User login
Maintaining stem cell pluripotency

Salk Institute
Retrotransposons—viral elements incorporated into the human genome—may play a key role in maintaining stem cell pluripotency, a new study suggests.
Previous research indicated that an important fraction of mammalian transcriptomes consists of transcripts derived from retrotransposon elements, but the biological function of these transcripts was unknown.
Now, experiments in induced pluripotent stem cells (iPSCs) and embryonic stem cells (ESCs) have provided some insight into the transcripts’ function.
Piero Carninci, PhD, of RIKEN Center for Life Science Technologies in Yokohama, Japan, and his colleagues described these findings in Nature Genetics.
The researchers found that thousands of transcripts in stem cells that have not yet been annotated are transcribed from retrotransposons, presumably to elicit nuclear functions. These transcripts were expressed in iPSCs and ESCs but not in differentiated cells.
Furthermore, several of the transcripts were shown to be involved in the maintenance of pluripotency. Degrading them using RNA interference caused iPSCs to lose their pluripotency and differentiate.
The researchers said these transcripts appear to have been recruited, both in the human and mouse genome, where they are used to maintain the pluripotency of stem cells. But more research is needed to determine exactly how and why this occurs.
“Our work has just begun to unravel the scale of unexpected functions carried out by retrotransposons and their derived transcripts in stem cell biology,” Dr Carninci said.
“We were extremely surprised to learn from our data that what was once considered genetic junk—namely, ancient retroviruses that were thought to just parasite the genome—are, in reality, symbiotic elements that work closely with other genes to maintain [iPSCs and ESCs] in their undifferentiated state.” ![]()
Salk Institute
Retrotransposons—viral elements incorporated into the human genome—may play a key role in maintaining stem cell pluripotency, a new study suggests.
Previous research indicated that an important fraction of mammalian transcriptomes consists of transcripts derived from retrotransposon elements, but the biological function of these transcripts was unknown.
Now, experiments in induced pluripotent stem cells (iPSCs) and embryonic stem cells (ESCs) have provided some insight into the transcripts’ function.
Piero Carninci, PhD, of RIKEN Center for Life Science Technologies in Yokohama, Japan, and his colleagues described these findings in Nature Genetics.
The researchers found that thousands of transcripts in stem cells that have not yet been annotated are transcribed from retrotransposons, presumably to elicit nuclear functions. These transcripts were expressed in iPSCs and ESCs but not in differentiated cells.
Furthermore, several of the transcripts were shown to be involved in the maintenance of pluripotency. Degrading them using RNA interference caused iPSCs to lose their pluripotency and differentiate.
The researchers said these transcripts appear to have been recruited, both in the human and mouse genome, where they are used to maintain the pluripotency of stem cells. But more research is needed to determine exactly how and why this occurs.
“Our work has just begun to unravel the scale of unexpected functions carried out by retrotransposons and their derived transcripts in stem cell biology,” Dr Carninci said.
“We were extremely surprised to learn from our data that what was once considered genetic junk—namely, ancient retroviruses that were thought to just parasite the genome—are, in reality, symbiotic elements that work closely with other genes to maintain [iPSCs and ESCs] in their undifferentiated state.” ![]()
Salk Institute
Retrotransposons—viral elements incorporated into the human genome—may play a key role in maintaining stem cell pluripotency, a new study suggests.
Previous research indicated that an important fraction of mammalian transcriptomes consists of transcripts derived from retrotransposon elements, but the biological function of these transcripts was unknown.
Now, experiments in induced pluripotent stem cells (iPSCs) and embryonic stem cells (ESCs) have provided some insight into the transcripts’ function.
Piero Carninci, PhD, of RIKEN Center for Life Science Technologies in Yokohama, Japan, and his colleagues described these findings in Nature Genetics.
The researchers found that thousands of transcripts in stem cells that have not yet been annotated are transcribed from retrotransposons, presumably to elicit nuclear functions. These transcripts were expressed in iPSCs and ESCs but not in differentiated cells.
Furthermore, several of the transcripts were shown to be involved in the maintenance of pluripotency. Degrading them using RNA interference caused iPSCs to lose their pluripotency and differentiate.
The researchers said these transcripts appear to have been recruited, both in the human and mouse genome, where they are used to maintain the pluripotency of stem cells. But more research is needed to determine exactly how and why this occurs.
“Our work has just begun to unravel the scale of unexpected functions carried out by retrotransposons and their derived transcripts in stem cell biology,” Dr Carninci said.
“We were extremely surprised to learn from our data that what was once considered genetic junk—namely, ancient retroviruses that were thought to just parasite the genome—are, in reality, symbiotic elements that work closely with other genes to maintain [iPSCs and ESCs] in their undifferentiated state.” ![]()
Study links serum phosphorous levels and anemia risk

Graham Colm
LAS VEGAS—New research suggests a link between serum phosphorous levels and anemia in patients without chronic kidney disease (CKD).
Previous studies have shown that elevations in serum phosphorous are associated with anemia in patients with end-stage renal disease, but whether the link exists in patients without CKD has been unclear.
Now, results of a large study indicate that patients without CKD who have elevated serum phosphorus also have an increased risk of anemia.
John J. Sim, MD, of the Kaiser Permanente Los Angeles Medical Center, and his colleagues presented these findings at the National Kidney Foundation’s 2014 Spring Clinical Meetings (abstract 1708).
The researchers evaluated 32,907 patients with documented serum phosphorus levels, hemoglobin values, and estimated glomerular filtration rates of 60 mL/min or greater. Anemia was defined as having a hemoglobin level below 11 g/dL.
The mean age was 52 years, and 62% of patients were female. The majority of patients were classified as white, 26% as Hispanic, 15% as black, and 7% as Asian.
Serum phosphorus levels ranged from 1.9 mg/dL to 5.7 mg/dL. And 13% of subjects met the criteria for anemia.
Multivariable analysis revealed that each 0.5 mg/dL increase in serum phosphorus level was associated with a 7% increase in the risk of anemia.
The researchers also divided subjects into quartiles according to serum phosphorous levels and calculated the odds ratios (ORs) for anemia.
For the 3.1 mg/dL to 3.5 mg/dL quartile, the OR was 0.85. For the 3.5 mg/dL to 3.9 mg/dL quartile, the OR was 0.90. And for the 3.9 mg/dL to 5.7 mg/dL quartile, the OR was 1.05.
The researchers noted that the link was “more pronounced” in men, but the results suggest that elevated serum phosphorous levels are associated with anemia in non-CKD patients of both sexes. ![]()
Graham Colm
LAS VEGAS—New research suggests a link between serum phosphorous levels and anemia in patients without chronic kidney disease (CKD).
Previous studies have shown that elevations in serum phosphorous are associated with anemia in patients with end-stage renal disease, but whether the link exists in patients without CKD has been unclear.
Now, results of a large study indicate that patients without CKD who have elevated serum phosphorus also have an increased risk of anemia.
John J. Sim, MD, of the Kaiser Permanente Los Angeles Medical Center, and his colleagues presented these findings at the National Kidney Foundation’s 2014 Spring Clinical Meetings (abstract 1708).
The researchers evaluated 32,907 patients with documented serum phosphorus levels, hemoglobin values, and estimated glomerular filtration rates of 60 mL/min or greater. Anemia was defined as having a hemoglobin level below 11 g/dL.
The mean age was 52 years, and 62% of patients were female. The majority of patients were classified as white, 26% as Hispanic, 15% as black, and 7% as Asian.
Serum phosphorus levels ranged from 1.9 mg/dL to 5.7 mg/dL. And 13% of subjects met the criteria for anemia.
Multivariable analysis revealed that each 0.5 mg/dL increase in serum phosphorus level was associated with a 7% increase in the risk of anemia.
The researchers also divided subjects into quartiles according to serum phosphorous levels and calculated the odds ratios (ORs) for anemia.
For the 3.1 mg/dL to 3.5 mg/dL quartile, the OR was 0.85. For the 3.5 mg/dL to 3.9 mg/dL quartile, the OR was 0.90. And for the 3.9 mg/dL to 5.7 mg/dL quartile, the OR was 1.05.
