 are increasingly prevalent in healthcare settings, and particularly troublesome to manage due to increasing resistance. Data from the Centers for Disease Control and Prevention's (CDC) National Healthcare Safety Network (NHSN) have shown that, in intensive care units (ICUs), 16% of HAIs are due to multidrug‐resistant (MDR) pathogens.4 These 16% have the highest mortality and length of hospital stay, and are associated with the highest healthcare costs.24, 25 Infections caused by MDR pathogens are more important than their actual numbers, because treatment decisions are driven by the intent to cover these MDR pathogens, even if that means providing excessively broad coverage for most patients. Moreover, the 16% mentioned above are only the tip of the iceberg, as many more HAIs will occur outside of the ICU, particularly catheter‐associated urinary tract infections (CAUTI) and surgical site infections, as these patients are often not sick enough to require ICU care. There is little information on the prevalence of HAIs outside of the ICU setting, the role of MDR bacteria in these infections, and the associated costs, mortality, and effects on length of stay.
K pneumoniae Carbapenemases and Community‐Acquired Methicillin‐Resistant Staphylococcus aureus
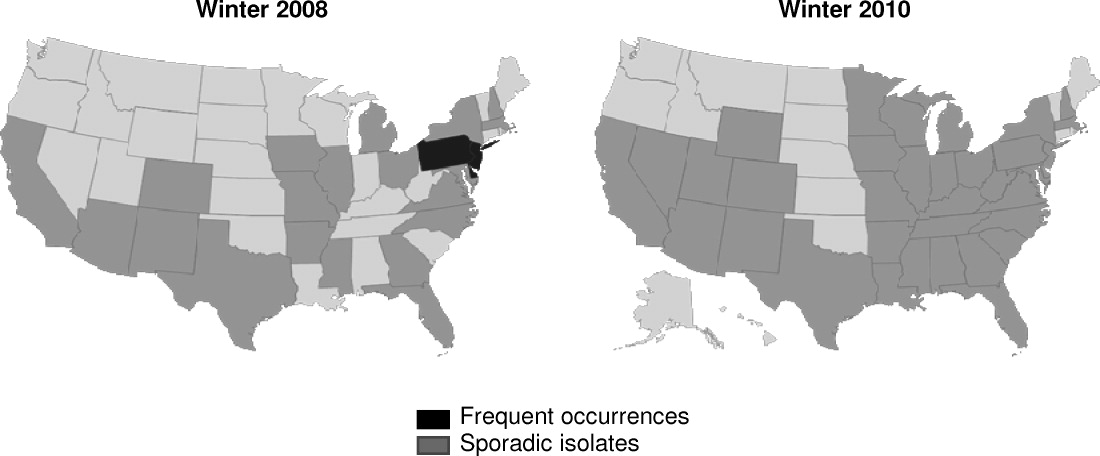
K pneumoniae carbapenemase (KPC) is a prime example of the emergence and rapid spread of a new resistance pattern that affects prescribing patterns. Emergence of KPC as the primary source of carbapenem resistance in Enterobacteriaceae26 is critically significant, as carbapenems are recommended first‐line therapy for serious infections caused by extended‐spectrum ‐lactamase (ESBL)‐producing K pneumoniae or other Enterobacteriaceae. One particularly remarkable fact about KPC‐producing bacteria is the speed at which they have spread since first emerging. Figure 1 from the CDC illustrates the rapid spread of KPC‐producing bacteria within the United States, from winter 2008 to May 2010. International spread has also been rapid and extensive. The first case of a KPC‐producing bacteria outside the United States was reported in France in February 2005, in an 80‐year‐old man who was admitted to a Parisian hospital 2 to 3 months after having a medical procedure performed in a New York City hospital, suggesting intercontinental transfer from the United States.27 Since then, KPC‐producing pathogenic bacteria have been identified in the Caribbean, South America, Europe, Israel, and China.2830 It is clear that once resistant bacteria emerge, they have the potential to spread very rapidly within and between countries, challenging currently available antimicrobial agents and complicating the treatment of serious infections.
Consideration of S aureus skin and skin‐structure infections highlights the fact that the barrier between hospital and community is now beginning to be crossed, further complicating prescribing decisions. The classic risk factors for resistance may no longer be reliable in determining best empiric treatment. In a landmark study, Moran et al. demonstrated the large percentages of outpatients in the United States with skin or soft‐tissue infections (SSTIs) involving community‐acquired methicillin‐resistant Staphylococcus aureus (CA‐MRSA).31 S aureus was isolated from 76% (320/422) of adults presenting to 11 university‐affiliated emergency departments with acute, purulent SSTIs in August 2004, 59% of whom were infected with MRSA. More than half the patients in the study (57%) were initially treated with antibiotics to which MRSA isolates were not susceptible.31 In the hospital, it has been shown that most invasive MRSA infections now actually have their onset outside of the healthcare setting,32 and that increasing numbers of hospitalized patients are now developing infections associated with CA‐MRSA strains >72 hours after admission.3338 Thus, it is becoming increasingly difficult to determine whether an invasive S aureus infection encountered in either a healthcare facility or community setting involves a sensitive organism, healthcare‐associated MRSA, or a CA‐MRSA pathogen, directly impacting treatment choices across all patients we care for with skin and skin‐structure infections.
Clostridium difficile‐Associated Disease
Indiscriminate and unnecessary use of antibiotics offer our patients no benefit, while exposing them to adverse effects of antibiotics, including allergies, rashes, and diarrhea among many potential other unintended consequences. C difficile‐associated disease is an increasingly problematic pathogen in the hospital setting that has been linked to unintended antibiotic effects.22, 39, 40 C difficile infection is not only costly in dollars, it is also a potentially fatal condition and has been linked to prolonged hospital stays and increased healthcare costs.4144 Improved infection control measures4549 and better use of antibiotics through antibiotic stewardship programs5055 have been shown to reduce the incidence of C difficile infection.
COSTS OF HAIs AND ANTIMICROBIAL RESISTANCE
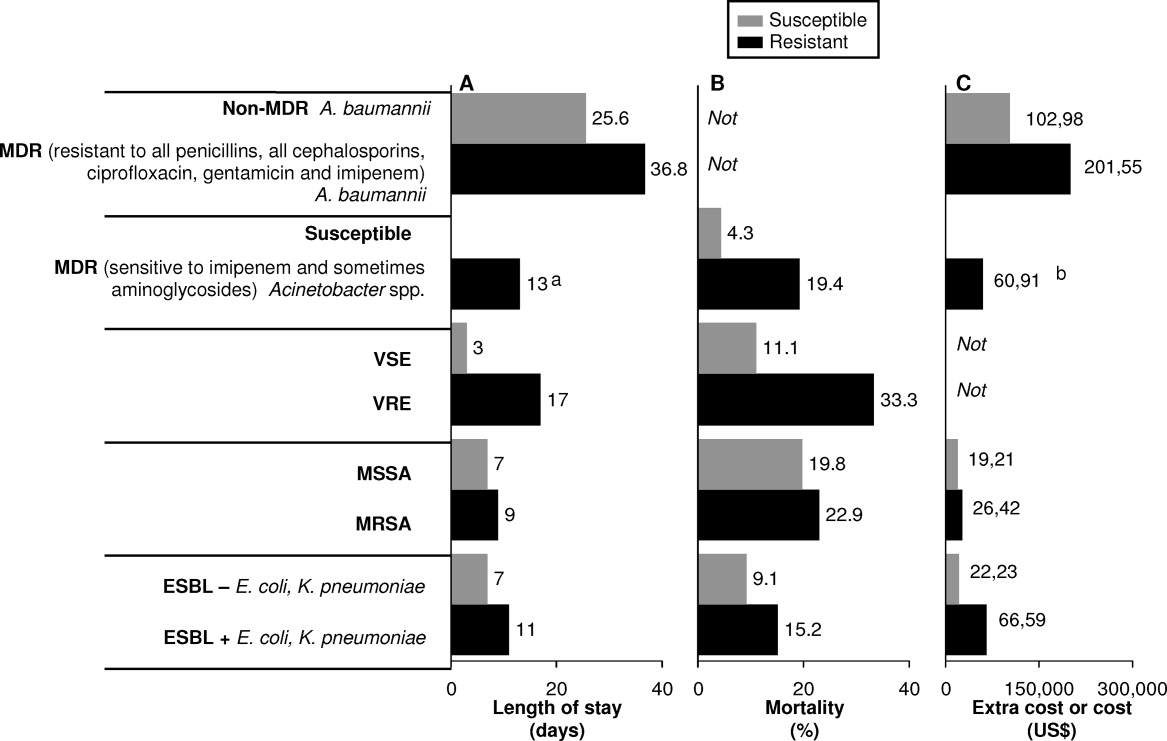
HAIs are an important and growing problem in the United States.56 Klevens et al. estimated that approximately 1.7 million individuals hospitalized in the United States in 2002 had HAI, leading to 98,987 deaths.1 Estimates of annual hospital costs in the United States related to HAIs range from $28 to $48 billion.57 Antimicrobial resistance is a major driver of mortality, increased length of hospital stay, and hospital costs associated with HAIs.24, 25 A recent review by Sipahi25 summarizes recent studies examining the impact of resistant and MDR bacterial infections (Figure 2).5866 It is dramatically clear that infections due to resistant and MDR bacteria more often result in death, are associated with longer hospital stays, and are considerably more expensive to treat.
A number of factors can lead to the increased hospital costs associated with infection with a resistant or MDR bacteria. These include the need to use more expensive antibiotics, increased length of hospital stay, delayed appropriate antibiotic therapy, increased treatment toxicity (and costs associated with managing these toxicities), and increased frequency of surgical interventions required to control infection.25, 67
The savings that could be realized through reduction in antimicrobial resistance was evaluated recently by Roberts et al.68 Using a sensitivity analysis for a sample of high‐risk adult patients hospitalized in an urban public teaching hospital in 2000, the authors determined that reducing the antimicrobial‐resistant infection rate by 3.5% (from 13.5% to 10.0%) would have saved the study hospital $910,812 (in 2008 US$), when using lowest cost and length of stay figures. The calculated societal savings, for reduced mortality and lost productivity associated with the reduced antimicrobial‐resistant rate, was $1.8 million. Hence, the analysis showed a minimum overall medical (hospital) and societal savings of $2.7 million for this single hospital with a cohort of 1391 patients. The projected savings would be dramatically higher if the reduced antimicrobial‐resistant rate was generalized to all hospitals throughout the United States.
ORGANIZATIONAL AND GOVERNMENTAL EFFORTS ADDRESSING ANTIMICROBIAL RESISTANCE AND HAIs
Given the relationships between antimicrobial use and resistance, and between antimicrobial resistance and morbidity, mortality, length of hospital stay, and healthcare costs, it is not surprising that we have seen a variety of programs and initiatives begun by either government agencies or healthcare organizations aimed at reducing antimicrobial resistance and HAIs.
The Joint Commission
The Joint Commission is an independent, not‐for‐profit organization that accredits and certifies >18,000 healthcare organizations/programs in the United States.69 The Joint Commission issues annual National Patient Safety Goals (NPSG). Hospital compliance with these goals is a critical component of the accreditation process.70
The seventh goal of The Joint Commission's NPSG is to reduce the risk of HAIs,70 the key features of which are listed in Table 2. The methodology recommended to achieve compliance includes infection control programs and implementation of evidence‐based practices to prevent HAIs due to MDR microorganisms in acute‐care hospitals. This presumably could include development and implementation of an institutional antimicrobial stewardship, or components of a program, to reduce antimicrobial resistance within the hospital.
| Goal 7: Reduce the Risk of Healthcare‐Associated Infections |
|---|
|
| NPSG.07.03.01 |
| Implement evidence‐based practices to prevent healthcare‐associated infections due to multidrug‐resistant organisms in acute‐care hospitals |
| Note: This requirement applies to, but is not limited to, epidemiologically important organisms such as methicillin‐resistant Staphylococcus aureus, Clostridium difficile, vancomycin‐resistant enterococci (VRE), and multidrug‐resistant Gram‐negative bacteria |
| NPSG.07.04.01 |
| Implement evidence‐based practices to prevent central line‐associated bloodstream infection |
| Note: This requirement covers short‐ and long‐term central venous catheters and peripherally inserted central catheter (PICC) lines |
Centers for Medicare and Medicaid Services
The Deficit Reduction Act of 2005, Section 5001(c), requires the Secretary of Health and Human Services to identify conditions that are: (1) high cost or high volume, or both; (2) result in assignment of a case to a diagnosis‐related group that has higher payment when the code is present as a secondary diagnosis; and (3) could reasonably have been prevented through application of evidence‐based guidelines.71 The Centers for Medicare and Medicaid Services (CMS), which develops and administers Medicare and Medicaid payment and coverage policies, encourages hospitals to reduce the occurrence of these preventable problems through reduced payments when these events occur. Among the Hospital Acquired Conditions (HAC) that CMS considers reasonably preventable are a number of HAIs, particularly CAUTI, vascular catheter‐associated infections, and various surgery‐related SSTIs. Importantly, the CMS policy is still in effect as of April 2011, and there are no signs of its being repealed or modified in the foreseeable future.
The CDC Get Smart and Get Smart for Healthcare Programs
The Get Smart campaign, initiated by the CDC in 1995, focused on providing information to parents about the appropriate and inappropriate use of antibiotics to treat common childhood infections, as well as about the dangers of antibiotic resistance.72 The goal of Get Smart is to reduce unnecessary antibiotic use and the spread of antibiotic resistance in the community by reducing the pressure exerted by parents on physicians to overuse or misuse antibiotics. Hence, the primary focus in this setting is on patient/parent education. The Get Smart campaign has been highly successful, with a significant reduction in antibiotic prescriptions after initiation of the campaign, across a range of infections for which antibiotics are generally or often not warranted.73 The success of Get Smart is also largely responsible for the improvement in antibiotic prescribing for childhood middle ear infections observed in the CDC Healthy People 2010 program.74 The actual performance achieved in 2007 (the latest year reported) exceeded the Healthy People 2010 target.75
Building on the success of Get Smart for community‐acquired infections, a similar CDC campaign (Get Smart for Healthcare) has been undertaken to improve antibiotic usage and reduce antibiotic resistance in inpatient healthcare facilities.76 The specific goals of Get Smart for Healthcare are to improve patient safety through better treatment of infections, reduce emergence of antimicrobial‐resistant pathogens and C difficile, and heighten awareness of the challenges posed by antimicrobial resistance in healthcare settings. To help accomplish these ends, the CDC has partnered with the Institute for Healthcare Improvement (IHI), an independent, not‐for‐profit organization dedicated to closing the gap between the healthcare that currently exists and the healthcare that should exist.77 Together, they have identified a number of primary drivers to improve antibiotic use: timely and appropriate initiation of antibiotics; appropriate administration and de‐escalation; data monitoring and transparency; and improving knowledge of, and engagement in, antimicrobial stewardship efforts, which are the focus of the next section. With respect to data monitoring, many in the healthcare community hope that, through the Get Smart program, we will soon have better sources of data, not just for the ICU, but across the entire hospital setting. This would help providers get a better sense of where resistance is located, thereby enabling better development of action plans to deal with the problem.
The CDC has recently expanded its Web site on antimicrobial stewardship, now providing extensive support and resources for program development and implementation at:
All Clinicians Should:
Dose, Duration, Indication
Too often antibiotics in hospitals are continued unnecessarily simply because clinicians caring for the patient do not have information indicating why the antibiotics were started initially or for how long they were to be continued. This challenge is compounded in today's healthcare system where primary responsibility for patient care is frequently transitioned from one clinician to another. Ensuring that all antibiotic orders are always accompanied by a dose, duration, and indication will help clinicians change or stop therapy when appropriate.
Get Cultures
Antibiotic therapy can be best optimized when it can be tailored to specific culture results. Knowing the susceptibility of the infecting organisms can lead to narrowing of broad‐spectrum therapy, changing therapy to better treat resistant pathogens and to stopping antibiotics when cultures suggest an infection is unlikely.
A number of other government initiatives have been developed to address the issues of HAIs, antimicrobial resistance, and improved antimicrobial stewardship. These are beyond the scope of the present article, but include the United States Department of Health and Human Services (HHS) action plan to prevent HAIs,79 and the CDC campaign and action plan to prevent and combat antimicrobial resistance,80, 81 among others.
ANTIMICROBIAL STEWARDSHIP IN HOSPITALS AND THE HOSPITALIST'S ROLE
As recently defined, antimicrobial stewardship is a system of personnel, informatics, data collection, and policy/procedures that promote the optimal selection, dosing, and duration of therapy for antimicrobial agents throughout the course of their use.20 In simple words, the right antibiotic, at the right dose, at the right time, and for the right duration. The primary goals of antimicrobial stewardship are to reduce patient morbidity and mortality, prevent or slow the emergence of antimicrobial resistance, and reduce adverse drug effects, including secondary infections, such as C difficile‐associated diarrhea.18, 20 Secondary goals include a reduction in hospital length of stay and healthcare expenditures, without adversely impacting quality of care. These goals are entirely in line with those of the hospitalist, who can play a critical role in the prevention and successful management of these infections. Optimal effects are expected when antimicrobial stewardship is combined with implementation of effective infection control measures within the hospital setting.
Antimicrobial Stewardship Strategies
Table 3 provides an overview of various general strategies/procedures employed as components of antimicrobial stewardship programs.82 The 2 most common are: (1) formulary restriction and preauthorization for specific agents; and (2) prospective audit with intervention and feedback.18, 20 Both approaches can and have been used to improve antimicrobial stewardship and to achieve at least some of its goals, and each is associated with advantages and disadvantages, as outlined in Table 3 and reviewed elsewhere.18, 20, 21, 83 Other strategies, such as education and use of guidelines and clinical pathways, tend to be used to supplement or complement either a general formulary restriction/preauthorization, or prospective audit/review and feedback approach to antimicrobial stewardship. It is important to note that, as in other areas such as venous thromboembolism prophylaxis, education alone is insufficient to drive changes in prescribing patterns and thereby reduce resistance. Healthcare informatics are increasingly being utilized to improve the management of infectious diseases. These can be simple programs that better assemble information about hospital‐pathogen epidemiology. They can also be sophisticated systems, designed to standardize the antimicrobial order sets and medical logic modules, that guide treatment options by connecting patient‐specific information with guideline recommendations and local resistance patterns.18, 20, 84, 85
| Strategy | Procedure | Personnel | Advantages | Disadvantages |
|---|---|---|---|---|
| ||||
| Education/ guidelines | Creation of guidelines for antimicrobial use | Antimicrobial committee to create guidelines | May alter behavior patterns | Passive education likely ineffective |
| Group or individual education of clinicians by educators | Educators (physicians, pharmacists) | Avoids loss of prescriber autonomy | ||
| Formulary restriction | Restrict dispensing of targeted antimicrobials to approved indications | Antimicrobial committee to create guidelines Approval personnel (physician, infectious diseases fellow, clinical pharmacist) | Most direct control over antimicrobial use Individual educational opportunities | Perceived loss of autonomy for prescribers Need for all‐hours consultant availability |
| Review and feedback | Daily review of targeted antimicrobials for appropriateness Contact prescribers with recommendations for alternative therapy | Antimicrobial committee to create guidelines Review personnel (usually clinical pharmacist) | Avoids loss of autonomy for prescribers Individual educational opportunities | Compliance with recommendations |
| Computer assistance | Use of information technology to implement previous strategies | Antimicrobial committee to create rules for computer systems | Provides patient‐specific data where most likely to impact care (point of care) | Significant time and resource investment to implement sophisticated systems |
| Expert systems provide patient‐specific recommendations at point of entry (order entry) | Personnel for approval or review (physicians, pharmacists) Computer programmers | Facilitates other strategies | ||
Two early, randomized, prospective studies illustrate the potential benefits and general receptiveness of clinicians to use of an audit/review and feedback approach to institutional antimicrobial stewardship. The first study randomized adult inpatients receiving 1 parenteral antibiotic for 3 days to an intervention (n = 141) or control group (n = 111).86 In the intervention group, a clinical pharmacist and infectious diseases fellow reviewed the initial therapy prescribed by the primary care physician and the patient's progress 3 days after therapy initiation, and at that point offered suggestions for subsequent antibiotic therapy. The feedback or suggestions were communicated via nonpermanent chart note. In total, 85% of the physicians implemented the suggestions, and there were no significant differences between the intervention and control group for clinical or microbiologic endpoints. However, per‐patient antibiotic charges were significantly lower in the intervention versus control group ($1287.17 vs $1673.97; P = 0.05), which yields an estimated $390,000 in annualized savings for the 600‐bed tertiary‐care hospital.
Similarly, a randomized, prospective study by Gums et al. showed that therapeutic intervention by a multidisciplinary antimicrobial team for inpatients receiving suboptimal intravenous antibiotic therapy was associated with a median hospital cost savings of $2642 per intervention, compared with costs for similar inpatients who did not receive such intervention.87 The multidisciplinary team in the study consisted of pharmacists, a clinical microbiologist, and an infectious diseases specialist, who provided the treating physician with recommendations of possible optimal antibiotics, dosages, and rationales based on timely, detailed reviews of relevant microbiologic and clinical data. In total, 89% of physicians in the study implemented the suggestions from the multidisciplinary antimicrobial team. In addition to reduced costs, the intervention versus control group was also associated with significant reductions in the overall length of stay (10.1 vs 14.5 days; P = 0.0001), and total non‐ICU length of stay (5.7 vs 9.0; P = 0.0001). There was no significant difference between the 2 groups for mortality rate.
The results from these studies86, 87 demonstrate how a prospective audit/review and feedback approach to antimicrobial stewardship can be associated with high physician participation and significant cost reductions for participating hospitals,88 and potentially improve patient outcomes. Antimicrobial stewardship programs overall have a long track record in improving patient outcomes and reducing antimicrobial resistance at the patient level.8991
The Hospitalist's Role in Antimicrobial Stewardship
Hospitalists can participate in antimicrobial stewardship at a number of levels. On the direct patient care level, they can consistently apply the principles of appropriate empiric therapy, de‐escalation, and duration of therapy as presented by Drs Snydman, Kaye, and File in this supplement. As hospitalists assume a continually increasing role in the care of hospitalized patients throughout the United States,92 they can directly influence the way medicine is practiced on a daily basis, patient by patient. A 2007 survey conducted by the American Hospital Association (AHA) showed that 58% of the 4897 community hospitals surveyed had hospital medicine programs, and that 83% of hospitals with 200 or more beds had such a program.93, 94 Estimates from the Society of Hospital Medicine (SHM) in July 2010 indicated that currently there were more than 30,000 hospitalists, practicing in 3300 large hospitals.95 This affords hospitalists the opportunity to improve care across a huge segment of hospitalized patients.
On a departmental or institutional level, hospitalists appear to be especially well positioned to contribute to, and in some cases direct, a hospital's antimicrobial stewardship program. Unique to hospital medicine, and incorporated into the definition of the profession, is the commitment to quality and process improvement, efficient use of hospital and healthcare resources, and an interdisciplinary approach to care.96 In line with this, hospitalists frequently serve on hospital committees and task forces, are experienced in developing and implementing clinical guidelines, and lead multidisciplinary teams to optimize patient care. For example, as reported in a recent review, a 2007 Pediatric Research in the Inpatient Setting survey of 208 pediatric hospitalists in the United States and Canada indicated that 92% spend at least some time in administration, 85% serve on hospital committees, and 61% and 52% lead initiatives in practice guidelines and quality improvement, respectively.97 Hospitalists are therefore especially well positioned to participate, and provide leadership, in hospital antimicrobial stewardship programs.
In 2007, the Infectious Diseases Society of America (IDSA)/Society for Healthcare Epidemiology of America (SHEA) released guidelines for developing institutional programs to enhance antimicrobial stewardship.18 According to these guidelines, the ideal institutional antimicrobial stewardship program contains an infectious diseases physician and clinical pharmacist with infectious diseases training as core members, along with a clinical microbiologist, an information system specialist, infection control professional, and a hospital epidemiologist. The infectious diseases physician and clinical pharmacist with infectious diseases training are expected to serve as leaders of the team and should be appropriately compensated for time dedicated to the program. Clearly, this is an extensive team requiring a lot of staff. Although optimal, many institutions do not have an infectious diseases physician on staff or an attending who is interested and willing to participate. For many institutions, an even bigger issue is identifying an infectious diseases pharmacist with sufficient skill to manage an antimicrobial stewardship program. As a consequence, many institutions wanting to develop an antimicrobial stewardship program to improve clinical outcomes, reduce antimicrobial resistance, and lower costs will need to think outside the box and look for nontraditional leaders to champion and lead their programs. Potential nontraditional leaders include general clinical pharmacists, intensivists, and hospitalists.98
Although hospitalists are not explicitly mentioned in the IDSA/SHEA guidelines, they seem to be implicitly included. The guidelines state that the development, maintenance, and ultimate success of such programs fundamentally depends on the support and collaboration of hospital administration, medical staff leadership, and local providers.18 Furthermore, they indicate the desirability for antimicrobial stewardship programs to function under the auspices of quality assurance and patient safety. As defined above, these are characteristics that are inherent to hospital medicine. Hence, there appears to be a good match between the activities performed by hospitalists and what the 2007 guidelines indicate is important for an effective antimicrobial stewardship program.
Now is the time for individuals to begin thinking about how best to prepare hospitalists for leadership roles in hospital antimicrobial stewardship programs. We need a well‐defined process for either training hospitalists for independent establishment of stewardship programs or establishing partnership with infectious disease specialists for the development of these programs. We need high‐level training programs in focused areas of infectious diseases that hospitalists encounter frequently (skin and skin‐structure infections, pneumonia, catheter‐associated infections, among others). Detailed understanding of the pathogens and their optimal treatment could form the core of such training. Additional education in infection control and the antimicrobial stewardship processes would round out the knowledge needed for a hospitalist to best implement and provide leadership for an antimicrobial stewardship program at his/her own institution. These training programs could be developed and delivered locally, or preferably they could be provided at national training sessions developed and supported through SHM, infectious disease societies, or the CDC.
Partnering with infectious diseases specialists is essential for protocol development and clinical support. This could allow the hospitalist to start a stewardship program on a small scale. It begins with identifying a single important problematic infection area, based on available local data (antibiotic usage, resistance levels, length of stay, C difficile rates, mortality, etc). The hospitalist would then work with the infectious disease department/staff to establish a protocol focusing on several of the key areas: diagnosis, optimal empiric therapy, de‐escalation (based on cultures and clinical response), transitioning intravenous antibiotics to oral, optimal duration of therapy, and transitioning therapy to the posthospital setting. The protocol would establish best treatment practices and the strategies to implement them (education, standardized order sets, computer decision support, monitoring and feedback, etc). The level of complexity and targeted outcomes need to be tailored to the resources available for implementation. Successful implementation and goal achievement in a small area could then be used to justify additional resources to expand the program. If hospitalists can be engaged in antimicrobial stewardship, both through individual patient care as well as program development, the large and growing number of hospitalists throughout the United States should allow for widespread implementation of antimicrobial stewardship programs.
CONCLUSIONS
Healthcare‐associated infections are increasingly a cause of morbidity and mortality in the United States and other countries, and the management of HAIs is increasingly complicated by involvement of MDR pathogens. Antimicrobial‐resistant pathogens are also increasingly involved in infections occurring outside the hospital setting. Infections caused by resistant or MDR pathogens are associated with increased mortality, longer length of hospital stay, and higher healthcare costs. The prevalence of these dangerous bacteria affects antimicrobial choices across a wider range of patients, particularly when choosing empiric therapy. Together with infection control, antimicrobial stewardship is an attractive solution to the challenges posed by antimicrobial resistance. Development and implementation of an effective institutional antimicrobial stewardship program can improve clinical outcome, reduce antimicrobial resistance and other unintended consequences of antimicrobial overuse/misuse, and lower healthcare costs.
At the forefront of inpatient care, hospitalists are positioned as excellent champions of the principles and practices of antimicrobial stewardship. By adhering to the principles of optimal antimicrobial therapy in their clinical practice, hospitalists can improve care and help reduce resistance on a patient‐by‐patient basis. At the same time, they may achieve other key hospitalist goals by reducing length of stay and decreasing costs and utilization. Moreover, they are well positioned to participate in, and at times lead, hospital‐based antimicrobial stewardship programs. As such, hospitalists are expected to play a critical role in helping to solve the problems of antimicrobial resistance and suboptimal inpatient care, as we move further into the 21st century.
- ,,, et al.Estimating health care‐associated infections and deaths in U.S. hospitals, 2002.Public Health Rep.2007;122:160–166.
- .Historical and changing epidemiology of healthcare‐associated infections.J Hosp Infect.2009;73:296–304.
- ,,, et al.Four country healthcare associated infection prevalence survey 2006: overview of the results.J Hosp Infect.2008;69:230–248.
- ,,, et al.NHSN annual update: antimicrobial‐resistant pathogens associated with healthcare‐associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006‐2007.Infect Control Hosp Epidemiol.2008;29:996–1011.
- ,,, et al.Detection and characterization of class A extended‐spectrum‐beta‐lactamase‐producing Pseudomonas aeruginosa isolates in Belgian hospitals.J Antimicrob Chemother.2010;65:866–871.
- ,,, et al.Multidrug‐resistant Acinetobacter baumannii in New York City—10 years into the epidemic.Infect Control Hosp Epidemiol.2009;30:196–197.
- ,,. Emergence of extensively drug‐resistant and pandrug‐resistant Gram‐negative bacilli in Europe. Euro Surveill. 2008;13(47):pii=19045. Available at: http://www.eurosurveillance.org/viewarticle.aspx?articleid=19045. Accessed on March 29, 2011.
- ,,,,.Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis.BMJ.2010;340:c2096.
- ,,,,,.Fluoroquinolone‐resistant Pseudomonas aeruginosa: assessment of risk factors and clinical impact.Am J Med.2006;119:526.e519–526.e525.
- ,,,,,.Imipenem resistance among Pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes.Infect Control Hosp Epidemiol.2006;27:893–900.
- ,,,,.Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals.Clin Infect Dis.2005;41:435–440.
- ,,,,,.Antibiotic resistance among Gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888.
- ,,.Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem‐resistant Pseudomonas aeruginosa.Antimicrob Agents Chemother.2009;53:1983–1986.
- ,,,,.Predicting hospital rates of fluoroquinolone‐resistant Pseudomonas aeruginosa from fluoroquinolone use in US hospitals and their surrounding communities.Clin Infect Dis.2004;39:497–503.
- ,,.The effect of an antimicrobial restriction program on Pseudomonas aeruginosa resistance to beta‐lactams in a large teaching hospital.Pharmacotherapy.2003;23:618–624.
- ,,, et al.Relationship between rates of antimicrobial consumption and the incidence of antimicrobial resistance in Staphylococcus aureus and Pseudomonas aeruginosa isolates from 47 French hospitals.Infect Control Hosp Epidemiol.2007;28:1389–1395.
- ,,, et al.The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. Finnish Study Group for Antimicrobial Resistance.N Engl J Med.1997;337:441–446.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- ,,, et al.Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals.Clin Infect Dis.1997;25:584–599.
- ,.Antimicrobial stewardship for inpatient facilities.J Hosp Med.2011;6(suppl 1):S4–S15.
- ,.Antimicrobial stewardship.Infect Dis Clin North Am.2011;25:245–260.
- .Bad bugs, no drugs: no ESCAPE revisited.Clin Infect Dis.2009;49:992–993.
- .Federal funding for the study of antimicrobial resistance in nosocomial pathogens: no ESKAPE.J Infect Dis.2008;197:1079–1081.
- ,,.Clinical and economic burden of antimicrobial resistance.Expert Rev Anti Infect Ther.2008;6:751–763.
- .Economics of antibiotic resistance.Expert Rev Anti Infect Ther.2008;6:523–539.
- ,,,,.Antimicrobial activities of tigecycline and other broad‐spectrum antimicrobials tested against serine carbapenemase‐ and metallo‐beta‐lactamase‐producing Enterobacteriaceae: report from the SENTRY Antimicrobial Surveillance Program.Antimicrob Agents Chemother.2008;52:570–573.
- ,,,.Plasmid‐mediated carbapenem‐hydrolyzing beta‐lactamase KPC in a Klebsiella pneumoniae isolate from France.Antimicrob Agents Chemother.2005;49:4423–4424.
- ,,, et al.Emergence of KPC‐producing Pseudomonas aeruginosa in Trinidad and Tobago.J Clin Microbiol.2009;47:2670–2671.
- ,,, et al.First report on a hyperepidemic clone of KPC‐3‐producing Klebsiella pneumoniae in Israel genetically related to a strain causing outbreaks in the United States.Antimicrob Agents Chemother.2009;53:818–820.
- ,,.The real threat of Klebsiella pneumoniae carbapenemase‐producing bacteria.Lancet Infect Dis.2009;9:228–236.
- ,,, et al.Methicillin‐resistant S. aureus infections among patients in the emergency department.N Engl J Med.2006;355:666–674.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,, et al.Epidemiology of healthcare‐associated bloodstream infection caused by USA300 strains of methicillin‐resistant Staphylococcus aureus in 3 affiliated hospitals.Infect Control Hosp Epidemiol.2009;30:233–241.
- ,,.Community‐associated methicillin‐resistant Staphylococcus aureus in outpatients, United States, 1999‐2006.Emerg Infect Dis.2009;15:1925–1930.
- ,,,,.Community‐associated methicillin‐resistant Staphylococcus aureus isolates causing healthcare‐associated infections.Emerg Infect Dis.2007;13:236–242.
- ,,, et al.Emergence of community‐associated methicillin‐resistant Staphylococcus aureus strains as a cause of healthcare‐associated bloodstream infections in Korea.Infect Control Hosp Epidemiol.2009;30:146–155.
- ,,.Are community‐associated methicillin‐resistant Staphylococcus aureus (MRSA) strains replacing traditional nosocomial MRSA strains?Clin Infect Dis.2008;46:787–794.
- ,,, et al.Emergence of community‐associated methicillin‐resistant Staphylococcus aureus USA300 genotype as a major cause of health care‐associated bloodstream infections.Clin Infect Dis.2006;42:647–656.
- ,.Clostridium difficile infection in the intensive care unit.Infect Dis Clin North Am.2009;23:727–743.
- .Established and potential risk factors for Clostridum difficile infection.Indian J Med Microbiol.2009;27:289–300.
- ,,,.Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States.Arch Surg.2007;142:624–631.
- ,,.Increase in adult Clostridium difficile‐related hospitalizations and case‐fatality rate, United States, 2000‐2005.Emerg Infect Dis.2008;14:929–931.
- ,,.Increase in Clostridium difficile‐related hospitalizations among infants in the United States, 2000‐2005.Pediatr Infect Dis J.2008;27:1111–1113.
- ,,,.Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile.Clin Infect Dis.2002;34:346–353.
- ,,, et al.Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).Infect Control Hosp Epidemiol.2010;31:431–455.
- ,,,.Prevention of endemic healthcare‐associated Clostridium difficile infection: reviewing the evidence.Am J Gastroenterol.2010;105:2327–2340.
- ,,, et al.A predominantly clonal multi‐institutional outbreak of Clostridium difficile‐associated diarrhea with high morbidity and mortality.N Engl J Med.2005;353:2442–2449.
- ,,,.Analysis of an outbreak of Clostridium difficile infection controlled with enhanced infection control measures.Am J Infect Control.2009;37:458–464.
- ,,, et al.Multipronged intervention strategy to control an outbreak of Clostridium difficile infection (CDI) and its impact on the rates of CDI from 2002 to 2007.Infect Control Hosp Epidemiol.2009;30:156–162.
- ,,,,,.Hospital‐wide restriction of clindamycin: effect on the incidence of Clostridium difficile‐associated diarrhea and cost.Ann Intern Med.1998;128:989–995.
- ,,, et al.Successful use of feedback to improve antibiotic prescribing and reduce Clostridium difficile infection: a controlled interrupted time series.J Antimicrob Chemother.2007;59:990–995.
- ,.Impact of changes in antibiotic policy on Clostridium difficile‐associated diarrhoea (CDAD) over a five‐year period in a district general hospital.J Hosp Infect.2003;54:104–108.
- ,,,,,.An antibiotic policy associated with reduced risk of Clostridium difficile‐associated diarrhoea.Age Ageing.1999;28:578–580.
- ,,,,,.Antibiotic prescribing policy and Clostridium difficile diarrhoea.Q J Med.2004;97:423–429.
- ,,,,.Impact of a reduction in the use of high‐risk antibiotics on the course of an epidemic of Clostridium difficile‐associated disease caused by the hypervirulent NAP1/027 strain.Clin Infect Dis.2007;45(suppl 2):S112–S121.
- .Economic burden of healthcare‐associated infections: an American perspective.Expert Rev Pharmacoecon Outcomes Res.2009;9:417–422.
- .The Direct Medical Costs of Healthcare‐Associated Infections in US Hospitals and the Benefits of Prevention. Division of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases, Coordinating Center for Infectious Diseases, Centers for Disease Control and Prevention. Polock DA, Stone PW, eds.London, UK:Economist;2009.
- ,,,,.Multidrug‐resistant Pseudomonas aeruginosa: risk factors and clinical impact.Antimicrob Agents Chemother.2006;50:43–48.
- ,,,,,.The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges.Infect Control Hosp Epidemiol.2005;26:166–174.
- ,,, et al.Impact of imipenem resistance on mortality in patients with Acinetobacter bacteraemia.J Antimicrob Chemother.2007;59:525–530.
- ,,,,.Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes.Clin Infect Dis.2001;32:1162–1171.
- ,.Clinical and economic impact of methicillin resistance in patients with Staphylococcus aureus bacteremia.Diagn Microbiol Infect Dis.2005;52:113–122.
- ,,,,,.Clinical and economic impact of bacteremia with extended‐spectrum‐beta‐lactamase‐producing Enterobacteriaceae.Antimicrob Agents Chemother.2006;50:1257–1262.
- ,,, et al.Determinants of vancomycin resistance and mortality rates in enterococcal bacteremia: a prospective multicenter study.Ann Intern Med.2001;135:484–492.
- ,,, et al.Direct costs of multidrug‐resistant Acinetobacter baumannii in the burn unit of a public teaching hospital.Am J Infect Control.2004;32:342–344.
- ,,.Epidemiologic, clinical, and economic evaluation of an outbreak of clonal multidrug‐resistant Acinetobacter baumannii infection in a surgical intensive care unit.Infect Control Hosp Epidemiol.2007;28:1247–1254.
- .The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.Clin Infect Dis.2006;42(suppl 2):S82–S89.
- ,,, et al.Hospital and societal costs of antimicrobial‐resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship.Clin Infect Dis.2009;49:1175–1184.
- The Joint Commission. About The Joint Commission. Available at: http://www.jointcommission.org/facts_about_the_joint_commission/. Accessed March 29,2011.
- The Joint Commission. Accreditation Program: Hospital. National Patient Safety Goals. Effective January 1, 2011. Available at: http://www.jointcommission.org/assets/1/6/2011_NPSGs_HAP.pdf. Accessed January 24,2011.
- Deficit Reduction Act. Sec. 5001. Hospital Quality Improvement. Available at: http://www.cms.gov/HospitalAcqCond/Downloads/DeficitReductionAct2005. pdf. Accessed March 29,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart: Know When Antibiotics Work. Available at: http://www.cdc.gov/getsmart/. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). National Ambulatory Medical Care Survey. Available at: http://www.cdc.gov/nchs/ahcd. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). About Healthy People 2010. Available at: http://www.cdc.gov/nchs/healthy_people/hp2010.htm. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). DATA2010…the Healthy People 2010 Database. Available at: http://wonder.cdc.gov/DATA2010/ by searching for antibiotic. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare. Available at: http://www.cdc.gov/getsmart/healthcare/. Accessed March 29,2011.
- The Institute for Healthcare Improvement (IHI). About IHI. Available at: http://www.ihi.org/ihi/about. Accessed March 29,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare: All Clinicians Should…. Available at: http://www. cdc.gov/getsmart/healthcare/improve‐efforts/clinicians.html. Accessed May 3,2011.
- United States Department of Health 18:638–656.
- .Antimicrobial stewardship: application in the intensive care unit.Infect Dis Clin North Am.2009;23:683–702.
- ,,.Information technology for optimizing the management of infectious diseases.Am J Health Syst Pharm.2006;63:957–965.
- ,.Informatics and epidemiology in infection control.Infect Dis Clin North Am.2011;25:261–270.
- ,,,,,.Antibiotic optimization. An evaluation of patient safety and economic outcomes.Arch Intern Med.1997;157:1689–1694.
- ,,,.A randomized, prospective study measuring outcomes after antibiotic therapy intervention by a multidisciplinary consult team.Pharmacotherapy.1999;19:1369–1377.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare: Impact of Antibiotic Stewardship Program Interventions on Costs. Available at: http://www.cdc.gov/getsmart/healthcare/support‐efforts/asp‐int‐costs.html. Accessed May 3,2011.
- ,,,,.Favorable impact of a multidisciplinary antibiotic management program conducted during 7 years.Infect Control Hosp Epidemiol.2003;24:699–706.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,,,,.Effects of requiring prior authorization for selected antimicrobials: expenditures, susceptibilities, and clinical outcomes.Clin Infect Dis.1997;25:230–239.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360:1102–1112.
- Society of Hospital Medicine (SHM). Information About SHM and Hospitalists. Available at: http://www.hospitalmedicine.org/. Accessed April 1,2011.
- Society of Hospital Medicine (SHM). New Study Finds Over Half of US Hospitals Utilize Hospitalists. Available at: http://www.hospital medicine.org/AM/Template.cfm?Section=Press_Releases56:893–904.
- .Engaging hospitalists in antimicrobial stewardship: the CDC perspective.J Hosp Med.2011;6(suppl 1):S31–S33.
Healthcare‐associated infections (HAIs) are important causes of morbidity and mortality in the United States and other countries.13 Moreover, treatment of HAIs is frequently complicated by involvement of bacterial pathogens resistant to 1 or more antibiotics or antibiotic classes,4 and sometimes bacteria resistant to all or nearly all currently available agents.57 The rapid emergence of resistant bacteria both in and out of the hospital setting can affect empiric antimicrobial choices across all patients. The effort to avoid undertreating or not covering resistant bacteria can lead to overuse of wide‐spectrum antimicrobials. Antimicrobial useand especially antimicrobial overuse or misusehas been linked with increased antimicrobial resistance,817 leading to worsened clinical outcomes with increased length of hospital stay and healthcare costs. Table 1 defines the various lines of evidence supporting a causal relationship between antibiotic use and emergence of antimicrobial resistance.18, 19
|
| Changes in antimicrobial use are paralleled by changes in the prevalence of resistance |
| Antimicrobial resistance is more prevalent in healthcare‐associated bacterial infections vs community‐acquired infections |
| Patients with healthcare‐associated infections caused by resistant strains are more likely than control patients to have received prior antimicrobials |
| Areas within hospitals that have the highest rates of antimicrobial resistance also have the highest rates of antimicrobial use |
| Increasing duration of patient exposure to antimicrobials increases the likelihood of colonization with resistant organisms |
Optimal management of patients with bacterial infections, both HAIs and those that originate in the community, involves a focus on treatment that maximizes clinical outcomes for the individual patient, while also inhibiting or slowing the development of antimicrobial resistance and its spread to other patients. Antimicrobial stewardship is a term describing the various clinical strategies that have been devised to maximize the benefits and minimize the costs of antimicrobial therapy through judicious use of these agents.18, 20, 21 This article examines the developing patterns of resistance among key bacterial pathogens in the hospital and associated healthcare settings, the costs associated with HAIs (specifically, those caused by resistant pathogens), and the various strategies or programs that have been developed by governmental agencies, individual healthcare institutions, and other organizations to optimize the use of antibiotics to improve patient outcomes and minimize healthcare costs. The value that the hospitalist can bring to the development and/or implementation of institutional antimicrobial stewardship programs is explored.
ANTIMICROBIAL RESISTANCE AND HAI TRENDS FOR KEY BACTERIAL PATHOGENS
Bacterial pathogens including Enterobacteriaceae (Klebsiella pneumoniae, Enterobacter spp, Escherichia coli, and Proteus spp, among others), Acinetobacter baumannii, Pseudomonas aeruginosa, Staphylococcus aureus, and Enterococcus faecium22, 23 are increasingly prevalent in healthcare settings, and particularly troublesome to manage due to increasing resistance. Data from the Centers for Disease Control and Prevention's (CDC) National Healthcare Safety Network (NHSN) have shown that, in intensive care units (ICUs), 16% of HAIs are due to multidrug‐resistant (MDR) pathogens.4 These 16% have the highest mortality and length of hospital stay, and are associated with the highest healthcare costs.24, 25 Infections caused by MDR pathogens are more important than their actual numbers, because treatment decisions are driven by the intent to cover these MDR pathogens, even if that means providing excessively broad coverage for most patients. Moreover, the 16% mentioned above are only the tip of the iceberg, as many more HAIs will occur outside of the ICU, particularly catheter‐associated urinary tract infections (CAUTI) and surgical site infections, as these patients are often not sick enough to require ICU care. There is little information on the prevalence of HAIs outside of the ICU setting, the role of MDR bacteria in these infections, and the associated costs, mortality, and effects on length of stay.
K pneumoniae Carbapenemases and Community‐Acquired Methicillin‐Resistant Staphylococcus aureus
K pneumoniae carbapenemase (KPC) is a prime example of the emergence and rapid spread of a new resistance pattern that affects prescribing patterns. Emergence of KPC as the primary source of carbapenem resistance in Enterobacteriaceae26 is critically significant, as carbapenems are recommended first‐line therapy for serious infections caused by extended‐spectrum ‐lactamase (ESBL)‐producing K pneumoniae or other Enterobacteriaceae. One particularly remarkable fact about KPC‐producing bacteria is the speed at which they have spread since first emerging. Figure 1 from the CDC illustrates the rapid spread of KPC‐producing bacteria within the United States, from winter 2008 to May 2010. International spread has also been rapid and extensive. The first case of a KPC‐producing bacteria outside the United States was reported in France in February 2005, in an 80‐year‐old man who was admitted to a Parisian hospital 2 to 3 months after having a medical procedure performed in a New York City hospital, suggesting intercontinental transfer from the United States.27 Since then, KPC‐producing pathogenic bacteria have been identified in the Caribbean, South America, Europe, Israel, and China.2830 It is clear that once resistant bacteria emerge, they have the potential to spread very rapidly within and between countries, challenging currently available antimicrobial agents and complicating the treatment of serious infections.
Consideration of S aureus skin and skin‐structure infections highlights the fact that the barrier between hospital and community is now beginning to be crossed, further complicating prescribing decisions. The classic risk factors for resistance may no longer be reliable in determining best empiric treatment. In a landmark study, Moran et al. demonstrated the large percentages of outpatients in the United States with skin or soft‐tissue infections (SSTIs) involving community‐acquired methicillin‐resistant Staphylococcus aureus (CA‐MRSA).31 S aureus was isolated from 76% (320/422) of adults presenting to 11 university‐affiliated emergency departments with acute, purulent SSTIs in August 2004, 59% of whom were infected with MRSA. More than half the patients in the study (57%) were initially treated with antibiotics to which MRSA isolates were not susceptible.31 In the hospital, it has been shown that most invasive MRSA infections now actually have their onset outside of the healthcare setting,32 and that increasing numbers of hospitalized patients are now developing infections associated with CA‐MRSA strains >72 hours after admission.3338 Thus, it is becoming increasingly difficult to determine whether an invasive S aureus infection encountered in either a healthcare facility or community setting involves a sensitive organism, healthcare‐associated MRSA, or a CA‐MRSA pathogen, directly impacting treatment choices across all patients we care for with skin and skin‐structure infections.
Clostridium difficile‐Associated Disease
Indiscriminate and unnecessary use of antibiotics offer our patients no benefit, while exposing them to adverse effects of antibiotics, including allergies, rashes, and diarrhea among many potential other unintended consequences. C difficile‐associated disease is an increasingly problematic pathogen in the hospital setting that has been linked to unintended antibiotic effects.22, 39, 40 C difficile infection is not only costly in dollars, it is also a potentially fatal condition and has been linked to prolonged hospital stays and increased healthcare costs.4144 Improved infection control measures4549 and better use of antibiotics through antibiotic stewardship programs5055 have been shown to reduce the incidence of C difficile infection.
COSTS OF HAIs AND ANTIMICROBIAL RESISTANCE
HAIs are an important and growing problem in the United States.56 Klevens et al. estimated that approximately 1.7 million individuals hospitalized in the United States in 2002 had HAI, leading to 98,987 deaths.1 Estimates of annual hospital costs in the United States related to HAIs range from $28 to $48 billion.57 Antimicrobial resistance is a major driver of mortality, increased length of hospital stay, and hospital costs associated with HAIs.24, 25 A recent review by Sipahi25 summarizes recent studies examining the impact of resistant and MDR bacterial infections (Figure 2).5866 It is dramatically clear that infections due to resistant and MDR bacteria more often result in death, are associated with longer hospital stays, and are considerably more expensive to treat.
A number of factors can lead to the increased hospital costs associated with infection with a resistant or MDR bacteria. These include the need to use more expensive antibiotics, increased length of hospital stay, delayed appropriate antibiotic therapy, increased treatment toxicity (and costs associated with managing these toxicities), and increased frequency of surgical interventions required to control infection.25, 67
The savings that could be realized through reduction in antimicrobial resistance was evaluated recently by Roberts et al.68 Using a sensitivity analysis for a sample of high‐risk adult patients hospitalized in an urban public teaching hospital in 2000, the authors determined that reducing the antimicrobial‐resistant infection rate by 3.5% (from 13.5% to 10.0%) would have saved the study hospital $910,812 (in 2008 US$), when using lowest cost and length of stay figures. The calculated societal savings, for reduced mortality and lost productivity associated with the reduced antimicrobial‐resistant rate, was $1.8 million. Hence, the analysis showed a minimum overall medical (hospital) and societal savings of $2.7 million for this single hospital with a cohort of 1391 patients. The projected savings would be dramatically higher if the reduced antimicrobial‐resistant rate was generalized to all hospitals throughout the United States.
ORGANIZATIONAL AND GOVERNMENTAL EFFORTS ADDRESSING ANTIMICROBIAL RESISTANCE AND HAIs
Given the relationships between antimicrobial use and resistance, and between antimicrobial resistance and morbidity, mortality, length of hospital stay, and healthcare costs, it is not surprising that we have seen a variety of programs and initiatives begun by either government agencies or healthcare organizations aimed at reducing antimicrobial resistance and HAIs.
The Joint Commission
The Joint Commission is an independent, not‐for‐profit organization that accredits and certifies >18,000 healthcare organizations/programs in the United States.69 The Joint Commission issues annual National Patient Safety Goals (NPSG). Hospital compliance with these goals is a critical component of the accreditation process.70
The seventh goal of The Joint Commission's NPSG is to reduce the risk of HAIs,70 the key features of which are listed in Table 2. The methodology recommended to achieve compliance includes infection control programs and implementation of evidence‐based practices to prevent HAIs due to MDR microorganisms in acute‐care hospitals. This presumably could include development and implementation of an institutional antimicrobial stewardship, or components of a program, to reduce antimicrobial resistance within the hospital.
| Goal 7: Reduce the Risk of Healthcare‐Associated Infections |
|---|
|
| NPSG.07.03.01 |
| Implement evidence‐based practices to prevent healthcare‐associated infections due to multidrug‐resistant organisms in acute‐care hospitals |
| Note: This requirement applies to, but is not limited to, epidemiologically important organisms such as methicillin‐resistant Staphylococcus aureus, Clostridium difficile, vancomycin‐resistant enterococci (VRE), and multidrug‐resistant Gram‐negative bacteria |
| NPSG.07.04.01 |
| Implement evidence‐based practices to prevent central line‐associated bloodstream infection |
| Note: This requirement covers short‐ and long‐term central venous catheters and peripherally inserted central catheter (PICC) lines |
Centers for Medicare and Medicaid Services
The Deficit Reduction Act of 2005, Section 5001(c), requires the Secretary of Health and Human Services to identify conditions that are: (1) high cost or high volume, or both; (2) result in assignment of a case to a diagnosis‐related group that has higher payment when the code is present as a secondary diagnosis; and (3) could reasonably have been prevented through application of evidence‐based guidelines.71 The Centers for Medicare and Medicaid Services (CMS), which develops and administers Medicare and Medicaid payment and coverage policies, encourages hospitals to reduce the occurrence of these preventable problems through reduced payments when these events occur. Among the Hospital Acquired Conditions (HAC) that CMS considers reasonably preventable are a number of HAIs, particularly CAUTI, vascular catheter‐associated infections, and various surgery‐related SSTIs. Importantly, the CMS policy is still in effect as of April 2011, and there are no signs of its being repealed or modified in the foreseeable future.
The CDC Get Smart and Get Smart for Healthcare Programs
The Get Smart campaign, initiated by the CDC in 1995, focused on providing information to parents about the appropriate and inappropriate use of antibiotics to treat common childhood infections, as well as about the dangers of antibiotic resistance.72 The goal of Get Smart is to reduce unnecessary antibiotic use and the spread of antibiotic resistance in the community by reducing the pressure exerted by parents on physicians to overuse or misuse antibiotics. Hence, the primary focus in this setting is on patient/parent education. The Get Smart campaign has been highly successful, with a significant reduction in antibiotic prescriptions after initiation of the campaign, across a range of infections for which antibiotics are generally or often not warranted.73 The success of Get Smart is also largely responsible for the improvement in antibiotic prescribing for childhood middle ear infections observed in the CDC Healthy People 2010 program.74 The actual performance achieved in 2007 (the latest year reported) exceeded the Healthy People 2010 target.75
Building on the success of Get Smart for community‐acquired infections, a similar CDC campaign (Get Smart for Healthcare) has been undertaken to improve antibiotic usage and reduce antibiotic resistance in inpatient healthcare facilities.76 The specific goals of Get Smart for Healthcare are to improve patient safety through better treatment of infections, reduce emergence of antimicrobial‐resistant pathogens and C difficile, and heighten awareness of the challenges posed by antimicrobial resistance in healthcare settings. To help accomplish these ends, the CDC has partnered with the Institute for Healthcare Improvement (IHI), an independent, not‐for‐profit organization dedicated to closing the gap between the healthcare that currently exists and the healthcare that should exist.77 Together, they have identified a number of primary drivers to improve antibiotic use: timely and appropriate initiation of antibiotics; appropriate administration and de‐escalation; data monitoring and transparency; and improving knowledge of, and engagement in, antimicrobial stewardship efforts, which are the focus of the next section. With respect to data monitoring, many in the healthcare community hope that, through the Get Smart program, we will soon have better sources of data, not just for the ICU, but across the entire hospital setting. This would help providers get a better sense of where resistance is located, thereby enabling better development of action plans to deal with the problem.
The CDC has recently expanded its Web site on antimicrobial stewardship, now providing extensive support and resources for program development and implementation at:
All Clinicians Should:
Dose, Duration, Indication
Too often antibiotics in hospitals are continued unnecessarily simply because clinicians caring for the patient do not have information indicating why the antibiotics were started initially or for how long they were to be continued. This challenge is compounded in today's healthcare system where primary responsibility for patient care is frequently transitioned from one clinician to another. Ensuring that all antibiotic orders are always accompanied by a dose, duration, and indication will help clinicians change or stop therapy when appropriate.
Get Cultures
Antibiotic therapy can be best optimized when it can be tailored to specific culture results. Knowing the susceptibility of the infecting organisms can lead to narrowing of broad‐spectrum therapy, changing therapy to better treat resistant pathogens and to stopping antibiotics when cultures suggest an infection is unlikely.
A number of other government initiatives have been developed to address the issues of HAIs, antimicrobial resistance, and improved antimicrobial stewardship. These are beyond the scope of the present article, but include the United States Department of Health and Human Services (HHS) action plan to prevent HAIs,79 and the CDC campaign and action plan to prevent and combat antimicrobial resistance,80, 81 among others.
ANTIMICROBIAL STEWARDSHIP IN HOSPITALS AND THE HOSPITALIST'S ROLE
As recently defined, antimicrobial stewardship is a system of personnel, informatics, data collection, and policy/procedures that promote the optimal selection, dosing, and duration of therapy for antimicrobial agents throughout the course of their use.20 In simple words, the right antibiotic, at the right dose, at the right time, and for the right duration. The primary goals of antimicrobial stewardship are to reduce patient morbidity and mortality, prevent or slow the emergence of antimicrobial resistance, and reduce adverse drug effects, including secondary infections, such as C difficile‐associated diarrhea.18, 20 Secondary goals include a reduction in hospital length of stay and healthcare expenditures, without adversely impacting quality of care. These goals are entirely in line with those of the hospitalist, who can play a critical role in the prevention and successful management of these infections. Optimal effects are expected when antimicrobial stewardship is combined with implementation of effective infection control measures within the hospital setting.
Antimicrobial Stewardship Strategies
Table 3 provides an overview of various general strategies/procedures employed as components of antimicrobial stewardship programs.82 The 2 most common are: (1) formulary restriction and preauthorization for specific agents; and (2) prospective audit with intervention and feedback.18, 20 Both approaches can and have been used to improve antimicrobial stewardship and to achieve at least some of its goals, and each is associated with advantages and disadvantages, as outlined in Table 3 and reviewed elsewhere.18, 20, 21, 83 Other strategies, such as education and use of guidelines and clinical pathways, tend to be used to supplement or complement either a general formulary restriction/preauthorization, or prospective audit/review and feedback approach to antimicrobial stewardship. It is important to note that, as in other areas such as venous thromboembolism prophylaxis, education alone is insufficient to drive changes in prescribing patterns and thereby reduce resistance. Healthcare informatics are increasingly being utilized to improve the management of infectious diseases. These can be simple programs that better assemble information about hospital‐pathogen epidemiology. They can also be sophisticated systems, designed to standardize the antimicrobial order sets and medical logic modules, that guide treatment options by connecting patient‐specific information with guideline recommendations and local resistance patterns.18, 20, 84, 85
| Strategy | Procedure | Personnel | Advantages | Disadvantages |
|---|---|---|---|---|
| ||||
| Education/ guidelines | Creation of guidelines for antimicrobial use | Antimicrobial committee to create guidelines | May alter behavior patterns | Passive education likely ineffective |
| Group or individual education of clinicians by educators | Educators (physicians, pharmacists) | Avoids loss of prescriber autonomy | ||
| Formulary restriction | Restrict dispensing of targeted antimicrobials to approved indications | Antimicrobial committee to create guidelines Approval personnel (physician, infectious diseases fellow, clinical pharmacist) | Most direct control over antimicrobial use Individual educational opportunities | Perceived loss of autonomy for prescribers Need for all‐hours consultant availability |
| Review and feedback | Daily review of targeted antimicrobials for appropriateness Contact prescribers with recommendations for alternative therapy | Antimicrobial committee to create guidelines Review personnel (usually clinical pharmacist) | Avoids loss of autonomy for prescribers Individual educational opportunities | Compliance with recommendations |
| Computer assistance | Use of information technology to implement previous strategies | Antimicrobial committee to create rules for computer systems | Provides patient‐specific data where most likely to impact care (point of care) | Significant time and resource investment to implement sophisticated systems |
| Expert systems provide patient‐specific recommendations at point of entry (order entry) | Personnel for approval or review (physicians, pharmacists) Computer programmers | Facilitates other strategies | ||
Two early, randomized, prospective studies illustrate the potential benefits and general receptiveness of clinicians to use of an audit/review and feedback approach to institutional antimicrobial stewardship. The first study randomized adult inpatients receiving 1 parenteral antibiotic for 3 days to an intervention (n = 141) or control group (n = 111).86 In the intervention group, a clinical pharmacist and infectious diseases fellow reviewed the initial therapy prescribed by the primary care physician and the patient's progress 3 days after therapy initiation, and at that point offered suggestions for subsequent antibiotic therapy. The feedback or suggestions were communicated via nonpermanent chart note. In total, 85% of the physicians implemented the suggestions, and there were no significant differences between the intervention and control group for clinical or microbiologic endpoints. However, per‐patient antibiotic charges were significantly lower in the intervention versus control group ($1287.17 vs $1673.97; P = 0.05), which yields an estimated $390,000 in annualized savings for the 600‐bed tertiary‐care hospital.
Similarly, a randomized, prospective study by Gums et al. showed that therapeutic intervention by a multidisciplinary antimicrobial team for inpatients receiving suboptimal intravenous antibiotic therapy was associated with a median hospital cost savings of $2642 per intervention, compared with costs for similar inpatients who did not receive such intervention.87 The multidisciplinary team in the study consisted of pharmacists, a clinical microbiologist, and an infectious diseases specialist, who provided the treating physician with recommendations of possible optimal antibiotics, dosages, and rationales based on timely, detailed reviews of relevant microbiologic and clinical data. In total, 89% of physicians in the study implemented the suggestions from the multidisciplinary antimicrobial team. In addition to reduced costs, the intervention versus control group was also associated with significant reductions in the overall length of stay (10.1 vs 14.5 days; P = 0.0001), and total non‐ICU length of stay (5.7 vs 9.0; P = 0.0001). There was no significant difference between the 2 groups for mortality rate.
The results from these studies86, 87 demonstrate how a prospective audit/review and feedback approach to antimicrobial stewardship can be associated with high physician participation and significant cost reductions for participating hospitals,88 and potentially improve patient outcomes. Antimicrobial stewardship programs overall have a long track record in improving patient outcomes and reducing antimicrobial resistance at the patient level.8991
The Hospitalist's Role in Antimicrobial Stewardship
Hospitalists can participate in antimicrobial stewardship at a number of levels. On the direct patient care level, they can consistently apply the principles of appropriate empiric therapy, de‐escalation, and duration of therapy as presented by Drs Snydman, Kaye, and File in this supplement. As hospitalists assume a continually increasing role in the care of hospitalized patients throughout the United States,92 they can directly influence the way medicine is practiced on a daily basis, patient by patient. A 2007 survey conducted by the American Hospital Association (AHA) showed that 58% of the 4897 community hospitals surveyed had hospital medicine programs, and that 83% of hospitals with 200 or more beds had such a program.93, 94 Estimates from the Society of Hospital Medicine (SHM) in July 2010 indicated that currently there were more than 30,000 hospitalists, practicing in 3300 large hospitals.95 This affords hospitalists the opportunity to improve care across a huge segment of hospitalized patients.
On a departmental or institutional level, hospitalists appear to be especially well positioned to contribute to, and in some cases direct, a hospital's antimicrobial stewardship program. Unique to hospital medicine, and incorporated into the definition of the profession, is the commitment to quality and process improvement, efficient use of hospital and healthcare resources, and an interdisciplinary approach to care.96 In line with this, hospitalists frequently serve on hospital committees and task forces, are experienced in developing and implementing clinical guidelines, and lead multidisciplinary teams to optimize patient care. For example, as reported in a recent review, a 2007 Pediatric Research in the Inpatient Setting survey of 208 pediatric hospitalists in the United States and Canada indicated that 92% spend at least some time in administration, 85% serve on hospital committees, and 61% and 52% lead initiatives in practice guidelines and quality improvement, respectively.97 Hospitalists are therefore especially well positioned to participate, and provide leadership, in hospital antimicrobial stewardship programs.
In 2007, the Infectious Diseases Society of America (IDSA)/Society for Healthcare Epidemiology of America (SHEA) released guidelines for developing institutional programs to enhance antimicrobial stewardship.18 According to these guidelines, the ideal institutional antimicrobial stewardship program contains an infectious diseases physician and clinical pharmacist with infectious diseases training as core members, along with a clinical microbiologist, an information system specialist, infection control professional, and a hospital epidemiologist. The infectious diseases physician and clinical pharmacist with infectious diseases training are expected to serve as leaders of the team and should be appropriately compensated for time dedicated to the program. Clearly, this is an extensive team requiring a lot of staff. Although optimal, many institutions do not have an infectious diseases physician on staff or an attending who is interested and willing to participate. For many institutions, an even bigger issue is identifying an infectious diseases pharmacist with sufficient skill to manage an antimicrobial stewardship program. As a consequence, many institutions wanting to develop an antimicrobial stewardship program to improve clinical outcomes, reduce antimicrobial resistance, and lower costs will need to think outside the box and look for nontraditional leaders to champion and lead their programs. Potential nontraditional leaders include general clinical pharmacists, intensivists, and hospitalists.98
Although hospitalists are not explicitly mentioned in the IDSA/SHEA guidelines, they seem to be implicitly included. The guidelines state that the development, maintenance, and ultimate success of such programs fundamentally depends on the support and collaboration of hospital administration, medical staff leadership, and local providers.18 Furthermore, they indicate the desirability for antimicrobial stewardship programs to function under the auspices of quality assurance and patient safety. As defined above, these are characteristics that are inherent to hospital medicine. Hence, there appears to be a good match between the activities performed by hospitalists and what the 2007 guidelines indicate is important for an effective antimicrobial stewardship program.
Now is the time for individuals to begin thinking about how best to prepare hospitalists for leadership roles in hospital antimicrobial stewardship programs. We need a well‐defined process for either training hospitalists for independent establishment of stewardship programs or establishing partnership with infectious disease specialists for the development of these programs. We need high‐level training programs in focused areas of infectious diseases that hospitalists encounter frequently (skin and skin‐structure infections, pneumonia, catheter‐associated infections, among others). Detailed understanding of the pathogens and their optimal treatment could form the core of such training. Additional education in infection control and the antimicrobial stewardship processes would round out the knowledge needed for a hospitalist to best implement and provide leadership for an antimicrobial stewardship program at his/her own institution. These training programs could be developed and delivered locally, or preferably they could be provided at national training sessions developed and supported through SHM, infectious disease societies, or the CDC.
Partnering with infectious diseases specialists is essential for protocol development and clinical support. This could allow the hospitalist to start a stewardship program on a small scale. It begins with identifying a single important problematic infection area, based on available local data (antibiotic usage, resistance levels, length of stay, C difficile rates, mortality, etc). The hospitalist would then work with the infectious disease department/staff to establish a protocol focusing on several of the key areas: diagnosis, optimal empiric therapy, de‐escalation (based on cultures and clinical response), transitioning intravenous antibiotics to oral, optimal duration of therapy, and transitioning therapy to the posthospital setting. The protocol would establish best treatment practices and the strategies to implement them (education, standardized order sets, computer decision support, monitoring and feedback, etc). The level of complexity and targeted outcomes need to be tailored to the resources available for implementation. Successful implementation and goal achievement in a small area could then be used to justify additional resources to expand the program. If hospitalists can be engaged in antimicrobial stewardship, both through individual patient care as well as program development, the large and growing number of hospitalists throughout the United States should allow for widespread implementation of antimicrobial stewardship programs.
CONCLUSIONS
Healthcare‐associated infections are increasingly a cause of morbidity and mortality in the United States and other countries, and the management of HAIs is increasingly complicated by involvement of MDR pathogens. Antimicrobial‐resistant pathogens are also increasingly involved in infections occurring outside the hospital setting. Infections caused by resistant or MDR pathogens are associated with increased mortality, longer length of hospital stay, and higher healthcare costs. The prevalence of these dangerous bacteria affects antimicrobial choices across a wider range of patients, particularly when choosing empiric therapy. Together with infection control, antimicrobial stewardship is an attractive solution to the challenges posed by antimicrobial resistance. Development and implementation of an effective institutional antimicrobial stewardship program can improve clinical outcome, reduce antimicrobial resistance and other unintended consequences of antimicrobial overuse/misuse, and lower healthcare costs.
At the forefront of inpatient care, hospitalists are positioned as excellent champions of the principles and practices of antimicrobial stewardship. By adhering to the principles of optimal antimicrobial therapy in their clinical practice, hospitalists can improve care and help reduce resistance on a patient‐by‐patient basis. At the same time, they may achieve other key hospitalist goals by reducing length of stay and decreasing costs and utilization. Moreover, they are well positioned to participate in, and at times lead, hospital‐based antimicrobial stewardship programs. As such, hospitalists are expected to play a critical role in helping to solve the problems of antimicrobial resistance and suboptimal inpatient care, as we move further into the 21st century.
Healthcare‐associated infections (HAIs) are important causes of morbidity and mortality in the United States and other countries.13 Moreover, treatment of HAIs is frequently complicated by involvement of bacterial pathogens resistant to 1 or more antibiotics or antibiotic classes,4 and sometimes bacteria resistant to all or nearly all currently available agents.57 The rapid emergence of resistant bacteria both in and out of the hospital setting can affect empiric antimicrobial choices across all patients. The effort to avoid undertreating or not covering resistant bacteria can lead to overuse of wide‐spectrum antimicrobials. Antimicrobial useand especially antimicrobial overuse or misusehas been linked with increased antimicrobial resistance,817 leading to worsened clinical outcomes with increased length of hospital stay and healthcare costs. Table 1 defines the various lines of evidence supporting a causal relationship between antibiotic use and emergence of antimicrobial resistance.18, 19
|
| Changes in antimicrobial use are paralleled by changes in the prevalence of resistance |
| Antimicrobial resistance is more prevalent in healthcare‐associated bacterial infections vs community‐acquired infections |
| Patients with healthcare‐associated infections caused by resistant strains are more likely than control patients to have received prior antimicrobials |
| Areas within hospitals that have the highest rates of antimicrobial resistance also have the highest rates of antimicrobial use |
| Increasing duration of patient exposure to antimicrobials increases the likelihood of colonization with resistant organisms |
Optimal management of patients with bacterial infections, both HAIs and those that originate in the community, involves a focus on treatment that maximizes clinical outcomes for the individual patient, while also inhibiting or slowing the development of antimicrobial resistance and its spread to other patients. Antimicrobial stewardship is a term describing the various clinical strategies that have been devised to maximize the benefits and minimize the costs of antimicrobial therapy through judicious use of these agents.18, 20, 21 This article examines the developing patterns of resistance among key bacterial pathogens in the hospital and associated healthcare settings, the costs associated with HAIs (specifically, those caused by resistant pathogens), and the various strategies or programs that have been developed by governmental agencies, individual healthcare institutions, and other organizations to optimize the use of antibiotics to improve patient outcomes and minimize healthcare costs. The value that the hospitalist can bring to the development and/or implementation of institutional antimicrobial stewardship programs is explored.
