User login
Electronic Order Set for AMI
Although the prevalence of coronary heart disease and death from acute myocardial infarction (AMI) have declined steadily, about 935,000 heart attacks still occur annually in the United States, with approximately one‐third of these being fatal.[1, 2, 3] Studies have demonstrated decreased 30‐day and longer‐term mortality in AMI patients who receive evidence‐based treatment, including aspirin, ‐blockers, angiotensin‐converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), anticoagulation therapy, and statins.[4, 5, 6, 7] Despite clinical practice guidelines (CPGs) outlining evidence‐based care and considerable efforts to implement processes that improve patient outcomes, delivery of effective therapy remains suboptimal.[8] For example, the Hospital Quality Alliance Program[9] found that in AMI patients, use of aspirin on admission was only 81% to 92%, ‐blocker on admission 75% to 85%, and ACE inhibitors for left ventricular dysfunction 71% to 74%.
Efforts to increase adherence to CPGs and improve patient outcomes in AMI have resulted in variable degrees of success. They include promotion of CPGs,[4, 5, 6, 7] physician education with feedback, report cards, care paths, registries,[10] Joint Commission standardized measures,[11] and paper checklists or order sets (OS).[12, 13]
In this report, we describe the association between use of an evidence‐based, electronic OS for AMI (AMI‐OS) and better adherence to CPGs. This AMI‐OS was implemented in the inpatient electronic medical records (EMRs) of a large integrated healthcare delivery system, Kaiser Permanente Northern California (KPNC). The purpose of our investigation was to determine (1) whether use of the AMI‐OS was associated with improved AMI processes and patient outcomes, and (2) whether these associations persisted after risk adjustment using a comprehensive severity of illness scoring system.
MATERIALS AND METHODS
This project was approved by the KPNC institutional review board.
Under a mutual exclusivity arrangement, salaried physicians of The Permanente Medical Group, Inc., care for 3.4 million Kaiser Foundation Health Plan, Inc. members at facilities owned by Kaiser Foundation Hospitals, Inc. All KPNC facilities employ the same information systems with a common medical record number and can track care covered by the plan but delivered elsewhere.[14] Our setting consisted of 21 KPNC hospitals described in previous reports,[15, 16, 17, 18] using the same commercially available EMR system that includes computerized physician order entry (CPOE). Deployment of the customized inpatient Epic EMR (
In this EMR's CPOE, physicians have options to select individual orders (a la carte) or they can utilize an OS, which is a collection of the most appropriate orders associated with specific diagnoses, procedures, or treatments. The evidence‐based AMI‐OS studied in this project was developed by a multidisciplinary team (for detailed components see Supporting Appendix 1Appendix 5 in the online version of this article).
Our study focused on the first set of hospital admission orders for patients with AMI. The study sample consisted of patients meeting these criteria: (1) age 18 years at admission; (2) admitted to a KPNC hospital for an overnight stay between September 28, 2008 and December 31, 2010; (3) principal diagnosis was AMI (International Classification of Diseases, 9th Revision [ICD‐9][19] codes 410.00, 01, 10, 11, 20, 21, 30, 31, 40, 41, 50, 51, 60, 61, 70, 71, 80, 90, and 91); and (4) KPHC had been operational at the hospital for at least 3 months to be included (for assembly descriptions see Supporting Appendices 15 in the online version of this article). At the study hospitals, troponin I was measured using the Beckman Access AccuTnI assay (Beckman Coulter, Inc., Brea, CA), whose upper reference limit (99th percentile) is 0.04 ng/mL. We excluded patients initially hospitalized for AMI at a non‐KPNC site and transferred into a study hospital.
The data processing methods we employed have been detailed elsewhere.[14, 15, 17, 20, 21, 22] The dependent outcome variables were total hospital length of stay, inpatient mortality, 30‐day mortality, and all‐cause rehospitalization within 30 days of discharge. Linked state mortality data were unavailable for the entire study period, so we ascertained 30‐day mortality based on the combination of KPNC patient demographic data and publicly available Social Security Administration decedent files. We ascertained rehospitalization by scanning KPNC hospitalization databases, which also track out‐of‐plan use.
The dependent process variables were use of aspirin within 24 hours of admission, ‐blockers, anticoagulation, ACE inhibitors or ARBs, and statins. The primary independent variable of interest was whether or not the admitting physician employed the AMI‐OS when admission orders were entered. Consequently, this variable is dichotomous (AMI‐OS vs a la carte).
We controlled for acute illness severity and chronic illness burden using a recent modification[22] of an externally validated risk‐adjustment system applicable to all hospitalized patients.[15, 16, 23, 24, 25] Our methodology included vital signs, neurological status checks, and laboratory test results obtained in the 72 hours preceding hospital admission; comorbidities were captured longitudinally using data from the year preceding hospitalization (for comparison purposes, we also assigned a Charlson Comorbidity Index score[26]).
End‐of‐life care directives are mandatory on admission at KPNC hospitals. Physicians have 4 options: full code, partial code, do not resuscitate, and comfort care only. Because of small numbers in some categories, we collapsed these 4 categories into full code and not full code. Because patients' care directives may change, we elected to capture the care directive in effect when a patient first entered a hospital unit other than the emergency department (ED).
Two authors (M.B., P.C.L.), one of whom is a board‐certified cardiologist, reviewed all admission electrocardiograms and made a consensus determination as to whether or not criteria for ST‐segment elevation myocardial infarction (STEMI) were present (ie, new ST‐segment elevation or left bundle branch block); we also reviewed the records of all patients with missing troponin I data to confirm the AMI diagnosis.
Statistical Methods
We performed unadjusted comparisons between AMI‐OS and nonAMI‐OS patients using the t test or the [2] test, as appropriate.
We hypothesized that the AMI‐OS plays a mediating role on patient outcomes through its effect on adherence to recommended treatment. We evaluated this hypothesis for inpatient mortality by first fitting a multivariable logistic regression model for inpatient mortality as the outcome and either the 5 evidence‐based therapies or the total number of evidence‐based therapies used (ranging from 02, 3, 4, or 5) as the dependent variable controlling for age, gender, presence of STEMI, troponin I, comorbidities, illness severity, ED length of stay (LOS), care directive status, and timing of cardiac catheterization referral as covariates to confirm the protective effect of these therapies on mortality. We then used the same model to estimate the effect of AMI‐OS on inpatient mortality, substituting the therapies with AMI‐OS as the dependent variable and using the same covariates. Last, we included both the therapies and the AMI‐OS in the model to evaluate their combined effects.[27]
We used 2 different methods to estimate the effects of AMI‐OS and number of therapies provided on the outcomes while adjusting for observed baseline differences between the 2 groups of patients: propensity risk score matching, which estimates the average treatment effect for the treated,[28, 29] and inverse probability of treatment weighting, which is used to estimate the average treatment effect.[30, 31, 32] The propensity score was defined as the probability of receiving the intervention for a patient with specific predictive factors.[33, 34] We computed a propensity score for each patient by using logistic regression, with the dependent variable being receipt of AMI‐OS and the independent variables being the covariates used for the multivariate logistic regression as well as ICD‐9 code for final diagnosis. We calculated the Mahalanobis distance between patients who received AMI‐OS (cases) and patients who did not received AMI‐OS (controls) using the same set of covariates. We matched each case to a single control within the same facility based on the nearest available Mahalanobis metric matching within calipers defied as the maximum width of 0.2 standard deviations of the logit of the estimated propensity score.[29, 35] We estimated the odds ratios for the binary dependent variables based on a conditional logistic regression model to account for the matched pairs design.[28] We used a generalized linear model with the log‐transformed LOS as the outcome to estimate the ratio of the LOS geometric mean of the cases to the controls. We calculated the relative risk for patients receiving AMI‐OS via the inverse probability weighting method by first defining a weight for each patient. [We assigned a weight of 1/psi to patients who received the AMI‐OS and a weight of 1/(1psi) to patients who did not receive the AMI‐OS, where psi denotes the propensity score for patient i]. We used a logistic regression model for the binary dependent variables with the same set of covariates described above to estimate the adjusted odds ratios while weighting each observation by its corresponding weight. Last, we used a weighted generalized linear model to estimate the AMI‐OS effect on the log‐transformed LOS.
RESULTS
Table 1 summarizes the characteristics of the 5879 patients. It shows that AMI‐OS patients were more likely to receive evidence‐based therapies for AMI (aspirin, ‐blockers, ACE inhibitors or ARBs, anticoagulation, and statins) and had a 46% lower mortality rate in hospital (3.51 % vs 6.52%) and 33% lower rate at 30 days (5.66% vs 8.48%). AMI‐OS patients were also found to be at lower risk for an adverse outcome than nonAMI‐OS patients. The AMI‐OS patients had lower peak troponin I values, severity of illness (lower Laboratory‐Based Acute Physiology Score, version 2 [LAPS2] scores), comorbidity burdens (lower Comorbidity Point Score, version 2 [COPS2] and Charlson scores), and global predicted mortality risk. AMI‐OS patients were also less likely to have required intensive care. AMI‐OS patients were at higher risk of death than nonAMI‐OS patients with respect to only 1 variable (being full code at the time of admission), but although this difference was statistically significant, it was of minor clinical impact (86% vs 88%).
| Patients Initially Managed Using | P Valuea | ||
|---|---|---|---|
| AMI Order Set, N=3,531b | A La Carte Orders, N=2,348b | ||
| |||
| Age, y, median (meanSD) | 70 (69.413.8) | 70 (69.213.8) | 0.5603 |
| Age (% >65 years) | 2,134 (60.4%) | 1,415 (60.3%) | 0.8949 |
| Sex (% male) | 2,202 (62.4%) | 1,451 (61.8%) | 0.6620 |
| STEMI (% with)c | 166 (4.7%) | 369 (15.7%) | <0.0001 |
| Troponin I (% missing) | 111 (3.1%) | 151 (6.4%) | <0.0001 |
| Troponin I median (meanSD) | 0.57 (3.08.2) | 0.27 (2.58.9) | 0.0651 |
| Charlson score median (meanSD)d | 2.0 (2.51.5) | 2.0 (2.71.6) | <0.0001 |
| COPS2, median (meanSD)e | 14.0 (29.831.7) | 17.0 (34.334.4) | <0.0001 |
| LAPS2, median (meanSD)e | 0.0 (35.643.5) | 27.0 (40.948.1) | <0.0001 |
| Length of stay in ED, h, median (meanSD) | 5.7 (5.93.0) | 5.7 (5.43.1) | <0.0001 |
| Patients receiving aspirin within 24 hoursf | 3,470 (98.3%) | 2,202 (93.8%) | <0.0001 |
| Patients receiving anticoagulation therapyf | 2,886 (81.7%) | 1,846 (78.6%) | 0.0032 |
| Patients receiving ‐blockersf | 3,196 (90.5%) | 1,926 (82.0%) | <0.0001 |
| Patients receiving ACE inhibitors or ARBsf | 2,395 (67.8%) | 1,244 (53.0%) | <0.0001 |
| Patients receiving statinsf | 3,337 (94.5%) | 1,975 (84.1%) | <0.0001 |
| Patient received 1 or more therapies | 3,531 (100.0%) | 2,330 (99.2%) | <0.0001 |
| Patient received 2 or more therapies | 3,521 (99.7%) | 2,266 (96.5%) | <0.0001 |
| Patient received 3 or more therapies | 3,440 (97.4%) | 2,085 (88.8%) | <0.0001 |
| Patient received 4 or more therapies | 3,015 (85.4%) | 1,646 (70.1%) | <0.0001 |
| Patient received all 5 therapies | 1,777 (50.3%) | 866 (35.9%) | <0.0001 |
| Predicted mortality risk, %, median, (meanSD)f | 0.86 (3.27.4) | 1.19 (4.810.8) | <0.0001 |
| Full code at time of hospital entry (%)g | 3,041 (86.1%) | 2,066 (88.0%) | 0.0379 |
| Admitted to ICU (%)i | |||
| Direct admit | 826 (23.4%) | 567 (24.2%) | 0.5047 |
| Unplanned transfer | 222 (6.3%) | 133 (5.7%) | 0.3262 |
| Ever | 1,283 (36.3%) | 1,169 (49.8%) | <0.0001 |
| Length of stay, h, median (meanSD) | 68.3 (109.4140.9) | 68.9 (113.8154.3) | 0.2615 |
| Inpatient mortality (%) | 124 (3.5%) | 153 (6.5%) | <0.0001 |
| 30‐day mortality (%) | 200 (5.7%) | 199 (8.5%) | <0.0001 |
| All‐cause rehospitalization within 30 days (%) | 576 (16.3%) | 401 (17.1%) | 0.4398 |
| Cardiac catheterization procedure referral timing | |||
| 1 day preadmission to discharge | 2,018 (57.2%) | 1,348 (57.4%) | 0.1638 |
| 2 days preadmission or earlier | 97 (2.8%) | 87 (3.7%) | |
| After discharge | 149 (4.2%) | 104 (4.4%) | |
| No referral | 1,267 (35.9%) | 809 (34.5%) | |
Table 2 shows the result of a logistic regression model in which the dependent variable was inpatient mortality and either the 5 evidence‐based therapies or the total number of evidence‐based therapies are the dependent variables. ‐blocker, statin, and ACE inhibitor or ARB therapies all had a protective effect on mortality, with odds ratios ranging from 0.48 (95% confidence interval [CI]: 0.36‐0.64), 0.63 (95% CI: 0.45‐0.89), and 0.40 (95% CI: 0.30‐0.53), respectively. An increased number of therapies also had a beneficial effect on inpatient mortality, with patients having 3 or more of the evidence‐based therapies showing an adjusted odds ratio (AOR) of 0.49 (95% CI: 0.33‐0.73), 4 or more therapies an AOR of 0.29 (95% CI: 0.20‐0.42), and 0.17 (95% CI: 0.11‐0.25) for 5 or more therapies.
| Multiple Therapies Effect | Individual Therapies Effect | |||
|---|---|---|---|---|
| Outcome | Death | Death | ||
| Number of outcomes | 277 | 277 | ||
| AORa | 95% CIb | AORa | 95% CIb | |
| ||||
| Age in years | ||||
| 1839 | Ref | Ref | ||
| 4064 | 1.02 | (0.147.73) | 1.01 | (0.137.66) |
| 6584 | 4.05 | (0.5529.72) | 3.89 | (0.5328.66) |
| 85+ | 4.99 | (0.6737.13) | 4.80 | (0.6435.84) |
| Sex | ||||
| Female | Ref | |||
| Male | 1.05 | (0.811.37) | 1.07 | (0.821.39) |
| STEMIc | ||||
| Absent | Ref | Ref | ||
| Present | 4.00 | (2.755.81) | 3.86 | (2.645.63) |
| Troponin I | ||||
| 0.1 ng/ml | Ref | Ref | ||
| >0.1 ng/ml | 1.01 | (0.721.42) | 1.02 | (0.731.43) |
| COPS2d (AOR per 10 points) | 1.05 | (1.011.08) | 1.04 | (1.011.08) |
| LAPS2d (AOR per 10 points) | 1.09 | (1.061.11) | 1.09 | (1.061.11) |
| ED LOSe (hours) | ||||
| <6 | Ref | Ref | ||
| 67 | 0.74 | (0.531.03) | 0.76 | (0.541.06) |
| >=12 | 0.82 | (0.391.74) | 0.83 | (0.391.78) |
| Code Statusf | ||||
| Full Code | Ref | |||
| Not Full Code | 1.08 | (0.781.49) | 1.09 | (0.791.51) |
| Cardiac procedure referral | ||||
| None during stay | Ref | |||
| 1 day pre adm until discharge | 0.40 | (0.290.54) | 0.39 | (0.280.53) |
| Number of therapies received | ||||
| 2 or less | Ref | |||
| 3 | 0.49 | (0.330.73) | ||
| 4 | 0.29 | (0.200.42) | ||
| 5 | 0.17 | (0.110.25) | ||
| Aspirin therapy | 0.80 | (0.491.32) | ||
| Anticoagulation therapy | 0.86 | (0.641.16) | ||
| Beta Blocker therapy | 0.48 | (0.360.64) | ||
| Statin therapy | 0.63 | (0.450.89) | ||
| ACE inhibitors or ARBs | 0.40 | (0.300.53) | ||
| C Statistic | 0.814 | 0.822 | ||
| Hosmer‐Lemeshow p value | 0.509 | 0.934 | ||
Table 3 shows that the use of the AMI‐OS is protective, with an AOR of 0.59 and a 95% CI of 0.45‐0.76. Table 3 also shows that the most potent predictors were comorbidity burden (AOR: 1.07, 95% CI: 1.03‐1.10 per 10 COPS2 points), severity of illness (AOR: 1.09, 95% CI: 1.07‐1.12 per 10 LAPS2 points), STEMI (AOR: 3.86, 95% CI: 2.68‐5.58), and timing of cardiac catheterization referral occurring immediately prior to or during the admission (AOR: 0.37, 95% CI: 0.27‐0.51). The statistical significance of the AMI‐OS effect disappears when both AMI‐OS and the individual therapies are included in the same model (see Supporting Information, Appendices 15, in the online version of this article).
| Outcome | Death | |
|---|---|---|
| Number of outcomes | 277 | |
| AORa | 95% CIb | |
| ||
| Age in years | ||
| 1839 | Ref | |
| 4064 | 1.16 | (0.158.78) |
| 6584 | 4.67 | (0.6334.46) |
| 85+ | 5.45 | (0.7340.86) |
| Sex | ||
| Female | Ref | |
| Male | 1.05 | (0.811.36) |
| STEMIc | ||
| Absent | Ref | |
| Present | 3.86 | (2.685.58) |
| Troponin I | ||
| 0.1 ng/ml | Ref | |
| >0.1 ng/ml | 1.16 | (0.831.62) |
| COPS2d (AOR per 10 points) | 1.07 | (1.031.10) |
| LAPS2d (AOR per 10 points) | 1.09 | (1.071.12) |
| ED LOSe (hours) | ||
| <6 | Ref | |
| 67 | 0.72 | (0.521.00) |
| >=12 | 0.70 | (0.331.48) |
| Code statusf | ||
| Full code | Ref | |
| Not full code | 1.22 | (0.891.68) |
| Cardiac procedure referral | ||
| None during stay | Ref | |
| 1 day pre adm until discharge | 0.37 | (0.270.51) |
| Order set employedg | ||
| No | Ref | |
| Yes | 0.59 | (0.450.76) |
| C Statistic | 0.792 | |
| Hosmer‐Lemeshow p value | 0.273 | |
Table 4 shows separately the average treatment effect (ATE) and average treatment effect for the treated (ATT) of AMI‐OS and of increasing number of therapies on other outcomes (30‐day mortality, LOS, and readmission). Both the ATE and ATT show that the use of the AMI‐OS was significantly protective with respect to mortality and total hospital LOS but not significant with respect to readmission. The effect of the number of therapies on mortality is significantly higher with increasing number of therapies. For example, patients who received 5 therapies had an average treatment effect on 30‐day inpatient mortality of 0.23 (95% CI: 0.15‐0.35) compared to 0.64 (95% CI: 0.43‐0.96) for 3 therapies, almost a 3‐fold difference. The effects of increasing number of therapies were not significant for LOS or readmission. A sensitivity analysis in which the 535 STEMI patients were removed showed essentially the same results, so it is not reported here.
| Outcome | Order Seta | 3 Therapiesb | 4 Therapiesb | 5 Therapiesb |
|---|---|---|---|---|
| ||||
| Average treatment effectc | ||||
| Inpatient mortality | 0.67 (0.520.86) | 0.64 (0.430.96) | 0.37 (0.250.54) | 0.23 (0.150.35) |
| 30‐day mortality | 0.77 (0.620.96) | 0.68 (0.480.98) | 0.34 (0.240.48) | 0.26 (0.180.37) |
| Readmission | 1.03 (0.901.19) | 1.20 (0.871.66) | 1.19 (0.881.60) | 1.30 (0.961.76) |
| LOS, ratio of the geometric means | 0.91 (0.870.95) | 1.16 (1.031.30) | 1.17 (1.051.30) | 1.12 (1.001.24) |
| Average treatment effect on the treatedd | ||||
| Inpatient mortality | 0.69 (0.520.92) | 0.35 (0.130.93) | 0.17 (0.070.43) | 0.08 (0.030.20) |
| 30‐day mortality | 0.84 (0.661.06) | 0.35 (0.150.79) | 0.17 (0.070.37) | 0.09 (0.040.20) |
| Readmission | 1.02 (0.871.20) | 1.39 (0.852.26) | 1.36 (0.882.12) | 1.23 (0.801.89) |
| LOS, ratio of the geometric meanse | 0.92 (0.870.97) | 1.18 (1.021.37) | 1.16 (1.011.33) | 1.04 (0.911.19) |
To further elucidate possible reasons why physicians did not use the AMI‐OS, the lead author reviewed 105 randomly selected records where the AMI‐OS was not used, 5 records from each of the 21 study hospitals. This review found that in 36% of patients, the AMI‐OS was not used because emergent catheterization or transfer to a facility with percutaneous coronary intervention capability occurred. Presence of other significant medical conditions, including critical illness, was the reason in 17% of these cases, patient or family refusal of treatments in 8%, issues around end‐of‐life care in 3%, and specific medical contraindications in 1%. In the remaining 34%, no reason for not using the AMI‐OS could be identified.
