User login
Partial Flexor Tendon Laceration Assessment: Interobserver and Intraobserver Reliability
How to manage complete flexor tendon lacerations in the hand is well documented and a subject of relative agreement among authors. However, treatment of partial flexor tendon lacerations is controversial and lacking clear consensus in the literature. Managing these injuries can be challenging, as clinicians must weigh the diminished tensile strength in the injured tendon and the potential for later complications (eg, entrapment, triggering, rupture) against the negative effects of tenorrhaphy.1 Several studies have found impaired tendon gliding on the basis of bulk and inflammatory reaction secondary to suture material within the flexor sheath as well as decreased tendon strength after tenorrhaphy.2-6 This finding led the investigators to recommend nonsurgical management for partial lacerations up to as much as 95% of the cross-sectional area (CSA) of the tendon. According to a survey by McCarthy and colleagues,7 45% of 591 members of the American Society for Surgery of the Hand (ASSH) indicated they would perform tenorrhaphy for a laceration that involved more than 50% of the tendon.
However, accurate assessment of partial-thickness flexor tendon lacerations is difficult owing to the subjectivity of evaluation. In the survey just mentioned,7 the majority of surgeons used the naked eye to make assessments, and only 14% used other means, such as a ruler, a pair of calipers, or loupe magnification. In addition, flexor tendon injuries are often evaluated under less than ideal circumstances—a dirty or bloody field, poor lighting, an uncomfortable patient.
We conducted a study to determine the interobserver and intraobserver reliability of surgeons assessing the percentage of CSA injured in partially lacerated digital flexor tendons. We hypothesized that participants’ accuracy and agreement would be poor.
Materials and Methods
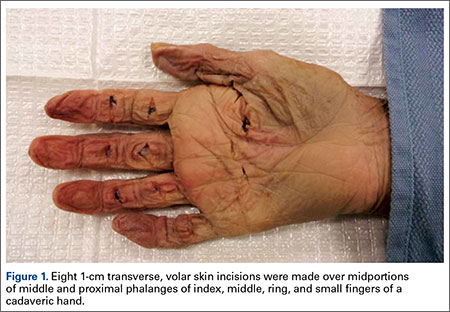
Eight 1-cm transverse, volar skin incisions were made over the midportions of the middle and proximal phalanges of the index, middle, ring, and small fingers of a fresh-frozen human cadaver hand (Figure 1). The tendon sheaths were incised, and the flexor digitorum profundus tendons to each digit were delivered through the wound. With use of a method described previously by Manning and colleagues,8 the tendon was then placed over a flat metal post to be used as a cutting board, and the proposed laceration site was marked with ink. Under loupe magnification, a No. 15 blade was used to create a partial transverse, volar-to-dorsal laceration in each tendon.8 The goal was to create lacerations of about 30%, 50%, and 70% of the total CSA of the tendon. The tendons were then returned to the wound, and visibility of the marked laceration within the wound was ensured. A similar exercise was performed at the level of the proximal palmar crease. Four flexor digitorum superficialis tendons were exposed through 1-cm transverse incisions, and partial lacerations were made in the volar substance of the tendons. The tendons were then returned to the wound, resulting in 12 partially lacerated tendons (8 flexor digitorum profundus, 4 flexor digitorum superficialis).
Six orthopedic surgery residents (2 postgraduate year 1 [PGY-1], 2 PGY-3, 2 PGY-5) and 4 fellowship-trained hand surgeons participated in our study. Each was asked to evaluate the tendons and determine the percentage of total CSA lacerated. Loupe magnification and measuring tools were not permitted, but participants were allowed to handle the tendons. In addition, they were asked if they would perform tenorrhaphy on the injured tendons, given only the amount of injury. The participants repeated this exercise 4 weeks later.
After all measurements were made, a longitudinal incision was made down each of the digits, and the flexor tendons were exposed within the flexor sheath. The transverse incisions in the palm were connected to expose the flexor digitorum superficialis tendons. Under an operating microscope, a pair of digital microcalipers (Kobalt 0.5-ft Metric and SAE Caliper; Figure 2) accurate to 0.01 mm was used to measure the external width (a) and height (b + bˈ) of the tendons just proximal to the lacerations. Measurements were made with the caliper blades just touching the edges of the lacerated tendon, thus minimizing deformation of the tendon. Other measurements made at the laceration site were width of the remaining tendon (c) and height of the remaining tendon (bˈ). CSA of the tendon was calculated assuming a regular ellipsoid shape and using the equation:
Area = 1/2π(b+b')
The area of the tendon injured was determined by calculating the area under a parabola and using the equation:
Area = 2/3c[(b+b')-b']
Last, the percentage of total CSA lacerated was calculated using the equation:
Area (total area)
Statistical analysis was performed to determine accuracy and interobserver and intraobserver reliability. Paired t tests were used in the assessment of accuracy to determine if there were differences between estimated and calibrated measurements.

Results
The 10 participants’ estimates differed significantly (P < .0006) from the calibrated measurements, as did residents’ estimates (P < .0025) and fellowship-trained hand surgeons’ estimates (P < .0002). Estimates were scored 1 to 5 on the basis of proximity to calibrated measurements (Table 1). Thus, more accurate estimates received lower scores. Individual estimates were then scored and stratified into groups for comparison. Third-year residents were the most accurate residents, and there was no difference in accuracy between residents and fellowship-trained hand surgeons. These results are listed in Table 2. Once overall and grouped accuracy was analyzed, κ statistics were calculated to compare interobserver and intraobserver reliability. Overall interobserver agreement was poor for both initial readings (κ = 0.16) and secondary readings (κ = 0.16), indicating poor strength of agreement between individuals both initially and secondarily. Table 3 presents the κ interpretations. There was moderate overall intraobserver agreement (45.83%), indicating participants’ secondary estimates agreed with their primary estimates 46% of the time. Fellowship-trained hand surgeons and first-year residents had the highest intraobserver agreement (50.0%). These results are listed in Table 4.




