User login
The Cruise With No Snooze
ANSWER
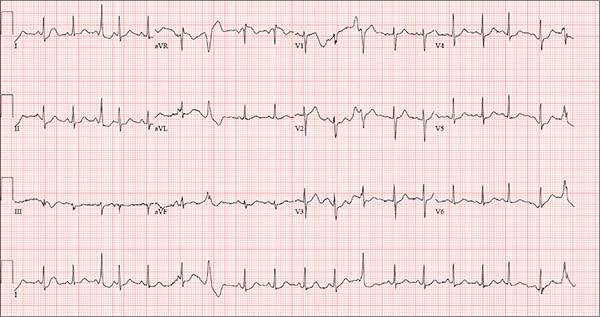
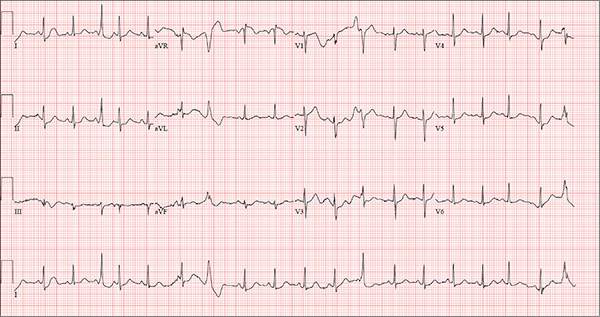
The correct interpretation of this ECG includes sinus tachycardia with premature supraventricular complexes, some with aberrant conduction.
The first, third, fourth, and 17th beats on lead I at the bottom of the rhythm strip are consistent with premature atrial contractions (PACs), while the sixth, seventh, 12th, and 19th beats represent PACs with aberrancy. The change in the QRS complex in the latter is due to the delay through the conduction system.
This patient was treated with low-dose ß-blockers and instructed to discontinue use of his holistic medication. His symptoms resolved, and follow-up ECGs have shown no evidence of sinus tachycardia or PACs.
ANSWER
The correct interpretation of this ECG includes sinus tachycardia with premature supraventricular complexes, some with aberrant conduction.
The first, third, fourth, and 17th beats on lead I at the bottom of the rhythm strip are consistent with premature atrial contractions (PACs), while the sixth, seventh, 12th, and 19th beats represent PACs with aberrancy. The change in the QRS complex in the latter is due to the delay through the conduction system.
This patient was treated with low-dose ß-blockers and instructed to discontinue use of his holistic medication. His symptoms resolved, and follow-up ECGs have shown no evidence of sinus tachycardia or PACs.
ANSWER
The correct interpretation of this ECG includes sinus tachycardia with premature supraventricular complexes, some with aberrant conduction.
The first, third, fourth, and 17th beats on lead I at the bottom of the rhythm strip are consistent with premature atrial contractions (PACs), while the sixth, seventh, 12th, and 19th beats represent PACs with aberrancy. The change in the QRS complex in the latter is due to the delay through the conduction system.
This patient was treated with low-dose ß-blockers and instructed to discontinue use of his holistic medication. His symptoms resolved, and follow-up ECGs have shown no evidence of sinus tachycardia or PACs.
Three weeks ago, while on a Caribbean cruise with his family, a 55-year-old man started experiencing an irregular heart rate, fluttering in his chest, and fullness in his throat. At the time, he was eating to excess, drinking heavily, and consuming three to five cups of coffee each morning to shake off the effects of the previous night. The palpitations were not noticeable during the day but were prevalent at night, when he tried to sleep. On more than one occasion, they woke him.
Since his return home, the symptoms have persisted; they now occur nightly. The patient is so concerned about them that he dreads going to bed. He has lost the 13 lb he gained on vacation and has abstained from alcohol, but he continues to drink four to six cups of coffee per day.
He denies syncope, near-syncope, chest pain, shortness of breath, and exertional dyspnea. On presentation, he is anxious to determine the cause of his symptoms and alleviate them.
The patient describes himself as active; he says he watches his diet, exercises regularly, and has never smoked. His medical history is unremarkable. He has never had surgery, and aside from sprained ankles, has had no medical treatment. His alcohol consumption, which tends to be limited to weekends, consists of four or five highballs at a time.
He is not currently taking any prescription medications, but he does admit to taking a proprietary herbal supplement that he purchases from a local Asian market. He says it “increases energy and libido.” He denies illicit drug use, now or ever.
The patient is married with three teenaged children who are all in the gifted program in high school. He and his wife are both accountants. His parents have no known medical problems; however, he is uncertain about the medical history of his grandparents.
A review of systems is unremarkable and reveals no complaints. The physical exam reveals an anxious male in no distress. His weight is 179 lb and his height, 74 in. Vital signs include a blood pressure of 140/86 mm Hg; pulse, 120 beats/min; respiratory rate, 14 breaths/min-1; and temperature, 98.2°F.
The HEENT exam is remarkable for contacts but is otherwise normal. There is no thyromegaly or jugular venous distention. His lungs are clear in all fields, and there are no wheezes.
His cardiac exam reveals an irregular rhythm at a rate of 120 beats/min. There are no appreciable murmurs or rubs, given his heart rate.
The abdomen is soft and nontender, with no palpable masses. The peripheral pulses are strong bilaterally in the upper and lower extremities, and the neurologic exam is normal.
Bloodwork is performed to assess blood chemistries, complete blood count, and thyroid and liver function. All results are within normal limits. An ECG shows a ventricular rate of 123 beats/min; PR interval, 128 ms; QRS duration, 72 ms; QT/QTc interval, 308/440 ms; P axis, 43°; R axis, –2°; and T axis, 46°.
What is your interpretation of this ECG?
Altered Mental Status Demands Closer Look
Answer
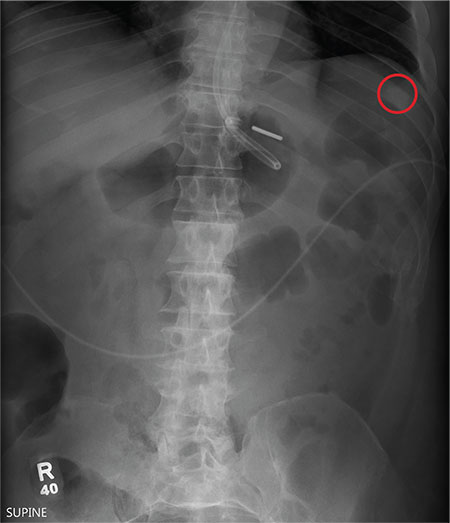
The radiograph demonstrates a normal gas pattern with a properly placed enteric feeding tube, which appears to be within the stomach. Of note is a sclerotic-appearing lesion on the posterior aspect of the left eighth rib. In a patient with a possible tumor, this lesion poses concern for potential metastasis and warrants appropriate work-up.
Answer
The radiograph demonstrates a normal gas pattern with a properly placed enteric feeding tube, which appears to be within the stomach. Of note is a sclerotic-appearing lesion on the posterior aspect of the left eighth rib. In a patient with a possible tumor, this lesion poses concern for potential metastasis and warrants appropriate work-up.
Answer
The radiograph demonstrates a normal gas pattern with a properly placed enteric feeding tube, which appears to be within the stomach. Of note is a sclerotic-appearing lesion on the posterior aspect of the left eighth rib. In a patient with a possible tumor, this lesion poses concern for potential metastasis and warrants appropriate work-up.

You receive a call from an ICU nurse regarding a patient your service is following—a 60-year-old man who was admitted for altered mental status and is being worked up for a possible brain mass. He has no other significant medical history. The nurse has placed a nasogastric feeding tube to facilitate nutrition and medication administration and has ordered a portable abdominal radiograph to confirm its placement. The completed radiograph is shown. What is your impression?

If at First You Don’t Succeed … Don’t Just Treat Again
ANSWER
Punch biopsy (choice “d”) is the correct answer for one simple reason: Correct diagnosis dictates correct treatment. What we’re missing is a diagnosis we can rely on.
DISCUSSION
This case demonstrates a major difference in outlook between the generalist and the specialist. The former is more interested in treating the problem, while the latter first wants to know what the problem is, then tailors the treatment to that problem and/or reassures the patient of the problem’s benign nature.
Had these lesions been of fungal origin, terbinafine would have had a positive effect. Furthermore, fungal infections are caused by organisms that only affect the outer layer of skin and create scaling, which was notably missing in this case.
Round to oval lesions suggest a number of diagnostic possibilities, only one of which is fungal (dermatophytosis). Others include T-cell lymphoma, psoriasis (though its lesions are almost always scaly), sarcoidosis, Hansen disease, lupus, and lichen planus. In cases like this one, these options need to be sorted through—and the only sure way to do that is with biopsy.
This patient’s biopsy showed a palisaded granulomatous process consistent with granuloma annulare (GA), a very commonly diagnosed benign condition. Since there are no ideal treatments for GA, he opted to do nothing, although he agreed to present for a biannual check-up. He was happy just to rule out all the things he didn’t have and thereby reduce his worries.
ANSWER
Punch biopsy (choice “d”) is the correct answer for one simple reason: Correct diagnosis dictates correct treatment. What we’re missing is a diagnosis we can rely on.
DISCUSSION
This case demonstrates a major difference in outlook between the generalist and the specialist. The former is more interested in treating the problem, while the latter first wants to know what the problem is, then tailors the treatment to that problem and/or reassures the patient of the problem’s benign nature.
Had these lesions been of fungal origin, terbinafine would have had a positive effect. Furthermore, fungal infections are caused by organisms that only affect the outer layer of skin and create scaling, which was notably missing in this case.
Round to oval lesions suggest a number of diagnostic possibilities, only one of which is fungal (dermatophytosis). Others include T-cell lymphoma, psoriasis (though its lesions are almost always scaly), sarcoidosis, Hansen disease, lupus, and lichen planus. In cases like this one, these options need to be sorted through—and the only sure way to do that is with biopsy.
This patient’s biopsy showed a palisaded granulomatous process consistent with granuloma annulare (GA), a very commonly diagnosed benign condition. Since there are no ideal treatments for GA, he opted to do nothing, although he agreed to present for a biannual check-up. He was happy just to rule out all the things he didn’t have and thereby reduce his worries.
ANSWER
Punch biopsy (choice “d”) is the correct answer for one simple reason: Correct diagnosis dictates correct treatment. What we’re missing is a diagnosis we can rely on.
DISCUSSION
This case demonstrates a major difference in outlook between the generalist and the specialist. The former is more interested in treating the problem, while the latter first wants to know what the problem is, then tailors the treatment to that problem and/or reassures the patient of the problem’s benign nature.
Had these lesions been of fungal origin, terbinafine would have had a positive effect. Furthermore, fungal infections are caused by organisms that only affect the outer layer of skin and create scaling, which was notably missing in this case.
Round to oval lesions suggest a number of diagnostic possibilities, only one of which is fungal (dermatophytosis). Others include T-cell lymphoma, psoriasis (though its lesions are almost always scaly), sarcoidosis, Hansen disease, lupus, and lichen planus. In cases like this one, these options need to be sorted through—and the only sure way to do that is with biopsy.
This patient’s biopsy showed a palisaded granulomatous process consistent with granuloma annulare (GA), a very commonly diagnosed benign condition. Since there are no ideal treatments for GA, he opted to do nothing, although he agreed to present for a biannual check-up. He was happy just to rule out all the things he didn’t have and thereby reduce his worries.

A 39-year-old man presents with asymptomatic lesions on both arms. When they manifested about six months ago, the patient diagnosed himself with “ringworm” and began treating them with an OTC clotrimazole cream his pharmacist recommended. Twice-daily application for two weeks did not result in a change, so the patient consulted his primary care provider (PCP), who also thought the problem was fungal. The PCP prescribed oral terbinafine (250 mg/d), which the patient took for a month without improvement. He then requested a referral to dermatology. The patient denies fever, malaise, shortness of breath, or unexplained weight loss. He is not taking any prescription medications. Both medial triceps have almost identical lesions: brownish red and oval, with well-defined margins. The margins are slightly raised relative to the central portions. The lesions, which measure 8 x 10 cm, exhibit no epidermal changes (eg, scale or papularity); they are totally intradermal. The rest of the examination is unremarkable.

Expanding Treatment Options
Q) One of my diabetic patients read about finerenone in The New York Times. Apparently, it’s the “newest cure for albuminuria”! Is this just hype, or do the trials on this medication really show progress against kidney disease? Should I buy stock in the company?
Albuminuria (> 500 mg/d) associated with diabetic nephropathy and other glomerular diseases increases patient risk for chronic kidney disease (CKD) and its progression to end-stage renal disease (ESRD). Reduction of albuminuria has been shown to slow the progression of CKD.
Renin-angiotensin-aldosterone system (RAAS) blockers, such as ACE inhibitors or angiotensin receptor blockers, are considered firstline therapy to reduce albuminuria. Additional treatment modalities include diuretics, nondihydropyridine calcium channel blockers, ß-blockers, and aldosterone antagonist therapy. Limiting dietary sodium helps control blood pressure, thus slowing disease progression. In addition, some studies show that limiting phosphorus and protein (for the latter, intake of no more than 0.7 g/kg ideal body weight per day) may slow the progression of CKD. Unfortunately, despite these interventions, patients may still advance to ESRD.1
The aldosterone and steroidal mineralocorticoid receptor antagonists (MRA) spironolactone and eplerenone have been found to reduce albuminuria when used in conjunction with RAAS blockade. However, patients using this combination are up to eight times more likely to experience hyperkalemia—a serious, potentially life-threatening adverse condition—than those not using an MRA.2 The presence of hyperkalemia requires discontinuation of the RAAS blocker and the MRA, at least temporarily.
Finerenone, a nonsteroidal MRA with “greater receptor selectivity than spironolactone and better receptor affinity than eplerenone in vitro,” is in phase III trials for the treatment of systolic and diastolic dysfunction and reduction of morbidity and mortality associated with heart failure.2 One study has already demonstrated that finerenone (5 to 10 mg/d) is at least as effective as spironolactone (25 mg/d) for heart failure patients.3
The Mineralocorticoid Receptor Antagonist Tolerability Study-Diabetic Nephropathy (ARTS-DN) found that finerenone at 10 to 20 mg/d was superior to spironolactone and eplerenone, partly due to the decreased incidence of hyperkalemia. However, it should be noted that the lower incidence of hyperkalemia may be attributable to the fact that 66% of the study participants had an estimated glomerular filtration rate (eGFR) greater than 60 mL/min and that potential participants with a serum potassium level of more than 4.8 mEq/L were not included in the study.2
Additional research is needed to confirm superiority of finerenone over spironolactone and eplerenone, in conjunction with RAAS blockers, in the treatment of albuminuria and hyperkalemia. Including subjects with lower eGFR (such as patients with stage IV CKD who are at higher risk for hyperkalemia) would give a better indication of finerenone’s efficacy. In the meantime, it’s probably too soon to corner the market on this stock! —SEB
Susan E. Brown, MS, ARNP, ACNP-BC, CCRN
Great River Nephrology, West Burlington, Iowa
References
1. Parikh SV, Haddad NJ, Hebert LA. Retarding progression of kidney disease. In: Johnson RJ, Feehally J, Floege J, eds. Comprehensive Clinical Nephrology. 5th ed. Philadelphia, PA: Saunders; 2015:931-940.
