User login
Guideline recommends 2-mm negative margins for DCIS
Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ (DCIS), according to a multidisciplinary consensus panel.
Despite the widespread use of surgical excision in breast-conserving therapy among patients with DCIS, there is no consensus on the optimal negative margin to prevent recurrence and re-excision. Therefore, the Society of Surgical Oncology, the American Society for Radiation Oncology, and the American Society of Clinical Oncology convened a panel to answer the following question: What margin width minimizes the risk of ipsilateral breast tumor recurrence in patients with DCIS receiving breast-conserving surgery?

The guideline panel reviewed 20 studies including 7,883 DCIS patients. A median of 100% of patients received whole-breast radiation therapy and a median of 21% received endocrine therapy. Patients were followed for a median of 6.5 years and the median incidence of recurrence was 8.3%.
“There is no debate that a positive margin ... implies a potentially incomplete resection and is associated with a higher rate of [recurrence],” according to Monica Morrow, MD, of Memorial Sloan-Kettering Cancer Center, and her fellow panelists. Further, the addition of whole-breast irradiation did not negate this increased risk, the panelists noted (J Clin Oncol. 2016 Aug. doi: 10.1200/JCO.2016.68.3573).
According to the meta-analysis, patients with 2-mm negative margins plus whole-breast irradiation were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
“Margins of at least 2 mm are associated with a reduced risk of [recurrence] relative to narrower negative margin widths in patients receiving [whole-breast radiotherapy]. The routine practice of obtaining negative margin widths wider than 2 mm is not supported by the evidence,” they wrote.
The panel also noted that treatment with excision alone is associated with higher rates of recurrence compared with treatment involving with both excision and whole-breast radiation therapy. However, if patients are treated with excision alone, the optimal margin, which is unknown for this subset of patients, should be at least 2 millimeters, according to the guideline.
Due to variability in specimen sampling and in margin evaluation and assessment, “clinical judgment must be used in determining whether patients with smaller negative margin widths (0 or 1 mm) require re-excision,” the panelists noted. “The findings should not be extrapolated to DCIS patients treated with [accelerated partial breast irradiation] or those with invasive carcinoma for whom a separate guideline has been developed,” Dr. Morrow and her associates wrote.
The guideline development process was funded by the Susan G. Komen Foundation. The authors had no relevant disclosures to report.
On Twitter @jessnicolecraig
Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ (DCIS), according to a multidisciplinary consensus panel.
Despite the widespread use of surgical excision in breast-conserving therapy among patients with DCIS, there is no consensus on the optimal negative margin to prevent recurrence and re-excision. Therefore, the Society of Surgical Oncology, the American Society for Radiation Oncology, and the American Society of Clinical Oncology convened a panel to answer the following question: What margin width minimizes the risk of ipsilateral breast tumor recurrence in patients with DCIS receiving breast-conserving surgery?
The guideline panel reviewed 20 studies including 7,883 DCIS patients. A median of 100% of patients received whole-breast radiation therapy and a median of 21% received endocrine therapy. Patients were followed for a median of 6.5 years and the median incidence of recurrence was 8.3%.
“There is no debate that a positive margin ... implies a potentially incomplete resection and is associated with a higher rate of [recurrence],” according to Monica Morrow, MD, of Memorial Sloan-Kettering Cancer Center, and her fellow panelists. Further, the addition of whole-breast irradiation did not negate this increased risk, the panelists noted (J Clin Oncol. 2016 Aug. doi: 10.1200/JCO.2016.68.3573).
According to the meta-analysis, patients with 2-mm negative margins plus whole-breast irradiation were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
“Margins of at least 2 mm are associated with a reduced risk of [recurrence] relative to narrower negative margin widths in patients receiving [whole-breast radiotherapy]. The routine practice of obtaining negative margin widths wider than 2 mm is not supported by the evidence,” they wrote.
The panel also noted that treatment with excision alone is associated with higher rates of recurrence compared with treatment involving with both excision and whole-breast radiation therapy. However, if patients are treated with excision alone, the optimal margin, which is unknown for this subset of patients, should be at least 2 millimeters, according to the guideline.
Due to variability in specimen sampling and in margin evaluation and assessment, “clinical judgment must be used in determining whether patients with smaller negative margin widths (0 or 1 mm) require re-excision,” the panelists noted. “The findings should not be extrapolated to DCIS patients treated with [accelerated partial breast irradiation] or those with invasive carcinoma for whom a separate guideline has been developed,” Dr. Morrow and her associates wrote.
The guideline development process was funded by the Susan G. Komen Foundation. The authors had no relevant disclosures to report.
On Twitter @jessnicolecraig
Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ (DCIS), according to a multidisciplinary consensus panel.
Despite the widespread use of surgical excision in breast-conserving therapy among patients with DCIS, there is no consensus on the optimal negative margin to prevent recurrence and re-excision. Therefore, the Society of Surgical Oncology, the American Society for Radiation Oncology, and the American Society of Clinical Oncology convened a panel to answer the following question: What margin width minimizes the risk of ipsilateral breast tumor recurrence in patients with DCIS receiving breast-conserving surgery?
The guideline panel reviewed 20 studies including 7,883 DCIS patients. A median of 100% of patients received whole-breast radiation therapy and a median of 21% received endocrine therapy. Patients were followed for a median of 6.5 years and the median incidence of recurrence was 8.3%.
“There is no debate that a positive margin ... implies a potentially incomplete resection and is associated with a higher rate of [recurrence],” according to Monica Morrow, MD, of Memorial Sloan-Kettering Cancer Center, and her fellow panelists. Further, the addition of whole-breast irradiation did not negate this increased risk, the panelists noted (J Clin Oncol. 2016 Aug. doi: 10.1200/JCO.2016.68.3573).
According to the meta-analysis, patients with 2-mm negative margins plus whole-breast irradiation were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
“Margins of at least 2 mm are associated with a reduced risk of [recurrence] relative to narrower negative margin widths in patients receiving [whole-breast radiotherapy]. The routine practice of obtaining negative margin widths wider than 2 mm is not supported by the evidence,” they wrote.
The panel also noted that treatment with excision alone is associated with higher rates of recurrence compared with treatment involving with both excision and whole-breast radiation therapy. However, if patients are treated with excision alone, the optimal margin, which is unknown for this subset of patients, should be at least 2 millimeters, according to the guideline.
Due to variability in specimen sampling and in margin evaluation and assessment, “clinical judgment must be used in determining whether patients with smaller negative margin widths (0 or 1 mm) require re-excision,” the panelists noted. “The findings should not be extrapolated to DCIS patients treated with [accelerated partial breast irradiation] or those with invasive carcinoma for whom a separate guideline has been developed,” Dr. Morrow and her associates wrote.
The guideline development process was funded by the Susan G. Komen Foundation. The authors had no relevant disclosures to report.
On Twitter @jessnicolecraig
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Surgical excision with 2-mm clear margins combined with whole-breast irradiation may be the optimal standard to reduce recurrence in patients with ductal carcinoma in situ.
Major finding: Patients with 2-mm clear margins were significantly less likely to experience ipsilateral breast tumor recurrence compared with patients who had excisions with positive margins.
Data source: Meta-analysis of 20 studies and other published literature.
Disclosures: The Susan G. Komen Foundation funded the guideline development process. The panel members had no relevant disclosures.

Pilot program helps children better understand food allergies
Elementary school students had improved attitudes toward food allergies and felt more confident in taking action during a food allergy emergency after completing an education program on the subject, results of a pilot study in Japan suggest.
At present there is no standard school curriculum for children regarding food allergy, wrote Dr. Kiwako Yamamoto-Hanada of the National Center for Child Health and Development, Tokyo, and associates, so they developed such a program consisting of two 60-minute sessions. A total of 36 elementary school children, 8 of whom had a history of food allergies, filled out questionnaires before and after participating in the program.
After completing the program, 79% of the students stated that it should be included in the school curriculum. Students also demonstrated improved knowledge about food allergies, with a greater percentage knowing what an EpiPen is (100% vs. 0%), understanding that food allergy is related to death (100% vs. 43%), and feeling confident that they could take immediate action if they saw a food allergy emergency (61% vs. 4%). “This is the first report to find that a [food allergy] program for elementary schoolchildren was well tolerated and that perceptions and attitudes toward [food allergies] improved,” the investigators wrote.
The authors stated that they had no financial conflicts of interest.
Read the full story here: http://dx.doi.org/10.1016/j.anai.2016.06.018
Elementary school students had improved attitudes toward food allergies and felt more confident in taking action during a food allergy emergency after completing an education program on the subject, results of a pilot study in Japan suggest.
At present there is no standard school curriculum for children regarding food allergy, wrote Dr. Kiwako Yamamoto-Hanada of the National Center for Child Health and Development, Tokyo, and associates, so they developed such a program consisting of two 60-minute sessions. A total of 36 elementary school children, 8 of whom had a history of food allergies, filled out questionnaires before and after participating in the program.
After completing the program, 79% of the students stated that it should be included in the school curriculum. Students also demonstrated improved knowledge about food allergies, with a greater percentage knowing what an EpiPen is (100% vs. 0%), understanding that food allergy is related to death (100% vs. 43%), and feeling confident that they could take immediate action if they saw a food allergy emergency (61% vs. 4%). “This is the first report to find that a [food allergy] program for elementary schoolchildren was well tolerated and that perceptions and attitudes toward [food allergies] improved,” the investigators wrote.
The authors stated that they had no financial conflicts of interest.
Read the full story here: http://dx.doi.org/10.1016/j.anai.2016.06.018
Elementary school students had improved attitudes toward food allergies and felt more confident in taking action during a food allergy emergency after completing an education program on the subject, results of a pilot study in Japan suggest.
At present there is no standard school curriculum for children regarding food allergy, wrote Dr. Kiwako Yamamoto-Hanada of the National Center for Child Health and Development, Tokyo, and associates, so they developed such a program consisting of two 60-minute sessions. A total of 36 elementary school children, 8 of whom had a history of food allergies, filled out questionnaires before and after participating in the program.
After completing the program, 79% of the students stated that it should be included in the school curriculum. Students also demonstrated improved knowledge about food allergies, with a greater percentage knowing what an EpiPen is (100% vs. 0%), understanding that food allergy is related to death (100% vs. 43%), and feeling confident that they could take immediate action if they saw a food allergy emergency (61% vs. 4%). “This is the first report to find that a [food allergy] program for elementary schoolchildren was well tolerated and that perceptions and attitudes toward [food allergies] improved,” the investigators wrote.
The authors stated that they had no financial conflicts of interest.
Read the full story here: http://dx.doi.org/10.1016/j.anai.2016.06.018
FROM ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Antipsychotics in pregnancy pose no meaningful malformation risk
Antipsychotic use early in pregnancy does not appear to meaningfully increase the risk of congenital malformations, according to findings from a large Medicaid pregnancy cohort.
A possible exception is with the use of risperidone; a small increase in the risk for malformations seen with the drug should be viewed as “an initial safety signal that will require confirmation in other studies,” Krista F. Huybrechts, PhD, of Brigham and Women’s Hospital and Harvard Medical School, Boston, and her colleagues reported online Aug. 17 in JAMA Psychiatry.

