User login
Navigating chronic cough in primary care
Chronic cough took center stage at the European Respiratory Society Congress session titled “Conditions We Are Just Dealing With the Tip of the Iceberg in Primary Care: Frequently Mismanaged Conditions in Primary Health Care.”
“When it comes to chronic cough, general practitioners often feel lost,” Miguel Román Rodríguez, family doctor and an associate professor of family medicine at the University of the Balearic Islands, Palma, Mallorca, Spain, and one of the chairs of the session, said to this news organization.
“GPs are central in diagnosing conditions like chronic cough. We bring something that the specialists don’t bring: the knowledge of the context, of the family, the longitudinal history,” echoed the second chair of the session, Hilary Pinnock, family physician and professor of primary care respiratory medicine at the University of Edinburgh.
Understanding the multifaceted nature of chronic cough
Imran Satia, an assistant professor at McMaster University, Hamilton, Ont., guided attendees at the Milan, Italy, meeting through a comprehensive exploration of chronic cough. The first issue he addressed was the definition of the condition, emphasizing that it is defined by its duration, with chronic cough typically lasting for more than 8 weeks. Prof. Satia pointed out common associations of chronic cough, including asthma, nasal disease, and reflux disease.
Delving into epidemiology, he cited a meta-analysis indicating a global prevalence of approximately 10% in the adult population, with significant regional variability: from 18.1% in Australia to 2.3% in Africa. Notably, the Canadian Longitudinal Study on Aging found an overall prevalence of 16% at baseline. “The most common risk factor was smoke, but even in nonsmokers the prevalence reached 10%,” Prof. Satia added, highlighting that it increased with age and changed depending on location. “The most common associated comorbidities were heart failure and hypertension, but also conditions related to chronic pain, mood, and anxiety,” he explained.
Mental health was identified as a crucial factor in chronic cough, with psychological distress and depressive symptoms emerging as risk factors for developing chronic cough over the next 3 years, contributing to a 20% increased risk.
Effective management strategies
Prof. Satia proposed the use of algorithms to aid in the management of patients with chronic cough in primary care. He introduced a Canadian algorithm that offers specific recommendations for both primary and secondary care.
The algorithm’s primary care assessment, step 1, includes a comprehensive evaluation of the cough history (duration, severity, triggers, nature, location); cardiorespiratory, gastrointestinal, and nasal symptoms; and use of angiotensin-converting enzyme inhibitors and smoking status. Essential diagnostic tests, such as chest radiography (to check for structural disease), complete blood cell count, and spirometry (with or without bronchodilator reversibility), were emphasized. Urgent referral criteria encompassed symptoms like hemoptysis, weight loss, fever, or abnormal chest radiography findings.
“When checking for cough history, GPs should always consider factors like the presence of dry or productive cough, mental health, presence of chronic pain, stroke, and swallowing,” said Prof. Satia, stressing the importance of documenting the impact of chronic cough on quality of life, work life, social life, and family life. “This is something that doctors sometimes do not ask about. They may think that these are not major problems, but acknowledging their importance can help the patient,” he added.
Step 2 of the algorithm focuses on treatment options tailored to specific diagnoses, such as asthma or chronic obstructive pulmonary disease. Prof. Satia urged caution, emphasizing that treatment should only be initiated when evidence of these conditions is present. Additionally, he encouraged early consideration of cough hypersensitivity syndrome when patients exhibit coughing in response to low levels of mechanical stimulation.
Current treatments and future prospects
Prof. Satia presented an overview of existing treatments for chronic cough, outlining their respective advantages and disadvantages. For instance, speech therapy is a patient-led approach with no side effects but entails challenges related to access, costs, and patient motivation. On the other hand, low-dose morphine offers rapid relief but is associated with issues like nausea, stigma, and constipation.
Looking ahead, Prof. Satia shared the results of COUGH-1 and COUGH-2, pivotal phase 3 trials evaluating the oral, peripherally acting P2X3-receptor antagonist gefapixant. This drug, currently approved in Switzerland and Japan, demonstrated a significant reduction in cough frequency, compared with placebo, with rapid and sustained effects. “The estimated relative reduction for 45 mg was 18.45% in COUGH-1 (12 weeks) and 14.64% in COUGH-2 (24 weeks). Of note, cough reduction is very quick and sustained with gefapixant, but a 40% reduction is observed in the placebo arm,” commented Prof. Satia.
Experts unanimously stressed the importance for specialists and GPs of effective communication in managing chronic cough, involving both patients and their families.
“As GPs, we are crucial to manage the common problems, but we are also crucial to spot the needle in the haystack: this is extremely difficult and challenging, and we need support from our colleagues,” Dr. Pinnock concluded.
Prof. Satia reported funding from Merck MSD, AstraZeneca, and GSK; consulting fees from Merck MSD, Genentech, and Respiplus; and speaker fees from AstraZeneca, GSK, and Merck MSD.
A version of this article first appeared on Medscape.com.
Chronic cough took center stage at the European Respiratory Society Congress session titled “Conditions We Are Just Dealing With the Tip of the Iceberg in Primary Care: Frequently Mismanaged Conditions in Primary Health Care.”
“When it comes to chronic cough, general practitioners often feel lost,” Miguel Román Rodríguez, family doctor and an associate professor of family medicine at the University of the Balearic Islands, Palma, Mallorca, Spain, and one of the chairs of the session, said to this news organization.
“GPs are central in diagnosing conditions like chronic cough. We bring something that the specialists don’t bring: the knowledge of the context, of the family, the longitudinal history,” echoed the second chair of the session, Hilary Pinnock, family physician and professor of primary care respiratory medicine at the University of Edinburgh.
Understanding the multifaceted nature of chronic cough
Imran Satia, an assistant professor at McMaster University, Hamilton, Ont., guided attendees at the Milan, Italy, meeting through a comprehensive exploration of chronic cough. The first issue he addressed was the definition of the condition, emphasizing that it is defined by its duration, with chronic cough typically lasting for more than 8 weeks. Prof. Satia pointed out common associations of chronic cough, including asthma, nasal disease, and reflux disease.
Delving into epidemiology, he cited a meta-analysis indicating a global prevalence of approximately 10% in the adult population, with significant regional variability: from 18.1% in Australia to 2.3% in Africa. Notably, the Canadian Longitudinal Study on Aging found an overall prevalence of 16% at baseline. “The most common risk factor was smoke, but even in nonsmokers the prevalence reached 10%,” Prof. Satia added, highlighting that it increased with age and changed depending on location. “The most common associated comorbidities were heart failure and hypertension, but also conditions related to chronic pain, mood, and anxiety,” he explained.
Mental health was identified as a crucial factor in chronic cough, with psychological distress and depressive symptoms emerging as risk factors for developing chronic cough over the next 3 years, contributing to a 20% increased risk.
Effective management strategies
Prof. Satia proposed the use of algorithms to aid in the management of patients with chronic cough in primary care. He introduced a Canadian algorithm that offers specific recommendations for both primary and secondary care.
The algorithm’s primary care assessment, step 1, includes a comprehensive evaluation of the cough history (duration, severity, triggers, nature, location); cardiorespiratory, gastrointestinal, and nasal symptoms; and use of angiotensin-converting enzyme inhibitors and smoking status. Essential diagnostic tests, such as chest radiography (to check for structural disease), complete blood cell count, and spirometry (with or without bronchodilator reversibility), were emphasized. Urgent referral criteria encompassed symptoms like hemoptysis, weight loss, fever, or abnormal chest radiography findings.
“When checking for cough history, GPs should always consider factors like the presence of dry or productive cough, mental health, presence of chronic pain, stroke, and swallowing,” said Prof. Satia, stressing the importance of documenting the impact of chronic cough on quality of life, work life, social life, and family life. “This is something that doctors sometimes do not ask about. They may think that these are not major problems, but acknowledging their importance can help the patient,” he added.
Step 2 of the algorithm focuses on treatment options tailored to specific diagnoses, such as asthma or chronic obstructive pulmonary disease. Prof. Satia urged caution, emphasizing that treatment should only be initiated when evidence of these conditions is present. Additionally, he encouraged early consideration of cough hypersensitivity syndrome when patients exhibit coughing in response to low levels of mechanical stimulation.
Current treatments and future prospects
Prof. Satia presented an overview of existing treatments for chronic cough, outlining their respective advantages and disadvantages. For instance, speech therapy is a patient-led approach with no side effects but entails challenges related to access, costs, and patient motivation. On the other hand, low-dose morphine offers rapid relief but is associated with issues like nausea, stigma, and constipation.
Looking ahead, Prof. Satia shared the results of COUGH-1 and COUGH-2, pivotal phase 3 trials evaluating the oral, peripherally acting P2X3-receptor antagonist gefapixant. This drug, currently approved in Switzerland and Japan, demonstrated a significant reduction in cough frequency, compared with placebo, with rapid and sustained effects. “The estimated relative reduction for 45 mg was 18.45% in COUGH-1 (12 weeks) and 14.64% in COUGH-2 (24 weeks). Of note, cough reduction is very quick and sustained with gefapixant, but a 40% reduction is observed in the placebo arm,” commented Prof. Satia.
Experts unanimously stressed the importance for specialists and GPs of effective communication in managing chronic cough, involving both patients and their families.
“As GPs, we are crucial to manage the common problems, but we are also crucial to spot the needle in the haystack: this is extremely difficult and challenging, and we need support from our colleagues,” Dr. Pinnock concluded.
Prof. Satia reported funding from Merck MSD, AstraZeneca, and GSK; consulting fees from Merck MSD, Genentech, and Respiplus; and speaker fees from AstraZeneca, GSK, and Merck MSD.
A version of this article first appeared on Medscape.com.
Chronic cough took center stage at the European Respiratory Society Congress session titled “Conditions We Are Just Dealing With the Tip of the Iceberg in Primary Care: Frequently Mismanaged Conditions in Primary Health Care.”
“When it comes to chronic cough, general practitioners often feel lost,” Miguel Román Rodríguez, family doctor and an associate professor of family medicine at the University of the Balearic Islands, Palma, Mallorca, Spain, and one of the chairs of the session, said to this news organization.
“GPs are central in diagnosing conditions like chronic cough. We bring something that the specialists don’t bring: the knowledge of the context, of the family, the longitudinal history,” echoed the second chair of the session, Hilary Pinnock, family physician and professor of primary care respiratory medicine at the University of Edinburgh.
Understanding the multifaceted nature of chronic cough
Imran Satia, an assistant professor at McMaster University, Hamilton, Ont., guided attendees at the Milan, Italy, meeting through a comprehensive exploration of chronic cough. The first issue he addressed was the definition of the condition, emphasizing that it is defined by its duration, with chronic cough typically lasting for more than 8 weeks. Prof. Satia pointed out common associations of chronic cough, including asthma, nasal disease, and reflux disease.
Delving into epidemiology, he cited a meta-analysis indicating a global prevalence of approximately 10% in the adult population, with significant regional variability: from 18.1% in Australia to 2.3% in Africa. Notably, the Canadian Longitudinal Study on Aging found an overall prevalence of 16% at baseline. “The most common risk factor was smoke, but even in nonsmokers the prevalence reached 10%,” Prof. Satia added, highlighting that it increased with age and changed depending on location. “The most common associated comorbidities were heart failure and hypertension, but also conditions related to chronic pain, mood, and anxiety,” he explained.
Mental health was identified as a crucial factor in chronic cough, with psychological distress and depressive symptoms emerging as risk factors for developing chronic cough over the next 3 years, contributing to a 20% increased risk.
Effective management strategies
Prof. Satia proposed the use of algorithms to aid in the management of patients with chronic cough in primary care. He introduced a Canadian algorithm that offers specific recommendations for both primary and secondary care.
The algorithm’s primary care assessment, step 1, includes a comprehensive evaluation of the cough history (duration, severity, triggers, nature, location); cardiorespiratory, gastrointestinal, and nasal symptoms; and use of angiotensin-converting enzyme inhibitors and smoking status. Essential diagnostic tests, such as chest radiography (to check for structural disease), complete blood cell count, and spirometry (with or without bronchodilator reversibility), were emphasized. Urgent referral criteria encompassed symptoms like hemoptysis, weight loss, fever, or abnormal chest radiography findings.
“When checking for cough history, GPs should always consider factors like the presence of dry or productive cough, mental health, presence of chronic pain, stroke, and swallowing,” said Prof. Satia, stressing the importance of documenting the impact of chronic cough on quality of life, work life, social life, and family life. “This is something that doctors sometimes do not ask about. They may think that these are not major problems, but acknowledging their importance can help the patient,” he added.
Step 2 of the algorithm focuses on treatment options tailored to specific diagnoses, such as asthma or chronic obstructive pulmonary disease. Prof. Satia urged caution, emphasizing that treatment should only be initiated when evidence of these conditions is present. Additionally, he encouraged early consideration of cough hypersensitivity syndrome when patients exhibit coughing in response to low levels of mechanical stimulation.
Current treatments and future prospects
Prof. Satia presented an overview of existing treatments for chronic cough, outlining their respective advantages and disadvantages. For instance, speech therapy is a patient-led approach with no side effects but entails challenges related to access, costs, and patient motivation. On the other hand, low-dose morphine offers rapid relief but is associated with issues like nausea, stigma, and constipation.
Looking ahead, Prof. Satia shared the results of COUGH-1 and COUGH-2, pivotal phase 3 trials evaluating the oral, peripherally acting P2X3-receptor antagonist gefapixant. This drug, currently approved in Switzerland and Japan, demonstrated a significant reduction in cough frequency, compared with placebo, with rapid and sustained effects. “The estimated relative reduction for 45 mg was 18.45% in COUGH-1 (12 weeks) and 14.64% in COUGH-2 (24 weeks). Of note, cough reduction is very quick and sustained with gefapixant, but a 40% reduction is observed in the placebo arm,” commented Prof. Satia.
Experts unanimously stressed the importance for specialists and GPs of effective communication in managing chronic cough, involving both patients and their families.
“As GPs, we are crucial to manage the common problems, but we are also crucial to spot the needle in the haystack: this is extremely difficult and challenging, and we need support from our colleagues,” Dr. Pinnock concluded.
Prof. Satia reported funding from Merck MSD, AstraZeneca, and GSK; consulting fees from Merck MSD, Genentech, and Respiplus; and speaker fees from AstraZeneca, GSK, and Merck MSD.
A version of this article first appeared on Medscape.com.
FROM ERS 2023
Hepatic presentations of celiac disease
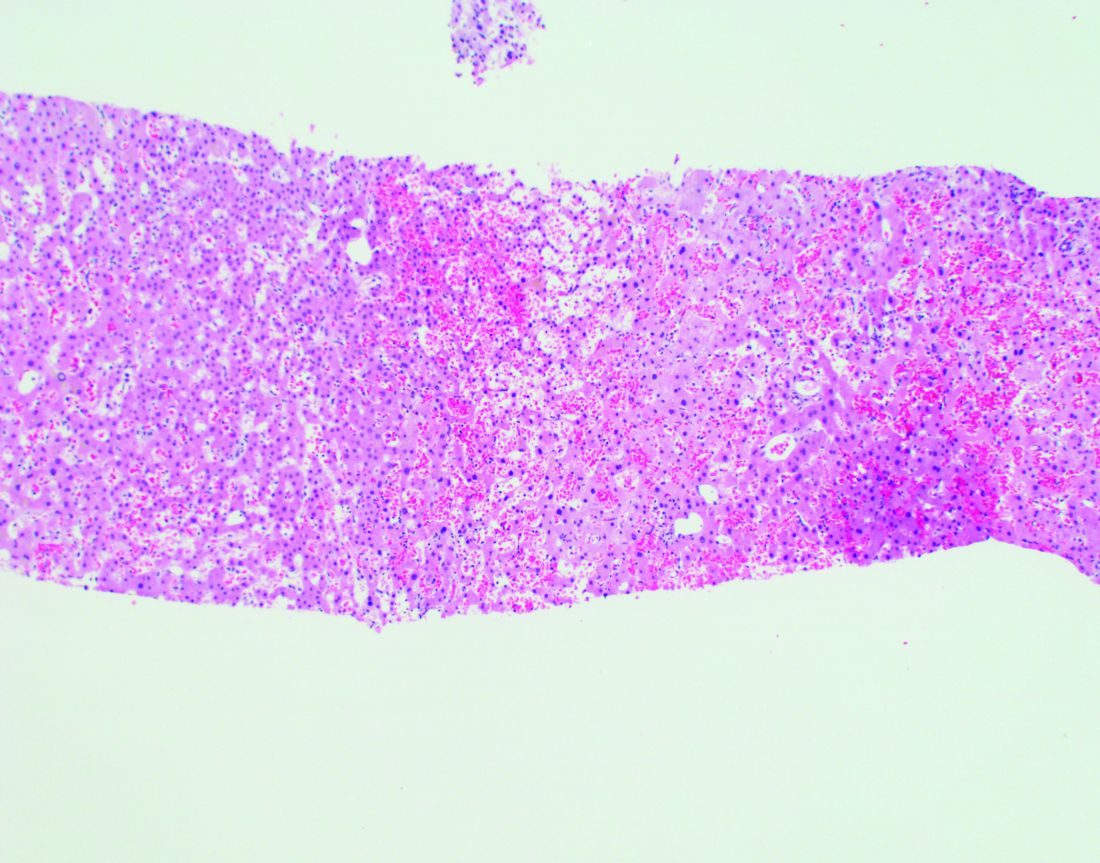
Liver biopsy findings may include variable degrees of steatosis, inflammation, and fibrosis.