DISCUSSION
We evaluated the use of an evidence‐based electronic AMI‐OS embedded in a comprehensive EMR and found that it was beneficial. Its use was associated with increased adherence to evidence‐based therapies, which in turn were associated with improved outcomes. Using data from a large cohort of hospitalized AMI patients in 21 community hospitals, we were able to use risk adjustment that included physiologic illness severity to adjust for baseline mortality risk. Patients in whom the AMI‐OS was employed tended to be at lower risk; nonetheless, after controlling for confounding variables and adjusting for bias using propensity scores, the AMI‐OS was associated with increased use of evidence‐based therapies and decreased mortality. Most importantly, it appears that the benefits of the OS were not just due to increased receipt of individual recommended therapies, but to increased concurrent receipt of multiple recommended therapies.
Modern EMRs have great potential for significant improvements in the quality, efficiency, and safety of care provided,[36] and our study highlights this potential. However, a number of important limitations to our study must be considered. Although we had access to a very rich dataset, we could not control for all possible confounders, and our risk adjustment cannot match the level of information available to clinicians. In particular, the measurements available to us with respect to cardiac risk are limited. Thus, we have to recognize that the strength of our findings does not approximate that of a randomized trial, and one would expect that the magnitude of the beneficial association would fall under more controlled conditions. Resource limitations also did not permit us to gather more time course data (eg, sequential measurements of patient instability, cardiac damage, or use of recommended therapies), which could provide a better delineation of differences in both processes and outcomes.
Limitations also exist to the generalizability of the use of order sets in other settings that go beyond the availability of a comprehensive EMR. Our study population was cared for in a setting with an unusually high level of integration.[1] For example, KPNC has an elaborate administrative infrastructure for training in the use of the EMR as well as ensuring that order sets are not just evidence‐based, but that they are perceived by clinicians to be of significant value. This infrastructure, established to ensure physician buy‐in, may not be easy to replicate in smaller or less‐integrated settings. Thus, it is conceivable that factors other than the degree of support during the EMR deployments can affect rates of order set use.
Although our use of counterfactual methods included illness severity (LAPS2) and longitudinal comorbidity burden (COPS2), which are not yet available outside highly integrated delivery services employing comprehensive EMRs, it is possible they are insufficient. We cannot exclude the possibility that other biases or patient characteristics were present that led clinicians to preferentially employ the electronic order set in some patients but not in others. One could also argue that future studies should consider using overall adherence to recommended AMI treatment guidelines as a risk adjustment tool that would permit one to analyze what other factors may be playing a role in residual differences in patient outcomes. Last, one could object to our inclusion of STEMI patients; however, this was not a study on optimum treatment strategies for STEMI patients. Rather, it was a study on the impact on AMI outcomes of a specific component of computerized order entry outside the research setting.
Despite these limitations, we believe that our findings provide strong support for the continued use of electronic evidence‐based order sets in the inpatient medical setting. Once the initial implementation of a comprehensive EMR has occurred, deployment of these electronic order sets is a relatively inexpensive but effective method to foster compliance with evidence‐based care.
Future research in healthcare information technology can take a number of directions. One important area, of course, revolves around ways to promote enhanced physician adoption of EMRs. Our audit of records where the AMI‐OS was not used found that specific reasons for not using the order set (eg, treatment refusals, emergent intervention) were present in two‐thirds of the cases. This suggests that future analyses of adherence involving EMRs and CPOE implementation should take a more nuanced look at how order entry is actually enabled. It may be that understanding how order sets affect care enhances clinician acceptance and thus could serve as an incentive to EMR adoption. However, once an EMR is adopted, a need exists to continue evaluations such as this because, ultimately, the gold standard should be improved patient care processes and better outcomes for patients.
Acknowledgement
The authors give special thanks to Dr. Brian Hoberman for sponsoring this work, Dr. Alan S. Go for providing assistance with obtaining copies of electrocardiograms for review, Drs. Tracy Lieu and Vincent Liu for reviewing the manuscript, and Ms. Rachel Lesser for formatting the manuscript.
Disclosures: This work was supported by The Permanente Medical Group, Inc. and Kaiser Foundation Hospitals, Inc. The algorithms used to extract data and perform risk adjustment were developed with funding from the Sidney Garfield Memorial Fund (Early Detection of Impending Physiologic Deterioration in Hospitalized Patients, 1159518), the Agency for Healthcare Quality and Research (Rapid Clinical Snapshots From the EMR Among Pneumonia Patients, 1R01HS018480‐01), and the Gordon and Betty Moore Foundation (Early Detection of Impending Physiologic Deterioration: Electronic Early Warning System).
- , , , , , . Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362(23):2155–2165.
- , , , et al. Twenty‐two‐year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987–2008. Circulation. 2012;125(15):1848–1857.
- , , , et al. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation. 2012;125(1):e2–e220.
- , , , et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non‐ST‐Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non‐ST‐Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50(7):e1–e157.
- , , , et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2008;51(2):210–247.
- , , , , , . Association between adoption of evidence‐based treatment and survival for patients with ST‐elevation myocardial infarction. JAMA. 2011;305(16):1677–1684.
- , , , et al. Association of changes in clinical characteristics and management with improvement in survival among patients with ST‐elevation myocardial infarction. JAMA. 2012;308(10):998–1006.
- , , , et al. Changes in myocardial infarction guideline adherence as a function of patient risk: an end to paradoxical care? J Am Coll Cardiol. 2011;58(17):1760–1765.
- , , , . Care in U.S. hospitals—the Hospital Quality Alliance program. N Engl J Med. 2005;353(3):265–274.
- , , et al. Challenges in the treatment of NSTEMI patients at high risk for both ischemic and bleeding events: insights from the ACTION Registry‐GWTG. J Am Coll Cardiol. 2011;57:E913–E913.
- , , , , . Quality of care in U.S. hospitals as reflected by standardized measures, 2002–2004. N Engl J Med. 2005;353(3):255–264.
- , , . Guideline‐based standardized care is associated with substantially lower mortality in medicare patients with acute myocardial infarction. J Am Coll Cardiol. 2005;46(7):1242–1248.
- , , , et al. Impact of a standardized heart failure order set on mortality, readmission, and quality and costs of care. Int J Qual Health Care. 2010;22(6):437–444.
- . Linking automated databases for research in managed care settings. Ann Intern Med. 1997;127(8 pt 2):719–724.
- , , , , , . Risk adjusting hospital inpatient mortality using automated inpatient, outpatient, and laboratory databases. Med Care. 2008;46(3):232–239.
- , , , . Length of stay predictions: improvements through the use of automated laboratory and comorbidity variables. Med Care. 2010;48(8):739–744.
- , , , , , . Intra‐hospital transfers to a higher level of care: contribution to total hospital and intensive care unit (ICU) mortality and length of stay (LOS). J Hosp Med. 2011;6(2):74–80.
- , , , . Adverse outcomes associated with delayed intensive care unit transfers in an integrated healthcare system. J Hosp Med. 2012;7(3):224–230.
- International Classification of Diseases, 9th Revision‐Clinical Modification. 4th ed. 3 Vols. Los Angeles, CA: Practice Management Information Corporation; 2006.
- , , , et al. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. 2003;290(20):2685–2692.
- , , , , , . Early detection of impending physiologic deterioration among patients who are not in intensive care: development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012;7(5):388–395.
- , , , , . Risk‐adjusting hospital mortality using a comprehensive electronic record in an integrated healthcare delivery system. Med Care. 2013;51(5):446–453.
- , , . Effect of choice of estimation method on inter‐hospital mortality rate comparisons. Med Care. 2010;48(5):456–485.
- , , , . The Kaiser Permanente inpatient risk adjustment methodology was valid in an external patient population. J Clin Epidemiol. 2010;63(7):798–803.
- , , , , . Derivation and validation of a model to predict daily risk of death in hospital. Med Care. 2011;49(8):734–743.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
- . Introduction to Statistical Mediation Analysis. New York, NY: Lawrence Erlbaum Associates; 2008.
- . Nonparametric estimation of average treatment effects under exogenity: a review. Rev Econ Stat. 2004;86:25.
- . Design of Observational Studies. New York, NY: Springer Science+Business Media; 2010.
- . Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity‐score matched samples. Stat Med. 2009;28:24.
- , , . Estimation of regression coefficients when some regressors are not always observed. J Am Stat Assoc. 1994(89):846–866.
- , . Stratification and weighting via the propensity score in estimation of causal treatment effects: a comparative study. Stat Med. 2004;23(19):2937–2960.
- . Discussing hidden bias in observational studies. Ann Intern Med. 1991;115(11):901–905.
- . Propensity score methods for bias reduction in the comparison of a treatment to a non‐randomized control group. Stat Med. 1998;17(19):2265–2281.
- , , . A method/macro based on propensity score and Mahalanobis distance to reduce bias in treatment comparison in observational study, 2005. www.lexjansen.com/pharmasug/2006/publichealthresearch/pr05.pdf. Accessed on September 14, 2013.
- . Using health information technology to improve health care. Arch Intern Med. 2012;172(22):1728–1730.
Although the prevalence of coronary heart disease and death from acute myocardial infarction (AMI) have declined steadily, about 935,000 heart attacks still occur annually in the United States, with approximately one‐third of these being fatal.[1, 2, 3] Studies have demonstrated decreased 30‐day and longer‐term mortality in AMI patients who receive evidence‐based treatment, including aspirin, ‐blockers, angiotensin‐converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), anticoagulation therapy, and statins.[4, 5, 6, 7] Despite clinical practice guidelines (CPGs) outlining evidence‐based care and considerable efforts to implement processes that improve patient outcomes, delivery of effective therapy remains suboptimal.[8] For example, the Hospital Quality Alliance Program[9] found that in AMI patients, use of aspirin on admission was only 81% to 92%, ‐blocker on admission 75% to 85%, and ACE inhibitors for left ventricular dysfunction 71% to 74%.
Efforts to increase adherence to CPGs and improve patient outcomes in AMI have resulted in variable degrees of success. They include promotion of CPGs,[4, 5, 6, 7] physician education with feedback, report cards, care paths, registries,[10] Joint Commission standardized measures,[11] and paper checklists or order sets (OS).[12, 13]
In this report, we describe the association between use of an evidence‐based, electronic OS for AMI (AMI‐OS) and better adherence to CPGs. This AMI‐OS was implemented in the inpatient electronic medical records (EMRs) of a large integrated healthcare delivery system, Kaiser Permanente Northern California (KPNC). The purpose of our investigation was to determine (1) whether use of the AMI‐OS was associated with improved AMI processes and patient outcomes, and (2) whether these associations persisted after risk adjustment using a comprehensive severity of illness scoring system.
MATERIALS AND METHODS
This project was approved by the KPNC institutional review board.
Under a mutual exclusivity arrangement, salaried physicians of The Permanente Medical Group, Inc., care for 3.4 million Kaiser Foundation Health Plan, Inc. members at facilities owned by Kaiser Foundation Hospitals, Inc. All KPNC facilities employ the same information systems with a common medical record number and can track care covered by the plan but delivered elsewhere.[14] Our setting consisted of 21 KPNC hospitals described in previous reports,[15, 16, 17, 18] using the same commercially available EMR system that includes computerized physician order entry (CPOE). Deployment of the customized inpatient Epic EMR (
In this EMR's CPOE, physicians have options to select individual orders (a la carte) or they can utilize an OS, which is a collection of the most appropriate orders associated with specific diagnoses, procedures, or treatments. The evidence‐based AMI‐OS studied in this project was developed by a multidisciplinary team (for detailed components see Supporting Appendix 1Appendix 5 in the online version of this article).
Our study focused on the first set of hospital admission orders for patients with AMI. The study sample consisted of patients meeting these criteria: (1) age 18 years at admission; (2) admitted to a KPNC hospital for an overnight stay between September 28, 2008 and December 31, 2010; (3) principal diagnosis was AMI (International Classification of Diseases, 9th Revision [ICD‐9][19] codes 410.00, 01, 10, 11, 20, 21, 30, 31, 40, 41, 50, 51, 60, 61, 70, 71, 80, 90, and 91); and (4) KPHC had been operational at the hospital for at least 3 months to be included (for assembly descriptions see Supporting Appendices 15 in the online version of this article). At the study hospitals, troponin I was measured using the Beckman Access AccuTnI assay (Beckman Coulter, Inc., Brea, CA), whose upper reference limit (99th percentile) is 0.04 ng/mL. We excluded patients initially hospitalized for AMI at a non‐KPNC site and transferred into a study hospital.
The data processing methods we employed have been detailed elsewhere.[14, 15, 17, 20, 21, 22] The dependent outcome variables were total hospital length of stay, inpatient mortality, 30‐day mortality, and all‐cause rehospitalization within 30 days of discharge. Linked state mortality data were unavailable for the entire study period, so we ascertained 30‐day mortality based on the combination of KPNC patient demographic data and publicly available Social Security Administration decedent files. We ascertained rehospitalization by scanning KPNC hospitalization databases, which also track out‐of‐plan use.
The dependent process variables were use of aspirin within 24 hours of admission, ‐blockers, anticoagulation, ACE inhibitors or ARBs, and statins. The primary independent variable of interest was whether or not the admitting physician employed the AMI‐OS when admission orders were entered. Consequently, this variable is dichotomous (AMI‐OS vs a la carte).
We controlled for acute illness severity and chronic illness burden using a recent modification[22] of an externally validated risk‐adjustment system applicable to all hospitalized patients.[15, 16, 23, 24, 25] Our methodology included vital signs, neurological status checks, and laboratory test results obtained in the 72 hours preceding hospital admission; comorbidities were captured longitudinally using data from the year preceding hospitalization (for comparison purposes, we also assigned a Charlson Comorbidity Index score[26]).
End‐of‐life care directives are mandatory on admission at KPNC hospitals. Physicians have 4 options: full code, partial code, do not resuscitate, and comfort care only. Because of small numbers in some categories, we collapsed these 4 categories into full code and not full code. Because patients' care directives may change, we elected to capture the care directive in effect when a patient first entered a hospital unit other than the emergency department (ED).
Two authors (M.B., P.C.L.), one of whom is a board‐certified cardiologist, reviewed all admission electrocardiograms and made a consensus determination as to whether or not criteria for ST‐segment elevation myocardial infarction (STEMI) were present (ie, new ST‐segment elevation or left bundle branch block); we also reviewed the records of all patients with missing troponin I data to confirm the AMI diagnosis.
Statistical Methods
We performed unadjusted comparisons between AMI‐OS and nonAMI‐OS patients using the t test or the [2] test, as appropriate.
We hypothesized that the AMI‐OS plays a mediating role on patient outcomes through its effect on adherence to recommended treatment. We evaluated this hypothesis for inpatient mortality by first fitting a multivariable logistic regression model for inpatient mortality as the outcome and either the 5 evidence‐based therapies or the total number of evidence‐based therapies used (ranging from 02, 3, 4, or 5) as the dependent variable controlling for age, gender, presence of STEMI, troponin I, comorbidities, illness severity, ED length of stay (LOS), care directive status, and timing of cardiac catheterization referral as covariates to confirm the protective effect of these therapies on mortality. We then used the same model to estimate the effect of AMI‐OS on inpatient mortality, substituting the therapies with AMI‐OS as the dependent variable and using the same covariates. Last, we included both the therapies and the AMI‐OS in the model to evaluate their combined effects.[27]
We used 2 different methods to estimate the effects of AMI‐OS and number of therapies provided on the outcomes while adjusting for observed baseline differences between the 2 groups of patients: propensity risk score matching, which estimates the average treatment effect for the treated,[28, 29] and inverse probability of treatment weighting, which is used to estimate the average treatment effect.[30, 31, 32] The propensity score was defined as the probability of receiving the intervention for a patient with specific predictive factors.[33, 34] We computed a propensity score for each patient by using logistic regression, with the dependent variable being receipt of AMI‐OS and the independent variables being the covariates used for the multivariate logistic regression as well as ICD‐9 code for final diagnosis. We calculated the Mahalanobis distance between patients who received AMI‐OS (cases) and patients who did not received AMI‐OS (controls) using the same set of covariates. We matched each case to a single control within the same facility based on the nearest available Mahalanobis metric matching within calipers defied as the maximum width of 0.2 standard deviations of the logit of the estimated propensity score.[29, 35] We estimated the odds ratios for the binary dependent variables based on a conditional logistic regression model to account for the matched pairs design.[28] We used a generalized linear model with the log‐transformed LOS as the outcome to estimate the ratio of the LOS geometric mean of the cases to the controls. We calculated the relative risk for patients receiving AMI‐OS via the inverse probability weighting method by first defining a weight for each patient. [We assigned a weight of 1/psi to patients who received the AMI‐OS and a weight of 1/(1psi) to patients who did not receive the AMI‐OS, where psi denotes the propensity score for patient i]. We used a logistic regression model for the binary dependent variables with the same set of covariates described above to estimate the adjusted odds ratios while weighting each observation by its corresponding weight. Last, we used a weighted generalized linear model to estimate the AMI‐OS effect on the log‐transformed LOS.
