User login
Psoriasis cardiovascular risk parallels type 2 diabetes
Psoriasis increased the measures of coronary artery calcium at a level similar to that seen in type 2 diabetes mellitus, independent of cardiovascular disease risk factors, based on data from a trio of cross-sectional studies including 387 adults. .
“Psoriasis and type 2 diabetes share similar cardiovascular risk profiles, which may predispose patients to developing coronary atherosclerosis at a relatively young age,” wrote Bobbak Mansouri, MD, of Baylor University Medical Center in Dallas and his associates (JAMA Dermatol. 2016. [doi: 10.1001/jamadermatol.2016.2907]).

The researchers compared coronary artery calcium (CAC) levels in patients with psoriasis, patients with type 2 diabetes, and healthy controls. CAC has become an accepted measure of atherosclerosis and “the cornerstone for screening the risk of future cardiac events and improving cardiovascular risk stratification beyond traditional risk factors, especially in higher-risk groups,” according to the investigators. The average age of the patients was 52 years, 50% were female, and at least 92% were white.
The researchers used a hierarchical Tobit regression analysis to determine the association between disease and CAC level, as measured by the Agatston score. After controlling for confounding variables, including cardiovascular risk factors (low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, systolic blood pressure, and tobacco use), the association with CAC was similar in psoriasis patients and type 2 diabetes patients (Tobit regression ratio [TRR], 0.89 and 0.79, respectively).
In a logistic multivariate regression analysis, patients with either psoriasis or type 2 diabetes were approximately twice as likely to have evidence of CAC as were healthy controls (odds ratio, 2.35 and 2.18, respectively), and psoriasis remained independently associated with the presence of CAC.
“When we added use of systemic or biological therapy to the models, the TRR and OR increased; however, these analyses were exploratory,” wrote Dr. Mansouri and his associates.
The study was limited by factors including the cross-sectional design and lack of diversity in the patient population, the investigators noted. However, the results suggest that “CAC assessment may be considered in patients with psoriasis who have two or more traditional cardiovascular risk factors given the high prevalence of CAC observed in this study,” they said.
Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
Psoriasis increased the measures of coronary artery calcium at a level similar to that seen in type 2 diabetes mellitus, independent of cardiovascular disease risk factors, based on data from a trio of cross-sectional studies including 387 adults. .
“Psoriasis and type 2 diabetes share similar cardiovascular risk profiles, which may predispose patients to developing coronary atherosclerosis at a relatively young age,” wrote Bobbak Mansouri, MD, of Baylor University Medical Center in Dallas and his associates (JAMA Dermatol. 2016. [doi: 10.1001/jamadermatol.2016.2907]).
The researchers compared coronary artery calcium (CAC) levels in patients with psoriasis, patients with type 2 diabetes, and healthy controls. CAC has become an accepted measure of atherosclerosis and “the cornerstone for screening the risk of future cardiac events and improving cardiovascular risk stratification beyond traditional risk factors, especially in higher-risk groups,” according to the investigators. The average age of the patients was 52 years, 50% were female, and at least 92% were white.
The researchers used a hierarchical Tobit regression analysis to determine the association between disease and CAC level, as measured by the Agatston score. After controlling for confounding variables, including cardiovascular risk factors (low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, systolic blood pressure, and tobacco use), the association with CAC was similar in psoriasis patients and type 2 diabetes patients (Tobit regression ratio [TRR], 0.89 and 0.79, respectively).
In a logistic multivariate regression analysis, patients with either psoriasis or type 2 diabetes were approximately twice as likely to have evidence of CAC as were healthy controls (odds ratio, 2.35 and 2.18, respectively), and psoriasis remained independently associated with the presence of CAC.
“When we added use of systemic or biological therapy to the models, the TRR and OR increased; however, these analyses were exploratory,” wrote Dr. Mansouri and his associates.
The study was limited by factors including the cross-sectional design and lack of diversity in the patient population, the investigators noted. However, the results suggest that “CAC assessment may be considered in patients with psoriasis who have two or more traditional cardiovascular risk factors given the high prevalence of CAC observed in this study,” they said.
Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
Psoriasis increased the measures of coronary artery calcium at a level similar to that seen in type 2 diabetes mellitus, independent of cardiovascular disease risk factors, based on data from a trio of cross-sectional studies including 387 adults. .
“Psoriasis and type 2 diabetes share similar cardiovascular risk profiles, which may predispose patients to developing coronary atherosclerosis at a relatively young age,” wrote Bobbak Mansouri, MD, of Baylor University Medical Center in Dallas and his associates (JAMA Dermatol. 2016. [doi: 10.1001/jamadermatol.2016.2907]).
The researchers compared coronary artery calcium (CAC) levels in patients with psoriasis, patients with type 2 diabetes, and healthy controls. CAC has become an accepted measure of atherosclerosis and “the cornerstone for screening the risk of future cardiac events and improving cardiovascular risk stratification beyond traditional risk factors, especially in higher-risk groups,” according to the investigators. The average age of the patients was 52 years, 50% were female, and at least 92% were white.
The researchers used a hierarchical Tobit regression analysis to determine the association between disease and CAC level, as measured by the Agatston score. After controlling for confounding variables, including cardiovascular risk factors (low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, systolic blood pressure, and tobacco use), the association with CAC was similar in psoriasis patients and type 2 diabetes patients (Tobit regression ratio [TRR], 0.89 and 0.79, respectively).
In a logistic multivariate regression analysis, patients with either psoriasis or type 2 diabetes were approximately twice as likely to have evidence of CAC as were healthy controls (odds ratio, 2.35 and 2.18, respectively), and psoriasis remained independently associated with the presence of CAC.
“When we added use of systemic or biological therapy to the models, the TRR and OR increased; however, these analyses were exploratory,” wrote Dr. Mansouri and his associates.
The study was limited by factors including the cross-sectional design and lack of diversity in the patient population, the investigators noted. However, the results suggest that “CAC assessment may be considered in patients with psoriasis who have two or more traditional cardiovascular risk factors given the high prevalence of CAC observed in this study,” they said.
Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
FROM JAMA DERMATOLOGY
Key clinical point: Psoriasis patients have increased coronary artery calcium levels similar to those seen in type 2 diabetes patients, suggesting subclinical atherosclerosis.
Major finding: Psoriasis patients were more than twice as likely (odds ratio, 2.35) to have evidence of coronary artery calcium, compared with healthy controls.
Data source: A set of three single-center, cross-sectional studies totaling 387 adults and including individuals with psoriasis or type 2 diabetes, and healthy controls.
Disclosures: Dr. Mansouri disclosed serving on an advisory board and receiving an honorarium from Celgene, maker of the psoriasis drug apremilast (Otezl). Study coauthors disclosed financial relationships with multiple pharmaceutical companies.
Cycling accounts for the most sports-related ED visits
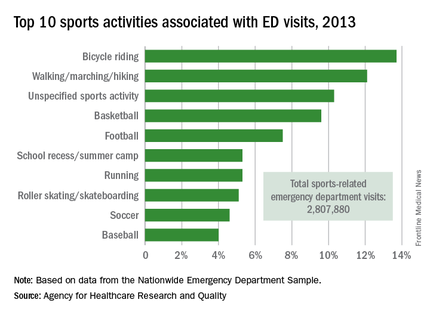
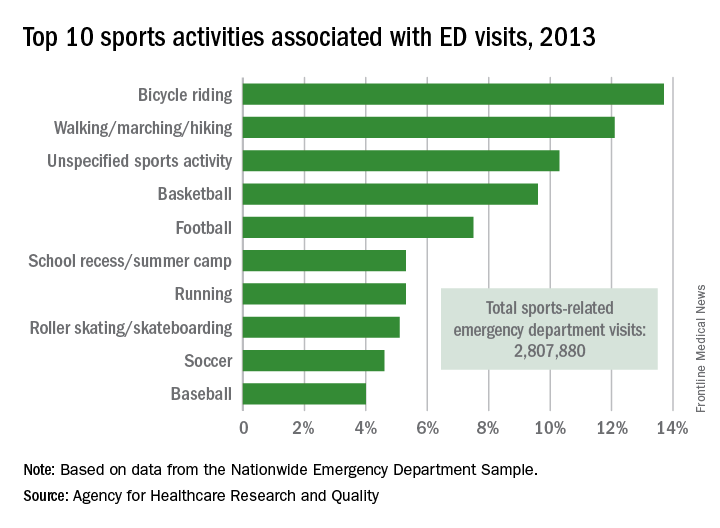
Bicycle riding results in more visits to the emergency department than any other sports activity, according to the Agency for Healthcare Research and Quality.
In 2013, cycling accounted for 13.7% of the 2.8 million ED visits in which the patient was discharged. Walking/marching/hiking was next with 12.1% of ED visits, while unspecified sports activities were third with 10.3% of visits. Team sports took the next two spots: basketball accounted for 9.6% of visits and football accounted for 7.5%, the AHRQ reported.
Among those under age 18 years, who accounted for over 1.5 million ED visits (54.7%) in 2013, football was associated with the most visits for boys (16.4%) and school recess/summer camp led to the most visits (12.8%) for girls. Bicycle riding was the leading reason for males aged 18-44 (16%) and 45-64 (34.9%), while walking/marching/hiking was the leading reason for females aged 18-44 (25.6%) and 45-64 years (49%). For those older than 65 years, walking/marching/hiking was the most common reason for ED visits among both men (54.3%) and women (79.7%), according to data from the Nationwide Emergency Department Sample.
The most common injuries in 2013 for sports-related ED visits (discharged) were sprains (24%), fractures (21%), and superficial injuries (18%). Among the top 10 injury-producing sports activities, cycling had the highest rate of superficial injuries at 26%, school recess/summer camp had the highest fracture rate (42%), and basketball led with a sprain rate of 40%, the AHRQ said.
Bicycle riding results in more visits to the emergency department than any other sports activity, according to the Agency for Healthcare Research and Quality.
In 2013, cycling accounted for 13.7% of the 2.8 million ED visits in which the patient was discharged. Walking/marching/hiking was next with 12.1% of ED visits, while unspecified sports activities were third with 10.3% of visits. Team sports took the next two spots: basketball accounted for 9.6% of visits and football accounted for 7.5%, the AHRQ reported.
Among those under age 18 years, who accounted for over 1.5 million ED visits (54.7%) in 2013, football was associated with the most visits for boys (16.4%) and school recess/summer camp led to the most visits (12.8%) for girls. Bicycle riding was the leading reason for males aged 18-44 (16%) and 45-64 (34.9%), while walking/marching/hiking was the leading reason for females aged 18-44 (25.6%) and 45-64 years (49%). For those older than 65 years, walking/marching/hiking was the most common reason for ED visits among both men (54.3%) and women (79.7%), according to data from the Nationwide Emergency Department Sample.
The most common injuries in 2013 for sports-related ED visits (discharged) were sprains (24%), fractures (21%), and superficial injuries (18%). Among the top 10 injury-producing sports activities, cycling had the highest rate of superficial injuries at 26%, school recess/summer camp had the highest fracture rate (42%), and basketball led with a sprain rate of 40%, the AHRQ said.
Bicycle riding results in more visits to the emergency department than any other sports activity, according to the Agency for Healthcare Research and Quality.
In 2013, cycling accounted for 13.7% of the 2.8 million ED visits in which the patient was discharged. Walking/marching/hiking was next with 12.1% of ED visits, while unspecified sports activities were third with 10.3% of visits. Team sports took the next two spots: basketball accounted for 9.6% of visits and football accounted for 7.5%, the AHRQ reported.
Among those under age 18 years, who accounted for over 1.5 million ED visits (54.7%) in 2013, football was associated with the most visits for boys (16.4%) and school recess/summer camp led to the most visits (12.8%) for girls. Bicycle riding was the leading reason for males aged 18-44 (16%) and 45-64 (34.9%), while walking/marching/hiking was the leading reason for females aged 18-44 (25.6%) and 45-64 years (49%). For those older than 65 years, walking/marching/hiking was the most common reason for ED visits among both men (54.3%) and women (79.7%), according to data from the Nationwide Emergency Department Sample.
The most common injuries in 2013 for sports-related ED visits (discharged) were sprains (24%), fractures (21%), and superficial injuries (18%). Among the top 10 injury-producing sports activities, cycling had the highest rate of superficial injuries at 26%, school recess/summer camp had the highest fracture rate (42%), and basketball led with a sprain rate of 40%, the AHRQ said.
Vaccine refusals and pediatrician dismissals increasing
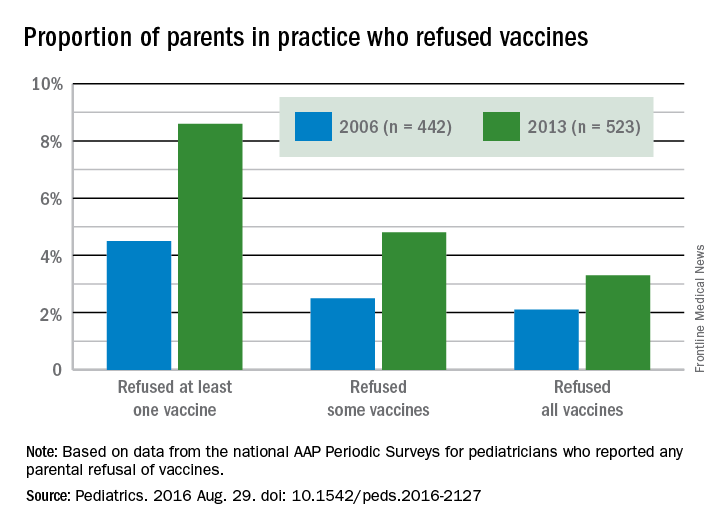
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).