In one case we have seen, the patient presented with unexplained ascites and features suggestive of Budd-Chiari syndrome. The serum ascites albumin gradient was 2.3 with a total protein of 0.8 g/dL, and albumin 0.5 g/dL, with an ascitic WBC count of 88/mm3.

Echocardiography showed an ejection fraction of 80%. Transjugular liver biopsy revealed a normal hepatic venous pressure gradient but marked sinusoidal dilatation and congestion with hepatocyte atrophy and focal necrosis suggestive of vascular outlet obstruction (Figure 1).
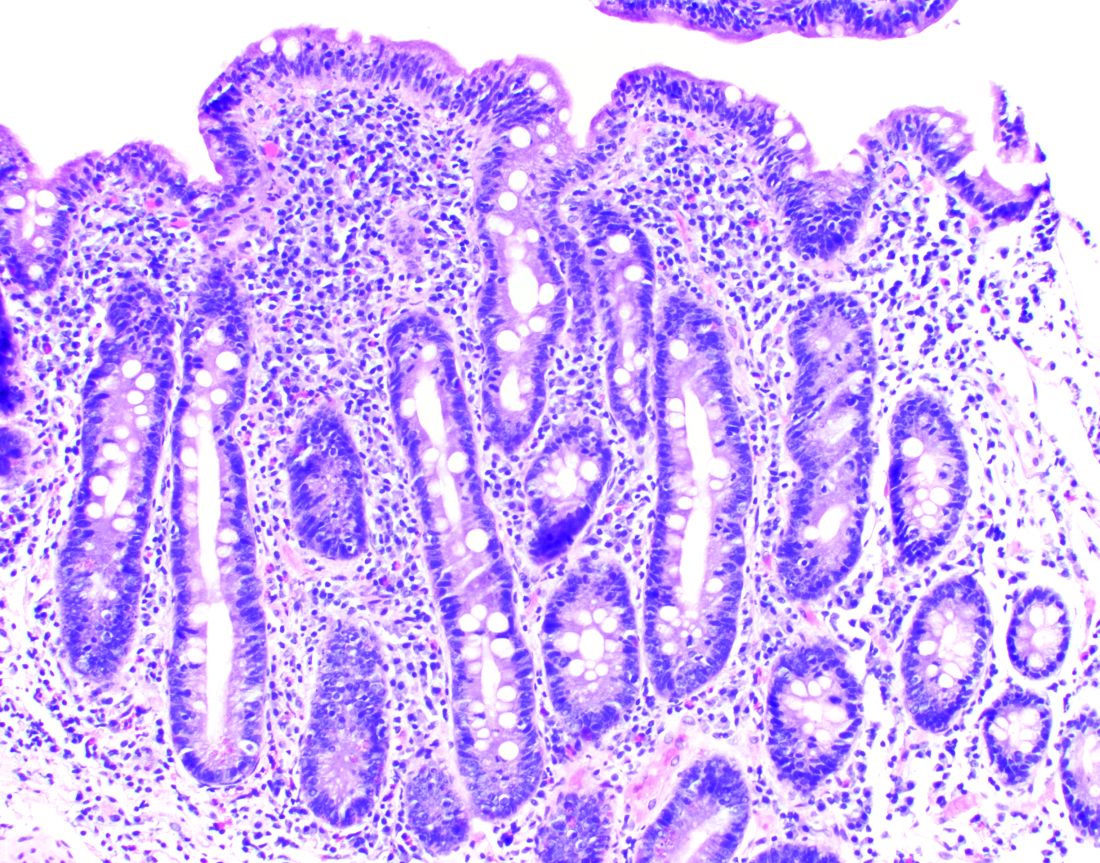
Hepatic venography, however, showed no evidence of Budd-Chiari syndrome. When seen in consultation, pertinent observations included Irish ancestry, a history of occasional diarrhea, short stature, osteoporosis, and an atrophic spleen on computed tomography. An IgA transglutaminase antibody was positive, and a small-bowel biopsy confirmed celiac disease (Figure 2).
On a gluten-free diet, the patient’s symptoms resolved, with clinical and laboratory abnormalities returning to normal. She lived another 20 years before dying of primary pulmonary hypertension. Recognition of an unusual hepatic manifestation of celiac disease led to effective management.
Dr. Friedman is the Anton R. Fried, MD, Chair of the department of medicine at Newton-Wellesley Hospital in Newton, Mass., and assistant chief of medicine at Massachusetts General Hospital, and a professor of medicine at Harvard Medical School and Tufts University School of Medicine, all in Boston. Dr. Martin is chief of the division of digestive health and liver diseases at the Miller School of Medicine, University of Miami, where he is the Mandel Chair of Gastroenterology. The authors disclose no conflicts.
Previously published in Gastro Hep Advances. 2023. doi: 10.1016/j.gastha.2023.03.018.
Liver biopsy findings may include variable degrees of steatosis, inflammation, and fibrosis.
In one case we have seen, the patient presented with unexplained ascites and features suggestive of Budd-Chiari syndrome. The serum ascites albumin gradient was 2.3 with a total protein of 0.8 g/dL, and albumin 0.5 g/dL, with an ascitic WBC count of 88/mm3.
Echocardiography showed an ejection fraction of 80%. Transjugular liver biopsy revealed a normal hepatic venous pressure gradient but marked sinusoidal dilatation and congestion with hepatocyte atrophy and focal necrosis suggestive of vascular outlet obstruction (Figure 1).
Hepatic venography, however, showed no evidence of Budd-Chiari syndrome. When seen in consultation, pertinent observations included Irish ancestry, a history of occasional diarrhea, short stature, osteoporosis, and an atrophic spleen on computed tomography. An IgA transglutaminase antibody was positive, and a small-bowel biopsy confirmed celiac disease (Figure 2).
On a gluten-free diet, the patient’s symptoms resolved, with clinical and laboratory abnormalities returning to normal. She lived another 20 years before dying of primary pulmonary hypertension. Recognition of an unusual hepatic manifestation of celiac disease led to effective management.
Dr. Friedman is the Anton R. Fried, MD, Chair of the department of medicine at Newton-Wellesley Hospital in Newton, Mass., and assistant chief of medicine at Massachusetts General Hospital, and a professor of medicine at Harvard Medical School and Tufts University School of Medicine, all in Boston. Dr. Martin is chief of the division of digestive health and liver diseases at the Miller School of Medicine, University of Miami, where he is the Mandel Chair of Gastroenterology. The authors disclose no conflicts.
Previously published in Gastro Hep Advances. 2023. doi: 10.1016/j.gastha.2023.03.018.
Liver biopsy findings may include variable degrees of steatosis, inflammation, and fibrosis.
In one case we have seen, the patient presented with unexplained ascites and features suggestive of Budd-Chiari syndrome. The serum ascites albumin gradient was 2.3 with a total protein of 0.8 g/dL, and albumin 0.5 g/dL, with an ascitic WBC count of 88/mm3.
Echocardiography showed an ejection fraction of 80%. Transjugular liver biopsy revealed a normal hepatic venous pressure gradient but marked sinusoidal dilatation and congestion with hepatocyte atrophy and focal necrosis suggestive of vascular outlet obstruction (Figure 1).
Hepatic venography, however, showed no evidence of Budd-Chiari syndrome. When seen in consultation, pertinent observations included Irish ancestry, a history of occasional diarrhea, short stature, osteoporosis, and an atrophic spleen on computed tomography. An IgA transglutaminase antibody was positive, and a small-bowel biopsy confirmed celiac disease (Figure 2).
On a gluten-free diet, the patient’s symptoms resolved, with clinical and laboratory abnormalities returning to normal. She lived another 20 years before dying of primary pulmonary hypertension. Recognition of an unusual hepatic manifestation of celiac disease led to effective management.
Dr. Friedman is the Anton R. Fried, MD, Chair of the department of medicine at Newton-Wellesley Hospital in Newton, Mass., and assistant chief of medicine at Massachusetts General Hospital, and a professor of medicine at Harvard Medical School and Tufts University School of Medicine, all in Boston. Dr. Martin is chief of the division of digestive health and liver diseases at the Miller School of Medicine, University of Miami, where he is the Mandel Chair of Gastroenterology. The authors disclose no conflicts.
Previously published in Gastro Hep Advances. 2023. doi: 10.1016/j.gastha.2023.03.018.
Is additional treatment needed, pretransplant, for r/r AML?
This critically important question was debated at the annual meeting of the Society of Hematologic Oncology, held in Houston and online.
Johannes Schetelig, MD, argued in favor of proceeding to transplant, even without a complete remission.
“In the past, I’ve told many patients with relapsed or refractory AML that we do need to induce a [complete remission] prior to transplantation,” said Dr. Schetelig, from the Clinical Trials Unit at DKMS in Dresden, Germany. “But is it true?”
According to findings from a recent randomized trial, it may not be. The trial, led by Dr. Schetelig, found that patients with AML who received immediate allogeneic transplant without first having achieved a complete response following induction therapy did just as well as those who received intensive salvage induction therapy to establish remission before transplant.
If this finding holds, it “completely upends” how experts have traditionally approached patients with AML, Mikkael A. Sekeres, MD, of the University of Miami said at a conference press briefing last year.
The phase 3 ASAP trial, presented at last year’s American Society of Hematology meeting, included patients with AML who had had a poor response or who had experienced a relapse after first induction therapy. Patients were randomly assigned to a remission-induction strategy prior to allogeneic stem cell transplant (alloHCT) or a disease-control approach of watchful waiting followed by sequential conditioning and alloHCT. The primary endpoint was treatment success, defined as a complete response at day 56 following alloHCT.
In an intention-to-treat analysis, 83.5% of patients in the disease-control group and 81% in the remission-induction group achieved treatment success. Similarly, in the per-protocol analysis, 84.1% and 81.3%, respectively, achieved a complete response at day 56 after alloHCT. After a median follow-up of 4 years, there were no differences in leukemia-free survival or overall survival between the two groups.
Another advantage to forgoing an intensive salvage induction regimen: Patients in the disease-control arm experienced significantly fewer severe adverse events (23% vs. 64% in the remission induction arm) and spent a mean of 27 fewer days in the hospital prior to transplantation.
At last year’s press briefing, Dr. Schetelig said his team did not expect that a complete response on day 56 after transplantation would translate into “equal long-term benefit” for these groups. “This is what I was really astonished about,” he said.
Delving further into the findings, Dr. Schetelig explained that in the remission-induction arm patients who had had a complete response prior to transplantation demonstrated significantly better overall survival at 4 years than those who had not had a complete response at that point: 60% vs. 40%.
The study also revealed that in the disease-control arm, for patients under watchful waiting who did not need low-dose cytarabine and mitoxantrone for disease control, overall survival outcomes were similar to those of patients in the remission-induction arm who achieved a complete response.
These findings suggest that patients who can be bridged with watchful waiting may have a more favorable disease biology, and chemosensitivity could just be a biomarker for disease biology. In other words, “AML biology matters for transplant outcome and not tumor load,” Dr. Schetelig explained.
A recent study that found that having minimal residual disease (MRD) prior to transplant “had no independent effect on leukemia-free survival” supports this idea, he added.
Overall, Dr. Schetelig concluded that data from the ASAP trial suggest that watchful waiting prior to alloHCT represents “an alternative” for some patients.
Counterpoint: Aim for complete remission
Ronald B. Walter, MD, PhD, argued the counterpoint: that residual disease before transplantation is associated with worse posttransplant outcomes and represents a meaningful pretransplant therapeutic target.
The goal of intensifying treatment for patients with residual disease is to erase disease vestiges prior to transplantation.
“The idea is that by doing so you might optimize the benefit-to-risk ratio and ultimately improve outcomes,” said Dr. Walter, of the translational science and therapeutics division at the Fred Hutchinson Cancer Research Center in Seattle.
Several reports support this view that patients who are MRD negative at the time of transplant have significantly better survival outcomes than patients with residual disease who undergo transplant.
A 2016 study from Dr. Walter and colleagues at Fred Hutchinson, for instance, found that 3-year overall survival was significantly higher among patients with no MRD who underwent myeloablative alloHCT: 73% vs. 26% of those in MRD-positive morphologic remission and 23% of patients with active AML.
Another study, published the year before by a different research team, also revealed that “adult patients with AML in morphologic [complete remission] but with detectable MRD who undergo alloHCT have poor outcomes, which approximates those who undergo transplantation with active disease,” the authors of the 2015 study wrote in a commentary highlighting findings from both studies.
Still, providing intensive therapy prior to transplant comes with drawbacks, Dr. Walter noted. These downsides include potential toxicity from more intense therapy, which may prevent further therapy with curative intent, as well as the possibility that deintensifying therapy could lead to difficult-to-treat relapse.
It may, however, be possible to reduce the intensity of therapy before transplant and still achieve good outcomes after transplant, though the data remain mixed.
One trial found that a reduced-intensity conditioning regimen was associated with a greater risk of relapse post transplant and worse overall survival, compared with standard myeloablative conditioning.
However, another recent trial in which patients with AML or high-risk myelodysplastic syndrome were randomly assigned to either a reduced-intensity conditioning regimen or an intensified version of that regimen prior to transplant demonstrated no difference in relapse rates and overall survival, regardless of patients’ MRD status prior to transplant.
“To me, it’s still key to go into transplant with as little disease as possible,” Dr. Walter said. How much value there is in targeted treatment to further reduce disease burden prior to transplant “will really require further careful study,” he said.
The ASAP trial was sponsored by DKMS. Dr. Schetelig has received honoraria from BeiGene, BMS, Janssen, AstraZeneca, AbbVie, and DKMS. Dr. Walter reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
This critically important question was debated at the annual meeting of the Society of Hematologic Oncology, held in Houston and online.
Johannes Schetelig, MD, argued in favor of proceeding to transplant, even without a complete remission.
“In the past, I’ve told many patients with relapsed or refractory AML that we do need to induce a [complete remission] prior to transplantation,” said Dr. Schetelig, from the Clinical Trials Unit at DKMS in Dresden, Germany. “But is it true?”
According to findings from a recent randomized trial, it may not be. The trial, led by Dr. Schetelig, found that patients with AML who received immediate allogeneic transplant without first having achieved a complete response following induction therapy did just as well as those who received intensive salvage induction therapy to establish remission before transplant.
If this finding holds, it “completely upends” how experts have traditionally approached patients with AML, Mikkael A. Sekeres, MD, of the University of Miami said at a conference press briefing last year.