2. Bakris GL, Agarwal R, Chan JC, et al. Effect of finerenone on albuminuria in patients with diabetic nephropathy: a randomized clinical trial. JAMA. 2015;314(9):884-894.
3. Kolkhof P, Delbeck M, Kretschmer A, et al. Finerenone, a novel selective nonsteroidal mineralocorticoid receptor antagonist, protects from rat cardiorenal injury. J Cardiovasc Pharmacol. 2014;64(1):69-78.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired PA who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Christine Corbett, MSN, APRN, FNP-BC, CNN-NP, who practices at Kansas City Veterans Affairs in Kansas City, Missouri, and Susan E. Brown, MS, ARNP, ACNP-BC, CCRN, who practices at Great River Nephrology in West Burlington, Iowa.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired PA who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Christine Corbett, MSN, APRN, FNP-BC, CNN-NP, who practices at Kansas City Veterans Affairs in Kansas City, Missouri, and Susan E. Brown, MS, ARNP, ACNP-BC, CCRN, who practices at Great River Nephrology in West Burlington, Iowa.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired PA who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Christine Corbett, MSN, APRN, FNP-BC, CNN-NP, who practices at Kansas City Veterans Affairs in Kansas City, Missouri, and Susan E. Brown, MS, ARNP, ACNP-BC, CCRN, who practices at Great River Nephrology in West Burlington, Iowa.
Q) One of my diabetic patients read about finerenone in The New York Times. Apparently, it’s the “newest cure for albuminuria”! Is this just hype, or do the trials on this medication really show progress against kidney disease? Should I buy stock in the company?
Albuminuria (> 500 mg/d) associated with diabetic nephropathy and other glomerular diseases increases patient risk for chronic kidney disease (CKD) and its progression to end-stage renal disease (ESRD). Reduction of albuminuria has been shown to slow the progression of CKD.
Renin-angiotensin-aldosterone system (RAAS) blockers, such as ACE inhibitors or angiotensin receptor blockers, are considered firstline therapy to reduce albuminuria. Additional treatment modalities include diuretics, nondihydropyridine calcium channel blockers, ß-blockers, and aldosterone antagonist therapy. Limiting dietary sodium helps control blood pressure, thus slowing disease progression. In addition, some studies show that limiting phosphorus and protein (for the latter, intake of no more than 0.7 g/kg ideal body weight per day) may slow the progression of CKD. Unfortunately, despite these interventions, patients may still advance to ESRD.1
The aldosterone and steroidal mineralocorticoid receptor antagonists (MRA) spironolactone and eplerenone have been found to reduce albuminuria when used in conjunction with RAAS blockade. However, patients using this combination are up to eight times more likely to experience hyperkalemia—a serious, potentially life-threatening adverse condition—than those not using an MRA.2 The presence of hyperkalemia requires discontinuation of the RAAS blocker and the MRA, at least temporarily.
Finerenone, a nonsteroidal MRA with “greater receptor selectivity than spironolactone and better receptor affinity than eplerenone in vitro,” is in phase III trials for the treatment of systolic and diastolic dysfunction and reduction of morbidity and mortality associated with heart failure.2 One study has already demonstrated that finerenone (5 to 10 mg/d) is at least as effective as spironolactone (25 mg/d) for heart failure patients.3
The Mineralocorticoid Receptor Antagonist Tolerability Study-Diabetic Nephropathy (ARTS-DN) found that finerenone at 10 to 20 mg/d was superior to spironolactone and eplerenone, partly due to the decreased incidence of hyperkalemia. However, it should be noted that the lower incidence of hyperkalemia may be attributable to the fact that 66% of the study participants had an estimated glomerular filtration rate (eGFR) greater than 60 mL/min and that potential participants with a serum potassium level of more than 4.8 mEq/L were not included in the study.2
Additional research is needed to confirm superiority of finerenone over spironolactone and eplerenone, in conjunction with RAAS blockers, in the treatment of albuminuria and hyperkalemia. Including subjects with lower eGFR (such as patients with stage IV CKD who are at higher risk for hyperkalemia) would give a better indication of finerenone’s efficacy. In the meantime, it’s probably too soon to corner the market on this stock! —SEB
Susan E. Brown, MS, ARNP, ACNP-BC, CCRN
Great River Nephrology, West Burlington, Iowa
References
1. Parikh SV, Haddad NJ, Hebert LA. Retarding progression of kidney disease. In: Johnson RJ, Feehally J, Floege J, eds. Comprehensive Clinical Nephrology. 5th ed. Philadelphia, PA: Saunders; 2015:931-940.
2. Bakris GL, Agarwal R, Chan JC, et al. Effect of finerenone on albuminuria in patients with diabetic nephropathy: a randomized clinical trial. JAMA. 2015;314(9):884-894.
3. Kolkhof P, Delbeck M, Kretschmer A, et al. Finerenone, a novel selective nonsteroidal mineralocorticoid receptor antagonist, protects from rat cardiorenal injury. J Cardiovasc Pharmacol. 2014;64(1):69-78.
Q) One of my diabetic patients read about finerenone in The New York Times. Apparently, it’s the “newest cure for albuminuria”! Is this just hype, or do the trials on this medication really show progress against kidney disease? Should I buy stock in the company?
Albuminuria (> 500 mg/d) associated with diabetic nephropathy and other glomerular diseases increases patient risk for chronic kidney disease (CKD) and its progression to end-stage renal disease (ESRD). Reduction of albuminuria has been shown to slow the progression of CKD.
Renin-angiotensin-aldosterone system (RAAS) blockers, such as ACE inhibitors or angiotensin receptor blockers, are considered firstline therapy to reduce albuminuria. Additional treatment modalities include diuretics, nondihydropyridine calcium channel blockers, ß-blockers, and aldosterone antagonist therapy. Limiting dietary sodium helps control blood pressure, thus slowing disease progression. In addition, some studies show that limiting phosphorus and protein (for the latter, intake of no more than 0.7 g/kg ideal body weight per day) may slow the progression of CKD. Unfortunately, despite these interventions, patients may still advance to ESRD.1
The aldosterone and steroidal mineralocorticoid receptor antagonists (MRA) spironolactone and eplerenone have been found to reduce albuminuria when used in conjunction with RAAS blockade. However, patients using this combination are up to eight times more likely to experience hyperkalemia—a serious, potentially life-threatening adverse condition—than those not using an MRA.2 The presence of hyperkalemia requires discontinuation of the RAAS blocker and the MRA, at least temporarily.
Finerenone, a nonsteroidal MRA with “greater receptor selectivity than spironolactone and better receptor affinity than eplerenone in vitro,” is in phase III trials for the treatment of systolic and diastolic dysfunction and reduction of morbidity and mortality associated with heart failure.2 One study has already demonstrated that finerenone (5 to 10 mg/d) is at least as effective as spironolactone (25 mg/d) for heart failure patients.3
The Mineralocorticoid Receptor Antagonist Tolerability Study-Diabetic Nephropathy (ARTS-DN) found that finerenone at 10 to 20 mg/d was superior to spironolactone and eplerenone, partly due to the decreased incidence of hyperkalemia. However, it should be noted that the lower incidence of hyperkalemia may be attributable to the fact that 66% of the study participants had an estimated glomerular filtration rate (eGFR) greater than 60 mL/min and that potential participants with a serum potassium level of more than 4.8 mEq/L were not included in the study.2
Additional research is needed to confirm superiority of finerenone over spironolactone and eplerenone, in conjunction with RAAS blockers, in the treatment of albuminuria and hyperkalemia. Including subjects with lower eGFR (such as patients with stage IV CKD who are at higher risk for hyperkalemia) would give a better indication of finerenone’s efficacy. In the meantime, it’s probably too soon to corner the market on this stock! —SEB
Susan E. Brown, MS, ARNP, ACNP-BC, CCRN
Great River Nephrology, West Burlington, Iowa
References
1. Parikh SV, Haddad NJ, Hebert LA. Retarding progression of kidney disease. In: Johnson RJ, Feehally J, Floege J, eds. Comprehensive Clinical Nephrology. 5th ed. Philadelphia, PA: Saunders; 2015:931-940.
2. Bakris GL, Agarwal R, Chan JC, et al. Effect of finerenone on albuminuria in patients with diabetic nephropathy: a randomized clinical trial. JAMA. 2015;314(9):884-894.
3. Kolkhof P, Delbeck M, Kretschmer A, et al. Finerenone, a novel selective nonsteroidal mineralocorticoid receptor antagonist, protects from rat cardiorenal injury. J Cardiovasc Pharmacol. 2014;64(1):69-78.
Nutrition Guidelines for CKD
Q) I see patients with diabetes, hypertension, chronic kidney disease (CKD), obesity ... often all within the same patient! I keep hearing that the DASH diet is best for these patients. Is this true? Do you have any suggestions (or handouts) for teaching good eating habits in a 15-minute office visit?
It is always nice to focus on what patients can do, rather than what they can’t. Patients with diabetes, kidney disease, heart disease, and obesity hear a lot of “can’t” messages, making “can” messages particularly important to emphasize.
Healthy diets for diabetes, heart, and kidney patients include foods low in trans and saturated fats and sodium. Not all CKD patients are required to follow a low-potassium diet; dietary restrictions are based on laboratory values, medications, and other factors. As we know, adding an ACE inhibitor or an angiotensin receptor blocker (ARB) to the treatment regimen can cause an elevation in serum potassium.
For adults with CKD, it is recommended that sodium intake be restricted to < 2,000 mg/d.4 And in this population, salt substitutes are not recommended, since they often contain large amounts of potassium chloride, which increases risk for hyperkalemia.5 Other spices (eg, garlic, pepper, lemon) are better substitutes for salt.
The late Paul Prudhomme, an award-winning chef from New Orleans, struggled with obesity and health issues for years. He developed wonderful, kidney-friendly spices free of salt and potassium. His line of spices, Magic Seasoning Blends, is sold in many grocery stores. You can recommend them without worry.
Studies have shown that the usual Western diet (which features an abundance of processed foods, fats, and sugars) contributes to kidney disease.6 The DASH (Dietary Approaches to Stop Hypertension) diet, developed by cardio experts, replaces these foods with healthier alternatives.
Recent research has shown that the DASH diet does, in fact, slow the progression of kidney disease.7 It also lowers blood pressure and decreases kidney stone formation, which are risk factors for kidney disease.
So, the DASH diet is protective for your patients (from both a kidney and a cardiac standpoint)—but how do you explain this in a 15-minute office visit?
Here are a few quick tips:
• Increase fruit and vegetable intake to include all colors on your plate (and no, tan is not really a color)
• If you eat meat, the cooking method should start with “B” (ie, bake, boil, broil, barbeque [without salty sauce]) ... Note that “fried” does not start with “B”!
• Use a smaller plate and you will not eat as much
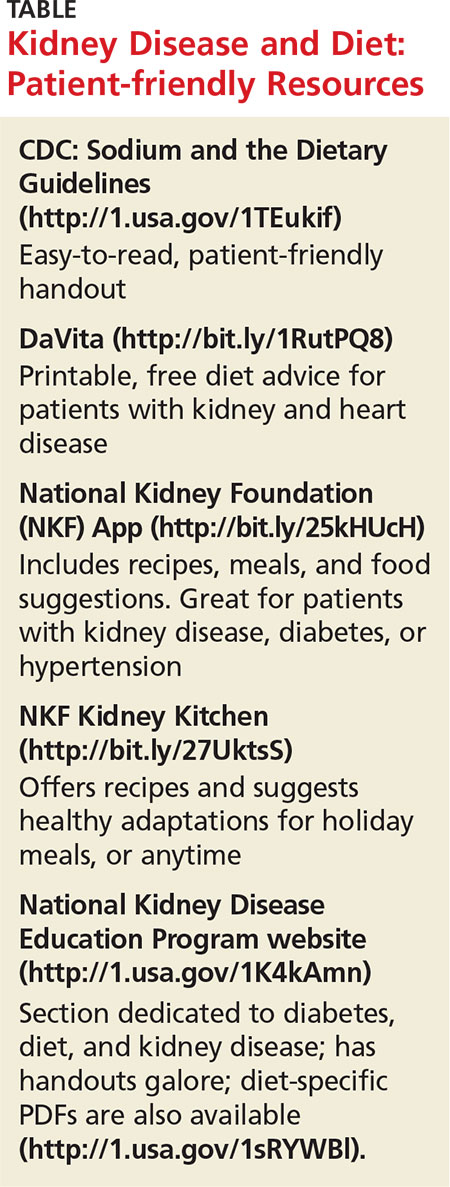
• Use technology in your favor. There are great apps and downloads you can recommend (see Table). —CC
Christine Corbett, MSN, APRN, FNP-BC, CNN-NP
Kansas City Veterans Affairs, Kansas City, Missouri
References
4. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;(3):1-150.
5. National Kidney Disease Education Program. Potassium: tips for people with chronic kidney disease (CKD). www.niddk.nih.gov/health-information/health-communication-programs/nkdep/a-z/nutrition-potassium/Documents/nutrition-potassium-508.pdf. Accessed June 20, 2016.
6. Odermatt A. The Western-style diet: a major risk factor for impaired kidney function and chronic kidney disease. Am J Physiol Renal Physiol. 2011;301(5):F919-F931.