Discussion
Accurate assessment of partial flexor tendon lacerations is difficult and subjective. There is no standardized method for determining the extent of injury, regardless of whether the evaluation is performed in an emergency department or in the operating room. As McCarthy and colleagues7 noted in their survey of ASSH members, naked eye assessment was by far the most popular means of estimating percentage injured in partial lacerations, and only 10% of the survey respondents used intraoperative measuring devices. Our study showed that participants agreed with one another less than 50% of the time when evaluating injuries without the aid of measuring devices. In addition, interobserver agreement in this study was about 50%, highlighting the difficulty in making an accurate and reproducible assessment.
In a study of canine flexor tendons, McCarthy and colleagues9 found calipers are inaccurate as well and do not provide a reliable means of assessing partial flexor tendon lacerations. They compared caliper measurements with laser micrometer measurements, and the differences averaged 29.3%. They suggested that methods for calculating loss of CSA and for creating precise lacerations must be developed in order to evaluate treatments. One such method is the “tenotome,” devised by Hitchcock and colleagues10: A device with standard scalpel blades is used to make uniform lacerations in tendons by leaving a constant area of the tendon intact, regardless of the size or shape of the original tendon. Measurements made with calipers or rulers assume the tendon has a regular ellipsoid shape, but in reality the shape is a double-ellipse, particularly within the flexor sheath.
Dobyns and colleagues11 observed that changes in CSA size can be related to changes in the size of the bundle pattern of the tendon. They found that, on average, the radial bundle comprised about 60% of the total CSA of the tendon. This finding was clarified by Grewal and colleagues.12 Using histologic sections of tendons plus photomicrographs, they determined that, in zone II of the index and small fingers, the ulnar bundle had an area consistently larger than 50% and the radial bundle less than 50% of the total tendon area. In the ring and middle fingers, the areas of both bundles were almost 50% of the total tendon area. The authors suggested that, using this bundle pattern theory of injury, surgeons could more accurately evaluate the extent of injury with the naked eye.
One of the questions that prompted our study is how reliable is the information a surgeon receives regarding a partial flexor tendon injury evaluated by someone else in another setting. What is done with this information is another question. The scenario can be considered in 2 settings: emergency department and operating room.
Given the poor accuracy and interobserver agreement found in our study, along with the inaccuracy of caliper and ruler measurements, it seems decisions to perform tenorrhaphy based on reported percentages lacerated are unreliable. Our results showed that the ability to accurately assess partial tendon injuries does not improve with surgeon experience, as fellowship-trained hand surgeons were not statistically more accurate or consistent than residents. To this effect, one institution treats all its partial flexor tendon lacerations with wound inspection and irrigation in the emergency department, under digital block and after neurovascular injury has been excluded.8 If the patient is able to actively flex and extend the digit without triggering, then the wound is closed without closing the tendon sheath, a dorsal blocking splint is applied, and motion is begun early, 48 hours later, regardless of laceration severity.
Once the decision has been made to go to the operating room and the injury is being evaluated, what should be done with the information from the measurement, whether made with loupe magnification, calipers, rulers, or the naked eye? Surgeons must weigh the risks for triggering, entrapment, and rupture of untreated partial tendon lacerations1 with the added bulk and potential for adhesions, along with the tensile strength reduction that accompanies tendon repair. Both Reynolds and colleagues13 and Ollinger and colleagues14 found tensile strength significantly diminished in sutured tendons. Ollinger and colleagues14 showed a decrease in tendon gliding after surgical exposure and tenorrhaphy for partial tendon lacerations. Reynolds and colleagues13 concluded that surgical repair leads to poorer results than nonsurgical treatment.
Clinical studies have demonstrated excellent results with nonintervention, and in vivo and in vitro studies have indicated that early motion can be initiated in partial lacerations of up to 95% of total CSA. Wray and Weeks6 treated 26 patients with partial lacerations varying from 25% to 95% of total CSA and noted 1 incidence of trigger finger (which resolved) and no late ruptures. They advocated treatment with early motion and excision or repair of beveled partial lacerations with simple sutures. Stahl and colleagues2 reported comparable outcomes in children with partial lacerations up to 75% of total CSA treated with and without surgery and noted no complications in either group. In a biomechanical study, Hariharan and colleagues4 found lacerations up to 75% can withstand forces associated with active unresisted mobilization.
Conversely, how many patients or surgeons want to return to the operating room to fix a late rupture when it could have been repaired in the primary setting? Schlenker and colleagues,1 reporting on a late flexor pollicus tendon rupture that required tendon grafting, recommended exploration and primary repair of all partial flexor tendon lacerations. Often, it is difficult to determine whether surgical repair is necessary to ensure the best outcome for the patient.
Our study results showed that, in the evaluation of flexor tendon lacerations, both accuracy and interobserver agreement were poor among residents and fellowship-trained hand surgeons, and intraobserver agreement was moderate. Third-year residents were the most accurate residents, and there was no difference in accuracy between residents and fellowship-trained hand surgeons. Our results highlight the difficulty in making accurate assessments of flexor tendon lacerations owing to the subjectivity of evaluation, which appear not to improve with surgeon experience.
1. Schlenker JD, Lister GD, Kleinert HE. Three complications of untreated partial laceration of flexor tendon—entrapment, rupture, and triggering. J Hand Surg Am. 1981;6(4):392-398.
2. Stahl S, Kaufman T, Bialik V. Partial lacerations of flexor tendons in children. Primary repair versus conservative treatment. J Hand Surg Br. 1997;22(3):377-380.
3. Al-Qattan MM. Conservative management of zone II partial flexor tendon lacerations greater than half the width of the tendon. J Hand Surg Am. 2000;25(6):1118-1121.
4. Hariharan JS, Diao E, Soejima O, Lotz JC. Partial lacerations of human digital flexor tendons: a biomechanical analysis. J Hand Surg Am. 1997;22(6):1011-1015.
5. Bishop AT, Cooney WP 3rd, Wood MB. Treatment of partial flexor tendon lacerations: the effect of tenorrhaphy and early protected mobilization. J Trauma. 1986;26(4):301-312.
6. Wray RC Jr, Weeks PM. Treatment of partial tendon lacerations. Hand. 1980;12(2):163-166.
7. McCarthy DM, Boardman ND 3rd, Tramaglini DM, Sotereanos DG, Herndon JH. Clinical management of partially lacerated digital flexor tendons: a survey of hand surgeons. J Hand Surg Am. 1995;20(2):273-275.
8. Manning DW, Spiguel AR, Mass DP. Biomechanical analysis of partial flexor tendon lacerations in zone II of human cadavers. J Hand Surg Am. 2010;35(1):11-18.
9. McCarthy DM, Tramaglini DM, Chan SS, Schmidt CC, Sotereanos DG, Herndon JH. Effect of partial laceration on the structural properties of the canine FDP tendon: an in vitro study. J Hand Surg Am. 1995;20(5):795-800.
10. Hitchcock TF, Candel AG, Light TR, Blevens AD. New technique for producing uniform partial lacerations of tendons. J Orthop Res. 1989;7(3):451-455.
11. Dobyns RC, Cooney WC, Wood MB. Effect of partial lacerations on canine flexor tendons. Minn Med. 1982;65(1):27-32.
12. Grewal R, Sotereanos DG, Rao U, Herndon JH, Woo SL. Bundle pattern of the flexor digitorum profundus tendon in zone II of the hand: a quantitative assessment of the size of a laceration. J Hand Surg Am. 1996;21(6):978-983.
13. Reynolds B, Wray RC Jr, Weeks PM. Should an incompletely severed tendon be sutured? Plast Reconstr Surg. 1976;57(1):36-38.
14. Ollinger H, Wray RC Jr, Weeks PM. Effects of suture on tensile strength gain of partially and completely severed tendons. Surg Forum. 1975;26:63-64.
How to manage complete flexor tendon lacerations in the hand is well documented and a subject of relative agreement among authors. However, treatment of partial flexor tendon lacerations is controversial and lacking clear consensus in the literature. Managing these injuries can be challenging, as clinicians must weigh the diminished tensile strength in the injured tendon and the potential for later complications (eg, entrapment, triggering, rupture) against the negative effects of tenorrhaphy.1 Several studies have found impaired tendon gliding on the basis of bulk and inflammatory reaction secondary to suture material within the flexor sheath as well as decreased tendon strength after tenorrhaphy.2-6 This finding led the investigators to recommend nonsurgical management for partial lacerations up to as much as 95% of the cross-sectional area (CSA) of the tendon. According to a survey by McCarthy and colleagues,7 45% of 591 members of the American Society for Surgery of the Hand (ASSH) indicated they would perform tenorrhaphy for a laceration that involved more than 50% of the tendon.
However, accurate assessment of partial-thickness flexor tendon lacerations is difficult owing to the subjectivity of evaluation. In the survey just mentioned,7 the majority of surgeons used the naked eye to make assessments, and only 14% used other means, such as a ruler, a pair of calipers, or loupe magnification. In addition, flexor tendon injuries are often evaluated under less than ideal circumstances—a dirty or bloody field, poor lighting, an uncomfortable patient.
We conducted a study to determine the interobserver and intraobserver reliability of surgeons assessing the percentage of CSA injured in partially lacerated digital flexor tendons. We hypothesized that participants’ accuracy and agreement would be poor.
Materials and Methods
Eight 1-cm transverse, volar skin incisions were made over the midportions of the middle and proximal phalanges of the index, middle, ring, and small fingers of a fresh-frozen human cadaver hand (Figure 1). The tendon sheaths were incised, and the flexor digitorum profundus tendons to each digit were delivered through the wound. With use of a method described previously by Manning and colleagues,8 the tendon was then placed over a flat metal post to be used as a cutting board, and the proposed laceration site was marked with ink. Under loupe magnification, a No. 15 blade was used to create a partial transverse, volar-to-dorsal laceration in each tendon.8 The goal was to create lacerations of about 30%, 50%, and 70% of the total CSA of the tendon. The tendons were then returned to the wound, and visibility of the marked laceration within the wound was ensured. A similar exercise was performed at the level of the proximal palmar crease. Four flexor digitorum superficialis tendons were exposed through 1-cm transverse incisions, and partial lacerations were made in the volar substance of the tendons. The tendons were then returned to the wound, resulting in 12 partially lacerated tendons (8 flexor digitorum profundus, 4 flexor digitorum superficialis).
Six orthopedic surgery residents (2 postgraduate year 1 [PGY-1], 2 PGY-3, 2 PGY-5) and 4 fellowship-trained hand surgeons participated in our study. Each was asked to evaluate the tendons and determine the percentage of total CSA lacerated. Loupe magnification and measuring tools were not permitted, but participants were allowed to handle the tendons. In addition, they were asked if they would perform tenorrhaphy on the injured tendons, given only the amount of injury. The participants repeated this exercise 4 weeks later.
After all measurements were made, a longitudinal incision was made down each of the digits, and the flexor tendons were exposed within the flexor sheath. The transverse incisions in the palm were connected to expose the flexor digitorum superficialis tendons. Under an operating microscope, a pair of digital microcalipers (Kobalt 0.5-ft Metric and SAE Caliper; Figure 2) accurate to 0.01 mm was used to measure the external width (a) and height (b + bˈ) of the tendons just proximal to the lacerations. Measurements were made with the caliper blades just touching the edges of the lacerated tendon, thus minimizing deformation of the tendon. Other measurements made at the laceration site were width of the remaining tendon (c) and height of the remaining tendon (bˈ). CSA of the tendon was calculated assuming a regular ellipsoid shape and using the equation:
Area = 1/2π(b+b')
The area of the tendon injured was determined by calculating the area under a parabola and using the equation:
Area = 2/3c[(b+b')-b']
Last, the percentage of total CSA lacerated was calculated using the equation:
Area (total area)
Statistical analysis was performed to determine accuracy and interobserver and intraobserver reliability. Paired t tests were used in the assessment of accuracy to determine if there were differences between estimated and calibrated measurements.
Results
The 10 participants’ estimates differed significantly (P < .0006) from the calibrated measurements, as did residents’ estimates (P < .0025) and fellowship-trained hand surgeons’ estimates (P < .0002). Estimates were scored 1 to 5 on the basis of proximity to calibrated measurements (Table 1). Thus, more accurate estimates received lower scores. Individual estimates were then scored and stratified into groups for comparison. Third-year residents were the most accurate residents, and there was no difference in accuracy between residents and fellowship-trained hand surgeons. These results are listed in Table 2. Once overall and grouped accuracy was analyzed, κ statistics were calculated to compare interobserver and intraobserver reliability. Overall interobserver agreement was poor for both initial readings (κ = 0.16) and secondary readings (κ = 0.16), indicating poor strength of agreement between individuals both initially and secondarily. Table 3 presents the κ interpretations. There was moderate overall intraobserver agreement (45.83%), indicating participants’ secondary estimates agreed with their primary estimates 46% of the time. Fellowship-trained hand surgeons and first-year residents had the highest intraobserver agreement (50.0%). These results are listed in Table 4.
Discussion
Accurate assessment of partial flexor tendon lacerations is difficult and subjective. There is no standardized method for determining the extent of injury, regardless of whether the evaluation is performed in an emergency department or in the operating room. As McCarthy and colleagues7 noted in their survey of ASSH members, naked eye assessment was by far the most popular means of estimating percentage injured in partial lacerations, and only 10% of the survey respondents used intraoperative measuring devices. Our study showed that participants agreed with one another less than 50% of the time when evaluating injuries without the aid of measuring devices. In addition, interobserver agreement in this study was about 50%, highlighting the difficulty in making an accurate and reproducible assessment.
In a study of canine flexor tendons, McCarthy and colleagues9 found calipers are inaccurate as well and do not provide a reliable means of assessing partial flexor tendon lacerations. They compared caliper measurements with laser micrometer measurements, and the differences averaged 29.3%. They suggested that methods for calculating loss of CSA and for creating precise lacerations must be developed in order to evaluate treatments. One such method is the “tenotome,” devised by Hitchcock and colleagues10: A device with standard scalpel blades is used to make uniform lacerations in tendons by leaving a constant area of the tendon intact, regardless of the size or shape of the original tendon. Measurements made with calipers or rulers assume the tendon has a regular ellipsoid shape, but in reality the shape is a double-ellipse, particularly within the flexor sheath.
Dobyns and colleagues11 observed that changes in CSA size can be related to changes in the size of the bundle pattern of the tendon. They found that, on average, the radial bundle comprised about 60% of the total CSA of the tendon. This finding was clarified by Grewal and colleagues.12 Using histologic sections of tendons plus photomicrographs, they determined that, in zone II of the index and small fingers, the ulnar bundle had an area consistently larger than 50% and the radial bundle less than 50% of the total tendon area. In the ring and middle fingers, the areas of both bundles were almost 50% of the total tendon area. The authors suggested that, using this bundle pattern theory of injury, surgeons could more accurately evaluate the extent of injury with the naked eye.
One of the questions that prompted our study is how reliable is the information a surgeon receives regarding a partial flexor tendon injury evaluated by someone else in another setting. What is done with this information is another question. The scenario can be considered in 2 settings: emergency department and operating room.
Given the poor accuracy and interobserver agreement found in our study, along with the inaccuracy of caliper and ruler measurements, it seems decisions to perform tenorrhaphy based on reported percentages lacerated are unreliable. Our results showed that the ability to accurately assess partial tendon injuries does not improve with surgeon experience, as fellowship-trained hand surgeons were not statistically more accurate or consistent than residents. To this effect, one institution treats all its partial flexor tendon lacerations with wound inspection and irrigation in the emergency department, under digital block and after neurovascular injury has been excluded.8 If the patient is able to actively flex and extend the digit without triggering, then the wound is closed without closing the tendon sheath, a dorsal blocking splint is applied, and motion is begun early, 48 hours later, regardless of laceration severity.
Once the decision has been made to go to the operating room and the injury is being evaluated, what should be done with the information from the measurement, whether made with loupe magnification, calipers, rulers, or the naked eye? Surgeons must weigh the risks for triggering, entrapment, and rupture of untreated partial tendon lacerations1 with the added bulk and potential for adhesions, along with the tensile strength reduction that accompanies tendon repair. Both Reynolds and colleagues13 and Ollinger and colleagues14 found tensile strength significantly diminished in sutured tendons. Ollinger and colleagues14 showed a decrease in tendon gliding after surgical exposure and tenorrhaphy for partial tendon lacerations. Reynolds and colleagues13 concluded that surgical repair leads to poorer results than nonsurgical treatment.
Clinical studies have demonstrated excellent results with nonintervention, and in vivo and in vitro studies have indicated that early motion can be initiated in partial lacerations of up to 95% of total CSA. Wray and Weeks6 treated 26 patients with partial lacerations varying from 25% to 95% of total CSA and noted 1 incidence of trigger finger (which resolved) and no late ruptures. They advocated treatment with early motion and excision or repair of beveled partial lacerations with simple sutures. Stahl and colleagues2 reported comparable outcomes in children with partial lacerations up to 75% of total CSA treated with and without surgery and noted no complications in either group. In a biomechanical study, Hariharan and colleagues4 found lacerations up to 75% can withstand forces associated with active unresisted mobilization.
Conversely, how many patients or surgeons want to return to the operating room to fix a late rupture when it could have been repaired in the primary setting? Schlenker and colleagues,1 reporting on a late flexor pollicus tendon rupture that required tendon grafting, recommended exploration and primary repair of all partial flexor tendon lacerations. Often, it is difficult to determine whether surgical repair is necessary to ensure the best outcome for the patient.
Our study results showed that, in the evaluation of flexor tendon lacerations, both accuracy and interobserver agreement were poor among residents and fellowship-trained hand surgeons, and intraobserver agreement was moderate. Third-year residents were the most accurate residents, and there was no difference in accuracy between residents and fellowship-trained hand surgeons. Our results highlight the difficulty in making accurate assessments of flexor tendon lacerations owing to the subjectivity of evaluation, which appear not to improve with surgeon experience.
How to manage complete flexor tendon lacerations in the hand is well documented and a subject of relative agreement among authors. However, treatment of partial flexor tendon lacerations is controversial and lacking clear consensus in the literature. Managing these injuries can be challenging, as clinicians must weigh the diminished tensile strength in the injured tendon and the potential for later complications (eg, entrapment, triggering, rupture) against the negative effects of tenorrhaphy.1 Several studies have found impaired tendon gliding on the basis of bulk and inflammatory reaction secondary to suture material within the flexor sheath as well as decreased tendon strength after tenorrhaphy.2-6 This finding led the investigators to recommend nonsurgical management for partial lacerations up to as much as 95% of the cross-sectional area (CSA) of the tendon. According to a survey by McCarthy and colleagues,7 45% of 591 members of the American Society for Surgery of the Hand (ASSH) indicated they would perform tenorrhaphy for a laceration that involved more than 50% of the tendon.
However, accurate assessment of partial-thickness flexor tendon lacerations is difficult owing to the subjectivity of evaluation. In the survey just mentioned,7 the majority of surgeons used the naked eye to make assessments, and only 14% used other means, such as a ruler, a pair of calipers, or loupe magnification. In addition, flexor tendon injuries are often evaluated under less than ideal circumstances—a dirty or bloody field, poor lighting, an uncomfortable patient.
We conducted a study to determine the interobserver and intraobserver reliability of surgeons assessing the percentage of CSA injured in partially lacerated digital flexor tendons. We hypothesized that participants’ accuracy and agreement would be poor.
Materials and Methods
Eight 1-cm transverse, volar skin incisions were made over the midportions of the middle and proximal phalanges of the index, middle, ring, and small fingers of a fresh-frozen human cadaver hand (Figure 1). The tendon sheaths were incised, and the flexor digitorum profundus tendons to each digit were delivered through the wound. With use of a method described previously by Manning and colleagues,8 the tendon was then placed over a flat metal post to be used as a cutting board, and the proposed laceration site was marked with ink. Under loupe magnification, a No. 15 blade was used to create a partial transverse, volar-to-dorsal laceration in each tendon.8 The goal was to create lacerations of about 30%, 50%, and 70% of the total CSA of the tendon. The tendons were then returned to the wound, and visibility of the marked laceration within the wound was ensured. A similar exercise was performed at the level of the proximal palmar crease. Four flexor digitorum superficialis tendons were exposed through 1-cm transverse incisions, and partial lacerations were made in the volar substance of the tendons. The tendons were then returned to the wound, resulting in 12 partially lacerated tendons (8 flexor digitorum profundus, 4 flexor digitorum superficialis).
Six orthopedic surgery residents (2 postgraduate year 1 [PGY-1], 2 PGY-3, 2 PGY-5) and 4 fellowship-trained hand surgeons participated in our study. Each was asked to evaluate the tendons and determine the percentage of total CSA lacerated. Loupe magnification and measuring tools were not permitted, but participants were allowed to handle the tendons. In addition, they were asked if they would perform tenorrhaphy on the injured tendons, given only the amount of injury. The participants repeated this exercise 4 weeks later.
After all measurements were made, a longitudinal incision was made down each of the digits, and the flexor tendons were exposed within the flexor sheath. The transverse incisions in the palm were connected to expose the flexor digitorum superficialis tendons. Under an operating microscope, a pair of digital microcalipers (Kobalt 0.5-ft Metric and SAE Caliper; Figure 2) accurate to 0.01 mm was used to measure the external width (a) and height (b + bˈ) of the tendons just proximal to the lacerations. Measurements were made with the caliper blades just touching the edges of the lacerated tendon, thus minimizing deformation of the tendon. Other measurements made at the laceration site were width of the remaining tendon (c) and height of the remaining tendon (bˈ). CSA of the tendon was calculated assuming a regular ellipsoid shape and using the equation:
Area = 1/2π(b+b')
The area of the tendon injured was determined by calculating the area under a parabola and using the equation:
Area = 2/3c[(b+b')-b']
Last, the percentage of total CSA lacerated was calculated using the equation:
Area (total area)
Statistical analysis was performed to determine accuracy and interobserver and intraobserver reliability. Paired t tests were used in the assessment of accuracy to determine if there were differences between estimated and calibrated measurements.
Results
The 10 participants’ estimates differed significantly (P < .0006) from the calibrated measurements, as did residents’ estimates (P < .0025) and fellowship-trained hand surgeons’ estimates (P < .0002). Estimates were scored 1 to 5 on the basis of proximity to calibrated measurements (Table 1). Thus, more accurate estimates received lower scores. Individual estimates were then scored and stratified into groups for comparison. Third-year residents were the most accurate residents, and there was no difference in accuracy between residents and fellowship-trained hand surgeons. These results are listed in Table 2. Once overall and grouped accuracy was analyzed, κ statistics were calculated to compare interobserver and intraobserver reliability. Overall interobserver agreement was poor for both initial readings (κ = 0.16) and secondary readings (κ = 0.16), indicating poor strength of agreement between individuals both initially and secondarily. Table 3 presents the κ interpretations. There was moderate overall intraobserver agreement (45.83%), indicating participants’ secondary estimates agreed with their primary estimates 46% of the time. Fellowship-trained hand surgeons and first-year residents had the highest intraobserver agreement (50.0%). These results are listed in Table 4.
Discussion
Accurate assessment of partial flexor tendon lacerations is difficult and subjective. There is no standardized method for determining the extent of injury, regardless of whether the evaluation is performed in an emergency department or in the operating room. As McCarthy and colleagues7 noted in their survey of ASSH members, naked eye assessment was by far the most popular means of estimating percentage injured in partial lacerations, and only 10% of the survey respondents used intraoperative measuring devices. Our study showed that participants agreed with one another less than 50% of the time when evaluating injuries without the aid of measuring devices. In addition, interobserver agreement in this study was about 50%, highlighting the difficulty in making an accurate and reproducible assessment.
In a study of canine flexor tendons, McCarthy and colleagues9 found calipers are inaccurate as well and do not provide a reliable means of assessing partial flexor tendon lacerations. They compared caliper measurements with laser micrometer measurements, and the differences averaged 29.3%. They suggested that methods for calculating loss of CSA and for creating precise lacerations must be developed in order to evaluate treatments. One such method is the “tenotome,” devised by Hitchcock and colleagues10: A device with standard scalpel blades is used to make uniform lacerations in tendons by leaving a constant area of the tendon intact, regardless of the size or shape of the original tendon. Measurements made with calipers or rulers assume the tendon has a regular ellipsoid shape, but in reality the shape is a double-ellipse, particularly within the flexor sheath.
Dobyns and colleagues11 observed that changes in CSA size can be related to changes in the size of the bundle pattern of the tendon. They found that, on average, the radial bundle comprised about 60% of the total CSA of the tendon. This finding was clarified by Grewal and colleagues.12 Using histologic sections of tendons plus photomicrographs, they determined that, in zone II of the index and small fingers, the ulnar bundle had an area consistently larger than 50% and the radial bundle less than 50% of the total tendon area. In the ring and middle fingers, the areas of both bundles were almost 50% of the total tendon area. The authors suggested that, using this bundle pattern theory of injury, surgeons could more accurately evaluate the extent of injury with the naked eye.
One of the questions that prompted our study is how reliable is the information a surgeon receives regarding a partial flexor tendon injury evaluated by someone else in another setting. What is done with this information is another question. The scenario can be considered in 2 settings: emergency department and operating room.
Given the poor accuracy and interobserver agreement found in our study, along with the inaccuracy of caliper and ruler measurements, it seems decisions to perform tenorrhaphy based on reported percentages lacerated are unreliable. Our results showed that the ability to accurately assess partial tendon injuries does not improve with surgeon experience, as fellowship-trained hand surgeons were not statistically more accurate or consistent than residents. To this effect, one institution treats all its partial flexor tendon lacerations with wound inspection and irrigation in the emergency department, under digital block and after neurovascular injury has been excluded.8 If the patient is able to actively flex and extend the digit without triggering, then the wound is closed without closing the tendon sheath, a dorsal blocking splint is applied, and motion is begun early, 48 hours later, regardless of laceration severity.
Once the decision has been made to go to the operating room and the injury is being evaluated, what should be done with the information from the measurement, whether made with loupe magnification, calipers, rulers, or the naked eye? Surgeons must weigh the risks for triggering, entrapment, and rupture of untreated partial tendon lacerations1 with the added bulk and potential for adhesions, along with the tensile strength reduction that accompanies tendon repair. Both Reynolds and colleagues13 and Ollinger and colleagues14 found tensile strength significantly diminished in sutured tendons. Ollinger and colleagues14 showed a decrease in tendon gliding after surgical exposure and tenorrhaphy for partial tendon lacerations. Reynolds and colleagues13 concluded that surgical repair leads to poorer results than nonsurgical treatment.
Clinical studies have demonstrated excellent results with nonintervention, and in vivo and in vitro studies have indicated that early motion can be initiated in partial lacerations of up to 95% of total CSA. Wray and Weeks6 treated 26 patients with partial lacerations varying from 25% to 95% of total CSA and noted 1 incidence of trigger finger (which resolved) and no late ruptures. They advocated treatment with early motion and excision or repair of beveled partial lacerations with simple sutures. Stahl and colleagues2 reported comparable outcomes in children with partial lacerations up to 75% of total CSA treated with and without surgery and noted no complications in either group. In a biomechanical study, Hariharan and colleagues4 found lacerations up to 75% can withstand forces associated with active unresisted mobilization.
Conversely, how many patients or surgeons want to return to the operating room to fix a late rupture when it could have been repaired in the primary setting? Schlenker and colleagues,1 reporting on a late flexor pollicus tendon rupture that required tendon grafting, recommended exploration and primary repair of all partial flexor tendon lacerations. Often, it is difficult to determine whether surgical repair is necessary to ensure the best outcome for the patient.
Our study results showed that, in the evaluation of flexor tendon lacerations, both accuracy and interobserver agreement were poor among residents and fellowship-trained hand surgeons, and intraobserver agreement was moderate. Third-year residents were the most accurate residents, and there was no difference in accuracy between residents and fellowship-trained hand surgeons. Our results highlight the difficulty in making accurate assessments of flexor tendon lacerations owing to the subjectivity of evaluation, which appear not to improve with surgeon experience.
1. Schlenker JD, Lister GD, Kleinert HE. Three complications of untreated partial laceration of flexor tendon—entrapment, rupture, and triggering. J Hand Surg Am. 1981;6(4):392-398.
2. Stahl S, Kaufman T, Bialik V. Partial lacerations of flexor tendons in children. Primary repair versus conservative treatment. J Hand Surg Br. 1997;22(3):377-380.
3. Al-Qattan MM. Conservative management of zone II partial flexor tendon lacerations greater than half the width of the tendon. J Hand Surg Am. 2000;25(6):1118-1121.
4. Hariharan JS, Diao E, Soejima O, Lotz JC. Partial lacerations of human digital flexor tendons: a biomechanical analysis. J Hand Surg Am. 1997;22(6):1011-1015.
5. Bishop AT, Cooney WP 3rd, Wood MB. Treatment of partial flexor tendon lacerations: the effect of tenorrhaphy and early protected mobilization. J Trauma. 1986;26(4):301-312.
6. Wray RC Jr, Weeks PM. Treatment of partial tendon lacerations. Hand. 1980;12(2):163-166.
7. McCarthy DM, Boardman ND 3rd, Tramaglini DM, Sotereanos DG, Herndon JH. Clinical management of partially lacerated digital flexor tendons: a survey of hand surgeons. J Hand Surg Am. 1995;20(2):273-275.
8. Manning DW, Spiguel AR, Mass DP. Biomechanical analysis of partial flexor tendon lacerations in zone II of human cadavers. J Hand Surg Am. 2010;35(1):11-18.
9. McCarthy DM, Tramaglini DM, Chan SS, Schmidt CC, Sotereanos DG, Herndon JH. Effect of partial laceration on the structural properties of the canine FDP tendon: an in vitro study. J Hand Surg Am. 1995;20(5):795-800.
10. Hitchcock TF, Candel AG, Light TR, Blevens AD. New technique for producing uniform partial lacerations of tendons. J Orthop Res. 1989;7(3):451-455.
11. Dobyns RC, Cooney WC, Wood MB. Effect of partial lacerations on canine flexor tendons. Minn Med. 1982;65(1):27-32.
12. Grewal R, Sotereanos DG, Rao U, Herndon JH, Woo SL. Bundle pattern of the flexor digitorum profundus tendon in zone II of the hand: a quantitative assessment of the size of a laceration. J Hand Surg Am. 1996;21(6):978-983.
13. Reynolds B, Wray RC Jr, Weeks PM. Should an incompletely severed tendon be sutured? Plast Reconstr Surg. 1976;57(1):36-38.
14. Ollinger H, Wray RC Jr, Weeks PM. Effects of suture on tensile strength gain of partially and completely severed tendons. Surg Forum. 1975;26:63-64.
1. Schlenker JD, Lister GD, Kleinert HE. Three complications of untreated partial laceration of flexor tendon—entrapment, rupture, and triggering. J Hand Surg Am. 1981;6(4):392-398.
2. Stahl S, Kaufman T, Bialik V. Partial lacerations of flexor tendons in children. Primary repair versus conservative treatment. J Hand Surg Br. 1997;22(3):377-380.
3. Al-Qattan MM. Conservative management of zone II partial flexor tendon lacerations greater than half the width of the tendon. J Hand Surg Am. 2000;25(6):1118-1121.
4. Hariharan JS, Diao E, Soejima O, Lotz JC. Partial lacerations of human digital flexor tendons: a biomechanical analysis. J Hand Surg Am. 1997;22(6):1011-1015.
5. Bishop AT, Cooney WP 3rd, Wood MB. Treatment of partial flexor tendon lacerations: the effect of tenorrhaphy and early protected mobilization. J Trauma. 1986;26(4):301-312.
6. Wray RC Jr, Weeks PM. Treatment of partial tendon lacerations. Hand. 1980;12(2):163-166.
7. McCarthy DM, Boardman ND 3rd, Tramaglini DM, Sotereanos DG, Herndon JH. Clinical management of partially lacerated digital flexor tendons: a survey of hand surgeons. J Hand Surg Am. 1995;20(2):273-275.
8. Manning DW, Spiguel AR, Mass DP. Biomechanical analysis of partial flexor tendon lacerations in zone II of human cadavers. J Hand Surg Am. 2010;35(1):11-18.
9. McCarthy DM, Tramaglini DM, Chan SS, Schmidt CC, Sotereanos DG, Herndon JH. Effect of partial laceration on the structural properties of the canine FDP tendon: an in vitro study. J Hand Surg Am. 1995;20(5):795-800.
10. Hitchcock TF, Candel AG, Light TR, Blevens AD. New technique for producing uniform partial lacerations of tendons. J Orthop Res. 1989;7(3):451-455.
11. Dobyns RC, Cooney WC, Wood MB. Effect of partial lacerations on canine flexor tendons. Minn Med. 1982;65(1):27-32.
12. Grewal R, Sotereanos DG, Rao U, Herndon JH, Woo SL. Bundle pattern of the flexor digitorum profundus tendon in zone II of the hand: a quantitative assessment of the size of a laceration. J Hand Surg Am. 1996;21(6):978-983.
13. Reynolds B, Wray RC Jr, Weeks PM. Should an incompletely severed tendon be sutured? Plast Reconstr Surg. 1976;57(1):36-38.
14. Ollinger H, Wray RC Jr, Weeks PM. Effects of suture on tensile strength gain of partially and completely severed tendons. Surg Forum. 1975;26:63-64.