The phase 3 ASAP trial, presented at last year’s American Society of Hematology meeting, included patients with AML who had had a poor response or who had experienced a relapse after first induction therapy. Patients were randomly assigned to a remission-induction strategy prior to allogeneic stem cell transplant (alloHCT) or a disease-control approach of watchful waiting followed by sequential conditioning and alloHCT. The primary endpoint was treatment success, defined as a complete response at day 56 following alloHCT.
In an intention-to-treat analysis, 83.5% of patients in the disease-control group and 81% in the remission-induction group achieved treatment success. Similarly, in the per-protocol analysis, 84.1% and 81.3%, respectively, achieved a complete response at day 56 after alloHCT. After a median follow-up of 4 years, there were no differences in leukemia-free survival or overall survival between the two groups.
Another advantage to forgoing an intensive salvage induction regimen: Patients in the disease-control arm experienced significantly fewer severe adverse events (23% vs. 64% in the remission induction arm) and spent a mean of 27 fewer days in the hospital prior to transplantation.
At last year’s press briefing, Dr. Schetelig said his team did not expect that a complete response on day 56 after transplantation would translate into “equal long-term benefit” for these groups. “This is what I was really astonished about,” he said.
Delving further into the findings, Dr. Schetelig explained that in the remission-induction arm patients who had had a complete response prior to transplantation demonstrated significantly better overall survival at 4 years than those who had not had a complete response at that point: 60% vs. 40%.
The study also revealed that in the disease-control arm, for patients under watchful waiting who did not need low-dose cytarabine and mitoxantrone for disease control, overall survival outcomes were similar to those of patients in the remission-induction arm who achieved a complete response.
These findings suggest that patients who can be bridged with watchful waiting may have a more favorable disease biology, and chemosensitivity could just be a biomarker for disease biology. In other words, “AML biology matters for transplant outcome and not tumor load,” Dr. Schetelig explained.
A recent study that found that having minimal residual disease (MRD) prior to transplant “had no independent effect on leukemia-free survival” supports this idea, he added.
Overall, Dr. Schetelig concluded that data from the ASAP trial suggest that watchful waiting prior to alloHCT represents “an alternative” for some patients.
Counterpoint: Aim for complete remission
Ronald B. Walter, MD, PhD, argued the counterpoint: that residual disease before transplantation is associated with worse posttransplant outcomes and represents a meaningful pretransplant therapeutic target.
The goal of intensifying treatment for patients with residual disease is to erase disease vestiges prior to transplantation.
“The idea is that by doing so you might optimize the benefit-to-risk ratio and ultimately improve outcomes,” said Dr. Walter, of the translational science and therapeutics division at the Fred Hutchinson Cancer Research Center in Seattle.
Several reports support this view that patients who are MRD negative at the time of transplant have significantly better survival outcomes than patients with residual disease who undergo transplant.
A 2016 study from Dr. Walter and colleagues at Fred Hutchinson, for instance, found that 3-year overall survival was significantly higher among patients with no MRD who underwent myeloablative alloHCT: 73% vs. 26% of those in MRD-positive morphologic remission and 23% of patients with active AML.
Another study, published the year before by a different research team, also revealed that “adult patients with AML in morphologic [complete remission] but with detectable MRD who undergo alloHCT have poor outcomes, which approximates those who undergo transplantation with active disease,” the authors of the 2015 study wrote in a commentary highlighting findings from both studies.
Still, providing intensive therapy prior to transplant comes with drawbacks, Dr. Walter noted. These downsides include potential toxicity from more intense therapy, which may prevent further therapy with curative intent, as well as the possibility that deintensifying therapy could lead to difficult-to-treat relapse.
It may, however, be possible to reduce the intensity of therapy before transplant and still achieve good outcomes after transplant, though the data remain mixed.
One trial found that a reduced-intensity conditioning regimen was associated with a greater risk of relapse post transplant and worse overall survival, compared with standard myeloablative conditioning.
However, another recent trial in which patients with AML or high-risk myelodysplastic syndrome were randomly assigned to either a reduced-intensity conditioning regimen or an intensified version of that regimen prior to transplant demonstrated no difference in relapse rates and overall survival, regardless of patients’ MRD status prior to transplant.
“To me, it’s still key to go into transplant with as little disease as possible,” Dr. Walter said. How much value there is in targeted treatment to further reduce disease burden prior to transplant “will really require further careful study,” he said.
The ASAP trial was sponsored by DKMS. Dr. Schetelig has received honoraria from BeiGene, BMS, Janssen, AstraZeneca, AbbVie, and DKMS. Dr. Walter reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
This critically important question was debated at the annual meeting of the Society of Hematologic Oncology, held in Houston and online.
Johannes Schetelig, MD, argued in favor of proceeding to transplant, even without a complete remission.
“In the past, I’ve told many patients with relapsed or refractory AML that we do need to induce a [complete remission] prior to transplantation,” said Dr. Schetelig, from the Clinical Trials Unit at DKMS in Dresden, Germany. “But is it true?”
According to findings from a recent randomized trial, it may not be. The trial, led by Dr. Schetelig, found that patients with AML who received immediate allogeneic transplant without first having achieved a complete response following induction therapy did just as well as those who received intensive salvage induction therapy to establish remission before transplant.
If this finding holds, it “completely upends” how experts have traditionally approached patients with AML, Mikkael A. Sekeres, MD, of the University of Miami said at a conference press briefing last year.
The phase 3 ASAP trial, presented at last year’s American Society of Hematology meeting, included patients with AML who had had a poor response or who had experienced a relapse after first induction therapy. Patients were randomly assigned to a remission-induction strategy prior to allogeneic stem cell transplant (alloHCT) or a disease-control approach of watchful waiting followed by sequential conditioning and alloHCT. The primary endpoint was treatment success, defined as a complete response at day 56 following alloHCT.
In an intention-to-treat analysis, 83.5% of patients in the disease-control group and 81% in the remission-induction group achieved treatment success. Similarly, in the per-protocol analysis, 84.1% and 81.3%, respectively, achieved a complete response at day 56 after alloHCT. After a median follow-up of 4 years, there were no differences in leukemia-free survival or overall survival between the two groups.
Another advantage to forgoing an intensive salvage induction regimen: Patients in the disease-control arm experienced significantly fewer severe adverse events (23% vs. 64% in the remission induction arm) and spent a mean of 27 fewer days in the hospital prior to transplantation.
At last year’s press briefing, Dr. Schetelig said his team did not expect that a complete response on day 56 after transplantation would translate into “equal long-term benefit” for these groups. “This is what I was really astonished about,” he said.
Delving further into the findings, Dr. Schetelig explained that in the remission-induction arm patients who had had a complete response prior to transplantation demonstrated significantly better overall survival at 4 years than those who had not had a complete response at that point: 60% vs. 40%.
The study also revealed that in the disease-control arm, for patients under watchful waiting who did not need low-dose cytarabine and mitoxantrone for disease control, overall survival outcomes were similar to those of patients in the remission-induction arm who achieved a complete response.
These findings suggest that patients who can be bridged with watchful waiting may have a more favorable disease biology, and chemosensitivity could just be a biomarker for disease biology. In other words, “AML biology matters for transplant outcome and not tumor load,” Dr. Schetelig explained.
A recent study that found that having minimal residual disease (MRD) prior to transplant “had no independent effect on leukemia-free survival” supports this idea, he added.
Overall, Dr. Schetelig concluded that data from the ASAP trial suggest that watchful waiting prior to alloHCT represents “an alternative” for some patients.
Counterpoint: Aim for complete remission
Ronald B. Walter, MD, PhD, argued the counterpoint: that residual disease before transplantation is associated with worse posttransplant outcomes and represents a meaningful pretransplant therapeutic target.
The goal of intensifying treatment for patients with residual disease is to erase disease vestiges prior to transplantation.
“The idea is that by doing so you might optimize the benefit-to-risk ratio and ultimately improve outcomes,” said Dr. Walter, of the translational science and therapeutics division at the Fred Hutchinson Cancer Research Center in Seattle.
Several reports support this view that patients who are MRD negative at the time of transplant have significantly better survival outcomes than patients with residual disease who undergo transplant.
A 2016 study from Dr. Walter and colleagues at Fred Hutchinson, for instance, found that 3-year overall survival was significantly higher among patients with no MRD who underwent myeloablative alloHCT: 73% vs. 26% of those in MRD-positive morphologic remission and 23% of patients with active AML.
Another study, published the year before by a different research team, also revealed that “adult patients with AML in morphologic [complete remission] but with detectable MRD who undergo alloHCT have poor outcomes, which approximates those who undergo transplantation with active disease,” the authors of the 2015 study wrote in a commentary highlighting findings from both studies.
Still, providing intensive therapy prior to transplant comes with drawbacks, Dr. Walter noted. These downsides include potential toxicity from more intense therapy, which may prevent further therapy with curative intent, as well as the possibility that deintensifying therapy could lead to difficult-to-treat relapse.
It may, however, be possible to reduce the intensity of therapy before transplant and still achieve good outcomes after transplant, though the data remain mixed.
One trial found that a reduced-intensity conditioning regimen was associated with a greater risk of relapse post transplant and worse overall survival, compared with standard myeloablative conditioning.
However, another recent trial in which patients with AML or high-risk myelodysplastic syndrome were randomly assigned to either a reduced-intensity conditioning regimen or an intensified version of that regimen prior to transplant demonstrated no difference in relapse rates and overall survival, regardless of patients’ MRD status prior to transplant.
“To me, it’s still key to go into transplant with as little disease as possible,” Dr. Walter said. How much value there is in targeted treatment to further reduce disease burden prior to transplant “will really require further careful study,” he said.
The ASAP trial was sponsored by DKMS. Dr. Schetelig has received honoraria from BeiGene, BMS, Janssen, AstraZeneca, AbbVie, and DKMS. Dr. Walter reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM SOHO 2023
Does remote blood pressure monitoring improve patient outcomes postpartum?
Hirshberg A, Zhu Y, Smith-McLallen A, et al. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstet Gynecol. 2023;141:1163-1170. doi:10.1097/AOG.0000000000005197.
EXPERT COMMENTARY
Courtney Bisson, MD, is a Maternal-Fetal Medicine Fellow, University of Chicago/NorthShore University HealthSystem, Chicago, Illinois.
Sarosh Rana, MD, MPH, is Professor of Obstetrics and Gynecology and Section Chief, Maternal-Fetal Medicine, University of Chicago.
Hypertensive disorders of pregnancy account for a significant amount of morbidity during pregnancy and postpartum. In the pregnant population, data have shown that the implementation of a standardized blood pressure education program, provision of a blood pressure cuff, and assistance with postpartum follow-up result in improved blood pressures and postpartum follow-up for up to 6 weeks. In the nonpregnant population, literature suggests that RBPM in patients with hypertension results in improved outcomes, although the long-term impact of RBPM in the postpartum population remains unclear.
Recently, Hirshberg and colleagues published the results of a retrospective cohort study that assessed the impact of RBPM with text message reminders for 10 days postpartum on a composite of adverse maternal outcomes, readmissions, and follow-up within 1 year postpartum.1

Details of the study
The retrospective cohort study was conducted during 2017–2021 based on insurance claims of patients with hypertensive disorders of pregnancy who were enrolled in a twice-daily text message–based RBPM program for 10 days postpartum.
Data from 1,700 patients enrolled in RBPM were compared with that of propensity score matched controls that included 2,297 women not enrolled in RBPM. Of these controls, 1,276 patients (cohort C) simultaneously received care at other institutions without RBPM, and 1,021 patients (cohort A) received care at the same institution prior to implementation of RBPM.
Results. Patients in the RBPM group were found to have a significantly lower rate of composite adverse maternal outcomes compared with their matched cohorts in the year after delivery. (Individual adverse outcomes included stroke, disseminated intravascular coagulation, eclampsia, pulmonary edema, renal injury or liver failure, HELLP [hemolysis, elevated liver enzymes, low platelet count] syndrome, myocardial infarction, and cardiomyopathy.) Rates were 2.9% versus 4.7% (odds ratio [OR], 0.61; 95% confidence interval [CI], 0.40–0.98) in the RBPM group compared with cohort A; rates in the RBPM group compared with cohort C were 3.2% versus 4.5% (OR, 0.71; 95% CI, 0.47–1.07).
Although not statistically significant, rates of emergency department visits and readmissions also were lower in the RBPM patients. Those enrolled in the RBPM program were more likely to have follow-up with cardiologists or specialist visits within 6 months postpartum. Fewer emergency department visits and readmissions resulted in lower health care utilization costs.
Study strengths and limitations
This study’s strength lies in its design and implementation of standardized protocols that allowed assessment of clinically meaningful outcomes postpartum. Although the program for RBPM was for only 10 days postpartum, it showed effects beyond the timeframe of the direct care. No such prior data exist evaluating a program’s effectiveness in improving postpartum clinical outcomes and costs through 1 year postdelivery.
Study limitations include residual bias from unobserved confounders, analysis of only 1 payer type, lack of patient level data, and evaluation of disparity. ●
Previous work by Suresh and colleagues illustrated that a standardized postpartum blood pressure monitoring quality improvement initiative resulted in better blood pressures, improved postpartum visit adherence, and reduced disparity.2 The study by Hirshberg and colleagues furthers these findings, illustrating how uniform protocols surrounding preeclampsia management in the postpartum setting could further improve morbidity and mortality in the year following childbirth. Such protocols should be incorporated hospital-wide in standard obstetrical management.
COURTNEY BISSON, MD; SAROSH RANA, MD, MPH
- Hirshberg A, Zhu Y, Smith-McLallen A, et al. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstet Gynecol. 2023;141:1163-1170. doi:10.1097/AOG.0000000000005197.
- Suresh SC, Duncan C, Kaur H, et al. Postpartum outcomes with systematic treatment and management of postpartum hypertension. Obstet Gynecol. 2021;138:777-787. doi:10.1097 /AOG.0000000000004574.
Hirshberg A, Zhu Y, Smith-McLallen A, et al. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstet Gynecol. 2023;141:1163-1170. doi:10.1097/AOG.0000000000005197.
EXPERT COMMENTARY
Courtney Bisson, MD, is a Maternal-Fetal Medicine Fellow, University of Chicago/NorthShore University HealthSystem, Chicago, Illinois.
Sarosh Rana, MD, MPH, is Professor of Obstetrics and Gynecology and Section Chief, Maternal-Fetal Medicine, University of Chicago.
Hypertensive disorders of pregnancy account for a significant amount of morbidity during pregnancy and postpartum. In the pregnant population, data have shown that the implementation of a standardized blood pressure education program, provision of a blood pressure cuff, and assistance with postpartum follow-up result in improved blood pressures and postpartum follow-up for up to 6 weeks. In the nonpregnant population, literature suggests that RBPM in patients with hypertension results in improved outcomes, although the long-term impact of RBPM in the postpartum population remains unclear.
Recently, Hirshberg and colleagues published the results of a retrospective cohort study that assessed the impact of RBPM with text message reminders for 10 days postpartum on a composite of adverse maternal outcomes, readmissions, and follow-up within 1 year postpartum.1
Details of the study
The retrospective cohort study was conducted during 2017–2021 based on insurance claims of patients with hypertensive disorders of pregnancy who were enrolled in a twice-daily text message–based RBPM program for 10 days postpartum.
Data from 1,700 patients enrolled in RBPM were compared with that of propensity score matched controls that included 2,297 women not enrolled in RBPM. Of these controls, 1,276 patients (cohort C) simultaneously received care at other institutions without RBPM, and 1,021 patients (cohort A) received care at the same institution prior to implementation of RBPM.
Results. Patients in the RBPM group were found to have a significantly lower rate of composite adverse maternal outcomes compared with their matched cohorts in the year after delivery. (Individual adverse outcomes included stroke, disseminated intravascular coagulation, eclampsia, pulmonary edema, renal injury or liver failure, HELLP [hemolysis, elevated liver enzymes, low platelet count] syndrome, myocardial infarction, and cardiomyopathy.) Rates were 2.9% versus 4.7% (odds ratio [OR], 0.61; 95% confidence interval [CI], 0.40–0.98) in the RBPM group compared with cohort A; rates in the RBPM group compared with cohort C were 3.2% versus 4.5% (OR, 0.71; 95% CI, 0.47–1.07).