7. Steiber A. DASH-style diet effective in preventing, delaying CKD progression. Renal and Urology News. 2012.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired PA who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Christine Corbett, MSN, APRN, FNP-BC, CNN-NP, who practices at Kansas City Veterans Affairs in Kansas City, Missouri, and Susan E. Brown, MS, ARNP, ACNP-BC, CCRN, who practices at Great River Nephrology in West Burlington, Iowa.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired PA who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Christine Corbett, MSN, APRN, FNP-BC, CNN-NP, who practices at Kansas City Veterans Affairs in Kansas City, Missouri, and Susan E. Brown, MS, ARNP, ACNP-BC, CCRN, who practices at Great River Nephrology in West Burlington, Iowa.
| Clinician Reviews in partnership with |
Renal Consult is edited by Jane S. Davis, CRNP, DNP, a member of the Clinician Reviews editorial board, who is a nurse practitioner in the Division of Nephrology at the University of Alabama at Birmingham and is the communications chairperson for the National Kidney Foundation’s Council of Advanced Practitioners (NKF-CAP); and Kim Zuber, PA-C, MSPS, DFAAPA, a retired PA who works with the American Academy of Nephrology PAs and is also past chair of the NKF-CAP. This month’s responses were authored by Christine Corbett, MSN, APRN, FNP-BC, CNN-NP, who practices at Kansas City Veterans Affairs in Kansas City, Missouri, and Susan E. Brown, MS, ARNP, ACNP-BC, CCRN, who practices at Great River Nephrology in West Burlington, Iowa.
Q) I see patients with diabetes, hypertension, chronic kidney disease (CKD), obesity ... often all within the same patient! I keep hearing that the DASH diet is best for these patients. Is this true? Do you have any suggestions (or handouts) for teaching good eating habits in a 15-minute office visit?
It is always nice to focus on what patients can do, rather than what they can’t. Patients with diabetes, kidney disease, heart disease, and obesity hear a lot of “can’t” messages, making “can” messages particularly important to emphasize.
Healthy diets for diabetes, heart, and kidney patients include foods low in trans and saturated fats and sodium. Not all CKD patients are required to follow a low-potassium diet; dietary restrictions are based on laboratory values, medications, and other factors. As we know, adding an ACE inhibitor or an angiotensin receptor blocker (ARB) to the treatment regimen can cause an elevation in serum potassium.
For adults with CKD, it is recommended that sodium intake be restricted to < 2,000 mg/d.4 And in this population, salt substitutes are not recommended, since they often contain large amounts of potassium chloride, which increases risk for hyperkalemia.5 Other spices (eg, garlic, pepper, lemon) are better substitutes for salt.
The late Paul Prudhomme, an award-winning chef from New Orleans, struggled with obesity and health issues for years. He developed wonderful, kidney-friendly spices free of salt and potassium. His line of spices, Magic Seasoning Blends, is sold in many grocery stores. You can recommend them without worry.
Studies have shown that the usual Western diet (which features an abundance of processed foods, fats, and sugars) contributes to kidney disease.6 The DASH (Dietary Approaches to Stop Hypertension) diet, developed by cardio experts, replaces these foods with healthier alternatives.
Recent research has shown that the DASH diet does, in fact, slow the progression of kidney disease.7 It also lowers blood pressure and decreases kidney stone formation, which are risk factors for kidney disease.
So, the DASH diet is protective for your patients (from both a kidney and a cardiac standpoint)—but how do you explain this in a 15-minute office visit?
Here are a few quick tips:
• Increase fruit and vegetable intake to include all colors on your plate (and no, tan is not really a color)
• If you eat meat, the cooking method should start with “B” (ie, bake, boil, broil, barbeque [without salty sauce]) ... Note that “fried” does not start with “B”!
• Use a smaller plate and you will not eat as much
• Use technology in your favor. There are great apps and downloads you can recommend (see Table). —CC
Christine Corbett, MSN, APRN, FNP-BC, CNN-NP
Kansas City Veterans Affairs, Kansas City, Missouri
References
4. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;(3):1-150.
5. National Kidney Disease Education Program. Potassium: tips for people with chronic kidney disease (CKD). www.niddk.nih.gov/health-information/health-communication-programs/nkdep/a-z/nutrition-potassium/Documents/nutrition-potassium-508.pdf. Accessed June 20, 2016.
6. Odermatt A. The Western-style diet: a major risk factor for impaired kidney function and chronic kidney disease. Am J Physiol Renal Physiol. 2011;301(5):F919-F931.
7. Steiber A. DASH-style diet effective in preventing, delaying CKD progression. Renal and Urology News. 2012.
Q) I see patients with diabetes, hypertension, chronic kidney disease (CKD), obesity ... often all within the same patient! I keep hearing that the DASH diet is best for these patients. Is this true? Do you have any suggestions (or handouts) for teaching good eating habits in a 15-minute office visit?
It is always nice to focus on what patients can do, rather than what they can’t. Patients with diabetes, kidney disease, heart disease, and obesity hear a lot of “can’t” messages, making “can” messages particularly important to emphasize.
Healthy diets for diabetes, heart, and kidney patients include foods low in trans and saturated fats and sodium. Not all CKD patients are required to follow a low-potassium diet; dietary restrictions are based on laboratory values, medications, and other factors. As we know, adding an ACE inhibitor or an angiotensin receptor blocker (ARB) to the treatment regimen can cause an elevation in serum potassium.
For adults with CKD, it is recommended that sodium intake be restricted to < 2,000 mg/d.4 And in this population, salt substitutes are not recommended, since they often contain large amounts of potassium chloride, which increases risk for hyperkalemia.5 Other spices (eg, garlic, pepper, lemon) are better substitutes for salt.
The late Paul Prudhomme, an award-winning chef from New Orleans, struggled with obesity and health issues for years. He developed wonderful, kidney-friendly spices free of salt and potassium. His line of spices, Magic Seasoning Blends, is sold in many grocery stores. You can recommend them without worry.
Studies have shown that the usual Western diet (which features an abundance of processed foods, fats, and sugars) contributes to kidney disease.6 The DASH (Dietary Approaches to Stop Hypertension) diet, developed by cardio experts, replaces these foods with healthier alternatives.
Recent research has shown that the DASH diet does, in fact, slow the progression of kidney disease.7 It also lowers blood pressure and decreases kidney stone formation, which are risk factors for kidney disease.
So, the DASH diet is protective for your patients (from both a kidney and a cardiac standpoint)—but how do you explain this in a 15-minute office visit?
Here are a few quick tips:
• Increase fruit and vegetable intake to include all colors on your plate (and no, tan is not really a color)
• If you eat meat, the cooking method should start with “B” (ie, bake, boil, broil, barbeque [without salty sauce]) ... Note that “fried” does not start with “B”!
• Use a smaller plate and you will not eat as much
• Use technology in your favor. There are great apps and downloads you can recommend (see Table). —CC
Christine Corbett, MSN, APRN, FNP-BC, CNN-NP
Kansas City Veterans Affairs, Kansas City, Missouri
References
4. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;(3):1-150.
5. National Kidney Disease Education Program. Potassium: tips for people with chronic kidney disease (CKD). www.niddk.nih.gov/health-information/health-communication-programs/nkdep/a-z/nutrition-potassium/Documents/nutrition-potassium-508.pdf. Accessed June 20, 2016.
6. Odermatt A. The Western-style diet: a major risk factor for impaired kidney function and chronic kidney disease. Am J Physiol Renal Physiol. 2011;301(5):F919-F931.
7. Steiber A. DASH-style diet effective in preventing, delaying CKD progression. Renal and Urology News. 2012.
More Isn’t Better With Acute Low Back Pain Treatment
PRACTICE CHANGER
Consider treating patients with acute low back pain with naproxen only, as adding cyclobenzaprine or oxycodone/acetaminophen to scheduled naproxen increases adverse effects and does not improve functional assessment at seven days or three months.
Strength of Recommendation
B: Based on a high-quality, randomized controlled trial (RCT).1
A 46-year-old man presents to the emergency department (ED) with low back pain (LBP) after helping a friend move a couch three days ago. He denies any direct trauma to his back and describes the pain as a “spasm” in his lumbar spinal region with no radicular symptoms. The pain worsens with prolonged standing and position changes. He has tried acetaminophen with no benefit. You diagnose a lumbar muscular strain. What medications should you prescribe to help relieve his LBP and improve his overall function?
Acute LBP prompts nearly 2.7 million ED visits in the United States each year.2 It leads to persistent subjective impairment and continued analgesic use at seven days (impairment, 70%; analgesic use, 69%) and three months (48% and 46%, respectively) after ED discharge.3 Systematic reviews show that monotherapy with NSAIDs or muscle relaxants is more effective than placebo for pain relief.4,5 A secondary analysis of patients (N = 715) from a prospective cohort study showed worse functioning at six months in those who were prescribed opiates for LBP than in those who were not.6
Monotherapy or combination therapy for LBP?
Because medications used for LBP have different mechanisms of action, clinicians frequently combine them in an attempt to improve symptoms and function.2 Current evidence on combination therapy shows mixed results. A large RCT (N = 867) showed that the combination of cyclobenzaprine and ibuprofen led to lower subjective pain intensity, but it did not result in self-reported pain improvement, compared to cyclobenzaprine alone. However, a small RCT (N = 40) demonstrated improved LBP and spasm with naprozen plus cyclobenzaprine, compared to naproxen alone.7,8
This study sought to determine the benefit of treating acute LBP with cyclobenzaprine or oxycodone/acetaminophen in combination with an NSAID, compared to treatment with an NSAID alone.
Continue for the study summary >>
STUDY SUMMARY
Adding second pain reliever provided no significant benefit
This double-blinded RCT enrolled 323 adults presenting to an ED with two weeks or less of nontraumatic, nonradicular LBP.1 Subjects had a score of > 5 on the Roland-Morris Disability Questionnaire (RMDQ), which measures functional impairment due to LBP (range, 0-24). Patients were excluded if they had radicular pain radiating below the gluteal folds, direct trauma to the back within the previous month, pain lasting > 2 wk, a recent history of multiple LBP episodes per month, or a history of opioid use.
All subjects received 10 days’ worth of naproxen (500 mg bid). They were then randomized to receive either oxycodone/acetaminophen (5 mg/325 mg), cyclobenzaprine (5 mg), or placebo, with instructions to take one to two tablets as needed every eight hours for 10 days. All patients also received a 10-minute educational session emphasizing the role of nonpharmacologic interventions.
The primary outcome was change in the RMDQ between ED discharge and a phone call seven days later; a 5-point improvement in the RMDQ was considered clinically significant. Secondary outcomes included subjective description of worst pain, frequency of LBP, frequency of analgesic use, satisfaction with treatment, median number of days to return to work and usual activities, need for follow-up health care visits, and opioid use. Investigators also asked about any adverse effects.
At seven days, reported RMDQ scores had improved by 9.8 points in patients taking naproxen plus placebo, 10.1 points in those receiving naproxen plus cyclobenzaprine, and 11.1 points in those using naproxen plus oxycodone/acetaminophen. There were no statistically significant between-group differences for placebo vs cyclobenzaprine or oxycodone/acetaminophen (0.3 points and 1.3 points, respectively) or cyclobenzaprine vs oxycodone/acetaminophen (0.9 points).
Secondary outcomes. At seven days, there was no significant difference between study groups in subjective pain assessment, frequency of LBP, or use of as-needed medications in the prior 24 hours. There was also no difference in the median number of days to return to work or need for follow-up health care visits.
Among patients who took more than one dose of the study medication, those who took oxycodone/acetaminophen were more likely to describe their worst pain in the last 24 hours as mild/none, compared to patients taking placebo (number needed to treat, 6). About 72% of all subjects reported that they would choose the same treatment option again, with no difference between groups. At three months, there was no difference between groups in subjective pain assessment, frequency of LBP, use of as-needed medications, or opioid use during the previous 72 hours.
Adverse effects, including drowsiness, dizziness, stomach irritation, and nausea or vomiting, were more common in the oxycodone/acetaminophen and the cyclobenzaprine treatment groups, with a number needed to harm of 5.3 and 7.8, respectively.
Continue for what's new >>
WHAT’S NEW
Second med adds nothing
This RCT found that adding cyclobenzaprine or oxycodone/acetaminophen to naproxen for the treatment of nontraumatic, nonradicular acute LBP did not significantly improve functional assessment at seven days or three months after the initial ED visit. But it did increase adverse effects.
CAVEATS
Specific subset studied
This study was performed in a single urban ED and included a very specific subset of LBP patients, which limits the generalizability of the results. However, patients often present to primary care with similar LBP complaints, and the results of the study should reasonably apply to other settings.
The findings may not generalize to all NSAIDs, but there is no evidence to suggest that other NSAIDs would behave differently when combined with cyclobenzaprine or oxycodone/acetaminophen. In this analysis, only about one-third of patients used the as-needed medication more than once daily; another third used it intermittently or never.
CHALLENGES TO IMPLEMENTATION
Patients may expect more
Patients expect to receive prescriptions, and clinicians are inclined to write them if they believe doing so will help their patients. The evidence, however, does not demonstrate a benefit to these prescription-only medications for LBP.
REFERENCES
1. Friedman BW, Dym AA, Davitt M, et al. Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial. JAMA. 2015;314:1572-1580.
2. Friedman BW, Chilstrom M, Bijur PE, et al. Diagnostic testing and treatment of low back pain in United States emergency departments: a national perspective. Spine (Phila Pa 1976). 2010;35:E1406-E1411.
3. Friedman BW, O’Mahony S, Mulvey L, et al. One-week and 3-month outcomes after an emergency department visit for undifferentiated musculoskeletal low back pain. Ann Emerg Med. 2012;59:128-133.
4. Roelofs PD, Deyo RA, Koes BW, et al. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine (Phila Pa 1976). 2008;33:1766-1774.
5. van Tulder MW, Touray T, Furlan AD, et al. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane collaboration. Spine (Phila Pa 1976). 2003;28:1978-1992.
6. Ashworth J, Green DJ, Dunn KM, et al. Opioid use among low back pain patients in primary care: is opioid prescription associated with disability at 6-month follow-up? Pain. 2013; 154:1038-1044.
7. Childers MK, Borenstein D, Brown RL, et al. Low-dose cyclobenzaprine versus combination therapy with ibuprofen for acute neck or back pain with muscle spasm: a randomized trial. Curr Med Res Opin. 2005;21:1485-1493.
8. Borenstein DG, Lacks S, Wiesel SW. Cyclobenzaprine and naproxen versus naproxen alone in the treatment of acute low back pain and muscle spasm. Clin Ther. 1990;12:125-131.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(6):404-406.
PRACTICE CHANGER
Consider treating patients with acute low back pain with naproxen only, as adding cyclobenzaprine or oxycodone/acetaminophen to scheduled naproxen increases adverse effects and does not improve functional assessment at seven days or three months.
Strength of Recommendation
B: Based on a high-quality, randomized controlled trial (RCT).1
A 46-year-old man presents to the emergency department (ED) with low back pain (LBP) after helping a friend move a couch three days ago. He denies any direct trauma to his back and describes the pain as a “spasm” in his lumbar spinal region with no radicular symptoms. The pain worsens with prolonged standing and position changes. He has tried acetaminophen with no benefit. You diagnose a lumbar muscular strain. What medications should you prescribe to help relieve his LBP and improve his overall function?