“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.

Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).
“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.
Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).
“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.
Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
FROM PEDIATRICS
Key clinical point: More parents have been refusing vaccines, and more pediatricians have been dismissing vaccine-refusing patients, since 2006.
Major finding: 11.7% of pediatricians reported dismissing patients for refusing vaccines in 2013, compared with 6.1% in 2006, and 8.6% of parents refused at least one vaccine in 2013, compared with 4.5% in 2006.
Data source: The findings are based on surveys of practicing members of the American Academy of Pediatrics, with 629 pediatricians in 2006 and 627 pediatricians in 2013.
Disclosures: The research was funded by the AAP and the Centers for Disease Control and Prevention Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
Navigating the obstacle course of diagnosing, managing pediatric hypertension
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.

One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.

Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.

“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.

“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.
One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.
Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.
“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.
“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.
One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.
Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.
“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.
“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler

Is stem-cell transplant curative for HIV infection?
DURBAN, SOUTH AFRICA – The 15 HIV-infected patients who have undergone allogeneic stem-cell transplant for life-threatening hematologic cancers under the auspices of the European EpiStem Consortium have uniformly demonstrated a profound and durable reduction in viral reservoir to a degree that hasn’t been approached by any other investigational cure strategy, Annemarie Wensing, MD, said at the 21st International AIDS Conference.
“We see an enormous reduction in the viral reservoir, and in two patients we cannot find any viable HIV in the blood using ultrasensitive tests. But we don’t know whether these patients are cured because they are still on antiretroviral therapy,” said Dr. Wensing of Utrecht (The Netherlands) University.