Although not statistically significant, rates of emergency department visits and readmissions also were lower in the RBPM patients. Those enrolled in the RBPM program were more likely to have follow-up with cardiologists or specialist visits within 6 months postpartum. Fewer emergency department visits and readmissions resulted in lower health care utilization costs.
Study strengths and limitations
This study’s strength lies in its design and implementation of standardized protocols that allowed assessment of clinically meaningful outcomes postpartum. Although the program for RBPM was for only 10 days postpartum, it showed effects beyond the timeframe of the direct care. No such prior data exist evaluating a program’s effectiveness in improving postpartum clinical outcomes and costs through 1 year postdelivery.
Study limitations include residual bias from unobserved confounders, analysis of only 1 payer type, lack of patient level data, and evaluation of disparity. ●
Previous work by Suresh and colleagues illustrated that a standardized postpartum blood pressure monitoring quality improvement initiative resulted in better blood pressures, improved postpartum visit adherence, and reduced disparity.2 The study by Hirshberg and colleagues furthers these findings, illustrating how uniform protocols surrounding preeclampsia management in the postpartum setting could further improve morbidity and mortality in the year following childbirth. Such protocols should be incorporated hospital-wide in standard obstetrical management.
COURTNEY BISSON, MD; SAROSH RANA, MD, MPH
Hirshberg A, Zhu Y, Smith-McLallen A, et al. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstet Gynecol. 2023;141:1163-1170. doi:10.1097/AOG.0000000000005197.
EXPERT COMMENTARY
Courtney Bisson, MD, is a Maternal-Fetal Medicine Fellow, University of Chicago/NorthShore University HealthSystem, Chicago, Illinois.
Sarosh Rana, MD, MPH, is Professor of Obstetrics and Gynecology and Section Chief, Maternal-Fetal Medicine, University of Chicago.
Hypertensive disorders of pregnancy account for a significant amount of morbidity during pregnancy and postpartum. In the pregnant population, data have shown that the implementation of a standardized blood pressure education program, provision of a blood pressure cuff, and assistance with postpartum follow-up result in improved blood pressures and postpartum follow-up for up to 6 weeks. In the nonpregnant population, literature suggests that RBPM in patients with hypertension results in improved outcomes, although the long-term impact of RBPM in the postpartum population remains unclear.
Recently, Hirshberg and colleagues published the results of a retrospective cohort study that assessed the impact of RBPM with text message reminders for 10 days postpartum on a composite of adverse maternal outcomes, readmissions, and follow-up within 1 year postpartum.1
Details of the study
The retrospective cohort study was conducted during 2017–2021 based on insurance claims of patients with hypertensive disorders of pregnancy who were enrolled in a twice-daily text message–based RBPM program for 10 days postpartum.
Data from 1,700 patients enrolled in RBPM were compared with that of propensity score matched controls that included 2,297 women not enrolled in RBPM. Of these controls, 1,276 patients (cohort C) simultaneously received care at other institutions without RBPM, and 1,021 patients (cohort A) received care at the same institution prior to implementation of RBPM.
Results. Patients in the RBPM group were found to have a significantly lower rate of composite adverse maternal outcomes compared with their matched cohorts in the year after delivery. (Individual adverse outcomes included stroke, disseminated intravascular coagulation, eclampsia, pulmonary edema, renal injury or liver failure, HELLP [hemolysis, elevated liver enzymes, low platelet count] syndrome, myocardial infarction, and cardiomyopathy.) Rates were 2.9% versus 4.7% (odds ratio [OR], 0.61; 95% confidence interval [CI], 0.40–0.98) in the RBPM group compared with cohort A; rates in the RBPM group compared with cohort C were 3.2% versus 4.5% (OR, 0.71; 95% CI, 0.47–1.07).
Although not statistically significant, rates of emergency department visits and readmissions also were lower in the RBPM patients. Those enrolled in the RBPM program were more likely to have follow-up with cardiologists or specialist visits within 6 months postpartum. Fewer emergency department visits and readmissions resulted in lower health care utilization costs.
Study strengths and limitations
This study’s strength lies in its design and implementation of standardized protocols that allowed assessment of clinically meaningful outcomes postpartum. Although the program for RBPM was for only 10 days postpartum, it showed effects beyond the timeframe of the direct care. No such prior data exist evaluating a program’s effectiveness in improving postpartum clinical outcomes and costs through 1 year postdelivery.
Study limitations include residual bias from unobserved confounders, analysis of only 1 payer type, lack of patient level data, and evaluation of disparity. ●
Previous work by Suresh and colleagues illustrated that a standardized postpartum blood pressure monitoring quality improvement initiative resulted in better blood pressures, improved postpartum visit adherence, and reduced disparity.2 The study by Hirshberg and colleagues furthers these findings, illustrating how uniform protocols surrounding preeclampsia management in the postpartum setting could further improve morbidity and mortality in the year following childbirth. Such protocols should be incorporated hospital-wide in standard obstetrical management.
COURTNEY BISSON, MD; SAROSH RANA, MD, MPH
- Hirshberg A, Zhu Y, Smith-McLallen A, et al. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstet Gynecol. 2023;141:1163-1170. doi:10.1097/AOG.0000000000005197.
- Suresh SC, Duncan C, Kaur H, et al. Postpartum outcomes with systematic treatment and management of postpartum hypertension. Obstet Gynecol. 2021;138:777-787. doi:10.1097 /AOG.0000000000004574.
- Hirshberg A, Zhu Y, Smith-McLallen A, et al. Association of a remote blood pressure monitoring program with postpartum adverse outcomes. Obstet Gynecol. 2023;141:1163-1170. doi:10.1097/AOG.0000000000005197.
- Suresh SC, Duncan C, Kaur H, et al. Postpartum outcomes with systematic treatment and management of postpartum hypertension. Obstet Gynecol. 2021;138:777-787. doi:10.1097 /AOG.0000000000004574.

Hemostatic powder superior in controlling tumor bleeding
The findings, published online in Gastroenterology (2023 Jun 3. doi: 10.1053/j.gastro.2023.05.042), come from the largest randomized trial to date of TC-325 (Hemospray, Cook Medical), compared with standard endoscopic hemostatic interventions for tumor bleeding.
For their research, Rapat Pittayanon, MD, of Chulalongkorn University in Bangkok and her colleagues, randomized patients (60% male, mean age 63) with active malignant upper or lower GI bleeding and low disability levels related to their cancers (ECOG score 0-2). The study was conducted at nine hospitals in Thailand.
The 106 patients who passed screening underwent either TC-325 or standard endoscopic hemostasis, which could involve use of thermal or mechanical methods or adrenaline injection, alone or combined with another modality, at the endoscopist’s discretion. Crossover between treatment allocations was permitted if hemostasis was not achieved. Investigators assessed rates of immediate hemostasis and rebleeding at 30 days.
Dr. Pittayanon and colleagues found rebleeding to be significantly lower among TC-325 treated patients, at 2.1%, compared with 21.3% for standard care (odds ratio, 0.09; 95% confidence interval, 0.01-0.80; P = .03). Rates of immediate hemostasis were 100% for TC-325–treated subjects, compared with 68.6% in the conventional-treatment group (OR, 1.45; 95% CI, 0.93-2.29; P < .001).
None of the 55 patients in the TC-325 group underwent crossover treatment, but 15 patients in the standard care group were crossed over to TC-325 after their endoscopic treatment was deemed to have failed. One-fifth of patients who got TC-325 as a crossover treatment developed rebleeding at 30 days, which the investigators surmised was related to mucosal damage incurred during the endoscopic procedure.
The study was not powered to adequately assess survival outcomes. Seven patients in the TC-325 group and four in the conventional care group died before 30 days’ follow-up, and no death was directly related to recurrent tumor bleeding.
“To our knowledge, our trial is the first to show such significant findings in an RCT setting, which now provide a long-awaited efficacious hemostatic approach where one had been lacking when managing patients with malignant GI bleeding,” the investigators wrote in their analysis.
“Perhaps most importantly, this carefully controlled study also highlights the unreliable hemostatic effect of standard endoscopic modalities available for GI tumor hemostasis, with high 30-day rebleeding rates in our patient population.”
Dr. Pittayanon and colleagues noted several limitations of their study. These included the inability to blind patients to an endoscopist, which “may have influenced subsequent management decisions … including the decision to cross over.”
Only in 5 of 15 cases of crossover did the treating endoscopist provide photo evidence of treatment failure as required by the trial’s protocol. Also, the use of adrenaline injection alone was permitted in the study, in contrast to best practice guidelines for endoscopic hemostasis to treat peptic ulcer bleeding. Finally, the study was conducted in Thailand, potentially reducing the generalizability of the results.
The study was funded by King Chulalongkorn Memorial Hospital; the Thai Red Cross; and Chulalongkorn University. Cook Medical donated some of the TC-325 kits used in the study.
One study coauthor, Alan N. Barkun, disclosed consulting work for Medtronic and past paid work for Cook Medical. The remaining authors disclosed no conflicts of interest.
Gastrointestinal tumor bleeding is a challenging problem that can lead to prolonged hospitalization and interruption of curative or palliative oncologic interventions. Standard endoscopic hemostasis interventions, such as subepithelial epinephrine injection and mechanical and thermal treatments, can be limited because of the underlying tumor biology that alters angiogenesis, distorts the surrounding mucosa, and undermines the normal coagulation process. This randomized trial by Pittayanon et al. demonstrated that the hemostatic powder TC-325 (Hemospray, Cook Medical) was superior to standard endoscopic intervention in achieving immediate hemostasis (100% vs. 69%) and reducing 30-day rebleeding rate (2% vs. 21%).

As clinicians and endoscopists, our ultimate goals in treating GI tumor bleeding are to provide safe and efficient hemostasis, to decrease hospital stay and to minimize delay and interruption of oncologic or palliative treatments. This study advocates that TC-325 may be a better primary option than standard endoscopic treatments for GI tumor bleeding in the appropriate setting. Safety, efficacy, and feasibility studies comparing TC-325 to the other hemostatic powder products are needed.
Malorie K. Simons, MD, is an interventional endoscopist with Fox Chase Cancer Center, Temple University Health System, Philadelphia. She specializes in colorectal cancer, esophageal cancer, and gastric cancer. She has no conflicts of interest.
Gastrointestinal tumor bleeding is a challenging problem that can lead to prolonged hospitalization and interruption of curative or palliative oncologic interventions. Standard endoscopic hemostasis interventions, such as subepithelial epinephrine injection and mechanical and thermal treatments, can be limited because of the underlying tumor biology that alters angiogenesis, distorts the surrounding mucosa, and undermines the normal coagulation process. This randomized trial by Pittayanon et al. demonstrated that the hemostatic powder TC-325 (Hemospray, Cook Medical) was superior to standard endoscopic intervention in achieving immediate hemostasis (100% vs. 69%) and reducing 30-day rebleeding rate (2% vs. 21%).
As clinicians and endoscopists, our ultimate goals in treating GI tumor bleeding are to provide safe and efficient hemostasis, to decrease hospital stay and to minimize delay and interruption of oncologic or palliative treatments. This study advocates that TC-325 may be a better primary option than standard endoscopic treatments for GI tumor bleeding in the appropriate setting. Safety, efficacy, and feasibility studies comparing TC-325 to the other hemostatic powder products are needed.
Malorie K. Simons, MD, is an interventional endoscopist with Fox Chase Cancer Center, Temple University Health System, Philadelphia. She specializes in colorectal cancer, esophageal cancer, and gastric cancer. She has no conflicts of interest.
Gastrointestinal tumor bleeding is a challenging problem that can lead to prolonged hospitalization and interruption of curative or palliative oncologic interventions. Standard endoscopic hemostasis interventions, such as subepithelial epinephrine injection and mechanical and thermal treatments, can be limited because of the underlying tumor biology that alters angiogenesis, distorts the surrounding mucosa, and undermines the normal coagulation process. This randomized trial by Pittayanon et al. demonstrated that the hemostatic powder TC-325 (Hemospray, Cook Medical) was superior to standard endoscopic intervention in achieving immediate hemostasis (100% vs. 69%) and reducing 30-day rebleeding rate (2% vs. 21%).
As clinicians and endoscopists, our ultimate goals in treating GI tumor bleeding are to provide safe and efficient hemostasis, to decrease hospital stay and to minimize delay and interruption of oncologic or palliative treatments. This study advocates that TC-325 may be a better primary option than standard endoscopic treatments for GI tumor bleeding in the appropriate setting. Safety, efficacy, and feasibility studies comparing TC-325 to the other hemostatic powder products are needed.
Malorie K. Simons, MD, is an interventional endoscopist with Fox Chase Cancer Center, Temple University Health System, Philadelphia. She specializes in colorectal cancer, esophageal cancer, and gastric cancer. She has no conflicts of interest.
The findings, published online in Gastroenterology (2023 Jun 3. doi: 10.1053/j.gastro.2023.05.042), come from the largest randomized trial to date of TC-325 (Hemospray, Cook Medical), compared with standard endoscopic hemostatic interventions for tumor bleeding.
For their research, Rapat Pittayanon, MD, of Chulalongkorn University in Bangkok and her colleagues, randomized patients (60% male, mean age 63) with active malignant upper or lower GI bleeding and low disability levels related to their cancers (ECOG score 0-2). The study was conducted at nine hospitals in Thailand.
The 106 patients who passed screening underwent either TC-325 or standard endoscopic hemostasis, which could involve use of thermal or mechanical methods or adrenaline injection, alone or combined with another modality, at the endoscopist’s discretion. Crossover between treatment allocations was permitted if hemostasis was not achieved. Investigators assessed rates of immediate hemostasis and rebleeding at 30 days.
Dr. Pittayanon and colleagues found rebleeding to be significantly lower among TC-325 treated patients, at 2.1%, compared with 21.3% for standard care (odds ratio, 0.09; 95% confidence interval, 0.01-0.80; P = .03). Rates of immediate hemostasis were 100% for TC-325–treated subjects, compared with 68.6% in the conventional-treatment group (OR, 1.45; 95% CI, 0.93-2.29; P < .001).
None of the 55 patients in the TC-325 group underwent crossover treatment, but 15 patients in the standard care group were crossed over to TC-325 after their endoscopic treatment was deemed to have failed. One-fifth of patients who got TC-325 as a crossover treatment developed rebleeding at 30 days, which the investigators surmised was related to mucosal damage incurred during the endoscopic procedure.
The study was not powered to adequately assess survival outcomes. Seven patients in the TC-325 group and four in the conventional care group died before 30 days’ follow-up, and no death was directly related to recurrent tumor bleeding.
“To our knowledge, our trial is the first to show such significant findings in an RCT setting, which now provide a long-awaited efficacious hemostatic approach where one had been lacking when managing patients with malignant GI bleeding,” the investigators wrote in their analysis.
“Perhaps most importantly, this carefully controlled study also highlights the unreliable hemostatic effect of standard endoscopic modalities available for GI tumor hemostasis, with high 30-day rebleeding rates in our patient population.”
Dr. Pittayanon and colleagues noted several limitations of their study. These included the inability to blind patients to an endoscopist, which “may have influenced subsequent management decisions … including the decision to cross over.”
Only in 5 of 15 cases of crossover did the treating endoscopist provide photo evidence of treatment failure as required by the trial’s protocol. Also, the use of adrenaline injection alone was permitted in the study, in contrast to best practice guidelines for endoscopic hemostasis to treat peptic ulcer bleeding. Finally, the study was conducted in Thailand, potentially reducing the generalizability of the results.
The study was funded by King Chulalongkorn Memorial Hospital; the Thai Red Cross; and Chulalongkorn University. Cook Medical donated some of the TC-325 kits used in the study.
One study coauthor, Alan N. Barkun, disclosed consulting work for Medtronic and past paid work for Cook Medical. The remaining authors disclosed no conflicts of interest.