The researchers noted that the link was “more pronounced” in men, but the results suggest that elevated serum phosphorous levels are associated with anemia in non-CKD patients of both sexes. ![]()
Graham Colm
LAS VEGAS—New research suggests a link between serum phosphorous levels and anemia in patients without chronic kidney disease (CKD).
Previous studies have shown that elevations in serum phosphorous are associated with anemia in patients with end-stage renal disease, but whether the link exists in patients without CKD has been unclear.
Now, results of a large study indicate that patients without CKD who have elevated serum phosphorus also have an increased risk of anemia.
John J. Sim, MD, of the Kaiser Permanente Los Angeles Medical Center, and his colleagues presented these findings at the National Kidney Foundation’s 2014 Spring Clinical Meetings (abstract 1708).
The researchers evaluated 32,907 patients with documented serum phosphorus levels, hemoglobin values, and estimated glomerular filtration rates of 60 mL/min or greater. Anemia was defined as having a hemoglobin level below 11 g/dL.
The mean age was 52 years, and 62% of patients were female. The majority of patients were classified as white, 26% as Hispanic, 15% as black, and 7% as Asian.
Serum phosphorus levels ranged from 1.9 mg/dL to 5.7 mg/dL. And 13% of subjects met the criteria for anemia.
Multivariable analysis revealed that each 0.5 mg/dL increase in serum phosphorus level was associated with a 7% increase in the risk of anemia.
The researchers also divided subjects into quartiles according to serum phosphorous levels and calculated the odds ratios (ORs) for anemia.
For the 3.1 mg/dL to 3.5 mg/dL quartile, the OR was 0.85. For the 3.5 mg/dL to 3.9 mg/dL quartile, the OR was 0.90. And for the 3.9 mg/dL to 5.7 mg/dL quartile, the OR was 1.05.
The researchers noted that the link was “more pronounced” in men, but the results suggest that elevated serum phosphorous levels are associated with anemia in non-CKD patients of both sexes. ![]()
New guidelines for NOAC use in surgical patients

Andre E.X. Brown
After reviewing relevant studies, researchers have developed guidelines for the use of new oral anticoagulants (NOACs) in patients undergoing surgery.
The team analyzed 14 years’ worth of data and devised recommendations pertaining to apixaban, dabigatran, and rivaroxaban.
Their guidelines include recommendations for coagulation monitoring, reversing the effects of NOACs, stopping NOACs before surgery, resuming treatment after surgery, and managing bleeding complications.
Aida Lai, MBChB, of the North Bristol NHS Trust in the UK, and her colleagues detailed these recommendations in the British Journal of Surgery.
The researchers looked at studies published between January 2000 and January 2014 that reported on the use of apixaban, dabigatran, and rivaroxaban.
“As these drugs are still relatively new in the market, knowledge about how they work and their associated bleeding risks are still limited in the medical and surgical community,” Dr Lai said. “Our review covers recommendation for the discontinuation of new oral anticoagulant drugs before surgical procedures and resuming of these drugs after procedures.”
Monitoring coagulation
Dr Lai and her colleagues noted that routine coagulation monitoring is not required in patients on NOACs. However, physicians can use these tests to estimate the drugs’ anticoagulation effect in the event of bleeding, suspected overdose, or the need for emergency surgery.
For dabigatran, thrombin clotting time and ecarin clotting time can be used to test the anticoagulation effect. But prothrombin time (PT) is relatively insensitive to the drug, and sensitivity is variable with the activated partial thromboplastin time (APTT) assay. The diluted thrombin time (dTT) provides a direct assessment of thrombin activity, but the assay is not always available.
For rivaroxaban, PT has higher sensitivity than APTT, but there is variability among PT reagents. The anti-Xa chromogenic assay can help estimate the anticoagulation effect of rivaroxaban and apixaban, but this requires calibration with drug-specific reagents.
Reversibility of NOACs
The researchers pointed out that, as NOACs have short half-lives, drug concentrations will decline rapidly in patients with normal renal function. There are few options for reversing the effects of NOACs, but studies are underway investigating the use of antifibrinolytic agents and monoclonal antibodies.
Activated charcoal can decrease the absorption of dabigatran, and hemodialysis can eliminate it from the system, to a large extent. Research has shown that prothrombin complex concentrate (PCC) can reverse the anticoagulation effect of rivaroxaban, although only in healthy subjects thus far.
Discontinuing NOACs before surgery
The decision of when to discontinue NOACs before elective surgery depends on the procedure and the drug in question, Dr Lai and her colleagues said. Physicians must also take into account the individual patient’s risk of bleeding. Recommendations for discontinuation range from 18 hours to 5 days before surgery.
As for emergency and trauma surgery, withholding NOAC doses and initiating supportive care may be sufficient for most patients, due to NOACs’ relatively short half-lives. However, if possible, surgery should be deferred at least 12 hours, ideally 24 hours, from the last dose of a NOAC.
If a patient has taken dabigatran within 2 hours, oral activated charcoal can be used to decrease absorption. Physicians should also consider hemodialysis in patients on dabigatran who have impaired renal function and will require more time for drug clearance. But dialysis will likely be ineffective for clearing rivaroxaban or apixaban.
The researchers recommend the use of PCC or fresh-frozen plasma only in the event of severe hemorrhage. They recommend hemodynamic support in the presence of major bleeding and note that massively transfused patients may require plasma or platelets in addition to red blood cells. Activated PCC or factor VIIa should be considered a last resort.
Restarting NOACs after surgery
The researchers said NOACs can be restarted at a therapeutic dose 24 hours after procedures that confer a low bleeding risk and 48 to 72 hours after procedures that confer a high bleeding risk, as long as adequate hemostasis has been achieved.
If patients have undergone procedures associated with immobilization, they should be given low-molecular-weight heparins 6 to 8 hours after surgery, once hemostasis has been achieved. Then, they can receive NOACs 48 to 72 hours after the procedure.
Managing bleeding complications
NOACs pose a lower risk of intracranial bleeding than warfarin, but they also confer an increased risk of gastrointestinal bleeding. If any bleeding occurs, physicians should enquire about the exact time and amount of the patient’s last NOAC dose.
“As NOACs have short elimination half-lives, time is the most important antidote,” Dr Lai and her colleagues noted.
If the bleeding is not life-threatening, withholding the NOAC and initiating standard supportive measures, such as fluid resuscitation and hemostatic measures, may be sufficient. Patients may receive red cell and platelet transfusions if necessary. And fresh-frozen plasma is appropriate as a plasma expander but not as a reversal agent.
If a patient is experiencing severe or life-threatening bleeding, physicians should withhold the NOAC and initiate standard supportive measures. But they should also try to reverse the anticoagulant effect with activated PCC (50 units/kg) or PCC (25 units/kg) in the case of rivaroxaban and hemodialysis in the case of dabigatran. ![]()
Andre E.X. Brown
After reviewing relevant studies, researchers have developed guidelines for the use of new oral anticoagulants (NOACs) in patients undergoing surgery.
The team analyzed 14 years’ worth of data and devised recommendations pertaining to apixaban, dabigatran, and rivaroxaban.
Their guidelines include recommendations for coagulation monitoring, reversing the effects of NOACs, stopping NOACs before surgery, resuming treatment after surgery, and managing bleeding complications.
Aida Lai, MBChB, of the North Bristol NHS Trust in the UK, and her colleagues detailed these recommendations in the British Journal of Surgery.
The researchers looked at studies published between January 2000 and January 2014 that reported on the use of apixaban, dabigatran, and rivaroxaban.
“As these drugs are still relatively new in the market, knowledge about how they work and their associated bleeding risks are still limited in the medical and surgical community,” Dr Lai said. “Our review covers recommendation for the discontinuation of new oral anticoagulant drugs before surgical procedures and resuming of these drugs after procedures.”
Monitoring coagulation
Dr Lai and her colleagues noted that routine coagulation monitoring is not required in patients on NOACs. However, physicians can use these tests to estimate the drugs’ anticoagulation effect in the event of bleeding, suspected overdose, or the need for emergency surgery.
