User login
The balm of reassurance
A toddler has had several brief episodes of mild perioral cyanosis noticed at day care. The parents see the primary care provider. The exam is normal. The child is admitted for a work-up. The CBC and comprehensive metabolic profile are unremarkable. The chest x-ray is normal. An ECG is normal. An echocardiogram is normal. The EEG is normal. Now what?
I was taught that an uncommon presentation of a common disease is still more common than a common presentation of an uncommon disease. Or simply, odd-looking horses are more common than zebras unless you practice in the savanna. There is a point in any safari at which you have to decide whether you are hunting a zebra or chasing a shadow. Clinical judgment is balancing the risk of missing something preventable that will actually harm the child against the harms of more tests.

The modern hospital has an array of equipment available. They are Greek Sirens calling to us. There is the video EEG room, the MR angiogram, the cardiac cath lab, and an endless list of blood tests. We are not even stopped by the walls of the hospital. We can order a follow-up ambulatory Holter ECG to search for intermittent arrhythmias. But are these Sirens really good medicine? At what point should we simply reassure the parents that the child is fine?
Physicians all worry about missing something. This fear was instilled when we were medical students and reinforced with the stress of residency. With years of experience, all physicians acquire a list of missed diagnoses. But I also have collected a list of times when the diagnostic tests themselves have caused harm, including death. I have a list of cases where nonspecific diagnostic testing has mislabeled a child with an obscure diagnosis that was later proven false, but not before harm was caused. There were patients with Stevens-Johnson syndrome who suffered serious harm from treatments for minor illnesses. Then there were the terrified families who, after extensive testing, became convinced that the child must have some horrible unknown disease because surely we wouldn’t have traumatized the child with all this work-up if there wasn’t really something seriously wrong. Each new test stoked their fear rather than soothed it.
A careful history is still the weapon of choice in the zebra hunt. On a first presentation of mild cyanosis, sepsis is the charging rhinoceros of preventable harm that will run you over if you are too slow to react. But this child has now had several episodes that have occurred: 1. in multiple settings, 2. with no distress, 3. while the child remained playful, and 4. that were self-limited. That history is incompatible with sepsis, so reflexively ordering a blood culture is an illogical choice. The history should be progressively explored using the differential diagnosis and an organ-based systematic approach to guide it. The thoroughness and thoughtfulness I put into the history taking can be key to finding the correct diagnosis. They also are a means of building trust and rapport with the parents. That will be important later if no definitive diagnosis is found.
Unclear and unusual presentations may merit a consult. The cardiologist knows the limits of an echo. Along with the technical expertise comes a new set of eyes and the additional perspective of a second opinion. It is great when a colleague can tell you that he or she too had a case like this years ago that was never solved, but did resolve on its own.
One advantage of being an office-based pediatrician, with an established relationship with a family over several years and a couple other children, is that parents do value and trust your clinical judgment. As a pediatrician, I know the most common product I sell is reassurance. It is not snake oil. There is a bedside manner in selling it. Put a positive spin on all the negative tests. Indicate that you and the parents can be vigilant in watching for new signs. Instruct the parents to bring the child back if the events are distressing for the child, which could justify more invasive testing. Arrange to recheck the child in the office in a week, then a month, then at the next well visit. Parents know that medicine isn’t perfect. Humans deal with fear and uncertainty better by knowing we aren’t facing the future alone. And that is why even with all this technology, I still lay a stethoscope on every child.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures.
A toddler has had several brief episodes of mild perioral cyanosis noticed at day care. The parents see the primary care provider. The exam is normal. The child is admitted for a work-up. The CBC and comprehensive metabolic profile are unremarkable. The chest x-ray is normal. An ECG is normal. An echocardiogram is normal. The EEG is normal. Now what?
I was taught that an uncommon presentation of a common disease is still more common than a common presentation of an uncommon disease. Or simply, odd-looking horses are more common than zebras unless you practice in the savanna. There is a point in any safari at which you have to decide whether you are hunting a zebra or chasing a shadow. Clinical judgment is balancing the risk of missing something preventable that will actually harm the child against the harms of more tests.
The modern hospital has an array of equipment available. They are Greek Sirens calling to us. There is the video EEG room, the MR angiogram, the cardiac cath lab, and an endless list of blood tests. We are not even stopped by the walls of the hospital. We can order a follow-up ambulatory Holter ECG to search for intermittent arrhythmias. But are these Sirens really good medicine? At what point should we simply reassure the parents that the child is fine?
Physicians all worry about missing something. This fear was instilled when we were medical students and reinforced with the stress of residency. With years of experience, all physicians acquire a list of missed diagnoses. But I also have collected a list of times when the diagnostic tests themselves have caused harm, including death. I have a list of cases where nonspecific diagnostic testing has mislabeled a child with an obscure diagnosis that was later proven false, but not before harm was caused. There were patients with Stevens-Johnson syndrome who suffered serious harm from treatments for minor illnesses. Then there were the terrified families who, after extensive testing, became convinced that the child must have some horrible unknown disease because surely we wouldn’t have traumatized the child with all this work-up if there wasn’t really something seriously wrong. Each new test stoked their fear rather than soothed it.
A careful history is still the weapon of choice in the zebra hunt. On a first presentation of mild cyanosis, sepsis is the charging rhinoceros of preventable harm that will run you over if you are too slow to react. But this child has now had several episodes that have occurred: 1. in multiple settings, 2. with no distress, 3. while the child remained playful, and 4. that were self-limited. That history is incompatible with sepsis, so reflexively ordering a blood culture is an illogical choice. The history should be progressively explored using the differential diagnosis and an organ-based systematic approach to guide it. The thoroughness and thoughtfulness I put into the history taking can be key to finding the correct diagnosis. They also are a means of building trust and rapport with the parents. That will be important later if no definitive diagnosis is found.
Unclear and unusual presentations may merit a consult. The cardiologist knows the limits of an echo. Along with the technical expertise comes a new set of eyes and the additional perspective of a second opinion. It is great when a colleague can tell you that he or she too had a case like this years ago that was never solved, but did resolve on its own.
One advantage of being an office-based pediatrician, with an established relationship with a family over several years and a couple other children, is that parents do value and trust your clinical judgment. As a pediatrician, I know the most common product I sell is reassurance. It is not snake oil. There is a bedside manner in selling it. Put a positive spin on all the negative tests. Indicate that you and the parents can be vigilant in watching for new signs. Instruct the parents to bring the child back if the events are distressing for the child, which could justify more invasive testing. Arrange to recheck the child in the office in a week, then a month, then at the next well visit. Parents know that medicine isn’t perfect. Humans deal with fear and uncertainty better by knowing we aren’t facing the future alone. And that is why even with all this technology, I still lay a stethoscope on every child.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures.
A toddler has had several brief episodes of mild perioral cyanosis noticed at day care. The parents see the primary care provider. The exam is normal. The child is admitted for a work-up. The CBC and comprehensive metabolic profile are unremarkable. The chest x-ray is normal. An ECG is normal. An echocardiogram is normal. The EEG is normal. Now what?
I was taught that an uncommon presentation of a common disease is still more common than a common presentation of an uncommon disease. Or simply, odd-looking horses are more common than zebras unless you practice in the savanna. There is a point in any safari at which you have to decide whether you are hunting a zebra or chasing a shadow. Clinical judgment is balancing the risk of missing something preventable that will actually harm the child against the harms of more tests.
The modern hospital has an array of equipment available. They are Greek Sirens calling to us. There is the video EEG room, the MR angiogram, the cardiac cath lab, and an endless list of blood tests. We are not even stopped by the walls of the hospital. We can order a follow-up ambulatory Holter ECG to search for intermittent arrhythmias. But are these Sirens really good medicine? At what point should we simply reassure the parents that the child is fine?
Physicians all worry about missing something. This fear was instilled when we were medical students and reinforced with the stress of residency. With years of experience, all physicians acquire a list of missed diagnoses. But I also have collected a list of times when the diagnostic tests themselves have caused harm, including death. I have a list of cases where nonspecific diagnostic testing has mislabeled a child with an obscure diagnosis that was later proven false, but not before harm was caused. There were patients with Stevens-Johnson syndrome who suffered serious harm from treatments for minor illnesses. Then there were the terrified families who, after extensive testing, became convinced that the child must have some horrible unknown disease because surely we wouldn’t have traumatized the child with all this work-up if there wasn’t really something seriously wrong. Each new test stoked their fear rather than soothed it.
A careful history is still the weapon of choice in the zebra hunt. On a first presentation of mild cyanosis, sepsis is the charging rhinoceros of preventable harm that will run you over if you are too slow to react. But this child has now had several episodes that have occurred: 1. in multiple settings, 2. with no distress, 3. while the child remained playful, and 4. that were self-limited. That history is incompatible with sepsis, so reflexively ordering a blood culture is an illogical choice. The history should be progressively explored using the differential diagnosis and an organ-based systematic approach to guide it. The thoroughness and thoughtfulness I put into the history taking can be key to finding the correct diagnosis. They also are a means of building trust and rapport with the parents. That will be important later if no definitive diagnosis is found.
Unclear and unusual presentations may merit a consult. The cardiologist knows the limits of an echo. Along with the technical expertise comes a new set of eyes and the additional perspective of a second opinion. It is great when a colleague can tell you that he or she too had a case like this years ago that was never solved, but did resolve on its own.
One advantage of being an office-based pediatrician, with an established relationship with a family over several years and a couple other children, is that parents do value and trust your clinical judgment. As a pediatrician, I know the most common product I sell is reassurance. It is not snake oil. There is a bedside manner in selling it. Put a positive spin on all the negative tests. Indicate that you and the parents can be vigilant in watching for new signs. Instruct the parents to bring the child back if the events are distressing for the child, which could justify more invasive testing. Arrange to recheck the child in the office in a week, then a month, then at the next well visit. Parents know that medicine isn’t perfect. Humans deal with fear and uncertainty better by knowing we aren’t facing the future alone. And that is why even with all this technology, I still lay a stethoscope on every child.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures.