ANTIMICROBIAL RESISTANCE AND HAI TRENDS FOR KEY BACTERIAL PATHOGENS
Bacterial pathogens including Enterobacteriaceae (Klebsiella pneumoniae, Enterobacter spp, Escherichia coli, and Proteus spp, among others), Acinetobacter baumannii, Pseudomonas aeruginosa, Staphylococcus aureus, and Enterococcus faecium22, 23 are increasingly prevalent in healthcare settings, and particularly troublesome to manage due to increasing resistance. Data from the Centers for Disease Control and Prevention's (CDC) National Healthcare Safety Network (NHSN) have shown that, in intensive care units (ICUs), 16% of HAIs are due to multidrug‐resistant (MDR) pathogens.4 These 16% have the highest mortality and length of hospital stay, and are associated with the highest healthcare costs.24, 25 Infections caused by MDR pathogens are more important than their actual numbers, because treatment decisions are driven by the intent to cover these MDR pathogens, even if that means providing excessively broad coverage for most patients. Moreover, the 16% mentioned above are only the tip of the iceberg, as many more HAIs will occur outside of the ICU, particularly catheter‐associated urinary tract infections (CAUTI) and surgical site infections, as these patients are often not sick enough to require ICU care. There is little information on the prevalence of HAIs outside of the ICU setting, the role of MDR bacteria in these infections, and the associated costs, mortality, and effects on length of stay.
K pneumoniae Carbapenemases and Community‐Acquired Methicillin‐Resistant Staphylococcus aureus
K pneumoniae carbapenemase (KPC) is a prime example of the emergence and rapid spread of a new resistance pattern that affects prescribing patterns. Emergence of KPC as the primary source of carbapenem resistance in Enterobacteriaceae26 is critically significant, as carbapenems are recommended first‐line therapy for serious infections caused by extended‐spectrum ‐lactamase (ESBL)‐producing K pneumoniae or other Enterobacteriaceae. One particularly remarkable fact about KPC‐producing bacteria is the speed at which they have spread since first emerging. Figure 1 from the CDC illustrates the rapid spread of KPC‐producing bacteria within the United States, from winter 2008 to May 2010. International spread has also been rapid and extensive. The first case of a KPC‐producing bacteria outside the United States was reported in France in February 2005, in an 80‐year‐old man who was admitted to a Parisian hospital 2 to 3 months after having a medical procedure performed in a New York City hospital, suggesting intercontinental transfer from the United States.27 Since then, KPC‐producing pathogenic bacteria have been identified in the Caribbean, South America, Europe, Israel, and China.2830 It is clear that once resistant bacteria emerge, they have the potential to spread very rapidly within and between countries, challenging currently available antimicrobial agents and complicating the treatment of serious infections.
Consideration of S aureus skin and skin‐structure infections highlights the fact that the barrier between hospital and community is now beginning to be crossed, further complicating prescribing decisions. The classic risk factors for resistance may no longer be reliable in determining best empiric treatment. In a landmark study, Moran et al. demonstrated the large percentages of outpatients in the United States with skin or soft‐tissue infections (SSTIs) involving community‐acquired methicillin‐resistant Staphylococcus aureus (CA‐MRSA).31 S aureus was isolated from 76% (320/422) of adults presenting to 11 university‐affiliated emergency departments with acute, purulent SSTIs in August 2004, 59% of whom were infected with MRSA. More than half the patients in the study (57%) were initially treated with antibiotics to which MRSA isolates were not susceptible.31 In the hospital, it has been shown that most invasive MRSA infections now actually have their onset outside of the healthcare setting,32 and that increasing numbers of hospitalized patients are now developing infections associated with CA‐MRSA strains >72 hours after admission.3338 Thus, it is becoming increasingly difficult to determine whether an invasive S aureus infection encountered in either a healthcare facility or community setting involves a sensitive organism, healthcare‐associated MRSA, or a CA‐MRSA pathogen, directly impacting treatment choices across all patients we care for with skin and skin‐structure infections.
Clostridium difficile‐Associated Disease
Indiscriminate and unnecessary use of antibiotics offer our patients no benefit, while exposing them to adverse effects of antibiotics, including allergies, rashes, and diarrhea among many potential other unintended consequences. C difficile‐associated disease is an increasingly problematic pathogen in the hospital setting that has been linked to unintended antibiotic effects.22, 39, 40 C difficile infection is not only costly in dollars, it is also a potentially fatal condition and has been linked to prolonged hospital stays and increased healthcare costs.4144 Improved infection control measures4549 and better use of antibiotics through antibiotic stewardship programs5055 have been shown to reduce the incidence of C difficile infection.
COSTS OF HAIs AND ANTIMICROBIAL RESISTANCE
HAIs are an important and growing problem in the United States.56 Klevens et al. estimated that approximately 1.7 million individuals hospitalized in the United States in 2002 had HAI, leading to 98,987 deaths.1 Estimates of annual hospital costs in the United States related to HAIs range from $28 to $48 billion.57 Antimicrobial resistance is a major driver of mortality, increased length of hospital stay, and hospital costs associated with HAIs.24, 25 A recent review by Sipahi25 summarizes recent studies examining the impact of resistant and MDR bacterial infections (Figure 2).5866 It is dramatically clear that infections due to resistant and MDR bacteria more often result in death, are associated with longer hospital stays, and are considerably more expensive to treat.
A number of factors can lead to the increased hospital costs associated with infection with a resistant or MDR bacteria. These include the need to use more expensive antibiotics, increased length of hospital stay, delayed appropriate antibiotic therapy, increased treatment toxicity (and costs associated with managing these toxicities), and increased frequency of surgical interventions required to control infection.25, 67
The savings that could be realized through reduction in antimicrobial resistance was evaluated recently by Roberts et al.68 Using a sensitivity analysis for a sample of high‐risk adult patients hospitalized in an urban public teaching hospital in 2000, the authors determined that reducing the antimicrobial‐resistant infection rate by 3.5% (from 13.5% to 10.0%) would have saved the study hospital $910,812 (in 2008 US$), when using lowest cost and length of stay figures. The calculated societal savings, for reduced mortality and lost productivity associated with the reduced antimicrobial‐resistant rate, was $1.8 million. Hence, the analysis showed a minimum overall medical (hospital) and societal savings of $2.7 million for this single hospital with a cohort of 1391 patients. The projected savings would be dramatically higher if the reduced antimicrobial‐resistant rate was generalized to all hospitals throughout the United States.
ORGANIZATIONAL AND GOVERNMENTAL EFFORTS ADDRESSING ANTIMICROBIAL RESISTANCE AND HAIs
Given the relationships between antimicrobial use and resistance, and between antimicrobial resistance and morbidity, mortality, length of hospital stay, and healthcare costs, it is not surprising that we have seen a variety of programs and initiatives begun by either government agencies or healthcare organizations aimed at reducing antimicrobial resistance and HAIs.
The Joint Commission
The Joint Commission is an independent, not‐for‐profit organization that accredits and certifies >18,000 healthcare organizations/programs in the United States.69 The Joint Commission issues annual National Patient Safety Goals (NPSG). Hospital compliance with these goals is a critical component of the accreditation process.70
The seventh goal of The Joint Commission's NPSG is to reduce the risk of HAIs,70 the key features of which are listed in Table 2. The methodology recommended to achieve compliance includes infection control programs and implementation of evidence‐based practices to prevent HAIs due to MDR microorganisms in acute‐care hospitals. This presumably could include development and implementation of an institutional antimicrobial stewardship, or components of a program, to reduce antimicrobial resistance within the hospital.
| Goal 7: Reduce the Risk of Healthcare‐Associated Infections |
|---|
|
| NPSG.07.03.01 |
| Implement evidence‐based practices to prevent healthcare‐associated infections due to multidrug‐resistant organisms in acute‐care hospitals |
| Note: This requirement applies to, but is not limited to, epidemiologically important organisms such as methicillin‐resistant Staphylococcus aureus, Clostridium difficile, vancomycin‐resistant enterococci (VRE), and multidrug‐resistant Gram‐negative bacteria |
| NPSG.07.04.01 |
| Implement evidence‐based practices to prevent central line‐associated bloodstream infection |
| Note: This requirement covers short‐ and long‐term central venous catheters and peripherally inserted central catheter (PICC) lines |
Centers for Medicare and Medicaid Services
The Deficit Reduction Act of 2005, Section 5001(c), requires the Secretary of Health and Human Services to identify conditions that are: (1) high cost or high volume, or both; (2) result in assignment of a case to a diagnosis‐related group that has higher payment when the code is present as a secondary diagnosis; and (3) could reasonably have been prevented through application of evidence‐based guidelines.71 The Centers for Medicare and Medicaid Services (CMS), which develops and administers Medicare and Medicaid payment and coverage policies, encourages hospitals to reduce the occurrence of these preventable problems through reduced payments when these events occur. Among the Hospital Acquired Conditions (HAC) that CMS considers reasonably preventable are a number of HAIs, particularly CAUTI, vascular catheter‐associated infections, and various surgery‐related SSTIs. Importantly, the CMS policy is still in effect as of April 2011, and there are no signs of its being repealed or modified in the foreseeable future.
The CDC Get Smart and Get Smart for Healthcare Programs
The Get Smart campaign, initiated by the CDC in 1995, focused on providing information to parents about the appropriate and inappropriate use of antibiotics to treat common childhood infections, as well as about the dangers of antibiotic resistance.72 The goal of Get Smart is to reduce unnecessary antibiotic use and the spread of antibiotic resistance in the community by reducing the pressure exerted by parents on physicians to overuse or misuse antibiotics. Hence, the primary focus in this setting is on patient/parent education. The Get Smart campaign has been highly successful, with a significant reduction in antibiotic prescriptions after initiation of the campaign, across a range of infections for which antibiotics are generally or often not warranted.73 The success of Get Smart is also largely responsible for the improvement in antibiotic prescribing for childhood middle ear infections observed in the CDC Healthy People 2010 program.74 The actual performance achieved in 2007 (the latest year reported) exceeded the Healthy People 2010 target.75
Building on the success of Get Smart for community‐acquired infections, a similar CDC campaign (Get Smart for Healthcare) has been undertaken to improve antibiotic usage and reduce antibiotic resistance in inpatient healthcare facilities.76 The specific goals of Get Smart for Healthcare are to improve patient safety through better treatment of infections, reduce emergence of antimicrobial‐resistant pathogens and C difficile, and heighten awareness of the challenges posed by antimicrobial resistance in healthcare settings. To help accomplish these ends, the CDC has partnered with the Institute for Healthcare Improvement (IHI), an independent, not‐for‐profit organization dedicated to closing the gap between the healthcare that currently exists and the healthcare that should exist.77 Together, they have identified a number of primary drivers to improve antibiotic use: timely and appropriate initiation of antibiotics; appropriate administration and de‐escalation; data monitoring and transparency; and improving knowledge of, and engagement in, antimicrobial stewardship efforts, which are the focus of the next section. With respect to data monitoring, many in the healthcare community hope that, through the Get Smart program, we will soon have better sources of data, not just for the ICU, but across the entire hospital setting. This would help providers get a better sense of where resistance is located, thereby enabling better development of action plans to deal with the problem.
The CDC has recently expanded its Web site on antimicrobial stewardship, now providing extensive support and resources for program development and implementation at:
All Clinicians Should:
Dose, Duration, Indication
Too often antibiotics in hospitals are continued unnecessarily simply because clinicians caring for the patient do not have information indicating why the antibiotics were started initially or for how long they were to be continued. This challenge is compounded in today's healthcare system where primary responsibility for patient care is frequently transitioned from one clinician to another. Ensuring that all antibiotic orders are always accompanied by a dose, duration, and indication will help clinicians change or stop therapy when appropriate.
Get Cultures
Antibiotic therapy can be best optimized when it can be tailored to specific culture results. Knowing the susceptibility of the infecting organisms can lead to narrowing of broad‐spectrum therapy, changing therapy to better treat resistant pathogens and to stopping antibiotics when cultures suggest an infection is unlikely.
A number of other government initiatives have been developed to address the issues of HAIs, antimicrobial resistance, and improved antimicrobial stewardship. These are beyond the scope of the present article, but include the United States Department of Health and Human Services (HHS) action plan to prevent HAIs,79 and the CDC campaign and action plan to prevent and combat antimicrobial resistance,80, 81 among others.
ANTIMICROBIAL STEWARDSHIP IN HOSPITALS AND THE HOSPITALIST'S ROLE
As recently defined, antimicrobial stewardship is a system of personnel, informatics, data collection, and policy/procedures that promote the optimal selection, dosing, and duration of therapy for antimicrobial agents throughout the course of their use.20 In simple words, the right antibiotic, at the right dose, at the right time, and for the right duration. The primary goals of antimicrobial stewardship are to reduce patient morbidity and mortality, prevent or slow the emergence of antimicrobial resistance, and reduce adverse drug effects, including secondary infections, such as C difficile‐associated diarrhea.18, 20 Secondary goals include a reduction in hospital length of stay and healthcare expenditures, without adversely impacting quality of care. These goals are entirely in line with those of the hospitalist, who can play a critical role in the prevention and successful management of these infections. Optimal effects are expected when antimicrobial stewardship is combined with implementation of effective infection control measures within the hospital setting.
Antimicrobial Stewardship Strategies
Table 3 provides an overview of various general strategies/procedures employed as components of antimicrobial stewardship programs.82 The 2 most common are: (1) formulary restriction and preauthorization for specific agents; and (2) prospective audit with intervention and feedback.18, 20 Both approaches can and have been used to improve antimicrobial stewardship and to achieve at least some of its goals, and each is associated with advantages and disadvantages, as outlined in Table 3 and reviewed elsewhere.18, 20, 21, 83 Other strategies, such as education and use of guidelines and clinical pathways, tend to be used to supplement or complement either a general formulary restriction/preauthorization, or prospective audit/review and feedback approach to antimicrobial stewardship. It is important to note that, as in other areas such as venous thromboembolism prophylaxis, education alone is insufficient to drive changes in prescribing patterns and thereby reduce resistance. Healthcare informatics are increasingly being utilized to improve the management of infectious diseases. These can be simple programs that better assemble information about hospital‐pathogen epidemiology. They can also be sophisticated systems, designed to standardize the antimicrobial order sets and medical logic modules, that guide treatment options by connecting patient‐specific information with guideline recommendations and local resistance patterns.18, 20, 84, 85
| Strategy | Procedure | Personnel | Advantages | Disadvantages |
|---|---|---|---|---|
| ||||
| Education/ guidelines | Creation of guidelines for antimicrobial use | Antimicrobial committee to create guidelines | May alter behavior patterns | Passive education likely ineffective |
| Group or individual education of clinicians by educators | Educators (physicians, pharmacists) | Avoids loss of prescriber autonomy | ||
| Formulary restriction | Restrict dispensing of targeted antimicrobials to approved indications | Antimicrobial committee to create guidelines Approval personnel (physician, infectious diseases fellow, clinical pharmacist) | Most direct control over antimicrobial use Individual educational opportunities | Perceived loss of autonomy for prescribers Need for all‐hours consultant availability |
| Review and feedback | Daily review of targeted antimicrobials for appropriateness Contact prescribers with recommendations for alternative therapy | Antimicrobial committee to create guidelines Review personnel (usually clinical pharmacist) | Avoids loss of autonomy for prescribers Individual educational opportunities | Compliance with recommendations |
| Computer assistance | Use of information technology to implement previous strategies | Antimicrobial committee to create rules for computer systems | Provides patient‐specific data where most likely to impact care (point of care) | Significant time and resource investment to implement sophisticated systems |
| Expert systems provide patient‐specific recommendations at point of entry (order entry) | Personnel for approval or review (physicians, pharmacists) Computer programmers | Facilitates other strategies | ||
Two early, randomized, prospective studies illustrate the potential benefits and general receptiveness of clinicians to use of an audit/review and feedback approach to institutional antimicrobial stewardship. The first study randomized adult inpatients receiving 1 parenteral antibiotic for 3 days to an intervention (n = 141) or control group (n = 111).86 In the intervention group, a clinical pharmacist and infectious diseases fellow reviewed the initial therapy prescribed by the primary care physician and the patient's progress 3 days after therapy initiation, and at that point offered suggestions for subsequent antibiotic therapy. The feedback or suggestions were communicated via nonpermanent chart note. In total, 85% of the physicians implemented the suggestions, and there were no significant differences between the intervention and control group for clinical or microbiologic endpoints. However, per‐patient antibiotic charges were significantly lower in the intervention versus control group ($1287.17 vs $1673.97; P = 0.05), which yields an estimated $390,000 in annualized savings for the 600‐bed tertiary‐care hospital.
Similarly, a randomized, prospective study by Gums et al. showed that therapeutic intervention by a multidisciplinary antimicrobial team for inpatients receiving suboptimal intravenous antibiotic therapy was associated with a median hospital cost savings of $2642 per intervention, compared with costs for similar inpatients who did not receive such intervention.87 The multidisciplinary team in the study consisted of pharmacists, a clinical microbiologist, and an infectious diseases specialist, who provided the treating physician with recommendations of possible optimal antibiotics, dosages, and rationales based on timely, detailed reviews of relevant microbiologic and clinical data. In total, 89% of physicians in the study implemented the suggestions from the multidisciplinary antimicrobial team. In addition to reduced costs, the intervention versus control group was also associated with significant reductions in the overall length of stay (10.1 vs 14.5 days; P = 0.0001), and total non‐ICU length of stay (5.7 vs 9.0; P = 0.0001). There was no significant difference between the 2 groups for mortality rate.
The results from these studies86, 87 demonstrate how a prospective audit/review and feedback approach to antimicrobial stewardship can be associated with high physician participation and significant cost reductions for participating hospitals,88 and potentially improve patient outcomes. Antimicrobial stewardship programs overall have a long track record in improving patient outcomes and reducing antimicrobial resistance at the patient level.8991
The Hospitalist's Role in Antimicrobial Stewardship
Hospitalists can participate in antimicrobial stewardship at a number of levels. On the direct patient care level, they can consistently apply the principles of appropriate empiric therapy, de‐escalation, and duration of therapy as presented by Drs Snydman, Kaye, and File in this supplement. As hospitalists assume a continually increasing role in the care of hospitalized patients throughout the United States,92 they can directly influence the way medicine is practiced on a daily basis, patient by patient. A 2007 survey conducted by the American Hospital Association (AHA) showed that 58% of the 4897 community hospitals surveyed had hospital medicine programs, and that 83% of hospitals with 200 or more beds had such a program.93, 94 Estimates from the Society of Hospital Medicine (SHM) in July 2010 indicated that currently there were more than 30,000 hospitalists, practicing in 3300 large hospitals.95 This affords hospitalists the opportunity to improve care across a huge segment of hospitalized patients.
On a departmental or institutional level, hospitalists appear to be especially well positioned to contribute to, and in some cases direct, a hospital's antimicrobial stewardship program. Unique to hospital medicine, and incorporated into the definition of the profession, is the commitment to quality and process improvement, efficient use of hospital and healthcare resources, and an interdisciplinary approach to care.96 In line with this, hospitalists frequently serve on hospital committees and task forces, are experienced in developing and implementing clinical guidelines, and lead multidisciplinary teams to optimize patient care. For example, as reported in a recent review, a 2007 Pediatric Research in the Inpatient Setting survey of 208 pediatric hospitalists in the United States and Canada indicated that 92% spend at least some time in administration, 85% serve on hospital committees, and 61% and 52% lead initiatives in practice guidelines and quality improvement, respectively.97 Hospitalists are therefore especially well positioned to participate, and provide leadership, in hospital antimicrobial stewardship programs.
In 2007, the Infectious Diseases Society of America (IDSA)/Society for Healthcare Epidemiology of America (SHEA) released guidelines for developing institutional programs to enhance antimicrobial stewardship.18 According to these guidelines, the ideal institutional antimicrobial stewardship program contains an infectious diseases physician and clinical pharmacist with infectious diseases training as core members, along with a clinical microbiologist, an information system specialist, infection control professional, and a hospital epidemiologist. The infectious diseases physician and clinical pharmacist with infectious diseases training are expected to serve as leaders of the team and should be appropriately compensated for time dedicated to the program. Clearly, this is an extensive team requiring a lot of staff. Although optimal, many institutions do not have an infectious diseases physician on staff or an attending who is interested and willing to participate. For many institutions, an even bigger issue is identifying an infectious diseases pharmacist with sufficient skill to manage an antimicrobial stewardship program. As a consequence, many institutions wanting to develop an antimicrobial stewardship program to improve clinical outcomes, reduce antimicrobial resistance, and lower costs will need to think outside the box and look for nontraditional leaders to champion and lead their programs. Potential nontraditional leaders include general clinical pharmacists, intensivists, and hospitalists.98
Although hospitalists are not explicitly mentioned in the IDSA/SHEA guidelines, they seem to be implicitly included. The guidelines state that the development, maintenance, and ultimate success of such programs fundamentally depends on the support and collaboration of hospital administration, medical staff leadership, and local providers.18 Furthermore, they indicate the desirability for antimicrobial stewardship programs to function under the auspices of quality assurance and patient safety. As defined above, these are characteristics that are inherent to hospital medicine. Hence, there appears to be a good match between the activities performed by hospitalists and what the 2007 guidelines indicate is important for an effective antimicrobial stewardship program.
Now is the time for individuals to begin thinking about how best to prepare hospitalists for leadership roles in hospital antimicrobial stewardship programs. We need a well‐defined process for either training hospitalists for independent establishment of stewardship programs or establishing partnership with infectious disease specialists for the development of these programs. We need high‐level training programs in focused areas of infectious diseases that hospitalists encounter frequently (skin and skin‐structure infections, pneumonia, catheter‐associated infections, among others). Detailed understanding of the pathogens and their optimal treatment could form the core of such training. Additional education in infection control and the antimicrobial stewardship processes would round out the knowledge needed for a hospitalist to best implement and provide leadership for an antimicrobial stewardship program at his/her own institution. These training programs could be developed and delivered locally, or preferably they could be provided at national training sessions developed and supported through SHM, infectious disease societies, or the CDC.
Partnering with infectious diseases specialists is essential for protocol development and clinical support. This could allow the hospitalist to start a stewardship program on a small scale. It begins with identifying a single important problematic infection area, based on available local data (antibiotic usage, resistance levels, length of stay, C difficile rates, mortality, etc). The hospitalist would then work with the infectious disease department/staff to establish a protocol focusing on several of the key areas: diagnosis, optimal empiric therapy, de‐escalation (based on cultures and clinical response), transitioning intravenous antibiotics to oral, optimal duration of therapy, and transitioning therapy to the posthospital setting. The protocol would establish best treatment practices and the strategies to implement them (education, standardized order sets, computer decision support, monitoring and feedback, etc). The level of complexity and targeted outcomes need to be tailored to the resources available for implementation. Successful implementation and goal achievement in a small area could then be used to justify additional resources to expand the program. If hospitalists can be engaged in antimicrobial stewardship, both through individual patient care as well as program development, the large and growing number of hospitalists throughout the United States should allow for widespread implementation of antimicrobial stewardship programs.
CONCLUSIONS
Healthcare‐associated infections are increasingly a cause of morbidity and mortality in the United States and other countries, and the management of HAIs is increasingly complicated by involvement of MDR pathogens. Antimicrobial‐resistant pathogens are also increasingly involved in infections occurring outside the hospital setting. Infections caused by resistant or MDR pathogens are associated with increased mortality, longer length of hospital stay, and higher healthcare costs. The prevalence of these dangerous bacteria affects antimicrobial choices across a wider range of patients, particularly when choosing empiric therapy. Together with infection control, antimicrobial stewardship is an attractive solution to the challenges posed by antimicrobial resistance. Development and implementation of an effective institutional antimicrobial stewardship program can improve clinical outcome, reduce antimicrobial resistance and other unintended consequences of antimicrobial overuse/misuse, and lower healthcare costs.
At the forefront of inpatient care, hospitalists are positioned as excellent champions of the principles and practices of antimicrobial stewardship. By adhering to the principles of optimal antimicrobial therapy in their clinical practice, hospitalists can improve care and help reduce resistance on a patient‐by‐patient basis. At the same time, they may achieve other key hospitalist goals by reducing length of stay and decreasing costs and utilization. Moreover, they are well positioned to participate in, and at times lead, hospital‐based antimicrobial stewardship programs. As such, hospitalists are expected to play a critical role in helping to solve the problems of antimicrobial resistance and suboptimal inpatient care, as we move further into the 21st century.
- ,,, et al.Estimating health care‐associated infections and deaths in U.S. hospitals, 2002.Public Health Rep.2007;122:160–166.
- .Historical and changing epidemiology of healthcare‐associated infections.J Hosp Infect.2009;73:296–304.
- ,,, et al.Four country healthcare associated infection prevalence survey 2006: overview of the results.J Hosp Infect.2008;69:230–248.
- ,,, et al.NHSN annual update: antimicrobial‐resistant pathogens associated with healthcare‐associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006‐2007.Infect Control Hosp Epidemiol.2008;29:996–1011.
- ,,, et al.Detection and characterization of class A extended‐spectrum‐beta‐lactamase‐producing Pseudomonas aeruginosa isolates in Belgian hospitals.J Antimicrob Chemother.2010;65:866–871.
- ,,, et al.Multidrug‐resistant Acinetobacter baumannii in New York City—10 years into the epidemic.Infect Control Hosp Epidemiol.2009;30:196–197.
- ,,. Emergence of extensively drug‐resistant and pandrug‐resistant Gram‐negative bacilli in Europe. Euro Surveill. 2008;13(47):pii=19045. Available at: http://www.eurosurveillance.org/viewarticle.aspx?articleid=19045. Accessed on March 29, 2011.
- ,,,,.Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis.BMJ.2010;340:c2096.
- ,,,,,.Fluoroquinolone‐resistant Pseudomonas aeruginosa: assessment of risk factors and clinical impact.Am J Med.2006;119:526.e519–526.e525.
- ,,,,,.Imipenem resistance among Pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes.Infect Control Hosp Epidemiol.2006;27:893–900.
- ,,,,.Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals.Clin Infect Dis.2005;41:435–440.
- ,,,,,.Antibiotic resistance among Gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888.
- ,,.Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem‐resistant Pseudomonas aeruginosa.Antimicrob Agents Chemother.2009;53:1983–1986.
- ,,,,.Predicting hospital rates of fluoroquinolone‐resistant Pseudomonas aeruginosa from fluoroquinolone use in US hospitals and their surrounding communities.Clin Infect Dis.2004;39:497–503.
- ,,.The effect of an antimicrobial restriction program on Pseudomonas aeruginosa resistance to beta‐lactams in a large teaching hospital.Pharmacotherapy.2003;23:618–624.
- ,,, et al.Relationship between rates of antimicrobial consumption and the incidence of antimicrobial resistance in Staphylococcus aureus and Pseudomonas aeruginosa isolates from 47 French hospitals.Infect Control Hosp Epidemiol.2007;28:1389–1395.
- ,,, et al.The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. Finnish Study Group for Antimicrobial Resistance.N Engl J Med.1997;337:441–446.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- ,,, et al.Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals.Clin Infect Dis.1997;25:584–599.
- ,.Antimicrobial stewardship for inpatient facilities.J Hosp Med.2011;6(suppl 1):S4–S15.
- ,.Antimicrobial stewardship.Infect Dis Clin North Am.2011;25:245–260.
- .Bad bugs, no drugs: no ESCAPE revisited.Clin Infect Dis.2009;49:992–993.
- .Federal funding for the study of antimicrobial resistance in nosocomial pathogens: no ESKAPE.J Infect Dis.2008;197:1079–1081.
- ,,.Clinical and economic burden of antimicrobial resistance.Expert Rev Anti Infect Ther.2008;6:751–763.
- .Economics of antibiotic resistance.Expert Rev Anti Infect Ther.2008;6:523–539.
- ,,,,.Antimicrobial activities of tigecycline and other broad‐spectrum antimicrobials tested against serine carbapenemase‐ and metallo‐beta‐lactamase‐producing Enterobacteriaceae: report from the SENTRY Antimicrobial Surveillance Program.Antimicrob Agents Chemother.2008;52:570–573.
- ,,,.Plasmid‐mediated carbapenem‐hydrolyzing beta‐lactamase KPC in a Klebsiella pneumoniae isolate from France.Antimicrob Agents Chemother.2005;49:4423–4424.
- ,,, et al.Emergence of KPC‐producing Pseudomonas aeruginosa in Trinidad and Tobago.J Clin Microbiol.2009;47:2670–2671.
- ,,, et al.First report on a hyperepidemic clone of KPC‐3‐producing Klebsiella pneumoniae in Israel genetically related to a strain causing outbreaks in the United States.Antimicrob Agents Chemother.2009;53:818–820.
- ,,.The real threat of Klebsiella pneumoniae carbapenemase‐producing bacteria.Lancet Infect Dis.2009;9:228–236.
- ,,, et al.Methicillin‐resistant S. aureus infections among patients in the emergency department.N Engl J Med.2006;355:666–674.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,, et al.Epidemiology of healthcare‐associated bloodstream infection caused by USA300 strains of methicillin‐resistant Staphylococcus aureus in 3 affiliated hospitals.Infect Control Hosp Epidemiol.2009;30:233–241.
- ,,.Community‐associated methicillin‐resistant Staphylococcus aureus in outpatients, United States, 1999‐2006.Emerg Infect Dis.2009;15:1925–1930.
- ,,,,.Community‐associated methicillin‐resistant Staphylococcus aureus isolates causing healthcare‐associated infections.Emerg Infect Dis.2007;13:236–242.
- ,,, et al.Emergence of community‐associated methicillin‐resistant Staphylococcus aureus strains as a cause of healthcare‐associated bloodstream infections in Korea.Infect Control Hosp Epidemiol.2009;30:146–155.
- ,,.Are community‐associated methicillin‐resistant Staphylococcus aureus (MRSA) strains replacing traditional nosocomial MRSA strains?Clin Infect Dis.2008;46:787–794.
- ,,, et al.Emergence of community‐associated methicillin‐resistant Staphylococcus aureus USA300 genotype as a major cause of health care‐associated bloodstream infections.Clin Infect Dis.2006;42:647–656.
- ,.Clostridium difficile infection in the intensive care unit.Infect Dis Clin North Am.2009;23:727–743.
- .Established and potential risk factors for Clostridum difficile infection.Indian J Med Microbiol.2009;27:289–300.
- ,,,.Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States.Arch Surg.2007;142:624–631.
- ,,.Increase in adult Clostridium difficile‐related hospitalizations and case‐fatality rate, United States, 2000‐2005.Emerg Infect Dis.2008;14:929–931.
- ,,.Increase in Clostridium difficile‐related hospitalizations among infants in the United States, 2000‐2005.Pediatr Infect Dis J.2008;27:1111–1113.
- ,,,.Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile.Clin Infect Dis.2002;34:346–353.
- ,,, et al.Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).Infect Control Hosp Epidemiol.2010;31:431–455.
- ,,,.Prevention of endemic healthcare‐associated Clostridium difficile infection: reviewing the evidence.Am J Gastroenterol.2010;105:2327–2340.
- ,,, et al.A predominantly clonal multi‐institutional outbreak of Clostridium difficile‐associated diarrhea with high morbidity and mortality.N Engl J Med.2005;353:2442–2449.
- ,,,.Analysis of an outbreak of Clostridium difficile infection controlled with enhanced infection control measures.Am J Infect Control.2009;37:458–464.
- ,,, et al.Multipronged intervention strategy to control an outbreak of Clostridium difficile infection (CDI) and its impact on the rates of CDI from 2002 to 2007.Infect Control Hosp Epidemiol.2009;30:156–162.
- ,,,,,.Hospital‐wide restriction of clindamycin: effect on the incidence of Clostridium difficile‐associated diarrhea and cost.Ann Intern Med.1998;128:989–995.
- ,,, et al.Successful use of feedback to improve antibiotic prescribing and reduce Clostridium difficile infection: a controlled interrupted time series.J Antimicrob Chemother.2007;59:990–995.
- ,.Impact of changes in antibiotic policy on Clostridium difficile‐associated diarrhoea (CDAD) over a five‐year period in a district general hospital.J Hosp Infect.2003;54:104–108.
- ,,,,,.An antibiotic policy associated with reduced risk of Clostridium difficile‐associated diarrhoea.Age Ageing.1999;28:578–580.
- ,,,,,.Antibiotic prescribing policy and Clostridium difficile diarrhoea.Q J Med.2004;97:423–429.
- ,,,,.Impact of a reduction in the use of high‐risk antibiotics on the course of an epidemic of Clostridium difficile‐associated disease caused by the hypervirulent NAP1/027 strain.Clin Infect Dis.2007;45(suppl 2):S112–S121.
- .Economic burden of healthcare‐associated infections: an American perspective.Expert Rev Pharmacoecon Outcomes Res.2009;9:417–422.
- .The Direct Medical Costs of Healthcare‐Associated Infections in US Hospitals and the Benefits of Prevention. Division of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases, Coordinating Center for Infectious Diseases, Centers for Disease Control and Prevention. Polock DA, Stone PW, eds.London, UK:Economist;2009.
- ,,,,.Multidrug‐resistant Pseudomonas aeruginosa: risk factors and clinical impact.Antimicrob Agents Chemother.2006;50:43–48.
- ,,,,,.The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges.Infect Control Hosp Epidemiol.2005;26:166–174.
- ,,, et al.Impact of imipenem resistance on mortality in patients with Acinetobacter bacteraemia.J Antimicrob Chemother.2007;59:525–530.
- ,,,,.Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes.Clin Infect Dis.2001;32:1162–1171.
- ,.Clinical and economic impact of methicillin resistance in patients with Staphylococcus aureus bacteremia.Diagn Microbiol Infect Dis.2005;52:113–122.
- ,,,,,.Clinical and economic impact of bacteremia with extended‐spectrum‐beta‐lactamase‐producing Enterobacteriaceae.Antimicrob Agents Chemother.2006;50:1257–1262.
- ,,, et al.Determinants of vancomycin resistance and mortality rates in enterococcal bacteremia: a prospective multicenter study.Ann Intern Med.2001;135:484–492.
- ,,, et al.Direct costs of multidrug‐resistant Acinetobacter baumannii in the burn unit of a public teaching hospital.Am J Infect Control.2004;32:342–344.
- ,,.Epidemiologic, clinical, and economic evaluation of an outbreak of clonal multidrug‐resistant Acinetobacter baumannii infection in a surgical intensive care unit.Infect Control Hosp Epidemiol.2007;28:1247–1254.
- .The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.Clin Infect Dis.2006;42(suppl 2):S82–S89.
- ,,, et al.Hospital and societal costs of antimicrobial‐resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship.Clin Infect Dis.2009;49:1175–1184.
- The Joint Commission. About The Joint Commission. Available at: http://www.jointcommission.org/facts_about_the_joint_commission/. Accessed March 29,2011.
- The Joint Commission. Accreditation Program: Hospital. National Patient Safety Goals. Effective January 1, 2011. Available at: http://www.jointcommission.org/assets/1/6/2011_NPSGs_HAP.pdf. Accessed January 24,2011.
- Deficit Reduction Act. Sec. 5001. Hospital Quality Improvement. Available at: http://www.cms.gov/HospitalAcqCond/Downloads/DeficitReductionAct2005. pdf. Accessed March 29,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart: Know When Antibiotics Work. Available at: http://www.cdc.gov/getsmart/. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). National Ambulatory Medical Care Survey. Available at: http://www.cdc.gov/nchs/ahcd. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). About Healthy People 2010. Available at: http://www.cdc.gov/nchs/healthy_people/hp2010.htm. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). DATA2010…the Healthy People 2010 Database. Available at: http://wonder.cdc.gov/DATA2010/ by searching for antibiotic. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare. Available at: http://www.cdc.gov/getsmart/healthcare/. Accessed March 29,2011.
- The Institute for Healthcare Improvement (IHI). About IHI. Available at: http://www.ihi.org/ihi/about. Accessed March 29,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare: All Clinicians Should…. Available at: http://www. cdc.gov/getsmart/healthcare/improve‐efforts/clinicians.html. Accessed May 3,2011.
- United States Department of Health 18:638–656.
- .Antimicrobial stewardship: application in the intensive care unit.Infect Dis Clin North Am.2009;23:683–702.
- ,,.Information technology for optimizing the management of infectious diseases.Am J Health Syst Pharm.2006;63:957–965.
- ,.Informatics and epidemiology in infection control.Infect Dis Clin North Am.2011;25:261–270.
- ,,,,,.Antibiotic optimization. An evaluation of patient safety and economic outcomes.Arch Intern Med.1997;157:1689–1694.
- ,,,.A randomized, prospective study measuring outcomes after antibiotic therapy intervention by a multidisciplinary consult team.Pharmacotherapy.1999;19:1369–1377.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare: Impact of Antibiotic Stewardship Program Interventions on Costs. Available at: http://www.cdc.gov/getsmart/healthcare/support‐efforts/asp‐int‐costs.html. Accessed May 3,2011.
- ,,,,.Favorable impact of a multidisciplinary antibiotic management program conducted during 7 years.Infect Control Hosp Epidemiol.2003;24:699–706.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,,,,.Effects of requiring prior authorization for selected antimicrobials: expenditures, susceptibilities, and clinical outcomes.Clin Infect Dis.1997;25:230–239.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360:1102–1112.
- Society of Hospital Medicine (SHM). Information About SHM and Hospitalists. Available at: http://www.hospitalmedicine.org/. Accessed April 1,2011.
- Society of Hospital Medicine (SHM). New Study Finds Over Half of US Hospitals Utilize Hospitalists. Available at: http://www.hospital medicine.org/AM/Template.cfm?Section=Press_Releases56:893–904.
- .Engaging hospitalists in antimicrobial stewardship: the CDC perspective.J Hosp Med.2011;6(suppl 1):S31–S33.
- ,,, et al.Estimating health care‐associated infections and deaths in U.S. hospitals, 2002.Public Health Rep.2007;122:160–166.
- .Historical and changing epidemiology of healthcare‐associated infections.J Hosp Infect.2009;73:296–304.
- ,,, et al.Four country healthcare associated infection prevalence survey 2006: overview of the results.J Hosp Infect.2008;69:230–248.
- ,,, et al.NHSN annual update: antimicrobial‐resistant pathogens associated with healthcare‐associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006‐2007.Infect Control Hosp Epidemiol.2008;29:996–1011.
- ,,, et al.Detection and characterization of class A extended‐spectrum‐beta‐lactamase‐producing Pseudomonas aeruginosa isolates in Belgian hospitals.J Antimicrob Chemother.2010;65:866–871.
- ,,, et al.Multidrug‐resistant Acinetobacter baumannii in New York City—10 years into the epidemic.Infect Control Hosp Epidemiol.2009;30:196–197.
- ,,. Emergence of extensively drug‐resistant and pandrug‐resistant Gram‐negative bacilli in Europe. Euro Surveill. 2008;13(47):pii=19045. Available at: http://www.eurosurveillance.org/viewarticle.aspx?articleid=19045. Accessed on March 29, 2011.
- ,,,,.Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis.BMJ.2010;340:c2096.
- ,,,,,.Fluoroquinolone‐resistant Pseudomonas aeruginosa: assessment of risk factors and clinical impact.Am J Med.2006;119:526.e519–526.e525.
- ,,,,,.Imipenem resistance among Pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes.Infect Control Hosp Epidemiol.2006;27:893–900.
- ,,,,.Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals.Clin Infect Dis.2005;41:435–440.
- ,,,,,.Antibiotic resistance among Gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888.
- ,,.Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem‐resistant Pseudomonas aeruginosa.Antimicrob Agents Chemother.2009;53:1983–1986.
- ,,,,.Predicting hospital rates of fluoroquinolone‐resistant Pseudomonas aeruginosa from fluoroquinolone use in US hospitals and their surrounding communities.Clin Infect Dis.2004;39:497–503.
- ,,.The effect of an antimicrobial restriction program on Pseudomonas aeruginosa resistance to beta‐lactams in a large teaching hospital.Pharmacotherapy.2003;23:618–624.
- ,,, et al.Relationship between rates of antimicrobial consumption and the incidence of antimicrobial resistance in Staphylococcus aureus and Pseudomonas aeruginosa isolates from 47 French hospitals.Infect Control Hosp Epidemiol.2007;28:1389–1395.
- ,,, et al.The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. Finnish Study Group for Antimicrobial Resistance.N Engl J Med.1997;337:441–446.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- ,,, et al.Society for Healthcare Epidemiology of America and Infectious Diseases Society of America Joint Committee on the Prevention of Antimicrobial Resistance: guidelines for the prevention of antimicrobial resistance in hospitals.Clin Infect Dis.1997;25:584–599.
- ,.Antimicrobial stewardship for inpatient facilities.J Hosp Med.2011;6(suppl 1):S4–S15.
- ,.Antimicrobial stewardship.Infect Dis Clin North Am.2011;25:245–260.
- .Bad bugs, no drugs: no ESCAPE revisited.Clin Infect Dis.2009;49:992–993.
- .Federal funding for the study of antimicrobial resistance in nosocomial pathogens: no ESKAPE.J Infect Dis.2008;197:1079–1081.
- ,,.Clinical and economic burden of antimicrobial resistance.Expert Rev Anti Infect Ther.2008;6:751–763.
- .Economics of antibiotic resistance.Expert Rev Anti Infect Ther.2008;6:523–539.
- ,,,,.Antimicrobial activities of tigecycline and other broad‐spectrum antimicrobials tested against serine carbapenemase‐ and metallo‐beta‐lactamase‐producing Enterobacteriaceae: report from the SENTRY Antimicrobial Surveillance Program.Antimicrob Agents Chemother.2008;52:570–573.
- ,,,.Plasmid‐mediated carbapenem‐hydrolyzing beta‐lactamase KPC in a Klebsiella pneumoniae isolate from France.Antimicrob Agents Chemother.2005;49:4423–4424.
- ,,, et al.Emergence of KPC‐producing Pseudomonas aeruginosa in Trinidad and Tobago.J Clin Microbiol.2009;47:2670–2671.
- ,,, et al.First report on a hyperepidemic clone of KPC‐3‐producing Klebsiella pneumoniae in Israel genetically related to a strain causing outbreaks in the United States.Antimicrob Agents Chemother.2009;53:818–820.
- ,,.The real threat of Klebsiella pneumoniae carbapenemase‐producing bacteria.Lancet Infect Dis.2009;9:228–236.
- ,,, et al.Methicillin‐resistant S. aureus infections among patients in the emergency department.N Engl J Med.2006;355:666–674.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,, et al.Epidemiology of healthcare‐associated bloodstream infection caused by USA300 strains of methicillin‐resistant Staphylococcus aureus in 3 affiliated hospitals.Infect Control Hosp Epidemiol.2009;30:233–241.
- ,,.Community‐associated methicillin‐resistant Staphylococcus aureus in outpatients, United States, 1999‐2006.Emerg Infect Dis.2009;15:1925–1930.
- ,,,,.Community‐associated methicillin‐resistant Staphylococcus aureus isolates causing healthcare‐associated infections.Emerg Infect Dis.2007;13:236–242.
- ,,, et al.Emergence of community‐associated methicillin‐resistant Staphylococcus aureus strains as a cause of healthcare‐associated bloodstream infections in Korea.Infect Control Hosp Epidemiol.2009;30:146–155.
- ,,.Are community‐associated methicillin‐resistant Staphylococcus aureus (MRSA) strains replacing traditional nosocomial MRSA strains?Clin Infect Dis.2008;46:787–794.
- ,,, et al.Emergence of community‐associated methicillin‐resistant Staphylococcus aureus USA300 genotype as a major cause of health care‐associated bloodstream infections.Clin Infect Dis.2006;42:647–656.
- ,.Clostridium difficile infection in the intensive care unit.Infect Dis Clin North Am.2009;23:727–743.
- .Established and potential risk factors for Clostridum difficile infection.Indian J Med Microbiol.2009;27:289–300.
- ,,,.Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States.Arch Surg.2007;142:624–631.
- ,,.Increase in adult Clostridium difficile‐related hospitalizations and case‐fatality rate, United States, 2000‐2005.Emerg Infect Dis.2008;14:929–931.
- ,,.Increase in Clostridium difficile‐related hospitalizations among infants in the United States, 2000‐2005.Pediatr Infect Dis J.2008;27:1111–1113.
- ,,,.Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile.Clin Infect Dis.2002;34:346–353.
- ,,, et al.Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).Infect Control Hosp Epidemiol.2010;31:431–455.
- ,,,.Prevention of endemic healthcare‐associated Clostridium difficile infection: reviewing the evidence.Am J Gastroenterol.2010;105:2327–2340.
- ,,, et al.A predominantly clonal multi‐institutional outbreak of Clostridium difficile‐associated diarrhea with high morbidity and mortality.N Engl J Med.2005;353:2442–2449.
- ,,,.Analysis of an outbreak of Clostridium difficile infection controlled with enhanced infection control measures.Am J Infect Control.2009;37:458–464.
- ,,, et al.Multipronged intervention strategy to control an outbreak of Clostridium difficile infection (CDI) and its impact on the rates of CDI from 2002 to 2007.Infect Control Hosp Epidemiol.2009;30:156–162.
- ,,,,,.Hospital‐wide restriction of clindamycin: effect on the incidence of Clostridium difficile‐associated diarrhea and cost.Ann Intern Med.1998;128:989–995.
- ,,, et al.Successful use of feedback to improve antibiotic prescribing and reduce Clostridium difficile infection: a controlled interrupted time series.J Antimicrob Chemother.2007;59:990–995.
- ,.Impact of changes in antibiotic policy on Clostridium difficile‐associated diarrhoea (CDAD) over a five‐year period in a district general hospital.J Hosp Infect.2003;54:104–108.
- ,,,,,.An antibiotic policy associated with reduced risk of Clostridium difficile‐associated diarrhoea.Age Ageing.1999;28:578–580.
- ,,,,,.Antibiotic prescribing policy and Clostridium difficile diarrhoea.Q J Med.2004;97:423–429.
- ,,,,.Impact of a reduction in the use of high‐risk antibiotics on the course of an epidemic of Clostridium difficile‐associated disease caused by the hypervirulent NAP1/027 strain.Clin Infect Dis.2007;45(suppl 2):S112–S121.
- .Economic burden of healthcare‐associated infections: an American perspective.Expert Rev Pharmacoecon Outcomes Res.2009;9:417–422.
- .The Direct Medical Costs of Healthcare‐Associated Infections in US Hospitals and the Benefits of Prevention. Division of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases, Coordinating Center for Infectious Diseases, Centers for Disease Control and Prevention. Polock DA, Stone PW, eds.London, UK:Economist;2009.
- ,,,,.Multidrug‐resistant Pseudomonas aeruginosa: risk factors and clinical impact.Antimicrob Agents Chemother.2006;50:43–48.
- ,,,,,.The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges.Infect Control Hosp Epidemiol.2005;26:166–174.
- ,,, et al.Impact of imipenem resistance on mortality in patients with Acinetobacter bacteraemia.J Antimicrob Chemother.2007;59:525–530.
- ,,,,.Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes.Clin Infect Dis.2001;32:1162–1171.
- ,.Clinical and economic impact of methicillin resistance in patients with Staphylococcus aureus bacteremia.Diagn Microbiol Infect Dis.2005;52:113–122.
- ,,,,,.Clinical and economic impact of bacteremia with extended‐spectrum‐beta‐lactamase‐producing Enterobacteriaceae.Antimicrob Agents Chemother.2006;50:1257–1262.
- ,,, et al.Determinants of vancomycin resistance and mortality rates in enterococcal bacteremia: a prospective multicenter study.Ann Intern Med.2001;135:484–492.
- ,,, et al.Direct costs of multidrug‐resistant Acinetobacter baumannii in the burn unit of a public teaching hospital.Am J Infect Control.2004;32:342–344.
- ,,.Epidemiologic, clinical, and economic evaluation of an outbreak of clonal multidrug‐resistant Acinetobacter baumannii infection in a surgical intensive care unit.Infect Control Hosp Epidemiol.2007;28:1247–1254.
- .The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.Clin Infect Dis.2006;42(suppl 2):S82–S89.
- ,,, et al.Hospital and societal costs of antimicrobial‐resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship.Clin Infect Dis.2009;49:1175–1184.
- The Joint Commission. About The Joint Commission. Available at: http://www.jointcommission.org/facts_about_the_joint_commission/. Accessed March 29,2011.
- The Joint Commission. Accreditation Program: Hospital. National Patient Safety Goals. Effective January 1, 2011. Available at: http://www.jointcommission.org/assets/1/6/2011_NPSGs_HAP.pdf. Accessed January 24,2011.
- Deficit Reduction Act. Sec. 5001. Hospital Quality Improvement. Available at: http://www.cms.gov/HospitalAcqCond/Downloads/DeficitReductionAct2005. pdf. Accessed March 29,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart: Know When Antibiotics Work. Available at: http://www.cdc.gov/getsmart/. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). National Ambulatory Medical Care Survey. Available at: http://www.cdc.gov/nchs/ahcd. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). About Healthy People 2010. Available at: http://www.cdc.gov/nchs/healthy_people/hp2010.htm. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). DATA2010…the Healthy People 2010 Database. Available at: http://wonder.cdc.gov/DATA2010/ by searching for antibiotic. Accessed March 30,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare. Available at: http://www.cdc.gov/getsmart/healthcare/. Accessed March 29,2011.
- The Institute for Healthcare Improvement (IHI). About IHI. Available at: http://www.ihi.org/ihi/about. Accessed March 29,2011.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare: All Clinicians Should…. Available at: http://www. cdc.gov/getsmart/healthcare/improve‐efforts/clinicians.html. Accessed May 3,2011.
- United States Department of Health 18:638–656.
- .Antimicrobial stewardship: application in the intensive care unit.Infect Dis Clin North Am.2009;23:683–702.
- ,,.Information technology for optimizing the management of infectious diseases.Am J Health Syst Pharm.2006;63:957–965.
- ,.Informatics and epidemiology in infection control.Infect Dis Clin North Am.2011;25:261–270.
- ,,,,,.Antibiotic optimization. An evaluation of patient safety and economic outcomes.Arch Intern Med.1997;157:1689–1694.
- ,,,.A randomized, prospective study measuring outcomes after antibiotic therapy intervention by a multidisciplinary consult team.Pharmacotherapy.1999;19:1369–1377.
- Centers for Disease Control and Prevention (CDC). Get Smart for Healthcare: Impact of Antibiotic Stewardship Program Interventions on Costs. Available at: http://www.cdc.gov/getsmart/healthcare/support‐efforts/asp‐int‐costs.html. Accessed May 3,2011.
- ,,,,.Favorable impact of a multidisciplinary antibiotic management program conducted during 7 years.Infect Control Hosp Epidemiol.2003;24:699–706.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,,,,.Effects of requiring prior authorization for selected antimicrobials: expenditures, susceptibilities, and clinical outcomes.Clin Infect Dis.1997;25:230–239.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360:1102–1112.
- Society of Hospital Medicine (SHM). Information About SHM and Hospitalists. Available at: http://www.hospitalmedicine.org/. Accessed April 1,2011.
- Society of Hospital Medicine (SHM). New Study Finds Over Half of US Hospitals Utilize Hospitalists. Available at: http://www.hospital medicine.org/AM/Template.cfm?Section=Press_Releases56:893–904.
- .Engaging hospitalists in antimicrobial stewardship: the CDC perspective.J Hosp Med.2011;6(suppl 1):S31–S33.
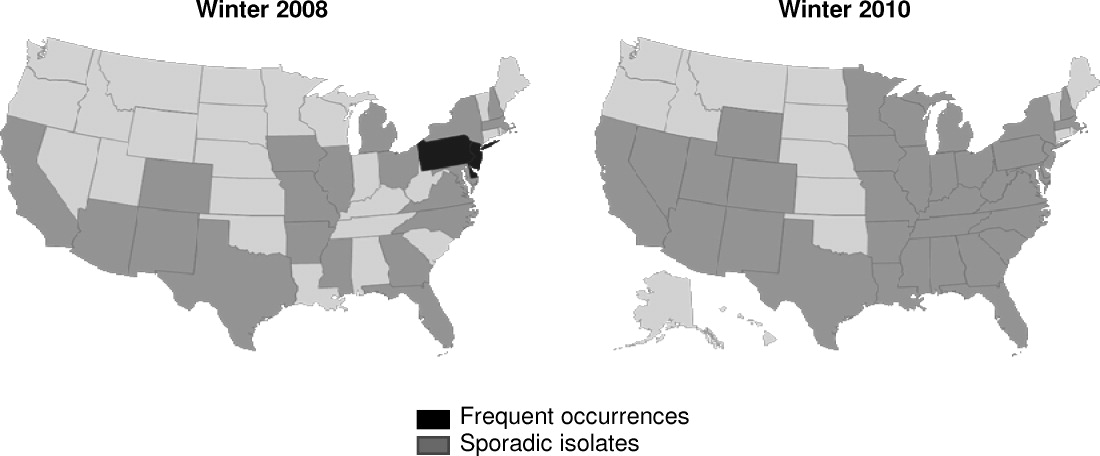
Antimicrobial De‐Escalation Strategies
Two conflicting aims collide when choosing initial empiric therapy for patients with a potential life‐threatening infection. On the one hand, the clinical picture and seriousness of the suspected infectionsometimes with a multi‐drug resistant (MDR) pathogenpoint to the need for immediate empiric therapy with a broad‐spectrum regimen covering the most likely pathogens. This getting it right the first time approach1 is clearly a reasonable one given the significant negative impact of inappropriate or inadequate initial therapy on patient outcomes and costs,24 and the apparent inability to remedy the initial error by subsequent antimicrobial regimen adjustment.57 On the other hand, use of a broad‐spectrum regimen increases the risk of emergent antimicrobial‐resistant pathogens, with potential harm for the immediate patient and all subsequent patients who become exposed and infected with the resistant pathogen. Hence, the aim of optimizing initial empiric therapy comes into conflict with an important aim of antimicrobial stewardship, namely, to use antimicrobials in a manner that does not excessively promote development or selection of antimicrobial‐resistant pathogens.
The de‐escalation strategy is an approach that attempts to balance these conflicting aims by providing optimal initial patient management without inordinately promoting development of antimicrobial resistance. As discussed more fully in the corresponding supplement article by Dr Syndman, the first part of this strategy involves collecting cultures from suitable patients prior to initiating broad‐spectrum empiric antimicrobial therapy designed to cover the most likely pathogenic microorganisms, based on local patterns of prevalence and susceptibility, and the presence of risk factors for infection with drug‐resistant species.810 The second critical step involves modification of initial empiric therapy (when warranted) based on clinical status and when culture results are available.810 In this manner, the initial broad‐spectrum regimen can often be streamlined or de‐escalated to a more narrow‐spectrum regimen or, in some cases, terminated when negative cultures suggest no infection. Frequently, initial combination therapy can be replaced by monotherapy targeting the pathogenic organism identified in culture. Sometimes culture results indicate that initial empiric therapy was inappropriate/emnadequate and requires replacement or other modification. Thus, by modifying empiric antimicrobial therapy on the basis of culture results and clinical criteria, the de‐escalation strategy enables more effective targeting of the causative pathogen(s), elimination of redundant therapy, a decrease in antimicrobial pressure for emergence of resistance, and cost savings.10, 11 Decreasing the number of antimicrobial agents and/or the spectrum of coverage is also expected to decrease the risk of adverse events, drugdrug interactions, and Clostridium difficile‐associated disease.12, 13 A number of studies have demonstrated that de‐escalation of initially appropriate therapy can be successfully accomplished with either improved outcomes14, 15 or with comparable effectiveness as continued initial therapy,1618 but with reduced antimicrobial exposure and costs.19
The timing of streamlining or other modification of initial empiric therapy typically occurs when microbiological culture results become available. Assuming blood or other relevant tissue cultures were obtained prior to initiating empiric therapy, this means de‐escalation or other modifications of initial therapy generally occurs 24 days after hospitalization and/or the beginning of empiric therapy. If rapid diagnostic tests are used to identify or rule out particular pathogens, then de‐escalation may occur slightly sooner. In addition to culture results, observation of the patient in the hospital setting and improved clarity as to his or her clinical status also affect the decision about whether and how to modify the initial empiric antimicrobial regimen. The clinical scenario of the patient and his or her response to initial antimicrobial therapy is also typically clearer by day 3 of antibiotic therapy. If, for some reason, cultures were not obtained prior to beginning empiric therapy, then observations of clinical status and consideration of patient risk factors for resistant pathogens become predominant in the decision‐making process. With respect to the timing of culture attainment, this should occur prior to beginning antimicrobial therapy, because therapy may reduce culture yield and result in false negative or other misleading findings.20, 21
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Case 1 is a 72‐year‐old woman admitted with findings consistent with healthcare‐associated pneumonia (HCAP). Empiric therapy was initiated with vancomycin and piperacillin/tazobactam. Figure 1 provides the laboratory (white blood cell [WBC] counts) and body temperature data for the patient since she entered the hospital and began empiric antibiotic therapy 3 days earlier. The WBC counts suggest the patient is responding to the antibiotic regimen, as demonstrated by a progressive reduction over the time period. However, her counts were still elevated above normal at last measurement, suggesting an incompletely resolved infection at this time. In addition, the patient is still coughing, but has less sputum production, and has some energy to get up and move around. Crackles are apparent at the right lung base. The patient's fever curve has trended down, but still shows notable fever spikes, with a temperature maximum of 101.4F for the past 24 hours. Her blood pressure (135/84 mmHg), pulse (74 bpm), and respiratory rate (14 breaths per minute) are normal, with slightly decreased oxygen saturation (94%) on room air, although improved from initial examination 3 days earlier (92%). The blood culture shows no growth; the sputum culture simply shows oropharyngeal flora. In other words, the culture results have not isolated a causative pathogen. In addition to vancomycin and piperacillin/tazobactam, the patient continues to receive her usual medications for a past history of myocardial infarction (low‐dose aspirin, metoprolol) and hypertension (enalapril, furosemide).
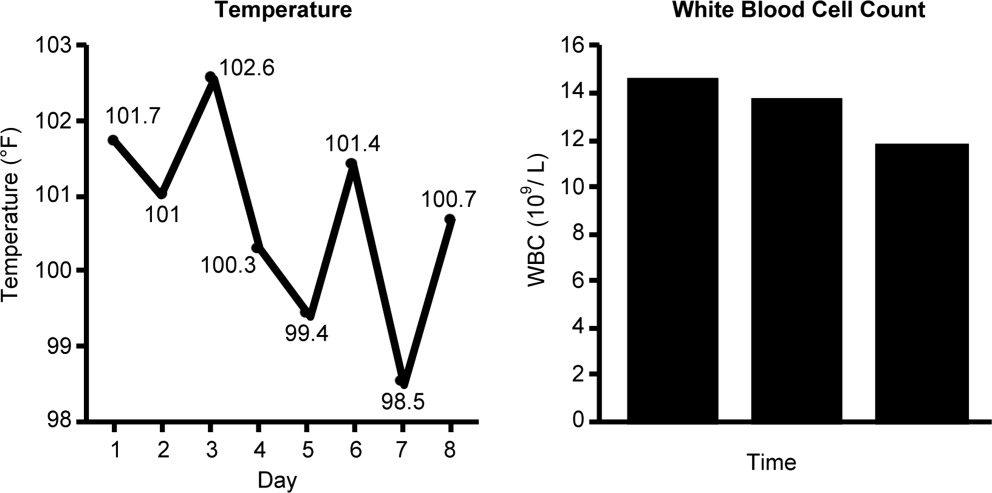
HCAP is a common infection often requiring initial empiric therapy with a broad‐spectrum regimen that covers possible involvement of resistant bacteria. As such, HCAP frequently provides excellent opportunities for de‐escalation. Figure 2 presents the general strategy from the 2005 American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA) guidelines for the management of HCAP, hospital‐acquired pneumonia (HAP), or ventilator‐associated pneumonia (VAP).22 According to the guidelines, HCAP, HAP, and VAP should be similarly managed. Broad‐spectrum initial empiric antibiotic therapy is recommended for patients with late‐onset disease or those with risk factors for MDR pathogens (including high prevalence of resistance based on local antibiograms), while limited‐spectrum antibiotic therapy is recommended for all other patients. Note that consideration of de‐escalation or streamlining of initial therapy begins 2‐3 days after initiation of therapy. Data that should be reviewed prior to instituting de‐escalation include blood cultures and respiratory cultures, as well as the clinical status of the patient. The adequacy of respiratory samples used for culturing should factor into the decision‐making process. For example, in patients who are not intubated or mechanically ventilated, it can be challenging to obtain a quality respiratory specimen for culture. If clinicians are uncertain as to the quality of the respiratory specimen that was cultured, then de‐escalation decisions should be based more on the clinical status of the patient.
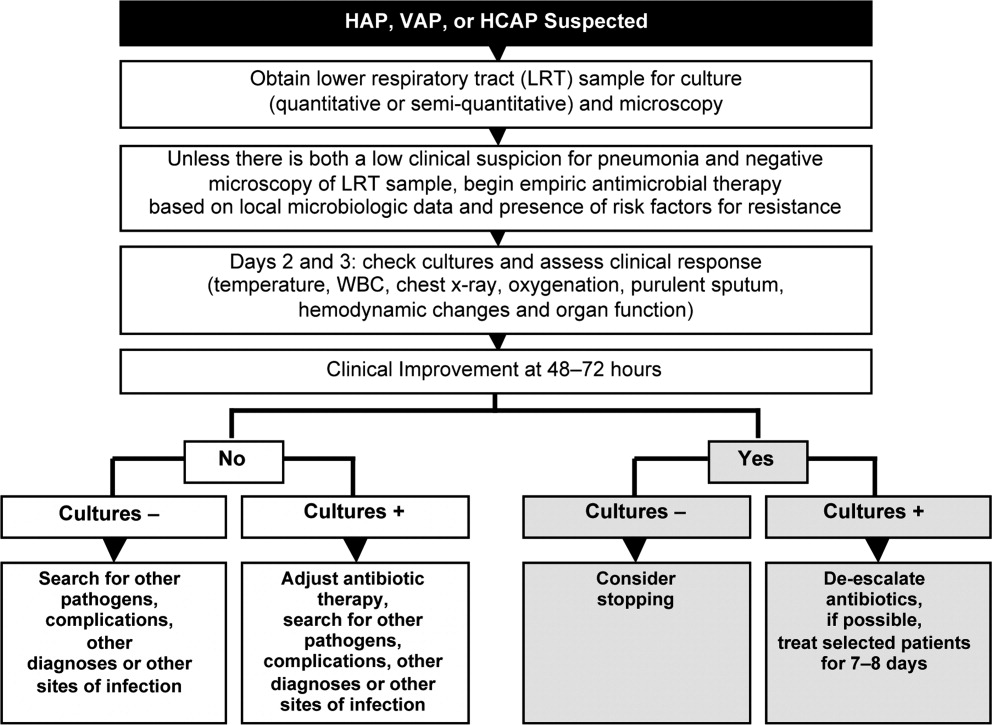
The clinical status of the patient, 2 days after beginning treatment, and culture results are critical in guiding the de‐escalation process.9, 22 The ATS/IDSA guidelines recommend serial assessments of clinical parameters to define the response to initial empiric therapy. If the therapy regimen is effective, an improvement in clinical response should be apparent within 2‐3 days of its initiation.22 Hence, no change in antimicrobial therapy should be undertaken before 3 days, unless there is evidence of rapid deterioration in clinical status or infectious diseases experts recommend a change. With respect to culture results, failure to isolate a group of MDR pathogens for which initial broad‐spectrum empiric therapy was selected affords an opportunity to now streamline therapy or treat with a more narrow‐spectrum regimen.9 Similarly, isolation of a particular pathogen can guide treatment modifications (when necessary), while a negative culture raises the possibility of terminating antimicrobial therapy, provided the culture was collected before initiating therapy. Confidence in this latter decision is bolstered when the patient exhibits rapid improvement in clinical status that is backed by radiographic resolution of lung abnormalities, or an alternative diagnosis has been established for which antimicrobial therapy is not indicated.9
At this stage in the process3 days after initiating empiric therapy, and with culture results in hand and evidence of clinical improvementthe first decision or question is whether antimicrobial therapy can be stopped altogether, ie, do the current data suggest a noninfectious diagnosis (eg, pulmonary embolism, atelectasis) or that bacterial pneumonia is unlikely or has resolved. A 2000 study by Singh et al. highlighted the feasibility of using operational criteria in the form of clinical pulmonary infection score (CPIS) to decide whether to terminate or shorten the duration of initial empiric antibiotic therapy for suspected VAP.23 More specifically, patients with pulmonary infiltrates but a low likelihood of pneumonia (CPIS 6) were randomized to receive either standard antibiotic therapy or ciprofloxacin monotherapy. The situation was re‐evaluated at 3 days, and ciprofloxacin therapy was discontinued if the CPIS remained 6. Results showed no difference in mortality between the ciprofloxacin and standard therapy groups, despite shorter duration of therapy for the former, together with lower antimicrobial exposure and costs for the ciprofloxacin group. (Use of the CPIS to shorten the duration of empiric therapy and limit antimicrobial exposure is discussed in greater detail in the corresponding article in this supplement by Dr File.) Having said that, the case study before us describes a patient with pneumonia by clinical criteria who has responded to broad‐spectrum therapy. Alternative noninfectious diagnoses are not apparent, and even though cultures have returned without significant growth, the patient should continue to receive antimicrobial treatment. The question now is whether to de‐escalate/streamline to a more narrow‐spectrum regimen, or continue the current one.
De‐escalation often targets antimicrobials that provide unnecessarily broad coverage, eg, those with antipseudomonal activity (particularly antipseudomonal carbapenems) and/or agents with activity against methicillin‐resistant Staphylococcus aureus (MRSA). In the absence of definitive culture results isolating a particular pathogen(s), decisions regarding which antibiotics to stop or change often depends, in large part, on patient characteristics (eg, history of prior infection with resistant pathogens, as well as drug allergies or renal insufficiency) and local antibiograms indicating the prevalence and antimicrobial susceptibility of different pneumonia pathogens in the hospital at large or particular wards within the hospital. However, negative culture results can also be useful in guiding subsequent therapy decisions or modifications. In the present case, MRSA was not grown from any cultures, and there was no evidence of Gram‐positive cocci clusters with Gram staining. This suggests that vancomycin should be stopped, and antimicrobial therapy continued with a single antibiotic or antibiotic product that does include MRSA coverage. The question then is whether to continue piperacillin/tazobactam or replace it with another antibiotic.
Because Pseudomonas aeruginosa was not isolated, the clinician might consider streamlining piperacillin/tazobactam to an antibiotic with less pseudomonal and anaerobic coverage, possibly a nonpseudomonal third‐generation cephalosporin or nonpseudomonal carbapenem, such as ertapenem. Given the activity of piperacillin/tazobactam against aerobic Gram‐positive and Gram‐negative pathogens, continuing piperacillin‐tazobactam as single‐agent therapy would also be a viable alternative. However, in the spirit of stewardship and lack of need for pseudomonal coverage, a decision was made to replace piperacillin/tazobactam with ceftriaxone. Ceftriaxone is a nonpseudomonal third‐generation cephalosporin with activity against most other Gram‐negative bacteria. Note that in this case, only oropharyngeal flora grew from the respiratory culture, and the blood culture was negative. However, if a pathogen had grown from either respiratory or blood cultures, then single‐agent therapy could have been used to target that specific pathogen. For example, if Klebsiella spp susceptible to ceftriaxone was isolated from the respiratory culture, then ceftriaxone would have been the obvious choice. If MRSA was isolated, then vancomycin (or another appropriate active agent, such as linezolid or clindamycin) could be administered as a single agent.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman who presents with a diverticular abscess and walled off perforation. Interventional radiology inserts a drain, and the patient is treated with ciprofloxacin plus metronidazole. This regimen is consistent with guidelines from the Surgical Infection Society and IDSA for initial empiric treatment of complicated intra‐abdominal infection of mild‐to‐moderate severity.24 On day 3 following hospital admission and initiation of empiric therapy, the patient seems to show treatment response, as evidenced by downward trends in body temperature and WBC count (Figure 3). However, although the body temperature measures are trending in the right direction, there is still concern about continuing fever spikes and fever at last measure (100.9F). In addition, the WBC count is still elevated, though improving. The patient's blood pressure has normalized (112/72 mmHg vs 84/58 mmHg at admission), and oxygen saturation (98%) measures are normal. The patient's lungs are clear, and her abdominal examination results are improving, though there is still some diffuse tenderness. Microbiological data show blood cultures with no growth, and isolation of Gram‐negative rods from cultures of the abdominal abscess.