Technical Errors May Affect Accuracy of Torque Limiter in Locking Plate Osteosynthesis
Proper surgical technique must be used to ensure that surgical fracture management is long-lasting. Plate implantation and screw implantation are among the most common orthopedic procedures performed. Plate and screw osteosynthesis can be done with nonlocking or locking plate and screw constructs or with hybrid fixation that incorporates both methods.
Nonlocking plate and screw osteosynthesis uses friction-fit for fixation. In osteoporotic bone, less torque is generated because of poor bone quality, and thus less friction force between plate and bone.1,2 Locked plating has dramatically changed fracture management, especially in frail and comminuted osteoporotic bone, with significant advantages over conventional plating.3-7
Development of locked plating systems, including the Less Invasive Stabilization System (LISS; DePuy Synthes) with its soft-tissue and fracture-fragment preservation, has changed treatment of distal femur and proximal tibia fractures. Cole and colleagues8 reported stable fixation and union in 97% of their patients. The LISS system proved to be stable, but there were cases of implant removal difficulty with this titanium construct. In 1 of the 10 cases in which the LISS plate was removed, 4 of the 11 locking screws were welded to the plate.8
Cold welding, in which similar metals are chemically bonded together under extreme pressure, is a complication associated with use of titanium-only plates and screws.9 This process, which is more likely to happen if cross-threading occurs within the screw–plate interface, can make screw removal extremely difficult. Screw removal difficulty strips screw heads, and often the surgeon must use either metal cutting instruments or trephines to remove screw remnants, which often results in retained implant or debris and damage or necrosis to surrounding bone.9,10
Locking screws are often inserted under power with a torque-limiting device attached to the drill mechanism to reduce the risk of lock screw overtightening and to try to prevent difficult implant removal. Although standard practice is to insert the screw and stop just before screw head engagement, with final tightening with a torque limiter and hand power, final tightening is often inadvertently done under power.3 Most technique guides instruct surgeons how to insert screws under power while using a torque limiter, but the exact technique is not emphasized.
We conducted a study to determine if rotational speed of screw insertion affects maximum torque on screw with use of a torque limiter. We describe proper use of a torque limiter as well as possible pitfalls. We hypothesized that improper use would result in substantially higher than expected insertion torque.
Materials and Methods
Torque-Limiting Attachments, Torque Wrench, and Drill
The Small Fragment Locking Compression Plate System (Synthes) includes a 1.5-Nm torque-limiting attachment and quick-coupling wooden handles and Star Drive attachments. All devices in this study were in active use at 6 urban institutions (3 level I trauma centers, 2 level II trauma centers, 1 level III hospital). Permission to obtain and test each device was granted by each institution.
A 0.25-inch dial torque wrench (751LDIN; CDI Torque Products) was purchased through an established distributor. The manufacturer includes a traceable certificate of accuracy to verify correct calibration. The torque wrench has a torque range of 0 to 9 Nm with visual increment demarcations of 0.2 Nm and a memory needle to retain maximum torque measurement. The same torque wrench was used in each experiment in order to maintain consistent measurements between devices. It was reset to zero after each use.
This study used a 0.5-inch, 19.2-V lithium drill (Craftsman C3) with 2 speed options: 0 to 440 rpm high torque and 0 to 1600 rpm high speed. This device provides variable torque output with a maximum output of 38.4 Nm. For this study, all measurements were done with the device on its high torque setting.
Maximum Torque Determination for Different Scenarios
Each torque limiter was evaluated for variations in maximum torque under 4 different scenarios. In each scenario, the torque limiter was coupled to the Star Drive attachment and then to that scenario’s rotating force. The completed system was then inserted into the torque wrench, which was secured to a flat working surface and rotated in accordance with each scenario; maximum torque was measured and recorded (Figures 1, 2). A torque-limiting event was defined as a single audible click on the torque limiter.
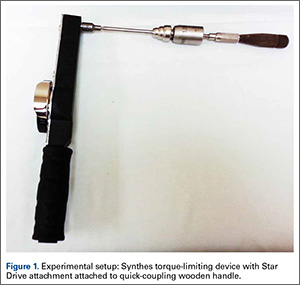
In scenario 1, each torque-limiting attachment system was attached to a quick-coupling wooden handle. The completed system was then rotated at controlled low velocity under hand power until 1 torque-limiting event occurred. This scenario was also used as an internal control to verify that the torque limiters were calibrated correctly.
In Scenario 2, the device was again attached to a quick-coupling wooden handle. The completed system was rotated at high velocity under hand power until multiple torque-limiting events occurred in a row. High velocity was defined as the operator freely rotating the wooden handle in a single action with full power resulting in multiple torque-limiting events.
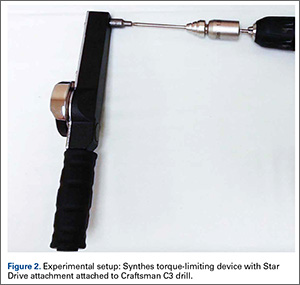
In Scenario 3, the device was attached to a power drill braced to the flat working surface and rotated at low velocity under power until 1 torque-limiting event occurred.
In Scenario 4, the device was again attached to a power drill braced to the flat working surface. The completed system was rotated at high velocity under power until multiple torque-limiting events occurred.
After each trial, we recorded maximum torque achieved before each device’s torque-limiting event. Either an orthopedic surgery resident or a qualified medical student tested each torque-limiting device in each standardized testing scenario.
Statistical Analysis
Experiments for each torque limiter were repeated for 3 trials of each of the 4 different scenarios. For comparative statistics between experiments, maximum torque measurements were expressed as means and SDs; 95% confidence interval (95% CI) was calculated and reported to determine extent of variation within a single group. One-way analysis of variance (ANOVA) and Tukey post hoc tests were performed between groups for comparison of the normally distributed data. Significance was set at P ≤ .05.
Results
During simulation, we successfully measured maximum torque achieved with each torque limiter under the 4 different scenarios. All testing was done by 2 operators. ANOVA demonstrated significant (P ≤ .001) differences in torque among the scenarios.
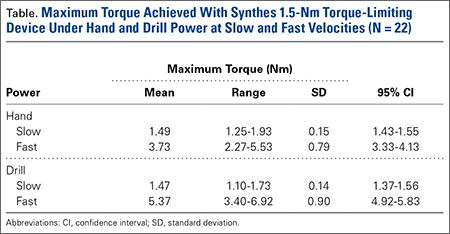
In scenario 1, mean (SD) maximum torque under hand power at low velocity was 1.49 (0.15) Nm (95% CI, 1.43-1.55), near the advertised maximum torque of 1.5 Nm, with relatively minimal variation between devices. This scenario confirmed proper calibration of properly used torque limiters. Mean maximum torque ranged from 1.25 to 1.93 Nm.
In scenario 2, mean (SD) maximum torque under hand power at high velocity was 3.73 (0.79) Nm (95% CI, 3.33-4.13), a 2.5-fold increase compared with scenario 1 (P < .0001) (Figure 3). There also was an increase in variation of maximum torque between trials of individual devices and between different devices. Mean maximum torque ranged from 2.27 to 5.53 Nm.
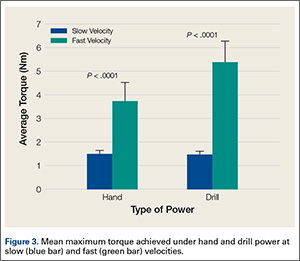
In scenario 3, mean (SD) maximum torque under drill power at controlled low velocity was 1.47 (0.14) Nm (95% CI, 1.37-1.56), again near the advertised maximum torque of 1.5 Nm, with relatively minimal variation. Mean maximum torque ranged from 1.10 to 1.73 Nm.
In scenario 4, mean (SD) maximum torque under drill power at full power/high velocity was 5.37 (0.90) Nm (95% CI, 4.92-5.83), a 3.65-fold increase compared with scenario 3 (P < .0001) (Figure 3). Mean maximum torque measured in 3 tests ranged from 3.40 to 6.92 Nm.
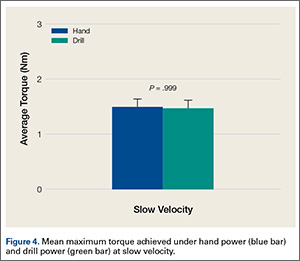
There was no significant difference in mean maximum torque between the scenarios of hand power at low velocity and drill power at low velocities (P = .999) (Figure 4). Highest maximum torque from any device was 9.0 Nm (drill at full power). Results are summarized in the Table. There was no statistical significance in the test between the 2 test operators.
Discussion
Maximum torque was measured using a torque-limiting attachment under 4 different simulated scenarios. Our goals were to determine if varying practice and rotational velocity would affect maximum insertional torque and to measure consistency among torque limiters. We designed the scenarios to mimic practice patterns, including hand insertion and power insertion of locking screws. Results demonstrated that misuse of a torque-limiting device may inadvertently produce insertional torque substantially higher than recommended. Highest maximum torque was 9.0 Nm, which is 6.0-fold higher than expected for a locking screw using a 1.5-Nm torque limiter.
Our study results showed that insertion under controlled hand power (and low-velocity drill power) until 1 torque-limiting event occurred produced the most consistent and predictable results. Insertion under drill power or high-velocity hand power produced multiple sequential torque-limiting events, yielding inaccurate insertion torque. Low-velocity insertion under hand power, or carefully controlled drill power, consistently produced torque similar to advertised values.
Manufacturers’ technique guides are available for proximal humerus locking compression plate (LCP) systems, small-fragment LCP systems, the Proximal Humeral Interlocking System (PHILOS; DePuy Synthes), and the LISS. These technique guides clearly state that insertion can be performed under power. Only the PHILOS and LISS guides state that insertion should be performed under power until a single click is heard or that final tightening should be completed under hand power. The proximal humerus LCP guide states that surgeons should insert the locking screw under power until the torque-limiting device clicks. The small-fragment LCP guide states that insertion under power should always be completed with the torque-limiting attachment; there is no mention of reducing power or a single click (this may give the surgeon a false sense of security).
Screw overtightening and head/thread stripping can make screw removal challenging.10 Removal rates for LISS plates range from 8% to 26%, and removal is often reported as taking longer than the index procedure, with complication rates as high as 47%.11-13 Bae and colleagues3 reported significant difficulty in removing 24 of 279 self-tapping locking screws (3.5 mm).
It is important to note that these complications, most notably cold welding, are mostly associated with titanium locking plate and screw constructs. Although stainless steel constructs have gained favor, titanium constructs are still widely used around the world.14,15
In 10% of cases in a laboratory setting, insertion of a 3.5-mm locking screw at 4 to 6 Nm damaged the screw.9 Removal of 3.5-mm locking screws had a stripping rate of 8.6%, and use of the torque limiter did not make removal easy all the time.3 Torque limiters are set specific to each screw diameter to reduce the risk of damage/stripping or even overtightening. Even when a surgeon intends to stop a drill before locking, final tightening often inadvertently occurs under power.3
Cold welding is often described as a cause of difficult implant removal.3,12 According to a newer definition, this process is independent of temperature and can occur when 2 metallic surfaces are in direct contact.16 High contact pressures between 2 similar metals can lead to this solid state welding.17 Theoretically, improper use of torque limiters can increase the risk of welding; however, it appears to be associated only with titanium locking plate and screw constructs.
Locked plating osteosynthesis is a valuable tool for fracture management, but improper use can have significant consequences, including morbid implant removal procedures, which are more difficult and time-consuming than the index surgery. We determined that proper use of torque limiters involves insertion under hand or power control at slow velocity until 1 torque-limiting event occurs. Many orthopedic surgeons may assume that torque limiters are accurate no matter how screws are inserted into locking plates. In addition, they may be unaware guidelines exist, as these are often deeply embedded within text. Therefore, we must emphasize that torque limiters can be inaccurate when used improperly.
One limitation of this study is that it tested only the Synthes 1.5-Nm torque-limiting attachment, though we can speculate that torque limiters designed for larger screws and limiters manufactured by different companies will behave similarly. Another limitation is that we did not obtain the hospitals’ service records for the tested equipment and assumed the equipment was properly checked for accuracy by the providing company. However, we hypothesized that, if maintenance were an issue, then our results would not be similar across all sites tested.
These tests involved a torque limiter linked to a torque-measuring device and may not perfectly represent actual torque measured at the locked screw–thread interface. However, we think our construct accurately determines the torque produced at the level of the driver tip. Also, we can speculate that the torque produced with improper use will lead to the complications mentioned and demonstrated in previous studies. Welding of the screw–plate interface may simply be a result of improper trajectory and cross-threading. However, if we assume that torque limiters prevent excessive torque no matter how they are used, high insertion speeds may compound the effect of welding. Additional biomechanical studies with full locked plate osteosynthesis constructs on bone specimens are planned to further characterize the potential complications of this issue.
1. Sommer C, Babst R, Müller M, Hanson B. Locking compression plate loosening and plate breakage: a report of four cases. J Orthop Trauma. 2004;18(8):571-577.
2. Schütz M, Südkamp NP. Revolution in plate osteosynthesis: new internal fixator systems. J Orthop Sci. 2003;8(2):252-258.
3. Bae JH, Oh JK, Oh CW, Hur CR. Technical difficulties of removal of locking screw after locking compression plating. Arch Orthop Trauma Surg. 2009;129(1):91-95.
4. Frigg R. Locking compression plate (LCP). An osteosynthesis plate based on the dynamic compression plate and the point contact fixator (PC-Fix). Injury. 2001;32(suppl 2):63-66.
5. Frigg R. Development of the locking compression plate. Injury. 2003;34(suppl 2):B6-B10.
6. Korner J, Lill H, Müller LP, Rommens PM, Schneider E, Linke B. The LCP-concept in the operative treatment of distal humerus fractures—biological, biomechanical and surgical aspects. Injury. 2003;34(suppl 2):B20-B30.
7. Egol KA, Kubiak EN, Fulkerson E, Kummer FJ, Koval KJ. Biomechanics of locked plates and screws. J Orthop Trauma. 2004;18(8):488-493.
8. Cole PA, Zlowodzki M, Kregor PJ. Treatment of proximal tibia fractures using the Less Invasive Stabilization System: surgical experience and early clinical results in 77 fractures. J Orthop Trauma. 2004;18(8):528-535.
9. Ehlinger M, Adam P, Simon P, Bonnomet F. Technical difficulties in hardware removal in titanium compression plates with locking screws. Orthop Traumatol Surg Res. 2009;95(5):373-376.
10. Gopinathan NR, Dhillon MS, Kumar R. Surgical technique: simple technique for removing a locking recon plate with damaged screw heads. Clin Orthop Relat Res. 2013;471(5):1572-1575.
11. Pattison G, Reynolds J, Hardy J. Salvaging a stripped drive connection when removing screws. Injury. 1999;30(1):74-75.
12. Raja S, Imbuldeniya AM, Garg S, Groom G. Difficulties encountered removing locked plates. Ann R Coll Surg Engl. 2012;94(7):502-505.
13. Kumar G, Dunlop C. Case report: a technique to remove a jammed locking screw from a locking plate. Clin Orthop Relat Res. 2011;469(2):613-616.
14. Disegi JA. Titanium alloys for fracture fixation implants. Injury. 2000;31(suppl 4):14-17.
15. El-Zayat BF, Ruchholtz S, Efe T, Paletta J, Kreslo D, Zettl R. Results of titanium locking plate and stainless steel cerclage wire combination in femoral fractures. Indian J Orthop. 2013;47(5):454-458.
16. Van Nortwick SS, Yao J, Ladd AL. Titanium integration with bone, welding, and screw head destruction complicating hardware removal of the distal radius: report of 2 cases. J Hand Surg. 2012;37(7):1388-1392.
17. Ferguson GS, Chaudhury MK, Sigal GB, Whitesides GM. Contact adhesion of thin gold films on elastomeric supports: cold welding under ambient conditions. Science. 1991;253(5021):776-778.
Proper surgical technique must be used to ensure that surgical fracture management is long-lasting. Plate implantation and screw implantation are among the most common orthopedic procedures performed. Plate and screw osteosynthesis can be done with nonlocking or locking plate and screw constructs or with hybrid fixation that incorporates both methods.
Nonlocking plate and screw osteosynthesis uses friction-fit for fixation. In osteoporotic bone, less torque is generated because of poor bone quality, and thus less friction force between plate and bone.1,2 Locked plating has dramatically changed fracture management, especially in frail and comminuted osteoporotic bone, with significant advantages over conventional plating.3-7
Development of locked plating systems, including the Less Invasive Stabilization System (LISS; DePuy Synthes) with its soft-tissue and fracture-fragment preservation, has changed treatment of distal femur and proximal tibia fractures. Cole and colleagues8 reported stable fixation and union in 97% of their patients. The LISS system proved to be stable, but there were cases of implant removal difficulty with this titanium construct. In 1 of the 10 cases in which the LISS plate was removed, 4 of the 11 locking screws were welded to the plate.8
Cold welding, in which similar metals are chemically bonded together under extreme pressure, is a complication associated with use of titanium-only plates and screws.9 This process, which is more likely to happen if cross-threading occurs within the screw–plate interface, can make screw removal extremely difficult. Screw removal difficulty strips screw heads, and often the surgeon must use either metal cutting instruments or trephines to remove screw remnants, which often results in retained implant or debris and damage or necrosis to surrounding bone.9,10
Locking screws are often inserted under power with a torque-limiting device attached to the drill mechanism to reduce the risk of lock screw overtightening and to try to prevent difficult implant removal. Although standard practice is to insert the screw and stop just before screw head engagement, with final tightening with a torque limiter and hand power, final tightening is often inadvertently done under power.3 Most technique guides instruct surgeons how to insert screws under power while using a torque limiter, but the exact technique is not emphasized.
We conducted a study to determine if rotational speed of screw insertion affects maximum torque on screw with use of a torque limiter. We describe proper use of a torque limiter as well as possible pitfalls. We hypothesized that improper use would result in substantially higher than expected insertion torque.
Materials and Methods
Torque-Limiting Attachments, Torque Wrench, and Drill
The Small Fragment Locking Compression Plate System (Synthes) includes a 1.5-Nm torque-limiting attachment and quick-coupling wooden handles and Star Drive attachments. All devices in this study were in active use at 6 urban institutions (3 level I trauma centers, 2 level II trauma centers, 1 level III hospital). Permission to obtain and test each device was granted by each institution.
A 0.25-inch dial torque wrench (751LDIN; CDI Torque Products) was purchased through an established distributor. The manufacturer includes a traceable certificate of accuracy to verify correct calibration. The torque wrench has a torque range of 0 to 9 Nm with visual increment demarcations of 0.2 Nm and a memory needle to retain maximum torque measurement. The same torque wrench was used in each experiment in order to maintain consistent measurements between devices. It was reset to zero after each use.
This study used a 0.5-inch, 19.2-V lithium drill (Craftsman C3) with 2 speed options: 0 to 440 rpm high torque and 0 to 1600 rpm high speed. This device provides variable torque output with a maximum output of 38.4 Nm. For this study, all measurements were done with the device on its high torque setting.
Maximum Torque Determination for Different Scenarios
Each torque limiter was evaluated for variations in maximum torque under 4 different scenarios. In each scenario, the torque limiter was coupled to the Star Drive attachment and then to that scenario’s rotating force. The completed system was then inserted into the torque wrench, which was secured to a flat working surface and rotated in accordance with each scenario; maximum torque was measured and recorded (Figures 1, 2). A torque-limiting event was defined as a single audible click on the torque limiter.
In scenario 1, each torque-limiting attachment system was attached to a quick-coupling wooden handle. The completed system was then rotated at controlled low velocity under hand power until 1 torque-limiting event occurred. This scenario was also used as an internal control to verify that the torque limiters were calibrated correctly.
In Scenario 2, the device was again attached to a quick-coupling wooden handle. The completed system was rotated at high velocity under hand power until multiple torque-limiting events occurred in a row. High velocity was defined as the operator freely rotating the wooden handle in a single action with full power resulting in multiple torque-limiting events.
In Scenario 3, the device was attached to a power drill braced to the flat working surface and rotated at low velocity under power until 1 torque-limiting event occurred.
In Scenario 4, the device was again attached to a power drill braced to the flat working surface. The completed system was rotated at high velocity under power until multiple torque-limiting events occurred.
After each trial, we recorded maximum torque achieved before each device’s torque-limiting event. Either an orthopedic surgery resident or a qualified medical student tested each torque-limiting device in each standardized testing scenario.
Statistical Analysis
Experiments for each torque limiter were repeated for 3 trials of each of the 4 different scenarios. For comparative statistics between experiments, maximum torque measurements were expressed as means and SDs; 95% confidence interval (95% CI) was calculated and reported to determine extent of variation within a single group. One-way analysis of variance (ANOVA) and Tukey post hoc tests were performed between groups for comparison of the normally distributed data. Significance was set at P ≤ .05.
Results
During simulation, we successfully measured maximum torque achieved with each torque limiter under the 4 different scenarios. All testing was done by 2 operators. ANOVA demonstrated significant (P ≤ .001) differences in torque among the scenarios.
In scenario 1, mean (SD) maximum torque under hand power at low velocity was 1.49 (0.15) Nm (95% CI, 1.43-1.55), near the advertised maximum torque of 1.5 Nm, with relatively minimal variation between devices. This scenario confirmed proper calibration of properly used torque limiters. Mean maximum torque ranged from 1.25 to 1.93 Nm.
In scenario 2, mean (SD) maximum torque under hand power at high velocity was 3.73 (0.79) Nm (95% CI, 3.33-4.13), a 2.5-fold increase compared with scenario 1 (P < .0001) (Figure 3). There also was an increase in variation of maximum torque between trials of individual devices and between different devices. Mean maximum torque ranged from 2.27 to 5.53 Nm.
In scenario 3, mean (SD) maximum torque under drill power at controlled low velocity was 1.47 (0.14) Nm (95% CI, 1.37-1.56), again near the advertised maximum torque of 1.5 Nm, with relatively minimal variation. Mean maximum torque ranged from 1.10 to 1.73 Nm.
In scenario 4, mean (SD) maximum torque under drill power at full power/high velocity was 5.37 (0.90) Nm (95% CI, 4.92-5.83), a 3.65-fold increase compared with scenario 3 (P < .0001) (Figure 3). Mean maximum torque measured in 3 tests ranged from 3.40 to 6.92 Nm.
There was no significant difference in mean maximum torque between the scenarios of hand power at low velocity and drill power at low velocities (P = .999) (Figure 4). Highest maximum torque from any device was 9.0 Nm (drill at full power). Results are summarized in the Table. There was no statistical significance in the test between the 2 test operators.
Discussion
Maximum torque was measured using a torque-limiting attachment under 4 different simulated scenarios. Our goals were to determine if varying practice and rotational velocity would affect maximum insertional torque and to measure consistency among torque limiters. We designed the scenarios to mimic practice patterns, including hand insertion and power insertion of locking screws. Results demonstrated that misuse of a torque-limiting device may inadvertently produce insertional torque substantially higher than recommended. Highest maximum torque was 9.0 Nm, which is 6.0-fold higher than expected for a locking screw using a 1.5-Nm torque limiter.
Our study results showed that insertion under controlled hand power (and low-velocity drill power) until 1 torque-limiting event occurred produced the most consistent and predictable results. Insertion under drill power or high-velocity hand power produced multiple sequential torque-limiting events, yielding inaccurate insertion torque. Low-velocity insertion under hand power, or carefully controlled drill power, consistently produced torque similar to advertised values.
Manufacturers’ technique guides are available for proximal humerus locking compression plate (LCP) systems, small-fragment LCP systems, the Proximal Humeral Interlocking System (PHILOS; DePuy Synthes), and the LISS. These technique guides clearly state that insertion can be performed under power. Only the PHILOS and LISS guides state that insertion should be performed under power until a single click is heard or that final tightening should be completed under hand power. The proximal humerus LCP guide states that surgeons should insert the locking screw under power until the torque-limiting device clicks. The small-fragment LCP guide states that insertion under power should always be completed with the torque-limiting attachment; there is no mention of reducing power or a single click (this may give the surgeon a false sense of security).
Screw overtightening and head/thread stripping can make screw removal challenging.10 Removal rates for LISS plates range from 8% to 26%, and removal is often reported as taking longer than the index procedure, with complication rates as high as 47%.11-13 Bae and colleagues3 reported significant difficulty in removing 24 of 279 self-tapping locking screws (3.5 mm).
It is important to note that these complications, most notably cold welding, are mostly associated with titanium locking plate and screw constructs. Although stainless steel constructs have gained favor, titanium constructs are still widely used around the world.14,15
In 10% of cases in a laboratory setting, insertion of a 3.5-mm locking screw at 4 to 6 Nm damaged the screw.9 Removal of 3.5-mm locking screws had a stripping rate of 8.6%, and use of the torque limiter did not make removal easy all the time.3 Torque limiters are set specific to each screw diameter to reduce the risk of damage/stripping or even overtightening. Even when a surgeon intends to stop a drill before locking, final tightening often inadvertently occurs under power.3
Cold welding is often described as a cause of difficult implant removal.3,12 According to a newer definition, this process is independent of temperature and can occur when 2 metallic surfaces are in direct contact.16 High contact pressures between 2 similar metals can lead to this solid state welding.17 Theoretically, improper use of torque limiters can increase the risk of welding; however, it appears to be associated only with titanium locking plate and screw constructs.
Locked plating osteosynthesis is a valuable tool for fracture management, but improper use can have significant consequences, including morbid implant removal procedures, which are more difficult and time-consuming than the index surgery. We determined that proper use of torque limiters involves insertion under hand or power control at slow velocity until 1 torque-limiting event occurs. Many orthopedic surgeons may assume that torque limiters are accurate no matter how screws are inserted into locking plates. In addition, they may be unaware guidelines exist, as these are often deeply embedded within text. Therefore, we must emphasize that torque limiters can be inaccurate when used improperly.
One limitation of this study is that it tested only the Synthes 1.5-Nm torque-limiting attachment, though we can speculate that torque limiters designed for larger screws and limiters manufactured by different companies will behave similarly. Another limitation is that we did not obtain the hospitals’ service records for the tested equipment and assumed the equipment was properly checked for accuracy by the providing company. However, we hypothesized that, if maintenance were an issue, then our results would not be similar across all sites tested.
These tests involved a torque limiter linked to a torque-measuring device and may not perfectly represent actual torque measured at the locked screw–thread interface. However, we think our construct accurately determines the torque produced at the level of the driver tip. Also, we can speculate that the torque produced with improper use will lead to the complications mentioned and demonstrated in previous studies. Welding of the screw–plate interface may simply be a result of improper trajectory and cross-threading. However, if we assume that torque limiters prevent excessive torque no matter how they are used, high insertion speeds may compound the effect of welding. Additional biomechanical studies with full locked plate osteosynthesis constructs on bone specimens are planned to further characterize the potential complications of this issue.
Proper surgical technique must be used to ensure that surgical fracture management is long-lasting. Plate implantation and screw implantation are among the most common orthopedic procedures performed. Plate and screw osteosynthesis can be done with nonlocking or locking plate and screw constructs or with hybrid fixation that incorporates both methods.
Nonlocking plate and screw osteosynthesis uses friction-fit for fixation. In osteoporotic bone, less torque is generated because of poor bone quality, and thus less friction force between plate and bone.1,2 Locked plating has dramatically changed fracture management, especially in frail and comminuted osteoporotic bone, with significant advantages over conventional plating.3-7
Development of locked plating systems, including the Less Invasive Stabilization System (LISS; DePuy Synthes) with its soft-tissue and fracture-fragment preservation, has changed treatment of distal femur and proximal tibia fractures. Cole and colleagues8 reported stable fixation and union in 97% of their patients. The LISS system proved to be stable, but there were cases of implant removal difficulty with this titanium construct. In 1 of the 10 cases in which the LISS plate was removed, 4 of the 11 locking screws were welded to the plate.8
Cold welding, in which similar metals are chemically bonded together under extreme pressure, is a complication associated with use of titanium-only plates and screws.9 This process, which is more likely to happen if cross-threading occurs within the screw–plate interface, can make screw removal extremely difficult. Screw removal difficulty strips screw heads, and often the surgeon must use either metal cutting instruments or trephines to remove screw remnants, which often results in retained implant or debris and damage or necrosis to surrounding bone.9,10
Locking screws are often inserted under power with a torque-limiting device attached to the drill mechanism to reduce the risk of lock screw overtightening and to try to prevent difficult implant removal. Although standard practice is to insert the screw and stop just before screw head engagement, with final tightening with a torque limiter and hand power, final tightening is often inadvertently done under power.3 Most technique guides instruct surgeons how to insert screws under power while using a torque limiter, but the exact technique is not emphasized.
We conducted a study to determine if rotational speed of screw insertion affects maximum torque on screw with use of a torque limiter. We describe proper use of a torque limiter as well as possible pitfalls. We hypothesized that improper use would result in substantially higher than expected insertion torque.
Materials and Methods
Torque-Limiting Attachments, Torque Wrench, and Drill
The Small Fragment Locking Compression Plate System (Synthes) includes a 1.5-Nm torque-limiting attachment and quick-coupling wooden handles and Star Drive attachments. All devices in this study were in active use at 6 urban institutions (3 level I trauma centers, 2 level II trauma centers, 1 level III hospital). Permission to obtain and test each device was granted by each institution.
A 0.25-inch dial torque wrench (751LDIN; CDI Torque Products) was purchased through an established distributor. The manufacturer includes a traceable certificate of accuracy to verify correct calibration. The torque wrench has a torque range of 0 to 9 Nm with visual increment demarcations of 0.2 Nm and a memory needle to retain maximum torque measurement. The same torque wrench was used in each experiment in order to maintain consistent measurements between devices. It was reset to zero after each use.
This study used a 0.5-inch, 19.2-V lithium drill (Craftsman C3) with 2 speed options: 0 to 440 rpm high torque and 0 to 1600 rpm high speed. This device provides variable torque output with a maximum output of 38.4 Nm. For this study, all measurements were done with the device on its high torque setting.
Maximum Torque Determination for Different Scenarios
Each torque limiter was evaluated for variations in maximum torque under 4 different scenarios. In each scenario, the torque limiter was coupled to the Star Drive attachment and then to that scenario’s rotating force. The completed system was then inserted into the torque wrench, which was secured to a flat working surface and rotated in accordance with each scenario; maximum torque was measured and recorded (Figures 1, 2). A torque-limiting event was defined as a single audible click on the torque limiter.
In scenario 1, each torque-limiting attachment system was attached to a quick-coupling wooden handle. The completed system was then rotated at controlled low velocity under hand power until 1 torque-limiting event occurred. This scenario was also used as an internal control to verify that the torque limiters were calibrated correctly.
In Scenario 2, the device was again attached to a quick-coupling wooden handle. The completed system was rotated at high velocity under hand power until multiple torque-limiting events occurred in a row. High velocity was defined as the operator freely rotating the wooden handle in a single action with full power resulting in multiple torque-limiting events.
In Scenario 3, the device was attached to a power drill braced to the flat working surface and rotated at low velocity under power until 1 torque-limiting event occurred.
In Scenario 4, the device was again attached to a power drill braced to the flat working surface. The completed system was rotated at high velocity under power until multiple torque-limiting events occurred.
After each trial, we recorded maximum torque achieved before each device’s torque-limiting event. Either an orthopedic surgery resident or a qualified medical student tested each torque-limiting device in each standardized testing scenario.
Statistical Analysis
Experiments for each torque limiter were repeated for 3 trials of each of the 4 different scenarios. For comparative statistics between experiments, maximum torque measurements were expressed as means and SDs; 95% confidence interval (95% CI) was calculated and reported to determine extent of variation within a single group. One-way analysis of variance (ANOVA) and Tukey post hoc tests were performed between groups for comparison of the normally distributed data. Significance was set at P ≤ .05.
Results
During simulation, we successfully measured maximum torque achieved with each torque limiter under the 4 different scenarios. All testing was done by 2 operators. ANOVA demonstrated significant (P ≤ .001) differences in torque among the scenarios.
In scenario 1, mean (SD) maximum torque under hand power at low velocity was 1.49 (0.15) Nm (95% CI, 1.43-1.55), near the advertised maximum torque of 1.5 Nm, with relatively minimal variation between devices. This scenario confirmed proper calibration of properly used torque limiters. Mean maximum torque ranged from 1.25 to 1.93 Nm.
In scenario 2, mean (SD) maximum torque under hand power at high velocity was 3.73 (0.79) Nm (95% CI, 3.33-4.13), a 2.5-fold increase compared with scenario 1 (P < .0001) (Figure 3). There also was an increase in variation of maximum torque between trials of individual devices and between different devices. Mean maximum torque ranged from 2.27 to 5.53 Nm.
In scenario 3, mean (SD) maximum torque under drill power at controlled low velocity was 1.47 (0.14) Nm (95% CI, 1.37-1.56), again near the advertised maximum torque of 1.5 Nm, with relatively minimal variation. Mean maximum torque ranged from 1.10 to 1.73 Nm.
In scenario 4, mean (SD) maximum torque under drill power at full power/high velocity was 5.37 (0.90) Nm (95% CI, 4.92-5.83), a 3.65-fold increase compared with scenario 3 (P < .0001) (Figure 3). Mean maximum torque measured in 3 tests ranged from 3.40 to 6.92 Nm.
There was no significant difference in mean maximum torque between the scenarios of hand power at low velocity and drill power at low velocities (P = .999) (Figure 4). Highest maximum torque from any device was 9.0 Nm (drill at full power). Results are summarized in the Table. There was no statistical significance in the test between the 2 test operators.
Discussion
Maximum torque was measured using a torque-limiting attachment under 4 different simulated scenarios. Our goals were to determine if varying practice and rotational velocity would affect maximum insertional torque and to measure consistency among torque limiters. We designed the scenarios to mimic practice patterns, including hand insertion and power insertion of locking screws. Results demonstrated that misuse of a torque-limiting device may inadvertently produce insertional torque substantially higher than recommended. Highest maximum torque was 9.0 Nm, which is 6.0-fold higher than expected for a locking screw using a 1.5-Nm torque limiter.
Our study results showed that insertion under controlled hand power (and low-velocity drill power) until 1 torque-limiting event occurred produced the most consistent and predictable results. Insertion under drill power or high-velocity hand power produced multiple sequential torque-limiting events, yielding inaccurate insertion torque. Low-velocity insertion under hand power, or carefully controlled drill power, consistently produced torque similar to advertised values.
Manufacturers’ technique guides are available for proximal humerus locking compression plate (LCP) systems, small-fragment LCP systems, the Proximal Humeral Interlocking System (PHILOS; DePuy Synthes), and the LISS. These technique guides clearly state that insertion can be performed under power. Only the PHILOS and LISS guides state that insertion should be performed under power until a single click is heard or that final tightening should be completed under hand power. The proximal humerus LCP guide states that surgeons should insert the locking screw under power until the torque-limiting device clicks. The small-fragment LCP guide states that insertion under power should always be completed with the torque-limiting attachment; there is no mention of reducing power or a single click (this may give the surgeon a false sense of security).
Screw overtightening and head/thread stripping can make screw removal challenging.10 Removal rates for LISS plates range from 8% to 26%, and removal is often reported as taking longer than the index procedure, with complication rates as high as 47%.11-13 Bae and colleagues3 reported significant difficulty in removing 24 of 279 self-tapping locking screws (3.5 mm).
It is important to note that these complications, most notably cold welding, are mostly associated with titanium locking plate and screw constructs. Although stainless steel constructs have gained favor, titanium constructs are still widely used around the world.14,15
In 10% of cases in a laboratory setting, insertion of a 3.5-mm locking screw at 4 to 6 Nm damaged the screw.9 Removal of 3.5-mm locking screws had a stripping rate of 8.6%, and use of the torque limiter did not make removal easy all the time.3 Torque limiters are set specific to each screw diameter to reduce the risk of damage/stripping or even overtightening. Even when a surgeon intends to stop a drill before locking, final tightening often inadvertently occurs under power.3
Cold welding is often described as a cause of difficult implant removal.3,12 According to a newer definition, this process is independent of temperature and can occur when 2 metallic surfaces are in direct contact.16 High contact pressures between 2 similar metals can lead to this solid state welding.17 Theoretically, improper use of torque limiters can increase the risk of welding; however, it appears to be associated only with titanium locking plate and screw constructs.
Locked plating osteosynthesis is a valuable tool for fracture management, but improper use can have significant consequences, including morbid implant removal procedures, which are more difficult and time-consuming than the index surgery. We determined that proper use of torque limiters involves insertion under hand or power control at slow velocity until 1 torque-limiting event occurs. Many orthopedic surgeons may assume that torque limiters are accurate no matter how screws are inserted into locking plates. In addition, they may be unaware guidelines exist, as these are often deeply embedded within text. Therefore, we must emphasize that torque limiters can be inaccurate when used improperly.
One limitation of this study is that it tested only the Synthes 1.5-Nm torque-limiting attachment, though we can speculate that torque limiters designed for larger screws and limiters manufactured by different companies will behave similarly. Another limitation is that we did not obtain the hospitals’ service records for the tested equipment and assumed the equipment was properly checked for accuracy by the providing company. However, we hypothesized that, if maintenance were an issue, then our results would not be similar across all sites tested.
These tests involved a torque limiter linked to a torque-measuring device and may not perfectly represent actual torque measured at the locked screw–thread interface. However, we think our construct accurately determines the torque produced at the level of the driver tip. Also, we can speculate that the torque produced with improper use will lead to the complications mentioned and demonstrated in previous studies. Welding of the screw–plate interface may simply be a result of improper trajectory and cross-threading. However, if we assume that torque limiters prevent excessive torque no matter how they are used, high insertion speeds may compound the effect of welding. Additional biomechanical studies with full locked plate osteosynthesis constructs on bone specimens are planned to further characterize the potential complications of this issue.
1. Sommer C, Babst R, Müller M, Hanson B. Locking compression plate loosening and plate breakage: a report of four cases. J Orthop Trauma. 2004;18(8):571-577.
2. Schütz M, Südkamp NP. Revolution in plate osteosynthesis: new internal fixator systems. J Orthop Sci. 2003;8(2):252-258.
3. Bae JH, Oh JK, Oh CW, Hur CR. Technical difficulties of removal of locking screw after locking compression plating. Arch Orthop Trauma Surg. 2009;129(1):91-95.
4. Frigg R. Locking compression plate (LCP). An osteosynthesis plate based on the dynamic compression plate and the point contact fixator (PC-Fix). Injury. 2001;32(suppl 2):63-66.
5. Frigg R. Development of the locking compression plate. Injury. 2003;34(suppl 2):B6-B10.
6. Korner J, Lill H, Müller LP, Rommens PM, Schneider E, Linke B. The LCP-concept in the operative treatment of distal humerus fractures—biological, biomechanical and surgical aspects. Injury. 2003;34(suppl 2):B20-B30.
7. Egol KA, Kubiak EN, Fulkerson E, Kummer FJ, Koval KJ. Biomechanics of locked plates and screws. J Orthop Trauma. 2004;18(8):488-493.
8. Cole PA, Zlowodzki M, Kregor PJ. Treatment of proximal tibia fractures using the Less Invasive Stabilization System: surgical experience and early clinical results in 77 fractures. J Orthop Trauma. 2004;18(8):528-535.
9. Ehlinger M, Adam P, Simon P, Bonnomet F. Technical difficulties in hardware removal in titanium compression plates with locking screws. Orthop Traumatol Surg Res. 2009;95(5):373-376.
10. Gopinathan NR, Dhillon MS, Kumar R. Surgical technique: simple technique for removing a locking recon plate with damaged screw heads. Clin Orthop Relat Res. 2013;471(5):1572-1575.
11. Pattison G, Reynolds J, Hardy J. Salvaging a stripped drive connection when removing screws. Injury. 1999;30(1):74-75.
12. Raja S, Imbuldeniya AM, Garg S, Groom G. Difficulties encountered removing locked plates. Ann R Coll Surg Engl. 2012;94(7):502-505.
13. Kumar G, Dunlop C. Case report: a technique to remove a jammed locking screw from a locking plate. Clin Orthop Relat Res. 2011;469(2):613-616.
14. Disegi JA. Titanium alloys for fracture fixation implants. Injury. 2000;31(suppl 4):14-17.
15. El-Zayat BF, Ruchholtz S, Efe T, Paletta J, Kreslo D, Zettl R. Results of titanium locking plate and stainless steel cerclage wire combination in femoral fractures. Indian J Orthop. 2013;47(5):454-458.
16. Van Nortwick SS, Yao J, Ladd AL. Titanium integration with bone, welding, and screw head destruction complicating hardware removal of the distal radius: report of 2 cases. J Hand Surg. 2012;37(7):1388-1392.
17. Ferguson GS, Chaudhury MK, Sigal GB, Whitesides GM. Contact adhesion of thin gold films on elastomeric supports: cold welding under ambient conditions. Science. 1991;253(5021):776-778.
1. Sommer C, Babst R, Müller M, Hanson B. Locking compression plate loosening and plate breakage: a report of four cases. J Orthop Trauma. 2004;18(8):571-577.
2. Schütz M, Südkamp NP. Revolution in plate osteosynthesis: new internal fixator systems. J Orthop Sci. 2003;8(2):252-258.
3. Bae JH, Oh JK, Oh CW, Hur CR. Technical difficulties of removal of locking screw after locking compression plating. Arch Orthop Trauma Surg. 2009;129(1):91-95.
4. Frigg R. Locking compression plate (LCP). An osteosynthesis plate based on the dynamic compression plate and the point contact fixator (PC-Fix). Injury. 2001;32(suppl 2):63-66.
5. Frigg R. Development of the locking compression plate. Injury. 2003;34(suppl 2):B6-B10.
6. Korner J, Lill H, Müller LP, Rommens PM, Schneider E, Linke B. The LCP-concept in the operative treatment of distal humerus fractures—biological, biomechanical and surgical aspects. Injury. 2003;34(suppl 2):B20-B30.
7. Egol KA, Kubiak EN, Fulkerson E, Kummer FJ, Koval KJ. Biomechanics of locked plates and screws. J Orthop Trauma. 2004;18(8):488-493.
8. Cole PA, Zlowodzki M, Kregor PJ. Treatment of proximal tibia fractures using the Less Invasive Stabilization System: surgical experience and early clinical results in 77 fractures. J Orthop Trauma. 2004;18(8):528-535.
9. Ehlinger M, Adam P, Simon P, Bonnomet F. Technical difficulties in hardware removal in titanium compression plates with locking screws. Orthop Traumatol Surg Res. 2009;95(5):373-376.
10. Gopinathan NR, Dhillon MS, Kumar R. Surgical technique: simple technique for removing a locking recon plate with damaged screw heads. Clin Orthop Relat Res. 2013;471(5):1572-1575.
11. Pattison G, Reynolds J, Hardy J. Salvaging a stripped drive connection when removing screws. Injury. 1999;30(1):74-75.
12. Raja S, Imbuldeniya AM, Garg S, Groom G. Difficulties encountered removing locked plates. Ann R Coll Surg Engl. 2012;94(7):502-505.
13. Kumar G, Dunlop C. Case report: a technique to remove a jammed locking screw from a locking plate. Clin Orthop Relat Res. 2011;469(2):613-616.
14. Disegi JA. Titanium alloys for fracture fixation implants. Injury. 2000;31(suppl 4):14-17.
15. El-Zayat BF, Ruchholtz S, Efe T, Paletta J, Kreslo D, Zettl R. Results of titanium locking plate and stainless steel cerclage wire combination in femoral fractures. Indian J Orthop. 2013;47(5):454-458.
16. Van Nortwick SS, Yao J, Ladd AL. Titanium integration with bone, welding, and screw head destruction complicating hardware removal of the distal radius: report of 2 cases. J Hand Surg. 2012;37(7):1388-1392.
17. Ferguson GS, Chaudhury MK, Sigal GB, Whitesides GM. Contact adhesion of thin gold films on elastomeric supports: cold welding under ambient conditions. Science. 1991;253(5021):776-778.