Non-Hodgkin’s lymphoma and Hodgkin’s lymphoma are 7-9 times more frequent in HIV-positive patients than in the general population. But allogeneic stem cell transplantation is an even higher-risk treatment in HIV-positive patients with life-threatening leukemia or lymphoma than in the HIV-negative population. Only 6 of the 15 EuroStem patients remain alive. Eight died within 4 months of the procedure and another died 2.5 years post-transplant, all from progression of their cancer or as a result of opportunistic infections arising during the immunosuppressive chemoablation that’s central to stem-cell transplantation. However, 3 of the 15 patients have survived longer than 3 years. In two of them, no HIV can be detected in blood or intestinal tissue using ultrasensitive tests, while in the third there is “only a slight trace,” according to Dr. Wensing, a clinical virologist.
EpiStem (the European Project to Guide and Investigate the Potential for HIV Cure by Stem-Cell Transplantation) is a multinational collaboration of European oncologists, infectious disease physicians, and other specialists. It was formed in response to the successful outcome of allogeneic stem cell transplantation for acute myeloid leukemia in HIV-positive Timothy Brown, more famously known as “the Berlin patient” (N Engl J Med. 2009 Feb 12;360(7):692-8). He has thus far survived 7 years off antiretroviral therapy.
Much has been made of the fact that Mr. Brown’s donor cells were homozygous for the CCR5 delta32 mutation, which confers natural resistance to HIV infection because it prevents the virus from infecting T cells. Only 1% or less of the population is homozygous for this mutation. But Dr. Wensing isn’t convinced that using donor cells with the mutation is a prerequisite for success. Indeed, while 4 of the 15 EpiStem patients received stem cells from donors homozygous for the mutation and another got donor cells heterozygous for the CCR5 delta32 mutation, the other 10 received stem cells capable of being infected by HIV – yet all 15 experienced an enormous reduction in their viral reservoir. And two of the three patients who have survived longer than 3 years got stem cells without the CCR5 delta32 mutation.
Dr. Wensing observed that a common denominator shared by Timothy Brown and the two EpiStem patients who have trace or undetectable HIV in blood or tissue samples more than 3 years post-transplant is that all three developed severe graft-versus-host disease in conjunction with their stem cell transplantation. She suspects this may have helped them to clear the infection, a hypothesis she intends to pursue further as EpiStem gathers more patients.
Eventually, if patients continue to test negative for HIV using ultrasensitive tests, it will be time to have a discussion with patients and their treating physicians as to whether they should continue on antiretroviral therapy.
“In the end it’s the patients’ decision, but they should be very well counseled because it can have medical and also psychological consequences if HIV returns,” she said.
EpiStem is funded by the American Foundation for AIDS Research Conssortium on HIV Eradication. Dr. Wensing reported having no financial conflicts regarding her presentation.
DURBAN, SOUTH AFRICA – The 15 HIV-infected patients who have undergone allogeneic stem-cell transplant for life-threatening hematologic cancers under the auspices of the European EpiStem Consortium have uniformly demonstrated a profound and durable reduction in viral reservoir to a degree that hasn’t been approached by any other investigational cure strategy, Annemarie Wensing, MD, said at the 21st International AIDS Conference.
“We see an enormous reduction in the viral reservoir, and in two patients we cannot find any viable HIV in the blood using ultrasensitive tests. But we don’t know whether these patients are cured because they are still on antiretroviral therapy,” said Dr. Wensing of Utrecht (The Netherlands) University.
Non-Hodgkin’s lymphoma and Hodgkin’s lymphoma are 7-9 times more frequent in HIV-positive patients than in the general population. But allogeneic stem cell transplantation is an even higher-risk treatment in HIV-positive patients with life-threatening leukemia or lymphoma than in the HIV-negative population. Only 6 of the 15 EuroStem patients remain alive. Eight died within 4 months of the procedure and another died 2.5 years post-transplant, all from progression of their cancer or as a result of opportunistic infections arising during the immunosuppressive chemoablation that’s central to stem-cell transplantation. However, 3 of the 15 patients have survived longer than 3 years. In two of them, no HIV can be detected in blood or intestinal tissue using ultrasensitive tests, while in the third there is “only a slight trace,” according to Dr. Wensing, a clinical virologist.
EpiStem (the European Project to Guide and Investigate the Potential for HIV Cure by Stem-Cell Transplantation) is a multinational collaboration of European oncologists, infectious disease physicians, and other specialists. It was formed in response to the successful outcome of allogeneic stem cell transplantation for acute myeloid leukemia in HIV-positive Timothy Brown, more famously known as “the Berlin patient” (N Engl J Med. 2009 Feb 12;360(7):692-8). He has thus far survived 7 years off antiretroviral therapy.
Much has been made of the fact that Mr. Brown’s donor cells were homozygous for the CCR5 delta32 mutation, which confers natural resistance to HIV infection because it prevents the virus from infecting T cells. Only 1% or less of the population is homozygous for this mutation. But Dr. Wensing isn’t convinced that using donor cells with the mutation is a prerequisite for success. Indeed, while 4 of the 15 EpiStem patients received stem cells from donors homozygous for the mutation and another got donor cells heterozygous for the CCR5 delta32 mutation, the other 10 received stem cells capable of being infected by HIV – yet all 15 experienced an enormous reduction in their viral reservoir. And two of the three patients who have survived longer than 3 years got stem cells without the CCR5 delta32 mutation.
Dr. Wensing observed that a common denominator shared by Timothy Brown and the two EpiStem patients who have trace or undetectable HIV in blood or tissue samples more than 3 years post-transplant is that all three developed severe graft-versus-host disease in conjunction with their stem cell transplantation. She suspects this may have helped them to clear the infection, a hypothesis she intends to pursue further as EpiStem gathers more patients.
Eventually, if patients continue to test negative for HIV using ultrasensitive tests, it will be time to have a discussion with patients and their treating physicians as to whether they should continue on antiretroviral therapy.
“In the end it’s the patients’ decision, but they should be very well counseled because it can have medical and also psychological consequences if HIV returns,” she said.
EpiStem is funded by the American Foundation for AIDS Research Conssortium on HIV Eradication. Dr. Wensing reported having no financial conflicts regarding her presentation.
DURBAN, SOUTH AFRICA – The 15 HIV-infected patients who have undergone allogeneic stem-cell transplant for life-threatening hematologic cancers under the auspices of the European EpiStem Consortium have uniformly demonstrated a profound and durable reduction in viral reservoir to a degree that hasn’t been approached by any other investigational cure strategy, Annemarie Wensing, MD, said at the 21st International AIDS Conference.
“We see an enormous reduction in the viral reservoir, and in two patients we cannot find any viable HIV in the blood using ultrasensitive tests. But we don’t know whether these patients are cured because they are still on antiretroviral therapy,” said Dr. Wensing of Utrecht (The Netherlands) University.
Non-Hodgkin’s lymphoma and Hodgkin’s lymphoma are 7-9 times more frequent in HIV-positive patients than in the general population. But allogeneic stem cell transplantation is an even higher-risk treatment in HIV-positive patients with life-threatening leukemia or lymphoma than in the HIV-negative population. Only 6 of the 15 EuroStem patients remain alive. Eight died within 4 months of the procedure and another died 2.5 years post-transplant, all from progression of their cancer or as a result of opportunistic infections arising during the immunosuppressive chemoablation that’s central to stem-cell transplantation. However, 3 of the 15 patients have survived longer than 3 years. In two of them, no HIV can be detected in blood or intestinal tissue using ultrasensitive tests, while in the third there is “only a slight trace,” according to Dr. Wensing, a clinical virologist.
EpiStem (the European Project to Guide and Investigate the Potential for HIV Cure by Stem-Cell Transplantation) is a multinational collaboration of European oncologists, infectious disease physicians, and other specialists. It was formed in response to the successful outcome of allogeneic stem cell transplantation for acute myeloid leukemia in HIV-positive Timothy Brown, more famously known as “the Berlin patient” (N Engl J Med. 2009 Feb 12;360(7):692-8). He has thus far survived 7 years off antiretroviral therapy.
Much has been made of the fact that Mr. Brown’s donor cells were homozygous for the CCR5 delta32 mutation, which confers natural resistance to HIV infection because it prevents the virus from infecting T cells. Only 1% or less of the population is homozygous for this mutation. But Dr. Wensing isn’t convinced that using donor cells with the mutation is a prerequisite for success. Indeed, while 4 of the 15 EpiStem patients received stem cells from donors homozygous for the mutation and another got donor cells heterozygous for the CCR5 delta32 mutation, the other 10 received stem cells capable of being infected by HIV – yet all 15 experienced an enormous reduction in their viral reservoir. And two of the three patients who have survived longer than 3 years got stem cells without the CCR5 delta32 mutation.
Dr. Wensing observed that a common denominator shared by Timothy Brown and the two EpiStem patients who have trace or undetectable HIV in blood or tissue samples more than 3 years post-transplant is that all three developed severe graft-versus-host disease in conjunction with their stem cell transplantation. She suspects this may have helped them to clear the infection, a hypothesis she intends to pursue further as EpiStem gathers more patients.
Eventually, if patients continue to test negative for HIV using ultrasensitive tests, it will be time to have a discussion with patients and their treating physicians as to whether they should continue on antiretroviral therapy.
“In the end it’s the patients’ decision, but they should be very well counseled because it can have medical and also psychological consequences if HIV returns,” she said.
EpiStem is funded by the American Foundation for AIDS Research Conssortium on HIV Eradication. Dr. Wensing reported having no financial conflicts regarding her presentation.
AT AIDS 2016
Key clinical point: It doesn’t appear to be necessary to use donor stem cells that are homozygous for the CCR5 delta32 mutation to achieve enormous sustained reductions in the viral reservoir in HIV-infected patients undergoing allogeneic stem cell transplantation for hematologic cancers.
Major finding: Two of three patients in a European series who have survived for longer than 3 years after stem-cell transplantation with undetectable or only trace HIV in their blood received donor cells lacking the rare CCR5 delta32 mutation.
Data source: EpiStem is an ongoing observational study of HIV-infected patients who undergo allogeneic stem cell transplantation for life-threatening hematologic cancers.
Disclosures: The EpiStem project is funded by the American Foundation for AIDS Research Conssortium on HIV Eradication. The presenter reported having no financial conflicts regarding her presentation.

HPV vaccination rates grow slowly
Over half, 56% of adolescents aged 13-17 years in the United States had received at least one dose of HPV vaccine, based on 2015 data from the Centers for Disease Control and Prevention’s 2015 National Immunization Survey-Teen.
From 2014 to 2015, the percentage of boys who had received at least one dose of HPV vaccine increased from 42% to 50% and the percentage in girls increased from 60% to 63%. In 2015, 35% of all adolescents (28% of boys and 42% of girls) received at least three doses of HPV vaccine.

Despite the increases, “coverage with at least one HPV vaccine dose was lower than coverage with Tdap and MenACWY,” wrote Dr. Sarah Reagan-Steiner of the CDC and colleagues. During the time of the study, vaccination with at least one dose of the quadrivalent meningococcal conjugate vaccine (MenACWY) increased from 79% to 81% for all adolescents.
“These gaps in coverage demonstrate ongoing missed opportunities for HPV vaccination at visits when other recommended vaccines are administered,” the researchers said. “Strong clinician recommendations for HPV vaccination, and coadministration of the first HPV vaccine dose with Tdap and MenACWY vaccine at age 11-12 years during the same visit would improve HPV coverage,” they added.
Clinician resources to promote conversations with parents and adolescents about vaccination are available on the CDC website.
The findings were published Aug. 25 in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report (MMWR 2016;65:850-8).
Over half, 56% of adolescents aged 13-17 years in the United States had received at least one dose of HPV vaccine, based on 2015 data from the Centers for Disease Control and Prevention’s 2015 National Immunization Survey-Teen.
From 2014 to 2015, the percentage of boys who had received at least one dose of HPV vaccine increased from 42% to 50% and the percentage in girls increased from 60% to 63%. In 2015, 35% of all adolescents (28% of boys and 42% of girls) received at least three doses of HPV vaccine.
Despite the increases, “coverage with at least one HPV vaccine dose was lower than coverage with Tdap and MenACWY,” wrote Dr. Sarah Reagan-Steiner of the CDC and colleagues. During the time of the study, vaccination with at least one dose of the quadrivalent meningococcal conjugate vaccine (MenACWY) increased from 79% to 81% for all adolescents.
“These gaps in coverage demonstrate ongoing missed opportunities for HPV vaccination at visits when other recommended vaccines are administered,” the researchers said. “Strong clinician recommendations for HPV vaccination, and coadministration of the first HPV vaccine dose with Tdap and MenACWY vaccine at age 11-12 years during the same visit would improve HPV coverage,” they added.
Clinician resources to promote conversations with parents and adolescents about vaccination are available on the CDC website.
The findings were published Aug. 25 in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report (MMWR 2016;65:850-8).
Over half, 56% of adolescents aged 13-17 years in the United States had received at least one dose of HPV vaccine, based on 2015 data from the Centers for Disease Control and Prevention’s 2015 National Immunization Survey-Teen.
From 2014 to 2015, the percentage of boys who had received at least one dose of HPV vaccine increased from 42% to 50% and the percentage in girls increased from 60% to 63%. In 2015, 35% of all adolescents (28% of boys and 42% of girls) received at least three doses of HPV vaccine.
Despite the increases, “coverage with at least one HPV vaccine dose was lower than coverage with Tdap and MenACWY,” wrote Dr. Sarah Reagan-Steiner of the CDC and colleagues. During the time of the study, vaccination with at least one dose of the quadrivalent meningococcal conjugate vaccine (MenACWY) increased from 79% to 81% for all adolescents.
“These gaps in coverage demonstrate ongoing missed opportunities for HPV vaccination at visits when other recommended vaccines are administered,” the researchers said. “Strong clinician recommendations for HPV vaccination, and coadministration of the first HPV vaccine dose with Tdap and MenACWY vaccine at age 11-12 years during the same visit would improve HPV coverage,” they added.
Clinician resources to promote conversations with parents and adolescents about vaccination are available on the CDC website.
The findings were published Aug. 25 in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report (MMWR 2016;65:850-8).
FROM MMWR

Antipsychotic agents key for treating delusional infestation
Boston – Patients with delusional infestation often resist referral to a psychiatrist and insist on treatment by a dermatologist, according to Mark D. P. Davis, MD.
Dermatologists, conversely, often don’t want to treat these challenging patients because they aren’t really sure how to manage them, Dr. Davis said during a “practice gaps” session at the American Academy of Dermatology summer meeting.

