User login
Crowdsourcing Medical Expertise
The volume of existing knowledge and the pace of discovery in medical science challenge a clinician's ability to access relevant information at the point of care. Knowledge gaps that arise in practice usually involve matters related to diagnosis, drug therapy, or treatment.[1] In the clinical setting, healthcare providers (HCPs) answer questions using a variety of online and print resources. Ironically, HCPs often lack the training required to find details regarding uncommon disorders or complex medical decisions that are not easily found or well represented in the published literature.[2] Instead, HCPs turn to trusted colleagues who possess the necessary expertise.[3]
Closing the knowledge‐to‐practice gap involves a range of factual information and data derived from published evidence, anecdotal experience, as well as organization‐ and region‐specific practices.[4] The inability to codify both explicit and tacit information has been linked to variability in prescription practices, excessive use of surgical services, and delayed decisions involving the appropriate provision of end‐of‐life care.[5] Although electronic medical record systems are not configured to support peer collaboration,[6] alternative strategies including crowdsourcing has been used successfully in other domains to tap collective intelligence of skilled workers.[7] Crowdsourcing allows organizations to explore problems at low cost, gain access a wide range of complementary expertise, and capture large amounts of data for analysis.[8, 9] Although an increasing number of physicians use either smartphones or tablets on the job,[10] peer‐to‐peer medical crowdsourcing has not been investigated, despite the fact that processes involving team‐based clinical decision making are associated with better outcomes.[11] Here we field tested the mobile crowdsourcing application DocCHIRP (Crowdsourcing Health Information Retrieval Protocol for Doctors) and assessed user opinion regarding its utility in the clinical setting.
MATERIALS AND METHODS
DocCHIRP Program Design
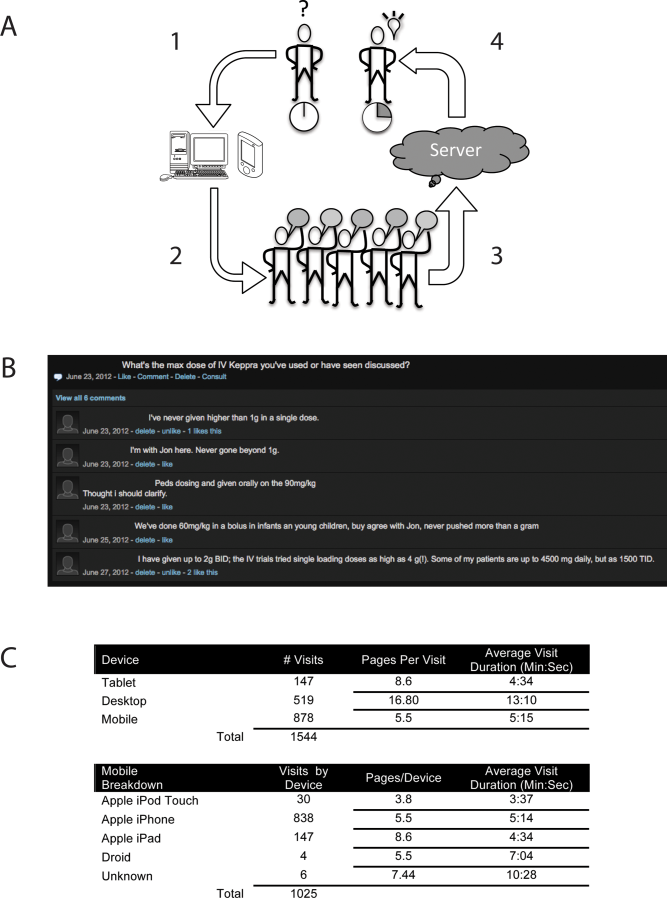
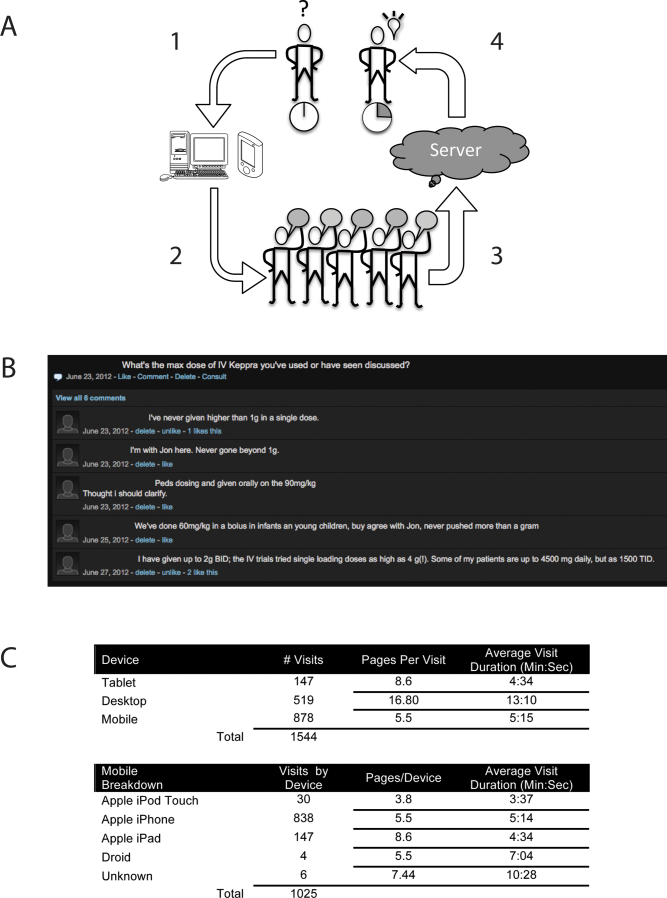
The authors (M.W.H., J.B., H.K.) conceptualized and designed DocCHIRP for mobile (iOS [Apple Inc., Cupertino, CA] and Android [Google Inc., Mountain View, CA]) and desktop use. Email prompts and push notifications, which were modeled after the application VizWiz (Rochester Human Computer Interaction Group, University of Rochester, Rochester, NY), supported near real‐time communication between HCPs. According to recent US Food and Drug Administration guidelines, DocCHIRP is considered a medical reference,[12] intended to share domain‐specific knowledge on diagnosis, therapy, and other medically relevant topics. Devices were password protected and encrypted according to university standards. A typical workflow involves an index provider faced with a clinical question that sends a consult question to 1 or more trusted providers. The crowd receiving the notification responds when available using either free‐text responses or agree/disagree prompts (Figure 1A,B). Providers use preference settings to manage crowd membership, notification settings, and demographics describing their expertise.
Trial Recruitment
The University of Rochester Research Subjects Review Board approved the study, in which prospective users were required to review and agree to a statement regarding potential liability as part of the consent process. In this pilot study, we invited a cross‐section of providers (n = 145) from the Departments of Neurology (including the Division of Pediatric Neurology), Pediatrics, Neuroradiology, Psychiatry, Orthopedics, Emergency Medicine, Internal Medicine, and Family Medicine to participate. E‐mail invitations were sent to HCPs in 3 phases in April (phase I), June (phase II), and August (phase III) over 244 consecutive days. At the conclusion of the trial, 85 HCPs (59%) had created accounts including attending physicians (n = 63), residents (n = 13), fellows (n = 1), and nurse practitioners (n = 8). We did not seek parity in either age or gender representation.
Data Analysis
Mobile device and network usage data, question and response strings, as well as data regarding hardware and browser identity were collected using Google Analytics (Google Inc.,
RESULTS
Attending and resident physicians represented the majority of DocCHIRP account holders (91%), with nurse practitioners accounting for the remaining sample (9%). There were 50 male and 35 female participants, with an age range of 28 to 78 years (median age, 43 years). Departmental affiliations included Pediatrics (n = 28, 33%), Neurology (n = 27, 32%), Internal Medicine (n = 10, 12%), Psychiatry (n = 4, 5%), the Division of Pediatric Neurology (n = 11, 13%), and others (n = 5, 6%). Of the 1544 total visits to the DocCHIRP site, providers favored using smart phones (56.8%) and tablets (9.5%) over the desktop interface (33.6%; Figure 1C). iPhone use (81.7%) surpassed the other platforms combined. Desktop users visited twice as many pages (16.8 pages/visit) compared to those using smart phones (5.5 pages/visit) or tablets (8.6 pages/visit). Desktop users remained engaged longer than mobile users (13 vs 5 minutes). In the post‐trial user survey, we received 72 valid surveys from 85 potential participants (85% response rate).
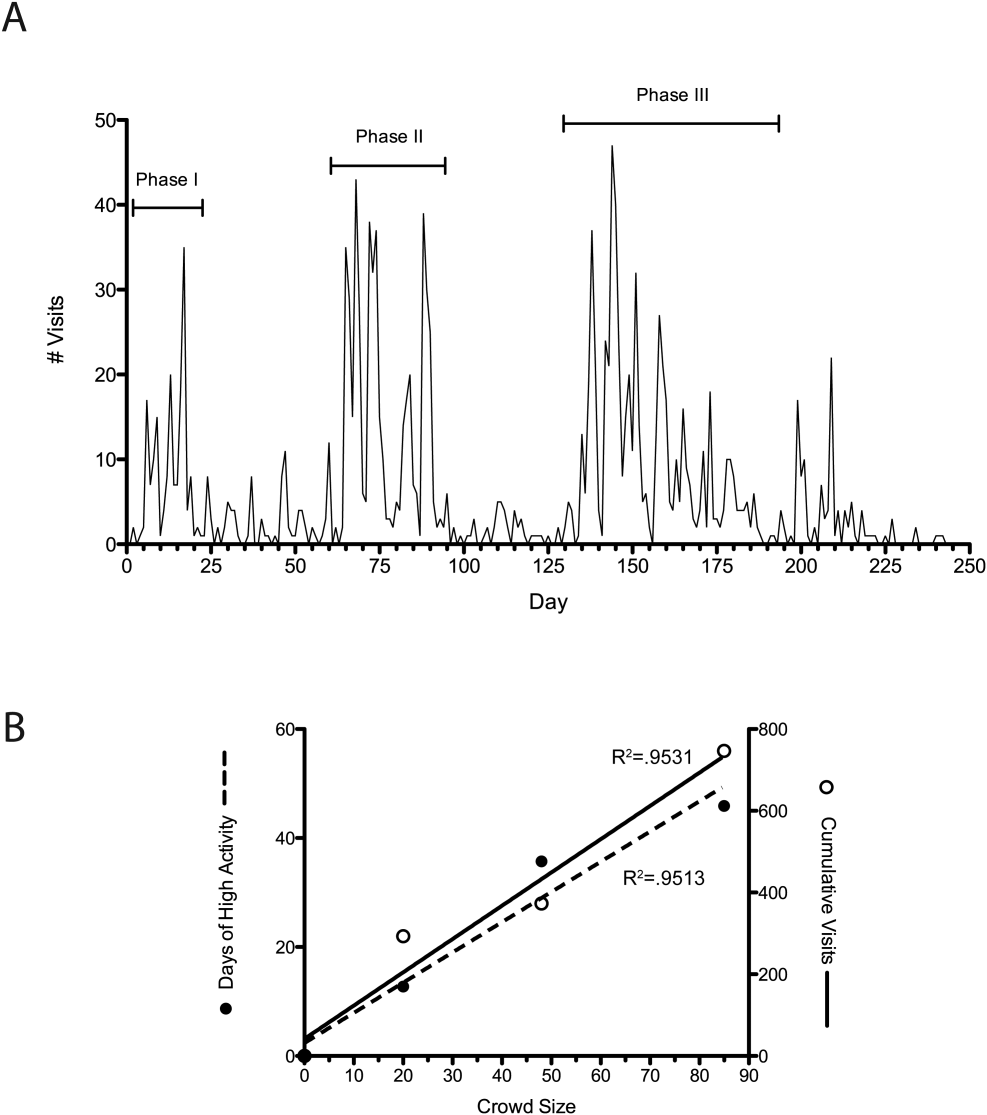
We used a tiered enrollment design, sending invitations to potential participants in 3 phases to study the relationship between the size of the HCP crowd and sustained use as reported in other social networks.[13] Using a cutoff of >3 visits per week to demarcate active periods of use, we saw during the initial phase of enrollment that 20 providers generated a total of 170 visits over 22 days (Figure 2A). The addition of 28 members (phase II, n = 48 total) extended active use by 28 days, with a total of 476 page visits. The addition of 32 members (phase III, n = 85 total) resulted in 56 days of active participation with 612 visits to the site. When plotted (Figure 2B), the relationship between crowd size (total number of registered users) and cumulative visits (R2 = 0.951), as well as crowd size and days of high activity (R2 = 0.953) were linear and direct. We also investigated the timing of user engagement by pooling the data and breaking down use by time of day and day of the week (Figure 3A,B). In addition to observing peak engagement during the midmorning and afternoon, times of anticipated physician‐patient contact, we observed a third use peak in the evening. With the exception of sporadic weekend use, DocCHIRP use clustered during midweek.
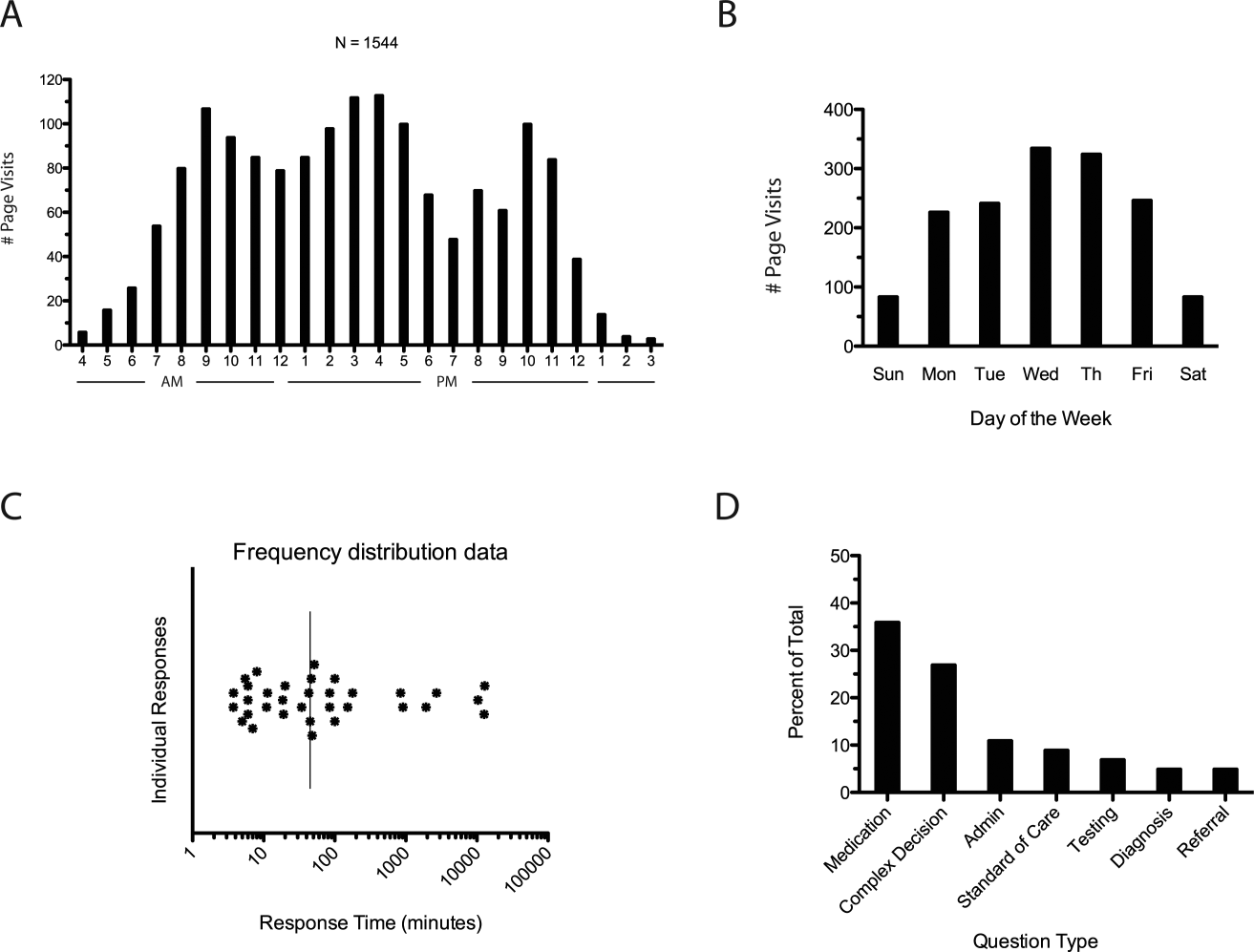
DocCHIRP users generated 45 questions. The fastest first response was returned in less than 4 minutes, with a median first response time of 19 minutes (Figure 3C). Analysis of the consult requests received revealed a clustering of 7 principal question‐response groups: (1) the effective use of medications, (2) complex medical decision making, (3) use of the application itself, (4) guidance regarding the standard of care, (5) selection and interpretation of diagnostic tests, (6) differential diagnosis, and (7) patient referral (Figure 3D). Consults regarding medication use and complex decision making were dominant themes (63%). Several consults generated multiple responses, broadening the scope of the original query or requesting additional information (Table 1).
