User login
Psychosis resolves, but menses stop
CASE Paranoid and hallucinating
Ms. S, age 30, is an unmarried graduate student who has been given a diagnosis of schizophrenia, paranoid type, during inpatient hospitalization that was prompted by impairment in school functioning (difficulty turning in assignments, poor concentration, making careless mistakes on tests), paranoid delusions, and multisensory hallucinations. She says that her roommate and classmates are working together to make her leave school, and recalls seeing them “snare and smirk” as she passes by. Ms. S says that she feels her classmates are calling her names and talking badly about her as soon as she is out of sight.
Ms. S is antipsychotic-naïve and has a baseline body mass index of 17.8 kg/m2, indicating that she is underweight. We believe that olanzapine, 20 mg/d, is a good initial treatment because of its propensity for weight gain; however, she experiences only marginal improvement. Ms. S does not have health insurance, and cannot afford a brand name medication; therefore, she is cross-tapered to perphenazine, 8 mg, and benzatropine, 0.5 mg, both taken twice daily (olanzapine was not available as a generic at the time).
At discharge, Ms. S does not report any hallucinatory experiences, but is guarded, voices suspicions about the treatment team, and asks “What are they doing with all my blood?”—referring to blood draws for laboratory testing during hospitalization.
As an outpatient, Ms. S is continued on the same medications until she has to be switched because she cannot afford the out-of-pocket cost of the antipsychotic, perphenazine ($80 a month). Clozapine is recommended, but Ms. S refuses because of the mandatory weekly blood monitoring. She briefly tries fluphenazine, 2.5 mg/d, but it is discontinued because of malaise and lightheadedness without extrapyramidal symptoms.
Clozapine is again recommended, but Ms. S remains suspicious of the necessary blood draws and refuses. After several trials of antipsychotics, Ms. S starts paliperidone using samples from the clinic, titrated to 6 mg at bedtime. Once tolerance and therapeutic improvement are observed, she is continued on this medication through the manufacturer’s patient assistance program.
Within 3 months, Ms. S and her family find that she has improved significantly. She no longer reports hallucinatory experiences, is less guarded during sessions, and has followed through with paid and volunteer job applications and interviews. She soon finds a job teaching entry-level classes at a community college and is looking forward to a summer trip abroad.
During a follow-up appointment, Ms. S reports that she had missed 2 consecutive menstrual cycles without galactorrhea or fractures. A urine pregnancy test is negative; the prolactin level is 72 μg/L.
Hyperprolactinemia in women is defined as a plasma prolactin level of
a)>2.5 µg/L
b) >5 µg/L
c) >10 µg/L
d) >20 µg/L
e) >25 µg/L
The authors’ observations
A prolactin level >25 μg/L is considered abnormal.1 A level of >250 μg/L may identify a prolactinoma; however, levels >200 μg/L have been observed in patients taking an antipsychotic.1 Given Ms. S’s clinically significant elevation of prolactin, she is referred to her primary care physician. We decide to augment her regimen with aripiprazole, 10 mg/d, because this drug has been noted to help in cases of hyperprolactinemia associated with other antipsychotics.2,3
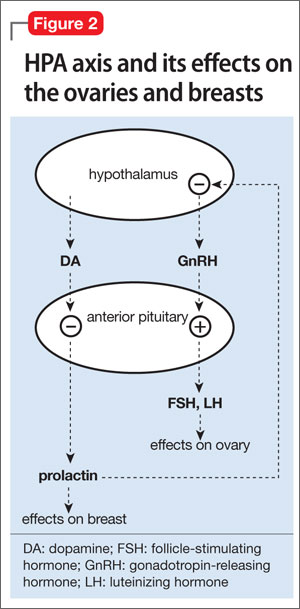
Prolactin serves several roles in the body, including but not limited to lactation, sexual gratification, proliferation of oligodendrocyte precursor cells, surfactant synthesis of fetal lungs at the end of pregnancy, and neurogenesis in maternal and fetal brains (Figure 1 and Figure 2). A 2004 review reported secondary amenorrhea, galactorrhea, and osteopenia as common symptoms of hyperprolactinemia.5 Hyperprolactinemia has been seen with most antipsychotics, both typical and atypical. Although several studies document prolactin elevation with risperidone, fewer have examined the active metabolite (9-hydroxyrisperidone) paliperidone.5-7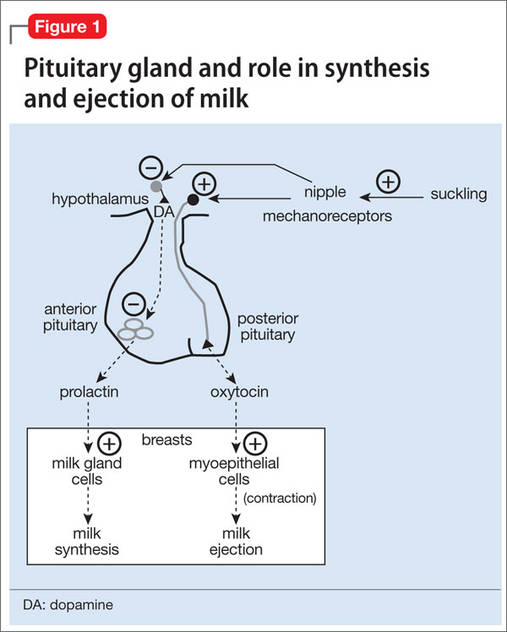
In women, a high prolactin level can cause
a) menstrual disturbance
b) galactorrhea
c) breast engorgement
d) sexual dysfunction
e) all of the above
The authors’ observations
Acutely, hyperprolactinemia can cause menstrual abnormalities, decreased libido, breast engorgement, galactorrhea, and sexual dysfunction in women.8 In men, the most common symptoms of hyperprolactinemia are loss of interest in sex, erectile dysfunction, infertility, and gynecomastia. Osteoporosis has been associated with chronic elevation of the prolactin level8 (Table).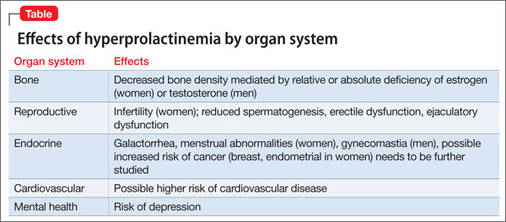
TREATMENT Adjunctive aripiprazole
After 8 weeks of adjunctive aripiprazole, Ms. S’s prolactin level decreases to 42 μg/L, but menses do not return. Because her family and primary care providers are eager to have the prolactin level return to normal, reducing her risk of complications, we decide to decrease paliperidone to 3 mg at bedtime.
Eight weeks later, Ms. S shows functional improvement. A repeat test of prolactin is 24 μg/L; she reports a 4-day period of spotting 1 week ago. One month later, the prolactin level is 21 μg/L, and she reports having a normal menstrual period. She continues treatment with paliperidone, 3 mg/d, and aripiprazole, 10 mg/d, experiences regular menses, and continues teaching.
Pharmacotherapy of hyperprolactinemia includes
a) haloperidol
b) perphenazine
c) bromocriptine
d) olanzapine
e) risperidone
The authors' observations
Our goal in treating Ms. S was to address her schizophrenia symptoms and improve her overall functioning. Often, finding an effective treatment can be challenging, and there is little evidence to support the efficacy of one antipsychotic over another.4 In Ms. S’s case, our care was stymied by the cost of medication, challenges related to delusions intrinsic to the illness (she refused clozapine because of required blood draws), and adverse effects. When Ms. S developed amenorrhea while taking paliperidone— the only medication that showed significant improvement in her psychotic symptoms—our goal was to maintain her functional level without significant long-term adverse effects.
Managing hyperprolactinemia
Management of iatrogenic hyperprolactinemia includes decreasing the dosage of the offending agent, using a prolactin-sparing antipsychotic, or initiating a dopamine agonist, such as bromocriptine or cabergoline, in addition to an antipsychotic.1,4 Aripiprazole is considered to be a prolactin-sparing agent because of its propensity to increase the prolactin level to less of a degree than what is seen with other antipsychotics; in fact, it has been shown to reduce an elevated prolactin level.9-11
Most typical and atypical antipsychotics are dopamine—specifically D2—receptor antagonists. These antipsychotics prevent dopamine from binding to the D2 receptor and from inhibiting prolactin release, therefore causing hyperprolactinemia. Aripiprazole differs from other antipsychotics: It is a partial D2 receptor agonist with high affinity, and therefore suppresses prolactin release.8 In a randomized controlled trial, aripiprazole had a lower rate of prolactin elevation compared with placebo.12
Aripiprazole’s ability to reduce an elevated prolactin level caused by other antipsychotics has been demonstrated in several studies with haloperidol,13 olanzapine,14,15 and risperidone.15-17 There has been 1 case report,18 but no controlled studies, of aripiprazole being used to decrease the prolactin level in patients treated with paliperidone.
In Ms. S’s case, adding aripiprazole, 10 mg/d, reduced her prolactin level by approximately 50%. Because several studies have shown that adjunctive aripiprazole with a D2 antagonist normalizes the prolactin level,19 it is reasonable to conclude that adding aripiprazole facilitated reduction of her prolactin level and might have continued to do so if given more time. Regrettably, because of patient and family concerns, paliperidone was reduced before this could be determined. It is unclear whether normalization of Ms. S’s prolactin level and return of her menstrual cycle was caused by adding aripiprazole or by reducing the dosage of paliperidone.
Although additional randomized controlled trials should be conducted on the utility of this approach, it is reasonable to consider augmentation with aripiprazole when treating a patient who is stable on an antipsychotic, including paliperidone, but has developed hyperprolactinemia secondary to treatment.
BOTTOM LINE
Hyperprolactinemia is a relatively common, underreported side effect of both typical and atypical antipsychotics. Paliperidone and risperidone have been shown to have the highest risk among the atypical antipsychotics; aripiprazole has the lowest risk. Treatment of an elevated prolactin level should include reduction or discontinuation of the offending agent and augmentation with aripiprazole.
Related Resources
• Peuskens J, Pani L, Detraux J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review [published online March 28, 2014]. CNS Drugs. doi: 10.1007/s40263-014-0157-3.
• Li X, Tang Y, Wang C. Adjunctive aripiprazole versus placebo for antipsychotic-induced hyperprolactinemia: meta-analysis of randomized controlled trials. PLoS One. 2013;8(8):e70179. doi: 10.1371/journal.pone.0070179.
Drug Brand Names
Aripiprazole • Abilify Haloperidol • Haldol
Benzatropine • Cogentin Olanzapine • Zyprexa
Bromocriptine • Parlodel Paliperidone • Invega
Cabergoline • Dostinex Perphenazine • Trilafon
Clozapine • Clozaril Risperidone • Risperdal
Fluphenazine • Prolixin
DisclosureThe authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273-288.
2. Madhusoodanan S, Parida S, Jimenez C. Hyperprolactinemia associated with psychotropics—a review. Hum Psychopharmacol. 2010;25(4):281-297.
3. Hanssens L, L’Italien G, Loze JY, et al. The effect of antipsychotic medication on sexual function and serum prolactin levels in community-treated schizophrenic patients: results from the Schizophrenia Trial of Aripiprazole (STAR) study (NCT00237913). BMC Psychiatry. 2008;8:95. doi: 10.1186/1471-244X-8-95.
4. Lieberman JA, Stroup TS, McEvoy JP, et al; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
5. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291-2314.
6. Knegtering R, Baselmans P, Castelein S, et al. Predominant role of the 9-hydroxy metabolite of risperidone in elevating blood prolactin levels. Am J Psychiatry. 2005;162(5): 1010-1012.
7. Berwaerts J, Cleton A, Rossenu S, et al. A comparison of serum prolactin concentrations after administration of paliperidone extended-release and risperidone tablets in patients with schizophrenia. J Psychopharmacol. 2010; 24(7):1011-1018.
8. Holt RI, Peveler RC. Antipsychotics and hyperprolactinaemia: mechanisms, consequences and management. Clin Endocrinol (Oxf). 2011;74(2):141-147.
9. Friberg LE, Vermeulen AM, Petersson KJ, et al. An agonist-antagonist interaction model for prolactin release following risperidone and paliperidone treatment. Clin Pharmacol Ther. 2009;85(4):409-417.
10. Skopek M, Manoj P. Hyperprolactinaemia during treatment with paliperidone. Australas Psychiatry. 2010; 18(3):261-263.
11. Aihara K, Shimada J, Miwa T, et al. The novel antipsychotic aripiprazole is a partial agonist at short and long isoforms of D2 receptors linked to the regulation of adenylyl cyclase activity and prolactin release. Brain Res. 2004;1003(1-2):9-17.
12. Bushe C, Shaw M, Peveler RC. A review of the association between antipsychotic use and hyperprolactinaemia. J Psychopharmacol. 2008;22(2 suppl):46-55.
13. Yasui-Furukori N, Furukori H, Sugawara N, et al. Dose-dependent effects of adjunctive treatment with aripiprazole on hyperprolactinemia induced by risperidone in female patients with schizophrenia. J Clin Psychopharmacol. 2010;30(5):596-599.
14. Lorenz RA, Weinstein B. Resolution of haloperidol-induced hyperprolactinemia with aripiprazole. J Clin Psychopharmacol. 2007;27(5):524-525.
15. Aggarwal A, Jain M, Garg A, et al. Aripiprazole for olanzapine-induced symptomatic hyper prolactinemia. Indian J Pharmacol. 2010;42(1):58-59.
16. Byerly MJ, Marcus RN, Tran QV, et al. Effects of aripiprazole on prolactin levels in subjects with schizophrenia during cross-titration with risperidone or olanzapine: analysis of a randomized, open-label study. Schizophr Res. 2009; 107(2-3):218-222.
17. Chen CK, Huang YS, Ree SC, et al. Differential add-on effects of aripiprazole in resolving hyperprolactinemia induced by risperidone in comparison to benzamide antipsychotics. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(8):1495-1499.
18. Chen CY, Lin TY, Wang CC, et al. Improvement of serum prolactin and sexual function after switching to aripiprazole from risperidone in schizophrenia: a case series. Psychiatry Clin Neurosci. 2011;65(1):95-97.
19. Rocha FL, Hara C, Ramos MG. Using aripiprazole to attenuate paliperidone-induced hyperprolactinemia. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(6):1153-1154.
CASE Paranoid and hallucinating
Ms. S, age 30, is an unmarried graduate student who has been given a diagnosis of schizophrenia, paranoid type, during inpatient hospitalization that was prompted by impairment in school functioning (difficulty turning in assignments, poor concentration, making careless mistakes on tests), paranoid delusions, and multisensory hallucinations. She says that her roommate and classmates are working together to make her leave school, and recalls seeing them “snare and smirk” as she passes by. Ms. S says that she feels her classmates are calling her names and talking badly about her as soon as she is out of sight.
Ms. S is antipsychotic-naïve and has a baseline body mass index of 17.8 kg/m2, indicating that she is underweight. We believe that olanzapine, 20 mg/d, is a good initial treatment because of its propensity for weight gain; however, she experiences only marginal improvement. Ms. S does not have health insurance, and cannot afford a brand name medication; therefore, she is cross-tapered to perphenazine, 8 mg, and benzatropine, 0.5 mg, both taken twice daily (olanzapine was not available as a generic at the time).
At discharge, Ms. S does not report any hallucinatory experiences, but is guarded, voices suspicions about the treatment team, and asks “What are they doing with all my blood?”—referring to blood draws for laboratory testing during hospitalization.
As an outpatient, Ms. S is continued on the same medications until she has to be switched because she cannot afford the out-of-pocket cost of the antipsychotic, perphenazine ($80 a month). Clozapine is recommended, but Ms. S refuses because of the mandatory weekly blood monitoring. She briefly tries fluphenazine, 2.5 mg/d, but it is discontinued because of malaise and lightheadedness without extrapyramidal symptoms.
Clozapine is again recommended, but Ms. S remains suspicious of the necessary blood draws and refuses. After several trials of antipsychotics, Ms. S starts paliperidone using samples from the clinic, titrated to 6 mg at bedtime. Once tolerance and therapeutic improvement are observed, she is continued on this medication through the manufacturer’s patient assistance program.
Within 3 months, Ms. S and her family find that she has improved significantly. She no longer reports hallucinatory experiences, is less guarded during sessions, and has followed through with paid and volunteer job applications and interviews. She soon finds a job teaching entry-level classes at a community college and is looking forward to a summer trip abroad.