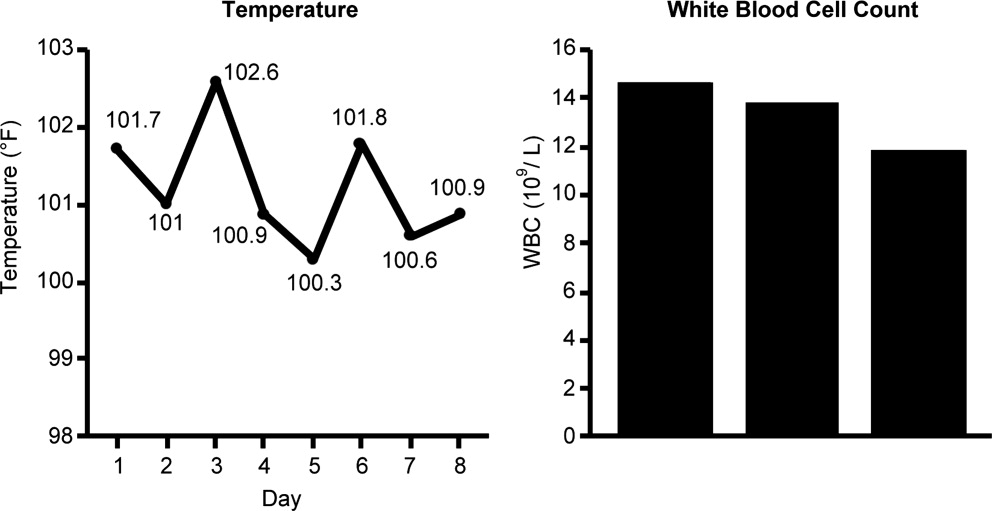
We now have preliminary microbiological data for a patient who remains febrile and has continuing abdominal tenderness, but who is otherwise clinically stable. Can her antimicrobial regimen be de‐escalated at this point, based on what is currently known? When managing a patient after the first 3 or 4 days of empiric treatment, it is important to realize that the patient's condition with regards to infection might reflect issues unrelated to inadequate antimicrobial coverage. If the patient's clinical status has not improved, or if he or she remains febrile even 3 or 4 days into therapy, the clinician should not automatically assume the lack of improvement is due to antibiotic failure. At this point, it is important to consider possible nonantibiotic causes of persistent clinical abnormalities and fever, and for the case here, one possibility is inadequate abscess drainage. The patient should be evaluated with abdominal imaging to ascertain whether the abscess is being adequately drained. With respect to antimicrobial therapy, the patient's blood pressure has stabilized, and her fever is trending downward. In many cases, a lingering fever such as the one observed here, in the context of improving WBC counts and clinical stabilization, may reflect inadequate mechanical drainage of the abscess. Certainly the antimicrobial therapy should not be broadened at this time, and consideration should be given to de‐escalation based on the available microbiological data.
If a type of pathogenic organism is preliminarily identified from culture, but the exact identification of the organism is pending, adjustments of therapy can still be made. Adjustments can also be made based on what is not growing. In this case, the abscess culture has grown Gram‐negative rods, but no Gram‐positive organisms. Hence, continued coverage of Gram‐negative organisms is warranted. In addition, anaerobes often will not readily grow in clinical cultures, and because anaerobes are frequent co‐pathogens, it is appropriate to continue to provide anaerobic coverage. Based on this information, continuation of both ciprofloxacin (for aerobic Gram‐negative coverage) and metronidazole (to cover for anaerobic bacteria) is appropriate in the present case. In other words, the initial empiric therapy should be continued until subsequent culture identifies a particular pathogen, at which time the therapy can be streamlined.
Now, 1 day later (day 4 of hospital admission and empiric therapy), the patient's clinical status is essentially unchangedexcept for a spike in fever to 103.2F. The WBC count is unchanged. Moreover, additional abscess culture data are available, showing definitive identification of an extended‐spectrum ‐lactamase (ESBL)‐producing Escherichia coli organism. The blood culture is still negative. The first observation is that ESBL‐producing E coli is a relatively unusual pathogen in a community‐based infection. However, the patient here did have risk factors for antibiotic‐resistant pathogens, notably prior antimicrobial therapy as an outpatient. It is also important to recognize that community‐acquired infections with ESBL‐producing bacteria (mostly isolated from the urinary tract) have been reported in many parts of the world, and even in some parts of the United States.25
Based on these additional microbiological data, the patient was switched to treatment with ertapenem, a nonpseudomonal carbapenem with activity against ESBL‐producing Enterobacteriaceae.26 In addition, ertapenem, and other carbapenems, have excellent activity against anaerobes,26 and it is prudent to continue coverage for anaerobes even though anaerobes were not grown in the culture. As mentioned above, these organisms are difficult to grow in clinical culture, and they are common pathogens or co‐pathogens in intra‐abdominal infections. Carbapenems are widely regarded as the antimicrobials of choice for treatment of serious, invasive infections with ESBL‐producing bacteria.27 Furthermore, by choosing a nonpseudomonal carbapenem, compared with an antipseudomonal carbapenem, the new antibiotic regimen provides coverage of the isolated ESBL‐producing E coli organismas well as covering possible anaerobe involvementwithout exposing host bacteria to unnecessarily broad antipseudomonal activity. Cephalosporins, monobactams, and fluoroquinolones are generally not active against ESBL‐producing Enterobacteriaceae, and ‐lactam/‐lactamase inhibitor combinations (eg, ampicillin/sulbactam, piperacillin/tazobactam) do not have reliable activity in serious, high inoculum infections caused by ESBL‐producing Enterobacteriaceae.27
CASE 3: CENTRAL LINE‐ASSOCIATED BLOODSTREAM INFECTION
Case 3 is a 56‐year‐old man who presented to the hospital emergency department with status epilepticus. He was intubated, had a central line placed in the internal jugular vein, and was admitted to the intensive care unit (ICU). The seizure was successfully broken by aggressive treatment with repeated intravenous dosing of lorazepam and loading with fosphenytoin. Empiric antibiotic therapy was initiated with vancomycin and piperacillin/tazobactam on day 5, after spiking a fever of 103.4F. No clear source of the fever was identified. While in the ICU with a central line in place, 2 sets of blood cultures were drawn. Now on hospital day 6, the patient is still spiking fever, although the fever trend appears to be decreasing. The patient is hemodynamically stable, with no other abnormal findings (besides persistent fever) on physical examination. WBC count remains elevated, and both sets of blood cultures are notable for growth of Gram‐positive cocci.
Bloodstream infection is a serious condition in hospitalized patients that is associated with significant morbidity and mortality.28 Patients with suspected bloodstream infection typically receive empiric broad‐spectrum antimicrobial therapy, and are thus good candidates for de‐escalation based on subsequent clinical status and blood culture results. Because of the seriousness of bloodstream infection, healthcare workers are sometimes hesitant to de‐escalate initial empiric therapy, even when cultures isolate a pathogen susceptible to narrower‐spectrum agents, particularly if the patient appears to be improving on such therapy. This is true for various serious hospital or healthcare‐associated infections,16, 29 but particularly for bloodstream infections. Moreover, when central line‐associated bloodstream infection (CLABSI) is suspected, the most important initial intervention is to remove the infected central venous catheter. For a patient with a short‐term catheter and a CLABSI due to Gram‐negative bacilli, S aureus (which appears to be a likely pathogen for the case patient here), enterococci, fungi, or mycobacteria, the 2009 IDSA guidelines for management of intravascular catheter‐related infections recommend catheter removal.30 Catheter removal is even more important than antibiotic coverage; this point cannot be stressed enough. In some extreme cases, when the line cannot be removed for clinical reasons, antibiotic lock therapy can be used to supplement systemic antimicrobial therapy.30 This involves instilling a high antibiotic solution into the catheter lumen for a period of time in order to sterilize the lumen and prevent biofilm formation.31
The first step taken for the patient here was to remove the central venous catheter. Then, turning to the preliminary culture data, there is evidence for Gram‐positive cocci in the patient's blood. The blood culture did not grow any Gram‐negative organisms. Gram‐positive cocci (coagulase‐negative staphylococci, S aureus [methicillin‐susceptible or MRSA]) are the most common causes of CLABSI.32 Can the physician de‐escalate antibiotic therapy in this patient with CLABSI based on the preliminary information? Yes. The information is solid enough to suggest removal of the catheter which was providing coverage for Gram‐negative bacteria (piperacillin/tazobactam), while continuing vancomycin for coverage of possible MRSA, pending further review, ie, until the Gram‐positive cocci are speciated. Rapid diagnostic methods, including polymerase chain reaction (PCR) and nucleic acid probes, can be used to provide more information about certain pathogens (such as MRSA33, 34) before final culture and susceptibility results are available, but these are not routinely available in many clinical microbiology laboratories. Furthermore, these newer technologies remain fairly expensive.
Revisiting the patient 1 day later (hospital day 7), after narrowing the initial combination antibiotic regimen to vancomycin monotherapy, the physical examination indicates the patient is clinically stable, with continued improvement in fever and WBC count (Figure 4). Blood culture analysis now isolates methicillin‐susceptible S aureus (MSSA). Methicillin resistance mediates resistance to all ‐lactams, including carbapenems, greatly limiting treatment options. Vancomycin is the most commonly utilized antibiotic for the treatment of MRSA, and the recent clinical practice guidelines from the IDSA recommend either vancomycin or daptomycin for management of MRSA bacteremia in adult patients.35 However, antistaphylococcal penicillins and first‐generation cephalosporins are the antibiotics of choice for MSSA infections, and particularly for MSSA bloodstream infections.
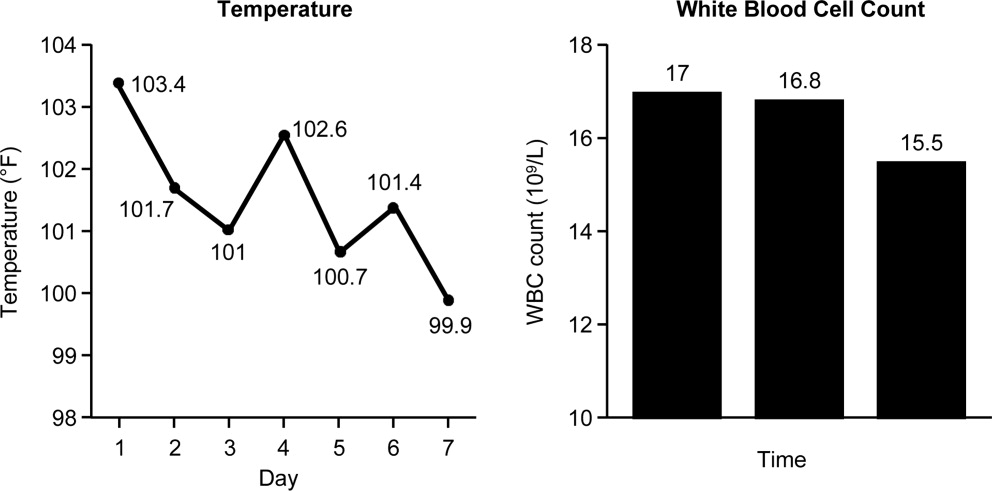
The activity provided by vancomycin (or daptomycin) is overly broad if MSSA is involved, and importantly, it is not as effective as treatment with an antistaphylococcal penicillin or first‐generation cephalosporin. A recent study by Stryjewski et al., of hemodialysis patients with MSSA bacteremia, reported a higher proportion of treatment failure with vancomycin versus first‐generation cephalosporin therapy (31% vs 13%; P = 0.02).36 Furthermore, multivariate analysis identified vancomycin (vs first‐generation cephalosporin) use as a significant independent predictor of treatment failure (odds ratio [OR], 3.53; 95% confidence interval [CI], 1.1513.45; P = 0.04). Similarly, Chang et al. reported nafcillin, an antistaphylococcal penicillin, was superior to vancomycin in preventing bacteriologic failure (persistent failure and/or relapse) in patients with MSSA bacteremia (0% vs 19%; P = 0.058), and used multivariate analysis to identify vancomycin as a significant independent predictor of relapse (OR, 6.5; 95% CI, 1.052.8; P 0.05).37 Another recent study by Lodise et al. reported that initial empiric therapy with vancomycin for endocarditis caused by MSSA was associated with a higher infection‐related mortality rate than initial empiric therapy with a ‐lactam‐containing regimen (39% vs 11%; P = 0.005).38 The negative impact of initial treatment with vancomycin persisted even in patients switched to a ‐lactam therapy after culture results became available.
Hence, if a patient is being treated with vancomycin for a bloodstream (or other) infection due to MSSA, the therapy is suboptimal. In such a scenariowhich corresponds to that for the case patient herevancomycin should be discontinued and replaced with an antistaphylococcal penicillin or first‐generation cephalosporin. Many times, clinicians are resistant to terminating vancomycin and de‐escalating to antistaphylococcal penicillin/first‐generation cephalosporin therapy in a patient with bacteremia who is apparently responding to vancomycin. However, as the studies just reviewed make clear, not only is vancomycin treatment overly broad for the circumstance, it is also suboptimal and does not represent best clinical practice or patient care. Furthermore, continuing vancomycin in this situation unnecessarily exposes the patient to possible renal toxicity, particularly when aggressive dosing or prolonged vancomycin treatment is involved.39 Because of these issues and concerns, case 3 was de‐escalated from vancomycin to cefazolin, a first‐generation cephalosporin. One word of caution, however, is that there is some controversy over using cefazolin in patients with S aureus native valve endocarditis, given the possibility of a Type A ‐lactamase‐producing species causing cefazolin degradation.40 As a result, the clinician should first rule out endocarditis in the patient here before proceeding with cefazolin therapy. Another alternative would be to use an antistaphylococcal penicillin, such as nafcillin.
Finally, when dealing with bacteremia, and particularly when dealing with a possible CLABSI, the issue of potential culture contamination needs to be seriously considered and answered. Treating an actual infection, not what appears to be an infection because of culture contamination, is particularly important when dealing with possible CLABSI, because coagulase‐negative staphylococci (CoNS) are the most common cause of these types of infections,32 and CoNS are also frequent blood‐culture contaminants.41 Therefore, one needs to determine whether a blood culture growing a CoNS represents true bacteremia or simply contaminationwhich will obviously impact de‐escalation decisions.
In addition, when determining whether a blood culture is truly positive and clinically significant, it is important to consider whether the isolated pathogens are unlikely to be contaminants, likely to be contaminants, or the situation is unclear. A 2000 study by Kim et al.42 suggested that, among patients with 2 positive blood cultures for CoNS, routine identification of CoNS species and genotyping selected isolates using pulsed‐field gel electrophoresis may improve the process of discriminating contaminants from pathogens. Various additional factors need to be weighed when trying to interpret CoNS blood culture results, including patient risk factors, presence of prosthetic devices, number of blood cultures and number positive, and the antimicrobial sensitivity patterns of different isolates. For example, if the sensitivity patterns of 2 CoNS strains isolated from a patient are the same, the likelihood is increased that they represent true pathogens rather than contaminants. Figure 5 presents a schematic of this general approach.42
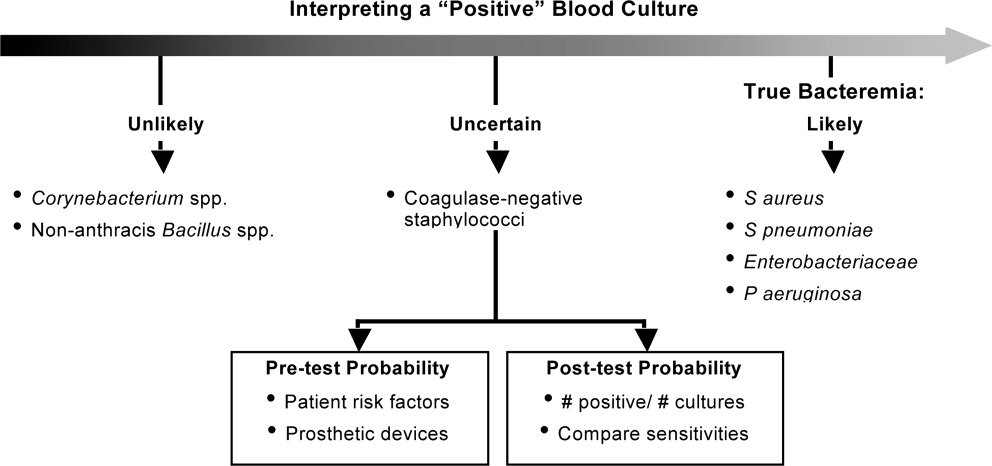
CONCLUSIONS
De‐escalation is a critical component of antimicrobial stewardship. As the prevalence of antimicrobial resistance grows in the hospital and community, de‐escalation will have an increasingly important role in limiting the further emergence of antimicrobial resistance. Pneumonia, intra‐abdominal infection, and bloodstream infection are commonly managed in the hospital setting. Each of these infection types presents excellent opportunities for de‐escalation, and each presents unique challenges and caveats. Concerted efforts must be made by clinicians and stewardship personnel to de‐escalate as soon as possible, based on culture results and clinical status. Although not discussed here, successful de‐escalation programs utilize structured process, guidelines, and algorithms to consistently implement de‐escalation efforts. These tools of implementation are more fully discussed in the corresponding article in this supplement by Dr Rosenberg.
- .Appropriate empirical antibacterial therapy for nosocomial infections: getting it right the first time.Drugs.2003;63:2157–2168.
- ,,, et al.Mortality and morbidity attributable to inadequate empirical antimicrobial therapy in patients admitted to the ICU with sepsis: a matched cohort study.J Antimicrob Chemother.2008;61:436–441.
- ,,,,,.Predictors of 30‐day mortality and hospital costs in patients with ventilator‐associated pneumonia attributed to potentially antibiotic‐resistant gram‐negative bacteria.Chest.2008;134:281–287.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.Impact of BAL data on the therapy and outcome of ventilator‐associated pneumonia.Chest.1997;111:676–685.
- ,,,,,.Emergence of antibiotic‐resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy.Clin Infect Dis.1996;23:486–494.
- ,,,,.Antimicrobial therapy escalation and hospital mortality among patients with health‐care‐associated pneumonia: a single‐center experience.Chest.2008;134:963–968.
- ,.De‐escalation in lower respiratory tract infections.Curr Opin Pulm Med.2006;12:364–368.
- .The importance of de‐escalating antimicrobial therapy in patients with ventilator‐associated pneumonia.Semin Respir Crit Care Med.2006;27:45–50.
- .Impact of antibiotic resistance in gram‐negative bacilli on empirical and definitive antibiotic therapy.Clin Infect Dis.2008;47(suppl 1):S14–S20.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- Bad Bugs, No Drugs: As Antibiotic R46:155–164.
- ,,, et al.De‐escalation therapy rates are significantly higher by bronchoalveolar lavage than by tracheal aspirate.Intensive Care Med.2007;33:1533–1540.
- ,,, et al.Clinical characteristics and treatment patterns among patients with ventilator‐associated pneumonia.Chest.2006;129:1210–1218.
- ,,, et al.Empiric broad‐spectrum antibiotic therapy of nosocomial pneumonia in the intensive care unit: a prospective observational study.Crit Care.2006;10:R78.
- ,,,.Does de‐escalation of antibiotic therapy for ventilator‐associated pneumonia affect the likelihood of recurrent pneumonia or mortality in critically ill surgical patients?J Trauma.2009;66:1343–1348.
- ,,, et al.Ventilator‐associated pneumonia: breaking the vicious circle of antibiotic overuse.Crit Care Med.2007;35:379–385; quiz 386.
- ,,,,.Adjustment of antibiotic treatment according to the results of blood cultures leads to decreased antibiotic use and costs.J Antimicrob Chemother.2006;57:326–330.
- ,,,,.Diagnostic yield of blood cultures from antibiotic‐naive and antibiotically treated patients with haematological malignancies and high‐risk neutropenia.Scand J Infect Dis.2009;41:650–655.
- ,,, et al.Diagnostic accuracy of protected specimen brush and bronchoalveolar lavage in nosocomial pneumonia: impact of previous antimicrobial treatments.Crit Care Med.1998;26:236–244.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,,.Molecular characteristics of extended‐spectrum beta‐lactamase‐producing Escherichia coli from the Chicago area: high prevalence of ST131 producing CTX‐M‐15 in community hospitals.Int J Antimicrob Agents.2010;36:19–23.
- ,.Ertapenem: a review of its use in the treatment of bacterial infections.Drugs.2005;65:2151–2178.
- .Infections with extended‐spectrum beta‐lactamase‐producing Enterobacteriaceae: changing epidemiology and drug treatment choices.Drugs.2010;70:313–333.
- ,.Bloodstream infection in the ICU.Infect Dis Clin North Am.2009;23:557–569.
- ,,,,.Insights from the Society of Infectious Diseases Pharmacists on antimicrobial stewardship guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America.Pharmacotherapy.2009;29:593–607.
- ,,, et al.Clinical practice guidelines for the diagnosis and management of intravascular catheter‐related infection: 2009 Update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,,,,,.Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients undergoing hemodialysis: systematic review and meta‐analysis of randomized, controlled trials.Clin Infect Dis.2008;47:83–93.
- ,.Catheter‐related bloodstream infections: catheter management according to pathogen.Int J Antimicrob Agents.2010;36(suppl 2):S26–S32.
- ,,,.Detection of methicillin‐resistant Staphylococcus aureus (MRSA) in specimens from various body sites: performance characteristics of the BD GeneOhm MRSA assay, the Xpert MRSA assay, and broth‐enriched culture in an area with a low prevalence of MRSA infections.J Clin Microbiol.2010;48:3882–3887.
- ,,,,.Clinical validation of the molecular BD GeneOhm StaphSR assay for direct detection of Staphylococcus aureus and methicillin‐resistant Staphylococcus aureus in positive blood cultures.J Clin Microbiol.2007;45:2191–2196.
- ,,, et al.Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin‐resistant Staphylococcus aureus infections in adults and children.Clin Infect Dis.2011;52:e18–e55.
- ,,, et al.Use of vancomycin or first‐generation cephalosporins for the treatment of hemodialysis‐dependent patients with methicillin‐susceptible Staphylococcus aureus bacteremia.Clin Infect Dis.2007;44:190–196.
- ,,, et al.Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study.Medicine (Baltimore).2003;82:333–339.
- ,,,.Impact of empirical‐therapy selection on outcomes of intravenous drug users with infective endocarditis caused by methicillin‐susceptible Staphylococcus aureus.Antimicrob Agents Chemother.2007;51:3731–3733.
- ,,,,.A retrospective analysis of possible renal toxicity associated with vancomycin in patients with health care‐associated methicillin‐resistant Staphylococcus aureus pneumonia.Clin Ther.2007;29:1107–1115.
- ,,.Relapse of type A beta‐lactamase‐producing Staphylococcus aureus native valve endocarditis during cefazolin therapy: revisiting the issue.Clin Infect Dis.2003;37:1194–1198.
- ,.The origin of coagulase‐negative staphylococci isolated from blood cultures.J Hosp Infect.1995;30:217–223.
- ,,, et al.Determining the significance of coagulase‐negative staphylococci isolated from blood cultures at a community hospital: a role for species and strain identification.Infect Control Hosp Epidemiol.2000;21:213–217.
Two conflicting aims collide when choosing initial empiric therapy for patients with a potential life‐threatening infection. On the one hand, the clinical picture and seriousness of the suspected infectionsometimes with a multi‐drug resistant (MDR) pathogenpoint to the need for immediate empiric therapy with a broad‐spectrum regimen covering the most likely pathogens. This getting it right the first time approach1 is clearly a reasonable one given the significant negative impact of inappropriate or inadequate initial therapy on patient outcomes and costs,24 and the apparent inability to remedy the initial error by subsequent antimicrobial regimen adjustment.57 On the other hand, use of a broad‐spectrum regimen increases the risk of emergent antimicrobial‐resistant pathogens, with potential harm for the immediate patient and all subsequent patients who become exposed and infected with the resistant pathogen. Hence, the aim of optimizing initial empiric therapy comes into conflict with an important aim of antimicrobial stewardship, namely, to use antimicrobials in a manner that does not excessively promote development or selection of antimicrobial‐resistant pathogens.
The de‐escalation strategy is an approach that attempts to balance these conflicting aims by providing optimal initial patient management without inordinately promoting development of antimicrobial resistance. As discussed more fully in the corresponding supplement article by Dr Syndman, the first part of this strategy involves collecting cultures from suitable patients prior to initiating broad‐spectrum empiric antimicrobial therapy designed to cover the most likely pathogenic microorganisms, based on local patterns of prevalence and susceptibility, and the presence of risk factors for infection with drug‐resistant species.810 The second critical step involves modification of initial empiric therapy (when warranted) based on clinical status and when culture results are available.810 In this manner, the initial broad‐spectrum regimen can often be streamlined or de‐escalated to a more narrow‐spectrum regimen or, in some cases, terminated when negative cultures suggest no infection. Frequently, initial combination therapy can be replaced by monotherapy targeting the pathogenic organism identified in culture. Sometimes culture results indicate that initial empiric therapy was inappropriate/emnadequate and requires replacement or other modification. Thus, by modifying empiric antimicrobial therapy on the basis of culture results and clinical criteria, the de‐escalation strategy enables more effective targeting of the causative pathogen(s), elimination of redundant therapy, a decrease in antimicrobial pressure for emergence of resistance, and cost savings.10, 11 Decreasing the number of antimicrobial agents and/or the spectrum of coverage is also expected to decrease the risk of adverse events, drugdrug interactions, and Clostridium difficile‐associated disease.12, 13 A number of studies have demonstrated that de‐escalation of initially appropriate therapy can be successfully accomplished with either improved outcomes14, 15 or with comparable effectiveness as continued initial therapy,1618 but with reduced antimicrobial exposure and costs.19
The timing of streamlining or other modification of initial empiric therapy typically occurs when microbiological culture results become available. Assuming blood or other relevant tissue cultures were obtained prior to initiating empiric therapy, this means de‐escalation or other modifications of initial therapy generally occurs 24 days after hospitalization and/or the beginning of empiric therapy. If rapid diagnostic tests are used to identify or rule out particular pathogens, then de‐escalation may occur slightly sooner. In addition to culture results, observation of the patient in the hospital setting and improved clarity as to his or her clinical status also affect the decision about whether and how to modify the initial empiric antimicrobial regimen. The clinical scenario of the patient and his or her response to initial antimicrobial therapy is also typically clearer by day 3 of antibiotic therapy. If, for some reason, cultures were not obtained prior to beginning empiric therapy, then observations of clinical status and consideration of patient risk factors for resistant pathogens become predominant in the decision‐making process. With respect to the timing of culture attainment, this should occur prior to beginning antimicrobial therapy, because therapy may reduce culture yield and result in false negative or other misleading findings.20, 21
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Case 1 is a 72‐year‐old woman admitted with findings consistent with healthcare‐associated pneumonia (HCAP). Empiric therapy was initiated with vancomycin and piperacillin/tazobactam. Figure 1 provides the laboratory (white blood cell [WBC] counts) and body temperature data for the patient since she entered the hospital and began empiric antibiotic therapy 3 days earlier. The WBC counts suggest the patient is responding to the antibiotic regimen, as demonstrated by a progressive reduction over the time period. However, her counts were still elevated above normal at last measurement, suggesting an incompletely resolved infection at this time. In addition, the patient is still coughing, but has less sputum production, and has some energy to get up and move around. Crackles are apparent at the right lung base. The patient's fever curve has trended down, but still shows notable fever spikes, with a temperature maximum of 101.4F for the past 24 hours. Her blood pressure (135/84 mmHg), pulse (74 bpm), and respiratory rate (14 breaths per minute) are normal, with slightly decreased oxygen saturation (94%) on room air, although improved from initial examination 3 days earlier (92%). The blood culture shows no growth; the sputum culture simply shows oropharyngeal flora. In other words, the culture results have not isolated a causative pathogen. In addition to vancomycin and piperacillin/tazobactam, the patient continues to receive her usual medications for a past history of myocardial infarction (low‐dose aspirin, metoprolol) and hypertension (enalapril, furosemide).
HCAP is a common infection often requiring initial empiric therapy with a broad‐spectrum regimen that covers possible involvement of resistant bacteria. As such, HCAP frequently provides excellent opportunities for de‐escalation. Figure 2 presents the general strategy from the 2005 American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA) guidelines for the management of HCAP, hospital‐acquired pneumonia (HAP), or ventilator‐associated pneumonia (VAP).22 According to the guidelines, HCAP, HAP, and VAP should be similarly managed. Broad‐spectrum initial empiric antibiotic therapy is recommended for patients with late‐onset disease or those with risk factors for MDR pathogens (including high prevalence of resistance based on local antibiograms), while limited‐spectrum antibiotic therapy is recommended for all other patients. Note that consideration of de‐escalation or streamlining of initial therapy begins 2‐3 days after initiation of therapy. Data that should be reviewed prior to instituting de‐escalation include blood cultures and respiratory cultures, as well as the clinical status of the patient. The adequacy of respiratory samples used for culturing should factor into the decision‐making process. For example, in patients who are not intubated or mechanically ventilated, it can be challenging to obtain a quality respiratory specimen for culture. If clinicians are uncertain as to the quality of the respiratory specimen that was cultured, then de‐escalation decisions should be based more on the clinical status of the patient.
The clinical status of the patient, 2 days after beginning treatment, and culture results are critical in guiding the de‐escalation process.9, 22 The ATS/IDSA guidelines recommend serial assessments of clinical parameters to define the response to initial empiric therapy. If the therapy regimen is effective, an improvement in clinical response should be apparent within 2‐3 days of its initiation.22 Hence, no change in antimicrobial therapy should be undertaken before 3 days, unless there is evidence of rapid deterioration in clinical status or infectious diseases experts recommend a change. With respect to culture results, failure to isolate a group of MDR pathogens for which initial broad‐spectrum empiric therapy was selected affords an opportunity to now streamline therapy or treat with a more narrow‐spectrum regimen.9 Similarly, isolation of a particular pathogen can guide treatment modifications (when necessary), while a negative culture raises the possibility of terminating antimicrobial therapy, provided the culture was collected before initiating therapy. Confidence in this latter decision is bolstered when the patient exhibits rapid improvement in clinical status that is backed by radiographic resolution of lung abnormalities, or an alternative diagnosis has been established for which antimicrobial therapy is not indicated.9
At this stage in the process3 days after initiating empiric therapy, and with culture results in hand and evidence of clinical improvementthe first decision or question is whether antimicrobial therapy can be stopped altogether, ie, do the current data suggest a noninfectious diagnosis (eg, pulmonary embolism, atelectasis) or that bacterial pneumonia is unlikely or has resolved. A 2000 study by Singh et al. highlighted the feasibility of using operational criteria in the form of clinical pulmonary infection score (CPIS) to decide whether to terminate or shorten the duration of initial empiric antibiotic therapy for suspected VAP.23 More specifically, patients with pulmonary infiltrates but a low likelihood of pneumonia (CPIS 6) were randomized to receive either standard antibiotic therapy or ciprofloxacin monotherapy. The situation was re‐evaluated at 3 days, and ciprofloxacin therapy was discontinued if the CPIS remained 6. Results showed no difference in mortality between the ciprofloxacin and standard therapy groups, despite shorter duration of therapy for the former, together with lower antimicrobial exposure and costs for the ciprofloxacin group. (Use of the CPIS to shorten the duration of empiric therapy and limit antimicrobial exposure is discussed in greater detail in the corresponding article in this supplement by Dr File.) Having said that, the case study before us describes a patient with pneumonia by clinical criteria who has responded to broad‐spectrum therapy. Alternative noninfectious diagnoses are not apparent, and even though cultures have returned without significant growth, the patient should continue to receive antimicrobial treatment. The question now is whether to de‐escalate/streamline to a more narrow‐spectrum regimen, or continue the current one.
De‐escalation often targets antimicrobials that provide unnecessarily broad coverage, eg, those with antipseudomonal activity (particularly antipseudomonal carbapenems) and/or agents with activity against methicillin‐resistant Staphylococcus aureus (MRSA). In the absence of definitive culture results isolating a particular pathogen(s), decisions regarding which antibiotics to stop or change often depends, in large part, on patient characteristics (eg, history of prior infection with resistant pathogens, as well as drug allergies or renal insufficiency) and local antibiograms indicating the prevalence and antimicrobial susceptibility of different pneumonia pathogens in the hospital at large or particular wards within the hospital. However, negative culture results can also be useful in guiding subsequent therapy decisions or modifications. In the present case, MRSA was not grown from any cultures, and there was no evidence of Gram‐positive cocci clusters with Gram staining. This suggests that vancomycin should be stopped, and antimicrobial therapy continued with a single antibiotic or antibiotic product that does include MRSA coverage. The question then is whether to continue piperacillin/tazobactam or replace it with another antibiotic.
Because Pseudomonas aeruginosa was not isolated, the clinician might consider streamlining piperacillin/tazobactam to an antibiotic with less pseudomonal and anaerobic coverage, possibly a nonpseudomonal third‐generation cephalosporin or nonpseudomonal carbapenem, such as ertapenem. Given the activity of piperacillin/tazobactam against aerobic Gram‐positive and Gram‐negative pathogens, continuing piperacillin‐tazobactam as single‐agent therapy would also be a viable alternative. However, in the spirit of stewardship and lack of need for pseudomonal coverage, a decision was made to replace piperacillin/tazobactam with ceftriaxone. Ceftriaxone is a nonpseudomonal third‐generation cephalosporin with activity against most other Gram‐negative bacteria. Note that in this case, only oropharyngeal flora grew from the respiratory culture, and the blood culture was negative. However, if a pathogen had grown from either respiratory or blood cultures, then single‐agent therapy could have been used to target that specific pathogen. For example, if Klebsiella spp susceptible to ceftriaxone was isolated from the respiratory culture, then ceftriaxone would have been the obvious choice. If MRSA was isolated, then vancomycin (or another appropriate active agent, such as linezolid or clindamycin) could be administered as a single agent.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman who presents with a diverticular abscess and walled off perforation. Interventional radiology inserts a drain, and the patient is treated with ciprofloxacin plus metronidazole. This regimen is consistent with guidelines from the Surgical Infection Society and IDSA for initial empiric treatment of complicated intra‐abdominal infection of mild‐to‐moderate severity.24 On day 3 following hospital admission and initiation of empiric therapy, the patient seems to show treatment response, as evidenced by downward trends in body temperature and WBC count (Figure 3). However, although the body temperature measures are trending in the right direction, there is still concern about continuing fever spikes and fever at last measure (100.9F). In addition, the WBC count is still elevated, though improving. The patient's blood pressure has normalized (112/72 mmHg vs 84/58 mmHg at admission), and oxygen saturation (98%) measures are normal. The patient's lungs are clear, and her abdominal examination results are improving, though there is still some diffuse tenderness. Microbiological data show blood cultures with no growth, and isolation of Gram‐negative rods from cultures of the abdominal abscess.
We now have preliminary microbiological data for a patient who remains febrile and has continuing abdominal tenderness, but who is otherwise clinically stable. Can her antimicrobial regimen be de‐escalated at this point, based on what is currently known? When managing a patient after the first 3 or 4 days of empiric treatment, it is important to realize that the patient's condition with regards to infection might reflect issues unrelated to inadequate antimicrobial coverage. If the patient's clinical status has not improved, or if he or she remains febrile even 3 or 4 days into therapy, the clinician should not automatically assume the lack of improvement is due to antibiotic failure. At this point, it is important to consider possible nonantibiotic causes of persistent clinical abnormalities and fever, and for the case here, one possibility is inadequate abscess drainage. The patient should be evaluated with abdominal imaging to ascertain whether the abscess is being adequately drained. With respect to antimicrobial therapy, the patient's blood pressure has stabilized, and her fever is trending downward. In many cases, a lingering fever such as the one observed here, in the context of improving WBC counts and clinical stabilization, may reflect inadequate mechanical drainage of the abscess. Certainly the antimicrobial therapy should not be broadened at this time, and consideration should be given to de‐escalation based on the available microbiological data.
If a type of pathogenic organism is preliminarily identified from culture, but the exact identification of the organism is pending, adjustments of therapy can still be made. Adjustments can also be made based on what is not growing. In this case, the abscess culture has grown Gram‐negative rods, but no Gram‐positive organisms. Hence, continued coverage of Gram‐negative organisms is warranted. In addition, anaerobes often will not readily grow in clinical cultures, and because anaerobes are frequent co‐pathogens, it is appropriate to continue to provide anaerobic coverage. Based on this information, continuation of both ciprofloxacin (for aerobic Gram‐negative coverage) and metronidazole (to cover for anaerobic bacteria) is appropriate in the present case. In other words, the initial empiric therapy should be continued until subsequent culture identifies a particular pathogen, at which time the therapy can be streamlined.
Now, 1 day later (day 4 of hospital admission and empiric therapy), the patient's clinical status is essentially unchangedexcept for a spike in fever to 103.2F. The WBC count is unchanged. Moreover, additional abscess culture data are available, showing definitive identification of an extended‐spectrum ‐lactamase (ESBL)‐producing Escherichia coli organism. The blood culture is still negative. The first observation is that ESBL‐producing E coli is a relatively unusual pathogen in a community‐based infection. However, the patient here did have risk factors for antibiotic‐resistant pathogens, notably prior antimicrobial therapy as an outpatient. It is also important to recognize that community‐acquired infections with ESBL‐producing bacteria (mostly isolated from the urinary tract) have been reported in many parts of the world, and even in some parts of the United States.25
Based on these additional microbiological data, the patient was switched to treatment with ertapenem, a nonpseudomonal carbapenem with activity against ESBL‐producing Enterobacteriaceae.26 In addition, ertapenem, and other carbapenems, have excellent activity against anaerobes,26 and it is prudent to continue coverage for anaerobes even though anaerobes were not grown in the culture. As mentioned above, these organisms are difficult to grow in clinical culture, and they are common pathogens or co‐pathogens in intra‐abdominal infections. Carbapenems are widely regarded as the antimicrobials of choice for treatment of serious, invasive infections with ESBL‐producing bacteria.27 Furthermore, by choosing a nonpseudomonal carbapenem, compared with an antipseudomonal carbapenem, the new antibiotic regimen provides coverage of the isolated ESBL‐producing E coli organismas well as covering possible anaerobe involvementwithout exposing host bacteria to unnecessarily broad antipseudomonal activity. Cephalosporins, monobactams, and fluoroquinolones are generally not active against ESBL‐producing Enterobacteriaceae, and ‐lactam/‐lactamase inhibitor combinations (eg, ampicillin/sulbactam, piperacillin/tazobactam) do not have reliable activity in serious, high inoculum infections caused by ESBL‐producing Enterobacteriaceae.27
CASE 3: CENTRAL LINE‐ASSOCIATED BLOODSTREAM INFECTION
Case 3 is a 56‐year‐old man who presented to the hospital emergency department with status epilepticus. He was intubated, had a central line placed in the internal jugular vein, and was admitted to the intensive care unit (ICU). The seizure was successfully broken by aggressive treatment with repeated intravenous dosing of lorazepam and loading with fosphenytoin. Empiric antibiotic therapy was initiated with vancomycin and piperacillin/tazobactam on day 5, after spiking a fever of 103.4F. No clear source of the fever was identified. While in the ICU with a central line in place, 2 sets of blood cultures were drawn. Now on hospital day 6, the patient is still spiking fever, although the fever trend appears to be decreasing. The patient is hemodynamically stable, with no other abnormal findings (besides persistent fever) on physical examination. WBC count remains elevated, and both sets of blood cultures are notable for growth of Gram‐positive cocci.
Bloodstream infection is a serious condition in hospitalized patients that is associated with significant morbidity and mortality.28 Patients with suspected bloodstream infection typically receive empiric broad‐spectrum antimicrobial therapy, and are thus good candidates for de‐escalation based on subsequent clinical status and blood culture results. Because of the seriousness of bloodstream infection, healthcare workers are sometimes hesitant to de‐escalate initial empiric therapy, even when cultures isolate a pathogen susceptible to narrower‐spectrum agents, particularly if the patient appears to be improving on such therapy. This is true for various serious hospital or healthcare‐associated infections,16, 29 but particularly for bloodstream infections. Moreover, when central line‐associated bloodstream infection (CLABSI) is suspected, the most important initial intervention is to remove the infected central venous catheter. For a patient with a short‐term catheter and a CLABSI due to Gram‐negative bacilli, S aureus (which appears to be a likely pathogen for the case patient here), enterococci, fungi, or mycobacteria, the 2009 IDSA guidelines for management of intravascular catheter‐related infections recommend catheter removal.30 Catheter removal is even more important than antibiotic coverage; this point cannot be stressed enough. In some extreme cases, when the line cannot be removed for clinical reasons, antibiotic lock therapy can be used to supplement systemic antimicrobial therapy.30 This involves instilling a high antibiotic solution into the catheter lumen for a period of time in order to sterilize the lumen and prevent biofilm formation.31
The first step taken for the patient here was to remove the central venous catheter. Then, turning to the preliminary culture data, there is evidence for Gram‐positive cocci in the patient's blood. The blood culture did not grow any Gram‐negative organisms. Gram‐positive cocci (coagulase‐negative staphylococci, S aureus [methicillin‐susceptible or MRSA]) are the most common causes of CLABSI.32 Can the physician de‐escalate antibiotic therapy in this patient with CLABSI based on the preliminary information? Yes. The information is solid enough to suggest removal of the catheter which was providing coverage for Gram‐negative bacteria (piperacillin/tazobactam), while continuing vancomycin for coverage of possible MRSA, pending further review, ie, until the Gram‐positive cocci are speciated. Rapid diagnostic methods, including polymerase chain reaction (PCR) and nucleic acid probes, can be used to provide more information about certain pathogens (such as MRSA33, 34) before final culture and susceptibility results are available, but these are not routinely available in many clinical microbiology laboratories. Furthermore, these newer technologies remain fairly expensive.
Revisiting the patient 1 day later (hospital day 7), after narrowing the initial combination antibiotic regimen to vancomycin monotherapy, the physical examination indicates the patient is clinically stable, with continued improvement in fever and WBC count (Figure 4). Blood culture analysis now isolates methicillin‐susceptible S aureus (MSSA). Methicillin resistance mediates resistance to all ‐lactams, including carbapenems, greatly limiting treatment options. Vancomycin is the most commonly utilized antibiotic for the treatment of MRSA, and the recent clinical practice guidelines from the IDSA recommend either vancomycin or daptomycin for management of MRSA bacteremia in adult patients.35 However, antistaphylococcal penicillins and first‐generation cephalosporins are the antibiotics of choice for MSSA infections, and particularly for MSSA bloodstream infections.
The activity provided by vancomycin (or daptomycin) is overly broad if MSSA is involved, and importantly, it is not as effective as treatment with an antistaphylococcal penicillin or first‐generation cephalosporin. A recent study by Stryjewski et al., of hemodialysis patients with MSSA bacteremia, reported a higher proportion of treatment failure with vancomycin versus first‐generation cephalosporin therapy (31% vs 13%; P = 0.02).36 Furthermore, multivariate analysis identified vancomycin (vs first‐generation cephalosporin) use as a significant independent predictor of treatment failure (odds ratio [OR], 3.53; 95% confidence interval [CI], 1.1513.45; P = 0.04). Similarly, Chang et al. reported nafcillin, an antistaphylococcal penicillin, was superior to vancomycin in preventing bacteriologic failure (persistent failure and/or relapse) in patients with MSSA bacteremia (0% vs 19%; P = 0.058), and used multivariate analysis to identify vancomycin as a significant independent predictor of relapse (OR, 6.5; 95% CI, 1.052.8; P 0.05).37 Another recent study by Lodise et al. reported that initial empiric therapy with vancomycin for endocarditis caused by MSSA was associated with a higher infection‐related mortality rate than initial empiric therapy with a ‐lactam‐containing regimen (39% vs 11%; P = 0.005).38 The negative impact of initial treatment with vancomycin persisted even in patients switched to a ‐lactam therapy after culture results became available.
Hence, if a patient is being treated with vancomycin for a bloodstream (or other) infection due to MSSA, the therapy is suboptimal. In such a scenariowhich corresponds to that for the case patient herevancomycin should be discontinued and replaced with an antistaphylococcal penicillin or first‐generation cephalosporin. Many times, clinicians are resistant to terminating vancomycin and de‐escalating to antistaphylococcal penicillin/first‐generation cephalosporin therapy in a patient with bacteremia who is apparently responding to vancomycin. However, as the studies just reviewed make clear, not only is vancomycin treatment overly broad for the circumstance, it is also suboptimal and does not represent best clinical practice or patient care. Furthermore, continuing vancomycin in this situation unnecessarily exposes the patient to possible renal toxicity, particularly when aggressive dosing or prolonged vancomycin treatment is involved.39 Because of these issues and concerns, case 3 was de‐escalated from vancomycin to cefazolin, a first‐generation cephalosporin. One word of caution, however, is that there is some controversy over using cefazolin in patients with S aureus native valve endocarditis, given the possibility of a Type A ‐lactamase‐producing species causing cefazolin degradation.40 As a result, the clinician should first rule out endocarditis in the patient here before proceeding with cefazolin therapy. Another alternative would be to use an antistaphylococcal penicillin, such as nafcillin.
Finally, when dealing with bacteremia, and particularly when dealing with a possible CLABSI, the issue of potential culture contamination needs to be seriously considered and answered. Treating an actual infection, not what appears to be an infection because of culture contamination, is particularly important when dealing with possible CLABSI, because coagulase‐negative staphylococci (CoNS) are the most common cause of these types of infections,32 and CoNS are also frequent blood‐culture contaminants.41 Therefore, one needs to determine whether a blood culture growing a CoNS represents true bacteremia or simply contaminationwhich will obviously impact de‐escalation decisions.
In addition, when determining whether a blood culture is truly positive and clinically significant, it is important to consider whether the isolated pathogens are unlikely to be contaminants, likely to be contaminants, or the situation is unclear. A 2000 study by Kim et al.42 suggested that, among patients with 2 positive blood cultures for CoNS, routine identification of CoNS species and genotyping selected isolates using pulsed‐field gel electrophoresis may improve the process of discriminating contaminants from pathogens. Various additional factors need to be weighed when trying to interpret CoNS blood culture results, including patient risk factors, presence of prosthetic devices, number of blood cultures and number positive, and the antimicrobial sensitivity patterns of different isolates. For example, if the sensitivity patterns of 2 CoNS strains isolated from a patient are the same, the likelihood is increased that they represent true pathogens rather than contaminants. Figure 5 presents a schematic of this general approach.42
CONCLUSIONS
De‐escalation is a critical component of antimicrobial stewardship. As the prevalence of antimicrobial resistance grows in the hospital and community, de‐escalation will have an increasingly important role in limiting the further emergence of antimicrobial resistance. Pneumonia, intra‐abdominal infection, and bloodstream infection are commonly managed in the hospital setting. Each of these infection types presents excellent opportunities for de‐escalation, and each presents unique challenges and caveats. Concerted efforts must be made by clinicians and stewardship personnel to de‐escalate as soon as possible, based on culture results and clinical status. Although not discussed here, successful de‐escalation programs utilize structured process, guidelines, and algorithms to consistently implement de‐escalation efforts. These tools of implementation are more fully discussed in the corresponding article in this supplement by Dr Rosenberg.
Two conflicting aims collide when choosing initial empiric therapy for patients with a potential life‐threatening infection. On the one hand, the clinical picture and seriousness of the suspected infectionsometimes with a multi‐drug resistant (MDR) pathogenpoint to the need for immediate empiric therapy with a broad‐spectrum regimen covering the most likely pathogens. This getting it right the first time approach1 is clearly a reasonable one given the significant negative impact of inappropriate or inadequate initial therapy on patient outcomes and costs,24 and the apparent inability to remedy the initial error by subsequent antimicrobial regimen adjustment.57 On the other hand, use of a broad‐spectrum regimen increases the risk of emergent antimicrobial‐resistant pathogens, with potential harm for the immediate patient and all subsequent patients who become exposed and infected with the resistant pathogen. Hence, the aim of optimizing initial empiric therapy comes into conflict with an important aim of antimicrobial stewardship, namely, to use antimicrobials in a manner that does not excessively promote development or selection of antimicrobial‐resistant pathogens.
The de‐escalation strategy is an approach that attempts to balance these conflicting aims by providing optimal initial patient management without inordinately promoting development of antimicrobial resistance. As discussed more fully in the corresponding supplement article by Dr Syndman, the first part of this strategy involves collecting cultures from suitable patients prior to initiating broad‐spectrum empiric antimicrobial therapy designed to cover the most likely pathogenic microorganisms, based on local patterns of prevalence and susceptibility, and the presence of risk factors for infection with drug‐resistant species.810 The second critical step involves modification of initial empiric therapy (when warranted) based on clinical status and when culture results are available.810 In this manner, the initial broad‐spectrum regimen can often be streamlined or de‐escalated to a more narrow‐spectrum regimen or, in some cases, terminated when negative cultures suggest no infection. Frequently, initial combination therapy can be replaced by monotherapy targeting the pathogenic organism identified in culture. Sometimes culture results indicate that initial empiric therapy was inappropriate/emnadequate and requires replacement or other modification. Thus, by modifying empiric antimicrobial therapy on the basis of culture results and clinical criteria, the de‐escalation strategy enables more effective targeting of the causative pathogen(s), elimination of redundant therapy, a decrease in antimicrobial pressure for emergence of resistance, and cost savings.10, 11 Decreasing the number of antimicrobial agents and/or the spectrum of coverage is also expected to decrease the risk of adverse events, drugdrug interactions, and Clostridium difficile‐associated disease.12, 13 A number of studies have demonstrated that de‐escalation of initially appropriate therapy can be successfully accomplished with either improved outcomes14, 15 or with comparable effectiveness as continued initial therapy,1618 but with reduced antimicrobial exposure and costs.19
The timing of streamlining or other modification of initial empiric therapy typically occurs when microbiological culture results become available. Assuming blood or other relevant tissue cultures were obtained prior to initiating empiric therapy, this means de‐escalation or other modifications of initial therapy generally occurs 24 days after hospitalization and/or the beginning of empiric therapy. If rapid diagnostic tests are used to identify or rule out particular pathogens, then de‐escalation may occur slightly sooner. In addition to culture results, observation of the patient in the hospital setting and improved clarity as to his or her clinical status also affect the decision about whether and how to modify the initial empiric antimicrobial regimen. The clinical scenario of the patient and his or her response to initial antimicrobial therapy is also typically clearer by day 3 of antibiotic therapy. If, for some reason, cultures were not obtained prior to beginning empiric therapy, then observations of clinical status and consideration of patient risk factors for resistant pathogens become predominant in the decision‐making process. With respect to the timing of culture attainment, this should occur prior to beginning antimicrobial therapy, because therapy may reduce culture yield and result in false negative or other misleading findings.20, 21
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Case 1 is a 72‐year‐old woman admitted with findings consistent with healthcare‐associated pneumonia (HCAP). Empiric therapy was initiated with vancomycin and piperacillin/tazobactam. Figure 1 provides the laboratory (white blood cell [WBC] counts) and body temperature data for the patient since she entered the hospital and began empiric antibiotic therapy 3 days earlier. The WBC counts suggest the patient is responding to the antibiotic regimen, as demonstrated by a progressive reduction over the time period. However, her counts were still elevated above normal at last measurement, suggesting an incompletely resolved infection at this time. In addition, the patient is still coughing, but has less sputum production, and has some energy to get up and move around. Crackles are apparent at the right lung base. The patient's fever curve has trended down, but still shows notable fever spikes, with a temperature maximum of 101.4F for the past 24 hours. Her blood pressure (135/84 mmHg), pulse (74 bpm), and respiratory rate (14 breaths per minute) are normal, with slightly decreased oxygen saturation (94%) on room air, although improved from initial examination 3 days earlier (92%). The blood culture shows no growth; the sputum culture simply shows oropharyngeal flora. In other words, the culture results have not isolated a causative pathogen. In addition to vancomycin and piperacillin/tazobactam, the patient continues to receive her usual medications for a past history of myocardial infarction (low‐dose aspirin, metoprolol) and hypertension (enalapril, furosemide).
HCAP is a common infection often requiring initial empiric therapy with a broad‐spectrum regimen that covers possible involvement of resistant bacteria. As such, HCAP frequently provides excellent opportunities for de‐escalation. Figure 2 presents the general strategy from the 2005 American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA) guidelines for the management of HCAP, hospital‐acquired pneumonia (HAP), or ventilator‐associated pneumonia (VAP).22 According to the guidelines, HCAP, HAP, and VAP should be similarly managed. Broad‐spectrum initial empiric antibiotic therapy is recommended for patients with late‐onset disease or those with risk factors for MDR pathogens (including high prevalence of resistance based on local antibiograms), while limited‐spectrum antibiotic therapy is recommended for all other patients. Note that consideration of de‐escalation or streamlining of initial therapy begins 2‐3 days after initiation of therapy. Data that should be reviewed prior to instituting de‐escalation include blood cultures and respiratory cultures, as well as the clinical status of the patient. The adequacy of respiratory samples used for culturing should factor into the decision‐making process. For example, in patients who are not intubated or mechanically ventilated, it can be challenging to obtain a quality respiratory specimen for culture. If clinicians are uncertain as to the quality of the respiratory specimen that was cultured, then de‐escalation decisions should be based more on the clinical status of the patient.
The clinical status of the patient, 2 days after beginning treatment, and culture results are critical in guiding the de‐escalation process.9, 22 The ATS/IDSA guidelines recommend serial assessments of clinical parameters to define the response to initial empiric therapy. If the therapy regimen is effective, an improvement in clinical response should be apparent within 2‐3 days of its initiation.22 Hence, no change in antimicrobial therapy should be undertaken before 3 days, unless there is evidence of rapid deterioration in clinical status or infectious diseases experts recommend a change. With respect to culture results, failure to isolate a group of MDR pathogens for which initial broad‐spectrum empiric therapy was selected affords an opportunity to now streamline therapy or treat with a more narrow‐spectrum regimen.9 Similarly, isolation of a particular pathogen can guide treatment modifications (when necessary), while a negative culture raises the possibility of terminating antimicrobial therapy, provided the culture was collected before initiating therapy. Confidence in this latter decision is bolstered when the patient exhibits rapid improvement in clinical status that is backed by radiographic resolution of lung abnormalities, or an alternative diagnosis has been established for which antimicrobial therapy is not indicated.9
At this stage in the process3 days after initiating empiric therapy, and with culture results in hand and evidence of clinical improvementthe first decision or question is whether antimicrobial therapy can be stopped altogether, ie, do the current data suggest a noninfectious diagnosis (eg, pulmonary embolism, atelectasis) or that bacterial pneumonia is unlikely or has resolved. A 2000 study by Singh et al. highlighted the feasibility of using operational criteria in the form of clinical pulmonary infection score (CPIS) to decide whether to terminate or shorten the duration of initial empiric antibiotic therapy for suspected VAP.23 More specifically, patients with pulmonary infiltrates but a low likelihood of pneumonia (CPIS 6) were randomized to receive either standard antibiotic therapy or ciprofloxacin monotherapy. The situation was re‐evaluated at 3 days, and ciprofloxacin therapy was discontinued if the CPIS remained 6. Results showed no difference in mortality between the ciprofloxacin and standard therapy groups, despite shorter duration of therapy for the former, together with lower antimicrobial exposure and costs for the ciprofloxacin group. (Use of the CPIS to shorten the duration of empiric therapy and limit antimicrobial exposure is discussed in greater detail in the corresponding article in this supplement by Dr File.) Having said that, the case study before us describes a patient with pneumonia by clinical criteria who has responded to broad‐spectrum therapy. Alternative noninfectious diagnoses are not apparent, and even though cultures have returned without significant growth, the patient should continue to receive antimicrobial treatment. The question now is whether to de‐escalate/streamline to a more narrow‐spectrum regimen, or continue the current one.
De‐escalation often targets antimicrobials that provide unnecessarily broad coverage, eg, those with antipseudomonal activity (particularly antipseudomonal carbapenems) and/or agents with activity against methicillin‐resistant Staphylococcus aureus (MRSA). In the absence of definitive culture results isolating a particular pathogen(s), decisions regarding which antibiotics to stop or change often depends, in large part, on patient characteristics (eg, history of prior infection with resistant pathogens, as well as drug allergies or renal insufficiency) and local antibiograms indicating the prevalence and antimicrobial susceptibility of different pneumonia pathogens in the hospital at large or particular wards within the hospital. However, negative culture results can also be useful in guiding subsequent therapy decisions or modifications. In the present case, MRSA was not grown from any cultures, and there was no evidence of Gram‐positive cocci clusters with Gram staining. This suggests that vancomycin should be stopped, and antimicrobial therapy continued with a single antibiotic or antibiotic product that does include MRSA coverage. The question then is whether to continue piperacillin/tazobactam or replace it with another antibiotic.
Because Pseudomonas aeruginosa was not isolated, the clinician might consider streamlining piperacillin/tazobactam to an antibiotic with less pseudomonal and anaerobic coverage, possibly a nonpseudomonal third‐generation cephalosporin or nonpseudomonal carbapenem, such as ertapenem. Given the activity of piperacillin/tazobactam against aerobic Gram‐positive and Gram‐negative pathogens, continuing piperacillin‐tazobactam as single‐agent therapy would also be a viable alternative. However, in the spirit of stewardship and lack of need for pseudomonal coverage, a decision was made to replace piperacillin/tazobactam with ceftriaxone. Ceftriaxone is a nonpseudomonal third‐generation cephalosporin with activity against most other Gram‐negative bacteria. Note that in this case, only oropharyngeal flora grew from the respiratory culture, and the blood culture was negative. However, if a pathogen had grown from either respiratory or blood cultures, then single‐agent therapy could have been used to target that specific pathogen. For example, if Klebsiella spp susceptible to ceftriaxone was isolated from the respiratory culture, then ceftriaxone would have been the obvious choice. If MRSA was isolated, then vancomycin (or another appropriate active agent, such as linezolid or clindamycin) could be administered as a single agent.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman who presents with a diverticular abscess and walled off perforation. Interventional radiology inserts a drain, and the patient is treated with ciprofloxacin plus metronidazole. This regimen is consistent with guidelines from the Surgical Infection Society and IDSA for initial empiric treatment of complicated intra‐abdominal infection of mild‐to‐moderate severity.24 On day 3 following hospital admission and initiation of empiric therapy, the patient seems to show treatment response, as evidenced by downward trends in body temperature and WBC count (Figure 3). However, although the body temperature measures are trending in the right direction, there is still concern about continuing fever spikes and fever at last measure (100.9F). In addition, the WBC count is still elevated, though improving. The patient's blood pressure has normalized (112/72 mmHg vs 84/58 mmHg at admission), and oxygen saturation (98%) measures are normal. The patient's lungs are clear, and her abdominal examination results are improving, though there is still some diffuse tenderness. Microbiological data show blood cultures with no growth, and isolation of Gram‐negative rods from cultures of the abdominal abscess.
We now have preliminary microbiological data for a patient who remains febrile and has continuing abdominal tenderness, but who is otherwise clinically stable. Can her antimicrobial regimen be de‐escalated at this point, based on what is currently known? When managing a patient after the first 3 or 4 days of empiric treatment, it is important to realize that the patient's condition with regards to infection might reflect issues unrelated to inadequate antimicrobial coverage. If the patient's clinical status has not improved, or if he or she remains febrile even 3 or 4 days into therapy, the clinician should not automatically assume the lack of improvement is due to antibiotic failure. At this point, it is important to consider possible nonantibiotic causes of persistent clinical abnormalities and fever, and for the case here, one possibility is inadequate abscess drainage. The patient should be evaluated with abdominal imaging to ascertain whether the abscess is being adequately drained. With respect to antimicrobial therapy, the patient's blood pressure has stabilized, and her fever is trending downward. In many cases, a lingering fever such as the one observed here, in the context of improving WBC counts and clinical stabilization, may reflect inadequate mechanical drainage of the abscess. Certainly the antimicrobial therapy should not be broadened at this time, and consideration should be given to de‐escalation based on the available microbiological data.
If a type of pathogenic organism is preliminarily identified from culture, but the exact identification of the organism is pending, adjustments of therapy can still be made. Adjustments can also be made based on what is not growing. In this case, the abscess culture has grown Gram‐negative rods, but no Gram‐positive organisms. Hence, continued coverage of Gram‐negative organisms is warranted. In addition, anaerobes often will not readily grow in clinical cultures, and because anaerobes are frequent co‐pathogens, it is appropriate to continue to provide anaerobic coverage. Based on this information, continuation of both ciprofloxacin (for aerobic Gram‐negative coverage) and metronidazole (to cover for anaerobic bacteria) is appropriate in the present case. In other words, the initial empiric therapy should be continued until subsequent culture identifies a particular pathogen, at which time the therapy can be streamlined.
Now, 1 day later (day 4 of hospital admission and empiric therapy), the patient's clinical status is essentially unchangedexcept for a spike in fever to 103.2F. The WBC count is unchanged. Moreover, additional abscess culture data are available, showing definitive identification of an extended‐spectrum ‐lactamase (ESBL)‐producing Escherichia coli organism. The blood culture is still negative. The first observation is that ESBL‐producing E coli is a relatively unusual pathogen in a community‐based infection. However, the patient here did have risk factors for antibiotic‐resistant pathogens, notably prior antimicrobial therapy as an outpatient. It is also important to recognize that community‐acquired infections with ESBL‐producing bacteria (mostly isolated from the urinary tract) have been reported in many parts of the world, and even in some parts of the United States.25
Based on these additional microbiological data, the patient was switched to treatment with ertapenem, a nonpseudomonal carbapenem with activity against ESBL‐producing Enterobacteriaceae.26 In addition, ertapenem, and other carbapenems, have excellent activity against anaerobes,26 and it is prudent to continue coverage for anaerobes even though anaerobes were not grown in the culture. As mentioned above, these organisms are difficult to grow in clinical culture, and they are common pathogens or co‐pathogens in intra‐abdominal infections. Carbapenems are widely regarded as the antimicrobials of choice for treatment of serious, invasive infections with ESBL‐producing bacteria.27 Furthermore, by choosing a nonpseudomonal carbapenem, compared with an antipseudomonal carbapenem, the new antibiotic regimen provides coverage of the isolated ESBL‐producing E coli organismas well as covering possible anaerobe involvementwithout exposing host bacteria to unnecessarily broad antipseudomonal activity. Cephalosporins, monobactams, and fluoroquinolones are generally not active against ESBL‐producing Enterobacteriaceae, and ‐lactam/‐lactamase inhibitor combinations (eg, ampicillin/sulbactam, piperacillin/tazobactam) do not have reliable activity in serious, high inoculum infections caused by ESBL‐producing Enterobacteriaceae.27
CASE 3: CENTRAL LINE‐ASSOCIATED BLOODSTREAM INFECTION
Case 3 is a 56‐year‐old man who presented to the hospital emergency department with status epilepticus. He was intubated, had a central line placed in the internal jugular vein, and was admitted to the intensive care unit (ICU). The seizure was successfully broken by aggressive treatment with repeated intravenous dosing of lorazepam and loading with fosphenytoin. Empiric antibiotic therapy was initiated with vancomycin and piperacillin/tazobactam on day 5, after spiking a fever of 103.4F. No clear source of the fever was identified. While in the ICU with a central line in place, 2 sets of blood cultures were drawn. Now on hospital day 6, the patient is still spiking fever, although the fever trend appears to be decreasing. The patient is hemodynamically stable, with no other abnormal findings (besides persistent fever) on physical examination. WBC count remains elevated, and both sets of blood cultures are notable for growth of Gram‐positive cocci.
Bloodstream infection is a serious condition in hospitalized patients that is associated with significant morbidity and mortality.28 Patients with suspected bloodstream infection typically receive empiric broad‐spectrum antimicrobial therapy, and are thus good candidates for de‐escalation based on subsequent clinical status and blood culture results. Because of the seriousness of bloodstream infection, healthcare workers are sometimes hesitant to de‐escalate initial empiric therapy, even when cultures isolate a pathogen susceptible to narrower‐spectrum agents, particularly if the patient appears to be improving on such therapy. This is true for various serious hospital or healthcare‐associated infections,16, 29 but particularly for bloodstream infections. Moreover, when central line‐associated bloodstream infection (CLABSI) is suspected, the most important initial intervention is to remove the infected central venous catheter. For a patient with a short‐term catheter and a CLABSI due to Gram‐negative bacilli, S aureus (which appears to be a likely pathogen for the case patient here), enterococci, fungi, or mycobacteria, the 2009 IDSA guidelines for management of intravascular catheter‐related infections recommend catheter removal.30 Catheter removal is even more important than antibiotic coverage; this point cannot be stressed enough. In some extreme cases, when the line cannot be removed for clinical reasons, antibiotic lock therapy can be used to supplement systemic antimicrobial therapy.30 This involves instilling a high antibiotic solution into the catheter lumen for a period of time in order to sterilize the lumen and prevent biofilm formation.31
The first step taken for the patient here was to remove the central venous catheter. Then, turning to the preliminary culture data, there is evidence for Gram‐positive cocci in the patient's blood. The blood culture did not grow any Gram‐negative organisms. Gram‐positive cocci (coagulase‐negative staphylococci, S aureus [methicillin‐susceptible or MRSA]) are the most common causes of CLABSI.32 Can the physician de‐escalate antibiotic therapy in this patient with CLABSI based on the preliminary information? Yes. The information is solid enough to suggest removal of the catheter which was providing coverage for Gram‐negative bacteria (piperacillin/tazobactam), while continuing vancomycin for coverage of possible MRSA, pending further review, ie, until the Gram‐positive cocci are speciated. Rapid diagnostic methods, including polymerase chain reaction (PCR) and nucleic acid probes, can be used to provide more information about certain pathogens (such as MRSA33, 34) before final culture and susceptibility results are available, but these are not routinely available in many clinical microbiology laboratories. Furthermore, these newer technologies remain fairly expensive.
Revisiting the patient 1 day later (hospital day 7), after narrowing the initial combination antibiotic regimen to vancomycin monotherapy, the physical examination indicates the patient is clinically stable, with continued improvement in fever and WBC count (Figure 4). Blood culture analysis now isolates methicillin‐susceptible S aureus (MSSA). Methicillin resistance mediates resistance to all ‐lactams, including carbapenems, greatly limiting treatment options. Vancomycin is the most commonly utilized antibiotic for the treatment of MRSA, and the recent clinical practice guidelines from the IDSA recommend either vancomycin or daptomycin for management of MRSA bacteremia in adult patients.35 However, antistaphylococcal penicillins and first‐generation cephalosporins are the antibiotics of choice for MSSA infections, and particularly for MSSA bloodstream infections.
The activity provided by vancomycin (or daptomycin) is overly broad if MSSA is involved, and importantly, it is not as effective as treatment with an antistaphylococcal penicillin or first‐generation cephalosporin. A recent study by Stryjewski et al., of hemodialysis patients with MSSA bacteremia, reported a higher proportion of treatment failure with vancomycin versus first‐generation cephalosporin therapy (31% vs 13%; P = 0.02).36 Furthermore, multivariate analysis identified vancomycin (vs first‐generation cephalosporin) use as a significant independent predictor of treatment failure (odds ratio [OR], 3.53; 95% confidence interval [CI], 1.1513.45; P = 0.04). Similarly, Chang et al. reported nafcillin, an antistaphylococcal penicillin, was superior to vancomycin in preventing bacteriologic failure (persistent failure and/or relapse) in patients with MSSA bacteremia (0% vs 19%; P = 0.058), and used multivariate analysis to identify vancomycin as a significant independent predictor of relapse (OR, 6.5; 95% CI, 1.052.8; P 0.05).37 Another recent study by Lodise et al. reported that initial empiric therapy with vancomycin for endocarditis caused by MSSA was associated with a higher infection‐related mortality rate than initial empiric therapy with a ‐lactam‐containing regimen (39% vs 11%; P = 0.005).38 The negative impact of initial treatment with vancomycin persisted even in patients switched to a ‐lactam therapy after culture results became available.
Hence, if a patient is being treated with vancomycin for a bloodstream (or other) infection due to MSSA, the therapy is suboptimal. In such a scenariowhich corresponds to that for the case patient herevancomycin should be discontinued and replaced with an antistaphylococcal penicillin or first‐generation cephalosporin. Many times, clinicians are resistant to terminating vancomycin and de‐escalating to antistaphylococcal penicillin/first‐generation cephalosporin therapy in a patient with bacteremia who is apparently responding to vancomycin. However, as the studies just reviewed make clear, not only is vancomycin treatment overly broad for the circumstance, it is also suboptimal and does not represent best clinical practice or patient care. Furthermore, continuing vancomycin in this situation unnecessarily exposes the patient to possible renal toxicity, particularly when aggressive dosing or prolonged vancomycin treatment is involved.39 Because of these issues and concerns, case 3 was de‐escalated from vancomycin to cefazolin, a first‐generation cephalosporin. One word of caution, however, is that there is some controversy over using cefazolin in patients with S aureus native valve endocarditis, given the possibility of a Type A ‐lactamase‐producing species causing cefazolin degradation.40 As a result, the clinician should first rule out endocarditis in the patient here before proceeding with cefazolin therapy. Another alternative would be to use an antistaphylococcal penicillin, such as nafcillin.