RESULTS
Table 1 summarizes the characteristics of the 5879 patients. It shows that AMI‐OS patients were more likely to receive evidence‐based therapies for AMI (aspirin, ‐blockers, ACE inhibitors or ARBs, anticoagulation, and statins) and had a 46% lower mortality rate in hospital (3.51 % vs 6.52%) and 33% lower rate at 30 days (5.66% vs 8.48%). AMI‐OS patients were also found to be at lower risk for an adverse outcome than nonAMI‐OS patients. The AMI‐OS patients had lower peak troponin I values, severity of illness (lower Laboratory‐Based Acute Physiology Score, version 2 [LAPS2] scores), comorbidity burdens (lower Comorbidity Point Score, version 2 [COPS2] and Charlson scores), and global predicted mortality risk. AMI‐OS patients were also less likely to have required intensive care. AMI‐OS patients were at higher risk of death than nonAMI‐OS patients with respect to only 1 variable (being full code at the time of admission), but although this difference was statistically significant, it was of minor clinical impact (86% vs 88%).
| Patients Initially Managed Using | P Valuea | ||
|---|---|---|---|
| AMI Order Set, N=3,531b | A La Carte Orders, N=2,348b | ||
| |||
| Age, y, median (meanSD) | 70 (69.413.8) | 70 (69.213.8) | 0.5603 |
| Age (% >65 years) | 2,134 (60.4%) | 1,415 (60.3%) | 0.8949 |
| Sex (% male) | 2,202 (62.4%) | 1,451 (61.8%) | 0.6620 |
| STEMI (% with)c | 166 (4.7%) | 369 (15.7%) | <0.0001 |
| Troponin I (% missing) | 111 (3.1%) | 151 (6.4%) | <0.0001 |
| Troponin I median (meanSD) | 0.57 (3.08.2) | 0.27 (2.58.9) | 0.0651 |
| Charlson score median (meanSD)d | 2.0 (2.51.5) | 2.0 (2.71.6) | <0.0001 |
| COPS2, median (meanSD)e | 14.0 (29.831.7) | 17.0 (34.334.4) | <0.0001 |
| LAPS2, median (meanSD)e | 0.0 (35.643.5) | 27.0 (40.948.1) | <0.0001 |
| Length of stay in ED, h, median (meanSD) | 5.7 (5.93.0) | 5.7 (5.43.1) | <0.0001 |
| Patients receiving aspirin within 24 hoursf | 3,470 (98.3%) | 2,202 (93.8%) | <0.0001 |
| Patients receiving anticoagulation therapyf | 2,886 (81.7%) | 1,846 (78.6%) | 0.0032 |
| Patients receiving ‐blockersf | 3,196 (90.5%) | 1,926 (82.0%) | <0.0001 |
| Patients receiving ACE inhibitors or ARBsf | 2,395 (67.8%) | 1,244 (53.0%) | <0.0001 |
| Patients receiving statinsf | 3,337 (94.5%) | 1,975 (84.1%) | <0.0001 |
| Patient received 1 or more therapies | 3,531 (100.0%) | 2,330 (99.2%) | <0.0001 |
| Patient received 2 or more therapies | 3,521 (99.7%) | 2,266 (96.5%) | <0.0001 |
| Patient received 3 or more therapies | 3,440 (97.4%) | 2,085 (88.8%) | <0.0001 |
| Patient received 4 or more therapies | 3,015 (85.4%) | 1,646 (70.1%) | <0.0001 |
| Patient received all 5 therapies | 1,777 (50.3%) | 866 (35.9%) | <0.0001 |
| Predicted mortality risk, %, median, (meanSD)f | 0.86 (3.27.4) | 1.19 (4.810.8) | <0.0001 |
| Full code at time of hospital entry (%)g | 3,041 (86.1%) | 2,066 (88.0%) | 0.0379 |
| Admitted to ICU (%)i | |||
| Direct admit | 826 (23.4%) | 567 (24.2%) | 0.5047 |
| Unplanned transfer | 222 (6.3%) | 133 (5.7%) | 0.3262 |
| Ever | 1,283 (36.3%) | 1,169 (49.8%) | <0.0001 |
| Length of stay, h, median (meanSD) | 68.3 (109.4140.9) | 68.9 (113.8154.3) | 0.2615 |
| Inpatient mortality (%) | 124 (3.5%) | 153 (6.5%) | <0.0001 |
| 30‐day mortality (%) | 200 (5.7%) | 199 (8.5%) | <0.0001 |
| All‐cause rehospitalization within 30 days (%) | 576 (16.3%) | 401 (17.1%) | 0.4398 |
| Cardiac catheterization procedure referral timing | |||
| 1 day preadmission to discharge | 2,018 (57.2%) | 1,348 (57.4%) | 0.1638 |
| 2 days preadmission or earlier | 97 (2.8%) | 87 (3.7%) | |
| After discharge | 149 (4.2%) | 104 (4.4%) | |
| No referral | 1,267 (35.9%) | 809 (34.5%) | |
Table 2 shows the result of a logistic regression model in which the dependent variable was inpatient mortality and either the 5 evidence‐based therapies or the total number of evidence‐based therapies are the dependent variables. ‐blocker, statin, and ACE inhibitor or ARB therapies all had a protective effect on mortality, with odds ratios ranging from 0.48 (95% confidence interval [CI]: 0.36‐0.64), 0.63 (95% CI: 0.45‐0.89), and 0.40 (95% CI: 0.30‐0.53), respectively. An increased number of therapies also had a beneficial effect on inpatient mortality, with patients having 3 or more of the evidence‐based therapies showing an adjusted odds ratio (AOR) of 0.49 (95% CI: 0.33‐0.73), 4 or more therapies an AOR of 0.29 (95% CI: 0.20‐0.42), and 0.17 (95% CI: 0.11‐0.25) for 5 or more therapies.
| Multiple Therapies Effect | Individual Therapies Effect | |||
|---|---|---|---|---|
| Outcome | Death | Death | ||
| Number of outcomes | 277 | 277 | ||
| AORa | 95% CIb | AORa | 95% CIb | |
| ||||
| Age in years | ||||
| 1839 | Ref | Ref | ||
| 4064 | 1.02 | (0.147.73) | 1.01 | (0.137.66) |
| 6584 | 4.05 | (0.5529.72) | 3.89 | (0.5328.66) |
| 85+ | 4.99 | (0.6737.13) | 4.80 | (0.6435.84) |
| Sex | ||||
| Female | Ref | |||
| Male | 1.05 | (0.811.37) | 1.07 | (0.821.39) |
| STEMIc | ||||
| Absent | Ref | Ref | ||
| Present | 4.00 | (2.755.81) | 3.86 | (2.645.63) |
| Troponin I | ||||
| 0.1 ng/ml | Ref | Ref | ||
| >0.1 ng/ml | 1.01 | (0.721.42) | 1.02 | (0.731.43) |
| COPS2d (AOR per 10 points) | 1.05 | (1.011.08) | 1.04 | (1.011.08) |
| LAPS2d (AOR per 10 points) | 1.09 | (1.061.11) | 1.09 | (1.061.11) |
| ED LOSe (hours) | ||||
| <6 | Ref | Ref | ||
| 67 | 0.74 | (0.531.03) | 0.76 | (0.541.06) |
| >=12 | 0.82 | (0.391.74) | 0.83 | (0.391.78) |
| Code Statusf | ||||
| Full Code | Ref | |||
| Not Full Code | 1.08 | (0.781.49) | 1.09 | (0.791.51) |
| Cardiac procedure referral | ||||
| None during stay | Ref | |||
| 1 day pre adm until discharge | 0.40 | (0.290.54) | 0.39 | (0.280.53) |
| Number of therapies received | ||||
| 2 or less | Ref | |||
| 3 | 0.49 | (0.330.73) | ||
| 4 | 0.29 | (0.200.42) | ||
| 5 | 0.17 | (0.110.25) | ||
| Aspirin therapy | 0.80 | (0.491.32) | ||
| Anticoagulation therapy | 0.86 | (0.641.16) | ||
| Beta Blocker therapy | 0.48 | (0.360.64) | ||
| Statin therapy | 0.63 | (0.450.89) | ||
| ACE inhibitors or ARBs | 0.40 | (0.300.53) | ||
| C Statistic | 0.814 | 0.822 | ||
| Hosmer‐Lemeshow p value | 0.509 | 0.934 | ||
Table 3 shows that the use of the AMI‐OS is protective, with an AOR of 0.59 and a 95% CI of 0.45‐0.76. Table 3 also shows that the most potent predictors were comorbidity burden (AOR: 1.07, 95% CI: 1.03‐1.10 per 10 COPS2 points), severity of illness (AOR: 1.09, 95% CI: 1.07‐1.12 per 10 LAPS2 points), STEMI (AOR: 3.86, 95% CI: 2.68‐5.58), and timing of cardiac catheterization referral occurring immediately prior to or during the admission (AOR: 0.37, 95% CI: 0.27‐0.51). The statistical significance of the AMI‐OS effect disappears when both AMI‐OS and the individual therapies are included in the same model (see Supporting Information, Appendices 15, in the online version of this article).
| Outcome | Death | |
|---|---|---|
| Number of outcomes | 277 | |
| AORa | 95% CIb | |
| ||
| Age in years | ||
| 1839 | Ref | |
| 4064 | 1.16 | (0.158.78) |
| 6584 | 4.67 | (0.6334.46) |
| 85+ | 5.45 | (0.7340.86) |
| Sex | ||
| Female | Ref | |
| Male | 1.05 | (0.811.36) |
| STEMIc | ||
| Absent | Ref | |
| Present | 3.86 | (2.685.58) |
| Troponin I | ||
| 0.1 ng/ml | Ref | |
| >0.1 ng/ml | 1.16 | (0.831.62) |
| COPS2d (AOR per 10 points) | 1.07 | (1.031.10) |
| LAPS2d (AOR per 10 points) | 1.09 | (1.071.12) |
| ED LOSe (hours) | ||
| <6 | Ref | |
| 67 | 0.72 | (0.521.00) |
| >=12 | 0.70 | (0.331.48) |
| Code statusf | ||
| Full code | Ref | |
| Not full code | 1.22 | (0.891.68) |
| Cardiac procedure referral | ||
| None during stay | Ref | |
| 1 day pre adm until discharge | 0.37 | (0.270.51) |
| Order set employedg | ||
| No | Ref | |
| Yes | 0.59 | (0.450.76) |
| C Statistic | 0.792 | |
| Hosmer‐Lemeshow p value | 0.273 | |
Table 4 shows separately the average treatment effect (ATE) and average treatment effect for the treated (ATT) of AMI‐OS and of increasing number of therapies on other outcomes (30‐day mortality, LOS, and readmission). Both the ATE and ATT show that the use of the AMI‐OS was significantly protective with respect to mortality and total hospital LOS but not significant with respect to readmission. The effect of the number of therapies on mortality is significantly higher with increasing number of therapies. For example, patients who received 5 therapies had an average treatment effect on 30‐day inpatient mortality of 0.23 (95% CI: 0.15‐0.35) compared to 0.64 (95% CI: 0.43‐0.96) for 3 therapies, almost a 3‐fold difference. The effects of increasing number of therapies were not significant for LOS or readmission. A sensitivity analysis in which the 535 STEMI patients were removed showed essentially the same results, so it is not reported here.
| Outcome | Order Seta | 3 Therapiesb | 4 Therapiesb | 5 Therapiesb |
|---|---|---|---|---|
| ||||
| Average treatment effectc | ||||
| Inpatient mortality | 0.67 (0.520.86) | 0.64 (0.430.96) | 0.37 (0.250.54) | 0.23 (0.150.35) |
| 30‐day mortality | 0.77 (0.620.96) | 0.68 (0.480.98) | 0.34 (0.240.48) | 0.26 (0.180.37) |
| Readmission | 1.03 (0.901.19) | 1.20 (0.871.66) | 1.19 (0.881.60) | 1.30 (0.961.76) |
| LOS, ratio of the geometric means | 0.91 (0.870.95) | 1.16 (1.031.30) | 1.17 (1.051.30) | 1.12 (1.001.24) |
| Average treatment effect on the treatedd | ||||
| Inpatient mortality | 0.69 (0.520.92) | 0.35 (0.130.93) | 0.17 (0.070.43) | 0.08 (0.030.20) |
| 30‐day mortality | 0.84 (0.661.06) | 0.35 (0.150.79) | 0.17 (0.070.37) | 0.09 (0.040.20) |
| Readmission | 1.02 (0.871.20) | 1.39 (0.852.26) | 1.36 (0.882.12) | 1.23 (0.801.89) |
| LOS, ratio of the geometric meanse | 0.92 (0.870.97) | 1.18 (1.021.37) | 1.16 (1.011.33) | 1.04 (0.911.19) |
To further elucidate possible reasons why physicians did not use the AMI‐OS, the lead author reviewed 105 randomly selected records where the AMI‐OS was not used, 5 records from each of the 21 study hospitals. This review found that in 36% of patients, the AMI‐OS was not used because emergent catheterization or transfer to a facility with percutaneous coronary intervention capability occurred. Presence of other significant medical conditions, including critical illness, was the reason in 17% of these cases, patient or family refusal of treatments in 8%, issues around end‐of‐life care in 3%, and specific medical contraindications in 1%. In the remaining 34%, no reason for not using the AMI‐OS could be identified.
DISCUSSION
We evaluated the use of an evidence‐based electronic AMI‐OS embedded in a comprehensive EMR and found that it was beneficial. Its use was associated with increased adherence to evidence‐based therapies, which in turn were associated with improved outcomes. Using data from a large cohort of hospitalized AMI patients in 21 community hospitals, we were able to use risk adjustment that included physiologic illness severity to adjust for baseline mortality risk. Patients in whom the AMI‐OS was employed tended to be at lower risk; nonetheless, after controlling for confounding variables and adjusting for bias using propensity scores, the AMI‐OS was associated with increased use of evidence‐based therapies and decreased mortality. Most importantly, it appears that the benefits of the OS were not just due to increased receipt of individual recommended therapies, but to increased concurrent receipt of multiple recommended therapies.
Modern EMRs have great potential for significant improvements in the quality, efficiency, and safety of care provided,[36] and our study highlights this potential. However, a number of important limitations to our study must be considered. Although we had access to a very rich dataset, we could not control for all possible confounders, and our risk adjustment cannot match the level of information available to clinicians. In particular, the measurements available to us with respect to cardiac risk are limited. Thus, we have to recognize that the strength of our findings does not approximate that of a randomized trial, and one would expect that the magnitude of the beneficial association would fall under more controlled conditions. Resource limitations also did not permit us to gather more time course data (eg, sequential measurements of patient instability, cardiac damage, or use of recommended therapies), which could provide a better delineation of differences in both processes and outcomes.
Limitations also exist to the generalizability of the use of order sets in other settings that go beyond the availability of a comprehensive EMR. Our study population was cared for in a setting with an unusually high level of integration.[1] For example, KPNC has an elaborate administrative infrastructure for training in the use of the EMR as well as ensuring that order sets are not just evidence‐based, but that they are perceived by clinicians to be of significant value. This infrastructure, established to ensure physician buy‐in, may not be easy to replicate in smaller or less‐integrated settings. Thus, it is conceivable that factors other than the degree of support during the EMR deployments can affect rates of order set use.
Although our use of counterfactual methods included illness severity (LAPS2) and longitudinal comorbidity burden (COPS2), which are not yet available outside highly integrated delivery services employing comprehensive EMRs, it is possible they are insufficient. We cannot exclude the possibility that other biases or patient characteristics were present that led clinicians to preferentially employ the electronic order set in some patients but not in others. One could also argue that future studies should consider using overall adherence to recommended AMI treatment guidelines as a risk adjustment tool that would permit one to analyze what other factors may be playing a role in residual differences in patient outcomes. Last, one could object to our inclusion of STEMI patients; however, this was not a study on optimum treatment strategies for STEMI patients. Rather, it was a study on the impact on AMI outcomes of a specific component of computerized order entry outside the research setting.
Despite these limitations, we believe that our findings provide strong support for the continued use of electronic evidence‐based order sets in the inpatient medical setting. Once the initial implementation of a comprehensive EMR has occurred, deployment of these electronic order sets is a relatively inexpensive but effective method to foster compliance with evidence‐based care.
Future research in healthcare information technology can take a number of directions. One important area, of course, revolves around ways to promote enhanced physician adoption of EMRs. Our audit of records where the AMI‐OS was not used found that specific reasons for not using the order set (eg, treatment refusals, emergent intervention) were present in two‐thirds of the cases. This suggests that future analyses of adherence involving EMRs and CPOE implementation should take a more nuanced look at how order entry is actually enabled. It may be that understanding how order sets affect care enhances clinician acceptance and thus could serve as an incentive to EMR adoption. However, once an EMR is adopted, a need exists to continue evaluations such as this because, ultimately, the gold standard should be improved patient care processes and better outcomes for patients.
Acknowledgement
The authors give special thanks to Dr. Brian Hoberman for sponsoring this work, Dr. Alan S. Go for providing assistance with obtaining copies of electrocardiograms for review, Drs. Tracy Lieu and Vincent Liu for reviewing the manuscript, and Ms. Rachel Lesser for formatting the manuscript.
Disclosures: This work was supported by The Permanente Medical Group, Inc. and Kaiser Foundation Hospitals, Inc. The algorithms used to extract data and perform risk adjustment were developed with funding from the Sidney Garfield Memorial Fund (Early Detection of Impending Physiologic Deterioration in Hospitalized Patients, 1159518), the Agency for Healthcare Quality and Research (Rapid Clinical Snapshots From the EMR Among Pneumonia Patients, 1R01HS018480‐01), and the Gordon and Betty Moore Foundation (Early Detection of Impending Physiologic Deterioration: Electronic Early Warning System).
Although the prevalence of coronary heart disease and death from acute myocardial infarction (AMI) have declined steadily, about 935,000 heart attacks still occur annually in the United States, with approximately one‐third of these being fatal.[1, 2, 3] Studies have demonstrated decreased 30‐day and longer‐term mortality in AMI patients who receive evidence‐based treatment, including aspirin, ‐blockers, angiotensin‐converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), anticoagulation therapy, and statins.[4, 5, 6, 7] Despite clinical practice guidelines (CPGs) outlining evidence‐based care and considerable efforts to implement processes that improve patient outcomes, delivery of effective therapy remains suboptimal.[8] For example, the Hospital Quality Alliance Program[9] found that in AMI patients, use of aspirin on admission was only 81% to 92%, ‐blocker on admission 75% to 85%, and ACE inhibitors for left ventricular dysfunction 71% to 74%.
Efforts to increase adherence to CPGs and improve patient outcomes in AMI have resulted in variable degrees of success. They include promotion of CPGs,[4, 5, 6, 7] physician education with feedback, report cards, care paths, registries,[10] Joint Commission standardized measures,[11] and paper checklists or order sets (OS).[12, 13]
In this report, we describe the association between use of an evidence‐based, electronic OS for AMI (AMI‐OS) and better adherence to CPGs. This AMI‐OS was implemented in the inpatient electronic medical records (EMRs) of a large integrated healthcare delivery system, Kaiser Permanente Northern California (KPNC). The purpose of our investigation was to determine (1) whether use of the AMI‐OS was associated with improved AMI processes and patient outcomes, and (2) whether these associations persisted after risk adjustment using a comprehensive severity of illness scoring system.
MATERIALS AND METHODS
This project was approved by the KPNC institutional review board.
Under a mutual exclusivity arrangement, salaried physicians of The Permanente Medical Group, Inc., care for 3.4 million Kaiser Foundation Health Plan, Inc. members at facilities owned by Kaiser Foundation Hospitals, Inc. All KPNC facilities employ the same information systems with a common medical record number and can track care covered by the plan but delivered elsewhere.[14] Our setting consisted of 21 KPNC hospitals described in previous reports,[15, 16, 17, 18] using the same commercially available EMR system that includes computerized physician order entry (CPOE). Deployment of the customized inpatient Epic EMR (
In this EMR's CPOE, physicians have options to select individual orders (a la carte) or they can utilize an OS, which is a collection of the most appropriate orders associated with specific diagnoses, procedures, or treatments. The evidence‐based AMI‐OS studied in this project was developed by a multidisciplinary team (for detailed components see Supporting Appendix 1Appendix 5 in the online version of this article).