Poor Sun Protection Practices in Hispanic Patients Increases Risk for Skin Cancer
The most common type of skin cancer in Hispanic patients is basal cell carcinoma, according to Maritza Perez, MD, Associate Clinical Professor of Dermatology at the Icahn School of Medicine at Mount Sinai, New York, New York. Dr. Perez reviewed skin cancer in Hispanics as part of the “Skin Issues in Latino Patients” forum at the 74th Annual Meeting of the American Academy of Dermatology (AAD)(March 4-8, 2016) in Washington, DC. The head and neck region is the most common location of BCC in Hispanics, and it is more common among Hispanic males. Squamous cell carcinomas are the second most common, and melanomas are third most common.
The mortality rate from squamous cell carcinoma is higher in Hispanic patients compared to white patients. Dr. Perez indicated that UV light exposure is a predisposing factor for these types of skin cancer, and poor sun protection practices in this population are to blame.
“Patients [in this population] do not perceive that they are prone to skin cancer,” said Dr. Perez. This erroneous perception has led to delayed diagnosis and treatment of patients in this group, which has caused increased mortality and decreased survival.
Marta Rendon, MD, director of the session at the AAD and Medical Director of The Rendon Center for Dermatology & Aesthetic Medicine, Boca Raton, Florida, noted that Latinos are the fastest growing minority population in the United States and it is estimated that they will be approximately 30% of the population by the year 2050. As a result, dermatologists must emphasize sun protection, avoidance of midday sun, and avoidance of UV radiation.
In his Cutis practical pearls, “Patient Compliance With Photoprotection,” Vincent A. DeLeo, MD, provided tips on sunscreen use. “Patients need a realistic approach to photoprotection based on their genetics, including Fitzpatrick skin type and family history . . . and lifestyle history, which should include location of residence as well as occupation and recreational pursuits,” he said. “These inquiries should lead to a frank discussion of the patient’s risk for developing photodamage and skin cancer.”
Encourage routine use of a sunscreen with a sun protection factor of 30 or higher that carries a “broad spectrum” label. “There is evidence that sunscreens prevent squamous cell carcinoma, actinic keratosis, and photoaging. Early evidence, less strong but positive, also suggests protection against basal cell carcinoma and melanoma,” Dr. DeLeo reported.
The most common type of skin cancer in Hispanic patients is basal cell carcinoma, according to Maritza Perez, MD, Associate Clinical Professor of Dermatology at the Icahn School of Medicine at Mount Sinai, New York, New York. Dr. Perez reviewed skin cancer in Hispanics as part of the “Skin Issues in Latino Patients” forum at the 74th Annual Meeting of the American Academy of Dermatology (AAD)(March 4-8, 2016) in Washington, DC. The head and neck region is the most common location of BCC in Hispanics, and it is more common among Hispanic males. Squamous cell carcinomas are the second most common, and melanomas are third most common.
The mortality rate from squamous cell carcinoma is higher in Hispanic patients compared to white patients. Dr. Perez indicated that UV light exposure is a predisposing factor for these types of skin cancer, and poor sun protection practices in this population are to blame.
“Patients [in this population] do not perceive that they are prone to skin cancer,” said Dr. Perez. This erroneous perception has led to delayed diagnosis and treatment of patients in this group, which has caused increased mortality and decreased survival.
Marta Rendon, MD, director of the session at the AAD and Medical Director of The Rendon Center for Dermatology & Aesthetic Medicine, Boca Raton, Florida, noted that Latinos are the fastest growing minority population in the United States and it is estimated that they will be approximately 30% of the population by the year 2050. As a result, dermatologists must emphasize sun protection, avoidance of midday sun, and avoidance of UV radiation.
In his Cutis practical pearls, “Patient Compliance With Photoprotection,” Vincent A. DeLeo, MD, provided tips on sunscreen use. “Patients need a realistic approach to photoprotection based on their genetics, including Fitzpatrick skin type and family history . . . and lifestyle history, which should include location of residence as well as occupation and recreational pursuits,” he said. “These inquiries should lead to a frank discussion of the patient’s risk for developing photodamage and skin cancer.”
Encourage routine use of a sunscreen with a sun protection factor of 30 or higher that carries a “broad spectrum” label. “There is evidence that sunscreens prevent squamous cell carcinoma, actinic keratosis, and photoaging. Early evidence, less strong but positive, also suggests protection against basal cell carcinoma and melanoma,” Dr. DeLeo reported.
The most common type of skin cancer in Hispanic patients is basal cell carcinoma, according to Maritza Perez, MD, Associate Clinical Professor of Dermatology at the Icahn School of Medicine at Mount Sinai, New York, New York. Dr. Perez reviewed skin cancer in Hispanics as part of the “Skin Issues in Latino Patients” forum at the 74th Annual Meeting of the American Academy of Dermatology (AAD)(March 4-8, 2016) in Washington, DC. The head and neck region is the most common location of BCC in Hispanics, and it is more common among Hispanic males. Squamous cell carcinomas are the second most common, and melanomas are third most common.
The mortality rate from squamous cell carcinoma is higher in Hispanic patients compared to white patients. Dr. Perez indicated that UV light exposure is a predisposing factor for these types of skin cancer, and poor sun protection practices in this population are to blame.
“Patients [in this population] do not perceive that they are prone to skin cancer,” said Dr. Perez. This erroneous perception has led to delayed diagnosis and treatment of patients in this group, which has caused increased mortality and decreased survival.
Marta Rendon, MD, director of the session at the AAD and Medical Director of The Rendon Center for Dermatology & Aesthetic Medicine, Boca Raton, Florida, noted that Latinos are the fastest growing minority population in the United States and it is estimated that they will be approximately 30% of the population by the year 2050. As a result, dermatologists must emphasize sun protection, avoidance of midday sun, and avoidance of UV radiation.
In his Cutis practical pearls, “Patient Compliance With Photoprotection,” Vincent A. DeLeo, MD, provided tips on sunscreen use. “Patients need a realistic approach to photoprotection based on their genetics, including Fitzpatrick skin type and family history . . . and lifestyle history, which should include location of residence as well as occupation and recreational pursuits,” he said. “These inquiries should lead to a frank discussion of the patient’s risk for developing photodamage and skin cancer.”
Encourage routine use of a sunscreen with a sun protection factor of 30 or higher that carries a “broad spectrum” label. “There is evidence that sunscreens prevent squamous cell carcinoma, actinic keratosis, and photoaging. Early evidence, less strong but positive, also suggests protection against basal cell carcinoma and melanoma,” Dr. DeLeo reported.