An important practice gap is the lack of a standard approach to the investigation and management of these patients, he said.
An audience poll showed that respondents were divided as to whether patients presenting with delusional infestation, also known as delusional parasitosis, should be confronted, referred to a psychiatrist, treated with an antipsychotic, or approached in some other way.
The condition, which involves the delusional belief that one’s skin is “infested” with parasites, fibers, or some other materials, can result from another cause, said Dr. Davis of the Mayo Clinic, Rochester, Minn, noting that anxiety, depression, and medications such as opioids or treatments for attention deficit/hyperactivity disorder can contribute to the delusions.
Skin diseases themselves can also cause the sensation of infestation.
A good history should assess medical comorbidities, electrolyte abnormalities, or medication use that might be contributing to the problem.
For dermatologists who are not well-versed in “picking up on psychiatric comorbidities,” validated measures can be useful. Tools such as the Personal Health Questionnaire (PHQ)-9 for depression and Generalized Anxiety Disorder (GAD)-7 can be useful, Dr. Davis said.
However, delusions, by definition, are “fixed false beliefs.” Challenging a patient regarding their delusions is likely pointless, as the patients’ minds cannot be changed.
For cases of primary delusional infestation, the goal generally is to decrease the patient’s preoccupation with the delusion and to improve social and occupational functions. Treatment with antipsychotic drugs is usually helpful–if patients will comply with treatment. “I’ve been very unsuccessful” at getting patients to use antipsychotics, he said.
A good treatment option is risperidone, which has low cost and good efficacy and tolerability. Start with a daily dose of 1 mg/day and gradually increase up to 6 mg daily if necessary, he said.
Establishing a rapport over multiple visits may help with compliance. For example, take a history on the first visit, order laboratory tests at a second visit, perform a biopsy at a third, and then broach the subject of treatment at a subsequent visit, he suggested.
Getting the patient on board with taking risperidone or another antipsychotic may be easier if you ask the patient early on whether they would like treatment for their symptoms in the event a definitive cause for their symptoms can’t be identified, he said.
Dr. Davis reported having no disclosures.
Boston – Patients with delusional infestation often resist referral to a psychiatrist and insist on treatment by a dermatologist, according to Mark D. P. Davis, MD.
Dermatologists, conversely, often don’t want to treat these challenging patients because they aren’t really sure how to manage them, Dr. Davis said during a “practice gaps” session at the American Academy of Dermatology summer meeting.
An important practice gap is the lack of a standard approach to the investigation and management of these patients, he said.
An audience poll showed that respondents were divided as to whether patients presenting with delusional infestation, also known as delusional parasitosis, should be confronted, referred to a psychiatrist, treated with an antipsychotic, or approached in some other way.
The condition, which involves the delusional belief that one’s skin is “infested” with parasites, fibers, or some other materials, can result from another cause, said Dr. Davis of the Mayo Clinic, Rochester, Minn, noting that anxiety, depression, and medications such as opioids or treatments for attention deficit/hyperactivity disorder can contribute to the delusions.
Skin diseases themselves can also cause the sensation of infestation.
A good history should assess medical comorbidities, electrolyte abnormalities, or medication use that might be contributing to the problem.
For dermatologists who are not well-versed in “picking up on psychiatric comorbidities,” validated measures can be useful. Tools such as the Personal Health Questionnaire (PHQ)-9 for depression and Generalized Anxiety Disorder (GAD)-7 can be useful, Dr. Davis said.
However, delusions, by definition, are “fixed false beliefs.” Challenging a patient regarding their delusions is likely pointless, as the patients’ minds cannot be changed.
For cases of primary delusional infestation, the goal generally is to decrease the patient’s preoccupation with the delusion and to improve social and occupational functions. Treatment with antipsychotic drugs is usually helpful–if patients will comply with treatment. “I’ve been very unsuccessful” at getting patients to use antipsychotics, he said.
A good treatment option is risperidone, which has low cost and good efficacy and tolerability. Start with a daily dose of 1 mg/day and gradually increase up to 6 mg daily if necessary, he said.
Establishing a rapport over multiple visits may help with compliance. For example, take a history on the first visit, order laboratory tests at a second visit, perform a biopsy at a third, and then broach the subject of treatment at a subsequent visit, he suggested.
Getting the patient on board with taking risperidone or another antipsychotic may be easier if you ask the patient early on whether they would like treatment for their symptoms in the event a definitive cause for their symptoms can’t be identified, he said.
Dr. Davis reported having no disclosures.
Boston – Patients with delusional infestation often resist referral to a psychiatrist and insist on treatment by a dermatologist, according to Mark D. P. Davis, MD.
Dermatologists, conversely, often don’t want to treat these challenging patients because they aren’t really sure how to manage them, Dr. Davis said during a “practice gaps” session at the American Academy of Dermatology summer meeting.
An important practice gap is the lack of a standard approach to the investigation and management of these patients, he said.
An audience poll showed that respondents were divided as to whether patients presenting with delusional infestation, also known as delusional parasitosis, should be confronted, referred to a psychiatrist, treated with an antipsychotic, or approached in some other way.
The condition, which involves the delusional belief that one’s skin is “infested” with parasites, fibers, or some other materials, can result from another cause, said Dr. Davis of the Mayo Clinic, Rochester, Minn, noting that anxiety, depression, and medications such as opioids or treatments for attention deficit/hyperactivity disorder can contribute to the delusions.
Skin diseases themselves can also cause the sensation of infestation.
A good history should assess medical comorbidities, electrolyte abnormalities, or medication use that might be contributing to the problem.
For dermatologists who are not well-versed in “picking up on psychiatric comorbidities,” validated measures can be useful. Tools such as the Personal Health Questionnaire (PHQ)-9 for depression and Generalized Anxiety Disorder (GAD)-7 can be useful, Dr. Davis said.
However, delusions, by definition, are “fixed false beliefs.” Challenging a patient regarding their delusions is likely pointless, as the patients’ minds cannot be changed.
For cases of primary delusional infestation, the goal generally is to decrease the patient’s preoccupation with the delusion and to improve social and occupational functions. Treatment with antipsychotic drugs is usually helpful–if patients will comply with treatment. “I’ve been very unsuccessful” at getting patients to use antipsychotics, he said.
A good treatment option is risperidone, which has low cost and good efficacy and tolerability. Start with a daily dose of 1 mg/day and gradually increase up to 6 mg daily if necessary, he said.
Establishing a rapport over multiple visits may help with compliance. For example, take a history on the first visit, order laboratory tests at a second visit, perform a biopsy at a third, and then broach the subject of treatment at a subsequent visit, he suggested.
Getting the patient on board with taking risperidone or another antipsychotic may be easier if you ask the patient early on whether they would like treatment for their symptoms in the event a definitive cause for their symptoms can’t be identified, he said.
Dr. Davis reported having no disclosures.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2016

