User login
Sudden Unexpected Death in Epilepsy

Management of wound complications following obstetric anal sphincter injury (OASIS)
During vaginal delivery spontaneous perineal trauma and extension of episiotomy incisions are common. A severe perineal laceration that extends into or through the anal sphincter complex is referred to as an obstetric anal sphincter injury (OASIS) and requires meticulous repair. Following the repair of an OASIS, serious wound complications, including dehiscence and infection, may occur. In Europe the reported rate of OASIS varies widely among countries, with a rate of 0.1% in Romania, possibly due to underreporting, and 4.9% in Iceland.1 In the United States the rates of 3rd- and 4th-degree lacerations were reported to be 3.3% and 1.1%, respectively.2
Risk factors for OASIS include forceps delivery (odds ratio [OR], 5.50), vacuum-assisted delivery (OR, 3.98), and midline episiotomy (OR, 3.82).3 Additional risk factors for severe perineal injury at vaginal delivery include nulliparity (adjusted odds ratio [aOR], 2.58), delivery from a persistent occiput posterior position (aOR, 2.24), and above-average newborn birth weight (aOR, 1.28).4
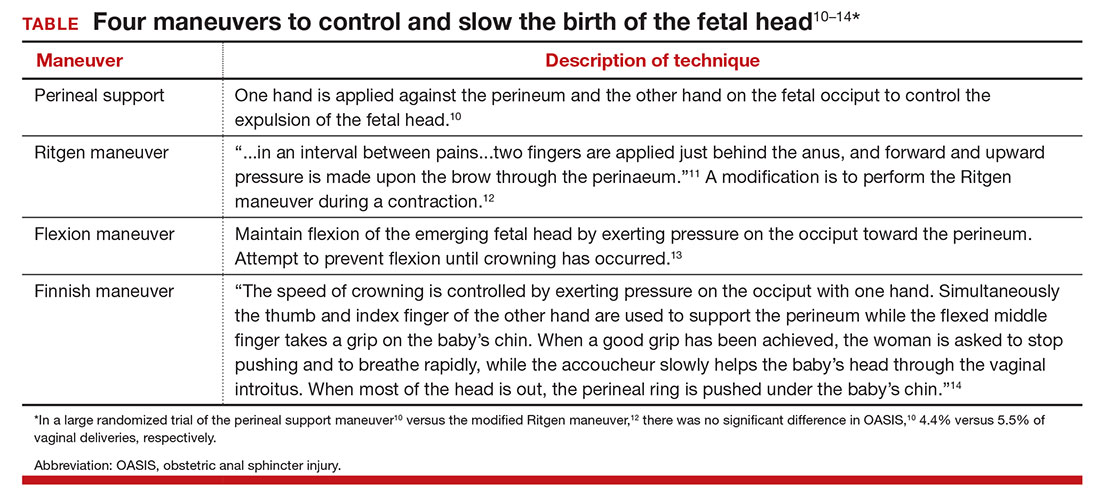
In a meta-analysis of randomized trials, the researchers reported that restrictive use of episiotomy reduced the risk of severe perineal trauma (relative risk [RR], 0.67) but increased the risk of anterior perineal trauma (RR, 1.84).5 The American College of Obstetricians and Gynecologists (ACOG) recommends that episiotomy should not be a routine practice and is best restricted to use in a limited number of cases where fetal and maternal benefit is likely.6 In addition, ACOG recommends that if episiotomy is indicated, a mediolateral incision is favored over a midline incision. In my practice I perform only mediolateral episiotomy incisions. However, mediolateral episiotomy may be associated with an increased risk of postpartum perineal pain and dyspareunia.7 Use of warm compresses applied to the perineum during the second stage of labor may reduce the risk of 3rd- and 4th-degree lacerations.8 Techniques to ensure that the fetal head and shoulders are birthed in a slow and controlled fashion may decrease the risk of OASIS.9 See the TABLE, “Four maneuvers to control and slow the birth of the fetal head.”10–14
Related article:
Stop performing median episiotomy!
Wound complications following the repair of a 3rd- or 4th-degree laceration are reported to occur in approximately 5% to 10% of cases.15 The most common wound complications are dehiscence, infection, abscess formation, pain, sexual dysfunction, and anal incontinence. Minor wound complications, including superficial epithelial separation, can be managed expectantly. However, major wound complications need intensive treatment.
In one study of 21 women who had a major wound complication following the repair of a 4th-degree laceration, 53% had dehiscence plus infection, 33% had dehiscence alone, and 14% had infection alone.16 Major wound complications present at a mean of 5 days after delivery, with a wide range from 1 to 17 days following delivery.17 In a study of 144 cases of wound breakdown following a perineal laceration repair, the major risk factors for wound breakdown were episiotomy (aOR, 11.1), smoking (aOR, 6.4), midwife repair of laceration (aOR, 4.7), use of chromic suture (aOR, 3.9), and operative vaginal delivery (aOR, 3.4).18 In one study of 66 women with a wound complication following the repair of a 3rd- or 4th-degree laceration, clinical risk factors for a wound complication were cigarette smoking (OR, 4.04), 4th-degree laceration (OR, 1.89), and operative vaginal delivery (OR, 1.76).19 The use of intrapartum antibiotics appears to be protective (OR, 0.29) against wound complications following a major perineal laceration.19
Approach to the patient with a dehisced and infected perineal wound
Historically, wound dehiscence following surgical repair of a perineal injury was managed by allowing the wound to slowly close. This approach adversely impacts the quality of life of the affected woman because it may take weeks for the wound to heal. One small randomized trial17 and multiple case series20–24 report that an active multistep management algorithm permits early closure of the majority of these wounds, thereby accelerating the patient’s full recovery. Delayed primary (within 72 hours postpartum) or early secondary reconstruction (within 14 days of delivery) has been demonstrated to be safe with acceptable long-term functional out-comes.25 The modern approach to the treatment of a patient with an infected wound dehiscence following a severe perineal injury involves 3 steps.
Related article:
It’s time to restrict the use of episiotomy
Step 1. Restore tissue to health
The dehisced wound is cultured and, if infection is present, treatment is initiated with intravenous antibiotics appropriate for an infection with colorectal flora. One antibiotic option includes a cephalosporin (cefotetan 2 g IV every 6 hours) plus metronidazole (500 mg IV every 8 hours).
In the operating room, the wound should be thoroughly assessed, cleansed, and debrided. This step includes irrigation of the wound with a warm fluid, mechanical debridement, and sharp dissection of necrotic tissue. If the wound is infected, removal of stitches that are visible in the open wound is recommended.
Often more than one session of debridement may be needed to obtain wound edges that are free from exudate and show granulation at the wound margins. Between debridement sessions, wet-to-dry dressings are utilized. Two to 10 days of wound care may be needed before an attempt is made to close the wound. The wound is suitable for repair when there is no infected tissue and granulation tissue is present. Some surgeons prefer a mechanical bowel preparation regimen just before surgically closing the open wound. This may prevent early bowel movements and provide for tissue healing after surgery.26 The same preparations recommended for colonoscopy can be considered prior to surgical repair.
Step 2. Surgically close the wound
The wound is surgically closed in the operating room. If in Step 1 the assessment of the wound shows major trauma, assistance from a urogynecologist may be warranted. Surgical management of a perineal wound dehiscence requires a clear understanding of perineal anatomy and the structures contained between the vagina and the anorectum.
Six key structures may be involved in perineal injury: the anorectal mucosa, internal anal sphincter, external anal sphincter, vaginal wall and perineal skin, bulbocavernosus muscle, and transverse perineal muscles. It is important to definitively identify the individual structures that need to be repaired. Careful dissection is then carried out to mobilize these structures for repair. Additional debridement may be necessary to remove excess granulation tissue.
Anorectal mucosa repair. With repair of a 4th-degree perineal wound dehiscence, the apex of the defect in the anorectal mucosa is identified. The defect is repaired beginning at the apex using closely spaced interrupted sutures or a running suture of 3-0 or 4-0 polyglactin 910. Adequate tissue bites that will resist tearing should be taken. If interrupted sutures are used, tying the knots within the anorectal canal prevents them from being located within the healing wound.
Internal anal sphincter repair. After the anorectal mucosa is closed, attention is turned to reapproximation of the internal anal sphincter. The ends of a torn internal anal sphincter are often located lateral to the anorectal mucosa and appear as shiny gray-white fibrous tissue. The surgeon’s gloved index finger can be placed within the anorectal canal to aid in identification of the internal anal sphincter, as it tends to have a rubbery feel. Additionally, while the surgeon’s gloved index finger is in the anorectal canal, the surgeon’s gloved thumb can be used to retract the anorectal mucosa slightly medial and inferior so that adequate bites of the internal anal sphincter can be taken on each side.
Alternatively, Allis clamps canbe placed on the ends of the retracted internal anal sphincter to facilitate repair. Suture selection for repair of the internal anal sphincter can include 3-0 polyglactin 910 or 3-0 monofilament, delayed-absorbable suture such as polydioxanone sulfate (PDS). Some surgeons prefer delayed-absorbable suture (PDS) for this layer given the internal anal sphincter is constantly contracting and relaxing as it samples stool.26 This layer also can be closed with either interrupted sutures or a running suture.
External anal sphincter repair. After the anorectal mucosa and internal anal sphincter defects are reapproximated, attention is turned to the external anal sphincter. Like the internal anal sphincter, the ends of the external anal sphincter are often retracted laterally and must be definitively identified and mobilized in order to ensure an adequate tension-free repair. It is important to include the fascial sheath in the repair of the external anal sphincter.27 Allis clamps can be used to grasp the ends of the torn muscle after they are identified.
We recommend 0 or 2-0 PDS for repair of the external sphincter. Repair can be performed using either an end-to-end or overlapping technique. An end-to-end repair traditionally involves reapproximating the ends of the torn muscle and its overlying fascial sheath using interrupted sutures placed at four quadrants (12:00, 3:00, 6:00, 9:00).
In contrast, in an overlapping repair, the ends of the muscle are brought together with mattress sutures. Suture is passed top down through the medial aspect of the more superior muscle flap and top down through the inferior muscle flap more laterally. The same suture is then passed bottom up through the inferior muscle flap more laterally and finally bottom up through the medial aspect of the more superior muscle flap. Two to four mattress sutures are usually placed. After all sutures are placed, they are tied securely.
An overlapping repair results in a greater amount of tissue contact between the two torn muscle ends. However, adequate mobility of the external anal sphincter is necessary to perform this type of repair.
Vaginal wall and perineal body repair. After the anal sphincters have been repaired, the vaginal wall and remainder of the perineal body are reconstructed using the same techniques involved in a 2nd-degree laceration repair. Care must be taken to retrieve and reapproximate the torn ends of the bulbocavernosus muscles, which are also often retracted laterally and superiorly. After the bulbocavernosus and transverse perineal muscles are brought together in the midline, the posterior vaginal wall should be perpendicular to the perineum.
An alternative to surgical closure of a 2nd-degree dehiscence is the use of vacuum-assisted wound closure. Disadvantages of this approach include difficulty in maintaining a vacuum seal in the perineal region and the risk of wound contamination with feces. In one case report, 3 weeks of vacuum-assisted wound closure resulted in healing of a 10-cm wound dehiscence that occurred 5 days following a forceps-assisted vaginal delivery with a mediolateral episiotomy.28
Step 3. Ensure complete healing of the wound
Superb postoperative wound care helps to ensure a quick return to full recovery. Wound care should include regularly scheduled sitz baths (at least 3 times daily) followed by drying the perineum. It is preferable to provide a liquid diet that avoids frequent bowel movements in the initial 3 postoperative days. Stool softeners and fiber supplementation are recommended when a full diet is resumed. Some surgeons have found mineral oil (1 to 2 tablespoons daily) effective in producing soft stools that are easy to pass.26 Ensuring soft stool consistency is important to help prevent repair breakdown that may occur with passage of hard stools, fecal impaction, and/or straining during defecation.
We recommend follow-up 1 to 2 weeks after surgery to assess wound healing. No vaginal intercourseis permitted until complete healing is achieved.
Use a surgical checklist
All obstetricians and midwives strive to reduce the risk of OASIS at vaginal birth. When OASIS occurs, it is often useful to use a surgical checklist to ensure the execution of all steps in the management of the repair and recovery process.29 It is heartbreaking to see an OASIS repair breakdown in the week following a vaginal delivery. But by following the 3 steps outlined here, the secondary repair is likely to be successful and will quickly return most patients to full health.
Related article:
Develop and use a checklist for 3rd- and 4th-degree perineal lacerations
The authors report no financial relationships relevant to this article.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Blondel B, Alexander S, Bjarnadottir RI, et al; Euro-Peristat Scientific Committee. Variations in rates of severe perineal tears and episiotomies in 20 European countries: a study based on routine national data in Euro-Perstat Project. Acta Obstet Gynecol Scand. 2016;95(7):746–754.
- Friedman AM, Ananth CV, Predergast E, D’Alton ME, Wright JD. Evaluation of third-degree and fourth-degree laceration rates as quality indicators. Obstet Gynecol. 2015;125(4):927–937.
- Pergialiotis V, Vlachos D, Protopapas A, Pappa K, Vlachos G. Risk factors for severe perineal lacerations during childbirth. Int J Gynecol Obstet. 2014;125(1):6–14.
- Schmitz T, Alberti C, Andriss B, Moutafoff C, Oury JF, Sibony O. Identification of women at high risk for severe perineal lacerations. Eur J Obstet Gynecol Reprod Biol. 2014;182:11–15.
- Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.
- ACOG Committee on Practice Bulletins—Obstetrics. Practice bulletin no. 165: Prevention and management of obstetric lacerations at vaginal delivery. Obstet Gynecol. 2016;128(1):e1–e15.
- Sartore A, De Seta F, Maso G, Pregazzi R, Grimaldi E, Guaschino S. The effects of mediolateral episiotomy on pelvic floor function after vaginal delivery. Obstet Gynecol. 2004;103(4):669–673.
- Aasheim V, Nilsen AB, Lukasse M, Reinar LM. Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Database Syst Rev. 2011;(12):CD006672.
- Harvey MA, Pierce M, Alter JE, et al; Society of Obstetricians and Gynaecologists of Canada. Obstetrical anal sphincter injuries (OASIS): prevention, recognition and repair. J Obstet Gynaecol Can. 2015;37(12):1131–1148.