Obesity, oral contraceptive use are risk factors for cerebral venous thrombosis in women
Obese women taking oral contraceptives had a 30-fold increased odds for cerebral venous thrombosis (CVT), compared with normal-weight women, in an unmatched case-control study of 186 CVT cases and 6,134 controls.
The association between a body-mass index of 30 kg/m2 or higher and increased odds of CVT “appears to be fully attributable to a strongly increased risk in women who use oral contraceptives [OCs],” said Dr. Susanna M. Zuurbier of the Academic Medical Centre in Amsterdam, and her colleagues.

“Although the relative risks are increased substantially, the absolute risks of CVT are still small,” the researchers said. “Moreover, withholding oral contraceptives may lead to an increase in unintended pregnancies and thus the number of pregnancy-related thrombosis cases.”
After controlling for multiple variables, CVT was 2.63 times more likely to occur in obese individuals, compared with those of normal weight. When the findings were stratified by sex, a BMI greater than 30 kg/m2 had no significant impact on CVT in men, but the odds rose 3.5-fold in women, the investigators reported online March 14 in JAMA Neurology (JAMA Neurol. 2016 Mar 14. doi: 10.1001/jamaneurol.2016.000100).
On further analysis, overweight and obesity had a dose-dependent impact on the odds of CVT among women who used OCs. Adjusted odds ratios were 11.87 for those with BMIs ranging from 25 kg/m2 to 29 kg/m2, and 29.26 for those with BMIs of 30 kg/m2 or higher when compared against normal-weight women who did not use OCs. No association was found between obesity and CVT risk in women who did not use OCs, the researchers noted.
Patients with CVT were recruited in 2006-2014 from two medical centers, one in the Netherlands and the other in Switzerland. The controls were part of the Dutch Multiple Environmental and Genetic Assessment of Risk Factors for Venous Thrombosis (MEGA) study. Overall, patients with CVT were more likely to be younger than controls (median age 40 years vs. 48 years). They also were more likely than controls to be female (72% vs. 53%), users of oral contraceptives (73% vs. 24%) and have a history of cancer (9% vs. 4%).
The study was limited by several factors, including the small number of CVT cases, the lack of complete BMI data for the study population, and time difference in recruitment of cases and controls, the researchers noted, but they advised clinicians to keep the risk in mind when counseling obese women about OC use.
“Alternative methods of contraception that are not associated with thrombosis, such as an intrauterine device, might be offered to these women,” they wrote.
The study was funded by grants from the Netherlands Organisation for Scientific Research, the Dutch Thrombosis Society, the Remmert Adriaan Laan Foundation, and the Swiss Heart Foundation. Study coauthor Dr. Marcel Arnold disclosed receiving honoraria for giving lectures and serving on advisory boards for Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Covidien.
“The discovery of increased rates of asymptomatic atherosclerosis in patients with VTE led to the systematic study of cardiovascular risk factors, such as obesity, in VTE,” but the possible association between obesity and CVT has not been explored, Dr. Chirantan Banerjee wrote in an accompanying editorial.
The current study results are “novel and in concordance with prior studies on obesity and OC use as risk factors for VTE,” Dr. Banerjee noted. The study’s strengths lie in the inclusion of appropriate subgroups, controls, and confounding variables. In addition to further research to validate the findings, “studies investigating the effect of inherited thrombophilia on the association between obesity and CVT would also be important because the current study did not have this data,” he noted. “Other potential confounders, such as obstructive sleep apnea and anemia, should be included in future studies.
In the meantime, “the authors correctly point out that despite the manifold increased relative risk, the absolute risk of CVT in obese women taking OCs still remains low and should not preclude OC use among them,” Dr. Banerjee said.
Dr. Banerjee is a member of the department of neurology at the Medical University of Charleston, S.C., and had no financial conflicts to disclose. These comments were taken from his editorial accompanying Dr. Zuurbier and colleagues’ report (JAMA Neurol. 2016 Mar 14. doi: 10.1001/jamaneurol.2015.5107).
“The discovery of increased rates of asymptomatic atherosclerosis in patients with VTE led to the systematic study of cardiovascular risk factors, such as obesity, in VTE,” but the possible association between obesity and CVT has not been explored, Dr. Chirantan Banerjee wrote in an accompanying editorial.
The current study results are “novel and in concordance with prior studies on obesity and OC use as risk factors for VTE,” Dr. Banerjee noted. The study’s strengths lie in the inclusion of appropriate subgroups, controls, and confounding variables. In addition to further research to validate the findings, “studies investigating the effect of inherited thrombophilia on the association between obesity and CVT would also be important because the current study did not have this data,” he noted. “Other potential confounders, such as obstructive sleep apnea and anemia, should be included in future studies.
In the meantime, “the authors correctly point out that despite the manifold increased relative risk, the absolute risk of CVT in obese women taking OCs still remains low and should not preclude OC use among them,” Dr. Banerjee said.
Dr. Banerjee is a member of the department of neurology at the Medical University of Charleston, S.C., and had no financial conflicts to disclose. These comments were taken from his editorial accompanying Dr. Zuurbier and colleagues’ report (JAMA Neurol. 2016 Mar 14. doi: 10.1001/jamaneurol.2015.5107).
“The discovery of increased rates of asymptomatic atherosclerosis in patients with VTE led to the systematic study of cardiovascular risk factors, such as obesity, in VTE,” but the possible association between obesity and CVT has not been explored, Dr. Chirantan Banerjee wrote in an accompanying editorial.
The current study results are “novel and in concordance with prior studies on obesity and OC use as risk factors for VTE,” Dr. Banerjee noted. The study’s strengths lie in the inclusion of appropriate subgroups, controls, and confounding variables. In addition to further research to validate the findings, “studies investigating the effect of inherited thrombophilia on the association between obesity and CVT would also be important because the current study did not have this data,” he noted. “Other potential confounders, such as obstructive sleep apnea and anemia, should be included in future studies.
In the meantime, “the authors correctly point out that despite the manifold increased relative risk, the absolute risk of CVT in obese women taking OCs still remains low and should not preclude OC use among them,” Dr. Banerjee said.
Dr. Banerjee is a member of the department of neurology at the Medical University of Charleston, S.C., and had no financial conflicts to disclose. These comments were taken from his editorial accompanying Dr. Zuurbier and colleagues’ report (JAMA Neurol. 2016 Mar 14. doi: 10.1001/jamaneurol.2015.5107).
Obese women taking oral contraceptives had a 30-fold increased odds for cerebral venous thrombosis (CVT), compared with normal-weight women, in an unmatched case-control study of 186 CVT cases and 6,134 controls.
The association between a body-mass index of 30 kg/m2 or higher and increased odds of CVT “appears to be fully attributable to a strongly increased risk in women who use oral contraceptives [OCs],” said Dr. Susanna M. Zuurbier of the Academic Medical Centre in Amsterdam, and her colleagues.
“Although the relative risks are increased substantially, the absolute risks of CVT are still small,” the researchers said. “Moreover, withholding oral contraceptives may lead to an increase in unintended pregnancies and thus the number of pregnancy-related thrombosis cases.”
After controlling for multiple variables, CVT was 2.63 times more likely to occur in obese individuals, compared with those of normal weight. When the findings were stratified by sex, a BMI greater than 30 kg/m2 had no significant impact on CVT in men, but the odds rose 3.5-fold in women, the investigators reported online March 14 in JAMA Neurology (JAMA Neurol. 2016 Mar 14. doi: 10.1001/jamaneurol.2016.000100).
On further analysis, overweight and obesity had a dose-dependent impact on the odds of CVT among women who used OCs. Adjusted odds ratios were 11.87 for those with BMIs ranging from 25 kg/m2 to 29 kg/m2, and 29.26 for those with BMIs of 30 kg/m2 or higher when compared against normal-weight women who did not use OCs. No association was found between obesity and CVT risk in women who did not use OCs, the researchers noted.
Patients with CVT were recruited in 2006-2014 from two medical centers, one in the Netherlands and the other in Switzerland. The controls were part of the Dutch Multiple Environmental and Genetic Assessment of Risk Factors for Venous Thrombosis (MEGA) study. Overall, patients with CVT were more likely to be younger than controls (median age 40 years vs. 48 years). They also were more likely than controls to be female (72% vs. 53%), users of oral contraceptives (73% vs. 24%) and have a history of cancer (9% vs. 4%).
The study was limited by several factors, including the small number of CVT cases, the lack of complete BMI data for the study population, and time difference in recruitment of cases and controls, the researchers noted, but they advised clinicians to keep the risk in mind when counseling obese women about OC use.
“Alternative methods of contraception that are not associated with thrombosis, such as an intrauterine device, might be offered to these women,” they wrote.
The study was funded by grants from the Netherlands Organisation for Scientific Research, the Dutch Thrombosis Society, the Remmert Adriaan Laan Foundation, and the Swiss Heart Foundation. Study coauthor Dr. Marcel Arnold disclosed receiving honoraria for giving lectures and serving on advisory boards for Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Covidien.
Obese women taking oral contraceptives had a 30-fold increased odds for cerebral venous thrombosis (CVT), compared with normal-weight women, in an unmatched case-control study of 186 CVT cases and 6,134 controls.
The association between a body-mass index of 30 kg/m2 or higher and increased odds of CVT “appears to be fully attributable to a strongly increased risk in women who use oral contraceptives [OCs],” said Dr. Susanna M. Zuurbier of the Academic Medical Centre in Amsterdam, and her colleagues.
“Although the relative risks are increased substantially, the absolute risks of CVT are still small,” the researchers said. “Moreover, withholding oral contraceptives may lead to an increase in unintended pregnancies and thus the number of pregnancy-related thrombosis cases.”
After controlling for multiple variables, CVT was 2.63 times more likely to occur in obese individuals, compared with those of normal weight. When the findings were stratified by sex, a BMI greater than 30 kg/m2 had no significant impact on CVT in men, but the odds rose 3.5-fold in women, the investigators reported online March 14 in JAMA Neurology (JAMA Neurol. 2016 Mar 14. doi: 10.1001/jamaneurol.2016.000100).
On further analysis, overweight and obesity had a dose-dependent impact on the odds of CVT among women who used OCs. Adjusted odds ratios were 11.87 for those with BMIs ranging from 25 kg/m2 to 29 kg/m2, and 29.26 for those with BMIs of 30 kg/m2 or higher when compared against normal-weight women who did not use OCs. No association was found between obesity and CVT risk in women who did not use OCs, the researchers noted.
Patients with CVT were recruited in 2006-2014 from two medical centers, one in the Netherlands and the other in Switzerland. The controls were part of the Dutch Multiple Environmental and Genetic Assessment of Risk Factors for Venous Thrombosis (MEGA) study. Overall, patients with CVT were more likely to be younger than controls (median age 40 years vs. 48 years). They also were more likely than controls to be female (72% vs. 53%), users of oral contraceptives (73% vs. 24%) and have a history of cancer (9% vs. 4%).
The study was limited by several factors, including the small number of CVT cases, the lack of complete BMI data for the study population, and time difference in recruitment of cases and controls, the researchers noted, but they advised clinicians to keep the risk in mind when counseling obese women about OC use.
“Alternative methods of contraception that are not associated with thrombosis, such as an intrauterine device, might be offered to these women,” they wrote.
The study was funded by grants from the Netherlands Organisation for Scientific Research, the Dutch Thrombosis Society, the Remmert Adriaan Laan Foundation, and the Swiss Heart Foundation. Study coauthor Dr. Marcel Arnold disclosed receiving honoraria for giving lectures and serving on advisory boards for Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Covidien.
FROM JAMA NEUROLOGY
Key clinical point: Obesity and oral contraceptive use significantly increased the odds for cerebral venous thrombosis in adults.
Major finding: The risk of CVT was 2.63 times more likely among obese women compared to nonobese women, and nearly 30 times more likely in women taking oral contraceptives.
Data source: An unmatched, case-control study of 186 CVT patients and 6,134 healthy controls.
Disclosures: The study was funded by grants from the Netherlands Organisation for Scientific Research, the Dutch Thrombosis Society, the Remmert Adriaan Laan Foundation, and the Swiss Heart Foundation. Study coauthor Dr. Marcel Arnold disclosed receiving honoraria for giving lectures and serving on advisory boards for Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and Covidien.