During a follow-up appointment, Ms. S reports that she had missed 2 consecutive menstrual cycles without galactorrhea or fractures. A urine pregnancy test is negative; the prolactin level is 72 μg/L.
Hyperprolactinemia in women is defined as a plasma prolactin level of
a)>2.5 µg/L
b) >5 µg/L
c) >10 µg/L
d) >20 µg/L
e) >25 µg/L
The authors’ observations
A prolactin level >25 μg/L is considered abnormal.1 A level of >250 μg/L may identify a prolactinoma; however, levels >200 μg/L have been observed in patients taking an antipsychotic.1 Given Ms. S’s clinically significant elevation of prolactin, she is referred to her primary care physician. We decide to augment her regimen with aripiprazole, 10 mg/d, because this drug has been noted to help in cases of hyperprolactinemia associated with other antipsychotics.2,3
Prolactin serves several roles in the body, including but not limited to lactation, sexual gratification, proliferation of oligodendrocyte precursor cells, surfactant synthesis of fetal lungs at the end of pregnancy, and neurogenesis in maternal and fetal brains (Figure 1 and Figure 2). A 2004 review reported secondary amenorrhea, galactorrhea, and osteopenia as common symptoms of hyperprolactinemia.5 Hyperprolactinemia has been seen with most antipsychotics, both typical and atypical. Although several studies document prolactin elevation with risperidone, fewer have examined the active metabolite (9-hydroxyrisperidone) paliperidone.5-7
In women, a high prolactin level can cause
a) menstrual disturbance
b) galactorrhea
c) breast engorgement
d) sexual dysfunction
e) all of the above
The authors’ observations
Acutely, hyperprolactinemia can cause menstrual abnormalities, decreased libido, breast engorgement, galactorrhea, and sexual dysfunction in women.8 In men, the most common symptoms of hyperprolactinemia are loss of interest in sex, erectile dysfunction, infertility, and gynecomastia. Osteoporosis has been associated with chronic elevation of the prolactin level8 (Table).
TREATMENT Adjunctive aripiprazole
After 8 weeks of adjunctive aripiprazole, Ms. S’s prolactin level decreases to 42 μg/L, but menses do not return. Because her family and primary care providers are eager to have the prolactin level return to normal, reducing her risk of complications, we decide to decrease paliperidone to 3 mg at bedtime.
Eight weeks later, Ms. S shows functional improvement. A repeat test of prolactin is 24 μg/L; she reports a 4-day period of spotting 1 week ago. One month later, the prolactin level is 21 μg/L, and she reports having a normal menstrual period. She continues treatment with paliperidone, 3 mg/d, and aripiprazole, 10 mg/d, experiences regular menses, and continues teaching.
Pharmacotherapy of hyperprolactinemia includes
a) haloperidol
b) perphenazine
c) bromocriptine
d) olanzapine
e) risperidone
The authors' observations
Our goal in treating Ms. S was to address her schizophrenia symptoms and improve her overall functioning. Often, finding an effective treatment can be challenging, and there is little evidence to support the efficacy of one antipsychotic over another.4 In Ms. S’s case, our care was stymied by the cost of medication, challenges related to delusions intrinsic to the illness (she refused clozapine because of required blood draws), and adverse effects. When Ms. S developed amenorrhea while taking paliperidone— the only medication that showed significant improvement in her psychotic symptoms—our goal was to maintain her functional level without significant long-term adverse effects.
Managing hyperprolactinemia
Management of iatrogenic hyperprolactinemia includes decreasing the dosage of the offending agent, using a prolactin-sparing antipsychotic, or initiating a dopamine agonist, such as bromocriptine or cabergoline, in addition to an antipsychotic.1,4 Aripiprazole is considered to be a prolactin-sparing agent because of its propensity to increase the prolactin level to less of a degree than what is seen with other antipsychotics; in fact, it has been shown to reduce an elevated prolactin level.9-11
Most typical and atypical antipsychotics are dopamine—specifically D2—receptor antagonists. These antipsychotics prevent dopamine from binding to the D2 receptor and from inhibiting prolactin release, therefore causing hyperprolactinemia. Aripiprazole differs from other antipsychotics: It is a partial D2 receptor agonist with high affinity, and therefore suppresses prolactin release.8 In a randomized controlled trial, aripiprazole had a lower rate of prolactin elevation compared with placebo.12
Aripiprazole’s ability to reduce an elevated prolactin level caused by other antipsychotics has been demonstrated in several studies with haloperidol,13 olanzapine,14,15 and risperidone.15-17 There has been 1 case report,18 but no controlled studies, of aripiprazole being used to decrease the prolactin level in patients treated with paliperidone.
In Ms. S’s case, adding aripiprazole, 10 mg/d, reduced her prolactin level by approximately 50%. Because several studies have shown that adjunctive aripiprazole with a D2 antagonist normalizes the prolactin level,19 it is reasonable to conclude that adding aripiprazole facilitated reduction of her prolactin level and might have continued to do so if given more time. Regrettably, because of patient and family concerns, paliperidone was reduced before this could be determined. It is unclear whether normalization of Ms. S’s prolactin level and return of her menstrual cycle was caused by adding aripiprazole or by reducing the dosage of paliperidone.
Although additional randomized controlled trials should be conducted on the utility of this approach, it is reasonable to consider augmentation with aripiprazole when treating a patient who is stable on an antipsychotic, including paliperidone, but has developed hyperprolactinemia secondary to treatment.
BOTTOM LINE
Hyperprolactinemia is a relatively common, underreported side effect of both typical and atypical antipsychotics. Paliperidone and risperidone have been shown to have the highest risk among the atypical antipsychotics; aripiprazole has the lowest risk. Treatment of an elevated prolactin level should include reduction or discontinuation of the offending agent and augmentation with aripiprazole.
Related Resources
• Peuskens J, Pani L, Detraux J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review [published online March 28, 2014]. CNS Drugs. doi: 10.1007/s40263-014-0157-3.
• Li X, Tang Y, Wang C. Adjunctive aripiprazole versus placebo for antipsychotic-induced hyperprolactinemia: meta-analysis of randomized controlled trials. PLoS One. 2013;8(8):e70179. doi: 10.1371/journal.pone.0070179.
Drug Brand Names
Aripiprazole • Abilify Haloperidol • Haldol
Benzatropine • Cogentin Olanzapine • Zyprexa
Bromocriptine • Parlodel Paliperidone • Invega
Cabergoline • Dostinex Perphenazine • Trilafon
Clozapine • Clozaril Risperidone • Risperdal
Fluphenazine • Prolixin
DisclosureThe authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE Paranoid and hallucinating
Ms. S, age 30, is an unmarried graduate student who has been given a diagnosis of schizophrenia, paranoid type, during inpatient hospitalization that was prompted by impairment in school functioning (difficulty turning in assignments, poor concentration, making careless mistakes on tests), paranoid delusions, and multisensory hallucinations. She says that her roommate and classmates are working together to make her leave school, and recalls seeing them “snare and smirk” as she passes by. Ms. S says that she feels her classmates are calling her names and talking badly about her as soon as she is out of sight.
Ms. S is antipsychotic-naïve and has a baseline body mass index of 17.8 kg/m2, indicating that she is underweight. We believe that olanzapine, 20 mg/d, is a good initial treatment because of its propensity for weight gain; however, she experiences only marginal improvement. Ms. S does not have health insurance, and cannot afford a brand name medication; therefore, she is cross-tapered to perphenazine, 8 mg, and benzatropine, 0.5 mg, both taken twice daily (olanzapine was not available as a generic at the time).
At discharge, Ms. S does not report any hallucinatory experiences, but is guarded, voices suspicions about the treatment team, and asks “What are they doing with all my blood?”—referring to blood draws for laboratory testing during hospitalization.
As an outpatient, Ms. S is continued on the same medications until she has to be switched because she cannot afford the out-of-pocket cost of the antipsychotic, perphenazine ($80 a month). Clozapine is recommended, but Ms. S refuses because of the mandatory weekly blood monitoring. She briefly tries fluphenazine, 2.5 mg/d, but it is discontinued because of malaise and lightheadedness without extrapyramidal symptoms.
Clozapine is again recommended, but Ms. S remains suspicious of the necessary blood draws and refuses. After several trials of antipsychotics, Ms. S starts paliperidone using samples from the clinic, titrated to 6 mg at bedtime. Once tolerance and therapeutic improvement are observed, she is continued on this medication through the manufacturer’s patient assistance program.
Within 3 months, Ms. S and her family find that she has improved significantly. She no longer reports hallucinatory experiences, is less guarded during sessions, and has followed through with paid and volunteer job applications and interviews. She soon finds a job teaching entry-level classes at a community college and is looking forward to a summer trip abroad.
During a follow-up appointment, Ms. S reports that she had missed 2 consecutive menstrual cycles without galactorrhea or fractures. A urine pregnancy test is negative; the prolactin level is 72 μg/L.
Hyperprolactinemia in women is defined as a plasma prolactin level of
a)>2.5 µg/L
b) >5 µg/L
c) >10 µg/L
d) >20 µg/L
e) >25 µg/L
The authors’ observations
A prolactin level >25 μg/L is considered abnormal.1 A level of >250 μg/L may identify a prolactinoma; however, levels >200 μg/L have been observed in patients taking an antipsychotic.1 Given Ms. S’s clinically significant elevation of prolactin, she is referred to her primary care physician. We decide to augment her regimen with aripiprazole, 10 mg/d, because this drug has been noted to help in cases of hyperprolactinemia associated with other antipsychotics.2,3
Prolactin serves several roles in the body, including but not limited to lactation, sexual gratification, proliferation of oligodendrocyte precursor cells, surfactant synthesis of fetal lungs at the end of pregnancy, and neurogenesis in maternal and fetal brains (Figure 1 and Figure 2). A 2004 review reported secondary amenorrhea, galactorrhea, and osteopenia as common symptoms of hyperprolactinemia.5 Hyperprolactinemia has been seen with most antipsychotics, both typical and atypical. Although several studies document prolactin elevation with risperidone, fewer have examined the active metabolite (9-hydroxyrisperidone) paliperidone.5-7
In women, a high prolactin level can cause
a) menstrual disturbance
b) galactorrhea
c) breast engorgement
d) sexual dysfunction
e) all of the above
The authors’ observations
Acutely, hyperprolactinemia can cause menstrual abnormalities, decreased libido, breast engorgement, galactorrhea, and sexual dysfunction in women.8 In men, the most common symptoms of hyperprolactinemia are loss of interest in sex, erectile dysfunction, infertility, and gynecomastia. Osteoporosis has been associated with chronic elevation of the prolactin level8 (Table).
TREATMENT Adjunctive aripiprazole
After 8 weeks of adjunctive aripiprazole, Ms. S’s prolactin level decreases to 42 μg/L, but menses do not return. Because her family and primary care providers are eager to have the prolactin level return to normal, reducing her risk of complications, we decide to decrease paliperidone to 3 mg at bedtime.
Eight weeks later, Ms. S shows functional improvement. A repeat test of prolactin is 24 μg/L; she reports a 4-day period of spotting 1 week ago. One month later, the prolactin level is 21 μg/L, and she reports having a normal menstrual period. She continues treatment with paliperidone, 3 mg/d, and aripiprazole, 10 mg/d, experiences regular menses, and continues teaching.
Pharmacotherapy of hyperprolactinemia includes
a) haloperidol
b) perphenazine
c) bromocriptine
d) olanzapine
e) risperidone
The authors' observations
Our goal in treating Ms. S was to address her schizophrenia symptoms and improve her overall functioning. Often, finding an effective treatment can be challenging, and there is little evidence to support the efficacy of one antipsychotic over another.4 In Ms. S’s case, our care was stymied by the cost of medication, challenges related to delusions intrinsic to the illness (she refused clozapine because of required blood draws), and adverse effects. When Ms. S developed amenorrhea while taking paliperidone— the only medication that showed significant improvement in her psychotic symptoms—our goal was to maintain her functional level without significant long-term adverse effects.
Managing hyperprolactinemia
Management of iatrogenic hyperprolactinemia includes decreasing the dosage of the offending agent, using a prolactin-sparing antipsychotic, or initiating a dopamine agonist, such as bromocriptine or cabergoline, in addition to an antipsychotic.1,4 Aripiprazole is considered to be a prolactin-sparing agent because of its propensity to increase the prolactin level to less of a degree than what is seen with other antipsychotics; in fact, it has been shown to reduce an elevated prolactin level.9-11
Most typical and atypical antipsychotics are dopamine—specifically D2—receptor antagonists. These antipsychotics prevent dopamine from binding to the D2 receptor and from inhibiting prolactin release, therefore causing hyperprolactinemia. Aripiprazole differs from other antipsychotics: It is a partial D2 receptor agonist with high affinity, and therefore suppresses prolactin release.8 In a randomized controlled trial, aripiprazole had a lower rate of prolactin elevation compared with placebo.12
Aripiprazole’s ability to reduce an elevated prolactin level caused by other antipsychotics has been demonstrated in several studies with haloperidol,13 olanzapine,14,15 and risperidone.15-17 There has been 1 case report,18 but no controlled studies, of aripiprazole being used to decrease the prolactin level in patients treated with paliperidone.
In Ms. S’s case, adding aripiprazole, 10 mg/d, reduced her prolactin level by approximately 50%. Because several studies have shown that adjunctive aripiprazole with a D2 antagonist normalizes the prolactin level,19 it is reasonable to conclude that adding aripiprazole facilitated reduction of her prolactin level and might have continued to do so if given more time. Regrettably, because of patient and family concerns, paliperidone was reduced before this could be determined. It is unclear whether normalization of Ms. S’s prolactin level and return of her menstrual cycle was caused by adding aripiprazole or by reducing the dosage of paliperidone.
Although additional randomized controlled trials should be conducted on the utility of this approach, it is reasonable to consider augmentation with aripiprazole when treating a patient who is stable on an antipsychotic, including paliperidone, but has developed hyperprolactinemia secondary to treatment.
BOTTOM LINE
Hyperprolactinemia is a relatively common, underreported side effect of both typical and atypical antipsychotics. Paliperidone and risperidone have been shown to have the highest risk among the atypical antipsychotics; aripiprazole has the lowest risk. Treatment of an elevated prolactin level should include reduction or discontinuation of the offending agent and augmentation with aripiprazole.
Related Resources
• Peuskens J, Pani L, Detraux J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review [published online March 28, 2014]. CNS Drugs. doi: 10.1007/s40263-014-0157-3.
• Li X, Tang Y, Wang C. Adjunctive aripiprazole versus placebo for antipsychotic-induced hyperprolactinemia: meta-analysis of randomized controlled trials. PLoS One. 2013;8(8):e70179. doi: 10.1371/journal.pone.0070179.
Drug Brand Names
Aripiprazole • Abilify Haloperidol • Haldol
Benzatropine • Cogentin Olanzapine • Zyprexa
Bromocriptine • Parlodel Paliperidone • Invega
Cabergoline • Dostinex Perphenazine • Trilafon
Clozapine • Clozaril Risperidone • Risperdal
Fluphenazine • Prolixin
DisclosureThe authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273-288.
2. Madhusoodanan S, Parida S, Jimenez C. Hyperprolactinemia associated with psychotropics—a review. Hum Psychopharmacol. 2010;25(4):281-297.
3. Hanssens L, L’Italien G, Loze JY, et al. The effect of antipsychotic medication on sexual function and serum prolactin levels in community-treated schizophrenic patients: results from the Schizophrenia Trial of Aripiprazole (STAR) study (NCT00237913). BMC Psychiatry. 2008;8:95. doi: 10.1186/1471-244X-8-95.
4. Lieberman JA, Stroup TS, McEvoy JP, et al; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
5. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291-2314.
6. Knegtering R, Baselmans P, Castelein S, et al. Predominant role of the 9-hydroxy metabolite of risperidone in elevating blood prolactin levels. Am J Psychiatry. 2005;162(5): 1010-1012.
7. Berwaerts J, Cleton A, Rossenu S, et al. A comparison of serum prolactin concentrations after administration of paliperidone extended-release and risperidone tablets in patients with schizophrenia. J Psychopharmacol. 2010; 24(7):1011-1018.
8. Holt RI, Peveler RC. Antipsychotics and hyperprolactinaemia: mechanisms, consequences and management. Clin Endocrinol (Oxf). 2011;74(2):141-147.
9. Friberg LE, Vermeulen AM, Petersson KJ, et al. An agonist-antagonist interaction model for prolactin release following risperidone and paliperidone treatment. Clin Pharmacol Ther. 2009;85(4):409-417.