Finally, when dealing with bacteremia, and particularly when dealing with a possible CLABSI, the issue of potential culture contamination needs to be seriously considered and answered. Treating an actual infection, not what appears to be an infection because of culture contamination, is particularly important when dealing with possible CLABSI, because coagulase‐negative staphylococci (CoNS) are the most common cause of these types of infections,32 and CoNS are also frequent blood‐culture contaminants.41 Therefore, one needs to determine whether a blood culture growing a CoNS represents true bacteremia or simply contaminationwhich will obviously impact de‐escalation decisions.
In addition, when determining whether a blood culture is truly positive and clinically significant, it is important to consider whether the isolated pathogens are unlikely to be contaminants, likely to be contaminants, or the situation is unclear. A 2000 study by Kim et al.42 suggested that, among patients with 2 positive blood cultures for CoNS, routine identification of CoNS species and genotyping selected isolates using pulsed‐field gel electrophoresis may improve the process of discriminating contaminants from pathogens. Various additional factors need to be weighed when trying to interpret CoNS blood culture results, including patient risk factors, presence of prosthetic devices, number of blood cultures and number positive, and the antimicrobial sensitivity patterns of different isolates. For example, if the sensitivity patterns of 2 CoNS strains isolated from a patient are the same, the likelihood is increased that they represent true pathogens rather than contaminants. Figure 5 presents a schematic of this general approach.42
CONCLUSIONS
De‐escalation is a critical component of antimicrobial stewardship. As the prevalence of antimicrobial resistance grows in the hospital and community, de‐escalation will have an increasingly important role in limiting the further emergence of antimicrobial resistance. Pneumonia, intra‐abdominal infection, and bloodstream infection are commonly managed in the hospital setting. Each of these infection types presents excellent opportunities for de‐escalation, and each presents unique challenges and caveats. Concerted efforts must be made by clinicians and stewardship personnel to de‐escalate as soon as possible, based on culture results and clinical status. Although not discussed here, successful de‐escalation programs utilize structured process, guidelines, and algorithms to consistently implement de‐escalation efforts. These tools of implementation are more fully discussed in the corresponding article in this supplement by Dr Rosenberg.
- .Appropriate empirical antibacterial therapy for nosocomial infections: getting it right the first time.Drugs.2003;63:2157–2168.
- ,,, et al.Mortality and morbidity attributable to inadequate empirical antimicrobial therapy in patients admitted to the ICU with sepsis: a matched cohort study.J Antimicrob Chemother.2008;61:436–441.
- ,,,,,.Predictors of 30‐day mortality and hospital costs in patients with ventilator‐associated pneumonia attributed to potentially antibiotic‐resistant gram‐negative bacteria.Chest.2008;134:281–287.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.Impact of BAL data on the therapy and outcome of ventilator‐associated pneumonia.Chest.1997;111:676–685.
- ,,,,,.Emergence of antibiotic‐resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy.Clin Infect Dis.1996;23:486–494.
- ,,,,.Antimicrobial therapy escalation and hospital mortality among patients with health‐care‐associated pneumonia: a single‐center experience.Chest.2008;134:963–968.
- ,.De‐escalation in lower respiratory tract infections.Curr Opin Pulm Med.2006;12:364–368.
- .The importance of de‐escalating antimicrobial therapy in patients with ventilator‐associated pneumonia.Semin Respir Crit Care Med.2006;27:45–50.
- .Impact of antibiotic resistance in gram‐negative bacilli on empirical and definitive antibiotic therapy.Clin Infect Dis.2008;47(suppl 1):S14–S20.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- Bad Bugs, No Drugs: As Antibiotic R46:155–164.
- ,,, et al.De‐escalation therapy rates are significantly higher by bronchoalveolar lavage than by tracheal aspirate.Intensive Care Med.2007;33:1533–1540.
- ,,, et al.Clinical characteristics and treatment patterns among patients with ventilator‐associated pneumonia.Chest.2006;129:1210–1218.
- ,,, et al.Empiric broad‐spectrum antibiotic therapy of nosocomial pneumonia in the intensive care unit: a prospective observational study.Crit Care.2006;10:R78.
- ,,,.Does de‐escalation of antibiotic therapy for ventilator‐associated pneumonia affect the likelihood of recurrent pneumonia or mortality in critically ill surgical patients?J Trauma.2009;66:1343–1348.
- ,,, et al.Ventilator‐associated pneumonia: breaking the vicious circle of antibiotic overuse.Crit Care Med.2007;35:379–385; quiz 386.
- ,,,,.Adjustment of antibiotic treatment according to the results of blood cultures leads to decreased antibiotic use and costs.J Antimicrob Chemother.2006;57:326–330.
- ,,,,.Diagnostic yield of blood cultures from antibiotic‐naive and antibiotically treated patients with haematological malignancies and high‐risk neutropenia.Scand J Infect Dis.2009;41:650–655.
- ,,, et al.Diagnostic accuracy of protected specimen brush and bronchoalveolar lavage in nosocomial pneumonia: impact of previous antimicrobial treatments.Crit Care Med.1998;26:236–244.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,,.Molecular characteristics of extended‐spectrum beta‐lactamase‐producing Escherichia coli from the Chicago area: high prevalence of ST131 producing CTX‐M‐15 in community hospitals.Int J Antimicrob Agents.2010;36:19–23.
- ,.Ertapenem: a review of its use in the treatment of bacterial infections.Drugs.2005;65:2151–2178.
- .Infections with extended‐spectrum beta‐lactamase‐producing Enterobacteriaceae: changing epidemiology and drug treatment choices.Drugs.2010;70:313–333.
- ,.Bloodstream infection in the ICU.Infect Dis Clin North Am.2009;23:557–569.
- ,,,,.Insights from the Society of Infectious Diseases Pharmacists on antimicrobial stewardship guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America.Pharmacotherapy.2009;29:593–607.
- ,,, et al.Clinical practice guidelines for the diagnosis and management of intravascular catheter‐related infection: 2009 Update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,,,,,.Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients undergoing hemodialysis: systematic review and meta‐analysis of randomized, controlled trials.Clin Infect Dis.2008;47:83–93.
- ,.Catheter‐related bloodstream infections: catheter management according to pathogen.Int J Antimicrob Agents.2010;36(suppl 2):S26–S32.
- ,,,.Detection of methicillin‐resistant Staphylococcus aureus (MRSA) in specimens from various body sites: performance characteristics of the BD GeneOhm MRSA assay, the Xpert MRSA assay, and broth‐enriched culture in an area with a low prevalence of MRSA infections.J Clin Microbiol.2010;48:3882–3887.
- ,,,,.Clinical validation of the molecular BD GeneOhm StaphSR assay for direct detection of Staphylococcus aureus and methicillin‐resistant Staphylococcus aureus in positive blood cultures.J Clin Microbiol.2007;45:2191–2196.
- ,,, et al.Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin‐resistant Staphylococcus aureus infections in adults and children.Clin Infect Dis.2011;52:e18–e55.
- ,,, et al.Use of vancomycin or first‐generation cephalosporins for the treatment of hemodialysis‐dependent patients with methicillin‐susceptible Staphylococcus aureus bacteremia.Clin Infect Dis.2007;44:190–196.
- ,,, et al.Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study.Medicine (Baltimore).2003;82:333–339.
- ,,,.Impact of empirical‐therapy selection on outcomes of intravenous drug users with infective endocarditis caused by methicillin‐susceptible Staphylococcus aureus.Antimicrob Agents Chemother.2007;51:3731–3733.
- ,,,,.A retrospective analysis of possible renal toxicity associated with vancomycin in patients with health care‐associated methicillin‐resistant Staphylococcus aureus pneumonia.Clin Ther.2007;29:1107–1115.
- ,,.Relapse of type A beta‐lactamase‐producing Staphylococcus aureus native valve endocarditis during cefazolin therapy: revisiting the issue.Clin Infect Dis.2003;37:1194–1198.
- ,.The origin of coagulase‐negative staphylococci isolated from blood cultures.J Hosp Infect.1995;30:217–223.
- ,,, et al.Determining the significance of coagulase‐negative staphylococci isolated from blood cultures at a community hospital: a role for species and strain identification.Infect Control Hosp Epidemiol.2000;21:213–217.
- .Appropriate empirical antibacterial therapy for nosocomial infections: getting it right the first time.Drugs.2003;63:2157–2168.
- ,,, et al.Mortality and morbidity attributable to inadequate empirical antimicrobial therapy in patients admitted to the ICU with sepsis: a matched cohort study.J Antimicrob Chemother.2008;61:436–441.
- ,,,,,.Predictors of 30‐day mortality and hospital costs in patients with ventilator‐associated pneumonia attributed to potentially antibiotic‐resistant gram‐negative bacteria.Chest.2008;134:281–287.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.Impact of BAL data on the therapy and outcome of ventilator‐associated pneumonia.Chest.1997;111:676–685.
- ,,,,,.Emergence of antibiotic‐resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy.Clin Infect Dis.1996;23:486–494.
- ,,,,.Antimicrobial therapy escalation and hospital mortality among patients with health‐care‐associated pneumonia: a single‐center experience.Chest.2008;134:963–968.
- ,.De‐escalation in lower respiratory tract infections.Curr Opin Pulm Med.2006;12:364–368.
- .The importance of de‐escalating antimicrobial therapy in patients with ventilator‐associated pneumonia.Semin Respir Crit Care Med.2006;27:45–50.
- .Impact of antibiotic resistance in gram‐negative bacilli on empirical and definitive antibiotic therapy.Clin Infect Dis.2008;47(suppl 1):S14–S20.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- Bad Bugs, No Drugs: As Antibiotic R46:155–164.
- ,,, et al.De‐escalation therapy rates are significantly higher by bronchoalveolar lavage than by tracheal aspirate.Intensive Care Med.2007;33:1533–1540.
- ,,, et al.Clinical characteristics and treatment patterns among patients with ventilator‐associated pneumonia.Chest.2006;129:1210–1218.
- ,,, et al.Empiric broad‐spectrum antibiotic therapy of nosocomial pneumonia in the intensive care unit: a prospective observational study.Crit Care.2006;10:R78.
- ,,,.Does de‐escalation of antibiotic therapy for ventilator‐associated pneumonia affect the likelihood of recurrent pneumonia or mortality in critically ill surgical patients?J Trauma.2009;66:1343–1348.
- ,,, et al.Ventilator‐associated pneumonia: breaking the vicious circle of antibiotic overuse.Crit Care Med.2007;35:379–385; quiz 386.
- ,,,,.Adjustment of antibiotic treatment according to the results of blood cultures leads to decreased antibiotic use and costs.J Antimicrob Chemother.2006;57:326–330.
- ,,,,.Diagnostic yield of blood cultures from antibiotic‐naive and antibiotically treated patients with haematological malignancies and high‐risk neutropenia.Scand J Infect Dis.2009;41:650–655.
- ,,, et al.Diagnostic accuracy of protected specimen brush and bronchoalveolar lavage in nosocomial pneumonia: impact of previous antimicrobial treatments.Crit Care Med.1998;26:236–244.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,,.Molecular characteristics of extended‐spectrum beta‐lactamase‐producing Escherichia coli from the Chicago area: high prevalence of ST131 producing CTX‐M‐15 in community hospitals.Int J Antimicrob Agents.2010;36:19–23.
- ,.Ertapenem: a review of its use in the treatment of bacterial infections.Drugs.2005;65:2151–2178.
- .Infections with extended‐spectrum beta‐lactamase‐producing Enterobacteriaceae: changing epidemiology and drug treatment choices.Drugs.2010;70:313–333.
- ,.Bloodstream infection in the ICU.Infect Dis Clin North Am.2009;23:557–569.
- ,,,,.Insights from the Society of Infectious Diseases Pharmacists on antimicrobial stewardship guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America.Pharmacotherapy.2009;29:593–607.
- ,,, et al.Clinical practice guidelines for the diagnosis and management of intravascular catheter‐related infection: 2009 Update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,,,,,.Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients undergoing hemodialysis: systematic review and meta‐analysis of randomized, controlled trials.Clin Infect Dis.2008;47:83–93.
- ,.Catheter‐related bloodstream infections: catheter management according to pathogen.Int J Antimicrob Agents.2010;36(suppl 2):S26–S32.
- ,,,.Detection of methicillin‐resistant Staphylococcus aureus (MRSA) in specimens from various body sites: performance characteristics of the BD GeneOhm MRSA assay, the Xpert MRSA assay, and broth‐enriched culture in an area with a low prevalence of MRSA infections.J Clin Microbiol.2010;48:3882–3887.
- ,,,,.Clinical validation of the molecular BD GeneOhm StaphSR assay for direct detection of Staphylococcus aureus and methicillin‐resistant Staphylococcus aureus in positive blood cultures.J Clin Microbiol.2007;45:2191–2196.
- ,,, et al.Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin‐resistant Staphylococcus aureus infections in adults and children.Clin Infect Dis.2011;52:e18–e55.
- ,,, et al.Use of vancomycin or first‐generation cephalosporins for the treatment of hemodialysis‐dependent patients with methicillin‐susceptible Staphylococcus aureus bacteremia.Clin Infect Dis.2007;44:190–196.
- ,,, et al.Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study.Medicine (Baltimore).2003;82:333–339.
- ,,,.Impact of empirical‐therapy selection on outcomes of intravenous drug users with infective endocarditis caused by methicillin‐susceptible Staphylococcus aureus.Antimicrob Agents Chemother.2007;51:3731–3733.
- ,,,,.A retrospective analysis of possible renal toxicity associated with vancomycin in patients with health care‐associated methicillin‐resistant Staphylococcus aureus pneumonia.Clin Ther.2007;29:1107–1115.
- ,,.Relapse of type A beta‐lactamase‐producing Staphylococcus aureus native valve endocarditis during cefazolin therapy: revisiting the issue.Clin Infect Dis.2003;37:1194–1198.
- ,.The origin of coagulase‐negative staphylococci isolated from blood cultures.J Hosp Infect.1995;30:217–223.
- ,,, et al.Determining the significance of coagulase‐negative staphylococci isolated from blood cultures at a community hospital: a role for species and strain identification.Infect Control Hosp Epidemiol.2000;21:213–217.
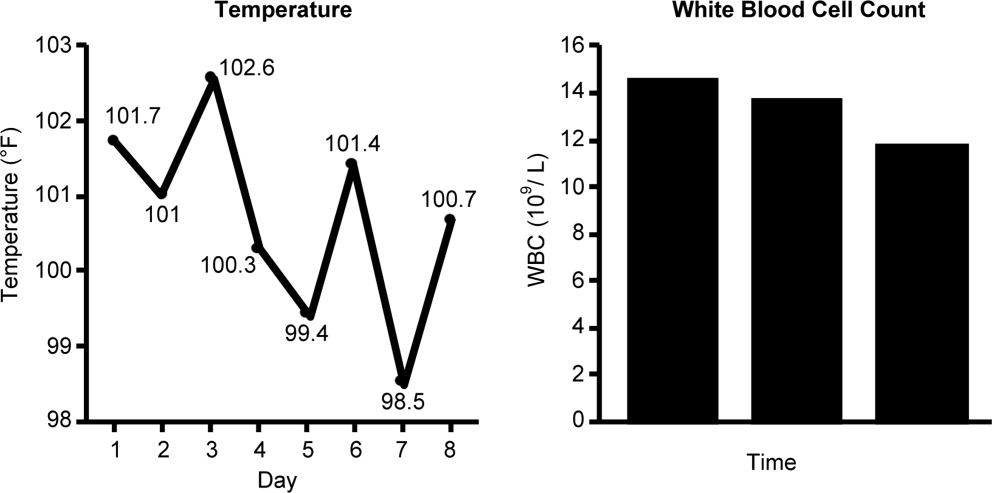
Duration and Cessation of Treatment
The appropriate duration of antimicrobial therapy for serious infections such as hospital‐ or healthcare‐associated pneumonia, complicated intra‐abdominal infection, and bacteremia has not been well studied. To the extent that guidelines for treatment duration exist, they are largely based on observational studies, clinical experience, and consensus, rather than data from well‐designed clinical studiesalthough such studies and data are beginning to emerge, more so in some areas (pneumonia) than others (intra‐abdominal infections and catheter‐related bacteremia). Additional studies supporting treatment durations for these and other important infections are encouraged, given the widely recognized relationships between antimicrobial use and development of antimicrobial resistance, and between antimicrobial resistance and increased morbidity, mortality, and healthcare costs.13 Duration is a component of antimicrobial exposure, and together with optimal dosing, has been linked with antimicrobial resistance and other adverse or unintended consequences of antimicrobial therapy. The general idea is to eradicate (kill) the pathogen as soon as possible, and then stop therapy, since dead bugs don't mutate.
An overwhelming body of work has established a link between antimicrobial use and emergence of antimicrobial‐resistant bacteria. This relationship holds for most, if not all, antimicrobial,47 but appears to be particularly strong for broader‐spectrum agents like fluoroquinolones,814 extended‐spectrum cephalosporins,1518 and carbapenems.4, 1822 Using an antimicrobial from a particular drug class typically promotes development of resistance to all members of the class, but can also lead to more broad‐based resistance including other drug classes, depending on the mechanisms of resistance. Emergence of resistance is expected to be especially high when a suboptimal antimicrobial regimen is administered for a prolonged time or duration,7, 23 as these conditions optimize pressure for selection of preexistent resistant strains or development of new ones.
Optimal efficacy and safety of antimicrobial therapy depends, first, on avoiding antimicrobials when they are not indicated, and second, when they are used, focusing on the 4 Ds of optimal antimicrobial therapy: right Drug, right Dose, De‐escalation to pathogen‐directed therapy, and right Duration of therapy.24 Corresponding articles in this supplement have focused on the first 3 Ds: Dr Syndman on selection of the right drug and dose, and Dr Kaye on de‐escalation of initial empiric therapy, when circumstances warrant it. The current article examines the rationale for reducing the duration of antimicrobial therapy (when possible), and current evidence or guidelines supporting the use of shorter courses of antimicrobial therapy for such infections as pneumonia (community‐, hospital‐, or healthcare‐acquired/associated), complicated intra‐abdominal infection, and bacteremia or sepsis. Key points will be illustrated through 3 case studies dealing with each of these general infection categories.
ADJUSTING DURATION TO OPTIMIZE ANTIMICROBIAL THERAPY
The ultimate goals of short‐course antimicrobial therapy are to rapidly eradicate pathogenic microorganisms and reduce selective pressure for emergence of resistance. The primary potential advantages of shorter duration antimicrobial therapy include lower cost, less toxicity, better adherence, reduced antimicrobial resistance, and reduced disruption of endogenous flora and risk of superinfections, such as Clostridium difficile‐associated disease.23 Other potential benefits of shorter antimicrobial durations include a shorter length of hospital stay and (perhaps) earlier removal of an intravenous catheter, which would be expected to reduce risk of iatrogenic complications and facilitate early mobility and earlier return to full health. Effective short‐course antimicrobial therapy also appears to better meet patient expectations of therapy than longer courses.25
Rapid or early eradication of pathogens depends not only on selecting an agent or combination of agents with activity against the causative pathogen, but also administering the agent in a manner that enables it to achieve its pharmacodynamic (PD) target for pathogen eradication in a rapid fashion.23, 26 The PD parameter that best predicts efficacy will vary for different antimicrobial classes, but the general idea is to use a dose, dosing schedule, and route of administration that rapidly achieves adequate tissue penetration and drug concentration at the infection site for a sufficient length of time for maximum efficacy. In brief, the general concept for short‐course antimicrobial therapy is to hit hard and fast then leave as soon as possible.23
The World Health Organization (WHO) 2000 report on overcoming antimicrobial resistance also recognizes that ideal antimicrobial usage includes using the correct drug, administered by the best route, in the right amount, at optimal intervals, for the appropriate period, after an accurate diagnosis.27 Administering antimicrobials for the wrong period of time (ie, duration) increases risk of resistance. In essence, the WHO report is another call to treat aggressively with shorter courses to help reduce antimicrobial resistance, and to avoid antimicrobial therapy when it is not warranted.
However, while there is general agreement about the utility of using as short an antimicrobial course as is consistent with efficacy, there has been a general dearth of information about exactly what the optimal duration is for particular agents (or drug classes) used to treat particular infections. This is especially the case for most infections occurring in critically ill patients in the hospital setting. Appropriate duration of therapy has been established for some infections, notably group A streptococcus pharyngitis, urinary tract infections, and some sexually transmitted diseases,2831 but treatment duration has not been firmly established for most serious infections. Furthermore, clinicians are often reluctant to shorten the duration of antimicrobial therapy in patients with serious infections for fear of incompletely eradicating the pathogen, thereby leading to relapses and significant morbidity or mortality.
Nevertheless, several studies have now been published that point to the effectiveness of shorter‐course antimicrobial therapy for community‐acquired pneumonia (CAP)3235 and hospital‐acquired pneumonia (HAP) or ventilator‐associated pneumonia (VAP),3645 and a more limited number pointing to the effectiveness of shorter‐course therapy for intra‐abdominal infections38, 46, 47 or bacteremia.4851 In addition, clinical practice guidelines recommend shorter‐course antimicrobial therapy for most patients with CAP,52 uncomplicated healthcare‐associated pneumonia (HCAP) or HAP/VAP,53 and complicated intra‐abdominal infections54and clinical practice guidelines for the management of intravascular catheter‐related infection, including bacteremia, specify a standard duration of therapy and conditions under which a shorter (or longer) course may be considered.55 Shorter‐course therapy can be best implemented based on clinical parameters (eg, resolution of fever, reduction of leukocytosis) along with clinical judgment of the well‐informed clinician with guidance from evidenced‐based guidelines.
The remainder of this section will examine some of the preclinical and clinical evidence supporting shorter‐course therapy for CAP. Subsequent sections of the article utilize 3 case studies to discuss current guidelines and supportive evidence for use of shorter‐course antimicrobial therapy in patients with HCAP or HAP/VAP, complicated intra‐abdominal infections, and bacteremia. The discussion of CAP is intended as an introduction that lays down some general concepts concerning shorter‐duration therapy before delving into the serious hospital‐ or healthcare‐related infections outlined above. Because there is more clinical research on duration of treatment for patients with HAP/VAP than for complicated intra‐abdominal infections or bacteremia, the section on HCAP/HAP/VAP is much longer and detailed than the ones for complicated intra‐abdominal infections or bacteremia.
CAP is defined as pneumonia developing in individuals who are not residents in a nursing home or extended‐care facility, and who have not recently been hospitalized or had significant exposure to the healthcare setting. Pneumonia developing after 48 hours of hospital admission, and that was not incubating at the time of admission, is known as HAP,53, 56 and VAP is a subset of HAP, more precisely defined as HAP that arises after endotracheal intubation.53 HCAP includes patients characterized by residence in a nursing home or extended‐care facility or hospitalization for 2 days in the preceding 90 days or other significant exposure to the healthcare setting.53, 57, 58
DURATION OF THERAPY FOR CAP
A number of studies have reported similar efficacy with shortened versus longer durations of antimicrobial therapy for CAP.33, 5964 Consistent with this, 2 recent meta‐analyses of studies comparing shorter‐ versus longer‐course therapy for mild‐to‐moderate CAP (22 randomized controlled trials and >8000 patients between them) reported similar efficacy and safety with shorter‐course therapy.65, 66 In addition, other studies have reported an association between longer durations of antimicrobial therapy and development of resistance by community respiratory pathogens, especially when lower doses have been used.67, 68 These findings are consistent with the belief that prolonged treatment with a suboptimal antimicrobial regimen creates particularly fertile conditions for selection or development of antimicrobial‐resistant strains.65, 66
Data from preclinical studies provide a basis for understanding the effectiveness of shorter‐dosing regimens of adequate antimicrobial therapy for CAP or other forms of pneumonia. In particular, in vitro time‐kill studies6974 and animal models of infection7577 have demonstrated that Streptococcus pneumoniae can be rapidly eradicated without use of long‐term therapy when appropriate antimicrobials are used. Consistent with these preclinical data, various clinical studies have also shown that S pneumoniae and other respiratory pathogens are rapidly eradicated from lower respiratory tract secretions after initiation of appropriate antimicrobial treatment. For example, Montravers et al. reported that 94% of respiratory pathogens were eradicated from the lungs of 76 patients with VAP after just 3 days of antimicrobial therapy.78
Based on the available data, the 2007 Infectious Diseases Society of America (IDSA)/America Thoracic Society (ATS) guidelines for CAP management recommend a minimum of 5 days of antimicrobial treatment, while noting that most patients become clinically stable within 3‐7 days of treatment onset and rarely require longer durations.52 The guidelines further recommend that CAP patients should be afebrile for 4872 hours and should have no more than 1 CAP‐associated sign of clinical instability before discontinuation of therapy. Although the general movement is toward use of shorter‐duration treatment courses than the traditional 710 days or longer, the IDSA/ATS guidelines acknowledge that longer durations may be needed in certain situations.79
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Case 1 is a 72‐year‐old woman admitted with findings consistent with HCAP who was initiated on an empiric therapy regimen of vancomycin and piperacillin‐tazobactam. Results from blood and sputum cultures obtained prior to treatment initiation came back on day 3, and were negative for pathogenic bacteria. White blood cell (WBC) counts were trending downward, and the patient appeared to be stabilizing. She still had an elevated WBC count, slight fever (temperature maximum of 101.4F for the past 24 hours), and lung crackles at the right lung base. Because Gram stain failed to identify Gram‐positive cocci clusters, and there was no culture evidence of methicillin‐resistant Staphylococcus aureus (MRSA) or Pseudomonas aeruginosa, vancomycin treatment was terminated and the patient was switched to single‐agent therapy with intravenous ceftriaxone, a nonpseudomonal third‐generation cephalosporin. On hospital day 5, there was continuing evidence of response to antimicrobial therapy. The patient reported feeling better and she was breathing comfortably. Her cough was much improved, sputum production was markedly decreased, and her fever had resolved. Now, on day 7, the patient is still afebrile, her WBC count is normal, and she has 96% oxygen saturation on room air.
The question before the clinician is whether to terminate or continue antimicrobial therapy, and if continued, with what regimen and for how long? In addition, if a decision is made to continue antimicrobial therapy, there is a possibility of switching from an intravenous to oral treatment regimen. An examination of the literature and current treatment guidelines for HCAP/HAP/VAP should enable a more informed decision, one that optimally benefits not only this patient, but all subsequent ones who might be exposed and infected with a resistant pathogen that develops when treatment is continued longer than necessary.
Using Clinical Parameters to Shorten Antimicrobial Therapy
A prospective study by Dennesen et al., published 10 years ago, was one of the first suggesting the possibility of shortened duration of antimicrobial therapy for VAP.80 At the time, duration of antimicrobial therapy for VAP typically ranged from 7 to 21 days, and was most commonly 14 to 21 days. In this study, Dennesen and coworkers examined symptom resolution in 27 patients diagnosed with VAP based on clinical, radiologic, and microbiological criteria, each of whom received appropriate antimicrobial therapy based on culture susceptibility data.80 Significant improvements were observed for all clinical parameters examined (highest temperature, leukocyte count, pressure of arterial oxygen to fractional inspired oxygen [PaO2/FIO2] ratio, semiquantitative culture result of endotracheal aspirate), usually first appearing within the first 6 days of antimicrobial therapy. Furthermore, analyses of specific pathogens showed that appropriate antimicrobial therapy rapidly eradicated endotracheal colonization with S pneumoniae, Haemophilus influenzae, and S aureus, but not of P aeruginosa or Enterobacteriaceae. Moreover, endotracheal colonization with resistant pathogens tended to occur when antimicrobial therapy was continued beyond the first week. Taken together, these results suggested that prolonged antimicrobials beyond 7 days usually did not benefit VAP patients, and in fact increased risk of superinfection with a resistant strain. However, it is important to make a distinction between VAP and, for example, skin or bloodstream infections involving S aureus. While improved signs and symptoms generally indicate clinical cure for VAP, this reasoning should not be applied to S aureus bacteremia.
The findings from Dennesen et al. are generally consistent with those from Montravers et al., which showed that 94% of respiratory pathogens were eradicated from the lungs of VAP patients 3 days after initiation of antimicrobial therapy.78 They are also consistent with the findings from a 2005 study by Vidaur et al., which demonstrated resolution of fever (38C), PaO2/FIO2 (>250 mmHg), and WBC/leukocyte count (10,000) in 73%, 75%, and 53% of VAP patients, respectively, without acute respiratory distress syndrome (ARDS; n = 75) after 3 days of appropriate antimicrobial therapy.81 However, Vidaur et al. reported that fever took roughly twice as long to resolve in VAP patients with ARDS (n = 20) versus without ARDS, and that hypoxia resolution was less useful when evaluating treatment response in ARDS patients. As with the Dennesen et al. study,80 the results from Vidaur et al. suggest that measures of core body temperature and oxygenation can be useful guides for clinicians in determining whether to shorten the duration of antimicrobial therapy for patients with VAP, HAP, or HCAP.81
Along the same lines, the clinical pulmonary infection score (CPIS) has established itself as a means for the early termination (shortening) of initial empiric antimicrobial therapy in particular VAP patients. The CPIS is derived by scoring 57 clinical indices relevant for the diagnosis of VAP, as illustrated in Table 1.82 A score of >6 is considered suggestive of pneumonia, while one 6 implies low likelihood of pneumonia. A 2000 study by Singh et al. randomized 81 consecutive patients with pulmonary infiltrates and a CPIS 6 to receive either standard antimicrobial therapy (at discretion of the clinician) or ciprofloxacin monotherapy, with the intention of reevaluating patients at day 3.45 For patients in the ciprofloxacin (experimental) group, antimicrobial therapy was terminated at day 3 if the CPIS remained 6. As a result, only 28% of patients in the experimental group had antimicrobial therapy continued beyond day 3, compared with 90% of patients in the standard therapy group (P = 0.0001). More importantly, there were no significant differences in mortality between patients in the 2 treatment groups, despite a significantly shorter treatment duration for those in the experimental group (3.0 vs 9.8 days, P = 0.0001). In addition, mean length of intensive care unit (ICU) stay was significantly shorter (9.4 vs 14.7 days, P= 0.04) and mean antimicrobial cost was significantly lower ($259 vs $640, P = 0.0001) for patients in the experimental versus standard therapy group.
| Points | |
|---|---|
| |
| Temperature C | |
| 36.5 and 38.4 | 0 |
| 38.5 and 38.9 | 1 |
| 39 or 36.0 | 2 |
| Tracheal secretions | |
| Absence of secretions | 0 |
| Presence of non‐purulent secretions | 1 |
| Presence of purulent secretions | 2 |
| Pulmonary radiography (chest X‐ray) | |
| No infiltrate | 0 |
| Diffused (or patchy) infiltrate | 1 |
| Localized infiltrate | 2 |
| WBCs, leukocytes/mm3 | |
| 4000 and 11,000 | 0 |
| 4000 or >11,000 | 1 |
| +Band forms 500 | 2 |
| Oxygenation: PaO2/FIO2 mmHg | |
| >240 or ARDS | 0 |
| 240 and no evidence of ARDS | 2 |
| Culture of tracheal aspirate (semiquantitative: 012 or 3+) | |
| Pathogenic bacteria cultured 1+ or no growth | 0 |
| Pathogenic bacteria cultured >1+ + same pathogenic bacteria seen on the gram stain >1+ | 1 2 |
| Progression of pulmonary infiltrate | |
| No radiographic progression | 0 |
| Radiographic progression (ARDS excluded) | 2 |
Furthermore, a significantly greater proportion of patients in the standard versus experimental therapy group exhibited evidence of antimicrobial resistance or superinfections (38% vs 14%, P = 0.017). The 2005 clinical practice guidelines for HAP, VAP, or HCAP state, A modified CPIS of 6 or less for 3 days, proposed by Singh and coworkers, is an objective criterion to select patients at low risk for early discontinuation of empiric treatment of HAP.53 While the Singh et al. study provides the rationale for shorter‐course therapy in ICU patients with pulmonary infiltrates who have low likelihood of pneumonia (CPIS 6), this criterion may or may not pertain to HAP/VAP more strictly, and still requires validation in patients with more severe forms of VAP. Incidentally, although the CPIS was designed to define VAP, and there are no data validating its use for other types of pneumonia, the clinical experience by this author indicates that it can be helpful in evaluating HCAP and non‐VAP HAP as well.
Clinical Trial to Support Shortened Duration of HCAP/HAP/VAP Therapy
A French study published in JAMA in 2003 provides more direct support that approximately 1 week of antimicrobial therapy produces effectiveness comparable to more traditional 23‐week therapy for most patients with VAP.37 In this prospective, multicenter, randomized, double‐blind (until day 8) clinical trial, 401 patients with microbiologically proven VAP were randomly assigned to receive either 8 days (n = 197) or 15 days (n = 204) of initial empiric antimicrobial therapy selected by the treating physician. No significant differences were observed between the 8‐day and 15‐day treatment groups for the 2 primary efficacy endpoints of death from any cause (18.8% vs 17.2%) and microbiologically documented pulmonary infection recurrence (28.9% vs 26.0%). There were also no differences between the groups for number of mechanical ventilation‐free days (8.7 vs 9.1 days), number of organ‐failure‐free days (8.7 vs 8.9 days), length of ICU stay (30.0 vs 27.5 days), unfavorable outcome (death, pulmonary infection recurrence, or prescription of a new antimicrobial) (46.2% vs 43.6%), mortality rate on day 60 (25.4% vs 27.9%), or in‐hospital mortality (32% vs 29.9%).
Conversely, patients in the 8‐day treatment group had significantly more antimicrobial‐free days (13.1 vs 8.7 days, P 0.001), and among patients who developed recurrent infections, multidrug‐resistant pathogens emerged more frequently in patients in the 15‐day versus 8‐day treatment group (62.0% vs 42.1%, P = 0.04). However, there was an apparent exception to the general comparable efficacy of the 8‐ and 15‐day treatment regimens for infections caused by nonfermenting Gram‐negative bacilli, including P aeruginosa. For primary infections caused by nonfermenting Gram‐negative bacilli, the 8‐day versus 15‐day regimen was associated with higher rates of pulmonary recurrence (40.6% vs 25.4%). Interestingly, the 8‐day regimen was not associated with more adverse outcomes here, just a higher recurrence rate. With respect to primary infections caused by MRSA, no differences were observed between the 2 treatment regimens for death for all causes (23.4% vs 30.2%) or pulmonary infection recurrence (33.3% vs 42.9%). Figure 1 presents the probability of survival data for the 8‐day and 15‐day treatment groups.
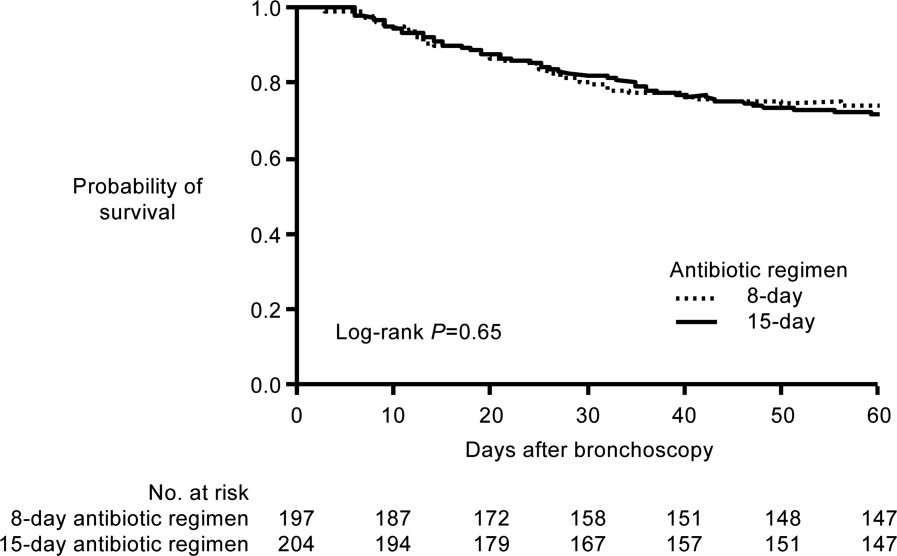
Hence, the data from the Chastre et al. study37 support use of an 8‐day (or shortened) regimen as standard antimicrobial therapy for most patients with VAP, with some possible exceptions. Additional studies provide further support for this general conclusion. For example, a prospective, randomized, controlled trial by Micek et al. evaluated the impact of using an antimicrobial discontinuation policy based on clinical criteria (discontinuation group; n = 150)versus the decision of treating physicians (conventional group, n = 140)to determine the duration of antimicrobial therapy for VAP, and observed a statistically shorter treatment duration in the discontinuation versus conventional management group (6.0 vs 8.0 days, P = 0.001), but no difference between the groups for hospital mortality (32.0% vs 37.1%), ICU length of stay (6.8 vs 7.0 days), or VAP recurrence (17.3% vs 19.3%).42 A prior study by the same group reported a shorter duration of antimicrobial therapy for VAP following implementation of an antimicrobial guideline (vs prior to implementation) (8.6 vs 14.8 days, P 0.001), and a lower rate of VAP recurrence among patients in the after period (7.7% vs 24.0%, P = 0.03). However, interpretation of the results was complicated by the fact that initial empiric therapy was more often appropriate during the after versus before guideline implementation period (94.2% vs 48.0%, P 0.001).40
A limited number of studies have focused further on shortened duration of therapy for patients with VAP caused by Gram‐negative bacteria, and particularly by nonfermenting Gram‐negative bacilli. A retrospective study by Hedrick et al. analyzed the relationship between antimicrobial duration and outcomes of 452 episodes of VAP in the ICU, 154 caused by nonfermenting Gram‐negative bacilli.39 In the study, 127 patients infected with a nonfermenting Gram‐negative bacillus received 9 days (mean 17.1 0.7 days) of antimicrobial therapy, while 27 received 3‐8 days (mean 6.4 0.3 days) of therapy. No significant differences were observed between the shorter‐ and longer‐duration groups for mortality (22% vs 14%, P = 0.38) or VAP recurrence (22% vs 34%, P = 0.27) for these patient populations. Table 2 provides the results for all 452 VAP episodes based on 8 days or 9 days of antimicrobial therapy.
| Patient Characteristic | 8 Days (n = 98) | 9 Days (n = 354) | P Value |
|---|---|---|---|
| |||
| Mean antimicrobial days | 6.2 | 16.8 | 0.0001 |
| Mean APACHE II | 18 | 20 | 0.0009 |
| % Trauma | 71 | 68 | 0.63 |
| Mean time to onset, days | 17.7 | 17.8 | 0.97 |
| Recurrence | 11% | 25% | 0.004 |
| Death | 13% | 11% | 0.59 |
| Nonfermenting Gram‐negative bacilli recurrence | 22% (n = 27) | 34% (n = 127) | 0.27 |
| Staphylococcus aureus recurrence | 20% (n = 10) | 38% (n = 47) | 0.47 |
The retrospective nature of the study limits the ability to more confidently interpret the results, but the data appear to be consistent with the conclusion that short‐duration therapy does not necessarily increase recurrence or worsen other outcomes in patients with VAP caused by nonfermenting Gram‐negative bacilli. The most common Gram‐negative bacilli associated with VAP in the study were P aeruginosa (18% of all infections), Enterobacter cloacae (11%), Acinetobacter spp (11%), Klebsiella pneumoniae (7%), Stenotrophomonas maltophilia (7%), Serratia spp (7%), H influenzae (6%), and Escherichia coli (4%). In addition, the study results suggest that short‐duration therapy is at least as effective as longer‐duration therapy for the overall VAP population, with potential benefits in terms of reduced antimicrobial use and lower rate of recurrence.
Another recent retrospective analysis examining an even shorter course of antimicrobial therapy (5 days) for patients with HAP associated with Gram‐negative bacteria reported a low overall recurrence rate (14%) and a critical care mortality rate (34.2%) in line with prior studies of short‐term therapy for VAP/HAP.44 However, the HAP relapse rate was significantly higher in patients with HAP caused by nonfermenting Gram‐negative bacilli versus other Gram‐negative species (17% vs 2%, P = 0.03).
A recent US pilot study explored the use of repeat bronchoalveolar lavage (BAL) to guide antimicrobial duration in 52 patients with VAP, and compared the results with a matched control group of 52 VAP patients treated before institution of the BAL pathway.43 Antimicrobial therapy in the pathway patients was discontinued if pathogen growth was 10,000 colony forming units/mL on the repeat BAL performed on day 4 of therapy. One objective was to determine whether a repeat BAL strategy, such as the one here, might be able to identify patients with VAP due to nonfermenting Gram‐negative bacilli or other microorganisms who could be safely and effectively treated with shorter‐duration therapy.
Results showed that the antimicrobial duration was significantly shorter for patients in the pathway group than the matched control group (9.8 vs 3.8 days, P 0.001), including the subset of patients with VAP associated with nonfermenting Gram‐negative bacilli (10.7 vs 14.4 days, P 0.001). No significant differences were observed between the overall treatment populations for VAP recurrence, mechanical ventilator‐free ICU days, ICU‐free hospital days, or mortality. Repeat BAL showed most VAP isolates in the study group (83%) responded to initial therapy with a mean duration of 8.8 days. Nonresponders without concomitant infections received significantly longer treatment than pure responding isolates (14.4 vs 7.3 days, P 0.001), and the most common nonresponding microorganisms were P aeruginosa (41% response rate) and S maltophilia (50% response rate), 2 nonfermenting Gram‐negative bacilli.
Most nonfermenting Gram‐negative bacilli‐associated VAP isolates in the study group did respond on repeat BAL (59%). These responders were treated for a mean duration of 8.2 days, and exhibited a similar recurrence rate versus that observed for the matched control group (12.0% vs 17.9%, P = 0.71). These pilot study results suggest that repeat BAL might be used to identify patients likely to benefit from short‐duration therapy, including patients infected with nonfermenting Gram‐negative bacilli. Further study on this is needed.
ATS/IDSA Guidelines for Duration of HCAP/HAP/VAP Therapy
Based largely on the studies by Dennesen et al.80 and Luna et al.83 indicating most VAP patients who respond to appropriate antimicrobial therapy do so within the first 6 days, and those by Chastre et al.37 and Singh et al.45 pointing to the efficacy and safety of shorter‐duration VAP therapy, the 2005 ATS/IDSA guidelines recommend the use of shorter‐duration antimicrobial therapy for most patients with HCAP or HAP/VAP.53 More specifically, the guidelines state, If patients receive an initially appropriate antimicrobial regimen, efforts should be made to shorten the duration of therapy from the traditional 14 to 21 days to periods as short as 7 days, provided that the etiologic pathogen is not P. aeruginosa, and that the patient has a good clinical response with resolution of clinical features of infection.53 Figure 2 presents an overview of the ATS/IDSA guidelines for HCAP/HAP/VAP management 48 to 72 hours after initiation of empiric antimicrobial therapy.53
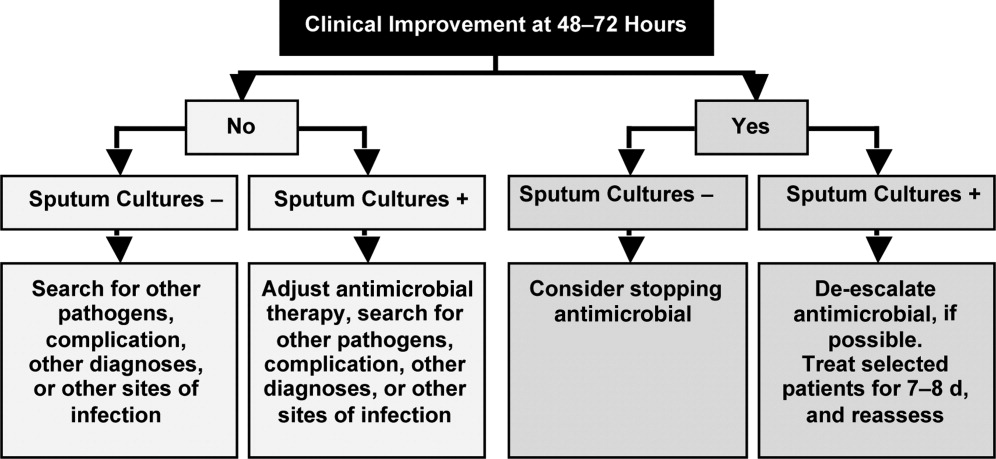
Note that the clinician should consider terminating antimicrobial therapy in patients with clinical improvement and negative cultures or other evidence suggestive of a noninfectious cause. CPIS can also be helpful when deciding whether to terminate initial empiric therapy in a patient with clinical improvement after 23 days of therapy and negative cultures. If cultures are positive, the clinician should consider whether antimicrobial de‐escalation is possible (as discussed by Dr Kaye in the corresponding supplement article), and aim to treat selected patients with an antimicrobial course lasting 78 days. After 78 days, patients should be reassessed for treatment termination or other appropriate actions.
The ATS/IDSA guidelines also provide recommendations for route of drug administration, and if and when to switch from an intravenous to oral agent. In particular, the guidelines state that all patients with HCAP, HAP, or VAP should initially receive therapy intravenously, but conversion to oral/enteral therapy may be possible in certain responding patients, ie, those with a good clinical response and a functioning intestinal tract.53 Fluoroquinolones and linezolid have oral formulations with bioavailability equivalent to the intravenous form, meaning the oral formulations are capable of achieving high levels at the site of infection. This may facilitate conversion to oral therapy in select patients. Early step‐down is safe and effective with fluoroquinolones.84, 85
Based on the information just reviewed, the antimicrobial can be terminated on day 7 for case 1. She is afebrile, and her WBC and oxygenation are normal. In fact, since her records show she was responding at day 5, consideration could have been given to switching from intravenous to oral therapy at that time, and perhaps even discharging her to the rehabilitation center.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman who presents with sepsis and diverticular abscess with walled‐off perforation. Upon hospital arrival, Interventional Radiology inserted a drain, and the patient was initiated on ciprofloxacin and metronidazole therapy. Day 3 examination showed improvement in WBC count and normal vital signs, but the patient still had a low‐grade fever (100.9F). Abdominal examination results were improved, but with some diffuse tenderness. Initial cultures of the abdominal abscess isolated Gram‐negative rods, and the patient was continued on ciprofloxacin/metronidazole. Further cultures on day 4 identified an extended‐spectrum ‐lactamase (ESBL)‐producing E coli organism as the causative pathogen. The patient was switched from ciprofloxacin/metronidazole to ertapenem. It is now hospital day 8, and the patient continues to show good response to treatment. She is afebrile and WBC count is normal. The abscess catheter is no longer draining. Her abdominal pain is improved, and she is complaining that she is hungry. A repeat computed tomography scan shows resolution of the abscess and no evidence of bowel perforation. Should antimicrobial therapy be continued in this patient, and if so, with what agent and for how long?
Guidelines from the Surgical Infection Society and IDSA state that antimicrobial therapy of established or complicated intra‐abdominal infection in adults should be limited to 47 days, unless it is difficult to achieve adequate source control.54 This is because extended antimicrobial exposure increases antimicrobial cost and risk of resistance, superinfection, C difficile‐associated colitis, or other untoward and unintended consequences of antimicrobial therapy, and there is no evidence that longer treatment durations improve outcomes.46, 47, 54, 86 Runyon et al. randomized 90 patients with spontaneous bacterial peritonitis or culture‐negative neutrocytic ascites to receive 5 days or 10 days of cefotaxime monotherapy, and reported similar rates of infection‐related mortality (0% vs 4.3%), hospitalization mortality (33% vs 43%), bacteriologic cure (93% vs 92%), and recurrence of ascitic fluid infection (12% vs 13%).46 Furthermore, shorter‐course therapy was associated with significantly lower antimicrobial administration and costs. Similarly, a recent prospective, randomized, double‐blind trial comparing 3 versus 5 days of ertapenem therapy in 111 patients with community‐acquired intra‐abdominal infection reported similar cure (93% vs 90%) and eradication rates (95% vs 94%).86 However, it should be noted that the mean duration of antimicrobial therapy in the longer‐duration group was still relatively short (5.7 days, range of 5‐10 days).
Studies also indicate there is a very low risk of infection recurrence or treatment failure when antimicrobial therapy is terminated in a patient diagnosed with a complicated intra‐abdominal infection who no longer shows signs of continuing infection.38, 87 Lennard et al. compared postoperative outcomes in 65 patients with or without leukocytosis and fever at the conclusion of antimicrobial therapy for intra‐abdominal sepsis, and reported development of intra‐abdominal infection in 7 of 21 (33%) with persistent leukocytosis.87 None of the 30 patients with normal WBC counts at the end of therapy developed an intra‐abdominal infection postoperatively. Furthermore, intra‐abdominal infection occurred postoperatively in 11 of 14 patients (79%) who responded to treatment but were still febrile at the time of antimicrobial discontinuation.
Similar results were obtained in a much larger, more recent study that retrospectively analyzed the relationship between duration of antimicrobial therapy and infectious complications for patients with intra‐abdominal infections.38 In the study, 929 patients with intra‐abdominal infections associated with either fever or leukocytosis were organized into 4 quartiles based on total duration of antimicrobial therapy (quartile 1: 07 days, n = 218; quartile 2: 812 days, n = 217; quartile 3: 1317 days, n = 246; and quartile 4: >17 days, n = 248) or antimicrobial duration after resolution of leukocytosis (quartile 1: 05 days, n = 130; quartile 2: 610 days, n = 127; quartile 3: 1115 days, n = 124; and quartile 4: >15 days, n = 118). Based on either total duration of antimicrobial therapy or duration after leukocytosis resolution, risk of recurrence was significantly higher for patients in quartiles 3 or 4 versus those in quartile 1, and there was no difference between quartiles 1 and 2.
Taken together, these results suggest that antimicrobial therapy for intra‐abdominal sepsis can be shortened in patients exhibiting a clinical response to treatment, if there are no signs of persistent leukocytosis or fever. Hence, clinicians should use the resolution of clinical signs of infection as a guide to determine when during the 47‐day window antimicrobial therapy should be terminated.54 In practical terms, this usually means treatment can be terminated when the patient is afebrile, has normal WBC counts, and is able to tolerate an oral diet.
Based on the clinical status of case 2 after 8 days of antimicrobial therapy (afebrile with normal WBC counts and requesting oral diet), the ertapenem regimen should be stopped. There is no reason to consider further outpatient antimicrobial therapy for this particular patient, but the Surgical Infection Society and IDSA guidelines discuss the type of patient who should be considered for oral or outpatient antimicrobial therapy. According to the guidelines, the patient convalescing from a complicated intra‐abdominal infection may receive oral antimicrobial therapy, but that therapy should only be included as a component within the brief treatment duration already mentioned, ie, in total, it should rarely exceed 7 days.54 Such therapy is rarely indicated for patients who are afebrile, with normal peripheral WBC/leukocyte counts, and with return of bowel function. These recommendations make it clear that no further antimicrobial therapy is warranted for case 2.
However, for appropriate patients who are recovering from a complicated intra‐abdominal infection and are able to tolerate an oral diet, an oral antimicrobial regimen selected on the basis of identified primary isolates may be used for completion of therapy.54 In the absence of cultures, an oral regimen that covers commonly isolated pathogens (eg, E coli, streptococci, and Bacteroides fragilis) should be considered. Common regimens include an oral cephalosporin or fluoroquinolone with metronidazole, or amoxicillin‐clavulanic acid, assuming susceptibility studies do not demonstrate resistance. Given the identification of an ESBL‐producing E coli for case 2a pathogen relatively resistant to oral antimicrobialan oral regimen probably would not have been viable for this patient even earlier in the treatment course. Lastly, a repeat computed tomography scan was used for the case here. It should be noted that there are currently no well‐established criteria for determining when repeat imaging is needed to confirm resolution of fluid collections. This should be a clinical decision. A general practice is that the catheter is left in place until there is minimal drainage (eg, 10 mL/day); catheter sinograms can also be helpful in determining the status of the abscess.
CASE 3: CENTRAL LINE‐ASSOCIATED BACTEREMIA
Case 3 is a 56‐year‐old man with status epilepticus, intubation, and ICU stay. He was initially treated with vancomycin and piperacillin‐tazobactam for a fever of 103.4F on day 5 of hospitalization. Blood cultures grew Gram‐positive cocci. The central venous catheter was removed, and the initial antimicrobial regimen was de‐escalated to vancomycin monotherapy, which was associated with continued improvement in fever and WBC count, and clinical stability on hospital day 7. At that time, further blood culture analyses isolated methicillin‐susceptible S aureus (MSSA), and the antimicrobial regimen was switched/de‐escalated from vancomycin to cefazolin. It is now hospital day 9 (day 3 of cefazolin) and the patient continues to respond and is afebrile. Repeat blood cultures show no bacterial growth, and a transesophageal echocardiograph (TEE) was performed and revealed normal heart valves. Should the antimicrobial therapy be continued for this patient, and if so, with what agent and for how long?
The IDSA guidelines for management of intravascular catheter‐related infections recommend catheter removal and 46 weeks of antimicrobial therapy for patients with S aureus catheter‐related bloodstream infection (CRBSI), unless the patient has exceptions allowing consideration of shorter‐duration therapy (minimum of 14 days, with day 1 being the first day of negative blood culture results).55 These exceptions include absence of diabetes; immunocompetence (no immunosuppression); removal of the infected catheter; no prosthetic intravascular device (eg, pacemaker or recently placed vascular graft); no evidence of endocarditis or suppurative thrombophlebitis on TEE and ultrasound, respectively; fever and bacteremia resolved within 72 hours after initiation of appropriate antimicrobial therapy; and no evidence of metastatic infection on physical examination and sign‐ or symptom‐directed diagnostic tests.
Short‐duration (10‐16 day) antimicrobial therapy has been reported to yield similarly low recurrence or relapse rates as longer courses of therapy in patients with uncomplicated catheter‐associated S aureus bacteremia.50, 51, 88, 89 A small 1989 study by Ehni and Reller prospectively followed 13 patients with S aureus CRBSI who had received short‐course therapy (17 days), and reported only 1 case of relapse with endocarditis (8% relapse rate).50 A subsequent study by Malanoski et al. retrospectively analyzed the data from 55 patients with S aureus CRBSI.51 Excluding the 8 patients with early complications, the authors observed similar rates of relapse in patients treated for 1015 days and those receiving longer courses of antimicrobial therapy (0% vs 4.7%). The clinical characteristics of the 2 treatment duration groups were similar, and delayed catheter removal was linked with persistence of bacteremia (P = 0.01).
A more recent multicenter, prospective observational study by Chang et al. examined recurrence and the impact of antimicrobial treatment in 505 consecutive patients with S aureus bacteremia, and determined that duration of antimicrobial therapy was not a factor associated with relapse.88 This was true both for patients with bacteremia resulting from endocarditis, bacteremia with no apparent source, or bacteremia due to a focus that could not be cured or removed (28 days therapy after defervescence, 28 days therapy, or 28 days therapy), or those with bacteremia resulting from a source amenable to definitive cure, such as an intravascular device that could be removed, an abscess that could be incised and drained, or an infected bone that could be resected (>14 days, 1014 days, or 10 days therapy). Similarly, a 2005 prospective study by Thomas and Morris determined there was no relationship between treatment duration (7 vs 8 days, 10 vs 10 days, or 14 vs 15 days; P = 0.62, 0.87, and 0.16, respectively) and rate of relapse for 276 patients with cannula‐associated S aureus bacteremia.89 Longer‐duration antimicrobial therapy is warranted in patients with CRBSI and an early complicated course, eg, fever and/or bacteremia persisting for >3 days after catheter removal.90
According to the IDSA guidelines, a TEE should be obtained for all patients with CRBSI involving S aureus who are being considered for a shorter duration of therapy, and the TEE should be performed at least 57 days after onset of bacteremia to minimize risk of false‐negative results.55 High rates of infective endocarditis are observed in patients with S aureus bacteremia,89, 9193 with higher rates in patients with MSSA versus MRSA bacteremia (43.4% vs 19.6%, P 0.009).91 TEE is essential to diagnose endocarditis and detect other complications of bacteremia.92, 93 This recommendation for use of TEE does not necessarily apply to all patients with CRBSI when S aureus is not involved.
Figure 3 summarizes the general recommendations from the IDSA guidelines for the management of CRBSI in patients with a short‐term catheter.55 The figure illustrates the varied recommendations for treatment duration depending on whether the infection is complicated or uncomplicated, and based on the pathogenic microorganism. Returning to case 3, the patient meets the general criteria for shorter duration of antimicrobial therapy: he is not diabetic or immunosuppressed, his catheter has been removed, he does not have any prosthetic intravascular devices, his fever and bacteremia (based on blood cultures) resolved within 3 days of initiating cefazolin therapy, and there is no evidence of endocarditis or other complications of bacteremia. Hence, he is an excellent example of a patient with uncomplicated MSSA CRBSI who meets the criteria for consideration of shortened antimicrobial therapy. Based on the clinical practice guidelines, the patient should continue on intravenous cefazolin for a 14‐day course of therapy, at which time he can be re‐evaluated. A recent review of bloodstream infections caused by various pathogens similarly concluded that the minimum treatment duration for low‐risk patients with S aureus CRBSI is 14 days.48 As a final point, it is also important to note that there is no role for oral therapy in patients with CRBSI, so whether shortened or not, the chosen regimen should be administered intravenously.
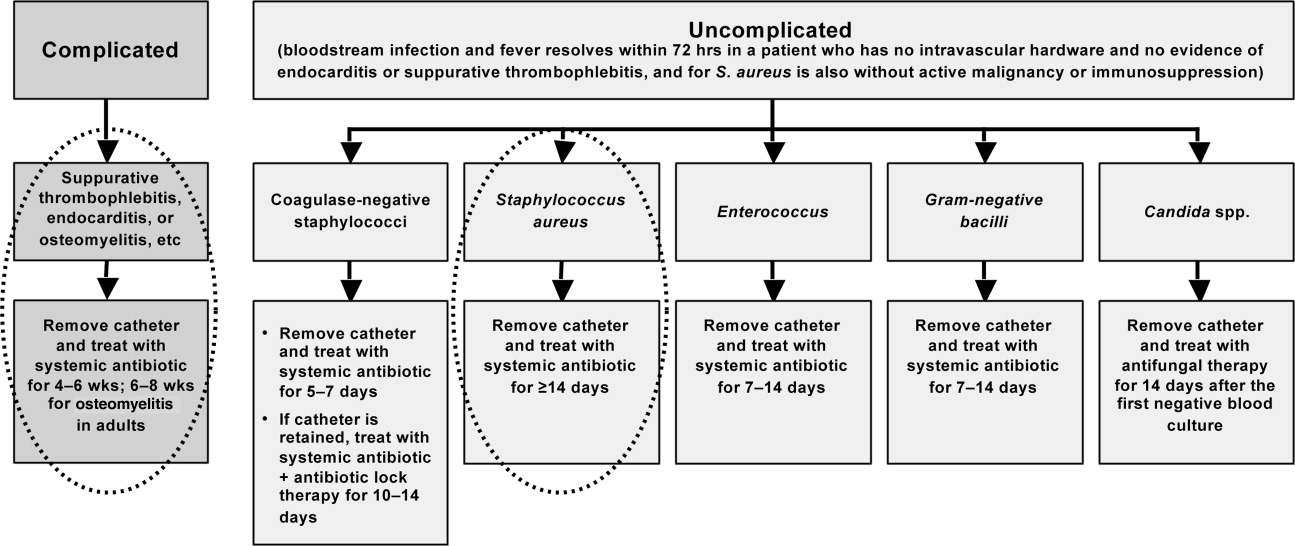
CONCLUSIONS
Shortening the duration of appropriate and adequate antimicrobial therapy represents one strategy for reducing pressure for selection or development of resistant pathogenic microorganisms. Other potential benefits of shorter courses of antimicrobial therapy include reduced risk of antimicrobial‐associated infections (superinfection, C difficile‐associated diarrhea) and other antimicrobial‐related adverse events, improved compliance, and reduced antimicrobial costs. Clinicians are sometimes concerned that reducing antimicrobial courses for patients with serious infections, such as HCAP/HAP/VAP, complicated intra‐abdominal infection, and CRBSI, will lead to incomplete eradication of pathogenic microorganisms, leading to disease recurrence and increased morbidity and mortality. When managing patients with these serious infections, clinicians often turn to the literature and recommendations from professional organizations for guidance. Available data from randomized controlled and nonrandomized clinical trials indicate that shorter‐course therapy is effective and safe for patients with CAP, HCAP/HAP/VAP, complicated intra‐abdominal infections, and CRBSI. Based on these data, and consensus/expert opinion, clinical practice guidelines have been developed that recommend specific durations of antimicrobial therapy for each of these infections.
Although greater study of antimicrobial therapy duration is needed, the current and developing literature and current treatment guidelines should enable clinicians to recognize patients who would benefit from shortened courses of antimicrobial therapy. In doing so, they would help to lower antimicrobial costs and reduce the growing problem of antimicrobial resistance, with its wide‐ranging, negative consequences for current and future patients, and the clinicians who treat them.
- .The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.Clin Infect Dis.2006;42(suppl 2):S82–S89.
- ,,.Clinical and economic burden of antimicrobial resistance.Expert Rev Anti Infect Ther.2008;6:751–763.
- .Economics of antibiotic resistance.Expert Rev Anti Infect Ther.2008;6:523–539.
- ,,,.Emergence of antibiotic‐resistant Pseudomonas aeruginosa: comparison of risks associated with different antipseudomonal agents.Antimicrob Agents Chemother.1999;43:1379–1382.
- ,,,,.Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis.BMJ.2010;340:c2096.
- ,,,,,.Risk factors for invasive pneumococcal disease in children: a population‐based case‐control study in North America.Pediatrics.1999;103:E28.
- ,,.Antimicrobial resistance: consideration as an adverse drug event.Crit Care Med.2010;38:S155–S161.
- ,,,,,.Fluoroquinolone‐resistant Pseudomonas aeruginosa: assessment of risk factors and clinical impact.Am J Med.2006;119:526.e519–526.525.
- ,,, et al.Emergence of fluoroquinolone resistance in outpatient urinary Escherichia coli isolates.Am J Med.2008;121:876–884.
- ,,,,,.Imipenem resistance among Pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes.Infect Control Hosp Epidemiol.2006;27:893–900.
- ,,,,.Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals.Clin Infect Dis.2005;41:435–440.
- ,,,.Evaluation of an intervention designed to decrease the rate of nosocomial methicillin‐resistant Staphylococcus aureus infection by encouraging decreased fluoroquinolone use.Infect Control Hosp Epidemiol.2006;27:155–169.
- ,,,,,.Antibiotic resistance among gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888.
- ,,, et al.Relationship between rates of antimicrobial consumption and the incidence of antimicrobial resistance in Staphylococcus aureus and Pseudomonas aeruginosa isolates from 47 French hospitals.Infect Control Hosp Epidemiol.2007;28:1389–1395.
- ,,, et al.Citywide clonal outbreak of multiresistant Acinetobacter baumannii and Pseudomonas aeruginosa in Brooklyn, NY: the preantibiotic era has returned.Arch Intern Med.2002;162:1515–1520.
- ,,,,.Nosocomial outbreak of Klebsiella infection resistant to late‐generation cephalosporins.Ann Intern Med.1993;119:353–358.
- ,,.The effect of an antimicrobial restriction program on Pseudomonas aeruginosa resistance to beta‐lactams in a large teaching hospital.Pharmacotherapy.2003;23:618–624.
- ,,,.Association between antibiotic usage and subsequent colonization or infection of extensive drug‐resistant Acinetobacter baumannii: a matched case‐control study in intensive care units.Diagn Microbiol Infect Dis.2008;62:298–305.
- ,,.Relationships between antimicrobial use and antimicrobial resistance in Gram‐negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan.Int J Antimicrob Agents.2005;26:463–472.
- ,,, et al.Risk factors for acquisition of imipenem‐resistant Acinetobacter baumannii: a case‐control study.Antimicrob Agents Chemother.2004;48:224–228.
- ,,,,.Consumption of imipenem correlates with beta‐lactam resistance in Pseudomonas aeruginosa.Antimicrob Agents Chemother.2002;46:2920–2925.
- ,,.Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem‐resistant Pseudomonas aeruginosa.Antimicrob Agents Chemother.2009;53:1983–1986.
- .Clinical efficacy of newer agents in short‐duration therapy for community‐acquired pneumonia.Clin Infect Dis.2004;39(suppl 3):S159–S164.
- ,.The role of carbapenems in the treatment of severe nosocomial respiratory tract infections.Expert Opin Pharmacother.2008;9:561–575.
- ,.Does short‐course antibiotic therapy better meet patient expectations?Int J Antimicrob Agents.2003;21:222–228.
- ,,,.Tackling empirical antibiotic therapy for ventilator‐associated pneumonia in your ICU: guidance for implementing the guidelines.Semin Respir Crit Care Med.2009;30:102–115.
- World Health Organization (WHO) report on infectious diseases 2000. Overcoming antimicrobial resistance. Chapter 5. Call to action: A massive effort to provide proper treatment. Available at: http://www.who.int/infectious‐disease‐report/2000/index.html. Accessed January 14,2011.
- ,,,,.Diagnosis and management of group A streptococcal pharyngitis: a practice guideline. Infectious Diseases Society of America.Clin Infect Dis.1997;25:574–583.
- ,,,,,.Shorter‐course antibiotic therapy (SCAT): principles, current data, and caveats. In: Owens RCJ, Lautenbach E, editors.Antimicrobial Resistance: Problem Pathogens and Clinical Countermeasures.New York, NY:Informa Healthcare;2008:337–370.
- ,,, et al.International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases.Clin Infect Dis.2011;52:e103–e120.
- ,.Sexually transmitted diseases treatment guidelines, 2006.MMWR Recomm Rep.2006;55:1–94.
- ,,,,.Novel, single‐dose microsphere formulation of azithromycin versus 7‐day levofloxacin therapy for treatment of mild to moderate community‐acquired pneumonia in adults.Antimicrob Agents Chemother.2005;49:4035–4041.
- ,,, et al.High‐dose, short‐course levofloxacin for community‐acquired pneumonia: a new treatment paradigm.Clin Infect Dis.2003;37:752–760.
- ,.Randomized, multicentre study of the efficacy and tolerance of azithromycin versus clarithromycin in the treatment of adults with mild to moderate community‐acquired pneumonia. Azithromycin Study Group.Eur J Clin Microbiol Infect Dis.1998;17:828–833.
- ,,,,,.A prospective randomized study of inpatient IV antibiotics for community‐acquired pneumonia. The optimal duration of therapy.Chest.1996;110:965–971.
- ,,,.Use of quantitative cultures and reduced duration of antibiotic regimens for patients with ventilator‐associated pneumonia to decrease resistance in the intensive care unit.Clin Infect Dis.2006;43(suppl 2):S75–S81.
- ,,, et al.Comparison of 8 vs 15 days of antibiotic therapy for ventilator‐associated pneumonia in adults: a randomized trial.JAMA.2003;290:2588–2598.
- ,,, et al.Can we define the ideal duration of antibiotic therapy?Surg Infect (Larchmt).2006;7:419–432.
- ,,,,,.Duration of antibiotic therapy for ventilator‐associated pneumonia caused by non‐fermentative gram‐negative bacilli.Surg Infect (Larchmt).2007;8:589–597.
- ,,,,,.Experience with a clinical guideline for the treatment of ventilator‐associated pneumonia.Crit Care Med.2001;29:1109–1115.
- ,.Antibiotic utilization and outcomes for patients with clinically suspected ventilator‐associated pneumonia and negative quantitative BAL culture results.Chest.2005;128:2706–2713.
- ,,,.A randomized controlled trial of an antibiotic discontinuation policy for clinically suspected ventilator‐associated pneumonia.Chest.2004;125:1791–1799.
- ,,, et al.Repeat bronchoalveolar lavage to guide antibiotic duration for ventilator‐associated pneumonia.J Trauma.2007;63:1329–1337.
- ,,.Short course antibiotic therapy for Gram‐negative hospital‐acquired pneumonia in the critically ill.J Hosp Infect.2010;74:337–343.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,,,.Short‐course versus long‐course antibiotic treatment of spontaneous bacterial peritonitis. A randomized controlled study of 100 patients.Gastroenterology.1991;100:1737–1742.
- ,,,,.Complicated appendicitis: is there a minimum intravenous antibiotic requirement? A prospective randomized trial.Am Surg.2000;66:887–890.
- ,,.Short‐course therapy for bloodstream infections in immunocompetent adults.Int J Antimicrob Agents.2009;34(suppl 4):S47–S51.
- ,,,.Short‐course monotherapy strategy for treating bacteremia in the critically ill.Minerva Anestesiol.2006;72:841–857.