The findings, published online in Gastroenterology (2023 Jun 3. doi: 10.1053/j.gastro.2023.05.042), come from the largest randomized trial to date of TC-325 (Hemospray, Cook Medical), compared with standard endoscopic hemostatic interventions for tumor bleeding.
For their research, Rapat Pittayanon, MD, of Chulalongkorn University in Bangkok and her colleagues, randomized patients (60% male, mean age 63) with active malignant upper or lower GI bleeding and low disability levels related to their cancers (ECOG score 0-2). The study was conducted at nine hospitals in Thailand.
The 106 patients who passed screening underwent either TC-325 or standard endoscopic hemostasis, which could involve use of thermal or mechanical methods or adrenaline injection, alone or combined with another modality, at the endoscopist’s discretion. Crossover between treatment allocations was permitted if hemostasis was not achieved. Investigators assessed rates of immediate hemostasis and rebleeding at 30 days.
Dr. Pittayanon and colleagues found rebleeding to be significantly lower among TC-325 treated patients, at 2.1%, compared with 21.3% for standard care (odds ratio, 0.09; 95% confidence interval, 0.01-0.80; P = .03). Rates of immediate hemostasis were 100% for TC-325–treated subjects, compared with 68.6% in the conventional-treatment group (OR, 1.45; 95% CI, 0.93-2.29; P < .001).
None of the 55 patients in the TC-325 group underwent crossover treatment, but 15 patients in the standard care group were crossed over to TC-325 after their endoscopic treatment was deemed to have failed. One-fifth of patients who got TC-325 as a crossover treatment developed rebleeding at 30 days, which the investigators surmised was related to mucosal damage incurred during the endoscopic procedure.
The study was not powered to adequately assess survival outcomes. Seven patients in the TC-325 group and four in the conventional care group died before 30 days’ follow-up, and no death was directly related to recurrent tumor bleeding.
“To our knowledge, our trial is the first to show such significant findings in an RCT setting, which now provide a long-awaited efficacious hemostatic approach where one had been lacking when managing patients with malignant GI bleeding,” the investigators wrote in their analysis.
“Perhaps most importantly, this carefully controlled study also highlights the unreliable hemostatic effect of standard endoscopic modalities available for GI tumor hemostasis, with high 30-day rebleeding rates in our patient population.”
Dr. Pittayanon and colleagues noted several limitations of their study. These included the inability to blind patients to an endoscopist, which “may have influenced subsequent management decisions … including the decision to cross over.”
Only in 5 of 15 cases of crossover did the treating endoscopist provide photo evidence of treatment failure as required by the trial’s protocol. Also, the use of adrenaline injection alone was permitted in the study, in contrast to best practice guidelines for endoscopic hemostasis to treat peptic ulcer bleeding. Finally, the study was conducted in Thailand, potentially reducing the generalizability of the results.
The study was funded by King Chulalongkorn Memorial Hospital; the Thai Red Cross; and Chulalongkorn University. Cook Medical donated some of the TC-325 kits used in the study.
One study coauthor, Alan N. Barkun, disclosed consulting work for Medtronic and past paid work for Cook Medical. The remaining authors disclosed no conflicts of interest.
FROM GASTROENTEROLOGY
Exercise tied to lower mortality risk across cancer types
TOPLINE:
Regular exercise can significantly reduce a cancer survivor’s mortality from cancer or other causes, a large analysis finds.
METHODOLOGY:
- Following a cancer diagnosis, the impact of exercise on all cause and cause-specific mortality among survivors, and whether the benefit of exercise differs by cancer site, remains unclear.
- To investigate, researchers leveraged data from 11,480 cancer survivors in the Prostate, Lung, Colorectal, and Ovarian cancer screening trial.
- Postdiagnosis exercise levels were quantified via a questionnaire. The primary outcome was all-cause mortality; secondary endpoints were deaths from cancer and other causes.
- Cox models estimated cause-specific hazard ratio for all-cause mortality as well as cancer and noncancer mortality based on whether survivors met or did not meet exercise guidelines.
- Meeting national exercise guidelines meant moderate-intensity exercise 4 or more days per week with sessions lasting, on average, 30 minutes or longer; and/or strenuous-intensity exercise 2 or more days per week with sessions lasting, on average, 20 minutes or longer.
TAKEAWAY:
- Overall, 62% of participants were deemed nonexercisers (no exercise or exercise below guidelines) and 38% were classified as exercisers (meeting or exceeding guidelines). After a median follow-up of 16 years from diagnosis, researchers documented 4,665 deaths – 1,940 from cancer and 2,725 from other causes.
- Exercise at recommended levels was associated with “near-universal” all-cause mortality benefit for most cancers represented, including prostate, breast, endometrial, renal, and head and neck cancers.
- In multivariate analysis, compared with nonexercisers, exercisers had a 25% reduced risk of all-cause mortality (HR, 0.75), with the benefit apparent within 5 years and persisting for at least 20 years after diagnosis.
- Exercise was associated with a 21% reduction in cancer mortality and a 28% reduction in mortality from other causes, with more exercise demonstrating a greater benefit on cancer-specific mortality risk.
IN PRACTICE:
Overall, “our findings show exercise is a holistic strategy that may complement contemporary management approaches to further reduce cancer mortality (in select sites) while simultaneously lowering risk of death from other competing causes, which combine to improve all-cause mortality,” the authors conclude. “This benefit was observed within a few years after diagnosis and sustained for at least 20 years.”
SOURCE:
The study, led by Jessica Lavery, MS, Memorial Sloan Kettering Cancer Center, New York, was published online in the Journal of Clinical Oncology.
LIMITATIONS:
Exercise habits were self-reported at one time point, not measured more objectively over time using wearable devices. The population studied was predominantly non-Hispanic White. The researchers could not determine whether exercise habits reflected lower disease and/or treatment-related toxicities as opposed to direct exercise-induced effects or better adherence to a healthy lifestyle.
DISCLOSURES:
Support for the study was provided by AKTIV Against Cancer and grants from Memorial Sloan Kettering Cancer Center and UCLA Jonsson Comprehensive Cancer Center. Disclosures for the study authors are available with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
Regular exercise can significantly reduce a cancer survivor’s mortality from cancer or other causes, a large analysis finds.
METHODOLOGY:
- Following a cancer diagnosis, the impact of exercise on all cause and cause-specific mortality among survivors, and whether the benefit of exercise differs by cancer site, remains unclear.
- To investigate, researchers leveraged data from 11,480 cancer survivors in the Prostate, Lung, Colorectal, and Ovarian cancer screening trial.
- Postdiagnosis exercise levels were quantified via a questionnaire. The primary outcome was all-cause mortality; secondary endpoints were deaths from cancer and other causes.
- Cox models estimated cause-specific hazard ratio for all-cause mortality as well as cancer and noncancer mortality based on whether survivors met or did not meet exercise guidelines.
- Meeting national exercise guidelines meant moderate-intensity exercise 4 or more days per week with sessions lasting, on average, 30 minutes or longer; and/or strenuous-intensity exercise 2 or more days per week with sessions lasting, on average, 20 minutes or longer.
TAKEAWAY:
- Overall, 62% of participants were deemed nonexercisers (no exercise or exercise below guidelines) and 38% were classified as exercisers (meeting or exceeding guidelines). After a median follow-up of 16 years from diagnosis, researchers documented 4,665 deaths – 1,940 from cancer and 2,725 from other causes.
- Exercise at recommended levels was associated with “near-universal” all-cause mortality benefit for most cancers represented, including prostate, breast, endometrial, renal, and head and neck cancers.
- In multivariate analysis, compared with nonexercisers, exercisers had a 25% reduced risk of all-cause mortality (HR, 0.75), with the benefit apparent within 5 years and persisting for at least 20 years after diagnosis.
- Exercise was associated with a 21% reduction in cancer mortality and a 28% reduction in mortality from other causes, with more exercise demonstrating a greater benefit on cancer-specific mortality risk.
IN PRACTICE:
Overall, “our findings show exercise is a holistic strategy that may complement contemporary management approaches to further reduce cancer mortality (in select sites) while simultaneously lowering risk of death from other competing causes, which combine to improve all-cause mortality,” the authors conclude. “This benefit was observed within a few years after diagnosis and sustained for at least 20 years.”
SOURCE:
The study, led by Jessica Lavery, MS, Memorial Sloan Kettering Cancer Center, New York, was published online in the Journal of Clinical Oncology.
LIMITATIONS:
Exercise habits were self-reported at one time point, not measured more objectively over time using wearable devices. The population studied was predominantly non-Hispanic White. The researchers could not determine whether exercise habits reflected lower disease and/or treatment-related toxicities as opposed to direct exercise-induced effects or better adherence to a healthy lifestyle.
DISCLOSURES:
Support for the study was provided by AKTIV Against Cancer and grants from Memorial Sloan Kettering Cancer Center and UCLA Jonsson Comprehensive Cancer Center. Disclosures for the study authors are available with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
Regular exercise can significantly reduce a cancer survivor’s mortality from cancer or other causes, a large analysis finds.
METHODOLOGY:
- Following a cancer diagnosis, the impact of exercise on all cause and cause-specific mortality among survivors, and whether the benefit of exercise differs by cancer site, remains unclear.
- To investigate, researchers leveraged data from 11,480 cancer survivors in the Prostate, Lung, Colorectal, and Ovarian cancer screening trial.
- Postdiagnosis exercise levels were quantified via a questionnaire. The primary outcome was all-cause mortality; secondary endpoints were deaths from cancer and other causes.
- Cox models estimated cause-specific hazard ratio for all-cause mortality as well as cancer and noncancer mortality based on whether survivors met or did not meet exercise guidelines.
- Meeting national exercise guidelines meant moderate-intensity exercise 4 or more days per week with sessions lasting, on average, 30 minutes or longer; and/or strenuous-intensity exercise 2 or more days per week with sessions lasting, on average, 20 minutes or longer.
TAKEAWAY:
- Overall, 62% of participants were deemed nonexercisers (no exercise or exercise below guidelines) and 38% were classified as exercisers (meeting or exceeding guidelines). After a median follow-up of 16 years from diagnosis, researchers documented 4,665 deaths – 1,940 from cancer and 2,725 from other causes.
- Exercise at recommended levels was associated with “near-universal” all-cause mortality benefit for most cancers represented, including prostate, breast, endometrial, renal, and head and neck cancers.
- In multivariate analysis, compared with nonexercisers, exercisers had a 25% reduced risk of all-cause mortality (HR, 0.75), with the benefit apparent within 5 years and persisting for at least 20 years after diagnosis.
- Exercise was associated with a 21% reduction in cancer mortality and a 28% reduction in mortality from other causes, with more exercise demonstrating a greater benefit on cancer-specific mortality risk.
IN PRACTICE:
Overall, “our findings show exercise is a holistic strategy that may complement contemporary management approaches to further reduce cancer mortality (in select sites) while simultaneously lowering risk of death from other competing causes, which combine to improve all-cause mortality,” the authors conclude. “This benefit was observed within a few years after diagnosis and sustained for at least 20 years.”
SOURCE:
The study, led by Jessica Lavery, MS, Memorial Sloan Kettering Cancer Center, New York, was published online in the Journal of Clinical Oncology.
LIMITATIONS:
Exercise habits were self-reported at one time point, not measured more objectively over time using wearable devices. The population studied was predominantly non-Hispanic White. The researchers could not determine whether exercise habits reflected lower disease and/or treatment-related toxicities as opposed to direct exercise-induced effects or better adherence to a healthy lifestyle.
DISCLOSURES:
Support for the study was provided by AKTIV Against Cancer and grants from Memorial Sloan Kettering Cancer Center and UCLA Jonsson Comprehensive Cancer Center. Disclosures for the study authors are available with the original article.
A version of this article first appeared on Medscape.com.
CHEST SEEK releases key points feature and new print edition
Two exciting updates have come to the CHEST SEEK™ portfolio this summer.
The latest book, CHEST SEEK™ Pulmonary Medicine: 33rd Edition, was released in August. And in this newest book and certain CHEST SEEK Library collections, a feature called key points is included in the recently published 150 pulmonary medicine questions.
Key points are concise summaries of the most important takeaways of SEEK questions. Knowing the key point can help learners focus their studies.
“SEEK questions can be quite robust and intentionally detailed in their response as to why the answer options are correct or incorrect. But because of the level of detail, it can be difficult at times for the learner to correctly hone in on the author’s teaching point,” said CHEST Director, Product Strategy and Evaluation, Martha Zaborowski Pascale, CPM.
“Key points concisely summarize each question’s most important details, potentially saving the learner study time.”
CHEST SEEK™ Pulmonary Medicine: 33rd Edition was developed from the pulmonary medicine board subspecialty examination content blueprints. It tests recall, interpretation, and problem-solving skills.
Rationales provide thorough explanations and reasoning for the correct and incorrect answers. Key points are easy to find at the bottom of the pages and in a tab within SEEK Library questions.
From a printed booklet to the classic book and subscription-based library, learners have engaged with case-based questions in multiple ways. As SEEK has transformed through the years, it’s continued to be a timeless, reliable study partner.
“SEEK has evolved in many ways over its 30-year history. As technologic involvement has permitted greater advances in imaging and data presentation, SEEK has sought to make such advances from the bedside as part of the SEEK experience,” said Pascale.
“The strength of peer-reviewed, expert-written content has remained the same, but modalities such as digital flash cards and behind-the-scenes peer review discussions have enhanced this enduring product in ways that help it stand the test of time.”
Based on CHEST evaluation data, more than 90% of SEEK learners said their practice will change based on content found in the library. Plus, more than 95% of SEEK learners agreed that SEEK question authors are effective instructors.
“The success of SEEK in the past and the ability of this tool to be adapted to the changing needs of learners makes one excited about the editions to come,” said Jesse B. Hall, MD, FCCP, SEEK Editor-in-Chief and Chair of CHEST SEEK™ Pulmonary Medicine: 33rd Edition.
Looking toward the future, SEEK will continue to develop and serve the needs of chest medicine clinicians.
“One of the joys of our professional lives is the constant new discoveries and trials that change the way we practice,” said SEEK Pulmonary Medicine Vice-Chair and Deputy Editor, Jess Mandel, MD.
“However, with this comes the challenge of keeping up and staying current as the field evolves. SEEK is a terrific resource for keeping up with changes in practice and the underlying data that justify them.”
Subscribe to the SEEK Library and find CHEST SEEK™ Pulmonary Medicine: 33rd Edition at chestnet.org/Learning-and-Events/Learning/Seek-App.
Two exciting updates have come to the CHEST SEEK™ portfolio this summer.
The latest book, CHEST SEEK™ Pulmonary Medicine: 33rd Edition, was released in August. And in this newest book and certain CHEST SEEK Library collections, a feature called key points is included in the recently published 150 pulmonary medicine questions.
Key points are concise summaries of the most important takeaways of SEEK questions. Knowing the key point can help learners focus their studies.
“SEEK questions can be quite robust and intentionally detailed in their response as to why the answer options are correct or incorrect. But because of the level of detail, it can be difficult at times for the learner to correctly hone in on the author’s teaching point,” said CHEST Director, Product Strategy and Evaluation, Martha Zaborowski Pascale, CPM.
“Key points concisely summarize each question’s most important details, potentially saving the learner study time.”
CHEST SEEK™ Pulmonary Medicine: 33rd Edition was developed from the pulmonary medicine board subspecialty examination content blueprints. It tests recall, interpretation, and problem-solving skills.
Rationales provide thorough explanations and reasoning for the correct and incorrect answers. Key points are easy to find at the bottom of the pages and in a tab within SEEK Library questions.
From a printed booklet to the classic book and subscription-based library, learners have engaged with case-based questions in multiple ways. As SEEK has transformed through the years, it’s continued to be a timeless, reliable study partner.
“SEEK has evolved in many ways over its 30-year history. As technologic involvement has permitted greater advances in imaging and data presentation, SEEK has sought to make such advances from the bedside as part of the SEEK experience,” said Pascale.