Finding Synchronous Cancers
Up to 6% of patients with head and neck squamous cell carcinoma (SCC) also have synchronous second primary cancers (SPCs). However, the synchronous cancers may be missed in a usual examination that relies on CT and MRI scans.
Related: Complex Malignancies: A Diagnostic and Therapeutic Trilemma
Clinicians from Odense University Hospital in Denmark report on a patient who presented with only tongue pain as a symptom but was found to have 4 SPCs. The CT and MRI results were inconclusive due to artifacts from metal dental fillings. However, a positron emission tomography (PET)-CT scan “easily revealed” the 3 coinciding malignancies because of their increased metabolic activity, the authors say.
Their patient had 4 primary cancers: 1 SCC on the left side of the tongue, 1 in the fold between the tongue and the floor of the mouth (the 2 tumors were near each other but separate entities), a third SCC in the right aryepiglottic fold, and a grade 2 follicular lymphoma diagnosed “by coincidence” in the lymph nodes of the neck.
The 3 SCCs in the upper aerodigestive tract were in line with the concept of field cancerization, the clinicians note. Multiple adjacent but independent tumors in the mucosa may arise from exposure to carcinogens, which can induce dysplastic changes that lead to malignancy. Moreover, although synchronous cancer of the head and neck regions and follicular lymphoma are rare, one of the potential risk factors for follicular lymphoma is smoking, the authors say. Their patient had been a smoker for 56 years.
The authors recommend a “more liberal approach” to examination and a “generous use” of PET-CT for patients with malignancies of the head and neck regions, particularly in patients with obvious risk factors, such as a long history of smoking or alcohol abuse. They add that PET-CT is also a useful tool in assessing tumor dissemination and prognosis of individual carcinomas—an important benefit in planning different treatments.
Source:
Heidemann LN, Johansen J, Larsen SR, Sørensen JA. BMJ Case Rep. 2016;pii: bcr2015214047.
doi: 10.1136/bcr-2015-214047.
Up to 6% of patients with head and neck squamous cell carcinoma (SCC) also have synchronous second primary cancers (SPCs). However, the synchronous cancers may be missed in a usual examination that relies on CT and MRI scans.
Related: Complex Malignancies: A Diagnostic and Therapeutic Trilemma
Clinicians from Odense University Hospital in Denmark report on a patient who presented with only tongue pain as a symptom but was found to have 4 SPCs. The CT and MRI results were inconclusive due to artifacts from metal dental fillings. However, a positron emission tomography (PET)-CT scan “easily revealed” the 3 coinciding malignancies because of their increased metabolic activity, the authors say.
Their patient had 4 primary cancers: 1 SCC on the left side of the tongue, 1 in the fold between the tongue and the floor of the mouth (the 2 tumors were near each other but separate entities), a third SCC in the right aryepiglottic fold, and a grade 2 follicular lymphoma diagnosed “by coincidence” in the lymph nodes of the neck.
The 3 SCCs in the upper aerodigestive tract were in line with the concept of field cancerization, the clinicians note. Multiple adjacent but independent tumors in the mucosa may arise from exposure to carcinogens, which can induce dysplastic changes that lead to malignancy. Moreover, although synchronous cancer of the head and neck regions and follicular lymphoma are rare, one of the potential risk factors for follicular lymphoma is smoking, the authors say. Their patient had been a smoker for 56 years.
The authors recommend a “more liberal approach” to examination and a “generous use” of PET-CT for patients with malignancies of the head and neck regions, particularly in patients with obvious risk factors, such as a long history of smoking or alcohol abuse. They add that PET-CT is also a useful tool in assessing tumor dissemination and prognosis of individual carcinomas—an important benefit in planning different treatments.
Source:
Heidemann LN, Johansen J, Larsen SR, Sørensen JA. BMJ Case Rep. 2016;pii: bcr2015214047.
doi: 10.1136/bcr-2015-214047.
Up to 6% of patients with head and neck squamous cell carcinoma (SCC) also have synchronous second primary cancers (SPCs). However, the synchronous cancers may be missed in a usual examination that relies on CT and MRI scans.
Related: Complex Malignancies: A Diagnostic and Therapeutic Trilemma
Clinicians from Odense University Hospital in Denmark report on a patient who presented with only tongue pain as a symptom but was found to have 4 SPCs. The CT and MRI results were inconclusive due to artifacts from metal dental fillings. However, a positron emission tomography (PET)-CT scan “easily revealed” the 3 coinciding malignancies because of their increased metabolic activity, the authors say.
Their patient had 4 primary cancers: 1 SCC on the left side of the tongue, 1 in the fold between the tongue and the floor of the mouth (the 2 tumors were near each other but separate entities), a third SCC in the right aryepiglottic fold, and a grade 2 follicular lymphoma diagnosed “by coincidence” in the lymph nodes of the neck.
The 3 SCCs in the upper aerodigestive tract were in line with the concept of field cancerization, the clinicians note. Multiple adjacent but independent tumors in the mucosa may arise from exposure to carcinogens, which can induce dysplastic changes that lead to malignancy. Moreover, although synchronous cancer of the head and neck regions and follicular lymphoma are rare, one of the potential risk factors for follicular lymphoma is smoking, the authors say. Their patient had been a smoker for 56 years.
The authors recommend a “more liberal approach” to examination and a “generous use” of PET-CT for patients with malignancies of the head and neck regions, particularly in patients with obvious risk factors, such as a long history of smoking or alcohol abuse. They add that PET-CT is also a useful tool in assessing tumor dissemination and prognosis of individual carcinomas—an important benefit in planning different treatments.
Source:
Heidemann LN, Johansen J, Larsen SR, Sørensen JA. BMJ Case Rep. 2016;pii: bcr2015214047.
doi: 10.1136/bcr-2015-214047.
The promise of peanut allergy prevention lies in draft guidelines
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.

“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.
“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.
Updated guidelines from the National Institute of Allergy and Infectious Diseases for the early introduction of peanut-containing foods to children at increased risk for peanut allergies are on the horizon, pending final approval.
“Two studies recently showed that infants at high risk of developing peanut allergy [infants with egg allergy and or severe eczema] were much less likely to have peanut allergy at age 5 years if they were able to incorporate peanut regularly into the diet between 4 and 11 months of age,” said Dr. Scott H. Sicherer, the Elliot and Roslyn Jaffe Professor of Pediatrics, Allergy and Immunology, and chief of the division of allergy and immunology in the department of pediatrics at the Icahn School of Medicine at Mount Sinai, New York.
“However, adding peanut to the diet at this age requires caution because these infants may already be allergic to peanut, and so allergy testing and care in adding peanut to the diet with medical supervision is needed in this high-risk group,” noted Dr. Sicherer, a member of the expert panel that worked on the guidelines.
The draft guidelines include 43 clinical recommendations for the diagnosis and management of food allergies in children, according to the NIAID website. In particular, the draft guidelines recommend introducing peanut-containing foods to infants aged 4-6 months who are at increased risk for peanut allergy because of severe eczema and/or egg allergies, after an evaluation with skin prick testing or peanut-specific IgE testing.
“Peanut allergy is relatively common and often persistent, and so a strategy that could prevent the allergy is very important,” Dr. Sicherer said in an interview. “However, peanut can be a choking hazard as peanuts or peanut butter, and so families should talk to their pediatrician about how and when to incorporate peanut into the diet, and whether allergy testing and referral to an allergist is needed.”
Support for the guidelines comes from several large studies with promising results, notably the LEAP (Learning Early about Peanut Allergy) trial. A recent extension of that study, known as LEAP-On (Persistence of Oral Tolerance to Peanut), showed that regular consumption of peanut-containing foods from infancy to 5 years provided ongoing protection against allergies, even 6 years after peanut consumption was discontinued for a 1-year period in 550 children (N Eng J Med. 2016 Apr 14;374:1435-43).
In the original LEAP study, 640 infants aged 4-11 months with severe eczema, egg allergy, or both were randomized to dietary peanut consumption or avoidance (N Engl J Med. 2015 Feb 26;372[9]:803-13). The prevalence of peanut allergy at 5 years of age was approximately 2% in the peanut-consumption group, compared with 14% in the peanut-avoidance group.
Another significant randomized trial, the EAT study (Enquiring About Tolerance) tested not only peanut, but also the early introduction of cooked egg, cow’s milk, sesame, wheat, and fish to 1,303 infants aged 3 months and older in the general population. The study’s strict protocol made adherence difficult, but researchers found a significant 67% reduction in the prevalence of food allergies at age 3 years among the children who followed the protocol, compared with controls, with relative risk reductions of 100% and 75%, respectively, for peanut and egg allergies (N Engl J Med. 2016 May 5;374:1733-43).
The next steps for research should make early introduction of peanut-containing foods even more effective at allergy prevention, Dr. Sicherer noted.
“We need to learn more about how much peanut should be incorporated into the diet, how long the protein has to be kept in the diet to have the best preventative effect, and whether this strategy applies to other foods,” he said.

Acalabrutinib shows efficacy as monotherapy in untreated CLL
CHICAGO – Acalabrutinib, which has shown efficacy in relapsed chronic lymphocytic leukemia, has now shown efficacy as a monotherapy for patients with previously untreated CLL, based on results from an ongoing phase I-II study presented as a poster at the annual meeting of the American Society of Clinical Oncology.
In a 74-patient study, best overall response rate was 96%, and median time to response was 2 months. CLL has not progressed in any of the patients, and none have experienced Richter’s transformation, Dr. John C. Byrd, the D. Warren Brown Chair of Leukemia Research at The Ohio State University, Columbus, and his colleagues reported. Based on its favorable safety profile and durable response rates, a phase III trialof acalabrutinib therapy has been initiated (NCT02475681).