Acute LBP prompts nearly 2.7 million ED visits in the United States each year.2 It leads to persistent subjective impairment and continued analgesic use at seven days (impairment, 70%; analgesic use, 69%) and three months (48% and 46%, respectively) after ED discharge.3 Systematic reviews show that monotherapy with NSAIDs or muscle relaxants is more effective than placebo for pain relief.4,5 A secondary analysis of patients (N = 715) from a prospective cohort study showed worse functioning at six months in those who were prescribed opiates for LBP than in those who were not.6
Monotherapy or combination therapy for LBP?
Because medications used for LBP have different mechanisms of action, clinicians frequently combine them in an attempt to improve symptoms and function.2 Current evidence on combination therapy shows mixed results. A large RCT (N = 867) showed that the combination of cyclobenzaprine and ibuprofen led to lower subjective pain intensity, but it did not result in self-reported pain improvement, compared to cyclobenzaprine alone. However, a small RCT (N = 40) demonstrated improved LBP and spasm with naprozen plus cyclobenzaprine, compared to naproxen alone.7,8
This study sought to determine the benefit of treating acute LBP with cyclobenzaprine or oxycodone/acetaminophen in combination with an NSAID, compared to treatment with an NSAID alone.
Continue for the study summary >>
STUDY SUMMARY
Adding second pain reliever provided no significant benefit
This double-blinded RCT enrolled 323 adults presenting to an ED with two weeks or less of nontraumatic, nonradicular LBP.1 Subjects had a score of > 5 on the Roland-Morris Disability Questionnaire (RMDQ), which measures functional impairment due to LBP (range, 0-24). Patients were excluded if they had radicular pain radiating below the gluteal folds, direct trauma to the back within the previous month, pain lasting > 2 wk, a recent history of multiple LBP episodes per month, or a history of opioid use.
All subjects received 10 days’ worth of naproxen (500 mg bid). They were then randomized to receive either oxycodone/acetaminophen (5 mg/325 mg), cyclobenzaprine (5 mg), or placebo, with instructions to take one to two tablets as needed every eight hours for 10 days. All patients also received a 10-minute educational session emphasizing the role of nonpharmacologic interventions.
The primary outcome was change in the RMDQ between ED discharge and a phone call seven days later; a 5-point improvement in the RMDQ was considered clinically significant. Secondary outcomes included subjective description of worst pain, frequency of LBP, frequency of analgesic use, satisfaction with treatment, median number of days to return to work and usual activities, need for follow-up health care visits, and opioid use. Investigators also asked about any adverse effects.
At seven days, reported RMDQ scores had improved by 9.8 points in patients taking naproxen plus placebo, 10.1 points in those receiving naproxen plus cyclobenzaprine, and 11.1 points in those using naproxen plus oxycodone/acetaminophen. There were no statistically significant between-group differences for placebo vs cyclobenzaprine or oxycodone/acetaminophen (0.3 points and 1.3 points, respectively) or cyclobenzaprine vs oxycodone/acetaminophen (0.9 points).
Secondary outcomes. At seven days, there was no significant difference between study groups in subjective pain assessment, frequency of LBP, or use of as-needed medications in the prior 24 hours. There was also no difference in the median number of days to return to work or need for follow-up health care visits.
Among patients who took more than one dose of the study medication, those who took oxycodone/acetaminophen were more likely to describe their worst pain in the last 24 hours as mild/none, compared to patients taking placebo (number needed to treat, 6). About 72% of all subjects reported that they would choose the same treatment option again, with no difference between groups. At three months, there was no difference between groups in subjective pain assessment, frequency of LBP, use of as-needed medications, or opioid use during the previous 72 hours.
Adverse effects, including drowsiness, dizziness, stomach irritation, and nausea or vomiting, were more common in the oxycodone/acetaminophen and the cyclobenzaprine treatment groups, with a number needed to harm of 5.3 and 7.8, respectively.
Continue for what's new >>
WHAT’S NEW
Second med adds nothing
This RCT found that adding cyclobenzaprine or oxycodone/acetaminophen to naproxen for the treatment of nontraumatic, nonradicular acute LBP did not significantly improve functional assessment at seven days or three months after the initial ED visit. But it did increase adverse effects.
CAVEATS
Specific subset studied
This study was performed in a single urban ED and included a very specific subset of LBP patients, which limits the generalizability of the results. However, patients often present to primary care with similar LBP complaints, and the results of the study should reasonably apply to other settings.
The findings may not generalize to all NSAIDs, but there is no evidence to suggest that other NSAIDs would behave differently when combined with cyclobenzaprine or oxycodone/acetaminophen. In this analysis, only about one-third of patients used the as-needed medication more than once daily; another third used it intermittently or never.
CHALLENGES TO IMPLEMENTATION
Patients may expect more
Patients expect to receive prescriptions, and clinicians are inclined to write them if they believe doing so will help their patients. The evidence, however, does not demonstrate a benefit to these prescription-only medications for LBP.
REFERENCES
1. Friedman BW, Dym AA, Davitt M, et al. Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial. JAMA. 2015;314:1572-1580.
2. Friedman BW, Chilstrom M, Bijur PE, et al. Diagnostic testing and treatment of low back pain in United States emergency departments: a national perspective. Spine (Phila Pa 1976). 2010;35:E1406-E1411.
3. Friedman BW, O’Mahony S, Mulvey L, et al. One-week and 3-month outcomes after an emergency department visit for undifferentiated musculoskeletal low back pain. Ann Emerg Med. 2012;59:128-133.
4. Roelofs PD, Deyo RA, Koes BW, et al. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine (Phila Pa 1976). 2008;33:1766-1774.
5. van Tulder MW, Touray T, Furlan AD, et al. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane collaboration. Spine (Phila Pa 1976). 2003;28:1978-1992.
6. Ashworth J, Green DJ, Dunn KM, et al. Opioid use among low back pain patients in primary care: is opioid prescription associated with disability at 6-month follow-up? Pain. 2013; 154:1038-1044.
7. Childers MK, Borenstein D, Brown RL, et al. Low-dose cyclobenzaprine versus combination therapy with ibuprofen for acute neck or back pain with muscle spasm: a randomized trial. Curr Med Res Opin. 2005;21:1485-1493.
8. Borenstein DG, Lacks S, Wiesel SW. Cyclobenzaprine and naproxen versus naproxen alone in the treatment of acute low back pain and muscle spasm. Clin Ther. 1990;12:125-131.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(6):404-406.
PRACTICE CHANGER
Consider treating patients with acute low back pain with naproxen only, as adding cyclobenzaprine or oxycodone/acetaminophen to scheduled naproxen increases adverse effects and does not improve functional assessment at seven days or three months.
Strength of Recommendation
B: Based on a high-quality, randomized controlled trial (RCT).1
A 46-year-old man presents to the emergency department (ED) with low back pain (LBP) after helping a friend move a couch three days ago. He denies any direct trauma to his back and describes the pain as a “spasm” in his lumbar spinal region with no radicular symptoms. The pain worsens with prolonged standing and position changes. He has tried acetaminophen with no benefit. You diagnose a lumbar muscular strain. What medications should you prescribe to help relieve his LBP and improve his overall function?
Acute LBP prompts nearly 2.7 million ED visits in the United States each year.2 It leads to persistent subjective impairment and continued analgesic use at seven days (impairment, 70%; analgesic use, 69%) and three months (48% and 46%, respectively) after ED discharge.3 Systematic reviews show that monotherapy with NSAIDs or muscle relaxants is more effective than placebo for pain relief.4,5 A secondary analysis of patients (N = 715) from a prospective cohort study showed worse functioning at six months in those who were prescribed opiates for LBP than in those who were not.6
Monotherapy or combination therapy for LBP?
Because medications used for LBP have different mechanisms of action, clinicians frequently combine them in an attempt to improve symptoms and function.2 Current evidence on combination therapy shows mixed results. A large RCT (N = 867) showed that the combination of cyclobenzaprine and ibuprofen led to lower subjective pain intensity, but it did not result in self-reported pain improvement, compared to cyclobenzaprine alone. However, a small RCT (N = 40) demonstrated improved LBP and spasm with naprozen plus cyclobenzaprine, compared to naproxen alone.7,8
This study sought to determine the benefit of treating acute LBP with cyclobenzaprine or oxycodone/acetaminophen in combination with an NSAID, compared to treatment with an NSAID alone.
Continue for the study summary >>
STUDY SUMMARY
Adding second pain reliever provided no significant benefit
This double-blinded RCT enrolled 323 adults presenting to an ED with two weeks or less of nontraumatic, nonradicular LBP.1 Subjects had a score of > 5 on the Roland-Morris Disability Questionnaire (RMDQ), which measures functional impairment due to LBP (range, 0-24). Patients were excluded if they had radicular pain radiating below the gluteal folds, direct trauma to the back within the previous month, pain lasting > 2 wk, a recent history of multiple LBP episodes per month, or a history of opioid use.
All subjects received 10 days’ worth of naproxen (500 mg bid). They were then randomized to receive either oxycodone/acetaminophen (5 mg/325 mg), cyclobenzaprine (5 mg), or placebo, with instructions to take one to two tablets as needed every eight hours for 10 days. All patients also received a 10-minute educational session emphasizing the role of nonpharmacologic interventions.
The primary outcome was change in the RMDQ between ED discharge and a phone call seven days later; a 5-point improvement in the RMDQ was considered clinically significant. Secondary outcomes included subjective description of worst pain, frequency of LBP, frequency of analgesic use, satisfaction with treatment, median number of days to return to work and usual activities, need for follow-up health care visits, and opioid use. Investigators also asked about any adverse effects.
At seven days, reported RMDQ scores had improved by 9.8 points in patients taking naproxen plus placebo, 10.1 points in those receiving naproxen plus cyclobenzaprine, and 11.1 points in those using naproxen plus oxycodone/acetaminophen. There were no statistically significant between-group differences for placebo vs cyclobenzaprine or oxycodone/acetaminophen (0.3 points and 1.3 points, respectively) or cyclobenzaprine vs oxycodone/acetaminophen (0.9 points).
Secondary outcomes. At seven days, there was no significant difference between study groups in subjective pain assessment, frequency of LBP, or use of as-needed medications in the prior 24 hours. There was also no difference in the median number of days to return to work or need for follow-up health care visits.
Among patients who took more than one dose of the study medication, those who took oxycodone/acetaminophen were more likely to describe their worst pain in the last 24 hours as mild/none, compared to patients taking placebo (number needed to treat, 6). About 72% of all subjects reported that they would choose the same treatment option again, with no difference between groups. At three months, there was no difference between groups in subjective pain assessment, frequency of LBP, use of as-needed medications, or opioid use during the previous 72 hours.
Adverse effects, including drowsiness, dizziness, stomach irritation, and nausea or vomiting, were more common in the oxycodone/acetaminophen and the cyclobenzaprine treatment groups, with a number needed to harm of 5.3 and 7.8, respectively.
Continue for what's new >>
WHAT’S NEW
Second med adds nothing
This RCT found that adding cyclobenzaprine or oxycodone/acetaminophen to naproxen for the treatment of nontraumatic, nonradicular acute LBP did not significantly improve functional assessment at seven days or three months after the initial ED visit. But it did increase adverse effects.
CAVEATS
Specific subset studied
This study was performed in a single urban ED and included a very specific subset of LBP patients, which limits the generalizability of the results. However, patients often present to primary care with similar LBP complaints, and the results of the study should reasonably apply to other settings.
The findings may not generalize to all NSAIDs, but there is no evidence to suggest that other NSAIDs would behave differently when combined with cyclobenzaprine or oxycodone/acetaminophen. In this analysis, only about one-third of patients used the as-needed medication more than once daily; another third used it intermittently or never.
CHALLENGES TO IMPLEMENTATION
Patients may expect more
Patients expect to receive prescriptions, and clinicians are inclined to write them if they believe doing so will help their patients. The evidence, however, does not demonstrate a benefit to these prescription-only medications for LBP.
REFERENCES
1. Friedman BW, Dym AA, Davitt M, et al. Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial. JAMA. 2015;314:1572-1580.
2. Friedman BW, Chilstrom M, Bijur PE, et al. Diagnostic testing and treatment of low back pain in United States emergency departments: a national perspective. Spine (Phila Pa 1976). 2010;35:E1406-E1411.
3. Friedman BW, O’Mahony S, Mulvey L, et al. One-week and 3-month outcomes after an emergency department visit for undifferentiated musculoskeletal low back pain. Ann Emerg Med. 2012;59:128-133.
4. Roelofs PD, Deyo RA, Koes BW, et al. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine (Phila Pa 1976). 2008;33:1766-1774.
5. van Tulder MW, Touray T, Furlan AD, et al. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane collaboration. Spine (Phila Pa 1976). 2003;28:1978-1992.
6. Ashworth J, Green DJ, Dunn KM, et al. Opioid use among low back pain patients in primary care: is opioid prescription associated with disability at 6-month follow-up? Pain. 2013; 154:1038-1044.
7. Childers MK, Borenstein D, Brown RL, et al. Low-dose cyclobenzaprine versus combination therapy with ibuprofen for acute neck or back pain with muscle spasm: a randomized trial. Curr Med Res Opin. 2005;21:1485-1493.
8. Borenstein DG, Lacks S, Wiesel SW. Cyclobenzaprine and naproxen versus naproxen alone in the treatment of acute low back pain and muscle spasm. Clin Ther. 1990;12:125-131.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2016. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice. 2016;65(6):404-406.
VIDEO: No major malformations ascribed to bisphosphonate use in pregnancy
LONDON – One of the largest studies of pregnancy outcomes after bisphosphonate exposure has found no evidence for major teratogenic effects in women with inflammatory diseases and glucocorticoid-induced osteoporosis and women with bone diseases.
However, the investigators for the French case-control study did find higher rates of neonatal complications and spontaneous abortion among infants of mothers with systemic inflammatory diseases and bisphosphonate use, but the results could be the result of confounding because of the severity of underlying disease and exposure to other medications.
“I think if a women is worried about bisphosphonate exposure during pregnancy, this study can bring her some reassuring news,” although it does not necessarily mean that bisphosphonates are safe during pregnancy, first author Aurélien Sokal said in an interview at the European Congress of Rheumatology. He is a medical student at Beaujon Hospital, Clichy, France, but conducted the study with colleagues during his time in training in the rheumatology department at Paris-Sud University.