In a nationwide sample of more than 1.3 million pregnant women with a live-born infant between January 1, 2000 and December 31, 2010, the rate of congenital malformations identified within 90 days after delivery was 32.7 per 1,000 births among 1,331,724 women with no antipsychotic (AP) exposure, compared with a rate of 44.5 per 1,000 births among 9,258 women who filled at least one prescription for an atypical AP during their first trimester, and 38.2 per 1,000 in 733 women who filled at least one prescription for a typical AP during their first trimester, the researchers found (JAMA Psychiatry. 2016 Aug 17. doi: 10.1001/jamapsychiatry.2016.1520).
On unadjusted analyses, an overall risk was seen with atypical AP exposure (relative risk, 1.36), but not with typical AP exposure (RR, 1.17). After adjusting for confounding variables, the risk was not statistically significant (RR, 1.05 and 0.90, respectively). The findings were similar for cardiac malformations, the researchers noted.
When agents were analyzed individually, a small increased risk in overall malformations and cardiac malformations was found with risperidone (RR, 1.26 for each).
“The findings for risperidone should be viewed as an initial safety signal that will require confirmation in other studies,” the researchers wrote.
The study was supported by grants from the National Institutes of Health and the Swiss National Science Foundation. Dr. Huybrechts reported having no financial disclosures. Other authors disclosed receiving consulting fees and/or grant support from AstraZeneca, UCB, Alkermes, Bristol-Myers Squibb/Otsuka, Sunovion, Bayer, Ortho-McNeil Janssen, Pfizer, Forest Laboratories, Cephalon, GlaxoSmithKline, Takeda/Lundbeck, the National Institutes of Health, JDS Therapeutics, Noven Pharmaceuticals, and PamLab.
This “landmark report” by Huybrechts et al involves the largest population of women exposed to APs published to date, and addresses a “major source of concern for women and prescribers,” Katherine L. Wisner, MD, and her colleagues wrote in an editorial.
With the exception of risperidone, which was found to be associated with a 26% increase in the risk of overall and cardiac malformations, and possibly even greater risk among those who filled at least two AP prescriptions – and thus merits further exploration – AP use was found in the study to be safe.
“This study increases the field’s appetite for additional high-quality data on other maternal and offspring outcomes to improve the sophistication of risk-benefit decision making,” the authors wrote.
Nowhere in medicine is there a greater need for personalization of care, particularly when it comes to the treatment of serious mental illness with consideration of “pregnancy physiology and the mother’s capacity to provide sustenance for the growing fetus and newborn,” they wrote.
Dr. Wisner is with Northwestern University, Chicago. She reported that her department at Northwestern received contractual fees for her consultation to Quinn Emanuel Urquhart & Sullivan, LLP, who represented Pfizer Pharmaceutical Company in 2015. A coauthor, Christina Chambers, PhD, reported receiving research funding from AbbVie, Bristol-Myers Squibb, Celgene, GlaxoSmithKline, Janssen, Pfizer, Sandoz, and Teva. No other disclosures were reported. Their comments are excerpted from an accompanying editorial (JAMA Psychiatry. 2016 Aug 17. doi: 10.1001/jamapsychiatry.2016.1538).
This “landmark report” by Huybrechts et al involves the largest population of women exposed to APs published to date, and addresses a “major source of concern for women and prescribers,” Katherine L. Wisner, MD, and her colleagues wrote in an editorial.
With the exception of risperidone, which was found to be associated with a 26% increase in the risk of overall and cardiac malformations, and possibly even greater risk among those who filled at least two AP prescriptions – and thus merits further exploration – AP use was found in the study to be safe.
“This study increases the field’s appetite for additional high-quality data on other maternal and offspring outcomes to improve the sophistication of risk-benefit decision making,” the authors wrote.
Nowhere in medicine is there a greater need for personalization of care, particularly when it comes to the treatment of serious mental illness with consideration of “pregnancy physiology and the mother’s capacity to provide sustenance for the growing fetus and newborn,” they wrote.
Dr. Wisner is with Northwestern University, Chicago. She reported that her department at Northwestern received contractual fees for her consultation to Quinn Emanuel Urquhart & Sullivan, LLP, who represented Pfizer Pharmaceutical Company in 2015. A coauthor, Christina Chambers, PhD, reported receiving research funding from AbbVie, Bristol-Myers Squibb, Celgene, GlaxoSmithKline, Janssen, Pfizer, Sandoz, and Teva. No other disclosures were reported. Their comments are excerpted from an accompanying editorial (JAMA Psychiatry. 2016 Aug 17. doi: 10.1001/jamapsychiatry.2016.1538).
This “landmark report” by Huybrechts et al involves the largest population of women exposed to APs published to date, and addresses a “major source of concern for women and prescribers,” Katherine L. Wisner, MD, and her colleagues wrote in an editorial.
With the exception of risperidone, which was found to be associated with a 26% increase in the risk of overall and cardiac malformations, and possibly even greater risk among those who filled at least two AP prescriptions – and thus merits further exploration – AP use was found in the study to be safe.
“This study increases the field’s appetite for additional high-quality data on other maternal and offspring outcomes to improve the sophistication of risk-benefit decision making,” the authors wrote.
Nowhere in medicine is there a greater need for personalization of care, particularly when it comes to the treatment of serious mental illness with consideration of “pregnancy physiology and the mother’s capacity to provide sustenance for the growing fetus and newborn,” they wrote.
Dr. Wisner is with Northwestern University, Chicago. She reported that her department at Northwestern received contractual fees for her consultation to Quinn Emanuel Urquhart & Sullivan, LLP, who represented Pfizer Pharmaceutical Company in 2015. A coauthor, Christina Chambers, PhD, reported receiving research funding from AbbVie, Bristol-Myers Squibb, Celgene, GlaxoSmithKline, Janssen, Pfizer, Sandoz, and Teva. No other disclosures were reported. Their comments are excerpted from an accompanying editorial (JAMA Psychiatry. 2016 Aug 17. doi: 10.1001/jamapsychiatry.2016.1538).
Antipsychotic use early in pregnancy does not appear to meaningfully increase the risk of congenital malformations, according to findings from a large Medicaid pregnancy cohort.
A possible exception is with the use of risperidone; a small increase in the risk for malformations seen with the drug should be viewed as “an initial safety signal that will require confirmation in other studies,” Krista F. Huybrechts, PhD, of Brigham and Women’s Hospital and Harvard Medical School, Boston, and her colleagues reported online Aug. 17 in JAMA Psychiatry.
In a nationwide sample of more than 1.3 million pregnant women with a live-born infant between January 1, 2000 and December 31, 2010, the rate of congenital malformations identified within 90 days after delivery was 32.7 per 1,000 births among 1,331,724 women with no antipsychotic (AP) exposure, compared with a rate of 44.5 per 1,000 births among 9,258 women who filled at least one prescription for an atypical AP during their first trimester, and 38.2 per 1,000 in 733 women who filled at least one prescription for a typical AP during their first trimester, the researchers found (JAMA Psychiatry. 2016 Aug 17. doi: 10.1001/jamapsychiatry.2016.1520).
On unadjusted analyses, an overall risk was seen with atypical AP exposure (relative risk, 1.36), but not with typical AP exposure (RR, 1.17). After adjusting for confounding variables, the risk was not statistically significant (RR, 1.05 and 0.90, respectively). The findings were similar for cardiac malformations, the researchers noted.
When agents were analyzed individually, a small increased risk in overall malformations and cardiac malformations was found with risperidone (RR, 1.26 for each).
“The findings for risperidone should be viewed as an initial safety signal that will require confirmation in other studies,” the researchers wrote.
The study was supported by grants from the National Institutes of Health and the Swiss National Science Foundation. Dr. Huybrechts reported having no financial disclosures. Other authors disclosed receiving consulting fees and/or grant support from AstraZeneca, UCB, Alkermes, Bristol-Myers Squibb/Otsuka, Sunovion, Bayer, Ortho-McNeil Janssen, Pfizer, Forest Laboratories, Cephalon, GlaxoSmithKline, Takeda/Lundbeck, the National Institutes of Health, JDS Therapeutics, Noven Pharmaceuticals, and PamLab.
Antipsychotic use early in pregnancy does not appear to meaningfully increase the risk of congenital malformations, according to findings from a large Medicaid pregnancy cohort.
A possible exception is with the use of risperidone; a small increase in the risk for malformations seen with the drug should be viewed as “an initial safety signal that will require confirmation in other studies,” Krista F. Huybrechts, PhD, of Brigham and Women’s Hospital and Harvard Medical School, Boston, and her colleagues reported online Aug. 17 in JAMA Psychiatry.
In a nationwide sample of more than 1.3 million pregnant women with a live-born infant between January 1, 2000 and December 31, 2010, the rate of congenital malformations identified within 90 days after delivery was 32.7 per 1,000 births among 1,331,724 women with no antipsychotic (AP) exposure, compared with a rate of 44.5 per 1,000 births among 9,258 women who filled at least one prescription for an atypical AP during their first trimester, and 38.2 per 1,000 in 733 women who filled at least one prescription for a typical AP during their first trimester, the researchers found (JAMA Psychiatry. 2016 Aug 17. doi: 10.1001/jamapsychiatry.2016.1520).
On unadjusted analyses, an overall risk was seen with atypical AP exposure (relative risk, 1.36), but not with typical AP exposure (RR, 1.17). After adjusting for confounding variables, the risk was not statistically significant (RR, 1.05 and 0.90, respectively). The findings were similar for cardiac malformations, the researchers noted.
When agents were analyzed individually, a small increased risk in overall malformations and cardiac malformations was found with risperidone (RR, 1.26 for each).
“The findings for risperidone should be viewed as an initial safety signal that will require confirmation in other studies,” the researchers wrote.
The study was supported by grants from the National Institutes of Health and the Swiss National Science Foundation. Dr. Huybrechts reported having no financial disclosures. Other authors disclosed receiving consulting fees and/or grant support from AstraZeneca, UCB, Alkermes, Bristol-Myers Squibb/Otsuka, Sunovion, Bayer, Ortho-McNeil Janssen, Pfizer, Forest Laboratories, Cephalon, GlaxoSmithKline, Takeda/Lundbeck, the National Institutes of Health, JDS Therapeutics, Noven Pharmaceuticals, and PamLab.
FROM JAMA PSYCHIATRY
Key clinical point: Antipsychotic use in the first trimester does not appear to meaningfully increase the risk of congenital malformations.
Major finding: The adjusted relative risk for malformations is 1.05 and 0.90 with atypical and typical antipsychotic drug exposure, respectively.
Data source: A total of 1,341,715 pregnancies from the Medicaid Analytic Extract database pregnancy cohort.
Disclosures: The study was supported by grants from the National Institutes of Health and the Swiss National Science Foundation. Dr. Huybrechts reported having no financial disclosures. Other authors disclosed receiving consulting fees and/or grant support from AstraZeneca, UCB, Alkermes, Bristol-Myers Squibb/Otsuka, Sunovion, Bayer, Ortho-McNeil Janssen, Pfizer, Forest Laboratories, Cephalon, GlaxoSmithKline, Takeda/Lundbeck, the National Institutes of Health, JDS Therapeutics, Noven Pharmaceuticals, and PamLab.