Maraviroc shows potential for HIV PrEP in women
DURBAN, SOUTH AFRICA – Maraviroc-containing regimens for daily oral pre-exposure prophylaxis in women at risk for HIV infection showed good safety and tolerability in a phase 2 study, the first randomized trial of PrEP ever conducted in U.S. women, Roy M. Gulick, MD, reported at the 21st International AIDS Conference.
No new HIV infections occurred in the 188 women who participated in the 48-week, randomized, double-blind, placebo-controlled study known as the HPTN 069/ACTG A5305 trial.
However, the results shouldn’t be taken as evidence of efficacy. The relatively low 2% incidence of new STIs diagnosed during 48 weeks of close followup – three cases of chlamydia, one of gonorrhea – suggests that the study population probably wasn’t at high risk for acquiring HIV. Further, the study wasn’t powered to determine efficacy. That determination will have to await a larger phase 3 trial, observed Dr. Gulick, professor of medicine at Cornell University in New York.
Maraviroc (Selzentry) is categorized as an HIV entry inhibitor. It’s an antagonist of the CCR5 receptor found on the surface of T cells, which is the route of HIV infection. The rationale for exploring the drug for HIV PrEP, according to Dr. Gulick, is that it concentrates in both the genital tract and rectum, doesn’t select for drug-resistant viral strains, is well tolerated, and it isn’t commonly used for treatment of HIV infection.
Additional options for oral daily HIV PrEP are clearly desirable, he added. The only approved agent is Truvada (tenofovir/emtricitabine), which is often used in HIV therapy as well, and there is concern it may select for drug resistance. Plus, it has renal, GI, and bone side effects.
Study participants were HIV-negative adult women who were born female and considered at risk for HIV acquisition because of a history of condomless vaginal or anal intercourse with at least one HIV-positive or unknown status man within the previous 90 days. The women were randomized to one of four study arms: maraviroc at the standard dose of 300 mg/day plus two placebo pills; maraviroc plus emtricitabine at the standard dose of 200 mg/day plus one placebo pill; maraviroc plus tenofovir at 300 mg/day plus a placebo pill, or a control regimen of fixed-dose Truvada (tenofovir 300 mg/emtricitabine 200 mg) plus two placebo pills. Thus, everyone took three pills once daily.
The three-pill regimen might help explain the less than stellar patient adherence. Study drugs were detectable – and not necessarily at therapeutic levels – in the plasma of 65% of subjects at 24 weeks and 60% at 48 weeks, with no differences between the study arms.
Maraviroc alone was associated with fewer grade 2-4 adverse events than the other regimens.
There were 11 grade 3 or 4 adverse events deemed by investigators to be related to study drugs. They included abnormal weight loss, depression, hypophosphatemia, a rise in LDL cholesterol, headache, vitamin D deficiency, back pain, two spontaneous abortions, and two dissimilar cases of congenital anomaly, with no obvious differences between the study groups in rate or pattern. Rates of specific renal and GI toxicities were comparable across the four study arms.
Earlier in 2016, Dr. Gulick presented the results of the men’s arm of HPTN 069/ACTG A5305, a parallel 48-week randomized trial in 406 men who have sex with men. Five men in the maraviroc monotherapy arm seroconverted during the 48-week study, for an incidence of 1.4%. All had no or low plasma drug concentrations, and all five were infected with HIV lacking antiretroviral drug resistance.
Dr. Gulick and coinvestigators plan to present the findings of an analysis of rectal and vaginal biopsies from 42 women in the trial, along with a bone mineral density substudy in 200 men and 200 women men in the trial, plus detailed quality-of-life, behavioral, and adherence data in the full men’s and women’s cohorts.
The trial was sponsored by the HIV Prevention Trials Network and the AIDS Clinical Trials Group with funding from the National Institute of Allergic and Infectious Diseases. Dr. Gulick reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Maraviroc-containing regimens for daily oral pre-exposure prophylaxis in women at risk for HIV infection showed good safety and tolerability in a phase 2 study, the first randomized trial of PrEP ever conducted in U.S. women, Roy M. Gulick, MD, reported at the 21st International AIDS Conference.
No new HIV infections occurred in the 188 women who participated in the 48-week, randomized, double-blind, placebo-controlled study known as the HPTN 069/ACTG A5305 trial.
However, the results shouldn’t be taken as evidence of efficacy. The relatively low 2% incidence of new STIs diagnosed during 48 weeks of close followup – three cases of chlamydia, one of gonorrhea – suggests that the study population probably wasn’t at high risk for acquiring HIV. Further, the study wasn’t powered to determine efficacy. That determination will have to await a larger phase 3 trial, observed Dr. Gulick, professor of medicine at Cornell University in New York.
Maraviroc (Selzentry) is categorized as an HIV entry inhibitor. It’s an antagonist of the CCR5 receptor found on the surface of T cells, which is the route of HIV infection. The rationale for exploring the drug for HIV PrEP, according to Dr. Gulick, is that it concentrates in both the genital tract and rectum, doesn’t select for drug-resistant viral strains, is well tolerated, and it isn’t commonly used for treatment of HIV infection.
Additional options for oral daily HIV PrEP are clearly desirable, he added. The only approved agent is Truvada (tenofovir/emtricitabine), which is often used in HIV therapy as well, and there is concern it may select for drug resistance. Plus, it has renal, GI, and bone side effects.
Study participants were HIV-negative adult women who were born female and considered at risk for HIV acquisition because of a history of condomless vaginal or anal intercourse with at least one HIV-positive or unknown status man within the previous 90 days. The women were randomized to one of four study arms: maraviroc at the standard dose of 300 mg/day plus two placebo pills; maraviroc plus emtricitabine at the standard dose of 200 mg/day plus one placebo pill; maraviroc plus tenofovir at 300 mg/day plus a placebo pill, or a control regimen of fixed-dose Truvada (tenofovir 300 mg/emtricitabine 200 mg) plus two placebo pills. Thus, everyone took three pills once daily.
The three-pill regimen might help explain the less than stellar patient adherence. Study drugs were detectable – and not necessarily at therapeutic levels – in the plasma of 65% of subjects at 24 weeks and 60% at 48 weeks, with no differences between the study arms.
Maraviroc alone was associated with fewer grade 2-4 adverse events than the other regimens.
There were 11 grade 3 or 4 adverse events deemed by investigators to be related to study drugs. They included abnormal weight loss, depression, hypophosphatemia, a rise in LDL cholesterol, headache, vitamin D deficiency, back pain, two spontaneous abortions, and two dissimilar cases of congenital anomaly, with no obvious differences between the study groups in rate or pattern. Rates of specific renal and GI toxicities were comparable across the four study arms.
Earlier in 2016, Dr. Gulick presented the results of the men’s arm of HPTN 069/ACTG A5305, a parallel 48-week randomized trial in 406 men who have sex with men. Five men in the maraviroc monotherapy arm seroconverted during the 48-week study, for an incidence of 1.4%. All had no or low plasma drug concentrations, and all five were infected with HIV lacking antiretroviral drug resistance.
Dr. Gulick and coinvestigators plan to present the findings of an analysis of rectal and vaginal biopsies from 42 women in the trial, along with a bone mineral density substudy in 200 men and 200 women men in the trial, plus detailed quality-of-life, behavioral, and adherence data in the full men’s and women’s cohorts.
The trial was sponsored by the HIV Prevention Trials Network and the AIDS Clinical Trials Group with funding from the National Institute of Allergic and Infectious Diseases. Dr. Gulick reported having no financial conflicts of interest.
DURBAN, SOUTH AFRICA – Maraviroc-containing regimens for daily oral pre-exposure prophylaxis in women at risk for HIV infection showed good safety and tolerability in a phase 2 study, the first randomized trial of PrEP ever conducted in U.S. women, Roy M. Gulick, MD, reported at the 21st International AIDS Conference.
No new HIV infections occurred in the 188 women who participated in the 48-week, randomized, double-blind, placebo-controlled study known as the HPTN 069/ACTG A5305 trial.
However, the results shouldn’t be taken as evidence of efficacy. The relatively low 2% incidence of new STIs diagnosed during 48 weeks of close followup – three cases of chlamydia, one of gonorrhea – suggests that the study population probably wasn’t at high risk for acquiring HIV. Further, the study wasn’t powered to determine efficacy. That determination will have to await a larger phase 3 trial, observed Dr. Gulick, professor of medicine at Cornell University in New York.
Maraviroc (Selzentry) is categorized as an HIV entry inhibitor. It’s an antagonist of the CCR5 receptor found on the surface of T cells, which is the route of HIV infection. The rationale for exploring the drug for HIV PrEP, according to Dr. Gulick, is that it concentrates in both the genital tract and rectum, doesn’t select for drug-resistant viral strains, is well tolerated, and it isn’t commonly used for treatment of HIV infection.
Additional options for oral daily HIV PrEP are clearly desirable, he added. The only approved agent is Truvada (tenofovir/emtricitabine), which is often used in HIV therapy as well, and there is concern it may select for drug resistance. Plus, it has renal, GI, and bone side effects.
Study participants were HIV-negative adult women who were born female and considered at risk for HIV acquisition because of a history of condomless vaginal or anal intercourse with at least one HIV-positive or unknown status man within the previous 90 days. The women were randomized to one of four study arms: maraviroc at the standard dose of 300 mg/day plus two placebo pills; maraviroc plus emtricitabine at the standard dose of 200 mg/day plus one placebo pill; maraviroc plus tenofovir at 300 mg/day plus a placebo pill, or a control regimen of fixed-dose Truvada (tenofovir 300 mg/emtricitabine 200 mg) plus two placebo pills. Thus, everyone took three pills once daily.
The three-pill regimen might help explain the less than stellar patient adherence. Study drugs were detectable – and not necessarily at therapeutic levels – in the plasma of 65% of subjects at 24 weeks and 60% at 48 weeks, with no differences between the study arms.
Maraviroc alone was associated with fewer grade 2-4 adverse events than the other regimens.
There were 11 grade 3 or 4 adverse events deemed by investigators to be related to study drugs. They included abnormal weight loss, depression, hypophosphatemia, a rise in LDL cholesterol, headache, vitamin D deficiency, back pain, two spontaneous abortions, and two dissimilar cases of congenital anomaly, with no obvious differences between the study groups in rate or pattern. Rates of specific renal and GI toxicities were comparable across the four study arms.
Earlier in 2016, Dr. Gulick presented the results of the men’s arm of HPTN 069/ACTG A5305, a parallel 48-week randomized trial in 406 men who have sex with men. Five men in the maraviroc monotherapy arm seroconverted during the 48-week study, for an incidence of 1.4%. All had no or low plasma drug concentrations, and all five were infected with HIV lacking antiretroviral drug resistance.
Dr. Gulick and coinvestigators plan to present the findings of an analysis of rectal and vaginal biopsies from 42 women in the trial, along with a bone mineral density substudy in 200 men and 200 women men in the trial, plus detailed quality-of-life, behavioral, and adherence data in the full men’s and women’s cohorts.
The trial was sponsored by the HIV Prevention Trials Network and the AIDS Clinical Trials Group with funding from the National Institute of Allergic and Infectious Diseases. Dr. Gulick reported having no financial conflicts of interest.
AT AIDS 2016
Key clinical point: Maraviroc shows promise as an alternative to Truvada for HIV pre-exposure prophylaxis.
Major finding: No new HIV infections occurred in at-risk women in a 48-week study of daily oral HIV pre-exposure prophylaxis comparing three maraviroc-containing regimens and tenofovir/emtricitabine.
Data source: This was a randomized, double-blind, placebo-controlled, multicenter, 48-week clinical trial involving 188 women at risk for HIV infection.
Disclosures: The trial was sponsored by the HIV Prevention Trials Network and the AIDS Clinical Trials Group with funding from the National Institute of Allergy and Infectious Diseases. The presenter reported having no financial conflicts of interest.
VIDEO: ICDs cut mortality in younger, healthier heart failure patients
ROME – Implantable cardioverter-defibrillators failed to significantly cut total mortality in patients with nonischemic systolic heart failure in the first large, randomized trial designed specifically to test the treatment in this setting. But the devices did show significant efficacy for doing what thy are specifically designed to do: prevent sudden cardiac death.
Results from the Danish Study to Assess the Efficacy of ICDs in Patients with Non-ischemic Systolic Heart Failure on Mortality (DANISH) also highlighted the importance of targeting implantable cardioverter-defibrillator (ICD) treatment to the patients with nonischemic systolic heart failure who are most likely to benefit from it, younger patients who can be expected to live substantially longer than 1 year after they receive the device.