| Question Type | Consult | Response(s) |
|---|---|---|
| ||
| Medication | How do you treat headache from viral meningitis? | R1: Any analgesic will work; need to clarify that the headache is not post‐LP, which may require blood patch. |
| Anyone know how oral fluconazole (liquid) tastes? We needed to prescribe for a young 13 year old. | R1: We should get a pharmacist on the chat. I would call the pharmacy and see if they can compound it with flavoring. | |
| How frequently do your patients complain of myalgias on statins? Have you prescribed coenzyme Q in this situation? | R1: Did you see the editorial in the Green Journal yesterday?Took the position that statins were not to blame. I usually give a trial off to make sure symptoms resolve. Usually I try them on a different statin.Have not routinely rx'd Q10. | |
| Complex medical decision making | Has anyone seen tapeworm infection from raw pork? Do we need to report this? We treated with mebendazole. | R1: You can check with CDC here: |
| R2: First‐line treatment for Tsolium is praziquantel or albendazole.However, mebendazole has also been used to successfully treat T solium. | ||
| R3: Whipworm is another common pork tapeworm.It is also covered by mebendazole | ||
| What are the current guidelines regarding the use of statins in patients with a history of lobar hemorrhage. | R1: Larger studies (SPARCL, HPS) both showed higher hemorrhage risks in statin treated patients.Cohort studies generally don't show an obvious risk to statins. I've generally taken patients off their statins when they come in with lobar ICH, and more neutral when it's a hypertensive bleed. | |
| Standard of care | How often would someone have to fall before you felt uncomfortable anticoagulating for AFib? | R1: The risk of falls alone should not automatically disqualify a person from being treated with warfarin. |
| R2: I recall reading a meta‐analysis that suggested 300 falls/year would start to favor not anticoagulating, but short of that, falls were not an important factor. | ||
| Anyone used IVIG for any of the following: autoimmune encephalopathy, NMO, paraneoplastic limbic encephalitis, PANDAS? | R1: We had a patient recently with a history of autoimmune encephalopathy who was treated with IVIG. | |
| Administrative | What medical apps do you have on your phone? | R1: DocCHIRP, Epocrates, NIH stroke calculator. |
| R2: I have Merck Medicus, Micromedex drugs, growth charts, and shotsall those are free.I also have Red Book from AAPand Sanford Guide, which I paid for. | ||
| R3: Instant ECG, ACLS Advisor, 10‐Second EM. | ||
| Testing | What would be considered a normal vitamin D level in a 2 year old? | R1: We typically treat at a level less than 30, with likely greater treatment if less than 21. I'm sure our phone nurses would be willing to share [our protocol]. |
| I have an obese 13‐year‐old AA girl with acanthosis nigricans. Do you check HbA1c? | R1: Yes. Sign of insulin resistance. HbA1c along with fasting blood glucose are a good start.Close monitoring indicated regardless. Endo may have more insight as to whether or not other labs are useful, such as fasting C‐peptide. | |
| Referral | Has anyone ever seen preteen or teen patients with ADHD‐like symptoms and poor sleep referred for a sleep study for possible restless leg syndrome? | R1: RLS seen in kids, but criteria are different for children than adults.Sleep studies may be warranted. |
| R2: I've also heard about a link between restless leg and iron deficiency. Is it a girl? | ||
| R3: Checking CBC, ferritin, and iron is a good start. | ||
To better understand factors influencing use of the mobile crowdsourcing application, we surveyed users, receiving 68 comments related to the overall approach and barriers to adoption among other aspects (Table 2). The 40 comments regarding the use of medical crowdsourcing were divided evenly between supporters and critics. Enthusiasm for cross‐discipline collaboration, having tools to codify expert knowledge, and discovering consensus opinion from the expert crowd was offset by concerns that push notifications would distract providers, compromise efficiency, and potentially lead providers to act on inaccurate information.
| Category | Comments | |
|---|---|---|
| Overall approach | Pro | This is a process whose time has come; we need it to adapt to the exponential increase in information content that impacts our clinical decisionmaking |
| I found [the application] it to be both useful and interesting. | ||
| Con | I just don't like these types of thingsemail already takes up too much time. | |
| Curbside consults result in worse outcomes for the patient and the physician. I found myself uncomfortable using this approach. | ||
| My biggest concern is the interruption in one's thinking.distractions are becoming increasingly common. | ||
| I do appreciate colleagues input; but ask for it verbally.I am struggling to learn even texting. | ||
| Barriers to adoption | Pro | I think premise is great, it is just a matter of enough people participating to make it worthwhile to use. |
| There is power in numbers here‐people won't use it unless there is lots of activity or feedback. | ||
| I think it will be very useful if the whole department or sections are involved in promoting and participating. | ||
| Con | I did not test it much since the posts were not very frequent at the time that I tried it. | |
| The barrier to use is quality control; how to substantiate the quality of input provided is key. | ||
| Anonymous posting | Pro | I would not have [posts] always be anonymous, but allow the user the option. |
| Anonymity would be greatI was concerned that some of my questions were "dumb." | ||
| Con | Anonymous posting would increase the risk of trolling. | |
| Suggested uses | I see a role for this app in relaying questions to subspecialty groups for judgment call questions. | |
| Best place to talk about weird cases, odd presentations; to ask have you ever seen anything like this before. | ||
| Consider rolling it out to entire family medicine department and/or primary care network. |
DISCUSSION
In the current study, we developed and field‐tested the application DocCHIRP, which helps HCPs crowdsource information from each other in near real time. The average response latency in this pilot trial was 20 minutes, which was unexpectedly fast given the relatively small size of the participating crowd. Additionally, nearly one‐third of users accessed the server in the evening using the web interface rather than their mobile phone. This suggests that although HCPs liked having direct access to colleagues in near real time, the also valued the opportunity to connect asynchronously after hours.
Relative to the total number of page views, the number of HCPs using the technology for peer‐to‐peer consultation was low. Feedback provided in the post‐trial survey suggested several reasons for this effect. Some providers viewed the application without posting because they were reluctant to disclose knowledge gaps to their peers. Several users suggested implementing a system that supports anonymous posting, but others thought this would undermine the value of the information provided. Additionally, users recognized the potential for crowdsourcing to adversely effect HCP's productivity and daily workflow. This is relevant given growing concerns about distracted doctoring and association with reduced safety and quality of medical care.[14] This concept is further echoed in a paper by Wu et al. demonstrating that frequent interruptions offset the perceived benefit of increased mobility afforded by the use of mobile technology.[15] However, it is worth considering that if implemented properly, study participants believe crowdsourcing could have a net neutral impact on clinical workflow by improving the efficiency of provider communication and saving time otherwise spent problem solving. Participants also felt the approach could infringe on an already threatened work‐life boundary, and could also lead to unprofessional and antisocial behaviors.[16] Collectively, these problems are not unique to medical crowdsourcing, and prior experience in this area may offer several viable solutions. First, because crowd burnout is inversely proportional to crowd size, successful adoption in practice will require growing a provider base of sufficient depth and expertise to handle the consult demand. With the expansion of accountable care organizations across the United States, this will not likely be a limiting factor. And although not implemented here, flexible notification settings, user‐defined identity rules, and other higher‐level software design elements should alleviate the issues related to provider reputation and workflow interruptions.
Overall, HCPs are optimistic that mobile handheld technologies will benefit their practice.[17] Yet, software‐based approaches including expert decision support systems must overcome particular hurdles including lack of provider trust in the algorithms used in these approaches.[18] In the end, trust is ultimately a human phenomena; users will only trust the system if they know the information came from a trusted and highly reputable individual or institution. By tapping the expertise of a network of institutional colleagues, crowdsourcing addresses this issue of trust. Appropriately, providers were also concerned about the legality and personal risk of using crowdsourcing to discuss matters related to patient care. The technology was not intended to share protected health information, and as with other forms of digital communication, providers were cautioned during the consent process to monitor their behavior in this regard. Although soliciting advice from the medical crowd has an inherently higher level of risk compared to the use of crowdsourcing in education, research, or business, the index provider is ultimately responsible for considering all available information before making any treatment decision.
Though our pilot trial was not designed to assess effects on HCP efficiency or on the quality of care delivered, our work provides a unique window on the information‐seeking behaviors HCPs and highlights potential modifications that could enhance the utility of future crowdsourcing programs. Because the trial was performed within the context of an academic health center, it remains to be seen how medical crowdsourcing will translate in private practice, rural clinics, and other clinical environments where peer‐to‐peer consultation is sought. Given the potential for high‐stakes information exchanges, further study regarding the use of medical crowdsourcing in a controlled environment will be required before the technology can be disseminated to a broader audience. If future iterations of the mobile crowdsourcing application can address the aforementioned adoption barriers and support the organic growth of the crowd of HCPs, we believe the approach could have a positive and transformative effect on how providers acquire relevant knowledge and care for patients.
Acknowledgements
The authors thank the physicians and nurse practitioners at the University of Rochester who participated in the trial. The authors also acknowledge Dr. Dan Goldstein at the Microsoft Research Group (New York, NY) for many helpful discussions.
Disclosures: This study was funded in part by grant support from the University of Rochester Robert B. Goergen Reach Fund (M.H.S.). Collaborative Informatics, LLC provided integrated mobile and server software used in this study. Dr. Halterman is co‐owner of Collaborative Informatics, LLC and oversaw the specifications and construction of the software used in this study. Dr. Halterman has provided the necessary conflict of interest documentation in keeping with the requirements of the University of Rochester. The DocCHIRP study was reviewed by the institutional review board at the University of Rochester and received approval posing minimal risk.
- , . The information‐seeking behaviour of doctors: a review of the evidence. Health Info Libr J. 2007;24(2):78–94.
- , , , . Information‐seeking behaviors of practitioners in a primary care practice‐based research network (PBRN). J Med Libr Assoc. 2005;93(2):206–212.
- . Physician use of the curbside consultation to address information needs: report on a collective case study. J Med Libr Assoc. 2006;94(2):137–144.
- , , , , . Uncovering tacit knowledge: a pilot study to broaden the concept of knowledge in knowledge translation. BMC Health Serv Res. 2011;11:198.
- , , , et al. Hospital variation and temporal trends in palliative and end‐of‐life care in the ICU. Crit Care Med. 2013;41(6):1405–1411.
- , , , et al. Comparison of user groups' perspectives of barriers and facilitators to implementing electronic health records: a systematic review. BMC Med. 2011;9:46.
- . The Rise of Crowdsourcing. Wired magazine. 2006;14(6):1–4.
- , , , , , . Novel web‐based tools combining chemistry informatics, biology and social networks for drug discovery. Drug Discov Today. 2009;14(5–6):261–270.
- , , , et al. Crowdsourcing—harnessing the masses to advance health and medicine: a systematic review. J Gen Intern Med. 2014;29(1):187–203.
- , , , . Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595–599.
- . Biomedical informatics in the education of physicians. JAMA. 2010;304(11):1227–1228.
- . Mobile medical applications: guidance for industry and Food and Drug Administration staff. Washington, DC: U.S. Department of Health and Human Services, Food and Drug Administration; 2013.
- , , , , , . Limits of social mobilization. Proc Natl Acad Sci U S A. 2013;110(16):6281–6286.
- . the rise of electronic distraction in health care is addiction to devices contributing. J Anesth Clin Res. 2013;4:e112.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- , . Instant mobile communication, efficiency, and quality of life. JAMA. 2008;299(10):1179–1181.
- , , . The impact of mobile handheld technology on hospital physicians' work practices and patient care: a systematic review. J Am Med Inform Assoc. 2009;16(6):792–801.
- . Issues of trust and ethics in computerized clinical decision support systems. Nurs Adm Q. 2006;30(1):21–29.
The volume of existing knowledge and the pace of discovery in medical science challenge a clinician's ability to access relevant information at the point of care. Knowledge gaps that arise in practice usually involve matters related to diagnosis, drug therapy, or treatment.[1] In the clinical setting, healthcare providers (HCPs) answer questions using a variety of online and print resources. Ironically, HCPs often lack the training required to find details regarding uncommon disorders or complex medical decisions that are not easily found or well represented in the published literature.[2] Instead, HCPs turn to trusted colleagues who possess the necessary expertise.[3]
Closing the knowledge‐to‐practice gap involves a range of factual information and data derived from published evidence, anecdotal experience, as well as organization‐ and region‐specific practices.[4] The inability to codify both explicit and tacit information has been linked to variability in prescription practices, excessive use of surgical services, and delayed decisions involving the appropriate provision of end‐of‐life care.[5] Although electronic medical record systems are not configured to support peer collaboration,[6] alternative strategies including crowdsourcing has been used successfully in other domains to tap collective intelligence of skilled workers.[7] Crowdsourcing allows organizations to explore problems at low cost, gain access a wide range of complementary expertise, and capture large amounts of data for analysis.[8, 9] Although an increasing number of physicians use either smartphones or tablets on the job,[10] peer‐to‐peer medical crowdsourcing has not been investigated, despite the fact that processes involving team‐based clinical decision making are associated with better outcomes.[11] Here we field tested the mobile crowdsourcing application DocCHIRP (Crowdsourcing Health Information Retrieval Protocol for Doctors) and assessed user opinion regarding its utility in the clinical setting.