Cancer trends shifting in HIV-positive patients
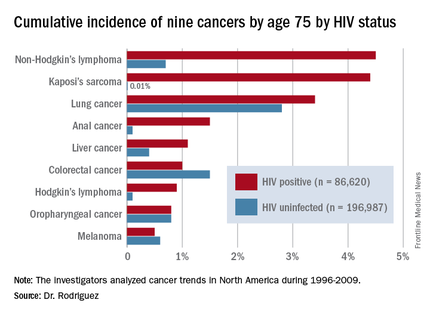
DURBAN, SOUTH AFRICA – The rates of the AIDS-defining cancers Kaposi’s sarcoma and non-Hodgkin’s lymphoma have plummeted in the antiretroviral era, yet they are still the two top cancers in terms of cumulative incidence in HIV-infected patients by age 75, Benigno Rodriguez, MD, said at the 21st International AIDS Conference.
Lung cancer also remains a major concern in the HIV-infected population. Each of these three cancers carries about a 1 in 25 lifetime risk to age 75, the estimated lifespan of HIV-positive patients on combination antiretroviral therapy (ART), according to Dr. Rodriguez of Case Western Reserve University in Cleveland.

ART has resulted in a marked change in cancer trends among HIV-infected patients. The incidence of AIDS-defining cancers has decreased “massively,” Dr. Rodriguez observed; but because ART has extended the lifespan, patients are now living long enough to get other cancers. And they do so at a higher rate than that of the general population because of their impaired immune function, higher rate of risk factors such as smoking, and greater prevalence of oncogenic viral coinfections such as hepatitis B and C and Epstein-Barr virus.
The increase in the incidence and risk of colorectal, liver, and anal cancers among HIV-positive individuals since the introduction of combination ART can largely be explained by the population’s longer exposure to risk due to increasing survival, he said.
Dr. Rodriguez presented highlights of an analysis of cancer trends in North America during 1996-2009. The study was based on 86,620 HIV-infected persons with 475,660 person-years of follow-up and 196,987 subjects without HIV infection and with more than 1.8 million person-years of follow-up. Trends over time were assessed for nine cancers: Kaposi’s sarcoma, non-Hodgkin’s lymphoma, Hodgkin’s lymphoma, and melanoma, as well as anal, lung, colorectal, liver, and oropharyngeal cancers (Ann Intern Med. 2015;163:507-18).
Examining trends in three periods – 1996-1999, 2000-2004, and 2005-2009 – the investigators looked at the impact of ART over time on rates of AIDS-related and non–AIDS-related cancers in HIV-infected patients and compared them to results in the general HIV-uninfected population.
By conducting a competing risk analysis, Dr. Rodriguez and his coworkers were able to estimate the cumulative lifetime risk of the various cancers by age 75, a metric that provides readily understandable information for counseling HIV-infected patients about their long-term cancer risk.
The measure “is more intuitive than using incidence rates,” Dr. Rodriguez said. In a study of 1,578 HIV-infected patients who received the hepatitis B vaccine, for example, those patients whose immune function did not to respond to the vaccine were more likely to be among the 6% of patients who subsequently developed cancer during up to 20 years of follow-up.
The findings on cancer trends in the ART era have clinical implications for cancer screening and prevention in HIV-infected patients. The high rates of smoking and lung cancer in this population make HIV-positive smokers a logical target for lung cancer screening. The rising risk of colorectal cancer – the cumulative lifetime risk to age 75 was 0.4% in 1996-1999, 0.7% in 2000-2004, and 1.3% in 2005-2009 – suggests a need for increased colorectal cancer screening in the older HIV-positive population.
Early and sustained HIV suppression with combination ART remains the only known method of preventing AIDS-defining cancers. Dr. Rodriguez and his coinvestigators in the Centers for AIDS Research Network of Integrated Clinical Systems demonstrated the crucial role of suppressing HIV in a study of 6,036 HIV-infected patients who started on ART and were followed for more than 21,000 person-years. Compared with HIV-infected patients with a 3-month lagged HIV viremia of no more than 50 copies/mL, patients’ risk of developing non-Hodgkin’s lymphoma was 2.1-fold greater if their 3-month lagged HIV viremia was 51-500 copies/mL and 3.56-fold greater if it exceeded 500 copies/mL (Clin Infect Dis. 2014 Jun;58[11]:1599-606).
The study on cancer trends over time was funded by the National Institutes of Health. Dr. Rodriguez reported receiving honoraria from Gilead Sciences.
DURBAN, SOUTH AFRICA – The rates of the AIDS-defining cancers Kaposi’s sarcoma and non-Hodgkin’s lymphoma have plummeted in the antiretroviral era, yet they are still the two top cancers in terms of cumulative incidence in HIV-infected patients by age 75, Benigno Rodriguez, MD, said at the 21st International AIDS Conference.
Lung cancer also remains a major concern in the HIV-infected population. Each of these three cancers carries about a 1 in 25 lifetime risk to age 75, the estimated lifespan of HIV-positive patients on combination antiretroviral therapy (ART), according to Dr. Rodriguez of Case Western Reserve University in Cleveland.
ART has resulted in a marked change in cancer trends among HIV-infected patients. The incidence of AIDS-defining cancers has decreased “massively,” Dr. Rodriguez observed; but because ART has extended the lifespan, patients are now living long enough to get other cancers. And they do so at a higher rate than that of the general population because of their impaired immune function, higher rate of risk factors such as smoking, and greater prevalence of oncogenic viral coinfections such as hepatitis B and C and Epstein-Barr virus.
The increase in the incidence and risk of colorectal, liver, and anal cancers among HIV-positive individuals since the introduction of combination ART can largely be explained by the population’s longer exposure to risk due to increasing survival, he said.
Dr. Rodriguez presented highlights of an analysis of cancer trends in North America during 1996-2009. The study was based on 86,620 HIV-infected persons with 475,660 person-years of follow-up and 196,987 subjects without HIV infection and with more than 1.8 million person-years of follow-up. Trends over time were assessed for nine cancers: Kaposi’s sarcoma, non-Hodgkin’s lymphoma, Hodgkin’s lymphoma, and melanoma, as well as anal, lung, colorectal, liver, and oropharyngeal cancers (Ann Intern Med. 2015;163:507-18).
Examining trends in three periods – 1996-1999, 2000-2004, and 2005-2009 – the investigators looked at the impact of ART over time on rates of AIDS-related and non–AIDS-related cancers in HIV-infected patients and compared them to results in the general HIV-uninfected population.
By conducting a competing risk analysis, Dr. Rodriguez and his coworkers were able to estimate the cumulative lifetime risk of the various cancers by age 75, a metric that provides readily understandable information for counseling HIV-infected patients about their long-term cancer risk.
The measure “is more intuitive than using incidence rates,” Dr. Rodriguez said. In a study of 1,578 HIV-infected patients who received the hepatitis B vaccine, for example, those patients whose immune function did not to respond to the vaccine were more likely to be among the 6% of patients who subsequently developed cancer during up to 20 years of follow-up.
The findings on cancer trends in the ART era have clinical implications for cancer screening and prevention in HIV-infected patients. The high rates of smoking and lung cancer in this population make HIV-positive smokers a logical target for lung cancer screening. The rising risk of colorectal cancer – the cumulative lifetime risk to age 75 was 0.4% in 1996-1999, 0.7% in 2000-2004, and 1.3% in 2005-2009 – suggests a need for increased colorectal cancer screening in the older HIV-positive population.
Early and sustained HIV suppression with combination ART remains the only known method of preventing AIDS-defining cancers. Dr. Rodriguez and his coinvestigators in the Centers for AIDS Research Network of Integrated Clinical Systems demonstrated the crucial role of suppressing HIV in a study of 6,036 HIV-infected patients who started on ART and were followed for more than 21,000 person-years. Compared with HIV-infected patients with a 3-month lagged HIV viremia of no more than 50 copies/mL, patients’ risk of developing non-Hodgkin’s lymphoma was 2.1-fold greater if their 3-month lagged HIV viremia was 51-500 copies/mL and 3.56-fold greater if it exceeded 500 copies/mL (Clin Infect Dis. 2014 Jun;58[11]:1599-606).
The study on cancer trends over time was funded by the National Institutes of Health. Dr. Rodriguez reported receiving honoraria from Gilead Sciences.
DURBAN, SOUTH AFRICA – The rates of the AIDS-defining cancers Kaposi’s sarcoma and non-Hodgkin’s lymphoma have plummeted in the antiretroviral era, yet they are still the two top cancers in terms of cumulative incidence in HIV-infected patients by age 75, Benigno Rodriguez, MD, said at the 21st International AIDS Conference.
Lung cancer also remains a major concern in the HIV-infected population. Each of these three cancers carries about a 1 in 25 lifetime risk to age 75, the estimated lifespan of HIV-positive patients on combination antiretroviral therapy (ART), according to Dr. Rodriguez of Case Western Reserve University in Cleveland.
ART has resulted in a marked change in cancer trends among HIV-infected patients. The incidence of AIDS-defining cancers has decreased “massively,” Dr. Rodriguez observed; but because ART has extended the lifespan, patients are now living long enough to get other cancers. And they do so at a higher rate than that of the general population because of their impaired immune function, higher rate of risk factors such as smoking, and greater prevalence of oncogenic viral coinfections such as hepatitis B and C and Epstein-Barr virus.
The increase in the incidence and risk of colorectal, liver, and anal cancers among HIV-positive individuals since the introduction of combination ART can largely be explained by the population’s longer exposure to risk due to increasing survival, he said.
Dr. Rodriguez presented highlights of an analysis of cancer trends in North America during 1996-2009. The study was based on 86,620 HIV-infected persons with 475,660 person-years of follow-up and 196,987 subjects without HIV infection and with more than 1.8 million person-years of follow-up. Trends over time were assessed for nine cancers: Kaposi’s sarcoma, non-Hodgkin’s lymphoma, Hodgkin’s lymphoma, and melanoma, as well as anal, lung, colorectal, liver, and oropharyngeal cancers (Ann Intern Med. 2015;163:507-18).
Examining trends in three periods – 1996-1999, 2000-2004, and 2005-2009 – the investigators looked at the impact of ART over time on rates of AIDS-related and non–AIDS-related cancers in HIV-infected patients and compared them to results in the general HIV-uninfected population.
By conducting a competing risk analysis, Dr. Rodriguez and his coworkers were able to estimate the cumulative lifetime risk of the various cancers by age 75, a metric that provides readily understandable information for counseling HIV-infected patients about their long-term cancer risk.
The measure “is more intuitive than using incidence rates,” Dr. Rodriguez said. In a study of 1,578 HIV-infected patients who received the hepatitis B vaccine, for example, those patients whose immune function did not to respond to the vaccine were more likely to be among the 6% of patients who subsequently developed cancer during up to 20 years of follow-up.
The findings on cancer trends in the ART era have clinical implications for cancer screening and prevention in HIV-infected patients. The high rates of smoking and lung cancer in this population make HIV-positive smokers a logical target for lung cancer screening. The rising risk of colorectal cancer – the cumulative lifetime risk to age 75 was 0.4% in 1996-1999, 0.7% in 2000-2004, and 1.3% in 2005-2009 – suggests a need for increased colorectal cancer screening in the older HIV-positive population.