Our study focused on the first set of hospital admission orders for patients with AMI. The study sample consisted of patients meeting these criteria: (1) age 18 years at admission; (2) admitted to a KPNC hospital for an overnight stay between September 28, 2008 and December 31, 2010; (3) principal diagnosis was AMI (International Classification of Diseases, 9th Revision [ICD‐9][19] codes 410.00, 01, 10, 11, 20, 21, 30, 31, 40, 41, 50, 51, 60, 61, 70, 71, 80, 90, and 91); and (4) KPHC had been operational at the hospital for at least 3 months to be included (for assembly descriptions see Supporting Appendices 15 in the online version of this article). At the study hospitals, troponin I was measured using the Beckman Access AccuTnI assay (Beckman Coulter, Inc., Brea, CA), whose upper reference limit (99th percentile) is 0.04 ng/mL. We excluded patients initially hospitalized for AMI at a non‐KPNC site and transferred into a study hospital.
The data processing methods we employed have been detailed elsewhere.[14, 15, 17, 20, 21, 22] The dependent outcome variables were total hospital length of stay, inpatient mortality, 30‐day mortality, and all‐cause rehospitalization within 30 days of discharge. Linked state mortality data were unavailable for the entire study period, so we ascertained 30‐day mortality based on the combination of KPNC patient demographic data and publicly available Social Security Administration decedent files. We ascertained rehospitalization by scanning KPNC hospitalization databases, which also track out‐of‐plan use.
The dependent process variables were use of aspirin within 24 hours of admission, ‐blockers, anticoagulation, ACE inhibitors or ARBs, and statins. The primary independent variable of interest was whether or not the admitting physician employed the AMI‐OS when admission orders were entered. Consequently, this variable is dichotomous (AMI‐OS vs a la carte).
We controlled for acute illness severity and chronic illness burden using a recent modification[22] of an externally validated risk‐adjustment system applicable to all hospitalized patients.[15, 16, 23, 24, 25] Our methodology included vital signs, neurological status checks, and laboratory test results obtained in the 72 hours preceding hospital admission; comorbidities were captured longitudinally using data from the year preceding hospitalization (for comparison purposes, we also assigned a Charlson Comorbidity Index score[26]).
End‐of‐life care directives are mandatory on admission at KPNC hospitals. Physicians have 4 options: full code, partial code, do not resuscitate, and comfort care only. Because of small numbers in some categories, we collapsed these 4 categories into full code and not full code. Because patients' care directives may change, we elected to capture the care directive in effect when a patient first entered a hospital unit other than the emergency department (ED).
Two authors (M.B., P.C.L.), one of whom is a board‐certified cardiologist, reviewed all admission electrocardiograms and made a consensus determination as to whether or not criteria for ST‐segment elevation myocardial infarction (STEMI) were present (ie, new ST‐segment elevation or left bundle branch block); we also reviewed the records of all patients with missing troponin I data to confirm the AMI diagnosis.
Statistical Methods
We performed unadjusted comparisons between AMI‐OS and nonAMI‐OS patients using the t test or the [2] test, as appropriate.
We hypothesized that the AMI‐OS plays a mediating role on patient outcomes through its effect on adherence to recommended treatment. We evaluated this hypothesis for inpatient mortality by first fitting a multivariable logistic regression model for inpatient mortality as the outcome and either the 5 evidence‐based therapies or the total number of evidence‐based therapies used (ranging from 02, 3, 4, or 5) as the dependent variable controlling for age, gender, presence of STEMI, troponin I, comorbidities, illness severity, ED length of stay (LOS), care directive status, and timing of cardiac catheterization referral as covariates to confirm the protective effect of these therapies on mortality. We then used the same model to estimate the effect of AMI‐OS on inpatient mortality, substituting the therapies with AMI‐OS as the dependent variable and using the same covariates. Last, we included both the therapies and the AMI‐OS in the model to evaluate their combined effects.[27]
We used 2 different methods to estimate the effects of AMI‐OS and number of therapies provided on the outcomes while adjusting for observed baseline differences between the 2 groups of patients: propensity risk score matching, which estimates the average treatment effect for the treated,[28, 29] and inverse probability of treatment weighting, which is used to estimate the average treatment effect.[30, 31, 32] The propensity score was defined as the probability of receiving the intervention for a patient with specific predictive factors.[33, 34] We computed a propensity score for each patient by using logistic regression, with the dependent variable being receipt of AMI‐OS and the independent variables being the covariates used for the multivariate logistic regression as well as ICD‐9 code for final diagnosis. We calculated the Mahalanobis distance between patients who received AMI‐OS (cases) and patients who did not received AMI‐OS (controls) using the same set of covariates. We matched each case to a single control within the same facility based on the nearest available Mahalanobis metric matching within calipers defied as the maximum width of 0.2 standard deviations of the logit of the estimated propensity score.[29, 35] We estimated the odds ratios for the binary dependent variables based on a conditional logistic regression model to account for the matched pairs design.[28] We used a generalized linear model with the log‐transformed LOS as the outcome to estimate the ratio of the LOS geometric mean of the cases to the controls. We calculated the relative risk for patients receiving AMI‐OS via the inverse probability weighting method by first defining a weight for each patient. [We assigned a weight of 1/psi to patients who received the AMI‐OS and a weight of 1/(1psi) to patients who did not receive the AMI‐OS, where psi denotes the propensity score for patient i]. We used a logistic regression model for the binary dependent variables with the same set of covariates described above to estimate the adjusted odds ratios while weighting each observation by its corresponding weight. Last, we used a weighted generalized linear model to estimate the AMI‐OS effect on the log‐transformed LOS.
RESULTS
Table 1 summarizes the characteristics of the 5879 patients. It shows that AMI‐OS patients were more likely to receive evidence‐based therapies for AMI (aspirin, ‐blockers, ACE inhibitors or ARBs, anticoagulation, and statins) and had a 46% lower mortality rate in hospital (3.51 % vs 6.52%) and 33% lower rate at 30 days (5.66% vs 8.48%). AMI‐OS patients were also found to be at lower risk for an adverse outcome than nonAMI‐OS patients. The AMI‐OS patients had lower peak troponin I values, severity of illness (lower Laboratory‐Based Acute Physiology Score, version 2 [LAPS2] scores), comorbidity burdens (lower Comorbidity Point Score, version 2 [COPS2] and Charlson scores), and global predicted mortality risk. AMI‐OS patients were also less likely to have required intensive care. AMI‐OS patients were at higher risk of death than nonAMI‐OS patients with respect to only 1 variable (being full code at the time of admission), but although this difference was statistically significant, it was of minor clinical impact (86% vs 88%).
| Patients Initially Managed Using | P Valuea | ||
|---|---|---|---|
| AMI Order Set, N=3,531b | A La Carte Orders, N=2,348b | ||
| |||
| Age, y, median (meanSD) | 70 (69.413.8) | 70 (69.213.8) | 0.5603 |
| Age (% >65 years) | 2,134 (60.4%) | 1,415 (60.3%) | 0.8949 |
| Sex (% male) | 2,202 (62.4%) | 1,451 (61.8%) | 0.6620 |
| STEMI (% with)c | 166 (4.7%) | 369 (15.7%) | <0.0001 |
| Troponin I (% missing) | 111 (3.1%) | 151 (6.4%) | <0.0001 |
| Troponin I median (meanSD) | 0.57 (3.08.2) | 0.27 (2.58.9) | 0.0651 |
| Charlson score median (meanSD)d | 2.0 (2.51.5) | 2.0 (2.71.6) | <0.0001 |
| COPS2, median (meanSD)e | 14.0 (29.831.7) | 17.0 (34.334.4) | <0.0001 |
| LAPS2, median (meanSD)e | 0.0 (35.643.5) | 27.0 (40.948.1) | <0.0001 |
| Length of stay in ED, h, median (meanSD) | 5.7 (5.93.0) | 5.7 (5.43.1) | <0.0001 |
| Patients receiving aspirin within 24 hoursf | 3,470 (98.3%) | 2,202 (93.8%) | <0.0001 |
| Patients receiving anticoagulation therapyf | 2,886 (81.7%) | 1,846 (78.6%) | 0.0032 |
| Patients receiving ‐blockersf | 3,196 (90.5%) | 1,926 (82.0%) | <0.0001 |
| Patients receiving ACE inhibitors or ARBsf | 2,395 (67.8%) | 1,244 (53.0%) | <0.0001 |
| Patients receiving statinsf | 3,337 (94.5%) | 1,975 (84.1%) | <0.0001 |
| Patient received 1 or more therapies | 3,531 (100.0%) | 2,330 (99.2%) | <0.0001 |
| Patient received 2 or more therapies | 3,521 (99.7%) | 2,266 (96.5%) | <0.0001 |
| Patient received 3 or more therapies | 3,440 (97.4%) | 2,085 (88.8%) | <0.0001 |
| Patient received 4 or more therapies | 3,015 (85.4%) | 1,646 (70.1%) | <0.0001 |
| Patient received all 5 therapies | 1,777 (50.3%) | 866 (35.9%) | <0.0001 |
| Predicted mortality risk, %, median, (meanSD)f | 0.86 (3.27.4) | 1.19 (4.810.8) | <0.0001 |
| Full code at time of hospital entry (%)g | 3,041 (86.1%) | 2,066 (88.0%) | 0.0379 |
| Admitted to ICU (%)i | |||
| Direct admit | 826 (23.4%) | 567 (24.2%) | 0.5047 |
| Unplanned transfer | 222 (6.3%) | 133 (5.7%) | 0.3262 |
| Ever | 1,283 (36.3%) | 1,169 (49.8%) | <0.0001 |
| Length of stay, h, median (meanSD) | 68.3 (109.4140.9) | 68.9 (113.8154.3) | 0.2615 |
| Inpatient mortality (%) | 124 (3.5%) | 153 (6.5%) | <0.0001 |
| 30‐day mortality (%) | 200 (5.7%) | 199 (8.5%) | <0.0001 |
| All‐cause rehospitalization within 30 days (%) | 576 (16.3%) | 401 (17.1%) | 0.4398 |
| Cardiac catheterization procedure referral timing | |||
| 1 day preadmission to discharge | 2,018 (57.2%) | 1,348 (57.4%) | 0.1638 |
| 2 days preadmission or earlier | 97 (2.8%) | 87 (3.7%) | |
| After discharge | 149 (4.2%) | 104 (4.4%) | |
| No referral | 1,267 (35.9%) | 809 (34.5%) | |
Table 2 shows the result of a logistic regression model in which the dependent variable was inpatient mortality and either the 5 evidence‐based therapies or the total number of evidence‐based therapies are the dependent variables. ‐blocker, statin, and ACE inhibitor or ARB therapies all had a protective effect on mortality, with odds ratios ranging from 0.48 (95% confidence interval [CI]: 0.36‐0.64), 0.63 (95% CI: 0.45‐0.89), and 0.40 (95% CI: 0.30‐0.53), respectively. An increased number of therapies also had a beneficial effect on inpatient mortality, with patients having 3 or more of the evidence‐based therapies showing an adjusted odds ratio (AOR) of 0.49 (95% CI: 0.33‐0.73), 4 or more therapies an AOR of 0.29 (95% CI: 0.20‐0.42), and 0.17 (95% CI: 0.11‐0.25) for 5 or more therapies.
| Multiple Therapies Effect | Individual Therapies Effect | |||
|---|---|---|---|---|
| Outcome | Death | Death | ||
| Number of outcomes | 277 | 277 | ||
| AORa | 95% CIb | AORa | 95% CIb | |
| ||||
| Age in years | ||||
| 1839 | Ref | Ref | ||
| 4064 | 1.02 | (0.147.73) | 1.01 | (0.137.66) |
| 6584 | 4.05 | (0.5529.72) | 3.89 | (0.5328.66) |
| 85+ | 4.99 | (0.6737.13) | 4.80 | (0.6435.84) |
| Sex | ||||
| Female | Ref | |||
| Male | 1.05 | (0.811.37) | 1.07 | (0.821.39) |
| STEMIc | ||||
| Absent | Ref | Ref | ||
| Present | 4.00 | (2.755.81) | 3.86 | (2.645.63) |
| Troponin I | ||||
| 0.1 ng/ml | Ref | Ref | ||
| >0.1 ng/ml | 1.01 | (0.721.42) | 1.02 | (0.731.43) |
| COPS2d (AOR per 10 points) | 1.05 | (1.011.08) | 1.04 | (1.011.08) |
| LAPS2d (AOR per 10 points) | 1.09 | (1.061.11) | 1.09 | (1.061.11) |
| ED LOSe (hours) | ||||
| <6 | Ref | Ref | ||
| 67 | 0.74 | (0.531.03) | 0.76 | (0.541.06) |
| >=12 | 0.82 | (0.391.74) | 0.83 | (0.391.78) |
| Code Statusf | ||||
| Full Code | Ref | |||
| Not Full Code | 1.08 | (0.781.49) | 1.09 | (0.791.51) |
| Cardiac procedure referral | ||||
| None during stay | Ref | |||
| 1 day pre adm until discharge | 0.40 | (0.290.54) | 0.39 | (0.280.53) |
| Number of therapies received | ||||
| 2 or less | Ref | |||
| 3 | 0.49 | (0.330.73) | ||
| 4 | 0.29 | (0.200.42) | ||
| 5 | 0.17 | (0.110.25) | ||
| Aspirin therapy | 0.80 | (0.491.32) | ||
| Anticoagulation therapy | 0.86 | (0.641.16) | ||
| Beta Blocker therapy | 0.48 | (0.360.64) | ||
| Statin therapy | 0.63 | (0.450.89) | ||
| ACE inhibitors or ARBs | 0.40 | (0.300.53) | ||
| C Statistic | 0.814 | 0.822 | ||
| Hosmer‐Lemeshow p value | 0.509 | 0.934 | ||
Table 3 shows that the use of the AMI‐OS is protective, with an AOR of 0.59 and a 95% CI of 0.45‐0.76. Table 3 also shows that the most potent predictors were comorbidity burden (AOR: 1.07, 95% CI: 1.03‐1.10 per 10 COPS2 points), severity of illness (AOR: 1.09, 95% CI: 1.07‐1.12 per 10 LAPS2 points), STEMI (AOR: 3.86, 95% CI: 2.68‐5.58), and timing of cardiac catheterization referral occurring immediately prior to or during the admission (AOR: 0.37, 95% CI: 0.27‐0.51). The statistical significance of the AMI‐OS effect disappears when both AMI‐OS and the individual therapies are included in the same model (see Supporting Information, Appendices 15, in the online version of this article).
| Outcome | Death | |
|---|---|---|
| Number of outcomes | 277 | |
| AORa | 95% CIb | |
| ||
| Age in years | ||
| 1839 | Ref | |
| 4064 | 1.16 | (0.158.78) |
| 6584 | 4.67 | (0.6334.46) |
| 85+ | 5.45 | (0.7340.86) |
| Sex | ||
| Female | Ref | |
| Male | 1.05 | (0.811.36) |
| STEMIc | ||
| Absent | Ref | |
| Present | 3.86 | (2.685.58) |
| Troponin I | ||
| 0.1 ng/ml | Ref | |
| >0.1 ng/ml | 1.16 | (0.831.62) |
| COPS2d (AOR per 10 points) | 1.07 | (1.031.10) |
| LAPS2d (AOR per 10 points) | 1.09 | (1.071.12) |
| ED LOSe (hours) | ||
| <6 | Ref | |
| 67 | 0.72 | (0.521.00) |
| >=12 | 0.70 | (0.331.48) |
| Code statusf | ||
| Full code | Ref | |
| Not full code | 1.22 | (0.891.68) |
| Cardiac procedure referral | ||
| None during stay | Ref | |
| 1 day pre adm until discharge | 0.37 | (0.270.51) |
| Order set employedg | ||
| No | Ref | |
| Yes | 0.59 | (0.450.76) |
| C Statistic | 0.792 | |
| Hosmer‐Lemeshow p value | 0.273 | |
Table 4 shows separately the average treatment effect (ATE) and average treatment effect for the treated (ATT) of AMI‐OS and of increasing number of therapies on other outcomes (30‐day mortality, LOS, and readmission). Both the ATE and ATT show that the use of the AMI‐OS was significantly protective with respect to mortality and total hospital LOS but not significant with respect to readmission. The effect of the number of therapies on mortality is significantly higher with increasing number of therapies. For example, patients who received 5 therapies had an average treatment effect on 30‐day inpatient mortality of 0.23 (95% CI: 0.15‐0.35) compared to 0.64 (95% CI: 0.43‐0.96) for 3 therapies, almost a 3‐fold difference. The effects of increasing number of therapies were not significant for LOS or readmission. A sensitivity analysis in which the 535 STEMI patients were removed showed essentially the same results, so it is not reported here.
| Outcome | Order Seta | 3 Therapiesb | 4 Therapiesb | 5 Therapiesb |
|---|---|---|---|---|
| ||||
| Average treatment effectc | ||||
| Inpatient mortality | 0.67 (0.520.86) | 0.64 (0.430.96) | 0.37 (0.250.54) | 0.23 (0.150.35) |
| 30‐day mortality | 0.77 (0.620.96) | 0.68 (0.480.98) | 0.34 (0.240.48) | 0.26 (0.180.37) |
| Readmission | 1.03 (0.901.19) | 1.20 (0.871.66) | 1.19 (0.881.60) | 1.30 (0.961.76) |
| LOS, ratio of the geometric means | 0.91 (0.870.95) | 1.16 (1.031.30) | 1.17 (1.051.30) | 1.12 (1.001.24) |
| Average treatment effect on the treatedd | ||||
| Inpatient mortality | 0.69 (0.520.92) | 0.35 (0.130.93) | 0.17 (0.070.43) | 0.08 (0.030.20) |
| 30‐day mortality | 0.84 (0.661.06) | 0.35 (0.150.79) | 0.17 (0.070.37) | 0.09 (0.040.20) |
| Readmission | 1.02 (0.871.20) | 1.39 (0.852.26) | 1.36 (0.882.12) | 1.23 (0.801.89) |
| LOS, ratio of the geometric meanse | 0.92 (0.870.97) | 1.18 (1.021.37) | 1.16 (1.011.33) | 1.04 (0.911.19) |
To further elucidate possible reasons why physicians did not use the AMI‐OS, the lead author reviewed 105 randomly selected records where the AMI‐OS was not used, 5 records from each of the 21 study hospitals. This review found that in 36% of patients, the AMI‐OS was not used because emergent catheterization or transfer to a facility with percutaneous coronary intervention capability occurred. Presence of other significant medical conditions, including critical illness, was the reason in 17% of these cases, patient or family refusal of treatments in 8%, issues around end‐of‐life care in 3%, and specific medical contraindications in 1%. In the remaining 34%, no reason for not using the AMI‐OS could be identified.
DISCUSSION
We evaluated the use of an evidence‐based electronic AMI‐OS embedded in a comprehensive EMR and found that it was beneficial. Its use was associated with increased adherence to evidence‐based therapies, which in turn were associated with improved outcomes. Using data from a large cohort of hospitalized AMI patients in 21 community hospitals, we were able to use risk adjustment that included physiologic illness severity to adjust for baseline mortality risk. Patients in whom the AMI‐OS was employed tended to be at lower risk; nonetheless, after controlling for confounding variables and adjusting for bias using propensity scores, the AMI‐OS was associated with increased use of evidence‐based therapies and decreased mortality. Most importantly, it appears that the benefits of the OS were not just due to increased receipt of individual recommended therapies, but to increased concurrent receipt of multiple recommended therapies.