10. Skopek M, Manoj P. Hyperprolactinaemia during treatment with paliperidone. Australas Psychiatry. 2010; 18(3):261-263.
11. Aihara K, Shimada J, Miwa T, et al. The novel antipsychotic aripiprazole is a partial agonist at short and long isoforms of D2 receptors linked to the regulation of adenylyl cyclase activity and prolactin release. Brain Res. 2004;1003(1-2):9-17.
12. Bushe C, Shaw M, Peveler RC. A review of the association between antipsychotic use and hyperprolactinaemia. J Psychopharmacol. 2008;22(2 suppl):46-55.
13. Yasui-Furukori N, Furukori H, Sugawara N, et al. Dose-dependent effects of adjunctive treatment with aripiprazole on hyperprolactinemia induced by risperidone in female patients with schizophrenia. J Clin Psychopharmacol. 2010;30(5):596-599.
14. Lorenz RA, Weinstein B. Resolution of haloperidol-induced hyperprolactinemia with aripiprazole. J Clin Psychopharmacol. 2007;27(5):524-525.
15. Aggarwal A, Jain M, Garg A, et al. Aripiprazole for olanzapine-induced symptomatic hyper prolactinemia. Indian J Pharmacol. 2010;42(1):58-59.
16. Byerly MJ, Marcus RN, Tran QV, et al. Effects of aripiprazole on prolactin levels in subjects with schizophrenia during cross-titration with risperidone or olanzapine: analysis of a randomized, open-label study. Schizophr Res. 2009; 107(2-3):218-222.
17. Chen CK, Huang YS, Ree SC, et al. Differential add-on effects of aripiprazole in resolving hyperprolactinemia induced by risperidone in comparison to benzamide antipsychotics. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(8):1495-1499.
18. Chen CY, Lin TY, Wang CC, et al. Improvement of serum prolactin and sexual function after switching to aripiprazole from risperidone in schizophrenia: a case series. Psychiatry Clin Neurosci. 2011;65(1):95-97.
19. Rocha FL, Hara C, Ramos MG. Using aripiprazole to attenuate paliperidone-induced hyperprolactinemia. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(6):1153-1154.
1. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273-288.
2. Madhusoodanan S, Parida S, Jimenez C. Hyperprolactinemia associated with psychotropics—a review. Hum Psychopharmacol. 2010;25(4):281-297.
3. Hanssens L, L’Italien G, Loze JY, et al. The effect of antipsychotic medication on sexual function and serum prolactin levels in community-treated schizophrenic patients: results from the Schizophrenia Trial of Aripiprazole (STAR) study (NCT00237913). BMC Psychiatry. 2008;8:95. doi: 10.1186/1471-244X-8-95.
4. Lieberman JA, Stroup TS, McEvoy JP, et al; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
5. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291-2314.
6. Knegtering R, Baselmans P, Castelein S, et al. Predominant role of the 9-hydroxy metabolite of risperidone in elevating blood prolactin levels. Am J Psychiatry. 2005;162(5): 1010-1012.
7. Berwaerts J, Cleton A, Rossenu S, et al. A comparison of serum prolactin concentrations after administration of paliperidone extended-release and risperidone tablets in patients with schizophrenia. J Psychopharmacol. 2010; 24(7):1011-1018.
8. Holt RI, Peveler RC. Antipsychotics and hyperprolactinaemia: mechanisms, consequences and management. Clin Endocrinol (Oxf). 2011;74(2):141-147.
9. Friberg LE, Vermeulen AM, Petersson KJ, et al. An agonist-antagonist interaction model for prolactin release following risperidone and paliperidone treatment. Clin Pharmacol Ther. 2009;85(4):409-417.
10. Skopek M, Manoj P. Hyperprolactinaemia during treatment with paliperidone. Australas Psychiatry. 2010; 18(3):261-263.
11. Aihara K, Shimada J, Miwa T, et al. The novel antipsychotic aripiprazole is a partial agonist at short and long isoforms of D2 receptors linked to the regulation of adenylyl cyclase activity and prolactin release. Brain Res. 2004;1003(1-2):9-17.
12. Bushe C, Shaw M, Peveler RC. A review of the association between antipsychotic use and hyperprolactinaemia. J Psychopharmacol. 2008;22(2 suppl):46-55.
13. Yasui-Furukori N, Furukori H, Sugawara N, et al. Dose-dependent effects of adjunctive treatment with aripiprazole on hyperprolactinemia induced by risperidone in female patients with schizophrenia. J Clin Psychopharmacol. 2010;30(5):596-599.
14. Lorenz RA, Weinstein B. Resolution of haloperidol-induced hyperprolactinemia with aripiprazole. J Clin Psychopharmacol. 2007;27(5):524-525.
15. Aggarwal A, Jain M, Garg A, et al. Aripiprazole for olanzapine-induced symptomatic hyper prolactinemia. Indian J Pharmacol. 2010;42(1):58-59.
16. Byerly MJ, Marcus RN, Tran QV, et al. Effects of aripiprazole on prolactin levels in subjects with schizophrenia during cross-titration with risperidone or olanzapine: analysis of a randomized, open-label study. Schizophr Res. 2009; 107(2-3):218-222.
17. Chen CK, Huang YS, Ree SC, et al. Differential add-on effects of aripiprazole in resolving hyperprolactinemia induced by risperidone in comparison to benzamide antipsychotics. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(8):1495-1499.
18. Chen CY, Lin TY, Wang CC, et al. Improvement of serum prolactin and sexual function after switching to aripiprazole from risperidone in schizophrenia: a case series. Psychiatry Clin Neurosci. 2011;65(1):95-97.
19. Rocha FL, Hara C, Ramos MG. Using aripiprazole to attenuate paliperidone-induced hyperprolactinemia. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(6):1153-1154.
100 years of solicitude: Do global traumatic events have a transgenerational effect?
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
Yet, important questions about the impact of these events have not been asked: Can there be a transgenerational neurobiological effect on the children and grandchildren of people who have been subjected to life-threatening, traumatic societal events? Could the psychobiology of widespread anxiety and worry (solicitude) be experienced not only by the generation that witnessed and lived through those devastating events, but also by their progeny, who were not yet born during the traumatic events? And could there be epigenetic consequences on a large scale, producing a generation that shares traits induced by the trauma experienced by the previous generation?
Did the rise of delinquency in the 1950s, followed by the anti-war rebellion, unprecedented sexual promiscuity, and substance abuse of the 1960s, be the result of genetic changes in the previous generation induced by living through World War II—after which the generation that grew up in the 1960s was born?
In the late Gabriel García Márquez’s masterpiece novel, One Hundred Years of Solitude, the 1982 Nobel Laureate’s chronicle of the Buendía family across 7 generations is replete with dark and insalubrious events. The fictional family’s story is considered a metaphor for the tumultuous evolution of Márquez’s native Colombia, but that story is consistent with the concept of transgenerational transmission of the biologic effects of stress, as each generation of the Buendía family manifests unusual, even pathological behaviors.
One hundred years of alarm, panic, and anxiety
Psychiatrists are keenly aware of the impact of stressful events on their patients’ mood and behavior, and of the association of life-threatening events with posttraumatic stress disorder (PTSD). For persons who suffer the generalized anxiety of PTSD, further stressful life events can aggravate their condition and result in additional anxiety and solicitude.
It is not surprising that anxiety has been documented as the most common psychiatric condition in the United States.1 Consider the variety of perturbations that have induced alarm, panic, fear, and simmering anxiety on a global scale over the past 100 years— starting with World War I, exactly a century ago.
War. The ruinous 4-year Great War was followed 20 years later by World War II, which caused tens of millions of casualties and the annihilation of Hiroshima and Nagasaki by the atomic bomb— escalating fear of nuclear warfare and radiation poisoning for decades to come. Add to that the Korean War, the Vietnam conflict, the First Gulf War, and the Iraq and Afghanistan wars. The war fatigue and mental exhaustion of the population are palpable.
Economic upheaval. After the Stock Market Crash of 1929 came the Great Depression, the recessions of the 1970s and early 1980s, another stock market crash in 1987, and, most recently, the financial crisis of 2008. Millions saw their wealth wiped out and their livelihoods disrupted, exerting enormous life-changing stresses on countless families.
Disasters. The sinking of the Titanic in 1912, the crash of the Hindenburg, the Three Mile Island nuclear accident, the meltdown of the Chernobyl and Fukushima Daiichi reactors, the space shuttle disasters, and the 9/11 terrorist attacks—all these trigger and perpetuate fear and worry about the one’s own, and one’s loved ones, abrupt and premature mortality.
Epidemics. Millions died in the 1918 influenza pandemic, prompting widespread societal fears that re-intensified during subsequent epidemics: polio in the 1950s, swine flu in the 1970s, SARS (severe acute respiratory syndrome) in the 1990s, West Nile Virus, and avian influenza.
Assassination. The shooting of Archduke Franz Ferdinand of Austria sparked World War I a century ago, but what baby boomers, such as me, vividly remember is our angst over the assassinations of President John F. Kennedy, his brother Robert, and Rev. Dr. Martin Luther King, Jr; the attempted assassination of President Ronald Reagan; and the murder of John Lennon. Each assassination leaves a communal scar on millions, forever reminding them of the ephemeral nature of life at any rung of the social ladder.
Mass murder. The past 100 years began with the Armenian genocide in 1918, followed by the Holocaust of World War II, the Munich Olympics killings, the Jonestown massacre, the Oklahoma City bombing, and, to name a few, the mass murders at Columbine, Virginia Tech, Newtown, and Fort Hood.
Natural disasters can wreak havoc on peoples’ lives. Consider the annual tally of hurricanes (a long list, some—such as Katrina and Sandy—more infamous than others). Add to those storms the earthquakes, tsunamis, erupting volcanoes, floods, and blizzards, and the result is suffering and anxiety on a massive scale, even among those who are not affected directly.
A surprising facet of these disquieting events is the resiliency of people. Life goes on, despite the agony, despair, and solicitude instigated by deadly events. But of those who buckle under the weight of adversity, many end up in a psychiatric clinic or hospital, and are disabled by their symptoms.
Even ‘good’ change can be disquieting
Juxtaposed against these awful events are 100 years of an array of positive, uplifting discoveries, inventions, and medical advances that have completely transformed our lives. Consider: electricity, clean water, women’s right to vote, automobiles, air and space travel, air conditioning, and highway systems; the momentous discoveries of penicillin, antipsychotics, antidepressants, and mood stabilizers; television, the telephone (evolving from dumb to smart), vaccines, oral contraceptives, genetic discoveries, brain imaging technology, and home appliances (refrigerators, microwave ovens, dishwashers); and not at all least, personal computers and the Internet.
But even these advances can generate anxiety and solicitude: Fear of flying, anyone? Embarrassment about a selfie gone viral on the Web? Worry about being a carrier of a breast cancer gene? Claustrophobia inside an MRI scanner?
Hypothesizing about the transfer of anxiety
Could PTSD and solicitude in one generation be transmitted to the next via epigenetic mechanisms (that is, by over-expression or silencing of genes involved in brain development) and could this transmission result in unusual wide-scale stress reactivity? Might this be an example of the infamous Lamarckian “inheritance of acquired characteristics” at the molecular genetic level, in which the anxiety of traumatized parents is transmitted to their offspring? Or could transmission be mediated by being reared in the emotionally oppressive environment of a family still reeling from the effects of war, disaster, and mass murder?
Such questions might sound rhetorical, but they present a reasonable hypothesis that can be answered by research. Findings from animal studies suggest that such a phenomenon might occur in humans.2 If those findings are validated, opportunities for preventing societal solicitude might emerge.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
1. Robins LN, Regier DA, eds. Psychiatric disorders in America: The Epidemiologic Catchment Area Study. New York, New York: The Free Press; 1991.
2. Rechavi O, Minevich G, Hobert O. Transgenerational inheritance of an acquired small RNA-based antiviral response in C. elegans. Cell. 2011;147(6):1248-1256.
HDAC inhibitors aid expansion of HSCs from cord blood

Credit: NHS
New research suggests that histone deacetylase (HDAC) inhibitors can be used to expand hematopoietic stem cells (HSCs) isolated from cord blood.
Investigators found that valproic acid (VPA), in particular, could greatly expand HSCs from cord blood.
These HSCs expressed markers of pluripotency and were more efficient than conventionally expanded HSCs in repopulating the bone marrow and establishing hematopoiesis in immune-deficient mice.
Pratima Chaurasia, PhD, of the Mount Sinai School of Medicine in New York, and colleagues reported these results in The Journal of Clinical Investigation.
For several decades, investigators have used a variety of strategies to expand the numbers of HSCs isolated from cord blood, with limited success. Evidence has suggested the accumulation of epigenetic modifications influences preservation of stem-cell characteristics in HSC daughter cells.
So Dr Chaurasia’s group tested the effects of HDAC inhibitors on CD34+ cells derived from cord blood. The team primed the cells for 16 hours with cytokines, then treated the cells for 7 days, with or without additional cytokines and in the presence or absence of HDAC inhibitors.
The inhibitors included VPA, scriptaid (SCR), trichostatin A, suberoylanilide hydroxamic acid, CAY10433 (C433), CAY10398, and CAY10603 .
VPA, SCR, and C433 were the most active inhibitors. Treatment with these agents led to a similar percentage of CD34+CD90+ cells—75.2% ± 10.7%, 73.4% ± 13.9%, and 70.1% ± 18.4%, respectively—which was significantly higher than control conditions—16.2% ± 9.2% (P<0.0001).
VPA, SCR, and C433 also generated a greater absolute number of CD34+ and CD34+CD90+ cells per cord blood collection, when compared to control conditions (P≤0.0007). And the inhibitors generated a greater absolute number of CD34+CD90+CD184+ cells (P<0.0001)
The investigators conducted subsequent experiments with VPA only. And they found that VPA was more effective under serum-free conditions and in the presence of cytokines.
Additional experiments revealed that VPA influences the expression of pluripotency genes—SOX2, OCT4, and NANOG. And these genes proved essential for the expansion of CD34+ CD90+ cells.
Lastly, the investigators tested VPA-expanded cells by transplanting them into immune-deficient mice. The cells were more efficient than conventionally expanded cord blood HSCs in repopulating the bone marrow and establishing hematopoietic populations.
Specifically, at 13 to 14 weeks after transplant, VPA-treated cord blood CD34+ cells resulted in a greater degree of human CD45+ cell chimerism—32.2% ± 11.3%—when compared to primary cord blood CD34+ cells—19.4% ± 4.9%—and to cells from control cultures—13.2% ± 6.4% (P=0.006 and P=0.0008, respectively).
The investigators evaluated the self-renewal potential of the expanded grafts by transplanting donor-derived cells from primary recipients into secondary recipients.
After 15 to 16 weeks, the secondary recipients transplanted with VPA-treated cord blood CD34+ cells had achieved the greatest degree of human CD45+ cell chimerism, compared to primary cord blood CD34+ cells and cells from control cultures (P<0.0001).
The team also noted that the VPA-treated cells belonged to multiple hematopoietic lineages. And this pattern was distinct from that observed in mice that had received primary cord blood CD34+ cells or cells from control cultures (P<0.0001).
In addition, the VPA-treated HSCs did not cause hematologic malignancies or teratomas in the mice.
The investigators said these results suggest that cord blood cells can be epigenetically reprogrammed by VPA to generate greater numbers of functional HSCs for transplantation.
In a related commentary, Hal Broxmeyer, PhD, of the Indiana University School of Medicine in Indianapolis, discussed how these findings enhance our understanding of HSC function and could potentially provide clinical benefit. ![]()
Credit: NHS
New research suggests that histone deacetylase (HDAC) inhibitors can be used to expand hematopoietic stem cells (HSCs) isolated from cord blood.
Investigators found that valproic acid (VPA), in particular, could greatly expand HSCs from cord blood.
These HSCs expressed markers of pluripotency and were more efficient than conventionally expanded HSCs in repopulating the bone marrow and establishing hematopoiesis in immune-deficient mice.
Pratima Chaurasia, PhD, of the Mount Sinai School of Medicine in New York, and colleagues reported these results in The Journal of Clinical Investigation.
For several decades, investigators have used a variety of strategies to expand the numbers of HSCs isolated from cord blood, with limited success. Evidence has suggested the accumulation of epigenetic modifications influences preservation of stem-cell characteristics in HSC daughter cells.