High false positives found for Medtronic’s implantable AF detectors
LOS ANGELES – Medtronic’s Reveal LINQ implantable loop recorders misidentified 84% of rhythm anomalies as atrial fibrillation in 52 stroke patients at Emory University in Atlanta, according to a presentation at the International Stroke Conference.
Two electrophysiologists reviewed a random sample of 166 rhythm strips from those patients that were identified by Reveal as atrial fibrillation (AF) over a 2-month period; 140 (84%) were false positives. Eighty (57%) of the false positives were premature atrial complexes, 31 (22%) were due to T wave over-sensing, 14 (10%) to noise, 7 (5%) to premature ventricular complexes, 4 (2.9%) to under-sensing, and 4 (2.9%) to sinus arrhythmias.
There wasn’t a mix-and-match of true and false positives in the same patient; false and true positives were consistent in patients over the study period.
The take-home message from the study is that the high sensitivity of Medtronic’s implantable loop recorders means that they are good at detecting possible AF, but their findings must be reviewed and confirmed before being acted upon.

“There are high rates of false positives, but the results can be easily adjudicated by electrophysiologists as evidenced by our observer agreement,” which was 100%. “These strips need to be adjudicated by somebody, and not taken at face value,” said investigator Dr. Spencer Maddox, an Emory resident.
The devices look mainly at RR intervals and the presence or absence of P waves. Runs of 2 minutes are required for AF. One of the issues in the study was that T waves were identified as QRS complexes, which changed the RR interval and trigged the device to report AF, he said.
Medtronic could reduce the false positive rate by, for instance, extending the run required for AF, but it would be a bad idea. “The goal here is to not miss atrial fibrillation,” Dr. Maddox said. “There are false positives, but as long as you go back and reread, I think that’s fine. I wouldn’t mess with the sensitivity of the device.”
The company said the same thing when asked for comment on the study.
“The AF detection algorithm ... is tuned to favor sensitivity because manual review can subsequently rule out any false positives. This is one reason it is important to have trained cardiologists or electrophysiologists involved in reviewing reports of irregular heart rhythms to determine a diagnosis of AF,” said Medtronic spokesman Ryan Mathre, who also noted that company data suggest a lower false positive rate (Cerebrovasc Dis. 2015;40:175-81).

Even so, confirmation doesn’t always happen, “and that’s the scary part. In practice almost all the time,” the report comes in “and it’s acted on,” said Dr. Robert Hart, a neurology professor at McMaster University in Hamilton, Ont., and comoderator of the study presentation.
The Emory patients were all recovering from ischemic strokes or TIAs. They were about 70 years old on average, about 60% were men, and almost all were white. A total of 38 had implantable loop recorders for cryptogenic strokes; the devices detected true AF in 4 (11%) after a mean of 92 days. Early Holter monitoring missed it.
Emory generally prescribes anticoagulants if AF is confirmed, but, as several audience members noted, the burden of AF that requires anticoagulation is unclear. “It’s an area with a lot of thought now, but no good answers,” Dr. Maddox said at the conference, sponsored by the American Heart Association.
The investigators had no disclosures, and there was no outside funding for the work.
LOS ANGELES – Medtronic’s Reveal LINQ implantable loop recorders misidentified 84% of rhythm anomalies as atrial fibrillation in 52 stroke patients at Emory University in Atlanta, according to a presentation at the International Stroke Conference.
Two electrophysiologists reviewed a random sample of 166 rhythm strips from those patients that were identified by Reveal as atrial fibrillation (AF) over a 2-month period; 140 (84%) were false positives. Eighty (57%) of the false positives were premature atrial complexes, 31 (22%) were due to T wave over-sensing, 14 (10%) to noise, 7 (5%) to premature ventricular complexes, 4 (2.9%) to under-sensing, and 4 (2.9%) to sinus arrhythmias.
There wasn’t a mix-and-match of true and false positives in the same patient; false and true positives were consistent in patients over the study period.
The take-home message from the study is that the high sensitivity of Medtronic’s implantable loop recorders means that they are good at detecting possible AF, but their findings must be reviewed and confirmed before being acted upon.
“There are high rates of false positives, but the results can be easily adjudicated by electrophysiologists as evidenced by our observer agreement,” which was 100%. “These strips need to be adjudicated by somebody, and not taken at face value,” said investigator Dr. Spencer Maddox, an Emory resident.
The devices look mainly at RR intervals and the presence or absence of P waves. Runs of 2 minutes are required for AF. One of the issues in the study was that T waves were identified as QRS complexes, which changed the RR interval and trigged the device to report AF, he said.
Medtronic could reduce the false positive rate by, for instance, extending the run required for AF, but it would be a bad idea. “The goal here is to not miss atrial fibrillation,” Dr. Maddox said. “There are false positives, but as long as you go back and reread, I think that’s fine. I wouldn’t mess with the sensitivity of the device.”
The company said the same thing when asked for comment on the study.
“The AF detection algorithm ... is tuned to favor sensitivity because manual review can subsequently rule out any false positives. This is one reason it is important to have trained cardiologists or electrophysiologists involved in reviewing reports of irregular heart rhythms to determine a diagnosis of AF,” said Medtronic spokesman Ryan Mathre, who also noted that company data suggest a lower false positive rate (Cerebrovasc Dis. 2015;40:175-81).
Even so, confirmation doesn’t always happen, “and that’s the scary part. In practice almost all the time,” the report comes in “and it’s acted on,” said Dr. Robert Hart, a neurology professor at McMaster University in Hamilton, Ont., and comoderator of the study presentation.
The Emory patients were all recovering from ischemic strokes or TIAs. They were about 70 years old on average, about 60% were men, and almost all were white. A total of 38 had implantable loop recorders for cryptogenic strokes; the devices detected true AF in 4 (11%) after a mean of 92 days. Early Holter monitoring missed it.
Emory generally prescribes anticoagulants if AF is confirmed, but, as several audience members noted, the burden of AF that requires anticoagulation is unclear. “It’s an area with a lot of thought now, but no good answers,” Dr. Maddox said at the conference, sponsored by the American Heart Association.
The investigators had no disclosures, and there was no outside funding for the work.
LOS ANGELES – Medtronic’s Reveal LINQ implantable loop recorders misidentified 84% of rhythm anomalies as atrial fibrillation in 52 stroke patients at Emory University in Atlanta, according to a presentation at the International Stroke Conference.
Two electrophysiologists reviewed a random sample of 166 rhythm strips from those patients that were identified by Reveal as atrial fibrillation (AF) over a 2-month period; 140 (84%) were false positives. Eighty (57%) of the false positives were premature atrial complexes, 31 (22%) were due to T wave over-sensing, 14 (10%) to noise, 7 (5%) to premature ventricular complexes, 4 (2.9%) to under-sensing, and 4 (2.9%) to sinus arrhythmias.
There wasn’t a mix-and-match of true and false positives in the same patient; false and true positives were consistent in patients over the study period.
The take-home message from the study is that the high sensitivity of Medtronic’s implantable loop recorders means that they are good at detecting possible AF, but their findings must be reviewed and confirmed before being acted upon.
“There are high rates of false positives, but the results can be easily adjudicated by electrophysiologists as evidenced by our observer agreement,” which was 100%. “These strips need to be adjudicated by somebody, and not taken at face value,” said investigator Dr. Spencer Maddox, an Emory resident.
The devices look mainly at RR intervals and the presence or absence of P waves. Runs of 2 minutes are required for AF. One of the issues in the study was that T waves were identified as QRS complexes, which changed the RR interval and trigged the device to report AF, he said.
Medtronic could reduce the false positive rate by, for instance, extending the run required for AF, but it would be a bad idea. “The goal here is to not miss atrial fibrillation,” Dr. Maddox said. “There are false positives, but as long as you go back and reread, I think that’s fine. I wouldn’t mess with the sensitivity of the device.”
The company said the same thing when asked for comment on the study.
“The AF detection algorithm ... is tuned to favor sensitivity because manual review can subsequently rule out any false positives. This is one reason it is important to have trained cardiologists or electrophysiologists involved in reviewing reports of irregular heart rhythms to determine a diagnosis of AF,” said Medtronic spokesman Ryan Mathre, who also noted that company data suggest a lower false positive rate (Cerebrovasc Dis. 2015;40:175-81).
Even so, confirmation doesn’t always happen, “and that’s the scary part. In practice almost all the time,” the report comes in “and it’s acted on,” said Dr. Robert Hart, a neurology professor at McMaster University in Hamilton, Ont., and comoderator of the study presentation.
The Emory patients were all recovering from ischemic strokes or TIAs. They were about 70 years old on average, about 60% were men, and almost all were white. A total of 38 had implantable loop recorders for cryptogenic strokes; the devices detected true AF in 4 (11%) after a mean of 92 days. Early Holter monitoring missed it.
Emory generally prescribes anticoagulants if AF is confirmed, but, as several audience members noted, the burden of AF that requires anticoagulation is unclear. “It’s an area with a lot of thought now, but no good answers,” Dr. Maddox said at the conference, sponsored by the American Heart Association.
The investigators had no disclosures, and there was no outside funding for the work.
AT The INTERNATIONAL STROKE CONFERENCE
Key clinical point: The high sensitivity of Medtronic’s implantable loop recorders means that they’re good at detecting possible AF, but their findings must be reviewed and confirmed before being acted upon.
Major finding: Two electrophysiologists reviewed a random sample of 166 rhythm strips identified by Reveal as atrial fibrillation; 140 (84%) were false positives.
Data source: Fifty-two ischemic stroke and TIA patients.
Disclosures: The investigators had no disclosures. There was no outside funding for the work.

Lenalidomide, thalidomide in melphalan regimen yields similar progression-free survival
Swapping lenalidomide for thalidomide in a standard regimen for transplant-ineligible patients with untreated multiple myeloma did not improve efficacy, but the toxicity profile may favor the use of lenalidomide in a maintenance regimen, results of a randomized trial suggest.
Among patients with previously untreated multiple myeloma who were not eligible for autologous stem cell transplant, neither median progression-free survival (PFS) nor overall survival (OS) were significantly different for patients treated with either melphalan, prednisone, and thalidomide (MPT-T) followed by thalidomide maintenance, or with the same regimen with lenalidomide (Revlimid) substituted for thalidomide (MPR-R), reported Dr. Sonja Zweegman of Vrije University Medical Center in Amsterdam.
“MPR-R has no advantage over MPT-T with respect to response rate, PFS, and OS. However, the use of thalidomide as maintenance therapy was associated with a high rate of clinically significant neuropathy and is therefore not preferred for maintenance strategies,” they wrote (Blood 2016;127[9];1109-16).
The investigators randomly assigned 637 transplant-ineligible patients with newly-diagnosed multiple myeloma to receive nine 4-week cycles of either MPT-T (318 patients) or MPR-R (319 patients). At 36 months’ median follow-up, median PFS, the primary endpoint, was 20 months for patients treated with MPT-T, compared with 23 months for those treated with MPR-R. This translated into a hazard ratio (HR) of 0.87, P = .12).
The overall response rates were 81% for MPT-T and 84% for MPR-R. Very good partial responses or better were seen in 47% and 45%, of patients, respectively. The complete response rate with MPT-T was 10%, compared with 13% for MPR-R. Median time to response and time to maximum response were similar between the arms.
OS at 2, 3, and 4 years in the MPT-T and MPR-R arms was 73% vs. 84%, 64% vs 69%, and 52% vs. 56%, respectively. These differences were not statistically significant.
The proportion of patients with one or more grade 3 or 4 adverse events was 81% with thalidomide and 86% with lenalidomide.
The investigators noted, however, that there was a high rate of discontinuation during induction therapy in each arm, with 49% of those starting on MPT-T and 41% of those starting on MPR-R halting therapy. Most of the patients who discontinued were older than age 75. Early treatment deaths (within three cycles) occurred in 13 patients on MPT-T, and 8 on MPR-R.
Among patients who started on maintenance therapy, significantly more patients on thalidomide had to discontinue thalidomide than did patients who started on lenalidomide maintenance (60% vs, 17%, P = .017).
The primary reason for the higher rate of discontinuation of MPT-T maintenance was neuropathy, which occurred in 87% of the discontinuations in this study arm, compared with 3% of those in the lenalidomide arm. Neuropathy of at least grade 3 was 16% in the MPT-T arm vs. 2% in MPR-R, resulting in a significantly shorter duration of maintenance therapy (5 vs. 17 months in MPR-R), irrespective of age.
Hematologic toxicities were higher in the MPR-R group, especially grades 3 and 4 neutropenia (64% vs 27%), but this did not translate into a higher clinical infection rate, and the toxicities were manageable in older patients, the investigators reported.
Swapping lenalidomide for thalidomide in a standard regimen for transplant-ineligible patients with untreated multiple myeloma did not improve efficacy, but the toxicity profile may favor the use of lenalidomide in a maintenance regimen, results of a randomized trial suggest.
Among patients with previously untreated multiple myeloma who were not eligible for autologous stem cell transplant, neither median progression-free survival (PFS) nor overall survival (OS) were significantly different for patients treated with either melphalan, prednisone, and thalidomide (MPT-T) followed by thalidomide maintenance, or with the same regimen with lenalidomide (Revlimid) substituted for thalidomide (MPR-R), reported Dr. Sonja Zweegman of Vrije University Medical Center in Amsterdam.
“MPR-R has no advantage over MPT-T with respect to response rate, PFS, and OS. However, the use of thalidomide as maintenance therapy was associated with a high rate of clinically significant neuropathy and is therefore not preferred for maintenance strategies,” they wrote (Blood 2016;127[9];1109-16).
The investigators randomly assigned 637 transplant-ineligible patients with newly-diagnosed multiple myeloma to receive nine 4-week cycles of either MPT-T (318 patients) or MPR-R (319 patients). At 36 months’ median follow-up, median PFS, the primary endpoint, was 20 months for patients treated with MPT-T, compared with 23 months for those treated with MPR-R. This translated into a hazard ratio (HR) of 0.87, P = .12).
The overall response rates were 81% for MPT-T and 84% for MPR-R. Very good partial responses or better were seen in 47% and 45%, of patients, respectively. The complete response rate with MPT-T was 10%, compared with 13% for MPR-R. Median time to response and time to maximum response were similar between the arms.
OS at 2, 3, and 4 years in the MPT-T and MPR-R arms was 73% vs. 84%, 64% vs 69%, and 52% vs. 56%, respectively. These differences were not statistically significant.
The proportion of patients with one or more grade 3 or 4 adverse events was 81% with thalidomide and 86% with lenalidomide.
The investigators noted, however, that there was a high rate of discontinuation during induction therapy in each arm, with 49% of those starting on MPT-T and 41% of those starting on MPR-R halting therapy. Most of the patients who discontinued were older than age 75. Early treatment deaths (within three cycles) occurred in 13 patients on MPT-T, and 8 on MPR-R.
Among patients who started on maintenance therapy, significantly more patients on thalidomide had to discontinue thalidomide than did patients who started on lenalidomide maintenance (60% vs, 17%, P = .017).
The primary reason for the higher rate of discontinuation of MPT-T maintenance was neuropathy, which occurred in 87% of the discontinuations in this study arm, compared with 3% of those in the lenalidomide arm. Neuropathy of at least grade 3 was 16% in the MPT-T arm vs. 2% in MPR-R, resulting in a significantly shorter duration of maintenance therapy (5 vs. 17 months in MPR-R), irrespective of age.
Hematologic toxicities were higher in the MPR-R group, especially grades 3 and 4 neutropenia (64% vs 27%), but this did not translate into a higher clinical infection rate, and the toxicities were manageable in older patients, the investigators reported.
Swapping lenalidomide for thalidomide in a standard regimen for transplant-ineligible patients with untreated multiple myeloma did not improve efficacy, but the toxicity profile may favor the use of lenalidomide in a maintenance regimen, results of a randomized trial suggest.
Among patients with previously untreated multiple myeloma who were not eligible for autologous stem cell transplant, neither median progression-free survival (PFS) nor overall survival (OS) were significantly different for patients treated with either melphalan, prednisone, and thalidomide (MPT-T) followed by thalidomide maintenance, or with the same regimen with lenalidomide (Revlimid) substituted for thalidomide (MPR-R), reported Dr. Sonja Zweegman of Vrije University Medical Center in Amsterdam.
“MPR-R has no advantage over MPT-T with respect to response rate, PFS, and OS. However, the use of thalidomide as maintenance therapy was associated with a high rate of clinically significant neuropathy and is therefore not preferred for maintenance strategies,” they wrote (Blood 2016;127[9];1109-16).
The investigators randomly assigned 637 transplant-ineligible patients with newly-diagnosed multiple myeloma to receive nine 4-week cycles of either MPT-T (318 patients) or MPR-R (319 patients). At 36 months’ median follow-up, median PFS, the primary endpoint, was 20 months for patients treated with MPT-T, compared with 23 months for those treated with MPR-R. This translated into a hazard ratio (HR) of 0.87, P = .12).
The overall response rates were 81% for MPT-T and 84% for MPR-R. Very good partial responses or better were seen in 47% and 45%, of patients, respectively. The complete response rate with MPT-T was 10%, compared with 13% for MPR-R. Median time to response and time to maximum response were similar between the arms.
OS at 2, 3, and 4 years in the MPT-T and MPR-R arms was 73% vs. 84%, 64% vs 69%, and 52% vs. 56%, respectively. These differences were not statistically significant.
The proportion of patients with one or more grade 3 or 4 adverse events was 81% with thalidomide and 86% with lenalidomide.
The investigators noted, however, that there was a high rate of discontinuation during induction therapy in each arm, with 49% of those starting on MPT-T and 41% of those starting on MPR-R halting therapy. Most of the patients who discontinued were older than age 75. Early treatment deaths (within three cycles) occurred in 13 patients on MPT-T, and 8 on MPR-R.
Among patients who started on maintenance therapy, significantly more patients on thalidomide had to discontinue thalidomide than did patients who started on lenalidomide maintenance (60% vs, 17%, P = .017).
The primary reason for the higher rate of discontinuation of MPT-T maintenance was neuropathy, which occurred in 87% of the discontinuations in this study arm, compared with 3% of those in the lenalidomide arm. Neuropathy of at least grade 3 was 16% in the MPT-T arm vs. 2% in MPR-R, resulting in a significantly shorter duration of maintenance therapy (5 vs. 17 months in MPR-R), irrespective of age.
Hematologic toxicities were higher in the MPR-R group, especially grades 3 and 4 neutropenia (64% vs 27%), but this did not translate into a higher clinical infection rate, and the toxicities were manageable in older patients, the investigators reported.
FROM BLOOD
Key clinical point: Lenalidomide or thalidomide added to a melphalan backbone regimen yielded similar outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma.
Major finding: At 36 months median follow-up, median PFS was 20 months for patients treated with thalidomide, compared with 23 months for those treated with lenalidomide.
Data source: Randomized controlled trial of 637 patients with multiple myeloma who were not candidates for autologous stem cell transplantation.
Disclosures: The Dutch Cancer Society, Norwegian Cancer Society, and Celgene supported the study. Dr. Zweegman and other colleagues reported financial relationships with Celgene.
MACRA Provides New Direction for U.S. Healthcare
Last year, Congress passed legislation to permanently eliminate the Sustainable Growth Rate (SGR) formula, created in 1997 and designed to hold Medicare Part B or outpatient spending under control. Allowing the SGR to go into effect would have severely cut physician reimbursements in recent years, but Congress passed legislation each year to temporarily avert these cuts (also known annually as the “doc fix”). In search of a permanent solution, the passage of bipartisan legislation permanently repealing the SGR in 2015 was hailed as a way to ensure more certainty around the future of Medicare payments for physicians.
This legislation (H.R. 2, 114th Congress), sponsored by Rep. Michael C. Burgess (R-Texas) and entitled “Medicare Access and CHIP Reauthorization Act of 2015,” or MACRA, does much more than simply remove the SGR’s threat of broader Medicare payment cuts. The law changes the ways physicians are reimbursed by Medicare and continues to shift our healthcare system away from volume-based reimbursements and toward a value-based payment system.
What Is MIPS?
MACRA creates two value-based payment tracks for physicians. The first, the Merit-Based Incentive Payment System (MIPS), is closer to the old fee-for-service model of reimbursement. However, MIPS takes into account both volume and quality (i.e., payment is adjusted based on physician-quality scores). These physician-specific scores broaden the scope of quality measurement by including new measures related to resource utilization, electronic health record (EHR) use, and clinical improvement practices, along with the traditional clinical quality markers.
Under MIPS, the current Physician Quality Reporting System (PQRS), EHR Incentive Program, and Physician Value-Based Modifier all will be integrated into this single-payment adjustment.
The range of potential payment adjustments based on a physician’s MIPS score grows each year through 2022 (in 2022, adjustments can range from +9% to -9%). The program is budget neutral, which means that increases in payments to high-scoring providers will be offset by decreases in payments to low-scoring providers. For 2019 to 2024, there also will be an additional payment adjustment given to the highest MIPS performers for exceptional performance.
A benefit of MIPS is that it will streamline the various quality-reporting programs currently in place into one single program and does not ask physicians to assume any additional financial risk related to outcomes when taking care of patients. However, the particulars of how the MIPS score will be calculated are yet to be determined, and much of the utility and palatability of this score will depend on the chosen metrics. The goal of these metrics should be that they are meaningful, valid, and attributable to specific providers.
What Are APMs?
The other payment option MACRA provides for physicians allows them to opt out of MIPS and participate in the Alternative Payment Models (APMs) track. To incentivize physicians to take part in this riskier track, providers taking part in APMs will receive some extra money for their participation: a 5% annual lump sum bonus on reimbursement payments. To clarify, qualifying APMs are those where providers take on “more than nominal” financial risk, report on their quality measures, and use certified EHR technology.
To qualify as a participant in an APM (for example, the Medicare Shared Savings Program), providers must hit a threshold for percentage of total revenue received or percentage of patients from qualifying APMs. This threshold will increase over time. For example, from 2019 to 2020, providers must obtain at least 25% of their Medicare revenue or patients via APMs, whereas in 2023, 75% of their Medicare revenue or \ patients will need to come from APMs.
Providers will benefit from the increased reimbursement offered if they participate in APMs. There also is funding allocated in MACRA to help develop quality measures, with a call for physician leads to develop quality standards. This payment model, however, does come with increased financial risk for the provider contingent on patient outcomes. In addition, it may be difficult for all providers to hit the thresholds for participation.
Stick with MIPS? Or Take the Plunge with APM?
How MACRA affects you will depend a lot on the practice environment. As described above, MACRA is designed to move physicians into risk-based payment structures if possible. If possible, or otherwise, to simplify the current fee-for-service mechanism of payment by consolidating various Medicare pay-for-performance programs.
Let’s look at a few scenarios:
Hospitalist A works for a physician group that assumes risk for patients in a MACRA-approved APM and sees only those inpatients as opposed to unassigned patients. Therefore, almost all of hospitalist A’s patients are covered by risk-based contracts, and hospitalist A might be well positioned for the new APM structure.
Hospitalist B works for a group, or a university, and sees whatever patients are admitted to the hospital. Hospitalist B’s eligibility to participate in the APM will depend on the percentage of patients in alternative payment models in their market. If hospitalist B’s market has many Medicare accountable care organizations, and Medicaid and the commercial insurers compensate through a risk-sharing model, hospitalist B might reach the threshold. This is more accidental than planned, however, and hospitalist B might not be able to consistently hit this threshold year after year.
In addition, just working within the model will probably not be enough to qualify. Hospitalist B will need to also take on “more than nominal risk” as a participant in the model. In an employed academic setting, where the hospital is taking on risk as part of an APM, it is unlikely hospitalist B will qualify just by virtue of hospital employment. Hospitalist B must also meet/exceed the patient or payment thresholds under the model.
Bottom line: Given the current situation, we expect many hospitalists will likely be required to participate in MIPS and not qualify for APMs. Understanding the details and expectations now will help them be successful in the future.
Is MACRA Good for Hospitalists?
Most of organized medicine is happy to be free from the annual threat of reimbursement cuts. In addition, the new law might streamline quality reporting. But the specific upside depends on your perspective.
With APMs, a hospitalist might enjoy more upside potential, particularly for high-quality work and EHR use. However, whether it is realistic for most hospitalists to even participate in the model depends on many factors, as described previously, and SHM is advocating for the law to be implemented in ways that will more readily accommodate hospitalist practice and employment structures.
For example, the SHM Public Policy Committee has provided the Centers for Medicare & Medicaid Services (CMS) with realistic options for implementing the APM framework that would allow hospitalist B in the above example to qualify as an APM participant.
With MIPS, the benefit to hospitalists depends a fair amount on the way the law is implemented: how quality reporting happens, what metrics will count as quality improvement efforts, and how utilization of EHRs is measured.
What Issues Should Hospitalists Be Aware Of?
As MACRA is further developed, the main issue for hospitalists will be to ensure fairness in assessing quality and incentive payments. As previously encountered with quality reporting, hospitalists are not differentiated clearly from outpatient providers. As a result, they could suffer from the comparison of their quality outcomes for their sicker hospitalized patients to the patients cared for in a typical primary-care internal medicine practice. This inaccurate comparison poses problems in both models.
A potential solution would be a hospitalist-specific billing code, which would make it easier to identify hospitalists. SHM applied for and advocated for the approval of such a billing code and the request was recently approved by CMS.
In addition, as hospitalists mostly work in groups with shift-based schedules, thus sharing care of patients, individual identifiers may not be as significant as possibly looking at hospital, system, or team-based metrics. Using facility performance measures for both clinical quality and performance improvement—where hospitalists can opt to align with their hospital, which is already reporting quality outcomes—might be one way out of this conundrum. It would take into account the type of facility-level quality improvement work many hospitalists participate in. This also would decrease reporting burden for hospitalist groups.
SHM has advocated for this solution and was able to ensure this concept was included in the law; however, it is unclear when or how CMS will implement it.
To summarize, looking good in quality reporting will continue to be a challenge for hospitalists. It will be critical to keep pressure on CMS to implement solutions that account for the unique situation of our specialty.
Another issue to be aware of is the ability of hospitalists to participate in APMs. As with other facility-based providers, hospitalists have little control over whether their facility participates in an APM. Ways to ensure hospitalists can reach thresholds for participation could include allowing the various APMs that hospitalist patients are aligned with count toward an individual hospitalists’ APM participation total—a solution that SHM is advocating for Medicare to include in the APM framework.
What’s Next?
Much remains to be solidified regarding implementation of MACRA, despite the fact it goes live in a few short years (see Figure 1). CMS has asked for comments and stakeholder input regarding MIPS and APMs, and it will be releasing the first round of rules around MACRA this year.
SHM is actively working with CMS to ensure this legislation will reflect the work we are doing as hospitalists to provide high-quality clinical care for our patients and enhance the performance of our hospitals and health system. TH