Oral acalabrutinib was given at doses of 100 mg twice daily to 37 patients or 200 mg daily to 37 other patients. About half of the patients had bulky lymph nodes of at least 5 cm and 38 of 67 patients had an unmutated IGHV gene. Median time on the study was 11 months.
All patients had rapid declines in lymphadenopathy. Both dose schedules were associated with clinical activity, with Bruton’s tyrosine kinase occupancy highest at 98% with twice-daily dosing and 93% with once-daily dosing. Treatment-related lymphocytosis occurred in 39 of 74 patients and resolved in 38 of the 39. In general, lymphocytosis peaked at a median of 1 week and resolved by a median of 7 weeks.
Acalabrutinib was well tolerated with 72 of 74 patients continuing on the drug. Most adverse events were grade 2 or less, and included headache (42%), diarrhea (35%), arthralgia (22%), contusion (18%), nausea (18%) and increased weight (18%). Grade 3-4 adverse events that occurred in at least two patients included syncope (two patients) and hypertension (two patients). There was one grade 3 upper GI bleed from a gastric ulcer and aspirin use, and one grade 5 case of pneumonia. No atrial fibrillation was reported.
Dr. Byrd receives research funding from Acerta Pharma, the maker of acalabrutinib, as well as from Genentech and Pharmacyclics.
On Twitter @maryjodales
CHICAGO – Acalabrutinib, which has shown efficacy in relapsed chronic lymphocytic leukemia, has now shown efficacy as a monotherapy for patients with previously untreated CLL, based on results from an ongoing phase I-II study presented as a poster at the annual meeting of the American Society of Clinical Oncology.
In a 74-patient study, best overall response rate was 96%, and median time to response was 2 months. CLL has not progressed in any of the patients, and none have experienced Richter’s transformation, Dr. John C. Byrd, the D. Warren Brown Chair of Leukemia Research at The Ohio State University, Columbus, and his colleagues reported. Based on its favorable safety profile and durable response rates, a phase III trialof acalabrutinib therapy has been initiated (NCT02475681).
Oral acalabrutinib was given at doses of 100 mg twice daily to 37 patients or 200 mg daily to 37 other patients. About half of the patients had bulky lymph nodes of at least 5 cm and 38 of 67 patients had an unmutated IGHV gene. Median time on the study was 11 months.
All patients had rapid declines in lymphadenopathy. Both dose schedules were associated with clinical activity, with Bruton’s tyrosine kinase occupancy highest at 98% with twice-daily dosing and 93% with once-daily dosing. Treatment-related lymphocytosis occurred in 39 of 74 patients and resolved in 38 of the 39. In general, lymphocytosis peaked at a median of 1 week and resolved by a median of 7 weeks.
Acalabrutinib was well tolerated with 72 of 74 patients continuing on the drug. Most adverse events were grade 2 or less, and included headache (42%), diarrhea (35%), arthralgia (22%), contusion (18%), nausea (18%) and increased weight (18%). Grade 3-4 adverse events that occurred in at least two patients included syncope (two patients) and hypertension (two patients). There was one grade 3 upper GI bleed from a gastric ulcer and aspirin use, and one grade 5 case of pneumonia. No atrial fibrillation was reported.
Dr. Byrd receives research funding from Acerta Pharma, the maker of acalabrutinib, as well as from Genentech and Pharmacyclics.
On Twitter @maryjodales
CHICAGO – Acalabrutinib, which has shown efficacy in relapsed chronic lymphocytic leukemia, has now shown efficacy as a monotherapy for patients with previously untreated CLL, based on results from an ongoing phase I-II study presented as a poster at the annual meeting of the American Society of Clinical Oncology.
In a 74-patient study, best overall response rate was 96%, and median time to response was 2 months. CLL has not progressed in any of the patients, and none have experienced Richter’s transformation, Dr. John C. Byrd, the D. Warren Brown Chair of Leukemia Research at The Ohio State University, Columbus, and his colleagues reported. Based on its favorable safety profile and durable response rates, a phase III trialof acalabrutinib therapy has been initiated (NCT02475681).
Oral acalabrutinib was given at doses of 100 mg twice daily to 37 patients or 200 mg daily to 37 other patients. About half of the patients had bulky lymph nodes of at least 5 cm and 38 of 67 patients had an unmutated IGHV gene. Median time on the study was 11 months.
All patients had rapid declines in lymphadenopathy. Both dose schedules were associated with clinical activity, with Bruton’s tyrosine kinase occupancy highest at 98% with twice-daily dosing and 93% with once-daily dosing. Treatment-related lymphocytosis occurred in 39 of 74 patients and resolved in 38 of the 39. In general, lymphocytosis peaked at a median of 1 week and resolved by a median of 7 weeks.
Acalabrutinib was well tolerated with 72 of 74 patients continuing on the drug. Most adverse events were grade 2 or less, and included headache (42%), diarrhea (35%), arthralgia (22%), contusion (18%), nausea (18%) and increased weight (18%). Grade 3-4 adverse events that occurred in at least two patients included syncope (two patients) and hypertension (two patients). There was one grade 3 upper GI bleed from a gastric ulcer and aspirin use, and one grade 5 case of pneumonia. No atrial fibrillation was reported.
Dr. Byrd receives research funding from Acerta Pharma, the maker of acalabrutinib, as well as from Genentech and Pharmacyclics.
On Twitter @maryjodales
FROM 2016 ASCO ANNUAL MEETING
Key clinical point: Acalabrutinib, which has shown efficacy in relapsed CLL, has now shown efficacy as a monotherapy for patients with previously untreated CLL.
Major finding: In a 74-patient study, best overall response rate was 96%, and median time to response was 2 months.
Data source: An ongoing phase I-II study.
Disclosures: Dr. Byrd receives research funding from Acerta Pharma, the maker of acalabrutinib, as well as from Genentech and Pharmacyclics.
Interim PET-CT can spare HL patients intensive chemo

The use of interim PET-CT scans can spare some advanced Hodgkin lymphoma (HL) patients the toxicity associated with bleomycin, according to researchers.
The team found that patients with negative PET-CT scans after 2 cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) could go on to receive AVD (doxorubicin, vinblastine, and dacarbazine) without experiencing a significant decrease in progression-free survival (PFS) or overall survival (OS).
Peter Johnson, MD, of the University of Southampton in the UK, and his colleagues reported these findings in NEJM.
“The good news is that the majority of people diagnosed with Hodgkin lymphoma can be cured,” Dr Johnson said. “In this trial, more than 95% of patients are alive after 3 years.”
“But we worry about the long-term side effects from the treatments we use. As we’ve done in this trial, personalizing treatment based on how well it works is a major development for patients with Hodgkin lymphoma and sets a new standard of care.”
Patients and treatment
For this study, Dr Johnson and his colleagues enrolled 1214 patients with newly diagnosed, advanced, classic HL. The patients’ median age was 33 (range, 18 to 79), and 54.5% were male. More patients had stage II disease (41.6%) than stage III (30.2%) or IV (28.3%).
A total of 1119 patients underwent a baseline PET-CT scan, received 2 cycles of ABVD, and underwent an interim PET-CT scan.
The patients with negative interim scans were then randomized to continue treatment with ABVD (n=470) or with AVD (n=465) in cycles 3 through 6.
Patients with positive interim scans (n=182) went on to receive BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, n=172), salvage treatments (n=6), or ABVD (n=4).
Results
The study’s primary outcome was the difference in 3-year PFS between the randomized groups of PET-CT-negative patients.
With a median follow-up of 41 months, the 3-year PFS was 85.7% in the ABVD group and 84.4% in the AVD group. The hazard ratio was 1.13 (95% CI, 0.81 to 1.57; P=0.48) in the intention-to-treat analysis and 1.10 (95% CI, 0.79 to 1.53; P=0.58) in the per-protocol analysis.
The absolute difference in 3-year PFS (ABVD minus AVD) was 1.6 percentage points (95% CI, −3.2 to 5.3).
The OS rates were 97.2% in the ABVD group and 97.6% in the AVD group. The hazard ratio in the intention-to-treat analysis was 0.90 (95% CI, 0.47 to 1.74; P=0.76).
Patients in the ABVD group had a significantly higher rate of clinical adverse events than patients in the AVD group—31% and 21%, respectively (P<0.005).
Patients in the ABVD group also had significantly (P<0.05) higher rates of fatigue (3% vs 1%), febrile neutropenia (5% vs 2%), pulmonary/upper respiratory events (3% vs 1%), and dyspnea (2% vs <0.5%). But patients in the AVD group had a significantly higher rate of thrombocytopenia (3% vs 1%).
For patients who had positive interim PET-CT scans, the 3-year PFS was 67.5%, and the OS was 87.8%. Among the 172 patients who went on to receive BEACOPP, 74.4% had negative findings on a third PET-CT scan.
Overall, 62 patients died during the trial—24 from HL. So, for the entire study cohort, the 3-year PFS was 82.6%, and the OS was 95.8%. ![]()
The use of interim PET-CT scans can spare some advanced Hodgkin lymphoma (HL) patients the toxicity associated with bleomycin, according to researchers.
The team found that patients with negative PET-CT scans after 2 cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) could go on to receive AVD (doxorubicin, vinblastine, and dacarbazine) without experiencing a significant decrease in progression-free survival (PFS) or overall survival (OS).
Peter Johnson, MD, of the University of Southampton in the UK, and his colleagues reported these findings in NEJM.
“The good news is that the majority of people diagnosed with Hodgkin lymphoma can be cured,” Dr Johnson said. “In this trial, more than 95% of patients are alive after 3 years.”