So Dr Chaurasia’s group tested the effects of HDAC inhibitors on CD34+ cells derived from cord blood. The team primed the cells for 16 hours with cytokines, then treated the cells for 7 days, with or without additional cytokines and in the presence or absence of HDAC inhibitors.
The inhibitors included VPA, scriptaid (SCR), trichostatin A, suberoylanilide hydroxamic acid, CAY10433 (C433), CAY10398, and CAY10603 .
VPA, SCR, and C433 were the most active inhibitors. Treatment with these agents led to a similar percentage of CD34+CD90+ cells—75.2% ± 10.7%, 73.4% ± 13.9%, and 70.1% ± 18.4%, respectively—which was significantly higher than control conditions—16.2% ± 9.2% (P<0.0001).
VPA, SCR, and C433 also generated a greater absolute number of CD34+ and CD34+CD90+ cells per cord blood collection, when compared to control conditions (P≤0.0007). And the inhibitors generated a greater absolute number of CD34+CD90+CD184+ cells (P<0.0001)
The investigators conducted subsequent experiments with VPA only. And they found that VPA was more effective under serum-free conditions and in the presence of cytokines.
Additional experiments revealed that VPA influences the expression of pluripotency genes—SOX2, OCT4, and NANOG. And these genes proved essential for the expansion of CD34+ CD90+ cells.
Lastly, the investigators tested VPA-expanded cells by transplanting them into immune-deficient mice. The cells were more efficient than conventionally expanded cord blood HSCs in repopulating the bone marrow and establishing hematopoietic populations.
Specifically, at 13 to 14 weeks after transplant, VPA-treated cord blood CD34+ cells resulted in a greater degree of human CD45+ cell chimerism—32.2% ± 11.3%—when compared to primary cord blood CD34+ cells—19.4% ± 4.9%—and to cells from control cultures—13.2% ± 6.4% (P=0.006 and P=0.0008, respectively).
The investigators evaluated the self-renewal potential of the expanded grafts by transplanting donor-derived cells from primary recipients into secondary recipients.
After 15 to 16 weeks, the secondary recipients transplanted with VPA-treated cord blood CD34+ cells had achieved the greatest degree of human CD45+ cell chimerism, compared to primary cord blood CD34+ cells and cells from control cultures (P<0.0001).
The team also noted that the VPA-treated cells belonged to multiple hematopoietic lineages. And this pattern was distinct from that observed in mice that had received primary cord blood CD34+ cells or cells from control cultures (P<0.0001).
In addition, the VPA-treated HSCs did not cause hematologic malignancies or teratomas in the mice.
The investigators said these results suggest that cord blood cells can be epigenetically reprogrammed by VPA to generate greater numbers of functional HSCs for transplantation.
In a related commentary, Hal Broxmeyer, PhD, of the Indiana University School of Medicine in Indianapolis, discussed how these findings enhance our understanding of HSC function and could potentially provide clinical benefit. ![]()
Credit: NHS
New research suggests that histone deacetylase (HDAC) inhibitors can be used to expand hematopoietic stem cells (HSCs) isolated from cord blood.
Investigators found that valproic acid (VPA), in particular, could greatly expand HSCs from cord blood.
These HSCs expressed markers of pluripotency and were more efficient than conventionally expanded HSCs in repopulating the bone marrow and establishing hematopoiesis in immune-deficient mice.
Pratima Chaurasia, PhD, of the Mount Sinai School of Medicine in New York, and colleagues reported these results in The Journal of Clinical Investigation.
For several decades, investigators have used a variety of strategies to expand the numbers of HSCs isolated from cord blood, with limited success. Evidence has suggested the accumulation of epigenetic modifications influences preservation of stem-cell characteristics in HSC daughter cells.
So Dr Chaurasia’s group tested the effects of HDAC inhibitors on CD34+ cells derived from cord blood. The team primed the cells for 16 hours with cytokines, then treated the cells for 7 days, with or without additional cytokines and in the presence or absence of HDAC inhibitors.
The inhibitors included VPA, scriptaid (SCR), trichostatin A, suberoylanilide hydroxamic acid, CAY10433 (C433), CAY10398, and CAY10603 .
VPA, SCR, and C433 were the most active inhibitors. Treatment with these agents led to a similar percentage of CD34+CD90+ cells—75.2% ± 10.7%, 73.4% ± 13.9%, and 70.1% ± 18.4%, respectively—which was significantly higher than control conditions—16.2% ± 9.2% (P<0.0001).
VPA, SCR, and C433 also generated a greater absolute number of CD34+ and CD34+CD90+ cells per cord blood collection, when compared to control conditions (P≤0.0007). And the inhibitors generated a greater absolute number of CD34+CD90+CD184+ cells (P<0.0001)
The investigators conducted subsequent experiments with VPA only. And they found that VPA was more effective under serum-free conditions and in the presence of cytokines.
Additional experiments revealed that VPA influences the expression of pluripotency genes—SOX2, OCT4, and NANOG. And these genes proved essential for the expansion of CD34+ CD90+ cells.
Lastly, the investigators tested VPA-expanded cells by transplanting them into immune-deficient mice. The cells were more efficient than conventionally expanded cord blood HSCs in repopulating the bone marrow and establishing hematopoietic populations.
Specifically, at 13 to 14 weeks after transplant, VPA-treated cord blood CD34+ cells resulted in a greater degree of human CD45+ cell chimerism—32.2% ± 11.3%—when compared to primary cord blood CD34+ cells—19.4% ± 4.9%—and to cells from control cultures—13.2% ± 6.4% (P=0.006 and P=0.0008, respectively).
The investigators evaluated the self-renewal potential of the expanded grafts by transplanting donor-derived cells from primary recipients into secondary recipients.
After 15 to 16 weeks, the secondary recipients transplanted with VPA-treated cord blood CD34+ cells had achieved the greatest degree of human CD45+ cell chimerism, compared to primary cord blood CD34+ cells and cells from control cultures (P<0.0001).
The team also noted that the VPA-treated cells belonged to multiple hematopoietic lineages. And this pattern was distinct from that observed in mice that had received primary cord blood CD34+ cells or cells from control cultures (P<0.0001).
In addition, the VPA-treated HSCs did not cause hematologic malignancies or teratomas in the mice.
The investigators said these results suggest that cord blood cells can be epigenetically reprogrammed by VPA to generate greater numbers of functional HSCs for transplantation.
In a related commentary, Hal Broxmeyer, PhD, of the Indiana University School of Medicine in Indianapolis, discussed how these findings enhance our understanding of HSC function and could potentially provide clinical benefit. ![]()
Tracking protein movement to improve patient monitoring, drug development

Credit: Virginia Tech
A novel technique that can detect the subcellular location of a protein may help improve the study of therapies for cancer and other diseases, according to a paper published in Chemical Science.
“Modulation of protein transport inside a cell is practiced as an important therapeutic approach for cancer treatment,” explained Chang Lu, PhD, of Virginia Tech in Blacksburg.
“The subcellular location of a target protein can also serve as a useful read-out for high-content screening of cancer drugs.”
With that in mind, Dr Lu and his colleagues set out to develop a simple and accessible protein detection method that can rapidly screen a large cell population and offers single-cell resolution.
Dr Lu noted that such techniques have been seriously lacking. For instance, fluorescence microscopy can only be used to analyze a limited number of cells.
And data collected by subcellular fractionation only reflects the average properties of the cell populations without revealing the heterogeneity that often exists among cells that seem identical.
Dr Lu and his colleagues had previously made some progress in screening cell populations using an electroporation-based technique, but it did not allow for the examination of native proteins and primary cells isolated from animals and from patients.
Their new work uses a method that “incorporates selective chemical release of cytosolic proteins with a standard procedure for fluorescent labeling of the protein,” Dr Lu said.
This simple tweak to the conventional cell-staining process allowed the researchers to pinpoint the subcellular location of the protein by measuring the amount of the residual protein after release. Using a flow cytometer, the speed of such measurement could reach 10,000 to 100,000 cells per second.
A key ingredient for the team’s process is saponin, an amphipathic glycoside. Saponin dissolves cholesterol and permeates the plasma membrane to allow protein release. And it “shows minimal effects on the state of the cell,” Dr Lu said. ![]()
Credit: Virginia Tech
A novel technique that can detect the subcellular location of a protein may help improve the study of therapies for cancer and other diseases, according to a paper published in Chemical Science.
“Modulation of protein transport inside a cell is practiced as an important therapeutic approach for cancer treatment,” explained Chang Lu, PhD, of Virginia Tech in Blacksburg.
“The subcellular location of a target protein can also serve as a useful read-out for high-content screening of cancer drugs.”
With that in mind, Dr Lu and his colleagues set out to develop a simple and accessible protein detection method that can rapidly screen a large cell population and offers single-cell resolution.
Dr Lu noted that such techniques have been seriously lacking. For instance, fluorescence microscopy can only be used to analyze a limited number of cells.
And data collected by subcellular fractionation only reflects the average properties of the cell populations without revealing the heterogeneity that often exists among cells that seem identical.
Dr Lu and his colleagues had previously made some progress in screening cell populations using an electroporation-based technique, but it did not allow for the examination of native proteins and primary cells isolated from animals and from patients.
Their new work uses a method that “incorporates selective chemical release of cytosolic proteins with a standard procedure for fluorescent labeling of the protein,” Dr Lu said.
This simple tweak to the conventional cell-staining process allowed the researchers to pinpoint the subcellular location of the protein by measuring the amount of the residual protein after release. Using a flow cytometer, the speed of such measurement could reach 10,000 to 100,000 cells per second.
A key ingredient for the team’s process is saponin, an amphipathic glycoside. Saponin dissolves cholesterol and permeates the plasma membrane to allow protein release. And it “shows minimal effects on the state of the cell,” Dr Lu said. ![]()
Credit: Virginia Tech
A novel technique that can detect the subcellular location of a protein may help improve the study of therapies for cancer and other diseases, according to a paper published in Chemical Science.
“Modulation of protein transport inside a cell is practiced as an important therapeutic approach for cancer treatment,” explained Chang Lu, PhD, of Virginia Tech in Blacksburg.
“The subcellular location of a target protein can also serve as a useful read-out for high-content screening of cancer drugs.”
With that in mind, Dr Lu and his colleagues set out to develop a simple and accessible protein detection method that can rapidly screen a large cell population and offers single-cell resolution.
Dr Lu noted that such techniques have been seriously lacking. For instance, fluorescence microscopy can only be used to analyze a limited number of cells.
And data collected by subcellular fractionation only reflects the average properties of the cell populations without revealing the heterogeneity that often exists among cells that seem identical.
Dr Lu and his colleagues had previously made some progress in screening cell populations using an electroporation-based technique, but it did not allow for the examination of native proteins and primary cells isolated from animals and from patients.
Their new work uses a method that “incorporates selective chemical release of cytosolic proteins with a standard procedure for fluorescent labeling of the protein,” Dr Lu said.
This simple tweak to the conventional cell-staining process allowed the researchers to pinpoint the subcellular location of the protein by measuring the amount of the residual protein after release. Using a flow cytometer, the speed of such measurement could reach 10,000 to 100,000 cells per second.
A key ingredient for the team’s process is saponin, an amphipathic glycoside. Saponin dissolves cholesterol and permeates the plasma membrane to allow protein release. And it “shows minimal effects on the state of the cell,” Dr Lu said. ![]()
New insight into PTEN’s role in cancers
Researchers say they’ve uncovered new details that help explain how the PTEN gene exerts its anticancer effects and how PTEN loss or alteration can set cells on a cancerous course.
The team’s study, published in Cell, reveals that PTEN loss and PTEN mutations are not synonymous.
This discovery provides additional insight into basic tumor biology and offers a potential new direction in the pursuit of cancer therapies, according to the researchers.
“By characterizing the ways that 2 specific PTEN mutations regulate the tumor suppressor function of the normal PTEN protein, our findings suggest that different PTEN mutations contribute to tumorigenesis by regulating different aspects of PTEN biology,” said study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center in Boston.
“It has been suggested that cancer patients harboring mutations in PTEN had poorer outcomes than cancer patients with PTEN loss. Now, using mouse modeling, we are able to demonstrate that this is indeed the case. Because PTEN mutations are extremely frequent in various types of tumors, this discovery could help pave the way for a new level of personalized cancer treatment.”
Several of the proteins that PTEN acts upon, both lipids and proteins, are known to promote cancer when bound to a phosphate. Consequently, when PTEN removes their phosphates, it is acting as a tumor suppressor to prevent cancer. When PTEN is mutated, it loses this suppressive ability, and the cancer-promoting proteins are left intact and uninhibited.
This new study showed that the PTEN mutant protein is not only functionally impaired, it also acquires the ability to affect the function of normal PTEN proteins, thereby gaining a pro-tumorigenic function. But the researchers also wanted to determine the difference between PTEN mutation and PTEN loss.
“We wanted to know, would outcomes differ in cases when PTEN was not expressed, compared with cases when PTEN was expressed but encoded a mutation within its sequence?” said study author Antonella Papa, PhD, an investigator in the Pandolfi lab.
To find out, the team created several genetically modified strains of mice to mimic the PTEN mutations found in human cancer patients.
“All mice [and humans] have 2 copies of the PTEN gene,” Dr Papa explained. “The genetically modified mice in our study had 1 copy of the PTEN gene that contained a cancer-associated mutation [either PTENC124S or PTENG129E] and 1 normal copy of PTEN. Other mice in the study had only 1 copy of the normal PTEN gene, and the second copy was removed.”
The researchers found that the mice with a single mutated copy of PTEN were more tumor-prone than the mice with a deleted copy of PTEN. They also discovered that the mutated protein that was produced by PTENC124S or PTENG129E was binding to and inhibiting the PTEN protein made from the normal copy of the PTEN gene.
“This was very surprising, as we were expecting a reduction in tumorigenesis,” Dr Papa said. “Instead, mechanistically, we found that PTEN exists as a dimer, and, in this new conformation, the mutated protein prevents the normal protein from functioning.”
At the molecular level, this generates an increased activation of a PTEN target—the protein Akt—which is what leads to the augmented tumorigenesis in the mice. Akt is part of a signaling pathway that regulates cell growth, division and metabolism.
When PTEN is prevented from inhibiting Akt, the pathway becomes overactive. As a result, targeting Akt and its pathway may be an effective treatment strategy for patients with PTEN mutations, the researchers said, adding that inhibitors to affect this pathway are currently being tested and developed.
“This defines a new working model for the function and regulation of PTEN and tells us that PTEN mutational status can be used to determine which cancer patients might benefit from earlier and more radical therapeutic interventions and, ultimately, better prognosis,” Dr Pandolfi said.
“Our findings may help to better identify and stratify patients and their response to treatment based on the different genetic alterations found in the PTEN gene. Importantly, our study shows that cancer therapy should be tailored on the basis of the very specific type of mutations that the tumor harbors.”
“This adds a new layer of complexity but also a new opportunity for precision medicine. I would say that, based on these thorough genetic analyses, this story represents the ultimate example of why personalized cancer medicine is so urgently needed.” ![]()
Researchers say they’ve uncovered new details that help explain how the PTEN gene exerts its anticancer effects and how PTEN loss or alteration can set cells on a cancerous course.
The team’s study, published in Cell, reveals that PTEN loss and PTEN mutations are not synonymous.
This discovery provides additional insight into basic tumor biology and offers a potential new direction in the pursuit of cancer therapies, according to the researchers.
“By characterizing the ways that 2 specific PTEN mutations regulate the tumor suppressor function of the normal PTEN protein, our findings suggest that different PTEN mutations contribute to tumorigenesis by regulating different aspects of PTEN biology,” said study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center in Boston.
“It has been suggested that cancer patients harboring mutations in PTEN had poorer outcomes than cancer patients with PTEN loss. Now, using mouse modeling, we are able to demonstrate that this is indeed the case. Because PTEN mutations are extremely frequent in various types of tumors, this discovery could help pave the way for a new level of personalized cancer treatment.”
Several of the proteins that PTEN acts upon, both lipids and proteins, are known to promote cancer when bound to a phosphate. Consequently, when PTEN removes their phosphates, it is acting as a tumor suppressor to prevent cancer. When PTEN is mutated, it loses this suppressive ability, and the cancer-promoting proteins are left intact and uninhibited.
This new study showed that the PTEN mutant protein is not only functionally impaired, it also acquires the ability to affect the function of normal PTEN proteins, thereby gaining a pro-tumorigenic function. But the researchers also wanted to determine the difference between PTEN mutation and PTEN loss.