For dabigatran, thrombin clotting time and ecarin clotting time can be used to test the anticoagulation effect. But prothrombin time (PT) is relatively insensitive to the drug, and sensitivity is variable with the activated partial thromboplastin time (APTT) assay. The diluted thrombin time (dTT) provides a direct assessment of thrombin activity, but the assay is not always available.
For rivaroxaban, PT has higher sensitivity than APTT, but there is variability among PT reagents. The anti-Xa chromogenic assay can help estimate the anticoagulation effect of rivaroxaban and apixaban, but this requires calibration with drug-specific reagents.
Reversibility of NOACs
The researchers pointed out that, as NOACs have short half-lives, drug concentrations will decline rapidly in patients with normal renal function. There are few options for reversing the effects of NOACs, but studies are underway investigating the use of antifibrinolytic agents and monoclonal antibodies.
Activated charcoal can decrease the absorption of dabigatran, and hemodialysis can eliminate it from the system, to a large extent. Research has shown that prothrombin complex concentrate (PCC) can reverse the anticoagulation effect of rivaroxaban, although only in healthy subjects thus far.
Discontinuing NOACs before surgery
The decision of when to discontinue NOACs before elective surgery depends on the procedure and the drug in question, Dr Lai and her colleagues said. Physicians must also take into account the individual patient’s risk of bleeding. Recommendations for discontinuation range from 18 hours to 5 days before surgery.
As for emergency and trauma surgery, withholding NOAC doses and initiating supportive care may be sufficient for most patients, due to NOACs’ relatively short half-lives. However, if possible, surgery should be deferred at least 12 hours, ideally 24 hours, from the last dose of a NOAC.
If a patient has taken dabigatran within 2 hours, oral activated charcoal can be used to decrease absorption. Physicians should also consider hemodialysis in patients on dabigatran who have impaired renal function and will require more time for drug clearance. But dialysis will likely be ineffective for clearing rivaroxaban or apixaban.
The researchers recommend the use of PCC or fresh-frozen plasma only in the event of severe hemorrhage. They recommend hemodynamic support in the presence of major bleeding and note that massively transfused patients may require plasma or platelets in addition to red blood cells. Activated PCC or factor VIIa should be considered a last resort.
Restarting NOACs after surgery
The researchers said NOACs can be restarted at a therapeutic dose 24 hours after procedures that confer a low bleeding risk and 48 to 72 hours after procedures that confer a high bleeding risk, as long as adequate hemostasis has been achieved.
If patients have undergone procedures associated with immobilization, they should be given low-molecular-weight heparins 6 to 8 hours after surgery, once hemostasis has been achieved. Then, they can receive NOACs 48 to 72 hours after the procedure.
Managing bleeding complications
NOACs pose a lower risk of intracranial bleeding than warfarin, but they also confer an increased risk of gastrointestinal bleeding. If any bleeding occurs, physicians should enquire about the exact time and amount of the patient’s last NOAC dose.
“As NOACs have short elimination half-lives, time is the most important antidote,” Dr Lai and her colleagues noted.
If the bleeding is not life-threatening, withholding the NOAC and initiating standard supportive measures, such as fluid resuscitation and hemostatic measures, may be sufficient. Patients may receive red cell and platelet transfusions if necessary. And fresh-frozen plasma is appropriate as a plasma expander but not as a reversal agent.
If a patient is experiencing severe or life-threatening bleeding, physicians should withhold the NOAC and initiate standard supportive measures. But they should also try to reverse the anticoagulant effect with activated PCC (50 units/kg) or PCC (25 units/kg) in the case of rivaroxaban and hemodialysis in the case of dabigatran. ![]()
Andre E.X. Brown
After reviewing relevant studies, researchers have developed guidelines for the use of new oral anticoagulants (NOACs) in patients undergoing surgery.
The team analyzed 14 years’ worth of data and devised recommendations pertaining to apixaban, dabigatran, and rivaroxaban.
Their guidelines include recommendations for coagulation monitoring, reversing the effects of NOACs, stopping NOACs before surgery, resuming treatment after surgery, and managing bleeding complications.
Aida Lai, MBChB, of the North Bristol NHS Trust in the UK, and her colleagues detailed these recommendations in the British Journal of Surgery.
The researchers looked at studies published between January 2000 and January 2014 that reported on the use of apixaban, dabigatran, and rivaroxaban.
“As these drugs are still relatively new in the market, knowledge about how they work and their associated bleeding risks are still limited in the medical and surgical community,” Dr Lai said. “Our review covers recommendation for the discontinuation of new oral anticoagulant drugs before surgical procedures and resuming of these drugs after procedures.”
Monitoring coagulation
Dr Lai and her colleagues noted that routine coagulation monitoring is not required in patients on NOACs. However, physicians can use these tests to estimate the drugs’ anticoagulation effect in the event of bleeding, suspected overdose, or the need for emergency surgery.
For dabigatran, thrombin clotting time and ecarin clotting time can be used to test the anticoagulation effect. But prothrombin time (PT) is relatively insensitive to the drug, and sensitivity is variable with the activated partial thromboplastin time (APTT) assay. The diluted thrombin time (dTT) provides a direct assessment of thrombin activity, but the assay is not always available.
For rivaroxaban, PT has higher sensitivity than APTT, but there is variability among PT reagents. The anti-Xa chromogenic assay can help estimate the anticoagulation effect of rivaroxaban and apixaban, but this requires calibration with drug-specific reagents.
Reversibility of NOACs
The researchers pointed out that, as NOACs have short half-lives, drug concentrations will decline rapidly in patients with normal renal function. There are few options for reversing the effects of NOACs, but studies are underway investigating the use of antifibrinolytic agents and monoclonal antibodies.
Activated charcoal can decrease the absorption of dabigatran, and hemodialysis can eliminate it from the system, to a large extent. Research has shown that prothrombin complex concentrate (PCC) can reverse the anticoagulation effect of rivaroxaban, although only in healthy subjects thus far.
Discontinuing NOACs before surgery
The decision of when to discontinue NOACs before elective surgery depends on the procedure and the drug in question, Dr Lai and her colleagues said. Physicians must also take into account the individual patient’s risk of bleeding. Recommendations for discontinuation range from 18 hours to 5 days before surgery.
As for emergency and trauma surgery, withholding NOAC doses and initiating supportive care may be sufficient for most patients, due to NOACs’ relatively short half-lives. However, if possible, surgery should be deferred at least 12 hours, ideally 24 hours, from the last dose of a NOAC.
If a patient has taken dabigatran within 2 hours, oral activated charcoal can be used to decrease absorption. Physicians should also consider hemodialysis in patients on dabigatran who have impaired renal function and will require more time for drug clearance. But dialysis will likely be ineffective for clearing rivaroxaban or apixaban.
The researchers recommend the use of PCC or fresh-frozen plasma only in the event of severe hemorrhage. They recommend hemodynamic support in the presence of major bleeding and note that massively transfused patients may require plasma or platelets in addition to red blood cells. Activated PCC or factor VIIa should be considered a last resort.
Restarting NOACs after surgery
The researchers said NOACs can be restarted at a therapeutic dose 24 hours after procedures that confer a low bleeding risk and 48 to 72 hours after procedures that confer a high bleeding risk, as long as adequate hemostasis has been achieved.
If patients have undergone procedures associated with immobilization, they should be given low-molecular-weight heparins 6 to 8 hours after surgery, once hemostasis has been achieved. Then, they can receive NOACs 48 to 72 hours after the procedure.
Managing bleeding complications
NOACs pose a lower risk of intracranial bleeding than warfarin, but they also confer an increased risk of gastrointestinal bleeding. If any bleeding occurs, physicians should enquire about the exact time and amount of the patient’s last NOAC dose.
“As NOACs have short elimination half-lives, time is the most important antidote,” Dr Lai and her colleagues noted.
If the bleeding is not life-threatening, withholding the NOAC and initiating standard supportive measures, such as fluid resuscitation and hemostatic measures, may be sufficient. Patients may receive red cell and platelet transfusions if necessary. And fresh-frozen plasma is appropriate as a plasma expander but not as a reversal agent.