As a consequence, although the DANISH outcome was neutral for the study’s primary endpoint of decreased all-cause mortality several experts who commented on the findings as well as its lead investigator saw the overall results as providing important new evidence that ICDs are beneficial as long as they get placed in relative young nonischemic heart failure patients who don’t have comorbidities that threaten a quick demise.
The DANISH results “tell us ICDs can benefit patients if we can be a little better in selecting the right patients,” said Lars Køber, MD, while presenting the results at the annual congress of the European Society of Cardiology.
He noted that “for us [in Denmark] the results actually mean we’ll implant more ICDs. We had not been using ICDs [in patients with nonischemic systolic heart failure] because we were not convinced we should use them on everyone,” said Dr. Køber, a professor of cardiology at the University of Copenhagen.
“The primary outcome was neutral, but the reduction in sudden cardiac death, the primary objective of an ICD, was significant, so placing an ICD should be taken into consideration,” commented Michel Komajda, MD, professor of cardiology at Pierre and Marie Curie University in Paris.
“This is the first trial to look at ICDs in the setting of modern therapy. Most of the ICD trials are very old now,” commented Mariell L. Jessup, MD, a heart failure specialist and professor of medicine at the University of Pennsylvania in Philadelphia. “In DANISH the ICDs significantly reduced the incidence of sudden cardiac death; that is what ICDs do.”
DANISH randomized 1,116 patients with nonischemic systolic heart failure at any of five Danish hospitals to either receive or not receive an ICD on top of optimal medical therapy and, when judged appropriate, placement of a cardiac resynchronization therapy (CRT) device. The patients averaged about 64 years of age, they all had New York Heart Association class II or III heart failure, and their maximum left ventricular ejection fraction was 35%. The researchers followed patients for a median of about 68 months (5.7 years).
The study’s primary endpoint, death from any cause, occurred in 22% of the ICD recipients and in 23% of control patients, a nonsignificant difference. The two prespecified secondary endpoints were cardiovascular death, which was a relative 23% lower in the ICD patients and also not statistically significant, but the rate of sudden cardiac death during follow-up was 4% in the ICD patients and 8% in the controls, a statistically significant 50% relative risk reduction. Concurrent with Dr. Køber’s report of these results at the meeting they also appeared online (N Engl J Med. 2016 Aug 28;doi: 10.1056/NEJMoa1608029).
The study design also included a set of prespecified subset analyses, and one of these showed a statistically significant interaction: When the analysis stratified patients into tertiles by age, those younger than 59 years old had a statistically significant 49% cut in all-cause mortality with ICD use, and patients 59-67 years old had a nonsignificant 25% reduction in all cause mortality when on ICD treatment. A second analysis that included all these patients less than 68 years old showed that ICD use linked with a statistically significant 36% relative cut in all-cause death, compared with the patients who did not receive an ICD. Older patients, those at least age 68 years, had a relative 20% increased rate of all-cause mortality with ICD use but not a statistically significant difference.

The results also showed a downside to ICD use. Among the 42% of patients who did not receive a CRT device, the rate of serious infection was 2.6% in the ICD recipients and 0.8% in the control. Serious infection rates with and without ICD placement were similar in the subgroup of patients who received a CRT device.
The results underscored the ability of ICDs to provide a substantial benefit to well-selected patients based on factors such as age. “Clearly we need more accurate selection of nonischemic systolic heart failure patients before implanting ICDs,” said Christophe Leclerqc, MD, designated discussant for the study and professor of cardiology at Central University Hospital of Rennes, France.
“It’s all about patient selection,” agreed Dr. Jessup, who added that currently many nonischemic heart failure patients worldwide who could benefit from an ICD and have a life expectancy beyond 1 year do not receive a device.
On Twitter @mitchelzoler
The message from this study is that in younger, nonischemic heart failure patients at risk for sudden cardiac death but with relatively less morbidity and more life expectancy, the placement of an implantable cardioverter-defibrillator produced a substantial reduction in all-cause mortality.
Although the all-cause mortality benefit was not statistically significant in the entire study population, the study results were very consistent with what we know about sudden cardiac death and why we give ICD therapy to heart failure patients. In DANISH the ICDs did what they are supposed to do, which is prevent sudden cardiac death.
The guidelines say that ICD treatment is appropriate when a patient’s life expectancy is “substantially” more than 1 year. They don’t specify an age cutoff because some 80-year-olds can have a good life expectancy while some younger patients may have comorbidities that make them unlikely to live more than 6 months. ICDs should be targeted to patients at high enough risk from sudden cardiac death to potentially get benefit from the device but not so high-risk that an ICD would be unlikely to make a difference in survival.
Many heart failure patients who could potentially get a benefit from an ICD still do not receive them. ICDs remain an underused treatment for heart failure patients in U.S. practice including patients with nonischemic systolic heart failure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Javed Butler, MD, is a professor of medicine and chief of cardiology at Stony Brook (N.Y.) University. He made these comments in an interview. He has been a consultant to several drug and therapeutics companies but had no relevant disclosures.
The message from this study is that in younger, nonischemic heart failure patients at risk for sudden cardiac death but with relatively less morbidity and more life expectancy, the placement of an implantable cardioverter-defibrillator produced a substantial reduction in all-cause mortality.
Although the all-cause mortality benefit was not statistically significant in the entire study population, the study results were very consistent with what we know about sudden cardiac death and why we give ICD therapy to heart failure patients. In DANISH the ICDs did what they are supposed to do, which is prevent sudden cardiac death.
The guidelines say that ICD treatment is appropriate when a patient’s life expectancy is “substantially” more than 1 year. They don’t specify an age cutoff because some 80-year-olds can have a good life expectancy while some younger patients may have comorbidities that make them unlikely to live more than 6 months. ICDs should be targeted to patients at high enough risk from sudden cardiac death to potentially get benefit from the device but not so high-risk that an ICD would be unlikely to make a difference in survival.
Many heart failure patients who could potentially get a benefit from an ICD still do not receive them. ICDs remain an underused treatment for heart failure patients in U.S. practice including patients with nonischemic systolic heart failure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Javed Butler, MD, is a professor of medicine and chief of cardiology at Stony Brook (N.Y.) University. He made these comments in an interview. He has been a consultant to several drug and therapeutics companies but had no relevant disclosures.
The message from this study is that in younger, nonischemic heart failure patients at risk for sudden cardiac death but with relatively less morbidity and more life expectancy, the placement of an implantable cardioverter-defibrillator produced a substantial reduction in all-cause mortality.
Although the all-cause mortality benefit was not statistically significant in the entire study population, the study results were very consistent with what we know about sudden cardiac death and why we give ICD therapy to heart failure patients. In DANISH the ICDs did what they are supposed to do, which is prevent sudden cardiac death.
The guidelines say that ICD treatment is appropriate when a patient’s life expectancy is “substantially” more than 1 year. They don’t specify an age cutoff because some 80-year-olds can have a good life expectancy while some younger patients may have comorbidities that make them unlikely to live more than 6 months. ICDs should be targeted to patients at high enough risk from sudden cardiac death to potentially get benefit from the device but not so high-risk that an ICD would be unlikely to make a difference in survival.
Many heart failure patients who could potentially get a benefit from an ICD still do not receive them. ICDs remain an underused treatment for heart failure patients in U.S. practice including patients with nonischemic systolic heart failure.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Javed Butler, MD, is a professor of medicine and chief of cardiology at Stony Brook (N.Y.) University. He made these comments in an interview. He has been a consultant to several drug and therapeutics companies but had no relevant disclosures.
ROME – Implantable cardioverter-defibrillators failed to significantly cut total mortality in patients with nonischemic systolic heart failure in the first large, randomized trial designed specifically to test the treatment in this setting. But the devices did show significant efficacy for doing what thy are specifically designed to do: prevent sudden cardiac death.
Results from the Danish Study to Assess the Efficacy of ICDs in Patients with Non-ischemic Systolic Heart Failure on Mortality (DANISH) also highlighted the importance of targeting implantable cardioverter-defibrillator (ICD) treatment to the patients with nonischemic systolic heart failure who are most likely to benefit from it, younger patients who can be expected to live substantially longer than 1 year after they receive the device.
As a consequence, although the DANISH outcome was neutral for the study’s primary endpoint of decreased all-cause mortality several experts who commented on the findings as well as its lead investigator saw the overall results as providing important new evidence that ICDs are beneficial as long as they get placed in relative young nonischemic heart failure patients who don’t have comorbidities that threaten a quick demise.
The DANISH results “tell us ICDs can benefit patients if we can be a little better in selecting the right patients,” said Lars Køber, MD, while presenting the results at the annual congress of the European Society of Cardiology.
He noted that “for us [in Denmark] the results actually mean we’ll implant more ICDs. We had not been using ICDs [in patients with nonischemic systolic heart failure] because we were not convinced we should use them on everyone,” said Dr. Køber, a professor of cardiology at the University of Copenhagen.
“The primary outcome was neutral, but the reduction in sudden cardiac death, the primary objective of an ICD, was significant, so placing an ICD should be taken into consideration,” commented Michel Komajda, MD, professor of cardiology at Pierre and Marie Curie University in Paris.
“This is the first trial to look at ICDs in the setting of modern therapy. Most of the ICD trials are very old now,” commented Mariell L. Jessup, MD, a heart failure specialist and professor of medicine at the University of Pennsylvania in Philadelphia. “In DANISH the ICDs significantly reduced the incidence of sudden cardiac death; that is what ICDs do.”
DANISH randomized 1,116 patients with nonischemic systolic heart failure at any of five Danish hospitals to either receive or not receive an ICD on top of optimal medical therapy and, when judged appropriate, placement of a cardiac resynchronization therapy (CRT) device. The patients averaged about 64 years of age, they all had New York Heart Association class II or III heart failure, and their maximum left ventricular ejection fraction was 35%. The researchers followed patients for a median of about 68 months (5.7 years).
The study’s primary endpoint, death from any cause, occurred in 22% of the ICD recipients and in 23% of control patients, a nonsignificant difference. The two prespecified secondary endpoints were cardiovascular death, which was a relative 23% lower in the ICD patients and also not statistically significant, but the rate of sudden cardiac death during follow-up was 4% in the ICD patients and 8% in the controls, a statistically significant 50% relative risk reduction. Concurrent with Dr. Køber’s report of these results at the meeting they also appeared online (N Engl J Med. 2016 Aug 28;doi: 10.1056/NEJMoa1608029).
The study design also included a set of prespecified subset analyses, and one of these showed a statistically significant interaction: When the analysis stratified patients into tertiles by age, those younger than 59 years old had a statistically significant 49% cut in all-cause mortality with ICD use, and patients 59-67 years old had a nonsignificant 25% reduction in all cause mortality when on ICD treatment. A second analysis that included all these patients less than 68 years old showed that ICD use linked with a statistically significant 36% relative cut in all-cause death, compared with the patients who did not receive an ICD. Older patients, those at least age 68 years, had a relative 20% increased rate of all-cause mortality with ICD use but not a statistically significant difference.
The results also showed a downside to ICD use. Among the 42% of patients who did not receive a CRT device, the rate of serious infection was 2.6% in the ICD recipients and 0.8% in the control. Serious infection rates with and without ICD placement were similar in the subgroup of patients who received a CRT device.
The results underscored the ability of ICDs to provide a substantial benefit to well-selected patients based on factors such as age. “Clearly we need more accurate selection of nonischemic systolic heart failure patients before implanting ICDs,” said Christophe Leclerqc, MD, designated discussant for the study and professor of cardiology at Central University Hospital of Rennes, France.
“It’s all about patient selection,” agreed Dr. Jessup, who added that currently many nonischemic heart failure patients worldwide who could benefit from an ICD and have a life expectancy beyond 1 year do not receive a device.
On Twitter @mitchelzoler
ROME – Implantable cardioverter-defibrillators failed to significantly cut total mortality in patients with nonischemic systolic heart failure in the first large, randomized trial designed specifically to test the treatment in this setting. But the devices did show significant efficacy for doing what thy are specifically designed to do: prevent sudden cardiac death.
Results from the Danish Study to Assess the Efficacy of ICDs in Patients with Non-ischemic Systolic Heart Failure on Mortality (DANISH) also highlighted the importance of targeting implantable cardioverter-defibrillator (ICD) treatment to the patients with nonischemic systolic heart failure who are most likely to benefit from it, younger patients who can be expected to live substantially longer than 1 year after they receive the device.
As a consequence, although the DANISH outcome was neutral for the study’s primary endpoint of decreased all-cause mortality several experts who commented on the findings as well as its lead investigator saw the overall results as providing important new evidence that ICDs are beneficial as long as they get placed in relative young nonischemic heart failure patients who don’t have comorbidities that threaten a quick demise.
The DANISH results “tell us ICDs can benefit patients if we can be a little better in selecting the right patients,” said Lars Køber, MD, while presenting the results at the annual congress of the European Society of Cardiology.
He noted that “for us [in Denmark] the results actually mean we’ll implant more ICDs. We had not been using ICDs [in patients with nonischemic systolic heart failure] because we were not convinced we should use them on everyone,” said Dr. Køber, a professor of cardiology at the University of Copenhagen.
“The primary outcome was neutral, but the reduction in sudden cardiac death, the primary objective of an ICD, was significant, so placing an ICD should be taken into consideration,” commented Michel Komajda, MD, professor of cardiology at Pierre and Marie Curie University in Paris.
“This is the first trial to look at ICDs in the setting of modern therapy. Most of the ICD trials are very old now,” commented Mariell L. Jessup, MD, a heart failure specialist and professor of medicine at the University of Pennsylvania in Philadelphia. “In DANISH the ICDs significantly reduced the incidence of sudden cardiac death; that is what ICDs do.”
DANISH randomized 1,116 patients with nonischemic systolic heart failure at any of five Danish hospitals to either receive or not receive an ICD on top of optimal medical therapy and, when judged appropriate, placement of a cardiac resynchronization therapy (CRT) device. The patients averaged about 64 years of age, they all had New York Heart Association class II or III heart failure, and their maximum left ventricular ejection fraction was 35%. The researchers followed patients for a median of about 68 months (5.7 years).
The study’s primary endpoint, death from any cause, occurred in 22% of the ICD recipients and in 23% of control patients, a nonsignificant difference. The two prespecified secondary endpoints were cardiovascular death, which was a relative 23% lower in the ICD patients and also not statistically significant, but the rate of sudden cardiac death during follow-up was 4% in the ICD patients and 8% in the controls, a statistically significant 50% relative risk reduction. Concurrent with Dr. Køber’s report of these results at the meeting they also appeared online (N Engl J Med. 2016 Aug 28;doi: 10.1056/NEJMoa1608029).
The study design also included a set of prespecified subset analyses, and one of these showed a statistically significant interaction: When the analysis stratified patients into tertiles by age, those younger than 59 years old had a statistically significant 49% cut in all-cause mortality with ICD use, and patients 59-67 years old had a nonsignificant 25% reduction in all cause mortality when on ICD treatment. A second analysis that included all these patients less than 68 years old showed that ICD use linked with a statistically significant 36% relative cut in all-cause death, compared with the patients who did not receive an ICD. Older patients, those at least age 68 years, had a relative 20% increased rate of all-cause mortality with ICD use but not a statistically significant difference.
The results also showed a downside to ICD use. Among the 42% of patients who did not receive a CRT device, the rate of serious infection was 2.6% in the ICD recipients and 0.8% in the control. Serious infection rates with and without ICD placement were similar in the subgroup of patients who received a CRT device.
The results underscored the ability of ICDs to provide a substantial benefit to well-selected patients based on factors such as age. “Clearly we need more accurate selection of nonischemic systolic heart failure patients before implanting ICDs,” said Christophe Leclerqc, MD, designated discussant for the study and professor of cardiology at Central University Hospital of Rennes, France.
“It’s all about patient selection,” agreed Dr. Jessup, who added that currently many nonischemic heart failure patients worldwide who could benefit from an ICD and have a life expectancy beyond 1 year do not receive a device.
On Twitter @mitchelzoler
AT THE ESC CONGRESS 2016
Key clinical point: Implantable cardioverter-defibrillators significantly cut the rate of sudden cardiac death in patients with nonishemic systolic heart failure, and reduced all-cause mortality in patients younger than 68 years.
Major finding: Sudden cardiac death was halved in patients who received an ICD compared with control patients.
Data source: DANISH, a multicenter, randomized trial in 1,116 patients with nonischemic systolic heart failure.
Disclosures: DANISH received partial funding from Medtronic and St. Jude, companies that market ICDs. Dr. Køber, Dr. Komajda, and Dr. Jessup had no relevant disclosures. Dr. Leclercq has been a consultant to or spoken on behalf of Biotronik, Boston Scientific, Medtronic, St. Jude, Livanova and several drug companies.