Early and sustained HIV suppression with combination ART remains the only known method of preventing AIDS-defining cancers. Dr. Rodriguez and his coinvestigators in the Centers for AIDS Research Network of Integrated Clinical Systems demonstrated the crucial role of suppressing HIV in a study of 6,036 HIV-infected patients who started on ART and were followed for more than 21,000 person-years. Compared with HIV-infected patients with a 3-month lagged HIV viremia of no more than 50 copies/mL, patients’ risk of developing non-Hodgkin’s lymphoma was 2.1-fold greater if their 3-month lagged HIV viremia was 51-500 copies/mL and 3.56-fold greater if it exceeded 500 copies/mL (Clin Infect Dis. 2014 Jun;58[11]:1599-606).
The study on cancer trends over time was funded by the National Institutes of Health. Dr. Rodriguez reported receiving honoraria from Gilead Sciences.
AT AIDS 2016
Key clinical point: HIV-infected persons in North America have roughly a 1 in 25 cumulative lifetime risk of developing lung cancer, Kaposi’s sarcoma, or non-Hodgkin’s lymphoma.
Major finding: The cumulative lifetime risk of developing non-Hodgkin’s lymphoma in HIV-infected patients on combination antiretroviral therapy is sevenfold greater than the risk in the general population.
Data source: A competing risk analysis for nine cancers based upon 86,620 HIV-infected persons followed for 475,660 person-years and 196,987 subjects not infected with HIV and with more than 1.8 million person-years of follow-up.
Disclosures: The National Institutes of Health funded the study. The presenter reported receiving honoraria from Gilead Sciences.

Ankylosing spondylitis patients develop multiple comorbidities after diagnosis
DENVER – Evidence continues to mount that ankylosing spondylitis patients are at increased risk for developing various comorbidities, compared with the general adult population.
Patients newly diagnosed with ankylosing spondylitis (AS) had twice the rate of new-onset depression during the first 3 years following diagnosis, compared with matched people from the general population in a study of more than 21,000 American adults. Patients with newly diagnosed AS also had a 60% higher rate of developing a new cardiovascular disease, compared with the matched general population, Jessica A. Walsh, MD, said at the annual meeting of the Spondyloarthritis Research and Treatment Network.

“We need to figure out what to do about all the comorbidities. Rheumatologists need to either screen their AS patients for comorbidities, or they need to be sure their patients are plugged in with another physician who will screen them,” said Dr. Walsh, director of the spondyloarthritis clinic at the University of Utah in Salt Lake City.
Her analysis used data from the Truven Health MarketScan databases for U.S. patients covered by Medicare or commercial health insurance, and included 6,370 patients with newly diagnosed AS and 14,988 adults matched by age and sex. The analysis only included AS patients who were free from comorbidities during the 2 years prior to their AS diagnosis. The average age of the people in the study was 52 years, and 54% were men.
During an average follow-up of 2.9 years following initial AS diagnosis, the most common comorbidity among the AS patients was uveitis, which occurred nearly 15-fold more frequently among the AS patients than in the controls. Other common incident comorbidities included inflammatory bowel disease, nearly sixfold more common among the AS patients, and osteoporosis, which was nearly threefold more common during follow-up after AS diagnosis, compared with the controls.
Other comorbidities with increased incidence in the AS patients included sleep apnea (80% more common among the AS patients during follow-up), asthma (50% more often), hypertension (44% more common), malignancy (23% more common), diabetes (20% more common), and dyslipidemia (11% more common). All these incidence rates represented statistically significant increases in the AS patients, compared with the controls.
A related analysis reported by Dr. Walsh also used data from the Truven Health databases for a somewhat larger group of AS patients, 6,679 followed for 1 year after their AS diagnosis, and 19,951 matched controls. The AS patients had a significantly higher rate of hospital admissions – 12%, compared with 6% among the controls – and a significantly higher rate of emergency department visits, at 23%, compared with 15% among the controls. The AS patients also had double the rate of physician office visits and prescribed medications.
“Obviously, the AS patients are not as healthy,” Dr. Walsh said in an interview. “We adjusted for their comorbidities, but that did not affect the hospitalization rates. We need to look into this more; I don’t know why the AS patients are being hospitalized. Typically AS itself does not lead to hospitalization, so I suspect it’s because of comorbidities, or perhaps because of adverse events from treatment.”
Dr. Walsh is a consultant to AbbVie and Novartis.
On Twitter @mitchelzoler
DENVER – Evidence continues to mount that ankylosing spondylitis patients are at increased risk for developing various comorbidities, compared with the general adult population.
Patients newly diagnosed with ankylosing spondylitis (AS) had twice the rate of new-onset depression during the first 3 years following diagnosis, compared with matched people from the general population in a study of more than 21,000 American adults. Patients with newly diagnosed AS also had a 60% higher rate of developing a new cardiovascular disease, compared with the matched general population, Jessica A. Walsh, MD, said at the annual meeting of the Spondyloarthritis Research and Treatment Network.
“We need to figure out what to do about all the comorbidities. Rheumatologists need to either screen their AS patients for comorbidities, or they need to be sure their patients are plugged in with another physician who will screen them,” said Dr. Walsh, director of the spondyloarthritis clinic at the University of Utah in Salt Lake City.
Her analysis used data from the Truven Health MarketScan databases for U.S. patients covered by Medicare or commercial health insurance, and included 6,370 patients with newly diagnosed AS and 14,988 adults matched by age and sex. The analysis only included AS patients who were free from comorbidities during the 2 years prior to their AS diagnosis. The average age of the people in the study was 52 years, and 54% were men.
During an average follow-up of 2.9 years following initial AS diagnosis, the most common comorbidity among the AS patients was uveitis, which occurred nearly 15-fold more frequently among the AS patients than in the controls. Other common incident comorbidities included inflammatory bowel disease, nearly sixfold more common among the AS patients, and osteoporosis, which was nearly threefold more common during follow-up after AS diagnosis, compared with the controls.
Other comorbidities with increased incidence in the AS patients included sleep apnea (80% more common among the AS patients during follow-up), asthma (50% more often), hypertension (44% more common), malignancy (23% more common), diabetes (20% more common), and dyslipidemia (11% more common). All these incidence rates represented statistically significant increases in the AS patients, compared with the controls.
A related analysis reported by Dr. Walsh also used data from the Truven Health databases for a somewhat larger group of AS patients, 6,679 followed for 1 year after their AS diagnosis, and 19,951 matched controls. The AS patients had a significantly higher rate of hospital admissions – 12%, compared with 6% among the controls – and a significantly higher rate of emergency department visits, at 23%, compared with 15% among the controls. The AS patients also had double the rate of physician office visits and prescribed medications.
“Obviously, the AS patients are not as healthy,” Dr. Walsh said in an interview. “We adjusted for their comorbidities, but that did not affect the hospitalization rates. We need to look into this more; I don’t know why the AS patients are being hospitalized. Typically AS itself does not lead to hospitalization, so I suspect it’s because of comorbidities, or perhaps because of adverse events from treatment.”
Dr. Walsh is a consultant to AbbVie and Novartis.
On Twitter @mitchelzoler
DENVER – Evidence continues to mount that ankylosing spondylitis patients are at increased risk for developing various comorbidities, compared with the general adult population.
Patients newly diagnosed with ankylosing spondylitis (AS) had twice the rate of new-onset depression during the first 3 years following diagnosis, compared with matched people from the general population in a study of more than 21,000 American adults. Patients with newly diagnosed AS also had a 60% higher rate of developing a new cardiovascular disease, compared with the matched general population, Jessica A. Walsh, MD, said at the annual meeting of the Spondyloarthritis Research and Treatment Network.
“We need to figure out what to do about all the comorbidities. Rheumatologists need to either screen their AS patients for comorbidities, or they need to be sure their patients are plugged in with another physician who will screen them,” said Dr. Walsh, director of the spondyloarthritis clinic at the University of Utah in Salt Lake City.
Her analysis used data from the Truven Health MarketScan databases for U.S. patients covered by Medicare or commercial health insurance, and included 6,370 patients with newly diagnosed AS and 14,988 adults matched by age and sex. The analysis only included AS patients who were free from comorbidities during the 2 years prior to their AS diagnosis. The average age of the people in the study was 52 years, and 54% were men.
During an average follow-up of 2.9 years following initial AS diagnosis, the most common comorbidity among the AS patients was uveitis, which occurred nearly 15-fold more frequently among the AS patients than in the controls. Other common incident comorbidities included inflammatory bowel disease, nearly sixfold more common among the AS patients, and osteoporosis, which was nearly threefold more common during follow-up after AS diagnosis, compared with the controls.
Other comorbidities with increased incidence in the AS patients included sleep apnea (80% more common among the AS patients during follow-up), asthma (50% more often), hypertension (44% more common), malignancy (23% more common), diabetes (20% more common), and dyslipidemia (11% more common). All these incidence rates represented statistically significant increases in the AS patients, compared with the controls.
A related analysis reported by Dr. Walsh also used data from the Truven Health databases for a somewhat larger group of AS patients, 6,679 followed for 1 year after their AS diagnosis, and 19,951 matched controls. The AS patients had a significantly higher rate of hospital admissions – 12%, compared with 6% among the controls – and a significantly higher rate of emergency department visits, at 23%, compared with 15% among the controls. The AS patients also had double the rate of physician office visits and prescribed medications.
“Obviously, the AS patients are not as healthy,” Dr. Walsh said in an interview. “We adjusted for their comorbidities, but that did not affect the hospitalization rates. We need to look into this more; I don’t know why the AS patients are being hospitalized. Typically AS itself does not lead to hospitalization, so I suspect it’s because of comorbidities, or perhaps because of adverse events from treatment.”
Dr. Walsh is a consultant to AbbVie and Novartis.
On Twitter @mitchelzoler
AT THE 2016 SPARTAN ANNUAL MEETING
Key clinical point: In the 3 years after initial ankylosing spondylitis diagnosis, the incidence of several comorbidities rises significantly above those in the general population.
Major finding: The incidence of new-onset depression among newly diagnosed ankylosing spondylitis patients was twice as high as it was among matched controls.
Data source: Observational data collected by Truven Health MarketScan, with a total of 21,358 patients and controls.
Disclosures: Dr. Walsh is a consultant to AbbVie and Novartis.

BM transplants provide better quality of life

Photo by Chad McNeeley
Patients receiving hematopoietic stem cell transplants from unrelated donors have better quality of life if they receive cells derived from bone marrow (BM) rather than peripheral blood (PB), according to a large study.
Recipients of BM transplants reported better psychological well-being, had fewer symptoms of graft-versus-host disease (GVHD), and were more likely to be back at work 5 years after their transplant.
However, there was no significant difference in overall survival, treatment-related death, or relapse between patients who received BM grafts and those who received PB transplants.
Stephanie Lee, MD, of Fred Hutchinson Cancer Research Center in Seattle, Washington, and her colleagues reported these results in JAMA Oncology.
“We’re hoping that, once we provide information about long-term quality of life and recovery, patients and their doctors can take this into account when they’re planning their transplants,” Dr Lee said.