If a patient is experiencing severe or life-threatening bleeding, physicians should withhold the NOAC and initiate standard supportive measures. But they should also try to reverse the anticoagulant effect with activated PCC (50 units/kg) or PCC (25 units/kg) in the case of rivaroxaban and hemodialysis in the case of dabigatran. ![]()
Team uncovers novel function of p53

Andrei Thomas Tikhonenko
Investigators have uncovered a novel role for the tumor suppressor p53, according to a paper published in Nature Cell Biology.
The research showed that loss of p53 function caused overproduction of the Aurora A kinase, an enzyme involved in cell division.
That overproduction led to mitotic spindle malformation and aberrant separation of duplicated chromosomes over daughter cells, a phenomenon that predicts tumor metastasis and poor patient outcomes.
“Attempts to identify which genetic defects drive chromosome reshuffling in human cancer led us to focus on cyclin B1 and B2, two key regulators of the stage in the cell cycle where duplicated chromosomes normally separate,” said principal investigator Jan van Deursen, PhD, of the Mayo Clinic in Rochester, Minnesota.
Dr van Deursen and his colleague, Hyun-Ja Nam, PhD, used mouse models to mimic the cyclin B1 and B2 gene defects observed in treatment-resistant human cancers. And the pair discovered that both cyclin B1 and B2 induce chromosome reshuffling and tumor formation.
Subsequent experiments investigating cyclin B2’s mechanism of action pinpointed Aurora A kinase hyperactivity as the main culprit and showed that damage or loss of p53 is a mimetic of cyclin B2 gene defects.
The investigators said the next step for this research will be testing whether anticancer drugs that inhibit Aurora A kinase can be effective in treating cancer patients whose tumors have defects in p53. ![]()
Andrei Thomas Tikhonenko
Investigators have uncovered a novel role for the tumor suppressor p53, according to a paper published in Nature Cell Biology.
The research showed that loss of p53 function caused overproduction of the Aurora A kinase, an enzyme involved in cell division.
That overproduction led to mitotic spindle malformation and aberrant separation of duplicated chromosomes over daughter cells, a phenomenon that predicts tumor metastasis and poor patient outcomes.
“Attempts to identify which genetic defects drive chromosome reshuffling in human cancer led us to focus on cyclin B1 and B2, two key regulators of the stage in the cell cycle where duplicated chromosomes normally separate,” said principal investigator Jan van Deursen, PhD, of the Mayo Clinic in Rochester, Minnesota.
Dr van Deursen and his colleague, Hyun-Ja Nam, PhD, used mouse models to mimic the cyclin B1 and B2 gene defects observed in treatment-resistant human cancers. And the pair discovered that both cyclin B1 and B2 induce chromosome reshuffling and tumor formation.
Subsequent experiments investigating cyclin B2’s mechanism of action pinpointed Aurora A kinase hyperactivity as the main culprit and showed that damage or loss of p53 is a mimetic of cyclin B2 gene defects.
The investigators said the next step for this research will be testing whether anticancer drugs that inhibit Aurora A kinase can be effective in treating cancer patients whose tumors have defects in p53. ![]()
Andrei Thomas Tikhonenko
Investigators have uncovered a novel role for the tumor suppressor p53, according to a paper published in Nature Cell Biology.
The research showed that loss of p53 function caused overproduction of the Aurora A kinase, an enzyme involved in cell division.
That overproduction led to mitotic spindle malformation and aberrant separation of duplicated chromosomes over daughter cells, a phenomenon that predicts tumor metastasis and poor patient outcomes.
“Attempts to identify which genetic defects drive chromosome reshuffling in human cancer led us to focus on cyclin B1 and B2, two key regulators of the stage in the cell cycle where duplicated chromosomes normally separate,” said principal investigator Jan van Deursen, PhD, of the Mayo Clinic in Rochester, Minnesota.
Dr van Deursen and his colleague, Hyun-Ja Nam, PhD, used mouse models to mimic the cyclin B1 and B2 gene defects observed in treatment-resistant human cancers. And the pair discovered that both cyclin B1 and B2 induce chromosome reshuffling and tumor formation.
Subsequent experiments investigating cyclin B2’s mechanism of action pinpointed Aurora A kinase hyperactivity as the main culprit and showed that damage or loss of p53 is a mimetic of cyclin B2 gene defects.
The investigators said the next step for this research will be testing whether anticancer drugs that inhibit Aurora A kinase can be effective in treating cancer patients whose tumors have defects in p53. ![]()
Practice Question Answers: Medications in Dermatology, Part 2
1. A 40-year-old woman is diagnosed with systemic lupus erythematosus. You discuss treatment options and decide to start hydroxychloroquine. What laboratory tests and monitoring are required prior to starting this medication?
a. complete blood cell count with differential and glucose-6-phosphate dehydrogenase
b. complete blood cell count with differential and complete metabolic profile
c. ophthalmology evaluation and glucose-6-phosphate dehydrogenase
d. b and c
2. Two months ago you saw a 30-year-old woman with a history of severe atopic dermatitis. She had been using topical steroids with not much improvement. You decided to start a systemic medication. Within 1 month of drug initiation, she called your office to tell you that she is much better but has noticed unwanted hair on her face lately. Which medication is most likely implicated?
a. cyclosporine
b. dapsone
c. hydroxychloroquine
d. methotrexate
3. A 70-year-old man with type 2 diabetes mellitus who drinks 10 cans of beer per week presents to the emergency department with a 3-day history of diffuse tense bullae and pruritus on the legs and trunk. Direct immunofluorescence displayed linear deposition of IgG and C3 at the dermoepidermal junction, confirming your clinical diagnosis. What is the best long-term treatment option for this patient?
a. combination of oral steroids plus methotrexate
b. oral steroids and mycophenolate mofetil
c. oral steroids only
d. topical steroids only
4. A 45-year-old Venezuelan man presents with painful nodules on his bilateral lower legs. A biopsy demonstrates acid-fast bacilli, and a multidrug regimen is initiated for erythema nodosum leprosum. Which of the following is the mechanism of action of the treatment that is US Food and Drug Administration approved for this condition?
a. inhibits chemotaxis
b. inhibits dihydrofolate reductase
c. inhibits tumor necrosis factor α
d. suppresses T-cell function and B-cell antibody production
5. A patient consults her physician because of several side effects from a medication she started 2 weeks ago due to erythematous to violaceous papules on the legs from palpable purpura. She reports diarrhea, abdominal pain, and fatigue. Which medication is she taking?
a. azathioprine
b. colchicine
c. dapsone
d. methotrexate
1. A 40-year-old woman is diagnosed with systemic lupus erythematosus. You discuss treatment options and decide to start hydroxychloroquine. What laboratory tests and monitoring are required prior to starting this medication?
a. complete blood cell count with differential and glucose-6-phosphate dehydrogenase
b. complete blood cell count with differential and complete metabolic profile
c. ophthalmology evaluation and glucose-6-phosphate dehydrogenase
d. b and c
2. Two months ago you saw a 30-year-old woman with a history of severe atopic dermatitis. She had been using topical steroids with not much improvement. You decided to start a systemic medication. Within 1 month of drug initiation, she called your office to tell you that she is much better but has noticed unwanted hair on her face lately. Which medication is most likely implicated?
a. cyclosporine
b. dapsone
c. hydroxychloroquine
d. methotrexate
3. A 70-year-old man with type 2 diabetes mellitus who drinks 10 cans of beer per week presents to the emergency department with a 3-day history of diffuse tense bullae and pruritus on the legs and trunk. Direct immunofluorescence displayed linear deposition of IgG and C3 at the dermoepidermal junction, confirming your clinical diagnosis. What is the best long-term treatment option for this patient?
a. combination of oral steroids plus methotrexate
b. oral steroids and mycophenolate mofetil
c. oral steroids only
d. topical steroids only
4. A 45-year-old Venezuelan man presents with painful nodules on his bilateral lower legs. A biopsy demonstrates acid-fast bacilli, and a multidrug regimen is initiated for erythema nodosum leprosum. Which of the following is the mechanism of action of the treatment that is US Food and Drug Administration approved for this condition?