- Jonsson ER, Elfaghi I, Rydhstrom H, Herbst A. Modified Ritgen’s maneuver for anal sphincter injury at delivery: a randomized controlled trial. Obstet Gynecol. 2008;112(2 pt 1):212–217.
- Williams JW. Obstetrics: A Text-book for the Use of Students and Practitioners. New York, NY: D Appleton and Co; 1903:288.
- Cunningham FG. The Ritgen maneuver: another sacred cow questioned. Obstet Gynecol. 2008;112(2 pt 1):210–211.
- Myrfield K, Brook C, Creedy D. Reducing perineal trauma: implications of flexion and extension of the fetal head during birth. Midwifery. 1997;13:197–201.
- Ostergaard Poulsen M, Lund Madsen M, Skriver-Moller AC, Overgaard C. Does the Finnish intervention prevent obstetrical anal sphincter injuries? A systematic review of the literature. BMJ Open. 2015;5:e008346.
- Kamel A, Khaled M. Episiotomy and obstetric perineal wound dehiscence: beyond soreness. J Obstet Gynaecol. 2014;34(3):215–217.
- Goldaber KG, Wendel PJ, McIntire DD, Wendel GD Jr. Postpartum perineal morbidity after fourth-degree perineal repair. Am J Obstet Gynecol. 1993;168(2):489–493.
- Monberg J, Hammen S. Ruptured episiotomia resutured primarily. Acta Obstet Gynecol Scand. 1987;66(2):163–164.
- Jallad K, Steele SE, Barber MD. Breakdown of perineal laceration repair after vaginal delivery: a case-control study. Female Pelvic Med Reconstr Surg. 2016;22(4):276–279.
- Stock L, Basham E, Gossett DR, Lewicky-Gaupp C. Factors associated with wound complications in women with obstetric anal sphincter injuries (OASIS). Am J Obstet Gynecol. 2013;208(4):327.e1–e8.
- Hauth JC, Gilstrap LC 3rd, Ward SC, Hankins GD. Early repair of an external sphincter ani muscle and rectal mucosal dehiscence. Obstet Gynecol. 1986;67(6):806–809.
- Hankins GD, Hauth JC, Gilstrap LC 3rd, Hammond TL, Yeomans ER, Snyder RR. Early repair of episiotomy dehiscence. Obstet Gynecol. 1990;75(1):48–51.
- Ramin SM, Ramus RM, Little BB, Gilstrap LC 3rd. Early repair of episiotomy dehiscence associated with infection. Am J Obstet Gynecol. 1992;167(4 pt 1):1104–1107.
- Arona AJ, Al-Marayati L, Grimes DA, Ballard CA. Early secondary repair of third- and fourth-degree perineal lacerations after outpatient wound preparation. Obstet Gynecol. 1995;86(2):294–296.
- Uygur D, Yesildaglar N, Kis S, Sipahi T. Early repair of episiotomy dehiscence. Aust N Z J Obstet Gynaecol. 2004;44(3):244–246.
- Soerensen MM, Bek KM, Buntzen S, Hojberg KE, Laurberg S. Long-term outcome of delayed primary or early secondary reconstruction of the anal sphincter after obstetrical injury. Dis Colon Rectum. 2008;51(3):312–317.
- Delancey JOL, Berger MB. Surgical approaches to postobstetrical perineal body defects (rectovaginal fistula and chronic third and fourth-degree lacerations). Clin Obstet Gynecol. 2010;53(1):134–144.
- Leeman L, Spearman M, Rogers R. Repair of obstetric perineal lacerations. Am Fam Physician. 2003;68(8):1585–1590.
- Aviki EM, Batalden RP, del Carmen MG, Berkowitz LR. Vacuum-assisted closure for episiotomy dehiscence. Obstet Gynecol. 2015;126(3):530–533.
- Barbieri RL. Develop and use a checklist for 3rd- and 4th-degree perineal lacerations. OBG Manag. 2013;25(8):8–12.


During vaginal delivery spontaneous perineal trauma and extension of episiotomy incisions are common. A severe perineal laceration that extends into or through the anal sphincter complex is referred to as an obstetric anal sphincter injury (OASIS) and requires meticulous repair. Following the repair of an OASIS, serious wound complications, including dehiscence and infection, may occur. In Europe the reported rate of OASIS varies widely among countries, with a rate of 0.1% in Romania, possibly due to underreporting, and 4.9% in Iceland.1 In the United States the rates of 3rd- and 4th-degree lacerations were reported to be 3.3% and 1.1%, respectively.2
Risk factors for OASIS include forceps delivery (odds ratio [OR], 5.50), vacuum-assisted delivery (OR, 3.98), and midline episiotomy (OR, 3.82).3 Additional risk factors for severe perineal injury at vaginal delivery include nulliparity (adjusted odds ratio [aOR], 2.58), delivery from a persistent occiput posterior position (aOR, 2.24), and above-average newborn birth weight (aOR, 1.28).4
In a meta-analysis of randomized trials, the researchers reported that restrictive use of episiotomy reduced the risk of severe perineal trauma (relative risk [RR], 0.67) but increased the risk of anterior perineal trauma (RR, 1.84).5 The American College of Obstetricians and Gynecologists (ACOG) recommends that episiotomy should not be a routine practice and is best restricted to use in a limited number of cases where fetal and maternal benefit is likely.6 In addition, ACOG recommends that if episiotomy is indicated, a mediolateral incision is favored over a midline incision. In my practice I perform only mediolateral episiotomy incisions. However, mediolateral episiotomy may be associated with an increased risk of postpartum perineal pain and dyspareunia.7 Use of warm compresses applied to the perineum during the second stage of labor may reduce the risk of 3rd- and 4th-degree lacerations.8 Techniques to ensure that the fetal head and shoulders are birthed in a slow and controlled fashion may decrease the risk of OASIS.9 See the TABLE, “Four maneuvers to control and slow the birth of the fetal head.”10–14
Related article:
Stop performing median episiotomy!
Wound complications following the repair of a 3rd- or 4th-degree laceration are reported to occur in approximately 5% to 10% of cases.15 The most common wound complications are dehiscence, infection, abscess formation, pain, sexual dysfunction, and anal incontinence. Minor wound complications, including superficial epithelial separation, can be managed expectantly. However, major wound complications need intensive treatment.
In one study of 21 women who had a major wound complication following the repair of a 4th-degree laceration, 53% had dehiscence plus infection, 33% had dehiscence alone, and 14% had infection alone.16 Major wound complications present at a mean of 5 days after delivery, with a wide range from 1 to 17 days following delivery.17 In a study of 144 cases of wound breakdown following a perineal laceration repair, the major risk factors for wound breakdown were episiotomy (aOR, 11.1), smoking (aOR, 6.4), midwife repair of laceration (aOR, 4.7), use of chromic suture (aOR, 3.9), and operative vaginal delivery (aOR, 3.4).18 In one study of 66 women with a wound complication following the repair of a 3rd- or 4th-degree laceration, clinical risk factors for a wound complication were cigarette smoking (OR, 4.04), 4th-degree laceration (OR, 1.89), and operative vaginal delivery (OR, 1.76).19 The use of intrapartum antibiotics appears to be protective (OR, 0.29) against wound complications following a major perineal laceration.19
Approach to the patient with a dehisced and infected perineal wound
Historically, wound dehiscence following surgical repair of a perineal injury was managed by allowing the wound to slowly close. This approach adversely impacts the quality of life of the affected woman because it may take weeks for the wound to heal. One small randomized trial17 and multiple case series20–24 report that an active multistep management algorithm permits early closure of the majority of these wounds, thereby accelerating the patient’s full recovery. Delayed primary (within 72 hours postpartum) or early secondary reconstruction (within 14 days of delivery) has been demonstrated to be safe with acceptable long-term functional out-comes.25 The modern approach to the treatment of a patient with an infected wound dehiscence following a severe perineal injury involves 3 steps.
Related article:
It’s time to restrict the use of episiotomy
Step 1. Restore tissue to health
The dehisced wound is cultured and, if infection is present, treatment is initiated with intravenous antibiotics appropriate for an infection with colorectal flora. One antibiotic option includes a cephalosporin (cefotetan 2 g IV every 6 hours) plus metronidazole (500 mg IV every 8 hours).
In the operating room, the wound should be thoroughly assessed, cleansed, and debrided. This step includes irrigation of the wound with a warm fluid, mechanical debridement, and sharp dissection of necrotic tissue. If the wound is infected, removal of stitches that are visible in the open wound is recommended.
Often more than one session of debridement may be needed to obtain wound edges that are free from exudate and show granulation at the wound margins. Between debridement sessions, wet-to-dry dressings are utilized. Two to 10 days of wound care may be needed before an attempt is made to close the wound. The wound is suitable for repair when there is no infected tissue and granulation tissue is present. Some surgeons prefer a mechanical bowel preparation regimen just before surgically closing the open wound. This may prevent early bowel movements and provide for tissue healing after surgery.26 The same preparations recommended for colonoscopy can be considered prior to surgical repair.
Step 2. Surgically close the wound
The wound is surgically closed in the operating room. If in Step 1 the assessment of the wound shows major trauma, assistance from a urogynecologist may be warranted. Surgical management of a perineal wound dehiscence requires a clear understanding of perineal anatomy and the structures contained between the vagina and the anorectum.
Six key structures may be involved in perineal injury: the anorectal mucosa, internal anal sphincter, external anal sphincter, vaginal wall and perineal skin, bulbocavernosus muscle, and transverse perineal muscles. It is important to definitively identify the individual structures that need to be repaired. Careful dissection is then carried out to mobilize these structures for repair. Additional debridement may be necessary to remove excess granulation tissue.
Anorectal mucosa repair. With repair of a 4th-degree perineal wound dehiscence, the apex of the defect in the anorectal mucosa is identified. The defect is repaired beginning at the apex using closely spaced interrupted sutures or a running suture of 3-0 or 4-0 polyglactin 910. Adequate tissue bites that will resist tearing should be taken. If interrupted sutures are used, tying the knots within the anorectal canal prevents them from being located within the healing wound.
Internal anal sphincter repair. After the anorectal mucosa is closed, attention is turned to reapproximation of the internal anal sphincter. The ends of a torn internal anal sphincter are often located lateral to the anorectal mucosa and appear as shiny gray-white fibrous tissue. The surgeon’s gloved index finger can be placed within the anorectal canal to aid in identification of the internal anal sphincter, as it tends to have a rubbery feel. Additionally, while the surgeon’s gloved index finger is in the anorectal canal, the surgeon’s gloved thumb can be used to retract the anorectal mucosa slightly medial and inferior so that adequate bites of the internal anal sphincter can be taken on each side.
Alternatively, Allis clamps canbe placed on the ends of the retracted internal anal sphincter to facilitate repair. Suture selection for repair of the internal anal sphincter can include 3-0 polyglactin 910 or 3-0 monofilament, delayed-absorbable suture such as polydioxanone sulfate (PDS). Some surgeons prefer delayed-absorbable suture (PDS) for this layer given the internal anal sphincter is constantly contracting and relaxing as it samples stool.26 This layer also can be closed with either interrupted sutures or a running suture.
External anal sphincter repair. After the anorectal mucosa and internal anal sphincter defects are reapproximated, attention is turned to the external anal sphincter. Like the internal anal sphincter, the ends of the external anal sphincter are often retracted laterally and must be definitively identified and mobilized in order to ensure an adequate tension-free repair. It is important to include the fascial sheath in the repair of the external anal sphincter.27 Allis clamps can be used to grasp the ends of the torn muscle after they are identified.
We recommend 0 or 2-0 PDS for repair of the external sphincter. Repair can be performed using either an end-to-end or overlapping technique. An end-to-end repair traditionally involves reapproximating the ends of the torn muscle and its overlying fascial sheath using interrupted sutures placed at four quadrants (12:00, 3:00, 6:00, 9:00).
In contrast, in an overlapping repair, the ends of the muscle are brought together with mattress sutures. Suture is passed top down through the medial aspect of the more superior muscle flap and top down through the inferior muscle flap more laterally. The same suture is then passed bottom up through the inferior muscle flap more laterally and finally bottom up through the medial aspect of the more superior muscle flap. Two to four mattress sutures are usually placed. After all sutures are placed, they are tied securely.
An overlapping repair results in a greater amount of tissue contact between the two torn muscle ends. However, adequate mobility of the external anal sphincter is necessary to perform this type of repair.
Vaginal wall and perineal body repair. After the anal sphincters have been repaired, the vaginal wall and remainder of the perineal body are reconstructed using the same techniques involved in a 2nd-degree laceration repair. Care must be taken to retrieve and reapproximate the torn ends of the bulbocavernosus muscles, which are also often retracted laterally and superiorly. After the bulbocavernosus and transverse perineal muscles are brought together in the midline, the posterior vaginal wall should be perpendicular to the perineum.
An alternative to surgical closure of a 2nd-degree dehiscence is the use of vacuum-assisted wound closure. Disadvantages of this approach include difficulty in maintaining a vacuum seal in the perineal region and the risk of wound contamination with feces. In one case report, 3 weeks of vacuum-assisted wound closure resulted in healing of a 10-cm wound dehiscence that occurred 5 days following a forceps-assisted vaginal delivery with a mediolateral episiotomy.28
Step 3. Ensure complete healing of the wound
Superb postoperative wound care helps to ensure a quick return to full recovery. Wound care should include regularly scheduled sitz baths (at least 3 times daily) followed by drying the perineum. It is preferable to provide a liquid diet that avoids frequent bowel movements in the initial 3 postoperative days. Stool softeners and fiber supplementation are recommended when a full diet is resumed. Some surgeons have found mineral oil (1 to 2 tablespoons daily) effective in producing soft stools that are easy to pass.26 Ensuring soft stool consistency is important to help prevent repair breakdown that may occur with passage of hard stools, fecal impaction, and/or straining during defecation.
We recommend follow-up 1 to 2 weeks after surgery to assess wound healing. No vaginal intercourseis permitted until complete healing is achieved.
Use a surgical checklist
All obstetricians and midwives strive to reduce the risk of OASIS at vaginal birth. When OASIS occurs, it is often useful to use a surgical checklist to ensure the execution of all steps in the management of the repair and recovery process.29 It is heartbreaking to see an OASIS repair breakdown in the week following a vaginal delivery. But by following the 3 steps outlined here, the secondary repair is likely to be successful and will quickly return most patients to full health.