She noted, however, that the results would only be applicable to transplant patients who are similar to those enrolled in this study.
The study included 551 patients, ages 16 to 66, who were receiving transplants from unrelated donors to treat hematologic neoplasms. The patients were randomly assigned to receive PB or BM grafts.
From 6 months to 5 years after transplant, researchers called the patients periodically to assess how they were doing.
At the 5-year mark, 102 BM recipients and 93 PB recipients were still alive and eligible for assessment.
At a median follow-up of 73 months (range, 30-121 months), there was no significant difference in survival rate, relapse incidence, or treatment-related mortality between BM and PB recipients.
The survival rate was 40% for BM recipients and 39% for PB recipients (P=0.84). The relapse rates were 32% and 29%, respectively (P=0.47). And the treatment-related mortality rates were 29% and 32%, respectively (P=0.44).
However, BM recipients were more likely to report better psychological well-being, earning higher Mental Health Inventory Psychological Well-Being scores than PB recipients. The mean scores were 78.9 and 72.2, respectively (P=0.01).
In addition, BM recipients had fewer symptoms of GVHD, earning lower Lee Chronic GVHD symptom scores than PB recipients. The mean scores were 13.1 and 19.3, respectively (P=0.004).
The researchers suspected, but could not confirm, that BM recipients had better psychological well-being because they experienced fewer self-reported symptoms of chronic GVHD.
The researchers also found that BM recipients were more likely than PB recipients to be working full-time or part-time 5 years after transplant. When the team adjusted for work status before transplant, the odds ratio was 1.5 (P=0.002).
“Results of this study set bone marrow as the standard source of stem cells for transplantation from unrelated donors,” said study author Claudio Anasetti, MD, of Moffitt Cancer Center in Tampa, Florida.
“When both your disease and the recommended treatment are life-threatening, I don’t think people are necessarily asking, ‘Which treatment is going to give me better quality of life years from now?’” Dr Lee added.
“Yet, if you’re going to make it through, as many patients do, you want to do it with good quality of life. That’s the whole point of having the transplant. It’s not just to cure your disease but also to try to get back to as normal a lifestyle as you can.” ![]()
Photo by Chad McNeeley
Patients receiving hematopoietic stem cell transplants from unrelated donors have better quality of life if they receive cells derived from bone marrow (BM) rather than peripheral blood (PB), according to a large study.
Recipients of BM transplants reported better psychological well-being, had fewer symptoms of graft-versus-host disease (GVHD), and were more likely to be back at work 5 years after their transplant.
However, there was no significant difference in overall survival, treatment-related death, or relapse between patients who received BM grafts and those who received PB transplants.
Stephanie Lee, MD, of Fred Hutchinson Cancer Research Center in Seattle, Washington, and her colleagues reported these results in JAMA Oncology.
“We’re hoping that, once we provide information about long-term quality of life and recovery, patients and their doctors can take this into account when they’re planning their transplants,” Dr Lee said.
She noted, however, that the results would only be applicable to transplant patients who are similar to those enrolled in this study.
The study included 551 patients, ages 16 to 66, who were receiving transplants from unrelated donors to treat hematologic neoplasms. The patients were randomly assigned to receive PB or BM grafts.
From 6 months to 5 years after transplant, researchers called the patients periodically to assess how they were doing.
At the 5-year mark, 102 BM recipients and 93 PB recipients were still alive and eligible for assessment.
At a median follow-up of 73 months (range, 30-121 months), there was no significant difference in survival rate, relapse incidence, or treatment-related mortality between BM and PB recipients.
The survival rate was 40% for BM recipients and 39% for PB recipients (P=0.84). The relapse rates were 32% and 29%, respectively (P=0.47). And the treatment-related mortality rates were 29% and 32%, respectively (P=0.44).
However, BM recipients were more likely to report better psychological well-being, earning higher Mental Health Inventory Psychological Well-Being scores than PB recipients. The mean scores were 78.9 and 72.2, respectively (P=0.01).
In addition, BM recipients had fewer symptoms of GVHD, earning lower Lee Chronic GVHD symptom scores than PB recipients. The mean scores were 13.1 and 19.3, respectively (P=0.004).
The researchers suspected, but could not confirm, that BM recipients had better psychological well-being because they experienced fewer self-reported symptoms of chronic GVHD.
The researchers also found that BM recipients were more likely than PB recipients to be working full-time or part-time 5 years after transplant. When the team adjusted for work status before transplant, the odds ratio was 1.5 (P=0.002).
“Results of this study set bone marrow as the standard source of stem cells for transplantation from unrelated donors,” said study author Claudio Anasetti, MD, of Moffitt Cancer Center in Tampa, Florida.
“When both your disease and the recommended treatment are life-threatening, I don’t think people are necessarily asking, ‘Which treatment is going to give me better quality of life years from now?’” Dr Lee added.
“Yet, if you’re going to make it through, as many patients do, you want to do it with good quality of life. That’s the whole point of having the transplant. It’s not just to cure your disease but also to try to get back to as normal a lifestyle as you can.” ![]()
Photo by Chad McNeeley
Patients receiving hematopoietic stem cell transplants from unrelated donors have better quality of life if they receive cells derived from bone marrow (BM) rather than peripheral blood (PB), according to a large study.
Recipients of BM transplants reported better psychological well-being, had fewer symptoms of graft-versus-host disease (GVHD), and were more likely to be back at work 5 years after their transplant.
However, there was no significant difference in overall survival, treatment-related death, or relapse between patients who received BM grafts and those who received PB transplants.
Stephanie Lee, MD, of Fred Hutchinson Cancer Research Center in Seattle, Washington, and her colleagues reported these results in JAMA Oncology.
“We’re hoping that, once we provide information about long-term quality of life and recovery, patients and their doctors can take this into account when they’re planning their transplants,” Dr Lee said.
She noted, however, that the results would only be applicable to transplant patients who are similar to those enrolled in this study.
The study included 551 patients, ages 16 to 66, who were receiving transplants from unrelated donors to treat hematologic neoplasms. The patients were randomly assigned to receive PB or BM grafts.
From 6 months to 5 years after transplant, researchers called the patients periodically to assess how they were doing.
At the 5-year mark, 102 BM recipients and 93 PB recipients were still alive and eligible for assessment.
At a median follow-up of 73 months (range, 30-121 months), there was no significant difference in survival rate, relapse incidence, or treatment-related mortality between BM and PB recipients.
The survival rate was 40% for BM recipients and 39% for PB recipients (P=0.84). The relapse rates were 32% and 29%, respectively (P=0.47). And the treatment-related mortality rates were 29% and 32%, respectively (P=0.44).
However, BM recipients were more likely to report better psychological well-being, earning higher Mental Health Inventory Psychological Well-Being scores than PB recipients. The mean scores were 78.9 and 72.2, respectively (P=0.01).
In addition, BM recipients had fewer symptoms of GVHD, earning lower Lee Chronic GVHD symptom scores than PB recipients. The mean scores were 13.1 and 19.3, respectively (P=0.004).
The researchers suspected, but could not confirm, that BM recipients had better psychological well-being because they experienced fewer self-reported symptoms of chronic GVHD.
The researchers also found that BM recipients were more likely than PB recipients to be working full-time or part-time 5 years after transplant. When the team adjusted for work status before transplant, the odds ratio was 1.5 (P=0.002).
“Results of this study set bone marrow as the standard source of stem cells for transplantation from unrelated donors,” said study author Claudio Anasetti, MD, of Moffitt Cancer Center in Tampa, Florida.
“When both your disease and the recommended treatment are life-threatening, I don’t think people are necessarily asking, ‘Which treatment is going to give me better quality of life years from now?’” Dr Lee added.
“Yet, if you’re going to make it through, as many patients do, you want to do it with good quality of life. That’s the whole point of having the transplant. It’s not just to cure your disease but also to try to get back to as normal a lifestyle as you can.” ![]()
Assay can aid blood biomarker research

Photo by Graham Colm
A new assay can overcome a limitation in blood biomarker research, according to a study published in Scientific Reports.
Researchers noted that transcriptome sequencing of whole-blood RNA holds promise for the identification and tracking of biomarkers.
Unfortunately, the high globin mRNA (gmRNA) content of erythrocytes can be problematic, causing technical bias and leaving biologically relevant molecules undetectable.
With this in mind, the researchers developed an assay known as GlobinLock, which is designed to preserve RNA quality by reducing globin content.
“The globin reduction rate of GlobinLock is sufficient for any application,” said study author Kaarel Krjutškov, PhD, of Karolinska Institutet in Huddinge, Sweden.
“It reduces the globin prevalence from 63% . . . to 5%, which makes it an effective tool for biotechnology companies as an additive to their kits.”
GlobinLock consists of a pair of gmRNA-specific oligonucleotides that silence the majority of globin RNA molecules by highly specific binding.
The oligonucleotides are introduced to a purified RNA sample and, according to the researchers, are effective immediately after RNA denaturation.
“We show that globin locking is fully effective not only for human samples but also for widely used animal models, like mouse and rat, cow, dog, and even zebrafish,” said study author Juha Kere, MD, PhD, of Karolinska Institutet. ![]()
Photo by Graham Colm
A new assay can overcome a limitation in blood biomarker research, according to a study published in Scientific Reports.
Researchers noted that transcriptome sequencing of whole-blood RNA holds promise for the identification and tracking of biomarkers.
Unfortunately, the high globin mRNA (gmRNA) content of erythrocytes can be problematic, causing technical bias and leaving biologically relevant molecules undetectable.
With this in mind, the researchers developed an assay known as GlobinLock, which is designed to preserve RNA quality by reducing globin content.
“The globin reduction rate of GlobinLock is sufficient for any application,” said study author Kaarel Krjutškov, PhD, of Karolinska Institutet in Huddinge, Sweden.
“It reduces the globin prevalence from 63% . . . to 5%, which makes it an effective tool for biotechnology companies as an additive to their kits.”
GlobinLock consists of a pair of gmRNA-specific oligonucleotides that silence the majority of globin RNA molecules by highly specific binding.
The oligonucleotides are introduced to a purified RNA sample and, according to the researchers, are effective immediately after RNA denaturation.
“We show that globin locking is fully effective not only for human samples but also for widely used animal models, like mouse and rat, cow, dog, and even zebrafish,” said study author Juha Kere, MD, PhD, of Karolinska Institutet. ![]()
Photo by Graham Colm
A new assay can overcome a limitation in blood biomarker research, according to a study published in Scientific Reports.
Researchers noted that transcriptome sequencing of whole-blood RNA holds promise for the identification and tracking of biomarkers.
Unfortunately, the high globin mRNA (gmRNA) content of erythrocytes can be problematic, causing technical bias and leaving biologically relevant molecules undetectable.
With this in mind, the researchers developed an assay known as GlobinLock, which is designed to preserve RNA quality by reducing globin content.
“The globin reduction rate of GlobinLock is sufficient for any application,” said study author Kaarel Krjutškov, PhD, of Karolinska Institutet in Huddinge, Sweden.
“It reduces the globin prevalence from 63% . . . to 5%, which makes it an effective tool for biotechnology companies as an additive to their kits.”