Novel treatment strategy to reduce infarct size in STEMI
ROME – Early administration of high-dose N-acetylcysteine and low-dose glyceryl trinitrate in ST-segment elevation acute myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (PCI) achieved a 30% reduction in myocardial infarct size, compared with placebo in a randomized, double-blind, multicenter clinical trial, Sivabaskari Pasupathy reported at the annual congress of the European Society of Cardiology.
The adjunctive regimen also resulted in a doubling of myocardial salvage, the secondary endpoint in the NACIAM (N-acetylcysteine in acute myocardial infarction) trial, said Ms. Pasupathy of the University of Adelaide, Australia.

NACIAM, which she stressed was a pilot study, included 75 randomized STEMI patients with follow-up cardiac MRIs obtained at about 5 days post-PCI, most of whom had another MRI at about 8 months.
All participants received IV glycerol trinitrate at a rate of 25 mcg/min for 48 hours starting in the emergency department. Patients in the active treatment arm received IV N-acetylcysteine (NAC) at 20 mg/min for the first hour and 10 mg/min for the next 47 hours. Controls got placebo at 40 mL/hour for the first hour and 20 mL/hour thereafter.
Cardiac MRI at 5 days showed a myocardial infarct size of 16.5% in the control group and 11% with active treatment. This absolute 5.5% reduction in infarct size in NAC recipients was achieved despite no difference between the two groups in myocardial area at risk by MRI, which was roughly 24%. Nor did the groups differ in rates of anterior MI or microvascular obstruction. The myocardial salvage rate was 60% in the NAC group and just 27% in controls.
Creatine kinase levels, measured hourly during the first 24 hours of hospitalization, were consistently lower in the NAC group, although the difference didn’t reach statistical significance.
In-hospital rates of hypotension, bleeding, or renal dysfunction were similar in the two study arms. However, at 2 years of follow-up the composite rate of death or cardiac rehospitalization was 27% in the control group, compared with 6% in patients who got NAC.
A key to the demonstrable success of the adjunctive NAC/nitrate treatment strategy was that it began early, in the emergency department, when patients initially presented with STEMI. The mean total ischemia time for study participants was 2.4 hours, and the shorter the duration of ischemia, the larger the reduction seen in infarct size, according to Ms. Pasupathy.
The rationale for this therapy is that NAC is thought to reduce oxidative stress by scavenging reactive oxygen species and inhibiting their release, thereby minimizing reperfusion injury. The Australian investigators also believe that NAC potentiates the effects of glycerol trinitrate in improving tissue reperfusion through enhanced vasodilation, inhibition of platelet aggregation, and dampening of inflammation. A reduction in reperfusion injury accompanied by increased tissue reperfusion could result in reduced infarct size, she explained.