MATERIALS AND METHODS
DocCHIRP Program Design
The authors (M.W.H., J.B., H.K.) conceptualized and designed DocCHIRP for mobile (iOS [Apple Inc., Cupertino, CA] and Android [Google Inc., Mountain View, CA]) and desktop use. Email prompts and push notifications, which were modeled after the application VizWiz (Rochester Human Computer Interaction Group, University of Rochester, Rochester, NY), supported near real‐time communication between HCPs. According to recent US Food and Drug Administration guidelines, DocCHIRP is considered a medical reference,[12] intended to share domain‐specific knowledge on diagnosis, therapy, and other medically relevant topics. Devices were password protected and encrypted according to university standards. A typical workflow involves an index provider faced with a clinical question that sends a consult question to 1 or more trusted providers. The crowd receiving the notification responds when available using either free‐text responses or agree/disagree prompts (Figure 1A,B). Providers use preference settings to manage crowd membership, notification settings, and demographics describing their expertise.
Trial Recruitment
The University of Rochester Research Subjects Review Board approved the study, in which prospective users were required to review and agree to a statement regarding potential liability as part of the consent process. In this pilot study, we invited a cross‐section of providers (n = 145) from the Departments of Neurology (including the Division of Pediatric Neurology), Pediatrics, Neuroradiology, Psychiatry, Orthopedics, Emergency Medicine, Internal Medicine, and Family Medicine to participate. E‐mail invitations were sent to HCPs in 3 phases in April (phase I), June (phase II), and August (phase III) over 244 consecutive days. At the conclusion of the trial, 85 HCPs (59%) had created accounts including attending physicians (n = 63), residents (n = 13), fellows (n = 1), and nurse practitioners (n = 8). We did not seek parity in either age or gender representation.
Data Analysis
Mobile device and network usage data, question and response strings, as well as data regarding hardware and browser identity were collected using Google Analytics (Google Inc.,
RESULTS
Attending and resident physicians represented the majority of DocCHIRP account holders (91%), with nurse practitioners accounting for the remaining sample (9%). There were 50 male and 35 female participants, with an age range of 28 to 78 years (median age, 43 years). Departmental affiliations included Pediatrics (n = 28, 33%), Neurology (n = 27, 32%), Internal Medicine (n = 10, 12%), Psychiatry (n = 4, 5%), the Division of Pediatric Neurology (n = 11, 13%), and others (n = 5, 6%). Of the 1544 total visits to the DocCHIRP site, providers favored using smart phones (56.8%) and tablets (9.5%) over the desktop interface (33.6%; Figure 1C). iPhone use (81.7%) surpassed the other platforms combined. Desktop users visited twice as many pages (16.8 pages/visit) compared to those using smart phones (5.5 pages/visit) or tablets (8.6 pages/visit). Desktop users remained engaged longer than mobile users (13 vs 5 minutes). In the post‐trial user survey, we received 72 valid surveys from 85 potential participants (85% response rate).
We used a tiered enrollment design, sending invitations to potential participants in 3 phases to study the relationship between the size of the HCP crowd and sustained use as reported in other social networks.[13] Using a cutoff of >3 visits per week to demarcate active periods of use, we saw during the initial phase of enrollment that 20 providers generated a total of 170 visits over 22 days (Figure 2A). The addition of 28 members (phase II, n = 48 total) extended active use by 28 days, with a total of 476 page visits. The addition of 32 members (phase III, n = 85 total) resulted in 56 days of active participation with 612 visits to the site. When plotted (Figure 2B), the relationship between crowd size (total number of registered users) and cumulative visits (R2 = 0.951), as well as crowd size and days of high activity (R2 = 0.953) were linear and direct. We also investigated the timing of user engagement by pooling the data and breaking down use by time of day and day of the week (Figure 3A,B). In addition to observing peak engagement during the midmorning and afternoon, times of anticipated physician‐patient contact, we observed a third use peak in the evening. With the exception of sporadic weekend use, DocCHIRP use clustered during midweek.
DocCHIRP users generated 45 questions. The fastest first response was returned in less than 4 minutes, with a median first response time of 19 minutes (Figure 3C). Analysis of the consult requests received revealed a clustering of 7 principal question‐response groups: (1) the effective use of medications, (2) complex medical decision making, (3) use of the application itself, (4) guidance regarding the standard of care, (5) selection and interpretation of diagnostic tests, (6) differential diagnosis, and (7) patient referral (Figure 3D). Consults regarding medication use and complex decision making were dominant themes (63%). Several consults generated multiple responses, broadening the scope of the original query or requesting additional information (Table 1).
| Question Type | Consult | Response(s) |
|---|---|---|
| ||
| Medication | How do you treat headache from viral meningitis? | R1: Any analgesic will work; need to clarify that the headache is not post‐LP, which may require blood patch. |
| Anyone know how oral fluconazole (liquid) tastes? We needed to prescribe for a young 13 year old. | R1: We should get a pharmacist on the chat. I would call the pharmacy and see if they can compound it with flavoring. | |
| How frequently do your patients complain of myalgias on statins? Have you prescribed coenzyme Q in this situation? | R1: Did you see the editorial in the Green Journal yesterday?Took the position that statins were not to blame. I usually give a trial off to make sure symptoms resolve. Usually I try them on a different statin.Have not routinely rx'd Q10. | |
| Complex medical decision making | Has anyone seen tapeworm infection from raw pork? Do we need to report this? We treated with mebendazole. | R1: You can check with CDC here: |
| R2: First‐line treatment for Tsolium is praziquantel or albendazole.However, mebendazole has also been used to successfully treat T solium. | ||
| R3: Whipworm is another common pork tapeworm.It is also covered by mebendazole | ||
| What are the current guidelines regarding the use of statins in patients with a history of lobar hemorrhage. | R1: Larger studies (SPARCL, HPS) both showed higher hemorrhage risks in statin treated patients.Cohort studies generally don't show an obvious risk to statins. I've generally taken patients off their statins when they come in with lobar ICH, and more neutral when it's a hypertensive bleed. | |
| Standard of care | How often would someone have to fall before you felt uncomfortable anticoagulating for AFib? | R1: The risk of falls alone should not automatically disqualify a person from being treated with warfarin. |
| R2: I recall reading a meta‐analysis that suggested 300 falls/year would start to favor not anticoagulating, but short of that, falls were not an important factor. | ||
| Anyone used IVIG for any of the following: autoimmune encephalopathy, NMO, paraneoplastic limbic encephalitis, PANDAS? | R1: We had a patient recently with a history of autoimmune encephalopathy who was treated with IVIG. | |
| Administrative | What medical apps do you have on your phone? | R1: DocCHIRP, Epocrates, NIH stroke calculator. |
| R2: I have Merck Medicus, Micromedex drugs, growth charts, and shotsall those are free.I also have Red Book from AAPand Sanford Guide, which I paid for. | ||
| R3: Instant ECG, ACLS Advisor, 10‐Second EM. | ||
| Testing | What would be considered a normal vitamin D level in a 2 year old? | R1: We typically treat at a level less than 30, with likely greater treatment if less than 21. I'm sure our phone nurses would be willing to share [our protocol]. |
| I have an obese 13‐year‐old AA girl with acanthosis nigricans. Do you check HbA1c? | R1: Yes. Sign of insulin resistance. HbA1c along with fasting blood glucose are a good start.Close monitoring indicated regardless. Endo may have more insight as to whether or not other labs are useful, such as fasting C‐peptide. | |
| Referral | Has anyone ever seen preteen or teen patients with ADHD‐like symptoms and poor sleep referred for a sleep study for possible restless leg syndrome? | R1: RLS seen in kids, but criteria are different for children than adults.Sleep studies may be warranted. |
| R2: I've also heard about a link between restless leg and iron deficiency. Is it a girl? | ||
| R3: Checking CBC, ferritin, and iron is a good start. | ||
To better understand factors influencing use of the mobile crowdsourcing application, we surveyed users, receiving 68 comments related to the overall approach and barriers to adoption among other aspects (Table 2). The 40 comments regarding the use of medical crowdsourcing were divided evenly between supporters and critics. Enthusiasm for cross‐discipline collaboration, having tools to codify expert knowledge, and discovering consensus opinion from the expert crowd was offset by concerns that push notifications would distract providers, compromise efficiency, and potentially lead providers to act on inaccurate information.
| Category | Comments | |
|---|---|---|
| Overall approach | Pro | This is a process whose time has come; we need it to adapt to the exponential increase in information content that impacts our clinical decisionmaking |
| I found [the application] it to be both useful and interesting. | ||
| Con | I just don't like these types of thingsemail already takes up too much time. | |
| Curbside consults result in worse outcomes for the patient and the physician. I found myself uncomfortable using this approach. | ||
| My biggest concern is the interruption in one's thinking.distractions are becoming increasingly common. | ||
| I do appreciate colleagues input; but ask for it verbally.I am struggling to learn even texting. | ||
| Barriers to adoption | Pro | I think premise is great, it is just a matter of enough people participating to make it worthwhile to use. |
| There is power in numbers here‐people won't use it unless there is lots of activity or feedback. | ||
| I think it will be very useful if the whole department or sections are involved in promoting and participating. | ||
| Con | I did not test it much since the posts were not very frequent at the time that I tried it. | |
| The barrier to use is quality control; how to substantiate the quality of input provided is key. | ||
| Anonymous posting | Pro | I would not have [posts] always be anonymous, but allow the user the option. |
| Anonymity would be greatI was concerned that some of my questions were "dumb." | ||
| Con | Anonymous posting would increase the risk of trolling. | |
| Suggested uses | I see a role for this app in relaying questions to subspecialty groups for judgment call questions. | |
| Best place to talk about weird cases, odd presentations; to ask have you ever seen anything like this before. | ||
| Consider rolling it out to entire family medicine department and/or primary care network. |
DISCUSSION
In the current study, we developed and field‐tested the application DocCHIRP, which helps HCPs crowdsource information from each other in near real time. The average response latency in this pilot trial was 20 minutes, which was unexpectedly fast given the relatively small size of the participating crowd. Additionally, nearly one‐third of users accessed the server in the evening using the web interface rather than their mobile phone. This suggests that although HCPs liked having direct access to colleagues in near real time, the also valued the opportunity to connect asynchronously after hours.
Relative to the total number of page views, the number of HCPs using the technology for peer‐to‐peer consultation was low. Feedback provided in the post‐trial survey suggested several reasons for this effect. Some providers viewed the application without posting because they were reluctant to disclose knowledge gaps to their peers. Several users suggested implementing a system that supports anonymous posting, but others thought this would undermine the value of the information provided. Additionally, users recognized the potential for crowdsourcing to adversely effect HCP's productivity and daily workflow. This is relevant given growing concerns about distracted doctoring and association with reduced safety and quality of medical care.[14] This concept is further echoed in a paper by Wu et al. demonstrating that frequent interruptions offset the perceived benefit of increased mobility afforded by the use of mobile technology.[15] However, it is worth considering that if implemented properly, study participants believe crowdsourcing could have a net neutral impact on clinical workflow by improving the efficiency of provider communication and saving time otherwise spent problem solving. Participants also felt the approach could infringe on an already threatened work‐life boundary, and could also lead to unprofessional and antisocial behaviors.[16] Collectively, these problems are not unique to medical crowdsourcing, and prior experience in this area may offer several viable solutions. First, because crowd burnout is inversely proportional to crowd size, successful adoption in practice will require growing a provider base of sufficient depth and expertise to handle the consult demand. With the expansion of accountable care organizations across the United States, this will not likely be a limiting factor. And although not implemented here, flexible notification settings, user‐defined identity rules, and other higher‐level software design elements should alleviate the issues related to provider reputation and workflow interruptions.
Overall, HCPs are optimistic that mobile handheld technologies will benefit their practice.[17] Yet, software‐based approaches including expert decision support systems must overcome particular hurdles including lack of provider trust in the algorithms used in these approaches.[18] In the end, trust is ultimately a human phenomena; users will only trust the system if they know the information came from a trusted and highly reputable individual or institution. By tapping the expertise of a network of institutional colleagues, crowdsourcing addresses this issue of trust. Appropriately, providers were also concerned about the legality and personal risk of using crowdsourcing to discuss matters related to patient care. The technology was not intended to share protected health information, and as with other forms of digital communication, providers were cautioned during the consent process to monitor their behavior in this regard. Although soliciting advice from the medical crowd has an inherently higher level of risk compared to the use of crowdsourcing in education, research, or business, the index provider is ultimately responsible for considering all available information before making any treatment decision.
Though our pilot trial was not designed to assess effects on HCP efficiency or on the quality of care delivered, our work provides a unique window on the information‐seeking behaviors HCPs and highlights potential modifications that could enhance the utility of future crowdsourcing programs. Because the trial was performed within the context of an academic health center, it remains to be seen how medical crowdsourcing will translate in private practice, rural clinics, and other clinical environments where peer‐to‐peer consultation is sought. Given the potential for high‐stakes information exchanges, further study regarding the use of medical crowdsourcing in a controlled environment will be required before the technology can be disseminated to a broader audience. If future iterations of the mobile crowdsourcing application can address the aforementioned adoption barriers and support the organic growth of the crowd of HCPs, we believe the approach could have a positive and transformative effect on how providers acquire relevant knowledge and care for patients.
Acknowledgements
The authors thank the physicians and nurse practitioners at the University of Rochester who participated in the trial. The authors also acknowledge Dr. Dan Goldstein at the Microsoft Research Group (New York, NY) for many helpful discussions.
Disclosures: This study was funded in part by grant support from the University of Rochester Robert B. Goergen Reach Fund (M.H.S.). Collaborative Informatics, LLC provided integrated mobile and server software used in this study. Dr. Halterman is co‐owner of Collaborative Informatics, LLC and oversaw the specifications and construction of the software used in this study. Dr. Halterman has provided the necessary conflict of interest documentation in keeping with the requirements of the University of Rochester. The DocCHIRP study was reviewed by the institutional review board at the University of Rochester and received approval posing minimal risk.
The volume of existing knowledge and the pace of discovery in medical science challenge a clinician's ability to access relevant information at the point of care. Knowledge gaps that arise in practice usually involve matters related to diagnosis, drug therapy, or treatment.[1] In the clinical setting, healthcare providers (HCPs) answer questions using a variety of online and print resources. Ironically, HCPs often lack the training required to find details regarding uncommon disorders or complex medical decisions that are not easily found or well represented in the published literature.[2] Instead, HCPs turn to trusted colleagues who possess the necessary expertise.[3]
Closing the knowledge‐to‐practice gap involves a range of factual information and data derived from published evidence, anecdotal experience, as well as organization‐ and region‐specific practices.[4] The inability to codify both explicit and tacit information has been linked to variability in prescription practices, excessive use of surgical services, and delayed decisions involving the appropriate provision of end‐of‐life care.[5] Although electronic medical record systems are not configured to support peer collaboration,[6] alternative strategies including crowdsourcing has been used successfully in other domains to tap collective intelligence of skilled workers.[7] Crowdsourcing allows organizations to explore problems at low cost, gain access a wide range of complementary expertise, and capture large amounts of data for analysis.[8, 9] Although an increasing number of physicians use either smartphones or tablets on the job,[10] peer‐to‐peer medical crowdsourcing has not been investigated, despite the fact that processes involving team‐based clinical decision making are associated with better outcomes.[11] Here we field tested the mobile crowdsourcing application DocCHIRP (Crowdsourcing Health Information Retrieval Protocol for Doctors) and assessed user opinion regarding its utility in the clinical setting.