“Very little is known about the effect of bisphosphonates on pregnancy outcomes and fetal development,” Mr. Sokal said, and they are feared for possible teratogenic effects in pregnancy because of their long half-life in bone – where they can be released even 1 year after their administration – as well as their ability to cross the placenta and high affinity for high-turnover bones, such as those in a growing fetus. He also noted that abnormalities in bone length, low birth weights, and bone diseases have been observed in rats exposed to bisphosphonates during gestation.
The study compared 23 patients with inflammatory diseases and bisphosphonate exposure during pregnancy against 92 controls with inflammatory diseases but no exposure, and 16 with bone diseases and exposure to bisphosphonates against 64 healthy controls with no underlying disease or bisphosphonate use. The patients came from a database assembled by the French Reference Center of Teratogenic Agents (CRAT) in Paris that has collected information since 1975 on patients referred for any drug exposure during pregnancy and followed their care through the end of pregnancy. The 39 patients who were exposed to bisphosphonates took the drugs during 1987-2014 within the 6 weeks preceding (n = 6) or during pregnancy (n = 33). They had a mean age of 33 years.
Systemic inflammatory diseases
The systemic inflammatory diseases found in women in the study included systemic lupus erythematosus (SLE), rheumatoid arthritis, antiphospholipid syndrome, systemic vasculitis, and other diseases. Of the 23 cases with systemic inflammatory diseases, 16 took risedronate, 5 took alendronate, 1 took etidronate, and the bisphosphonate was unknown in 1. Bisphosphonate exposure occurred before pregnancy in 2, during the first trimester in 21, second trimester in 4, third trimester in 4, and in all trimesters in 1.
Other types of medications were used significantly more often by patients with systemic inflammatory diseases than by controls: steroids (78% vs. 47%), methotrexate (26% vs. 5%), colchicine (17% vs. 2%), proton pump inhibitors (22% vs. 5%), and reproductive hormones (17% vs. 2%). Controls took antimalarials significantly more often (50% vs. 22%).
Voluntary abortions occurred at a similar rate in both exposed and unexposed women (12% vs. 9%), whereas significantly more therapeutic pregnancy terminations occurred among women exposed to bisphosphonates (17% vs. 1%). Live births occurred in 94% of the remaining exposed pregnant women, compared with 80% of controls.
Newborns were delivered at a mean of 38 weeks in both cases and controls, and there were no differences in birth weight, length, or rate of congenital malformation (9% vs. 2%).
The two malformations in neonates from exposed women had an uncertain link to bisphosphonates. One involved a neonate with severe malformative syndrome and advanced bone maturation who had a mother with SLE and was exposed to multiple drugs, including mycophenolate mofetil. The other neonate had ductus arteriosus, inguinal hernia, and negative otoacoustic emission; the baby’s mother had Crohn’s disease but had not taken known teratogenic drugs.
Two neonatal malformations among control women involved one neonate with severe malformative syndrome who had a mother with SLE but who was without exposure to known teratogenic drugs, and another with convulsant encephalopathy whose mother had systemic sclerosis and took pentoxifylline, cisapride, dihydroergocryptine, and colchicine.
However, cases had a 25% rate of neonatal complications, compared with a significantly lower 5% in controls. No infants had hypocalcemia.
Bone diseases
The 16 women with bone diseases included 9 with osteoporosis, 3 with malignancy, and 4 with miscellaneous bone conditions. A total of 5 received intravenous bisphosphonates and 11 received oral drugs (9 alendronate, 2 other). Most received a bisphosphonate in the first trimester (9 patients), but also 4 received it before pregnancy and 3 in the second trimester. More pregnancy terminations (voluntary or therapeutic) occurred among women with bone disease when compared with controls (19% vs. 3%), but the difference was not statistically significant. However in the remaining patients, live births occurred significantly less often in cases than in controls (69% vs. 100%). Birth weight, length, gestational age at birth, and the rates of congenital malformation and neonatal complications were otherwise similar.
The results of the study fall in line with those from the two major previous controlled studies on 24 women (Reprod Toxicol. 2006 Nov;22:578-9) and 21 women (Bone. 2009 Mar;44:428-30). Another series of 10 bisphosphonate-exposed pregnancies described 2 malformations, including 1 ventricular septal defect and 1 kidney and cardiac malformation (Autoimmun Rev. 2010 Jun;9:547-52). Another single case report described a neonate with bilateral talipes equinovarus (J Bone Miner Res. 2004 Oct;19:1742-5). A literature review of 78 cases of bisphosphonate exposure during or prior to pregnancy reported three malformations (Hormones [Athens]. 2011 Oct-Dec;10:280-91).
The study is ongoing and continues to collect data on the follow-up of children, Mr. Sokal said.
The study had no specific funding, and none of the investigators had disclosures to report.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LONDON – One of the largest studies of pregnancy outcomes after bisphosphonate exposure has found no evidence for major teratogenic effects in women with inflammatory diseases and glucocorticoid-induced osteoporosis and women with bone diseases.
However, the investigators for the French case-control study did find higher rates of neonatal complications and spontaneous abortion among infants of mothers with systemic inflammatory diseases and bisphosphonate use, but the results could be the result of confounding because of the severity of underlying disease and exposure to other medications.
“I think if a women is worried about bisphosphonate exposure during pregnancy, this study can bring her some reassuring news,” although it does not necessarily mean that bisphosphonates are safe during pregnancy, first author Aurélien Sokal said in an interview at the European Congress of Rheumatology. He is a medical student at Beaujon Hospital, Clichy, France, but conducted the study with colleagues during his time in training in the rheumatology department at Paris-Sud University.
“Very little is known about the effect of bisphosphonates on pregnancy outcomes and fetal development,” Mr. Sokal said, and they are feared for possible teratogenic effects in pregnancy because of their long half-life in bone – where they can be released even 1 year after their administration – as well as their ability to cross the placenta and high affinity for high-turnover bones, such as those in a growing fetus. He also noted that abnormalities in bone length, low birth weights, and bone diseases have been observed in rats exposed to bisphosphonates during gestation.
The study compared 23 patients with inflammatory diseases and bisphosphonate exposure during pregnancy against 92 controls with inflammatory diseases but no exposure, and 16 with bone diseases and exposure to bisphosphonates against 64 healthy controls with no underlying disease or bisphosphonate use. The patients came from a database assembled by the French Reference Center of Teratogenic Agents (CRAT) in Paris that has collected information since 1975 on patients referred for any drug exposure during pregnancy and followed their care through the end of pregnancy. The 39 patients who were exposed to bisphosphonates took the drugs during 1987-2014 within the 6 weeks preceding (n = 6) or during pregnancy (n = 33). They had a mean age of 33 years.
Systemic inflammatory diseases
The systemic inflammatory diseases found in women in the study included systemic lupus erythematosus (SLE), rheumatoid arthritis, antiphospholipid syndrome, systemic vasculitis, and other diseases. Of the 23 cases with systemic inflammatory diseases, 16 took risedronate, 5 took alendronate, 1 took etidronate, and the bisphosphonate was unknown in 1. Bisphosphonate exposure occurred before pregnancy in 2, during the first trimester in 21, second trimester in 4, third trimester in 4, and in all trimesters in 1.
Other types of medications were used significantly more often by patients with systemic inflammatory diseases than by controls: steroids (78% vs. 47%), methotrexate (26% vs. 5%), colchicine (17% vs. 2%), proton pump inhibitors (22% vs. 5%), and reproductive hormones (17% vs. 2%). Controls took antimalarials significantly more often (50% vs. 22%).
Voluntary abortions occurred at a similar rate in both exposed and unexposed women (12% vs. 9%), whereas significantly more therapeutic pregnancy terminations occurred among women exposed to bisphosphonates (17% vs. 1%). Live births occurred in 94% of the remaining exposed pregnant women, compared with 80% of controls.
Newborns were delivered at a mean of 38 weeks in both cases and controls, and there were no differences in birth weight, length, or rate of congenital malformation (9% vs. 2%).
The two malformations in neonates from exposed women had an uncertain link to bisphosphonates. One involved a neonate with severe malformative syndrome and advanced bone maturation who had a mother with SLE and was exposed to multiple drugs, including mycophenolate mofetil. The other neonate had ductus arteriosus, inguinal hernia, and negative otoacoustic emission; the baby’s mother had Crohn’s disease but had not taken known teratogenic drugs.
Two neonatal malformations among control women involved one neonate with severe malformative syndrome who had a mother with SLE but who was without exposure to known teratogenic drugs, and another with convulsant encephalopathy whose mother had systemic sclerosis and took pentoxifylline, cisapride, dihydroergocryptine, and colchicine.
However, cases had a 25% rate of neonatal complications, compared with a significantly lower 5% in controls. No infants had hypocalcemia.
Bone diseases
The 16 women with bone diseases included 9 with osteoporosis, 3 with malignancy, and 4 with miscellaneous bone conditions. A total of 5 received intravenous bisphosphonates and 11 received oral drugs (9 alendronate, 2 other). Most received a bisphosphonate in the first trimester (9 patients), but also 4 received it before pregnancy and 3 in the second trimester. More pregnancy terminations (voluntary or therapeutic) occurred among women with bone disease when compared with controls (19% vs. 3%), but the difference was not statistically significant. However in the remaining patients, live births occurred significantly less often in cases than in controls (69% vs. 100%). Birth weight, length, gestational age at birth, and the rates of congenital malformation and neonatal complications were otherwise similar.
The results of the study fall in line with those from the two major previous controlled studies on 24 women (Reprod Toxicol. 2006 Nov;22:578-9) and 21 women (Bone. 2009 Mar;44:428-30). Another series of 10 bisphosphonate-exposed pregnancies described 2 malformations, including 1 ventricular septal defect and 1 kidney and cardiac malformation (Autoimmun Rev. 2010 Jun;9:547-52). Another single case report described a neonate with bilateral talipes equinovarus (J Bone Miner Res. 2004 Oct;19:1742-5). A literature review of 78 cases of bisphosphonate exposure during or prior to pregnancy reported three malformations (Hormones [Athens]. 2011 Oct-Dec;10:280-91).
The study is ongoing and continues to collect data on the follow-up of children, Mr. Sokal said.
The study had no specific funding, and none of the investigators had disclosures to report.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LONDON – One of the largest studies of pregnancy outcomes after bisphosphonate exposure has found no evidence for major teratogenic effects in women with inflammatory diseases and glucocorticoid-induced osteoporosis and women with bone diseases.
However, the investigators for the French case-control study did find higher rates of neonatal complications and spontaneous abortion among infants of mothers with systemic inflammatory diseases and bisphosphonate use, but the results could be the result of confounding because of the severity of underlying disease and exposure to other medications.
“I think if a women is worried about bisphosphonate exposure during pregnancy, this study can bring her some reassuring news,” although it does not necessarily mean that bisphosphonates are safe during pregnancy, first author Aurélien Sokal said in an interview at the European Congress of Rheumatology. He is a medical student at Beaujon Hospital, Clichy, France, but conducted the study with colleagues during his time in training in the rheumatology department at Paris-Sud University.
“Very little is known about the effect of bisphosphonates on pregnancy outcomes and fetal development,” Mr. Sokal said, and they are feared for possible teratogenic effects in pregnancy because of their long half-life in bone – where they can be released even 1 year after their administration – as well as their ability to cross the placenta and high affinity for high-turnover bones, such as those in a growing fetus. He also noted that abnormalities in bone length, low birth weights, and bone diseases have been observed in rats exposed to bisphosphonates during gestation.
The study compared 23 patients with inflammatory diseases and bisphosphonate exposure during pregnancy against 92 controls with inflammatory diseases but no exposure, and 16 with bone diseases and exposure to bisphosphonates against 64 healthy controls with no underlying disease or bisphosphonate use. The patients came from a database assembled by the French Reference Center of Teratogenic Agents (CRAT) in Paris that has collected information since 1975 on patients referred for any drug exposure during pregnancy and followed their care through the end of pregnancy. The 39 patients who were exposed to bisphosphonates took the drugs during 1987-2014 within the 6 weeks preceding (n = 6) or during pregnancy (n = 33). They had a mean age of 33 years.
Systemic inflammatory diseases
The systemic inflammatory diseases found in women in the study included systemic lupus erythematosus (SLE), rheumatoid arthritis, antiphospholipid syndrome, systemic vasculitis, and other diseases. Of the 23 cases with systemic inflammatory diseases, 16 took risedronate, 5 took alendronate, 1 took etidronate, and the bisphosphonate was unknown in 1. Bisphosphonate exposure occurred before pregnancy in 2, during the first trimester in 21, second trimester in 4, third trimester in 4, and in all trimesters in 1.
Other types of medications were used significantly more often by patients with systemic inflammatory diseases than by controls: steroids (78% vs. 47%), methotrexate (26% vs. 5%), colchicine (17% vs. 2%), proton pump inhibitors (22% vs. 5%), and reproductive hormones (17% vs. 2%). Controls took antimalarials significantly more often (50% vs. 22%).
Voluntary abortions occurred at a similar rate in both exposed and unexposed women (12% vs. 9%), whereas significantly more therapeutic pregnancy terminations occurred among women exposed to bisphosphonates (17% vs. 1%). Live births occurred in 94% of the remaining exposed pregnant women, compared with 80% of controls.
Newborns were delivered at a mean of 38 weeks in both cases and controls, and there were no differences in birth weight, length, or rate of congenital malformation (9% vs. 2%).
The two malformations in neonates from exposed women had an uncertain link to bisphosphonates. One involved a neonate with severe malformative syndrome and advanced bone maturation who had a mother with SLE and was exposed to multiple drugs, including mycophenolate mofetil. The other neonate had ductus arteriosus, inguinal hernia, and negative otoacoustic emission; the baby’s mother had Crohn’s disease but had not taken known teratogenic drugs.
Two neonatal malformations among control women involved one neonate with severe malformative syndrome who had a mother with SLE but who was without exposure to known teratogenic drugs, and another with convulsant encephalopathy whose mother had systemic sclerosis and took pentoxifylline, cisapride, dihydroergocryptine, and colchicine.
However, cases had a 25% rate of neonatal complications, compared with a significantly lower 5% in controls. No infants had hypocalcemia.
Bone diseases
The 16 women with bone diseases included 9 with osteoporosis, 3 with malignancy, and 4 with miscellaneous bone conditions. A total of 5 received intravenous bisphosphonates and 11 received oral drugs (9 alendronate, 2 other). Most received a bisphosphonate in the first trimester (9 patients), but also 4 received it before pregnancy and 3 in the second trimester. More pregnancy terminations (voluntary or therapeutic) occurred among women with bone disease when compared with controls (19% vs. 3%), but the difference was not statistically significant. However in the remaining patients, live births occurred significantly less often in cases than in controls (69% vs. 100%). Birth weight, length, gestational age at birth, and the rates of congenital malformation and neonatal complications were otherwise similar.