Modern EMRs have great potential for significant improvements in the quality, efficiency, and safety of care provided,[36] and our study highlights this potential. However, a number of important limitations to our study must be considered. Although we had access to a very rich dataset, we could not control for all possible confounders, and our risk adjustment cannot match the level of information available to clinicians. In particular, the measurements available to us with respect to cardiac risk are limited. Thus, we have to recognize that the strength of our findings does not approximate that of a randomized trial, and one would expect that the magnitude of the beneficial association would fall under more controlled conditions. Resource limitations also did not permit us to gather more time course data (eg, sequential measurements of patient instability, cardiac damage, or use of recommended therapies), which could provide a better delineation of differences in both processes and outcomes.
Limitations also exist to the generalizability of the use of order sets in other settings that go beyond the availability of a comprehensive EMR. Our study population was cared for in a setting with an unusually high level of integration.[1] For example, KPNC has an elaborate administrative infrastructure for training in the use of the EMR as well as ensuring that order sets are not just evidence‐based, but that they are perceived by clinicians to be of significant value. This infrastructure, established to ensure physician buy‐in, may not be easy to replicate in smaller or less‐integrated settings. Thus, it is conceivable that factors other than the degree of support during the EMR deployments can affect rates of order set use.
Although our use of counterfactual methods included illness severity (LAPS2) and longitudinal comorbidity burden (COPS2), which are not yet available outside highly integrated delivery services employing comprehensive EMRs, it is possible they are insufficient. We cannot exclude the possibility that other biases or patient characteristics were present that led clinicians to preferentially employ the electronic order set in some patients but not in others. One could also argue that future studies should consider using overall adherence to recommended AMI treatment guidelines as a risk adjustment tool that would permit one to analyze what other factors may be playing a role in residual differences in patient outcomes. Last, one could object to our inclusion of STEMI patients; however, this was not a study on optimum treatment strategies for STEMI patients. Rather, it was a study on the impact on AMI outcomes of a specific component of computerized order entry outside the research setting.
Despite these limitations, we believe that our findings provide strong support for the continued use of electronic evidence‐based order sets in the inpatient medical setting. Once the initial implementation of a comprehensive EMR has occurred, deployment of these electronic order sets is a relatively inexpensive but effective method to foster compliance with evidence‐based care.
Future research in healthcare information technology can take a number of directions. One important area, of course, revolves around ways to promote enhanced physician adoption of EMRs. Our audit of records where the AMI‐OS was not used found that specific reasons for not using the order set (eg, treatment refusals, emergent intervention) were present in two‐thirds of the cases. This suggests that future analyses of adherence involving EMRs and CPOE implementation should take a more nuanced look at how order entry is actually enabled. It may be that understanding how order sets affect care enhances clinician acceptance and thus could serve as an incentive to EMR adoption. However, once an EMR is adopted, a need exists to continue evaluations such as this because, ultimately, the gold standard should be improved patient care processes and better outcomes for patients.
Acknowledgement
The authors give special thanks to Dr. Brian Hoberman for sponsoring this work, Dr. Alan S. Go for providing assistance with obtaining copies of electrocardiograms for review, Drs. Tracy Lieu and Vincent Liu for reviewing the manuscript, and Ms. Rachel Lesser for formatting the manuscript.
Disclosures: This work was supported by The Permanente Medical Group, Inc. and Kaiser Foundation Hospitals, Inc. The algorithms used to extract data and perform risk adjustment were developed with funding from the Sidney Garfield Memorial Fund (Early Detection of Impending Physiologic Deterioration in Hospitalized Patients, 1159518), the Agency for Healthcare Quality and Research (Rapid Clinical Snapshots From the EMR Among Pneumonia Patients, 1R01HS018480‐01), and the Gordon and Betty Moore Foundation (Early Detection of Impending Physiologic Deterioration: Electronic Early Warning System).
- , , , , , . Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362(23):2155–2165.
- , , , et al. Twenty‐two‐year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987–2008. Circulation. 2012;125(15):1848–1857.
- , , , et al. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation. 2012;125(1):e2–e220.
- , , , et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non‐ST‐Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non‐ST‐Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50(7):e1–e157.
- , , , et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2008;51(2):210–247.
- , , , , , . Association between adoption of evidence‐based treatment and survival for patients with ST‐elevation myocardial infarction. JAMA. 2011;305(16):1677–1684.
- , , , et al. Association of changes in clinical characteristics and management with improvement in survival among patients with ST‐elevation myocardial infarction. JAMA. 2012;308(10):998–1006.
- , , , et al. Changes in myocardial infarction guideline adherence as a function of patient risk: an end to paradoxical care? J Am Coll Cardiol. 2011;58(17):1760–1765.
- , , , . Care in U.S. hospitals—the Hospital Quality Alliance program. N Engl J Med. 2005;353(3):265–274.
- , , et al. Challenges in the treatment of NSTEMI patients at high risk for both ischemic and bleeding events: insights from the ACTION Registry‐GWTG. J Am Coll Cardiol. 2011;57:E913–E913.
- , , , , . Quality of care in U.S. hospitals as reflected by standardized measures, 2002–2004. N Engl J Med. 2005;353(3):255–264.
- , , . Guideline‐based standardized care is associated with substantially lower mortality in medicare patients with acute myocardial infarction. J Am Coll Cardiol. 2005;46(7):1242–1248.
- , , , et al. Impact of a standardized heart failure order set on mortality, readmission, and quality and costs of care. Int J Qual Health Care. 2010;22(6):437–444.
- . Linking automated databases for research in managed care settings. Ann Intern Med. 1997;127(8 pt 2):719–724.
- , , , , , . Risk adjusting hospital inpatient mortality using automated inpatient, outpatient, and laboratory databases. Med Care. 2008;46(3):232–239.
- , , , . Length of stay predictions: improvements through the use of automated laboratory and comorbidity variables. Med Care. 2010;48(8):739–744.
- , , , , , . Intra‐hospital transfers to a higher level of care: contribution to total hospital and intensive care unit (ICU) mortality and length of stay (LOS). J Hosp Med. 2011;6(2):74–80.
- , , , . Adverse outcomes associated with delayed intensive care unit transfers in an integrated healthcare system. J Hosp Med. 2012;7(3):224–230.
- International Classification of Diseases, 9th Revision‐Clinical Modification. 4th ed. 3 Vols. Los Angeles, CA: Practice Management Information Corporation; 2006.
- , , , et al. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. 2003;290(20):2685–2692.
- , , , , , . Early detection of impending physiologic deterioration among patients who are not in intensive care: development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012;7(5):388–395.
- , , , , . Risk‐adjusting hospital mortality using a comprehensive electronic record in an integrated healthcare delivery system. Med Care. 2013;51(5):446–453.
- , , . Effect of choice of estimation method on inter‐hospital mortality rate comparisons. Med Care. 2010;48(5):456–485.
- , , , . The Kaiser Permanente inpatient risk adjustment methodology was valid in an external patient population. J Clin Epidemiol. 2010;63(7):798–803.
- , , , , . Derivation and validation of a model to predict daily risk of death in hospital. Med Care. 2011;49(8):734–743.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
- . Introduction to Statistical Mediation Analysis. New York, NY: Lawrence Erlbaum Associates; 2008.
- . Nonparametric estimation of average treatment effects under exogenity: a review. Rev Econ Stat. 2004;86:25.
- . Design of Observational Studies. New York, NY: Springer Science+Business Media; 2010.
- . Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity‐score matched samples. Stat Med. 2009;28:24.
- , , . Estimation of regression coefficients when some regressors are not always observed. J Am Stat Assoc. 1994(89):846–866.
- , . Stratification and weighting via the propensity score in estimation of causal treatment effects: a comparative study. Stat Med. 2004;23(19):2937–2960.
- . Discussing hidden bias in observational studies. Ann Intern Med. 1991;115(11):901–905.
- . Propensity score methods for bias reduction in the comparison of a treatment to a non‐randomized control group. Stat Med. 1998;17(19):2265–2281.
- , , . A method/macro based on propensity score and Mahalanobis distance to reduce bias in treatment comparison in observational study, 2005. www.lexjansen.com/pharmasug/2006/publichealthresearch/pr05.pdf. Accessed on September 14, 2013.
- . Using health information technology to improve health care. Arch Intern Med. 2012;172(22):1728–1730.
- , , , , , . Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362(23):2155–2165.
- , , , et al. Twenty‐two‐year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987–2008. Circulation. 2012;125(15):1848–1857.
- , , , et al. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation. 2012;125(1):e2–e220.
- , , , et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non‐ST‐Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non‐ST‐Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50(7):e1–e157.
- , , , et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2008;51(2):210–247.
- , , , , , . Association between adoption of evidence‐based treatment and survival for patients with ST‐elevation myocardial infarction. JAMA. 2011;305(16):1677–1684.
- , , , et al. Association of changes in clinical characteristics and management with improvement in survival among patients with ST‐elevation myocardial infarction. JAMA. 2012;308(10):998–1006.
- , , , et al. Changes in myocardial infarction guideline adherence as a function of patient risk: an end to paradoxical care? J Am Coll Cardiol. 2011;58(17):1760–1765.
- , , , . Care in U.S. hospitals—the Hospital Quality Alliance program. N Engl J Med. 2005;353(3):265–274.
- , , et al. Challenges in the treatment of NSTEMI patients at high risk for both ischemic and bleeding events: insights from the ACTION Registry‐GWTG. J Am Coll Cardiol. 2011;57:E913–E913.
- , , , , . Quality of care in U.S. hospitals as reflected by standardized measures, 2002–2004. N Engl J Med. 2005;353(3):255–264.
- , , . Guideline‐based standardized care is associated with substantially lower mortality in medicare patients with acute myocardial infarction. J Am Coll Cardiol. 2005;46(7):1242–1248.
- , , , et al. Impact of a standardized heart failure order set on mortality, readmission, and quality and costs of care. Int J Qual Health Care. 2010;22(6):437–444.
- . Linking automated databases for research in managed care settings. Ann Intern Med. 1997;127(8 pt 2):719–724.
- , , , , , . Risk adjusting hospital inpatient mortality using automated inpatient, outpatient, and laboratory databases. Med Care. 2008;46(3):232–239.
- , , , . Length of stay predictions: improvements through the use of automated laboratory and comorbidity variables. Med Care. 2010;48(8):739–744.
- , , , , , . Intra‐hospital transfers to a higher level of care: contribution to total hospital and intensive care unit (ICU) mortality and length of stay (LOS). J Hosp Med. 2011;6(2):74–80.
- , , , . Adverse outcomes associated with delayed intensive care unit transfers in an integrated healthcare system. J Hosp Med. 2012;7(3):224–230.
- International Classification of Diseases, 9th Revision‐Clinical Modification. 4th ed. 3 Vols. Los Angeles, CA: Practice Management Information Corporation; 2006.
- , , , et al. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. 2003;290(20):2685–2692.
- , , , , , . Early detection of impending physiologic deterioration among patients who are not in intensive care: development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012;7(5):388–395.
- , , , , . Risk‐adjusting hospital mortality using a comprehensive electronic record in an integrated healthcare delivery system. Med Care. 2013;51(5):446–453.
- , , . Effect of choice of estimation method on inter‐hospital mortality rate comparisons. Med Care. 2010;48(5):456–485.
- , , , . The Kaiser Permanente inpatient risk adjustment methodology was valid in an external patient population. J Clin Epidemiol. 2010;63(7):798–803.
- , , , , . Derivation and validation of a model to predict daily risk of death in hospital. Med Care. 2011;49(8):734–743.
- , , . Adapting a clinical comorbidity index for use with ICD‐9‐CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
- . Introduction to Statistical Mediation Analysis. New York, NY: Lawrence Erlbaum Associates; 2008.
- . Nonparametric estimation of average treatment effects under exogenity: a review. Rev Econ Stat. 2004;86:25.
- . Design of Observational Studies. New York, NY: Springer Science+Business Media; 2010.
- . Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity‐score matched samples. Stat Med. 2009;28:24.
- , , . Estimation of regression coefficients when some regressors are not always observed. J Am Stat Assoc. 1994(89):846–866.
- , . Stratification and weighting via the propensity score in estimation of causal treatment effects: a comparative study. Stat Med. 2004;23(19):2937–2960.
- . Discussing hidden bias in observational studies. Ann Intern Med. 1991;115(11):901–905.
- . Propensity score methods for bias reduction in the comparison of a treatment to a non‐randomized control group. Stat Med. 1998;17(19):2265–2281.
- , , . A method/macro based on propensity score and Mahalanobis distance to reduce bias in treatment comparison in observational study, 2005. www.lexjansen.com/pharmasug/2006/publichealthresearch/pr05.pdf. Accessed on September 14, 2013.
- . Using health information technology to improve health care. Arch Intern Med. 2012;172(22):1728–1730.
© 2014 Society of Hospital Medicine
Group ‘rewrites rules’ on pluripotency
Credit: Haruko Obokata
Researchers say they have developed a novel technique for inducing pluripotency in somatic cells.
Unlike methods for creating induced pluripotent stem cells (iPSCs), the new process—called stimulus-triggered acquisition of pluripotency (STAP)—does not require the introduction of genetic material.
Instead, adult cells must only be injured in order to revert to a pluripotent state.
The investigators tested STAP in preclinical models and reported the results in both a letter and an article published in Nature.
Inspired by plants
Haruko Obokata, PhD, of the RIKEN Center for Developmental Biology in Japan, and her colleagues said this research was inspired by the ability of a plant callus—a node of plant cells created by injuring an existing plant—to grow into a new plant.
The researchers thought this phenomenon suggested that any somatic cell could be de-differentiated through injury.
To find out, they tested cells derived from mice. The team chose hematopoietic cells positive for CD45 because these are lineage-committed, somatic cells that do not express pluripotency-related markers unless they are reprogrammed.
The investigators stressed the cells almost to the point of death by exposing them to various stimuli in vitro, including trauma, a low-oxygen environment, and a low-pH environment.
Within a few days, the cells had recovered from the stressful stimuli by naturally reverting to a pluripotent state. These stem cells were then able to re-differentiate and mature into any type of cell and grow into any type of tissue, depending on the environment into which they were placed.
“It was really surprising to see that such a remarkable transformation could be triggered simply by stimuli from outside of the cell,” Dr Obokata said.
She and her colleagues found that the low-pH environment was most effective for inducing pluripotency.
“Once again, Japanese scientists have unexpectedly rewritten the rules on making pluripotent cells from adult cells,” said Chris Mason, MD, PhD, of the University College London in the UK, who was not involved in this research.
“In 2006, [Shinya] Yamanaka used 4 genes [to create iPSCs]. And now, the far simpler and quicker route discovered by Obokata . . . requires only transient exposure of adult cells to an acidic solution.”
Growth in mice
To examine the cells’ growth potential in vivo, Dr Obokata and her colleagues used CD45+ cells from GFP+ mice. The team exposed the cells to a low-pH environment and found that, in the days following the stress, the cells reverted back to a pluripotent state.
These stem cells then began growing in spherical clusters, similar to a plant callus. The researchers introduced the cell clusters into the developing embryo of a non-GFP mouse and found the clusters could create GFP+ tissues in all organs tested, thereby confirming that the cells are pluripotent.
The investigators think these findings raise the possibility that unknown cellular functions activated through external stress may set somatic cells free from their current commitment and permit them to revert to their naïve state.
“Our findings suggest that, somehow, through part of a natural repair process, mature cells turn off some of the epigenetic controls that inhibit expression of certain nuclear genes that result in differentiation,” said study author Charles Vacanti, MD, of Brigham and Women’s Hospital in Boston.
If this process can be replicated in human cells, researchers might one day be able to use a skin biopsy or blood sample to create stem cells specific to each individual. And this could have implications for treating cancers and other diseases.
The investigators are now testing the STAP technique in human cells. ![]()
Credit: Haruko Obokata
Researchers say they have developed a novel technique for inducing pluripotency in somatic cells.
Unlike methods for creating induced pluripotent stem cells (iPSCs), the new process—called stimulus-triggered acquisition of pluripotency (STAP)—does not require the introduction of genetic material.
Instead, adult cells must only be injured in order to revert to a pluripotent state.
The investigators tested STAP in preclinical models and reported the results in both a letter and an article published in Nature.
Inspired by plants
Haruko Obokata, PhD, of the RIKEN Center for Developmental Biology in Japan, and her colleagues said this research was inspired by the ability of a plant callus—a node of plant cells created by injuring an existing plant—to grow into a new plant.
The researchers thought this phenomenon suggested that any somatic cell could be de-differentiated through injury.
To find out, they tested cells derived from mice. The team chose hematopoietic cells positive for CD45 because these are lineage-committed, somatic cells that do not express pluripotency-related markers unless they are reprogrammed.
The investigators stressed the cells almost to the point of death by exposing them to various stimuli in vitro, including trauma, a low-oxygen environment, and a low-pH environment.
Within a few days, the cells had recovered from the stressful stimuli by naturally reverting to a pluripotent state. These stem cells were then able to re-differentiate and mature into any type of cell and grow into any type of tissue, depending on the environment into which they were placed.
“It was really surprising to see that such a remarkable transformation could be triggered simply by stimuli from outside of the cell,” Dr Obokata said.
She and her colleagues found that the low-pH environment was most effective for inducing pluripotency.
“Once again, Japanese scientists have unexpectedly rewritten the rules on making pluripotent cells from adult cells,” said Chris Mason, MD, PhD, of the University College London in the UK, who was not involved in this research.
“In 2006, [Shinya] Yamanaka used 4 genes [to create iPSCs]. And now, the far simpler and quicker route discovered by Obokata . . . requires only transient exposure of adult cells to an acidic solution.”
Growth in mice
To examine the cells’ growth potential in vivo, Dr Obokata and her colleagues used CD45+ cells from GFP+ mice. The team exposed the cells to a low-pH environment and found that, in the days following the stress, the cells reverted back to a pluripotent state.
These stem cells then began growing in spherical clusters, similar to a plant callus. The researchers introduced the cell clusters into the developing embryo of a non-GFP mouse and found the clusters could create GFP+ tissues in all organs tested, thereby confirming that the cells are pluripotent.
The investigators think these findings raise the possibility that unknown cellular functions activated through external stress may set somatic cells free from their current commitment and permit them to revert to their naïve state.
“Our findings suggest that, somehow, through part of a natural repair process, mature cells turn off some of the epigenetic controls that inhibit expression of certain nuclear genes that result in differentiation,” said study author Charles Vacanti, MD, of Brigham and Women’s Hospital in Boston.
If this process can be replicated in human cells, researchers might one day be able to use a skin biopsy or blood sample to create stem cells specific to each individual. And this could have implications for treating cancers and other diseases.
The investigators are now testing the STAP technique in human cells. ![]()
Credit: Haruko Obokata
Researchers say they have developed a novel technique for inducing pluripotency in somatic cells.
Unlike methods for creating induced pluripotent stem cells (iPSCs), the new process—called stimulus-triggered acquisition of pluripotency (STAP)—does not require the introduction of genetic material.
Instead, adult cells must only be injured in order to revert to a pluripotent state.
The investigators tested STAP in preclinical models and reported the results in both a letter and an article published in Nature.
Inspired by plants
Haruko Obokata, PhD, of the RIKEN Center for Developmental Biology in Japan, and her colleagues said this research was inspired by the ability of a plant callus—a node of plant cells created by injuring an existing plant—to grow into a new plant.
The researchers thought this phenomenon suggested that any somatic cell could be de-differentiated through injury.