MATERIALS AND METHODS
DocCHIRP Program Design
The authors (M.W.H., J.B., H.K.) conceptualized and designed DocCHIRP for mobile (iOS [Apple Inc., Cupertino, CA] and Android [Google Inc., Mountain View, CA]) and desktop use. Email prompts and push notifications, which were modeled after the application VizWiz (Rochester Human Computer Interaction Group, University of Rochester, Rochester, NY), supported near real‐time communication between HCPs. According to recent US Food and Drug Administration guidelines, DocCHIRP is considered a medical reference,[12] intended to share domain‐specific knowledge on diagnosis, therapy, and other medically relevant topics. Devices were password protected and encrypted according to university standards. A typical workflow involves an index provider faced with a clinical question that sends a consult question to 1 or more trusted providers. The crowd receiving the notification responds when available using either free‐text responses or agree/disagree prompts (Figure 1A,B). Providers use preference settings to manage crowd membership, notification settings, and demographics describing their expertise.
Trial Recruitment
The University of Rochester Research Subjects Review Board approved the study, in which prospective users were required to review and agree to a statement regarding potential liability as part of the consent process. In this pilot study, we invited a cross‐section of providers (n = 145) from the Departments of Neurology (including the Division of Pediatric Neurology), Pediatrics, Neuroradiology, Psychiatry, Orthopedics, Emergency Medicine, Internal Medicine, and Family Medicine to participate. E‐mail invitations were sent to HCPs in 3 phases in April (phase I), June (phase II), and August (phase III) over 244 consecutive days. At the conclusion of the trial, 85 HCPs (59%) had created accounts including attending physicians (n = 63), residents (n = 13), fellows (n = 1), and nurse practitioners (n = 8). We did not seek parity in either age or gender representation.
Data Analysis
Mobile device and network usage data, question and response strings, as well as data regarding hardware and browser identity were collected using Google Analytics (Google Inc.,
RESULTS
Attending and resident physicians represented the majority of DocCHIRP account holders (91%), with nurse practitioners accounting for the remaining sample (9%). There were 50 male and 35 female participants, with an age range of 28 to 78 years (median age, 43 years). Departmental affiliations included Pediatrics (n = 28, 33%), Neurology (n = 27, 32%), Internal Medicine (n = 10, 12%), Psychiatry (n = 4, 5%), the Division of Pediatric Neurology (n = 11, 13%), and others (n = 5, 6%). Of the 1544 total visits to the DocCHIRP site, providers favored using smart phones (56.8%) and tablets (9.5%) over the desktop interface (33.6%; Figure 1C). iPhone use (81.7%) surpassed the other platforms combined. Desktop users visited twice as many pages (16.8 pages/visit) compared to those using smart phones (5.5 pages/visit) or tablets (8.6 pages/visit). Desktop users remained engaged longer than mobile users (13 vs 5 minutes). In the post‐trial user survey, we received 72 valid surveys from 85 potential participants (85% response rate).
We used a tiered enrollment design, sending invitations to potential participants in 3 phases to study the relationship between the size of the HCP crowd and sustained use as reported in other social networks.[13] Using a cutoff of >3 visits per week to demarcate active periods of use, we saw during the initial phase of enrollment that 20 providers generated a total of 170 visits over 22 days (Figure 2A). The addition of 28 members (phase II, n = 48 total) extended active use by 28 days, with a total of 476 page visits. The addition of 32 members (phase III, n = 85 total) resulted in 56 days of active participation with 612 visits to the site. When plotted (Figure 2B), the relationship between crowd size (total number of registered users) and cumulative visits (R2 = 0.951), as well as crowd size and days of high activity (R2 = 0.953) were linear and direct. We also investigated the timing of user engagement by pooling the data and breaking down use by time of day and day of the week (Figure 3A,B). In addition to observing peak engagement during the midmorning and afternoon, times of anticipated physician‐patient contact, we observed a third use peak in the evening. With the exception of sporadic weekend use, DocCHIRP use clustered during midweek.
DocCHIRP users generated 45 questions. The fastest first response was returned in less than 4 minutes, with a median first response time of 19 minutes (Figure 3C). Analysis of the consult requests received revealed a clustering of 7 principal question‐response groups: (1) the effective use of medications, (2) complex medical decision making, (3) use of the application itself, (4) guidance regarding the standard of care, (5) selection and interpretation of diagnostic tests, (6) differential diagnosis, and (7) patient referral (Figure 3D). Consults regarding medication use and complex decision making were dominant themes (63%). Several consults generated multiple responses, broadening the scope of the original query or requesting additional information (Table 1).
| Question Type | Consult | Response(s) |
|---|---|---|
| ||
| Medication | How do you treat headache from viral meningitis? | R1: Any analgesic will work; need to clarify that the headache is not post‐LP, which may require blood patch. |
| Anyone know how oral fluconazole (liquid) tastes? We needed to prescribe for a young 13 year old. | R1: We should get a pharmacist on the chat. I would call the pharmacy and see if they can compound it with flavoring. | |
| How frequently do your patients complain of myalgias on statins? Have you prescribed coenzyme Q in this situation? | R1: Did you see the editorial in the Green Journal yesterday?Took the position that statins were not to blame. I usually give a trial off to make sure symptoms resolve. Usually I try them on a different statin.Have not routinely rx'd Q10. | |
| Complex medical decision making | Has anyone seen tapeworm infection from raw pork? Do we need to report this? We treated with mebendazole. | R1: You can check with CDC here: |
| R2: First‐line treatment for Tsolium is praziquantel or albendazole.However, mebendazole has also been used to successfully treat T solium. | ||
| R3: Whipworm is another common pork tapeworm.It is also covered by mebendazole | ||
| What are the current guidelines regarding the use of statins in patients with a history of lobar hemorrhage. | R1: Larger studies (SPARCL, HPS) both showed higher hemorrhage risks in statin treated patients.Cohort studies generally don't show an obvious risk to statins. I've generally taken patients off their statins when they come in with lobar ICH, and more neutral when it's a hypertensive bleed. | |
| Standard of care | How often would someone have to fall before you felt uncomfortable anticoagulating for AFib? | R1: The risk of falls alone should not automatically disqualify a person from being treated with warfarin. |
| R2: I recall reading a meta‐analysis that suggested 300 falls/year would start to favor not anticoagulating, but short of that, falls were not an important factor. | ||
| Anyone used IVIG for any of the following: autoimmune encephalopathy, NMO, paraneoplastic limbic encephalitis, PANDAS? | R1: We had a patient recently with a history of autoimmune encephalopathy who was treated with IVIG. | |
| Administrative | What medical apps do you have on your phone? | R1: DocCHIRP, Epocrates, NIH stroke calculator. |
| R2: I have Merck Medicus, Micromedex drugs, growth charts, and shotsall those are free.I also have Red Book from AAPand Sanford Guide, which I paid for. | ||
| R3: Instant ECG, ACLS Advisor, 10‐Second EM. | ||
| Testing | What would be considered a normal vitamin D level in a 2 year old? | R1: We typically treat at a level less than 30, with likely greater treatment if less than 21. I'm sure our phone nurses would be willing to share [our protocol]. |
| I have an obese 13‐year‐old AA girl with acanthosis nigricans. Do you check HbA1c? | R1: Yes. Sign of insulin resistance. HbA1c along with fasting blood glucose are a good start.Close monitoring indicated regardless. Endo may have more insight as to whether or not other labs are useful, such as fasting C‐peptide. | |
| Referral | Has anyone ever seen preteen or teen patients with ADHD‐like symptoms and poor sleep referred for a sleep study for possible restless leg syndrome? | R1: RLS seen in kids, but criteria are different for children than adults.Sleep studies may be warranted. |
| R2: I've also heard about a link between restless leg and iron deficiency. Is it a girl? | ||
| R3: Checking CBC, ferritin, and iron is a good start. | ||
To better understand factors influencing use of the mobile crowdsourcing application, we surveyed users, receiving 68 comments related to the overall approach and barriers to adoption among other aspects (Table 2). The 40 comments regarding the use of medical crowdsourcing were divided evenly between supporters and critics. Enthusiasm for cross‐discipline collaboration, having tools to codify expert knowledge, and discovering consensus opinion from the expert crowd was offset by concerns that push notifications would distract providers, compromise efficiency, and potentially lead providers to act on inaccurate information.
| Category | Comments | |
|---|---|---|
| Overall approach | Pro | This is a process whose time has come; we need it to adapt to the exponential increase in information content that impacts our clinical decisionmaking |
| I found [the application] it to be both useful and interesting. | ||
| Con | I just don't like these types of thingsemail already takes up too much time. | |
| Curbside consults result in worse outcomes for the patient and the physician. I found myself uncomfortable using this approach. | ||
| My biggest concern is the interruption in one's thinking.distractions are becoming increasingly common. | ||
| I do appreciate colleagues input; but ask for it verbally.I am struggling to learn even texting. | ||
| Barriers to adoption | Pro | I think premise is great, it is just a matter of enough people participating to make it worthwhile to use. |
| There is power in numbers here‐people won't use it unless there is lots of activity or feedback. | ||
| I think it will be very useful if the whole department or sections are involved in promoting and participating. | ||
| Con | I did not test it much since the posts were not very frequent at the time that I tried it. | |
| The barrier to use is quality control; how to substantiate the quality of input provided is key. | ||
| Anonymous posting | Pro | I would not have [posts] always be anonymous, but allow the user the option. |
| Anonymity would be greatI was concerned that some of my questions were "dumb." | ||
| Con | Anonymous posting would increase the risk of trolling. | |
| Suggested uses | I see a role for this app in relaying questions to subspecialty groups for judgment call questions. | |
| Best place to talk about weird cases, odd presentations; to ask have you ever seen anything like this before. | ||
| Consider rolling it out to entire family medicine department and/or primary care network. |
DISCUSSION
In the current study, we developed and field‐tested the application DocCHIRP, which helps HCPs crowdsource information from each other in near real time. The average response latency in this pilot trial was 20 minutes, which was unexpectedly fast given the relatively small size of the participating crowd. Additionally, nearly one‐third of users accessed the server in the evening using the web interface rather than their mobile phone. This suggests that although HCPs liked having direct access to colleagues in near real time, the also valued the opportunity to connect asynchronously after hours.
Relative to the total number of page views, the number of HCPs using the technology for peer‐to‐peer consultation was low. Feedback provided in the post‐trial survey suggested several reasons for this effect. Some providers viewed the application without posting because they were reluctant to disclose knowledge gaps to their peers. Several users suggested implementing a system that supports anonymous posting, but others thought this would undermine the value of the information provided. Additionally, users recognized the potential for crowdsourcing to adversely effect HCP's productivity and daily workflow. This is relevant given growing concerns about distracted doctoring and association with reduced safety and quality of medical care.[14] This concept is further echoed in a paper by Wu et al. demonstrating that frequent interruptions offset the perceived benefit of increased mobility afforded by the use of mobile technology.[15] However, it is worth considering that if implemented properly, study participants believe crowdsourcing could have a net neutral impact on clinical workflow by improving the efficiency of provider communication and saving time otherwise spent problem solving. Participants also felt the approach could infringe on an already threatened work‐life boundary, and could also lead to unprofessional and antisocial behaviors.[16] Collectively, these problems are not unique to medical crowdsourcing, and prior experience in this area may offer several viable solutions. First, because crowd burnout is inversely proportional to crowd size, successful adoption in practice will require growing a provider base of sufficient depth and expertise to handle the consult demand. With the expansion of accountable care organizations across the United States, this will not likely be a limiting factor. And although not implemented here, flexible notification settings, user‐defined identity rules, and other higher‐level software design elements should alleviate the issues related to provider reputation and workflow interruptions.
Overall, HCPs are optimistic that mobile handheld technologies will benefit their practice.[17] Yet, software‐based approaches including expert decision support systems must overcome particular hurdles including lack of provider trust in the algorithms used in these approaches.[18] In the end, trust is ultimately a human phenomena; users will only trust the system if they know the information came from a trusted and highly reputable individual or institution. By tapping the expertise of a network of institutional colleagues, crowdsourcing addresses this issue of trust. Appropriately, providers were also concerned about the legality and personal risk of using crowdsourcing to discuss matters related to patient care. The technology was not intended to share protected health information, and as with other forms of digital communication, providers were cautioned during the consent process to monitor their behavior in this regard. Although soliciting advice from the medical crowd has an inherently higher level of risk compared to the use of crowdsourcing in education, research, or business, the index provider is ultimately responsible for considering all available information before making any treatment decision.
Though our pilot trial was not designed to assess effects on HCP efficiency or on the quality of care delivered, our work provides a unique window on the information‐seeking behaviors HCPs and highlights potential modifications that could enhance the utility of future crowdsourcing programs. Because the trial was performed within the context of an academic health center, it remains to be seen how medical crowdsourcing will translate in private practice, rural clinics, and other clinical environments where peer‐to‐peer consultation is sought. Given the potential for high‐stakes information exchanges, further study regarding the use of medical crowdsourcing in a controlled environment will be required before the technology can be disseminated to a broader audience. If future iterations of the mobile crowdsourcing application can address the aforementioned adoption barriers and support the organic growth of the crowd of HCPs, we believe the approach could have a positive and transformative effect on how providers acquire relevant knowledge and care for patients.
Acknowledgements
The authors thank the physicians and nurse practitioners at the University of Rochester who participated in the trial. The authors also acknowledge Dr. Dan Goldstein at the Microsoft Research Group (New York, NY) for many helpful discussions.
Disclosures: This study was funded in part by grant support from the University of Rochester Robert B. Goergen Reach Fund (M.H.S.). Collaborative Informatics, LLC provided integrated mobile and server software used in this study. Dr. Halterman is co‐owner of Collaborative Informatics, LLC and oversaw the specifications and construction of the software used in this study. Dr. Halterman has provided the necessary conflict of interest documentation in keeping with the requirements of the University of Rochester. The DocCHIRP study was reviewed by the institutional review board at the University of Rochester and received approval posing minimal risk.
- , . The information‐seeking behaviour of doctors: a review of the evidence. Health Info Libr J. 2007;24(2):78–94.
- , , , . Information‐seeking behaviors of practitioners in a primary care practice‐based research network (PBRN). J Med Libr Assoc. 2005;93(2):206–212.
- . Physician use of the curbside consultation to address information needs: report on a collective case study. J Med Libr Assoc. 2006;94(2):137–144.
- , , , , . Uncovering tacit knowledge: a pilot study to broaden the concept of knowledge in knowledge translation. BMC Health Serv Res. 2011;11:198.
- , , , et al. Hospital variation and temporal trends in palliative and end‐of‐life care in the ICU. Crit Care Med. 2013;41(6):1405–1411.
- , , , et al. Comparison of user groups' perspectives of barriers and facilitators to implementing electronic health records: a systematic review. BMC Med. 2011;9:46.