Related article:
Develop and use a checklist for 3rd- and 4th-degree perineal lacerations
The authors report no financial relationships relevant to this article.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
During vaginal delivery spontaneous perineal trauma and extension of episiotomy incisions are common. A severe perineal laceration that extends into or through the anal sphincter complex is referred to as an obstetric anal sphincter injury (OASIS) and requires meticulous repair. Following the repair of an OASIS, serious wound complications, including dehiscence and infection, may occur. In Europe the reported rate of OASIS varies widely among countries, with a rate of 0.1% in Romania, possibly due to underreporting, and 4.9% in Iceland.1 In the United States the rates of 3rd- and 4th-degree lacerations were reported to be 3.3% and 1.1%, respectively.2
Risk factors for OASIS include forceps delivery (odds ratio [OR], 5.50), vacuum-assisted delivery (OR, 3.98), and midline episiotomy (OR, 3.82).3 Additional risk factors for severe perineal injury at vaginal delivery include nulliparity (adjusted odds ratio [aOR], 2.58), delivery from a persistent occiput posterior position (aOR, 2.24), and above-average newborn birth weight (aOR, 1.28).4
In a meta-analysis of randomized trials, the researchers reported that restrictive use of episiotomy reduced the risk of severe perineal trauma (relative risk [RR], 0.67) but increased the risk of anterior perineal trauma (RR, 1.84).5 The American College of Obstetricians and Gynecologists (ACOG) recommends that episiotomy should not be a routine practice and is best restricted to use in a limited number of cases where fetal and maternal benefit is likely.6 In addition, ACOG recommends that if episiotomy is indicated, a mediolateral incision is favored over a midline incision. In my practice I perform only mediolateral episiotomy incisions. However, mediolateral episiotomy may be associated with an increased risk of postpartum perineal pain and dyspareunia.7 Use of warm compresses applied to the perineum during the second stage of labor may reduce the risk of 3rd- and 4th-degree lacerations.8 Techniques to ensure that the fetal head and shoulders are birthed in a slow and controlled fashion may decrease the risk of OASIS.9 See the TABLE, “Four maneuvers to control and slow the birth of the fetal head.”10–14
Related article:
Stop performing median episiotomy!
Wound complications following the repair of a 3rd- or 4th-degree laceration are reported to occur in approximately 5% to 10% of cases.15 The most common wound complications are dehiscence, infection, abscess formation, pain, sexual dysfunction, and anal incontinence. Minor wound complications, including superficial epithelial separation, can be managed expectantly. However, major wound complications need intensive treatment.
In one study of 21 women who had a major wound complication following the repair of a 4th-degree laceration, 53% had dehiscence plus infection, 33% had dehiscence alone, and 14% had infection alone.16 Major wound complications present at a mean of 5 days after delivery, with a wide range from 1 to 17 days following delivery.17 In a study of 144 cases of wound breakdown following a perineal laceration repair, the major risk factors for wound breakdown were episiotomy (aOR, 11.1), smoking (aOR, 6.4), midwife repair of laceration (aOR, 4.7), use of chromic suture (aOR, 3.9), and operative vaginal delivery (aOR, 3.4).18 In one study of 66 women with a wound complication following the repair of a 3rd- or 4th-degree laceration, clinical risk factors for a wound complication were cigarette smoking (OR, 4.04), 4th-degree laceration (OR, 1.89), and operative vaginal delivery (OR, 1.76).19 The use of intrapartum antibiotics appears to be protective (OR, 0.29) against wound complications following a major perineal laceration.19
Approach to the patient with a dehisced and infected perineal wound
Historically, wound dehiscence following surgical repair of a perineal injury was managed by allowing the wound to slowly close. This approach adversely impacts the quality of life of the affected woman because it may take weeks for the wound to heal. One small randomized trial17 and multiple case series20–24 report that an active multistep management algorithm permits early closure of the majority of these wounds, thereby accelerating the patient’s full recovery. Delayed primary (within 72 hours postpartum) or early secondary reconstruction (within 14 days of delivery) has been demonstrated to be safe with acceptable long-term functional out-comes.25 The modern approach to the treatment of a patient with an infected wound dehiscence following a severe perineal injury involves 3 steps.
Related article:
It’s time to restrict the use of episiotomy
Step 1. Restore tissue to health
The dehisced wound is cultured and, if infection is present, treatment is initiated with intravenous antibiotics appropriate for an infection with colorectal flora. One antibiotic option includes a cephalosporin (cefotetan 2 g IV every 6 hours) plus metronidazole (500 mg IV every 8 hours).
In the operating room, the wound should be thoroughly assessed, cleansed, and debrided. This step includes irrigation of the wound with a warm fluid, mechanical debridement, and sharp dissection of necrotic tissue. If the wound is infected, removal of stitches that are visible in the open wound is recommended.
Often more than one session of debridement may be needed to obtain wound edges that are free from exudate and show granulation at the wound margins. Between debridement sessions, wet-to-dry dressings are utilized. Two to 10 days of wound care may be needed before an attempt is made to close the wound. The wound is suitable for repair when there is no infected tissue and granulation tissue is present. Some surgeons prefer a mechanical bowel preparation regimen just before surgically closing the open wound. This may prevent early bowel movements and provide for tissue healing after surgery.26 The same preparations recommended for colonoscopy can be considered prior to surgical repair.
Step 2. Surgically close the wound
The wound is surgically closed in the operating room. If in Step 1 the assessment of the wound shows major trauma, assistance from a urogynecologist may be warranted. Surgical management of a perineal wound dehiscence requires a clear understanding of perineal anatomy and the structures contained between the vagina and the anorectum.
Six key structures may be involved in perineal injury: the anorectal mucosa, internal anal sphincter, external anal sphincter, vaginal wall and perineal skin, bulbocavernosus muscle, and transverse perineal muscles. It is important to definitively identify the individual structures that need to be repaired. Careful dissection is then carried out to mobilize these structures for repair. Additional debridement may be necessary to remove excess granulation tissue.
Anorectal mucosa repair. With repair of a 4th-degree perineal wound dehiscence, the apex of the defect in the anorectal mucosa is identified. The defect is repaired beginning at the apex using closely spaced interrupted sutures or a running suture of 3-0 or 4-0 polyglactin 910. Adequate tissue bites that will resist tearing should be taken. If interrupted sutures are used, tying the knots within the anorectal canal prevents them from being located within the healing wound.
Internal anal sphincter repair. After the anorectal mucosa is closed, attention is turned to reapproximation of the internal anal sphincter. The ends of a torn internal anal sphincter are often located lateral to the anorectal mucosa and appear as shiny gray-white fibrous tissue. The surgeon’s gloved index finger can be placed within the anorectal canal to aid in identification of the internal anal sphincter, as it tends to have a rubbery feel. Additionally, while the surgeon’s gloved index finger is in the anorectal canal, the surgeon’s gloved thumb can be used to retract the anorectal mucosa slightly medial and inferior so that adequate bites of the internal anal sphincter can be taken on each side.
Alternatively, Allis clamps canbe placed on the ends of the retracted internal anal sphincter to facilitate repair. Suture selection for repair of the internal anal sphincter can include 3-0 polyglactin 910 or 3-0 monofilament, delayed-absorbable suture such as polydioxanone sulfate (PDS). Some surgeons prefer delayed-absorbable suture (PDS) for this layer given the internal anal sphincter is constantly contracting and relaxing as it samples stool.26 This layer also can be closed with either interrupted sutures or a running suture.
External anal sphincter repair. After the anorectal mucosa and internal anal sphincter defects are reapproximated, attention is turned to the external anal sphincter. Like the internal anal sphincter, the ends of the external anal sphincter are often retracted laterally and must be definitively identified and mobilized in order to ensure an adequate tension-free repair. It is important to include the fascial sheath in the repair of the external anal sphincter.27 Allis clamps can be used to grasp the ends of the torn muscle after they are identified.
We recommend 0 or 2-0 PDS for repair of the external sphincter. Repair can be performed using either an end-to-end or overlapping technique. An end-to-end repair traditionally involves reapproximating the ends of the torn muscle and its overlying fascial sheath using interrupted sutures placed at four quadrants (12:00, 3:00, 6:00, 9:00).
In contrast, in an overlapping repair, the ends of the muscle are brought together with mattress sutures. Suture is passed top down through the medial aspect of the more superior muscle flap and top down through the inferior muscle flap more laterally. The same suture is then passed bottom up through the inferior muscle flap more laterally and finally bottom up through the medial aspect of the more superior muscle flap. Two to four mattress sutures are usually placed. After all sutures are placed, they are tied securely.
An overlapping repair results in a greater amount of tissue contact between the two torn muscle ends. However, adequate mobility of the external anal sphincter is necessary to perform this type of repair.
Vaginal wall and perineal body repair. After the anal sphincters have been repaired, the vaginal wall and remainder of the perineal body are reconstructed using the same techniques involved in a 2nd-degree laceration repair. Care must be taken to retrieve and reapproximate the torn ends of the bulbocavernosus muscles, which are also often retracted laterally and superiorly. After the bulbocavernosus and transverse perineal muscles are brought together in the midline, the posterior vaginal wall should be perpendicular to the perineum.
An alternative to surgical closure of a 2nd-degree dehiscence is the use of vacuum-assisted wound closure. Disadvantages of this approach include difficulty in maintaining a vacuum seal in the perineal region and the risk of wound contamination with feces. In one case report, 3 weeks of vacuum-assisted wound closure resulted in healing of a 10-cm wound dehiscence that occurred 5 days following a forceps-assisted vaginal delivery with a mediolateral episiotomy.28
Step 3. Ensure complete healing of the wound
Superb postoperative wound care helps to ensure a quick return to full recovery. Wound care should include regularly scheduled sitz baths (at least 3 times daily) followed by drying the perineum. It is preferable to provide a liquid diet that avoids frequent bowel movements in the initial 3 postoperative days. Stool softeners and fiber supplementation are recommended when a full diet is resumed. Some surgeons have found mineral oil (1 to 2 tablespoons daily) effective in producing soft stools that are easy to pass.26 Ensuring soft stool consistency is important to help prevent repair breakdown that may occur with passage of hard stools, fecal impaction, and/or straining during defecation.
We recommend follow-up 1 to 2 weeks after surgery to assess wound healing. No vaginal intercourseis permitted until complete healing is achieved.
Use a surgical checklist
All obstetricians and midwives strive to reduce the risk of OASIS at vaginal birth. When OASIS occurs, it is often useful to use a surgical checklist to ensure the execution of all steps in the management of the repair and recovery process.29 It is heartbreaking to see an OASIS repair breakdown in the week following a vaginal delivery. But by following the 3 steps outlined here, the secondary repair is likely to be successful and will quickly return most patients to full health.
Related article:
Develop and use a checklist for 3rd- and 4th-degree perineal lacerations
The authors report no financial relationships relevant to this article.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Blondel B, Alexander S, Bjarnadottir RI, et al; Euro-Peristat Scientific Committee. Variations in rates of severe perineal tears and episiotomies in 20 European countries: a study based on routine national data in Euro-Perstat Project. Acta Obstet Gynecol Scand. 2016;95(7):746–754.
- Friedman AM, Ananth CV, Predergast E, D’Alton ME, Wright JD. Evaluation of third-degree and fourth-degree laceration rates as quality indicators. Obstet Gynecol. 2015;125(4):927–937.
- Pergialiotis V, Vlachos D, Protopapas A, Pappa K, Vlachos G. Risk factors for severe perineal lacerations during childbirth. Int J Gynecol Obstet. 2014;125(1):6–14.
- Schmitz T, Alberti C, Andriss B, Moutafoff C, Oury JF, Sibony O. Identification of women at high risk for severe perineal lacerations. Eur J Obstet Gynecol Reprod Biol. 2014;182:11–15.
- Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.
- ACOG Committee on Practice Bulletins—Obstetrics. Practice bulletin no. 165: Prevention and management of obstetric lacerations at vaginal delivery. Obstet Gynecol. 2016;128(1):e1–e15.
- Sartore A, De Seta F, Maso G, Pregazzi R, Grimaldi E, Guaschino S. The effects of mediolateral episiotomy on pelvic floor function after vaginal delivery. Obstet Gynecol. 2004;103(4):669–673.
- Aasheim V, Nilsen AB, Lukasse M, Reinar LM. Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Database Syst Rev. 2011;(12):CD006672.
- Harvey MA, Pierce M, Alter JE, et al; Society of Obstetricians and Gynaecologists of Canada. Obstetrical anal sphincter injuries (OASIS): prevention, recognition and repair. J Obstet Gynaecol Can. 2015;37(12):1131–1148.
- Jonsson ER, Elfaghi I, Rydhstrom H, Herbst A. Modified Ritgen’s maneuver for anal sphincter injury at delivery: a randomized controlled trial. Obstet Gynecol. 2008;112(2 pt 1):212–217.
- Williams JW. Obstetrics: A Text-book for the Use of Students and Practitioners. New York, NY: D Appleton and Co; 1903:288.
- Cunningham FG. The Ritgen maneuver: another sacred cow questioned. Obstet Gynecol. 2008;112(2 pt 1):210–211.
- Myrfield K, Brook C, Creedy D. Reducing perineal trauma: implications of flexion and extension of the fetal head during birth. Midwifery. 1997;13:197–201.
- Ostergaard Poulsen M, Lund Madsen M, Skriver-Moller AC, Overgaard C. Does the Finnish intervention prevent obstetrical anal sphincter injuries? A systematic review of the literature. BMJ Open. 2015;5:e008346.
- Kamel A, Khaled M. Episiotomy and obstetric perineal wound dehiscence: beyond soreness. J Obstet Gynaecol. 2014;34(3):215–217.
- Goldaber KG, Wendel PJ, McIntire DD, Wendel GD Jr. Postpartum perineal morbidity after fourth-degree perineal repair. Am J Obstet Gynecol. 1993;168(2):489–493.
- Monberg J, Hammen S. Ruptured episiotomia resutured primarily. Acta Obstet Gynecol Scand. 1987;66(2):163–164.
- Jallad K, Steele SE, Barber MD. Breakdown of perineal laceration repair after vaginal delivery: a case-control study. Female Pelvic Med Reconstr Surg. 2016;22(4):276–279.
- Stock L, Basham E, Gossett DR, Lewicky-Gaupp C. Factors associated with wound complications in women with obstetric anal sphincter injuries (OASIS). Am J Obstet Gynecol. 2013;208(4):327.e1–e8.