To find out, they tested cells derived from mice. The team chose hematopoietic cells positive for CD45 because these are lineage-committed, somatic cells that do not express pluripotency-related markers unless they are reprogrammed.
The investigators stressed the cells almost to the point of death by exposing them to various stimuli in vitro, including trauma, a low-oxygen environment, and a low-pH environment.
Within a few days, the cells had recovered from the stressful stimuli by naturally reverting to a pluripotent state. These stem cells were then able to re-differentiate and mature into any type of cell and grow into any type of tissue, depending on the environment into which they were placed.
“It was really surprising to see that such a remarkable transformation could be triggered simply by stimuli from outside of the cell,” Dr Obokata said.
She and her colleagues found that the low-pH environment was most effective for inducing pluripotency.
“Once again, Japanese scientists have unexpectedly rewritten the rules on making pluripotent cells from adult cells,” said Chris Mason, MD, PhD, of the University College London in the UK, who was not involved in this research.
“In 2006, [Shinya] Yamanaka used 4 genes [to create iPSCs]. And now, the far simpler and quicker route discovered by Obokata . . . requires only transient exposure of adult cells to an acidic solution.”
Growth in mice
To examine the cells’ growth potential in vivo, Dr Obokata and her colleagues used CD45+ cells from GFP+ mice. The team exposed the cells to a low-pH environment and found that, in the days following the stress, the cells reverted back to a pluripotent state.
These stem cells then began growing in spherical clusters, similar to a plant callus. The researchers introduced the cell clusters into the developing embryo of a non-GFP mouse and found the clusters could create GFP+ tissues in all organs tested, thereby confirming that the cells are pluripotent.
The investigators think these findings raise the possibility that unknown cellular functions activated through external stress may set somatic cells free from their current commitment and permit them to revert to their naïve state.
“Our findings suggest that, somehow, through part of a natural repair process, mature cells turn off some of the epigenetic controls that inhibit expression of certain nuclear genes that result in differentiation,” said study author Charles Vacanti, MD, of Brigham and Women’s Hospital in Boston.
If this process can be replicated in human cells, researchers might one day be able to use a skin biopsy or blood sample to create stem cells specific to each individual. And this could have implications for treating cancers and other diseases.
The investigators are now testing the STAP technique in human cells. ![]()
Listen Now! Dining and Nightlife Recommendations for HM14
Listen Up! What Hospitalists Need to Know About Healthcare Post-Obamacare
Click here to listen to more of our interview with Dr. Morrison
Click here to listen to more of our interview with Dr. Morrison
Click here to listen to more of our interview with Dr. Morrison
Likelihood for Readmission of Hospitalized Medicare Patients with Multiple Chronic Conditions Up 600%
600%
The increased likelihood of 30-day hospital readmission for hospitalized Medicare patients who have 10 or more chronic conditions, compared with those who have only one to four chronic conditions.4 These patients with multiple chronic conditions represent only 8.9% of Medicare beneficiaries but account for 50% of all rehospitalizations. The numbers are drawn from a 5% sample of Medicare fee-for-service beneficiaries during the first nine months of 2008. Those with five to nine chronic conditions had 2.5 times the odds for being readmitted.
Larry Beresford is a freelance writer in Alameda, Calif.
- Shieh L, Pummer E, Tsui J, et al. Septris: improving sepsis recognition and management through a mobile educational game [abstract]. J Hosp Med. 2013;8(Suppl 1):1053.
- Mitchell SE, Gardiner PM, Sadikova E, et al. Patient activation and 30-day post-discharge hospital utilization. J Gen Intern Med. 2014;29(2):349-355.
- Daniels KR, Lee GC, Frei CR. Trends in catheter-associated urinary tract infections among a national cohort of hospitalized adults, 2001-2010. Am J Infect Control. 2014;42(1):17-22.
- Berkowitz SA. Anderson GF. Medicare beneficiaries most likely to be readmitted. J Hosp Med. 2013;8(11):639-641.
600%
The increased likelihood of 30-day hospital readmission for hospitalized Medicare patients who have 10 or more chronic conditions, compared with those who have only one to four chronic conditions.4 These patients with multiple chronic conditions represent only 8.9% of Medicare beneficiaries but account for 50% of all rehospitalizations. The numbers are drawn from a 5% sample of Medicare fee-for-service beneficiaries during the first nine months of 2008. Those with five to nine chronic conditions had 2.5 times the odds for being readmitted.
Larry Beresford is a freelance writer in Alameda, Calif.
- Shieh L, Pummer E, Tsui J, et al. Septris: improving sepsis recognition and management through a mobile educational game [abstract]. J Hosp Med. 2013;8(Suppl 1):1053.
- Mitchell SE, Gardiner PM, Sadikova E, et al. Patient activation and 30-day post-discharge hospital utilization. J Gen Intern Med. 2014;29(2):349-355.
- Daniels KR, Lee GC, Frei CR. Trends in catheter-associated urinary tract infections among a national cohort of hospitalized adults, 2001-2010. Am J Infect Control. 2014;42(1):17-22.
- Berkowitz SA. Anderson GF. Medicare beneficiaries most likely to be readmitted. J Hosp Med. 2013;8(11):639-641.
600%
The increased likelihood of 30-day hospital readmission for hospitalized Medicare patients who have 10 or more chronic conditions, compared with those who have only one to four chronic conditions.4 These patients with multiple chronic conditions represent only 8.9% of Medicare beneficiaries but account for 50% of all rehospitalizations. The numbers are drawn from a 5% sample of Medicare fee-for-service beneficiaries during the first nine months of 2008. Those with five to nine chronic conditions had 2.5 times the odds for being readmitted.
Larry Beresford is a freelance writer in Alameda, Calif.
- Shieh L, Pummer E, Tsui J, et al. Septris: improving sepsis recognition and management through a mobile educational game [abstract]. J Hosp Med. 2013;8(Suppl 1):1053.
- Mitchell SE, Gardiner PM, Sadikova E, et al. Patient activation and 30-day post-discharge hospital utilization. J Gen Intern Med. 2014;29(2):349-355.
- Daniels KR, Lee GC, Frei CR. Trends in catheter-associated urinary tract infections among a national cohort of hospitalized adults, 2001-2010. Am J Infect Control. 2014;42(1):17-22.
- Berkowitz SA. Anderson GF. Medicare beneficiaries most likely to be readmitted. J Hosp Med. 2013;8(11):639-641.
Shift from Productivity to Value-Based Compensation Gains Momentum
At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
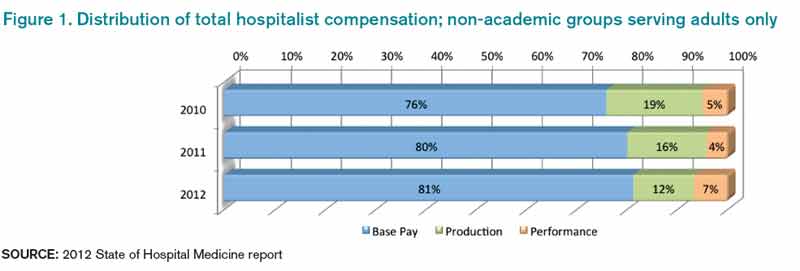
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.

At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.
At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.
Mid-Flight Medical Emergencies Benefit from Hospitalist on Board
We were still climbing from the airport tarmac, and the movie on my iPad, “Star Trek II: The Wrath of Khan,” was at an exciting point where Klingons are attacking the USS Enterprise when it came: “Is there a doctor on the plane?”
If you talk to your physician and healthcare colleagues who fly, you’ll hear about this scenario enough to know that it is not a rare event. Healthcare providers who fly routinely are more likely to tend to a sick airline passenger than they are to diagnose pheochromocytoma in their day jobs. Pheo is a two-in-a-million disease, but getting ill on a plane happens to one to two people in every 20,000. In fact, the sick airline passenger is relatively common, with an FAA study estimating 13 events per day in the 1990s (Anesthesiology. 2008;108(4):749-755). There have been a number of interesting articles written about the doctor-on-the-plane scenario. Our own Bob Wachter, MD, MHM, blogged about it in his usual humorous and insightful way a few years ago here, (http://community.the-hospitalist.org/2010/08/22/if-there-s-a-doctor-on-board-please-ring-your-call-button), and The New England Journal of Medicine published a perspective on it at www.nejm.org/doi/full/10.1056/NEJMp1006331?query=TOC (NEJM; 2010;363(21):1988-1989).
My most recent experience happened on a flight just before the New Year, and because many of us will be flying to and from the annual meeting in Las Vegas and it seems to fit naturally (in many cases) with what we do as hospitalists, I thought I’d put pen to paper regarding the sick airline passenger in flight.
Fasten Your Seatbelt
As I was walked up to the first row, the flight attendant said a passenger had almost passed out. A doctor was tending to the sick woman already, as were two very concerned flight attendants. I have been through this before, so I knew I couldn’t go back to my seat just yet. I asked the physician if everything was OK and if he needed help. In my previous experiences, the initial doctor was often a specialist, or retired, or both. They often were relieved to see a hospitalist and happily handed over the care of the airline patient once they heard I’m a hospitalist. Sound familiar from your day job?
This episode was no different: Although pleasant and concerned, the initial doctor was retired, and he made it clear this was outside of his area of expertise. He didn’t exactly sprint back to his seat, but you get the picture.
The patient was pale, looked ill, and was semi-conscious. She was about 70 (later confirmed at 73) and was sitting with her son, who worriedly showed me the auto-blood pressure cuff they had brought with her; it read 81/60. She denied chest pain or shortness of breath. Her pulse was 65, and her breathing was not labored.
For a hospitalist, attending to the ill airline passenger can be quite rewarding. Most diagnoses are those we see every day: syncope/pre-syncope, respiratory, and GI complaints make up more than half of the calls. Death is rare (0.3%), and other “big” decisions, like whether to force the plane to land early (landing a plane still full of fuel or at a smaller airport is not to be taken lightly), are uncommon (7.3%). Still, the illnesses can be real, and more than a quarter of aircraft patients are transported to a hospital upon landing (N Engl J Med. 2013;368(22):2075-2083). Our skills at diagnosis are undoubtedly valuable in the air.
Also, as Dr. Wachter said in his blog on the subject, tending to the ill airline passenger is “one of the purest expressions of our Hippocratic oath, and our professionalism. We have no obligation to respond, and no contractual relationship. It’s just you, armed with your wits and experience, a sick and scared patient and family member, and about 200 interested observers.”
We broke open the aircraft medical kit, which was surprisingly well supplied, complete with a manual BP cuff and medications any registered respiratory therapist or code responder would find familiar. Bronchodilators, epinephrine and lidocaine, the usual aspirin, even IV tubing and needles. The one thing I was shocked to find was that there is limited supplemental oxygen: only enough to supply a nasal cannula at 4L max, and that for only a few hours.
As with the vast majority of medical cases, a thorough history of my 73-year-old air traveler proved invaluable. She felt light-headed but never lost consciousness. She had no other symptoms. Her past medical history was significant for hypertension but no heart disease. Was there anything else? She had been discharged from a hospital three days before for severe hypertension. Her ACE inhibitor and beta-blocker doses had been doubled and HCTZ added (her hospitalist had done an excellent job educating her on her disease, her medication changes, and possible side effects).
Anything else? She had been traveling more than 12 hours with little to drink, but she had taken all of her meds just before boarding the flight. After some oral rehydration, leaning back, and elevating her feet, her blood pressure increased to 125/71. I checked on her frequently for the rest of the flight, and she was talking happily to neighbors and her son long before we deplaned. They were en route to Boston, where she was moving and had no doctor, but she had an appointment scheduled with a new one soon. I gave her my card and my cell number and instructed them to call me if there were any problems. She and her son were thankful (and her neighbors were too!), and I was glad to have helped.
The Aftermath
The only thing left was the administrative paperwork for the airline. Would I please sign here? What was my license number (they were confused as to whether to take my NPI, my state license number, or DEA number, so I gave them all three), and where was I employed?
After getting home and recovering from my jet lag, I did some research on this topic. Colleagues of mine expressed concern over the legal liability of providing assistance in flight, but, compared to our day jobs, that concern seems to be unwarranted. The Aviation Medical Assistance Act of 1998 (www.gpo.gov) protects healthcare providers who render care in good faith.
As of the 2008 article by Ruskin, no physician providing care for an airline patient had been successfully sued. I learned that the medical kits are fairly well stocked and are set up for the physician/medical professional. I also learned that supplemental oxygen, so ubiquitous in the hospital, is more limited on an airplane. And, I found out that, while airlines contract with ground-based medical services, half of all emergencies are cared for by Good Samaritan doctors, licensed providers, nurses, and EMTs.
So, before my next flight, in addition to packing my iPad and thumb drive, boarding pass, and ID, I plan to pack those reference articles by Ruskin and Peterson.

We were still climbing from the airport tarmac, and the movie on my iPad, “Star Trek II: The Wrath of Khan,” was at an exciting point where Klingons are attacking the USS Enterprise when it came: “Is there a doctor on the plane?”
If you talk to your physician and healthcare colleagues who fly, you’ll hear about this scenario enough to know that it is not a rare event. Healthcare providers who fly routinely are more likely to tend to a sick airline passenger than they are to diagnose pheochromocytoma in their day jobs. Pheo is a two-in-a-million disease, but getting ill on a plane happens to one to two people in every 20,000. In fact, the sick airline passenger is relatively common, with an FAA study estimating 13 events per day in the 1990s (Anesthesiology. 2008;108(4):749-755). There have been a number of interesting articles written about the doctor-on-the-plane scenario. Our own Bob Wachter, MD, MHM, blogged about it in his usual humorous and insightful way a few years ago here, (http://community.the-hospitalist.org/2010/08/22/if-there-s-a-doctor-on-board-please-ring-your-call-button), and The New England Journal of Medicine published a perspective on it at www.nejm.org/doi/full/10.1056/NEJMp1006331?query=TOC (NEJM; 2010;363(21):1988-1989).
My most recent experience happened on a flight just before the New Year, and because many of us will be flying to and from the annual meeting in Las Vegas and it seems to fit naturally (in many cases) with what we do as hospitalists, I thought I’d put pen to paper regarding the sick airline passenger in flight.
Fasten Your Seatbelt
As I was walked up to the first row, the flight attendant said a passenger had almost passed out. A doctor was tending to the sick woman already, as were two very concerned flight attendants. I have been through this before, so I knew I couldn’t go back to my seat just yet. I asked the physician if everything was OK and if he needed help. In my previous experiences, the initial doctor was often a specialist, or retired, or both. They often were relieved to see a hospitalist and happily handed over the care of the airline patient once they heard I’m a hospitalist. Sound familiar from your day job?
This episode was no different: Although pleasant and concerned, the initial doctor was retired, and he made it clear this was outside of his area of expertise. He didn’t exactly sprint back to his seat, but you get the picture.
The patient was pale, looked ill, and was semi-conscious. She was about 70 (later confirmed at 73) and was sitting with her son, who worriedly showed me the auto-blood pressure cuff they had brought with her; it read 81/60. She denied chest pain or shortness of breath. Her pulse was 65, and her breathing was not labored.
For a hospitalist, attending to the ill airline passenger can be quite rewarding. Most diagnoses are those we see every day: syncope/pre-syncope, respiratory, and GI complaints make up more than half of the calls. Death is rare (0.3%), and other “big” decisions, like whether to force the plane to land early (landing a plane still full of fuel or at a smaller airport is not to be taken lightly), are uncommon (7.3%). Still, the illnesses can be real, and more than a quarter of aircraft patients are transported to a hospital upon landing (N Engl J Med. 2013;368(22):2075-2083). Our skills at diagnosis are undoubtedly valuable in the air.
Also, as Dr. Wachter said in his blog on the subject, tending to the ill airline passenger is “one of the purest expressions of our Hippocratic oath, and our professionalism. We have no obligation to respond, and no contractual relationship. It’s just you, armed with your wits and experience, a sick and scared patient and family member, and about 200 interested observers.”
We broke open the aircraft medical kit, which was surprisingly well supplied, complete with a manual BP cuff and medications any registered respiratory therapist or code responder would find familiar. Bronchodilators, epinephrine and lidocaine, the usual aspirin, even IV tubing and needles. The one thing I was shocked to find was that there is limited supplemental oxygen: only enough to supply a nasal cannula at 4L max, and that for only a few hours.
As with the vast majority of medical cases, a thorough history of my 73-year-old air traveler proved invaluable. She felt light-headed but never lost consciousness. She had no other symptoms. Her past medical history was significant for hypertension but no heart disease. Was there anything else? She had been discharged from a hospital three days before for severe hypertension. Her ACE inhibitor and beta-blocker doses had been doubled and HCTZ added (her hospitalist had done an excellent job educating her on her disease, her medication changes, and possible side effects).
Anything else? She had been traveling more than 12 hours with little to drink, but she had taken all of her meds just before boarding the flight. After some oral rehydration, leaning back, and elevating her feet, her blood pressure increased to 125/71. I checked on her frequently for the rest of the flight, and she was talking happily to neighbors and her son long before we deplaned. They were en route to Boston, where she was moving and had no doctor, but she had an appointment scheduled with a new one soon. I gave her my card and my cell number and instructed them to call me if there were any problems. She and her son were thankful (and her neighbors were too!), and I was glad to have helped.
The Aftermath
The only thing left was the administrative paperwork for the airline. Would I please sign here? What was my license number (they were confused as to whether to take my NPI, my state license number, or DEA number, so I gave them all three), and where was I employed?
After getting home and recovering from my jet lag, I did some research on this topic. Colleagues of mine expressed concern over the legal liability of providing assistance in flight, but, compared to our day jobs, that concern seems to be unwarranted. The Aviation Medical Assistance Act of 1998 (www.gpo.gov) protects healthcare providers who render care in good faith.
As of the 2008 article by Ruskin, no physician providing care for an airline patient had been successfully sued. I learned that the medical kits are fairly well stocked and are set up for the physician/medical professional. I also learned that supplemental oxygen, so ubiquitous in the hospital, is more limited on an airplane. And, I found out that, while airlines contract with ground-based medical services, half of all emergencies are cared for by Good Samaritan doctors, licensed providers, nurses, and EMTs.
So, before my next flight, in addition to packing my iPad and thumb drive, boarding pass, and ID, I plan to pack those reference articles by Ruskin and Peterson.
We were still climbing from the airport tarmac, and the movie on my iPad, “Star Trek II: The Wrath of Khan,” was at an exciting point where Klingons are attacking the USS Enterprise when it came: “Is there a doctor on the plane?”
If you talk to your physician and healthcare colleagues who fly, you’ll hear about this scenario enough to know that it is not a rare event. Healthcare providers who fly routinely are more likely to tend to a sick airline passenger than they are to diagnose pheochromocytoma in their day jobs. Pheo is a two-in-a-million disease, but getting ill on a plane happens to one to two people in every 20,000. In fact, the sick airline passenger is relatively common, with an FAA study estimating 13 events per day in the 1990s (Anesthesiology. 2008;108(4):749-755). There have been a number of interesting articles written about the doctor-on-the-plane scenario. Our own Bob Wachter, MD, MHM, blogged about it in his usual humorous and insightful way a few years ago here, (http://community.the-hospitalist.org/2010/08/22/if-there-s-a-doctor-on-board-please-ring-your-call-button), and The New England Journal of Medicine published a perspective on it at www.nejm.org/doi/full/10.1056/NEJMp1006331?query=TOC (NEJM; 2010;363(21):1988-1989).