John F. Beltrame, MD, lead investigator in the NACIAM study, noted that infarct size and myocardial salvage are surrogate endpoints. The investigators plan to conduct a larger trial with hard clinical outcomes.
“The key thing we need to do before we start using this in widespread fashion and changing practice guidelines is to look at clinical endpoints,” said Dr. Beltrame, professor of medicine at the University of Adelaide.
Nonetheless, he added, this therapy is given routinely in the setting of primary PCI for STEMI where he practices. That has been the case for 20 years because he and colleagues in his department did some of the early studies suggesting NAC was beneficial.
“Hospitals have different practices, and this is one of our particular practices,” the cardiologist said.
It all sounded pretty good to Jorge A. Belardi, MD, who co-chaired a press conference devoted to the NACIAM trial and other hotline presentations.
“It’s a very benign combination of medicines to use. So why not use it? We already use it to prevent contrast nephropathy. And there are no contraindications, to my knowledge,” said Dr. Belardi, director of the department of cardiology at the Buenos Aires Cardiovascular Institute.
Michel Ovize, MD, of the University of Lyon (France), the formal discussant designated for NACIAM, took a more flinty eyed view, noting that the study was small and previous studies of NAC during the past 2 decades have yielded conflicting results.
Ms. Pasupathy responded that a likely explanation for the disparate results is the fact that other investigators didn’t start NAC at the soonest possible time in the ED.
The NACIAM trial was funded by the Australian National Heart Foundation. Ms. Pasupathy and Dr. Beltrame reported having no financial conflicts of interest.
ROME – Early administration of high-dose N-acetylcysteine and low-dose glyceryl trinitrate in ST-segment elevation acute myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (PCI) achieved a 30% reduction in myocardial infarct size, compared with placebo in a randomized, double-blind, multicenter clinical trial, Sivabaskari Pasupathy reported at the annual congress of the European Society of Cardiology.
The adjunctive regimen also resulted in a doubling of myocardial salvage, the secondary endpoint in the NACIAM (N-acetylcysteine in acute myocardial infarction) trial, said Ms. Pasupathy of the University of Adelaide, Australia.
NACIAM, which she stressed was a pilot study, included 75 randomized STEMI patients with follow-up cardiac MRIs obtained at about 5 days post-PCI, most of whom had another MRI at about 8 months.
All participants received IV glycerol trinitrate at a rate of 25 mcg/min for 48 hours starting in the emergency department. Patients in the active treatment arm received IV N-acetylcysteine (NAC) at 20 mg/min for the first hour and 10 mg/min for the next 47 hours. Controls got placebo at 40 mL/hour for the first hour and 20 mL/hour thereafter.
Cardiac MRI at 5 days showed a myocardial infarct size of 16.5% in the control group and 11% with active treatment. This absolute 5.5% reduction in infarct size in NAC recipients was achieved despite no difference between the two groups in myocardial area at risk by MRI, which was roughly 24%. Nor did the groups differ in rates of anterior MI or microvascular obstruction. The myocardial salvage rate was 60% in the NAC group and just 27% in controls.
Creatine kinase levels, measured hourly during the first 24 hours of hospitalization, were consistently lower in the NAC group, although the difference didn’t reach statistical significance.
In-hospital rates of hypotension, bleeding, or renal dysfunction were similar in the two study arms. However, at 2 years of follow-up the composite rate of death or cardiac rehospitalization was 27% in the control group, compared with 6% in patients who got NAC.
A key to the demonstrable success of the adjunctive NAC/nitrate treatment strategy was that it began early, in the emergency department, when patients initially presented with STEMI. The mean total ischemia time for study participants was 2.4 hours, and the shorter the duration of ischemia, the larger the reduction seen in infarct size, according to Ms. Pasupathy.
The rationale for this therapy is that NAC is thought to reduce oxidative stress by scavenging reactive oxygen species and inhibiting their release, thereby minimizing reperfusion injury. The Australian investigators also believe that NAC potentiates the effects of glycerol trinitrate in improving tissue reperfusion through enhanced vasodilation, inhibition of platelet aggregation, and dampening of inflammation. A reduction in reperfusion injury accompanied by increased tissue reperfusion could result in reduced infarct size, she explained.
John F. Beltrame, MD, lead investigator in the NACIAM study, noted that infarct size and myocardial salvage are surrogate endpoints. The investigators plan to conduct a larger trial with hard clinical outcomes.
“The key thing we need to do before we start using this in widespread fashion and changing practice guidelines is to look at clinical endpoints,” said Dr. Beltrame, professor of medicine at the University of Adelaide.
Nonetheless, he added, this therapy is given routinely in the setting of primary PCI for STEMI where he practices. That has been the case for 20 years because he and colleagues in his department did some of the early studies suggesting NAC was beneficial.
“Hospitals have different practices, and this is one of our particular practices,” the cardiologist said.
It all sounded pretty good to Jorge A. Belardi, MD, who co-chaired a press conference devoted to the NACIAM trial and other hotline presentations.
“It’s a very benign combination of medicines to use. So why not use it? We already use it to prevent contrast nephropathy. And there are no contraindications, to my knowledge,” said Dr. Belardi, director of the department of cardiology at the Buenos Aires Cardiovascular Institute.
Michel Ovize, MD, of the University of Lyon (France), the formal discussant designated for NACIAM, took a more flinty eyed view, noting that the study was small and previous studies of NAC during the past 2 decades have yielded conflicting results.
Ms. Pasupathy responded that a likely explanation for the disparate results is the fact that other investigators didn’t start NAC at the soonest possible time in the ED.
The NACIAM trial was funded by the Australian National Heart Foundation. Ms. Pasupathy and Dr. Beltrame reported having no financial conflicts of interest.
ROME – Early administration of high-dose N-acetylcysteine and low-dose glyceryl trinitrate in ST-segment elevation acute myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (PCI) achieved a 30% reduction in myocardial infarct size, compared with placebo in a randomized, double-blind, multicenter clinical trial, Sivabaskari Pasupathy reported at the annual congress of the European Society of Cardiology.
The adjunctive regimen also resulted in a doubling of myocardial salvage, the secondary endpoint in the NACIAM (N-acetylcysteine in acute myocardial infarction) trial, said Ms. Pasupathy of the University of Adelaide, Australia.
NACIAM, which she stressed was a pilot study, included 75 randomized STEMI patients with follow-up cardiac MRIs obtained at about 5 days post-PCI, most of whom had another MRI at about 8 months.
All participants received IV glycerol trinitrate at a rate of 25 mcg/min for 48 hours starting in the emergency department. Patients in the active treatment arm received IV N-acetylcysteine (NAC) at 20 mg/min for the first hour and 10 mg/min for the next 47 hours. Controls got placebo at 40 mL/hour for the first hour and 20 mL/hour thereafter.
Cardiac MRI at 5 days showed a myocardial infarct size of 16.5% in the control group and 11% with active treatment. This absolute 5.5% reduction in infarct size in NAC recipients was achieved despite no difference between the two groups in myocardial area at risk by MRI, which was roughly 24%. Nor did the groups differ in rates of anterior MI or microvascular obstruction. The myocardial salvage rate was 60% in the NAC group and just 27% in controls.
Creatine kinase levels, measured hourly during the first 24 hours of hospitalization, were consistently lower in the NAC group, although the difference didn’t reach statistical significance.
In-hospital rates of hypotension, bleeding, or renal dysfunction were similar in the two study arms. However, at 2 years of follow-up the composite rate of death or cardiac rehospitalization was 27% in the control group, compared with 6% in patients who got NAC.
A key to the demonstrable success of the adjunctive NAC/nitrate treatment strategy was that it began early, in the emergency department, when patients initially presented with STEMI. The mean total ischemia time for study participants was 2.4 hours, and the shorter the duration of ischemia, the larger the reduction seen in infarct size, according to Ms. Pasupathy.
The rationale for this therapy is that NAC is thought to reduce oxidative stress by scavenging reactive oxygen species and inhibiting their release, thereby minimizing reperfusion injury. The Australian investigators also believe that NAC potentiates the effects of glycerol trinitrate in improving tissue reperfusion through enhanced vasodilation, inhibition of platelet aggregation, and dampening of inflammation. A reduction in reperfusion injury accompanied by increased tissue reperfusion could result in reduced infarct size, she explained.
John F. Beltrame, MD, lead investigator in the NACIAM study, noted that infarct size and myocardial salvage are surrogate endpoints. The investigators plan to conduct a larger trial with hard clinical outcomes.
“The key thing we need to do before we start using this in widespread fashion and changing practice guidelines is to look at clinical endpoints,” said Dr. Beltrame, professor of medicine at the University of Adelaide.
Nonetheless, he added, this therapy is given routinely in the setting of primary PCI for STEMI where he practices. That has been the case for 20 years because he and colleagues in his department did some of the early studies suggesting NAC was beneficial.
“Hospitals have different practices, and this is one of our particular practices,” the cardiologist said.
It all sounded pretty good to Jorge A. Belardi, MD, who co-chaired a press conference devoted to the NACIAM trial and other hotline presentations.
“It’s a very benign combination of medicines to use. So why not use it? We already use it to prevent contrast nephropathy. And there are no contraindications, to my knowledge,” said Dr. Belardi, director of the department of cardiology at the Buenos Aires Cardiovascular Institute.
Michel Ovize, MD, of the University of Lyon (France), the formal discussant designated for NACIAM, took a more flinty eyed view, noting that the study was small and previous studies of NAC during the past 2 decades have yielded conflicting results.
Ms. Pasupathy responded that a likely explanation for the disparate results is the fact that other investigators didn’t start NAC at the soonest possible time in the ED.
The NACIAM trial was funded by the Australian National Heart Foundation. Ms. Pasupathy and Dr. Beltrame reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2016
Key clinical point: Early use of N-acetylcysteine with glyceryl trinitrate resulted in reduced myocardial infarct size in STEMI patients undergoing primary PCI.
Major finding: Early use of N-acetylcysteine with glyceryl trinitrate in STEMI patients undergoing primary PCI resulted in a myocardial infarct size of 11% as assessed on day 5, compared with 16.5% in placebo-treated controls.
Data source: The NACIAM trial was a 75-patient, randomized, double-blind, multicenter study.
Disclosures: The study was supported by the Australian National Heart Foundation. The presenter reported having no financial conflicts of interest.