“We wanted to know, would outcomes differ in cases when PTEN was not expressed, compared with cases when PTEN was expressed but encoded a mutation within its sequence?” said study author Antonella Papa, PhD, an investigator in the Pandolfi lab.
To find out, the team created several genetically modified strains of mice to mimic the PTEN mutations found in human cancer patients.
“All mice [and humans] have 2 copies of the PTEN gene,” Dr Papa explained. “The genetically modified mice in our study had 1 copy of the PTEN gene that contained a cancer-associated mutation [either PTENC124S or PTENG129E] and 1 normal copy of PTEN. Other mice in the study had only 1 copy of the normal PTEN gene, and the second copy was removed.”
The researchers found that the mice with a single mutated copy of PTEN were more tumor-prone than the mice with a deleted copy of PTEN. They also discovered that the mutated protein that was produced by PTENC124S or PTENG129E was binding to and inhibiting the PTEN protein made from the normal copy of the PTEN gene.
“This was very surprising, as we were expecting a reduction in tumorigenesis,” Dr Papa said. “Instead, mechanistically, we found that PTEN exists as a dimer, and, in this new conformation, the mutated protein prevents the normal protein from functioning.”
At the molecular level, this generates an increased activation of a PTEN target—the protein Akt—which is what leads to the augmented tumorigenesis in the mice. Akt is part of a signaling pathway that regulates cell growth, division and metabolism.
When PTEN is prevented from inhibiting Akt, the pathway becomes overactive. As a result, targeting Akt and its pathway may be an effective treatment strategy for patients with PTEN mutations, the researchers said, adding that inhibitors to affect this pathway are currently being tested and developed.
“This defines a new working model for the function and regulation of PTEN and tells us that PTEN mutational status can be used to determine which cancer patients might benefit from earlier and more radical therapeutic interventions and, ultimately, better prognosis,” Dr Pandolfi said.
“Our findings may help to better identify and stratify patients and their response to treatment based on the different genetic alterations found in the PTEN gene. Importantly, our study shows that cancer therapy should be tailored on the basis of the very specific type of mutations that the tumor harbors.”
“This adds a new layer of complexity but also a new opportunity for precision medicine. I would say that, based on these thorough genetic analyses, this story represents the ultimate example of why personalized cancer medicine is so urgently needed.” ![]()
Researchers say they’ve uncovered new details that help explain how the PTEN gene exerts its anticancer effects and how PTEN loss or alteration can set cells on a cancerous course.
The team’s study, published in Cell, reveals that PTEN loss and PTEN mutations are not synonymous.
This discovery provides additional insight into basic tumor biology and offers a potential new direction in the pursuit of cancer therapies, according to the researchers.
“By characterizing the ways that 2 specific PTEN mutations regulate the tumor suppressor function of the normal PTEN protein, our findings suggest that different PTEN mutations contribute to tumorigenesis by regulating different aspects of PTEN biology,” said study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center in Boston.
“It has been suggested that cancer patients harboring mutations in PTEN had poorer outcomes than cancer patients with PTEN loss. Now, using mouse modeling, we are able to demonstrate that this is indeed the case. Because PTEN mutations are extremely frequent in various types of tumors, this discovery could help pave the way for a new level of personalized cancer treatment.”
Several of the proteins that PTEN acts upon, both lipids and proteins, are known to promote cancer when bound to a phosphate. Consequently, when PTEN removes their phosphates, it is acting as a tumor suppressor to prevent cancer. When PTEN is mutated, it loses this suppressive ability, and the cancer-promoting proteins are left intact and uninhibited.
This new study showed that the PTEN mutant protein is not only functionally impaired, it also acquires the ability to affect the function of normal PTEN proteins, thereby gaining a pro-tumorigenic function. But the researchers also wanted to determine the difference between PTEN mutation and PTEN loss.
“We wanted to know, would outcomes differ in cases when PTEN was not expressed, compared with cases when PTEN was expressed but encoded a mutation within its sequence?” said study author Antonella Papa, PhD, an investigator in the Pandolfi lab.
To find out, the team created several genetically modified strains of mice to mimic the PTEN mutations found in human cancer patients.
“All mice [and humans] have 2 copies of the PTEN gene,” Dr Papa explained. “The genetically modified mice in our study had 1 copy of the PTEN gene that contained a cancer-associated mutation [either PTENC124S or PTENG129E] and 1 normal copy of PTEN. Other mice in the study had only 1 copy of the normal PTEN gene, and the second copy was removed.”
The researchers found that the mice with a single mutated copy of PTEN were more tumor-prone than the mice with a deleted copy of PTEN. They also discovered that the mutated protein that was produced by PTENC124S or PTENG129E was binding to and inhibiting the PTEN protein made from the normal copy of the PTEN gene.
“This was very surprising, as we were expecting a reduction in tumorigenesis,” Dr Papa said. “Instead, mechanistically, we found that PTEN exists as a dimer, and, in this new conformation, the mutated protein prevents the normal protein from functioning.”
At the molecular level, this generates an increased activation of a PTEN target—the protein Akt—which is what leads to the augmented tumorigenesis in the mice. Akt is part of a signaling pathway that regulates cell growth, division and metabolism.
When PTEN is prevented from inhibiting Akt, the pathway becomes overactive. As a result, targeting Akt and its pathway may be an effective treatment strategy for patients with PTEN mutations, the researchers said, adding that inhibitors to affect this pathway are currently being tested and developed.
“This defines a new working model for the function and regulation of PTEN and tells us that PTEN mutational status can be used to determine which cancer patients might benefit from earlier and more radical therapeutic interventions and, ultimately, better prognosis,” Dr Pandolfi said.
“Our findings may help to better identify and stratify patients and their response to treatment based on the different genetic alterations found in the PTEN gene. Importantly, our study shows that cancer therapy should be tailored on the basis of the very specific type of mutations that the tumor harbors.”
“This adds a new layer of complexity but also a new opportunity for precision medicine. I would say that, based on these thorough genetic analyses, this story represents the ultimate example of why personalized cancer medicine is so urgently needed.” ![]()
AACAP disagrees with marijuana legalization, cites harmful effects on children
The American Academy of Child and Adolescent Psychiatry has released a policy opposing efforts to legalize marijuana.
The AACAP policy statement, released April 15, opposes marijuana legalization while supporting initiatives aimed at increasing awareness of marijuana’s effects on adolescents and improving access to evidence-based treatment, rather than focusing on criminal charges for adolescent users. AACAP also supports the careful monitoring of marijuana-related policy changes on the mental health of children and adolescents.
The policy stresses that significant early use of the drug is associated with increased incidence and worsened psychotic, mood, anxiety, and substance use disorders "across the lifespan." In addition, one in six adolescent marijuana users develops cannabis use disorder, a syndrome involving tolerance, withdrawal, and continued marijuana use despite significant associated impairments.
"Often lost in the discussion on marijuana are the concerning potential implications of policy changes on children and adolescents, who are particularly vulnerable to marijuana’s adverse effects," Dr. Kevin Gray, cochair of AACAP’s Substance Abuse and Addiction Committee, said in a statement. "With this in mind, AACAP felt it was critically important to communicate our organization’s position, given our role as advocates for children and adolescent mental health."
The American Academy of Child and Adolescent Psychiatry has released a policy opposing efforts to legalize marijuana.
The AACAP policy statement, released April 15, opposes marijuana legalization while supporting initiatives aimed at increasing awareness of marijuana’s effects on adolescents and improving access to evidence-based treatment, rather than focusing on criminal charges for adolescent users. AACAP also supports the careful monitoring of marijuana-related policy changes on the mental health of children and adolescents.
The policy stresses that significant early use of the drug is associated with increased incidence and worsened psychotic, mood, anxiety, and substance use disorders "across the lifespan." In addition, one in six adolescent marijuana users develops cannabis use disorder, a syndrome involving tolerance, withdrawal, and continued marijuana use despite significant associated impairments.
"Often lost in the discussion on marijuana are the concerning potential implications of policy changes on children and adolescents, who are particularly vulnerable to marijuana’s adverse effects," Dr. Kevin Gray, cochair of AACAP’s Substance Abuse and Addiction Committee, said in a statement. "With this in mind, AACAP felt it was critically important to communicate our organization’s position, given our role as advocates for children and adolescent mental health."
The American Academy of Child and Adolescent Psychiatry has released a policy opposing efforts to legalize marijuana.
The AACAP policy statement, released April 15, opposes marijuana legalization while supporting initiatives aimed at increasing awareness of marijuana’s effects on adolescents and improving access to evidence-based treatment, rather than focusing on criminal charges for adolescent users. AACAP also supports the careful monitoring of marijuana-related policy changes on the mental health of children and adolescents.
The policy stresses that significant early use of the drug is associated with increased incidence and worsened psychotic, mood, anxiety, and substance use disorders "across the lifespan." In addition, one in six adolescent marijuana users develops cannabis use disorder, a syndrome involving tolerance, withdrawal, and continued marijuana use despite significant associated impairments.
"Often lost in the discussion on marijuana are the concerning potential implications of policy changes on children and adolescents, who are particularly vulnerable to marijuana’s adverse effects," Dr. Kevin Gray, cochair of AACAP’s Substance Abuse and Addiction Committee, said in a statement. "With this in mind, AACAP felt it was critically important to communicate our organization’s position, given our role as advocates for children and adolescent mental health."
New and Noteworthy Information—May 2014
PET is a promising tool for determining which severely brain damaged individuals in vegetative states have the potential to recover consciousness, according to research published online ahead of print April 16 in Lancet. Investigators examined 81 patients in a minimally conscious state, 41 patients with unresponsive wakefulness syndrome, and four patients with locked-in syndrome. The researchers performed repeated standardized clinical assessments with the Coma Recovery Scale–Revised (CRS-R), cerebral 18F-fluorodeoxyglucose (FDG) PET, and fMRI while the patients performed mental activation tasks. Mental imagery fMRI was less sensitive at diagnosing a minimally conscious state than FDG-PET (45% vs 93%) and had less agreement with behavioral CRS-R scores than FDG-PET (63% vs 85%). 18F-FDG PET correctly predicted outcome in 75 of 102 patients, and fMRI in 36 of 65 patients.
The risk of epilepsy may be heightened significantly among patients with autoimmune diseases, especially children, according to data published online ahead of print March 31 in JAMA Neurology. Researchers conducted a retrospective population-based study using claims from a nationwide employer-provided health insurance plan in the United States. All 2,518,034 participants included in the study were beneficiaries enrolled between 1999 and 2006. The investigators examined the relationship between epilepsy and type 1 diabetes mellitus, psoriasis, rheumatoid arthritis, Graves disease, Hashimoto thyroiditis, Crohn disease, ulcerative colitis, systemic lupus erythematosus, antiphospholipid syndrome, Sjögren syndrome, myasthenia gravis, and celiac disease. The odds ratio of epilepsy was 3.8 among patients with autoimmune diseases and 5.2 among children. Based on their findings, the authors recommended that patients with epilepsy undergo surveillance for autoimmune disease, and vice versa.
Migraineurs whose stress decreases from one day to the next have a significantly increased risk of migraine onset on the subsequent day, according to a study published online ahead of print March 26 in Neurology. Twenty-two patients with migraine participated in a three-month electronic diary study. Participants entered data daily regarding migraine attack experience, as well as subjective stress ratings. Stress was assessed using the Perceived Stress Scale and the Self-Reported Stress Scale. Level of stress was generally not associated with migraine occurrence. Decline in stress from one evening diary to the next was associated with increased migraine onset during the subsequent six, 12, and 18 hours for the Perceived Stress Scale. Decline in stress was associated with migraine onset after controlling for level of stress for all time points.
Patients older than 60 with stroke resulting from blockage of the middle cerebral artery (MCA) benefit from hemicraniectomy, researchers reported March 20 in the New England Journal of Medicine. Investigators randomly assigned 112 patients age 61 or older with malignant MCA infarction to conservative treatment in the ICU or hemicraniectomy. The primary end point was survival without severe disability (defined as a score of 0 to 4 on the modified Rankin scale). The proportion of patients who survived without severe disability was 38% in the hemicraniectomy group, compared with 18% in the control group. This difference resulted from lower mortality in the surgery group (33% vs 70%). Infections were more frequent in the hemicraniectomy group, and herniation was more frequent in the control group.
The FDA has approved Topamax (topiramate) for the prevention of migraine headaches in adolescents ages 12 to 17. Topamax is the first drug with FDA approval for migraine prevention in this age group. The medication is taken daily to reduce the frequency of migraine headaches. A clinical trial that enrolled 103 participants established the safety and effectiveness of Topamax in preventing migraine headaches in adolescents ages 12 to 17. Participants treated with Topamax had a decrease in migraine frequency of approximately 72%, compared with 44% in participants who took placebo. The most common adverse reactions with the approved dose of Topamax (100 mg) were paresthesia, upper respiratory infection, anorexia, and abdominal pain. Topamax is manufactured by Janssen Pharmaceuticals of Titusville, New Jersey.
The FDA has approved Evzio (naloxone hydrochloride injection), a prescription treatment that family members or caregivers can use to treat a person suspected to have had an opioid overdose. Evzio rapidly delivers a single dose of naloxone through a handheld autoinjector that can be carried in a pocket or stored in a medicine cabinet. Evzio provides intramuscular or subcutaneous administration. Once turned on, the device provides verbal instruction about how to deliver the medication. In one pharmacokinetic study of 30 patients, a single Evzio injection provided equivalent naloxone, compared with a single dose of naloxone injection using a standard syringe. Administering Evzio to patients who are opioid dependent may result in severe opioid withdrawal. Evzio is manufactured by kaléo, which is based in Richmond, Virginia.
The International League Against Epilepsy has altered its practical definition of epilepsy per the recommendation of a task force, according to an article published online ahead of print April 14 in Epilepsia. Recognizing the limitations of the practical definition of epilepsy as two unprovoked seizures more than 24 hours apart, the task force proposed that epilepsy be considered to be a disease of the brain defined by any of the following conditions: (1) At least two unprovoked (or reflex) seizures occurring more than 24 h apart; (2) one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (ie, at least 60%) after two unprovoked seizures, occurring over the next 10 years; (3) diagnosis of an epilepsy syndrome.
Older people who have apathy but not depression may have smaller brain volumes than those without apathy, according to data published online ahead of print April 16 in Neurology. Investigators performed cross-sectional analyses of data from 4,354 persons without dementia (average age, 76) participating in a population-based study. Apathy symptoms were assessed with the Geriatric Depression Scale. Brain volumes and total white matter lesion (WML) volume were estimated on 1.5-T MRI using an automated segmentation program. Regional WML load was calculated using a semiquantitative scale. Compared with individuals with fewer than two apathy symptoms, participants with two or more apathy symptoms had significantly smaller gray matter volumes, smaller white matter volumes, and smaller thalamus volumes. The latter individuals also were more likely to have WMLs in the frontal lobe.
The APOE4 gene variant confers a substantially greater risk for Alzheimer’s disease to women than it does to men, researchers reported online ahead of print April 14 in Annals of Neurology. The group performed Cox proportional hazards analysis to compute hazard ratios (HRs) for an APOE-by-sex interaction on conversion in 5,496 healthy individuals and 2,588 patients with mild cognitive impairment (MCI). The investigators also tested the interaction in CSF biomarker levels of 980 subjects from the Alzheimer’s Disease Neuroimaging Initiative. Among controls, male and female carriers were more likely to convert to MCI or Alzheimer’s disease, but the effect was stronger in women (HR, 1.81 for women; HR, 1.27 for men). The interaction remained significant in a predefined subanalysis that was restricted to APOE3/3 and APOE3/4 genotypes.
The size and shape of the nucleus accumbens and the amygdala may differ in young adults who smoke marijuana at least once a week, according to a study published April 16 in the Journal of Neuroscience. Investigators collected high-resolution MRI scans on young adults who used recreational marijuana and on controls. The researchers conducted three independent analyses of morphometry in gray matter density, volume (total brain and regional volumes), and surface morphometry. The study authors found greater gray matter density in marijuana users than in control participants in the left nucleus accumbens extending to the subcallosal cortex, hypothalamus, sublenticular extended amygdala, and left amygdala, even after controlling for age, sex, alcohol use, and cigarette smoking. Trend-level effects were observed for a volume increase in the left nucleus accumbens only.