- . The Rise of Crowdsourcing. Wired magazine. 2006;14(6):1–4.
- , , , , , . Novel web‐based tools combining chemistry informatics, biology and social networks for drug discovery. Drug Discov Today. 2009;14(5–6):261–270.
- , , , et al. Crowdsourcing—harnessing the masses to advance health and medicine: a systematic review. J Gen Intern Med. 2014;29(1):187–203.
- , , , . Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595–599.
- . Biomedical informatics in the education of physicians. JAMA. 2010;304(11):1227–1228.
- . Mobile medical applications: guidance for industry and Food and Drug Administration staff. Washington, DC: U.S. Department of Health and Human Services, Food and Drug Administration; 2013.
- , , , , , . Limits of social mobilization. Proc Natl Acad Sci U S A. 2013;110(16):6281–6286.
- . the rise of electronic distraction in health care is addiction to devices contributing. J Anesth Clin Res. 2013;4:e112.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- , . Instant mobile communication, efficiency, and quality of life. JAMA. 2008;299(10):1179–1181.
- , , . The impact of mobile handheld technology on hospital physicians' work practices and patient care: a systematic review. J Am Med Inform Assoc. 2009;16(6):792–801.
- . Issues of trust and ethics in computerized clinical decision support systems. Nurs Adm Q. 2006;30(1):21–29.
- , . The information‐seeking behaviour of doctors: a review of the evidence. Health Info Libr J. 2007;24(2):78–94.
- , , , . Information‐seeking behaviors of practitioners in a primary care practice‐based research network (PBRN). J Med Libr Assoc. 2005;93(2):206–212.
- . Physician use of the curbside consultation to address information needs: report on a collective case study. J Med Libr Assoc. 2006;94(2):137–144.
- , , , , . Uncovering tacit knowledge: a pilot study to broaden the concept of knowledge in knowledge translation. BMC Health Serv Res. 2011;11:198.
- , , , et al. Hospital variation and temporal trends in palliative and end‐of‐life care in the ICU. Crit Care Med. 2013;41(6):1405–1411.
- , , , et al. Comparison of user groups' perspectives of barriers and facilitators to implementing electronic health records: a systematic review. BMC Med. 2011;9:46.
- . The Rise of Crowdsourcing. Wired magazine. 2006;14(6):1–4.
- , , , , , . Novel web‐based tools combining chemistry informatics, biology and social networks for drug discovery. Drug Discov Today. 2009;14(5–6):261–270.
- , , , et al. Crowdsourcing—harnessing the masses to advance health and medicine: a systematic review. J Gen Intern Med. 2014;29(1):187–203.
- , , , . Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595–599.
- . Biomedical informatics in the education of physicians. JAMA. 2010;304(11):1227–1228.
- . Mobile medical applications: guidance for industry and Food and Drug Administration staff. Washington, DC: U.S. Department of Health and Human Services, Food and Drug Administration; 2013.
- , , , , , . Limits of social mobilization. Proc Natl Acad Sci U S A. 2013;110(16):6281–6286.
- . the rise of electronic distraction in health care is addiction to devices contributing. J Anesth Clin Res. 2013;4:e112.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- , . Instant mobile communication, efficiency, and quality of life. JAMA. 2008;299(10):1179–1181.
- , , . The impact of mobile handheld technology on hospital physicians' work practices and patient care: a systematic review. J Am Med Inform Assoc. 2009;16(6):792–801.
- . Issues of trust and ethics in computerized clinical decision support systems. Nurs Adm Q. 2006;30(1):21–29.
Type 2 diabetes begins in utero?
A new study1 provides the first evidence of a direct effect of maternal metabolism on fetal brain activity, suggesting that insulin resistance, the precursor to type 2 diabetes, begins its formation prenatally.
DETAILS OF THE STUDY
Dr. Katarzyna Linder from the University Hospital Tübingen in Germany and colleagues included in their study 13 healthy pregnant women with normal, singleton pregnancies of between 27 and 36 weeks. All of the women underwent an oral glucose tolerance test, meaning that after a 5-hour overnight fast, each woman drank a solution containing 75 g glucose. The investigators ascertained blood glucose and plasma insulin levels from blood samples taken at 0, 60, and 120 minutes.
At approximately the same time points, but before they drew each blood sample, the authors obtained a fetal magnetoencephalography (fMEG) measurement in an effort to noninvasively record brain activity in utero. During each measurement, they presented an auditory sequence to the fetus. Most (75%) of the time, the sound presented had a frequency of 500 Hz, but 25% of the time the researchers presented a deviant tone with a frequency of 750 Hz to prevent habituation.
The researchers found that maternal insulin sensitivity significantly correlated with response latency of the fetus at the 60-minute time point, so that the higher the insulin sensitivity of the mother, the shorter the response time of the fetus to the sound. The association remained significant even after the investigators controlled for relative maternal weight gain, gestational age, and the child’s birth weight. No significant correlation existed at baseline or at 120 minutes.
The investigators then split the women into 2 groups: those who were insulin-resistant and those who were insulin-sensitive. They found that the fetuses of the insulin-resistant moms were almost 40% slower to respond to the auditory stimuli than those of the insulin-sensitive moms (mean [SD], 283 [79] ms vs 178 [46] ms; P=.03).
INTERPRETING THE FINDINGS
According to the US Centers for Disease Control and Prevention, almost one-third (30.3%) of US adults between the ages of 20 and 39 years—the primary child-bearing years—are obese,2 as are 17% of our children and adolescents—triple the rate of 1 generation previous.3 Furthermore, 25.8 million people in the United States have diabetes, including 1 in every 400 children and adolescents.4
Experts know that the children of obese or diabetic mothers are at increased risk for obesity and type 2 diabetes as adults, and that the connection is not purely genetic; environmental and epigenetic (environmental elements that affect genetics) factors also play key roles. The latter is the basis for the fetal or developmental origins hypothesis,5 which posits that a pregnant woman’s exposure to certain environmental factors can affect the programming of her unborn child and impact adult health.
The authors of the current study demonstrate that the metabolism of a pregnant woman after a sugar load directly affects the response time and brain activity of her developing fetus. They suggest as a mechanism for the effect that “insulin-resistant mothers have higher glucose levels accompanied by increased insulin levels in the postprandial state. As glucose passes the placenta, these postprandially increased glucose levels induce hyperinsulinaemia in the fetus.” The resulting chronic hyperinsulinemia “might induce insulin resistance in the fetal brain.”
1. Linder K, Schleger F, Ketterer C, et al. Maternal insulin sensitivity is associated with oral glucose-induced changes in fetal brain activity. Diabetologia. 2014. [Epub ahead of print]
2. Adult obesity facts. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/obesity/data/adult.html. Accessed April 12, 2014.
3. Childhood overweight and obesity. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/obesity/childhood/index.html. Accessed April 12, 2014.
4. Statistics about diabetes. American Diabetes Association Web site. http://www.diabetes.org/diabetes-basics/statistics/. Accessed April 12, 2014.
5. Wadhwa PD, Buss C, Entringer S, Swanson JM. Developmental origins of health and disease: brief history of the approach and current focus on epigenetic mechanisms. Semin Reprod Med. 2009;27(5):358–368.
A new study1 provides the first evidence of a direct effect of maternal metabolism on fetal brain activity, suggesting that insulin resistance, the precursor to type 2 diabetes, begins its formation prenatally.
DETAILS OF THE STUDY
Dr. Katarzyna Linder from the University Hospital Tübingen in Germany and colleagues included in their study 13 healthy pregnant women with normal, singleton pregnancies of between 27 and 36 weeks. All of the women underwent an oral glucose tolerance test, meaning that after a 5-hour overnight fast, each woman drank a solution containing 75 g glucose. The investigators ascertained blood glucose and plasma insulin levels from blood samples taken at 0, 60, and 120 minutes.
At approximately the same time points, but before they drew each blood sample, the authors obtained a fetal magnetoencephalography (fMEG) measurement in an effort to noninvasively record brain activity in utero. During each measurement, they presented an auditory sequence to the fetus. Most (75%) of the time, the sound presented had a frequency of 500 Hz, but 25% of the time the researchers presented a deviant tone with a frequency of 750 Hz to prevent habituation.
The researchers found that maternal insulin sensitivity significantly correlated with response latency of the fetus at the 60-minute time point, so that the higher the insulin sensitivity of the mother, the shorter the response time of the fetus to the sound. The association remained significant even after the investigators controlled for relative maternal weight gain, gestational age, and the child’s birth weight. No significant correlation existed at baseline or at 120 minutes.
The investigators then split the women into 2 groups: those who were insulin-resistant and those who were insulin-sensitive. They found that the fetuses of the insulin-resistant moms were almost 40% slower to respond to the auditory stimuli than those of the insulin-sensitive moms (mean [SD], 283 [79] ms vs 178 [46] ms; P=.03).
INTERPRETING THE FINDINGS
According to the US Centers for Disease Control and Prevention, almost one-third (30.3%) of US adults between the ages of 20 and 39 years—the primary child-bearing years—are obese,2 as are 17% of our children and adolescents—triple the rate of 1 generation previous.3 Furthermore, 25.8 million people in the United States have diabetes, including 1 in every 400 children and adolescents.4
Experts know that the children of obese or diabetic mothers are at increased risk for obesity and type 2 diabetes as adults, and that the connection is not purely genetic; environmental and epigenetic (environmental elements that affect genetics) factors also play key roles. The latter is the basis for the fetal or developmental origins hypothesis,5 which posits that a pregnant woman’s exposure to certain environmental factors can affect the programming of her unborn child and impact adult health.
The authors of the current study demonstrate that the metabolism of a pregnant woman after a sugar load directly affects the response time and brain activity of her developing fetus. They suggest as a mechanism for the effect that “insulin-resistant mothers have higher glucose levels accompanied by increased insulin levels in the postprandial state. As glucose passes the placenta, these postprandially increased glucose levels induce hyperinsulinaemia in the fetus.” The resulting chronic hyperinsulinemia “might induce insulin resistance in the fetal brain.”
A new study1 provides the first evidence of a direct effect of maternal metabolism on fetal brain activity, suggesting that insulin resistance, the precursor to type 2 diabetes, begins its formation prenatally.
DETAILS OF THE STUDY
Dr. Katarzyna Linder from the University Hospital Tübingen in Germany and colleagues included in their study 13 healthy pregnant women with normal, singleton pregnancies of between 27 and 36 weeks. All of the women underwent an oral glucose tolerance test, meaning that after a 5-hour overnight fast, each woman drank a solution containing 75 g glucose. The investigators ascertained blood glucose and plasma insulin levels from blood samples taken at 0, 60, and 120 minutes.
At approximately the same time points, but before they drew each blood sample, the authors obtained a fetal magnetoencephalography (fMEG) measurement in an effort to noninvasively record brain activity in utero. During each measurement, they presented an auditory sequence to the fetus. Most (75%) of the time, the sound presented had a frequency of 500 Hz, but 25% of the time the researchers presented a deviant tone with a frequency of 750 Hz to prevent habituation.
The researchers found that maternal insulin sensitivity significantly correlated with response latency of the fetus at the 60-minute time point, so that the higher the insulin sensitivity of the mother, the shorter the response time of the fetus to the sound. The association remained significant even after the investigators controlled for relative maternal weight gain, gestational age, and the child’s birth weight. No significant correlation existed at baseline or at 120 minutes.
The investigators then split the women into 2 groups: those who were insulin-resistant and those who were insulin-sensitive. They found that the fetuses of the insulin-resistant moms were almost 40% slower to respond to the auditory stimuli than those of the insulin-sensitive moms (mean [SD], 283 [79] ms vs 178 [46] ms; P=.03).
INTERPRETING THE FINDINGS
According to the US Centers for Disease Control and Prevention, almost one-third (30.3%) of US adults between the ages of 20 and 39 years—the primary child-bearing years—are obese,2 as are 17% of our children and adolescents—triple the rate of 1 generation previous.3 Furthermore, 25.8 million people in the United States have diabetes, including 1 in every 400 children and adolescents.4
Experts know that the children of obese or diabetic mothers are at increased risk for obesity and type 2 diabetes as adults, and that the connection is not purely genetic; environmental and epigenetic (environmental elements that affect genetics) factors also play key roles. The latter is the basis for the fetal or developmental origins hypothesis,5 which posits that a pregnant woman’s exposure to certain environmental factors can affect the programming of her unborn child and impact adult health.
The authors of the current study demonstrate that the metabolism of a pregnant woman after a sugar load directly affects the response time and brain activity of her developing fetus. They suggest as a mechanism for the effect that “insulin-resistant mothers have higher glucose levels accompanied by increased insulin levels in the postprandial state. As glucose passes the placenta, these postprandially increased glucose levels induce hyperinsulinaemia in the fetus.” The resulting chronic hyperinsulinemia “might induce insulin resistance in the fetal brain.”
1. Linder K, Schleger F, Ketterer C, et al. Maternal insulin sensitivity is associated with oral glucose-induced changes in fetal brain activity. Diabetologia. 2014. [Epub ahead of print]
2. Adult obesity facts. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/obesity/data/adult.html. Accessed April 12, 2014.
3. Childhood overweight and obesity. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/obesity/childhood/index.html. Accessed April 12, 2014.
4. Statistics about diabetes. American Diabetes Association Web site. http://www.diabetes.org/diabetes-basics/statistics/. Accessed April 12, 2014.
5. Wadhwa PD, Buss C, Entringer S, Swanson JM. Developmental origins of health and disease: brief history of the approach and current focus on epigenetic mechanisms. Semin Reprod Med. 2009;27(5):358–368.
1. Linder K, Schleger F, Ketterer C, et al. Maternal insulin sensitivity is associated with oral glucose-induced changes in fetal brain activity. Diabetologia. 2014. [Epub ahead of print]
2. Adult obesity facts. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/obesity/data/adult.html. Accessed April 12, 2014.
3. Childhood overweight and obesity. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/obesity/childhood/index.html. Accessed April 12, 2014.
4. Statistics about diabetes. American Diabetes Association Web site. http://www.diabetes.org/diabetes-basics/statistics/. Accessed April 12, 2014.
5. Wadhwa PD, Buss C, Entringer S, Swanson JM. Developmental origins of health and disease: brief history of the approach and current focus on epigenetic mechanisms. Semin Reprod Med. 2009;27(5):358–368.
Frustration Grows with SGR Fix, ICD-10 Transition
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula, but this time, the vote by lawmakers to patch the ailing physician reimbursement program rather than scrap it also pushes back the pending debut of ICD-10.
And that's frustrating some hospitalists.
"For about 12 hours, I felt relief about the ICD-10 and then I just realized, it's still coming, presumably," says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash. "[It's] like a patient who needs surgery and finds out it's canceled for the day and he'll have it tomorrow. Well, that's good for right now, but [he] still has to face this eventually."
The SGR extension through year's end means that physicians do not face a 24% cut to physician payments under Medicare. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 could mean the upgraded system may not go into effect until at least Oct. 1, 2015. This comes after the Centers for Medicare & Medicaid Services already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, SFHM, says he expects the majority of doctors to be content with the delay, particularly in light of some estimates that show only 20% or so of physicians "have actually initiated the ICD-10 transition," but that it's unfair to those health systems that have prepared.
"ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes...and over 72,000 procedural codes," Dr. Lenchus writes in an e-mail to The Hospitalist's eWire. "So, it is not surprising that many take solace in the delay."
"It's distressing and frustrating for hospitalists, but less disruptive than it might be for hospitals," Dr. Nelson says. "And, of course in some places, hospitalists may be the physician leads on ICD-10 efforts, so [they are] very much wrapped up in the problem of 'What do we do now?'"
Visit our website for more information about ICD-10.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula, but this time, the vote by lawmakers to patch the ailing physician reimbursement program rather than scrap it also pushes back the pending debut of ICD-10.
And that's frustrating some hospitalists.
"For about 12 hours, I felt relief about the ICD-10 and then I just realized, it's still coming, presumably," says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash. "[It's] like a patient who needs surgery and finds out it's canceled for the day and he'll have it tomorrow. Well, that's good for right now, but [he] still has to face this eventually."
The SGR extension through year's end means that physicians do not face a 24% cut to physician payments under Medicare. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 could mean the upgraded system may not go into effect until at least Oct. 1, 2015. This comes after the Centers for Medicare & Medicaid Services already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, SFHM, says he expects the majority of doctors to be content with the delay, particularly in light of some estimates that show only 20% or so of physicians "have actually initiated the ICD-10 transition," but that it's unfair to those health systems that have prepared.
"ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes...and over 72,000 procedural codes," Dr. Lenchus writes in an e-mail to The Hospitalist's eWire. "So, it is not surprising that many take solace in the delay."
"It's distressing and frustrating for hospitalists, but less disruptive than it might be for hospitals," Dr. Nelson says. "And, of course in some places, hospitalists may be the physician leads on ICD-10 efforts, so [they are] very much wrapped up in the problem of 'What do we do now?'"
Visit our website for more information about ICD-10.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula, but this time, the vote by lawmakers to patch the ailing physician reimbursement program rather than scrap it also pushes back the pending debut of ICD-10.
And that's frustrating some hospitalists.
"For about 12 hours, I felt relief about the ICD-10 and then I just realized, it's still coming, presumably," says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash. "[It's] like a patient who needs surgery and finds out it's canceled for the day and he'll have it tomorrow. Well, that's good for right now, but [he] still has to face this eventually."
The SGR extension through year's end means that physicians do not face a 24% cut to physician payments under Medicare. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 could mean the upgraded system may not go into effect until at least Oct. 1, 2015. This comes after the Centers for Medicare & Medicaid Services already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, SFHM, says he expects the majority of doctors to be content with the delay, particularly in light of some estimates that show only 20% or so of physicians "have actually initiated the ICD-10 transition," but that it's unfair to those health systems that have prepared.
"ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes...and over 72,000 procedural codes," Dr. Lenchus writes in an e-mail to The Hospitalist's eWire. "So, it is not surprising that many take solace in the delay."
"It's distressing and frustrating for hospitalists, but less disruptive than it might be for hospitals," Dr. Nelson says. "And, of course in some places, hospitalists may be the physician leads on ICD-10 efforts, so [they are] very much wrapped up in the problem of 'What do we do now?'"
Visit our website for more information about ICD-10.
New SHM Board Member Danielle Scheurer, MD, MSRC, SFHM, Expands Commitment to Patient-Centered Care
Danielle Scheurer, MD, MSCR, SFHM, has her sights set on quality improvement when it comes to serving on SHM's Board of Directors over the next three years. As a representative of a society she considers well managed and efficient, Dr. Scheurer plans to continue fulfilling the goals she set for herself when she began her career in hospital medicine.
"I realized very quickly that I was not going to be satisfied being a good doctor with individual patients because of the barriers to good care and became compelled to attack the issues at the system level," says Dr. Scheurer, who also serves as physician editor of The Hospitalist.

Since becoming involved with SHM in 2003, Dr. Scheurer has spent time educating hospitalists on tactics to make hospital systems more effective and she blogs about clinical and practice issues. Dr. Scheurer also serves on SHM’s Education Committee, a role that she plans to continue in tandem with her work on the board.
Dr. Scheurer's hard work for the society not gone unnoticed. SHM President Burke T. Kealey, MD, SFHM, notes, "I'm very pleased to have Danielle on the board with us. I think she is going to add a great voice. Danielle has already been a great contributor to SHM. She has done a great job of getting out the message about SHM to our members and to others."
One of Dr. Scheurer's biggest accomplishments has been her role developing medical knowledge modules on quality and patient safety for the American Board of Internal Medicine's Recognition in Focused Practice in Hospital Medicine maintenance of certification (MOC) program. She has presented numerous MOC pre-courses at SHM's annual meetings. She says her involvement with fledgling hospitalists has made her optimistic about the future of the specialty.
"People in hospital medicine are already very focused on quality," she says. "We are getting better at understanding that it's not just about being a good doctor, its about creating systems that can effectively and reliably deliver high-quality care."
Danielle Scheurer, MD, MSCR, SFHM, has her sights set on quality improvement when it comes to serving on SHM's Board of Directors over the next three years. As a representative of a society she considers well managed and efficient, Dr. Scheurer plans to continue fulfilling the goals she set for herself when she began her career in hospital medicine.
"I realized very quickly that I was not going to be satisfied being a good doctor with individual patients because of the barriers to good care and became compelled to attack the issues at the system level," says Dr. Scheurer, who also serves as physician editor of The Hospitalist.
Since becoming involved with SHM in 2003, Dr. Scheurer has spent time educating hospitalists on tactics to make hospital systems more effective and she blogs about clinical and practice issues. Dr. Scheurer also serves on SHM’s Education Committee, a role that she plans to continue in tandem with her work on the board.
Dr. Scheurer's hard work for the society not gone unnoticed. SHM President Burke T. Kealey, MD, SFHM, notes, "I'm very pleased to have Danielle on the board with us. I think she is going to add a great voice. Danielle has already been a great contributor to SHM. She has done a great job of getting out the message about SHM to our members and to others."
One of Dr. Scheurer's biggest accomplishments has been her role developing medical knowledge modules on quality and patient safety for the American Board of Internal Medicine's Recognition in Focused Practice in Hospital Medicine maintenance of certification (MOC) program. She has presented numerous MOC pre-courses at SHM's annual meetings. She says her involvement with fledgling hospitalists has made her optimistic about the future of the specialty.
"People in hospital medicine are already very focused on quality," she says. "We are getting better at understanding that it's not just about being a good doctor, its about creating systems that can effectively and reliably deliver high-quality care."
Danielle Scheurer, MD, MSCR, SFHM, has her sights set on quality improvement when it comes to serving on SHM's Board of Directors over the next three years. As a representative of a society she considers well managed and efficient, Dr. Scheurer plans to continue fulfilling the goals she set for herself when she began her career in hospital medicine.
"I realized very quickly that I was not going to be satisfied being a good doctor with individual patients because of the barriers to good care and became compelled to attack the issues at the system level," says Dr. Scheurer, who also serves as physician editor of The Hospitalist.
Since becoming involved with SHM in 2003, Dr. Scheurer has spent time educating hospitalists on tactics to make hospital systems more effective and she blogs about clinical and practice issues. Dr. Scheurer also serves on SHM’s Education Committee, a role that she plans to continue in tandem with her work on the board.
Dr. Scheurer's hard work for the society not gone unnoticed. SHM President Burke T. Kealey, MD, SFHM, notes, "I'm very pleased to have Danielle on the board with us. I think she is going to add a great voice. Danielle has already been a great contributor to SHM. She has done a great job of getting out the message about SHM to our members and to others."
One of Dr. Scheurer's biggest accomplishments has been her role developing medical knowledge modules on quality and patient safety for the American Board of Internal Medicine's Recognition in Focused Practice in Hospital Medicine maintenance of certification (MOC) program. She has presented numerous MOC pre-courses at SHM's annual meetings. She says her involvement with fledgling hospitalists has made her optimistic about the future of the specialty.
"People in hospital medicine are already very focused on quality," she says. "We are getting better at understanding that it's not just about being a good doctor, its about creating systems that can effectively and reliably deliver high-quality care."
Marriage protects against vascular disease
WASHINGTON – Being married is independently associated with a significantly reduced rate of vascular disease across all arterial beds, according to a population-based study of more than 3.5 million subjects.
This apparent protective effect was strongest in younger individuals. In a multivariate regression analysis adjusted for demographics and cardiovascular risk factors, married subjects under age 50 years were 12% less likely to have prevalent vascular disease than were those who were single. The risk advantage shrank with advancing age such that married participants above age 70 years had a 4% lower risk of vascular disease than did those who were single, a difference that was statistically significant because of the huge size of the study population. And those who were single were at lower risk than were widowed or divorced subjects, Dr. Carlos L. Alviar reported at the annual meeting of the American College of Cardiology.
He presented an analysis of slightly more than 3.5 million participants in the Life Line Screening Diabetes Mellitus and Vascular Disease survey conducted during 2003-2008. Unlike most other studies of the relationship between marital status and health, which have focused on the risk of coronary disease, this study also included screening for peripheral artery disease, abdominal aortic aneurysm, and cerebrovascular disease.
Among participants of all ages, the risk of prevalent vascular disease was 5% less in those who were married than in those who were single. The risk was 3.2% greater in subjects who were divorced than in those who were single, and 5.1% greater in subjects who were widowed, according to Dr. Alviar of New York University.
The mean age of the study population was 63.7 years. Among women, 63.4% were married, 8.1% were single, 10.5% divorced, and 18% widowed. The male demographics were somewhat different: 80.4% of the men were married, 8.8% single, 6.1% divorced, and 4.7% were widowed.
Being widowed was associated with a higher prevalence of diabetes, hypertension, physical inactivity, and dyslipidemia, although investigators adjusted for that in their multivariate analysis. Divorced subjects were more likely to be smokers and have a family history of premature cardiovascular disease.
Dr. Alviar proposed as potential explanations for the reduced prevalence of vascular disease among married individuals their possibly lower levels of psychologic and physical stress, better access to medical care, and improved adherence to medication.
He reported having no financial disclosures regarding this study.
WASHINGTON – Being married is independently associated with a significantly reduced rate of vascular disease across all arterial beds, according to a population-based study of more than 3.5 million subjects.
This apparent protective effect was strongest in younger individuals. In a multivariate regression analysis adjusted for demographics and cardiovascular risk factors, married subjects under age 50 years were 12% less likely to have prevalent vascular disease than were those who were single. The risk advantage shrank with advancing age such that married participants above age 70 years had a 4% lower risk of vascular disease than did those who were single, a difference that was statistically significant because of the huge size of the study population. And those who were single were at lower risk than were widowed or divorced subjects, Dr. Carlos L. Alviar reported at the annual meeting of the American College of Cardiology.
He presented an analysis of slightly more than 3.5 million participants in the Life Line Screening Diabetes Mellitus and Vascular Disease survey conducted during 2003-2008. Unlike most other studies of the relationship between marital status and health, which have focused on the risk of coronary disease, this study also included screening for peripheral artery disease, abdominal aortic aneurysm, and cerebrovascular disease.
Among participants of all ages, the risk of prevalent vascular disease was 5% less in those who were married than in those who were single. The risk was 3.2% greater in subjects who were divorced than in those who were single, and 5.1% greater in subjects who were widowed, according to Dr. Alviar of New York University.
The mean age of the study population was 63.7 years. Among women, 63.4% were married, 8.1% were single, 10.5% divorced, and 18% widowed. The male demographics were somewhat different: 80.4% of the men were married, 8.8% single, 6.1% divorced, and 4.7% were widowed.
Being widowed was associated with a higher prevalence of diabetes, hypertension, physical inactivity, and dyslipidemia, although investigators adjusted for that in their multivariate analysis. Divorced subjects were more likely to be smokers and have a family history of premature cardiovascular disease.
Dr. Alviar proposed as potential explanations for the reduced prevalence of vascular disease among married individuals their possibly lower levels of psychologic and physical stress, better access to medical care, and improved adherence to medication.
He reported having no financial disclosures regarding this study.
WASHINGTON – Being married is independently associated with a significantly reduced rate of vascular disease across all arterial beds, according to a population-based study of more than 3.5 million subjects.
This apparent protective effect was strongest in younger individuals. In a multivariate regression analysis adjusted for demographics and cardiovascular risk factors, married subjects under age 50 years were 12% less likely to have prevalent vascular disease than were those who were single. The risk advantage shrank with advancing age such that married participants above age 70 years had a 4% lower risk of vascular disease than did those who were single, a difference that was statistically significant because of the huge size of the study population. And those who were single were at lower risk than were widowed or divorced subjects, Dr. Carlos L. Alviar reported at the annual meeting of the American College of Cardiology.
He presented an analysis of slightly more than 3.5 million participants in the Life Line Screening Diabetes Mellitus and Vascular Disease survey conducted during 2003-2008. Unlike most other studies of the relationship between marital status and health, which have focused on the risk of coronary disease, this study also included screening for peripheral artery disease, abdominal aortic aneurysm, and cerebrovascular disease.
Among participants of all ages, the risk of prevalent vascular disease was 5% less in those who were married than in those who were single. The risk was 3.2% greater in subjects who were divorced than in those who were single, and 5.1% greater in subjects who were widowed, according to Dr. Alviar of New York University.
The mean age of the study population was 63.7 years. Among women, 63.4% were married, 8.1% were single, 10.5% divorced, and 18% widowed. The male demographics were somewhat different: 80.4% of the men were married, 8.8% single, 6.1% divorced, and 4.7% were widowed.
Being widowed was associated with a higher prevalence of diabetes, hypertension, physical inactivity, and dyslipidemia, although investigators adjusted for that in their multivariate analysis. Divorced subjects were more likely to be smokers and have a family history of premature cardiovascular disease.
Dr. Alviar proposed as potential explanations for the reduced prevalence of vascular disease among married individuals their possibly lower levels of psychologic and physical stress, better access to medical care, and improved adherence to medication.
He reported having no financial disclosures regarding this study.
AT ACC 14
Major finding: Married men under age 50 years were 14.4% less likely than their single counterparts were to have vascular disease, and married women were 10.7% less likely. This advantage remained significant, albeit attenuated, in older married individuals.
Data source: This was an analysis of 3,532,189 adult participants in the Life Line Screening Diabetes Mellitus and Vascular Disease survey.
Disclosures: The study presenter reported having no financial conflicts of interest.
VIDEO: Concise guide to lasers: cellulite, tattoo removal, and skin tightening
DENVER – In 15 minutes, Dr. M. Christine Lee brings you a definitive guide to lasers for various patient needs, including tattoo removal, treatment of cellulite, skin tightening, and skin resurfacing. Learn more about lasers that you might want to add to your practice and get ideas on how to make the most of devices you already have.
Dr. Lee is with the department of dermatologic surgery at the University of California, San Francisco, and director of East Bay Laser & Skin Care Center in Walnut Creek, Calif. In this video, she also shares clinical pearls about different types of laser procedures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
DENVER – In 15 minutes, Dr. M. Christine Lee brings you a definitive guide to lasers for various patient needs, including tattoo removal, treatment of cellulite, skin tightening, and skin resurfacing. Learn more about lasers that you might want to add to your practice and get ideas on how to make the most of devices you already have.