- ,.Short‐course therapy for catheter‐associated Staphylococcus aureus bacteremia.Arch Intern Med.1989;149:533–536.
- ,,,.Staphylococcus aureus catheter‐associated bacteremia. Minimal effective therapy and unusual infectious complications associated with arterial sheath catheters.Arch Intern Med.1995;155:1161–1166.
- ,,, et al.Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults.Clin Infect Dis.2007;44(suppl 2):S27–S72.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,,, et al.Clinical practice guidelines for the diagnosis and management of intravascular catheter‐related infection: 2009 update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,.Hospital‐acquired pneumonia: pathophysiology, diagnosis, and treatment.Surg Clin North Am.2009;89:439–461, ix.
- ,,.Healthcare‐associated pneumonia in adults: management principles to improve outcomes.Infect Dis Clin North Am.2004;18:939–962.
- ,,.Healthcare‐associated infections. A useful concept?Curr Opin Crit Care.2009;15:419–424.
- ,,,,,.Efficacy of 750‐mg, 5‐day levofloxacin in the treatment of community‐acquired pneumonia caused by atypical pathogens.Curr Med Res Opin.2004;20:555–563.
- ,,, et al.Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate‐severe community acquired pneumonia: randomised, double blind study.BMJ.2006;332:1355.
- ,,,,.Gemifloxacin once daily for 5 days versus 7 days for the treatment of community‐acquired pneumonia: a randomized, multicentre, double‐blind study.J Antimicrob Chemother.2007;60:112–120.
- ,,.Gemifloxacin once daily for 7 days compared to amoxicillin/clavulanic acid thrice daily for 10 days for the treatment of community‐acquired pneumonia of suspected pneumococcal origin.Respir Med.2004;98:708–720.
- ,,,.Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community‐acquired pneumonia: a prospective, randomized, double‐blind study.Am J Ther.1999;6:217–222.
- ,,,,.Clinical and bacteriological efficacy and safety of 5 and 7 day regimens of telithromycin once daily compared with a 10 day regimen of clarithromycin twice daily in patients with mild to moderate community‐acquired pneumonia.J Antimicrob Chemother.2004;54:515–523.
- ,,,,,.Short‐ versus long‐course antibacterial therapy for community‐acquired pneumonia: a meta‐analysis.Drugs.2008;68:1841–1854.
- ,,,.Efficacy of short‐course antibiotic regimens for community‐acquired pneumonia: a meta‐analysis.Am J Med.2007;120:783–790.
- ,,, et al.Low dosage and long treatment duration of beta‐lactam: risk factors for carriage of penicillin‐resistant Streptococcus pneumoniae.JAMA.1998;279:365–370.
- ,,, et al.Effect of short‐course, high‐dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial.JAMA.2001;286:49–56.
- ,,,.Antipneumococcal activity of ertapenem (MK‐0826) compared to those of other agents.Antimicrob Agents Chemother.2002;46:42–46.
- ,,.MIC and time‐kill study of antipneumococcal activities of RPR 106972 (a new oral streptogramin), RP 59500 (quinupristin‐dalfopristin), pyostacine (RP 7293), penicillin G, cefotaxime, erythromycin, and clarithromycin against 10 penicillin‐susceptible and ‐resistant pneumococci.Antimicrob Agents Chemother.1996;40:2071–2074.
- ,,.Bactericidal activity of daptomycin against Streptococcus pneumoniae compared with eight other antimicrobials.J Antimicrob Chemother.2003;51:443–446.
- ,,.Antipneumococcal activity of ertapenem compared to nine other compounds by time‐kill [abstract E‐800]. In:Program and Abstracts of the 41st Interscience Conference on Antimicrobial Agents and Chemotherapy (Chicago).Washington, DC:American Society for Microbiology,2001:184.
- ,,.Time‐kill analysis of the antipneumococcal activity of daptomycin compared with 8 other agents. In:Program and Abstracts of the 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego).Washington, DC:American Society for Microbiology,2002:161.
- ,,.Post‐antibiotic effect of garenoxacin against gram‐positive and gram‐negative organisms [abstract A‐496]. In:Program and Abstracts of the 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego).Washington, DC:American Society for Microbiology,2002:42.
- ,,, et al.Short‐course therapy of gemifloxacin effective against pneumococcal pneumonia in mice.J Chemother.2006;18:634–640.
- ,,.Animal models of Streptococcus pneumoniae disease.Clin Microbiol Rev.2008;21:666–685.
- ,,,,.Protective effect of trovafloxacin, ciprofloxacin and ampicillin against Streptococcus pneumoniae in a murine sepsis model.J Antimicrob Chemother.1999;44:477–481.
- ,,, et al.Follow‐up protected specimen brushes to assess treatment in nosocomial pneumonia.Am Rev Respir Dis.1993;147:38–44.
- ,.Antimicrobial therapy of community‐acquired pneumonia.Infect Dis Clin North Am.2004;18:993–1016, xi.
- ,,,,.Resolution of infectious parameters after antimicrobial therapy in patients with ventilator‐associated pneumonia.Am J Respir Crit Care Med.2001;163:1371–1375.
- ,,, et al.Clinical resolution in patients with suspicion of ventilator‐associated pneumonia: a cohort study comparing patients with and without acute respiratory distress syndrome.Crit Care Med.2005;33:1248–1253.
- ,,,,,.Diagnosis of ventilator‐associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid.Am Rev Respir Dis.1991;143:1121–1129.
- ,,, et al.Resolution of ventilator‐associated pneumonia: prospective evaluation of the clinical pulmonary infection score as an early clinical predictor of outcome.Crit Care Med.2003;31:676–682.
- .Pharmacoeconomic comparison of sequential IV/oral ciprofloxacin versus ceftazidime in the treatment of nosocomial pneumonia.Can J Hosp Pharm.1995;48:276–283.
- ,,, et al.Clinical and economic evaluation of oral ciprofloxacin after an abbreviated course of intravenous antibiotics.Am J Med.1991;91:462–470.
- ,,, et al.A prospective, double‐blind, multicenter, randomized trial comparing ertapenem 3 vs > or = 5 days in community‐acquired intraabdominal infection.J Gastrointest Surg.2008;12:592–600.
- ,,,.Implications of leukocytosis and fever at conclusion of antibiotic therapy for intra‐abdominal sepsis.Ann Surg.1982;195:19–24.
- ,,, et al.Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study.Medicine (Baltimore).2003;82:333–339.
- ,.Cannula‐associated Staphylococcus aureus bacteraemia: outcome in relation to treatment.Intern Med J.2005;35:319–330.
- ,.Optimal duration of therapy for catheter‐related Staphylococcus aureus bacteremia: a study of 55 cases and review.Clin Infect Dis.1992;14:75–82.
- ,,,,.Staphylococcus aureus bacteremia and endocarditis: the Grady Memorial Hospital experience with methicillin‐sensitive S aureus and methicillin‐resistant S aureus bacteremia.Am Heart J.2004;147:536–539.
- ,,, et al.Role of echocardiography in evaluation of patients with Staphylococcus aureus bacteremia: experience in 103 patients.J Am Coll Cardiol.1997;30:1072–1078.
- ,,, et al.Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow‐up.Clin Infect Dis.1999;28:106–114.
The appropriate duration of antimicrobial therapy for serious infections such as hospital‐ or healthcare‐associated pneumonia, complicated intra‐abdominal infection, and bacteremia has not been well studied. To the extent that guidelines for treatment duration exist, they are largely based on observational studies, clinical experience, and consensus, rather than data from well‐designed clinical studiesalthough such studies and data are beginning to emerge, more so in some areas (pneumonia) than others (intra‐abdominal infections and catheter‐related bacteremia). Additional studies supporting treatment durations for these and other important infections are encouraged, given the widely recognized relationships between antimicrobial use and development of antimicrobial resistance, and between antimicrobial resistance and increased morbidity, mortality, and healthcare costs.13 Duration is a component of antimicrobial exposure, and together with optimal dosing, has been linked with antimicrobial resistance and other adverse or unintended consequences of antimicrobial therapy. The general idea is to eradicate (kill) the pathogen as soon as possible, and then stop therapy, since dead bugs don't mutate.
An overwhelming body of work has established a link between antimicrobial use and emergence of antimicrobial‐resistant bacteria. This relationship holds for most, if not all, antimicrobial,47 but appears to be particularly strong for broader‐spectrum agents like fluoroquinolones,814 extended‐spectrum cephalosporins,1518 and carbapenems.4, 1822 Using an antimicrobial from a particular drug class typically promotes development of resistance to all members of the class, but can also lead to more broad‐based resistance including other drug classes, depending on the mechanisms of resistance. Emergence of resistance is expected to be especially high when a suboptimal antimicrobial regimen is administered for a prolonged time or duration,7, 23 as these conditions optimize pressure for selection of preexistent resistant strains or development of new ones.
Optimal efficacy and safety of antimicrobial therapy depends, first, on avoiding antimicrobials when they are not indicated, and second, when they are used, focusing on the 4 Ds of optimal antimicrobial therapy: right Drug, right Dose, De‐escalation to pathogen‐directed therapy, and right Duration of therapy.24 Corresponding articles in this supplement have focused on the first 3 Ds: Dr Syndman on selection of the right drug and dose, and Dr Kaye on de‐escalation of initial empiric therapy, when circumstances warrant it. The current article examines the rationale for reducing the duration of antimicrobial therapy (when possible), and current evidence or guidelines supporting the use of shorter courses of antimicrobial therapy for such infections as pneumonia (community‐, hospital‐, or healthcare‐acquired/associated), complicated intra‐abdominal infection, and bacteremia or sepsis. Key points will be illustrated through 3 case studies dealing with each of these general infection categories.
ADJUSTING DURATION TO OPTIMIZE ANTIMICROBIAL THERAPY
The ultimate goals of short‐course antimicrobial therapy are to rapidly eradicate pathogenic microorganisms and reduce selective pressure for emergence of resistance. The primary potential advantages of shorter duration antimicrobial therapy include lower cost, less toxicity, better adherence, reduced antimicrobial resistance, and reduced disruption of endogenous flora and risk of superinfections, such as Clostridium difficile‐associated disease.23 Other potential benefits of shorter antimicrobial durations include a shorter length of hospital stay and (perhaps) earlier removal of an intravenous catheter, which would be expected to reduce risk of iatrogenic complications and facilitate early mobility and earlier return to full health. Effective short‐course antimicrobial therapy also appears to better meet patient expectations of therapy than longer courses.25
Rapid or early eradication of pathogens depends not only on selecting an agent or combination of agents with activity against the causative pathogen, but also administering the agent in a manner that enables it to achieve its pharmacodynamic (PD) target for pathogen eradication in a rapid fashion.23, 26 The PD parameter that best predicts efficacy will vary for different antimicrobial classes, but the general idea is to use a dose, dosing schedule, and route of administration that rapidly achieves adequate tissue penetration and drug concentration at the infection site for a sufficient length of time for maximum efficacy. In brief, the general concept for short‐course antimicrobial therapy is to hit hard and fast then leave as soon as possible.23
The World Health Organization (WHO) 2000 report on overcoming antimicrobial resistance also recognizes that ideal antimicrobial usage includes using the correct drug, administered by the best route, in the right amount, at optimal intervals, for the appropriate period, after an accurate diagnosis.27 Administering antimicrobials for the wrong period of time (ie, duration) increases risk of resistance. In essence, the WHO report is another call to treat aggressively with shorter courses to help reduce antimicrobial resistance, and to avoid antimicrobial therapy when it is not warranted.
However, while there is general agreement about the utility of using as short an antimicrobial course as is consistent with efficacy, there has been a general dearth of information about exactly what the optimal duration is for particular agents (or drug classes) used to treat particular infections. This is especially the case for most infections occurring in critically ill patients in the hospital setting. Appropriate duration of therapy has been established for some infections, notably group A streptococcus pharyngitis, urinary tract infections, and some sexually transmitted diseases,2831 but treatment duration has not been firmly established for most serious infections. Furthermore, clinicians are often reluctant to shorten the duration of antimicrobial therapy in patients with serious infections for fear of incompletely eradicating the pathogen, thereby leading to relapses and significant morbidity or mortality.
Nevertheless, several studies have now been published that point to the effectiveness of shorter‐course antimicrobial therapy for community‐acquired pneumonia (CAP)3235 and hospital‐acquired pneumonia (HAP) or ventilator‐associated pneumonia (VAP),3645 and a more limited number pointing to the effectiveness of shorter‐course therapy for intra‐abdominal infections38, 46, 47 or bacteremia.4851 In addition, clinical practice guidelines recommend shorter‐course antimicrobial therapy for most patients with CAP,52 uncomplicated healthcare‐associated pneumonia (HCAP) or HAP/VAP,53 and complicated intra‐abdominal infections54and clinical practice guidelines for the management of intravascular catheter‐related infection, including bacteremia, specify a standard duration of therapy and conditions under which a shorter (or longer) course may be considered.55 Shorter‐course therapy can be best implemented based on clinical parameters (eg, resolution of fever, reduction of leukocytosis) along with clinical judgment of the well‐informed clinician with guidance from evidenced‐based guidelines.
The remainder of this section will examine some of the preclinical and clinical evidence supporting shorter‐course therapy for CAP. Subsequent sections of the article utilize 3 case studies to discuss current guidelines and supportive evidence for use of shorter‐course antimicrobial therapy in patients with HCAP or HAP/VAP, complicated intra‐abdominal infections, and bacteremia. The discussion of CAP is intended as an introduction that lays down some general concepts concerning shorter‐duration therapy before delving into the serious hospital‐ or healthcare‐related infections outlined above. Because there is more clinical research on duration of treatment for patients with HAP/VAP than for complicated intra‐abdominal infections or bacteremia, the section on HCAP/HAP/VAP is much longer and detailed than the ones for complicated intra‐abdominal infections or bacteremia.
CAP is defined as pneumonia developing in individuals who are not residents in a nursing home or extended‐care facility, and who have not recently been hospitalized or had significant exposure to the healthcare setting. Pneumonia developing after 48 hours of hospital admission, and that was not incubating at the time of admission, is known as HAP,53, 56 and VAP is a subset of HAP, more precisely defined as HAP that arises after endotracheal intubation.53 HCAP includes patients characterized by residence in a nursing home or extended‐care facility or hospitalization for 2 days in the preceding 90 days or other significant exposure to the healthcare setting.53, 57, 58
DURATION OF THERAPY FOR CAP
A number of studies have reported similar efficacy with shortened versus longer durations of antimicrobial therapy for CAP.33, 5964 Consistent with this, 2 recent meta‐analyses of studies comparing shorter‐ versus longer‐course therapy for mild‐to‐moderate CAP (22 randomized controlled trials and >8000 patients between them) reported similar efficacy and safety with shorter‐course therapy.65, 66 In addition, other studies have reported an association between longer durations of antimicrobial therapy and development of resistance by community respiratory pathogens, especially when lower doses have been used.67, 68 These findings are consistent with the belief that prolonged treatment with a suboptimal antimicrobial regimen creates particularly fertile conditions for selection or development of antimicrobial‐resistant strains.65, 66
Data from preclinical studies provide a basis for understanding the effectiveness of shorter‐dosing regimens of adequate antimicrobial therapy for CAP or other forms of pneumonia. In particular, in vitro time‐kill studies6974 and animal models of infection7577 have demonstrated that Streptococcus pneumoniae can be rapidly eradicated without use of long‐term therapy when appropriate antimicrobials are used. Consistent with these preclinical data, various clinical studies have also shown that S pneumoniae and other respiratory pathogens are rapidly eradicated from lower respiratory tract secretions after initiation of appropriate antimicrobial treatment. For example, Montravers et al. reported that 94% of respiratory pathogens were eradicated from the lungs of 76 patients with VAP after just 3 days of antimicrobial therapy.78
Based on the available data, the 2007 Infectious Diseases Society of America (IDSA)/America Thoracic Society (ATS) guidelines for CAP management recommend a minimum of 5 days of antimicrobial treatment, while noting that most patients become clinically stable within 3‐7 days of treatment onset and rarely require longer durations.52 The guidelines further recommend that CAP patients should be afebrile for 4872 hours and should have no more than 1 CAP‐associated sign of clinical instability before discontinuation of therapy. Although the general movement is toward use of shorter‐duration treatment courses than the traditional 710 days or longer, the IDSA/ATS guidelines acknowledge that longer durations may be needed in certain situations.79
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Case 1 is a 72‐year‐old woman admitted with findings consistent with HCAP who was initiated on an empiric therapy regimen of vancomycin and piperacillin‐tazobactam. Results from blood and sputum cultures obtained prior to treatment initiation came back on day 3, and were negative for pathogenic bacteria. White blood cell (WBC) counts were trending downward, and the patient appeared to be stabilizing. She still had an elevated WBC count, slight fever (temperature maximum of 101.4F for the past 24 hours), and lung crackles at the right lung base. Because Gram stain failed to identify Gram‐positive cocci clusters, and there was no culture evidence of methicillin‐resistant Staphylococcus aureus (MRSA) or Pseudomonas aeruginosa, vancomycin treatment was terminated and the patient was switched to single‐agent therapy with intravenous ceftriaxone, a nonpseudomonal third‐generation cephalosporin. On hospital day 5, there was continuing evidence of response to antimicrobial therapy. The patient reported feeling better and she was breathing comfortably. Her cough was much improved, sputum production was markedly decreased, and her fever had resolved. Now, on day 7, the patient is still afebrile, her WBC count is normal, and she has 96% oxygen saturation on room air.
The question before the clinician is whether to terminate or continue antimicrobial therapy, and if continued, with what regimen and for how long? In addition, if a decision is made to continue antimicrobial therapy, there is a possibility of switching from an intravenous to oral treatment regimen. An examination of the literature and current treatment guidelines for HCAP/HAP/VAP should enable a more informed decision, one that optimally benefits not only this patient, but all subsequent ones who might be exposed and infected with a resistant pathogen that develops when treatment is continued longer than necessary.
Using Clinical Parameters to Shorten Antimicrobial Therapy
A prospective study by Dennesen et al., published 10 years ago, was one of the first suggesting the possibility of shortened duration of antimicrobial therapy for VAP.80 At the time, duration of antimicrobial therapy for VAP typically ranged from 7 to 21 days, and was most commonly 14 to 21 days. In this study, Dennesen and coworkers examined symptom resolution in 27 patients diagnosed with VAP based on clinical, radiologic, and microbiological criteria, each of whom received appropriate antimicrobial therapy based on culture susceptibility data.80 Significant improvements were observed for all clinical parameters examined (highest temperature, leukocyte count, pressure of arterial oxygen to fractional inspired oxygen [PaO2/FIO2] ratio, semiquantitative culture result of endotracheal aspirate), usually first appearing within the first 6 days of antimicrobial therapy. Furthermore, analyses of specific pathogens showed that appropriate antimicrobial therapy rapidly eradicated endotracheal colonization with S pneumoniae, Haemophilus influenzae, and S aureus, but not of P aeruginosa or Enterobacteriaceae. Moreover, endotracheal colonization with resistant pathogens tended to occur when antimicrobial therapy was continued beyond the first week. Taken together, these results suggested that prolonged antimicrobials beyond 7 days usually did not benefit VAP patients, and in fact increased risk of superinfection with a resistant strain. However, it is important to make a distinction between VAP and, for example, skin or bloodstream infections involving S aureus. While improved signs and symptoms generally indicate clinical cure for VAP, this reasoning should not be applied to S aureus bacteremia.
The findings from Dennesen et al. are generally consistent with those from Montravers et al., which showed that 94% of respiratory pathogens were eradicated from the lungs of VAP patients 3 days after initiation of antimicrobial therapy.78 They are also consistent with the findings from a 2005 study by Vidaur et al., which demonstrated resolution of fever (38C), PaO2/FIO2 (>250 mmHg), and WBC/leukocyte count (10,000) in 73%, 75%, and 53% of VAP patients, respectively, without acute respiratory distress syndrome (ARDS; n = 75) after 3 days of appropriate antimicrobial therapy.81 However, Vidaur et al. reported that fever took roughly twice as long to resolve in VAP patients with ARDS (n = 20) versus without ARDS, and that hypoxia resolution was less useful when evaluating treatment response in ARDS patients. As with the Dennesen et al. study,80 the results from Vidaur et al. suggest that measures of core body temperature and oxygenation can be useful guides for clinicians in determining whether to shorten the duration of antimicrobial therapy for patients with VAP, HAP, or HCAP.81
Along the same lines, the clinical pulmonary infection score (CPIS) has established itself as a means for the early termination (shortening) of initial empiric antimicrobial therapy in particular VAP patients. The CPIS is derived by scoring 57 clinical indices relevant for the diagnosis of VAP, as illustrated in Table 1.82 A score of >6 is considered suggestive of pneumonia, while one 6 implies low likelihood of pneumonia. A 2000 study by Singh et al. randomized 81 consecutive patients with pulmonary infiltrates and a CPIS 6 to receive either standard antimicrobial therapy (at discretion of the clinician) or ciprofloxacin monotherapy, with the intention of reevaluating patients at day 3.45 For patients in the ciprofloxacin (experimental) group, antimicrobial therapy was terminated at day 3 if the CPIS remained 6. As a result, only 28% of patients in the experimental group had antimicrobial therapy continued beyond day 3, compared with 90% of patients in the standard therapy group (P = 0.0001). More importantly, there were no significant differences in mortality between patients in the 2 treatment groups, despite a significantly shorter treatment duration for those in the experimental group (3.0 vs 9.8 days, P = 0.0001). In addition, mean length of intensive care unit (ICU) stay was significantly shorter (9.4 vs 14.7 days, P= 0.04) and mean antimicrobial cost was significantly lower ($259 vs $640, P = 0.0001) for patients in the experimental versus standard therapy group.
| Points | |
|---|---|
| |
| Temperature C | |
| 36.5 and 38.4 | 0 |
| 38.5 and 38.9 | 1 |
| 39 or 36.0 | 2 |
| Tracheal secretions | |
| Absence of secretions | 0 |
| Presence of non‐purulent secretions | 1 |
| Presence of purulent secretions | 2 |
| Pulmonary radiography (chest X‐ray) | |
| No infiltrate | 0 |
| Diffused (or patchy) infiltrate | 1 |
| Localized infiltrate | 2 |
| WBCs, leukocytes/mm3 | |
| 4000 and 11,000 | 0 |
| 4000 or >11,000 | 1 |
| +Band forms 500 | 2 |
| Oxygenation: PaO2/FIO2 mmHg | |
| >240 or ARDS | 0 |
| 240 and no evidence of ARDS | 2 |
| Culture of tracheal aspirate (semiquantitative: 012 or 3+) | |
| Pathogenic bacteria cultured 1+ or no growth | 0 |
| Pathogenic bacteria cultured >1+ + same pathogenic bacteria seen on the gram stain >1+ | 1 2 |
| Progression of pulmonary infiltrate | |
| No radiographic progression | 0 |
| Radiographic progression (ARDS excluded) | 2 |
Furthermore, a significantly greater proportion of patients in the standard versus experimental therapy group exhibited evidence of antimicrobial resistance or superinfections (38% vs 14%, P = 0.017). The 2005 clinical practice guidelines for HAP, VAP, or HCAP state, A modified CPIS of 6 or less for 3 days, proposed by Singh and coworkers, is an objective criterion to select patients at low risk for early discontinuation of empiric treatment of HAP.53 While the Singh et al. study provides the rationale for shorter‐course therapy in ICU patients with pulmonary infiltrates who have low likelihood of pneumonia (CPIS 6), this criterion may or may not pertain to HAP/VAP more strictly, and still requires validation in patients with more severe forms of VAP. Incidentally, although the CPIS was designed to define VAP, and there are no data validating its use for other types of pneumonia, the clinical experience by this author indicates that it can be helpful in evaluating HCAP and non‐VAP HAP as well.
Clinical Trial to Support Shortened Duration of HCAP/HAP/VAP Therapy
A French study published in JAMA in 2003 provides more direct support that approximately 1 week of antimicrobial therapy produces effectiveness comparable to more traditional 23‐week therapy for most patients with VAP.37 In this prospective, multicenter, randomized, double‐blind (until day 8) clinical trial, 401 patients with microbiologically proven VAP were randomly assigned to receive either 8 days (n = 197) or 15 days (n = 204) of initial empiric antimicrobial therapy selected by the treating physician. No significant differences were observed between the 8‐day and 15‐day treatment groups for the 2 primary efficacy endpoints of death from any cause (18.8% vs 17.2%) and microbiologically documented pulmonary infection recurrence (28.9% vs 26.0%). There were also no differences between the groups for number of mechanical ventilation‐free days (8.7 vs 9.1 days), number of organ‐failure‐free days (8.7 vs 8.9 days), length of ICU stay (30.0 vs 27.5 days), unfavorable outcome (death, pulmonary infection recurrence, or prescription of a new antimicrobial) (46.2% vs 43.6%), mortality rate on day 60 (25.4% vs 27.9%), or in‐hospital mortality (32% vs 29.9%).
Conversely, patients in the 8‐day treatment group had significantly more antimicrobial‐free days (13.1 vs 8.7 days, P 0.001), and among patients who developed recurrent infections, multidrug‐resistant pathogens emerged more frequently in patients in the 15‐day versus 8‐day treatment group (62.0% vs 42.1%, P = 0.04). However, there was an apparent exception to the general comparable efficacy of the 8‐ and 15‐day treatment regimens for infections caused by nonfermenting Gram‐negative bacilli, including P aeruginosa. For primary infections caused by nonfermenting Gram‐negative bacilli, the 8‐day versus 15‐day regimen was associated with higher rates of pulmonary recurrence (40.6% vs 25.4%). Interestingly, the 8‐day regimen was not associated with more adverse outcomes here, just a higher recurrence rate. With respect to primary infections caused by MRSA, no differences were observed between the 2 treatment regimens for death for all causes (23.4% vs 30.2%) or pulmonary infection recurrence (33.3% vs 42.9%). Figure 1 presents the probability of survival data for the 8‐day and 15‐day treatment groups.
Hence, the data from the Chastre et al. study37 support use of an 8‐day (or shortened) regimen as standard antimicrobial therapy for most patients with VAP, with some possible exceptions. Additional studies provide further support for this general conclusion. For example, a prospective, randomized, controlled trial by Micek et al. evaluated the impact of using an antimicrobial discontinuation policy based on clinical criteria (discontinuation group; n = 150)versus the decision of treating physicians (conventional group, n = 140)to determine the duration of antimicrobial therapy for VAP, and observed a statistically shorter treatment duration in the discontinuation versus conventional management group (6.0 vs 8.0 days, P = 0.001), but no difference between the groups for hospital mortality (32.0% vs 37.1%), ICU length of stay (6.8 vs 7.0 days), or VAP recurrence (17.3% vs 19.3%).42 A prior study by the same group reported a shorter duration of antimicrobial therapy for VAP following implementation of an antimicrobial guideline (vs prior to implementation) (8.6 vs 14.8 days, P 0.001), and a lower rate of VAP recurrence among patients in the after period (7.7% vs 24.0%, P = 0.03). However, interpretation of the results was complicated by the fact that initial empiric therapy was more often appropriate during the after versus before guideline implementation period (94.2% vs 48.0%, P 0.001).40
A limited number of studies have focused further on shortened duration of therapy for patients with VAP caused by Gram‐negative bacteria, and particularly by nonfermenting Gram‐negative bacilli. A retrospective study by Hedrick et al. analyzed the relationship between antimicrobial duration and outcomes of 452 episodes of VAP in the ICU, 154 caused by nonfermenting Gram‐negative bacilli.39 In the study, 127 patients infected with a nonfermenting Gram‐negative bacillus received 9 days (mean 17.1 0.7 days) of antimicrobial therapy, while 27 received 3‐8 days (mean 6.4 0.3 days) of therapy. No significant differences were observed between the shorter‐ and longer‐duration groups for mortality (22% vs 14%, P = 0.38) or VAP recurrence (22% vs 34%, P = 0.27) for these patient populations. Table 2 provides the results for all 452 VAP episodes based on 8 days or 9 days of antimicrobial therapy.
| Patient Characteristic | 8 Days (n = 98) | 9 Days (n = 354) | P Value |
|---|---|---|---|
| |||
| Mean antimicrobial days | 6.2 | 16.8 | 0.0001 |
| Mean APACHE II | 18 | 20 | 0.0009 |
| % Trauma | 71 | 68 | 0.63 |
| Mean time to onset, days | 17.7 | 17.8 | 0.97 |
| Recurrence | 11% | 25% | 0.004 |
| Death | 13% | 11% | 0.59 |
| Nonfermenting Gram‐negative bacilli recurrence | 22% (n = 27) | 34% (n = 127) | 0.27 |
| Staphylococcus aureus recurrence | 20% (n = 10) | 38% (n = 47) | 0.47 |
The retrospective nature of the study limits the ability to more confidently interpret the results, but the data appear to be consistent with the conclusion that short‐duration therapy does not necessarily increase recurrence or worsen other outcomes in patients with VAP caused by nonfermenting Gram‐negative bacilli. The most common Gram‐negative bacilli associated with VAP in the study were P aeruginosa (18% of all infections), Enterobacter cloacae (11%), Acinetobacter spp (11%), Klebsiella pneumoniae (7%), Stenotrophomonas maltophilia (7%), Serratia spp (7%), H influenzae (6%), and Escherichia coli (4%). In addition, the study results suggest that short‐duration therapy is at least as effective as longer‐duration therapy for the overall VAP population, with potential benefits in terms of reduced antimicrobial use and lower rate of recurrence.
Another recent retrospective analysis examining an even shorter course of antimicrobial therapy (5 days) for patients with HAP associated with Gram‐negative bacteria reported a low overall recurrence rate (14%) and a critical care mortality rate (34.2%) in line with prior studies of short‐term therapy for VAP/HAP.44 However, the HAP relapse rate was significantly higher in patients with HAP caused by nonfermenting Gram‐negative bacilli versus other Gram‐negative species (17% vs 2%, P = 0.03).
A recent US pilot study explored the use of repeat bronchoalveolar lavage (BAL) to guide antimicrobial duration in 52 patients with VAP, and compared the results with a matched control group of 52 VAP patients treated before institution of the BAL pathway.43 Antimicrobial therapy in the pathway patients was discontinued if pathogen growth was 10,000 colony forming units/mL on the repeat BAL performed on day 4 of therapy. One objective was to determine whether a repeat BAL strategy, such as the one here, might be able to identify patients with VAP due to nonfermenting Gram‐negative bacilli or other microorganisms who could be safely and effectively treated with shorter‐duration therapy.
Results showed that the antimicrobial duration was significantly shorter for patients in the pathway group than the matched control group (9.8 vs 3.8 days, P 0.001), including the subset of patients with VAP associated with nonfermenting Gram‐negative bacilli (10.7 vs 14.4 days, P 0.001). No significant differences were observed between the overall treatment populations for VAP recurrence, mechanical ventilator‐free ICU days, ICU‐free hospital days, or mortality. Repeat BAL showed most VAP isolates in the study group (83%) responded to initial therapy with a mean duration of 8.8 days. Nonresponders without concomitant infections received significantly longer treatment than pure responding isolates (14.4 vs 7.3 days, P 0.001), and the most common nonresponding microorganisms were P aeruginosa (41% response rate) and S maltophilia (50% response rate), 2 nonfermenting Gram‐negative bacilli.
Most nonfermenting Gram‐negative bacilli‐associated VAP isolates in the study group did respond on repeat BAL (59%). These responders were treated for a mean duration of 8.2 days, and exhibited a similar recurrence rate versus that observed for the matched control group (12.0% vs 17.9%, P = 0.71). These pilot study results suggest that repeat BAL might be used to identify patients likely to benefit from short‐duration therapy, including patients infected with nonfermenting Gram‐negative bacilli. Further study on this is needed.
ATS/IDSA Guidelines for Duration of HCAP/HAP/VAP Therapy
Based largely on the studies by Dennesen et al.80 and Luna et al.83 indicating most VAP patients who respond to appropriate antimicrobial therapy do so within the first 6 days, and those by Chastre et al.37 and Singh et al.45 pointing to the efficacy and safety of shorter‐duration VAP therapy, the 2005 ATS/IDSA guidelines recommend the use of shorter‐duration antimicrobial therapy for most patients with HCAP or HAP/VAP.53 More specifically, the guidelines state, If patients receive an initially appropriate antimicrobial regimen, efforts should be made to shorten the duration of therapy from the traditional 14 to 21 days to periods as short as 7 days, provided that the etiologic pathogen is not P. aeruginosa, and that the patient has a good clinical response with resolution of clinical features of infection.53 Figure 2 presents an overview of the ATS/IDSA guidelines for HCAP/HAP/VAP management 48 to 72 hours after initiation of empiric antimicrobial therapy.53
Note that the clinician should consider terminating antimicrobial therapy in patients with clinical improvement and negative cultures or other evidence suggestive of a noninfectious cause. CPIS can also be helpful when deciding whether to terminate initial empiric therapy in a patient with clinical improvement after 23 days of therapy and negative cultures. If cultures are positive, the clinician should consider whether antimicrobial de‐escalation is possible (as discussed by Dr Kaye in the corresponding supplement article), and aim to treat selected patients with an antimicrobial course lasting 78 days. After 78 days, patients should be reassessed for treatment termination or other appropriate actions.
The ATS/IDSA guidelines also provide recommendations for route of drug administration, and if and when to switch from an intravenous to oral agent. In particular, the guidelines state that all patients with HCAP, HAP, or VAP should initially receive therapy intravenously, but conversion to oral/enteral therapy may be possible in certain responding patients, ie, those with a good clinical response and a functioning intestinal tract.53 Fluoroquinolones and linezolid have oral formulations with bioavailability equivalent to the intravenous form, meaning the oral formulations are capable of achieving high levels at the site of infection. This may facilitate conversion to oral therapy in select patients. Early step‐down is safe and effective with fluoroquinolones.84, 85
Based on the information just reviewed, the antimicrobial can be terminated on day 7 for case 1. She is afebrile, and her WBC and oxygenation are normal. In fact, since her records show she was responding at day 5, consideration could have been given to switching from intravenous to oral therapy at that time, and perhaps even discharging her to the rehabilitation center.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman who presents with sepsis and diverticular abscess with walled‐off perforation. Upon hospital arrival, Interventional Radiology inserted a drain, and the patient was initiated on ciprofloxacin and metronidazole therapy. Day 3 examination showed improvement in WBC count and normal vital signs, but the patient still had a low‐grade fever (100.9F). Abdominal examination results were improved, but with some diffuse tenderness. Initial cultures of the abdominal abscess isolated Gram‐negative rods, and the patient was continued on ciprofloxacin/metronidazole. Further cultures on day 4 identified an extended‐spectrum ‐lactamase (ESBL)‐producing E coli organism as the causative pathogen. The patient was switched from ciprofloxacin/metronidazole to ertapenem. It is now hospital day 8, and the patient continues to show good response to treatment. She is afebrile and WBC count is normal. The abscess catheter is no longer draining. Her abdominal pain is improved, and she is complaining that she is hungry. A repeat computed tomography scan shows resolution of the abscess and no evidence of bowel perforation. Should antimicrobial therapy be continued in this patient, and if so, with what agent and for how long?
Guidelines from the Surgical Infection Society and IDSA state that antimicrobial therapy of established or complicated intra‐abdominal infection in adults should be limited to 47 days, unless it is difficult to achieve adequate source control.54 This is because extended antimicrobial exposure increases antimicrobial cost and risk of resistance, superinfection, C difficile‐associated colitis, or other untoward and unintended consequences of antimicrobial therapy, and there is no evidence that longer treatment durations improve outcomes.46, 47, 54, 86 Runyon et al. randomized 90 patients with spontaneous bacterial peritonitis or culture‐negative neutrocytic ascites to receive 5 days or 10 days of cefotaxime monotherapy, and reported similar rates of infection‐related mortality (0% vs 4.3%), hospitalization mortality (33% vs 43%), bacteriologic cure (93% vs 92%), and recurrence of ascitic fluid infection (12% vs 13%).46 Furthermore, shorter‐course therapy was associated with significantly lower antimicrobial administration and costs. Similarly, a recent prospective, randomized, double‐blind trial comparing 3 versus 5 days of ertapenem therapy in 111 patients with community‐acquired intra‐abdominal infection reported similar cure (93% vs 90%) and eradication rates (95% vs 94%).86 However, it should be noted that the mean duration of antimicrobial therapy in the longer‐duration group was still relatively short (5.7 days, range of 5‐10 days).
Studies also indicate there is a very low risk of infection recurrence or treatment failure when antimicrobial therapy is terminated in a patient diagnosed with a complicated intra‐abdominal infection who no longer shows signs of continuing infection.38, 87 Lennard et al. compared postoperative outcomes in 65 patients with or without leukocytosis and fever at the conclusion of antimicrobial therapy for intra‐abdominal sepsis, and reported development of intra‐abdominal infection in 7 of 21 (33%) with persistent leukocytosis.87 None of the 30 patients with normal WBC counts at the end of therapy developed an intra‐abdominal infection postoperatively. Furthermore, intra‐abdominal infection occurred postoperatively in 11 of 14 patients (79%) who responded to treatment but were still febrile at the time of antimicrobial discontinuation.
Similar results were obtained in a much larger, more recent study that retrospectively analyzed the relationship between duration of antimicrobial therapy and infectious complications for patients with intra‐abdominal infections.38 In the study, 929 patients with intra‐abdominal infections associated with either fever or leukocytosis were organized into 4 quartiles based on total duration of antimicrobial therapy (quartile 1: 07 days, n = 218; quartile 2: 812 days, n = 217; quartile 3: 1317 days, n = 246; and quartile 4: >17 days, n = 248) or antimicrobial duration after resolution of leukocytosis (quartile 1: 05 days, n = 130; quartile 2: 610 days, n = 127; quartile 3: 1115 days, n = 124; and quartile 4: >15 days, n = 118). Based on either total duration of antimicrobial therapy or duration after leukocytosis resolution, risk of recurrence was significantly higher for patients in quartiles 3 or 4 versus those in quartile 1, and there was no difference between quartiles 1 and 2.
Taken together, these results suggest that antimicrobial therapy for intra‐abdominal sepsis can be shortened in patients exhibiting a clinical response to treatment, if there are no signs of persistent leukocytosis or fever. Hence, clinicians should use the resolution of clinical signs of infection as a guide to determine when during the 47‐day window antimicrobial therapy should be terminated.54 In practical terms, this usually means treatment can be terminated when the patient is afebrile, has normal WBC counts, and is able to tolerate an oral diet.
Based on the clinical status of case 2 after 8 days of antimicrobial therapy (afebrile with normal WBC counts and requesting oral diet), the ertapenem regimen should be stopped. There is no reason to consider further outpatient antimicrobial therapy for this particular patient, but the Surgical Infection Society and IDSA guidelines discuss the type of patient who should be considered for oral or outpatient antimicrobial therapy. According to the guidelines, the patient convalescing from a complicated intra‐abdominal infection may receive oral antimicrobial therapy, but that therapy should only be included as a component within the brief treatment duration already mentioned, ie, in total, it should rarely exceed 7 days.54 Such therapy is rarely indicated for patients who are afebrile, with normal peripheral WBC/leukocyte counts, and with return of bowel function. These recommendations make it clear that no further antimicrobial therapy is warranted for case 2.
However, for appropriate patients who are recovering from a complicated intra‐abdominal infection and are able to tolerate an oral diet, an oral antimicrobial regimen selected on the basis of identified primary isolates may be used for completion of therapy.54 In the absence of cultures, an oral regimen that covers commonly isolated pathogens (eg, E coli, streptococci, and Bacteroides fragilis) should be considered. Common regimens include an oral cephalosporin or fluoroquinolone with metronidazole, or amoxicillin‐clavulanic acid, assuming susceptibility studies do not demonstrate resistance. Given the identification of an ESBL‐producing E coli for case 2a pathogen relatively resistant to oral antimicrobialan oral regimen probably would not have been viable for this patient even earlier in the treatment course. Lastly, a repeat computed tomography scan was used for the case here. It should be noted that there are currently no well‐established criteria for determining when repeat imaging is needed to confirm resolution of fluid collections. This should be a clinical decision. A general practice is that the catheter is left in place until there is minimal drainage (eg, 10 mL/day); catheter sinograms can also be helpful in determining the status of the abscess.
CASE 3: CENTRAL LINE‐ASSOCIATED BACTEREMIA
Case 3 is a 56‐year‐old man with status epilepticus, intubation, and ICU stay. He was initially treated with vancomycin and piperacillin‐tazobactam for a fever of 103.4F on day 5 of hospitalization. Blood cultures grew Gram‐positive cocci. The central venous catheter was removed, and the initial antimicrobial regimen was de‐escalated to vancomycin monotherapy, which was associated with continued improvement in fever and WBC count, and clinical stability on hospital day 7. At that time, further blood culture analyses isolated methicillin‐susceptible S aureus (MSSA), and the antimicrobial regimen was switched/de‐escalated from vancomycin to cefazolin. It is now hospital day 9 (day 3 of cefazolin) and the patient continues to respond and is afebrile. Repeat blood cultures show no bacterial growth, and a transesophageal echocardiograph (TEE) was performed and revealed normal heart valves. Should the antimicrobial therapy be continued for this patient, and if so, with what agent and for how long?
The IDSA guidelines for management of intravascular catheter‐related infections recommend catheter removal and 46 weeks of antimicrobial therapy for patients with S aureus catheter‐related bloodstream infection (CRBSI), unless the patient has exceptions allowing consideration of shorter‐duration therapy (minimum of 14 days, with day 1 being the first day of negative blood culture results).55 These exceptions include absence of diabetes; immunocompetence (no immunosuppression); removal of the infected catheter; no prosthetic intravascular device (eg, pacemaker or recently placed vascular graft); no evidence of endocarditis or suppurative thrombophlebitis on TEE and ultrasound, respectively; fever and bacteremia resolved within 72 hours after initiation of appropriate antimicrobial therapy; and no evidence of metastatic infection on physical examination and sign‐ or symptom‐directed diagnostic tests.
Short‐duration (10‐16 day) antimicrobial therapy has been reported to yield similarly low recurrence or relapse rates as longer courses of therapy in patients with uncomplicated catheter‐associated S aureus bacteremia.50, 51, 88, 89 A small 1989 study by Ehni and Reller prospectively followed 13 patients with S aureus CRBSI who had received short‐course therapy (17 days), and reported only 1 case of relapse with endocarditis (8% relapse rate).50 A subsequent study by Malanoski et al. retrospectively analyzed the data from 55 patients with S aureus CRBSI.51 Excluding the 8 patients with early complications, the authors observed similar rates of relapse in patients treated for 1015 days and those receiving longer courses of antimicrobial therapy (0% vs 4.7%). The clinical characteristics of the 2 treatment duration groups were similar, and delayed catheter removal was linked with persistence of bacteremia (P = 0.01).
A more recent multicenter, prospective observational study by Chang et al. examined recurrence and the impact of antimicrobial treatment in 505 consecutive patients with S aureus bacteremia, and determined that duration of antimicrobial therapy was not a factor associated with relapse.88 This was true both for patients with bacteremia resulting from endocarditis, bacteremia with no apparent source, or bacteremia due to a focus that could not be cured or removed (28 days therapy after defervescence, 28 days therapy, or 28 days therapy), or those with bacteremia resulting from a source amenable to definitive cure, such as an intravascular device that could be removed, an abscess that could be incised and drained, or an infected bone that could be resected (>14 days, 1014 days, or 10 days therapy). Similarly, a 2005 prospective study by Thomas and Morris determined there was no relationship between treatment duration (7 vs 8 days, 10 vs 10 days, or 14 vs 15 days; P = 0.62, 0.87, and 0.16, respectively) and rate of relapse for 276 patients with cannula‐associated S aureus bacteremia.89 Longer‐duration antimicrobial therapy is warranted in patients with CRBSI and an early complicated course, eg, fever and/or bacteremia persisting for >3 days after catheter removal.90
According to the IDSA guidelines, a TEE should be obtained for all patients with CRBSI involving S aureus who are being considered for a shorter duration of therapy, and the TEE should be performed at least 57 days after onset of bacteremia to minimize risk of false‐negative results.55 High rates of infective endocarditis are observed in patients with S aureus bacteremia,89, 9193 with higher rates in patients with MSSA versus MRSA bacteremia (43.4% vs 19.6%, P 0.009).91 TEE is essential to diagnose endocarditis and detect other complications of bacteremia.92, 93 This recommendation for use of TEE does not necessarily apply to all patients with CRBSI when S aureus is not involved.
Figure 3 summarizes the general recommendations from the IDSA guidelines for the management of CRBSI in patients with a short‐term catheter.55 The figure illustrates the varied recommendations for treatment duration depending on whether the infection is complicated or uncomplicated, and based on the pathogenic microorganism. Returning to case 3, the patient meets the general criteria for shorter duration of antimicrobial therapy: he is not diabetic or immunosuppressed, his catheter has been removed, he does not have any prosthetic intravascular devices, his fever and bacteremia (based on blood cultures) resolved within 3 days of initiating cefazolin therapy, and there is no evidence of endocarditis or other complications of bacteremia. Hence, he is an excellent example of a patient with uncomplicated MSSA CRBSI who meets the criteria for consideration of shortened antimicrobial therapy. Based on the clinical practice guidelines, the patient should continue on intravenous cefazolin for a 14‐day course of therapy, at which time he can be re‐evaluated. A recent review of bloodstream infections caused by various pathogens similarly concluded that the minimum treatment duration for low‐risk patients with S aureus CRBSI is 14 days.48 As a final point, it is also important to note that there is no role for oral therapy in patients with CRBSI, so whether shortened or not, the chosen regimen should be administered intravenously.
CONCLUSIONS
Shortening the duration of appropriate and adequate antimicrobial therapy represents one strategy for reducing pressure for selection or development of resistant pathogenic microorganisms. Other potential benefits of shorter courses of antimicrobial therapy include reduced risk of antimicrobial‐associated infections (superinfection, C difficile‐associated diarrhea) and other antimicrobial‐related adverse events, improved compliance, and reduced antimicrobial costs. Clinicians are sometimes concerned that reducing antimicrobial courses for patients with serious infections, such as HCAP/HAP/VAP, complicated intra‐abdominal infection, and CRBSI, will lead to incomplete eradication of pathogenic microorganisms, leading to disease recurrence and increased morbidity and mortality. When managing patients with these serious infections, clinicians often turn to the literature and recommendations from professional organizations for guidance. Available data from randomized controlled and nonrandomized clinical trials indicate that shorter‐course therapy is effective and safe for patients with CAP, HCAP/HAP/VAP, complicated intra‐abdominal infections, and CRBSI. Based on these data, and consensus/expert opinion, clinical practice guidelines have been developed that recommend specific durations of antimicrobial therapy for each of these infections.
Although greater study of antimicrobial therapy duration is needed, the current and developing literature and current treatment guidelines should enable clinicians to recognize patients who would benefit from shortened courses of antimicrobial therapy. In doing so, they would help to lower antimicrobial costs and reduce the growing problem of antimicrobial resistance, with its wide‐ranging, negative consequences for current and future patients, and the clinicians who treat them.
The appropriate duration of antimicrobial therapy for serious infections such as hospital‐ or healthcare‐associated pneumonia, complicated intra‐abdominal infection, and bacteremia has not been well studied. To the extent that guidelines for treatment duration exist, they are largely based on observational studies, clinical experience, and consensus, rather than data from well‐designed clinical studiesalthough such studies and data are beginning to emerge, more so in some areas (pneumonia) than others (intra‐abdominal infections and catheter‐related bacteremia). Additional studies supporting treatment durations for these and other important infections are encouraged, given the widely recognized relationships between antimicrobial use and development of antimicrobial resistance, and between antimicrobial resistance and increased morbidity, mortality, and healthcare costs.13 Duration is a component of antimicrobial exposure, and together with optimal dosing, has been linked with antimicrobial resistance and other adverse or unintended consequences of antimicrobial therapy. The general idea is to eradicate (kill) the pathogen as soon as possible, and then stop therapy, since dead bugs don't mutate.
An overwhelming body of work has established a link between antimicrobial use and emergence of antimicrobial‐resistant bacteria. This relationship holds for most, if not all, antimicrobial,47 but appears to be particularly strong for broader‐spectrum agents like fluoroquinolones,814 extended‐spectrum cephalosporins,1518 and carbapenems.4, 1822 Using an antimicrobial from a particular drug class typically promotes development of resistance to all members of the class, but can also lead to more broad‐based resistance including other drug classes, depending on the mechanisms of resistance. Emergence of resistance is expected to be especially high when a suboptimal antimicrobial regimen is administered for a prolonged time or duration,7, 23 as these conditions optimize pressure for selection of preexistent resistant strains or development of new ones.
Optimal efficacy and safety of antimicrobial therapy depends, first, on avoiding antimicrobials when they are not indicated, and second, when they are used, focusing on the 4 Ds of optimal antimicrobial therapy: right Drug, right Dose, De‐escalation to pathogen‐directed therapy, and right Duration of therapy.24 Corresponding articles in this supplement have focused on the first 3 Ds: Dr Syndman on selection of the right drug and dose, and Dr Kaye on de‐escalation of initial empiric therapy, when circumstances warrant it. The current article examines the rationale for reducing the duration of antimicrobial therapy (when possible), and current evidence or guidelines supporting the use of shorter courses of antimicrobial therapy for such infections as pneumonia (community‐, hospital‐, or healthcare‐acquired/associated), complicated intra‐abdominal infection, and bacteremia or sepsis. Key points will be illustrated through 3 case studies dealing with each of these general infection categories.
ADJUSTING DURATION TO OPTIMIZE ANTIMICROBIAL THERAPY
The ultimate goals of short‐course antimicrobial therapy are to rapidly eradicate pathogenic microorganisms and reduce selective pressure for emergence of resistance. The primary potential advantages of shorter duration antimicrobial therapy include lower cost, less toxicity, better adherence, reduced antimicrobial resistance, and reduced disruption of endogenous flora and risk of superinfections, such as Clostridium difficile‐associated disease.23 Other potential benefits of shorter antimicrobial durations include a shorter length of hospital stay and (perhaps) earlier removal of an intravenous catheter, which would be expected to reduce risk of iatrogenic complications and facilitate early mobility and earlier return to full health. Effective short‐course antimicrobial therapy also appears to better meet patient expectations of therapy than longer courses.25
Rapid or early eradication of pathogens depends not only on selecting an agent or combination of agents with activity against the causative pathogen, but also administering the agent in a manner that enables it to achieve its pharmacodynamic (PD) target for pathogen eradication in a rapid fashion.23, 26 The PD parameter that best predicts efficacy will vary for different antimicrobial classes, but the general idea is to use a dose, dosing schedule, and route of administration that rapidly achieves adequate tissue penetration and drug concentration at the infection site for a sufficient length of time for maximum efficacy. In brief, the general concept for short‐course antimicrobial therapy is to hit hard and fast then leave as soon as possible.23
The World Health Organization (WHO) 2000 report on overcoming antimicrobial resistance also recognizes that ideal antimicrobial usage includes using the correct drug, administered by the best route, in the right amount, at optimal intervals, for the appropriate period, after an accurate diagnosis.27 Administering antimicrobials for the wrong period of time (ie, duration) increases risk of resistance. In essence, the WHO report is another call to treat aggressively with shorter courses to help reduce antimicrobial resistance, and to avoid antimicrobial therapy when it is not warranted.
However, while there is general agreement about the utility of using as short an antimicrobial course as is consistent with efficacy, there has been a general dearth of information about exactly what the optimal duration is for particular agents (or drug classes) used to treat particular infections. This is especially the case for most infections occurring in critically ill patients in the hospital setting. Appropriate duration of therapy has been established for some infections, notably group A streptococcus pharyngitis, urinary tract infections, and some sexually transmitted diseases,2831 but treatment duration has not been firmly established for most serious infections. Furthermore, clinicians are often reluctant to shorten the duration of antimicrobial therapy in patients with serious infections for fear of incompletely eradicating the pathogen, thereby leading to relapses and significant morbidity or mortality.
Nevertheless, several studies have now been published that point to the effectiveness of shorter‐course antimicrobial therapy for community‐acquired pneumonia (CAP)3235 and hospital‐acquired pneumonia (HAP) or ventilator‐associated pneumonia (VAP),3645 and a more limited number pointing to the effectiveness of shorter‐course therapy for intra‐abdominal infections38, 46, 47 or bacteremia.4851 In addition, clinical practice guidelines recommend shorter‐course antimicrobial therapy for most patients with CAP,52 uncomplicated healthcare‐associated pneumonia (HCAP) or HAP/VAP,53 and complicated intra‐abdominal infections54and clinical practice guidelines for the management of intravascular catheter‐related infection, including bacteremia, specify a standard duration of therapy and conditions under which a shorter (or longer) course may be considered.55 Shorter‐course therapy can be best implemented based on clinical parameters (eg, resolution of fever, reduction of leukocytosis) along with clinical judgment of the well‐informed clinician with guidance from evidenced‐based guidelines.
The remainder of this section will examine some of the preclinical and clinical evidence supporting shorter‐course therapy for CAP. Subsequent sections of the article utilize 3 case studies to discuss current guidelines and supportive evidence for use of shorter‐course antimicrobial therapy in patients with HCAP or HAP/VAP, complicated intra‐abdominal infections, and bacteremia. The discussion of CAP is intended as an introduction that lays down some general concepts concerning shorter‐duration therapy before delving into the serious hospital‐ or healthcare‐related infections outlined above. Because there is more clinical research on duration of treatment for patients with HAP/VAP than for complicated intra‐abdominal infections or bacteremia, the section on HCAP/HAP/VAP is much longer and detailed than the ones for complicated intra‐abdominal infections or bacteremia.
CAP is defined as pneumonia developing in individuals who are not residents in a nursing home or extended‐care facility, and who have not recently been hospitalized or had significant exposure to the healthcare setting. Pneumonia developing after 48 hours of hospital admission, and that was not incubating at the time of admission, is known as HAP,53, 56 and VAP is a subset of HAP, more precisely defined as HAP that arises after endotracheal intubation.53 HCAP includes patients characterized by residence in a nursing home or extended‐care facility or hospitalization for 2 days in the preceding 90 days or other significant exposure to the healthcare setting.53, 57, 58
DURATION OF THERAPY FOR CAP
A number of studies have reported similar efficacy with shortened versus longer durations of antimicrobial therapy for CAP.33, 5964 Consistent with this, 2 recent meta‐analyses of studies comparing shorter‐ versus longer‐course therapy for mild‐to‐moderate CAP (22 randomized controlled trials and >8000 patients between them) reported similar efficacy and safety with shorter‐course therapy.65, 66 In addition, other studies have reported an association between longer durations of antimicrobial therapy and development of resistance by community respiratory pathogens, especially when lower doses have been used.67, 68 These findings are consistent with the belief that prolonged treatment with a suboptimal antimicrobial regimen creates particularly fertile conditions for selection or development of antimicrobial‐resistant strains.65, 66
Data from preclinical studies provide a basis for understanding the effectiveness of shorter‐dosing regimens of adequate antimicrobial therapy for CAP or other forms of pneumonia. In particular, in vitro time‐kill studies6974 and animal models of infection7577 have demonstrated that Streptococcus pneumoniae can be rapidly eradicated without use of long‐term therapy when appropriate antimicrobials are used. Consistent with these preclinical data, various clinical studies have also shown that S pneumoniae and other respiratory pathogens are rapidly eradicated from lower respiratory tract secretions after initiation of appropriate antimicrobial treatment. For example, Montravers et al. reported that 94% of respiratory pathogens were eradicated from the lungs of 76 patients with VAP after just 3 days of antimicrobial therapy.78
Based on the available data, the 2007 Infectious Diseases Society of America (IDSA)/America Thoracic Society (ATS) guidelines for CAP management recommend a minimum of 5 days of antimicrobial treatment, while noting that most patients become clinically stable within 3‐7 days of treatment onset and rarely require longer durations.52 The guidelines further recommend that CAP patients should be afebrile for 4872 hours and should have no more than 1 CAP‐associated sign of clinical instability before discontinuation of therapy. Although the general movement is toward use of shorter‐duration treatment courses than the traditional 710 days or longer, the IDSA/ATS guidelines acknowledge that longer durations may be needed in certain situations.79
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Case 1 is a 72‐year‐old woman admitted with findings consistent with HCAP who was initiated on an empiric therapy regimen of vancomycin and piperacillin‐tazobactam. Results from blood and sputum cultures obtained prior to treatment initiation came back on day 3, and were negative for pathogenic bacteria. White blood cell (WBC) counts were trending downward, and the patient appeared to be stabilizing. She still had an elevated WBC count, slight fever (temperature maximum of 101.4F for the past 24 hours), and lung crackles at the right lung base. Because Gram stain failed to identify Gram‐positive cocci clusters, and there was no culture evidence of methicillin‐resistant Staphylococcus aureus (MRSA) or Pseudomonas aeruginosa, vancomycin treatment was terminated and the patient was switched to single‐agent therapy with intravenous ceftriaxone, a nonpseudomonal third‐generation cephalosporin. On hospital day 5, there was continuing evidence of response to antimicrobial therapy. The patient reported feeling better and she was breathing comfortably. Her cough was much improved, sputum production was markedly decreased, and her fever had resolved. Now, on day 7, the patient is still afebrile, her WBC count is normal, and she has 96% oxygen saturation on room air.
The question before the clinician is whether to terminate or continue antimicrobial therapy, and if continued, with what regimen and for how long? In addition, if a decision is made to continue antimicrobial therapy, there is a possibility of switching from an intravenous to oral treatment regimen. An examination of the literature and current treatment guidelines for HCAP/HAP/VAP should enable a more informed decision, one that optimally benefits not only this patient, but all subsequent ones who might be exposed and infected with a resistant pathogen that develops when treatment is continued longer than necessary.
Using Clinical Parameters to Shorten Antimicrobial Therapy
A prospective study by Dennesen et al., published 10 years ago, was one of the first suggesting the possibility of shortened duration of antimicrobial therapy for VAP.80 At the time, duration of antimicrobial therapy for VAP typically ranged from 7 to 21 days, and was most commonly 14 to 21 days. In this study, Dennesen and coworkers examined symptom resolution in 27 patients diagnosed with VAP based on clinical, radiologic, and microbiological criteria, each of whom received appropriate antimicrobial therapy based on culture susceptibility data.80 Significant improvements were observed for all clinical parameters examined (highest temperature, leukocyte count, pressure of arterial oxygen to fractional inspired oxygen [PaO2/FIO2] ratio, semiquantitative culture result of endotracheal aspirate), usually first appearing within the first 6 days of antimicrobial therapy. Furthermore, analyses of specific pathogens showed that appropriate antimicrobial therapy rapidly eradicated endotracheal colonization with S pneumoniae, Haemophilus influenzae, and S aureus, but not of P aeruginosa or Enterobacteriaceae. Moreover, endotracheal colonization with resistant pathogens tended to occur when antimicrobial therapy was continued beyond the first week. Taken together, these results suggested that prolonged antimicrobials beyond 7 days usually did not benefit VAP patients, and in fact increased risk of superinfection with a resistant strain. However, it is important to make a distinction between VAP and, for example, skin or bloodstream infections involving S aureus. While improved signs and symptoms generally indicate clinical cure for VAP, this reasoning should not be applied to S aureus bacteremia.
The findings from Dennesen et al. are generally consistent with those from Montravers et al., which showed that 94% of respiratory pathogens were eradicated from the lungs of VAP patients 3 days after initiation of antimicrobial therapy.78 They are also consistent with the findings from a 2005 study by Vidaur et al., which demonstrated resolution of fever (38C), PaO2/FIO2 (>250 mmHg), and WBC/leukocyte count (10,000) in 73%, 75%, and 53% of VAP patients, respectively, without acute respiratory distress syndrome (ARDS; n = 75) after 3 days of appropriate antimicrobial therapy.81 However, Vidaur et al. reported that fever took roughly twice as long to resolve in VAP patients with ARDS (n = 20) versus without ARDS, and that hypoxia resolution was less useful when evaluating treatment response in ARDS patients. As with the Dennesen et al. study,80 the results from Vidaur et al. suggest that measures of core body temperature and oxygenation can be useful guides for clinicians in determining whether to shorten the duration of antimicrobial therapy for patients with VAP, HAP, or HCAP.81
Along the same lines, the clinical pulmonary infection score (CPIS) has established itself as a means for the early termination (shortening) of initial empiric antimicrobial therapy in particular VAP patients. The CPIS is derived by scoring 57 clinical indices relevant for the diagnosis of VAP, as illustrated in Table 1.82 A score of >6 is considered suggestive of pneumonia, while one 6 implies low likelihood of pneumonia. A 2000 study by Singh et al. randomized 81 consecutive patients with pulmonary infiltrates and a CPIS 6 to receive either standard antimicrobial therapy (at discretion of the clinician) or ciprofloxacin monotherapy, with the intention of reevaluating patients at day 3.45 For patients in the ciprofloxacin (experimental) group, antimicrobial therapy was terminated at day 3 if the CPIS remained 6. As a result, only 28% of patients in the experimental group had antimicrobial therapy continued beyond day 3, compared with 90% of patients in the standard therapy group (P = 0.0001). More importantly, there were no significant differences in mortality between patients in the 2 treatment groups, despite a significantly shorter treatment duration for those in the experimental group (3.0 vs 9.8 days, P = 0.0001). In addition, mean length of intensive care unit (ICU) stay was significantly shorter (9.4 vs 14.7 days, P= 0.04) and mean antimicrobial cost was significantly lower ($259 vs $640, P = 0.0001) for patients in the experimental versus standard therapy group.
| Points | |
|---|---|
| |
| Temperature C | |
| 36.5 and 38.4 | 0 |
| 38.5 and 38.9 | 1 |
| 39 or 36.0 | 2 |
| Tracheal secretions | |
| Absence of secretions | 0 |
| Presence of non‐purulent secretions | 1 |
| Presence of purulent secretions | 2 |
| Pulmonary radiography (chest X‐ray) | |
| No infiltrate | 0 |
| Diffused (or patchy) infiltrate | 1 |
| Localized infiltrate | 2 |
| WBCs, leukocytes/mm3 | |
| 4000 and 11,000 | 0 |
| 4000 or >11,000 | 1 |
| +Band forms 500 | 2 |
| Oxygenation: PaO2/FIO2 mmHg | |
| >240 or ARDS | 0 |
| 240 and no evidence of ARDS | 2 |
| Culture of tracheal aspirate (semiquantitative: 012 or 3+) | |
| Pathogenic bacteria cultured 1+ or no growth | 0 |
| Pathogenic bacteria cultured >1+ + same pathogenic bacteria seen on the gram stain >1+ | 1 2 |
| Progression of pulmonary infiltrate | |
| No radiographic progression | 0 |
| Radiographic progression (ARDS excluded) | 2 |
Furthermore, a significantly greater proportion of patients in the standard versus experimental therapy group exhibited evidence of antimicrobial resistance or superinfections (38% vs 14%, P = 0.017). The 2005 clinical practice guidelines for HAP, VAP, or HCAP state, A modified CPIS of 6 or less for 3 days, proposed by Singh and coworkers, is an objective criterion to select patients at low risk for early discontinuation of empiric treatment of HAP.53 While the Singh et al. study provides the rationale for shorter‐course therapy in ICU patients with pulmonary infiltrates who have low likelihood of pneumonia (CPIS 6), this criterion may or may not pertain to HAP/VAP more strictly, and still requires validation in patients with more severe forms of VAP. Incidentally, although the CPIS was designed to define VAP, and there are no data validating its use for other types of pneumonia, the clinical experience by this author indicates that it can be helpful in evaluating HCAP and non‐VAP HAP as well.
Clinical Trial to Support Shortened Duration of HCAP/HAP/VAP Therapy
A French study published in JAMA in 2003 provides more direct support that approximately 1 week of antimicrobial therapy produces effectiveness comparable to more traditional 23‐week therapy for most patients with VAP.37 In this prospective, multicenter, randomized, double‐blind (until day 8) clinical trial, 401 patients with microbiologically proven VAP were randomly assigned to receive either 8 days (n = 197) or 15 days (n = 204) of initial empiric antimicrobial therapy selected by the treating physician. No significant differences were observed between the 8‐day and 15‐day treatment groups for the 2 primary efficacy endpoints of death from any cause (18.8% vs 17.2%) and microbiologically documented pulmonary infection recurrence (28.9% vs 26.0%). There were also no differences between the groups for number of mechanical ventilation‐free days (8.7 vs 9.1 days), number of organ‐failure‐free days (8.7 vs 8.9 days), length of ICU stay (30.0 vs 27.5 days), unfavorable outcome (death, pulmonary infection recurrence, or prescription of a new antimicrobial) (46.2% vs 43.6%), mortality rate on day 60 (25.4% vs 27.9%), or in‐hospital mortality (32% vs 29.9%).
Conversely, patients in the 8‐day treatment group had significantly more antimicrobial‐free days (13.1 vs 8.7 days, P 0.001), and among patients who developed recurrent infections, multidrug‐resistant pathogens emerged more frequently in patients in the 15‐day versus 8‐day treatment group (62.0% vs 42.1%, P = 0.04). However, there was an apparent exception to the general comparable efficacy of the 8‐ and 15‐day treatment regimens for infections caused by nonfermenting Gram‐negative bacilli, including P aeruginosa. For primary infections caused by nonfermenting Gram‐negative bacilli, the 8‐day versus 15‐day regimen was associated with higher rates of pulmonary recurrence (40.6% vs 25.4%). Interestingly, the 8‐day regimen was not associated with more adverse outcomes here, just a higher recurrence rate. With respect to primary infections caused by MRSA, no differences were observed between the 2 treatment regimens for death for all causes (23.4% vs 30.2%) or pulmonary infection recurrence (33.3% vs 42.9%). Figure 1 presents the probability of survival data for the 8‐day and 15‐day treatment groups.
Hence, the data from the Chastre et al. study37 support use of an 8‐day (or shortened) regimen as standard antimicrobial therapy for most patients with VAP, with some possible exceptions. Additional studies provide further support for this general conclusion. For example, a prospective, randomized, controlled trial by Micek et al. evaluated the impact of using an antimicrobial discontinuation policy based on clinical criteria (discontinuation group; n = 150)versus the decision of treating physicians (conventional group, n = 140)to determine the duration of antimicrobial therapy for VAP, and observed a statistically shorter treatment duration in the discontinuation versus conventional management group (6.0 vs 8.0 days, P = 0.001), but no difference between the groups for hospital mortality (32.0% vs 37.1%), ICU length of stay (6.8 vs 7.0 days), or VAP recurrence (17.3% vs 19.3%).42 A prior study by the same group reported a shorter duration of antimicrobial therapy for VAP following implementation of an antimicrobial guideline (vs prior to implementation) (8.6 vs 14.8 days, P 0.001), and a lower rate of VAP recurrence among patients in the after period (7.7% vs 24.0%, P = 0.03). However, interpretation of the results was complicated by the fact that initial empiric therapy was more often appropriate during the after versus before guideline implementation period (94.2% vs 48.0%, P 0.001).40
A limited number of studies have focused further on shortened duration of therapy for patients with VAP caused by Gram‐negative bacteria, and particularly by nonfermenting Gram‐negative bacilli. A retrospective study by Hedrick et al. analyzed the relationship between antimicrobial duration and outcomes of 452 episodes of VAP in the ICU, 154 caused by nonfermenting Gram‐negative bacilli.39 In the study, 127 patients infected with a nonfermenting Gram‐negative bacillus received 9 days (mean 17.1 0.7 days) of antimicrobial therapy, while 27 received 3‐8 days (mean 6.4 0.3 days) of therapy. No significant differences were observed between the shorter‐ and longer‐duration groups for mortality (22% vs 14%, P = 0.38) or VAP recurrence (22% vs 34%, P = 0.27) for these patient populations. Table 2 provides the results for all 452 VAP episodes based on 8 days or 9 days of antimicrobial therapy.
| Patient Characteristic | 8 Days (n = 98) | 9 Days (n = 354) | P Value |
|---|---|---|---|
| |||
| Mean antimicrobial days | 6.2 | 16.8 | 0.0001 |
| Mean APACHE II | 18 | 20 | 0.0009 |
| % Trauma | 71 | 68 | 0.63 |
| Mean time to onset, days | 17.7 | 17.8 | 0.97 |
| Recurrence | 11% | 25% | 0.004 |
| Death | 13% | 11% | 0.59 |
| Nonfermenting Gram‐negative bacilli recurrence | 22% (n = 27) | 34% (n = 127) | 0.27 |
| Staphylococcus aureus recurrence | 20% (n = 10) | 38% (n = 47) | 0.47 |
The retrospective nature of the study limits the ability to more confidently interpret the results, but the data appear to be consistent with the conclusion that short‐duration therapy does not necessarily increase recurrence or worsen other outcomes in patients with VAP caused by nonfermenting Gram‐negative bacilli. The most common Gram‐negative bacilli associated with VAP in the study were P aeruginosa (18% of all infections), Enterobacter cloacae (11%), Acinetobacter spp (11%), Klebsiella pneumoniae (7%), Stenotrophomonas maltophilia (7%), Serratia spp (7%), H influenzae (6%), and Escherichia coli (4%). In addition, the study results suggest that short‐duration therapy is at least as effective as longer‐duration therapy for the overall VAP population, with potential benefits in terms of reduced antimicrobial use and lower rate of recurrence.