Neuronal death in Parkinson’s disease may occur when the immune system mistakes neurons for foreign invaders and kills them, according to a study published April 16 in Nature Communications. An examination of postmortem brain tissue revealed major histocompatibility complex class I (MHC-1) proteins in catecholaminergic substantia nigra and locus coeruleus neurons. When researchers conducted in vitro experiments with mouse neurons and human neurons created from embryonic stem cells, they found that under certain circumstances, including conditions that occur in Parkinson’s disease, the neurons use MHC-1 to display antigens. Among the different types of neurons tested, the two types affected in Parkinson’s disease were far more responsive than other neurons to signals that triggered antigen display. The researchers also confirmed that T cells recognized and attacked neurons displaying specific antigens.
People who have had a stroke who consistently control their blood pressure may reduce the likelihood of a second stroke by more than half, according to research published online ahead of print March 27 in Stroke. In a post hoc analysis, 3,680 individuals with recent stroke who were followed up for two years were grouped according to the proportion of visits during which their blood pressure was controlled (ie, <140/90 mm Hg). Consistency of blood pressure control affected outcomes in individuals with baseline systolic blood pressure greater than 132 mm Hg. Among individuals with baseline systolic blood pressure higher than 153 mm Hg, risks of stroke, myocardial infarction, or vascular death were lower in those with blood pressure controlled during 75% or more visits, versus less than 25% of visits.
Individuals between ages 18 and 24 who occasionally use stimulant drugs may have impaired neuronal activity in the parts of the brain associated with anticipatory functioning, according to research published March 26 in the Journal of Neuroscience. Investigators recruited 158 nondependent occasional stimulant users and 47 stimulant-naive controls. Participants completed a stop signal task while undergoing functional MRI. Compared with controls, occasional stimulant users showed attenuated neural activation related to the magnitude of probabilistic expectations of inhibitory demand in several areas, including the left prefrontal cortex and left caudate. The results indicate that clinicians may be able to use brain activity patterns as a means of identifying at-risk youth long before they have any obvious outward signs of addictive behaviors, according to the investigators.
—Erik Greb
PET is a promising tool for determining which severely brain damaged individuals in vegetative states have the potential to recover consciousness, according to research published online ahead of print April 16 in Lancet. Investigators examined 81 patients in a minimally conscious state, 41 patients with unresponsive wakefulness syndrome, and four patients with locked-in syndrome. The researchers performed repeated standardized clinical assessments with the Coma Recovery Scale–Revised (CRS-R), cerebral 18F-fluorodeoxyglucose (FDG) PET, and fMRI while the patients performed mental activation tasks. Mental imagery fMRI was less sensitive at diagnosing a minimally conscious state than FDG-PET (45% vs 93%) and had less agreement with behavioral CRS-R scores than FDG-PET (63% vs 85%). 18F-FDG PET correctly predicted outcome in 75 of 102 patients, and fMRI in 36 of 65 patients.
The risk of epilepsy may be heightened significantly among patients with autoimmune diseases, especially children, according to data published online ahead of print March 31 in JAMA Neurology. Researchers conducted a retrospective population-based study using claims from a nationwide employer-provided health insurance plan in the United States. All 2,518,034 participants included in the study were beneficiaries enrolled between 1999 and 2006. The investigators examined the relationship between epilepsy and type 1 diabetes mellitus, psoriasis, rheumatoid arthritis, Graves disease, Hashimoto thyroiditis, Crohn disease, ulcerative colitis, systemic lupus erythematosus, antiphospholipid syndrome, Sjögren syndrome, myasthenia gravis, and celiac disease. The odds ratio of epilepsy was 3.8 among patients with autoimmune diseases and 5.2 among children. Based on their findings, the authors recommended that patients with epilepsy undergo surveillance for autoimmune disease, and vice versa.
Migraineurs whose stress decreases from one day to the next have a significantly increased risk of migraine onset on the subsequent day, according to a study published online ahead of print March 26 in Neurology. Twenty-two patients with migraine participated in a three-month electronic diary study. Participants entered data daily regarding migraine attack experience, as well as subjective stress ratings. Stress was assessed using the Perceived Stress Scale and the Self-Reported Stress Scale. Level of stress was generally not associated with migraine occurrence. Decline in stress from one evening diary to the next was associated with increased migraine onset during the subsequent six, 12, and 18 hours for the Perceived Stress Scale. Decline in stress was associated with migraine onset after controlling for level of stress for all time points.
Patients older than 60 with stroke resulting from blockage of the middle cerebral artery (MCA) benefit from hemicraniectomy, researchers reported March 20 in the New England Journal of Medicine. Investigators randomly assigned 112 patients age 61 or older with malignant MCA infarction to conservative treatment in the ICU or hemicraniectomy. The primary end point was survival without severe disability (defined as a score of 0 to 4 on the modified Rankin scale). The proportion of patients who survived without severe disability was 38% in the hemicraniectomy group, compared with 18% in the control group. This difference resulted from lower mortality in the surgery group (33% vs 70%). Infections were more frequent in the hemicraniectomy group, and herniation was more frequent in the control group.
The FDA has approved Topamax (topiramate) for the prevention of migraine headaches in adolescents ages 12 to 17. Topamax is the first drug with FDA approval for migraine prevention in this age group. The medication is taken daily to reduce the frequency of migraine headaches. A clinical trial that enrolled 103 participants established the safety and effectiveness of Topamax in preventing migraine headaches in adolescents ages 12 to 17. Participants treated with Topamax had a decrease in migraine frequency of approximately 72%, compared with 44% in participants who took placebo. The most common adverse reactions with the approved dose of Topamax (100 mg) were paresthesia, upper respiratory infection, anorexia, and abdominal pain. Topamax is manufactured by Janssen Pharmaceuticals of Titusville, New Jersey.
The FDA has approved Evzio (naloxone hydrochloride injection), a prescription treatment that family members or caregivers can use to treat a person suspected to have had an opioid overdose. Evzio rapidly delivers a single dose of naloxone through a handheld autoinjector that can be carried in a pocket or stored in a medicine cabinet. Evzio provides intramuscular or subcutaneous administration. Once turned on, the device provides verbal instruction about how to deliver the medication. In one pharmacokinetic study of 30 patients, a single Evzio injection provided equivalent naloxone, compared with a single dose of naloxone injection using a standard syringe. Administering Evzio to patients who are opioid dependent may result in severe opioid withdrawal. Evzio is manufactured by kaléo, which is based in Richmond, Virginia.
The International League Against Epilepsy has altered its practical definition of epilepsy per the recommendation of a task force, according to an article published online ahead of print April 14 in Epilepsia. Recognizing the limitations of the practical definition of epilepsy as two unprovoked seizures more than 24 hours apart, the task force proposed that epilepsy be considered to be a disease of the brain defined by any of the following conditions: (1) At least two unprovoked (or reflex) seizures occurring more than 24 h apart; (2) one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (ie, at least 60%) after two unprovoked seizures, occurring over the next 10 years; (3) diagnosis of an epilepsy syndrome.
Older people who have apathy but not depression may have smaller brain volumes than those without apathy, according to data published online ahead of print April 16 in Neurology. Investigators performed cross-sectional analyses of data from 4,354 persons without dementia (average age, 76) participating in a population-based study. Apathy symptoms were assessed with the Geriatric Depression Scale. Brain volumes and total white matter lesion (WML) volume were estimated on 1.5-T MRI using an automated segmentation program. Regional WML load was calculated using a semiquantitative scale. Compared with individuals with fewer than two apathy symptoms, participants with two or more apathy symptoms had significantly smaller gray matter volumes, smaller white matter volumes, and smaller thalamus volumes. The latter individuals also were more likely to have WMLs in the frontal lobe.
The APOE4 gene variant confers a substantially greater risk for Alzheimer’s disease to women than it does to men, researchers reported online ahead of print April 14 in Annals of Neurology. The group performed Cox proportional hazards analysis to compute hazard ratios (HRs) for an APOE-by-sex interaction on conversion in 5,496 healthy individuals and 2,588 patients with mild cognitive impairment (MCI). The investigators also tested the interaction in CSF biomarker levels of 980 subjects from the Alzheimer’s Disease Neuroimaging Initiative. Among controls, male and female carriers were more likely to convert to MCI or Alzheimer’s disease, but the effect was stronger in women (HR, 1.81 for women; HR, 1.27 for men). The interaction remained significant in a predefined subanalysis that was restricted to APOE3/3 and APOE3/4 genotypes.
The size and shape of the nucleus accumbens and the amygdala may differ in young adults who smoke marijuana at least once a week, according to a study published April 16 in the Journal of Neuroscience. Investigators collected high-resolution MRI scans on young adults who used recreational marijuana and on controls. The researchers conducted three independent analyses of morphometry in gray matter density, volume (total brain and regional volumes), and surface morphometry. The study authors found greater gray matter density in marijuana users than in control participants in the left nucleus accumbens extending to the subcallosal cortex, hypothalamus, sublenticular extended amygdala, and left amygdala, even after controlling for age, sex, alcohol use, and cigarette smoking. Trend-level effects were observed for a volume increase in the left nucleus accumbens only.
Neuronal death in Parkinson’s disease may occur when the immune system mistakes neurons for foreign invaders and kills them, according to a study published April 16 in Nature Communications. An examination of postmortem brain tissue revealed major histocompatibility complex class I (MHC-1) proteins in catecholaminergic substantia nigra and locus coeruleus neurons. When researchers conducted in vitro experiments with mouse neurons and human neurons created from embryonic stem cells, they found that under certain circumstances, including conditions that occur in Parkinson’s disease, the neurons use MHC-1 to display antigens. Among the different types of neurons tested, the two types affected in Parkinson’s disease were far more responsive than other neurons to signals that triggered antigen display. The researchers also confirmed that T cells recognized and attacked neurons displaying specific antigens.
People who have had a stroke who consistently control their blood pressure may reduce the likelihood of a second stroke by more than half, according to research published online ahead of print March 27 in Stroke. In a post hoc analysis, 3,680 individuals with recent stroke who were followed up for two years were grouped according to the proportion of visits during which their blood pressure was controlled (ie, <140/90 mm Hg). Consistency of blood pressure control affected outcomes in individuals with baseline systolic blood pressure greater than 132 mm Hg. Among individuals with baseline systolic blood pressure higher than 153 mm Hg, risks of stroke, myocardial infarction, or vascular death were lower in those with blood pressure controlled during 75% or more visits, versus less than 25% of visits.
Individuals between ages 18 and 24 who occasionally use stimulant drugs may have impaired neuronal activity in the parts of the brain associated with anticipatory functioning, according to research published March 26 in the Journal of Neuroscience. Investigators recruited 158 nondependent occasional stimulant users and 47 stimulant-naive controls. Participants completed a stop signal task while undergoing functional MRI. Compared with controls, occasional stimulant users showed attenuated neural activation related to the magnitude of probabilistic expectations of inhibitory demand in several areas, including the left prefrontal cortex and left caudate. The results indicate that clinicians may be able to use brain activity patterns as a means of identifying at-risk youth long before they have any obvious outward signs of addictive behaviors, according to the investigators.
—Erik Greb
PET is a promising tool for determining which severely brain damaged individuals in vegetative states have the potential to recover consciousness, according to research published online ahead of print April 16 in Lancet. Investigators examined 81 patients in a minimally conscious state, 41 patients with unresponsive wakefulness syndrome, and four patients with locked-in syndrome. The researchers performed repeated standardized clinical assessments with the Coma Recovery Scale–Revised (CRS-R), cerebral 18F-fluorodeoxyglucose (FDG) PET, and fMRI while the patients performed mental activation tasks. Mental imagery fMRI was less sensitive at diagnosing a minimally conscious state than FDG-PET (45% vs 93%) and had less agreement with behavioral CRS-R scores than FDG-PET (63% vs 85%). 18F-FDG PET correctly predicted outcome in 75 of 102 patients, and fMRI in 36 of 65 patients.
The risk of epilepsy may be heightened significantly among patients with autoimmune diseases, especially children, according to data published online ahead of print March 31 in JAMA Neurology. Researchers conducted a retrospective population-based study using claims from a nationwide employer-provided health insurance plan in the United States. All 2,518,034 participants included in the study were beneficiaries enrolled between 1999 and 2006. The investigators examined the relationship between epilepsy and type 1 diabetes mellitus, psoriasis, rheumatoid arthritis, Graves disease, Hashimoto thyroiditis, Crohn disease, ulcerative colitis, systemic lupus erythematosus, antiphospholipid syndrome, Sjögren syndrome, myasthenia gravis, and celiac disease. The odds ratio of epilepsy was 3.8 among patients with autoimmune diseases and 5.2 among children. Based on their findings, the authors recommended that patients with epilepsy undergo surveillance for autoimmune disease, and vice versa.
Migraineurs whose stress decreases from one day to the next have a significantly increased risk of migraine onset on the subsequent day, according to a study published online ahead of print March 26 in Neurology. Twenty-two patients with migraine participated in a three-month electronic diary study. Participants entered data daily regarding migraine attack experience, as well as subjective stress ratings. Stress was assessed using the Perceived Stress Scale and the Self-Reported Stress Scale. Level of stress was generally not associated with migraine occurrence. Decline in stress from one evening diary to the next was associated with increased migraine onset during the subsequent six, 12, and 18 hours for the Perceived Stress Scale. Decline in stress was associated with migraine onset after controlling for level of stress for all time points.
Patients older than 60 with stroke resulting from blockage of the middle cerebral artery (MCA) benefit from hemicraniectomy, researchers reported March 20 in the New England Journal of Medicine. Investigators randomly assigned 112 patients age 61 or older with malignant MCA infarction to conservative treatment in the ICU or hemicraniectomy. The primary end point was survival without severe disability (defined as a score of 0 to 4 on the modified Rankin scale). The proportion of patients who survived without severe disability was 38% in the hemicraniectomy group, compared with 18% in the control group. This difference resulted from lower mortality in the surgery group (33% vs 70%). Infections were more frequent in the hemicraniectomy group, and herniation was more frequent in the control group.
The FDA has approved Topamax (topiramate) for the prevention of migraine headaches in adolescents ages 12 to 17. Topamax is the first drug with FDA approval for migraine prevention in this age group. The medication is taken daily to reduce the frequency of migraine headaches. A clinical trial that enrolled 103 participants established the safety and effectiveness of Topamax in preventing migraine headaches in adolescents ages 12 to 17. Participants treated with Topamax had a decrease in migraine frequency of approximately 72%, compared with 44% in participants who took placebo. The most common adverse reactions with the approved dose of Topamax (100 mg) were paresthesia, upper respiratory infection, anorexia, and abdominal pain. Topamax is manufactured by Janssen Pharmaceuticals of Titusville, New Jersey.
The FDA has approved Evzio (naloxone hydrochloride injection), a prescription treatment that family members or caregivers can use to treat a person suspected to have had an opioid overdose. Evzio rapidly delivers a single dose of naloxone through a handheld autoinjector that can be carried in a pocket or stored in a medicine cabinet. Evzio provides intramuscular or subcutaneous administration. Once turned on, the device provides verbal instruction about how to deliver the medication. In one pharmacokinetic study of 30 patients, a single Evzio injection provided equivalent naloxone, compared with a single dose of naloxone injection using a standard syringe. Administering Evzio to patients who are opioid dependent may result in severe opioid withdrawal. Evzio is manufactured by kaléo, which is based in Richmond, Virginia.
The International League Against Epilepsy has altered its practical definition of epilepsy per the recommendation of a task force, according to an article published online ahead of print April 14 in Epilepsia. Recognizing the limitations of the practical definition of epilepsy as two unprovoked seizures more than 24 hours apart, the task force proposed that epilepsy be considered to be a disease of the brain defined by any of the following conditions: (1) At least two unprovoked (or reflex) seizures occurring more than 24 h apart; (2) one unprovoked (or reflex) seizure and a probability of further seizures similar to the general recurrence risk (ie, at least 60%) after two unprovoked seizures, occurring over the next 10 years; (3) diagnosis of an epilepsy syndrome.
Older people who have apathy but not depression may have smaller brain volumes than those without apathy, according to data published online ahead of print April 16 in Neurology. Investigators performed cross-sectional analyses of data from 4,354 persons without dementia (average age, 76) participating in a population-based study. Apathy symptoms were assessed with the Geriatric Depression Scale. Brain volumes and total white matter lesion (WML) volume were estimated on 1.5-T MRI using an automated segmentation program. Regional WML load was calculated using a semiquantitative scale. Compared with individuals with fewer than two apathy symptoms, participants with two or more apathy symptoms had significantly smaller gray matter volumes, smaller white matter volumes, and smaller thalamus volumes. The latter individuals also were more likely to have WMLs in the frontal lobe.