“The strength of peer-reviewed, expert-written content has remained the same, but modalities such as digital flash cards and behind-the-scenes peer review discussions have enhanced this enduring product in ways that help it stand the test of time.”
Based on CHEST evaluation data, more than 90% of SEEK learners said their practice will change based on content found in the library. Plus, more than 95% of SEEK learners agreed that SEEK question authors are effective instructors.
“The success of SEEK in the past and the ability of this tool to be adapted to the changing needs of learners makes one excited about the editions to come,” said Jesse B. Hall, MD, FCCP, SEEK Editor-in-Chief and Chair of CHEST SEEK™ Pulmonary Medicine: 33rd Edition.
Looking toward the future, SEEK will continue to develop and serve the needs of chest medicine clinicians.
“One of the joys of our professional lives is the constant new discoveries and trials that change the way we practice,” said SEEK Pulmonary Medicine Vice-Chair and Deputy Editor, Jess Mandel, MD.
“However, with this comes the challenge of keeping up and staying current as the field evolves. SEEK is a terrific resource for keeping up with changes in practice and the underlying data that justify them.”
Subscribe to the SEEK Library and find CHEST SEEK™ Pulmonary Medicine: 33rd Edition at chestnet.org/Learning-and-Events/Learning/Seek-App.
Two exciting updates have come to the CHEST SEEK™ portfolio this summer.
The latest book, CHEST SEEK™ Pulmonary Medicine: 33rd Edition, was released in August. And in this newest book and certain CHEST SEEK Library collections, a feature called key points is included in the recently published 150 pulmonary medicine questions.
Key points are concise summaries of the most important takeaways of SEEK questions. Knowing the key point can help learners focus their studies.
“SEEK questions can be quite robust and intentionally detailed in their response as to why the answer options are correct or incorrect. But because of the level of detail, it can be difficult at times for the learner to correctly hone in on the author’s teaching point,” said CHEST Director, Product Strategy and Evaluation, Martha Zaborowski Pascale, CPM.
“Key points concisely summarize each question’s most important details, potentially saving the learner study time.”
CHEST SEEK™ Pulmonary Medicine: 33rd Edition was developed from the pulmonary medicine board subspecialty examination content blueprints. It tests recall, interpretation, and problem-solving skills.
Rationales provide thorough explanations and reasoning for the correct and incorrect answers. Key points are easy to find at the bottom of the pages and in a tab within SEEK Library questions.
From a printed booklet to the classic book and subscription-based library, learners have engaged with case-based questions in multiple ways. As SEEK has transformed through the years, it’s continued to be a timeless, reliable study partner.
“SEEK has evolved in many ways over its 30-year history. As technologic involvement has permitted greater advances in imaging and data presentation, SEEK has sought to make such advances from the bedside as part of the SEEK experience,” said Pascale.
“The strength of peer-reviewed, expert-written content has remained the same, but modalities such as digital flash cards and behind-the-scenes peer review discussions have enhanced this enduring product in ways that help it stand the test of time.”
Based on CHEST evaluation data, more than 90% of SEEK learners said their practice will change based on content found in the library. Plus, more than 95% of SEEK learners agreed that SEEK question authors are effective instructors.
“The success of SEEK in the past and the ability of this tool to be adapted to the changing needs of learners makes one excited about the editions to come,” said Jesse B. Hall, MD, FCCP, SEEK Editor-in-Chief and Chair of CHEST SEEK™ Pulmonary Medicine: 33rd Edition.
Looking toward the future, SEEK will continue to develop and serve the needs of chest medicine clinicians.
“One of the joys of our professional lives is the constant new discoveries and trials that change the way we practice,” said SEEK Pulmonary Medicine Vice-Chair and Deputy Editor, Jess Mandel, MD.
“However, with this comes the challenge of keeping up and staying current as the field evolves. SEEK is a terrific resource for keeping up with changes in practice and the underlying data that justify them.”
Subscribe to the SEEK Library and find CHEST SEEK™ Pulmonary Medicine: 33rd Edition at chestnet.org/Learning-and-Events/Learning/Seek-App.
Are you ready for CHEST 2023 in Hawai’i?
Just a few weeks ahead of CHEST 2023, we’re sharing the can’t-miss opportunities available on site at the meeting.
Beyond the top-tier education, CHEST 2023 has a lot to offer attendees in the way of networking, development, and unique experiences that will all make for a memorable meeting.
We’re sharing a preview of the many opportunities that will be available over the 4 days of the meeting. For more specifics on these events, including locations, visit the CHEST 2023 website. You can also download the CHEST 2023 mobile app, which will be available in mid-September.
Networking and development
• For those who want to get more involved with the CHEST community, the Networks Mixer (Monday, October 9, 4 PM HST) is open to all who’d like to learn more about the seven CHEST Networks and the 21 clinically-focused Sections within them.
• The annual Women in Chest Medicine Luncheon (Monday, October 9, 12:45 PM HST) will feature a panel of three women speaking about their experiences, their advice, how to support other women in the field, and more. This event is free, but preregistration is required. Scan the QR code to sign up.
• The first-ever Ohana Mixer (Tuesday, October 10, 6 PM HST) is an opportunity for CHEST attendees to celebrate the spirit of community that unites us across our differences. Attendees can network with each other, meet the members of our newly formed Interest Groups – including the leaders of our Women in Chest Medicine Interest Group and Respiratory Care Interest Group – and socialize with presenters from our three local CHEST Community Connections organizations.
• The Trainee Lounge will feature activities like speed mentoring, a lunch and learn with the Keynote Speaker, Dr. Cedric “Jamie” Rutland, financial wellness presentations, and more.
CHEST experiences
• The Opening Session (Sunday, October 8, 3:15 PM HST) will showcase traditional Hawaiian performances and the Keynote Address from Dr. Rutland. Immediately following, the CHEST Welcome Reception will feature live music and a traditional Hawaiian luau.
• For the second year, CHEST After Hours (Monday, October 9, 3 PM HST) will feature clinicians sharing stories of their personal triumphs, tribulations, and more experiences within medicine.
• Each year, the CHEST Challenge Championship (Tuesday, October 10, 7 PM HST) gives pulmonary and critical care medicine fellows-in-training an opportunity to compete in a live Jeopardy-style game – with bragging rights and cash prizes on the line.
• The Wellness Zone has a packed schedule of events, including beachy workouts, food demonstrations, meditation, and more.
Exhibit hall activities
• Opportunities to network with and hear presentations from local Hawaiian organizations, such as the Waianae Coast Comprehensive Health Center
• Hands-on, experiential education escape rooms
• Live educational games, including Hocus POCUS Diagnosis, PulmMemory, Peer Pressure, and more
• Simulation experiences, including Aspirated and Need for Speed – Airway Bleed
Mark your calendars now to participate in all that CHEST 2023 has to offer. We’ll see you in Hawai’i!
Just a few weeks ahead of CHEST 2023, we’re sharing the can’t-miss opportunities available on site at the meeting.
Beyond the top-tier education, CHEST 2023 has a lot to offer attendees in the way of networking, development, and unique experiences that will all make for a memorable meeting.
We’re sharing a preview of the many opportunities that will be available over the 4 days of the meeting. For more specifics on these events, including locations, visit the CHEST 2023 website. You can also download the CHEST 2023 mobile app, which will be available in mid-September.
Networking and development
• For those who want to get more involved with the CHEST community, the Networks Mixer (Monday, October 9, 4 PM HST) is open to all who’d like to learn more about the seven CHEST Networks and the 21 clinically-focused Sections within them.
• The annual Women in Chest Medicine Luncheon (Monday, October 9, 12:45 PM HST) will feature a panel of three women speaking about their experiences, their advice, how to support other women in the field, and more. This event is free, but preregistration is required. Scan the QR code to sign up.
• The first-ever Ohana Mixer (Tuesday, October 10, 6 PM HST) is an opportunity for CHEST attendees to celebrate the spirit of community that unites us across our differences. Attendees can network with each other, meet the members of our newly formed Interest Groups – including the leaders of our Women in Chest Medicine Interest Group and Respiratory Care Interest Group – and socialize with presenters from our three local CHEST Community Connections organizations.
• The Trainee Lounge will feature activities like speed mentoring, a lunch and learn with the Keynote Speaker, Dr. Cedric “Jamie” Rutland, financial wellness presentations, and more.
CHEST experiences
• The Opening Session (Sunday, October 8, 3:15 PM HST) will showcase traditional Hawaiian performances and the Keynote Address from Dr. Rutland. Immediately following, the CHEST Welcome Reception will feature live music and a traditional Hawaiian luau.
• For the second year, CHEST After Hours (Monday, October 9, 3 PM HST) will feature clinicians sharing stories of their personal triumphs, tribulations, and more experiences within medicine.
• Each year, the CHEST Challenge Championship (Tuesday, October 10, 7 PM HST) gives pulmonary and critical care medicine fellows-in-training an opportunity to compete in a live Jeopardy-style game – with bragging rights and cash prizes on the line.
• The Wellness Zone has a packed schedule of events, including beachy workouts, food demonstrations, meditation, and more.
Exhibit hall activities
• Opportunities to network with and hear presentations from local Hawaiian organizations, such as the Waianae Coast Comprehensive Health Center
• Hands-on, experiential education escape rooms
• Live educational games, including Hocus POCUS Diagnosis, PulmMemory, Peer Pressure, and more
• Simulation experiences, including Aspirated and Need for Speed – Airway Bleed
Mark your calendars now to participate in all that CHEST 2023 has to offer. We’ll see you in Hawai’i!
Just a few weeks ahead of CHEST 2023, we’re sharing the can’t-miss opportunities available on site at the meeting.
Beyond the top-tier education, CHEST 2023 has a lot to offer attendees in the way of networking, development, and unique experiences that will all make for a memorable meeting.
We’re sharing a preview of the many opportunities that will be available over the 4 days of the meeting. For more specifics on these events, including locations, visit the CHEST 2023 website. You can also download the CHEST 2023 mobile app, which will be available in mid-September.
Networking and development
• For those who want to get more involved with the CHEST community, the Networks Mixer (Monday, October 9, 4 PM HST) is open to all who’d like to learn more about the seven CHEST Networks and the 21 clinically-focused Sections within them.
• The annual Women in Chest Medicine Luncheon (Monday, October 9, 12:45 PM HST) will feature a panel of three women speaking about their experiences, their advice, how to support other women in the field, and more. This event is free, but preregistration is required. Scan the QR code to sign up.
• The first-ever Ohana Mixer (Tuesday, October 10, 6 PM HST) is an opportunity for CHEST attendees to celebrate the spirit of community that unites us across our differences. Attendees can network with each other, meet the members of our newly formed Interest Groups – including the leaders of our Women in Chest Medicine Interest Group and Respiratory Care Interest Group – and socialize with presenters from our three local CHEST Community Connections organizations.
• The Trainee Lounge will feature activities like speed mentoring, a lunch and learn with the Keynote Speaker, Dr. Cedric “Jamie” Rutland, financial wellness presentations, and more.
CHEST experiences
• The Opening Session (Sunday, October 8, 3:15 PM HST) will showcase traditional Hawaiian performances and the Keynote Address from Dr. Rutland. Immediately following, the CHEST Welcome Reception will feature live music and a traditional Hawaiian luau.
• For the second year, CHEST After Hours (Monday, October 9, 3 PM HST) will feature clinicians sharing stories of their personal triumphs, tribulations, and more experiences within medicine.
• Each year, the CHEST Challenge Championship (Tuesday, October 10, 7 PM HST) gives pulmonary and critical care medicine fellows-in-training an opportunity to compete in a live Jeopardy-style game – with bragging rights and cash prizes on the line.
• The Wellness Zone has a packed schedule of events, including beachy workouts, food demonstrations, meditation, and more.
Exhibit hall activities
• Opportunities to network with and hear presentations from local Hawaiian organizations, such as the Waianae Coast Comprehensive Health Center
• Hands-on, experiential education escape rooms
• Live educational games, including Hocus POCUS Diagnosis, PulmMemory, Peer Pressure, and more
• Simulation experiences, including Aspirated and Need for Speed – Airway Bleed
Mark your calendars now to participate in all that CHEST 2023 has to offer. We’ll see you in Hawai’i!
Seeking help for burnout may be a gamble for doctors
By the end of 2021, Anuj Peddada, MD, had hit a wall. He couldn’t sleep, couldn’t concentrate, erupted in anger, and felt isolated personally and professionally. To temper pandemic-driven pressures, the Colorado radiation oncologist took an 8-week stress management and resiliency course, but the feelings kept creeping back.
Still, Dr. Peddada, in his own private practice, pushed through, working 60-hour weeks and carrying the workload of two physicians. It wasn’t until he caught himself making uncharacteristic medical errors, including radiation planning for the wrong site, that he knew he needed help – and possibly a temporary break from medicine.
There was just one hitch: He was closing his private practice to start a new in-house job with Centura Health, the Colorado Springs hospital he’d contracted with for over 20 years.
Given the long-standing relationship – Dr. Peddada’s image graced some of the company’s marketing billboards – he expected Centura would understand when, on his doctor’s recommendation, he requested a short-term medical leave that would delay his start date by 1 month.
Instead, Centura abruptly rescinded the employment offer, leaving Dr. Peddada jobless and with no recourse but to sue.
“I was blindsided. The hospital had a physician resiliency program that claimed to encourage physicians to seek help, [so] I thought they would be completely supportive and understanding,” Dr. Peddada said.
He told this news organization that he was naive to have been so honest with the hospital he’d long served as a contractor, including the decade-plus he›d spent directing its radiation oncology department.
“It is exceedingly painful to see hospital leadership use me in their advertisement[s] ... trying to profit off my reputation and work after devastating my career.”
The lawsuit Dr. Peddada filed in July in Colorado federal district court may offer a rare glimpse of the potential career ramifications of seeking help for physician burnout. Despite employers’ oft-stated support for physician wellness, Dr. Peddada’s experience may serve as a cautionary tale for doctors who are open about their struggles.
Centura Health did not respond to requests for comment. In court documents, the health system’s attorneys asked for more time to respond to Dr. Peddada’s complaint.
A plea for help
In the complaint, Dr. Peddada and his attorneys claim that Centura violated the state’s Anti-Discrimination Act and the Americans with Disabilities Act (ADA) when it failed to offer reasonable accommodations after he began experiencing “physiological and psychological symptoms corresponding to burnout.”
Since 1999, Dr. Peddada had contracted exclusively with Centura to provide oncology services at its hospital, Penrose Cancer Center, and began covering a second Centura location in 2021. As medical director of Penrose’s radiation oncology department, he helped establish a community nurse navigator program and accounted for 75% of Centura’s radiation oncology referrals, according to the complaint.
But when his symptoms and fear for the safety of his patients became unbearable, Dr. Peddada requested an urgent evaluation from his primary care physician, who diagnosed him with “physician burnout” and recommended medical leave.
Shortly after presenting the leave request to Centura, rumors began circulating that he was having a “nervous breakdown,” the complaint noted. Dr. Peddada worried that perhaps his private health information was being shared with hospital employees.
After meeting with the hospital’s head of physician resiliency and agreeing to undergo a peer review evaluation by the Colorado Physician Health Program, which would decide the reinstatement timeline and if further therapy was necessary, Dr. Peddada was assured his leave would be approved.
Five days later, his job offer was revoked.
In an email from hospital leadership, the oncologist was informed that he had “declined employment” by failing to sign a revised employment contract sent to him 2 weeks prior when he was out of state on a preapproved vacation, according to the lawsuit.
The lawsuit alleges that Dr. Peddada was wrongfully discharged due to his disability after Centura “exploited [his] extensive patient base, referral network, and reputation to generate growth and profit.”
Colorado employment law attorney Deborah Yim, Esq., who is not involved in Peddada’s case, told this news organization that the ADA requires employers to provide reasonable accommodations for physical or mental impairments that substantially limit at least one major life activity, except when the request imposes an undue hardship on the employer.
“Depression and related mental health conditions would qualify, depending on the circumstances, and courts have certainly found them to be qualifying disabilities entitled to ADA protection in the past,” she said.