Dr. Lee is with the department of dermatologic surgery at the University of California, San Francisco, and director of East Bay Laser & Skin Care Center in Walnut Creek, Calif. In this video, she also shares clinical pearls about different types of laser procedures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
DENVER – In 15 minutes, Dr. M. Christine Lee brings you a definitive guide to lasers for various patient needs, including tattoo removal, treatment of cellulite, skin tightening, and skin resurfacing. Learn more about lasers that you might want to add to your practice and get ideas on how to make the most of devices you already have.
Dr. Lee is with the department of dermatologic surgery at the University of California, San Francisco, and director of East Bay Laser & Skin Care Center in Walnut Creek, Calif. In this video, she also shares clinical pearls about different types of laser procedures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @naseemmiller
EXPERT ANALYSIS FROM THE AAD ANNUAL MEETING

Group describes mechanism of resistance in CLL
SAN DIEGO—Preclinical research has revealed a mechanism of rituximab resistance in chronic lymphocytic leukemia (CLL), as well as a possible new treatment approach.
The study suggests the TNF-family member BAFF contributes to CLL cells’ resistance to direct and rituximab-induced natural killer (NK) cell reactivity.
However, the BAFF-specific antibody belimumab can overcome this resistance and restore CLL cells’ sensitivity to chemotherapy.
Julia Wild, a PhD student at Eberhard Karls University in Tuebingen, Germany, and her colleagues presented these findings at the AACR Annual Meeting 2014 as abstract 148.
“It is widely known that NK cells’ ability to react against lymphoblastic leukemia is impaired, as compared to myeloid leukemia,” Wild said. “And we now think we’ve identified a factor involved in this—a member of the tumor necrosis factor family called BAFF.”
Previous research showed that NK cells’ ability to target malignant cells and mediate antibody-dependent cellular cytotoxicity (ADCC) is compromised in CLL, but the underlying mechanisms were not clear. Wild and her colleagues therefore speculated that BAFF, which regulates B-cell proliferation and survival, plays a role.
The researchers’ initial experiments revealed that NK cells express BAFF at the mRNA level and release the protein in a soluble form, with levels depending on the state of activation.
The team then assessed BAFF expression in primary CLL cells. They collected cells from 17 CLL patients and analyzed surface expression of the 3 BAFF receptors. All 17 samples were positive for BAFF-R and TACI, and about 53% (9/17) were positive for BCMA.
Additional experiments revealed that BAFF enhances the metabolic activity of primary CLL cells. To uncover this result, the researchers incubated the cells with increasing concentrations of BAFF. And they compared untreated cells to cells treated with belimumab, isotype control, BAFF, BAFF plus belimumab, and BAFF plus isotype control.
The team then compared untreated CLL cells to cells treated with fludarabine and cyclophosphamide (Flu/Cy); Flu/Cy plus BAFF; and Flu/Cy, BAFF, and belimumab.
They found that BAFF protects CLL cells from chemotherapy-induced death. However, belimumab inhibits the protective effects of BAFF and restores CLL cells’ sensitivity to chemotherapy.
The researchers then performed cytotoxicity assays in primary CLL cells, comparing untreated cells to cells exposed to BAFF alone; rituximab alone; BAFF and rituximab; BAFF and belimumab; and rituximab, BAFF, and belimumab.
They found that lysis was highest among cells treated with rituximab alone or rituximab, BAFF, and belimumab, with comparable results in these 2 groups.
The team also evaluated CLL cell lysis due to ADCC induction. They analyzed peripheral blood mononuclear cells from CLL patients, comparing untreated cells to cells exposed to rituximab alone; rituximab and BAFF; rituximab, belimumab, and BAFF; and rituximab, bevacizumab, and BAFF.
Results showed that CLL cell survival was lowest (and comparable) in cells treated with rituximab alone or rituximab, belimumab, and BAFF.
“When CLL cells are cultured in the presence of BAFF, cytotoxicity is decreased as compared to untreated cells, and this is not only for direct NK-cell activity, but also for ADCC-mediated activity,” Wild summarized.
“But we can block this effect with belimumab, which suggests we could use this antibody for CLL treatment.” ![]()
SAN DIEGO—Preclinical research has revealed a mechanism of rituximab resistance in chronic lymphocytic leukemia (CLL), as well as a possible new treatment approach.
The study suggests the TNF-family member BAFF contributes to CLL cells’ resistance to direct and rituximab-induced natural killer (NK) cell reactivity.
However, the BAFF-specific antibody belimumab can overcome this resistance and restore CLL cells’ sensitivity to chemotherapy.
Julia Wild, a PhD student at Eberhard Karls University in Tuebingen, Germany, and her colleagues presented these findings at the AACR Annual Meeting 2014 as abstract 148.
“It is widely known that NK cells’ ability to react against lymphoblastic leukemia is impaired, as compared to myeloid leukemia,” Wild said. “And we now think we’ve identified a factor involved in this—a member of the tumor necrosis factor family called BAFF.”
Previous research showed that NK cells’ ability to target malignant cells and mediate antibody-dependent cellular cytotoxicity (ADCC) is compromised in CLL, but the underlying mechanisms were not clear. Wild and her colleagues therefore speculated that BAFF, which regulates B-cell proliferation and survival, plays a role.
The researchers’ initial experiments revealed that NK cells express BAFF at the mRNA level and release the protein in a soluble form, with levels depending on the state of activation.
The team then assessed BAFF expression in primary CLL cells. They collected cells from 17 CLL patients and analyzed surface expression of the 3 BAFF receptors. All 17 samples were positive for BAFF-R and TACI, and about 53% (9/17) were positive for BCMA.
Additional experiments revealed that BAFF enhances the metabolic activity of primary CLL cells. To uncover this result, the researchers incubated the cells with increasing concentrations of BAFF. And they compared untreated cells to cells treated with belimumab, isotype control, BAFF, BAFF plus belimumab, and BAFF plus isotype control.
The team then compared untreated CLL cells to cells treated with fludarabine and cyclophosphamide (Flu/Cy); Flu/Cy plus BAFF; and Flu/Cy, BAFF, and belimumab.
They found that BAFF protects CLL cells from chemotherapy-induced death. However, belimumab inhibits the protective effects of BAFF and restores CLL cells’ sensitivity to chemotherapy.
The researchers then performed cytotoxicity assays in primary CLL cells, comparing untreated cells to cells exposed to BAFF alone; rituximab alone; BAFF and rituximab; BAFF and belimumab; and rituximab, BAFF, and belimumab.
They found that lysis was highest among cells treated with rituximab alone or rituximab, BAFF, and belimumab, with comparable results in these 2 groups.
The team also evaluated CLL cell lysis due to ADCC induction. They analyzed peripheral blood mononuclear cells from CLL patients, comparing untreated cells to cells exposed to rituximab alone; rituximab and BAFF; rituximab, belimumab, and BAFF; and rituximab, bevacizumab, and BAFF.
Results showed that CLL cell survival was lowest (and comparable) in cells treated with rituximab alone or rituximab, belimumab, and BAFF.
“When CLL cells are cultured in the presence of BAFF, cytotoxicity is decreased as compared to untreated cells, and this is not only for direct NK-cell activity, but also for ADCC-mediated activity,” Wild summarized.
“But we can block this effect with belimumab, which suggests we could use this antibody for CLL treatment.” ![]()
SAN DIEGO—Preclinical research has revealed a mechanism of rituximab resistance in chronic lymphocytic leukemia (CLL), as well as a possible new treatment approach.
The study suggests the TNF-family member BAFF contributes to CLL cells’ resistance to direct and rituximab-induced natural killer (NK) cell reactivity.
However, the BAFF-specific antibody belimumab can overcome this resistance and restore CLL cells’ sensitivity to chemotherapy.
Julia Wild, a PhD student at Eberhard Karls University in Tuebingen, Germany, and her colleagues presented these findings at the AACR Annual Meeting 2014 as abstract 148.
“It is widely known that NK cells’ ability to react against lymphoblastic leukemia is impaired, as compared to myeloid leukemia,” Wild said. “And we now think we’ve identified a factor involved in this—a member of the tumor necrosis factor family called BAFF.”
Previous research showed that NK cells’ ability to target malignant cells and mediate antibody-dependent cellular cytotoxicity (ADCC) is compromised in CLL, but the underlying mechanisms were not clear. Wild and her colleagues therefore speculated that BAFF, which regulates B-cell proliferation and survival, plays a role.
The researchers’ initial experiments revealed that NK cells express BAFF at the mRNA level and release the protein in a soluble form, with levels depending on the state of activation.
The team then assessed BAFF expression in primary CLL cells. They collected cells from 17 CLL patients and analyzed surface expression of the 3 BAFF receptors. All 17 samples were positive for BAFF-R and TACI, and about 53% (9/17) were positive for BCMA.
Additional experiments revealed that BAFF enhances the metabolic activity of primary CLL cells. To uncover this result, the researchers incubated the cells with increasing concentrations of BAFF. And they compared untreated cells to cells treated with belimumab, isotype control, BAFF, BAFF plus belimumab, and BAFF plus isotype control.
The team then compared untreated CLL cells to cells treated with fludarabine and cyclophosphamide (Flu/Cy); Flu/Cy plus BAFF; and Flu/Cy, BAFF, and belimumab.
They found that BAFF protects CLL cells from chemotherapy-induced death. However, belimumab inhibits the protective effects of BAFF and restores CLL cells’ sensitivity to chemotherapy.
The researchers then performed cytotoxicity assays in primary CLL cells, comparing untreated cells to cells exposed to BAFF alone; rituximab alone; BAFF and rituximab; BAFF and belimumab; and rituximab, BAFF, and belimumab.
They found that lysis was highest among cells treated with rituximab alone or rituximab, BAFF, and belimumab, with comparable results in these 2 groups.
The team also evaluated CLL cell lysis due to ADCC induction. They analyzed peripheral blood mononuclear cells from CLL patients, comparing untreated cells to cells exposed to rituximab alone; rituximab and BAFF; rituximab, belimumab, and BAFF; and rituximab, bevacizumab, and BAFF.
Results showed that CLL cell survival was lowest (and comparable) in cells treated with rituximab alone or rituximab, belimumab, and BAFF.
“When CLL cells are cultured in the presence of BAFF, cytotoxicity is decreased as compared to untreated cells, and this is not only for direct NK-cell activity, but also for ADCC-mediated activity,” Wild summarized.
“But we can block this effect with belimumab, which suggests we could use this antibody for CLL treatment.” ![]()
NICE supports use of ESAs in cancer patients

Anemic cancer patients in the UK may soon have 6 erythropoiesis-stimulating agents (ESAs) available through the National Health Service.
The National Institute for Health and Care Excellence (NICE) has drafted a guidance recommending 5 epoetins—2 alfas, 1 beta, 1 theta, and 1 zeta—and 1 darbepoetin to treat anemia in adult cancer patients receiving chemotherapy.
NICE has started a consultation on the guidance, and it will be open for comment until May 9.
To inform NICE on the clinical effectiveness of the 6 ESAs, an independent appraisal committee looked at results from several clinical trials and reviewed the existing guidance.
The committee concluded that the ESAs were effective at increasing hemoglobin levels and managing anemia when compared to current standards of care. The drugs reduced the need for blood transfusions in patients receiving cancer treatment.
Furthermore, analyses suggested the ESAs are cost-effective. However, the draft guidance recommends that healthcare professionals offer patients the appropriate ESA with the lowest cost.
The guidance recommends the ESAs for their approved indications.
Epoetin alfa (marketed as Eprex and Binocrit) and epoetin zeta (marketed as Retacrit) are approved in the UK to treat anemia and reduce transfusion requirements in adult patients receiving chemotherapy for solid tumors, malignant lymphoma, or multiple myeloma. Patients must be at risk of transfusion, as assessed by their general status (eg, cardiovascular status, pre-existing anemia at the start of chemotherapy).
Eprex, Binocrit, and Retacrit are available in pre-filled syringes at net prices of £5.53, £5.09, and £5.66 per 1000 units, respectively.
Epoetin beta (marketed as NeoRecormon) and Epoetin theta (marketed as Eporatio) are approved to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy.
NeoRecormo is available in a pre-filled syringe at a net price of £3.51 per 500 units, and Eporatio is available in a pre-filled syringe at a net price of £5.99 per 1000 units.
Darbepoetin alfa (marketed as Aranesp) is approved to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy. It is recommended for use at hemoglobin concentrations of 100 g/l or lower, with target values up to 120 g/l. Aranesp is available in a pre-filled syringe at a net price of £14.68 per 10 micrograms.
Costs exclude tax and may vary in different settings. For more information, see the draft guidance. ![]()
Anemic cancer patients in the UK may soon have 6 erythropoiesis-stimulating agents (ESAs) available through the National Health Service.
The National Institute for Health and Care Excellence (NICE) has drafted a guidance recommending 5 epoetins—2 alfas, 1 beta, 1 theta, and 1 zeta—and 1 darbepoetin to treat anemia in adult cancer patients receiving chemotherapy.
NICE has started a consultation on the guidance, and it will be open for comment until May 9.
To inform NICE on the clinical effectiveness of the 6 ESAs, an independent appraisal committee looked at results from several clinical trials and reviewed the existing guidance.
The committee concluded that the ESAs were effective at increasing hemoglobin levels and managing anemia when compared to current standards of care. The drugs reduced the need for blood transfusions in patients receiving cancer treatment.
Furthermore, analyses suggested the ESAs are cost-effective. However, the draft guidance recommends that healthcare professionals offer patients the appropriate ESA with the lowest cost.
The guidance recommends the ESAs for their approved indications.
Epoetin alfa (marketed as Eprex and Binocrit) and epoetin zeta (marketed as Retacrit) are approved in the UK to treat anemia and reduce transfusion requirements in adult patients receiving chemotherapy for solid tumors, malignant lymphoma, or multiple myeloma. Patients must be at risk of transfusion, as assessed by their general status (eg, cardiovascular status, pre-existing anemia at the start of chemotherapy).
Eprex, Binocrit, and Retacrit are available in pre-filled syringes at net prices of £5.53, £5.09, and £5.66 per 1000 units, respectively.
Epoetin beta (marketed as NeoRecormon) and Epoetin theta (marketed as Eporatio) are approved to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy.
NeoRecormo is available in a pre-filled syringe at a net price of £3.51 per 500 units, and Eporatio is available in a pre-filled syringe at a net price of £5.99 per 1000 units.
Darbepoetin alfa (marketed as Aranesp) is approved to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy. It is recommended for use at hemoglobin concentrations of 100 g/l or lower, with target values up to 120 g/l. Aranesp is available in a pre-filled syringe at a net price of £14.68 per 10 micrograms.
Costs exclude tax and may vary in different settings. For more information, see the draft guidance. ![]()
Anemic cancer patients in the UK may soon have 6 erythropoiesis-stimulating agents (ESAs) available through the National Health Service.
The National Institute for Health and Care Excellence (NICE) has drafted a guidance recommending 5 epoetins—2 alfas, 1 beta, 1 theta, and 1 zeta—and 1 darbepoetin to treat anemia in adult cancer patients receiving chemotherapy.
NICE has started a consultation on the guidance, and it will be open for comment until May 9.