“But we worry about the long-term side effects from the treatments we use. As we’ve done in this trial, personalizing treatment based on how well it works is a major development for patients with Hodgkin lymphoma and sets a new standard of care.”
Patients and treatment
For this study, Dr Johnson and his colleagues enrolled 1214 patients with newly diagnosed, advanced, classic HL. The patients’ median age was 33 (range, 18 to 79), and 54.5% were male. More patients had stage II disease (41.6%) than stage III (30.2%) or IV (28.3%).
A total of 1119 patients underwent a baseline PET-CT scan, received 2 cycles of ABVD, and underwent an interim PET-CT scan.
The patients with negative interim scans were then randomized to continue treatment with ABVD (n=470) or with AVD (n=465) in cycles 3 through 6.
Patients with positive interim scans (n=182) went on to receive BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, n=172), salvage treatments (n=6), or ABVD (n=4).
Results
The study’s primary outcome was the difference in 3-year PFS between the randomized groups of PET-CT-negative patients.
With a median follow-up of 41 months, the 3-year PFS was 85.7% in the ABVD group and 84.4% in the AVD group. The hazard ratio was 1.13 (95% CI, 0.81 to 1.57; P=0.48) in the intention-to-treat analysis and 1.10 (95% CI, 0.79 to 1.53; P=0.58) in the per-protocol analysis.
The absolute difference in 3-year PFS (ABVD minus AVD) was 1.6 percentage points (95% CI, −3.2 to 5.3).
The OS rates were 97.2% in the ABVD group and 97.6% in the AVD group. The hazard ratio in the intention-to-treat analysis was 0.90 (95% CI, 0.47 to 1.74; P=0.76).
Patients in the ABVD group had a significantly higher rate of clinical adverse events than patients in the AVD group—31% and 21%, respectively (P<0.005).
Patients in the ABVD group also had significantly (P<0.05) higher rates of fatigue (3% vs 1%), febrile neutropenia (5% vs 2%), pulmonary/upper respiratory events (3% vs 1%), and dyspnea (2% vs <0.5%). But patients in the AVD group had a significantly higher rate of thrombocytopenia (3% vs 1%).
For patients who had positive interim PET-CT scans, the 3-year PFS was 67.5%, and the OS was 87.8%. Among the 172 patients who went on to receive BEACOPP, 74.4% had negative findings on a third PET-CT scan.
Overall, 62 patients died during the trial—24 from HL. So, for the entire study cohort, the 3-year PFS was 82.6%, and the OS was 95.8%. ![]()
The use of interim PET-CT scans can spare some advanced Hodgkin lymphoma (HL) patients the toxicity associated with bleomycin, according to researchers.
The team found that patients with negative PET-CT scans after 2 cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) could go on to receive AVD (doxorubicin, vinblastine, and dacarbazine) without experiencing a significant decrease in progression-free survival (PFS) or overall survival (OS).
Peter Johnson, MD, of the University of Southampton in the UK, and his colleagues reported these findings in NEJM.
“The good news is that the majority of people diagnosed with Hodgkin lymphoma can be cured,” Dr Johnson said. “In this trial, more than 95% of patients are alive after 3 years.”
“But we worry about the long-term side effects from the treatments we use. As we’ve done in this trial, personalizing treatment based on how well it works is a major development for patients with Hodgkin lymphoma and sets a new standard of care.”
Patients and treatment
For this study, Dr Johnson and his colleagues enrolled 1214 patients with newly diagnosed, advanced, classic HL. The patients’ median age was 33 (range, 18 to 79), and 54.5% were male. More patients had stage II disease (41.6%) than stage III (30.2%) or IV (28.3%).
A total of 1119 patients underwent a baseline PET-CT scan, received 2 cycles of ABVD, and underwent an interim PET-CT scan.
The patients with negative interim scans were then randomized to continue treatment with ABVD (n=470) or with AVD (n=465) in cycles 3 through 6.
Patients with positive interim scans (n=182) went on to receive BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone, n=172), salvage treatments (n=6), or ABVD (n=4).
Results
The study’s primary outcome was the difference in 3-year PFS between the randomized groups of PET-CT-negative patients.
With a median follow-up of 41 months, the 3-year PFS was 85.7% in the ABVD group and 84.4% in the AVD group. The hazard ratio was 1.13 (95% CI, 0.81 to 1.57; P=0.48) in the intention-to-treat analysis and 1.10 (95% CI, 0.79 to 1.53; P=0.58) in the per-protocol analysis.
The absolute difference in 3-year PFS (ABVD minus AVD) was 1.6 percentage points (95% CI, −3.2 to 5.3).
The OS rates were 97.2% in the ABVD group and 97.6% in the AVD group. The hazard ratio in the intention-to-treat analysis was 0.90 (95% CI, 0.47 to 1.74; P=0.76).
Patients in the ABVD group had a significantly higher rate of clinical adverse events than patients in the AVD group—31% and 21%, respectively (P<0.005).
Patients in the ABVD group also had significantly (P<0.05) higher rates of fatigue (3% vs 1%), febrile neutropenia (5% vs 2%), pulmonary/upper respiratory events (3% vs 1%), and dyspnea (2% vs <0.5%). But patients in the AVD group had a significantly higher rate of thrombocytopenia (3% vs 1%).
For patients who had positive interim PET-CT scans, the 3-year PFS was 67.5%, and the OS was 87.8%. Among the 172 patients who went on to receive BEACOPP, 74.4% had negative findings on a third PET-CT scan.
Overall, 62 patients died during the trial—24 from HL. So, for the entire study cohort, the 3-year PFS was 82.6%, and the OS was 95.8%. ![]()
SHM SPARK Helps Bridge Gap for Hospitalist MOC Exam Prep

SHM SPARK delivers 175 vignette-style, multiple-choice questions that bridge the primary knowledge gaps found within existing MOC exam-preparation products. It offers up to 10.5 AMA PRA Category 1 Credits of CME. Content areas covered include:
- Palliative care, ethics, and decision making
- Patient safety
- Perioperative care and consultative co-management
- Quality, cost, and clinical reasoning
The Hospitalist recently spoke with three SHM SPARK users about its impact on their exam-preparation efforts: Louis O’Boyle, DO, SFHM, CLHM, medical director of Advanced Inpatient Medicine, a hospitalist management company in Lakeville, Pa.; Timothy Crone, MD, SFHM, medical director of Enterprise Intelligence and Analytics and former vice-chairman of the Department of Hospital Medicine at Cleveland Clinic; and Aroop Pal, MD, FHM, hospitalist, associate professor, and program director of transitions of care services at University of Kansas Medical Center.
Question: Why did you choose to purchase SHM SPARK?
Dr. O’Boyle: I was expecting the FPHM exam to be more challenging than the traditional exam, so I wanted to get as much help as possible, particularly in those areas that are less utilized in day-to-day hospitalist practice. This exam covered the 40% or so that is not covered in a typical review course.
Dr. Crone: I was selected to receive SHM SPARK as a test user, but had I not been, I probably would have purchased it as there was not another single tool that addressed the content gap preparing for the exam that SHM SPARK did. On HMX and in conversations with other hospitalists, I was aware of “collections” of tools, like books and websites, that people had put together to review information not covered in MKSAP or other standard test-prep materials. SHM SPARK brought that content together in a single space, which allowed me to take a systematic approach to reviewing the content areas covered as opposed to a potentially incomplete, piecemeal approach.
Dr. Pal: There are no board review products focused on the 40% of the FPHM exam not based on traditional clinical knowledge. Thus, it made sense to give SHM SPARK a try, especially since it was affordable for members.
Q: During your preparation, what was the most useful aspect of SHM SPARK?
Dr. Crone: I find that working through computer-based questions similar in format to the actual exam is most helpful to me. Both in terms of knowledge acquisition and comfort level with the exam itself, the “context-dependent learning” aspect is important for me. SHM SPARK allowed me to work through its content areas in that way and also helped me identify and correct gaps in my knowledge as opposed to guessing what was important and searching for source material on my own.
Dr. Pal: SHM SPARK helped frame how quality and patient safety questions would or could be posed on the FPHM exam. This made it helpful to determine what content is fair game for the exam and the key competencies ABIM was focusing on—especially since traditional board review materials do not cover as much quality-specific content.
Dr. O’Boyle: The most useful aspects were the topics that are not encountered specifically in everyday practice, such as the sections on quality, cost, and clinical reasoning, as well as patient safety.
Q: After taking the exam, in retrospect, how effective was SHM SPARK in preparing you?
Dr. Pal: SHM SPARK was valuable to me and worth the time and effort. The board exam itself is a little bit of a blur; if nothing else, it helped me identify areas that I needed more information on and reinforced some knowledge I had prior to taking the exam.
Dr. O’Boyle: The SHM SPARK review absolutely helped me perform well on the sections that were covered. I think it is almost essential to prepare for the Focused Practice in Hospital Medicine exam.
Dr. Crone: I passed, so I’d label that effective! In some cases, using SHM SPARK, I scored 90% or better on a first pass on questions with no review; that has not been my experience with MKSAP or Med Study questions. The only recommendation I would have is to make some of the questions a bit more rigorous. However, SHM SPARK clearly met a need nothing else did.
Q: If you were to tell a fellow hospitalist one thing about SHM SPARK, what would it be?
Dr. O’Boyle: I encourage everyone to purchase it. It is an excellent resource guide. The way the exam is currently designed, you may need the additional 40% of exam content covered by SHM SPARK in order to pass. By that, I mean that some of the medical questions were so complicated and cumbersome that they were at the specialist level and not at all representative of what a typical hospitalist routinely encounters, in my opinion. Therefore, knowing this portion of the exam content through SHM SPARK made up for the questions that I felt should not have been fair game. I, for one, would likely not have passed without SHM SPARK.
Dr. Crone: It’s worth the time, effort, and cost. Although much or most of the exam content was couched in a clinical scenario, substantive content existed on the MOC exam around these subject areas. To not use some form of structured approach to covering this material would have been a mistake.