The APOE4 gene variant confers a substantially greater risk for Alzheimer’s disease to women than it does to men, researchers reported online ahead of print April 14 in Annals of Neurology. The group performed Cox proportional hazards analysis to compute hazard ratios (HRs) for an APOE-by-sex interaction on conversion in 5,496 healthy individuals and 2,588 patients with mild cognitive impairment (MCI). The investigators also tested the interaction in CSF biomarker levels of 980 subjects from the Alzheimer’s Disease Neuroimaging Initiative. Among controls, male and female carriers were more likely to convert to MCI or Alzheimer’s disease, but the effect was stronger in women (HR, 1.81 for women; HR, 1.27 for men). The interaction remained significant in a predefined subanalysis that was restricted to APOE3/3 and APOE3/4 genotypes.
The size and shape of the nucleus accumbens and the amygdala may differ in young adults who smoke marijuana at least once a week, according to a study published April 16 in the Journal of Neuroscience. Investigators collected high-resolution MRI scans on young adults who used recreational marijuana and on controls. The researchers conducted three independent analyses of morphometry in gray matter density, volume (total brain and regional volumes), and surface morphometry. The study authors found greater gray matter density in marijuana users than in control participants in the left nucleus accumbens extending to the subcallosal cortex, hypothalamus, sublenticular extended amygdala, and left amygdala, even after controlling for age, sex, alcohol use, and cigarette smoking. Trend-level effects were observed for a volume increase in the left nucleus accumbens only.
Neuronal death in Parkinson’s disease may occur when the immune system mistakes neurons for foreign invaders and kills them, according to a study published April 16 in Nature Communications. An examination of postmortem brain tissue revealed major histocompatibility complex class I (MHC-1) proteins in catecholaminergic substantia nigra and locus coeruleus neurons. When researchers conducted in vitro experiments with mouse neurons and human neurons created from embryonic stem cells, they found that under certain circumstances, including conditions that occur in Parkinson’s disease, the neurons use MHC-1 to display antigens. Among the different types of neurons tested, the two types affected in Parkinson’s disease were far more responsive than other neurons to signals that triggered antigen display. The researchers also confirmed that T cells recognized and attacked neurons displaying specific antigens.
People who have had a stroke who consistently control their blood pressure may reduce the likelihood of a second stroke by more than half, according to research published online ahead of print March 27 in Stroke. In a post hoc analysis, 3,680 individuals with recent stroke who were followed up for two years were grouped according to the proportion of visits during which their blood pressure was controlled (ie, <140/90 mm Hg). Consistency of blood pressure control affected outcomes in individuals with baseline systolic blood pressure greater than 132 mm Hg. Among individuals with baseline systolic blood pressure higher than 153 mm Hg, risks of stroke, myocardial infarction, or vascular death were lower in those with blood pressure controlled during 75% or more visits, versus less than 25% of visits.
Individuals between ages 18 and 24 who occasionally use stimulant drugs may have impaired neuronal activity in the parts of the brain associated with anticipatory functioning, according to research published March 26 in the Journal of Neuroscience. Investigators recruited 158 nondependent occasional stimulant users and 47 stimulant-naive controls. Participants completed a stop signal task while undergoing functional MRI. Compared with controls, occasional stimulant users showed attenuated neural activation related to the magnitude of probabilistic expectations of inhibitory demand in several areas, including the left prefrontal cortex and left caudate. The results indicate that clinicians may be able to use brain activity patterns as a means of identifying at-risk youth long before they have any obvious outward signs of addictive behaviors, according to the investigators.
—Erik Greb

FDA, hospitals caution against laparoscopic power morcellation during hysterectomy and myomectomy
The use of power morcellation to remove the uterus or uterine tumors during hysterectomy and myomectomy may be riskier than many have thought. That’s the conclusion reached by the US Food and Drug Administration (FDA) in a safety communication issued April 17, 2014. In its communication, the FDA “discouraged” use of power morcellation during hysterectomy and myomectomy. Shortly afterward, Brigham and Women’s and Massachusetts General hospitals in Boston banned power morcellation in all hysterectomy and myomectomy procedures. The hospitals may resume power morcellation at some future date using a containment system, pending guidance from the Institutional Review Board.
Robert L. Barbieri, MD, who is chair of obstetrics and gynecology at Brigham and Women’s Hospital, recently wrote about this concern for OBG Management in his capacity as editor in chief of the journal.
“When used to treat tumors presumed to be fibroids, open power morcellation [without a containment system] is associated with an increased risk of dispersing benign myoma tissue and occult malignant leiomyosarcoma tissue throughout the abdominal cavity,” he wrote.1 “Dispersion of benign myoma tissue may result in the growth of fibroids on the peritoneal surface, omentum, and bowel, causing abdominal and pelvic pain and necessitating reoperation. Dispersion of leiomyosarcoma tissue throughout the abdominal cavity may result in a Stage I cancer being upstaged to a Stage IV malignancy, requiring additional surgery and chemotherapy. In cases in which open power morcellation causes the upstaging of a leiomyosarcoma, the death rate is increased.”1
The two Boston hospitals are not the only institutions reconsidering the use of power morcellation. Temple University Hospital in Philadelphia banned use of the procedure without a containment system in late February 2014.
And in December 2013, the Society of Gynecologic Oncology issued a position statement on the issue, which said, “power morcellation or other techniques that cut up the uterus in the abdomen have the potential to disseminate an otherwise contained malignancy throughout the abdominal cavity. For this reason, the Society of Gynecologic Oncology (SGO) asserts that it is generally contraindicated in the presence of documented or highly suspected malignancy, and may be inadvisable in premalignant conditions or risk-reducing surgery.”2
For its part, at the time of this writing, the AAGL, previously known as the American Association of Gynecologic Laparoscopists, “is reviewing the scientific evidence and best practices reported by our members,” stated an article in its Association News. “We recognize that, in rare cases, the use of power morcellators can lead to the dissemination of an occult malignancy of endometrial or myometrial origin, and also to dissemination of benign morcellated tissues. We encourage our members to fully research and understand the risks of power morcellation and to learn more about when alternative methods of tissue extraction may be appropriate.”3
FDA STOPS SHORT OF A BAN
In laying out its concerns, the FDA stopped short of an outright ban on power morcellation. Instead, it stated that, “based on currently available information, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids.”4
It also noted that approximately 1 in 350 women “undergoing hysterectomy or myomectomy for the treatment of fibroids is found to have an unsuspected uterine sarcoma.”4
Among its recommendations for health-care providers:
- avoid laparoscopic uterine power morcellation in women with suspected or known uterine cancer
- carefully consider all available treatment options for women with symptomatic uterine fibroids
- thoroughly discuss the benefits and risks of all treatments with patients.4
The FDA also noted that “some clinicians and medical institutions now advocate using a specimen ‘bag’ during morcellation in an attempt to contain the uterine tissue and minimize the risk of spread in the abdomen and pelvis.”4
ACOG HAS YET TO WEIGH IN
At the time of this writing, the most recent committee opinion on choosing a hysterectomy route from the American College of Obstetricians and Gynecologists (ACOG) to touch on the issue states that, “the decision to perform a hysterectomy via [minimally invasive surgery] (with or without morcellation) is based on a patient evaluation, including the patient’s history and general health, tests, and procedures, such as pre-surgery biopsies. The evaluation and diagnostic process also provides an opportunity to identify any cautions or contraindications, such as finding a gynecological cancer.”5
FILLING THE TECHNOLOGY GAP
Now that power morcellation appears to be receding as an option for minimally invasive gynecologic surgeons, what is the best approach?
In its position statement, the SGO recommends that, “Patients being considered for minimally invasive surgery performed by laparoscopic or robotic techniques who might require intracorporeal morcellation should be appropriately evaluated for the possibility of coexisting uterine or cervical malignancy. Other options to intracorporeal morcellation include removing the uterus through a mini-laparotomy or morcellating the uterus inside a laparoscopic bag.”2
K. Anthony Shibley, MD, a Minneapolis-area ObGyn, has developed a novel strategy to prevent tissue dissemination during open power morcellation, which is demonstrated in a video at obgmanagement.com. Similarly, Ceana Nezhat, MD, and Erica Dun, MD, demonstrate enclosed vaginal morcellation of a large uterus. Click here to access these and other features in the Morcellation Topic Collection.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, and the city and state in which you practice.
- Barbieri RL. Options for reducing the use of open power morcellation of uterine tumors. OBG Manag. 2014;26(3):10,11,20.
- Society of Gynecologic Oncology. Position Statement: Morcellation. https://www.sgo.org/newsroom/position-statements-2/morcellation/. Published December 2013. Accessed April 8, 2014.
- AAGL Member Update: Disseminated Leiomyosarcoma with Power Morcellation. http://www.aagl.org/aaglnews/aagl-member-update-disseminated-leiomyosarcoma-with-power-morcellation/. Accessed April 11, 2014.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. April 17, 2014.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009;114(5):1156–1158.
The use of power morcellation to remove the uterus or uterine tumors during hysterectomy and myomectomy may be riskier than many have thought. That’s the conclusion reached by the US Food and Drug Administration (FDA) in a safety communication issued April 17, 2014. In its communication, the FDA “discouraged” use of power morcellation during hysterectomy and myomectomy. Shortly afterward, Brigham and Women’s and Massachusetts General hospitals in Boston banned power morcellation in all hysterectomy and myomectomy procedures. The hospitals may resume power morcellation at some future date using a containment system, pending guidance from the Institutional Review Board.
Robert L. Barbieri, MD, who is chair of obstetrics and gynecology at Brigham and Women’s Hospital, recently wrote about this concern for OBG Management in his capacity as editor in chief of the journal.
“When used to treat tumors presumed to be fibroids, open power morcellation [without a containment system] is associated with an increased risk of dispersing benign myoma tissue and occult malignant leiomyosarcoma tissue throughout the abdominal cavity,” he wrote.1 “Dispersion of benign myoma tissue may result in the growth of fibroids on the peritoneal surface, omentum, and bowel, causing abdominal and pelvic pain and necessitating reoperation. Dispersion of leiomyosarcoma tissue throughout the abdominal cavity may result in a Stage I cancer being upstaged to a Stage IV malignancy, requiring additional surgery and chemotherapy. In cases in which open power morcellation causes the upstaging of a leiomyosarcoma, the death rate is increased.”1
The two Boston hospitals are not the only institutions reconsidering the use of power morcellation. Temple University Hospital in Philadelphia banned use of the procedure without a containment system in late February 2014.
And in December 2013, the Society of Gynecologic Oncology issued a position statement on the issue, which said, “power morcellation or other techniques that cut up the uterus in the abdomen have the potential to disseminate an otherwise contained malignancy throughout the abdominal cavity. For this reason, the Society of Gynecologic Oncology (SGO) asserts that it is generally contraindicated in the presence of documented or highly suspected malignancy, and may be inadvisable in premalignant conditions or risk-reducing surgery.”2
For its part, at the time of this writing, the AAGL, previously known as the American Association of Gynecologic Laparoscopists, “is reviewing the scientific evidence and best practices reported by our members,” stated an article in its Association News. “We recognize that, in rare cases, the use of power morcellators can lead to the dissemination of an occult malignancy of endometrial or myometrial origin, and also to dissemination of benign morcellated tissues. We encourage our members to fully research and understand the risks of power morcellation and to learn more about when alternative methods of tissue extraction may be appropriate.”3
FDA STOPS SHORT OF A BAN
In laying out its concerns, the FDA stopped short of an outright ban on power morcellation. Instead, it stated that, “based on currently available information, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids.”4
It also noted that approximately 1 in 350 women “undergoing hysterectomy or myomectomy for the treatment of fibroids is found to have an unsuspected uterine sarcoma.”4
Among its recommendations for health-care providers:
- avoid laparoscopic uterine power morcellation in women with suspected or known uterine cancer
- carefully consider all available treatment options for women with symptomatic uterine fibroids
- thoroughly discuss the benefits and risks of all treatments with patients.4
The FDA also noted that “some clinicians and medical institutions now advocate using a specimen ‘bag’ during morcellation in an attempt to contain the uterine tissue and minimize the risk of spread in the abdomen and pelvis.”4
ACOG HAS YET TO WEIGH IN
At the time of this writing, the most recent committee opinion on choosing a hysterectomy route from the American College of Obstetricians and Gynecologists (ACOG) to touch on the issue states that, “the decision to perform a hysterectomy via [minimally invasive surgery] (with or without morcellation) is based on a patient evaluation, including the patient’s history and general health, tests, and procedures, such as pre-surgery biopsies. The evaluation and diagnostic process also provides an opportunity to identify any cautions or contraindications, such as finding a gynecological cancer.”5
FILLING THE TECHNOLOGY GAP
Now that power morcellation appears to be receding as an option for minimally invasive gynecologic surgeons, what is the best approach?
In its position statement, the SGO recommends that, “Patients being considered for minimally invasive surgery performed by laparoscopic or robotic techniques who might require intracorporeal morcellation should be appropriately evaluated for the possibility of coexisting uterine or cervical malignancy. Other options to intracorporeal morcellation include removing the uterus through a mini-laparotomy or morcellating the uterus inside a laparoscopic bag.”2
K. Anthony Shibley, MD, a Minneapolis-area ObGyn, has developed a novel strategy to prevent tissue dissemination during open power morcellation, which is demonstrated in a video at obgmanagement.com. Similarly, Ceana Nezhat, MD, and Erica Dun, MD, demonstrate enclosed vaginal morcellation of a large uterus. Click here to access these and other features in the Morcellation Topic Collection.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, and the city and state in which you practice.
The use of power morcellation to remove the uterus or uterine tumors during hysterectomy and myomectomy may be riskier than many have thought. That’s the conclusion reached by the US Food and Drug Administration (FDA) in a safety communication issued April 17, 2014. In its communication, the FDA “discouraged” use of power morcellation during hysterectomy and myomectomy. Shortly afterward, Brigham and Women’s and Massachusetts General hospitals in Boston banned power morcellation in all hysterectomy and myomectomy procedures. The hospitals may resume power morcellation at some future date using a containment system, pending guidance from the Institutional Review Board.
Robert L. Barbieri, MD, who is chair of obstetrics and gynecology at Brigham and Women’s Hospital, recently wrote about this concern for OBG Management in his capacity as editor in chief of the journal.
“When used to treat tumors presumed to be fibroids, open power morcellation [without a containment system] is associated with an increased risk of dispersing benign myoma tissue and occult malignant leiomyosarcoma tissue throughout the abdominal cavity,” he wrote.1 “Dispersion of benign myoma tissue may result in the growth of fibroids on the peritoneal surface, omentum, and bowel, causing abdominal and pelvic pain and necessitating reoperation. Dispersion of leiomyosarcoma tissue throughout the abdominal cavity may result in a Stage I cancer being upstaged to a Stage IV malignancy, requiring additional surgery and chemotherapy. In cases in which open power morcellation causes the upstaging of a leiomyosarcoma, the death rate is increased.”1
The two Boston hospitals are not the only institutions reconsidering the use of power morcellation. Temple University Hospital in Philadelphia banned use of the procedure without a containment system in late February 2014.