Another recent retrospective analysis examining an even shorter course of antimicrobial therapy (5 days) for patients with HAP associated with Gram‐negative bacteria reported a low overall recurrence rate (14%) and a critical care mortality rate (34.2%) in line with prior studies of short‐term therapy for VAP/HAP.44 However, the HAP relapse rate was significantly higher in patients with HAP caused by nonfermenting Gram‐negative bacilli versus other Gram‐negative species (17% vs 2%, P = 0.03).
A recent US pilot study explored the use of repeat bronchoalveolar lavage (BAL) to guide antimicrobial duration in 52 patients with VAP, and compared the results with a matched control group of 52 VAP patients treated before institution of the BAL pathway.43 Antimicrobial therapy in the pathway patients was discontinued if pathogen growth was 10,000 colony forming units/mL on the repeat BAL performed on day 4 of therapy. One objective was to determine whether a repeat BAL strategy, such as the one here, might be able to identify patients with VAP due to nonfermenting Gram‐negative bacilli or other microorganisms who could be safely and effectively treated with shorter‐duration therapy.
Results showed that the antimicrobial duration was significantly shorter for patients in the pathway group than the matched control group (9.8 vs 3.8 days, P 0.001), including the subset of patients with VAP associated with nonfermenting Gram‐negative bacilli (10.7 vs 14.4 days, P 0.001). No significant differences were observed between the overall treatment populations for VAP recurrence, mechanical ventilator‐free ICU days, ICU‐free hospital days, or mortality. Repeat BAL showed most VAP isolates in the study group (83%) responded to initial therapy with a mean duration of 8.8 days. Nonresponders without concomitant infections received significantly longer treatment than pure responding isolates (14.4 vs 7.3 days, P 0.001), and the most common nonresponding microorganisms were P aeruginosa (41% response rate) and S maltophilia (50% response rate), 2 nonfermenting Gram‐negative bacilli.
Most nonfermenting Gram‐negative bacilli‐associated VAP isolates in the study group did respond on repeat BAL (59%). These responders were treated for a mean duration of 8.2 days, and exhibited a similar recurrence rate versus that observed for the matched control group (12.0% vs 17.9%, P = 0.71). These pilot study results suggest that repeat BAL might be used to identify patients likely to benefit from short‐duration therapy, including patients infected with nonfermenting Gram‐negative bacilli. Further study on this is needed.
ATS/IDSA Guidelines for Duration of HCAP/HAP/VAP Therapy
Based largely on the studies by Dennesen et al.80 and Luna et al.83 indicating most VAP patients who respond to appropriate antimicrobial therapy do so within the first 6 days, and those by Chastre et al.37 and Singh et al.45 pointing to the efficacy and safety of shorter‐duration VAP therapy, the 2005 ATS/IDSA guidelines recommend the use of shorter‐duration antimicrobial therapy for most patients with HCAP or HAP/VAP.53 More specifically, the guidelines state, If patients receive an initially appropriate antimicrobial regimen, efforts should be made to shorten the duration of therapy from the traditional 14 to 21 days to periods as short as 7 days, provided that the etiologic pathogen is not P. aeruginosa, and that the patient has a good clinical response with resolution of clinical features of infection.53 Figure 2 presents an overview of the ATS/IDSA guidelines for HCAP/HAP/VAP management 48 to 72 hours after initiation of empiric antimicrobial therapy.53
Note that the clinician should consider terminating antimicrobial therapy in patients with clinical improvement and negative cultures or other evidence suggestive of a noninfectious cause. CPIS can also be helpful when deciding whether to terminate initial empiric therapy in a patient with clinical improvement after 23 days of therapy and negative cultures. If cultures are positive, the clinician should consider whether antimicrobial de‐escalation is possible (as discussed by Dr Kaye in the corresponding supplement article), and aim to treat selected patients with an antimicrobial course lasting 78 days. After 78 days, patients should be reassessed for treatment termination or other appropriate actions.
The ATS/IDSA guidelines also provide recommendations for route of drug administration, and if and when to switch from an intravenous to oral agent. In particular, the guidelines state that all patients with HCAP, HAP, or VAP should initially receive therapy intravenously, but conversion to oral/enteral therapy may be possible in certain responding patients, ie, those with a good clinical response and a functioning intestinal tract.53 Fluoroquinolones and linezolid have oral formulations with bioavailability equivalent to the intravenous form, meaning the oral formulations are capable of achieving high levels at the site of infection. This may facilitate conversion to oral therapy in select patients. Early step‐down is safe and effective with fluoroquinolones.84, 85
Based on the information just reviewed, the antimicrobial can be terminated on day 7 for case 1. She is afebrile, and her WBC and oxygenation are normal. In fact, since her records show she was responding at day 5, consideration could have been given to switching from intravenous to oral therapy at that time, and perhaps even discharging her to the rehabilitation center.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman who presents with sepsis and diverticular abscess with walled‐off perforation. Upon hospital arrival, Interventional Radiology inserted a drain, and the patient was initiated on ciprofloxacin and metronidazole therapy. Day 3 examination showed improvement in WBC count and normal vital signs, but the patient still had a low‐grade fever (100.9F). Abdominal examination results were improved, but with some diffuse tenderness. Initial cultures of the abdominal abscess isolated Gram‐negative rods, and the patient was continued on ciprofloxacin/metronidazole. Further cultures on day 4 identified an extended‐spectrum ‐lactamase (ESBL)‐producing E coli organism as the causative pathogen. The patient was switched from ciprofloxacin/metronidazole to ertapenem. It is now hospital day 8, and the patient continues to show good response to treatment. She is afebrile and WBC count is normal. The abscess catheter is no longer draining. Her abdominal pain is improved, and she is complaining that she is hungry. A repeat computed tomography scan shows resolution of the abscess and no evidence of bowel perforation. Should antimicrobial therapy be continued in this patient, and if so, with what agent and for how long?
Guidelines from the Surgical Infection Society and IDSA state that antimicrobial therapy of established or complicated intra‐abdominal infection in adults should be limited to 47 days, unless it is difficult to achieve adequate source control.54 This is because extended antimicrobial exposure increases antimicrobial cost and risk of resistance, superinfection, C difficile‐associated colitis, or other untoward and unintended consequences of antimicrobial therapy, and there is no evidence that longer treatment durations improve outcomes.46, 47, 54, 86 Runyon et al. randomized 90 patients with spontaneous bacterial peritonitis or culture‐negative neutrocytic ascites to receive 5 days or 10 days of cefotaxime monotherapy, and reported similar rates of infection‐related mortality (0% vs 4.3%), hospitalization mortality (33% vs 43%), bacteriologic cure (93% vs 92%), and recurrence of ascitic fluid infection (12% vs 13%).46 Furthermore, shorter‐course therapy was associated with significantly lower antimicrobial administration and costs. Similarly, a recent prospective, randomized, double‐blind trial comparing 3 versus 5 days of ertapenem therapy in 111 patients with community‐acquired intra‐abdominal infection reported similar cure (93% vs 90%) and eradication rates (95% vs 94%).86 However, it should be noted that the mean duration of antimicrobial therapy in the longer‐duration group was still relatively short (5.7 days, range of 5‐10 days).
Studies also indicate there is a very low risk of infection recurrence or treatment failure when antimicrobial therapy is terminated in a patient diagnosed with a complicated intra‐abdominal infection who no longer shows signs of continuing infection.38, 87 Lennard et al. compared postoperative outcomes in 65 patients with or without leukocytosis and fever at the conclusion of antimicrobial therapy for intra‐abdominal sepsis, and reported development of intra‐abdominal infection in 7 of 21 (33%) with persistent leukocytosis.87 None of the 30 patients with normal WBC counts at the end of therapy developed an intra‐abdominal infection postoperatively. Furthermore, intra‐abdominal infection occurred postoperatively in 11 of 14 patients (79%) who responded to treatment but were still febrile at the time of antimicrobial discontinuation.
Similar results were obtained in a much larger, more recent study that retrospectively analyzed the relationship between duration of antimicrobial therapy and infectious complications for patients with intra‐abdominal infections.38 In the study, 929 patients with intra‐abdominal infections associated with either fever or leukocytosis were organized into 4 quartiles based on total duration of antimicrobial therapy (quartile 1: 07 days, n = 218; quartile 2: 812 days, n = 217; quartile 3: 1317 days, n = 246; and quartile 4: >17 days, n = 248) or antimicrobial duration after resolution of leukocytosis (quartile 1: 05 days, n = 130; quartile 2: 610 days, n = 127; quartile 3: 1115 days, n = 124; and quartile 4: >15 days, n = 118). Based on either total duration of antimicrobial therapy or duration after leukocytosis resolution, risk of recurrence was significantly higher for patients in quartiles 3 or 4 versus those in quartile 1, and there was no difference between quartiles 1 and 2.
Taken together, these results suggest that antimicrobial therapy for intra‐abdominal sepsis can be shortened in patients exhibiting a clinical response to treatment, if there are no signs of persistent leukocytosis or fever. Hence, clinicians should use the resolution of clinical signs of infection as a guide to determine when during the 47‐day window antimicrobial therapy should be terminated.54 In practical terms, this usually means treatment can be terminated when the patient is afebrile, has normal WBC counts, and is able to tolerate an oral diet.
Based on the clinical status of case 2 after 8 days of antimicrobial therapy (afebrile with normal WBC counts and requesting oral diet), the ertapenem regimen should be stopped. There is no reason to consider further outpatient antimicrobial therapy for this particular patient, but the Surgical Infection Society and IDSA guidelines discuss the type of patient who should be considered for oral or outpatient antimicrobial therapy. According to the guidelines, the patient convalescing from a complicated intra‐abdominal infection may receive oral antimicrobial therapy, but that therapy should only be included as a component within the brief treatment duration already mentioned, ie, in total, it should rarely exceed 7 days.54 Such therapy is rarely indicated for patients who are afebrile, with normal peripheral WBC/leukocyte counts, and with return of bowel function. These recommendations make it clear that no further antimicrobial therapy is warranted for case 2.
However, for appropriate patients who are recovering from a complicated intra‐abdominal infection and are able to tolerate an oral diet, an oral antimicrobial regimen selected on the basis of identified primary isolates may be used for completion of therapy.54 In the absence of cultures, an oral regimen that covers commonly isolated pathogens (eg, E coli, streptococci, and Bacteroides fragilis) should be considered. Common regimens include an oral cephalosporin or fluoroquinolone with metronidazole, or amoxicillin‐clavulanic acid, assuming susceptibility studies do not demonstrate resistance. Given the identification of an ESBL‐producing E coli for case 2a pathogen relatively resistant to oral antimicrobialan oral regimen probably would not have been viable for this patient even earlier in the treatment course. Lastly, a repeat computed tomography scan was used for the case here. It should be noted that there are currently no well‐established criteria for determining when repeat imaging is needed to confirm resolution of fluid collections. This should be a clinical decision. A general practice is that the catheter is left in place until there is minimal drainage (eg, 10 mL/day); catheter sinograms can also be helpful in determining the status of the abscess.
CASE 3: CENTRAL LINE‐ASSOCIATED BACTEREMIA
Case 3 is a 56‐year‐old man with status epilepticus, intubation, and ICU stay. He was initially treated with vancomycin and piperacillin‐tazobactam for a fever of 103.4F on day 5 of hospitalization. Blood cultures grew Gram‐positive cocci. The central venous catheter was removed, and the initial antimicrobial regimen was de‐escalated to vancomycin monotherapy, which was associated with continued improvement in fever and WBC count, and clinical stability on hospital day 7. At that time, further blood culture analyses isolated methicillin‐susceptible S aureus (MSSA), and the antimicrobial regimen was switched/de‐escalated from vancomycin to cefazolin. It is now hospital day 9 (day 3 of cefazolin) and the patient continues to respond and is afebrile. Repeat blood cultures show no bacterial growth, and a transesophageal echocardiograph (TEE) was performed and revealed normal heart valves. Should the antimicrobial therapy be continued for this patient, and if so, with what agent and for how long?
The IDSA guidelines for management of intravascular catheter‐related infections recommend catheter removal and 46 weeks of antimicrobial therapy for patients with S aureus catheter‐related bloodstream infection (CRBSI), unless the patient has exceptions allowing consideration of shorter‐duration therapy (minimum of 14 days, with day 1 being the first day of negative blood culture results).55 These exceptions include absence of diabetes; immunocompetence (no immunosuppression); removal of the infected catheter; no prosthetic intravascular device (eg, pacemaker or recently placed vascular graft); no evidence of endocarditis or suppurative thrombophlebitis on TEE and ultrasound, respectively; fever and bacteremia resolved within 72 hours after initiation of appropriate antimicrobial therapy; and no evidence of metastatic infection on physical examination and sign‐ or symptom‐directed diagnostic tests.
Short‐duration (10‐16 day) antimicrobial therapy has been reported to yield similarly low recurrence or relapse rates as longer courses of therapy in patients with uncomplicated catheter‐associated S aureus bacteremia.50, 51, 88, 89 A small 1989 study by Ehni and Reller prospectively followed 13 patients with S aureus CRBSI who had received short‐course therapy (17 days), and reported only 1 case of relapse with endocarditis (8% relapse rate).50 A subsequent study by Malanoski et al. retrospectively analyzed the data from 55 patients with S aureus CRBSI.51 Excluding the 8 patients with early complications, the authors observed similar rates of relapse in patients treated for 1015 days and those receiving longer courses of antimicrobial therapy (0% vs 4.7%). The clinical characteristics of the 2 treatment duration groups were similar, and delayed catheter removal was linked with persistence of bacteremia (P = 0.01).
A more recent multicenter, prospective observational study by Chang et al. examined recurrence and the impact of antimicrobial treatment in 505 consecutive patients with S aureus bacteremia, and determined that duration of antimicrobial therapy was not a factor associated with relapse.88 This was true both for patients with bacteremia resulting from endocarditis, bacteremia with no apparent source, or bacteremia due to a focus that could not be cured or removed (28 days therapy after defervescence, 28 days therapy, or 28 days therapy), or those with bacteremia resulting from a source amenable to definitive cure, such as an intravascular device that could be removed, an abscess that could be incised and drained, or an infected bone that could be resected (>14 days, 1014 days, or 10 days therapy). Similarly, a 2005 prospective study by Thomas and Morris determined there was no relationship between treatment duration (7 vs 8 days, 10 vs 10 days, or 14 vs 15 days; P = 0.62, 0.87, and 0.16, respectively) and rate of relapse for 276 patients with cannula‐associated S aureus bacteremia.89 Longer‐duration antimicrobial therapy is warranted in patients with CRBSI and an early complicated course, eg, fever and/or bacteremia persisting for >3 days after catheter removal.90
According to the IDSA guidelines, a TEE should be obtained for all patients with CRBSI involving S aureus who are being considered for a shorter duration of therapy, and the TEE should be performed at least 57 days after onset of bacteremia to minimize risk of false‐negative results.55 High rates of infective endocarditis are observed in patients with S aureus bacteremia,89, 9193 with higher rates in patients with MSSA versus MRSA bacteremia (43.4% vs 19.6%, P 0.009).91 TEE is essential to diagnose endocarditis and detect other complications of bacteremia.92, 93 This recommendation for use of TEE does not necessarily apply to all patients with CRBSI when S aureus is not involved.
Figure 3 summarizes the general recommendations from the IDSA guidelines for the management of CRBSI in patients with a short‐term catheter.55 The figure illustrates the varied recommendations for treatment duration depending on whether the infection is complicated or uncomplicated, and based on the pathogenic microorganism. Returning to case 3, the patient meets the general criteria for shorter duration of antimicrobial therapy: he is not diabetic or immunosuppressed, his catheter has been removed, he does not have any prosthetic intravascular devices, his fever and bacteremia (based on blood cultures) resolved within 3 days of initiating cefazolin therapy, and there is no evidence of endocarditis or other complications of bacteremia. Hence, he is an excellent example of a patient with uncomplicated MSSA CRBSI who meets the criteria for consideration of shortened antimicrobial therapy. Based on the clinical practice guidelines, the patient should continue on intravenous cefazolin for a 14‐day course of therapy, at which time he can be re‐evaluated. A recent review of bloodstream infections caused by various pathogens similarly concluded that the minimum treatment duration for low‐risk patients with S aureus CRBSI is 14 days.48 As a final point, it is also important to note that there is no role for oral therapy in patients with CRBSI, so whether shortened or not, the chosen regimen should be administered intravenously.
CONCLUSIONS
Shortening the duration of appropriate and adequate antimicrobial therapy represents one strategy for reducing pressure for selection or development of resistant pathogenic microorganisms. Other potential benefits of shorter courses of antimicrobial therapy include reduced risk of antimicrobial‐associated infections (superinfection, C difficile‐associated diarrhea) and other antimicrobial‐related adverse events, improved compliance, and reduced antimicrobial costs. Clinicians are sometimes concerned that reducing antimicrobial courses for patients with serious infections, such as HCAP/HAP/VAP, complicated intra‐abdominal infection, and CRBSI, will lead to incomplete eradication of pathogenic microorganisms, leading to disease recurrence and increased morbidity and mortality. When managing patients with these serious infections, clinicians often turn to the literature and recommendations from professional organizations for guidance. Available data from randomized controlled and nonrandomized clinical trials indicate that shorter‐course therapy is effective and safe for patients with CAP, HCAP/HAP/VAP, complicated intra‐abdominal infections, and CRBSI. Based on these data, and consensus/expert opinion, clinical practice guidelines have been developed that recommend specific durations of antimicrobial therapy for each of these infections.
Although greater study of antimicrobial therapy duration is needed, the current and developing literature and current treatment guidelines should enable clinicians to recognize patients who would benefit from shortened courses of antimicrobial therapy. In doing so, they would help to lower antimicrobial costs and reduce the growing problem of antimicrobial resistance, with its wide‐ranging, negative consequences for current and future patients, and the clinicians who treat them.
- .The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.Clin Infect Dis.2006;42(suppl 2):S82–S89.
- ,,.Clinical and economic burden of antimicrobial resistance.Expert Rev Anti Infect Ther.2008;6:751–763.
- .Economics of antibiotic resistance.Expert Rev Anti Infect Ther.2008;6:523–539.
- ,,,.Emergence of antibiotic‐resistant Pseudomonas aeruginosa: comparison of risks associated with different antipseudomonal agents.Antimicrob Agents Chemother.1999;43:1379–1382.
- ,,,,.Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis.BMJ.2010;340:c2096.
- ,,,,,.Risk factors for invasive pneumococcal disease in children: a population‐based case‐control study in North America.Pediatrics.1999;103:E28.
- ,,.Antimicrobial resistance: consideration as an adverse drug event.Crit Care Med.2010;38:S155–S161.
- ,,,,,.Fluoroquinolone‐resistant Pseudomonas aeruginosa: assessment of risk factors and clinical impact.Am J Med.2006;119:526.e519–526.525.
- ,,, et al.Emergence of fluoroquinolone resistance in outpatient urinary Escherichia coli isolates.Am J Med.2008;121:876–884.
- ,,,,,.Imipenem resistance among Pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes.Infect Control Hosp Epidemiol.2006;27:893–900.
- ,,,,.Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals.Clin Infect Dis.2005;41:435–440.
- ,,,.Evaluation of an intervention designed to decrease the rate of nosocomial methicillin‐resistant Staphylococcus aureus infection by encouraging decreased fluoroquinolone use.Infect Control Hosp Epidemiol.2006;27:155–169.
- ,,,,,.Antibiotic resistance among gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888.
- ,,, et al.Relationship between rates of antimicrobial consumption and the incidence of antimicrobial resistance in Staphylococcus aureus and Pseudomonas aeruginosa isolates from 47 French hospitals.Infect Control Hosp Epidemiol.2007;28:1389–1395.
- ,,, et al.Citywide clonal outbreak of multiresistant Acinetobacter baumannii and Pseudomonas aeruginosa in Brooklyn, NY: the preantibiotic era has returned.Arch Intern Med.2002;162:1515–1520.
- ,,,,.Nosocomial outbreak of Klebsiella infection resistant to late‐generation cephalosporins.Ann Intern Med.1993;119:353–358.
- ,,.The effect of an antimicrobial restriction program on Pseudomonas aeruginosa resistance to beta‐lactams in a large teaching hospital.Pharmacotherapy.2003;23:618–624.
- ,,,.Association between antibiotic usage and subsequent colonization or infection of extensive drug‐resistant Acinetobacter baumannii: a matched case‐control study in intensive care units.Diagn Microbiol Infect Dis.2008;62:298–305.
- ,,.Relationships between antimicrobial use and antimicrobial resistance in Gram‐negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan.Int J Antimicrob Agents.2005;26:463–472.
- ,,, et al.Risk factors for acquisition of imipenem‐resistant Acinetobacter baumannii: a case‐control study.Antimicrob Agents Chemother.2004;48:224–228.
- ,,,,.Consumption of imipenem correlates with beta‐lactam resistance in Pseudomonas aeruginosa.Antimicrob Agents Chemother.2002;46:2920–2925.
- ,,.Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem‐resistant Pseudomonas aeruginosa.Antimicrob Agents Chemother.2009;53:1983–1986.
- .Clinical efficacy of newer agents in short‐duration therapy for community‐acquired pneumonia.Clin Infect Dis.2004;39(suppl 3):S159–S164.
- ,.The role of carbapenems in the treatment of severe nosocomial respiratory tract infections.Expert Opin Pharmacother.2008;9:561–575.
- ,.Does short‐course antibiotic therapy better meet patient expectations?Int J Antimicrob Agents.2003;21:222–228.
- ,,,.Tackling empirical antibiotic therapy for ventilator‐associated pneumonia in your ICU: guidance for implementing the guidelines.Semin Respir Crit Care Med.2009;30:102–115.
- World Health Organization (WHO) report on infectious diseases 2000. Overcoming antimicrobial resistance. Chapter 5. Call to action: A massive effort to provide proper treatment. Available at: http://www.who.int/infectious‐disease‐report/2000/index.html. Accessed January 14,2011.
- ,,,,.Diagnosis and management of group A streptococcal pharyngitis: a practice guideline. Infectious Diseases Society of America.Clin Infect Dis.1997;25:574–583.
- ,,,,,.Shorter‐course antibiotic therapy (SCAT): principles, current data, and caveats. In: Owens RCJ, Lautenbach E, editors.Antimicrobial Resistance: Problem Pathogens and Clinical Countermeasures.New York, NY:Informa Healthcare;2008:337–370.
- ,,, et al.International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases.Clin Infect Dis.2011;52:e103–e120.
- ,.Sexually transmitted diseases treatment guidelines, 2006.MMWR Recomm Rep.2006;55:1–94.
- ,,,,.Novel, single‐dose microsphere formulation of azithromycin versus 7‐day levofloxacin therapy for treatment of mild to moderate community‐acquired pneumonia in adults.Antimicrob Agents Chemother.2005;49:4035–4041.
- ,,, et al.High‐dose, short‐course levofloxacin for community‐acquired pneumonia: a new treatment paradigm.Clin Infect Dis.2003;37:752–760.
- ,.Randomized, multicentre study of the efficacy and tolerance of azithromycin versus clarithromycin in the treatment of adults with mild to moderate community‐acquired pneumonia. Azithromycin Study Group.Eur J Clin Microbiol Infect Dis.1998;17:828–833.
- ,,,,,.A prospective randomized study of inpatient IV antibiotics for community‐acquired pneumonia. The optimal duration of therapy.Chest.1996;110:965–971.
- ,,,.Use of quantitative cultures and reduced duration of antibiotic regimens for patients with ventilator‐associated pneumonia to decrease resistance in the intensive care unit.Clin Infect Dis.2006;43(suppl 2):S75–S81.
- ,,, et al.Comparison of 8 vs 15 days of antibiotic therapy for ventilator‐associated pneumonia in adults: a randomized trial.JAMA.2003;290:2588–2598.
- ,,, et al.Can we define the ideal duration of antibiotic therapy?Surg Infect (Larchmt).2006;7:419–432.
- ,,,,,.Duration of antibiotic therapy for ventilator‐associated pneumonia caused by non‐fermentative gram‐negative bacilli.Surg Infect (Larchmt).2007;8:589–597.
- ,,,,,.Experience with a clinical guideline for the treatment of ventilator‐associated pneumonia.Crit Care Med.2001;29:1109–1115.
- ,.Antibiotic utilization and outcomes for patients with clinically suspected ventilator‐associated pneumonia and negative quantitative BAL culture results.Chest.2005;128:2706–2713.
- ,,,.A randomized controlled trial of an antibiotic discontinuation policy for clinically suspected ventilator‐associated pneumonia.Chest.2004;125:1791–1799.
- ,,, et al.Repeat bronchoalveolar lavage to guide antibiotic duration for ventilator‐associated pneumonia.J Trauma.2007;63:1329–1337.
- ,,.Short course antibiotic therapy for Gram‐negative hospital‐acquired pneumonia in the critically ill.J Hosp Infect.2010;74:337–343.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,,,.Short‐course versus long‐course antibiotic treatment of spontaneous bacterial peritonitis. A randomized controlled study of 100 patients.Gastroenterology.1991;100:1737–1742.
- ,,,,.Complicated appendicitis: is there a minimum intravenous antibiotic requirement? A prospective randomized trial.Am Surg.2000;66:887–890.
- ,,.Short‐course therapy for bloodstream infections in immunocompetent adults.Int J Antimicrob Agents.2009;34(suppl 4):S47–S51.
- ,,,.Short‐course monotherapy strategy for treating bacteremia in the critically ill.Minerva Anestesiol.2006;72:841–857.
- ,.Short‐course therapy for catheter‐associated Staphylococcus aureus bacteremia.Arch Intern Med.1989;149:533–536.
- ,,,.Staphylococcus aureus catheter‐associated bacteremia. Minimal effective therapy and unusual infectious complications associated with arterial sheath catheters.Arch Intern Med.1995;155:1161–1166.
- ,,, et al.Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults.Clin Infect Dis.2007;44(suppl 2):S27–S72.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,,, et al.Clinical practice guidelines for the diagnosis and management of intravascular catheter‐related infection: 2009 update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,.Hospital‐acquired pneumonia: pathophysiology, diagnosis, and treatment.Surg Clin North Am.2009;89:439–461, ix.
- ,,.Healthcare‐associated pneumonia in adults: management principles to improve outcomes.Infect Dis Clin North Am.2004;18:939–962.
- ,,.Healthcare‐associated infections. A useful concept?Curr Opin Crit Care.2009;15:419–424.
- ,,,,,.Efficacy of 750‐mg, 5‐day levofloxacin in the treatment of community‐acquired pneumonia caused by atypical pathogens.Curr Med Res Opin.2004;20:555–563.
- ,,, et al.Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate‐severe community acquired pneumonia: randomised, double blind study.BMJ.2006;332:1355.
- ,,,,.Gemifloxacin once daily for 5 days versus 7 days for the treatment of community‐acquired pneumonia: a randomized, multicentre, double‐blind study.J Antimicrob Chemother.2007;60:112–120.
- ,,.Gemifloxacin once daily for 7 days compared to amoxicillin/clavulanic acid thrice daily for 10 days for the treatment of community‐acquired pneumonia of suspected pneumococcal origin.Respir Med.2004;98:708–720.
- ,,,.Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community‐acquired pneumonia: a prospective, randomized, double‐blind study.Am J Ther.1999;6:217–222.
- ,,,,.Clinical and bacteriological efficacy and safety of 5 and 7 day regimens of telithromycin once daily compared with a 10 day regimen of clarithromycin twice daily in patients with mild to moderate community‐acquired pneumonia.J Antimicrob Chemother.2004;54:515–523.
- ,,,,,.Short‐ versus long‐course antibacterial therapy for community‐acquired pneumonia: a meta‐analysis.Drugs.2008;68:1841–1854.
- ,,,.Efficacy of short‐course antibiotic regimens for community‐acquired pneumonia: a meta‐analysis.Am J Med.2007;120:783–790.
- ,,, et al.Low dosage and long treatment duration of beta‐lactam: risk factors for carriage of penicillin‐resistant Streptococcus pneumoniae.JAMA.1998;279:365–370.
- ,,, et al.Effect of short‐course, high‐dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial.JAMA.2001;286:49–56.
- ,,,.Antipneumococcal activity of ertapenem (MK‐0826) compared to those of other agents.Antimicrob Agents Chemother.2002;46:42–46.
- ,,.MIC and time‐kill study of antipneumococcal activities of RPR 106972 (a new oral streptogramin), RP 59500 (quinupristin‐dalfopristin), pyostacine (RP 7293), penicillin G, cefotaxime, erythromycin, and clarithromycin against 10 penicillin‐susceptible and ‐resistant pneumococci.Antimicrob Agents Chemother.1996;40:2071–2074.
- ,,.Bactericidal activity of daptomycin against Streptococcus pneumoniae compared with eight other antimicrobials.J Antimicrob Chemother.2003;51:443–446.
- ,,.Antipneumococcal activity of ertapenem compared to nine other compounds by time‐kill [abstract E‐800]. In:Program and Abstracts of the 41st Interscience Conference on Antimicrobial Agents and Chemotherapy (Chicago).Washington, DC:American Society for Microbiology,2001:184.
- ,,.Time‐kill analysis of the antipneumococcal activity of daptomycin compared with 8 other agents. In:Program and Abstracts of the 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego).Washington, DC:American Society for Microbiology,2002:161.
- ,,.Post‐antibiotic effect of garenoxacin against gram‐positive and gram‐negative organisms [abstract A‐496]. In:Program and Abstracts of the 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego).Washington, DC:American Society for Microbiology,2002:42.
- ,,, et al.Short‐course therapy of gemifloxacin effective against pneumococcal pneumonia in mice.J Chemother.2006;18:634–640.
- ,,.Animal models of Streptococcus pneumoniae disease.Clin Microbiol Rev.2008;21:666–685.
- ,,,,.Protective effect of trovafloxacin, ciprofloxacin and ampicillin against Streptococcus pneumoniae in a murine sepsis model.J Antimicrob Chemother.1999;44:477–481.
- ,,, et al.Follow‐up protected specimen brushes to assess treatment in nosocomial pneumonia.Am Rev Respir Dis.1993;147:38–44.
- ,.Antimicrobial therapy of community‐acquired pneumonia.Infect Dis Clin North Am.2004;18:993–1016, xi.
- ,,,,.Resolution of infectious parameters after antimicrobial therapy in patients with ventilator‐associated pneumonia.Am J Respir Crit Care Med.2001;163:1371–1375.
- ,,, et al.Clinical resolution in patients with suspicion of ventilator‐associated pneumonia: a cohort study comparing patients with and without acute respiratory distress syndrome.Crit Care Med.2005;33:1248–1253.
- ,,,,,.Diagnosis of ventilator‐associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid.Am Rev Respir Dis.1991;143:1121–1129.
- ,,, et al.Resolution of ventilator‐associated pneumonia: prospective evaluation of the clinical pulmonary infection score as an early clinical predictor of outcome.Crit Care Med.2003;31:676–682.
- .Pharmacoeconomic comparison of sequential IV/oral ciprofloxacin versus ceftazidime in the treatment of nosocomial pneumonia.Can J Hosp Pharm.1995;48:276–283.
- ,,, et al.Clinical and economic evaluation of oral ciprofloxacin after an abbreviated course of intravenous antibiotics.Am J Med.1991;91:462–470.
- ,,, et al.A prospective, double‐blind, multicenter, randomized trial comparing ertapenem 3 vs > or = 5 days in community‐acquired intraabdominal infection.J Gastrointest Surg.2008;12:592–600.
- ,,,.Implications of leukocytosis and fever at conclusion of antibiotic therapy for intra‐abdominal sepsis.Ann Surg.1982;195:19–24.
- ,,, et al.Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study.Medicine (Baltimore).2003;82:333–339.
- ,.Cannula‐associated Staphylococcus aureus bacteraemia: outcome in relation to treatment.Intern Med J.2005;35:319–330.
- ,.Optimal duration of therapy for catheter‐related Staphylococcus aureus bacteremia: a study of 55 cases and review.Clin Infect Dis.1992;14:75–82.
- ,,,,.Staphylococcus aureus bacteremia and endocarditis: the Grady Memorial Hospital experience with methicillin‐sensitive S aureus and methicillin‐resistant S aureus bacteremia.Am Heart J.2004;147:536–539.
- ,,, et al.Role of echocardiography in evaluation of patients with Staphylococcus aureus bacteremia: experience in 103 patients.J Am Coll Cardiol.1997;30:1072–1078.
- ,,, et al.Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow‐up.Clin Infect Dis.1999;28:106–114.
- .The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.Clin Infect Dis.2006;42(suppl 2):S82–S89.
- ,,.Clinical and economic burden of antimicrobial resistance.Expert Rev Anti Infect Ther.2008;6:751–763.
- .Economics of antibiotic resistance.Expert Rev Anti Infect Ther.2008;6:523–539.
- ,,,.Emergence of antibiotic‐resistant Pseudomonas aeruginosa: comparison of risks associated with different antipseudomonal agents.Antimicrob Agents Chemother.1999;43:1379–1382.
- ,,,,.Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis.BMJ.2010;340:c2096.
- ,,,,,.Risk factors for invasive pneumococcal disease in children: a population‐based case‐control study in North America.Pediatrics.1999;103:E28.
- ,,.Antimicrobial resistance: consideration as an adverse drug event.Crit Care Med.2010;38:S155–S161.
- ,,,,,.Fluoroquinolone‐resistant Pseudomonas aeruginosa: assessment of risk factors and clinical impact.Am J Med.2006;119:526.e519–526.525.
- ,,, et al.Emergence of fluoroquinolone resistance in outpatient urinary Escherichia coli isolates.Am J Med.2008;121:876–884.
- ,,,,,.Imipenem resistance among Pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes.Infect Control Hosp Epidemiol.2006;27:893–900.
- ,,,,.Hospital and community fluoroquinolone use and resistance in Staphylococcus aureus and Escherichia coli in 17 US hospitals.Clin Infect Dis.2005;41:435–440.
- ,,,.Evaluation of an intervention designed to decrease the rate of nosocomial methicillin‐resistant Staphylococcus aureus infection by encouraging decreased fluoroquinolone use.Infect Control Hosp Epidemiol.2006;27:155–169.
- ,,,,,.Antibiotic resistance among gram‐negative bacilli in US intensive care units: implications for fluoroquinolone use.JAMA.2003;289:885–888.
- ,,, et al.Relationship between rates of antimicrobial consumption and the incidence of antimicrobial resistance in Staphylococcus aureus and Pseudomonas aeruginosa isolates from 47 French hospitals.Infect Control Hosp Epidemiol.2007;28:1389–1395.
- ,,, et al.Citywide clonal outbreak of multiresistant Acinetobacter baumannii and Pseudomonas aeruginosa in Brooklyn, NY: the preantibiotic era has returned.Arch Intern Med.2002;162:1515–1520.
- ,,,,.Nosocomial outbreak of Klebsiella infection resistant to late‐generation cephalosporins.Ann Intern Med.1993;119:353–358.
- ,,.The effect of an antimicrobial restriction program on Pseudomonas aeruginosa resistance to beta‐lactams in a large teaching hospital.Pharmacotherapy.2003;23:618–624.
- ,,,.Association between antibiotic usage and subsequent colonization or infection of extensive drug‐resistant Acinetobacter baumannii: a matched case‐control study in intensive care units.Diagn Microbiol Infect Dis.2008;62:298–305.
- ,,.Relationships between antimicrobial use and antimicrobial resistance in Gram‐negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan.Int J Antimicrob Agents.2005;26:463–472.
- ,,, et al.Risk factors for acquisition of imipenem‐resistant Acinetobacter baumannii: a case‐control study.Antimicrob Agents Chemother.2004;48:224–228.
- ,,,,.Consumption of imipenem correlates with beta‐lactam resistance in Pseudomonas aeruginosa.Antimicrob Agents Chemother.2002;46:2920–2925.
- ,,.Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem‐resistant Pseudomonas aeruginosa.Antimicrob Agents Chemother.2009;53:1983–1986.
- .Clinical efficacy of newer agents in short‐duration therapy for community‐acquired pneumonia.Clin Infect Dis.2004;39(suppl 3):S159–S164.
- ,.The role of carbapenems in the treatment of severe nosocomial respiratory tract infections.Expert Opin Pharmacother.2008;9:561–575.
- ,.Does short‐course antibiotic therapy better meet patient expectations?Int J Antimicrob Agents.2003;21:222–228.
- ,,,.Tackling empirical antibiotic therapy for ventilator‐associated pneumonia in your ICU: guidance for implementing the guidelines.Semin Respir Crit Care Med.2009;30:102–115.
- World Health Organization (WHO) report on infectious diseases 2000. Overcoming antimicrobial resistance. Chapter 5. Call to action: A massive effort to provide proper treatment. Available at: http://www.who.int/infectious‐disease‐report/2000/index.html. Accessed January 14,2011.
- ,,,,.Diagnosis and management of group A streptococcal pharyngitis: a practice guideline. Infectious Diseases Society of America.Clin Infect Dis.1997;25:574–583.
- ,,,,,.Shorter‐course antibiotic therapy (SCAT): principles, current data, and caveats. In: Owens RCJ, Lautenbach E, editors.Antimicrobial Resistance: Problem Pathogens and Clinical Countermeasures.New York, NY:Informa Healthcare;2008:337–370.
- ,,, et al.International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases.Clin Infect Dis.2011;52:e103–e120.
- ,.Sexually transmitted diseases treatment guidelines, 2006.MMWR Recomm Rep.2006;55:1–94.
- ,,,,.Novel, single‐dose microsphere formulation of azithromycin versus 7‐day levofloxacin therapy for treatment of mild to moderate community‐acquired pneumonia in adults.Antimicrob Agents Chemother.2005;49:4035–4041.
- ,,, et al.High‐dose, short‐course levofloxacin for community‐acquired pneumonia: a new treatment paradigm.Clin Infect Dis.2003;37:752–760.
- ,.Randomized, multicentre study of the efficacy and tolerance of azithromycin versus clarithromycin in the treatment of adults with mild to moderate community‐acquired pneumonia. Azithromycin Study Group.Eur J Clin Microbiol Infect Dis.1998;17:828–833.
- ,,,,,.A prospective randomized study of inpatient IV antibiotics for community‐acquired pneumonia. The optimal duration of therapy.Chest.1996;110:965–971.
- ,,,.Use of quantitative cultures and reduced duration of antibiotic regimens for patients with ventilator‐associated pneumonia to decrease resistance in the intensive care unit.Clin Infect Dis.2006;43(suppl 2):S75–S81.
- ,,, et al.Comparison of 8 vs 15 days of antibiotic therapy for ventilator‐associated pneumonia in adults: a randomized trial.JAMA.2003;290:2588–2598.
- ,,, et al.Can we define the ideal duration of antibiotic therapy?Surg Infect (Larchmt).2006;7:419–432.
- ,,,,,.Duration of antibiotic therapy for ventilator‐associated pneumonia caused by non‐fermentative gram‐negative bacilli.Surg Infect (Larchmt).2007;8:589–597.
- ,,,,,.Experience with a clinical guideline for the treatment of ventilator‐associated pneumonia.Crit Care Med.2001;29:1109–1115.
- ,.Antibiotic utilization and outcomes for patients with clinically suspected ventilator‐associated pneumonia and negative quantitative BAL culture results.Chest.2005;128:2706–2713.
- ,,,.A randomized controlled trial of an antibiotic discontinuation policy for clinically suspected ventilator‐associated pneumonia.Chest.2004;125:1791–1799.
- ,,, et al.Repeat bronchoalveolar lavage to guide antibiotic duration for ventilator‐associated pneumonia.J Trauma.2007;63:1329–1337.
- ,,.Short course antibiotic therapy for Gram‐negative hospital‐acquired pneumonia in the critically ill.J Hosp Infect.2010;74:337–343.
- ,,,,.Short‐course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription.Am J Respir Crit Care Med.2000;162:505–511.
- ,,,,.Short‐course versus long‐course antibiotic treatment of spontaneous bacterial peritonitis. A randomized controlled study of 100 patients.Gastroenterology.1991;100:1737–1742.
- ,,,,.Complicated appendicitis: is there a minimum intravenous antibiotic requirement? A prospective randomized trial.Am Surg.2000;66:887–890.
- ,,.Short‐course therapy for bloodstream infections in immunocompetent adults.Int J Antimicrob Agents.2009;34(suppl 4):S47–S51.
- ,,,.Short‐course monotherapy strategy for treating bacteremia in the critically ill.Minerva Anestesiol.2006;72:841–857.
- ,.Short‐course therapy for catheter‐associated Staphylococcus aureus bacteremia.Arch Intern Med.1989;149:533–536.
- ,,,.Staphylococcus aureus catheter‐associated bacteremia. Minimal effective therapy and unusual infectious complications associated with arterial sheath catheters.Arch Intern Med.1995;155:1161–1166.
- ,,, et al.Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community‐acquired pneumonia in adults.Clin Infect Dis.2007;44(suppl 2):S27–S72.
- Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,,, et al.Clinical practice guidelines for the diagnosis and management of intravascular catheter‐related infection: 2009 update by the Infectious Diseases Society of America.Clin Infect Dis.2009;49:1–45.
- ,.Hospital‐acquired pneumonia: pathophysiology, diagnosis, and treatment.Surg Clin North Am.2009;89:439–461, ix.
- ,,.Healthcare‐associated pneumonia in adults: management principles to improve outcomes.Infect Dis Clin North Am.2004;18:939–962.
- ,,.Healthcare‐associated infections. A useful concept?Curr Opin Crit Care.2009;15:419–424.
- ,,,,,.Efficacy of 750‐mg, 5‐day levofloxacin in the treatment of community‐acquired pneumonia caused by atypical pathogens.Curr Med Res Opin.2004;20:555–563.
- ,,, et al.Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate‐severe community acquired pneumonia: randomised, double blind study.BMJ.2006;332:1355.
- ,,,,.Gemifloxacin once daily for 5 days versus 7 days for the treatment of community‐acquired pneumonia: a randomized, multicentre, double‐blind study.J Antimicrob Chemother.2007;60:112–120.
- ,,.Gemifloxacin once daily for 7 days compared to amoxicillin/clavulanic acid thrice daily for 10 days for the treatment of community‐acquired pneumonia of suspected pneumococcal origin.Respir Med.2004;98:708–720.
- ,,,.Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community‐acquired pneumonia: a prospective, randomized, double‐blind study.Am J Ther.1999;6:217–222.
- ,,,,.Clinical and bacteriological efficacy and safety of 5 and 7 day regimens of telithromycin once daily compared with a 10 day regimen of clarithromycin twice daily in patients with mild to moderate community‐acquired pneumonia.J Antimicrob Chemother.2004;54:515–523.
- ,,,,,.Short‐ versus long‐course antibacterial therapy for community‐acquired pneumonia: a meta‐analysis.Drugs.2008;68:1841–1854.
- ,,,.Efficacy of short‐course antibiotic regimens for community‐acquired pneumonia: a meta‐analysis.Am J Med.2007;120:783–790.
- ,,, et al.Low dosage and long treatment duration of beta‐lactam: risk factors for carriage of penicillin‐resistant Streptococcus pneumoniae.JAMA.1998;279:365–370.
- ,,, et al.Effect of short‐course, high‐dose amoxicillin therapy on resistant pneumococcal carriage: a randomized trial.JAMA.2001;286:49–56.
- ,,,.Antipneumococcal activity of ertapenem (MK‐0826) compared to those of other agents.Antimicrob Agents Chemother.2002;46:42–46.
- ,,.MIC and time‐kill study of antipneumococcal activities of RPR 106972 (a new oral streptogramin), RP 59500 (quinupristin‐dalfopristin), pyostacine (RP 7293), penicillin G, cefotaxime, erythromycin, and clarithromycin against 10 penicillin‐susceptible and ‐resistant pneumococci.Antimicrob Agents Chemother.1996;40:2071–2074.
- ,,.Bactericidal activity of daptomycin against Streptococcus pneumoniae compared with eight other antimicrobials.J Antimicrob Chemother.2003;51:443–446.
- ,,.Antipneumococcal activity of ertapenem compared to nine other compounds by time‐kill [abstract E‐800]. In:Program and Abstracts of the 41st Interscience Conference on Antimicrobial Agents and Chemotherapy (Chicago).Washington, DC:American Society for Microbiology,2001:184.
- ,,.Time‐kill analysis of the antipneumococcal activity of daptomycin compared with 8 other agents. In:Program and Abstracts of the 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego).Washington, DC:American Society for Microbiology,2002:161.
- ,,.Post‐antibiotic effect of garenoxacin against gram‐positive and gram‐negative organisms [abstract A‐496]. In:Program and Abstracts of the 42nd Interscience Conference on Antimicrobial Agents and Chemotherapy (San Diego).Washington, DC:American Society for Microbiology,2002:42.
- ,,, et al.Short‐course therapy of gemifloxacin effective against pneumococcal pneumonia in mice.J Chemother.2006;18:634–640.
- ,,.Animal models of Streptococcus pneumoniae disease.Clin Microbiol Rev.2008;21:666–685.
- ,,,,.Protective effect of trovafloxacin, ciprofloxacin and ampicillin against Streptococcus pneumoniae in a murine sepsis model.J Antimicrob Chemother.1999;44:477–481.
- ,,, et al.Follow‐up protected specimen brushes to assess treatment in nosocomial pneumonia.Am Rev Respir Dis.1993;147:38–44.
- ,.Antimicrobial therapy of community‐acquired pneumonia.Infect Dis Clin North Am.2004;18:993–1016, xi.
- ,,,,.Resolution of infectious parameters after antimicrobial therapy in patients with ventilator‐associated pneumonia.Am J Respir Crit Care Med.2001;163:1371–1375.
- ,,, et al.Clinical resolution in patients with suspicion of ventilator‐associated pneumonia: a cohort study comparing patients with and without acute respiratory distress syndrome.Crit Care Med.2005;33:1248–1253.
- ,,,,,.Diagnosis of ventilator‐associated pneumonia by bacteriologic analysis of bronchoscopic and nonbronchoscopic “blind” bronchoalveolar lavage fluid.Am Rev Respir Dis.1991;143:1121–1129.
- ,,, et al.Resolution of ventilator‐associated pneumonia: prospective evaluation of the clinical pulmonary infection score as an early clinical predictor of outcome.Crit Care Med.2003;31:676–682.
- .Pharmacoeconomic comparison of sequential IV/oral ciprofloxacin versus ceftazidime in the treatment of nosocomial pneumonia.Can J Hosp Pharm.1995;48:276–283.
- ,,, et al.Clinical and economic evaluation of oral ciprofloxacin after an abbreviated course of intravenous antibiotics.Am J Med.1991;91:462–470.
- ,,, et al.A prospective, double‐blind, multicenter, randomized trial comparing ertapenem 3 vs > or = 5 days in community‐acquired intraabdominal infection.J Gastrointest Surg.2008;12:592–600.
- ,,,.Implications of leukocytosis and fever at conclusion of antibiotic therapy for intra‐abdominal sepsis.Ann Surg.1982;195:19–24.
- ,,, et al.Staphylococcus aureus bacteremia: recurrence and the impact of antibiotic treatment in a prospective multicenter study.Medicine (Baltimore).2003;82:333–339.
- ,.Cannula‐associated Staphylococcus aureus bacteraemia: outcome in relation to treatment.Intern Med J.2005;35:319–330.
- ,.Optimal duration of therapy for catheter‐related Staphylococcus aureus bacteremia: a study of 55 cases and review.Clin Infect Dis.1992;14:75–82.
- ,,,,.Staphylococcus aureus bacteremia and endocarditis: the Grady Memorial Hospital experience with methicillin‐sensitive S aureus and methicillin‐resistant S aureus bacteremia.Am Heart J.2004;147:536–539.
- ,,, et al.Role of echocardiography in evaluation of patients with Staphylococcus aureus bacteremia: experience in 103 patients.J Am Coll Cardiol.1997;30:1072–1078.
- ,,, et al.Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow‐up.Clin Infect Dis.1999;28:106–114.
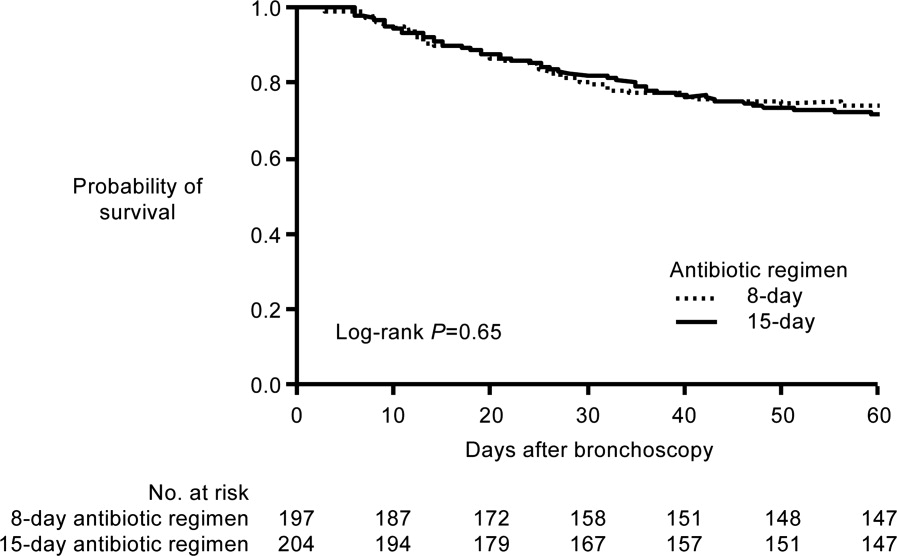
Initiation and Selection of Antibiotics
Early appropriate antimicrobial therapy is necessary to minimize the morbidity and mortality associated with hospital‐ or healthcare‐associated infections (HAIs). A number of studies have demonstrated that delayed or inadequate antimicrobial therapy leads to worse clinical outcomes and higher healthcare costs.1, 2 Inadequate antimicrobial therapy can also promote or enhance the development of resistance,2 with potential wide‐ranging impact beyond the immediate patient under care. Because delaying treatment until availability of culture results decreases the likelihood of a successful outcome, patients with a suspected invasive HAI commonly receive empiric therapy with a regimen expected to cover the most likely causative pathogens. Based on characteristics of the patient and healthcare facility or unit, likely pathogens may include bacteria or other pathogens resistant to 1 or more antimicrobial drug classes. This article discusses the various processes and factors that need to be considered when choosing empiric antibiotics in the hospital or other healthcare setting, and uses 3 case studies dealing with pneumonia, intra‐abdominal infection, and bacteremia, respectively, to illustrate points of interest.
IMPORTANCE OF EARLY ADEQUATE ANTIBIOTIC USE
The initial selection and early deployment of adequate antimicrobial therapy is critical for successful resolution of HAIs. The terms inadequate and inappropriate antimicrobial therapy are commonly used interchangeably in the literature, and can be defined as use of antimicrobial treatment without (sufficient) activity against the identified pathogen.2 Using an antibiotic for a fungal infection would be inadequate, as would using a drug or dosing regimen that is ineffective against the identified bacterial species due to resistance or a failure to achieve the drug's pharmacokinetic/pharmacodynamic target for efficacy against the pathogen. The complete absence of antimicrobial therapy is also considered inadequate therapy. Some investigators consider inappropriate therapy a more general term that includes excessive treatment as well as inadequate treatment.1 Others reserve the term inappropriate for use of an antimicrobial without activity against the identified pathogen, and the term inadequate for use of an insufficient regimen, either in terms of optimal dose, route of administration, timeliness, or failure to use combination therapy when appropriate.3 However, many or most research articles do not make the distinction, and the current article does not make a distinction.
In addition, some articles arbitrarily define inadequate therapy as either use (or absence) of a treatment without activity against the identified pathogen or a delay in appropriate or adequate treatment, eg, no patient exposure to adequate treatment within 24 hours of hospital admission. It is important to recognize this when evaluating articles in the literature. Other studies separate inadequate and delayed therapy as variables. However, when dealing with empiric therapy, the adequacy of initial empiric therapy cannot be fully determined until subsequent possession of the tissue/blood culture results.
Inadequate Antibiotic Treatment
A 1999 study by Kollef et al. identified inadequate antimicrobial treatment as the most important independent predictor of hospital mortality, in a group of patients with a nosocomial or community‐acquired infection, while in the medical or surgical intensive care unit (ICU).4 Infection sites included in the study were lung, bloodstream, urinary tract, gastrointestinal (GI) tract, and wound. Various other studies have confirmed an association between inadequate antibiotic therapy and increased hospital mortality, and some demonstrated a relationship between inadequate antibiotic therapy and longer hospital or ICU stays57 and higher hospital‐related costs.8 More specifically, initial inappropriate antibiotic therapy has been associated with increased mortality in patients with healthcare‐associated9 or ventilator‐associated pneumonia (VAP)5, 7, 8, 1014 and those with bacteremia/sepsis.6, 10, 1524 Inadequate empiric therapy has also been linked with worsened outcomes,19, 2529 longer hospital stays,2527, 29 and increased healthcare costs25, 29 in patients with infections of the GI tract.
With respect to specific bacterial pathogens, inappropriate antibiotic therapy has been shown to increase risk of hospital mortality for patients with VAP or bacteremia caused by Pseudomonas aeruginosa,20, 30 extended‐spectrum ‐lactamase (ESBL)‐producing or multidrug‐resistant (MDR) Klebsiella pneumoniae or Escherichia coli,21, 31, 32 and methicillin‐resistant Staphylococcus aureus (MRSA).15, 23 In fact, infection with resistant bacteria, and particularly MDR bacteria, is a principal risk factor for inadequate initial antibiotic therapy.14, 16, 33, 34 A recent study by Teixeira and coworkers showed that inadequate therapy was more than twice as common for additional episodes of VAP caused by MDR pathogens as for those involving drug‐susceptible pathogens (56% vs 25.5%).14 Moreover, VAP caused by MDR pathogens was identified as a significant independent predictor of inadequate antimicrobial therapy (odds ratio [OR], 3.07; 95% confidence interval [CI], 1.29‐7.30; P = 0.01). Infections caused by drug‐resistant versus susceptible bacteria have generally been associated with increased morbidity, longer hospital or ICU stays, and higher costs.24, 3437 At least part of the reason for these worsened outcomes appears to be an increased likelihood that initial therapy is inadequate for the causative agent. Because of this, it is particularly important to consider the probability of infection with resistant bacteria when initiating empiric antibiotic therapy.
Delayed Antibiotic Treatment
In addition to inadequate initial therapy, a delay in the onset of adequate therapy has also been shown to have negative impact on outcome in patients with VAP, bacteremia, or intra‐abdominal infections.12, 13, 27, 38, 39 For example, Iregui et al. identified administration of initially delayed appropriate antibiotic treatment (treatment delayed for 24 hours after initial diagnosis of VAP) as a significant predictor of hospital mortality (OR, 7.68; 95% CI, 4.50‐13.09; P 0.001) in patients with VAP at a US teaching hospital.38 Similarly, Lodise et al. identified delayed antibiotic treatment as an independent predictor of infection‐related mortality in patients with hospital‐acquired S aureus bacteremia (OR, 3.8; 95% CI, 1.3‐11.0; P = 0.01).39 Delayed versus early antibiotic therapy was also associated with significantly longer hospital stay (20.2 vs 14.3 days, P = 0.05). Classification and regression tree analysis identified 44.75 hours from the initial positive blood culture result to appropriate therapy as the breakpoint between delayed and early treatment for bacteremia.
Of particular interest, evidence suggests that the negative impact of initial delay or initial use of inadequate therapy often cannot be remedied by subsequent treatment alterations. For example, Luna et al. reported a significantly lower hospital mortality rate for VAP patients who received early adequate antibiotic therapy compared with those who received early inadequate therapy (38% vs 91%, P 0.001).13 In this study, early treatment referred to drug administration prior to bronchoscopy, which was performed within 24 hours of clinical diagnosis of VAP. A subset of patients only received treatment after bronchoscopy, and the mortality rate for VAP‐positive patients who received adequate antibiotic therapy after this initial delay was similar to that for VAP‐positive patients who received inadequate therapy postbronchoscopy (71% vs 70%). In other words, the negative impact of an initial delay in adequate therapy could not be subsequently overcome by using adequate antibiotic therapy later in the disease process. Similarly, a recent study by Zilberberg et al. of healthcare‐associated pneumonia reported that the negative effect of initial inadequate antibiotic therapy on hospital mortality could not be mitigated by subsequent escalation of adequate antibiotic therapy after reception of culture results.9 Finally, a study of inadequate initial empiric antibiotic therapy of postoperative intra‐abdominal infection (peritonitis) also showed that adverse outcomes could not be abrogated by changes in antibiotic therapy based on culture results.27 Taken together, the results from these studies emphasize the importance of early adequate antibiotic therapy.
PRACTICAL GUIDELINES FOR CHOOSING EMPIRIC ANTIBIOTICS
When choosing initial empiric therapy for a suspected hospital‐ or healthcare‐related bacterial infection, it is first important to determine if the patient has received prior antibiotic therapy, and if the patient has, then the clinician should consider choosing an antibiotic from a different drug class. This is because prior antibiotic therapy increases risk of infection with a pathogen resistant to the initial antibiotic drug and other members of its class. Also, depending on the site of the infection and likely pathogenic bacteria, the clinician will need to decide whether to initiate empiric therapy with a single antibiotic or combination of agents. A number of patient‐ and institution‐related factors can be utilized by clinicians to better identify the likely pathogen responsible for the infection, and it is critical to use this information when selecting initial empiric therapy. Finally, as is true whenever choosing antimicrobial or other drug therapies, clinicians need to consider and weigh the safety/tolerability profile, potential for drugdrug interactions, and relative cost of different treatment options. These will vary for individual patients receiving the same drug or drug combination.
MINIMIZING ANTIMICROBIAL RESISTANCE IN THE HOSPITAL OR HEALTHCARE SETTING
It is also important to consider the potential for development of antibiotic resistance when choosing initial empiric therapy. The current paradigm for treatment of serious hospital or healthcare infections is to prescribe broad‐spectrum antimicrobial therapy upfront while awaiting culture results, and to de‐escalate (or terminate) therapy once culture results are available4042or as 2 authors recently put it, get it right the first time, hit hard up front, and use large doses of broad‐spectrum antibiotics for a short period.41 The initial empiric antibiotic regimen should have a high likelihood of covering the most likely causative pathogens, including resistant species or strains. Furthermore, emergence of resistance is minimized when the initial regimen effectively covers the most likely causative pathogens, and subsequent culture results are utilized to streamline or narrow the initial regimen, when possible.40, 42 Emergence of resistance is also minimized by using the shortest duration of treatment with maximal clinical effect. (These latter 2 points are discussed in greater detail in the Kaye and File articles in this supplement.)
Factoring in Institution‐ and Patient‐Specific Factors
Local antibiograms are useful in determining the most likely infection‐causing pathogens, within different wards of the hospital, and their susceptibility or resistance to various antibiotics. Local patterns of pathogen susceptibility and resistance can differ markedly from national averages, so local antibiograms are more useful than national or even regional surveillance data when making choices about the initial agent and dosing regimen for initial empiric therapy.43 Hospitals are required by the Joint Commission to create antibiograms on at least an annual basis, although more frequent antibiograms are particularly useful, given that susceptibility or resistance patterns change over time. It is also important that hospital microbiologists create antibiograms specifically for different hospital wards or departments, as well as hospital‐wide. The incidence and susceptibility of pathogenic bacteria has been shown to vary across different wards within a hospital, as well as within different regions of a given country.4446
Patient‐specific factors should also be considered in the decision‐making process for selection of initial empiric therapy for a suspected bacterial infection. Relevant patient characteristics or factors may differ somewhat when examining risk for particular types of infection (eg, healthcare/hospital‐acquired pneumonia, VAP, or bacteremia) or particular antibiotic‐resistant pathogens (eg, MRSA, ESBL‐producing E coli or Klebsiella spp, P aeruginosa and MDR P aeruginosa, and carbapenem‐resistant Acinetobacter baumannii). Nonetheless, several risk factors appear to generally increase risk of infection with a resistant pathogen across these subcategories, including prior antibiotic treatment (with agents sometimes varying depending on the particular pathogen of interest); recent hospital admission or residence in a nursing home or extended‐care facility; prolonged hospital stay (particularly in the ICU); prior colonization with the pathogen; presence of an indwelling catheter (central venous, arterial, or urinary); and mechanical ventilation; among others.2, 47, 48 Patients who are immunocompromised, either due to their condition or immunosuppressive therapy, are also generally at increased risk of infection with resistant bacteria.47
Patient age and presence of comorbidities can also affect initial selection of empiric therapy. Cell‐mediated immunity tends to decline with age, and elderly individuals are also more likely to have conditions or comorbidities associated with diminished host immunity, both of which may contribute to increased susceptibility to infection and infection involving resistant bacteria.49 Furthermore, elderly individuals are more likely to have decline in renal or hepatic function or other physiologic changes that can alter drug pharmacokinetics and pharmacodynamics,50 and these factors need to be considered when selecting an initial empiric therapy regimen that covers likely pathogens, without increasing risk of drug toxicity. In addition, the increased number of comorbidities in elderly patients typically translates into polypharmacy, with potential for drugdrug interactions that need to be weighed when selecting initial empiric therapy.
Treat Infection, Not Contamination or Colonization
It is important to limit antimicrobial use to treatment of actual infections, and not for treatment of colonization or contamination. Treatment of colonization is a significant source of antimicrobial overuse. Hence, it is important that healthcare teams take appropriate steps to ensure they are treating pneumonia, bacteremia, or a urinary tract infection, not colonization of the tracheal aspirate, catheter tip or hub, or indwelling urinary catheter that is unassociated with actual infection. Strategies to employ when considering how to differentiate between true infection and colonization include using Gram stain in sputum specimens to look for evidence of polymorphonuclear leukocytes (inflammation), understanding that certain organisms, such as Enterococcus and Candida are not respiratory pathogens, recognizing that urinary catheters may be colonized in the absence of infection, and remaining vigilant regarding blood culture contamination. Since antibiotic use is generally linked to increased risk of resistance,51, 52 antibiotics should only be used when there is a clear clinical benefit associated with their use; treatment of colonization does not fit this description. When in doubt, an infectious diseases (ID) specialist consultation is recommended.
Similarly, overuse/misuse of antibiotics that occurs due to false‐positive culture results also increases development of resistance in hospitalized patients. In particular, contamination of blood cultures is relatively common in hospitalized patients, particularly in hospital emergency rooms,53 and frequently results in administration of antibiotics to treat an apparent infection that actually represents a contaminated culture. Antimicrobial treatment due to false‐positive blood culture results has been associated with prolonged hospitalization and elevated laboratory and hospital costs,54, 55 and provides an environment for development of antimicrobial resistance. Contamination of blood cultures often occurs at the point of blood collection via venipuncture or through indwelling catheters,56, 57 but can occur later in the process during laboratory handling or processing of specimens.58 Hence, it is important to use proper antisepsis when collecting blood or other cultures, to make sure it is blood and not skin or the catheter hub that is being cultured, and to make sure to use proper methods when processing all cultures.
Consult Infectious Diseases Experts
The 2007 guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America (IDSA/SHEA) for the development of institutional antimicrobial stewardship programs recommend inclusion of an ID physician and a clinical pharmacist with ID training as core members of a multidisciplinary antimicrobial stewardship team.59 Consultation with an ID expert or inclusion of an ID specialist into an institutional antimicrobial stewardship program has been shown to improve antibiotic usage and reduce morbidity and mortality, length of hospital stay, healthcare costs, and resistance.6064 In hospitals without easy access to an ID specialist, hospitalists with ID training may be able to fulfill the role provided by ID physicians or clinical pharmacists with ID training.
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Table 1 provides the key initial data for Case 1. The patient has a history of hypertension, congestive heart failure (CHF), and myocardial infarction (MI), and is receiving medications consistent with such a history. In terms of her acute presentation, cough, fever, chills, dyspnea, lung crackles (rales), X‐ray evidence of lung infiltrate, reduced oxygen saturation, elevated white blood cell (WBC) count, and increased percentage of WBC bands are all consistent with a diagnosis of pneumonia of relatively recent origin. Progressive worsening of symptoms within the previous 36 hours is also consistent with infection of recent origin. There are no neurologic symptoms, and cardiac function appears relatively normal, with no evidence of MI or cardiac arrhythmia based on electrocardiogram or heart rate, although there is evidence of continuing hypertension and perhaps CHF.
| |
| History | A 72‐yr‐old woman recently hospitalized for congestive heart failure (CHF), returns to the emergency department from rehab with cough, fever, chills, shortness of breath, all progressively worsening over the past 36 hr |
| Past history of CHF (ejection fraction 44%), myocardial infarction 2 yr ago, hypertension, past smoking | |
| Medications: metoprolol 50 mg BID; furosemide 40 mg daily; aspirin 81 mg daily; enalapril 20 mg daily | |
| Physical | Vitals: BP 148/88, P 82, RR 16, T 101.7, O2 sat 92% on room air |
| Heart: S1, S2 no murmurs | |
| Lungs: crackles at R lung base | |
| Abdomen: bowel sounds present, non‐tender | |
| Extremities: trace edema bilaterally | |
| Neurologic: no focal findings | |
| Labs | EKG: NSR, no acute ST‐T changes |
| Chemistry, hemoglobin, platelets, within normal limits | |
| WBC: 14,700/mm3, 10% bands | |
| Cardiac enzymes negative | |
| ‐Natriuretic peptide within normal limits for age | |
| Chest X‐ray: right lower lung infiltrate | |
Given the patient's history of recent hospitalization, the clinician should consider that the pneumonia is most likely hospital‐ or healthcare‐acquired. Because she was described as developing the problem while in rehabilitation, it can be assumed that hospitalization occurred relatively recently. Hospital‐acquired pneumonia (HAP) is defined as pneumonia that occurs within 48 hours of hospital admission, and that was not incubating at the time of admission.47, 65 HAP accounts for approximately of 15% of all nosocomial/hospital‐acquired infections in the United States and up to 27% in the ICU,65, 66 and is a frequent cause of morbidity and mortality in this setting.65 In addition to hospitalization, other characteristics or risk factors for HAP include severe illness, hemodynamic compromise, depressed immune function, use of nasogastric tubes, and mechanical ventilation for the important subset of HAP patients with VAP.65 VAP is more precisely defined as HAP that arises >48‐72 hours after endotracheal intubation.47
Healthcare‐associated pneumonia (HCAP) is a more recently defined category that includes patients with HAP and VAP, and is characterized by hospitalization for 2 days in the preceding 90 days, or residence in a nursing home or extended‐care facility.47, 67, 68 Additional risk factors for HCAP include intravenous therapy at home (including antibiotics); intravenous chemotherapy or wound care within 30 days of the current infection; and recent attendance at a hospital or hemodialysis clinic.47 Most HAP or HCAP data have been derived from patients with VAP, and the 2005 American Thoracic Society (ATS)/IDSA guidelines for management of HAP, VAP, and HCAP recommend similar approaches for the initial treatment of patients with nonintubated HAP, VAP, and HCAP.47 There are general similarities between these 3 disease categories with respect to etiology, epidemiology of likely pathogens, and prognosis, and important differences compared with community‐acquired pneumonia (CAP), which in turn gives rise to different treatment strategies for HAP/VAP/HCAP and CAP.
Given an initial diagnosis of HAP or HCAP, the clinician should be considering the following questions: 1) What are the appropriate choices of antimicrobials? 2) What are the clinical parameters that should alert one to resistant organisms? 3) What are the appropriate cultures to order? 4) What is the role of Gram stain, if any?
Selection of Initial Empiric Therapy for Likely Pathogens
HAP is usually caused by bacterial pathogens, and much more rarely involves viruses or fungi in immunocompetent patients. Therefore, from the start, the focus should be on empiric therapy with an antibiotic or combination of antibiotics that has a high probability of covering the most likely pathogens. Empiric therapy is warranted because of the risk of mortality or other negative consequences when antibiotic therapy is delayed, particularly in an aged patient with a chronic illness like CHF (such as the case study here). Clues as to likely pathogensand hence most appropriate antibiotic regimencan be discerned by looking at the onset of HAP/VAP (early vs late) and whether the patient has risk factors for infection with a MDR or antibiotic‐susceptible bacterial pathogen. A significant proportion of patients with HAP, VAP, or HCAP are infected with MDR pathogens, and identifying these patients and providing them with appropriate broad‐spectrum empiric therapy is a key to successful management.