My most recent experience happened on a flight just before the New Year, and because many of us will be flying to and from the annual meeting in Las Vegas and it seems to fit naturally (in many cases) with what we do as hospitalists, I thought I’d put pen to paper regarding the sick airline passenger in flight.
Fasten Your Seatbelt
As I was walked up to the first row, the flight attendant said a passenger had almost passed out. A doctor was tending to the sick woman already, as were two very concerned flight attendants. I have been through this before, so I knew I couldn’t go back to my seat just yet. I asked the physician if everything was OK and if he needed help. In my previous experiences, the initial doctor was often a specialist, or retired, or both. They often were relieved to see a hospitalist and happily handed over the care of the airline patient once they heard I’m a hospitalist. Sound familiar from your day job?
This episode was no different: Although pleasant and concerned, the initial doctor was retired, and he made it clear this was outside of his area of expertise. He didn’t exactly sprint back to his seat, but you get the picture.
The patient was pale, looked ill, and was semi-conscious. She was about 70 (later confirmed at 73) and was sitting with her son, who worriedly showed me the auto-blood pressure cuff they had brought with her; it read 81/60. She denied chest pain or shortness of breath. Her pulse was 65, and her breathing was not labored.
For a hospitalist, attending to the ill airline passenger can be quite rewarding. Most diagnoses are those we see every day: syncope/pre-syncope, respiratory, and GI complaints make up more than half of the calls. Death is rare (0.3%), and other “big” decisions, like whether to force the plane to land early (landing a plane still full of fuel or at a smaller airport is not to be taken lightly), are uncommon (7.3%). Still, the illnesses can be real, and more than a quarter of aircraft patients are transported to a hospital upon landing (N Engl J Med. 2013;368(22):2075-2083). Our skills at diagnosis are undoubtedly valuable in the air.
Also, as Dr. Wachter said in his blog on the subject, tending to the ill airline passenger is “one of the purest expressions of our Hippocratic oath, and our professionalism. We have no obligation to respond, and no contractual relationship. It’s just you, armed with your wits and experience, a sick and scared patient and family member, and about 200 interested observers.”
We broke open the aircraft medical kit, which was surprisingly well supplied, complete with a manual BP cuff and medications any registered respiratory therapist or code responder would find familiar. Bronchodilators, epinephrine and lidocaine, the usual aspirin, even IV tubing and needles. The one thing I was shocked to find was that there is limited supplemental oxygen: only enough to supply a nasal cannula at 4L max, and that for only a few hours.
As with the vast majority of medical cases, a thorough history of my 73-year-old air traveler proved invaluable. She felt light-headed but never lost consciousness. She had no other symptoms. Her past medical history was significant for hypertension but no heart disease. Was there anything else? She had been discharged from a hospital three days before for severe hypertension. Her ACE inhibitor and beta-blocker doses had been doubled and HCTZ added (her hospitalist had done an excellent job educating her on her disease, her medication changes, and possible side effects).
Anything else? She had been traveling more than 12 hours with little to drink, but she had taken all of her meds just before boarding the flight. After some oral rehydration, leaning back, and elevating her feet, her blood pressure increased to 125/71. I checked on her frequently for the rest of the flight, and she was talking happily to neighbors and her son long before we deplaned. They were en route to Boston, where she was moving and had no doctor, but she had an appointment scheduled with a new one soon. I gave her my card and my cell number and instructed them to call me if there were any problems. She and her son were thankful (and her neighbors were too!), and I was glad to have helped.
The Aftermath
The only thing left was the administrative paperwork for the airline. Would I please sign here? What was my license number (they were confused as to whether to take my NPI, my state license number, or DEA number, so I gave them all three), and where was I employed?
After getting home and recovering from my jet lag, I did some research on this topic. Colleagues of mine expressed concern over the legal liability of providing assistance in flight, but, compared to our day jobs, that concern seems to be unwarranted. The Aviation Medical Assistance Act of 1998 (www.gpo.gov) protects healthcare providers who render care in good faith.
As of the 2008 article by Ruskin, no physician providing care for an airline patient had been successfully sued. I learned that the medical kits are fairly well stocked and are set up for the physician/medical professional. I also learned that supplemental oxygen, so ubiquitous in the hospital, is more limited on an airplane. And, I found out that, while airlines contract with ground-based medical services, half of all emergencies are cared for by Good Samaritan doctors, licensed providers, nurses, and EMTs.
So, before my next flight, in addition to packing my iPad and thumb drive, boarding pass, and ID, I plan to pack those reference articles by Ruskin and Peterson.
What Physicians Should Know About Buying into Hospitalist Practice
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Physicians who join a hospitalist practice often have the opportunity to purchase an equity interest after some period of employment. The future possibility of the physician-employee becoming an owner of the practice is sometimes addressed in the physician’s employment agreement. The amount of detail in the employment agreement regarding potential ownership will vary depending on the practice and the negotiating power of the individual physician. Clearly, the more specificity found in the contract, the better the hospitalist is served.
Because the circumstances of the individual parties will govern the terms of the buy-in, there is no standard contract language universally used in physician employment agreements. Specific aspects exist in many buy-in provisions contained in physician employment agreements, however. Such issues include: (i) the opportunity to purchase an ownership interest; (ii) performance reviews; (iii) how the interest will be valued; and (iv) payment terms.
Ownership Interest
The employment agreement should specify whether and when the employee-physician will be eligible to acquire an interest in the practice. The idea of remaining an employee may be attractive to some physicians who prefer to have less involvement in the business and financial aspects of the hospitalist practice. Sometimes cost becomes a critical issue.
However, if the parties do intend for the physician to have the right to purchase an ownership interest, the timeframe and conditions for exercising that right should be specified in writing. The following is an example of a provision addressing the opportunity to purchase an equity interest:
“The parties agree that it is their intent that upon X years of continuous employment pursuant to the terms and conditions of this Agreement, Hospitalist shall be given the opportunity to purchase [a partnership interest or stock] in Practice.”
Performance Reviews
One condition precedent to the right to purchase an equity interest may be satisfactory performance reviews by senior physicians. Although these reviews frequently are based on subjective standards, the employee-physician should seek a contractual commitment describing the criteria to be evaluated in order to make the reviews as objective as possible. Standard criteria include statistical analysis (e.g. number of patients seen a day), the quality of patient care rendered, and contributions to the practice’s operations (e.g. marketing, community outreach).
In addition, the physician’s employment agreement should specify the frequency of performance reviews. Physician reviews commonly occur on an annual, and sometimes semi-annual, basis, especially during the initial years of employment. Regardless of how often the reviews are conducted, it is highly beneficial to both the practice and the physician-employee that the time periods for evaluations be strictly enforced. Consistent, formal performance reviews promote improvement and synergy between the physician and the practice.
Equity Interest
Typically, an employment agreement will either provide an exact purchase price or, more often, state the future method to be used for calculating the buy-in price. Ordinarily, the buy-in price will be a function of the valuation of the total equity of the practice and the percentage of that equity, which is represented by the interests to be acquired by the purchasing physician. While there are a few formulas for valuing the equity of a hospitalist practice, the most common method is discounted present value of net revenue stream.
The appropriate valuation method will depend on a number of factors unique to the individual practice. Therefore, the practice should seek the assistance of an accountant or practice valuation specialist when determining the value. Stating an agreed-upon valuation method in the employment agreement will limit surprises and “sticker shock” to the buy-in price when the ownership decision is made down the road.
Payment Terms
In the event that the physician-employee exercises the opportunity to buy in, the employment or purchase agreement should provide terms governing how the purchase price will be paid. Often, the practice will be flexible in negotiating payment terms that meet the physician’s individual financial needs; however, the parties frequently agree that the physician will either pay the owners in full up front or make installment payments over a specified number of years.
If the physician is required to pay the total purchase price up front, he or she will be personally responsible for obtaining the necessary funding through bank loans or other sources. If the purchasing physician is permitted to make installment payments, he or she will be required to sign a promissory note in which the payee is the practice and the note is secured by a security interest in the equity granted to the physician. There are important tax strategies that can be implemented when installment payments are agreed upon. In the event that the physician fails to make the installment payments, the practice may be able to recover the equity interest.
In Sum
Both parties should review and understand the terms and conditions of the buy-in so that all parties enter the employment relationship with the same expectations for future ownership.
Steven Harris is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Tips for Landing Your First Job in Hospital Medicine
Finding the right hospitalist position can help make the transition from resident to attending enjoyable as you adjust to a new level of responsibility. But the wrong job can leave you feeling overwhelmed and unsupported. So what is a busy senior resident to do? Here we offer selected pearls and pitfalls to help you find a great position.
Initial Steps and Things to Consider
Start applying in the fall of your PGY-3 year. The process of interviewing applicants, finalizing contracts, arranging for hospital privileges, and enrolling a new hire in insurance plans can take many months. Many employers start looking early.
Meet with your residency program director and your hospitalist group director to discuss your plans. They can help you clarify your goals, serving as coaches throughout the process, and they may know people at the places you are interested in. Recruiters can be helpful, but remember—many are incentivized to find you a position. Advertisements in the back of journals and professional society publications are useful resources.
Obtain your medical license as early as possible. Getting licensed in the state you will be working in can be much faster if you already have a license from another state. Applicants have lost positions because they didn’t have their medical license in time.
Don’t shop for a job based on schedule and salary alone. There are reasons some jobs pay better than most, and they aren’t always good (home call, for example). A seven-on, seven-off schedule affords a lot of free time, but while you are on service, family life often takes a back seat. Conversely, working every Monday to Friday offers less free time for travel or moonlighting.
Think about the care model you prefer. Do you want to work with residents, physician assistants, nurse practitioners, or in a “direct care” model where it’s just you and the nurses caring for patients? Salaries often are inversely related to the number of providers between you and the patients. Positions without resident support might require procedural competence. Demonstrating academic productivity, especially in the area of quality improvement or patient safety, can help you secure a position working with residents. Some programs first place new hires on the non-teaching service to earn the chance to work with residents and medical students.
Think about what type of career you want. Do you only want to see patients, or do you want a career that includes a non-clinical role for which you will be paid? Some hospitalists find that becoming a patient safety officer or residency program director, trying out a medical student clerkship, or growing into another administrative role is a great complement to their clinical time and prevents burnout.
How to Stand Out
Start off by getting the basics right. Make sure your e-mail address sounds professional. A well-formatted CV, with no spelling errors or unexplained time gaps, is a must. A cover letter that succinctly describes the type of position you are looking for, highlights your strengths, and does not wax on about why you wanted to become a doctor—that was your personal statement for med school—is helpful. Don’t correspond with employers using your smartphone if you’re prone to autocorrect or spelling errors, or if you tend to write too casually from a mobile device. Before you shoot off that immediate e-mail response, make sure you’re addressing people properly and not mixing up employers.
Join SHM (they have trainee rates!), and attend an SHM conference or local chapter meeting if you can (www.hospitalmedicine.org/events). SHM membership reflects your commitment to the specialty. Membership in other professional societies is a plus as well.
Quality improvement (QI), patient safety, and patient satisfaction are central to hospital medicine. Medication reconciliation, infection control, handoff, transitions of care, listening carefully to patients, and explaining things to them are likely things you’ve done throughout residency. Communicate to employers your experience in and appreciation of these areas. Completing a QI or patient safety project and participating on a hospital committee will help make you a competitive applicant.
Interview Do’s and Don’ts
The advice most were given when applying to residency still holds. Be on time, dress professionally, research the program, and be prepared to speak about why you want to work at a particular place. Speak to hospitalists in the group, and be very courteous to everyone.
Don’t start off by asking about salary—if you move along in the process, compensation will be discussed. Get a clear picture of the schedule and how time off/non-clinical time occurs, but don’t come off as inflexible or too needy.
Ask why hospitalists have left a group. Frequent turnover without good reason could be a red flag. If the hospitalist director and/or department chair are new or will be leaving, you should ask how that might affect the group. If the current leadership has been stable, ask what growth has occurred for the group overall and among individuals during their tenure.
Find out whether hospitalists have been promoted academically and if there are career growth opportunities in areas you are interested in. Try to determine if the group has a “voice” with administration by asking for examples of how hospitalist concerns have been positively addressed.
Having a clear picture of how much nursing, social work, case management, subspecialist, and intensivist support is available is critical. Whether billing is done electronically or on paper is important, as is the degree of instruction and support for billing.
Take the opportunity to meet the current hospitalists—and note that their input often is solicited as to whether or not to hire a candidate—and ask them questions away from the ears of the program leadership; most hospitalists like to meet potential colleagues.
Closing the Deal
If you make it past the interview stage, be sure additional deliverables, such as letters of recommendation, are on time. Now is the time to ask about salary. Don’t be afraid to inquire about relocation or sign-on bonuses. At this point, the employer likes you and has invested time in recruiting you. You can gently leverage this in your negotiations. Consult your program director or other mentors at this point—they can provide guidance.
If you are uncertain about accepting an offer, be open about this with the employer. Your honesty in the process is essential, will be viewed positively, and can trigger additional dialogue that may help you decide. Juggling multiple offers dishonestly is not ethical and can backfire, as many hospitalist directors know each other.
Have an attorney familiar with physician contracts review yours. Look at whether “tail coverage,” which insures legal actions brought against you after you have left, is provided. Take note of “non-compete” clauses; they may limit your ability to practice in the area if you leave a practice. Find out if moonlighting is allowed and if the hospital requires you to give them a percentage of your outside earnings.
If you secure a position, whether as a career hospitalist or just for a year or two before fellowship, you should be excited. HM is a wonderful field with tremendous and varied opportunities. Dive in, enjoy, and explore everything it has to offer!
Dr. Bryson is medical director of teaching services, associate program director of internal medicine residency, and assistant professor at Tufts University, and a hospitalist at Baystate Medical Center in Springfield, Mass. Dr. Steinberg is residency program director in the Department of Medicine at Beth Israel Medical Center, and associate professor of medicine at the Icahn School of Medicine at Mount Sinai in New York City. Both are members of SHM’s Physicians in Training Committee.
Finding the right hospitalist position can help make the transition from resident to attending enjoyable as you adjust to a new level of responsibility. But the wrong job can leave you feeling overwhelmed and unsupported. So what is a busy senior resident to do? Here we offer selected pearls and pitfalls to help you find a great position.
Initial Steps and Things to Consider
Start applying in the fall of your PGY-3 year. The process of interviewing applicants, finalizing contracts, arranging for hospital privileges, and enrolling a new hire in insurance plans can take many months. Many employers start looking early.
Meet with your residency program director and your hospitalist group director to discuss your plans. They can help you clarify your goals, serving as coaches throughout the process, and they may know people at the places you are interested in. Recruiters can be helpful, but remember—many are incentivized to find you a position. Advertisements in the back of journals and professional society publications are useful resources.
Obtain your medical license as early as possible. Getting licensed in the state you will be working in can be much faster if you already have a license from another state. Applicants have lost positions because they didn’t have their medical license in time.
Don’t shop for a job based on schedule and salary alone. There are reasons some jobs pay better than most, and they aren’t always good (home call, for example). A seven-on, seven-off schedule affords a lot of free time, but while you are on service, family life often takes a back seat. Conversely, working every Monday to Friday offers less free time for travel or moonlighting.
Think about the care model you prefer. Do you want to work with residents, physician assistants, nurse practitioners, or in a “direct care” model where it’s just you and the nurses caring for patients? Salaries often are inversely related to the number of providers between you and the patients. Positions without resident support might require procedural competence. Demonstrating academic productivity, especially in the area of quality improvement or patient safety, can help you secure a position working with residents. Some programs first place new hires on the non-teaching service to earn the chance to work with residents and medical students.
Think about what type of career you want. Do you only want to see patients, or do you want a career that includes a non-clinical role for which you will be paid? Some hospitalists find that becoming a patient safety officer or residency program director, trying out a medical student clerkship, or growing into another administrative role is a great complement to their clinical time and prevents burnout.
How to Stand Out
Start off by getting the basics right. Make sure your e-mail address sounds professional. A well-formatted CV, with no spelling errors or unexplained time gaps, is a must. A cover letter that succinctly describes the type of position you are looking for, highlights your strengths, and does not wax on about why you wanted to become a doctor—that was your personal statement for med school—is helpful. Don’t correspond with employers using your smartphone if you’re prone to autocorrect or spelling errors, or if you tend to write too casually from a mobile device. Before you shoot off that immediate e-mail response, make sure you’re addressing people properly and not mixing up employers.
Join SHM (they have trainee rates!), and attend an SHM conference or local chapter meeting if you can (www.hospitalmedicine.org/events). SHM membership reflects your commitment to the specialty. Membership in other professional societies is a plus as well.
Quality improvement (QI), patient safety, and patient satisfaction are central to hospital medicine. Medication reconciliation, infection control, handoff, transitions of care, listening carefully to patients, and explaining things to them are likely things you’ve done throughout residency. Communicate to employers your experience in and appreciation of these areas. Completing a QI or patient safety project and participating on a hospital committee will help make you a competitive applicant.
Interview Do’s and Don’ts
The advice most were given when applying to residency still holds. Be on time, dress professionally, research the program, and be prepared to speak about why you want to work at a particular place. Speak to hospitalists in the group, and be very courteous to everyone.
Don’t start off by asking about salary—if you move along in the process, compensation will be discussed. Get a clear picture of the schedule and how time off/non-clinical time occurs, but don’t come off as inflexible or too needy.
Ask why hospitalists have left a group. Frequent turnover without good reason could be a red flag. If the hospitalist director and/or department chair are new or will be leaving, you should ask how that might affect the group. If the current leadership has been stable, ask what growth has occurred for the group overall and among individuals during their tenure.
Find out whether hospitalists have been promoted academically and if there are career growth opportunities in areas you are interested in. Try to determine if the group has a “voice” with administration by asking for examples of how hospitalist concerns have been positively addressed.
Having a clear picture of how much nursing, social work, case management, subspecialist, and intensivist support is available is critical. Whether billing is done electronically or on paper is important, as is the degree of instruction and support for billing.
Take the opportunity to meet the current hospitalists—and note that their input often is solicited as to whether or not to hire a candidate—and ask them questions away from the ears of the program leadership; most hospitalists like to meet potential colleagues.
Closing the Deal
If you make it past the interview stage, be sure additional deliverables, such as letters of recommendation, are on time. Now is the time to ask about salary. Don’t be afraid to inquire about relocation or sign-on bonuses. At this point, the employer likes you and has invested time in recruiting you. You can gently leverage this in your negotiations. Consult your program director or other mentors at this point—they can provide guidance.
If you are uncertain about accepting an offer, be open about this with the employer. Your honesty in the process is essential, will be viewed positively, and can trigger additional dialogue that may help you decide. Juggling multiple offers dishonestly is not ethical and can backfire, as many hospitalist directors know each other.
Have an attorney familiar with physician contracts review yours. Look at whether “tail coverage,” which insures legal actions brought against you after you have left, is provided. Take note of “non-compete” clauses; they may limit your ability to practice in the area if you leave a practice. Find out if moonlighting is allowed and if the hospital requires you to give them a percentage of your outside earnings.
If you secure a position, whether as a career hospitalist or just for a year or two before fellowship, you should be excited. HM is a wonderful field with tremendous and varied opportunities. Dive in, enjoy, and explore everything it has to offer!
Dr. Bryson is medical director of teaching services, associate program director of internal medicine residency, and assistant professor at Tufts University, and a hospitalist at Baystate Medical Center in Springfield, Mass. Dr. Steinberg is residency program director in the Department of Medicine at Beth Israel Medical Center, and associate professor of medicine at the Icahn School of Medicine at Mount Sinai in New York City. Both are members of SHM’s Physicians in Training Committee.