GlobinLock consists of a pair of gmRNA-specific oligonucleotides that silence the majority of globin RNA molecules by highly specific binding.
The oligonucleotides are introduced to a purified RNA sample and, according to the researchers, are effective immediately after RNA denaturation.
“We show that globin locking is fully effective not only for human samples but also for widely used animal models, like mouse and rat, cow, dog, and even zebrafish,” said study author Juha Kere, MD, PhD, of Karolinska Institutet. ![]()
Drug can worsen allo-HSCT outcomes in ATLL
![]()
Photo by Chad McNeeley
Results of a large, retrospective study suggest that receiving mogamulizumab before allogeneic hematopoietic stem cell transplant (allo-HSCT) can worsen outcomes in patients with adult T-cell leukemia/lymphoma (ATLL).
Patients who received mogamulizumab had a higher risk of grade 3/4 acute graft-versus-host disease (GVHD), a higher incidence of nonrelapse mortality, and worse overall survival than patients who did not take the drug.
Researchers reported these findings in the Journal of Clinical Oncology.
Previous research suggested that pre-HSCT mogamulizumab can produce adverse effects, but these studies had small patient numbers. Researchers have suggested the adverse effects may occur because mogamulizumab depletes regulatory T cells for several months, but there has been no direct evidence supporting this idea.
To investigate the issue, Shigeo Fuji, MD, of National Cancer Center Hospital in Tokyo, Japan, and colleagues assessed the impact of pre-HSCT mogamulizumab in a large group of ATLL patients undergoing allo-HSCT.
The study included 996 patients age 70 and younger. Patients had aggressive ATLL diagnosed between 2000 and 2013. They received intensive chemotherapy as first-line treatment.
Eighty-two of the patients received mogamulizumab before HSCT, with a median of 45 days from the last mogamulizumab treatment to allo-HSCT.
Pre-HSCT mogamulizumab was associated with an increased risk of grade 3/4 acute GVHD, with a relative risk of 1.80 (P<0.01).
Patients who received mogamulizumab were also more likely to be refractory to the systemic corticosteroids given to treat acute GVHD, with a relative risk of 2.09 (P<0.01).
The 1-year cumulative incidence of nonrelapse mortality was significantly higher among patients who received mogamulizumab than among those who did not—43.7% and 25.1%, respectively (P<0.01).
And the probability of 1-year overall survival was significantly lower in patients who received mogamulizumab than in those who did not—32.3% and 49.4%, respectively (P<0.01).
The researchers noted that outcomes were particularly poor when patients received mogamulizumab within less than 50 days of allo-HSCT.
The team said this study appears to confirm that pre-HSCT mogamulizumab significantly worsens clinical outcomes, mainly because of an increased risk of severe/corticosteroid-refractory acute GVHD. And the results support the idea that the drug depletes regulatory T cells.
The researchers concluded that mogamulizumab should be used with caution in ATLL patients who are eligible for allo-HSCT. And the possibility of intensifying GVHD prophylaxis in patients who do receive pre-HSCT mogamulizumab should be explored. ![]()
![]()
Photo by Chad McNeeley
Results of a large, retrospective study suggest that receiving mogamulizumab before allogeneic hematopoietic stem cell transplant (allo-HSCT) can worsen outcomes in patients with adult T-cell leukemia/lymphoma (ATLL).
Patients who received mogamulizumab had a higher risk of grade 3/4 acute graft-versus-host disease (GVHD), a higher incidence of nonrelapse mortality, and worse overall survival than patients who did not take the drug.
Researchers reported these findings in the Journal of Clinical Oncology.
Previous research suggested that pre-HSCT mogamulizumab can produce adverse effects, but these studies had small patient numbers. Researchers have suggested the adverse effects may occur because mogamulizumab depletes regulatory T cells for several months, but there has been no direct evidence supporting this idea.
To investigate the issue, Shigeo Fuji, MD, of National Cancer Center Hospital in Tokyo, Japan, and colleagues assessed the impact of pre-HSCT mogamulizumab in a large group of ATLL patients undergoing allo-HSCT.
The study included 996 patients age 70 and younger. Patients had aggressive ATLL diagnosed between 2000 and 2013. They received intensive chemotherapy as first-line treatment.
Eighty-two of the patients received mogamulizumab before HSCT, with a median of 45 days from the last mogamulizumab treatment to allo-HSCT.
Pre-HSCT mogamulizumab was associated with an increased risk of grade 3/4 acute GVHD, with a relative risk of 1.80 (P<0.01).
Patients who received mogamulizumab were also more likely to be refractory to the systemic corticosteroids given to treat acute GVHD, with a relative risk of 2.09 (P<0.01).
The 1-year cumulative incidence of nonrelapse mortality was significantly higher among patients who received mogamulizumab than among those who did not—43.7% and 25.1%, respectively (P<0.01).
And the probability of 1-year overall survival was significantly lower in patients who received mogamulizumab than in those who did not—32.3% and 49.4%, respectively (P<0.01).
The researchers noted that outcomes were particularly poor when patients received mogamulizumab within less than 50 days of allo-HSCT.
The team said this study appears to confirm that pre-HSCT mogamulizumab significantly worsens clinical outcomes, mainly because of an increased risk of severe/corticosteroid-refractory acute GVHD. And the results support the idea that the drug depletes regulatory T cells.
The researchers concluded that mogamulizumab should be used with caution in ATLL patients who are eligible for allo-HSCT. And the possibility of intensifying GVHD prophylaxis in patients who do receive pre-HSCT mogamulizumab should be explored. ![]()
![]()
Photo by Chad McNeeley
Results of a large, retrospective study suggest that receiving mogamulizumab before allogeneic hematopoietic stem cell transplant (allo-HSCT) can worsen outcomes in patients with adult T-cell leukemia/lymphoma (ATLL).
Patients who received mogamulizumab had a higher risk of grade 3/4 acute graft-versus-host disease (GVHD), a higher incidence of nonrelapse mortality, and worse overall survival than patients who did not take the drug.
Researchers reported these findings in the Journal of Clinical Oncology.
Previous research suggested that pre-HSCT mogamulizumab can produce adverse effects, but these studies had small patient numbers. Researchers have suggested the adverse effects may occur because mogamulizumab depletes regulatory T cells for several months, but there has been no direct evidence supporting this idea.
To investigate the issue, Shigeo Fuji, MD, of National Cancer Center Hospital in Tokyo, Japan, and colleagues assessed the impact of pre-HSCT mogamulizumab in a large group of ATLL patients undergoing allo-HSCT.
The study included 996 patients age 70 and younger. Patients had aggressive ATLL diagnosed between 2000 and 2013. They received intensive chemotherapy as first-line treatment.
Eighty-two of the patients received mogamulizumab before HSCT, with a median of 45 days from the last mogamulizumab treatment to allo-HSCT.
Pre-HSCT mogamulizumab was associated with an increased risk of grade 3/4 acute GVHD, with a relative risk of 1.80 (P<0.01).
Patients who received mogamulizumab were also more likely to be refractory to the systemic corticosteroids given to treat acute GVHD, with a relative risk of 2.09 (P<0.01).
The 1-year cumulative incidence of nonrelapse mortality was significantly higher among patients who received mogamulizumab than among those who did not—43.7% and 25.1%, respectively (P<0.01).
And the probability of 1-year overall survival was significantly lower in patients who received mogamulizumab than in those who did not—32.3% and 49.4%, respectively (P<0.01).
The researchers noted that outcomes were particularly poor when patients received mogamulizumab within less than 50 days of allo-HSCT.
The team said this study appears to confirm that pre-HSCT mogamulizumab significantly worsens clinical outcomes, mainly because of an increased risk of severe/corticosteroid-refractory acute GVHD. And the results support the idea that the drug depletes regulatory T cells.
The researchers concluded that mogamulizumab should be used with caution in ATLL patients who are eligible for allo-HSCT. And the possibility of intensifying GVHD prophylaxis in patients who do receive pre-HSCT mogamulizumab should be explored. ![]()
Mortality rates higher among influenza B patients than influenza A patients
Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A, investigators found.
Among those with influenza B, patients aged 10-16 years were most likely to require ICU admission, suggesting this subpopulation may be a target for immunization programs.

The percentage of clinical cases attributed to influenza B range from less than 1% to 44%, according to data published by the Centers for Disease Control and Prevention. However, influenza B is considered less virulent and less capable of causing pandemics and has therefore been less studied and outcomes of its disease less characterized, Dat Tran, MD, MSc, of the Hospital for Sick Children in Canada and his associates reported (Pediatrics. 2016 August. doi: 10.1542/peds.2015-4643).
The purpose of this study was to further understand the prevalence and severity of influenza B cases in comparison with influenza A and to identify pediatric subpopulations most at risk for contracting influenza B.
Children aged 16 years or younger hospitalized from laboratory-confirmed influenza A or B from September 2004 to June 2013 (excluding the pandemic year 2009-2010) were identified through active surveillance of admissions at the 12 pediatric referral centers of the Canadian Immunization Monitoring Program Active (IMPACT), a national surveillance initiative. Information regarding demographics, health status, vaccination status, presenting signs and symptoms, illness severity and mortality, treatment regimens, and ICU admission were collected and analyzed.
Of 4,155 influenza-related admissions during this time period, influenza B accounted for 1,510 (36.3%) cases and influenza A accounted for 2,645 (63.7%) cases.
Children admitted with influenza B tended to be older with a median age 3.9 years (interquartile range, 1.4-7.2), compared with a median of 2 years (IQR, 0.6-4.8 years) for children admitted with influenza A.
Children admitted with influenza B, compared with influenza A, had higher odds of having a vaccine-indicated condition (odds ratio, 1.30; 95% confidence interval, 1.14-1.47) and lower odds of having no underlying medical condition (OR, 0.80; 95% CI, 0.71-0.91), Dr. Tran and his associates reported.
“Compared with influenza A cases, children admitted with influenza B had greater adjusted odds of presenting with headache, abdominal pain, and myalgia, ranging from 1.38 for abdominal pain to 3.19 for myalgia,” they added. “There were no significant differences in antiviral or antibiotic prescription or use between influenza A and B cases.”
There was no significant difference in the proportion of influenza A or B patients admitted to the ICU (12.7% vs. 12.6%). Rather, multivariate modeling identified age and presence of an underlying condition as independent predictors of ICU admission.
Finally, influenza-attributable mortality was significantly greater in children with influenza B (adjusted OR, 2.65; 95% CI, 1.18-5.94). Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. All-cause mortality followed a similar trend.
“Among hospitalized children, influenza A and B infections resulted in similar morbidity while mortality was greater for influenza B disease. Among healthy children hospitalized with influenza B, those aged 10-16 years were most likely to require ICU admission,” the investigators summarized.
“These children should be considered at high risk for complicated influenza B infection and be specifically targeted by immunization programs to receive influenza vaccination, and in particular, a [quadrivalent influenza vaccine],” they recommended.
This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.
Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A, investigators found.
Among those with influenza B, patients aged 10-16 years were most likely to require ICU admission, suggesting this subpopulation may be a target for immunization programs.