Early‐onset HAP/VAP (occurring 5 days after hospitalization) is more likely to be due to antibiotic‐sensitive bacteria than late‐onset HAP/VAP (occurring 5 days after hospitalization), which often occurs due to MDR species.47, 69, 70 Not surprisingly, risk of inappropriate initial antibiotic therapy14 is higher, and mortality is also higher in patients with late‐onset HAP/VAP.47, 71 Patients with early‐onset HAP/VAP who have received prior antibiotics or been hospitalized within the past 90 days are also at risk for infection due to MDR bacteria, and hence should be treated the same as patients with late‐onset HAP/VAP.47 Additional risk factors for infection with MDR pathogens include antimicrobial therapy in the preceding 90 days (particularly with broad‐spectrum agents), current hospitalization 5 days, high prevalence of antibiotic resistance in the specific hospital unit, immunosuppression, and presence of risk factors for HCAP (hospitalization 2 days in the preceding 90 days, residence in a nursing home or extended‐care facility, home infusion therapy, chronic dialysis within 30 days, home wound care, or family member with MDR pathogen).47 For VAP patients, duration of ventilator support 7 days is an additional risk factor for infection with a MDR pathogen.70, 72 A second episode of VAP is more likely to be due either to MRSA or P aeruginosa; therefore, these organisms need to be considered when selecting initial empiric therapy.
The most common bacterial causes of HAP, VAP, or HCAP include aerobic Gram‐negative bacilli, such as P aeruginosa, Acinetobacter spp, and Enterobacteriaceae (eg, K pneumoniae, E coli, Enterobacter spp), and Gram‐positive cocci, such as S aureus and Streptococcus pneumoniae.47, 73 MDR bacterial species are more likely when certain risk factors are present, and the ATS/IDSA guidelines recommend using a risk‐stratification process when selecting empiric antibiotic therapy for patients with suspected HAP, VAP, or HCAP.47 The guidelines also emphasize that local conditions can greatly impact whether a patient is infected with an antibiotic‐sensitive or antibiotic‐resistant species, regardless of other risk factors, thereby highlighting the importance of using recent hospital and hospital unit‐specific antibiograms when stratifying a patient based on risk.
Other guiding principles of initial empiric treatment, as outlined in the ATS/IDSA guidelines, include not delaying therapy while awaiting culture results and administration of therapy as soon as possible following diagnosis; making sure the dosing regimen as well as drug selection is appropriate/adequate for the patient and suspected pathogen; and using a different class of antibiotic for patients with prior antibiotic exposure.47 The guidelines further indicate that combination therapy is appropriate initial therapy in patients at high risk for infection with MDR bacteria, and that for patients receiving combination therapy including an aminoglycoside, the aminoglycoside can be stopped after 5‐7 days in responding patients. Table 2 highlights ATS/IDSA recommendations for initial empiric antibiotic therapy in patients with suspected HAP/VAP who have early‐onset disease and no risk factors for MDR pathogens.47 Table 3 highlights recommendations for initial empiric antibiotic therapy in patients with suspected HAP/VAP/HCAP who have late‐onset disease and/or risk factors for MDR pathogens.47
| Potential Pathogen | Recommended Antibiotic |
|---|---|
| |
| Streptococcus pneumoniae* | |
| Haemophilus influenzae | Ceftriaxone |
| Methicillin‐sensitive Staphylococcus aureus | or |
| Antibiotic‐sensitive enteric Gram‐negative bacilli | Levofloxacin, moxifloxacin, or ciprofloxacin |
| Escherichia coli | or |
| Klebsiella pneumoniae | Ampicillin/sulbactam |
| Enterobacter spp | or |
| Proteus spp | Ertapenem |
| Serratia marcescens | |
| Potential Pathogen | Combination Antibiotic Therapy |
|---|---|
| |
| Pathogens listed in Table 2, plus MDR pathogens | Antipseudomonal cephalosporin (cefepime, ceftazidime) |
| Pseudomonas aeruginosa | or |
| Klebsiella pneumoniae (ESBL‐positive)* | Antipseudomonal carbapenem (imipenem or meropenem) |
| Acinetobacter spp* | or |
| ‐Lactam/‐lactamase inhibitor (piperacillin‐tazobactam) | |
| plus | |
| Antipseudomonal fluoroquinolone* (ciprofloxacin or levofloxacin) | |
| or | |
| Aminoglycoside (amikacin, gentamicin, or tobramycin) | |
| plus | |
| Methicillin‐resistant Staphylococcus aureus (MRSA) | Linezolid or vancomycin |
| Legionella pneumophila* | |
Returning to Case 1, given a clinical diagnosis of HAP/HCAP and the patient's heightened risk for infection with MRSA or resistant Gram‐negative bacteria, she was initiated on a regimen consisting of piperacillin/tazobactam plus vancomycin and ciprofloxacin. The choice of 3 agents is consistent with ATS and IDSA guidelines to cover the potential for an ESBL‐producer or Acinetobacter, or Pseudomonas. Individual choices should be dictated by one's own institutional antibiogram or some knowledge of the rehabilitation facility from which the patient was transferred.
Guiding Principles for Culture Management
Culture collection and management plays an important role in diagnosis and subsequent treatment of HAP/VAP or HCAP. As outlined in the ATS/IDSA guidelines, patient management typically proceeds using either a clinical strategy or bacteriologic strategy, or a combination thereof.47 The clinical strategy makes use of cultures of endotracheal aspirates or sputum, with initial microscopic examination and Gram staining to identify bacterial growth and guide initiation of empiric antibiotic therapy. Cultures should always be performed before instituting antibiotic therapy. Microorganism growth is described as light, moderate, or heavy by microbiology laboratories using semiquantitative analysis. Gram staining should be performed only if the specimen is of good quality; most microbiology laboratories will do screening tests to ensure they are of good quality, or else will reject the specimen. When correlated with culture results, Gram staining can improve diagnostic accuracy.74
The bacteriologic strategy uses quantitative means to analyze and describe cultures of lower respiratory secretions or specimens obtained via endotracheal aspirates, mini‐bronchoalveolar lavage specimens (mini‐BAL), bronchoalveolar lavage, or protected‐specimen bronchial brushing, collected with or without a bronchoscope, ie, with or without invasive techniques. Hence, whereas the clinical strategy uses noninvasive tracheal aspirates to culture microorganisms for analysis, the bacteriologic strategy often employs a relatively noninvasive strategy like a mini‐BAL, or invasive (bronchoscopic) lower respiratory tract samples for quantitative culture analysis. Diagnosis of HAP/VAP or HCAP, and determination of the causative microorganism(s), requires growth above a certain threshold when using the semi‐quantitative analysis. The clinical approach is more sensitive, but can result in overtreatment, while the bacteriologic strategy is associated with risk of undertreatment due to false‐negative culture results. On the other hand, quantitative cultures increase the specificity of diagnosis.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman with no past medical history of note, who presented to her physician about 3 days ago, after 5 days of abdominal pain and fever (101.7F). She had an outpatient computed tomography (CT) scan, and the results suggested diverticulitis. After the CT scan, she was given amoxicillin/clavulanate. She now presents to the emergency department (3 days later) with worsening pain, fever, and severe weakness. A physical exam shows low blood pressure (84/58 mmHg) and tachycardia (132 bpm). Her respiratory rate is 22 breaths per minute. Oxygenation (O2 saturation 99% on room air) is normal, and the patient's lungs are clear. Abdominal examination reveals bowel sounds and diffuse tenderness, particularly at the left lower quadrant, and there is evidence of guarding and rebound. Her blood chemistry is generally normal, although the WBC count is elevated (15,200/mm3). No abnormalities are evident on chest X‐ray. The patient's blood pressure increases to 96/64 mmHg after she is infused with 2 liters of normal saline. She undergoes another CT scan and is admitted to the ICU. The CT scan shows diverticulitis with abscess and walled‐off perforation. An interventional radiologist inserts a pigtail catheter into the abscess for sample collection, and the samples are sent to the microbiology laboratory for culture.
The radiology results indicate that the patient has what may be considered a complicated intra‐abdominal infection (diverticulitis with abscess), community‐acquired. Because empiric therapy is usually necessary for patients with complicated or even uncomplicated intra‐abdominal infections, the clinician should now be asking: What is optimal empiric antimicrobial therapy for this patient? Both prior75 and current guidelines76 for the management of intra‐abdominal infection indicate that antimicrobial therapy should be initiated when a patient receives such a diagnosis or when such an infection is considered likely. In making the determination of initial empiric therapy, the clinician should also be considering whether there is likely involvement of resistant Gram‐negative bacteria, and if so, how that would change the choice of antibiotic therapy.
Enteric Gram‐negative bacilli such as E coli and K pneumoniae are the most common microorganisms isolated from patients with intra‐abdominal infections, although Gram‐positive cocci (Staphylococcus or Streptococcus spp, and less commonly, enterococci) and obligate anaerobic organisms (particularly, Bacteroides fragilis) are also frequent components of intra‐abdominal infections.77 The relative frequency of bacterial pathogens shifts in patients who acquired their intra‐abdominal infection in the hospital versus community setting, with greater prevalence of Enterobacter, P aeruginosa, and Enterococcus spp, and less frequent isolation of E coli and streptococci.77 Recent results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) indicate a general increase in resistance among Gram‐negative bacilli isolated from patients with intra‐abdominal infections treated in medical centers, primarily due to acquisition of ESBLs.78, 79 This is true both in the United States79 and worldwide.78 Carbapenems continue to exhibit consistent activity against Gram‐negative bacilli isolated from intra‐abdominal infections, including ESBL‐producers.
Selection of initial empiric therapy should incorporate information from the literature and local antibiograms to determine the most likely causative pathogen(s), including ones with reduced susceptibility or resistance to commonly employed antibiotics. Then an antibiotic regimen should be selected that provides coverage of likely pathogens with minimal adverse events, including risk of collateral damage such as Clostridium difficile‐associated disease. Dose and dosing interval considerations are also important, particularly in patients with reduced renal or hepatic function. The general approach is to select an antibiotic or combination of antibiotic agents to provide coverage of the bacterial pathogens most commonly isolated from patients with intra‐abdominal infections, ie, aerobic/facultative anaerobic Gram‐negative bacilli, aerobic Gram‐positive cocci, and obligate anaerobic organisms.77 Table 4 presents the antibiotic treatment recommendations from the Surgical Infection Society and IDSA 2010 guidelines for management of patients with complicated intra‐abdominal infections.76 The guidelines are based on whether the patient has mild‐to‐moderate or high‐risk/severe community‐acquired complicated intra‐abdominal infections. Recommendations for the empiric treatment of hospital or healthcare‐associated complicated intra‐abdominal infections are largely based on local antibiogram (microbiologic) results, and include some similarities and differences compared with recommended treatment of high‐risk community‐acquired infections, as illustrated in Table 5.76 A patient with mild‐to‐moderate infection would be someone who does not require intensive care, and has community‐acquired intra‐abdominal infection due to secondary peritonitis. Severe intra‐abdominal infection would be defined by requiring intensive care, having sepsis, or having healthcare‐acquired peritonitis (such as a bowel leak following surgery). In line with these guidelines, and considering the case patient's risk profile, ciprofloxacin plus metronidazole was selected as initial empiric therapy, because she had not been hospitalized previously. Although she was hypotensive, the blood pressure was easily raised with fluids.
| Community‐Acquired Infection in Adults | ||
|---|---|---|
| Regimen | Mild‐to‐Moderate Severity* | High Risk or Severity |
| ||
| Single agent | Cefoxitin, ertapenem, moxifloxacin, tigecycline, and ticarcillin‐clavulanate | Imipenem‐cilastatin, meropenem, doripenem, and piperacillin‐tazobactam |
| Combination | Cefazolin, cefuroxime, ceftriaxone, cefotaxime, ciprofloxacin, or levofloxacin, each in combination with metronidazole | Cefepime, ceftazidime, ciprofloxacin, or levofloxacin, each in combination with metronidazole |
| Organisms Seen in the Hospital/Healthcare Infection at the Local Institution | Regimen | ||||
|---|---|---|---|---|---|
| Carbapenem* | Piperacillin‐Tazobactam | Ceftazidime or Cefepime + Metronidazole | Aminoglycoside | Vancomycin | |
| |||||
| 20% Resistant Pseudomonas aeruginosa, ESBL‐producing Enterobacteriaceae, Acinetobacter, or other multidrug‐resistant Gram‐negative bacteria | Recommended | Recommended | Recommended | Not recommended | Not recommended |
| ESBL‐producing Enterobacteriaceae | Recommended | Recommended | Not recommended | Recommended | Not recommended |
| P aeruginosa >20% resistant to ceftazidime | Recommended | Recommended | Not recommended | Recommended | Not recommended |
| Methicillin‐resistant Staphylococcus aureus | Not recommended | Not recommended | Not recommended | Not recommended | Recommended |
There are a number of controversies in intra‐abdominal sepsis management. These include whether or when initial empiric therapy should provide coverage of Enterococcus/vancomycin‐resistant enterococci or MRSA, when the regimen should include an antifungal to cover possible Candida spp infection, the role of resistant Bacteroides in intra‐abdominal infections, and when clinicians should be particularly concerned about ESBL‐producing or other resistant Gram‐negative bacteria. These topics are beyond the reach of the present article, but are and will continue to be important issues for clinicians to grapple with when selecting initial empiric therapy for patients with intra‐abdominal infections.
CASE 3: CENTRAL LINE‐ASSOCIATED BACTEREMIA
The third case is a 56‐year‐old man with epilepsy who presents to the emergency department with status epilepticus. Subsequent resuscitative efforts included intubation and placement of an internal jugular central line. The patient was admitted to the ICU, and aggressive treatment was initiated with repeated intravenous dosing of lorazepam and loading with fosphenytoin, which successfully broke the seizure. Subsequent imaging and laboratory tests failed to reveal any specific cause for the status epilepticus. The patient was extubated on day 4 and transferred out of the ICU. On day 5, he spiked a fever of 103.4F. He did not report any new symptoms, and there was no evidence of cough, sputum, shortness of breath, abdominal pain, diarrhea, or urinary symptoms. Physical examination revealed normal blood pressure (122/68 mmHg) and oxygen saturation (95% on room air), a normal respiratory rate (12 breaths per minute), clear lungs, no edema, no heart murmur, and normal neurologic findings. The patient's heart rate was somewhat high (102 bpm), and his temperature remained elevated (103.4F). Abdominal examination revealed no tenderness, and bowel sounds were present. Laboratory results were normal, except for an elevated WBC count (17,000/mm3 of blood). The chest X‐ray was clear.
This is an example of a patient with fever and leukocytosis of unknown origin. There are no focal findings indicative of a particular infection site or process. The patient was treated in the ICU, including use of a central catheter. Differential diagnosis of fever and leukocytosis without source, in a patient from the ICU with a central line, should consider catheter‐associated bacteremia; C difficile‐associated disease; a silent intra‐abdominal process, such as cholangitis or gangrenous cholecystitis; drug fever related to (in this patient) anticonvulsant therapy; urinary tract infection (no evidence for in this patient); or pulmonary embolism. The clinician needs to make a decision as to the relative benefits of empiric antibiotic or other antimicrobial treatment versus observation. If the patient is to be treated with an antibiotic, then a choice has to be made as to the best agent for the patient at hand.
In terms of the choice of antibiotics for a patient such as the one here, the clinician needs to assess the severity of illness and, when doing so, determine what infection site or sites should be covered, and the most likely sites of infection. A determination of likely pathogens also needs to be made. Cultures should be obtained prior to initiating therapy with a regimen providing broad coverage of the most likely pathogen(s), while allowing for the possibility of later de‐escalation based on clinical evaluation and culture results. This is similar to the situation for initial empiric treatment of pneumonia or intra‐abdominal infection. In general, the clinician should obtain blood, urine, and possibly sputum cultures to aid in future decision making. Furthermore, if the patient has diarrhea (which the current one does not), the clinician should obtain a stool for C difficile toxin analysis.
For the case illustrated here, the clinician determined catheter‐associated bacteremia was a strong possibility, and decided to initiate empiric therapy with vancomycin and piperacillin‐tazobactam to provide coverage of MRSA and resistant Gram‐negative bacteria. The most common causes of nosocomial or catheter‐associated bloodstream infections (BSIs) are coagulase‐negative staphylococci, S aureus, enterococci, and Candida spp,8082 but Gram‐negative bacilli like P aeruginosa, Klebsiella spp, and E coli (among others) are also frequently involved, particularly in patients with catheter‐associated BSIs.81 Moreover, significant and increasing percentages of Gram‐negative bacilli exhibit resistance to 1 or more antibiotic classes,8385 and >50% of S aureus are typically MRSA,82, 83, 85, 86 although there has been some decline in MRSA central line‐associated BSIs in US ICUs in recent years.87
Clinical practice guidelines from the IDSA recommend vancomycin (or daptomycin) for the management of MRSA bacteremia,88 while piperacillin‐tazobactam is frequently empirically added to Gram‐positive coverage for serious hospital‐acquired infections because of its broad activity against many pathogenic bacteria, including some ESBL‐producing Gram‐negative bacteria and P aeruginosa,89 which are significant causes of patient morbidity and mortality.36, 90 However, to be effective, both vancomycin and piperacillin‐tazobactam need to be properly dosed to maximize their pharmacodynamic properties. Guidelines from the American Society of Health‐System Pharmacists, IDSA, and Society of Infectious Diseases Pharmacists recommend vancomycin serum trough concentrations of 15‐20 mg/L for patients with bacteremia due to MRSA.91 These levels are recommended to improve penetration, increase the probability of obtaining optimal target serum concentrations, and improve clinical outcomes. To achieve these trough levels, the guidelines recommend doses of 15‐20 mg/kg of actual body weight given every 8‐12 hours for most patients with normal renal function, assuming a minimum inhibitory concentration (MIC) of 1 mg/L. In seriously ill patients, the guidelines recommend using a loading dose of 25‐30 mg/kg to facilitate rapid attainment of the target trough serum vancomycin level. (If the MIC is 2 mg/L, then the targeted pharmacodynamic parameter for vancomycin is unachievable, and an alternative therapy should be considered.)
The pharmacodynamic parameter that best predicts efficacy for ‐lactams like piperacillin is the duration of time that free drug concentrations remain above the MIC (T>MIC), with near maximal bactericidal effects for penicillins when the free drug concentrations remain above the MIC for 50% of the dosing interval.92 The target pharmacodynamic parameter for piperacillin‐tazobactam (50% T>MIC) may be better achieved with use of prolonged or extended infusion regimens than with intermittent, more rapidly infused, administration schedules. Lodise and coworkers recently reported that extended infusion (3.375 g intravenously [IV] for 4 hours every 8 hours) versus intermittent infusion of piperacillin‐tazobactam (3.375 g IV for 30 minutes every 4 to 6 hours) was associated with a significantly lower 14‐day mortality rate (12.2% vs 31.6%, P = 0.04) and median duration of hospital stay (21 vs 38 days, P = 0.02) in a cohort of hospitalized patients with a P aeruginosa infection.93 Based on data such as these, the case patient here was initiated on vancomycin (15‐20 mg/kg every 812 hours) and piperacillin‐tazobactam (3.375 g IV for 4 hours every 8 hours).
CONCLUSIONS
Successful treatment of patients with serious, life‐threatening hospital‐ or healthcare‐associated infections depends on early adequate antimicrobial treatment. To accomplish this, empiric therapy is typically employed with a broad‐spectrum regimen intended to cover likely causative pathogen(s) based on local antibiograms and risk factors for involvement of resistant microorganisms. Choice of empiric therapy should also be based on the site of infection, and make use of clinical practice guidelines, when available. Although this approach often means treatment with a regimen that is unnecessarily broad, based on subsequent culture findings, it is warranted based on the significant negative impact of initial inadequate/emnappropriate empiric therapy, and the inability to remedy this negative effect by later modification of antimicrobial therapy. The possibility of de‐escalating the initial broad‐spectrum regimen is revisited after the results from cultures collected prior to beginning empiric therapy become available, generally 2‐4 days after beginning the process. In this manner, both the dangers of initial inadequate empiric therapy and overuse or misuse of antimicrobials are minimized. To further minimize the risk of antimicrobial resistance linked to overuse or misuse of antimicrobial agents, care should be taken to avoid treatment of colonization or culture contamination.
- ,.Appropriate vs. inappropriate antimicrobial therapy.Clin Microbiol Infect.2008;14(suppl 3):15–21.
- .Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients.Clin Infect Dis.2000;31(suppl 4):S131–S138.
- .Treatment options for nosocomial pneumonia due to MRSA.J Infect.2009;59(suppl 1):S25–S31.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,,.Impact of appropriateness of initial antibiotic therapy on the outcome of ventilator‐associated pneumonia.Intensive Care Med.2001;27:355–362.
- ,,, et al.Mortality and morbidity attributable to inadequate empirical antimicrobial therapy in patients admitted to the ICU with sepsis: a matched cohort study.J Antimicrob Chemother.2008;61:436–441.
- ,,,,,.Effect from multiple episodes of inadequate empiric antibiotic therapy for ventilator‐associated pneumonia on morbidity and mortality among critically ill trauma patients.J Trauma.2005;58:94–101.
- ,,,,,.Predictors of 30‐day mortality and hospital costs in patients with ventilator‐associated pneumonia attributed to potentially antibiotic‐resistant gram‐negative bacteria.Chest.2008;134:281–287.
- ,,,,.Antimicrobial therapy escalation and hospital mortality among patients with health‐care‐associated pneumonia: a single‐center experience.Chest.2008;134:963–968.
- ,,.Impact of inappropriate antibiotic therapy on mortality in patients with ventilator‐associated pneumonia and blood stream infection: a meta‐analysis.J Crit Care.2008;23:91–100.
- ,,, et al.Ventilator‐associated pneumonia: breaking the vicious circle of antibiotic overuse.Crit Care Med.2007;35:379–385; quiz 386.
- ,,, et al.Appropriateness and delay to initiate therapy in ventilator‐associated pneumonia.Eur Respir J.2006;27:158–164.
- ,,, et al.Impact of BAL data on the therapy and outcome of ventilator‐associated pneumonia.Chest.1997;111:676–685.
- ,,,,.Inadequate treatment of ventilator‐associated pneumonia: risk factors and impact on outcomes.J Hosp Infect.2007;65:361–367.
- ,,, et al.Predictors of mortality in patients with methicillin‐resistant Staphylococcus aureus (MRSA) bacteraemia: the role of empiric antibiotic therapy.Eur J Clin Microbiol Infect Dis.2007;26:239–245.
- ,,,,,.Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med.2003;115:529–535.
- ,,,,.The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting.Chest.2000;118:146–155.
- ,,, et al.Bloodstream infections caused by antibiotic‐resistant gram‐negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome.Antimicrob Agents Chemother.2005;49:760–766.
- ,,,,,.The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection.J Intern Med.1998;244:379–386.
- ,,,,,.Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment.Antimicrob Agents Chemother.2005;49:1306–1311.
- ,,, et al.Antibiotic therapy for Klebsiella pneumoniae bacteremia: implications of production of extended‐spectrum beta‐lactamases.Clin Infect Dis.2004;39:31–37.
- ,,, et al.Impact of inappropriate empirical therapy for sepsis due to health care‐associated methicillin‐resistant Staphylococcus aureus.J Infect.2009;58:131–137.
- ,,, et al.Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46:193–200.
- ,,, et al.Multidrug‐resistant Pseudomonas aeruginosa bloodstream infections: risk factors and mortality.Epidemiol Infect.2011; Jan 13:1–10.
- ,,,,,.Economic consequences of failure of initial antibiotic therapy in hospitalized adults with complicated intra‐abdominal infections.Surg Infect (Larchmt).2008;9:335–347.
- ,,, et al.Effect of inappropriate initial empiric antibiotic therapy on outcome of patients with community‐acquired intra‐abdominal infections requiring surgery.Eur J Clin Microbiol Infect Dis.2004;23:682–687.
- ,,,,,.Emergence of antibiotic‐resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy.Clin Infect Dis.1996;23:486–494.
- ,,, et al.Antibiotic treatment for surgical peritonitis.Ann Surg.1991;214:543–549.
- ,,, et al.Inappropriate initial treatment of secondary intra‐abdominal infections leads to increased risk of clinical failure and costs.Br J Clin Pharmacol.2005;60:438–443.
- ,,, et al.Optimal management therapy for Pseudomonas aeruginosa ventilator‐associated pneumonia: an observational, multicenter study comparing monotherapy with combination antibiotic therapy.Crit Care Med.2007;35:1888–1895.
- ,,,,,.Risk factors for and outcomes of healthcare‐associated infection due to extended‐spectrum beta‐lactamase‐producing Escherichia coli or Klebsiella pneumoniae in Thailand.Infect Control Hosp Epidemiol.2007;28:873–876.
- ,,, et al.Impact of antibiotic resistance and of adequate empirical antibiotic treatment in the prognosis of patients with Escherichia coli bacteraemia.J Antimicrob Chemother.2007;60:855–863.
- .Predicting methicillin resistance and the effect of inadequate empiric therapy on survival in patients with Staphylococcus aureus bacteremia.Arch Intern Med.2000;160:1001–1004.
- ,,,,,.Impact of multiresistance of gram‐negative bacteria in bloodstream infection on mortality rates and length of stay.Infection.2008;36:31–35.
- ,,,.Clinical and economic impact of common multidrug‐resistant gram‐negative bacilli.Antimicrob Agents Chemother.2008;52:813–821.
- .Review of studies of the impact on Gram‐negative bacterial resistance on outcomes in the intensive care unit.Crit Care Med.2009;37:1463–1469.
- ,,,,,.Impact of multidrug‐resistant Pseudomonas aeruginosa bacteremia on patient outcomes.Antimicrob Agents Chemother.2010;54:3717–3722.
- ,,,,.Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator‐associated pneumonia.Chest.2002;122:262–268.
- ,,,.Outcomes analysis of delayed antibiotic treatment for hospital‐acquired Staphylococcus aureus bacteremia.Clin Infect Dis.2003;36:1418–1423.
- .Broad‐spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front.Clin Infect Dis.2008;47(suppl 1):S3–S13.
- ,.A new paradigm for treating infections: “go hard and go home.”Crit Care Resusc.2009;11:276–281.
- .Use of broad‐spectrum antimicrobials for the treatment of pneumonia in seriously ill patients: maximizing clinical outcomes and minimizing selection of resistant organisms.Clin Infect Dis.2006;42(suppl 2):S72–S81.
- ,.Antibiotic resistance: location, location, location.Clin Microbiol Infect.2007;13(suppl 2):7–16.
- ,,,,,.Ventilator‐associated pneumonia in a multi‐hospital system: differences in microbiology by location.Infect Control Hosp Epidemiol.2003;24:853–858.
- ,,, et al.Incidence and susceptibility of pathogenic bacteria vary between intensive care units within a single hospital: implications for empiric antibiotic strategies.J Trauma.2000;49:638–645; discussion645–646.
- ,,,,.Variations in etiology of ventilator‐associated pneumonia across four treatment sites: implications for antimicrobial prescribing practices.Am J Respir Crit Care Med.1999;160:608–613.
- Hospital‐Acquired Pneumonia Guideline Committee of the American Thoracic Society and Infectious Diseases Society of America.Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- .The dilemma of multidrug‐resistant gram‐negative bacteria.Am J Med Sci.2010;340:232–237.
- .Antimicrobial resistance and aging: beginning of the end of the antibiotic era?J Am Geriatr Soc.2002;50:S226–S229.
- ,.Principles of antimicrobial use in older adults.Clin Geriatr Med.2007;23:481–497,v.
- .Antimicrobial use: risk driver of multidrug resistant microorganisms in healthcare settings.Curr Opin Infect Dis.2009;22:352–358.
- .Collateral damage and what the future might hold. The need to balance prudent antibiotic utilization and stewardship with effective patient management.Int J Infect Dis.2006;10:S17–S24.
- ,,,.Blood culture contamination in Tanzania, Malawi, and the United States: a microbiological tale of three cities.J Clin Microbiol.2006;44:4425–4429.
- ,,, et al.Clinical and economic impact of contaminated blood cultures within the hospital setting.J Hosp Infect.2011;77:233–236.
- ,,.Contaminant blood cultures and resource utilization. The true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,,,.Contamination of catheter‐drawn blood cultures.J Clin Microbiol.2001;39:3393–3394.
- ,,.Comparison of utility of blood cultures from intravascular catheters and peripheral veins: a systematic review and decision analysis.J Med Microbiol.2008;57:1–8.
- ,,.Contamination of blood cultures during venepuncture: fact or myth?Postgrad Med J.1990;66:1053–1058.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- ,,,,.The value of infectious diseases consultation in Staphylococcus aureus bacteremia.Am J Med.2010;123:631–637.
- ,,,,.Infectious diseases consultation lowers mortality from Staphylococcus aureus bacteremia.Medicine (Baltimore).2009;88:263–267.
- ,,,,,.The value of infectious diseases specialists: non‐patient care activities.Clin Infect Dis.2008;47:1051–1063.
- ,,, et al.The value of an infectious diseases specialist.Clin Infect Dis.2003;36:1013–1017.
- ,,, et al.Mortality of S. aureus bacteremia and infectious diseases specialist consultation—a study of 521 patients in Germany.J Infect.2009;59:232–239.
- ,.Hospital‐acquired pneumonia: pathophysiology, diagnosis, and treatment.Surg Clin North Am.2009;89:439–461,ix.
- ,,,.Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System.Crit Care Med.1999;27:887–892.
- ,,.Healthcare‐associated pneumonia in adults: management principles to improve outcomes.Infect Dis Clin North Am.2004;18:939–962.
- ,,.Healthcare‐associated infections. A useful concept?Curr Opin Crit Care.2009;15:419–424.
- ,,,,.Ventilator‐associated pneumonia: incidence, risk factors, and microbiology.Semin Respir Infect.2000;15:272–279.
- ,,, et al.Ventilator‐associated pneumonia caused by potentially drug‐resistant bacteria.Am J Respir Crit Care Med.1998;157:531–539.
- ,,.A study of ventilator‐associated pneumonia: incidence, outcome, risk factors and measures to be taken for prevention.Indian J Anaesth.2010;54:535–540.
- ,,, et al.Risk factors for infection by Pseudomonas aeruginosa in patients with ventilator‐associated pneumonia.Intensive Care Med.1994;20:193–198.
- ,,,.Tackling empirical antibiotic therapy for ventilator‐associated pneumonia in your ICU: guidance for implementing the guidelines.Semin Respir Crit Care Med.2009;30:102–115.
- ,,,,,.Diagnosing pneumonia during mechanical ventilation: the clinical pulmonary infection score revisited.Am J Respir Crit Care Med.2003;168:173–179.
- ,,,,.Guidelines for clinical care: anti‐infective agents for intra‐abdominal infection. A Surgical Infection Society policy statement.Arch Surg.1992;127:83–89.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,.Intra‐abdominal infections.Surg Clin North Am.2009;89:421–437,ix.
- ,,,.In vitro susceptibilities of aerobic and facultative anaerobic Gram‐negative bacilli from patients with intra‐abdominal infections worldwide from 2005–2007: results from the SMART study.Int J Antimicrob Agents.2009;34:585–588.
- ,,,,,.Susceptibility of gram‐negative pathogens isolated from patients with complicated intra‐abdominal infections in the United States, 2007–2008: results of the Study for Monitoring Antimicrobial Resistance Trends (SMART).Antimicrob Agents Chemother.2010;54:3031–3034.
- ,,, et al.NHSN annual update: antimicrobial‐resistant pathogens associated with healthcare‐associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007.Infect Control Hosp Epidemiol.2008;29:996–1011.
- ,.Central line‐associated bloodstream infections: prevention and management.Infect Dis Clin North Am.2011;25:77–102.
- ,,,,,.Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.Clin Infect Dis.2004;39:309–317.
- National Nosocomial Infections Surveillance (NNIS) system report,data summary from January 1992 through June 2004, issued October 2004.Am J Infect Control.2004;32:470–485.
- ,,,.Antimicrobial resistance trends of Escherichia coli bloodstream isolates: a population‐based study, 1998–2007.J Antimicrob Chemother.2009;64:169–174.
- ,,, et al.International Nosocomial Infection Control Consortium (INICC) report, data summary for 2003–2008, issued June 2009.Am J Infect Control.2010;38:95–104,e102.
- ,,.The impact of antimicrobial‐resistant, health care‐associated infections on mortality in the United States.Clin Infect Dis.2008;47:927–930.
- ,,,,.Methicillin‐resistant Staphylococcus aureus central line‐associated bloodstream infections in US intensive care units, 1997–2007.JAMA.2009;301:727–736.
- ,,, et al.Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin‐resistant Staphylococcus aureus infections in adults and children: executive summary.Clin Infect Dis.2011;52:285–292.
- ,,,.Pharmacokinetic evaluation of piperacillin‐tazobactam.Expert Opin Drug Metab Toxicol.2010;6:1017–1031.
- ,,, et al.Morbidity associated with Pseudomonas aeruginosa bloodstream infections.Diagn Microbiol Infect Dis.2009;64:311–319.
- ,,, et al.Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health‐System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists.Am J Health Syst Pharm.2009;66:82–98.
- ,.Pharmacokinetic and pharmacodynamic parameters of antimicrobials: potential for providing dosing regimens that are less vulnerable to resistance.Clin Pharmacokinet.2009;48:517–528.
- ,,.Piperacillin‐tazobactam for Pseudomonas aeruginosa infection: clinical implications of an extended‐infusion dosing strategy.Clin Infect Dis.2007;44:357–363.
Early appropriate antimicrobial therapy is necessary to minimize the morbidity and mortality associated with hospital‐ or healthcare‐associated infections (HAIs). A number of studies have demonstrated that delayed or inadequate antimicrobial therapy leads to worse clinical outcomes and higher healthcare costs.1, 2 Inadequate antimicrobial therapy can also promote or enhance the development of resistance,2 with potential wide‐ranging impact beyond the immediate patient under care. Because delaying treatment until availability of culture results decreases the likelihood of a successful outcome, patients with a suspected invasive HAI commonly receive empiric therapy with a regimen expected to cover the most likely causative pathogens. Based on characteristics of the patient and healthcare facility or unit, likely pathogens may include bacteria or other pathogens resistant to 1 or more antimicrobial drug classes. This article discusses the various processes and factors that need to be considered when choosing empiric antibiotics in the hospital or other healthcare setting, and uses 3 case studies dealing with pneumonia, intra‐abdominal infection, and bacteremia, respectively, to illustrate points of interest.
IMPORTANCE OF EARLY ADEQUATE ANTIBIOTIC USE
The initial selection and early deployment of adequate antimicrobial therapy is critical for successful resolution of HAIs. The terms inadequate and inappropriate antimicrobial therapy are commonly used interchangeably in the literature, and can be defined as use of antimicrobial treatment without (sufficient) activity against the identified pathogen.2 Using an antibiotic for a fungal infection would be inadequate, as would using a drug or dosing regimen that is ineffective against the identified bacterial species due to resistance or a failure to achieve the drug's pharmacokinetic/pharmacodynamic target for efficacy against the pathogen. The complete absence of antimicrobial therapy is also considered inadequate therapy. Some investigators consider inappropriate therapy a more general term that includes excessive treatment as well as inadequate treatment.1 Others reserve the term inappropriate for use of an antimicrobial without activity against the identified pathogen, and the term inadequate for use of an insufficient regimen, either in terms of optimal dose, route of administration, timeliness, or failure to use combination therapy when appropriate.3 However, many or most research articles do not make the distinction, and the current article does not make a distinction.
In addition, some articles arbitrarily define inadequate therapy as either use (or absence) of a treatment without activity against the identified pathogen or a delay in appropriate or adequate treatment, eg, no patient exposure to adequate treatment within 24 hours of hospital admission. It is important to recognize this when evaluating articles in the literature. Other studies separate inadequate and delayed therapy as variables. However, when dealing with empiric therapy, the adequacy of initial empiric therapy cannot be fully determined until subsequent possession of the tissue/blood culture results.
Inadequate Antibiotic Treatment
A 1999 study by Kollef et al. identified inadequate antimicrobial treatment as the most important independent predictor of hospital mortality, in a group of patients with a nosocomial or community‐acquired infection, while in the medical or surgical intensive care unit (ICU).4 Infection sites included in the study were lung, bloodstream, urinary tract, gastrointestinal (GI) tract, and wound. Various other studies have confirmed an association between inadequate antibiotic therapy and increased hospital mortality, and some demonstrated a relationship between inadequate antibiotic therapy and longer hospital or ICU stays57 and higher hospital‐related costs.8 More specifically, initial inappropriate antibiotic therapy has been associated with increased mortality in patients with healthcare‐associated9 or ventilator‐associated pneumonia (VAP)5, 7, 8, 1014 and those with bacteremia/sepsis.6, 10, 1524 Inadequate empiric therapy has also been linked with worsened outcomes,19, 2529 longer hospital stays,2527, 29 and increased healthcare costs25, 29 in patients with infections of the GI tract.
With respect to specific bacterial pathogens, inappropriate antibiotic therapy has been shown to increase risk of hospital mortality for patients with VAP or bacteremia caused by Pseudomonas aeruginosa,20, 30 extended‐spectrum ‐lactamase (ESBL)‐producing or multidrug‐resistant (MDR) Klebsiella pneumoniae or Escherichia coli,21, 31, 32 and methicillin‐resistant Staphylococcus aureus (MRSA).15, 23 In fact, infection with resistant bacteria, and particularly MDR bacteria, is a principal risk factor for inadequate initial antibiotic therapy.14, 16, 33, 34 A recent study by Teixeira and coworkers showed that inadequate therapy was more than twice as common for additional episodes of VAP caused by MDR pathogens as for those involving drug‐susceptible pathogens (56% vs 25.5%).14 Moreover, VAP caused by MDR pathogens was identified as a significant independent predictor of inadequate antimicrobial therapy (odds ratio [OR], 3.07; 95% confidence interval [CI], 1.29‐7.30; P = 0.01). Infections caused by drug‐resistant versus susceptible bacteria have generally been associated with increased morbidity, longer hospital or ICU stays, and higher costs.24, 3437 At least part of the reason for these worsened outcomes appears to be an increased likelihood that initial therapy is inadequate for the causative agent. Because of this, it is particularly important to consider the probability of infection with resistant bacteria when initiating empiric antibiotic therapy.
Delayed Antibiotic Treatment
In addition to inadequate initial therapy, a delay in the onset of adequate therapy has also been shown to have negative impact on outcome in patients with VAP, bacteremia, or intra‐abdominal infections.12, 13, 27, 38, 39 For example, Iregui et al. identified administration of initially delayed appropriate antibiotic treatment (treatment delayed for 24 hours after initial diagnosis of VAP) as a significant predictor of hospital mortality (OR, 7.68; 95% CI, 4.50‐13.09; P 0.001) in patients with VAP at a US teaching hospital.38 Similarly, Lodise et al. identified delayed antibiotic treatment as an independent predictor of infection‐related mortality in patients with hospital‐acquired S aureus bacteremia (OR, 3.8; 95% CI, 1.3‐11.0; P = 0.01).39 Delayed versus early antibiotic therapy was also associated with significantly longer hospital stay (20.2 vs 14.3 days, P = 0.05). Classification and regression tree analysis identified 44.75 hours from the initial positive blood culture result to appropriate therapy as the breakpoint between delayed and early treatment for bacteremia.
Of particular interest, evidence suggests that the negative impact of initial delay or initial use of inadequate therapy often cannot be remedied by subsequent treatment alterations. For example, Luna et al. reported a significantly lower hospital mortality rate for VAP patients who received early adequate antibiotic therapy compared with those who received early inadequate therapy (38% vs 91%, P 0.001).13 In this study, early treatment referred to drug administration prior to bronchoscopy, which was performed within 24 hours of clinical diagnosis of VAP. A subset of patients only received treatment after bronchoscopy, and the mortality rate for VAP‐positive patients who received adequate antibiotic therapy after this initial delay was similar to that for VAP‐positive patients who received inadequate therapy postbronchoscopy (71% vs 70%). In other words, the negative impact of an initial delay in adequate therapy could not be subsequently overcome by using adequate antibiotic therapy later in the disease process. Similarly, a recent study by Zilberberg et al. of healthcare‐associated pneumonia reported that the negative effect of initial inadequate antibiotic therapy on hospital mortality could not be mitigated by subsequent escalation of adequate antibiotic therapy after reception of culture results.9 Finally, a study of inadequate initial empiric antibiotic therapy of postoperative intra‐abdominal infection (peritonitis) also showed that adverse outcomes could not be abrogated by changes in antibiotic therapy based on culture results.27 Taken together, the results from these studies emphasize the importance of early adequate antibiotic therapy.
PRACTICAL GUIDELINES FOR CHOOSING EMPIRIC ANTIBIOTICS
When choosing initial empiric therapy for a suspected hospital‐ or healthcare‐related bacterial infection, it is first important to determine if the patient has received prior antibiotic therapy, and if the patient has, then the clinician should consider choosing an antibiotic from a different drug class. This is because prior antibiotic therapy increases risk of infection with a pathogen resistant to the initial antibiotic drug and other members of its class. Also, depending on the site of the infection and likely pathogenic bacteria, the clinician will need to decide whether to initiate empiric therapy with a single antibiotic or combination of agents. A number of patient‐ and institution‐related factors can be utilized by clinicians to better identify the likely pathogen responsible for the infection, and it is critical to use this information when selecting initial empiric therapy. Finally, as is true whenever choosing antimicrobial or other drug therapies, clinicians need to consider and weigh the safety/tolerability profile, potential for drugdrug interactions, and relative cost of different treatment options. These will vary for individual patients receiving the same drug or drug combination.
MINIMIZING ANTIMICROBIAL RESISTANCE IN THE HOSPITAL OR HEALTHCARE SETTING
It is also important to consider the potential for development of antibiotic resistance when choosing initial empiric therapy. The current paradigm for treatment of serious hospital or healthcare infections is to prescribe broad‐spectrum antimicrobial therapy upfront while awaiting culture results, and to de‐escalate (or terminate) therapy once culture results are available4042or as 2 authors recently put it, get it right the first time, hit hard up front, and use large doses of broad‐spectrum antibiotics for a short period.41 The initial empiric antibiotic regimen should have a high likelihood of covering the most likely causative pathogens, including resistant species or strains. Furthermore, emergence of resistance is minimized when the initial regimen effectively covers the most likely causative pathogens, and subsequent culture results are utilized to streamline or narrow the initial regimen, when possible.40, 42 Emergence of resistance is also minimized by using the shortest duration of treatment with maximal clinical effect. (These latter 2 points are discussed in greater detail in the Kaye and File articles in this supplement.)
Factoring in Institution‐ and Patient‐Specific Factors
Local antibiograms are useful in determining the most likely infection‐causing pathogens, within different wards of the hospital, and their susceptibility or resistance to various antibiotics. Local patterns of pathogen susceptibility and resistance can differ markedly from national averages, so local antibiograms are more useful than national or even regional surveillance data when making choices about the initial agent and dosing regimen for initial empiric therapy.43 Hospitals are required by the Joint Commission to create antibiograms on at least an annual basis, although more frequent antibiograms are particularly useful, given that susceptibility or resistance patterns change over time. It is also important that hospital microbiologists create antibiograms specifically for different hospital wards or departments, as well as hospital‐wide. The incidence and susceptibility of pathogenic bacteria has been shown to vary across different wards within a hospital, as well as within different regions of a given country.4446
Patient‐specific factors should also be considered in the decision‐making process for selection of initial empiric therapy for a suspected bacterial infection. Relevant patient characteristics or factors may differ somewhat when examining risk for particular types of infection (eg, healthcare/hospital‐acquired pneumonia, VAP, or bacteremia) or particular antibiotic‐resistant pathogens (eg, MRSA, ESBL‐producing E coli or Klebsiella spp, P aeruginosa and MDR P aeruginosa, and carbapenem‐resistant Acinetobacter baumannii). Nonetheless, several risk factors appear to generally increase risk of infection with a resistant pathogen across these subcategories, including prior antibiotic treatment (with agents sometimes varying depending on the particular pathogen of interest); recent hospital admission or residence in a nursing home or extended‐care facility; prolonged hospital stay (particularly in the ICU); prior colonization with the pathogen; presence of an indwelling catheter (central venous, arterial, or urinary); and mechanical ventilation; among others.2, 47, 48 Patients who are immunocompromised, either due to their condition or immunosuppressive therapy, are also generally at increased risk of infection with resistant bacteria.47
Patient age and presence of comorbidities can also affect initial selection of empiric therapy. Cell‐mediated immunity tends to decline with age, and elderly individuals are also more likely to have conditions or comorbidities associated with diminished host immunity, both of which may contribute to increased susceptibility to infection and infection involving resistant bacteria.49 Furthermore, elderly individuals are more likely to have decline in renal or hepatic function or other physiologic changes that can alter drug pharmacokinetics and pharmacodynamics,50 and these factors need to be considered when selecting an initial empiric therapy regimen that covers likely pathogens, without increasing risk of drug toxicity. In addition, the increased number of comorbidities in elderly patients typically translates into polypharmacy, with potential for drugdrug interactions that need to be weighed when selecting initial empiric therapy.
Treat Infection, Not Contamination or Colonization
It is important to limit antimicrobial use to treatment of actual infections, and not for treatment of colonization or contamination. Treatment of colonization is a significant source of antimicrobial overuse. Hence, it is important that healthcare teams take appropriate steps to ensure they are treating pneumonia, bacteremia, or a urinary tract infection, not colonization of the tracheal aspirate, catheter tip or hub, or indwelling urinary catheter that is unassociated with actual infection. Strategies to employ when considering how to differentiate between true infection and colonization include using Gram stain in sputum specimens to look for evidence of polymorphonuclear leukocytes (inflammation), understanding that certain organisms, such as Enterococcus and Candida are not respiratory pathogens, recognizing that urinary catheters may be colonized in the absence of infection, and remaining vigilant regarding blood culture contamination. Since antibiotic use is generally linked to increased risk of resistance,51, 52 antibiotics should only be used when there is a clear clinical benefit associated with their use; treatment of colonization does not fit this description. When in doubt, an infectious diseases (ID) specialist consultation is recommended.
Similarly, overuse/misuse of antibiotics that occurs due to false‐positive culture results also increases development of resistance in hospitalized patients. In particular, contamination of blood cultures is relatively common in hospitalized patients, particularly in hospital emergency rooms,53 and frequently results in administration of antibiotics to treat an apparent infection that actually represents a contaminated culture. Antimicrobial treatment due to false‐positive blood culture results has been associated with prolonged hospitalization and elevated laboratory and hospital costs,54, 55 and provides an environment for development of antimicrobial resistance. Contamination of blood cultures often occurs at the point of blood collection via venipuncture or through indwelling catheters,56, 57 but can occur later in the process during laboratory handling or processing of specimens.58 Hence, it is important to use proper antisepsis when collecting blood or other cultures, to make sure it is blood and not skin or the catheter hub that is being cultured, and to make sure to use proper methods when processing all cultures.
Consult Infectious Diseases Experts
The 2007 guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America (IDSA/SHEA) for the development of institutional antimicrobial stewardship programs recommend inclusion of an ID physician and a clinical pharmacist with ID training as core members of a multidisciplinary antimicrobial stewardship team.59 Consultation with an ID expert or inclusion of an ID specialist into an institutional antimicrobial stewardship program has been shown to improve antibiotic usage and reduce morbidity and mortality, length of hospital stay, healthcare costs, and resistance.6064 In hospitals without easy access to an ID specialist, hospitalists with ID training may be able to fulfill the role provided by ID physicians or clinical pharmacists with ID training.
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Table 1 provides the key initial data for Case 1. The patient has a history of hypertension, congestive heart failure (CHF), and myocardial infarction (MI), and is receiving medications consistent with such a history. In terms of her acute presentation, cough, fever, chills, dyspnea, lung crackles (rales), X‐ray evidence of lung infiltrate, reduced oxygen saturation, elevated white blood cell (WBC) count, and increased percentage of WBC bands are all consistent with a diagnosis of pneumonia of relatively recent origin. Progressive worsening of symptoms within the previous 36 hours is also consistent with infection of recent origin. There are no neurologic symptoms, and cardiac function appears relatively normal, with no evidence of MI or cardiac arrhythmia based on electrocardiogram or heart rate, although there is evidence of continuing hypertension and perhaps CHF.
| |
| History | A 72‐yr‐old woman recently hospitalized for congestive heart failure (CHF), returns to the emergency department from rehab with cough, fever, chills, shortness of breath, all progressively worsening over the past 36 hr |
| Past history of CHF (ejection fraction 44%), myocardial infarction 2 yr ago, hypertension, past smoking | |
| Medications: metoprolol 50 mg BID; furosemide 40 mg daily; aspirin 81 mg daily; enalapril 20 mg daily | |
| Physical | Vitals: BP 148/88, P 82, RR 16, T 101.7, O2 sat 92% on room air |
| Heart: S1, S2 no murmurs | |
| Lungs: crackles at R lung base | |
| Abdomen: bowel sounds present, non‐tender | |
| Extremities: trace edema bilaterally | |
| Neurologic: no focal findings | |
| Labs | EKG: NSR, no acute ST‐T changes |
| Chemistry, hemoglobin, platelets, within normal limits | |
| WBC: 14,700/mm3, 10% bands | |
| Cardiac enzymes negative | |
| ‐Natriuretic peptide within normal limits for age | |
| Chest X‐ray: right lower lung infiltrate | |
Given the patient's history of recent hospitalization, the clinician should consider that the pneumonia is most likely hospital‐ or healthcare‐acquired. Because she was described as developing the problem while in rehabilitation, it can be assumed that hospitalization occurred relatively recently. Hospital‐acquired pneumonia (HAP) is defined as pneumonia that occurs within 48 hours of hospital admission, and that was not incubating at the time of admission.47, 65 HAP accounts for approximately of 15% of all nosocomial/hospital‐acquired infections in the United States and up to 27% in the ICU,65, 66 and is a frequent cause of morbidity and mortality in this setting.65 In addition to hospitalization, other characteristics or risk factors for HAP include severe illness, hemodynamic compromise, depressed immune function, use of nasogastric tubes, and mechanical ventilation for the important subset of HAP patients with VAP.65 VAP is more precisely defined as HAP that arises >48‐72 hours after endotracheal intubation.47
Healthcare‐associated pneumonia (HCAP) is a more recently defined category that includes patients with HAP and VAP, and is characterized by hospitalization for 2 days in the preceding 90 days, or residence in a nursing home or extended‐care facility.47, 67, 68 Additional risk factors for HCAP include intravenous therapy at home (including antibiotics); intravenous chemotherapy or wound care within 30 days of the current infection; and recent attendance at a hospital or hemodialysis clinic.47 Most HAP or HCAP data have been derived from patients with VAP, and the 2005 American Thoracic Society (ATS)/IDSA guidelines for management of HAP, VAP, and HCAP recommend similar approaches for the initial treatment of patients with nonintubated HAP, VAP, and HCAP.47 There are general similarities between these 3 disease categories with respect to etiology, epidemiology of likely pathogens, and prognosis, and important differences compared with community‐acquired pneumonia (CAP), which in turn gives rise to different treatment strategies for HAP/VAP/HCAP and CAP.
Given an initial diagnosis of HAP or HCAP, the clinician should be considering the following questions: 1) What are the appropriate choices of antimicrobials? 2) What are the clinical parameters that should alert one to resistant organisms? 3) What are the appropriate cultures to order? 4) What is the role of Gram stain, if any?
Selection of Initial Empiric Therapy for Likely Pathogens
HAP is usually caused by bacterial pathogens, and much more rarely involves viruses or fungi in immunocompetent patients. Therefore, from the start, the focus should be on empiric therapy with an antibiotic or combination of antibiotics that has a high probability of covering the most likely pathogens. Empiric therapy is warranted because of the risk of mortality or other negative consequences when antibiotic therapy is delayed, particularly in an aged patient with a chronic illness like CHF (such as the case study here). Clues as to likely pathogensand hence most appropriate antibiotic regimencan be discerned by looking at the onset of HAP/VAP (early vs late) and whether the patient has risk factors for infection with a MDR or antibiotic‐susceptible bacterial pathogen. A significant proportion of patients with HAP, VAP, or HCAP are infected with MDR pathogens, and identifying these patients and providing them with appropriate broad‐spectrum empiric therapy is a key to successful management.
Early‐onset HAP/VAP (occurring 5 days after hospitalization) is more likely to be due to antibiotic‐sensitive bacteria than late‐onset HAP/VAP (occurring 5 days after hospitalization), which often occurs due to MDR species.47, 69, 70 Not surprisingly, risk of inappropriate initial antibiotic therapy14 is higher, and mortality is also higher in patients with late‐onset HAP/VAP.47, 71 Patients with early‐onset HAP/VAP who have received prior antibiotics or been hospitalized within the past 90 days are also at risk for infection due to MDR bacteria, and hence should be treated the same as patients with late‐onset HAP/VAP.47 Additional risk factors for infection with MDR pathogens include antimicrobial therapy in the preceding 90 days (particularly with broad‐spectrum agents), current hospitalization 5 days, high prevalence of antibiotic resistance in the specific hospital unit, immunosuppression, and presence of risk factors for HCAP (hospitalization 2 days in the preceding 90 days, residence in a nursing home or extended‐care facility, home infusion therapy, chronic dialysis within 30 days, home wound care, or family member with MDR pathogen).47 For VAP patients, duration of ventilator support 7 days is an additional risk factor for infection with a MDR pathogen.70, 72 A second episode of VAP is more likely to be due either to MRSA or P aeruginosa; therefore, these organisms need to be considered when selecting initial empiric therapy.
The most common bacterial causes of HAP, VAP, or HCAP include aerobic Gram‐negative bacilli, such as P aeruginosa, Acinetobacter spp, and Enterobacteriaceae (eg, K pneumoniae, E coli, Enterobacter spp), and Gram‐positive cocci, such as S aureus and Streptococcus pneumoniae.47, 73 MDR bacterial species are more likely when certain risk factors are present, and the ATS/IDSA guidelines recommend using a risk‐stratification process when selecting empiric antibiotic therapy for patients with suspected HAP, VAP, or HCAP.47 The guidelines also emphasize that local conditions can greatly impact whether a patient is infected with an antibiotic‐sensitive or antibiotic‐resistant species, regardless of other risk factors, thereby highlighting the importance of using recent hospital and hospital unit‐specific antibiograms when stratifying a patient based on risk.
Other guiding principles of initial empiric treatment, as outlined in the ATS/IDSA guidelines, include not delaying therapy while awaiting culture results and administration of therapy as soon as possible following diagnosis; making sure the dosing regimen as well as drug selection is appropriate/adequate for the patient and suspected pathogen; and using a different class of antibiotic for patients with prior antibiotic exposure.47 The guidelines further indicate that combination therapy is appropriate initial therapy in patients at high risk for infection with MDR bacteria, and that for patients receiving combination therapy including an aminoglycoside, the aminoglycoside can be stopped after 5‐7 days in responding patients. Table 2 highlights ATS/IDSA recommendations for initial empiric antibiotic therapy in patients with suspected HAP/VAP who have early‐onset disease and no risk factors for MDR pathogens.47 Table 3 highlights recommendations for initial empiric antibiotic therapy in patients with suspected HAP/VAP/HCAP who have late‐onset disease and/or risk factors for MDR pathogens.47
| Potential Pathogen | Recommended Antibiotic |
|---|---|
| |
| Streptococcus pneumoniae* | |
| Haemophilus influenzae | Ceftriaxone |
| Methicillin‐sensitive Staphylococcus aureus | or |
| Antibiotic‐sensitive enteric Gram‐negative bacilli | Levofloxacin, moxifloxacin, or ciprofloxacin |
| Escherichia coli | or |
| Klebsiella pneumoniae | Ampicillin/sulbactam |
| Enterobacter spp | or |
| Proteus spp | Ertapenem |
| Serratia marcescens | |
| Potential Pathogen | Combination Antibiotic Therapy |
|---|---|
| |
| Pathogens listed in Table 2, plus MDR pathogens | Antipseudomonal cephalosporin (cefepime, ceftazidime) |
| Pseudomonas aeruginosa | or |
| Klebsiella pneumoniae (ESBL‐positive)* | Antipseudomonal carbapenem (imipenem or meropenem) |
| Acinetobacter spp* | or |
| ‐Lactam/‐lactamase inhibitor (piperacillin‐tazobactam) | |
| plus | |
| Antipseudomonal fluoroquinolone* (ciprofloxacin or levofloxacin) | |
| or | |
| Aminoglycoside (amikacin, gentamicin, or tobramycin) | |
| plus | |
| Methicillin‐resistant Staphylococcus aureus (MRSA) | Linezolid or vancomycin |
| Legionella pneumophila* | |
Returning to Case 1, given a clinical diagnosis of HAP/HCAP and the patient's heightened risk for infection with MRSA or resistant Gram‐negative bacteria, she was initiated on a regimen consisting of piperacillin/tazobactam plus vancomycin and ciprofloxacin. The choice of 3 agents is consistent with ATS and IDSA guidelines to cover the potential for an ESBL‐producer or Acinetobacter, or Pseudomonas. Individual choices should be dictated by one's own institutional antibiogram or some knowledge of the rehabilitation facility from which the patient was transferred.
Guiding Principles for Culture Management
Culture collection and management plays an important role in diagnosis and subsequent treatment of HAP/VAP or HCAP. As outlined in the ATS/IDSA guidelines, patient management typically proceeds using either a clinical strategy or bacteriologic strategy, or a combination thereof.47 The clinical strategy makes use of cultures of endotracheal aspirates or sputum, with initial microscopic examination and Gram staining to identify bacterial growth and guide initiation of empiric antibiotic therapy. Cultures should always be performed before instituting antibiotic therapy. Microorganism growth is described as light, moderate, or heavy by microbiology laboratories using semiquantitative analysis. Gram staining should be performed only if the specimen is of good quality; most microbiology laboratories will do screening tests to ensure they are of good quality, or else will reject the specimen. When correlated with culture results, Gram staining can improve diagnostic accuracy.74
The bacteriologic strategy uses quantitative means to analyze and describe cultures of lower respiratory secretions or specimens obtained via endotracheal aspirates, mini‐bronchoalveolar lavage specimens (mini‐BAL), bronchoalveolar lavage, or protected‐specimen bronchial brushing, collected with or without a bronchoscope, ie, with or without invasive techniques. Hence, whereas the clinical strategy uses noninvasive tracheal aspirates to culture microorganisms for analysis, the bacteriologic strategy often employs a relatively noninvasive strategy like a mini‐BAL, or invasive (bronchoscopic) lower respiratory tract samples for quantitative culture analysis. Diagnosis of HAP/VAP or HCAP, and determination of the causative microorganism(s), requires growth above a certain threshold when using the semi‐quantitative analysis. The clinical approach is more sensitive, but can result in overtreatment, while the bacteriologic strategy is associated with risk of undertreatment due to false‐negative culture results. On the other hand, quantitative cultures increase the specificity of diagnosis.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman with no past medical history of note, who presented to her physician about 3 days ago, after 5 days of abdominal pain and fever (101.7F). She had an outpatient computed tomography (CT) scan, and the results suggested diverticulitis. After the CT scan, she was given amoxicillin/clavulanate. She now presents to the emergency department (3 days later) with worsening pain, fever, and severe weakness. A physical exam shows low blood pressure (84/58 mmHg) and tachycardia (132 bpm). Her respiratory rate is 22 breaths per minute. Oxygenation (O2 saturation 99% on room air) is normal, and the patient's lungs are clear. Abdominal examination reveals bowel sounds and diffuse tenderness, particularly at the left lower quadrant, and there is evidence of guarding and rebound. Her blood chemistry is generally normal, although the WBC count is elevated (15,200/mm3). No abnormalities are evident on chest X‐ray. The patient's blood pressure increases to 96/64 mmHg after she is infused with 2 liters of normal saline. She undergoes another CT scan and is admitted to the ICU. The CT scan shows diverticulitis with abscess and walled‐off perforation. An interventional radiologist inserts a pigtail catheter into the abscess for sample collection, and the samples are sent to the microbiology laboratory for culture.
The radiology results indicate that the patient has what may be considered a complicated intra‐abdominal infection (diverticulitis with abscess), community‐acquired. Because empiric therapy is usually necessary for patients with complicated or even uncomplicated intra‐abdominal infections, the clinician should now be asking: What is optimal empiric antimicrobial therapy for this patient? Both prior75 and current guidelines76 for the management of intra‐abdominal infection indicate that antimicrobial therapy should be initiated when a patient receives such a diagnosis or when such an infection is considered likely. In making the determination of initial empiric therapy, the clinician should also be considering whether there is likely involvement of resistant Gram‐negative bacteria, and if so, how that would change the choice of antibiotic therapy.
Enteric Gram‐negative bacilli such as E coli and K pneumoniae are the most common microorganisms isolated from patients with intra‐abdominal infections, although Gram‐positive cocci (Staphylococcus or Streptococcus spp, and less commonly, enterococci) and obligate anaerobic organisms (particularly, Bacteroides fragilis) are also frequent components of intra‐abdominal infections.77 The relative frequency of bacterial pathogens shifts in patients who acquired their intra‐abdominal infection in the hospital versus community setting, with greater prevalence of Enterobacter, P aeruginosa, and Enterococcus spp, and less frequent isolation of E coli and streptococci.77 Recent results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) indicate a general increase in resistance among Gram‐negative bacilli isolated from patients with intra‐abdominal infections treated in medical centers, primarily due to acquisition of ESBLs.78, 79 This is true both in the United States79 and worldwide.78 Carbapenems continue to exhibit consistent activity against Gram‐negative bacilli isolated from intra‐abdominal infections, including ESBL‐producers.
Selection of initial empiric therapy should incorporate information from the literature and local antibiograms to determine the most likely causative pathogen(s), including ones with reduced susceptibility or resistance to commonly employed antibiotics. Then an antibiotic regimen should be selected that provides coverage of likely pathogens with minimal adverse events, including risk of collateral damage such as Clostridium difficile‐associated disease. Dose and dosing interval considerations are also important, particularly in patients with reduced renal or hepatic function. The general approach is to select an antibiotic or combination of antibiotic agents to provide coverage of the bacterial pathogens most commonly isolated from patients with intra‐abdominal infections, ie, aerobic/facultative anaerobic Gram‐negative bacilli, aerobic Gram‐positive cocci, and obligate anaerobic organisms.77 Table 4 presents the antibiotic treatment recommendations from the Surgical Infection Society and IDSA 2010 guidelines for management of patients with complicated intra‐abdominal infections.76 The guidelines are based on whether the patient has mild‐to‐moderate or high‐risk/severe community‐acquired complicated intra‐abdominal infections. Recommendations for the empiric treatment of hospital or healthcare‐associated complicated intra‐abdominal infections are largely based on local antibiogram (microbiologic) results, and include some similarities and differences compared with recommended treatment of high‐risk community‐acquired infections, as illustrated in Table 5.76 A patient with mild‐to‐moderate infection would be someone who does not require intensive care, and has community‐acquired intra‐abdominal infection due to secondary peritonitis. Severe intra‐abdominal infection would be defined by requiring intensive care, having sepsis, or having healthcare‐acquired peritonitis (such as a bowel leak following surgery). In line with these guidelines, and considering the case patient's risk profile, ciprofloxacin plus metronidazole was selected as initial empiric therapy, because she had not been hospitalized previously. Although she was hypotensive, the blood pressure was easily raised with fluids.
| Community‐Acquired Infection in Adults | ||
|---|---|---|
| Regimen | Mild‐to‐Moderate Severity* | High Risk or Severity |
| ||
| Single agent | Cefoxitin, ertapenem, moxifloxacin, tigecycline, and ticarcillin‐clavulanate | Imipenem‐cilastatin, meropenem, doripenem, and piperacillin‐tazobactam |
| Combination | Cefazolin, cefuroxime, ceftriaxone, cefotaxime, ciprofloxacin, or levofloxacin, each in combination with metronidazole | Cefepime, ceftazidime, ciprofloxacin, or levofloxacin, each in combination with metronidazole |
| Organisms Seen in the Hospital/Healthcare Infection at the Local Institution | Regimen | ||||
|---|---|---|---|---|---|
| Carbapenem* | Piperacillin‐Tazobactam | Ceftazidime or Cefepime + Metronidazole | Aminoglycoside | Vancomycin | |
| |||||
| 20% Resistant Pseudomonas aeruginosa, ESBL‐producing Enterobacteriaceae, Acinetobacter, or other multidrug‐resistant Gram‐negative bacteria | Recommended | Recommended | Recommended | Not recommended | Not recommended |
| ESBL‐producing Enterobacteriaceae | Recommended | Recommended | Not recommended | Recommended | Not recommended |
| P aeruginosa >20% resistant to ceftazidime | Recommended | Recommended | Not recommended | Recommended | Not recommended |
| Methicillin‐resistant Staphylococcus aureus | Not recommended | Not recommended | Not recommended | Not recommended | Recommended |
There are a number of controversies in intra‐abdominal sepsis management. These include whether or when initial empiric therapy should provide coverage of Enterococcus/vancomycin‐resistant enterococci or MRSA, when the regimen should include an antifungal to cover possible Candida spp infection, the role of resistant Bacteroides in intra‐abdominal infections, and when clinicians should be particularly concerned about ESBL‐producing or other resistant Gram‐negative bacteria. These topics are beyond the reach of the present article, but are and will continue to be important issues for clinicians to grapple with when selecting initial empiric therapy for patients with intra‐abdominal infections.
CASE 3: CENTRAL LINE‐ASSOCIATED BACTEREMIA
The third case is a 56‐year‐old man with epilepsy who presents to the emergency department with status epilepticus. Subsequent resuscitative efforts included intubation and placement of an internal jugular central line. The patient was admitted to the ICU, and aggressive treatment was initiated with repeated intravenous dosing of lorazepam and loading with fosphenytoin, which successfully broke the seizure. Subsequent imaging and laboratory tests failed to reveal any specific cause for the status epilepticus. The patient was extubated on day 4 and transferred out of the ICU. On day 5, he spiked a fever of 103.4F. He did not report any new symptoms, and there was no evidence of cough, sputum, shortness of breath, abdominal pain, diarrhea, or urinary symptoms. Physical examination revealed normal blood pressure (122/68 mmHg) and oxygen saturation (95% on room air), a normal respiratory rate (12 breaths per minute), clear lungs, no edema, no heart murmur, and normal neurologic findings. The patient's heart rate was somewhat high (102 bpm), and his temperature remained elevated (103.4F). Abdominal examination revealed no tenderness, and bowel sounds were present. Laboratory results were normal, except for an elevated WBC count (17,000/mm3 of blood). The chest X‐ray was clear.
This is an example of a patient with fever and leukocytosis of unknown origin. There are no focal findings indicative of a particular infection site or process. The patient was treated in the ICU, including use of a central catheter. Differential diagnosis of fever and leukocytosis without source, in a patient from the ICU with a central line, should consider catheter‐associated bacteremia; C difficile‐associated disease; a silent intra‐abdominal process, such as cholangitis or gangrenous cholecystitis; drug fever related to (in this patient) anticonvulsant therapy; urinary tract infection (no evidence for in this patient); or pulmonary embolism. The clinician needs to make a decision as to the relative benefits of empiric antibiotic or other antimicrobial treatment versus observation. If the patient is to be treated with an antibiotic, then a choice has to be made as to the best agent for the patient at hand.
In terms of the choice of antibiotics for a patient such as the one here, the clinician needs to assess the severity of illness and, when doing so, determine what infection site or sites should be covered, and the most likely sites of infection. A determination of likely pathogens also needs to be made. Cultures should be obtained prior to initiating therapy with a regimen providing broad coverage of the most likely pathogen(s), while allowing for the possibility of later de‐escalation based on clinical evaluation and culture results. This is similar to the situation for initial empiric treatment of pneumonia or intra‐abdominal infection. In general, the clinician should obtain blood, urine, and possibly sputum cultures to aid in future decision making. Furthermore, if the patient has diarrhea (which the current one does not), the clinician should obtain a stool for C difficile toxin analysis.
For the case illustrated here, the clinician determined catheter‐associated bacteremia was a strong possibility, and decided to initiate empiric therapy with vancomycin and piperacillin‐tazobactam to provide coverage of MRSA and resistant Gram‐negative bacteria. The most common causes of nosocomial or catheter‐associated bloodstream infections (BSIs) are coagulase‐negative staphylococci, S aureus, enterococci, and Candida spp,8082 but Gram‐negative bacilli like P aeruginosa, Klebsiella spp, and E coli (among others) are also frequently involved, particularly in patients with catheter‐associated BSIs.81 Moreover, significant and increasing percentages of Gram‐negative bacilli exhibit resistance to 1 or more antibiotic classes,8385 and >50% of S aureus are typically MRSA,82, 83, 85, 86 although there has been some decline in MRSA central line‐associated BSIs in US ICUs in recent years.87
Clinical practice guidelines from the IDSA recommend vancomycin (or daptomycin) for the management of MRSA bacteremia,88 while piperacillin‐tazobactam is frequently empirically added to Gram‐positive coverage for serious hospital‐acquired infections because of its broad activity against many pathogenic bacteria, including some ESBL‐producing Gram‐negative bacteria and P aeruginosa,89 which are significant causes of patient morbidity and mortality.36, 90 However, to be effective, both vancomycin and piperacillin‐tazobactam need to be properly dosed to maximize their pharmacodynamic properties. Guidelines from the American Society of Health‐System Pharmacists, IDSA, and Society of Infectious Diseases Pharmacists recommend vancomycin serum trough concentrations of 15‐20 mg/L for patients with bacteremia due to MRSA.91 These levels are recommended to improve penetration, increase the probability of obtaining optimal target serum concentrations, and improve clinical outcomes. To achieve these trough levels, the guidelines recommend doses of 15‐20 mg/kg of actual body weight given every 8‐12 hours for most patients with normal renal function, assuming a minimum inhibitory concentration (MIC) of 1 mg/L. In seriously ill patients, the guidelines recommend using a loading dose of 25‐30 mg/kg to facilitate rapid attainment of the target trough serum vancomycin level. (If the MIC is 2 mg/L, then the targeted pharmacodynamic parameter for vancomycin is unachievable, and an alternative therapy should be considered.)