- Hauth JC, Gilstrap LC 3rd, Ward SC, Hankins GD. Early repair of an external sphincter ani muscle and rectal mucosal dehiscence. Obstet Gynecol. 1986;67(6):806–809.
- Hankins GD, Hauth JC, Gilstrap LC 3rd, Hammond TL, Yeomans ER, Snyder RR. Early repair of episiotomy dehiscence. Obstet Gynecol. 1990;75(1):48–51.
- Ramin SM, Ramus RM, Little BB, Gilstrap LC 3rd. Early repair of episiotomy dehiscence associated with infection. Am J Obstet Gynecol. 1992;167(4 pt 1):1104–1107.
- Arona AJ, Al-Marayati L, Grimes DA, Ballard CA. Early secondary repair of third- and fourth-degree perineal lacerations after outpatient wound preparation. Obstet Gynecol. 1995;86(2):294–296.
- Uygur D, Yesildaglar N, Kis S, Sipahi T. Early repair of episiotomy dehiscence. Aust N Z J Obstet Gynaecol. 2004;44(3):244–246.
- Soerensen MM, Bek KM, Buntzen S, Hojberg KE, Laurberg S. Long-term outcome of delayed primary or early secondary reconstruction of the anal sphincter after obstetrical injury. Dis Colon Rectum. 2008;51(3):312–317.
- Delancey JOL, Berger MB. Surgical approaches to postobstetrical perineal body defects (rectovaginal fistula and chronic third and fourth-degree lacerations). Clin Obstet Gynecol. 2010;53(1):134–144.
- Leeman L, Spearman M, Rogers R. Repair of obstetric perineal lacerations. Am Fam Physician. 2003;68(8):1585–1590.
- Aviki EM, Batalden RP, del Carmen MG, Berkowitz LR. Vacuum-assisted closure for episiotomy dehiscence. Obstet Gynecol. 2015;126(3):530–533.
- Barbieri RL. Develop and use a checklist for 3rd- and 4th-degree perineal lacerations. OBG Manag. 2013;25(8):8–12.
- Blondel B, Alexander S, Bjarnadottir RI, et al; Euro-Peristat Scientific Committee. Variations in rates of severe perineal tears and episiotomies in 20 European countries: a study based on routine national data in Euro-Perstat Project. Acta Obstet Gynecol Scand. 2016;95(7):746–754.
- Friedman AM, Ananth CV, Predergast E, D’Alton ME, Wright JD. Evaluation of third-degree and fourth-degree laceration rates as quality indicators. Obstet Gynecol. 2015;125(4):927–937.
- Pergialiotis V, Vlachos D, Protopapas A, Pappa K, Vlachos G. Risk factors for severe perineal lacerations during childbirth. Int J Gynecol Obstet. 2014;125(1):6–14.
- Schmitz T, Alberti C, Andriss B, Moutafoff C, Oury JF, Sibony O. Identification of women at high risk for severe perineal lacerations. Eur J Obstet Gynecol Reprod Biol. 2014;182:11–15.
- Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.
- ACOG Committee on Practice Bulletins—Obstetrics. Practice bulletin no. 165: Prevention and management of obstetric lacerations at vaginal delivery. Obstet Gynecol. 2016;128(1):e1–e15.
- Sartore A, De Seta F, Maso G, Pregazzi R, Grimaldi E, Guaschino S. The effects of mediolateral episiotomy on pelvic floor function after vaginal delivery. Obstet Gynecol. 2004;103(4):669–673.
- Aasheim V, Nilsen AB, Lukasse M, Reinar LM. Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Database Syst Rev. 2011;(12):CD006672.
- Harvey MA, Pierce M, Alter JE, et al; Society of Obstetricians and Gynaecologists of Canada. Obstetrical anal sphincter injuries (OASIS): prevention, recognition and repair. J Obstet Gynaecol Can. 2015;37(12):1131–1148.
- Jonsson ER, Elfaghi I, Rydhstrom H, Herbst A. Modified Ritgen’s maneuver for anal sphincter injury at delivery: a randomized controlled trial. Obstet Gynecol. 2008;112(2 pt 1):212–217.
- Williams JW. Obstetrics: A Text-book for the Use of Students and Practitioners. New York, NY: D Appleton and Co; 1903:288.
- Cunningham FG. The Ritgen maneuver: another sacred cow questioned. Obstet Gynecol. 2008;112(2 pt 1):210–211.
- Myrfield K, Brook C, Creedy D. Reducing perineal trauma: implications of flexion and extension of the fetal head during birth. Midwifery. 1997;13:197–201.
- Ostergaard Poulsen M, Lund Madsen M, Skriver-Moller AC, Overgaard C. Does the Finnish intervention prevent obstetrical anal sphincter injuries? A systematic review of the literature. BMJ Open. 2015;5:e008346.
- Kamel A, Khaled M. Episiotomy and obstetric perineal wound dehiscence: beyond soreness. J Obstet Gynaecol. 2014;34(3):215–217.
- Goldaber KG, Wendel PJ, McIntire DD, Wendel GD Jr. Postpartum perineal morbidity after fourth-degree perineal repair. Am J Obstet Gynecol. 1993;168(2):489–493.
- Monberg J, Hammen S. Ruptured episiotomia resutured primarily. Acta Obstet Gynecol Scand. 1987;66(2):163–164.
- Jallad K, Steele SE, Barber MD. Breakdown of perineal laceration repair after vaginal delivery: a case-control study. Female Pelvic Med Reconstr Surg. 2016;22(4):276–279.
- Stock L, Basham E, Gossett DR, Lewicky-Gaupp C. Factors associated with wound complications in women with obstetric anal sphincter injuries (OASIS). Am J Obstet Gynecol. 2013;208(4):327.e1–e8.
- Hauth JC, Gilstrap LC 3rd, Ward SC, Hankins GD. Early repair of an external sphincter ani muscle and rectal mucosal dehiscence. Obstet Gynecol. 1986;67(6):806–809.
- Hankins GD, Hauth JC, Gilstrap LC 3rd, Hammond TL, Yeomans ER, Snyder RR. Early repair of episiotomy dehiscence. Obstet Gynecol. 1990;75(1):48–51.
- Ramin SM, Ramus RM, Little BB, Gilstrap LC 3rd. Early repair of episiotomy dehiscence associated with infection. Am J Obstet Gynecol. 1992;167(4 pt 1):1104–1107.
- Arona AJ, Al-Marayati L, Grimes DA, Ballard CA. Early secondary repair of third- and fourth-degree perineal lacerations after outpatient wound preparation. Obstet Gynecol. 1995;86(2):294–296.
- Uygur D, Yesildaglar N, Kis S, Sipahi T. Early repair of episiotomy dehiscence. Aust N Z J Obstet Gynaecol. 2004;44(3):244–246.
- Soerensen MM, Bek KM, Buntzen S, Hojberg KE, Laurberg S. Long-term outcome of delayed primary or early secondary reconstruction of the anal sphincter after obstetrical injury. Dis Colon Rectum. 2008;51(3):312–317.
- Delancey JOL, Berger MB. Surgical approaches to postobstetrical perineal body defects (rectovaginal fistula and chronic third and fourth-degree lacerations). Clin Obstet Gynecol. 2010;53(1):134–144.
- Leeman L, Spearman M, Rogers R. Repair of obstetric perineal lacerations. Am Fam Physician. 2003;68(8):1585–1590.
- Aviki EM, Batalden RP, del Carmen MG, Berkowitz LR. Vacuum-assisted closure for episiotomy dehiscence. Obstet Gynecol. 2015;126(3):530–533.
- Barbieri RL. Develop and use a checklist for 3rd- and 4th-degree perineal lacerations. OBG Manag. 2013;25(8):8–12.

SYNTAX analysis: Making the case for CABG over PCI
Whenever seminal clinical trials report results that challenge conventional thinking, physicians face the challenge of actually applying those findings in the clinic. A team of cardiac surgeons from Baylor University in Plano, Tex., has offered its take on the clinical implications of recent findings from the cause-of-death analysis of the SYNTAX trial that compared coronary artery bypass grafting with stenting: When counseling higher-risk patients with coronary artery disease about revascularization procedures, cardiologists and cardiac surgeons should clearly elucidate the dramatic advantage of coronary artery bypass grafting over stenting that SYNTAX had demonstrated.
Michael Mack, MD, and coauthors made their case in a featured expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1237-40).

“In fact, there was a significant survival advantage for CABG in the patients with intermediate and high SYNTAX scores, with the death rate of CABG versus PCI being 9.6% versus 16.3% (P less than .047) and 8.8% versus 17.8% (P less than .02), respectively,” they wrote.
The advantages of surgery “have been most striking for patients with intermediate or high SYNTAX scores, but seem to exist for patients with low scores as well, although requiring more follow-up,” Dr. Mack and colleagues said. But the situation is less clear in other subgroups, particularly in patients with less diffuse distal disease and lower SYNTAX scores, they added.
Complete revascularization after the procedure may explain the better outcomes with CABG, as 43.3% of those in the PCI arm had incomplete revascularization vs. 36.8% in the CABG arm. “Incomplete revascularization was associated with increased risk for major adverse cardiac or cerebrovascular events three years after PCI, but incomplete revascularization in the CABG group could not be identified as a predictor for worse outcomes,” Dr. Mack and colleagues noted.
The expert opinion authors debunk one of the recent criticisms of SYNTAX: that its reliance on first-generation drug-eluting stents is dated and not relevant today. They noted the more recent Bypass Surgery Vs. Everolimus-Eluting Stent Implantation for Multivessel Coronary Artery Disease trial found a similarly higher rate of death, heart attack, and target vessel revascularization occurred more frequently in the PCI group (15.3% vs. 10.6% in the CABG group) (N Engl J Med. 2015;372:1204-12).
Nonetheless, Dr. Mack and coauthors found room for improvement for CABG through increased use of atrial revascularization and appropriate measures to minimize stroke.
The latest SYNTAX findings can inform the approach surgeons take with high-risk patients, they said. This should include “a discussion of these data, particularly in regard to survival.” And physicians should base their therapeutic recommendations on these data. “At present, there are data seeming to indicate that the majority of patients with three-vessel disease receiving invasive treatment in the United States are being treated with PCI, an outcome that is not congruent with these outcome findings,” they said.
Taking into consideration other SYNTAX analyses that have shown that completeness of revascularization is a determining factor in post-PCI outcomes, Dr. Mack and coauthors said that physicians should calculate the degree of coronary artery disease (CAD) left untreated after intervention, “and those patients who are likely to have a high residual SYNTAX score should be strongly considered for CABG.” Doctors should also focus “intensive efforts” on adherence to optimal medical therapy after both CABG and PCI.
“Finally, although there is a strong patient preference for a less-invasive treatment of their CAD, patients with advanced disease should be made aware that the choice of PCI puts them at an increased risk of death relative to CABG, and a full and transparent discussion should occur regarding the implications of their decision,” Dr. Mack and coauthors concluded.
They had no relevant financial relationships to disclose.
In their invited editorial commentary, Saswata Deb, MD, and Stephen E. Fremes, MD, of the Schulich Heart Center at the University of Toronto, concurred with the conclusions of Dr. Mack and colleagues (J Thorac Cardiovasc Surg. 2016;152:1241-2). And Joseph F. Sabik III, MD, of the Cleveland Clinic arrived at a similar conclusion in an accompanying editorial (J. Thorac Cardiovasc Surg. 2016;152:1227-8).
Dr. Deb and Dr. Fremes found noteworthy the point Dr. Mack and coauthors raised about cardiologists and internists continuing to recommend PCI to patients with complex multivessel CAD despite evidence from SYNTAX and other trials. “This raises the importance of having a multidisciplinary heart team,” Dr. Deb and Dr. Fremes said.
But they also raised an important question about the difference in outcomes between CABG and PCI in complex multivessel disease. CABG should be the preferred intervention if the high rates of late fatal myocardial infarction after PCI are due to incomplete revascularization; however, if late stent thrombosis was the cause of this disparity in outcomes, then improvements in PCI could close that gap.
In his editorial, Dr. Sabik attributed the difference in outcomes between PCI and CABG to the ability of the former to both treat existing and prevent future stenosis. PCI can be “difficult, dangerous, and even impossible” when the target vessel is totally occluded or the stenosis is complex, hence leading to incomplete revascularization and residual ischemia. “Performing CABG to these vessels is no more difficult than for an isolated, noncomplex stenosis,” Dr. Sabik said.
Dr. Sabik disclosed he is the principal investigator for an Abbott Laboratories–sponsored trial of left main coronary disease, and is on the scientific advisory board of Medtronic.
Dr. Deb and Dr. Fremes had no relationships to disclose.
In their invited editorial commentary, Saswata Deb, MD, and Stephen E. Fremes, MD, of the Schulich Heart Center at the University of Toronto, concurred with the conclusions of Dr. Mack and colleagues (J Thorac Cardiovasc Surg. 2016;152:1241-2). And Joseph F. Sabik III, MD, of the Cleveland Clinic arrived at a similar conclusion in an accompanying editorial (J. Thorac Cardiovasc Surg. 2016;152:1227-8).
Dr. Deb and Dr. Fremes found noteworthy the point Dr. Mack and coauthors raised about cardiologists and internists continuing to recommend PCI to patients with complex multivessel CAD despite evidence from SYNTAX and other trials. “This raises the importance of having a multidisciplinary heart team,” Dr. Deb and Dr. Fremes said.
But they also raised an important question about the difference in outcomes between CABG and PCI in complex multivessel disease. CABG should be the preferred intervention if the high rates of late fatal myocardial infarction after PCI are due to incomplete revascularization; however, if late stent thrombosis was the cause of this disparity in outcomes, then improvements in PCI could close that gap.
In his editorial, Dr. Sabik attributed the difference in outcomes between PCI and CABG to the ability of the former to both treat existing and prevent future stenosis. PCI can be “difficult, dangerous, and even impossible” when the target vessel is totally occluded or the stenosis is complex, hence leading to incomplete revascularization and residual ischemia. “Performing CABG to these vessels is no more difficult than for an isolated, noncomplex stenosis,” Dr. Sabik said.
Dr. Sabik disclosed he is the principal investigator for an Abbott Laboratories–sponsored trial of left main coronary disease, and is on the scientific advisory board of Medtronic.
Dr. Deb and Dr. Fremes had no relationships to disclose.