The percentage of clinical cases attributed to influenza B range from less than 1% to 44%, according to data published by the Centers for Disease Control and Prevention. However, influenza B is considered less virulent and less capable of causing pandemics and has therefore been less studied and outcomes of its disease less characterized, Dat Tran, MD, MSc, of the Hospital for Sick Children in Canada and his associates reported (Pediatrics. 2016 August. doi: 10.1542/peds.2015-4643).
The purpose of this study was to further understand the prevalence and severity of influenza B cases in comparison with influenza A and to identify pediatric subpopulations most at risk for contracting influenza B.
Children aged 16 years or younger hospitalized from laboratory-confirmed influenza A or B from September 2004 to June 2013 (excluding the pandemic year 2009-2010) were identified through active surveillance of admissions at the 12 pediatric referral centers of the Canadian Immunization Monitoring Program Active (IMPACT), a national surveillance initiative. Information regarding demographics, health status, vaccination status, presenting signs and symptoms, illness severity and mortality, treatment regimens, and ICU admission were collected and analyzed.
Of 4,155 influenza-related admissions during this time period, influenza B accounted for 1,510 (36.3%) cases and influenza A accounted for 2,645 (63.7%) cases.
Children admitted with influenza B tended to be older with a median age 3.9 years (interquartile range, 1.4-7.2), compared with a median of 2 years (IQR, 0.6-4.8 years) for children admitted with influenza A.
Children admitted with influenza B, compared with influenza A, had higher odds of having a vaccine-indicated condition (odds ratio, 1.30; 95% confidence interval, 1.14-1.47) and lower odds of having no underlying medical condition (OR, 0.80; 95% CI, 0.71-0.91), Dr. Tran and his associates reported.
“Compared with influenza A cases, children admitted with influenza B had greater adjusted odds of presenting with headache, abdominal pain, and myalgia, ranging from 1.38 for abdominal pain to 3.19 for myalgia,” they added. “There were no significant differences in antiviral or antibiotic prescription or use between influenza A and B cases.”
There was no significant difference in the proportion of influenza A or B patients admitted to the ICU (12.7% vs. 12.6%). Rather, multivariate modeling identified age and presence of an underlying condition as independent predictors of ICU admission.
Finally, influenza-attributable mortality was significantly greater in children with influenza B (adjusted OR, 2.65; 95% CI, 1.18-5.94). Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. All-cause mortality followed a similar trend.
“Among hospitalized children, influenza A and B infections resulted in similar morbidity while mortality was greater for influenza B disease. Among healthy children hospitalized with influenza B, those aged 10-16 years were most likely to require ICU admission,” the investigators summarized.
“These children should be considered at high risk for complicated influenza B infection and be specifically targeted by immunization programs to receive influenza vaccination, and in particular, a [quadrivalent influenza vaccine],” they recommended.
This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.
Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A, investigators found.
Among those with influenza B, patients aged 10-16 years were most likely to require ICU admission, suggesting this subpopulation may be a target for immunization programs.
The percentage of clinical cases attributed to influenza B range from less than 1% to 44%, according to data published by the Centers for Disease Control and Prevention. However, influenza B is considered less virulent and less capable of causing pandemics and has therefore been less studied and outcomes of its disease less characterized, Dat Tran, MD, MSc, of the Hospital for Sick Children in Canada and his associates reported (Pediatrics. 2016 August. doi: 10.1542/peds.2015-4643).
The purpose of this study was to further understand the prevalence and severity of influenza B cases in comparison with influenza A and to identify pediatric subpopulations most at risk for contracting influenza B.
Children aged 16 years or younger hospitalized from laboratory-confirmed influenza A or B from September 2004 to June 2013 (excluding the pandemic year 2009-2010) were identified through active surveillance of admissions at the 12 pediatric referral centers of the Canadian Immunization Monitoring Program Active (IMPACT), a national surveillance initiative. Information regarding demographics, health status, vaccination status, presenting signs and symptoms, illness severity and mortality, treatment regimens, and ICU admission were collected and analyzed.
Of 4,155 influenza-related admissions during this time period, influenza B accounted for 1,510 (36.3%) cases and influenza A accounted for 2,645 (63.7%) cases.
Children admitted with influenza B tended to be older with a median age 3.9 years (interquartile range, 1.4-7.2), compared with a median of 2 years (IQR, 0.6-4.8 years) for children admitted with influenza A.
Children admitted with influenza B, compared with influenza A, had higher odds of having a vaccine-indicated condition (odds ratio, 1.30; 95% confidence interval, 1.14-1.47) and lower odds of having no underlying medical condition (OR, 0.80; 95% CI, 0.71-0.91), Dr. Tran and his associates reported.
“Compared with influenza A cases, children admitted with influenza B had greater adjusted odds of presenting with headache, abdominal pain, and myalgia, ranging from 1.38 for abdominal pain to 3.19 for myalgia,” they added. “There were no significant differences in antiviral or antibiotic prescription or use between influenza A and B cases.”
There was no significant difference in the proportion of influenza A or B patients admitted to the ICU (12.7% vs. 12.6%). Rather, multivariate modeling identified age and presence of an underlying condition as independent predictors of ICU admission.
Finally, influenza-attributable mortality was significantly greater in children with influenza B (adjusted OR, 2.65; 95% CI, 1.18-5.94). Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. All-cause mortality followed a similar trend.
“Among hospitalized children, influenza A and B infections resulted in similar morbidity while mortality was greater for influenza B disease. Among healthy children hospitalized with influenza B, those aged 10-16 years were most likely to require ICU admission,” the investigators summarized.
“These children should be considered at high risk for complicated influenza B infection and be specifically targeted by immunization programs to receive influenza vaccination, and in particular, a [quadrivalent influenza vaccine],” they recommended.
This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.
FROM PEDIATRICS
Key clinical point: Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A.
Major finding: Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. Influenza-attributable mortality was significantly greater in children with influenza B (adjusted odds ratio, 2.65, 95% confidence interval, 1.18-5.94).
Data source: An observational study of 4,155 children admitted to the hospital with influenza A or B during nonpandemic years between September 2004 and June 2013.
Disclosures: This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.

Providing Effective Palliative Care in the Era of Value
Although effective palliative care has always been a must-have for patients and caregivers facing serious illness, it hasn’t always been readily available. With the emergence of value-based healthcare models—and their potent incentives to reduce avoidable readmissions—there is renewed hope that such care will be accessible to those who need it.
Palliative and end-of-life care have long been promoted as core skills for hospitalists. The topic has regularly been included at SHM annual meetings and other prominent hospital medicine conferences, in the American Board of Internal Medicine blueprint for recognition of focused practice in hospital medicine, and in a number of influential references for hospitalists. Still, as I look at hospitalist programs around the country, there is a clear need to improve hospitalists’ delivery of palliative and end-of-life care.
Care of patients with chronic illness in their last two years of life accounts for a third of all Medicare spending.1 As hospitalists, we encounter many of these patients as they are hospitalized—and often re-hospitalized. Palliative care, which can improve quality of life and decrease costs for patients while leading to increased satisfaction and better outcomes for caregivers, can help alleviate unneeded and unwanted aggressive interventions like hospitalization.2,3
In its 2014 report, Dying in America, the Institute of Medicine (IOM) identified several areas for improvement, including better advance care planning and payment systems supporting high quality end-of-life care.4 As I write this column in mid 2016, there are two notable achievements since the IOM report: two E&M codes for advance care planning and a substantial and growing number of hospitalist patients in alternative payment models like bundled payments or ACOs.5 I believe we are entering a time when the availability of good palliative care will be accelerated due to broader forces in healthcare that for the first time align incentives between patients’ wishes and how care is paid for.
Palliative Care Skills for Hospitalists
The following are key actions for physicians in addressing palliative care for the hospitalized patient. At the risk of oversimplifying the discipline, I offer a few key actions for hospitalists to keep in mind.
Identify patients who would benefit from palliative care. The surprise question—“Would I be surprised if this patient died in the next year?”—has the ability to predict which patients would benefit from palliative care. In one observation from a group of patients with cancer, a “no” answer identified 60% of patients who died within a year.6 The surprise question has previously been shown to be predictive in other cancer and non-cancer populations.7,8
Weisman and Meier suggest using the following in a checklist at the time of hospital admission as “primary criteria to screen for unmet palliative care needs”:9
- The surprise question
- Frequent admissions
- Admission prompted by difficult-to-control physical or psychological symptoms
- Complex care requirements
- Decline in function, feeding intolerance, or unintended decline in weight
Hold a “goals of care” meeting. A notable step forward for supporting conversations between physicians and patients occurred on Jan. 1, when the Centers for Medicare & Medicaid Services (CMS) announced the Advance Care Planning E&M codes. These are CPT codes 99497 and 99498. They can be used on the same day as other E&M codes and cover discussions regarding advance care planning issues including discussing advance directives, appointing a healthcare proxy or durable power of attorney, discussing a living will, or addressing orders for life-sustaining treatment like the role of hydration or future hospitalizations. (For more information on how to use them, visit the CMS website and search for the FAQ.)
What should hospitalists concentrate on when having “goals of care” conversations with patients and caregivers? Ariadne Labs, a Harvard-affiliated health innovation group, offers the following as elements of a serious illness conversation:10
- Patients’ understanding of their illness
- Patients’ preferences for information and for family involvement
- Personal life goals, fears, and anxieties
- Trade-offs they are willing to accept
For hospitalists, an important area to pay particular attention to is the role of future hospitalizations in patients’ wishes for care, as some patients, if offered appropriate symptom control, would prefer to remain at home.
Two other crucial elements of inpatient palliative care—offer psychosocial support and symptom relief and hand off patient to effective post-hospital palliative care—are outside the scope of this article. However, they should be kept in mind and, of course, applied.
Understand the role of the palliative care consultation. Busy hospitalists might reasonably think, “I simply don’t have time to address palliative care in patients who aren’t likely to die during this hospitalization or soon after.” The palliative care consult service, if available, should be accessed when patients are identified as palliative care candidates but the primary hospitalist does not have the time or resources—including specialized knowledge in some cases—to deliver adequate palliative care. Palliative care specialists can also help bridge the gap between inpatient and outpatient palliative care resources.
In sum, the move to value-based payment models and the new advance care planning E&M codes provide a renewed focus—with more aligned incentives—and the opportunity to provide good palliative care to all who need it.
For hospitalists, identifying those who would benefit from palliative care and working with the healthcare team to ensure the care is delivered are at the heart of our professional mission. TH
References
- End-of-life care. The Darmouth Atlas of Health Care website. Accessed June 23, 2016.
- Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180-190.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Int Med. 2008;168(16):1783-1790.
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. 2014.
- BPCI Model 2: Retrospective acute & post acute care episode. Centers for Medicare & Medicaid Services website. Accessed June 24, 2016.
- Vick JB, Pertsch N, Hutchings M, et al. The utility of the surprise question in identifying patients most at risk of death. J Clin Oncol. 2015;33(suppl):8.
- Moss AH, Ganjoo J, Sharma S, et al. Utility of the “surprise” question to identify dialysis patients with high mortality. Clin J Am Soc Nephrol. 2008;3:1379-1384.
- Moss AH, Lunney JR, Culp S, et al. Prognostic significance of the “surprise” question in cancer patients. J Palliat Med. 2010;13(7):837-840.