The results of the study fall in line with those from the two major previous controlled studies on 24 women (Reprod Toxicol. 2006 Nov;22:578-9) and 21 women (Bone. 2009 Mar;44:428-30). Another series of 10 bisphosphonate-exposed pregnancies described 2 malformations, including 1 ventricular septal defect and 1 kidney and cardiac malformation (Autoimmun Rev. 2010 Jun;9:547-52). Another single case report described a neonate with bilateral talipes equinovarus (J Bone Miner Res. 2004 Oct;19:1742-5). A literature review of 78 cases of bisphosphonate exposure during or prior to pregnancy reported three malformations (Hormones [Athens]. 2011 Oct-Dec;10:280-91).
The study is ongoing and continues to collect data on the follow-up of children, Mr. Sokal said.
The study had no specific funding, and none of the investigators had disclosures to report.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE EULAR 2016 CONGRESS
Key clinical point: One of the largest controlled studies on pregnancy outcomes following bisphosphonate use found no increase in major malformations.
Major finding: Congenital malformations occurred at similar rates for both cases and controls with systemic inflammatory disease and also for women with bone diseases and bisphosphonate exposure in comparison with healthy control women.
Data source: A French case-control study involving 23 patients with systemic inflammatory diseases and bisphosphonate exposure during pregnancy, 92 controls with systemic inflammatory diseases but no exposure, 16 with bone diseases and exposure to bisphosphonates, and 64 healthy controls with no underlying disease or bisphosphonate exposure.
Disclosures: The study had no specific funding and none of the investigators had disclosures to report.

Bariatric surgery good deal for diabetes, but…
NEW ORLEANS – If the yardstick for measuring the cost-effectiveness of an operation or a medical treatment is that it costs less than $50,000 for each quality-adjusted life-year gained, then weight-loss surgery as a treatment for type 2 diabetes is cost-effective.
However, more long-term follow-up is needed to determine the true value of metabolic or bariatric surgery such as gastric bypass, compared with medical treatment for type 2 diabetes. Studies of bariatric surgery in the nondiabetic population found it was most cost-effective in the following scenarios: in women; in the morbidly obese vs. the moderately obese; in patients with obesity-related comorbidities including diabetes; when the procedures were performed laparoscopically; and when the studies themselves received industry support.

In people with diabetes, the results were similar. “Diabetes metabolic surgery is more cost-effective early in the course of type 2 diabetes compared to later in the course, when performed laparoscopically, and again when the study received support from industry,” reported Dr. William H. Herman, professor of epidemiology and internal medicine at the University of Michigan School of Public Health in Ann Arbor and director of the Michigan Center for Diabetes Translational Research.
He reviewed 11 economic analyses of bariatric surgery and concluded that all exceeded the benchmark for cost-effectiveness based on the cost per quality-adjusted life-year (QALY) gained. Six studies evaluated the general population of obese people and found that the cost-effectiveness ratios ranged from $1,600 to $44,000 per QALY gained. The remaining five studies involved obese patients with type 2 diabetes, two of which reported cost-effectiveness ratios of $2,000 to $23,000 per QALY gained; and the remaining three studies actually reporting a cost-savings. “In other words, the money spent on these interventions was more than recouped in the savings resulting from reduced downstream medical costs,” Dr. Herman reported at the American Diabetes Association scientific sessions.
The studies that found gastric bypass cost-saving in diabetes are noteworthy, Dr. Herman said. “If an intervention is more effective and less costly than a comparator intervention, then it is cost-saving, and that really is an unusual finding in health or medicine; perhaps 10% or 15% of interventions turn out to be cost-saving,” he said. “These are interventions that we want to adopt and put into practice pretty much without question.”
By the same measure, if an intervention is more costly and less effective, it’s easy to dismiss “out of hand,” Dr. Herman said. However, interpreting some of the studies he evaluated was more nuanced. “The problem occurs when a new treatment is both more effective but more costly, which was the case with two of the five analyses of metabolic surgery, and all of the analysis of bariatric surgery in the nondiabetic population,” he said
While gastric bypass surgery for type 2 diabetes is a good value, Dr. Herman added a few caveats. “When one looks at other interventions in similar categories, metformin for diabetes prevention has recently been shown to be cost-saving,” he said. He also said surgery is more cost-effective than marginally cost-effective interventions like intensive glycemic management for people with newly diagnosed type 2 diabetes or retinal screening every year vs. every 2 years.
One key issue with the existing evidence on cost-effectiveness of metabolic surgery for type 2 diabetes that Dr. Herman elucidated is how the studies accounted for participants lost to follow-up. “We know that a patient lost to follow-up may have a less favorable outcome than one who returns for follow-up,” he said. There are two ways studies can account for lost patients: the available-case analysis, which assumes that the patients lost to follow-up have the same rates of remission; and the attrition-adjusted available case follow-up, which uses a worst-case imputation. “I would argue that to account for attrition bias, remission rates calculated using the cases available for follow-up should be adjusted using worst-case imputation,” Dr. Herman said.
He pointed out another limitation when calculating the value of gastric bypass surgery for type 2 diabetes: “There are no randomized clinical trials of metabolic surgery that describe its long-term impact on diabetes treatments, complications, comorbidities, and survival. And it really is going be very important to get these data to confirm the cost-effectiveness of metabolic surgery.”
Among the shortcomings of the existing literature he noted are the assumptions that treatment-related adverse events are self-limited, that body mass index (BMI) achieved up to 5 years after surgery will remain stable, and that diabetes will not relapse. “The data are pretty good now on reversal, remission, hernia repair, and those sorts of things, but we need to look at longer downstream costs associated with surgery, including the need for cholecystectomy, joint replacements, and nutritional deficiencies that may occur and do clearly have financial implications,” he said.
At the same time, the analyses on gastric bypass surgery for type 2 diabetes could be more favorable if they account for improvements in health-related quality-of-life and rely less on cross-sectional data. Dr. Herman said, “I would argue that using cross-sectional data to estimate changes in health-related quality of life as a function of BMI underestimates the improvements on health-related quality-of-life associated with weight loss and will in fact underestimate the cost utility of interventions for obesity treatment,” he said.
Dr. Herman added, “Clearly the evidence to date suggests that metabolic surgery is cost-effective, but I’ll be more assured when I see longer-term follow-up.”
Dr. Herman has no financial relationships to disclose.
NEW ORLEANS – If the yardstick for measuring the cost-effectiveness of an operation or a medical treatment is that it costs less than $50,000 for each quality-adjusted life-year gained, then weight-loss surgery as a treatment for type 2 diabetes is cost-effective.
However, more long-term follow-up is needed to determine the true value of metabolic or bariatric surgery such as gastric bypass, compared with medical treatment for type 2 diabetes. Studies of bariatric surgery in the nondiabetic population found it was most cost-effective in the following scenarios: in women; in the morbidly obese vs. the moderately obese; in patients with obesity-related comorbidities including diabetes; when the procedures were performed laparoscopically; and when the studies themselves received industry support.
In people with diabetes, the results were similar. “Diabetes metabolic surgery is more cost-effective early in the course of type 2 diabetes compared to later in the course, when performed laparoscopically, and again when the study received support from industry,” reported Dr. William H. Herman, professor of epidemiology and internal medicine at the University of Michigan School of Public Health in Ann Arbor and director of the Michigan Center for Diabetes Translational Research.
He reviewed 11 economic analyses of bariatric surgery and concluded that all exceeded the benchmark for cost-effectiveness based on the cost per quality-adjusted life-year (QALY) gained. Six studies evaluated the general population of obese people and found that the cost-effectiveness ratios ranged from $1,600 to $44,000 per QALY gained. The remaining five studies involved obese patients with type 2 diabetes, two of which reported cost-effectiveness ratios of $2,000 to $23,000 per QALY gained; and the remaining three studies actually reporting a cost-savings. “In other words, the money spent on these interventions was more than recouped in the savings resulting from reduced downstream medical costs,” Dr. Herman reported at the American Diabetes Association scientific sessions.
The studies that found gastric bypass cost-saving in diabetes are noteworthy, Dr. Herman said. “If an intervention is more effective and less costly than a comparator intervention, then it is cost-saving, and that really is an unusual finding in health or medicine; perhaps 10% or 15% of interventions turn out to be cost-saving,” he said. “These are interventions that we want to adopt and put into practice pretty much without question.”
By the same measure, if an intervention is more costly and less effective, it’s easy to dismiss “out of hand,” Dr. Herman said. However, interpreting some of the studies he evaluated was more nuanced. “The problem occurs when a new treatment is both more effective but more costly, which was the case with two of the five analyses of metabolic surgery, and all of the analysis of bariatric surgery in the nondiabetic population,” he said
While gastric bypass surgery for type 2 diabetes is a good value, Dr. Herman added a few caveats. “When one looks at other interventions in similar categories, metformin for diabetes prevention has recently been shown to be cost-saving,” he said. He also said surgery is more cost-effective than marginally cost-effective interventions like intensive glycemic management for people with newly diagnosed type 2 diabetes or retinal screening every year vs. every 2 years.
One key issue with the existing evidence on cost-effectiveness of metabolic surgery for type 2 diabetes that Dr. Herman elucidated is how the studies accounted for participants lost to follow-up. “We know that a patient lost to follow-up may have a less favorable outcome than one who returns for follow-up,” he said. There are two ways studies can account for lost patients: the available-case analysis, which assumes that the patients lost to follow-up have the same rates of remission; and the attrition-adjusted available case follow-up, which uses a worst-case imputation. “I would argue that to account for attrition bias, remission rates calculated using the cases available for follow-up should be adjusted using worst-case imputation,” Dr. Herman said.
He pointed out another limitation when calculating the value of gastric bypass surgery for type 2 diabetes: “There are no randomized clinical trials of metabolic surgery that describe its long-term impact on diabetes treatments, complications, comorbidities, and survival. And it really is going be very important to get these data to confirm the cost-effectiveness of metabolic surgery.”
Among the shortcomings of the existing literature he noted are the assumptions that treatment-related adverse events are self-limited, that body mass index (BMI) achieved up to 5 years after surgery will remain stable, and that diabetes will not relapse. “The data are pretty good now on reversal, remission, hernia repair, and those sorts of things, but we need to look at longer downstream costs associated with surgery, including the need for cholecystectomy, joint replacements, and nutritional deficiencies that may occur and do clearly have financial implications,” he said.
At the same time, the analyses on gastric bypass surgery for type 2 diabetes could be more favorable if they account for improvements in health-related quality-of-life and rely less on cross-sectional data. Dr. Herman said, “I would argue that using cross-sectional data to estimate changes in health-related quality of life as a function of BMI underestimates the improvements on health-related quality-of-life associated with weight loss and will in fact underestimate the cost utility of interventions for obesity treatment,” he said.
Dr. Herman added, “Clearly the evidence to date suggests that metabolic surgery is cost-effective, but I’ll be more assured when I see longer-term follow-up.”
Dr. Herman has no financial relationships to disclose.
NEW ORLEANS – If the yardstick for measuring the cost-effectiveness of an operation or a medical treatment is that it costs less than $50,000 for each quality-adjusted life-year gained, then weight-loss surgery as a treatment for type 2 diabetes is cost-effective.
However, more long-term follow-up is needed to determine the true value of metabolic or bariatric surgery such as gastric bypass, compared with medical treatment for type 2 diabetes. Studies of bariatric surgery in the nondiabetic population found it was most cost-effective in the following scenarios: in women; in the morbidly obese vs. the moderately obese; in patients with obesity-related comorbidities including diabetes; when the procedures were performed laparoscopically; and when the studies themselves received industry support.
In people with diabetes, the results were similar. “Diabetes metabolic surgery is more cost-effective early in the course of type 2 diabetes compared to later in the course, when performed laparoscopically, and again when the study received support from industry,” reported Dr. William H. Herman, professor of epidemiology and internal medicine at the University of Michigan School of Public Health in Ann Arbor and director of the Michigan Center for Diabetes Translational Research.
He reviewed 11 economic analyses of bariatric surgery and concluded that all exceeded the benchmark for cost-effectiveness based on the cost per quality-adjusted life-year (QALY) gained. Six studies evaluated the general population of obese people and found that the cost-effectiveness ratios ranged from $1,600 to $44,000 per QALY gained. The remaining five studies involved obese patients with type 2 diabetes, two of which reported cost-effectiveness ratios of $2,000 to $23,000 per QALY gained; and the remaining three studies actually reporting a cost-savings. “In other words, the money spent on these interventions was more than recouped in the savings resulting from reduced downstream medical costs,” Dr. Herman reported at the American Diabetes Association scientific sessions.
The studies that found gastric bypass cost-saving in diabetes are noteworthy, Dr. Herman said. “If an intervention is more effective and less costly than a comparator intervention, then it is cost-saving, and that really is an unusual finding in health or medicine; perhaps 10% or 15% of interventions turn out to be cost-saving,” he said. “These are interventions that we want to adopt and put into practice pretty much without question.”
By the same measure, if an intervention is more costly and less effective, it’s easy to dismiss “out of hand,” Dr. Herman said. However, interpreting some of the studies he evaluated was more nuanced. “The problem occurs when a new treatment is both more effective but more costly, which was the case with two of the five analyses of metabolic surgery, and all of the analysis of bariatric surgery in the nondiabetic population,” he said
While gastric bypass surgery for type 2 diabetes is a good value, Dr. Herman added a few caveats. “When one looks at other interventions in similar categories, metformin for diabetes prevention has recently been shown to be cost-saving,” he said. He also said surgery is more cost-effective than marginally cost-effective interventions like intensive glycemic management for people with newly diagnosed type 2 diabetes or retinal screening every year vs. every 2 years.
One key issue with the existing evidence on cost-effectiveness of metabolic surgery for type 2 diabetes that Dr. Herman elucidated is how the studies accounted for participants lost to follow-up. “We know that a patient lost to follow-up may have a less favorable outcome than one who returns for follow-up,” he said. There are two ways studies can account for lost patients: the available-case analysis, which assumes that the patients lost to follow-up have the same rates of remission; and the attrition-adjusted available case follow-up, which uses a worst-case imputation. “I would argue that to account for attrition bias, remission rates calculated using the cases available for follow-up should be adjusted using worst-case imputation,” Dr. Herman said.
He pointed out another limitation when calculating the value of gastric bypass surgery for type 2 diabetes: “There are no randomized clinical trials of metabolic surgery that describe its long-term impact on diabetes treatments, complications, comorbidities, and survival. And it really is going be very important to get these data to confirm the cost-effectiveness of metabolic surgery.”