a. inhibits chemotaxis
b. inhibits dihydrofolate reductase
c. inhibits tumor necrosis factor α
d. suppresses T-cell function and B-cell antibody production
5. A patient consults her physician because of several side effects from a medication she started 2 weeks ago due to erythematous to violaceous papules on the legs from palpable purpura. She reports diarrhea, abdominal pain, and fatigue. Which medication is she taking?
a. azathioprine
b. colchicine
c. dapsone
d. methotrexate
1. A 40-year-old woman is diagnosed with systemic lupus erythematosus. You discuss treatment options and decide to start hydroxychloroquine. What laboratory tests and monitoring are required prior to starting this medication?
a. complete blood cell count with differential and glucose-6-phosphate dehydrogenase
b. complete blood cell count with differential and complete metabolic profile
c. ophthalmology evaluation and glucose-6-phosphate dehydrogenase
d. b and c
2. Two months ago you saw a 30-year-old woman with a history of severe atopic dermatitis. She had been using topical steroids with not much improvement. You decided to start a systemic medication. Within 1 month of drug initiation, she called your office to tell you that she is much better but has noticed unwanted hair on her face lately. Which medication is most likely implicated?
a. cyclosporine
b. dapsone
c. hydroxychloroquine
d. methotrexate
3. A 70-year-old man with type 2 diabetes mellitus who drinks 10 cans of beer per week presents to the emergency department with a 3-day history of diffuse tense bullae and pruritus on the legs and trunk. Direct immunofluorescence displayed linear deposition of IgG and C3 at the dermoepidermal junction, confirming your clinical diagnosis. What is the best long-term treatment option for this patient?
a. combination of oral steroids plus methotrexate
b. oral steroids and mycophenolate mofetil
c. oral steroids only
d. topical steroids only
4. A 45-year-old Venezuelan man presents with painful nodules on his bilateral lower legs. A biopsy demonstrates acid-fast bacilli, and a multidrug regimen is initiated for erythema nodosum leprosum. Which of the following is the mechanism of action of the treatment that is US Food and Drug Administration approved for this condition?
a. inhibits chemotaxis
b. inhibits dihydrofolate reductase
c. inhibits tumor necrosis factor α
d. suppresses T-cell function and B-cell antibody production
5. A patient consults her physician because of several side effects from a medication she started 2 weeks ago due to erythematous to violaceous papules on the legs from palpable purpura. She reports diarrhea, abdominal pain, and fatigue. Which medication is she taking?
a. azathioprine
b. colchicine
c. dapsone
d. methotrexate

Medications in Dermatology, Part 2: Immunosuppressives
6 ‘M’s to keep in mind when you next see a patient with anorexia nervosa
Anorexia nervosa is associated with comorbid psychiatric disorders, severe physical complications, and high mortality. To help you remember important clinical information when working with patients with anorexia, we propose this “6 M” model for screening, treatment, and prognosis.
Monitor closely. Anorexia can go undiagnosed and untreated for years. During your patients’ office visits, ask about body image, exercise habits, and menstrual irregularities, especially when seeing at-risk youth. During physical examination, reluctance to be weighed, vital sign abnormalities (eg, orthostatic hypotension, variability in pulse), skin abnormalities (lanugo hair, dryness), and marks indicating self-harm can serve as diagnostic indicators. Consider hospitalization for patients at <75% of their ideal body weight, who refuse to eat, or who show vital signs and laboratory abnormalities.
Media. By providing information on healthy eating and nutrition, the Internet can be an excellent resource for people with an eating disorder; however, you should also be aware of the impact of so-called pro-ana Web sites. People with anorexia use these Web sites to discuss their illness, but the sites sometimes glorify eating disorders as a lifestyle choice, and can be a place to share tips and tricks on extreme dieting, and might promote what is known as “thinspiration” in popular culture.
Meals. The American Dietetic Association recommends that anorexic patients begin oral intake at no more than 30 to 40 kcal/kg/day, and then gradually increase it, with a weight gain goal of 0.5 to 1 lb per week.
This graduated weight gain is done to prevent refeeding syndrome. After chronic starvation, intracellular phosphate stores are depleted and once carbohydrate intake resumes, insulin release causes phosphate to enter cells, thereby leading to hypophosphatemia. This electrolyte abnormality can result in cardiac failure. As a result, consider regular monitoring of phosphate levels, especially during the first week of reintroducing food.
Multimodal therapy. Despite being notoriously difficult to treat, patients with anorexia might respond to psychotherapy—especially family therapy—with an increased remission rate and faster return to health, compared with other forms of treatment. With a multimodal regimen involving proper refeeding techniques, family therapy, and medications as appropriate, recovery is possible.
Medications might be a helpful adjunct in patients who do not gain weight despite psychotherapy and proper nutritional measures. For example:
• There is some research on medications such as olanzapine and anxiolytics for treating anorexia.
• A low-dose anxiolytic might benefit patients with preprandial anxiety.
• Comorbid psychiatric disorders might improve during treatment of the eating disorder.
• Selective serotonin reuptake inhibitors and second-generation antipsychotics might help manage severe comorbid psychiatric disorders.
Because of low body weight and altered plasma protein binding, start medications at a low dosage. The risk of adverse effects can increase because more “free” medication is available. Consider avoiding medications such as bupropion and tricyclic antidepressants, because they carry an increased risk of seizures and cardiac effects, respectively.
Morbidity and mortality. Untreated anorexia has the highest mortality among psychiatric disorders: approximately 5.1 deaths for every 1,000 people.1 Recent meta-analyses show that patients with anorexia may have a 5.86 times greater risk of death than the general population.1 Serious sequelae include cardiac complications; osteoporosis; infertility; and comorbid psychiatric conditions such as substance abuse, depression, and obsessive-compulsive disorder.2
1. Arcelus J, Mitchell AJ, Wales J, et al. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry. 2011; 68(7):724-731.
2. Yager J, Andersen AE. Clinical practice. Anorexia nervosa. N Engl J Med. 2005;353(14):1481-1488.
Anorexia nervosa is associated with comorbid psychiatric disorders, severe physical complications, and high mortality. To help you remember important clinical information when working with patients with anorexia, we propose this “6 M” model for screening, treatment, and prognosis.
Monitor closely. Anorexia can go undiagnosed and untreated for years. During your patients’ office visits, ask about body image, exercise habits, and menstrual irregularities, especially when seeing at-risk youth. During physical examination, reluctance to be weighed, vital sign abnormalities (eg, orthostatic hypotension, variability in pulse), skin abnormalities (lanugo hair, dryness), and marks indicating self-harm can serve as diagnostic indicators. Consider hospitalization for patients at <75% of their ideal body weight, who refuse to eat, or who show vital signs and laboratory abnormalities.
Media. By providing information on healthy eating and nutrition, the Internet can be an excellent resource for people with an eating disorder; however, you should also be aware of the impact of so-called pro-ana Web sites. People with anorexia use these Web sites to discuss their illness, but the sites sometimes glorify eating disorders as a lifestyle choice, and can be a place to share tips and tricks on extreme dieting, and might promote what is known as “thinspiration” in popular culture.
Meals. The American Dietetic Association recommends that anorexic patients begin oral intake at no more than 30 to 40 kcal/kg/day, and then gradually increase it, with a weight gain goal of 0.5 to 1 lb per week.
This graduated weight gain is done to prevent refeeding syndrome. After chronic starvation, intracellular phosphate stores are depleted and once carbohydrate intake resumes, insulin release causes phosphate to enter cells, thereby leading to hypophosphatemia. This electrolyte abnormality can result in cardiac failure. As a result, consider regular monitoring of phosphate levels, especially during the first week of reintroducing food.
Multimodal therapy. Despite being notoriously difficult to treat, patients with anorexia might respond to psychotherapy—especially family therapy—with an increased remission rate and faster return to health, compared with other forms of treatment. With a multimodal regimen involving proper refeeding techniques, family therapy, and medications as appropriate, recovery is possible.