Dr. Pal: SHM SPARK is extremely valuable if you plan to take the FPHM exam as it highlights many areas not covered by any other review material. It offers great CME, too! TH
Brett Radler is SHM’s communications specialist.
More Info
For more information about how SHM SPARK can help you master your preparation for the FPHM MOC exam this fall, visit www.hospitalmedicine.org/SPARK.
SHM SPARK delivers 175 vignette-style, multiple-choice questions that bridge the primary knowledge gaps found within existing MOC exam-preparation products. It offers up to 10.5 AMA PRA Category 1 Credits of CME. Content areas covered include:
- Palliative care, ethics, and decision making
- Patient safety
- Perioperative care and consultative co-management
- Quality, cost, and clinical reasoning
The Hospitalist recently spoke with three SHM SPARK users about its impact on their exam-preparation efforts: Louis O’Boyle, DO, SFHM, CLHM, medical director of Advanced Inpatient Medicine, a hospitalist management company in Lakeville, Pa.; Timothy Crone, MD, SFHM, medical director of Enterprise Intelligence and Analytics and former vice-chairman of the Department of Hospital Medicine at Cleveland Clinic; and Aroop Pal, MD, FHM, hospitalist, associate professor, and program director of transitions of care services at University of Kansas Medical Center.
Question: Why did you choose to purchase SHM SPARK?
Dr. O’Boyle: I was expecting the FPHM exam to be more challenging than the traditional exam, so I wanted to get as much help as possible, particularly in those areas that are less utilized in day-to-day hospitalist practice. This exam covered the 40% or so that is not covered in a typical review course.
Dr. Crone: I was selected to receive SHM SPARK as a test user, but had I not been, I probably would have purchased it as there was not another single tool that addressed the content gap preparing for the exam that SHM SPARK did. On HMX and in conversations with other hospitalists, I was aware of “collections” of tools, like books and websites, that people had put together to review information not covered in MKSAP or other standard test-prep materials. SHM SPARK brought that content together in a single space, which allowed me to take a systematic approach to reviewing the content areas covered as opposed to a potentially incomplete, piecemeal approach.
Dr. Pal: There are no board review products focused on the 40% of the FPHM exam not based on traditional clinical knowledge. Thus, it made sense to give SHM SPARK a try, especially since it was affordable for members.
Q: During your preparation, what was the most useful aspect of SHM SPARK?
Dr. Crone: I find that working through computer-based questions similar in format to the actual exam is most helpful to me. Both in terms of knowledge acquisition and comfort level with the exam itself, the “context-dependent learning” aspect is important for me. SHM SPARK allowed me to work through its content areas in that way and also helped me identify and correct gaps in my knowledge as opposed to guessing what was important and searching for source material on my own.
Dr. Pal: SHM SPARK helped frame how quality and patient safety questions would or could be posed on the FPHM exam. This made it helpful to determine what content is fair game for the exam and the key competencies ABIM was focusing on—especially since traditional board review materials do not cover as much quality-specific content.
Dr. O’Boyle: The most useful aspects were the topics that are not encountered specifically in everyday practice, such as the sections on quality, cost, and clinical reasoning, as well as patient safety.
Q: After taking the exam, in retrospect, how effective was SHM SPARK in preparing you?
Dr. Pal: SHM SPARK was valuable to me and worth the time and effort. The board exam itself is a little bit of a blur; if nothing else, it helped me identify areas that I needed more information on and reinforced some knowledge I had prior to taking the exam.
Dr. O’Boyle: The SHM SPARK review absolutely helped me perform well on the sections that were covered. I think it is almost essential to prepare for the Focused Practice in Hospital Medicine exam.
Dr. Crone: I passed, so I’d label that effective! In some cases, using SHM SPARK, I scored 90% or better on a first pass on questions with no review; that has not been my experience with MKSAP or Med Study questions. The only recommendation I would have is to make some of the questions a bit more rigorous. However, SHM SPARK clearly met a need nothing else did.
Q: If you were to tell a fellow hospitalist one thing about SHM SPARK, what would it be?
Dr. O’Boyle: I encourage everyone to purchase it. It is an excellent resource guide. The way the exam is currently designed, you may need the additional 40% of exam content covered by SHM SPARK in order to pass. By that, I mean that some of the medical questions were so complicated and cumbersome that they were at the specialist level and not at all representative of what a typical hospitalist routinely encounters, in my opinion. Therefore, knowing this portion of the exam content through SHM SPARK made up for the questions that I felt should not have been fair game. I, for one, would likely not have passed without SHM SPARK.
Dr. Crone: It’s worth the time, effort, and cost. Although much or most of the exam content was couched in a clinical scenario, substantive content existed on the MOC exam around these subject areas. To not use some form of structured approach to covering this material would have been a mistake.
Dr. Pal: SHM SPARK is extremely valuable if you plan to take the FPHM exam as it highlights many areas not covered by any other review material. It offers great CME, too! TH
Brett Radler is SHM’s communications specialist.
More Info
For more information about how SHM SPARK can help you master your preparation for the FPHM MOC exam this fall, visit www.hospitalmedicine.org/SPARK.
SHM SPARK delivers 175 vignette-style, multiple-choice questions that bridge the primary knowledge gaps found within existing MOC exam-preparation products. It offers up to 10.5 AMA PRA Category 1 Credits of CME. Content areas covered include:
- Palliative care, ethics, and decision making
- Patient safety
- Perioperative care and consultative co-management
- Quality, cost, and clinical reasoning
The Hospitalist recently spoke with three SHM SPARK users about its impact on their exam-preparation efforts: Louis O’Boyle, DO, SFHM, CLHM, medical director of Advanced Inpatient Medicine, a hospitalist management company in Lakeville, Pa.; Timothy Crone, MD, SFHM, medical director of Enterprise Intelligence and Analytics and former vice-chairman of the Department of Hospital Medicine at Cleveland Clinic; and Aroop Pal, MD, FHM, hospitalist, associate professor, and program director of transitions of care services at University of Kansas Medical Center.
Question: Why did you choose to purchase SHM SPARK?
Dr. O’Boyle: I was expecting the FPHM exam to be more challenging than the traditional exam, so I wanted to get as much help as possible, particularly in those areas that are less utilized in day-to-day hospitalist practice. This exam covered the 40% or so that is not covered in a typical review course.
Dr. Crone: I was selected to receive SHM SPARK as a test user, but had I not been, I probably would have purchased it as there was not another single tool that addressed the content gap preparing for the exam that SHM SPARK did. On HMX and in conversations with other hospitalists, I was aware of “collections” of tools, like books and websites, that people had put together to review information not covered in MKSAP or other standard test-prep materials. SHM SPARK brought that content together in a single space, which allowed me to take a systematic approach to reviewing the content areas covered as opposed to a potentially incomplete, piecemeal approach.
Dr. Pal: There are no board review products focused on the 40% of the FPHM exam not based on traditional clinical knowledge. Thus, it made sense to give SHM SPARK a try, especially since it was affordable for members.
Q: During your preparation, what was the most useful aspect of SHM SPARK?
Dr. Crone: I find that working through computer-based questions similar in format to the actual exam is most helpful to me. Both in terms of knowledge acquisition and comfort level with the exam itself, the “context-dependent learning” aspect is important for me. SHM SPARK allowed me to work through its content areas in that way and also helped me identify and correct gaps in my knowledge as opposed to guessing what was important and searching for source material on my own.
Dr. Pal: SHM SPARK helped frame how quality and patient safety questions would or could be posed on the FPHM exam. This made it helpful to determine what content is fair game for the exam and the key competencies ABIM was focusing on—especially since traditional board review materials do not cover as much quality-specific content.
Dr. O’Boyle: The most useful aspects were the topics that are not encountered specifically in everyday practice, such as the sections on quality, cost, and clinical reasoning, as well as patient safety.
Q: After taking the exam, in retrospect, how effective was SHM SPARK in preparing you?
Dr. Pal: SHM SPARK was valuable to me and worth the time and effort. The board exam itself is a little bit of a blur; if nothing else, it helped me identify areas that I needed more information on and reinforced some knowledge I had prior to taking the exam.
Dr. O’Boyle: The SHM SPARK review absolutely helped me perform well on the sections that were covered. I think it is almost essential to prepare for the Focused Practice in Hospital Medicine exam.
Dr. Crone: I passed, so I’d label that effective! In some cases, using SHM SPARK, I scored 90% or better on a first pass on questions with no review; that has not been my experience with MKSAP or Med Study questions. The only recommendation I would have is to make some of the questions a bit more rigorous. However, SHM SPARK clearly met a need nothing else did.
Q: If you were to tell a fellow hospitalist one thing about SHM SPARK, what would it be?
Dr. O’Boyle: I encourage everyone to purchase it. It is an excellent resource guide. The way the exam is currently designed, you may need the additional 40% of exam content covered by SHM SPARK in order to pass. By that, I mean that some of the medical questions were so complicated and cumbersome that they were at the specialist level and not at all representative of what a typical hospitalist routinely encounters, in my opinion. Therefore, knowing this portion of the exam content through SHM SPARK made up for the questions that I felt should not have been fair game. I, for one, would likely not have passed without SHM SPARK.
Dr. Crone: It’s worth the time, effort, and cost. Although much or most of the exam content was couched in a clinical scenario, substantive content existed on the MOC exam around these subject areas. To not use some form of structured approach to covering this material would have been a mistake.
Dr. Pal: SHM SPARK is extremely valuable if you plan to take the FPHM exam as it highlights many areas not covered by any other review material. It offers great CME, too! TH
Brett Radler is SHM’s communications specialist.
More Info
For more information about how SHM SPARK can help you master your preparation for the FPHM MOC exam this fall, visit www.hospitalmedicine.org/SPARK.