Not all employers are receptive to doctors’ needs, says the leadership team at Physicians Just Equity, an organization providing peer support to doctors experiencing workplace conflicts like discrimination and retaliation. They say that Dr. Peddada’s experience, where disclosing burnout results in being “ostracized, penalized, and ultimately ousted,” is the rule rather than the exception.
“Dr. Peddada’s case represents the unfortunate reality faced by many physicians in today’s clinical landscape,” the organization’s board of directors said in a written statement. “The imbalance of unreasonable professional demands, the lack of autonomy, moral injury, and disintegrating practice rewards is unsustainable for the medical professional.”
“Retaliation by employers after speaking up against this imbalance [and] requesting support and time to rejuvenate is a grave failure of health care systems that prioritize the business of delivering health care over the health, well-being, and satisfaction of their most valuable resource – the physician,” the board added in their statement.
Dr. Peddada has since closed his private practice and works as an independent contractor and consultant, his attorney, Iris Halpern, JD, said in an interview. She says Centura could have honored the accommodation request or suggested another option that met his needs, but “not only were they unsupportive, they terminated him.”
Ms. Yim says the parties will have opportunities to reach a settlement and resolve the dispute as the case works through the court system. Otherwise, Dr. Peddada and Centura may eventually head to trial.
Current state of physician burnout
The state of physician burnout is certainly a concerning one. More than half (53%) of physicians responding to this year’s Medscape Physician Burnout & Depression Report said they are burned out. Nearly one-quarter reported feeling depressed. Some of the top reasons they cited were too many bureaucratic tasks (61%), too many work hours (37%), and lack of autonomy (31%).
A 2022 study by the Mayo Clinic found a substantial increase in physician burnout in the first 2 years of the pandemic, with doctors reporting rising emotional exhaustion and depersonalization.
Although burnout affects many physicians and is a priority focus of the National Academy of Medicine’s plan to restore workforce well-being, admitting it is often seen as taboo and can imperil a doctor’s career. In the Medscape report, for example, 39% of physicians said they would not even consider professional treatment for burnout, with many commenting that they would just deal with it themselves.
“Many physicians are frightened to take time out for self-care because [they] fear losing their job, being stigmatized, and potentially ending their careers,” said Dr. Peddada, adding that physicians are commonly asked questions about their mental health when applying for hospital privileges. He says this dynamic forces them to choose between getting help or ignoring their true feelings, leading to poor quality of care and patient safety risks.
Medical licensing boards probe physicians’ mental health, too. As part of its #FightingForDocs campaign, the American Medical Association hopes to remove the stigma around burnout and depression and advocates for licensing boards to revise questions that may discourage physicians from seeking assistance. The AMA recommends that physicians only disclose current physical or mental conditions affecting their ability to practice.
Pringl Miller, MD, founder and executive director of Physician Just Equity, told Medscape that improving physician wellness requires structural change.
“Physicians (who) experience burnout without the proper accommodations run the risk of personal harm, because most physicians will prioritize the health and well-being of their patients over themselves ... [resulting in] suboptimal and unsafe patient care,” she said.
Helping doctors regain a sense of purpose
One change involves reframing how the health care industry thinks about and approaches burnout, says Steven Siegel, MD, chief mental health and wellness officer with Keck Medicine of USC. He told this news organization that these discussions should enhance the physician’s sense of purpose.
“Some people treat burnout as a concrete disorder like cancer, instead of saying, ‘I’m feeling exhausted, demoralized, and don’t enjoy my job anymore. What can we do to restore my enthusiasm for work?’ ”
Dr. Siegel recognizes that these issues existed before the pandemic and have only worsened as physicians feel less connected to and satisfied with their profession – a byproduct, he says, of the commercialization of medicine.
“We’ve moved from practices to systems, then from small to large systems, where it seems the path to survival is cutting costs and increasing margins, even among nonprofits.”
The road ahead
Making headway on these problems will take time. Last year, Keck Medicine received a $2 million grant to launch a 3-year randomized clinical trial to help reconnect physicians and other clinicians with their work. Dr. Siegel says the trial may serve as a national pilot program and will eventually grow to include 400 volunteers.
The trial will investigate the effectiveness of three possible interventions: (1) teaching people how to regulate their internal narratives and emotions through techniques like cognitive behavioral therapy and acceptance and commitment therapy; (2) providing customized EHR training to reduce the burden of navigating the system; and (3) allowing physicians to weigh in on workflow changes.
“We put physicians on teams that make the decisions about workflows,” said Dr. Siegel. The arrangement can give people the agency they desire and help them understand why an idea might not be plausible, which enriches future suggestions and discussions, he says.
A version of this article first appeared on Medscape.com.
By the end of 2021, Anuj Peddada, MD, had hit a wall. He couldn’t sleep, couldn’t concentrate, erupted in anger, and felt isolated personally and professionally. To temper pandemic-driven pressures, the Colorado radiation oncologist took an 8-week stress management and resiliency course, but the feelings kept creeping back.
Still, Dr. Peddada, in his own private practice, pushed through, working 60-hour weeks and carrying the workload of two physicians. It wasn’t until he caught himself making uncharacteristic medical errors, including radiation planning for the wrong site, that he knew he needed help – and possibly a temporary break from medicine.
There was just one hitch: He was closing his private practice to start a new in-house job with Centura Health, the Colorado Springs hospital he’d contracted with for over 20 years.
Given the long-standing relationship – Dr. Peddada’s image graced some of the company’s marketing billboards – he expected Centura would understand when, on his doctor’s recommendation, he requested a short-term medical leave that would delay his start date by 1 month.
Instead, Centura abruptly rescinded the employment offer, leaving Dr. Peddada jobless and with no recourse but to sue.
“I was blindsided. The hospital had a physician resiliency program that claimed to encourage physicians to seek help, [so] I thought they would be completely supportive and understanding,” Dr. Peddada said.
He told this news organization that he was naive to have been so honest with the hospital he’d long served as a contractor, including the decade-plus he›d spent directing its radiation oncology department.
“It is exceedingly painful to see hospital leadership use me in their advertisement[s] ... trying to profit off my reputation and work after devastating my career.”
The lawsuit Dr. Peddada filed in July in Colorado federal district court may offer a rare glimpse of the potential career ramifications of seeking help for physician burnout. Despite employers’ oft-stated support for physician wellness, Dr. Peddada’s experience may serve as a cautionary tale for doctors who are open about their struggles.
Centura Health did not respond to requests for comment. In court documents, the health system’s attorneys asked for more time to respond to Dr. Peddada’s complaint.
A plea for help
In the complaint, Dr. Peddada and his attorneys claim that Centura violated the state’s Anti-Discrimination Act and the Americans with Disabilities Act (ADA) when it failed to offer reasonable accommodations after he began experiencing “physiological and psychological symptoms corresponding to burnout.”
Since 1999, Dr. Peddada had contracted exclusively with Centura to provide oncology services at its hospital, Penrose Cancer Center, and began covering a second Centura location in 2021. As medical director of Penrose’s radiation oncology department, he helped establish a community nurse navigator program and accounted for 75% of Centura’s radiation oncology referrals, according to the complaint.
But when his symptoms and fear for the safety of his patients became unbearable, Dr. Peddada requested an urgent evaluation from his primary care physician, who diagnosed him with “physician burnout” and recommended medical leave.
Shortly after presenting the leave request to Centura, rumors began circulating that he was having a “nervous breakdown,” the complaint noted. Dr. Peddada worried that perhaps his private health information was being shared with hospital employees.
After meeting with the hospital’s head of physician resiliency and agreeing to undergo a peer review evaluation by the Colorado Physician Health Program, which would decide the reinstatement timeline and if further therapy was necessary, Dr. Peddada was assured his leave would be approved.
Five days later, his job offer was revoked.
In an email from hospital leadership, the oncologist was informed that he had “declined employment” by failing to sign a revised employment contract sent to him 2 weeks prior when he was out of state on a preapproved vacation, according to the lawsuit.
The lawsuit alleges that Dr. Peddada was wrongfully discharged due to his disability after Centura “exploited [his] extensive patient base, referral network, and reputation to generate growth and profit.”
Colorado employment law attorney Deborah Yim, Esq., who is not involved in Peddada’s case, told this news organization that the ADA requires employers to provide reasonable accommodations for physical or mental impairments that substantially limit at least one major life activity, except when the request imposes an undue hardship on the employer.
“Depression and related mental health conditions would qualify, depending on the circumstances, and courts have certainly found them to be qualifying disabilities entitled to ADA protection in the past,” she said.
Not all employers are receptive to doctors’ needs, says the leadership team at Physicians Just Equity, an organization providing peer support to doctors experiencing workplace conflicts like discrimination and retaliation. They say that Dr. Peddada’s experience, where disclosing burnout results in being “ostracized, penalized, and ultimately ousted,” is the rule rather than the exception.
“Dr. Peddada’s case represents the unfortunate reality faced by many physicians in today’s clinical landscape,” the organization’s board of directors said in a written statement. “The imbalance of unreasonable professional demands, the lack of autonomy, moral injury, and disintegrating practice rewards is unsustainable for the medical professional.”
“Retaliation by employers after speaking up against this imbalance [and] requesting support and time to rejuvenate is a grave failure of health care systems that prioritize the business of delivering health care over the health, well-being, and satisfaction of their most valuable resource – the physician,” the board added in their statement.
Dr. Peddada has since closed his private practice and works as an independent contractor and consultant, his attorney, Iris Halpern, JD, said in an interview. She says Centura could have honored the accommodation request or suggested another option that met his needs, but “not only were they unsupportive, they terminated him.”
Ms. Yim says the parties will have opportunities to reach a settlement and resolve the dispute as the case works through the court system. Otherwise, Dr. Peddada and Centura may eventually head to trial.
Current state of physician burnout
The state of physician burnout is certainly a concerning one. More than half (53%) of physicians responding to this year’s Medscape Physician Burnout & Depression Report said they are burned out. Nearly one-quarter reported feeling depressed. Some of the top reasons they cited were too many bureaucratic tasks (61%), too many work hours (37%), and lack of autonomy (31%).
A 2022 study by the Mayo Clinic found a substantial increase in physician burnout in the first 2 years of the pandemic, with doctors reporting rising emotional exhaustion and depersonalization.
Although burnout affects many physicians and is a priority focus of the National Academy of Medicine’s plan to restore workforce well-being, admitting it is often seen as taboo and can imperil a doctor’s career. In the Medscape report, for example, 39% of physicians said they would not even consider professional treatment for burnout, with many commenting that they would just deal with it themselves.
“Many physicians are frightened to take time out for self-care because [they] fear losing their job, being stigmatized, and potentially ending their careers,” said Dr. Peddada, adding that physicians are commonly asked questions about their mental health when applying for hospital privileges. He says this dynamic forces them to choose between getting help or ignoring their true feelings, leading to poor quality of care and patient safety risks.
Medical licensing boards probe physicians’ mental health, too. As part of its #FightingForDocs campaign, the American Medical Association hopes to remove the stigma around burnout and depression and advocates for licensing boards to revise questions that may discourage physicians from seeking assistance. The AMA recommends that physicians only disclose current physical or mental conditions affecting their ability to practice.
Pringl Miller, MD, founder and executive director of Physician Just Equity, told Medscape that improving physician wellness requires structural change.
“Physicians (who) experience burnout without the proper accommodations run the risk of personal harm, because most physicians will prioritize the health and well-being of their patients over themselves ... [resulting in] suboptimal and unsafe patient care,” she said.
Helping doctors regain a sense of purpose
One change involves reframing how the health care industry thinks about and approaches burnout, says Steven Siegel, MD, chief mental health and wellness officer with Keck Medicine of USC. He told this news organization that these discussions should enhance the physician’s sense of purpose.
“Some people treat burnout as a concrete disorder like cancer, instead of saying, ‘I’m feeling exhausted, demoralized, and don’t enjoy my job anymore. What can we do to restore my enthusiasm for work?’ ”
Dr. Siegel recognizes that these issues existed before the pandemic and have only worsened as physicians feel less connected to and satisfied with their profession – a byproduct, he says, of the commercialization of medicine.
“We’ve moved from practices to systems, then from small to large systems, where it seems the path to survival is cutting costs and increasing margins, even among nonprofits.”
The road ahead
Making headway on these problems will take time. Last year, Keck Medicine received a $2 million grant to launch a 3-year randomized clinical trial to help reconnect physicians and other clinicians with their work. Dr. Siegel says the trial may serve as a national pilot program and will eventually grow to include 400 volunteers.
The trial will investigate the effectiveness of three possible interventions: (1) teaching people how to regulate their internal narratives and emotions through techniques like cognitive behavioral therapy and acceptance and commitment therapy; (2) providing customized EHR training to reduce the burden of navigating the system; and (3) allowing physicians to weigh in on workflow changes.
“We put physicians on teams that make the decisions about workflows,” said Dr. Siegel. The arrangement can give people the agency they desire and help them understand why an idea might not be plausible, which enriches future suggestions and discussions, he says.
A version of this article first appeared on Medscape.com.
By the end of 2021, Anuj Peddada, MD, had hit a wall. He couldn’t sleep, couldn’t concentrate, erupted in anger, and felt isolated personally and professionally. To temper pandemic-driven pressures, the Colorado radiation oncologist took an 8-week stress management and resiliency course, but the feelings kept creeping back.
Still, Dr. Peddada, in his own private practice, pushed through, working 60-hour weeks and carrying the workload of two physicians. It wasn’t until he caught himself making uncharacteristic medical errors, including radiation planning for the wrong site, that he knew he needed help – and possibly a temporary break from medicine.
There was just one hitch: He was closing his private practice to start a new in-house job with Centura Health, the Colorado Springs hospital he’d contracted with for over 20 years.
Given the long-standing relationship – Dr. Peddada’s image graced some of the company’s marketing billboards – he expected Centura would understand when, on his doctor’s recommendation, he requested a short-term medical leave that would delay his start date by 1 month.
Instead, Centura abruptly rescinded the employment offer, leaving Dr. Peddada jobless and with no recourse but to sue.
“I was blindsided. The hospital had a physician resiliency program that claimed to encourage physicians to seek help, [so] I thought they would be completely supportive and understanding,” Dr. Peddada said.
He told this news organization that he was naive to have been so honest with the hospital he’d long served as a contractor, including the decade-plus he›d spent directing its radiation oncology department.
“It is exceedingly painful to see hospital leadership use me in their advertisement[s] ... trying to profit off my reputation and work after devastating my career.”
The lawsuit Dr. Peddada filed in July in Colorado federal district court may offer a rare glimpse of the potential career ramifications of seeking help for physician burnout. Despite employers’ oft-stated support for physician wellness, Dr. Peddada’s experience may serve as a cautionary tale for doctors who are open about their struggles.
Centura Health did not respond to requests for comment. In court documents, the health system’s attorneys asked for more time to respond to Dr. Peddada’s complaint.
A plea for help
In the complaint, Dr. Peddada and his attorneys claim that Centura violated the state’s Anti-Discrimination Act and the Americans with Disabilities Act (ADA) when it failed to offer reasonable accommodations after he began experiencing “physiological and psychological symptoms corresponding to burnout.”
Since 1999, Dr. Peddada had contracted exclusively with Centura to provide oncology services at its hospital, Penrose Cancer Center, and began covering a second Centura location in 2021. As medical director of Penrose’s radiation oncology department, he helped establish a community nurse navigator program and accounted for 75% of Centura’s radiation oncology referrals, according to the complaint.
But when his symptoms and fear for the safety of his patients became unbearable, Dr. Peddada requested an urgent evaluation from his primary care physician, who diagnosed him with “physician burnout” and recommended medical leave.
Shortly after presenting the leave request to Centura, rumors began circulating that he was having a “nervous breakdown,” the complaint noted. Dr. Peddada worried that perhaps his private health information was being shared with hospital employees.
After meeting with the hospital’s head of physician resiliency and agreeing to undergo a peer review evaluation by the Colorado Physician Health Program, which would decide the reinstatement timeline and if further therapy was necessary, Dr. Peddada was assured his leave would be approved.