Medications might be a helpful adjunct in patients who do not gain weight despite psychotherapy and proper nutritional measures. For example:
• There is some research on medications such as olanzapine and anxiolytics for treating anorexia.
• A low-dose anxiolytic might benefit patients with preprandial anxiety.
• Comorbid psychiatric disorders might improve during treatment of the eating disorder.
• Selective serotonin reuptake inhibitors and second-generation antipsychotics might help manage severe comorbid psychiatric disorders.
Because of low body weight and altered plasma protein binding, start medications at a low dosage. The risk of adverse effects can increase because more “free” medication is available. Consider avoiding medications such as bupropion and tricyclic antidepressants, because they carry an increased risk of seizures and cardiac effects, respectively.
Morbidity and mortality. Untreated anorexia has the highest mortality among psychiatric disorders: approximately 5.1 deaths for every 1,000 people.1 Recent meta-analyses show that patients with anorexia may have a 5.86 times greater risk of death than the general population.1 Serious sequelae include cardiac complications; osteoporosis; infertility; and comorbid psychiatric conditions such as substance abuse, depression, and obsessive-compulsive disorder.2
Anorexia nervosa is associated with comorbid psychiatric disorders, severe physical complications, and high mortality. To help you remember important clinical information when working with patients with anorexia, we propose this “6 M” model for screening, treatment, and prognosis.
Monitor closely. Anorexia can go undiagnosed and untreated for years. During your patients’ office visits, ask about body image, exercise habits, and menstrual irregularities, especially when seeing at-risk youth. During physical examination, reluctance to be weighed, vital sign abnormalities (eg, orthostatic hypotension, variability in pulse), skin abnormalities (lanugo hair, dryness), and marks indicating self-harm can serve as diagnostic indicators. Consider hospitalization for patients at <75% of their ideal body weight, who refuse to eat, or who show vital signs and laboratory abnormalities.
Media. By providing information on healthy eating and nutrition, the Internet can be an excellent resource for people with an eating disorder; however, you should also be aware of the impact of so-called pro-ana Web sites. People with anorexia use these Web sites to discuss their illness, but the sites sometimes glorify eating disorders as a lifestyle choice, and can be a place to share tips and tricks on extreme dieting, and might promote what is known as “thinspiration” in popular culture.
Meals. The American Dietetic Association recommends that anorexic patients begin oral intake at no more than 30 to 40 kcal/kg/day, and then gradually increase it, with a weight gain goal of 0.5 to 1 lb per week.
This graduated weight gain is done to prevent refeeding syndrome. After chronic starvation, intracellular phosphate stores are depleted and once carbohydrate intake resumes, insulin release causes phosphate to enter cells, thereby leading to hypophosphatemia. This electrolyte abnormality can result in cardiac failure. As a result, consider regular monitoring of phosphate levels, especially during the first week of reintroducing food.
Multimodal therapy. Despite being notoriously difficult to treat, patients with anorexia might respond to psychotherapy—especially family therapy—with an increased remission rate and faster return to health, compared with other forms of treatment. With a multimodal regimen involving proper refeeding techniques, family therapy, and medications as appropriate, recovery is possible.
Medications might be a helpful adjunct in patients who do not gain weight despite psychotherapy and proper nutritional measures. For example:
• There is some research on medications such as olanzapine and anxiolytics for treating anorexia.
• A low-dose anxiolytic might benefit patients with preprandial anxiety.
• Comorbid psychiatric disorders might improve during treatment of the eating disorder.
• Selective serotonin reuptake inhibitors and second-generation antipsychotics might help manage severe comorbid psychiatric disorders.
Because of low body weight and altered plasma protein binding, start medications at a low dosage. The risk of adverse effects can increase because more “free” medication is available. Consider avoiding medications such as bupropion and tricyclic antidepressants, because they carry an increased risk of seizures and cardiac effects, respectively.
Morbidity and mortality. Untreated anorexia has the highest mortality among psychiatric disorders: approximately 5.1 deaths for every 1,000 people.1 Recent meta-analyses show that patients with anorexia may have a 5.86 times greater risk of death than the general population.1 Serious sequelae include cardiac complications; osteoporosis; infertility; and comorbid psychiatric conditions such as substance abuse, depression, and obsessive-compulsive disorder.2
1. Arcelus J, Mitchell AJ, Wales J, et al. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry. 2011; 68(7):724-731.
2. Yager J, Andersen AE. Clinical practice. Anorexia nervosa. N Engl J Med. 2005;353(14):1481-1488.
1. Arcelus J, Mitchell AJ, Wales J, et al. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch Gen Psychiatry. 2011; 68(7):724-731.
2. Yager J, Andersen AE. Clinical practice. Anorexia nervosa. N Engl J Med. 2005;353(14):1481-1488.
Rethink clonidine for patients undergoing noncardiac surgery
Close to 1 in 3 Americans has hypertension, and the American Heart Association estimates that number will increase by more than 7% by 2030. The prevalence of obesity, a sedentary lifestyle, cigarette smoking, and a variety of other risk factors create a perfect storm for cardiovascular topsy-turviness.
Hypertension is so common among hospitalized patients, most of us have already chosen our "drugs of choice" to treat it. Unlike the case in primary care, in which physicians may have the luxury of starting with a first-line drug, and perhaps adding a second-line agent a few months later, in the hospital setting, we are often faced with hypertensive emergencies and urgencies that require immediate treatment. The expert opinions outlined in the new JNC-8 guidelines may not be appropriate for our acutely ill patient with a blood pressure of 240/135.
While decreasing the blood pressure is a top priority, there are frequently complicating factors, such as uncontrolled pain, intravenous fluids, or glucocorticoid use that make maintaining a consistently safe blood pressure challenging, to say the least. One reading may be an acceptable 140/85, while a few hours later it may spike to 200/120, and this roller coaster ride may continue for days on end. That\'s when we often reach for a PRN medication to help keep the patient out of danger as we manage a host of other conditions.
Many remember when sublingual nifedipine was the drug of choice for rapid reduction of severe blood pressure elevations, until the rapid drop proved to be devastating to the cerebral perfusion for some very unfortunate patients. Over the years, clonidine has become a highly favored drug if an oral agent is deemed appropriate. Its onset is rapid, and it drops the blood pressure to a moderate degree in most patients. However, a recent article in the New England Journal of Medicine, Clonidine in Patients Undergoing Noncardiac Surgery, may make many rethink their use of clonidine in this subpopulation of patients.
Researchers found clonidine 0.2 mg daily started just before surgery and continued until 72 hours postop was associated with an increase in nonfatal cardiac arrest (0.3% vs. 0.1%) and clinically significant hypotension (47.6% vs. 37.1%). Myocardial infarction occurred in 5.9% in the placebo group, compared to 6.6% in the clonidine group (N. Engl. J. Med. 2014;370:1504-13).
This article is highly significant to me, a frequent prescriber of PRN clonidine. Though the article did not address PRN use of clonidine perioperatively, in my opinion, the results are concerning enough to warrant thoughtful consideration. While it will not likely affect my prescribing practice for most patients, I plan to expand my armamentarium of drugs for those who I think may require surgery in the near future.
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at [email protected].
Close to 1 in 3 Americans has hypertension, and the American Heart Association estimates that number will increase by more than 7% by 2030. The prevalence of obesity, a sedentary lifestyle, cigarette smoking, and a variety of other risk factors create a perfect storm for cardiovascular topsy-turviness.
Hypertension is so common among hospitalized patients, most of us have already chosen our "drugs of choice" to treat it. Unlike the case in primary care, in which physicians may have the luxury of starting with a first-line drug, and perhaps adding a second-line agent a few months later, in the hospital setting, we are often faced with hypertensive emergencies and urgencies that require immediate treatment. The expert opinions outlined in the new JNC-8 guidelines may not be appropriate for our acutely ill patient with a blood pressure of 240/135.