Measure Hospitalist Engagement with SHM’s Engagement Benchmarking Service
One of the most important questions for leaders of hospital medicine groups is, “How can I measure the level of engagement of my hospitalists?” Measuring hospitalist engagement can be difficult, and many leaders are not satisfied with the tools they currently have at their disposal.
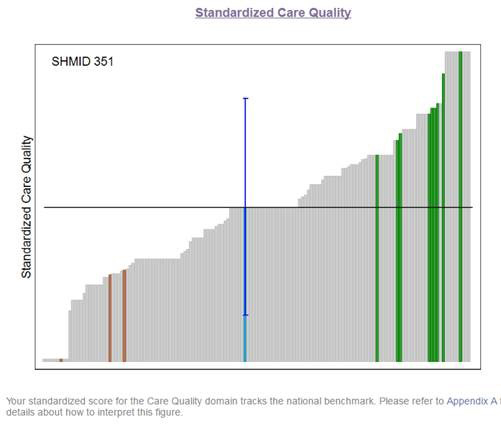
SHM is here to help. SHM developed an Engagement Benchmarking Service to evaluate relationships with leaders, care quality, autonomy, effective motivation, burnout risk, and more. You can see your standardized score in the various domains and where it falls within the national benchmark. This helps you know what is working well and identifies the areas for improvement in your hospital medicine group.
More than 80% of respondents from 2015 indicated that they will utilize the service again and plan to recommend it to a colleague. Help ensure hospitalists are engaged in your HM group by registering now for the next cohort at www.hospitalmedicine.org/pmad3.
One of the most important questions for leaders of hospital medicine groups is, “How can I measure the level of engagement of my hospitalists?” Measuring hospitalist engagement can be difficult, and many leaders are not satisfied with the tools they currently have at their disposal.
SHM is here to help. SHM developed an Engagement Benchmarking Service to evaluate relationships with leaders, care quality, autonomy, effective motivation, burnout risk, and more. You can see your standardized score in the various domains and where it falls within the national benchmark. This helps you know what is working well and identifies the areas for improvement in your hospital medicine group.
More than 80% of respondents from 2015 indicated that they will utilize the service again and plan to recommend it to a colleague. Help ensure hospitalists are engaged in your HM group by registering now for the next cohort at www.hospitalmedicine.org/pmad3.
One of the most important questions for leaders of hospital medicine groups is, “How can I measure the level of engagement of my hospitalists?” Measuring hospitalist engagement can be difficult, and many leaders are not satisfied with the tools they currently have at their disposal.
SHM is here to help. SHM developed an Engagement Benchmarking Service to evaluate relationships with leaders, care quality, autonomy, effective motivation, burnout risk, and more. You can see your standardized score in the various domains and where it falls within the national benchmark. This helps you know what is working well and identifies the areas for improvement in your hospital medicine group.
More than 80% of respondents from 2015 indicated that they will utilize the service again and plan to recommend it to a colleague. Help ensure hospitalists are engaged in your HM group by registering now for the next cohort at www.hospitalmedicine.org/pmad3.
Stopping TKI therapy can be safe, study suggests

COPENHAGEN—Results of a large study suggest that stopping treatment with tyrosine kinase inhibitors (TKIs) can be safe for patients with chronic myeloid leukemia (CML) in deep molecular response (MR4).
Six months after patients stopped receiving a TKI, the relapse-free survival was 62%. At 12 months, it was 56%.
Havinga longer duration of TKI treatment and a longer duration of deep molecular response were both associated with a higher likelihood of relapse-free survival.
These results, from the EURO-SKI trial, were presented at the 21st Congress of the European Hematology Association (abstract S145*) by Johan Richter, MD, PhD, of Skåne University Hospital in Lund, Sweden.
The goal of the EURO-SKI study was to define prognostic markers to increase the proportion of patients in durable deep molecular response after stopping TKI treatment.
The trial included 760 adults with chronic phase CML who were on TKI treatment for at least 3 years. Patients were either on their first TKI or on their second TKI due to toxicity with their first. (None had failed TKI treatment.)
Patients had been in MR4 (BCR/ABL <0.01%) for at least a year, which was confirmed by 3 consecutive polymerase chain reaction (PCR) results during the last 12 months. The final MR4 confirmation was performed in a EUTOS standardized laboratory.
After the final MR4 confirmation, patients stopped TKI treatment. They underwent real-time quantitative PCR (RQ-PCR) every 4 weeks for the first 6 months and every 6 weeks for the next 6 months. In years 2 and 3, they underwent RQ-PCR every third month.
The patients had a median age at diagnosis of 52 (range, 11.2-85.5) and a median age at TKI stop of 60.3 (range, 19.5-89.9). The median duration of TKI therapy was 7.6 years (range, 3.0-14.2), and the median duration of MR4 before TKI stop was 4.7 years (range, 1.0-13.3).
Most patients had received imatinib (n=710) as first-line TKI treatment, though some received nilotinib (n=35) or dasatinib (n=14). The type of first-line TKI was unknown in 1 patient. Second-line TKI treatment included imatinib (n=7), nilotinib (n=47), and dasatinib (n=57).
Relapse, survival, and safety
Six months after stopping TKI treatment, the cumulative incidence of molecular relapse was 37%. It was 43% at 12 months, 47% at 24 months, and 50% at 36 months.
In all, 347 patients had a molecular relapse. Seventy-two patients had BCR/ABL >1%, and 11 lost their complete cytogenetic response. None of the patients progressed to accelerated phase or blast crisis.
Among patients who restarted TKI treatment, the median time to restart was 4.1 months. Fourteen patients restarted treatment without a loss of major molecular response.
Dr Richter noted that the study is still ongoing, but, thus far, more than 80% of patients who restarted TKI therapy have achieved MR4 again.
The molecular relapse-free survival was 62% at 6 months after TKI stop, 56% at 12 months, 52% at 24 months, and 49% at 36 months.
There were 9 on-trial deaths, none of which were related to CML. Five patients died while in remission.
Previous studies revealed a TKI withdrawal syndrome that consists of (mostly transient) musculoskeletal pain or discomfort. In this study, 30.9% of patients (n=235) reported musculoskeletal symptoms, 226 with grade 1-2 events and 9 with grade 3 events.
Prognostic factors
The researchers performed prognostic modeling in 448 patients who previously received imatinib. Univariate analysis revealed no significant association between molecular relapse-free survival at 6 months and age, gender, depth of molecular response, Sokal score, EURO score, EUTOS score, or ELTS score.
However, TKI treatment duration and MR4 duration were both significantly (P<0.001) associated with major molecular response status at 6 months.
The odds ratio for treatment duration was 1.16 (95% CI, 1.08-1.25), which means that an additional year of imatinib treatment increases a patient’s odds of staying in major molecular response at 6 months by 16%.
The odds ratio for MR4 duration was also 1.16 (95% CI, 1.076-1.253), which means that an additional year in MR4 before TKI stop increases a patient’s odds of staying in major molecular response at 6 months by 16%.
Dr Richter noted that treatment duration and MR4 duration were highly correlated, which prevented a significant multiple model including both variables. He said the researchers will conduct further analyses to overcome the correlation between the 2 variables and determine an optimal cutoff for MR4 duration.
The team also plans to collect more data on pretreatment with interferon, as there is reason to suspect it has an influence on major molecular response duration after TKI discontinuation. ![]()
*Data in the abstract differ from data presented at the meeting.
COPENHAGEN—Results of a large study suggest that stopping treatment with tyrosine kinase inhibitors (TKIs) can be safe for patients with chronic myeloid leukemia (CML) in deep molecular response (MR4).
Six months after patients stopped receiving a TKI, the relapse-free survival was 62%. At 12 months, it was 56%.
Havinga longer duration of TKI treatment and a longer duration of deep molecular response were both associated with a higher likelihood of relapse-free survival.
These results, from the EURO-SKI trial, were presented at the 21st Congress of the European Hematology Association (abstract S145*) by Johan Richter, MD, PhD, of Skåne University Hospital in Lund, Sweden.
The goal of the EURO-SKI study was to define prognostic markers to increase the proportion of patients in durable deep molecular response after stopping TKI treatment.
The trial included 760 adults with chronic phase CML who were on TKI treatment for at least 3 years. Patients were either on their first TKI or on their second TKI due to toxicity with their first. (None had failed TKI treatment.)
Patients had been in MR4 (BCR/ABL <0.01%) for at least a year, which was confirmed by 3 consecutive polymerase chain reaction (PCR) results during the last 12 months. The final MR4 confirmation was performed in a EUTOS standardized laboratory.
After the final MR4 confirmation, patients stopped TKI treatment. They underwent real-time quantitative PCR (RQ-PCR) every 4 weeks for the first 6 months and every 6 weeks for the next 6 months. In years 2 and 3, they underwent RQ-PCR every third month.
The patients had a median age at diagnosis of 52 (range, 11.2-85.5) and a median age at TKI stop of 60.3 (range, 19.5-89.9). The median duration of TKI therapy was 7.6 years (range, 3.0-14.2), and the median duration of MR4 before TKI stop was 4.7 years (range, 1.0-13.3).
Most patients had received imatinib (n=710) as first-line TKI treatment, though some received nilotinib (n=35) or dasatinib (n=14). The type of first-line TKI was unknown in 1 patient. Second-line TKI treatment included imatinib (n=7), nilotinib (n=47), and dasatinib (n=57).
Relapse, survival, and safety
Six months after stopping TKI treatment, the cumulative incidence of molecular relapse was 37%. It was 43% at 12 months, 47% at 24 months, and 50% at 36 months.
In all, 347 patients had a molecular relapse. Seventy-two patients had BCR/ABL >1%, and 11 lost their complete cytogenetic response. None of the patients progressed to accelerated phase or blast crisis.