Five days later, his job offer was revoked.
In an email from hospital leadership, the oncologist was informed that he had “declined employment” by failing to sign a revised employment contract sent to him 2 weeks prior when he was out of state on a preapproved vacation, according to the lawsuit.
The lawsuit alleges that Dr. Peddada was wrongfully discharged due to his disability after Centura “exploited [his] extensive patient base, referral network, and reputation to generate growth and profit.”
Colorado employment law attorney Deborah Yim, Esq., who is not involved in Peddada’s case, told this news organization that the ADA requires employers to provide reasonable accommodations for physical or mental impairments that substantially limit at least one major life activity, except when the request imposes an undue hardship on the employer.
“Depression and related mental health conditions would qualify, depending on the circumstances, and courts have certainly found them to be qualifying disabilities entitled to ADA protection in the past,” she said.
Not all employers are receptive to doctors’ needs, says the leadership team at Physicians Just Equity, an organization providing peer support to doctors experiencing workplace conflicts like discrimination and retaliation. They say that Dr. Peddada’s experience, where disclosing burnout results in being “ostracized, penalized, and ultimately ousted,” is the rule rather than the exception.
“Dr. Peddada’s case represents the unfortunate reality faced by many physicians in today’s clinical landscape,” the organization’s board of directors said in a written statement. “The imbalance of unreasonable professional demands, the lack of autonomy, moral injury, and disintegrating practice rewards is unsustainable for the medical professional.”
“Retaliation by employers after speaking up against this imbalance [and] requesting support and time to rejuvenate is a grave failure of health care systems that prioritize the business of delivering health care over the health, well-being, and satisfaction of their most valuable resource – the physician,” the board added in their statement.
Dr. Peddada has since closed his private practice and works as an independent contractor and consultant, his attorney, Iris Halpern, JD, said in an interview. She says Centura could have honored the accommodation request or suggested another option that met his needs, but “not only were they unsupportive, they terminated him.”
Ms. Yim says the parties will have opportunities to reach a settlement and resolve the dispute as the case works through the court system. Otherwise, Dr. Peddada and Centura may eventually head to trial.
Current state of physician burnout
The state of physician burnout is certainly a concerning one. More than half (53%) of physicians responding to this year’s Medscape Physician Burnout & Depression Report said they are burned out. Nearly one-quarter reported feeling depressed. Some of the top reasons they cited were too many bureaucratic tasks (61%), too many work hours (37%), and lack of autonomy (31%).
A 2022 study by the Mayo Clinic found a substantial increase in physician burnout in the first 2 years of the pandemic, with doctors reporting rising emotional exhaustion and depersonalization.
Although burnout affects many physicians and is a priority focus of the National Academy of Medicine’s plan to restore workforce well-being, admitting it is often seen as taboo and can imperil a doctor’s career. In the Medscape report, for example, 39% of physicians said they would not even consider professional treatment for burnout, with many commenting that they would just deal with it themselves.
“Many physicians are frightened to take time out for self-care because [they] fear losing their job, being stigmatized, and potentially ending their careers,” said Dr. Peddada, adding that physicians are commonly asked questions about their mental health when applying for hospital privileges. He says this dynamic forces them to choose between getting help or ignoring their true feelings, leading to poor quality of care and patient safety risks.
Medical licensing boards probe physicians’ mental health, too. As part of its #FightingForDocs campaign, the American Medical Association hopes to remove the stigma around burnout and depression and advocates for licensing boards to revise questions that may discourage physicians from seeking assistance. The AMA recommends that physicians only disclose current physical or mental conditions affecting their ability to practice.
Pringl Miller, MD, founder and executive director of Physician Just Equity, told Medscape that improving physician wellness requires structural change.
“Physicians (who) experience burnout without the proper accommodations run the risk of personal harm, because most physicians will prioritize the health and well-being of their patients over themselves ... [resulting in] suboptimal and unsafe patient care,” she said.
Helping doctors regain a sense of purpose
One change involves reframing how the health care industry thinks about and approaches burnout, says Steven Siegel, MD, chief mental health and wellness officer with Keck Medicine of USC. He told this news organization that these discussions should enhance the physician’s sense of purpose.
“Some people treat burnout as a concrete disorder like cancer, instead of saying, ‘I’m feeling exhausted, demoralized, and don’t enjoy my job anymore. What can we do to restore my enthusiasm for work?’ ”
Dr. Siegel recognizes that these issues existed before the pandemic and have only worsened as physicians feel less connected to and satisfied with their profession – a byproduct, he says, of the commercialization of medicine.
“We’ve moved from practices to systems, then from small to large systems, where it seems the path to survival is cutting costs and increasing margins, even among nonprofits.”
The road ahead
Making headway on these problems will take time. Last year, Keck Medicine received a $2 million grant to launch a 3-year randomized clinical trial to help reconnect physicians and other clinicians with their work. Dr. Siegel says the trial may serve as a national pilot program and will eventually grow to include 400 volunteers.
The trial will investigate the effectiveness of three possible interventions: (1) teaching people how to regulate their internal narratives and emotions through techniques like cognitive behavioral therapy and acceptance and commitment therapy; (2) providing customized EHR training to reduce the burden of navigating the system; and (3) allowing physicians to weigh in on workflow changes.
“We put physicians on teams that make the decisions about workflows,” said Dr. Siegel. The arrangement can give people the agency they desire and help them understand why an idea might not be plausible, which enriches future suggestions and discussions, he says.
A version of this article first appeared on Medscape.com.
Using JAK inhibitors for myelofibrosis
“We are thankfully starting to be blessed with more options than we’ve ever had,” he said, but “in the front-line proliferative setting, ruxolitinib has remained the standard of care.” It’s “well established in higher-risk patients and very much an option for very symptomatic lower-risk patients.”
Dr. Hunter helped his colleagues navigate the evolving field of JAK inhibition for myelofibrosis in a presentation titled “Choosing and Properly Using a JAK Inhibitor in Myelofibrosis,”at the Society of Hematologic Oncology annual meeting.
Ruxolitinib was the first JAK inhibitor for myelofibrosis on the U.S. market, approved in 2011. Two more have followed, fedratinib in 2019 and pacritinib in 2022.
A fourth JAK inhibitor for myelofibrosis, momelotinib, is under Food and Drug Administration review with a decision expected shortly.
JAK inhibitors disrupt a key pathogenic pathway in myelofibrosis and are a mainstay of treatment, but Dr. Hunter noted that they should not replace allogeneic transplants in patients who are candidates because transplants remain “the best way to achieve long term survival, especially in higher risk patients.”
He noted that not every patient needs a JAK inhibitor, especially “lower-risk, more asymptomatic patients who are predominantly manifesting with cytopenias. [They] are less likely to benefit.”
Dr. Hunter said that although ruxolitinib remains a treatment of choice, fedratinib “is certainly an option” with comparable rates of symptom control and splenomegaly reduction. Also, while ruxolitinib is dosed according to platelet levels, fedratinib allows for full dosing down to a platelet count of 50 x 109/L.
“But there’s more GI toxicity than with ruxolitinib, especially in the first couple of months,” he said, as well as a black box warning of Wernicke’s encephalopathy. “I generally put all my [fedratinib] patients on thiamine repletion as a precaution.”
One of the most challenging aspects of using JAK inhibitors for myelofibrosis is their tendency to cause cytopenia, particularly anemia and thrombocytopenia, which, ironically, are also hallmarks of myelofibrosis itself.
Although there’s an alternative low-dose ruxolitinib regimen that can be effective in anemic settings, the approval of pacritinib and most likely momelotinib is particularly helpful for cytopenic patients, “a population which historically has been very hard to treat with our prior agents,” Dr. Hunter said.
Pacritinib is approved specifically for patients with platelet counts below 50 x 109/L; momelotinib also included lower platelet counts in several studies. Both agents indirectly boost erythropoiesis with subsequent amelioration of anemia.
“Momelotinib is an important emerging agent for these more anemic patients,” with a spleen response comparable to ruxolitinib and significantly higher rates of transfusion independence, but with lower rates of symptom control, Dr. Hunter said.
Pacritinib “really helps extend the benefit of JAK inhibitors to a group of thrombocytopenic patients who have been hard to treat with ruxolitinib,” with the added potential of improving anemia, although, like fedratinib, it has more GI toxicity, he said.
There are multiple add-on options for JAK inhibitor patients with anemia, including luspatercept, an erythropoiesis-stimulating agent approved for anemia in patients with myelodysplastic syndromes; promising results were reported recently for myelofibrosis.
Fedratinib, pacritinib, and momelotinib all have activity in the second line after ruxolitinib failure, Dr. Hunter noted, but he cautioned that ruxolitinib must be tapered over a few weeks, not stopped abruptly, to avoid withdrawal symptoms. Some clinicians overlap JAK inhibitors a day or two to avoid issues.
“Clinical trials should still be considered in many of these settings,” he said, adding that emerging agents are under development, including multiple combination therapies, often with JAK inhibitors as the background.
No disclosure information was reported.
“We are thankfully starting to be blessed with more options than we’ve ever had,” he said, but “in the front-line proliferative setting, ruxolitinib has remained the standard of care.” It’s “well established in higher-risk patients and very much an option for very symptomatic lower-risk patients.”
Dr. Hunter helped his colleagues navigate the evolving field of JAK inhibition for myelofibrosis in a presentation titled “Choosing and Properly Using a JAK Inhibitor in Myelofibrosis,”at the Society of Hematologic Oncology annual meeting.
Ruxolitinib was the first JAK inhibitor for myelofibrosis on the U.S. market, approved in 2011. Two more have followed, fedratinib in 2019 and pacritinib in 2022.
A fourth JAK inhibitor for myelofibrosis, momelotinib, is under Food and Drug Administration review with a decision expected shortly.
JAK inhibitors disrupt a key pathogenic pathway in myelofibrosis and are a mainstay of treatment, but Dr. Hunter noted that they should not replace allogeneic transplants in patients who are candidates because transplants remain “the best way to achieve long term survival, especially in higher risk patients.”
He noted that not every patient needs a JAK inhibitor, especially “lower-risk, more asymptomatic patients who are predominantly manifesting with cytopenias. [They] are less likely to benefit.”
Dr. Hunter said that although ruxolitinib remains a treatment of choice, fedratinib “is certainly an option” with comparable rates of symptom control and splenomegaly reduction. Also, while ruxolitinib is dosed according to platelet levels, fedratinib allows for full dosing down to a platelet count of 50 x 109/L.
“But there’s more GI toxicity than with ruxolitinib, especially in the first couple of months,” he said, as well as a black box warning of Wernicke’s encephalopathy. “I generally put all my [fedratinib] patients on thiamine repletion as a precaution.”
One of the most challenging aspects of using JAK inhibitors for myelofibrosis is their tendency to cause cytopenia, particularly anemia and thrombocytopenia, which, ironically, are also hallmarks of myelofibrosis itself.
Although there’s an alternative low-dose ruxolitinib regimen that can be effective in anemic settings, the approval of pacritinib and most likely momelotinib is particularly helpful for cytopenic patients, “a population which historically has been very hard to treat with our prior agents,” Dr. Hunter said.
Pacritinib is approved specifically for patients with platelet counts below 50 x 109/L; momelotinib also included lower platelet counts in several studies. Both agents indirectly boost erythropoiesis with subsequent amelioration of anemia.
“Momelotinib is an important emerging agent for these more anemic patients,” with a spleen response comparable to ruxolitinib and significantly higher rates of transfusion independence, but with lower rates of symptom control, Dr. Hunter said.
Pacritinib “really helps extend the benefit of JAK inhibitors to a group of thrombocytopenic patients who have been hard to treat with ruxolitinib,” with the added potential of improving anemia, although, like fedratinib, it has more GI toxicity, he said.
There are multiple add-on options for JAK inhibitor patients with anemia, including luspatercept, an erythropoiesis-stimulating agent approved for anemia in patients with myelodysplastic syndromes; promising results were reported recently for myelofibrosis.
Fedratinib, pacritinib, and momelotinib all have activity in the second line after ruxolitinib failure, Dr. Hunter noted, but he cautioned that ruxolitinib must be tapered over a few weeks, not stopped abruptly, to avoid withdrawal symptoms. Some clinicians overlap JAK inhibitors a day or two to avoid issues.
“Clinical trials should still be considered in many of these settings,” he said, adding that emerging agents are under development, including multiple combination therapies, often with JAK inhibitors as the background.
No disclosure information was reported.
“We are thankfully starting to be blessed with more options than we’ve ever had,” he said, but “in the front-line proliferative setting, ruxolitinib has remained the standard of care.” It’s “well established in higher-risk patients and very much an option for very symptomatic lower-risk patients.”
Dr. Hunter helped his colleagues navigate the evolving field of JAK inhibition for myelofibrosis in a presentation titled “Choosing and Properly Using a JAK Inhibitor in Myelofibrosis,”at the Society of Hematologic Oncology annual meeting.
Ruxolitinib was the first JAK inhibitor for myelofibrosis on the U.S. market, approved in 2011. Two more have followed, fedratinib in 2019 and pacritinib in 2022.
A fourth JAK inhibitor for myelofibrosis, momelotinib, is under Food and Drug Administration review with a decision expected shortly.
JAK inhibitors disrupt a key pathogenic pathway in myelofibrosis and are a mainstay of treatment, but Dr. Hunter noted that they should not replace allogeneic transplants in patients who are candidates because transplants remain “the best way to achieve long term survival, especially in higher risk patients.”
He noted that not every patient needs a JAK inhibitor, especially “lower-risk, more asymptomatic patients who are predominantly manifesting with cytopenias. [They] are less likely to benefit.”
Dr. Hunter said that although ruxolitinib remains a treatment of choice, fedratinib “is certainly an option” with comparable rates of symptom control and splenomegaly reduction. Also, while ruxolitinib is dosed according to platelet levels, fedratinib allows for full dosing down to a platelet count of 50 x 109/L.
“But there’s more GI toxicity than with ruxolitinib, especially in the first couple of months,” he said, as well as a black box warning of Wernicke’s encephalopathy. “I generally put all my [fedratinib] patients on thiamine repletion as a precaution.”
One of the most challenging aspects of using JAK inhibitors for myelofibrosis is their tendency to cause cytopenia, particularly anemia and thrombocytopenia, which, ironically, are also hallmarks of myelofibrosis itself.
Although there’s an alternative low-dose ruxolitinib regimen that can be effective in anemic settings, the approval of pacritinib and most likely momelotinib is particularly helpful for cytopenic patients, “a population which historically has been very hard to treat with our prior agents,” Dr. Hunter said.
Pacritinib is approved specifically for patients with platelet counts below 50 x 109/L; momelotinib also included lower platelet counts in several studies. Both agents indirectly boost erythropoiesis with subsequent amelioration of anemia.
“Momelotinib is an important emerging agent for these more anemic patients,” with a spleen response comparable to ruxolitinib and significantly higher rates of transfusion independence, but with lower rates of symptom control, Dr. Hunter said.
Pacritinib “really helps extend the benefit of JAK inhibitors to a group of thrombocytopenic patients who have been hard to treat with ruxolitinib,” with the added potential of improving anemia, although, like fedratinib, it has more GI toxicity, he said.
There are multiple add-on options for JAK inhibitor patients with anemia, including luspatercept, an erythropoiesis-stimulating agent approved for anemia in patients with myelodysplastic syndromes; promising results were reported recently for myelofibrosis.
Fedratinib, pacritinib, and momelotinib all have activity in the second line after ruxolitinib failure, Dr. Hunter noted, but he cautioned that ruxolitinib must be tapered over a few weeks, not stopped abruptly, to avoid withdrawal symptoms. Some clinicians overlap JAK inhibitors a day or two to avoid issues.
“Clinical trials should still be considered in many of these settings,” he said, adding that emerging agents are under development, including multiple combination therapies, often with JAK inhibitors as the background.
No disclosure information was reported.
FROM SOHO 2023