In their invited editorial commentary, Saswata Deb, MD, and Stephen E. Fremes, MD, of the Schulich Heart Center at the University of Toronto, concurred with the conclusions of Dr. Mack and colleagues (J Thorac Cardiovasc Surg. 2016;152:1241-2). And Joseph F. Sabik III, MD, of the Cleveland Clinic arrived at a similar conclusion in an accompanying editorial (J. Thorac Cardiovasc Surg. 2016;152:1227-8).
Dr. Deb and Dr. Fremes found noteworthy the point Dr. Mack and coauthors raised about cardiologists and internists continuing to recommend PCI to patients with complex multivessel CAD despite evidence from SYNTAX and other trials. “This raises the importance of having a multidisciplinary heart team,” Dr. Deb and Dr. Fremes said.
But they also raised an important question about the difference in outcomes between CABG and PCI in complex multivessel disease. CABG should be the preferred intervention if the high rates of late fatal myocardial infarction after PCI are due to incomplete revascularization; however, if late stent thrombosis was the cause of this disparity in outcomes, then improvements in PCI could close that gap.
In his editorial, Dr. Sabik attributed the difference in outcomes between PCI and CABG to the ability of the former to both treat existing and prevent future stenosis. PCI can be “difficult, dangerous, and even impossible” when the target vessel is totally occluded or the stenosis is complex, hence leading to incomplete revascularization and residual ischemia. “Performing CABG to these vessels is no more difficult than for an isolated, noncomplex stenosis,” Dr. Sabik said.
Dr. Sabik disclosed he is the principal investigator for an Abbott Laboratories–sponsored trial of left main coronary disease, and is on the scientific advisory board of Medtronic.
Dr. Deb and Dr. Fremes had no relationships to disclose.
Whenever seminal clinical trials report results that challenge conventional thinking, physicians face the challenge of actually applying those findings in the clinic. A team of cardiac surgeons from Baylor University in Plano, Tex., has offered its take on the clinical implications of recent findings from the cause-of-death analysis of the SYNTAX trial that compared coronary artery bypass grafting with stenting: When counseling higher-risk patients with coronary artery disease about revascularization procedures, cardiologists and cardiac surgeons should clearly elucidate the dramatic advantage of coronary artery bypass grafting over stenting that SYNTAX had demonstrated.
Michael Mack, MD, and coauthors made their case in a featured expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1237-40).
“In fact, there was a significant survival advantage for CABG in the patients with intermediate and high SYNTAX scores, with the death rate of CABG versus PCI being 9.6% versus 16.3% (P less than .047) and 8.8% versus 17.8% (P less than .02), respectively,” they wrote.
The advantages of surgery “have been most striking for patients with intermediate or high SYNTAX scores, but seem to exist for patients with low scores as well, although requiring more follow-up,” Dr. Mack and colleagues said. But the situation is less clear in other subgroups, particularly in patients with less diffuse distal disease and lower SYNTAX scores, they added.
Complete revascularization after the procedure may explain the better outcomes with CABG, as 43.3% of those in the PCI arm had incomplete revascularization vs. 36.8% in the CABG arm. “Incomplete revascularization was associated with increased risk for major adverse cardiac or cerebrovascular events three years after PCI, but incomplete revascularization in the CABG group could not be identified as a predictor for worse outcomes,” Dr. Mack and colleagues noted.
The expert opinion authors debunk one of the recent criticisms of SYNTAX: that its reliance on first-generation drug-eluting stents is dated and not relevant today. They noted the more recent Bypass Surgery Vs. Everolimus-Eluting Stent Implantation for Multivessel Coronary Artery Disease trial found a similarly higher rate of death, heart attack, and target vessel revascularization occurred more frequently in the PCI group (15.3% vs. 10.6% in the CABG group) (N Engl J Med. 2015;372:1204-12).
Nonetheless, Dr. Mack and coauthors found room for improvement for CABG through increased use of atrial revascularization and appropriate measures to minimize stroke.
The latest SYNTAX findings can inform the approach surgeons take with high-risk patients, they said. This should include “a discussion of these data, particularly in regard to survival.” And physicians should base their therapeutic recommendations on these data. “At present, there are data seeming to indicate that the majority of patients with three-vessel disease receiving invasive treatment in the United States are being treated with PCI, an outcome that is not congruent with these outcome findings,” they said.
Taking into consideration other SYNTAX analyses that have shown that completeness of revascularization is a determining factor in post-PCI outcomes, Dr. Mack and coauthors said that physicians should calculate the degree of coronary artery disease (CAD) left untreated after intervention, “and those patients who are likely to have a high residual SYNTAX score should be strongly considered for CABG.” Doctors should also focus “intensive efforts” on adherence to optimal medical therapy after both CABG and PCI.
“Finally, although there is a strong patient preference for a less-invasive treatment of their CAD, patients with advanced disease should be made aware that the choice of PCI puts them at an increased risk of death relative to CABG, and a full and transparent discussion should occur regarding the implications of their decision,” Dr. Mack and coauthors concluded.
They had no relevant financial relationships to disclose.
Whenever seminal clinical trials report results that challenge conventional thinking, physicians face the challenge of actually applying those findings in the clinic. A team of cardiac surgeons from Baylor University in Plano, Tex., has offered its take on the clinical implications of recent findings from the cause-of-death analysis of the SYNTAX trial that compared coronary artery bypass grafting with stenting: When counseling higher-risk patients with coronary artery disease about revascularization procedures, cardiologists and cardiac surgeons should clearly elucidate the dramatic advantage of coronary artery bypass grafting over stenting that SYNTAX had demonstrated.
Michael Mack, MD, and coauthors made their case in a featured expert opinion in the Journal of Thoracic and Cardiovascular Surgery (2016;152:1237-40).
“In fact, there was a significant survival advantage for CABG in the patients with intermediate and high SYNTAX scores, with the death rate of CABG versus PCI being 9.6% versus 16.3% (P less than .047) and 8.8% versus 17.8% (P less than .02), respectively,” they wrote.
The advantages of surgery “have been most striking for patients with intermediate or high SYNTAX scores, but seem to exist for patients with low scores as well, although requiring more follow-up,” Dr. Mack and colleagues said. But the situation is less clear in other subgroups, particularly in patients with less diffuse distal disease and lower SYNTAX scores, they added.
Complete revascularization after the procedure may explain the better outcomes with CABG, as 43.3% of those in the PCI arm had incomplete revascularization vs. 36.8% in the CABG arm. “Incomplete revascularization was associated with increased risk for major adverse cardiac or cerebrovascular events three years after PCI, but incomplete revascularization in the CABG group could not be identified as a predictor for worse outcomes,” Dr. Mack and colleagues noted.
The expert opinion authors debunk one of the recent criticisms of SYNTAX: that its reliance on first-generation drug-eluting stents is dated and not relevant today. They noted the more recent Bypass Surgery Vs. Everolimus-Eluting Stent Implantation for Multivessel Coronary Artery Disease trial found a similarly higher rate of death, heart attack, and target vessel revascularization occurred more frequently in the PCI group (15.3% vs. 10.6% in the CABG group) (N Engl J Med. 2015;372:1204-12).
Nonetheless, Dr. Mack and coauthors found room for improvement for CABG through increased use of atrial revascularization and appropriate measures to minimize stroke.
The latest SYNTAX findings can inform the approach surgeons take with high-risk patients, they said. This should include “a discussion of these data, particularly in regard to survival.” And physicians should base their therapeutic recommendations on these data. “At present, there are data seeming to indicate that the majority of patients with three-vessel disease receiving invasive treatment in the United States are being treated with PCI, an outcome that is not congruent with these outcome findings,” they said.
Taking into consideration other SYNTAX analyses that have shown that completeness of revascularization is a determining factor in post-PCI outcomes, Dr. Mack and coauthors said that physicians should calculate the degree of coronary artery disease (CAD) left untreated after intervention, “and those patients who are likely to have a high residual SYNTAX score should be strongly considered for CABG.” Doctors should also focus “intensive efforts” on adherence to optimal medical therapy after both CABG and PCI.
“Finally, although there is a strong patient preference for a less-invasive treatment of their CAD, patients with advanced disease should be made aware that the choice of PCI puts them at an increased risk of death relative to CABG, and a full and transparent discussion should occur regarding the implications of their decision,” Dr. Mack and coauthors concluded.
They had no relevant financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Physicians should clearly communicate to patients with complex multivessel artery disease the key findings of the SYNTAX trial.
Major finding: The SYNTAX trials showed the risk of cardiac death from myocardial infarction after percutaneous coronary intervention (PCI) is 10 times greater than that after coronary artery bypass grafting in higher-risk patients.
Data source: A post hoc analysis of causes of death in all 3,075 trial and registry patients in the Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery (SYNTAX) trial.
Disclosures: Dr. Mack and coauthors reported having no financial disclosures.
Letters to the Editor: Update on contraception
“UPDATE ON CONTRACEPTION”
Mitchell D. Creinin, MD; Natasha R. Schimmoeller, MD, MPH, MA (August 2016)
Interesting anatomic variation and management for IUD placement
I recently saw a patient for insertion of an intrauterine device (IUD). On examination with a speculum, I could not find the patient’s cervix. On bimanual exam, I found the cervix to be extremely anterior. I again placed a speculum and, even knowing where to look, could not bring the cervix into view. I did a second bimanual exam and noticed that I could move the cervix into a more axial plane if I exerted suprapubic pressure. The patient’s uterus was retroverted and her cervix was behind her symphysis. When I placed the speculum again, I asked the patient to apply suprapubic pressure, as I just had. With this procedure I then found her cervix easily, grasped it with a tenaculum, and inserted the IUD, which went well.
Jeffrey Joseph, MD
Wakefield, Rhode Island
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“UPDATE ON CONTRACEPTION”
Mitchell D. Creinin, MD; Natasha R. Schimmoeller, MD, MPH, MA (August 2016)
Interesting anatomic variation and management for IUD placement
I recently saw a patient for insertion of an intrauterine device (IUD). On examination with a speculum, I could not find the patient’s cervix. On bimanual exam, I found the cervix to be extremely anterior. I again placed a speculum and, even knowing where to look, could not bring the cervix into view. I did a second bimanual exam and noticed that I could move the cervix into a more axial plane if I exerted suprapubic pressure. The patient’s uterus was retroverted and her cervix was behind her symphysis. When I placed the speculum again, I asked the patient to apply suprapubic pressure, as I just had. With this procedure I then found her cervix easily, grasped it with a tenaculum, and inserted the IUD, which went well.
Jeffrey Joseph, MD
Wakefield, Rhode Island
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“UPDATE ON CONTRACEPTION”
Mitchell D. Creinin, MD; Natasha R. Schimmoeller, MD, MPH, MA (August 2016)
Interesting anatomic variation and management for IUD placement
I recently saw a patient for insertion of an intrauterine device (IUD). On examination with a speculum, I could not find the patient’s cervix. On bimanual exam, I found the cervix to be extremely anterior. I again placed a speculum and, even knowing where to look, could not bring the cervix into view. I did a second bimanual exam and noticed that I could move the cervix into a more axial plane if I exerted suprapubic pressure. The patient’s uterus was retroverted and her cervix was behind her symphysis. When I placed the speculum again, I asked the patient to apply suprapubic pressure, as I just had. With this procedure I then found her cervix easily, grasped it with a tenaculum, and inserted the IUD, which went well.
Jeffrey Joseph, MD
Wakefield, Rhode Island
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Letters to the Editor: Rectal misoprostol for postpartum hemorrhage
“STOP USING RECTAL MISOPROSTOL FOR THE TREATMENT OF POSTPARTUM HEMORRHAGE CAUSED BY UTERINE ATONY”
ROBERT L. BARBIERI, MD (JULY 2016)
More on rectal misoprostol for postpartum hemorrhage
We applaud Dr. Barbieri’s July Editorial urging providers to stop administering misoprostol rectally for the treatment of postpartum hemorrhage (PPH) given the well-documented evidence and pharmacokinetics that recommend the sublingual route. Confusion among providers may derive from the fact that not all international guidelines, including the American College of Obstetricians and Gynecologists clinical guidelines on the management of PPH, have been updated to reflect the latest evidence.1 Guidelines from the World Health Organization and the International Federation of Gynecology and Obstetrics reflect the latest evidence and clearly recommend the evidence-based regimen of 800 μg misoprostol sublingually for treatment of PPH,2 which has been shown to be comparable to 40 IU oxytocin intravenously in women who receive oxytocin for PPH prophylaxis.3
Although oxytocin remains the first-line treatment for PPH, evidence suggests that sublingual misoprostol should be considered a viable first alternative if oxytocin is not available or fails. There is little evidence on the benefit of methergine or carboprost over misoprostol for PPH treatment, and inclusion of these drugs in treatment guidelines and practice is based on extrapolations from studies on PPH prevention.4 As Dr. Barbieri noted, pyrexia from misoprostol has been cited in the literature; however, contrary to contraindications for methergine, for example, this rare event does not pose serious risks to women, is self-limiting, and appears to be most acute among certain populations.5
It is paramount that safe, effective, and evidence-based PPH treatments be available and known to providers both in the United States and globally in order to provide women with timely treatment. Greater discussion and research is warranted about the hierarchy of use for these drugs and the possible impact of routine use of uterotonics before and during delivery, given that overexposure to uterotonics may in fact be making PPH harder to treat.6
Gillian Burkhardt, MD, and Rasha Dabash, MPH
New York, New York
Dr. Barbieri responds
I thank Drs. Burkhardt and Dabash for sharing their expert perspective with our readers. They advocate for the use of sublingual misoprostol for the treatment of PPH “if oxytocin is not available or fails.” I agree that at a home birth, if oxytocin is not available, sublingual misoprostol would be of great benefit. I remain concerned that misoprostol has little clinical utility for the treatment of PPH in the hospital setting in which oxytocin, methergine, and carboprost are available alternatives. Misoprostol causes fever in many women, and women who develop a postpartum fever due to misoprostol will receive unnecessary antibiotic treatment. I recommend that our readers stop using misoprostol for the treatment of PPH in the hospital setting.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- ACOG Committee on Practice Bulletins–Obstetrics. ACOG Practice Bulletin No. 76: Postpartum hemorrhage. Obstet Gynecol. 2006;108(4):1039–1048. Reaffirmed 2015.
- World Health Organization. WHO recommendations for the prevention and treatment of postpartum haemorrhage. Geneva, Switzerland: World Health Organization; 2012.