While decreasing the blood pressure is a top priority, there are frequently complicating factors, such as uncontrolled pain, intravenous fluids, or glucocorticoid use that make maintaining a consistently safe blood pressure challenging, to say the least. One reading may be an acceptable 140/85, while a few hours later it may spike to 200/120, and this roller coaster ride may continue for days on end. That\'s when we often reach for a PRN medication to help keep the patient out of danger as we manage a host of other conditions.
Many remember when sublingual nifedipine was the drug of choice for rapid reduction of severe blood pressure elevations, until the rapid drop proved to be devastating to the cerebral perfusion for some very unfortunate patients. Over the years, clonidine has become a highly favored drug if an oral agent is deemed appropriate. Its onset is rapid, and it drops the blood pressure to a moderate degree in most patients. However, a recent article in the New England Journal of Medicine, Clonidine in Patients Undergoing Noncardiac Surgery, may make many rethink their use of clonidine in this subpopulation of patients.
Researchers found clonidine 0.2 mg daily started just before surgery and continued until 72 hours postop was associated with an increase in nonfatal cardiac arrest (0.3% vs. 0.1%) and clinically significant hypotension (47.6% vs. 37.1%). Myocardial infarction occurred in 5.9% in the placebo group, compared to 6.6% in the clonidine group (N. Engl. J. Med. 2014;370:1504-13).
This article is highly significant to me, a frequent prescriber of PRN clonidine. Though the article did not address PRN use of clonidine perioperatively, in my opinion, the results are concerning enough to warrant thoughtful consideration. While it will not likely affect my prescribing practice for most patients, I plan to expand my armamentarium of drugs for those who I think may require surgery in the near future.
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at [email protected].
Close to 1 in 3 Americans has hypertension, and the American Heart Association estimates that number will increase by more than 7% by 2030. The prevalence of obesity, a sedentary lifestyle, cigarette smoking, and a variety of other risk factors create a perfect storm for cardiovascular topsy-turviness.
Hypertension is so common among hospitalized patients, most of us have already chosen our "drugs of choice" to treat it. Unlike the case in primary care, in which physicians may have the luxury of starting with a first-line drug, and perhaps adding a second-line agent a few months later, in the hospital setting, we are often faced with hypertensive emergencies and urgencies that require immediate treatment. The expert opinions outlined in the new JNC-8 guidelines may not be appropriate for our acutely ill patient with a blood pressure of 240/135.
While decreasing the blood pressure is a top priority, there are frequently complicating factors, such as uncontrolled pain, intravenous fluids, or glucocorticoid use that make maintaining a consistently safe blood pressure challenging, to say the least. One reading may be an acceptable 140/85, while a few hours later it may spike to 200/120, and this roller coaster ride may continue for days on end. That\'s when we often reach for a PRN medication to help keep the patient out of danger as we manage a host of other conditions.
Many remember when sublingual nifedipine was the drug of choice for rapid reduction of severe blood pressure elevations, until the rapid drop proved to be devastating to the cerebral perfusion for some very unfortunate patients. Over the years, clonidine has become a highly favored drug if an oral agent is deemed appropriate. Its onset is rapid, and it drops the blood pressure to a moderate degree in most patients. However, a recent article in the New England Journal of Medicine, Clonidine in Patients Undergoing Noncardiac Surgery, may make many rethink their use of clonidine in this subpopulation of patients.
Researchers found clonidine 0.2 mg daily started just before surgery and continued until 72 hours postop was associated with an increase in nonfatal cardiac arrest (0.3% vs. 0.1%) and clinically significant hypotension (47.6% vs. 37.1%). Myocardial infarction occurred in 5.9% in the placebo group, compared to 6.6% in the clonidine group (N. Engl. J. Med. 2014;370:1504-13).
This article is highly significant to me, a frequent prescriber of PRN clonidine. Though the article did not address PRN use of clonidine perioperatively, in my opinion, the results are concerning enough to warrant thoughtful consideration. While it will not likely affect my prescribing practice for most patients, I plan to expand my armamentarium of drugs for those who I think may require surgery in the near future.
Dr. Hester is a hospitalist with Baltimore-Washington Medical Center who has a passion for empowering patients to partner in their health care. She is the creator of the Patient Whiz, a patient-engagement app for iOS. Reach her at [email protected].

What are the benefits and risks of inhaled corticosteroids for COPD?
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
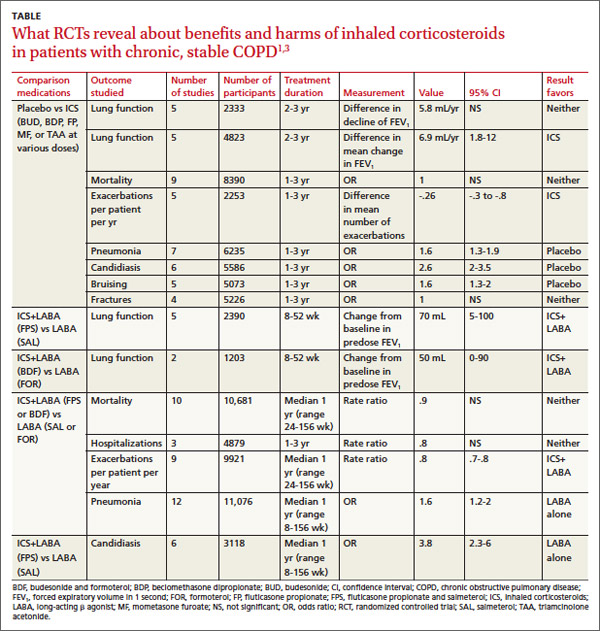
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
RECOMMENDATIONS
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
RECOMMENDATIONS
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
Inhaled corticosteroids (ICS), either alone or with a long-acting β agonist (LABA), reduce the frequency of exacerbations of chronic obstructive pulmonary disease (COPD) and statistically, but not clinically, improve quality of life (QOL) (strength of recommendation [SOR]: B, meta-analyses of heterogeneous studies).
However, ICS have no mortality benefit and don’t consistently improve forced expiratory volume in 1 second (FEV1) (SOR: B, meta-analyses of secondary outcomes). They increase the risk of pneumonia, oropharyngeal candidiasis, and bruising (SOR: B, meta-analyses of secondary outcomes).
Withdrawal of ICS doesn’t significantly increase the risk of COPD exacerbation (SOR: B, a meta-analysis).
EVIDENCE SUMMARY
A Cochrane meta-analysis designed to determine the efficacy of ICS in patients with stable COPD found 55 randomized, controlled trials (RCTs) with a total of 16,154 participants that compared ICS with placebo for 2 weeks to 3 years duration.1 COPD varied from moderate to severe in most studies.
In pooled data, ICS for 2 or more years didn’t consistently improve lung function, the primary outcome (TABLE). However, the largest RCT (N=2617) of 3 years duration showed a small decrease in decline of FEV1 (55 mL compared with 42 mL, P value not provided). Regarding the secondary outcomes of mortality and exacerbations, ICS for a year or longer didn’t reduce mortality but decreased exacerbations by 19%.
Clinically significant adverse effects of ICS use included pneumonia, oropharyngeal candidiasis, and bruising; for ICS treatment longer than one year, the numbers needed to harm (NNH) compared with placebo were 30, 27, and 32, respectively. Bone fractures weren’t more common among ICS users. Investigators observed a statistical, but not clinical, QOL benefit as measured by the St. George’s Respiratory Questionnaire (SGRQ) in 5 RCTs with a total of 2507 patients (mean difference, ‒1.22 units/year; 95% confidence interval, ‒1.83 to ‒.60). The minimum clinically important difference on the 76-item questionnaire was 4 units.2
Adding ICS to LABA increases risk of pneumonia and candidiasis
A Cochrane meta-analysis of 14 double-blind RCTs comprising a total of 11,794 participants with severe COPD compared LABA plus ICS with LABA alone over 8 weeks to 3 years.3 Primary outcomes were exacerbations, mortality, hospitalizations, and pneumonia. Secondary outcomes included oropharyngeal candidiasis and health-related QOL.