Among patients who restarted TKI treatment, the median time to restart was 4.1 months. Fourteen patients restarted treatment without a loss of major molecular response.
Dr Richter noted that the study is still ongoing, but, thus far, more than 80% of patients who restarted TKI therapy have achieved MR4 again.
The molecular relapse-free survival was 62% at 6 months after TKI stop, 56% at 12 months, 52% at 24 months, and 49% at 36 months.
There were 9 on-trial deaths, none of which were related to CML. Five patients died while in remission.
Previous studies revealed a TKI withdrawal syndrome that consists of (mostly transient) musculoskeletal pain or discomfort. In this study, 30.9% of patients (n=235) reported musculoskeletal symptoms, 226 with grade 1-2 events and 9 with grade 3 events.
Prognostic factors
The researchers performed prognostic modeling in 448 patients who previously received imatinib. Univariate analysis revealed no significant association between molecular relapse-free survival at 6 months and age, gender, depth of molecular response, Sokal score, EURO score, EUTOS score, or ELTS score.
However, TKI treatment duration and MR4 duration were both significantly (P<0.001) associated with major molecular response status at 6 months.
The odds ratio for treatment duration was 1.16 (95% CI, 1.08-1.25), which means that an additional year of imatinib treatment increases a patient’s odds of staying in major molecular response at 6 months by 16%.
The odds ratio for MR4 duration was also 1.16 (95% CI, 1.076-1.253), which means that an additional year in MR4 before TKI stop increases a patient’s odds of staying in major molecular response at 6 months by 16%.
Dr Richter noted that treatment duration and MR4 duration were highly correlated, which prevented a significant multiple model including both variables. He said the researchers will conduct further analyses to overcome the correlation between the 2 variables and determine an optimal cutoff for MR4 duration.
The team also plans to collect more data on pretreatment with interferon, as there is reason to suspect it has an influence on major molecular response duration after TKI discontinuation. ![]()
*Data in the abstract differ from data presented at the meeting.
COPENHAGEN—Results of a large study suggest that stopping treatment with tyrosine kinase inhibitors (TKIs) can be safe for patients with chronic myeloid leukemia (CML) in deep molecular response (MR4).
Six months after patients stopped receiving a TKI, the relapse-free survival was 62%. At 12 months, it was 56%.
Havinga longer duration of TKI treatment and a longer duration of deep molecular response were both associated with a higher likelihood of relapse-free survival.
These results, from the EURO-SKI trial, were presented at the 21st Congress of the European Hematology Association (abstract S145*) by Johan Richter, MD, PhD, of Skåne University Hospital in Lund, Sweden.
The goal of the EURO-SKI study was to define prognostic markers to increase the proportion of patients in durable deep molecular response after stopping TKI treatment.
The trial included 760 adults with chronic phase CML who were on TKI treatment for at least 3 years. Patients were either on their first TKI or on their second TKI due to toxicity with their first. (None had failed TKI treatment.)
Patients had been in MR4 (BCR/ABL <0.01%) for at least a year, which was confirmed by 3 consecutive polymerase chain reaction (PCR) results during the last 12 months. The final MR4 confirmation was performed in a EUTOS standardized laboratory.
After the final MR4 confirmation, patients stopped TKI treatment. They underwent real-time quantitative PCR (RQ-PCR) every 4 weeks for the first 6 months and every 6 weeks for the next 6 months. In years 2 and 3, they underwent RQ-PCR every third month.
The patients had a median age at diagnosis of 52 (range, 11.2-85.5) and a median age at TKI stop of 60.3 (range, 19.5-89.9). The median duration of TKI therapy was 7.6 years (range, 3.0-14.2), and the median duration of MR4 before TKI stop was 4.7 years (range, 1.0-13.3).
Most patients had received imatinib (n=710) as first-line TKI treatment, though some received nilotinib (n=35) or dasatinib (n=14). The type of first-line TKI was unknown in 1 patient. Second-line TKI treatment included imatinib (n=7), nilotinib (n=47), and dasatinib (n=57).
Relapse, survival, and safety
Six months after stopping TKI treatment, the cumulative incidence of molecular relapse was 37%. It was 43% at 12 months, 47% at 24 months, and 50% at 36 months.
In all, 347 patients had a molecular relapse. Seventy-two patients had BCR/ABL >1%, and 11 lost their complete cytogenetic response. None of the patients progressed to accelerated phase or blast crisis.
Among patients who restarted TKI treatment, the median time to restart was 4.1 months. Fourteen patients restarted treatment without a loss of major molecular response.
Dr Richter noted that the study is still ongoing, but, thus far, more than 80% of patients who restarted TKI therapy have achieved MR4 again.
The molecular relapse-free survival was 62% at 6 months after TKI stop, 56% at 12 months, 52% at 24 months, and 49% at 36 months.
There were 9 on-trial deaths, none of which were related to CML. Five patients died while in remission.
Previous studies revealed a TKI withdrawal syndrome that consists of (mostly transient) musculoskeletal pain or discomfort. In this study, 30.9% of patients (n=235) reported musculoskeletal symptoms, 226 with grade 1-2 events and 9 with grade 3 events.
Prognostic factors
The researchers performed prognostic modeling in 448 patients who previously received imatinib. Univariate analysis revealed no significant association between molecular relapse-free survival at 6 months and age, gender, depth of molecular response, Sokal score, EURO score, EUTOS score, or ELTS score.
However, TKI treatment duration and MR4 duration were both significantly (P<0.001) associated with major molecular response status at 6 months.
The odds ratio for treatment duration was 1.16 (95% CI, 1.08-1.25), which means that an additional year of imatinib treatment increases a patient’s odds of staying in major molecular response at 6 months by 16%.
The odds ratio for MR4 duration was also 1.16 (95% CI, 1.076-1.253), which means that an additional year in MR4 before TKI stop increases a patient’s odds of staying in major molecular response at 6 months by 16%.
Dr Richter noted that treatment duration and MR4 duration were highly correlated, which prevented a significant multiple model including both variables. He said the researchers will conduct further analyses to overcome the correlation between the 2 variables and determine an optimal cutoff for MR4 duration.
The team also plans to collect more data on pretreatment with interferon, as there is reason to suspect it has an influence on major molecular response duration after TKI discontinuation. ![]()
*Data in the abstract differ from data presented at the meeting.
Therapy granted fast track designation to treat GVHD
![]()
Photo by Chad McNeeley
The US Food and Drug Administration (FDA) has granted fast track designation for ProTmune™, a programmed cellular immunotherapy, to reduce the incidence and severity of acute graft-versus-host disease (GVHD) in patients undergoing allogeneic hematopoietic stem cell transplant (HSCT).
ProTmune is produced by modulating a donor-sourced, mobilized peripheral blood (mPB) graft ex vivo with 2 small molecules (FT1050 and FT4145) to enhance the biological properties and therapeutic function of the graft’s immune cells.
The programmed mPB graft is adoptively transferred and administered to a patient as a one-time intravenous infusion.
ProTmune is being developed by Fate Therapeutics, Inc.
The company is conducting a phase 1/2 trial testing ProTmune for the prevention of acute GVHD and cytomegalovirus infection in adults with hematologic malignancies who are undergoing HSCT.
The trial design consists of an initial 10-subject, phase 1 stage, during which all subjects undergoing allogeneic mPB HSCT will receive ProTmune.
Following an independent data monitoring committee safety review, a 60-subject, randomized, controlled phase 2 stage is expected to begin. In this stage, subjects undergoing allogeneic mPB HSCT will be assigned to receive either ProTmune or a conventional mPB cell graft in a 1:1 ratio.
About fast track designation
The FDA’s fast track program is designed to facilitate and expedite the development and review of new drugs intended to treat serious or life-threatening conditions and address unmet medical need.
Through the fast track program, a product may be eligible for priority review. In addition, the company developing the drug may be allowed to submit sections of the biologic license application or new drug application on a rolling basis as data become available.
Fast track designation also provides the company with opportunities for more frequent meetings with the FDA to discuss the drug’s development plan and ensure collection of the appropriate data needed to support drug approval. And the designation allows for more frequent written communication from the FDA about things such as the design of proposed clinical trials and the use of biomarkers. ![]()
![]()
Photo by Chad McNeeley
The US Food and Drug Administration (FDA) has granted fast track designation for ProTmune™, a programmed cellular immunotherapy, to reduce the incidence and severity of acute graft-versus-host disease (GVHD) in patients undergoing allogeneic hematopoietic stem cell transplant (HSCT).
ProTmune is produced by modulating a donor-sourced, mobilized peripheral blood (mPB) graft ex vivo with 2 small molecules (FT1050 and FT4145) to enhance the biological properties and therapeutic function of the graft’s immune cells.
The programmed mPB graft is adoptively transferred and administered to a patient as a one-time intravenous infusion.
ProTmune is being developed by Fate Therapeutics, Inc.
The company is conducting a phase 1/2 trial testing ProTmune for the prevention of acute GVHD and cytomegalovirus infection in adults with hematologic malignancies who are undergoing HSCT.
The trial design consists of an initial 10-subject, phase 1 stage, during which all subjects undergoing allogeneic mPB HSCT will receive ProTmune.
Following an independent data monitoring committee safety review, a 60-subject, randomized, controlled phase 2 stage is expected to begin. In this stage, subjects undergoing allogeneic mPB HSCT will be assigned to receive either ProTmune or a conventional mPB cell graft in a 1:1 ratio.
About fast track designation
The FDA’s fast track program is designed to facilitate and expedite the development and review of new drugs intended to treat serious or life-threatening conditions and address unmet medical need.
Through the fast track program, a product may be eligible for priority review. In addition, the company developing the drug may be allowed to submit sections of the biologic license application or new drug application on a rolling basis as data become available.