And in December 2013, the Society of Gynecologic Oncology issued a position statement on the issue, which said, “power morcellation or other techniques that cut up the uterus in the abdomen have the potential to disseminate an otherwise contained malignancy throughout the abdominal cavity. For this reason, the Society of Gynecologic Oncology (SGO) asserts that it is generally contraindicated in the presence of documented or highly suspected malignancy, and may be inadvisable in premalignant conditions or risk-reducing surgery.”2
For its part, at the time of this writing, the AAGL, previously known as the American Association of Gynecologic Laparoscopists, “is reviewing the scientific evidence and best practices reported by our members,” stated an article in its Association News. “We recognize that, in rare cases, the use of power morcellators can lead to the dissemination of an occult malignancy of endometrial or myometrial origin, and also to dissemination of benign morcellated tissues. We encourage our members to fully research and understand the risks of power morcellation and to learn more about when alternative methods of tissue extraction may be appropriate.”3
FDA STOPS SHORT OF A BAN
In laying out its concerns, the FDA stopped short of an outright ban on power morcellation. Instead, it stated that, “based on currently available information, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids.”4
It also noted that approximately 1 in 350 women “undergoing hysterectomy or myomectomy for the treatment of fibroids is found to have an unsuspected uterine sarcoma.”4
Among its recommendations for health-care providers:
- avoid laparoscopic uterine power morcellation in women with suspected or known uterine cancer
- carefully consider all available treatment options for women with symptomatic uterine fibroids
- thoroughly discuss the benefits and risks of all treatments with patients.4
The FDA also noted that “some clinicians and medical institutions now advocate using a specimen ‘bag’ during morcellation in an attempt to contain the uterine tissue and minimize the risk of spread in the abdomen and pelvis.”4
ACOG HAS YET TO WEIGH IN
At the time of this writing, the most recent committee opinion on choosing a hysterectomy route from the American College of Obstetricians and Gynecologists (ACOG) to touch on the issue states that, “the decision to perform a hysterectomy via [minimally invasive surgery] (with or without morcellation) is based on a patient evaluation, including the patient’s history and general health, tests, and procedures, such as pre-surgery biopsies. The evaluation and diagnostic process also provides an opportunity to identify any cautions or contraindications, such as finding a gynecological cancer.”5
FILLING THE TECHNOLOGY GAP
Now that power morcellation appears to be receding as an option for minimally invasive gynecologic surgeons, what is the best approach?
In its position statement, the SGO recommends that, “Patients being considered for minimally invasive surgery performed by laparoscopic or robotic techniques who might require intracorporeal morcellation should be appropriately evaluated for the possibility of coexisting uterine or cervical malignancy. Other options to intracorporeal morcellation include removing the uterus through a mini-laparotomy or morcellating the uterus inside a laparoscopic bag.”2
K. Anthony Shibley, MD, a Minneapolis-area ObGyn, has developed a novel strategy to prevent tissue dissemination during open power morcellation, which is demonstrated in a video at obgmanagement.com. Similarly, Ceana Nezhat, MD, and Erica Dun, MD, demonstrate enclosed vaginal morcellation of a large uterus. Click here to access these and other features in the Morcellation Topic Collection.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, and the city and state in which you practice.
- Barbieri RL. Options for reducing the use of open power morcellation of uterine tumors. OBG Manag. 2014;26(3):10,11,20.
- Society of Gynecologic Oncology. Position Statement: Morcellation. https://www.sgo.org/newsroom/position-statements-2/morcellation/. Published December 2013. Accessed April 8, 2014.
- AAGL Member Update: Disseminated Leiomyosarcoma with Power Morcellation. http://www.aagl.org/aaglnews/aagl-member-update-disseminated-leiomyosarcoma-with-power-morcellation/. Accessed April 11, 2014.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. April 17, 2014.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009;114(5):1156–1158.
- Barbieri RL. Options for reducing the use of open power morcellation of uterine tumors. OBG Manag. 2014;26(3):10,11,20.
- Society of Gynecologic Oncology. Position Statement: Morcellation. https://www.sgo.org/newsroom/position-statements-2/morcellation/. Published December 2013. Accessed April 8, 2014.
- AAGL Member Update: Disseminated Leiomyosarcoma with Power Morcellation. http://www.aagl.org/aaglnews/aagl-member-update-disseminated-leiomyosarcoma-with-power-morcellation/. Accessed April 11, 2014.
- US Food and Drug Administration. Laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. April 17, 2014.
- American College of Obstetricians and Gynecologists. Committee Opinion No. 444: Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009;114(5):1156–1158.
To access articles, videos, and audiocasts in the Morcellation Topic Collection, click here.
Autism May Start in Utero
Autism may begin in utero, according to a study of postmortem brain tissue from children with and without autism published online ahead of print March 27 in the New England Journal of Medicine.
The findings imply that layer formation and layer-specific neuronal differentiation are dysregulated during prenatal development. The study also suggests that early recognition and treatment of autism may allow the developing brains of autistic children to construct alternative brain pathways around the patchy defects in the cortex. The result could be improved social functioning and communication, the researchers theorized.
Researchers used gene expression to examine cellular markers in each of the cortical layers, as well as genes that are associated with autism. Markers for several layers of the cortex were absent in the brain tissue of 10 of 11 (91%) children with autism and in one of 11 (9%) control children. The areas of disorganization were seen in multiple cortical layers, with most abnormal expression noted in layers 4 and 5 and focal disruption of cortical laminar architecture as patches that were 5 to 7 mm long.
—Mary Jo M. Dales
Suggested Reading
Stoner R, Chow ML, Boyle MP, et al. Patches of disorganization in the neocortex of children with autism. N Engl J Med. 2014;370(13):1209-1219.
Autism may begin in utero, according to a study of postmortem brain tissue from children with and without autism published online ahead of print March 27 in the New England Journal of Medicine.
The findings imply that layer formation and layer-specific neuronal differentiation are dysregulated during prenatal development. The study also suggests that early recognition and treatment of autism may allow the developing brains of autistic children to construct alternative brain pathways around the patchy defects in the cortex. The result could be improved social functioning and communication, the researchers theorized.
Researchers used gene expression to examine cellular markers in each of the cortical layers, as well as genes that are associated with autism. Markers for several layers of the cortex were absent in the brain tissue of 10 of 11 (91%) children with autism and in one of 11 (9%) control children. The areas of disorganization were seen in multiple cortical layers, with most abnormal expression noted in layers 4 and 5 and focal disruption of cortical laminar architecture as patches that were 5 to 7 mm long.
—Mary Jo M. Dales
Autism may begin in utero, according to a study of postmortem brain tissue from children with and without autism published online ahead of print March 27 in the New England Journal of Medicine.
The findings imply that layer formation and layer-specific neuronal differentiation are dysregulated during prenatal development. The study also suggests that early recognition and treatment of autism may allow the developing brains of autistic children to construct alternative brain pathways around the patchy defects in the cortex. The result could be improved social functioning and communication, the researchers theorized.
Researchers used gene expression to examine cellular markers in each of the cortical layers, as well as genes that are associated with autism. Markers for several layers of the cortex were absent in the brain tissue of 10 of 11 (91%) children with autism and in one of 11 (9%) control children. The areas of disorganization were seen in multiple cortical layers, with most abnormal expression noted in layers 4 and 5 and focal disruption of cortical laminar architecture as patches that were 5 to 7 mm long.
—Mary Jo M. Dales
Suggested Reading
Stoner R, Chow ML, Boyle MP, et al. Patches of disorganization in the neocortex of children with autism. N Engl J Med. 2014;370(13):1209-1219.
Suggested Reading
Stoner R, Chow ML, Boyle MP, et al. Patches of disorganization in the neocortex of children with autism. N Engl J Med. 2014;370(13):1209-1219.

Prevalence of Autism Spectrum Disorder Is Increasing
The CDC estimates that about one in 68 US children has autism spectrum disorder, according to findings published in the March 28 issue of Morbidity and Mortality Weekly Report Surveillance Summaries. This prevalence is a 30% increase from the CDC’s estimate of one in 88 children using 2008 data.
The findings also show that autism spectrum disorder continues to be more prevalent in boys than in girls: one in 42 boys had autism spectrum disorder in the latest report, compared with one in 189 girls.
The increased prevalence could be attributed to improved clinician identification of autism, a growing number of autistic children with average to above-average intellectual ability, or a combination of both factors, said Coleen Boyle, PhD, Director of the CDC’s National Center on Birth Defects and Developmental Disabilities (NCBDDD).
The CDC analyzed 2010 data collected by its Autism and Developmental Disabilities Monitoring (ADDM) Network, which provides population-based estimates of autism spectrum disorder prevalence in children age 8 at 11 sites in the United States based on records from community sources that diagnose and provide services to children with developmental disabilities.
Of the 11 sites studied, seven had information available on the intellectual ability of at least 70% of children with autism spectrum disorder. Of the 3,604 children for whom data were available, 31% were classified as having intellectual disability (IQ of 70 or lower), 23% were considered borderline (IQ = 71 to 85), and 46% had IQ scores of greater than 85, considered average or above average intellectual ability.
“We recognize now that autism is a spectrum, no longer limited to the severely affected,” said Marshalyn Yeargin-Allsopp, MD, Chief of the Developmental Disabilities branch of NCBDDD. “There are children with higher IQs being diagnosed who may not even be receiving special education services, and the numbers may reflect that.”
Non-Hispanic white children were 30% more likely to be diagnosed with autism spectrum disorder than were non-Hispanic black children and about 50% more likely to be diagnosed with autism spectrum disorder than were Hispanic children.
Dr. Boyle stressed the importance of early screening and identification of autism spectrum disorder in children (it can be diagnosed by the time a child reaches age 2) and urged parents to take action if a child shows any signs of developmental delays.
“Community leaders, health professionals, educators, and childcare providers should use these data to ensure that children with autism spectrum disorder are identified as early as possible and connected to the services they need,” said Dr. Boyle.
To help promote early intervention in autism spectrum disorder, the CDC will be launching an awareness initiative called “Birth to Five, Watch Me Thrive,” which aims to provide parents, teachers, and community members with information and resources about developmental milestones and screening for autism.
“Most children with autism are not diagnosed until after age 4,” said Dr. Boyle. “The CDC will continue to promote early identification and research. The earlier a child is identified and connected with services, the better.”
The CDC cited several limitations to the report. First, the surveillance sites were not selected to be representative of the entire United States. Second, population denominators used for this report were based on the 2010 decennial census. Comparisons with previous ADDM findings thus should be interpreted with caution because ADDM reports from nondecennial surveillance years are likely influenced by greater error in the population denominators used for those previous surveillance years, which were based on postcensus estimates. Third, three of the nine sites with access to review children’s education records did not receive permission to do so in all school districts within the site’s overall surveillance area. Fourth, findings that address intellectual ability might not be generalizable to all ADDM sites. Finally, race and ethnicity are presented in broad terms and should not be interpreted as generalizable to all persons within those categories.
—Madhu Rajaraman
Suggested Reading
Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators. Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014; Mar 28;63 Suppl 2:1-21.
The CDC estimates that about one in 68 US children has autism spectrum disorder, according to findings published in the March 28 issue of Morbidity and Mortality Weekly Report Surveillance Summaries. This prevalence is a 30% increase from the CDC’s estimate of one in 88 children using 2008 data.
The findings also show that autism spectrum disorder continues to be more prevalent in boys than in girls: one in 42 boys had autism spectrum disorder in the latest report, compared with one in 189 girls.
The increased prevalence could be attributed to improved clinician identification of autism, a growing number of autistic children with average to above-average intellectual ability, or a combination of both factors, said Coleen Boyle, PhD, Director of the CDC’s National Center on Birth Defects and Developmental Disabilities (NCBDDD).
The CDC analyzed 2010 data collected by its Autism and Developmental Disabilities Monitoring (ADDM) Network, which provides population-based estimates of autism spectrum disorder prevalence in children age 8 at 11 sites in the United States based on records from community sources that diagnose and provide services to children with developmental disabilities.
Of the 11 sites studied, seven had information available on the intellectual ability of at least 70% of children with autism spectrum disorder. Of the 3,604 children for whom data were available, 31% were classified as having intellectual disability (IQ of 70 or lower), 23% were considered borderline (IQ = 71 to 85), and 46% had IQ scores of greater than 85, considered average or above average intellectual ability.
“We recognize now that autism is a spectrum, no longer limited to the severely affected,” said Marshalyn Yeargin-Allsopp, MD, Chief of the Developmental Disabilities branch of NCBDDD. “There are children with higher IQs being diagnosed who may not even be receiving special education services, and the numbers may reflect that.”
Non-Hispanic white children were 30% more likely to be diagnosed with autism spectrum disorder than were non-Hispanic black children and about 50% more likely to be diagnosed with autism spectrum disorder than were Hispanic children.
Dr. Boyle stressed the importance of early screening and identification of autism spectrum disorder in children (it can be diagnosed by the time a child reaches age 2) and urged parents to take action if a child shows any signs of developmental delays.
“Community leaders, health professionals, educators, and childcare providers should use these data to ensure that children with autism spectrum disorder are identified as early as possible and connected to the services they need,” said Dr. Boyle.
To help promote early intervention in autism spectrum disorder, the CDC will be launching an awareness initiative called “Birth to Five, Watch Me Thrive,” which aims to provide parents, teachers, and community members with information and resources about developmental milestones and screening for autism.
“Most children with autism are not diagnosed until after age 4,” said Dr. Boyle. “The CDC will continue to promote early identification and research. The earlier a child is identified and connected with services, the better.”
The CDC cited several limitations to the report. First, the surveillance sites were not selected to be representative of the entire United States. Second, population denominators used for this report were based on the 2010 decennial census. Comparisons with previous ADDM findings thus should be interpreted with caution because ADDM reports from nondecennial surveillance years are likely influenced by greater error in the population denominators used for those previous surveillance years, which were based on postcensus estimates. Third, three of the nine sites with access to review children’s education records did not receive permission to do so in all school districts within the site’s overall surveillance area. Fourth, findings that address intellectual ability might not be generalizable to all ADDM sites. Finally, race and ethnicity are presented in broad terms and should not be interpreted as generalizable to all persons within those categories.
—Madhu Rajaraman
The CDC estimates that about one in 68 US children has autism spectrum disorder, according to findings published in the March 28 issue of Morbidity and Mortality Weekly Report Surveillance Summaries. This prevalence is a 30% increase from the CDC’s estimate of one in 88 children using 2008 data.
The findings also show that autism spectrum disorder continues to be more prevalent in boys than in girls: one in 42 boys had autism spectrum disorder in the latest report, compared with one in 189 girls.
The increased prevalence could be attributed to improved clinician identification of autism, a growing number of autistic children with average to above-average intellectual ability, or a combination of both factors, said Coleen Boyle, PhD, Director of the CDC’s National Center on Birth Defects and Developmental Disabilities (NCBDDD).
The CDC analyzed 2010 data collected by its Autism and Developmental Disabilities Monitoring (ADDM) Network, which provides population-based estimates of autism spectrum disorder prevalence in children age 8 at 11 sites in the United States based on records from community sources that diagnose and provide services to children with developmental disabilities.
Of the 11 sites studied, seven had information available on the intellectual ability of at least 70% of children with autism spectrum disorder. Of the 3,604 children for whom data were available, 31% were classified as having intellectual disability (IQ of 70 or lower), 23% were considered borderline (IQ = 71 to 85), and 46% had IQ scores of greater than 85, considered average or above average intellectual ability.
“We recognize now that autism is a spectrum, no longer limited to the severely affected,” said Marshalyn Yeargin-Allsopp, MD, Chief of the Developmental Disabilities branch of NCBDDD. “There are children with higher IQs being diagnosed who may not even be receiving special education services, and the numbers may reflect that.”
Non-Hispanic white children were 30% more likely to be diagnosed with autism spectrum disorder than were non-Hispanic black children and about 50% more likely to be diagnosed with autism spectrum disorder than were Hispanic children.
Dr. Boyle stressed the importance of early screening and identification of autism spectrum disorder in children (it can be diagnosed by the time a child reaches age 2) and urged parents to take action if a child shows any signs of developmental delays.
“Community leaders, health professionals, educators, and childcare providers should use these data to ensure that children with autism spectrum disorder are identified as early as possible and connected to the services they need,” said Dr. Boyle.
To help promote early intervention in autism spectrum disorder, the CDC will be launching an awareness initiative called “Birth to Five, Watch Me Thrive,” which aims to provide parents, teachers, and community members with information and resources about developmental milestones and screening for autism.
“Most children with autism are not diagnosed until after age 4,” said Dr. Boyle. “The CDC will continue to promote early identification and research. The earlier a child is identified and connected with services, the better.”
The CDC cited several limitations to the report. First, the surveillance sites were not selected to be representative of the entire United States. Second, population denominators used for this report were based on the 2010 decennial census. Comparisons with previous ADDM findings thus should be interpreted with caution because ADDM reports from nondecennial surveillance years are likely influenced by greater error in the population denominators used for those previous surveillance years, which were based on postcensus estimates. Third, three of the nine sites with access to review children’s education records did not receive permission to do so in all school districts within the site’s overall surveillance area. Fourth, findings that address intellectual ability might not be generalizable to all ADDM sites. Finally, race and ethnicity are presented in broad terms and should not be interpreted as generalizable to all persons within those categories.
—Madhu Rajaraman
Suggested Reading
Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators. Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014; Mar 28;63 Suppl 2:1-21.
Suggested Reading
Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators. Prevalence of autism spectrum disorder among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014; Mar 28;63 Suppl 2:1-21.