- Weissman D, Meier C. Identifying patients in need of a palliative care assessment in the hospital setting: a consensus report from the Center to Advance Palliative Care. J Palliat Med. 2011;14(1):17-23.
- Serious illness care resources. Ariadne Labs website. Accessed June 24, 2016.
Although effective palliative care has always been a must-have for patients and caregivers facing serious illness, it hasn’t always been readily available. With the emergence of value-based healthcare models—and their potent incentives to reduce avoidable readmissions—there is renewed hope that such care will be accessible to those who need it.
Palliative and end-of-life care have long been promoted as core skills for hospitalists. The topic has regularly been included at SHM annual meetings and other prominent hospital medicine conferences, in the American Board of Internal Medicine blueprint for recognition of focused practice in hospital medicine, and in a number of influential references for hospitalists. Still, as I look at hospitalist programs around the country, there is a clear need to improve hospitalists’ delivery of palliative and end-of-life care.
Care of patients with chronic illness in their last two years of life accounts for a third of all Medicare spending.1 As hospitalists, we encounter many of these patients as they are hospitalized—and often re-hospitalized. Palliative care, which can improve quality of life and decrease costs for patients while leading to increased satisfaction and better outcomes for caregivers, can help alleviate unneeded and unwanted aggressive interventions like hospitalization.2,3
In its 2014 report, Dying in America, the Institute of Medicine (IOM) identified several areas for improvement, including better advance care planning and payment systems supporting high quality end-of-life care.4 As I write this column in mid 2016, there are two notable achievements since the IOM report: two E&M codes for advance care planning and a substantial and growing number of hospitalist patients in alternative payment models like bundled payments or ACOs.5 I believe we are entering a time when the availability of good palliative care will be accelerated due to broader forces in healthcare that for the first time align incentives between patients’ wishes and how care is paid for.
Palliative Care Skills for Hospitalists
The following are key actions for physicians in addressing palliative care for the hospitalized patient. At the risk of oversimplifying the discipline, I offer a few key actions for hospitalists to keep in mind.
Identify patients who would benefit from palliative care. The surprise question—“Would I be surprised if this patient died in the next year?”—has the ability to predict which patients would benefit from palliative care. In one observation from a group of patients with cancer, a “no” answer identified 60% of patients who died within a year.6 The surprise question has previously been shown to be predictive in other cancer and non-cancer populations.7,8
Weisman and Meier suggest using the following in a checklist at the time of hospital admission as “primary criteria to screen for unmet palliative care needs”:9
- The surprise question
- Frequent admissions
- Admission prompted by difficult-to-control physical or psychological symptoms
- Complex care requirements
- Decline in function, feeding intolerance, or unintended decline in weight
Hold a “goals of care” meeting. A notable step forward for supporting conversations between physicians and patients occurred on Jan. 1, when the Centers for Medicare & Medicaid Services (CMS) announced the Advance Care Planning E&M codes. These are CPT codes 99497 and 99498. They can be used on the same day as other E&M codes and cover discussions regarding advance care planning issues including discussing advance directives, appointing a healthcare proxy or durable power of attorney, discussing a living will, or addressing orders for life-sustaining treatment like the role of hydration or future hospitalizations. (For more information on how to use them, visit the CMS website and search for the FAQ.)
What should hospitalists concentrate on when having “goals of care” conversations with patients and caregivers? Ariadne Labs, a Harvard-affiliated health innovation group, offers the following as elements of a serious illness conversation:10
- Patients’ understanding of their illness
- Patients’ preferences for information and for family involvement
- Personal life goals, fears, and anxieties
- Trade-offs they are willing to accept
For hospitalists, an important area to pay particular attention to is the role of future hospitalizations in patients’ wishes for care, as some patients, if offered appropriate symptom control, would prefer to remain at home.
Two other crucial elements of inpatient palliative care—offer psychosocial support and symptom relief and hand off patient to effective post-hospital palliative care—are outside the scope of this article. However, they should be kept in mind and, of course, applied.
Understand the role of the palliative care consultation. Busy hospitalists might reasonably think, “I simply don’t have time to address palliative care in patients who aren’t likely to die during this hospitalization or soon after.” The palliative care consult service, if available, should be accessed when patients are identified as palliative care candidates but the primary hospitalist does not have the time or resources—including specialized knowledge in some cases—to deliver adequate palliative care. Palliative care specialists can also help bridge the gap between inpatient and outpatient palliative care resources.
In sum, the move to value-based payment models and the new advance care planning E&M codes provide a renewed focus—with more aligned incentives—and the opportunity to provide good palliative care to all who need it.
For hospitalists, identifying those who would benefit from palliative care and working with the healthcare team to ensure the care is delivered are at the heart of our professional mission. TH
References
- End-of-life care. The Darmouth Atlas of Health Care website. Accessed June 23, 2016.
- Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180-190.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Int Med. 2008;168(16):1783-1790.
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. 2014.
- BPCI Model 2: Retrospective acute & post acute care episode. Centers for Medicare & Medicaid Services website. Accessed June 24, 2016.
- Vick JB, Pertsch N, Hutchings M, et al. The utility of the surprise question in identifying patients most at risk of death. J Clin Oncol. 2015;33(suppl):8.
- Moss AH, Ganjoo J, Sharma S, et al. Utility of the “surprise” question to identify dialysis patients with high mortality. Clin J Am Soc Nephrol. 2008;3:1379-1384.
- Moss AH, Lunney JR, Culp S, et al. Prognostic significance of the “surprise” question in cancer patients. J Palliat Med. 2010;13(7):837-840.
- Weissman D, Meier C. Identifying patients in need of a palliative care assessment in the hospital setting: a consensus report from the Center to Advance Palliative Care. J Palliat Med. 2011;14(1):17-23.
- Serious illness care resources. Ariadne Labs website. Accessed June 24, 2016.
Although effective palliative care has always been a must-have for patients and caregivers facing serious illness, it hasn’t always been readily available. With the emergence of value-based healthcare models—and their potent incentives to reduce avoidable readmissions—there is renewed hope that such care will be accessible to those who need it.
Palliative and end-of-life care have long been promoted as core skills for hospitalists. The topic has regularly been included at SHM annual meetings and other prominent hospital medicine conferences, in the American Board of Internal Medicine blueprint for recognition of focused practice in hospital medicine, and in a number of influential references for hospitalists. Still, as I look at hospitalist programs around the country, there is a clear need to improve hospitalists’ delivery of palliative and end-of-life care.
Care of patients with chronic illness in their last two years of life accounts for a third of all Medicare spending.1 As hospitalists, we encounter many of these patients as they are hospitalized—and often re-hospitalized. Palliative care, which can improve quality of life and decrease costs for patients while leading to increased satisfaction and better outcomes for caregivers, can help alleviate unneeded and unwanted aggressive interventions like hospitalization.2,3
In its 2014 report, Dying in America, the Institute of Medicine (IOM) identified several areas for improvement, including better advance care planning and payment systems supporting high quality end-of-life care.4 As I write this column in mid 2016, there are two notable achievements since the IOM report: two E&M codes for advance care planning and a substantial and growing number of hospitalist patients in alternative payment models like bundled payments or ACOs.5 I believe we are entering a time when the availability of good palliative care will be accelerated due to broader forces in healthcare that for the first time align incentives between patients’ wishes and how care is paid for.
Palliative Care Skills for Hospitalists
The following are key actions for physicians in addressing palliative care for the hospitalized patient. At the risk of oversimplifying the discipline, I offer a few key actions for hospitalists to keep in mind.
Identify patients who would benefit from palliative care. The surprise question—“Would I be surprised if this patient died in the next year?”—has the ability to predict which patients would benefit from palliative care. In one observation from a group of patients with cancer, a “no” answer identified 60% of patients who died within a year.6 The surprise question has previously been shown to be predictive in other cancer and non-cancer populations.7,8
Weisman and Meier suggest using the following in a checklist at the time of hospital admission as “primary criteria to screen for unmet palliative care needs”:9
- The surprise question
- Frequent admissions
- Admission prompted by difficult-to-control physical or psychological symptoms
- Complex care requirements
- Decline in function, feeding intolerance, or unintended decline in weight
Hold a “goals of care” meeting. A notable step forward for supporting conversations between physicians and patients occurred on Jan. 1, when the Centers for Medicare & Medicaid Services (CMS) announced the Advance Care Planning E&M codes. These are CPT codes 99497 and 99498. They can be used on the same day as other E&M codes and cover discussions regarding advance care planning issues including discussing advance directives, appointing a healthcare proxy or durable power of attorney, discussing a living will, or addressing orders for life-sustaining treatment like the role of hydration or future hospitalizations. (For more information on how to use them, visit the CMS website and search for the FAQ.)
What should hospitalists concentrate on when having “goals of care” conversations with patients and caregivers? Ariadne Labs, a Harvard-affiliated health innovation group, offers the following as elements of a serious illness conversation:10
- Patients’ understanding of their illness
- Patients’ preferences for information and for family involvement
- Personal life goals, fears, and anxieties
- Trade-offs they are willing to accept
For hospitalists, an important area to pay particular attention to is the role of future hospitalizations in patients’ wishes for care, as some patients, if offered appropriate symptom control, would prefer to remain at home.
Two other crucial elements of inpatient palliative care—offer psychosocial support and symptom relief and hand off patient to effective post-hospital palliative care—are outside the scope of this article. However, they should be kept in mind and, of course, applied.
Understand the role of the palliative care consultation. Busy hospitalists might reasonably think, “I simply don’t have time to address palliative care in patients who aren’t likely to die during this hospitalization or soon after.” The palliative care consult service, if available, should be accessed when patients are identified as palliative care candidates but the primary hospitalist does not have the time or resources—including specialized knowledge in some cases—to deliver adequate palliative care. Palliative care specialists can also help bridge the gap between inpatient and outpatient palliative care resources.
In sum, the move to value-based payment models and the new advance care planning E&M codes provide a renewed focus—with more aligned incentives—and the opportunity to provide good palliative care to all who need it.
For hospitalists, identifying those who would benefit from palliative care and working with the healthcare team to ensure the care is delivered are at the heart of our professional mission. TH
References
- End-of-life care. The Darmouth Atlas of Health Care website. Accessed June 23, 2016.
- Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180-190.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Int Med. 2008;168(16):1783-1790.
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. 2014.
- BPCI Model 2: Retrospective acute & post acute care episode. Centers for Medicare & Medicaid Services website. Accessed June 24, 2016.
- Vick JB, Pertsch N, Hutchings M, et al. The utility of the surprise question in identifying patients most at risk of death. J Clin Oncol. 2015;33(suppl):8.
- Moss AH, Ganjoo J, Sharma S, et al. Utility of the “surprise” question to identify dialysis patients with high mortality. Clin J Am Soc Nephrol. 2008;3:1379-1384.
- Moss AH, Lunney JR, Culp S, et al. Prognostic significance of the “surprise” question in cancer patients. J Palliat Med. 2010;13(7):837-840.
- Weissman D, Meier C. Identifying patients in need of a palliative care assessment in the hospital setting: a consensus report from the Center to Advance Palliative Care. J Palliat Med. 2011;14(1):17-23.
- Serious illness care resources. Ariadne Labs website. Accessed June 24, 2016.