Among the shortcomings of the existing literature he noted are the assumptions that treatment-related adverse events are self-limited, that body mass index (BMI) achieved up to 5 years after surgery will remain stable, and that diabetes will not relapse. “The data are pretty good now on reversal, remission, hernia repair, and those sorts of things, but we need to look at longer downstream costs associated with surgery, including the need for cholecystectomy, joint replacements, and nutritional deficiencies that may occur and do clearly have financial implications,” he said.
At the same time, the analyses on gastric bypass surgery for type 2 diabetes could be more favorable if they account for improvements in health-related quality-of-life and rely less on cross-sectional data. Dr. Herman said, “I would argue that using cross-sectional data to estimate changes in health-related quality of life as a function of BMI underestimates the improvements on health-related quality-of-life associated with weight loss and will in fact underestimate the cost utility of interventions for obesity treatment,” he said.
Dr. Herman added, “Clearly the evidence to date suggests that metabolic surgery is cost-effective, but I’ll be more assured when I see longer-term follow-up.”
Dr. Herman has no financial relationships to disclose.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: Bariatric or metabolic surgery is a cost-effective treatment for type 2 diabetes.
Major finding: Cost-effectiveness ratios of $2,000-$23,000 for bariatric surgery in people with type 2 diabetes fall below the cost-effectiveness threshold.
Data source: Review of 11 economic analyses of bariatric surgery, including six studies of bariatric surgery in people with type 2 diabetes.
Disclosures: Dr. Herman reported having no financial disclosures.

Supreme Court deadlocks on immigration policy case
Supreme Court justices have deadlocked on whether protections for undocumented immigrants can be expanded under an executive order by the President.
In a June 23 decision, justices were equally divided on the constitutionality of two of President Obama’s immigration policies: the Deferred Action for Parents of Americans and Lawful Permanent Residents (DAPA) and an expanded version of the Deferred Action for Childhood Arrivals (DACA). The former protects undocumented immigrants who are parents of U.S. citizens from deportation, if they meet certain criteria. The second extends work authorization under the original DACA program from 2 years to 3 years and broadens age requirements.

The 4-to-4 split decision in Texas v. United States mean the policies remain blocked by the lower court, and the expanded programs will not go forward anytime soon. The decision does not affect original DACA, which protects from deportation undocumented immigrants brought to the United States as children and offers access to work authorization.
President Obama expressed disappointment at the lack of agreement, saying the tie vote underscores the need for nine justices on the court.
“As disappointing as it was to be challenged for taking the kind of action that other administrations have taken, the country was looking to the Supreme Court to resolve the important legal questions raised in this case,” President Obama said during a June 23 press conference. “Today, the Supreme Court was unable to reach a decision ... it means the expanded set of common sense deferred action policies that I announced 2 years ago cannot go forward at this stage until there is a ninth justice on the court to break the tie.”
Texas Attorney General Ken Paxton was satisfied with the decision, calling it a victory for the state plaintiffs.
“Today’s decision keeps in place what we have maintained from the very start: one person, even a president, cannot unilaterally change the law,” Mr. Paxton said in a statement. “This is a major setback to President Obama’s attempts to expand executive power, and a victory for those who believe in the separation of powers and the rule of law.”
Texas was 1 of 26 states that sued over DAPA and expanded DACA. The states argued the president does not have the authority to issue the new immigration policies, and that the programs violate the Constitution as well as the Administrative Procedure Act for notice-and-comment rule making. Justices heard oral arguments April 18.
Immigration advocates were worried that if expanded DACA were struck down, a similar fate would follow for the original DACA policy. As it stands, undocumented immigrants who benefit from deportation protection and work authorization under original DACA, including undocumented medical students, will not be affected by the Supreme Court decision.
Marielena Hincapié, executive director for the National Immigration Law Center, vowed to continue fighting for the policies to take effect.
“Immigrants and allies fought for and won these significant policy victories, which would have brought much-needed emotional and economic stability to millions of our community members, and we will not sit back,” she said in a statement. “We urge the Department of Justice to seek a rehearing for when a ninth justice is confirmed for the Supreme Court.”
Federation for American Immigration Reform President Dan Stein said the split decision upholds the rule of law and helps preserve the balance of power in the United States.
“By ruling in favor of the federal court’s injunction, half of the nation’s Supreme Court Justices have shown that they have deep concerns about this president’s attempt at a power grab by his efforts to amend federal laws from the Oval Office,” Mr. Stein said in a statement.
Texas v. United States will be sent back to U.S. District Court Judge Andrew Hanen in Texas who will hear the case on its merits. The case could wind its way back to the U.S. Supreme Court for a rehearing after a ninth justice is confirmed.
On Twitter @legal_med
Supreme Court justices have deadlocked on whether protections for undocumented immigrants can be expanded under an executive order by the President.
In a June 23 decision, justices were equally divided on the constitutionality of two of President Obama’s immigration policies: the Deferred Action for Parents of Americans and Lawful Permanent Residents (DAPA) and an expanded version of the Deferred Action for Childhood Arrivals (DACA). The former protects undocumented immigrants who are parents of U.S. citizens from deportation, if they meet certain criteria. The second extends work authorization under the original DACA program from 2 years to 3 years and broadens age requirements.
The 4-to-4 split decision in Texas v. United States mean the policies remain blocked by the lower court, and the expanded programs will not go forward anytime soon. The decision does not affect original DACA, which protects from deportation undocumented immigrants brought to the United States as children and offers access to work authorization.
President Obama expressed disappointment at the lack of agreement, saying the tie vote underscores the need for nine justices on the court.
“As disappointing as it was to be challenged for taking the kind of action that other administrations have taken, the country was looking to the Supreme Court to resolve the important legal questions raised in this case,” President Obama said during a June 23 press conference. “Today, the Supreme Court was unable to reach a decision ... it means the expanded set of common sense deferred action policies that I announced 2 years ago cannot go forward at this stage until there is a ninth justice on the court to break the tie.”
Texas Attorney General Ken Paxton was satisfied with the decision, calling it a victory for the state plaintiffs.
“Today’s decision keeps in place what we have maintained from the very start: one person, even a president, cannot unilaterally change the law,” Mr. Paxton said in a statement. “This is a major setback to President Obama’s attempts to expand executive power, and a victory for those who believe in the separation of powers and the rule of law.”
Texas was 1 of 26 states that sued over DAPA and expanded DACA. The states argued the president does not have the authority to issue the new immigration policies, and that the programs violate the Constitution as well as the Administrative Procedure Act for notice-and-comment rule making. Justices heard oral arguments April 18.
Immigration advocates were worried that if expanded DACA were struck down, a similar fate would follow for the original DACA policy. As it stands, undocumented immigrants who benefit from deportation protection and work authorization under original DACA, including undocumented medical students, will not be affected by the Supreme Court decision.
Marielena Hincapié, executive director for the National Immigration Law Center, vowed to continue fighting for the policies to take effect.
“Immigrants and allies fought for and won these significant policy victories, which would have brought much-needed emotional and economic stability to millions of our community members, and we will not sit back,” she said in a statement. “We urge the Department of Justice to seek a rehearing for when a ninth justice is confirmed for the Supreme Court.”
Federation for American Immigration Reform President Dan Stein said the split decision upholds the rule of law and helps preserve the balance of power in the United States.
“By ruling in favor of the federal court’s injunction, half of the nation’s Supreme Court Justices have shown that they have deep concerns about this president’s attempt at a power grab by his efforts to amend federal laws from the Oval Office,” Mr. Stein said in a statement.
Texas v. United States will be sent back to U.S. District Court Judge Andrew Hanen in Texas who will hear the case on its merits. The case could wind its way back to the U.S. Supreme Court for a rehearing after a ninth justice is confirmed.
On Twitter @legal_med
Supreme Court justices have deadlocked on whether protections for undocumented immigrants can be expanded under an executive order by the President.
In a June 23 decision, justices were equally divided on the constitutionality of two of President Obama’s immigration policies: the Deferred Action for Parents of Americans and Lawful Permanent Residents (DAPA) and an expanded version of the Deferred Action for Childhood Arrivals (DACA). The former protects undocumented immigrants who are parents of U.S. citizens from deportation, if they meet certain criteria. The second extends work authorization under the original DACA program from 2 years to 3 years and broadens age requirements.
The 4-to-4 split decision in Texas v. United States mean the policies remain blocked by the lower court, and the expanded programs will not go forward anytime soon. The decision does not affect original DACA, which protects from deportation undocumented immigrants brought to the United States as children and offers access to work authorization.
President Obama expressed disappointment at the lack of agreement, saying the tie vote underscores the need for nine justices on the court.
“As disappointing as it was to be challenged for taking the kind of action that other administrations have taken, the country was looking to the Supreme Court to resolve the important legal questions raised in this case,” President Obama said during a June 23 press conference. “Today, the Supreme Court was unable to reach a decision ... it means the expanded set of common sense deferred action policies that I announced 2 years ago cannot go forward at this stage until there is a ninth justice on the court to break the tie.”
Texas Attorney General Ken Paxton was satisfied with the decision, calling it a victory for the state plaintiffs.
“Today’s decision keeps in place what we have maintained from the very start: one person, even a president, cannot unilaterally change the law,” Mr. Paxton said in a statement. “This is a major setback to President Obama’s attempts to expand executive power, and a victory for those who believe in the separation of powers and the rule of law.”
Texas was 1 of 26 states that sued over DAPA and expanded DACA. The states argued the president does not have the authority to issue the new immigration policies, and that the programs violate the Constitution as well as the Administrative Procedure Act for notice-and-comment rule making. Justices heard oral arguments April 18.
Immigration advocates were worried that if expanded DACA were struck down, a similar fate would follow for the original DACA policy. As it stands, undocumented immigrants who benefit from deportation protection and work authorization under original DACA, including undocumented medical students, will not be affected by the Supreme Court decision.
Marielena Hincapié, executive director for the National Immigration Law Center, vowed to continue fighting for the policies to take effect.
“Immigrants and allies fought for and won these significant policy victories, which would have brought much-needed emotional and economic stability to millions of our community members, and we will not sit back,” she said in a statement. “We urge the Department of Justice to seek a rehearing for when a ninth justice is confirmed for the Supreme Court.”
Federation for American Immigration Reform President Dan Stein said the split decision upholds the rule of law and helps preserve the balance of power in the United States.
“By ruling in favor of the federal court’s injunction, half of the nation’s Supreme Court Justices have shown that they have deep concerns about this president’s attempt at a power grab by his efforts to amend federal laws from the Oval Office,” Mr. Stein said in a statement.
Texas v. United States will be sent back to U.S. District Court Judge Andrew Hanen in Texas who will hear the case on its merits. The case could wind its way back to the U.S. Supreme Court for a rehearing after a ninth justice is confirmed.
On Twitter @legal_med

Guns are psychiatry’s domain, like it or not
Truly, the right to bear firearms is not something that should be in the domain of the psychiatrist, but in our current landscape, it’s fallen into our realm. Personally, (as opposed to professionally), it seems to me that there is no reason that someone needs to own an assault weapon, and Americans somehow survived without them for 10 years from 1994 to 2004 during a national ban on assault weapons, inspired in part by the massacre of children in a 1989 mass shooting at a Stockton, Calif., school, followed in 1993 by a street shooting where eight people were killed in San Francisco.
A CNN poll conducted in 1993 revealed that 73% of those polled opposed the manufacture, sale, or possession of assault weapons, and back then, the politics of gun control were less partisan: Former Republican President Ronald Reagan supported legislation to make them illegal. The ban on assault weapons expired in 2004, and mass shooters have been able to obtain these weapons legally and have used them for many of the highly publicized massacres we read about, now several times a year.

What shocks me is that we manufacture these weapons to allow for rapid and efficient discharge, we make these firearms easily accessible to anyone who wants them in more than 40 states, and then we are surprised when people use them to do exactly what they were designed to do: kill lots of people quickly. Those who oppose bans on these weapons insist that terrorists will find other ways: They will use illegal weapons, bombs made from pressure cookers, biologic agents, or explosives. They may be right; that doesn’t mean our government needs to make it easy for gunmen to massacre innocent people.
Until recently, the discussion about mass murder somehow pitted mental illness against gun control, so like it or not, psychiatry was pulled into the discussion of mass murder. Does this make sense? Very little of gun violence takes the form of these highly publicized mass murders – perhaps 1%. But if you’ve turned on CNN lately, they get a lot of air time, while the deaths of countless others – dozens a day in our gun-drenched cities – are now just part of the routine risks of life. If you hold your definition of mass murders to the deaths of four victims in a public place, then most mass murders are what we see in the news: Aurora, Newtown, Fort Hood, Isla Vista, and the list goes on. Of those shooters, roughly half had some history of some kind of mental illness. If you enlarge the definition, as some do, to include any shooting where four or more victims die, then the association with mental illness drops. Many of these killings are domestic and gang violence, or deaths that occur during the commission of another crime.
Overall, it is estimated that less than 10% of gun murders are caused by mental illness, and the politically correct mantra of the time is to point out that people with mental illness are more likely to be the victims of violence than to perpetrate it. Finally, most gun deaths are suicides and not homicides – a distinction not made by CNN.
Despite the staggering rise in gun deaths in our country, and the clear link between gun availability and gun deaths, our federal legislators are stuck; no new gun legislation has passed. Our Congress has made the quiet statement after Newtown that the National Rifle Association (NRA) is remarkably powerful, and perhaps the story was over when we decided that killing children is acceptable. If that’s not enough, Congress was not propelled to action when one of their own was shot in the head during a massacre.
If I feel frustrated and let off steam by tweeting, how awful former U.S. Rep. Gabby Giffords must feel that her former colleagues have not embraced her advocacy actions with Americans for Responsible Solutions.
Over the last week, we’ve seen Sen. Chris Murphy (D-Conn.) stage a 15-hour filibuster on two gun safety amendments. One would close the terror gap; the other sought to expand background checks for firearms purchases. Both measures failed, as did two other gun control measures in the Senate. We’ve also seen House Democrats conduct a sit-in in an effort to force gun control votes. We can’t even agree that those under FBI surveillance for terrorist activities and those on a no-fly list should not be allowed to purchase firearms of any type, including assault rifles. The response is that the right to own guns is protected by the Constitution and can’t be denied without a judicial process.
In the case of those with mental illnesses, individual states do not allow for such protections. In New York, the NYSAFE Act allows that patients can be reported to the state, then placed on the National Instant Criminal Background Check System, to prevent gun purchases if a therapist believes a patient is at risk of violence. There needs to be no dangerous act and no history of hospitalization to set this in motion, just a therapist’s belief. And all patients who are involuntarily hospitalized in New York are placed in the database.