- Blum J, Winikoff B, Raghavan S, et al. Treatment of post-partum haemorrhage with sublingual misoprostol versus oxytocin in women receiving prophylactic oxytocin: a double-blind placebo-controlled randomized non-inferiority trial. Lancet. 2010;375(9710):217–223.
- Weeks A. The prevention and treatment of postpartum haemorrhage: what do we know, and where do we go to next? BJOG. 2015;122(2):202–210.
- Durocher J, Bynum J, León W, Barrera G, Winikoff B. High fever following postpartum administration of sublingual misoprostol. BJOG. 2010;117(7):845–852.
- Balki M, Erik-Soussi M, Kingdom J, Carvalho JC. Oxytocin pretreatment attenuates oxytocin-induced contractions in human myometrium in vitro. Anesthesiology. 2013;119(3):552–561.
“STOP USING RECTAL MISOPROSTOL FOR THE TREATMENT OF POSTPARTUM HEMORRHAGE CAUSED BY UTERINE ATONY”
ROBERT L. BARBIERI, MD (JULY 2016)
More on rectal misoprostol for postpartum hemorrhage
We applaud Dr. Barbieri’s July Editorial urging providers to stop administering misoprostol rectally for the treatment of postpartum hemorrhage (PPH) given the well-documented evidence and pharmacokinetics that recommend the sublingual route. Confusion among providers may derive from the fact that not all international guidelines, including the American College of Obstetricians and Gynecologists clinical guidelines on the management of PPH, have been updated to reflect the latest evidence.1 Guidelines from the World Health Organization and the International Federation of Gynecology and Obstetrics reflect the latest evidence and clearly recommend the evidence-based regimen of 800 μg misoprostol sublingually for treatment of PPH,2 which has been shown to be comparable to 40 IU oxytocin intravenously in women who receive oxytocin for PPH prophylaxis.3
Although oxytocin remains the first-line treatment for PPH, evidence suggests that sublingual misoprostol should be considered a viable first alternative if oxytocin is not available or fails. There is little evidence on the benefit of methergine or carboprost over misoprostol for PPH treatment, and inclusion of these drugs in treatment guidelines and practice is based on extrapolations from studies on PPH prevention.4 As Dr. Barbieri noted, pyrexia from misoprostol has been cited in the literature; however, contrary to contraindications for methergine, for example, this rare event does not pose serious risks to women, is self-limiting, and appears to be most acute among certain populations.5
It is paramount that safe, effective, and evidence-based PPH treatments be available and known to providers both in the United States and globally in order to provide women with timely treatment. Greater discussion and research is warranted about the hierarchy of use for these drugs and the possible impact of routine use of uterotonics before and during delivery, given that overexposure to uterotonics may in fact be making PPH harder to treat.6
Gillian Burkhardt, MD, and Rasha Dabash, MPH
New York, New York
Dr. Barbieri responds
I thank Drs. Burkhardt and Dabash for sharing their expert perspective with our readers. They advocate for the use of sublingual misoprostol for the treatment of PPH “if oxytocin is not available or fails.” I agree that at a home birth, if oxytocin is not available, sublingual misoprostol would be of great benefit. I remain concerned that misoprostol has little clinical utility for the treatment of PPH in the hospital setting in which oxytocin, methergine, and carboprost are available alternatives. Misoprostol causes fever in many women, and women who develop a postpartum fever due to misoprostol will receive unnecessary antibiotic treatment. I recommend that our readers stop using misoprostol for the treatment of PPH in the hospital setting.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
“STOP USING RECTAL MISOPROSTOL FOR THE TREATMENT OF POSTPARTUM HEMORRHAGE CAUSED BY UTERINE ATONY”
ROBERT L. BARBIERI, MD (JULY 2016)
More on rectal misoprostol for postpartum hemorrhage
We applaud Dr. Barbieri’s July Editorial urging providers to stop administering misoprostol rectally for the treatment of postpartum hemorrhage (PPH) given the well-documented evidence and pharmacokinetics that recommend the sublingual route. Confusion among providers may derive from the fact that not all international guidelines, including the American College of Obstetricians and Gynecologists clinical guidelines on the management of PPH, have been updated to reflect the latest evidence.1 Guidelines from the World Health Organization and the International Federation of Gynecology and Obstetrics reflect the latest evidence and clearly recommend the evidence-based regimen of 800 μg misoprostol sublingually for treatment of PPH,2 which has been shown to be comparable to 40 IU oxytocin intravenously in women who receive oxytocin for PPH prophylaxis.3
Although oxytocin remains the first-line treatment for PPH, evidence suggests that sublingual misoprostol should be considered a viable first alternative if oxytocin is not available or fails. There is little evidence on the benefit of methergine or carboprost over misoprostol for PPH treatment, and inclusion of these drugs in treatment guidelines and practice is based on extrapolations from studies on PPH prevention.4 As Dr. Barbieri noted, pyrexia from misoprostol has been cited in the literature; however, contrary to contraindications for methergine, for example, this rare event does not pose serious risks to women, is self-limiting, and appears to be most acute among certain populations.5
It is paramount that safe, effective, and evidence-based PPH treatments be available and known to providers both in the United States and globally in order to provide women with timely treatment. Greater discussion and research is warranted about the hierarchy of use for these drugs and the possible impact of routine use of uterotonics before and during delivery, given that overexposure to uterotonics may in fact be making PPH harder to treat.6
Gillian Burkhardt, MD, and Rasha Dabash, MPH
New York, New York
Dr. Barbieri responds
I thank Drs. Burkhardt and Dabash for sharing their expert perspective with our readers. They advocate for the use of sublingual misoprostol for the treatment of PPH “if oxytocin is not available or fails.” I agree that at a home birth, if oxytocin is not available, sublingual misoprostol would be of great benefit. I remain concerned that misoprostol has little clinical utility for the treatment of PPH in the hospital setting in which oxytocin, methergine, and carboprost are available alternatives. Misoprostol causes fever in many women, and women who develop a postpartum fever due to misoprostol will receive unnecessary antibiotic treatment. I recommend that our readers stop using misoprostol for the treatment of PPH in the hospital setting.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- ACOG Committee on Practice Bulletins–Obstetrics. ACOG Practice Bulletin No. 76: Postpartum hemorrhage. Obstet Gynecol. 2006;108(4):1039–1048. Reaffirmed 2015.
- World Health Organization. WHO recommendations for the prevention and treatment of postpartum haemorrhage. Geneva, Switzerland: World Health Organization; 2012.
- Blum J, Winikoff B, Raghavan S, et al. Treatment of post-partum haemorrhage with sublingual misoprostol versus oxytocin in women receiving prophylactic oxytocin: a double-blind placebo-controlled randomized non-inferiority trial. Lancet. 2010;375(9710):217–223.
- Weeks A. The prevention and treatment of postpartum haemorrhage: what do we know, and where do we go to next? BJOG. 2015;122(2):202–210.
- Durocher J, Bynum J, León W, Barrera G, Winikoff B. High fever following postpartum administration of sublingual misoprostol. BJOG. 2010;117(7):845–852.
- Balki M, Erik-Soussi M, Kingdom J, Carvalho JC. Oxytocin pretreatment attenuates oxytocin-induced contractions in human myometrium in vitro. Anesthesiology. 2013;119(3):552–561.
- ACOG Committee on Practice Bulletins–Obstetrics. ACOG Practice Bulletin No. 76: Postpartum hemorrhage. Obstet Gynecol. 2006;108(4):1039–1048. Reaffirmed 2015.
- World Health Organization. WHO recommendations for the prevention and treatment of postpartum haemorrhage. Geneva, Switzerland: World Health Organization; 2012.
- Blum J, Winikoff B, Raghavan S, et al. Treatment of post-partum haemorrhage with sublingual misoprostol versus oxytocin in women receiving prophylactic oxytocin: a double-blind placebo-controlled randomized non-inferiority trial. Lancet. 2010;375(9710):217–223.
- Weeks A. The prevention and treatment of postpartum haemorrhage: what do we know, and where do we go to next? BJOG. 2015;122(2):202–210.
- Durocher J, Bynum J, León W, Barrera G, Winikoff B. High fever following postpartum administration of sublingual misoprostol. BJOG. 2010;117(7):845–852.
- Balki M, Erik-Soussi M, Kingdom J, Carvalho JC. Oxytocin pretreatment attenuates oxytocin-induced contractions in human myometrium in vitro. Anesthesiology. 2013;119(3):552–561.
Product Update: JUST…Love, pjur med
MASSAGE AND MOISTURING OIL

Just Pure Essentials suggests that JUST…Love be used to moisturize the face and body and for facial cleansing and shaving. It has been recommended by women’s health professionals as a lubricant and moisturizer to relieve vaginal dryness, says the manufacturer.
Just Pure Essentials products are 100% vegan; chemical and preservative free; and without alcohols, additives, or phytoestrogens. The base of each product is coconut medium-chain triglyceride (MCT) oil pressed from nongenetically modified coconut oil by a steam distillation process. The oil is blended with other organic oils and botanical ingredients, including green tea see oil, French plum oil, argan, and marshmallow leaf. It does not contain dyes, perfumes, or artificial flavors. Just Pure Essentials says its formulas do not dry up and turn sticky.
FOR MORE INFORMATION, VISIT: www.justpureessentials.com
SEXUAL HEALTH AND WELLBEING

pjur med says that PREMIUM glide is specially formulated for dry or highly sensitive genital mucous membranes and is made of non–pore-blocking, high-quality silicones. SENSITIVE glide is specifically developed for those with very sensitive genital mucous membranes, according to the manufacturer. Both products are available in 3.4 fl oz bottles. pjur med suggests its products are suitable for every skin type and maintains that they are dermatologically tested and paraben-, glycerin-, and preservative-free. In addition, pjur med says its formulas have been kept as neutral as possible and the ingredients have been put together in a way that microbial growth cannot occur.
FOR MORE INFORMATION, VISIT: www.pjurmed.com
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
MASSAGE AND MOISTURING OIL
Just Pure Essentials suggests that JUST…Love be used to moisturize the face and body and for facial cleansing and shaving. It has been recommended by women’s health professionals as a lubricant and moisturizer to relieve vaginal dryness, says the manufacturer.
Just Pure Essentials products are 100% vegan; chemical and preservative free; and without alcohols, additives, or phytoestrogens. The base of each product is coconut medium-chain triglyceride (MCT) oil pressed from nongenetically modified coconut oil by a steam distillation process. The oil is blended with other organic oils and botanical ingredients, including green tea see oil, French plum oil, argan, and marshmallow leaf. It does not contain dyes, perfumes, or artificial flavors. Just Pure Essentials says its formulas do not dry up and turn sticky.
FOR MORE INFORMATION, VISIT: www.justpureessentials.com
SEXUAL HEALTH AND WELLBEING
pjur med says that PREMIUM glide is specially formulated for dry or highly sensitive genital mucous membranes and is made of non–pore-blocking, high-quality silicones. SENSITIVE glide is specifically developed for those with very sensitive genital mucous membranes, according to the manufacturer. Both products are available in 3.4 fl oz bottles. pjur med suggests its products are suitable for every skin type and maintains that they are dermatologically tested and paraben-, glycerin-, and preservative-free. In addition, pjur med says its formulas have been kept as neutral as possible and the ingredients have been put together in a way that microbial growth cannot occur.
FOR MORE INFORMATION, VISIT: www.pjurmed.com
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
MASSAGE AND MOISTURING OIL
Just Pure Essentials suggests that JUST…Love be used to moisturize the face and body and for facial cleansing and shaving. It has been recommended by women’s health professionals as a lubricant and moisturizer to relieve vaginal dryness, says the manufacturer.
Just Pure Essentials products are 100% vegan; chemical and preservative free; and without alcohols, additives, or phytoestrogens. The base of each product is coconut medium-chain triglyceride (MCT) oil pressed from nongenetically modified coconut oil by a steam distillation process. The oil is blended with other organic oils and botanical ingredients, including green tea see oil, French plum oil, argan, and marshmallow leaf. It does not contain dyes, perfumes, or artificial flavors. Just Pure Essentials says its formulas do not dry up and turn sticky.
FOR MORE INFORMATION, VISIT: www.justpureessentials.com
SEXUAL HEALTH AND WELLBEING
pjur med says that PREMIUM glide is specially formulated for dry or highly sensitive genital mucous membranes and is made of non–pore-blocking, high-quality silicones. SENSITIVE glide is specifically developed for those with very sensitive genital mucous membranes, according to the manufacturer. Both products are available in 3.4 fl oz bottles. pjur med suggests its products are suitable for every skin type and maintains that they are dermatologically tested and paraben-, glycerin-, and preservative-free. In addition, pjur med says its formulas have been kept as neutral as possible and the ingredients have been put together in a way that microbial growth cannot occur.
FOR MORE INFORMATION, VISIT: www.pjurmed.com
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Vaccine/PD-1 inhibitor combo shows early promise against mCRPC
NATIONAL HARBOR, MD. – To date, checkpoint inhibitors have shown little clinical activity as single agents against metastatic, castration-resistant prostate cancer, but a combination of a DNA vaccine and a programmed-death 1 inhibitor shows promise for enhancing anti-tumor immune responses, report investigators in a phase I trial.
“If you vaccinate animals, PD-1 expression transiently goes up, and if you block it at that point you get a better anti-tumor response, and that was in models where anti PD-1 therapy alone didn’t do anything. So we thought this could be a good approach for prostate cancer,” Douglas G. McNeel, MD, PhD, of the University of Wisconsin, Madison, said in an interview at the annual meeting of the Society for Immunotherapy of Cancer.
Dr. McNeel and colleagues are exploring the therapeutic potential of combining the PD-1 inhibitor pembrolizumab (Keytruda) with an investigational DNA vaccine targeted against prostatic acid phosphatase (PAP), the same antigen targeted by sipuleucel-T (Provenge).
They presented data in a scientific poster from a pilot study of the combination in patients with metastatic, castration-resistant prostate cancer (mCRPC).
Vaccine ramps up PD-1 expression
The investigators had previously shown that patients immunized with a DNA vaccine encoding PAP (pTVG-HP; currently in phase II clinical trials) developed PD-1-regulated, PAP-specific T cells and had increased PD-L1 expression in circulating tumor cells. They also demonstrated in preclinical studies with mouse models that increased PD-1 expression on vaccine-induced CD8-positive T cells led to inferior anti-tumor immune responses, and that blocking PD-1 at the time of T-cell activation with vaccine improved anti-tumor responses.