To inform NICE on the clinical effectiveness of the 6 ESAs, an independent appraisal committee looked at results from several clinical trials and reviewed the existing guidance.
The committee concluded that the ESAs were effective at increasing hemoglobin levels and managing anemia when compared to current standards of care. The drugs reduced the need for blood transfusions in patients receiving cancer treatment.
Furthermore, analyses suggested the ESAs are cost-effective. However, the draft guidance recommends that healthcare professionals offer patients the appropriate ESA with the lowest cost.
The guidance recommends the ESAs for their approved indications.
Epoetin alfa (marketed as Eprex and Binocrit) and epoetin zeta (marketed as Retacrit) are approved in the UK to treat anemia and reduce transfusion requirements in adult patients receiving chemotherapy for solid tumors, malignant lymphoma, or multiple myeloma. Patients must be at risk of transfusion, as assessed by their general status (eg, cardiovascular status, pre-existing anemia at the start of chemotherapy).
Eprex, Binocrit, and Retacrit are available in pre-filled syringes at net prices of £5.53, £5.09, and £5.66 per 1000 units, respectively.
Epoetin beta (marketed as NeoRecormon) and Epoetin theta (marketed as Eporatio) are approved to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy.
NeoRecormo is available in a pre-filled syringe at a net price of £3.51 per 500 units, and Eporatio is available in a pre-filled syringe at a net price of £5.99 per 1000 units.
Darbepoetin alfa (marketed as Aranesp) is approved to treat symptomatic anemia in adult patients with non-myeloid malignancies who are receiving chemotherapy. It is recommended for use at hemoglobin concentrations of 100 g/l or lower, with target values up to 120 g/l. Aranesp is available in a pre-filled syringe at a net price of £14.68 per 10 micrograms.
Costs exclude tax and may vary in different settings. For more information, see the draft guidance. ![]()
Patient perception of control affects satisfaction

patient and her father
Credit: Rhoda Baer
Feeling as though they play an active role in their treatment decisions increases satisfaction among cancer patients undergoing radiotherapy (RT), according to research published in Cancer.
In a study of more than 300 RT patients, those who were involved in their treatment decisions—or perceived they had some control over their treatment—were more satisfied than their peers.
On the other hand, patients who wanted control over their treatment but did not feel they had any were more likely than their peers to experience anxiety, depression, and fatigue.
“Our findings emphasize the value of patient-physician relationships and communication, specifically in radiation oncology, and their impact on patient experience in a way that hasn’t been shown before,” said study author Neha Vapiwala, MD, of the Perelman School of Medicine at the University of Pennsylvania.
Dr Vapiwala and her colleagues noted that past studies of shared decision-making (SDM)—in which patients and providers make healthcare decisions together, taking into account scientific evidence and patient preferences—have shown an association between patient satisfaction and quality of life.
However, none of these studies has evaluated the impact of SDM on patients undergoing RT. Often, radiation oncology is seen as a treatment avenue that is ultimately left to the physician to dictate. But there are tailored options, decisions, and discussions that can apply to individual patients.
With this in mind, the researchers conducted a survey of SDM in 305 patients undergoing RT. In all, 31% of patients said they experienced SDM, 32% perceived control in their treatment decisions, and 76% reported feeling very satisfied with their radiation treatment course overall.
Patient satisfaction was significantly higher among those who perceived SDM than among those who did not—84.4% and 71.4%, respectively (P<0.02).
And satisfaction was higher among patients who perceived control over their treatment than among those who did not—89.7% and 69.2%, respectively (P<0.001).
Patients who expressed a desire for control over their treatment decisions but did not perceive having any control were significantly more likely than their peers to experience symptoms tied to psychological distress.
Anxiety was reported in 44% and 20% of patients, respectively (P<0.02). Depression was reported in 44% and 15%, respectively (P<0.01). And fatigue was reported in 68% and 39.2%, respectively (P<0.01).
The researchers said one of this study’s strengths is the diverse group of patients enrolled. Ages ranged from 18 to 87 years, and a variety of ethnic/racial groups were represented. Patients had a range of cancers at all stages, and could participate in the study as long as they were well enough.
The team said the next step for this research is to determine both physician and patient barriers to SDM and identify methods to break down these barriers.
“As providers, it doesn’t matter what treatment you are offering, or how complicated it is, or how busy you may be,” Dr Vapiwala said. “It’s worth taking even a few minutes to talk to patients about seemingly minor decisions in which they can provide some input.”
“It’s not only critical in today’s healthcare setting, where both information and misinformation are rampant, but will very likely lead to the patient feeling positively about the encounter.” ![]()
patient and her father
Credit: Rhoda Baer
Feeling as though they play an active role in their treatment decisions increases satisfaction among cancer patients undergoing radiotherapy (RT), according to research published in Cancer.
In a study of more than 300 RT patients, those who were involved in their treatment decisions—or perceived they had some control over their treatment—were more satisfied than their peers.
On the other hand, patients who wanted control over their treatment but did not feel they had any were more likely than their peers to experience anxiety, depression, and fatigue.
“Our findings emphasize the value of patient-physician relationships and communication, specifically in radiation oncology, and their impact on patient experience in a way that hasn’t been shown before,” said study author Neha Vapiwala, MD, of the Perelman School of Medicine at the University of Pennsylvania.
Dr Vapiwala and her colleagues noted that past studies of shared decision-making (SDM)—in which patients and providers make healthcare decisions together, taking into account scientific evidence and patient preferences—have shown an association between patient satisfaction and quality of life.
However, none of these studies has evaluated the impact of SDM on patients undergoing RT. Often, radiation oncology is seen as a treatment avenue that is ultimately left to the physician to dictate. But there are tailored options, decisions, and discussions that can apply to individual patients.
With this in mind, the researchers conducted a survey of SDM in 305 patients undergoing RT. In all, 31% of patients said they experienced SDM, 32% perceived control in their treatment decisions, and 76% reported feeling very satisfied with their radiation treatment course overall.
Patient satisfaction was significantly higher among those who perceived SDM than among those who did not—84.4% and 71.4%, respectively (P<0.02).
And satisfaction was higher among patients who perceived control over their treatment than among those who did not—89.7% and 69.2%, respectively (P<0.001).
Patients who expressed a desire for control over their treatment decisions but did not perceive having any control were significantly more likely than their peers to experience symptoms tied to psychological distress.
Anxiety was reported in 44% and 20% of patients, respectively (P<0.02). Depression was reported in 44% and 15%, respectively (P<0.01). And fatigue was reported in 68% and 39.2%, respectively (P<0.01).
The researchers said one of this study’s strengths is the diverse group of patients enrolled. Ages ranged from 18 to 87 years, and a variety of ethnic/racial groups were represented. Patients had a range of cancers at all stages, and could participate in the study as long as they were well enough.
The team said the next step for this research is to determine both physician and patient barriers to SDM and identify methods to break down these barriers.
“As providers, it doesn’t matter what treatment you are offering, or how complicated it is, or how busy you may be,” Dr Vapiwala said. “It’s worth taking even a few minutes to talk to patients about seemingly minor decisions in which they can provide some input.”
“It’s not only critical in today’s healthcare setting, where both information and misinformation are rampant, but will very likely lead to the patient feeling positively about the encounter.” ![]()
patient and her father
Credit: Rhoda Baer
Feeling as though they play an active role in their treatment decisions increases satisfaction among cancer patients undergoing radiotherapy (RT), according to research published in Cancer.
In a study of more than 300 RT patients, those who were involved in their treatment decisions—or perceived they had some control over their treatment—were more satisfied than their peers.
On the other hand, patients who wanted control over their treatment but did not feel they had any were more likely than their peers to experience anxiety, depression, and fatigue.
“Our findings emphasize the value of patient-physician relationships and communication, specifically in radiation oncology, and their impact on patient experience in a way that hasn’t been shown before,” said study author Neha Vapiwala, MD, of the Perelman School of Medicine at the University of Pennsylvania.
Dr Vapiwala and her colleagues noted that past studies of shared decision-making (SDM)—in which patients and providers make healthcare decisions together, taking into account scientific evidence and patient preferences—have shown an association between patient satisfaction and quality of life.
However, none of these studies has evaluated the impact of SDM on patients undergoing RT. Often, radiation oncology is seen as a treatment avenue that is ultimately left to the physician to dictate. But there are tailored options, decisions, and discussions that can apply to individual patients.
With this in mind, the researchers conducted a survey of SDM in 305 patients undergoing RT. In all, 31% of patients said they experienced SDM, 32% perceived control in their treatment decisions, and 76% reported feeling very satisfied with their radiation treatment course overall.
Patient satisfaction was significantly higher among those who perceived SDM than among those who did not—84.4% and 71.4%, respectively (P<0.02).
And satisfaction was higher among patients who perceived control over their treatment than among those who did not—89.7% and 69.2%, respectively (P<0.001).
Patients who expressed a desire for control over their treatment decisions but did not perceive having any control were significantly more likely than their peers to experience symptoms tied to psychological distress.
Anxiety was reported in 44% and 20% of patients, respectively (P<0.02). Depression was reported in 44% and 15%, respectively (P<0.01). And fatigue was reported in 68% and 39.2%, respectively (P<0.01).
The researchers said one of this study’s strengths is the diverse group of patients enrolled. Ages ranged from 18 to 87 years, and a variety of ethnic/racial groups were represented. Patients had a range of cancers at all stages, and could participate in the study as long as they were well enough.
The team said the next step for this research is to determine both physician and patient barriers to SDM and identify methods to break down these barriers.
“As providers, it doesn’t matter what treatment you are offering, or how complicated it is, or how busy you may be,” Dr Vapiwala said. “It’s worth taking even a few minutes to talk to patients about seemingly minor decisions in which they can provide some input.”
“It’s not only critical in today’s healthcare setting, where both information and misinformation are rampant, but will very likely lead to the patient feeling positively about the encounter.” ![]()
Team finds Achilles’ heel in malaria parasite protein
Credit: Ute Frevert
and Margaret Shear
Changing the administration of chloroquine might prevent resistance to the antimalarial agent, according to a study published in PNAS.
Investigators found the parasite protein that causes chloroquine resistance—the Plasmodium falciparum chloroquine resistance transporter (PfCRT)—has an Achilles’ heel.
“We studied diverse versions of this protein and, in all cases, found that it is limited in its capacity to remove the drug from the parasite,” said Rowena Martin, PhD, of The Australian National University in Canberra.
“This means malaria could once again be treated with chloroquine if it is administered twice-daily, rather than just once a day.”
Dr Martin and her colleagues noted that a number of distinct PfCRT haplotypes, containing between 4 and 10 mutations, have given rise to chloroquine resistance.
So they set out to characterize these forms of PfCRT and determine the number of mutations, as well as the order of their addition, required to confer chloroquine transport activity.
The investigators analyzed more than 100 variants of PfCRT, measuring their ability to transport chloroquine.
The team identified multiple mutational pathways that led to chloroquine transport via PfCRT but divided these pathways into 2 main lineages.
“We found that the protein gains the ability to move chloroquine out of the parasite through 1 of 2 evolutionary pathways but that this process is rigid,” Dr Martin said. “One wrong turn, and the protein is rendered useless.”
In fact, the investigators found that, if mutations did not occur in a precise order, chloroquine transport activity decreased.
The number of mutations played a key role as well. A minimum of 2 mutations was sufficient for chloroquine transport activity, but as few as 4 conferred full activity.
“This indicates that the protein is under conflicting pressures, which is a weakness that could be exploited in future antimalarial strategies,” Dr Martin said.
She also noted that these findings might not apply only to chloroquine. They might apply to several chloroquine-like drugs that are also becoming less effective as the malaria parasite builds up resistance. ![]()
Credit: Ute Frevert
and Margaret Shear
Changing the administration of chloroquine might prevent resistance to the antimalarial agent, according to a study published in PNAS.
Investigators found the parasite protein that causes chloroquine resistance—the Plasmodium falciparum chloroquine resistance transporter (PfCRT)—has an Achilles’ heel.
“We studied diverse versions of this protein and, in all cases, found that it is limited in its capacity to remove the drug from the parasite,” said Rowena Martin, PhD, of The Australian National University in Canberra.
“This means malaria could once again be treated with chloroquine if it is administered twice-daily, rather than just once a day.”
Dr Martin and her colleagues noted that a number of distinct PfCRT haplotypes, containing between 4 and 10 mutations, have given rise to chloroquine resistance.
So they set out to characterize these forms of PfCRT and determine the number of mutations, as well as the order of their addition, required to confer chloroquine transport activity.
The investigators analyzed more than 100 variants of PfCRT, measuring their ability to transport chloroquine.
The team identified multiple mutational pathways that led to chloroquine transport via PfCRT but divided these pathways into 2 main lineages.
“We found that the protein gains the ability to move chloroquine out of the parasite through 1 of 2 evolutionary pathways but that this process is rigid,” Dr Martin said. “One wrong turn, and the protein is rendered useless.”
In fact, the investigators found that, if mutations did not occur in a precise order, chloroquine transport activity decreased.
The number of mutations played a key role as well. A minimum of 2 mutations was sufficient for chloroquine transport activity, but as few as 4 conferred full activity.
“This indicates that the protein is under conflicting pressures, which is a weakness that could be exploited in future antimalarial strategies,” Dr Martin said.
She also noted that these findings might not apply only to chloroquine. They might apply to several chloroquine-like drugs that are also becoming less effective as the malaria parasite builds up resistance. ![]()
Credit: Ute Frevert
and Margaret Shear
Changing the administration of chloroquine might prevent resistance to the antimalarial agent, according to a study published in PNAS.
Investigators found the parasite protein that causes chloroquine resistance—the Plasmodium falciparum chloroquine resistance transporter (PfCRT)—has an Achilles’ heel.
“We studied diverse versions of this protein and, in all cases, found that it is limited in its capacity to remove the drug from the parasite,” said Rowena Martin, PhD, of The Australian National University in Canberra.
“This means malaria could once again be treated with chloroquine if it is administered twice-daily, rather than just once a day.”
Dr Martin and her colleagues noted that a number of distinct PfCRT haplotypes, containing between 4 and 10 mutations, have given rise to chloroquine resistance.
So they set out to characterize these forms of PfCRT and determine the number of mutations, as well as the order of their addition, required to confer chloroquine transport activity.
The investigators analyzed more than 100 variants of PfCRT, measuring their ability to transport chloroquine.
The team identified multiple mutational pathways that led to chloroquine transport via PfCRT but divided these pathways into 2 main lineages.
“We found that the protein gains the ability to move chloroquine out of the parasite through 1 of 2 evolutionary pathways but that this process is rigid,” Dr Martin said. “One wrong turn, and the protein is rendered useless.”
In fact, the investigators found that, if mutations did not occur in a precise order, chloroquine transport activity decreased.
The number of mutations played a key role as well. A minimum of 2 mutations was sufficient for chloroquine transport activity, but as few as 4 conferred full activity.
“This indicates that the protein is under conflicting pressures, which is a weakness that could be exploited in future antimalarial strategies,” Dr Martin said.
She also noted that these findings might not apply only to chloroquine. They might apply to several chloroquine-like drugs that are also becoming less effective as the malaria parasite builds up resistance. ![]()