Dr. Doctoroff is a hospitalist at Beth Israel Deaconess Medical Center and an instructor of medicine at Harvard Medical School in Boston. Dr. Dutta is a hospitalist at Rush University Medical Center and an assistant professor of medicine at Rush Medical College in Chicago. Both are members of the SHM Public Policy Committee.
Last year, Congress passed legislation to permanently eliminate the Sustainable Growth Rate (SGR) formula, created in 1997 and designed to hold Medicare Part B or outpatient spending under control. Allowing the SGR to go into effect would have severely cut physician reimbursements in recent years, but Congress passed legislation each year to temporarily avert these cuts (also known annually as the “doc fix”). In search of a permanent solution, the passage of bipartisan legislation permanently repealing the SGR in 2015 was hailed as a way to ensure more certainty around the future of Medicare payments for physicians.
This legislation (H.R. 2, 114th Congress), sponsored by Rep. Michael C. Burgess (R-Texas) and entitled “Medicare Access and CHIP Reauthorization Act of 2015,” or MACRA, does much more than simply remove the SGR’s threat of broader Medicare payment cuts. The law changes the ways physicians are reimbursed by Medicare and continues to shift our healthcare system away from volume-based reimbursements and toward a value-based payment system.
What Is MIPS?
MACRA creates two value-based payment tracks for physicians. The first, the Merit-Based Incentive Payment System (MIPS), is closer to the old fee-for-service model of reimbursement. However, MIPS takes into account both volume and quality (i.e., payment is adjusted based on physician-quality scores). These physician-specific scores broaden the scope of quality measurement by including new measures related to resource utilization, electronic health record (EHR) use, and clinical improvement practices, along with the traditional clinical quality markers.
Under MIPS, the current Physician Quality Reporting System (PQRS), EHR Incentive Program, and Physician Value-Based Modifier all will be integrated into this single-payment adjustment.
The range of potential payment adjustments based on a physician’s MIPS score grows each year through 2022 (in 2022, adjustments can range from +9% to -9%). The program is budget neutral, which means that increases in payments to high-scoring providers will be offset by decreases in payments to low-scoring providers. For 2019 to 2024, there also will be an additional payment adjustment given to the highest MIPS performers for exceptional performance.
A benefit of MIPS is that it will streamline the various quality-reporting programs currently in place into one single program and does not ask physicians to assume any additional financial risk related to outcomes when taking care of patients. However, the particulars of how the MIPS score will be calculated are yet to be determined, and much of the utility and palatability of this score will depend on the chosen metrics. The goal of these metrics should be that they are meaningful, valid, and attributable to specific providers.
What Are APMs?
The other payment option MACRA provides for physicians allows them to opt out of MIPS and participate in the Alternative Payment Models (APMs) track. To incentivize physicians to take part in this riskier track, providers taking part in APMs will receive some extra money for their participation: a 5% annual lump sum bonus on reimbursement payments. To clarify, qualifying APMs are those where providers take on “more than nominal” financial risk, report on their quality measures, and use certified EHR technology.
To qualify as a participant in an APM (for example, the Medicare Shared Savings Program), providers must hit a threshold for percentage of total revenue received or percentage of patients from qualifying APMs. This threshold will increase over time. For example, from 2019 to 2020, providers must obtain at least 25% of their Medicare revenue or patients via APMs, whereas in 2023, 75% of their Medicare revenue or \ patients will need to come from APMs.
Providers will benefit from the increased reimbursement offered if they participate in APMs. There also is funding allocated in MACRA to help develop quality measures, with a call for physician leads to develop quality standards. This payment model, however, does come with increased financial risk for the provider contingent on patient outcomes. In addition, it may be difficult for all providers to hit the thresholds for participation.
Stick with MIPS? Or Take the Plunge with APM?
How MACRA affects you will depend a lot on the practice environment. As described above, MACRA is designed to move physicians into risk-based payment structures if possible. If possible, or otherwise, to simplify the current fee-for-service mechanism of payment by consolidating various Medicare pay-for-performance programs.
Let’s look at a few scenarios:
Hospitalist A works for a physician group that assumes risk for patients in a MACRA-approved APM and sees only those inpatients as opposed to unassigned patients. Therefore, almost all of hospitalist A’s patients are covered by risk-based contracts, and hospitalist A might be well positioned for the new APM structure.
Hospitalist B works for a group, or a university, and sees whatever patients are admitted to the hospital. Hospitalist B’s eligibility to participate in the APM will depend on the percentage of patients in alternative payment models in their market. If hospitalist B’s market has many Medicare accountable care organizations, and Medicaid and the commercial insurers compensate through a risk-sharing model, hospitalist B might reach the threshold. This is more accidental than planned, however, and hospitalist B might not be able to consistently hit this threshold year after year.
In addition, just working within the model will probably not be enough to qualify. Hospitalist B will need to also take on “more than nominal risk” as a participant in the model. In an employed academic setting, where the hospital is taking on risk as part of an APM, it is unlikely hospitalist B will qualify just by virtue of hospital employment. Hospitalist B must also meet/exceed the patient or payment thresholds under the model.
Bottom line: Given the current situation, we expect many hospitalists will likely be required to participate in MIPS and not qualify for APMs. Understanding the details and expectations now will help them be successful in the future.
Is MACRA Good for Hospitalists?
Most of organized medicine is happy to be free from the annual threat of reimbursement cuts. In addition, the new law might streamline quality reporting. But the specific upside depends on your perspective.
With APMs, a hospitalist might enjoy more upside potential, particularly for high-quality work and EHR use. However, whether it is realistic for most hospitalists to even participate in the model depends on many factors, as described previously, and SHM is advocating for the law to be implemented in ways that will more readily accommodate hospitalist practice and employment structures.
For example, the SHM Public Policy Committee has provided the Centers for Medicare & Medicaid Services (CMS) with realistic options for implementing the APM framework that would allow hospitalist B in the above example to qualify as an APM participant.
With MIPS, the benefit to hospitalists depends a fair amount on the way the law is implemented: how quality reporting happens, what metrics will count as quality improvement efforts, and how utilization of EHRs is measured.
What Issues Should Hospitalists Be Aware Of?
As MACRA is further developed, the main issue for hospitalists will be to ensure fairness in assessing quality and incentive payments. As previously encountered with quality reporting, hospitalists are not differentiated clearly from outpatient providers. As a result, they could suffer from the comparison of their quality outcomes for their sicker hospitalized patients to the patients cared for in a typical primary-care internal medicine practice. This inaccurate comparison poses problems in both models.
A potential solution would be a hospitalist-specific billing code, which would make it easier to identify hospitalists. SHM applied for and advocated for the approval of such a billing code and the request was recently approved by CMS.
In addition, as hospitalists mostly work in groups with shift-based schedules, thus sharing care of patients, individual identifiers may not be as significant as possibly looking at hospital, system, or team-based metrics. Using facility performance measures for both clinical quality and performance improvement—where hospitalists can opt to align with their hospital, which is already reporting quality outcomes—might be one way out of this conundrum. It would take into account the type of facility-level quality improvement work many hospitalists participate in. This also would decrease reporting burden for hospitalist groups.
SHM has advocated for this solution and was able to ensure this concept was included in the law; however, it is unclear when or how CMS will implement it.
To summarize, looking good in quality reporting will continue to be a challenge for hospitalists. It will be critical to keep pressure on CMS to implement solutions that account for the unique situation of our specialty.
Another issue to be aware of is the ability of hospitalists to participate in APMs. As with other facility-based providers, hospitalists have little control over whether their facility participates in an APM. Ways to ensure hospitalists can reach thresholds for participation could include allowing the various APMs that hospitalist patients are aligned with count toward an individual hospitalists’ APM participation total—a solution that SHM is advocating for Medicare to include in the APM framework.
What’s Next?
Much remains to be solidified regarding implementation of MACRA, despite the fact it goes live in a few short years (see Figure 1). CMS has asked for comments and stakeholder input regarding MIPS and APMs, and it will be releasing the first round of rules around MACRA this year.
SHM is actively working with CMS to ensure this legislation will reflect the work we are doing as hospitalists to provide high-quality clinical care for our patients and enhance the performance of our hospitals and health system. TH
Dr. Doctoroff is a hospitalist at Beth Israel Deaconess Medical Center and an instructor of medicine at Harvard Medical School in Boston. Dr. Dutta is a hospitalist at Rush University Medical Center and an assistant professor of medicine at Rush Medical College in Chicago. Both are members of the SHM Public Policy Committee.
Last year, Congress passed legislation to permanently eliminate the Sustainable Growth Rate (SGR) formula, created in 1997 and designed to hold Medicare Part B or outpatient spending under control. Allowing the SGR to go into effect would have severely cut physician reimbursements in recent years, but Congress passed legislation each year to temporarily avert these cuts (also known annually as the “doc fix”). In search of a permanent solution, the passage of bipartisan legislation permanently repealing the SGR in 2015 was hailed as a way to ensure more certainty around the future of Medicare payments for physicians.
This legislation (H.R. 2, 114th Congress), sponsored by Rep. Michael C. Burgess (R-Texas) and entitled “Medicare Access and CHIP Reauthorization Act of 2015,” or MACRA, does much more than simply remove the SGR’s threat of broader Medicare payment cuts. The law changes the ways physicians are reimbursed by Medicare and continues to shift our healthcare system away from volume-based reimbursements and toward a value-based payment system.
What Is MIPS?
MACRA creates two value-based payment tracks for physicians. The first, the Merit-Based Incentive Payment System (MIPS), is closer to the old fee-for-service model of reimbursement. However, MIPS takes into account both volume and quality (i.e., payment is adjusted based on physician-quality scores). These physician-specific scores broaden the scope of quality measurement by including new measures related to resource utilization, electronic health record (EHR) use, and clinical improvement practices, along with the traditional clinical quality markers.
Under MIPS, the current Physician Quality Reporting System (PQRS), EHR Incentive Program, and Physician Value-Based Modifier all will be integrated into this single-payment adjustment.
The range of potential payment adjustments based on a physician’s MIPS score grows each year through 2022 (in 2022, adjustments can range from +9% to -9%). The program is budget neutral, which means that increases in payments to high-scoring providers will be offset by decreases in payments to low-scoring providers. For 2019 to 2024, there also will be an additional payment adjustment given to the highest MIPS performers for exceptional performance.
A benefit of MIPS is that it will streamline the various quality-reporting programs currently in place into one single program and does not ask physicians to assume any additional financial risk related to outcomes when taking care of patients. However, the particulars of how the MIPS score will be calculated are yet to be determined, and much of the utility and palatability of this score will depend on the chosen metrics. The goal of these metrics should be that they are meaningful, valid, and attributable to specific providers.
What Are APMs?
The other payment option MACRA provides for physicians allows them to opt out of MIPS and participate in the Alternative Payment Models (APMs) track. To incentivize physicians to take part in this riskier track, providers taking part in APMs will receive some extra money for their participation: a 5% annual lump sum bonus on reimbursement payments. To clarify, qualifying APMs are those where providers take on “more than nominal” financial risk, report on their quality measures, and use certified EHR technology.
To qualify as a participant in an APM (for example, the Medicare Shared Savings Program), providers must hit a threshold for percentage of total revenue received or percentage of patients from qualifying APMs. This threshold will increase over time. For example, from 2019 to 2020, providers must obtain at least 25% of their Medicare revenue or patients via APMs, whereas in 2023, 75% of their Medicare revenue or \ patients will need to come from APMs.
Providers will benefit from the increased reimbursement offered if they participate in APMs. There also is funding allocated in MACRA to help develop quality measures, with a call for physician leads to develop quality standards. This payment model, however, does come with increased financial risk for the provider contingent on patient outcomes. In addition, it may be difficult for all providers to hit the thresholds for participation.
Stick with MIPS? Or Take the Plunge with APM?
How MACRA affects you will depend a lot on the practice environment. As described above, MACRA is designed to move physicians into risk-based payment structures if possible. If possible, or otherwise, to simplify the current fee-for-service mechanism of payment by consolidating various Medicare pay-for-performance programs.
Let’s look at a few scenarios:
Hospitalist A works for a physician group that assumes risk for patients in a MACRA-approved APM and sees only those inpatients as opposed to unassigned patients. Therefore, almost all of hospitalist A’s patients are covered by risk-based contracts, and hospitalist A might be well positioned for the new APM structure.
Hospitalist B works for a group, or a university, and sees whatever patients are admitted to the hospital. Hospitalist B’s eligibility to participate in the APM will depend on the percentage of patients in alternative payment models in their market. If hospitalist B’s market has many Medicare accountable care organizations, and Medicaid and the commercial insurers compensate through a risk-sharing model, hospitalist B might reach the threshold. This is more accidental than planned, however, and hospitalist B might not be able to consistently hit this threshold year after year.
In addition, just working within the model will probably not be enough to qualify. Hospitalist B will need to also take on “more than nominal risk” as a participant in the model. In an employed academic setting, where the hospital is taking on risk as part of an APM, it is unlikely hospitalist B will qualify just by virtue of hospital employment. Hospitalist B must also meet/exceed the patient or payment thresholds under the model.
Bottom line: Given the current situation, we expect many hospitalists will likely be required to participate in MIPS and not qualify for APMs. Understanding the details and expectations now will help them be successful in the future.
Is MACRA Good for Hospitalists?
Most of organized medicine is happy to be free from the annual threat of reimbursement cuts. In addition, the new law might streamline quality reporting. But the specific upside depends on your perspective.
With APMs, a hospitalist might enjoy more upside potential, particularly for high-quality work and EHR use. However, whether it is realistic for most hospitalists to even participate in the model depends on many factors, as described previously, and SHM is advocating for the law to be implemented in ways that will more readily accommodate hospitalist practice and employment structures.
For example, the SHM Public Policy Committee has provided the Centers for Medicare & Medicaid Services (CMS) with realistic options for implementing the APM framework that would allow hospitalist B in the above example to qualify as an APM participant.
With MIPS, the benefit to hospitalists depends a fair amount on the way the law is implemented: how quality reporting happens, what metrics will count as quality improvement efforts, and how utilization of EHRs is measured.
What Issues Should Hospitalists Be Aware Of?
As MACRA is further developed, the main issue for hospitalists will be to ensure fairness in assessing quality and incentive payments. As previously encountered with quality reporting, hospitalists are not differentiated clearly from outpatient providers. As a result, they could suffer from the comparison of their quality outcomes for their sicker hospitalized patients to the patients cared for in a typical primary-care internal medicine practice. This inaccurate comparison poses problems in both models.
A potential solution would be a hospitalist-specific billing code, which would make it easier to identify hospitalists. SHM applied for and advocated for the approval of such a billing code and the request was recently approved by CMS.
In addition, as hospitalists mostly work in groups with shift-based schedules, thus sharing care of patients, individual identifiers may not be as significant as possibly looking at hospital, system, or team-based metrics. Using facility performance measures for both clinical quality and performance improvement—where hospitalists can opt to align with their hospital, which is already reporting quality outcomes—might be one way out of this conundrum. It would take into account the type of facility-level quality improvement work many hospitalists participate in. This also would decrease reporting burden for hospitalist groups.
SHM has advocated for this solution and was able to ensure this concept was included in the law; however, it is unclear when or how CMS will implement it.
To summarize, looking good in quality reporting will continue to be a challenge for hospitalists. It will be critical to keep pressure on CMS to implement solutions that account for the unique situation of our specialty.
Another issue to be aware of is the ability of hospitalists to participate in APMs. As with other facility-based providers, hospitalists have little control over whether their facility participates in an APM. Ways to ensure hospitalists can reach thresholds for participation could include allowing the various APMs that hospitalist patients are aligned with count toward an individual hospitalists’ APM participation total—a solution that SHM is advocating for Medicare to include in the APM framework.
What’s Next?
Much remains to be solidified regarding implementation of MACRA, despite the fact it goes live in a few short years (see Figure 1). CMS has asked for comments and stakeholder input regarding MIPS and APMs, and it will be releasing the first round of rules around MACRA this year.
SHM is actively working with CMS to ensure this legislation will reflect the work we are doing as hospitalists to provide high-quality clinical care for our patients and enhance the performance of our hospitals and health system. TH
Dr. Doctoroff is a hospitalist at Beth Israel Deaconess Medical Center and an instructor of medicine at Harvard Medical School in Boston. Dr. Dutta is a hospitalist at Rush University Medical Center and an assistant professor of medicine at Rush Medical College in Chicago. Both are members of the SHM Public Policy Committee.
SHM’s Twitter Contest Encourages Appropriate Antibiotic Prescribing