“The current pilot trial was designed to evaluate whether delivery of PD-1 blockade after immunization (when PD-1-regulated T cells are elicited and when PD-L1 expression is induced with vaccination on tumor cells) or with immunization (when PD-1 expression increases on antigen-specific CD8+ T cells with activation) results in anti-tumor responses in patients with advanced, metastatic, castration-resistant prostate cancer,” Dr. McNeel and his colleagues wrote.
They reported preliminary impressions of the efficacy and safety of the combination in 12 patients with mCRPC. The patients all had evidence of progressive disease and were at least 6 months out from chemotherapy. Patients could have previously been treated with enzalutamide (Xtandi) or abiraterone (Zytiga), but were excluded if they had received sipuleucel-T vaccine.
Patients in the ongoing trial are randomized to receive six doses of pTVG-HP over 10 weeks with either four doses of concurrent pembrolizumab, or four doses of pembrolizumab delivered every 3 weeks beginning 2 weeks after the last vaccine dose.
The authors reported that treatment with the combination evokes changes in serum prostate-specific antigen (PSA) that are associated with objective radiographic changes, and “elicits robust and persistent PAP-specific Th1-based immunity.”
They also found evidence to suggest that concurrent administration of the vaccine and the PD-1 inhibitor may be more effective than sequential administration, based on differences in serum PSA and PAP.
Adverse events were generally mild and similar to those seen in other studies of pembrolizumab and DNA vaccine, with only three grade 3 events and no grade 4 events.
The investigators hope to expand the pilot study beyond the 12 weeks originally scheduled, and plan to explore potential biomarkers for vaccine response based on T-cell proliferation in tumors and in regional lymph nodes as seen on imaging modalities.
The study is funded by a 2014 Movember Prostate Cancer Foundation Challenge Award and Madison Vaccines Inc. Dr. McNeel reports an ownership interest and funding support from Madison Vaccines. All other coauthors reported no conflicts of interest.
NATIONAL HARBOR, MD. – To date, checkpoint inhibitors have shown little clinical activity as single agents against metastatic, castration-resistant prostate cancer, but a combination of a DNA vaccine and a programmed-death 1 inhibitor shows promise for enhancing anti-tumor immune responses, report investigators in a phase I trial.
“If you vaccinate animals, PD-1 expression transiently goes up, and if you block it at that point you get a better anti-tumor response, and that was in models where anti PD-1 therapy alone didn’t do anything. So we thought this could be a good approach for prostate cancer,” Douglas G. McNeel, MD, PhD, of the University of Wisconsin, Madison, said in an interview at the annual meeting of the Society for Immunotherapy of Cancer.
Dr. McNeel and colleagues are exploring the therapeutic potential of combining the PD-1 inhibitor pembrolizumab (Keytruda) with an investigational DNA vaccine targeted against prostatic acid phosphatase (PAP), the same antigen targeted by sipuleucel-T (Provenge).
They presented data in a scientific poster from a pilot study of the combination in patients with metastatic, castration-resistant prostate cancer (mCRPC).
Vaccine ramps up PD-1 expression
The investigators had previously shown that patients immunized with a DNA vaccine encoding PAP (pTVG-HP; currently in phase II clinical trials) developed PD-1-regulated, PAP-specific T cells and had increased PD-L1 expression in circulating tumor cells. They also demonstrated in preclinical studies with mouse models that increased PD-1 expression on vaccine-induced CD8-positive T cells led to inferior anti-tumor immune responses, and that blocking PD-1 at the time of T-cell activation with vaccine improved anti-tumor responses.
“The current pilot trial was designed to evaluate whether delivery of PD-1 blockade after immunization (when PD-1-regulated T cells are elicited and when PD-L1 expression is induced with vaccination on tumor cells) or with immunization (when PD-1 expression increases on antigen-specific CD8+ T cells with activation) results in anti-tumor responses in patients with advanced, metastatic, castration-resistant prostate cancer,” Dr. McNeel and his colleagues wrote.
They reported preliminary impressions of the efficacy and safety of the combination in 12 patients with mCRPC. The patients all had evidence of progressive disease and were at least 6 months out from chemotherapy. Patients could have previously been treated with enzalutamide (Xtandi) or abiraterone (Zytiga), but were excluded if they had received sipuleucel-T vaccine.
Patients in the ongoing trial are randomized to receive six doses of pTVG-HP over 10 weeks with either four doses of concurrent pembrolizumab, or four doses of pembrolizumab delivered every 3 weeks beginning 2 weeks after the last vaccine dose.
The authors reported that treatment with the combination evokes changes in serum prostate-specific antigen (PSA) that are associated with objective radiographic changes, and “elicits robust and persistent PAP-specific Th1-based immunity.”
They also found evidence to suggest that concurrent administration of the vaccine and the PD-1 inhibitor may be more effective than sequential administration, based on differences in serum PSA and PAP.
Adverse events were generally mild and similar to those seen in other studies of pembrolizumab and DNA vaccine, with only three grade 3 events and no grade 4 events.
The investigators hope to expand the pilot study beyond the 12 weeks originally scheduled, and plan to explore potential biomarkers for vaccine response based on T-cell proliferation in tumors and in regional lymph nodes as seen on imaging modalities.
The study is funded by a 2014 Movember Prostate Cancer Foundation Challenge Award and Madison Vaccines Inc. Dr. McNeel reports an ownership interest and funding support from Madison Vaccines. All other coauthors reported no conflicts of interest.
NATIONAL HARBOR, MD. – To date, checkpoint inhibitors have shown little clinical activity as single agents against metastatic, castration-resistant prostate cancer, but a combination of a DNA vaccine and a programmed-death 1 inhibitor shows promise for enhancing anti-tumor immune responses, report investigators in a phase I trial.
“If you vaccinate animals, PD-1 expression transiently goes up, and if you block it at that point you get a better anti-tumor response, and that was in models where anti PD-1 therapy alone didn’t do anything. So we thought this could be a good approach for prostate cancer,” Douglas G. McNeel, MD, PhD, of the University of Wisconsin, Madison, said in an interview at the annual meeting of the Society for Immunotherapy of Cancer.
Dr. McNeel and colleagues are exploring the therapeutic potential of combining the PD-1 inhibitor pembrolizumab (Keytruda) with an investigational DNA vaccine targeted against prostatic acid phosphatase (PAP), the same antigen targeted by sipuleucel-T (Provenge).
They presented data in a scientific poster from a pilot study of the combination in patients with metastatic, castration-resistant prostate cancer (mCRPC).
Vaccine ramps up PD-1 expression
The investigators had previously shown that patients immunized with a DNA vaccine encoding PAP (pTVG-HP; currently in phase II clinical trials) developed PD-1-regulated, PAP-specific T cells and had increased PD-L1 expression in circulating tumor cells. They also demonstrated in preclinical studies with mouse models that increased PD-1 expression on vaccine-induced CD8-positive T cells led to inferior anti-tumor immune responses, and that blocking PD-1 at the time of T-cell activation with vaccine improved anti-tumor responses.
“The current pilot trial was designed to evaluate whether delivery of PD-1 blockade after immunization (when PD-1-regulated T cells are elicited and when PD-L1 expression is induced with vaccination on tumor cells) or with immunization (when PD-1 expression increases on antigen-specific CD8+ T cells with activation) results in anti-tumor responses in patients with advanced, metastatic, castration-resistant prostate cancer,” Dr. McNeel and his colleagues wrote.
They reported preliminary impressions of the efficacy and safety of the combination in 12 patients with mCRPC. The patients all had evidence of progressive disease and were at least 6 months out from chemotherapy. Patients could have previously been treated with enzalutamide (Xtandi) or abiraterone (Zytiga), but were excluded if they had received sipuleucel-T vaccine.
Patients in the ongoing trial are randomized to receive six doses of pTVG-HP over 10 weeks with either four doses of concurrent pembrolizumab, or four doses of pembrolizumab delivered every 3 weeks beginning 2 weeks after the last vaccine dose.
The authors reported that treatment with the combination evokes changes in serum prostate-specific antigen (PSA) that are associated with objective radiographic changes, and “elicits robust and persistent PAP-specific Th1-based immunity.”
They also found evidence to suggest that concurrent administration of the vaccine and the PD-1 inhibitor may be more effective than sequential administration, based on differences in serum PSA and PAP.
Adverse events were generally mild and similar to those seen in other studies of pembrolizumab and DNA vaccine, with only three grade 3 events and no grade 4 events.
The investigators hope to expand the pilot study beyond the 12 weeks originally scheduled, and plan to explore potential biomarkers for vaccine response based on T-cell proliferation in tumors and in regional lymph nodes as seen on imaging modalities.
The study is funded by a 2014 Movember Prostate Cancer Foundation Challenge Award and Madison Vaccines Inc. Dr. McNeel reports an ownership interest and funding support from Madison Vaccines. All other coauthors reported no conflicts of interest.
AT SITC 2016
Key clinical point:. Adding the PD-1 inhibitor pembrolizumab to a DNA vaccine may enhance vaccine-induced immunity against metastatic castration-resistant prostate cancer (mCRPC).
Major finding: Treatment with a vaccine targeted to prostatic acid phosphatase and pembrolizumab elicited changes in PAP that are associated with objective radiographic responses.
Data source: Ongoing open-label, randomized pilot study in men with mCRPC.
Disclosures: The study is funded by a 2014 Movember Prostate Cancer Foundation Challenge Award and Madison Vaccines Inc. Dr. McNeel reports an ownership interest and funding support from Madison Vaccines. All other coauthors reported no conflicts of interest.
The art of persuasion
With the advent of the Internet, many parents and teen patients come in armed with information and sometimes even a diagnosis. Much of our time is spent dispelling falsehoods that were posted on the Internet or clarifying information that was misinterpreted. Although generally more information is a good thing, too much false information can result in limiting health care.
Vaccine administration has suffered significantly because of this. With a simple Google search, you can find articles that do everything just short of proving that vaccines are harmful, and tear-jerking stories about children who were harmed by the administration of vaccines. Many sites – Vaxtruth.org, healthwyze.org, naturalnews.com – all present convincing data that would scare any concerned parent to not vaccinate their child. So how do medical professionals regain the trust of their parents and/or patients?

The strategies put forth by the Centers for Disease Control and Prevention for talking to parents about vaccines begin with listening.1 Many parents come with fears that are unfounded and unrealistic that can simply be discussed and resolved. Others present with information from the Internet that discourages vaccines or life experiences such as another family member who was thought to be harmed by vaccines; this discussion is more complex.
It is imperative to become familiar with the most popular information sources on the Internet so that you can speak directly to the validity of the source. As well, countering with a more reliable source will substantiate your position. Healthychildren.org2 is an excellent reference for the AAP recommendations and further references. Vaccinesafety.edu is an independent source that reviews vaccine safety and current research.

Being proactive also builds trust. Provide families with the list of ingredients (vaccinesafety.edu), what their role is in keeping vaccines safe (tell them to go to cdc.gov and search under “vaccines for parents”), and help them understand how vaccines work. Parents then see that you are well informed and are passionate about the health of their children. The AAP provides physicians with a tool kit for the HPV vaccine, and the CDC has an HPV tipsheet entitled “Addressing Parents’ Top Questions about HPV Vaccine” that gives suggestions for what you can say or that can save you time if you provide it while the family waits to be seen.
Probably the most important strategy is believing in what you’re doing. No matter what you’re promoting, if you truly believe in it, then you will encourage others to believe in it as well. This requires educating yourself on current research and recommendations, as well as what is being reported in the news so you can be armed with factual data when parents have questions.
Today, health care is a partnership, and we must embrace our role as educators to empower patients to make good choices for themselves as well as their families.
References
1. http://www.cdc.gov/vaccines/hcp/conversations/conv-materials.html
2. https://www.healthychildren.org/English/safety-prevention/immunizations/Pages/Vaccine-Safety-The-Facts.aspx
3. http://www.immunize.org
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at [email protected].
With the advent of the Internet, many parents and teen patients come in armed with information and sometimes even a diagnosis. Much of our time is spent dispelling falsehoods that were posted on the Internet or clarifying information that was misinterpreted. Although generally more information is a good thing, too much false information can result in limiting health care.
Vaccine administration has suffered significantly because of this. With a simple Google search, you can find articles that do everything just short of proving that vaccines are harmful, and tear-jerking stories about children who were harmed by the administration of vaccines. Many sites – Vaxtruth.org, healthwyze.org, naturalnews.com – all present convincing data that would scare any concerned parent to not vaccinate their child. So how do medical professionals regain the trust of their parents and/or patients?
The strategies put forth by the Centers for Disease Control and Prevention for talking to parents about vaccines begin with listening.1 Many parents come with fears that are unfounded and unrealistic that can simply be discussed and resolved. Others present with information from the Internet that discourages vaccines or life experiences such as another family member who was thought to be harmed by vaccines; this discussion is more complex.
It is imperative to become familiar with the most popular information sources on the Internet so that you can speak directly to the validity of the source. As well, countering with a more reliable source will substantiate your position. Healthychildren.org2 is an excellent reference for the AAP recommendations and further references. Vaccinesafety.edu is an independent source that reviews vaccine safety and current research.
Being proactive also builds trust. Provide families with the list of ingredients (vaccinesafety.edu), what their role is in keeping vaccines safe (tell them to go to cdc.gov and search under “vaccines for parents”), and help them understand how vaccines work. Parents then see that you are well informed and are passionate about the health of their children. The AAP provides physicians with a tool kit for the HPV vaccine, and the CDC has an HPV tipsheet entitled “Addressing Parents’ Top Questions about HPV Vaccine” that gives suggestions for what you can say or that can save you time if you provide it while the family waits to be seen.
Probably the most important strategy is believing in what you’re doing. No matter what you’re promoting, if you truly believe in it, then you will encourage others to believe in it as well. This requires educating yourself on current research and recommendations, as well as what is being reported in the news so you can be armed with factual data when parents have questions.
Today, health care is a partnership, and we must embrace our role as educators to empower patients to make good choices for themselves as well as their families.
References
1. http://www.cdc.gov/vaccines/hcp/conversations/conv-materials.html
2. https://www.healthychildren.org/English/safety-prevention/immunizations/Pages/Vaccine-Safety-The-Facts.aspx
3. http://www.immunize.org
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at [email protected].