The LABA-plus-ICS group had lower rates of exacerbations than the LABA group, but the data were of low quality because of significant heterogeneity among studies and high rates of attrition. No significant difference in mortality or hospitalizations was found between the groups. The risk of pneumonia in the LABA-plus-ICS group was higher than in the LABA-alone group, with a NNH of 48.
Candidiasis occurred more often in patients on combination fluticasone and salmeterol than salmeterol alone, with a NNH of 22. QOL scores (measured by the SGRQ) in patients on combination therapy were statistically better, but clinically insignificant.
Discontinuing ICS doesn’t increase exacerbations
A meta-analysis of 3 RCTs that enrolled a total of 877 patients with COPD compared the number of exacerbations in patients who continued fluticasone 500 mcg inhaled twice daily and patients who were withdrawn from the medication. All patients had been treated with ICS for at least 3 months, and had been on fluticasone for at least 2 weeks. Subjects had a baseline FEV1 between 25% and 80% predicted. No significant increase in exacerbations occurred after discontinuing ICS.4
RECOMMENDATIONS
The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society, in a joint guideline, recommend against using ICS as monotherapy for patients with stable COPD. They acknowledge that these drugs are superior to placebo in reducing exacerbations, but note that concerns about their side-effect profile (thrush, potential for bone loss, and moderate to severe easy bruisability) make them less desirable than LABAs or long-acting inhaled anticholinergics.5
The Global Initiative for Chronic Obstructive Lung Disease likewise discourages long-term use of ICS because of the risk of pneumonia and fractures.6 Both groups note that patients with severe COPD may benefit from a combination of ICS and a long-acting medication (usually a LABA).
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
1. Yang IA, Clarke MS, Sim EH, et al. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(7):CD002991.
2. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2:75-79.
3. Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;9:CD006829.
4. Nadeem NJ, Taylor SJ, Eldridge SM. Withdrawal of inhaled corticosteroids in individuals with COPD—a systemic review and comment on trial methodology. Respir Res. 2011;12:107.
5. Qaseem A, Wilt TJ, Weinberger SE, et al; American College of Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med. 2011;155:179-191.
6. Global Initiative for Chronic Obstructive Lung Disease Web site. Global strategy for the diagnosis, management and prevention of COPD. 2014. Available at: www.goldcopd.org/uploads/users/files/GOLD_Report2014_Feb07.pdf. Accessed April 4, 2013.
Evidence-based answers from the Family Physicians Inquiries Network
Bruises Be Gone! Treatment of Bruising

An article in Dermatologic Surgery, “Comparative Study on Bruise Reduction Treatments After Bruise Induction Using the Pulsed Dye Laser,” (2013;39:1459-1464) compared the of effectiveness different modalities in reducing time for bruise resolution. The investigators compared cold compresses; hydrogen peroxide; over-the-counter bruise serum containing primrose oil, vitamin E oil, and glycerin; and pulsed dye laser (PDL). Seventeen patients (Fitzpatrick skin types I–IV) were enrolled and had bruise induction with a PDL to produce five 2×2-cm zones of bruising on the lower abdomen. Excluding the control, bruises were randomly treated using a cold compress, bruise serum, 3% hydrogen peroxide–soaked gauze, or PDL. Subjects and 2 blinded physician evaluators graded the bruise severity using a visual scale on days 0, 3, and 7. The investigators found that treatment did not result in statistically significantly shorter bruise resolution time than in controls. They reported that PDL-treated bruises took a longer time to resolve than controls.
What’s the issue?
Although this study found that the PDL-treated bruises took a longer time to resolve, there have been other studies that have shown PDL to hasten time to bruise resolution, which could be due to the fact that the initial bruises in this particular study were actually induced by PDL. In another study, DeFatta et al (Arch Facial Plast Surg. 2009;11:99-103) found maximal efficacy when PDL was performed on or after postoperative day 5. It was reasoned that treatment before then was less effective because of the depth of red blood cell extravasation and overlying inflammation and edema. Karen and Hale (Dermatol Surg. 2010;36:1328-1331) reported that the optimal time for PDL treatment was between 48 and 72 hours, suggesting that hemoglobin predominates during this period instead of the bilirubin predominance seen in the later stages of ecchymosis. Their parameters were 7.5 J/cm2, 10-mm spot, 6-millisecond pulse duration, and cryogen 30 milliseconds with a 20-millisecond delay for a single pass. What do you use for posttreatment bruising?
An article in Dermatologic Surgery, “Comparative Study on Bruise Reduction Treatments After Bruise Induction Using the Pulsed Dye Laser,” (2013;39:1459-1464) compared the of effectiveness different modalities in reducing time for bruise resolution. The investigators compared cold compresses; hydrogen peroxide; over-the-counter bruise serum containing primrose oil, vitamin E oil, and glycerin; and pulsed dye laser (PDL). Seventeen patients (Fitzpatrick skin types I–IV) were enrolled and had bruise induction with a PDL to produce five 2×2-cm zones of bruising on the lower abdomen. Excluding the control, bruises were randomly treated using a cold compress, bruise serum, 3% hydrogen peroxide–soaked gauze, or PDL. Subjects and 2 blinded physician evaluators graded the bruise severity using a visual scale on days 0, 3, and 7. The investigators found that treatment did not result in statistically significantly shorter bruise resolution time than in controls. They reported that PDL-treated bruises took a longer time to resolve than controls.
What’s the issue?
Although this study found that the PDL-treated bruises took a longer time to resolve, there have been other studies that have shown PDL to hasten time to bruise resolution, which could be due to the fact that the initial bruises in this particular study were actually induced by PDL. In another study, DeFatta et al (Arch Facial Plast Surg. 2009;11:99-103) found maximal efficacy when PDL was performed on or after postoperative day 5. It was reasoned that treatment before then was less effective because of the depth of red blood cell extravasation and overlying inflammation and edema. Karen and Hale (Dermatol Surg. 2010;36:1328-1331) reported that the optimal time for PDL treatment was between 48 and 72 hours, suggesting that hemoglobin predominates during this period instead of the bilirubin predominance seen in the later stages of ecchymosis. Their parameters were 7.5 J/cm2, 10-mm spot, 6-millisecond pulse duration, and cryogen 30 milliseconds with a 20-millisecond delay for a single pass. What do you use for posttreatment bruising?
An article in Dermatologic Surgery, “Comparative Study on Bruise Reduction Treatments After Bruise Induction Using the Pulsed Dye Laser,” (2013;39:1459-1464) compared the of effectiveness different modalities in reducing time for bruise resolution. The investigators compared cold compresses; hydrogen peroxide; over-the-counter bruise serum containing primrose oil, vitamin E oil, and glycerin; and pulsed dye laser (PDL). Seventeen patients (Fitzpatrick skin types I–IV) were enrolled and had bruise induction with a PDL to produce five 2×2-cm zones of bruising on the lower abdomen. Excluding the control, bruises were randomly treated using a cold compress, bruise serum, 3% hydrogen peroxide–soaked gauze, or PDL. Subjects and 2 blinded physician evaluators graded the bruise severity using a visual scale on days 0, 3, and 7. The investigators found that treatment did not result in statistically significantly shorter bruise resolution time than in controls. They reported that PDL-treated bruises took a longer time to resolve than controls.
What’s the issue?
Although this study found that the PDL-treated bruises took a longer time to resolve, there have been other studies that have shown PDL to hasten time to bruise resolution, which could be due to the fact that the initial bruises in this particular study were actually induced by PDL. In another study, DeFatta et al (Arch Facial Plast Surg. 2009;11:99-103) found maximal efficacy when PDL was performed on or after postoperative day 5. It was reasoned that treatment before then was less effective because of the depth of red blood cell extravasation and overlying inflammation and edema. Karen and Hale (Dermatol Surg. 2010;36:1328-1331) reported that the optimal time for PDL treatment was between 48 and 72 hours, suggesting that hemoglobin predominates during this period instead of the bilirubin predominance seen in the later stages of ecchymosis. Their parameters were 7.5 J/cm2, 10-mm spot, 6-millisecond pulse duration, and cryogen 30 milliseconds with a 20-millisecond delay for a single pass. What do you use for posttreatment bruising?