Fast track designation also provides the company with opportunities for more frequent meetings with the FDA to discuss the drug’s development plan and ensure collection of the appropriate data needed to support drug approval. And the designation allows for more frequent written communication from the FDA about things such as the design of proposed clinical trials and the use of biomarkers. ![]()
![]()
Photo by Chad McNeeley
The US Food and Drug Administration (FDA) has granted fast track designation for ProTmune™, a programmed cellular immunotherapy, to reduce the incidence and severity of acute graft-versus-host disease (GVHD) in patients undergoing allogeneic hematopoietic stem cell transplant (HSCT).
ProTmune is produced by modulating a donor-sourced, mobilized peripheral blood (mPB) graft ex vivo with 2 small molecules (FT1050 and FT4145) to enhance the biological properties and therapeutic function of the graft’s immune cells.
The programmed mPB graft is adoptively transferred and administered to a patient as a one-time intravenous infusion.
ProTmune is being developed by Fate Therapeutics, Inc.
The company is conducting a phase 1/2 trial testing ProTmune for the prevention of acute GVHD and cytomegalovirus infection in adults with hematologic malignancies who are undergoing HSCT.
The trial design consists of an initial 10-subject, phase 1 stage, during which all subjects undergoing allogeneic mPB HSCT will receive ProTmune.
Following an independent data monitoring committee safety review, a 60-subject, randomized, controlled phase 2 stage is expected to begin. In this stage, subjects undergoing allogeneic mPB HSCT will be assigned to receive either ProTmune or a conventional mPB cell graft in a 1:1 ratio.
About fast track designation
The FDA’s fast track program is designed to facilitate and expedite the development and review of new drugs intended to treat serious or life-threatening conditions and address unmet medical need.
Through the fast track program, a product may be eligible for priority review. In addition, the company developing the drug may be allowed to submit sections of the biologic license application or new drug application on a rolling basis as data become available.
Fast track designation also provides the company with opportunities for more frequent meetings with the FDA to discuss the drug’s development plan and ensure collection of the appropriate data needed to support drug approval. And the designation allows for more frequent written communication from the FDA about things such as the design of proposed clinical trials and the use of biomarkers. ![]()
A new approach to treat AML?

Preclinical research suggests that activating the STING pathway may be a feasible approach for treating acute myeloid leukemia (AML).
The STING protein has been shown to play a crucial role in the immune system’s ability to “sense” cancer by recognizing and responding to DNA from tumor cells.
In past studies, researchers injected compounds that activate the STING pathway directly into solid tumors in mice, and this produced potent anti-tumor immune responses.
In a new study, researchers injected substances that mimic tumor-cell DNA into the bloodstream and found they could stimulate STING to provoke a life-extending immune response in mice with AML.
“Delivery of these substances into the blood led to massive immune responses,” said study author Justin Kline, MD, of the University of Chicago in Illinois.
“I’ve worked extensively with animal models of this disease, and have never seen responses like this.”
This research, published in Cell Reports, is the first demonstration that activating the STING pathway could be effective in hematologic malignancies.
STING (short for STimulator of INterferon Genes) plays a role in detecting threats, such as viral infections or cancer. STING is activated when DNA turns up in the wrong place, inside the cell but outside the nucleus.
When it encounters such misplaced DNA, STING induces the production of interferon-beta and other chemical signals that recruit certain components of the immune system to manage the threat, such as leukemia-specific killer T cells.
In this study, the researchers found that mice with established AML were rarely able to launch an effective immune response against the disease.
But when the team exposed the mice to DMXAA (5,6-dimethylxanthenone-4-acetic acid), a molecule that activates STING, the immune system responded aggressively, culminating in the activation of highly potent, cancer-cell killing T cells.
This response prolonged survival and, in some cases, cured the mice of their leukemia. About 60% of DMXAA-treated mice survived long-term. They were even able to protect themselves when “re-challenged” with AML cells.
Because of significant differences between mice and humans, DMXAA does not activate the human STING pathway, but researchers have found that several cyclic dinucleotides—signaling molecules produced by bacteria—have a comparable effect in stimulating the STING pathway.
This leads to an immune response that begins with the production of type I interferons and proceeds to later, more powerful stages, ultimately including leukemia-specific T cells.
“Our results provide strong rationale for the clinical translation of STING agonists as immune therapy for leukemia and possibly other hematologic
malignancies,” said study author Emily Curran, MD, of the University of Chicago.
However, Dr Kline noted that this approach is “not without risk.” He said it can induce “a lot of inflammation, fever, even shock.” Such a stimulated immune system can be “too effective,” especially when the therapy is given through the blood stream, rather than injected into a solid tumor.
“I think drug makers will want to focus on intra-tumoral injection studies before they are ready to bet on systemic infusion,” Dr Kline said. “But this is an important first step.” ![]()
Preclinical research suggests that activating the STING pathway may be a feasible approach for treating acute myeloid leukemia (AML).
The STING protein has been shown to play a crucial role in the immune system’s ability to “sense” cancer by recognizing and responding to DNA from tumor cells.
In past studies, researchers injected compounds that activate the STING pathway directly into solid tumors in mice, and this produced potent anti-tumor immune responses.
In a new study, researchers injected substances that mimic tumor-cell DNA into the bloodstream and found they could stimulate STING to provoke a life-extending immune response in mice with AML.
“Delivery of these substances into the blood led to massive immune responses,” said study author Justin Kline, MD, of the University of Chicago in Illinois.
“I’ve worked extensively with animal models of this disease, and have never seen responses like this.”
This research, published in Cell Reports, is the first demonstration that activating the STING pathway could be effective in hematologic malignancies.
STING (short for STimulator of INterferon Genes) plays a role in detecting threats, such as viral infections or cancer. STING is activated when DNA turns up in the wrong place, inside the cell but outside the nucleus.
When it encounters such misplaced DNA, STING induces the production of interferon-beta and other chemical signals that recruit certain components of the immune system to manage the threat, such as leukemia-specific killer T cells.
In this study, the researchers found that mice with established AML were rarely able to launch an effective immune response against the disease.
But when the team exposed the mice to DMXAA (5,6-dimethylxanthenone-4-acetic acid), a molecule that activates STING, the immune system responded aggressively, culminating in the activation of highly potent, cancer-cell killing T cells.
This response prolonged survival and, in some cases, cured the mice of their leukemia. About 60% of DMXAA-treated mice survived long-term. They were even able to protect themselves when “re-challenged” with AML cells.
Because of significant differences between mice and humans, DMXAA does not activate the human STING pathway, but researchers have found that several cyclic dinucleotides—signaling molecules produced by bacteria—have a comparable effect in stimulating the STING pathway.
This leads to an immune response that begins with the production of type I interferons and proceeds to later, more powerful stages, ultimately including leukemia-specific T cells.
“Our results provide strong rationale for the clinical translation of STING agonists as immune therapy for leukemia and possibly other hematologic
malignancies,” said study author Emily Curran, MD, of the University of Chicago.
However, Dr Kline noted that this approach is “not without risk.” He said it can induce “a lot of inflammation, fever, even shock.” Such a stimulated immune system can be “too effective,” especially when the therapy is given through the blood stream, rather than injected into a solid tumor.
“I think drug makers will want to focus on intra-tumoral injection studies before they are ready to bet on systemic infusion,” Dr Kline said. “But this is an important first step.” ![]()
Preclinical research suggests that activating the STING pathway may be a feasible approach for treating acute myeloid leukemia (AML).
The STING protein has been shown to play a crucial role in the immune system’s ability to “sense” cancer by recognizing and responding to DNA from tumor cells.
In past studies, researchers injected compounds that activate the STING pathway directly into solid tumors in mice, and this produced potent anti-tumor immune responses.
In a new study, researchers injected substances that mimic tumor-cell DNA into the bloodstream and found they could stimulate STING to provoke a life-extending immune response in mice with AML.
“Delivery of these substances into the blood led to massive immune responses,” said study author Justin Kline, MD, of the University of Chicago in Illinois.
“I’ve worked extensively with animal models of this disease, and have never seen responses like this.”
This research, published in Cell Reports, is the first demonstration that activating the STING pathway could be effective in hematologic malignancies.
STING (short for STimulator of INterferon Genes) plays a role in detecting threats, such as viral infections or cancer. STING is activated when DNA turns up in the wrong place, inside the cell but outside the nucleus.
When it encounters such misplaced DNA, STING induces the production of interferon-beta and other chemical signals that recruit certain components of the immune system to manage the threat, such as leukemia-specific killer T cells.
In this study, the researchers found that mice with established AML were rarely able to launch an effective immune response against the disease.
But when the team exposed the mice to DMXAA (5,6-dimethylxanthenone-4-acetic acid), a molecule that activates STING, the immune system responded aggressively, culminating in the activation of highly potent, cancer-cell killing T cells.
This response prolonged survival and, in some cases, cured the mice of their leukemia. About 60% of DMXAA-treated mice survived long-term. They were even able to protect themselves when “re-challenged” with AML cells.
Because of significant differences between mice and humans, DMXAA does not activate the human STING pathway, but researchers have found that several cyclic dinucleotides—signaling molecules produced by bacteria—have a comparable effect in stimulating the STING pathway.
This leads to an immune response that begins with the production of type I interferons and proceeds to later, more powerful stages, ultimately including leukemia-specific T cells.
“Our results provide strong rationale for the clinical translation of STING agonists as immune therapy for leukemia and possibly other hematologic
malignancies,” said study author Emily Curran, MD, of the University of Chicago.
However, Dr Kline noted that this approach is “not without risk.” He said it can induce “a lot of inflammation, fever, even shock.” Such a stimulated immune system can be “too effective,” especially when the therapy is given through the blood stream, rather than injected into a solid tumor.
“I think drug makers will want to focus on intra-tumoral injection studies before they are ready to bet on systemic infusion,” Dr Kline said. “But this is an important first step.” ![]()