With the advent of the Internet, many parents and teen patients come in armed with information and sometimes even a diagnosis. Much of our time is spent dispelling falsehoods that were posted on the Internet or clarifying information that was misinterpreted. Although generally more information is a good thing, too much false information can result in limiting health care.
Vaccine administration has suffered significantly because of this. With a simple Google search, you can find articles that do everything just short of proving that vaccines are harmful, and tear-jerking stories about children who were harmed by the administration of vaccines. Many sites – Vaxtruth.org, healthwyze.org, naturalnews.com – all present convincing data that would scare any concerned parent to not vaccinate their child. So how do medical professionals regain the trust of their parents and/or patients?
The strategies put forth by the Centers for Disease Control and Prevention for talking to parents about vaccines begin with listening.1 Many parents come with fears that are unfounded and unrealistic that can simply be discussed and resolved. Others present with information from the Internet that discourages vaccines or life experiences such as another family member who was thought to be harmed by vaccines; this discussion is more complex.
It is imperative to become familiar with the most popular information sources on the Internet so that you can speak directly to the validity of the source. As well, countering with a more reliable source will substantiate your position. Healthychildren.org2 is an excellent reference for the AAP recommendations and further references. Vaccinesafety.edu is an independent source that reviews vaccine safety and current research.
Being proactive also builds trust. Provide families with the list of ingredients (vaccinesafety.edu), what their role is in keeping vaccines safe (tell them to go to cdc.gov and search under “vaccines for parents”), and help them understand how vaccines work. Parents then see that you are well informed and are passionate about the health of their children. The AAP provides physicians with a tool kit for the HPV vaccine, and the CDC has an HPV tipsheet entitled “Addressing Parents’ Top Questions about HPV Vaccine” that gives suggestions for what you can say or that can save you time if you provide it while the family waits to be seen.
Probably the most important strategy is believing in what you’re doing. No matter what you’re promoting, if you truly believe in it, then you will encourage others to believe in it as well. This requires educating yourself on current research and recommendations, as well as what is being reported in the news so you can be armed with factual data when parents have questions.
Today, health care is a partnership, and we must embrace our role as educators to empower patients to make good choices for themselves as well as their families.
References
1. http://www.cdc.gov/vaccines/hcp/conversations/conv-materials.html
2. https://www.healthychildren.org/English/safety-prevention/immunizations/Pages/Vaccine-Safety-The-Facts.aspx
3. http://www.immunize.org
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at [email protected].
HCV patients with early-stage hepatocellular carcinoma can achieve SVR
BOSTON – Among patients with hepatocellular carcinoma (HCC), rates of sustained viral response (SVR) to direct-acting regimens for hepatitis C virus were 79% for genotype 1, 69% for genotype 2, and 47% for genotype 3 infections, reported George N. Ioannou, MD.
“These rates are lower than in patients who do not have hepatocellular carcinoma [HCC], but are still remarkably high,” Dr. Ioannou said during an oral presentation at the annual meeting of the American Association for the Study of Liver Diseases. “Antiviral therapy should be considered in patients with early-stage hepatocellular carcinoma, ideally after adequate locoregional treatments.”
The study included Veterans Affairs Health Care System data on 17,487 recipients of direct-acting anti-HCV regimens. When patients did not have HCC, SVR rates were 93% for genotype 1 infection, 87% for genotype 2 (GT2), and 76% for GT3. Among the 624 (3.6%) patients with a history of HCC, 142 underwent antiviral treatment after transplantation and 482 received other types of cancer therapy.
Why HCC is associated with lower SVR in HCV patients remains unclear, Dr. Ioannou noted. Age does not seem to explain the effect, and neither does sex, race, or ethnicity; cirrhosis or decompensated cirrhosis; renal disease; diabetes; HCV viral load; genotype or subgenotype; HCV regimen; or treatment experience, he said.
Dr. Ioannou noted several study limitations. Nine percent of patients lacked data on SVR, and the imputation to correct for this lowered SVR rates by about 1%-2%. The dataset also did not include information on HCC tumor size or number, and the researchers have not yet examined how antiviral therapy affects the likelihood of de novo HCC, recurrent HCC, or progression of cirrhosis and liver dysfunction.
The Veterans Affairs Office of Research and Development sponsored the study. Dr. Ioannou had no disclosures.
BOSTON – Among patients with hepatocellular carcinoma (HCC), rates of sustained viral response (SVR) to direct-acting regimens for hepatitis C virus were 79% for genotype 1, 69% for genotype 2, and 47% for genotype 3 infections, reported George N. Ioannou, MD.
“These rates are lower than in patients who do not have hepatocellular carcinoma [HCC], but are still remarkably high,” Dr. Ioannou said during an oral presentation at the annual meeting of the American Association for the Study of Liver Diseases. “Antiviral therapy should be considered in patients with early-stage hepatocellular carcinoma, ideally after adequate locoregional treatments.”
The study included Veterans Affairs Health Care System data on 17,487 recipients of direct-acting anti-HCV regimens. When patients did not have HCC, SVR rates were 93% for genotype 1 infection, 87% for genotype 2 (GT2), and 76% for GT3. Among the 624 (3.6%) patients with a history of HCC, 142 underwent antiviral treatment after transplantation and 482 received other types of cancer therapy.
Why HCC is associated with lower SVR in HCV patients remains unclear, Dr. Ioannou noted. Age does not seem to explain the effect, and neither does sex, race, or ethnicity; cirrhosis or decompensated cirrhosis; renal disease; diabetes; HCV viral load; genotype or subgenotype; HCV regimen; or treatment experience, he said.
Dr. Ioannou noted several study limitations. Nine percent of patients lacked data on SVR, and the imputation to correct for this lowered SVR rates by about 1%-2%. The dataset also did not include information on HCC tumor size or number, and the researchers have not yet examined how antiviral therapy affects the likelihood of de novo HCC, recurrent HCC, or progression of cirrhosis and liver dysfunction.
The Veterans Affairs Office of Research and Development sponsored the study. Dr. Ioannou had no disclosures.
BOSTON – Among patients with hepatocellular carcinoma (HCC), rates of sustained viral response (SVR) to direct-acting regimens for hepatitis C virus were 79% for genotype 1, 69% for genotype 2, and 47% for genotype 3 infections, reported George N. Ioannou, MD.
“These rates are lower than in patients who do not have hepatocellular carcinoma [HCC], but are still remarkably high,” Dr. Ioannou said during an oral presentation at the annual meeting of the American Association for the Study of Liver Diseases. “Antiviral therapy should be considered in patients with early-stage hepatocellular carcinoma, ideally after adequate locoregional treatments.”
The study included Veterans Affairs Health Care System data on 17,487 recipients of direct-acting anti-HCV regimens. When patients did not have HCC, SVR rates were 93% for genotype 1 infection, 87% for genotype 2 (GT2), and 76% for GT3. Among the 624 (3.6%) patients with a history of HCC, 142 underwent antiviral treatment after transplantation and 482 received other types of cancer therapy.
Why HCC is associated with lower SVR in HCV patients remains unclear, Dr. Ioannou noted. Age does not seem to explain the effect, and neither does sex, race, or ethnicity; cirrhosis or decompensated cirrhosis; renal disease; diabetes; HCV viral load; genotype or subgenotype; HCV regimen; or treatment experience, he said.
Dr. Ioannou noted several study limitations. Nine percent of patients lacked data on SVR, and the imputation to correct for this lowered SVR rates by about 1%-2%. The dataset also did not include information on HCC tumor size or number, and the researchers have not yet examined how antiviral therapy affects the likelihood of de novo HCC, recurrent HCC, or progression of cirrhosis and liver dysfunction.
The Veterans Affairs Office of Research and Development sponsored the study. Dr. Ioannou had no disclosures.
AT THE LIVER MEETING
Key clinical point: Consider direct-acting antiviral therapy in HCV-infected patients with early-stage HCC.
Major finding: Rates of sustained viral response were 79% in HCC patients with GT1 HCV infection, 69% in GT2 patients, and 47% in GT3 patients.
Data source: An analysis of Veterans Affairs Health Care System data on 17,487 recipients of direct-acting antiviral regimens, including 624 patients with HCC.
Disclosures: The Veterans Affairs Office of Research and Development sponsored the study.
Early TIPS effective in high-risk cirrhosis patients, but still underutilized
BOSTON – High-risk cirrhosis patients treated early with a transjugular intrahepatic portosystemic shunt (TIPS) showed increased survival rates and reduced rates of adverse events, according to a study.
The data were presented at the American Association for the Study of Liver Diseases by Virginia Hernandez-Gea, MD, a hepatologist at the Hospital Clinic in Barcelona.

In each study arm, three-quarters were men in their mid-50s. Cirrhosis in the non-TIPS group was alcohol-related in 57.4% of the cohort, compared with 71.2% of the group given early TIPS; roughly half of each group mentioned alcohol use in the past 3 months.
Also similar were Model for End-stage Liver Disease (MELD) scores: an average of 15.5 in the non-TIPS group, compared with 15 on average in the TIPS group. Nearly three-quarters of the TIPS group had a Child-Pugh C score, compared with 64% in the non-TIPS group. A Child-Pugh score with active bleeding was recorded in 28.8% of the TIPS group, compared with 36% in the non-TIPS group.
The transplant-free survival rate at 1 year in the standard care group was 61%, compared with 76% in the early TIPS group (P = .0175). The failure and bleeding rate at 1 year was significantly higher in the standard care group: 91%, compared with 68% in the early TIPS group (P = .004). Failure and bleeding rates in the Child-Pugh B and C groups across the study were similar.
Ascites at 1 year was seen in 88% of the standard care group, compared with in 64% of the study group. Rates of hepatic encephalopathy were similar in those with Child-Pugh B with active bleeding, and Child-Pugh C across both groups: 22% in the standard care group vs. 25% in the early TIPS group.
That there was no associated significant risk of hepatic encephalopathy in persons with acute variceal bleeding who were given early TIPS “strongly suggests that early TIPS should be included in clinical practice,” Dr. Hernandez-Gea said, noting that only 10% of the 34 sites in the study had used early TIPS. “We don’t really know why centers are not using this, since it is very difficult to find treatments that extend survival rates in this population.”
[email protected]
On Twitter @whitneymcknight
BOSTON – High-risk cirrhosis patients treated early with a transjugular intrahepatic portosystemic shunt (TIPS) showed increased survival rates and reduced rates of adverse events, according to a study.
The data were presented at the American Association for the Study of Liver Diseases by Virginia Hernandez-Gea, MD, a hepatologist at the Hospital Clinic in Barcelona.
In each study arm, three-quarters were men in their mid-50s. Cirrhosis in the non-TIPS group was alcohol-related in 57.4% of the cohort, compared with 71.2% of the group given early TIPS; roughly half of each group mentioned alcohol use in the past 3 months.
Also similar were Model for End-stage Liver Disease (MELD) scores: an average of 15.5 in the non-TIPS group, compared with 15 on average in the TIPS group. Nearly three-quarters of the TIPS group had a Child-Pugh C score, compared with 64% in the non-TIPS group. A Child-Pugh score with active bleeding was recorded in 28.8% of the TIPS group, compared with 36% in the non-TIPS group.
The transplant-free survival rate at 1 year in the standard care group was 61%, compared with 76% in the early TIPS group (P = .0175). The failure and bleeding rate at 1 year was significantly higher in the standard care group: 91%, compared with 68% in the early TIPS group (P = .004). Failure and bleeding rates in the Child-Pugh B and C groups across the study were similar.
Ascites at 1 year was seen in 88% of the standard care group, compared with in 64% of the study group. Rates of hepatic encephalopathy were similar in those with Child-Pugh B with active bleeding, and Child-Pugh C across both groups: 22% in the standard care group vs. 25% in the early TIPS group.
That there was no associated significant risk of hepatic encephalopathy in persons with acute variceal bleeding who were given early TIPS “strongly suggests that early TIPS should be included in clinical practice,” Dr. Hernandez-Gea said, noting that only 10% of the 34 sites in the study had used early TIPS. “We don’t really know why centers are not using this, since it is very difficult to find treatments that extend survival rates in this population.”
[email protected]
On Twitter @whitneymcknight
BOSTON – High-risk cirrhosis patients treated early with a transjugular intrahepatic portosystemic shunt (TIPS) showed increased survival rates and reduced rates of adverse events, according to a study.
The data were presented at the American Association for the Study of Liver Diseases by Virginia Hernandez-Gea, MD, a hepatologist at the Hospital Clinic in Barcelona.
In each study arm, three-quarters were men in their mid-50s. Cirrhosis in the non-TIPS group was alcohol-related in 57.4% of the cohort, compared with 71.2% of the group given early TIPS; roughly half of each group mentioned alcohol use in the past 3 months.
Also similar were Model for End-stage Liver Disease (MELD) scores: an average of 15.5 in the non-TIPS group, compared with 15 on average in the TIPS group. Nearly three-quarters of the TIPS group had a Child-Pugh C score, compared with 64% in the non-TIPS group. A Child-Pugh score with active bleeding was recorded in 28.8% of the TIPS group, compared with 36% in the non-TIPS group.
The transplant-free survival rate at 1 year in the standard care group was 61%, compared with 76% in the early TIPS group (P = .0175). The failure and bleeding rate at 1 year was significantly higher in the standard care group: 91%, compared with 68% in the early TIPS group (P = .004). Failure and bleeding rates in the Child-Pugh B and C groups across the study were similar.
Ascites at 1 year was seen in 88% of the standard care group, compared with in 64% of the study group. Rates of hepatic encephalopathy were similar in those with Child-Pugh B with active bleeding, and Child-Pugh C across both groups: 22% in the standard care group vs. 25% in the early TIPS group.
That there was no associated significant risk of hepatic encephalopathy in persons with acute variceal bleeding who were given early TIPS “strongly suggests that early TIPS should be included in clinical practice,” Dr. Hernandez-Gea said, noting that only 10% of the 34 sites in the study had used early TIPS. “We don’t really know why centers are not using this, since it is very difficult to find treatments that extend survival rates in this population.”
[email protected]
On Twitter @whitneymcknight
AT THE LIVER MEETING
Key clinical point:
Major finding: At 1 year post procedure, early TIPS was associated with better rates of survival and lower rates of adverse events, compared with those who did not receive early TIPS.
Data source: Multicenter, international observational study between 2011 and 2015 of 671 high-risk patients with cirrhosis managed according to current guidelines.
Disclosures: Dr. Hernandez-Gea did not have any relevant disclosures.