Finding the right hospitalist position can help make the transition from resident to attending enjoyable as you adjust to a new level of responsibility. But the wrong job can leave you feeling overwhelmed and unsupported. So what is a busy senior resident to do? Here we offer selected pearls and pitfalls to help you find a great position.
Initial Steps and Things to Consider
Start applying in the fall of your PGY-3 year. The process of interviewing applicants, finalizing contracts, arranging for hospital privileges, and enrolling a new hire in insurance plans can take many months. Many employers start looking early.
Meet with your residency program director and your hospitalist group director to discuss your plans. They can help you clarify your goals, serving as coaches throughout the process, and they may know people at the places you are interested in. Recruiters can be helpful, but remember—many are incentivized to find you a position. Advertisements in the back of journals and professional society publications are useful resources.
Obtain your medical license as early as possible. Getting licensed in the state you will be working in can be much faster if you already have a license from another state. Applicants have lost positions because they didn’t have their medical license in time.
Don’t shop for a job based on schedule and salary alone. There are reasons some jobs pay better than most, and they aren’t always good (home call, for example). A seven-on, seven-off schedule affords a lot of free time, but while you are on service, family life often takes a back seat. Conversely, working every Monday to Friday offers less free time for travel or moonlighting.
Think about the care model you prefer. Do you want to work with residents, physician assistants, nurse practitioners, or in a “direct care” model where it’s just you and the nurses caring for patients? Salaries often are inversely related to the number of providers between you and the patients. Positions without resident support might require procedural competence. Demonstrating academic productivity, especially in the area of quality improvement or patient safety, can help you secure a position working with residents. Some programs first place new hires on the non-teaching service to earn the chance to work with residents and medical students.
Think about what type of career you want. Do you only want to see patients, or do you want a career that includes a non-clinical role for which you will be paid? Some hospitalists find that becoming a patient safety officer or residency program director, trying out a medical student clerkship, or growing into another administrative role is a great complement to their clinical time and prevents burnout.
How to Stand Out
Start off by getting the basics right. Make sure your e-mail address sounds professional. A well-formatted CV, with no spelling errors or unexplained time gaps, is a must. A cover letter that succinctly describes the type of position you are looking for, highlights your strengths, and does not wax on about why you wanted to become a doctor—that was your personal statement for med school—is helpful. Don’t correspond with employers using your smartphone if you’re prone to autocorrect or spelling errors, or if you tend to write too casually from a mobile device. Before you shoot off that immediate e-mail response, make sure you’re addressing people properly and not mixing up employers.
Join SHM (they have trainee rates!), and attend an SHM conference or local chapter meeting if you can (www.hospitalmedicine.org/events). SHM membership reflects your commitment to the specialty. Membership in other professional societies is a plus as well.
Quality improvement (QI), patient safety, and patient satisfaction are central to hospital medicine. Medication reconciliation, infection control, handoff, transitions of care, listening carefully to patients, and explaining things to them are likely things you’ve done throughout residency. Communicate to employers your experience in and appreciation of these areas. Completing a QI or patient safety project and participating on a hospital committee will help make you a competitive applicant.
Interview Do’s and Don’ts
The advice most were given when applying to residency still holds. Be on time, dress professionally, research the program, and be prepared to speak about why you want to work at a particular place. Speak to hospitalists in the group, and be very courteous to everyone.
Don’t start off by asking about salary—if you move along in the process, compensation will be discussed. Get a clear picture of the schedule and how time off/non-clinical time occurs, but don’t come off as inflexible or too needy.
Ask why hospitalists have left a group. Frequent turnover without good reason could be a red flag. If the hospitalist director and/or department chair are new or will be leaving, you should ask how that might affect the group. If the current leadership has been stable, ask what growth has occurred for the group overall and among individuals during their tenure.
Find out whether hospitalists have been promoted academically and if there are career growth opportunities in areas you are interested in. Try to determine if the group has a “voice” with administration by asking for examples of how hospitalist concerns have been positively addressed.
Having a clear picture of how much nursing, social work, case management, subspecialist, and intensivist support is available is critical. Whether billing is done electronically or on paper is important, as is the degree of instruction and support for billing.
Take the opportunity to meet the current hospitalists—and note that their input often is solicited as to whether or not to hire a candidate—and ask them questions away from the ears of the program leadership; most hospitalists like to meet potential colleagues.
Closing the Deal
If you make it past the interview stage, be sure additional deliverables, such as letters of recommendation, are on time. Now is the time to ask about salary. Don’t be afraid to inquire about relocation or sign-on bonuses. At this point, the employer likes you and has invested time in recruiting you. You can gently leverage this in your negotiations. Consult your program director or other mentors at this point—they can provide guidance.
If you are uncertain about accepting an offer, be open about this with the employer. Your honesty in the process is essential, will be viewed positively, and can trigger additional dialogue that may help you decide. Juggling multiple offers dishonestly is not ethical and can backfire, as many hospitalist directors know each other.
Have an attorney familiar with physician contracts review yours. Look at whether “tail coverage,” which insures legal actions brought against you after you have left, is provided. Take note of “non-compete” clauses; they may limit your ability to practice in the area if you leave a practice. Find out if moonlighting is allowed and if the hospital requires you to give them a percentage of your outside earnings.
If you secure a position, whether as a career hospitalist or just for a year or two before fellowship, you should be excited. HM is a wonderful field with tremendous and varied opportunities. Dive in, enjoy, and explore everything it has to offer!
Dr. Bryson is medical director of teaching services, associate program director of internal medicine residency, and assistant professor at Tufts University, and a hospitalist at Baystate Medical Center in Springfield, Mass. Dr. Steinberg is residency program director in the Department of Medicine at Beth Israel Medical Center, and associate professor of medicine at the Icahn School of Medicine at Mount Sinai in New York City. Both are members of SHM’s Physicians in Training Committee.
Beware Mid-Career
Middle age is typically a difficult passage for many professionals. It is a developmental phase involving the mourning of lost opportunities and the acceptance of one’s limits. One also reflects on his or her identity, takes note of regrets, and reevaluates how one will apportion time in the future.—Glen Gabbard, MD1

Hospital medicine is a relatively young specialty, but we are growing up, with many hospitalists now firmly in the middle phase of their careers. In 1999, 15% of our peers had been hospitalists for more than five years; by 2010, that number had grown to 50%.2 As the ranks of hospitalists grow older, we are faced with questions reflecting a life station marked by a little more wisdom, a few more gray hairs, and an occasional reflection on the legacy we will leave.
Drybye and colleagues recently released further analysis on a survey that had been previously reported, shedding new light on mid-career physician satisfaction and burnout and revealing important implications for hospital medicine.3 The study looked at responses to the Maslach Burnout Inventory for physicians from a range of specialties who had been in practice 10 years or less (early career), 11 to 20 years (mid-career), and 21 years or more (late career).
The study demonstrated that while early and late career have their challenges, middle career is a particularly difficult time for physicians. Mid-career physicians had the lowest satisfaction with their specialty choice and their work-life balance and the highest rates of emotional exhaustion and burnout. Strikingly, mid-career physicians were more than twice as likely as those in early and late career to plan to leave the practice of medicine for reasons other than retirement in the next 24 months.
What does this mean for hospital medicine? Because the survey findings are drawn from multiple specialties, we must use caution in extrapolating the results to hospitalists; however, if hospitalists are leaving the specialty mid-career, a more pressing problem may exist for hospital medicine than for other specialties. Why? First, the specialty has grown so rapidly over the last 15 years that it has been difficult to generate a sufficient supply of physicians to meet the demand. If a large number of mid-career hospitalists leave the specialty, our field may be stuck in a state of “arrested development” without the sufficient presence of mature clinicians. Second, effective hospitalists possess “system” skills that are learned on the job, so seasoned hospitalists often play an integrative and problem-solving role within the hospital. Third, there could be a downward spiral of career satisfaction in the specialty if onlookers like trainees and stakeholders in the healthcare ecosystem see hospitalists as dissatisfied and disengaged. Will the promise of hospital medicine be fulfilled?
In an accompanying editorial, Spinelli suggests three principles for physician well-being, which hospitalist programs would do well to consider:4
- Elevate well-being metrics to the same level of importance as financial, quality, and patient satisfaction metrics. (Place such metrics on the organizational dashboard.)
- Design system and care processes that include intentional plans for physician and staff wellness. (Redesign of care models and workflows should consider physician and staff wellness.)
- Adopt a robust set of self-care strategies for those experiencing burnout.
SHM’s Role
SHM has taken up the issue of hospitalist career satisfaction on a number of occasions over the years, initially engendered by field observations of the stressful nature of hospitalist work and a 2001 study reporting that 25% of hospitalists were “at risk” of burnout and 13% were “burned out.”5 Subsequently, SHM released a white paper with a number of specific recommendations organized around a career satisfaction framework consisting of autonomy, reward/recognition, occupational solidarity, and connection with one’s professional and broader community.6
Recently, the SHM Practice Management Committee has once again taken up the issue of “physician engagement.” Over the next few months, the committee plans to:
- Create a repository of related resources on the SHM website, including physician engagement profiles for some hospitalist practices;
- Initiate a dialogue on the topic of physician engagement on HMX (connect.hospitalmedicine.org), SHM’s social networking platform; and
- Publish a “public domain” survey questionnaire that hospitalist practices can use. This is a crucial matter that remains a central concern for our specialty and for the safety and well-being of our patients.
Conclusion
The Institute for Healthcare Improvement advanced the idea of the Triple Aim (better care, better health, lower costs) several years ago as a guiding principle in the transformation of healthcare. More recently, a growing number of voices suggest that physician satisfaction is a crucial foundation of the Triple Aim.4 I submit that for hospitalists to fulfill their potential as healthcare change agents, we will need to build a professional experience that enables them to traverse mid-career challenges and make it to the professional finish line as engaged and well-adjusted members of the healthcare community.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at [email protected].
References
- Gabbard GO. Medicine and its discontents. Mayo Clin Proc. 2013;88(12):1347-1349.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: Toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Drybye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
- Spinelli WM. The phantom limb of the triple aim. Mayo Clin Proc. 2013;88(12):1356-1357.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Society of Hospital Medicine. A challenge for a new specialty: a white paper on hospitalist career satisfaction. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed January 4, 2014.
Middle age is typically a difficult passage for many professionals. It is a developmental phase involving the mourning of lost opportunities and the acceptance of one’s limits. One also reflects on his or her identity, takes note of regrets, and reevaluates how one will apportion time in the future.—Glen Gabbard, MD1
Hospital medicine is a relatively young specialty, but we are growing up, with many hospitalists now firmly in the middle phase of their careers. In 1999, 15% of our peers had been hospitalists for more than five years; by 2010, that number had grown to 50%.2 As the ranks of hospitalists grow older, we are faced with questions reflecting a life station marked by a little more wisdom, a few more gray hairs, and an occasional reflection on the legacy we will leave.
Drybye and colleagues recently released further analysis on a survey that had been previously reported, shedding new light on mid-career physician satisfaction and burnout and revealing important implications for hospital medicine.3 The study looked at responses to the Maslach Burnout Inventory for physicians from a range of specialties who had been in practice 10 years or less (early career), 11 to 20 years (mid-career), and 21 years or more (late career).
The study demonstrated that while early and late career have their challenges, middle career is a particularly difficult time for physicians. Mid-career physicians had the lowest satisfaction with their specialty choice and their work-life balance and the highest rates of emotional exhaustion and burnout. Strikingly, mid-career physicians were more than twice as likely as those in early and late career to plan to leave the practice of medicine for reasons other than retirement in the next 24 months.
What does this mean for hospital medicine? Because the survey findings are drawn from multiple specialties, we must use caution in extrapolating the results to hospitalists; however, if hospitalists are leaving the specialty mid-career, a more pressing problem may exist for hospital medicine than for other specialties. Why? First, the specialty has grown so rapidly over the last 15 years that it has been difficult to generate a sufficient supply of physicians to meet the demand. If a large number of mid-career hospitalists leave the specialty, our field may be stuck in a state of “arrested development” without the sufficient presence of mature clinicians. Second, effective hospitalists possess “system” skills that are learned on the job, so seasoned hospitalists often play an integrative and problem-solving role within the hospital. Third, there could be a downward spiral of career satisfaction in the specialty if onlookers like trainees and stakeholders in the healthcare ecosystem see hospitalists as dissatisfied and disengaged. Will the promise of hospital medicine be fulfilled?
In an accompanying editorial, Spinelli suggests three principles for physician well-being, which hospitalist programs would do well to consider:4
- Elevate well-being metrics to the same level of importance as financial, quality, and patient satisfaction metrics. (Place such metrics on the organizational dashboard.)
- Design system and care processes that include intentional plans for physician and staff wellness. (Redesign of care models and workflows should consider physician and staff wellness.)
- Adopt a robust set of self-care strategies for those experiencing burnout.
SHM’s Role
SHM has taken up the issue of hospitalist career satisfaction on a number of occasions over the years, initially engendered by field observations of the stressful nature of hospitalist work and a 2001 study reporting that 25% of hospitalists were “at risk” of burnout and 13% were “burned out.”5 Subsequently, SHM released a white paper with a number of specific recommendations organized around a career satisfaction framework consisting of autonomy, reward/recognition, occupational solidarity, and connection with one’s professional and broader community.6
Recently, the SHM Practice Management Committee has once again taken up the issue of “physician engagement.” Over the next few months, the committee plans to:
- Create a repository of related resources on the SHM website, including physician engagement profiles for some hospitalist practices;
- Initiate a dialogue on the topic of physician engagement on HMX (connect.hospitalmedicine.org), SHM’s social networking platform; and
- Publish a “public domain” survey questionnaire that hospitalist practices can use. This is a crucial matter that remains a central concern for our specialty and for the safety and well-being of our patients.
Conclusion
The Institute for Healthcare Improvement advanced the idea of the Triple Aim (better care, better health, lower costs) several years ago as a guiding principle in the transformation of healthcare. More recently, a growing number of voices suggest that physician satisfaction is a crucial foundation of the Triple Aim.4 I submit that for hospitalists to fulfill their potential as healthcare change agents, we will need to build a professional experience that enables them to traverse mid-career challenges and make it to the professional finish line as engaged and well-adjusted members of the healthcare community.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at [email protected].
References
- Gabbard GO. Medicine and its discontents. Mayo Clin Proc. 2013;88(12):1347-1349.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: Toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Drybye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
- Spinelli WM. The phantom limb of the triple aim. Mayo Clin Proc. 2013;88(12):1356-1357.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Society of Hospital Medicine. A challenge for a new specialty: a white paper on hospitalist career satisfaction. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed January 4, 2014.
Middle age is typically a difficult passage for many professionals. It is a developmental phase involving the mourning of lost opportunities and the acceptance of one’s limits. One also reflects on his or her identity, takes note of regrets, and reevaluates how one will apportion time in the future.—Glen Gabbard, MD1
Hospital medicine is a relatively young specialty, but we are growing up, with many hospitalists now firmly in the middle phase of their careers. In 1999, 15% of our peers had been hospitalists for more than five years; by 2010, that number had grown to 50%.2 As the ranks of hospitalists grow older, we are faced with questions reflecting a life station marked by a little more wisdom, a few more gray hairs, and an occasional reflection on the legacy we will leave.
Drybye and colleagues recently released further analysis on a survey that had been previously reported, shedding new light on mid-career physician satisfaction and burnout and revealing important implications for hospital medicine.3 The study looked at responses to the Maslach Burnout Inventory for physicians from a range of specialties who had been in practice 10 years or less (early career), 11 to 20 years (mid-career), and 21 years or more (late career).
The study demonstrated that while early and late career have their challenges, middle career is a particularly difficult time for physicians. Mid-career physicians had the lowest satisfaction with their specialty choice and their work-life balance and the highest rates of emotional exhaustion and burnout. Strikingly, mid-career physicians were more than twice as likely as those in early and late career to plan to leave the practice of medicine for reasons other than retirement in the next 24 months.
What does this mean for hospital medicine? Because the survey findings are drawn from multiple specialties, we must use caution in extrapolating the results to hospitalists; however, if hospitalists are leaving the specialty mid-career, a more pressing problem may exist for hospital medicine than for other specialties. Why? First, the specialty has grown so rapidly over the last 15 years that it has been difficult to generate a sufficient supply of physicians to meet the demand. If a large number of mid-career hospitalists leave the specialty, our field may be stuck in a state of “arrested development” without the sufficient presence of mature clinicians. Second, effective hospitalists possess “system” skills that are learned on the job, so seasoned hospitalists often play an integrative and problem-solving role within the hospital. Third, there could be a downward spiral of career satisfaction in the specialty if onlookers like trainees and stakeholders in the healthcare ecosystem see hospitalists as dissatisfied and disengaged. Will the promise of hospital medicine be fulfilled?
In an accompanying editorial, Spinelli suggests three principles for physician well-being, which hospitalist programs would do well to consider:4
- Elevate well-being metrics to the same level of importance as financial, quality, and patient satisfaction metrics. (Place such metrics on the organizational dashboard.)
- Design system and care processes that include intentional plans for physician and staff wellness. (Redesign of care models and workflows should consider physician and staff wellness.)
- Adopt a robust set of self-care strategies for those experiencing burnout.
SHM’s Role
SHM has taken up the issue of hospitalist career satisfaction on a number of occasions over the years, initially engendered by field observations of the stressful nature of hospitalist work and a 2001 study reporting that 25% of hospitalists were “at risk” of burnout and 13% were “burned out.”5 Subsequently, SHM released a white paper with a number of specific recommendations organized around a career satisfaction framework consisting of autonomy, reward/recognition, occupational solidarity, and connection with one’s professional and broader community.6
Recently, the SHM Practice Management Committee has once again taken up the issue of “physician engagement.” Over the next few months, the committee plans to:
- Create a repository of related resources on the SHM website, including physician engagement profiles for some hospitalist practices;
- Initiate a dialogue on the topic of physician engagement on HMX (connect.hospitalmedicine.org), SHM’s social networking platform; and
- Publish a “public domain” survey questionnaire that hospitalist practices can use. This is a crucial matter that remains a central concern for our specialty and for the safety and well-being of our patients.
Conclusion
The Institute for Healthcare Improvement advanced the idea of the Triple Aim (better care, better health, lower costs) several years ago as a guiding principle in the transformation of healthcare. More recently, a growing number of voices suggest that physician satisfaction is a crucial foundation of the Triple Aim.4 I submit that for hospitalists to fulfill their potential as healthcare change agents, we will need to build a professional experience that enables them to traverse mid-career challenges and make it to the professional finish line as engaged and well-adjusted members of the healthcare community.
Dr. Whitcomb is Chief Medical Officer of Remedy Partners. He is co-founder and past president of SHM. Email him at [email protected].
References
- Gabbard GO. Medicine and its discontents. Mayo Clin Proc. 2013;88(12):1347-1349.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: Toward flourishing careers. J Gen Intern Med. 2012;27(1):28-36.
- Drybye LN, Varkey P, Boone SL, Satele DV, Sloan JA, Shanafelt TD. Physician satisfaction and burnout at different career stages. Mayo Clin Proc. 2013;88(12):1358-1367.
- Spinelli WM. The phantom limb of the triple aim. Mayo Clin Proc. 2013;88(12):1356-1357.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Society of Hospital Medicine. A challenge for a new specialty: a white paper on hospitalist career satisfaction. Available at: http://www.hospitalmedicine.org/Content/NavigationMenu/Publications/WhitePapers/White_Papers.htm. Accessed January 4, 2014.