- Identify opportunities to engage with all hospital-based clinicians to improve antibiotic stewardship in your hospital.
- Pay attention to appropriate antibiotic choice and resistance patterns and identify mechanisms to educate providers on overprescribing in your hospital.
- Consider the following:
Adhere to antibiotic treatment guidelines.
Track the day.
Set a stop date.
Reevaluate therapy.
Streamline therapy.
Avoid automatic time courses.

Not only did participants receive recognition for their efforts hanging up the posters and engaging their teams, the posters’ presence in various hospitals and offices around the country created thousands of impressions among hospital-based staff and others directly responsible for proper antibiotic prescribing.
Although the contest is over, you can still help facilitate culture change related to appropriate antibiotic prescribing. Follow SHM on Twitter @SHMLive, and continue to visit FightTheResistance.org for the latest updates on the campaign and new tools to promote antibiotic stewardship. TH
Brett Radler is SHM’s communications coordinator.
- Identify opportunities to engage with all hospital-based clinicians to improve antibiotic stewardship in your hospital.
- Pay attention to appropriate antibiotic choice and resistance patterns and identify mechanisms to educate providers on overprescribing in your hospital.
- Consider the following:
Adhere to antibiotic treatment guidelines.
Track the day.
Set a stop date.
Reevaluate therapy.
Streamline therapy.
Avoid automatic time courses.
Not only did participants receive recognition for their efforts hanging up the posters and engaging their teams, the posters’ presence in various hospitals and offices around the country created thousands of impressions among hospital-based staff and others directly responsible for proper antibiotic prescribing.
Although the contest is over, you can still help facilitate culture change related to appropriate antibiotic prescribing. Follow SHM on Twitter @SHMLive, and continue to visit FightTheResistance.org for the latest updates on the campaign and new tools to promote antibiotic stewardship. TH
Brett Radler is SHM’s communications coordinator.
- Identify opportunities to engage with all hospital-based clinicians to improve antibiotic stewardship in your hospital.
- Pay attention to appropriate antibiotic choice and resistance patterns and identify mechanisms to educate providers on overprescribing in your hospital.
- Consider the following:
Adhere to antibiotic treatment guidelines.
Track the day.
Set a stop date.
Reevaluate therapy.
Streamline therapy.
Avoid automatic time courses.
Not only did participants receive recognition for their efforts hanging up the posters and engaging their teams, the posters’ presence in various hospitals and offices around the country created thousands of impressions among hospital-based staff and others directly responsible for proper antibiotic prescribing.
Although the contest is over, you can still help facilitate culture change related to appropriate antibiotic prescribing. Follow SHM on Twitter @SHMLive, and continue to visit FightTheResistance.org for the latest updates on the campaign and new tools to promote antibiotic stewardship. TH
Brett Radler is SHM’s communications coordinator.
Gut microbes affect platelet function, thrombosis risk

Image by Andre E.X. Brown
New research indicates that gut microbes alter platelet function, which affects the risk of thrombosis and related events like heart attack and stroke.
When the nutrient choline, which is abundant in animal products like meat and egg yolk, is ingested, gut microbes play a role in breaking it down and producing the compound TMAO.
Recent studies have shown that blood TMAO levels are associated with a heightened risk of heart attack and stroke.
The new study, published in Cell, suggests that TMAO encourages hyper-reactive platelet function, thereby increasing the likelihood of thrombosis.
Researchers said this could be the mechanism by which TMAO increases the risk of heart attack and stroke. And these findings reveal a previously unrecognized mechanistic link between specific dietary nutrients, gut microbes, platelet function, and thrombosis risk.
“It is remarkable that gut microbes produce a compound that alters platelet function and thrombotic heart attack and stroke risk,” said study author Stanley Hazen, MD, PhD, of the Cleveland Clinic in Ohio.
“This new link helps explain how diet-induced TMAO generation is mechanistically linked to development of lethal adverse complications of heart disease.”
Dr Hazen and his colleagues first discovered a link between TMAO, gut microbes, and heart disease 5 years ago.
For the current study, the researchers analyzed blood levels of TMAO in more than 4000 patients and saw a significant correlation between higher TMAO and thrombosis potential. This led to the hypothesis that TMAO may directly impact platelet function.
Subsequent studies with both human platelets and animal models confirmed that TMAO makes platelets hyper-reactive, heightening thrombosis potential and accelerating clotting rates.
“We have shown that TMAO fundamentally alters calcium signaling within platelets,” Dr Hazen said. “When TMAO is elevated, platelet responsiveness to known triggers like thrombin, collagen, or ADP is heightened.”
“In general, there’s a broad range for how quickly different people will form clots. However, across the board, when TMAO is elevated, platelet responsiveness jumps to the hyper-reactive side of normal.”
Dr Hazen and his colleagues said these results suggest that lowering TMAO—via dietary manipulation, alteration in microbial community with a probiotic or prebiotic, or direct pharmacological inhibition of microbial enzymes involved in TMA production—may be a way to reduce the risk of thrombotic events.
They noted that, unlike current antiplatelet therapies, targeting TMAO would likely reduce platelet hyper-responsiveness to the normal range and not induce impairment in overall platelet function. So the intervention could attenuate pro-thrombotic tendencies without increasing the risk of bleeding complications. ![]()
Image by Andre E.X. Brown
New research indicates that gut microbes alter platelet function, which affects the risk of thrombosis and related events like heart attack and stroke.
When the nutrient choline, which is abundant in animal products like meat and egg yolk, is ingested, gut microbes play a role in breaking it down and producing the compound TMAO.
Recent studies have shown that blood TMAO levels are associated with a heightened risk of heart attack and stroke.
The new study, published in Cell, suggests that TMAO encourages hyper-reactive platelet function, thereby increasing the likelihood of thrombosis.
Researchers said this could be the mechanism by which TMAO increases the risk of heart attack and stroke. And these findings reveal a previously unrecognized mechanistic link between specific dietary nutrients, gut microbes, platelet function, and thrombosis risk.
“It is remarkable that gut microbes produce a compound that alters platelet function and thrombotic heart attack and stroke risk,” said study author Stanley Hazen, MD, PhD, of the Cleveland Clinic in Ohio.
“This new link helps explain how diet-induced TMAO generation is mechanistically linked to development of lethal adverse complications of heart disease.”
Dr Hazen and his colleagues first discovered a link between TMAO, gut microbes, and heart disease 5 years ago.
For the current study, the researchers analyzed blood levels of TMAO in more than 4000 patients and saw a significant correlation between higher TMAO and thrombosis potential. This led to the hypothesis that TMAO may directly impact platelet function.
Subsequent studies with both human platelets and animal models confirmed that TMAO makes platelets hyper-reactive, heightening thrombosis potential and accelerating clotting rates.
“We have shown that TMAO fundamentally alters calcium signaling within platelets,” Dr Hazen said. “When TMAO is elevated, platelet responsiveness to known triggers like thrombin, collagen, or ADP is heightened.”
“In general, there’s a broad range for how quickly different people will form clots. However, across the board, when TMAO is elevated, platelet responsiveness jumps to the hyper-reactive side of normal.”
Dr Hazen and his colleagues said these results suggest that lowering TMAO—via dietary manipulation, alteration in microbial community with a probiotic or prebiotic, or direct pharmacological inhibition of microbial enzymes involved in TMA production—may be a way to reduce the risk of thrombotic events.
They noted that, unlike current antiplatelet therapies, targeting TMAO would likely reduce platelet hyper-responsiveness to the normal range and not induce impairment in overall platelet function. So the intervention could attenuate pro-thrombotic tendencies without increasing the risk of bleeding complications. ![]()
Image by Andre E.X. Brown
New research indicates that gut microbes alter platelet function, which affects the risk of thrombosis and related events like heart attack and stroke.
When the nutrient choline, which is abundant in animal products like meat and egg yolk, is ingested, gut microbes play a role in breaking it down and producing the compound TMAO.
Recent studies have shown that blood TMAO levels are associated with a heightened risk of heart attack and stroke.
The new study, published in Cell, suggests that TMAO encourages hyper-reactive platelet function, thereby increasing the likelihood of thrombosis.
Researchers said this could be the mechanism by which TMAO increases the risk of heart attack and stroke. And these findings reveal a previously unrecognized mechanistic link between specific dietary nutrients, gut microbes, platelet function, and thrombosis risk.
“It is remarkable that gut microbes produce a compound that alters platelet function and thrombotic heart attack and stroke risk,” said study author Stanley Hazen, MD, PhD, of the Cleveland Clinic in Ohio.
“This new link helps explain how diet-induced TMAO generation is mechanistically linked to development of lethal adverse complications of heart disease.”
Dr Hazen and his colleagues first discovered a link between TMAO, gut microbes, and heart disease 5 years ago.
For the current study, the researchers analyzed blood levels of TMAO in more than 4000 patients and saw a significant correlation between higher TMAO and thrombosis potential. This led to the hypothesis that TMAO may directly impact platelet function.
Subsequent studies with both human platelets and animal models confirmed that TMAO makes platelets hyper-reactive, heightening thrombosis potential and accelerating clotting rates.
“We have shown that TMAO fundamentally alters calcium signaling within platelets,” Dr Hazen said. “When TMAO is elevated, platelet responsiveness to known triggers like thrombin, collagen, or ADP is heightened.”
“In general, there’s a broad range for how quickly different people will form clots. However, across the board, when TMAO is elevated, platelet responsiveness jumps to the hyper-reactive side of normal.”
Dr Hazen and his colleagues said these results suggest that lowering TMAO—via dietary manipulation, alteration in microbial community with a probiotic or prebiotic, or direct pharmacological inhibition of microbial enzymes involved in TMA production—may be a way to reduce the risk of thrombotic events.
They noted that, unlike current antiplatelet therapies, targeting TMAO would likely reduce platelet hyper-responsiveness to the normal range and not induce impairment in overall platelet function. So the intervention could attenuate pro-thrombotic tendencies without increasing the risk of bleeding complications. ![]()
Negative cancer trials have long-term impact

for a clinical trial
Photo by Esther Dyson
Cancer trials with negative results don’t make an immediate splash in the scientific literature, but they do have a long-term impact on research, according to a study published in JAMA Oncology.
Researchers found that first reports of positive phase 3 cancer trials were twice as likely as first reports of negative phase 3 cancer trials
to be cited in scientific journals.
But over time, when all articles associated with the trials were considered, the scientific impact of negative trials and positive trials was about the same.
“Negative trials aren’t scientific failures,” said study author Joseph Unger, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington.
“We found that they have a positive, lasting impact on cancer research.”
Dr Unger and his colleagues analyzed every randomized, phase 3 cancer trial completed by the cooperative group SWOG from 1984 to 2014. This amounted to 94 studies involving 46,424 patients.
Of those 94 studies, 26 were positive, meaning that the treatment tested performed measurably better than the standard treatment at the time.
Analyses revealed that primary manuscripts first announcing these encouraging results were published in journals with higher impact factors and were cited twice as often as primary manuscripts of negative trials.
The mean 2-year impact factor of the journals was 28 for positive trials and 18 for negative trials (P=0.007). And the mean number of citations per year was 43 for positive trials and 21 for negative trials (P=0.03).
However, when the researchers looked at the number of citations from all primary and secondary manuscripts, they did not see a significant difference between positive and negative trials. The mean number of citations per year was 55 and 45, respectively (P=0.53).
“Negative trials matter because they tell us what doesn’t work, which can be as important as what does,” said study author Dawn Hershman, MD, of Columbia University Medical Center in New York, New York.
“Negative trials are also critical for secondary research, which mines existing trial data to answer new questions in cancer care and prevention. Negative trials are used frequently in secondary research and add great value to the scientific community.” ![]()
for a clinical trial
Photo by Esther Dyson
Cancer trials with negative results don’t make an immediate splash in the scientific literature, but they do have a long-term impact on research, according to a study published in JAMA Oncology.
Researchers found that first reports of positive phase 3 cancer trials were twice as likely as first reports of negative phase 3 cancer trials
to be cited in scientific journals.
But over time, when all articles associated with the trials were considered, the scientific impact of negative trials and positive trials was about the same.
“Negative trials aren’t scientific failures,” said study author Joseph Unger, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington.
“We found that they have a positive, lasting impact on cancer research.”
Dr Unger and his colleagues analyzed every randomized, phase 3 cancer trial completed by the cooperative group SWOG from 1984 to 2014. This amounted to 94 studies involving 46,424 patients.
Of those 94 studies, 26 were positive, meaning that the treatment tested performed measurably better than the standard treatment at the time.
Analyses revealed that primary manuscripts first announcing these encouraging results were published in journals with higher impact factors and were cited twice as often as primary manuscripts of negative trials.
The mean 2-year impact factor of the journals was 28 for positive trials and 18 for negative trials (P=0.007). And the mean number of citations per year was 43 for positive trials and 21 for negative trials (P=0.03).
However, when the researchers looked at the number of citations from all primary and secondary manuscripts, they did not see a significant difference between positive and negative trials. The mean number of citations per year was 55 and 45, respectively (P=0.53).
“Negative trials matter because they tell us what doesn’t work, which can be as important as what does,” said study author Dawn Hershman, MD, of Columbia University Medical Center in New York, New York.
“Negative trials are also critical for secondary research, which mines existing trial data to answer new questions in cancer care and prevention. Negative trials are used frequently in secondary research and add great value to the scientific community.” ![]()
for a clinical trial
Photo by Esther Dyson
Cancer trials with negative results don’t make an immediate splash in the scientific literature, but they do have a long-term impact on research, according to a study published in JAMA Oncology.
Researchers found that first reports of positive phase 3 cancer trials were twice as likely as first reports of negative phase 3 cancer trials
to be cited in scientific journals.
But over time, when all articles associated with the trials were considered, the scientific impact of negative trials and positive trials was about the same.
“Negative trials aren’t scientific failures,” said study author Joseph Unger, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington.
“We found that they have a positive, lasting impact on cancer research.”
Dr Unger and his colleagues analyzed every randomized, phase 3 cancer trial completed by the cooperative group SWOG from 1984 to 2014. This amounted to 94 studies involving 46,424 patients.
Of those 94 studies, 26 were positive, meaning that the treatment tested performed measurably better than the standard treatment at the time.
Analyses revealed that primary manuscripts first announcing these encouraging results were published in journals with higher impact factors and were cited twice as often as primary manuscripts of negative trials.
The mean 2-year impact factor of the journals was 28 for positive trials and 18 for negative trials (P=0.007). And the mean number of citations per year was 43 for positive trials and 21 for negative trials (P=0.03).
However, when the researchers looked at the number of citations from all primary and secondary manuscripts, they did not see a significant difference between positive and negative trials. The mean number of citations per year was 55 and 45, respectively (P=0.53).
“Negative trials matter because they tell us what doesn’t work, which can be as important as what does,” said study author Dawn Hershman, MD, of Columbia University Medical Center in New York, New York.
“Negative trials are also critical for secondary research, which mines existing trial data to answer new questions in cancer care and prevention. Negative trials are used frequently in secondary research and add great value to the scientific community.” ![]()