The pharmacodynamic parameter that best predicts efficacy for ‐lactams like piperacillin is the duration of time that free drug concentrations remain above the MIC (T>MIC), with near maximal bactericidal effects for penicillins when the free drug concentrations remain above the MIC for 50% of the dosing interval.92 The target pharmacodynamic parameter for piperacillin‐tazobactam (50% T>MIC) may be better achieved with use of prolonged or extended infusion regimens than with intermittent, more rapidly infused, administration schedules. Lodise and coworkers recently reported that extended infusion (3.375 g intravenously [IV] for 4 hours every 8 hours) versus intermittent infusion of piperacillin‐tazobactam (3.375 g IV for 30 minutes every 4 to 6 hours) was associated with a significantly lower 14‐day mortality rate (12.2% vs 31.6%, P = 0.04) and median duration of hospital stay (21 vs 38 days, P = 0.02) in a cohort of hospitalized patients with a P aeruginosa infection.93 Based on data such as these, the case patient here was initiated on vancomycin (15‐20 mg/kg every 812 hours) and piperacillin‐tazobactam (3.375 g IV for 4 hours every 8 hours).
CONCLUSIONS
Successful treatment of patients with serious, life‐threatening hospital‐ or healthcare‐associated infections depends on early adequate antimicrobial treatment. To accomplish this, empiric therapy is typically employed with a broad‐spectrum regimen intended to cover likely causative pathogen(s) based on local antibiograms and risk factors for involvement of resistant microorganisms. Choice of empiric therapy should also be based on the site of infection, and make use of clinical practice guidelines, when available. Although this approach often means treatment with a regimen that is unnecessarily broad, based on subsequent culture findings, it is warranted based on the significant negative impact of initial inadequate/emnappropriate empiric therapy, and the inability to remedy this negative effect by later modification of antimicrobial therapy. The possibility of de‐escalating the initial broad‐spectrum regimen is revisited after the results from cultures collected prior to beginning empiric therapy become available, generally 2‐4 days after beginning the process. In this manner, both the dangers of initial inadequate empiric therapy and overuse or misuse of antimicrobials are minimized. To further minimize the risk of antimicrobial resistance linked to overuse or misuse of antimicrobial agents, care should be taken to avoid treatment of colonization or culture contamination.
Early appropriate antimicrobial therapy is necessary to minimize the morbidity and mortality associated with hospital‐ or healthcare‐associated infections (HAIs). A number of studies have demonstrated that delayed or inadequate antimicrobial therapy leads to worse clinical outcomes and higher healthcare costs.1, 2 Inadequate antimicrobial therapy can also promote or enhance the development of resistance,2 with potential wide‐ranging impact beyond the immediate patient under care. Because delaying treatment until availability of culture results decreases the likelihood of a successful outcome, patients with a suspected invasive HAI commonly receive empiric therapy with a regimen expected to cover the most likely causative pathogens. Based on characteristics of the patient and healthcare facility or unit, likely pathogens may include bacteria or other pathogens resistant to 1 or more antimicrobial drug classes. This article discusses the various processes and factors that need to be considered when choosing empiric antibiotics in the hospital or other healthcare setting, and uses 3 case studies dealing with pneumonia, intra‐abdominal infection, and bacteremia, respectively, to illustrate points of interest.
IMPORTANCE OF EARLY ADEQUATE ANTIBIOTIC USE
The initial selection and early deployment of adequate antimicrobial therapy is critical for successful resolution of HAIs. The terms inadequate and inappropriate antimicrobial therapy are commonly used interchangeably in the literature, and can be defined as use of antimicrobial treatment without (sufficient) activity against the identified pathogen.2 Using an antibiotic for a fungal infection would be inadequate, as would using a drug or dosing regimen that is ineffective against the identified bacterial species due to resistance or a failure to achieve the drug's pharmacokinetic/pharmacodynamic target for efficacy against the pathogen. The complete absence of antimicrobial therapy is also considered inadequate therapy. Some investigators consider inappropriate therapy a more general term that includes excessive treatment as well as inadequate treatment.1 Others reserve the term inappropriate for use of an antimicrobial without activity against the identified pathogen, and the term inadequate for use of an insufficient regimen, either in terms of optimal dose, route of administration, timeliness, or failure to use combination therapy when appropriate.3 However, many or most research articles do not make the distinction, and the current article does not make a distinction.
In addition, some articles arbitrarily define inadequate therapy as either use (or absence) of a treatment without activity against the identified pathogen or a delay in appropriate or adequate treatment, eg, no patient exposure to adequate treatment within 24 hours of hospital admission. It is important to recognize this when evaluating articles in the literature. Other studies separate inadequate and delayed therapy as variables. However, when dealing with empiric therapy, the adequacy of initial empiric therapy cannot be fully determined until subsequent possession of the tissue/blood culture results.
Inadequate Antibiotic Treatment
A 1999 study by Kollef et al. identified inadequate antimicrobial treatment as the most important independent predictor of hospital mortality, in a group of patients with a nosocomial or community‐acquired infection, while in the medical or surgical intensive care unit (ICU).4 Infection sites included in the study were lung, bloodstream, urinary tract, gastrointestinal (GI) tract, and wound. Various other studies have confirmed an association between inadequate antibiotic therapy and increased hospital mortality, and some demonstrated a relationship between inadequate antibiotic therapy and longer hospital or ICU stays57 and higher hospital‐related costs.8 More specifically, initial inappropriate antibiotic therapy has been associated with increased mortality in patients with healthcare‐associated9 or ventilator‐associated pneumonia (VAP)5, 7, 8, 1014 and those with bacteremia/sepsis.6, 10, 1524 Inadequate empiric therapy has also been linked with worsened outcomes,19, 2529 longer hospital stays,2527, 29 and increased healthcare costs25, 29 in patients with infections of the GI tract.
With respect to specific bacterial pathogens, inappropriate antibiotic therapy has been shown to increase risk of hospital mortality for patients with VAP or bacteremia caused by Pseudomonas aeruginosa,20, 30 extended‐spectrum ‐lactamase (ESBL)‐producing or multidrug‐resistant (MDR) Klebsiella pneumoniae or Escherichia coli,21, 31, 32 and methicillin‐resistant Staphylococcus aureus (MRSA).15, 23 In fact, infection with resistant bacteria, and particularly MDR bacteria, is a principal risk factor for inadequate initial antibiotic therapy.14, 16, 33, 34 A recent study by Teixeira and coworkers showed that inadequate therapy was more than twice as common for additional episodes of VAP caused by MDR pathogens as for those involving drug‐susceptible pathogens (56% vs 25.5%).14 Moreover, VAP caused by MDR pathogens was identified as a significant independent predictor of inadequate antimicrobial therapy (odds ratio [OR], 3.07; 95% confidence interval [CI], 1.29‐7.30; P = 0.01). Infections caused by drug‐resistant versus susceptible bacteria have generally been associated with increased morbidity, longer hospital or ICU stays, and higher costs.24, 3437 At least part of the reason for these worsened outcomes appears to be an increased likelihood that initial therapy is inadequate for the causative agent. Because of this, it is particularly important to consider the probability of infection with resistant bacteria when initiating empiric antibiotic therapy.
Delayed Antibiotic Treatment
In addition to inadequate initial therapy, a delay in the onset of adequate therapy has also been shown to have negative impact on outcome in patients with VAP, bacteremia, or intra‐abdominal infections.12, 13, 27, 38, 39 For example, Iregui et al. identified administration of initially delayed appropriate antibiotic treatment (treatment delayed for 24 hours after initial diagnosis of VAP) as a significant predictor of hospital mortality (OR, 7.68; 95% CI, 4.50‐13.09; P 0.001) in patients with VAP at a US teaching hospital.38 Similarly, Lodise et al. identified delayed antibiotic treatment as an independent predictor of infection‐related mortality in patients with hospital‐acquired S aureus bacteremia (OR, 3.8; 95% CI, 1.3‐11.0; P = 0.01).39 Delayed versus early antibiotic therapy was also associated with significantly longer hospital stay (20.2 vs 14.3 days, P = 0.05). Classification and regression tree analysis identified 44.75 hours from the initial positive blood culture result to appropriate therapy as the breakpoint between delayed and early treatment for bacteremia.
Of particular interest, evidence suggests that the negative impact of initial delay or initial use of inadequate therapy often cannot be remedied by subsequent treatment alterations. For example, Luna et al. reported a significantly lower hospital mortality rate for VAP patients who received early adequate antibiotic therapy compared with those who received early inadequate therapy (38% vs 91%, P 0.001).13 In this study, early treatment referred to drug administration prior to bronchoscopy, which was performed within 24 hours of clinical diagnosis of VAP. A subset of patients only received treatment after bronchoscopy, and the mortality rate for VAP‐positive patients who received adequate antibiotic therapy after this initial delay was similar to that for VAP‐positive patients who received inadequate therapy postbronchoscopy (71% vs 70%). In other words, the negative impact of an initial delay in adequate therapy could not be subsequently overcome by using adequate antibiotic therapy later in the disease process. Similarly, a recent study by Zilberberg et al. of healthcare‐associated pneumonia reported that the negative effect of initial inadequate antibiotic therapy on hospital mortality could not be mitigated by subsequent escalation of adequate antibiotic therapy after reception of culture results.9 Finally, a study of inadequate initial empiric antibiotic therapy of postoperative intra‐abdominal infection (peritonitis) also showed that adverse outcomes could not be abrogated by changes in antibiotic therapy based on culture results.27 Taken together, the results from these studies emphasize the importance of early adequate antibiotic therapy.
PRACTICAL GUIDELINES FOR CHOOSING EMPIRIC ANTIBIOTICS
When choosing initial empiric therapy for a suspected hospital‐ or healthcare‐related bacterial infection, it is first important to determine if the patient has received prior antibiotic therapy, and if the patient has, then the clinician should consider choosing an antibiotic from a different drug class. This is because prior antibiotic therapy increases risk of infection with a pathogen resistant to the initial antibiotic drug and other members of its class. Also, depending on the site of the infection and likely pathogenic bacteria, the clinician will need to decide whether to initiate empiric therapy with a single antibiotic or combination of agents. A number of patient‐ and institution‐related factors can be utilized by clinicians to better identify the likely pathogen responsible for the infection, and it is critical to use this information when selecting initial empiric therapy. Finally, as is true whenever choosing antimicrobial or other drug therapies, clinicians need to consider and weigh the safety/tolerability profile, potential for drugdrug interactions, and relative cost of different treatment options. These will vary for individual patients receiving the same drug or drug combination.
MINIMIZING ANTIMICROBIAL RESISTANCE IN THE HOSPITAL OR HEALTHCARE SETTING
It is also important to consider the potential for development of antibiotic resistance when choosing initial empiric therapy. The current paradigm for treatment of serious hospital or healthcare infections is to prescribe broad‐spectrum antimicrobial therapy upfront while awaiting culture results, and to de‐escalate (or terminate) therapy once culture results are available4042or as 2 authors recently put it, get it right the first time, hit hard up front, and use large doses of broad‐spectrum antibiotics for a short period.41 The initial empiric antibiotic regimen should have a high likelihood of covering the most likely causative pathogens, including resistant species or strains. Furthermore, emergence of resistance is minimized when the initial regimen effectively covers the most likely causative pathogens, and subsequent culture results are utilized to streamline or narrow the initial regimen, when possible.40, 42 Emergence of resistance is also minimized by using the shortest duration of treatment with maximal clinical effect. (These latter 2 points are discussed in greater detail in the Kaye and File articles in this supplement.)
Factoring in Institution‐ and Patient‐Specific Factors
Local antibiograms are useful in determining the most likely infection‐causing pathogens, within different wards of the hospital, and their susceptibility or resistance to various antibiotics. Local patterns of pathogen susceptibility and resistance can differ markedly from national averages, so local antibiograms are more useful than national or even regional surveillance data when making choices about the initial agent and dosing regimen for initial empiric therapy.43 Hospitals are required by the Joint Commission to create antibiograms on at least an annual basis, although more frequent antibiograms are particularly useful, given that susceptibility or resistance patterns change over time. It is also important that hospital microbiologists create antibiograms specifically for different hospital wards or departments, as well as hospital‐wide. The incidence and susceptibility of pathogenic bacteria has been shown to vary across different wards within a hospital, as well as within different regions of a given country.4446
Patient‐specific factors should also be considered in the decision‐making process for selection of initial empiric therapy for a suspected bacterial infection. Relevant patient characteristics or factors may differ somewhat when examining risk for particular types of infection (eg, healthcare/hospital‐acquired pneumonia, VAP, or bacteremia) or particular antibiotic‐resistant pathogens (eg, MRSA, ESBL‐producing E coli or Klebsiella spp, P aeruginosa and MDR P aeruginosa, and carbapenem‐resistant Acinetobacter baumannii). Nonetheless, several risk factors appear to generally increase risk of infection with a resistant pathogen across these subcategories, including prior antibiotic treatment (with agents sometimes varying depending on the particular pathogen of interest); recent hospital admission or residence in a nursing home or extended‐care facility; prolonged hospital stay (particularly in the ICU); prior colonization with the pathogen; presence of an indwelling catheter (central venous, arterial, or urinary); and mechanical ventilation; among others.2, 47, 48 Patients who are immunocompromised, either due to their condition or immunosuppressive therapy, are also generally at increased risk of infection with resistant bacteria.47
Patient age and presence of comorbidities can also affect initial selection of empiric therapy. Cell‐mediated immunity tends to decline with age, and elderly individuals are also more likely to have conditions or comorbidities associated with diminished host immunity, both of which may contribute to increased susceptibility to infection and infection involving resistant bacteria.49 Furthermore, elderly individuals are more likely to have decline in renal or hepatic function or other physiologic changes that can alter drug pharmacokinetics and pharmacodynamics,50 and these factors need to be considered when selecting an initial empiric therapy regimen that covers likely pathogens, without increasing risk of drug toxicity. In addition, the increased number of comorbidities in elderly patients typically translates into polypharmacy, with potential for drugdrug interactions that need to be weighed when selecting initial empiric therapy.
Treat Infection, Not Contamination or Colonization
It is important to limit antimicrobial use to treatment of actual infections, and not for treatment of colonization or contamination. Treatment of colonization is a significant source of antimicrobial overuse. Hence, it is important that healthcare teams take appropriate steps to ensure they are treating pneumonia, bacteremia, or a urinary tract infection, not colonization of the tracheal aspirate, catheter tip or hub, or indwelling urinary catheter that is unassociated with actual infection. Strategies to employ when considering how to differentiate between true infection and colonization include using Gram stain in sputum specimens to look for evidence of polymorphonuclear leukocytes (inflammation), understanding that certain organisms, such as Enterococcus and Candida are not respiratory pathogens, recognizing that urinary catheters may be colonized in the absence of infection, and remaining vigilant regarding blood culture contamination. Since antibiotic use is generally linked to increased risk of resistance,51, 52 antibiotics should only be used when there is a clear clinical benefit associated with their use; treatment of colonization does not fit this description. When in doubt, an infectious diseases (ID) specialist consultation is recommended.
Similarly, overuse/misuse of antibiotics that occurs due to false‐positive culture results also increases development of resistance in hospitalized patients. In particular, contamination of blood cultures is relatively common in hospitalized patients, particularly in hospital emergency rooms,53 and frequently results in administration of antibiotics to treat an apparent infection that actually represents a contaminated culture. Antimicrobial treatment due to false‐positive blood culture results has been associated with prolonged hospitalization and elevated laboratory and hospital costs,54, 55 and provides an environment for development of antimicrobial resistance. Contamination of blood cultures often occurs at the point of blood collection via venipuncture or through indwelling catheters,56, 57 but can occur later in the process during laboratory handling or processing of specimens.58 Hence, it is important to use proper antisepsis when collecting blood or other cultures, to make sure it is blood and not skin or the catheter hub that is being cultured, and to make sure to use proper methods when processing all cultures.
Consult Infectious Diseases Experts
The 2007 guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America (IDSA/SHEA) for the development of institutional antimicrobial stewardship programs recommend inclusion of an ID physician and a clinical pharmacist with ID training as core members of a multidisciplinary antimicrobial stewardship team.59 Consultation with an ID expert or inclusion of an ID specialist into an institutional antimicrobial stewardship program has been shown to improve antibiotic usage and reduce morbidity and mortality, length of hospital stay, healthcare costs, and resistance.6064 In hospitals without easy access to an ID specialist, hospitalists with ID training may be able to fulfill the role provided by ID physicians or clinical pharmacists with ID training.
CASE 1: HEALTHCARE‐ASSOCIATED PNEUMONIA
Table 1 provides the key initial data for Case 1. The patient has a history of hypertension, congestive heart failure (CHF), and myocardial infarction (MI), and is receiving medications consistent with such a history. In terms of her acute presentation, cough, fever, chills, dyspnea, lung crackles (rales), X‐ray evidence of lung infiltrate, reduced oxygen saturation, elevated white blood cell (WBC) count, and increased percentage of WBC bands are all consistent with a diagnosis of pneumonia of relatively recent origin. Progressive worsening of symptoms within the previous 36 hours is also consistent with infection of recent origin. There are no neurologic symptoms, and cardiac function appears relatively normal, with no evidence of MI or cardiac arrhythmia based on electrocardiogram or heart rate, although there is evidence of continuing hypertension and perhaps CHF.
| |
| History | A 72‐yr‐old woman recently hospitalized for congestive heart failure (CHF), returns to the emergency department from rehab with cough, fever, chills, shortness of breath, all progressively worsening over the past 36 hr |
| Past history of CHF (ejection fraction 44%), myocardial infarction 2 yr ago, hypertension, past smoking | |
| Medications: metoprolol 50 mg BID; furosemide 40 mg daily; aspirin 81 mg daily; enalapril 20 mg daily | |
| Physical | Vitals: BP 148/88, P 82, RR 16, T 101.7, O2 sat 92% on room air |
| Heart: S1, S2 no murmurs | |
| Lungs: crackles at R lung base | |
| Abdomen: bowel sounds present, non‐tender | |
| Extremities: trace edema bilaterally | |
| Neurologic: no focal findings | |
| Labs | EKG: NSR, no acute ST‐T changes |
| Chemistry, hemoglobin, platelets, within normal limits | |
| WBC: 14,700/mm3, 10% bands | |
| Cardiac enzymes negative | |
| ‐Natriuretic peptide within normal limits for age | |
| Chest X‐ray: right lower lung infiltrate | |
Given the patient's history of recent hospitalization, the clinician should consider that the pneumonia is most likely hospital‐ or healthcare‐acquired. Because she was described as developing the problem while in rehabilitation, it can be assumed that hospitalization occurred relatively recently. Hospital‐acquired pneumonia (HAP) is defined as pneumonia that occurs within 48 hours of hospital admission, and that was not incubating at the time of admission.47, 65 HAP accounts for approximately of 15% of all nosocomial/hospital‐acquired infections in the United States and up to 27% in the ICU,65, 66 and is a frequent cause of morbidity and mortality in this setting.65 In addition to hospitalization, other characteristics or risk factors for HAP include severe illness, hemodynamic compromise, depressed immune function, use of nasogastric tubes, and mechanical ventilation for the important subset of HAP patients with VAP.65 VAP is more precisely defined as HAP that arises >48‐72 hours after endotracheal intubation.47
Healthcare‐associated pneumonia (HCAP) is a more recently defined category that includes patients with HAP and VAP, and is characterized by hospitalization for 2 days in the preceding 90 days, or residence in a nursing home or extended‐care facility.47, 67, 68 Additional risk factors for HCAP include intravenous therapy at home (including antibiotics); intravenous chemotherapy or wound care within 30 days of the current infection; and recent attendance at a hospital or hemodialysis clinic.47 Most HAP or HCAP data have been derived from patients with VAP, and the 2005 American Thoracic Society (ATS)/IDSA guidelines for management of HAP, VAP, and HCAP recommend similar approaches for the initial treatment of patients with nonintubated HAP, VAP, and HCAP.47 There are general similarities between these 3 disease categories with respect to etiology, epidemiology of likely pathogens, and prognosis, and important differences compared with community‐acquired pneumonia (CAP), which in turn gives rise to different treatment strategies for HAP/VAP/HCAP and CAP.
Given an initial diagnosis of HAP or HCAP, the clinician should be considering the following questions: 1) What are the appropriate choices of antimicrobials? 2) What are the clinical parameters that should alert one to resistant organisms? 3) What are the appropriate cultures to order? 4) What is the role of Gram stain, if any?
Selection of Initial Empiric Therapy for Likely Pathogens
HAP is usually caused by bacterial pathogens, and much more rarely involves viruses or fungi in immunocompetent patients. Therefore, from the start, the focus should be on empiric therapy with an antibiotic or combination of antibiotics that has a high probability of covering the most likely pathogens. Empiric therapy is warranted because of the risk of mortality or other negative consequences when antibiotic therapy is delayed, particularly in an aged patient with a chronic illness like CHF (such as the case study here). Clues as to likely pathogensand hence most appropriate antibiotic regimencan be discerned by looking at the onset of HAP/VAP (early vs late) and whether the patient has risk factors for infection with a MDR or antibiotic‐susceptible bacterial pathogen. A significant proportion of patients with HAP, VAP, or HCAP are infected with MDR pathogens, and identifying these patients and providing them with appropriate broad‐spectrum empiric therapy is a key to successful management.
Early‐onset HAP/VAP (occurring 5 days after hospitalization) is more likely to be due to antibiotic‐sensitive bacteria than late‐onset HAP/VAP (occurring 5 days after hospitalization), which often occurs due to MDR species.47, 69, 70 Not surprisingly, risk of inappropriate initial antibiotic therapy14 is higher, and mortality is also higher in patients with late‐onset HAP/VAP.47, 71 Patients with early‐onset HAP/VAP who have received prior antibiotics or been hospitalized within the past 90 days are also at risk for infection due to MDR bacteria, and hence should be treated the same as patients with late‐onset HAP/VAP.47 Additional risk factors for infection with MDR pathogens include antimicrobial therapy in the preceding 90 days (particularly with broad‐spectrum agents), current hospitalization 5 days, high prevalence of antibiotic resistance in the specific hospital unit, immunosuppression, and presence of risk factors for HCAP (hospitalization 2 days in the preceding 90 days, residence in a nursing home or extended‐care facility, home infusion therapy, chronic dialysis within 30 days, home wound care, or family member with MDR pathogen).47 For VAP patients, duration of ventilator support 7 days is an additional risk factor for infection with a MDR pathogen.70, 72 A second episode of VAP is more likely to be due either to MRSA or P aeruginosa; therefore, these organisms need to be considered when selecting initial empiric therapy.
The most common bacterial causes of HAP, VAP, or HCAP include aerobic Gram‐negative bacilli, such as P aeruginosa, Acinetobacter spp, and Enterobacteriaceae (eg, K pneumoniae, E coli, Enterobacter spp), and Gram‐positive cocci, such as S aureus and Streptococcus pneumoniae.47, 73 MDR bacterial species are more likely when certain risk factors are present, and the ATS/IDSA guidelines recommend using a risk‐stratification process when selecting empiric antibiotic therapy for patients with suspected HAP, VAP, or HCAP.47 The guidelines also emphasize that local conditions can greatly impact whether a patient is infected with an antibiotic‐sensitive or antibiotic‐resistant species, regardless of other risk factors, thereby highlighting the importance of using recent hospital and hospital unit‐specific antibiograms when stratifying a patient based on risk.
Other guiding principles of initial empiric treatment, as outlined in the ATS/IDSA guidelines, include not delaying therapy while awaiting culture results and administration of therapy as soon as possible following diagnosis; making sure the dosing regimen as well as drug selection is appropriate/adequate for the patient and suspected pathogen; and using a different class of antibiotic for patients with prior antibiotic exposure.47 The guidelines further indicate that combination therapy is appropriate initial therapy in patients at high risk for infection with MDR bacteria, and that for patients receiving combination therapy including an aminoglycoside, the aminoglycoside can be stopped after 5‐7 days in responding patients. Table 2 highlights ATS/IDSA recommendations for initial empiric antibiotic therapy in patients with suspected HAP/VAP who have early‐onset disease and no risk factors for MDR pathogens.47 Table 3 highlights recommendations for initial empiric antibiotic therapy in patients with suspected HAP/VAP/HCAP who have late‐onset disease and/or risk factors for MDR pathogens.47
| Potential Pathogen | Recommended Antibiotic |
|---|---|
| |
| Streptococcus pneumoniae* | |
| Haemophilus influenzae | Ceftriaxone |
| Methicillin‐sensitive Staphylococcus aureus | or |
| Antibiotic‐sensitive enteric Gram‐negative bacilli | Levofloxacin, moxifloxacin, or ciprofloxacin |
| Escherichia coli | or |
| Klebsiella pneumoniae | Ampicillin/sulbactam |
| Enterobacter spp | or |
| Proteus spp | Ertapenem |
| Serratia marcescens | |
| Potential Pathogen | Combination Antibiotic Therapy |
|---|---|
| |
| Pathogens listed in Table 2, plus MDR pathogens | Antipseudomonal cephalosporin (cefepime, ceftazidime) |
| Pseudomonas aeruginosa | or |
| Klebsiella pneumoniae (ESBL‐positive)* | Antipseudomonal carbapenem (imipenem or meropenem) |
| Acinetobacter spp* | or |
| ‐Lactam/‐lactamase inhibitor (piperacillin‐tazobactam) | |
| plus | |
| Antipseudomonal fluoroquinolone* (ciprofloxacin or levofloxacin) | |
| or | |
| Aminoglycoside (amikacin, gentamicin, or tobramycin) | |
| plus | |
| Methicillin‐resistant Staphylococcus aureus (MRSA) | Linezolid or vancomycin |
| Legionella pneumophila* | |
Returning to Case 1, given a clinical diagnosis of HAP/HCAP and the patient's heightened risk for infection with MRSA or resistant Gram‐negative bacteria, she was initiated on a regimen consisting of piperacillin/tazobactam plus vancomycin and ciprofloxacin. The choice of 3 agents is consistent with ATS and IDSA guidelines to cover the potential for an ESBL‐producer or Acinetobacter, or Pseudomonas. Individual choices should be dictated by one's own institutional antibiogram or some knowledge of the rehabilitation facility from which the patient was transferred.
Guiding Principles for Culture Management
Culture collection and management plays an important role in diagnosis and subsequent treatment of HAP/VAP or HCAP. As outlined in the ATS/IDSA guidelines, patient management typically proceeds using either a clinical strategy or bacteriologic strategy, or a combination thereof.47 The clinical strategy makes use of cultures of endotracheal aspirates or sputum, with initial microscopic examination and Gram staining to identify bacterial growth and guide initiation of empiric antibiotic therapy. Cultures should always be performed before instituting antibiotic therapy. Microorganism growth is described as light, moderate, or heavy by microbiology laboratories using semiquantitative analysis. Gram staining should be performed only if the specimen is of good quality; most microbiology laboratories will do screening tests to ensure they are of good quality, or else will reject the specimen. When correlated with culture results, Gram staining can improve diagnostic accuracy.74
The bacteriologic strategy uses quantitative means to analyze and describe cultures of lower respiratory secretions or specimens obtained via endotracheal aspirates, mini‐bronchoalveolar lavage specimens (mini‐BAL), bronchoalveolar lavage, or protected‐specimen bronchial brushing, collected with or without a bronchoscope, ie, with or without invasive techniques. Hence, whereas the clinical strategy uses noninvasive tracheal aspirates to culture microorganisms for analysis, the bacteriologic strategy often employs a relatively noninvasive strategy like a mini‐BAL, or invasive (bronchoscopic) lower respiratory tract samples for quantitative culture analysis. Diagnosis of HAP/VAP or HCAP, and determination of the causative microorganism(s), requires growth above a certain threshold when using the semi‐quantitative analysis. The clinical approach is more sensitive, but can result in overtreatment, while the bacteriologic strategy is associated with risk of undertreatment due to false‐negative culture results. On the other hand, quantitative cultures increase the specificity of diagnosis.
CASE 2: INTRA‐ABDOMINAL INFECTION (DIVERTICULITIS)
Case 2 is a 56‐year‐old woman with no past medical history of note, who presented to her physician about 3 days ago, after 5 days of abdominal pain and fever (101.7F). She had an outpatient computed tomography (CT) scan, and the results suggested diverticulitis. After the CT scan, she was given amoxicillin/clavulanate. She now presents to the emergency department (3 days later) with worsening pain, fever, and severe weakness. A physical exam shows low blood pressure (84/58 mmHg) and tachycardia (132 bpm). Her respiratory rate is 22 breaths per minute. Oxygenation (O2 saturation 99% on room air) is normal, and the patient's lungs are clear. Abdominal examination reveals bowel sounds and diffuse tenderness, particularly at the left lower quadrant, and there is evidence of guarding and rebound. Her blood chemistry is generally normal, although the WBC count is elevated (15,200/mm3). No abnormalities are evident on chest X‐ray. The patient's blood pressure increases to 96/64 mmHg after she is infused with 2 liters of normal saline. She undergoes another CT scan and is admitted to the ICU. The CT scan shows diverticulitis with abscess and walled‐off perforation. An interventional radiologist inserts a pigtail catheter into the abscess for sample collection, and the samples are sent to the microbiology laboratory for culture.
The radiology results indicate that the patient has what may be considered a complicated intra‐abdominal infection (diverticulitis with abscess), community‐acquired. Because empiric therapy is usually necessary for patients with complicated or even uncomplicated intra‐abdominal infections, the clinician should now be asking: What is optimal empiric antimicrobial therapy for this patient? Both prior75 and current guidelines76 for the management of intra‐abdominal infection indicate that antimicrobial therapy should be initiated when a patient receives such a diagnosis or when such an infection is considered likely. In making the determination of initial empiric therapy, the clinician should also be considering whether there is likely involvement of resistant Gram‐negative bacteria, and if so, how that would change the choice of antibiotic therapy.
Enteric Gram‐negative bacilli such as E coli and K pneumoniae are the most common microorganisms isolated from patients with intra‐abdominal infections, although Gram‐positive cocci (Staphylococcus or Streptococcus spp, and less commonly, enterococci) and obligate anaerobic organisms (particularly, Bacteroides fragilis) are also frequent components of intra‐abdominal infections.77 The relative frequency of bacterial pathogens shifts in patients who acquired their intra‐abdominal infection in the hospital versus community setting, with greater prevalence of Enterobacter, P aeruginosa, and Enterococcus spp, and less frequent isolation of E coli and streptococci.77 Recent results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) indicate a general increase in resistance among Gram‐negative bacilli isolated from patients with intra‐abdominal infections treated in medical centers, primarily due to acquisition of ESBLs.78, 79 This is true both in the United States79 and worldwide.78 Carbapenems continue to exhibit consistent activity against Gram‐negative bacilli isolated from intra‐abdominal infections, including ESBL‐producers.
Selection of initial empiric therapy should incorporate information from the literature and local antibiograms to determine the most likely causative pathogen(s), including ones with reduced susceptibility or resistance to commonly employed antibiotics. Then an antibiotic regimen should be selected that provides coverage of likely pathogens with minimal adverse events, including risk of collateral damage such as Clostridium difficile‐associated disease. Dose and dosing interval considerations are also important, particularly in patients with reduced renal or hepatic function. The general approach is to select an antibiotic or combination of antibiotic agents to provide coverage of the bacterial pathogens most commonly isolated from patients with intra‐abdominal infections, ie, aerobic/facultative anaerobic Gram‐negative bacilli, aerobic Gram‐positive cocci, and obligate anaerobic organisms.77 Table 4 presents the antibiotic treatment recommendations from the Surgical Infection Society and IDSA 2010 guidelines for management of patients with complicated intra‐abdominal infections.76 The guidelines are based on whether the patient has mild‐to‐moderate or high‐risk/severe community‐acquired complicated intra‐abdominal infections. Recommendations for the empiric treatment of hospital or healthcare‐associated complicated intra‐abdominal infections are largely based on local antibiogram (microbiologic) results, and include some similarities and differences compared with recommended treatment of high‐risk community‐acquired infections, as illustrated in Table 5.76 A patient with mild‐to‐moderate infection would be someone who does not require intensive care, and has community‐acquired intra‐abdominal infection due to secondary peritonitis. Severe intra‐abdominal infection would be defined by requiring intensive care, having sepsis, or having healthcare‐acquired peritonitis (such as a bowel leak following surgery). In line with these guidelines, and considering the case patient's risk profile, ciprofloxacin plus metronidazole was selected as initial empiric therapy, because she had not been hospitalized previously. Although she was hypotensive, the blood pressure was easily raised with fluids.
| Community‐Acquired Infection in Adults | ||
|---|---|---|
| Regimen | Mild‐to‐Moderate Severity* | High Risk or Severity |
| ||
| Single agent | Cefoxitin, ertapenem, moxifloxacin, tigecycline, and ticarcillin‐clavulanate | Imipenem‐cilastatin, meropenem, doripenem, and piperacillin‐tazobactam |
| Combination | Cefazolin, cefuroxime, ceftriaxone, cefotaxime, ciprofloxacin, or levofloxacin, each in combination with metronidazole | Cefepime, ceftazidime, ciprofloxacin, or levofloxacin, each in combination with metronidazole |
| Organisms Seen in the Hospital/Healthcare Infection at the Local Institution | Regimen | ||||
|---|---|---|---|---|---|
| Carbapenem* | Piperacillin‐Tazobactam | Ceftazidime or Cefepime + Metronidazole | Aminoglycoside | Vancomycin | |
| |||||
| 20% Resistant Pseudomonas aeruginosa, ESBL‐producing Enterobacteriaceae, Acinetobacter, or other multidrug‐resistant Gram‐negative bacteria | Recommended | Recommended | Recommended | Not recommended | Not recommended |
| ESBL‐producing Enterobacteriaceae | Recommended | Recommended | Not recommended | Recommended | Not recommended |
| P aeruginosa >20% resistant to ceftazidime | Recommended | Recommended | Not recommended | Recommended | Not recommended |
| Methicillin‐resistant Staphylococcus aureus | Not recommended | Not recommended | Not recommended | Not recommended | Recommended |
There are a number of controversies in intra‐abdominal sepsis management. These include whether or when initial empiric therapy should provide coverage of Enterococcus/vancomycin‐resistant enterococci or MRSA, when the regimen should include an antifungal to cover possible Candida spp infection, the role of resistant Bacteroides in intra‐abdominal infections, and when clinicians should be particularly concerned about ESBL‐producing or other resistant Gram‐negative bacteria. These topics are beyond the reach of the present article, but are and will continue to be important issues for clinicians to grapple with when selecting initial empiric therapy for patients with intra‐abdominal infections.
CASE 3: CENTRAL LINE‐ASSOCIATED BACTEREMIA
The third case is a 56‐year‐old man with epilepsy who presents to the emergency department with status epilepticus. Subsequent resuscitative efforts included intubation and placement of an internal jugular central line. The patient was admitted to the ICU, and aggressive treatment was initiated with repeated intravenous dosing of lorazepam and loading with fosphenytoin, which successfully broke the seizure. Subsequent imaging and laboratory tests failed to reveal any specific cause for the status epilepticus. The patient was extubated on day 4 and transferred out of the ICU. On day 5, he spiked a fever of 103.4F. He did not report any new symptoms, and there was no evidence of cough, sputum, shortness of breath, abdominal pain, diarrhea, or urinary symptoms. Physical examination revealed normal blood pressure (122/68 mmHg) and oxygen saturation (95% on room air), a normal respiratory rate (12 breaths per minute), clear lungs, no edema, no heart murmur, and normal neurologic findings. The patient's heart rate was somewhat high (102 bpm), and his temperature remained elevated (103.4F). Abdominal examination revealed no tenderness, and bowel sounds were present. Laboratory results were normal, except for an elevated WBC count (17,000/mm3 of blood). The chest X‐ray was clear.
This is an example of a patient with fever and leukocytosis of unknown origin. There are no focal findings indicative of a particular infection site or process. The patient was treated in the ICU, including use of a central catheter. Differential diagnosis of fever and leukocytosis without source, in a patient from the ICU with a central line, should consider catheter‐associated bacteremia; C difficile‐associated disease; a silent intra‐abdominal process, such as cholangitis or gangrenous cholecystitis; drug fever related to (in this patient) anticonvulsant therapy; urinary tract infection (no evidence for in this patient); or pulmonary embolism. The clinician needs to make a decision as to the relative benefits of empiric antibiotic or other antimicrobial treatment versus observation. If the patient is to be treated with an antibiotic, then a choice has to be made as to the best agent for the patient at hand.
In terms of the choice of antibiotics for a patient such as the one here, the clinician needs to assess the severity of illness and, when doing so, determine what infection site or sites should be covered, and the most likely sites of infection. A determination of likely pathogens also needs to be made. Cultures should be obtained prior to initiating therapy with a regimen providing broad coverage of the most likely pathogen(s), while allowing for the possibility of later de‐escalation based on clinical evaluation and culture results. This is similar to the situation for initial empiric treatment of pneumonia or intra‐abdominal infection. In general, the clinician should obtain blood, urine, and possibly sputum cultures to aid in future decision making. Furthermore, if the patient has diarrhea (which the current one does not), the clinician should obtain a stool for C difficile toxin analysis.
For the case illustrated here, the clinician determined catheter‐associated bacteremia was a strong possibility, and decided to initiate empiric therapy with vancomycin and piperacillin‐tazobactam to provide coverage of MRSA and resistant Gram‐negative bacteria. The most common causes of nosocomial or catheter‐associated bloodstream infections (BSIs) are coagulase‐negative staphylococci, S aureus, enterococci, and Candida spp,8082 but Gram‐negative bacilli like P aeruginosa, Klebsiella spp, and E coli (among others) are also frequently involved, particularly in patients with catheter‐associated BSIs.81 Moreover, significant and increasing percentages of Gram‐negative bacilli exhibit resistance to 1 or more antibiotic classes,8385 and >50% of S aureus are typically MRSA,82, 83, 85, 86 although there has been some decline in MRSA central line‐associated BSIs in US ICUs in recent years.87
Clinical practice guidelines from the IDSA recommend vancomycin (or daptomycin) for the management of MRSA bacteremia,88 while piperacillin‐tazobactam is frequently empirically added to Gram‐positive coverage for serious hospital‐acquired infections because of its broad activity against many pathogenic bacteria, including some ESBL‐producing Gram‐negative bacteria and P aeruginosa,89 which are significant causes of patient morbidity and mortality.36, 90 However, to be effective, both vancomycin and piperacillin‐tazobactam need to be properly dosed to maximize their pharmacodynamic properties. Guidelines from the American Society of Health‐System Pharmacists, IDSA, and Society of Infectious Diseases Pharmacists recommend vancomycin serum trough concentrations of 15‐20 mg/L for patients with bacteremia due to MRSA.91 These levels are recommended to improve penetration, increase the probability of obtaining optimal target serum concentrations, and improve clinical outcomes. To achieve these trough levels, the guidelines recommend doses of 15‐20 mg/kg of actual body weight given every 8‐12 hours for most patients with normal renal function, assuming a minimum inhibitory concentration (MIC) of 1 mg/L. In seriously ill patients, the guidelines recommend using a loading dose of 25‐30 mg/kg to facilitate rapid attainment of the target trough serum vancomycin level. (If the MIC is 2 mg/L, then the targeted pharmacodynamic parameter for vancomycin is unachievable, and an alternative therapy should be considered.)
The pharmacodynamic parameter that best predicts efficacy for ‐lactams like piperacillin is the duration of time that free drug concentrations remain above the MIC (T>MIC), with near maximal bactericidal effects for penicillins when the free drug concentrations remain above the MIC for 50% of the dosing interval.92 The target pharmacodynamic parameter for piperacillin‐tazobactam (50% T>MIC) may be better achieved with use of prolonged or extended infusion regimens than with intermittent, more rapidly infused, administration schedules. Lodise and coworkers recently reported that extended infusion (3.375 g intravenously [IV] for 4 hours every 8 hours) versus intermittent infusion of piperacillin‐tazobactam (3.375 g IV for 30 minutes every 4 to 6 hours) was associated with a significantly lower 14‐day mortality rate (12.2% vs 31.6%, P = 0.04) and median duration of hospital stay (21 vs 38 days, P = 0.02) in a cohort of hospitalized patients with a P aeruginosa infection.93 Based on data such as these, the case patient here was initiated on vancomycin (15‐20 mg/kg every 812 hours) and piperacillin‐tazobactam (3.375 g IV for 4 hours every 8 hours).
CONCLUSIONS
Successful treatment of patients with serious, life‐threatening hospital‐ or healthcare‐associated infections depends on early adequate antimicrobial treatment. To accomplish this, empiric therapy is typically employed with a broad‐spectrum regimen intended to cover likely causative pathogen(s) based on local antibiograms and risk factors for involvement of resistant microorganisms. Choice of empiric therapy should also be based on the site of infection, and make use of clinical practice guidelines, when available. Although this approach often means treatment with a regimen that is unnecessarily broad, based on subsequent culture findings, it is warranted based on the significant negative impact of initial inadequate/emnappropriate empiric therapy, and the inability to remedy this negative effect by later modification of antimicrobial therapy. The possibility of de‐escalating the initial broad‐spectrum regimen is revisited after the results from cultures collected prior to beginning empiric therapy become available, generally 2‐4 days after beginning the process. In this manner, both the dangers of initial inadequate empiric therapy and overuse or misuse of antimicrobials are minimized. To further minimize the risk of antimicrobial resistance linked to overuse or misuse of antimicrobial agents, care should be taken to avoid treatment of colonization or culture contamination.
- ,.Appropriate vs. inappropriate antimicrobial therapy.Clin Microbiol Infect.2008;14(suppl 3):15–21.
- .Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients.Clin Infect Dis.2000;31(suppl 4):S131–S138.
- .Treatment options for nosocomial pneumonia due to MRSA.J Infect.2009;59(suppl 1):S25–S31.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,,.Impact of appropriateness of initial antibiotic therapy on the outcome of ventilator‐associated pneumonia.Intensive Care Med.2001;27:355–362.
- ,,, et al.Mortality and morbidity attributable to inadequate empirical antimicrobial therapy in patients admitted to the ICU with sepsis: a matched cohort study.J Antimicrob Chemother.2008;61:436–441.
- ,,,,,.Effect from multiple episodes of inadequate empiric antibiotic therapy for ventilator‐associated pneumonia on morbidity and mortality among critically ill trauma patients.J Trauma.2005;58:94–101.
- ,,,,,.Predictors of 30‐day mortality and hospital costs in patients with ventilator‐associated pneumonia attributed to potentially antibiotic‐resistant gram‐negative bacteria.Chest.2008;134:281–287.
- ,,,,.Antimicrobial therapy escalation and hospital mortality among patients with health‐care‐associated pneumonia: a single‐center experience.Chest.2008;134:963–968.
- ,,.Impact of inappropriate antibiotic therapy on mortality in patients with ventilator‐associated pneumonia and blood stream infection: a meta‐analysis.J Crit Care.2008;23:91–100.
- ,,, et al.Ventilator‐associated pneumonia: breaking the vicious circle of antibiotic overuse.Crit Care Med.2007;35:379–385; quiz 386.
- ,,, et al.Appropriateness and delay to initiate therapy in ventilator‐associated pneumonia.Eur Respir J.2006;27:158–164.
- ,,, et al.Impact of BAL data on the therapy and outcome of ventilator‐associated pneumonia.Chest.1997;111:676–685.
- ,,,,.Inadequate treatment of ventilator‐associated pneumonia: risk factors and impact on outcomes.J Hosp Infect.2007;65:361–367.
- ,,, et al.Predictors of mortality in patients with methicillin‐resistant Staphylococcus aureus (MRSA) bacteraemia: the role of empiric antibiotic therapy.Eur J Clin Microbiol Infect Dis.2007;26:239–245.
- ,,,,,.Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med.2003;115:529–535.
- ,,,,.The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting.Chest.2000;118:146–155.
- ,,, et al.Bloodstream infections caused by antibiotic‐resistant gram‐negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome.Antimicrob Agents Chemother.2005;49:760–766.
- ,,,,,.The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection.J Intern Med.1998;244:379–386.
- ,,,,,.Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment.Antimicrob Agents Chemother.2005;49:1306–1311.
- ,,, et al.Antibiotic therapy for Klebsiella pneumoniae bacteremia: implications of production of extended‐spectrum beta‐lactamases.Clin Infect Dis.2004;39:31–37.
- ,,, et al.Impact of inappropriate empirical therapy for sepsis due to health care‐associated methicillin‐resistant Staphylococcus aureus.J Infect.2009;58:131–137.
- ,,, et al.Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46:193–200.
- ,,, et al.Multidrug‐resistant Pseudomonas aeruginosa bloodstream infections: risk factors and mortality.Epidemiol Infect.2011; Jan 13:1–10.
- ,,,,,.Economic consequences of failure of initial antibiotic therapy in hospitalized adults with complicated intra‐abdominal infections.Surg Infect (Larchmt).2008;9:335–347.
- ,,, et al.Effect of inappropriate initial empiric antibiotic therapy on outcome of patients with community‐acquired intra‐abdominal infections requiring surgery.Eur J Clin Microbiol Infect Dis.2004;23:682–687.
- ,,,,,.Emergence of antibiotic‐resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy.Clin Infect Dis.1996;23:486–494.
- ,,, et al.Antibiotic treatment for surgical peritonitis.Ann Surg.1991;214:543–549.
- ,,, et al.Inappropriate initial treatment of secondary intra‐abdominal infections leads to increased risk of clinical failure and costs.Br J Clin Pharmacol.2005;60:438–443.
- ,,, et al.Optimal management therapy for Pseudomonas aeruginosa ventilator‐associated pneumonia: an observational, multicenter study comparing monotherapy with combination antibiotic therapy.Crit Care Med.2007;35:1888–1895.
- ,,,,,.Risk factors for and outcomes of healthcare‐associated infection due to extended‐spectrum beta‐lactamase‐producing Escherichia coli or Klebsiella pneumoniae in Thailand.Infect Control Hosp Epidemiol.2007;28:873–876.
- ,,, et al.Impact of antibiotic resistance and of adequate empirical antibiotic treatment in the prognosis of patients with Escherichia coli bacteraemia.J Antimicrob Chemother.2007;60:855–863.
- .Predicting methicillin resistance and the effect of inadequate empiric therapy on survival in patients with Staphylococcus aureus bacteremia.Arch Intern Med.2000;160:1001–1004.
- ,,,,,.Impact of multiresistance of gram‐negative bacteria in bloodstream infection on mortality rates and length of stay.Infection.2008;36:31–35.
- ,,,.Clinical and economic impact of common multidrug‐resistant gram‐negative bacilli.Antimicrob Agents Chemother.2008;52:813–821.
- .Review of studies of the impact on Gram‐negative bacterial resistance on outcomes in the intensive care unit.Crit Care Med.2009;37:1463–1469.
- ,,,,,.Impact of multidrug‐resistant Pseudomonas aeruginosa bacteremia on patient outcomes.Antimicrob Agents Chemother.2010;54:3717–3722.
- ,,,,.Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator‐associated pneumonia.Chest.2002;122:262–268.
- ,,,.Outcomes analysis of delayed antibiotic treatment for hospital‐acquired Staphylococcus aureus bacteremia.Clin Infect Dis.2003;36:1418–1423.
- .Broad‐spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front.Clin Infect Dis.2008;47(suppl 1):S3–S13.
- ,.A new paradigm for treating infections: “go hard and go home.”Crit Care Resusc.2009;11:276–281.
- .Use of broad‐spectrum antimicrobials for the treatment of pneumonia in seriously ill patients: maximizing clinical outcomes and minimizing selection of resistant organisms.Clin Infect Dis.2006;42(suppl 2):S72–S81.
- ,.Antibiotic resistance: location, location, location.Clin Microbiol Infect.2007;13(suppl 2):7–16.
- ,,,,,.Ventilator‐associated pneumonia in a multi‐hospital system: differences in microbiology by location.Infect Control Hosp Epidemiol.2003;24:853–858.
- ,,, et al.Incidence and susceptibility of pathogenic bacteria vary between intensive care units within a single hospital: implications for empiric antibiotic strategies.J Trauma.2000;49:638–645; discussion645–646.
- ,,,,.Variations in etiology of ventilator‐associated pneumonia across four treatment sites: implications for antimicrobial prescribing practices.Am J Respir Crit Care Med.1999;160:608–613.
- Hospital‐Acquired Pneumonia Guideline Committee of the American Thoracic Society and Infectious Diseases Society of America.Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- .The dilemma of multidrug‐resistant gram‐negative bacteria.Am J Med Sci.2010;340:232–237.
- .Antimicrobial resistance and aging: beginning of the end of the antibiotic era?J Am Geriatr Soc.2002;50:S226–S229.
- ,.Principles of antimicrobial use in older adults.Clin Geriatr Med.2007;23:481–497,v.
- .Antimicrobial use: risk driver of multidrug resistant microorganisms in healthcare settings.Curr Opin Infect Dis.2009;22:352–358.
- .Collateral damage and what the future might hold. The need to balance prudent antibiotic utilization and stewardship with effective patient management.Int J Infect Dis.2006;10:S17–S24.
- ,,,.Blood culture contamination in Tanzania, Malawi, and the United States: a microbiological tale of three cities.J Clin Microbiol.2006;44:4425–4429.
- ,,, et al.Clinical and economic impact of contaminated blood cultures within the hospital setting.J Hosp Infect.2011;77:233–236.
- ,,.Contaminant blood cultures and resource utilization. The true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,,,.Contamination of catheter‐drawn blood cultures.J Clin Microbiol.2001;39:3393–3394.
- ,,.Comparison of utility of blood cultures from intravascular catheters and peripheral veins: a systematic review and decision analysis.J Med Microbiol.2008;57:1–8.
- ,,.Contamination of blood cultures during venepuncture: fact or myth?Postgrad Med J.1990;66:1053–1058.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- ,,,,.The value of infectious diseases consultation in Staphylococcus aureus bacteremia.Am J Med.2010;123:631–637.
- ,,,,.Infectious diseases consultation lowers mortality from Staphylococcus aureus bacteremia.Medicine (Baltimore).2009;88:263–267.
- ,,,,,.The value of infectious diseases specialists: non‐patient care activities.Clin Infect Dis.2008;47:1051–1063.
- ,,, et al.The value of an infectious diseases specialist.Clin Infect Dis.2003;36:1013–1017.
- ,,, et al.Mortality of S. aureus bacteremia and infectious diseases specialist consultation—a study of 521 patients in Germany.J Infect.2009;59:232–239.
- ,.Hospital‐acquired pneumonia: pathophysiology, diagnosis, and treatment.Surg Clin North Am.2009;89:439–461,ix.
- ,,,.Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System.Crit Care Med.1999;27:887–892.
- ,,.Healthcare‐associated pneumonia in adults: management principles to improve outcomes.Infect Dis Clin North Am.2004;18:939–962.
- ,,.Healthcare‐associated infections. A useful concept?Curr Opin Crit Care.2009;15:419–424.
- ,,,,.Ventilator‐associated pneumonia: incidence, risk factors, and microbiology.Semin Respir Infect.2000;15:272–279.
- ,,, et al.Ventilator‐associated pneumonia caused by potentially drug‐resistant bacteria.Am J Respir Crit Care Med.1998;157:531–539.
- ,,.A study of ventilator‐associated pneumonia: incidence, outcome, risk factors and measures to be taken for prevention.Indian J Anaesth.2010;54:535–540.
- ,,, et al.Risk factors for infection by Pseudomonas aeruginosa in patients with ventilator‐associated pneumonia.Intensive Care Med.1994;20:193–198.
- ,,,.Tackling empirical antibiotic therapy for ventilator‐associated pneumonia in your ICU: guidance for implementing the guidelines.Semin Respir Crit Care Med.2009;30:102–115.
- ,,,,,.Diagnosing pneumonia during mechanical ventilation: the clinical pulmonary infection score revisited.Am J Respir Crit Care Med.2003;168:173–179.
- ,,,,.Guidelines for clinical care: anti‐infective agents for intra‐abdominal infection. A Surgical Infection Society policy statement.Arch Surg.1992;127:83–89.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,.Intra‐abdominal infections.Surg Clin North Am.2009;89:421–437,ix.
- ,,,.In vitro susceptibilities of aerobic and facultative anaerobic Gram‐negative bacilli from patients with intra‐abdominal infections worldwide from 2005–2007: results from the SMART study.Int J Antimicrob Agents.2009;34:585–588.
- ,,,,,.Susceptibility of gram‐negative pathogens isolated from patients with complicated intra‐abdominal infections in the United States, 2007–2008: results of the Study for Monitoring Antimicrobial Resistance Trends (SMART).Antimicrob Agents Chemother.2010;54:3031–3034.
- ,,, et al.NHSN annual update: antimicrobial‐resistant pathogens associated with healthcare‐associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007.Infect Control Hosp Epidemiol.2008;29:996–1011.
- ,.Central line‐associated bloodstream infections: prevention and management.Infect Dis Clin North Am.2011;25:77–102.
- ,,,,,.Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.Clin Infect Dis.2004;39:309–317.
- National Nosocomial Infections Surveillance (NNIS) system report,data summary from January 1992 through June 2004, issued October 2004.Am J Infect Control.2004;32:470–485.
- ,,,.Antimicrobial resistance trends of Escherichia coli bloodstream isolates: a population‐based study, 1998–2007.J Antimicrob Chemother.2009;64:169–174.
- ,,, et al.International Nosocomial Infection Control Consortium (INICC) report, data summary for 2003–2008, issued June 2009.Am J Infect Control.2010;38:95–104,e102.
- ,,.The impact of antimicrobial‐resistant, health care‐associated infections on mortality in the United States.Clin Infect Dis.2008;47:927–930.
- ,,,,.Methicillin‐resistant Staphylococcus aureus central line‐associated bloodstream infections in US intensive care units, 1997–2007.JAMA.2009;301:727–736.
- ,,, et al.Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin‐resistant Staphylococcus aureus infections in adults and children: executive summary.Clin Infect Dis.2011;52:285–292.
- ,,,.Pharmacokinetic evaluation of piperacillin‐tazobactam.Expert Opin Drug Metab Toxicol.2010;6:1017–1031.
- ,,, et al.Morbidity associated with Pseudomonas aeruginosa bloodstream infections.Diagn Microbiol Infect Dis.2009;64:311–319.
- ,,, et al.Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health‐System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists.Am J Health Syst Pharm.2009;66:82–98.
- ,.Pharmacokinetic and pharmacodynamic parameters of antimicrobials: potential for providing dosing regimens that are less vulnerable to resistance.Clin Pharmacokinet.2009;48:517–528.
- ,,.Piperacillin‐tazobactam for Pseudomonas aeruginosa infection: clinical implications of an extended‐infusion dosing strategy.Clin Infect Dis.2007;44:357–363.
- ,.Appropriate vs. inappropriate antimicrobial therapy.Clin Microbiol Infect.2008;14(suppl 3):15–21.
- .Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients.Clin Infect Dis.2000;31(suppl 4):S131–S138.
- .Treatment options for nosocomial pneumonia due to MRSA.J Infect.2009;59(suppl 1):S25–S31.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,,.Impact of appropriateness of initial antibiotic therapy on the outcome of ventilator‐associated pneumonia.Intensive Care Med.2001;27:355–362.
- ,,, et al.Mortality and morbidity attributable to inadequate empirical antimicrobial therapy in patients admitted to the ICU with sepsis: a matched cohort study.J Antimicrob Chemother.2008;61:436–441.
- ,,,,,.Effect from multiple episodes of inadequate empiric antibiotic therapy for ventilator‐associated pneumonia on morbidity and mortality among critically ill trauma patients.J Trauma.2005;58:94–101.
- ,,,,,.Predictors of 30‐day mortality and hospital costs in patients with ventilator‐associated pneumonia attributed to potentially antibiotic‐resistant gram‐negative bacteria.Chest.2008;134:281–287.
- ,,,,.Antimicrobial therapy escalation and hospital mortality among patients with health‐care‐associated pneumonia: a single‐center experience.Chest.2008;134:963–968.
- ,,.Impact of inappropriate antibiotic therapy on mortality in patients with ventilator‐associated pneumonia and blood stream infection: a meta‐analysis.J Crit Care.2008;23:91–100.
- ,,, et al.Ventilator‐associated pneumonia: breaking the vicious circle of antibiotic overuse.Crit Care Med.2007;35:379–385; quiz 386.
- ,,, et al.Appropriateness and delay to initiate therapy in ventilator‐associated pneumonia.Eur Respir J.2006;27:158–164.
- ,,, et al.Impact of BAL data on the therapy and outcome of ventilator‐associated pneumonia.Chest.1997;111:676–685.
- ,,,,.Inadequate treatment of ventilator‐associated pneumonia: risk factors and impact on outcomes.J Hosp Infect.2007;65:361–367.
- ,,, et al.Predictors of mortality in patients with methicillin‐resistant Staphylococcus aureus (MRSA) bacteraemia: the role of empiric antibiotic therapy.Eur J Clin Microbiol Infect Dis.2007;26:239–245.
- ,,,,,.Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med.2003;115:529–535.
- ,,,,.The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting.Chest.2000;118:146–155.
- ,,, et al.Bloodstream infections caused by antibiotic‐resistant gram‐negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome.Antimicrob Agents Chemother.2005;49:760–766.
- ,,,,,.The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection.J Intern Med.1998;244:379–386.
- ,,,,,.Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment.Antimicrob Agents Chemother.2005;49:1306–1311.
- ,,, et al.Antibiotic therapy for Klebsiella pneumoniae bacteremia: implications of production of extended‐spectrum beta‐lactamases.Clin Infect Dis.2004;39:31–37.
- ,,, et al.Impact of inappropriate empirical therapy for sepsis due to health care‐associated methicillin‐resistant Staphylococcus aureus.J Infect.2009;58:131–137.
- ,,, et al.Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46:193–200.
- ,,, et al.Multidrug‐resistant Pseudomonas aeruginosa bloodstream infections: risk factors and mortality.Epidemiol Infect.2011; Jan 13:1–10.
- ,,,,,.Economic consequences of failure of initial antibiotic therapy in hospitalized adults with complicated intra‐abdominal infections.Surg Infect (Larchmt).2008;9:335–347.
- ,,, et al.Effect of inappropriate initial empiric antibiotic therapy on outcome of patients with community‐acquired intra‐abdominal infections requiring surgery.Eur J Clin Microbiol Infect Dis.2004;23:682–687.
- ,,,,,.Emergence of antibiotic‐resistant bacteria in cases of peritonitis after intraabdominal surgery affects the efficacy of empirical antimicrobial therapy.Clin Infect Dis.1996;23:486–494.
- ,,, et al.Antibiotic treatment for surgical peritonitis.Ann Surg.1991;214:543–549.
- ,,, et al.Inappropriate initial treatment of secondary intra‐abdominal infections leads to increased risk of clinical failure and costs.Br J Clin Pharmacol.2005;60:438–443.
- ,,, et al.Optimal management therapy for Pseudomonas aeruginosa ventilator‐associated pneumonia: an observational, multicenter study comparing monotherapy with combination antibiotic therapy.Crit Care Med.2007;35:1888–1895.
- ,,,,,.Risk factors for and outcomes of healthcare‐associated infection due to extended‐spectrum beta‐lactamase‐producing Escherichia coli or Klebsiella pneumoniae in Thailand.Infect Control Hosp Epidemiol.2007;28:873–876.
- ,,, et al.Impact of antibiotic resistance and of adequate empirical antibiotic treatment in the prognosis of patients with Escherichia coli bacteraemia.J Antimicrob Chemother.2007;60:855–863.
- .Predicting methicillin resistance and the effect of inadequate empiric therapy on survival in patients with Staphylococcus aureus bacteremia.Arch Intern Med.2000;160:1001–1004.
- ,,,,,.Impact of multiresistance of gram‐negative bacteria in bloodstream infection on mortality rates and length of stay.Infection.2008;36:31–35.
- ,,,.Clinical and economic impact of common multidrug‐resistant gram‐negative bacilli.Antimicrob Agents Chemother.2008;52:813–821.
- .Review of studies of the impact on Gram‐negative bacterial resistance on outcomes in the intensive care unit.Crit Care Med.2009;37:1463–1469.
- ,,,,,.Impact of multidrug‐resistant Pseudomonas aeruginosa bacteremia on patient outcomes.Antimicrob Agents Chemother.2010;54:3717–3722.
- ,,,,.Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator‐associated pneumonia.Chest.2002;122:262–268.
- ,,,.Outcomes analysis of delayed antibiotic treatment for hospital‐acquired Staphylococcus aureus bacteremia.Clin Infect Dis.2003;36:1418–1423.
- .Broad‐spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front.Clin Infect Dis.2008;47(suppl 1):S3–S13.
- ,.A new paradigm for treating infections: “go hard and go home.”Crit Care Resusc.2009;11:276–281.
- .Use of broad‐spectrum antimicrobials for the treatment of pneumonia in seriously ill patients: maximizing clinical outcomes and minimizing selection of resistant organisms.Clin Infect Dis.2006;42(suppl 2):S72–S81.
- ,.Antibiotic resistance: location, location, location.Clin Microbiol Infect.2007;13(suppl 2):7–16.
- ,,,,,.Ventilator‐associated pneumonia in a multi‐hospital system: differences in microbiology by location.Infect Control Hosp Epidemiol.2003;24:853–858.
- ,,, et al.Incidence and susceptibility of pathogenic bacteria vary between intensive care units within a single hospital: implications for empiric antibiotic strategies.J Trauma.2000;49:638–645; discussion645–646.
- ,,,,.Variations in etiology of ventilator‐associated pneumonia across four treatment sites: implications for antimicrobial prescribing practices.Am J Respir Crit Care Med.1999;160:608–613.
- Hospital‐Acquired Pneumonia Guideline Committee of the American Thoracic Society and Infectious Diseases Society of America.Guidelines for the management of adults with hospital‐acquired, ventilator‐associated, and healthcare‐associated pneumonia.Am J Respir Crit Care Med.2005;171:388–416.
- .The dilemma of multidrug‐resistant gram‐negative bacteria.Am J Med Sci.2010;340:232–237.
- .Antimicrobial resistance and aging: beginning of the end of the antibiotic era?J Am Geriatr Soc.2002;50:S226–S229.
- ,.Principles of antimicrobial use in older adults.Clin Geriatr Med.2007;23:481–497,v.
- .Antimicrobial use: risk driver of multidrug resistant microorganisms in healthcare settings.Curr Opin Infect Dis.2009;22:352–358.
- .Collateral damage and what the future might hold. The need to balance prudent antibiotic utilization and stewardship with effective patient management.Int J Infect Dis.2006;10:S17–S24.
- ,,,.Blood culture contamination in Tanzania, Malawi, and the United States: a microbiological tale of three cities.J Clin Microbiol.2006;44:4425–4429.
- ,,, et al.Clinical and economic impact of contaminated blood cultures within the hospital setting.J Hosp Infect.2011;77:233–236.
- ,,.Contaminant blood cultures and resource utilization. The true consequences of false‐positive results.JAMA.1991;265:365–369.
- ,,,.Contamination of catheter‐drawn blood cultures.J Clin Microbiol.2001;39:3393–3394.
- ,,.Comparison of utility of blood cultures from intravascular catheters and peripheral veins: a systematic review and decision analysis.J Med Microbiol.2008;57:1–8.
- ,,.Contamination of blood cultures during venepuncture: fact or myth?Postgrad Med J.1990;66:1053–1058.
- ,,, et al.Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship.Clin Infect Dis.2007;44:159–177.
- ,,,,.The value of infectious diseases consultation in Staphylococcus aureus bacteremia.Am J Med.2010;123:631–637.
- ,,,,.Infectious diseases consultation lowers mortality from Staphylococcus aureus bacteremia.Medicine (Baltimore).2009;88:263–267.
- ,,,,,.The value of infectious diseases specialists: non‐patient care activities.Clin Infect Dis.2008;47:1051–1063.
- ,,, et al.The value of an infectious diseases specialist.Clin Infect Dis.2003;36:1013–1017.
- ,,, et al.Mortality of S. aureus bacteremia and infectious diseases specialist consultation—a study of 521 patients in Germany.J Infect.2009;59:232–239.
- ,.Hospital‐acquired pneumonia: pathophysiology, diagnosis, and treatment.Surg Clin North Am.2009;89:439–461,ix.
- ,,,.Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System.Crit Care Med.1999;27:887–892.
- ,,.Healthcare‐associated pneumonia in adults: management principles to improve outcomes.Infect Dis Clin North Am.2004;18:939–962.
- ,,.Healthcare‐associated infections. A useful concept?Curr Opin Crit Care.2009;15:419–424.
- ,,,,.Ventilator‐associated pneumonia: incidence, risk factors, and microbiology.Semin Respir Infect.2000;15:272–279.
- ,,, et al.Ventilator‐associated pneumonia caused by potentially drug‐resistant bacteria.Am J Respir Crit Care Med.1998;157:531–539.
- ,,.A study of ventilator‐associated pneumonia: incidence, outcome, risk factors and measures to be taken for prevention.Indian J Anaesth.2010;54:535–540.
- ,,, et al.Risk factors for infection by Pseudomonas aeruginosa in patients with ventilator‐associated pneumonia.Intensive Care Med.1994;20:193–198.
- ,,,.Tackling empirical antibiotic therapy for ventilator‐associated pneumonia in your ICU: guidance for implementing the guidelines.Semin Respir Crit Care Med.2009;30:102–115.
- ,,,,,.Diagnosing pneumonia during mechanical ventilation: the clinical pulmonary infection score revisited.Am J Respir Crit Care Med.2003;168:173–179.
- ,,,,.Guidelines for clinical care: anti‐infective agents for intra‐abdominal infection. A Surgical Infection Society policy statement.Arch Surg.1992;127:83–89.
- ,,, et al.Diagnosis and management of complicated intra‐abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America.Clin Infect Dis.2010;50:133–164.
- ,.Intra‐abdominal infections.Surg Clin North Am.2009;89:421–437,ix.
- ,,,.In vitro susceptibilities of aerobic and facultative anaerobic Gram‐negative bacilli from patients with intra‐abdominal infections worldwide from 2005–2007: results from the SMART study.Int J Antimicrob Agents.2009;34:585–588.
- ,,,,,.Susceptibility of gram‐negative pathogens isolated from patients with complicated intra‐abdominal infections in the United States, 2007–2008: results of the Study for Monitoring Antimicrobial Resistance Trends (SMART).Antimicrob Agents Chemother.2010;54:3031–3034.
- ,,, et al.NHSN annual update: antimicrobial‐resistant pathogens associated with healthcare‐associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007.Infect Control Hosp Epidemiol.2008;29:996–1011.
- ,.Central line‐associated bloodstream infections: prevention and management.Infect Dis Clin North Am.2011;25:77–102.
- ,,,,,.Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.Clin Infect Dis.2004;39:309–317.
- National Nosocomial Infections Surveillance (NNIS) system report,data summary from January 1992 through June 2004, issued October 2004.Am J Infect Control.2004;32:470–485.
- ,,,.Antimicrobial resistance trends of Escherichia coli bloodstream isolates: a population‐based study, 1998–2007.J Antimicrob Chemother.2009;64:169–174.
- ,,, et al.International Nosocomial Infection Control Consortium (INICC) report, data summary for 2003–2008, issued June 2009.Am J Infect Control.2010;38:95–104,e102.
- ,,.The impact of antimicrobial‐resistant, health care‐associated infections on mortality in the United States.Clin Infect Dis.2008;47:927–930.
- ,,,,.Methicillin‐resistant Staphylococcus aureus central line‐associated bloodstream infections in US intensive care units, 1997–2007.JAMA.2009;301:727–736.
- ,,, et al.Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin‐resistant Staphylococcus aureus infections in adults and children: executive summary.Clin Infect Dis.2011;52:285–292.
- ,,,.Pharmacokinetic evaluation of piperacillin‐tazobactam.Expert Opin Drug Metab Toxicol.2010;6:1017–1031.
- ,,, et al.Morbidity associated with Pseudomonas aeruginosa bloodstream infections.Diagn Microbiol Infect Dis.2009;64:311–319.
- ,,, et al.Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health‐System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists.Am J Health Syst Pharm.2009;66:82–98.
- ,.Pharmacokinetic and pharmacodynamic parameters of antimicrobials: potential for providing dosing regimens that are less vulnerable to resistance.Clin Pharmacokinet.2009;48:517–528.
- ,,.Piperacillin‐tazobactam for Pseudomonas aeruginosa infection: clinical implications of an extended‐infusion dosing strategy.Clin Infect Dis.2007;44:357–363.