California is different with its efforts to keep guns from those with mental disorders: Anyone brought in for a psychiatric evaluation by law enforcement or involuntarily hospitalized from an ER on what is commonly known as a “5150 hold,” loses the right to own a gun for 5 years. There is no hearing at that point, and those who are later released at the commitment hearing do not get their gun rights back.
In Maryland, where I live, the restrictions are a mixed bag: Anyone who remains in a psychiatric hospital for more than 30 days, voluntarily or otherwise and without regard to dangerousness, loses his right to own a gun. In addition, more recent legislation has added that at commitment hearings, the administrative law judge determines whether the patient may retain gun rights based on an assessment of his dangerousness toward others.
Each state is different, but for psychiatric patients who are lawful gun owners, seeking help can be a mixed bag, and they certainly do not get the national civil rights protections that we afford terror suspects. Does the fear of losing the right to bear arms play into a hunter’s decision to seek mental health care? It’s hard to imagine that it would not. While we advocate for decreasing stigma and getting care for those who need help, we also erect barriers and increase stigma in this odd mixed-message public health endeavor.
Given the vocal nature of gun control advocates, it’s hard not to wonder whether the unwillingness of Congress to pass laws that might make us safer is about the will of the people or the dollar amount that legislatures receive from the NRA. I am sure there are readers who disagree with me and feel that more guns in the hands of “good guys” make us all safer, but I continue to find it interesting that mental illness does not cause mass murder – at least not with the numbers we see in the United States – in countries with stricter gun control.
Those who advocate for gun rights remain unconcerned about the high incidence of guns and suicide. Many believe that people should have the right to take their own lives, and if a gun were not available, another means would be found. In some cases, there is no doubt that this is true. In others, we worry that an easily accessible gun in the hands of a suicidal person has a very high rate of mortality, and there is no room for second thoughts or chances after an impulsive decision.
Psychiatry has been lassoed here – guns are our domain whether we want them to be or not – and we already are starting to see patients who want us to advocate for their right to retain their firearms. While I can’t imagine taking on the responsibility or liability of saying my patient (or anyone else) is safe with a firearm, there may be moments where it seems there is little choice, especially when a firearm is required for the patient’s employment. In the meantime, I keep hoping our legislators will wake up and come to their senses.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care,” forthcoming from Johns Hopkins University Press in fall 2016.
Truly, the right to bear firearms is not something that should be in the domain of the psychiatrist, but in our current landscape, it’s fallen into our realm. Personally, (as opposed to professionally), it seems to me that there is no reason that someone needs to own an assault weapon, and Americans somehow survived without them for 10 years from 1994 to 2004 during a national ban on assault weapons, inspired in part by the massacre of children in a 1989 mass shooting at a Stockton, Calif., school, followed in 1993 by a street shooting where eight people were killed in San Francisco.
A CNN poll conducted in 1993 revealed that 73% of those polled opposed the manufacture, sale, or possession of assault weapons, and back then, the politics of gun control were less partisan: Former Republican President Ronald Reagan supported legislation to make them illegal. The ban on assault weapons expired in 2004, and mass shooters have been able to obtain these weapons legally and have used them for many of the highly publicized massacres we read about, now several times a year.
What shocks me is that we manufacture these weapons to allow for rapid and efficient discharge, we make these firearms easily accessible to anyone who wants them in more than 40 states, and then we are surprised when people use them to do exactly what they were designed to do: kill lots of people quickly. Those who oppose bans on these weapons insist that terrorists will find other ways: They will use illegal weapons, bombs made from pressure cookers, biologic agents, or explosives. They may be right; that doesn’t mean our government needs to make it easy for gunmen to massacre innocent people.
Until recently, the discussion about mass murder somehow pitted mental illness against gun control, so like it or not, psychiatry was pulled into the discussion of mass murder. Does this make sense? Very little of gun violence takes the form of these highly publicized mass murders – perhaps 1%. But if you’ve turned on CNN lately, they get a lot of air time, while the deaths of countless others – dozens a day in our gun-drenched cities – are now just part of the routine risks of life. If you hold your definition of mass murders to the deaths of four victims in a public place, then most mass murders are what we see in the news: Aurora, Newtown, Fort Hood, Isla Vista, and the list goes on. Of those shooters, roughly half had some history of some kind of mental illness. If you enlarge the definition, as some do, to include any shooting where four or more victims die, then the association with mental illness drops. Many of these killings are domestic and gang violence, or deaths that occur during the commission of another crime.
Overall, it is estimated that less than 10% of gun murders are caused by mental illness, and the politically correct mantra of the time is to point out that people with mental illness are more likely to be the victims of violence than to perpetrate it. Finally, most gun deaths are suicides and not homicides – a distinction not made by CNN.
Despite the staggering rise in gun deaths in our country, and the clear link between gun availability and gun deaths, our federal legislators are stuck; no new gun legislation has passed. Our Congress has made the quiet statement after Newtown that the National Rifle Association (NRA) is remarkably powerful, and perhaps the story was over when we decided that killing children is acceptable. If that’s not enough, Congress was not propelled to action when one of their own was shot in the head during a massacre.
If I feel frustrated and let off steam by tweeting, how awful former U.S. Rep. Gabby Giffords must feel that her former colleagues have not embraced her advocacy actions with Americans for Responsible Solutions.
Over the last week, we’ve seen Sen. Chris Murphy (D-Conn.) stage a 15-hour filibuster on two gun safety amendments. One would close the terror gap; the other sought to expand background checks for firearms purchases. Both measures failed, as did two other gun control measures in the Senate. We’ve also seen House Democrats conduct a sit-in in an effort to force gun control votes. We can’t even agree that those under FBI surveillance for terrorist activities and those on a no-fly list should not be allowed to purchase firearms of any type, including assault rifles. The response is that the right to own guns is protected by the Constitution and can’t be denied without a judicial process.
In the case of those with mental illnesses, individual states do not allow for such protections. In New York, the NYSAFE Act allows that patients can be reported to the state, then placed on the National Instant Criminal Background Check System, to prevent gun purchases if a therapist believes a patient is at risk of violence. There needs to be no dangerous act and no history of hospitalization to set this in motion, just a therapist’s belief. And all patients who are involuntarily hospitalized in New York are placed in the database.
California is different with its efforts to keep guns from those with mental disorders: Anyone brought in for a psychiatric evaluation by law enforcement or involuntarily hospitalized from an ER on what is commonly known as a “5150 hold,” loses the right to own a gun for 5 years. There is no hearing at that point, and those who are later released at the commitment hearing do not get their gun rights back.
In Maryland, where I live, the restrictions are a mixed bag: Anyone who remains in a psychiatric hospital for more than 30 days, voluntarily or otherwise and without regard to dangerousness, loses his right to own a gun. In addition, more recent legislation has added that at commitment hearings, the administrative law judge determines whether the patient may retain gun rights based on an assessment of his dangerousness toward others.
Each state is different, but for psychiatric patients who are lawful gun owners, seeking help can be a mixed bag, and they certainly do not get the national civil rights protections that we afford terror suspects. Does the fear of losing the right to bear arms play into a hunter’s decision to seek mental health care? It’s hard to imagine that it would not. While we advocate for decreasing stigma and getting care for those who need help, we also erect barriers and increase stigma in this odd mixed-message public health endeavor.
Given the vocal nature of gun control advocates, it’s hard not to wonder whether the unwillingness of Congress to pass laws that might make us safer is about the will of the people or the dollar amount that legislatures receive from the NRA. I am sure there are readers who disagree with me and feel that more guns in the hands of “good guys” make us all safer, but I continue to find it interesting that mental illness does not cause mass murder – at least not with the numbers we see in the United States – in countries with stricter gun control.
Those who advocate for gun rights remain unconcerned about the high incidence of guns and suicide. Many believe that people should have the right to take their own lives, and if a gun were not available, another means would be found. In some cases, there is no doubt that this is true. In others, we worry that an easily accessible gun in the hands of a suicidal person has a very high rate of mortality, and there is no room for second thoughts or chances after an impulsive decision.
Psychiatry has been lassoed here – guns are our domain whether we want them to be or not – and we already are starting to see patients who want us to advocate for their right to retain their firearms. While I can’t imagine taking on the responsibility or liability of saying my patient (or anyone else) is safe with a firearm, there may be moments where it seems there is little choice, especially when a firearm is required for the patient’s employment. In the meantime, I keep hoping our legislators will wake up and come to their senses.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care,” forthcoming from Johns Hopkins University Press in fall 2016.
Truly, the right to bear firearms is not something that should be in the domain of the psychiatrist, but in our current landscape, it’s fallen into our realm. Personally, (as opposed to professionally), it seems to me that there is no reason that someone needs to own an assault weapon, and Americans somehow survived without them for 10 years from 1994 to 2004 during a national ban on assault weapons, inspired in part by the massacre of children in a 1989 mass shooting at a Stockton, Calif., school, followed in 1993 by a street shooting where eight people were killed in San Francisco.
A CNN poll conducted in 1993 revealed that 73% of those polled opposed the manufacture, sale, or possession of assault weapons, and back then, the politics of gun control were less partisan: Former Republican President Ronald Reagan supported legislation to make them illegal. The ban on assault weapons expired in 2004, and mass shooters have been able to obtain these weapons legally and have used them for many of the highly publicized massacres we read about, now several times a year.
What shocks me is that we manufacture these weapons to allow for rapid and efficient discharge, we make these firearms easily accessible to anyone who wants them in more than 40 states, and then we are surprised when people use them to do exactly what they were designed to do: kill lots of people quickly. Those who oppose bans on these weapons insist that terrorists will find other ways: They will use illegal weapons, bombs made from pressure cookers, biologic agents, or explosives. They may be right; that doesn’t mean our government needs to make it easy for gunmen to massacre innocent people.
Until recently, the discussion about mass murder somehow pitted mental illness against gun control, so like it or not, psychiatry was pulled into the discussion of mass murder. Does this make sense? Very little of gun violence takes the form of these highly publicized mass murders – perhaps 1%. But if you’ve turned on CNN lately, they get a lot of air time, while the deaths of countless others – dozens a day in our gun-drenched cities – are now just part of the routine risks of life. If you hold your definition of mass murders to the deaths of four victims in a public place, then most mass murders are what we see in the news: Aurora, Newtown, Fort Hood, Isla Vista, and the list goes on. Of those shooters, roughly half had some history of some kind of mental illness. If you enlarge the definition, as some do, to include any shooting where four or more victims die, then the association with mental illness drops. Many of these killings are domestic and gang violence, or deaths that occur during the commission of another crime.
Overall, it is estimated that less than 10% of gun murders are caused by mental illness, and the politically correct mantra of the time is to point out that people with mental illness are more likely to be the victims of violence than to perpetrate it. Finally, most gun deaths are suicides and not homicides – a distinction not made by CNN.
Despite the staggering rise in gun deaths in our country, and the clear link between gun availability and gun deaths, our federal legislators are stuck; no new gun legislation has passed. Our Congress has made the quiet statement after Newtown that the National Rifle Association (NRA) is remarkably powerful, and perhaps the story was over when we decided that killing children is acceptable. If that’s not enough, Congress was not propelled to action when one of their own was shot in the head during a massacre.
If I feel frustrated and let off steam by tweeting, how awful former U.S. Rep. Gabby Giffords must feel that her former colleagues have not embraced her advocacy actions with Americans for Responsible Solutions.
Over the last week, we’ve seen Sen. Chris Murphy (D-Conn.) stage a 15-hour filibuster on two gun safety amendments. One would close the terror gap; the other sought to expand background checks for firearms purchases. Both measures failed, as did two other gun control measures in the Senate. We’ve also seen House Democrats conduct a sit-in in an effort to force gun control votes. We can’t even agree that those under FBI surveillance for terrorist activities and those on a no-fly list should not be allowed to purchase firearms of any type, including assault rifles. The response is that the right to own guns is protected by the Constitution and can’t be denied without a judicial process.
In the case of those with mental illnesses, individual states do not allow for such protections. In New York, the NYSAFE Act allows that patients can be reported to the state, then placed on the National Instant Criminal Background Check System, to prevent gun purchases if a therapist believes a patient is at risk of violence. There needs to be no dangerous act and no history of hospitalization to set this in motion, just a therapist’s belief. And all patients who are involuntarily hospitalized in New York are placed in the database.
California is different with its efforts to keep guns from those with mental disorders: Anyone brought in for a psychiatric evaluation by law enforcement or involuntarily hospitalized from an ER on what is commonly known as a “5150 hold,” loses the right to own a gun for 5 years. There is no hearing at that point, and those who are later released at the commitment hearing do not get their gun rights back.
In Maryland, where I live, the restrictions are a mixed bag: Anyone who remains in a psychiatric hospital for more than 30 days, voluntarily or otherwise and without regard to dangerousness, loses his right to own a gun. In addition, more recent legislation has added that at commitment hearings, the administrative law judge determines whether the patient may retain gun rights based on an assessment of his dangerousness toward others.
Each state is different, but for psychiatric patients who are lawful gun owners, seeking help can be a mixed bag, and they certainly do not get the national civil rights protections that we afford terror suspects. Does the fear of losing the right to bear arms play into a hunter’s decision to seek mental health care? It’s hard to imagine that it would not. While we advocate for decreasing stigma and getting care for those who need help, we also erect barriers and increase stigma in this odd mixed-message public health endeavor.
Given the vocal nature of gun control advocates, it’s hard not to wonder whether the unwillingness of Congress to pass laws that might make us safer is about the will of the people or the dollar amount that legislatures receive from the NRA. I am sure there are readers who disagree with me and feel that more guns in the hands of “good guys” make us all safer, but I continue to find it interesting that mental illness does not cause mass murder – at least not with the numbers we see in the United States – in countries with stricter gun control.
Those who advocate for gun rights remain unconcerned about the high incidence of guns and suicide. Many believe that people should have the right to take their own lives, and if a gun were not available, another means would be found. In some cases, there is no doubt that this is true. In others, we worry that an easily accessible gun in the hands of a suicidal person has a very high rate of mortality, and there is no room for second thoughts or chances after an impulsive decision.
Psychiatry has been lassoed here – guns are our domain whether we want them to be or not – and we already are starting to see patients who want us to advocate for their right to retain their firearms. While I can’t imagine taking on the responsibility or liability of saying my patient (or anyone else) is safe with a firearm, there may be moments where it seems there is little choice, especially when a firearm is required for the patient’s employment. In the meantime, I keep hoping our legislators will wake up and come to their senses.
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care,” forthcoming from Johns Hopkins University Press in fall 2016.
